Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Prevalence and determinants of hypertension in the Algerian Sahara Mohamed Temmar a , Carlos Labat b , Salim Benkhedda c , Meriem Charifi d , Frederique Thomas e , Mohamed Tahar Bouafia d , Kathy Bean e , Bernadette Darne f , Michel E. Safar f and Athanase Benetos b,g Background In-Salah is a city-oasis located in the middle of the Algerian Sahara, a desert area whose drinking water has a high sodium content. No cardiovascular epidemiological studies have ever been conducted in this region. Methods A randomized sample of 635 men and 711 women, aged 40–99 years, was studied. Blood pressure measurements, combined with a clinical questionnaire that included educational and socio-economic data, and standard blood samples for the detection of dyslipidemia and diabetes mellitus, were collected. Results The mean age was 55 W 12 years. The prevalence of hypertension was 44% and was highly influenced by age, sex, skin colour, educational status, obesity and metabolic parameters. The higher prevalence of hypertension among black individuals was independent of socio-economic and educational levels, and of metabolic parameters. The presence of antihypertensive treatment was three times more frequent in women than in men, and there was no difference according to skin colour. Among treated subjects, 25% were well controlled, and this percentage was similar among both black and white individuals. Conclusion Epidemiological studies in such an emergent population indicate that hypertension is a major public health problem. The high sodium content in drinking water in this region could play a major role in the development of hypertension. J Hypertens 25:2218–2226 Q 2007 Wolters Kluwer Health | Lippincott Williams & Wilkins. Journal of Hypertension 2007, 25:2218–2226 Keywords: age, Algerian Sahara, cardiovascular risk factors, high blood pressure, NaCl intake, skin colour a Cardiology Centre, Ghardaia, Algeria, b INSERM U684, Nancy, France, c Cardiology Department, University Hospital Mustafa, Alger, d Cardiology Department, University Hospital of Blida, Blida, Algeria, e IPC Center, Paris, f Ho ˆ tel Dieu Hospital, Paris and g Geriatric Department, University Hospital of Nancy, Nancy, France Correspondence to Athanase Benetos, MD, PhD, INSERM Unit 684, University of Nancy, 54511 Nancy-les-Vandoeuvre, France E-mail: [email protected] Received 14 November 2006 Revised 29 May 2007 Accepted 10 June 2007 Introduction Hypertension is a major cardiovascular disorder in Africa [1–9]. Parallel to this, the incidence of diabetes mellitus is on the rise [10], thus increasing the severity of renal and cardiac damage caused by any given blood pressure level. Most of the existing data on hypertension and diabetes mellitus in Africa has been collected in sub-Saharan countries. Hypertension is also a problem in supra- Saharan nations such as Egypt [11]. Algeria is made up of two different geographical regions. The northern region is situated primarily along the Mediterranean sea. The southern region represents the Algerian portion of the Sahara, between Ghardaia in the north and Tamanrasset in the south. In- Salah, a city located in the middle of this Saharan country, is an oasis in a desert area where temperatures range between 258 and 498C in summer (mean 388) and between 28 and 288C in winter (mean 158). The population is composed of 50% black and 50% white individuals. The aim of this study was to estimate the prevalence of hypertension and assess the determinants of blood pres- sure levels in a random population over 40 years old living in In-Salah city. Methods The population sample was randomly selected and was composed of 1346 subjects (635 men and 711 women, aged 40–99 years). All subjects were aware of the time and the purpose of the visit several weeks before. All subjects had been asked to be under fasting conditions the day of the examination. If an individual had not respected the fasting conditions, the investigators returned a few days later for the blood tests. The total the population of In-Salah is approximately 30 000 inhabitants. According to the city records, 5210 individuals were 40 years of age or older (approximately 17% of the entire population) at the time this study was undertaken. The city is divided into 38 districts; each 2218 Original article 0263-6352 ß 2007 Wolters Kluwer Health | Lippincott Williams & Wilkins

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

C
2218 Original article
Prevalence and determinants of hypertension in theAlgerian SaharaMohamed Temmara, Carlos Labatb, Salim Benkheddac, Meriem Charifid,Frederique Thomase, Mohamed Tahar Bouafiad, Kathy Beane,Bernadette Darnef, Michel E. Safarf and Athanase Benetosb,g
Background In-Salah is a city-oasis located in the middle
of the Algerian Sahara, a desert area whose drinking
water has a high sodium content. No cardiovascular
epidemiological studies have ever been conducted in
this region.
Methods A randomized sample of 635 men and
711 women, aged 40–99 years, was studied. Blood
pressure measurements, combined with a clinical
questionnaire that included educational and
socio-economic data, and standard blood samples for
the detection of dyslipidemia and diabetes mellitus,
were collected.
Results The mean age was 55 W 12 years. The prevalence
of hypertension was 44% and was highly influenced by age,
sex, skin colour, educational status, obesity and metabolic
parameters. The higher prevalence of hypertension among
black individuals was independent of socio-economic and
educational levels, and of metabolic parameters. The
presence of antihypertensive treatment was three times
more frequent in women than in men, and there was no
difference according to skin colour. Among treated subjects,
opyright © Lippincott Williams & Wilkins. Unautho
0263-6352 � 2007 Wolters Kluwer Health | Lippincott Williams & Wilkins
25% were well controlled, and this percentage was similar
among both black and white individuals.
Conclusion Epidemiological studies in such an emergent
population indicate that hypertension is a major public
health problem. The high sodium content in drinking water
in this region could play a major role in the development of
hypertension. J Hypertens 25:2218–2226 Q 2007 Wolters
Kluwer Health | Lippincott Williams & Wilkins.
Journal of Hypertension 2007, 25:2218–2226
Keywords: age, Algerian Sahara, cardiovascular risk factors, high bloodpressure, NaCl intake, skin colour
aCardiology Centre, Ghardaia, Algeria, bINSERM U684, Nancy, France,cCardiology Department, University Hospital Mustafa, Alger, dCardiologyDepartment, University Hospital of Blida, Blida, Algeria, eIPC Center, Paris,fHotel Dieu Hospital, Paris and gGeriatric Department, University Hospital ofNancy, Nancy, France
Correspondence to Athanase Benetos, MD, PhD, INSERM Unit 684, Universityof Nancy, 54511 Nancy-les-Vandoeuvre, FranceE-mail: [email protected]
Received 14 November 2006 Revised 29 May 2007Accepted 10 June 2007
IntroductionHypertension is a major cardiovascular disorder in Africa
[1–9]. Parallel to this, the incidence of diabetes mellitus
is on the rise [10], thus increasing the severity of renal and
cardiac damage caused by any given blood pressure level.
Most of the existing data on hypertension and diabetes
mellitus in Africa has been collected in sub-Saharan
countries. Hypertension is also a problem in supra-
Saharan nations such as Egypt [11].
Algeria is made up of two different geographical
regions. The northern region is situated primarily
along the Mediterranean sea. The southern region
represents the Algerian portion of the Sahara, between
Ghardaia in the north and Tamanrasset in the south. In-
Salah, a city located in the middle of this Saharan
country, is an oasis in a desert area where temperatures
range between 258 and 498C in summer (mean 388)and between 28 and 288C in winter (mean 158). The
population is composed of 50% black and 50% white
individuals.
The aim of this study was to estimate the prevalence of
hypertension and assess the determinants of blood pres-
sure levels in a random population over 40 years old living
in In-Salah city.
MethodsThe population sample was randomly selected and was
composed of 1346 subjects (635 men and 711 women,
aged 40–99 years). All subjects were aware of the time
and the purpose of the visit several weeks before. All
subjects had been asked to be under fasting conditions
the day of the examination. If an individual had not
respected the fasting conditions, the investigators
returned a few days later for the blood tests.
The total the population of In-Salah is approximately
30 000 inhabitants. According to the city records, 5210
individuals were 40 years of age or older (approximately
17% of the entire population) at the time this study was
undertaken. The city is divided into 38 districts; each
rized reproduction of this article is prohibited.

C
Prevalence of hypertension in the Algerian Sahara Temmar et al. 2219
district is subdivided into several neighbourhoods. For
the purpose of this study, 25% of the total population over
40 years of age was included. A sample of 1400 subjects
was drawn proportionally from each district. Among these
subjects, 54 were not included (39 were absent at the time
of the examination and 16 did not give their consent to
participate in the study). The study duration was 6 weeks,
from April to May. All subjects were examined between
0700 and 1230 h.
During the study, outdoor temperatures were recorded
using professional thermometers provided by the
National Meteorological Society (Meterologie Natio-
nale). Measurements were taken during short periods
of time in order to avoid major differences in temperature
during the study.
A questionnaire, which included life habits, personal and
family medical history as well as data for the socio-
economic and educational level, was completed. Subjects
were asked if they currently smoked more than five
cigarettes per day. Subjects who gave a negative answer
to this question were considered non-smokers. Alcohol
intake was not assessed with this questionnaire. In this
traditional Muslim area where alcohol intake is prohib-
ited by religious rules (even though not officially prohib-
ited by law), subjects might not be truthful and therefore
we judged that the answers to the question would be very
difficult to interpret.
Three categories of socio-economic level were defined
according to the following question included in the
questionnaire: (i) high socio-economic level: house with
refrigerator, air conditioning, and a maximum of two
individuals per room; (ii) mid level: either a refrigerator
or air conditioning; (iii) low level: neither of these two.
We chose these criteria because in this very hot area of
the world they constitute a priority for families. In the
Results section, we combined groups of the high and
mid level.
Educational level was defined as follows: (i) low level: no
school at all or only elementary school (4–5 years); (ii)
mid level: high school level (þ3 years); (iii) high level:
college, university. As the large majority of subjects
belonged to the first group, mid and high level subjects
were grouped together.
Three blood pressure measurements were taken at 2-min
intervals, after a 5-min rest in the sitting position, using
an electronic blood pressure monitor (Omron 705
CP; Omron Healthcare Europe BV, Amsterdam, the
Netherlands) [12]. The mean of the last two measure-
ments was used for statistical analysis. Hypertension was
defined as systolic blood pressure (SBP) of 140 mmHg
or greater or diastolic blood pressure (DBP) of 90 mmHg
opyright © Lippincott Williams & Wilkins. Unauth
or greater, or both, or the presence of chronic antihyper-
tensive drug treatment. Height, weight and waist and
hip circumference were also measured the same day.
Blood chemistry [plasma cholesterol, high-density lipo-
protein (HDL)-cholesterol, triglycerides and glucose]
was measured under fasting conditions according to stan-
dard techniques. The metabolic syndrome was defined
according the National Cholesterol Education Program
2001 definition [13].
For the present analysis, subjects were divided into four
subgroups according to sex and skin colour. Skin pig-
mentation and general characteristics were the main
criteria the investigators of the present study used to
classify the examined subjects as ‘black’ or ‘white’. When
these criteria were not conclusive (in less than 10% of the
cases), the examined subjects were asked if they defined
themselves as white or black. Following this procedure,
all subjects were classified as black or white.
For the statistical evaluation, mean values� standard
deviation are presented. The prevalence between differ-
ent groups was compared using a chisquared test. Black
men and women and white men and women were studied
using a two-way analysis of variance, involving a sex
effect, a skin colour effect and their interaction. Multiple
regression analyses were performed using a two-tailed
test. A P value of 0.05 or less was considered significant.
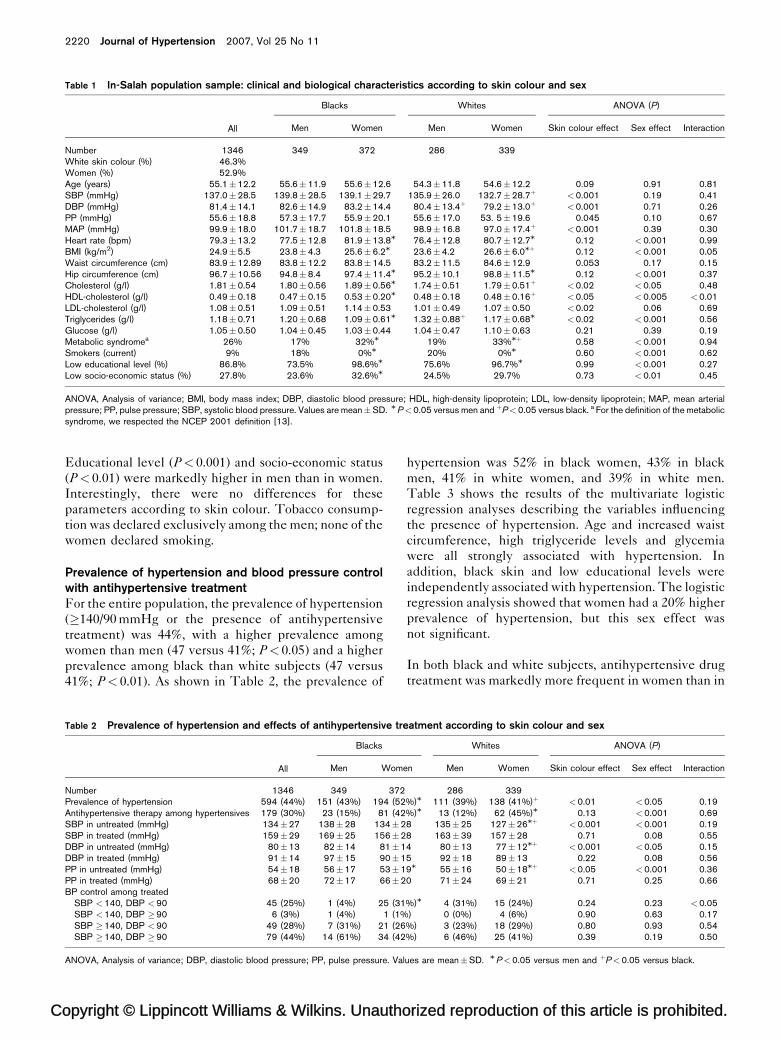
ResultsDescription of the populationTable 1 shows the main clinical and biological charac-
teristics of the population, as well as their distribution
according to sex and skin colour.
Age was similar in the four groups of subjects. SBP, DBP
and mean arterial pressure were significantly higher in
black than in white subjects (P< 0.001; Table 1). This
difference was less important for pulse pressure
(P¼ 0.045). There was no sex effect on SBP, DBP, mean
arterial pressure and pulse pressure levels. As expected,
heart rate was markedly higher (P< 0.001) in women
than in men. Body mass index and waist circumference
were also significantly higher in women than in men
(P< 0.001).
In both sexes, plasma glucose did not differ in black and
white subjects. Total and HDL-cholesterol were signifi-
cantly higher in blacks than in whites (P< 0.01 for total
cholesterol and P< 0.05 for HDL-cholesterol) and in
women than in men (sex effect P< 0.05). The contrary
was found for plasma triglyceride levels, which were
higher in men than in women (P< 0.001) and higher
in white than in black subjects (P< 0.02). No significant
sex–skin colour interaction was observed for these
parameters.
orized reproduction of this article is prohibited.
C
2220 Journal of Hypertension 2007, Vol 25 No 11
Table 1 In-Salah population sample: clinical and biological characteristics according to skin colour and sex
All
Blacks Whites ANOVA (P)
Men Women Men Women Skin colour effect Sex effect Interaction
Number 1346 349 372 286 339White skin colour (%) 46.3%Women (%) 52.9%Age (years) 55.1�12.2 55.6�11.9 55.6�12.6 54.3�11.8 54.6�12.2 0.09 0.91 0.81SBP (mmHg) 137.0�28.5 139.8�28.5 139.1�29.7 135.9�26.0 132.7�28.7þ <0.001 0.19 0.41DBP (mmHg) 81.4�14.1 82.6�14.9 83.2�14.4 80.4�13.4þ 79.2�13.0þ <0.001 0.71 0.26PP (mmHg) 55.6�18.8 57.3�17.7 55.9�20.1 55.6�17.0 53. 5�19.6 0.045 0.10 0.67MAP (mmHg) 99.9�18.0 101.7�18.7 101.8�18.5 98.9�16.8 97.0�17.4þ <0.001 0.39 0.30Heart rate (bpm) 79.3�13.2 77.5�12.8 81.9�13.8M 76.4�12.8 80.7�12.7M 0.12 <0.001 0.99BMI (kg/m2) 24.9�5.5 23.8�4.3 25.6�6.2M 23.6�4.2 26.6�6.0Mþ 0.12 <0.001 0.05Waist circumference (cm) 83.9�12.89 83.8�12.2 83.8�14.5 83.2�11.5 84.6�12.9 0.053 0.17 0.15Hip circumference (cm) 96.7�10.56 94.8�8.4 97.4�11.4M 95.2�10.1 98.8�11.5M 0.12 <0.001 0.37Cholesterol (g/l) 1.81�0.54 1.80�0.56 1.89�0.56M 1.74�0.51 1.79�0.51þ <0.02 <0.05 0.48HDL-cholesterol (g/l) 0.49�0.18 0.47�0.15 0.53�0.20M 0.48�0.18 0.48�0.16þ <0.05 <0.005 <0.01LDL-cholesterol (g/l) 1.08�0.51 1.09�0.51 1.14�0.53 1.01�0.49 1.07�0.50 <0.02 0.06 0.69Triglycerides (g/l) 1.18�0.71 1.20�0.68 1.09�0.61M 1.32�0.88þ 1.17�0.68M <0.02 <0.001 0.56Glucose (g/l) 1.05�0.50 1.04�0.45 1.03�0.44 1.04�0.47 1.10�0.63 0.21 0.39 0.19Metabolic syndromea 26% 17% 32%M 19% 33%Mþ 0.58 <0.001 0.94Smokers (current) 9% 18% 0%M 20% 0%M 0.60 <0.001 0.62Low educational level (%) 86.8% 73.5% 98.6%M 75.6% 96.7%M 0.99 <0.001 0.27Low socio-economic status (%) 27.8% 23.6% 32.6%M 24.5% 29.7% 0.73 <0.01 0.45
ANOVA, Analysis of variance; BMI, body mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MAP, mean arterialpressure; PP, pulse pressure; SBP, systolic blood pressure. Values are mean�SD. MP<0.05 versus men and þP<0.05 versus black. a For the definition of the metabolicsyndrome, we respected the NCEP 2001 definition [13].
Educational level (P< 0.001) and socio-economic status
(P< 0.01) were markedly higher in men than in women.
Interestingly, there were no differences for these
parameters according to skin colour. Tobacco consump-
tion was declared exclusively among the men; none of the
women declared smoking.
Prevalence of hypertension and blood pressure controlwith antihypertensive treatmentFor the entire population, the prevalence of hypertension
(�140/90 mmHg or the presence of antihypertensive
treatment) was 44%, with a higher prevalence among
women than men (47 versus 41%; P< 0.05) and a higher
prevalence among black than white subjects (47 versus
41%; P< 0.01). As shown in Table 2, the prevalence of
opyright © Lippincott Williams & Wilkins. Unautho
Table 2 Prevalence of hypertension and effects of antihypertensive tre
All
Blacks
Men Wome
Number 1346 349 372Prevalence of hypertension 594 (44%) 151 (43%) 194 (52Antihypertensive therapy among hypertensives 179 (30%) 23 (15%) 81 (42SBP in untreated (mmHg) 134�27 138�28 134�2SBP in treated (mmHg) 159�29 169�25 156�2DBP in untreated (mmHg) 80�13 82�14 81�1DBP in treated (mmHg) 91�14 97�15 90�1PP in untreated (mmHg) 54�18 56�17 53�1PP in treated (mmHg) 68�20 72�17 66�2BP control among treated
SBP <140, DBP <90 45 (25%) 1 (4%) 25 (31SBP <140, DBP �90 6 (3%) 1 (4%) 1 (1%SBP �140, DBP <90 49 (28%) 7 (31%) 21 (26SBP �140, DBP �90 79 (44%) 14 (61%) 34 (42
ANOVA, Analysis of variance; DBP, diastolic blood pressure; PP, pulse pressure. Val
hypertension was 52% in black women, 43% in black
men, 41% in white women, and 39% in white men.
Table 3 shows the results of the multivariate logistic
regression analyses describing the variables influencing
the presence of hypertension. Age and increased waist
circumference, high triglyceride levels and glycemia
were all strongly associated with hypertension. In
addition, black skin and low educational levels were
independently associated with hypertension. The logistic
regression analysis showed that women had a 20% higher
prevalence of hypertension, but this sex effect was
not significant.
In both black and white subjects, antihypertensive drug
treatment was markedly more frequent in women than in
rized reproduction of this article is prohibited.
atment according to skin colour and sex
Whites ANOVA (P)
n Men Women Skin colour effect Sex effect Interaction
286 339%)M 111 (39%) 138 (41%)þ <0.01 <0.05 0.19%)M 13 (12%) 62 (45%)M 0.13 <0.001 0.698 135�25 127�26Mþ <0.001 <0.001 0.198 163�39 157�28 0.71 0.08 0.554 80�13 77�12Mþ <0.001 <0.05 0.155 92�18 89�13 0.22 0.08 0.569M 55�16 50�18Mþ <0.05 <0.001 0.360 71�24 69�21 0.71 0.25 0.66
%)M 4 (31%) 15 (24%) 0.24 0.23 <0.05) 0 (0%) 4 (6%) 0.90 0.63 0.17
%) 3 (23%) 18 (29%) 0.80 0.93 0.54%) 6 (46%) 25 (41%) 0.39 0.19 0.50
ues are mean�SD. MP<0.05 versus men and þP<0.05 versus black.
C
Prevalence of hypertension in the Algerian Sahara Temmar et al. 2221
Table 3 Variables associated with presence of hypertensionfollowing a logistic multivariate regression
OR 95% CI Z P
Sex (women vs men) 1.18 0.90–1.54 1.20 0.23Age (1 year) 1.06 1.05–1.07 9.907 <0.001Skin colour (black/white) 1.41 1.09–1.82 2.66 <0.01Education level (low vs others) 1.68 1.08–2.61 2.29 <0.05Waist (1 cm) 1.03 1.02–1.05 6.17 <0.001Triglycerides (1 g/l) 1.32 1.08–1.60 2.76 <0.01Glucose (1 g/l) 1.57 1.19–2.06 3.24 <0.001
CI, Confidence interval; OR, odds ratio.
men (sex effect P< 0.001), with no difference according
to the skin colour (Table 2). Among treated subjects, 25%
were well controlled (SBP < 140 and DBP < 90 mmHg),
and this percentage was similar among both black and
white individuals. Forty-two per cent of the treated white
subjects and 46% of the treated black subjects had
uncontrolled SBP and DBP, whereas 27 and 28%,
respectively, presented with uncontrolled SBP but had
controlled DBP under treatment. Finally, 5% of the
white and 2% of the black subjects had high DBP and
controlled SBP under treatment. Blood pressure values in
the four groups, according to sex and skin colour, are also
illustrated in Table 2. These data show a better control of
blood pressure in black women than in black men. No
opyright © Lippincott Williams & Wilkins. Unauth
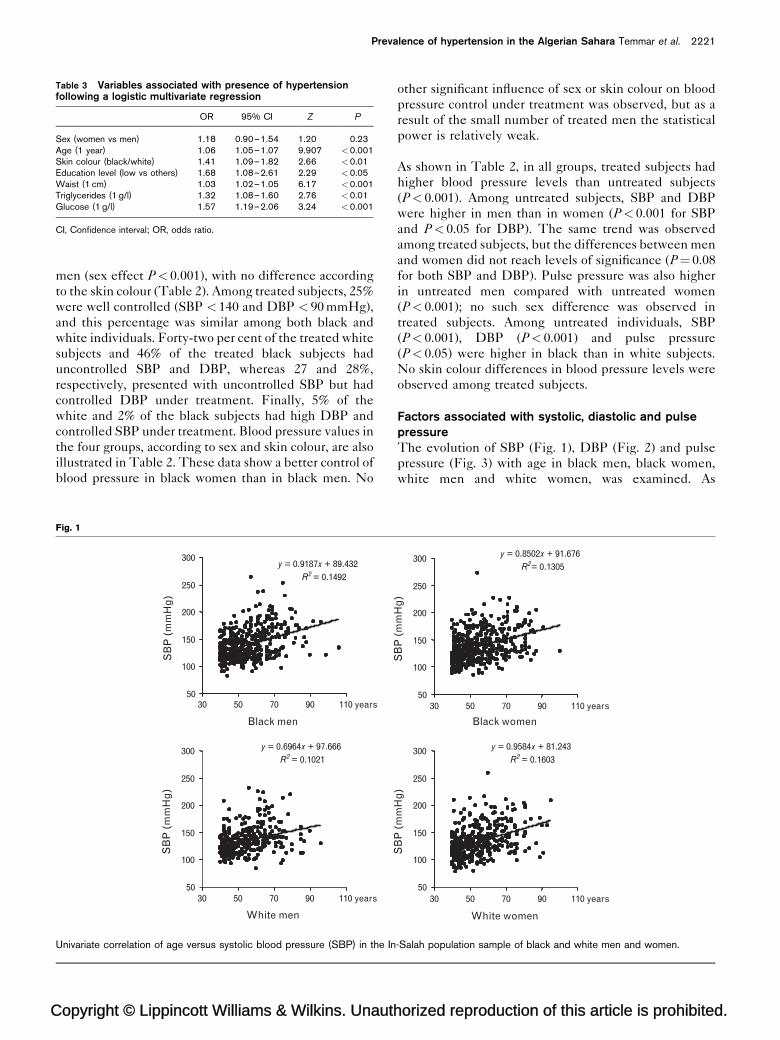
Fig. 1
Black men
White men
y = 0.9187x + 89.432R2 = 0.1492
50
100
150
200
250
300
110 years90705030
y = 0.6964x + 97.666R2 = 0.1021
50
100
150
200
250
300
110 years90705030
SB
P (
mm
Hg
) S
BP
(m
mH
g)
Univariate correlation of age versus systolic blood pressure (SBP) in the In
other significant influence of sex or skin colour on blood
pressure control under treatment was observed, but as a
result of the small number of treated men the statistical
power is relatively weak.
As shown in Table 2, in all groups, treated subjects had
higher blood pressure levels than untreated subjects
(P< 0.001). Among untreated subjects, SBP and DBP
were higher in men than in women (P< 0.001 for SBP
and P< 0.05 for DBP). The same trend was observed
among treated subjects, but the differences between men
and women did not reach levels of significance (P¼ 0.08
for both SBP and DBP). Pulse pressure was also higher
in untreated men compared with untreated women
(P< 0.001); no such sex difference was observed in
treated subjects. Among untreated individuals, SBP
(P< 0.001), DBP (P< 0.001) and pulse pressure
(P< 0.05) were higher in black than in white subjects.
No skin colour differences in blood pressure levels were
observed among treated subjects.
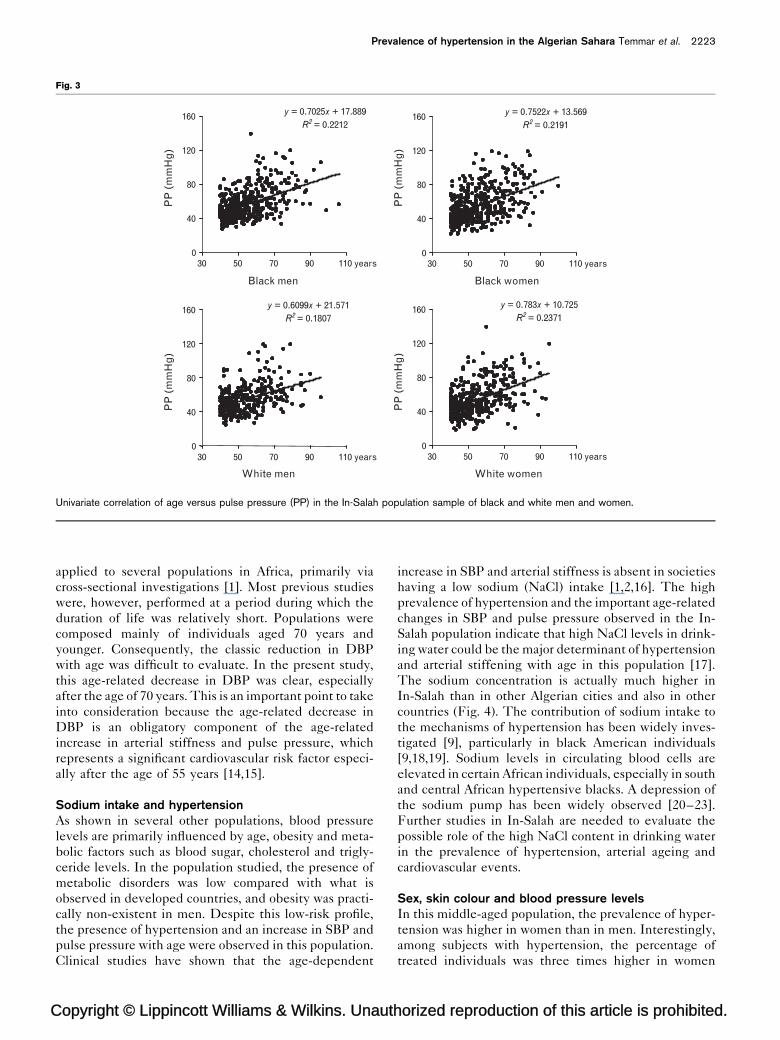
Factors associated with systolic, diastolic and pulsepressureThe evolution of SBP (Fig. 1), DBP (Fig. 2) and pulse
pressure (Fig. 3) with age in black men, black women,
white men and white women, was examined. As
orized reproduction of this article is prohibited.
Black women
White women
y = 0.8502x + 91.676R2= 0.1305
50
100
150
200
250
300
110 years90705030
y = 0.9584x + 81.243R2 = 0.1603
50
100
150
200
250
300
110 years90705030
SB
P (
mm
Hg
) S
BP
(m
mH
g)
-Salah population sample of black and white men and women.
C
2222 Journal of Hypertension 2007, Vol 25 No 11
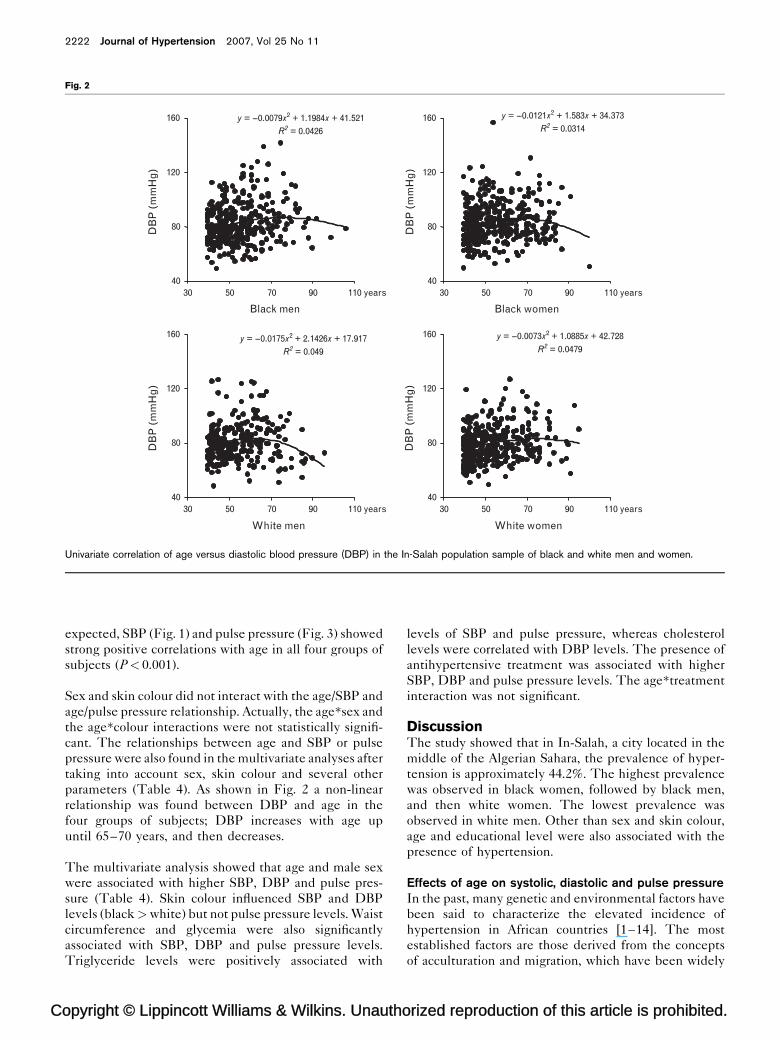
Fig. 2
Black men
DB
P (
mm
Hg
)
y = --0.0079x2 + 1.1984x + 41.521R2 = 0.0426
40
80
120
160
110 years90705030
White men
DB
P (
mm
Hg
)
y = --0.0175x2 + 2.1426x + 17.917R2 = 0.049
40
80
120
160
110 years90705030
Black women
DB
P (
mm
Hg
)
y = --0.0121x2 + 1.583x + 34.373R2 = 0.0314
40
80
120
160
110 years90705030
White women
DB
P (
mm
Hg
)
y = --0.0073x2 + 1.0885x + 42.728R2 = 0.0479
40
80
120
160
110 years90705030
Univariate correlation of age versus diastolic blood pressure (DBP) in the In-Salah population sample of black and white men and women.
expected, SBP (Fig. 1) and pulse pressure (Fig. 3) showed
strong positive correlations with age in all four groups of
subjects (P< 0.001).
Sex and skin colour did not interact with the age/SBP and
age/pulse pressure relationship. Actually, the age�sex and
the age�colour interactions were not statistically signifi-
cant. The relationships between age and SBP or pulse
pressure were also found in the multivariate analyses after
taking into account sex, skin colour and several other
parameters (Table 4). As shown in Fig. 2 a non-linear
relationship was found between DBP and age in the
four groups of subjects; DBP increases with age up
until 65–70 years, and then decreases.
The multivariate analysis showed that age and male sex
were associated with higher SBP, DBP and pulse pres-
sure (Table 4). Skin colour influenced SBP and DBP
levels (black >white) but not pulse pressure levels. Waist
circumference and glycemia were also significantly
associated with SBP, DBP and pulse pressure levels.
Triglyceride levels were positively associated with
opyright © Lippincott Williams & Wilkins. Unautho
levels of SBP and pulse pressure, whereas cholesterol
levels were correlated with DBP levels. The presence of
antihypertensive treatment was associated with higher
SBP, DBP and pulse pressure levels. The age�treatment
interaction was not significant.
DiscussionThe study showed that in In-Salah, a city located in the
middle of the Algerian Sahara, the prevalence of hyper-
tension is approximately 44.2%. The highest prevalence
was observed in black women, followed by black men,
and then white women. The lowest prevalence was
observed in white men. Other than sex and skin colour,
age and educational level were also associated with the
presence of hypertension.
Effects of age on systolic, diastolic and pulse pressureIn the past, many genetic and environmental factors have
been said to characterize the elevated incidence of
hypertension in African countries [1–14]. The most
established factors are those derived from the concepts
of acculturation and migration, which have been widely
rized reproduction of this article is prohibited.
C
Prevalence of hypertension in the Algerian Sahara Temmar et al. 2223
Fig. 3
Black men
White men
Black women
White women
y = 0.7025x + 17.889R2 = 0.2212
0
40
80
120
160
110 years90705030
y = 0.6099x + 21.571R2 = 0.1807
0
40
80
120
160
110 years90705030
y = 0.7522x + 13.569R2 = 0.2191
0
40
80
120
160
110 years90705030
y = 0.783x + 10.725R2 = 0.2371
0
40
80
120
160
110 years90705030
PP
(m
mH
g)
PP
(m
mH
g)
PP
(m
mH
g)
PP
(m
mH
g)
Univariate correlation of age versus pulse pressure (PP) in the In-Salah population sample of black and white men and women.
applied to several populations in Africa, primarily via
cross-sectional investigations [1]. Most previous studies
were, however, performed at a period during which the
duration of life was relatively short. Populations were
composed mainly of individuals aged 70 years and
younger. Consequently, the classic reduction in DBP
with age was difficult to evaluate. In the present study,
this age-related decrease in DBP was clear, especially
after the age of 70 years. This is an important point to take
into consideration because the age-related decrease in
DBP is an obligatory component of the age-related
increase in arterial stiffness and pulse pressure, which
represents a significant cardiovascular risk factor especi-
ally after the age of 55 years [14,15].
Sodium intake and hypertensionAs shown in several other populations, blood pressure
levels are primarily influenced by age, obesity and meta-
bolic factors such as blood sugar, cholesterol and trigly-
ceride levels. In the population studied, the presence of
metabolic disorders was low compared with what is
observed in developed countries, and obesity was practi-
cally non-existent in men. Despite this low-risk profile,
the presence of hypertension and an increase in SBP and
pulse pressure with age were observed in this population.
Clinical studies have shown that the age-dependent
opyright © Lippincott Williams & Wilkins. Unauth
increase in SBP and arterial stiffness is absent in societies
having a low sodium (NaCl) intake [1,2,16]. The high
prevalence of hypertension and the important age-related
changes in SBP and pulse pressure observed in the In-
Salah population indicate that high NaCl levels in drink-
ing water could be the major determinant of hypertension
and arterial stiffening with age in this population [17].
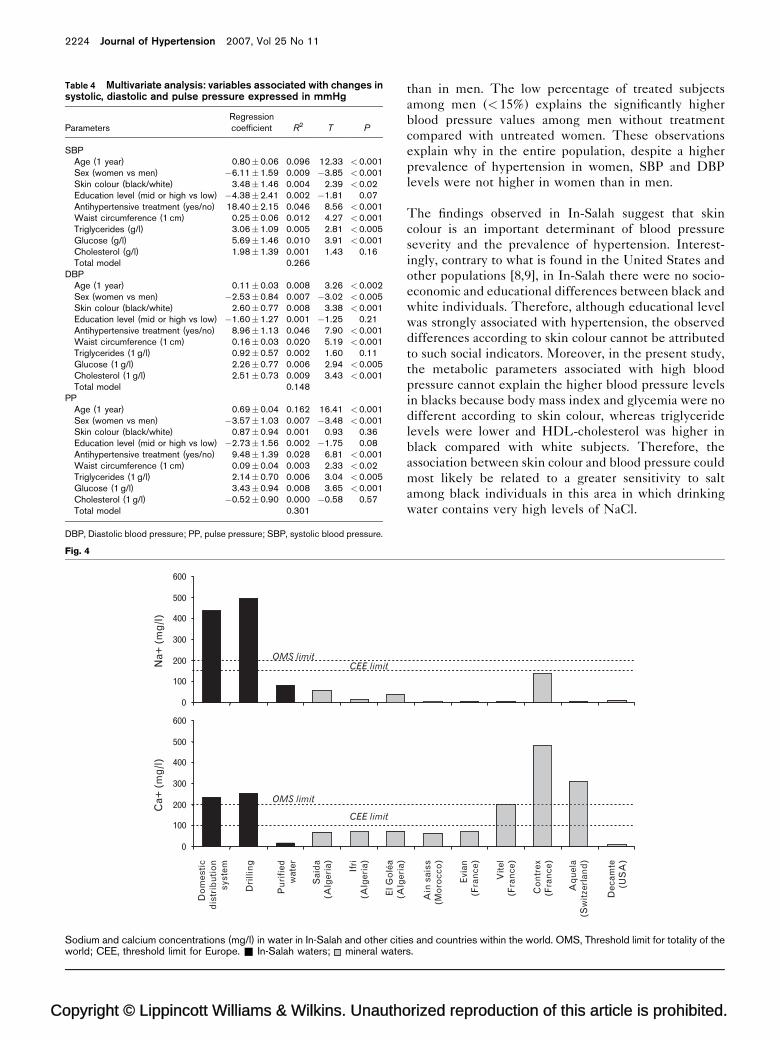
The sodium concentration is actually much higher in
In-Salah than in other Algerian cities and also in other
countries (Fig. 4). The contribution of sodium intake to
the mechanisms of hypertension has been widely inves-
tigated [9], particularly in black American individuals
[9,18,19]. Sodium levels in circulating blood cells are
elevated in certain African individuals, especially in south
and central African hypertensive blacks. A depression of
the sodium pump has been widely observed [20–23].
Further studies in In-Salah are needed to evaluate the
possible role of the high NaCl content in drinking water
in the prevalence of hypertension, arterial ageing and
cardiovascular events.
Sex, skin colour and blood pressure levelsIn this middle-aged population, the prevalence of hyper-
tension was higher in women than in men. Interestingly,
among subjects with hypertension, the percentage of
treated individuals was three times higher in women
orized reproduction of this article is prohibited.
Copyright © Lippincott Williams & Wilkins. Unautho
2224 Journal of Hypertension 2007, Vol 25 No 11
Table 4 Multivariate analysis: variables associated with changes insystolic, diastolic and pulse pressure expressed in mmHg
ParametersRegressioncoefficient R2 T P
SBPAge (1 year) 0.80�0.06 0.096 12.33 <0.001Sex (women vs men) �6.11�1.59 0.009 �3.85 <0.001Skin colour (black/white) 3.48�1.46 0.004 2.39 <0.02Education level (mid or high vs low) �4.38�2.41 0.002 �1.81 0.07Antihypertensive treatment (yes/no) 18.40�2.15 0.046 8.56 <0.001Waist circumference (1 cm) 0.25�0.06 0.012 4.27 <0.001Triglycerides (g/l) 3.06�1.09 0.005 2.81 <0.005Glucose (g/l) 5.69�1.46 0.010 3.91 <0.001Cholesterol (g/l) 1.98�1.39 0.001 1.43 0.16Total model 0.266
DBPAge (1 year) 0.11�0.03 0.008 3.26 <0.002Sex (women vs men) �2.53�0.84 0.007 �3.02 <0.005Skin colour (black/white) 2.60�0.77 0.008 3.38 <0.001Education level (mid or high vs low) �1.60�1.27 0.001 �1.25 0.21Antihypertensive treatment (yes/no) 8.96�1.13 0.046 7.90 <0.001Waist circumference (1 cm) 0.16�0.03 0.020 5.19 <0.001Triglycerides (1 g/l) 0.92�0.57 0.002 1.60 0.11Glucose (1 g/l) 2.26�0.77 0.006 2.94 <0.005Cholesterol (1 g/l) 2.51�0.73 0.009 3.43 <0.001Total model 0.148
PPAge (1 year) 0.69�0.04 0.162 16.41 <0.001Sex (women vs men) �3.57�1.03 0.007 �3.48 <0.001Skin colour (black/white) 0.87�0.94 0.001 0.93 0.36Education level (mid or high vs low) �2.73�1.56 0.002 �1.75 0.08Antihypertensive treatment (yes/no) 9.48�1.39 0.028 6.81 <0.001Waist circumference (1 cm) 0.09�0.04 0.003 2.33 <0.02Triglycerides (1 g/l) 2.14�0.70 0.006 3.04 <0.005Glucose (1 g/l) 3.43�0.94 0.008 3.65 <0.001Cholesterol (1 g/l) �0.52�0.90 0.000 �0.58 0.57Total model 0.301
DBP, Diastolic blood pressure; PP, pulse pressure; SBP, systolic blood pressure.
Fig. 4
0
100
200
300
400
500
600
Na+
(m
g/l
)
0
100
200
300
400
500
600
Do
mes
tic
dis
trib
uti
on
syst
em
Dri
llin
g
Pu
rifi
edw
ater
Sai
da
(Alg
eria
)
Ifri
(Alg
eria
)
El G
olé
a
Ca+
(m
g/l
)
OMS limit
CEE limit
OMS limitCEE limit
Sodium and calcium concentrations (mg/l) in water in In-Salah and other citiworld; CEE, threshold limit for Europe. & In-Salah waters; mineral water
than in men. The low percentage of treated subjects
among men (< 15%) explains the significantly higher
blood pressure values among men without treatment
compared with untreated women. These observations
explain why in the entire population, despite a higher
prevalence of hypertension in women, SBP and DBP
levels were not higher in women than in men.
The findings observed in In-Salah suggest that skin
colour is an important determinant of blood pressure
severity and the prevalence of hypertension. Interest-
ingly, contrary to what is found in the United States and
other populations [8,9], in In-Salah there were no socio-
economic and educational differences between black and
white individuals. Therefore, although educational level
was strongly associated with hypertension, the observed
differences according to skin colour cannot be attributed
to such social indicators. Moreover, in the present study,
the metabolic parameters associated with high blood
pressure cannot explain the higher blood pressure levels
in blacks because body mass index and glycemia were no
different according to skin colour, whereas triglyceride
levels were lower and HDL-cholesterol was higher in
black compared with white subjects. Therefore, the
association between skin colour and blood pressure could
most likely be related to a greater sensitivity to salt
among black individuals in this area in which drinking
water contains very high levels of NaCl.
rized reproduction of this article is prohibited.
Ain
sai
ss(M
oro
cco
)
(Alg
eria
)
Evi
an(F
ran
ce)
Vit
el(F
ran
ce)
Co
ntr
ex(F
ran
ce)
Dec
amte
(US
A)
Aq
uel
a(S
wit
zerl
and
)
es and countries within the world. OMS, Threshold limit for totality of thes.

C
Prevalence of hypertension in the Algerian Sahara Temmar et al. 2225
Blood pressure control with antihypertensive treatmentThe present analysis shows that among subjects receiving
antihypertensive treatment, 25% were well controlled,
and this percentage was similar in both black and white
individuals. Half the treated subjects had high levels of
both SBP and DBP, followed by those with high SBP and
controlled DBP, and the percentage of subjects with
uncontrolled DBP and controlled DBP was very low.
This clearly confirms that, as measured in a clinical
setting, the control of blood pressure, especially SBP,
is not obtained in a large majority of individuals. Data
from several countries have demonstrated similar results,
showing that among treated hypertensive individuals, the
proportion of those who are well controlled is less than
30% [24–27]. Interestingly, education level, sex and skin
colour had no significant influence on blood pressure
control through treatment.
Limitations of the studyOne limitation is that the present study can only suggest
but not confirm that the high prevalence of hypertension
in the population could be related to the high levels of salt
in the drinking water. Unfortunately, we do not have
urinary sodium measurements, and even if we did, it
would not be possible to detect the effects of high salt
levels in drinking water on blood pressure levels, because
in that area almost the entire population uses this water,
with very few exceptions who drink mineral or
‘filtered’ water.
The fact that blood pressure was measured three times in
only one visit is also a limitation, but we would like to
make the following comments. First, as mentioned in the
Methods section, blood pressure was measured using an
automatic device, after a 5-min rest period, and the
reported values were the mean of the second and third
measurements. As in most observational studies, subjects
had only one visit. In a subgroup of 89 subjects with high
blood pressure, measurements were repeated the day
after in order to evaluate the evolution of blood pressure.
The mean values of blood pressure in the 89 subjects
during the first visit were 164/96 mmHg. The mean
values (mean of the three measurements) during the
second visit were 160/93 mmHg. In 81 out of the 89
patients (> 90%), the diagnosis of hypertension was con-
firmed during the second visit. Although those with
normal blood pressure levels during the first visit did
not have a second visit, one might suggest that because of
the normal variability of blood pressure levels some of the
low blood pressure patients could have shown higher levels
during the second visit. The 3–4 mmHg differences in
blood pressure levels between the two visits observed in
the subgroup of 89 patients could be responsible for a
minor overestimation of the number of hypertensive
individuals in this population, but cannot explain the
high prevalence of hypertension in this population.
opyright © Lippincott Williams & Wilkins. Unauth
Clinical implicationsThe results of this study, which show a very high preva-
lence of hypertension in a Saharan population, confirm
results of other epidemiological studies that have shown
that not only is hypertension a frequent disease in devel-
oped countries, but it is also a major public health
problem in these developing countries [28,29]. These
results may also point out the harmful effects of high
sodium intake, especially in drinking water, and suggest
that the entire population, independently of age, sex,
skin colour and socio-economic level, is concerned.
AcknowledgementsThe authors would like to thank the public health direc-
tion of Ghardaia and Tamanrasset for their important
contribution.
This study was made possible with the help of INSERM
(Institut National de la Sante et de la Recherche Med-
icale), Groupe de Pharmacologie et d’Hemodynamique
Cardiovasculaire, Caisse Nationale d’Assurance Maladie
(CNAM), and the Caisse Primaire d’Assurance Maladie
de Paris (CPAM–Paris), France.
There are no conflicts of interest.
References1 Opie LH, Seedat YK. Hypertension in sub-Saharan African populations.
Circulation 2005; 112:3562–3568.2 Seedat YK. Hypertension in developing nations in sub-Saharan Africa.
J Hum Hypertens 2000; 14:739–747.3 Sever PS. Blood-pressure and its correlates in urban and tribal Africa.
Lancet 1980; 2:60–64.4 Kaminer B, Lutz WP. Blood pressure in Bushmen of the Kalahari Desert.
Circulation 1960; 22:289–295.5 Mbanya JC, Minkoulou EM, Salah JN, Balkau B. The prevalence of
hypertension in rural and urban Cameroon. Int J Epidemiol 1998; 27:181–185.
6 Edwards R, Unwin N, Mugusi F, Whiting D, Rashid S, Kissima J, et al.Hypertension prevalence and care in an urban and rural area of Tanzania.J Hypertens 2000; 18:145–152.
7 Cooper R, Rotimi C, Ataman S, McGee D, Osotimehin B, Kadiri S, et al. Theprevalence of hypertension in seven populations of west African origin.Am J Public Health 1997; 87:160–168.
8 Cooper R, Rotimi C. Hypertension in blacks. Am J Hypertens 1997;10:804–812.
9 Saunders E. Hypertension in African-Americans. Circulation 1991;83:1465–1467.
10 De Courten M, McCarty D, Zimmet P. In: Hitman G, editor. Diagnosis: thescale of the problem of furure risks, 1999 in type II diabetes, prediction andprevention. Chichester: John Wiley & Son. pp. 17–36.
11 Ibrahim MM. Hypertension surveys in the developing world. Lessons fromthe Egyptian National Hypertension Project (NHP). J Hum Hypertens1997; 11:709–726.
12 O’Brien E, Mee F, Atkins N, Thomas M. Evaluation of three devices for self-measurement of blood pressure according to the revised BritishHypertension Society Protocol: the Omron HEM-705CP, Philips HP5332,and Nissei DS-175. Blood Press Monit 1996; 1:55–61.
13 Executive Summary of the Third Report of the National CholesterolEducation Program (NCEP) Expert Panel on Detection, Evaluation, andTreatment of High Blood Cholesterol in Adults (Adult Treatment Panel III).JAMA 2001; 285: 2486–2497.
14 Franklin SS, Wilkinson IB, Cockcroft JR. Brachial and central pulsepressure, and cardiovascular risk. In: Safar ME, O’Rourke MF, editors.Arterial stiffness in hypertension. Sydney: Elsevier; 2006. pp. 225–240.
15 Stehouwer CD, Ferreira I. Diabetes, lipids and other cardiovascular riskfactors. In: Safar ME, O’Rourke ME, editors. Arterial stiffness inhypertension. Sydney: Elsevier; 2006. pp. 427–458.
orized reproduction of this article is prohibited.

C
2226 Journal of Hypertension 2007, Vol 25 No 11
16 Kaplan NM, Lieberman E. Clinical hypertension. 4th Ed. Williams andWilkins: Baltimore; 1986. pp. 71–72.
17 Worthington MG, Wendt MC, Opie LH. Sodium transport in hypertension:assessment of membrane-associated defects in South African black andwhite hypertensives. J Hum Hypertens 1993; 7:291–297.
18 Cooper R, Rotimi C. Hypertension in populations of West African origin: isthere a genetic predisposition? J Hypertens 1994; 12:215–227.
19 Burt VL, Cutler JA, Higgins M, Horlan MJ, Labarthe D, Whelton P, et al.Trends in the prevalence, awareness, treatment, and control ofhypertension in the adult US population. Data from the health examinationsurveys, 1960 to 1991. Hypertension 1995; 26:60–69.
20 M’Buyamba-Kabangu JR, Lepira B, Lijenen P, Tshiani K, Fagard R, Amery A.Intracellular sodium and the response to nitrendipine or atenolol in Africanblacks. Hypertension 1988; 11:100–105.
21 Touyz RM, Milne FJ, Reinach SG. Platelet and erythrocyte Mg2þ, Ca2þ,Naþ, Kþ and cell membrane adenosine triphosphatase activity in essentialhypertension in blacks. J Hypertens 1992; 10:571–578.
22 Hoosen S, Seedat YK, Bhigjee AI. A study of urinary and intracellularsodium and potassium, renin, aldosterone, and hypertension in blacks andIndians in Natal. Cardiovasc Drugs Ther 1990; 4 (Suppl 2):363–365.
23 Touyz RM, Milne FJ, Reinach SG. Racial differences in cell membraneATPases and cellular cation content in urban South African normotensiveand hypertensive subjects. Am J Hypertens 1993; 6:693–700.
24 Burt VL, Cutler JA, Higgins M, Horan MJ, Labarthe D, Whelton P, et al.Trends in the prevalence, awareness, treatment, and control ofhypertension in the adult US population. Data from the Health ExaminationSurveys, 1960 to 1991. Hypertension 1995; 26:60–69.
25 Marques-Vidal P, Tuomilehto J. Hypertension awareness, treatment andcontrol in the community: is the ‘rule of halves’ still valid? J Hum Hypertens1997; 11:213–220.
26 Colhoun HM, Dong W, Poulter NR. Blood pressure screening,management and control in England: results from the health survey forEngland 1994. J Hypertens 1998; 16:747–752.
27 Benetos A, Thomas F, Bean K, Gautier S, Smulyan H, Guize L. Prognosticvalue of systolic and diastolic pressure in treated hypertensive men.Arch Intern Med 2002; 162:577–581.
28 Douglas JG, Bakris GL, Epstein M, Ferdinand KC, Ferrario C, Flack JM,et al. Management of high blood pressure in African Americans: consensusstatement of the Hypertension in African Americans Working Group of theInternational Society on Hypertension in Blacks. Arch Intern Med 2003;163:525–541.
29 Cruickshank JK, Mbanya JC, Wilks R, Balkau B, Forrester T, Anderson SG,et al. Hypertension in four African-origin populations: current ‘Rule ofHalves’, quality of blood pressure control and attributable risk ofcardiovascular disease. J Hypertens 2001; 19:41–46.
opyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Related Documents