Prostate MRI: Revolution, now evolution XXVIIIth Congress of the Hungarian Society of Radiology 24 th June 2016 Tristan Barrett University Lecturer and Honorary NHS Consultant Addenbrooke’s Hospital, Cambridge, UK

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Prostate MRI:
Revolution, now evolution
XXVIIIth Congress of the Hungarian Society of Radiology
24th June 2016
Tristan Barrett
University Lecturer and Honorary NHS Consultant Addenbrooke’sHospital, Cambridge, UK

(R)Evolution of Prostate Talks
RSNA 2001 Understand the application of Prostate MR for staging
RSNA 2003 Imaging Prostate Cancer: What the Radiologist Should Know
RSNA 2005 Prostate Cancer Imaging: Past, Present, and Future
RSNA 2007 Prostate MR: Relevance, Current Practices, and Evolving
Techniques
RSNA 2010 Prostate MRI: Ready for Prime Time
BIR 2014 Prostate mp-MRI: Can it facilitate a paradigm shift in
management?
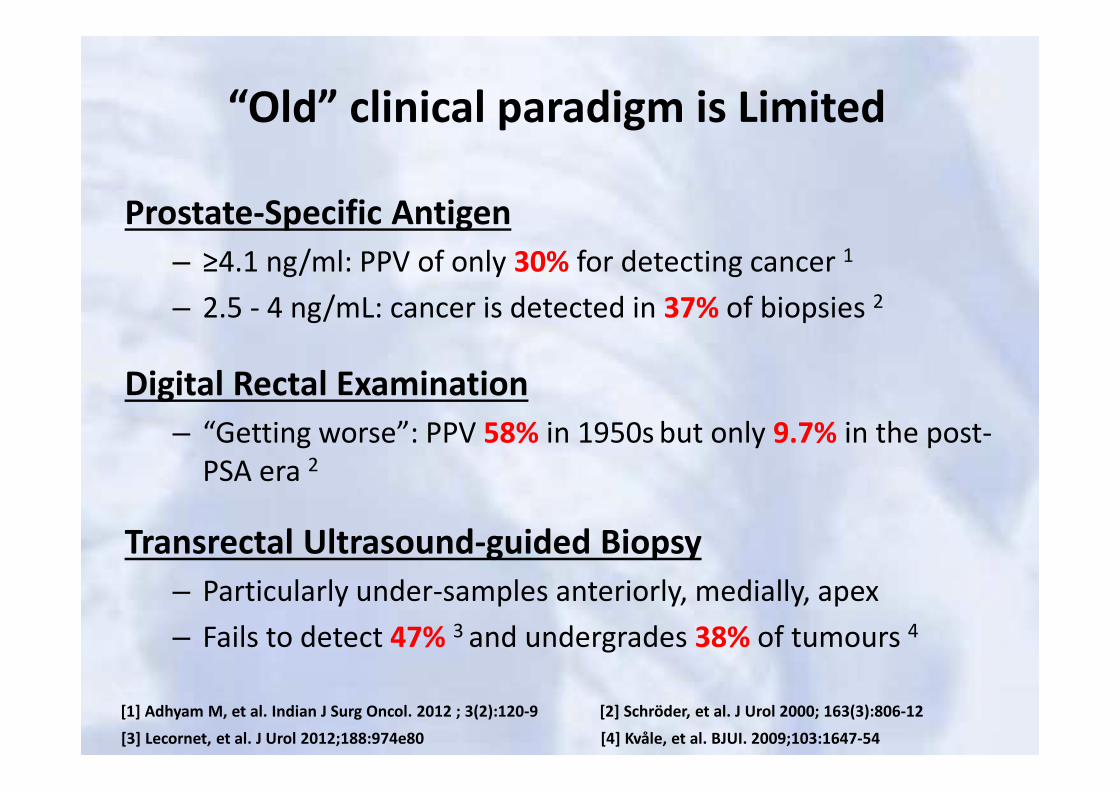
“Old” clinical paradigm is Limited
Prostate-Specific Antigen
– ≥4.1 ng/ml: PPV of only 30% for detecting cancer 1
– 2.5 - 4 ng/mL: cancer is detected in 37% of biopsies 2
Digital Rectal Examination
– “Getting worse”: PPV 58% in 1950s but only 9.7% in the post-
PSA era 2
Transrectal Ultrasound-guided Biopsy
– Particularly under-samples anteriorly, medially, apex
– Fails to detect 47% 3 and undergrades 38% of tumours 4
[1] Adhyam M, et al. Indian J Surg Oncol. 2012 ; 3(2):120-9 [2] Schröder, et al. J Urol 2000; 163(3):806-12
[4] Kvåle, et al. BJUI. 2009;103:1647-54[3] Lecornet, et al. J Urol 2012;188:974e80

• Prostate MRI previously used for local T-staging
• Anatomical imaging sensitive but not specific
– “multiparametric” MRI with functional imaging allows
↑lesion detec>on and (possibly) characterisa>on
• There are several drivers to lesion identification
– Targeting repeat biopsies in high risk patients
– Risk stratification at AS enrolment
– Potential for focal therapies
Evolving Role of Imaging

Diffusion-weighted imaging
• Paradigm: tumours show restricted diffusion
• ↑cellularity, ↑nuclear : cytoplasmic ratio
Dynamic contrast-enhanced (DCE) MRI
• Paradigm: tumours have “leaky” vessels
• ↑angiogenesis; disorganized neovasculature
MR Spectroscopy (MRSI)
• Paradigm: tumours have ↑ cells and ↑prolifera>on
• ↑Choline and ↓citrate (benign marker)
Available functional sequences

Khalifa MHK, Hafez A, Elnoueam K, A. Elabbady, et al. DOI: 10.1594/ecr2015/C-0590
Acc
ura
cy (
%)
100
90
80
70
60
50
40
30
20
10
0
↑ Sequences = ↑ Accuracy

Mowatt G, et al. Health Technol Assess. 2013; 17(20):vii-xix, 1-281
Est
ima
ted
He
alt
hca
re C
ost
(£
)↑ Sequences = ↑↑ £Cost

Current PIRADS (v2) recommends
• Axial T2WI and DWI, DCE 1
• Why has MRSI been dropped?
– Specificity 100% (!) - Good for characterisation 2
– Sensitivity 16% - Poor for lesion detection
• Should we also drop DCE?
[2] Turkbey B, et al. J Urol. 2011;186(5):1818-24[1] Barrett T, et al. Clin. Rad. 2015; 70: 1165-76

Should we also drop DCE?
The prostate is NOT the breast– Benign conditions such as prostatitis and BPH can demonstrate early
contrast wash-in and wash-out
– Tumours more commonly have a Type II curve
– Inability of curve-typing to accurately differentiate malignancy 2
[2] Hansford BG, et al. Radiology. 2015;275:448-57[1] Macura KJ, et al. Radiographics. 2006; 26:1719-34
Type I: 83% benign; 9% cancer
….………………………………..
Type III: 90.4% spec for cancer 13
2
1

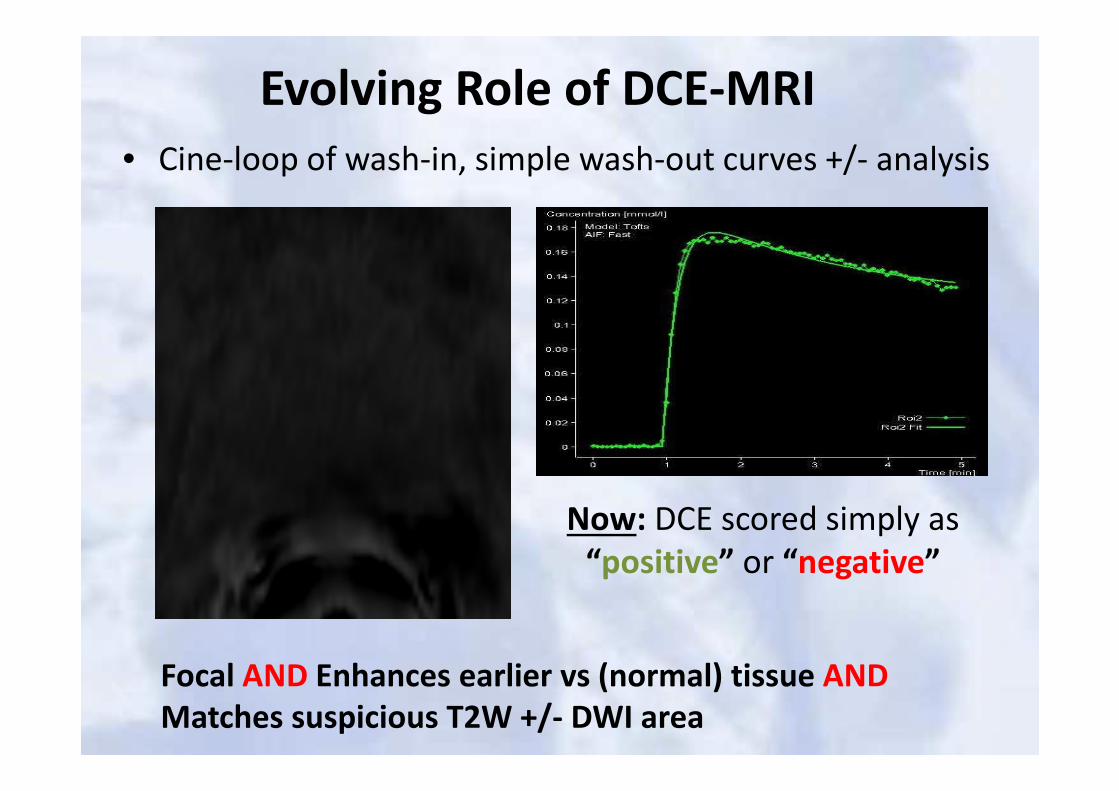
Evolving Role of DCE-MRI
• Cine-loop of wash-in, simple wash-out curves +/- analysis
Focal AND Enhances earlier vs (normal) tissue AND
Matches suspicious T2W +/- DWI area
Now: DCE scored simply as
“positive” or “negative”
Evolving Role of DCE-MRI
• Cine-loop of wash-in, simple wash-out curves +/- analysis
Focal AND Enhances earlier vs (normal) tissue AND
Matches suspicious T2W +/- DWI area
Now: DCE scored simply as
“positive” or “negative”

How good is mp-MRI?
• mp-MRI for lesion detection– Gleason 3+4 lesions ≥0.5 cm3 (≈ 10 mm sphere) 1
– Gleason ≥4+3 lesions ≥0.2cm3 (≈ 7 mm sphere) 1
– Sens 74%, spec 88% 2
– Will “never” detect all small vol GS 6… may be a good thing
• … But it’s difficult– Known learning curve for reporting 3
– Technical factors (coil, sequences), Patient factors (BPH, previous treatment, biopsy artefact)
[1] Puech, et al. Eur Rad. 2009;19:470-80 [2] de Rooij M, et al. AJR. 2014; 202(2):343-5
[3] Gaziev G, et al. BJU Int. 2016;117(1):80-6

Should we offer MRI before
biopsy?

MRI pre-biopsy
• “Most” who have TRUS Bx will go on to have MRI
– Why not MRI pre biopsy?
– Avoids biopsy related artefact
– Allows triage of biopsy “type” +/- targeting
• Even IF no increase in MRIs done
– Harder to schedule “within 5 days” vs “4-6 weeks”
– Report turnaround time

Local experience
• Official part of pathway since 5th October 2015
– Aim MRI in 5 days, clinic in 7 days (2 days to report)
• Pre-Pre-Biopsy MRI
– 607 MRs in 39 wks 5/1/15 - 4/10/15 (15.6 per week)
• Post-Pre-Biopsy MRI
– 661 MRs in 35 wks 5/10/15 – 5/6/16 (18.9 per week)
↑3.3/wk (↑ ~20%)

MRI numbers Pre vs Post

Totals
• Oct 2015 – Jan 2016 “Initial spike”
– 274 MRs in 14 wks 5/10/16 - 10/1/16 (19.9 per wk)
• Jan – June 2016
– 383 MRs in 21 wks 11/1/16 - 5/6/16 (18.2 per wk)
• Jan – June 2015
– 350 MRs in 21 wks 12/1/15 - 7/6/15 (16.7 per wk)
↑1.5/wk (↑ <10%)
… “Probably” no increase (vs background) after initial spike
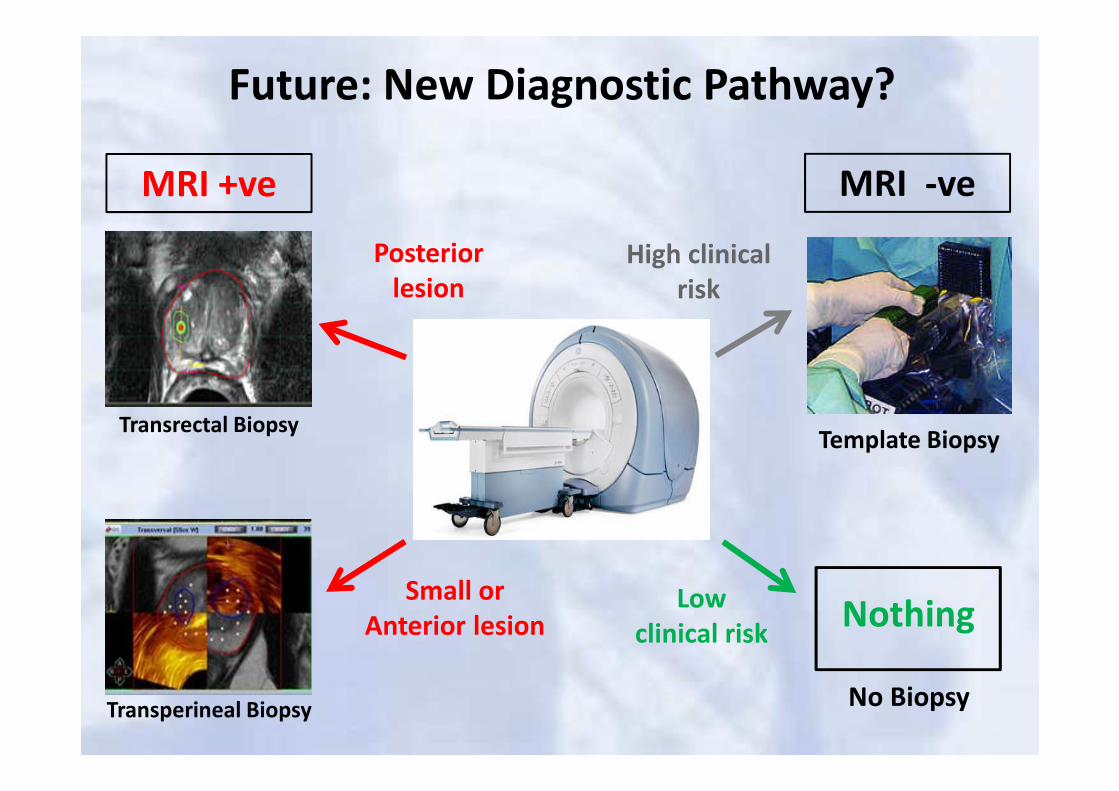
MRI +ve MRI -ve
Small or
Anterior lesion
Posterior
lesion
Transrectal Biopsy
Transperineal Biopsy
NothingLow
clinical risk
High clinical
risk
Template Biopsy
No Biopsy
Future: New Diagnostic Pathway?

Conclusions
• Revolution has occurred
– mpMRI established in the work-up of prostate cancer
• Evolution now in process
– Spectroscopy dropped
– DCE role significantly changed
• Further evolving considerations
– MRI pre-biopsy?
– Role of MRI in follow-up of AS needs defining
– Choice of “short” or “detailed” protocols?
Related Documents











