1 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 Prioritising gender, equity, and human rights in a GRADE-based framework to inform future research on self care for sexual and reproductive health and rights Nandi Siegfried , 1 Manjulaa Narasimhan, 2 Carmen H Logie, 3 Rebekah Thomas, 4 Laura Ferguson, 5 Kevin Moody, 6 Michelle Remme 7 Original research To cite: Siegfried N, Narasimhan M, Logie CH, et al. Prioritising gender, equity, and human rights in a GRADE- based framework to inform future research on self care for sexual and reproductive health and rights. BMJ Global Health 2020;5:e002128. doi:10.1136/ bmjgh-2019-002128 Handling editor Seye Abimbola Received 30 October 2019 Revised 28 January 2020 Accepted 15 February 2020 For numbered affiliations see end of article. Correspondence to Dr Nandi Siegfried; [email protected] © Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ. ABSTRACT Introduction In January 2019, the WHO reviewed evidence to develop global recommendations on self-care interventions for sexual and reproductive health and rights (SRHR). Identification of research gaps is part of the WHO guidelines development process, but reliable methods to do so are currently lacking with gender, equity and human rights (GER) infrequently prioritised. Methods We expanded a prior framework based on Grading of Evidence, Assessment, Development and Evaluation (GRADE) to include GER. The revised framework is applied systematically during the formulation of research questions and comprises: (1) assessment of the GRADE strength and quality rating of recommendations; (2) mandatory inclusion of research questions identified from a global stakeholder survey; and (3) selection of the GER standards and principles most relevant to the question through discussion and consensus. For each question, we articulated: (1) the most appropriate and robust study design; (2) an alternative pragmatic design if the ideal design was not feasible; and (3) the methodological challenges facing researchers through identifying potential biases. Results We identified 39 research questions, 7 overarching research approaches and 13 discrete feasible study designs. Availability and accessibility were most frequently identified as the GER standards and principles to consider when planning studies, followed by privacy and confidentiality. Selection and detection bias were the primary methodological challenges across mixed methods, quantitative and qualitative studies. A lack of generalisability potentially limits the use of study results with non-participation in research potentially highest in more vulnerable populations. Conclusion A framework based on GRADE that includes stakeholders’ values and identification of core GER standards and principles provides a practical, systematic approach to identifying research questions from a WHO guideline. Clear guidance for future studies will contribute to an anticipated ‘living guidelines’ approach within WHO. Foregrounding GER as a separate component of the framework is innovative but further elaboration to operationalise appropriate indicators for SRHR self-care interventions is required. INTRODUCTION The mandate of the WHO is to develop global clinical and public health guidance that informs country-level healthcare policies, guidelines, programmes and services. The systematic process of WHO guideline devel- opment includes the identification and docu- mentation of research gaps. 1 This is intended to focus research to inform and strengthen Key questions What is already known? ► Reliable methods to identify research gaps from WHO guidelines are lacking with gender, equity and human rights (GER) infrequently prioritised when for- mulating future research questions. What are the new findings? ► A prior Grading of Evidence, Assessment, Development and Evaluation (GRADE)-based frame- work was revised to include mandatory stakeholder input and selection of relevant GER standards and principles and successfully applied to a WHO guide- line on self-care interventions for sexual and repro- ductive health and rights (SRHR). ► 39 research questions, 6 research approaches and 16 discrete study designs for SRHR self-care were identified and the key methodological issues outlined. ► Availability and accessibility were the GER standards and principles most frequently identified as relevant. What do the new findings imply? ► Application of the GRADE-informed framework to future WHO guidelines development processes has potential to harmonise research question formula- tion and to ensure more consistent consideration of GER across the organisation. ► The dashboard outlining future SRHR studies is ex- pected to prove useful to researchers. on July 28, 2020 by guest. Protected by copyright. http://gh.bmj.com/ BMJ Glob Health: first published as 10.1136/bmjgh-2019-002128 on 30 March 2020. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
Prioritising gender, equity, and human rights in a GRADE- based framework to inform future research on self care for sexual and reproductive health and rights
Nandi Siegfried ,1 Manjulaa Narasimhan,2 Carmen H Logie,3 Rebekah Thomas,4 Laura Ferguson,5 Kevin Moody,6 Michelle Remme7
Original research
To cite: Siegfried N, Narasimhan M, Logie CH, et al. Prioritising gender, equity, and human rights in a GRADE- based framework to inform future research on self care for sexual and reproductive health and rights. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
Handling editor Seye Abimbola
Received 30 October 2019Revised 28 January 2020Accepted 15 February 2020
For numbered affiliations see end of article.
Correspondence toDr Nandi Siegfried; nandi. siegfried@ gmail. com
© Author(s) (or their employer(s)) 2020. Re- use permitted under CC BY. Published by BMJ.
AbsTrACTIntroduction In January 2019, the WHO reviewed evidence to develop global recommendations on self- care interventions for sexual and reproductive health and rights (SRHR). Identification of research gaps is part of the WHO guidelines development process, but reliable methods to do so are currently lacking with gender, equity and human rights (GER) infrequently prioritised.Methods We expanded a prior framework based on Grading of Evidence, Assessment, Development and Evaluation (GRADE) to include GER. The revised framework is applied systematically during the formulation of research questions and comprises: (1) assessment of the GRADE strength and quality rating of recommendations; (2) mandatory inclusion of research questions identified from a global stakeholder survey; and (3) selection of the GER standards and principles most relevant to the question through discussion and consensus. For each question, we articulated: (1) the most appropriate and robust study design; (2) an alternative pragmatic design if the ideal design was not feasible; and (3) the methodological challenges facing researchers through identifying potential biases.results We identified 39 research questions, 7 overarching research approaches and 13 discrete feasible study designs. Availability and accessibility were most frequently identified as the GER standards and principles to consider when planning studies, followed by privacy and confidentiality. Selection and detection bias were the primary methodological challenges across mixed methods, quantitative and qualitative studies. A lack of generalisability potentially limits the use of study results with non- participation in research potentially highest in more vulnerable populations.Conclusion A framework based on GRADE that includes stakeholders’ values and identification of core GER standards and principles provides a practical, systematic approach to identifying research questions from a WHO guideline. Clear guidance for future studies will contribute to an anticipated ‘living guidelines’ approach within WHO. Foregrounding GER as a separate component of the framework is innovative but further elaboration to operationalise appropriate indicators for SRHR self- care interventions is required.
InTroduCTIonThe mandate of the WHO is to develop global clinical and public health guidance that informs country- level healthcare policies, guidelines, programmes and services. The systematic process of WHO guideline devel-opment includes the identification and docu-mentation of research gaps.1 This is intended to focus research to inform and strengthen
Key questions
What is already known? ► Reliable methods to identify research gaps from WHO guidelines are lacking with gender, equity and human rights (GER) infrequently prioritised when for-mulating future research questions.
What are the new findings? ► A prior Grading of Evidence, Assessment, Development and Evaluation (GRADE)- based frame-work was revised to include mandatory stakeholder input and selection of relevant GER standards and principles and successfully applied to a WHO guide-line on self- care interventions for sexual and repro-ductive health and rights (SRHR).
► 39 research questions, 6 research approaches and 16 discrete study designs for SRHR self- care were identified and the key methodological issues outlined.
► Availability and accessibility were the GER standards and principles most frequently identified as relevant.
What do the new findings imply? ► Application of the GRADE- informed framework to future WHO guidelines development processes has potential to harmonise research question formula-tion and to ensure more consistent consideration of GER across the organisation.
► The dashboard outlining future SRHR studies is ex-pected to prove useful to researchers.
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

2 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
new and existing WHO recommendations. However, wide variation in the quality, robustness, presentation and dissemination of research priorities across sets of WHO guidelines has been noted.2 Currently within the WHO transformation process, systematic approaches to coherent research agenda formulation are being explored.
In 2018, the WHO Department of Reproductive Health and Research embarked on a process to: (1) develop evidence- based recommendations on self- care inter-ventions for sexual and reproductive health and rights (SRHR) and (2) delineate research gaps in the field. A Guidelines Development Group (GDG) was established comprising experts and stakeholders active in SRHR and/or self- care interventions. The GDG was regionally and gender representative and included representation from youth, vulnerable populations, healthcare providers, policymakers, programme managers, researchers and civil society, as well as experts in human rights, gender equality and health economics.3
The following definition of self- care was adopted for the guidelines: self- care is the ability of individuals, families and communities to promote health, prevent disease, maintain health and to cope with illness and disability with or without the support of a healthcare provider.4 The scope of self- care as described in this definition includes health promo-tion, disease prevention and control, self- medication, providing care to dependent persons, seeking hospital/specialist care if necessary and rehabilitation including palliative care.
Members of the GDG attended a scoping meeting in March 2018 to prioritise and refine the self- care inter-ventions to be evaluated in the guideline and to reflect on discussions arising from a prior WHO- led meeting on the ethical, legal, social accountability and human rights implications of self- care interventions.5 The GDG agreed that the systematic consideration of gender, equity and human rights (GER) in the provision of self- care interventions is key to ensuring better health for all. As defined by WHO, human rights- based approaches to health consider and address inequalities, power imbal-ances and discrimination, including those related to gender.6 Such approaches also aim to support better and more sustainable health and development outcomes and focus on capacity development, both of duty bearers to meet their obligations and of individuals to claim their rights.7 Attention to ways of empowering individuals and communities, particularly vulnerable populations, to understand and claim their rights requires special atten-tion in many domains, including in research. Sridharan and colleagues8 argue that WHO needs to develop concrete actions towards mainstreaming GER. The GDG selected the fulfilment of the following GER standards and principles as key to measuring the impact of self- care interventions in future research studies: (1) the right to highest attainable standard of health (including avail-ability, accessibility, acceptability and quality); (2) active and fully informed participation; (3) non- discrimination;
(4) the right to seek, receive and impart information; (5) informed decision- making; (6) privacy and confidenti-ality; and (7) accountability.9
At a final GDG meeting in January 2019, the GDG reviewed evidence from five systematic reviews on self- care interventions in order to formulate new consensus- based self- care recommendations.3 The new recommendations covered the following topics: (1) self- injectable hormonal contraception, (2) over- the- counter oral contraception, (3) home- based ovulation predictor kits (OPKs), (4) self- sampling for human papilloma virus (HPV) and (5) self- collection of samples for sexually transmitted infections (STIs). Each recom-mendation was formulated in response to an a priori clinical or public health question regarding the effec-tiveness of the intervention when offered as an addi-tional approach to current practice within the formal health sector. The questions were formulated using the Population, Interventions, Comparison and Outcomes (PICO) structure.1
To further inform the guidelines, the GDG also reviewed evidence from a global online survey of health-care providers and users of healthcare services, which was hosted on the WHO website and shared via several listservs between July and October 2018.10 The survey included a range of questions regarding respondents’ values and preferences for self- care interventions for sexual and reproductive health. Three of these were interventions evaluated in the systematic reviews: (1) self- injectable hormonal contraception, (2) oral contracep-tion (including over the counter), and (3) self- collection of samples for STIs (including HPV). The survey reached 294 (35.6%) healthcare providers and 531 (64.4%) users of healthcare services from 113 countries. There was diversity in WHO regional representation in responses from healthcare providers (Africa 30.0%, Europe 20.8%, Latin America and the Caribbean 20.8%, Asia 14.2%, Northern America 13.9% and Oceania 0.3%) and lay respondents (Europe 32.0%, Africa 23.0%, Asia 20.2%, Northern America 12.9%, Latin America and the Carib-bean 10.5% and Oceania 1.3%).10
In this article, we present a systematic approach to the formulation of research questions to guide future studies related to the five topics of the new WHO recommen-dations on self- care interventions. We demonstrate how evidence from systematic reviews, results from a global survey and consideration of GER, together informed question formulation. Our primary aim is to demon-strate both the feasibility and utility of using a structured process combined with a GER lens to identify research gaps within the context of developing a WHO guideline. A secondary aim is to provide researchers with a dash-board of potential evidence- informed research ques-tions and related feasible study designs—and associated methodological challenges and GER considerations—to ensure responsive future research in the rapidly evolving field of SRHR self- care.
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 3
BMJ Global Health
Table 1 Key domains that require consideration when formulating WHO recommendations
Factor How the factor influences the direction and strength of a recommendation
Quality of the evidence The quality of the evidence across outcomes critical to decision making will inform the strength of the recommendation. The higher the quality of the evidence, the greater the likelihood of a strong recommendation.
Values and preferences This describes the relative importance assigned to health outcomes by those affected by them; how such importance varies within and across populations; and whether this importance or variability is surrounded by uncertainty. The less uncertainty or variability there is about the values and preferences of people experiencing the critical or important outcomes, the greater the likelihood of a strong recommendation.
Balance of benefits versus harms
This requires an evaluation of the absolute effects of both benefits and harms (or downsides) of the intervention and their importance. The greater the net benefit or net harm associated with an intervention or exposure, the greater the likelihood of a strong recommendation in favour or against the intervention.
Resource implications This pertains to how resource intense an intervention is, whether it is cost–effective and whether it offers any incremental benefit. The more advantageous or clearly disadvantageous the resource implications are, the greater the likelihood of a strong recommendation either for or against the intervention.
Priority The problem’s priority is determined by its importance and frequency (ie, burden of disease, disease prevalence or baseline risk). The greater the importance of the problem, the greater the likelihood of a strong recommendation.
Equity and human rights The greater the likelihood that the intervention will reduce inequities, improve equity or contribute to the realisation of one or several human rights as defined under the international legal framework, the greater the likelihood of a strong recommendation.
Acceptability The greater the acceptability of an option to all or most stakeholders, the greater the likelihood of a strong recommendation.
Feasibility The greater the feasibility of an option from the standpoint of all or most stakeholders, the greater the likelihood of a strong recommendation. Feasibility overlaps with values and preferences, resource considerations, existing infrastructures, equity, cultural norms, legal frameworks and many other considerations.
Reproduced from the WHO 2014.1
MeTHodsWe adopted a similar methodological approach to research formulation used in two previously published WHO guidelines.11 12 Prior to the GDG meeting, a system-atic review, including meta- analysis where appropriate, was conducted for each of the five selected PICO ques-tions.13–17 The overall certainty of evidence was rated as high, moderate, low or very low according to the Grading of Evidence, Assessment, Development and Evalua-tion (GRADE) approach.18 The certainty of evidence is dependent on the risk of bias, precision, consistency, directness of the results and other considerations such as publication bias. During the meeting, the GDG formu-lated a recommendation in response to the following GRADE domains: certainty of the evidence, balance of benefits and harms, resource use implications, user values and preferences, acceptability among healthcare providers and key stakeholders, feasibility, equity and human rights (See table 1). Recommendations were then further categorised by the GDG as strong or conditional. In general, strong recommendations are made when the quality of evidence is high and the benefits of an intervention clearly outweigh the harms, whereas condi-tional recommendations recognise that the quality of the
evidence is low or that specific country contextual factors may determine the uptake of a recommendation.19
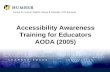
We used the GRADE framework as a starting point as it allows determination of research gaps based on the strength of the recommendation and the certainty of the evidence. For example, identification of a conditional recommendation, or low or very low certainty evidence, regardless of the strength of the recommendation, is indicative of where further research is required (see figure 1).
Previously, we had expanded the GRADE framework and included an additional component specific to the values and preferences of the community of users and potential users the recommendations intend to serve.12 We applied this step to the current guidelines on self- care interventions and reviewed results from the WHO- commissioned global online survey of users of sexual and reproductive self- care interventions.3 In addition, we captured specific research gaps identified by GDG participants during dedicated sessions at both the scoping and guidelines development meetings. We then viewed each research question through a GER lens and through discussion and consensus between authors of this paper identified the GER standards and principles
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

4 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Figure 1 Hierarchical decision making algorithm to formulate research questions based on the presence and strength of a WHO recommendation, combined with the source of the question. GDG, Guidelines Development Group; GER, gender, equity and human rights; PICO, Population, Interventions, Comparison and Outcomes.
essential to consider and measure when planning future research.
Following the GDG meeting, for each a priori PICO question, and for additional research questions identi-fied from the global survey and during the meeting, we tabulated the following:1. The clinical, programmatic, values- based or GER re-
search question.2. The related recommendation formulated by the GDG
(or a record that no recommendation was made) where applicable.
3. The strength of each recommendation where applica-ble.
4. The certainty of the evidence underpinning the rec-ommendation where applicable.
5. The GER standards and principles most relevant to the question as discussed during the scoping and guide-line development meetings and agreed on by authors of this paper.
From the above, a research gap was identified when one or more of the following conditions was met: (1) the recommendation was conditional; or (2) the certainty of evidence was low or very low (even in the presence of a strong recommendation); or (3) key GER principles were not considered or absent (even if the certainty of evidence was moderate or high for clinical or public health effectiveness outcomes); or (4) no recommendation was made and the GDG or survey had articulated a research gap during their deliberations. We also identified a gap for strong recommendations if the evidence only arose
from well- resourced settings. For each identified research gap, the authors then tabulated the following:6. The most robust study design to answer the research
question(s), including identification of GER princi-ples to consider.
7. Conceptualisation of a pragmatic alternative study de-sign if the ideal design was not feasible.
8. Consideration of the methodological challenges of the alternative study design with the potential bias(es) identified.
Following tabulation, we categorised the primary focus of each research question according to the relevant GRADE domain as outlined in table 1.
Patient and public involvementParticipation of the public in developing research gaps was achieved in several ways: (1) through completion of the global survey, (2) members of several civil society associations contributed to the GDG meeting as partic-ipants on the GDG, (3) one of the authors is a patient representative and (4) all authors identify as individuals who engage or may engage with SRHR self- care interven-tions.
resulTsTables 2–6 provide an overview of research gaps in SRHR self- care, the most relevant GER for each question and the study design(s) considered most feasible and appro-priate to answer each question. Thirty- nine research ques-tions were formulated with seven overarching research
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 5
BMJ Global Health
Tab
le 2
R
esea
rch
gap
s fo
r se
lf- ad
min
istr
atio
n of
inje
ctab
le c
ontr
acep
tion
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed o
r hu
man
rig
hts
que
stio
nC
urre
nt W
HO
re
com
men
dat
ion
Str
eng
th o
f re
com
men
dat
ion
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty a
nd p
ract
ical
co
nstr
aint
sA
lter
nati
ve s
tud
y d
esig
nM
etho
do
log
ical
issu
es a
risi
ng
in t
he a
lter
nati
ve s
tud
y d
esig
n
Ben
efits
ver
sus
harm
sP
ICO
: sho
uld
sel
f-
adm
inis
tere
d in
ject
able
co
ntra
cep
tion
be
mad
e av
aila
ble
as
an a
dd
ition
al
app
roac
h to
del
iver
in
ject
able
con
trac
eptio
n?
Sel
f- ad
min
iste
red
in
ject
able
con
trac
eptio
n sh
ould
be
mad
e av
aila
ble
as
an
add
ition
al a
pp
roac
h to
del
iver
inje
ctab
le
cont
race
ptio
n.
Str
ong.
Mod
erat
e.N
o d
ata
avai
lab
le
from
LM
IC;
avai
lab
ility
, ac
cess
ibili
ty,
priv
acy
and
co
nfid
entia
lity.
RC
T co
nduc
ted
in
LMIC
with
incl
usio
n of
ou
tcom
es t
o m
easu
re
acce
ssib
ility
, priv
acy
and
co
nfid
entia
lity.
As
a st
rong
WH
O
reco
mm
end
atio
n ex
ists
, it
wou
ld b
e un
ethi
cal t
o re
pea
t an
RC
T of
the
in
terv
entio
n.
Pro
spec
tive
non-
cont
rolle
d c
ohor
t st
udy
to b
e co
nduc
ted
in s
ever
al
low
- an
d m
idd
le- i
ncom
e co
untr
ies
whe
re t
he in
terv
entio
n is
or
will
be
imp
lem
ente
d. A
naly
sis
to c
omb
ine
qua
ntita
tive
surv
ey s
upp
lem
ente
d
with
focu
sed
in- d
epth
qua
litat
ive
inte
rvie
ws
with
wom
en (b
oth
thos
e w
ho h
ave
used
and
hav
e no
t us
ed s
elf-
adm
inis
tere
d in
ject
able
co
ntra
cep
tion
and
incl
udin
g ad
oles
cent
girl
s an
d y
oung
wom
en)
to e
xplo
re G
ER
out
com
es o
f av
aila
bili
ty, a
cces
sib
ility
, priv
acy
and
co
nfid
entia
lity.
Cos
t an
alys
es c
an b
e ne
sted
in t
he c
ohor
t st
udy.
Con
foun
din
g: p
artic
ipan
ts
in c
ohor
t se
lf- se
lect
to
self-
ad
min
iste
r in
ject
able
and
may
ha
ve o
ther
sim
ilar
char
acte
ristic
s th
at m
ay in
fluen
ce t
heir
abili
ty t
o ac
cess
inje
ctab
le c
ontr
acep
tion.
Mea
sur e
men
t b
ias:
sel
f- re
por
ting
bia
s an
issu
e fo
r q
ualit
ativ
e co
mp
onen
t. T
his
will
req
uire
w
ell t
rain
ed r
esea
rche
rs a
nd
valid
ated
too
ls. T
he t
riang
ulat
ion
of t
he q
ualit
ativ
e d
ata
with
th
e q
uant
itativ
e su
rvey
res
ults
p
rovi
des
an
elem
ent
of a
dd
ition
al
valid
atio
n of
out
com
es.
Valu
es a
nd
pre
fere
nces
Is t
here
an
imp
act
of
diff
eren
ces
bet
wee
n gr
oup
s of
wom
en (e
g,
age,
soc
ioec
onom
ic a
nd
occu
pat
iona
l sta
tus)
on
the
ir va
lues
and
p
refe
renc
es w
ith r
esp
ect
to s
elf-
adm
inis
trat
ion
of
inje
ctab
le c
ontr
acep
tion?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Acc
essi
bili
ty,
priv
acy
and
co
nfid
entia
lity,
non
- d
iscr
imin
atio
n.
Cro
ss- s
ectio
nal s
tud
y of
w
omen
usi
ng in
ject
able
co
ntra
cep
tion
to
eval
uate
ass
ocia
tions
b
etw
een
char
acte
ristic
s an
d u
se, o
r w
illin
gnes
s to
use
.
A s
urve
y m
ay n
ot p
rovi
de
an o
bje
ctiv
e m
easu
re
or a
tru
e re
flect
ion
of
beh
avio
urs
if d
riven
by
que
stio
ns r
equi
ring
soci
ally
ac
cep
tab
le r
esp
onse
s.
This
is a
feas
ible
stu
dy
des
ign
but
co
uld
be
sup
ple
men
ted
with
dia
ry
colle
ctio
n of
dat
a as
gre
ater
priv
acy
and
less
like
ly fo
r so
cial
des
irab
ility
to
influ
ence
sel
f- re
cord
ing.
Par
tner
ing
with
wom
en w
ho h
ave
used
or
are
will
ing
to s
elf-
adm
inis
ter
inje
ctab
le
cont
race
ptio
n is
imp
orta
nt t
o id
entif
y cr
itica
l and
non
- jud
gmen
tal q
uest
ions
.
Mea
sure
men
t b
ias:
for
bot
h su
rvey
and
dia
ry c
olle
ctio
n,
que
stio
ns w
ill n
eed
to
be
form
ulat
ed t
oget
her
with
wom
en
usin
g in
ject
able
con
trac
eptio
n to
ens
ure
trus
t, p
artic
ipat
ion
and
va
lidity
to
avoi
d s
ocia
l des
irab
ility
b
ias.
Wha
t ha
pp
ens
afte
r w
omen
dis
cont
inue
us
e of
sel
f- in
ject
able
co
ntra
cep
tion
– d
o th
ey
use
othe
r m
etho
ds?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Acc
essi
bili
ty.
Nat
iona
l pha
rmac
y or
cl
inic
- bas
ed r
egis
try
of w
omen
usi
ng s
elf-
ad
min
iste
red
inje
ctab
le
cont
race
ptio
n.
Reg
istr
ies
can
be
cost
ly
to e
stab
lish,
mai
ntai
n an
d
mon
itor.
A r
egis
try
req
uire
s p
oliti
cal w
ill a
nd c
apac
ity
to p
rovi
de
effe
ctiv
e d
ata
to
info
rm d
ecis
ions
.
Con
veni
ence
sam
ple
and
sur
vey
of
wom
en a
tten
din
g fa
mily
pla
nnin
g cl
inic
s to
elu
cid
ate
thei
r p
rior
mod
es
of c
ontr
acep
tion
and
rea
sons
for
dis
cont
inua
tion.
Sel
ectio
n b
ias:
suc
h a
sam
ple
w
ould
onl
y in
clud
e w
omen
who
at
tend
the
clin
ic t
o ch
ange
to
a d
iffer
ent
form
of c
ontr
acep
tion;
w
omen
who
cea
se t
o us
e se
lf-
adm
inis
tere
d c
ontr
acep
tion
and
d
o no
t re
turn
to
the
clin
ic w
ould
no
t b
e in
clud
ed. T
heir
choi
ces
may
diff
er fr
om t
hose
wom
en
who
do
atte
nd t
he c
linic
.
Wha
t is
the
imp
act
of
stig
ma
on t
he c
hoic
e of
se
lf- ad
min
istr
atio
n of
in
ject
able
con
trac
eptio
n?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G a
nd
surv
ey.
Acc
essi
bili
ty,
priv
acy
and
co
nfid
entia
lity
and
no
n- d
iscr
imin
atio
n.
Qua
litat
ive
stud
y of
in
terv
iew
s of
wom
en
self-
adm
inis
terin
g in
ject
able
con
trac
eptio
n to
elu
cid
ate
thei
r ex
per
ienc
es a
nd
obse
rvat
ions
.
This
is a
feas
ible
stu
dy.
Not
ap
plic
able
.S
elec
tion
bia
s: a
s w
ith a
ll q
ualit
ativ
e st
udie
s, p
artic
ipan
ts
are
pur
pos
ivel
y se
lect
ed.
How
ever
, thi
s is
an
adva
ntag
e in
thi
s st
udy
des
ign
as t
hose
w
omen
who
hav
e co
nsid
ered
thi
s is
sue
will
hav
e ric
h ex
per
ienc
es
and
ob
serv
atio
ns t
o sh
are.
Wha
t ar
e th
e op
timal
m
odel
s of
info
rmat
ion
pro
visi
on fo
r aw
aren
ess
rais
ing
and
incr
easi
ng
know
led
ge o
f sel
f-
adm
inis
trat
ion
of
inje
ctab
le c
ontr
acep
tion?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G a
nd
surv
ey.
Acc
essi
bili
ty, t
he
right
to
seek
, re
ceiv
e an
d im
par
t in
form
atio
n.
Com
par
ativ
e ef
fect
iven
ess
rese
arch
of
diff
eren
t m
odel
s of
in
form
atio
n p
rovi
sion
, op
timal
ly in
an
RC
T.
This
will
firs
t re
qui
re
dev
elop
men
t of
mod
els
of d
edic
ated
info
rmat
ion
pro
visi
on a
nd h
ealth
lit
erac
y (e
g, t
elep
honi
c,
inte
rnet
, pos
ters
and
co
unse
lling
) prio
r to
ex
per
imen
tal t
estin
g.
Exp
lora
tory
qua
litat
ive
inte
rvie
ws
with
wom
en s
elf-
adm
inis
terin
g or
will
ing
to s
elf-
adm
inis
ter
to
iden
tify
thei
r kn
owle
dge
, att
itud
es
and
und
erst
and
ing
of in
ject
able
co
ntra
cep
tion
are
req
uire
d t
o in
form
m
odel
s of
info
rmat
ion
pro
visi
on.
Sel
ectio
n b
ias:
as
with
all
qua
litat
ive
stud
ies,
par
ticip
ants
ar
e p
urp
osiv
ely
sele
cted
. H
owev
er, t
his
is a
n ad
vant
age
in t
his
stud
y d
esig
n as
tho
se
wom
en w
ho h
ave
cons
ider
ed t
his
issu
e w
ill h
ave
rich
exp
erie
nces
an
d o
bse
rvat
ions
to
shar
e w
hich
ca
n gu
ide
the
dev
elop
men
t of
he
alth
pro
mot
ion
inte
rven
tion
and
too
ls.
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

6 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed o
r hu
man
rig
hts
que
stio
nC
urre
nt W
HO
re
com
men
dat
ion
Str
eng
th o
f re
com
men
dat
ion
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty a
nd p
ract
ical
co
nstr
aint
sA
lter
nati
ve s
tud
y d
esig
nM
etho
do
log
ical
issu
es a
risi
ng
in t
he a
lter
nati
ve s
tud
y d
esig
n
Hum
an r
ight
s an
d e
qui
tyW
hat
imp
lem
enta
tion
mea
sure
s ca
n en
sure
th
at in
equi
ty is
red
uced
or
min
imis
ed w
hen
self-
adm
inis
trat
ion
is
intr
oduc
ed?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Non
- dis
crim
inat
ion.
Com
par
ativ
e ef
fect
iven
ess
rese
arch
of
diff
eren
t m
odel
s of
imp
lem
enta
tion,
op
timal
ly in
a c
lust
er
RC
T.
An
RC
T of
mod
els
of
imp
lem
enta
tion
may
b
e ve
ry c
ostly
due
to
the
com
ple
x na
ture
of
imp
lem
enta
tion
stra
tegi
es
that
are
dep
end
ent
on t
he
sett
ing,
typ
e of
pro
vid
er
and
tra
inin
g re
qui
red
, and
en
surin
g fid
elity
to
the
inte
rven
tion.
Des
crip
tive
case
stu
die
s of
d
emon
stra
tion
pro
ject
s us
ing
diff
eren
t st
rate
gies
to
imp
lem
ent
inje
ctab
le
cont
race
ptio
n in
pro
gram
mes
in
seve
ral c
ount
ries
to in
dic
ate
optim
al
mea
sure
s to
ens
ure
equi
tab
le a
cces
s an
d t
o fo
rmul
ate
less
ons
lear
nt fo
r sc
ale-
up e
lsew
here
Lack
of g
ener
alis
abili
ty: c
urre
nt
pra
ctic
es a
nd p
oten
tial f
or
scal
e w
ill d
iffer
mar
ked
ly
bet
wee
n co
untr
ies.
The
refo
re
sele
ctio
n of
cou
ntry
site
s fo
r d
emon
stra
tion
pro
ject
s w
ill
req
uire
cha
ract
eris
atio
n of
un
der
lyin
g re
sour
ce n
eed
s,
trai
ning
, sta
ff an
d s
ocio
pol
itica
l fa
ctor
s to
ens
ure
max
imal
d
iver
sity
and
tha
t re
ason
able
co
mp
aris
ons
can
be
mad
e b
etw
een
coun
trie
s. T
riang
ulat
ion
bet
wee
n d
ata
sour
ces
and
site
s w
ill b
e ne
cess
ary
to in
crea
se
gene
ralis
abili
ty.
Acc
epta
bili
tyIs
the
re a
n im
pac
t of
d
iffer
ence
s b
etw
een
heal
thca
re p
rovi
der
s (e
g, a
ge, i
ncom
e st
atus
of
cou
ntry
, priv
ate/
pub
lic s
ecto
r) o
n th
e ac
cep
tab
ility
of
self-
adm
inis
trat
ion
of
inje
ctab
le c
ontr
acep
tion?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Acc
epta
bili
ty a
nd
acce
ssib
ilty.
Cro
ss- s
ectio
nal s
tud
y of
hea
lthca
re p
rovi
der
s to
eva
luat
e as
soci
atio
ns
bet
wee
n ch
arac
teris
tics
and
will
ingn
ess
to
pre
scrib
e an
d p
rovi
de
inje
ctab
le c
ontr
acep
tion
for
self-
adm
inis
trat
ion.
A s
urve
y m
ay n
ot p
rovi
de
an o
bje
ctiv
e m
easu
re
or a
tru
e re
flect
ion
of
beh
avio
urs
if d
riven
by
que
stio
ns r
equi
ring
soci
ally
ac
cep
tab
le r
esp
onse
s.
This
is a
feas
ible
stu
dy
des
ign
but
co
uld
be
sup
ple
men
ted
with
focu
s gr
oup
s or
qua
litat
ive
inte
rvie
ws.
Mea
sure
men
t b
ias:
for
bot
h su
rvey
and
inte
rvie
ws,
que
stio
ns
will
nee
d t
o b
e fo
rmul
ated
to
geth
er w
ith h
ealth
care
p
rovi
der
s to
ens
ure
trus
t,
par
ticip
atio
n an
d v
alid
ity a
nd t
o av
oid
soc
ial d
esira
bili
ty b
ias.
Wha
t is
the
sca
le
and
con
seq
uenc
e of
in
corr
ect
use
of s
elf-
ad
min
istr
atio
n?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Acc
ount
abili
ty.
Nat
iona
l pha
rmac
y or
cl
inic
- bas
ed r
egis
try
of w
omen
usi
ng s
elf-
ad
min
iste
red
inje
ctab
le
cont
race
ptio
n.
Reg
istr
ies
can
be
cost
ly
to e
stab
lish,
mai
ntai
n an
d
mon
itor.
A r
egis
try
req
uire
s p
oliti
cal w
ill a
nd c
apac
ity
to p
rovi
de
effe
ctiv
e d
ata
to
info
rm d
ecis
ions
.
Sen
tinel
(act
ive)
sur
veill
ance
thr
ough
m
onito
ring
and
eva
luat
ion
of a
dve
rse
effe
cts
and
ad
vers
e ev
ents
at
clin
ic
or p
rovi
der
leve
l em
bed
ded
in lo
cal
and
nat
iona
l qua
lity
assu
ranc
e p
rogr
amm
es.
Rep
ortin
g b
ias:
the
dat
a co
llect
ed
is d
epen
den
t on
the
tra
inin
g an
d e
xper
tise
of p
rovi
der
s to
ad
equa
tely
rec
ogni
se a
dve
rse
even
ts. R
esou
rces
can
be
dire
cted
tow
ard
s ap
pro
pria
te
sent
inel
site
s to
ens
ure
staf
f are
sk
illed
and
tha
t d
ata
inte
grity
is
ensu
red
.
Tab
le 2
C
ontin
ued
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 7
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed o
r hu
man
rig
hts
que
stio
nC
urre
nt W
HO
re
com
men
dat
ion
Str
eng
th o
f re
com
men
dat
ion
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty a
nd p
ract
ical
co
nstr
aint
sA
lter
nati
ve s
tud
y d
esig
nM
etho
do
log
ical
issu
es a
risi
ng
in t
he a
lter
nati
ve s
tud
y d
esig
n
Res
ourc
e us
eW
hat
are
the
user
an
d p
rovi
der
cos
ts o
f se
lf- ad
min
istr
atio
n (a
s w
ell a
s ou
t- of
- poc
ket
exp
end
iture
s), c
omp
ared
w
ith p
rovi
der
- bas
ed
adm
inis
trat
ion?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G a
nd
surv
ey.
Acc
essi
bili
ty.
Em
piri
cal c
ostin
g st
udie
s to
est
imat
e us
er
and
pro
vid
er c
osts
, an
d fi
nanc
ing
sour
ces
for
each
(use
rs p
ay o
r he
alth
sys
tem
pay
s)D
ata
are
curr
ently
onl
y av
aila
ble
from
one
st
udy
in t
hree
cou
ntrie
s in
sub
- Sah
aran
Afr
ica.
G
iven
tha
t co
sts
vary
by
cont
ext
and
by
del
iver
y m
odel
, the
r e is
a n
eed
fo
r m
ore
rep
rese
ntat
ive
cost
est
imat
es t
o co
nfirm
tha
t us
er c
osts
an
d o
ut- o
f- p
ocke
t ex
pen
ditu
res
are
likel
y to
dec
reas
e w
ith s
elf-
ad
min
istr
atio
n.
This
is a
feas
ible
stu
dy
but
ca
n b
e co
stly
to
cond
uct
acr o
ss a
rep
rese
ntat
ive
sam
ple
of u
sers
and
fa
cilit
ies.
This
is fe
asib
le b
ut c
ould
be
sup
ple
men
ted
by
mod
ellin
g b
ased
on
the
exis
ting
emp
irica
l cos
t d
ata,
cos
t st
ruct
ures
and
exp
ert
cons
ulta
tion
on
exp
ecte
d v
aria
tion
in p
aram
eter
s.
Mea
sure
men
t b
ias:
the
res
ults
ar
e d
epen
den
t on
use
r re
call
and
sel
f- r e
por
ted
res
ourc
e us
e,
opp
ortu
nity
cos
ts, a
s w
ell a
s on
as
sum
ptio
ns r
egar
din
g sh
ared
co
sts
in h
ealth
faci
litie
s.
Wha
t is
the
cos
t-
effe
ctiv
enes
s of
sel
f-
adm
inis
trat
ion,
com
par
ed
with
pro
vid
er- b
ased
ad
min
istr
atio
n?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Acc
essi
bili
ty.
Mod
ellin
g st
udie
s of
co
st-
effe
ctiv
enes
s ac
ross
bro
ader
ran
ge o
f se
ttin
gs, t
akin
g b
oth
a he
alth
care
pro
vid
er a
nd
soci
etal
per
spec
tive.
This
is a
feas
ible
stu
dy
but
its
qua
lity
and
use
fuln
ess
dep
end
s on
the
rel
iab
ility
of
the
par
amet
ers
for
unit
cost
s an
d e
ffect
iven
ess,
w
hich
wou
ld b
e d
raw
n fr
om c
ostin
g st
udie
s (n
oted
ab
ove)
and
RC
Ts. I
t w
ill
also
req
uire
mor
e lo
ng-
term
mod
ellin
g to
cap
tur e
d
owns
trea
m e
ffect
s on
the
ty
pes
of c
ontr
acep
tives
se
lf- in
ject
ing
wom
en
switc
h to
com
par
ed w
ith
pro
vid
er- b
ased
inje
ctin
g w
omen
.
Mea
sure
men
t b
ias:
the
res
ults
ar
e d
epen
den
t on
sel
ectio
n of
var
iab
les
incl
uded
in t
he
mod
el, a
ssum
ptio
ns r
egar
din
g d
isco
unt
rate
s, c
ost-
effe
ctiv
enes
s th
resh
old
s an
d a
ccur
ate
estim
ates
of c
urre
nt a
nd
pro
ject
ed c
osts
and
effe
cts.
Wha
t is
the
en
viro
nmen
tal i
mp
act
of d
isp
osal
of s
elf-
ad
min
iste
r ed
inje
ctab
le
oral
con
trac
eptio
n?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Acc
ount
abili
ty.
Col
lect
ion
and
col
latio
n of
rep
orts
from
en
viro
nmen
tal r
egul
ator
y b
odie
s d
ocum
entin
g sc
ale
and
imp
act
of
med
ical
was
te a
nd
hous
ehol
d w
aste
.
Reg
ulat
ory
agen
cies
are
un
likel
y to
diff
eren
tiate
b
etw
een
whe
ther
inje
ctab
le
cont
race
ptiv
es p
rese
nt in
w
aste
are
sou
rced
dire
ctly
fr
om c
linic
s or
from
the
ho
mes
of u
sers
.
A q
ualit
ativ
e ho
useh
old
dia
ry
stud
y of
wom
en w
ho s
elf-
inje
ct in
w
hich
the
y re
cord
was
te fr
om t
he
pac
kagi
ng a
nd t
heir
man
agem
ent
of
it. T
his
coul
d b
e d
eliv
ered
with
the
in
ject
able
pac
kagi
ng a
nd w
omen
can
re
turn
it w
hen
colle
ctin
g th
eir
next
p
resc
riptio
n.
Rec
all b
ias:
wom
en m
ay n
ot
rem
emb
er w
hat
they
did
with
th
e p
acka
ging
if t
hey
do
not
reco
rd it
at
the
time.
Thi
s m
ay
req
uire
an
ince
ntiv
e d
urin
g th
e re
sear
ch p
erio
d in
ord
er t
o en
cour
age
wom
en t
o co
mp
lete
th
e ho
useh
old
was
te d
iary
.
GD
G, G
uid
elin
e D
evel
opm
ent
Gro
up; G
ER
, gen
der
, eq
uity
and
hum
an r
ight
s; R
CTs
, ran
dom
ised
con
trol
led
tria
ls.
Tab
le 2
C
ontin
ued
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

8 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Tab
le 3
R
esea
rch
gap
s fo
r se
lf- co
llect
ion
of S
TI s
amp
les
Clin
ical
, pro
gra
mm
atic
, val
ues-
b
ased
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty
and
pra
ctic
al
cons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Met
hod
olo
gic
al is
sues
ari
sing
in
the
alt
erna
tive
stu
dy
des
ign
Ben
efits
ve
rsus
har
ms
PIC
O: s
houl
d
self-
colle
ctio
n of
sa
mp
les
for
STI
s b
e m
ade
avai
lab
le
as a
n ad
diti
onal
ap
pro
ach
to
del
iver
STI
tes
ting
serv
ices
?
Sel
f- co
llect
ion
of
sam
ple
s fo
r N
eiss
eria
go
norr
hoea
e an
d
Chl
amyd
ia t
rach
omat
is
shou
ld b
e m
ade
avai
lab
le a
s an
ad
diti
onal
ap
pro
ach
to d
eliv
er S
TI t
estin
g se
rvic
es.
Str
ong.
Mod
erat
e.N
o d
ata
from
LM
IC. A
vaila
bili
ty
and
acc
essi
bili
ty.
RC
T co
nduc
ted
in
LM
IC w
ith
incl
usio
n of
ou
tcom
es
to m
easu
re
avai
lab
ility
and
ac
cess
ibili
ty.
As
a st
rong
WH
O
reco
mm
end
atio
n ex
ists
, it
wou
ld b
e un
ethi
cal t
o re
pea
t an
RC
T of
the
in
terv
entio
n.
Pro
spec
tive
non-
co
ntro
lled
coh
ort
stud
y to
be
cond
ucte
d in
se
vera
l LM
ICs
whe
re t
he
inte
rven
tion
is o
r w
ill b
e im
ple
men
ted
. Ana
lysi
s to
com
bin
e q
uant
itativ
e su
rvey
sup
ple
men
ted
w
ith fo
cuse
d in
- dep
th
qua
litat
ive
inte
rvie
ws
with
gen
eral
pop
ulat
ion
(with
att
entio
n gi
ven
to e
nsur
e sa
mp
ling
of
vuln
erab
le p
opul
atio
ns)
to e
xplo
re G
ER
ou
tcom
es o
f ava
ilab
ility
an
d a
cces
sib
ility
. Cos
t an
alys
es c
an b
e ne
sted
in
the
coho
rt s
tud
y.
Con
foun
din
g: p
artic
ipan
ts
in c
ohor
t se
lf- se
lect
to
self-
co
llect
and
may
hav
e ot
her
sim
ilar
char
acte
ristic
s th
at m
ay
influ
ence
the
ir ab
ility
to
acce
ss
STI
sel
f- co
llect
ion.
Mea
sure
men
t b
ias:
sel
f-
rep
ortin
g b
ias
an is
sue
for
qua
litat
ive
com
pon
ent.
Thi
s w
ill
req
uire
wel
l- tr
aine
d r
esea
rche
rs
and
val
idat
ed t
ools
. The
tr
iang
ulat
ion
of t
he q
ualit
ativ
e d
ata
with
the
qua
ntita
tive
surv
ey r
esul
ts p
rovi
des
an
elem
ent
of a
dd
ition
al v
alid
atio
n of
out
com
es.
Sel
f- co
llect
ion
of
sam
ple
s fo
r Tre
pon
ema
pal
lidum
(syp
hilis
) and
Tr
icho
mon
as v
agin
alis
m
ay b
e co
nsid
ered
as
an a
dd
ition
al a
pp
roac
h to
del
iver
STI
tes
ting
serv
ices
.
Con
diti
onal
.Lo
w.
Ava
ilab
ility
, ac
cess
ibili
ty a
nd
acce
pta
bili
ty.
Ran
dom
ised
co
ntro
lled
tria
l sp
ecifi
c to
se
lf- co
llect
ion
of t
hese
or
gani
sms.
This
is a
feas
ible
d
esig
n.
G
ener
alis
abili
ty: t
he c
hoic
e of
se
ttin
g an
d u
ser
pop
ulat
ion
will
det
erm
ine
how
wid
ely
the
resu
lts c
an b
e ap
plie
d. T
he
focu
s sh
ould
be
on t
estin
g th
is in
LM
IC s
ettin
gs a
nd w
ith
vuln
erab
le p
opul
atio
ns.
Wha
t is
the
imp
act
of s
elf-
sam
plin
g fo
r S
TIs
on p
artn
er
scre
enin
g?
GD
G.
Priv
acy
and
co
nfid
entia
lity.
Ran
dom
ised
co
ntro
lled
tria
l w
ith u
pta
ke
of p
artn
er
scre
enin
g in
clud
ed a
s an
ou
tcom
e.
As
a st
rong
WH
O
reco
mm
end
atio
n ex
ists
, it
wou
ld b
e un
ethi
cal t
o re
pea
t an
RC
T of
the
in
terv
entio
n.
Cro
ss- s
ectio
nal s
tud
y of
w
omen
who
res
pon
d t
o re
sults
follo
win
g S
TI s
elf-
co
llect
ion
to a
scer
tain
how
m
any
have
not
ified
the
ir p
artn
ers
to b
e sc
r een
ed,
and
of t
hose
how
man
y p
artn
ers
have
gon
e fo
r sc
reen
ing.
Acc
epta
bili
ty
of s
cree
ning
for
par
tner
s,
and
ava
ilab
ility
and
ac
cess
ibili
ty o
f par
tner
sc
reen
ing
will
be
imp
orta
nt
to m
easu
re.
Sel
ectio
n b
ias:
sur
veys
will
on
ly c
aptu
re t
hose
wom
en
who
hav
e re
spon
ded
act
ivel
y to
the
res
ults
and
may
not
be
rep
rese
ntat
ive
of t
hose
wom
en
who
do
not
resp
ond
act
ivel
y to
th
eir
resu
lts.
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 9
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
b
ased
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty
and
pra
ctic
al
cons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Met
hod
olo
gic
al is
sues
ari
sing
in
the
alt
erna
tive
stu
dy
des
ign
Wha
t is
the
imp
act
of s
elf-
sam
plin
g fo
r S
TIs
on li
nkag
e to
car
e an
d c
ase-
fin
din
g?
GD
G.
Acc
epta
bili
ty
and
non
- d
iscr
imin
atio
n.
RC
T w
ith
incl
usio
n of
ou
tcom
es
to m
easu
r e
linka
ge t
o ca
re
and
cas
e-
find
ing.
As
a st
rong
WH
O
reco
mm
end
atio
n ex
ists
, it
wou
ld
be
unet
hica
l to
rep
eat
an R
CT
of
effe
ctiv
enes
s of
the
in
terv
entio
n.
Inte
rrup
ted
tim
e se
ries
usin
g re
pea
ted
cro
ss-
sect
iona
l sur
veys
of
pop
ulat
ions
att
end
ing
STI
clin
ics
for
trea
tmen
t b
efor
e, d
urin
g an
d a
fter
im
ple
men
tatio
n of
pol
icy
to a
scer
tain
pro
por
tion
of
wom
en w
ho s
elf-
sam
ple
d
prio
r to
link
age
to c
are.
Att
ritio
n b
ias:
the
res
ults
may
in
dic
ate
that
mor
e p
eop
le w
ho
link
to c
are
used
sel
f- sa
mp
ling,
b
ut t
his
doe
s no
t p
r ovi
de
info
rmat
ion
on h
ow m
any
peo
ple
who
sel
f- sa
mp
led
with
a
pos
itive
res
ult
did
not
link
to
car
e.
Wha
t is
the
ben
efit
and
har
m o
f sel
f-
sam
plin
g fo
r S
TIs
of
vira
l aet
iolo
gy?
GD
G.
Ava
ilab
ility
, ac
cess
ibili
ty a
nd
acce
pta
bili
ty.
Ran
dom
ised
co
ntro
lled
tria
l sp
ecifi
c to
se
lf- co
llect
ion
of S
TIs
of
vira
l aet
iolo
gy.
Out
com
es
to in
clud
e m
easu
rem
ent
of a
vaila
bili
ty
and
ac
cess
ibili
ty,
as w
ell a
s ac
cep
tab
ility
of
self-
sam
plin
g,
esp
ecia
lly
rega
rdin
g sa
mp
ling
of
blo
ods
(eg,
he
pat
itis
B
viru
s).
This
is a
feas
ible
d
esig
n.
P
erfo
rman
ce b
ias:
it is
not
p
ossi
ble
to
mas
k us
ers
or
pro
vid
ers
to m
ode
of s
amp
ling.
Th
is c
an b
e m
itiga
ted
by
cons
ider
ing
cond
uctin
g a
clus
ter
RC
T ra
ther
tha
n an
in
div
idua
lly r
and
omis
ed t
rial,
or
a st
epp
ed w
edge
des
ign
whe
re
the
inte
rven
tion
is d
eliv
ered
at
stag
gere
d t
ime
per
iod
s.
Valu
es a
nd
pre
fere
nces
Wha
t ar
e th
e va
lues
an
d p
refe
renc
es
of m
argi
nalis
ed
pop
ulat
ions
(eg,
M
en w
ho h
ave
sex
with
men
, se
x w
orke
rs,
tran
s p
opul
atio
ns)
rega
rdin
g se
lf-
sam
plin
g?
Not
ap
plic
able
.
G
DG
and
su
rvey
.A
cces
sib
ility
ac
cep
tab
ility
, p
rivac
y an
d
confi
den
tialit
y,
and
non
- d
iscr
imin
atio
n.
Qua
litat
ive
key
info
rman
t st
udy
of w
omen
and
m
en w
ho a
re
mar
gina
lised
re
gard
ing
thei
r va
lues
and
p
refe
renc
es o
f se
lf- sa
mp
ling
and
the
bar
riers
th
at t
hey
exp
erie
nce
or
may
exp
erie
nce
whe
n ac
cess
ing
self-
sam
plin
g,
rece
ivin
g th
eir
resu
lts a
nd
whe
n lin
king
to
care
.
This
is a
feas
ible
st
udy.
Sel
ectio
n b
ias:
as
with
al
l qua
litat
ive
stud
ies,
p
artic
ipan
ts a
re p
urp
osiv
ely
sele
cted
. How
ever
, thi
s is
an
ad
vant
age
in t
his
stud
y d
esig
n as
mar
gina
lised
w
omen
and
men
—in
clud
ing
tran
s p
opul
atio
ns—
who
hav
e co
nsid
ered
thi
s is
sue
will
ha
ve r
ich
exp
erie
nces
and
ob
serv
atio
ns t
o sh
are.
Tab
le 3
C
ontin
ued
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

10 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
b
ased
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty
and
pra
ctic
al
cons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Met
hod
olo
gic
al is
sues
ari
sing
in
the
alt
erna
tive
stu
dy
des
ign
Hum
an r
ight
s an
d e
qui
tyW
hat
are
the
bes
t p
ract
ices
for
avoi
din
g co
erci
on in
se
lf- sa
mp
ling?
Not
ap
plic
able
.
G
DG
.N
on-
dis
crim
inat
ion,
p
rivac
y an
d
confi
den
tialit
y.
Qua
litat
ive
stud
y us
ing
focu
s gr
oup
s of
vul
nera
ble
p
opul
atio
ns in
co
ntex
ts w
here
se
lf- sa
mp
ling
is im
ple
men
ted
to
und
erst
and
ho
w t
hey
per
ceiv
e co
erci
on c
ould
b
e av
oid
ed.
This
can
allo
w
crea
tion
of
an e
xpan
ded
ve
rsio
n of
the
in
terv
entio
n fo
r fu
rthe
r ev
alua
tion
with
m
easu
rem
ent
of n
on- c
oerc
ion
incl
uded
as
an
outc
ome.
This
is a
feas
ible
d
esig
n.
S
elec
tion
bia
s: a
s w
ith a
ll q
ualit
ativ
e st
udie
s, p
artic
ipan
ts
are
pur
pos
ivel
y se
lect
ed.
How
ever
, thi
s is
an
adva
ntag
e in
thi
s st
udy
des
ign
as
mar
gina
lised
wom
en a
nd m
en
who
hav
e co
nsid
ered
thi
s is
sue
will
hav
e ric
h ex
per
ienc
es a
nd
obse
rvat
ions
to
shar
e.
Res
ourc
e us
eIs
sel
f- co
llect
ion
for
STI
s co
st- e
ffect
ive?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Acc
essi
bili
ty.
Mod
ellin
g st
udie
s of
cos
t-
effe
ctiv
enes
s ac
ross
b
road
er r
ange
of
set
tings
, ta
king
bot
h a
heal
thca
re
pro
vid
er
and
soc
ieta
l p
ersp
ectiv
e.
This
is a
feas
ible
st
udy,
but
its
qua
lity
and
us
eful
ness
dep
end
on
the
rel
iab
ility
of
the
par
amet
ers
for
unit
cost
s an
d
effe
ctiv
enes
s,
whi
ch w
ould
b
e d
raw
n fr
om
cost
ing
stud
ies
and
the
RC
Ts
with
effe
ctiv
enes
s d
ata.
It w
ill a
lso
req
uire
mor
e lo
ng-
term
mod
ellin
g to
cap
ture
d
owns
trea
m
effe
cts
on li
nkag
e to
car
e.
Mea
sure
men
t b
ias:
the
re
sults
are
dep
end
ent
on
sele
ctio
n of
var
iab
les
incl
uded
in
the
mod
el, a
ssum
ptio
ns
rega
rdin
g d
isco
unt
rate
s,
cost
- effe
ctiv
enes
s th
resh
old
s an
d a
ccur
ate
estim
ates
of
curr
ent
and
pro
ject
ed c
osts
. Fo
r ex
amp
le, v
ulne
rab
le
pop
ulat
ions
with
lim
ited
acc
ess
to c
are
are
likel
y to
gen
erat
e d
iffer
ent
resu
lts b
ased
on
the
pro
bab
ility
tha
t th
ey w
ould
hav
e lim
ited
or
no a
cces
s to
car
e w
ithou
t se
lf- sa
mp
ling.
Dat
a ac
cura
cy: u
nit
cost
s m
ay n
ot b
e av
aila
ble
for
man
y or
any
LM
IC, e
spec
ially
w
here
sel
f- sa
mp
ling
has
not
bee
n av
aila
ble
. To
avoi
d
assu
mp
tions
, thi
s m
ay r
equi
re
prio
r as
sess
men
t vi
a an
initi
al
imp
lem
enta
tion
pro
cess
to
asce
rtai
n re
ason
able
cos
tings
.
Tab
le 3
C
ontin
ued
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 11
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
b
ased
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty
and
pra
ctic
al
cons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Met
hod
olo
gic
al is
sues
ari
sing
in
the
alt
erna
tive
stu
dy
des
ign
Doe
s se
lf- co
llect
ion
offe
r a
cost
- effi
cien
t ap
pro
ach
to c
ase
det
ectio
n in
low
- in
com
e se
ttin
gs?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Ava
ilab
ility
and
ac
cess
ibili
ty.
Em
piri
cal
cost
ing
stud
ies
to e
stim
ate
the
cost
s an
d t
arge
ting
effic
ienc
y of
se
lf- co
llect
ion
in L
MIC
s us
ing
vario
us fe
asib
le
mod
els
of
del
iver
y.
As
abov
e.
A
s ab
ove.
GD
G, G
uid
elin
e D
evel
opm
ent
Gro
up; G
ER
, gen
der
, eq
uity
and
hum
an r
ight
s; P
ICO
, Pop
ulat
ion,
Inte
rven
tions
, Com
par
ison
and
Out
com
es; R
CTs
, ran
dom
ised
con
trol
led
tria
ls; S
TI, s
exua
lly t
rans
mitt
ed in
fect
ion.
Tab
le 3
C
ontin
ued
approaches and 13 discrete feasible study designs devel-oped:1. Survey approach (one prevalence survey; two inter-
rupted time series; five cross- sectional studies; one household diary study).
2. Qualitative approach (seven key informant interviews; three focus groups).
3. Implementation research approach (four prospective mixed methods cohort studies; one demonstration project).
4. Comparative effectiveness research (three non- randomised controlled trials (non- RCTs); two RCTs).
5. Economic approach (four cost- effectiveness studies; four costing studies).
6. Surveillance (one sentinel surveillance study).7. Standard patient study (1).
We identified selection bias and detection bias as the primary methodological challenges across mixed methods, quantitative and qualitative studies. Detection bias was driven by concerns around self- reported data that may be prone to social desirability bias when partici-pants provide answers they consider the assessors expect to hear. Selection bias in non- randomised studies limits generalisability and occurs when research participants who agree to participate differ qualitatively from those who do not agree to participate. Non- participation may be highest in those vulnerable populations who fear discrim-ination or have privacy and confidentiality concerns. This would then limit the utility of the results obtained from those who do participate, including in relation to GER.
The most frequent GER standards and principles considered relevant were availability and accessibility, followed by privacy and confidentiality.
dIsCussIonWe developed a structured approach to identification of research gaps and formulation of research questions and study designs during a WHO guidelines development process. Our approach builds on our previous work in this area and is rooted in the current GRADE framework used by WHO, further extending it to incorporate the user perspective and foregrounding GER throughout the process.
To the best of our knowledge, our approach is unique in providing practical systematised steps to research ques-tion formulation during WHO guideline development and elaboration of the design of future studies. Prior work in this area has been sparse and focused on identifi-cation and characterisation of research gaps arising from systematic reviews (not guidelines) and has not described the type of research that is required.20 Given that the aim of identification of research gaps is to reduce waste and increase research value,21 collation and possible registra-tion of research gaps on a publicly accessible platform should be encouraged to realign future studies with the existing body of evidence. This would increase access to suggested methodologies and processes to advance
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

12 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Tab
le 4
R
esea
rch
gap
s fo
r ov
er- t
he- c
ount
er (O
TC) o
ral c
ontr
acep
tion
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Cri
tica
l hum
an
rig
hts
and
eq
uity
co
nsid
erat
ions
Idea
l stu
dy
des
ign(
s)
Feas
ibili
ty
and
pra
ctic
al
cons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Met
hod
olo
gic
al
issu
es a
risi
ng in
the
al
tern
ativ
e st
udy
des
ign
Ben
efits
ve
rsus
har
ms
PIC
O: s
houl
d O
TC
cont
race
ptio
n b
e m
ade
avai
lab
le w
ithou
t a
pre
scrip
tion?
OTC
ora
l co
ntra
cep
tion
shou
ld
be
mad
e av
aila
ble
w
ithou
t a
pre
scrip
tion.
Str
ong.
Very
low
.P
rivac
y an
d
confi
den
tialit
y;
acce
ssib
ility
.
RC
T co
nduc
ted
in
LMIC
with
incl
usio
n of
out
com
es
to m
easu
re
acce
ssib
ility
, priv
acy
and
con
fiden
tialit
y.
As
a st
rong
WH
O
reco
mm
end
atio
n ex
ists
, it
wou
ld b
e un
ethi
cal t
o re
pea
t an
RC
T of
the
ef
fect
iven
ess
of t
he
inte
rven
tion.
Rep
eate
d c
ross
- sec
tiona
l su
rvey
s (c
an b
e ta
rget
ed
to s
pec
ific
sub
grou
ps
or
of w
omen
in t
he g
ener
al
pop
ulat
ion
incl
udin
g ad
oles
cent
girl
s an
d
youn
g w
omen
) att
end
ing
pha
rmac
ies
to e
valu
ate
priv
acy
and
con
fiden
tialit
y an
d c
hoic
e to
ob
tain
OTC
co
ntra
cep
tion
over
tim
e.
Sel
ectio
n b
ias:
w
omen
who
p
artic
ipat
e in
the
su
rvey
may
hav
e fe
wer
con
cern
s re
gard
ing
priv
acy
and
con
fiden
tialit
y th
an t
hose
who
w
ould
ref
use
to
par
ticip
ate,
lim
iting
ge
nera
lisab
ility
.
Are
the
re q
ualit
y d
iffer
ence
s b
etw
een
OTC
ora
l con
trac
eptio
n m
edic
atio
n an
d
pre
scrib
ed o
ral
cont
race
ptio
n m
edic
atio
n?
Not
ap
plic
able
.
G
DG
.
Not
ap
plic
able
.Th
is is
a q
ualit
y as
sess
men
t co
ncer
n an
d r
equi
res
lab
orat
ory
anal
ysis
and
is o
utsi
de
the
scop
e of
thi
s ar
ticle
. WH
O g
uid
elin
es fo
r na
tiona
l reg
ulat
ory
auth
oriti
es e
xist
to
guid
e na
tiona
l re
gula
tory
con
trol
to
ensu
re s
ubst
and
ard
pro
duc
ts a
re n
ot m
ade
avai
lab
le a
nd t
hat
dos
ages
are
co
rrec
t (s
ee h
ttp
s://
ww
w.w
ho.in
t/m
edic
ines
/are
as/
qua
lity_
safe
ty/q
ualit
y_as
sura
nce/
Goo
dR
egul
ator
y_P
ract
ices
Pub
licC
onsu
lt.p
df).
Wha
t ar
e th
e op
timal
w
ays
to p
rovi
de
advi
ce o
n sw
itchi
ng
to d
iffer
ent
oral
co
ntra
cep
tion
or u
sing
ot
her
cont
race
ptiv
e op
tions
(eg,
via
tex
t m
essa
ging
, in
per
son
in p
harm
acy)
?
Not
ap
plic
able
.
G
DG
.A
cces
sib
ility
and
in
form
ed d
ecis
ion
mak
ing.
Com
par
ativ
e ef
fect
iven
ess
rese
arch
to
com
par
e d
iffer
ent
typ
es o
f m
etho
ds
to p
rovi
de
advi
ce.
A c
ontr
olle
d t
rial
that
may
or
may
no
t b
e ra
ndom
ised
is
feas
ible
. Id
entifi
catio
n or
d
evel
opm
ent
of
mod
es o
f hea
lth
liter
acy
will
be
req
uire
d p
rior
to t
estin
g in
a
cont
rolle
d m
anne
r. In
LM
IC, p
harm
acy
tech
nici
ans
or c
ashi
ers
may
pro
vid
e ad
vice
inst
ead
of
pha
rmac
ists
th
at r
equi
res
cons
ider
atio
n w
hen
pla
nnin
g re
al- w
orld
st
udie
s.
Fid
elity
bia
s: d
eliv
ery
of h
ealth
ad
vice
is
dep
end
ent
on m
ode
of a
dvi
ce. I
f giv
en
by
pha
rmac
ists
, co
mm
unity
he
alth
wor
kers
or
tech
nici
ans,
the
n m
onito
ring
the
fidel
ity
of t
he in
terv
entio
n w
ill
ensu
re t
he r
igou
r of
th
e re
sults
. Out
com
es
mus
t in
clud
e a
mea
sure
men
t of
ac
cess
ibili
ty s
uch
as r
eque
sts
for
and
up
take
of a
dvi
ce.
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 13
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Cri
tica
l hum
an
rig
hts
and
eq
uity
co
nsid
erat
ions
Idea
l stu
dy
des
ign(
s)
Feas
ibili
ty
and
pra
ctic
al
cons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Met
hod
olo
gic
al
issu
es a
risi
ng in
the
al
tern
ativ
e st
udy
des
ign
Wha
t ad
vers
e ev
ents
ar
ise
from
pro
vid
ing
oral
con
trac
eptio
n O
TC?
Not
ap
plic
able
.
G
DG
.A
ccep
tab
ility
, in
form
ed d
ecis
ion
mak
ing
and
non
- d
iscr
imin
atio
n.
Con
veni
ence
sa
mp
le a
nd c
ross
- se
ctio
nal s
urve
y of
w
omen
ob
tain
ing
OTC
con
trac
eptio
n at
pha
rmac
ies
to
eluc
idat
e if
they
hav
e ex
per
ienc
ed a
dve
rse
even
ts r
elat
ed t
o th
e O
TC n
atur
e of
the
co
ntra
cep
tion.
This
is a
feas
ible
st
udy
des
ign.
N
ot a
pp
licab
le.
Sel
ectio
n b
ias:
suc
h a
sam
ple
wou
ld o
nly
incl
ude
wom
en w
ho
are
will
ing
to p
rovi
de
info
rmat
ion
and
w
ho fe
el s
uffic
ient
ly
confi
den
t to
voi
ce
thei
r co
ncer
ns;
wom
en w
ho h
ave
alre
ady
exp
erie
nced
st
igm
a or
who
fear
it
are
less
like
ly
to r
etur
n to
the
p
harm
acy
and
so
are
less
like
ly t
o b
e re
pre
sent
ed in
the
sa
mp
le.
Valu
es a
nd
pre
fere
nces
Wha
t ar
e th
e va
lues
an
d p
refe
renc
es o
f w
omen
livi
ng in
low
- in
com
e an
d m
idd
le-
inco
me
coun
trie
s re
late
d t
o O
TC o
ral
cont
race
ptio
n?
Not
ap
plic
able
.
G
DG
and
su
rvey
.A
cces
sib
ility
, p
rivac
y an
d
confi
den
tialit
y, a
nd
non-
dis
crim
inat
ion.
Qua
litat
ive
stud
y us
ing
key
info
rman
t in
terv
iew
s w
ith
wom
en s
eeki
ng
and
/or
usin
g co
ntra
cep
tion
and
w
ho li
ve in
LM
IC
rega
rdin
g th
eir
valu
es
and
pre
fere
nces
to
elu
cid
ate
thei
r ex
per
ienc
es a
nd
obse
rvat
ions
. A
que
stio
n re
gard
ing
rece
ipt
of a
pp
rop
riate
sc
reen
ing
for
cont
rain
dic
atio
ns
will
be
esse
ntia
l to
incl
ude.
This
is a
feas
ible
st
udy.
Not
ap
plic
able
.S
elec
tion
bia
s: a
s w
ith a
ll q
ualit
ativ
e st
udie
s, p
artic
ipan
ts
are
pur
pos
ivel
y se
lect
ed. H
owev
er,
this
is a
n ad
vant
age
in t
his
stud
y d
esig
n as
tho
se w
omen
who
ha
ve c
onsi
der
ed
this
issu
e w
ill h
ave
rich
exp
erie
nces
an
d o
bse
rvat
ions
to
shar
e.
Tab
le 4
C
ontin
ued
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

14 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Cri
tica
l hum
an
rig
hts
and
eq
uity
co
nsid
erat
ions
Idea
l stu
dy
des
ign(
s)
Feas
ibili
ty
and
pra
ctic
al
cons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Met
hod
olo
gic
al
issu
es a
risi
ng in
the
al
tern
ativ
e st
udy
des
ign
Hum
an r
ight
s an
d e
qui
tyW
ill w
omen
of a
ll ag
es
be
able
to
acce
ss O
TC
oral
con
trac
eptio
n?
Wha
t b
arrie
rs r
emai
n in
th
e he
alth
care
sec
tor?
Not
ap
plic
able
.
G
DG
.A
vaila
bili
ty,
acce
ssib
ility
and
no
n- d
iscr
imin
atio
n.
Una
nnou
nced
st
and
ard
pat
ient
(s
imul
atio
n) s
tud
y w
here
wom
en o
f d
iffer
ent
ages
pos
e as
use
rs w
ishi
ng
to p
rocu
re O
TC
cont
race
ptio
n in
d
iffer
ent
sett
ings
, re
gion
s an
d
coun
trie
s.
This
is a
feas
ible
st
udy
des
ign.
Whi
le t
his
des
ign
is
feas
ible
, cur
rent
ob
stac
les
to c
ond
uctin
g st
and
ard
p
atie
nt r
esea
rch
incl
ude
auto
mat
ed e
lect
roni
c m
edic
al r
ecor
ds
and
cr
eatio
n of
bel
ieva
ble
id
entit
ies.
How
ever
, thi
s sh
ould
be
less
rel
evan
t fo
r O
TC s
tud
ies
than
med
ical
p
ract
ice
stud
ies
whe
re
sim
ulat
ion
is w
idel
y us
ed.
Mea
sure
men
t er
ror:
th
e p
rese
ntat
ion
and
res
pon
ses
of
the
'sta
ndar
d u
ser'
m
ay d
iffer
bet
wee
n sc
enar
ios
and
se
ttin
gs le
adin
g to
ov
eres
timat
ing
or
und
eres
timat
ing
the
acce
ssib
ility
of
the
OTC
co
ntra
cep
tion.
Thi
s ca
n b
e ad
dre
ssed
by
ensu
ring
adeq
uate
tr
aini
ng fo
r 's
tand
ard
us
ers'
and
dev
elop
ing
tem
pla
tes
for
diff
eren
t re
spon
ses.
Acc
epta
bili
tyW
hat
do
heal
thca
re
pro
vid
ers
know
, th
ink
and
feel
ab
out
pro
visi
on o
f OTC
or
al c
ontr
acep
tion,
es
pec
ially
in lo
w-
inco
me
and
mid
dle
- in
com
e se
ttin
gs?
Not
ap
plic
able
.
S
urve
y.A
cces
sib
ility
, p
rivac
y, t
he r
ight
to
seek
, rec
eive
and
im
par
t in
form
atio
n.
Onl
ine
glob
al c
ross
- se
ctio
nal s
urve
y of
he
alth
care
pro
vid
ers
with
del
iver
y th
roug
h re
leva
nt
orga
nisa
tions
.
In m
any
sett
ings
of
dep
rivat
ion,
and
es
pec
ially
in L
MIC
, on
line
acce
ssib
ility
is
lim
ited
by
cost
s, in
adeq
uate
te
chno
logy
and
lack
of
kno
wle
dge
on
how
to
use
tool
s.
Focu
s gr
oup
s in
p
urp
osiv
ely
sam
ple
d
heal
thca
re p
rovi
der
p
opul
atio
ns a
nd r
egio
ns.
Focu
s gr
oup
s ar
e m
ost
suita
ble
to
driv
e co
nver
satio
ns a
nd
elic
it re
spon
ses
amon
g p
artic
ipan
ts w
ith s
hare
d
lived
exp
erie
nces
and
is
less
con
fron
tatio
nal a
s th
e ai
m is
not
to
gath
er in
- d
epth
per
sona
l exp
erie
nces
b
ut a
sses
s cu
rren
t cu
ltura
l an
d s
ocia
l nor
ms,
pra
ctic
es
and
con
cern
s w
ith r
esp
ect
to O
TC c
ontr
acep
tion.
S
pec
ific
que
stio
ns c
an b
e d
irect
ed r
egar
din
g at
titud
es
tow
ard
s vu
lner
able
p
opul
atio
ns, f
or e
xam
ple
, tr
ans-
men
and
bis
exua
l w
omen
.
Soc
ial a
ccep
tab
ility
b
ias:
giv
en t
hat
exp
erie
nces
are
sh
ared
in a
gro
up,
ther
e m
ay b
e a
relu
ctan
ce t
o d
iscl
ose
stig
mat
isin
g b
ehav
iour
s; h
owev
er,
dev
elop
men
t of
se
mis
truc
ture
d
inte
rvie
w q
uest
ions
in
con
sulta
tion
with
lo
cal h
ealth
care
p
rovi
der
s to
bes
t re
flect
loca
l bel
iefs
fo
r in
terr
ogat
ion
can
red
uce
this
bia
s. In
ad
diti
on, a
ski
lled
fo
cus
grou
p le
ader
ca
n cr
eate
a s
afe
spac
e fo
r d
iscl
osur
e.
Tab
le 4
C
ontin
ued
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 15
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Cri
tica
l hum
an
rig
hts
and
eq
uity
co
nsid
erat
ions
Idea
l stu
dy
des
ign(
s)
Feas
ibili
ty
and
pra
ctic
al
cons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Met
hod
olo
gic
al
issu
es a
risi
ng in
the
al
tern
ativ
e st
udy
des
ign
Res
ourc
e us
eW
ho b
ears
the
cos
t of
O
TC o
ral c
ontr
acep
tion
– is
the
cos
t sh
ifted
fr
om t
he h
ealth
sys
tem
to
the
use
r?
Not
ap
plic
able
.
G
DG
.A
cces
sib
ility
.R
egio
nal p
atie
nt
cost
ing
stud
y us
ing
cros
s- se
ctio
nal
surv
ey o
f wom
en
obta
inin
g O
TC
cont
race
ptio
n at
p
harm
acie
s to
d
eter
min
e 'u
ser
cost
p
athw
ay' (
incl
udin
g tr
ansp
ort;
loss
of
inco
me)
and
iden
tify
finan
cing
sou
rces
(e
g, u
ser
pay
s, t
ax-
bas
ed o
r co
ntrib
utor
y he
alth
insu
ranc
e sc
hem
e p
ays)
.
This
is a
feas
ible
st
udy .
Gen
eral
isab
ility
: the
re
sults
of a
ny c
ostin
g st
udy
will
be
spec
ific
to t
he c
onte
xt;
how
ever
, the
met
hod
of
dat
a co
llect
ion
can
be
rep
licat
ed in
oth
er
regi
ons
to d
eter
min
e lo
cally
sp
ecifi
c co
sts.
Mea
sure
men
t b
ias:
m
uch
of t
he d
ata
will
be
dep
end
ent
on p
artic
ipan
t re
colle
ctio
ns (r
ecal
l b
ias
may
be
a ris
k) a
nd t
heir
own
assu
mp
tions
ab
out
wha
t co
nstit
utes
op
por
tuni
ty c
ost,
for
exam
ple
.
GD
G, G
uid
elin
e D
evel
opm
ent
Gro
up; P
ICO
, Pop
ulat
ion,
Inte
rven
tions
, Com
par
ison
and
Out
com
es; R
CT,
ran
dom
ised
con
trol
led
tria
l.
Tab
le 4
C
ontin
ued
research from resource- constrained settings where we found gaps in existing evidence around self- care inter-ventions. Given that much of the evidence reviewed came from high- income countries, it will also be important for future research in these fields to develop capacity where needed and promote research appropriate to the local contexts in low- income and middle- income countries.
The application of a ‘living guidelines’ approach to WHO guideline development process will ensure greater responsiveness to new research findings.22 Current guid-ance for formulating and prioritising research gaps during WHO guideline development processes requires strengthening in the WHO Handbook of Guideline Devel-opment.1 Research gap identification is rarely prioritised during guideline development processes and the oppor-tunity to shape the future research agenda is missed.2 Our practical approach presents an opportunity to WHO (and other guidelines developers) to better inte-grate research identification and elaboration into the guidelines decision- making space, in particular research that is reflective of need and priorities. Time and cost constraints may preclude extensive discussion of research gaps during a guidelines meeting, but at a minimum a dedicated agenda item and a working group tasked to develop the research gaps further following the meeting should be considered. We can envision automation of the decision- making steps in our approach using the hierar-chical model outlined in figure 1. However, we would caution that such a process be viewed as a starting point to facilitate more in- depth discussions rather than a rigid template.
GER are recognised as key considerations in the SRHR field.23 24 SRHR self- care interventions present many opportunities to address common obstacles to delivering equitable, gender- responsive and rights- based healthcare. Provided users are fully informed, able to make auton-omous choices and are able to link to a health system when required, high- quality self- care interventions can offer available, accessible and acceptable healthcare to those individuals and groups who may be less likely to access formal healthcare due to fear of discrimination or privacy and confidentiality concerns. Benefits may flow to healthcare providers too as users become more engaged in their healthcare, with task- shifting reducing heavy workloads and consumer self- sampling potentially reducing the risk of personal injury to providers when obtaining samples (eg, via venepuncture).
We consistently identified accessibility as an important GER principle to measure across questions for all five interventions. From a human rights perspective, accessi-bility encompasses physical accessibility, economic acces-sibility (affordability), non- discrimination in access and information accessibility.25 This illustrates that multiple indicators are often required to measure a single outcome domain. Within a rights- based approach to measuring health, health indicators can be used to measure different standards and principles relating to GER.26 For example, some health surveys collect data on informed choice in
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

16 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Tab
le 5
R
esea
rch
gap
s fo
r se
lf- sa
mp
ling
for
hum
an p
apill
oma
viru
s (H
PV
) inf
ectio
n
Clin
ical
, pro
gra
mm
atic
, val
ues-
b
ased
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty a
nd
pra
ctic
al c
ons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Mai
n m
etho
do
log
ical
is
sues
ari
sing
in t
he
alte
rnat
ive
stud
y d
esig
n
Ben
efits
ve
rsus
har
ms
PIC
O: s
houl
d H
PV
se
lf- sa
mp
ling
be
mad
e av
aila
ble
to
ad
ult
wom
en
as a
n ad
diti
onal
ap
pro
ach
to
clin
icia
n- b
ased
sa
mp
ling
and
ce
rvic
al s
ervi
ces?
HP
V s
elf-
sam
plin
g sh
ould
be
mad
e av
aila
ble
to
adul
t w
omen
as
an a
dd
ition
al
app
roac
h to
clin
icia
n-
bas
ed s
amp
ling
and
ce
rvic
al s
ervi
ces.
Str
ong.
Mod
erat
e.N
o d
ata
from
LM
IC.
Ava
ilab
ility
and
ac
cess
ibili
ty.
RC
T co
nduc
ted
in
LM
IC w
ith
incl
usio
n of
ou
tcom
es
to m
easu
re
avai
lab
ility
and
ac
cess
ibili
ty.
As
a st
rong
WH
O
reco
mm
end
atio
n ex
ists
, it
wou
ld b
e un
ethi
cal t
o re
pea
t an
RC
T of
the
ef
fect
iven
ess
of t
he
inte
rven
tion.
Pro
spec
tive
non-
co
ntro
lled
coh
ort
stud
y to
be
cond
ucte
d in
se
vera
l LM
IC w
here
the
in
terv
entio
n is
or
will
be
imp
lem
ente
d. A
naly
sis
to c
omb
ine
qua
ntita
tive
surv
ey s
upp
lem
ente
d
with
focu
sed
in- d
epth
q
ualit
ativ
e in
terv
iew
s w
ith
wom
en t
o ex
plo
re G
ER
ou
tcom
es o
f ava
ilab
ility
an
d a
cces
sib
ility
. Cos
t an
alys
es c
an b
e ne
sted
in
the
coh
ort
stud
y.
Con
foun
din
g:
par
ticip
ants
in c
ohor
t se
lf- se
lect
to
self-
sa
mp
le a
nd m
ay
have
oth
er s
imila
r ch
arac
teris
tics
that
m
ay in
fluen
ce t
heir
abili
ty t
o ac
cess
HP
V
self-
sam
plin
g.M
easu
rem
ent
bia
s:
self-
rep
ortin
g b
ias
an
issu
e fo
r q
ualit
ativ
e co
mp
onen
t. T
his
will
re
qui
re w
ell t
rain
ed
rese
arch
ers
and
va
lidat
ed t
ools
. The
tr
iang
ulat
ion
of t
he
qua
litat
ive
dat
a w
ith
the
qua
ntita
tive
surv
ey
resu
lts p
rovi
des
an
elem
ent
of a
dd
ition
al
valid
atio
n of
out
com
es.
Valu
es a
nd
pre
fere
nces
Wha
t is
the
op
timal
way
(s) t
o en
gage
wom
en t
o se
lf- sa
mp
le, f
or
exam
ple
, via
tex
t or
via
com
mun
ity-
bas
ed m
eans
?
Not
ap
plic
able
.
G
DG
.A
cces
sib
ility
.C
omp
arat
ive
effe
ctiv
enes
s re
sear
ch t
o co
mp
are
diff
eren
t ty
pes
of m
etho
ds
to e
ngag
e w
omen
.
A c
ontr
olle
d t
rial
that
may
or
may
not
b
e ra
ndom
ised
is
feas
ible
. Id
entifi
catio
n or
dev
elop
men
t of
met
hod
s of
en
gage
men
t d
urin
g a
form
ativ
e st
age
will
b
e re
qui
red
prio
r to
te
stin
g in
a c
ontr
olle
d
man
ner.
Cur
rent
m
etho
ds
emp
loye
d
in H
IV a
dhe
renc
e p
rogr
amm
es m
ay b
e in
form
ativ
e.
Det
ectio
n b
ias:
the
ou
tcom
e w
ill b
e nu
mb
er o
f wom
en
enga
ged
for
each
m
etho
d. A
scer
tain
men
t of
eng
agem
ent
will
lik
ely
be
via
self-
rep
ort
and
as
wom
en w
ill b
e aw
are
of w
hat
met
hod
th
ey r
ecei
ved
, the
re is
a
risk
of d
etec
tion
bia
s.
This
can
be
red
uced
b
y en
surin
g th
at
outc
ome
asse
ssor
s ar
e m
aske
d t
o th
e al
loca
ted
gro
up, b
ut a
ris
k of
det
ectio
n b
ias
rem
ains
.
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 17
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
b
ased
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty a
nd
pra
ctic
al c
ons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Mai
n m
etho
do
log
ical
is
sues
ari
sing
in t
he
alte
rnat
ive
stud
y d
esig
n
Hum
an r
ight
s an
d e
qui
tyW
hat
are
the
optim
al m
etho
ds
to e
ncou
rage
w
omen
livi
ng
in h
uman
itaria
n se
ttin
gs t
o se
lf-
sam
ple
?
Ava
ilab
ility
, acc
essi
bili
ty,
acce
pta
bili
ty, n
on-
dis
crim
inat
ion,
priv
acy
and
con
fiden
tialit
y
Qua
litat
ive
key
info
rman
t st
udy
of u
sers
in
hum
anita
rian
sett
ings
reg
ard
ing
thei
r ex
per
ienc
es
of h
ealth
care
and
d
esire
s fo
r se
lf-
sam
plin
g.
This
is a
feas
ible
stu
dy .
Sel
ectio
n b
ias:
as
with
al
l qua
litat
ive
stud
ies,
p
artic
ipan
ts a
re
pur
pos
ivel
y se
lect
ed.
How
ever
, thi
s is
an
adva
ntag
e in
thi
s st
udy
des
ign
as u
sers
an
d p
oten
tial u
sers
liv
ing
in h
uman
itaria
n se
ttin
gs w
ill h
ave
rich
exp
erie
nces
and
ob
serv
atio
ns t
o sh
are.
How
can
link
age
to c
are
be
ensu
red
fo
llow
ing
HP
V s
elf-
sa
mp
ling?
GD
GA
cces
sib
ility
, ac
cep
tab
ility
and
non
- d
iscr
imin
atio
n.
Com
par
ativ
e ef
fect
iven
ess
rese
arch
of a
p
acka
ge o
f car
e th
at in
clud
es
self-
sam
plin
g co
mb
ined
with
d
iffer
ent s
trat
egie
s su
ch a
s tr
aini
ng
of c
linic
sta
ff to
en
cour
age
wom
en
and
faci
litat
e lin
kage
to
care
co
mp
ared
with
se
lf- sa
mp
ling
only
.
A c
ontr
olle
d t
rial
that
may
or
may
not
b
e ra
ndom
ised
is
a fe
asib
le d
esig
n.
Link
age
to c
are
need
s to
incl
ude
links
to
car
e fo
r w
omen
se
lf- sa
mp
ling
and
se
nsiti
satio
n to
HP
V
vacc
inat
ion
and
p
oten
tial m
essa
ging
to
par
tner
s.
Soc
ial d
esira
bili
ty
bia
s: w
omen
will
be
awar
e of
the
diff
eren
t st
rate
gies
the
y ha
ve
rece
ived
and
may
feel
co
mp
elle
d t
o re
por
t p
ositi
ve e
xper
ienc
es
from
sta
ff, r
athe
r th
an
dis
crim
inat
ion.
To
add
ress
thi
s, o
utco
me
asse
ssm
ent
shou
ld b
e d
one
by
thos
e b
lind
ed
to t
he g
roup
and
w
ho a
re n
ot p
art,
or
per
ceiv
ed t
o b
e p
art,
of
the
clin
ic s
taff.
Wha
t ar
e th
e op
timal
met
hod
s to
ac
cess
hom
eles
s w
omen
?
Acc
essi
bili
ty,
acce
pta
bili
ty a
nd n
on-
dis
crim
inat
ion.
This
is a
n un
der
- re
sear
ched
are
a.
Initi
al r
esea
rch
shou
ld in
clud
e id
entifi
catio
n of
cur
rent
he
alth
- see
king
p
ract
ices
of
hom
eles
s w
omen
vi
a q
ualit
ativ
e in
terv
iew
s w
ith
thos
e w
orki
ng
with
the
hom
eles
s an
d t
he h
omel
ess
to fi
nd o
ut h
ow
they
wou
ld li
ke t
o b
e re
ache
d a
nd t
o d
evel
op s
trat
egie
s p
rior
to fu
rthe
r ev
alua
tion.
This
is a
feas
ible
d
esig
n.
La
ck o
f gen
eral
isab
ility
: th
e re
sults
will
be
cont
ext
spec
ific
and
may
not
be
gene
ralis
able
to
othe
r re
gion
s; t
his
is e
spec
ially
tru
e of
ac
cess
to
serv
ices
. H
owev
er, t
he d
esire
fo
r ap
pro
ache
s to
ou
trea
ch m
ay b
e ge
nera
lisab
le t
o ot
her
sett
ings
.
Tab
le 5
C
ontin
ued
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

18 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
b
ased
or
hum
an r
ight
s q
uest
ion
Cur
rent
WH
O
reco
mm
end
atio
nS
tren
gth
of
reco
mm
end
atio
n
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty a
nd
pra
ctic
al c
ons
trai
nts
Alt
erna
tive
stu
dy
des
ign
Mai
n m
etho
do
log
ical
is
sues
ari
sing
in t
he
alte
rnat
ive
stud
y d
esig
n
Res
ourc
e us
eW
hat
is t
he c
ost-
ef
fect
iven
ess
of
self-
sam
plin
g w
hen
linka
ge t
o ca
re
is in
clud
ed a
s an
ou
tcom
e in
the
an
alys
is?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
Ava
ilab
ility
and
ac
cess
ibili
ty.
Mod
ellin
g st
udie
s of
cos
t-
effe
ctiv
enes
s ac
ross
bro
ader
ra
nge
of s
ettin
gs,
taki
ng b
oth
a he
alth
care
p
rovi
der
an
d s
ocie
tal
per
spec
tive.
This
is a
feas
ible
stu
dy,
b
ut it
s q
ualit
y an
d
usef
ulne
ss d
epen
d
on t
he r
elia
bili
ty
of t
he p
aram
eter
s fo
r un
it co
sts
and
ef
fect
iven
ess,
whi
ch
wou
ld b
e d
raw
n fr
om
cost
ing
stud
ies
and
th
e R
CTs
effe
ctiv
enes
s d
ata.
It w
ill a
lso
req
uire
mor
e lo
ng- t
erm
m
odel
ling
to c
aptu
r e
dow
nstr
eam
effe
cts
on
linka
ge t
o ca
re.
Mea
sure
men
t b
ias:
the
res
ults
ar
e d
epen
den
t on
se
lect
ion
of v
aria
ble
s in
clud
ed in
the
mod
el,
assu
mp
tions
reg
ard
ing
dis
coun
t ra
tes,
co
st- e
ffect
iven
ess
thre
shol
ds
and
ac
cura
te e
stim
ates
of
curr
ent
and
pro
ject
ed
cost
s. F
or e
xam
ple
, vu
lner
able
pop
ulat
ions
w
ith li
mite
d a
cces
s to
car
e ar
e lik
ely
to
gene
rate
diff
eren
t re
sults
bas
ed o
n th
e p
rob
abili
ty t
hat
they
w
ould
hav
e lim
ited
or
no
acce
ss t
o ca
re
with
out
self-
sam
plin
g.
Wha
t ar
e th
e d
iffer
ence
s in
ou
t- of
- poc
ket
exp
end
iture
s fo
r se
lf- sa
mp
ling
bet
wee
n hi
gh-
inco
me
and
low
- in
com
e re
gion
s?
Not
ap
plic
able
.N
ot a
pp
licab
le.
GD
G.
A
cces
sib
ility
.E
mp
irica
l cos
ting
stud
ies
to
estim
ate
user
and
p
rovi
der
cos
ts,
and
fina
ncin
g so
urce
s fo
r ea
ch
(use
rs p
ay, o
r he
alth
sys
tem
p
ays)
This
is a
feas
ible
stu
dy.
Mea
sure
men
t b
ias:
the
re
sults
are
dep
end
ent
on u
ser
reca
ll an
d s
elf-
r e
por
ted
res
ourc
e us
e,
opp
ortu
nity
cos
ts, a
s w
ell a
s on
ass
ump
tions
re
gard
ing
shar
ed c
osts
in
hea
lth fa
cilit
ies.
GD
G, G
uid
elin
e D
evel
opm
ent
Gro
up; G
ER
, gen
der
, eq
uity
and
hum
an r
ight
s; P
ICO
, Pop
ulat
ion,
Inte
rven
tions
, Com
par
ison
and
Out
com
es; R
CT,
ran
dom
ised
con
trol
led
tria
l.
Tab
le 5
C
ontin
ued
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 19
BMJ Global Health
Tab
le 6
R
esea
rch
gap
s fo
r ho
me-
bas
ed o
vula
tion
pre
dic
tor
kits
(OP
Ks)
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed o
r hu
man
rig
hts
que
stio
nC
urre
nt W
HO
re
com
men
dat
ion
Str
eng
th o
f re
com
men
dat
ion
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty a
nd p
ract
ical
co
nstr
aint
sA
lter
nati
ve s
tud
y d
esig
n
Mai
n m
etho
do
log
ical
issu
es
aris
ing
in t
he a
lter
nati
ve
stud
y d
esig
n
Ben
efits
ver
sus
harm
sP
ICO
: sho
uld
hom
e-
bas
ed O
PK
s b
e m
ade
avai
lab
le a
s an
ad
diti
onal
ap
pro
ach
to
fert
ility
man
agem
ent
for
wom
en a
nd c
oup
les
des
iring
pre
gnan
cy?
Hom
e- b
ased
OP
Ks
shou
ld
be
mad
e av
aila
ble
as
an
add
ition
al a
pp
r oac
h to
fert
ility
m
anag
emen
t fo
r w
omen
and
co
uple
s d
esiri
ng p
regn
ancy
.
Str
ong.
Very
low
.N
o d
ata
from
LM
IC. K
ey G
ER
co
nsid
erat
ions
in
clud
e av
aila
bili
ty
and
acc
essi
bili
ty.
RC
T co
nduc
ted
in
LMIC
with
incl
usio
n of
out
com
es t
o m
easu
re a
vaila
bili
ty
and
acc
essi
bili
ty, a
nd
exp
lora
tion
of p
oten
tial
for
coer
cion
.
As
a st
rong
WH
O
reco
mm
end
atio
n, it
wou
ld
be
unet
hica
l to
rep
eat
an
RC
T of
the
effe
ctiv
enes
s of
the
inte
rven
tion.
Pro
spec
tive
non-
cont
rolle
d
coho
rt s
tud
y to
be
cond
ucte
d
in s
ever
al L
MIC
whe
re t
he
inte
rven
tion
is o
r w
ill b
e im
ple
men
ted
. Ana
lysi
s to
com
bin
e q
uant
itativ
e su
rvey
sup
ple
men
ted
with
fo
cuse
d in
- dep
th q
ualit
ativ
e in
terv
iew
s w
ith w
omen
and
p
artn
ers
to e
xplo
re G
ER
ou
tcom
es o
f ava
ilab
ility
and
ac
cess
ibili
ty. E
xplo
ratio
n of
p
oten
tial f
or c
oerc
ion
wou
ld
be
adva
ntag
eous
to
det
erm
ine
pot
entia
l har
ms.
Cos
t an
alys
es
can
be
nest
ed in
the
coh
ort
stud
y.
Con
foun
din
g: p
artic
ipan
ts
in c
ohor
t se
lf- se
lect
to
use
OP
K a
nd m
ay h
ave
othe
r si
mila
r ch
arac
teris
tics
that
m
ay in
fluen
ce t
heir
abili
ty t
o ac
cess
OP
Ks.
Mea
sur e
men
t b
ias:
sel
f-
rep
ortin
g b
ias
an is
sue
for
qua
litat
ive
com
pon
ent
as w
ell
as s
ocia
l des
irab
ility
bia
s if
bot
h th
e w
omen
and
par
tner
s ar
e in
clud
ed. T
his
will
req
uire
w
ell t
rain
ed r
esea
rche
rs
and
val
idat
ed t
ools
. The
tr
iang
ulat
ion
of t
he q
ualit
ativ
e d
ata
with
the
qua
ntita
tive
surv
ey r
esul
ts p
rovi
des
an
ele
men
t of
ad
diti
onal
va
lidat
ion
of o
utco
mes
.
How
pre
vale
nt is
in
fert
ility
in lo
w- i
ncom
e an
d m
idd
le- i
ncom
e se
ttin
gs a
nd w
hat
are
the
cons
eque
nces
?
Not
ap
plic
able
.
G
DG
.N
ot a
pp
licab
le.
Cro
ss- s
ectio
nal s
urve
y of
wom
en fr
om g
ener
al
pop
ulat
ion
in L
MIC
to
asce
rtai
n se
lf- re
por
ted
p
reva
lenc
e of
infe
rtili
ty.
Cro
ss- s
ectio
nal
sem
en a
naly
sis
surv
ey
of s
elec
ted
you
ng
mal
e p
opul
atio
ns in
LM
IC (e
g, s
old
iers
) to
asc
erta
in m
ale
infe
rtili
ty.
A la
rge
gene
ral p
opul
atio
n su
rvey
is fe
asib
le b
ut
has
cost
imp
licat
ions
to
ach
ieve
a s
uffic
ient
ly
larg
e sa
mp
le t
o b
e re
pre
sent
ativ
e.
Focu
sed
cro
ss- s
ectio
nal
stud
y of
wom
en a
tten
din
g p
rimar
y ca
re c
linic
s, e
xclu
din
g an
tena
tal c
are,
to
asce
rtai
n se
lf- re
por
ted
pre
vale
nce
of
infe
rtili
ty.
Ber
kson
’s b
ias:
peo
ple
who
p
rese
nt w
ith o
ne c
ond
ition
ar
e m
ore
likel
y to
hav
e a
seco
nd c
ond
ition
. The
refo
re,
sam
plin
g fr
om a
clin
ic m
ay
over
- rep
rese
nt t
he p
reva
lenc
e of
infe
rtili
ty a
nd n
ot b
e re
pre
sent
ativ
e of
the
gen
eral
p
opul
atio
n.
Wha
t is
the
imp
act
of
usin
g a
hom
e- b
ased
O
PK
on
com
mun
icat
ion
bet
wee
n p
artn
ers?
Not
ap
plic
able
.
G
DG
.P
rivac
y an
d
confi
den
tialit
y.P
harm
acy-
led
su
rvey
of w
omen
's
exp
erie
nces
of p
artn
er
com
mun
icat
ion
whe
n p
urch
asin
g th
e O
PK
an
d a
fter
usi
ng t
he
OP
K.
Priv
acy
and
per
cep
tion
of la
ck o
f priv
acy,
may
co
mp
rom
ise
the
inte
grity
of
the
dat
a an
d w
omen
's
will
ingn
ess
to c
onse
nt
to p
artic
ipat
e. L
ack
of
trai
ned
pro
fess
iona
ls in
th
e p
harm
acy
may
als
o re
duc
e th
e up
take
and
q
ualit
y of
the
sur
vey.
Qua
litat
ive
key
info
rman
t in
terv
iew
s of
cou
ple
s in
vite
d t
o p
artic
ipat
e ei
ther
at
infe
rtili
ty
clin
ics
or a
t p
harm
acie
s.
Soc
ial a
ccep
tab
ility
bia
s:
this
stu
dy
will
req
uire
car
eful
in
terv
iew
ing
with
hig
hly
trai
ned
inte
rvie
wer
s to
elic
it re
spon
ses
that
are
tru
thfu
l an
d n
ot s
ocia
lly d
esira
ble
. In
terv
iew
ing
wom
en a
nd
men
sep
arat
ely
may
red
uce
this
but
con
seq
uent
ly
red
uces
the
ob
serv
atio
n of
co
mm
unic
atio
n p
atte
rns
bet
wee
n p
artn
ers.
Valu
es a
nd
pre
fere
nces
Wha
t ar
e th
e va
lues
an
d p
refe
renc
es o
f w
omen
and
men
re
gard
ing
infe
rtili
ty in
se
ttin
gs o
f dep
rivat
ion
(bot
h in
hig
h- in
com
e co
untr
ies
and
in lo
w-
inco
me
and
mid
dle
- in
com
e co
untr
ies)
?
Not
ap
plic
able
.
G
DG
.
Non
- d
iscr
imin
atio
n.O
nlin
e gl
obal
cro
ss-
sect
iona
l sur
vey
of
men
and
wom
en
del
iver
ed t
hrou
gh
rele
vant
org
anis
atio
ns.
The
par
ticip
ants
can
be
any
age
and
infe
rtili
ty
is n
ot a
n in
clus
ion
crite
ria.
In m
any
sett
ings
of
dep
rivat
ion,
and
es
pec
ially
in L
MIC
, onl
ine
acce
ssib
ility
is li
mite
d
by
cost
s, in
adeq
uate
te
chno
logy
and
lack
of
know
led
ge o
n ho
w t
o us
e to
ols.
Sp
ecifi
c gr
oup
s,
for
exam
ple
, tra
ns m
en,
may
not
be
reac
hed
by
a su
rvey
aim
ed a
t th
e ge
nera
l pop
ulat
ion.
Focu
s gr
oup
s in
pur
pos
ivel
y sa
mp
led
pop
ulat
ions
and
re
gion
s. F
ocus
gro
ups
are
mos
t su
itab
le t
o d
rive
conv
ersa
tions
and
elic
it re
spon
ses
amon
g p
artic
ipan
ts
with
sha
red
live
d e
xper
ienc
es
and
is le
ss c
onfr
onta
tiona
l as
the
aim
is n
ot t
o ga
ther
in-
dep
th p
erso
nal e
xper
ienc
es
of in
fert
ility
, but
ass
ess
curr
ent
cultu
ral a
nd s
ocia
l no
rms.
Rec
ruitm
ent
of
spec
ific
grou
ps,
for
exam
ple
, tr
ans
men
, can
be
targ
eted
ap
pro
pria
tely
.
Soc
ial a
ccep
tab
ility
bia
s:
give
n th
at e
xper
ienc
es a
re
shar
ed in
a g
roup
, the
re m
ay
be
a re
luct
ance
to
dis
clos
e st
igm
atis
ing
beh
avio
urs;
ho
wev
er, d
evel
opm
ent
of
sem
istr
uctu
red
inte
rvie
w
que
stio
ns in
con
sulta
tion
with
res
earc
hers
and
re
pre
sent
ativ
es o
f the
sa
mp
led
pop
ulat
ion
to
bes
t re
flect
loca
l bel
iefs
for
inte
rrog
atio
n ca
n re
duc
e th
is
bia
s. In
ad
diti
on, a
ski
lled
fo
cus
grou
p le
ader
can
cre
ate
a sa
fe s
pac
e fo
r d
iscl
osur
e.
Con
tinue
d
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

20 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
Clin
ical
, pro
gra
mm
atic
, val
ues-
bas
ed o
r hu
man
rig
hts
que
stio
nC
urre
nt W
HO
re
com
men
dat
ion
Str
eng
th o
f re
com
men
dat
ion
So
urce
or
qua
lity
of
evid
ence
Key
GE
R
cons
ider
atio
nsId
eal s
tud
y d
esig
n(s)
Feas
ibili
ty a
nd p
ract
ical
co
nstr
aint
sA
lter
nati
ve s
tud
y d
esig
n
Mai
n m
etho
do
log
ical
issu
es
aris
ing
in t
he a
lter
nati
ve
stud
y d
esig
n
Res
ourc
e us
eA
re h
ome-
bas
ed
OP
Ks
cost
- effe
ctiv
e co
mp
ared
with
oth
er
fert
ility
man
agem
ent
optio
ns?
Not
ap
plic
able
.
G
DG
.A
vaila
bili
ty a
nd
acce
ssib
ility
.M
odel
ling
stud
ies
of
cost
- effe
ctiv
enes
s.Th
is is
a fe
asib
le s
tud
y d
esig
n. M
odel
ling
will
re
qui
re id
entifi
catio
n of
sec
ond
ary
dat
a on
the
cos
ts o
f OP
K
and
oth
er fe
rtili
ty
man
agem
ent
optio
ns
in a
sp
ecifi
c co
untr
y se
ttin
g. A
ssum
ptio
ns
und
erly
ing
the
mod
el
will
incl
ude
sele
ctio
n of
a p
rimar
y ou
tcom
e (p
regn
ancy
or
live
birt
h)
or d
isab
ility
- ad
just
ed li
fe
year
s or
qua
lity-
adju
sted
lif
e ye
ars
(whi
ch c
an
cap
ture
red
uced
dis
abili
ty
or im
pro
ved
qua
lity
of
life
from
red
uctio
n in
an
xiet
y). A
sses
smen
t an
d
inco
rpor
atio
n of
hum
an
right
s m
easu
rem
ents
su
ch a
s p
rivac
y an
d
non-
coer
cion
will
b
e ch
alle
ngin
g. A
ny
mod
ellin
g w
ill e
ither
nee
d
to b
e co
untr
y- sp
ecifi
c or
st
ratifi
ed b
y co
untr
y.
Lack
of g
ener
alis
abili
ty: a
cos
t co
mp
aris
on w
ould
pro
vid
e in
dire
ct d
ata
for
man
y re
gion
s w
here
diff
eren
ces
bet
wee
n co
sts
of fe
rtili
ty m
anag
emen
t op
tions
and
cos
ts o
f acc
ess
to h
ealth
care
diff
er w
idel
y.
GD
G, G
uid
elin
e D
evel
opm
ent
Gro
up; G
ER
, gen
der
, eq
uity
and
hum
an r
ight
s; P
ICO
, Pop
ulat
ion,
Inte
rven
tions
, Com
par
ison
and
Out
com
es; R
CT,
ran
dom
ised
con
trol
led
tria
l.
Tab
le 6
C
ontin
ued
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 21
BMJ Global Health
contraception uptake (measured by the proportion of users who were informed of potential side effects, what to do in the case of side effects and alternative contra-ceptive options). This highlights the human rights stan-dard of acceptability as well as the principle of autonomy, expressed through free, full and informed decision making.27 Similarly, indicators commonly used in the fields of GER may be used to measure certain aspects of sexual and reproductive health; for example, measures of the existence, content and degree of implementation of relevant laws and policies governing access to sexual and reproductive health information and services can help elucidate patterns in uptake of services, including for self- care initiatives. An indicator that incorporates both sets of concern will allow for identification of interven-tions that are sensitive to issues relating to GER and most effective in terms of improving health.26
In our approach, we identified the GER standards and principles most relevant to each question but did not oper-ationalise measurement. This is an important next step. Development of, and agreement on, standardised indica-tors and the optimal instruments to measure these within the SRHR self- care intervention field will greatly enhance the usability and uptake of GER- informed evidence into future guidelines through streamlining meta- analysis and synthesis more broadly. The experience and guid-ance of the Core Outcome Measures in Effectiveness Trials (COMET) initiative are instructive in this regard. COMET advocates for the development and applica-tion of agreed, standardised sets of outcomes, known as ‘core outcome sets’, which represent the minimum that should be measured and reported in all clinical trials of a specific condition and are also suitable for use in clin-ical auditing or research other than randomised trials.28 Inclusion of GER in an SRHR self- care core outcome set will ensure GER are integral to all future evaluations. We welcome initiatives to bring researchers from the human rights, gender, health economics and epidemiology fields together to advance this.
The WHO aims to be representative when determining GDG composition, and for the guideline on self- care interventions, we believe reasonable representation was achieved. However, in general, the balance is in favour of healthcare providers rather than community members and users of interventions. We were also able to ensure participation of users and healthcare providers of SRHR self- care interventions by incorporating the findings of the global survey and focus group discussions with vulnerable populations into the formulation of research gaps. Active and informed participation of users is also an important consideration during implementation of recommendations and in planning future research studies. Many of the proposed future studies are focused on vulnerable populations, and participation in the study or assessment of an outcome may place participants at risk. This illustrates that outcome measurement and the process of research itself requires careful consideration of GER to minimise unintended harms. Community- based
participatory research is a useful strategy to conducting research that is relevant, appropriate and acceptable.
Prior to conducting studies on self- care, researchers need to consider the burdens faced by study participants, particularly for implementation research and qualitative methodologies. There is an opportunity cost to partic-ipants who may have to take time away from work or family care in order to contribute to research activities. We encourage meaningful involvement of individuals or groups representing target populations in the design and cocreation of research methodologies to optimise bene-fits to individuals and the wider group while minimising burdens to the participants. This approach is supported by ethical considerations29 and several frameworks that promote person- centred interventions.30 31
Each of the proposed study designs can be further expanded into a template for a study protocol and made publicly available. The WHO successfully achieved rapid deployment of ethically approved clinical trial protocols for the Ebola vaccine under emergency conditions.32 33 Under more controlled conditions, WHO may consider systematically developing field- specific study protocol templates that meet ethics standards. Researchers can then modify these templates to their context addressing any specific local ethics requirements before rapidly conducting studies during implementation of new WHO recommendations to inform programme scale- up or for testing new strategies well in advance of planned future GDG meetings.
Similar to our previous work where we applied the original framework to SRHR guidelines for women living with HIV, we found that many of the identified research questions require evaluation of complex, multifaceted and often multisectoral interventions that may be best suited to evaluation within an implementation research paradigm.12 Implementation science provides a platform to learn whether an intervention works in real- world settings and demonstrates how to ensure an intervention can effectively be brought to scale. Importantly, outcomes such as acceptability, feasibility and costs are encouraged in addition to conventional measures of effectiveness.34 RCTs are the optimal design for providing evidence of efficacy and will remain the gold standard for informing WHO recommendations. However, comparative effec-tiveness research (CER) where available interventions are compared with each other (instead of with usual care or placebo) can be viewed as a bridge between RCTs and implementation research.35 36 Five of our research ques-tions are best evaluated using CER (eg, comparison on OPKs with other fertility management options) with 10 studies requiring a multistudy approach best articulated in implementation science. The challenge for WHO will be how these types of study designs and approaches can best be incorporated into future WHO guidelines deci-sion making. Some progress has been made with the inclusion of the Risk of Bias in Non- randomised studies of interventions (ROBINS- I) tool for assessing risk of bias in non- randomised studies in GRADE,36 guidance
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

22 Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128
BMJ Global Health
for rating certainty of evidence when reviewing public health interventions37 and the development of the WHO- INTEGRATE framework to WHO guidelines develop-ment that includes specific methods to incorporate norms and values and a greater complexity perspective.38
Our approach is unique to the development of norma-tive guidance. As such it is limited by the scope of a guide-line, which may be intentionally narrow due to feasibility, resources and time constraints. The research gaps arising from such a process are specific to the scope of the guidelines and should not be viewed as a comprehensive research agenda for the relevant clinical or public health field nor as a research prioritisation exercise. However, the resultant research questions can provide a baseline list of questions that can then be further subjected to one of several research prioritisation methodologies.39–41
Lastly, while our overall decision- making process is structured and systematised, the selection of the most relevant GER standards and principles was done primarily through iterative discussion and ultimately consensus between study authors. Such decisions may not readily lend themselves to standardised processes, but we would advocate that in order to ensure the integrity and gener-alisability of the selected standards and principles, deci-sions should be made by a diverse and representative group as possible. We attempted to do so by reflecting a diversity of backgrounds, skills and experiences among the study authors, but we acknowledge that our selections are nonetheless subjective and may be best done by the broader GDG. Further exploration and development of ways to standardise such decisions such as initiated in the family planning field is now required.42
ConClusIonA framework based on GRADE that includes stake-holders’ values and identification of core GER standards and principles provides a practical, systematic approach to identifying research questions from a WHO guideline. Uptake of this framework has the potential to harmonise methods and ensure more consistent consideration of research question formulation across the organisation. Clear guidance for future studies, including anticipation of, and methods to reduce risks of bias, can contribute to an anticipated ‘living guidelines’ approach within WHO. Foregrounding GER as a separate component of the framework is key to ensuring it is considered as inte-gral to outcome evaluation, and further elaboration to operationalise appropriate indicators for SRHR self- care interventions is required.
Author affiliations1Independent Clinical Epidemiologist, Cape Town, South Africa2Department of Sexual and Reproductive Health and Research, including UNDP- UNFPA- UNICEF- WHO- World Bank Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization, Geneva, Switzerland3Factor- Inwentash Faculty of Social Work, University of Toronto, Toronto, Ontario, Canada
4Guideline Review Committee Secretariat (Science Division), World Health Organization, Geneva, Switzerland5Institute on Inequalities in Global Health, Keck School of Medicine, University of Southern California, Los Angeles, California, USA6Independent Consultant, Amsterdam, The Netherlands7International Institute for Global Health, United Nations University, Kuala Lumpur, Malaysia
Acknowledgements The authors are grateful to all members of the Guidelines Development Group for their contributions during the meeting. We would like to thank Rachel Beanland, Independent Public Health Consultant, for her helpful comments on the selection of study designs and elaboration of biases.
Contributors NS conceived the concept and developed the framework and methodology informed by prior work in the area. MN led the WHO guideline development process and initiated the use of the framework during the guideline process. All authors contributed to refining the framework and provided expertise- informed contributions to adapting the framework, formulating research questions and identifying study designs. All authors contributed to the final manuscript.
Funding This paper was funded by WHO/UNDP- UNFPA- UNICEF- WHO- World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP). The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
data availability statement The article describes development and application of a framework. The tables generated regarding study design may constitute data and are included in the published manuscript.
open access This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https:// creativecommons. org/ licenses/ by/ 4. 0/.
orCId idNandi Siegfried http:// orcid. org/ 0000- 0002- 4081- 1698
REFEREnCES 1 World Health Organization. WHO Handbook for Guideline
development. 2nd edn, 2014. Available: https://www. who. int/ publications/ guidelines/ guidelines_ review_ committee/ en/ [Accessed 19 Mar 2020]
2 Maher D, Ford N. A public health research agenda informed by guidelines in development. Bull World Health Organ 2017;95:795- A.
3 World Health Organization. WHO consolidated guideline on self- care interventions for health: sexual and reproductive health and rights. Geneva: World Health Organization, 2019Licence: CC BY- NC- SA 3.0 IGO
4 Hatch S IK. Self- help and health in Europe: new approaches in health care. Albany, NY: World Health Organization Publications Center USA, 1983.
5 World Health Organization. WHO meeting on ethical, legal, human rights and social accountability implications of self- care interventions for sexual and reproductive health: 12–14 March 2018, Brocher Foundation, Hermance, Switzerland: summary report. Geneva: World Health Organization, 2018. Licence: CC BY- NC- SA 3.0 IGO.
6 World Health Organization. Gender, equity and human rights, 2019. Available: https://www. who. int/ gender- equity- rights/ understanding/ human- rights- definition/ en/ [Accessed 5 Jun 2019].
7 World Health Organization. A human- rights based approach to health. Available: https://www. who. int/ hhr/ news/ hrba_ to_ health2. pdf [Accessed 22 Aug 2019].
8 Sridharan S, Maplazi J, Shirodkar A, et al. Incorporating gender, equity, and human rights into the action planning process: moving from rhetoric to action. Glob Health Action 2016;9:30870.
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from

Siegfried N, et al. BMJ Global Health 2020;5:e002128. doi:10.1136/bmjgh-2019-002128 23
BMJ Global Health
9 Ferguson L, Fried S, Matsaseng T, et al. Human rights and legal dimensions of self care interventions for sexual and reproductive health. BMJ 2019;365:l1941.
10 World Health Organization. WHO consolidated guideline on self- care interventions for health: sexual and reproductive health and rights web supplement: global values and preferences survey report. Geneva: World Health Organization, 2019. https:// apps. who. int/ iris/ bitstream/ handle/ 10665/ 329989/ WHO- RHR- 19. 24- eng. pdf? ua=1
11 Siegfried N, Beanland RL, Ford N, et al. Formulating the future research agenda for postexposure prophylaxis for HIV: methodological challenges and potential approaches. Clin Infect Dis 2015;60(Suppl 3):S205–11.
12 Siegfried N, Narasimhan M, Kennedy CE, et al. Using GRADE as a framework to guide research on the sexual and reproductive health and rights (SRHR) of women living with HIV - methodological opportunities and challenges. AIDS Care 2017;29:1088–93.
13 Yeh PT, Kennedy CE, Van der Poel S, et al. Should home- based ovulation predictor kits be offered as an additional approach for fertility management for women and couples desiring pregnancy? A systematic review and meta- analysis. BMJ Glob Health 2019;4:e001403.
14 Yeh PT, Kennedy CE, de Vuyst H, et al. Self- sampling for human papillomavirus (HPV) testing: a systematic review and meta- analysis. BMJ Glob Health 2019;4:e001351.
15 Ogale Y, Yeh PT, Kennedy CE, et al. Self- collection of samples as an additional approach to deliver testing services for sexually transmitted infections: a systematic review and meta- analysis. BMJ Glob Health 2019;4:e001349.
16 Kennedy CE, Yeh PT, Gonsalves L, et al. Should oral contraceptive pills be available without a prescription? A systematic review of over- the- counter and pharmacy access availability. BMJ Glob Health 2019;4:e001402.
17 Kennedy CE, Yeh PT, Gaffield ML, et al. Self- administration of injectable contraception: a systematic review and meta- analysis. BMJ Glob Health 2019;4:e001350.
18 Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336:924–6.
19 Andrews JC, Schünemann HJ, Oxman AD, et al. Grade guidelines: 15. going from evidence to recommendation- determinants of a recommendation's direction and strength. J Clin Epidemiol 2013;66:726–35.
20 Robinson KA, Saldanha IJ, McKoy NA. Frameworks for determining research gaps during systematic reviews. In: Methods future research needs report No. 2. Rockville MD: Agency for Healthcare Research and Quality, 2011. www. effectivehealthcare. ahrq. gov/ reports/ final. cfm
21 Dechartres A, Ravaud P. Better prioritization to increase research value and decrease waste. BMC Med 2015;13:244.
22 Akl EA, Meerpohl JJ, Elliott J, et al. Living systematic reviews: 4. living guideline recommendations. J Clin Epidemiol 2017;91:47–53.
23 World Health Organization. Ensuring human rights in the provision of contraceptive information and services: guidance and recommendations, 2019. Available: https:// apps. who. int/ iris/ bitstream/ handle/ 10665/ 102539/ 9789241506748_ eng. pdf; jsessionid= 36DD E4C1 852D 56BB 855F 5082 C1436DA7? sequence=1 [Accessed 30 Sep 2019].
24 World Health Organization. Reproductive, maternal, newborn and child health and human rights: a toolbox for examining laws, regulations and policies, 2016. Available: https:// apps. who. int/ iris/ bitstream/ handle/ 10665/ 126383/ 9789241507424_ eng. pdf; jsessionid= 7A1B FE94 AB89 3308 6237 F6D3 85966381? sequence=1 [Accessed 30 Sep 2019].
25 UN Committee on Economic, Social and Cultural Rights (CESCR). General Comment No. 14: the right to the highest attainable standard of health (art. 12 of the covenant), 11 August 2000, E/C.12/2000/4. Available: https://www. refworld. org/ docid/ 4538838d0. html [Accessed 10 Sep 2019].
26 Gruskin S, Ferguson L. Using indicators to determine the contribution of human rights to public health efforts. Bull World Health Organ 2009;87:714–9.
27 World Health Organization. Ensuring human rights within contraceptive programmes: a human rights analysis of existing quantitative indicators, 2014. Available: https:// apps. who. int/ iris/ bitstream/ handle/ 10665/ 126799/ 9789241507493_ eng. pdf? ua= 1& ua= 1? sequence=1 [Accessed 8 Oct 2019].
28 Williamson PR, Altman DG, Bagley H, et al. The COMET Handbook: version 1.0. Trials 2017;18:280.
29 Aluwihare- Samaranayake D. Ethics in qualitative research: a view of the participants' and researchers' world from a critical standpoint. Int J Qual Methods 2012;11:64–81.
30 Narasimhan M, Allotey P, Hardon A. Self care interventions to advance health and wellbeing: a conceptual framework to inform normative guidance. BMJ 2019;365:l688.
31 World Health Organization. Who framework on integrated person- centred services. Sixty- ninth World health assembly A69/39, 2016. Available: https://www. who. int/ serv iced eliv erys afety/ areas/ people- centred- care/ Overview_ IPCHS_ final. pdf? ua=1 [Accessed 20 Sep 2019].
32 Calain P. The Ebola clinical trials: a precedent for research ethics in disasters. J Med Ethics 2018;44:3–8.
33 Heymann DL, Rodier GR, Ryan MJ. Ebola vaccines: keep the clinical trial protocols on the shelf and ready to roll out. Lancet 2015;385:1913–5.
34 Peters DH, Adam T, Alonge O, et al. Implementation research: what it is and how to do it. BMJ 2013;347:f6753.
35 Glasgow RE, Rabin BA. Implementation science and comparative effectiveness research: a partnership capable of improving population health. J Comp Eff Res 2014;3:237–40.
36 Schünemann HJ, Cuello C, Akl EA, et al. GRADE guidelines: 18. How ROBINS- I and other tools to assess risk of bias in nonrandomized studies should be used to rate the certainty of a body of evidence. J Clin Epidemiol 2019;111:105–14.
37 Montgomery P, Movsisyan A, Grant SP, et al. Considerations of complexity in rating certainty of evidence in systematic reviews: a primer on using the grade approach in global health. BMJ Glob Health 2019;4:e000848.
38 Rehfuess EA, Stratil JM, Scheel IB, et al. The WHO- INTEGRATE evidence to decision framework version 1.0: integrating who norms and values and a complexity perspective. BMJ Glob Health 2019;4:e000844.
39 Nasser M, Welch V. Prioritization of systematic reviews leads prioritization of research gaps and needs. J Clin Epidemiol 2013;66:522–3.
40 Nasser M, Ueffing E, Welch V, et al. An equity lens can ensure an equity- oriented approach to agenda setting and priority setting of Cochrane reviews. J Clin Epidemiol 2013;66:511–21.
41 Bhaumik S, Rana S, Karimkhani C, et al. Ethics and equity in research priority- setting: stakeholder engagement and the needs of disadvantaged groups. Indian J Med Ethics 2015;12:110–3.
42 Gruskin S, Ferguson L, Kumar S, et al. A novel methodology for strengthening human rights based monitoring in public health: family planning indicators as an illustrative example. PLoS One 2017;12:e0186330.
on July 28, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2019-002128 on 30 March 2020. D
ownloaded from
Related Documents