PULMONARY HYPERTENSION & THALASSAEMIA 3rd Pan-American Thalassaemia Conference – Buenos Aires 2010 Dr Malcolm Walker Cardiologist University College & the Heart Hospital – LONDON Clinical Director Hatter Cardiovascular Institute - UCLH JMWalker 2010

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PULMONARY HYPERTENSION & THALASSAEMIA
3rd Pan-American Thalassaemia Conference – Buenos Aires 2010
Dr Malcolm Walker Cardiologist University College & the Heart Hospital – LONDON Clinical Director Hatter Cardiovascular Institute - UCLH
JMWalker 2010
Pulmonary hypertension & the haemoglobinopathies
Definition
Measurement
Pathophysiology
Consequences
Clinical prevalence & implications
Treatments
JMWalker 2010
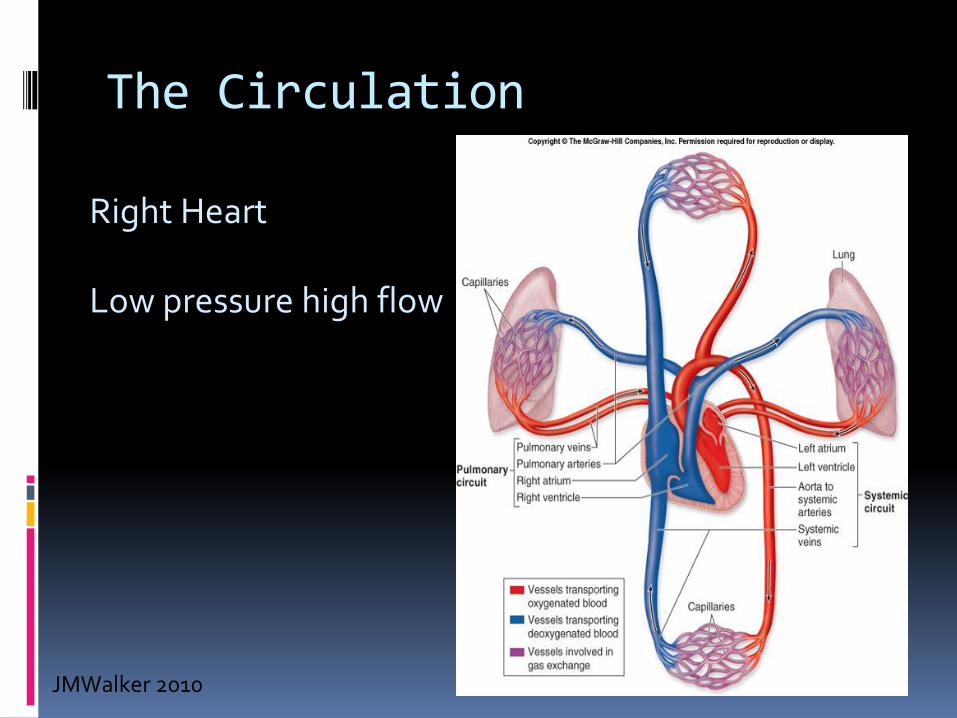
The Circulation
Right Heart Low pressure high flow
JMWalker 2010

The Circulation - pressures
JMWalker 2010

Pulmonary hypertension Definition
Normal values at rest:
Mean pulmonary artery pressure (mPAP):
= 8 – 20 mmHg
Pulmonary hypertension
mPAP >25 mmHg
JMWalker 2010

Pulmonary hypertension Measurement – Direct
Cardiac Catheterisation
JMWalker 2010
Pulmonary hypertension Measurement
Direct by cardiac catheterisation
“Gold Standard”
Can measure PA pressure & mPA, Cardiac output, saturations, indirect or direct left heart pressures
BUT
Invasive, with attendant small risk
Results may not be representative
Patient lying down, fasted, often dehydrated
May require provocation test – hypoxia, inhaled NO, fluid challenge
JMWalker 2010

Pulmonary hypertension Measurement
Direct by cardiac catheterisation
Echocardiography
JMWalker 2010

Doppler: tricuspid jet velocity
JMWalker 2010

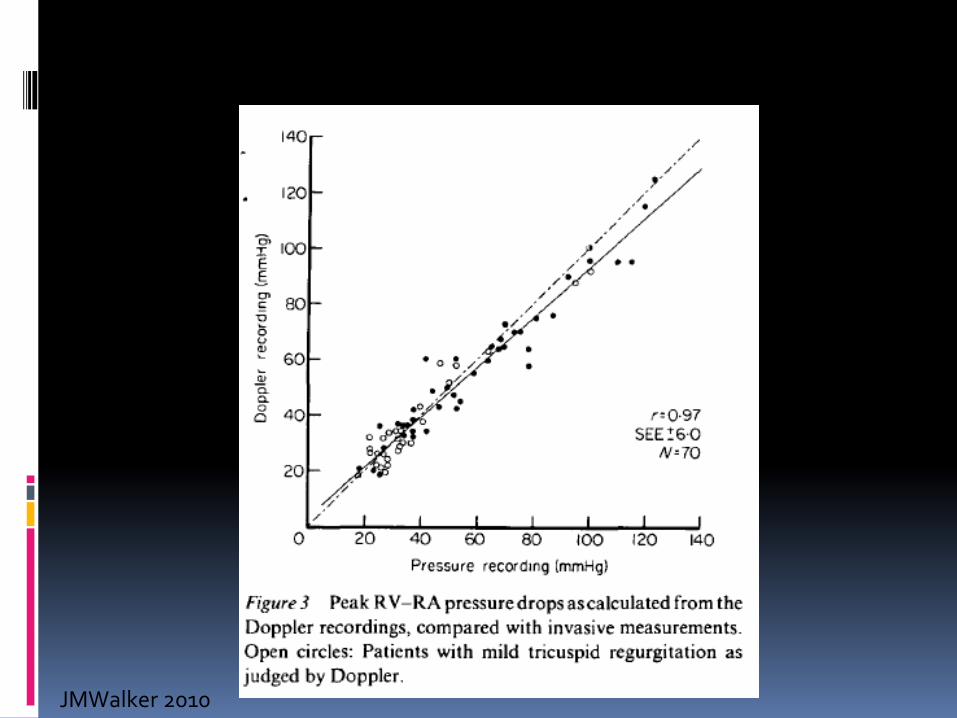
Correlation of tricuspid jet velocity & invasive measurement
Simplified Bernoulli equation: pressure drop = 4 x Vmax2
JMWalker 2010
JMWalker 2010

Doppler tricuspid jet velocity - advantages
ECHO technology widely available
Cheap and rapid (instant)
Completely safe & painless, so can repeat at any moment, at the bed-side if necessary
BUT does NOT measure mPAP
Gives peak pressure drop between RV & RA
Assume systolic pressure in RV = PA
To get sysPAP need to add RA pressure – often assumed to be 5 mmHg
JMWalker 2010
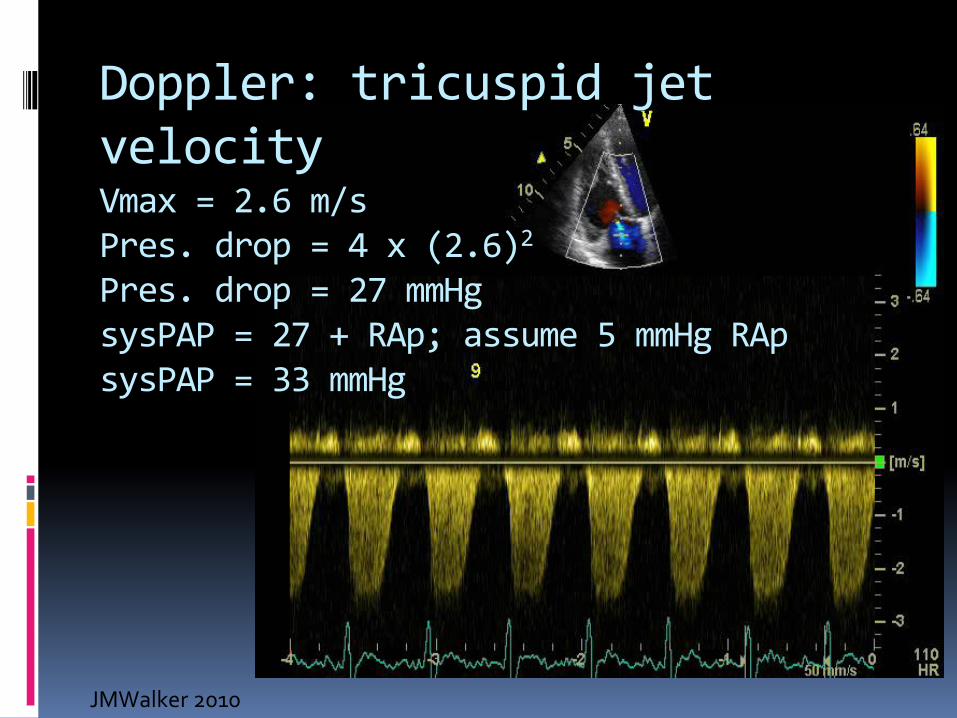
Doppler: tricuspid jet velocity Vmax = 2.6 m/s Pres. drop = 4 x (2.6)2
Pres. drop = 27 mmHg sysPAP = 27 + RAp; assume 5 mmHg RAp sysPAP = 33 mmHg
JMWalker 2010
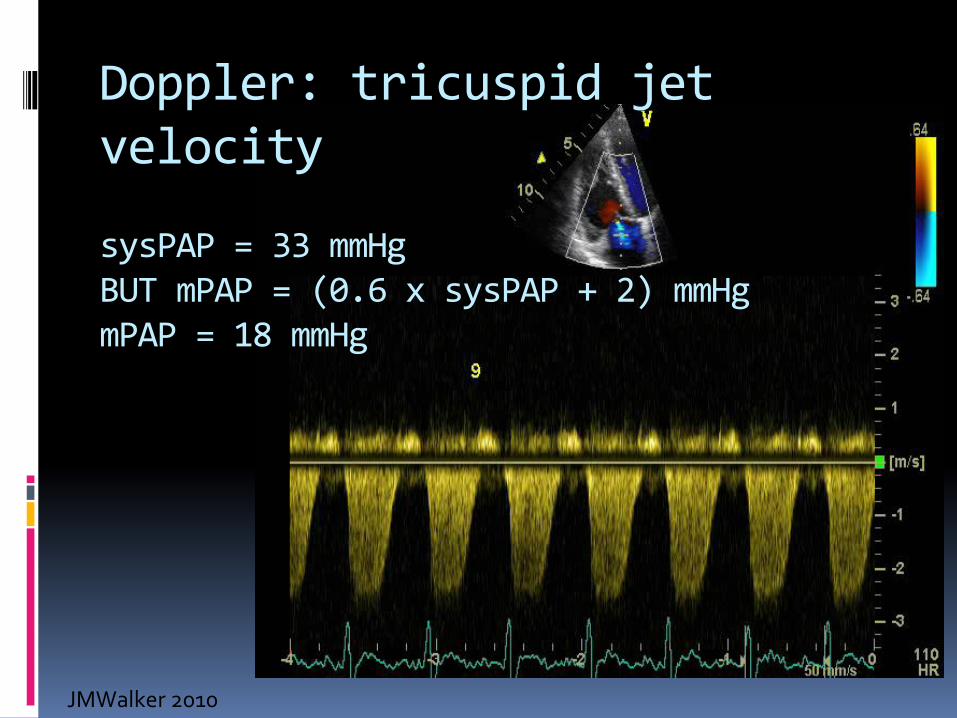
Doppler: tricuspid jet velocity sysPAP = 33 mmHg BUT mPAP = (0.6 x sysPAP + 2) mmHg mPAP = 18 mmHg
JMWalker 2010
Problems with Doppler tricuspid jet velocity
Tricuspid jet absent in about 20%
Poor indicator of pressure if tricuspid regurgitation (TR) is more than moderate
As RV dilates apparent fall in PA pressure may be seen – due to increased TR
JMWalker 2010
Problems with Doppler tricuspid jet velocity
Conversion from velocity to pressure amplifies errors of velocity (V) measurement (P = 4xV2)
RA pressure estimates from 5 to 15 mmHg – wildly inaccurate (sysPAP = P + Rap)
To get to mPAP: = (sysPAP x 0.6 + 2) mmHg
There is a case to stick to TR jet velocity without conversion to a pressure measurement
JMWalker 2010

Pulmonary hypertension Measurement Conclusions
ECHO TR jet velocity: practical tool for screening
Cardiac catheterisation: for special circumstances
Cardiac Magnetic Resonance imaging : techniques in development
Pulmonary hypertension Pathophysiology The cause of increased mPA
Mostly a condition of pulmonary arteries, this is termed pulmonary arterial hypertension PAH
Idiopathic & hereditable
Associated with connective tissue disease
Portal hypertension
Congenital heart disease (shunts)
Pulmonary hypertension PH may also be a consequence of severe left ventricular disease
JMWalker 2010
Pulmonary hypertension Pathophysiology
Whatever the cause of Pulmonary hypertension it results in:
Right ventricular failure
RV failure causes the symptoms & accounts for the mortality associated with PH
JMWalker 2010

Pulmonary hypertension Pathophysiology
Pulmonary arterial pathophysiology
JMWalker 2010
Pulmonary hypertension Pathophysiology
Pulmonary arterial hypertension (PAH)
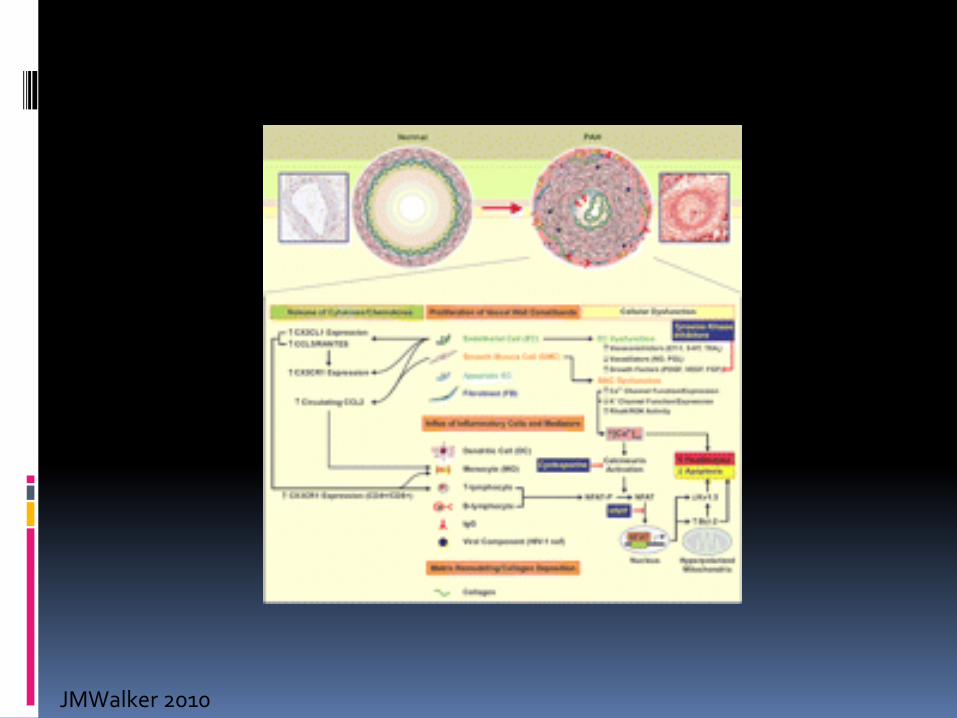
Initial reversible vasoconstriction
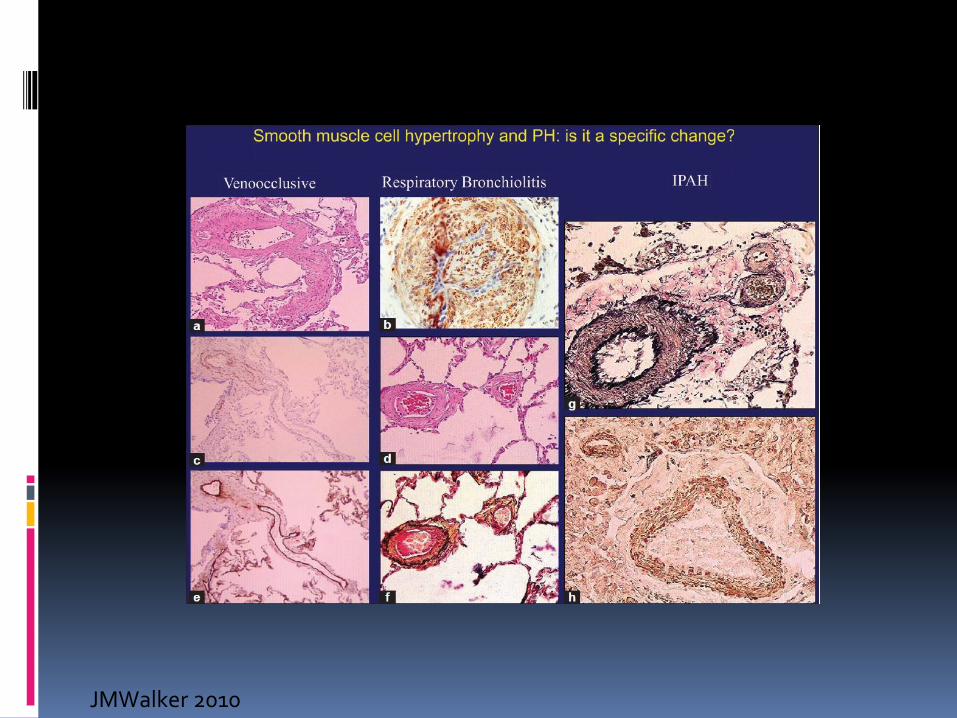
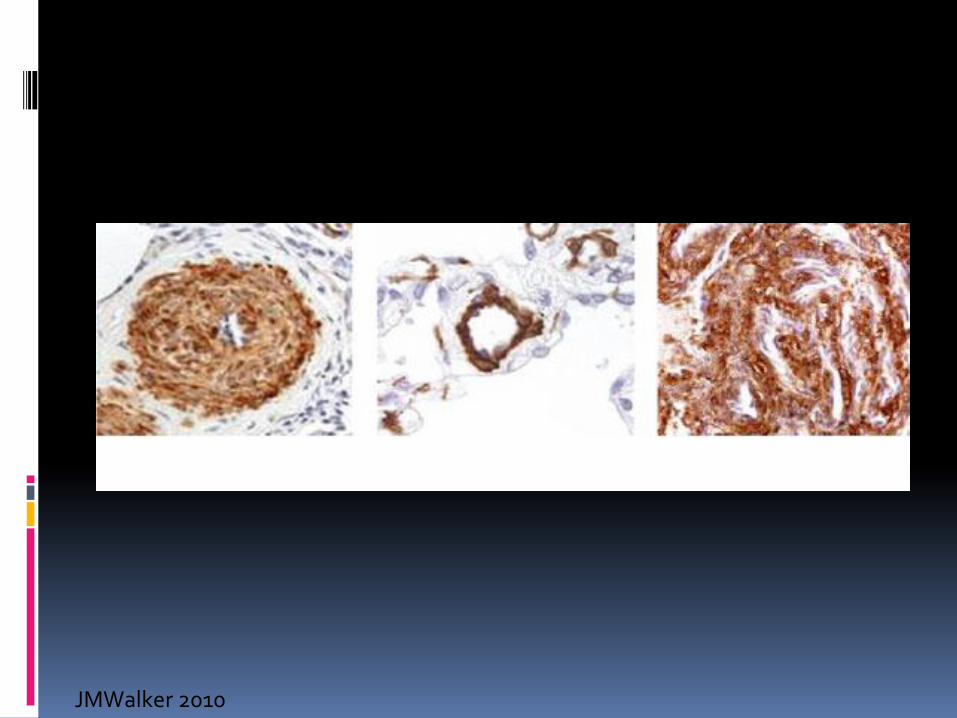
Pulmonary arterial remodelling
Thickening of vessel walls due to smooth muscle & fibroblast proliferation + increased extra-cellular matrix
Increased vascular stiffness & resistance
Increased resistance (PVR)
JMWalker 2010

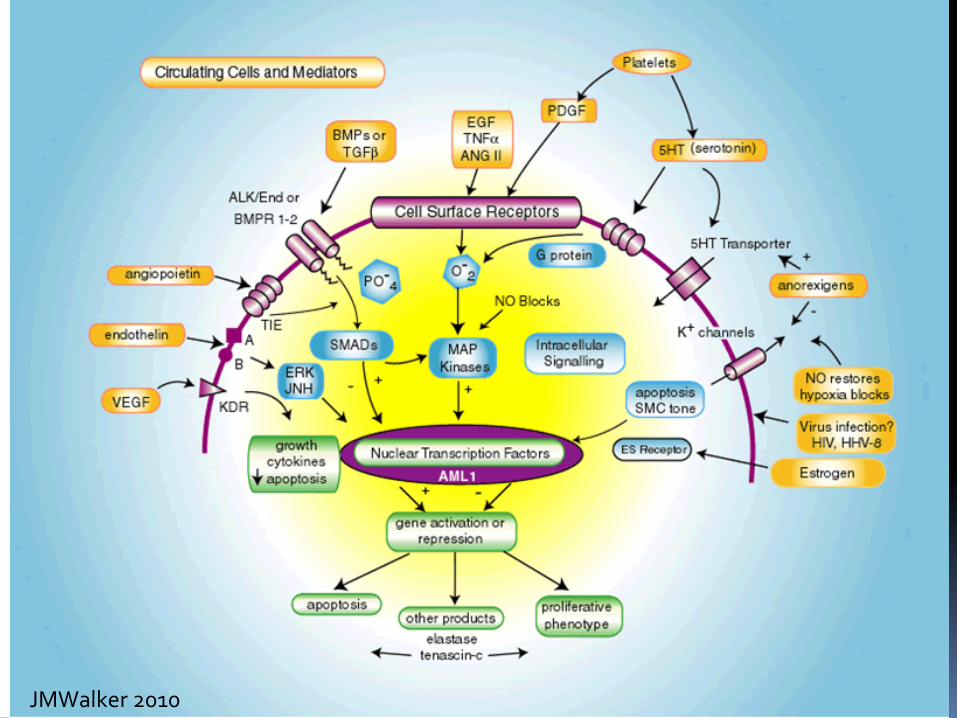
Pulmonary hypertension Pathophysiology
JMWalker 2010
Pulmonary hypertension Pathophysiology
Pulmonary arterial pathophysiology
Complex
JMWalker 2010

Pulmonary Hypertension: Etiology
RestrictiveLung Disease
Cardiac Output
HypoxemiaPulmonary ArteryCircumferential Stress
LV compliance
Iron Circulating plateletAggregates
Splenectomy Liver Dysfunction
Angiotoxic mediators or Trophic Factors
Endothelial Dysfunction/Toxicity
AbnormalMechanicalForces
Vasoconstriction = Pulmonary Hypertension
+
PulmonaryDiffusionBlock
Endothelial Shear Stress
LA pressure
Hemolysis
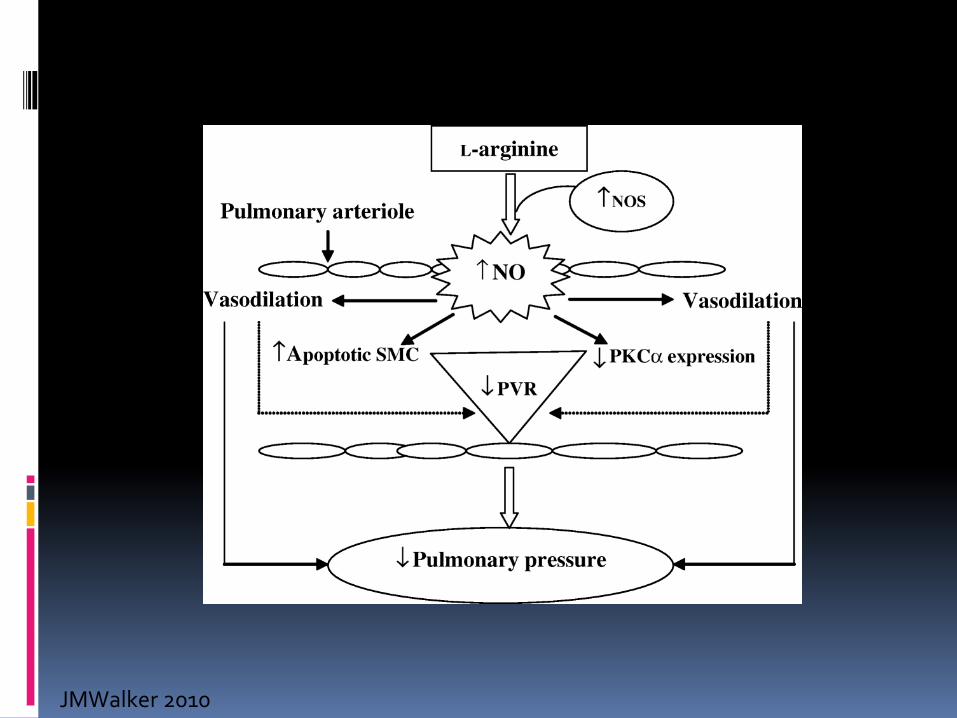
Arginine
NO
JMWalker 2010
Pulmonary hypertension Pathophysiology
Pulmonary arterial pathophysiology
Complex
JMWalker 2010
Pulmonary hypertension Pathophysiology
Pulmonary arterial pathophysiology
Complex
Main target for therapy
Right Ventricular adaptation & failure
Poorly studied
It is main cause of symptoms/ mortality in PH
Measurement of RV function is difficult
JMWalker 2010
Pulmonary hypertension
Haemoglobinopathies are prime candidates for the development of PH :
Release of free Hb from haemolysis (NO)
Hypoxia
Increased shear stress via high cardiac output
Thrombosis
JMWalker 2010
Pulmonary hypertension clinical correlates
Thalassaemia major (TM)
Variable incidence of PH complicating TM
Lebanese/ Egypt experience in children
TR jet velocity > 2.5 m/s (PAsp 25 mmHg): 12/20 (60%)
UK experience (UCLH)
Adult clinic population < 5% TR jet velocity > 2.5 m/s
Transient PH complicating Left Ventricular failure
US report 60% incidence in 1 study
Greek experience in HbS Thal
Severe PH in 2.9%; Mild PH 27% (TR jet > 2.6 m/s)
JMWalker 2010
Pulmonary hypertension clinical correlates
Thalassaemia major (TM)
Pulmonary hypertension (TR jet > 2.5 m/s)
Uncommon in uncomplicated TM
Good chelation
Low cardiac iron
Good LV function
Seen under certain circumstances:
Acute LV failure
Pulmonary embolism
JMWalker 2010

Pulmonary hypertension in TM
JMWalker 2010
Pulmonary hypertension clinical correlates
Thalassaemia major (TM)
Pulmonary hypertension
Uncommon in uncomplicated TM
Good chelation
Low cardiac iron
Good LV function
Seen under certain circumstances:
Acute LV failure
Pulmonary embolism
JMWalker 2010

Pulmonary hypertension clinical correlates
Thalassaemia intermedia (TI)
Accepted that much higher incidence of PH
Mechanisms might include:
1. Haemolysis – free Hb – interference with NO
2. Embolism – high risk of CTPE – splenectomy
3. PAH due to shear stress – high CO due to anaemia
4. Poor LV function - uncommon
JMWalker 2010
Pulmonary hypertension clinical correlates
All Thalassaemia
Definition of PH is lacking
Can 2.5m/s (25 mmHg) be accepted?
Is 2.9 m/s (34 mmHg) more appropriate?
REGULAR Screening by ECHO Doppler now essential
Establish if PHT due to poor LV function
Assess RV function with great care (difficult, but TDI RV systolic longitudunal velocity is promising)
BNP
JMWalker 2010

Pulmonary hypertension clinical plan
ECHO shows TR jet velocity > 2.5 m/s
Or ECHO shows worsening RV function
1. Establish LV function
2. Exclude pulmonary embolism
3. Assess baseline functional capacity
6 minute walk test distance in m
Treadmill test or Cpex – if available
JMWalker 2010
Pulmonary hypertension clinical plan
ECHO shows TR jet velocity > 2.5 m/s
Or ECHO shows worsening RV function
1. Establish LV function
2. Exclude pulmonary embolism
3. Assess baseline functional capacity
6 minute walk test distance in m
Treadmill test or Cpex – if available
JMWalker 2010

Pulmonary hypertension in thalassamia : treatment 1. Isolated PH – with normal LV function
1. Diminish haemolysis
2. Diminish hypoxia, thrombosis, high cardiac output state
3. Drugs
2. PH with impaired LV function
1. Chelate if iron overload is the problem
2. ACEi + beta-blockers (carvidelol)
3. Spironolactone
JMWalker 2010
Pulmonary hypertension in thalassaemia : drugs Drugs: no prospective trial data yet available
1. Warfarin
2. Digoxin
3. Phosphodiesterase inhibitors (PD5) – sildenafil (Viagra – marketed for PH as Revatio – 20 to 80mg tds)
4. Calcium channel blockers: Nifedipine, amlodipine
5. 5 hydroxyurea – (raising NO via arginine mechanism)
6. Endothelin receptor antagonists: bosentan, ambrisentan, sitaxentan
7. Thromboxane inhibitors: epoprostenol, iloprost, treprostinil
8. l-Carnitine
JMWalker 2010

Pulmonary hypertension in thalassaemia : treatment
Drugs costs pa. estimated in US$ 1. Warfarin: 800
2. Digoxin: 50
3. Sildenafil 15,000
4. CCB 500
5. 5 HU
6. ERA – bosentan 35,000
7. Thromboxane inhibitors 100,000
8. l-Carnitine ?50
JMWalker 2010
Conclusions
Pulmonary hypertension There remain more questions than answers What level of TR jet velocity? 2.5 m/s, >3.0 m/s?
Patients must be screened for this complication ; use ECHO – regularly! If detected, do the simple things first:
1. Optimise haematological care 2. Support LV 3. Warfarin, digoxin & vasodilate – if pulmonary vascular
reactivity +ve 4. STOP SMOKING!! 5. Improve diet 6. Consider the more complex & expensive therapies
JMWalker 2010
JMWalker 2010

JMWalker 2010
JMWalker 2010
JMWalker 2010
JMWalker 2010
Related Documents