Please see full prescribing information available in this kit. MRSA INFECTIONS: A LOCAL PROBLEM ECHEZONA EZEANOLUE, MD, MPH, FAAP ASSISTANT PROFESSOR OF PEDIATRICS DIRECTOR, PEDIATRIC & ADOLESCENT HIV SERVICES UNIVERSITY OF NEVADA SCHOOL OF MEDICINE

Please see full prescribing information available in this kit.
Jul 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Please see full prescribing information available in this kit.
MRSA INFECTIONS: A LOCAL PROBLEM
ECHEZONA EZEANOLUE, MD, MPH, FAAP
ASSISTANT PROFESSOR OF PEDIATRICSDIRECTOR, PEDIATRIC & ADOLESCENT HIV SERVICES
UNIVERSITY OF NEVADA SCHOOL OF MEDICINE
2Please see full prescribing information available in this kit.
CASE STUDY 1
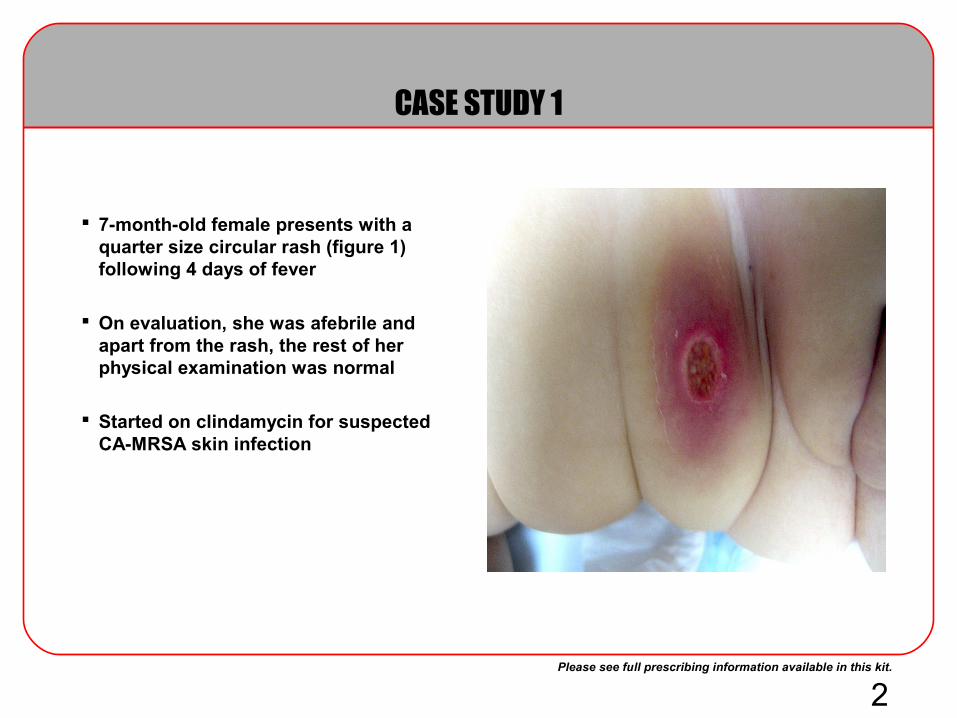
7-month-old female presents with a quarter size circular rash (figure 1) following 4 days of fever
On evaluation, she was afebrile and apart from the rash, the rest of her physical examination was normal
Started on clindamycin for suspected CA-MRSA skin infection

3Please see full prescribing information available in this kit.
CASE STUDY 2
10 year old female presents to the emergency room with a 2 days history of fever, left ankle swelling and pain. She complained of twisting her left ankle 1 day prior to onset of symptom
On physical examination, she had a temperature of 102˚F and her extremities revealed diffuse left ankle swelling, moderate tenderness and inability to bear weight
Radiological evaluation of her ankle revealed no fractures, marked ankle effusion with necrotic bone. Peripheral white count was 12,000/mm3 with 13% bands. C-reactive protein was 35mg/dl
She was admitted and empirically started on intravenous ceftriaxone and nafcillin for suspected osteomyelitis

4Please see full prescribing information available in this kit.
CASE STUDY 3
26 month-month-old female admitted with pneumonia complicated by empyema
She underwent decortication procedure and treated with vancomycin and ceftriaxone for six weeks and discharged
Readmitted with respiratory distress 2 weeks later and found to have empyema. She had a bronchoscopy, chest tube insertion and pleura fluid sent for culture. Started on vancomycin and ceftriaxone
Patient continues to have fever with persistent pleura effusion. Pleura cultures grew MRSA
5Please see full prescribing information available in this kit.Haddadin AS et al. Postgrad Med J. 2002;78:385-392.
Diekema DJ et al. Clin Infect Dis. 2001;32(suppl 2):S114-S132. Deresinski S. Clin Infect Dis. 2005;40:562-573.Zetola N et al. Lancet Infect Dis. 2005;5:275-286.
Nosocomial Infections and Resistance
2 million nosocomial infections per year in US hospitals
60% involve antibiotic-resistant bacteria– Staphylococcus aureus is the most common overall bacterial cause of
infection involving bloodstream, respiratory tract, and skin/soft tissue, according to the SENTRY Antimicrobial Surveillance Program
– Strains of S aureus that have acquired resistance to β-lactam antibiotics, most commonly through inheritance of the mecA resistance gene, are known as methicillin-resistant S aureus (MRSA)
– MRSA accounts for 29% to 35% of all clinical isolates of S aureus in US and European hospitals
Estimated excess costs related to antibiotic resistance approach $30 billion per year in US hospitals
6Please see full prescribing information available in this kit.
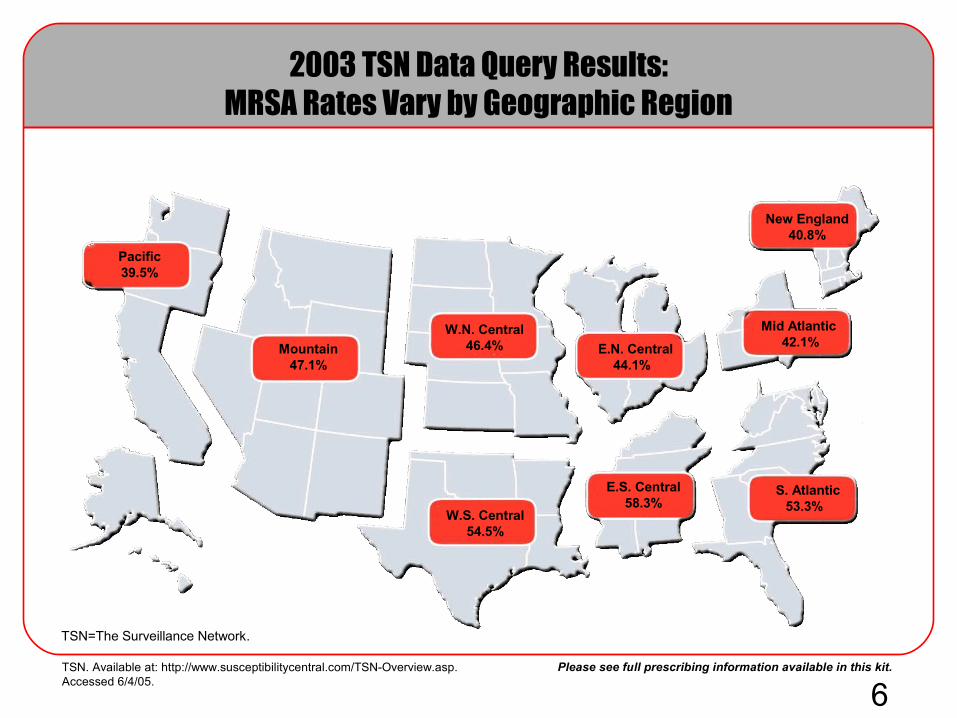
2003 TSN Data Query Results:MRSA Rates Vary by Geographic Region
Pacific39.5%
Mountain47.1%
W.N. Central46.4%
W.S. Central54.5%
E.N. Central44.1%
E.S. Central58.3%
New England40.8%
Mid Atlantic 42.1%
S. Atlantic53.3%
TSN. Available at: http://www.susceptibilitycentral.com/TSN-Overview.asp. Accessed 6/4/05.
TSN=The Surveillance Network.

7Please see full prescribing information available in this kit.
Physiology and Resistance Mechanisms of S aureus
WTA=wall teichoic acid; PVL=Panton-Valentine leukocidin; CHIP=chemotaxis inhibitory protein.
S aureus is an adaptive and successful human pathogen, with the ability to elaborate a range of virulence factors and toxins
Resistance to methicillin first appeared in 1961, attributed to inheritance of a mecA gene found on the mobile staphylococcal cassette chromosome mec (SCCmec)
Genetic analysis suggests that mecA has been transferred to S aureus over 20 times, resulting in 5 major lineages
Transfer of the mecA gene into S aureusstrains already well adapted to survival inhospital or community setting has given riseto 2 major MRSA categories:
– Health careassociate MRSA – Communityacquired MRSA
Zetola N et al. Lancet Infect Dis. 2005;5:275-286.Deresinski S. Clin Infect Dis. 2005;40:562-573. Foster TJ. J Clin Invest. 2004;114:1693-1696.

8Please see full prescribing information available in this kit.
An Emerging Resistance Problem with S aureus
VISA - vancomycin-intermediate S aureus (vancomycin MIC >8-16 µg/mL) has emerged in MRSA strains in the US, Japan, UK, France, etc. Because many of these strains are also resistant to teicoplanin, they are also known as glycopeptide intermediate S aureus (GISA)
VRSA – vancomycin-resistant S aureus (vancomycin MIC ≥32 µg/mL). Four cases of VRSA (associated with vanA genes) have occurred in the US
Following a report from the CDC, the FDA issued a letter to testing labswarning that 2 methods used for automated susceptibility testing can miss rising vancomycin MIC.
Haddadin et al. Postgrad Med J. 2002;78:385-392.CDC. Morb Mortal Wkly Rep. 2004;53:322-323.Rudrik JT. Michigan Dept of Community Health. March 3, 2005.FDA Web site. Available at http://www.fda.gov/cdrh/oivd/letters/062904-vrsa1.html, accessed August 25, 2005.
MIC=minimal inhibitory concentration.

9Please see full prescribing information available in this kit.
Settings Where MRSA Is Encountered
Multidrug resistant (MDR), including:– Clindamycin– Gentamicin– Fluoroquinolone
Usually PVL negative
Associated with nosocomial pneumonia (NP) and skin, surgical site, and bloodstream infections
Can typically be treated with common oral antibiotics. Usually only resistant to:
– Penicillin, oxacillin– Erythromycin, fluoroquinolones
Usually PVL positive and other toxin and virulence factors may be present
Associated with necrotizing skin, pulmonary, and bloodstream infections
Health CareAssociated MRSAHealth CareAssociated MRSA CommunityAcquired MRSACommunityAcquired MRSA
Naimi TS et al. JAMA. 2003;290:2976-2984.Deresinski S. Clin Infect Dis. 2005;40:562-573.Zetola N et al. Lancet Infect Dis. 2005;5:275-286.
10Please see full prescribing information available in this kit.
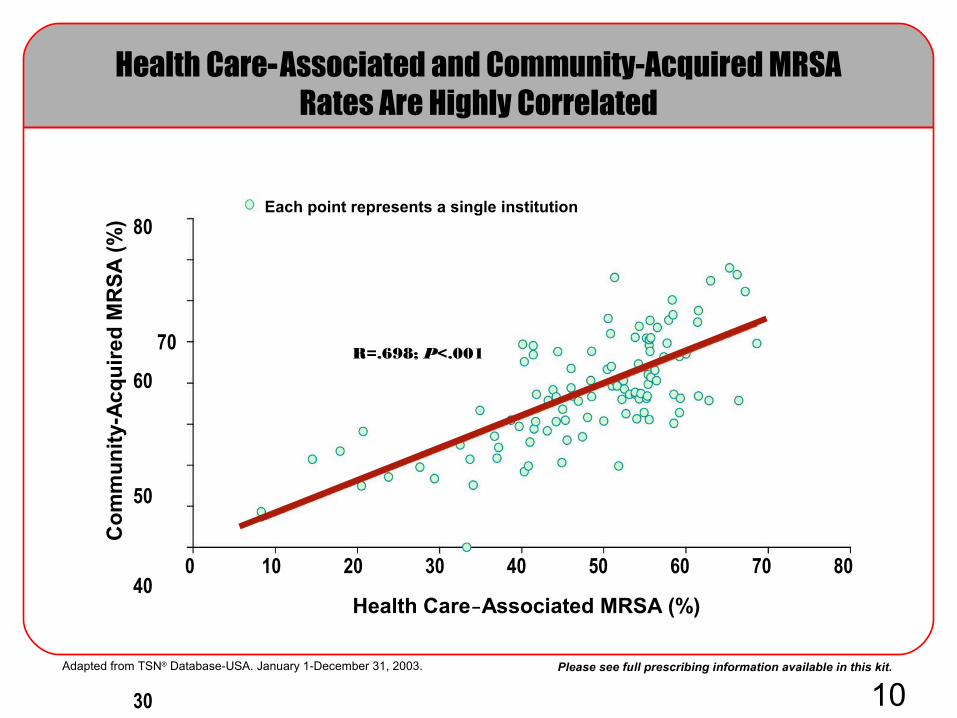
Health CareAssociated and CommunityAcquired MRSA Rates Are Highly Correlated
0 10 20 30 40 50 60 70 80
Health CareAssociated MRSA (%)
80
70
60
50
40
30
20
10
0
Co
mm
un
ity-
Acq
uir
ed M
RS
A (
%)
Each point represents a single institution
R=.698; P<.001
Adapted from TSN® Database-USA. January 1-December 31, 2003.

11Please see full prescribing information available in this kit.
Community–Acquired MRSA
In contrast to the rise in nosocomial MRSA from 1990 to the present (attributed to traditional risk factors in health care facilities), growing awareness of community-acquired MRSA has occurred through published reports of MRSA outbreaks over the past 2 decades, including skin and pneumonia outbreaks for which traditional risk factors were not identified.
Necrotizing pneumonia,United States and EuropeNecrotizing pneumonia,
United States and Europe
1980
Outbreak in Detroit, Mich• 2/3 of patients were IVDUOutbreak in Detroit, Mich
• 2/3 of patients were IVDU
Mid 1990s
Children• w/o identifiable risk factors
Children• w/o identifiable risk factors
Late 1990s
1998 - Athletes/sports teams 1999 - Native Americans
1998 - Athletes/sports teams 1999 - Native Americans
2000
Prison and jail populations Prison and jail populations
2003
IVDU=intravenous drug users.
Groom AV et al. JAMA. 2001;286:1201-1205. Herold BC et al. JAMA. 1998;279:593-598. CDC. Morb Mortal Wkly Rep. 2001;50:919-922.
Naimi TS et al. JAMA. 2003;290:2976-2984.Zetola N et al. Lancet Infect Dis. 2005;5:275-286.Levine DP et al. Ann Intern Med. 1982;97:330-338. CDC. Morb Mortal Wkly Rep. 2003;52:793-795.
Gillet Y et al. Lancet. 2002;359:753-759. CDC. Morb Mortal Wkly Rep. 1999;48:707-710.

13Please see full prescribing information available in this kit.
The Burden of MRSA
Increased hospitalization– MRSA infections increase the median length of hospital stay for nosocomial
infections (median: 12 days for MRSA versus 4 days for methicillin-susceptible S aureus [MSSA]) and surgical site infections (SSIs) (median: 23 days for MRSA versus 14 days for MSSA)
Increased cost– MRSA infections increase per-patient hospital costs in New York City
hospitals by approximately $2500 to $3700 (expressed in 1995 dollars) compared with MSSA
– Direct hospital cost from nosocomial MRSA bacteremia is 2.8 times greater than that for MSSA bacteremia
– MRSA SSIs increase median hospital cost by approximately $40,000 compared with MSSA infections
Increased mortality– Nosocomial MRSA infections are associated with higher mortality compared
with MSSA (21% versus 8%)– MRSA SSIs are associated with a higher 90-day mortality rate (20.7% for
MRSA versus 6.7% MSSA)
Abramson MA, Sexton DJ. Infect Control Hosp Epidemiol. 1999;20:408-411. Engemann JJ et al. Clin Infect Dis. 2003;36:592-598.Rubin RJ et al. Emerg Infect Dis. 1999;5:9-17.

14Please see full prescribing information available in this kit.
Clinical and Economic Outcomes and MRSA SSIs
Data for 479 patients were analyzed to assess the impact of MRSA on outcomes for patients with SSIs
MRSA infected SSI was associated with a >12-fold increase in the 90-day postoperative mortality rate
Patients with MRSA had longer durations of hospitalization
Median Hospital Charges
Engemann JJ et al. Clin Infect Dis. 2003;36:592-598.
20,000
40,000
60,000
80,000
100,000
Ho
sp
ital
Ch
arg
es (
do
llar
s)
0
No Infection MSSA MRSA
P<.001
P<.001
P<.001
15Please see full prescribing information available in this kit.
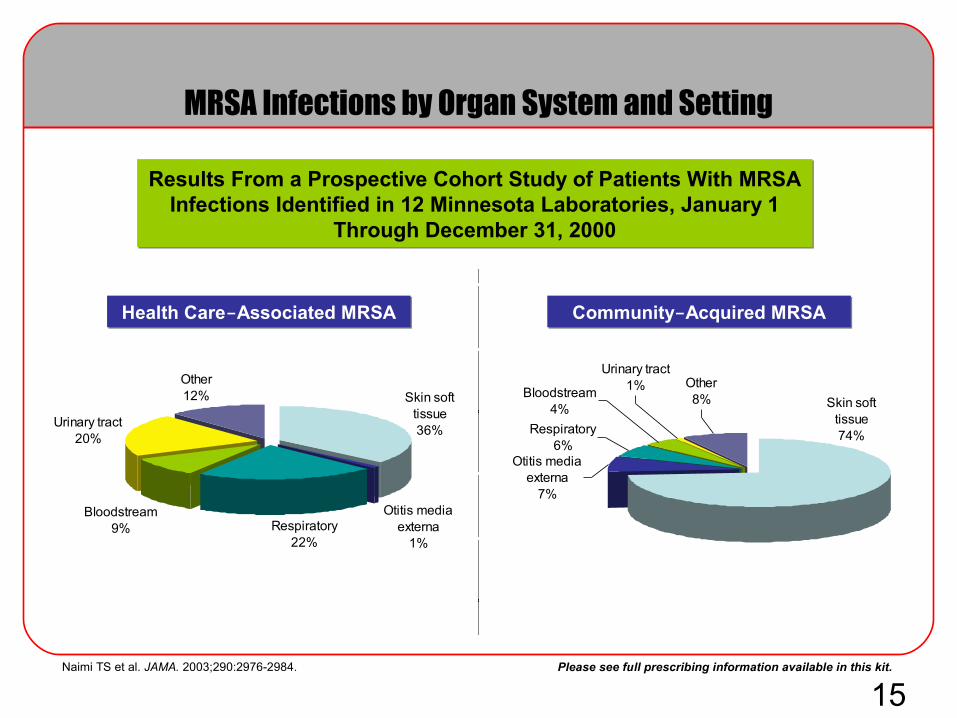
MRSA Infections by Organ System and Setting
Results From a Prospective Cohort Study of Patients With MRSA Infections Identified in 12 Minnesota Laboratories, January 1
Through December 31, 2000
Results From a Prospective Cohort Study of Patients With MRSA Infections Identified in 12 Minnesota Laboratories, January 1
Through December 31, 2000
Health CareAssociated MRSAHealth CareAssociated MRSA CommunityAcquired MRSACommunityAcquired MRSA
Skin soft tissue74%
Other8%Bloodstream
4%
Urinary tract1%
Respiratory6%
Otitis media externa
7%
Skin soft tissue36%
Other12%
Bloodstream9%
Urinary tract20%
Respiratory22%
Otitis media externa
1%
Naimi TS et al. JAMA. 2003;290:2976-2984.

16Please see full prescribing information available in this kit.
Nonsurgical superficial infections– Cellulitis– Impetiginous lesions
Uncomplicated
Classification of SSSIs: Uncomplicated
Cellulitis
Impetigo
FDA. Available at: http://www.fda.gov/cder/guidance/2566dft.pdf. Accessed June 14, 2005.Health-related pictures and definitions. Available at: http://health-pictures.com/cellulitis-pictures.htm. Accessed August 19, 2005.DermNet NZ. Available at: http://dermnetnz.org/bacterial/impetigo.html. Accessed August 19, 2005.

17Please see full prescribing information available in this kit.
Uncomplicated
Classification of SSSIs: Uncomplicated
Nonsurgical superficial infections– Cellulitis– Impetiginous lesions
Surgical superficial infections– Furuncles– Simple abscesses
Treatment usually requires antibiotics and/or simple incision and drainage
Furuncles
Simple AbscessesFDA. Available at: http://www.fda.gov/cder/guidance/2566dft.pdf. Accessed June 14, 2005.OneSkin.com. Available at: http://dermatology.netfirms.com/SkinA2Z/F/Furuncles.html. Accessed August 19, 2005.Otolaryngolgy Houston. Available at: http://ghorayeb.com/NECKABSCESS.html. Accessed June 14, 2005.

18Please see full prescribing information available in this kit.
Classification of SSSIs: Complicated
Complicated
Deep soft tissue infections
Infected ulcers
Infected burns
Major abscesses
May require extensive surgical debridement and reconstruction
Significant underlying disease state, which complicates response to treatment
Infected Burns
Infected Ulcer
FDA. Available at: http://www.fda.gov/cder/guidance/2566dft.pdf. Accessed June 14, 2005.Burn Surgery. Available at: http://burnsurgery.com/modules/burnwound%201/index.htm. Accessed August 3, 2005.AFIDS. Available at: http://afids.org/case8a.htm. Accessed August 3, 2005.
19Please see full prescribing information available in this kit.
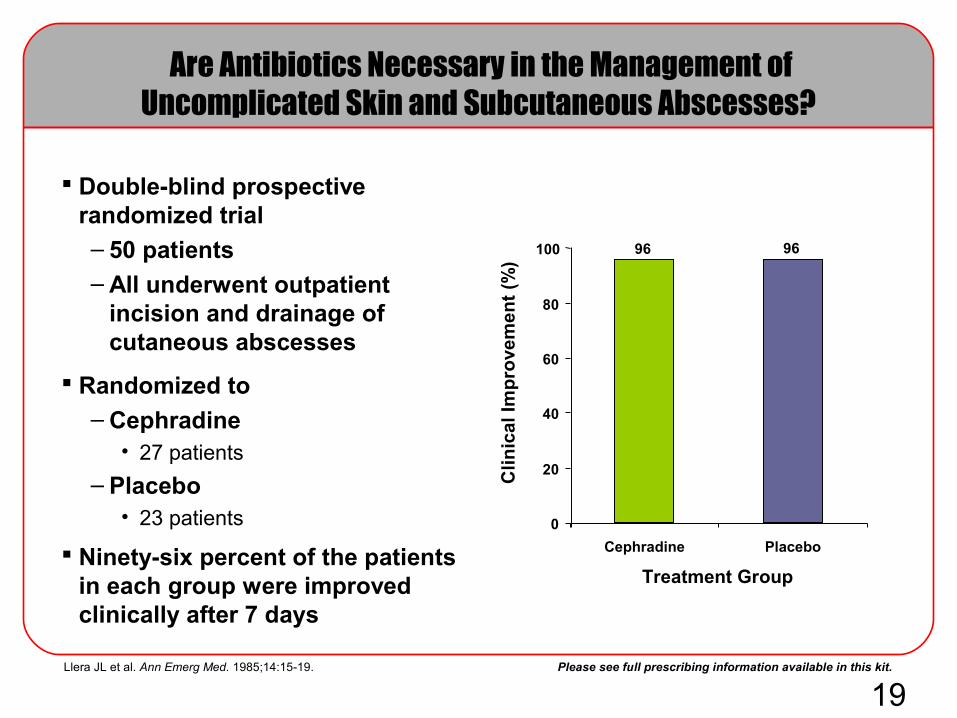
Are Antibiotics Necessary in the Management of Uncomplicated Skin and Subcutaneous Abscesses?
Double-blind prospective randomized trial
– 50 patients– All underwent outpatient
incision and drainage of cutaneous abscesses
Randomized to– Cephradine
• 27 patients
– Placebo• 23 patients
Ninety-six percent of the patients in each group were improved clinically after 7 days
Llera JL et al. Ann Emerg Med. 1985;14:15-19.
Cli
nic
al I
mp
rove
men
t (%
)0
20
40
60
80
100
Cephradine Placebo
Treatment Group
96 96
20Please see full prescribing information available in this kit.
Indications for Antibiotics in the Management of SSSI Abscesses
Antibiotics not necessary for majority of patients
– Surgical drainage and wound care is key to effective management
Systemic signs of infection– Fever– Elevated WBC
– Left shift on differential count– Septic shock
Cellulitis or phlegmon
Immunocompromised patient
Certain foreign bodies– ie, Marlex mesh
Baddour LM. Skin abscess. UpToDate® [serial online]. April 6, 2005;13.2.
21Please see full prescribing information available in this kit.
Which Antibiotics Should Be Used in the Management of SSSIs?
Therapy may be geared toward expected pathogens, guided by:
– Specific social history– Pre-existing medical condition– Drug allergies– Antecedent trauma
– Gram-stain of discharge or exudate– Local bacterial resistance patterns of the institution
Fung HB et al. Drugs. 2003;63:1459-1480.
22Please see full prescribing information available in this kit.
DRUG TREATMENT OF UNCOMPLICATED CA-MRSA
Clindamycin
Trimethoprim/sulfamethoxazole
Rifampin

23Please see full prescribing information available in this kit.
Current FDA-Approved Drug Treatmentsfor Health Care- Associated MRSA
Linezolid (IV, PO) Vancomycin (IV)
Linezolid (IV, PO) Vancomycin (IV) Daptomycin (IV) Tigecycline (IV)
cSSSI=complicated skin and skin structure infection.
NPNP cSSSIcSSSI
24Please see full prescribing information available in this kit.
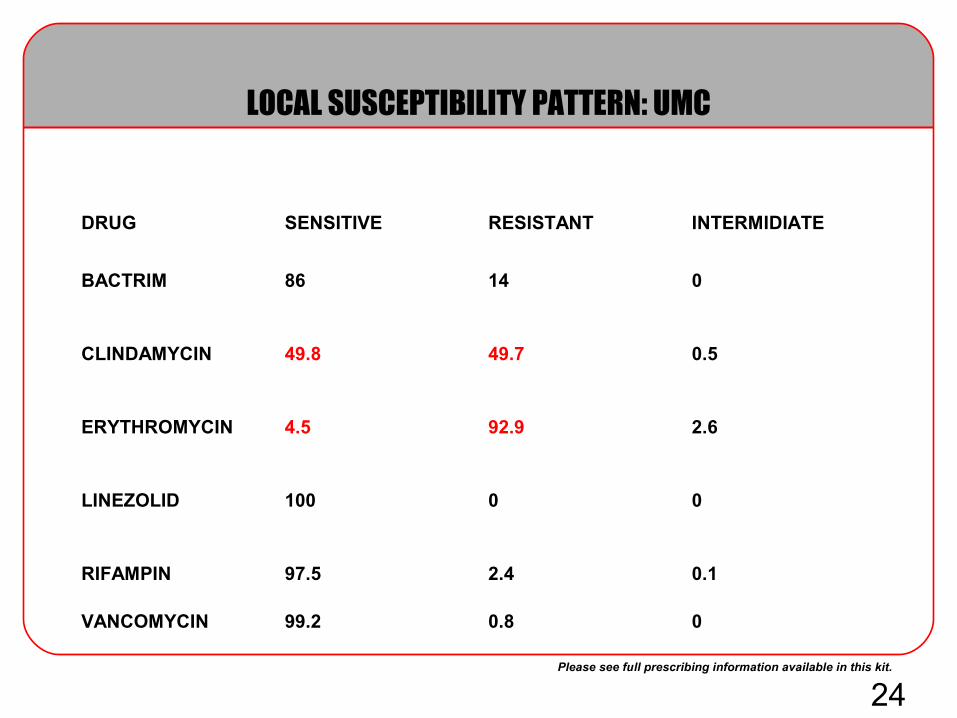
LOCAL SUSCEPTIBILITY PATTERN: UMC
DRUG SENSITIVE RESISTANT INTERMIDIATE
BACTRIM 86 14 0
CLINDAMYCIN 49.8 49.7 0.5
ERYTHROMYCIN 4.5 92.9 2.6
LINEZOLID 100 0 0
RIFAMPIN 97.5 2.4 0.1
VANCOMYCIN 99.2 0.8 0
25Please see full prescribing information available in this kit.
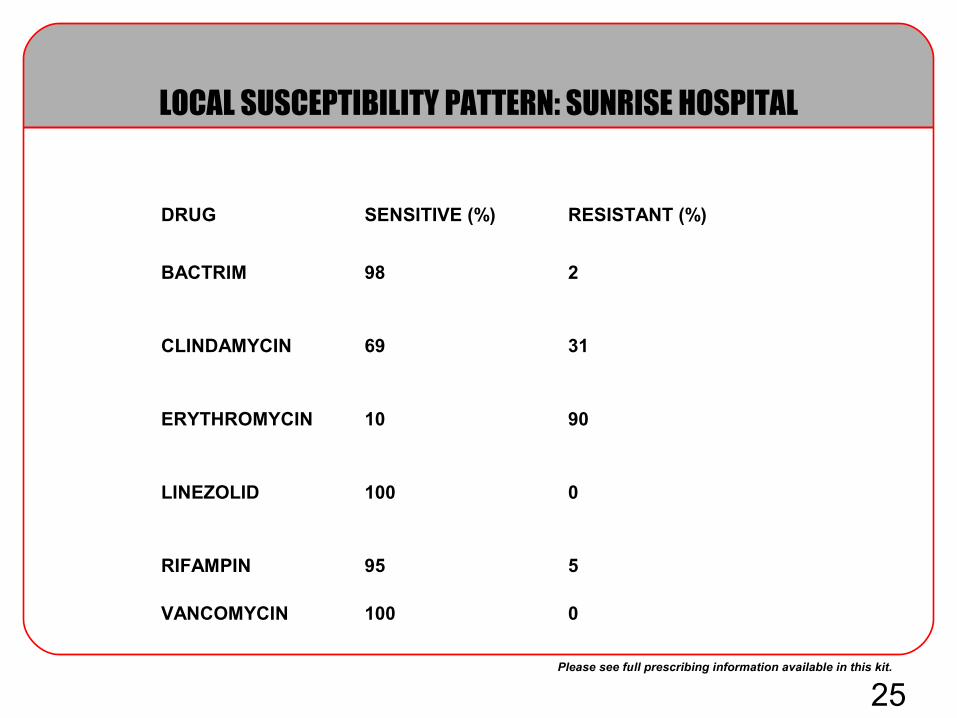
LOCAL SUSCEPTIBILITY PATTERN: SUNRISE HOSPITAL
DRUG SENSITIVE (%) RESISTANT (%)
BACTRIM 98 2
CLINDAMYCIN 69 31
ERYTHROMYCIN 10 90
LINEZOLID 100 0
RIFAMPIN 95 5
VANCOMYCIN 100 0
26Please see full prescribing information available in this kit.
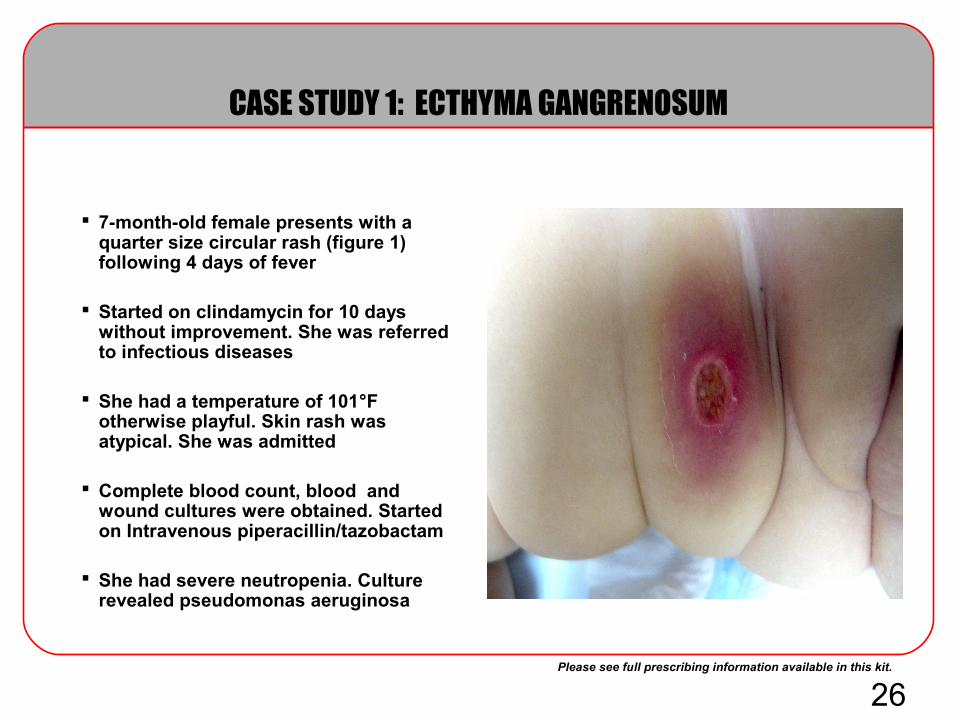
CASE STUDY 1: ECTHYMA GANGRENOSUM
7-month-old female presents with a quarter size circular rash (figure 1) following 4 days of fever
Started on clindamycin for 10 days without improvement. She was referred to infectious diseases
She had a temperature of 101°F otherwise playful. Skin rash was atypical. She was admitted
Complete blood count, blood and wound cultures were obtained. Started on Intravenous piperacillin/tazobactam
She had severe neutropenia. Culture revealed pseudomonas aeruginosa
31Please see full prescribing information available in this kit.Craven DE et al. Infect Dis Clin North Am. 2004;18:939-962.
Singh N et al. Am J Respir Crit Care Med. 2000;162:505-511.Lodise TP et al. Cin Infect Dis. 2003;36:1418-1423.Kollef MH et al. Chest. 1999;115:462-474.
Benefits of Early, Appropriate Therapy
Cumulative evidence from multiple studies has demonstrated that early, appropriate therapy is associated with:
Shorter duration of antibiotic therapy– Short-course therapy is only an option when the right antibiotic is
used from the start
Decreased length of ICU or hospital stay
Lower total cost
Decreased mortality– Appropriate antimicrobial therapy reduces infection-related and
all-cause mortality

32Please see full prescribing information available in this kit.Mangili A et al. Clin Infect Dis. 2005;40:1058-1060.
Meka VG et al. Clin Infect Dis. 2004;39:1010-1015.
Importance of Short-Course Therapy
Short-course therapy lowers the risk of developing resistance and superinfections:– Vancomycin
• Vancomycin failure is associated with small shifts in MIC into the 1 µg/mL to 2 µg/mL range, associated in part with the presence of a polymorphism in the accessory gene regulator locus
• Vancomycin failure can be anticipated for glycopeptide-resistant S aureus strains
– Daptomycin• Daptomycin-resistant MRSA has been reported already
– Linezolid• Cases of linezolid-resistant S aureus have been reported, typically
associated with single nucleotide changes in 23S ribosomal RNA• Linezolid inhibits bacterial protein synthesis through a mechanism of action
different from that of the other antibacterial agents; therefore, cross-resistance between linezolid and other classes of antibiotics is unlikely

33Please see full prescribing information available in this kit.
Controlling MRSA in the Hospital
Rigorous infection control policies– Surveillance of ICU infections to identify and quantify endemic
MDR pathogens – Strict adherence to barrier precautions (gown and glove) for infected or
colonized patients
Hand hygiene– Antiseptic-containing preparation before and after all patient contacts – Monitor compliance
Antibiotic stewardship– Avoid inappropriate or excessive antibiotic prophylaxis or therapy
Craven DE et al. Infect Dis Clin North Am. 2004;18:939-962.
Infection control and prevention in health care settings encompass several nonpharmacologic options, including, but not limited to:
Infection control and prevention in health care settings encompass several nonpharmacologic options, including, but not limited to:
34Please see full prescribing information available in this kit.
Local regulations
A child diagnosed with infected, untreated skin patches, skin rashes, (excluding diaper rash), lasting more than one (1) day or weeping or bleeding skin lesions that have not been treated by a Licensed Medical Practitioner, is not permitted to attend daycare until written documentation from a health care professional is received stating that the child’s condition is not infectious/communicable/contagious.
https://owa.unr.edu/exchweb/bin/redir.asp?URL=http://www.cchd.org/download/environmental_health/child_care_regs82202.pdf
https://owa.unr.edu/exchweb/bin/redir.asp?URL=http://www.cchd.org/download/disease_factsheets/ca-mrsa_patient_facts_05.pdf
35Please see full prescribing information available in this kit.
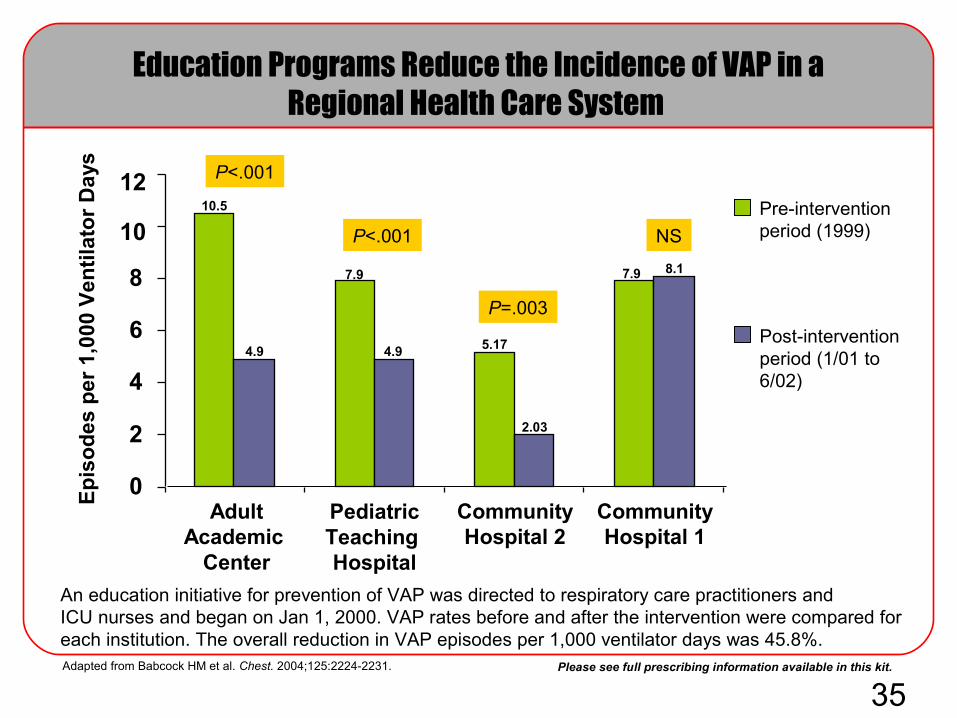
Education Programs Reduce the Incidence of VAP in a Regional Health Care System
Ep
iso
des
per
1,0
00 V
enti
lato
r D
ays
Adapted from Babcock HM et al. Chest. 2004;125:2224-2231.
Pre-intervention period (1999)
Post-intervention period (1/01 to 6/02)
An education initiative for prevention of VAP was directed to respiratory care practitioners andICU nurses and began on Jan 1, 2000. VAP rates before and after the intervention were compared for each institution. The overall reduction in VAP episodes per 1,000 ventilator days was 45.8%.
0
2
4
6
8
10
12
AdultAcademic
Center
CommunityHospital 2
CommunityHospital 1
PediatricTeaching Hospital
P<.001
P=.003
P<.001 NS
4.9
10.5
7.9
4.9 5.17
2.03
8.17.9

37Please see full prescribing information available in this kit.
MRSA SSTI Infection Rates Rising in the ED of a County-Owned Hospital
Prevalence of MRSA SSTI evaluated from August 2001 to March 2004 in a county hospital that services a largely uninsured low-income population with an annual census around 43,000 visits
MRSA was isolated from 44/96 (46%) of enrolled patients with single wound infections
– 8 were treated as out-patients, 36 were admitted
No clinical or epidemiologic features were predictive of MRSA infections
Moran EG et al. Emerg Infect Dis. 2005;11:928-930.
Other pathogens included: 15 MSSA, 19 Streptococcus spp, 4 coagulase-negative staphylococci, 2 diphtheroids, 2 Citrobacter spp, 2 Escherichia coli, 1 Enterococcus
29%(14/49)
Aug 2001 – Dec 2002
64%(30/47)
Jan 2003 – Mar 2004
16 Months
15 Months
The proportion of infections yielding MRSA increased as the study
progressed

Please see full prescribing information available in this kit.
THANK YOU
QUESTIONS AND DISCUSSION?
Related Documents











