Paediatric and Perinatal Epidemiology 1989, 3, 19-28 Original articles Pregnant women at work: rest periods to prevent preterm birth? N. Mamelle, I. Bertucat and F. Munoz UnitP de Recherches Epidirniologiques sur les Composantes physiques, psychologiques et sociales de la Santi, INSERM, Lyon, France Summary. The aim of this study is to identify social preventive measures in an attempt to prevent pre-term birth in pregnant women who work under strenubus conditions. A study carried out in 50 factories allowed us to gather data on 1168 pregnanaes that occurred during 1 year and to study the modifications in working conditions now granted to pregnant women in many firms in France. We observed a significant relationship between 'episodes of sick leave' prescribed especially for fatigue (without any pathological reason) and a lower preterm birth rate. The potential benefit of rest-periods, granted to pregnant women working in strenuous conditions, is discussed. Introduction Industrialised countries, where more than 504b of pregnant women work outside their home, are concerned with the problem of work during pregnancy. Chamberlain raises the problem of a necessary concilia tion between occupational activity and pregnancy, as many women wish to work during pregnancy and feel that doctors are overprotective and unnecessarily restrictive.' Women, policy-makers, trade unions and clinicians are looking for ways in which to prevent the adverse outcomes of pregnancy caused by harmful work conditions. At the same time, one must avoid protective legislation that could have adverse consequences on women's employment, as is suggested by Garcia.2 Address for correspondence: Dr N. Mamelle, Unite de Recherches Epidemiologiques sur les Composantes Physiques, Psychologiques et Sociales de la Sante, INSERM U 265, 151, cours Albert Thomas, 69424 Lyon cedex 3, France. 19

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Paediatric and Perinatal Epidemiology 1989, 3, 19-28
Original articles
Pregnant women at work: rest periods to prevent pre term birth?
N. Mamelle, I. Bertucat and F. Munoz UnitP de Recherches Epidirniologiques sur les Composantes physiques, psychologiques et sociales de la Santi , INSERM, Lyon, France
Summary. The aim of this study is to identify social preventive measures in an attempt to prevent pre-term birth in pregnant women who work under strenubus conditions. A study carried out in 50 factories allowed us to gather data on 1168 pregnanaes that occurred during 1 year and to study the modifications in working conditions now granted to pregnant women in many firms in France. We observed a significant relationship between 'episodes of sick leave' prescribed especially for fatigue (without any pathological reason) and a lower preterm birth rate. The potential benefit of rest-periods, granted to pregnant women working in strenuous conditions, is discussed.
Introduction
Industrialised countries, where more than 504b of pregnant women work outside their home, are concerned with the problem of work during pregnancy. Chamberlain raises the problem of a necessary concilia tion between occupational activity and pregnancy, as many women wish to work during pregnancy and feel that doctors are overprotective and unnecessarily restrictive.'
Women, policy-makers, trade unions and clinicians are looking for ways in which to prevent the adverse outcomes of pregnancy caused by harmful work conditions. At the same time, one must avoid protective legislation that could have adverse consequences on women's employment, as is suggested by Garcia.2
Address for correspondence: Dr N. Mamelle, Unite de Recherches Epidemiologiques sur les Composantes Physiques, Psychologiques et Sociales de la Sante, INSERM U 265, 151, cours Albert Thomas, 69424 Lyon cedex 3, France.
19

20 N . Mamelle, 1. Bertucat and F . Munoz
A recent review of epidemiological studies in this field has been published.' In most cases, the indicators describing the outcome of pregnancy are length of gestation and birthweight. Many studies have shown that occupational activity is not, in itself, a preterm birth risk factor.&' However, some authors have found a rela tionship between strenuous working conditions and pre-term delivery.'.'~~ In an earlier s t ~ d y ~ . ~ we found that the women most prone to pre-term birth were unskilled workers and cleaning staff and those working in hospitals and shops. Similar findings were reported in the French National S ~ r v e y . ~ In our study, we proposed a fatigue scoring system based on the accumulation of fatigue sources such as posture, work on a machine, physical exertion, mental stress and environment and found a significant relationship between our fatigue score and the pre-term birth rate. We also estimated that about 20% of women had an occupational activity which may have had a harmful effect on their p regnan~y.~ In a later study, we assessPd the reliability of this fatigue scoring system.I0
Therefore, besides the intensive prenatal care suggested by Papiernik," social preventive measures should be considered. The problem is to determine which social measures could be implemented to prevent pre-term birth among working women without creating adverse consequences for them. Should we give time off to women whose jobs are strenuous, reduce their weekly working hours, or lengthen their antenatal maternity leave?
Recently, in many firms in France, several modifications to working conditions have been routinely established. We call 'modification in working conditions' any change in relation to pregnancy, granted by the employers or by the doctors who take care of the pregnant women. These modifications can be:
1
2
a change of work station within the firm (this was usually a change in job to one which required less physical effort); a reduction in weekly working hours (half an hour a day from the sixth month of pregnancy in some organisations or 1 hour a day from the third month of pregnancy in others);
3 sick leave during pregnancy (referred to here as 'episodes of sick leave' when the woman comes back to work at the end of the time off and an 'increase in antenatal maternity leave', when this time off ends at the beginning of the legal maternity leave).
In France, the legal maternity leave starts 6 weeks before the estimated delivery date (8 weeks when the woman is expecting her third baby), and in the case of a pathological pregnancy, the doctor can grant an 'additional 2 weeks' of antenatal leave (remunerated by the Social Security, as the legal maternity leave). In actual fact, 'episodes of sick leave' during pregnancy, an 'additional 2 weeks', or a 'longer increase of maternity leave' are very often granted for fatigue, without any pathological reason, especially if the working conditions are strenuous. These could be considered as 'preventive rest periods'.

Pregnant women at work 21
In our previous study, results concerning women who stopped work before the third month of pregnancy (for personal reasons, without any real pathology), led us to observe a pre-term birth rate as high as that in women who remain at home.12 Many studies such as ours report a higher pre-term birth rate in women at home than in women at work. Therefore we ask how to take into account the potential beneficial psychological role of occupational environment, while at the same time stopping strenuous occupations.
In another paper13 we reported the results of a questionnaire concerning pregnant women’s preferences. It showed that women do not appreciate moving to a different work station and would prefer a reduction in weekly working hours. Moreover, interviews with trade unions reveal that women do not want a generalised increase in antenatal maternity leave, which they consider to be detrimental to their employment.
Thus, before recodmending a lengthening of the antenatal maternity leave, we wished to confirm our previous results in a new observational study and then attempt to elaborate appropriate preventive measures; this is the purpose of our paper.
Material and methods
Study design
We elected to conduct a prospective study in 50 firms in the Rh6ne-Alpes area in France. The firms were selected with regard to three criteria: they needed to employ a high percentage of women, to have standard working conditions where the women were mostly full-time, and to conduct types of activities considered to be harmful during pregnancy, as outlined in our previous r e p ~ r t . ~
The study population included 23000 women working in these firms. All women were taken into consideration, providing they worked at least 30 hours per week. With an annual pregnancy rate of about 59b among these working women, we could expect approximately 1150 pregnancies. Under these condi- tions, assuming an 8% pre-term birth rate in women for whom there would be no modifications in working conditions and a 4% rate in those benefiting from such modifications, we estimated the power of the study to be 80Y0, if at least 50% of women benefitted from modifications, with a two-sided test and a type I error equal to 5 YO.
Data collection The survey was carried out in 1982, in collaboration with occupational health physicians in the firms. One thousand and sixty-eight pregnancies were recorded (i.e. as many as we had expected), from six different activity sectors: 35Y0 from hospitals, 10% from supermarkets, 134b from clothing and shoe manufacture, 8%
22
from mechanics factories, l6Y0 from electrical and electronic factories and 18% from banks (included in the study because of the recent work on terminals).
N . Mamelle, 1. Bertucat and F. Munoz
The data were collected in three stages: prospective recording of working conditions through observation of work stations by occupational health physicians and concerned groups within the firms (before they knew if the women at these work stations were pregnant or not); prospective recording of data related to life-style, previous obstetrical pathology, course of pregnancy, modifications in working conditions (indud- ing sick leave and the reasons for it), through interviews of pregnant women by physicians during a special medical consultation at 5-6 months of pregnancy; and retrospective recording of data related to the course of the third trimester of pregnancy, and to the delivery, during a routine medical consultation 2 months after birth, when the woman returned to work. In the case of a woman who did not return to work or who lengthened her
i
postnatal maternity leave, the third part of the questionnaire was completed in an interview at home. About 104b of women were contacted in this way and less than 290 of pregnant women were lost to follow-up.
Analysis
This observational study enabled us to describe the baseline characteristics of women in the sample (in order to compare them to a national sample), describe modifications in their working conditions, and study the relationships between these modifications and the pre-term birth rate. The relationships observed were measured in terms of relative risks and 9596 confidence limits," and the adjustments used the Mantel-Haenszel method.lS
Results
Characteristics of the sample women
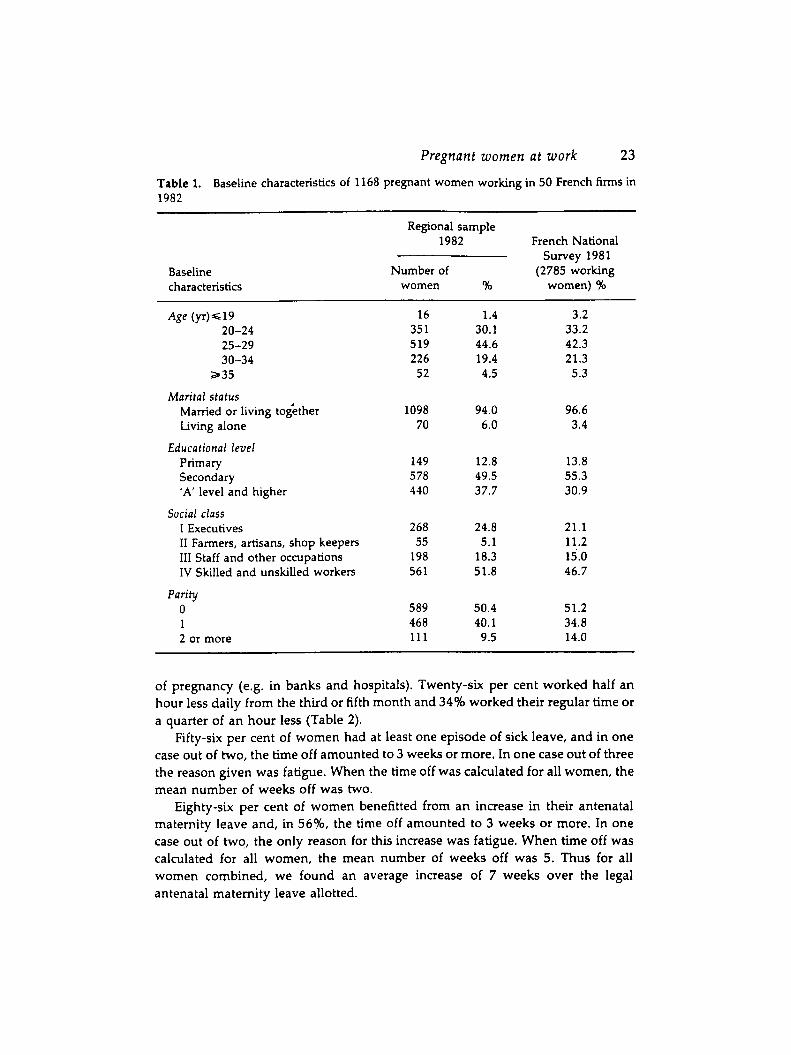
When we compared the baseline characteristics of the women in our sample with a representative sample of women who had given birth in 1981 from the French National Survey,16 we did not find any important differences with regard to age, marital status, educational level, social class or parity (Table 1).
Modifications of working conditions
We observed that 7.5% of women took advantage of a change in work station. A reduction in weekly working hours was often granted to women. Thus, 40% of the women in our sample worked 1 hour less every day, usually from the third month
Pregnant women at work 23
Table 1. Baseline characteristics of 1168 pregnant women working in 50 French firms in 1982
Baseline characteristics
Regional sample 1982 French National
Survey 1981 Number of (2785 working
women 90 women) %
Age (YrW19 20-24 25-29 30-34
a 3 5
Marital s tatus Married or living toiether Living alone
Educational level Primary Secondary ‘A’ level and higher
I Executives I1 Farmers, artisans, shop keepers 111 Staff and other occupations IV Skilled and unskilled workers
Social class
Parity 0 1 2 or more
16 35 1 519 226 52
1098 70
149 578 440
268 55
198 561
589 468 111
1.4 30.1 44.6 19.4 4.5
94.0 6.0
12.8 49.5 37.7
24.8 5.1
18.3 51.8
50.4 40.1
9.5
3.2 33.2 42.3 21.3 5.3
96.6 3.4
13.8 55.3 30.9
21.1 11.2
46.7 15.0
51.2 34.8 14.0
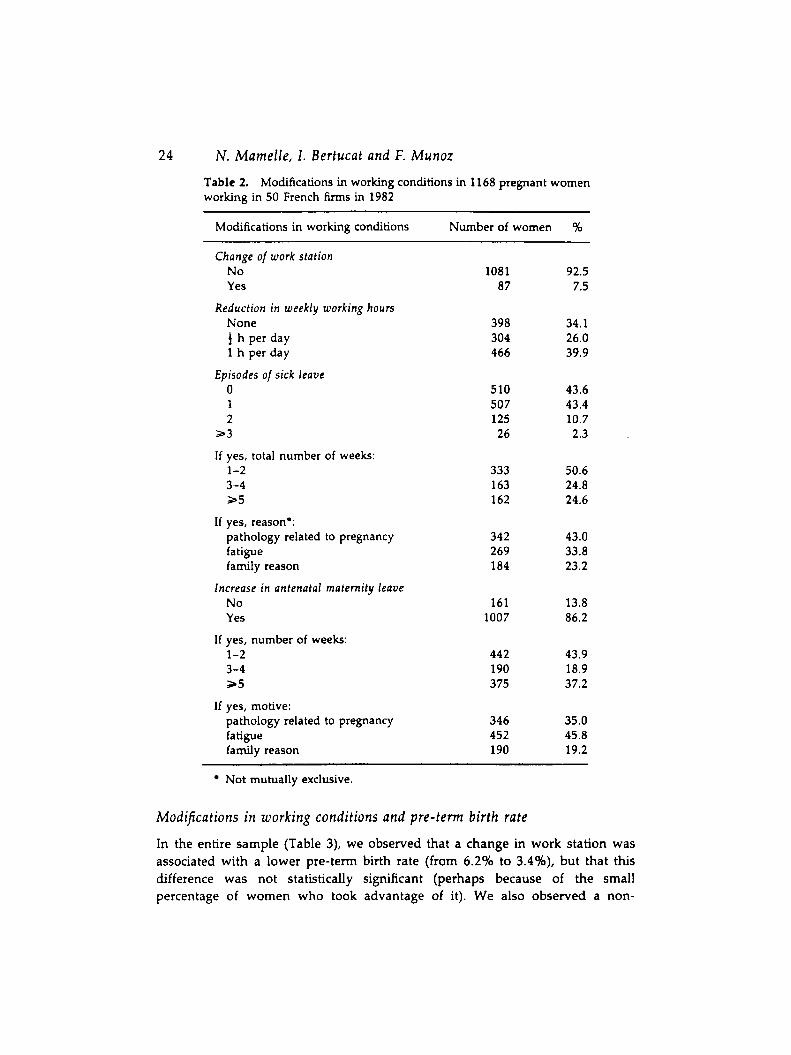
of pregnancy (e.g. in banks and hospitals). Twenty-six per cent worked half an hour less daily from the third or fifth month and 3446 worked their regular time or a quarter of an hour less (Table 2).
Fifty-six per cent of women had at least one episode of sick leave, and in one case out of two, the time off amounted to 3 weeks or more. In one case out of three the reason given was fatigue. When the time off was calculated for all women, the mean number of weeks off was two.
Eighty-six per cent of women benefitted from an increase in their antenatal maternity leave and, in 5696, the time off amounted to 3 weeks or more. In one case out of two, the only reason for this increase was fatigue. When time off was calculated for all women, the mean number of weeks off was 5 . Thus for all women combined, we found an average increase of 7 weeks over the legal antenatal maternity leave allotted.
24 N . Mamelle, I. Bertucat and F. Munoz
Table 2. working in 50 French f i rms in 1982
Modifications in working conditions in 1168 pregnant women
Modifications in working conditions Number of women %
Change of work station No Yes
Reduction in weekly working hours None f h per day 1 h per day
0 1 2
2 3
I f yes, total number of weeks:
Episodes of sick leave
1-2 3-4 3 5
If yes, reason*: pathology related to pregnancy fatigue family reason
No Yes
Increase in antenatal maternity leave
If yes, number of weeks: 1-2 3-4 a 5
If yes, motive: pathology related to pregnancy fatigue family reason
1081 87
398 304 466
510 507 125 26
333 163 162
342 269 184
161 1007
442 190 3 75
346 452 190
92.5 7.5
34.1 26.0 39.9
43.6 43.4 10.7 2.3
50.6 24.8 24.6
43.0 33.8 23.2
13.8 86.2
43.9 18.9 37.2
35.0 45.8 19.2
Not mutually exclusive.
Modifications in working conditions and pre-term birth rate
In the entire sample (Table 3), we observed that a change in work station was associated with a lower pre-term birth rate (from 6.2% to 3.4%), but that this difference was not statistically significant (perhaps because of the small percentage of women who took advantage of it). We also observed a non-
Pregnant women at work 25
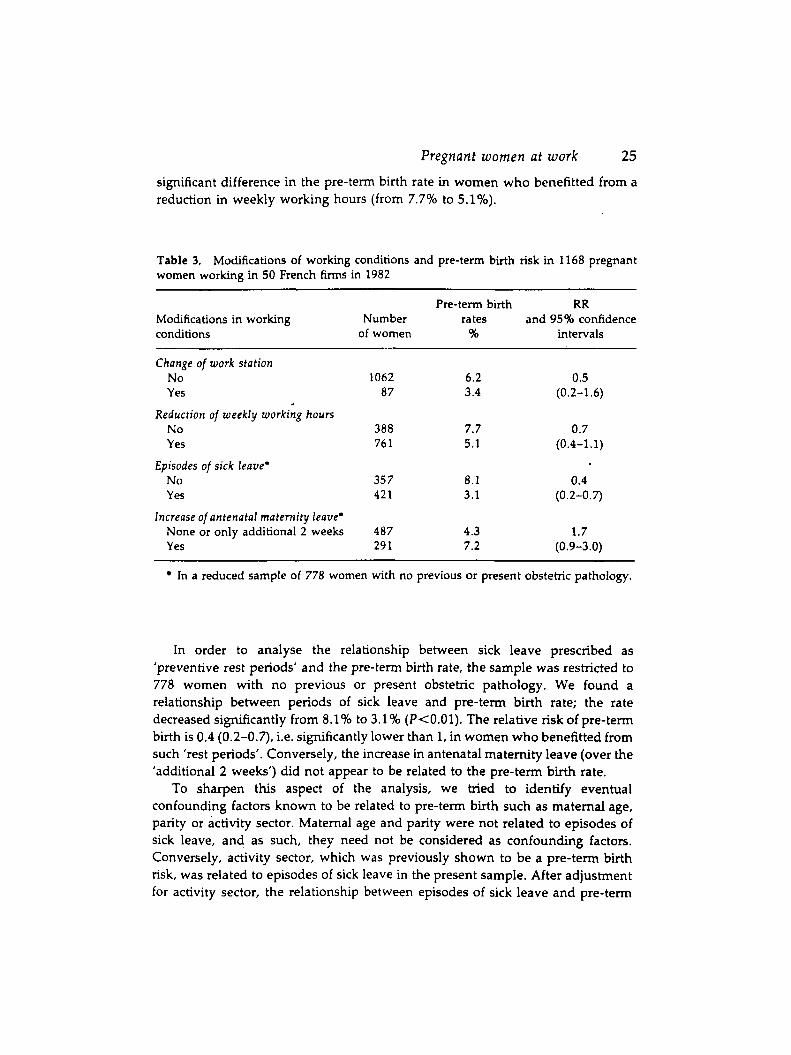
significant difference in the pre-term birth rate in women who benefitted from a reduction in weekly working hours (from 7.796 to 5.146).
Table 3. Modifications of working conditions and pre-term birth risk in 1168 pregnant women working in 50 French fums in 1982
Pre-term birth RR Modifications in working Number rates and 95% confidence conditions of women % intervals
Change of work station No Yes
Reduction of weekly working hours No Yes
Episodes of sick leave* No Yes
Increase of antenatal maternity leave’ None or only additional 2 weeks Yes
1062 87
388 76 1
35 7 42 1
487 29 1
6.2 0.5 3.4 (0.2-1.6)
7.7 0.7 5.1 (0.4-1.1)
8.1 0.4 3.1 (0.2-0.7)
4 .3 1.7 7.2 (0.9-3.0)
~~
In a reduced sample of 778 women with no previous or present obstetric pathology.
In order to analyse the relationship between sick leave prescribed as ’preventive rest periods’ and the pre-term birth rate, the sample was restricted to 778 women with no previous or present obstetric pathology. We found a relationship between periods of sick leave and pre-term birth rate; the rate decreased sigruficantly from 8.196 to 3.19’0 (P<O.Ol). The relative risk of pre-term birth is 0.4 (0.2-0.7), i.e. significantly lower than 1, in women who benefitted from such ’rest periods’. Conversely, the increase in antenatal maternity leave (over the ’additional 2 weeks’) did not appear to be related to the pre-term birth rate.
To sharpen this aspect of the analysis, we tried to identify eventual confounding factors known to be related to pre-term birth such as maternal age, parity or activity sector. Maternal age and parity were not related to episodes of sick leave, and as such, they need not be considered as confounding factors. Conversely, activity sector, which was previously shown to be a pre-term birth risk, was related to episodes of sick leave in the present sample. After adjustment for activity sector, the relationship between episodes of sick leave and pre-term

26
birth remains, with a relative risk of 0.65 (P<0.002) and a 95% confidence interval of 0.50-0.85 (Table 4).
N. Mamelle, 1. Bertucat and F . Munoz
Table 4. Episodes of sick leave and pre-term birth risk in 778 pregnant women with no previous or present obstetric patho- lorn
RR* 95% confidence interval
Episodes of sick leave 0.65 0.50-0.85
After adjustment for activity sector.
Discussion
Few studies have been concerned with modifications in working conditions and sick leave, in relation to the outcome of pregnancy. It appears that a reduction in weekly working hours has been granted more and more often over the last 10 years in France: 65Y0 of the women in our sample in 1982, compared to 40’70 in the National Survey1’ in 1981, and 104b in our previous survey in 1977-1978.‘ The National Report also indicated that 62’70 of women took sick leave during their pregnancy (this included episodes of sick leave and an increase in maternity leave, but did not take into account the ’additional 2 weeks’). In this national report, among women who took sick leave, the average duration of this sick leave was 5 weeks. Using the same definition in our survey, we found that 73’70 of the women took sick leave and the average duration was 7.5 weeks. Thus, we observed that women working under strenuous conditions turn to sick leave to shorten their working hours. The same findings were also reported by Saurel-Cubizolles in the French National Survey; the women exposed to strenuous working conditions had an increased duration of sick leave.9
In this observational study, we have demonstrated that women working under strenuous conditions resort more often to sick leave than the general population and that episodes of sick leave granted as rest periods (especially for fatigue) are associated with a lower pre-term birth rate.
In spite of the methodological difficulties, it would be necessary to carry out an experimental study in order to prove the effectiveness of such measures on the risk of pre-term birth. In the meantime, we have proposed a theoretical method to evaluate the effectiveness, cost and acceptability of social preventive measures, taking into account the national p01icy.l~
While waiting for such experimental evaluation, our proposition would be to systematically give time off to women whose jobs could be harmful to their pregnancy (this would encompass about 20’70 of working women) in order to
Pregnant women at work 27
make sure that every woman who needs a rest period has it. In practice, recommendations could be made to those with responsibilities for working condltions in firms that they detect harmful work stations and plan rest periods for pregnant women working in them. Parallel to this, obstetricians could be asked to question women about their working conditions (using our fatigue scoring system for example) and to prescribe ’rest periods’ in the case of strenuous conditions.
Acknowledgements
This study was constructed in collaboration with the ‘inspections midicales du travail‘ and the occupational health physicians in the firms which participated in the study. This work was supported by research grants from the French Ministry of Labour and the Regional Health Observatory. We are grateful to J. Cogan- Collet for her help in the translation of this text. The authors also wish to thank one of the reviewers for his very helpful suggestions.
References
1 Chamberlain, G. Women at work in pregnancy. In: Pregnant Women at Work, Editor: G. Chamberlain. London: Royal Society of Medicine, 1984; pp. 3-13. 2 Garcia, 1. Future research on work in pregnancy. In: Pregnant Women at Work, Editor: G. Chamberlain. London: Royal Society of Medicine, 1984; pp. 273-285. 3 Saurel-Cubizolles, M.J. Work in pregnancy: its evolving relationship with perinatal outcome. Social Science and Medicine 1986; 22431-442. 4 Marnelle, N., Munoz, F., Collin. D. Quantification de la charge de travail feminin pendant la grossesse. Archives des Maladies Professionnelles 1981; 42:205-210. 5 Mamelle, N., Laumon, B., Lazar, P. Prematurity and occupational activity during pregnancy, American Journal of Epidemiology 1984; 119309-322, 6 Marguet, G., Michel-Briand, C., Quichon, R., et al. Influence de la situation professionnelle de la femme sur l’enfant A naitre. Archives des Maladies Professionnelles
7 Naeye, R.L., Peters, E.C. Working during pregnancy: effects on the fetus. Pediatrics
8 Papiemik, E., Kaminski, M. Multifactorial study of the risk of prematurity at 32 weeks of gestation - 1, a study of the frequency of 30 predictive characteristics. Journal of Perinatal Medicine 1974; 2:30-36. 9 Saurel-Cubizolles, M.J., Kaminski, M. Pregnant women’s working conditions and their changes during pregnancy. A National Study in France. British Journal of Industrial Medicine 1987; 44:236-243. 10 Mamelle, N., Munoz, F. Occupational working conditions and preterm birth-a reliable scoring system. American Journal of Epidemiology 1987; 126150-152. 11 Papiemik, E., Maine, D., Rush, D. et al. Prenatal care and prevention of preterm delivery. International Journal of Gynaecology and Obstetrics 1985; 23~427-433. 12 Marnelle, N., Munoz, F., Collin, D. et al. Fatigue professionnelle et prematurite. Archives des Maladies Professionnelles 1981; 92211-216. 13 Marnelle, N., Bertucat, I., Auray, JP., et al. Quelles mesures de prevention de la
1977; 38~329-346.
1982; 69724-727.

28 N. Mamelle, 1. Bertucat and F . Munoz
prematuritb en milieu professionnel? Revue d’Epidemiologie et de Santi Publique 1986;
14 Miettinen, 0.5 Estimability and estimation in case referrant studies, American Journal of Epidemiology 1976; 103226-235. 15 Mantel, N., Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. Journal of the National Cancer Znstitute 1959; 22:719-748. 16 Stengel, B., Saurel-Cubizolles, M.J., Kaminski, M. Pregnant immigrant women: occupational activity, antenatal care and outcome. Znternational Journal of Epidemiology
17 Rumeau-Rouquette, C., du Mazaubrun, C., Rabarison, Y. Naitre en France, Ed Doin. INSERM, Pans, 1984.
34:286-293.
1986; 15533-539.
Literature review
Decline in urinary infections in childhodd
The Scandinavians keep wonderful population-based data. For example, the Finnish National Board of Health has a central data base for all hospital discharges in Finland. On the basis that almost all children under the age of 1 year will be admitted to hospital when they have a symptomatic urinary tract infection, these were analysed separately. The rate decreased from 8.9 per 1000 in 1978 to 6.7 in 1984. Data for older children showed a similar decline.
In order to assess that this wasn’t associated with changes in policy for hospital admission, the data on children receiving continuous medication for recurrent urinary tract infections was also obtained. This also showed a significant decline for girls, although no such decline was apparent for boys. It should be noted that, as in other population studies, girls had a substantially increased rate of urinary tract infection compared with that of boys, except in infancy when the rates were about the same. The same trend was found for the proportion of bacterial cultures that were positive. The authors feel that there is considerable evidence to support the conclusion that there has been a reduction in the frequency of urinary tract infection over time. They suggest that this may be connected with the advent of good quality disposable nappies.
Uhari, M., Nuutinen, M. Epidemiology of symptomatic infections of the urinary tract in children. British Medical journal 1988; 297:450-452.
Related Documents











