doi: 10.2522/ptj.20060006 Originally published online January 1, 2006 2007; 87:32-43. PHYS THER. Rana S Hinman, Sophie E Heywood and Anthony R Day Controlled Trial Osteoarthritis: Results of a Single-Blind Randomized Aquatic Physical Therapy for Hip and Knee http://ptjournal.apta.org/content/87/1/32 found online at: The online version of this article, along with updated information and services, can be Online-Only Material 60006.DC1.html http://ptjournal.apta.org/content/suppl/2007/01/23/ptj.200 Collections Therapeutic Exercise Osteoarthritis Osteoarthritis in the following collection(s): This article, along with others on similar topics, appears e-Letters "Responses" in the online version of this article. "Submit a response" in the right-hand menu under or click on here To submit an e-Letter on this article, click E-mail alerts to receive free e-mail alerts here Sign up by guest on March 29, 2015 http://ptjournal.apta.org/ Downloaded from by guest on March 29, 2015 http://ptjournal.apta.org/ Downloaded from

PHYS_THER-2007-Hinman-32-43.pdf
Dec 21, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

doi: 10.2522/ptj.20060006Originally published online January 1, 2006
2007; 87:32-43.PHYS THER. Rana S Hinman, Sophie E Heywood and Anthony R DayControlled TrialOsteoarthritis: Results of a Single-Blind Randomized Aquatic Physical Therapy for Hip and Knee
http://ptjournal.apta.org/content/87/1/32found online at: The online version of this article, along with updated information and services, can be
Online-Only Material 60006.DC1.html
http://ptjournal.apta.org/content/suppl/2007/01/23/ptj.200
Collections
Therapeutic Exercise Osteoarthritis Osteoarthritis
in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from
Aquatic Physical Therapy forHip and Knee Osteoarthritis:Results of a Single-BlindRandomized Controlled TrialRana S Hinman, Sophie E Heywood, Anthony R Day
Background and PurposeAquatic physical therapy is frequently used in the management of patients with hipand knee osteoarthritis (OA), yet there is little research establishing its efficacy forthis population. The purpose of this study was to evaluate the effects of aquaticphysical therapy on hip or knee OA.
SubjectsA total of 71 volunteers with symptomatic hip OA or knee OA participated in thisstudy.
MethodsThe study was designed as a randomized controlled trial in which participantsrandomly received 6 weeks of aquatic physical therapy or no aquatic physicaltherapy. Outcome measures included pain, physical function, physical activity levels,quality of life, and muscle strength.
ResultsThe intervention resulted in less pain and joint stiffness and greater physical function,quality of life, and hip muscle strength. Totals of 72% and 75% of participantsreported improvements in pain and function, respectively, compared with only 17%(each) of control participants. Benefits were maintained 6 weeks after the comple-tion of physical therapy, with 84% of participants continuing independently.
Discussion and ConclusionCompared with no intervention, a 6-week program of aquatic physical therapyresulted in significantly less pain and improved physical function, strength, andquality of life. It is unclear whether the benefits were attributable to interventioneffects or a placebo response.
RS Hinman, BPhysio(Hons), PhD,is Lecturer, Centre for Health Ex-ercise and Sports Medicine, Uni-versity of Melbourne, Melbourne,Victoria, Australia. Address all cor-respondence to Dr Hinman at:[email protected].
SE Heywood, BPhysio(Hons),MPhysio(Sports), Cert Hydrother-apy, is Senior Aquatic Physiother-apist, Physiotherapy Department,Sunshine Hospital, and Physio-therapist, Melbourne Sports Med-icine Centre, Melbourne, Victoria,Australia.
AR Day, BAppSci(Human Move-ment), BAppSci(Physio), MSportsPhysio, is Principal Physiotherapist,ProCare Physiotherapy, Newport,and Physiotherapist, ISIS PrimaryCare, Altona Meadows, Melbourne,Victoria, Australia.
[Hinman RS, Heywood SE, DayAR. Aquatic physical therapy forhip and knee osteoarthritis: re-sults of a single-blind randomizedcontrolled trial. Phys Ther. 2007;87:32–43.]
© 2007 American Physical TherapyAssociation
Research Report
For The Bottom Line:www.ptjournal.org
32 f Physical Therapy Volume 87 Number 1 January 2007 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

Osteoarthritis (OA) is one ofthe most prevalent musculo-skeletal conditions affecting
the elderly population worldwide,1
and its prevalence is predicted torise significantly in the future as thepopulation ages.2 Knee OA currentlyaffects about 40% of people agedover 75 years, and hip OA affectsabout 10%.3 People with OA fre-quently report joint pain, stiffness,loss of physical function, increasingimmobility, and muscle weakness.Such signs and symptoms of the dis-ease often culminate in reductions inquality of life. Contemporary man-agement of OA aims to alleviate painand disability while avoiding adverseeffects of therapy.4 Current guide-lines recommend nonpharmacologicmethods, such as physical therapy,as first-line options in the manage-ment of OA.5 Physical therapy forOA may be provided on land or in anaquatic environment.
“Hydrotherapy” is a term encom-passing a range of therapeutic andexercise activities carried out inheated pools by a variety of provid-ers. Experts rate hydrotherapy asone of the least toxic of 33 potentialtreatments for knee OA.6 Aquaticphysical therapy incorporates indi-vidual assessment, evidence-basedpractice, and clinical reasoning skillsto devise treatment plans based onthe principles of hydrostatics andhydrodynamics and the physiologiceffects of immersion.7 Aquatic phys-ical therapy offers several benefitsover land-based physical therapy forpeople with OA. Buoyancy reducesloading across joints affected by painand allows the performance of func-tional closed-chain exercises thatotherwise may be too difficult onland. Water turbulence can be usedas a method of increasing resistance,and percentage of body weightborne across the lower limbs can bedecreased or progressed in propor-tion to the depth of immersion.8,9
The warmth and pressure of the
water may further assist with painrelief, swelling reduction, and easeof movement.
Despite the widespread provision ofaquatic physical therapy for peoplewith hip or knee OA, there is littleevidence attesting to its efficacy inthis population. Although many stud-ies have reported positive effects ofhydrotherapy interventions in cohortswith various arthritic conditions,10 fewhave evaluated a sample selected onthe basis of knee or hip OA alone. Arecent study found no significant ben-efit of hydrotherapy over a gym-basedprogram or no intervention for symp-toms in people with hip or knee OA.11
However, the program tested by theauthors made use of nonfunctionalbody positions and had a limitedcapacity for progression, features thatmay explain their nonsignificant find-ings. Methodological limitations inother published studies on OA includeinadequate sample size, nonrandomallocation, and no intention-to-treatanalysis.12–15 Furthermore, most hydro-therapy programs demonstrate littleconsideration of hydrostatic or hydro-dynamic principles in their choice ofexercises, thus reducing the potentialfor benefit from the overall program.The present study was designed to ad-dress the limitations of previous stud-ies through the use of an adequatelypowered randomized controlled trialwith intention-to-treat analysis and afunctional progressive intervention thatmaximized the unique properties ofwater to optimize outcomes.
The aim of this study was to test theefficacy of a 6-week aquatic physicaltherapy program in a group of peo-ple with symptomatic hip OA, kneeOA, or both. The primary hypothesiswas that aquatic physical therapywould result in greater improve-ments in pain and physical functionthan would no aquatic physical ther-apy. The secondary hypothesis wasthat aquatic physical therapy wouldresult in greater improvements in
stiffness, quality of life, physical activ-ity, and muscle strength. Finally, weaimed to determine whether partici-pants were adherent to ongoing in-dependent aquatic physical therapyonce the program had ceased andwhether any benefits of the programremained 6 weeks later.
MethodParticipantsDiagnosis was based on AmericanCollege of Rheumatology classifica-tion criteria.16,17 Volunteers aged 50years and older and with hip OA orknee OA were recruited by adver-tisements in local clubs, libraries,general practitioner’s rooms, printand radio media, and the orthopedicclinic at a metropolitan hospital. Par-ticipants with knee OA wereincluded if they had knee pain onmost days of the previous month andosteophytes on radiographs. Partici-pants with hip OA were included ifthey had hip pain and osteophytesand joint space narrowing on radio-graphs. Other inclusion criteria forall participants were an averageseverity of pain of greater than 3 cmon a 10-cm visual analog scale (VAS)and difficulty with stair climbing,walking, or getting in or out of achair. Exclusion criteria includedcontraindications to aquatic physicaltherapy7; significant back or otherjoint pain; recent (preceding 6months) joint injections, surgery,physical therapy, or hydrotherapy;lower-limb joint replacement; inabil-ity to understand English; and inabil-ity to safely enter and exit the pool.
Between October 2003 and April2004, 312 volunteers were screened.Of these volunteers, 71 fulfilled theselection criteria and were enrolledin the study. Thirty-six participantswere randomly assigned to anaquatic physical therapy group(intervention group), and 35 partici-pants were randomly assigned to acontrol group. One aquatic physicaltherapy participant withdrew after
Aquatic Physical Therapy for Hip and Knee OA
January 2007 Volume 87 Number 1 Physical Therapy f 33 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

randomization, did not undergo theintervention as allocated, and did notreturn for reassessment. Four con-trol participants withdrew prior toreassessment; however, 2 of themcompleted reassessment question-naires only. All participants providedwritten informed consent.
ProtocolThe trial comprised a 6-week inter-vention period (Fig. 1). Participantswere assessed immediately beforetreatment (0 weeks) and immedi-ately after treatment was completed(6 weeks). Furthermore, the aquaticphysical therapy group underwentfollow-up assessment at 12 weeks(ie, 6 weeks after the interventionwas completed) to determinewhether any benefits of the interven-tion were maintained in the shortterm and to assess adherence toindependent aquatic physical ther-apy. Every effort was made to obtainreassessment data on primary out-comes from any participant whowithdrew from the study.
AssignmentFollowing the baseline assessment,participants were randomly assignedto either the aquatic physical ther-apy group or the control group. Blockrandomization (randomly alternatingblocks of 4 and 6) stratified for sexwas set up with a computer-generatedtable of random numbers. Assignmentwas concealed in sequential opaqueenvelopes and was revealed by anindependent researcher not involvedin eligibility assessment, outcome as-sessment, or intervention followingthe baseline assessment.
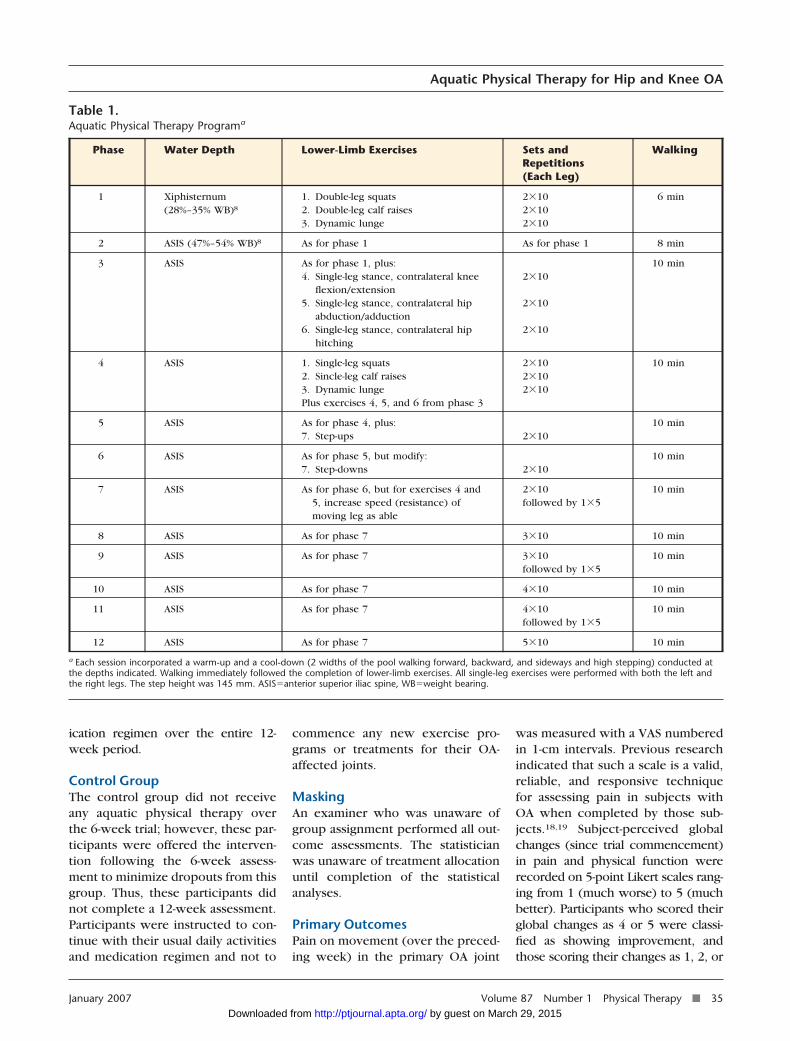
Aquatic Physical TherapyInterventionThe aquatic physical therapy pro-gram comprised functional weight-bearing and progressive exercises(Tab. 1) provided twice weekly(45–60 minutes each) for 6 weeks.An experienced aquatic physicaltherapist individually instructed par-
ticipants in the hydrotherapy pool(water temperature�34°C), with amaximum of 6 participants per ses-sion. Quality of movement was em-phasized, and the therapist palpatedthe lower-limb musculature to en-sure appropriate contraction through-out the exercises. Balance withoutthe aid of rails to maximize posturaland isometric leg stance control wasachieved with all participants. A neu-tral spinal position also was taught;feedback was provided on posture,transversus abdominis muscle contrac-tion, and trunk control. Individual pro-gression to subsequent phases of theprogram was clinically determined bythe therapist and occurred upon com-pletion of the prior phase with either
no or minimal symptom exacerbation.Attendance at intervention sessionsand adverse effects of the interventionwere recorded by the aquatic physicaltherapist.
Upon completion of the 6-week pro-gram, participants were encouragedto continue independent aquatic phys-ical therapy twice weekly at a localpool and were provided with detailsof local pools and a written descrip-tion of the exercises to maximize ad-herence. During the follow-up period,between week 6 and week 12, partic-ipants recorded in a logbook the ses-sions of independent aquatic physicaltherapy that they undertook. Partici-pants continued with their usual med-
Figure 1.Flow of participants through the trial.
Aquatic Physical Therapy for Hip and Knee OA
34 f Physical Therapy Volume 87 Number 1 January 2007 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from
ication regimen over the entire 12-week period.
Control GroupThe control group did not receiveany aquatic physical therapy overthe 6-week trial; however, these par-ticipants were offered the interven-tion following the 6-week assess-ment to minimize dropouts from thisgroup. Thus, these participants didnot complete a 12-week assessment.Participants were instructed to con-tinue with their usual daily activitiesand medication regimen and not to
commence any new exercise pro-grams or treatments for their OA-affected joints.
MaskingAn examiner who was unaware ofgroup assignment performed all out-come assessments. The statisticianwas unaware of treatment allocationuntil completion of the statisticalanalyses.
Primary OutcomesPain on movement (over the preced-ing week) in the primary OA joint
was measured with a VAS numberedin 1-cm intervals. Previous researchindicated that such a scale is a valid,reliable, and responsive techniquefor assessing pain in subjects withOA when completed by those sub-jects.18,19 Subject-perceived globalchanges (since trial commencement)in pain and physical function wererecorded on 5-point Likert scales rang-ing from 1 (much worse) to 5 (muchbetter). Participants who scored theirglobal changes as 4 or 5 were classi-fied as showing improvement, andthose scoring their changes as 1, 2, or
Table 1.Aquatic Physical Therapy Programa
Phase Water Depth Lower-Limb Exercises Sets andRepetitions(Each Leg)
Walking
1 Xiphisternum(28%–35% WB)8
1. Double-leg squats2. Double-leg calf raises3. Dynamic lunge
2�102�102�10
6 min
2 ASIS (47%–54% WB)8 As for phase 1 As for phase 1 8 min
3 ASIS As for phase 1, plus:4. Single-leg stance, contralateral knee
flexion/extension5. Single-leg stance, contralateral hip
abduction/adduction6. Single-leg stance, contralateral hip
hitching
2�10
2�10
2�10
10 min
4 ASIS 1. Single-leg squats2. Sincle-leg calf raises3. Dynamic lungePlus exercises 4, 5, and 6 from phase 3
2�102�102�10
10 min
5 ASIS As for phase 4, plus:7. Step-ups 2�10
10 min
6 ASIS As for phase 5, but modify:7. Step-downs 2�10
10 min
7 ASIS As for phase 6, but for exercises 4 and5, increase speed (resistance) ofmoving leg as able
2�10followed by 1�5
10 min
8 ASIS As for phase 7 3�10 10 min
9 ASIS As for phase 7 3�10followed by 1�5
10 min
10 ASIS As for phase 7 4�10 10 min
11 ASIS As for phase 7 4�10followed by 1�5
10 min
12 ASIS As for phase 7 5�10 10 min
a Each session incorporated a warm-up and a cool-down (2 widths of the pool walking forward, backward, and sideways and high stepping) conducted atthe depths indicated. Walking immediately followed the completion of lower-limb exercises. All single-leg exercises were performed with both the left andthe right legs. The step height was 145 mm. ASIS�anterior superior iliac spine, WB�weight bearing.
Aquatic Physical Therapy for Hip and Knee OA
January 2007 Volume 87 Number 1 Physical Therapy f 35 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

3 were classified as not showingimprovement.
Secondary OutcomesQuestionnaires. The 24-item disease-specific Western Ontario and McMas-ter Universities Osteoarthritis Index(WOMAC) was used to assess pain,stiffness, and physical function in theprimary OA joint over the previous48 hours. This measure has been vali-dated with respect to reliability, facevalidity, content validity, constructvalidity, and responsiveness for peo-ple with OA of the hip or knee.20
Health-related quality of life over theprevious week was assessed with the15-item Assessment of Quality of Lifescale.21 This scale has been validatedfor use in the general population.Physical activity levels over the previ-ous week were assessed with thePhysical Activity Scale for the Elderly(PASE) (with supervised aquatic phys-ical therapy sessions excluded fromthe analyses to accurately measureindependent activity). The PASE dem-onstrated good test-retest reliability,convergent validity, and construct va-lidity in older adults with knee pain.22
Musclestrength. Isometrichipab-duction and knee extension strength(force-generating capacity) was as-sessed bilaterally with a Nicholas Man-ual Muscle Tester (model 01160)*according to the protocol of Bohan-non.23 The hip abductors were chosenbecause some data have suggestedthat stronger hip abductors may assistin reducing the knee adduction mo-ment.24 The quadriceps femoris mus-cles were assessed because knee ex-tensor strength has been correlatedwith both pain severity and physi-cal function in knee OA.25–27 Thepeak strength of each muscle groupwas assessed 3 times, and the high-est score was recorded (in kilograms).Handheld dynamometry demon-
strated adequate test-retest reliabilityfor the muscles of the lower limbs ina community-dwelling group ofolder people (intraclass correlationcoefficients [ICCs]�.95–1.00).28
Balance. Dynamic standing bal-ance was assessed with the step test,a reliable and valid measure in olderpeople (ICC�.9)29 that is sensitiveenough to discriminate betweenthose with knee OA and those with-out knee OA.30 Participants stoodbarefoot on the osteoarthritic limb infront of a 7.5-cm step and wereinstructed to move the opposite footon and off the step as many times aspossible over 15 seconds. This testdoes not require the participant tomove body weight over the step butsimply to perform a potentiallydestabilizing foot placement activity.The number of times the participantcould place the foot on the step andreturn it to the floor was recorded,with higher scores indicating betterbalance.
Physical function. The Timed“Up & Go” Test was used to assessfunctional ability.31 This test demon-strated good intratester and inter-tester reliability (ICC�.99) for a geri-atric population as well as criterionvalidity. Participants were instructedto rise from a standard armchair,walk to a point on the floor 3 maway, return to the chair, and sitdown again while being timed with astopwatch. Participants performedthe test only once and at their ownpace.
Gait. The Six-Minute Walk Testwas used to evaluate how far partic-ipants could walk at a fast, comfort-able pace. This test was validated asa measure of physical function inpeople with heart failure and respi-ratory disease.32 Participants walkedback and forth over a 50-m stretch ofcarpeted corridor for 6 minutes, andthe total distance walked wasrecorded (in meters).
Sample SizeA pain reduction of 1.75 cm on aVAS is recommended as the mini-mum clinically important differenceto be detected in OA trials.33 With58 participants, the study had 90%power to detect a difference in painreduction of 1.75 cm between groups,assuming a standard deviation of 2.0cm and a significance level of 5%.Numbers were increased to 71 par-ticipants to allow for dropouts.
Data AnalysesData analyses were performed withSPSS software† and an alpha level of.05 on an intention-to-treat basis. Thelast observation carried forward wasused to impute data missing at reas-sessment; a score of 3 (“unchanged”)was allocated for missing globalchange measures. Data were checkedfor normality and homogeneity ofvariance prior to analyses. Baselinecomparability between groups wasdetermined with independent t tests(because most data were normally dis-tributed) or chi-square tests. Meanscores at 6 weeks were comparedbetween groups by use of univariateanalysis of variance; baseline scoreswere included as covariates to controlfor any group differences at baseline.Effect sizes were calculated; effectsizes of .2 were regarded as small,those of .5 were regarded as medium,and those of .8 were regarded as large.A comparison of the numbers of par-ticipants showing improvement be-tween groups was made with chi-square tests, and odds ratios (OR)(with 95% confidence intervals [CI])were calculated. Outcomes at 6 and12 weeks in the intervention groupwere compared by use of paired ttests.
ResultsGroups were found not to be signif-icantly different at baseline withregard to demographic characteris-
* Lafayette Instrument Co, 3700 SagamorePkwy North, PO Box 5729, Lafayette, IN47903.
† SPSS Inc, 233 S Wacker Dr, Chicago, IL60606.
Aquatic Physical Therapy for Hip and Knee OA
36 f Physical Therapy Volume 87 Number 1 January 2007 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

tics or outcome measures (Tab. 2),with the exception of quality of life,which was significantly poorer inthe aquatic physical therapy partici-pants (P �.01).
Primary OutcomesAquatic physical therapy partici-pants reported a mean reduction in
pain on movement of 33% from base-line and thus demonstrated signifi-cantly less pain at 6 weeks than con-trol participants (P �.01) (Tab. 3).This finding represented a smalleffect size (.24) for this outcome.Seventy-two percent (26 of 36) ofthe intervention participants re-ported a global improvement in
pain; only 17% (6 of 35) of the con-trol participants did so (P �.001)(Fig. 2). Similarly, 75% (27 of 36)of the intervention participants re-ported a global improvement inphysical function; only 17% (6 of 31)of the control participants did so(P �.001) (Fig. 2). Aquatic physicaltherapy participants were more than
Table 2.Baseline Comparability of Participant Groupsa
Parameter Control Group (n�35) Aquatic PhysicalTherapy Group (n�36)
Age, y 61.5 (7.8) 63.3 (9.5)
Height, m 1.61 (0.01) 1.63 (0.09)
Weight, kg 85 (17) 88 (15)
Body mass index, kg/m2 32.9 (6.6) 33.8 (6.5)
Symptom duration, y 8.0 (10.6) 8.0 (9.3)
Sex, no. (%) 24 (69) female, 11 (31) male 24 (67) female, 12 (33) male
Symptomatic joint, no. (%) 24 (69) knee, 11 (31) hip 31 (86) knee, 5 (14) hip
Medications, no. (%) 16 (46) analgesics,14 (40) NSAIDs,14 (40) nutraceuticalsb
20 (56) analgesics,18 (50) NSAIDs,14 (39) nutraceuticals
Primary outcomes
VAS movement pain, 0–10 cm 5 (2) 6 (2)
Secondary outcomes
WOMAC pain, 0–500 mm 199 (85) 202 (79)
WOMAC stiffness, 0–200 mm 100 (46) 99 (46)
WOMAC function, 0–1,700 mm 630 (315) 757 (327)
AQoL, �0.04 to 1.00 0.52 (0.20) 0.38 (0.17)c
PASE, 0–400 153 (79) 165 (80)
Hip abductor strength, kg
Right 21.0 (7.2) 20.3 (8.2)
Left 22.3 (8.3) 20.6 (8.4)
Quadriceps femoris muscle strength, kg
Right 24.5 (8.2) 26.6 (9.1)
Left 24.3 (8.3) 23.2 (9.3)
Timed “Up & Go” Test, s 10.38 (2.82) 11.26 (2.37)
Six-Minute Walk Test, m 448.09 (82.88) 420.56 (91.10)
Step test, no. of steps 13 (4) 13 (4)
a Data are presented as mean (SD) unless otherwise indicated. AQoL�Assessment of Quality of Life (with higher scores indicating better quality of life),NSAIDs�nonsteroidal anti-inflammatory drugs, PASE�Physical Activity Scale for the Elderly (with higher scores indicating greater physical activity),VAS�visual analog scale (with higher scores indicating more pain), WOMAC�Western Ontario and McMaster Universities Osteoarthritis Index (with higherscores indicating worse pain, stiffness, or physical function).b Nutraceutical can be defined as a food (or part of a food) that provides medical or health benefits, including the prevention or treatment of a disease;typically glucosamine in this population.c Significantly different from value for control group (P �.01).
Aquatic Physical Therapy for Hip and Knee OA
January 2007 Volume 87 Number 1 Physical Therapy f 37 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

12 times as likely as control partici-pants to report global improvementsin pain (OR�12.6, 95% CI�4.0–39.4), corresponding to a numberneeded to treat of 2 (95% CI�1–3),and physical function (OR�12.5,95% CI�3.9–40.2), correspondingto a number needed to treat of 2(95% CI�1–3).
Secondary OutcomesThe aquatic physical therapy partic-ipants reported significantly lesspain and significantly superior phys-ical function on many secondary out-comes (Tab. 3). Hip muscle strengthand quality of life also were signifi-cantly greater in this group than inthe control group at 6 weeks. Out-comes that were not significantly dif-ferent following the interventionwere quadriceps femoris muscle
Figure 2.Global improvement in pain and physical function at 6 weeks across groups.
Table 3.Outcome Scores at 6 Weeks Across Groupsa
Outcome X (SD) P EffectSize
Control Group(n�35)
Aquatic PhysicalTherapy Group(n�36)
Primary
VAS movement pain, 0–10 cm 5 (2) 4 (2) .003 .24
Secondary
WOMAC pain, 0–500 mm 198 (108) 143 (79) �.001 .28
WOMAC stiffness, 0–200 mm 95 (44) 73 (45) .007 .24
WOMAC function, 0–1,700 mm 656 (373) 598 (316) �.001 .08
AQoL, �0.04 to 1.00 0.50 (0.20) 0.43 (0.20) .018 .17
PASE, 0–400 142 (77) 165 (70) .351 .15
Hip abductor strength, kg
Right 20.3 (6.8) 22.7 (8.3) .012 .16
Left 21.0 (8.0) 22.2 (8.5) .011 .07
Quadriceps femoris muscle strength, kg
Right 24.7 (9.5) 29.9 (12.5) .059 .23
Left 24.9 (10.3) 25.7 (10.6) .193 .04
Timed “Up & Go” Test, s 10.30 (2.78) 10.32 (1.94) .053 .00
Six-Minute Walk Test, m 440.38 (79.03) 441.72 (87.25) .001 .01
Step test, no. of steps 14 (4) 13 (3) .998 .14
a AQoL�Assessment of Quality of Life (with higher scores indicating better quality of life), PASE�Physical Activity Scale for the Elderly (with higher scoresindicating greater physical activity), VAS�visual analog scale (with higher scores indicating more pain), WOMAC�Western Ontario and McMasterUniversities Osteoarthritis Index (with higher scores indicating worse pain, stiffness, or physical function).
Aquatic Physical Therapy for Hip and Knee OA
38 f Physical Therapy Volume 87 Number 1 January 2007 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

strength, the step test, the Timed“Up & Go” Test, and the PASE. Effectsizes for secondary outcomes weresmall at best.
Attendance and Adverse EffectsOnly 2 participants failed to attendall 12 aquatic physical therapy ses-sions (excluding the participant whowithdrew before attending any ses-sions); 1 of these 2 participantsattended 10 sessions (83%), and theother participant attended 11 ses-sions (92%). Adverse effects wereminor and did not affect ongoingparticipation. Seventeen (49%) par-ticipants reported mild joint discom-fort, 3 (9%) reported mild lumbarpain, and 2 (6%) reported cramps inthe calf or foot. Upon completion ofthe program, 11 participants (31%)had reached phase 12, and 1 (3%), 1(3%), 1 (3%), 2 (5%), 10 (29%), and 9
(26%) had reached phases 6, 7, 8, 9,10, and 11, respectively.
Ongoing Participation andOutcome at Follow-up in theAquatic Physical Therapy GroupAt follow-up, 84% of participants (28of 33) had continued to undertakeaquatic physical therapy indepen-dently since ceasing the supervisedprogram. Over the 6-week follow-upperiod, 24% (8 of 33) attended thelocal pool less than once per weekon average, 45% (15 of 33) attended1 or 2 times per week, and 15% (5 of33) attended 2 or 3 times per week;only 16% (5 of 33) failed to attend atall. Follow-up scores at 12 weeks forthe aquatic physical therapy groupwere generally unchanged fromscores obtained at 6 weeks (Tab. 4),suggesting that the benefits of the
program were maintained in theshort term.
DiscussionThis randomized controlled trialevaluated the efficacy of aquaticphysical therapy for hip OA andknee OA. Our findings demonstratedthat a 6-week, twice-weekly pro-gram leads to reduced pain and jointstiffness as well as improved physi-cal function, hip muscle strength,and quality of life in people withOA. Furthermore, the benefits ofaquatic physical therapy appear toremain 6 weeks after the cessationof the supervised program. Despitestatistically significant differencesbetween groups, effect size calcula-tions revealed only small benefits ofaquatic physical therapy for pain,stiffness, right hip abductor strength,and quality of life and doubtful clin-
Table 4.Outcome Scores at Follow-up (12 Weeks) in the Aquatic Physical Therapy Group (n�36)a
Outcome 6 wk 12 wk P
Primary
VAS movement pain, 0–10 cm 4 (2) 4 (2) .45
Secondary
WOMAC pain, 0–500 mm 143 (79) 132 (89) .23
WOMAC stiffness, 0–200 mm 73 (45) 65 (46) .05
WOMAC function, 0–1,700 mm 598 (316) 556 (341) .08
AQoL, �0.04 to 1.00 0.43 (0.20) 0.45 (0.22) .31
PASE, 0–400b 140 (104) 160 (150) .63
Hip abductor strength, kg
Right 22.7 (8.3) 23.4 (10.7) .44
Left 22.2 (8.5) 21.8 (8.8) .46
Quadriceps femoris muscle strength, kg
Right 29.9 (12.5) 29.2 (11.7) .47
Left 25.7 (10.6) 24.5 (9.4) .21
Timed “Up & Go” Test, s 10.32 (1.94) 9.98 (1.93) .03
Six-Minute Walk Test, m 441.72 (87.25) 447.39 (89.07) .18
Step test, no. of steps 13 (3) 14 (4) .03
a Data are presented as mean (SD) unless otherwise indicated. AQoL�Assessment of Quality of Life (with higher scores indicating better quality of life),PASE�Physical Activity Scale for the Elderly (with higher scores indicating greater physical activity), VAS�visual analog scale (with higher scores indicatingmore pain), WOMAC�Western Ontario and McMaster Universities Osteoarthritis Index (with higher scores indicating worse pain, stiffness, or physicalfunction).b Data are presented as median (interquartile range) and were analyzed with the Wilcoxon signed rank test.
Aquatic Physical Therapy for Hip and Knee OA
January 2007 Volume 87 Number 1 Physical Therapy f 39 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

ical benefits for physical functionand left hip abductor strength.
Few randomized controlled trials haveevaluated hydrotherapy interventionsin a sample selected on the basis of hipor knee OA alone.11,12,14,15 Our find-ings of reduced pain and improvedfunction with aquatic physical therapyconcur with the findings of others.14,15
However, the most rigorously de-signed randomized controlled trialpublished to date found no significantchange in WOMAC scores (pain, stiff-ness, or function) with hydrotherapycompared with a gym-based strength-ening program or no intervention in105 participants with clinical hip orknee OA.11 Nevertheless, hydrother-apy did result in improved walkingdistance and left quadriceps femorismuscle strength compared with nointervention.
In contrast to the program of Foleyet al,11 our aquatic physical therapyprogram primarily focused on exer-cises in functional positions, wasprogressed by increasing resistance(weight bearing or turbulence), andincorporated a walking component,features that may explain our find-ings of significant improvements inpain and most self-reported andobserved physical function mea-sures. Differences in study partici-pants also may account for theconflicting findings. Participants inour study were younger, were morefrequently female, and predomi-nantly had knee OA. Importantly,our volunteers were recruited pri-marily from the community ratherthan from an orthopedic surgerywaiting list (44% of participants inthe study of Foley et al11), suggest-ing that aquatic physical therapymay be more effective for lesssevere OA rather than end-stagedisease.
Several reasons may account for theimprovements in pain observed inthe aquatic physical therapy group.
Quadriceps femoris muscle strengthis associated with knee pain severityin knee OA,25,27 although whethermuscle weakness causes knee painor vice versa is unclear at present.Recent work demonstrated an associ-ation between hip abductor strengthand the knee adduction moment. Ithas been postulated that stronger hipabductors help to stabilize the con-tralateral pelvis during walking and,by virtue of the effect on the body’scenter of mass, can reduce the adduc-tion moment (or compressive force)at the knee.24 Thus, it is possible thatimprovements in hip and knee musclestrength were partially responsible forthe improvements in knee pain ob-served in the present study.
Although changes were not statisti-cally significant, aquatic physicaltherapy did demonstrate a smalleffect size (.23) for right quadricepsfemoris muscle strength and a smallbut statistically significant effect forthe right hip abductors. Conversely,it is also possible that reductions inknee pain were responsible for thesmall strength gains evident in thepresent study with aquatic physicaltherapy. It is difficult to identify themechanism underlying the observedimprovements in strength, but im-proved recruitment of motor units,muscle hypertrophy, pain allevia-tion, or reduced knee joint swellingare all possibilities.
A placebo effect of aquatic physicaltherapy cannot be ruled out becauseof the lack of a placebo control inthe present study. Placebo effectsare common in knee OA; reportedimprovements with sham interven-tion range from 16% to 40%.34–37
However, a meta-analysis of placebo-controlled clinical trials38 demon-strated that placebos have the great-est effect on continuous subjectiveoutcomes and in the treatment ofpain, with no significant effect onobjective measures. Given that ourstudy demonstrated beneficial ef-
fects of aquatic physical therapy onobserved objective measures (hipmuscle strength and 6-minute walk),it is unlikely that our findings areattributable to a placebo responsealone and likely that they may beattributed, at least partially, to theintervention itself.
Joint stiffness was reduced withaquatic physical therapy, and thisresult may be at least partially attrib-utable to the warm-water environ-ment of the hydrotherapy pool.Warm water may encourage musclerelaxation, thus reducing guardingaround joints and enhancing move-ment. It is also possible that painrelief was achieved by the tempera-ture and pressure of the water on theskin.39 Although it is possible thatsome benefits of aquatic physicaltherapy may be attributable to warm-water immersion alone, a previousrandomized controlled trial in rheu-matoid arthritis demonstrated supe-rior effects of hydrotherapy overseated immersion alone.40 Perhapsthe most important aspect of theaquatic environment is the buoyancyof the water, rather than its warmth,which reduces the weight-bearingstresses on the lower limbs and thuspromotes more pain-free and effectiveexercise of the muscles and joints thanwould otherwise be possible.
To our knowledge, this is the firststudy of aquatic physical therapythat has encouraged ongoing inde-pendent aquatic therapy followingcessation of the supervised programand incorporated a follow-up period.As part of the intervention, our par-ticipants were instructed in the ben-efits of ongoing therapy and exerciseself-management principles, providedwith detailed written instructions onhow to perform aquatic physical ther-apy exercises independently as wellas how to modify or progress theirprogram according to symptoms, andgiven written directions on conve-nient local pools in which to exercise.
Aquatic Physical Therapy for Hip and Knee OA
40 f Physical Therapy Volume 87 Number 1 January 2007 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

Although ongoing adherence amongparticipants was variable, 60% con-tinued aquatic physical therapy inde-pendently at least once per week onaverage. It was not possible to monitorcontrol participants at 12 weeks inthe present study, as most of the con-trol group had commenced aquaticphysical therapy by this stage. How-ever, follow-up (without a controlgroup) of the aquatic physical therapygroup at this time appeared to demon-strate that benefits at 6 weeks weremaintained.
Like that of land-based exercise pro-grams, the success of water-basedexercise programs is probably par-tially dependent on adherence to theprescribed exercises. Given the al-most perfect attendance demon-strated by our participants duringthe intervention period, it was notpossible to evaluate the relationshipbetween adherence and outcome. Inthis trial, it is likely that adherencewas enhanced by virtue of the closemonitoring associated with partici-pation in a research study, and suchextremely high levels of adherenceshould not be expected in the clini-cal setting. Thus, strategies to maxi-mize adherence are essential for suc-cess in clinical practice.
Setting specific exercise-related goalsthat are relatively easy to achieve hasbeen shown to increase aquatic exer-cise adherence in people with arthri-tis.41 In addition, as people improve intheir ability to exercise in the aquaticenvironment, adherence to exerciseincreases. Strategies that may promoteself-efficacy include beginning slowlywith exercises that are easily accom-plished, progressing exercise pro-grams slowly, and providing frequentencouragement.42 Our program wasdesigned to educate participantsabout the appropriate progression ofaquatic exercises, thus optimizing theability of people to adjust resistanceand advance the program themselvesor modify it according to symptoms.
Adverse effects associated with ouraquatic physical therapy interven-tion were minor and transient, andover half of the participants experi-enced no adverse effects at all. Asexpected, the most frequent com-plaint was aggravation of joint symp-toms with exercise. Some partici-pants also described back pain aftercommencing exercises; the backpain may have been related to theprompts that they were given toimprove their posture and spinalposition while walking and exercis-ing in the pool.
Our program did not involve the useof any specific exercise equipmentother than a step, which is a featureof most hydrotherapy pools. Thisstudy design was used to facilitateparticipants’ understanding of exer-cise progression in the aquatic envi-ronment in order to improve confi-dence as well as to maximizeadherence to the program indepen-dently at a local pool during follow-up. The use of equipment (flippers,boots, and floats) can be beneficialfor resistance training in the water,and greater strength gains mighthave been obtained in our study hadequipment been incorporated intothe program. The fact that quadri-ceps femoris muscle strength did notincrease significantly with our pro-gram may argue for the need forequipment for this muscle group inparticular. However, the additionalbenefits of equipment might be off-set by increased financial costs of theintervention or by reduced ongoingadherence to the program by partic-ipants.
There are a number of limitations ofthe present study. The lack of a pla-cebo group necessitated a single-blind design, which may have influ-enced the study outcomes. Thefollow-up period was short, and inchronic conditions such as OA,much longer periods are warrantedto evaluate lasting treatment effects.
Furthermore, the follow-up periodlacked a control group because offunding constraints. Relatively fewof our study participants presentedwith hip OA primarily; thus, it wasnot possible to perform subgroupanalyses to determine outcomes forhip OA and knee OA separately. It ispossible that knee OA and hip OAresponded differently to our aquaticphysical therapy program, but thepresent study did not have sufficientpower to detect such differences.
The question remains as to whetheraquatic physical therapy is superiorto land-based physical therapy forOA. Other authors have failed todemonstrate any additional benefitof hydrotherapy over home exercis-es12 or over a gym-based strengthen-ing program11 for people with OA;those results may have been relatedto the aquatic physical therapy pro-gram content in those published tri-als. Given the association of quadri-ceps femoris muscle strength withpain severity and physical functionin OA,25,27 it is essential that aquaticprograms incorporate a resistancetraining intensity comparable to thatof land-based programs. To increaseresistance for muscle strengtheningin the water, it may be necessary tofurther decrease the depth of immer-sion with closed-chain exercises, touse floats in buoyancy-resisted posi-tions, or to increase resistance fromturbulence by increasing speed orsurface area (with the addition offlippers or boots) with open-chainexercises. Further studies of aquaticphysical therapy should aim to refineprogram content by maximizing theuse of the hydrostatic and hydro-dynamic properties of water andthus the potential benefits of aquaticphysical therapy for people withlower-limb OA. Future research alsoshould be directed toward evaluat-ing the characteristics of peoplewho respond to land- and water-based exercises, as it is possible thatcertain types of exercise regimens
Aquatic Physical Therapy for Hip and Knee OA
January 2007 Volume 87 Number 1 Physical Therapy f 41 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

are more suitable for particular sub-groups of people.
ConclusionThe present study demonstrated thata 6-week program of aquatic physi-cal therapy results in small improve-ments in pain, stiffness, hip strength,and quality of life in people with hipOA or knee OA compared with nointervention. Aquatic physical ther-apy is a useful intervention optionfor such people; many people mayadhere to the intervention indepen-dently once the supervised programceases.
Dr Hinman and Ms Heywood provided con-cept/idea/research design and writing. MrDay provided data collection, and Dr Hin-man provided data analysis. Ms Heywoodprovided project management and fundprocurement. The authors thank KathrynRitchie for her assistance with data entry,Jenny Geytenbeek for her guidance, and theSunshine Hospital and Western Hospitalphysiotherapy department staff for theirsupport.
The local Human Research Ethics Committeeapproved the study.
This research, in part, was presented at the47th Annual Scientific Meeting of the Aus-tralian Rheumatology Association/Rheuma-tology Health Professionals Association; May22–25, 2005; Melbourne, Victoria, Australia.
This study was supported by a NationalArthritis and Musculoskeletal ConditionsImprovement Grant from the AustralianGovernment Department of Health andAging.
This article was received January 5, 2006, andwas accepted August 11, 2006.
DOI: 10.2522/ptj.20060006
References1 Vanhoof J, Declerck K, Geusens P. Preva-
lence of rheumatic diseases in a rheuma-tological outpatient practice. Ann RheumDis. 2002;61:453–455.
2 Hamerman D. Clinical implications ofosteoarthritis and aging. Ann Rheum Dis.1995;54:82–85.
3 Felson DT. Epidemiology of hip and kneeosteoarthritis. Epidemiol Rev. 1988;10:1–28.
4 American College of Rheumatology Sub-committee on Osteoarthritis. Recommen-dations for the medical management ofosteoarthritis of the hip and knee: 2000update. Arthritis Rheum. 2000;43:1905–1915.
5 Walker-Bone K, Javaid K, Arden N, CooperC. Medical management of osteoarthritis.BMJ. 2000;321:936–940.
6 Jordan K, Arden N, Doherty M, et al.EULAR recommendations 2003: an evi-dence based approach to the managementof knee osteoarthritis—report of a taskforce of the Standing Committee for Inter-national Clinical Studies Including Thera-peutic Trials (ESCISIT). Ann Rheum Dis.2003;62:1145–1155.
7 Larsen J, Pryce M, Harrison J, et al. Guide-lines for Physiotherapists Working inand/or Managing Hydrotherapy Pools.Melbourne, Victoria, Australia: AustralianPhysiotherapy Association; 2002.
8 Harrison R, Bulstrode S. Percentage weight-bearing during partial immersion. Phys-iother Pract. 1987;3:60–63.
9 Harrison R, Hillman M, Bulstrode S. Load-ing of the lower limb when walking par-tially immersed: implications for clinicalpractice. Physiotherapy. 1992;78:164–166.
10 Geytenbeek J. Evidence for effective hy-drotherapy. Physiotherapy. 2002;88:514–529.
11 Foley A, Halbert J, Hewitt T, Crotty M.Does hydrotherapy improve strength andphysical function in patients with osteo-arthritis: a randomised controlled trialcomparing a gym based and a hydrother-apy based strengthening program. AnnRheum Dis. 2003;62:1162–1167.
12 Green J, McKenna F, Refern E, Chamber-lain M. Home exercises are as effective asoutpatient hydrotherapy for osteoarthritisof the hip. Br J Rheumatol. 1993;32:812–815.
13 Lin S, Davey R, Cochrane T. Communityrehabilitation for older adults with osteo-arthritis of the lower limb: a controlledclinical trial. Clin Rehabil. 2004;18:92–101.
14 Sylvester K. Investigation of the effects ofhydrotherapy in the treatment of osteo-arthritic hips. Clin Rehabil. 1989;4:223–228.
15 Wyatt F, Milam S, Manske R, Deere R. Theeffects of aquatic and traditional exerciseprograms on persons with knee osteo-arthritis. J Strength Conditioning Res.2001;15:337–340.
16 Altman R, Alarcon G, Appelrouth D, et al.The American College of Rheumatologycriteria for the classification and reportingof osteoarthritis of the hip. ArthritisRheum. 1991;34:505–514.
17 Altman R, Asch E, Bloch D, et al. Develop-ment of criteria for the classification andreporting of osteoarthritis: classification ofosteoarthritis of the knee. ArthritisRheum. 1986;29:1039–1049.
18 Bellamy N. Osteoarthritis clinical trials:candidate variables and clinimetric prop-erties. J Rheumatol. 1997;24:768–778.
19 Huskisson EC. Visual analogue scales. In:Melzack R, ed. Pain Measurement andAssessment. New York, NY: Raven Press;1983:33–37.
20 Bellamy N, Buchanan WW, Goldsmith CH,et al. Validation study of WOMAC: a healthstatus instrument for measuring clinicallyimportant patient relevant outcomes toantirheumatic drug therapy in patientswith osteoarthritis of the hip or knee.J Rheumatol. 1988;15:1833–1840.
21 Hawthorne G, Richardson J, Day N. Acomparison of the Assessment of Qualityof Life (AQoL) with four other genericutility instruments. Ann Med. 2001;33:358–370.
22 Martin KA, Rejeski JW, Miller ME, et al.Validation of the PASE in older adults withknee pain and physical disability. Med SciSports Exerc. 1999;31:627–633.
23 Bohannon R. Reference values for extrem-ity muscle strength obtained by hand-helddynamometry from adults aged 20 to 79years. Arch Phys Med Rehabil. 1997;78:26–32.
24 Chang A, Hayes K, Dunlop D, et al. Hipabduction moment and protection againstmedial tibiofemoral osteoarthritis progres-sion. Arthritis Rheum. 2005;52:3515–3519.
25 Slemenda C, Brandt KD, Heilman DK,et al. Quadriceps weakness and oste-oarthritis of the knee. Ann Intern Med.1997;127:97–104.
26 McAlindon TE, Cooper C, Kirwan JR, et al.Determinants of disability in osteoarthritisof the knee. Ann Rheum Dis. 1993;52:258–262.
27 O’Reilly SC, Jones A, Muir KR, Doherty M.Quadriceps weakness in knee osteoarthri-tis: the effect on pain and disability. AnnRheum Dis. 1998;57:588–594.
28 Wang CY, Olson SL, Protas EJ. Test-reteststrength reliability: hand-held dynamome-try in community-dwelling elderly fallers.Arch Phys Med Rehabil. 2002;83:811–815.
29 Hill K, Bernhardt J, McGann AM, et al. Anew test of dynamic standing balance forstroke patients: reliability, validity andcomparison with healthy elderly. Phys-iother Can. 1996;48:257–262.
30 Hinman RS, Bennell KL, Metcalf BR, Cross-ley KM. Balance impairments in individu-als with symptomatic knee osteoarthritis:a comparison with matched controls usingclinical tests. Rheumatology. 2002;41:1388–1394.
31 Podsiadlo D, Richardson S. The timed “upand go”: a test of basic functional mobilityfor frail elderly persons. J Am Geriatr Soc.1991;39:142–148.
32 Guyatt GH, Thompson PJ, Berman LB,et al. How should we measure function inpatients with chronic heart and lung dis-ease? J Chronic Dis. 1985;38:517–524.
33 Bellamy N, Carette S, Ford PM, et al.Osteoarthritis antirheumatic drug trials.III. Setting the delta for clinical trials:results of a consensus development(Delphi) exercise. J Rheumatol. 1992;19:451–457.
Aquatic Physical Therapy for Hip and Knee OA
42 f Physical Therapy Volume 87 Number 1 January 2007 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from

34 Hassan B, Doherty S, Mockett S, DohertyM. Effect of pain reduction on posturalsway, proprioception, and quadricepsstrength in subjects with knee osteoarthri-tis. Ann Rheum Dis. 2002;61:422–428.
35 Moseley B, O’Malley K, Petersen N, et al. Acontrolled trial of arthroscopic surgery forosteoarthritis of the knee. N Engl J Med.2002;347:81–88.
36 Deyle GD, Henderson NE, Matekel RL,et al. Effectiveness of manual physicaltherapy and exercise in osteoarthritis ofthe knee: a randomized, controlled trial.Ann Intern Med. 2000;132:173–181.
37 Hughes R, Carr A. A randomized, double-blind, placebo-controlled trial of glu-cosamine sulphate as an analgesic inosteoarthritis of the knee. Rheumatology.2002;41:279–284.
38 Hrobjartsson A, Gotzsche P. Is the placebopowerless? An analysis of clinical trialscomparing placebo with no treatment.N Engl J Med. 2001;344:1594–1602.
39 Bender T, Karagulle Z, Balint GP, et al.Hydrotherapy, balneotherapy, and spatreatment in pain management. Rheuma-tol Int. 2005;25:220–224.
40 Hall J, Skevington S, Maddison P, Chap-man K. A randomized and controlled trialof hydrotherapy in rheumatoid arthritis.Arthritis Care Res. 1996;9:206–215.
41 Gyurcsik N, Estabrooks P, Frahm-TemplarM. Exercise-related goals and self-efficacyas correlates of aquatic exercise in individ-uals with arthritis. Arthritis Care Res.2003;49:306–313.
42 Nied R, Franklin B. Promoting and pre-scribing exercise for the elderly. Am FamPhysician. 2002;65:419–426.
Aquatic Physical Therapy for Hip and Knee OA
January 2007 Volume 87 Number 1 Physical Therapy f 43 by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from
doi: 10.2522/ptj.20060006Originally published online January 1, 2006
2007; 87:32-43.PHYS THER. Rana S Hinman, Sophie E Heywood and Anthony R DayControlled TrialOsteoarthritis: Results of a Single-Blind Randomized Aquatic Physical Therapy for Hip and Knee
References
http://ptjournal.apta.org/content/87/1/32#BIBLfor free at: This article cites 40 articles, 12 of which you can access
Cited by
http://ptjournal.apta.org/content/87/1/32#otherarticlesarticles: This article has been cited by 11 HighWire-hosted
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on March 29, 2015http://ptjournal.apta.org/Downloaded from
Related Documents











