Physical Function in Patients Following Surgery for Colorectal Cancer Kuan-Yin Lin Bachelor of Science in Physical Therapy Master of Science ORCID: 0000-0002-2902-3156 Submitted in total fulfilment of the requirements of the Degree of Doctor of Philosophy September 2016 Department of Physiotherapy Melbourne School of Health Sciences The University of Melbourne

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Physical Function in Patients Following Surgery for
Colorectal Cancer
Kuan-Yin Lin
Bachelor of Science in Physical Therapy
Master of Science
ORCID: 0000-0002-2902-3156
Submitted in total fulfilment of the requirements of the
Degree of Doctor of Philosophy
September 2016
Department of Physiotherapy
Melbourne School of Health Sciences
The University of Melbourne
i
Abstract
Colorectal cancer (CRC) is the third most commonly diagnosed cancer in males and
the second most common cancer in females worldwide. Surgery is the usual treatment
for CRC, however post-operative morbidity can be high. Post-operative problems can
include symptoms such as anxiety, depression, and bowel, bladder and sexual
dysfunction, poor functional exercise capacity, and low levels of physical activity.
These highly distressing problems can negatively impact patients’ health-related
quality of life (HRQoL). Although the current evidence is strong for physical activity
for patients with CRC, there is limited evidence for optimal bowel management in
patients who have undergone surgical treatment for CRC. In addition, there are no
validated instruments for measuring pelvic floor symptoms and functional exercise
capacity in both colon and rectal cancer.
This thesis aimed to (1) determine the validity and applicability of a bladder and
bowel symptom-specific questionnaire and three field walking tests for the CRC
population; (2) comprehensively understand the changes in pelvic floor symptoms and
physical and psychological outcomes in patients before and six months after surgery
for CRC; (3) investigate the feasibility of implementing a general rehabilitation
program incorporating the international physical activity guidelines for patients
following surgery for CRC; (4) explore changes in patient centred functional and
pelvic floor outcomes following the rehabilitation program; and (5) identify and
synthesize current evidence for the effectiveness of pelvic floor muscle training for
bowel dysfunction in patients who have undergone CRC surgery.

ii
Study 1 and Study 2 examined the validity and applicability of instruments/tests used
in the measurement of functional exercise capacity and bladder and bowel symptoms
of patients with CRC. The studies found that one pelvic floor symptom-specific
instrument and two functional exercise capacity field walking tests are suitable (valid
and applicable) for use with patients with CRC. The findings from Study 1 and Study
2 support the choice of outcome measures used in the subsequent studies in this thesis.
Study 3 examined the pelvic floor symptoms, physical and psychological outcomes of
patients undergoing surgery for CRC in a prospective observational study design.
Adult patients with stage I-III CRC completed pelvic floor symptom-specific
questionnaires (the Australian Pelvic Floor Questionnaire and the International
Consultation on Incontinence Questionnaire Bowel module and Urinary Incontinence
short form module) and questionnaires on physical activity levels, anxiety, depression,
and HRQoL before and six months following surgery. The main findings were that
patients experience significant bowel symptoms and persistent low physical activity
levels for up to 6 months following CRC surgery. These results suggest the need for
interventions such as rehabilitation programs or exercise interventions to increase
levels of physical activity and address bowel symptoms in patients following CRC
surgery.
Therefore, Study 4, a prospective non-randomized quasi-control study, was
undertaken to investigate the feasibility of implementing international guidelines
within an oncology rehabilitation program in patients following CRC surgery and to
explore changes in patient centred functional and pelvic floor outcomes following the
rehabilitation program. The findings showed that implementation in the oncology
rehabilitation program was feasible, and patients who have undergone the
iii
rehabilitation program had improvements in bladder and bowel symptoms, depression
and HRQoL.
Study 5, a pilot study nested within Study 4, was conducted to further explore the
changes in bladder and bowel symptoms and pelvic floor muscle clinical outcomes
measured using digital rectal examination, anorectal manometry and transperineal
ultrasound in patients following a general oncology rehabilitation program. Findings
demonstrated improved bowel symptoms from pre- to post-rehabilitation program in
patients following surgery for CRC. This suggests that general exercise may have
positive effects on pelvic floor symptoms in patients following surgery for CRC.
However, the evidence is stronger for targeted pelvic floor muscle training/exercise
than general exercise on pelvic floor symptoms in non-cancer populations, and
patients with CRC behave differently to those with non-cancer diagnoses in terms of
symptoms and treatment (i.e. surgical approaches and side effects of chemotherapy
(CT) and radiotherapy (RT)). Study 6 summarizes the current evidence on the
effectiveness of pelvic floor muscle training on bowel dysfunction in patients who
have undergone CRC surgery by systematic literature reviews. This review identified
eight studies of level III-2 to IV evidence that reported improvements in
patient-reported measures of bowel function and the HRQoL of patients who have
undergone pelvic floor muscle training following CRC surgery. This systematic
review identified gaps in the literature and revealed that there is a need for
randomized controlled trials to provide high levels of evidence of pelvic floor muscle
training for CRC populations.

iv
In conclusion, the studies outlined in this thesis identified the importance of bowel
problems following CRC surgery and suggest that an oncology rehabilitation program
may be clinically feasible for CRC. Pelvic floor muscle training is widely used in the
incontinence population, and the systematic review suggests that randomized
controlled trials are needed to confirm the effectiveness of pelvic floor muscle
training in CRC population. Given the small sample size, the evidence in this thesis
must be regarded as preliminary. Future research should investigate which subgroups
of patients with CRC (i.e. low functional exercise capacity or physical activity levels
or high levels of comorbidity at baseline) to target with exercise interventions and
which intervention (i.e. general exercise, pelvic floor muscle training, or a
combination of both) is more effective in improving pelvic floor outcomes in patients
with CRC.
v
Declaration
This is to certify that:
i. this thesis comprises only my original work towards the Doctor of Philosophy;
ii. due acknowledgment has been made in the text to all other material used; and
iii. this thesis is less than 100,000 words length, exclusive of tables, references and
appendices.
Kuan-Yin Lin
September 2016
vi
Acknowledgements
The PhD journey is a unique adventure and this journey would not have been possible
without the assistance and support of so many people I wish to thank. I would like to
express my deepest appreciation to all the members of my advisory committee,
especially my supervisors Professor Linda Denehy, Associate Professor Helena
Frawley, and Dr Catherine Granger who have constantly provided support, guidance,
encouragement and valuable suggestions at every turn of my PhD journey. I would
also like to thank my committee members, Professor Lynette Joubert, Professor Rana
Hinman and Associate Professor Jennifer Mcginley for their continuous support and
advice, thanks to you.
I would especially like to thank the participants and their families in my studies for
their generosity, courage, and support. I am extremely grateful for many of them who
expressed that they believe their participation would benefit future patients. I hope
that this work will contribute to improving survivorship care for CRC.
I would like to express my sincere gratitude and appreciation to the people who
assisted me in my research. I would like to thank the participating surgeons, especially
Professor Ian Hayes and Ms Susan Shedda, and the staff of the Department of General
Surgery at the Royal Melbourne Hospital and Melbourne Private Hospital. I would
like to thank Lisa Wilson and Annie Allman for providing patient contact details for
the study presented in Chapter 5. I would also like to thank the staff of the
Physiotherapy Department at the Royal Melbourne Hospital, especially Joel Martin,
for assisting with participant recruitment for the study presented in Chapter 4. I am
sincerely thankful to the participating surgeons and the staff from Cabrini Health and
vii
the Centre for Allied Health Research and Education at Cabrini Institute, especially
Rosemary Higgins, Michael Butler, Isabella Lees-Trinca, Hema Navaratnum,
Matthew Macauley, Ann-Marie Damatopoulos, Alice Saunder, Annika Dorey, Karen
Oliva, Jess Frydenberg, Amy Lipshutz, and Isabel LeonEscobar for their contribution
and assistance to the studies presented in Chapter 6 and Chapter 7. I would also like to
thank Dr Margaret Sherburn, Ms Angela Khera, Ms Anne-florence Plante, and Merete
Kolberg for their assistance in clinical examination training for the study presented in
Chapter 7. Thank you to Associate Professor Graham Hepworth of the Statistical
Consulting Centre at the University of Melbourne for his advice on the statistical
approach to the analyses in the studies presented in this thesis.
I would like to acknowledge and thank the grant funding from the Pat Cosh Trust,
Royal Melbourne Hospital Home Lottery Research Grant in Aid - Allied Health and
the Cabrini Foundation seed funding for supporting the studies presented in Chapter 4,
Chapter 5, Chapter 6, and Chapter 7. I would also like to acknowledge The University
of Melbourne for the Melbourne International Fee Remission Scholarship and the
Melbourne International Research Scholarships.
A special thanks to my other research colleagues and friends, in particular Katijjahbe
Binti MD Ali, Jennifer Jones, Elizabeth Proud, Elizabeth Madden, Pippa Nicolson,
Xinyang Wang, Sulakshana Balachandran, Doa El-Ansary, Raquel Sebio, Raquel
Annoni, Alexandra Eriksen, Selina Parry, Lara Edbrooke, Reiko Hara, Dolly Huang,
Chi-Yin Kao and Cristino Oliveira, thank you for your advice and friendship. Thank
you to my Taiwanese crew for their constant support and love.
viii
I would like to thank the examiners for taking time during their busy schedule to read
my thesis.
Finally, and most importantly, thank you to my family, my parents, and my sister
Kuan-Han who have always supported me all the way, through everything. Thank you
for your unconditional love and patience.
ix
Publications
Lin K-Y, Frawley H, Granger C, Denehy L. The Australian Pelvic Floor
Questionnaire is a valid measure of pelvic floor symptoms in patients following
surgery for colorectal cancer. Neurourology and Urodynamics. 2016. In press.
[Chapter 3]
Lin K-Y, Denehy L, Frawley H.C., Dimitriadis T, Martin J, Parry S, Irving L, Granger
C.L. How should functional exercise capacity be measured in colorectal cancer? a
pilot validation study. Jacobs Journal of Physiotherapy and Exercise. 2016;2(2): 017.
[Chapter 4]
Lin K-Y, Frawley H, Denehy L, Feil D, Granger C. Exercise interventions for patients
with gynecological cancer: a systematic review and meta-analysis. Physiotherapy.
2016;102(4):309-319.
Lin K-Y, Granger C, Denehy L, Frawley H. Pelvic floor muscle training for bowel
dysfunction following colorectal cancer surgery: a systematic review. Neurourology
and Urodynamics. 2015;34(8):703-12. [Chapter 8]
Publications under peer review
Lin K-Y, Denehy L, Frawley H.C., Wilson L, Granger C.L. Pelvic floor symptoms,
physical and psychological outcomes of patients following surgery for colorectal
cancer. Physiotherapy Theory and Practice. Submitted September 2016. [Chapter 5]

x
Lin K-Y, Denehy L, Granger C.L., Frawley H.C. Pelvic floor outcomes in patients
who have undergone general rehabilitation following surgery for colorectal cancer: a
pilot study. Physiotherapy Theory and Practice. Submitted December 2016. [Chapter
7]
xi
Conference Presentations
Lin K-Y, Frawley H, Granger C, Denehy L. (2016). The Australian Pelvic Floor
Questionnaire is a valid measure of pelvic floor symptoms in patients following
surgery for colorectal cancer. International Continence Society 2016. Tokyo, Japan.
Lin K-Y, Denehy L, Frawley H, Wilson L, Granger C. (2016). Pelvic floor symptoms,
physical and psychological outcomes of patients undergoing colorectal cancer surgery.
International Continence Society 2016. Tokyo, Japan.
Lin K-Y, Denehy L, Granger C, Frawley H. (2016). Pelvic floor muscle assessment in
patients who have undergone general rehabilitation following surgery for colorectal
cancer: a pilot study. International Continence Society 2016. Tokyo, Japan.
Lin K-Y, Denehy L, Frawley H, Wilson L, Granger C. (2016). Pelvic floor symptoms,
physical and psychological status of patients following surgery for colorectal cancer.
Melbourne Health Research Week Symposium 2016. Melbourne, Victoria.
Lin K-Y, Frawley H, Denehy L, Feil D, Granger C. (2015). Exercise interventions for
patients with gynaecological cancer: a systematic review and meta-analysis. APA
CONNECT Physiotherapy Conference 2015. Gold Coast, Queensland.
Lin K-Y, Granger C. Denehy L, Frawley H. (2014). Pelvic floor muscle training for
bowel dysfunction following colorectal cancer surgery: a systematic review.
Continence Foundation of Australia. Cairns, Queensland.
xii
Invited Presentations
Lin K-Y (2016). Physical Function in Patients Following Surgery for Colorectal
Cancer. St Vincent’s Hospital, Melbourne, Australia. 28th July 2016.
Lin K-Y (2015). Exercise interventions for patients with gynaecological cancer: a
systematic review and meta-analysis. CardioRespiratory Research Network,
Melbourne, Australia. 14th September 2015.
Lin K-Y (2014). Pelvic floor muscle training for bowel dysfunction following
colorectal cancer surgery. CardioRespiratory Research Network, Melbourne,
Australia. 30th July 2014.
xiii
Scholarships & Awards
Melbourne International Fee Remission Scholarship
The University of Melbourne (2013-2017)
Melbourne International Research Scholarships
The University of Melbourne (2013-2016)
Studying Abroad Scholarship
Ministry of Education, Taiwan (2013-2015)
Best Presentation Award
The University of Melbourne, School of Health Sciences (2015)
xiv
Glossary of abbreviations
6MWT 6 minute walk test
ACPS Australian clinicopathological staging
ANCOVA Analysis of covariance
ANOVA Analysis of variance
ANZCTR Australian New Zealand Clinical Trials Registry
A-P Anterior-posterior
APFQ Australian Pelvic Floor Questionnaire
APR Abdominoperineal resection
BMI Body mass index
CI Confidence interval
cmH2O Centimetre of water
COPD Chronic obstructive pulmonary disease
CPET Cardiopulmonary exercise testing
CRC Colorectal cancer
CROM Clinician reported outcome measures
CT Chemotherapy
DALY Disability-adjusted life year
DRE Digital rectal examination
EAS External anal sphincter
ECOG-PS Eastern Cooperate Oncology Group Performance Status
EMG Electromyography
EORTC QLQ-C30 European Organization for Research and Treatment of Cancer
Quality of Life Core Questionnaire
ESWT Endurance shuttle walk test
xv
FACT-C Functional Assessment of Cancer Therapy – Colorectal
questionnaire
FEV1 Forced expiratory volume in 1 second
FIQL Rockwood Faecal Incontinence Quality of Life Scale
FVC Forced vital capacity
HADS Hospital Anxiety and Depression Scale
HAR High anterior resection
HREC Human Research Ethics Committee
HRQoL Health-related quality of life
ICF International Classification of Functioning, Disability, and
Health
ICI International Consultation on Incontinence
ICIQ International Consultation on Incontinence Questionnaire
ICIQ-B International Consultation on Incontinence Questionnaire -
Bowel module
ICIQ-UI SF International Consultation on Incontinence Questionnaire Short
Form Questionnaire for urinary incontinence
ICS International Continence Society
IPAQ-SF International Physical Activity Questionnaire
IQR Interquartile range
ISWT Incremental shuttle walk test
JP J pouch
LAR Low anterior resection
MCID Minimal clinically important difference
MCIS Modified Cleveland Incontinence Score

xvi
MET Metabolic equivalent
MVC Maximum voluntary contraction
NA Not available
NCCN National Comprehensive Cancer Network
NES Nutrition Self-Efficacy Scale
NOS Newcastle-Ottawa Scale
NR Not reported
OR Odds ratio
PA Physical activity
PES Physical Exercise Self-Efficacy Scale
PFM Pelvic floor muscle
PhD Doctor of Philosophy
PRISMA Preferred Reporting Items for Systematic Reviews and
Meta-Analyses
PROM Patient reported outcome measures
PRS Perineal rectosigmoidectomy
QLQ-CR29 European Organization for Research and Treatment of Cancer
Quality of Life colorectal cancer modules
RCT Randomized controlled trial
RR Relative risk
RT Radiotherapy
SD Standard deviation
SF-36 Short Form 36 questionnaire
SpO2 Oxygen saturation
STROBE Strengthening the Reporting of Observational Studies in

xvii
Epidemiology
TAFE Technical and further education
TEM Transanal endoscopic microsurgery
TME Total mesorectal excision
TNM Tumour-node-metastasis
TPUS Transperineal ultrasound
TREND Transparent Reporting of Evaluations with Nonrandomized
Designs
UDI Urogenital Distress Inventory
ULAR Ultra-low anterior resection
VO2max Peak oxygen consumption
WHO World Health Organization
WIS Wexner Incontinence Scale

xviii
Table of contents
Chapter 1. Introduction .................................................................................................. 1
1.1 Background of the problem ............................................................................. 1
1.2 Evidence Gaps in the literature ........................................................................ 4
1.3 Significance of the research ............................................................................. 5
1.4 Research aims .................................................................................................. 6
1.5 Overview of the thesis ..................................................................................... 8
Chapter 2. Colorectal cancer ........................................................................................ 12
2.1 Introduction .................................................................................................... 12
2.2 Definition ....................................................................................................... 12
2.3 Epidemiology ................................................................................................. 13
2.3.1 Incidence ............................................................................................. 13
2.3.2 Mortality and survival ......................................................................... 16
2.3.3 Prevalence ........................................................................................... 18
2.4 Cost and burden of CRC ................................................................................ 19
2.5 Etiology / risk factors ..................................................................................... 20
2.5.1 Sociodemographic factors (age and gender) ....................................... 21
2.5.2 Medical factors (Inflammatory bowel disease, history of CRC,
hereditary factors, and diabetes) .................................................................. 22
2.5.3 Lifestyle factors (obesity, physical inactivity, smoking, alcohol
consumption, and diet) ................................................................................. 23
2.6 Histopathology ............................................................................................... 27
2.7 Cancer staging ................................................................................................ 28
2.8 Signs and symptoms of CRC at diagnosis ..................................................... 31
2.9 Treatment ....................................................................................................... 32

xix
2.9.1 Overview of CRC treatment ............................................................... 32
2.9.1.1 Surgical approaches for CRC ................................................... 32
2.9.2 Adjuvant medical treatment (radiotherapy and chemotherapy) .......... 37
2.10 Side effects and symptoms following treatment .......................................... 41
2.10.1 Pelvic floor dysfunction .................................................................... 41
2.10.2 Physical function (functional exercise capacity and muscle strength)
...................................................................................................................... 45
2.10.3 Level of physical activity .................................................................. 46
2.10.4 Anxiety and depression ..................................................................... 48
2.10.5 Health-related quality of life (HRQoL) ............................................ 49
2.11 Summary ...................................................................................................... 50
Chapter 3. Outcome Measures ..................................................................................... 51
3.1 Introduction .................................................................................................... 51
3.2 Patient reported outcome-measures (PROM) ................................................ 52
3.2.1 Pelvic floor symptoms ........................................................................ 52
3.2.2 Pelvic floor signs ................................................................................. 54
3.2.3 Levels of physical activity .................................................................. 55
3.2.4 Anxiety and depression ....................................................................... 56
3.2.5 Health related quality of life (HRQoL) ............................................... 56
3.2.6 Self efficacy ........................................................................................ 57
3.3 Clinical-reported outcome measures / performance-based outcome measures
............................................................................................................................. 58
3.3.1 Pelvic floor muscle function ............................................................... 58
3.3.2 Functional exercise capacity ............................................................... 60
3.3.3 Muscle strength ................................................................................... 62
3.4 Summary of outcome measures chosen for the studies in this thesis ............ 63

xx
3.5 Validation study of the Australian Pelvic Floor Questionnaire in patients
following surgery for colorectal cancer ............................................................... 63
3.5.1 Introduction ......................................................................................... 64
3.5.1.1 Study aims ................................................................................ 64
3.5.2 Materials and Methods ........................................................................ 65
3.5.3 Results ................................................................................................. 68
3.5.4 Discussion ........................................................................................... 80
3.5.5 Summary ............................................................................................. 83
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
a pilot validation study ................................................................................................. 84
4.1 Introduction .................................................................................................... 84
4.1.1 Study aims and hypotheses ................................................................. 85
4.2 Materials and Methods ................................................................................... 85
4.2.1 Study design, setting and participants ................................................. 86
4.2.2 Procedure ............................................................................................ 86
4.2.3 Measures ............................................................................................. 86
4.2.4 Statistical analyses .............................................................................. 89
4.3 Results ............................................................................................................ 90
4.4 Discussion .................................................................................................... 100
4.5 Summary ...................................................................................................... 103
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients
following surgery for colorectal cancer ..................................................................... 105
5.1 Introduction .................................................................................................. 105
5.1.1 Study aims and hypotheses ............................................................... 106
5.2 Materials and Methods ................................................................................. 106
5.2.1 Study design and participants ........................................................... 106
xxi
5.2.2 Outcome measures ............................................................................ 107
5.2.3 Statistical analysis ............................................................................. 109
5.3 Results .......................................................................................................... 110
5.3.1 Subgroup analysis over three assessment time points (before surgery,
6-week after surgery, and 6-month after surgery) ...................................... 117
5.4 Discussion .................................................................................................... 123
5.5 Summary ...................................................................................................... 126
Chapter 6. A general oncology rehabilitation program for patients following surgery
for colorectal cancer – a pilot study ........................................................................... 128
6.1 Introduction .................................................................................................. 128
6.1.1 Study aims and hypotheses ............................................................... 129
6.2 Methods ....................................................................................................... 130
6.2.1 Participants ........................................................................................ 130
6.2.2 Intervention ....................................................................................... 132
6.2.3 Outcomes .......................................................................................... 132
6.2.4 Sample size ....................................................................................... 137
6.2.5 Statistical Methods ............................................................................ 137
6.3 Results .......................................................................................................... 137
6.3.1 Participant flow ................................................................................. 137
6.3.2 Recruitment ....................................................................................... 140
6.3.3 Baseline Data and Baseline Equivalence .......................................... 140
6.3.4 Primary outcomes ............................................................................. 143
6.3.5 Secondary outcomes ......................................................................... 145
6.4 Discussion .................................................................................................... 154
6.5 Summary ...................................................................................................... 161

xxii
Chapter 7. Pelvic floor outcomes in patients who have undergone general oncology
rehabilitation following surgery for colorectal cancer: a pilot study ......................... 162
7.1 Introduction .................................................................................................. 162
7.1.1 Study aims ......................................................................................... 163
7.2 Materials and Methods ................................................................................. 163
7.2.1 Participants ........................................................................................ 163
7.2.2 Interventions ..................................................................................... 164
7.2.3 Outcomes .......................................................................................... 164
7.2.4 Statistical Methods ............................................................................ 167
7.3 Results .......................................................................................................... 168
7.3.1 Participant flow and recruitment ....................................................... 168
7.3.2 Baseline Data and Baseline Equivalence .......................................... 170
7.3.3 Outcomes .......................................................................................... 172
7.4 Discussion .................................................................................................... 191
7.5 Summary ...................................................................................................... 195
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal
cancer surgery: a systematic review .......................................................................... 196
8.1 Introduction .................................................................................................. 196
8.2 Review aim .................................................................................................. 197
8.3 Methods ....................................................................................................... 197
8.3.1 Literature search ................................................................................ 197
8.3.2 Selection criteria ............................................................................... 197
8.3.3 Screening of papers ........................................................................... 199
8.3.4 Risk of bias ....................................................................................... 199
8.3.5 Data extraction .................................................................................. 200
8.4 Results .......................................................................................................... 200
xxiii
8.4.1 Search strategy and study selection .................................................. 200
8.4.2 Study and participant characteristics ................................................ 203
8.4.3 Effects of pelvic floor muscle training in patients following colorectal
cancer surgery ............................................................................................ 214
8.5 Discussion .................................................................................................... 219
8.5.1 Study limitations ............................................................................... 222
8.6 Summary ...................................................................................................... 222
8.7 Additional papers published since the systematic review was undertaken .. 223
8.7.1 Summary of additional study ............................................................ 223
Chapter 9. Conclusion and future directions .............................................................. 225
9.1 Overview of main findings .......................................................................... 225
9.2 Strengths and limitations of the present research ........................................ 226
9.3 Future directions .......................................................................................... 226
References .................................................................................................................. 230
Appendices ................................................................................................................. 282
xxiv
List of Appendices
Appendix 4.1 Ethics Approval Documentation (Study 2) ......................................... 282
Appendix 4.2 Data collection sheets (Study 2) .......................................................... 283
Appendix 5.1 Ethics Approval Documentation (Study 3) ......................................... 314
Appendix 5.2 Data collection sheets (Study 3) .......................................................... 319
Appendix 6.1 Ethics Approval Documentation (Study 4) ......................................... 347
Appendix 6.2 “Exercise for home” sheet (Study 4) ................................................... 350
Appendix 6.3 Exercise diary (Study 4) ...................................................................... 354
Appendix 6.4 Data Collection Sheets (Study 4) ........................................................ 358
Appendix 7.1 Ethics Approval Documentation (Study 5) ......................................... 390
Appendix 7.2 Data Collection Sheets (Study 5) ........................................................ 395
Appendix 8.1 Systematic review article .................................................................... 404
Appendix 8.2 Example of search strategy ................................................................. 414
xxv
List of Tables
Table 2-1: Risk factors for colorectal cancer ............................................................... 21
Table 2-2: WHO histological classification of tumours of the colon and rectum ........ 28
Table 2-3: Australian clinicopathological staging ........................................................ 29
Table 2-4: TNM CRC staging ...................................................................................... 29
Table 2-5: TNM, Duke and ACPS cancer staging for CRC ......................................... 30
Table 2-6: Most common symptoms or side effects from cancer treatment ................ 40
Table 3-1: Demographic and clinical variables in participants with and without
bladder symptoms following surgery for colorectal cancer ......................................... 69
Table 3-2: Demographic and clinical variables in participants with and without bowel
symptoms following surgery for colorectal cancer ...................................................... 71
Table 3-3: Characteristics of participants..................................................................... 74
Table 3-4: Severity of bladder and bowel symptoms ................................................... 75
Table 3-5: Correlations between AFPQ bladder and bowel domains, ICIQ-UI SF and
ICIQ-B in total cohort (n=44) ...................................................................................... 76
Table 3-6: Correlations between AFPQ bladder and bowel domains, ICIQ-UI SF, and
ICIQ-B in males (n = 25) ............................................................................................. 77
Table 3-7: Correlations between AFPQ bladder and bowel domains, ICIQ-B, and
ICIQ-UI SF in females (n = 19) ................................................................................... 77
Table 3-8: Agreement between AFPQ bladder and bowel domains, ICIQ-B, and
ICIQ-UI SF for symptomatic participants ................................................................... 78
Table 3-9: Association between demographic and clinical variables and bladder and
bowel symptoms in participants following surgery for colorectal cancer ................... 79
Table 4-1: Medical and social demographics (n = 10) ................................................. 92
Table 4-2: Test results .................................................................................................. 93
xxvi
Table 4-3: Pearson’s correlations between CPET VO2peak and 6MWT distance,
ISWT distance, and ESWT time (N = 10) ................................................................... 97
Table 4-4: Pearson’s correlations between 6MWT distance, ISWT distance, ESWT
time, CPET VO2peak and respiratory function .............................................................. 97
Table 4-5: Pearson’s correlations between 6MWT distance, ISWT distance, ESWT
time, and CPET VO2peak and ECOG-PS, HRQoL physical function and global health
domain scores, and hand-grip strength ........................................................................ 97
Table 4-6: Discriminant validity: Difference between participants with or without
self-rated walking limitations in all walking tests ....................................................... 98
Table 4-7: Changes in BORG scores with each test .................................................. 100
Table 5-1: Demographic and medical data at baseline (n = 30)................................. 112
Table 5-2: Pelvic floor symptoms, physical activity levels, and psychological
outcomes .................................................................................................................... 114
Table 5-3: Number of participants categorized according to level of severity of
bladder and bowel symptoms and physical activity, n (%) ........................................ 116
Table 5-4: Health-related quality of life outcomes .................................................... 119
Table 6-1: Demographic and medical data at baseline .............................................. 141
Table 6-2: Adherence: Exercise diary, mean (SD) or n (%) ....................................... 145
Table 6-3: Outcomes: baseline to post-intervention .................................................. 147
Table 6-4: Health-related quality of life outcomes .................................................... 150
Table 6-5: Global rate of change immediately post-intervention or 8 weeks following
baseline ...................................................................................................................... 154
Table 7-1: Participant demographics and clinical characteristics .............................. 171
Table 7-2: Results of pelvic floor muscle clinical assessment in rehabilitation group
.................................................................................................................................... 173
Table 7-3: Pelvic floor symptom scores ..................................................................... 181

xxvii
Table 7-4: Bladder diary results in rehabilitation group ............................................ 183
Table 7-5: Bowel diary results in rehabilitation group .............................................. 184
Table 7-6: Pelvic floor muscle strength of rehabilitation group Spearman’s correlation
at baseline (n = 9) ....................................................................................................... 186
Table 7-7: Pelvic floor muscle strength Spearman’s correlation immediately post-
rehabilitation program (n = 9) .................................................................................... 187
Table 7-8: Pelvic floor muscle strength Spearman’s correlation at 6 months follow-up
(n = 8) ......................................................................................................................... 188
Table 7-9: Linear regression analyses examining the relationship between different
clinical measures of PFM function and severity of pelvic floor symptoms .............. 189
Table 8-1: Risk of bias in reviewed observational trials using the Newcastle-Ottawa
Scale ........................................................................................................................... 204
Table 8-2: Participants in reviewed studies................................................................ 206
Table 8-3: Intervention programs in reviewed studies ............................................... 210
Table 8-4: Results: patient-reported bowel function pre- and post-intervention ....... 215
xxviii
List of Figures
Figure 2.1: Incidence of top ten leading cancers in Victoria, Australia during the
period from 2009 to 2014 (Cancer Council Victoria, 2016) ........................................ 15
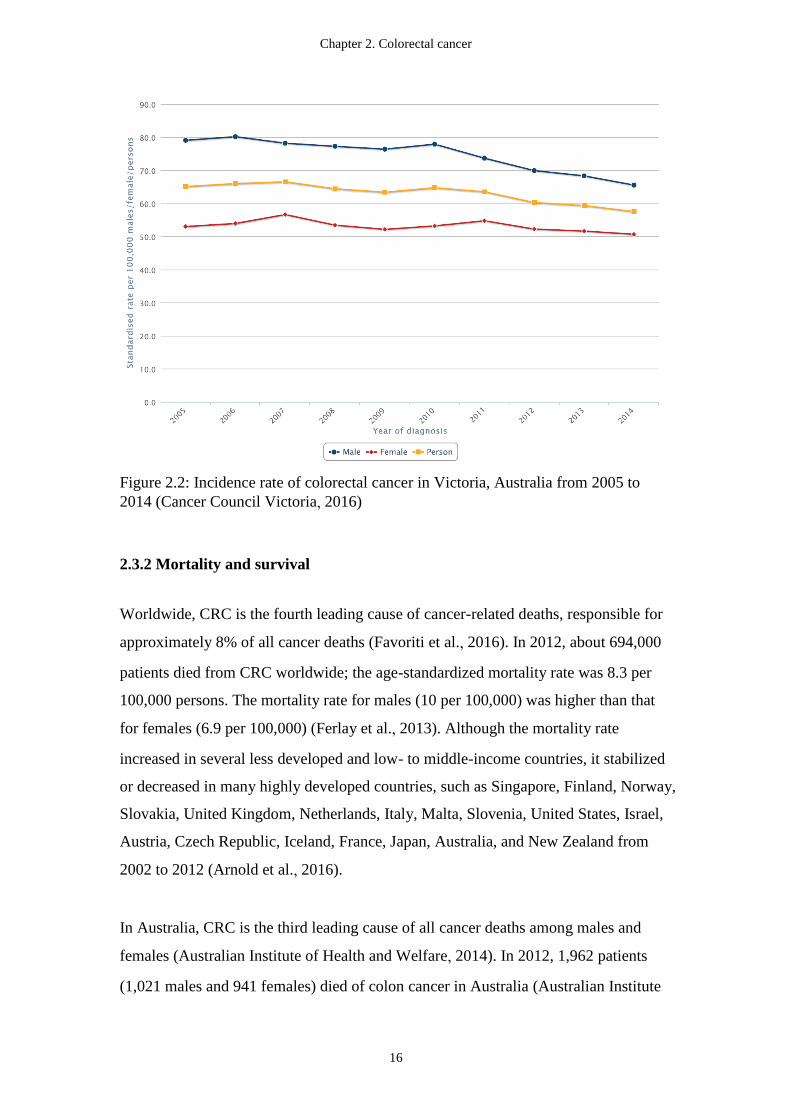
Figure 2.2: Incidence rate of colorectal cancer in Victoria, Australia from 2005 to
2014 (Cancer Council Victoria, 2016) ......................................................................... 16
Figure 2.3: Mortality from colorectal cancer in Victoria, Australia during the period
from 2005 to 2014 (Cancer Council Victoria, 2016) ................................................... 18
Figure 2.4: Average age-specific incidence rate of CRC in Victoria, Australia during
the period from 2009 to 2014 (Cancer Council Victoria, 2016) .................................. 22
Figure 2.5: Surgical procedures for colon cancer: (A) right hemicolectomy; (B)
transverse colectomy; (C) left hemicolectomy; (D) total colectomy (Cancer Council
Victoria, 2013). ............................................................................................................ 34
Figure 2.6: Surgical procedures for rectal cancer: (A) high anterior resection; (B)
ultra-low anterior resection; (C) abdominoperineal resection (Cancer Council Victoria,
2013). ........................................................................................................................... 35
Figure 3.1: Flow chart of the two studies .................................................................... 73
Figure 4.1: STROBE flow chart of the study .............................................................. 91
Figure 4.2: Relationship between 6MWT distance (A), ISWT distance (B), and ESWT
time (C) with CPET VO2peak. ....................................................................................... 96
Figure 5.1: Flow of patients throughout the study ..................................................... 111
Figure 5.2: Bar graph showing mean scores of role functioning for pre-and
post-operative assessments ........................................................................................ 118
Figure 6.1: Patient flow through the study ................................................................. 139
Figure 7.1: Pelvic floor measures in the sagittal plane .............................................. 167
Figure 7.2: Flow chart of the study ............................................................................ 169
xxix
Figure 7.3: Change in raw scores of anorectal manometry variables over time for
participants with CRC ................................................................................................ 175
Figure 7.4: Change in raw scores of ultrasound variables over time for participants
with CRC. .................................................................................................................. 178
Figure 7.5: Change in raw scores of bladder and bowel symptoms over time for
participants with CRC. ............................................................................................... 180
Figure 8.1: PRISMA flow diagram of study selection process. ................................. 202
Chapter 1. Introduction
1
Chapter 1. Introduction
1.1 Background of the problem
Worldwide, colorectal cancer (CRC) is the third most commonly diagnosed cancer
and the fourth leading cause of cancer mortality (Arnold et al., 2016; Torre et al.,
2015). The five-year survival for CRC is about 60% internationally (Favoriti et al.,
2016). In Australia, CRC is the second most commonly diagnosed cancer in both
males and females. The incidence rate of CRC in 2011 was 8,351 cases per 100,000
men and 6,800 cases per 100,000 women (Australian Institute of Health and Welfare,
2015a, 2015b). Despite the high incidence of CRC, the five-year survival for CRC is
improving in Australia; the rate was 66.4% for males and 67.4% for females in the
period 2007-2011 (Australian Institute of Health and Welfare, 2014). This indicates
that most patients with CRC today can expect to live many years after their diagnosis.
Due to the improving survival rates and aging of the population, the number of CRC
survivors in the community is expected to continue to increase (Favoriti et al., 2016;
Parry, Kent, Mariotto, Alfano, & Rowland, 2011).
The medical treatment for CRC includes surgery, chemotherapy (CT), and/or
radiotherapy (RT). The type of treatment combination depends on the patient’s stage
of the cancer disease, tumour location and characteristics, and their performance
status (Stintzing, 2014). In Australia in 2000, approximately 82% of patients had
undergone surgery for CRC and adjuvant CT was offered to 49% of patients with
rectal cancer and 39% of patients with colon cancer (McGrath, Leong, Armstrong, &
Spigelman, 2004). Although medical treatment is associated with survival benefits
(Aran, Victorino, Thuler, & Ferreira, 2016), patients often experience significant
morbidity following treatment. Problems include high levels of symptoms (anxiety,
depression, and bowel, bladder and sexual dysfunction), poor functional exercise
capacity, and low levels of physical activity (PA) (Bailey et al., 2015; Brant et al.,
2011; Hamaker et al., 2015; Jensen, Houborg, Norager, Henriksen, & Laurberg;
Lange & van de Velde, 2011; Lynch, Cerin, Owen, & Aitken, 2007; Siefert; Tomoda
Chapter 1. Introduction
2
& Furusawa, 1985; van Duijvendijk et al., 2003). These symptoms can significantly
impact on the patient’s daily functioning and health-related quality of life (HRQoL).
These symptoms can also be mapped into the main domains of the World Health
Organization (WHO)’s International Classification of Functioning, Disability, and
Health (ICF) framework: health condition, body structures and functions, activities,
participation, and environmental and personal factors (Bours et al., 2016; World
Health Organization, 2001). Due to the growing number of CRC survivors,
management of the disease burden and post-operative symptoms is a priority.
The Australian Physical Activity and Sedentary Behaviour Guidelines recommend
that older adults, 65 years and above, undertake at least 30 minutes of
moderate-intensity PA on most days of the week (Brown, Moorhead, & Marshall,
2008). Similar recommendations (exercise at least 150 minutes per week with
addition of strength training exercise at least 2 days per week) were made for cancer
survivors in the American College of Sports Medicine (Schmitz et al., 2010) and
American Cancer Society Guidelines (Rock et al., 2012), as well as with advice to
avoid sedentary time and return to normal daily activities as quickly as possible after
surgery. The guidelines suggest that exercise is safe and effective in improving
physical functioning, HRQoL, and cancer-related fatigue in cancer survivors both
during and after cancer treatment (Rock et al., 2012; Schmitz et al., 2010). Exercise
interventions in the adult cancer populations are associated with benefits on
cardiorespiratory fitness, HRQoL, mood, symptoms and treatment side-effects (Conn,
Hafdahl, Porock, McDaniel, & Nielsen, 2006; Knols, Aaronson, Uebelhart, Fransen,
& Aufdemkampe, 2005; Schmitz et al., 2005). A recent systematic review and
meta-analysis of five randomized controlled trials (RCT) with a total of 238 patients
with CRC found strong evidence for short-term improvements of physical fitness in
patients after exercise interventions compared with controls (Cramer, Lauche, Klose,
Dobos, & Langhorst, 2013). However, the effects of exercise on HRQoL and the
long-term effects of exercise interventions were inconclusive due to the small number
of trials (Cramer et al., 2013). Moreover, the feasibility of implementing an exercise
program in an Australian healthcare setting has not been reported.
Chapter 1. Introduction
3
In addition to impaired physical function and low levels of PA, pelvic floor
dysfunction (bladder, bowel, and sexual dysfunction) is prevalent in patients
following treatment for CRC (Fish & Temple, 2014). While it is widely recognized
that bladder, bowel, and sexual dysfunction is more common and severe in patients
following rectal cancer surgery than patients with colon cancer (Fish & Temple, 2014;
Martin, Haren, Marshall, Lange, & Wittert, 2011; Panjari et al., 2012; Scheer et al.,
2011; van Duijvendijk et al., 2003), small studies have shown that patients with colon
cancer also suffer from pelvic floor dysfunction following surgery (Phipps, Braitman,
Stites, & Leighton, 2008; Tomoda & Furusawa, 1985). Urinary dysfunction (38% -
60%) and sexual dysfunction (male: 44% - 63%; female: 25%) among patients
following surgery for CRC are common (Panjari et al., 2012; Perera et al., 2008). The
most frequently reported bowel problems after sphincter-saving surgery for CRC are
incomplete evacuation (75%), excessive flatus (75%), faecal urgency (73%), straining
at stool (61%), peri-anal soreness or itching (49%), bloating (44%), and faecal
incontinence (38%) (Nikoletti et al., 2008). A study by Phipps et al. also found that
bowel problems (63%) are common among colon cancer survivors (Phipps et al.,
2008). Altered bowel function and urogenital dysfunction may profoundly influence
CRC patients’ personal relationships, social activities (Vironen, Kairaluoma, Aalto, &
Kellokumpu, 2006), work, and HRQoL (Wilson, Alexander, & Kind, 2006), and
impose significant economic burden to the healthcare system and the community.
Although changes in pelvic floor symptoms before and after CRC surgery
(predominantly in rectal cancer) have been documented in the literature, currently
there are no studies that provide information regarding bladder, bowel and sexual
symptoms, and physical and psychological outcomes in one patient cohort which
includes both colon and rectal cancer populations. To date, there is a large body of
evidence regarding the effectiveness of PA or general exercise on physical and
psychological outcomes in patients with CRC, however the role of general exercise in
the management of pelvic floor dysfunction in CRC is not well understood.
To evaluate the effectiveness of an intervention or the appropriateness of care
provided to a specific patient cohort, it is necessary to measure changes in the
outcomes of an intervention using measurement instruments which are validated and
Chapter 1. Introduction
4
applicable to the population. Although many performance-based instruments and
patient-reported outcome measures have been used to measure symptoms, function
and HRQoL in mixed cancer populations or patients with rectal cancer in clinical
practice and research studies (Aaronson et al., 1993; Emmertsen & Laurberg, 2012;
Schmidt, Vogt, Thiel, Jäger, & Banzer, 2013; Whistance et al., 2009), to date, there
are no validated instruments for measuring pelvic floor symptoms and functional
exercise capacity in both colon and rectal cancer. As the ratio of colon to rectal cancer
in Australia is approximately 2:1 (Australian Institute of Health and Welfare, 2015a,
2015b), it is potentially useful to have measurements instruments which are valid and
applicable across both tumour streams.
In addition to the lack of appropriate instruments for measuring pelvic floor
symptoms and functional exercise capacity in CRC, based on the current literature,
there is limited evidence on the optimal management of pelvic floor dysfunction in
CRC. Although it is clear that exercise improves several important health outcomes of
patients following CRC treatment, no studies have investigated the effects of a
general exercise on pelvic floor dysfunction in CRC populations, and hence there is
limited understanding of the changes in pelvic floor dysfunction in patients following
a general oncology rehabilitation. The following section lists the evidence gaps
identified in the literature.
1.2 Evidence Gaps in the literature
The key gaps identified in the research and literature are as follows:
1. There is lack of evidence on the validity of the measurement instruments for
pelvic floor outcomes (bladder, bowel, and sexual dysfunction) and functional
exercise capacity for use in patients with CRC.
2. Information regarding pelvic floor symptoms and physical and psychological
outcomes in patients following surgery for both rectal and colon cancer is scarce.
Chapter 1. Introduction
5
3. The feasibility of implementing an exercise program incorporating the American
Cancer Society physical activity guidelines for patients with CRC in an Australian
healthcare setting has not been reported.
4. There are no studies investigating the potential impact of a general oncology
rehabilitation program on pelvic floor outcomes (bladder, bowel, and sexual
function) in patients with CRC.
5. Although evidence of the benefits of general exercise interventions for patients
with CRC is rapidly emerging, there are no exercise or physiotherapy guidelines
for treating pelvic floor symptoms after CRC surgery.
1.3 Significance of the research
Colorectal cancer is the second most commonly diagnosed cancer in Australia; one in
12 patients are diagnosed with CRC by the age of 85 (Australian Institute of Health
and Welfare, 2014). In Australia, cancer ranks sixth in terms of estimated total health
system expenditure on chronic diseases, with CRC accounting for the highest
expenditure (7.7%) (Australian Institute of Health and Welfare, 2013). Whilst
survivorship care has become a major area of interest due to the growing number of
CRC survivors, the prevalence of post-discharge unmet needs is high. Approximately
21% of patients’ unmet needs persist at least 6 months after their hospital discharge
(Harrison et al., 2011). Post-operative problems may include physical, psychological,
and pelvic floor symptoms (bladder, bowel and sexual dysfunction), which can
severely impact on the patient’s HRQoL. Therefore, it is important to understand the
natural history of pelvic floor symptoms and other physical and psychological
outcomes in this patient cohort in order to develop appropriate rehabilitation programs
or exercise interventions to address these de novo or residual symptoms for patients
with CRC.
Increased levels of PA after CRC diagnosis are associated with lower risk of mortality
(Van Blarigan & Meyerhardt, 2015). However, CRC survivors following cancer
diagnosis are more likely to be insufficiently active than community populations

Chapter 1. Introduction
6
(Hawkes, Lynch, Youlden, Owen, & Aitken, 2008). While cardiac or pulmonary
rehabilitation programs are offered as standard care to patients with coronary heart
disease (Anderson et al., 2016) and chronic obstructive pulmonary disease (COPD)
(Nici & ZuWallack, 2015), no rehabilitation program has been recommended and
implemented as routine care for patients after CRC treatment in Australia or in most
parts of the world. Such a program may be able to appropriately address the physical,
psychological, and social challenges and needs of patients after CRC treatment.
Hence, an oncology rehabilitation program which implements international
survivorship care and exercise guidelines and addresses the diverse range of concerns
related to CRC may change the clinical care pathway for this population.
Specific pelvic floor muscle (PFM) training has been used routinely for treatment of
incontinence in clinical practice (Bø & Herbert, 2013), however there is a paucity of
evidence on changes in pelvic floor outcomes (bladder, bowel, and sexual dysfunction)
in patients with CRC following a general oncology rehabilitation program, which
does not include specific PFM training. Information on the prospective changes in
pelvic floor outcomes following a general oncology rehabilitation program in patients
following CRC surgery will add evidence to the current literature regarding the role of
general exercise on pelvic floor outcomes.
The findings of this thesis will (1) provide suggestions on the choice of appropriate
instruments to measure functional exercise capacity and pelvic floor outcomes in
CRC and (2) add valuable evidence on the role of general exercise in CRC
rehabilitation with view to (3) evaluate the impact of an oncology rehabilitation
program on physical, psychological and pelvic floor outcomes; if found to be
beneficial, the program may be further translated into practice and be provided as part
of standard care in clinical pathway for patients with CRC.
1.4 Research aims
This thesis focuses on physical function of patients following surgery for CRC. The
first section of the thesis relates to measurement of pelvic floor symptoms and
Chapter 1. Introduction
7
physical and psychological outcomes of patients with CRC. The aims of these studies
were to:
1. Evaluate the construct validity and clinical utility of the Australian Pelvic Floor
Questionnaire (APFQ) against two alternative measures of the severity of bladder and
bowel symptoms in males and females following surgery for CRC;
2. Determine demographic and clinical variables as clinical predictors of bladder and
bowel symptoms following CRC surgery;
3. Explore the criterion validity of three field walking tests (6 minute walk test
[6MWT], incremental shuttle walk test [ISWT] and endurance shuttle walk test
[ESWT]) against the gold standard laboratory test (cardiopulmonary exercise testing
[CPET]) to measure functional exercise capacity in CRC;
4. Investigate the relationships of 6MWT, ISWT, ESWT, and CPET to
patient-reported physical function, hand grip strength and HRQoL, and to determine
the clinical applicability/practicality of these tests;
5. Prospectively measure pelvic floor symptoms in patients before and up to six
months after surgery for CRC;
6. Assess PA levels, psychological outcomes, and HRQoL in patients before and up to
six months after surgery for CRC.
The second section of the thesis relates to the impact of a general oncology
rehabilitation program on physical, psychological, and pelvic floor outcomes, and the
effectiveness of PFM training on pelvic floor outcomes in patients following surgery
for CRC through a systematic review of the evidence. The aims of these studies were
to:
1. Investigate the feasibility of implementing a general oncology rehabilitation
program incorporating the physical activity guidelines for patients following surgery
for CRC;

Chapter 1. Introduction
8
2. Explore changes in functional exercise capacity, muscle strength, psychological
outcomes, level of PA, self-efficacy, pelvic floor symptoms, and HRQoL in patients
before and after a general oncology rehabilitation program;
3. Explore changes in pelvic floor clinical outcomes in patients who have undergone a
general oncology rehabilitation program following surgery for CRC;
4. Assess the associations between different clinical measures of PFM function and
severity of pelvic floor symptoms at baseline, immediately post-oncology
rehabilitation, and at 6-months follow-up;
5. Identify, evaluate and synthesize the evidence examining the effectiveness of PFM
training on bowel dysfunction in patients who have undergone CRC surgery.
1.5 Overview of the thesis
There are six studies which form the main body of this thesis.
Chapter 2 provides an overview to the background of the studies and summarizes the
epidemiology, aetiology / risk factors, cancer staging, signs and symptoms of the
disease, the medical treatment of the disease, as well as the clinical impact of
treatment on the patient. The post-treatment symptoms including pelvic floor
dysfunction (bowel, bladder, and sexual dysfunction), impaired functional exercise
capacity, low levels of PA, anxiety, depression, and poor HRQoL are discussed.
Chapter 3 consists of two parts. The first part introduces the psychometric properties
of the measurement instruments specifically used in the studies. Part two reports on
Study 1 in which an exploratory analysis of data from two prospective studies (Study
3 and Study 4) was undertaken. The study sample consisted of 44 participants.
Bladder and bowel symptoms were measured using three validated questionnaires: the
APFQ, the International Consultation on Incontinence Questionnaire (ICIQ) Short
Form Questionnaire for urinary incontinence (ICIQ-UI SF), and the International

Chapter 1. Introduction
9
Consultation on Incontinence Questionnaire-Bowel Module (ICIQ-B) post-cancer
treatment. The relationships between these questionnaires are described and the
predictors of postoperative bladder or bowel symptoms following CRC surgery are
reported. Results of Study 1 support the choice of outcome measures used to assess
pelvic floor symptoms in Studies 3, 4, and 5.
Chapter 4 reports on Study 2 in which the criterion validity of three common field
walking tests was explored against CPET, the gold standard laboratory measure of
functional exercise capacity, in patients with CRC. The observational study included
ten participants with stage I-III CRC who were evaluated within six months of their
last treatment (surgery, CT, RT or targeted treatment). Functional exercise capacity
was assessed by the 6MWT, ISWT, ESWT, and CPET. Additional measures included
hand-grip strength, physical function, respiratory function and HRQoL. The results on
the participant stability between tests, criterion validity, construct validity,
discriminant validity, and clinical applicability are provided. The results of Study 2
support the use of 6MWT in Study 4.
Chapter 5 reports on Study 3 where pelvic floor symptoms, PA levels, psychological
outcomes, and HRQoL of patients undergoing CRC surgery were measured across the
natural history of disease. The prospective observational study included 30
participants with stage I-III CRC. The primary outcome was pelvic floor symptoms
measured with the APFQ. Supplementary data were also collected from the ICIQ-B
and ICIQ-UI SF. Secondary outcomes were PA levels, anxiety, depression, and
HRQoL evaluated with questionnaires. Outcomes were measured pre-operatively and
six-months post-operatively. Changes in outcomes of interest over 6 months of the
assessment period are described. Results from Study 3 provide justification for the
need for rehabilitation programs or exercise interventions to increase levels of PA and
address bowel symptoms in patients following CRC surgery.
Chapter 6 reports on Study 4 where the feasibility of implementing a general
oncology rehabilitation program incorporating the international physical activity
guidelines in an Australian healthcare setting for patients following CRC surgery was
undertaken. The changes in patient centred functional and pelvic floor outcomes
following the rehabilitation program were evaluated. The pilot non-randomized

Chapter 1. Introduction
10
quasi-control study included 12 participants in the ‘rehabilitation’ group and 10 in the
‘questionnaire’ (quasi-control) group. The rehabilitation group participated in an
8-week exercise and education program. The questionnaire group was asked to
complete the postal questionnaires only and did not undertake the rehabilitation
program. The outcome measures were obtained at baseline and immediately
post-intervention or at 8-weeks following the baseline assessment. The feasibility of
implementation of the general oncology rehabilitation program and the changes in the
outcomes of interest are described. Findings from Study 4 inform clinicians of the
feasibility and benefits of the general oncology rehabilitation, which should be
considered as a useful component in the standard care for patients with CRC.
Chapter 7 reports on Study 5 which explored the PFM outcomes measured using
digital rectal examination (DRE), anorectal manometry, transperineal ultrasound and
standardized questionnaires in an opportunistic sample of volunteers from the
‘rehabilitation’ group in Study 4. The changes in and differences between bladder and
bowel outcomes in patients following general oncology rehabilitation compared with
a questionnaire group are described. The results of Study 5 provide useful information
for future studies to design an appropriately powered large RCT to study the
long-term effect of a general oncology rehabilitation on pelvic floor outcomes in
patients with CRC. The correlations between different clinical PFM outcome
measures and the associations between clinical outcome measures and self-reported
pelvic floor symptoms are presented. Conclusion and recommendations for future
studies to establish the optimal outcome measure for pelvic floor outcomes in this
patient population are made.
Chapter 8 reports on Study 6 in which a systematic review was undertaken to identify,
evaluate and synthesize the evidence examining the effectiveness of PFM training on
bowel dysfunction in patients who have undergone CRC surgery. Eligible studies
were systematically reviewed, data were extracted, and risk of bias was assessed.
Results of studies were summarized. Results of Study 6 support the need for RCTs to
confirm the effects of PFM training for patients after CRC surgery.

Chapter 1. Introduction
11
Chapter 9 concludes the thesis by summarizing the findings from all studies,
discussing the major strengths and weaknesses of the studies and recommending the
directions of future research.
Chapters 3, 4, 5, 7, and 8 within this thesis contain content that is substantially
unchanged from the content of multi-author papers which have been either published
or are currently under review.
Chapter 2. Colorectal cancer
12
Chapter 2. Colorectal cancer
2.1 Introduction
This chapter provides an overview of CRC. The first half of the chapter focuses on the
epidemiology, aetiology and medical treatment including cancer staging. The second
half of the chapter focuses on the disease burden associated with CRC including
symptoms, treatment side effects. This chapter provides background information
relevant to the studies reported in this thesis.
2.2 Definition
The following definitions apply to this thesis:
Colon cancer: “cancer that forms in the tissues of the colon (the longest part of the
large intestine). Most colon cancers are adenocarcinomas (cancers that begin in cells
that make and release mucus and other fluids).” (Australian Institute of Health and
Welfare & Australian Government Department of Health, 2016)
Rectal cancer: “cancer that forms in the tissues of the rectum (the last several inches
of the large intestine closest to the anus).” (Australian Institute of Health and Welfare
& Australian Government Department of Health, 2016)
Right hemicolectomy: “surgical procedure performed for tumours of the cecum and
ascending colon; removal of the right side of the colon” (Cancer Council Victoria,
2013; McKenzie, Barnes, & Schwartz, 2005)
Transverse colectomy: “surgical procedure for tumours of the transverse colon;
removal of the middle part of the colon” (Cancer Council Victoria, 2013; McKenzie
et al., 2005)

Chapter 2. Colorectal cancer
13
Left hemicolectomy: “surgical procedure for descending or sigmoid colonic lesions;
removal of the left side of the colon” (Cancer Council Victoria, 2013; McKenzie et al.,
2005)
Total colectomy: “surgical procedure for the entire colon; removal of all of the colon”
(Cancer Council Victoria, 2013; McKenzie et al., 2005)
Low anterior resection: “removal of the sigmoid colon and upper rectum”(American
Cancer Society, 2014)
Abdominoperineal resection: “removal of the sigmoid colon and entire rectum and
anus” (Cancer Council Victoria, 2013)
Proctectomy with total mesorectal excision: “removal of the rectum together with the
mesorectum around it and the surrounding mesorectal fascia.” (American Cancer
Society, 2014)
Coloanal anastomosis: “the colon is connected to the anus.”(American Cancer Society,
2014)
Colostomy: “opening formed by diverting the end of colon to the abdominal
wall”(Cancer Council Victoria, 2013)
Ileostomy: “opening constructed by bringing the end of the ileum to the surface of the
skin”(Cancer Council Victoria, 2013)
2.3 Epidemiology
2.3.1 Incidence
Colorectal cancer is the third most commonly diagnosed cancer worldwide, with an
estimation of 1.4 million new cases diagnosed in 2012 (Arnold et al., 2016). In males,
Chapter 2. Colorectal cancer
14
CRC is the third most common cancer diagnosed after lung cancer and prostate cancer,
accounting for 10% of all new cancer diagnoses yearly (Ferlay et al., 2013). In
females, it is the second most common cancer diagnosed after breast cancer,
accounting for 9% of new cancer diagnoses worldwide (Ferlay et al., 2013). While the
incidence of CRC is increasing in several European, Latin American and Asian
countries, and Canada over the most recent 10-year period (2002-2012), the incidence
rate declined in the United States, Australia, New Zealand, Iceland, Czech Republic
and Japan (Arnold et al., 2016). The most marked decline occurred in the United
States, where CRC incidence rates have declined about 3.2% per year over the last 10
years (National Cancer Institute, 2016).
In Australia, CRC is the second most commonly diagnosed cancer after prostate
cancer in males, and after breast cancer in females (Australian Institute of Health and
Welfare, 2014). In 2011, 10,037 (66%) new cases of colon cancer and 5,114 (34%)
new cases of rectal cancer were diagnosed (Australian Institute of Health and Welfare,
2015a, 2015b). More than half (55%) of these cases were diagnosed in males
(Australian Institute of Health and Welfare, 2015a, 2015b). In 2016, the estimated
number of new cases of CRC is 17,520 (9,810 males and 7,710 females (Australian
Institute of Health and Welfare, 2014). In Australia, the age-standardised incidence
rates of CRC remained stable for males (75 cases per 100,000 males) but decreased
from 53 cases to 50 cases per 100,000 females from 2003 to 2012 (Australian Institute
of Health and Welfare, 2016b). The mean age of patients at time of first diagnosis of
CRC is 69 in males and 71 in females (Australian Institute of Health and Welfare,
2014).
In Victoria (the state of Australia where the studies which form this thesis were
undertaken), CRC is the third most commonly diagnosed cancer after prostate and
breast cancer (Farrugia et al., 2015) (Figure 2.1) with 3,712 new cases diagnosed in
2014 (2,004 males and 1,708 females). The age-standardised incidence rates were 68
and 53 per 100,000 Victorian males and females, respectively (Cancer Council
Victoria, 2016).

Chapter 2. Colorectal cancer
15
Figure 2.1: Incidence of top ten leading cancers in Victoria, Australia during the
period from 2009 to 2014 (Cancer Council Victoria, 2016)
Over the ten year period from 2005 to 2014, CRC incidence rates in Victoria declined
by 14.1% for males and 5.4% for females (Figure 2.2). The improvement in
diagnostic technology and the introduction of screening programs (i.e. the Australian
National Bowel Cancer Screening Program) may have contributed to the decline in
the incidence rate (Australian Institute of Health and Welfare & Australian
Government Department of Health, 2016). Despite the declining incidence rates
shown by the global, Australian, and Victorian data, CRC remains one of the leading
types of cancers internationally, nationally and regionally. Greater attention and
efforts are needed to put into this population in order to alleviate the burden of CRC
worldwide.
Chapter 2. Colorectal cancer
16
Figure 2.2: Incidence rate of colorectal cancer in Victoria, Australia from 2005 to
2014 (Cancer Council Victoria, 2016)
2.3.2 Mortality and survival
Worldwide, CRC is the fourth leading cause of cancer-related deaths, responsible for
approximately 8% of all cancer deaths (Favoriti et al., 2016). In 2012, about 694,000
patients died from CRC worldwide; the age-standardized mortality rate was 8.3 per
100,000 persons. The mortality rate for males (10 per 100,000) was higher than that
for females (6.9 per 100,000) (Ferlay et al., 2013). Although the mortality rate
increased in several less developed and low- to middle-income countries, it stabilized
or decreased in many highly developed countries, such as Singapore, Finland, Norway,
Slovakia, United Kingdom, Netherlands, Italy, Malta, Slovenia, United States, Israel,
Austria, Czech Republic, Iceland, France, Japan, Australia, and New Zealand from
2002 to 2012 (Arnold et al., 2016).
In Australia, CRC is the third leading cause of all cancer deaths among males and
females (Australian Institute of Health and Welfare, 2014). In 2012, 1,962 patients
(1,021 males and 941 females) died of colon cancer in Australia (Australian Institute
Chapter 2. Colorectal cancer
17
of Health and Welfare, 2015a). There were 2,018 deaths from rectal cancer in 2012
(1,187 males and 831 females) (Australian Institute of Health and Welfare, 2015b).
Although it was estimated that the number of patients who died from CRC would
increase to 4,120 deaths in 2016 (2,170 males and 1,950 females) (Australian Institute
of Health and Welfare, 2014), the age-standardized mortality rate of CRC decreased
from 24 deaths to 19 deaths per 100,000 males and 16 deaths to 13 deaths per 100,000
females between 2004 and 2013 (Australian Institute of Health and Welfare, 2016b).
The decreasing mortality rate may be due to the improvements in CRC treatment
and/or early detection of the disease (Center, Jemal, Smith, & Ward, 2009; Favoriti et
al., 2016). The decreasing mortality rates also reflect the increase in survival rate. In
Australia, the one-year and five-year relative survival rates for CRC were 85% and
67% in 2007 to 2011 (Australian Institute of Health and Welfare, 2014), which are
comparable to the worldwide data of one- and 5-year relative survival rates, 83% and
65%, respectively (Favoriti et al., 2016). This indicates that most patients with CRC
today can expect to live many years after their diagnosis. The one-year, five-year, and
ten-year relative survivals increased from 76%, 54%, and 49% in the period
1988-1993 to 85%, 66%, and 61% in the period 2006-2010 (Australian Institute of
Health and Welfare, 2012). However, the 5-year survival rate of CRC is highly
dependent upon stage of disease at time of diagnosis and ranges from 90% for
localized cancers detected at very early stage to 13% for patients diagnosed with
metastatic disease (National Cancer Institute, 2016).
In Victoria, CRC is the second most common cause of cancer death after lung cancer,
with age-standardised mortality rates of 24 per 100,000 males and 16 per 100,000
women in 2014 (Cancer Council Victoria, 2016). Over the ten year period from 2005
to 2014, mortality rates declined by 6.4% for males and 6.9% for females (Cancer
Council Victoria, 2016) (Figure 2.3). In 2013, the 5-year relative survival for CRC
was 67%; a significant increase from 50% in 1988-1992 to 67% in 2008-2012
(Farrugia et al., 2015). The number of CRC survivors living in the community in
Victoria is increasing. Therefore research which aims to address survivorship needs of
this growing population is warranted.
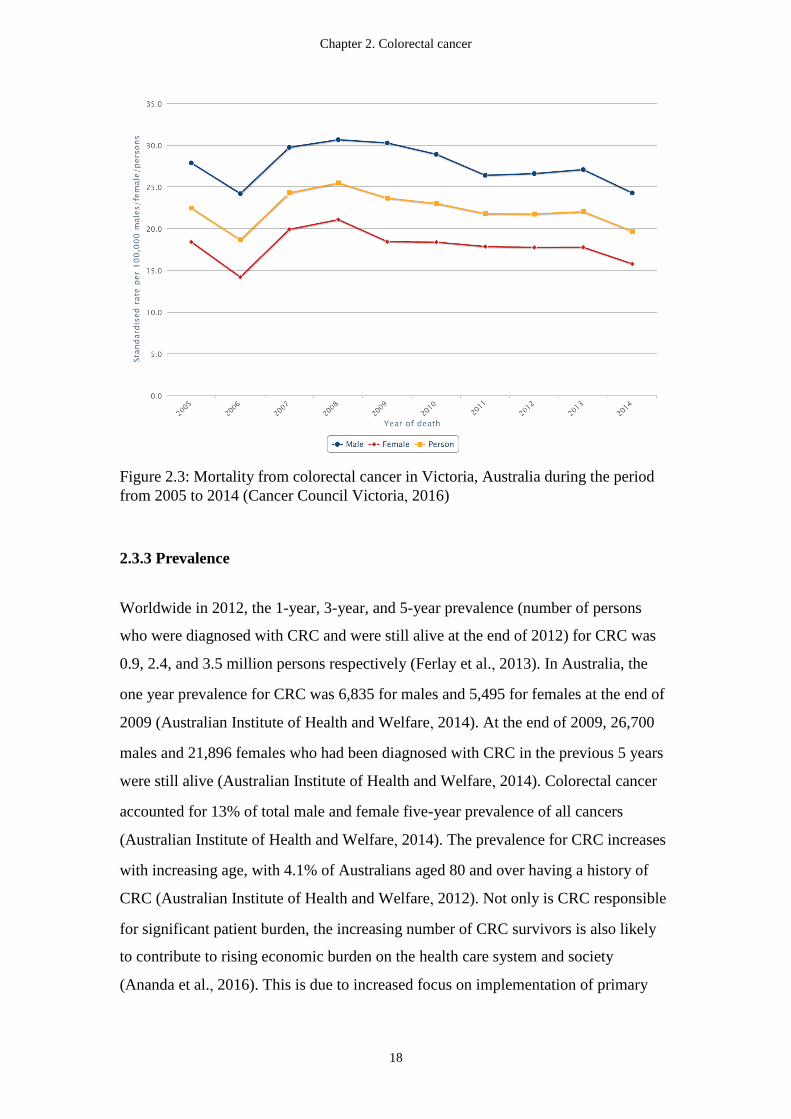
Chapter 2. Colorectal cancer
18
Figure 2.3: Mortality from colorectal cancer in Victoria, Australia during the period
from 2005 to 2014 (Cancer Council Victoria, 2016)
2.3.3 Prevalence
Worldwide in 2012, the 1-year, 3-year, and 5-year prevalence (number of persons
who were diagnosed with CRC and were still alive at the end of 2012) for CRC was
0.9, 2.4, and 3.5 million persons respectively (Ferlay et al., 2013). In Australia, the
one year prevalence for CRC was 6,835 for males and 5,495 for females at the end of
2009 (Australian Institute of Health and Welfare, 2014). At the end of 2009, 26,700
males and 21,896 females who had been diagnosed with CRC in the previous 5 years
were still alive (Australian Institute of Health and Welfare, 2014). Colorectal cancer
accounted for 13% of total male and female five-year prevalence of all cancers
(Australian Institute of Health and Welfare, 2014). The prevalence for CRC increases
with increasing age, with 4.1% of Australians aged 80 and over having a history of
CRC (Australian Institute of Health and Welfare, 2012). Not only is CRC responsible
for significant patient burden, the increasing number of CRC survivors is also likely
to contribute to rising economic burden on the health care system and society
(Ananda et al., 2016). This is due to increased focus on implementation of primary
Chapter 2. Colorectal cancer
19
(diet and PA) and secondary (screening program) prevention; increased requirements
for medical treatment and surveillance (which can last for many years after a
diagnosis), and the requirement for the development of new and improved curative
treatments (Tarraga Lopez, Albero, & Rodriguez-Montes, 2014; Van Cutsem et al.,
2013).
2.4 Cost and burden of CRC
Burden of disease can be analysed by quantifying the impact of a disease or injury on
an individual or population, using the disability-adjusted life year (DALY) measure
(Australian Institute of Health and Welfare, 2014). The DALY uses time as a
common currency; one DALY is one year of ‘healthy life’ lost due to premature death,
prolonged illness or disability (AIHW & AACR, 2012; Australian Institute of Health
and Welfare, 2016a). The more DALYs associated with a particular disease, the
greater the burden (AIHW & AACR, 2012).
Worldwide, it was estimated that 169 million years of healthy life were lost due to
cancer in 2008 (Soerjomataram et al., 2012). In Australia, cancer was the leading
cause of the burden of disease in 2011 (19% of the total DALYs) (Australian Institute
of Health and Welfare, 2016a). In 2011, CRC was estimated to account for 2.1% of
total DALYs in Australia. In males, CRC (53,084 DALYs) ranked twelfth (2.2% of
the total DALYs) in terms of top causes of total burden in 2011; in females, CRC
(39,338 DALYs) ranked sixteenth (1.9% of total DALYs) (Australian Institute of
Health and Welfare, 2016a). Moreover, CRC accounted for almost 11% of the total
cancer burden (dying early from cancer) and ranked second after lung cancer as the
top causes of total cancer burden in 2011 (Australian Institute of Health and Welfare,
2016a).
According to the Australian Institute of Health and Welfare report, the total
expenditure on CRC was $427.35 million, accounting for 9.4% of all cancer
expenditure and attributing to the highest expenditure for individuals aged 65 and
above in 2008-2009 (Australian Institute of Health and Welfare, 2013). The estimated
Chapter 2. Colorectal cancer
20
health system expenditures on CRC were $248 million (10%) for males and $180
million, (8.7%) for females (Australian Institute of Health and Welfare, 2013). In
2012 - 2013, there were 914,993 cancer-related hospitalizations, which indicated that
cancer was responsible for 1 in 10 hospitalizations in Australia (Australian Institute of
Health Welfare, 2015). The number of total hospitalizations with a principal diagnosis
of cancer was 415,130 and CRC was the fourth most common cancer type recorded as
principal diagnosis, accounting for 7% (28,213) of all hospitalizations in 2012 - 2013
(Australian Institute of Health Welfare, 2015). The costs of treating CRC in Australia
was estimated to be $34,337 per patient for stage I CRC, $43,776 for stage II colon
cancer, $79,375 for stage III colon cancer, $86,317 for stage II and III rectal cancer,
and $71,156 for stage IV CRC (Ananda et al., 2016). The cost of treatment is likely to
increase with the availability of more effective systemic treatments, improved
imaging modalities and other emerging treatment strategies (Ananda et al., 2016). As
the costs reported in the study by Ananda et al. were calculated using public hospital
data, the figures may be an underestimate of the true cost in private systems.
2.5 Etiology / risk factors
There are multiple factors associated with the development of CRC. These include
age, gender, inflammatory bowel disease, history of CRC in first-degree relatives,
diabetes, obesity, physical inactivity, smoking, high alcohol consumption, and diet
high in fat or animal products (Brenner, Kloor, & Pox, 2014; Johnson et al., 2013)
(Table 2-1).

Chapter 2. Colorectal cancer
21
Table 2-1: Risk factors for colorectal cancer
Sociodemographic factors Age
Gender
Medical factors Inflammatory bowel disease
History of CRC
Family history/hereditary factors
Diabetes Mellitus
Lifestyle factors Obesity
Physical inactivity
Smoking
Alcohol consumption
Diet
2.5.1 Sociodemographic factors (age and gender)
Advancing age is an independent risk factor associated with the development of CRC
(Day & Velayos, 2014). In Australia, the mean age at CRC diagnosis was 70 years in
2011 (69 years for males and 71 years for females) (Australian Institute of Health and
Welfare, 2014). In 2011, the risk for CRC was 1 in 23 before the age of 75 years and
1 in 12 before the age of 85 years (Australian Institute of Health and Welfare, 2014).
In males, the risk of being diagnosed with CRC before the age of 75 years and the age
of 85 years was 1 in 19 and 1 in 10, respectively. In comparison, the risk of a female
being diagnosed with CRC was 1 in 28 before the age of 75 years and 1 in 15 before
the age of 85 years (Australian Institute of Health and Welfare, 2014). In Victoria, the
median age at CRC diagnosis was 70 years for males and 72 years for females in 2013
(Cancer Council Victoria, 2016). The risk of being diagnosed with CRC by the age of
75 was 1 in 22 for males and 1 in 30 for females (Farrugia et al., 2015). Figure 2.4
shows the average age-specific incidence rate of CRC in Victoria, Australia.
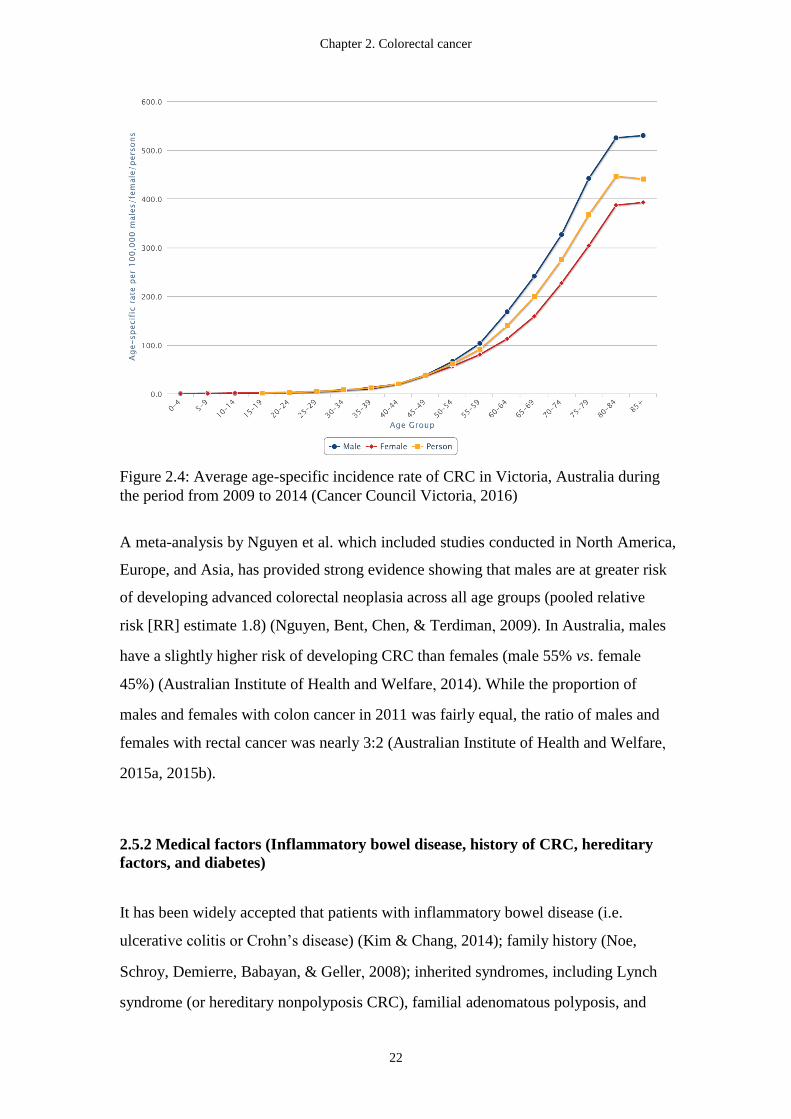
Chapter 2. Colorectal cancer
22
Figure 2.4: Average age-specific incidence rate of CRC in Victoria, Australia during
the period from 2009 to 2014 (Cancer Council Victoria, 2016)
A meta-analysis by Nguyen et al. which included studies conducted in North America,
Europe, and Asia, has provided strong evidence showing that males are at greater risk
of developing advanced colorectal neoplasia across all age groups (pooled relative
risk [RR] estimate 1.8) (Nguyen, Bent, Chen, & Terdiman, 2009). In Australia, males
have a slightly higher risk of developing CRC than females (male 55% vs. female
45%) (Australian Institute of Health and Welfare, 2014). While the proportion of
males and females with colon cancer in 2011 was fairly equal, the ratio of males and
females with rectal cancer was nearly 3:2 (Australian Institute of Health and Welfare,
2015a, 2015b).
2.5.2 Medical factors (Inflammatory bowel disease, history of CRC, hereditary
factors, and diabetes)
It has been widely accepted that patients with inflammatory bowel disease (i.e.
ulcerative colitis or Crohn’s disease) (Kim & Chang, 2014); family history (Noe,
Schroy, Demierre, Babayan, & Geller, 2008); inherited syndromes, including Lynch
syndrome (or hereditary nonpolyposis CRC), familial adenomatous polyposis, and
Chapter 2. Colorectal cancer
23
mutY Homolog-associated polyposis, juvenile polyposis, hereditary mixed polyposis,
and Peutz-Jeghers syndrome (Ballinger & Anggiansah, 2007; Jasperson, Tuohy,
Neklason, & Burt, 2010); or diabetes mellitus (Yuhara et al., 2011) have an increased
risk of developing CRC. As most of the medical factors are non-modifiable, the
details of which are not covered in this thesis. Nevertheless, identification of patients
with these medical factors who are at risk for CRC and surveillance for these patients
are critical in reducing the risk of developing CRC.
2.5.3 Lifestyle factors (obesity, physical inactivity, smoking, alcohol consumption,
and diet)
One in three cancers in Australia is attributable to a modifiable risk factor (Whiteman
et al., 2015). Colorectal cancer is the second leading potentially preventable cancer
after lung cancer, indicating that most cases of CRC in Australia could be prevented if
the population avoided exposure to known risk factors such as tobacco smoke, alcohol,
obesity, insufficient PA, and diet, which independently raise an individual’s risk of
the disease (Whiteman et al., 2015).
Obesity
Obesity is a major health issue in Australia, with 63% of adults being classified as
overweight or obese (body mass index [BMI] ≥ 25 kg/m2), among which 28% are
classified as obese (BMI ≥ 30 kg/m2) (Leung & Funder, 2014). In Victoria, the rates
of overweight and obesity are about 36% and 17% respectively (Rahman & Harding,
2013). A national longitudinal study has projected that the prevalence of obesity will
increase to 70% by 2025, with approximately less than one third of the Australian
population classified as normal weight (BMI 18.5-24.9 kg/m2) (Walls et al., 2012).
Substantial number of cancers are attributable to overweight or obesity in Australia,
amongst which the evidence is strong and convincing for a link with CRC (Kendall et
al., 2015). A meta-analysis has indicated that individuals with obesity have a 40%
greater risk of CRC compared with individuals with normal weight (RR = 1.4 (95%
confidence interval [CI]: 1.3 - 1.5) in males; RR = 1.1 (95% CI: 1.0 - 1.2) in females)
Chapter 2. Colorectal cancer
24
(Huxley et al., 2009). The RR was nonsignificantly higher for colon cancer than rectal
cancer: RR 1.2 (95% CI: 1.1 - 1.4) versus 1.1 (95% CI: 1.0 - 1.3) (Huxley et al., 2009).
A study with a large cohort of Australian adults has shown that high BMI is
associated with the development of CRC with a hazard ratio of 1.1 (95% CI 1.1 - 1.2)
in males and 1.1 (95% 1.0 - 1.1) in females (Harding et al., 2015).
Research which focuses on the mechanisms underlying the link between obesity and
CRC is emerging, and several pathways have been postulated, although the evidence
is inconsistent. These include mechanisms involving insulin and IGF signalling
pathways, adipokines secretion, chronic inflammation, metabolic syndrome and gut
microbiota (Laiyemo, 2014). Obesity-induced insulin resistance causes high levels of
plasma insulin, glucose and fatty acids; exposure of the colonocyte to increased
concentration of insulin, glucose, and fatty acid, which may induce a mitogenic effect
within these cells; metabolic perturbations; and alterations in cell signalling pathways
and oxidative stress (Gunter & Leitzmann, 2006). Chronic inflammation leads to the
secretion of inflammatory cytokines (i.e. tumour necrosis factor-a, monocyte
chemoattractant protein-1, and interleukin-6), which are associated with CRC (Guffey,
Fan, Singh, & Murphy, 2013). As prediagnosis BMI may be associated with higher
all-cause mortality, and CRC-specific mortality or recurrence (Campbell et al., 2012;
Vrieling & Kampman, 2010), maintaining a healthy body weight is important
throughout life.
Physical inactivity
Physical activity is beneficial for physical and psychological health and well-being of
the general population (Teixeira, Carraca, Markland, Silva, & Ryan, 2012). In
Australia between 2002 and 2004, the prevalence of "low PA" (< 600 metabolic
equivalent [MET]-minutes/week) of the adult population was 17%. Females were
more sedentary than males, with a prevalence of low PA 20% versus 14% in males
(Bauman et al., 2009). Low PA is associated with increased risk of CRC. A
meta-analysis found a significant negative correlation between PA and the risk of
developing CRC (RR = 0.9 per increase of 2 in the standardized PA score [95% CI:
Chapter 2. Colorectal cancer
25
0.8 - 0.9]) (Johnson et al., 2013). The negative association with PA is stronger for
colon cancer than for rectal cancer (RR reduction 24% (95% CI: 18% - 29%) versus
6% (95% CI: -3% - 14%) (Huxley et al., 2009). In Australia, approximately 5% of
CRC cases (4.2% in males and 5.4% in females) diagnosed in 2010 were attributable
to insufficient PA (< 300 minutes [5 hours ~ 30 MET-hours] of moderate activity per
week) (Whiteman et al., 2015). Possible mechanisms for the protective effect of PA
against CRC include changes in gastrointestinal transit time, modulation of chronic
inflammation, enhanced immune function, altered gene mutation, changes in insulin
levels, prostaglandin levels, insulin-like growth factors, bile acid secretion, serum
cholesterol and gastrointestinal and pancreatic hormone profiles, and weight loss
(Harriss et al., 2007; Quadrilatero & Hoffman-Goetz, 2003). However, due to the lack
of empirical data to support any of the proposed mechanisms, it is likely that the link
between PA and CRC is the results of a combination of these mechanisms
(Quadrilatero & Hoffman-Goetz, 2003). Research has shown that PA is not only
associated with the risk of CRC but may also influence survival after a diagnosis of
CRC and physical recovery after CRC surgery (Boyle, Fritschi, Platell, & Heyworth,
2013; Hardikar et al., 2015; Onerup et al., 2016). Therefore, PA is an important factor
in preventing CRC and promoting long-term health and survival after cancer
treatment.
Smoking
Smoking increases the risk of CRC (Boyle et al., 2013). In Australia, approximately
6.4% (6% in males and 7% in females) of CRC cases diagnosed in 2010 was
independently attributable to smoking (Whiteman et al., 2015). A meta-analysis has
shown that the pooled risk estimates for current smoker versus never smoker, former
smoker versus never smokers, and ever smokers versus never smokers were 1.1
(95% CI 1.0 - 1.2), 1.2 (95% CI 1.1 - 1.2), and 1.2 (95% CI 1.1 - 1.3) respectively
(Botteri et al., 2008). Moreover, significant dose-response relationship (i.e. increase in
risk with increasing smoking consumption) was observed in the meta-analysis, and
the risk increased by 7.8% (95% CI 5.7% - 10.0%) for every additional 10 cigarettes
(Botteri et al., 2008). The associated risk is higher for rectal cancers than for colon
Chapter 2. Colorectal cancer
26
cancer (Liang, Chen, & Giovannucci, 2009). The carcinogens in tobacco are
understood to form and to increase the growth rate of adenomatous polyps, the
precursor lesions of CRC (Botteri et al., 2008; Haggar & Boushey, 2009).
Alcohol consumption
Alcohol consumption is associated with an increase in risk for CRC (Fedirko et al.,
2011). In Australia, 9% of CRC cases (13% in males and 4% in females) diagnosed in
2010 were independently attributable to alcohol consumption (Whiteman et al., 2015).
A meta-analysis has shown that the pooled RRs of CRC for any alcohol drinking
versus no or occasional drinking was 1.1 (95% CI 1.1 - 1.2); the RRs were for light (≤
12.5 g/day), moderate (12.6 to 49.9 g/day) and heavy drinking (≥ 50 g/day) were 1.1
(95% CI 1.0 - 1.1), 1.2 (95% CI 1.2 - 1.3) and 1.4 (95% CI 1.3 - 1.5), respectively
(Wang, Duan, Yang, & Lin, 2015). Meta-analyses have indicated that the risk of CRC
increased dose-dependently and the association of alcohol drinking with the risk of
CRC did not differ by sex and tumour site (i.e. colon or rectum) (Fedirko et al., 2011;
Wang et al., 2015), however the World Cancer Research Fund /American Institute of
Cancer Research reported that alcohol consumption seems to have a stronger negative
effect in males compared to females (Roswall & Weiderpass, 2015). Potential
mechanisms connecting CRC with alcohol consumption have been studied in human,
animal, and cell line studies and these are related to acetaldehyde production in the
colon (i.e. the effect of acetaldehyde on the disruption of epithelial tight junctions and
cell adhesion, mucosal damage after ethanol consumption, increased degradation of
folate, stimulation of rectal carcinogenesis, increased effect of carcinogens by
acetaldehyde, and stimulation of acetaldehyde on cell proliferation in intestinal crypt
cells) (Oyesanmi et al., 2010).
Diet
Diet strongly influences the risk of CRC (Haggar & Boushey, 2009). In Australia,
35% of CRC cases (40% in males and 29% in females) in 2010 were independently
attributable to insufficient fibre and red and processed meat (Whiteman et al., 2015).
Chapter 2. Colorectal cancer
27
A meta-analysis has demonstrated that the pooled RR of CRC for the highest versus
lowest intake of red and processed meats was 1.2 (95% CI 1.1 - 1.3) and the RR for
every 100 g/day increase was 1.1 (95% CI = 1.0 - 1.2) (Chan et al., 2011). Similar
associations were observed for colon and rectal cancer (Chan et al., 2011). Potential
underlying mechanisms for the association between red meat consumption and CRC
include the presence of haeme iron in red meat, production of heterocyclic aromatic
amines and polycyclic aromatic hydrocarbons resulting from meat cooked at high
temperatures, and formation of N-nitroso compounds (Baena & Salinas, 2015; Haggar
& Boushey, 2009).
Fibre has been shown to have a protective effect on CRC (Baena & Salinas, 2015).
The RR of developing CRC was 0.9 (95% CI 0.9 - 0.9) for 10 g daily of total dietary
fibre, 0.9 (95% CI 0.8 - 1.1) for fruit fibre, 1.0 (95% CI 0.9 - 1.1) for vegetable fibre,
0.6 (95% CI 0.3 - 1.4) for legume fibre, and 0.9 (95% CI 0.8 - 1.0) for cereal fibre
(Aune et al., 2011). Whole grain foods are important sources of dietary fibre, and the
summary RR for CRC with an increment of three servings daily (90 g/day) of whole
grains was 0.8 (95% CI 0.8 - 0.9) (Aune et al., 2011). Proposed mechanisms for the
protective effects of fibre on CRC are increasing faecal bulk, diluting faecal
carcinogens, bacterial fermentation of fibre, and decreasing gut transit time (Aune et
al., 2011; Baena & Salinas, 2015). Other components of whole grains including
antioxidants, vitamins, trace minerals, phytate, phenolic acids, lignans, phytoestrogens,
folate, and magnesium may also have beneficial effects on reducing the risk of
developing CRC (Aune et al., 2011).
2.6 Histopathology
Table 2-2 shows the histological types of colorectal tumours according to the WHO
histological classification of tumours of the colon and rectum (Hamilton & Aaltonen,
2000). Adenocarcinoma is the most common CRC tumour type, accounting for 90%
of CRC (Resch, Schneider, & Langner, 2015). Mucinous adenocarcinomas constitute
4 -19 % of CRC (Langner et al., 2012) and are a subtype of adenocarcinomas that
secrete extracellular mucin (Resch et al., 2015). In Australia in the period 2006 - 2010,

Chapter 2. Colorectal cancer
28
the five-year survival from adenocarcinoma and mucinous adenocarcinoma was
similar (65% and 66%, respectively); survival was highest for adenocarcinoma in
tubulovillous adenoma and adenocarcinoma in adenomatous polyp (87% and 88%,
respectively), followed by adenocarcinoma in villous adenoma (79%) (Australian
Institute of Health and Welfare, 2012).
Table 2-2: WHO histological classification of tumours of the colon and rectum
Epithelial tumours Non-epithelial tumours
Adenoma Lipoma
Tubular Leiomyoma
Villous Gastrointestinal stromal tumour
Tubulovillous Leiomyosarcoma
Serrated Angiosarcoma
Intraepithelial neoplasia (dysplasia)
associated with chronic inflammatory
diseases
Kaposi sarcoma
Low-grade glandular intraepithelial
neoplasia
Malignant melanoma
High-grade glandular intraepithelial
neoplasia
Others
Carcinoma Malignant lymphomas
Adenocarcinoma Marginal zone B-cell lymphoma of
MALT Type
Mucinous adenocarcinoma Mantle cell lymphoma
Signet-ring cell carcinoma Diffuse large B-cell lymphoma
Small cell carcinoma Burkitt lymphoma
Squamous cell carcinoma Burkitt-like /atypical Burkitt-lymphoma
Adenosquamous carcinoma Others
Medullary carcinoma Secondary tumours
Undifferentiated carcinoma Polyps
Carcinoid (well differentiated endocrine
neoplasm)
Hyperplastic (metaplastic)
EC-cell, serotonin-producing neoplasm Peutz-Jeghers
L-cell, glucagon-like peptide and
PP/PYY producing tumour
Juvenile
Others
Mixed carcinoid-adenocarcinoma
Others
2.7 Cancer staging
Staging of CRC classifies the tumour according to the extent of disease spread, and
provides clinically useful prognostic information to assist in the clinical decision
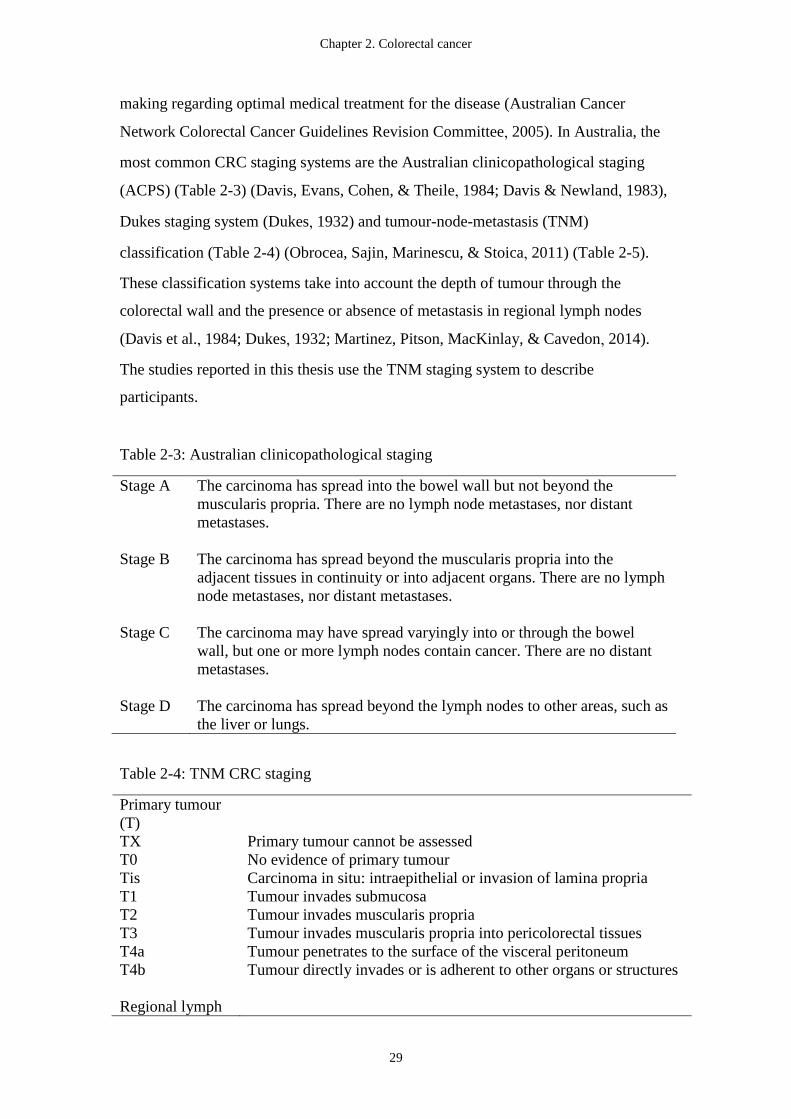
Chapter 2. Colorectal cancer
29
making regarding optimal medical treatment for the disease (Australian Cancer
Network Colorectal Cancer Guidelines Revision Committee, 2005). In Australia, the
most common CRC staging systems are the Australian clinicopathological staging
(ACPS) (Table 2-3) (Davis, Evans, Cohen, & Theile, 1984; Davis & Newland, 1983),
Dukes staging system (Dukes, 1932) and tumour-node-metastasis (TNM)
classification (Table 2-4) (Obrocea, Sajin, Marinescu, & Stoica, 2011) (Table 2-5).
These classification systems take into account the depth of tumour through the
colorectal wall and the presence or absence of metastasis in regional lymph nodes
(Davis et al., 1984; Dukes, 1932; Martinez, Pitson, MacKinlay, & Cavedon, 2014).
The studies reported in this thesis use the TNM staging system to describe
participants.
Table 2-3: Australian clinicopathological staging
Stage A The carcinoma has spread into the bowel wall but not beyond the
muscularis propria. There are no lymph node metastases, nor distant
metastases.
Stage B The carcinoma has spread beyond the muscularis propria into the
adjacent tissues in continuity or into adjacent organs. There are no lymph
node metastases, nor distant metastases.
Stage C The carcinoma may have spread varyingly into or through the bowel
wall, but one or more lymph nodes contain cancer. There are no distant
metastases.
Stage D The carcinoma has spread beyond the lymph nodes to other areas, such as
the liver or lungs.
Table 2-4: TNM CRC staging
Primary tumour
(T)
TX Primary tumour cannot be assessed
T0 No evidence of primary tumour
Tis Carcinoma in situ: intraepithelial or invasion of lamina propria
T1 Tumour invades submucosa
T2 Tumour invades muscularis propria
T3 Tumour invades muscularis propria into pericolorectal tissues
T4a Tumour penetrates to the surface of the visceral peritoneum
T4b Tumour directly invades or is adherent to other organs or structures
Regional lymph
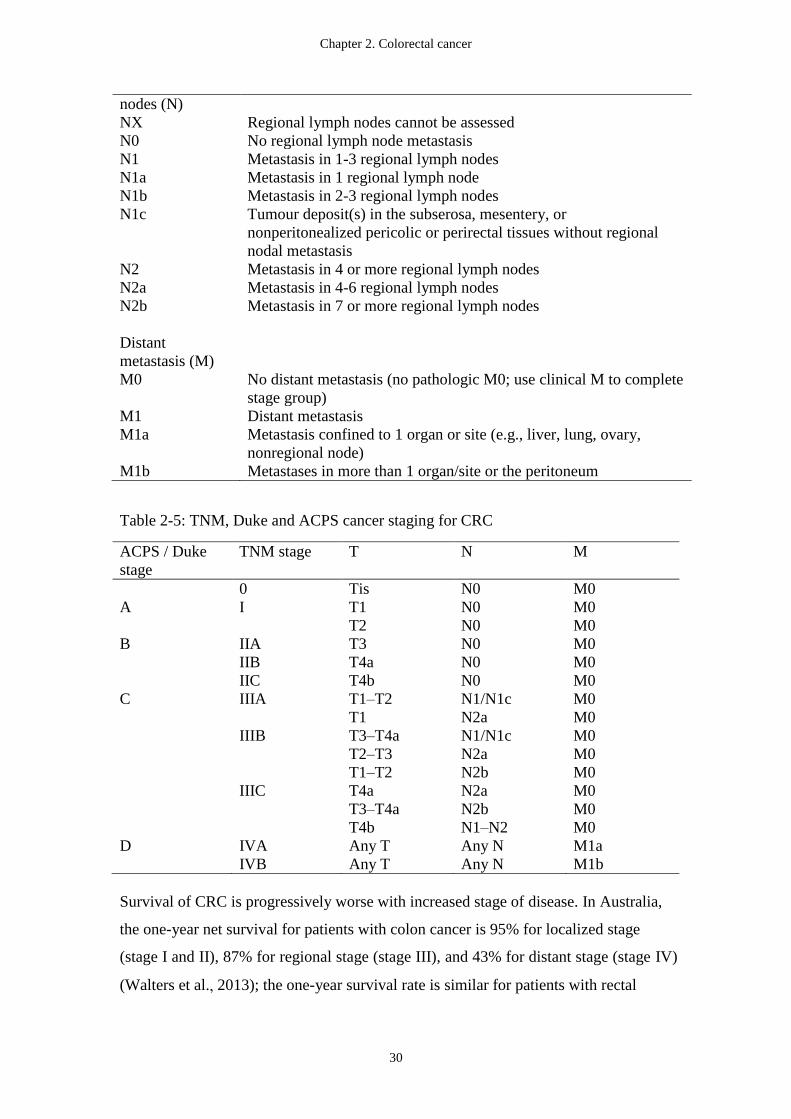
Chapter 2. Colorectal cancer
30
nodes (N)
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in 1-3 regional lymph nodes
N1a Metastasis in 1 regional lymph node
N1b Metastasis in 2-3 regional lymph nodes
N1c Tumour deposit(s) in the subserosa, mesentery, or
nonperitonealized pericolic or perirectal tissues without regional
nodal metastasis
N2 Metastasis in 4 or more regional lymph nodes
N2a Metastasis in 4-6 regional lymph nodes
N2b Metastasis in 7 or more regional lymph nodes
Distant
metastasis (M)
M0 No distant metastasis (no pathologic M0; use clinical M to complete
stage group)
M1 Distant metastasis
M1a Metastasis confined to 1 organ or site (e.g., liver, lung, ovary,
nonregional node)
M1b Metastases in more than 1 organ/site or the peritoneum
Table 2-5: TNM, Duke and ACPS cancer staging for CRC
ACPS / Duke
stage
TNM stage T N M
0 Tis N0 M0
A I T1 N0 M0
T2 N0 M0
B IIA T3 N0 M0
IIB T4a N0 M0
IIC T4b N0 M0
C IIIA T1–T2 N1/N1c M0
T1 N2a M0
IIIB T3–T4a N1/N1c M0
T2–T3 N2a M0
T1–T2 N2b M0
IIIC T4a N2a M0
T3–T4a N2b M0
T4b N1–N2 M0
D IVA Any T Any N M1a
IVB Any T Any N M1b
Survival of CRC is progressively worse with increased stage of disease. In Australia,
the one-year net survival for patients with colon cancer is 95% for localized stage
(stage I and II), 87% for regional stage (stage III), and 43% for distant stage (stage IV)
(Walters et al., 2013); the one-year survival rate is similar for patients with rectal
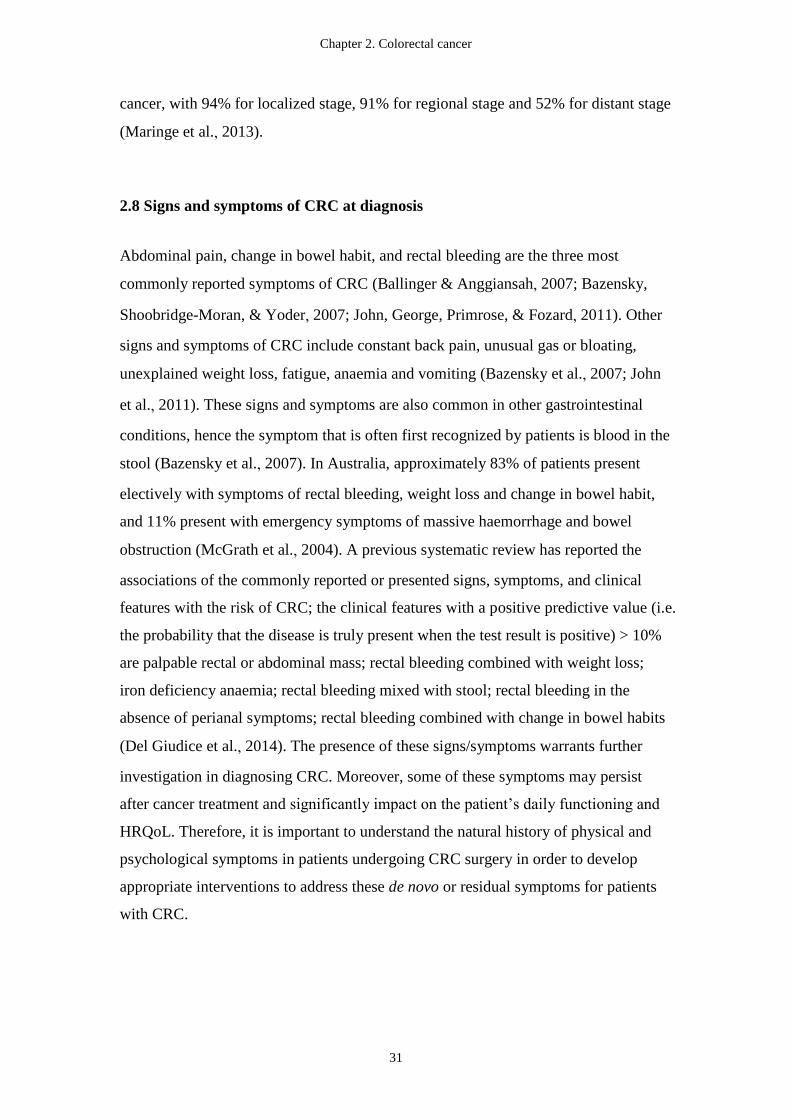
Chapter 2. Colorectal cancer
31
cancer, with 94% for localized stage, 91% for regional stage and 52% for distant stage
(Maringe et al., 2013).
2.8 Signs and symptoms of CRC at diagnosis
Abdominal pain, change in bowel habit, and rectal bleeding are the three most
commonly reported symptoms of CRC (Ballinger & Anggiansah, 2007; Bazensky,
Shoobridge-Moran, & Yoder, 2007; John, George, Primrose, & Fozard, 2011). Other
signs and symptoms of CRC include constant back pain, unusual gas or bloating,
unexplained weight loss, fatigue, anaemia and vomiting (Bazensky et al., 2007; John
et al., 2011). These signs and symptoms are also common in other gastrointestinal
conditions, hence the symptom that is often first recognized by patients is blood in the
stool (Bazensky et al., 2007). In Australia, approximately 83% of patients present
electively with symptoms of rectal bleeding, weight loss and change in bowel habit,
and 11% present with emergency symptoms of massive haemorrhage and bowel
obstruction (McGrath et al., 2004). A previous systematic review has reported the
associations of the commonly reported or presented signs, symptoms, and clinical
features with the risk of CRC; the clinical features with a positive predictive value (i.e.
the probability that the disease is truly present when the test result is positive) > 10%
are palpable rectal or abdominal mass; rectal bleeding combined with weight loss;
iron deficiency anaemia; rectal bleeding mixed with stool; rectal bleeding in the
absence of perianal symptoms; rectal bleeding combined with change in bowel habits
(Del Giudice et al., 2014). The presence of these signs/symptoms warrants further
investigation in diagnosing CRC. Moreover, some of these symptoms may persist
after cancer treatment and significantly impact on the patient’s daily functioning and
HRQoL. Therefore, it is important to understand the natural history of physical and
psychological symptoms in patients undergoing CRC surgery in order to develop
appropriate interventions to address these de novo or residual symptoms for patients
with CRC.

Chapter 2. Colorectal cancer
32
2.9 Treatment
2.9.1 Overview of CRC treatment
Colorectal cancer can be treated medically with a combination of surgery, RT, CT,
and or targeted therapy. Depending on the stage and location of the cancer, either one
or a combination of these treatments may be offered. According to the National
Comprehensive Cancer Network (NCCN) guidelines (National Comprehensive
Cancer Network (NCCN), 2016a, 2016b), surgery is recommended for resectable
stage I, II and III CRC (National Comprehensive Cancer Network (NCCN), 2016a,
2016b). After surgery, adjuvant (additional) treatment may be offered to patients with
stage II and III CRC if the cancer is likely to return (National Comprehensive Cancer
Network (NCCN), 2016a, 2016b). Neoadjuvant (preoperative) treatment is also
available for patients with stage IIIC (T4b) colon cancer (National Comprehensive
Cancer Network (NCCN), 2016a) and stage II and III rectal cancer (National
Comprehensive Cancer Network (NCCN), 2016b). A combination of surgery and CT,
CT with or without targeted therapy, and surgery plus CT with or without targeted
therapy are the treatment options for patients with stage IV CRC (National
Comprehensive Cancer Network (NCCN), 2016a, 2016b).
2.9.1.1 Surgical approaches for CRC
The aims of surgery are to cure and to avoid recurrence (Dorudi, Steele, & McArdle,
2002). Surgical resection is one of the most common treatments for CRC with a rate
of surgery ranging from 54% to 85%, depending on cancer site, stage, and patient age
(Chawla et al., 2013) and results in cure in approximately 50% of patients (Labianca
et al., 2010). In Australia, about 82% of patients undergo surgery with curative intent
(McGrath et al., 2004). However, the types of surgery used to treat colon and rectal
cancers are slightly different (Tamas et al., 2015).

Chapter 2. Colorectal cancer
33
Colon cancer surgery
In colon cancer surgery, the tumour and the corresponding lymph vessels are removed
by colectomy (sometimes called a hemicolectomy, partial colectomy, or segmental
resection) with lymphadenectomy (Brenner et al., 2014; National Comprehensive
Cancer Network (NCCN), 2016a). The extent of surgery is based on the tumour
location and the supplying blood vessels containing the regional lymph node
(National Comprehensive Cancer Network (NCCN), 2016a). If the surgery is
performed through a single incision in the abdomen, it is referred to as an open
colectomy (McKenzie et al., 2005). Right hemicolectomy, transverse colectomy, left
hemicolectomy, and total colectomy are the most common surgical procedures for
colon cancer (Figure 2.5) (De Rosa et al., 2015; McKenzie et al., 2005). Recently,
minimally invasive procedures (i.e. laparoscopic-assisted colectomy) have been
utilized as an alternative approach to removing part of the colon and nearby lymph
nodes by making several smaller incisions instead of one long incision in the
abdomen (Porpiglia & Sigurdson, 2015). A meta-analysis by Di et al. has suggested
that laparoscopic colectomy is as effective and as safe as open colectomy in terms of
the overall mortality (RR = 0.9), total recurrence rate (RR = 0.9), 5-year tumour free
survival rate (RR = 1.0), and overall 5-year survival (RR =1.0) (Di et al., 2013). The
overall mortality in laparoscopic colectomy and open colectomy is 25% to 26%; the
total recurrence rates are 19% to 20%; the 5-year tumour free survival rate is 62%;
and the overall 5-year survival rates are 74% to 75% (Di et al., 2013).
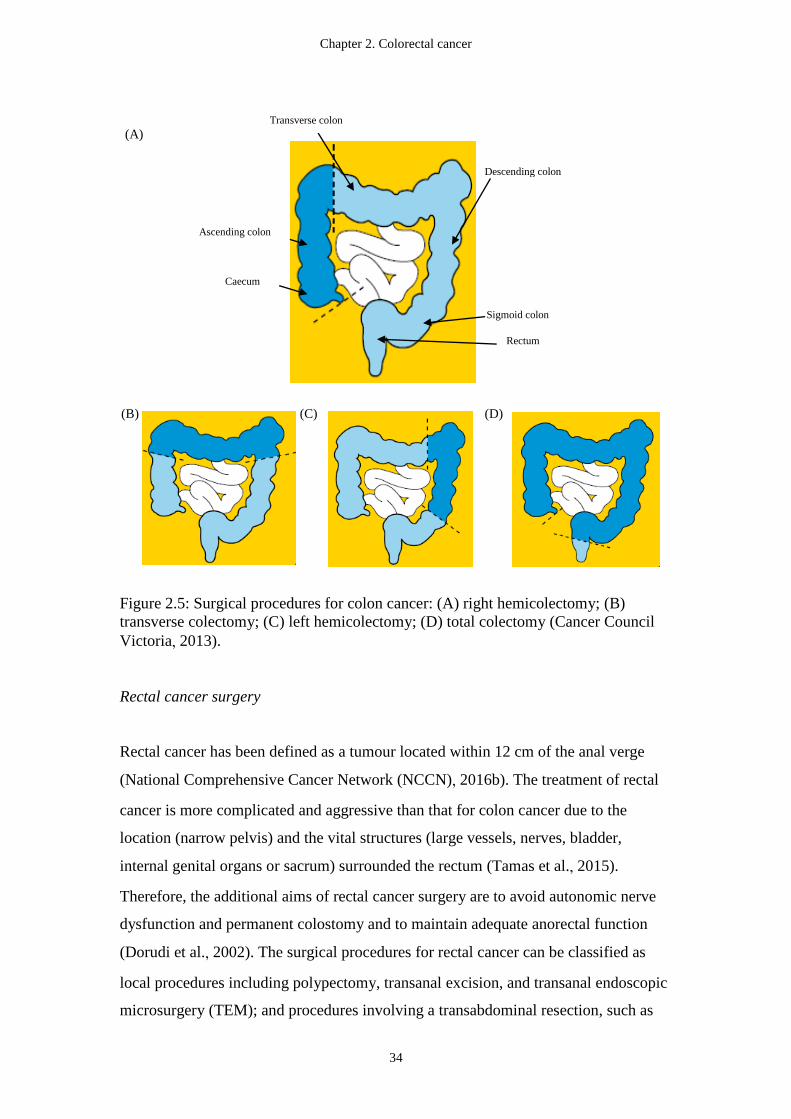
Chapter 2. Colorectal cancer
34
Figure 2.5: Surgical procedures for colon cancer: (A) right hemicolectomy; (B)
transverse colectomy; (C) left hemicolectomy; (D) total colectomy (Cancer Council
Victoria, 2013).
Rectal cancer surgery
Rectal cancer has been defined as a tumour located within 12 cm of the anal verge
(National Comprehensive Cancer Network (NCCN), 2016b). The treatment of rectal
cancer is more complicated and aggressive than that for colon cancer due to the
location (narrow pelvis) and the vital structures (large vessels, nerves, bladder,
internal genital organs or sacrum) surrounded the rectum (Tamas et al., 2015).
Therefore, the additional aims of rectal cancer surgery are to avoid autonomic nerve
dysfunction and permanent colostomy and to maintain adequate anorectal function
(Dorudi et al., 2002). The surgical procedures for rectal cancer can be classified as
local procedures including polypectomy, transanal excision, and transanal endoscopic
microsurgery (TEM); and procedures involving a transabdominal resection, such as
(A)
(B) (C) (D)
Descending colon
Transverse colon
Ascending colon
Caecum
Sigmoid colon
Rectum
Chapter 2. Colorectal cancer
35
high anterior resection (HAR) (Figure 2.6 A), low anterior resection (LAR), ultra-low
anterior resection (ULAR) (Figure 2.6 B), proctectomy with total mesorectal excision
(TME) and coloanal anastomosis, and abdominoperineal resection (APR) (Figure 2.6
C) (Brenner et al., 2014; National Comprehensive Cancer Network (NCCN), 2016b).
Figure 2.6: Surgical procedures for rectal cancer: (A) high anterior resection; (B)
ultra-low anterior resection; (C) abdominoperineal resection (Cancer Council Victoria,
2013).
The treatment of rectal cancer is heavily stage dependent (Porpiglia & Sigurdson,
2015). For stage I rectal cancer, local excision (i.e. transanal excision and TEM) can
be used (American Cancer Society, 2014). For most stage II or III rectal cancers, LAR
could be considered if the cancer is in the upper third of the rectum (American Cancer
Society, 2014); and the LAR is recommended to extend 4 to 5cm below the distal of
the tumour using TME followed by a colorectal anastomosis (National
Comprehensive Cancer Network (NCCN), 2016b). When the stage II or III rectal
cancer is in the middle and lower third of the rectum, proctectomy with TME and
coloanal anastomosis is required (American Cancer Society, 2014).
Abdominoperineal resection is considered when stage II or III rectal cancer is in the
lower third of the rectum and when the cancer is growing into the sphincter muscle
(American Cancer Society, 2014). As the anal sphincters are resected en bloc with
APR, a permanent colostomy is required (Damin & Lazzaron, 2014). As the goal of
rectal cancer surgery is to maintain anorectal function, sphincter-saving or sphincter
preservation surgery, which includes intersphincteric resection or ultra-LAR and
coloanal anastomosis, should be recommended if possible to patients with ultralow
tumours (< 1 cm from the dentate line or within 6 cm from the anal verge) (Damin &
(A) (B) (C)
Chapter 2. Colorectal cancer
36
Lazzaron, 2014; Porpiglia & Sigurdson, 2015). Colostomy or ileostomy is required if
creation of an anastomosis is not possible (National Comprehensive Cancer Network
(NCCN), 2016b). Colostomy/ileostomy can be permanent or temporary; if the ostomy
is temporary, the reversal is usually undertaken within 8 to 12 weeks after the primary
rectal resection (Damin & Lazzaron, 2014).
An Australian survey has shown that anterior resection is the most common procedure,
with approximately 61% of patients with rectal cancer undergoing an anterior
resection (McGrath et al., 2004) in 2000. About 24% of patients received APR, and
TME was used in 65% of patients with rectal cancer (McGrath et al., 2004). In
Victoria, the overall rate of anterior resection was 53%; APR was 23%; ultra-LAR
was 23%; total proctocolectomy 1.2%; and TEM was 0.2% in 2005 (Marwan, Staples,
Thursfield, & Bell, 2010).
Similar to colon cancer surgery, surgery for rectal cancer can be performed
laparoscopically or open (De Rosa et al., 2015). Meta-analyses have found no
significant differences in postoperative complications, oncological clearance, local
and distant recurrences, disease-free survival and overall survival between
laparoscopic and open surgery for rectal cancer (Jiang et al., 2015; Zhang et al., 2014),
which suggest that laparoscopic surgery is comparable to open surgery for treatment
of rectal cancer. The 5-year or longer time overall survival and disease-free survival
are similar for open surgery (65% and 67%) and for laparoscopic surgery (63% and
69%) (Zhang et al., 2014).
Although surgery is the mainstay of treatment for CRC, it is associated with
postoperative complications and morbidity (van Vugt, Reisinger, Derikx, Boerma, &
Stoot, 2014). In Australia, the average length of stay in hospital is 10 days after CRC
surgery (Rothwell, Bokey, Keshava, Chapuis, & Dent, 2006). Approximately 11% of
patients have a CRC surgery-related post-operative complication (i.e. wound infection,
deep venous thrombosis, pulmonary embolus, anastomotic leak. Wound infection is
the most commonly reported (7.4%) complication and anastomotic leak is the second
most commonly reported complication (2.1%) (McGrath et al., 2004). Postoperative
Chapter 2. Colorectal cancer
37
complications are classified as infective or non-infective. Infective complications
include wound infection, anastomotic leakage, Intra-abdominal collection, pneumonia,
septicaemia, and urinary tract infection (McSorley, Horgan, & McMillan, 2016).
Non-infective complications are seroma, dehiscence, haemorrhage, myocardial
infarction, arrhythmia, venous thromboembolism, cerebrovascular accident, renal
failure, acute urinary retention, and ileus (paralytic/non-mechanical small bowel
obstruction) (McSorley et al., 2016). McSorley et al. has reported that infective
complications have a detrimental impact on disease free and overall survival (hazard
rate = 1.4, 95%CI 1.1 - 1.8; hazard rate = 1.4, 95%CI 1.2 - 1.6) (McSorley et al.,
2016). Furthermore, open CRC surgery is associated with high levels of postoperative
fatigue, malnutrition (Garth, Newsome, Simmance, & Crowe, 2010), and a significant
reduction in physical performance, work capacity, muscle strength and lean body
mass (Jensen et al., 2011). Postoperative complications and morbidity have adverse
effects on HRQoL, particularly physical functioning, role functioning, social
functioning, body image, mobility, self-care, and pain/discomfort after curative CRC
surgery (Brown et al., 2014) which are detrimental to the patient. Post-operative
impairments and recovery following CRC in patient outcomes are investigated further
in Study 3 in this thesis.
2.9.2 Adjuvant medical treatment (radiotherapy and chemotherapy)
Neoadjuvant therapy
Neoadjuvant therapy (i.e. pre-operative RT with or without CT) is recommended by
the NCCN guideline for stage II and III rectal cancer (National Comprehensive
Cancer Network (NCCN), 2016b). Neoadjuvant therapy followed by radical resection
and subsequent adjuvant CT is standard care for patients with locally advanced rectal
cancer (Sclafani & Chau, 2016). Neoadjuvant treatment is also an option for patients
with resectable T4b colon cancer (National Comprehensive Cancer Network (NCCN),
2016a). However, neoadjuvant therapy is not recommended for patients with stage I
CRC given the low recurrence rate (about 3%) and small benefits (Brenner et al.,
2014). The role of the neoadjuvant RT is to inhibit cell proliferation and tumour
Chapter 2. Colorectal cancer
38
growth and to induce apoptotic cell death (Hendry & West, 1997). The potential
effects of a combination of neoadjuvant RT with CT are to sensitize local RT, to
induce tumour downsizing, to improve rates of sphincter preservation, and to increase
rates of pathological complete response (Gaertner, Kwaan, Madoff, & Melton, 2015).
In Australia, about 72% of patients with rectal cancer have received neoadjuvant RT
(McGrath et al., 2004). Although neoadjuvant therapy improves oncologic outcomes
(survival and recurrence rates) for patients with rectal cancer, it is associated with
treatment-related toxicity (Joye & Haustermans, 2014; National Comprehensive
Cancer Network (NCCN), 2016b); high rates of morbidity, such as impaired bowel
and sexual function, malnutrition, and reduced physical fitness (Gavaruzzi, Lotto,
Giandomenico, Perin, & Pucciarelli, 2014; West et al., 2014; Yamano et al., 2016);
and decreased HRQoL (Battersby et al., 2016). A systematic review by Gavaruzzi et
al. found that neoadjuvant therapy has a detrimental impact on bowel and sexual
function but less significant impact on bladder function (Gavaruzzi et al., 2014).
Adjuvant therapy
Adjuvant CT is recommended for all patients with stage II and III rectal cancer
(National Comprehensive Cancer Network (NCCN), 2016b), and patients with stage
III or stage II colon cancer with a high risk of relapse (Brenner et al., 2014). In
Australia, adjuvant CT is received by 29% of stage II colon cancer and 47% of stage
II rectal cancer, and 76% of stage III colon cancer and 90% of stage III rectal cancer
(McGrath et al., 2004). Chemotherapy regimen involving infusional 5-FU with
leucovorin (folinic acid) is the standard of care for patients with CRC (Gustavsson et
al., 2015), and a combination of CT regimen (Oxaliplatin/5-FU/Leucovorin) called
FOLFOX has been shown to further enhance the treatment (Brezden-Masley &
Polenz, 2014).
Despite the survival benefits of adjuvant CT, toxicities of the CT can significantly
impact on patient’s HRQoL (Mols et al., 2015). These include nausea, diarrhoea,
myelosuppression, fatigue, palmar-plantar syndrome (hand-foot syndrome),
Chapter 2. Colorectal cancer
39
peripheral neuropathy, and hypersensitivity (Aprile, Rihawi, De Carlo, & Sonis, 2015;
Goodwin & Asmis, 2009; Park et al., 2013; Tantoy, Cataldo, Aouizerat, Dhruva, &
Miaskowski, 2016). During CT, the most common physical and psychological
symptoms experienced by more than 40% of patients with CRC are
numbness/tingling in the hands/feet (64%), lack of energy (62%), feeling drowsy
(49%), nausea (45%), shortness of breath (43%), dry mouth (42%) difficulty sleeping
(46%) and worrying (44%) (Pettersson, Bertero, Unosson, & Borjeson, 2014). A
previous study has also shown that patients treated with CT who are not meeting the
PA guidelines of 150 min of moderate to vigorous PA per week experience higher CT
related toxicities (Mols et al., 2015).
In Australia, about 17% of patients with CRC present with a metastasis at the time of
diagnosis (McGrath et al., 2004). The main goals of treatment for stage IV CRC are to
prolong survival, to cure, to stop tumour progression, to improve cancer-related
symptoms, and to maintain HRQoL (Labianca et al., 2010; Van Cutsem, Cervantes,
Nordlinger, Arnold, & Group, 2014). Treatment options include surgical resection of
primary tumour, surgical resection of the metastases (liver or lung), palliative CT,
palliative RT, and targeted therapy (Labianca et al., 2010).
Targeted therapy
Biologic or targeted agents, such as monoclonal antibodies (cetuximab and
panitumumab) that inhibits epidermal growth factor receptor; a monoclonal antibody
(bevacizumab) and proteins (aflibercept) against vascular endothelial growth factor;
and a multi-kinase inhibitor (regorafenib), are used in combination with CT in
patients with stage IV CRC (Aparo & Goel, 2012; Fakih, 2015). The overall survival
in patients who have received targeted therapy ranges from 6 months to 26 months,
which is worse than curative treatment (Rolfo et al., 2014). Regardless of the survival
benefits from the introduction of targeted therapy (Kirstein et al., 2014), treatment of
stage IV CRC should be personalized depending on the age of patient, patient’s
molecular phenotype, comorbidities, performance status, extent of the disease, and
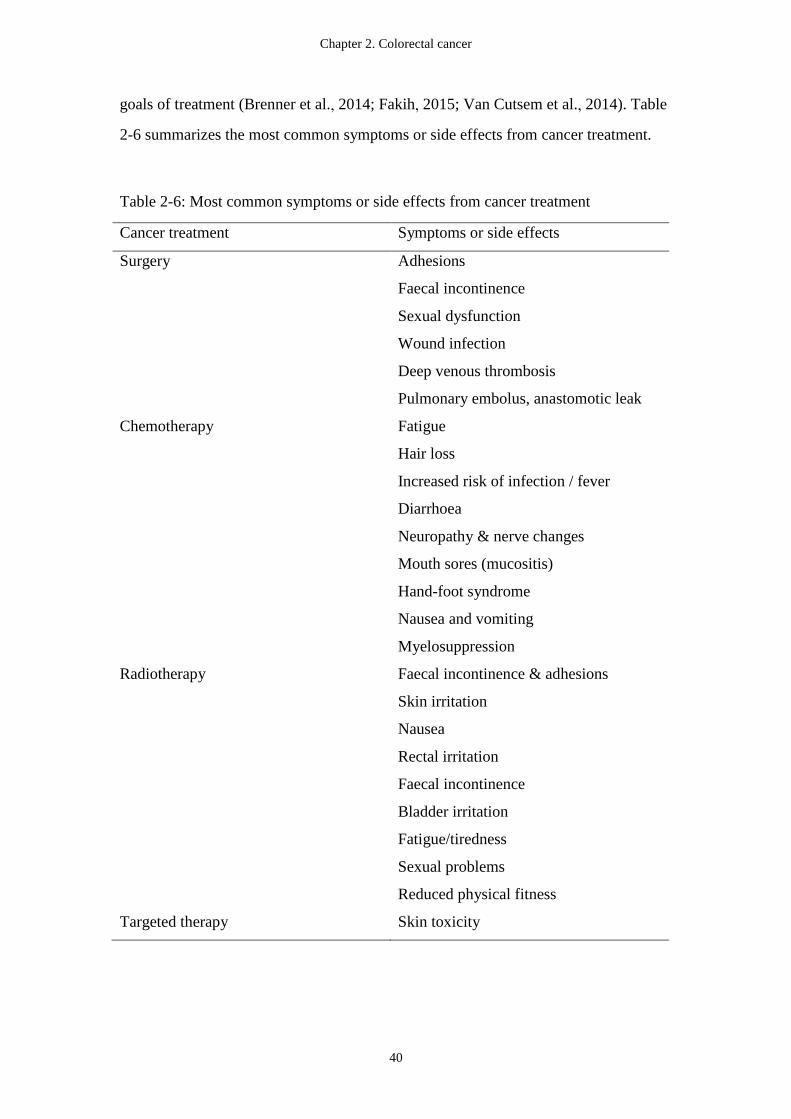
Chapter 2. Colorectal cancer
40
goals of treatment (Brenner et al., 2014; Fakih, 2015; Van Cutsem et al., 2014). Table
2-6 summarizes the most common symptoms or side effects from cancer treatment.
Table 2-6: Most common symptoms or side effects from cancer treatment
Cancer treatment Symptoms or side effects
Surgery Adhesions
Faecal incontinence
Sexual dysfunction
Wound infection
Deep venous thrombosis
Pulmonary embolus, anastomotic leak
Chemotherapy Fatigue
Hair loss
Increased risk of infection / fever
Diarrhoea
Neuropathy & nerve changes
Mouth sores (mucositis)
Hand-foot syndrome
Nausea and vomiting
Myelosuppression
Radiotherapy Faecal incontinence & adhesions
Skin irritation
Nausea
Rectal irritation
Faecal incontinence
Bladder irritation
Fatigue/tiredness
Sexual problems
Reduced physical fitness
Targeted therapy Skin toxicity
Chapter 2. Colorectal cancer
41
2.10 Side effects and symptoms following treatment
Patients with stage I-III CRC experience symptoms associated with their disease,
treatment, and comorbidities (Deshields, Potter, Olsen, Liu, & Dye, 2011). Research
has shown that patients with CRC 6 to 8 months following initial diagnosis report an
average of 12 symptoms (Deshields et al., 2011). Overall, lack of energy was the most
prevalent symptom for CRC, which was experienced by 79% of patients with CRC
(Deshields et al., 2011). In addition to the symptoms, comorbidity is also common
among patients with CRC; hypertension, diabetes, and cardiovascular diseases are the
most prevalent comorbodities (van Leersum et al., 2013). Symptoms and
comorbidities can significantly impact upon patients’ activities of daily living, reduce
their functional status, and decrease their HRQoL (Cheng & Lee, 2011). Based on the
ICF model, Bours et al. have identified potential predictors of low HRQoL in CRC
survivors (Bours et al., 2016), which include the presence of a stoma and comorbidity
(ICF domain: health condition); high BMI, high levels of fatigue, psychological
distress, anxiety, and depression (ICF domain: body structures/functions); low levels
of PA (ICF domain: activities); low perceived social support, and low perceived
quality of care (environmental factors); low optimism and negative cancer threat
appraisal (personal factors). The most common symptoms experienced by the patients
following CRC treatment are described below.
2.10.1 Pelvic floor dysfunction
Pelvic floor dysfunction refers to a wide variety of clinical conditions, including
bladder, bowel, and sexual dysfunction (Sung & Hampton, 2009).
Bowel function and symptoms
Bowel symptoms are common in the general population (Kepenekci et al., 2011). The
prevalence of faecal incontinence is 8% (male 8% and female 9%) in the community
(Ng, Sivakumaran, Nassar, & Gladman, 2015). Bowel symptoms or dysfunction,
including diarrhoea, abdominal pain, an alteration in the frequency of bowel

Chapter 2. Colorectal cancer
42
movements, incontinence, abnormal sensations, and difficulties with evacuation, are
commonly reported among CRC survivors (Kent, Mitchell, Oakley-Girvan, & Arora,
2014), and most of these symptoms are frequent and severe within the first year
following rectal cancer surgery, especially within the first six months, and stabilize
after one year though some may persist for years (Lai, Wong, & Ching, 2013).
Surgical treatment may damage anal sphincter or levator ani muscles and alter bowel
function in patients who have undergone surgery for rectal cancer (Hirano, Koda,
Kosugi, Yamazaki, & Yasuda, 2011; Koda et al., 2009; van Duijvendijk et al., 2003).
Bowel symptoms are commonly reported among patients undergoing LAR for rectal
cancer 8 to 16 months postoperatively, with 63% experienced incontinence of flatus,
42% incontinence of liquid stool, and 14% incontinence of solid stool (Lin, Chen, &
Liu, 2015). Bowel dysfunction after rectal cancer treatment is closely related to
tumour height, which determines preservation of the anal sphincters and rectal
capacity; pouch reconstruction; and RT (Fish & Temple, 2014).
While it is widely recognized that bowel dysfunction is more prevalent and severe in
patients following rectal cancer surgery than patients with colon cancer (Fish &
Temple, 2014; Scheer et al., 2011; van Duijvendijk et al., 2003), small studies have
documented that patients who have undergone surgery for colon cancer also
experience changes in bowel habits and other bowel problems (Phipps et al., 2008;
Thorsen et al., 2016). A study by Nikoletti et al. which included both colon and rectal
cancer cohorts reported that incomplete evacuation (75.2%), excessive flatus (75.2%),
urgency (73.3%), straining (61.4%), perianal soreness or itching (49.5%), bloating
(43.6%), and faecal incontinence (37.6%) are the most frequently reported bowel
symptoms in patients 6 to 24 months after surgery for CRC (Nikoletti et al., 2008).
Neoadjuvant chemoradiotherapy has also been documented to cause adverse effects
on bowel function by vascular toxicity and damage to the anal sphincter muscle,
which may lead to a decrease in anal resting pressure and colonic compliance and
inhibition of the impulse conduction (Knowles et al., 2013; Ozgen et al., 2015). Rectal
cancer surgery (i.e. TME) is probably the main contributing factor to major LAR
Chapter 2. Colorectal cancer
43
syndrome, a constellation of symptoms including faecal urgency, frequent bowel
movements, bowel fragmentation and incontinence (Ziv, Zbar, Bar-Shavit, & Igov,
2013), with preoperative RT and age > 75 years conferring further risks (Chen et al.,
2015). Two systematic reviews have concluded that TME and preoperative RT have
negative impact on long-term bowel function (Loos et al., 2013; Scheer et al., 2011).
Bowel dysfunction and symptoms following cancer treatment can lead to alterations
in daily activities, work, social relationships, and impact the patients’ HRQoL (Bailey
et al., 2015; Varpe et al., 2011).
Bladder function and symptoms
Bladder dysfunction is a common problem within the general population, and the
prevalence is lower in males (13% - 28%) (Martin et al., 2011) than in females (32% -
66%) (Teleman, Lidfeldt, Nerbrand, Samsioe, & Mattiasson, 2005), as vaginal
delivery and parity increase the risk of urinary symptoms in women (Kepenekci et al.,
2011; Lukacz, Lawrence, Contreras, Nager, & Luber, 2006). Bladder dysfunction and
symptoms include urinary incontinence, urgency and frequency, slow or intermittent
stream and straining, and feeling of incomplete emptying (Messelink et al., 2005);
among which, urinary incontinence is the main focus in the literature. Approximately
1% to 39% of male and 37% to 55% of female in general population experience
urinary incontinence (Tikkinen, Agarwal, & Griebling, 2013; Wood & Anger, 2014).
Although bladder dysfunction after CRC treatment remains poorly understood (Fish
& Temple, 2014), it is a significant clinical problem and has been shown to be related
to surgical nerve damage in rectal cancer (Lange et al., 2008). While bladder
symptoms are transient and less frequently reported (10.3%) in patients following
colon cancer treatment (Fish & Temple, 2014; Tomoda & Furusawa, 1985), patients
following rectal cancer surgery often experience worse bladder symptoms compared
to preoperative levels (Daniels, Woodward, Taylor, Raja, & Toomey, 2006). One
study has shown bladder symptoms developed following surgery for rectal cancer in
females included nocturia (59%) and stress incontinence (18%), and 80% of these
symptoms persisted longer than three months from surgery (Daniels et al., 2006).
Urgency and incontinence are the most frequent bladder symptoms reported in 77%
Chapter 2. Colorectal cancer
44
and 63% of patients who have undergone APR or LAR for rectal cancer (Bregendahl,
Emmertsen, Lindegaard, & Laurberg, 2015). Neoadjuvant RT for rectal cancer has
also been shown to be associated with voiding difficulties (odds ratio [OR] = 1.6,
95% CI 1.1 - 2.4) (Bregendahl et al., 2015). To date, post-operative bladder
dysfunction is prevalent in patients after rectal cancer treatment, however there is
limited evidence on bladder symptoms in patients following colon cancer treatment.
More research on changes in bladder symptoms in patients undergoing colon cancer
surgery is warranted.
Sexual function and symptoms
There is a limited number of studies evaluating sexual dysfunction in the community
(McCool, Theurich, & Apfelbacher, 2014). Among females, sexual dysfunction
includes hypoactive sexual desire disorder, sexual arousal disorder, orgasm disorder,
and pain disorders (Giraldi et al., 2011). The prevalence rates of sexual dysfunction in
females varies widely in the literature, with the prevalence of female arousal disorder
ranging from 11% to 48% (McCool et al., 2014), hypoactive sexual desire disorder
3% to 10% (Davison, 2012; McCabe & Goldhammer, 2013) and pain disorders 6.5%
to 45% (Boa, 2013). In males, sexual dysfunction can be classified into erectile
dysfunction and ejaculatory disorders such as premature ejaculation (Jannini, Maggi,
& Lenzi, 2011). The prevalence rates of erectile dysfunction and premature
ejaculation are about 34% and 30% respectively (Lee, Fahmy, & Brock, 2013).
The rates of sexual dysfunction can be high in patients with CRC given the
physiological changes following cancer treatment (Averyt & Nishimoto, 2014).
Similar to bladder dysfunction, sexual dysfunction after CRC treatment also remains
poorly understood due to insufficient measurement of preoperative function and
psychosocial confounders (Fish & Temple, 2014). Nevertheless, to date it appears that
both men and women experience sexual dysfunction after rectal cancer surgery
(Angenete, Asplund, Andersson, & Haglind, 2014). Following surgery for rectal
cancer, sexual function is worse in 23% to 69% of men and 19% to 62% of women
(Ho, Lee, Stein, & Temple, 2011). Moreover, rates of erectile dysfunction (54%

Chapter 2. Colorectal cancer
45
versus 25%) and ejaculation problems (68% versus 47%) are higher in male patients
with rectal cancer than those with colon cancer (Den Oudsten et al., 2012). Females
with rectal cancer have reported more vaginal dryness (35% versus 28%) and pain
during intercourse (30% versus 9%) than those with colon cancer (Den Oudsten et al.,
2012). Neoadjuvant RT, a stoma, complications during or after surgery, a higher age,
type of surgery, and a lower tumour location are the predictors of postoperative sexual
dysfunction in patients with CRC (Traa, De Vries, Roukema, & Den Oudsten, 2012).
As most of the existing studies on sexual dysfunction following CRC surgery suffer
from low methodological quality (i.e. cross-sectional design, small sample size, and
the use of nonstandardized measurements) (Traa et al., 2012), more well designed
research is needed to understand the natural history of sexual dysfunction in patients
undergoing CRC surgery before an appropriate intervention can be developed to
address this important issue in the CRC populations.
2.10.2 Physical function (functional exercise capacity and muscle strength)
Functional exercise capacity is defined as the maximal performance in a given
physical domain and is an important measure of an individual’s ability to achieve
essential tasks needed in daily living (Larson, 2007; Matheson, 1996). Functional
exercise capacity can be measured directly by determining peak oxygen consumption
(VO2max), estimated from the highest treadmill or cycle work rate achieved, or
measured using submaximal testing, such as timed field walking tests (Fleg et al.,
2000). Patients with stage I-II CRC have significantly lower functional exercise
capacity measured by 6MWT (325 meters) compared to a healthy control group
(6MWT distance = 469 meters) 6 months following completion of cancer treatment
(Sanchez-Jimenez et al., 2015). A pre-operative 6MWT distance shorter than 392
meters is predictive of cardiopulmonary complications for colorectal surgery patients
(Li et al., 2013). Moreover, neoadjuvant chemoradiotherapy has been shown to be
associated with a clinically significant reduction in VO2max (West et al., 2014).
Functional exercise capacity is a common target for exercise and physiotherapy
interventions in CRC as higher functional exercise capacity is associated with a lower
Chapter 2. Colorectal cancer
46
risk of cancer mortality and cardiovascular disease mortality following a diagnosis of
CRC (Lakoski et al., 2015). Moreover, exercise and PA has numerous documented
health-benefits among cancer survivors, including improved disease-free survival,
functional exercise capacity, muscular strength, and HRQoL (Brown, Winters-Stone,
Lee, & Schmitz), which is discussed in further detail later in the thesis.
Muscle strength refers to the maximal voluntary force or torque of short duration that
skeletal muscles can bring to bear on the environment (Bohannon, 2015). Grip
strength measured by dynamometry has been shown to reflect overall muscle strength
and physical performance particularly among older adults (Bohannon, Magasi, Bubela,
Wang, & Gershon, 2012; Kim et al., 2016) and is highly predictive of survival
(Bohannon, 2015). The normative values of grip strengths for individuals living in the
community are 28kg (female) and 47kg (male) for individuals aged 51 to 60 years,
and 26kg and 42kg for females and males aged 61 to 70 years (Leong et al., 2016). A
previous study has shown that the hand grip strength in a group of stage II-III CRC
patients (average age 56 years) who completed treatment within 2 years was 24kg in
females and 40kg in males (Ahn et al., 2016). Furthermore, sarcopenia defined as
reduced skeletal muscle mass plus low muscle strength and/or low physical
performance is highly prevalent among older patients with early stage CRC (56% -
60%) (Broughman et al., 2015). Sarcopenia is an independent risk factor for
complications after surgery for CRC (Huang et al., 2015) and a predictor for worse
overall survival in patients who have undergone an elective open colon resection for
CRC (hazard ratio = 8.54, 95% CI 1.07 - 68.32) (Boer et al., 2016). Resistance
training has been shown to be associated with clinically positive effects on muscle
strength in cancer survivors (Strasser, Steindorf, Wiskemann, & Ulrich, 2013);
therefore, international guidelines recommend CRC survivors to do strength exercises
at least 2 days per week in addition to at least 150 min of aerobic exercises per week
(El-Shami et al., 2015).
2.10.3 Level of physical activity
Chapter 2. Colorectal cancer
47
According to the WHO, PA is defined as any bodily movement produced by skeletal
muscles that requires energy expenditure (World Health Organization, 2010). The
WHO guidelines recommend that adults aged 65 years and above should do at least
150 minutes of moderate-intensity aerobic PA throughout the week or at least 75
minutes of vigorous-intensity aerobic PA throughout the week or an equivalent
combination of moderate- and vigorous-intensity activity, undertake muscle
strengthening activities involving major muscle groups on 2 or more days a week; and
avoid sedentary time (World Health Organization, 2010). The PA guidelines
specifically for patients with cancer and cancer survivors are the same (Buffart,
Galvao, Brug, Chinapaw, & Newton, 2014; El-Shami et al., 2015; Rock et al., 2012).
Previous studies have reported that CRC survivors are less likely to meet the PA
recommendations than their healthy peers (Chung et al., 2013; Grimmett, Bridgewater,
Steptoe, & Wardle, 2011; Hawkes et al., 2008). A study by Chung et al. found that
patients with CRC tend not to participate in the recommended levels of PA during
treatment (meeting the guideline: 20% pre-diagnosis; 7.6% during treatment) (Chung
et al., 2013). Furthermore, an Australian survey among CRC survivors demonstrated
that CRC survivors were more likely to be insufficiently active (1–149 min per week)
and inactive (0 min per week) compared to a non-cancer population; the percentage of
survivors who were sufficiently active reduced from 53% pre-diagnosis to 32% at 6
months and 38% at 12 months post-diagnosis (Hawkes et al., 2008). At 12 months,
CRC survivors were more likely than a matched population group to be insufficiently
active (OR = 1.6, 95% CI 1.3 - 1.8) (Hawkes et al., 2008). The most commonly
reported barriers to PA in patients with CRC are related to cancer and its treatments
(e.g. fatigue), age and mobility-related comorbidities (e.g. impaired mobility) (Fisher
et al., 2016).
In CRC, sedentary behaviour is associated with poorer overall and disease specific
survival, with higher all-cause mortality when spending 6 or more hours per day of
leisure time sitting compared with fewer than 3 hours per day (prediagnosis sitting
time: RR = 1.4; 95% CI 1.1 - 1.7; postdiagnosis sitting time: RR = 1.3; 95% CI, 1.0 -
1.6) (Campbell, Patel, Newton, Jacobs, & Gapstur, 2013). Conversely, increased PA
Chapter 2. Colorectal cancer
48
is associated with improved prognosis and HRQoL (Otto et al., 2015). A
meta-analysis estimated that each 10 MET - hour per week increase in PA after CRC
diagnosis (i.e. 150 minute of moderate intensity activity per week) is associated with a
28% lower total mortality risk in CRC survivors (Schmid & Leitzmann, 2014).
Despite that PA levels of CRC survivors have been documented across the cancer
continuum, it remains unknown how PA levels change in relation to the CRC surgery
in Australia.
2.10.4 Anxiety and depression
The prevalence rate of anxiety and depression among the general Australian
population are 20% and 6% respectively (Chiu, 2004; McEvoy, Grove, & Slade,
2011).The diagnosis of cancer is a highly distressing experience for most patients and
their families due to the uncertainties related to cancer prognosis and the possibility of
death (Graca Pereira, Figueiredo, & Fincham, 2012). While anxiety rates in patients
with CRC are similar to the general population, depression rates are higher in patients
with CRC (19% for anxiety and 37% for depression) than the general population
(Simon, Thompson, Flashman, & Wardle, 2009; Tsunoda et al., 2005). Anxiety and
depression have been shown to be different in patient with CRC according to the
treatment approaches and disease stage (Graca Pereira et al., 2012). Patients who have
undergone surgery and CT or RT have significantly more anxiety and depression
compared to the surgery only group (Graca Pereira et al., 2012; Medeiros, Oshima, &
Forones, 2010). Patients with more advanced disease (stage III and IV) are more
anxious and depressed than those with localized disease (Simon et al., 2009).
However, a study by Russel et al. reported that CRC survivors who have completed
treatment within 6 months have lower levels of anxiety and depression compared to
community norms (Russell et al., 2015). The inconsistency in the literature warrants
further research to explore this issue. Nevertheless, research has shown that anxiety
and depression are strong predictors of HRQoL in patients with CRC (Graca Pereira
et al., 2012; Tung et al., 2016). Moreover, one study has shown that depressive
symptoms increase the risk of mortality among 1- to 2-year CRC survivors and 1- to

Chapter 2. Colorectal cancer
49
10-year CRC survivors (hazard ratio = 2.6, 95 % CI 1.4 - 4.5; hazard ratio = 1.9, 95 %
CI 1.2 - 2.8) (Mols, Husson, Roukema, & van de Poll-Franse, 2013).
2.10.5 Health-related quality of life (HRQoL)
Health-related quality of life refers to the physical, emotional and social aspects of
quality of life that are influenced by disease or treatment (Kaplan & Ries, 2007).
Symptoms, surgical procedures, and the number of comorbidities can significantly
affect HRQoL in patients with CRC (Marventano et al., 2013). A study has shown
that CRC survivors who have completed treatment within 6 months still experience
lower role, cognitive and social functioning, and higher fatigue, nausea/vomiting,
appetite loss, diarrhoea, financial problems, pain, and constipation than community
norms (Russell et al., 2015). Nevertheless, a previous study has shown that HRQoL in
patient with CRC is quite satisfactory one year after the surgery (Di Fabio, Koller,
Nascimbeni, Talarico, & Salerni, 2008) despite that patients undergoing surgery for
rectal cancer tend to have more bowel-related HRQoL problems than those
undergoing surgery for colon cancer (Di Fabio et al., 2008). Health-related quality of
life is also poor in patients with a permanent stoma following APR (Konanz, Herrle,
Weiss, Post, & Kienle, 2013). Research has shown that post-operative pelvic floor
dysfunction was associated with an impaired HRQoL (Pucciarelli et al., 2011; Taylor
& Morgan, 2011; Varpe et al., 2011). The presence of a stoma, comorbidity, high
BMI, high levels of fatigue, psychological distress, anxiety, depression, low levels of
PA, low perceived social support, and shorter time since diagnosis are the potential
predictors of low HRQoL in CRC survivors (Bours et al., 2016). Furthermore,
financial stress is strongly associated poorer HRQoL and may prevent adherence to
recommended treatments (Regenbogen et al., 2014) and thereby compromise
treatment outcomes. Therefore, understanding the symptoms and comorbidities
experienced by CRC survivors is essential for implementing appropriate supportive
care interventions with a particular focus on decreasing symptoms and improving
patients’ HRQoL.
Chapter 2. Colorectal cancer
50
Studies have found that HRQoL has an independent prognostic value in predicting
mortality in patients with CRC (Fournier et al., 2016; Wong, Law, Wan, Poon, & Lam,
2014). Moreover, Fournier et al. reported that patients with role functioning scores
lower than the median had a 5-year relative survival of 49% compared with 80% for
patients with role functioning scores higher than the median (hazard ratio = 3.1)
(Fournier et al., 2016). Given the close relationships between HRQoL and survival,
symptom management and HRQoL improvement are important goals in developing
cancer rehabilitation programs as survival following any cancer treatment is the
primary concern of patients.
2.11 Summary
Colorectal cancer is the second most commonly diagnosed cancer in Australia and
responsible for 11% of the total cancer burden. Medical treatments usually include a
combination of surgery, RT, CT, and or targeted therapy. However the treatment of
CRC has significant consequences on patients’ pelvic floor function (bowel, bladder,
and sexual function), physical function, psychological outcomes and HRQoL.
Post-treatment pelvic floor dysfunction affects patients physically, socially and
psychologically (Fish & Temple, 2014). Impaired pelvic floor function, low
functional exercise capacity and PA levels, anxiety, and depression are prevalent in
CRC; these symptoms following CRC treatment can cause significant burden to
patient, family, and society. Supportive care interventions and symptom management
targeting patients unmet needs is critical throughout the continuum of oncology care.
The next section of the thesis focuses on measurement instruments which can be used
to assess patients’ physical and psychological function and symptoms in CRC. Such
instruments can be used to measure change in patient outcomes over time and the
efficacy of supportive care interventions such as rehabilitation programs.

Chapter 3. Outcome Measures
51
Chapter 3. Outcome Measures
3.1 Introduction
In CRC, the disease and its treatments cause significant physical and psychological
impairments (Cheville, Beck, Petersen, Marks, & Gamble, 2009; Sweeney et al., 2006;
Yabroff, Lawrence, Clauser, Davis, & Brown, 2004). As described in the previous
chapter some of the common side effects and impairments experienced by patients
following CRC treatment are pelvic floor dysfunction, lower PA levels, muscle
strength weakness, reduced functional exercise capacity, anxiety, depression, and
impaired HRQoL (Fish & Temple, 2014; Hamaker et al., 2015; Jensen et al., 2011).
Being able to accurately measure these variables at a single point in time, as
longitudinally over time, is important to understand the impact and response to natural
history or treatments.
Measurement instruments can be performance-based instruments such as tests of
functional exercise capacity and muscle strength; clinician reported outcome
measures (CROM) such as tests of PFM (PFM) function; or patient reported outcome
measures (PROM) such as standardized, validated questionnaires (Gilbert,
Sebag-Montefiore, Davidson, & Velikova, 2015; Minneci et al., 2015; Valderas &
Alonso, 2008). To date, evidence on the validity of the measurement instruments for
pelvic floor outcomes and functional exercise capacity in patients with CRC is not
available. As the validity of an instrument or test is purpose-, setting- and
population-specific (Jerosch-Herold, 2005; Portney & Watkins, 2009; Talmage &
Rasher, 1981), it is important to assess the applicability and validity of the outcome
measures with respect to the characteristics of the CRC population.
This chapter begins by reviewing the outcome measures used in the prospective
observational studies and the non-randomized quasi-control study reported in Chapter
3, Chapter 4, Chapter 5, Chapter 6, and Chapter 7. As PROMs are standard measures
in the assessment of CRC treatment (McNair et al., 2015), these outcome measures
are discussed first. The second half of the chapter and next chapter describe Study
Chapter 3. Outcome Measures
52
1and Study 2, which evaluated the validity of a pelvic floor symptom-specific
questionnaire and three field walking tests in CRC populations, the results of which
informed the choice of measures used in subsequent studies in this thesis.
3.2 Patient reported outcome-measures (PROM)
3.2.1 Pelvic floor symptoms
Clinical measures for PFM function, such as pad testing, urodynamic tests, anorectal
manometry, anorectal sensation and ultrasound are commonly used for classifying
pelvic floor symptom severity (Messelink et al., 2005). However, discrepancies often
exist between clinical measures of symptom severity and the subjective patient
perception of the condition (Avery et al., 2007; Chen, Emmertsen, & Laurberg, 2014).
In response to this, the measurement of pelvic floor symptoms through the use of
psychometrically robust self-completion questionnaires has become more common
and is now recognized as the gold standard of measuring the patient perspective of the
condition (Chen, Emmertsen, & Laurberg, 2015; Kelleher et al., 2013).
Avery et al. have reviewed and identified a total of 23 robust and relevant
questionnaires for the assessment of urinary and anal incontinence, and most of the
questionnaires are sex-specific (Avery et al., 2007). Among all questionnaires for
incontinence, the ICIQ-UI SF is recommended as a Grade A questionnaire to assess
combined symptoms of urinary incontinence/lower urinary tract symptoms/overactive
bladder in males and females (Avery et al., 2007).
The ICIQ-UI SF is the first module developed by the WHO-sponsored International
Consultation on Incontinence (ICI) to assess urinary incontinence and its impact on
HRQoL (Avery et al., 2004). The ICIQ-UI SF consists of three scored items related to
frequency and amount of urinary incontinence and quality of life and a self-diagnostic
item, not scored. An overall ICIQ-UI SF score is calculated as the summation of the
three scored items (Reis, Beji, & Coskun, 2010). The cut-off scores are set to ‘0’
meaning ‘no incontinence’ and ‘≥ 1’ meaning ‘urinary incontinence’ (Klovning,

Chapter 3. Outcome Measures
53
Avery, Sandvik, & Hunskaar, 2009). The ICIQ-UI SF has been shown to have good
construct validity, acceptable convergent validity, and good reliability (Avery et al.,
2004).
Subsequently, the ICIQ-Bowel module (ICIQ-B) was developed as one of the series
questionnaires included in the ICIQ project (Abrams, Avery, Gardener, & Donovan,
2006). The ICIQ-B (Grade A+) is highly recommended by the ICI as the outcome
measures for the symptoms and impact of urinary and faecal incontinence in clinical
practice and research trials (Kelleher et al., 2013). The ICIQ-B contains a total of 21
questions; 17 of which are scored and arranged in 3 domains: bowel pattern (score
range 1-21), bowel control (score range 1-28), and quality of life (score range 0-26).
Four unscored items include other bowel symptoms and sexual impact. Higher score
indicates greater symptoms or impairment (Cotterill, Norton, Avery, Abrams, &
Donovan, 2011). Validity and reliability of ICIQ-B has been demonstrated (Cotterill,
Norton, Avery, Abrams, & Donovan, 2008; Cotterill et al., 2011). Both ICIQ-UI SF
and ICIQ-B are non-gender-specific questionnaires which have undergone extensive
psychometric testing in different patient groups, however not in CRC-specific
populations (Cotterill et al., 2011; Kelleher et al., 2013).
The APFQ is one of the few validated questionnaires that integrate bladder, bowel,
and sexual function as well as pelvic organ prolapse symptoms (Baessler, O'Neill,
Maher, & Battistutta, 2009, 2010). The APFQ was first developed as an
interviewer-administered questionnaire in Australia to assess bladder, bowel, and
sexual function; pelvic organ prolapse; and condition-specific quality-of-life issues in
community-dwelling women (Baessler, O'Neill, Maher, & Battistutta, 2008) and had
been later validated in groups of urogynaecological patients and in self-administered
format (Baessler et al., 2009). The APFQ consists of 42 questions, and the scores
within each domain were divided by the number of relevant questions and multiplied
by 10; thus, the scores range from 0-10 for each domain, giving a maximum total
score of 40 (Baessler et al., 2009). A higher score indicates more severe symptoms.
Although the APFQ was designed for females in the community (Baessler et al., 2008)
and females with pelvic floor disorders (Baessler et al., 2009), the questions in the
Chapter 3. Outcome Measures
54
bladder and bowel function domains of the APFQ may also be applicable to males.
Baessler et al. reported that a difference of more than 3 in the total score of the APFQ
can distinguish the community and clinical populations; a difference of 0.9 in the
bowel domain score is considered clinically important (Baessler et al., 2009). The
test-retest reliability of the APFQ has also been reported (kappa coefficients 0.7 to 1.0)
(Baessler et al., 2009). Although the psychometric properties of the APFQ have been
previously established (Baessler et al., 2008, 2009, 2010), it has not been evaluated in
a sample of patients with CRC. The validation of the APFQ bladder and bowel
function domains was tested in a group of patients who have undergone surgery for
CRC later in this Chapter.
3.2.2 Pelvic floor signs
Objective bladder and bowel diaries are recommended by the ICI to be used with the
PROMs for assessment and measurement of the degree of symptoms, bother of
incontinence and impact of treatment (Staskin et al., 2013). The bladder diary is a
comprehensive instrument to document objective information such as the times of
micturition and voided volumes, leakage episodes, fluid intake, and degree of urgency
(Abrams et al., 2010). Moreover, diary patterns may characterise normal and
abnormal states (Staskin et al., 2013). A 3-day bladder diary is recommended for
accurate assessment of bladder symptoms and has been shown to be equivalent to a
7-day diary (Brown et al., 2003; Staskin et al., 2013; Wieslander, 2009).
A bowel diary is strongly recommended by the ICI (grade A) for accurate information
of faecal incontinence severity (Bliss et al., 2013). A bowel diary can be helpful in
investigating bowel symptoms (Messelink et al., 2005) and used to record bowel
movements with the time of day, time spent at toilet, presence of straining, soiling
episodes, pad usage and use of medications to assist with bowel movements (Ballard
et al., 2015), and the utilization of the Bristol Stool Form Scale is preferred to
document stool consistency (O'Donnell, Virjee, & Heaton, 1990).

Chapter 3. Outcome Measures
55
3.2.3 Levels of physical activity
Physical activity is defined as “any bodily movement produced by skeletal muscles
resulting in energy expenditure” (Caspersen, Powell, & Christenson, 1985) and can be
measured using the validated and well-defined reference methods (e.g. double
labelled water, direct calorimetry, indirect calorimetry), objective measurements
(direct observation, pedometers, accelerometers, heart rate monitors) (Trost & O'Neil,
2014), or self-report methods (daily diaries and recall questionnaires) (Reiser &
Schlenk, 2009). Reference methods are mostly expensive and limited to the laboratory
setting (Aparicio-Ugarriza et al., 2015). Objective measurements are commonly used
in research practice but have limitations particularly due to the cost of purchasing the
device and patient burden / feasibility since the patient is required to wear the device
during waking hours for a continuous period of four to seven days (Aparicio-Ugarriza
et al., 2015). Objective measurements are understood to be more valid than self-report
(over reporting with questionnaires) (Westerterp, 2009) however self-report methods
are more practical for wider use in clinical settings (Reiser & Schlenk, 2009).
The short form version of the International Physical Activity Questionnaire (IPAQ-SF)
is commonly used to assess levels of PA in research studies and clinical practice
(Silsbury, Goldsmith, & Rushton, 2015). This is a detailed self-report questionnaire
which asks the patient about the frequency and duration of strenuous, moderate, and
mild physical activity undertaken in the previous seven days. The IPAQ-SF has good
reliability and acceptable validity (Craig et al., 2003; Lee, Macfarlane, Lam, &
Stewart, 2011; Silsbury et al., 2015). The total IPAQ-SF score in MET-minutes per
week is the summation of walking (3.3 MET), moderate activity (4.0 MET), and
vigorous (8.0 MET) activity minutes per week. Total IPAQ scores are classified as
"low" (not meeting the criteria for moderate-intensity and vigorous-intensity activity
categories), "moderate" (achieving at least 600 MET-minutes/week) and "high"
(achieving at least 3000 MET-minutes/week) (IPAQ Research Committee, 2005). The
IPAQ-SF has been used by a previous study to examine the patterns of PA in a CRC
population (Kang, 2015). Given there is no gold standard questionnaire for the
assessment of physical activity in the general or specific CRC population, we chose to
Chapter 3. Outcome Measures
56
use the IPAQ due to its prior use in CRC, international context (to allow comparison
of data across studies) and ease of completion (Kang, 2015; Silsbury et al., 2015).
3.2.4 Anxiety and depression
There are numerous PROMs for measuring psychological morbidity in oncology
research, and Hospital Anxiety and Depression Scale (HADS) is one of the most
frequently used questionnaires to measure symptoms of anxiety, depression, and
psychological distress among patients with cancer (Yeh, Chung, Hsu, & Hsu, 2014).
The HADS includes a total of 14 items and is composed of an anxiety subscale and a
depression subscale (Zigmond & Snaith, 1983). Each subscale is scored from 0 to 21
(Zigmond & Snaith, 1983). Scores of 0–7 represent no anxiety or depression, 8–10
indicates a borderline anxiety or depression, and 11–21 indicates a clinical anxiety or
depression (Luckett et al., 2010; Zigmond & Snaith, 1983). The HADS has
demonstrated high internal consistency in patient populations including cancer
(Zigmond & Snaith, 1983) and it has also been widely used in patients with CRC
(Polat, Arpaci, Demir, Erdal, & Yalcin, 2014; Tsunoda et al., 2005). The minimal
clinically important difference (MCID) of HADS has not been established; however,
the minimal detectable change in HADS (HADS-Anxiety= 3.80; HADS-Depression=
3.99; HADS-Total= 5.68) has been reported in patients with coronary heart disease
(Wang, Chair, Thompson, & Twinn, 2009).
3.2.5 Health related quality of life (HRQoL)
European Organization for Research and Treatment of Cancer Quality of Life Core
Questionnaire (EORTC QLQ-C30) is one of the most frequently used HRQoL
instruments in CRC research (Sanoff, Goldberg, & Pignone, 2007). In this thesis,
HRQoL was evaluated using the EORTC QLQ-C30 and the CRC modules
(QLQ-CR29). The EORTC QLQ-C30 comprises 30 items assessing functional and
symptom aspects of HRQoL; the QLQ-CR29 consists of 18 items assessing
gastrointestinal symptoms, pain and problems with micturition, and separate scales for
the patients with or without a stoma and for men and women’s sexual function
Chapter 3. Outcome Measures
57
(Whistance et al., 2009). The QLQ-CR29 was implemented in conjunction with the
EORTC QLQ-C30, giving a total of 59 items. All EORTC scale/single item measures
range in score from 0-100. A higher score on the functional and the global HRQoL
scale represents a high level of functioning and high HRQoL, while a higher score on
the symptom scale represents a high level of symptomatology. Osoba et al. has shown
that a mean change of 5 to 10 points on the EORTC QLQ-C30 indicates a “little”
change; a change of 10 to 20 points indicates a “moderate” change; and a change of
greater than 20 points indicates a “large” change (Osoba, Rodrigues, Myles, Zee, &
Pater, 1998). The EORTC QLQ-C30 and QLQ-CR29 have been shown to valid and
reliable to assess HRQoL in clinical trials and research in patients with CRC (Ganesh
et al., 2016; Whistance et al., 2009).
3.2.6 Self efficacy
Self-efficacy determines whether an individual’s coping behaviour will be initiated,
how much effort will be expended, and how long it will be sustained in face of
obstacles and adverse experiences (Bandura, 1977). As efficacy beliefs are
task-specific, different self-efficacy measures are required to assess the outcomes of
interest (Lev, 1997). The Physical Exercise Self-Efficacy Scale (PES) and Nutrition
Self-Efficacy Scale (NES) of the Health-Specific Self-Efficacy Scale developed by
Schwarzer and Renner (Schwarzer & Renner, 2005) were used in the study presented
in Chapter 6 to assess changes in self-efficacy before and after an oncology
rehabilitation program which implemented an international guideline on nutrition and
PA for cancer survivors (Rock et al., 2012). The PES and NES each consists of five
items, which are scored on a 4-point Likert-type scale (1 = very uncertain, 2 = rather
uncertain, 3 = rather certain, and 4 = very certain) (Schwarzer & Renner, 2005). The
total score of each scale is the sum of the responses to the 5 items ranging from 5-20.
Higher score indicates higher self-efficacy. The Health-Specific Self Efficacy Scale
has been shown to have satisfactory psychometric properties, with a Cronbach’s alpha
of 0.87 for NES and 0.88 for PES (Schwarzer & Renner, 2005). The Health-Specific
Self-Efficacy Scale has been widely used in patients with chronic diseases (Clarke,
2009).
Chapter 3. Outcome Measures
58
3.3 Clinical-reported outcome measures / performance-based outcome measures
3.3.1 Pelvic floor muscle function
Pelvic floor muscle function can be measured using manual or digital muscle testing,
pressure manometry, and ultrasound (Bø & Sherburn, 2005; Messelink et al., 2005).
Digital rectal examination is a common basic examination performed by the
gastroenterologist in patients with CRC and by the physiotherapist in patients with
bowel dysfunction (Bols et al., 2007; Lindsetmo, Joh, & Delaney, 2008). The DRE is
performed with the patient in the left lateral position by inserting a lubricated, gloved
index finger into the rectum to determine resting and squeeze pressure (Talley, 2008).
Worldwide, several scales of digital muscle testing are in use for PFM strength testing.
In this thesis, the International Continence Society (ICS) scale, which has been
recommended by the ICS, was chosen to grade the PFM contraction. Resting pressure
is scored as “increased”, “normal” or “reduced” at the discretion of the investigator
(Dobben et al., 2007). Squeeze pressure or maximum voluntary contraction (MVC) is
scored as “absent”, “weak”, “moderate” or “strong” (Haylen et al., 2010; Messelink et
al., 2005). The reliability of DRE for the evaluation of anal sphincter tone is
conflicting. Some studies have shown poor correlations between manometric findings
and digital assessment (Eckardt & Kanzler, 1993), while some showed significant
correlations between digital and manometric assessment of resting and squeeze anal
sphincter function (Hallan, Marzouk, Waldron, Womack, & Williams, 1989).
An anorectal manometer is a reliable instrument in the assessment of anorectal
pressure and is widely used in patients with incontinence (Kerschan-Schindl et al.,
2002; Messelink et al., 2005; Probst et al., 2010). The Peritron was used as the
anorectal manometry in this thesis as it is inexpensive and simple to operate, has been
used mainly in the setting of outpatient manometry (Simpson, Kennedy, Nguyen,
Dinning, & Lubowski, 2006), and has satisfactory correlations with standard
manometry equipment (Simpson et al., 2006). The Peritron manometer

Chapter 3. Outcome Measures
59
(Cardio-Design, Australia) consists of an anal probe connecting to an electronic
device that shows the values of contraction in centimetre of water (cmH2O) (Cardio
Design, 2016). Anorectal manometry is tested in the same position as for DRE (i.e.
left lateral position). The anal resting and squeeze pressures are assessed by inserting
the anal probe of the Peritron in the anus. A single pressure recording (displayed
numerically in cm H2O) reflects the average pressure generated in the anal canal
(Simpson et al., 2006). The Peritron has been shown to be to be highly reliable in
measuring PFM strength and endurance (Hundley, Wu, & Visco, 2005; Rahmani &
Mohseni-Bandpei, 2011).
Transperineal ultrasound (TPUS) is useful in the clinical assessment of PFM function
(Thompson, O'Sullivan, Briffa, Neumann, & Court, 2005) and is increasingly used for
anorectal evaluation (Albuquerque & Pereira, 2016). The TPUS used in this thesis is a
GE Voluson-e System (GE Medical System) with a 4D transducer RAB4-8RS
(4-8MHz). The participant is tested in supine position with hips and knees flexed to
60 degrees. The ultrasound transducer is placed in the mid-sagittal plane at the
perineum (Dietz, 2010). A 2-dimensional image of the pelvic floor is visualized with
a field of view of 70 degrees in the sagittal plane. Anorectal angle (in degrees)
(Raizada et al., 2010), levator hiatus anterior-posterior (A-P) distance (in centimetres)
(Oversand, Kamisan Atan, Shek, & Dietz, 2015), and distance from anorectal angle to
the horizontal reference line (in centimetres) are measured at rest and at MVC (best of
three contractions) (van Delft, Thakar, & Sultan, 2015). The anorectal angle is formed
by the longitudinal axis of the anal canal and the posterior rectal wall (Raizada et al.,
2010). The levator hiatus A-P distance (in centimetres) is measured from the lower
edge of the pubic symphysis to the anorectal angle (Oversand et al., 2015). The
distance from anorectal angle to the horizontal reference line is measured from the
anorectal angle to a horizontal line drawn from pubic symphysis parallel to the
transducer surface (Raizada et al., 2010). Previous studies have found significant
correlations between the assessment of PFM strength by digital palpation and
objective 2D and 3D ultrasound parameters in urogynaecological patients (Albrich et
al., 2015) and healthy women (Volloyhaug, Morkved, Salvesen, & Salvesen, 2015).
Chapter 3. Outcome Measures
60
Transperineal ultrasound has also been shown to be reliable to measure the PFM
function in male and female populations (Roll et al., 2015; Thompson et al., 2005).
3.3.2 Functional exercise capacity
Physical function is a measure of functional exercise capacity. There is no common
definition of physical function. According to the Patient-Reported Outcomes
Measurement Information System, physical function is defined as “the ability to carry
out various activities that require physical capability, ranging from self-care to
more-vigorous activities that require increasing degrees of mobility, strength, or
endurance" (Bruce et al., 2009). Physical function can be measured in many ways.
One of the most fundamental measures is functional exercise capacity (Evans, 2002).
Functional exercise capacity is the maximal performance in a given domain (Larson,
2007) and can be measured directly by determining the VO2peak or estimated from the
highest treadmill or cycle work rate achieved (Fleg et al., 2000). The VO2peak is the
one of the gold standard in the assessment of exercise tolerance (Vanhees et al., 2005)
and can be measured by the CPET with continuous gas exchange analysis during
incremental exercise (Steins Bisschop et al., 2012). However, laboratory-based testing
(i.e. CPET) usually requires an experienced technician and is complex, time
consuming and expensive (Jones, Eves, Haykowsky, Joy, & Douglas, 2008). Details
of the CPET procedure are described in Chapter 4. The 6MWT (Holland et al., 2014),
ISWT (Singh, Morgan, Scott, Walters, & Hardman, 1992), and ESWT (Revill,
Morgan, Singh, Williams, & Hardman, 1999) are commonly performed field walking
tests in clinical settings for functional exercise capacity as these tests are easy to
perform, time efficient, and require only portable equipment.
The 6MWT is a self-paced field walking test. Participants are asked to walk as far as
possible over a 30-meter course in 6 minutes as per published guidelines (American
Thoracic Society) (ATS Committee on Proficiency Standards for Clinical Pulmonary
Function Laboratories, 2002). The total distance walked in meters is documented.
Participant’s heart rate, oxygen saturation (SpO2), and perceived exertion and leg

Chapter 3. Outcome Measures
61
fatigue are recorded before and after the test (Kendrick, Baxi, & Smith, 2000). The
6MWT is recommended to be performed on two occasions to account for a learning
effect and the best test result is used in analysis (Spencer, Alison, & McKeough, 2008;
Wu, Sanderson, & Bittner, 2003). In patients with cancer, the 6WMT is reliable (the
intraclass correlation coefficient [ICC] r = 0.93) and valid (CPET VO2peak r = 0.67)
(Schmidt et al., 2013). The 6MWT is well validated for patients with cardiac or
pulmonary disease (Fotheringham et al., 2015; Guazzi, Dickstein, Vicenzi, & Arena,
2009; Singh et al., 2014), and has been reported as a valid measure for patients post
colorectal surgery (Moriello, Mayo, Feldman, & Carli, 2008). The MCID has not
been reported specifically for patients with CRC, however in patients with coronary
artery disease who have undergone a cardiac rehabilitation program it is 25 meters
(Gremeaux et al., 2011), in patients with lung cancer (many following surgery) it is 22
meters to 42 meters (Granger, Holland, Gordon, & Denehy, 2015), and in patients
with respiratory disease it is 25 meters to 33 meters (Holland et al., 2014).
The ISWT is an externally-paced incremental field walking test (Singh et al., 1992).
The distance in meters that an individual can walk up and down a 10-meter course
paced according to an incremental walking speed dictated by an audio signal is
measured. The speed increases every minute, and the test finishes when the
participant is unable to maintain the required speed or limited by dyspnoea or a heart
rate >85% predicted maximum (Singh et al., 1992). Duplicate tests are completed to
account for the learning effect, and the best test result is used in analysis (McKeough,
Leung, & Alison, 2011; Singh et al., 2014). The MCID in the ISWT for patients
following cardiac rehabilitation is 70 meters (Houchen-Wolloff, Boyce, & Singh,
2015). The ISWT has been shown to have good reliability (ICC > 0.75) and strong
correlations with the VO2peak (r ≥ 0.70) in patients with various diseases, such as
COPD, chronic heart failure, cardiomyopathy, and cystic fibrosis, and in patients who
have undergone cardiovascular, abdominal, or lung cancer surgery (Parreira et al.,
2014). The ISWT has also been shown to be valid and reliable to assess maximal
exercise capacity in patients with advanced cancer (Booth & Adams, 2001; Parreira et
al., 2014).

Chapter 3. Outcome Measures
62
The ESWT is an externally-paced field walking test of endurance capacity. It is
performed along the same course as the ISWT according to published guidelines
(Revill et al., 1999). The walking speed is pre-set at the pace equivalent to 85% of the
VO2peak calculated from the ISWT (Hill et al., 2012b). Patients are instructed to walk
for as long as possible until they are unable to maintain the required speed or became
breathless, and the endurance time in seconds is recorded. A single ESWT is
performed as no learning effect is reported for ESWT (McKeough et al., 2011; Ngai,
Spencer, Jones, & Alison, 2015). The ESWT has been shown to be valid in patients
with COPD (Revill et al., 1999) and very responsive to bronchodilation (Borel, Pepin,
Mahler, Nadreau, & Maltais, 2014) and pulmonary rehabilitation (Altenburg, de Greef,
ten Hacken, & Wempe, 2012; Eaton, Young, Nicol, & Kolbe, 2006).
3.3.3 Muscle strength
Hand held dynamometry for manual muscle testing is a common, simple
measurement of strength and has been used in many patient populations including
cancer. Hand-grip strength as an indicator of general muscle strength is measured
using the Jamar dynamometer (Lafayette Instrument Company, USA). The participant
is tested in the position recommended by the American Society for Hand Therapists
(Peolsson, Hedlund, & Oberg, 2001). Three measurements are made from both hands
of each participant and only the maximum values obtained from each hand are used
(Vaz, Thangam, Prabhu, & Shetty, 1996). Grip strength has been shown to be a
predictor of postoperative complications, mortality, and functional decline (Bohannon,
2001) and a strong predictor of all-cause death, cardiovascular death, and
cardiovascular disease (Leong et al., 2015). Hand-held dynamometry has been shown
to be a reliable, objective instrument for hand-grip strength (Mathiowetz, 2002;
Roberts et al., 2011). The MCID in grip strength is 5.0 kg and 6.2 kg for the affected
dominant and non-dominant sides in stroke respectively (Lang, Edwards, Birkenmeier,
& Dromerick, 2008) and 6.5 kg in patients treated for distal radius fracture (Kim, Park,
& Shin, 2014).
Chapter 3. Outcome Measures
63
3.4 Summary of outcome measures chosen for the studies in this thesis
The first part of this chapter has summarised the outcome measures included in the
studies described in the second part of Chapter 3, Chapter 4, Chapter 5, Chapter 6,
and Chapter 7. The outcome measures are chosen from the previous CRC and pelvic
floor research studies to measure the wide range of dysfunction and symptoms which
are likely to present after surgery and respond to an intervention. There is a paucity of
literature available to guide selection of the outcome measures that would be valid
and applicable in the population undergoing CRC surgery or an oncology
rehabilitation following CRC surgery. Hence the validity and applicability of some
commonly used CROMs and PROMs were investigated and reported in the next
section of this chapter, as well as Chapter 4 and Chapter 7.
3.5 Validation study of the Australian Pelvic Floor Questionnaire in patients
following surgery for colorectal cancer
This study is currently in press:
Lin K-Y, Frawley H.C., Granger C.L., Denehy L. (2016). The APFQ is a valid
measure of pelvic floor symptoms in patients following surgery for colorectal cancer.
Neurourology and Urodynamics. Accepted (24/08/2016).
Author contributions for this chapter are the following: K-YL, HF, CG and LD
conceived the idea for the paper. K-YL, HF, CG and LD contributed to research
design. K-YL, HF and CG contributed to data acquisition. K-YL, HF, CG and LD
contributed to data analysis and interpretation. K-YL completed all statistical analyses.
K-YL wrote the first draft of the manuscript and managed manuscript submission. All
authors revised the paper and provided scientific input. All authors approved the final
version of the manuscript.
Chapter 3. Outcome Measures
64
3.5.1 Introduction
This chapter will describe an analysis of data from two prospective studies to assess
the construct validity (Frost et al., 2007), and clinical utility (Mullins-Sweatt, Lengel,
& DeShong, 2016) of the bladder and bowel function domains of the APFQ compared
with two existing bladder and bowel questionnaires (i.e. ICIQ-UI SF and ICIQ-B) in
patients following surgery for CRC. Many symptom-specific or HRQoL
questionnaires (i.e. LAR Syndrome Score and EORTC QLQ-CR29) have been
developed and used to measure bladder and/or bowel dysfunction in patients with
CRC (Emmertsen & Laurberg, 2012; Whistance et al., 2009), however these measures
are either designed specifically for use in patients with rectal cancer or are lengthy
and time-consuming to complete. The APFQ is one of the few validated
questionnaires that integrates bladder, bowel, and sexual function as well as pelvic
organ prolapse symptoms (Baessler et al., 2009, 2010). Although the psychometric
properties of the APFQ have been previously established (Baessler et al., 2008, 2009,
2010), it has not been evaluated in a sample of patients with CRC. We hypothesized
that the bladder and bowel domains of the APFQ, which are less lengthy and more
symptom specific than the corresponding questions in the LAR Syndrome Score and
the EORTC QLQ-CR29, are also valid and applicable to patients with CRC.
This chapter contains content that is substantially unchanged from the content of the
paper which has been accepted for publication.
3.5.1.1 Study aims
Aim 1: To assess the construct validity, and clinical utility of the bladder and bowel
function domains of the APFQ compared with two existing bladder and bowel
questionnaires (i.e. ICIQ-UI SF and ICIQ-B) in patients following surgery for CRC.
Aim 2: To determine the predictors of post-operative bladder and bowel symptoms in
patients undergoing surgery for CRC
Chapter 3. Outcome Measures
65
3.5.2 Materials and Methods
Study design
This was an analysis of data from two ongoing prospective clinical studies at three
large hospitals in Melbourne Australia, two private and one public.
Study 1 is a prospective observational study to assess pelvic floor symptoms,
anorectal muscle function, functional outcomes, emotional distress, and HRQoL in
patients who undergo surgery for CRC. The study was approved by the Melbourne
Health Human Research Ethics Committee (HREC).
Study 2 is a prospective observational pre-post study to investigate the feasibility of a
general oncology rehabilitation program for patients following surgery for
abdomino-pelvic cancer (Australian New Zealand Clinical Trials Registry [ANZCTR]:
12614000580673). The study had ethics approval from Cabrini Hospital HREC.
Participants
Participants included patients who had undergone surgery for histologically
confirmed stage I-III CRC; had an Eastern Cooperative Oncology Group performance
status of between 0-2 (0 = fully active, 2 = up and about for 50% of a day); and had
sufficient English language skills to participate. Patients were excluded if they were
aged 86 and over, were pregnant or up to 12 months postpartum, or had severe
physical/psychiatric impairments. Data from all participants who were eligible from
the two ongoing prospective clinical studies and recruited between October 2013 and
August 2015 were used for analysis. Written informed consent was obtained from all
participants before completing the measurements.
Measures
Bladder and bowel symptoms were assessed using the bladder and bowel function
domains of the APFQ, ICIQ-UI SF, and ICIQ-B at six to eight weeks post-cancer
treatment.
Chapter 3. Outcome Measures
66
The APFQ is an instrument consisting of 42 questions in 4 domains (bladder, bowel,
and sexual function and pelvic organ prolapse) (Baessler et al., 2009). The scores
within each domain are divided by the number of relevant questions and multiplied by
10; thus, the scores range from 0 to 10 for each domain, giving a maximum total score
of 40 (Baessler et al., 2009). We chose to focus on the bladder and bowel function
domains, which contain 15 and 12 questions respectively, and the maximum total
score for both bladder and bowel function domains combined is 20. A higher score
indicates more severe symptoms. The APFQ has been validated in groups of
urogynaecological patients (Baessler et al., 2009) and applied in broad populations
(Laterza, Schrutka, Umek, Albrich, & Koelbl, 2015; Yang, Lim, Rah, & Kim, 2012).
The ICIQ-UI SF was developed to evaluate the severity of urinary incontinence and
its impact on HRQoL. It consists of three scored items related to frequency and
amount of urinary incontinence and quality of life and a self-diagnostic item, not
scored. An overall ICIQ-UI SF score is calculated as the summation of the three
scored items and ranges from 0 to 21. Urinary incontinence is defined as either absent
(score 0) or present (score ≥ 1) on the ICIQ-UI SF (Avery et al., 2004). Higher score
indicates worse symptom severity or greater impact of symptoms on HRQoL. The
ICIQ-UI SF has been shown to have good psychometric properties in patients with
incontinence or other lower urinary tract symptoms and is suitable for use in clinical
practice and research (Avery et al., 2004).
The ICIQ-B is a non-gender-specific questionnaire developed to evaluate anal
incontinence symptoms and impact on quality of life and contains a total of 21
questions. Seventeen of 21 questions are scored and arranged in three domains: bowel
pattern (score range 1-21), bowel control (score range 0-28), and quality of life (score
range 0-26). Four unscored items include other bowel symptoms and sexual impact. A
five-point Likert scale is used for most questions to assess the presence or absence of
a symptom and its severity, followed by visual analogue scale of 0–10 to assess
associated bother (Cotterill et al., 2011). Higher scores indicate greater impairment or
symptoms (Cotterill et al., 2011). The ICIQ-B has been shown to be a
Chapter 3. Outcome Measures
67
psychometrically robust instrument for use in patients with anal incontinence of
varying causes (Cotterill et al., 2011).
Statistical analysis
Statistical analysis was performed using SPSS Windows Version 22.0 (SPSS,
Chicago, IL, USA). Demographic and clinical outcome data of the participants were
analysed using descriptive statistics, such as mean and standard deviation (SD),
median and interquartile range (IQR), or number and percentage. The differences in
the participants’ characteristics between male and females were compared using the
independent t-test or Mann-Whitney U test for continuous variables, and χ2 test for
categorical variables. Pearson's correlation coefficients were used to examine the
bivariate relationships among the bladder domain of the APFQ and the total score of
ICIQ- UI SF, as well as the correlations between the bowel domain of the APFQ and
ICIQ-B subscales. The strength of the correlation was determined by the correlation
coefficient values (0.00–0.30 = negligible; 0.30–0.50 = low positive correlation; 0.50–
0.70 = moderate positive correlation; 0.70–0.90 = high positive correlation; and 0.90–
1.00 = very high positive correlation) (Zou, Tuncali, & Silverman, 2003).
The score of each instrument was categorized as symptomatic or asymptomatic using
a cut-off score of greater than or equal to 1, based on the cut-off value reported in
previous studies (Avery et al., 2004; Baessler et al., 2009). Kappa coefficients were
calculated to determine the agreement between questionnaires. A kappa value of less
than 0.40 was considered poor-to-fair agreement, 0.41-0.60 moderate agreement,
0.61-0.80 substantial agreement, and 0.81-1.00 almost perfect agreement (Landis &
Koch, 1977).
A Logistic regression model was applied to calculate the ORs to estimate whether
variables (age, level of tumour, and stage of cancer) identified by univariate analysis
(p-value < 0.20) (Table 3-1and Table 3-2) could predict the occurrence of
dichotomised bladder or bowel symptoms following CRC surgery. As this study was
an exploratory analysis, no power calculation was carried out. P values < 0.05 were
considered statistically significant.
Chapter 3. Outcome Measures
68
3.5.3 Results
Participant characteristics
Data from 44 participants (25 males and 19 females) with a mean age of 64.8 years
(SD = 14.1, range 26-85 years) were collected from the two studies (Figure 3.1).
Eighty-two percent and 18% had a confirmed diagnosis of colon cancer and rectal
cancer respectively. Seventy-five percent had not undergone any adjuvant therapies at
the time of diagnosis. Thirty-six percent had bladder symptoms and 66% had bowel
symptoms as assessed using the APFQ bladder and bowel domains; conversely, 64%
did not have bladder symptoms and 34% did not have bowel symptoms six to eight
weeks following cancer treatment (Table 3-3). No statistically significant differences
were found in socio-demographic and clinical characteristics and the number of
participants being symptomatic (APFQ bladder and APFQ bowel ≥ 1) between male
and females. Table 3-4 shows the descriptive statistics for APFQ bladder and bowel
domains, total score of ICIQ-UI SF, and ICIQ-B subscales as well as the number of
participants with a score above the cut-off score of being symptomatic. No
statistically significant differences existed in the number of participants being
symptomatic as assessed using the APFQ, ICIQ-UI SF, and ICIQ-B between males
and females (Table 3-4). Age (p = 0.002) was significantly different between
participants with or without bladder symptoms (Table 3-1). However, no significant
differences were found in demographic and clinical variables between groups with or
without bowel symptoms (Table 3-2).

Chapter 3. Outcome Measures
69
Table 3-1: Demographic and clinical variables in participants with and without bladder symptoms following surgery for colorectal cancer
Variables Total Males Females
Symptomatic
APFQ
bladder Score
≥ 1
Asymptomatic
APFQ bladder
Score < 1
p-value Symptomatic
APFQ
bladder Score
≥ 1
Asymptomatic
APFQ bladder
Score < 1
p-value Symptomatic
APFQ
bladder Score
≥ 1
Asymptomatic
APFQ bladder
Score < 1
p-value
Age, years
(mean±SD)a
73.3 ± 8.6 59.7 ± 15.1 0.002 71.6 ± 9.2 59.1 ± 14.4 0.023 76.0 ± 7.4 61.2±15.0 0.036
Genderb 0.565 - -
Male 10 (62.5) 15 (53.6) - - - - - -
Female 6 (37.5) 13 (46.4) - - - - - -
Level of
tumour, n
(%)b
0.941 1.00 0.943
Colon 13 (81.3) 23 (82.1) 8 (80.0) 12 (80.0) 5 (83.3) 11 (84.6)
Rectum 3 (18.8) 5 (17.9) 2 (20.0) 3 (20.0) 1 (16.7) 2 (15.4)
Adjuvant
treatment, n
(%)b
1.000 0.610 0.554
Yes 4 (25.0) 7 (25.0) 3 (30.0) 6 (40.0) 1 (16.7) 1 (7.7)
No 12 (75.0) 21 (75.0) 7 (70.0) 9 (60.0) 5 (83.3) 12 (92.3)
Length of
stay, days
(median,
IQR)c
8 (5.3 - 10.8) 7 (6.0 - 12.5) 0.802 8 (5.8 - 10.3) 8 (6.0 - 15.0) 0.696 6 (4.5 - 17.8) 6 (4.8 - 12.3) 1.000
Type of
surgery, n
(%)b
0.820 0.622 0.419
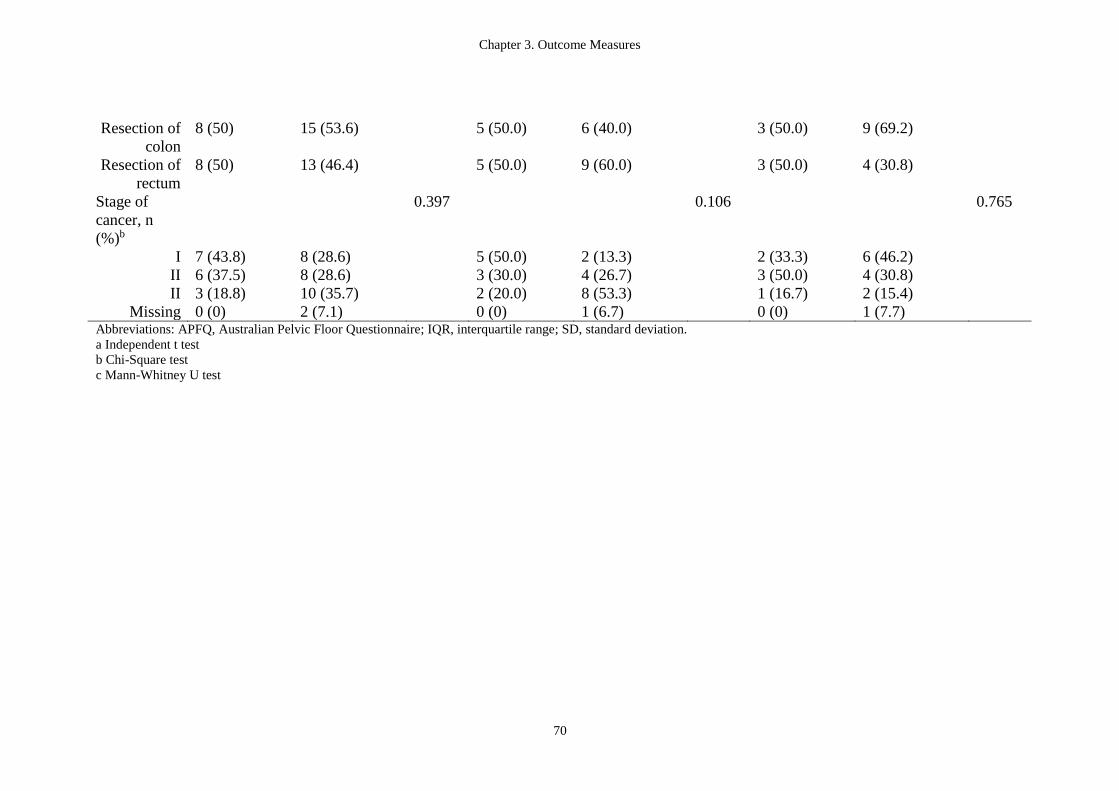
Chapter 3. Outcome Measures
70
Resection of
colon
8 (50) 15 (53.6) 5 (50.0) 6 (40.0) 3 (50.0) 9 (69.2)
Resection of
rectum
8 (50) 13 (46.4) 5 (50.0) 9 (60.0) 3 (50.0) 4 (30.8)
Stage of
cancer, n
(%)b
0.397 0.106 0.765
I 7 (43.8) 8 (28.6) 5 (50.0) 2 (13.3) 2 (33.3) 6 (46.2)
II 6 (37.5) 8 (28.6) 3 (30.0) 4 (26.7) 3 (50.0) 4 (30.8)
II 3 (18.8) 10 (35.7) 2 (20.0) 8 (53.3) 1 (16.7) 2 (15.4)
Missing 0 (0) 2 (7.1) 0 (0) 1 (6.7) 0 (0) 1 (7.7) Abbreviations: APFQ, Australian Pelvic Floor Questionnaire; IQR, interquartile range; SD, standard deviation.
a Independent t test
b Chi-Square test
c Mann-Whitney U test
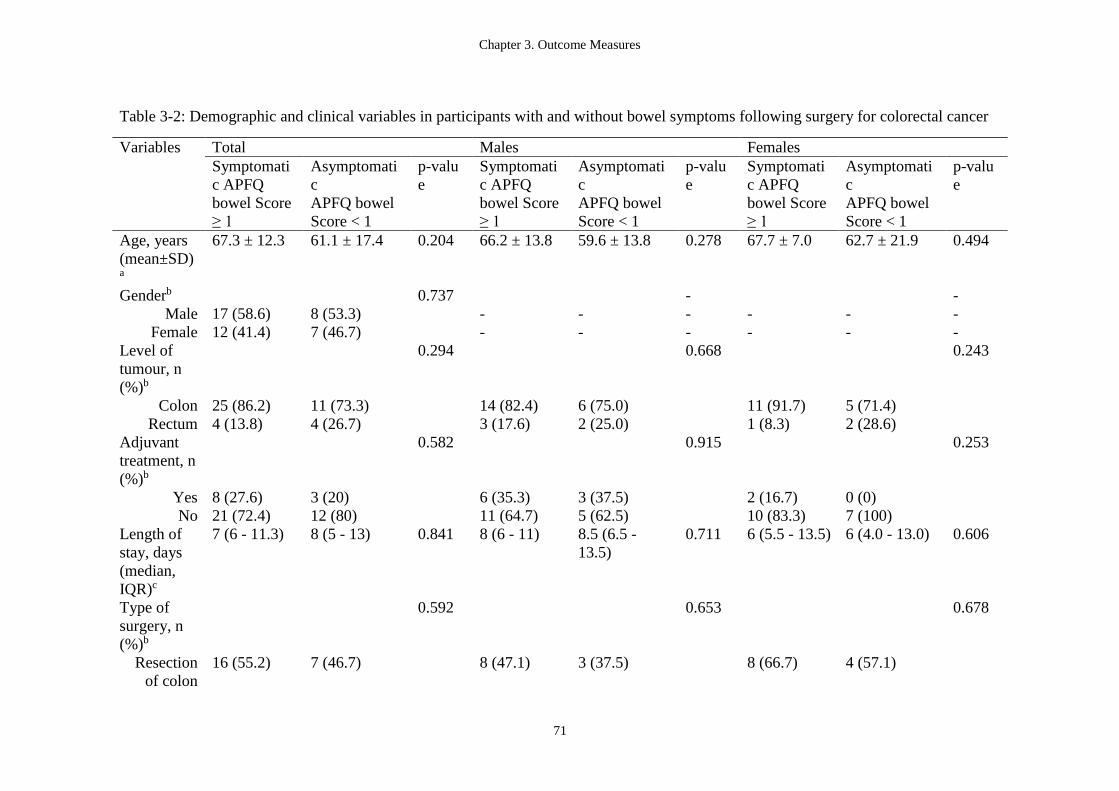
Chapter 3. Outcome Measures
71
Table 3-2: Demographic and clinical variables in participants with and without bowel symptoms following surgery for colorectal cancer
Variables Total Males Females
Symptomati
c APFQ
bowel Score
≥ 1
Asymptomati
c
APFQ bowel
Score < 1
p-valu
e
Symptomati
c APFQ
bowel Score
≥ 1
Asymptomati
c
APFQ bowel
Score < 1
p-valu
e
Symptomati
c APFQ
bowel Score
≥ 1
Asymptomati
c
APFQ bowel
Score < 1
p-valu
e
Age, years
(mean±SD)a
67.3 ± 12.3 61.1 ± 17.4 0.204 66.2 ± 13.8 59.6 ± 13.8 0.278 67.7 ± 7.0 62.7 ± 21.9 0.494
Genderb 0.737 - -
Male 17 (58.6) 8 (53.3) - - - - - -
Female 12 (41.4) 7 (46.7) - - - - - -
Level of
tumour, n
(%)b
0.294 0.668 0.243
Colon 25 (86.2) 11 (73.3) 14 (82.4) 6 (75.0) 11 (91.7) 5 (71.4)
Rectum 4 (13.8) 4 (26.7) 3 (17.6) 2 (25.0) 1 (8.3) 2 (28.6)
Adjuvant
treatment, n
(%)b
0.582 0.915 0.253
Yes 8 (27.6) 3 (20) 6 (35.3) 3 (37.5) 2 (16.7) 0 (0)
No 21 (72.4) 12 (80) 11 (64.7) 5 (62.5) 10 (83.3) 7 (100)
Length of
stay, days
(median,
IQR)c
7 (6 - 11.3) 8 (5 - 13) 0.841 8 (6 - 11) 8.5 (6.5 -
13.5)
0.711 6 (5.5 - 13.5) 6 (4.0 - 13.0) 0.606
Type of
surgery, n
(%)b
0.592 0.653 0.678
Resection
of colon
16 (55.2) 7 (46.7) 8 (47.1) 3 (37.5) 8 (66.7) 4 (57.1)
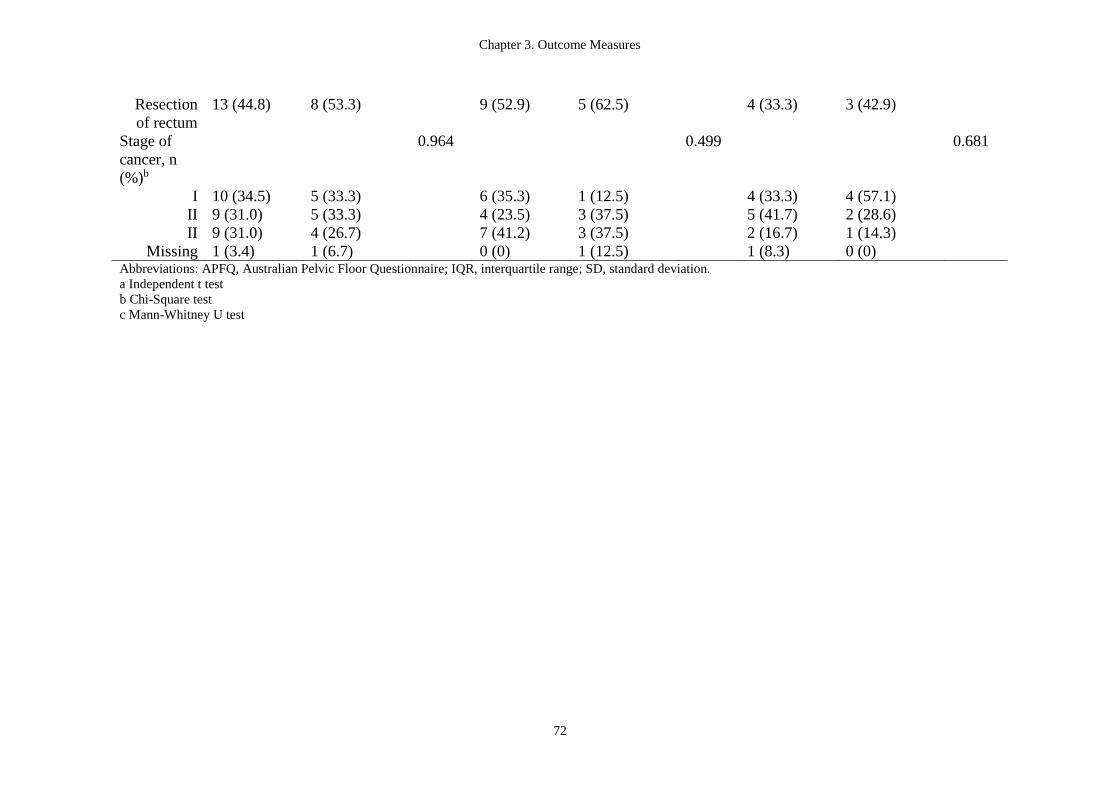
Chapter 3. Outcome Measures
72
Resection
of rectum
13 (44.8) 8 (53.3) 9 (52.9) 5 (62.5) 4 (33.3) 3 (42.9)
Stage of
cancer, n
(%)b
0.964 0.499 0.681
I 10 (34.5) 5 (33.3) 6 (35.3) 1 (12.5) 4 (33.3) 4 (57.1)
II 9 (31.0) 5 (33.3) 4 (23.5) 3 (37.5) 5 (41.7) 2 (28.6)
II 9 (31.0) 4 (26.7) 7 (41.2) 3 (37.5) 2 (16.7) 1 (14.3)
Missing 1 (3.4) 1 (6.7) 0 (0) 1 (12.5) 1 (8.3) 0 (0) Abbreviations: APFQ, Australian Pelvic Floor Questionnaire; IQR, interquartile range; SD, standard deviation.
a Independent t test
b Chi-Square test
c Mann-Whitney U test
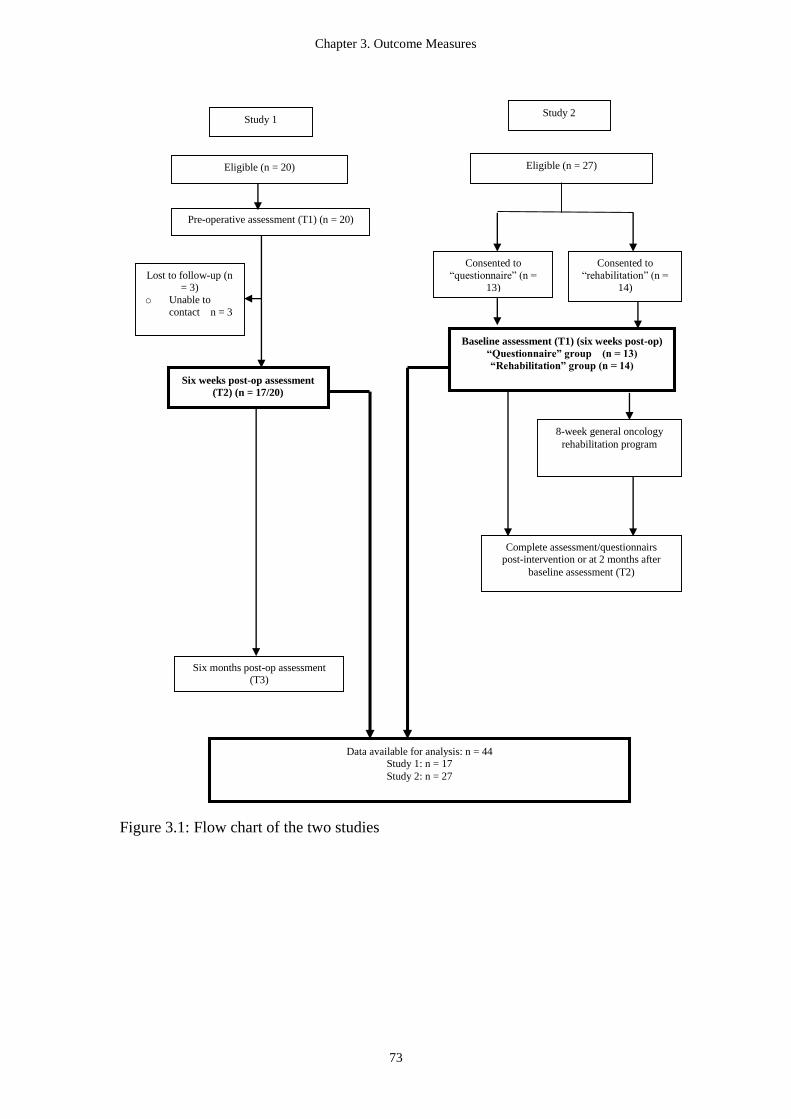
Chapter 3. Outcome Measures
73
Figure 3.1: Flow chart of the two studies
Study 1
Six weeks post-op assessment
(T2) (n = 17/20)
Six months post-op assessment (T3)
Data available for analysis: n = 44 Study 1: n = 17
Study 2: n = 27
Eligible (n = 20)
Lost to follow-up (n = 3)
o Unable to
contact n = 3
Study 2
Eligible (n = 27)
Consented to
“questionnaire” (n =
13)
Consented to
“rehabilitation” (n =
14)
8-week general oncology
rehabilitation program
Complete assessment/questionnairs post-intervention or at 2 months after
baseline assessment (T2)
Baseline assessment (T1) (six weeks post-op)
“Questionnaire” group (n = 13)
“Rehabilitation” group (n = 14)
Pre-operative assessment (T1) (n = 20)
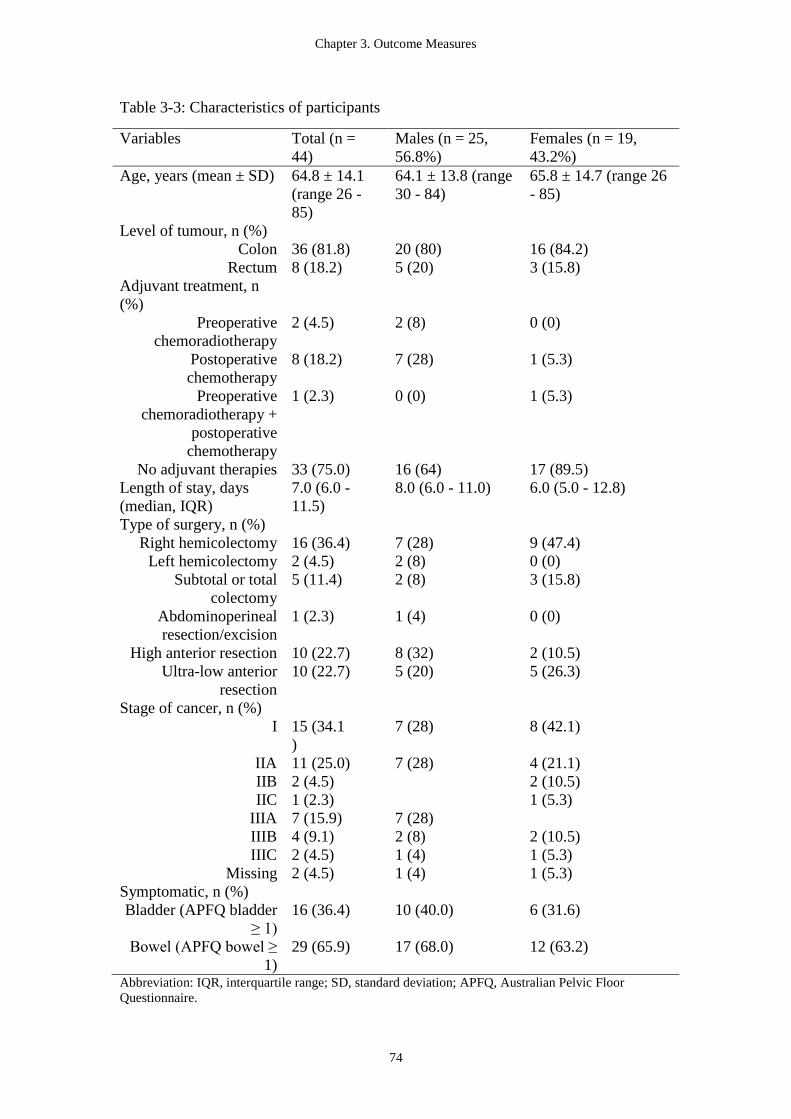
Chapter 3. Outcome Measures
74
Table 3-3: Characteristics of participants
Variables Total (n =
44)
Males (n = 25,
56.8%)
Females (n = 19,
43.2%)
Age, years (mean ± SD) 64.8 ± 14.1
(range 26 -
85)
64.1 ± 13.8 (range
30 - 84)
65.8 ± 14.7 (range 26
- 85)
Level of tumour, n (%)
Colon 36 (81.8) 20 (80) 16 (84.2)
Rectum 8 (18.2) 5 (20) 3 (15.8)
Adjuvant treatment, n
(%)
Preoperative
chemoradiotherapy
2 (4.5) 2 (8) 0 (0)
Postoperative
chemotherapy
8 (18.2) 7 (28) 1 (5.3)
Preoperative
chemoradiotherapy +
postoperative
chemotherapy
1 (2.3) 0 (0) 1 (5.3)
No adjuvant therapies 33 (75.0) 16 (64) 17 (89.5)
Length of stay, days
(median, IQR)
7.0 (6.0 -
11.5)
8.0 (6.0 - 11.0) 6.0 (5.0 - 12.8)
Type of surgery, n (%)
Right hemicolectomy 16 (36.4) 7 (28) 9 (47.4)
Left hemicolectomy 2 (4.5) 2 (8) 0 (0)
Subtotal or total
colectomy
5 (11.4) 2 (8) 3 (15.8)
Abdominoperineal
resection/excision
1 (2.3) 1 (4) 0 (0)
High anterior resection 10 (22.7) 8 (32) 2 (10.5)
Ultra-low anterior
resection
10 (22.7) 5 (20) 5 (26.3)
Stage of cancer, n (%)
I 15 (34.1
)
7 (28) 8 (42.1)
IIA 11 (25.0) 7 (28) 4 (21.1)
IIB 2 (4.5) 2 (10.5)
IIC 1 (2.3) 1 (5.3)
IIIA 7 (15.9) 7 (28)
IIIB 4 (9.1) 2 (8) 2 (10.5)
IIIC 2 (4.5) 1 (4) 1 (5.3)
Missing 2 (4.5) 1 (4) 1 (5.3)
Symptomatic, n (%)
Bladder (APFQ bladder
≥ 1)
16 (36.4) 10 (40.0) 6 (31.6)
Bowel (APFQ bowel ≥
1)
29 (65.9) 17 (68.0) 12 (63.2)
Abbreviation: IQR, interquartile range; SD, standard deviation; APFQ, Australian Pelvic Floor
Questionnaire.
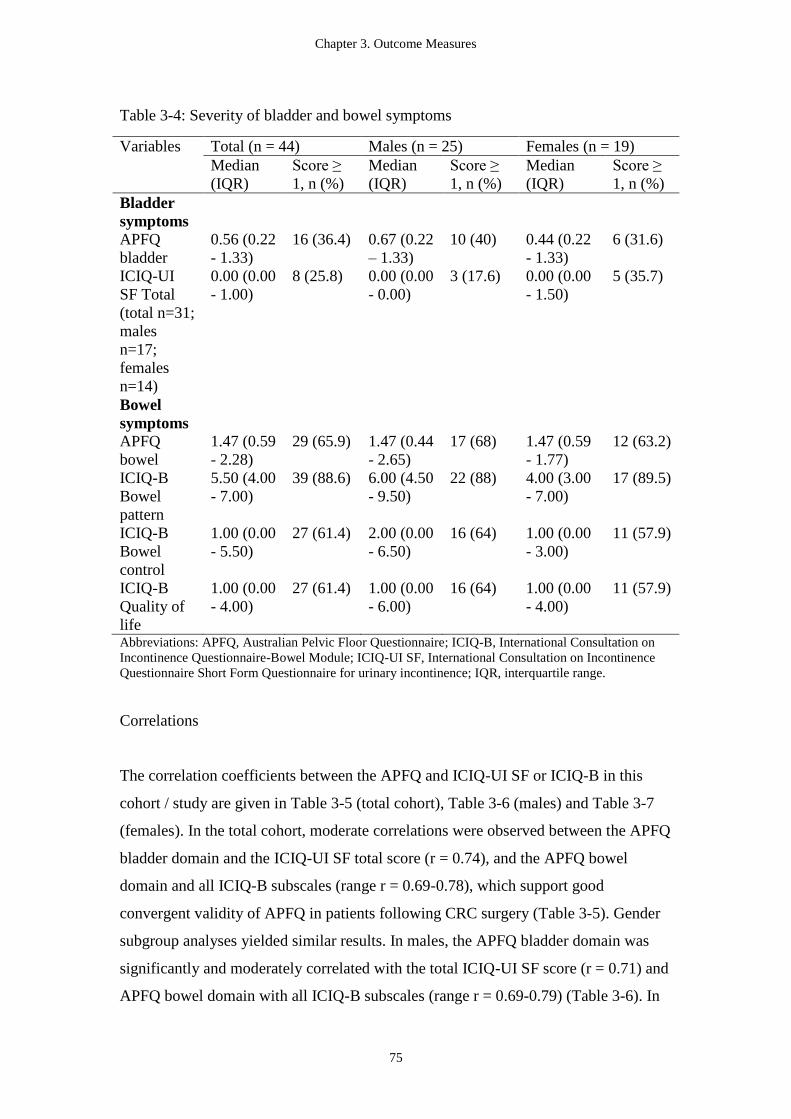
Chapter 3. Outcome Measures
75
Table 3-4: Severity of bladder and bowel symptoms
Variables Total (n = 44) Males (n = 25) Females (n = 19)
Median
(IQR)
Score ≥
1, n (%)
Median
(IQR)
Score ≥
1, n (%)
Median
(IQR)
Score ≥
1, n (%)
Bladder
symptoms
APFQ
bladder
0.56 (0.22
- 1.33)
16 (36.4) 0.67 (0.22
– 1.33)
10 (40) 0.44 (0.22
- 1.33)
6 (31.6)
ICIQ-UI
SF Total
(total n=31;
males
n=17;
females
n=14)
0.00 (0.00
- 1.00)
8 (25.8) 0.00 (0.00
- 0.00)
3 (17.6) 0.00 (0.00
- 1.50)
5 (35.7)
Bowel
symptoms
APFQ
bowel
1.47 (0.59
- 2.28)
29 (65.9) 1.47 (0.44
- 2.65)
17 (68) 1.47 (0.59
- 1.77)
12 (63.2)
ICIQ-B
Bowel
pattern
5.50 (4.00
- 7.00)
39 (88.6) 6.00 (4.50
- 9.50)
22 (88) 4.00 (3.00
- 7.00)
17 (89.5)
ICIQ-B
Bowel
control
1.00 (0.00
- 5.50)
27 (61.4) 2.00 (0.00
- 6.50)
16 (64) 1.00 (0.00
- 3.00)
11 (57.9)
ICIQ-B
Quality of
life
1.00 (0.00
- 4.00)
27 (61.4) 1.00 (0.00
- 6.00)
16 (64) 1.00 (0.00
- 4.00)
11 (57.9)
Abbreviations: APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on
Incontinence Questionnaire-Bowel Module; ICIQ-UI SF, International Consultation on Incontinence
Questionnaire Short Form Questionnaire for urinary incontinence; IQR, interquartile range.
Correlations
The correlation coefficients between the APFQ and ICIQ-UI SF or ICIQ-B in this
cohort / study are given in Table 3-5 (total cohort), Table 3-6 (males) and Table 3-7
(females). In the total cohort, moderate correlations were observed between the APFQ
bladder domain and the ICIQ-UI SF total score (r = 0.74), and the APFQ bowel
domain and all ICIQ-B subscales (range r = 0.69-0.78), which support good
convergent validity of APFQ in patients following CRC surgery (Table 3-5). Gender
subgroup analyses yielded similar results. In males, the APFQ bladder domain was
significantly and moderately correlated with the total ICIQ-UI SF score (r = 0.71) and
APFQ bowel domain with all ICIQ-B subscales (range r = 0.69-0.79) (Table 3-6). In
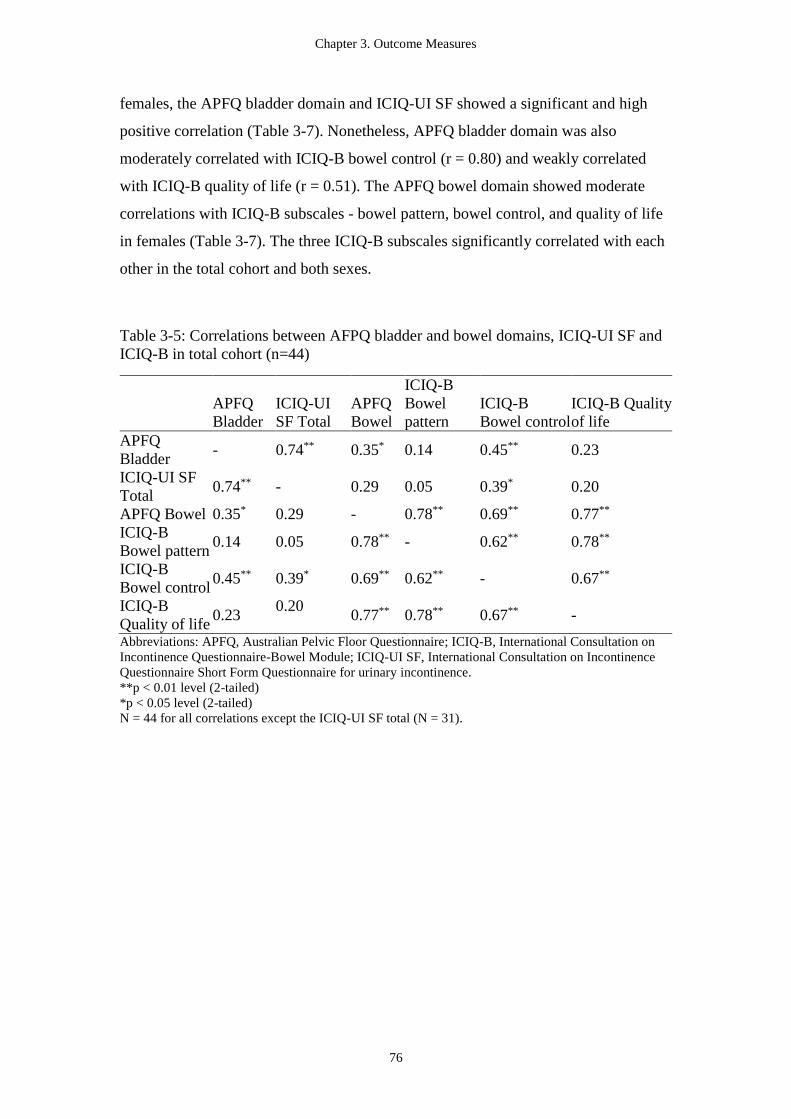
Chapter 3. Outcome Measures
76
females, the APFQ bladder domain and ICIQ-UI SF showed a significant and high
positive correlation (Table 3-7). Nonetheless, APFQ bladder domain was also
moderately correlated with ICIQ-B bowel control (r = 0.80) and weakly correlated
with ICIQ-B quality of life (r = 0.51). The APFQ bowel domain showed moderate
correlations with ICIQ-B subscales - bowel pattern, bowel control, and quality of life
in females (Table 3-7). The three ICIQ-B subscales significantly correlated with each
other in the total cohort and both sexes.
Table 3-5: Correlations between AFPQ bladder and bowel domains, ICIQ-UI SF and
ICIQ-B in total cohort (n=44)
APFQ
Bladder
ICIQ-UI
SF Total
APFQ
Bowel
ICIQ-B
Bowel
pattern
ICIQ-B
Bowel control
ICIQ-B Quality
of life
APFQ
Bladder - 0.74** 0.35* 0.14 0.45** 0.23
ICIQ-UI SF
Total 0.74** - 0.29 0.05 0.39* 0.20
APFQ Bowel 0.35* 0.29 - 0.78** 0.69** 0.77**
ICIQ-B
Bowel pattern 0.14 0.05 0.78** - 0.62** 0.78**
ICIQ-B
Bowel control 0.45** 0.39* 0.69** 0.62** - 0.67**
ICIQ-B
Quality of life 0.23
0.20 0.77** 0.78** 0.67** -
Abbreviations: APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on
Incontinence Questionnaire-Bowel Module; ICIQ-UI SF, International Consultation on Incontinence
Questionnaire Short Form Questionnaire for urinary incontinence.
**p < 0.01 level (2-tailed)
*p < 0.05 level (2-tailed)
N = 44 for all correlations except the ICIQ-UI SF total (N = 31).
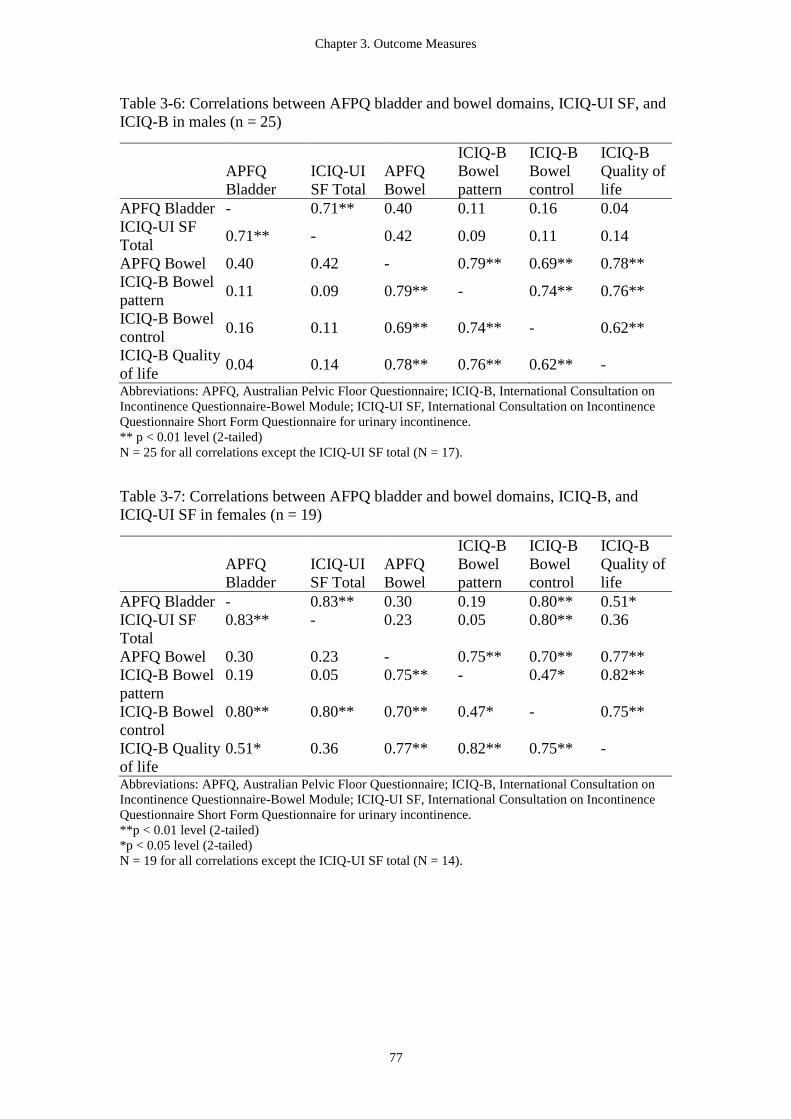
Chapter 3. Outcome Measures
77
Table 3-6: Correlations between AFPQ bladder and bowel domains, ICIQ-UI SF, and
ICIQ-B in males (n = 25)
APFQ
Bladder
ICIQ-UI
SF Total
APFQ
Bowel
ICIQ-B
Bowel
pattern
ICIQ-B
Bowel
control
ICIQ-B
Quality of
life
APFQ Bladder - 0.71** 0.40 0.11 0.16 0.04
ICIQ-UI SF
Total 0.71** - 0.42 0.09 0.11 0.14
APFQ Bowel 0.40 0.42 - 0.79** 0.69** 0.78**
ICIQ-B Bowel
pattern 0.11 0.09 0.79** - 0.74** 0.76**
ICIQ-B Bowel
control 0.16 0.11 0.69** 0.74** - 0.62**
ICIQ-B Quality
of life 0.04 0.14 0.78** 0.76** 0.62** -
Abbreviations: APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on
Incontinence Questionnaire-Bowel Module; ICIQ-UI SF, International Consultation on Incontinence
Questionnaire Short Form Questionnaire for urinary incontinence.
** p < 0.01 level (2-tailed)
N = 25 for all correlations except the ICIQ-UI SF total (N = 17).
Table 3-7: Correlations between AFPQ bladder and bowel domains, ICIQ-B, and
ICIQ-UI SF in females (n = 19)
APFQ
Bladder
ICIQ-UI
SF Total
APFQ
Bowel
ICIQ-B
Bowel
pattern
ICIQ-B
Bowel
control
ICIQ-B
Quality of
life
APFQ Bladder - 0.83** 0.30 0.19 0.80** 0.51*
ICIQ-UI SF
Total
0.83** - 0.23 0.05 0.80** 0.36
APFQ Bowel 0.30 0.23 - 0.75** 0.70** 0.77**
ICIQ-B Bowel
pattern
0.19 0.05 0.75** - 0.47* 0.82**
ICIQ-B Bowel
control
0.80** 0.80** 0.70** 0.47* - 0.75**
ICIQ-B Quality
of life
0.51* 0.36 0.77** 0.82** 0.75** -
Abbreviations: APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on
Incontinence Questionnaire-Bowel Module; ICIQ-UI SF, International Consultation on Incontinence
Questionnaire Short Form Questionnaire for urinary incontinence.
**p < 0.01 level (2-tailed)
*p < 0.05 level (2-tailed)
N = 19 for all correlations except the ICIQ-UI SF total (N = 14).

Chapter 3. Outcome Measures
78
Agreement
The results for agreement were similar to the correlation analysis: moderate level of
agreement between APFQ bladder domain and ICIQ-UI SF with a kappa coefficient
value of 0.56 in males and 0.51 in females. The agreement between APFQ bowel
domain and ICIQ-B subscales was low to moderate with a range of kappa values from
0.34 to 0.56 (Table 3-8). All agreements were statistically significant, except the
kappa values in females (p = 0.05).
Table 3-8: Agreement between AFPQ bladder and bowel domains, ICIQ-B, and
ICIQ-UI SF for symptomatic participants
Total Males Females
APFQ
domains
Comparison Kappa p value Kappa p value Kappa p value
Bladder
function
ICIQ-UI SF 0.53 0.003 0.56 0.01 0.51 0.05
Bowel
function
ICIQ-B
Bowel
pattern
0.40 0.001 0.45 0.007 0.34 0.05
ICIQ-B
Bowel
control
0.51 0.001 0.56 0.005 0.45 0.05
ICIQ-B
Quality of
life
0.51 0.001 0.56 0.005 0.45 0.05
Abbreviations: APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on
Incontinence Questionnaire-Bowel Module; ICIQ-UI SF, International Consultation on Incontinence
Questionnaire Short Form Questionnaire for urinary incontinence.
Predictors
The logistic regression analysis showed that the significant predictors for bladder
symptoms were increase in age per year in males (p = 0.03) and females (p = 0.045)
and stage of cancer in males: a diagnosis of stage III CRC (26.5 OR: 95% CI 1.29 to
543.65; p = 0.03) predicted bladder symptoms in males following CRC surgery
(Table 3-9).
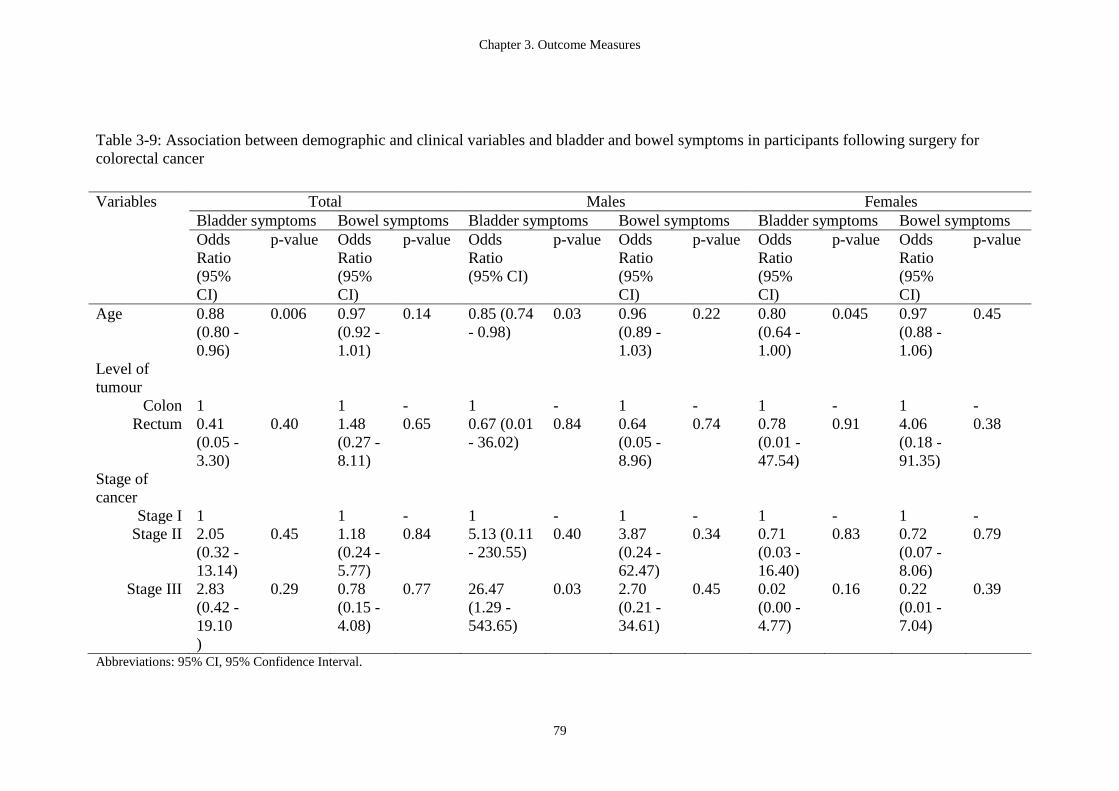
Chapter 3. Outcome Measures
79
Table 3-9: Association between demographic and clinical variables and bladder and bowel symptoms in participants following surgery for
colorectal cancer
Abbreviations: 95% CI, 95% Confidence Interval.
Variables Total Males Females
Bladder symptoms Bowel symptoms Bladder symptoms Bowel symptoms Bladder symptoms Bowel symptoms
Odds
Ratio
(95%
CI)
p-value Odds
Ratio
(95%
CI)
p-value Odds
Ratio
(95% CI)
p-value Odds
Ratio
(95%
CI)
p-value Odds
Ratio
(95%
CI)
p-value Odds
Ratio
(95%
CI)
p-value
Age 0.88
(0.80 -
0.96)
0.006 0.97
(0.92 -
1.01)
0.14 0.85 (0.74
- 0.98)
0.03 0.96
(0.89 -
1.03)
0.22 0.80
(0.64 -
1.00)
0.045 0.97
(0.88 -
1.06)
0.45
Level of
tumour
Colon 1 1 - 1 - 1 - 1 - 1 -
Rectum 0.41
(0.05 -
3.30)
0.40 1.48
(0.27 -
8.11)
0.65 0.67 (0.01
- 36.02)
0.84 0.64
(0.05 -
8.96)
0.74 0.78
(0.01 -
47.54)
0.91 4.06
(0.18 -
91.35)
0.38
Stage of
cancer
Stage I 1 1 - 1 - 1 - 1 - 1 -
Stage II 2.05
(0.32 -
13.14)
0.45 1.18
(0.24 -
5.77)
0.84 5.13 (0.11
- 230.55)
0.40 3.87
(0.24 -
62.47)
0.34 0.71
(0.03 -
16.40)
0.83 0.72
(0.07 -
8.06)
0.79
Stage III 2.83
(0.42 -
19.10
)
0.29 0.78
(0.15 -
4.08)
0.77 26.47
(1.29 -
543.65)
0.03 2.70
(0.21 -
34.61)
0.45 0.02
(0.00 -
4.77)
0.16 0.22
(0.01 -
7.04)
0.39
Chapter 3. Outcome Measures
80
3.5.4 Discussion
This exploratory analysis showed moderate correlations between the bladder and
bowel function domains of APFQ and the ICIQ-UI SF and ICIQ-B in patients
following surgery for CRC surgery. The positive associations observed with the
bladder and bowel function domains of APFQ and the other two symptom severity
questionnaires support the construct validity of the APFQ. The results of this study
suggest that the APFQ may be valid in the CRC population, and also that its utility
can be generalized beyond female CRC populations.
In the original validation for the APFQ, the bladder function domain score was
validated against the short version of the Urogenital Distress Inventory (UDI) in
females with pelvic floor disorders (Baessler et al., 2009), and the authors found a
significant correlation with the UDI score (Spearman’s rho 0.80; p < 0.001). The
findings of our study using a smaller cohort of males and females following surgery
for CRC suggested a significant and similar correlation of the APFQ bladder function
domain in comparison to the ICIQ-UI SF scores (total: r = 0.74; p < 0.01; male: r =
0.71; p < 0.01; female: r= 0.83; p < 0.01). The slightly lower correlation in males may
be accounted for by a relatively lower prevalence of urinary symptoms among the
majority of the males than females in the CRC populations (Lange & de Velde, 2010).
Baessler et al. validated the bowel function domain of the APFQ against the Heaton’s
bowel questionnaire, and found a high correlation between the two questionnaires
(Spearman’s rho 0.81-0.92, p < 0.001) (Baessler et al., 2009). Although the
correlations in our findings were lower (r = 0.69 - 0.78 in total cohort; r = 0.69 – 0.79
in males; r = 0.70 - 0.77 in females), it should be noted that our study may not be
directly comparable with the study by Baessler et al. due to the population differences
(Baessler et al., 2009). The inclusion of male participants and the effects of cancer and
cancer treatment (surgery, RT, CT) on bladder and bowel function in patients with
CRC (Bernard, Ouellet, Moffet, Roy, & Dumoulin, 2015; Lange et al., 2008) may
affect the comparisons.
Chapter 3. Outcome Measures
81
Nevertheless, the moderate correlations between APFQ, ICIQ-UI SF, and ICIQ-B in
our study suggested that these questionnaires measure similar constructs in the CRC
population. Although a combination of different self-reported questionnaires on
bladder and bowel symptoms are often used in research studies to obtain a
comprehensive understanding of a patient’s condition, these are likely to be too
time-consuming and burdensome for patients and clinicians in a clinical practice
setting. The use of one questionnaire (i.e. APFQ) which is applicable to male and
female CRC populations and evaluates both bladder and bowel domains instead of
two separate questionnaires (i.e. ICIQ-UI SF and ICIQ-B) can reduce participant
burden in both research and clinical settings.
In this study, the APFQ bladder domain was significantly correlated not only with
ICIQ-UI SF total score but also with some ICIQ-B subscales in the female cohort.
One possible explanation is that urinary and faecal incontinence are not only highly
prevalent but also co-existing among women in the community (Botlero, Bell,
Urquhart, & Davis, 2011; Malykhina, Wyndaele, Andersson, De Wachter, &
Dmochowski, 2012); therefore, preoperative bladder and bowel dysfunction may
influence post-operative function (Lange et al., 2008). Nevertheless, further
evaluation is required to determine the prevalence and the impact of preoperative
bladder and bowel dysfunction in females who are scheduled to undergo CRC
surgery.
With a score of greater than or equal to one as the cut-off value for symptomatic
participants, the APFQ bladder domain had a moderate agreement with ICIQ-UI SF,
and low to moderate agreement was found between APFQ bowel domain and ICIQ-B.
A cut-off score of one was chosen based on previous validation study (Avery et al.,
2004). However, it is important to note that no cut-off values have been established
for APFQ and ICIQ-B. All of the correlations and agreements should be interpreted
with caution due to the possible over- or under-estimation of the number of
symptomatic participants and the small sample size. More research is warranted to
establish the sensitivity, specificity, and positive and negative predictive values of the
APFQ in a cancer population.
Chapter 3. Outcome Measures
82
Our exploratory results revealed that age and stage III cancer had the potential to
predict the severity of male post-operative bladder symptoms using the APFQ bladder
domain following CRC surgery. The finding of this study on cancer stage as a
predictor of male bladder symptoms concurs with a previous study (Morino et al.,
2009), which reported that tumour stage and distance from the anal verge were
independently associated with postoperative bladder function in males. However,
Morino et al. found that age did not significantly affect bladder function (Morino et al.,
2009), which was in contrast to the finding of our study. This may be due to the
different types of surgery and the age range of the participants in the two studies.
Moreover, previous studies demonstrated that aging might be related to deterioration
in bladder function in community-dwelling men and women (Madersbacher et al.,
1998). As the preoperative bladder function was not available, our findings on the
association between age and postoperative bladder function could reflect a natural
history of bladder dysfunction and need to be confirmed with further studies.
This study has some limitations. First, as this study was a retrospective analysis of
two prospective studies, a selection bias must be considered. Second, other potential
confounding factors that may have an impact on post-operative bladder and bowel
symptoms, such as pre-operative bladder and bowel function (Fish & Temple, 2014;
Lange et al., 2008), history of childbirth and hormonal status of the female
participants (Daniels et al., 2006; Fish & Temple, 2014), were not addressed in the
study due to the lack of available pre-operative data. Moreover, given the small
sample size, it was difficult to conduct subgroup analyses to investigate the validity of
APFQ in patients who have undergone surgery for rectal cancer versus colon cancer
and those who have undergone adjuvant therapies versus no adjuvant therapies. Due
to a higher percentage of participants treated for colon cancer (82%) compared to
18% of participants with rectal cancer in our study, the findings of this study may not
be generalized to all CRC population. Lastly, the ICIQ-UI SF and ICIQ-B do not
include all bladder and bowel symptoms that could affect a patient following CRC
surgery. Despite the inherent differences between the three questionnaires and the
limitations, the relationships observed in this study were in the direction hypothesized.
This work has clinical implications for health care professionals working with the
CRC population. In view of reducing the burden for patient, researcher and clinician,

Chapter 3. Outcome Measures
83
the APFQ would be a potentially appropriate and easy to administer instrument to
measure the severity of bladder and bowel symptoms in patients following surgery for
CRC.
3.5.5 Summary
The APFQ is moderately correlated with the ICIQ-UI SF and ICIQ-B and appears to
be a useful instrument for clinical and research use. Age may be a potential predictor
for bladder symptoms in patients following surgery for CRC. While stage III cancer
might impact upon post-operative bladder symptoms in males, more robust and
prospective studies are needed to fully understand the roles of clinical and surgical
variables as predictors of bladder and bowel symptoms in patients following CRC
surgery. Further research using larger cohorts is warranted to evaluate additional
psychometric properties including sensitivity and specificity of the APFQ in CRC to
further demonstrate the utility of the instrument within this population.
The measurement instruments described in this chapter were utilised in Study 3, 4, 5,
6, and 7 in this thesis. In the following chapter, the validity of three most commonly
used field walking tests utilized to measure functional exercise capacity was explored
to assist in choosing the most appropriate alternatives to laboratory based CPET for
use in the studies within this thesis and in clinical practice.
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
84
Chapter 4. How should functional exercise capacity be measured in colorectal
cancer? a pilot validation study
This study was published in 2016:
Lin K-Y, Denehy L, Frawley H.C., Dimitriadis T, Martin J, Parry S, Irving L,
Granger C.L. How should functional exercise capacity be measured in colorectal
cancer? a pilot validation study. Jacobs Journal of Physiotherapy and Exercise.
2016;2(2): 017.
Author contributions for this chapter are the following: K-YL, LD, HF, SP and CG
conceived the idea for the paper. K-YL, LD, HF and CG contributed to research
design. K-YL, TD, JM, LI and CG contributed to data acquisition. K-YL, LD, HF and
CG contributed to data analysis and interpretation. K-YL completed all statistical
analyses. K-YL wrote the first draft of the manuscript and managed manuscript
submission. All authors revised the paper and provided scientific input. All authors
approved the final version of the manuscript.
This study was supported by grant funding from the Pat Cosh Trust, Victoria,
Australia.
4.1 Introduction
This chapter will describe a prospective observational cohort pilot study undertaken to
explore the criterion validity, construct validity and clinical applicability of three field
walking tests to measure functional exercise capacity in patients who had undergone
treatment for CRC. Functional exercise capacity is an important marker in CRC
particularly given its close relationship to surgical outcomes and survival (Mayo et al.,
2011; Meyerhardt, Giovannucci et al., 2006; Meyerhardt, Heseltine et al., 2006;
Rodriguez, Hawkins, Berkowitz, & Li, 2015). It is commonly measured for risk
stratification to determine if patients are fit for surgery or radical treatment (Reilly,
1997) and is also an important common target for exercise and physiotherapy
interventions. As such a simple, inexpensive, feasible and valid measure of functional
exercise capacity is important for use in clinical practice. Field walking tests are
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
85
walking tests performed to measure functional exercise capacity in a clinical and
non-laboratory setting. The three most commonly used tests are the 6MWT (2002),
ISWT, and ESWT (Singh et al., 1992). However, the validity of these tests as
measures of functional exercise capacity in CRC is not well understood. As the
validity of an instrument or test is purpose-, setting- and population-specific
(Jerosch-Herold, 2005; Portney & Watkins, 2009; Talmage & Rasher, 1981), it is
important to assess the applicability and validity of these measures with respect to the
characteristics of the CRC population.
This chapter contains content that is substantially unchanged from the content of the
paper which has been accepted for publication.
4.1.1 Study aims and hypotheses
Aim1: To explore the criterion validity of three field walking tests (6MWT, ISWT
and ESWT) against the gold standard test (laboratory CPET) to measure functional
exercise capacity in patients who had undergone treatment for CRC
Hypothesis 1: All three field walking tests would be moderately and positively
correlated with VO2peak measured by CPET
Aim 2: To investigate the relationships of 6MWT, ISWT, ESWT, and CPET to
patient-reported physical function, respiratory function, hand grip strength, and
HRQoL, and to determine the clinical applicability and practicality of the tests
Hypothesis 2: The 6MWT, ISWT, ESWT, and CPET would be moderately correlated
with patient-reported physical function, respiratory function, hand grip strength, and
HRQoL.
4.2 Materials and Methods
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
86
4.2.1 Study design, setting and participants
This prospective observational cohort pilot study was conducted at a tertiary
metropolitan hospital in Melbourne, Australia from May 2014 to February 2016. The
study was approved by the Melbourne Health HREC, and written informed consent
was obtained from all participants. A copy of the HREC approval letter (HREC
2013.052) from Melbourne Health is included in Appendix 4.1. This study was
conducted and is reported according to the Strengthening the Reporting of
Observational Studies in Epidemiology (STROBE) guidelines (von Elm, Altman,
Pocock, Gotzsche, & Vandenbroucke, 2007). Participants were eligible for the study
if they had histologically confirmed diagnosis of CRC; received treatment (surgery,
CT, and/or RT) within the past six months; and had an Eastern Cooperate Oncology
Group Performance Status (ECOG-PS) score of 0–2. Exclusion criteria included
co-morbidity preventing exercise testing; insufficient English language skills to
participate; and a contraindication to CPET as recommended by the American
Thoracic Society (ATS & ACCP, 2003).
4.2.2 Procedure
Ten participants were recruited from the colorectal outpatient clinics between May
2014 and August 2015, and tested within six months of their last treatment (surgery,
CT and/or RT). Each participant completed the 6MWT, ISWT, ESWT, CPET,
hand-grip strength test, and study questionnaires on the same day. The order of testing
was managed pragmatically. Participants rested for at least one hour before CPET. In
between field walking tests, participants were given a minimum of 15 minutes rest to
ensure they had recovered (assessed by return to resting heart rate and resting Borg
score [+/- 1]) prior to completing the next test. No treatment occurred in between
tests.
4.2.3 Measures
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
87
Socio-demographic and medical variables were collected. Participants were asked if
they had any limitations to walking. The ECOG-PS was used to measure participants’
physical function (Oken et al., 1982).
Field walking tests
Six minute walk test (6MWT)
The 6MWT, a self-paced field walking test, was performed according to the published
American Thoracic Society guidelines (2002). Participants were asked to walk as far
as possible over a 30-meter course in 6 minutes. The total distance walked in meters
(m) was documented. The 6MWT was performed on two occasions to account for the
learning effect, and the best test result was used in analyses (Spencer et al., 2008; Wu
et al., 2003). In patients with cancer, the 6WMT is a reliable measure (intraclass
correlation coefficient [ICC] r = 0.93) (Schmidt et al., 2013).
Incremental Shuttle Walk Test (ISWT) (Department of Respiratory Medicine,
Glenfield Hospital, Leicester, UK)
The ISWT, an externally-paced incremental field walking test, was performed around
a 10-meter course according to published guidelines (Singh et al., 1992). Participants
were asked to pace according to an incremental walking speed dictated by an audio
signal, and the distance in meters was measured. The test speed increased every
minute, and the test finished when the participant was unable to maintain the required
speed or limited by dyspnoea or a heart rate >85% predicted maximum (Singh et al.,
1992). The ISWT was performed twice to account for the learning effect and the best
test result was used in analyses (McKeough et al., 2011; Singh et al., 2014). A
previous systematic review has reported good reliability (ICC > 0.75) in patients with
various diseases, such as COPD, chronic heart failure, cardiomyopathy, and cystic
fibrosis, and patients who have undergone cardiovascular, abdominal, or lung cancer
surgery (Parreira et al., 2014).
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
88
Endurance Shuttle Walk Test (ESWT) (Department of Respiratory Medicine,
Glenfield Hospital, Leicester, UK)
The ESWT, an externally-paced field walking test of endurance capacity, was
performed along the same course as the ISWT (Revill et al., 1999) and performed
according to published guidelines (Revill et al., 1999). The walking speed was pre-set
at the pace equivalent to 85% of the calculated VO2peak from the ISWT (Hill et al.,
2012b). Participants were instructed to walk for as long as possible until they were
unable to maintain the required speed or became breathless, and the endurance time in
seconds was recorded. The cut-off time was 20 minutes, but patients were unaware of
the time limit. A single ESWT was performed as no learning effect is reported for
ESWT (McKeough et al., 2011; Ngai et al., 2015).
Laboratory-based exercise test
Cardiopulmonary Exercise Testing (CPET)
Cardiopulmonary Exercise Testing was performed to determine VO2peak using a
Sensormedics Vmax Encore, 229D (Sensormedics, Yorba Linda, Ca, USA) exercise
system and a Ergoline Via Sprint 150P cycle ergometer (Lindenstrabe 5, 72475 Bitz,
Germany) (ATS & ACCP, 2003). The test started with two minutes of rest followed
by cycling with the workload increments selected using the equations from Jones
(Jones, 1988), and the test continued to the point of symptom-limitation (Datta,
Normandin, & ZuWallack, 2015). Heart rate, blood pressure, and SpO2 were
monitored with a 12-lead electrocardiogram using a GE Cardiosoft Version 6.51
electrocardiography system (GE Healthcare, GE Marquette Medical Systems, 8200
West Tower Ave, Milwaukee, WI 53223. USA), a sphygmomanometer, and a pulse
oximeter throughout the test and during recovery. The CPET data were calculated by
averaging the results every 30 seconds, and the percentage of predicted VO2peak was
calculated according to normative equations by Jones (Jones, 1988). Maximal patient
effort was indicated by evidence of exhaustion, attaining predicted maximal heart rate,
and attaining predicted minute ventilation (Datta et al., 2015).
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
89
Throughout the field walking tests and laboratory-based exercise test, patient safety
was monitored. Before and after the test, participants’ heart rate and SpO2 were
recorded with a portable pulse monitor (Datex-Ohmeda TuffSat handheld pulse
oximeter [Fairfield, CT, USA]). Dyspnoea and leg fatigue were measured with the
Modified Borg Scale (10-point scale, with 0 as ‘nothing at all’ and 10 as ‘maximal’
breathing difficulty or leg fatigue) (Kendrick et al., 2000). Participant stability
between tests was assessed by the differences in the pre-test Borg scores. The time
and number of assessors required to conduct each test, and any adverse events were
recorded.
Additional measures
Hand-grip strength was measured using a Jamar hydraulic hand-grip dynamometer
(Roberts et al., 2011). The participant was tested in the position recommended by the
American Society for Hand Therapists (Peolsson et al., 2001), and the best of three
measures was taken. Health-related quality of life was evaluated by the European
Organization for the Research and Treatment of Cancer questionnaire and CRC
module (EORTC QLQ-C30 and QLQ-CR29). All scale/single item measures range in
score from 0-100. A high score on the functional and the global quality of life scale
represents a high level of functioning and high quality of life, while a high score on
the symptom scale represents a high level of symptomatology (Aaronson et al., 1993;
Whistance et al., 2009).
A standardized data collection sheet and a questionnaire booklet were used (Appendix
4.2).
4.2.4 Statistical analyses
Data analyses were performed using the SPSS Windows Version 22.0 (SPSS,
Chicago, IL, USA). Data were assessed for normality and homoscedasticity (equality
of variance) using the Shapiro-Wilk test, and bivariate scotterplot, residual plot, and
Levene’s tests, respectively (Exposito-Ruiz, Perez-Vicente, & Rivas-Ruiz, 2010;
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
90
Ghasemi & Zahediasl, 2012). Descriptive statistics, such as mean and SD and number
and percentage were used to summarise data. Participant exercise stability was
assessed by comparing Borg dyspnoea scores and Borg leg fatigue scores before each
test (6MWT x 2, ISWT x 2, ESWT and CPET) using paired t-tests. Pearson’s
correlation coefficients were calculated between 6MWT distance (meters), ISWT
distance (meters), ESWT time (seconds) and CPET VO2peak (ml∙kg-1∙min-1) to assess
criterion validity (Norman, 2010). Construct validity was examined by investigating
the relationships between field walking tests, CPET, respiratory function, physical
function (ECOG-PS), hand-grip strength, and HRQoL physical function and global
health domain scores using Pearson's correlation coefficients. The strength of the
correlation was determined by the correlation coefficient values (0.00–0.30 =
negligible; 0.30–0.50 = low positive correlation; 0.50–0.70 = moderate positive
correlation; 0.70–0.90 = high positive correlation; and 0.90–1.00 = very high positive
correlation) (Mukaka, 2012; Zou et al., 2003). The relationships between the CPET
and field walking tests were further analysed using simple linear regression with the
CPET VO2peak as the dependent variable, and 6MWT distance, ISWT distance or
ESWT time as the independent variables. The differences in the test results between
participants with or without self-rated walking limitations (to determine discriminant
validity) were compared using the independent t-test. The test floor and ceiling effects
were calculated as the percentage of participants scoring at the lowest [6MWT = 0 m,
ISWT= 0 m, ESWT= 0 s] or the highest [ISWT = 1020 m, ESWT = 1200 s] possible
results, respectively. The level of significance was set at p < 0.05.
4.3 Results
A total of 103 patients were screened between July 2013 and August 2015. Thirty-five
(n = 35/103) were eligible and approached (Figure 4.1). Twenty-five patients declined
to participate; the consent rate was 29% (n = 10/35). The main reasons for decline
were “not interested” 24 % (n = 6/25) and “initially agreed but failed to attend” 20 %
(n = 5/25). A total of 10 patients with CRC were enrolled in the study (Figure 4.1).
The mean age of the study cohort was 56.2 ± 15.5 years, and 70% were female.
Socio-demographic and medical variables including age, sex, BMI, social situation,
education, and employment status, cancer stage, treatment type/status, smoking
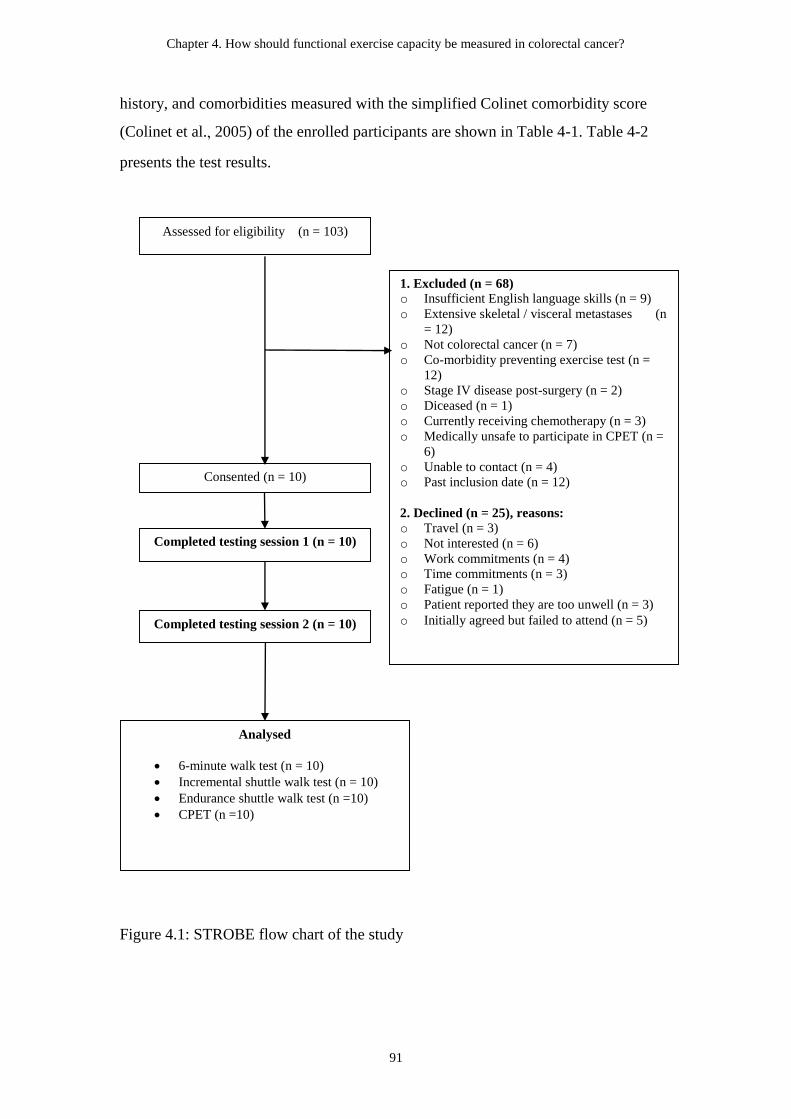
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
91
history, and comorbidities measured with the simplified Colinet comorbidity score
(Colinet et al., 2005) of the enrolled participants are shown in Table 4-1. Table 4-2
presents the test results.
Figure 4.1: STROBE flow chart of the study
Consented (n = 10)
Assessed for eligibility (n = 103)
Analysed
6-minute walk test (n = 10)
Incremental shuttle walk test (n = 10)
Endurance shuttle walk test (n =10)
CPET (n =10)
1. Excluded (n = 68)
o Insufficient English language skills (n = 9)
o Extensive skeletal / visceral metastases (n
= 12)
o Not colorectal cancer (n = 7)
o Co-morbidity preventing exercise test (n =
12)
o Stage IV disease post-surgery (n = 2)
o Diceased (n = 1)
o Currently receiving chemotherapy (n = 3)
o Medically unsafe to participate in CPET (n =
6)
o Unable to contact (n = 4)
o Past inclusion date (n = 12)
2. Declined (n = 25), reasons:
o Travel (n = 3)
o Not interested (n = 6)
o Work commitments (n = 4)
o Time commitments (n = 3)
o Fatigue (n = 1)
o Patient reported they are too unwell (n = 3)
o Initially agreed but failed to attend (n = 5)
Completed testing session 1 (n = 10)
Completed testing session 2 (n = 10)

Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
92
Table 4-1: Medical and social demographics (n = 10)
Variables Mean ± SD or n (%)
Age, years 56.2 ± 15.5
Sex, female:male 7 (70) : 3 (30)
Body mass index, kg/m2 24.6 ± 4.5
Colinet comorbidity score 1.2 ± 2.4
Smoking status
Never smoker 4 (40)
Ex-smoker 6 (60)
Cancer site
Colon 3 (30)
Rectum 7 (70)
Cancer stage
Stage I 3 (30)
Stage II 2 (20)
Stage III 5 (50)
Adjuvant treatment
Chemotherapy and radiotherapy 3 (30)
Chemotherapy only 5 (50)
No adjuvant treatment 2 (20)
Type of colorectal surgery
Colectomy 3 (30)
Anterior resection 5 (50)
Abdomino-perineal excision of rectum 2 (20)
Time since operation, days 271.6 ± 92.3
ECOG-PS, patient rated
Fully active 6 (60)
Walking but only light work 4 (40)
Self-reported limitation to walking 3 (30)
Use of a gait aid 1(10)
Physical activity levels
Sedentary (0 min/week) 1 (10)
Insufficient (1–149 min/week) 7 (70)
Sufficient (150+ min/week) 2 (20)
Time spent watching television, hours/day 3.9 ± 3.4
Social situation
Home with family 7 (70)
Home alone, independent 1 (10)
Home with supports 1 (10)
Nursing home-high level care 1 (10)
Employment status
Working full time 2 (20)
Working part time 1 (10)
Sick leave/leave of absence-temporary 1 (10)
Retired 5 (50)
Home duties 1 (10)
Highest level of education
Some primary schooling 1 (10)
Some secondary or high school 3 (30)
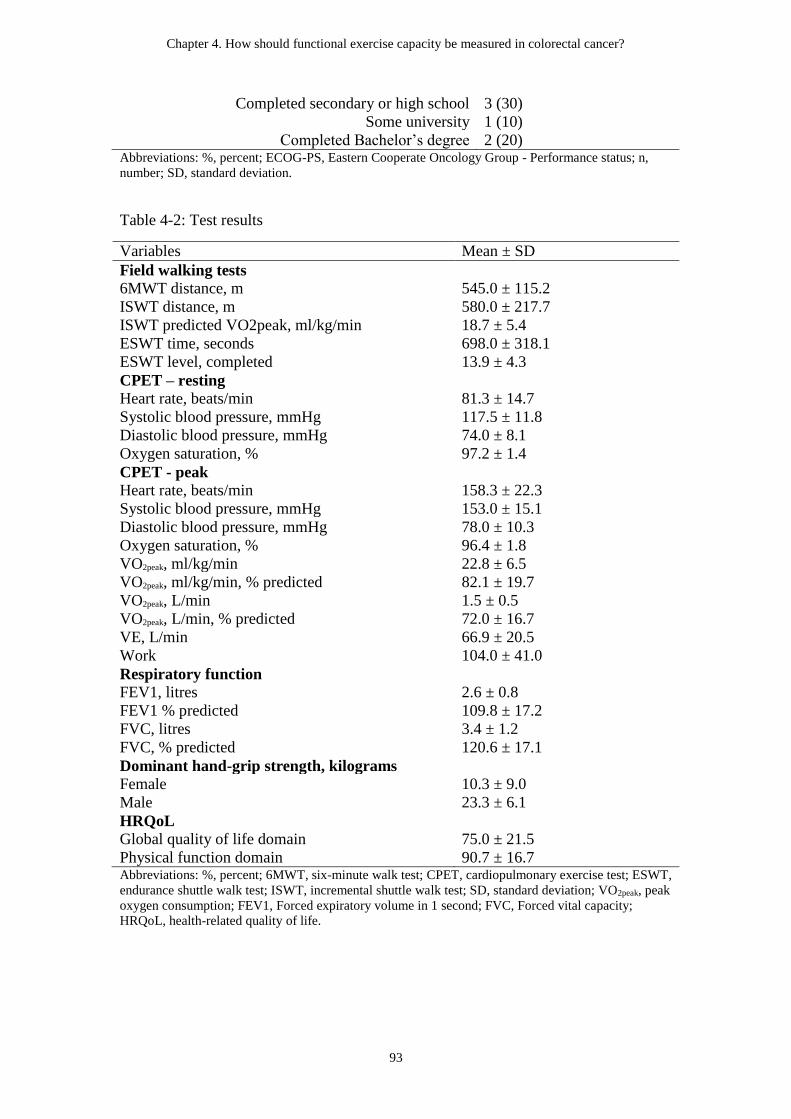
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
93
Completed secondary or high school 3 (30)
Some university 1 (10)
Completed Bachelor’s degree 2 (20) Abbreviations: %, percent; ECOG-PS, Eastern Cooperate Oncology Group - Performance status; n,
number; SD, standard deviation.
Table 4-2: Test results
Variables Mean ± SD
Field walking tests
6MWT distance, m 545.0 ± 115.2
ISWT distance, m 580.0 ± 217.7
ISWT predicted VO2peak, ml/kg/min 18.7 ± 5.4
ESWT time, seconds 698.0 ± 318.1
ESWT level, completed 13.9 ± 4.3
CPET – resting
Heart rate, beats/min 81.3 ± 14.7
Systolic blood pressure, mmHg 117.5 ± 11.8
Diastolic blood pressure, mmHg 74.0 ± 8.1
Oxygen saturation, % 97.2 ± 1.4
CPET - peak
Heart rate, beats/min 158.3 ± 22.3
Systolic blood pressure, mmHg 153.0 ± 15.1
Diastolic blood pressure, mmHg 78.0 ± 10.3
Oxygen saturation, % 96.4 ± 1.8
VO2peak, ml/kg/min 22.8 ± 6.5
VO2peak, ml/kg/min, % predicted 82.1 ± 19.7
VO2peak, L/min 1.5 ± 0.5
VO2peak, L/min, % predicted 72.0 ± 16.7
VE, L/min 66.9 ± 20.5
Work 104.0 ± 41.0
Respiratory function
FEV1, litres 2.6 ± 0.8
FEV1 % predicted 109.8 ± 17.2
FVC, litres 3.4 ± 1.2
FVC, % predicted 120.6 ± 17.1
Dominant hand-grip strength, kilograms
Female 10.3 ± 9.0
Male 23.3 ± 6.1
HRQoL
Global quality of life domain 75.0 ± 21.5
Physical function domain 90.7 ± 16.7 Abbreviations: %, percent; 6MWT, six-minute walk test; CPET, cardiopulmonary exercise test; ESWT,
endurance shuttle walk test; ISWT, incremental shuttle walk test; SD, standard deviation; VO2peak, peak
oxygen consumption; FEV1, Forced expiratory volume in 1 second; FVC, Forced vital capacity;
HRQoL, health-related quality of life.
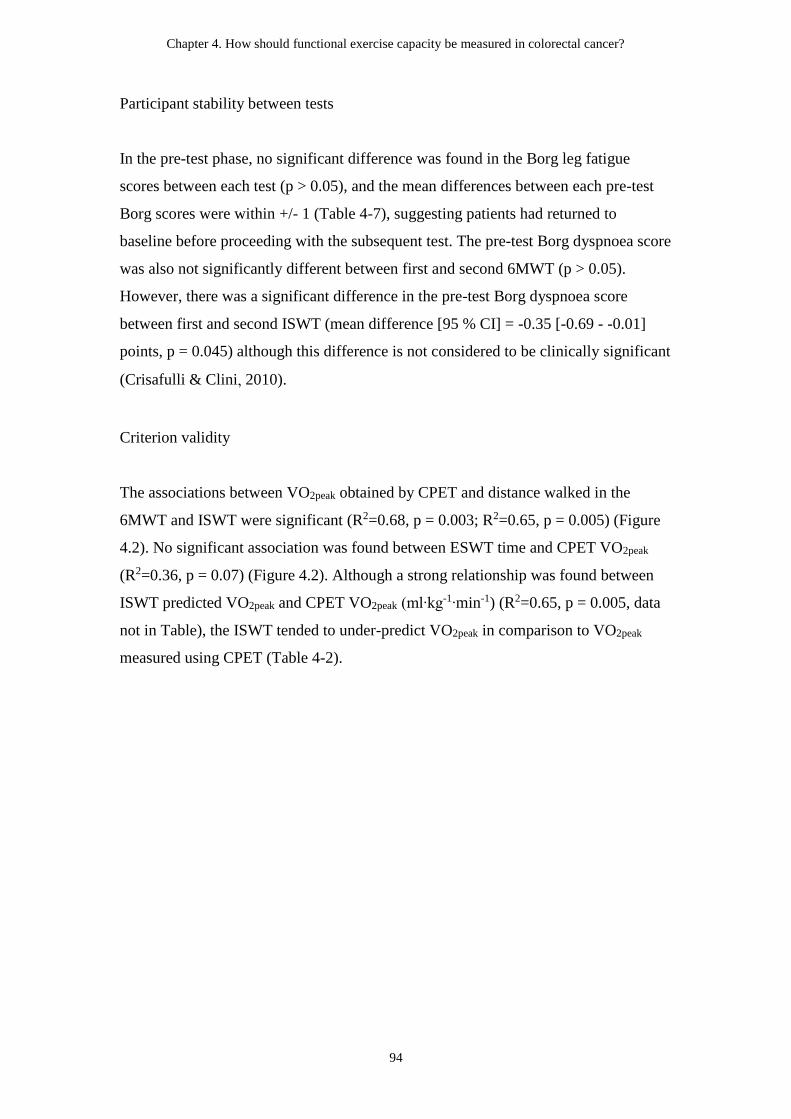
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
94
Participant stability between tests
In the pre-test phase, no significant difference was found in the Borg leg fatigue
scores between each test (p > 0.05), and the mean differences between each pre-test
Borg scores were within +/- 1 (Table 4-7), suggesting patients had returned to
baseline before proceeding with the subsequent test. The pre-test Borg dyspnoea score
was also not significantly different between first and second 6MWT (p > 0.05).
However, there was a significant difference in the pre-test Borg dyspnoea score
between first and second ISWT (mean difference [95 % CI] = -0.35 [-0.69 - -0.01]
points, p = 0.045) although this difference is not considered to be clinically significant
(Crisafulli & Clini, 2010).
Criterion validity
The associations between VO2peak obtained by CPET and distance walked in the
6MWT and ISWT were significant (R2=0.68, p = 0.003; R2=0.65, p = 0.005) (Figure
4.2). No significant association was found between ESWT time and CPET VO2peak
(R2=0.36, p = 0.07) (Figure 4.2). Although a strong relationship was found between
ISWT predicted VO2peak and CPET VO2peak (ml∙kg-1∙min-1) (R2=0.65, p = 0.005, data
not in Table), the ISWT tended to under-predict VO2peak in comparison to VO2peak
measured using CPET (Table 4-2).
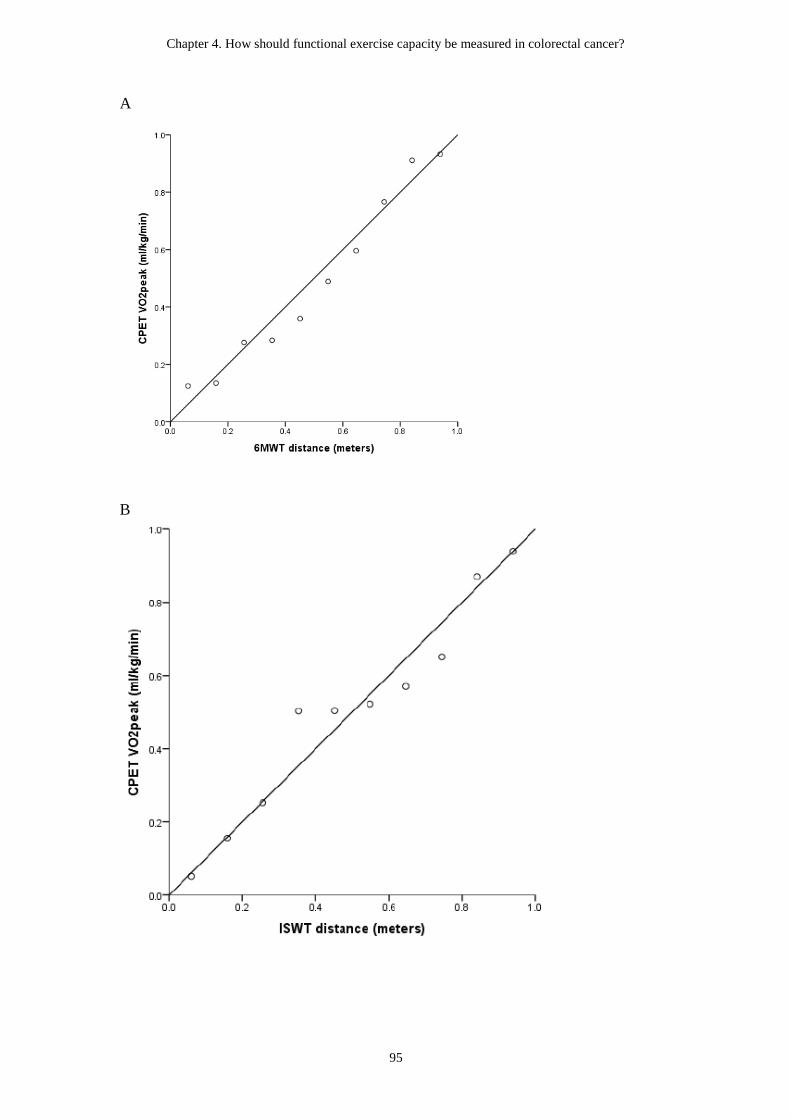
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
95
A
B
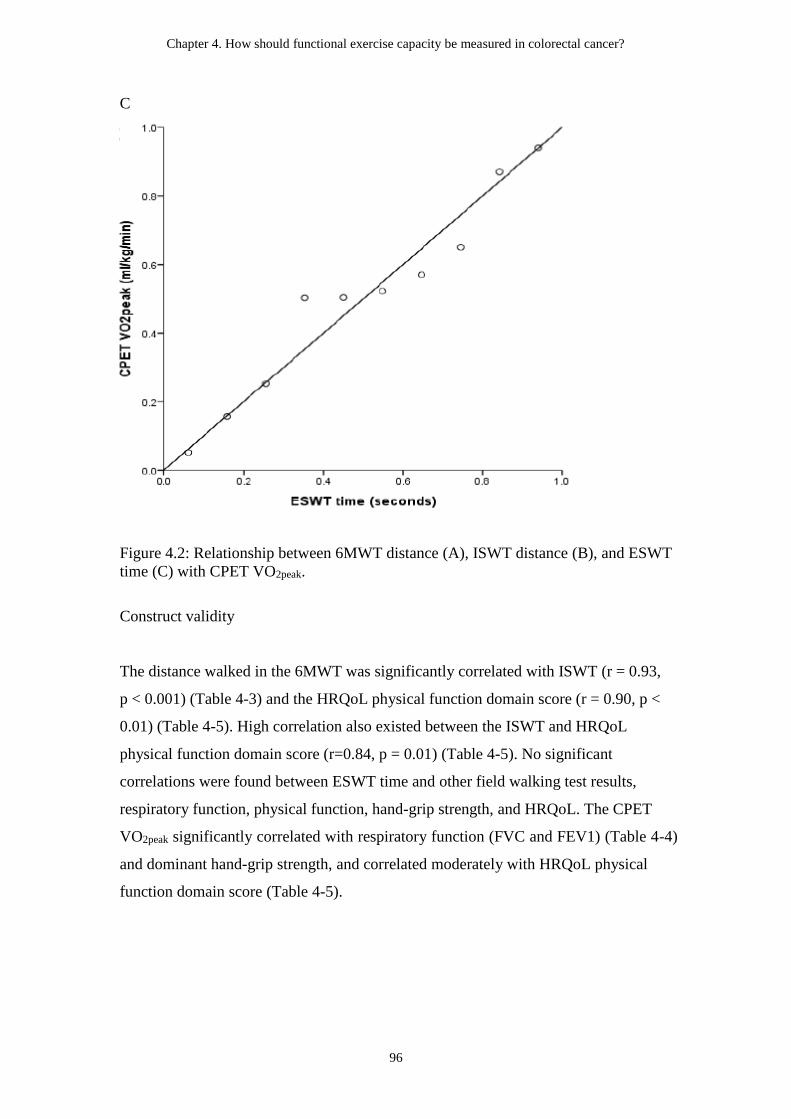
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
96
C
Figure 4.2: Relationship between 6MWT distance (A), ISWT distance (B), and ESWT
time (C) with CPET VO2peak.
Construct validity
The distance walked in the 6MWT was significantly correlated with ISWT (r = 0.93,
p < 0.001) (Table 4-3) and the HRQoL physical function domain score (r = 0.90, p <
0.01) (Table 4-5). High correlation also existed between the ISWT and HRQoL
physical function domain score (r=0.84, p = 0.01) (Table 4-5). No significant
correlations were found between ESWT time and other field walking test results,
respiratory function, physical function, hand-grip strength, and HRQoL. The CPET
VO2peak significantly correlated with respiratory function (FVC and FEV1) (Table 4-4)
and dominant hand-grip strength, and correlated moderately with HRQoL physical
function domain score (Table 4-5).

Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
97
Table 4-3: Pearson’s correlations between CPET VO2peak and 6MWT distance,
ISWT distance, and ESWT time (N = 10)
6MWT
distance, m
ISWT
distance, m
ESWT time,
seconds
CPET VO2peak,
ml/kg/min
6MWT distance, m - 0.93** 0.53 0.82**
ISWT distance, m - 0.49 0.81**
ESWT time,
seconds - 0.60
CPET VO2peak,
ml/kg/min -
Abbreviations: 6MWT, six-minute walk test; CPET, cardiopulmonary exercise test; ESWT, endurance
shuttle walk test; ISWT, incremental shuttle walk test; VO2peak, peak oxygen consumption.
** p < 0.01 level (2-tailed).
Table 4-4: Pearson’s correlations between 6MWT distance, ISWT distance, ESWT
time, CPET VO2peak and respiratory function
6MWT
Distance, m
ISWT Distance,
m
ESWT time,
seconds
CPET
VO2peak,
ml/kg/min
FVC, litres 0.36 0.31 0.22 0.70*
FEV1, litres 0.45 0.45 0.41 0.75*
FEV1/FVC 0.17 0.30 0.45 -0.07 Abbreviations: FEV1, Forced expiratory volume in 1 second; FVC, Forced vital capacity; 6MWT,
six-minute walk test; CPET, cardiopulmonary exercise test; ESWT, endurance shuttle walk test; ISWT,
incremental shuttle walk test; VO2peak, peak oxygen consumption.
*p < 0.05 level (2-tailed).
Table 4-5: Pearson’s correlations between 6MWT distance, ISWT distance, ESWT
time, and CPET VO2peak and ECOG-PS, HRQoL physical function and global health
domain scores, and hand-grip strength
6MWT
Distance, m
ISWT
Distance, m
ESWT time,
seconds
CPET VO2peak,
ml/kg/min
Dominant hand grip
strength, kg
0.50 0.60 0.32 0.82**
HRQoL Global quality
of life domain
0.15 0.13 -0.44 -0.23
HRQoL Physical
function domain
0.90** 0.84** 0.29 0.64*
ECOG-PS -0.61 -0.58 0.09 -0.33 Abbreviations: 6MWT, six-minute walk test; CPET, cardiopulmonary exercise test; ESWT, endurance
shuttle walk test; ISWT, incremental shuttle walk test; VO2peak, peak oxygen consumption; ECOG-PS,
Eastern Cooperate Oncology Group - Performance status; HRQoL, health-related quality of life.
* Correlation is significant at the 0.05 level (2-tailed).
** Correlation is significant at the 0.01 level (2-tailed).
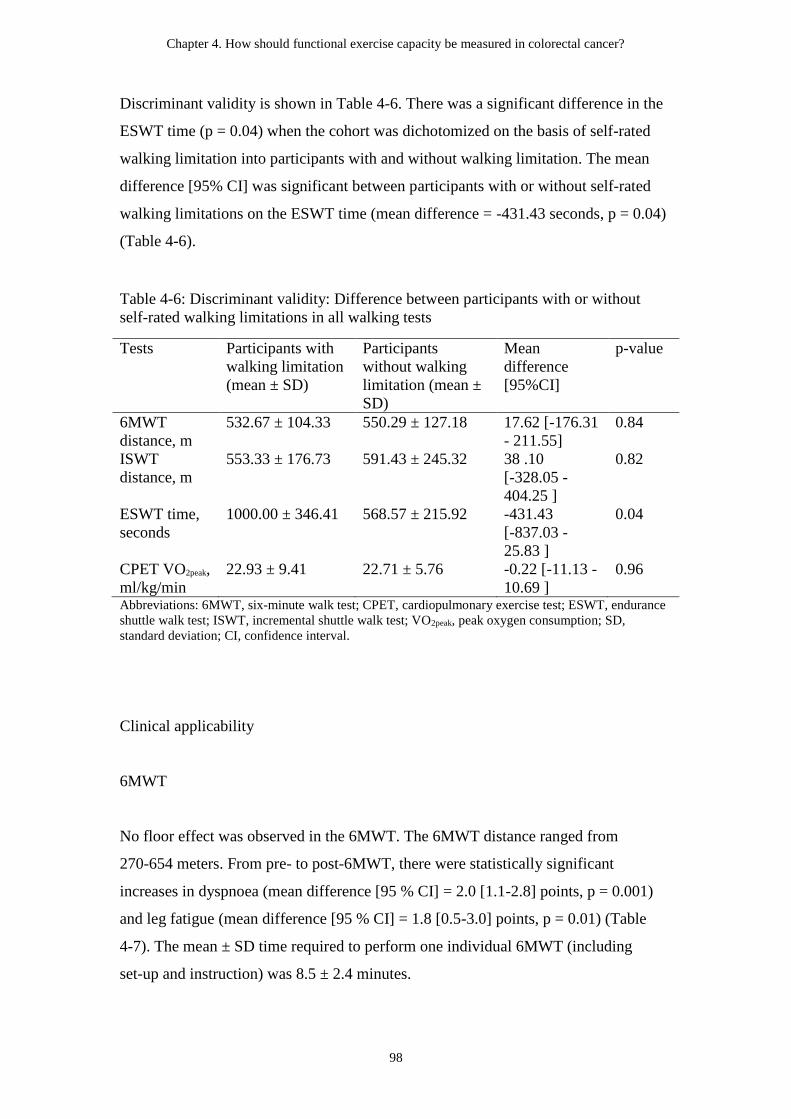
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
98
Discriminant validity is shown in Table 4-6. There was a significant difference in the
ESWT time (p = 0.04) when the cohort was dichotomized on the basis of self-rated
walking limitation into participants with and without walking limitation. The mean
difference [95% CI] was significant between participants with or without self-rated
walking limitations on the ESWT time (mean difference = -431.43 seconds, p = 0.04)
(Table 4-6).
Table 4-6: Discriminant validity: Difference between participants with or without
self-rated walking limitations in all walking tests
Tests Participants with
walking limitation
(mean ± SD)
Participants
without walking
limitation (mean ±
SD)
Mean
difference
[95%CI]
p-value
6MWT
distance, m
532.67 ± 104.33 550.29 ± 127.18 17.62 [-176.31
- 211.55]
0.84
ISWT
distance, m
553.33 ± 176.73 591.43 ± 245.32 38 .10
[-328.05 -
404.25 ]
0.82
ESWT time,
seconds
1000.00 ± 346.41 568.57 ± 215.92 -431.43
[-837.03 -
25.83 ]
0.04
CPET VO2peak,
ml/kg/min
22.93 ± 9.41 22.71 ± 5.76 -0.22 [-11.13 -
10.69 ]
0.96
Abbreviations: 6MWT, six-minute walk test; CPET, cardiopulmonary exercise test; ESWT, endurance
shuttle walk test; ISWT, incremental shuttle walk test; VO2peak, peak oxygen consumption; SD,
standard deviation; CI, confidence interval.
Clinical applicability
6MWT
No floor effect was observed in the 6MWT. The 6MWT distance ranged from
270-654 meters. From pre- to post-6MWT, there were statistically significant
increases in dyspnoea (mean difference [95 % CI] = 2.0 [1.1-2.8] points, p = 0.001)
and leg fatigue (mean difference [95 % CI] = 1.8 [0.5-3.0] points, p = 0.01) (Table
4-7). The mean ± SD time required to perform one individual 6MWT (including
set-up and instruction) was 8.5 ± 2.4 minutes.
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
99
ISWT
No floor or ceiling effects were observed in the ISWT. The ISWT distance ranged
from 110-890 meters, and the predicted VO2peak from this test ranged from 6.9-26.4
ml∙kg-1∙min-1. Significant increases were found from pre-ISWT dyspnoea and leg
fatigue to post-ISWT dyspnoea (p < 0.0005) and leg fatigue (p = 0.001) (Table 4-7).
The mean ± SD time required to perform one individual ISWT was 10.6 ± 3.5
minutes.
ESWT
Although no floor effect was seen in the ESWT, a ceiling effect was found with 70 %
(n = 7/10) of participants reaching the end of the test (1200 seconds). The ESWT time
ranged from 220-1200 seconds. The ESWT was performed on the ESWT tape levels
ranging from 3–16. From pre- to post-ESWT, there were statistically significant
increases in dyspnoea (mean difference [95 % CI] = 2.6 [1.7-3.5] points, p < 0.0005)
and leg fatigue (mean difference [95 % CI] = 2.3 [1.1-3.4], p = 0.002) (Table 4-7).
The mean ± SD time required to perform the ESWT was 13.1 ± 4.9 minutes.
CPET
In comparison, the time required to perform the CPET was 48.1 ± 9.4 minutes. No
adverse events were observed during the CPET. The increase in dyspnoea and leg
fatigue from pre- to post-CPET were mean difference [95 % CI] 5.0 [3.7-6.3] points
(p < 0.0005) and 5.4 [3.3-7.6] points (p < 0.0005) respectively (Table 4-7). Only one
assessor was required to perform the field walking tests, whereas the CPET required
two to three assessors.

Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
100
Table 4-7: Changes in BORG scores with each test
Test Pre-test
mean ± SD
Post-test
mean ± SD
Mean difference
[95%CI]
p-value
Dyspnoea
6MWT 0.4 ± 0.7 2.4 ± 1.4 2.0 [1.1 - 2.8] 0.001
ISWT 0.4 ± 0.4 3.1 ± 1.0 2.8 [2.1 - 3.4] < 0.0005
ESWT 0.6 ± 0.4 3.2 ± 1.4 2.6 [1.7 - 3.5] < 0.0005
CPET 0.8 ± 1.6 5.8 ± 1.5 5.0 [3.7 - 6.3] < 0.0005
Leg fatigue
6MWT 0.8 ± 1.2 2.6 ± 1.3 1.8 [0.5 - 3.0] 0.010
ISWT 0.7 ± 0.8 3.1 ± 1.9 2.4 [1.4 - 3.4] 0.001
ESWT 0.9 ± 0.5 3.2 ± 1.8 2.3 [1.1 - 3.4] 0.002
CPET 0.5 ± 1.0 5.9 ± 2.8 5.4 [3.3 - 7.4] < 0.0005 Abbreviations: 6MWT, six-minute walk test; CPET, cardiopulmonary exercise test; ESWT, endurance
shuttle walk test; ISWT, incremental shuttle walk test; SD, standard deviation; CI, confidence interval.
4.4 Discussion
This is the first study to explore the association of three common field walking tests
with CPET, the gold standard measure of functional exercise capacity, in patients with
CRC. Our results demonstrate significant relationships between the distance walked
in both the 6MWT and the ISWT and the VO2peak achieved on the CPET. This result
corresponds to findings reported in previous studies in patients with mixed cancer
diagnoses (26% CRC) (Schmidt et al., 2013), operable lung cancer (Win et al., 2006),
and non-small cell lung cancer (Granger, Denehy et al., 2015), and suggests that
6MWT and ISWT are both valid tests for assessing functional exercise capacity in
patients with CRC. As well as the similarity of our findings with previous studies in
cancer populations (Granger, Denehy et al., 2015; Schmidt et al., 2013; Win et al.,
2006), the criterion validity of the 6MWT and ISWT in our study is also comparable
to the studies in patients with COPD (Hill et al., 2012a; Luxton, Alison, Wu, &
Mackey, 2008), pulmonary arterial hypertension (Mainguy et al., 2014), and obesity
(Di Thommazo-Luporini et al., 2015). Therefore, both 6MWT and ISWT are useful
tests for the evaluation of functional exercise capacity in cancer and non- cancer
populations. Given the broad applicability and simplicity of 6MWT and ISWT, our
study adds further evidence to support their use by physiotherapists in the clinical and
research settings worldwide. There was no significant relationship between ESWT
and CPET. This could be expected since CPET is a test of exercise response involving
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
101
cardiorespiratory, musculoskeletal, neuropsychological, and haematological systems
(ATS & ACCP, 2003), while ESWT measures physical endurance only. Further, there
was a large ceiling effect (70%) for the ESWT (Witham, Sugden, Sumukadas,
Dryburgh, & McMurdo, 2012) and these findings indicate that the ESWT is not an
appropriate alternative to CPET and limited for use in this cohort. Therefore, our
finding, which showed a significant difference in the ESWT time between participants
with or without walking limitation, should be interpreted with caution. Further studies
with larger sample size are warranted to confirm this.
Although VO2peak measured by CPET is the gold standard for cardiorespiratory fitness
(ATS & ACCP, 2003), it is not commonly measured in CRC; whereas, despite lack of
proven validity to date, 6MWT is the most commonly used field walking test in CRC
research (Gillis et al., 2015; Lee et al., 2015; Li et al., 2013; Tomruk, Karadibak,
Yavuzsen, & Akman, 2015). Our results showed that compared to CPET, 6MWT and
ISWT required less time to complete (less than 15 minutes), fewer personnel to
conduct the test (only one assessor needed), and were safe for the patients. The
6MWT and ISWT may be useful and simpler alternatives to CPET in terms of the
time, costs and the equipment required in a clinical setting.
Furthermore, the 6MWT and ISWT measure a similar construct to each other as
shown by the high correlation between them. Nevertheless, use of CPET provides
more accurate physiological data and would be needed in some settings. For example,
preoperative use of CPET allows identification of patients with CRC at high risk of
requiring postoperative critical care unit admission (Chan, Pathak, Smart, Batchelor,
& Daniels, 2015). Moreover, our findings showed that VO2peak was moderately to
highly correlated to respiratory function, dominant hand-grip strength, and HRQoL
physical function domain, which is consistent with previous studies in population with
cardiopulmonary disease (Hager & Hess, 2005; Kato, Rodgers, Stickland, & Haennel,
2012; Tzani et al., 2010).
The results of this exploratory study demonstrate a significant relationship between
6MWT and ISWT, with the physical function domain of the EORTC QLQ-C30,
suggesting that greater functional exercise capacity is associated with better
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
102
self-reported physical function. Our findings are in line with previous studies, which
found significant correlations between 6MWT distance and HRQoL physical
well-being in CRC survivors (Lee et al., 2015), and ISWT distance and physical
functioning domain of the Short Form-36 health survey in patients with heart disease
(Costa et al., 2014). As the primary goal of physiotherapy is frequently to assist
patients to restore normal function or maximise residual function in order to prevent
limitations in activities of daily living in the long term (Higgs, Refshauge, & Ellis,
2001), our findings support physiotherapists to confidently use 6MWT and ISWT in
their assessment of function in CRC population in clinical practice. Although not
assessed in our study, the 6MWT and ISWT are known to be sensitive and responsive
to physiotherapy intervention in cardiorespiratory diseases (Bellet, Adams, & Morris,
2012; Fotheringham et al., 2015; Lee et al., 2015; Taylor, Frost, Taylor, & Barker,
2001); therefore, we hypothesize this may be the case in CRC. Further studies are
needed to investigate this. The results of our study may also inform future studies to
examine the effects of a physiotherapy program (e.g. a cardiopulmonary rehabilitation
program) in patients following surgery for CRC (Hubbard et al., 2016).
Physical function measured with ECOG-PS has been found to be the only predictor of
functional exercise capacity assessed by 6MWT in patients with CRC (Tomruk et al.,
2015). Eastern Cooperate Oncology Group Performance Status is frequently used by
clinicians to determine eligibility for treatment and prognosis of various types of
cancer (Correa et al., 2012; Sargent et al., 2009; Suh, Leblanc, Shelby, Samsa, &
Abernethy, 2011). However, our findings showed that there was no significant
relationship between ECOG-PS and field walking tests, or CPET measures, which
suggests that ECOG-PS is not interchangeable with these tests. Therefore, field
walking tests or CPET are needed for accurate assessment of functional exercise
capacity. Furthermore, it should be noted that the ECOG-PS was patient-rated in our
study; whereas, it has often been scored by clinicians in clinical practice and research
trials (Atkinson et al., 2015). The lack of congruency between patient-rated and
physician-rated ECOG-PS has been documented in the literature (Ando et al., 2001;
Dajczman et al., 2008). As better performance status at diagnosis is related to better
survival in patients with CRC (Eker et al., 2015), the relationships between ECOG-PS
Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
103
and functional exercise capacity in CRC should be clearly elucidated by future studies
with a larger sample size
Our study is strengthened by robust methodology performed following STROBE
guidelines (von Elm et al., 2007), conduct of testing over a full day (ensuring patients
are stable) and the assessment of participant stability between each test. In addition,
tests were performed according to published guidelines (ATS & ACCP, 2003; 2002;
Miller et al., 2005; Revill et al., 1999; Singh et al., 1992). As an exploratory study, the
small sample size is our primary limitation. A larger trial is warranted to confirm the
validity of the field walking tests in CRC. Moreover, there were more females and
patients who had undergone treatment for rectal cancer in our study, which affects the
generalizability of our findings. Due to the lack of randomisation of the testing order,
an order bias must be considered, however we assessed stability between tests to
account for this. Although rest periods were provided between tests, there was a small
statistically significant difference in pre-ISWT Borg dyspnoea between the first and
second ISWT; this may have impacted upon the test results.
Despite the limitations, this preliminary evidence has clinical implications for health
care professionals working with the CRC population. In view of reducing the burden
for patient, researcher and clinician, the 6MWT and ISWT would be potentially valid,
feasible, and applicable to measure the functional exercise capacity in patients with
CRC. Our results also provide a rationale for using the field walking tests in future
studies in CRC, and inform further exploration into the potential effectiveness of
post-operative cardiopulmonary rehabilitation in this population.
4.5 Summary
The 6MWT and ISWT appear to be feasible alternative tests to CPET in the
evaluation of functional exercise capacity in patients with CRC. The distances walked
in both the 6MWT and ISWT are significantly associated with CPET VO2peak and
highly-correlated with HRQoL physical function domain. Both 6MWT and ISWT are
simple, quick and safe to perform; and do not have a floor or ceiling effect in CRC
population. However, the small sample size limits the interpretation of our results,

Chapter 4. How should functional exercise capacity be measured in colorectal cancer?
104
hence further studies involving larger sample sizes are required to confirm the
findings of this pilot study.
As the findings of this study demonstrated that 6MWT is a valid test for functional
exercise capacity in patients with CRC, it was used to measure changes in functional
exercise capacity before and after an oncology rehabilitation program in Study 4. The
next chapter describes changes in pelvic floor symptoms, physical activity levels,
psychological status and HRQoL in patients with CRC from pre- to six months
post-operatively.
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
105
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of
patients following surgery for colorectal cancer
This study is under review for publication:
Lin K-Y, Denehy L, Frawley H.C., Wilson L, Granger C.L. (2016). Pelvic floor
symptoms, physical and psychological outcomes of patients following surgery for
colorectal cancer. Physiotherapy Theory and Practice. Under review. Submitted
September 2016.
Author contributions for this chapter are the following: K-YL, LD, HF and CG
conceived the idea for the paper. K-YL, LD, HF and CG contributed to research
design. K-YL, LW and CG contributed to data acquisition. K-YL, LD, HF and CG
contributed to data analysis and interpretation. K-YL completed all statistical analyses.
CG obtained project funding. K-YL wrote the first draft of the manuscript and
managed manuscript submission. All authors revised the paper and provided scientific
input. All authors approved the submitted version of the manuscript.
This study was supported by grant funding (GIA-00038-2014) from the Royal
Melbourne Hospital Home Lottery Research Grant in Aid - Allied Health, Victoria,
Australia.
5.1 Introduction
This chapter will describe a prospective observational study to prospectively assess
pelvic floor symptoms and physical and psychological outcomes in patients before
and up to six months after surgery for CRC. Despite the high prevalence of pelvic
floor symptoms in the community and in patients before and following rectal cancer
surgery (Bregendahl, Emmertsen, Lous, & Laurberg, 2013; Contin et al., 2014; John
et al., 2011; Maris et al., 2013; Murata, Brown, Raval, & Phang, 2008; Scheer et al.,
2011), only two small studies have shown that patients with colon cancer also suffer
from pelvic floor dysfunction following surgery (Phipps et al., 2008; Tomoda &
Furusawa, 1985). Furthermore, limited evidence is available regarding change of
pelvic floor symptoms (bladder, bowel, and sexual symptoms) and functional

Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
106
outcomes over time in CRC patients. As we seek to improve survivorship outcomes
for this population, it is important to understand the natural history of changes in
pelvic floor symptoms in patients who have undergone CRC surgery including any
potential natural recovery of physical and psychological status, in order to inform
clinical practice and research studies.
This chapter contains content that is substantially unchanged from the content of the
paper which is currently under review with the Physiotherapy Theory and Practice
journal.
5.1.1 Study aims and hypotheses
Primary aim
Aim 1: To prospectively assess pelvic floor symptoms in patients before and up to six
months after surgery for CRC.
Hypothesis 1: There would be deterioration in pelvic floor symptoms 6 months after
CRC surgery compared to pre-operative status.
Secondary aim
Aim 2: To assess PA levels, psychological outcomes, and HRQoL in patients before
and up to six months after surgery.
Hypothesis 2: There would be deterioration in PA levels, HRQoL and increased
anxiety and depression 6 months after CRC surgery compared to pre-operative status.
5.2 Materials and Methods
5.2.1 Study design and participants
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
107
This was a prospective observational study. Participants were eligible if they had
histologically confirmed stage I-III CRC and were undergoing CRC surgery. Patients
were excluded if they required a permanent ostomy, had insufficient English language
skills to participate, or had severe physical/psychiatric impairments. Participants were
recruited through Royal Melbourne Hospital and Melbourne Private Hospital between
October 2013 and August 2015. Potentially eligible patients were identified by the
treating surgeons or colorectal liaison nurse, who asked patients for their permission
to be contacted by a member of the research team. The researcher explained the study
and invited patients to participate. Written informed consent was obtained from all
participants. The study was approved by the Melbourne Health and Melbourne Private
Hospital HREC (number 2013.199) (Appendix 5.1).
5.2.2 Outcome measures
Outcomes were evaluated before and 6 months after surgery. In a subset of
participants (n=17), measures were also performed 6 weeks after surgery, to compare
the short-and medium-term changes in outcome measures over time. A questionnaire
booklet (Appendix 5.2) was given to participants at each time-point.
Pelvic floor symptoms
Pelvic floor symptoms were assessed using the APFQ (Baessler et al., 2010), ICIQ-B
(Cotterill et al., 2011) and ICIQ-UI SF (Avery et al., 2004). The APFQ is a valid and
reliable instrument consisting of 42 questions across 4 domains (bladder, bowel, and
sexual function and pelvic organ prolapse) (Baessler et al.). Scores within each
domain are divided by the number of relevant questions and multiplied by 10; thus,
the scores range from 0 to 10 for each domain, giving a maximum total score of 40
(higher scores represent worse severity/symptoms) (Baessler et al., 2009). ICIQ-B
was used in addition to APFQ to obtain more comprehensive evaluation of bowel
symptoms. ICIQ-B is a validated non-gender-specific questionnaire developed to
evaluate anal incontinence symptoms and impact on HRQoL. The ICIQ-B contains a
total of 21 questions, 17 of which are scored and form 3 domains: bowel pattern
(score range 1-21), bowel control (score range 0-28), and HRQoL (score range 0-26).
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
108
Four unscored items include other bowel symptoms and sexual impact (Cotterill et al.,
2011). Higher scores on the ICIQ-B represent worse bowel symptoms. As the APFQ
has only been validated in female populations (Baessler et al., 2010), the ICIQ-UI SF,
a validated non-gender-specific questionnaires, was introduced later in the study to
evaluate urinary incontinence symptoms. The ICIQ-UI SF consists of three scored
items related to frequency and amount of urinary incontinence and HRQoL and a
self-diagnostic item, which is not scored. An overall ICIQ-UI SF score is calculated
as the summation of the three scored items. Urinary incontinence is defined as either
absent (score 0) or present (score ≥ 1) on the ICIQ-UI SF (Avery et al., 2004).
Physical activity levels
The short form version of the IPAQ-SF was used to assess PA levels over the
previous 7 days. This self-report questionnaire measures frequency (days per week)
and duration (minutes per day) of PA (vigorous, moderate, and walking) and has
acceptable reliability and validity (Craig et al., 2003). The total IPAQ score in
MET-minutes per week is the summation of walking (3.3 MET), moderate activity
(4.0 MET), and vigorous (8.0 MET) activity minutes per week. Total IPAQ scores are
classified as “low” (not meeting the criteria for moderate-intensity and
vigorous-intensity activity categories), “moderate” (achieving at least 600
MET-minutes/week) and “high” (achieving at least 3000 MET-minutes/week) (IPAQ
Research Committee, 2005).
Psychological outcomes
Anxiety and depression were screened with the 14-item HADS, which is composed of
an anxiety subscale and a depression subscale. Each subscale is scored from 0 to 21.
The HADS has high internal consistency in patient populations including cancer
(Zigmond & Snaith, 1983).
Health-related quality of life
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
109
Health-related quality of life was evaluated by the EORTC QLQ-C30 and the
QLQ-CR29. As a supplement to EORTC QLQ-C30, QLQ-CR29 consists of 29
questions assessing the CRC-specific functional and symptom scales, such as,
gastrointestinal symptoms, pain, problems with micturition, symptoms with/without
stoma, and sexual function. All scale/single item measures of EORTC QLQ-C30 and
QLQ-CR29 range in score from 0-100. Higher scores on the functional and the global
quality of life scales represents higher level of functioning and higher HRQoL, while
higher scores on the symptom scales represents a higher levels of symptomatology.
The EORTC QLQ-C30 and QLQ-CR29 have good validity and reliability (Aaronson
et al., 1993; Whistance et al., 2009).
Socio-demographic and medical variables were collected including age; sex; BMI;
social situation; education, employment, marital, smoking and hormonal status
(female only); cancer stage; treatment type/status; length of in-patient stay; and the
ECOG-PS (Oken et al., 1982).
5.2.3 Statistical analysis
Data analyses were performed using the Statistical Package for Social Sciences
version 20.0 for Windows. Data were assessed for normality using
Kolmogorov-Smirnov (Ghasemi & Zahediasl, 2012). Descriptive statistics, such as
mean and SD, and number and percentage were used to summarize data. Paired-t tests
were used to compare changes in outcomes of interest before and 6 months after
surgery. A subgroup analysis (n=17) using repeated measures analysis of variance
(ANOVA) with Bonferroni post hoc comparisons was performed to compare changes
in outcome variables over three assessment time points (before surgery, 6-week after
surgery, and 6-month after surgery). All analyses were tested with a significance level
of p < 0.05. Data were also compared with published population norms for APFQ
(Baessler et al., 2009), ICIQ-UI SF (Osuga, Okamura, Ando, & Shimokata, 2013),
IPAQ (Tomioka, Iwamoto, Saeki, & Okamoto, 2011), HADS (Crawford, Henry,
Crombie, & Taylor, 2001) and EORTC QLQ-C30 (Hinz, Singer, & Brahler, 2014).
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
110
Sample size requirement was estimated from a previous study (Baessler et al., 2009).
Twenty-three participants were needed for a mean change (SD) of 1.0 ± 1.7 in the
bowel domain score of the APFQ with a power of 0.8 and alpha 0.05 (Hozo,
Djulbegovic, & Hozo, 2005). Allowing for 30% attrition, a total of 30 participants
was sought.
5.3 Results
One hundred and twenty-three patients were assessed for eligibility over the 22 month
recruitment period, 56 patients were ineligible and 56 were approached. The consent
rate was 53.6%. The main reasons for decline were “inability to read/write English”
31 % (n = 8/26) and “too busy” 27 % (n = 7/26). A total of 30 patients with CRC were
recruited (Figure 5.1).
Demographic characteristics are shown in Table 5-1. Fifty-three percent were males,
and 67% and 33% had a diagnosis of colon cancer and rectal cancer respectively.
Thirteen percent of the cohort received chemoradiotherapy before surgery, and 50%
received CT after surgery. The most common types of surgery were right
hemicolectomy (30%), HAR (27%), and ultra-low anterior resection (27%) (Table
5-1). None of the participants were referred to the local continence service or exercise
rehabilitation programs following surgery.
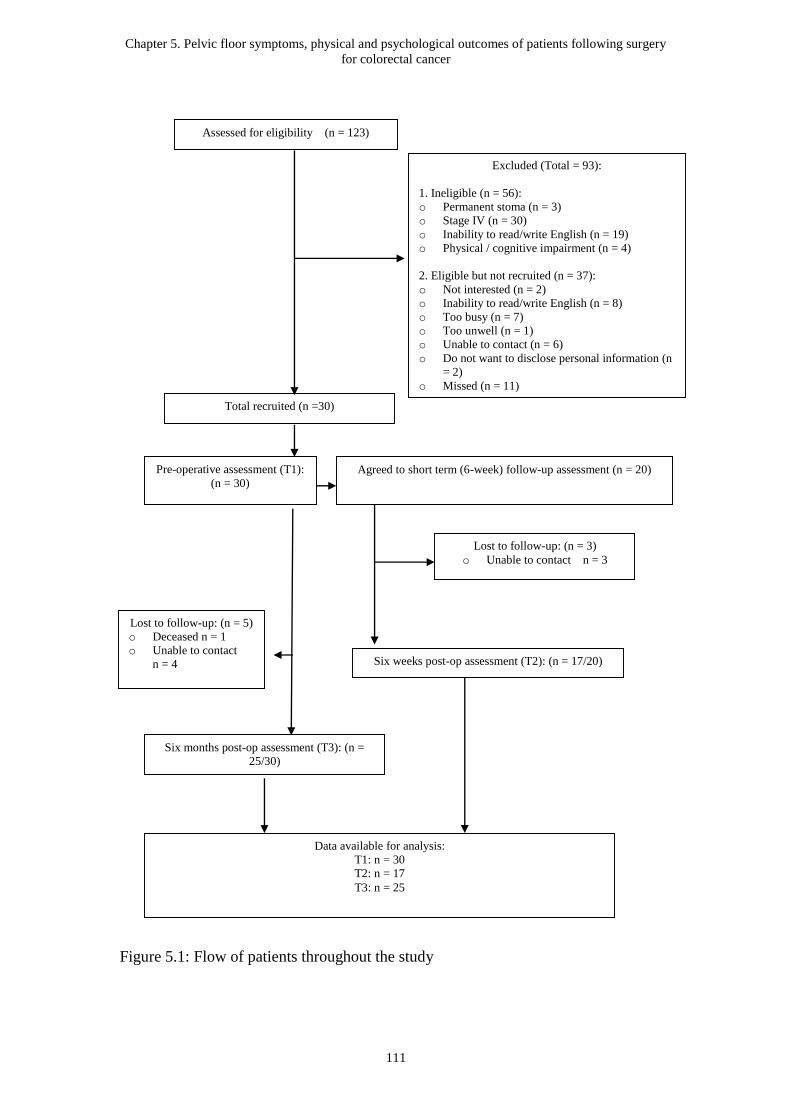
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
111
Figure 5.1: Flow of patients throughout the study
Total recruited (n =30)
Assessed for eligibility (n = 123)
Six weeks post-op assessment (T2): (n = 17/20)
Six months post-op assessment (T3): (n =
25/30)
Data available for analysis:
T1: n = 30
T2: n = 17
T3: n = 25
Excluded (Total = 93):
1. Ineligible (n = 56):
o Permanent stoma (n = 3)
o Stage IV (n = 30)
o Inability to read/write English (n = 19)
o Physical / cognitive impairment (n = 4)
2. Eligible but not recruited (n = 37):
o Not interested (n = 2)
o Inability to read/write English (n = 8)
o Too busy (n = 7)
o Too unwell (n = 1)
o Unable to contact (n = 6)
o Do not want to disclose personal information (n
= 2)
o Missed (n = 11)
Pre-operative assessment (T1):
(n = 30)
Lost to follow-up: (n = 3)
o Unable to contact n = 3
Lost to follow-up: (n = 5)
o Deceased n = 1
o Unable to contact
n = 4
Agreed to short term (6-week) follow-up assessment (n = 20)
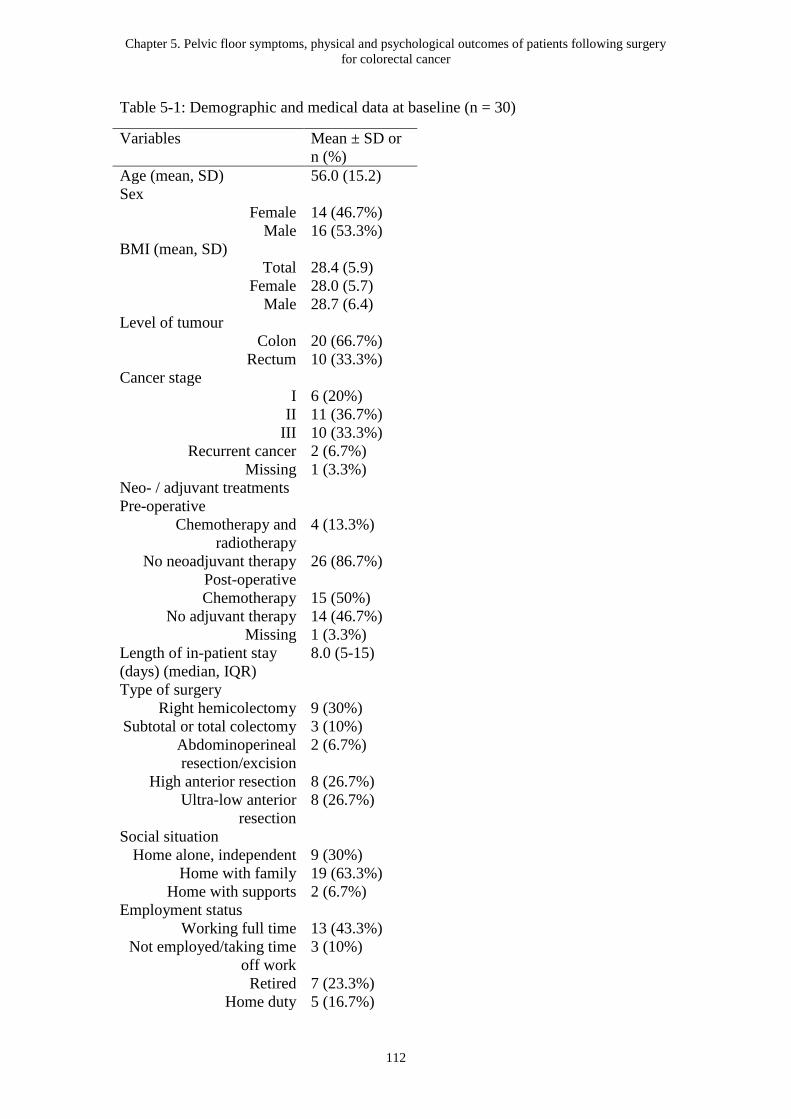
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
112
Table 5-1: Demographic and medical data at baseline (n = 30)
Variables Mean ± SD or
n (%)
Age (mean, SD) 56.0 (15.2)
Sex
Female 14 (46.7%)
Male 16 (53.3%)
BMI (mean, SD)
Total 28.4 (5.9)
Female 28.0 (5.7)
Male 28.7 (6.4)
Level of tumour
Colon 20 (66.7%)
Rectum 10 (33.3%)
Cancer stage
I 6 (20%)
II 11 (36.7%)
III 10 (33.3%)
Recurrent cancer 2 (6.7%)
Missing 1 (3.3%)
Neo- / adjuvant treatments
Pre-operative
Chemotherapy and
radiotherapy
4 (13.3%)
No neoadjuvant therapy 26 (86.7%)
Post-operative
Chemotherapy 15 (50%)
No adjuvant therapy 14 (46.7%)
Missing 1 (3.3%)
Length of in-patient stay
(days) (median, IQR)
8.0 (5-15)
Type of surgery
Right hemicolectomy 9 (30%)
Subtotal or total colectomy 3 (10%)
Abdominoperineal
resection/excision
2 (6.7%)
High anterior resection 8 (26.7%)
Ultra-low anterior
resection
8 (26.7%)
Social situation
Home alone, independent 9 (30%)
Home with family 19 (63.3%)
Home with supports 2 (6.7%)
Employment status
Working full time 13 (43.3%)
Not employed/taking time
off work
3 (10%)
Retired 7 (23.3%)
Home duty 5 (16.7%)
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
113
Studying 1 (3.3%)
Other 1 (3.3%)
Education
No formal schooling 1 (3.3%)
High school or less 11 (36.7%)
Some college or university 11 (36.7%)
Completed Bachelor’s
degree
5 (16.7%)
Completed Masters or PhD
degree
1 (3.3%)
Other 1 (3.3%)
Smoking status
Never smoked 17 (56.7%)
Ex-smoker 9 (30%)
Missing 4 (13.3%)
ECOG performance status
Fully active 20 (66.7%)
Walking, but only can do
light work
8 (26.7%)
Rest in bed LESS than half
the day, do not work but
can care for self
2 (6.7%)
Hormonal status (n = 14)
Menstruating regularly 3 (21.4%)
Post-menopausal 11 (78.6%) Abbreviation: IQR, interquartile range; SD, standard deviation; n, number; %, percent; ECOG, The
Eastern Cooperative Oncology Group; PhD, Doctor of Philosophy.
The outcomes of the study population and the published normative values – to act as a
reference point – are shown in Tables 5-2 and 5-4. Table 5-3 reports the number of
participants categorized according to level of severity of bladder and bowel symptoms
and PA, which are the first three major outcomes of interest.
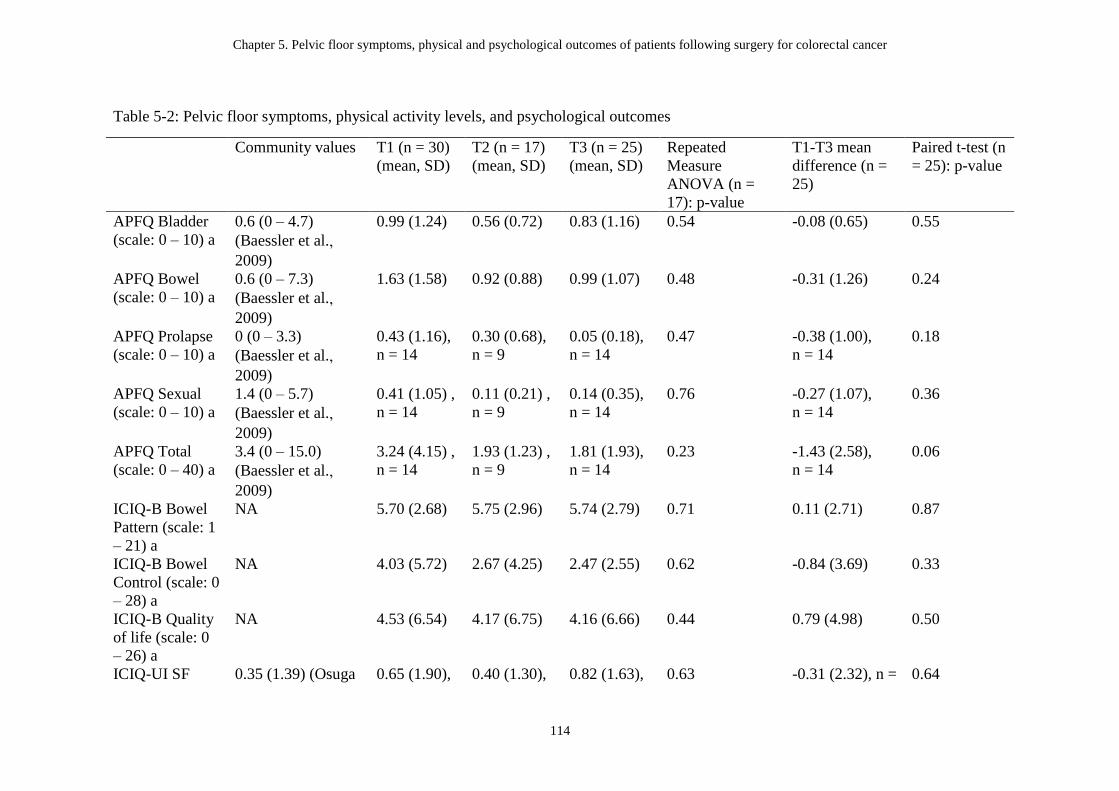
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery for colorectal cancer
114
Table 5-2: Pelvic floor symptoms, physical activity levels, and psychological outcomes
Community values T1 (n = 30)
(mean, SD)
T2 (n = 17)
(mean, SD)
T3 (n = 25)
(mean, SD)
Repeated
Measure
ANOVA (n =
17): p-value
T1-T3 mean
difference (n =
25)
Paired t-test (n
= 25): p-value
APFQ Bladder
(scale: 0 – 10) a
0.6 (0 – 4.7)
(Baessler et al., 2009)
0.99 (1.24) 0.56 (0.72) 0.83 (1.16) 0.54 -0.08 (0.65) 0.55
APFQ Bowel
(scale: 0 – 10) a
0.6 (0 – 7.3)
(Baessler et al., 2009)
1.63 (1.58) 0.92 (0.88) 0.99 (1.07) 0.48 -0.31 (1.26) 0.24
APFQ Prolapse
(scale: 0 – 10) a
0 (0 – 3.3)
(Baessler et al.,
2009)
0.43 (1.16),
n = 14
0.30 (0.68),
n = 9
0.05 (0.18),
n = 14
0.47 -0.38 (1.00),
n = 14
0.18
APFQ Sexual
(scale: 0 – 10) a
1.4 (0 – 5.7)
(Baessler et al.,
2009)
0.41 (1.05) ,
n = 14
0.11 (0.21) ,
n = 9
0.14 (0.35),
n = 14
0.76 -0.27 (1.07),
n = 14
0.36
APFQ Total
(scale: 0 – 40) a
3.4 (0 – 15.0)
(Baessler et al., 2009)
3.24 (4.15) ,
n = 14
1.93 (1.23) ,
n = 9
1.81 (1.93),
n = 14
0.23 -1.43 (2.58),
n = 14
0.06
ICIQ-B Bowel
Pattern (scale: 1
– 21) a
NA 5.70 (2.68) 5.75 (2.96) 5.74 (2.79) 0.71 0.11 (2.71) 0.87
ICIQ-B Bowel
Control (scale: 0
– 28) a
NA 4.03 (5.72) 2.67 (4.25) 2.47 (2.55) 0.62 -0.84 (3.69) 0.33
ICIQ-B Quality
of life (scale: 0
– 26) a
NA 4.53 (6.54) 4.17 (6.75) 4.16 (6.66) 0.44 0.79 (4.98) 0.50
ICIQ-UI SF 0.35 (1.39) (Osuga 0.65 (1.90), 0.40 (1.30), 0.82 (1.63), 0.63 -0.31 (2.32), n = 0.64
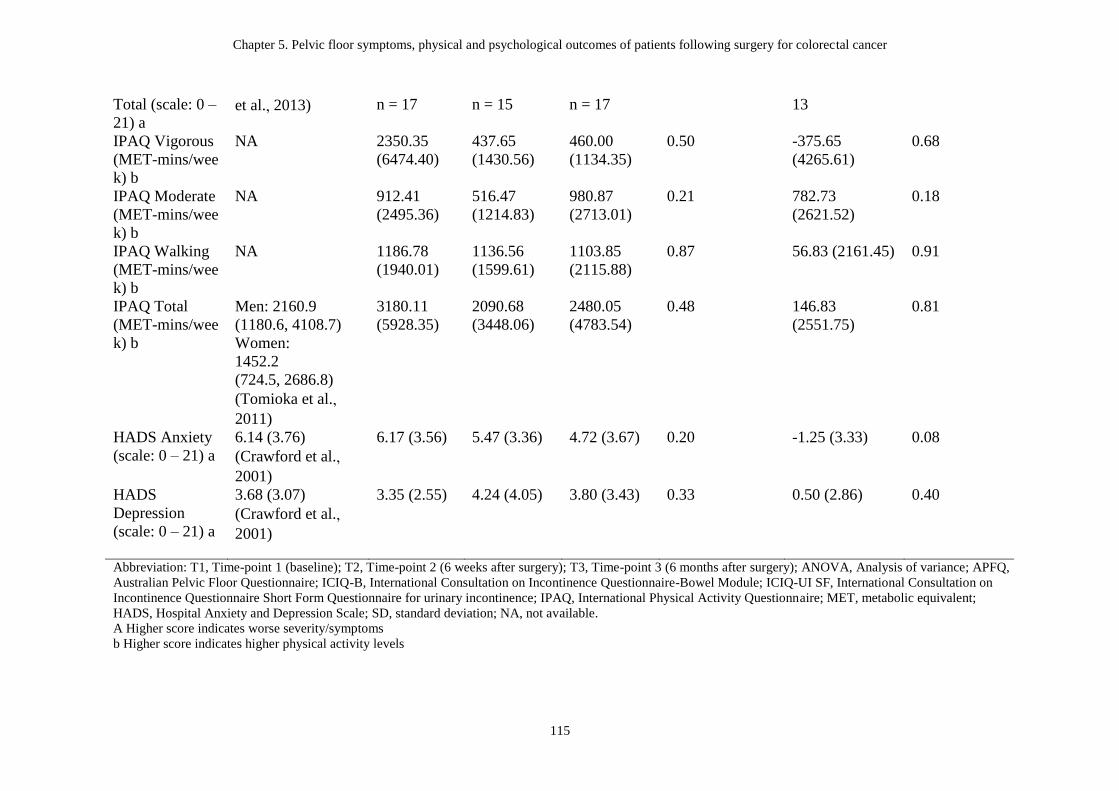
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery for colorectal cancer
115
Total (scale: 0 –
21) a et al., 2013) n = 17 n = 15 n = 17 13
IPAQ Vigorous
(MET-mins/wee
k) b
NA 2350.35
(6474.40)
437.65
(1430.56)
460.00
(1134.35)
0.50 -375.65
(4265.61)
0.68
IPAQ Moderate
(MET-mins/wee
k) b
NA 912.41
(2495.36)
516.47
(1214.83)
980.87
(2713.01)
0.21 782.73
(2621.52)
0.18
IPAQ Walking
(MET-mins/wee
k) b
NA 1186.78
(1940.01)
1136.56
(1599.61)
1103.85
(2115.88)
0.87 56.83 (2161.45) 0.91
IPAQ Total
(MET-mins/wee
k) b
Men: 2160.9
(1180.6, 4108.7)
Women:
1452.2
(724.5, 2686.8)
(Tomioka et al., 2011)
3180.11
(5928.35)
2090.68
(3448.06)
2480.05
(4783.54)
0.48 146.83
(2551.75)
0.81
HADS Anxiety
(scale: 0 – 21) a
6.14 (3.76)
(Crawford et al., 2001)
6.17 (3.56) 5.47 (3.36) 4.72 (3.67) 0.20 -1.25 (3.33) 0.08
HADS
Depression
(scale: 0 – 21) a
3.68 (3.07)
(Crawford et al., 2001)
3.35 (2.55) 4.24 (4.05) 3.80 (3.43) 0.33 0.50 (2.86) 0.40
Abbreviation: T1, Time-point 1 (baseline); T2, Time-point 2 (6 weeks after surgery); T3, Time-point 3 (6 months after surgery); ANOVA, Analysis of variance; APFQ,
Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on Incontinence Questionnaire-Bowel Module; ICIQ-UI SF, International Consultation on
Incontinence Questionnaire Short Form Questionnaire for urinary incontinence; IPAQ, International Physical Activity Questionnaire; MET, metabolic equivalent;
HADS, Hospital Anxiety and Depression Scale; SD, standard deviation; NA, not available.
A Higher score indicates worse severity/symptoms
b Higher score indicates higher physical activity levels

Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
116
Table 5-3: Number of participants categorized according to level of severity of
bladder and bowel symptoms and physical activity, n (%)
Variables T1 (n = 30)
n (%)
T2 (n = 17)
n (%)
T3 (n = 25)
n (%)
Symptomatic-bladdera
APFQ bladder score ≥
1
11 (36.7%) 3 (17.6%) 6 (24.0%)
ICIQ-UI SF Total ≥ 1 2 (11.8%), n = 17 2 (13.33%), n =
15
4 (23.5%), n = 17
Symptomatic-bowela
APFQ bowel score ≥ 1 18 (60.0%) 8 (47.1%) 11 (44.0%)
ICIQ-B bowel pattern
≥ 1
29 (96.7%) 12 (70.6%) 18 (72.2%)
ICIQ-B bowel control
≥ 1
18 (60.0%) 8 (47.1%) 13 (52.0%)
ICIQ-B quality of life
≥ 1
19 (63.3%) 10 (58.8%) 11 (44.0%)
IPAQ-Totalb
Low 11 (42.3%) 8 (47.1%) 9 (47.4%)
Moderate: at least 600
MET-min/week
8 (30.8%) 5 (29.4%) 6 (31.6%)
High: at least 3000
MET-min/week
7 (26.9%) 4 (23.5%) 4 (21.1%)
Abbreviation: T1, Time-point 1 (baseline); T2, Time-point 2 (6 weeks after surgery); T3, Time-point 3
(6 months after surgery); APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International
Consultation on Incontinence Questionnaire-Bowel Module; ICIQ-UI SF, International Consultation on
Incontinence Questionnaire Short Form Questionnaire for urinary incontinence; IPAQ, International
Physical Activity Questionnaire; MET, metabolic equivalent; n, number; %, percent.
A Higher score indicates worse severity/symptoms
b Higher score indicates higher physical activity levels
Pelvic floor symptoms
There were no statistically significant changes in the bladder (APFQ bladder domain
and ICIQ-UI SF) or bowel symptom scores (APFQ bowel domain and ICIQ-B) from
pre-operatively to 6-month post-operatively (Table 5-2). Changes in symptom status
are shown in Table 5-3. Prior to surgery, 37% of the participants had an APFQ
bladder score ≥ 1 and were thus classified as ‘symptomatic’. Six months after surgery,
this had declined to 24% (p > 0.05). In contrast to the APFQ results, the percentage of
participants who were symptomatic on the ICIQ-UI SF doubled (12% to 24%) from
pre-operatively to 6 months post-operatively, however this change was
non-significant (p > 0.05). Furthermore, as the ICIQ-UI SF was introduced later in the
study, there were a smaller number of participants compared to the APFQ. The
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
117
percentage of participants with bowel symptoms measured using APFQ decreased
from 60% pre-operatively to 44% of the participants 6 months after surgery (p >
0.05).
Psychological outcomes and PA levels
No significant changes were found in the HADS anxiety and depression scores and
PA levels assessed with the IPAQ from pre- to 6 months post-surgery (Table 5-2).
The percentage of participants engaged in low PA levels increased slightly from
42.3% pre-operatively to 47.4% at 6 months post-operatively (Table 5-3).
Health-related quality of life
The results of the changes in HRQoL scores over time are shown in Table 5-4. Six
months after surgery, patients had significantly less abdominal pain (mean difference
[SD] = -15.3 ± 31.1, p = 0.02) compared to pre-operative levels. However hair loss
(mean difference = 20.8 ± 30.8, p = 0.003) and faecal incontinence (mean difference
= 15.3 ± 32.6, p = 0.03) were significantly worse. The changes in anxiety, hair loss,
symptoms of peri-anal skin soreness, abdominal pain, faecal incontinence, stool
frequency, and embarrassment by bowel movement exceeded the minimal clinically
meaningful differences on the EORTC (≥ 10 points) (Osoba et al., 1998).
5.3.1 Subgroup analysis over three assessment time points (before surgery,
6-week after surgery, and 6-month after surgery)
From pre-operatively to 6 weeks post-operatively, the EORTC QLQ C-30 role
functioning (performing work or hobbies) (Figure 5.2) and QLQ-CR29 hair loss were
significantly worse; whereas, the QLQ-CR29 anxiety and urinary frequency were
significantly improved (Table 5-4). From 6 weeks to 6 months after surgery, the
anxiety and urinary frequency as measured with QLQ-CR29 were significantly worse;
the EORTC QLQ C-30 emotional functioning and QLQ-CR29 blood and mucus in
stool improved significantly (Table 5-4).
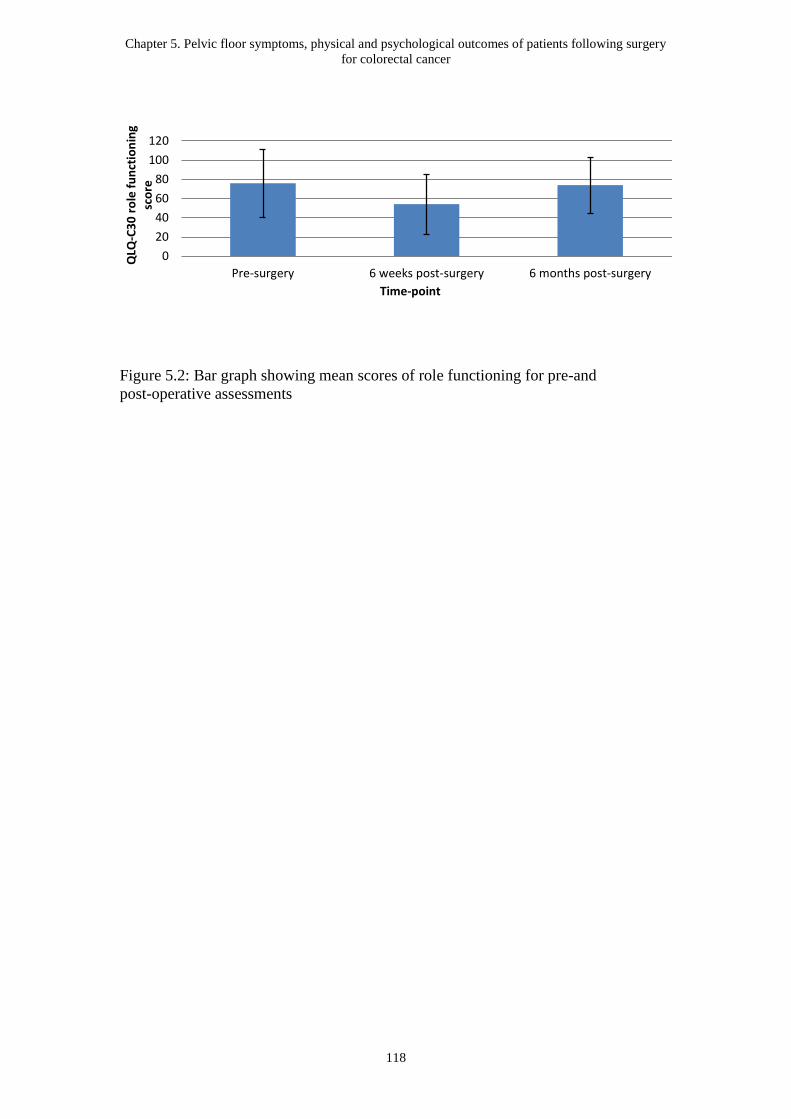
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
118
Figure 5.2: Bar graph showing mean scores of role functioning for pre-and
post-operative assessments
0
20
40
60
80
100
120
Pre-surgery 6 weeks post-surgery 6 months post-surgery
QLQ
-C3
0 r
ole
fu
nct
ion
ing
sco
re
Time-point
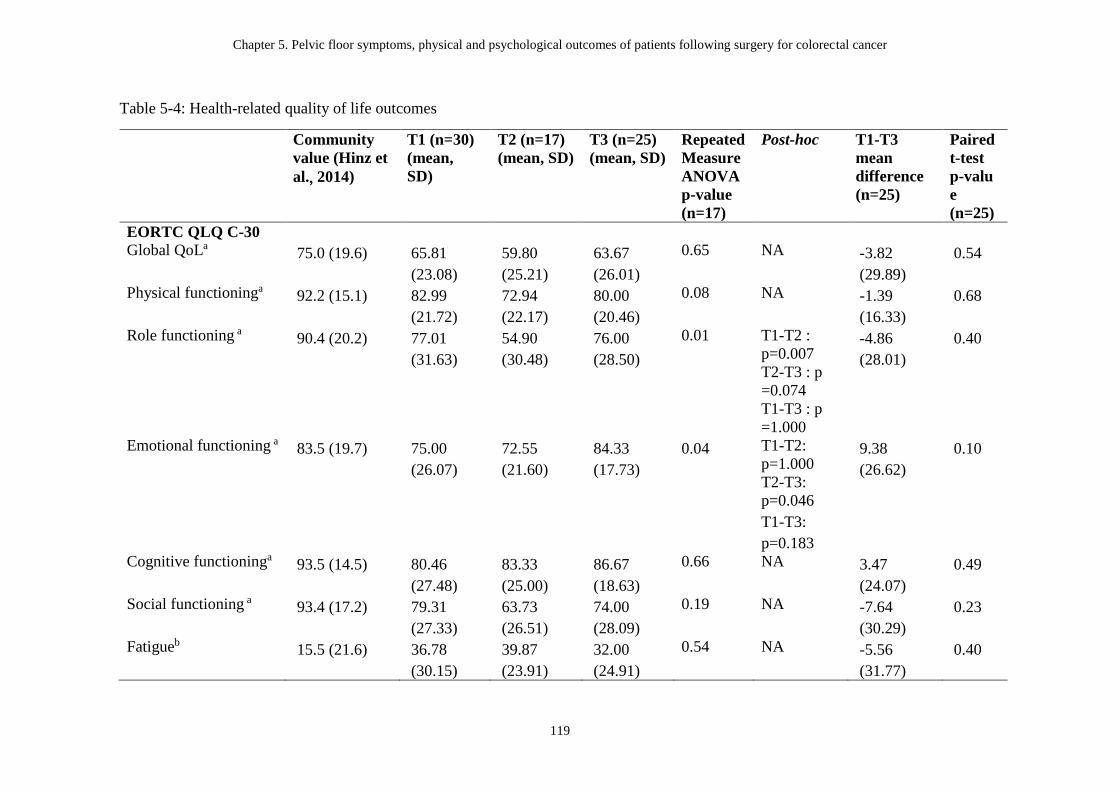
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery for colorectal cancer
119
Table 5-4: Health-related quality of life outcomes
Community
value (Hinz et
al., 2014)
T1 (n=30)
(mean,
SD)
T2 (n=17)
(mean, SD)
T3 (n=25)
(mean, SD)
Repeated
Measure
ANOVA
p-value
(n=17)
Post-hoc T1-T3
mean
difference
(n=25)
Paired
t-test
p-valu
e
(n=25)
EORTC QLQ C-30
Global QoLa 75.0 (19.6) 65.81
(23.08)
59.80
(25.21)
63.67
(26.01)
0.65 NA -3.82
(29.89)
0.54
Physical functioninga 92.2 (15.1) 82.99
(21.72)
72.94
(22.17)
80.00
(20.46)
0.08 NA -1.39
(16.33)
0.68
Role functioning a 90.4 (20.2) 77.01
(31.63)
54.90
(30.48)
76.00
(28.50)
0.01 T1-T2 :
p=0.007
T2-T3 : p
=0.074
T1-T3 : p
=1.000
-4.86
(28.01)
0.40
Emotional functioning a 83.5 (19.7) 75.00
(26.07)
72.55
(21.60)
84.33
(17.73)
0.04 T1-T2:
p=1.000
T2-T3:
p=0.046
T1-T3:
p=0.183
9.38
(26.62)
0.10
Cognitive functioninga 93.5 (14.5) 80.46
(27.48)
83.33
(25.00)
86.67
(18.63)
0.66 NA 3.47
(24.07)
0.49
Social functioning a 93.4 (17.2) 79.31
(27.33)
63.73
(26.51)
74.00
(28.09)
0.19 NA -7.64
(30.29)
0.23
Fatigueb 15.5 (21.6) 36.78
(30.15)
39.87
(23.91)
32.00
(24.91)
0.54 NA -5.56
(31.77)
0.40
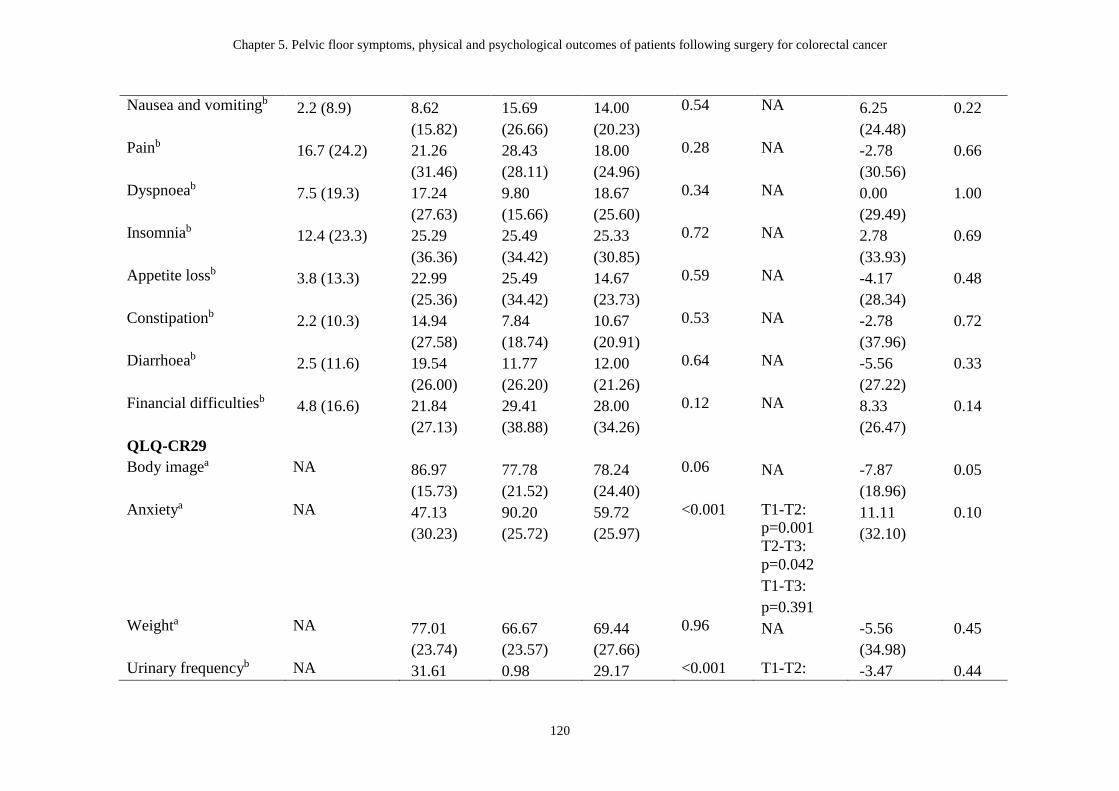
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery for colorectal cancer
120
Nausea and vomitingb 2.2 (8.9) 8.62
(15.82)
15.69
(26.66)
14.00
(20.23)
0.54 NA 6.25
(24.48)
0.22
Painb 16.7 (24.2) 21.26
(31.46)
28.43
(28.11)
18.00
(24.96)
0.28 NA -2.78
(30.56)
0.66
Dyspnoeab 7.5 (19.3) 17.24
(27.63)
9.80
(15.66)
18.67
(25.60)
0.34 NA 0.00
(29.49)
1.00
Insomniab 12.4 (23.3) 25.29
(36.36)
25.49
(34.42)
25.33
(30.85)
0.72 NA 2.78
(33.93)
0.69
Appetite lossb 3.8 (13.3) 22.99
(25.36)
25.49
(34.42)
14.67
(23.73)
0.59 NA -4.17
(28.34)
0.48
Constipationb 2.2 (10.3) 14.94
(27.58)
7.84
(18.74)
10.67
(20.91)
0.53 NA -2.78
(37.96)
0.72
Diarrhoeab 2.5 (11.6) 19.54
(26.00)
11.77
(26.20)
12.00
(21.26)
0.64 NA -5.56
(27.22)
0.33
Financial difficultiesb 4.8 (16.6) 21.84
(27.13)
29.41
(38.88)
28.00
(34.26)
0.12 NA 8.33
(26.47)
0.14
QLQ-CR29
Body imagea NA 86.97
(15.73)
77.78
(21.52)
78.24
(24.40)
0.06 NA -7.87
(18.96)
0.05
Anxietya NA 47.13
(30.23)
90.20
(25.72)
59.72
(25.97)
<0.001 T1-T2:
p=0.001
T2-T3:
p=0.042
T1-T3:
p=0.391
11.11
(32.10)
0.10
Weighta NA 77.01
(23.74)
66.67
(23.57)
69.44
(27.66)
0.96 NA -5.56
(34.98)
0.45
Urinary frequencyb NA 31.61 0.98 29.17 <0.001 T1-T2: -3.47 0.44
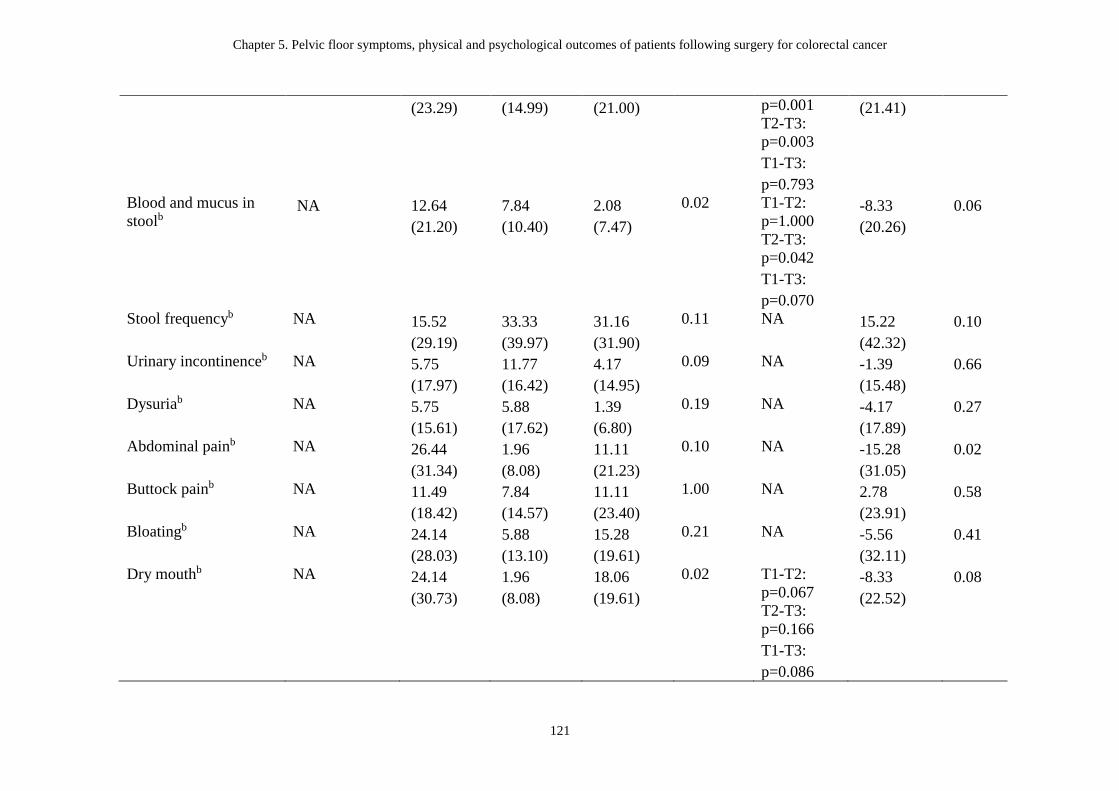
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery for colorectal cancer
121
(23.29) (14.99) (21.00) p=0.001
T2-T3:
p=0.003
T1-T3:
p=0.793
(21.41)
Blood and mucus in
stoolb NA 12.64
(21.20)
7.84
(10.40)
2.08
(7.47)
0.02 T1-T2:
p=1.000
T2-T3:
p=0.042
T1-T3:
p=0.070
-8.33
(20.26)
0.06
Stool frequencyb NA 15.52
(29.19)
33.33
(39.97)
31.16
(31.90)
0.11 NA 15.22
(42.32)
0.10
Urinary incontinenceb NA 5.75
(17.97)
11.77
(16.42)
4.17
(14.95)
0.09 NA -1.39
(15.48)
0.66
Dysuriab NA 5.75
(15.61)
5.88
(17.62)
1.39
(6.80)
0.19 NA -4.17
(17.89)
0.27
Abdominal painb NA 26.44
(31.34)
1.96
(8.08)
11.11
(21.23)
0.10 NA -15.28
(31.05)
0.02
Buttock painb NA 11.49
(18.42)
7.84
(14.57)
11.11
(23.40)
1.00 NA 2.78
(23.91)
0.58
Bloatingb NA 24.14
(28.03)
5.88
(13.10)
15.28
(19.61)
0.21 NA -5.56
(32.11)
0.41
Dry mouthb NA 24.14
(30.73)
1.96
(8.08)
18.06
(19.61)
0.02 T1-T2:
p=0.067
T2-T3:
p=0.166
T1-T3:
p=0.086
-8.33
(22.52)
0.08
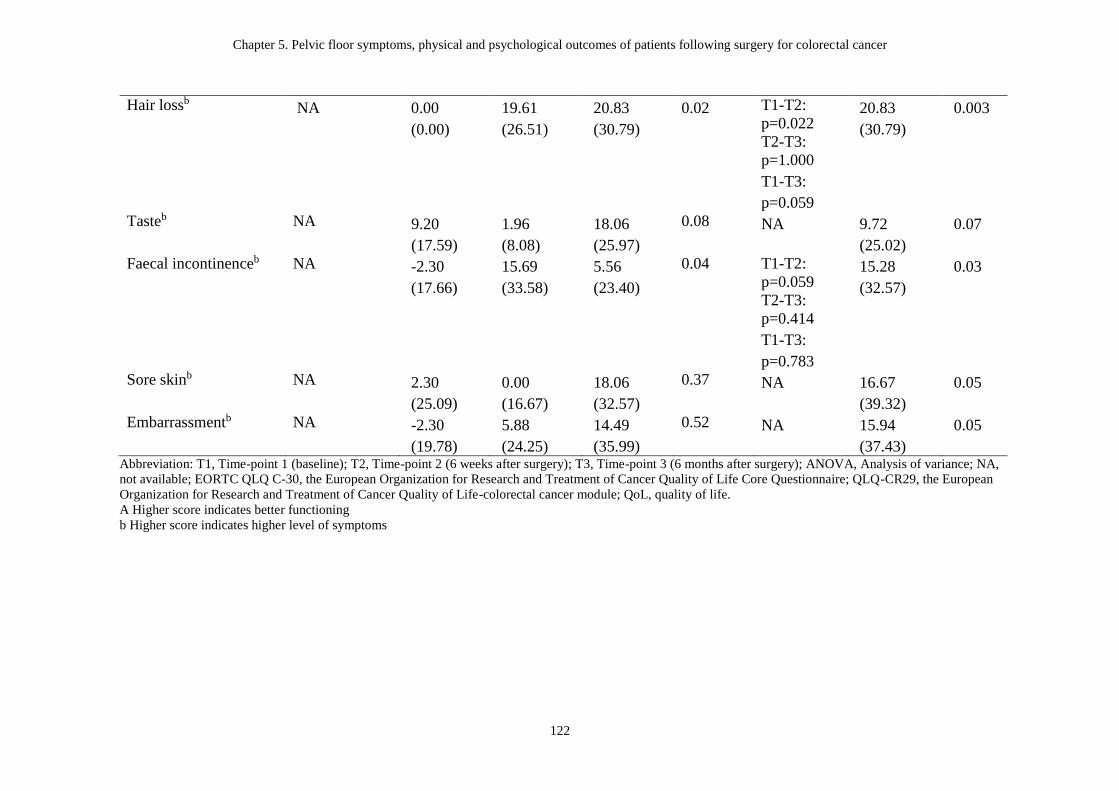
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery for colorectal cancer
122
Hair lossb NA 0.00
(0.00)
19.61
(26.51)
20.83
(30.79)
0.02 T1-T2:
p=0.022
T2-T3:
p=1.000
T1-T3:
p=0.059
20.83
(30.79)
0.003
Tasteb NA 9.20
(17.59)
1.96
(8.08)
18.06
(25.97)
0.08 NA 9.72
(25.02)
0.07
Faecal incontinenceb NA -2.30
(17.66)
15.69
(33.58)
5.56
(23.40)
0.04 T1-T2:
p=0.059
T2-T3:
p=0.414
T1-T3:
p=0.783
15.28
(32.57)
0.03
Sore skinb NA 2.30
(25.09)
0.00
(16.67)
18.06
(32.57)
0.37 NA 16.67
(39.32)
0.05
Embarrassmentb NA -2.30
(19.78)
5.88
(24.25)
14.49
(35.99)
0.52 NA 15.94
(37.43)
0.05
Abbreviation: T1, Time-point 1 (baseline); T2, Time-point 2 (6 weeks after surgery); T3, Time-point 3 (6 months after surgery); ANOVA, Analysis of variance; NA,
not available; EORTC QLQ C-30, the European Organization for Research and Treatment of Cancer Quality of Life Core Questionnaire; QLQ-CR29, the European
Organization for Research and Treatment of Cancer Quality of Life-colorectal cancer module; QoL, quality of life.
A Higher score indicates better functioning
b Higher score indicates higher level of symptoms
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
123
5.4 Discussion
To our knowledge, this is the first study assessing pelvic floor symptoms, physical
and psychological outcomes of Australian patients following surgery for CRC. Our
study showed that compared to pre-operative levels, clinically meaningful deficits
appeared with respect to stool frequency, hair loss, faecal incontinence, symptoms of
peri-anal skin soreness, and bowel embarrassment measured with HRQoL instrument
up to six months after CRC surgery. Due to the growing number of patients
undergoing CRC surgery, our results have significant clinical implications for the
supportive care and survivorship management of patients with CRC and provide
evidence to inform expectations about the course of recovery. Although overall
physical and psychological function may be recovered within 6 months following
surgery, patients still experience significant bowel symptoms for up to 6 months.
Pelvic floor muscle training has been shown to be associated with improvements in
pelvic floor dysfunction in patients following surgery for CRC (Lin, Granger, Denehy,
& Frawley, 2015) and other cancer populations with pelvic floor problems (Yang et
al., 2012). Our findings highlight the importance of the emerging field of survivorship
care in CRC and inform future research to evaluate the effects of PFM training plus or
minus pre-or post-operative general oncology rehabilitation programs in improving
recovery, bowel symptoms, and general health in patients with CRC. Oncology
rehabilitation is a growing area of physiotherapy practice and one that warrants
continued research.
In contrast to the incidence of post-operative bladder, bowel, and sexual dysfunction
observed in other studies (Nikoletti et al., 2008; Perera et al., 2008), no significant
changes were found in pelvic floor symptoms as measured by APFQ, ICIQ-B,
ICIQ-UI SF six weeks and six months after surgery in our study. This may be due to
the fact that our study included a higher percentage of patients treated for colon
cancer compared to patients with rectal cancer (ratio 2:1) and that the majority of our
participants (86.7%) did not receive CT and/or RT before surgery. It is recognized
that pelvic floor dysfunction is more prevalent and severe in patients with rectal
cancer than patients with colon cancer as the more distal tumour level and level of
anastomosis increase the risk of injury to the autonomic nerves, pelvic floor, and anal
Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
124
sphincter (Brown, Fenech, & McLeod, 2008; Fish & Temple, 2014). Pre-and
post-operative chemoradiotherapy has also been shown to have detrimental effects on
PFM function and symptoms (Bernard et al., 2015); however, only 13% of
participants in our study received preoperative chemoradiotherapy and half of the
cohort received post-operative CT. As expected the pre-operative bladder and bowel
symptoms of our cohort were higher than that of the community population (Baessler
et al., 2009; Osuga et al., 2013). Six months after surgery, the severity of some pelvic
floor symptoms (i.e. APFQ bladder and bowel domains and ICIQ-UI SF) remained
higher than the community values. As ICIQ-B is a relatively new questionnaire, there
are no published community data; hence, a comparison of our study cohort with the
community on ICIQ-B was not possible. Future studies are required to elucidate the
effects of surgery and/or adjuvant therapy on pelvic floor symptoms to improve our
understanding of this important issue.
As evidence has shown that low HRQoL scores are a risk-factor for poor survival in
older patients with CRC (Fournier et al., 2016), HRQoL has become an important
outcome measure for clinical research in CRC. We found that most of the EROTC
QLQ-C30 functioning domains returned to pre-operative level six months
post-operatively, however scores were still lower compared with community data
(Hinz et al., 2014). Our findings are similar to previous studies (Tsunoda, Nakao,
Hiratsuka, Tsunoda, & Kusano, 2007; Wilson & Alexander, 2008). Despite the
recovery of anxiety and abdominal pain by 6 months following CRC surgery, our
study showed that participants still suffered from hair loss and several bowel
symptoms, such as stool frequency, faecal incontinence, peri-anal skin soreness and
embarrassment by bowel movements 6 months following surgery. Bailey et al.
(Bailey et al., 2015) reported similar results in a group of long-term CRC survivors.
Although a previous study has indicated that the QLQ-CR29 is a useful questionnaire
in evaluating patients with rectal cancer who have undergone curative surgery (Peng
et al., 2011), more studies are warranted to evaluate the CRC-specific HRQoL
measured using QLQ-CR29 in patients with colon cancer.
While no significant differences were found in the bowel domains of the APFQ and
ICIQ-B subscales before and after CRC surgery, statistically and clinically worse

Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
125
faecal incontinence measured using QLQ-CR29 was found at 6 months following
surgery. Our finding is in contrast to the previous study by Chen et al. (Chen, Wiltink
et al., 2015), which found an association between bowel dysfunction, measured using
a bowel dysfunction-specific questionnaire and HRQoL measured using the EORTC
QLQ-C30 and QLQ-CR29. However, it should be noted that our results are not
directly comparable to that of Chen et al. due to the different pelvic floor symptom
questionnaires used and the higher proportion of patients with colon cancer were
included in our study. Moreover, different items of the questionnaires may also
account for the discrepancy in our findings on bowel symptoms given that the faecal
incontinence subscale in the QLQ-CR29 consists of only one question on stool
leakage; whereas, the APFQ and ICIQ-B provide a summed score of questions such
as defecation frequency, bowel consistency, faecal urgency, flatus incontinence in
additional to faecal incontinence. While the bowel function domain of APFQ may be
valid in patients with CRC as shown in Study 1 (Chapter 3), no universally accepted
questionnaire to measure CRC-specific bowel symptoms (e.g. peri-rectal bleeding and
abdominal pain) in CRC populations has been established. As bowel symptoms are
the common side-effects of CRC treatment (Fish & Temple, 2014), future studies are
required to investigate the optimal bowel-specific instrument that is valid and
applicable for patients with CRC.
In contrast to prior research which found patients with CRC reduced their
participation in strenuous-intensity PA during adjuvant therapy, and spent greater
time in mild intensity PA after treatment (Chung et al., 2013); we found no significant
changes in PA levels before and after CRC surgery. As the percentage of participants
with moderate PA levels was similar before and 6 months after surgery (31% and
32%), this suggests that participants may not have received advice or encouragement
from health care professionals to engage in regular PA following CRC surgery (Lynch,
Owen, Hawkes, & Aitken, 2010). Overall we found corresponding low levels of PA
in our cohort both before and after surgery. Physical activity is very important for
patients with CRC and is associated with improvements in physical fitness (Cramer et
al., 2013) and HRQoL (Otto et al., 2015). Physical activity may also influence
survival and a previous meta-analysis estimated that each 10 MET-hour per week
increase in PA (equivalent to at least 150 minutes/week of moderate intensity PA)

Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
126
after diagnosis was associated with 28% (95% CI = 11–36%) lower risk of mortality
among CRC survivors (Schmid & Leitzmann, 2014). Therefore our results suggest
patients following surgery for CRC should be either referred to physiotherapy or
exercise rehabilitation programs, or encouraged to engage in regular PA by their
treating physician (Fisher, Smith, & Wardle, 2016) as part of usual care.
This is the first study investigating pelvic floor symptoms, PA levels, psychological
outcomes and HRQoL in Australian patients who have undergone surgery for colon or
rectal cancer in a prospective study design. As mentioned previously, few studies
have evaluated pelvic floors symptoms in patients following surgery for colon cancer.
With a higher proportion of patients with colon cancer in our study, more information
is added to current literature about physical and psychological outcomes of this
patient group. There are several limitations in our study. The primary limitation of
this study is that the small sample size makes it difficult to conduct subgroup analyses
in patients with rectal cancer versus colon cancer or surgery only versus surgery plus
neo-adjuvant / adjuvant therapy. It is possible that different treatment regimens may
have an effect on patient symptoms and patterns of change in PA levels (Granger,
Parry, Edbrooke, & Denehy, 2016). Moreover, the findings of this study may not be
generalized to all CRC populations due to the possible selection bias and potential
confounders (i.e. comorbidities of patients) which were not collected. Although
participants were not referred to a continence service from the hospital, it is not
known if the participants received treatment from private clinics. Despite these
limitations, our findings inform future research to design appropriate interventions or
rehabilitation programs to treat the distressing bowel symptoms in patients post-CRC
surgery, as optimal bowel management following CRC surgery has not been
addressed in clinical pathway or guidelines (El-Shami et al., 2015).
5.5 Summary
Patients undergoing surgery for CRC experience worsened bowel symptoms
including incontinence from pre- to six months post-surgery. However, bladder and
sexual function, PA levels, and depression were unchanged. The findings of a higher
percentage of participants with persistent low PA levels and worse bowel symptoms

Chapter 5. Pelvic floor symptoms, physical and psychological outcomes of patients following surgery
for colorectal cancer
127
after CRC surgery compared to pre-operative levels indicate the need for healthcare
professionals to provide information about the benefits of increasing PA levels and
access to the continence service specialist for bowel management when required at
patient post-operative follow-ups. The next chapter describes a pilot non-randomized
quasi-control trial conducted in Australia, which provided a general oncology
rehabilitation program to patients following CRC surgery in attempt to address some
of these un-met patient needs.

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
128
Chapter 6. A general oncology rehabilitation program for patients following
surgery for colorectal cancer – a pilot study
6.1 Introduction
Oncology rehabilitation is a rapidly growing area of cancer management to mitigate
the symptoms and side effects caused by cancer and its treatment. Patients with CRC
often experience impaired physical function, malnutrition and psychosocial sequelae
of cancer and cancer treatment (Daudt, Cosby, Dennis, Payeur, & Nurullah, 2012;
Medeiros et al., 2010), which are associated with poor HRQoL in patients following
CRC treatment (Gupta et al., 2006). To address the physical, psychological, and social
challenges and needs of patients after cancer treatment, many oncology rehabilitation
programs which combine physical and psychosocial interventions have been
developed and assessed in various cancer populations (Dingman et al., 2008;
Hanssens et al., 2011; Spruit, Janssen, Willemsen, Hochstenbag, & Wouters, 2006).
Guidelines by Rock et al. (2012) have also addressed cancer survivors’ concerns
regarding food choices, dietary supplements and PA (Rock et al., 2012). However, a
recent study on utilization of supportive care after primary treatment for CRC has
reported that only 4.6 % of CRC survivors participated in an oncology rehabilitation
program consisting of physical exercise and psycho-education following CRC surgery
(Holla, van de Poll-Franse, Huijgens, Mols, & Dekker, 2016) and the clinical changes
after utilization of supportive care were not measured. Therefore, the effects of a
general oncology rehabilitation program including disciplines such as physiotherapy,
exercise physiology, dietetics, and psychology on physical and psychosocial
symptoms have not yet been evaluated specifically in patients with CRC.
Physical interventions including exercise therapy are one of the most common
components of oncology rehabilitation with solid evidence for efficacy (Gudbergsson
et al., 2015). Exercise training is recommended by the American College of Sports
Medicine as safe and effective in improving physical functioning, HRQoL, and
cancer-related fatigue in cancer survivors both during and after cancer treatment
(Schmitz et al., 2010). In addition, evidence is emerging regarding the positive effect
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
129
of PA on cancer recurrence and survival in several tumour streams (Rock et al., 2012).
Increases in PA after CRC diagnosis are found to be associated with reduced risk of
CRC recurrence and mortality (Van Blarigan & Meyerhardt, 2015; Vrieling &
Kampman, 2010).
Current evidence for the effectiveness of exercise training specifically in CRC
survivors is emerging. A recent systematic review and meta-analysis of five RCTs
with a total of 238 patients with CRC found strong evidence for short-term
improvements of physical fitness in patients after exercise interventions compared
with controls (Cramer et al., 2013). However, the effects of exercise on HRQoL and
the long-term effects of exercise interventions were inconclusive due to the small
number of trials (Cramer et al., 2013). No well-designed trials have been published
since those included in the Cramer systematic review. Although the health care and
cancer care systems may be different across countries, the recommendations on PA
for cancer and non-cancer populations in the international guidelines are very similar
(Rock et al., 2012; World Health Organization, 2010). Therefore, the American
Cancer Society Guidelines, which recommend cancer survivors engage in regular PA
for at least 150 minutes per week and muscle strengthening activities at least 2 days
per week (Rock et al., 2012), are likely to be applicable for other countries and were
implemented in this study. As the feasibility of implementing an exercise program for
patients with CRC has not been reported, the feasibility of implementing the
American Cancer Society guidelines in the oncology rehabilitation program was the
primary aim of this study with view to implementing the program as a clinical service
for patients with CRC should the pilot study be successful.
6.1.1 Study aims and hypotheses
Primary aim
Aim 1: To investigate the feasibility of implementing a general oncology
rehabilitation program for patients following surgery for CRC.
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
130
Hypothesis 1: The general oncology rehabilitation program will be a safe and feasible
therapy option for patients following surgery for CRC.
Secondary aims
Aim 2: To explore changes in functional exercise capacity, muscle strength,
psychological outcome, level of PA, self-efficacy, pelvic floor symptoms, and
HRQoL in patients before and after a general oncology rehabilitation program.
Hypothesis 2: Physical and psychological variables will show a trend towards
improvement following an 8-week general oncology rehabilitation program.
Aim 3: To investigate changes in psychological outcomes, level of PA, self-efficacy,
pelvic floor symptoms, and HRQoL between a ‘rehabilitation’ group and a
‘questionnaire’ only (quasi-control) group 8 weeks after the baseline assessment.
Hypothesis 3: The ‘rehabilitation’ group will show a trend towards improvement in
physical and psychological variables compared to the ‘questionnaire’ group.
6.2 Methods
This was a pilot non-randomized quasi-control study. This study is reported according
to the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND)
statement (Des Jarlais, Lyles, Crepaz, & Group, 2004).
6.2.1 Participants
Inclusion/exclusion criteria
Patients were eligible if they had undergone surgery for histologically confirmed,
stage I-III CRC; had an Eastern Cooperative Oncology Group performance status of
between 0-2 (0 = fully active to 2 = up and about for 50% of a day); and had sufficient
English language skills to participate. Patients were excluded if they were aged 86 and
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
131
over (von Gruenigen et al., 2012), were pregnant or up to 12 months postpartum, had
physical / psychiatric impairments that prevented participation in the exercise
programs, presence of other malignancies or had already been involved in a
rehabilitation program in the prior 12 months.
Recruitment and data collection
Potentially eligible patients were identified by the treating surgeons or ward / practice
nurses at Cabrini Hospital, Victoria, Australia. The surgeons provided the research
team with the patient details of interested eligible patients. An invitation letter and
summary information about the study was then posted from the surgeon’s rooms or
the research team 6 weeks after the cessation of patients’ surgical and medical
treatments. A follow-up telephone contact was made directly by the research team
approximately seven days after the study summary information had been posted, or
after the surgeon signified he had referred the patient to the study, in order to establish
if the information had been received; assess the patient’s interest and eligibility; and
make arrangements to post or email the Participant Information and Consent Form.
Once the patient had provided consent to participate, an appointment time for baseline
assessment was made. Eligible patients were recruited consecutively, and an 8-week
group-based education and exercise rehabilitation program was offered.
If patients were interested to participate in the study but declined to attend the
rehabilitation program due to distance or other factors, they were invited to complete
the postal questionnaires only and were used as a ‘quasi-control’ group in this study.
The outcome measures were obtained at baseline (time-point 1 [T1]) and immediately
post-intervention or at 8-weeks following baseline (time-point 2 [T2]). The study was
approved by the Cabrini HREC (Melbourne, Australia) (Appendix 6.1). All
participants provided signed informed consent. The protocol was registered with the
Australian and New Zealand Clinical Trial Registry (ACTRN12614000580673).

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
132
6.2.2 Intervention
The general oncology rehabilitation program consisted of an 8-week multidisciplinary
education and exercise program. Over the 8 week program, the education components
included 1-hour nutritional advice and management provided by a dietician; 1-hour
exercise education regarding the importance of exercise to well-being, bladder and
bowel advice, and adherence to exercise provided by a physiotherapist; 3-hour action
planning for PA and implementation of exercise provided by an exercise physiologist;
and 3-hour stress management and behavioural change techniques provided by a
psychologist. The exercise component was informed by the PA guidelines for cancer
survivors by Rock et al. (Rock et al., 2012), and consisted of a moderate intensity,
combined aerobic and resistance training program jointly supervised by a
physiotherapist and exercise physiologist. The exercise program was individualised
for patients based on the results of their baseline outcome measures. The intervention
was provided twice weekly, and each session lasted approximately one hour. Verbal
cueing was provided during exercise classes to encourage PFM activation prior to an
anticipated rise in intra-abdominal pressure (the technique is called the ‘knack’)
(Miller, Ashton-Miller, & DeLancey, 1998). In addition, participants were provided
with an “Exercises for home” sheet which included instructions and photo
demonstrations for major muscle group’s resistance training to be performed at home
(Appendix 6.2). To encourage adherence to the exercise program, participants were
instructed to record the number of steps taken daily with a simple “fit bit” pedometer
(Fitbit ZipTM), plus record weekly home-based exercise to supplement the supervised
sessions, in an exercise diary (Appendix 6.3).
6.2.3 Outcomes
Socio-demographic and medical variables were recorded including age; sex; BMI;
social situation; education, employment status; marital status; level of tumour; cancer
stage; treatment type/status; length of in-patient stay after surgery; time since
operation; surgical history; and distance of home from hospital. Clinical outcomes
were evaluated by a physiotherapist who was involved in the program before and
immediately after the intervention or at 8-week follow-up (Appendix 6.4).

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
133
Primary outcome measure
Feasibility
Feasibility measures included referral, recruitment, attendance, adherence,
withdrawals, and adverse events. Referral is the number of patients referred to the
program during the recruitment time. Recruitment rate is defined as the number of
participants consented divided by those eligible. Attendance is measured by the
number of sessions attended out of 16. Adherence was monitored through exercise
diaries completed by the participants and the reasons for not attending an exercise
session were assessed immediately after absence from a session. To be considered as
adherent to the international PA guidelines, the participants were required to do at
least 150 minutes of moderate intensity (BORG Scale ≥ 13) (Muyor, 2013) exercise
and at least two strength training sessions per week. Withdrawals during the study
period were tracked. Any adverse events were assessed and recorded by the
physiotherapist and exercise physiologist during or following intervention and
assessment (Stevinson & Fox, 2006).
Secondary outcome measures
Physical Activity
Self-reported level of PA was assessed using the short form version of the IPAQ-SF.
This is a detailed self-report questionnaire which measures frequency and duration of
several types of activity (strenuous, moderate, and mild) over the previous seven days,
and has acceptable reliability and validity (Craig et al., 2003). The total IPAQ in
MET-minutes per week is the sum of walking (3.3 MET), moderate activity (4.0
MET), and vigorous activity (8.0 MET) minutes per week (Craig et al., 2003).
Functional exercise capacity
Six-minute walk test
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
134
Functional exercise capacity was assessed using the six-minute walk distance (ATS
Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories,
2002). As per the published American Thoracic Society guideline (ATS Committee
on Proficiency Standards for Clinical Pulmonary Function Laboratories, 2002),
participants were asked to follow standardized instructions and walk as far as possible
over a 30-meter course in 6 minutes. The distance covered in meters was documented.
The 6MWT was performed on two occasions to account for the learning effect, and
the best test result was used in analysis (Spencer et al., 2008; Wu et al., 2003). The
6WMT is a reliable measure (intraclass correlation coefficient [ICC] r = 0.93) in
patients with cancer (Schmidt et al., 2013), and reflects functional exercise required
for daily physical activities (ATS Committee on Proficiency Standards for Clinical
Pulmonary Function Laboratories, 2002).
Muscle strength
Muscle strength was assessed using handgrip dynamometry. As an indicator of
general muscle strength, hand-grip strength has been shown to be a predictor of
postoperative complications, mortality, and functional decline (Bohannon, 2001).
Hand-held dynamometry is a common, simple measurement of strength and has been
used in many patient populations including cancer (Trutschnigg et al., 2008).
Hand-grip strength was measured using the Jamar dynamometer (Lafayette
Instrument Company, USA) (Roberts et al., 2011). The participant was tested in the
position recommended by the American Society for Hand Therapists, and the best
value of the three measures was used for analysis (Peolsson et al., 2001). Hand-grip
dynamometry is a reliable instrument for assessing hand-grip strength (Mathiowetz,
2002; Roberts et al., 2011).
Psychological outcomes
Psychological outcomes were assessed with the 14-item HADS, which is composed of
an anxiety subscale and a depression subscale. Each subscale is scored from 0 to 21.

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
135
As a screening instrument for emotional distress in patients with cancer (Vodermaier
& Millman, 2011), scores of 0–7 on the HADS represent a non-case of anxiety and
depression, 8–10 indicates a possible case, and 11–21 indicates a probable case
(Zigmond & Snaith, 1983). The HADS has demonstrated high internal consistency in
patient populations including cancer (Zigmond & Snaith, 1983).
Health-related quality of life
Health-related quality of life was assessed by the EORTC QLQ-C30 and QLQ-CR29.
The EORTC QLQ-C30 comprises 30 items assessing functional aspects and
symptoms of HRQoL. As a supplement to EORTC QLQ-C30, QLQ-CR29 consists of
29 questions assessing the CRC-specific functional and symptom scales, such as
gastrointestinal symptoms, pain, problems with micturition, symptoms with/without
stoma, and sexual function. In the questionnaires, all scale/single item measures range
in score from 0-100. Higher scores on the functional and the global quality of life
scales represent higher level of functioning and higher HRQoL, while higher scores
on the symptom scales represent higher (worse) levels of symptomatology. The
EORTC QLQ-C30 and QLQ-CR29 have been shown to have good validity and
reliability properties (Aaronson et al., 1993; Whistance et al., 2009).
Self-efficacy
Self-efficacy for exercise and nutrition was assessed using the PES and NES
subscales of the Health-Specific Self-Efficacy Scale developed by Schwarzer R. and
Renner B (Schwarzer & Renner, 2005). Each subscale consists of 5 items, which are
scored on a 4-point Likert-type scale (1 = very uncertain, 2 = rather uncertain, 3 =
rather certain, and 4 = very certain). The total score of each subscale is the sum of the
responses to the 5 items ranging from 5-20. Higher scores indicate higher
self-efficacy. The Health-Specific Self Efficacy Scale has satisfactory psychometric
properties (Schwarzer & Renner, 2005), and is widely used in patients with chronic
diseases (Clarke, 2009).
Pelvic floor symptoms
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
136
Pelvic floor symptoms were assessed using the APFQ (Baessler et al., 2009) and the
ICIQ-B (Cotterill et al., 2011). The APFQ is a validated, reliable, reproducible, and
sensitive to change instrument consisting of 42 questions in four domains (bladder,
bowel, pelvic organ prolapse and sexual function). The scores within each domain are
divided by the number of relevant questions and multiplied by 10; thus, the scores
range from 0-10 for each domain, giving a maximum total score of 40, and higher
scores represent worse symptoms (Baessler et al., 2009). Although the APFQ has only
been validated in female populations (Baessler et al., 2010), the questions in the
bladder and bowel domains may be applicable to males. Hence, only the bladder and
bowel domains of the APFQ were used and included in the data analysis. The ICIQ-B
was used in addition to the APFQ to obtain more comprehensive evaluation of bowel
symptoms. The ICIQ-B is a validated non-gender-specific questionnaire developed to
evaluate anal incontinence symptoms and impact on HRQoL. The ICIQ-B contains a
total of 21 questions; 17 of which are scored and arranged in 3 domains: bowel
pattern (score range 1-21), bowel control (score range 0-28), and HRQoL (score range
0-26). Four unscored items include other bowel symptoms and sexual impact. Higher
scores on the ICIQ-B represent worse bowel symptoms (Cotterill et al., 2011).
Global response change score
Participants’ self-perception of change in their overall pelvic floor symptoms and
fitness were assessed using a global rating of change scale. Global rating of change
scales are commonly used in clinical research to quantify a patient’s overall
improvement or deterioration over time (Kamper, Maher, & Mackay, 2009).
The global rating of change asks participants two single questions:
1: “How do your pelvic floor symptoms / control now, compare to your pelvic floor
symptoms / control at the start of the study?”
2: “How does your fitness now, compare to your fitness at the start of the study?”
Answers are rated on a 7-point Likert response scale (1 = Very much improved
through to 7 = Very much worse) (de Morton, Davidson, & Keating, 2010).
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
137
6.2.4 Sample size
This was a pilot feasibility of guideline implementation study; therefore, it was not
powered to identify statistically significant changes before and after the rehabilitation
program. However, it has been recommended that a minimum of 10 participants per
group be considered for pilot feasibility studies (Hertzog, 2008; Julious, 2005). The
results of this study may assist to determine the sample size for future trials to explore
clinical efficacy and efficiency.
6.2.5 Statistical Methods
Data were analysed using the Statistical Package for Social Sciences, version 20.0 for
Windows. Descriptive statistics, such as mean and SD, and number and percentage
were used to summarize data. Data were assessed for normality using
Kolmogorov-Smirnov (Ghasemi & Zahediasl, 2012). The baseline data of the two
groups were compared using independent t-tests for continuous variables, and
chi-squared test for categorical variables. Paired-t tests were used to compare changes
in outcomes within each group before and after the oncology rehabilitation program.
Changes to each measure across time (group by time interaction) were assessed with
repeated measures analysis of covariance (ANCOVA) adjusted for any statistically
significant differences between groups on outcomes at baseline. All analyses were
tested with a significance level of p < 0.05.
6.3 Results
6.3.1 Participant flow
Figure 6.1 shows the flow of participants through the study. One-hundred and
twenty-two participants were assessed for eligibility between July 2014 and August
2015. The main reasons for ineligibility were age (age > 85) (n = 19) and advanced
cancer stage (stage IV) (n = 7). Seventy-three (59.8%) potentially eligible patients
were approached. Seventeen (23.3%) were unable to be contacted. The two main

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
138
reasons for eligible patients declining to participate in the study were ‘too busy’ (n =
10) and ‘not interested’ (n = 8). Thirteen out of the 27 participants (48%) declined
specifically to participate in rehabilitation program but agreed to participate in the
postal questionnaires, hence the consent rate to the questionnaire group was 17.8% (n
= 13/73) and the consent rate to the rehabilitation program was 19.2% (n = 14/73),
giving a combined consent rate of 37% (n = 27/73). Two participants in the
rehabilitation group and three in the questionnaire group did not complete the study
(three were unable to be contacted at follow-up, one withdrew after the first session,
and one started CT before the first session) (Figure 6.1). The drop-out rate was 14.3%
for the rehabilitation group and 23.1% for the questionnaire group.
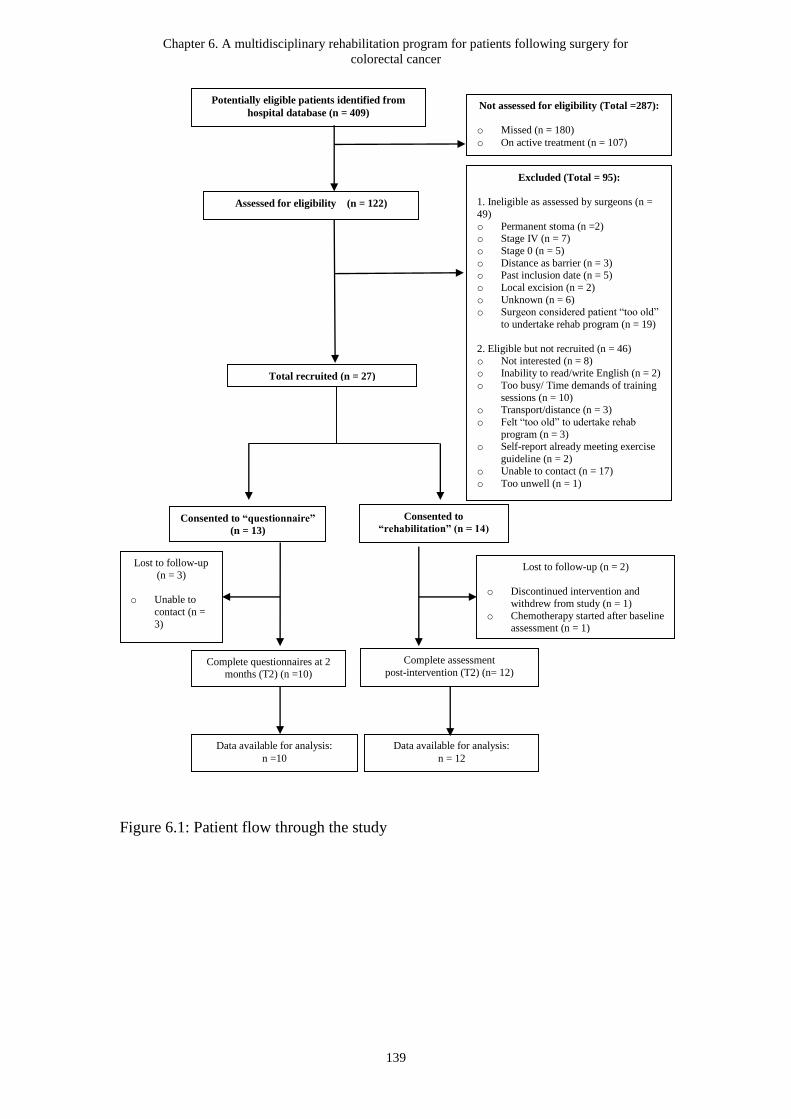
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
139
Figure 6.1: Patient flow through the study
Total recruited (n = 27)
Assessed for eligibility (n = 122)
Not assessed for eligibility (Total =287):
o Missed (n = 180)
o On active treatment (n = 107)
Excluded (Total = 95):
1. Ineligible as assessed by surgeons (n =
49)
o Permanent stoma (n =2) o Stage IV (n = 7)
o Stage 0 (n = 5)
o Distance as barrier (n = 3) o Past inclusion date (n = 5)
o Local excision (n = 2)
o Unknown (n = 6)
o Surgeon considered patient “too old”
to undertake rehab program (n = 19)
2. Eligible but not recruited (n = 46)
o Not interested (n = 8) o Inability to read/write English (n = 2)
o Too busy/ Time demands of training
sessions (n = 10) o Transport/distance (n = 3)
o Felt “too old” to udertake rehab
program (n = 3) o Self-report already meeting exercise
guideline (n = 2)
o Unable to contact (n = 17)
o Too unwell (n = 1)
Consented to “questionnaire”
(n = 13)
Complete questionnaires at 2
months (T2) (n =10)
Consented to
“rehabilitation” (n = 14)
Complete assessment
post-intervention (T2) (n= 12)
Data available for analysis:
n =10
Data available for analysis:
n = 12
Lost to follow-up (n = 2)
o Discontinued intervention and
withdrew from study (n = 1)
o Chemotherapy started after baseline assessment (n = 1)
Lost to follow-up
(n = 3)
o Unable to
contact (n =
3)
Potentially eligible patients identified from
hospital database (n = 409)
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
140
6.3.2 Recruitment
Eligible participants were recruited between July 2014 and August 2015 and the
follow-up period finished in October 2015.
6.3.3 Baseline Data and Baseline Equivalence
The baseline demographics and medical characteristics of the participants are
presented in Table 6-1. The mean (SD) age of the combined cohort was 70.4 ± 9.3
years, and 64% were male. Eighteen out of 22 participants (82%) had a diagnosis of
colon cancer. Fifty-five percent of the participants had undergone colectomy, and nine
(41%) participants had received adjuvant treatment (CT and RT) before and/or after
surgery (Table 6-1). There were no statistically significant differences in participant
characteristics between the rehabilitation and questionnaire groups at baseline except
the time since operation (Table 6-1).
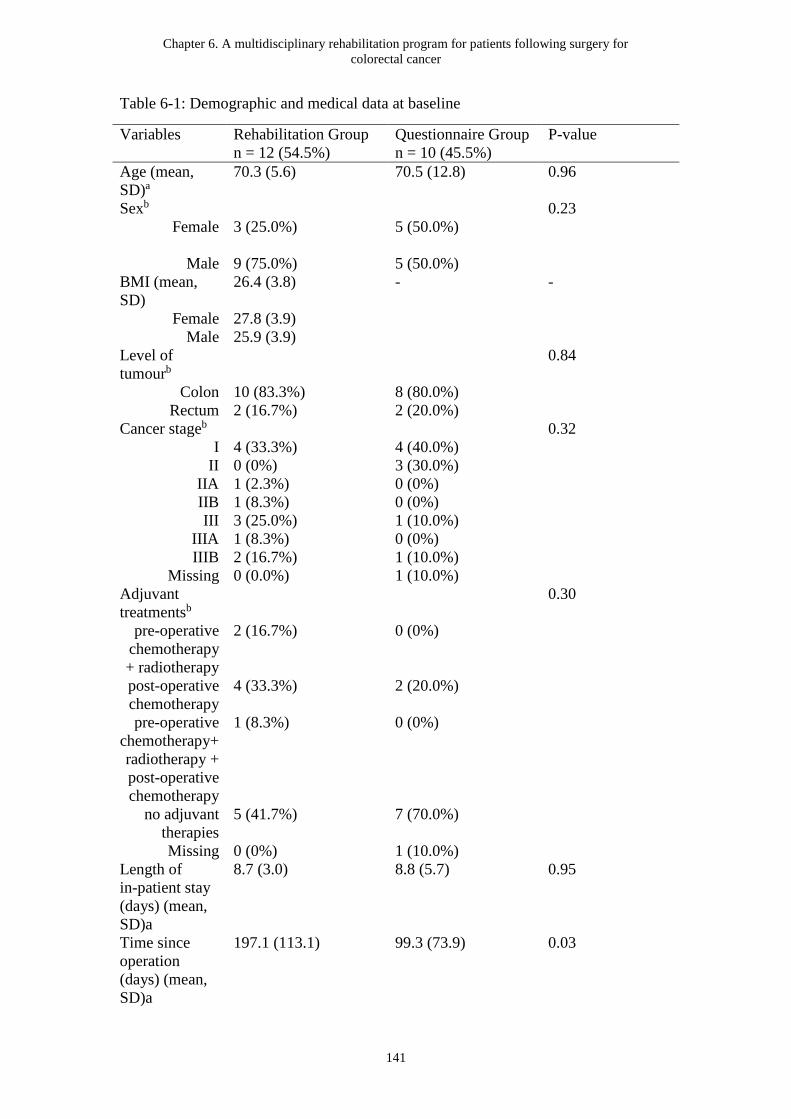
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
141
Table 6-1: Demographic and medical data at baseline
Variables Rehabilitation Group
n = 12 (54.5%)
Questionnaire Group
n = 10 (45.5%)
P-value
Age (mean,
SD)a
70.3 (5.6) 70.5 (12.8) 0.96
Sexb 0.23
Female 3 (25.0%) 5 (50.0%)
Male 9 (75.0%) 5 (50.0%)
BMI (mean,
SD)
26.4 (3.8) - -
Female 27.8 (3.9)
Male 25.9 (3.9)
Level of
tumourb
0.84
Colon 10 (83.3%) 8 (80.0%)
Rectum 2 (16.7%) 2 (20.0%)
Cancer stageb 0.32
I 4 (33.3%) 4 (40.0%)
II 0 (0%) 3 (30.0%)
IIA 1 (2.3%) 0 (0%)
IIB 1 (8.3%) 0 (0%)
III 3 (25.0%) 1 (10.0%)
IIIA 1 (8.3%) 0 (0%)
IIIB 2 (16.7%) 1 (10.0%)
Missing 0 (0.0%) 1 (10.0%)
Adjuvant
treatmentsb
0.30
pre-operative
chemotherapy
+ radiotherapy
2 (16.7%) 0 (0%)
post-operative
chemotherapy
4 (33.3%) 2 (20.0%)
pre-operative
chemotherapy+
radiotherapy +
post-operative
chemotherapy
1 (8.3%) 0 (0%)
no adjuvant
therapies
5 (41.7%) 7 (70.0%)
Missing 0 (0%) 1 (10.0%)
Length of
in-patient stay
(days) (mean,
SD)a
8.7 (3.0) 8.8 (5.7) 0.95
Time since
operation
(days) (mean,
SD)a
197.1 (113.1) 99.3 (73.9) 0.03

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
142
Type of
surgeryb
0.11
right
hemicolectomy
4 (33.3%) 4 (40.0%)
left
hemicolectomy
2 (16.7%) 0 (0%)
Subtotal or
total colectomy
0 (0%) 2 (20.0%)
high anterior
resection
1 (8.3%) 3 (30.0%)
ultra-low
anterior
resection
5 (41.7%) 1 (10.0%)
Social
situationb
0.43
home alone,
independent
1 (8.3%) 2 (20.0%)
home with
family
11 (91.7%) 8 (80.0%)
Employment
statusb
0.69
working full
time
3 (25.0%) 3 (30.0%)
working part
time or as a
casual
2 (16.7%) 1 (10.0%)
retired 6 (50.0%) 5 (50.0%)
retired, home
duty
0 (0%) 1 (10.0%)
other 1 (8.3%) 0 (0%)
Marital statusb 0.42
living with
partner
1 (8.3%) 3 (30.0%)
married for
first time
7 (58.3%) 6 (60.0%)
remarried 2 (16.7%) 0 (0%)
divorced 1 (8.3%) 0 (0%)
widowed 1 (8.3%) 1 (10.0%)
Educationb 0.76
some
secondary or
high school
1 (8.3%) 2 (20.0%)
completed
secondary or
high school
0 (0%) 1 (10.0%)
some trade,
community or
TAFE college
0 (0%) 1 (10.0%)
completed
trade,
1 (8.3%) 1 (10.0%)
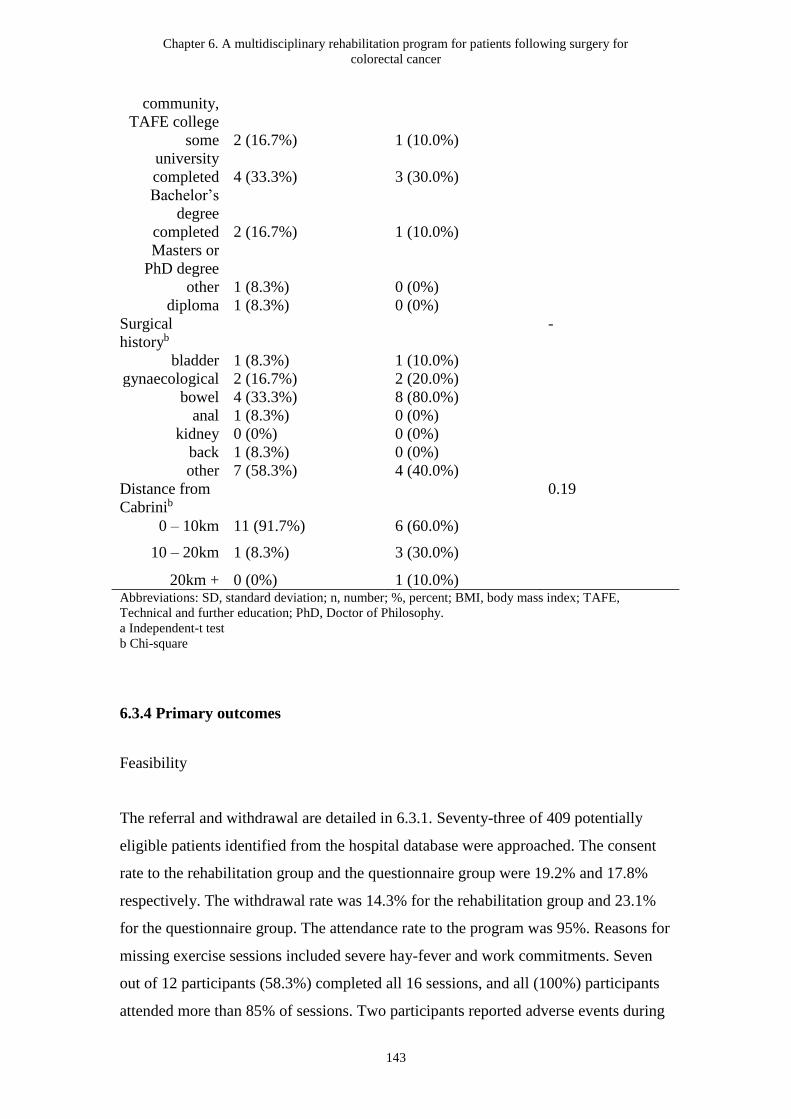
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
143
community,
TAFE college
some
university
2 (16.7%) 1 (10.0%)
completed
Bachelor’s
degree
4 (33.3%) 3 (30.0%)
completed
Masters or
PhD degree
2 (16.7%) 1 (10.0%)
other 1 (8.3%) 0 (0%)
diploma 1 (8.3%) 0 (0%)
Surgical
historyb
-
bladder 1 (8.3%) 1 (10.0%)
gynaecological 2 (16.7%) 2 (20.0%)
bowel 4 (33.3%) 8 (80.0%)
anal 1 (8.3%) 0 (0%)
kidney 0 (0%) 0 (0%)
back 1 (8.3%) 0 (0%)
other 7 (58.3%) 4 (40.0%)
Distance from
Cabrinib
0.19
0 – 10km 11 (91.7%) 6 (60.0%)
10 – 20km 1 (8.3%) 3 (30.0%)
20km + 0 (0%) 1 (10.0%) Abbreviations: SD, standard deviation; n, number; %, percent; BMI, body mass index; TAFE,
Technical and further education; PhD, Doctor of Philosophy.
a Independent-t test
b Chi-square
6.3.4 Primary outcomes
Feasibility
The referral and withdrawal are detailed in 6.3.1. Seventy-three of 409 potentially
eligible patients identified from the hospital database were approached. The consent
rate to the rehabilitation group and the questionnaire group were 19.2% and 17.8%
respectively. The withdrawal rate was 14.3% for the rehabilitation group and 23.1%
for the questionnaire group. The attendance rate to the program was 95%. Reasons for
missing exercise sessions included severe hay-fever and work commitments. Seven
out of 12 participants (58.3%) completed all 16 sessions, and all (100%) participants
attended more than 85% of sessions. Two participants reported adverse events during

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
144
the intervention period and none of the events were related to the participation in the
study (one described anal discomfort with bloody discharge on sitting and one
reported cardiac problems followed by low haemoglobin levels). These two
participants were advised to seek advice from their general practitioner and colorectal
surgeon before returning to classes. No serious adverse events attributable to the study
occurred.
Half of the participants in the rehabilitation group (6/12) completed and returned the
exercise diary after the completion of the rehabilitation program. Table 6-2 shows the
exercise adherence (exercise diary). The average daily steps collected from the Fitbit
pedometer, ranged from 8020 steps to 9788 steps (average of 8 weeks = 8773 steps)
and 50% to 83% (average of 8 weeks = 55%) of participants met the recommended
PA guidelines of 150 minutes moderate-intensity PA plus 2 strengthening sessions per
week during the intervention period.
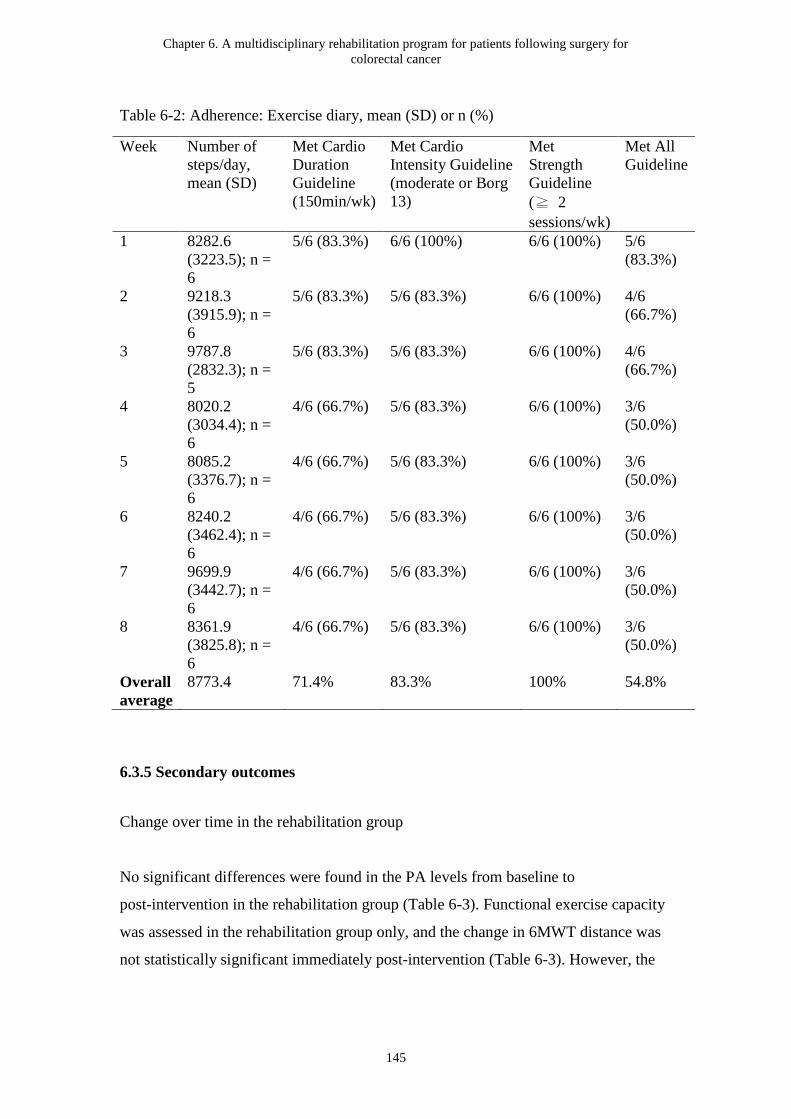
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
145
Table 6-2: Adherence: Exercise diary, mean (SD) or n (%)
Week Number of
steps/day,
mean (SD)
Met Cardio
Duration
Guideline
(150min/wk)
Met Cardio
Intensity Guideline
(moderate or Borg
13)
Met
Strength
Guideline
(≧ 2
sessions/wk)
Met All
Guideline
1 8282.6
(3223.5); n =
6
5/6 (83.3%) 6/6 (100%) 6/6 (100%) 5/6
(83.3%)
2 9218.3
(3915.9); n =
6
5/6 (83.3%) 5/6 (83.3%) 6/6 (100%) 4/6
(66.7%)
3 9787.8
(2832.3); n =
5
5/6 (83.3%) 5/6 (83.3%) 6/6 (100%) 4/6
(66.7%)
4 8020.2
(3034.4); n =
6
4/6 (66.7%) 5/6 (83.3%) 6/6 (100%) 3/6
(50.0%)
5 8085.2
(3376.7); n =
6
4/6 (66.7%) 5/6 (83.3%) 6/6 (100%) 3/6
(50.0%)
6 8240.2
(3462.4); n =
6
4/6 (66.7%) 5/6 (83.3%) 6/6 (100%) 3/6
(50.0%)
7 9699.9
(3442.7); n =
6
4/6 (66.7%) 5/6 (83.3%) 6/6 (100%) 3/6
(50.0%)
8 8361.9
(3825.8); n =
6
4/6 (66.7%) 5/6 (83.3%) 6/6 (100%) 3/6
(50.0%)
Overall
average
8773.4 71.4% 83.3% 100% 54.8%
6.3.5 Secondary outcomes
Change over time in the rehabilitation group
No significant differences were found in the PA levels from baseline to
post-intervention in the rehabilitation group (Table 6-3). Functional exercise capacity
was assessed in the rehabilitation group only, and the change in 6MWT distance was
not statistically significant immediately post-intervention (Table 6-3). However, the
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
146
mean difference from baseline to post intervention (27.3 m – improvement) was
greater than the MCID of 25 meters (Gremeaux et al., 2011).
Hand-grip strength was measured in the rehabilitation group only and did not change
significantly in either males or females following the intervention (Table 6-3). The
symptoms of depression (p = 0.01), APFQ bladder domain (p = 0.03), APFQ bowel
domain (p = 0.01), ICIQ-B bowel pattern domain (p = 0.03), ICIQ-B bowel control
domain (p = 0.02), and ICIQ-B quality of life (p = 0.02) were significantly improved
following the intervention (Table 6-3). Table 6-4 shows the results of HRQoL
outcomes. Global quality of life (p = 0.02), fatigue (p = 0.01), diarrhoea (p = 0.046),
dry mouth (p = 0.04), and urinary frequency (p = 0.02) were significantly improved
following the intervention.

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
147
Table 6-3: Outcomes: baseline to post-intervention
Variables Rehabilitation group Questionnaire group Between
group
ANCOV
A p
value**
T1
(mean,
SD)
T2
(mean,
SD)
Mean
differenc
e
(mean,
SD)
[95% CI]
Within-group
:
paired-t
p-value
T1
(mean,
SD)
T2
(mean,
SD)
Mean
differenc
e
(mean,
SD)
[95% CI]
Within-group
:
paired-t
p-value
6MWT Distance
(metres)
514.2
(78.1);
n = 12
541.4
(73.4);
n = 12
27.3
(59.0)
[-10.2 -
64.7]
0.14 - - - - -
Hand-grip
strength -
Dominant hand
(kg)
34.3
(11.0);
n = 12
34.8
(11.3);
n = 12
0.5 (3.4)
[-1.7 -
2.7]
0.62 - - - - -
Female 20.0
(4.0);
n = 3
20.7
(1.2);
n = 3
0.7 (3.1)
[-6.9 -
8.3]
0.74 - - - - -
Male 39.1
(7.8);
n = 9
39.6
(8.60);
n = 9
0.4 (3.7)
[-2.4 -
3.3]
0.73 - - - - -
APFQ Bladder
(scale: 0 - 10)a
1.4
(1.0);
n = 12
(1.3);
n = 12
-0.3 (0.4)
[-0.6 -
-0.05]
0.03 0.7
(0.6);
n = 10
1.0 (0.6);
n = 10
0.2 (0.5)
[-0.1 -
0.6]
0.15 0.009
APFQ Bowel
(scale: 0 - 10)a
2.4
(1.4);
n = 12
1.6
(0.7);
n = 12
-0.8 (0.9)
[-1.4 -
0.2]
0.01 1.5
(0.7);
n = 10
1.5 (0.6);
n = 10
0 (0.7)
[-0.5 -
0.5]
1.00 0.51
ICIQ-B Bowel
Pattern (scale: 1
- 21)a
8.4
(4.8);
n = 12
6.1
(2.5);
n = 12
-2.3 (3.3)
[-4.4 -
-0.3]
0.03 7.1
(3.2);
n = 10
6.6 (2.5);
n = 10
-0.5 (2.0)
[-1.9 -
0.9]
0.45 0.59
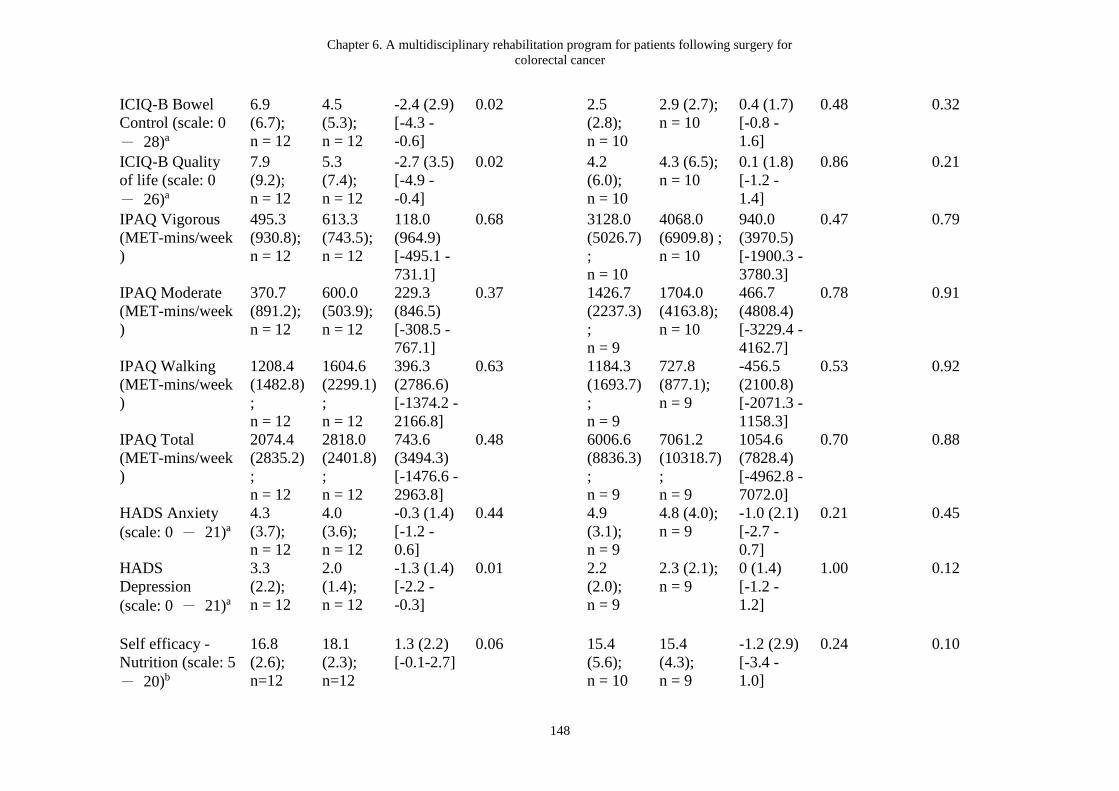
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
148
ICIQ-B Bowel
Control (scale: 0
- 28)a
6.9
(6.7);
n = 12
4.5
(5.3);
n = 12
-2.4 (2.9)
[-4.3 -
-0.6]
0.02 2.5
(2.8);
n = 10
2.9 (2.7);
n = 10
0.4 (1.7)
[-0.8 -
1.6]
0.48 0.32
ICIQ-B Quality
of life (scale: 0
- 26)a
7.9
(9.2);
n = 12
5.3
(7.4);
n = 12
-2.7 (3.5)
[-4.9 -
-0.4]
0.02 4.2
(6.0);
n = 10
4.3 (6.5);
n = 10
0.1 (1.8)
[-1.2 -
1.4]
0.86 0.21
IPAQ Vigorous
(MET-mins/week
)
495.3
(930.8);
n = 12
613.3
(743.5);
n = 12
118.0
(964.9)
[-495.1 -
731.1]
0.68 3128.0
(5026.7)
;
n = 10
4068.0
(6909.8) ;
n = 10
940.0
(3970.5)
[-1900.3 -
3780.3]
0.47 0.79
IPAQ Moderate
(MET-mins/week
)
370.7
(891.2);
n = 12
600.0
(503.9);
n = 12
229.3
(846.5)
[-308.5 -
767.1]
0.37 1426.7
(2237.3)
;
n = 9
1704.0
(4163.8);
n = 10
466.7
(4808.4)
[-3229.4 -
4162.7]
0.78 0.91
IPAQ Walking
(MET-mins/week
)
1208.4
(1482.8)
;
n = 12
1604.6
(2299.1)
;
n = 12
396.3
(2786.6)
[-1374.2 -
2166.8]
0.63 1184.3
(1693.7)
;
n = 9
727.8
(877.1);
n = 9
-456.5
(2100.8)
[-2071.3 -
1158.3]
0.53 0.92
IPAQ Total
(MET-mins/week
)
2074.4
(2835.2)
;
n = 12
2818.0
(2401.8)
;
n = 12
743.6
(3494.3)
[-1476.6 -
2963.8]
0.48 6006.6
(8836.3)
;
n = 9
7061.2
(10318.7)
;
n = 9
1054.6
(7828.4)
[-4962.8 -
7072.0]
0.70 0.88
HADS Anxiety
(scale: 0 - 21)a
4.3
(3.7);
n = 12
4.0
(3.6);
n = 12
-0.3 (1.4)
[-1.2 -
0.6]
0.44 4.9
(3.1);
n = 9
4.8 (4.0);
n = 9
-1.0 (2.1)
[-2.7 -
0.7]
0.21 0.45
HADS
Depression
(scale: 0 - 21)a
3.3
(2.2);
n = 12
2.0
(1.4);
n = 12
-1.3 (1.4)
[-2.2 -
-0.3]
0.01 2.2
(2.0);
n = 9
2.3 (2.1);
n = 9
0 (1.4)
[-1.2 -
1.2]
1.00 0.12
Self efficacy -
Nutrition (scale: 5
- 20)b
16.8
(2.6);
n=12
18.1
(2.3);
n=12
1.3 (2.2)
[-0.1-2.7]
0.06 15.4
(5.6);
n = 10
15.4
(4.3);
n = 9
-1.2 (2.9)
[-3.4 -
1.0]
0.24 0.10
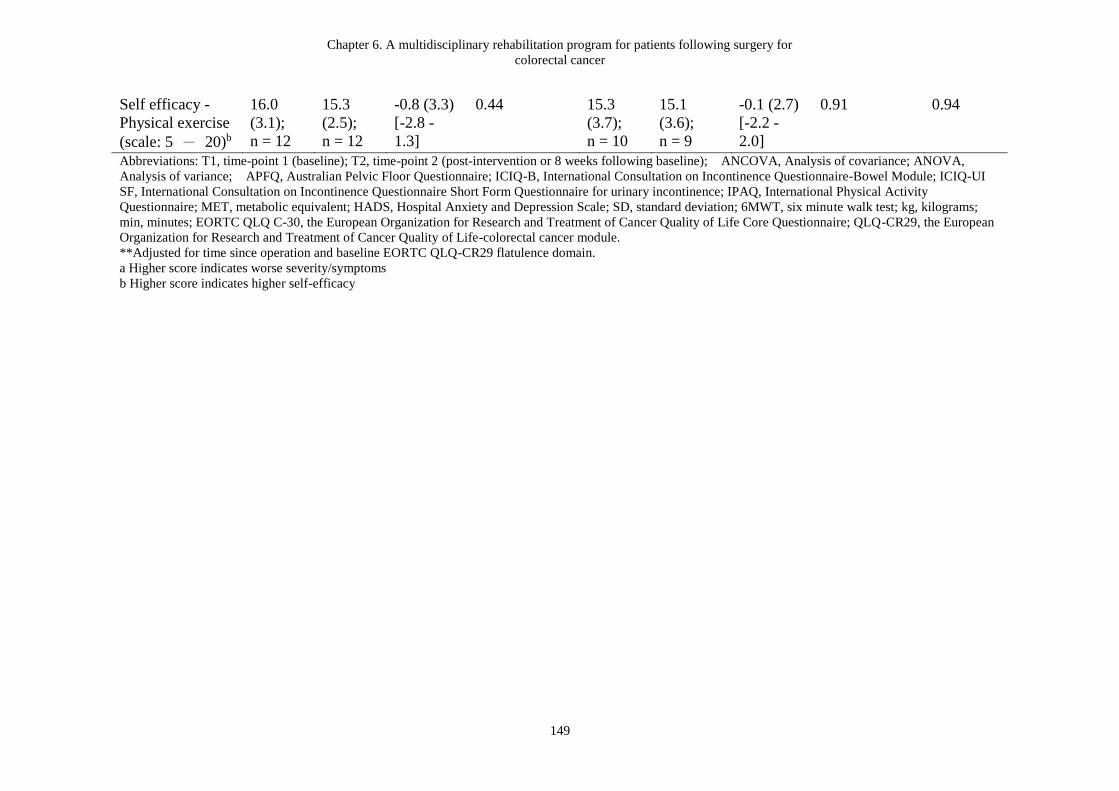
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
149
Self efficacy -
Physical exercise
(scale: 5 - 20)b
16.0
(3.1);
n = 12
15.3
(2.5);
n = 12
-0.8 (3.3)
[-2.8 -
1.3]
0.44 15.3
(3.7);
n = 10
15.1
(3.6);
n = 9
-0.1 (2.7)
[-2.2 -
2.0]
0.91 0.94
Abbreviations: T1, time-point 1 (baseline); T2, time-point 2 (post-intervention or 8 weeks following baseline); ANCOVA, Analysis of covariance; ANOVA,
Analysis of variance; APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on Incontinence Questionnaire-Bowel Module; ICIQ-UI
SF, International Consultation on Incontinence Questionnaire Short Form Questionnaire for urinary incontinence; IPAQ, International Physical Activity
Questionnaire; MET, metabolic equivalent; HADS, Hospital Anxiety and Depression Scale; SD, standard deviation; 6MWT, six minute walk test; kg, kilograms;
min, minutes; EORTC QLQ C-30, the European Organization for Research and Treatment of Cancer Quality of Life Core Questionnaire; QLQ-CR29, the European
Organization for Research and Treatment of Cancer Quality of Life-colorectal cancer module.
**Adjusted for time since operation and baseline EORTC QLQ-CR29 flatulence domain.
a Higher score indicates worse severity/symptoms
b Higher score indicates higher self-efficacy

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
150
Table 6-4: Health-related quality of life outcomes
Variables Rehabilitation group Questionnaire group Between
group
ANCOVA
p value**
T1
(mean, SD)
T2
(mean, SD)
Mean
difference
(mean, SD)
Within-gr
oup:
paired-t
p-value
T1
(mean, SD)
T2
(mean, SD)
Mean
difference
(mean, SD)
Within-gr
oup:
paired-t
p-value
EORTC QLQ
C-30
Global QoL (scale:
0 – 100) a*
73.6 (16.6);
n=12
81.9 (11.7);
n=12
8.3 (10.1)
[1.9-14.7] 0.02 86.7 (9.0);
n=10
81.5 (23.9);
n=9
-3.7 (23.2)
[-21.6-14.2]
0.65 0.16
Physical
functioning (scale:
0 – 100) a *
81.1 (17.9);
n=12
87.2 (12.2);
n=12
6.1 (20.4)
[-6.8-19.1]
0.32 95.3 (4.5);
n=10
92.6 (9.1);
n=9
-3.0 (10.1)
[-10.7-4.8]
0.40 0.59
Role functioning
(scale: 0 – 100) a
80.6 (30.0);
n=12
83.3 (21.3);
n=12
2.8 (30.0)
[-16.3-21.8]
0.75 95.0 (8.1);
n=10
96.3 (11.1);
n=9
1.9 (15.5)
[-10.0-13.7]
0.73 0.77
Emotional
functioning (scale:
0 – 100) a
84.0 (10.9);
n=12
83.3 (12.8);
n=12
-0.7 (11.5)
[-8.0-6.6]
0.84 80.8 (17.1);
n=10
75.9 (15.8);
n=9
-3.7 (11.9)
[-12.8-5.4]
0.38 0.11
Cognitive
functioning (scale:
0 – 100) a
81.9 (16.6);
n=12
88.9 (14.8);
n=12
6.9 (19.4)
[-5.4-19.3]
0.24 86.7 (10.5);
n=10
90.7 (12.1);
n=9
3.7 (13.9)
[-7.0-14.4]
0.45 0.85
Social functioning
(scale: 0 – 100) a *
77.8 (20.5);
n=12
91.7 (13.3);
n=12
13.9 (23.4)
[-1.0-28.8]
0.06 95.0 (8.1);
n=10
98.1 (5.6);
n=9
1.9 (5.6)
[-2.4-6.1]
0.35 0.63
Fatigue (scale: 0 –
100) b *
38.9 (19.8);
n=12
21.3 (15.3);
n=12
-17.6 (19.2)
[-29.8- -5.4] 0.01 18.9 (12.9);
n=10
12.3 (8.7);
n=9
-8.6 (12.1)
[-18.0-0.7]
0.07 0.20
Nausea and
vomiting (scale: 0
– 100) b
1.4 (4.8);
n=12
1.4 (4.8);
n=12
0 (7.1)
[-4.5-4.5]
1.00 3.3 (7.0);
n=10
0 (0);
n=9
-3.7 (7.3)
[-9.4-1.9]
0.17 0.19
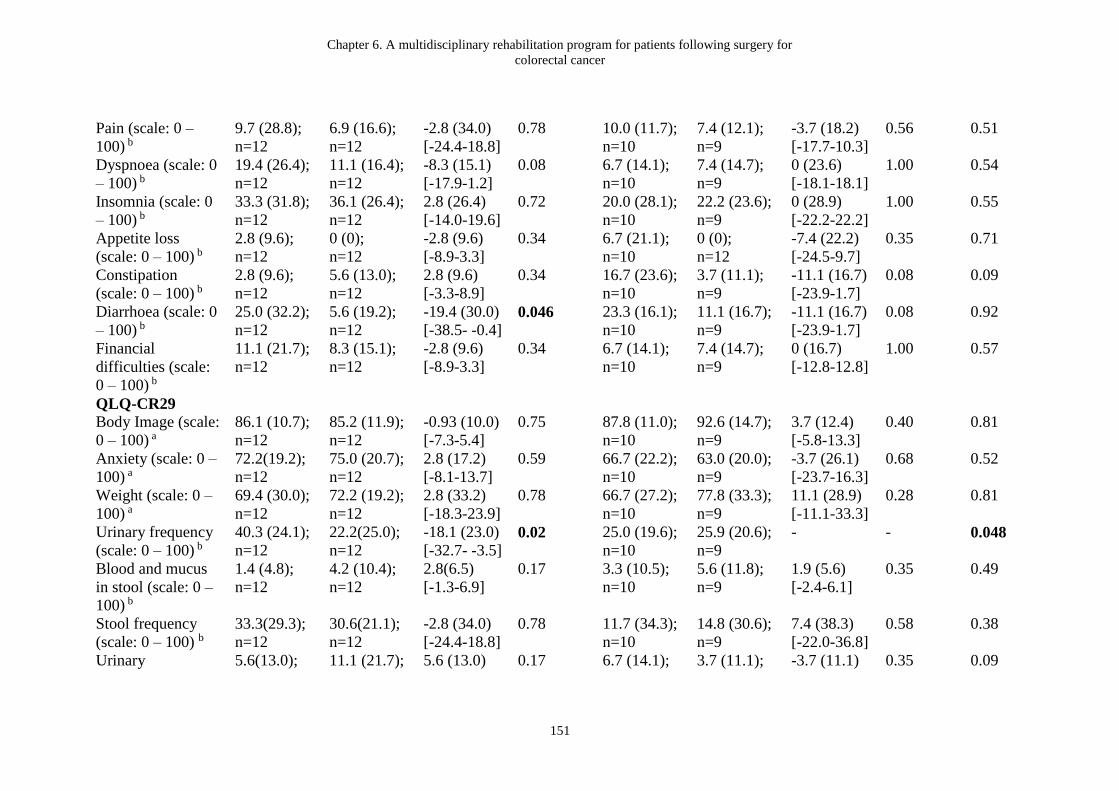
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
151
Pain (scale: 0 –
100) b
9.7 (28.8);
n=12
6.9 (16.6);
n=12
-2.8 (34.0)
[-24.4-18.8]
0.78 10.0 (11.7);
n=10
7.4 (12.1);
n=9
-3.7 (18.2)
[-17.7-10.3]
0.56 0.51
Dyspnoea (scale: 0
– 100) b
19.4 (26.4);
n=12
11.1 (16.4);
n=12
-8.3 (15.1)
[-17.9-1.2]
0.08 6.7 (14.1);
n=10
7.4 (14.7);
n=9
0 (23.6)
[-18.1-18.1]
1.00 0.54
Insomnia (scale: 0
– 100) b
33.3 (31.8);
n=12
36.1 (26.4);
n=12
2.8 (26.4)
[-14.0-19.6]
0.72 20.0 (28.1);
n=10
22.2 (23.6);
n=9
0 (28.9)
[-22.2-22.2]
1.00 0.55
Appetite loss
(scale: 0 – 100) b
2.8 (9.6);
n=12
0 (0);
n=12
-2.8 (9.6)
[-8.9-3.3]
0.34 6.7 (21.1);
n=10
0 (0);
n=12
-7.4 (22.2)
[-24.5-9.7]
0.35 0.71
Constipation
(scale: 0 – 100) b
2.8 (9.6);
n=12
5.6 (13.0);
n=12
2.8 (9.6)
[-3.3-8.9]
0.34 16.7 (23.6);
n=10
3.7 (11.1);
n=9
-11.1 (16.7)
[-23.9-1.7]
0.08 0.09
Diarrhoea (scale: 0
– 100) b
25.0 (32.2);
n=12
5.6 (19.2);
n=12
-19.4 (30.0)
[-38.5- -0.4] 0.046 23.3 (16.1);
n=10
11.1 (16.7);
n=9
-11.1 (16.7)
[-23.9-1.7]
0.08 0.92
Financial
difficulties (scale:
0 – 100) b
11.1 (21.7);
n=12
8.3 (15.1);
n=12
-2.8 (9.6)
[-8.9-3.3]
0.34 6.7 (14.1);
n=10
7.4 (14.7);
n=9
0 (16.7)
[-12.8-12.8]
1.00 0.57
QLQ-CR29
Body Image (scale:
0 – 100) a
86.1 (10.7);
n=12
85.2 (11.9);
n=12
-0.93 (10.0)
[-7.3-5.4]
0.75 87.8 (11.0);
n=10
92.6 (14.7);
n=9
3.7 (12.4)
[-5.8-13.3]
0.40 0.81
Anxiety (scale: 0 –
100) a
72.2(19.2);
n=12
75.0 (20.7);
n=12
2.8 (17.2)
[-8.1-13.7]
0.59 66.7 (22.2);
n=10
63.0 (20.0);
n=9
-3.7 (26.1)
[-23.7-16.3]
0.68 0.52
Weight (scale: 0 –
100) a
69.4 (30.0);
n=12
72.2 (19.2);
n=12
2.8 (33.2)
[-18.3-23.9]
0.78 66.7 (27.2);
n=10
77.8 (33.3);
n=9
11.1 (28.9)
[-11.1-33.3]
0.28 0.81
Urinary frequency
(scale: 0 – 100) b
40.3 (24.1);
n=12
22.2(25.0);
n=12
-18.1 (23.0)
[-32.7- -3.5] 0.02 25.0 (19.6);
n=10
25.9 (20.6);
n=9
- - 0.048
Blood and mucus
in stool (scale: 0 –
100) b
1.4 (4.8);
n=12
4.2 (10.4);
n=12
2.8(6.5)
[-1.3-6.9]
0.17 3.3 (10.5);
n=10
5.6 (11.8);
n=9
1.9 (5.6)
[-2.4-6.1]
0.35 0.49
Stool frequency
(scale: 0 – 100) b
33.3(29.3);
n=12
30.6(21.1);
n=12
-2.8 (34.0)
[-24.4-18.8]
0.78 11.7 (34.3);
n=10
14.8 (30.6);
n=9
7.4 (38.3)
[-22.0-36.8]
0.58 0.38
Urinary 5.6(13.0); 11.1 (21.7); 5.6 (13.0) 0.17 6.7 (14.1); 3.7 (11.1); -3.7 (11.1) 0.35 0.09
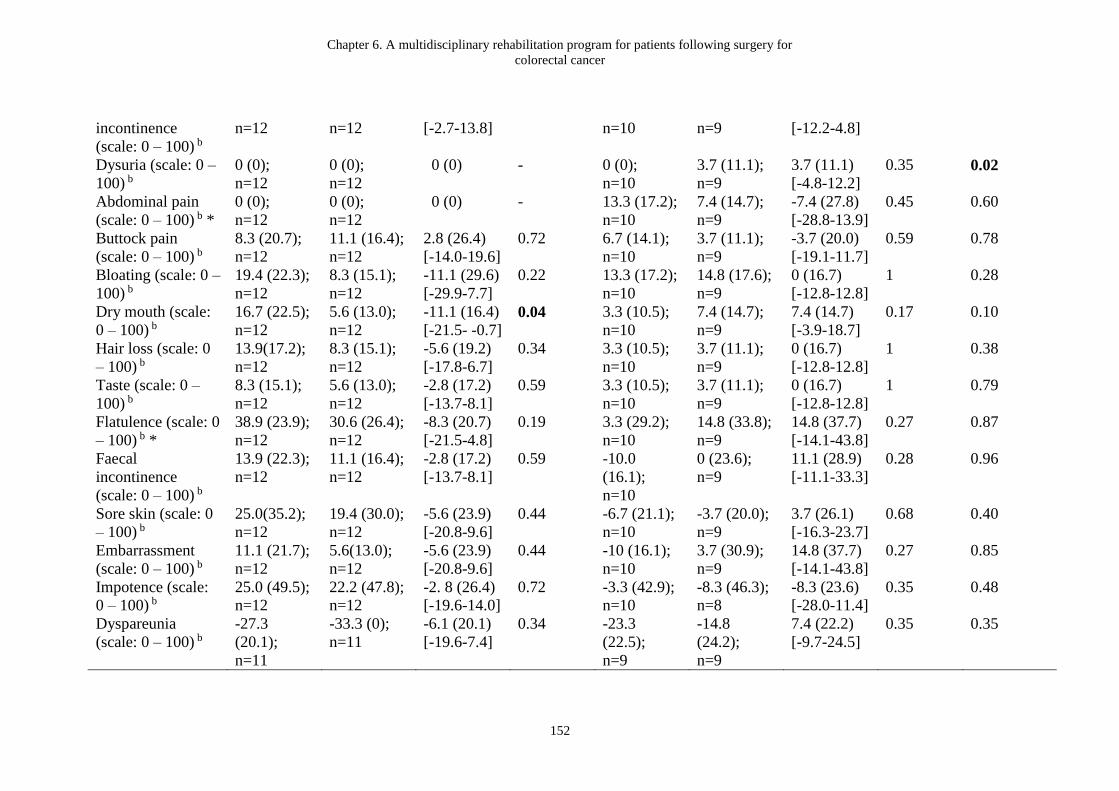
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
152
incontinence
(scale: 0 – 100) b
n=12 n=12 [-2.7-13.8] n=10 n=9 [-12.2-4.8]
Dysuria (scale: 0 –
100) b
0 (0);
n=12
0 (0);
n=12
0 (0)
- 0 (0);
n=10
3.7 (11.1);
n=9
3.7 (11.1)
[-4.8-12.2]
0.35 0.02
Abdominal pain
(scale: 0 – 100) b *
0 (0);
n=12
0 (0);
n=12
0 (0)
- 13.3 (17.2);
n=10
7.4 (14.7);
n=9
-7.4 (27.8)
[-28.8-13.9]
0.45 0.60
Buttock pain
(scale: 0 – 100) b
8.3 (20.7);
n=12
11.1 (16.4);
n=12
2.8 (26.4)
[-14.0-19.6]
0.72 6.7 (14.1);
n=10
3.7 (11.1);
n=9
-3.7 (20.0)
[-19.1-11.7]
0.59 0.78
Bloating (scale: 0 –
100) b
19.4 (22.3);
n=12
8.3 (15.1);
n=12
-11.1 (29.6)
[-29.9-7.7]
0.22 13.3 (17.2);
n=10
14.8 (17.6);
n=9
0 (16.7)
[-12.8-12.8]
1 0.28
Dry mouth (scale:
0 – 100) b
16.7 (22.5);
n=12
5.6 (13.0);
n=12
-11.1 (16.4)
[-21.5- -0.7] 0.04 3.3 (10.5);
n=10
7.4 (14.7);
n=9
7.4 (14.7)
[-3.9-18.7]
0.17 0.10
Hair loss (scale: 0
– 100) b
13.9(17.2);
n=12
8.3 (15.1);
n=12
-5.6 (19.2)
[-17.8-6.7]
0.34 3.3 (10.5);
n=10
3.7 (11.1);
n=9
0 (16.7)
[-12.8-12.8]
1 0.38
Taste (scale: 0 –
100) b
8.3 (15.1);
n=12
5.6 (13.0);
n=12
-2.8 (17.2)
[-13.7-8.1]
0.59 3.3 (10.5);
n=10
3.7 (11.1);
n=9
0 (16.7)
[-12.8-12.8]
1 0.79
Flatulence (scale: 0
– 100) b *
38.9 (23.9);
n=12
30.6 (26.4);
n=12
-8.3 (20.7)
[-21.5-4.8]
0.19 3.3 (29.2);
n=10
14.8 (33.8);
n=9
14.8 (37.7)
[-14.1-43.8]
0.27 0.87
Faecal
incontinence
(scale: 0 – 100) b
13.9 (22.3);
n=12
11.1 (16.4);
n=12
-2.8 (17.2)
[-13.7-8.1]
0.59 -10.0
(16.1);
n=10
0 (23.6);
n=9
11.1 (28.9)
[-11.1-33.3]
0.28 0.96
Sore skin (scale: 0
– 100) b
25.0(35.2);
n=12
19.4 (30.0);
n=12
-5.6 (23.9)
[-20.8-9.6]
0.44 -6.7 (21.1);
n=10
-3.7 (20.0);
n=9
3.7 (26.1)
[-16.3-23.7]
0.68 0.40
Embarrassment
(scale: 0 – 100) b
11.1 (21.7);
n=12
5.6(13.0);
n=12
-5.6 (23.9)
[-20.8-9.6]
0.44 -10 (16.1);
n=10
3.7 (30.9);
n=9
14.8 (37.7)
[-14.1-43.8]
0.27 0.85
Impotence (scale:
0 – 100) b
25.0 (49.5);
n=12
22.2 (47.8);
n=12
-2. 8 (26.4)
[-19.6-14.0]
0.72 -3.3 (42.9);
n=10
-8.3 (46.3);
n=8
-8.3 (23.6)
[-28.0-11.4]
0.35 0.48
Dyspareunia
(scale: 0 – 100) b
-27.3
(20.1);
n=11
-33.3 (0);
n=11
-6.1 (20.1)
[-19.6-7.4]
0.34 -23.3
(22.5);
n=9
-14.8
(24.2);
n=9
7.4 (22.2)
[-9.7-24.5]
0.35 0.35
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
153
Abbreviations: T1, time-point 1 (baseline); T2, time-point 2 (post-intervention or 8 weeks following baseline); ANCOVA, Analysis of covariance; ANOVA, Analysis of
variance; EORTC QLQ C-30, the European Organization for Research and Treatment of Cancer Quality of Life Core Questionnaire; QLQ-CR29, the European
Organization for Research and Treatment of Cancer Quality of Life-colorectal cancer module; QoL, quality of life.
*p < 0.05 at baseline. Baseline EORTC QLQ-30 quality of life domain (p = 0.038), physical functioning domain (p = 0.02), social functioning
domain (p = 0.018), and fatigue domain (p = 0.013), and QLQ-CR29 abdominal pain domain (p = 0.037) and flatulence domain (p = 0.005)
**Adjusted for time since operation and baseline EORTC QLQ-CR29 flatulence domain.
a Higher score indicates better functioning
b Higher score indicates higher level of symptoms

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
154
Comparison between the rehabilitation group and the questionnaire group
An ANCOVA adjusted for time since operation and baseline EORTC QLQ-CR29
flatulence domain showed significant group by time interaction in APFQ bladder
domain (p = 0.009). Global quality of life, physical functioning, social functioning,
fatigue, abdominal pain, and flatulence were significantly different (p < 0.05) between
the rehabilitation group and the questionnaire group at baseline. Significant group by
time interaction after controlling for time since operation and baseline EORTC
QLQ-CR29 flatulence was found in urinary frequency (p = 0.048) and dysuria (p =
0.02) as measured using QLQ-CR29. Table 6-5 summarizes participants’ global rate
of change at T2 compared with baseline. The proportion of participants who reported
better fitness was higher in the rehabilitation group (50%) than the questionnaire
group (10%).
Table 6-5: Global rate of change immediately post-intervention or 8 weeks following
baseline
Rehabilitation Group
n = 12
Questionnaire
Group n = 10
Global rate of change score-fitness, n
(%)
Much better 5 (41.7%) 3 (30.0%)
Better 6 (50.0%) 1 (10.0%)
A little better 1 (8.3%) 1 (10.0%)
No change 0 (0%) 4 (40.0%)
Missing 0 (0%) 1 (10.0%)
Global rate of change score-pelvic floor
symptoms, n (%)
Much better 2 (16.7%) 1 (10.0%)
Better 3 (25.0%) 2 (20.0%)
A little better 0 (0%) 1 (10.0%)
No change 7 (58.3%) 3 (30.0%)
A little worse 0 (0%) 1 (10.0%)
Missing 0 (0%) 2 (20.0%) Abbreviations: n, number; %, percent.
6.4 Discussion
This prospective pilot study aimed to investigate the feasibility of implementing a
general oncology rehabilitation program in CRC and to obtain preliminary data on

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
155
patient outcomes before and after the rehabilitation program. Although the consent
rate was low (37% to the study and 19% to the rehabilitation program), the adherence
to the supervised exercise component of the rehabilitation program was excellent and
the drop-out rate was low. Additionally, significant differences were noted in bladder
symptoms including urinary frequency and dysuria between the rehabilitation group
and the questionnaire group over the 8-week intervention period. Significant
within-group improvements were also observed in bladder and bowel symptoms,
symptoms of depression, and HRQoL in the rehabilitation group, and no within-group
improvements were observed in the questionnaire group. These results demonstrate
that such an oncology rehabilitation program is potentially feasible in patients
following surgery for CRC and may improve important health outcomes.
Feasibility
Although other literature reports that rehabilitation programs are of interest to CRC
survivors (McGowan et al., 2013), recruitment was challenging in this study and
slower than anticipated; only 14 participants (19.2% of the eligible pool) were
enrolled over the 13 months recruitment period. A previous study has shown that
patients with CRC are less willing to participate in clinical research than patients with
prostate or breast cancer (Snyder et al., 2009). Symptoms related to CRC and its
treatments (e.g. fatigue), age, and mobility-related comorbidities (e.g. impaired
mobility) are some of the perceived barriers to PA in CRC reported in the literature
(Fisher et al., 2016) and may be a potential explanation for the low recruitment rate.
However, as fatigue is prevalent among cancer survivors of many tumour streams
(Kuhnt et al., 2009), future studies should determine the potential barriers to clinical
research participation among patients with CRC specifically. Despite the low
recruitment rate, the consent rate was higher in our study than in large intervention
trials in cancer survivors (11.1%) (Adams et al., 2015). Future studies should examine
the predictors of CRC patients' willingness to participate in rehabilitation program by
undertaking a barriers and enablers analysis and specific qualitative evaluation to
inform future recruitment strategies and programs which will be of interest to
potential participants.
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
156
Adherence to the supervised exercise sessions was excellent, with a 95% attendance
rate and 100% of participants attended more than 85% of the rehabilitation sessions.
These findings are similar to a previous exercise intervention study in CRC survivors
that reported 90.7% adherence to a 12-week exercise intervention consisting of two
combined aerobic and resistance training sessions and one aerobic only session per
week, and 93% completed more than 80% of training sessions (Sellar et al., 2014).
The drop-out rate in our study (14.3%) was within the range of 3%-28% reported in
previous exercise or PA intervention research (Devin et al., 2015) that included
patients with CRC (Grimmett, Simon, Lawson, & Wardle, 2015). One participant in
the rehabilitation group became ineligible after the baseline assessment due to the
start of CT, giving our study a drop-out rate of 8% once the rehabilitation program
had commenced. Although the low drop-out rate and excellent adherence may be the
result of a recruitment bias, it also suggests that the program was acceptable to this
cohort.
Physical and psychological outcomes
The present study found no significant changes in the clinical outcome measures (i.e.
functional exercise capacity and muscle strength) after the oncology rehabilitation
program. Our finding on functional exercise capacity is in line with a previous study
in CRC that reported no significant change in functional exercise capacity as
measured with a cycle ergometer following 12 sessions of moderate-intensity exercise
training program, which was published after our study had commenced (Devin et al.,
2015). Moreover, participants in our study had relatively high functional exercise
capacity (514 meters) at baseline, which is comparable to that of the age-matched
community population (ranging 510-574 meters) (Tveter, Dagfinrud, Moseng, &
Holm, 2014). Therefore, the rehabilitation program may have had limited scope to
effect a significant change in functional exercise capacity, due to a ceiling effect of
the 6MWT. As previous studies in cardiac rehabilitation have shown that patients
with high baseline exercise capacity have less relative improvement in exercise
capacity than patients with low baseline exercise capacity following a rehabilitation
and exercise training program (Lavie & Milani, 1994) and that high initial fitness is
related to reduced training effect (Pierson, Miller, & Herbert, 2004), future research

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
157
investigating the effects of an exercise intervention in CRC should consider recruiting
participants with lower functional exercise capacity at baseline.
In addition to the relatively high baseline functional exercise capacity, participants in
the rehabilitation group also had a high average daily step count (> 8,000 steps/day),
which was comparable to the published data for community dwelling populations
(Aoyagi, Park, Watanabe, Park, & Shephard, 2009; Dwyer et al., 2015). One study
has suggested that the program exercise intensity could be set higher than that
recommended for the general population in order to improve functional exercise
capacity for physically active individuals (Azevedo et al., 2011). Although a
systematic review has demonstrated that moderate-intensity aerobic exercise is
effective in reducing fatigue and improving endurance in cancer survivors (Dennett,
Peiris, Shields, Prendergast, & Taylor, 2016), none of the studies included in that
review focused solely on patients with CRC. Devin et al. suggested that high-intensity
exercise training is more effective than current PA recommendations
(moderate-intensity exercise) in improving functional exercise capacity in CRC
survivors (Devin et al., 2015). Nevertheless, clinical improvement was observed in
the 6MWT distance in our study, which suggests that a moderate-intensity aerobic
and resistance training program may have a clinical effect on functional exercise
capacity. Although the 6MWT MCID has not yet been published specifically for
patients with CRC following a general oncology rehabilitation program, the mean
difference of the 6MWT distance (27.2 meters) was greater than the MCID of 25
meters as reported among coronary artery disease patients following cardiac
rehabilitation (Gremeaux et al., 2011).
Despite the fact that the baseline muscle strength of our study cohort (20kg in female
and 39kg in male) was lower than that of the community (26kg in female and 42kg in
male) (Leong et al., 2016), no significant change was found in dominant hand-grip
strength after intervention. Our finding is in contrast to the study by Sellar et al.,
which provided an exercise intervention with longer duration (12 weeks) and higher
frequency (3 sessions per week) and found significant improvements in upper and
lower body muscle strength (Sellar et al., 2014). Future studies should examine the

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
158
dose-response relationships between exercise intensity / frequency and muscle
strength.
A number of secondary outcomes in the rehabilitation group changed significantly
after the oncology rehabilitation program in the present study. Significant
improvements were observed in the APFQ bladder and bowel domains and all ICIQ-B
domains in the rehabilitation group following intervention. Significant between-group
difference was also observed in the APFQ bladder domain following intervention.
This suggests that in addition to numerous health benefits, general exercise may have
positive effects on pelvic floor symptoms in patients following surgery for CRC. The
physiotherapist and exercise physiologist who supervised the exercises sessions
provided PFM ‘cueing’ during exertional manoeuvres, which may have increased the
contractility of the PFMs and therefore improved bladder control. In addition, it has
been hypothesized that the increase in intra-abdominal pressure occurring during
general movements may lead to the co-contraction of the PFMs (Bø, 2004b). Most of
the current literature has examined the effect of targeted PFM training/exercise on
pelvic floor symptoms in non-cancer populations (Norton & Cody, 2012; Starr et al.,
2013). A recent systematic review evaluated the effects of PFM training for bowel
dysfunction in patients who have undergone surgery for CRC and found that PFM
training may improve the patient-reported measures of bowel function and the
HRQoL of CRC patients following surgery (Lin et al., 2015). Although
cross-sectional studies have reported that mild to moderate PA appeared to decrease
both the odds of having urinary and faecal incontinence in older women (Nygaard &
Shaw, 2016), the effects of general exercise on pelvic floor symptoms remains
unknown. Our exploratory findings add important information to the current literature
and provide a foundation for future studies to compare general exercise interventions
with greater statistical power to specific PFM training on detecting pelvic floor
symptom changes.
An alternative explanation for the observed improvement in the APFQ bladder
domain score could be as a result of one of the education sessions, which included a
brief description on the role of the PFMs in bladder and bowel function; this session
may have had an impact on participants’ awareness of bladder and bowel symptoms
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
159
and encouraged them to adhere to good bladder and bowel habits, or seek further
advice; neither of these outcomes were measured during our study. Moreover, as
participants in our study were not stratified according to the severity of pelvic floor
symptoms at baseline, future studies are required to allow subgroup analysis.
Despite the significant improvement found in bladder and bowel symptoms in the
rehabilitation group, no improvement in PA levels, symptoms of anxiety or
self-efficacy was observed; this concurs with findings from previous studies in mixed
cancer and CRC populations (Devin et al., 2015; Hanssens et al., 2011; Ligibel et al.,
2012). No differences in PA levels and self-efficacy between the rehabilitation and
questionnaire groups at T2 in our study suggest the possibility of natural recovery
over time in these domains. Moreover, some of the participants in the questionnaire
group might have been highly motivated to change exercise behaviour after surgery
and had resumed self-initiated normal daily activity and work; hence, they declined
the rehabilitation program as perhaps they believed that they were already active
enough, which has been reported in previous studies as one of the perceived barriers
to PA in patients with CRC (Appleton, Goodlad, Irvine, Poole, & Wall, 2013; Bhalla
et al., 2014; Lynch et al., 2010; Mizuno, Kakuta, Ono, Kato, & Inoue, 2007). While
anxiety did not change after the intervention, significant improvement in symptoms of
depression as assessed by the HADS was noted in the rehabilitation group. Similar
observations with regard to changes in depression but not anxiety have been made by
Midtgaard et al. who provided a 6-week supervised, group-based multimodal exercise
in cancer patients undergoing CT (Midtgaard et al., 2011). Nevertheless, the anxiety
score showed a trend towards a decrease in the rehabilitation group in our study. One
possible explanation for the discrepancy in the results between the anxiety and
depression is that the intensity of the rehabilitation program was insufficient to cause
changes in the anxiety, whereas the mechanism of effect of exercise on depression
may be due to the release of monoamine neurotransmitters (i.e. serotonin, dopamine,
and norepinephrine) and endorphins during aerobic exercise and the social support
network built during group exercise sessions (Brown et al., 2012; Makino et al., 2015;
North, McCullagh, & Tran, 1990).

Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
160
A previous meta-analysis reported no exercise intervention effect on HRQoL in CRC
(Cramer et al., 2013). However, we found significant changes in global quality of life,
diarrhoea, and urinary frequency following the oncology rehabilitation program, and
between-group differences for urinary frequency and dysuria. Diarrhoea and urinary
frequency improved after the oncology rehabilitation program, which is congruent
with the decreases in bladder and bowel symptoms as measured with the APFQ and
ICIQ-B. The improvement in HRQoL following the oncology rehabilitation program
may be due to the changes in bladder and bowel symptoms as a significant association
between bowel and bowel dysfunction and HRQoL following CRC surgery has been
reported (Juul et al., 2014; Vironen et al., 2006). Previous research has shown that
depression has a strong impact on the global quality of life of patients; therefore, the
change in global quality of life in our study may be attributable to the improvement in
symptoms of depression (Tsunoda et al., 2005).
This is the first study investing the feasibility of implementing a general oncology
rehabilitation program in patients following surgery for CRC. The low drop-out rate,
excellent program adherence, and patient-perceived improvement in fitness as
measured with global rating of change indicate that this rehabilitation program is
acceptable to the population. The low consent rate needs further investigation using
qualitative research in order to improve this aspect of feasibility in future research.
Nonetheless, the pilot nature (non-powered), small sample size, lack of a true control
(comparison) group, lack of adjustment for multiple testing and possible selection bias
are the strongest limitations of the study. Although participants were not randomized
to the two groups in our study, the questionnaire group functioned as a quasi-control
group given there were no significant differences in demographic and medical
characteristics except the time since operation (a covariate adjusted in this study)
between both groups. However, the between-group comparisons need to be
interpreted with caution due to the non-randomized design of the study. The results of
this study cannot be generalized for all patients with CRC, as the percentage of male
participants (75%) and patients who had a diagnosis of colon cancer (83%) are higher
than those reported in the population data (55% males and 66% colon cancer)
(Australian Institute of Health and Welfare, 2015a, 2015b). The 12 participants in the
rehabilitation group may have represented a group of highly motivated patients. It is
Chapter 6. A multidisciplinary rehabilitation program for patients following surgery for
colorectal cancer
161
unknown whether motivation played a role in the improvements of the outcomes as
we did not measure this construct. Furthermore, it was impossible to determine
whether the improvements observed in the rehabilitation group were from the
education components, exercise components, the effect of time, or a combination. The
study is further limited by the lack of long-term follow-up data available by the time
the data analysis was carried out for this thesis. A prospective RCT is needed to
determine the long-term effect of an oncology rehabilitation program for CRC.
6.5 Summary
An oncology rehabilitation program which includes implementation of international
PA guidelines may be feasible and potentially beneficial for improving bladder
symptoms including urinary frequency and dysuria in patients who complete a
rehabilitation program. Moreover, general oncology rehabilitation may positively
impact on bladder and bowel symptoms, depression and HRQoL in patients with CRC.
Despite the limitations (small sample size, pilot nature, lack of a true control group
[selection bias]), this pilot study adds valuable evidence to current literature in
oncology care and informs clinicians of the feasibility and potential clinical benefits
of general oncology rehabilitation, which could be considered as a useful component
in the standard care for patient with CRC. Fully powered RCTs are warranted to
determine the optimal exercise dosage to improve functional exercise capacity in
patients with CRC and to examine the effects of general exercise compared with PFM
training on pelvic floor outcomes in this population. The next chapter further
describes changes in pelvic floor outcomes in an opportunistic sample of volunteers
within the oncology rehabilitation program.

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
162
Chapter 7. Pelvic floor outcomes in patients who have undergone general
oncology rehabilitation following surgery for colorectal cancer: a pilot study
This study is under review for publication:
Lin K-Y, Denehy L, Granger C.L., Frawley H.C. (2016). Pelvic floor outcomes in
patients who have undergone general rehabilitation following surgery for colorectal
cancer: a pilot study. Physiotherapy Theory and Practice. Under review. Submitted
December 2016.
Author contributions for this chapter are the following: K-YL, LD, CG and HF
conceived the idea for the paper. K-YL, LD, CG and HF contributed to research
design. K-YL and HF contributed to data acquisition. K-YL, LD, CG and HF
contributed to data analysis and interpretation. K-YL completed all statistical analyses.
HF obtained project funding. K-YL wrote the first draft of the manuscript and
managed manuscript submission. All authors revised the paper and provided scientific
input. All authors approved the submitted version of the manuscript.
This study was supported by grant funding (Cabrini Foundation seed funding) from
the Cabrini Institute, Cabrini Health, Victoria, Australia.
7.1 Introduction
This chapter will describe a nested study to explore changes and differences between
bladder and bowel outcomes in patients who have undergone a general oncology
rehabilitation program compared with a questionnaire-only group following surgery
for CRC. Specific PFM training has been used routinely for treatment of incontinence
in clinical practice (Bø & Herbert, 2013). However, there is a paucity of evidence on
changes in pelvic floor outcomes (muscle function, bladder, bowel, and sexual
dysfunction) in patients with CRC following general oncology rehabilitation which
does not include specific PFM training. As general fitness training is considered to be
in the ‘development’ phase for treatment of pelvic floor outcomes (Bø & Herbert,
2013), the present study documents prospective changes in pelvic floor outcomes over
time in an opportunistic sample of volunteers undertaking a general oncology
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
163
rehabilitation program following CRC surgery. This study is reported according to the
TREND statement (Des Jarlais et al., 2004).
This chapter contains content that is substantially unchanged from the content of the
paper which is currently under review with the Neurourology and Urodynamics
journal.
7.1.1 Study aims
Aim 1: To explore changes and differences between bladder and bowel outcomes in
patients who have undergone a general oncology rehabilitation program compared
with a questionnaire only group following surgery for CRC
Aim 2: To investigate the correlation between different PFM clinical outcome
measures
Aim 3: To assess the association between PFM clinical outcome measures and
severity of pelvic floor symptoms
7.2 Materials and Methods
7.2.1 Participants
This study was conducted between July 2014 to February 2016 as part of a larger
prospective study evaluating the feasibility of a general oncology rehabilitation
program for patients following surgery for abdomino-pelvic cancer. In this nested
study, patients were eligible if they had undergone surgery for histologically
confirmed stage I-III CRC; had an Eastern Cooperative Oncology Group performance
status of between 0-2 (0 = fully active, 2 = up and about for 50% of a day) and
sufficient English language skills to participate. Patients were excluded if they were
aged 86 and over, were pregnant or up to 12 months postpartum, had a permanent
ostomy, had severe physical/psychiatric impairments that prevented participation in

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
164
the exercise programs, presence of other malignancies or had received post-operative
supervised exercise or rehabilitation similar to the program in this study in the
preceding 12 months. Participants with CRC from a non-intervention group who only
completed questionnaires in the main study were matched by gender and level of
cancer and used as a comparison control group in this study. The study was approved
by the institutional HREC (Appendix 7.1), and all participants provided written
informed consent.
7.2.2 Interventions
The general oncology rehabilitation program consisted of an 8-week multidisciplinary
education and exercise program. The education component included 1-hour of
nutritional advice and management provided by a dietician; 1-hour of exercise
education regarding the importance of exercise to well-being, bladder and bowel
advice, and adherence to exercise provided by a physiotherapist; 3-hours of action
planning for PA and implementation of exercise provided by an exercise physiologist;
and 3-hours of stress management and coping strategies provided by a psychologist.
The exercise component consisted of a moderate intensity aerobic and resistance
training program which was supervised by a physiotherapist and exercise physiologist,
and included PFM ‘cueing’ to encourage PFM activation prior to rises in
intra-abdominal pressure which may be caused by breath holding and/or straining
during strenuous exercise. The exercise program was individualised for patients based
on the results of their baseline outcome measures. The intervention was provided
twice weekly, and each session lasted approximately one hour.
7.2.3 Outcomes
All participants in the PFM measurement study were assessed for anorectal/PFM
function in addition to measures taken for participation in the pre-post study. These
included functional exercise capacity (6MWT); self-reported level of PA (IPAQ-SF);
muscle strength; psychological status; cancer specific HRQoL; global rating of
change; pelvic floor symptoms (APFQ (Baessler et al., 2009), ICIQ-B (Cotterill et al.,
2011) and ICIQ-UI SF (Reis et al., 2010)). The measurements were taken at baseline

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
165
(time-point 1), immediately post-rehabilitation (time-point 2), and at 6 months
following baseline (time-point 3). The bladder and bowel symptom data (i.e. APFQ
and ICIQ-B) of participants who completed only the questionnaires (collected at three
assessment time-points) were used for matched control data. Specific PFM function
measures for this nested study are described below. Data were collected by a trained
physiotherapist.
Digital rectal examination
For this measure, participants were asked to lie in the left lateral position. The
examination was performed by inserting a lubricated, gloved index finger into the
rectum to assess the resting sphincter tone and the strength of the puborectalis and
external anal sphincter (EAS) squeeze (Talley, 2008). Participants were asked to
perform three maximal contractions of external sphincter and puborectalis, and the
strongest contraction (MVC) was recorded. Squeeze pressure or MVC was scored
using the ICS scale as “absent”, “weak”, “moderate” or “strong” (Messelink et al.,
2005). If no correct contractions were obtained, the squeeze pressure was recorded as
absent. Digital rectal examination has been shown to be reliable for the assessment of
anal sphincter strength (Kaushal & Goldner, 1991).
Anorectal manometry
After DRE, anorectal pressure was measured at rest and at MVC using a Peritron
9300A manometer (Cardio-Design, Australia), which consists of an anal probe
connected to an electronic device that shows the values of contraction in cmH2O. For
anorectal manometry measurement, examination position was the same as for DRE.
Before insertion, the Peritron was zeroed. The lubricated, covered anal sensor was
then inserted until the sensor cuff rested at the anus. Participants were asked to relax
for 10 seconds during which the resting pressure (lowest value) was recorded. Then
the participants were asked to squeeze around the sensor and hold the contraction for
30 seconds. The MVC was obtained by subtracting the lowest value obtained during
the 10-second rest from the highest pressure achieved during the first 3 seconds of the
30-second squeeze. Area under curve (cmH2O-30sec) was calculated as the sum of
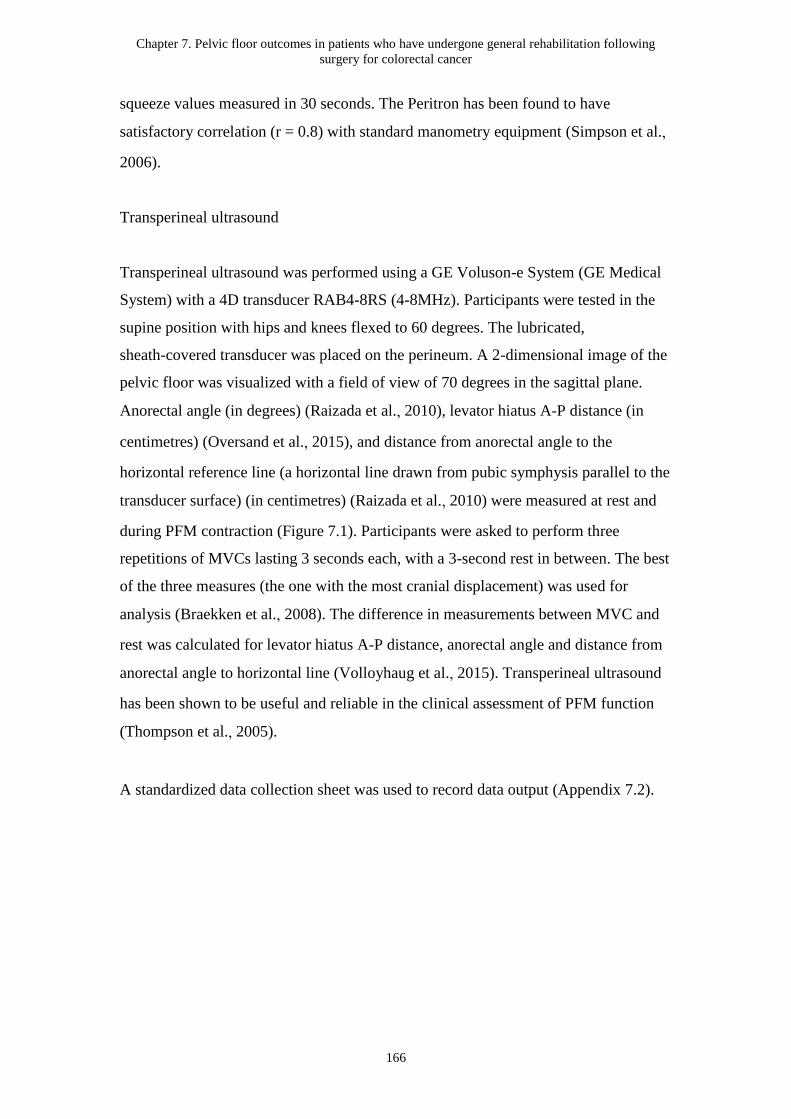
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
166
squeeze values measured in 30 seconds. The Peritron has been found to have
satisfactory correlation (r = 0.8) with standard manometry equipment (Simpson et al.,
2006).
Transperineal ultrasound
Transperineal ultrasound was performed using a GE Voluson-e System (GE Medical
System) with a 4D transducer RAB4-8RS (4-8MHz). Participants were tested in the
supine position with hips and knees flexed to 60 degrees. The lubricated,
sheath-covered transducer was placed on the perineum. A 2-dimensional image of the
pelvic floor was visualized with a field of view of 70 degrees in the sagittal plane.
Anorectal angle (in degrees) (Raizada et al., 2010), levator hiatus A-P distance (in
centimetres) (Oversand et al., 2015), and distance from anorectal angle to the
horizontal reference line (a horizontal line drawn from pubic symphysis parallel to the
transducer surface) (in centimetres) (Raizada et al., 2010) were measured at rest and
during PFM contraction (Figure 7.1). Participants were asked to perform three
repetitions of MVCs lasting 3 seconds each, with a 3-second rest in between. The best
of the three measures (the one with the most cranial displacement) was used for
analysis (Braekken et al., 2008). The difference in measurements between MVC and
rest was calculated for levator hiatus A-P distance, anorectal angle and distance from
anorectal angle to horizontal line (Volloyhaug et al., 2015). Transperineal ultrasound
has been shown to be useful and reliable in the clinical assessment of PFM function
(Thompson et al., 2005).
A standardized data collection sheet was used to record data output (Appendix 7.2).
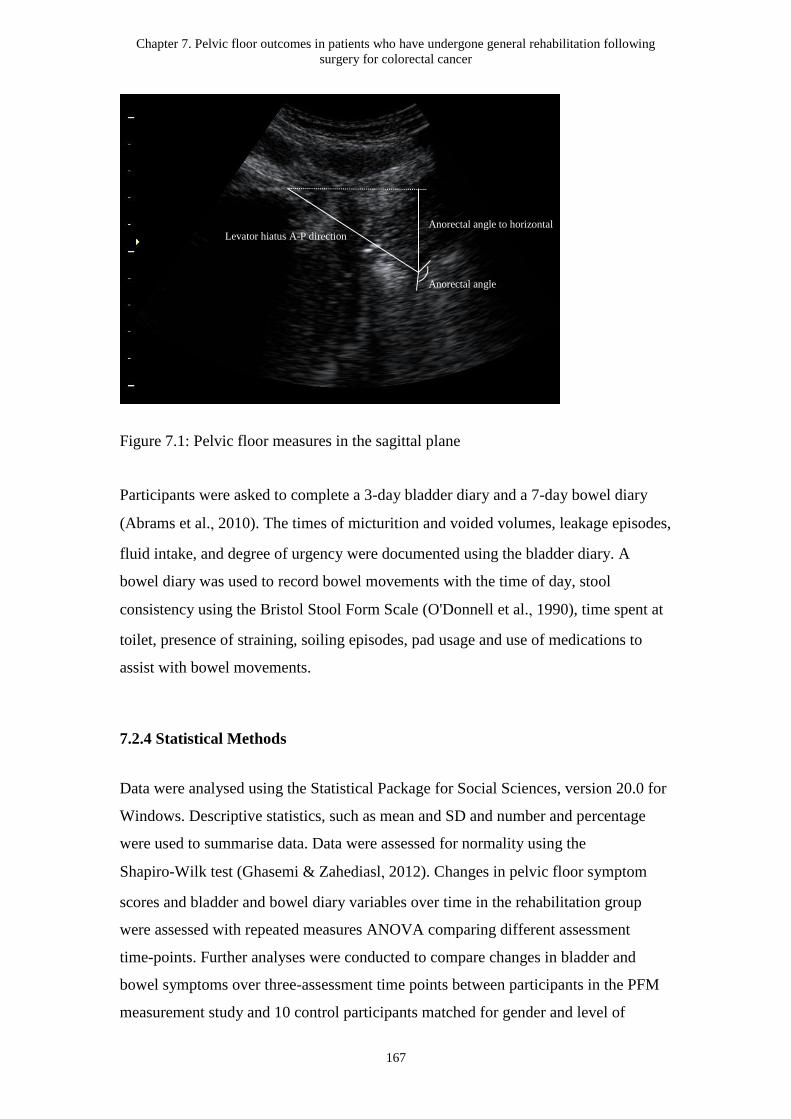
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
167
Figure 7.1: Pelvic floor measures in the sagittal plane
Participants were asked to complete a 3-day bladder diary and a 7-day bowel diary
(Abrams et al., 2010). The times of micturition and voided volumes, leakage episodes,
fluid intake, and degree of urgency were documented using the bladder diary. A
bowel diary was used to record bowel movements with the time of day, stool
consistency using the Bristol Stool Form Scale (O'Donnell et al., 1990), time spent at
toilet, presence of straining, soiling episodes, pad usage and use of medications to
assist with bowel movements.
7.2.4 Statistical Methods
Data were analysed using the Statistical Package for Social Sciences, version 20.0 for
Windows. Descriptive statistics, such as mean and SD and number and percentage
were used to summarise data. Data were assessed for normality using the
Shapiro-Wilk test (Ghasemi & Zahediasl, 2012). Changes in pelvic floor symptom
scores and bladder and bowel diary variables over time in the rehabilitation group
were assessed with repeated measures ANOVA comparing different assessment
time-points. Further analyses were conducted to compare changes in bladder and
bowel symptoms over three-assessment time points between participants in the PFM
measurement study and 10 control participants matched for gender and level of
Anorectal angle
Anorectal angle to horizontal Levator hiatus A-P direction
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
168
tumour using repeated measures ANOVA. Spearman’s rank correlation coefficient
rho was used to evaluate the correlations between the clinical outcome variables. The
strength of the correlation was determined by the correlation coefficient values (0.00–
0.30 = negligible; 0.30–0.50 = low positive correlation; 0.50–0.70 = moderate
positive correlation; 0.70–0.90 = high positive correlation; and 0.90–1.00 = very high
positive correlation) (Zou et al., 2003). The relationships between the clinical
measures of PFM function (anorectal manometry and TPUS) and pelvic floor
symptoms were analysed using simple linear regression with the pelvic floor
symptom scores as the dependent variable, and clinical outcome parameters as the
independent variables. All analyses were tested with a significance level of p < 0.05.
The PFM clinical outcomes are presented separately for male and female due to the
anatomical sex differences in pelvic floor structures (Seike et al., 2009).
7.3 Results
7.3.1 Participant flow and recruitment
A total of 20 participants in the pre-post study were screened between July 2014 and
August 2015. Seventeen were eligible and invited to participate in the PFM nested
measurement study (Figure 7.2). Seven of seventeen declined with a reason of ‘not
interested’ (71.4%) or ‘time demands of appointment’ (28.6%). Ten patients who
participated in the rehabilitation program agreed to undertake PFM measurements.
The consent rate was 58.8% (10/17). All participants completed 6-month follow-up
assessments.
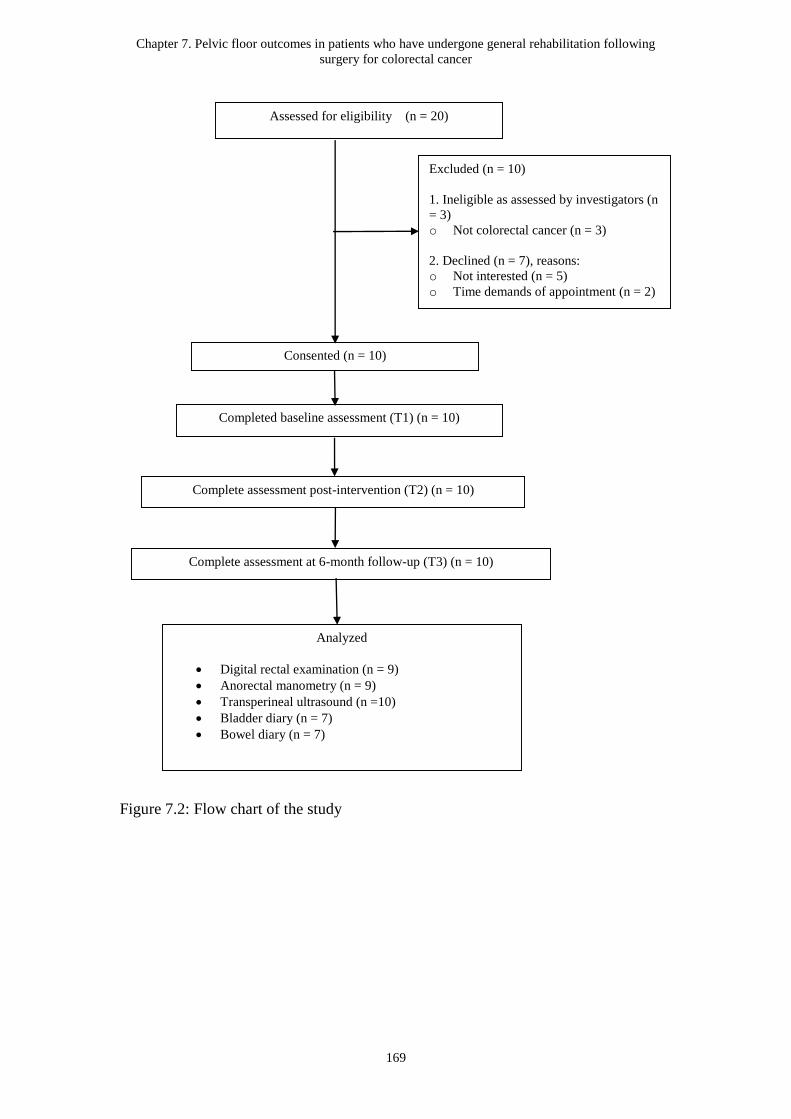
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
169
Figure 7.2: Flow chart of the study
Consented (n = 10)
Assessed for eligibility (n = 20)
Analyzed
Digital rectal examination (n = 9)
Anorectal manometry (n = 9)
Transperineal ultrasound (n =10)
Bladder diary (n = 7)
Bowel diary (n = 7)
Excluded (n = 10)
1. Ineligible as assessed by investigators (n
= 3)
o Not colorectal cancer (n = 3)
2. Declined (n = 7), reasons:
o Not interested (n = 5)
o Time demands of appointment (n = 2)
Completed baseline assessment (T1) (n = 10)
Complete assessment post-intervention (T2) (n = 10)
Complete assessment at 6-month follow-up (T3) (n = 10)
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
170
7.3.2 Baseline Data and Baseline Equivalence
Baseline Data and Baseline Equivalence
Participant demographics are shown in Table 7-1. Seven of 10 participants were
males and the mean (SD) age of the total cohort was 70.0 ± 6.2 years. Seventy percent
of participants had a diagnosis of colon cancer, and 30% had rectal cancer. All
participants had undergone surgery for CRC (50% hemicolectomy and 50% anterior
resection), and six participants had received adjuvant treatment (CT and/or RT) before
and/or after surgery. Of the 10 participants, six had prior pelvic/pelvic floor surgery
(i.e. bladder, gynaecological, bowel, and/or anal surgery). There were no significant
differences in participant characteristics or baseline bladder and bowel symptom
scores between participants in the rehabilitation group and the questionnaire group
(Table 7-1).
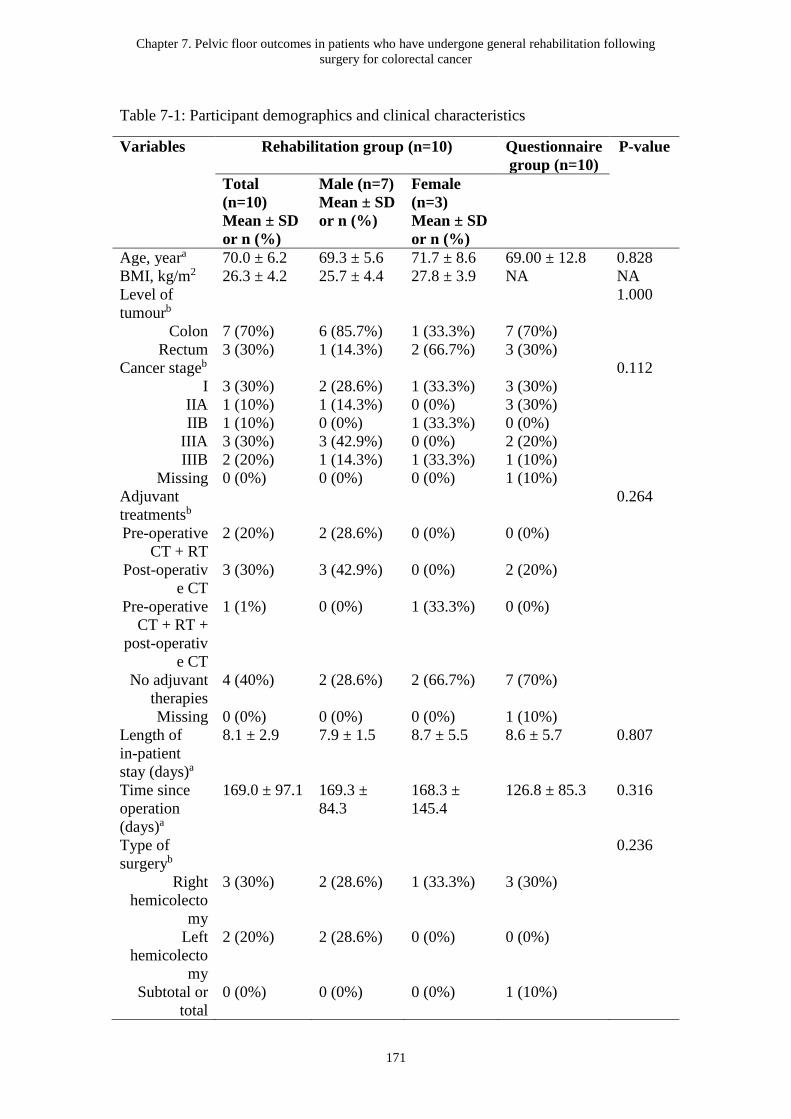
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
171
Table 7-1: Participant demographics and clinical characteristics
Variables Rehabilitation group (n=10) Questionnaire
group (n=10)
P-value
Total
(n=10)
Mean ± SD
or n (%)
Male (n=7)
Mean ± SD
or n (%)
Female
(n=3)
Mean ± SD
or n (%)
Age, yeara 70.0 ± 6.2 69.3 ± 5.6 71.7 ± 8.6 69.00 ± 12.8 0.828
BMI, kg/m2 26.3 ± 4.2 25.7 ± 4.4 27.8 ± 3.9 NA NA
Level of
tumourb
1.000
Colon 7 (70%) 6 (85.7%) 1 (33.3%) 7 (70%)
Rectum 3 (30%) 1 (14.3%) 2 (66.7%) 3 (30%)
Cancer stageb 0.112
I 3 (30%) 2 (28.6%) 1 (33.3%) 3 (30%)
IIA 1 (10%) 1 (14.3%) 0 (0%) 3 (30%)
IIB 1 (10%) 0 (0%) 1 (33.3%) 0 (0%)
IIIA 3 (30%) 3 (42.9%) 0 (0%) 2 (20%)
IIIB 2 (20%) 1 (14.3%) 1 (33.3%) 1 (10%)
Missing 0 (0%) 0 (0%) 0 (0%) 1 (10%)
Adjuvant
treatmentsb
0.264
Pre-operative
CT + RT
2 (20%) 2 (28.6%) 0 (0%) 0 (0%)
Post-operativ
e CT
3 (30%) 3 (42.9%) 0 (0%) 2 (20%)
Pre-operative
CT + RT +
post-operativ
e CT
1 (1%) 0 (0%) 1 (33.3%) 0 (0%)
No adjuvant
therapies
4 (40%) 2 (28.6%) 2 (66.7%) 7 (70%)
Missing 0 (0%) 0 (0%) 0 (0%) 1 (10%)
Length of
in-patient
stay (days)a
8.1 ± 2.9 7.9 ± 1.5 8.7 ± 5.5 8.6 ± 5.7 0.807
Time since
operation
(days)a
169.0 ± 97.1 169.3 ±
84.3
168.3 ±
145.4
126.8 ± 85.3 0.316
Type of
surgeryb
0.236
Right
hemicolecto
my
3 (30%) 2 (28.6%) 1 (33.3%) 3 (30%)
Left
hemicolecto
my
2 (20%) 2 (28.6%) 0 (0%) 0 (0%)
Subtotal or
total
0 (0%) 0 (0%) 0 (0%) 1 (10%)
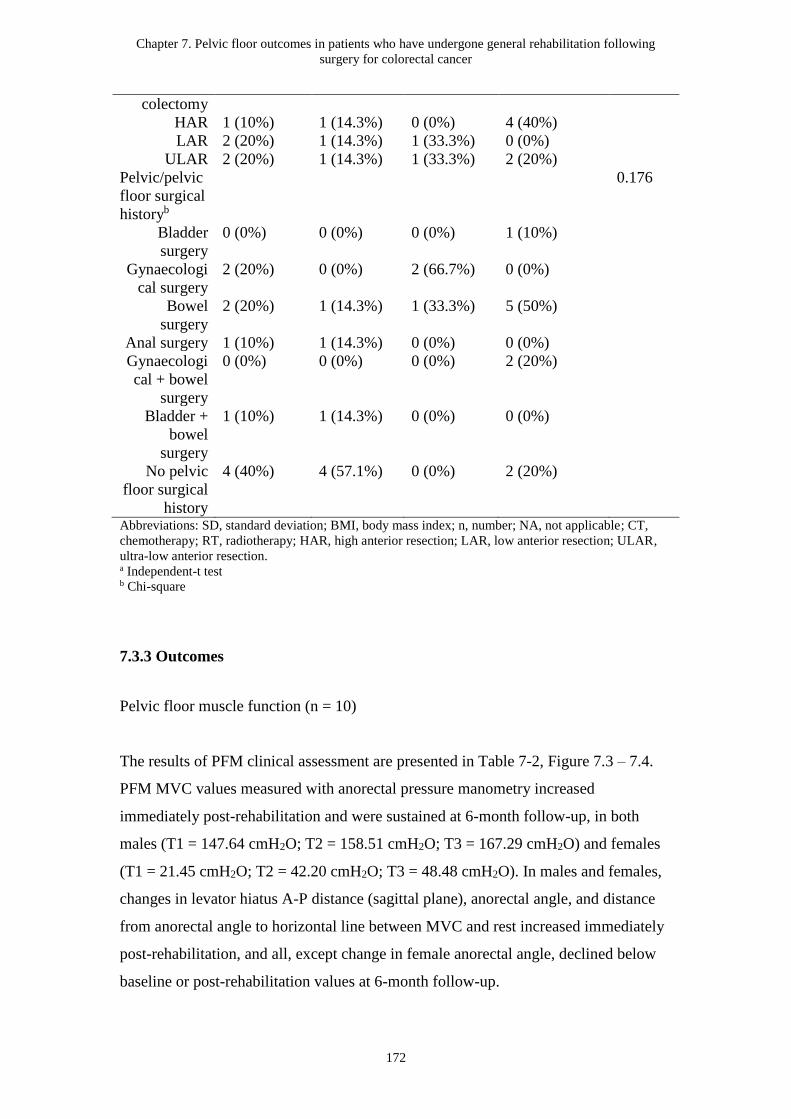
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
172
colectomy
HAR 1 (10%) 1 (14.3%) 0 (0%) 4 (40%)
LAR 2 (20%) 1 (14.3%) 1 (33.3%) 0 (0%)
ULAR 2 (20%) 1 (14.3%) 1 (33.3%) 2 (20%)
Pelvic/pelvic
floor surgical
historyb
0.176
Bladder
surgery
0 (0%) 0 (0%) 0 (0%) 1 (10%)
Gynaecologi
cal surgery
2 (20%) 0 (0%) 2 (66.7%) 0 (0%)
Bowel
surgery
2 (20%) 1 (14.3%) 1 (33.3%) 5 (50%)
Anal surgery 1 (10%) 1 (14.3%) 0 (0%) 0 (0%)
Gynaecologi
cal + bowel
surgery
0 (0%) 0 (0%) 0 (0%) 2 (20%)
Bladder +
bowel
surgery
1 (10%) 1 (14.3%) 0 (0%) 0 (0%)
No pelvic
floor surgical
history
4 (40%) 4 (57.1%) 0 (0%) 2 (20%)
Abbreviations: SD, standard deviation; BMI, body mass index; n, number; NA, not applicable; CT,
chemotherapy; RT, radiotherapy; HAR, high anterior resection; LAR, low anterior resection; ULAR,
ultra-low anterior resection. a Independent-t test b Chi-square
7.3.3 Outcomes
Pelvic floor muscle function (n = 10)
The results of PFM clinical assessment are presented in Table 7-2, Figure 7.3 – 7.4.
PFM MVC values measured with anorectal pressure manometry increased
immediately post-rehabilitation and were sustained at 6-month follow-up, in both
males (T1 = 147.64 cmH2O; T2 = 158.51 cmH2O; T3 = 167.29 cmH2O) and females
(T1 = 21.45 cmH2O; T2 = 42.20 cmH2O; T3 = 48.48 cmH2O). In males and females,
changes in levator hiatus A-P distance (sagittal plane), anorectal angle, and distance
from anorectal angle to horizontal line between MVC and rest increased immediately
post-rehabilitation, and all, except change in female anorectal angle, declined below
baseline or post-rehabilitation values at 6-month follow-up.
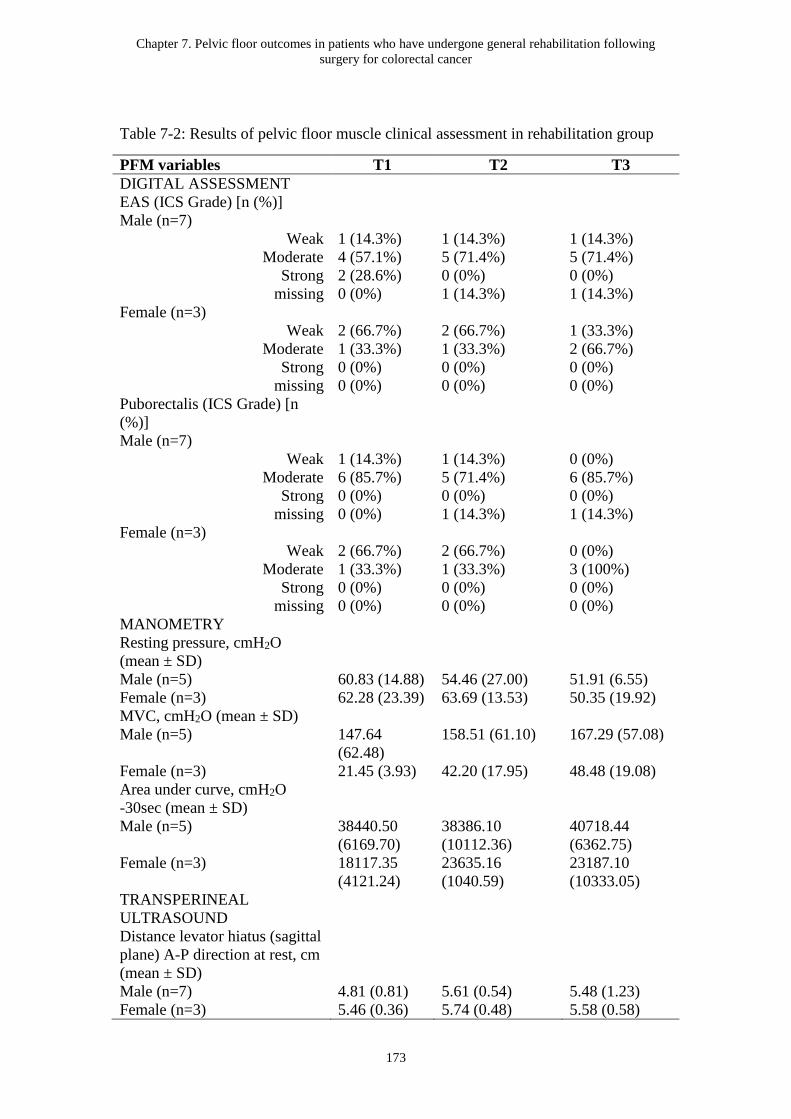
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
173
Table 7-2: Results of pelvic floor muscle clinical assessment in rehabilitation group
PFM variables T1 T2 T3
DIGITAL ASSESSMENT
EAS (ICS Grade) [n (%)]
Male (n=7)
Weak 1 (14.3%) 1 (14.3%) 1 (14.3%)
Moderate 4 (57.1%) 5 (71.4%) 5 (71.4%)
Strong 2 (28.6%) 0 (0%) 0 (0%)
missing 0 (0%) 1 (14.3%) 1 (14.3%)
Female (n=3)
Weak 2 (66.7%) 2 (66.7%) 1 (33.3%)
Moderate 1 (33.3%) 1 (33.3%) 2 (66.7%)
Strong 0 (0%) 0 (0%) 0 (0%)
missing 0 (0%) 0 (0%) 0 (0%)
Puborectalis (ICS Grade) [n
(%)]
Male (n=7)
Weak 1 (14.3%) 1 (14.3%) 0 (0%)
Moderate 6 (85.7%) 5 (71.4%) 6 (85.7%)
Strong 0 (0%) 0 (0%) 0 (0%)
missing 0 (0%) 1 (14.3%) 1 (14.3%)
Female (n=3)
Weak 2 (66.7%) 2 (66.7%) 0 (0%)
Moderate 1 (33.3%) 1 (33.3%) 3 (100%)
Strong 0 (0%) 0 (0%) 0 (0%)
missing 0 (0%) 0 (0%) 0 (0%)
MANOMETRY
Resting pressure, cmH2O
(mean ± SD)
Male (n=5) 60.83 (14.88) 54.46 (27.00) 51.91 (6.55)
Female (n=3) 62.28 (23.39) 63.69 (13.53) 50.35 (19.92)
MVC, cmH2O (mean ± SD)
Male (n=5) 147.64
(62.48)
158.51 (61.10) 167.29 (57.08)
Female (n=3) 21.45 (3.93) 42.20 (17.95) 48.48 (19.08)
Area under curve, cmH2O
-30sec (mean ± SD)
Male (n=5) 38440.50
(6169.70)
38386.10
(10112.36)
40718.44
(6362.75)
Female (n=3) 18117.35
(4121.24)
23635.16
(1040.59)
23187.10
(10333.05)
TRANSPERINEAL
ULTRASOUND
Distance levator hiatus (sagittal
plane) A-P direction at rest, cm
(mean ± SD)
Male (n=7) 4.81 (0.81) 5.61 (0.54) 5.48 (1.23)
Female (n=3) 5.46 (0.36) 5.74 (0.48) 5.58 (0.58)
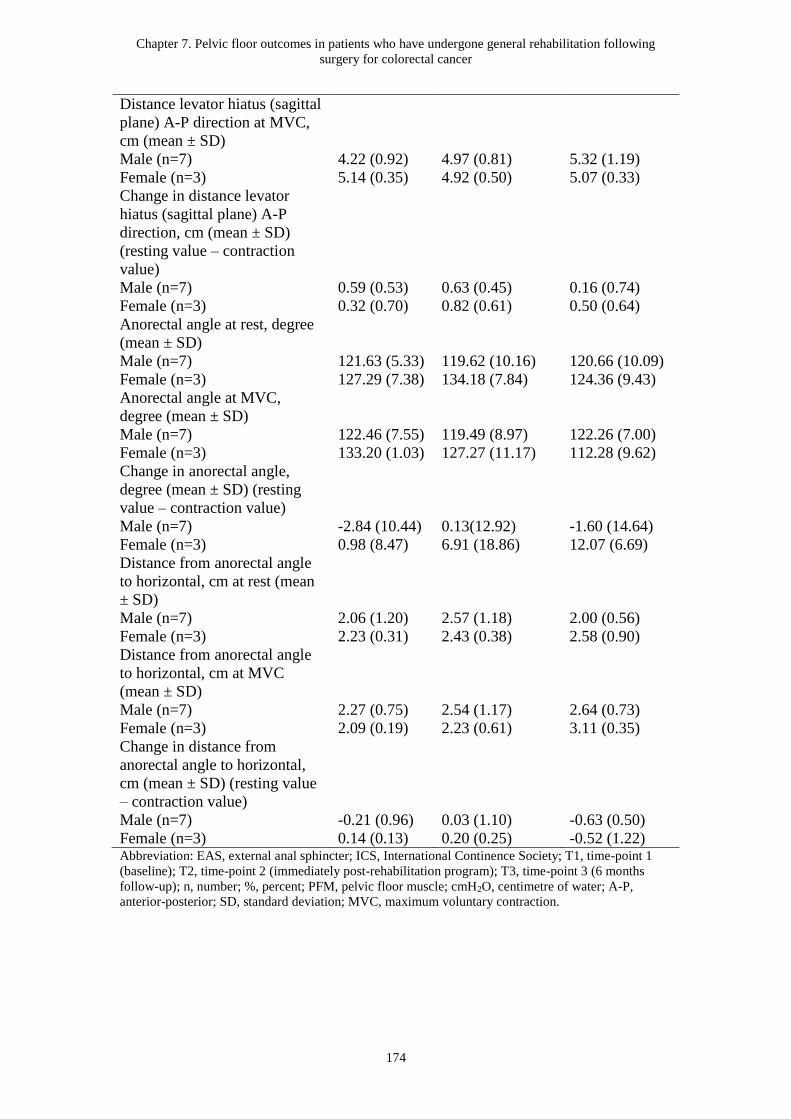
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
174
Distance levator hiatus (sagittal
plane) A-P direction at MVC,
cm (mean ± SD)
Male (n=7) 4.22 (0.92) 4.97 (0.81) 5.32 (1.19)
Female (n=3) 5.14 (0.35) 4.92 (0.50) 5.07 (0.33)
Change in distance levator
hiatus (sagittal plane) A-P
direction, cm (mean ± SD)
(resting value – contraction
value)
Male (n=7) 0.59 (0.53) 0.63 (0.45) 0.16 (0.74)
Female (n=3) 0.32 (0.70) 0.82 (0.61) 0.50 (0.64)
Anorectal angle at rest, degree
(mean ± SD)
Male (n=7) 121.63 (5.33) 119.62 (10.16) 120.66 (10.09)
Female (n=3) 127.29 (7.38) 134.18 (7.84) 124.36 (9.43)
Anorectal angle at MVC,
degree (mean ± SD)
Male (n=7) 122.46 (7.55) 119.49 (8.97) 122.26 (7.00)
Female (n=3) 133.20 (1.03) 127.27 (11.17) 112.28 (9.62)
Change in anorectal angle,
degree (mean ± SD) (resting
value – contraction value)
Male (n=7) -2.84 (10.44) 0.13(12.92) -1.60 (14.64)
Female (n=3) 0.98 (8.47) 6.91 (18.86) 12.07 (6.69)
Distance from anorectal angle
to horizontal, cm at rest (mean
± SD)
Male (n=7) 2.06 (1.20) 2.57 (1.18) 2.00 (0.56)
Female (n=3) 2.23 (0.31) 2.43 (0.38) 2.58 (0.90)
Distance from anorectal angle
to horizontal, cm at MVC
(mean ± SD)
Male (n=7) 2.27 (0.75) 2.54 (1.17) 2.64 (0.73)
Female (n=3) 2.09 (0.19) 2.23 (0.61) 3.11 (0.35)
Change in distance from
anorectal angle to horizontal,
cm (mean ± SD) (resting value
– contraction value)
Male (n=7) -0.21 (0.96) 0.03 (1.10) -0.63 (0.50)
Female (n=3) 0.14 (0.13) 0.20 (0.25) -0.52 (1.22) Abbreviation: EAS, external anal sphincter; ICS, International Continence Society; T1, time-point 1
(baseline); T2, time-point 2 (immediately post-rehabilitation program); T3, time-point 3 (6 months
follow-up); n, number; %, percent; PFM, pelvic floor muscle; cmH2O, centimetre of water; A-P,
anterior-posterior; SD, standard deviation; MVC, maximum voluntary contraction.
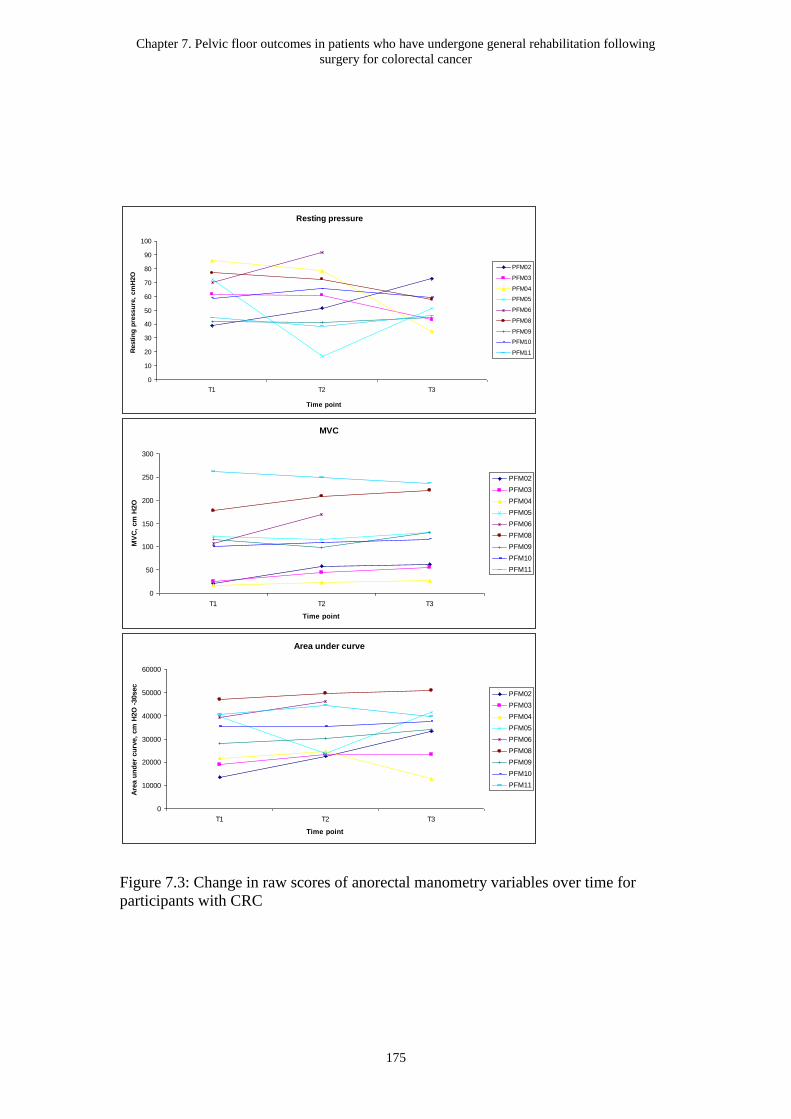
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
175
Figure 7.3: Change in raw scores of anorectal manometry variables over time for
participants with CRC
Resting pressure
0
10
20
30
40
50
60
70
80
90
100
T1 T2 T3
Time point
Resti
ng
pre
ssu
re,
cm
H2O
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
MVC
0
50
100
150
200
250
300
T1 T2 T3
Time point
MV
C,
cm
H2O
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
Area under curve
0
10000
20000
30000
40000
50000
60000
T1 T2 T3
Time point
Are
a u
nd
er
cu
rve,
cm
H2O
-30sec
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
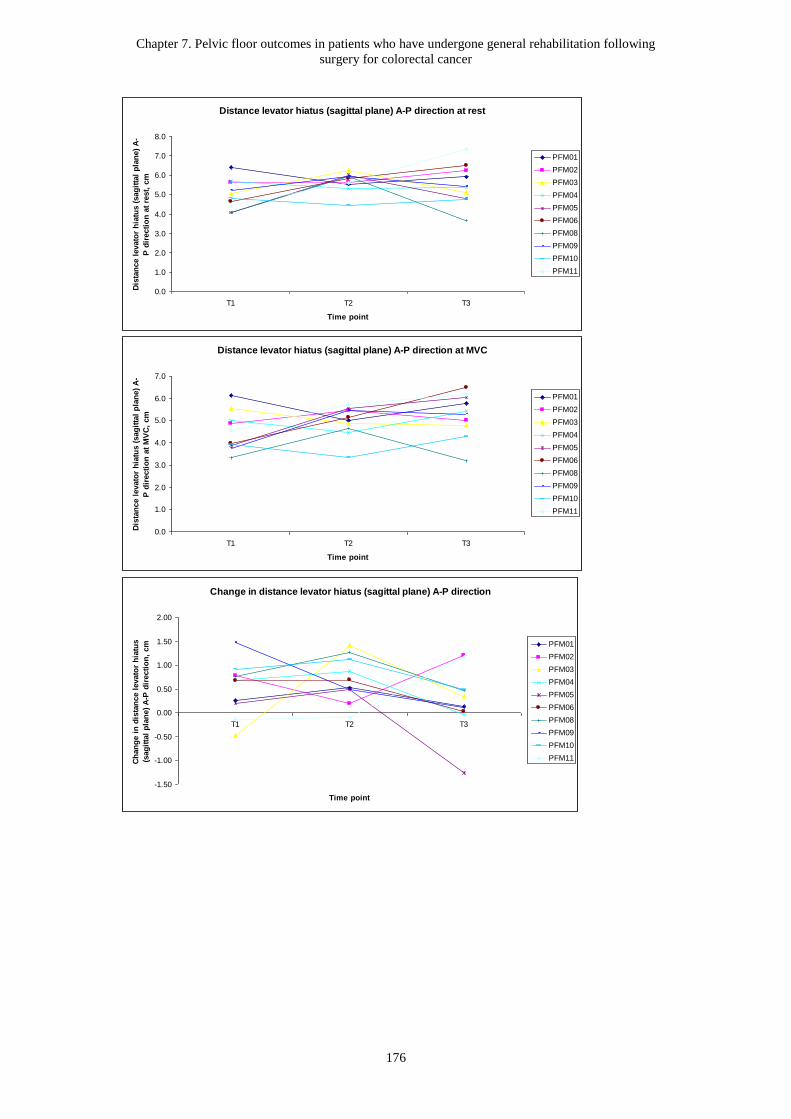
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
176
Distance levator hiatus (sagittal plane) A-P direction at rest
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
T1 T2 T3
Time point
Dis
tan
ce l
evato
r h
iatu
s (
sag
itta
l p
lan
e)
A-
P d
irecti
on
at
rest,
cm
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
Distance levator hiatus (sagittal plane) A-P direction at MVC
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
T1 T2 T3
Time point
Dis
tan
ce l
evato
r h
iatu
s (
sag
itta
l p
lan
e)
A-
P d
irecti
on
at
MV
C,
cm
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
Change in distance levator hiatus (sagittal plane) A-P direction
-1.50
-1.00
-0.50
0.00
0.50
1.00
1.50
2.00
T1 T2 T3
Time point
Ch
an
ge i
n d
ista
nce l
evato
r h
iatu
s
(sag
itta
l p
lan
e)
A-P
dir
ecti
on
, cm
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
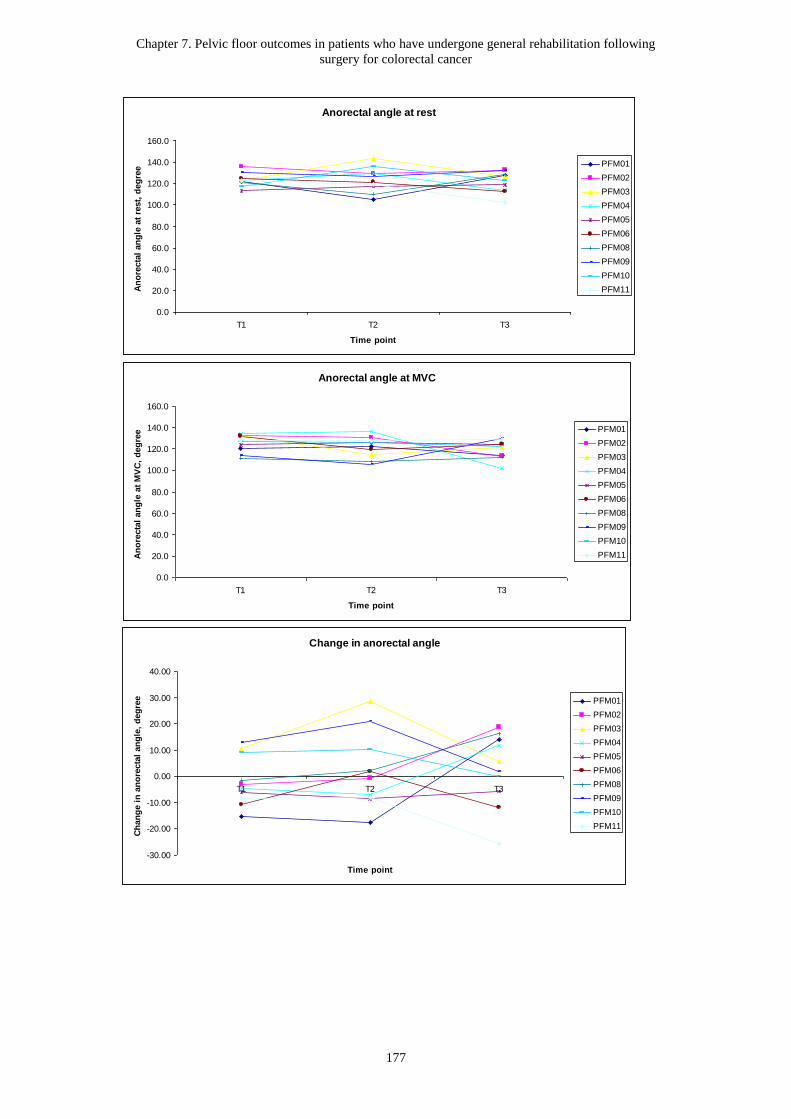
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
177
Anorectal angle at rest
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0
T1 T2 T3
Time point
An
ore
cta
l an
gle
at
rest,
deg
ree PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
Anorectal angle at MVC
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0
T1 T2 T3
Time point
An
ore
cta
l an
gle
at
MV
C,
deg
ree PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
Change in anorectal angle
-30.00
-20.00
-10.00
0.00
10.00
20.00
30.00
40.00
T1 T2 T3
Time point
Ch
an
ge i
n a
no
recta
l an
gle
, d
eg
ree PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
178
Figure 7.4: Change in raw scores of ultrasound variables over time for participants
with CRC.
Distance anorectal angle to horizontal at rest
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
T1 T2 T3
Time point
Dis
tan
ce a
no
recta
l an
gle
to
ho
rizo
nta
l,
cm
at
rest
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
Distance anorectal angle to horizontal at MVC
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
T1 T2 T3
Time point
Dis
tan
ce a
no
recta
l an
gle
to
ho
rizo
nta
l,
cm
at
MV
C
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
Change in distance anorectal angle to horizontal
-2.50
-2.00
-1.50
-1.00
-0.50
0.00
0.50
1.00
1.50
2.00
2.50
T1 T2 T3
Time point
Ch
an
ge i
n d
ista
nce a
no
recta
l an
gle
to
ho
rizo
nta
l, c
m
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
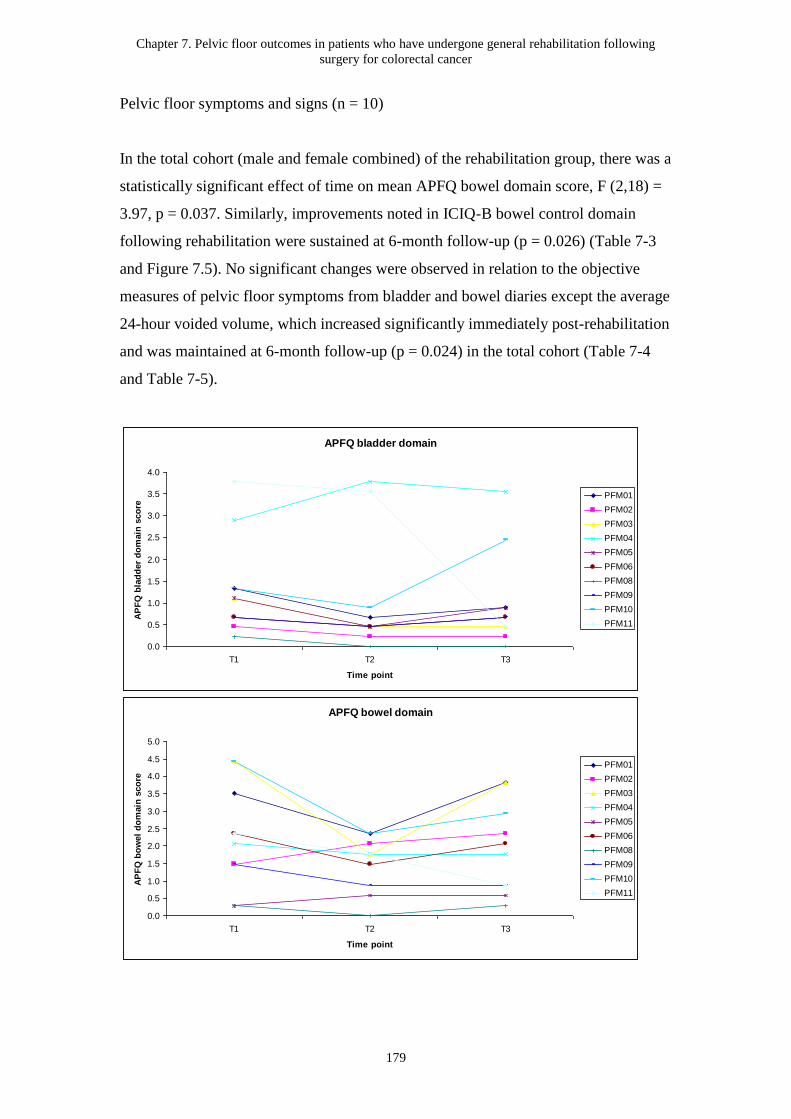
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
179
Pelvic floor symptoms and signs (n = 10)
In the total cohort (male and female combined) of the rehabilitation group, there was a
statistically significant effect of time on mean APFQ bowel domain score, F (2,18) =
3.97, p = 0.037. Similarly, improvements noted in ICIQ-B bowel control domain
following rehabilitation were sustained at 6-month follow-up (p = 0.026) (Table 7-3
and Figure 7.5). No significant changes were observed in relation to the objective
measures of pelvic floor symptoms from bladder and bowel diaries except the average
24-hour voided volume, which increased significantly immediately post-rehabilitation
and was maintained at 6-month follow-up (p = 0.024) in the total cohort (Table 7-4
and Table 7-5).
APFQ bladder domain
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
T1 T2 T3
Time point
AP
FQ
bla
dd
er
do
main
sco
re
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
APFQ bowel domain
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
T1 T2 T3
Time point
AP
FQ
bo
wel
do
main
sco
re
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
180
Figure 7.5: Change in raw scores of bladder and bowel symptoms over time for
participants with CRC.
ICIQ-B bowel pattern
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
T1 T2 T3
Time point
ICIQ
-B b
ow
el
patt
ern
sco
re
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
ICIQ-B bowel control
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
T1 T2 T3
Time point
ICIQ
-B b
ow
el
co
ntr
ol
sco
re
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
ICIQ-B quality of life
0.0
5.0
10.0
15.0
20.0
25.0
T1 T2 T3
Time point
ICIQ
-B q
uali
ty o
f li
fe s
co
re
PFM01
PFM02
PFM03
PFM04
PFM05
PFM06
PFM08
PFM09
PFM10
PFM11
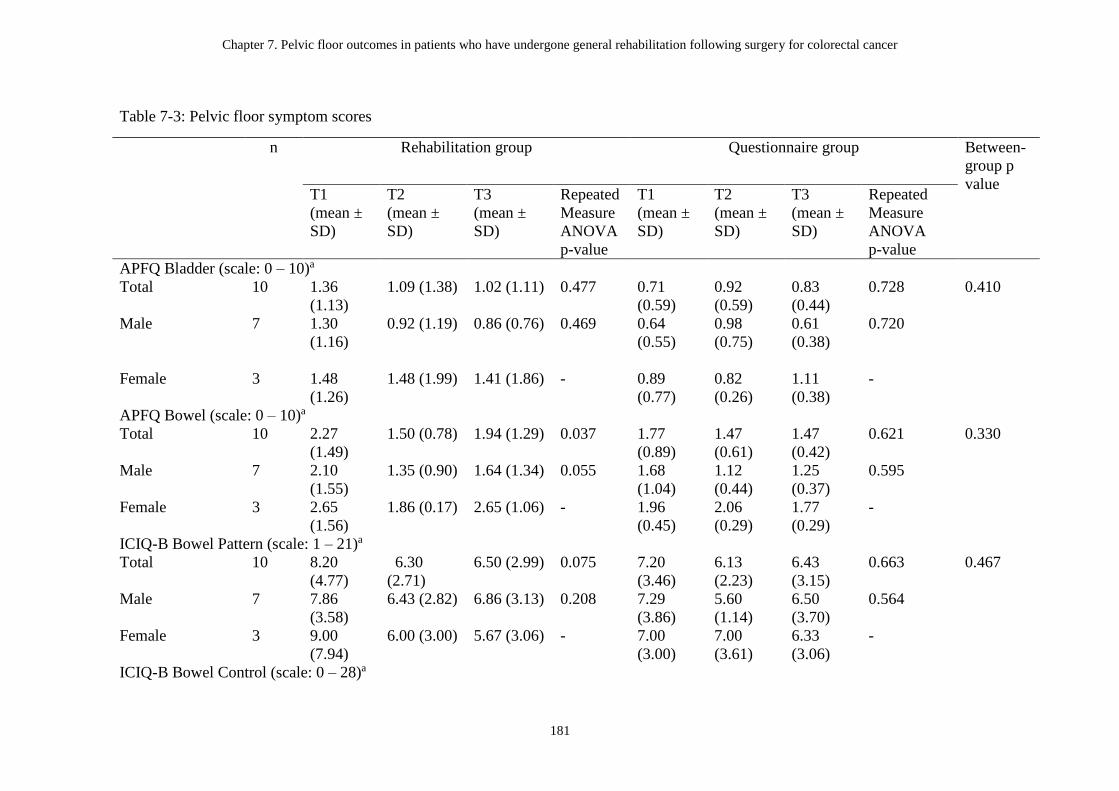
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following surgery for colorectal cancer
181
Table 7-3: Pelvic floor symptom scores
n Rehabilitation group Questionnaire group Between-
group p
value T1
(mean ±
SD)
T2
(mean ±
SD)
T3
(mean ±
SD)
Repeated
Measure
ANOVA
p-value
T1
(mean ±
SD)
T2
(mean ±
SD)
T3
(mean ±
SD)
Repeated
Measure
ANOVA
p-value
APFQ Bladder (scale: 0 – 10)a
Total 10 1.36
(1.13)
1.09 (1.38) 1.02 (1.11) 0.477 0.71
(0.59)
0.92
(0.59)
0.83
(0.44)
0.728 0.410
Male 7 1.30
(1.16)
0.92 (1.19) 0.86 (0.76) 0.469 0.64
(0.55)
0.98
(0.75)
0.61
(0.38)
0.720
Female 3 1.48
(1.26)
1.48 (1.99) 1.41 (1.86) - 0.89
(0.77)
0.82
(0.26)
1.11
(0.38)
-
APFQ Bowel (scale: 0 – 10)a
Total 10 2.27
(1.49)
1.50 (0.78) 1.94 (1.29) 0.037 1.77
(0.89)
1.47
(0.61)
1.47
(0.42)
0.621 0.330
Male 7 2.10
(1.55)
1.35 (0.90) 1.64 (1.34) 0.055 1.68
(1.04)
1.12
(0.44)
1.25
(0.37)
0.595
Female 3 2.65
(1.56)
1.86 (0.17) 2.65 (1.06) - 1.96
(0.45)
2.06
(0.29)
1.77
(0.29)
-
ICIQ-B Bowel Pattern (scale: 1 – 21)a
Total 10 8.20
(4.77)
6.30
(2.71)
6.50 (2.99) 0.075 7.20
(3.46)
6.13
(2.23)
6.43
(3.15)
0.663 0.467
Male 7 7.86
(3.58)
6.43 (2.82) 6.86 (3.13) 0.208 7.29
(3.86)
5.60
(1.14)
6.50
(3.70)
0.564
Female 3 9.00
(7.94)
6.00 (3.00) 5.67 (3.06) - 7.00
(3.00)
7.00
(3.61)
6.33
(3.06)
-
ICIQ-B Bowel Control (scale: 0 – 28)a

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following surgery for colorectal cancer
182
Total 10 7.40
(6.96)
4.90 (5.67) 4.70 (4.74) 0.026 4.00
(5.03)
2.75
(2.76)
3.14
(3.72)
0.719 0.099
Male 7 6.43
(6.75)
5.00 (6.51) 4.71 (5.02) 0.153 4.00
(5.80)
2.20
(2.77)
2.75
(4.19)
0.880
Female 3 9.67
(8.38)
4.67 (4.16) 4.67 (5.03) - 4.00
(3.61)
3.67
(3.06)
3.67
(3.79)
-
ICIQ-B Quality of Life (scale: 0 – 21)a
Total 10 8.00
(10.03)
6.20 (7.81) 5.90 (7.98) 0.213 4.00
(5.94)
4.13
(7.24)
4.57
(5.06)
0.992 0.398
Male 7 6.43
(10.03)
4.86 (7.84) 4.14 (6.49) 0.370 2.86
(3.93)
2.20
(4.38)
3.75
(5.68)
0.401
Female 3 11.67
(11.06)
9.33 (8.33) 10.00
(11.14)
- 6.67
(9.87)
7.33
(10.97)
5.67
(5.03)
-
Abbreviation: n, number of participants; T1, time-point 1 (baseline); T2, time-point 2 (immediately post-rehabilitation program); T3, time-point 3 (6 months
follow-up); ANOVA, Analysis of variance; APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on Incontinence Questionnaire-Bowel
Module. a Higher score indicates worse severity/symptoms
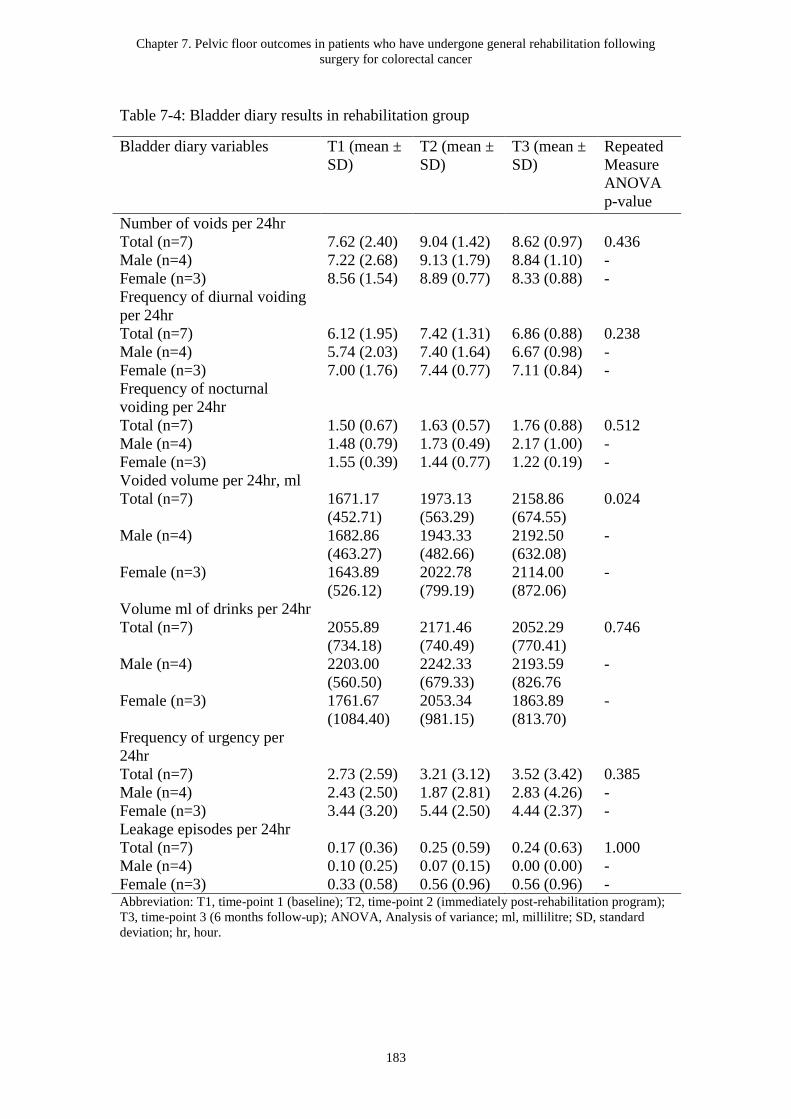
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
183
Table 7-4: Bladder diary results in rehabilitation group
Bladder diary variables T1 (mean ±
SD)
T2 (mean ±
SD)
T3 (mean ±
SD)
Repeated
Measure
ANOVA
p-value
Number of voids per 24hr
Total (n=7) 7.62 (2.40) 9.04 (1.42) 8.62 (0.97) 0.436
Male (n=4) 7.22 (2.68) 9.13 (1.79) 8.84 (1.10) -
Female (n=3) 8.56 (1.54) 8.89 (0.77) 8.33 (0.88) -
Frequency of diurnal voiding
per 24hr
Total (n=7) 6.12 (1.95) 7.42 (1.31) 6.86 (0.88) 0.238
Male (n=4) 5.74 (2.03) 7.40 (1.64) 6.67 (0.98) -
Female (n=3) 7.00 (1.76) 7.44 (0.77) 7.11 (0.84) -
Frequency of nocturnal
voiding per 24hr
Total (n=7) 1.50 (0.67) 1.63 (0.57) 1.76 (0.88) 0.512
Male (n=4) 1.48 (0.79) 1.73 (0.49) 2.17 (1.00) -
Female (n=3) 1.55 (0.39) 1.44 (0.77) 1.22 (0.19) -
Voided volume per 24hr, ml
Total (n=7) 1671.17
(452.71)
1973.13
(563.29)
2158.86
(674.55)
0.024
Male (n=4) 1682.86
(463.27)
1943.33
(482.66)
2192.50
(632.08)
-
Female (n=3) 1643.89
(526.12)
2022.78
(799.19)
2114.00
(872.06)
-
Volume ml of drinks per 24hr
Total (n=7) 2055.89
(734.18)
2171.46
(740.49)
2052.29
(770.41)
0.746
Male (n=4) 2203.00
(560.50)
2242.33
(679.33)
2193.59
(826.76
-
Female (n=3) 1761.67
(1084.40)
2053.34
(981.15)
1863.89
(813.70)
-
Frequency of urgency per
24hr
Total (n=7) 2.73 (2.59) 3.21 (3.12) 3.52 (3.42) 0.385
Male (n=4) 2.43 (2.50) 1.87 (2.81) 2.83 (4.26) -
Female (n=3) 3.44 (3.20) 5.44 (2.50) 4.44 (2.37) -
Leakage episodes per 24hr
Total (n=7) 0.17 (0.36) 0.25 (0.59) 0.24 (0.63) 1.000
Male (n=4) 0.10 (0.25) 0.07 (0.15) 0.00 (0.00) -
Female (n=3) 0.33 (0.58) 0.56 (0.96) 0.56 (0.96) - Abbreviation: T1, time-point 1 (baseline); T2, time-point 2 (immediately post-rehabilitation program);
T3, time-point 3 (6 months follow-up); ANOVA, Analysis of variance; ml, millilitre; SD, standard
deviation; hr, hour.
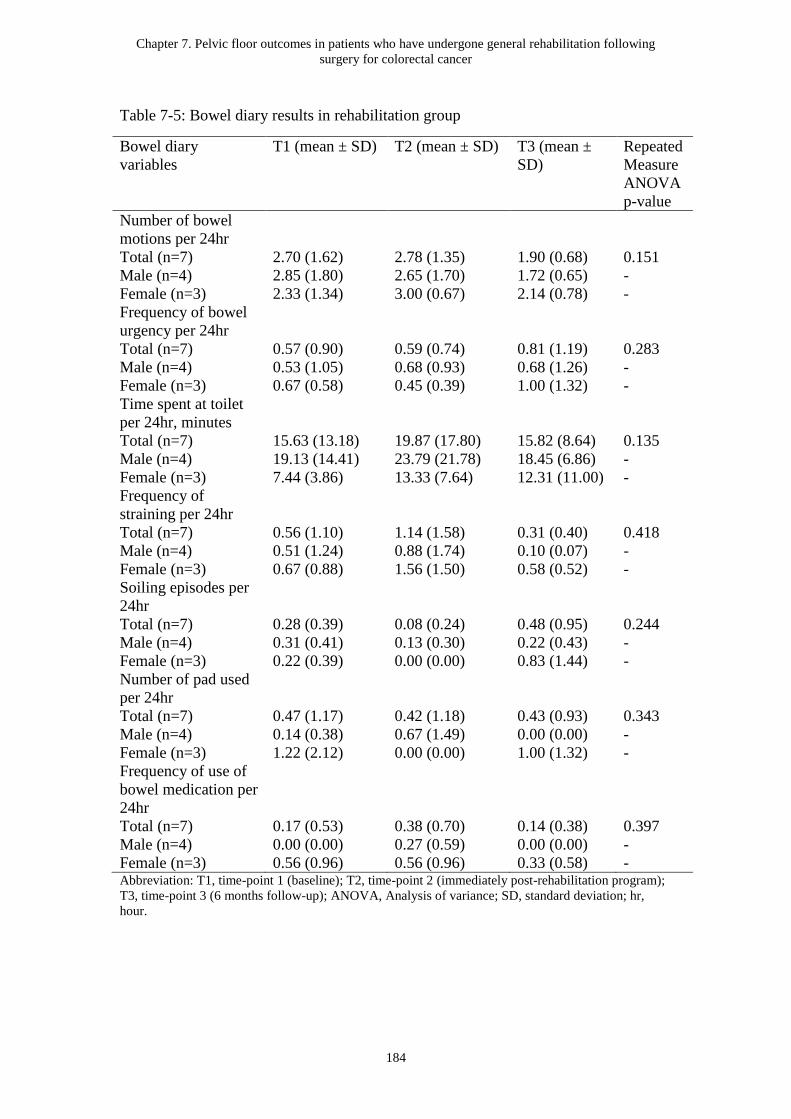
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
184
Table 7-5: Bowel diary results in rehabilitation group
Bowel diary
variables
T1 (mean ± SD)
T2 (mean ± SD) T3 (mean ±
SD)
Repeated
Measure
ANOVA
p-value
Number of bowel
motions per 24hr
Total (n=7) 2.70 (1.62) 2.78 (1.35) 1.90 (0.68) 0.151
Male (n=4) 2.85 (1.80) 2.65 (1.70) 1.72 (0.65) -
Female (n=3) 2.33 (1.34) 3.00 (0.67) 2.14 (0.78) -
Frequency of bowel
urgency per 24hr
Total (n=7) 0.57 (0.90) 0.59 (0.74) 0.81 (1.19) 0.283
Male (n=4) 0.53 (1.05) 0.68 (0.93) 0.68 (1.26) -
Female (n=3) 0.67 (0.58) 0.45 (0.39) 1.00 (1.32) -
Time spent at toilet
per 24hr, minutes
Total (n=7) 15.63 (13.18) 19.87 (17.80) 15.82 (8.64) 0.135
Male (n=4) 19.13 (14.41) 23.79 (21.78) 18.45 (6.86) -
Female (n=3) 7.44 (3.86) 13.33 (7.64) 12.31 (11.00) -
Frequency of
straining per 24hr
Total (n=7) 0.56 (1.10) 1.14 (1.58) 0.31 (0.40) 0.418
Male (n=4) 0.51 (1.24) 0.88 (1.74) 0.10 (0.07) -
Female (n=3) 0.67 (0.88) 1.56 (1.50) 0.58 (0.52) -
Soiling episodes per
24hr
Total (n=7) 0.28 (0.39) 0.08 (0.24) 0.48 (0.95) 0.244
Male (n=4) 0.31 (0.41) 0.13 (0.30) 0.22 (0.43) -
Female (n=3) 0.22 (0.39) 0.00 (0.00) 0.83 (1.44) -
Number of pad used
per 24hr
Total (n=7) 0.47 (1.17) 0.42 (1.18) 0.43 (0.93) 0.343
Male (n=4) 0.14 (0.38) 0.67 (1.49) 0.00 (0.00) -
Female (n=3) 1.22 (2.12) 0.00 (0.00) 1.00 (1.32) -
Frequency of use of
bowel medication per
24hr
Total (n=7) 0.17 (0.53) 0.38 (0.70) 0.14 (0.38) 0.397
Male (n=4) 0.00 (0.00) 0.27 (0.59) 0.00 (0.00) -
Female (n=3) 0.56 (0.96) 0.56 (0.96) 0.33 (0.58) - Abbreviation: T1, time-point 1 (baseline); T2, time-point 2 (immediately post-rehabilitation program);
T3, time-point 3 (6 months follow-up); ANOVA, Analysis of variance; SD, standard deviation; hr,
hour.
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
185
Comparison with the matched control (n = 20)
Further analyses showed no significant changes in PROMs (i.e. APFQ bladder and
bowel domains and ICIQ-B domains) between three time-points in the matched
control group (Table 7-3). However, a trend of difference was noted in ICIQ-B bowel
control between groups over time (p = 0.099).
Correlations between different PFM clinical outcome measures (n = 10)
Statistically significant moderate correlations for PFM strength were found between
MVC measured by anorectal pressure manometry and DRE measured muscle strength
of the EAS immediately post-rehabilitation (Spearman’s rho 0.73, p < 0.05). Change
in distance from anorectal angle to horizontal line between MVC and rest measured
by TPUS was also significantly and positively moderately correlated with DRE
measured muscle strength of the EAS at 6-month follow-up (Spearman’s rho 0.73, p <
0.05) (Table 7-6 , Table 7-7, and Table 7-8).
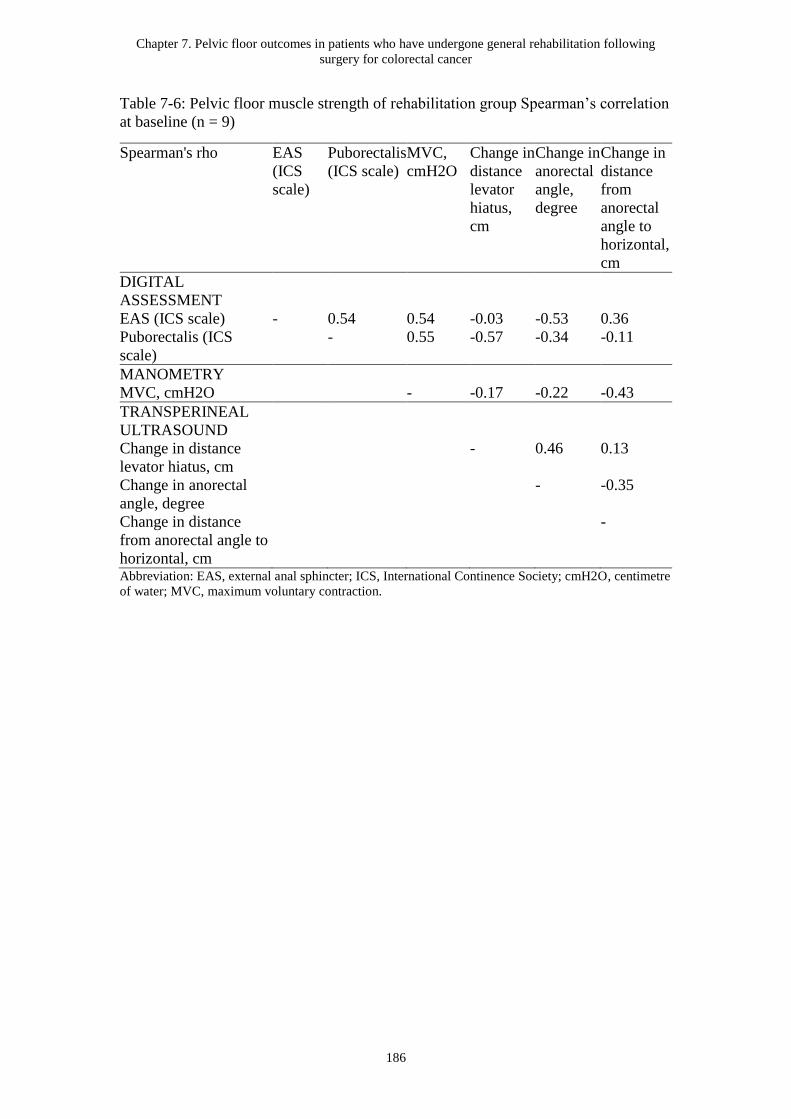
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
186
Table 7-6: Pelvic floor muscle strength of rehabilitation group Spearman’s correlation
at baseline (n = 9)
Spearman's rho EAS
(ICS
scale)
Puborectalis
(ICS scale)
MVC,
cmH2O
Change in
distance
levator
hiatus,
cm
Change in
anorectal
angle,
degree
Change in
distance
from
anorectal
angle to
horizontal,
cm
DIGITAL
ASSESSMENT
EAS (ICS scale) - 0.54 0.54 -0.03 -0.53 0.36
Puborectalis (ICS
scale)
- 0.55 -0.57 -0.34 -0.11
MANOMETRY
MVC, cmH2O - -0.17 -0.22 -0.43
TRANSPERINEAL
ULTRASOUND
Change in distance
levator hiatus, cm
- 0.46 0.13
Change in anorectal
angle, degree
- -0.35
Change in distance
from anorectal angle to
horizontal, cm
-
Abbreviation: EAS, external anal sphincter; ICS, International Continence Society; cmH2O, centimetre
of water; MVC, maximum voluntary contraction.
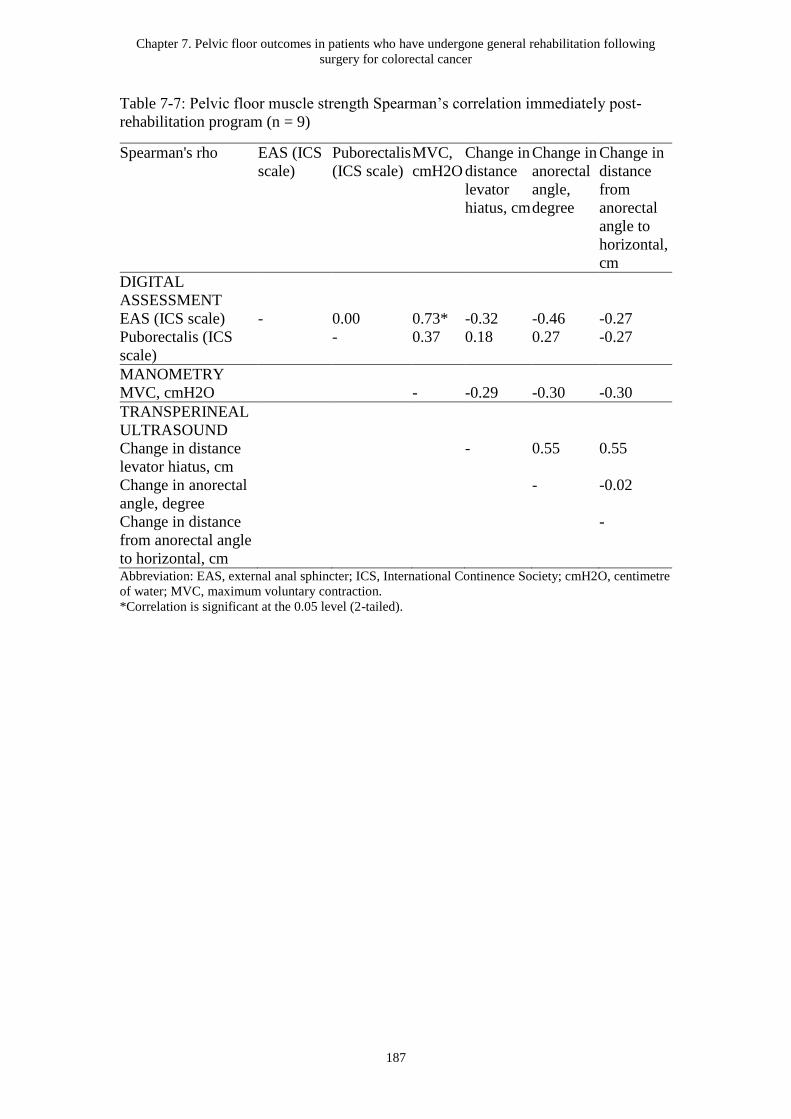
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
187
Table 7-7: Pelvic floor muscle strength Spearman’s correlation immediately post-
rehabilitation program (n = 9)
Spearman's rho EAS (ICS
scale)
Puborectalis
(ICS scale)
MVC,
cmH2O
Change in
distance
levator
hiatus, cm
Change in
anorectal
angle,
degree
Change in
distance
from
anorectal
angle to
horizontal,
cm
DIGITAL
ASSESSMENT
EAS (ICS scale) - 0.00 0.73* -0.32 -0.46 -0.27
Puborectalis (ICS
scale)
- 0.37 0.18 0.27 -0.27
MANOMETRY
MVC, cmH2O - -0.29 -0.30 -0.30
TRANSPERINEAL
ULTRASOUND
Change in distance
levator hiatus, cm
- 0.55 0.55
Change in anorectal
angle, degree
- -0.02
Change in distance
from anorectal angle
to horizontal, cm
-
Abbreviation: EAS, external anal sphincter; ICS, International Continence Society; cmH2O, centimetre
of water; MVC, maximum voluntary contraction.
*Correlation is significant at the 0.05 level (2-tailed).
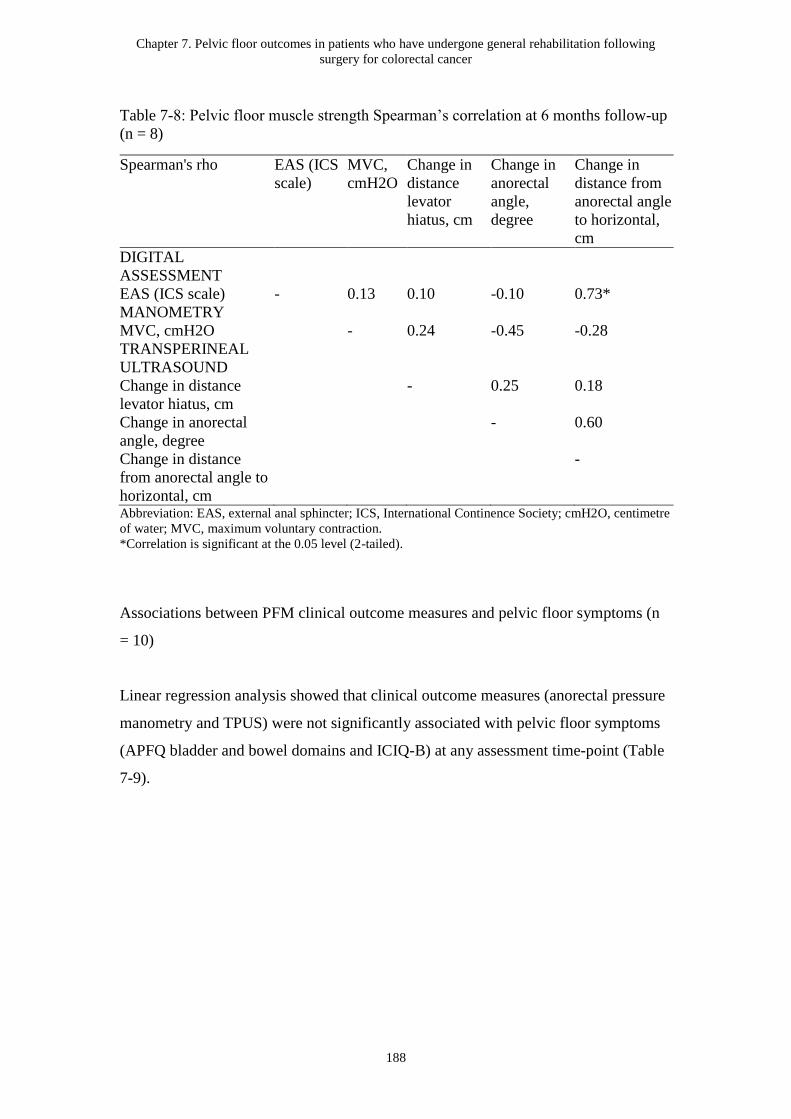
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
188
Table 7-8: Pelvic floor muscle strength Spearman’s correlation at 6 months follow-up
(n = 8)
Spearman's rho EAS (ICS
scale)
MVC,
cmH2O
Change in
distance
levator
hiatus, cm
Change in
anorectal
angle,
degree
Change in
distance from
anorectal angle
to horizontal,
cm
DIGITAL
ASSESSMENT
EAS (ICS scale) - 0.13 0.10 -0.10 0.73*
MANOMETRY
MVC, cmH2O - 0.24 -0.45 -0.28
TRANSPERINEAL
ULTRASOUND
Change in distance
levator hiatus, cm
- 0.25 0.18
Change in anorectal
angle, degree
- 0.60
Change in distance
from anorectal angle to
horizontal, cm
-
Abbreviation: EAS, external anal sphincter; ICS, International Continence Society; cmH2O, centimetre
of water; MVC, maximum voluntary contraction.
*Correlation is significant at the 0.05 level (2-tailed).
Associations between PFM clinical outcome measures and pelvic floor symptoms (n
= 10)
Linear regression analysis showed that clinical outcome measures (anorectal pressure
manometry and TPUS) were not significantly associated with pelvic floor symptoms
(APFQ bladder and bowel domains and ICIQ-B) at any assessment time-point (Table
7-9).

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following surgery for colorectal cancer
189
Table 7-9: Linear regression analyses examining the relationship between different clinical measures of PFM function and severity of
pelvic floor symptoms
Independent
variables
Dependent variables Baseline Immediately
post-intervention
6 months follow-up
Β
(regre
ssion
coeffi
cients)
95% CI P-Valu
e
Β
(regre
ssion
coeffi
cients)
95% CI P-Valu
e
Β
(regre
ssion
coeffi
cients
)
95% CI P-Valu
e
Anorectal
manometry - MVC,
cmH2O
APFQ Bladder 0.32 -0.01-0.02 0.400 0.05 -0.02-0.02 0.892 -0.51 -0.02-0.0
1
0.199
APFQ Bowel -0.28 -0.02-0.01 0.466 -0.37 -0.01-0.01 0.322 -0.66 -0.02-0.0
01
0.073
ICIQ-B Bowel
Pattern
-0.21 -0.07-0.04 0.585 -0.34 -0.04-0.02 0.365 -0.17 -0.05-0.0
3
0.696
ICIQ-B Bowel
Control
-0.55 -0.11-0.02 0.123 -0.56 -0.10-0.01 0.114 -0.40 -0.08-0.0
3
0.327
ICIQ-B Quality of
Life
-0.49 -0.16-0.04 0.181 -0.62 -0.14-0.01 0.077 -0.50 -0.14-0.0
4
0.210
Ultrasound -
Change in distance
levator hiatus
(sagittal plane) A-P
direction, cm
APFQ Bladder -0.81 -2.31-0.69 0.246 -0.91 -3.14-1.33 0.377 -0.38 -1.65-0.8
9
0.509
APFQ Bowel -0.90 -2.94-1.14 0.340 -0.29 -1.59-1.02 0.628 0.33 -1.17-1.8
3
0.622
ICIQ-B Bowel
Pattern
-4.01 -10.15-2.1
4
0.171 2.10 -2.20-6.39 0.293 -0.23 -3.75-3.2
8
0.884
ICIQ-B Bowel -1.19 -11.28-8.9 0.793 1.92 -7.62-11.4 0.655 -0.39 -5.96-5.1 0.876
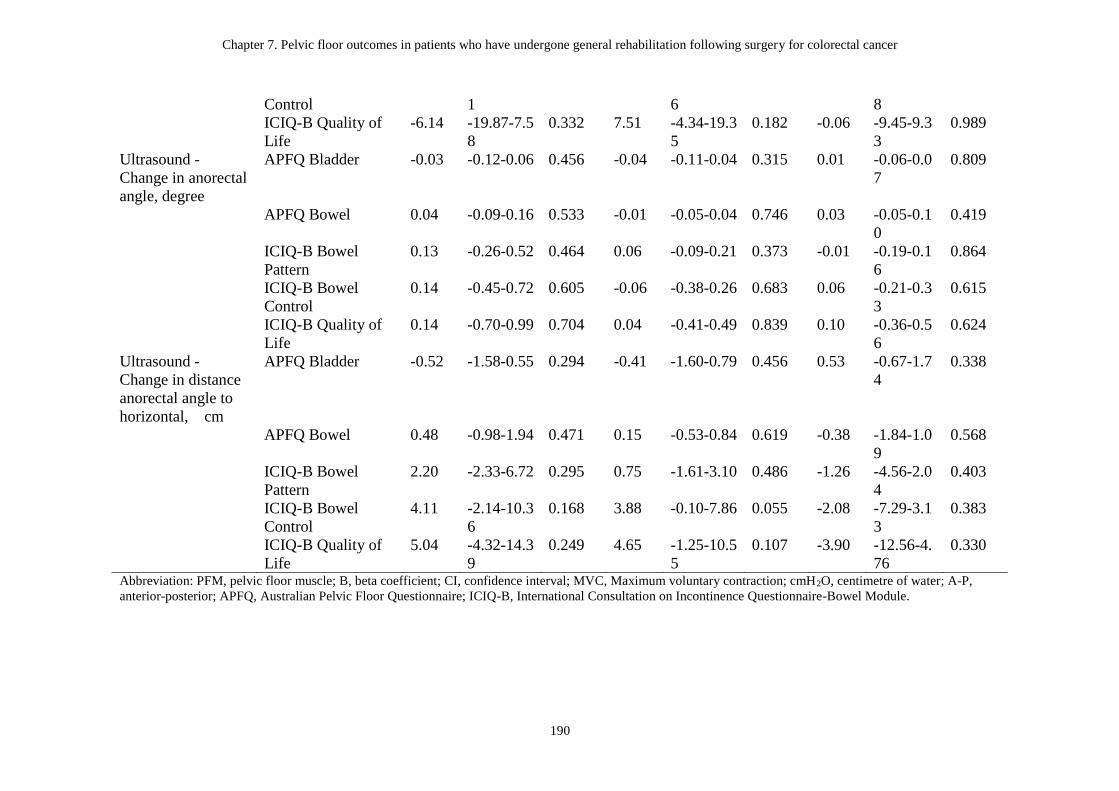
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following surgery for colorectal cancer
190
Control 1 6 8
ICIQ-B Quality of
Life
-6.14 -19.87-7.5
8
0.332 7.51 -4.34-19.3
5
0.182 -0.06 -9.45-9.3
3
0.989
Ultrasound -
Change in anorectal
angle, degree
APFQ Bladder -0.03 -0.12-0.06 0.456 -0.04 -0.11-0.04 0.315 0.01 -0.06-0.0
7
0.809
APFQ Bowel 0.04 -0.09-0.16 0.533 -0.01 -0.05-0.04 0.746 0.03 -0.05-0.1
0
0.419
ICIQ-B Bowel
Pattern
0.13 -0.26-0.52 0.464 0.06 -0.09-0.21 0.373 -0.01 -0.19-0.1
6
0.864
ICIQ-B Bowel
Control
0.14 -0.45-0.72 0.605 -0.06 -0.38-0.26 0.683 0.06 -0.21-0.3
3
0.615
ICIQ-B Quality of
Life
0.14 -0.70-0.99 0.704 0.04 -0.41-0.49 0.839 0.10 -0.36-0.5
6
0.624
Ultrasound -
Change in distance
anorectal angle to
horizontal, cm
APFQ Bladder -0.52 -1.58-0.55 0.294 -0.41 -1.60-0.79 0.456 0.53 -0.67-1.7
4
0.338
APFQ Bowel 0.48 -0.98-1.94 0.471 0.15 -0.53-0.84 0.619 -0.38 -1.84-1.0
9
0.568
ICIQ-B Bowel
Pattern
2.20 -2.33-6.72 0.295 0.75 -1.61-3.10 0.486 -1.26 -4.56-2.0
4
0.403
ICIQ-B Bowel
Control
4.11 -2.14-10.3
6
0.168 3.88 -0.10-7.86 0.055 -2.08 -7.29-3.1
3
0.383
ICIQ-B Quality of
Life
5.04 -4.32-14.3
9
0.249 4.65 -1.25-10.5
5
0.107 -3.90 -12.56-4.
76
0.330
Abbreviation: PFM, pelvic floor muscle; B, beta coefficient; CI, confidence interval; MVC, Maximum voluntary contraction; cmH2O, centimetre of water; A-P,
anterior-posterior; APFQ, Australian Pelvic Floor Questionnaire; ICIQ-B, International Consultation on Incontinence Questionnaire-Bowel Module.
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
191
7.4 Discussion
This is the first study to explore changes in PFM clinical measures and bladder and
bowel symptom outcomes in patients following a general oncology rehabilitation
program compared with a matched control group post–CRC surgery. The findings
showed significant improvements in patient-reported bowel symptoms immediately
post-rehabilitation and the improvements were maintained 6 months following
baseline. Significant correlations were found between muscle strength of the EAS
measured by DRE and MVC measured with anorectal pressure manometry, and DRE
and change in distance from anorectal angle to horizontal line between MVC and rest
measured using TPUS. No associations were found between clinical outcome
measures and patient-reported pelvic floor symptoms.
Despite the small numbers in male and female groups, our data showed maintenance
of the improvement in MVC measured by anorectal pressure manometry in males and
females immediately post-rehabilitation and at 6-month follow-up. A previous study
has shown a similar improvement in maximum squeeze pressure after a specific PFM
rehabilitation training program including electrical stimulation and biofeedback in
patients with faecal incontinence and defecation disorders following rectal cancer
surgery (Kuo et al., 2015), however we investigated changes in pelvic floor outcomes
following a general oncology rehabilitation program without specific PFM training. It
should be noted that the mean MVC value of our male cohort at baseline
(147.6cmH2O) was comparable to the MVC reading of 100-150 cmH2O reported as
normal in the Peritron Handbook (Cardio Design, 2016), while that of our female
cohort (21.45 cmH2O) was lower than the mean squeeze pressure 49 (range 7–91)
cmH2O reported by Ryhammer et al. in 75 women with no known anorectal disease
(Ryhammer, Laurberg, & Sorensen, 1997). Nevertheless, the mean MVC value of our
female cohort was closer to the mean maximum anal pressure of 24 cmH2O measured
using Peritron in patients with faecal incontinence (Simpson et al., 2006).
Furthermore, the difference in the baseline MVC values between male and female
was significant, however this accords with results from previous studies (Li, Yang,
Xu, Zhang, & Zhang, 2013; Ozgen et al., 2015). Randomized controlled trials with

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
192
subgroup analysis by sex are warranted to further explore the effects of general
exercise on anorectal pressure in patients following surgery for CRC.
In our study, the change in levator hiatus A-P distance and distance from anorectal
angle to horizontal line from rest to MVC increased in both males and females
post-rehabilitation. The mean values of change in levator hiatus A-P distance and
distance from anorectal angle to horizontal line from rest to MVC in females at
baseline (0.3 cm and 0.1 cm) were lower in our study compared to previous studies in
healthy women (Volloyhaug et al., 2015) and urogynaecologic patients (Albrich et al.,
2015), and the change in distance from anorectal angle to horizontal line in
nulliparous asymptomatic women (Raizada et al., 2010). The lower values in our
study may be due to the damage to the PFM structure and function caused by CRC
surgery and adjuvant therapy (Bernard et al., 2015; Hirano et al., 2011) as levator
trauma has been shown to be associated with reduced contractile function (Guzman
Rojas, Wong, Shek, & Dietz, 2014). However, there is scant knowledge on the
changes in levator hiatus and distance from anorectal angle to horizontal following
general exercise for CRC, and no strong conclusion can be drawn from our study due
to its small sample size.
Our study showed that both males and females had large anorectal angles at rest
ranging from 119.6 degree to 134.2 degree at three time-points. The widened
anorectal angle may be due to the damage to the puborectalis muscle caused by CRC
surgery (Hirano et al., 2011). Although an obtuse anorectal angle at rest suggests
weakening and increased laxity of the PFMs (Yang, Partanen, Farin, & Soimakallio,
1995), the clinical significance of the anorectal angle as an indicator of pelvic floor
dysfunction is uncertain. The normal values of anorectal angle at rest vary widely in
the literature, ranging from 60 degree to 114 degree (Pittman, Benson, & Sumners,
1990) and the findings of asymptomatic and symptomatic individuals may overlap
(Schreyer et al., 2012). Moreover, Pittman et al. have reported that patients who had
partial incontinence with an abnormally large anorectal angle were able to
compensate with normal sphincter pressures (Pittman et al., 1990). Despite the
increase in change in anorectal angle in both males and females from rest to MVC

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
193
post-rehabilitation, the improvements noted in PFM strength and MVC as measured
by DRE and anorectal manometry post-rehabilitation suggested a compensation by
non-injured muscle fibres of anal sphincters and puborectalis (Hilde et al., 2013).
Nevertheless, more studies are needed to further explore PFM function in the CRC
population.
As discrepancy often exists between clinicians’ assessment of patients’ outcomes and
the degree of bother perceived by patients (Avery et al., 2007), PROMs (severity of
symptoms) represent the most important clinical outcomes from a patient perspective
(Kelleher et al., 2013). Our findings of significant improvements in APFQ bowel
domain and ICIQ-B bowel control in the rehabilitation group and no changes in the
‘matched control’ group suggest that general exercise with the components we
provided, may have beneficial effects on bowel symptoms in patients following
surgery for CRC. A trend of difference in ICIQ-B bowel control was observed
between groups over time. With such a small group of participants in our study, this
finding is encouraging and supports the potential positive effect of a general exercise
program as we provided, on bowel symptoms. Nevertheless, a specific PFM training
program may provide a stronger effect, and this requires investigation.
Despite the observed improvements in bowel symptoms and MVC values measured
with anorectal manometry post-rehabilitation, no significant associations were found
between these measures. This finding concurs with that of Wasserberg et al. (2011)
who noted no correlation between squeeze pressures and bowel symptoms in a group
of patients with faecal incontinence (Wasserberg, Mazaheri, Petrone, Tulchinsky, &
Kaufman, 2011). Moreover, our finding is consistent with two previous studies, which
reported no significant relationships between subjective and clinical outcomes
following biofeedback treatment in patients with faecal incontinence (Norton,
Chelvanayagam, Wilson-Barnett, Redfern, & Kamm, 2003) and in patients with
faecal incontinence after surgery for CRC (Allgayer, Dietrich, Rohde, Koch, &
Tuschhoff, 2005). However, we acknowledge that our study was exploratory (not
powered). Further studies are required to identify the predictive values of clinical
measures on severity of bladder and bowel symptoms in patients with CRC.

Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
194
Our study showed that MVC as measured by DRE of the EAS is significantly
correlated with MVC values measured by anorectal manometry immediately
post-rehabilitation, and with ultrasound findings at 6-months follow-up. However, the
findings should be read with caution due to the small size of our study. Moreover, our
findings are unable to be compared directly with previous studies (Dobben et al., 2007;
Favetta, Amato, Interisano, & Pescatori, 1996), due to differences in study
populations, equipment used, and study purposes. The lack of studies that have
examined relationships between DRE, anorectal pressure manometry (Peritron) and
TPUS following surgery for CRC justifies the importance of this pilot study. Despite
the exploratory nature of our study, the high correlations between DRE, anorectal
pressure manometry and TPUS suggest that DRE, which is relatively simple and
inexpensive, may be useful for the assessment of PFM strength in a CRC population
if more sophisticated equipment (i.e. anorectal manometry and ultrasound) is not
readily available in clinical practice. However, further studies are warranted to
determine the optimum measurement instrument for PFM assessment following
surgery for CRC.
There are a number of limitations to this study. As a prospective observational
pre-post pilot study, the nature of the study does not allow us to establish a causal
effect of the changes in the outcomes of interest. Another limitation was the relatively
low consent rate (58.8%), which indicates that there may have been a selection bias in
terms of the patients who agreed to be in this nested PFM measurement study. The
researcher who performed the clinical assessments was aware of participants’ medical
history; hence, information bias must be considered. However, our findings add
valuable information to the current literature as the majority of research in this field
has focused on rectal cancer only. Moreover, given the small sample of female
participants in this study, it was difficult to account for the potential confounding
factors that may have an impact on pelvic floor function and symptoms, such as
history of childbirth and hormonal status (Fish & Temple, 2014). The effects of the
cancer treatment (RT and CT) on the outcomes of interest are unknown. Participants
included in this study were not stratified according to the presence of bladder and/or
bowel symptoms prior to enrolment; hence, pre-existing symptoms may have
impacted upon the pelvic floor outcomes following the rehabilitation program.
Chapter 7. Pelvic floor outcomes in patients who have undergone general rehabilitation following
surgery for colorectal cancer
195
Although PFM training was not provided as part of the rehabilitation program, the
program included advice on bladder and bowel habits, and verbal cueing during
exercise classes to encourage PFM activation prior to rises in intra-abdominal
pressure. Therefore it is unknown whether it was the general exercise component or
other components of the rehabilitation program which impacted on the pelvic floor
outcomes.
Despite the limitations, this is the first exploratory study investigating changes in
pelvic floor outcomes in patients with CRC who have undergone an oncology
rehabilitation program following surgery. Our findings provide a foundation for future
studies to evaluate the effects of general exercise compared with PFM training on
pelvic floor outcomes in patients with CRC.
7.5 Summary
From this exploratory analysis, patient-reported bowel symptoms improved after a
general oncology rehabilitation program in patients following surgery for CRC.
Moreover, it seems that there is a strong positive correlation between DRE and
anorectal pressure manometry following oncology rehabilitation, and DRE and TPUS
at 6-month follow-up. Further studies with larger sample sizes are needed to establish
the optimal outcome measure for pelvic floor outcomes in a CRC population. The
results of this pilot study provide useful information for future studies such as RCTs
to investigate the long-term effect of general oncology rehabilitations and or PFM
specific training programs on pelvic floor outcomes in patients with CRC. The role of
specific PFM training (as opposed to general oncology rehabilitation) in the CRC
population has been studied and the next chapter describes a systematic review of the
published studies to date.

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
196
Chapter 8. Pelvic floor muscle training for bowel dysfunction following
colorectal cancer surgery: a systematic review
This systematic review was published in 2015 (Appendix 8.1):
Lin KY, Granger C, Denehy L, Frawley H. Pelvic floor muscle training for bowel
dysfunction following colorectal cancer surgery: a systematic review. Neurourology
and Urodynamics. 2015;34(8):703-12.
Author contributions for this chapter are the following: K-YL, CG, LD and HF
conceived the idea for the paper. K-YL and CG performed the literature search and
quality assessment. K-YL wrote the first draft of the manuscript, managed manuscript
submission and subsequent reviews. All authors revised the paper and provided
scientific input. All authors approved the final version of the manuscript.
8.1 Introduction
This chapter will describe a systematic review undertaken to systematically
investigate the effect of PFM training on bowel dysfunction in patients after surgery
for CRC. Despite the publication of a previous systematic review evaluating the
conservative therapies such as pelvic floor re-education and colonic irrigation on
anorectal function in patients undergoing rectal resection for cancer and non-cancer
diagnoses (Maris, Devreese, D'Hoore, Penninckx, & Staes, 2013), this was the first
systematic review published investigating the benefit of PFM training in patients
specially with CRC. This systematic review was conducted according to the Preferred
Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
This chapter has the same content as that in the published systematic review. The new
recently published articles which were not included in the published manuscript are
briefly summarised at the end of the chapter.

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
197
8.2 Review aim
To identify, evaluate and synthesize the evidence examining the effectiveness of PFM
training on bowel dysfunction in patients who have undergone CRC surgery.
8.3 Methods
No protocol for this review has been registered or published (Moher, Liberati, Tetzlaff,
& Altman, 2009).
8.3.1 Literature search
Electronic databases, MEDLINE (1950-2014), CINAHL (1982-2014), EMBASE
(1980-2014), Scopus (1823-2014), PsycINFO (1806-2014), Web of Science
(1970-2014), Cochrane Library (2014), and Physiotherapy Evidence Database
(1999-2014) were searched in March 2014 by one reviewer (K-YL) using different
combinations of the following terms: pelvic floor muscle training; rehabilitation;
physical therapy modalities; biofeedback psychology; pelvic floor exercise; kegel;
biofeedback; bowel function; defecation; faecal incontinence; gastrointestinal
function; total mesorectal excision; sphincter-saving surgery; anterior resection; APR;
colectomy; colorectal surgery; sphincter-preserving surgery; colorectal neoplasms;
rectal neoplasms; colonic neoplasms. An example of search strategy is presented in
Appendix 8.2. Electronic databases were accessed via The University of Melbourne,
Australia, with the last search run on 10 March 2014. No restrictions on the
publication date were imposed. The search was limited to articles written in English.
The reference lists of identified articles were also hand searched.
8.3.2 Selection criteria
Studies were eligible if they met the following inclusion criteria:
Types of studies
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
198
Quantitative study designs including RCTs, cohort studies and case series were
eligible for inclusion. Case studies with only one participant were not eligible. Only
studies published in a peer reviewed journal were eligible.
Types of participants
Participants of any age, who had undergone surgery for colon or rectal cancer, were
eligible to be included in this review. Colorectal cancer was defined as cancer that
forms in the tissues of the colon or the rectum, and participants with any stage of CRC
were eligible (National Cancer Institute, 2014). Given the limited number of studies
available on this topic, we included studies with mixed cohorts of participants with
cancer and non-cancer diagnoses who had undergone colorectal surgery; for inclusion,
we required at least 50% of the participants in the study to have CRC, or data to be
reported separately for the cancer participants.
Types of intervention
Studies which included PFM training with or without biofeedback were eligible. This
included all types of visual, sensory, or auditory biofeedback. According to the 5th
ICI, PFM training (also known as Kegel exercise training) for treating faecal
incontinence involves the contraction of PFM including the EAS and puborectalis
(Bliss et al., 2013). For the purpose of this review, PFM training /Kegel exercise and
anal sphincter exercise will be considered together with the use of biofeedback for the
purpose of PFM strengthening (PFM training combined with anal canal pressure or
intra-anal electromyograph feedback device), sensory training (introducing a
balloon-tipped catheter into the rectum), or coordination training (employing a
pressure transducer to provide simultaneous feedback in intra-rectal and intra-anal
pressure during PFM contraction) made explicit (Bliss et al., 2013; Heymen &
Kuijpers, 2007). Studies that used solely electrical stimulation were not eligible for
inclusion.
Types of outcomes
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
199
Studies were eligible for inclusion if their primary outcome was bowel function
measured by a patient-reported outcome measure (such as a bowel diary,
questionnaire, patient report) or anal manometry.
8.3.3 Screening of papers
Two reviewers (K-YL and CG) independently assessed studies based on titles and
abstracts for inclusion. Full texts of potentially relevant studies were retrieved and
reviewed by the two reviewers to evaluate the eligibility. Disagreements were able to
be resolved by a third independent reviewer (HF) although this was not required.
Authors were contacted by e-mail if more information was needed to screen an article
(this occurred on one occasion).
8.3.4 Risk of bias
As non-randomized studies were the primary study design found, the risk of bias was
assessed by the two independent reviewers using the Newcastle-Ottawa Scale (NOS)
for non-randomized studies. A third review was available if any disagreements arose
between the two reviewers (although this was not required), and a consensus
score/point was assigned after discussion. Studies were also ranked on the National
Health and Medical Research Council Hierarchy of Evidence Scale (National Health
Medical Research Council, 2009). The scoring criteria used for synthesis of bias risk
of included studies were reported as “poor” to “excellent” based on the score
calculated in the NOS.
The NOS, a valid and reliable instrument, evaluates the risk of bias of studies based
on participant selection, comparability of study groups, and the assessment of
exposure (case-control studies) or outcome (cohort studies) (Wells et al., 2005). There
are a total of eight items for both case-control studies and cohort studies. A point can
be given to each item except the items in the category of comparability in which a
maximum of 2 points can be obtained (Wells et al., 2005). A total of 7 to 9 points

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
200
indicates high methodological quality (low risk of bias), a total of 4 to 6 indicates
moderate quality, and points below 4 indicate low quality (high risk of bias) (Suthar,
Granich, Mermin, & Van Rie).
8.3.5 Data extraction
An electronic data collection form was specifically developed and utilised. Data were
extracted from the included studies by one reviewer (K-YL) and crossed-checked by a
second independent reviewer (CG). Disagreements were resolved through discussion
or with the use of a third reviewer (HF). Data items extracted from the included
studies included the first author’s name; year published; number of participants;
gender; age; type of surgery; adjuvant therapy; type, duration, frequency, and length
of intervention program; and results of reviewed studies.
Statistics
Kappa statistics and percentage agreement were calculated to establish agreement
between reviewers for study selection and risk of bias using SPSS for Windows
statistical software package (SPSS Inc., Version 21, Chicago, IL) (Landis & Koch,
1977). Values of kappa greater than 0.8 reflect “excellent” agreement (Higgins &
Green, 2011). Mean and variance of pre- and post- intervention assessments were
obtained directly from the study results or calculated using the following equations
when not reported (Hozo et al., 2005; Moore, McCabe, & Craig, 2010):
Standard deviation = Range / 4
Standard deviation = Standard error of the mean (square root of the number of
samples).
8.4 Results
8.4.1 Search strategy and study selection

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
201
Study selection
A total of 51 studies were identified following the electronic database search, and an
additional four studies were identified though searching reference lists. After
exclusion of duplicate records and assessment of titles and abstracts, 10 studies met
inclusion criteria and were further assessed with full text. The author of one
potentially eligible study (Chiang, Yeh, & Wang, 1997) was contacted to clarify
whether the study had included any participants with CRC; the study was
subsequently excluded because the diagnosis of participants was unknown. The study
of Hwang et al. was excluded because only three of the fourteen participants (21%) in
their study had a diagnosis of rectal cancer (Hwang et al., 2005). After assessment of
the eligibility of full-text articles, eight studies were finally included for review.
Figure 8.1 shows the flow diagram of study selection. Kappa statistics for agreement
between the two independent reviewers on title/abstracts and full text were 0.94
(percentage agreement, 98.0%) and 1.000 (percentage agreement, 100%), respectively
(Landis & Koch, 1977).
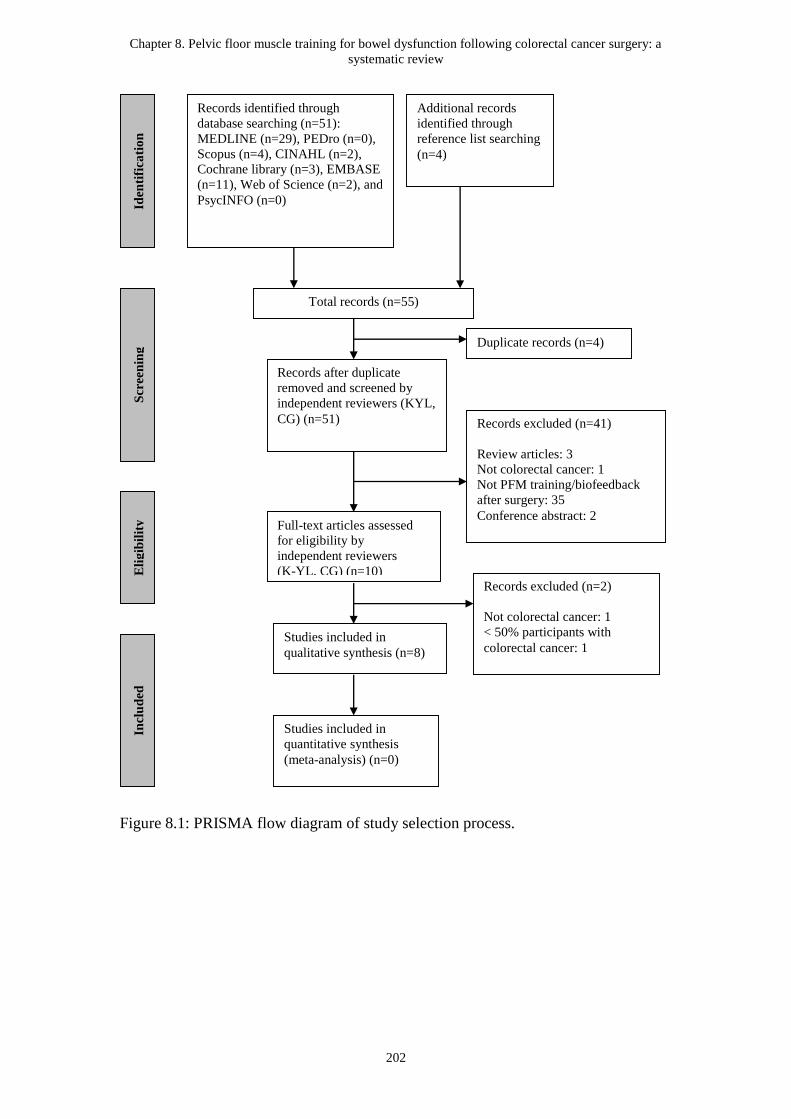
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
202
Figure 8.1: PRISMA flow diagram of study selection process.
Iden
tifi
cati
on
S
creen
ing
E
lig
ibil
ity
In
clu
ded
Full-text articles assessed
for eligibility by
independent reviewers
(K-YL, CG) (n=10)
Total records (n=55)
Records after duplicate
removed and screened by
independent reviewers (KYL,
CG) (n=51)
Duplicate records (n=4)
Records excluded (n=41)
Review articles: 3
Not colorectal cancer: 1
Not PFM training/biofeedback
after surgery: 35
Conference abstract: 2
Studies included in
qualitative synthesis (n=8)
Records identified through
database searching (n=51):
MEDLINE (n=29), PEDro (n=0),
Scopus (n=4), CINAHL (n=2),
Cochrane library (n=3), EMBASE
(n=11), Web of Science (n=2), and
PsycINFO (n=0)
Additional records
identified through
reference list searching
(n=4)
Records excluded (n=2)
Not colorectal cancer: 1
< 50% participants with
colorectal cancer: 1
Studies included in
quantitative synthesis
(meta-analysis) (n=0)

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
203
8.4.2 Study and participant characteristics
Study characteristics
Methods
No RCTs were found. Six prospective non-randomized studies (Bartlett, Sloots,
Nowak, & Ho, 2011; Ho, Chiang, Tan, & Low, 1996; Ho & Tan, 1997; Laforest et al.,
2012; Liu, Chen, & Lee, 2011; Pucciani, Ringressi, Redditi, Masi, & Giani, 2008) and
two retrospective review studies (Allgayer et al., 2005; Kim et al., 2011) were
included (Table 8-1).
Participants’ characteristics
The characteristics of the participants are presented in Table 8-2. A total of 374
participants were included in the studies. Six of eight studies reported data on cancer
patients only (Allgayer et al., 2005; Bartlett et al., 2011; Kim et al., 2011; Laforest et
al., 2012; Liu et al., 2011; Pucciani et al., 2008). The remaining two studies (Ho et al.,
1996; Ho & Tan, 1997) included 54% (7/13) and 91% (10/11) cancer patients,
respectively. The mean (SD) age of the participants across all studies ranged from
55.0 (11.3) to 67.0 (8.8) years. Of the eight studies, two included patients who had
undergone LAR (Allgayer et al., 2005; Ho & Tan, 1997), three following
sphincter-saving surgery (Kim et al., 2011; Laforest et al., 2012; Liu et al., 2011), and
three receiving mixed types of surgery (Bartlett et al., 2011; Ho et al., 1996; Pucciani
et al., 2008). Of the three studies with mixed types of surgery, one included patients
who had undergone colectomy for colon cancer (Bartlett et al., 2011). The majority of
studies (75%) included participants who had undergone CT and/or RT (Allgayer et al.,
2005; Ho et al., 1996; Ho & Tan, 1997; Kim et al., 2011; Laforest et al., 2012;
Pucciani et al., 2008).

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
204
Table 8-1: Risk of bias in reviewed observational trials using the Newcastle-Ottawa Scale
Auth
or
and
year
Count
ry
Design NOS score
Selection (0 - 4)
Comparability
(0 - 2)
Outcome (0 - 3)
Total
(0 - 9)
NHM
RC
grade
of
evide
nce
1)
Represent
ativeness
of the
exposed
cohort
2)
Selection
of the
non
exposed
cohort
3)
Ascert
ainme
nt of
expos
ure
4)
Demonst
ration
that
outcome
of
interest
was not
present
at start of
study
1)
Comparability
of cohorts on
the basis of the
design or
analysis
1)
Assessm
ent of
outcome
2) Was
follow-
up long
enough
for
outcom
es to
occur
3)
Adeq
uacy
of
follow
up of
cohort
s
Allga
yer et
al.
2005
Germ
any
Prospect
ive case
series
* - - * * * - * 5 IV
Bartl
ett et
al.
2011
Austra
lia
Retrospe
ctive
case
series
* - - - - * - * 3 IV
Ho et
al.
1996
Singa
pore
Prospect
ive case
series
* - * * - * - * 5 IV
Ho et Singa Prospect * - * * * * - * 6 IV
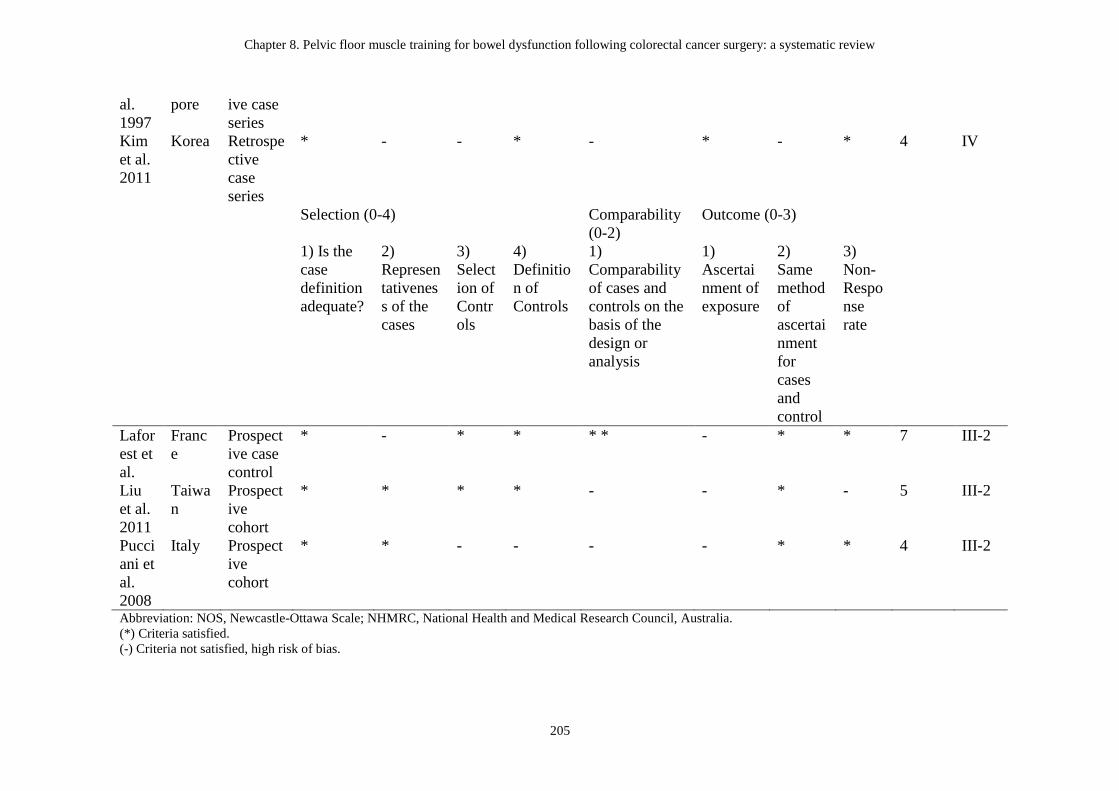
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
205
al.
1997
pore ive case
series
Kim
et al.
2011
Korea Retrospe
ctive
case
series
* - - * - * - * 4 IV
Selection (0-4)
Comparability
(0-2)
Outcome (0-3)
1) Is the
case
definition
adequate?
2)
Represen
tativenes
s of the
cases
3)
Select
ion of
Contr
ols
4)
Definitio
n of
Controls
1)
Comparability
of cases and
controls on the
basis of the
design or
analysis
1)
Ascertai
nment of
exposure
2)
Same
method
of
ascertai
nment
for
cases
and
control
3)
Non-
Respo
nse
rate
Lafor
est et
al.
Franc
e
Prospect
ive case
control
* - * * * * - * * 7 III-2
Liu
et al.
2011
Taiwa
n
Prospect
ive
cohort
* * * * - - * - 5 III-2
Pucci
ani et
al.
2008
Italy Prospect
ive
cohort
* * - - - - * * 4 III-2
Abbreviation: NOS, Newcastle-Ottawa Scale; NHMRC, National Health and Medical Research Council, Australia.
(*) Criteria satisfied.
(-) Criteria not satisfied, high risk of bias.

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
206
Table 8-2: Participants in reviewed studies
Author and year Number of
participants, (n) %
Gender, M/F Mean age, year ± SD Type of surgery, (n)
%
Adjuvant
therapy, (n) %
Symptoms at
baseline
Prospective
non-randomized
trials
Allgayer et al.,
2005
95
Irradiated patients
(41) 43.2%
Non-irradiated
patients (54) 56.8%
Irradiated:
28/13
Non-irradiated:
33/21
Irradiated: 58.5 ±
11.3* (range: 31.0 -
76.0)
Non-irradiated: 67.0
± 8.8* (range:
48.0-83.0)
Low anterior
resection (95) 100%
Post-op RT
(41) 43.2%
Faecal
incontinence
Ho et al., 1996 13
10/3 62.1 ± 16.6* Anterior resection
(7) 53.8%
Total colectomy (6)
46.2%
Post-op RT
(4) 30.8%
Frequent
bowel
movement
and / episode
of
incontinence
Ho et al., 1997 11
Incontinence (6)
54.5%
Constipation (5)
45.5%
5/6 64.8 ± 10.9* Low anterior
resection (11) 100%
Post-op RT
(2) 18.2%
Incontinence
or
constipation
Laforest et al.,
2012
46
Rehabilitation
group (22) 47.8%
Control group (24)
52.2%
Rehabilitation:
11/11
Control: 15/9
Rehabilitation: 55.0 ±
11.3* (range: 33.0 -
78.0)
Control: 60.0 ± 11.3*
(range: 35.0 - 80.0)
Laparoscopic
sphincter-saving
TME (46) 100%
Pre-op RCT
(32) 69.6%
Not specified
Liu et al., 2011 22
Exercise group (11)
Exercise: 4/7
Non-exercise:
Exercise: 55.3 ± 14.3
(range: 27.0 - 82.0)
Anal sphincter
preserving surgery
NR Frequent
defecation
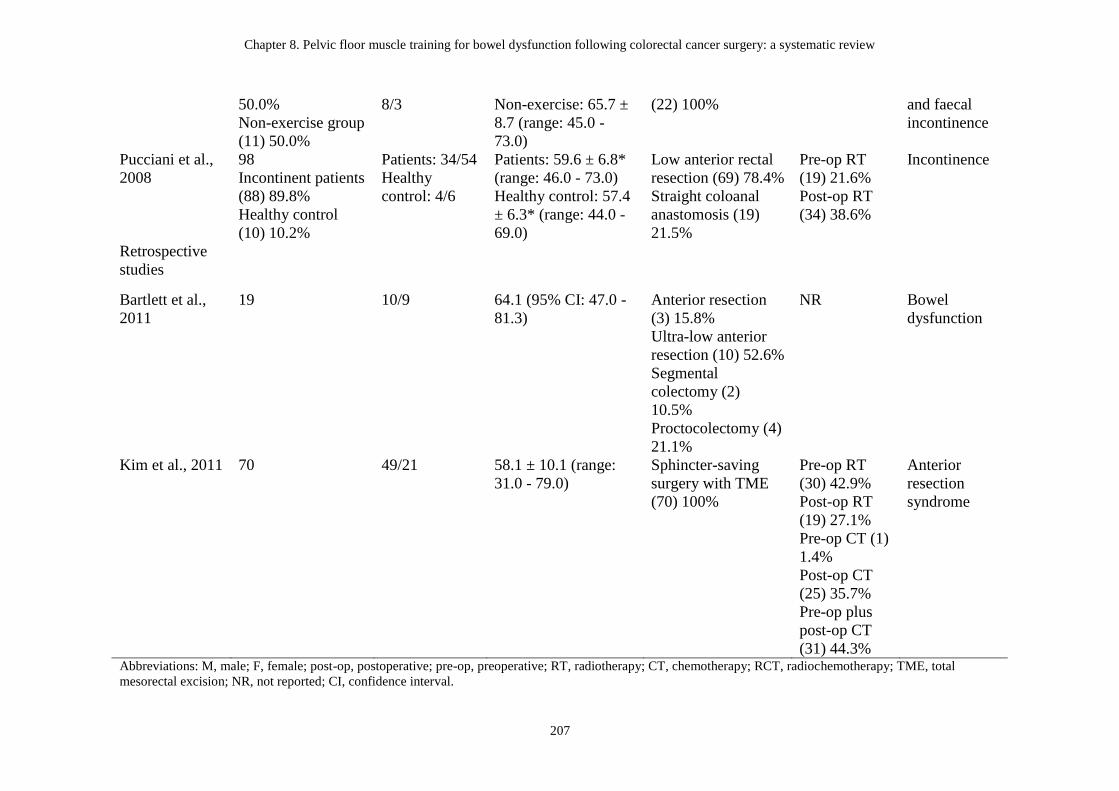
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
207
50.0%
Non-exercise group
(11) 50.0%
8/3 Non-exercise: 65.7 ±
8.7 (range: 45.0 -
73.0)
(22) 100% and faecal
incontinence
Pucciani et al.,
2008
98
Incontinent patients
(88) 89.8%
Healthy control
(10) 10.2%
Patients: 34/54
Healthy
control: 4/6
Patients: 59.6 ± 6.8*
(range: 46.0 - 73.0)
Healthy control: 57.4
± 6.3* (range: 44.0 -
69.0)
Low anterior rectal
resection (69) 78.4%
Straight coloanal
anastomosis (19)
21.5%
Pre-op RT
(19) 21.6%
Post-op RT
(34) 38.6%
Incontinence
Retrospective
studies
Bartlett et al.,
2011
19 10/9 64.1 (95% CI: 47.0 -
81.3)
Anterior resection
(3) 15.8%
Ultra-low anterior
resection (10) 52.6%
Segmental
colectomy (2)
10.5%
Proctocolectomy (4)
21.1%
NR Bowel
dysfunction
Kim et al., 2011 70 49/21 58.1 ± 10.1 (range:
31.0 - 79.0)
Sphincter-saving
surgery with TME
(70) 100%
Pre-op RT
(30) 42.9%
Post-op RT
(19) 27.1%
Pre-op CT (1)
1.4%
Post-op CT
(25) 35.7%
Pre-op plus
post-op CT
(31) 44.3%
Anterior
resection
syndrome
Abbreviations: M, male; F, female; post-op, postoperative; pre-op, preoperative; RT, radiotherapy; CT, chemotherapy; RCT, radiochemotherapy; TME, total
mesorectal excision; NR, not reported; CI, confidence interval.

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
208
* Value calculated (not reported in original study)

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
209
Intervention
The types, duration, and frequency of PFM training programs varied among all
studies (Table 8-3). One study used PFM training without biofeedback (Liu et al.,
2011). Six of eight studies provided PFM training with different types of biofeedback:
EMG biofeedback for strengthening (Allgayer et al., 2005); manometric pressure
biofeedback for coordination training (Bartlett et al., 2011; Ho et al., 1996; Ho & Tan,
1997; Laforest et al., 2012); and manometric biofeedback for coordination training,
sensory training, and strength training (Kim et al., 2011). One study used a
multimodal rehabilitative program including PFM training with manometric
biofeedback for strengthening (Pucciani et al., 2008). Length of intervention ranged
from three weeks to 20 months. The frequency of outpatient sessions ranged from
daily to once weekly, and that of home-based sessions ranged from 3-4 times daily to
once daily. In most studies, home practice was encouraged via a formal protocol
(Allgayer et al., 2005; Bartlett et al., 2011; Kim et al., 2011; Liu et al., 2011; Pucciani
et al., 2008) or with general encouragement (Ho et al., 1996; Ho & Tan, 1997).

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
210
Table 8-3: Intervention programs in reviewed studies
Author and year Intervention
program
Duration (min) Frequency (per
week)
Length Total number
of sessions
Home practice
(Y/N)
Prospective
non-randomized
trials
Allgayer et al.,
2005
Outpatient intensive
PFM training with
intra-anal EMG
biofeedback for
strengthening in
addition to routine
rehabilitation
program
(information,
psychological
support, and light
aerobic exercise)
30 - 40 (PFM
training)
Daily 3 weeks NR Y, PFM training
with biofeedback,
1-hour daily
Ho et al., 1996 Outpatient PFM
training using
manometric
pressure
biofeedback for
coordination
training
60 1 NR 4 Y, encouraged
Ho et al., 1997 Outpatient PFM
training using
manometric
pressure
biofeedback for
60 1 NR 4 Y, encouraged
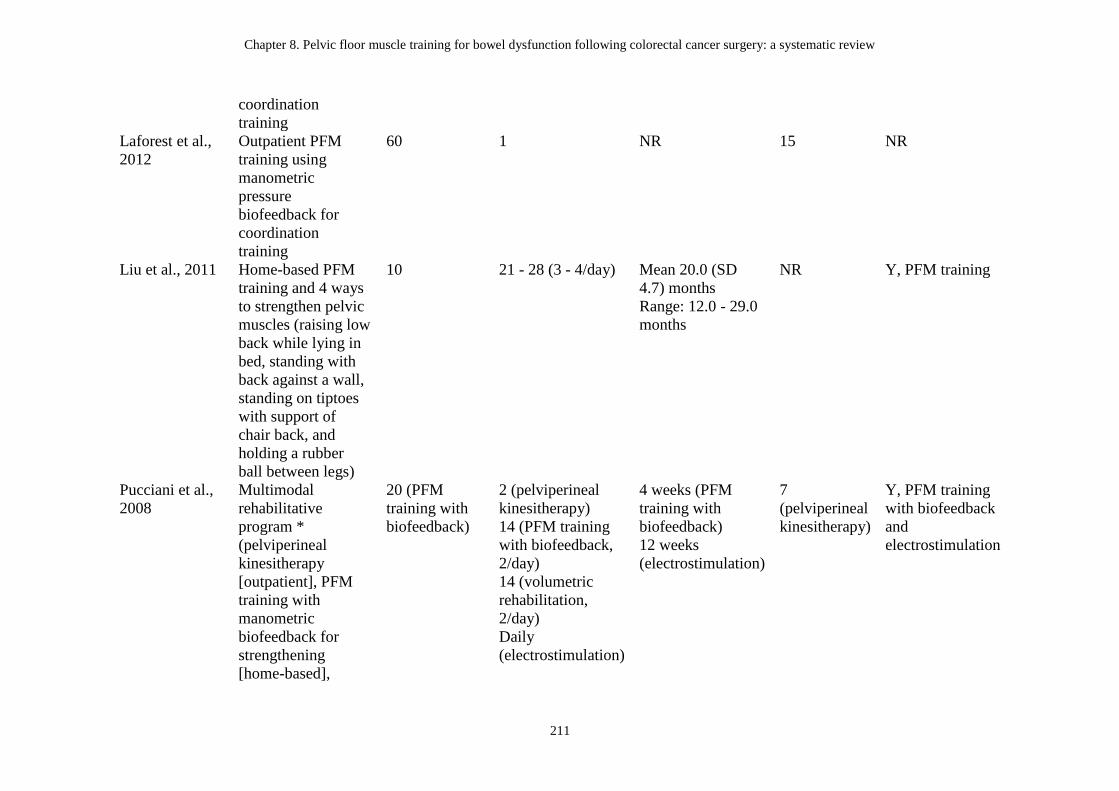
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
211
coordination
training
Laforest et al.,
2012
Outpatient PFM
training using
manometric
pressure
biofeedback for
coordination
training
60 1 NR 15 NR
Liu et al., 2011 Home-based PFM
training and 4 ways
to strengthen pelvic
muscles (raising low
back while lying in
bed, standing with
back against a wall,
standing on tiptoes
with support of
chair back, and
holding a rubber
ball between legs)
10 21 - 28 (3 - 4/day) Mean 20.0 (SD
4.7) months
Range: 12.0 - 29.0
months
NR Y, PFM training
Pucciani et al.,
2008
Multimodal
rehabilitative
program *
(pelviperineal
kinesitherapy
[outpatient], PFM
training with
manometric
biofeedback for
strengthening
[home-based],
20 (PFM
training with
biofeedback)
2 (pelviperineal
kinesitherapy)
14 (PFM training
with biofeedback,
2/day)
14 (volumetric
rehabilitation,
2/day)
Daily
(electrostimulation)
4 weeks (PFM
training with
biofeedback)
12 weeks
(electrostimulation)
7
(pelviperineal
kinesitherapy)
Y, PFM training
with biofeedback
and
electrostimulation
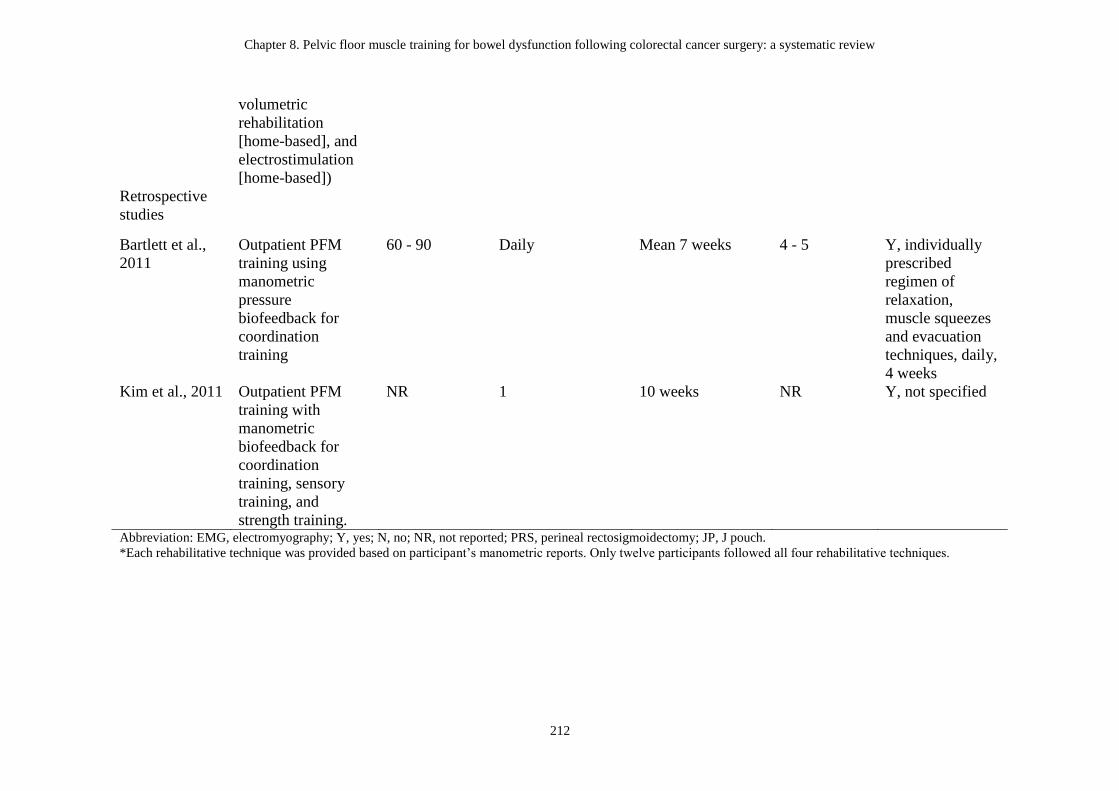
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
212
volumetric
rehabilitation
[home-based], and
electrostimulation
[home-based])
Retrospective
studies
Bartlett et al.,
2011
Outpatient PFM
training using
manometric
pressure
biofeedback for
coordination
training
60 - 90 Daily Mean 7 weeks 4 - 5 Y, individually
prescribed
regimen of
relaxation,
muscle squeezes
and evacuation
techniques, daily,
4 weeks
Kim et al., 2011 Outpatient PFM
training with
manometric
biofeedback for
coordination
training, sensory
training, and
strength training.
NR 1 10 weeks NR Y, not specified
Abbreviation: EMG, electromyography; Y, yes; N, no; NR, not reported; PRS, perineal rectosigmoidectomy; JP, J pouch.
*Each rehabilitative technique was provided based on participant’s manometric reports. Only twelve participants followed all four rehabilitative techniques.

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
213
Outcome measures
All included studies evaluated patient-reported measures of bowel function in terms
of stool frequency, incontinence episodes, and severity of faecal incontinence. Seven
of eight studies assessed stool frequency using a bowel diary Ho et al., 1996; Ho &
Tan, 1997), patient report (Kim et al., 2011; Liu et al., 2011; Pucciani et al., 2008), or
gastrointestinal questionnaires (Laforest et al., 2012). Three studies used a bowel
diary (Bartlett et al., 2011; Ho et al., 1996; Ho & Tan, 1997) to assess number of
incontinence episodes. Five studies included severity of faecal incontinence as a
patient-reported outcome (Allgayer et al., 2005; Bartlett et al., 2011; Kim et al., 2011;
Laforest et al., 2012; Pucciani et al., 2008). However, different faecal incontinence
severity scales including Modified Cleveland Incontinence Score (MCIS) (Allgayer et
al., 2005) and Wexner Incontinence Scale (WIS) (Bartlett et al., 2011; Kim et al.,
2011; Laforest et al., 2012; Pucciani et al., 2008) were used. In addition to the
patient-reported measures of bowel function, six studies used anorectal manometry to
measure anorectal physiological function (Allgayer et al., 2005; Bartlett et al., 2011;
Ho et al., 1996; Ho & Tan, 1997; Kim et al., 2011; Pucciani et al., 2008). Three
studies examined HRQoL after CRC surgery (Bartlett et al., 2011; Laforest et al.,
2012; Liu et al., 2011). The HRQoL was measured by the Functional Assessment of
Cancer Therapy – Colorectal (FACT-C) questionnaire (studies n = 1) (Liu et al.,
2011), Short Form 36 questionnaire (SF-36) (studies n = 1) (Laforest et al., 2012), and
Rockwood Faecal Incontinence Quality of Life Scale (FIQL) (studies n = 2) (Bartlett
et al., 2011; Laforest et al., 2012).
Risk of bias and Level of Evidence
Risk of bias of studies is presented in Table 8-1. The agreement using kappa statistics
between the two independent reviewers on risk of bias assessed using the NOS was
0.972 (percentage agreement, 98.6%). Minor disagreements were resolved with
consensus on 100% of occasions, and on all occasions, scores between reviewers
deviated by only one point. The results of risk of bias assessment showed a mean total
score of 4.9 (SD 1.2, range 3 to 7). Although most criteria within participant selection
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
214
and outcome measure categories were satisfied, the majority of studies were limited
by lack of a non-exposed cohort, lack of independent blinded assessment, and/or
inadequate longer-term follow-up (Allgayer et al., 2005; Bartlett et al., 2011; Ho et al.,
1996; Ho & Tan, 1997; Kim et al., 2011; Laforest et al., 2012; Liu et al., 2011;
Pucciani et al., 2008). Five studies also scored 0 points (out of possible two points) in
the category of comparability of study group (Bartlett et al., 2011; Ho et al., 1996;
Kim et al., 2011; Liu et al., 2011; Pucciani et al., 2008). At best, the level of evidence
was III-2 (range III-2 to IV) (Table 8-1).
8.4.3 Effects of pelvic floor muscle training in patients following colorectal cancer
surgery
Outcomes
Patient-reported outcomes measures
Study results on patient-reported measures of bowel function are presented in Table
8-4. Six studies showed improvement in stool frequency after intervention (Bartlett et
al., 2011; Ho et al., 1996; Ho & Tan, 1997; Kim et al., 2011; Laforest et al., 2012;
Pucciani et al., 2008), and four were statistically significant (p < 0.05) (Bartlett et al.,
2011; Ho et al., 1996; Kim et al., 2011; Laforest et al., 2012). Liu et al. reported no
significant differences in stool frequency between intervention and control groups
after home-based PFM training (Liu et al., 2011). Only one study reported the
long-term follow-up results of stool frequency, which increased at two years after the
final treatment session (Bartlett et al., 2011). Of the three studies that assessed
incontinence episodes, two showed a significant decrease in incontinence episodes (p
< 0.05) after PFM training using manometric biofeedback (Ho et al., 1996; Ho & Tan,
1997). Bartlett et al. reported no significant difference in incontinence episodes after
PFM training using manometric pressure biofeedback (Bartlett et al., 2011).
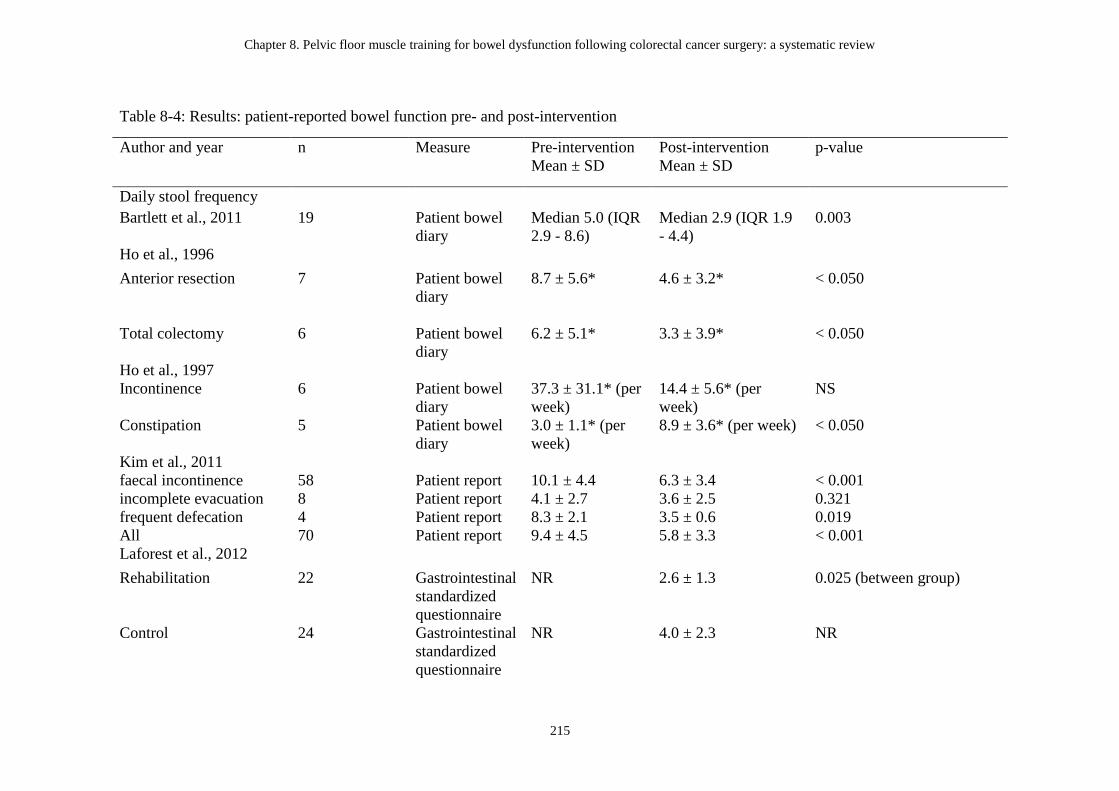
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
215
Table 8-4: Results: patient-reported bowel function pre- and post-intervention
Author and year n Measure Pre-intervention
Mean ± SD
Post-intervention
Mean ± SD
p-value
Daily stool frequency
Bartlett et al., 2011 19 Patient bowel
diary
Median 5.0 (IQR
2.9 - 8.6)
Median 2.9 (IQR 1.9
- 4.4)
0.003
Ho et al., 1996
Anterior resection 7 Patient bowel
diary
8.7 ± 5.6* 4.6 ± 3.2* < 0.050
Total colectomy 6 Patient bowel
diary
6.2 ± 5.1* 3.3 ± 3.9* < 0.050
Ho et al., 1997
Incontinence 6 Patient bowel
diary
37.3 ± 31.1* (per
week)
14.4 ± 5.6* (per
week)
NS
Constipation 5 Patient bowel
diary
3.0 ± 1.1* (per
week)
8.9 ± 3.6* (per week) < 0.050
Kim et al., 2011
faecal incontinence 58 Patient report 10.1 ± 4.4 6.3 ± 3.4 < 0.001
incomplete evacuation 8 Patient report 4.1 ± 2.7 3.6 ± 2.5 0.321
frequent defecation 4 Patient report 8.3 ± 2.1 3.5 ± 0.6 0.019
All 70 Patient report 9.4 ± 4.5 5.8 ± 3.3 < 0.001
Laforest et al., 2012
Rehabilitation 22 Gastrointestinal
standardized
questionnaire
NR 2.6 ± 1.3 0.025 (between group)
Control 24 Gastrointestinal
standardized
questionnaire
NR 4.0 ± 2.3 NR
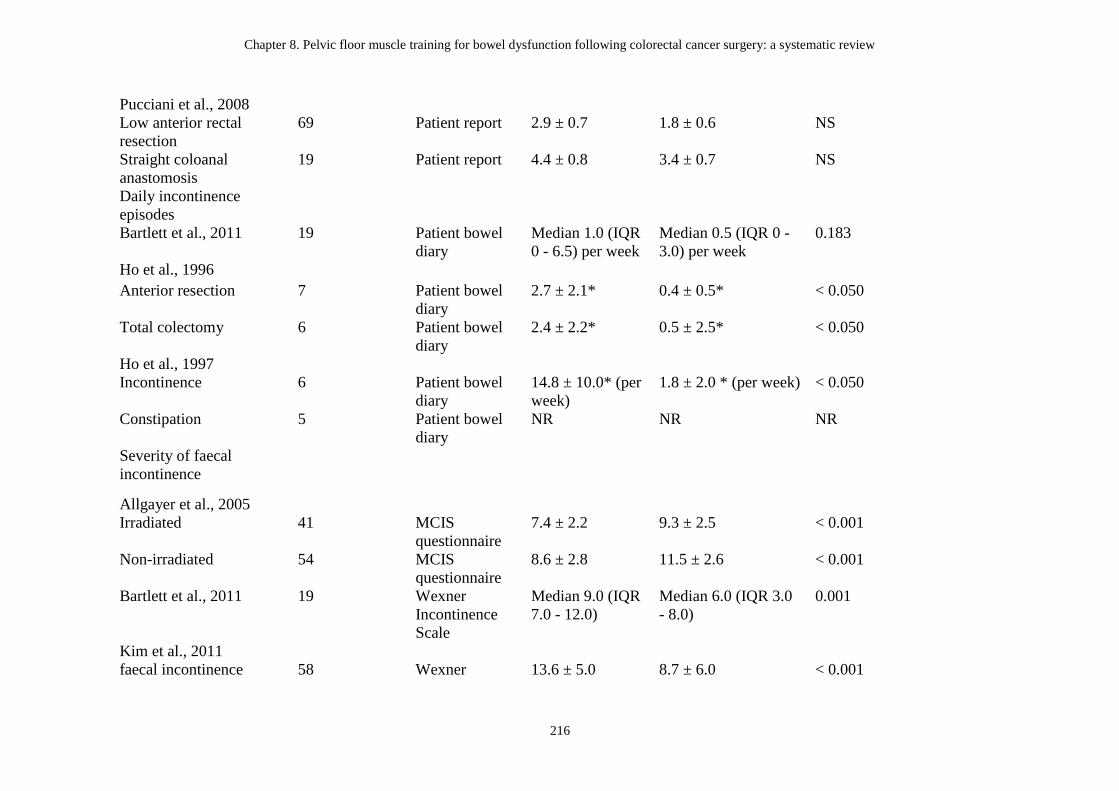
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
216
Pucciani et al., 2008
Low anterior rectal
resection
69 Patient report 2.9 ± 0.7 1.8 ± 0.6 NS
Straight coloanal
anastomosis
19 Patient report 4.4 ± 0.8 3.4 ± 0.7 NS
Daily incontinence
episodes
Bartlett et al., 2011 19 Patient bowel
diary
Median 1.0 (IQR
0 - 6.5) per week
Median 0.5 (IQR 0 -
3.0) per week
0.183
Ho et al., 1996
Anterior resection 7 Patient bowel
diary
2.7 ± 2.1* 0.4 ± 0.5* < 0.050
Total colectomy 6 Patient bowel
diary
2.4 ± 2.2* 0.5 ± 2.5* < 0.050
Ho et al., 1997
Incontinence 6 Patient bowel
diary
14.8 ± 10.0* (per
week)
1.8 ± 2.0 * (per week) < 0.050
Constipation 5 Patient bowel
diary
NR NR NR
Severity of faecal
incontinence
Allgayer et al., 2005
Irradiated 41 MCIS
questionnaire
7.4 ± 2.2 9.3 ± 2.5 < 0.001
Non-irradiated 54 MCIS
questionnaire
8.6 ± 2.8 11.5 ± 2.6 < 0.001
Bartlett et al., 2011 19 Wexner
Incontinence
Scale
Median 9.0 (IQR
7.0 - 12.0)
Median 6.0 (IQR 3.0
- 8.0)
0.001
Kim et al., 2011
faecal incontinence 58 Wexner 13.6 ± 5.0 8.7 ± 6.0 < 0.001
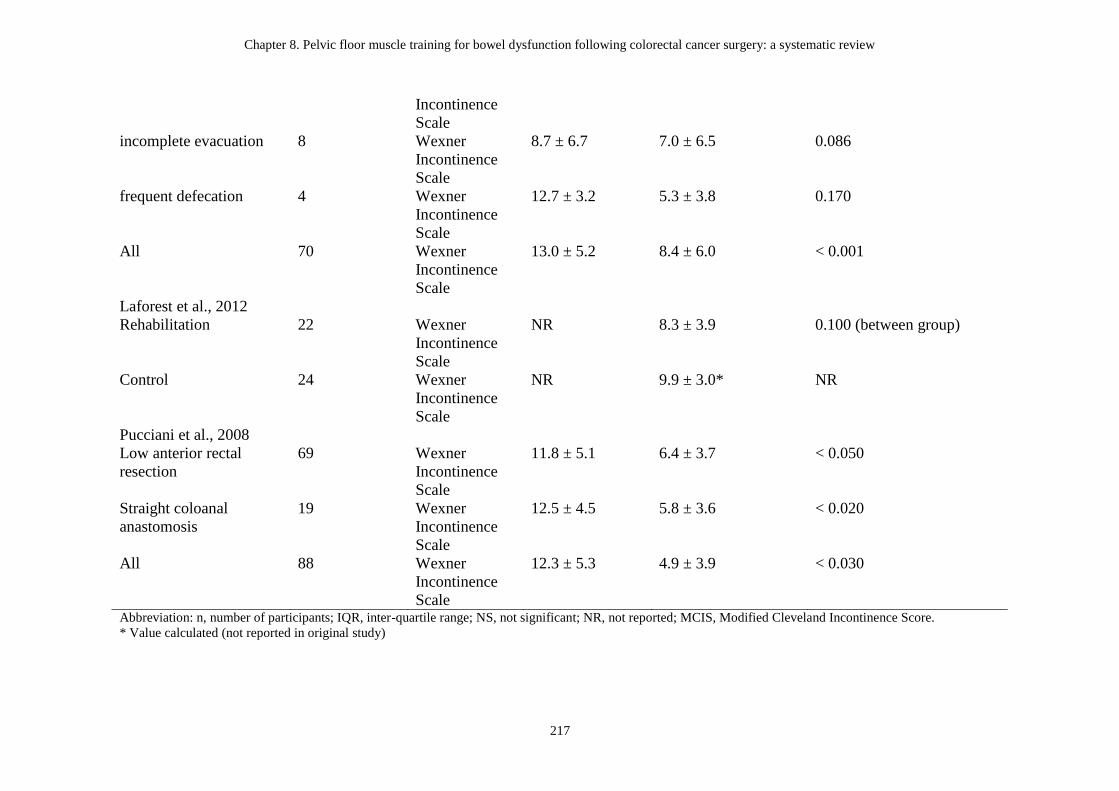
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review
217
Incontinence
Scale
incomplete evacuation 8 Wexner
Incontinence
Scale
8.7 ± 6.7 7.0 ± 6.5 0.086
frequent defecation 4 Wexner
Incontinence
Scale
12.7 ± 3.2 5.3 ± 3.8 0.170
All 70 Wexner
Incontinence
Scale
13.0 ± 5.2 8.4 ± 6.0 < 0.001
Laforest et al., 2012
Rehabilitation 22 Wexner
Incontinence
Scale
NR 8.3 ± 3.9 0.100 (between group)
Control 24 Wexner
Incontinence
Scale
NR 9.9 ± 3.0* NR
Pucciani et al., 2008
Low anterior rectal
resection
69 Wexner
Incontinence
Scale
11.8 ± 5.1 6.4 ± 3.7 < 0.050
Straight coloanal
anastomosis
19 Wexner
Incontinence
Scale
12.5 ± 4.5 5.8 ± 3.6 < 0.020
All 88 Wexner
Incontinence
Scale
12.3 ± 5.3 4.9 ± 3.9 < 0.030
Abbreviation: n, number of participants; IQR, inter-quartile range; NS, not significant; NR, not reported; MCIS, Modified Cleveland Incontinence Score.
* Value calculated (not reported in original study)
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
218
Five studies used MCIS or WIS to measure severity of faecal incontinence (Allgayer
et al., 2005; Bartlett et al., 2011; Kim et al., 2011; Laforest et al., 2012; Pucciani et al.,
2008). A higher score on MCIS indicates better continence; whereas a higher WIS
score indicates worse continence. In the study by Allgayer et al., the MCIS
significantly increased (p < 0.001) indicating improved incontinence in 95
participants after a 3-week intensive PFM training (Allgayer et al., 2005). The results
of studies using WIS also showed a significant improvement in severity of faecal
incontinence after intervention (p < 0.05) (Bartlett et al., 2011; Kim et al., 2011;
Pucciani et al., 2008), except for Laforest et al., who reported no significant difference
in WIS score between intervention and control groups (Laforest et al., 2012). Two
studies demonstrated conflicting long-term follow-up results of severity of faecal
incontinence (Allgayer et al., 2005; Bartlett et al., 2011). One study reported
maintenance of effects of PFM training with intra-anal EMG biofeedback after 1 year
(Allgayer et al., 2005), and the other study reported increased severity at 2 years
following last treatment session of PFM training using manometric biofeedback,
although the severity remained better than at baseline (Bartlett et al., 2011).
Manometric measures
Six studies used anorectal manometry to measure anorectal physiological function
(Allgayer et al., 2005; Bartlett et al., 2011; Ho et al., 1996; Ho & Tan, 1997; Kim et
al., 2011; Pucciani et al., 2008). The majority reported no significant differences in
mean resting pressure (Allgayer et al., 2005; Bartlett et al., 2011; Ho et al., 1996; Ho
& Tan, 1997; Pucciani et al., 2008), maximum squeeze pressure (Allgayer et al., 2005;
Bartlett et al., 2011; Ho et al., 1996; Ho & Tan, 1997; Pucciani et al., 2008), maximal
tolerable volume (Bartlett et al., 2011; Ho et al., 1996; Ho & Tan, 1997; Pucciani et
al., 2008), volume at initial sensation (Allgayer et al., 2005; Bartlett et al., 2011; Ho et
al., 1996; Ho & Tan, 1997; Pucciani et al., 2008), physiological length (Allgayer et al.,
2005; Ho et al., 1996; Ho & Tan, 1997), and compliance (Ho et al., 1996; Ho & Tan,
1997) in patients after intervention. Only one study by Kim et al. showed significant
differences in mean resting pressure (p = 0.01), maximum squeeze pressure (p =
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
219
0.006), and maximum tolerable volume (p = 0.003) in patients with anterior resection
after PFM training with manometric biofeedback (Kim et al., 2011).
Health-related quality of life (HRQoL)
Three studies examined HRQoL after CRC surgery (Bartlett et al., 2011; Laforest et
al., 2012; Liu et al., 2011). Two studies demonstrated significant improvement in
some domains of HRQoL (Bartlett et al., 2011; Laforest et al., 2012), and one found a
significant difference in total score of HRQoL (p = 0.038) measured using FACT-C
after intervention (Liu et al., 2011). Although not statistically significant, Bartlett et al.
reported further improvement in FIQL scores from the final session at two-year
follow-up.
8.5 Discussion
The aim of our review was to systematically evaluate the evidence for the effect of
PFM training on bowel dysfunction in patients who have undergone CRC surgery. No
RCTs were identified in this review, which reflects the urgent need for RCTs in this
field to provide high levels of evidence to direct PFM training for patients suffering
from this highly distressing problem. Despite the paucity of RCTs and the inherent
methodological shortcomings of the included observational studies, this systematic
review found that PFM training may improve the patient-reported measures of bowel
function and the HRQoL of colon as well as rectal cancer patients following surgery.
The findings in this review are in line with a previous systematic review on treatment
options for improving anorectal function after rectal surgery for patients with or
without cancer (Maris et al., 2013). The previous review examined fifteen studies,
which included heterogeneous treatment options, such as pelvic floor re-education
(seven out of fifteen studies), colonic irrigation, and sacral nerve stimulation.
Although the review reported beneficial effects of conservative therapies on anorectal
function after rectal resection, the papers reviewed were of limited methodological
quality with heterogeneous patient populations, such as patients with rectal cancer,
cervical cancer, and undefined pathology (Maris et al., 2013).

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
220
The findings of our systematic review on specific bowel cancer populations are
consistent with the 5th ICI, which recommends PFM training as an early intervention
in the treatment of faecal incontinence in general adult populations (Bliss et al., 2013).
The results of the present study demonstrate a modest reduction in stool frequency
and incontinence episodes measured by patient bowel diary or patient report after
PFM training. However, most studies that showed significant effects were
underpowered with small numbers of participants or used a retrospective study design;
hence, it is possible that the positive effects of PFM training on patient-reported
measure of bowel function are the results of natural recovery or the Hawthorne effect
(McCarney et al., 2007). Furthermore, the effectiveness of PFM training for the
severity of incontinence in CRC patients after surgery in this study was consistent
with the result of the systematic review conducted by Maris et al. (Maris et al., 2013);
however, our study found that PFM training may be beneficial to certain patient
populations - CRC patients. Only two studies included in our review had evaluated
whether the improvements in the patient-reported measures of bowel function were
maintained over time, and the results were conflicting. Randomized controlled trials
with longitudinal follow-ups are urgently needed to investigate if the long-term
effects of PFM training for patients after CRC surgery are maintained.
In contrast to the beneficial effects of PFM training on the patient-reported measures
of bowel function, all studies except one retrospective study reported no significant
changes in manometric measures following interventions (Allgayer et al., 2005;
Bartlett et al., 2011; Ho et al., 1996; Ho & Tan, 1997; Pucciani et al., 2008). The
inconsistent findings between patient-reported measures and objective manometric
measures of bowel function were consistent with previous studies, which
demonstrated no correlation between anorectal manometry and severity of faecal
incontinence (Lam, Mulder, & Felt-Bersma, 2012; Zutshi, Salcedo, Hammel, & Hull,
2010) or patients’ perception of relief (Deutekom et al., 2005). This may be due to the
multifactorial aetiology of bowel dysfunction or insufficient intensity of PFM training
to achieve a physiological effect. Further mechanistic studies are required to explain
the relationship between changes in symptoms and physiologic measures.

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
221
The findings on HRQoL after PFM training in our review were consistent with
previous studies (Bols et al., 2012; Heymen et al., 2009). As bowel dysfunction may
be the factor that most disturbs patients and impacts their HRQoL after CRC surgery
(Vironen et al., 2006), future studies aimed at investigating the effects of PFM
training on bowel dysfunction in patients with CRC should include HRQoL outcome
measures.
The majority of studies in this review provided PFM training with biofeedback
(Allgayer et al., 2005; Bartlett et al., 2011; Ho et al., 1996; Ho & Tan, 1997; Kim et
al., 2011; Laforest et al., 2012; Pucciani et al., 2008). Only one study focused on PFM
training alone (Liu et al., 2011). Although PFM training is recommended as a
treatment for patients with faecal incontinence (Bliss et al., 2013), a Cochrane review
reported that addition of biofeedback to PFM training may enhance the outcome of
treatment compared to PFM training alone in patients with faecal incontinence after
other conservative managements has failed (Norton & Cody, 2012). Due to limited
number of identified trials in this review, there is not enough evidence to comment on
the effect of PFM training alone and to suggest which modality of biofeedback is
optimal for bowel dysfunction after CRC surgery.
As a dose-response relationship exists in all forms of exercise training, the outcomes
of PFM training may be affected by the duration of treatment and the frequency of
supervision by the therapist (Bø et al., 1990; Bø, 2004a). It is possible that the positive
treatment effects of PFM training on patient-reported measures of bowel function in
this review may be due to the adequate treatment dosage. However, as no significant
changes were found in manometric measures after PFM training, an effective training
dosage for physiological parameters of anorectal function needs to be determined in
future studies. Although home practice was encouraged in most studies (Allgayer et
al., 2005; Bartlett et al., 2011; Ho et al., 1996; Ho & Tan, 1997; Kim et al., 2011;
Pucciani et al., 2008), the content and treatment dosage (frequency and duration) of
the home program were only specified in four studies (Allgayer et al., 2005; Bartlett
et al., 2011; Liu et al., 2011; Pucciani et al., 2008). The adherence to training sessions
and adverse events were not reported by any of the studies included in this review.

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
222
Randomized controlled trials are needed to develop and to investigate the optimal
training regimens and home practice for bowel dysfunction in patient who have
undergone CRC surgery.
Our systematic review adds to a previous systematic review (Maris et al., 2013) in
several ways: the inclusion of two additional studies published in 2011 (Bartlett et al.,
2011; Liu et al., 2011), the inclusion of colon as well as rectal cancer populations, and
a focus on PFM training as the primary intervention. In contrast to the prior review,
we excluded case studies due to the high potential for bias in this study design and
studies which had less than 50% of participants with CRC in order to maintain the
homogeneity of the target population.
8.5.1 Study limitations
The primary limitation is that all studies included were non-randomized observational
studies with small numbers of participants and with the findings predominantly
presented as within-group comparisons. However, according to the ClincalTrials.gov
and the ANZCTR, there are three RCTs currently in progress examining the effect of
PFM training, with or without biofeedback, for patients with rectal cancer, which will
add to the evidence base in the future. This systematic review is further limited by the
moderate methodological quality of the studies and the inclusion of articles published
in English only, which may have led to selection bias. Further limitations include
heterogeneous PFM training interventions program with regards to types of PFM
training, frequency, intensity and duration and few evidence for the long-term effects
of PFM training on bowel dysfunction after CRC surgery.
8.6 Summary
The paucity and limited methodological quality of the evidence does not allow a
robust conclusion to be drawn in support of PFM training in the treatment of bowel
dysfunction of patients following colon or rectal cancer surgery. However, promising
findings from non-randomized studies, suggest that PFM training may be effective in
Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
223
improving the patient-reported measures of bowel function and the HRQoL of
patients who have undergone colon or rectal cancer surgery. This intervention can be
viewed as being in the ‘development phase’ of research (Bø & Herbert, 2013; Craig et
al., 2013). Accordingly, the results and the conclusion of this systematic review
should be read with caution due to the lack of RCTs; lack of studies with long-term
follow-up; and the heterogeneity of methodological quality and PFM training
protocols in included studies. Well-designed RCTs with long-term follow-up are
urgently required to provide guidance for clinicians caring for this population in
clinical practice.
8.7 Additional papers published since the systematic review was undertaken
An additional search was run on 17th June 2016 and only two papers were relevant
and retrieved. One is a systematic review, which was published after our systematic
review was accepted for publication. This systematic review by Visser et al. (Visser,
Te Riele, Boerma, van Ramshorst, & van Westreenen, 2014) evaluated the
effectiveness of pelvic floor rehabilitation in improving functional outcome after
sphincter-preserving surgery for rectal cancer and included five studies (Allgayer et
al., 2005; Kim et al., 2011; Laforest et al., 2012; Liu et al., 2011; Pucciani et al., 2008),
which were also included in our systematic review. Although Visser’s systematic
review was limited to patients with rectal cancer, the same conclusion was drawn
(PFM training may be useful in improving continence, stool frequency and HRQoL
for rectal cancer population) (Visser et al., 2014). Only one original article, which met
our inclusion criteria, has been published since our systematic review was published.
This original article is briefly summarised in next section.
8.7.1 Summary of additional study
Kuo and colleagues (Kuo et al., 2015) conducted a prospective observational study to
assess the efficacy and benefits of pelvic rehabilitation programs in terms of
functional outcomes and quality of life for 32 patients with faecal incontinence and
defecation disorders after sphincter saving surgery (a rectal cancer surgery). The

Chapter 8. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a
systematic review
224
pelvic rehabilitation programs, which included electrical stimulation and biofeedback,
were conducted in an outpatient hospital setting and performed 2 to 3 times per week
for 4-6 weeks of electrical stimulation and 4-6 weeks of biofeedback. The outpatient
PFM training using manometric pressure biofeedback for coordination training and
sensory training was conducted after completion of electrical stimulation sessions.
Participants with a mean age of 56.5 years (53% males; 78% received neoadjuvant
chemoradiotherapy) experienced significant improvements in maximum squeeze
pressure measured with anorectal manometry (p = 0.014), mean stool frequency per
24h (p < 0.001), use of antidiarrhoeal medications (p < 0.001), stool fragmentation (p
= 0.016), and Wexner Incontinence score (p < 0.001) from pre to post intervention.
Results of this additional study provides further support to the findings of our
systematic review published in 2015 which concluded that pelvic rehabilitation
programs which include electrical stimulation and biofeedback are effective in
improving bowel function and quality of life for patients undergoing sphincter-saving
rectal cancer resection. The additional search shows that the number of studies
investigating the role of PFM training in the management of bowel function following
CRC surgery is slowing emerging. Due to the lack of RCTs, significant gaps still
remain in the literature. Furthermore, the majority of studies to date do not include a
control group; hence, the findings on the improvement in bowel function and HRQoL
following PFM training intervention programs in CRC must be interpreted with
caution. Nevertheless, attention has been drawn to this emerging field of supportive
care in CRC as several RCTs are in progress, which should improve the strength of
evidence in the coming years. The next chapter will provide summary of findings,
strengths and limitations of research design, recommendations and future directions of
CRC research.
Chapter 9. Conclusion and future directions
225
Chapter 9. Conclusion and future directions
9.1 Overview of main findings
Patients with CRC often experience significant morbidity including distressing
symptoms (anxiety, depression, and bowel, bladder and sexual dysfunction), poor
functional exercise capacity, low levels of PA, and decreased HRQoL following
cancer treatment. The findings in this thesis have demonstrated that:
The APFQ is a valid measurement instrument for use in evaluating bladder
and bowel symptoms in the CRC population.
Age (older) and advanced cancer stage have the potential to predict the
severity of post-operative bladder symptoms in CRC.
The 6MWT and ISWT are valid measures of functional exercise capacity in
patients with CRC.
Patients with CRC experience worsening bowel symptoms, including
incontinence, from pre- to six months post-surgery. They also have low PA
levels both before and after surgery.
Implementation of a general oncology rehabilitation program incorporating the
international PA guidelines is feasible in CRC and associated with
improvements in bladder and bowel symptoms, depression and HRQoL.
Digital rectal examination is positively correlated with both anorectal pressure
manometry and transperineal ultrasound following oncology rehabilitation and
at 6-month follow-up.
Pelvic floor muscle training for patients following surgery for CRC is
associated with improvements in bowel function and HRQoL (level of
evidence III-2 to IV).
In Australia, current clinical pathways or service for patients with CRC do not involve
referral to an oncology rehabilitation program or specific PFM training intervention
following surgery despite the fact that patients have significant unmet needs related to
symptom control and low PA levels. The findings of this thesis support the need for
Chapter 9. Conclusion and future directions
226
routine general oncology rehabilitation programs and PFM training to be offered to
patients in attempt to improve their bladder and bowel symptoms, minimise
symptoms of depression, maximise HRQoL and promote increases in PA levels. The
findings of this thesis also support the use of the APFQ, 6MWT and ISWT as
measurement instruments for use in the CRC population in research and clinical
practice.
9.2 Strengths and limitations of the present research
The mains strengths of this thesis are (1) highlighting the important issue of uptake
and adherence to exercise guidelines within the CRC population; (2) providing novel
findings on the changes in bladder and bowel symptoms and PFM clinical outcomes
in patients following a general oncology rehabilitation program; (3) identifying
promising outcomes regarding patient benefit from PFM training; (4) confirming the
significant bowel symptoms and inactivity in Australian patients with CRC, which are
comparable with international data; and (5) providing new findings on the validity and
applicability of measurement instruments for functional exercise capacity and pelvic
floor symptoms in patients following CRC surgery.
The limitations of each study have been outlined in the corresponding thesis chapters.
The major limitation is the small sample size making it difficult to conduct subgroup
analyses and generalize results. The pilot or exploratory nature (not powered) of all
studies and the lack of a true control (comparison) group in Study 4 and Study 5 limit
the ability to draw definitive conclusions. However, with a high proportion of patients
with colon cancer included in our studies, our findings add valuable information to the
current literature as the majority of research in this field has focused on rectal cancer
only.
9.3 Future directions
Colorectal cancer is the third most prevalent cancer worldwide, with more than 3.5
millions of CRC survivors (Ferlay et al., 2013). The number of patients living in the
community with CRC or as survivors is steadily increasing. Minimising disease
Chapter 9. Conclusion and future directions
227
burden and maximizing patient function and HRQoL are of upmost important to this
large patient population.
As the number of CRC survivors continues to grow (Miller et al., 2016), survivorship
care including oncology rehabilitation for CRC has become a major area of interest
(Jorgensen, Young, & Solomon, 2015). According to the American Cancer Society
CRC survivorship care guidelines (El-Shami et al., 2015), the evidence (level I) is
strong for clinicians to recommend PA to their patients, and to refer on to specialists
for psychosocial support and or rehabilitation as needed. An important question
remains regarding the impact of exercise training on survival in CRC. There is a small
amount of evidence on the association between PA levels and CRC survival
(Meyerhardt et al., 2006; Heseltine et al., 2006), however the effects of a general
oncology rehabilitation program on survival remain unknown. Well-designed RCTs
with long-term follow-up are urgently required to provide guidance for clinicians
caring for CRC populations in clinical practice. A search of the clinical trial registry
databases (ClinicalTrials.gov and the Australian and New Zealand Clinical Trials
Registry) showed that several RCTs on exercise interventions for survival in patients
with CRC are currently in progress, which will add new evidence to this emerging
field of CRC oncology rehabilitation in the near future. If conclusions can be found,
such that participation in rehabilitation is associated with prolong life, this will change
current referral pathways.
In addition, further work is required to determine if there are specific subgroups
within the CRC population (i.e. low functional exercise capacity or PA levels or high
levels of comorbidity at baseline) who are more likely to respond to exercise
interventions and develop a risk classification system to determine who is at greatest
need (Dittus et al., 2015).
Despite the strong evidence for PA and reduced sedentary time, there is limited
evidence (level III) for optimal management of bowel problems in CRC (El-Shami et
al., 2015). Although our findings in Study 4 and Study 6 add to the evidence by
showing that an oncology rehabilitation program or PFM training with or without
biofeedback may be beneficial for bladder and bowel symptoms, Study 4 is a pilot
Chapter 9. Conclusion and future directions
228
non-randomized quasi-control study and Study 6 is a systematic review including
nonrandomized observational studies with small numbers of participants. There were
no RCTs identified in the systematic review reflecting a need for higher levels of
evidence in this field to direct general oncology rehabilitation or PFM training for
patients suffering from the highly distressing bowel problems following CRC surgery.
However, according to the ClincalTrials.gov and the ANZCTR, there are RCTs
currently in progress examining the effect of PFM training with or without
biofeedback for patients with CRC, which will provide valuable evidence regarding
the role of PFM training in CRC rehabilitation. If the efficacy of the PFM training is
established, best practice for CRC rehabilitation may be developed and the referral
pathways and clinical service delivery for this population may change.
Across the cancer care continuum (Taplin et al., 2012), there are three phases
post-cancer diagnosis (i.e. pretreatment, treatment, and survivorship/end of life)
(Courneya & Friedenreich, 2007). Cancer prehabilitation is part of the cancer care
continuum that occurs between cancer diagnosis and the beginning of primary
treatment and provides interventions to promote physical and psychological health
and to reduce the incidence and/or severity of future impairments (Silver, Baima, &
Mayer, 2013). Research is emerging to investigate the impact of prehabilitation on
functional recovery in patients undergoing CRC surgery (Bruns et al., 2016; Gillis et
al., 2014; Li et al., 2013). A systematic review by Bruns et al.(Bruns et al., 2016)
identified five studies with moderate methodological quality and showed that
prehabilitation can improve physical condition (walking distance and respiratory
endurance) in patients aged over 60 years undergoing CRC surgery. However, no
studies have included PFM training as a component of the prehabilitation program
(Bruns et al., 2016). Although there is emerging evidence (Kim et al., 2015; Kye, Kim,
Kim, Yoo, & Cho, 2016) for the role of PFM training with biofeedback during the
temporary stoma period on bowel function in patients with CRC following stomal
closure, the results are contradictory with one study showing no effect of PFM
training on preventing bowel dysfunction after temporary stoma reversal (Kye et al.,
2016) and one reporting improvements in bowel symptoms 12 months after ileostomy
closure (Kim et al., 2015). As bowel symptoms are common in patients following
Chapter 9. Conclusion and future directions
229
CRC treatment, future studies should focus on the prevention of deterioration in
bowel symptoms following CRC surgery and determine the optimal timing of the
PFM training.
As the majority of participants in Study 4 felt that the general oncology rehabilitation
program was beneficial, future RCTs should consider investigating the
implementation and translations of such rehabilitation program to other pelvic cancers
(i.e. urological and gynaecological cancers).
“Excellent to take me from loss to confidence in how to manage my body. Great
opportunity to share issues relating to cancer with others. Valuable information and a
good time frame to learn new habits.” (Participant A)
“The entire program is well run and extremely beneficial. It should be compulsory for
all cancer patients!! I am very pleased I did it and grateful for what it taught me. All
the presenters were highly qualified, patient and caring. Quietly motivating!”
(Participant B)
References
230
References
Aaronson, N. K., Ahmedzai, S., Bergman, B., Bullinger, M., Cull, A., Duez, N. J.,
Filiberti, A., Flechtner, H., Fleishman, S. B., de Haes, J. C., Kaasa, S., Klee,
M., Osoba, D., Razavi, D., Rofe, P.B., Schraub, S., Sneeuw, K., Sullivan, M.
& Takeda, F. (1993). The European Organization for Research and Treatment
of Cancer QLQ-C30: a quality-of-life instrument for use in international
clinical trials in oncology. J Natl Cancer Inst, 85(5), 365-376.
Abrams, P., Andersson, K. E., Birder, L., Brubaker, L., Cardozo, L., Chapple, C.,
Cottenden, A., Davila, W., de Ridder, D., Dmochowski, R., Drake, M.,
Dubeau, C., Fry, C., Hanno, P., Smith, J. H., Herschorn, S., Hosker, G.,
Kelleher, C., Koelbl, H., Khoury, S., Madoff, R., Milsom, I., Moore, K.,
Newman, D., Nitti, V., Norton, C., Nygaard, I., Payne, C., Smith, A., Staskin,
D., Tekgul, S., Thuroff, J., Tubaro, A., Vodusek, D., Wein, A., Wyndaele, J. J.,
Members of Committees & Fourth International Consultation on Incontinence.
(2010). Fourth International Consultation on Incontinence Recommendations
of the International Scientific Committee: Evaluation and treatment of urinary
incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol
Urodyn, 29(1), 213-240.
Abrams, P., Avery, K., Gardener, N. & Donovan, J. (2006). The International
Consultation on Incontinence Modular Questionnaire: www.iciq.net. J Urol,
175(3 Pt 1), 1063-1066; discussion 1066.
Adams, R. N., Mosher, C. E., Blair, C. K., Snyder, D. C., Sloane, R. &
Demark-Wahnefried, W. (2015). Cancer survivors' uptake and adherence in
diet and exercise intervention trials: an integrative data analysis. Cancer,
121(1), 77-83.
Ahn, K. Y., Lee, M. K., Kim, D. I., Park, J., Min, J., In Yang, H., Lee, J., Oh, M., An,
J., Lee, J. W., Chu, S. H., Meyerhardt, J. A., Kim, N. K. & Jeon, J. Y. (2016).
Cardiopulmonary fitness, adiponectin, chemerin associated fasting insulin
level in colorectal cancer patients. Support Care Cancer, 24(7), 2927-2935.
AIHW. & AACR. (2012). Cancer in Australia: an overview 2012. Canberra: AIHW.

References
231
Albrich, S., Steetskamp, J., Knoechel, S. L., Porta, S., Hoffmann, G. & Skala, C.
(2015). Assessment of pelvic floor muscle contractility: digital palpation
versus 2D and 3D perineal ultrasound. Arch Gynecol Obstet, 293(4), 839-843.
Albuquerque, A. & Pereira, E. (2016). Current applications of transperineal
ultrasound in gastroenterology. World J Radiol, 8(4), 370-377.
Allgayer, H., Dietrich, C. F., Rohde, W., Koch, G. F. & Tuschhoff, T. (2005).
Prospective comparison of short- and long-term effects of pelvic floor
exercise/biofeedback training in patients with fecal incontinence after surgery
plus irradiation versus surgery alone for colorectal cancer: clinical, functional
and endoscopic/endosonographic findings. Scand J Gastroenterol, 40(10),
1168-1175.
Altenburg, W. A., de Greef, M. H., ten Hacken, N. H. & Wempe, J. B. (2012). A
better response in exercise capacity after pulmonary rehabilitation in more
severe COPD patients. Respir Med, 106(5), 694-700.
American Cancer Society (2014). Colorectal Cancer. Retrieved from
http://www.cancer.org/acs/groups/cid/documents/webcontent/003096-pdf.pdf.
Ananda, S., Kosmider, S., Tran, B., Field, K., Jones, I., Skinner, I., Guerrieri, M.,
Chapman, M. & Gibbs, P. (2016). The rapidly escalating cost of treating
colorectal cancer in Australia. Asia Pac J Clin Oncol, 12(1), 33-40.
Anderson, L., Oldridge, N., Thompson, D. R., Zwisler, A. D., Rees, K., Martin, N. &
Taylor, R. S. (2016). Exercise-Based Cardiac Rehabilitation for Coronary
Heart Disease: Cochrane Systematic Review and Meta-Analysis. J Am Coll
Cardiol, 67(1), 1-12.
Ando, M., Ando, Y., Hasegawa, Y., Shimokata, K., Minami, H., Wakai, K., Ohno, Y.
& Sakai, S. (2001). Prognostic value of performance status assessed by
patients themselves, nurses, and oncologists in advanced non-small cell lung
cancer. Br J Cancer, 85(11), 1634-1639.
Angenete, E., Asplund, D., Andersson, J. & Haglind, E. (2014). Self reported
experience of sexual function and quality after abdominoperineal excision in a
prospective cohort. Int J Surg, 12(11), 1221-1227.
Aoyagi, Y., Park, H., Watanabe, E., Park, S. & Shephard, R. J. (2009). Habitual
physical activity and physical fitness in older Japanese adults: the Nakanojo
Study. Gerontology, 55(5), 523-531.
References
232
Aparicio-Ugarriza, R., Mielgo-Ayuso, J., Benito, P. J., Pedrero-Chamizo, R., Ara, I.
& Gonzalez-Gross, M. (2015). Physical activity assessment in the general
population; instrumental methods and new technologies. Nutr Hosp, 31 Suppl
3, 219-226.
Aparo, S. & Goel, S. (2012). Evolvement of the treatment paradigm for metastatic
colon cancer. From chemotherapy to targeted therapy. Crit Rev Oncol
Hematol, 83(1), 47-58.
Appleton, L., Goodlad, S., Irvine, F., Poole, H. & Wall, C. (2013). Patients'
experiences of living beyond colorectal cancer: a qualitative study. Eur J
Oncol Nurs, 17(5), 610-617.
Aprile, G., Rihawi, K., De Carlo, E. & Sonis, S. T. (2015). Treatment-related
gastrointestinal toxicities and advanced colorectal or pancreatic cancer: A
critical update. World J Gastroenterol, 21(41), 11793-11803.
Aran, V., Victorino, A. P., Thuler, L. C. & Ferreira, C. G. (2016). Colorectal Cancer:
Epidemiology, Disease Mechanisms and Interventions to Reduce Onset and
Mortality. Clin Colorectal Cancer, 15(3), 195-203.
Arnold, M., Sierra, M. S., Laversanne, M., Soerjomataram, I., Jemal, A. & Bray, F.
(2016). Global patterns and trends in colorectal cancer incidence and mortality.
Gut. Advance online publication. doi: 10.1136/gutjnl-2015-310912.
Atkinson, T. M., Andreotti, C. F., Roberts, K. E., Saracino, R. M., Hernandez, M. &
Basch, E. (2015). The level of association between functional performance
status measures and patient-reported outcomes in cancer patients: a systematic
review. Support Care Cancer, 23(12), 3645-3652.
ATS & ACCP (2003). ATS/ACCP statement on cardiopulmonary exercise testing.
Am J Respir Crit Care Med, 167(2), 211-277.
ATS Committee on Proficiency Standards for Clinical Pulmonary Function
Laboratories (2002). ATS statement: guidelines for the six-minute walk test.
Am J Respir Crit Care Med, 166(1), 111-117.
Aune, D., Chan, D. S., Lau, R., Vieira, R., Greenwood, D. C., Kampman, E. & Norat,
T. (2011). Dietary fibre, whole grains, and risk of colorectal cancer:
systematic review and dose-response meta-analysis of prospective studies.
BMJ, 343, d6617.
Australian Cancer Network Colorectal Cancer Guidelines Revision Committee (2005).
Guidelines for the Prevention, Early Detection and Management of Colorectal
References
233
Cancer. Sydney: The Cancer Council Australia and Australian Cancer
Network Colorectal Cancer.
Australian Institute of Health and Welfare (2012). Cancer survival and prevalence in
Australia: period estimates from 1982 to 2010. Canberra: AIHW.
Australian Institute of Health and Welfare (2013). Health system expenditure on
cancer and other neoplasms in Australia: 2008–09. Canberra: AIHW.
Australian Institute of Health and Welfare (2014). Cancer in Australia: an overview
2014. Canberra: AIHW.
Australian Institute of Health and Welfare (2015a). Australian Cancer Incidence and
Mortality (ACIM) books: Colon cancer. Retrieved from
http://www.aihw.gov.au/acim-books/
Australian Institute of Health and Welfare (2015b). Australian Cancer Incidence and
Mortality (ACIM) books: Rectal cancer. Retrieved from
http://www.aihw.gov.au/acim-books/
Australian Institute of Health and Welfare (2016a). Australian Burden of Disease
Study: Impact and causes of illness and death in Australia 2011. Australian
Burden of Disease Study series no. 3. BOD 4. Retrieved from
http://www.aihw.gov.au/publication-detail/?id=60129555173.
Australian Institute of Health and Welfare (2016b). Australian Cancer Incidence and
Mortality (ACIM) book for colorectal cancer (also called bowel cancer).
Retrieved from http://www.aihw.gov.au/acim-books.
Australian Institute of Health and Welfare & Australian Government Department of
Health (2016). Analysis of colorectal cancer outcomes for the Australian
National Bowel Cancer Screening Program. Asia Pac J Clin Oncol, 12(1),
22-32.
Australian Institute of Health Welfare (2015). Cancer in Australia 2014: actual
incidence data from 1982 to 2011 and mortality data from 1982 to 2012 with
projections to 2014. Asia Pac J Clin Oncol, 11(3), 208-220.
Avery, K., Donovan, J., Peters, T. J., Shaw, C., Gotoh, M. & Abrams, P. (2004). ICIQ:
a brief and robust measure for evaluating the symptoms and impact of urinary
incontinence. Neurourol Urodyn, 23(4), 322-330.
Avery, K. N., Bosch, J. L., Gotoh, M., Naughton, M., Jackson, S., Radley, S. C.,
Valiquette, L., Batista, J. & Donovan, J. L. (2007). Questionnaires to assess
References
234
urinary and anal incontinence: review and recommendations. J Urol, 177(1),
39-49.
Averyt, J. C. & Nishimoto, P. W. (2014). Addressing sexual dysfunction in colorectal
cancer survivorship care. J Gastrointest Oncol, 5(5), 388-394.
Azevedo, L. F., Perlingeiro, P. S., Brum, P. C., Braga, A. M., Negrao, C. E. & de
Matos, L. D. (2011). Exercise intensity optimization for men with high
cardiorespiratory fitness. J Sports Sci, 29(6), 555-561.
Baena, R. & Salinas, P. (2015). Diet and colorectal cancer. Maturitas, 80(3), 258-264.
Baessler, K., O'Neill, S. M., Maher, C. F. & Battistutta, D. (2008). An
interviewer-administered validated female pelvic floor questionnaire for
community-based research. Menopause, 15(5), 973-977.
Baessler, K., O'Neill, S. M., Maher, C. F. & Battistutta, D. (2009). Australian pelvic
floor questionnaire: a validated interviewer-administered pelvic floor
questionnaire for routine clinic and research. Int Urogynecol J Pelvic Floor
Dysfunct, 20(2), 149-158.
Baessler, K., O'Neill, S. M., Maher, C. F. & Battistutta, D. (2010). A validated
self-administered female pelvic floor questionnaire. Int Urogynecol J, 21(2),
163-172.
Bailey, C. E., Cao, H. S. T., Hu, C. Y., Chang, G. J., Feig, B. W., Rodriguez-Bigas, M.
A., Nguyen, S. T., Skibber, J. M. & You, Y. N. (2015). Functional Deficits
and Symptoms of Long-Term Survivors of Colorectal Cancer Treated by
Multimodality Therapy Differ by Age at Diagnosis. J Gastrointest Surg, 19(1),
180-188.
Ballard, A., Parker-Autry, C., Lin, C. P., Markland, A. D., Ellington, D. R. & Richter,
H. E. (2015). Postoperative bowel function, symptoms, and habits in women
after vaginal reconstructive surgery. Int Urogynecol J, 26(6), 817-821.
Ballinger, A. B. & Anggiansah, C. (2007). Colorectal cancer. BMJ, 335(7622),
715-718.
Bandura, A. (1977). Self-efficacy: toward a unifying theory of behavioral change.
Psychol Rev, 84(2), 191-215.
Bartlett, L., Sloots, K., Nowak, M. & Ho, Y. H. (2011). Biofeedback therapy for
symptoms of bowel dysfunction following surgery for colorectal cancer. Tech
Coloproctol, 15(3), 319-326.
References
235
Battersby, N. J., Juul, T., Christensen, P., Janjua, A. Z., Branagan, G., Emmertsen, K.
J., Norton, C., Hughes, R., Laurberg, S. & Moran, B. J. (2016). Predicting the
Risk of Bowel-Related Quality-of-Life Impairment After Restorative
Resection for Rectal Cancer: A Multicenter Cross-Sectional Study. Dis Colon
Rectum, 59(4), 270-280.
Bauman, A., Bull, F., Chey, T., Craig, C. L., Ainsworth, B. E., Sallis, J. F., Bowles, H.
R., Hagstromer, M., Sjostrom, M., Pratt, M. & Group, I. P. S. (2009). The
International Prevalence Study on Physical Activity: results from 20 countries.
Int J Behav Nutr Phys Act, 6, 21.
Bazensky, I., Shoobridge-Moran, C. & Yoder, L. H. (2007). Colorectal cancer: an
overview of the epidemiology, risk factors, symptoms, and screening
guidelines. Medsurg Nurs, 16(1), 46-51.
Bellet, R. N., Adams, L. & Morris, N. R. (2012). The 6-minute walk test in outpatient
cardiac rehabilitation: validity, reliability and responsiveness--a systematic
review. Physiotherapy, 98(4), 277-286.
Bernard, S., Ouellet, M. P., Moffet, H., Roy, J. S. & Dumoulin, C. (2015). Effects of
radiation therapy on the structure and function of the pelvic floor muscles of
patients with cancer in the pelvic area: a systematic review. J Cancer Surviv.
Bhalla, A., Williams, J. P., Hurst, N. G., Speake, W. J., Tierney, G. M., Tou, S. &
Lund, J. N. (2014). One-third of patients fail to return to work 1 year after
surgery for colorectal cancer. Tech Coloproctol, 18(12), 1153-1159.
Bliss, D. Z., Mellgren, A., Whitehead, W. E., Chiarioni, G., Emmanuel, A., Santoro,
G. A., Zbar, A., Peden-McAlpine, C., Northwood, M., Slieker-ten Hove, M.,
Berghmans, B. & Mimura, T. (2013). Assessment and Conservative
Management of Faecal Incontinence and Quality of Life in Adults. Paris: 5th
International Consultation on Incontinence.
Bø, K. (2004a). Pelvic floor muscle training is effective in treatment of female stress
urinary incontinence, but how does it work? Int Urogynecol J, 15(2), 76-84.
Bø, K. (2004b). Urinary incontinence, pelvic floor dysfunction, exercise and sport.
Sports Med, 34(7), 451-464.
Bø, K., Hagen, R. H., Kvarstein, B., Jørgensen, J., Larsen, S. & Burgio, K. L. (1990).
Pelvic floor muscle exercise for the treatment of female stress urinary
incontinence: III. Effects of two different degrees of pelvic floor muscle
exercises. Neurourol Urodyn, 9(5), 489–502.
References
236
Bø, K. & Herbert, R. D. (2013). There is not yet strong evidence that exercise
regimens other than pelvic floor muscle training can reduce stress urinary
incontinence in women: a systematic review. J Physiother, 59(3), 159-168.
Bø, K. & Sherburn, M. (2005). Evaluation of female pelvic-floor muscle function and
strength. Phys Ther, 85(3), 269-282.
Boa, R. (2013). Female sexual pain disorders. Obstetrics & Gynaecology Forum, 23,
27-31.
Boer, B. C., de Graaff, F., Brusse-Keizer, M., Bouman, D. E., Slump, C. H.,
Slee-Valentijn, M. & Klaase, J. M. (2016). Skeletal muscle mass and quality
as risk factors for postoperative outcome after open colon resection for cancer.
Int J Colorectal Dis, 31(6), 1117-1124.
Bohannon, R. W. (2001). Dynamometer measurements of hand-grip strength predict
multiple outcomes. Percept Mot Skills, 93(2), 323-328.
Bohannon, R. W. (2015). Muscle strength: clinical and prognostic value of hand-grip
dynamometry. Curr Opin Clin Nutr Metab Care, 18(5), 465-470.
Bohannon, R. W., Magasi, S. R., Bubela, D. J., Wang, Y. C. & Gershon, R. C. (2012).
Grip and Knee Extension Muscle Strength Reflect a Common Construct
among Adults. Muscle & Nerve, 46(4), 555-558.
Bols, E., Berghmans, B., de Bie, R., Govaert, B., van Wunnik, B., Heymans, M.,
Hendriks, E. & Baeten, C. (2012). Rectal balloon training as add-on therapy to
pelvic floor muscle training in adults with fecal incontinence: a randomized
controlled trial. Neurourol Urodyn, 31(1), 132-138.
Bols, E. M., Berghmans, B. C., Hendriks, E. J., de Bie, R. A., Melenhorst, J., van
Gemert, W. G. & Baeten, C. G. (2007). A randomized physiotherapy trial in
patients with fecal incontinence: design of the PhysioFIT-study. BMC Public
Health, 7, 355.
Booth, S. & Adams, L. (2001). The shuttle walking test: a reproducible method for
evaluating the impact of shortness of breath on functional capacity in patients
with advanced cancer. Thorax, 56(2), 146-150.
Borel, B., Pepin, V., Mahler, D. A., Nadreau, E. & Maltais, F. (2014). Prospective
validation of the endurance shuttle walking test in the context of
bronchodilation in COPD. Eur Respir J, 44(5), 1166-1176.

References
237
Botlero, R., Bell, R. J., Urquhart, D. M. & Davis, S. R. (2011). Prevalence of fecal
incontinence and its relationship with urinary incontinence in women living in
the community. Menopause, 18(6), 685-689.
Botteri, E., Iodice, S., Bagnardi, V., Raimondi, S., Lowenfels, A. B. & Maisonneuve,
P. (2008). Smoking and colorectal cancer: a meta-analysis. JAMA, 300(23),
2765-2778.
Bours, M. J., van der Linden, B. W., Winkels, R. M., van Duijnhoven, F. J., Mols, F.,
van Roekel, E. H., Kampman, E., Beijer, S. & Weijenberg, M. P. (2016).
Candidate Predictors of Health-Related Quality of Life of Colorectal Cancer
Survivors: A Systematic Review. Oncologist, 21(4), 433-452.
Boyle, T., Fritschi, L., Platell, C. & Heyworth, J. (2013). Lifestyle factors associated
with survival after colorectal cancer diagnosis. Br J Cancer, 109(3), 814-822.
Braekken, I. H., Majida, M., Ellstrom-Engh, M., Dietz, H. P., Umek, W. & Bo, K.
(2008). Test-retest and intra-observer repeatability of two-, three- and
four-dimensional perineal ultrasound of pelvic floor muscle anatomy and
function. Int Urogynecol J Pelvic Floor Dysfunct, 19(2), 227-235.
Brant, J. M., Beck, S. L., Dudley, W. N., Cobb, P., Pepper, G. & Miaskowski, C.
(2011). Symptom trajectories during chemotherapy in outpatients with lung
cancer colorectal cancer, or lymphoma. Eur J Oncol Nurs, 15(5), 470-477.
Bregendahl, S., Emmertsen, K. J., Lindegaard, J. C. & Laurberg, S. (2015). Urinary
and sexual dysfunction in women after resection with and without
preoperative radiotherapy for rectal cancer: a population-based cross-sectional
study. Colorectal Dis, 17(1), 26-37.
Bregendahl, S., Emmertsen, K. J., Lous, J. & Laurberg, S. (2013). Bowel dysfunction
after low anterior resection with and without neoadjuvant therapy for rectal
cancer: a population-based cross-sectional study. Colorectal Dis,15(9),
1130-1139.
Brenner, H., Kloor, M. & Pox, C. P. (2014). Colorectal cancer. Lancet, 383(9927),
1490-1502.
Brezden-Masley, C. & Polenz, C. (2014). Current practices and challenges of
adjuvant chemotherapy in patients with colorectal cancer. Surg Oncol Clin N
Am, 23(1), 49-58.
References
238
Broughman, J. R., Williams, G. R., Deal, A. M., Yu, H., Nyrop, K. A., Alston, S. M.,
Gordon, B. B., Sanoff, H. K. & Muss, H. B. (2015). Prevalence of sarcopenia
in older patients with colorectal cancer. J Geriatr Oncol, 6(6), 442-445.
Brown, C. J., Fenech, D. S. & McLeod, R. S. (2008). Reconstructive techniques after
rectal resection for rectal cancer. Cochrane Database Syst Rev,16(2),
CD006040.
Brown, J. C., Huedo-Medina, T. B., Pescatello, L. S., Ryan, S. M., Pescatello, S. M.,
Moker, E., LaCroix, J. M., Ferrer, R. A. & Johnson, B. T. (2012). The
Efficacy of Exercise in Reducing Depressive Symptoms among Cancer
Survivors: A Meta-Analysis. Plos One, 7(1).
Brown, J. C., Winters-Stone, K., Lee, A. & Schmitz, K. H. Cancer, physical activity,
and exercise. Compr Physiol, 2(4), 2775-2809.
Brown, J. S., McNaughton, K. S., Wyman, J. F., Burgio, K. L., Harkaway, R.,
Bergner, D., Altman, D. S., Kaufman, J., Kaufman, K. & Girman, C. J. (2003).
Measurement characteristics of a voiding diary for use by men and women
with overactive bladder. Urology, 61(4), 802-809.
Brown, S. R., Mathew, R., Keding, A., Marshall, H. C., Brown, J. M. & Jayne, D. G.
(2014). The impact of postoperative complications on long-term quality of life
after curative colorectal cancer surgery. Ann Surg, 259(5), 916-923.
Brown, W. J., Moorhead, G. E. & Marshall, A. L. (2008). Choose Health: Be Active:
A Physical Activity Guide for Older Australians. Canberra: Commonwealth of
Australia and repatriation Commission.
Bruce, B., Fries, J. F., Ambrosini, D., Lingala, B., Gandek, B., Rose, M. & Ware, J. E.
(2009). Better assessment of physical function: item improvement is neglected
but essential. Arthritis Res Ther, 11(6), R191.
Bruns, E. R., van den Heuvel, B., Buskens, C. J., van Duijvendijk, P., Wassenaar, E.
B., van der Zaag, E. S., Bemelman, W. A. & van Munster, B. C. (2016). The
effects of physical prehabilitation in elderly patients undergoing colorectal
surgery: a systematic review. Colorectal Dis, 18(8), O267-77.
Buffart, L. M., Galvao, D. A., Brug, J., Chinapaw, M. J. & Newton, R. U. (2014).
Evidence-based physical activity guidelines for cancer survivors: current
guidelines, knowledge gaps and future research directions. Cancer Treat Rev,
40(2), 327-340.

References
239
Campbell, P. T., Newton, C. C., Dehal, A. N., Jacobs, E. J., Patel, A. V. & Gapstur, S.
M. (2012). Impact of body mass index on survival after colorectal cancer
diagnosis: the Cancer Prevention Study-II Nutrition Cohort. J Clin Oncol,
30(1), 42-52.
Campbell, P. T., Patel, A. V., Newton, C. C., Jacobs, E. J. & Gapstur, S. M. (2013).
Associations of Recreational Physical Activity and Leisure Time Spent Sitting
With Colorectal Cancer Survival. J Clin Oncol, 31(7), 876-885.
Cancer Council Victoria (2013). Understanding Bowel Cancer. Sydney: Cancer
Council Australia.
Cancer Council Victoria (2016). Victorian Cancer Statistics. Retrieved from
http://vcrdata.cancervic.org.au/vs/#view=leading_cancer&selectedWafers=8&
selectedColumns=0&topNSortColumn=0
Cardio Design (2016). Handbook for the Peritron. Victoria: Cardio design pty ltd.
Caspersen, C. J., Powell, K. E. & Christenson, G. M. (1985). Physical activity,
exercise, and physical fitness: definitions and distinctions for health-related
research. Public Health Rep, 100(2), 126-131.
Center, M. M., Jemal, A., Smith, R. A. & Ward, E. (2009). Worldwide variations in
colorectal cancer. CA Cancer J Clin, 59(6), 366-378.
Chan, D. S. M., Lau, R., Aune, D., Vieira, R., Greenwood, D. C., Kampman, E. &
Norat, T. (2011). Red and Processed Meat and Colorectal Cancer Incidence:
Meta-Analysis of Prospective Studies. PLoS One, 6(6), e20456.
Chan, K. E., Pathak, S., Smart, N. J., Batchelor, N. & Daniels, I. R. (2015). The
impact of Cardiopulmonary Exercise Testing (CPET) on patients over 80
years undergoing elective colorectal cancer surgery. Colorectal Dis, 18(6),
578-85.
Chawla, N., Butler, E. N., Lund, J., Warren, J. L., Harlan, L. C. & Yabroff, K. R.
(2013). Patterns of colorectal cancer care in Europe, Australia, and New
Zealand. J Natl Cancer Inst Monogr, 2013(46), 36-61.
Chen, T. Y., Emmertsen, K. J. & Laurberg, S. (2014). Bowel dysfunction after rectal
cancer treatment: a study comparing the specialist's versus patient's
perspective. BMJ Open, 4(1), e003374.
Chen, T. Y., Emmertsen, K. J. & Laurberg, S. (2015). What Are the Best
Questionnaires To Capture Anorectal Function After Surgery in Rectal Cancer?
Curr Colorectal Cancer Rep, 11, 37-43.

References
240
Chen, T. Y., Wiltink, L. M., Nout, R. A., Meershoek-Klein Kranenbarg, E., Laurberg,
S., Marijnen, C. A. & van de Velde, C. J. (2015). Bowel function 14 years
after preoperative short-course radiotherapy and total mesorectal excision for
rectal cancer: report of a multicenter randomized trial. Clin Colorectal Cancer,
14(2), 106-114.
Cheng, K. K. & Lee, D. T. (2011). Effects of pain, fatigue, insomnia, and mood
disturbance on functional status and quality of life of elderly patients with
cancer. Crit Rev Oncol Hematol, 78(2), 127-137.
Cheville, A. L., Beck, L. A., Petersen, T. L., Marks, R. S. & Gamble, G. L. (2009).
The detection and treatment of cancer-related functional problems in an
outpatient setting. Support Care Cancer, 17(1), 61-67.
Chiang JM, Yeh CY & JY, W. (1997). Anorectal manometric characteristics differ in
biofeedback for postoperative fecal incontinence. Journal of Surgical
Association Republic of China, 30, 316-321.
Chiu, E. (2004). Epidemiology of depression in the Asia Pacific region. Australas
Psychiatry, 12 Suppl, S4-10.
Chung, J. Y., Lee, D. H., Park, J. H., Lee, M. K., Kang, D. W., Min, J., Kim, D. I.,
Jeong, D. H., Kim, N. K., Meyerhardt, J. A., Jones, L. W. & Jeon, J. Y. (2013).
Patterns of physical activity participation across the cancer trajectory in
colorectal cancer survivors. Support Care Cancer, 21(6), 1605-1612.
Clarke, A. (2009). Effects of routine education on people newly diagnosed with type 2
diabetes. European Diabetes Nursing, 6(3), 88-94.
Colinet, B., Jacot, W., Bertrand, D., Lacombe, S., Bozonnat, M. C., Daures, J. P.,
Pujol, J. L. & Network, O. H. (2005). A new simplified comorbidity score as a
prognostic factor in non-small-cell lung cancer patients: description and
comparison with the Charlson's index. Br J Cancer, 93(10), 1098-1105.
Conn, V. S., Hafdahl, A. R., Porock, D. C., McDaniel, R. & Nielsen, P. J. (2006). A
meta-analysis of exercise interventions among people treated for cancer.
Support Care Cancer, 14(7), 699-712.
Contin, P., Kulu, Y., Bruckner, T., Sturm, M., Welsch, T., Müller-Stich, B. P., Huber,
J., Büchler, M. W. & Ulrich, A. (2014). Comparative analysis of late
functional outcome following preoperative radiation therapy or
chemoradiotherapy and surgery or surgery alone in rectal cancer. Int J
Colorectal Dis, 29(2), 165-175.
References
241
Correa, G. T., Bandeira, G. A., Cavalcanti, B. G., Santos, F. B., Rodrigues Neto, J. F.,
Guimaraes, A. L., Haikal, D. S. & De Paula, A. M. (2012). Analysis of ECOG
performance status in head and neck squamous cell carcinoma patients:
association with sociodemographical and clinical factors, and overall survival.
Support Care Cancer, 20(11), 2679-2685.
Costa, H. S., Alves, R. L., da Silva, S. A., Alencar, M. C., Nunes Mdo, C., Lima, M.
M. & Rocha, M. O. (2014). Assessment of Functional Capacity in Chagas
Heart Disease by Incremental Shuttle Walk Test and its Relation to
Quality-of-Life. Int J Prev Med, 5(2), 152-158.
Cotterill, N., Norton, C., Avery, K. N., Abrams, P. & Donovan, J. L. (2008). A
patient-centered approach to developing a comprehensive symptom and
quality of life assessment of anal incontinence. Dis Colon Rectum, 51(1),
82-87.
Cotterill, N., Norton, C., Avery, K. N., Abrams, P. & Donovan, J. L. (2011).
Psychometric evaluation of a new patient-completed questionnaire for
evaluating anal incontinence symptoms and impact on quality of life: the
ICIQ-B. Dis Colon Rectum, 54(10), 1235-1250.
Courneya, K. S. & Friedenreich, C. M. (2007). Physical activity and cancer control.
Semin Oncol Nurs, 23(4), 242-252.
Craig, C. L., Marshall, A. L., Sjostrom, M., Bauman, A. E., Booth, M. L., Ainsworth,
B. E., Pratt, M., Ekelund, U., Yngve, A., Sallis, J. F. & Oja, P. (2003).
International physical activity questionnaire: 12-country reliability and
validity. Med Sci Sports Exerc, 35(8), 1381-1395.
Craig, P., Dieppe, P., Macintyre, S., Michie, S., Nazareth, I. & Petticrew, M. (2013).
Developing and evaluating complex interventions: the new Medical Research
Council guidance. Int J Nurs Stud, 50(5), 587-592.
Cramer, H., Lauche, R., Klose, P., Dobos, G. & Langhorst, J. (2013). A systematic
review and meta-analysis of exercise interventions for colorectal cancer
patients. Eur J Cancer Care (Engl), 23(1), 3-14.
Crawford, J. R., Henry, J. D., Crombie, C. & Taylor, E. P. (2001). Normative data for
the HADS from a large non-clinical sample. Br J Clin Psychol, 40(Pt 4),
429-434.
Crisafulli, E. & Clini, E. M. (2010). Measures of dyspnea in pulmonary rehabilitation.
Multidiscip Respir Med, 5(3), 202-210.

References
242
Dajczman, E., Kasymjanova, G., Kreisman, H., Swinton, N., Pepe, C. & Small, D.
(2008). Should Patient-Rated Performance Status Affect Treatment Decisions
in Advanced Lung Cancer? J Thorac Oncol, 3(10), 1133-1136.
Damin, D. C. & Lazzaron, A. R. (2014). Evolving treatment strategies for colorectal
cancer: a critical review of current therapeutic options. World J Gastroenterol,
20(4), 877-887.
Daniels, I. R., Woodward, S., Taylor, F. G., Raja, A. & Toomey, P. (2006). Female
urogenital dysfunction following total mesorectal excision for rectal cancer.
World J Surg Oncol, 4, 6.
Datta, D., Normandin, E. & ZuWallack, R. (2015). Cardiopulmonary exercise testing
in the assessment of exertional dyspnea. Ann Thorac Med, 10(2), 77-86.
Daudt, H. M. L., Cosby, C., Dennis, D. L., Payeur, N. & Nurullah, R. (2012).
Nutritional and psychosocial status of colorectal cancer patients referred to an
outpatient oncology clinic. Support Care Cancer, 20(7), 1417-1423.
Davis, N. C., Evans, E. B., Cohen, J. R. & Theile, D. E. (1984). Staging of colorectal
cancer. The Australian clinico-pathological staging (ACPS) system compared
with Dukes' system. Dis Colon Rectum, 27(11), 707-713.
Davis, N. C. & Newland, R. C. (1983). Terminology and classification of colorectal
adenocarcinoma: the Australian clinico-pathological staging system. Aust N Z
J Surg, 53(3), 211-221.
Davison, S. L. (2012). Hypoactive sexual desire disorder. Curr Opin Obstet Gynecol,
24(4), 215-220.
Day, L. W. & Velayos, F. (2014). Colorectal Cancer and the Elderly. Clin Geriatr
Med, 30(1), 117-131.
de Morton, N. A., Davidson, M. & Keating, J. L. (2010). Validity, responsiveness and
the minimal clinically important difference for the de Morton Mobility Index
(DEMMI) in an older acute medical population. BMC Geriatr, 10, 72.
De Rosa, M., Pace, U., Rega, D., Costabile, V., Duraturo, F., Izzo, P. & Delrio, P.
(2015). Genetics, diagnosis and management of colorectal cancer (Review).
Oncol Rep, 34(3), 1087-1096.
Del Giudice, M. E., Vella, E. T., Hey, A., Simunovic, M., Harris, W. & Levitt, C.
(2014). Systematic review of clinical features of suspected colorectal cancer in
primary care. Can Fam Physician, 60(8), e405-415.
References
243
Den Oudsten, B. L., Traa, M. J., Thong, M. S., Martijn, H., De Hingh, I. H., Bosscha,
K. & van de Poll-Franse, L. V. (2012). Higher prevalence of sexual
dysfunction in colon and rectal cancer survivors compared with the normative
population: a population-based study. Eur J Cancer, 48(17), 3161-3170.
Dennett, A. M., Peiris, C. L., Shields, N., Prendergast, L. A. & Taylor, N. F. (2016).
Moderate-intensity exercise reduces fatigue and improves mobility in cancer
survivors: a systematic review and meta-regression. J Physiother, 62(2),
68-82.
Des Jarlais, D. C., Lyles, C., Crepaz, N. & Group, T. (2004). Improving the reporting
quality of nonrandomized evaluations of behavioral and public health
interventions: the TREND statement. Am J Public Health, 94(3), 361-366.
Deshields, T. L., Potter, P., Olsen, S., Liu, J. & Dye, L. (2011). Documenting the
symptom experience of cancer patients. J Support Oncol, 9(6), 216-223.
Deutekom, M., Terra, M. P., Dobben, A. C., Dijkgraaf, M. G., Felt-Bersma, R. J.,
Stoker, J. & Bossuyt, P. M. (2005). Selecting an outcome measure for
evaluating treatment in fecal incontinence. Dis Colon Rectum, 48(12),
2294-2301.
Devin, J. L., Sax, A. T., Hughes, G. I., Jenkins, D. G., Aitken, J. F., Chambers, S. K.,
Dunn, J. C., Bolam, K. A. & Skinner, T. L. (2015). The influence of
high-intensity compared with moderate-intensity exercise training on
cardiorespiratory fitness and body composition in colorectal cancer survivors:
a randomised controlled trial. J Cancer Surviv, 10(3), 467-79.
Di, B., Li, Y., Wei, K., Xiao, X., Shi, J., Zhang, Y., Yang, X., Gao, P., Zhang, K.,
Yuan, Y., Zhang, D., Wei, X., Liu, S., Wang, J., Wang, X., Zhang, Y. & Cai,
H. (2013). Laparoscopic versus open surgery for colon cancer: a meta-analysis
of 5-year follow-up outcomes. Surg Oncol, 22(3), e39-43.
Di Fabio, F., Koller, M., Nascimbeni, R., Talarico, C. & Salerni, B. (2008).
Long-term outcome after colorectal cancer resection. Patients' self-reported
quality of life, sexual dysfunction and surgeons' awareness of patients' needs.
Tumori, 94(1), 30-35.
Di Thommazo-Luporini, L., Carvalho, L. P., Luporini, R. L., Trimer, R., Pantoni, C.
B., Martinez, A. F., Catai, A. M., Arena, R. & Borghi-Silva, A. (2015). Are
cardiovascular and metabolic responses to field walking tests interchangeable
and obesity-dependent? Disabil Rehabil, 38(18), 1820-9.

References
244
Dietz, H. P. (2010). Pelvic floor ultrasound: a review. Am J Obstet Gynecol, 202(4),
321-334.
Dingman, C., Hegedus, P. D., Likes, C., McDowell, P., McCarthy, E. & Zwilling, C.
(2008). A coordinated, multidisciplinary approach to caring for the patient
with head and neck cancer. J Support Oncol, 6(3), 125-131.
Dittus, K. L., Lakoski, S. G., Savage, P. D., Kokinda, N., Toth, M., Stevens, D.,
Woods, K., O'Brien, P. & Ades, P. A. (2015). Exercise-based oncology
rehabilitation: leveraging the cardiac rehabilitation model. J Cardiopulm
Rehabil Prev, 35(2), 130-139.
Dobben, A. C., Terra, M. P., Deutekom, M., Gerhards, M. F., Bijnen, A. B.,
Felt-Bersma, R. J., Janssen, L. W., Bossuyt, P. M. & Stoker, J. (2007). Anal
inspection and digital rectal examination compared to anorectal physiology
tests and endoanal ultrasonography in evaluating fecal incontinence. Int J
Colorectal Dis, 22(7), 783-790.
Dorudi, S., Steele, R. J. & McArdle, C. S. (2002). Surgery for colorectal cancer. Br
Med Bull, 64, 101-118.
Dukes, C. E. (1932). The classification of cancer of the rectum. J Pathol Bacteriol,
35(3), 323-332.
Dwyer, T., Pezic, A., Sun, C., Cochrane, J., Venn, A., Srikanth, V., Jones, G., Shook,
R. P., Sui, X., Ortaglia, A., Blair, S. & Ponsonby, A. L. Objectively Measured
Daily Steps and Subsequent Long Term All-Cause Mortality: The Tasped
Prospective Cohort Study. PLoS One, 10(11), e0141274.
Eaton, T., Young, P., Nicol, K. & Kolbe, J. (2006). The endurance shuttle walking
test: a responsive measure in pulmonary rehabilitation for COPD patients.
Chron Respir Dis, 3(1), 3-9.
Eckardt, V. F. & Kanzler, G. (1993). How Reliable Is Digital Examination for the
Evaluation of Anal-Sphincter Tone. Int J Colorectal Dis, 8(2), 95-97.
Eker, B., Ozaslan, E., Karaca, H., Berk, V., Bozkurt, O., Inanc, M., Duran, A. O. &
Ozkan, M. (2015). Factors affecting prognosis in metastatic colorectal cancer
patients. Asian Pac J Cancer Prev, 16(7), 3015-3021.
El-Shami, K., Oeffinger, K. C., Erb, N. L., Willis, A., Bretsch, J. K., Pratt-Chapman,
M. L., Cannady, R. S., Wong, S. L., Rose, J., Barbour, A. L., Stein, K. D.,
Sharpe, K. B., Brooks, D. D. & Cowens-Alvarado, R. L. (2015). American
References
245
Cancer Society Colorectal Cancer Survivorship Care Guidelines. CA Cancer J
Clin, 65(6), 428-455.
Emmertsen, K. J. & Laurberg, S. (2012). Low anterior resection syndrome score:
development and validation of a symptom-based scoring system for bowel
dysfunction after low anterior resection for rectal cancer. Ann Surg, 255(5),
922-928.
Evans, W. J. (2002). Physical function in men and women with cancer. Effects of
anemia and conditioning. Oncology (Williston Park), 16(9 Suppl 10), 109-115.
Exposito-Ruiz, M., Perez-Vicente, S. & Rivas-Ruiz, F. (2010). Statistical inference:
hypothesis testing. Allergol Immunopathol (Madr), 38(5), 266-277.
Fakih, M. G. (2015). Metastatic colorectal cancer: current state and future directions.
J Clin Oncol, 33(16), 1809-1824.
Farrugia, H., Zalcberg, J., Milne, R., Thursfield, V., Martin, K., Staines, C. & Giles, G.
(2015). Cancer in Victoria: Cancer Risk 2015. Retrieved from
http://www.cancervic.org.au/downloads/cec/cancer-in-vic/Cancer-Risk-in-Vic
toria-2015.pdf.
Favetta, U., Amato, A., Interisano, A. & Pescatori, M. (1996). Clinical, manometric
and sonographic assessment of the anal sphincters. A comparative prospective
study. Int J Colorectal Dis, 11(4), 163-166.
Favoriti, P., Carbone, G., Greco, M., Pirozzi, F., Pirozzi, R. E. & Corcione, F. (2016).
Worldwide burden of colorectal cancer: a review. Updates Surg, 68(1), 7-11.
Fedirko, V., Tramacere, I., Bagnardi, V., Rota, M., Scotti, L., Islami, F., Negri, E.,
Straif, K., Romieu, I., La Vecchia, C., Boffetta, P. & Jenab, M. (2011).
Alcohol drinking and colorectal cancer risk: an overall and dose-response
meta-analysis of published studies. Ann Oncol, 22(9), 1958-1972.
Ferlay, J., Soerjomataram, I., Ervik, M., Dikshit, R., Eser, S., Mathers, C., Rebelo, M.,
Parkin, D., Forman, D. & Bray, F. (2013). GLOBOCAN 2012 v1.0, Cancer
Incidence and Mortality Worldwide: IARC CancerBase No. 11. Retrieved
from http://globocan.iarc.fr.
Fish, D. & Temple, L. K. (2014). Functional consequences of colorectal cancer
management. Surg Oncol Clin N Am, 23(1), 127-149.
Fisher, A., Smith, L. & Wardle, J. (2016). Physical activity advice could become part
of routine care for colorectal cancer survivors. Future Oncol, 12(2), 139-141.
References
246
Fisher, A., Wardle, J., Beeken, R. J., Croker, H., Williams, K. & Grimmett, C. (2016).
Perceived barriers and benefits to physical activity in colorectal cancer
patients. Support Care Cancer, 24(2), 903-910.
Fleg, J. L., Pina, I. L., Balady, G. J., Chaitman, B. R., Fletcher, B., Lavie, C.,
Limacher, M. C., Stein, R. A., Williams, M. & Bazzarre, T. (2000).
Assessment of functional capacity in clinical and research applications: An
advisory from the Committee on Exercise, Rehabilitation, and Prevention,
Council on Clinical Cardiology, American Heart Association. Circulation,
102(13), 1591-1597.
Fotheringham, I., Meakin, G., Punekar, Y. S., Riley, J. H., Cockle, S. M. & Singh, S.
J. (2015). Comparison of laboratory- and field-based exercise tests for COPD:
a systematic review. Int J Chron Obstruct Pulmon Dis, 10, 625-643.
Fournier, E., Jooste, V., Woronoff, A. S., Quipourt, V., Bouvier, A. M. & Mercier, M.
(2016). Health-related quality of life is a prognostic factor for survival in older
patients after colorectal cancer diagnosis: A population-based study. Dig Liver
Dis, 48(1), 87-93.
Frost, M. H., Reeve, B. B., Liepa, A. M., Stauffer, J. W., Hays, R. D. & Sloan, J. A.
(2007). What is sufficient evidence for the reliability and validity of
patient-reported outcome measures? Value Health, 10, S94-S105.
Gaertner, W. B., Kwaan, M. R., Madoff, R. D. & Melton, G. B. (2015). Rectal cancer:
An evidence-based update for primary care providers. World J Gastroenterol,
21(25), 7659-7671.
Ganesh, V., Agarwal, A., Popovic, M., Cella, D., McDonald, R., Vuong, S., Lam, H.,
Rowbottom, L., Chan, S., Barakat, T., DeAngelis, C., Borean, M., Chow, E. &
Bottomley, A. (2016). Comparison of the FACT-C, EORTC QLQ-CR38, and
QLQ-CR29 quality of life questionnaires for patients with colorectal cancer: a
literature review. Support Care Cancer, 24(8), 3661-3668.
Garth, A. K., Newsome, C. M., Simmance, N. & Crowe, T. C. (2010). Nutritional
status, nutrition practices and post-operative complications in patients with
gastrointestinal cancer. J Hum Nutr Diet, 23(4), 393-401.
Gavaruzzi, T., Lotto, L., Giandomenico, F., Perin, A. & Pucciarelli, S. (2014).
Patient-reported outcomes after neoadjuvant therapy for rectal cancer: a
systematic review. Expert Rev Anticancer Ther, 14(8), 901-918.
References
247
Ghasemi, A. & Zahediasl, S. (2012). Normality tests for statistical analysis: a guide
for non-statisticians. Int J Endocrinol Metab, 10(2), 486-489.
Gilbert, A., Sebag-Montefiore, D., Davidson, S. & Velikova, G. (2015). Use of
patient-reported outcomes to measure symptoms and health related quality of
life in the clinic. Gynecol Oncol, 136(3), 429-439.
Gillis, C., Li, C., Lee, L., Awasthi, R., Augustin, B., Gamsa, A., Liberman, A. S.,
Stein, B., Charlebois, P., Feldman, L. S. & Carli, F. (2014). Prehabilitation
versus rehabilitation: a randomized control trial in patients undergoing
colorectal resection for cancer. Anesthesiology, 121(5), 937-947.
Gillis, C., Loiselle, S. E., Fiore, J. F., Jr., Awasthi, R., Wykes, L., Liberman, A. S.,
Stein, B., Charlebois, P. & Carli, F. (2015). Prehabilitation with Whey Protein
Supplementation on Perioperative Functional Exercise Capacity in Patients
Undergoing Colorectal Resection for Cancer: A Pilot Double-Blinded
Randomized Placebo-Controlled Trial. J Acad Nutr Diet, 116(5), 802-12.
Giraldi, A., Rellini, A., Pfaus, J. G., Bitzer, J., Laan, E., Jannini, E. A. & Fugl-Meyer,
A. R. (2011). Questionnaires for assessment of female sexual dysfunction: a
review and proposal for a standardized screener. J Sex Med, 8(10), 2681-2706.
Goodwin, R. A. & Asmis, T. R. (2009). Overview of systemic therapy for colorectal
cancer. Clin Colon Rectal Surg, 22(4), 251-256.
Graca Pereira, M., Figueiredo, A. P. & Fincham, F. D. (2012). Anxiety, depression,
traumatic stress and quality of life in colorectal cancer after different
treatments: A study with Portuguese patients and their partners. Eur J Oncol
Nurs, 16(3), 227-232.
Granger, C. L., Denehy, L., Parry, S. M., Martin, J., Dimitriadis, T., Sorohan, M. &
Irving, L. (2015). Which field walking test should be used to assess functional
exercise capacity in lung cancer? an observational study. BMC Pulmonary
Medicine, 15, 89.
Granger, C. L., Holland, A. E., Gordon, I. R. & Denehy, L. (2015). Minimal
important difference of the 6-minute walk distance in lung cancer. Chron
Respir Dis, 12(2), 146-154.
Granger, C. L., Parry, S. M., Edbrooke, L. & Denehy, L. (2016). Deterioration in
physical activity and function differs according to treatment type in non-small
cell lung cancer - future directions for physiotherapy management.
Physiotherapy, 102(3), 256-263.
References
248
Gremeaux, V., Troisgros, O., Benaim, S., Hannequin, A., Laurent, Y., Casillas, J. M.
& Benaim, C. (2011). Determining the minimal clinically important difference
for the six-minute walk test and the 200-meter fast-walk test during cardiac
rehabilitation program in coronary artery disease patients after acute coronary
syndrome. Arch Phys Med Rehabil, 92(4), 611-619.
Grimmett, C., Bridgewater, J., Steptoe, A. & Wardle, J. (2011). Lifestyle and quality
of life in colorectal cancer survivors. Qual Life Res, 20(8), 1237-1245.
Grimmett, C., Simon, A., Lawson, V. & Wardle, J. (2015). Diet and physical activity
intervention in colorectal cancer survivors: a feasibility study. Eur J Oncol
Nurs, 19(1), 1-6.
Guazzi, M., Dickstein, K., Vicenzi, M. & Arena, R. (2009). Six-minute walk test and
cardiopulmonary exercise testing in patients with chronic heart failure: a
comparative analysis on clinical and prognostic insights. Circ Heart Fail, 2(6),
549-555.
Gudbergsson, S. B., Dahl, A. A., Loge, J. H., Thorsen, L., Oldervoll, L. & Grov, E. K.
(2015). What Is Covered by "Cancer Rehabilitation" in Pubmed? A Review of
Randomized Controlled Trials 1990-2011. J Rehabil Med, 47(2), 97-106.
Guffey, C. R., Fan, D., Singh, U. P. & Murphy, E. A. (2013). Linking obesity to
colorectal cancer: recent insights into plausible biological mechanisms. Curr
Opin Clin Nutr Metab Care, 16(5), 595-600.
Gunter, M. J. & Leitzmann, M. F. (2006). Obesity and colorectal cancer:
epidemiology, mechanisms and candidate genes. J Nutr Biochem, 17(3),
145-156.
Gupta, D., Lis, C. G., Granick, J., Grutsch, J. F., Vashi, P. G. & Lammersfeld, C. A.
(2006). Malnutrition was associated with poor quality of life in colorectal
cancer: a retrospective analysis. J Clin Epidemiol, 59(7), 704-709.
Gustavsson, B., Carlsson, G., Machover, D., Petrelli, N., Roth, A., Schmoll, H. J.,
Tveit, K. M. & Gibson, F. (2015). A review of the evolution of systemic
chemotherapy in the management of colorectal cancer. Clin Colorectal Cancer,
14(1), 1-10.
Guzman Rojas, R., Wong, V., Shek, K. L. & Dietz, H. P. (2014). Impact of levator
trauma on pelvic floor muscle function. Int Urogynecol J, 25(3), 375-380.
References
249
Hager, A. & Hess, J. (2005). Comparison of health related quality of life with
cardiopulmonary exercise testing in adolescents and adults with congenital
heart disease. Heart, 91(4), 517-520.
Haggar, F. A. & Boushey, R. P. (2009). Colorectal cancer epidemiology: incidence,
mortality, survival, and risk factors. Clin Colon Rectal Surg, 22(4), 191-197.
Hallan, R. I., Marzouk, D. E., Waldron, D. J., Womack, N. R. & Williams, N. S.
(1989). Comparison of digital and manometric assessment of anal sphincter
function. Br J Surg, 76(9), 973-975.
Hamaker, M. E., Prins, M. C., Schiphorst, A. H., van Tuyl, S. A., Pronk, A. & van
den Bos, F. (2015). Long-term changes in physical capacity after colorectal
cancer treatment. J Geriatr Oncol, 6(2), 153-164.
Hamilton, S. R. & Aaltonen, L. A. (2000). World Health Organization Classification
of Tumours. Pathology and Genetics of Tumours of the Digestive System.
Lyon, France: International Agency for Research on Cancer (IARC).
Hanssens, S., Luyten, R., Watthy, C., Fontaine, C., Decoster, L., Baillon, C.,
Trullemans, F., Cortoos, A. & De Greve, J. Evaluation of a comprehensive
rehabilitation program for post-treatment patients with cancer. Oncol Nurs
Forum, 38(6), E418-424.
Hardikar, S., Newcomb, P. A., Campbell, P. T., Win, A. K., Lindor, N. M., Buchanan,
D. D., Makar, K. W., Jenkins, M. A., Potter, J. D. & Phipps, A. I. (2015).
Prediagnostic Physical Activity and Colorectal Cancer Survival: Overall and
Stratified by Tumor Characteristics. Cancer Epidemiol Biomarkers Prev,
24(7), 1130-1137.
Harding, J. L., Shaw, J. E., Anstey, K. J., Adams, R., Balkau, B., Brennan-Olsen, S.
L., Briffa, T., Davis, T. M., Davis, W. A., Dobson, A., Flicker, L., Giles, G.,
Grant, J., Huxley, R., Knuiman, M., Luszcz, M., MacInnis, R. J., Mitchell, P.,
Pasco, J. A., Reid, C., Simmons, D., Simons, L., Tonkin, A., Woodward, M.,
Peeters, A. & Magliano, D. J. (2015). Comparison of anthropometric measures
as predictors of cancer incidence: A pooled collaborative analysis of 11
Australian cohorts. Int J Cancer, 137(7), 1699-1708.
Harrison, J. D., Young, J. M., Auld, S., Masya, L., Solomon, M. J. & Butow, P. N.
(2011). Quantifying postdischarge unmet supportive care needs of people with
colorectal cancer: a clinical audit. Colorectal Dis, 13(12), 1400-1406.
References
250
Harriss, D. J., Cable, N. T., George, K., Reilly, T., Renehan, A. G. & Haboubi, N.
(2007). Physical activity before and after diagnosis of colorectal cancer:
disease risk, clinical outcomes, response pathways and biomarkers. Sports
Med, 37(11), 947-960.
Hawkes, A. L., Lynch, B. M., Youlden, D. R., Owen, N. & Aitken, J. F. (2008).
Health behaviors of Australian colorectal cancer survivors, compared with
noncancer population controls. Support Care Cancer, 16(10), 1097-1104.
Haylen, B. T., de Ridder, D., Freeman, R. M., Swift, S. E., Berghmans, B., Lee, J.,
Monga, A., Petri, E., Rizk, D. E., Sand, P. K. & Schaer, G. N. (2010). An
International Urogynecological Association (IUGA)/International Continence
Society (ICS) Joint Report on the Terminology for Female Pelvic Floor
Dysfunction. Neurourol Urodyn, 29(1), 4-20.
Hendry, J. H. & West, C. M. L. (1997). Apoptosis and mitotic cell death: Their
relative contributions to normal-tissue and tumour radiation response. Int J
Radiat Biol, 71(6), 709-719.
Hertzog, M. A. (2008). Considerations in determining sample size for pilot studies.
Res Nurs Health, 31(2), 180-191.
Heymen, S. & Kuijpers, H. (2007). Biofeedback for pelvic floor disorders. New York:
Informa Healthcare.
Heymen, S., Scarlett, Y., Jones, K., Ringel, Y., Drossman, D. & Whitehead, W. E.
(2009). Randomized controlled trial shows biofeedback to be superior to
pelvic floor exercises for fecal incontinence. Dis Colon Rectum, 52(10),
1730-1737.
Higgins, J.P.T. & Green, S. (2011). Cochrane Handbook for Systematic Reviews of
Interventions Version 5.1.0. Retrieved from www.cochrane-handbook.org.
Higgs, J., Refshauge, K. & Ellis, E. (2001). Portrait of the physiotherapy profession. J
Interprof Care, 15(1), 79-89.
Hilde, G., Staer-Jensen, J., Siafarikas, F., Gjestland, K., Engh, M. E. & Bo, K. (2013).
How well can pelvic floor muscles with major defects contract? A
cross-sectional comparative study 6 weeks after delivery using transperineal
3D/4D ultrasound and manometer. BJOG, 120(11), 1423-1429.
Hill, K., Dolmage, T. E., Woon, L., Coutts, D., Goldstein, R. & Brooks, D. (2012a).
Comparing peak and submaximal cardiorespiratory responses during field
References
251
walking tests with incremental cycle ergometry in COPD. Respirology, 17(2),
278-284.
Hill, K., Dolmage, T. E., Woon, L., Coutts, D., Goldstein, R. & Brooks, D. (2012b).
A simple method to derive speed for the endurance shuttle walk test. Respir
Med, 106(12), 1665-1670.
Hinz, A., Singer, S. & Brahler, E. (2014). European reference values for the quality of
life questionnaire EORTC QLQ-C30: Results of a German investigation and a
summarizing analysis of six European general population normative studies.
Acta Oncol, 53(7), 958-965.
Hirano, A., Koda, K., Kosugi, C., Yamazaki, M. & Yasuda, H. (2011). Damage to
anal sphincter/levator ani muscles caused by operative procedure in anal
sphincter-preserving operation for rectal cancer. Am J Surg, 201(4), 508-513.
Ho, V. P., Lee, Y., Stein, S. L. & Temple, L. K. F. (2011). Sexual Function After
Treatment for Rectal Cancer: A Review. Dis Colon Rectum, 54(1), 113-125.
Ho, Y. H., Chiang, J. M., Tan, M. & Low, J. Y. (1996). Biofeedback therapy for
excessive stool frequency and incontinence following anterior resection or
total colectomy. Dis Colon Rectum, 39(11), 1289-1292.
Ho, Y. H. & Tan, M. (1997). Biofeedback therapy for bowel dysfunction following
low anterior resection. Ann Acad Med Singapore, 26(3), 299-302.
Holla, J. F., van de Poll-Franse, L. V., Huijgens, P. C., Mols, F. & Dekker, J. (2016).
Utilization of supportive care by survivors of colorectal cancer: results from
the PROFILES registry. Support Care Cancer, 24(7), 2883-2892.
Holland, A. E., Spruit, M. A., Troosters, T., Puhan, M. A., Pepin, V., Saey, D.,
McCormack, M. C., Carlin, B. W., Sciurba, F. C., Pitta, F., Wanger, J.,
MacIntyre, N., Kaminsky, D. A., Culver, B. H., Revill, S. M., Hernandes, N.
A., Andrianopoulos, V., Camillo, C. A., Mitchell, K. E., Lee, A. L., Hill, C. J.
& Singh, S. J. (2014). An official European Respiratory Society/American
Thoracic Society technical standard: field walking tests in chronic respiratory
disease. Eur Respir J, 44(6), 1428-1446.
Houchen-Wolloff, L., Boyce, S. & Singh, S. (2015). The minimum clinically
important improvement in the incremental shuttle walk test following cardiac
rehabilitation. Eur J Prev Cardiol, 22(8), 972-978.
References
252
Hozo, S. P., Djulbegovic, B. & Hozo, I. (2005). Estimating the mean and variance
from the median, range, and the size of a sample. BMC Med Res Methodol, 5,
13.
Huang, D. D., Wang, S. L., Zhuang, C. L., Zheng, B. S., Lu, J. X., Chen, F. F., Zhou,
C. J., Shen, X. & Yu, Z. (2015). Sarcopenia, as defined by low muscle mass,
strength and physical performance, predicts complications after surgery for
colorectal cancer. Colorectal Dis, 17(11), O256-O264.
Hubbard, G., Adams, R., Campbell, A., Kidd, L., Leslie, S. J., Munro, J. & Watson, A.
(2016). Is referral of postsurgical colorectal cancer survivors to cardiac
rehabilitation feasible and acceptable? A pragmatic pilot randomised
controlled trial with embedded qualitative study. BMJ Open, 6(1).
Hundley, A. F., Wu, J. M. & Visco, A. G. (2005). A comparison of perineometer to
brink score for assessment of pelvic floor muscle strength. Am J Obstet
Gynecol, 192(5), 1583-1591.
Huxley, R. R., Ansary-Moghaddam, A., Clifton, P., Czernichow, S., Parr, C. L. &
Woodward, M. (2009). The impact of dietary and lifestyle risk factors on risk
of colorectal cancer: a quantitative overview of the epidemiological evidence.
Int J Cancer, 125(1), 171-180.
Hwang, Y. H., Choi, J. S., Nam, Y. S., Salum, M. R., Weiss, E. G., Nogueras, J. J. &
Wexner, S. D. (2005). Biofeedback therapy after perineal rectosigmoidectomy
or J pouch procedure. Surg Innov, 12(2), 135-138.
IPAQ Research Committee (2005). Guidelines for Data Processing and Analysis of
the International Physical Activity Questionnaire (IPAQ). Retrieved from
https://docs.google.com/viewer?a=v&pid=sites&srcid=ZGVmYXVsdGRvbW
Fpbnx0aGVpcGFxfGd4OjE0NDgxMDk3NDU1YWRlZTM.
Jannini, E. A., Maggi, M. & Lenzi, A. (2011). Evaluation of premature ejaculation. J
Sex Med, 8 Suppl 4, 328-334.
Jasperson, K. W., Tuohy, T. M., Neklason, D. W. & Burt, R. W. (2010). Hereditary
and familial colon cancer. Gastroenterology, 138(6), 2044-2058.
Jensen, M. B., Houborg, K. B., Norager, C. B., Henriksen, M. G. & Laurberg, S.
Postoperative changes in fatigue, physical function and body composition: an
analysis of the amalgamated data from five randomized trials on patients
undergoing colorectal surgery. Colorectal Dis, 13(5), 588-593.

References
253
Jerosch-Herold, C. (2005). An Evidence-Based Approach to Choosing Outcome
Measures: a Checklist for the Critical Appraisal of Validity, Reliability and
Responsiveness Studies. Br J Occup Ther, 68(8), 347-353.
Jiang, J. B., Jiang, K., Dai, Y., Wang, R. X., Wu, W. Z., Wang, J. J., Xie, F. B. & Li,
X. M. (2015). Laparoscopic Versus Open Surgery for Mid-Low Rectal Cancer:
a Systematic Review and Meta-Analysis on Short- and Long-Term Outcomes.
J Gastrointest Surg, 19(8), 1497-1512.
John, S. K., George, S., Primrose, J. N. & Fozard, J. B. (2011). Symptoms and signs
in patients with colorectal cancer. Colorectal Dis, 13(1), 17-25.
Johnson, C. M., Wei, C., Ensor, J. E., Smolenski, D. J., Amos, C. I., Levin, B. &
Berry, D. A. (2013). Meta-analyses of colorectal cancer risk factors. Cancer
Causes Control, 24(6), 1207-1222.
Jones, L. W., Eves, N. D., Haykowsky, M., Joy, A. A. & Douglas, P. S. (2008).
Cardiorespiratory exercise testing in clinical oncology research: systematic
review and practice recommendations. Lancet Oncol, 9(8), 757-765.
Jones, N. (1988). Clinical Exercise Testing. Philadelphia: W.B. Saunders.
Jorgensen, M. L., Young, J. M. & Solomon, M. J. (2015). Optimal delivery of
colorectal cancer follow-up care: improving patient outcomes. Patient Relat
Outcome Meas, 6, 127-138.
Joye, I. & Haustermans, K. (2014). Early and late toxicity of radiotherapy for rectal
cancer. Recent Results Cancer Res, 203, 189-201.
Julious, S. A. (2005). Sample size of 12 per group rule of thumb for a pilot study.
Pharm Stat, 4, 287-291.
Juul, T., Ahlberg, M., Biondo, S., Espin, E., Jimenez, L. M., Matzel, K. E., Palmer, G.
J., Sauermann, A., Trenti, L., Zhang, W., Laurberg, S. & Christensen, P.
(2014). Low anterior resection syndrome and quality of life: an international
multicenter study. Dis Colon Rectum, 57(5), 585-591.
Kamper, S. J., Maher, C. G. & Mackay, G. (2009). Global rating of change scales: a
review of strengths and weaknesses and considerations for design. J Man
Manip Ther, 17(3), 163-170.
Kang, S. J. (2015). The association of physical activity and colorectal and breast
cancer: The Fifth Korea National Health and Nutrition Examination Survey
(2008-2011). J Exerc Rehabil, 11(3), 155-160.
References
254
Kaplan, R. M. & Ries, A. L. (2007). Quality of life: concept and definition. COPD,
4(3), 263-271.
Kato, D. J., Rodgers, W. M., Stickland, M. K. & Haennel, R. G. (2012). Impact of
peak oxygen uptake and muscular fitness on the performance of activities of
daily living in patients with chronic obstructive pulmonary disease. J
Cardiopulm Rehabil Prev, 32(6), 400-404.
Kaushal, J. N. & Goldner, F. (1991). Validation of the Digital Rectal Examination as
an Estimate of Anal-Sphincter Squeeze Pressure. Am J Gastroenterol, 86(7),
886-887.
Kelleher, C., Staskin, D., Cherian, P., Cotterill, N., Coyne, K. K., Z. & Symonds, T.
(2013). Patient-Reported Outcome Assessment. Paris: 5th International
Consultation on Incontinence.
Kendall, B. J., Wilson, L. F., Olsen, C. M., Webb, P. M., Neale, R. E., Bain, C. J. &
Whiteman, D. C. (2015). Cancers in Australia in 2010 attributable to
overweight and obesity. Aust N Z J Public Health, 39(5), 452-457.
Kendrick, K. R., Baxi, S. C. & Smith, R. M. (2000). Usefulness of the modified 0-10
Borg scale in assessing the degree of dyspnea in patients with COPD and
asthma. J Emerg Nurs, 26(3), 216-222.
Kent, E. E., Mitchell, S. A., Oakley-Girvan, I. & Arora, N. K. (2014). The importance
of symptom surveillance during follow-up care of leukemia, bladder, and
colorectal cancer survivors. Support Care Cancer, 22(1), 163-172.
Kepenekci, I., Keskinkilic, B., Akinsu, F., Cakir, P., Elhan, A. H., Erkek, A. B. &
Kuzu, M. A. (2011). Prevalence of pelvic floor disorders in the female
population and the impact of age, mode of delivery, and parity. Dis Colon
Rectum, 54(1), 85-94.
Kerschan-Schindl, K., Uher, E., Wiesinger, G., Kaider, A., Ebenbichler, G., Nicolakis,
P., Kollmitzer, J., Preisinger, E. & Fialka-Moser, V. (2002). Reliability of
pelvic floor muscle strength measurement in elderly incontinent women.
Neurourol Urodyn, 21(1), 42-47.
Kim, E. R. & Chang, D. K. (2014). Colorectal cancer in inflammatory bowel disease:
the risk, pathogenesis, prevention and diagnosis. World J Gastroenterol,
20(29), 9872-9881.
Kim, J. K., Jeon, B. G., Song, Y. S., Seo, M. S., Kwon, Y. H., Park, J. W., Ryoo, S. B.,
Jeong, S. Y. & Park, K. J. (2015). Biofeedback Therapy Before Ileostomy

References
255
Closure in Patients Undergoing Sphincter-Saving Surgery for Rectal Cancer:
A Pilot Study. Ann Coloproctol, 31(4), 138-143.
Kim, J. K., Park, M. G. & Shin, S. J. (2014). What is the Minimum Clinically
Important Difference in Grip Strength? Clin Orthop Relat Res, 472(8),
2536-2541.
Kim, K. H., Yu, C. S., Yoon, Y. S., Yoon, S. N., Lim, S. B. & Kim, J. C. (2011).
Effectiveness of biofeedback therapy in the treatment of anterior resection
syndrome after rectal cancer surgery. Dis Colon Rectum, 54(9), 1107-1113.
Kim, Y. H., Kim, K. I., Paik, N. J., Kim, K. W., Jang, H. C. & Lim, J. Y. (2016).
Muscle strength: A better index of low physical performance than muscle
mass in older adults. Geriatr Gerontol Int, 16(5), 577-585.
Kirstein, M. M., Lange, A., Prenzler, A., Manns, M. P., Kubicka, S. & Vogel, A.
(2014). Targeted therapies in metastatic colorectal cancer: a systematic review
and assessment of currently available data. Oncologist, 19(11), 1156-1168.
Klovning, A., Avery, K., Sandvik, H. & Hunskaar, S. (2009). Comparison of two
questionnaires for assessing the severity of urinary incontinence: The ICIQ-UI
SF versus the incontinence severity index. Neurourol Urodyn, 28(5), 411-415.
Knols, R., Aaronson, N. K., Uebelhart, D., Fransen, J. & Aufdemkampe, G. (2005).
Physical exercise in cancer patients during and after medical treatment: a
systematic review of randomized and controlled clinical trials. J Clin Oncol,
23(16), 3830-3842.
Knowles, G., Haigh, R., McLean, C., Phillips, H. A., Dunlop, M. G. & Din, F. V.
(2013). Long term effect of surgery and radiotherapy for colorectal cancer on
defecatory function and quality of life. Eur J Oncol Nurs, 17(5), 570-577.
Koda, K., Yasuda, H., Hirano, A., Kosugi, C., Suzuki, M., Yamazaki, M., Tezuka, T.,
Higuchi, R., Tsuchiya, H. & Saito, N. (2009). Evaluation of postoperative
damage to anal sphincter/levator ani muscles with three-dimensional vector
manometry after sphincter-preserving operation for rectal cancer. J Am Coll
Surg, 208(3), 362-367.
Konanz, J., Herrle, F., Weiss, C., Post, S. & Kienle, P. (2013). Quality of life of
patients after low anterior, intersphincteric, and abdominoperineal resection
for rectal cancer--a matched-pair analysis. Int J Colorectal Dis, 28(5),
679-688.
References
256
Kuhnt, S., Ernst, J., Singer, S., Ruffer, J. U., Kortmann, R. D., Stolzenburg, J. U. &
Schwarz, R. (2009). Fatigue in cancer survivors--prevalence and correlates.
Onkologie, 32(6), 312-317.
Kuo, L. J., Lin, Y. C., Lai, C. H., Lin, Y. K., Huang, Y. S., Hu, C. C. & Chen, S. C.
(2015). Improvement of fecal incontinence and quality of life by electrical
stimulation and biofeedback for patients with low rectal cancer after
intersphincteric resection. Arch Phys Med Rehabil, 96(8), 1442-1447.
Kye, B. H., Kim, H. J., Kim, G., Yoo, R. N. & Cho, H. M. (2016). The Effect of
Biofeedback Therapy on Anorectal Function After the Reversal of Temporary
Stoma When Administered During the Temporary Stoma Period in Rectal
Cancer Patients With Sphincter-Saving Surgery The Interim Report of a
Prospective Randomized Controlled Trial. Medicine (Baltimore), 95(18),
e3611.
Labianca, R., Beretta, G. D., Kildani, B., Milesi, L., Merlin, F., Mosconi, S., Pessi, M.
A., Prochilo, T., Quadri, A., Gatta, G., de Braud, F. & Wils, J. (2010). Colon
cancer. Crit Rev Oncol Hematol, 74(2), 106-133.
Laforest, A., Bretagnol, F., Mouazan, A. S., Maggiori, L., Ferron, M. & Panis, Y.
(2012). Functional disorders after rectal cancer resection: does a rehabilitation
programme improve anal continence and quality of life? Colorectal Dis,
14(10), 1231-1237.
Lai, X., Wong, F. K. & Ching, S. S. (2013). Review of bowel dysfunction of rectal
cancer patients during the first five years after sphincter-preserving surgery: a
population in need of nursing attention. Eur J Oncol Nurs, 17(5), 681-692.
Laiyemo, A. O. (2014). The risk of colonic adenomas and colonic cancer in obesity.
Best Pract Res Clin Gastroenterol, 28(4), 655-663.
Lakoski, S. G., Willis, B. L., Barlow, C. E., Leonard, D., Gao, A., Radford, N. B.,
Farrell, S. W., Douglas, P. S., Berry, J. D., DeFina, L. F. & Jones, L. W.
(2015). Midlife Cardiorespiratory Fitness, Incident Cancer, and Survival After
Cancer in Men: The Cooper Center Longitudinal Study. JAMA Oncol, 1(2),
231-237.
Lam, T. J., Mulder, C. J. & Felt-Bersma, R. J. (2012). Critical reappraisal of anorectal
function tests in patients with faecal incontinence who have failed
conservative treatment. Int J Colorectal Dis, 27(7), 931-937.
References
257
Landis, J. R. & Koch, G. G. (1977). The measurement of observer agreement for
categorical data. Biometrics, 33(1), 159-174.
Lang, C. E., Edwards, D. F., Birkenmeier, R. L. & Dromerick, A. W. (2008).
Estimating minimal clinically important differences of upper-extremity
measures early after stroke. Arch Phys Med Rehabil, 89(9), 1693-1700.
Lange, M. M. & de Velde, C. J. H. V. (2010). Long-Term Anorectal and Urogenital
Dysfunction After Rectal Cancer Treatment. Semin Colon Rectal Surg, 21(2),
87-94.
Lange, M. M., Maas, C. P., Marijnen, C. A. M., Wiggers, T., Rutten, H. J.,
Kranenbarg, E. K., van de Velde, C. J. H. & Tr, D. T. M. E. (2008). Urinary
dysfunction after rectal cancer treatment is mainly caused by surgery. Br J
Surg, 95(8), 1020-1028.
Lange, M. M. & van de Velde, C. J. (2011). Urinary and sexual dysfunction after
rectal cancer treatment. Nat Rev Urol, 8(1), 51-57.
Langner, C., Harbaum, L., Pollheimer, M. J., Kornprat, P., Lindtner, R. A.,
Schlemmer, A., Vieth, M. & Rehak, P. (2012). Mucinous differentiation in
colorectal cancer--indicator of poor prognosis? Histopathology, 60(7),
1060-1072.
Larson, J. L. (2007). Functional performance and physical activity in chronic
obstructive pulmonary disease: theoretical perspectives. COPD, 4(3), 237-242.
Laterza, R. M., Schrutka, L., Umek, W., Albrich, S. & Koelbl, H. (2015). Pelvic floor
dysfunction after levator trauma 1-year postpartum: a prospective case-control
study. Int Urogynecol J, 26(1), 41-47.
Lavie, C. J. & Milani, R. V. (1994). Patients with high baseline exercise capacity
benefit from cardiac rehabilitation and exercise training programs. Am Heart J,
128(6 Pt 1), 1105-1109.
Lee, A. L., Cecins, N., Holland, A. E., Hill, C. J., McDonald, C. F., Burge, A. T.,
Rautela, L., Thompson, P. J., Stirling, R. G. & Jenkins, S. (2015). Field
Walking Tests Are Reliable and Responsive to Exercise Training in People
With Non-Cystic Fibrosis Bronchiectasis. J Cardiopulm Rehabil Prev, 35(6),
439-445.
Lee, J., Lee, M., Hong, S., Kim, J. Y., Park, H., Oh, M., Yang, H. I., Kang, D. W.,
Park, J., Kim, D. I., Chu, S., Lee, J., Hur, H., Kim, N. K. & Jeon, J. Y. (2015).
References
258
Association between physical fitness, quality of life, and depression in stage
II-III colorectal cancer survivors. Support Care Cancer, 23(9), 2569-2577.
Lee, K. C., Fahmy, N. & Brock, G. B. (2013). Sexual dysfunction in 2013: Advances
in epidemiology, diagnosis and treatment. Arab J Urol, 11(3), 194-202.
Lee, P. H., Macfarlane, D. J., Lam, T. H. & Stewart, S. M. (2011). Validity of the
International Physical Activity Questionnaire Short Form (IPAQ-SF): a
systematic review. Int J Behav Nutr Phys Act, 8, 115.
Leong, D. P., Teo, K. K., Rangarajan, S., Kutty, V. R., Lanas, F., Hui, C., Quanyong,
X., Zhenzhen, Q., Jinhua, T., Noorhassim, I., AlHabib, K. F., Moss, S. J.,
Rosengren, A., Akalin, A. A., Rahman, O., Chifamba, J., Orlandini, A.,
Kumar, R., Yeates, K., Gupta, R., Yusufali, A., Dans, A., Avezum, A.,
Lopez-Jaramillo, P., Poirier, P., Heidari, H., Zatonska, K., Iqbal, R., Khatib, R.
& Yusuf, S. (2016). Reference ranges of handgrip strength from 125,462
healthy adults in 21 countries: a prospective urban rural epidemiologic (PURE)
study. J Cachexia Sarcopenia Muscle. Advance online publication. doi:
10.1002/jcsm.12112.
Leong, D. P., Teo, K. K., Rangarajan, S., Lopez-Jaramillo, P., Avezum, A., Orlandini,
A., Seron, P., Ahmed, S. H., Rosengren, A., Kelishadi, R., Rahman, O.,
Swaminathan, S., Iqbal, R., Gupta, R., Lear, S. A., Oguz, A., Yusoff, K.,
Zatonska, K., Chifamba, J., Igumbor, E., Mohan, V., Anjana, R. M., Gu, H. Q.,
Li, W., Yusuf, S. & Epidemiolo, P. U. R. (2015). Prognostic value of grip
strength: findings from the Prospective Urban Rural Epidemiology (PURE)
study. Lancet, 386(9990), 266-273.
Leung, J. & Funder, J. (2014). Obesity: A National Epidemic and its Impact on
Australia. Retrieved from
http://www.obesityaustralia.org/_literature_168776/No_Time_To_Weight_Re
port.
Lev, E. L. (1997). Bandura's theory of self-efficacy: applications to oncology. Sch Inq
Nurs Pract, 11(1), 21-37; discussion 39-43.
Li, C., Carli, F., Lee, L., Charlebois, P., Stein, B., Liberman, A. S., Kaneva, P.,
Augustin, B., Wongyingsinn, M., Gamsa, A., Kim do, J., Vassiliou, M. C. &
Feldman, L. S. (2013). Impact of a trimodal prehabilitation program on
functional recovery after colorectal cancer surgery: a pilot study. Surg Endosc,
27(4), 1072-1082.

References
259
Li, Y., Yang, X., Xu, C., Zhang, Y. & Zhang, X. (2013). Normal values and pressure
morphology for three-dimensional high-resolution anorectal manometry of
asymptomatic adults: a study in 110 subjects. Int J Colorectal Dis, 28(8),
1161-1168.
Liang, P. S., Chen, T. Y. & Giovannucci, E. (2009). Cigarette smoking and colorectal
cancer incidence and mortality: systematic review and meta-analysis. Int J
Cancer, 124(10), 2406-2415.
Ligibel, J. A., Meyerhardt, J., Pierce, J. P., Najita, J., Shockro, L., Campbell, N.,
Newman, V. A., Barbier, L., Hacker, E., Wood, M., Marshall, J., Paskett, E. &
Shapiro, C. (2012). Impact of a telephone-based physical activity intervention
upon exercise behaviors and fitness in cancer survivors enrolled in a
cooperative group setting. Breast Cancer Res Treat, 132(1), 205-213.
Lin, K. Y., Granger, C. L., Denehy, L. & Frawley, H. C. (2015). Pelvic floor muscle
training for bowel dysfunction following colorectal cancer surgery: A
systematic review. Neurourol Urodyn, 34(8), 703-712.
Lin, Y. H., Chen, H. P. & Liu, K. W. (2015). Fecal Incontinence and Quality of Life
in Adults With Rectal Cancer After Lower Anterior Resection. J Wound
Ostomy Continence Nurs, 42(4), 395-400.
Lindsetmo, R. O., Joh, Y. G. & Delaney, C. P. (2008). Surgical treatment for rectal
cancer: an international perspective on what the medical gastroenterologist
needs to know. World J Gastroenterol, 14(21), 3281-3289.
Liu, C. H., Chen, C. H. & Lee, J. C. (2011). Rehabilitation exercise on the quality of
life in anal sphincter-preserving surgery. Hepatogastroenterology,
58(110-111), 1461-1465.
Loos, M., Quentmeier, P., Schuster, T., Nitsche, U., Gertler, R., Keerl, A., Kocher, T.,
Friess, H. & Rosenberg, R. (2013). Effect of preoperative
radio(chemo)therapy on long-term functional outcome in rectal cancer patients:
a systematic review and meta-analysis. Ann Surg Oncol, 20(6), 1816-1828.
Luckett, T., Butow, P. N., King, M. T., Oguchi, M., Heading, G., Hackl, N. A.,
Rankin, N. & Price, M. A. (2010). A review and recommendations for optimal
outcome measures of anxiety, depression and general distress in studies
evaluating psychosocial interventions for English-speaking adults with
heterogeneous cancer diagnoses. Support Care Cancer, 18(10), 1241-1262.
References
260
Lukacz, E. S., Lawrence, J. M., Contreras, R., Nager, C. W. & Luber, K. M. (2006).
Parity, mode of delivery, and pelvic floor disorders. Obstet Gynecol, 107(6),
1253-1260.
Luxton, N., Alison, J. A., Wu, J. & Mackey, M. G. (2008). Relationship between field
walking tests and incremental cycle ergometry in COPD. Respirology, 13(6),
856-862.
Lynch, B. M., Cerin, E., Owen, N. & Aitken, J. F. (2007). Associations of
leisure-time physical activity with quality of life in a large, population-based
sample of colorectal cancer survivors. Cancer Causes Control, 18(7),
735-742.
Lynch, B. M., Owen, N., Hawkes, A. L. & Aitken, J. F. (2010). Perceived barriers to
physical activity for colorectal cancer survivors. Support Care Cancer, 18(6),
729-734.
Madersbacher, S., Pycha, A., Schatzl, G., Mian, C., Klingler, C. H. & Marberger, M.
(1998). The aging lower urinary tract: a comparative urodynamic study of men
and women. Urology, 51(2), 206-212.
Mainguy, V., Malenfant, S., Neyron, A. S., Saey, D., Maltais, F., Bonnet, S. &
Provencher, S. (2014). Alternatives to the six-minute walk test in pulmonary
arterial hypertension. PLoS One, 9(8), e103626.
Makino, K., Ihira, H., Mizumoto, A., Shimizu, K., Ishida, T. & Furuna, T. (2015).
Associations between the settings of exercise habits and health-related
outcomes in community-dwelling older adults. J Phys Ther Sci, 27(7),
2207-2211.
Malykhina, A. P., Wyndaele, J. J., Andersson, K. E., De Wachter, S. & Dmochowski,
R. R. (2012). Do the urinary bladder and large bowel interact, in sickness or in
health?: ICI-RS 2011. Neurourol Urodyn, 31(3), 352-358.
Maringe, C., Walters, S., Rachet, B., Butler, J., Fields, T., Finan, P., Maxwell, R.,
Nedrebo, B., Pahlman, L., Sjovall, A., Spigelman, A., Engholm, G., Gavin, A.,
Gjerstorff, M. L., Hatcher, J., Johannesen, T. B., Morris, E., McGahan, C. E.,
Tracey, E., Turner, D., Richards, M. A., Coleman, M. P. & Group, I. M. W.
(2013). Stage at diagnosis and colorectal cancer survival in six high-income
countries: a population-based study of patients diagnosed during 2000-2007.
Acta Oncol, 52(5), 919-932.
References
261
Maris, A., Devreese, A. M., D'Hoore, A., Penninckx, F. & Staes, F. (2013). Treatment
options to improve anorectal function following rectal resection: a systematic
review. Colorectal Dis, 15(2), e67-78.
Maris, A., Penninckx, F., Devreese, A. M., Staes, F., Moons, P., Van Cutsem, E.,
Haustermans, K. & D'Hoore, A. (2013). Persisting anorectal dysfunction after
rectal cancer surgery. Colorectal Dis, 15(11), e672-e679.
Martin, S. A., Haren, M. T., Marshall, V. R., Lange, K. & Wittert, G. A. (2011).
Prevalence and factors associated with uncomplicated storage and voiding
lower urinary tract symptoms in community-dwelling Australian men. World J
Urol, 29(2), 179-184.
Martinez, D., Pitson, G., MacKinlay, A. & Cavedon, L. (2014). Cross-hospital
portability of information extraction of cancer staging information. Artif Intell
Med, 62(1), 11-21.
Marventano, S., Forjaz, M., Grosso, G., Mistretta, A., Giorgianni, G., Platania, A.,
Gangi, S., Basile, F. & Biondi, A. (2013). Health related quality of life in
colorectal cancer patients: state of the art. BMC Surg, 13 Suppl 2, S15.
Marwan, K., Staples, M. P., Thursfield, V. & Bell, S. W. (2010). The rate of
abdominoperineal resections for rectal cancer in the state of Victoria, Australia:
a population-based study. Dis Colon Rectum, 53(12), 1645-1651.
Matheson, L. (1996). Functional capacity evaluation. Chicago: Mosby Yearbook.
Mathiowetz, V. (2002). Comparison of Rolyan and Jamar dynamometers for
measuring grip strength. Occup Ther Int, 9(3), 201-209.
Mayo, N. E., Feldman, L., Scott, S., Zavorsky, G., Kim do, J., Charlebois, P., Stein, B.
& Carli, F. (2011). Impact of preoperative change in physical function on
postoperative recovery: argument supporting prehabilitation for colorectal
surgery. Surgery, 150(3), 505-514.
McCabe, M. P. & Goldhammer, D. L. (2013). Prevalence of women's sexual desire
problems: what criteria do we use? Arch Sex Behav, 42(6), 1073-1078.
McCarney, R., Warner, J., Iliffe, S., van Haselen, R., Griffin, M. & Fisher, P. (2007).
The Hawthorne Effect: a randomised, controlled trial. BMC Med Res
Methodol, 7, 30.
McCool, M. E., Theurich, M. A. & Apfelbacher, C. (2014). Prevalence and predictors
of female sexual dysfunction: a protocol for a systematic review. Syst Rev, 3,
75.
References
262
McEvoy, P. M., Grove, R. & Slade, T. (2011). Epidemiology of anxiety disorders in
the Australian general population: findings of the 2007 Australian National
Survey of Mental Health and Wellbeing. Aust N Z J Psychiatry, 45(11),
957-967.
McGowan, E. L., Speed-Andrews, A. E., Blanchard, C. M., Rhodes, R. E.,
Friedenreich, C. M., Culos-Reed, S. N. & Courneya, K. S. (2013). Physical
activity preferences among a population-based sample of colorectal cancer
survivors. Oncol Nurs Forum, 40(1), 44-52.
McGrath, D. R., Leong, D. C., Armstrong, B. K. & Spigelman, A. D. (2004).
Management of colorectal cancer patients in Australia: the National Colorectal
Cancer Care Survey. ANZ J Surg, 74(1-2), 55-64.
McKenzie, S., Barnes, S. & Schwartz, R. (2005). An update on the surgical
management of colon cancer. Curr Surg, 62(3), 313-318.
McKeough, Z. J., Leung, R. W. M. & Alison, J. A. (2011). Shuttle Walk Tests as
Outcome Measures Are Two Incremental Shuttle Walk Tests and Two
Endurance Shuttle Walk Tests Necessary? Am J Phys Med Rehabil, 90(1),
35-39.
McNair, A. G., Whistance, R. N., Forsythe, R. O., Rees, J., Jones, J. E., Pullyblank, A.
M., Avery, K. N., Brookes, S. T., Thomas, M. G., Sylvester, P. A., Russell, A.,
Oliver, A., Morton, D., Kennedy, R., Jayne, D. G., Huxtable, R., Hackett, R.,
Dutton, S. J., Coleman, M. G., Card, M., Brown, J. & Blazeby, J. M. (2015).
Synthesis and summary of patient-reported outcome measures to inform the
development of a core outcome set in colorectal cancer surgery. Colorectal
Dis, 17(11), O217-229.
McSorley, S. T., Horgan, P. G. & McMillan, D. C. (2016). The impact of the type and
severity of postoperative complications on long-term outcomes following
surgery for colorectal cancer: A systematic review and meta-analysis. Crit Rev
Oncol Hematol, 97, 168-177.
Medeiros, M., Oshima, C. T. & Forones, N. M. (2010). Depression and anxiety in
colorectal cancer patients. J Gastrointest Cancer, 41(3), 179-184.
Messelink, B., Benson, T., Berghmans, B., Bo, K., Corcos, J., Fowler, C., Laycock, J.,
Lim, P. H. C., van Lunsen, R., Nijeholt, G. L., Pemberton, J., Wang, A.,
Watier, A. & Van Kerrebroeck, P. (2005). Standardization of terminology of
pelvic floor muscle function and dysfunction: Report from the pelvic floor
References
263
clinical assessment group of the international continence society. Neurourol
Urodyn, 24(4), 374-380.
Meyerhardt, J. A., Giovannucci, E. L., Holmes, M. D., Chan, A. T., Chan, J. A.,
Colditz, G. A. & Fuchs, C. S. (2006). Physical activity and survival after
colorectal cancer diagnosis. J Clin Oncol, 24(22), 3527-3534.
Meyerhardt, J. A., Heseltine, D., Niedzwiecki, D., Hollis, D., Saltz, L. B., Mayer, R.
J., Thomas, J., Nelson, H., Whittom, R., Hantel, A., Schilsky, R. L. & Fuchs,
C. S. (2006). Impact of physical activity on cancer recurrence and survival in
patients with stage III colon cancer: findings from CALGB 89803. J Clin
Oncol, 24(22), 3535-3541.
Midtgaard, J., Stage, M., Moller, T., Andersen, C., Quist, M., Rorth, M., Herrstedt, J.,
Vistisen, K., Christiansen, B. & Adamsen, L. (2011). Exercise may reduce
depression but not anxiety in self-referred cancer patients undergoing
chemotherapy. Post-hoc analysis of data from the 'Body & Cancer' trial. Acta
Oncol, 50(5), 660-669.
Miller, J. M., Ashton-Miller, J. A. & DeLancey, J. O. (1998). A pelvic muscle
precontraction can reduce cough-related urine loss in selected women with
mild SUI. J Am Geriatr Soc, 46(7), 870-874.
Miller, K. D., Siegel, R. L., Lin, C. C., Mariotto, A. B., Kramer, J. L., Rowland, J. H.,
Stein, K. D., Alteri, R. & Jemal, A. (2016). Cancer treatment and survivorship
statistics, 2016. CA Cancer J Clin, 66(4), 271-89.
Miller, M. R., Hankinson, J., Brusasco, V., Burgos, F., Casaburi, R., Coates, A.,
Crapo, R., Enright, P., van der Grinten, C. P. M., Gustafsson, P., Jensen, R.,
Johnson, D. C., MacIntyre, N., McKay, R., Navajas, D., Pedersen, O. F.,
Pellegrino, R., Viegi, G. & Wanger, J. (2005). Standardisation of spirometry.
Eur Respir J, 26(2), 319-338.
Minneci, C., Mello, A. M., Mossello, E., Baldasseroni, S., Macchi, L., Cipolletti, S.,
Marchionni, N. & Di Bari, M. (2015). Comparative Study of Four Physical
Performance Measures as Predictors of Death, Incident Disability, and Falls in
Unselected Older Persons: The Insufficienza Cardiaca negli Anziani Residenti
a Dicomano Study. J Am Geriatr Soc, 63(1), 136-141.
Mizuno, M., Kakuta, M., Ono, Y., Kato, A. & Inoue, Y. (2007). Experiences of
Japanese patients with colorectal cancer during the first six months after
surgery. Oncol Nurs Forum, 34(4), 869-876.
References
264
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. (2009). Preferred reporting items
for systematic reviews and meta-analyses: the PRISMA statement. BMJ, 339,
b2535.
Mols, F., Beijers, A. J., Vreugdenhil, G., Verhulst, A., Schep, G. & Husson, O. (2015).
Chemotherapy-induced peripheral neuropathy, physical activity and
health-related quality of life among colorectal cancer survivors from the
PROFILES registry. J Cancer Surviv, 9(3), 512-522.
Mols, F., Husson, O., Roukema, J. A. & van de Poll-Franse, L. V. (2013). Depressive
symptoms are a risk factor for all-cause mortality: results from a prospective
population-based study among 3,080 cancer survivors from the PROFILES
registry. J Cancer Surviv, 7(3), 484-492.
Moore DS, McCabe GP & BA, C. (2010). Introduction to the Basic Practice of
Statistics New York: W.H. Freeman & Co.
Moriello, C., Mayo, N. E., Feldman, L. & Carli, F. (2008). Validating the six-minute
walk test as a measure of recovery after elective colon resection surgery. Arch
Phys Med Rehabil, 89(6), 1083-1089.
Morino, M., Parini, U., Allaix, M. E., Monasterolo, G., Brachet Contul, R. & Garrone,
C. (2009). Male sexual and urinary function after laparoscopic total mesorectal
excision. Surg Endosc, 23(6), 1233-1240.
Mukaka, M. M. (2012). Statistics Corner: A guide to appropriate use of Correlation
coefficient in medical research. Malawi Med J, 24(3), 69-71.
Mullins-Sweatt, S. N., Lengel, G. J. & DeShong, H. L. (2016). The Importance of
Considering Clinical Utility in the Construction of a Diagnostic Manual. Annu
Rev Clin Psychol, 12, 133-155.
Murata, A., Brown, C. J., Raval, M. & Phang, P. T. (2008). Impact of short-course
radiotherapy and low anterior resection on quality of life and bowel function
in primary rectal cancer. Am J Surg, 195(5), 611-615.
Muyor, J. M. (2013). Exercise Intensity and Validity of the Ratings of Perceived
Exertion (Borg and OMNI Scales) in an Indoor Cycling Session. J Hum Kinet,
39, 93-101.
National Cancer Institute (2014). Colon and Rectal Cancer. Retrieved from
http://www.cancer.gov/cancertopics/types/colon-and-rectal.

References
265
National Cancer Institute (2016). SEER Cancer Statistics Factsheets: Colon and
Rectum Cancer. Retrieved from
http://seer.cancer.gov/statfacts/html/colorect.html.
National Comprehensive Cancer Network (NCCN) (2016a). NCCN Clinical Practice
Guidelines in Oncology. Colon Cancer Version 2.2016. Retrieved from
https://www.nccn.org/professionals/physician_gls/f_guidelines.asp#colon.
National Comprehensive Cancer Network (NCCN) (2016b). NCCN Clinical Practice
Guidelines in Oncology. Rectal Cancer Version 2.2016. Retrieved from
https://www.nccn.org/professionals/physician_gls/f_guidelines.asp#colon.
National Health Medical Research Council (2009). NHMRC additional levels of
evidence and grades for recommendations for developers of guidelines.
Canberra: National Health Medical Research Council.
Ng, K. S., Sivakumaran, Y., Nassar, N. & Gladman, M. A. (2015). Fecal Incontinence:
Community Prevalence and Associated Factors--A Systematic Review. Dis
Colon Rectum, 58(12), 1194-1209.
Ngai, S. P., Spencer, L. M., Jones, A. Y. & Alison, J. A. (2015). Repeatability of the
endurance shuttle walk test in people with Chronic Obstructive Pulmonary
Disease (COPD). Clin Respir J. Advance online publication. doi:
10.1111/crj.12430.
Nguyen, S. P., Bent, S., Chen, Y. H. & Terdiman, J. P. (2009). Gender as a Risk
Factor for Advanced Neoplasia and Colorectal Cancer: A Systematic Review
and Meta-analysis. Clin Gastroenterol Hepatol, 7(6), 676-681.
Nici, L. & ZuWallack, R. (2015). Chronic Obstructive Pulmonary Disease-Evolving
Concepts in Treatment: Advances in Pulmonary Rehabilitation. Semin Respir
Crit Care Med, 36(4), 567-574.
Nikoletti, S., Young, J., Levitt, M., King, M., Chidlow, C. & Hollingsworth, S. (2008).
Bowel problems, self-care practices, and information needs of colorectal
cancer survivors at 6 to 24 months after sphincter-saving surgery. Cancer Nurs,
31(5), 389-398.
Noe, M., Schroy, P., Demierre, M. F., Babayan, R. & Geller, A. C. (2008). Increased
cancer risk for individuals with a family history of prostate cancer, colorectal
cancer, and melanoma and their associated screening recommendations and
practices. Cancer Causes Control, 19(1), 1-12.
References
266
Norman, G. (2010). Likert scales, levels of measurement and the "laws" of statistics.
Adv Health Sci Educ Theory Pract, 15(5), 625-632.
North, T. C., McCullagh, P. & Tran, Z. V. (1990). Effect of exercise on depression.
Exerc Sport Sci Rev, 18, 379-415.
Norton, C., Chelvanayagam, S., Wilson-Barnett, J., Redfern, S. & Kamm, M. A.
(2003). Randomized controlled trial of biofeedback for fecal incontinence.
Gastroenterology, 125(5), 1320-1329.
Norton, C. & Cody, J. D. (2012). Biofeedback and/or sphincter exercises for the
treatment of faecal incontinence in adults. Cochrane Database Syst Rev, 11;(7),
CD002111.
Nygaard, I. E. & Shaw, J. M. (2016). Physical activity and the pelvic floor. Am J
Obstet Gynecol, 214(2), 164-171.
O'Donnell, L. J., Virjee, J. & Heaton, K. W. (1990). Detection of pseudodiarrhoea by
simple clinical assessment of intestinal transit rate. BMJ, 300(6722), 439-440.
Obrocea, F. L., Sajin, M., Marinescu, E. C. & Stoica, D. (2011). Colorectal cancer
and the 7th revision of the TNM staging system: review of changes and
suggestions for uniform pathologic reporting. Rom J Morphol Embryol, 52(2),
537-544.
Oken, M. M., Creech, R. H., Tormey, D. C., Horton, J., Davis, T. E., McFadden, E. T.
& Carbone, P. P. (1982). Toxicity and response criteria of the Eastern
Cooperative Oncology Group. Am J Clin Oncol, 5(6), 649-655.
Onerup, A., Bock, D., Borjesson, M., Fagevik Olsen, M., Gellerstedt, M., Haglind, E.,
Nilsson, H. & Angenete, E. (2016). Is preoperative physical activity related to
post-surgery recovery?-a cohort study of colorectal cancer patients. Int J
Colorectal Dis, 31(6), 1131-1140.
Osoba, D., Rodrigues, G., Myles, J., Zee, B. & Pater, J. (1998). Interpreting the
significance of changes in health-related quality-of-life scores. J Clin Oncol,
16(1), 139-144.
Osuga, Y., Okamura, K., Ando, F. & Shimokata, H. (2013). Prevalence of lower
urinary tract symptoms in middle-aged and elderly Japanese. Geriatr Gerontol
Int, 13(4), 1010-1017.
Otto, S. J., Korfage, I. J., Polinder, S., van der Heide, A., de Vries, E., Rietjens, J. A.
C. & Soerjomataram, I. (2015). Association of change in physical activity and
References
267
body weight with quality of life and mortality in colorectal cancer: a
systematic review and meta-analysis. Support Care Cancer, 23(5), 1237-1250.
Oversand, S., Kamisan Atan, I., Shek, K. L. & Dietz, H. P. (2015). The association of
urinary and anal incontinence with measures of pelvic floor muscle
contractility. Ultrasound Obstet Gynecol, 47(5), 642-645.
Oyesanmi, O., Snyder, D., Sullivan, N., Reston, J., Treadwell, J. & Schoelles, K. M.
(2010). Alcohol consumption and cancer risk: understanding possible causal
mechanisms for breast and colorectal cancers. Evid Rep Technol Assess (Full
Rep), (197), 1-151.
Ozgen, Z., Ozden, S., Atasoy, B. M., Ozyurt, H., Gencosmanoglu, R. & Imeryuz, N.
(2015). Long-term effects of neoadjuvant chemoradiotherapy followed by
sphincter-preserving resection on anal sphincter function in relation to quality
of life among locally advanced rectal cancer patients: a cross-sectional
analysis. Radiat Oncol, 10, 168.
Panjari, M., Bell, R. J., Burney, S., Bell, S., McMurrick, P. J. & Davis, S. R. (2012).
Sexual function, incontinence, and wellbeing in women after rectal cancer--a
review of the evidence. J Sex Med, 9(11), 2749-2758.
Park, S. B., Goldstein, D., Krishnan, A. V., Lin, C. S., Friedlander, M. L., Cassidy, J.,
Koltzenburg, M. & Kiernan, M. C. (2013). Chemotherapy-induced peripheral
neurotoxicity: a critical analysis. CA Cancer J Clin, 63(6), 419-437.
Parreira, V. F., Janaudis-Ferreira, T., Evans, R. A., Mathur, S., Goldstein, R. S. &
Brooks, D. (2014). Measurement properties of the incremental shuttle walk
test. a systematic review. Chest, 145(6), 1357-1369.
Parry, C., Kent, E. E., Mariotto, A. B., Alfano, C. M. & Rowland, J. H. (2011).
Cancer survivors: a booming population. Cancer Epidemiol Biomarkers Prev,
20(10), 1996-2005.
Peng, J., Shi, D., Goodman, K. A., Goldstein, D., Xiao, C., Guan, Z. & Cai, S. (2011).
Early results of quality of life for curatively treated rectal cancers in Chinese
patients with EORTC QLQ-CR29. Radiat Oncol, 6, 93.
Peolsson, A., Hedlund, R. & Oberg, B. (2001). Intra- and inter-tester reliability and
reference values for hand strength. J Rehabil Med, 33(1), 36-41.
Perera, M. T., Deen, K. I., Wijesuriya, S. R., Kumarage, S. K., De Zylva, S. T. &
Ariyaratne, M. H. (2008). Sexual and urinary dysfunction following rectal
References
268
dissection compared with segmental colectomy. Colorectal Dis, 10(7),
689-693.
Pettersson, G., Bertero, C., Unosson, M. & Borjeson, S. (2014). Symptom prevalence,
frequency, severity, and distress during chemotherapy for patients with
colorectal cancer. Support Care Cancer, 22(5), 1171-1179.
Phipps, E., Braitman, L. E., Stites, S. & Leighton, J. C. (2008). Quality of life and
symptom attribution in long-term colon cancer survivors. J Eval Clin Pract,
14(2), 254-258.
Pierson, L. M., Miller, L. E. & Herbert, W. G. (2004). Predicting exercise training
outcome from cardiac rehabilitation. J Cardiopulm Rehabil, 24(2), 113-118;
quiz 119-120.
Pittman, J. S., Benson, J. T. & Sumners, J. E. (1990). Physiologic evaluation of the
anorectum. A new ultrasound technique. Dis Colon Rectum, 33(6), 476-478.
Polat, U., Arpaci, A., Demir, S., Erdal, S. & Yalcin, S. (2014). Evaluation of quality
of life and anxiety and depression levels in patients receiving chemotherapy
for colorectal cancer: impact of patient education before treatment initiation. J
Gastrointest Oncol, 5(4), 270-275.
Porpiglia, A. S. & Sigurdson, E. R. (2015). Surgical Options in the Treatment of
Lower Gastrointestinal Tract Cancers. Curr Treat Options Oncol, 16(9), 46.
Portney, L. G. & Watkins, M. P. (2009). Foundations of Clinical Research:
Applications to Practice. Upper Saddle River, NJ: Prentice Hall.
Probst, M., Pages, H., Riemann, J. F., Eickhoff, A., Raulf, F. & Kolbert, G. (2010).
Fecal incontinence: part 4 of a series of articles on incontinence. Dtsch Arztebl
Int, 107(34-35), 596-601.
Pucciani, F., Ringressi, M. N., Redditi, S., Masi, A. & Giani, I. (2008). Rehabilitation
of fecal incontinence after sphincter-saving surgery for rectal cancer:
encouraging results. Dis Colon Rectum, 51(10), 1552-1558.
Pucciarelli, S., Del Bianco, P., Efficace, F., Serpentini, S., Capirci, C., De Paoli, A.,
Amato, A., Cuicchi, D. & Nitti, D. (2011). Patient-Reported Outcomes After
Neoadjuvant Chemoradiotherapy for Rectal Cancer A Multicenter Prospective
Observational Study. Ann Surg, 253(1), 71-77.
Quadrilatero, J. & Hoffman-Goetz, L. (2003). Physical activity and colon cancer. A
systematic review of potential mechanisms. J Sports Med Phys Fitness, 43(2),
121-138.
References
269
Rahman, A. & Harding, A. (2013). Prevalence of overweight and obesity epidemic in
Australia: some causes and consequences. JP Journal of Biostatistics, 10(1),
31-48.
Rahmani, N. & Mohseni-Bandpei, M. A. (2011). Application of perineometer in the
assessment of pelvic floor muscle strength and endurance: a reliability study. J
Bodyw Mov Ther, 15(2), 209-214.
Raizada, V., Bhargava, V., Jung, S. A., Karstens, A., Pretorius, D., Krysl, P. & Mittal,
R. K. (2010). Dynamic assessment of the vaginal high-pressure zone using
high-definition manometery, 3-dimensional ultrasound, and magnetic
resonance imaging of the pelvic floor muscles. Am J Obstet Gynecol, 203(2),
172 e171-178.
Regenbogen, S. E., Veenstra, C. M., Hawley, S. T., Banerjee, M., Ward, K. C., Kato,
I. & Morris, A. M. (2014). The personal financial burden of complications
after colorectal cancer surgery. Cancer, 120(19), 3074-3081.
Reilly, J. J., Jr. (1997). Preoperative and postoperative care of standard and high risk
surgical patients. Hematol Oncol Clin North Am, 11(3), 449-459.
Reis, N., Beji, N. K. & Coskun, A. (2010). Quality of life and sexual functioning in
gynecological cancer patients: results from quantitative and qualitative data.
Eur J Oncol Nurs, 14(2), 137-146.
Reiser, L. M. & Schlenk, E. A. (2009). Clinical use of physical activity measures. J
Am Acad Nurse Pract, 21(2), 87-94.
Resch, A., Schneider, N. I. & Langner, C. (2015). Pathological evaluation of
colorectal cancer specimens: advanced and early lesions. Cesk Patol, 51(1),
12-22.
Revill, S. M., Morgan, M. D., Singh, S. J., Williams, J. & Hardman, A. E. (1999). The
endurance shuttle walk: a new field test for the assessment of endurance
capacity in chronic obstructive pulmonary disease. Thorax, 54(3), 213-222.
Roberts, H. C., Denison, H. J., Martin, H. J., Patel, H. P., Syddall, H., Cooper, C. &
Sayer, A. A. (2011). A review of the measurement of grip strength in clinical
and epidemiological studies: towards a standardised approach. Age Ageing,
40(4), 423-429.
Rock, C. L., Doyle, C., Demark-Wahnefried, W., Meyerhardt, J., Courneya, K. S.,
Schwartz, A. L., Bandera, E. V., Hamilton, K. K., Grant, B., McCullough, M.,
References
270
Byers, T. & Gansler, T. (2012). Nutrition and physical activity guidelines for
cancer survivors. CA Cancer J Clin, 62(4), 243-274.
Rodriguez, J. L., Hawkins, N. A., Berkowitz, Z. & Li, C. Y. (2015). Factors
Associated with Health-Related Quality of Life Among Colorectal Cancer
Survivors. Am J Prev Med, 49(6), S518-S527.
Rolfo, C., Bronte, G., Sortino, G., Papadimitriou, K., Passiglia, F., Fiorentino, E.,
Marogy, G., Russo, A. & Peeters, M. (2014). The role of targeted therapy for
gastrointestinal tumors. Expert Rev Gastroenterol Hepatol, 8(8), 875-885.
Roll, S. C., Rana, M., Sigward, S. M., Yani, M. S., Kirages, D. J. & Kutchy, J. J.
(2015). Reliability of Superficial Male Pelvic Floor Structural Measurements
Using Linear-Array Transperineal Sonography. Ultrasound Med Biol, 41(2),
610-617.
Roswall, N. & Weiderpass, E. (2015). Alcohol as a Risk Factor for Cancer: Existing
Evidence in a Global Perspective. J Prev Med Public Health, 48(1), 1-9.
Rothwell, L. A., Bokey, E. L., Keshava, A., Chapuis, P. H. & Dent, O. F. (2006).
Outcomes after admission on the day of elective resection for colorectal
cancer. ANZ J Surg, 76(1-2), 14-19.
Russell, L., Gough, K., Drosdowsky, A., Schofield, P., Aranda, S., Butow, P. N.,
Westwood, J. A., Krishnasamy, M., Young, J. M., Phipps-Nelson, J., King, D.
& Jefford, M. (2015). Psychological distress, quality of life, symptoms and
unmet needs of colorectal cancer survivors near the end of treatment. J Cancer
Surviv, 9(3), 462-470.
Ryhammer, A. M., Laurberg, S. & Sorensen, F. H. (1997). Effects of age on anal
function in normal women. Int J Colorectal Dis, 12(4), 225-229.
Sanchez-Jimenez, A., Cantarero-Villanueva, I., Delgado-Garcia, G., Molina-Barea, R.,
Fernandez-Lao, C., Galiano-Castillo, N. & Arroyo-Morales, M. (2015).
Physical impairments and quality of life of colorectal cancer survivors: a
case-control study. Eur J Cancer Care (Engl), 24(5), 642-649.
Sanoff, H. K., Goldberg, R. M. & Pignone, M. P. (2007). A systematic review of the
use of quality of life measures in colorectal cancer research with attention to
outcomes in elderly patients. Clin Colorectal Cancer, 6(10), 700-709.
Sargent, D. J., Kohne, C. H., Sanoff, H. K., Bot, B. M., Seymour, M. T., de Gramont,
A., Porschen, R., Saltz, L. B., Rougier, P., Tournigand, C., Douillard, J. Y.,
Stephens, R. J., Grothey, A. & Goldberg, R. M. (2009). Pooled safety and
References
271
efficacy analysis examining the effect of performance status on outcomes in
nine first-line treatment trials using individual data from patients with
metastatic colorectal cancer. J Clin Oncol, 27(12), 1948-1955.
Scheer, A. S., Boushey, R. P., Liang, S. Y., Doucette, S., O'Connor, A. M. & Moher,
D. (2011). The Long-term Gastrointestinal Functional Outcomes Following
Curative Anterior Resection in Adults With Rectal Cancer: A Systematic
Review and Meta-analysis. Dis Colon Rectum, 54(12), 1589-1597.
Schmid, D. & Leitzmann, M. F. (2014). Association between physical activity and
mortality among breast cancer and colorectal cancer survivors: a systematic
review and meta-analysis. Ann Oncol, 25(7), 1293-1311.
Schmidt, K., Vogt, L., Thiel, C., Jäger, E. & Banzer, W. (2013). Validity of the
Six-Minute Walk Test in Cancer Patients. Int J Sports Med, 34(07), 631-636.
Schmitz, K. H., Courneya, K. S., Matthews, C., Demark-Wahnefried, W., Galvao, D.
A., Pinto, B. M., Irwin, M. L., Wolin, K. Y., Segal, R. J., Lucia, A., Schneider,
C. M., von Gruenigen, V. E. & Schwartz, A. L. (2010). American College of
Sports Medicine roundtable on exercise guidelines for cancer survivors. Med
Sci Sports Exerc, 42(7), 1409-1426.
Schmitz, K. H., Holtzman, J., Courneya, K. S., Masse, L. C., Duval, S. & Kane, R.
(2005). Controlled physical activity trials in cancer survivors: a systematic
review and meta-analysis. Cancer Epidemiol Biomarkers Prev, 14(7),
1588-1595.
Schreyer, A. G., Paetzel, C., Furst, A., Dendl, L. M., Hutzel, E., Muller-Wille, R.,
Wiggermann, P., Schleder, S., Stroszczynski, C. & Hoffstetter, P. (2012).
Dynamic magnetic resonance defecography in 10 asymptomatic volunteers.
World J Gastroenterol, 18(46), 6836-6842.
Schwarzer, R. & Renner, B. (2005). Health-specific self-efficacy scales. Retrieved
from http://userpage.fu-berlin.de/health/healself.pdf.
Sclafani, F. & Chau, I. (2016). Timing of Therapies in the Multidisciplinary
Treatment of Locally Advanced Rectal Cancer: Available Evidence and
Implications for Routine Practice. Semin Radiat Oncol, 26(3), 176-185.
Seike, K., Koda, K., Oda, K., Kosugi, C., Shimizu, K. & Miyazaki, M. (2009).
Gender differences in pelvic anatomy and effects on rectal cancer surgery.
Hepatogastroenterology, 56(89), 111-115.
References
272
Sellar, C. M., Bell, G. J., Haennel, R. G., Au, H. J., Chua, N. & Courneya, K. S.
(2014). Feasibility and efficacy of a 12-week supervised exercise intervention
for colorectal cancer survivors. Appl Physiol Nutr Metab, 39(6), 715-723.
Siefert, M. L. Fatigue, pain, and functional status during outpatient chemotherapy.
Oncol Nurs Forum, 37(2), E114-123.
Silsbury, Z., Goldsmith, R. & Rushton, A. (2015). Systematic review of the
measurement properties of self-report physical activity questionnaires in
healthy adult populations. BMJ Open, 5(9), e008430.
Silver, J. K., Baima, J. & Mayer, R. S. (2013). Impairment-driven cancer
rehabilitation: an essential component of quality care and survivorship. CA
Cancer J Clin, 63(5), 295-317.
Simon, A. E., Thompson, M. R., Flashman, K. & Wardle, J. (2009). Disease stage and
psychosocial outcomes in colorectal cancer. Colorectal Dis, 11(1), 19-25.
Simpson, R. R., Kennedy, M. L., Nguyen, M. H., Dinning, P. G. & Lubowski, D. Z.
(2006). Anal manometry: a comparison of techniques. Dis Colon Rectum,
49(7), 1033-1038.
Singh, S. J., Morgan, M. D., Scott, S., Walters, D. & Hardman, A. E. (1992).
Development of a shuttle walking test of disability in patients with chronic
airways obstruction. Thorax, 47(12), 1019-1024.
Singh, S. J., Puhan, M. A., Andrianopoulos, V., Hernandes, N. A., Mitchell, K. E.,
Hill, C. J., Lee, A. L., Camillo, C. A., Troosters, T., Spruit, M. A., Carlin, B.
W., Wanger, J., Pepin, V., Saey, D., Pitta, F., Kaminsky, D. A., McCormack,
M. C., MacIntyre, N., Culver, B. H., Sciurba, F. C., Revill, S. M., Delafosse,
V. & Holland, A. E. (2014). An official systematic review of the European
Respiratory Society/American Thoracic Society: measurement properties of
field walking tests in chronic respiratory disease. Eur Respir J, 44(6),
1447-1478.
Snyder, D. C., Morey, M. C., Sloane, R., Stull, V., Cohen, H. J., Peterson, B., Pieper,
C., Hartman, T. J., Miller, P. E., Mitchell, D. C. & Demark-Wahnefried, W.
(2009). Reach out to ENhancE Wellness in Older Cancer Survivors (RENEW):
design, methods and recruitment challenges of a home-based exercise and diet
intervention to improve physical function among long-term survivors of breast,
prostate, and colorectal cancer. Psychooncology, 18(4), 429-439.
References
273
Soerjomataram, I., Lortet-Tieulent, J., Parkin, D. M., Ferlay, J., Mathers, C., Forman,
D. & Bray, F. (2012). Global burden of cancer in 2008: a systematic analysis
of disability-adjusted life-years in 12 world regions. Lancet, 380(9856),
1840-1850.
Spencer, L. M., Alison, J. A. & McKeough, Z. J. (2008). Six-minute walk test as an
outcome measure - Are two six-minute walk tests necessary immediately after
pulmonary rehabilitation and at three-month follow-up? Am J Phys Med
Rehabil, 87(3), 224-228.
Spruit, M. A., Janssen, P. P., Willemsen, S. C., Hochstenbag, M. M. & Wouters, E. F.
(2006). Exercise capacity before and after an 8-week multidisciplinary
inpatient rehabilitation program in lung cancer patients: a pilot study. Lung
Cancer, 52(2), 257-260.
Starr, J. A., Drobnis, E. Z., Lenger, S., Parrot, J., Barrier, B. & Foster, R. (2013).
Outcomes of a comprehensive nonsurgical approach to pelvic floor
rehabilitation for urinary symptoms, defecatory dysfunction, and pelvic pain.
Female Pelvic Med Reconstr Surg, 19(5), 260-265.
Staskin, D., Kelleher, C., Bosch, R., Cotterill, N., Coyne, K., Kopp, Z., Rosenberg, M.,
Symonds, T., Tannenbaum, C., Yoshida, M., Basra, C. & Cherian, P. (2013).
Initial Assessment of Urinary Incontinence in Adult Male and Female Patients
(5A). Paris: 5th International Consultation on Incontinence.
Steins Bisschop, C. N., Velthuis, M. J., Wittink, H., Kuiper, K., Takken, T., van der
Meulen, W. J., Lindeman, E., Peeters, P. H. & May, A. M. (2012).
Cardiopulmonary exercise testing in cancer rehabilitation: a systematic review.
Sports Med, 42(5), 367-379.
Stevinson, C. & Fox, K. R. (2006). Feasibility of an exercise rehabilitation
programme for cancer patients. Eur J Cancer Care (Engl), 15(4), 386-396.
Stintzing, S. (2014). Management of colorectal cancer. F1000Prime Rep, 6, 108.
Strasser, B., Steindorf, K., Wiskemann, J. & Ulrich, C. M. (2013). Impact of
resistance training in cancer survivors: a meta-analysis. Med Sci Sports Exerc,
45(11), 2080-2090.
Suh, S. Y., Leblanc, T. W., Shelby, R. A., Samsa, G. P. & Abernethy, A. P. (2011).
Longitudinal patient-reported performance status assessment in the cancer
clinic is feasible and prognostic. J Oncol Pract, 7(6), 374-381.

References
274
Sung, V. W. & Hampton, B. S. (2009). Epidemiology of pelvic floor dysfunction.
Obstet Gynecol Clin North Am, 36(3), 421-443.
Suthar, A. B., Granich, R., Mermin, J. & Van Rie, A. Effect of cotrimoxazole on
mortality in HIV-infected adults on antiretroviral therapy: a systematic review
and meta-analysis. Bull World Health Organ, 90(2), 128C-138C.
Sweeney, C., Schmitz, K. H., Lazovich, D., Virnig, B. A., Wallace, R. B. & Folsom,
A. R. (2006). Functional limitations in elderly female cancer survivors. J Natl
Cancer Inst, 98(8), 521-529.
Talley, N. J. (2008). How to do and interpret a rectal examination in gastroenterology.
Am J Gastroenterol, 103(4), 820-822.
Talmage, H. & Rasher, S. P. (1981). Validity and Reliability Issues in Measurement
Instrumentation. J Nutr Educ, 13(3), 83-85.
Tamas, K., Walenkamp, A. M., de Vries, E. G., van Vugt, M. A., Beets-Tan, R. G.,
van Etten, B., de Groot, D. J. & Hospers, G. A. (2015). Rectal and colon
cancer: Not just a different anatomic site. Cancer Treat Rev, 41(8), 671-679.
Tantoy, I. Y., Cataldo, J. K., Aouizerat, B. E., Dhruva, A. & Miaskowski, C. (2016).
A Review of the Literature on Multiple Co-occurring Symptoms in Patients
With Colorectal Cancer Who Received Chemotherapy Alone or
Chemotherapy With Targeted Therapies. Cancer Nurs.Advance online
publication. doi: 10.1097/NCC.0000000000000343.
Taplin, S. H., Anhang Price, R., Edwards, H. M., Foster, M. K., Breslau, E. S.,
Chollette, V., Prabhu Das, I., Clauser, S. B., Fennell, M. L. & Zapka, J. (2012).
Introduction: Understanding and influencing multilevel factors across the
cancer care continuum. J Natl Cancer Inst Monogr, 2012(44), 2-10.
Tarraga Lopez, P. J., Albero, J. S. & Rodriguez-Montes, J. A. (2014). Primary and
secondary prevention of colorectal cancer. Clin Med Insights Gastroenterol, 7,
33-46.
Taylor, C. & Morgan, L. (2011). Quality of life following reversal of temporary stoma
after rectal cancer treatment. Eur J Oncol Nurs, 15(1), 59-66.
Taylor, S., Frost, H., Taylor, A. & Barker, K. (2001). Reliability and responsiveness
of the shuttle walking test in patients with chronic low back pain. Physiother
Res Int, 6(3), 170-178.
References
275
Teixeira, P. J., Carraca, E. V., Markland, D., Silva, M. N. & Ryan, R. M. (2012).
Exercise, physical activity, and self-determination theory: a systematic review.
Int J Behav Nutr Phys Act, 9, 78.
Teleman, P., Lidfeldt, J., Nerbrand, C., Samsioe, G. & Mattiasson, A. (2005). Lower
urinary tract symptoms in middle-aged women--prevalence and attitude
towards mild urinary incontinence: a community-based population study. Acta
Obstet Gynecol Scand, 84(11), 1108-1112.
Thompson, J. A., O'Sullivan, P. B., Briffa, K., Neumann, P. & Court, S. (2005).
Assessment of pelvic floor movement using transabdominal and transperineal
ultrasound. Int Urogynecol J Pelvic Floor Dysfunct, 16(4), 285-292.
Thorsen, Y., Stimec, B., Andersen, S. N., Lindstrom, J. C., Pfeffer, F., Oresland, T. &
Ignjatovic, D. (2016). Bowel function and quality of life after superior
mesenteric nerve plexus transection in right colectomy with D3 extended
mesenterectomy. Tech Coloproctol, 20(7), 445-453.
Tikkinen, K. A., Agarwal, A. & Griebling, T. L. (2013). Epidemiology of male
urinary incontinence. Curr Opin Urol, 23(6), 502-508.
Tomioka, K., Iwamoto, J., Saeki, K. & Okamoto, N. (2011). Reliability and validity
of the International Physical Activity Questionnaire (IPAQ) in elderly adults:
the Fujiwara-kyo Study. J Epidemiol, 21(6), 459-465.
Tomoda, H. & Furusawa, M. (1985). Sexual and urinary dysfunction following
surgery for sigmoid colon cancer. Jpn J Surg, 15(5), 355-360.
Tomruk, M., Karadibak, D., Yavuzsen, T. & Akman, T. (2015). Predictors of
functional capacity in colorectal cancer patients. Support Care Cancer, 23(9),
2747-54.
Torre, L. A., Bray, F., Siegel, R. L., Ferlay, J., Lortet-Tieulent, J. & Jemal, A. (2015).
Global cancer statistics, 2012. CA Cancer J Clin, 65(2), 87-108.
Traa, M. J., De Vries, J., Roukema, J. A. & Den Oudsten, B. L. (2012). Sexual
(dys)function and the quality of sexual life in patients with colorectal cancer: a
systematic review. Ann Oncol, 23(1), 19-27.
Trost, S. G. & O'Neil, M. (2014). Clinical use of objective measures of physical
activity. Br J Sports Med, 48(3), 178-181.
Trutschnigg, B., Kilgour, R. D., Reinglas, J., Rosenthall, L., Hornby, L., Morais, J. A.
& Vigano, A. (2008). Precision and reliability of strength (Jamar vs. Biodex
handgrip) and body composition (dual-energy X-ray absorptiometry vs.
References
276
bioimpedance analysis) measurements in advanced cancer patients. Appl
Physiol Nutr Metab, 33(6), 1232-1239.
Tsunoda, A., Nakao, K., Hiratsuka, K., Tsunoda, Y. & Kusano, M. (2007).
Prospective analysis of quality of life in the first year after colorectal cancer
surgery. Acta Oncol, 46(1), 77-82.
Tsunoda, A., Nakao, K., Hiratsuka, K., Yasuda, N., Shibusawa, M. & Kusano, M.
(2005). Anxiety, depression and quality of life in colorectal cancer patients. Int
J Clin Oncol, 10(6), 411-417.
Tung, H. Y., Chao, T. B., Lin, Y. H., Wu, S. F., Lee, H. Y., Ching, C. Y., Hung, K. W.
& Lin, T. J. (2016). Depression, Fatigue, and QoL in Colorectal Cancer
Patients During and After Treatment. West J Nurs Res, 38(7), 893-908.
Tveter, A. T., Dagfinrud, H., Moseng, T. & Holm, I. (2014). Health-Related Physical
Fitness Measures: Reference Values and Reference Equations for Use in
Clinical Practice. Arch Phys Med Rehabil, 95(7), 1366-1373.
Tzani, P., Piepoli, M. F., Longo, F., Aiello, M., Serra, W., Maurizio, A. R., Olivieri, D.
& Chetta, A. (2010). Resting lung function in the assessment of the exercise
capacity in patients with chronic heart failure. Am J Med Sci, 339(3), 210-215.
Valderas, J. M. & Alonso, J. (2008). Patient reported outcome measures: a
model-based classification system for research and clinical practice. Qual Life
Res, 17(9), 1125-1135.
Van Blarigan, E. L. & Meyerhardt, J. A. (2015). Role of Physical Activity and Diet
After Colorectal Cancer Diagnosis. Journal of Clinical Oncology, 33(16),
1825-1834.
Van Cutsem, E., Borras, J. M., Castells, A., Ciardiello, F., Ducreux, M., Haq, A.,
Schmoll, H. J. & Tabernero, J. (2013). Improving outcomes in colorectal
cancer: where do we go from here? Eur J Cancer, 49(11), 2476-2485.
Van Cutsem, E., Cervantes, A., Nordlinger, B., Arnold, D. & Group, E. G. W. (2014).
Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis,
treatment and follow-up. Ann Oncol, 25 Suppl 3, iii1-9.
van Delft, K., Thakar, R. & Sultan, A. H. (2015). Pelvic floor muscle contractility:
digital assessment vs transperineal ultrasound. Ultrasound Obstet Gynecol,
45(2), 217-222.
van Duijvendijk, P., Slors, F., Taat, C. W., Heisterkamp, S. H., Obertop, H. &
Boeckxstaens, G. E. (2003). A prospective evaluation of anorectal function
References
277
after total mesorectal excision in patients with a rectal carcinoma. Surgery,
133(1), 56-65.
van Leersum, N. J., Janssen-Heijnen, M. L., Wouters, M. W., Rutten, H. J., Coebergh,
J. W., Tollenaar, R. A. & Lemmens, V. E. (2013). Increasing prevalence of
comorbidity in patients with colorectal cancer in the South of the Netherlands
1995-2010. Int J Cancer, 132(9), 2157-2163.
van Vugt, J. L., Reisinger, K. W., Derikx, J. P., Boerma, D. & Stoot, J. H. (2014).
Improving the outcomes in oncological colorectal surgery. World J
Gastroenterol, 20(35), 12445-12457.
Vanhees, L., Lefevre, J., Philippaerts, R., Martens, M., Huygens, W., Troosters, T. &
Beunen, G. (2005). How to assess physical activity? How to assess physical
fitness? Eur J Cardiovasc Prev Rehabil, 12(2), 102-114.
Varpe, P., Huhtinen, H., Rantala, A., Salminen, P., Rautava, P., Hurme, S. &
Gronroos, J. (2011). Quality of life after surgery for rectal cancer with special
reference to pelvic floor dysfunction. Colorectal Dis, 13(4), 399-405.
Vaz, M., Thangam, S., Prabhu, A. & Shetty, P. S. (1996). Maximal voluntary
contraction as a functional indicator of adult chronic undernutrition. Br J Nutr,
76(1), 9-15.
Vironen, J. H., Kairaluoma, M., Aalto, A. M. & Kellokumpu, I. H. (2006). Impact of
functional results on quality of life after rectal cancer surgery. Dis Colon
Rectum, 49(5), 568-578.
Visser, W. S., Te Riele, W. W., Boerma, D., van Ramshorst, B. & van Westreenen, H.
L. (2014). Pelvic floor rehabilitation to improve functional outcome after a
low anterior resection: a systematic review. Ann Coloproctol, 30(3), 109-114.
Vodermaier, A. & Millman, R. D. (2011). Accuracy of the Hospital Anxiety and
Depression Scale as a screening tool in cancer patients: a systematic review
and meta-analysis. Support Care Cancer, 19(12), 1899-1908.
Volloyhaug, I., Morkved, S., Salvesen, O. & Salvesen, K. A. (2015). Assessment of
pelvic floor muscle contraction with palpation, perineometry and transperineal
ultrasound: a cross-sectional study. Ultrasound Obstet Gynecol, 47(6),
768-773.
von Elm, E., Altman, D. G., Pocock, S. J., Gotzsche, P. C. & Vandenbroucke, J. P.
(2007). Strengthening the reporting of observational studies in epidemiology
References
278
(STROBE) statement: guidelines for reporting observational studies. Br Med J,
335(7624), 806-808.
von Gruenigen, V., Frasure, H., Kavanagh, M. B., Janata, J., Waggoner, S., Rose, P.,
Lerner, E. & Courneya, K. S. (2012). Survivors of uterine cancer empowered
by exercise and healthy diet (SUCCEED): a randomized controlled trial.
Gynecol Oncol, 125(3), 699-704.
Vrieling, A. & Kampman, E. (2010). The role of body mass index, physical activity,
and diet in colorectal cancer recurrence and survival: a review of the literature.
Am J Clin Nutr, 92(3), 471-490.
Walls, H. L., Magliano, D. J., Stevenson, C. E., Backholer, K., Mannan, H. R., Shaw,
J. E. & Peeters, A. (2012). Projected progression of the prevalence of obesity
in Australia. Obesity (Silver Spring), 20(4), 872-878.
Walters, S., Maringe, C., Butler, J., Brierley, J. D., Rachet, B. & Coleman, M. P.
(2013). Comparability of stage data in cancer registries in six countries:
lessons from the International Cancer Benchmarking Partnership. Int J Cancer,
132(3), 676-685.
Wang, W., Chair, S. Y., Thompson, D. R. & Twinn, S. F. (2009). A psychometric
evaluation of the Chinese version of the Hospital Anxiety and Depression
Scale in patients with coronary heart disease. J Clin Nurs, 18(13), 1908-1915.
Wang, Y., Duan, H., Yang, H. & Lin, J. (2015). A pooled analysis of alcohol intake
and colorectal cancer. Int J Clin Exp Med, 8(5), 6878-6889.
Wasserberg, N., Mazaheri, A., Petrone, P., Tulchinsky, H. & Kaufman, H. S. (2011).
Three-dimensional endoanal ultrasonography of external anal sphincter
defects in patients with faecal incontinence: correlation with symptoms and
manometry. Colorectal Dis, 13(4), 449-453.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M & P, T. (2005). The
Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised
studies in meta-analyses. Retrieved from
http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
West, M. A., Loughney, L., Barben, C. P., Sripadam, R., Kemp, G. J., Grocott, M. P.
& Jack, S. (2014). The effects of neoadjuvant chemoradiotherapy on physical
fitness and morbidity in rectal cancer surgery patients. Eur J Surg Oncol,
40(11), 1421-1428.
References
279
Westerterp, K. R. (2009). Assessment of physical activity: a critical appraisal. Eur J
Appl Physiol, 105(6), 823-828.
Whistance, R. N., Conroy, T., Chie, W., Costantini, A., Sezer, O., Koller, M., Johnson,
C. D., Pilkington, S. A., Arraras, J., Ben-Josef, E., Pullyblank, A. M., Fayers,
P. & Blazeby, J. M. (2009). Clinical and psychometric validation of the
EORTC QLQ-CR29 questionnaire module to assess health-related quality of
life in patients with colorectal cancer. Eur J Cancer, 45(17), 3017-3026.
Whiteman, D. C., Webb, P. M., Green, A. C., Neale, R. E., Fritschi, L., Bain, C. J.,
Parkin, D. M., Wilson, L. F., Olsen, C. M., Nagle, C. M., Pandeya, N., Jordan,
S. J., Antonsson, A., Kendall, B. J., Hughes, M. C., Ibiebele, T. I., Miura, K.,
Peters, S. & Carey, R. N. (2015). Cancers in Australia in 2010 attributable to
modifiable factors: summary and conclusions. Aust N Z J Public Health, 39(5),
477-484.
Wieslander, C. K. (2009). Clinical approach and office evaluation of the patient with
pelvic floor dysfunction. Obstet Gynecol Clin North Am, 36(3), 445-462.
Wilson, T. R. & Alexander, D. J. (2008). Clinical and non-clinical factors influencing
postoperative health-related quality of life in patients with colorectal cancer.
Br J Surg, 95(11), 1408-1415.
Wilson, T. R., Alexander, D. J. & Kind, P. (2006). Measurement of health-related
quality of life in the early follow-up of colon and rectal cancer. Dis Colon
Rectum, 49(11), 1692-1702.
Win, T., Jackson, A., Groves, A. M., Sharples, L. D., Charman, S. C. & Laroche, C.
M. (2006). Comparison of shuttle walk with measured peak oxygen
consumption in patients with operable lung cancer. Thorax, 61(1), 57-60.
Witham, M. D., Sugden, J. A., Sumukadas, D., Dryburgh, M. & McMurdo, M. E.
(2012). A comparison of the Endurance Shuttle Walk test and the Six Minute
Walk test for assessment of exercise capacity in older people. Aging Clin Exp
Res, 24(2), 176-180.
Wong, C. K. H., Law, W. L., Wan, Y. F., Poon, J. T. C. & Lam, C. L. K. (2014).
Health-related quality of life and risk of colorectal cancer recurrence and
All-cause death among advanced stages of colorectal cancer 1-year after
diagnosis. BMC Cancer, 14, 337.
Wood, L. N. & Anger, J. T. (2014). Urinary incontinence in women. BMJ, 349,
g4531.
References
280
World Health Organization (2001). International Classification of Functioning,
Disability and Health: ICF. Geneva: World Health Organization.
World Health Organization. (2010). Global recommendations on physical activity for
health. Retrieved from
http://apps.who.int/iris/bitstream/10665/44399/1/9789241599979_eng.pdf.
Wu, G., Sanderson, B. & Bittner, V. (2003). The 6-minute walk test: How important
is the learning effect? Am Heart J, 146(1), 129-132.
Yabroff, K. R., Lawrence, W. F., Clauser, S., Davis, W. W. & Brown, M. L. (2004).
Burden of illness in cancer survivors: findings from a population-based
national sample. J Natl Cancer Inst, 96(17), 1322-1330.
Yamano, T., Yoshimura, M., Kobayashi, M., Beppu, N., Hamanaka, M., Babaya, A.,
Tsukamoto, K., Noda, M., Matsubara, N. & Tomita, N. Malnutrition in rectal
cancer patients receiving preoperative chemoradiotherapy is common and
associated with treatment tolerability and anastomotic leakage. Int J
Colorectal Dis, 31(4), 877-884.
Yang, E. J., Lim, J. Y., Rah, U. W. & Kim, Y. B. (2012). Effect of a pelvic floor
muscle training program on gynecologic cancer survivors with pelvic floor
dysfunction: A randomized controlled trial. Gynecol Oncol, 125(3), 705-711.
Yang, X. M., Partanen, K., Farin, P. & Soimakallio, S. (1995). Defecography. Acta
Radiol, 36(5), 460-468.
Yeh, M. L., Chung, Y. C., Hsu, M. Y. F. & Hsu, C. C. (2014). Quantifying
Psychological Distress among Cancer Patients in Interventions and Scales: A
Systematic Review. Curr Pain Headache Rep, 18(3), 399.
Yuhara, H., Steinmaus, C., Cohen, S. E., Corley, D. A., Tei, Y. & Buffler, P. A.
(2011). Is Diabetes Mellitus an Independent Risk Factor for Colon Cancer and
Rectal Cancer? Am J Gastroenterol, 106(11), 1911-1921.
Zhang, F. W., Zhou, Z. Y., Wang, H. L., Zhang, J. X., Di, B. S., Huang, W. H. &
Yang, K. H. (2014). Laparoscopic versus open surgery for rectal cancer: a
systematic review and meta-analysis of randomized controlled trials. Asian
Pac J Cancer Prev, 15(22), 9985-9996.
Zigmond, A. S. & Snaith, R. P. (1983). The hospital anxiety and depression scale.
Acta Psychiatr Scand, 67(6), 361-370.

References
281
Ziv, Y., Zbar, A., Bar-Shavit, Y. & Igov, I. (2013). Low anterior resection syndrome
(LARS): cause and effect and reconstructive considerations. Tech Coloproctol,
17(2), 151-162.
Zou, K. H., Tuncali, K. & Silverman, S. G. (2003). Correlation and simple linear
regression. Radiology, 227(3), 617-622.
Zutshi, M., Salcedo, L., Hammel, J. & Hull, T. (2010). Anal physiology testing in
fecal incontinence: is it of any value? Int J Colorectal Dis, 25(2), 277-282.
Appendix 4.1
282
Appendices
Appendix 4.1 Ethics Approval Documentation (Study 2)
Appendix 4.2
283
Appendix 4.2 Data collection sheets (Study 2)
VALIDATION OF EXERCISE TESTS TO BE USED WITH PATIENTS WITH
LUNG AND COLORECTAL CANCER
HREC 2013.052
Version 2
DATA COLLECTION SHEET
Participant trial number: ___________
Date of consent: ___________
Recruitment therapist: ___________
MEDICAL DEMOGRAPHICS
Please circle the number or tick the box (to be completed from the medical history)
Age ___________
Gender 1 = male 2 = female
Cancer type 1 = lung cancer 2 = colorectal cancer
Lung cancer histological
type
1 = squamous 2 = adenocarcinoma
3 = large cell
5 = not lung cancer
4 = other: ___________
Colorectal cancer
histological type
1 = medullary carcinoma 2 = adenocarcinoma
3 = mucinous (colloid)
adenocarcinoma
5 = squamous cell (epidermoid)
carcinoma
7 = small cell (oat cell)
carcinoma
9 = not colorectal cancer
4 = signet-ring cell carcinoma
6 = adenosquamous carcinoma
8 = undifferentiated carcinoma
10 = other: ___________
TNM stage of cancer (lung
and colorectal)
1 = stage IA includes: T1a/bN0M0
2 = stage IB includes: T2aN0M0
3 = stage IIA includes: T2bN0M0; T1a/bN1M0; T2aN1M0
4 = stage IIB Includes: T2bN1M0; T3N0M0
5 = stage IIIA Includes: T1a/bN2M0; T2a/bN2M0; T3N1/2M0;
T4N0/1M0
6 = stage IIIB Includes: Any T N3 MO; T4 any N M0
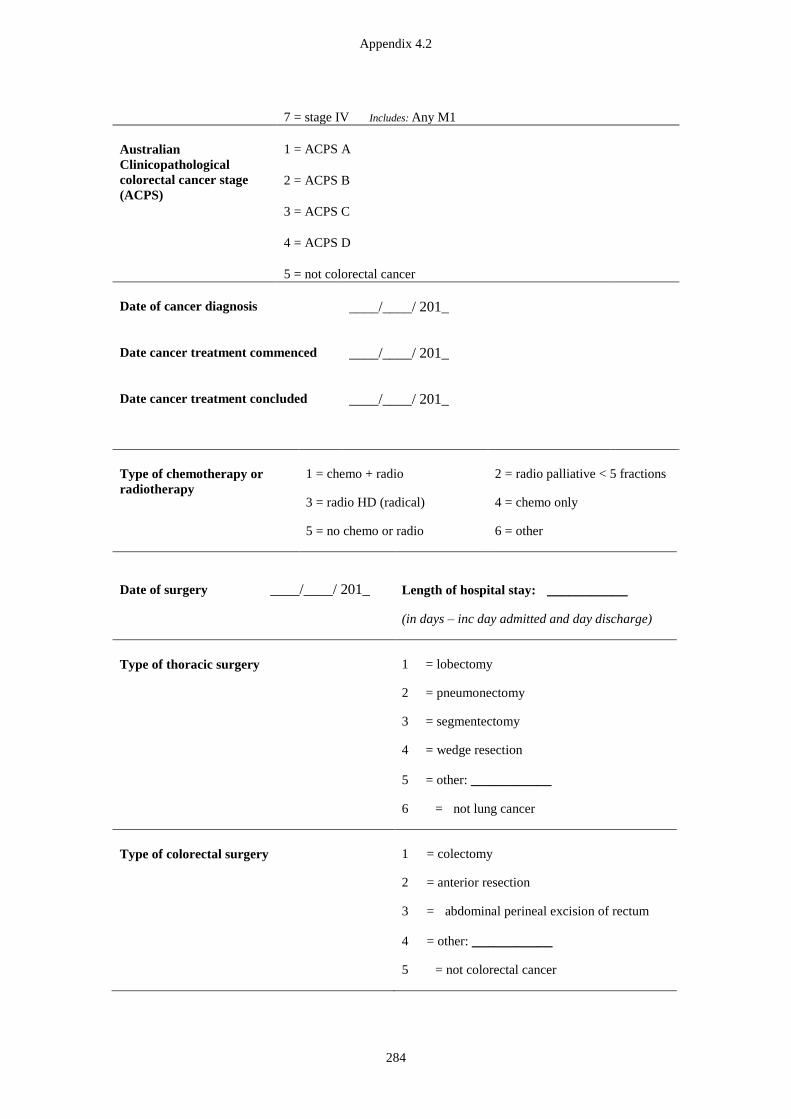
Appendix 4.2
284
7 = stage IV Includes: Any M1
Australian
Clinicopathological
colorectal cancer stage
(ACPS)
1 = ACPS A
2 = ACPS B
3 = ACPS C
4 = ACPS D
5 = not colorectal cancer
Date of cancer diagnosis ____/____/ 201_
Date cancer treatment commenced ____/____/ 201_
Date cancer treatment concluded ____/____/ 201_
Type of chemotherapy or
radiotherapy
1 = chemo + radio 2 = radio palliative < 5 fractions
3 = radio HD (radical) 4 = chemo only
5 = no chemo or radio 6 = other
Date of surgery ____/____/ 201_
Length of hospital stay: ___________
(in days – inc day admitted and day discharge)
Type of thoracic surgery 1 = lobectomy
2 = pneumonectomy
3 = segmentectomy
4 = wedge resection
5 = other: ___________
6 = not lung cancer
Type of colorectal surgery 1 = colectomy
2 = anterior resection
3 = abdominal perineal excision of rectum
4 = other: ___________
5 = not colorectal cancer
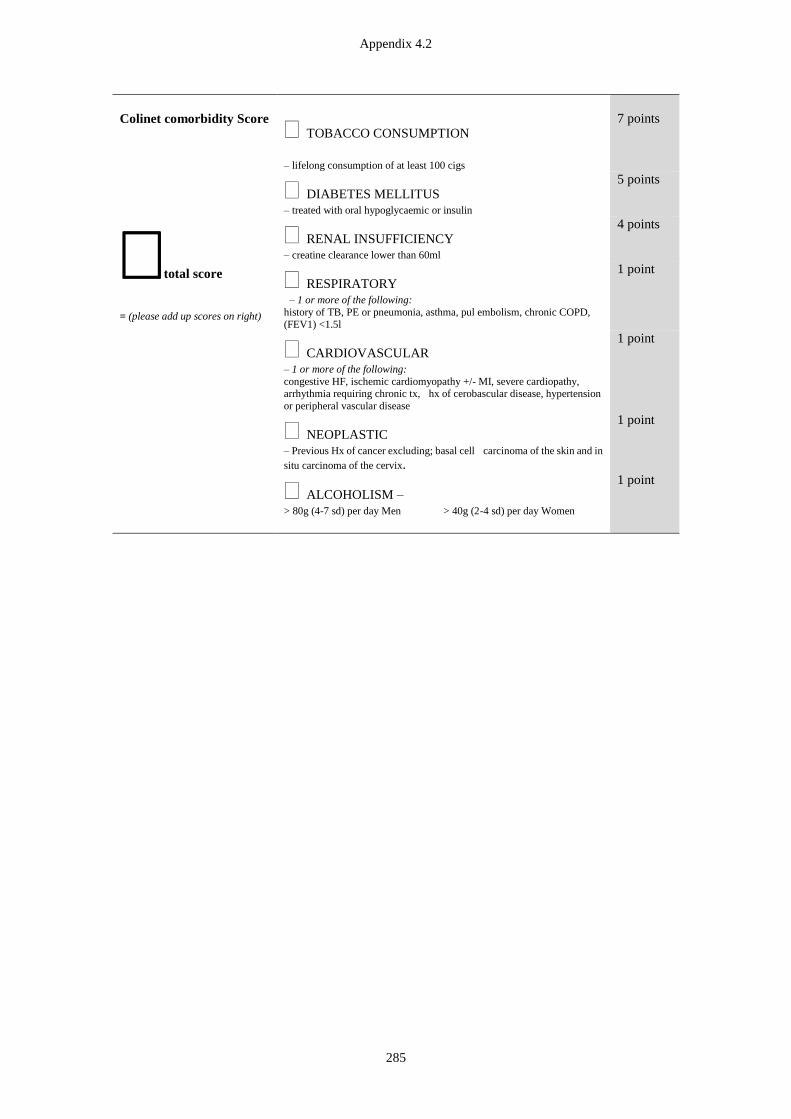
Appendix 4.2
285
Colinet comorbidity Score
total score
= (please add up scores on right)
TOBACCO CONSUMPTION
– lifelong consumption of at least 100 cigs
7 points
DIABETES MELLITUS
– treated with oral hypoglycaemic or insulin
5 points
RENAL INSUFFICIENCY
– creatine clearance lower than 60ml
4 points
RESPIRATORY
– 1 or more of the following:
history of TB, PE or pneumonia, asthma, pul embolism, chronic COPD,
(FEV1) <1.5l
1 point
CARDIOVASCULAR
– 1 or more of the following:
congestive HF, ischemic cardiomyopathy +/- MI, severe cardiopathy, arrhythmia requiring chronic tx, hx of cerobascular disease, hypertension
or peripheral vascular disease
1 point
NEOPLASTIC
– Previous Hx of cancer excluding; basal cell carcinoma of the skin and in
situ carcinoma of the cervix.
1 point
ALCOHOLISM –
> 80g (4-7 sd) per day Men > 40g (2-4 sd) per day Women
1 point
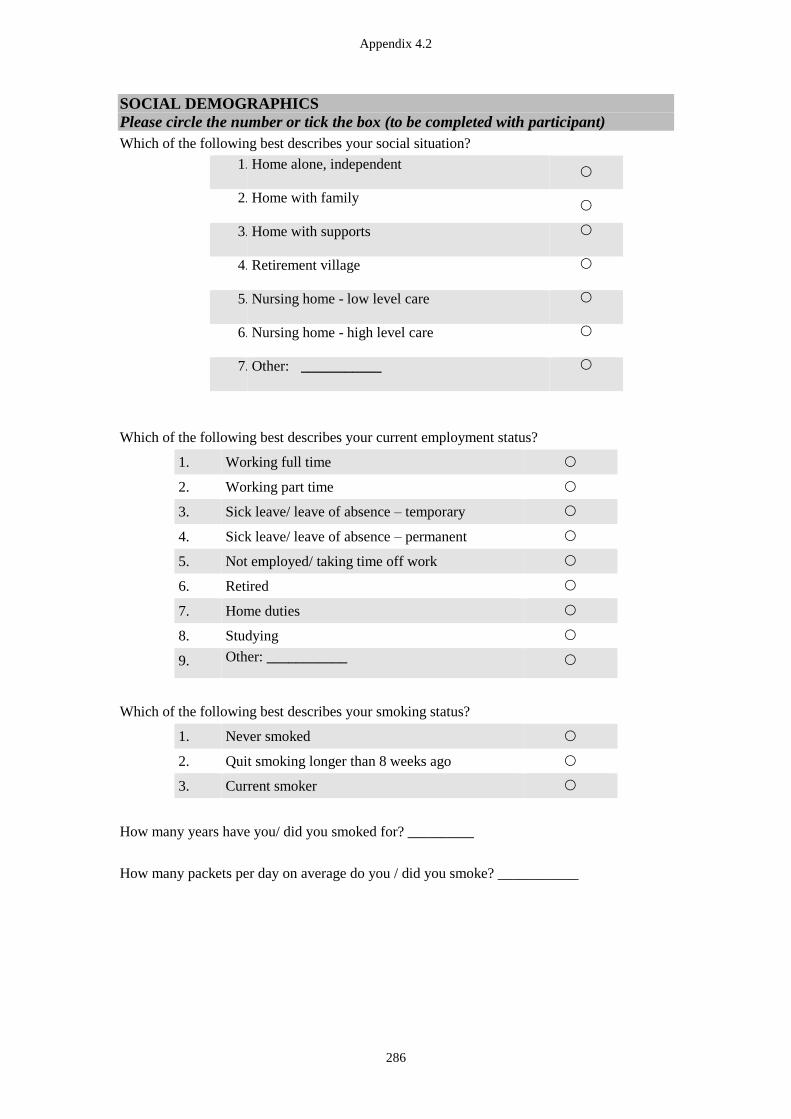
Appendix 4.2
286
SOCIAL DEMOGRAPHICS
Please circle the number or tick the box (to be completed with participant)
Which of the following best describes your social situation?
1. a
)
Home alone, independent
2. b
)
Home with family
3. c
)
Home with supports
4. d
)
Retirement village
5. e
)
Nursing home - low level care
6. f
)
Nursing home - high level care
7. i
)
Other: ___________
Which of the following best describes your current employment status?
1. Working full time
2. Working part time
3. Sick leave/ leave of absence – temporary
4. Sick leave/ leave of absence – permanent
5. Not employed/ taking time off work
6. Retired
7. Home duties
8. Studying
9. Other: ___________
Which of the following best describes your smoking status?
1. Never smoked
2. Quit smoking longer than 8 weeks ago
3. Current smoker
How many years have you/ did you smoked for? __________
How many packets per day on average do you / did you smoke? ___________
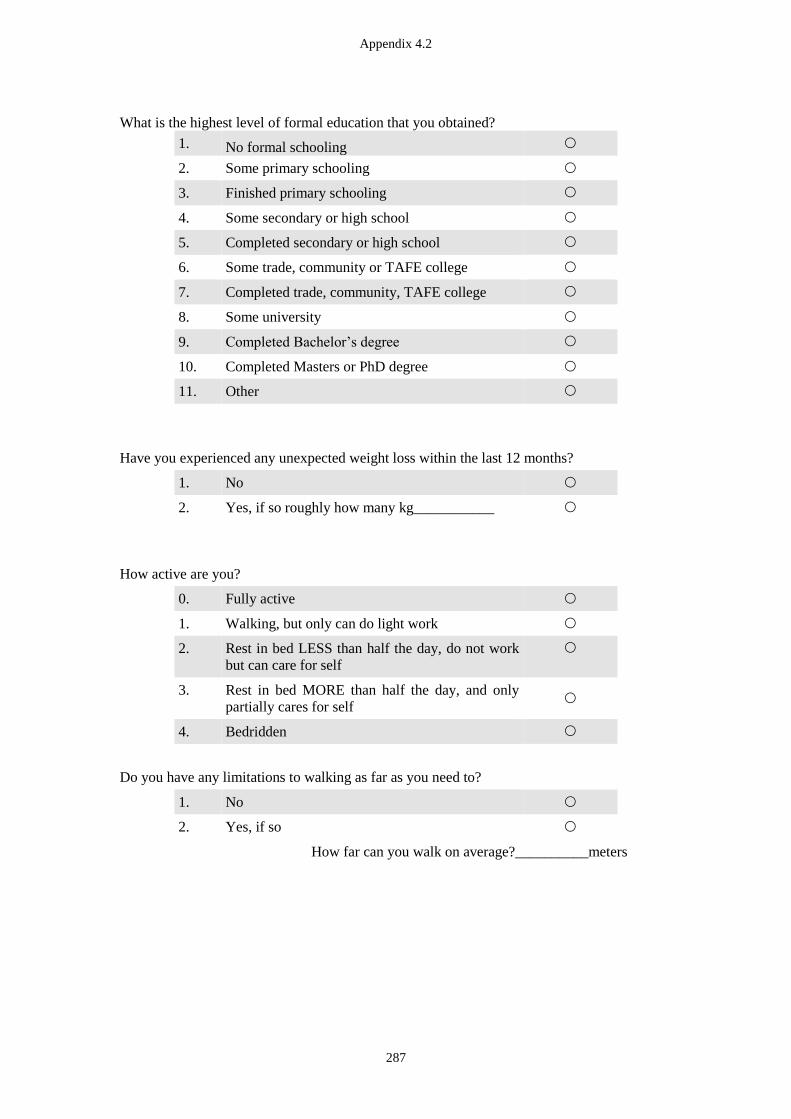
Appendix 4.2
287
What is the highest level of formal education that you obtained?
1. No formal schooling
2. Some primary schooling
3. Finished primary schooling
4. Some secondary or high school
5. Completed secondary or high school
6. Some trade, community or TAFE college
7. Completed trade, community, TAFE college
8. Some university
9. Completed Bachelor’s degree
10. Completed Masters or PhD degree
11. Other
Have you experienced any unexpected weight loss within the last 12 months?
1. No
2. Yes, if so roughly how many kg___________
How active are you?
0. Fully active
1. Walking, but only can do light work
2. Rest in bed LESS than half the day, do not work
but can care for self
3. Rest in bed MORE than half the day, and only
partially cares for self
4. Bedridden
Do you have any limitations to walking as far as you need to?
1. No
2. Yes, if so
How far can you walk on average?__________meters
Appendix 4.2
288
Do you need an aid to walk with?
1. No
2. Walking stick outdoors only
3. Walking stick
4. Walking frame
5. Other
In the last week, have you gone for a walk outside for more than 10 minutes? For example, this
could be walking the dog, walking to the shops or walking for exercise. This does not include
walking you do as part of your job or walking when you are doing the gardening?
1. No
2. Yes
If so:
How many times in the last week _____________days
On average for how long at one time __________minutes
How many hours did you watch television or videos in the last week?
= average_______________ hours per
day

Appendix 4.2
289
SIX MINUTE WALK TEST RECORDING SHEET (accessed from the Pulmonary Rehabilitation Toolkit http://www.pulmonaryrehab.com.au)
Walk 1 Walk 2
Time:___________ Time:___________
Bronchodilator/time since last dose:______ Bronchodilator/time since last
dose:___
BP
__/__
mmH
g
SupplementalOx
ygen
____l/min
Gait Aid
_________
__
BP
__/__
mmH
g
SupplementalOx
ygen
____l/min
Gait Aid
_________
___
Time (mins) SpO2
(%)
Dyspnoea
(Borg)
Rests Time
(mins)
SpO2
(%)
Dyspnoea
(Borg)
Rests
Rest Rest
1 1
2
2
3
3
4
4
5
5
6 6
Recovery 1 Recovery
1
Distance (m):________________ Distance (m):______________
Limiting factor to the test: Limiting factor to the test:
SOB Low SpO2 SOB Low SpO2
Leg fatigue Other: Leg fatigue Other:
Reason for test non-completion:
Patient deceased Patient lost to follow up
Patient refused Patient confusion
Other: ______________________

Appendix 4.2
290
INCREMENTAL SHUTTLE WALKING TEST RECORDING SHEET (accessed from the Pulmonary Rehabilitation Toolkit http://www.pulmonaryrehab.com.au)
Age: Predicted HRmax (220-age):
Walk 1 Walk 2
Time:___________ Time:___________
Bronchodilator/time since last dose:______ Bronchodilator/time since last dose:___
BP
__/__
mmH
g
SupplementalOx
ygen
____l/min
Gait Aid
_________
__
BP
__/__
mmH
g
SupplementalOx
ygen
____l/min
Gait Aid
_________
___
Time
mins
SpO2 HR Dyspnoea Time
mins
SpO2 HR Dyspnoea
Rest Rest
1 1
2 2
3 3
4 4
5
5
6 6
7 7
8 8
9 9
10 10
11 11
12 12
Recovery 1
Recovery
1
2 2
Number of shuttles completed: _______ Number of shuttles completed:
______
Distance (number of shuttles x 10):_____ Distance (m): _______
Limiting factor to the test: Limiting factor to the test:
SOB Low SpO2 SOB Low SpO2
Leg fatigue Other: Leg fatigue Other:
Appendix 4.2
291
Tick shuttles completed during test:
Clinical notes for using the recording sheet:
You do not need to record SpO2%, heart rate and dyspnoea every minute but there is
space on the table above if you wish to.
The box diagram above is designed to make sure you don’t lose track of the number
of shuttles completed. Tick a box each time the patient reaches a cone.
Level 1
Level 2
Level 3
Level 4
Level 5
Level 6
Level 7
Level 8
Level 9
Level 10
Level 11
Level 12
Level 13
Level 14
Level 15
Level 16
Level 1
Level 2
Level 3
Level 4
Level 5
Level 6
Level 7
Level 8
Level 9
Level 10
Level 11
Level 12
Level 13
Level 14
Level 15
Level 16
Appendix 4.2
292
ENDURANCE SHUTTLE WALKING TEST RECORDING SHEET (accessed from the Pulmonary Rehabilitation Toolkit http://www.pulmonaryrehab.com.au)
Therapist initials______________
Number and grade/classification of therapists taken to complete assessment:______
START time for this test:______END time for this test:______Test duration (min)___
Gait aid___________ BP________________
ESWT level:_____________
Time
mins
SpO2 (%) HR Rests Dyspnoea (Borg) Leg fatigue
(Borg)
Rest
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
Appendix 4.2
293
20
Test end
Recovery 1
Time for HR to recover to
resting level (min
Total time walked: ______ (this excludes the 90second warm up)
Limiting factor to the test:
SOB Low SpO2 Leg fatigue
Other:

Appendix 4.2
294
BODY COMPOSITION RECORDING SHEET
Participants with a permanent pacemaker or defibrillator must be excluded
from this test
Arm circumference __________cm (non dominant arm, measure midpoint between AC shoulder joint and olecranon while arm is resting by side )
Calf circumference __________cm (widest part around calf )
Height: ___________cm
Weight: ___________kg
Total body water: ____________L _________%
Extracellular fluid: ____________L _________%
Intracellular fluid: ____________L _________%
Fat free mass: ____________kg _________%
Fat mass: ____________kg _________%
BMI: ___________kg/m2
Ri: ___________
Re: ___________
Rinf: ___________

Appendix 4.2
295
EORTC QLQ-C30 (Version 3)
We are interested in some things about you and your health. Please answer all of the questions
yourself by circling the number that best applies to you. There are no "right" or "wrong"
answers. The information that you provide will remain strictly confidential.
Not
at all
A
Little
Quite
a bit
Very
much
1 Do you have any trouble doing strenuous activities,
like carrying a heavy shopping bag or a suitcase?
1 2 3 4
2 Do you have any trouble taking a long walk? 1 2 3 4
3 Do you have any trouble taking a short walk outside
of the house?
1 2 3 4
4 Do you need to stay in bed or a chair during the day? 1 2 3 4
5 Do you need help with eating, dressing, washing
yourself or using the toilet?
1 2 3 4
During the past week: Not
at all
A
Little
Quite
a bit
Very
much
6 Were you limited in doing either your work or other
daily activities?
1 2 3 4
7 Were you limited in pursuing your hobbies or other
leisure time activities?
1 2 3 4
8 Were you short of breath? 1 2 3 4
9 Have you had pain? 1 2 3 4
10 Did you need to rest? 1 2 3 4
11 Have you had trouble sleeping? 1 2 3 4
12 Have you felt weak? 1 2 3 4
13 Have you lacked appetite? 1 2 3 4
14 Have you felt nauseated? 1 2 3 4
15 Have you vomited? 1 2 3 4
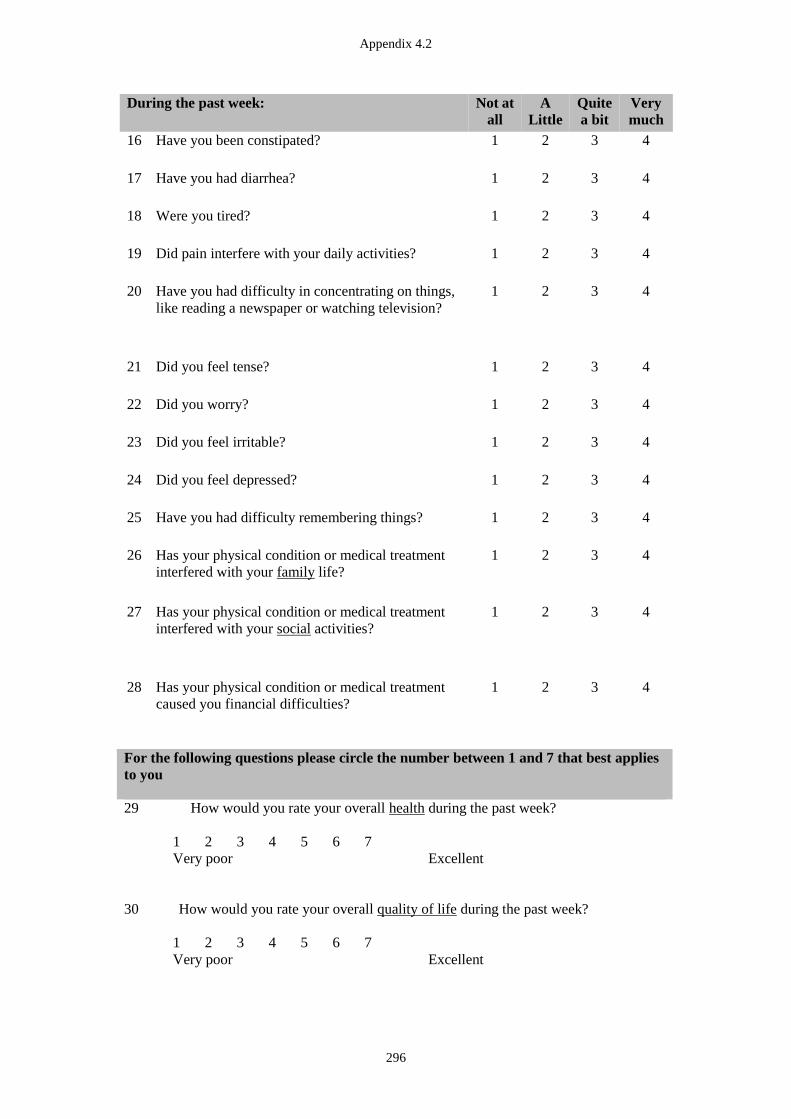
Appendix 4.2
296
During the past week: Not at
all
A
Little
Quite
a bit
Very
much
16 Have you been constipated? 1 2 3 4
17 Have you had diarrhea? 1 2 3 4
18 Were you tired? 1 2 3 4
19 Did pain interfere with your daily activities? 1 2 3 4
20 Have you had difficulty in concentrating on things,
like reading a newspaper or watching television?
1 2 3 4
21 Did you feel tense? 1 2 3 4
22 Did you worry? 1 2 3 4
23 Did you feel irritable? 1 2 3 4
24 Did you feel depressed? 1 2 3 4
25 Have you had difficulty remembering things? 1 2 3 4
26 Has your physical condition or medical treatment
interfered with your family life?
1 2 3 4
27 Has your physical condition or medical treatment
interfered with your social activities?
1 2 3 4
28 Has your physical condition or medical treatment
caused you financial difficulties?
1 2 3 4
For the following questions please circle the number between 1 and 7 that best applies
to you
29 How would you rate your overall health during the past week?
1 2 3 4 5 6 7
Very poor Excellent
30 How would you rate your overall quality of life during the past week?
1 2 3 4 5 6 7
Very poor Excellent
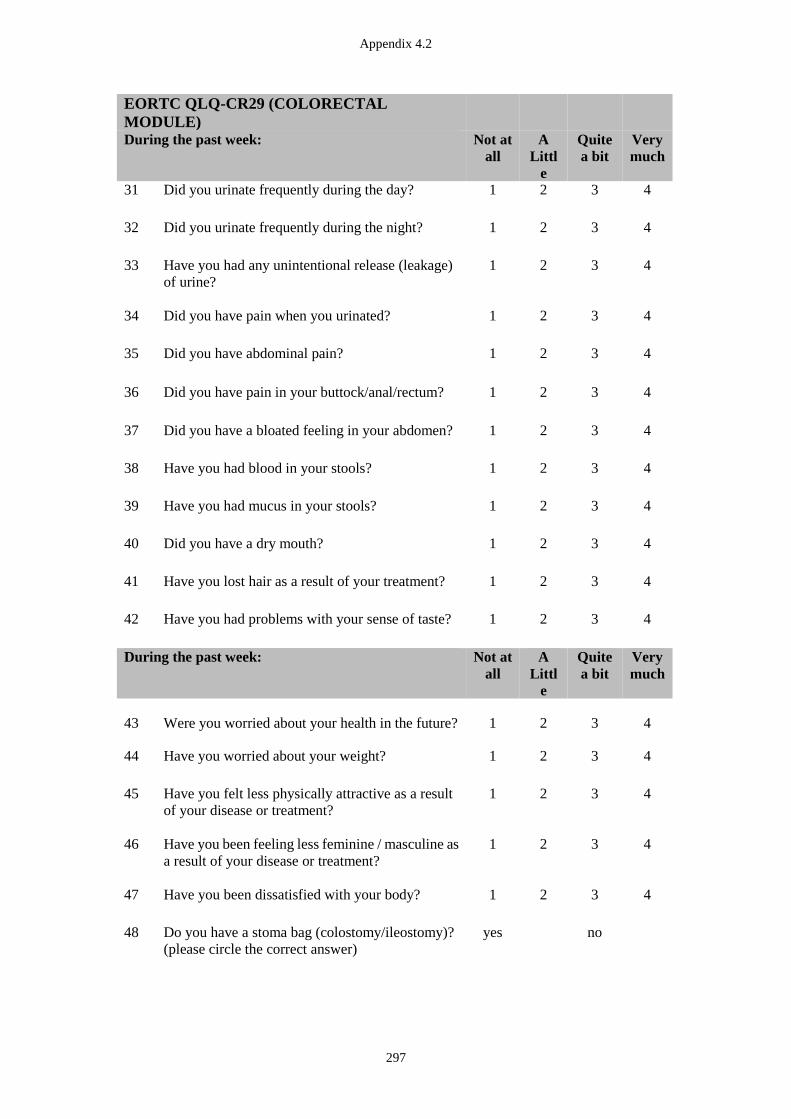
Appendix 4.2
297
EORTC QLQ-CR29 (COLORECTAL
MODULE)
During the past week: Not at
all
A
Littl
e
Quite
a bit
Very
much
31 Did you urinate frequently during the day? 1 2 3 4
32 Did you urinate frequently during the night? 1 2 3 4
33 Have you had any unintentional release (leakage)
of urine?
1 2 3 4
34 Did you have pain when you urinated? 1 2 3 4
35 Did you have abdominal pain? 1 2 3 4
36 Did you have pain in your buttock/anal/rectum? 1 2 3 4
37 Did you have a bloated feeling in your abdomen? 1 2 3 4
38 Have you had blood in your stools? 1 2 3 4
39 Have you had mucus in your stools? 1 2 3 4
40 Did you have a dry mouth? 1 2 3 4
41 Have you lost hair as a result of your treatment? 1 2 3 4
42 Have you had problems with your sense of taste?
1 2 3 4
During the past week: Not at
all
A
Littl
e
Quite
a bit
Very
much
43 Were you worried about your health in the future? 1 2 3 4
44 Have you worried about your weight?
1 2 3 4
45 Have you felt less physically attractive as a result
of your disease or treatment?
1 2 3 4
46 Have you been feeling less feminine / masculine as
a result of your disease or treatment?
1 2 3 4
47 Have you been dissatisfied with your body?
1 2 3 4
48 Do you have a stoma bag (colostomy/ileostomy)?
(please circle the correct answer)
yes no
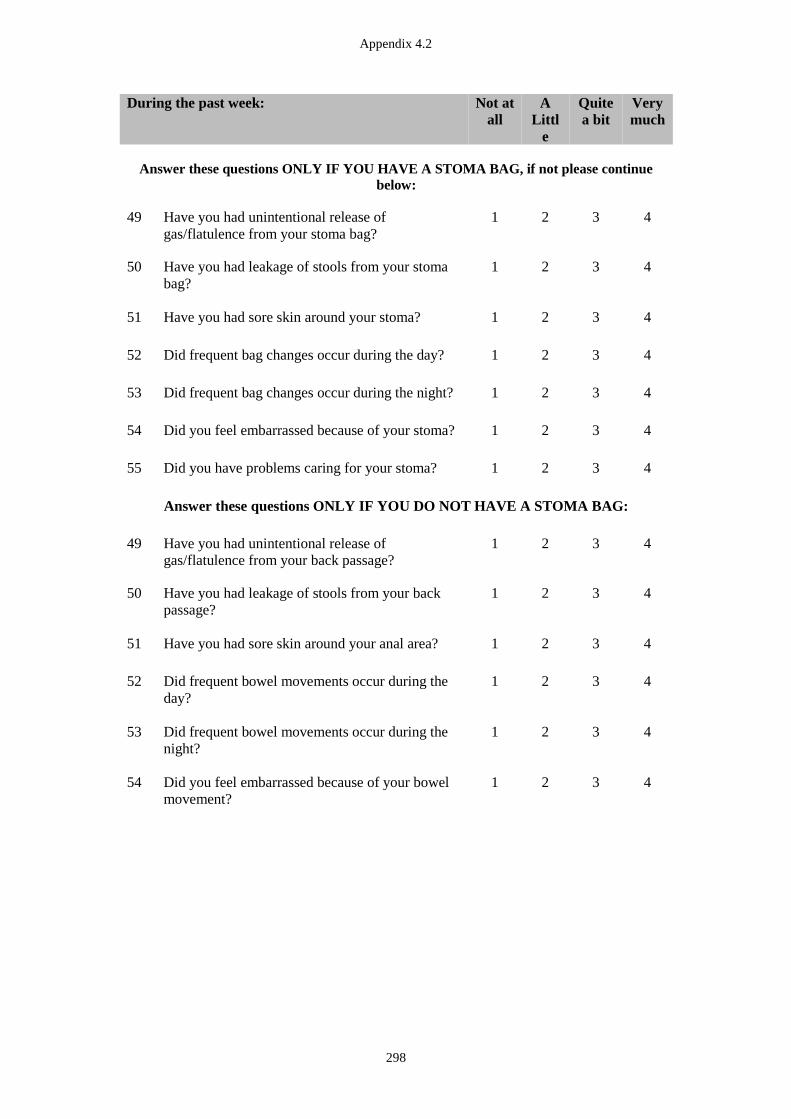
Appendix 4.2
298
During the past week: Not at
all
A
Littl
e
Quite
a bit
Very
much
Answer these questions ONLY IF YOU HAVE A STOMA BAG, if not please continue
below:
49 Have you had unintentional release of
gas/flatulence from your stoma bag?
1 2 3 4
50 Have you had leakage of stools from your stoma
bag?
1 2 3 4
51 Have you had sore skin around your stoma?
1 2 3 4
52 Did frequent bag changes occur during the day?
1 2 3 4
53 Did frequent bag changes occur during the night?
1 2 3 4
54 Did you feel embarrassed because of your stoma?
1 2 3 4
55 Did you have problems caring for your stoma?
1 2 3 4
Answer these questions ONLY IF YOU DO NOT HAVE A STOMA BAG:
49 Have you had unintentional release of
gas/flatulence from your back passage?
1 2 3 4
50 Have you had leakage of stools from your back
passage?
1 2 3 4
51 Have you had sore skin around your anal area?
1 2 3 4
52 Did frequent bowel movements occur during the
day?
1 2 3 4
53 Did frequent bowel movements occur during the
night?
1 2 3 4
54 Did you feel embarrassed because of your bowel
movement?
1 2 3 4
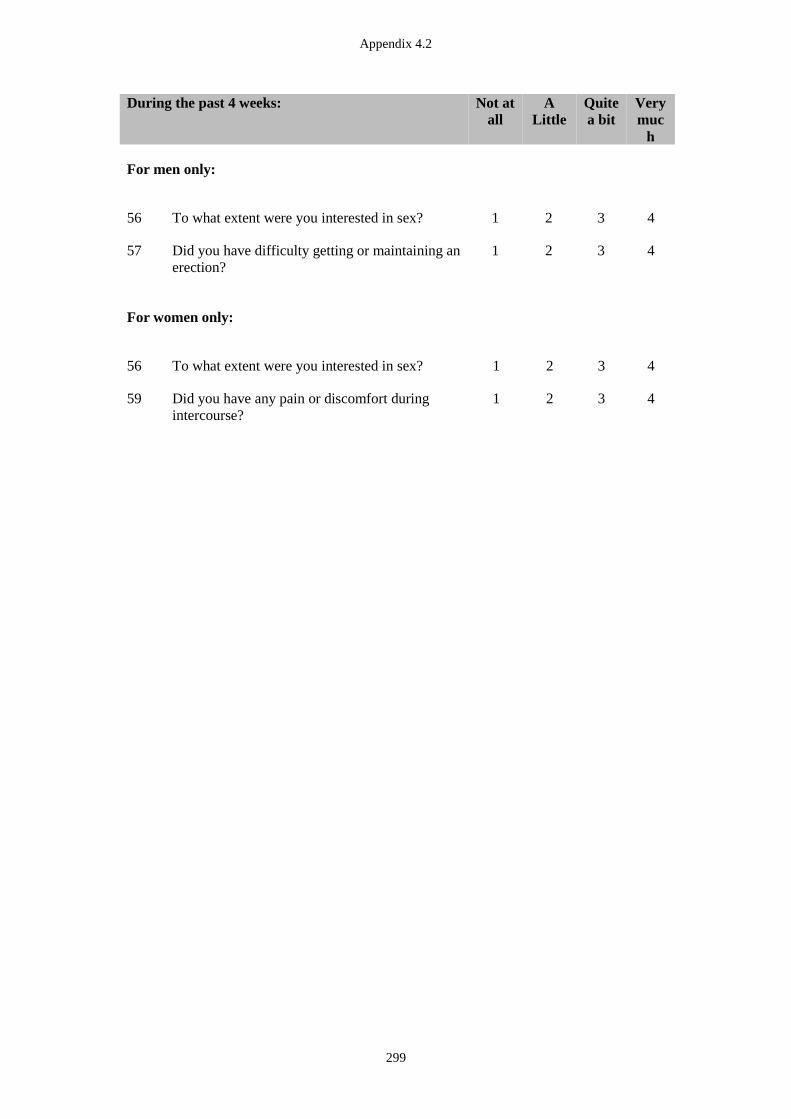
Appendix 4.2
299
During the past 4 weeks: Not at
all
A
Little
Quite
a bit
Very
muc
h
For men only:
56 To what extent were you interested in sex? 1 2 3 4
57 Did you have difficulty getting or maintaining an
erection?
1 2 3 4
For women only:
56 To what extent were you interested in sex? 1 2 3 4
59 Did you have any pain or discomfort during
intercourse?
1 2 3 4
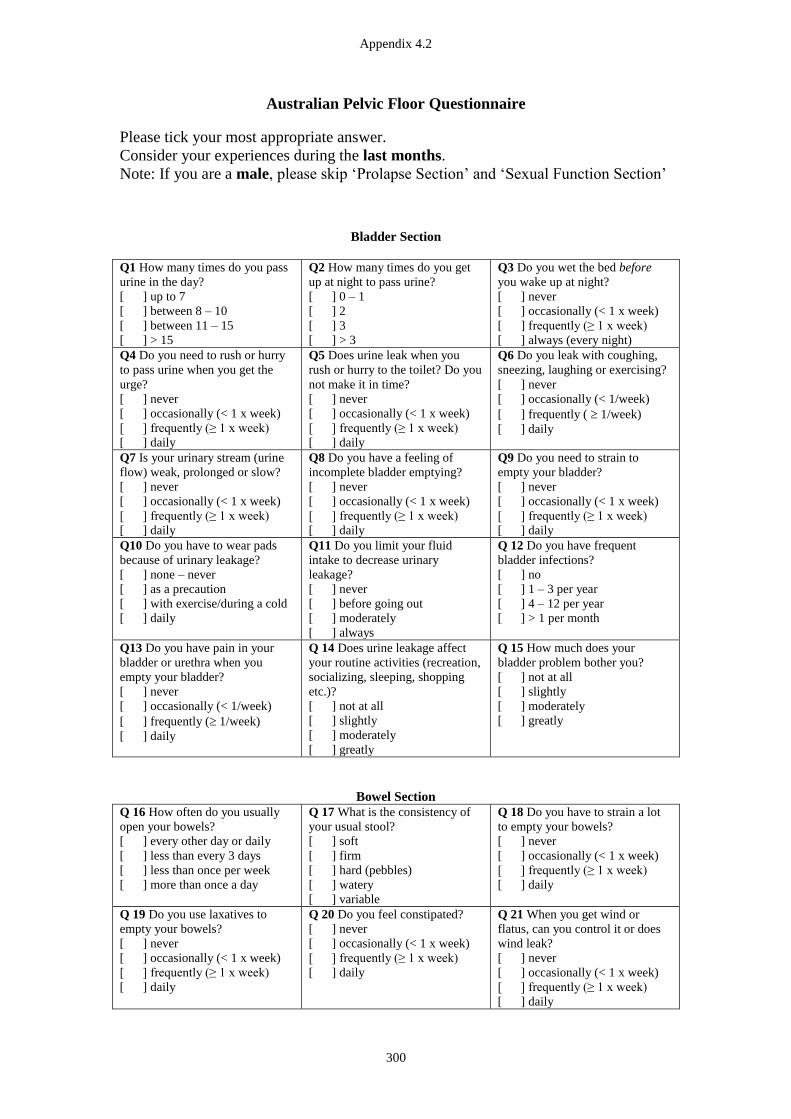
Appendix 4.2
300
Australian Pelvic Floor Questionnaire
Please tick your most appropriate answer.
Consider your experiences during the last months.
Note: If you are a male, please skip ‘Prolapse Section’ and ‘Sexual Function Section’
Bladder Section
Q1 How many times do you pass
urine in the day?
[ ] up to 7
[ ] between 8 – 10
[ ] between 11 – 15
[ ] > 15
Q2 How many times do you get
up at night to pass urine?
[ ] 0 – 1
[ ] 2
[ ] 3
[ ] > 3
Q3 Do you wet the bed before
you wake up at night?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] always (every night)
Q4 Do you need to rush or hurry
to pass urine when you get the
urge?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q5 Does urine leak when you
rush or hurry to the toilet? Do you
not make it in time?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q6 Do you leak with coughing,
sneezing, laughing or exercising?
[ ] never
[ ] occasionally (< 1/week)
[ ] frequently ( 1/week)
[ ] daily
Q7 Is your urinary stream (urine
flow) weak, prolonged or slow?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q8 Do you have a feeling of
incomplete bladder emptying?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q9 Do you need to strain to
empty your bladder?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q10 Do you have to wear pads
because of urinary leakage?
[ ] none – never
[ ] as a precaution
[ ] with exercise/during a cold
[ ] daily
Q11 Do you limit your fluid
intake to decrease urinary
leakage?
[ ] never
[ ] before going out
[ ] moderately
[ ] always
Q 12 Do you have frequent
bladder infections?
[ ] no
[ ] 1 – 3 per year
[ ] 4 – 12 per year
[ ] > 1 per month
Q13 Do you have pain in your
bladder or urethra when you
empty your bladder?
[ ] never
[ ] occasionally (< 1/week)
[ ] frequently ( 1/week)
[ ] daily
Q 14 Does urine leakage affect
your routine activities (recreation,
socializing, sleeping, shopping
etc.)?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Q 15 How much does your
bladder problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Bowel Section
Q 16 How often do you usually
open your bowels?
[ ] every other day or daily
[ ] less than every 3 days
[ ] less than once per week
[ ] more than once a day
Q 17 What is the consistency of
your usual stool?
[ ] soft
[ ] firm
[ ] hard (pebbles)
[ ] watery
[ ] variable
Q 18 Do you have to strain a lot
to empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 19 Do you use laxatives to
empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 20 Do you feel constipated?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 21 When you get wind or
flatus, can you control it or does
wind leak?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
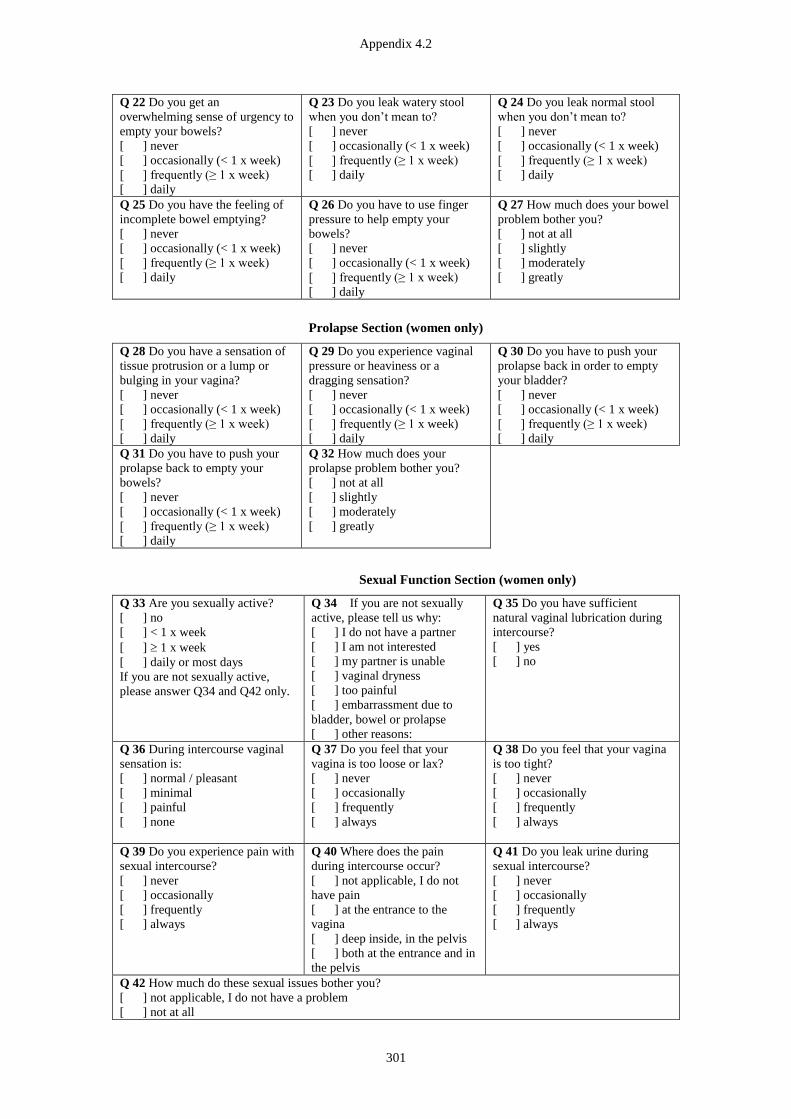
Appendix 4.2
301
Q 22 Do you get an
overwhelming sense of urgency to
empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 23 Do you leak watery stool
when you don’t mean to?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 24 Do you leak normal stool
when you don’t mean to?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 25 Do you have the feeling of
incomplete bowel emptying?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 26 Do you have to use finger
pressure to help empty your
bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 27 How much does your bowel
problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Prolapse Section (women only)
Q 28 Do you have a sensation of
tissue protrusion or a lump or
bulging in your vagina?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 29 Do you experience vaginal
pressure or heaviness or a
dragging sensation?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 30 Do you have to push your
prolapse back in order to empty
your bladder?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 31 Do you have to push your
prolapse back to empty your
bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 32 How much does your
prolapse problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Sexual Function Section (women only)
Q 33 Are you sexually active?
[ ] no
[ ] < 1 x week
[ ] 1 x week
[ ] daily or most days
If you are not sexually active,
please answer Q34 and Q42 only.
Q 34 If you are not sexually
active, please tell us why:
[ ] I do not have a partner
[ ] I am not interested
[ ] my partner is unable
[ ] vaginal dryness
[ ] too painful
[ ] embarrassment due to
bladder, bowel or prolapse
[ ] other reasons:
Q 35 Do you have sufficient
natural vaginal lubrication during
intercourse?
[ ] yes
[ ] no
Q 36 During intercourse vaginal
sensation is:
[ ] normal / pleasant
[ ] minimal
[ ] painful
[ ] none
Q 37 Do you feel that your
vagina is too loose or lax?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 38 Do you feel that your vagina
is too tight?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 39 Do you experience pain with
sexual intercourse?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 40 Where does the pain
during intercourse occur?
[ ] not applicable, I do not
have pain
[ ] at the entrance to the
vagina
[ ] deep inside, in the pelvis
[ ] both at the entrance and in
the pelvis
Q 41 Do you leak urine during
sexual intercourse?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 42 How much do these sexual issues bother you?
[ ] not applicable, I do not have a problem
[ ] not at all

Appendix 4.2
302
[ ] slightly
[ ] moderately
[ ] greatly

Appendix 4.2
303
INTERNATIONAL CONSULTATION ON INCONTINENCE
QUESTIONNAIRE-BOWELS
Many people experience bowel accidents or bowel leakages. We would be grateful if
you could answer the following questions, thinking about how you have been over the
PAST THREE MONTHS
Bowel pattern
3 On average how many times do you open your bowels in 24 hours?
(Tick one box for ‘usual’ and tick one box for ‘at worst’)
(a) (b)
Usual At worst
less than once 1 1
one to three times 2 2
three to ten times 3 3
ten or more times 4 4
(c) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
4 How often do you open your bowels during the night from going to bed to
sleep until you get up in the morning? (Tick one box)
(a)
never 0
once 1
twice 2
three times 3
four or more times 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal

Appendix 4.2
304
5 Do you have to rush to the toilet when you need to open your bowels?
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
6 Do you use medications (tablets or liquids) to stop you opening your
bowels? (Tick one box)
(a)
never 0
less than once a month 1
less than once a week 2
less than once a day 3
about once a day 4
several times a day 5
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
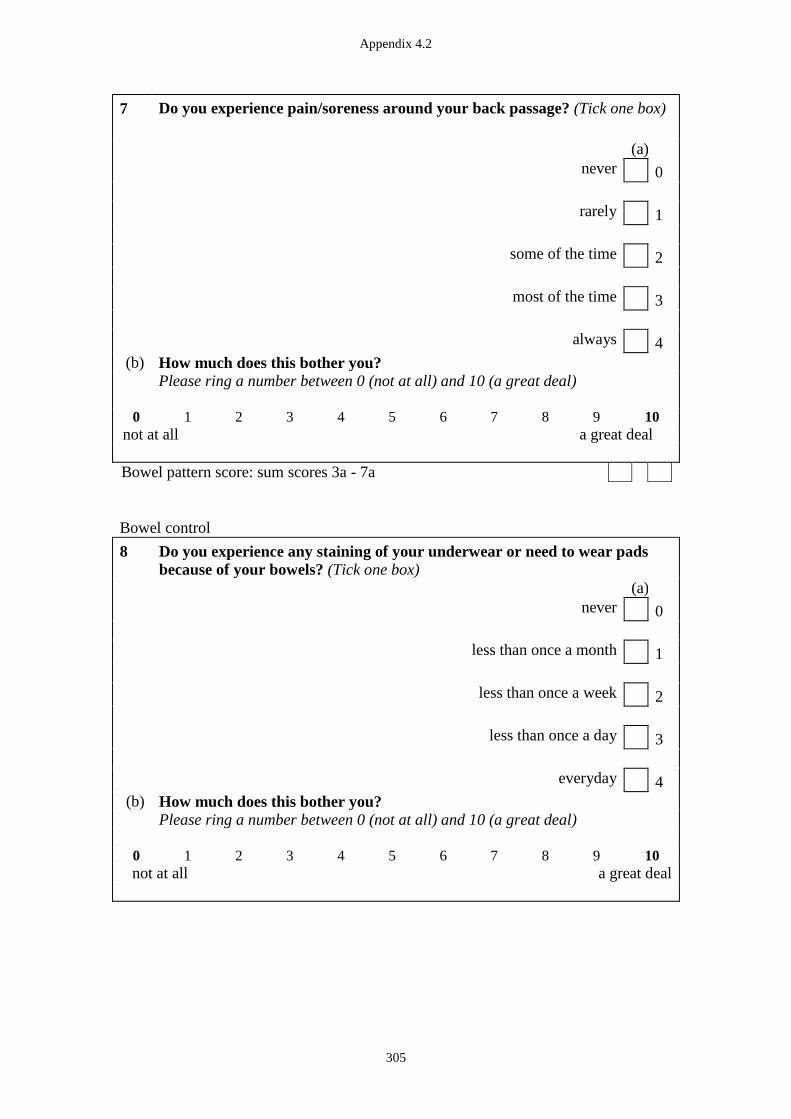
Appendix 4.2
305
7
Do you experience pain/soreness around your back passage? (Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Bowel pattern score: sum scores 3a - 7a
Bowel control
8 Do you experience any staining of your underwear or need to wear pads
because of your bowels? (Tick one box)
(a)
never 0
less than once a month 1
less than once a week 2
less than once a day 3
everyday 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
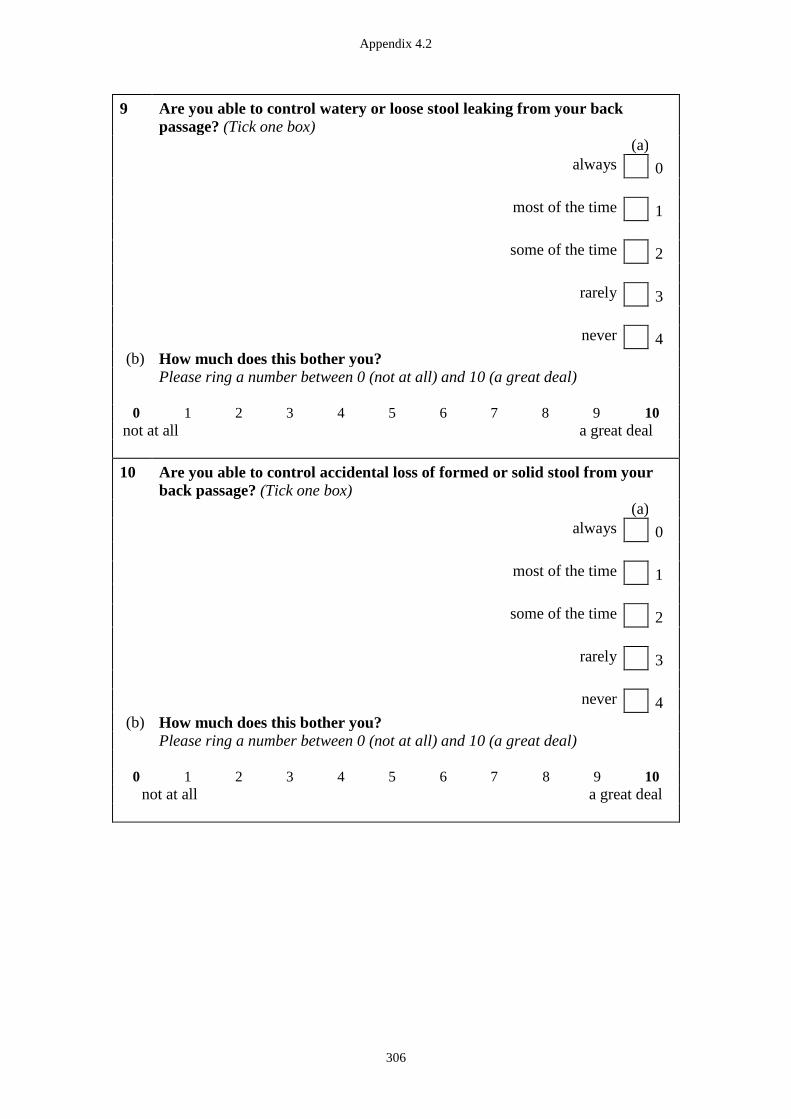
Appendix 4.2
306
9 Are you able to control watery or loose stool leaking from your back
passage? (Tick one box)
(a)
always 0
most of the time 1
some of the time 2
rarely 3
never 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
10 Are you able to control accidental loss of formed or solid stool from your
back passage? (Tick one box)
(a)
always 0
most of the time 1
some of the time 2
rarely 3
never 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
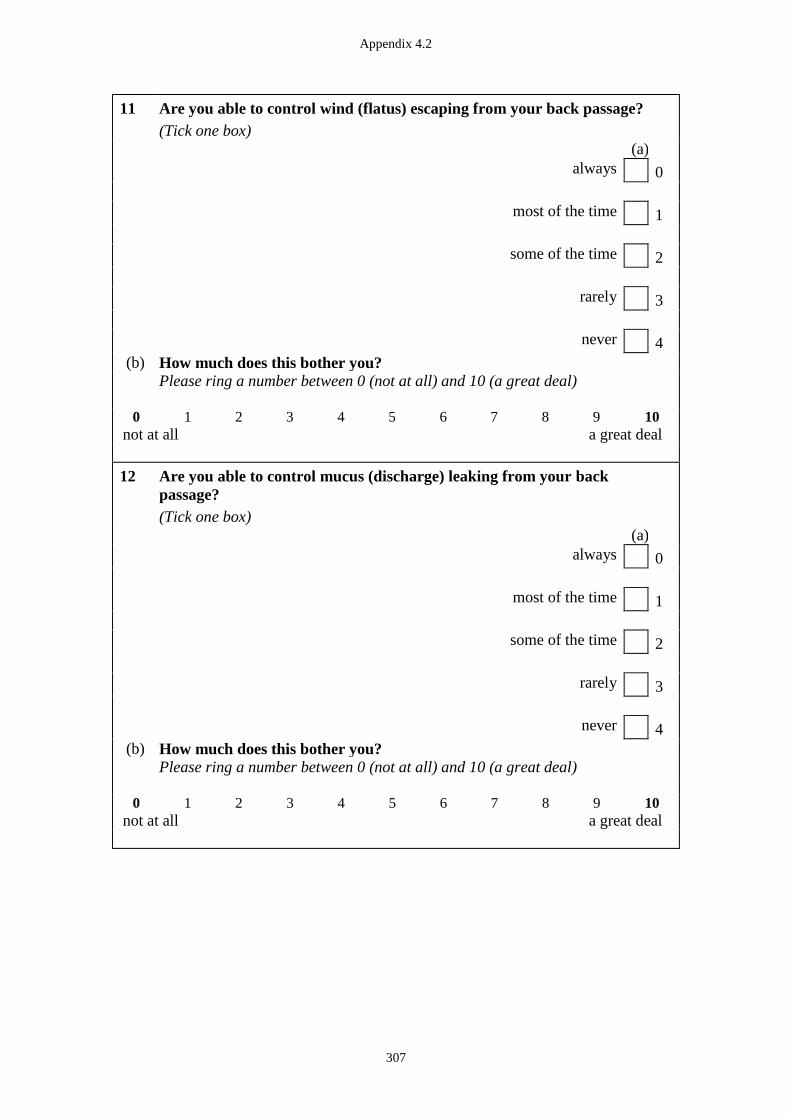
Appendix 4.2
307
11 Are you able to control wind (flatus) escaping from your back passage?
(Tick one box)
(a)
always 0
most of the time 1
some of the time 2
rarely 3
never 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
12 Are you able to control mucus (discharge) leaking from your back
passage?
(Tick one box)
(a)
always 0
most of the time 1
some of the time 2
rarely 3
never 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
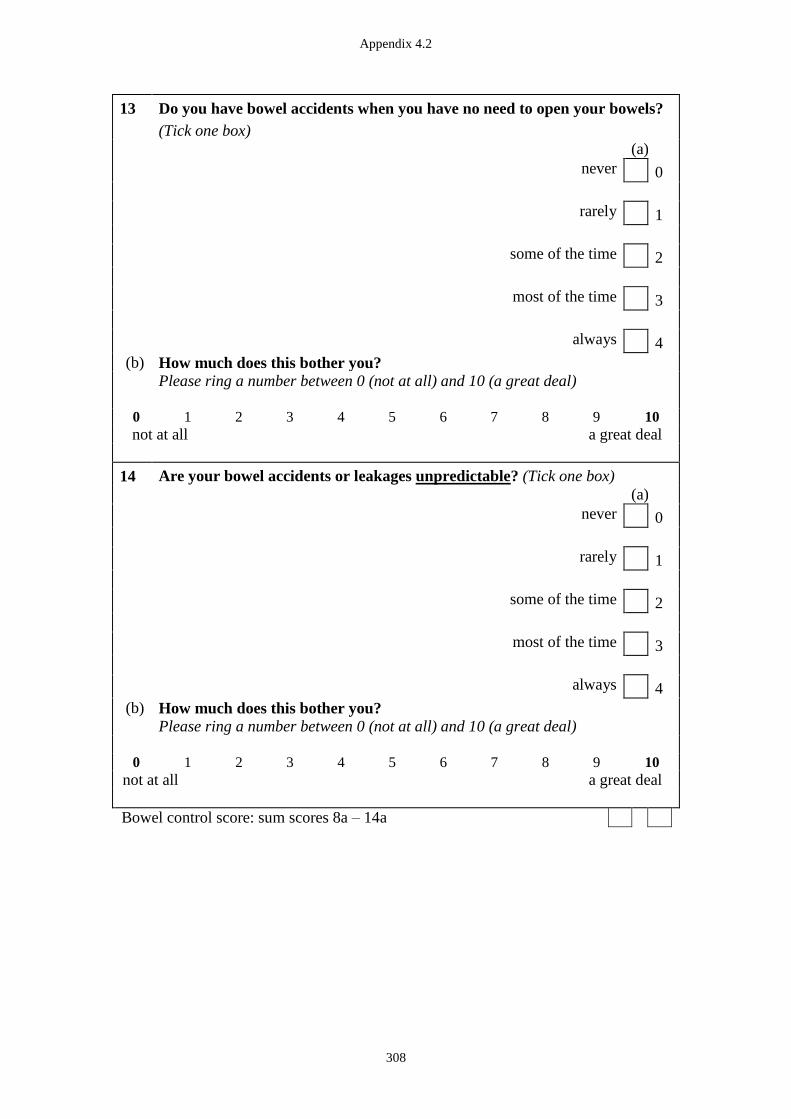
Appendix 4.2
308
13 Do you have bowel accidents when you have no need to open your bowels?
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
14 Are your bowel accidents or leakages unpredictable? (Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Bowel control score: sum scores 8a – 14a
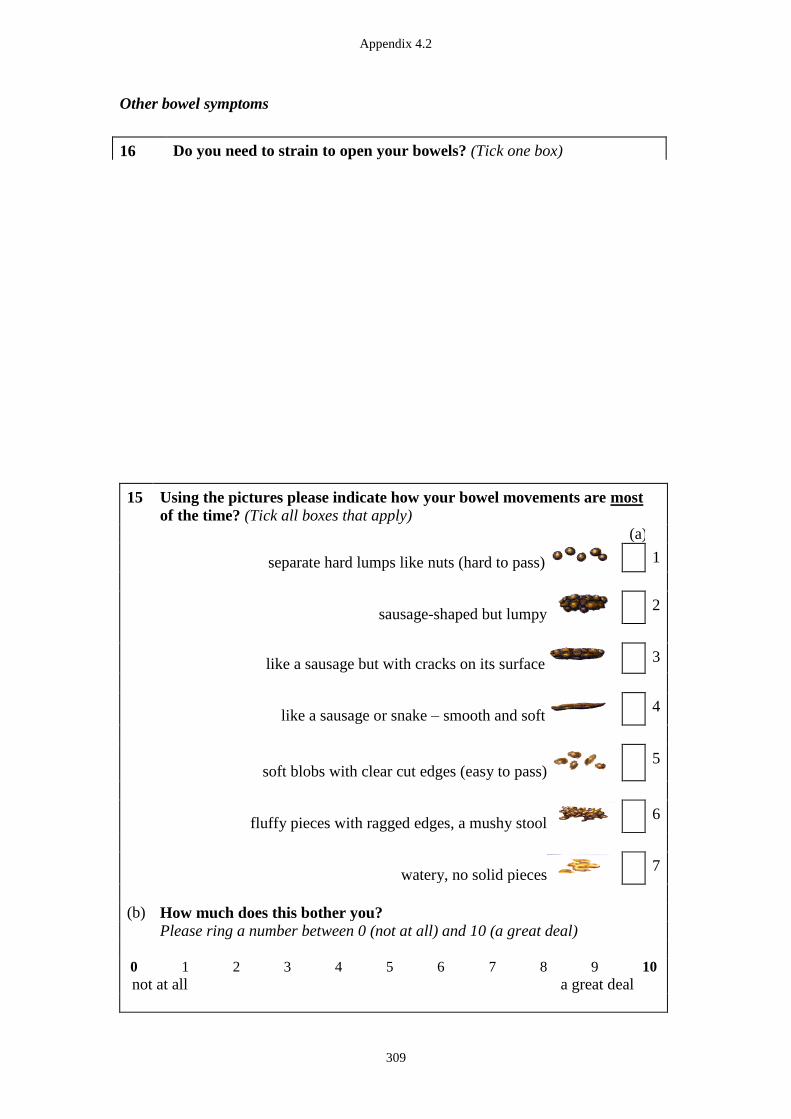
Appendix 4.2
309
Other bowel symptoms
15 Using the pictures please indicate how your bowel movements are most
of the time? (Tick all boxes that apply)
(a)
separate hard lumps like nuts (hard to pass) 1
sausage-shaped but lumpy 2
like a sausage but with cracks on its surface 3
like a sausage or snake – smooth and soft 4
soft blobs with clear cut edges (easy to pass) 5
fluffy pieces with ragged edges, a mushy stool 6
watery, no solid pieces 7
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
16 Do you need to strain to open your bowels? (Tick one box)
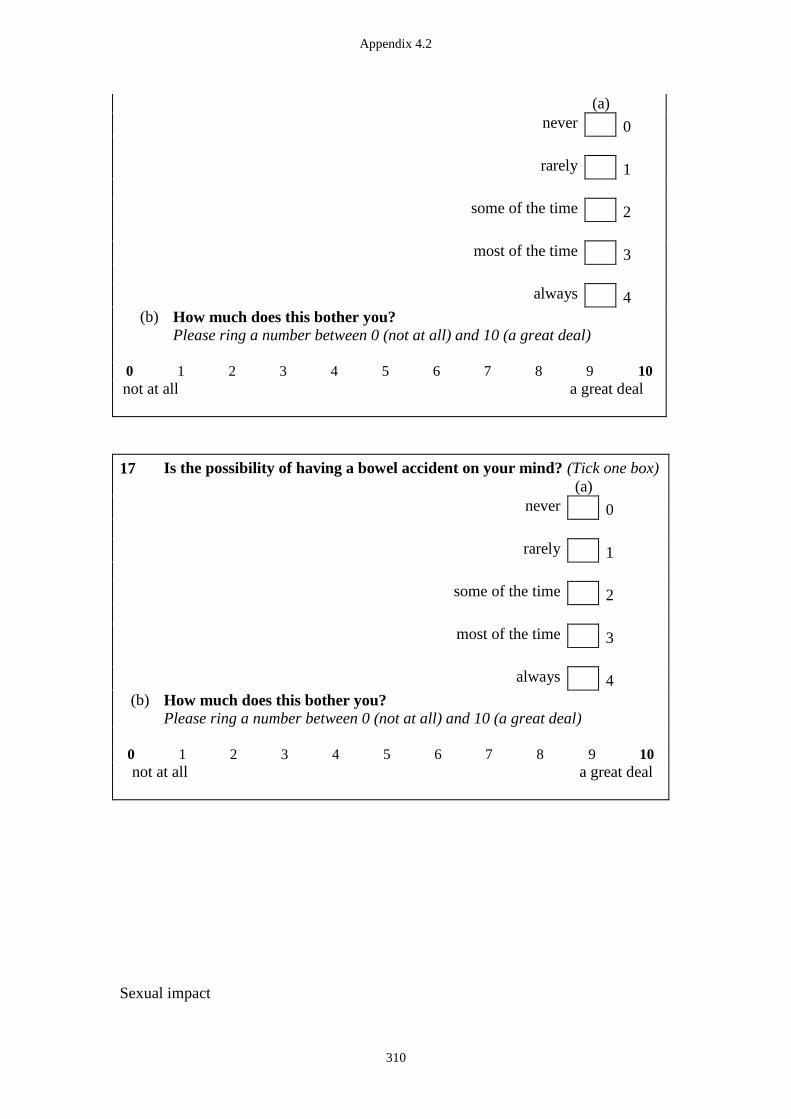
Appendix 4.2
310
17 Is the possibility of having a bowel accident on your mind? (Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Sexual impact
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Appendix 4.2
311
18 Do you restrict your sexual activities because of your bowels? (Tick one
box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
not applicable 5
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Quality of life
19 Do your bowels cause you to feel embarrassed? (Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
20 Do your bowels cause you to make sure you know where toilets are?

Appendix 4.2
312
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
21 Do your bowels cause you to make plans according to your bowels?
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
22 Do your bowels cause you to stay home more often than you would like?

Appendix 4.2
313
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
23. Overall, how much do your bowels interfere with your everyday life?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Quality of life score: sum scores 19a -23
24
Please use the space below to describe any worries you have about
bowel accidents or leakages, what you think may have caused your
bowel accidents or leakages, or anything else you think we should
know.
Appendix 5.1
314
Appendix 5.1 Ethics Approval Documentation (Study 3)

Appendix 5.1
315

Appendix 5.1
316
Appendix 5.1
317
Appendix 5.1
318
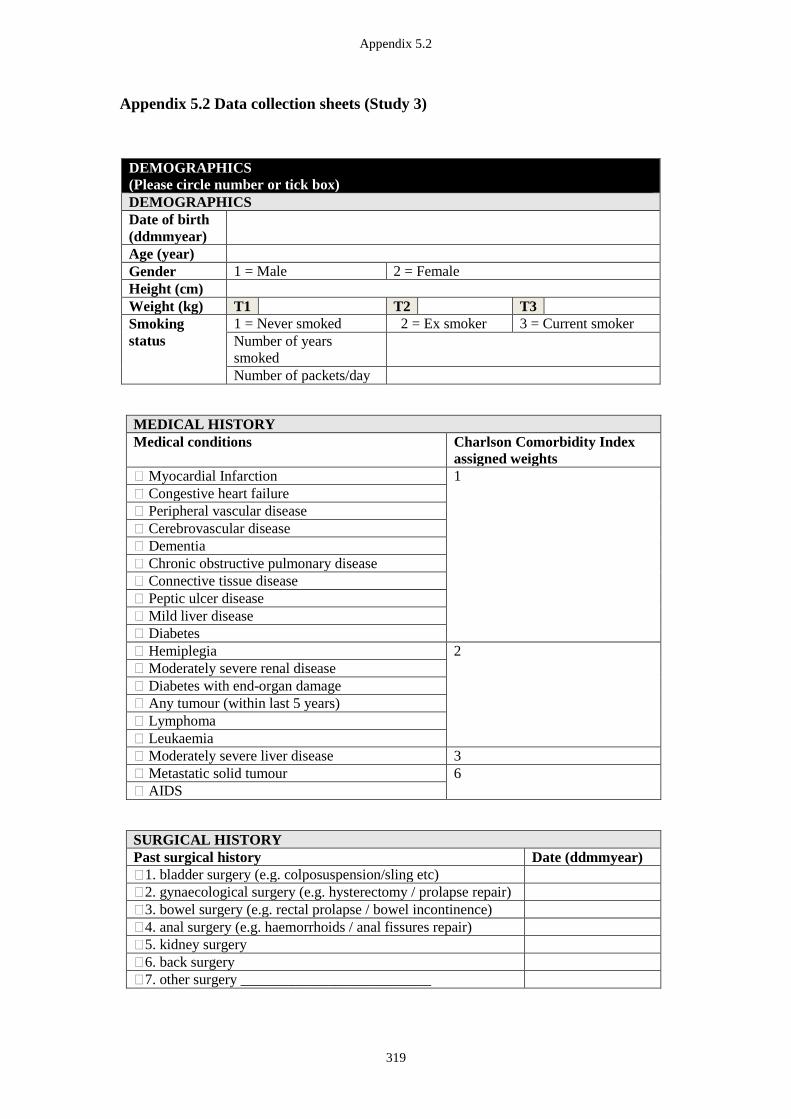
Appendix 5.2
319
Appendix 5.2 Data collection sheets (Study 3)
DEMOGRAPHICS
(Please circle number or tick box)
DEMOGRAPHICS
Date of birth
(ddmmyear)
Age (year)
Gender 1 = Male 2 = Female
Height (cm)
Weight (kg) T1 T2 T3
Smoking
status
1 = Never smoked 2 = Ex smoker 3 = Current smoker
Number of years
smoked
Number of packets/day
MEDICAL HISTORY
Medical conditions Charlson Comorbidity Index
assigned weights
� Myocardial Infarction 1
� Congestive heart failure
� Peripheral vascular disease
� Cerebrovascular disease
� Dementia
� Chronic obstructive pulmonary disease
� Connective tissue disease
� Peptic ulcer disease
� Mild liver disease
� Diabetes
� Hemiplegia 2
� Moderately severe renal disease
� Diabetes with end-organ damage
� Any tumour (within last 5 years)
� Lymphoma
� Leukaemia
� Moderately severe liver disease 3
� Metastatic solid tumour 6
� AIDS
SURGICAL HISTORY
Past surgical history Date (ddmmyear)
�1. bladder surgery (e.g. colposuspension/sling etc)
�2. gynaecological surgery (e.g. hysterectomy / prolapse repair)
�3. bowel surgery (e.g. rectal prolapse / bowel incontinence)
�4. anal surgery (e.g. haemorrhoids / anal fissures repair)
�5. kidney surgery
�6. back surgery
�7. other surgery __________________________
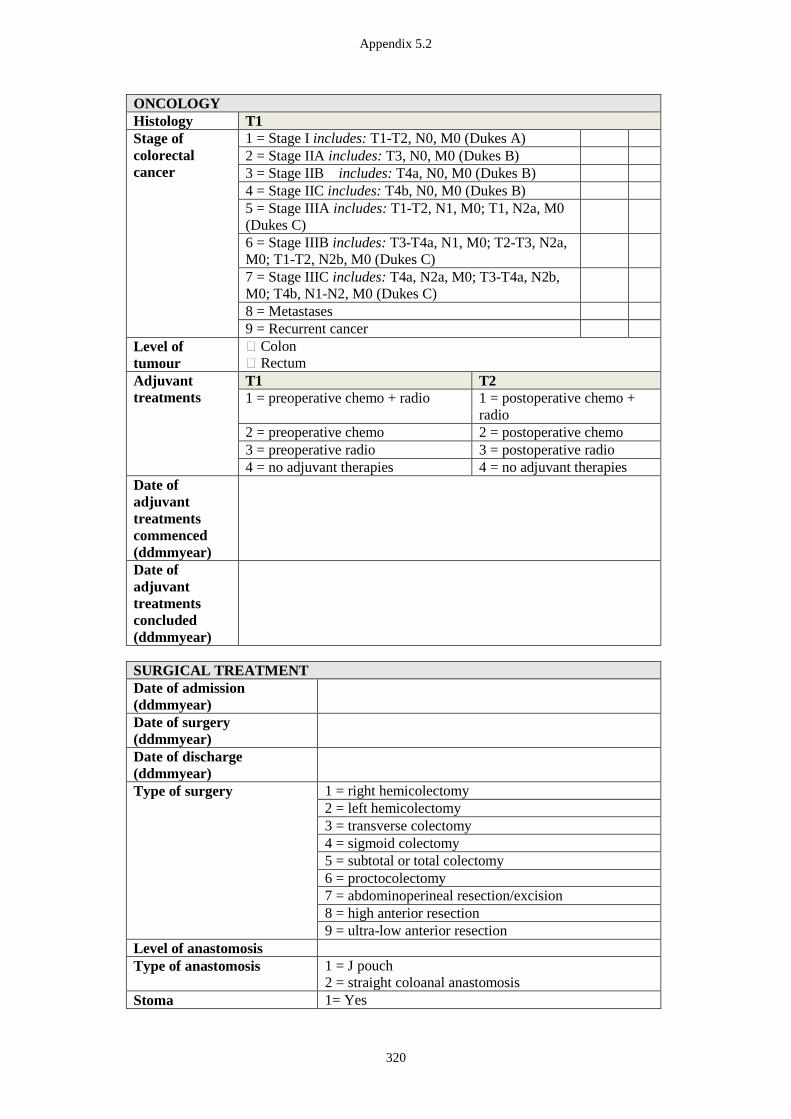
Appendix 5.2
320
ONCOLOGY
Histology T1
Stage of
colorectal
cancer
1 = Stage I includes: T1-T2, N0, M0 (Dukes A)
2 = Stage IIA includes: T3, N0, M0 (Dukes B)
3 = Stage IIB includes: T4a, N0, M0 (Dukes B)
4 = Stage IIC includes: T4b, N0, M0 (Dukes B)
5 = Stage IIIA includes: T1-T2, N1, M0; T1, N2a, M0
(Dukes C)
6 = Stage IIIB includes: T3-T4a, N1, M0; T2-T3, N2a,
M0; T1-T2, N2b, M0 (Dukes C)
7 = Stage IIIC includes: T4a, N2a, M0; T3-T4a, N2b,
M0; T4b, N1-N2, M0 (Dukes C)
8 = Metastases
9 = Recurrent cancer
Level of
tumour
� Colon
� Rectum
Adjuvant
treatments
T1 T2
1 = preoperative chemo + radio 1 = postoperative chemo +
radio
2 = preoperative chemo 2 = postoperative chemo
3 = preoperative radio 3 = postoperative radio
4 = no adjuvant therapies 4 = no adjuvant therapies Date of
adjuvant
treatments
commenced
(ddmmyear)
Date of
adjuvant
treatments
concluded
(ddmmyear)
SURGICAL TREATMENT
Date of admission
(ddmmyear)
Date of surgery
(ddmmyear)
Date of discharge
(ddmmyear)
Type of surgery 1 = right hemicolectomy
2 = left hemicolectomy
3 = transverse colectomy
4 = sigmoid colectomy
5 = subtotal or total colectomy
6 = proctocolectomy
7 = abdominoperineal resection/excision
8 = high anterior resection
9 = ultra-low anterior resection
Level of anastomosis
Type of anastomosis 1 = J pouch
2 = straight coloanal anastomosis
Stoma 1= Yes
Appendix 5.2
321
2 = No
Reason for stoma
Date of closure of ostomy
(ddmmyear)
Appendix 5.2
322
PARTICIPANT QUESTIONNAIRE BOOKLET
TIME POINT
Pre-operation (T1)
6 weeks post operation (T2)
6 months post operation (T2/T3)
`
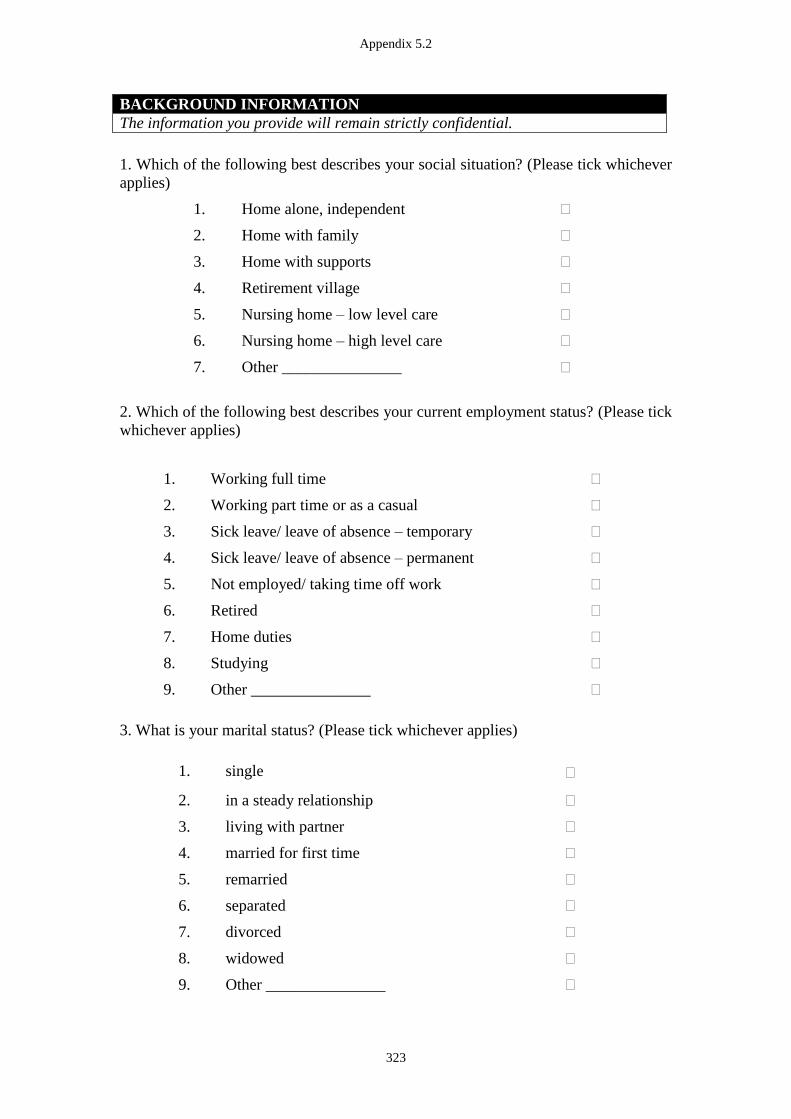
Appendix 5.2
323
BACKGROUND INFORMATION
The information you provide will remain strictly confidential.
1. Which of the following best describes your social situation? (Please tick whichever
applies)
1. Home alone, independent �
2. Home with family �
3. Home with supports �
4. Retirement village �
5. Nursing home – low level care �
6. Nursing home – high level care �
7. Other _______________ �
2. Which of the following best describes your current employment status? (Please tick
whichever applies)
1. Working full time �
2. Working part time or as a casual �
3. Sick leave/ leave of absence – temporary �
4. Sick leave/ leave of absence – permanent �
5. Not employed/ taking time off work �
6. Retired �
7. Home duties �
8. Studying �
9. Other _______________ �
3. What is your marital status? (Please tick whichever applies)
1. single �
2. in a steady relationship �
3. living with partner �
4. married for first time �
5. remarried �
6. separated �
7. divorced �
8. widowed �
9. Other _______________ �
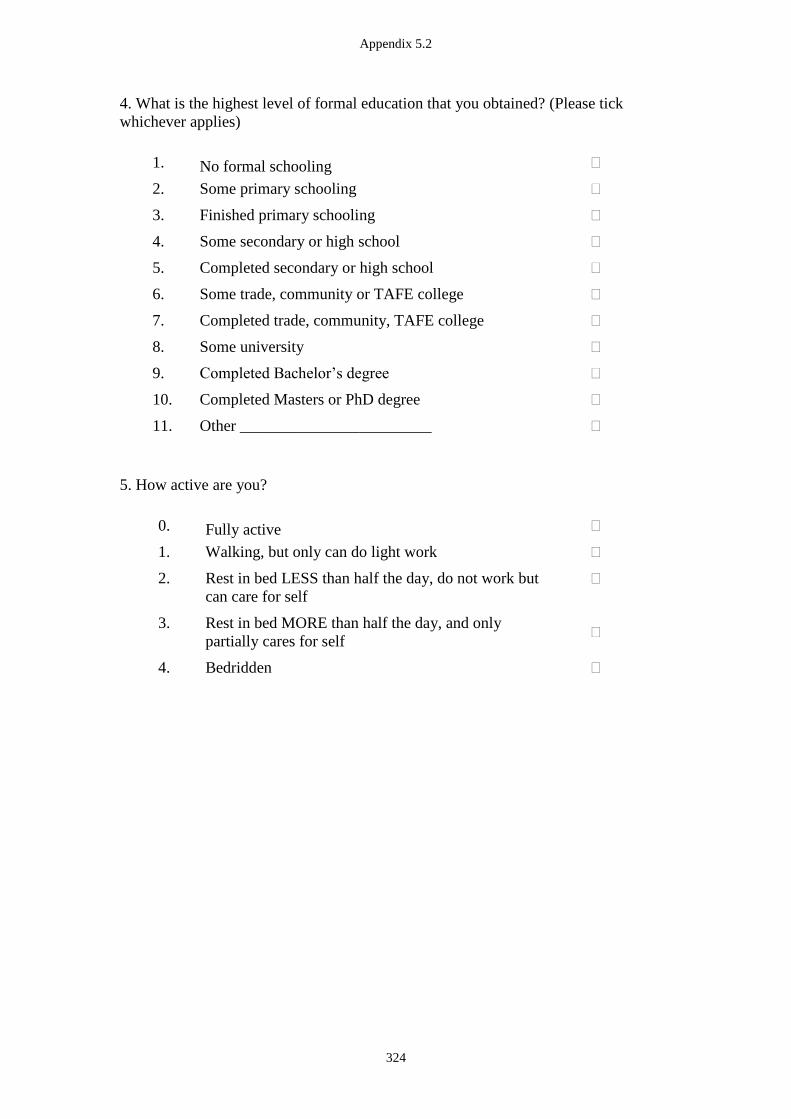
Appendix 5.2
324
4. What is the highest level of formal education that you obtained? (Please tick
whichever applies)
1. No formal schooling �
2. Some primary schooling �
3. Finished primary schooling �
4. Some secondary or high school �
5. Completed secondary or high school �
6. Some trade, community or TAFE college �
7. Completed trade, community, TAFE college �
8. Some university �
9. Completed Bachelor’s degree �
10. Completed Masters or PhD degree �
11. Other ________________________ �
5. How active are you?
0. Fully active �
1. Walking, but only can do light work �
2. Rest in bed LESS than half the day, do not work but
can care for self
�
3. Rest in bed MORE than half the day, and only
partially cares for self �
4. Bedridden �
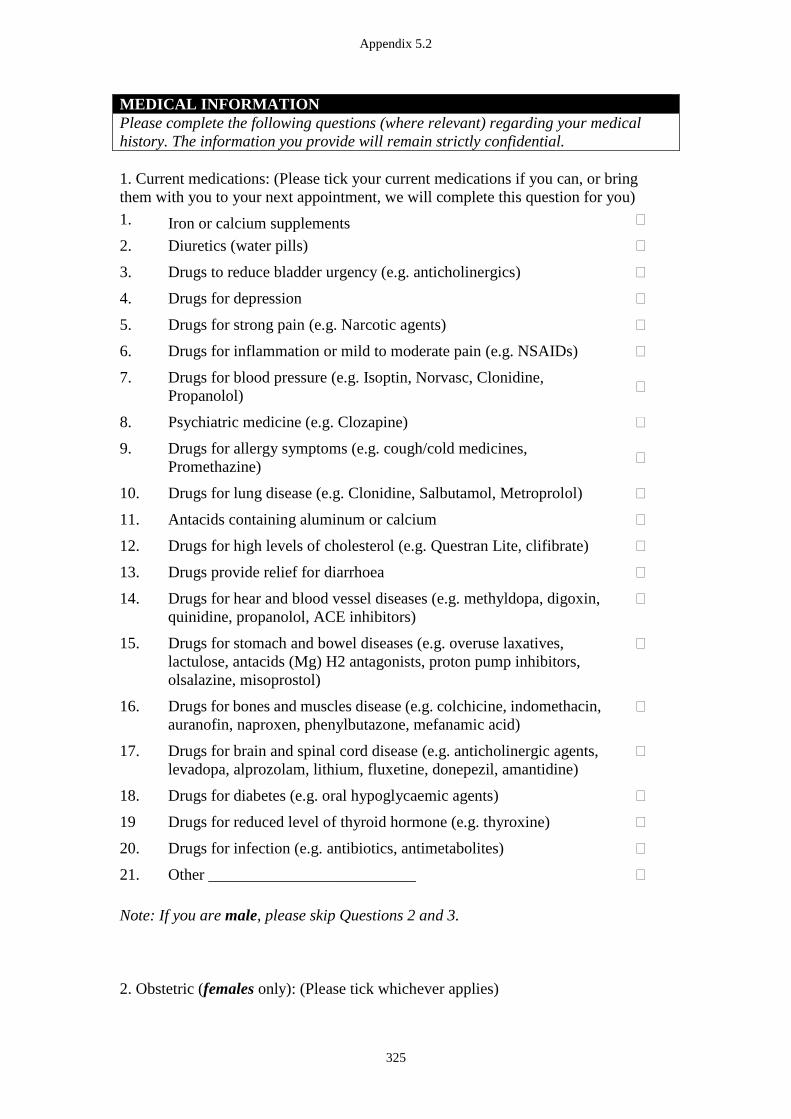
Appendix 5.2
325
MEDICAL INFORMATION
Please complete the following questions (where relevant) regarding your medical
history. The information you provide will remain strictly confidential.
1. Current medications: (Please tick your current medications if you can, or bring
them with you to your next appointment, we will complete this question for you)
1. Iron or calcium supplements �
2. Diuretics (water pills) �
3. Drugs to reduce bladder urgency (e.g. anticholinergics) �
4. Drugs for depression �
5. Drugs for strong pain (e.g. Narcotic agents) �
6. Drugs for inflammation or mild to moderate pain (e.g. NSAIDs) �
7. Drugs for blood pressure (e.g. Isoptin, Norvasc, Clonidine,
Propanolol) �
8. Psychiatric medicine (e.g. Clozapine) �
9. Drugs for allergy symptoms (e.g. cough/cold medicines,
Promethazine) �
10. Drugs for lung disease (e.g. Clonidine, Salbutamol, Metroprolol) �
11. Antacids containing aluminum or calcium �
12. Drugs for high levels of cholesterol (e.g. Questran Lite, clifibrate) �
13. Drugs provide relief for diarrhoea �
14. Drugs for hear and blood vessel diseases (e.g. methyldopa, digoxin,
quinidine, propanolol, ACE inhibitors)
�
15. Drugs for stomach and bowel diseases (e.g. overuse laxatives,
lactulose, antacids (Mg) H2 antagonists, proton pump inhibitors,
olsalazine, misoprostol)
�
16. Drugs for bones and muscles disease (e.g. colchicine, indomethacin,
auranofin, naproxen, phenylbutazone, mefanamic acid)
�
17. Drugs for brain and spinal cord disease (e.g. anticholinergic agents,
levadopa, alprozolam, lithium, fluxetine, donepezil, amantidine)
�
18. Drugs for diabetes (e.g. oral hypoglycaemic agents) �
19 Drugs for reduced level of thyroid hormone (e.g. thyroxine) �
20. Drugs for infection (e.g. antibiotics, antimetabolites) �
21. Other __________________________ �
Note: If you are male, please skip Questions 2 and 3.
2. Obstetric (females only): (Please tick whichever applies)
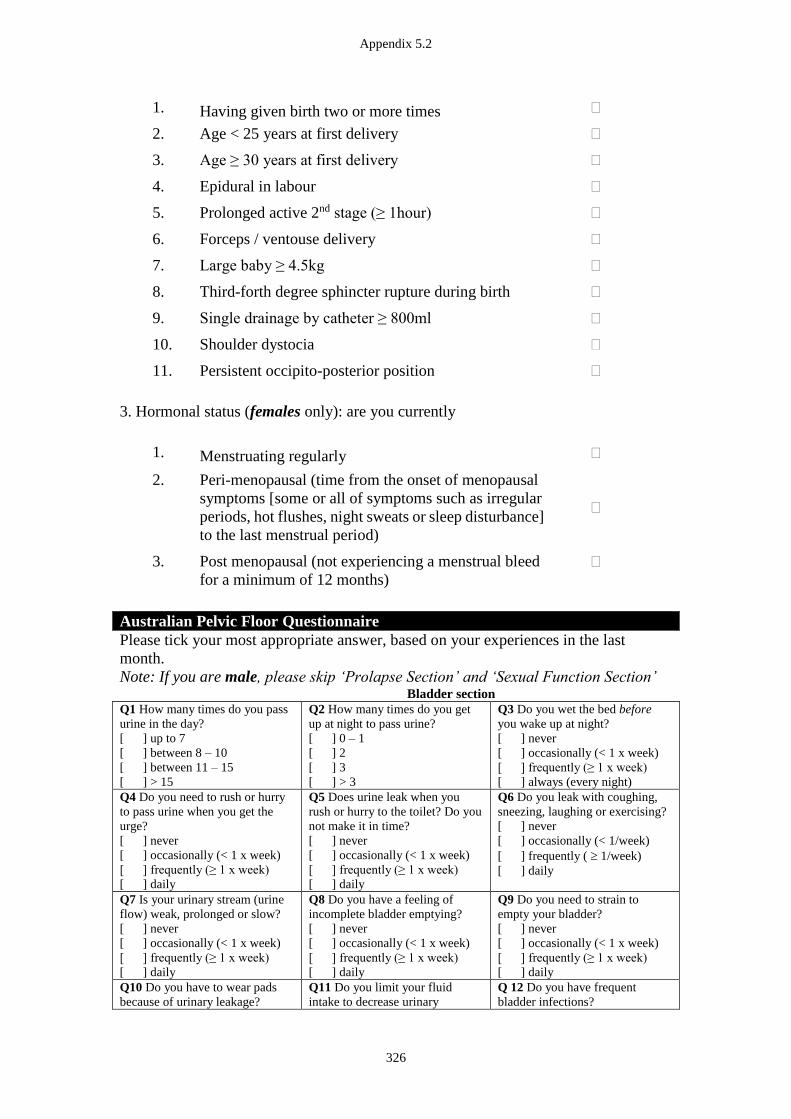
Appendix 5.2
326
1. Having given birth two or more times �
2. Age < 25 years at first delivery �
3. Age ≥ 30 years at first delivery �
4. Epidural in labour �
5. Prolonged active 2nd stage (≥ 1hour) �
6. Forceps / ventouse delivery �
7. Large baby ≥ 4.5kg �
8. Third-forth degree sphincter rupture during birth �
9. Single drainage by catheter ≥ 800ml �
10. Shoulder dystocia �
11. Persistent occipito-posterior position �
3. Hormonal status (females only): are you currently
1. Menstruating regularly �
2. Peri-menopausal (time from the onset of menopausal
symptoms [some or all of symptoms such as irregular
periods, hot flushes, night sweats or sleep disturbance]
to the last menstrual period)
�
3. Post menopausal (not experiencing a menstrual bleed
for a minimum of 12 months)
�
Australian Pelvic Floor Questionnaire
Please tick your most appropriate answer, based on your experiences in the last
month.
Note: If you are male, please skip ‘Prolapse Section’ and ‘Sexual Function Section’
Bladder section
Q1 How many times do you pass
urine in the day?
[ ] up to 7
[ ] between 8 – 10
[ ] between 11 – 15
[ ] > 15
Q2 How many times do you get
up at night to pass urine?
[ ] 0 – 1
[ ] 2
[ ] 3
[ ] > 3
Q3 Do you wet the bed before
you wake up at night?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] always (every night)
Q4 Do you need to rush or hurry
to pass urine when you get the
urge?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q5 Does urine leak when you
rush or hurry to the toilet? Do you
not make it in time?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q6 Do you leak with coughing,
sneezing, laughing or exercising?
[ ] never
[ ] occasionally (< 1/week)
[ ] frequently ( 1/week)
[ ] daily
Q7 Is your urinary stream (urine
flow) weak, prolonged or slow?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q8 Do you have a feeling of
incomplete bladder emptying?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q9 Do you need to strain to
empty your bladder?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q10 Do you have to wear pads
because of urinary leakage?
Q11 Do you limit your fluid
intake to decrease urinary
Q 12 Do you have frequent
bladder infections?
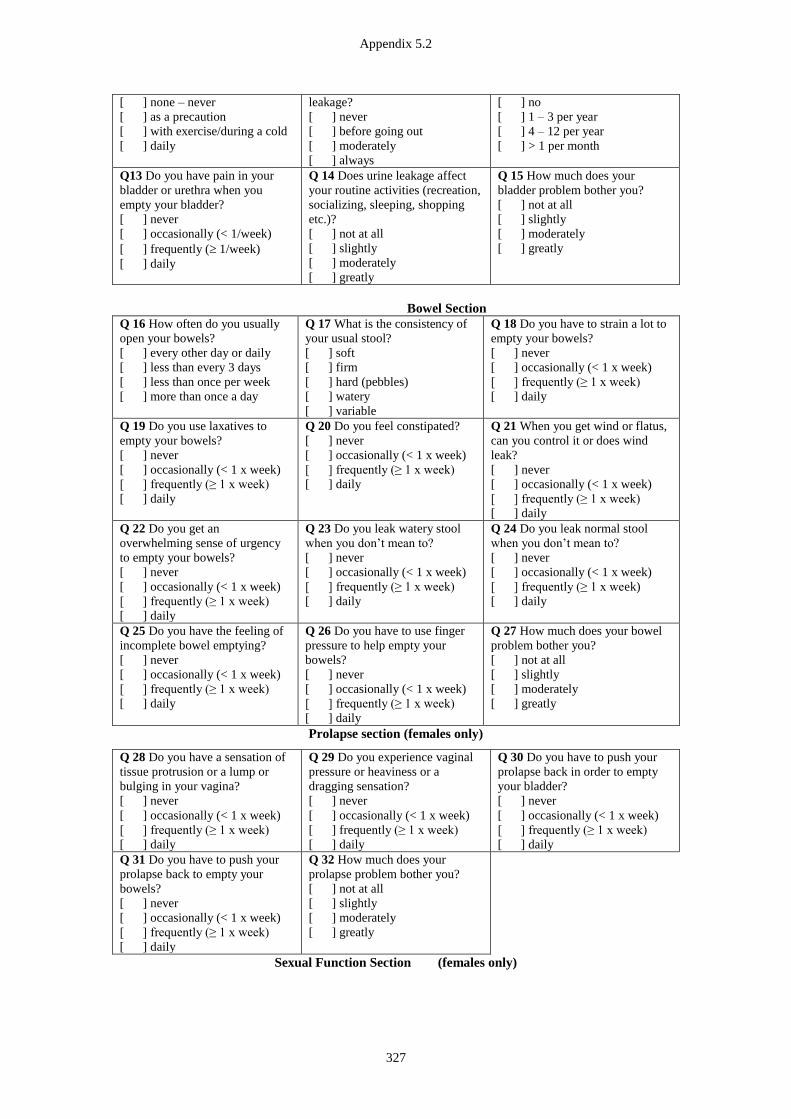
Appendix 5.2
327
[ ] none – never
[ ] as a precaution
[ ] with exercise/during a cold
[ ] daily
leakage?
[ ] never
[ ] before going out
[ ] moderately
[ ] always
[ ] no
[ ] 1 – 3 per year
[ ] 4 – 12 per year
[ ] > 1 per month
Q13 Do you have pain in your
bladder or urethra when you
empty your bladder?
[ ] never
[ ] occasionally (< 1/week)
[ ] frequently ( 1/week)
[ ] daily
Q 14 Does urine leakage affect
your routine activities (recreation,
socializing, sleeping, shopping
etc.)?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Q 15 How much does your
bladder problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Bowel Section
Q 16 How often do you usually
open your bowels?
[ ] every other day or daily
[ ] less than every 3 days
[ ] less than once per week
[ ] more than once a day
Q 17 What is the consistency of
your usual stool?
[ ] soft
[ ] firm
[ ] hard (pebbles)
[ ] watery
[ ] variable
Q 18 Do you have to strain a lot to
empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 19 Do you use laxatives to
empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 20 Do you feel constipated?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 21 When you get wind or flatus,
can you control it or does wind
leak?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 22 Do you get an
overwhelming sense of urgency
to empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 23 Do you leak watery stool
when you don’t mean to?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 24 Do you leak normal stool
when you don’t mean to?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 25 Do you have the feeling of
incomplete bowel emptying?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 26 Do you have to use finger
pressure to help empty your
bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 27 How much does your bowel
problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Prolapse section (females only)
Q 28 Do you have a sensation of
tissue protrusion or a lump or
bulging in your vagina?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 29 Do you experience vaginal
pressure or heaviness or a
dragging sensation?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 30 Do you have to push your
prolapse back in order to empty
your bladder?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 31 Do you have to push your
prolapse back to empty your
bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 32 How much does your
prolapse problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Sexual Function Section (females only)
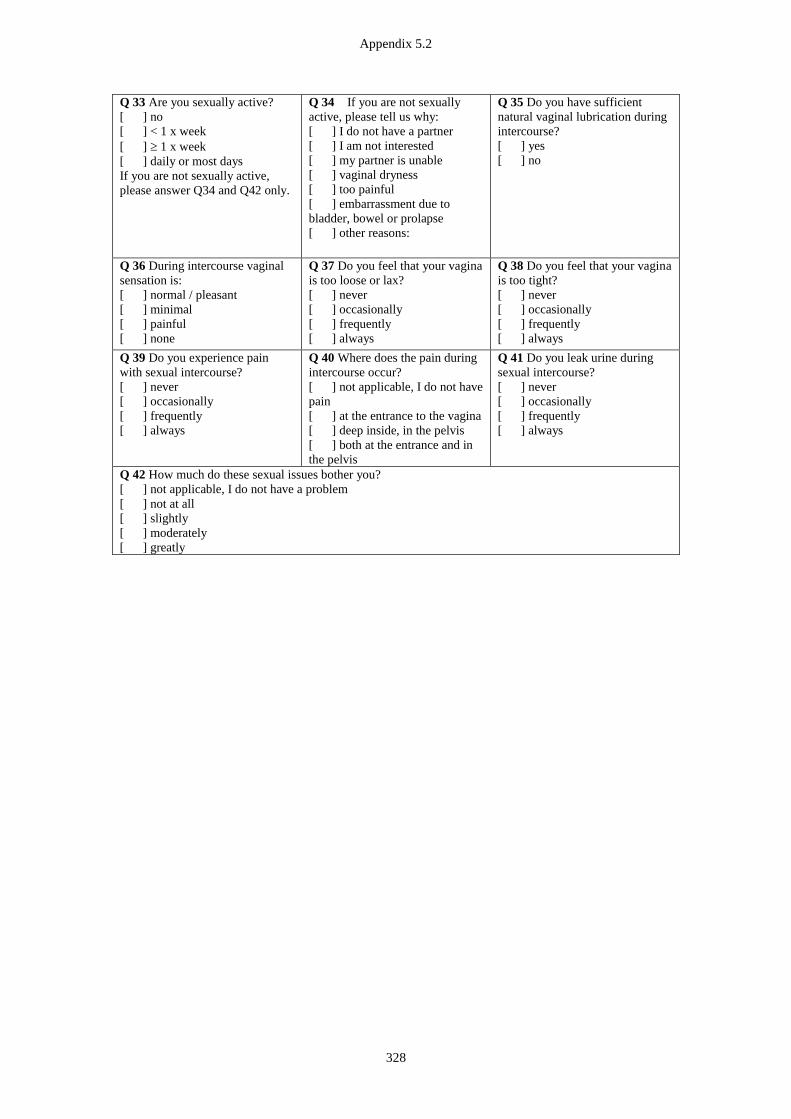
Appendix 5.2
328
Q 33 Are you sexually active?
[ ] no
[ ] < 1 x week
[ ] 1 x week
[ ] daily or most days
If you are not sexually active,
please answer Q34 and Q42 only.
Q 34 If you are not sexually
active, please tell us why:
[ ] I do not have a partner
[ ] I am not interested
[ ] my partner is unable
[ ] vaginal dryness
[ ] too painful
[ ] embarrassment due to
bladder, bowel or prolapse
[ ] other reasons:
Q 35 Do you have sufficient
natural vaginal lubrication during
intercourse?
[ ] yes
[ ] no
Q 36 During intercourse vaginal
sensation is:
[ ] normal / pleasant
[ ] minimal
[ ] painful
[ ] none
Q 37 Do you feel that your vagina
is too loose or lax?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 38 Do you feel that your vagina
is too tight?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 39 Do you experience pain
with sexual intercourse?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 40 Where does the pain during
intercourse occur?
[ ] not applicable, I do not have
pain
[ ] at the entrance to the vagina
[ ] deep inside, in the pelvis
[ ] both at the entrance and in
the pelvis
Q 41 Do you leak urine during
sexual intercourse?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 42 How much do these sexual issues bother you?
[ ] not applicable, I do not have a problem
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
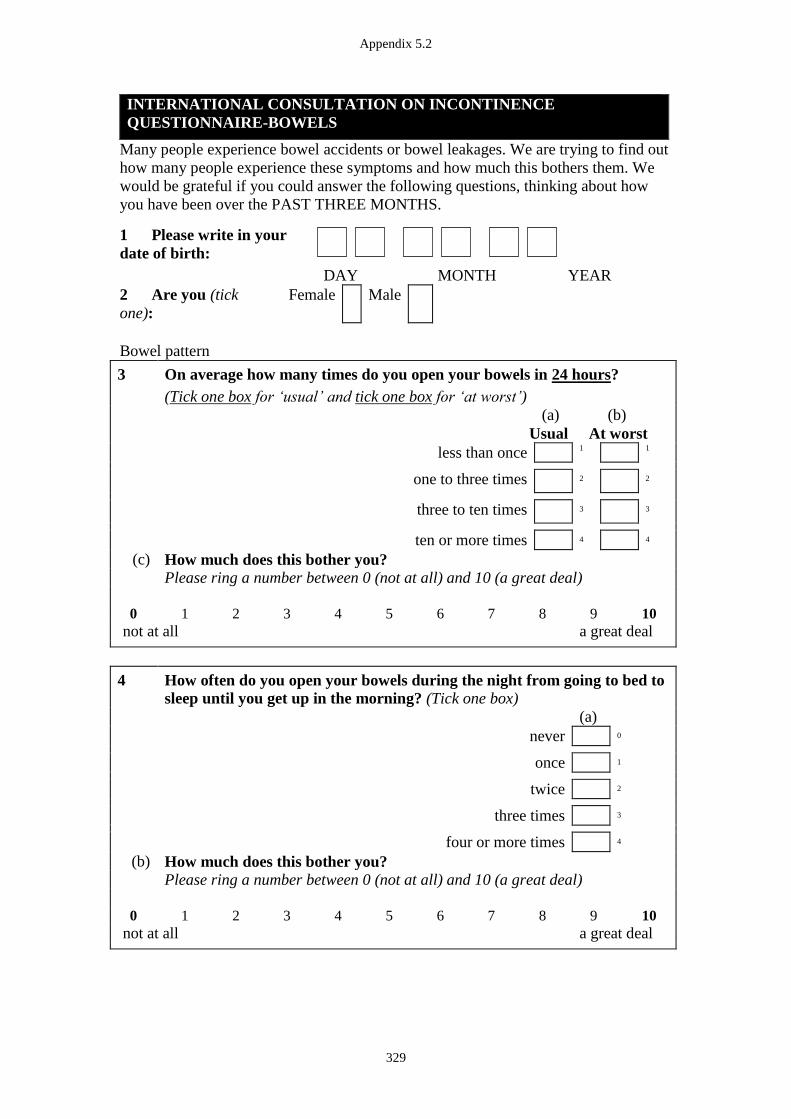
Appendix 5.2
329
INTERNATIONAL CONSULTATION ON INCONTINENCE
QUESTIONNAIRE-BOWELS
Many people experience bowel accidents or bowel leakages. We are trying to find out
how many people experience these symptoms and how much this bothers them. We
would be grateful if you could answer the following questions, thinking about how
you have been over the PAST THREE MONTHS.
1 Please write in your
date of birth:
DAY MONTH YEAR
2 Are you (tick
one):
Female Male
Bowel pattern
3 On average how many times do you open your bowels in 24 hours?
(Tick one box for ‘usual’ and tick one box for ‘at worst’)
(a) (b)
Usual At worst
less than once 1
1
one to three times 2 2
three to ten times 3 3
ten or more times 4 4
(c) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
4 How often do you open your bowels during the night from going to bed to
sleep until you get up in the morning? (Tick one box)
(a)
never 0
once 1
twice 2
three times 3
four or more times 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
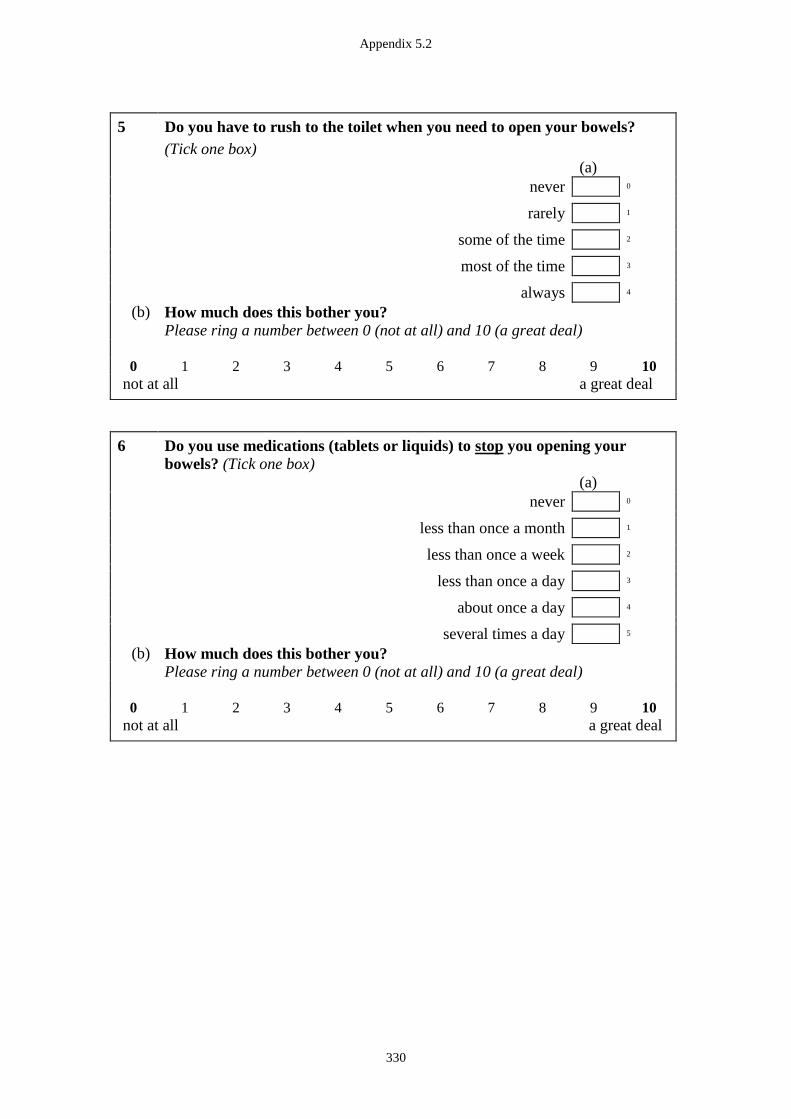
Appendix 5.2
330
5 Do you have to rush to the toilet when you need to open your bowels?
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
6 Do you use medications (tablets or liquids) to stop you opening your
bowels? (Tick one box)
(a)
never 0
less than once a month 1
less than once a week 2
less than once a day 3
about once a day 4
several times a day 5
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
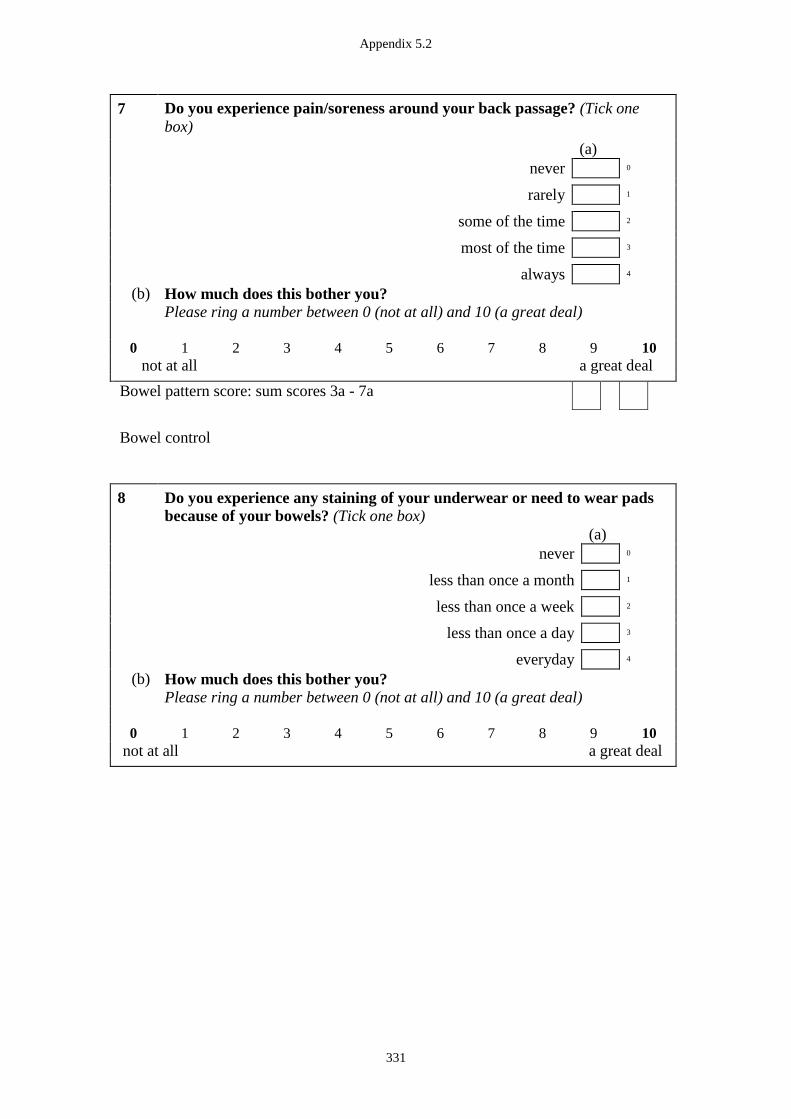
Appendix 5.2
331
7
Do you experience pain/soreness around your back passage? (Tick one
box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Bowel pattern score: sum scores 3a - 7a
Bowel control
8 Do you experience any staining of your underwear or need to wear pads
because of your bowels? (Tick one box)
(a)
never 0
less than once a month 1
less than once a week 2
less than once a day 3
everyday 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal

Appendix 5.2
332
9 Are you able to control watery or loose stool leaking from your back
passage? (Tick one box)
(a)
always 0
most of the time 1
some of the time 2
rarely 3
never 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
10 Are you able to control accidental loss of formed or solid stool from your
back passage? (Tick one box)
(a)
always 0
most of the time 1
some of the time 2
rarely 3
never 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
11 Are you able to control wind (flatus) escaping from your back passage?
(Tick one box)
(a)
always 0
most of the time 1
some of the time 2
rarely 3
never 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
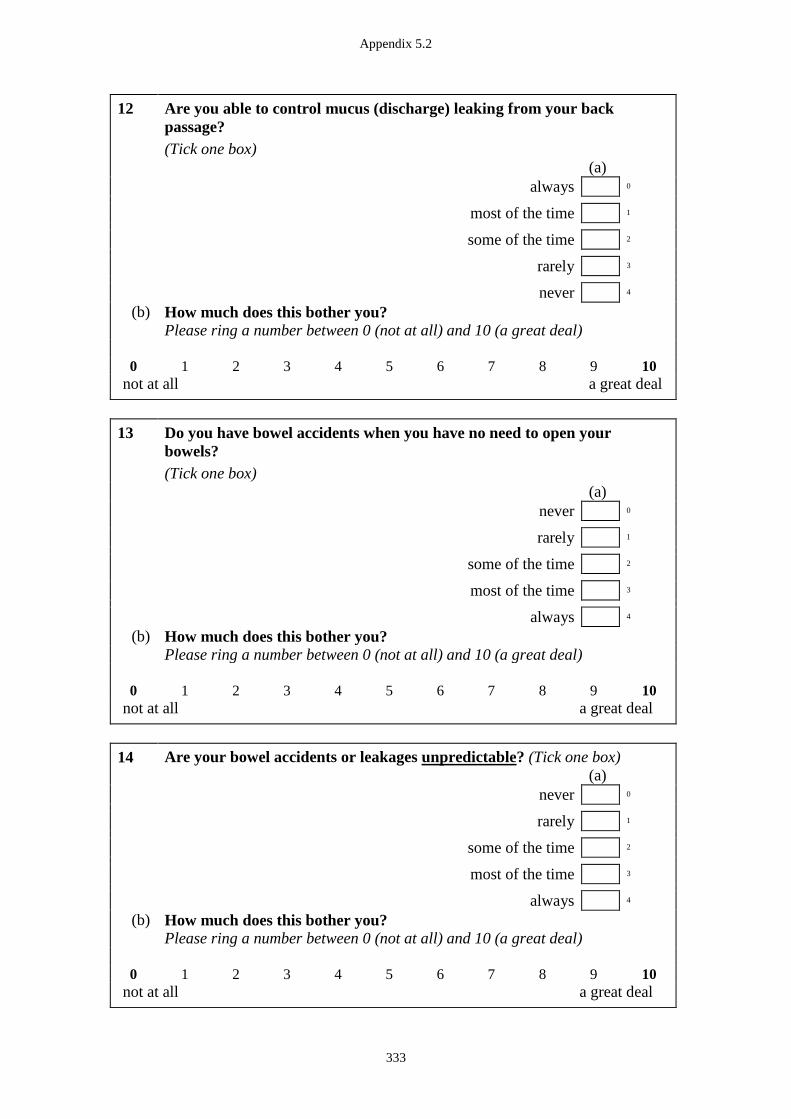
Appendix 5.2
333
12 Are you able to control mucus (discharge) leaking from your back
passage?
(Tick one box)
(a)
always 0
most of the time 1
some of the time 2
rarely 3
never 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
13 Do you have bowel accidents when you have no need to open your
bowels?
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
14 Are your bowel accidents or leakages unpredictable? (Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
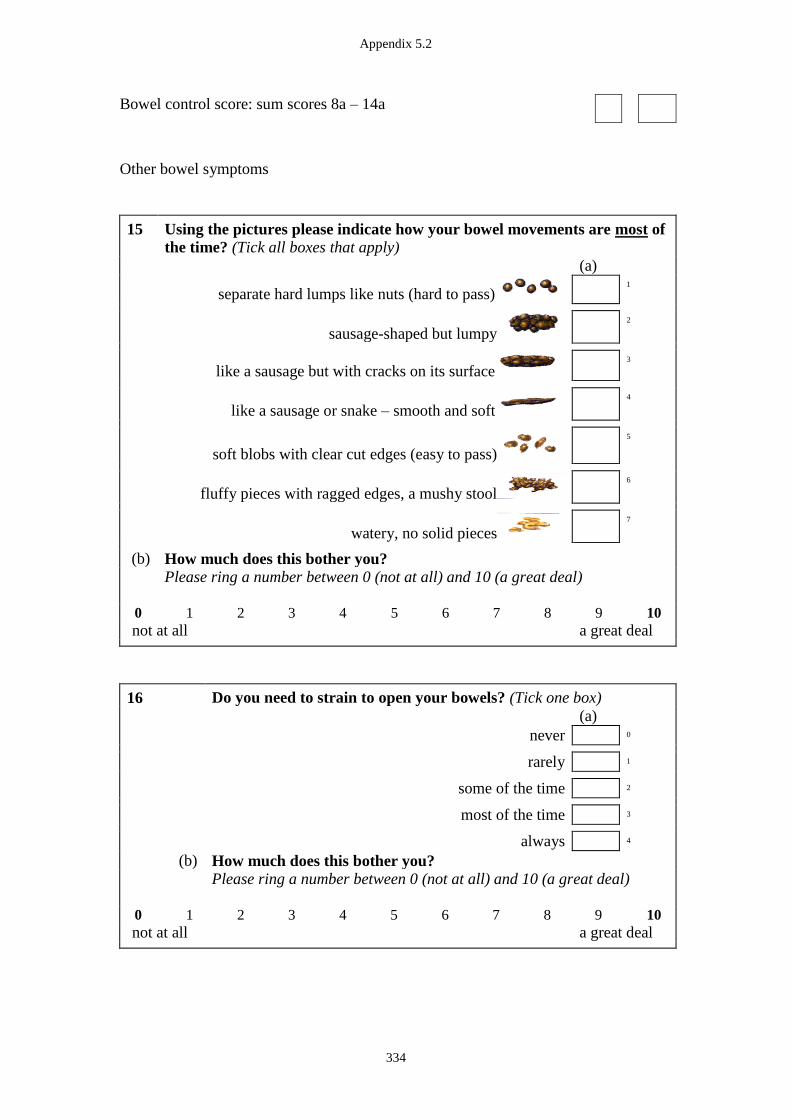
Appendix 5.2
334
Bowel control score: sum scores 8a – 14a
Other bowel symptoms
15 Using the pictures please indicate how your bowel movements are most of
the time? (Tick all boxes that apply)
(a)
separate hard lumps like nuts (hard to pass) 1
sausage-shaped but lumpy 2
like a sausage but with cracks on its surface 3
like a sausage or snake – smooth and soft 4
soft blobs with clear cut edges (easy to pass) 5
fluffy pieces with ragged edges, a mushy stool 6
watery, no solid pieces 7
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
16 Do you need to strain to open your bowels? (Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
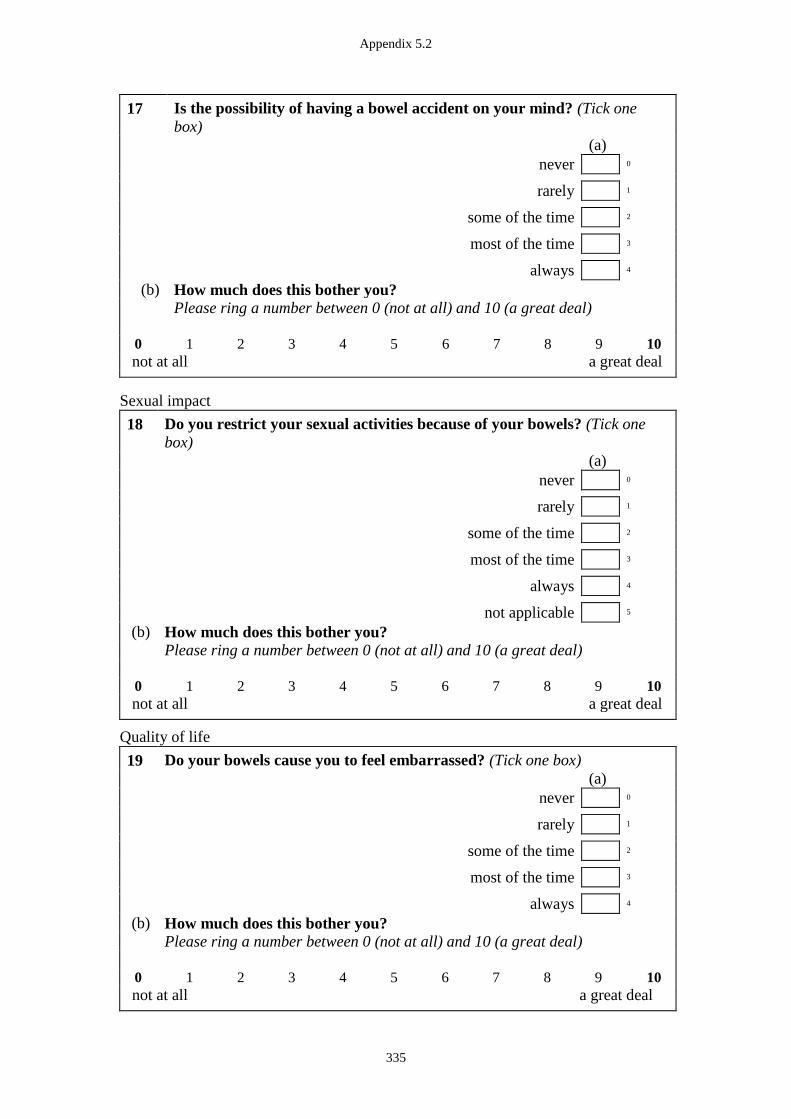
Appendix 5.2
335
17 Is the possibility of having a bowel accident on your mind? (Tick one
box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Sexual impact
18 Do you restrict your sexual activities because of your bowels? (Tick one
box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
not applicable 5
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Quality of life
19 Do your bowels cause you to feel embarrassed? (Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
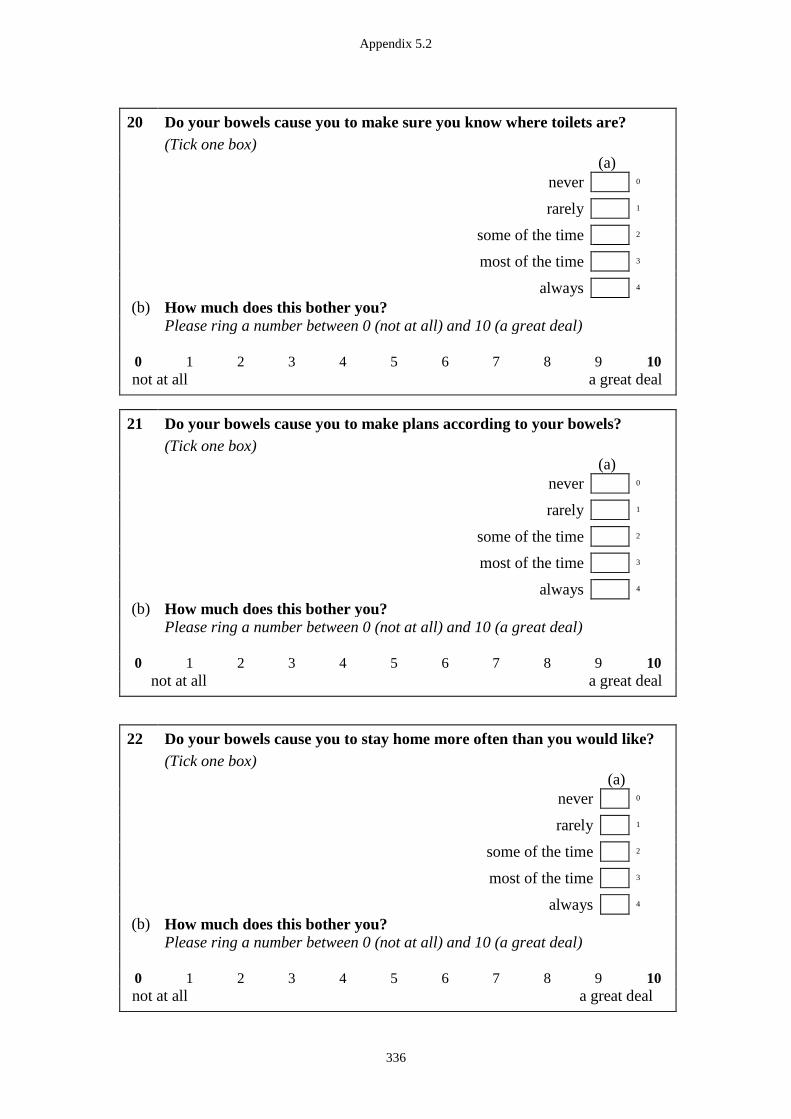
Appendix 5.2
336
20 Do your bowels cause you to make sure you know where toilets are?
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
21 Do your bowels cause you to make plans according to your bowels?
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
22 Do your bowels cause you to stay home more often than you would like?
(Tick one box)
(a)
never 0
rarely 1
some of the time 2
most of the time 3
always 4
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
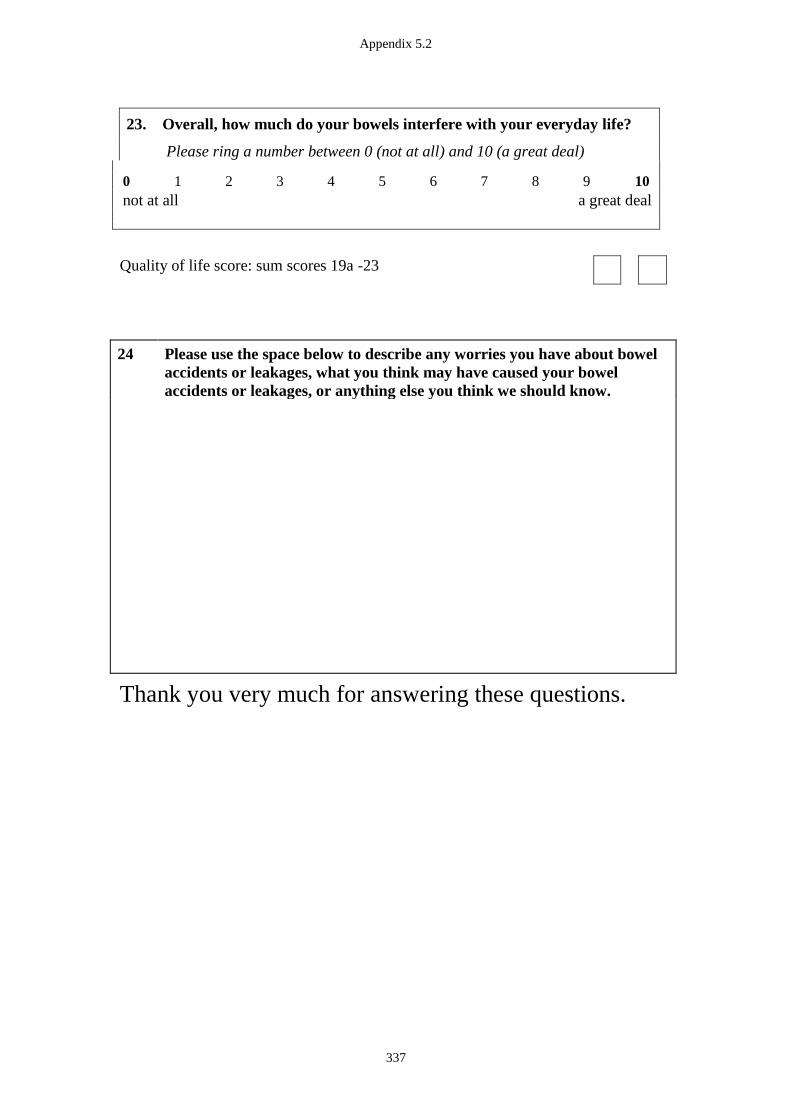
Appendix 5.2
337
23. Overall, how much do your bowels interfere with your everyday life?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Quality of life score: sum scores 19a -23
24
Please use the space below to describe any worries you have about bowel
accidents or leakages, what you think may have caused your bowel
accidents or leakages, or anything else you think we should know.
Thank you very much for answering these questions.
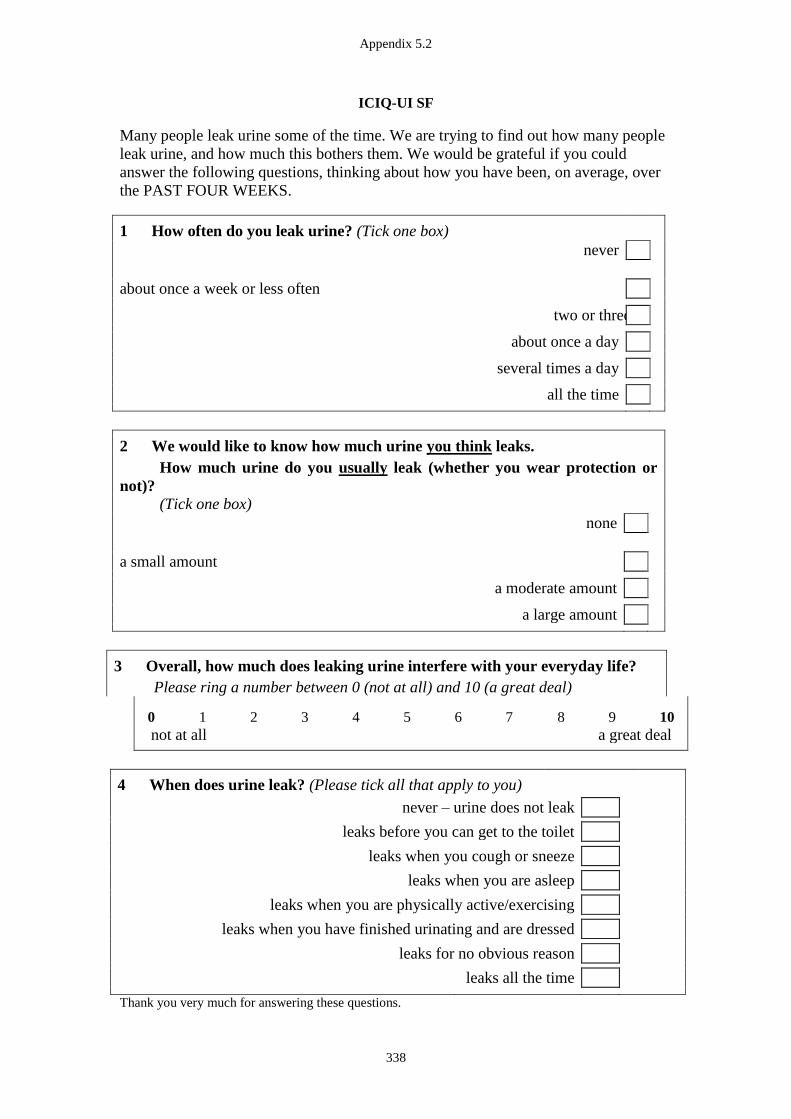
Appendix 5.2
338
ICIQ-UI SF
Many people leak urine some of the time. We are trying to find out how many people
leak urine, and how much this bothers them. We would be grateful if you could
answer the following questions, thinking about how you have been, on average, over
the PAST FOUR WEEKS.
1 How often do you leak urine? (Tick one box)
never
about once a week or less often
two or three times a week
about once a day
several times a day
all the time
2 We would like to know how much urine you think leaks.
How much urine do you usually leak (whether you wear protection or
not)?
(Tick one box)
none
a small amount
a moderate amount
a large amount
3 Overall, how much does leaking urine interfere with your everyday life?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
4 When does urine leak? (Please tick all that apply to you)
never – urine does not leak
leaks before you can get to the toilet leaks when you cough or sneeze leaks when you are asleep leaks when you are physically active/exercising leaks when you have finished urinating and are dressed leaks for no obvious reason
leaks all the time
Thank you very much for answering these questions.
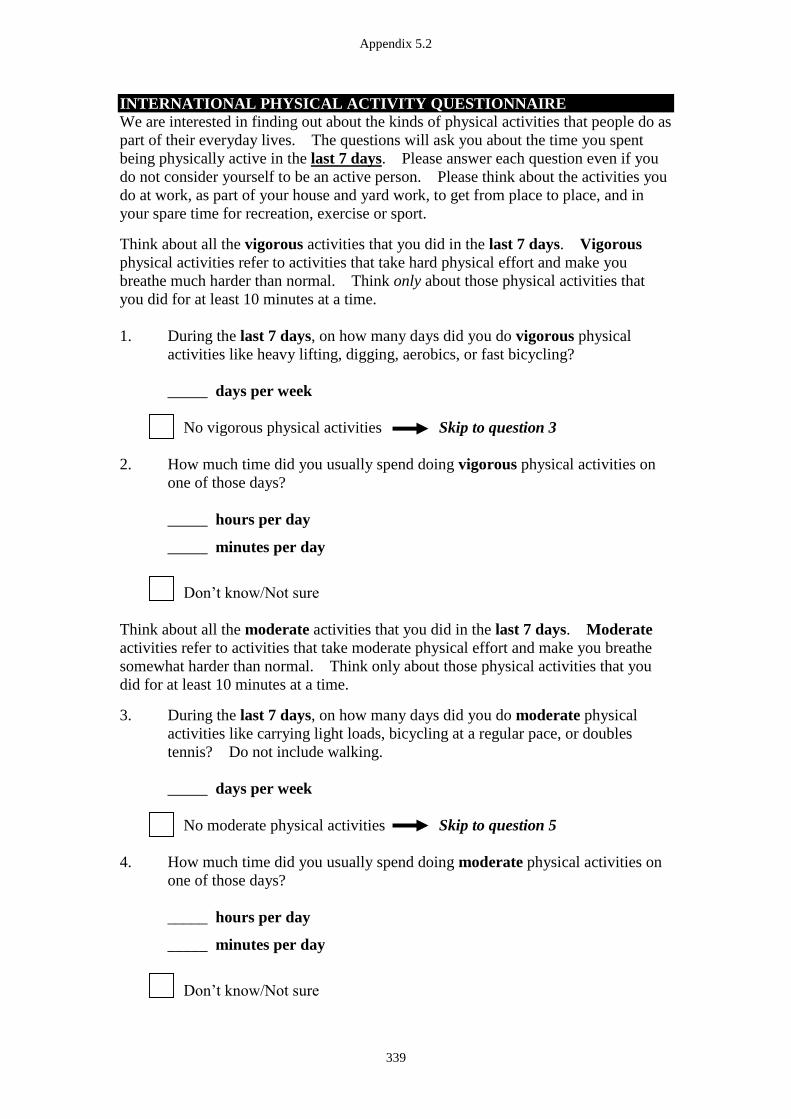
Appendix 5.2
339
INTERNATIONAL PHYSICAL ACTIVITY QUESTIONNAIRE
We are interested in finding out about the kinds of physical activities that people do as
part of their everyday lives. The questions will ask you about the time you spent
being physically active in the last 7 days. Please answer each question even if you
do not consider yourself to be an active person. Please think about the activities you
do at work, as part of your house and yard work, to get from place to place, and in
your spare time for recreation, exercise or sport.
Think about all the vigorous activities that you did in the last 7 days. Vigorous
physical activities refer to activities that take hard physical effort and make you
breathe much harder than normal. Think only about those physical activities that
you did for at least 10 minutes at a time.
1. During the last 7 days, on how many days did you do vigorous physical
activities like heavy lifting, digging, aerobics, or fast bicycling?
_____ days per week
No vigorous physical activities Skip to question 3
2. How much time did you usually spend doing vigorous physical activities on
one of those days?
_____ hours per day
_____ minutes per day
Don’t know/Not sure
Think about all the moderate activities that you did in the last 7 days. Moderate
activities refer to activities that take moderate physical effort and make you breathe
somewhat harder than normal. Think only about those physical activities that you
did for at least 10 minutes at a time.
3. During the last 7 days, on how many days did you do moderate physical
activities like carrying light loads, bicycling at a regular pace, or doubles
tennis? Do not include walking.
_____ days per week
No moderate physical activities Skip to question 5
4. How much time did you usually spend doing moderate physical activities on
one of those days?
_____ hours per day
_____ minutes per day
Don’t know/Not sure
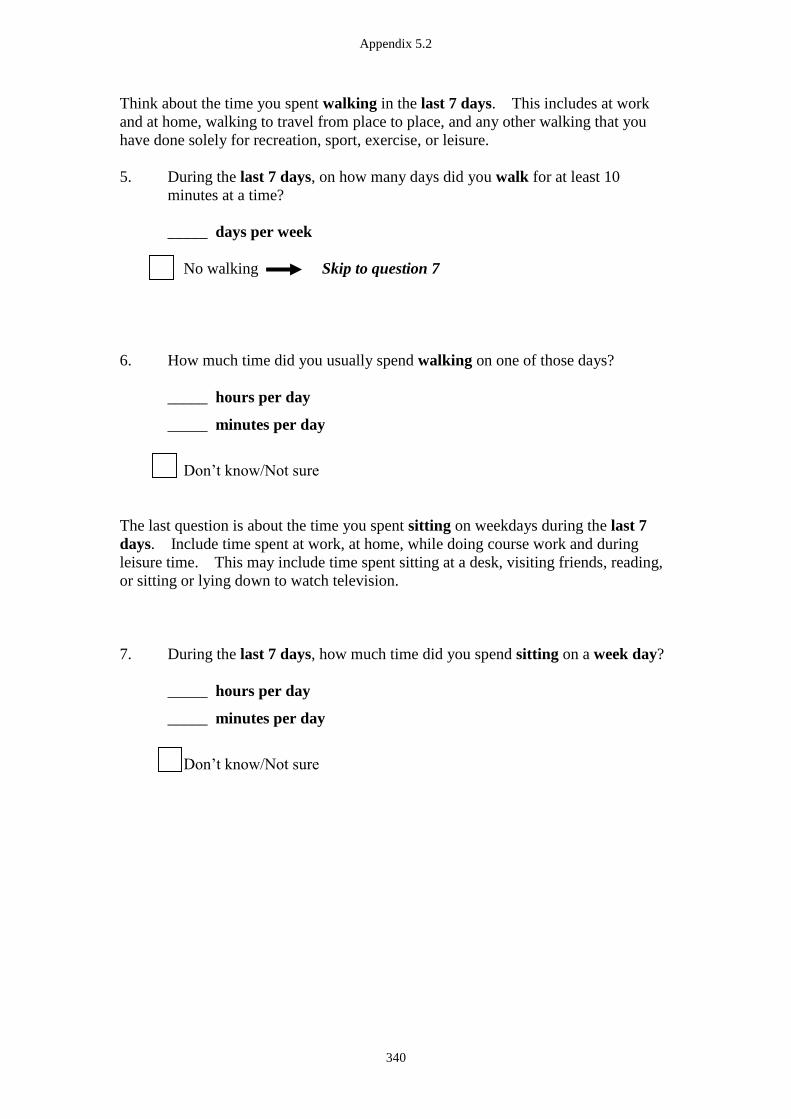
Appendix 5.2
340
Think about the time you spent walking in the last 7 days. This includes at work
and at home, walking to travel from place to place, and any other walking that you
have done solely for recreation, sport, exercise, or leisure.
5. During the last 7 days, on how many days did you walk for at least 10
minutes at a time?
_____ days per week
No walking Skip to question 7
6. How much time did you usually spend walking on one of those days?
_____ hours per day
_____ minutes per day
Don’t know/Not sure
The last question is about the time you spent sitting on weekdays during the last 7
days. Include time spent at work, at home, while doing course work and during
leisure time. This may include time spent sitting at a desk, visiting friends, reading,
or sitting or lying down to watch television.
7. During the last 7 days, how much time did you spend sitting on a week day?
_____ hours per day
_____ minutes per day
Don’t know/Not sure
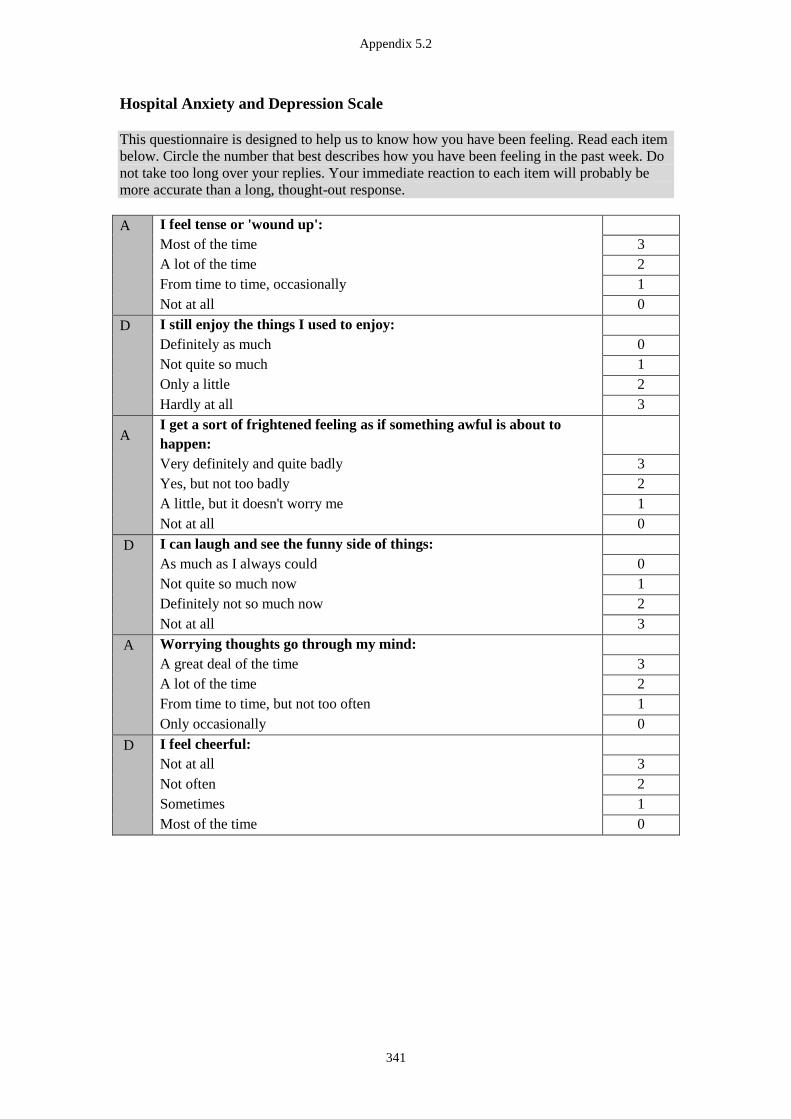
Appendix 5.2
341
Hospital Anxiety and Depression Scale
This questionnaire is designed to help us to know how you have been feeling. Read each item
below. Circle the number that best describes how you have been feeling in the past week. Do
not take too long over your replies. Your immediate reaction to each item will probably be
more accurate than a long, thought-out response.
A
I feel tense or 'wound up':
Most of the time 3
A lot of the time 2
From time to time, occasionally 1
Not at all 0
D
I still enjoy the things I used to enjoy:
Definitely as much 0
Not quite so much 1
Only a little 2
Hardly at all 3
A
I get a sort of frightened feeling as if something awful is about to
happen:
Very definitely and quite badly 3
Yes, but not too badly 2
A little, but it doesn't worry me 1
Not at all 0
D
I can laugh and see the funny side of things:
As much as I always could 0
Not quite so much now 1
Definitely not so much now 2
Not at all 3
A
Worrying thoughts go through my mind:
A great deal of the time 3
A lot of the time 2
From time to time, but not too often 1
Only occasionally 0
D
I feel cheerful:
Not at all 3
Not often 2
Sometimes 1
Most of the time 0
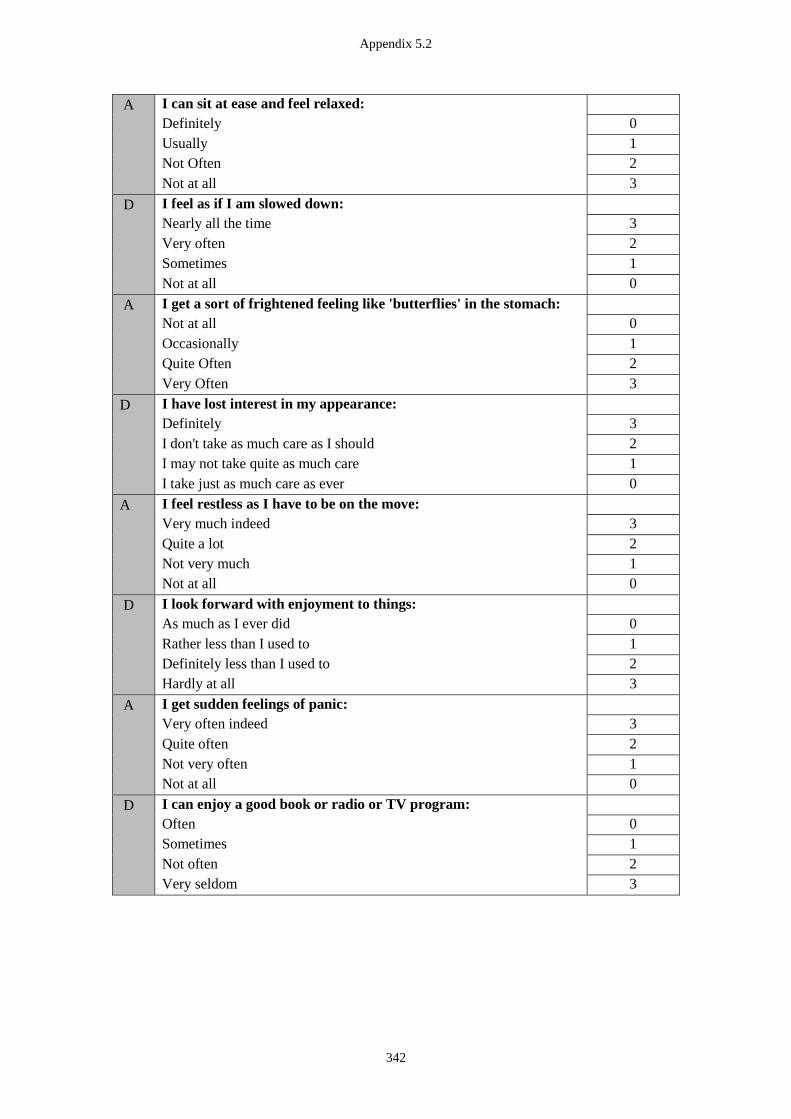
Appendix 5.2
342
A
I can sit at ease and feel relaxed:
Definitely 0
Usually 1
Not Often 2
Not at all 3
D
I feel as if I am slowed down:
Nearly all the time 3
Very often 2
Sometimes 1
Not at all 0
A
I get a sort of frightened feeling like 'butterflies' in the stomach:
Not at all 0
Occasionally 1
Quite Often 2
Very Often 3
D
I have lost interest in my appearance:
Definitely 3
I don't take as much care as I should 2
I may not take quite as much care 1
I take just as much care as ever 0
A
I feel restless as I have to be on the move:
Very much indeed 3
Quite a lot 2
Not very much 1
Not at all 0
D
I look forward with enjoyment to things:
As much as I ever did 0
Rather less than I used to 1
Definitely less than I used to 2
Hardly at all 3
A
I get sudden feelings of panic:
Very often indeed 3
Quite often 2
Not very often 1
Not at all 0
D
I can enjoy a good book or radio or TV program:
Often 0
Sometimes 1
Not often 2
Very seldom 3
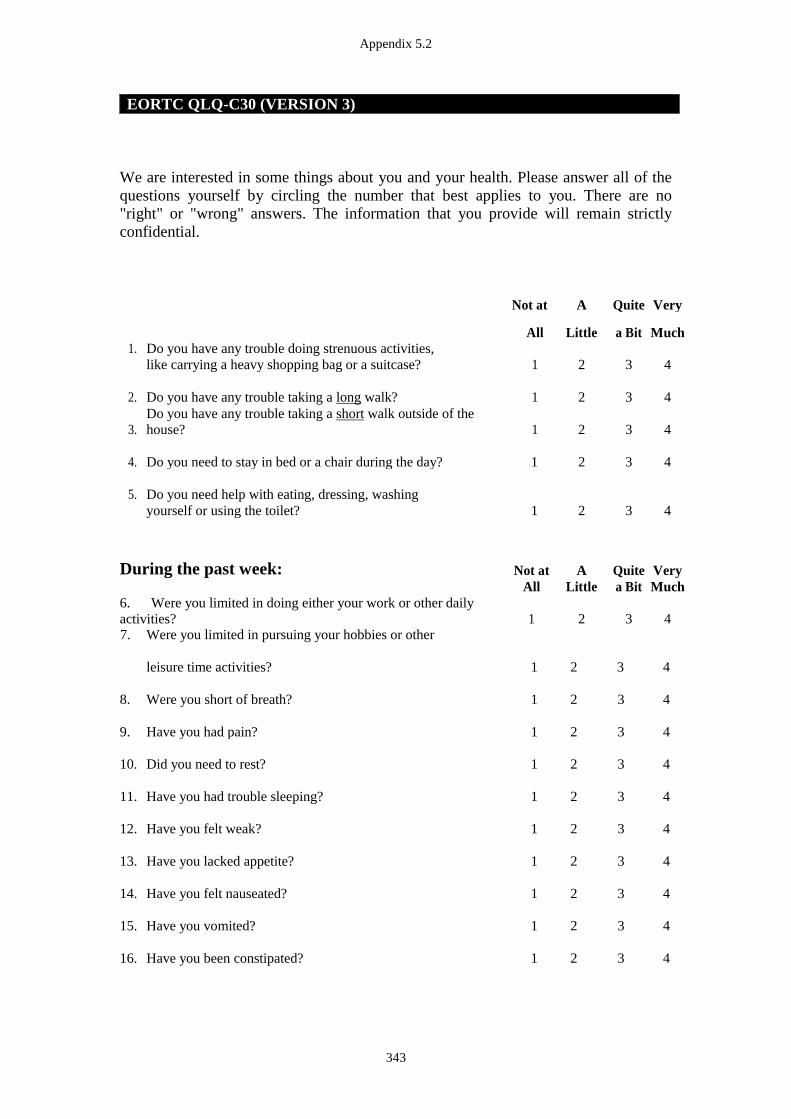
Appendix 5.2
343
EORTC QLQ-C30 (VERSION 3)
We are interested in some things about you and your health. Please answer all of the
questions yourself by circling the number that best applies to you. There are no "right" or "wrong" answers. The information that you provide will remain strictly
confidential.
Not at A Quite Very
All Little a Bit Much 1. Do you have any trouble doing strenuous activities,
like carrying a heavy shopping bag or a suitcase? 1 2 3 4
2. Do you have any trouble taking a long walk? 1 2 3 4
3. Do you have any trouble taking a short walk outside of the
house? 1 2 3 4
4. Do you need to stay in bed or a chair during the day? 1 2 3 4
5. Do you need help with eating, dressing, washing yourself or using the toilet? 1 2 3 4
During the past week: Not at A Quite Very All Little a Bit Much 6. Were you limited in doing either your work or other daily
activities? 1 2 3 4 7. Were you limited in pursuing your hobbies or other
leisure time activities?
1
2
3 4
8. Were you short of breath?
1
2
3 4
9. Have you had pain?
1
2
3 4
10. Did you need to rest?
1
2
3 4
11. Have you had trouble sleeping?
1
2
3 4
12. Have you felt weak?
1
2
3 4
13. Have you lacked appetite?
1
2
3 4
14. Have you felt nauseated?
1
2
3 4
15. Have you vomited?
1
2
3 4
16. Have you been constipated?
1
2
3 4

Appendix 5.2
344
During the past week: Not at A Quite Very All Little a Bit Much
17. Have you had diarrhoea? 1 2 3 4
18. Were you tired? 1 2 3 4
19. Did pain interfere with your daily activities? 1 2 3 4
20. Have you had difficulty in concentrating on things, like reading a newspaper or watching television? 1 2 3 4
21. Did you feel tense? 1 2 3 4
22. Did you worry? 1 2 3 4
23. Did you feel irritable? 1 2 3 4
24. Did you feel depressed? 1 2 3 4
25. Have you had difficulty remembering things? 1 2 3 4
26. Has your physical condition or medical treatment interfered with your family life? 1 2 3 4
27. Has your physical condition or medical treatment interfered with your social activities? 1 2 3 4
28. Has your physical condition or medical treatment caused you financial difficulties? 1 2 3 4
For the following questions please circle the
number between 1 and 7 that
best applies to you
29. How would you rate your overall health during the past week?
1 2 3 4 5 6 7
Very poor Excellent
30. How would you rate your overall quality of life during the past week?
1 2 3 4 5 6 7
Very poor Excellent © Copyright 1995 EORTC Quality of Life Group. All rights reserved. Version 3.0
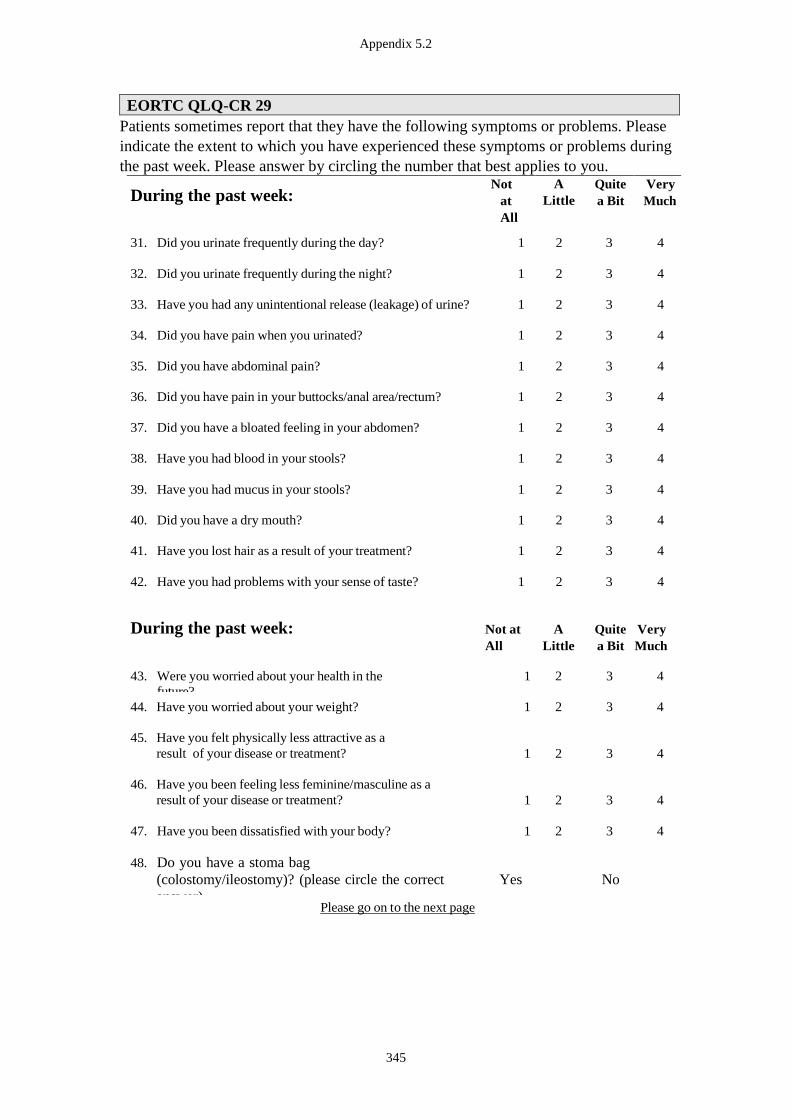
Appendix 5.2
345
EORTC QLQ-CR 29
Patients sometimes report that they have the following symptoms or problems. Please
indicate the extent to which you have experienced these symptoms or problems during
the past week. Please answer by circling the number that best applies to you.
During the past week: Not
at
All
A
Little Quite
a Bit Very
Much
31. Did you urinate frequently during the day? 1 2 3 4
32. Did you urinate frequently during the night? 1 2 3 4
33. Have you had any unintentional release (leakage) of urine? 1 2 3 4
34. Did you have pain when you urinated? 1 2 3 4
35. Did you have abdominal pain? 1 2 3 4
36. Did you have pain in your buttocks/anal area/rectum? 1 2 3 4
37. Did you have a bloated feeling in your abdomen? 1 2 3 4
38. Have you had blood in your stools? 1 2 3 4
39. Have you had mucus in your stools? 1 2 3 4
40. Did you have a dry mouth? 1 2 3 4
41. Have you lost hair as a result of your treatment? 1 2 3 4
42. Have you had problems with your sense of taste? 1 2 3 4
During the past week: Not at
All A
Little Quite
a Bit Very
Much
43. Were you worried about your health in the
future? 1 2 3 4
44. Have you worried about your weight? 1 2 3 4
45. Have you felt physically less attractive as a
result of your disease or treatment?
1
2
3
4
46. Have you been feeling less feminine/masculine as a
result of your disease or treatment?
1
2
3
4
47. Have you been dissatisfied with your body? 1 2 3 4
48. Do you have a stoma bag
(colostomy/ileostomy)? (please circle the correct
answer)
Yes
No
Please go on to the next page
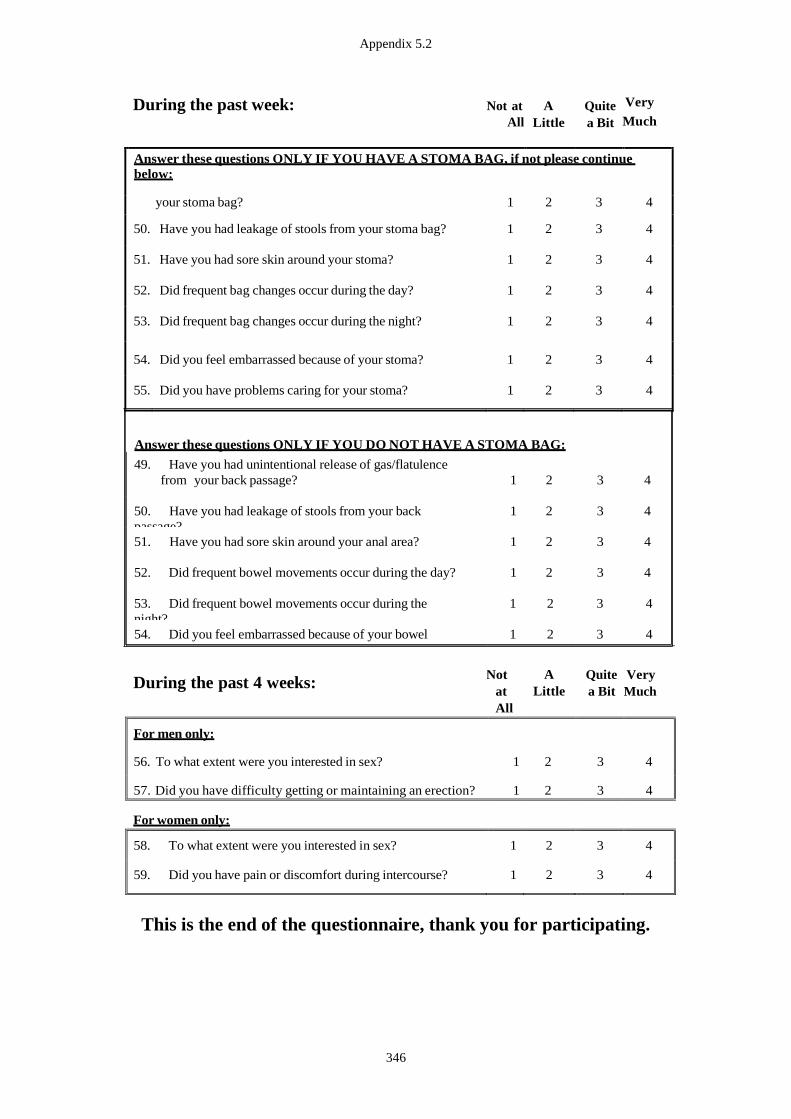
Appendix 5.2
346
During the past week: Not at
All A
Little Quite
a Bit
Very
Much
Answer these questions ONLY IF YOU HAVE A STOMA BAG, if not please continue
below:
49. Have you had unintentional release of gas/flatulence from your stoma bag? 1 2 3 4
50. Have you had leakage of stools from your stoma bag? 1 2 3 4
51. Have you had sore skin around your stoma? 1 2 3 4
52. Did frequent bag changes occur during the day? 1 2 3 4
53. Did frequent bag changes occur during the night? 1 2 3 4
54. Did you feel embarrassed because of your stoma? 1 2 3 4
55. Did you have problems caring for your stoma? 1 2 3 4
Answer these questions ONLY IF YOU DO NOT HAVE A STOMA BAG:
49. Have you had unintentional release of gas/flatulence
from your back passage?
1
2
3
4
50. Have you had leakage of stools from your back
passage? 1 2 3 4
51. Have you had sore skin around your anal area? 1 2 3 4
52. Did frequent bowel movements occur during the day? 1 2 3 4
53. Did frequent bowel movements occur during the
night? 1 2 3 4
54. Did you feel embarrassed because of your bowel
movement? 1 2 3 4
During the past 4 weeks:
Not
at
All
A
Little
Quite
a Bit
Very
Much
For men only:
56. To what extent were you interested in sex? 1 2 3 4
57. Did you have difficulty getting or maintaining an erection? 1 2 3 4
For women only:
58. To what extent were you interested in sex? 1 2 3 4
59. Did you have pain or discomfort during intercourse? 1 2 3 4
This is the end of the questionnaire, thank you for participating.
Appendix 6.1
347
Appendix 6.1 Ethics Approval Documentation (Study 4)
Appendix 6.1
348
Appendix 6.1
349
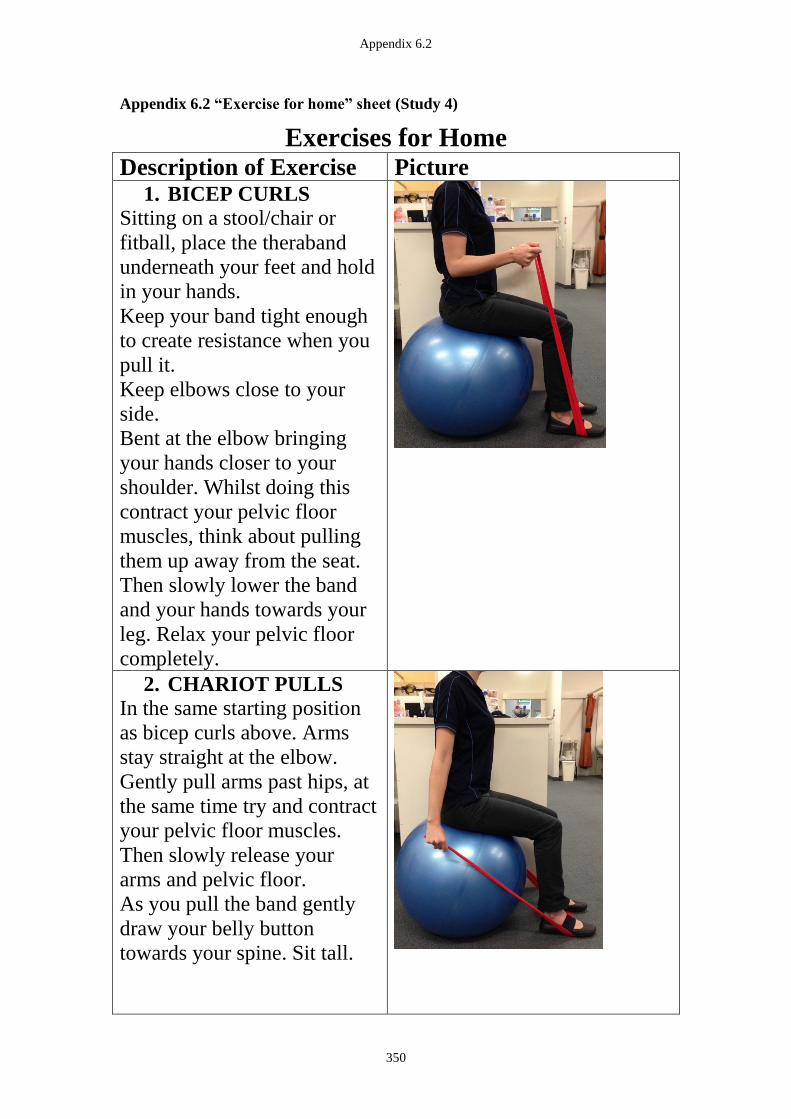
Appendix 6.2
350
Appendix 6.2 “Exercise for home” sheet (Study 4)
Exercises for Home Description of Exercise Picture
1. BICEP CURLS
Sitting on a stool/chair or
fitball, place the theraband
underneath your feet and hold
in your hands.
Keep your band tight enough
to create resistance when you
pull it.
Keep elbows close to your
side.
Bent at the elbow bringing
your hands closer to your
shoulder. Whilst doing this
contract your pelvic floor
muscles, think about pulling
them up away from the seat.
Then slowly lower the band
and your hands towards your
leg. Relax your pelvic floor
completely.
2. CHARIOT PULLS
In the same starting position
as bicep curls above. Arms
stay straight at the elbow.
Gently pull arms past hips, at
the same time try and contract
your pelvic floor muscles.
Then slowly release your
arms and pelvic floor.
As you pull the band gently
draw your belly button
towards your spine. Sit tall.

Appendix 6.2
351
3. SHOULDER
STABILITY
Sitting on the ball/stool or
standing if preferred.
Band is in hands at short
distance (approx 5cm).
Elbows bent to right angle
and tucked in at side.
Palms facing each other.
Pull the band by pulling hands
away from each other, keep
elbows still. Gently release.
Description of Exercise Picture 4. FORWARD RAISE
Sitting on fitball/stool. Place
band around back at bra level
and then hold each side in
each hand at the front.
Pull band out and forwards
from chest level.
Gently and slowly release.
Keep drawing in your lower
tummy muscles to engage
your core and also think about
engaging your pelvic floor.
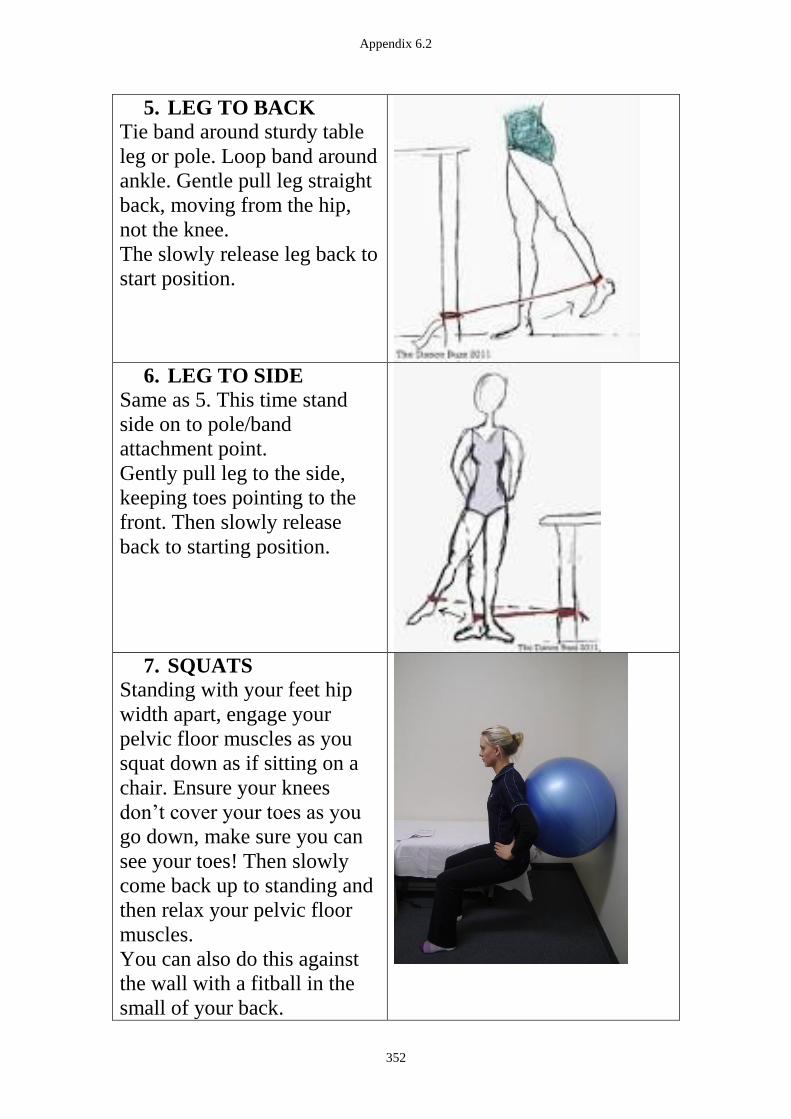
Appendix 6.2
352
5. LEG TO BACK
Tie band around sturdy table
leg or pole. Loop band around
ankle. Gentle pull leg straight
back, moving from the hip,
not the knee.
The slowly release leg back to
start position.
6. LEG TO SIDE
Same as 5. This time stand
side on to pole/band
attachment point.
Gently pull leg to the side,
keeping toes pointing to the
front. Then slowly release
back to starting position.
7. SQUATS
Standing with your feet hip
width apart, engage your
pelvic floor muscles as you
squat down as if sitting on a
chair. Ensure your knees
don’t cover your toes as you
go down, make sure you can
see your toes! Then slowly
come back up to standing and
then relax your pelvic floor
muscles.
You can also do this against
the wall with a fitball in the
small of your back.

Appendix 6.2
353
8. HEEL RAISES
Standing with your feet hip
width apart, lift your heels up
off the ground then slowly
lower. If you want to advance
this exercise try it on one leg.
Use a chair in-front or wall
for balance.
Think about staying tall and
not letting your heels fall
towards the floor, lower
gradually.
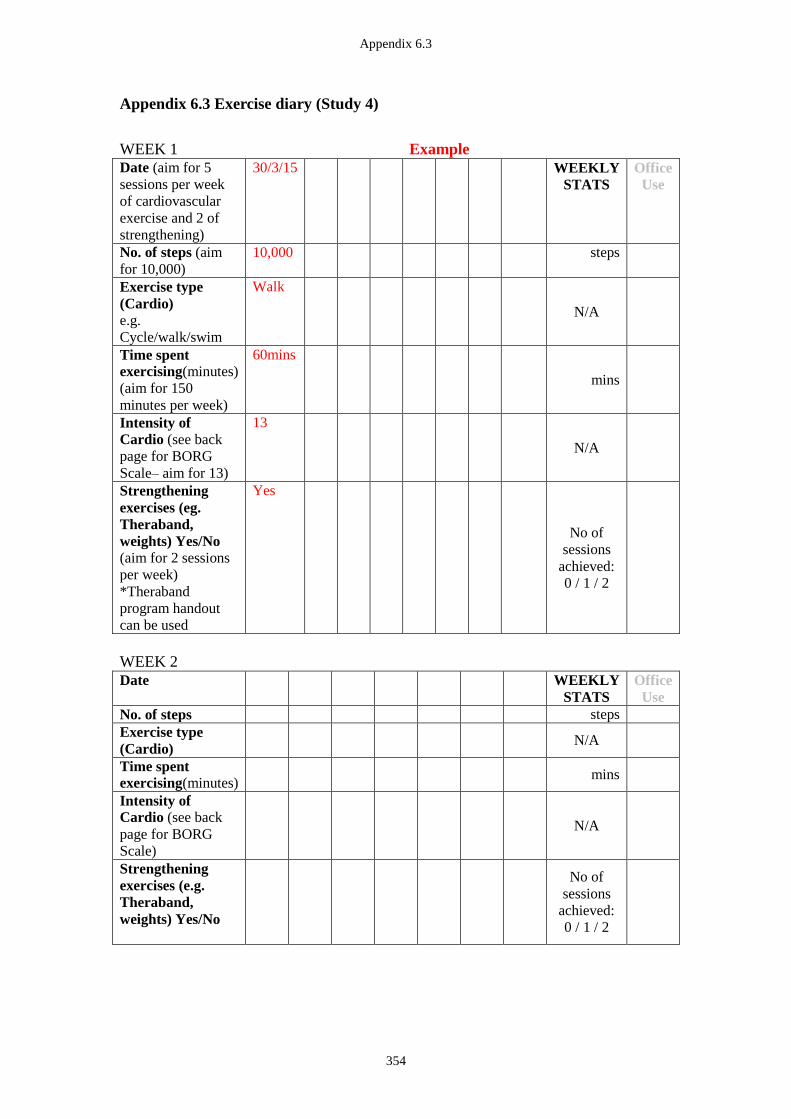
Appendix 6.3
354
Appendix 6.3 Exercise diary (Study 4)
WEEK 1 Example Date (aim for 5
sessions per week
of cardiovascular
exercise and 2 of
strengthening)
30/3/15 WEEKLY
STATS
Office
Use
No. of steps (aim
for 10,000)
10,000 steps
Exercise type
(Cardio)
e.g.
Cycle/walk/swim
Walk
N/A
Time spent
exercising(minutes)
(aim for 150
minutes per week)
60mins
mins
Intensity of
Cardio (see back
page for BORG
Scale– aim for 13)
13
N/A
Strengthening
exercises (eg.
Theraband,
weights) Yes/No
(aim for 2 sessions
per week)
*Theraband
program handout
can be used
Yes
No of
sessions
achieved:
0 / 1 / 2
WEEK 2
Date WEEKLY
STATS
Office
Use
No. of steps steps
Exercise type
(Cardio)
N/A
Time spent
exercising(minutes)
mins
Intensity of
Cardio (see back
page for BORG
Scale)
N/A
Strengthening
exercises (e.g.
Theraband,
weights) Yes/No
No of
sessions
achieved:
0 / 1 / 2
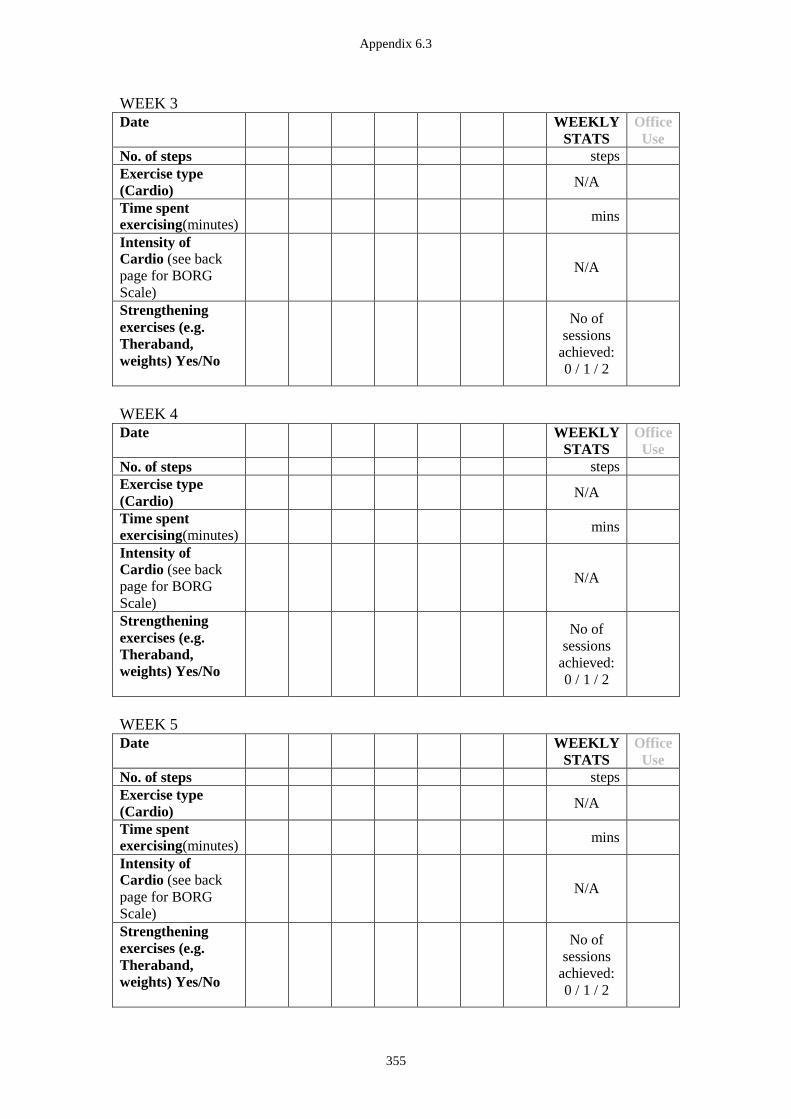
Appendix 6.3
355
WEEK 3
Date WEEKLY
STATS
Office
Use
No. of steps steps
Exercise type
(Cardio)
N/A
Time spent
exercising(minutes)
mins
Intensity of
Cardio (see back
page for BORG
Scale)
N/A
Strengthening
exercises (e.g.
Theraband,
weights) Yes/No
No of
sessions
achieved:
0 / 1 / 2
WEEK 4
Date WEEKLY
STATS
Office
Use
No. of steps steps
Exercise type
(Cardio)
N/A
Time spent
exercising(minutes)
mins
Intensity of
Cardio (see back
page for BORG
Scale)
N/A
Strengthening
exercises (e.g.
Theraband,
weights) Yes/No
No of
sessions
achieved:
0 / 1 / 2
WEEK 5
Date WEEKLY
STATS
Office
Use
No. of steps steps
Exercise type
(Cardio)
N/A
Time spent
exercising(minutes)
mins
Intensity of
Cardio (see back
page for BORG
Scale)
N/A
Strengthening
exercises (e.g.
Theraband,
weights) Yes/No
No of
sessions
achieved:
0 / 1 / 2
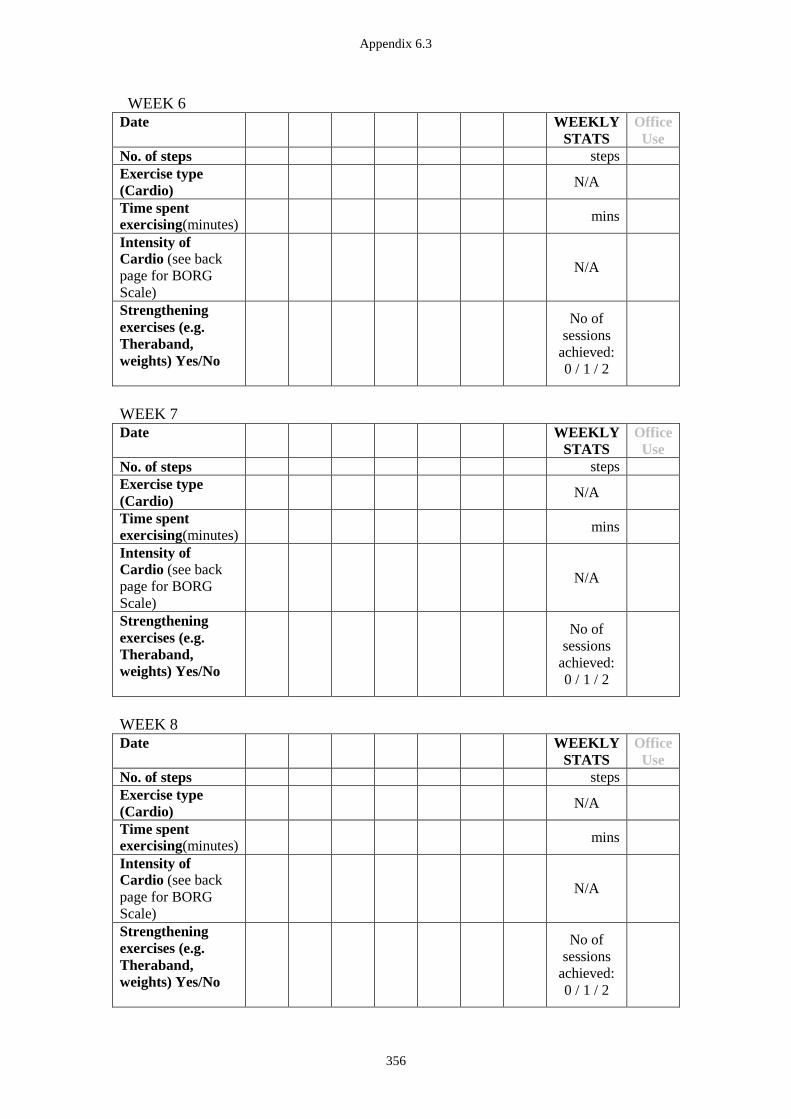
Appendix 6.3
356
WEEK 6
Date WEEKLY
STATS
Office
Use
No. of steps steps
Exercise type
(Cardio)
N/A
Time spent
exercising(minutes)
mins
Intensity of
Cardio (see back
page for BORG
Scale)
N/A
Strengthening
exercises (e.g.
Theraband,
weights) Yes/No
No of
sessions
achieved:
0 / 1 / 2
WEEK 7
Date WEEKLY
STATS
Office
Use
No. of steps steps
Exercise type
(Cardio)
N/A
Time spent
exercising(minutes)
mins
Intensity of
Cardio (see back
page for BORG
Scale)
N/A
Strengthening
exercises (e.g.
Theraband,
weights) Yes/No
No of
sessions
achieved:
0 / 1 / 2
WEEK 8
Date WEEKLY
STATS
Office
Use
No. of steps steps
Exercise type
(Cardio)
N/A
Time spent
exercising(minutes)
mins
Intensity of
Cardio (see back
page for BORG
Scale)
N/A
Strengthening
exercises (e.g.
Theraband,
weights) Yes/No
No of
sessions
achieved:
0 / 1 / 2
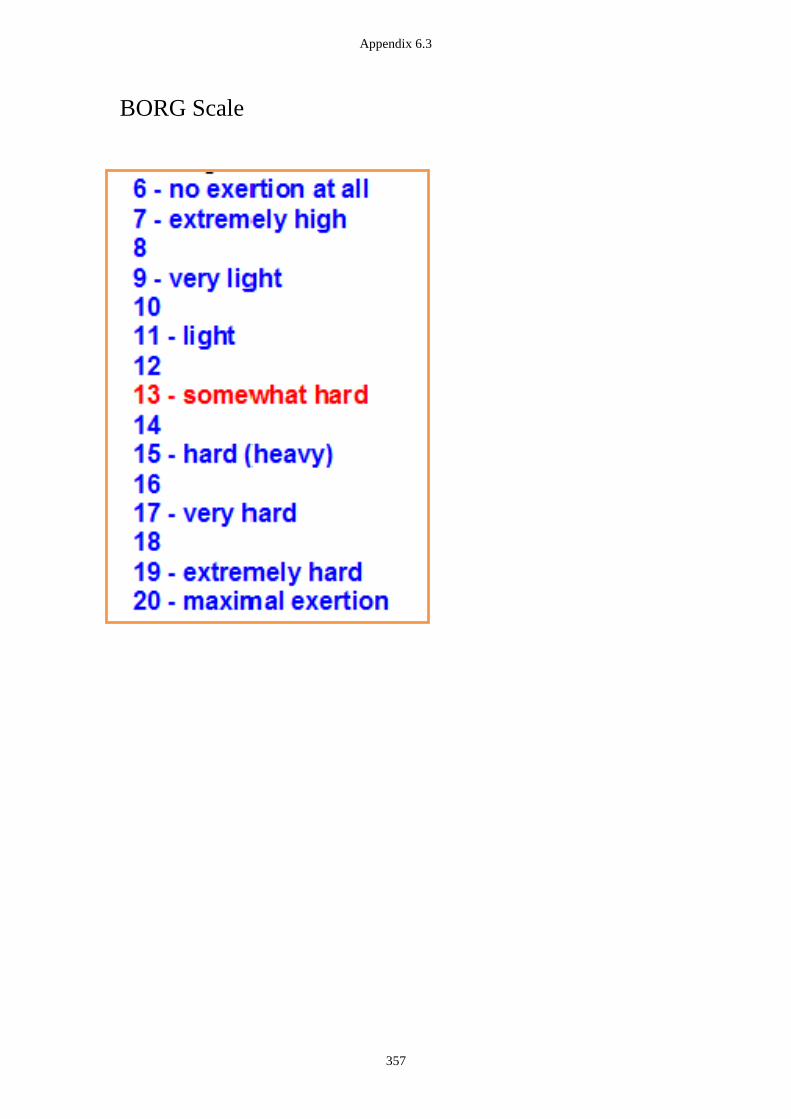
Appendix 6.3
357
BORG Scale
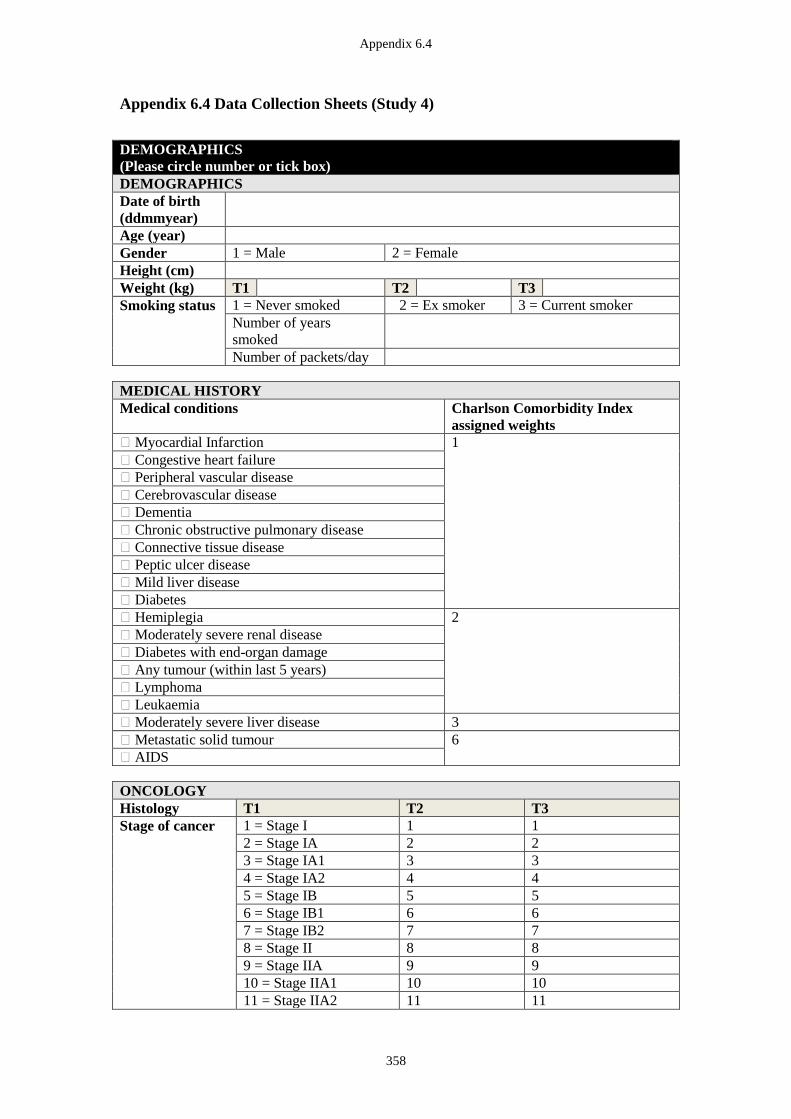
Appendix 6.4
358
Appendix 6.4 Data Collection Sheets (Study 4)
DEMOGRAPHICS
(Please circle number or tick box)
DEMOGRAPHICS
Date of birth
(ddmmyear)
Age (year)
Gender 1 = Male 2 = Female
Height (cm)
Weight (kg) T1 T2 T3
Smoking status 1 = Never smoked 2 = Ex smoker 3 = Current smoker
Number of years
smoked
Number of packets/day
MEDICAL HISTORY
Medical conditions Charlson Comorbidity Index
assigned weights
� Myocardial Infarction 1
� Congestive heart failure
� Peripheral vascular disease
� Cerebrovascular disease
� Dementia
� Chronic obstructive pulmonary disease
� Connective tissue disease
� Peptic ulcer disease
� Mild liver disease
� Diabetes
� Hemiplegia 2
� Moderately severe renal disease
� Diabetes with end-organ damage
� Any tumour (within last 5 years)
� Lymphoma
� Leukaemia
� Moderately severe liver disease 3
� Metastatic solid tumour 6
� AIDS
ONCOLOGY
Histology T1 T2 T3
Stage of cancer 1 = Stage I 1 1
2 = Stage IA 2 2
3 = Stage IA1 3 3
4 = Stage IA2 4 4
5 = Stage IB 5 5
6 = Stage IB1 6 6
7 = Stage IB2 7 7
8 = Stage II 8 8
9 = Stage IIA 9 9
10 = Stage IIA1 10 10
11 = Stage IIA2 11 11
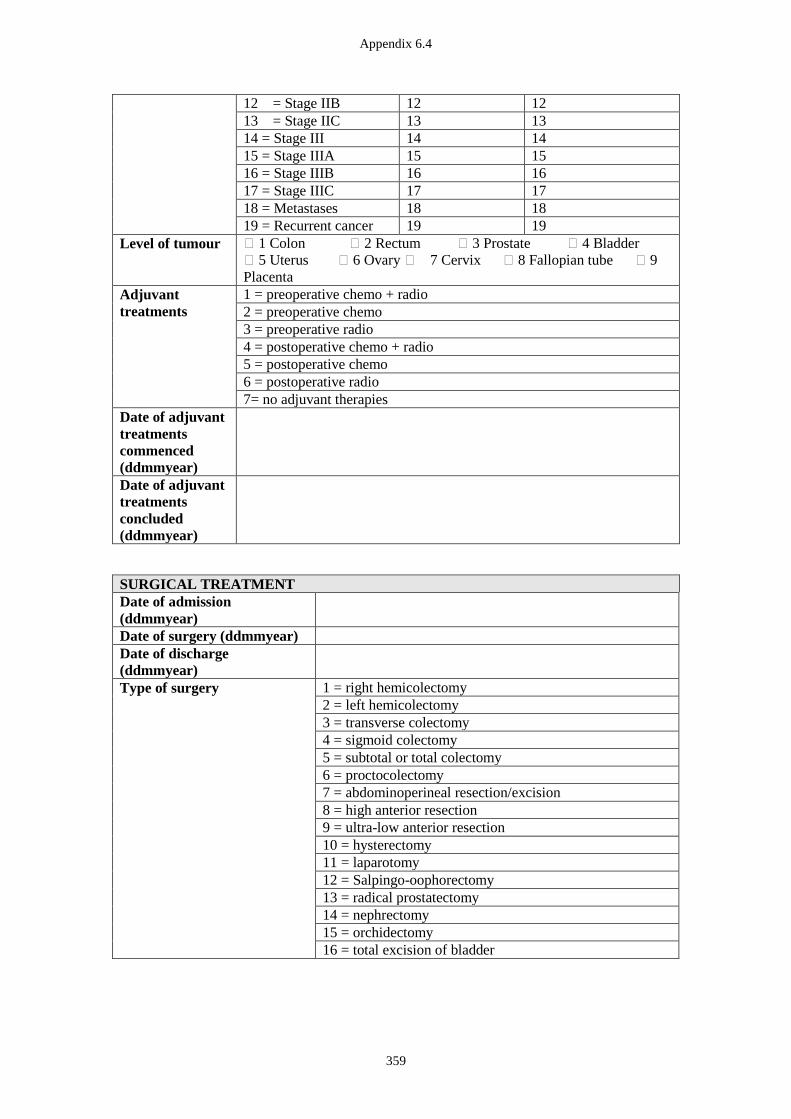
Appendix 6.4
359
12 = Stage IIB 12 12
13 = Stage IIC 13 13
14 = Stage III 14 14
15 = Stage IIIA 15 15
16 = Stage IIIB 16 16
17 = Stage IIIC 17 17
18 = Metastases 18 18
19 = Recurrent cancer 19 19
Level of tumour � 1 Colon � 2 Rectum � 3 Prostate � 4 Bladder
� 5 Uterus � 6 Ovary � 7 Cervix � 8 Fallopian tube � 9
Placenta
Adjuvant
treatments
1 = preoperative chemo + radio
2 = preoperative chemo
3 = preoperative radio
4 = postoperative chemo + radio
5 = postoperative chemo
6 = postoperative radio
7= no adjuvant therapies Date of adjuvant
treatments
commenced
(ddmmyear)
Date of adjuvant
treatments
concluded
(ddmmyear)
SURGICAL TREATMENT
Date of admission
(ddmmyear)
Date of surgery (ddmmyear)
Date of discharge
(ddmmyear)
Type of surgery 1 = right hemicolectomy
2 = left hemicolectomy
3 = transverse colectomy
4 = sigmoid colectomy
5 = subtotal or total colectomy
6 = proctocolectomy
7 = abdominoperineal resection/excision
8 = high anterior resection
9 = ultra-low anterior resection
10 = hysterectomy
11 = laparotomy
12 = Salpingo-oophorectomy
13 = radical prostatectomy
14 = nephrectomy
15 = orchidectomy
16 = total excision of bladder
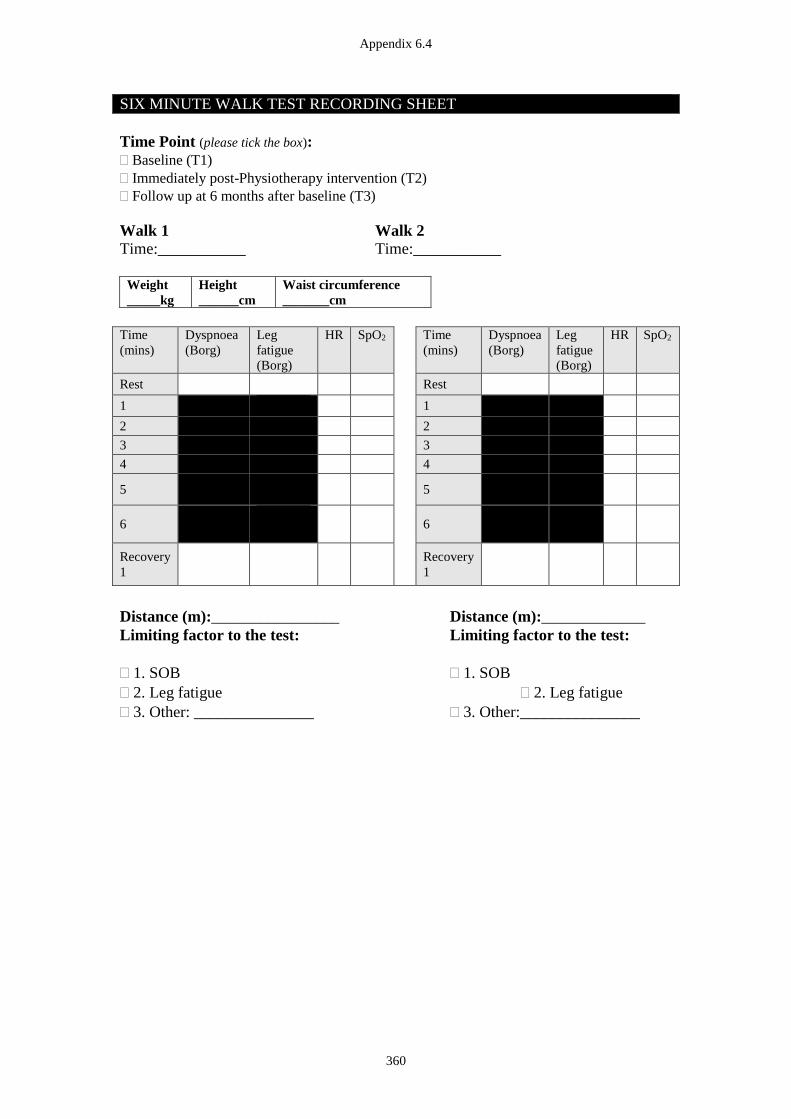
Appendix 6.4
360
SIX MINUTE WALK TEST RECORDING SHEET
Time Point (please tick the box):
Baseline (T1)
Immediately post-Physiotherapy intervention (T2)
Follow up at 6 months after baseline (T3)
Walk 1 Walk 2
Time:___________ Time:___________
Weight
_____kg
Height
______cm
Waist circumference
_______cm
Time
(mins)
Dyspnoea
(Borg)
Leg
fatigue
(Borg)
HR SpO2 Time
(mins)
Dyspnoea
(Borg)
Leg
fatigue
(Borg)
HR SpO2
Rest Rest
1 1
2 2
3 3
4 4
5
5
6
6
Recovery
1
Recovery
1
Distance (m):________________ Distance (m):_____________
Limiting factor to the test: Limiting factor to the test:
1. SOB 1. SOB
2. Leg fatigue 2. Leg fatigue
3. Other: _______________ 3. Other:_______________

Appendix 6.4
361
HAND-GRIP STRENGTH RECORDING SHEETS
Time Point (please tick the box):
Baseline (T1)
Immediately post-Physiotherapy intervention (T2)
Follow up at 6 months after baseline (T3)
Dominant Hand
Right Left
HAND-GRIP STRENGTH
RIGHT LEFT
1
(kg)
2
(kg)
3
(kg)
1
(kg)
2
(kg)
3
(kg)
Appendix 6.4
362
FOR OFFICE USE ONLY ID number:
Date:
Oncology Rehabilitation Research Project
for patients following surgery for pelvic cancer
PARTICIPANT QUESTIONNAIRE
BOOKLET (colorectal cancer)
We would be very grateful if you could complete and bring this questionnaire
booklet with you to your appointment.
Thank you for taking the time to help us with our research.
Appendix 6.4
363
Please start here
Date questionnaire filled in (dd/mm/yyyy): _ _ / _ _ / 2 0 1 _
Your date of birth (dd/mm/yyyy): _ _ / _ _ / 1 9 _ _
Sex: [ ] Male [ ] Female
BACKGROUND INFORMATION
The information you provide will remain strictly confidential.
1. Which of the following best describes your social situation? (Please tick whichever
applies)
1. Home alone, independent �
2. Home with family �
3. Home with supports �
4. Retirement village �
5. Nursing home – low level care �
6. Nursing home – high level care �
7. Other (please specify)_______________ �
2. Which of the following best describes your current employment status? (Please tick
whichever applies)
1. Working full time �
2. Working part time or as a casual �
3. Sick leave/ leave of absence – temporary �
4. Sick leave/ leave of absence – permanent �
5. Not employed/ taking time off work �
6. Retired �
7. Home duties �
8. Studying �
9. Other (please specify)_______________ �
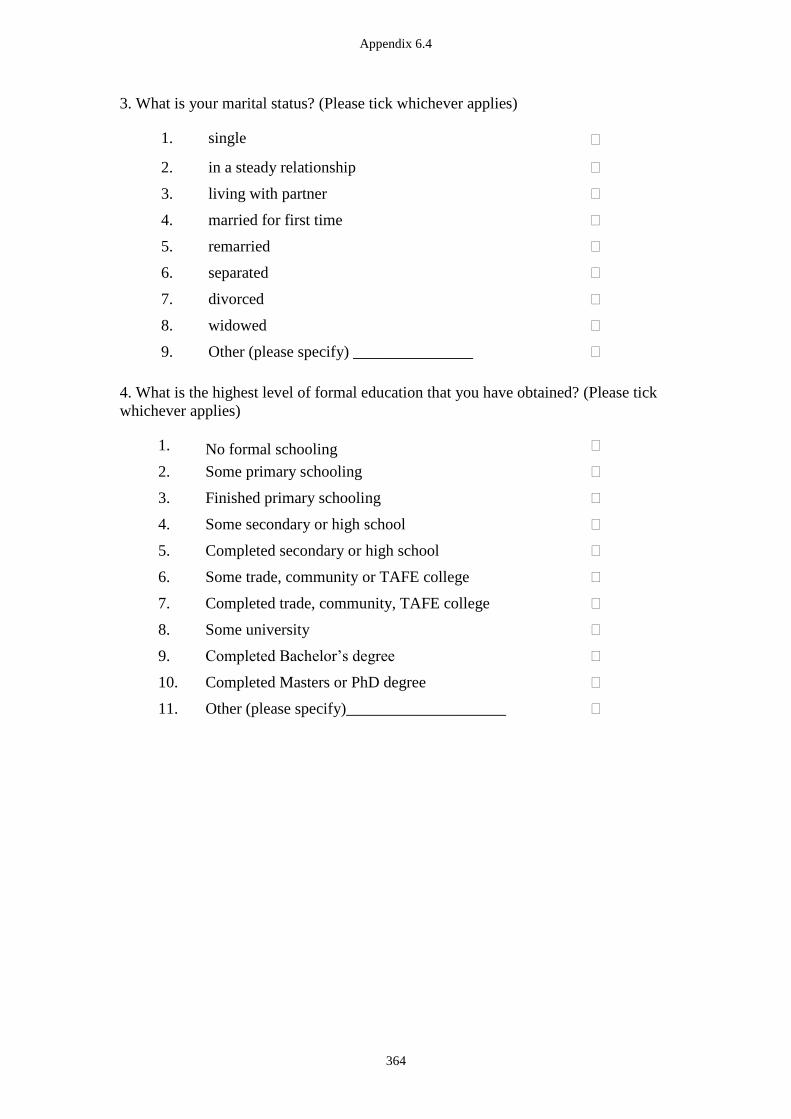
Appendix 6.4
364
3. What is your marital status? (Please tick whichever applies)
1. single �
2. in a steady relationship �
3. living with partner �
4. married for first time �
5. remarried �
6. separated �
7. divorced �
8. widowed �
9. Other (please specify) _______________ �
4. What is the highest level of formal education that you have obtained? (Please tick
whichever applies)
1. No formal schooling �
2. Some primary schooling �
3. Finished primary schooling �
4. Some secondary or high school �
5. Completed secondary or high school �
6. Some trade, community or TAFE college �
7. Completed trade, community, TAFE college �
8. Some university �
9. Completed Bachelor’s degree �
10. Completed Masters or PhD degree �
11. Other (please specify)____________________ �
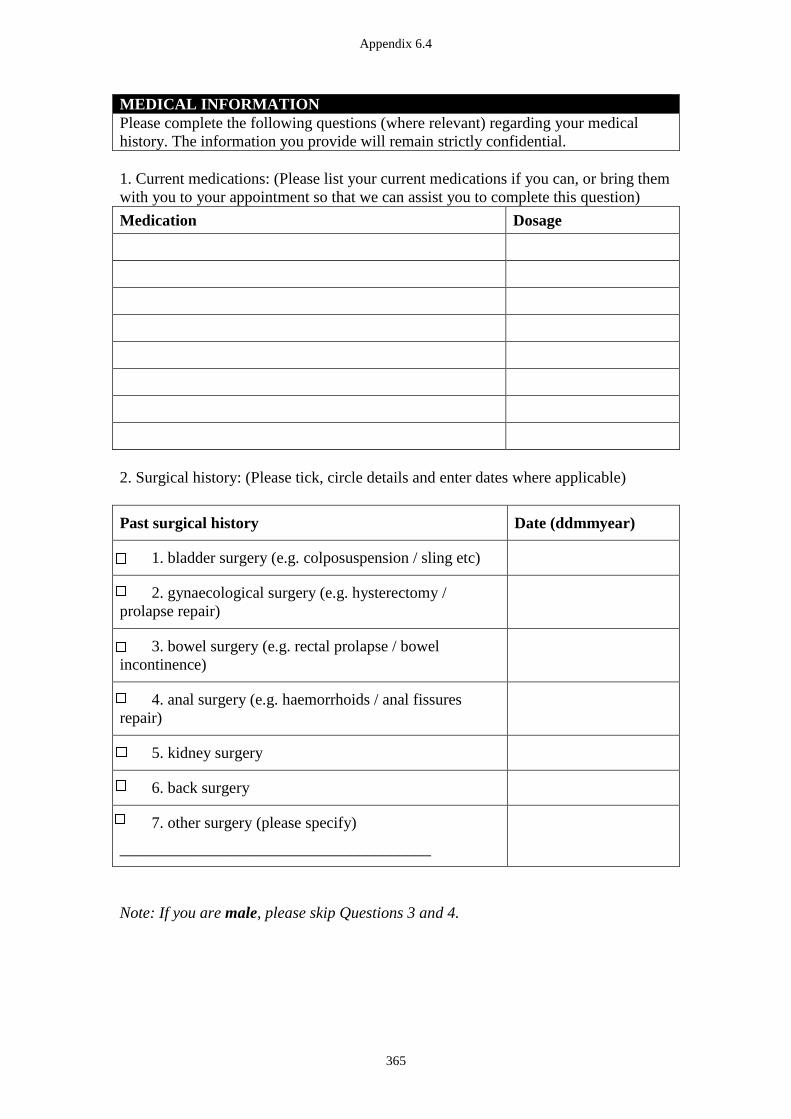
Appendix 6.4
365
MEDICAL INFORMATION
Please complete the following questions (where relevant) regarding your medical
history. The information you provide will remain strictly confidential.
1. Current medications: (Please list your current medications if you can, or bring them
with you to your appointment so that we can assist you to complete this question)
Medication Dosage
2. Surgical history: (Please tick, circle details and enter dates where applicable)
Past surgical history Date (ddmmyear)
1. bladder surgery (e.g. colposuspension / sling etc)
2. gynaecological surgery (e.g. hysterectomy /
prolapse repair)
3. bowel surgery (e.g. rectal prolapse / bowel
incontinence)
4. anal surgery (e.g. haemorrhoids / anal fissures
repair)
5. kidney surgery
6. back surgery
7. other surgery (please specify)
_______________________________________
Note: If you are male, please skip Questions 3 and 4.
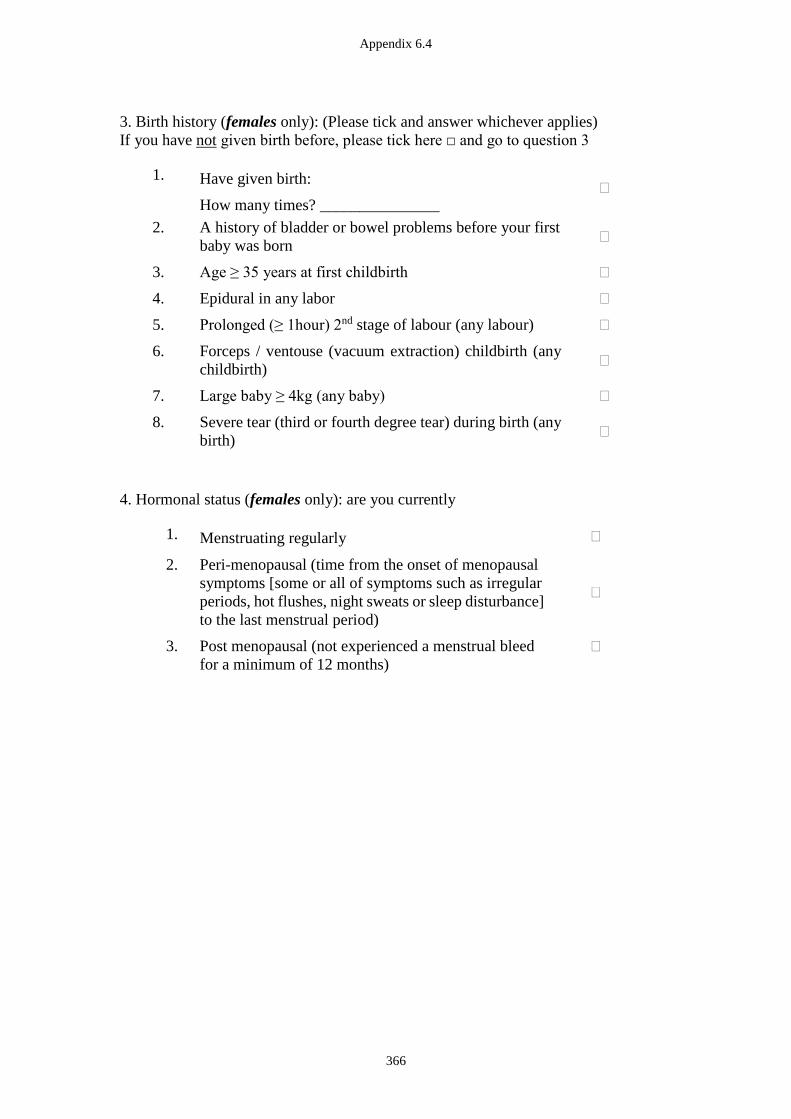
Appendix 6.4
366
3. Birth history (females only): (Please tick and answer whichever applies)
If you have not given birth before, please tick here □ and go to question 3
1. Have given birth:
How many times? _______________ �
2. A history of bladder or bowel problems before your first
baby was born �
3. Age ≥ 35 years at first childbirth �
4. Epidural in any labor �
5. Prolonged (≥ 1hour) 2nd stage of labour (any labour) �
6. Forceps / ventouse (vacuum extraction) childbirth (any
childbirth) �
7. Large baby ≥ 4kg (any baby) �
8. Severe tear (third or fourth degree tear) during birth (any
birth) �
4. Hormonal status (females only): are you currently
1. Menstruating regularly �
2. Peri-menopausal (time from the onset of menopausal
symptoms [some or all of symptoms such as irregular
periods, hot flushes, night sweats or sleep disturbance]
to the last menstrual period)
�
3. Post menopausal (not experienced a menstrual bleed
for a minimum of 12 months)
�
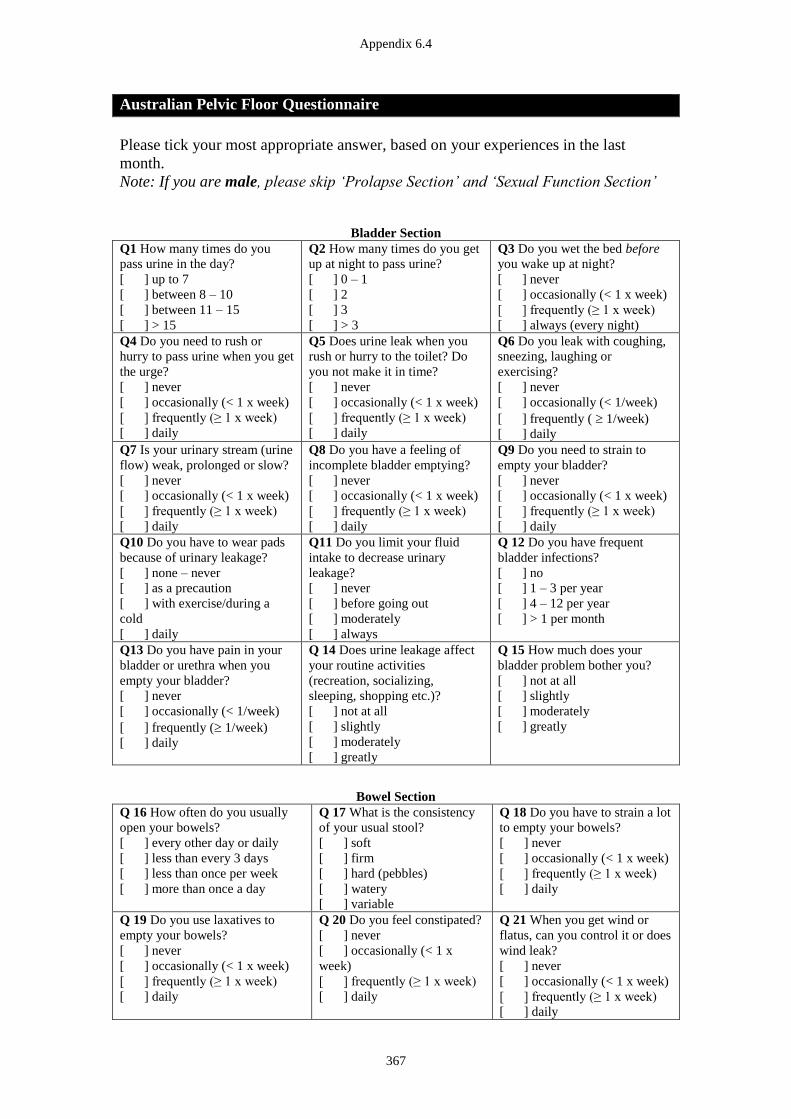
Appendix 6.4
367
Australian Pelvic Floor Questionnaire
Please tick your most appropriate answer, based on your experiences in the last
month.
Note: If you are male, please skip ‘Prolapse Section’ and ‘Sexual Function Section’
Bladder Section
Q1 How many times do you
pass urine in the day?
[ ] up to 7
[ ] between 8 – 10
[ ] between 11 – 15
[ ] > 15
Q2 How many times do you get
up at night to pass urine?
[ ] 0 – 1
[ ] 2
[ ] 3
[ ] > 3
Q3 Do you wet the bed before
you wake up at night?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] always (every night)
Q4 Do you need to rush or
hurry to pass urine when you get
the urge?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q5 Does urine leak when you
rush or hurry to the toilet? Do
you not make it in time?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q6 Do you leak with coughing,
sneezing, laughing or
exercising?
[ ] never
[ ] occasionally (< 1/week)
[ ] frequently ( 1/week)
[ ] daily
Q7 Is your urinary stream (urine
flow) weak, prolonged or slow?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q8 Do you have a feeling of
incomplete bladder emptying?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q9 Do you need to strain to
empty your bladder?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q10 Do you have to wear pads
because of urinary leakage?
[ ] none – never
[ ] as a precaution
[ ] with exercise/during a
cold
[ ] daily
Q11 Do you limit your fluid
intake to decrease urinary
leakage?
[ ] never
[ ] before going out
[ ] moderately
[ ] always
Q 12 Do you have frequent
bladder infections?
[ ] no
[ ] 1 – 3 per year
[ ] 4 – 12 per year
[ ] > 1 per month
Q13 Do you have pain in your
bladder or urethra when you
empty your bladder?
[ ] never
[ ] occasionally (< 1/week)
[ ] frequently ( 1/week)
[ ] daily
Q 14 Does urine leakage affect
your routine activities
(recreation, socializing,
sleeping, shopping etc.)?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Q 15 How much does your
bladder problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Bowel Section
Q 16 How often do you usually
open your bowels?
[ ] every other day or daily
[ ] less than every 3 days
[ ] less than once per week
[ ] more than once a day
Q 17 What is the consistency
of your usual stool?
[ ] soft
[ ] firm
[ ] hard (pebbles)
[ ] watery
[ ] variable
Q 18 Do you have to strain a lot
to empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 19 Do you use laxatives to
empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 20 Do you feel constipated?
[ ] never
[ ] occasionally (< 1 x
week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 21 When you get wind or
flatus, can you control it or does
wind leak?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
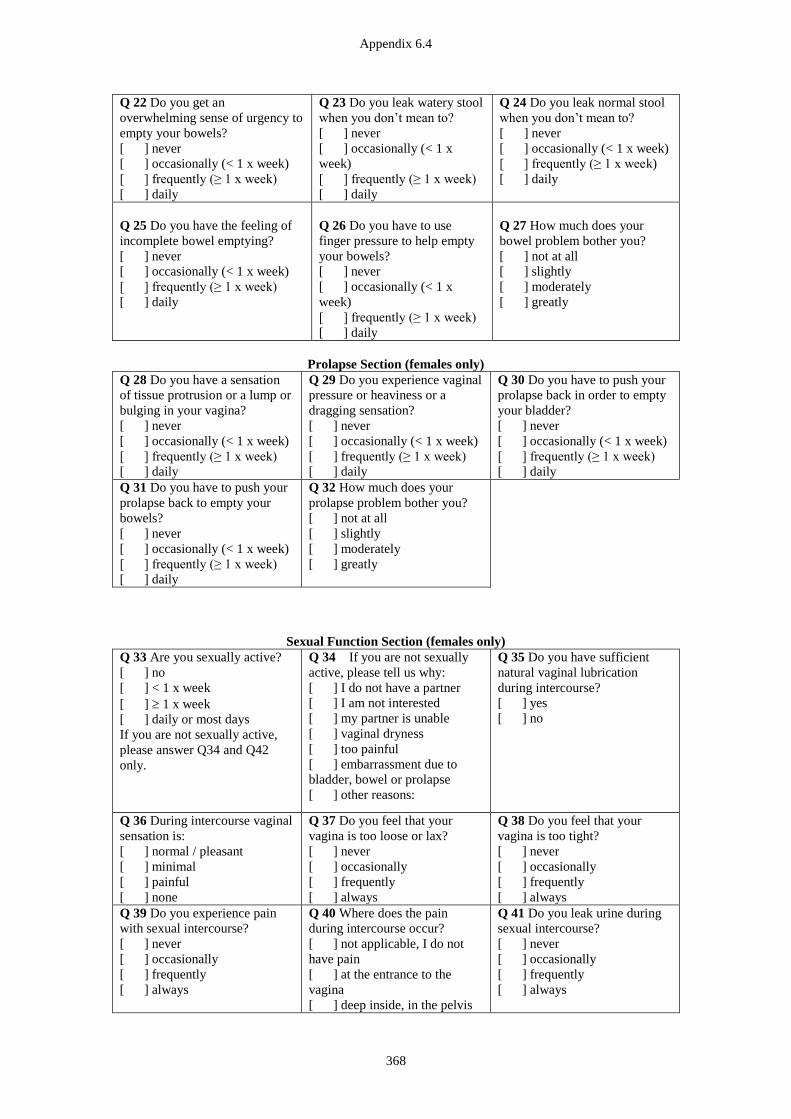
Appendix 6.4
368
Q 22 Do you get an
overwhelming sense of urgency to
empty your bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 23 Do you leak watery stool
when you don’t mean to?
[ ] never
[ ] occasionally (< 1 x
week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 24 Do you leak normal stool
when you don’t mean to?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 25 Do you have the feeling of
incomplete bowel emptying?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 26 Do you have to use
finger pressure to help empty
your bowels?
[ ] never
[ ] occasionally (< 1 x
week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 27 How much does your
bowel problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Prolapse Section (females only)
Q 28 Do you have a sensation
of tissue protrusion or a lump or
bulging in your vagina?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 29 Do you experience vaginal
pressure or heaviness or a
dragging sensation?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 30 Do you have to push your
prolapse back in order to empty
your bladder?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 31 Do you have to push your
prolapse back to empty your
bowels?
[ ] never
[ ] occasionally (< 1 x week)
[ ] frequently (≥ 1 x week)
[ ] daily
Q 32 How much does your
prolapse problem bother you?
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
Sexual Function Section (females only)
Q 33 Are you sexually active?
[ ] no
[ ] < 1 x week
[ ] 1 x week
[ ] daily or most days
If you are not sexually active,
please answer Q34 and Q42
only.
Q 34 If you are not sexually
active, please tell us why:
[ ] I do not have a partner
[ ] I am not interested
[ ] my partner is unable
[ ] vaginal dryness
[ ] too painful
[ ] embarrassment due to
bladder, bowel or prolapse
[ ] other reasons:
Q 35 Do you have sufficient
natural vaginal lubrication
during intercourse?
[ ] yes
[ ] no
Q 36 During intercourse vaginal
sensation is:
[ ] normal / pleasant
[ ] minimal
[ ] painful
[ ] none
Q 37 Do you feel that your
vagina is too loose or lax?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 38 Do you feel that your
vagina is too tight?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 39 Do you experience pain
with sexual intercourse?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
Q 40 Where does the pain
during intercourse occur?
[ ] not applicable, I do not
have pain
[ ] at the entrance to the
vagina
[ ] deep inside, in the pelvis
Q 41 Do you leak urine during
sexual intercourse?
[ ] never
[ ] occasionally
[ ] frequently
[ ] always
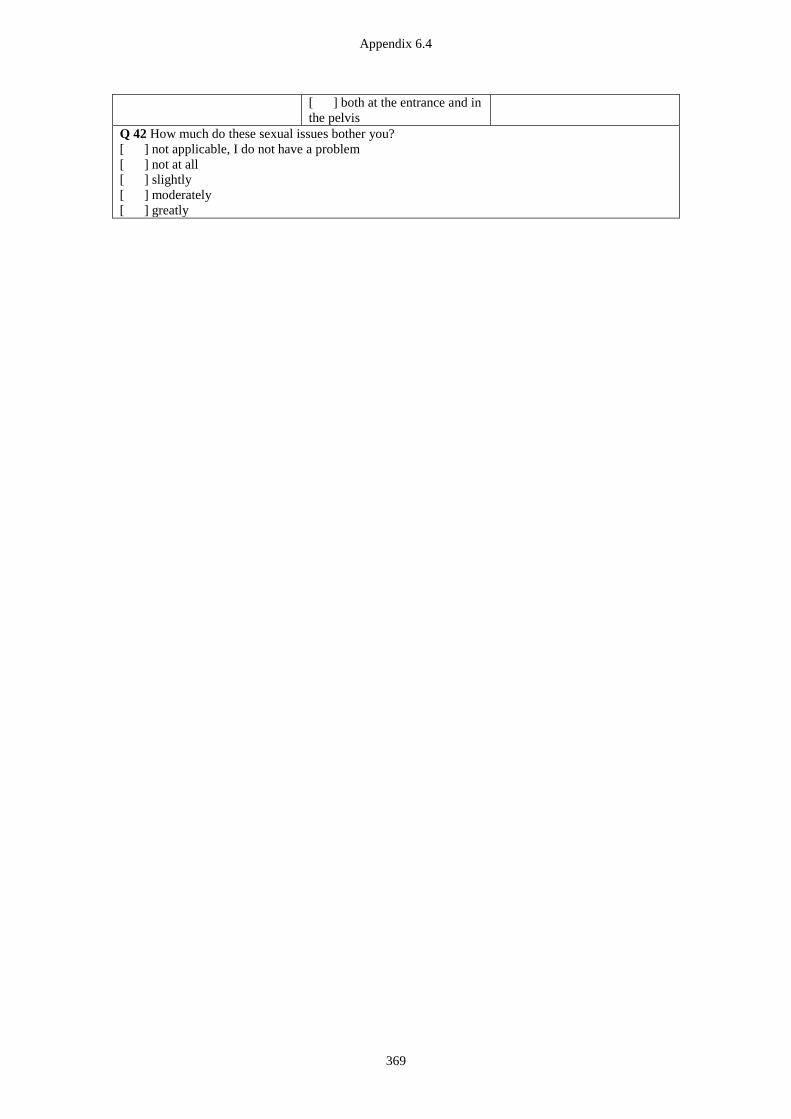
Appendix 6.4
369
[ ] both at the entrance and in
the pelvis
Q 42 How much do these sexual issues bother you?
[ ] not applicable, I do not have a problem
[ ] not at all
[ ] slightly
[ ] moderately
[ ] greatly
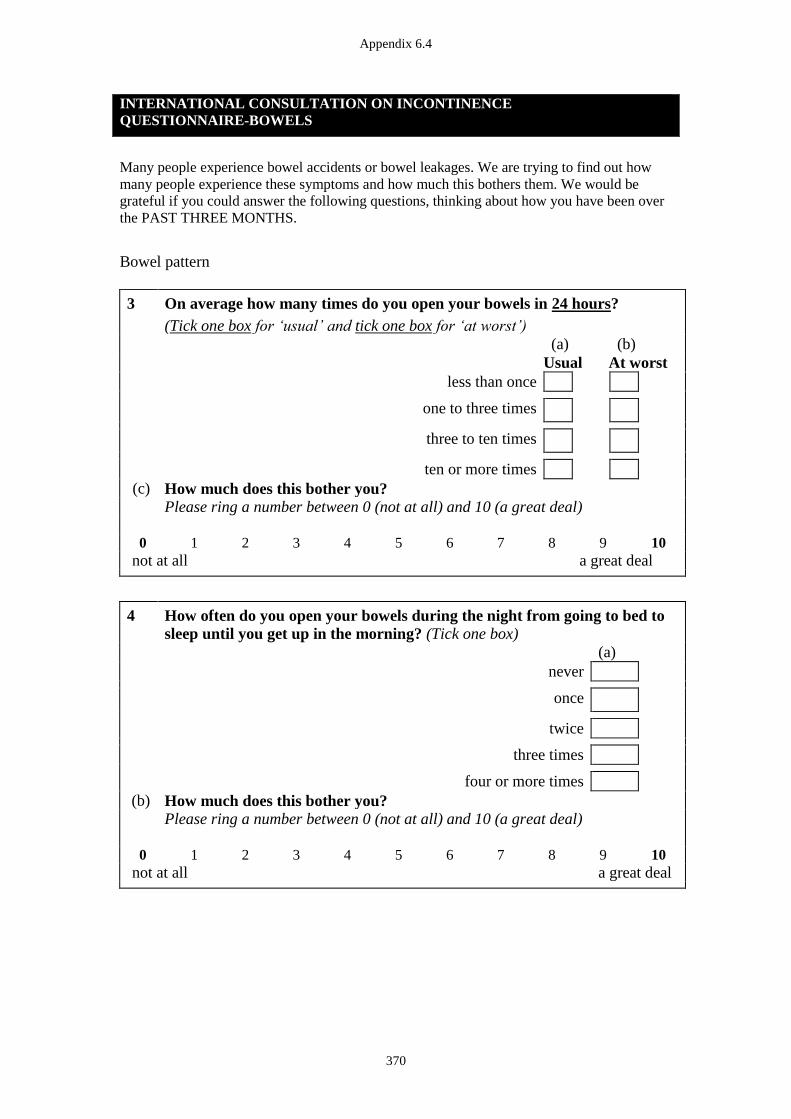
Appendix 6.4
370
INTERNATIONAL CONSULTATION ON INCONTINENCE
QUESTIONNAIRE-BOWELS
Many people experience bowel accidents or bowel leakages. We are trying to find out how
many people experience these symptoms and how much this bothers them. We would be
grateful if you could answer the following questions, thinking about how you have been over
the PAST THREE MONTHS.
Bowel pattern
3 On average how many times do you open your bowels in 24 hours?
(Tick one box for ‘usual’ and tick one box for ‘at worst’)
(a) (b)
Usual At worst
less than once
one to three times
three to ten times
ten or more times
(c) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
4 How often do you open your bowels during the night from going to bed to
sleep until you get up in the morning? (Tick one box)
(a)
never
once
twice
three times
four or more times
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
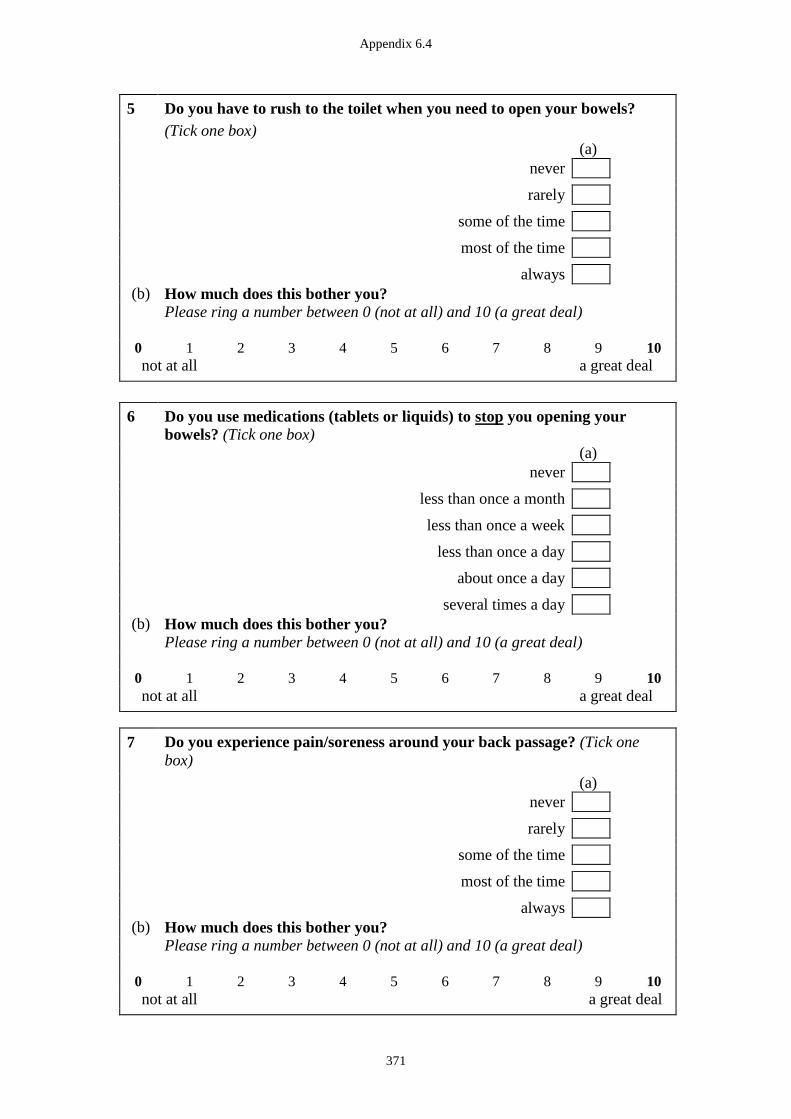
Appendix 6.4
371
5 Do you have to rush to the toilet when you need to open your bowels?
(Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
6 Do you use medications (tablets or liquids) to stop you opening your
bowels? (Tick one box)
(a)
never
less than once a month
less than once a week
less than once a day
about once a day
several times a day
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
7
Do you experience pain/soreness around your back passage? (Tick one
box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal

Appendix 6.4
372
Bowel control
8 Do you experience any staining of your underwear or need to wear pads
because of your bowels? (Tick one box)
(a)
never
less than once a month
less than once a week
less than once a day
everyday
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
9 Are you able to control watery or loose stool leaking from your back
passage? (Tick one box)
(a)
always
most of the time
some of the time
rarely
never
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
10 Are you able to control accidental loss of formed or solid stool from your
back passage? (Tick one box)
(a)
always
most of the time
some of the time
rarely
never
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
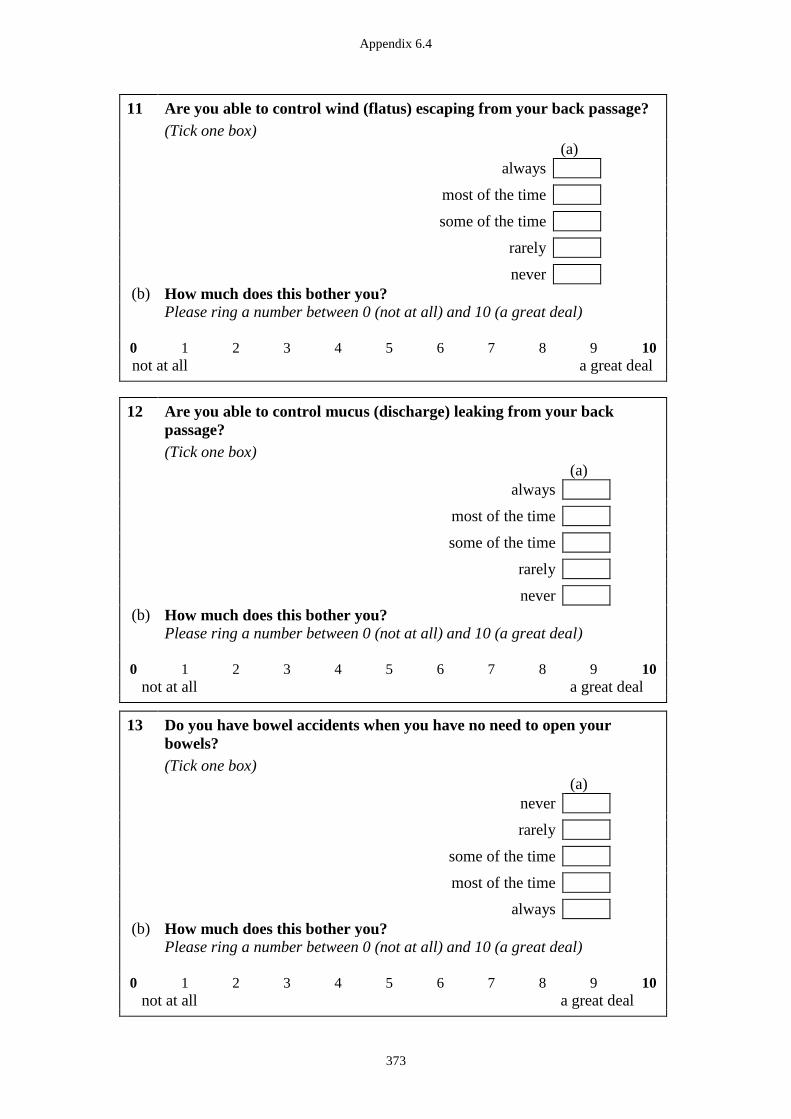
Appendix 6.4
373
11 Are you able to control wind (flatus) escaping from your back passage?
(Tick one box)
(a)
always
most of the time
some of the time
rarely
never
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
12 Are you able to control mucus (discharge) leaking from your back
passage?
(Tick one box)
(a)
always
most of the time
some of the time
rarely
never
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
13 Do you have bowel accidents when you have no need to open your
bowels?
(Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal

Appendix 6.4
374
14 Are your bowel accidents or leakages unpredictable? (Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Other bowel symptoms
15 Using the pictures please indicate how your bowel movements are most of
the time? (Tick all boxes that apply)
(a)
separate hard lumps like nuts (hard to pass)
sausage-shaped but lumpy
like a sausage but with cracks on its surface
like a sausage or snake – smooth and soft
soft blobs with clear cut edges (easy to pass)
fluffy pieces with ragged edges, a mushy stool
watery, no solid pieces
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal

Appendix 6.4
375
16 Do you need to strain to open your bowels? (Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
17 Is the possibility of having a bowel accident on your mind? (Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
Sexual impact
18 Do you restrict your sexual activities because of your bowels? (Tick one
box)
(a)
never
rarely
some of the time
most of the time
always
not applicable
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal

Appendix 6.4
376
Quality of life
19 Do your bowels cause you to feel embarrassed? (Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
20 Do your bowels cause you to make sure you know where toilets are?
(Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
21 Do your bowels cause you to make plans according to your bowels?
(Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
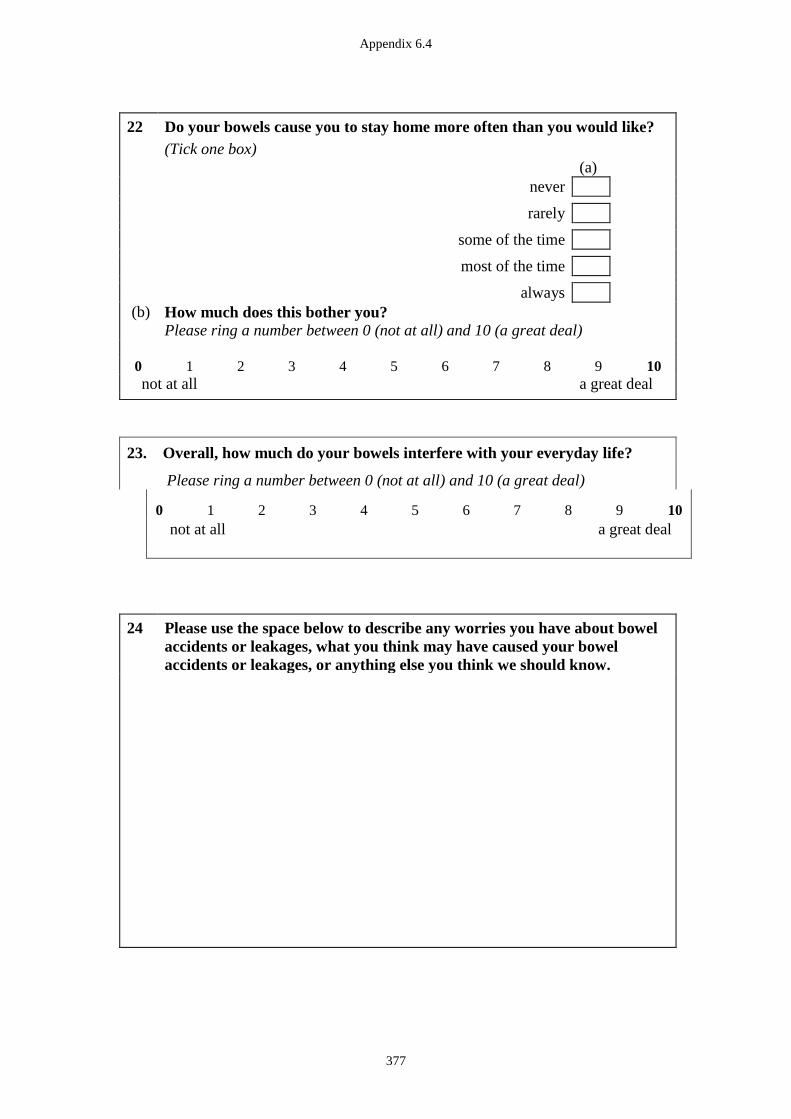
Appendix 6.4
377
22 Do your bowels cause you to stay home more often than you would like?
(Tick one box)
(a)
never
rarely
some of the time
most of the time
always
(b) How much does this bother you?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
23. Overall, how much do your bowels interfere with your everyday life?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
24
Please use the space below to describe any worries you have about bowel
accidents or leakages, what you think may have caused your bowel
accidents or leakages, or anything else you think we should know.
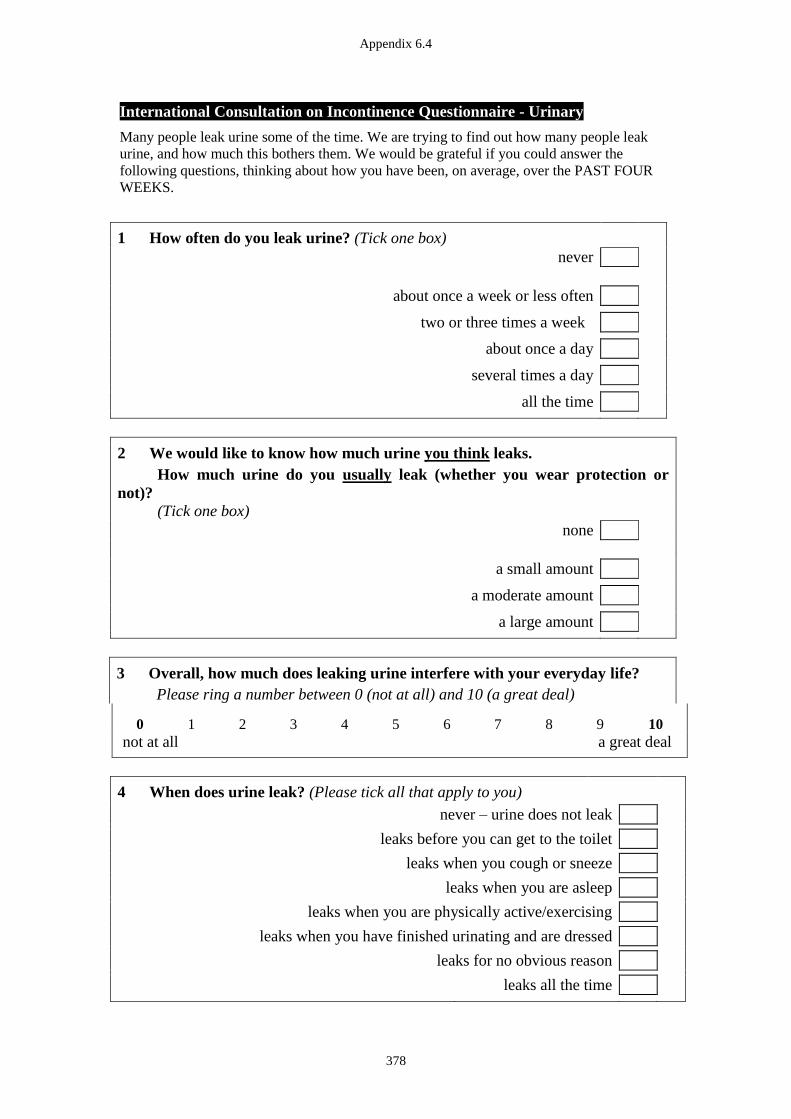
Appendix 6.4
378
International Consultation on Incontinence Questionnaire - Urinary
Many people leak urine some of the time. We are trying to find out how many people leak
urine, and how much this bothers them. We would be grateful if you could answer the
following questions, thinking about how you have been, on average, over the PAST FOUR
WEEKS.
1 How often do you leak urine? (Tick one box)
never
about once a week or less often
two or three times a week
about once a day
several times a day
all the time
2 We would like to know how much urine you think leaks.
How much urine do you usually leak (whether you wear protection or
not)?
(Tick one box)
none
a small amount
a moderate amount
a large amount
3 Overall, how much does leaking urine interfere with your everyday life?
Please ring a number between 0 (not at all) and 10 (a great deal)
0 1 2 3 4 5 6 7 8 9 10
not at all a great deal
4 When does urine leak? (Please tick all that apply to you)
never – urine does not leak
leaks before you can get to the toilet leaks when you cough or sneeze leaks when you are asleep leaks when you are physically active/exercising leaks when you have finished urinating and are dressed leaks for no obvious reason
leaks all the time
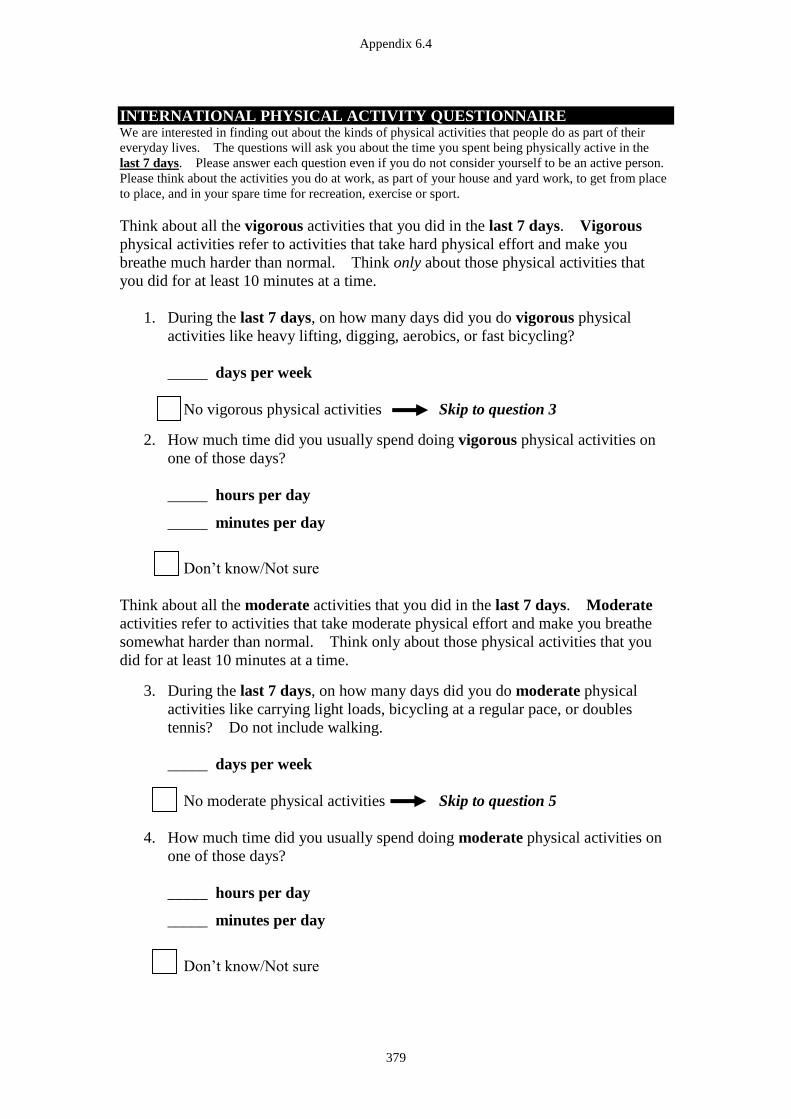
Appendix 6.4
379
INTERNATIONAL PHYSICAL ACTIVITY QUESTIONNAIRE We are interested in finding out about the kinds of physical activities that people do as part of their
everyday lives. The questions will ask you about the time you spent being physically active in the
last 7 days. Please answer each question even if you do not consider yourself to be an active person.
Please think about the activities you do at work, as part of your house and yard work, to get from place
to place, and in your spare time for recreation, exercise or sport.
Think about all the vigorous activities that you did in the last 7 days. Vigorous
physical activities refer to activities that take hard physical effort and make you
breathe much harder than normal. Think only about those physical activities that
you did for at least 10 minutes at a time.
1. During the last 7 days, on how many days did you do vigorous physical
activities like heavy lifting, digging, aerobics, or fast bicycling?
_____ days per week
No vigorous physical activities Skip to question 3
2. How much time did you usually spend doing vigorous physical activities on
one of those days?
_____ hours per day
_____ minutes per day
Don’t know/Not sure
Think about all the moderate activities that you did in the last 7 days. Moderate
activities refer to activities that take moderate physical effort and make you breathe
somewhat harder than normal. Think only about those physical activities that you
did for at least 10 minutes at a time.
3. During the last 7 days, on how many days did you do moderate physical
activities like carrying light loads, bicycling at a regular pace, or doubles
tennis? Do not include walking.
_____ days per week
No moderate physical activities Skip to question 5
4. How much time did you usually spend doing moderate physical activities on
one of those days?
_____ hours per day
_____ minutes per day
Don’t know/Not sure

Appendix 6.4
380
Think about the time you spent walking in the last 7 days. This includes at work
and at home, walking to travel from place to place, and any other walking that you
have done solely for recreation, sport, exercise, or leisure.
5. During the last 7 days, on how many days did you walk for at least 10
minutes at a time?
_____ days per week
No walking Skip to question 7
8. How much time did you usually spend walking on one of those days?
_____ hours per day
_____ minutes per day
Don’t know/Not sure
The last question is about the time you spent sitting on weekdays during the last 7
days. Include time spent at work, at home, while doing course work and during
leisure time. This may include time spent sitting at a desk, visiting friends, reading,
or sitting or lying down to watch television.
9. During the last 7 days, how much time did you spend sitting on a week day?
_____ hours per day
_____ minutes per day
Don’t know/Not sure
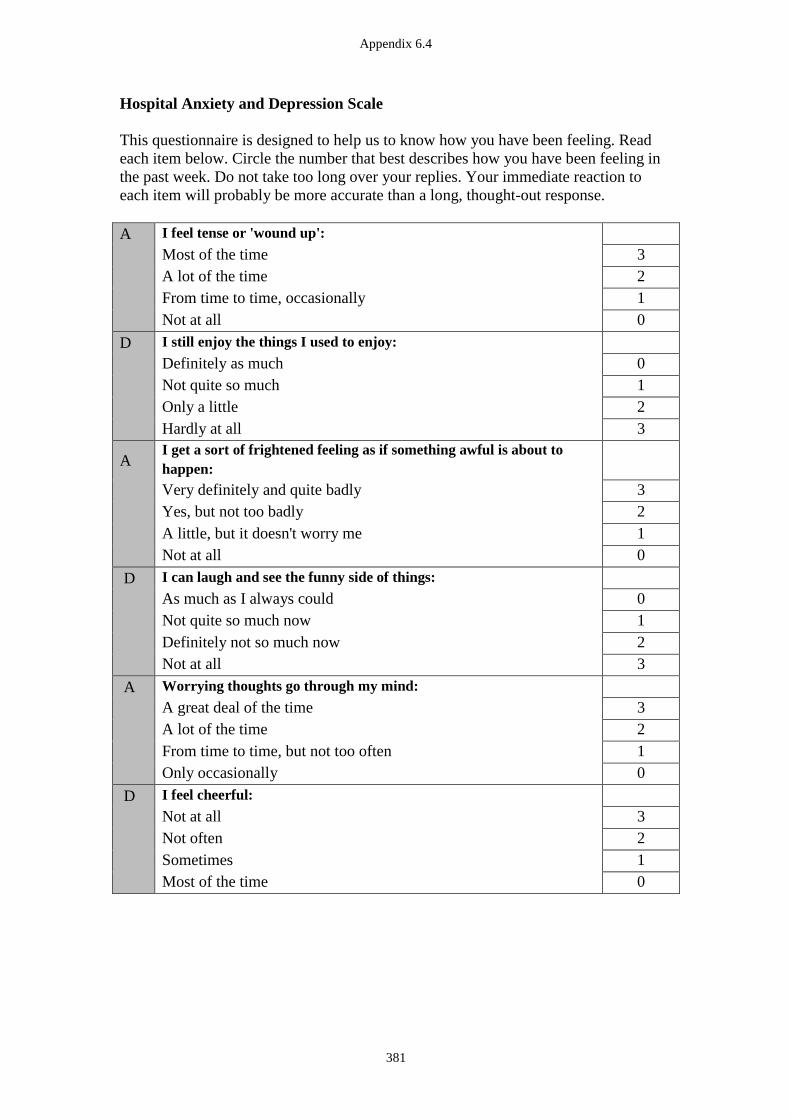
Appendix 6.4
381
Hospital Anxiety and Depression Scale
This questionnaire is designed to help us to know how you have been feeling. Read
each item below. Circle the number that best describes how you have been feeling in
the past week. Do not take too long over your replies. Your immediate reaction to
each item will probably be more accurate than a long, thought-out response.
A
I feel tense or 'wound up':
Most of the time 3
A lot of the time 2
From time to time, occasionally 1
Not at all 0
D
I still enjoy the things I used to enjoy:
Definitely as much 0
Not quite so much 1
Only a little 2
Hardly at all 3
A
I get a sort of frightened feeling as if something awful is about to
happen:
Very definitely and quite badly 3
Yes, but not too badly 2
A little, but it doesn't worry me 1
Not at all 0
D
I can laugh and see the funny side of things:
As much as I always could 0
Not quite so much now 1
Definitely not so much now 2
Not at all 3
A
Worrying thoughts go through my mind:
A great deal of the time 3
A lot of the time 2
From time to time, but not too often 1
Only occasionally 0
D
I feel cheerful:
Not at all 3
Not often 2
Sometimes 1
Most of the time 0

Appendix 6.4
382
A
I can sit at ease and feel relaxed:
Definitely 0
Usually 1
Not Often 2
Not at all 3
D
I feel as if I am slowed down:
Nearly all the time 3
Very often 2
Sometimes 1
Not at all 0
A
I get a sort of frightened feeling like 'butterflies' in the stomach:
Not at all 0
Occasionally 1
Quite Often 2
Very Often 3
D
I have lost interest in my appearance:
Definitely 3
I don't take as much care as I should 2
I may not take quite as much care 1
I take just as much care as ever 0
A
I feel restless as I have to be on the move:
Very much indeed 3
Quite a lot 2
Not very much 1
Not at all 0
D
I look forward with enjoyment to things:
As much as I ever did 0
Rather less than I used to 1
Definitely less than I used to 2
Hardly at all 3
A
I get sudden feelings of panic:
Very often indeed 3
Quite often 2
Not very often 1
Not at all 0
D
I can enjoy a good book or radio or TV program:
Often 0
Sometimes 1
Not often 2
Very seldom 3

Appendix 6.4
383
EORTC QLQ-C30 (Version 3)
We are interested in some things about you and your health. Please answer all of the
questions yourself by circling the number that best applies to you. There are no "right"
or "wrong" answers. The information that you provide will remain strictly confidential.
Not
at all
A
Little
Quite
a bit
Very
much
1 Do you have any trouble doing strenuous
activities, like carrying a heavy shopping bag or
a suitcase?
1 2 3 4
2 Do you have any trouble taking a long walk? 1 2 3 4
3 Do you have any trouble taking a short walk
outside of the house?
1 2 3 4
4 Do you need to stay in bed or a chair during the
day?
1 2 3 4
5 Do you need help with eating, dressing,
washing yourself or using the toilet?
1 2 3 4
During the past week: Not
at all
A
Little
Quite
a bit
Very
much
6 Were you limited in doing either your work or
other daily activities?
1 2 3 4
7 Were you limited in pursuing your hobbies or
other leisure time activities?
1 2 3 4
8 Were you short of breath? 1 2 3 4
9 Have you had pain? 1 2 3 4
10 Did you need to rest? 1 2 3 4
11 Have you had trouble sleeping? 1 2 3 4
12 Have you felt weak? 1 2 3 4
13 Have you lacked appetite? 1 2 3 4
14 Have you felt nauseated? 1 2 3 4
15 Have you vomited? 1 2 3 4
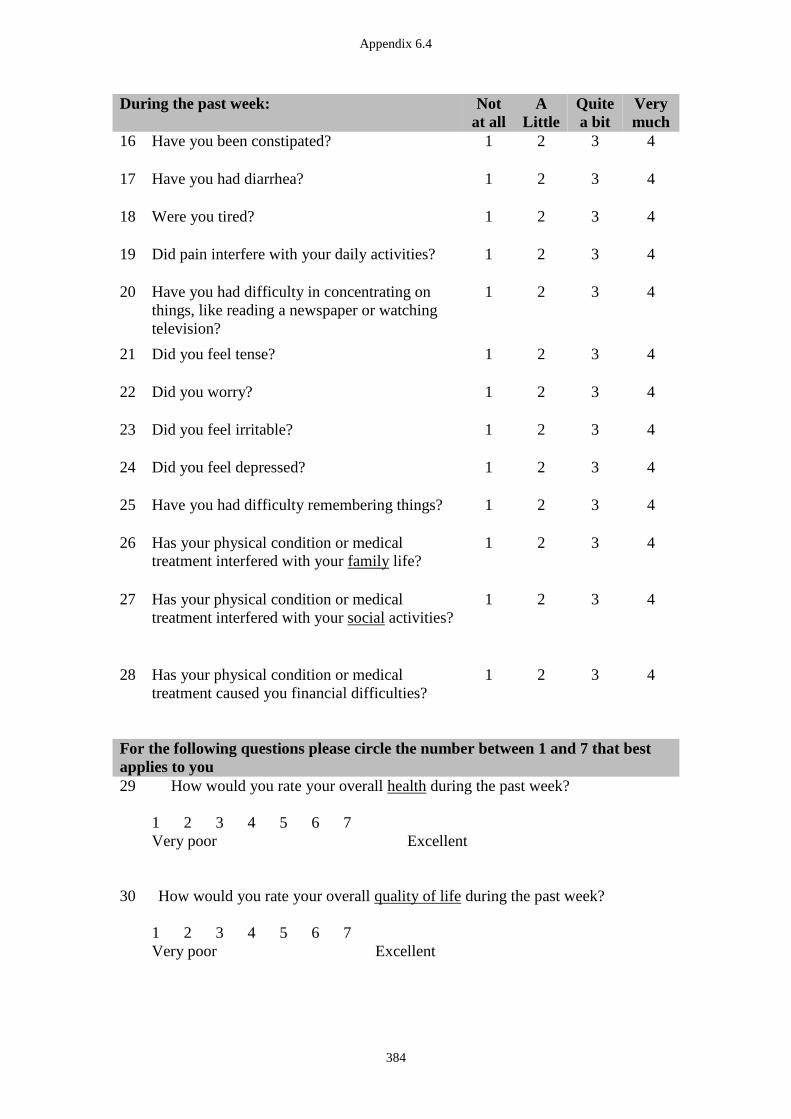
Appendix 6.4
384
During the past week: Not
at all
A
Little
Quite
a bit
Very
much
16 Have you been constipated? 1 2 3 4
17 Have you had diarrhea? 1 2 3 4
18 Were you tired? 1 2 3 4
19 Did pain interfere with your daily activities? 1 2 3 4
20 Have you had difficulty in concentrating on
things, like reading a newspaper or watching
television?
1 2 3 4
21 Did you feel tense? 1 2 3 4
22 Did you worry? 1 2 3 4
23 Did you feel irritable? 1 2 3 4
24 Did you feel depressed? 1 2 3 4
25 Have you had difficulty remembering things? 1 2 3 4
26 Has your physical condition or medical
treatment interfered with your family life?
1 2 3 4
27 Has your physical condition or medical
treatment interfered with your social activities?
1 2 3 4
28 Has your physical condition or medical
treatment caused you financial difficulties?
1 2 3 4
For the following questions please circle the number between 1 and 7 that best
applies to you
29 How would you rate your overall health during the past week?
1 2 3 4 5 6 7
Very poor Excellent
30 How would you rate your overall quality of life during the past week?
1 2 3 4 5 6 7
Very poor Excellent

Appendix 6.4
385
EORTC QLQ-CR29
During the past week: Not
at all
A
Little
Quite
a bit
Very
much
31 Did you urinate frequently during the day? 1 2 3 4
32 Did you urinate frequently during the night? 1 2 3 4
33 Have you had any unintentional release
(leakage) of urine?
1 2 3 4
34 Did you have pain when you urinated? 1 2 3 4
35 Did you have abdominal pain? 1 2 3 4
36 Did you have pain in your buttock/anal/rectum? 1 2 3 4
37 Did you have a bloated feeling in your
abdomen?
1 2 3 4
38 Have you had blood in your stools? 1 2 3 4
39 Have you had mucus in your stools? 1 2 3 4
40 Did you have a dry mouth? 1 2 3 4
41 Have you lost hair as a result of your treatment? 1 2 3 4
42 Have you had problems with your sense of
taste?
1 2 3 4
During the past week: Not
at all
A
Little
Quite
a bit
Very
much
43 Were you worried about your health in the
future?
1 2 3 4
44 Have you worried about your weight?
1 2 3 4
45 Have you felt less physically attractive as a
result of your disease or treatment?
1 2 3 4
46 Have you been feeling less feminine /
masculine as a result of your disease or
treatment?
1 2 3 4
47 Have you been dissatisfied with your body?
1 2 3 4
48 Do you have a stoma bag (colostomy /
ileostomy)? (please circle the correct answer)
yes no
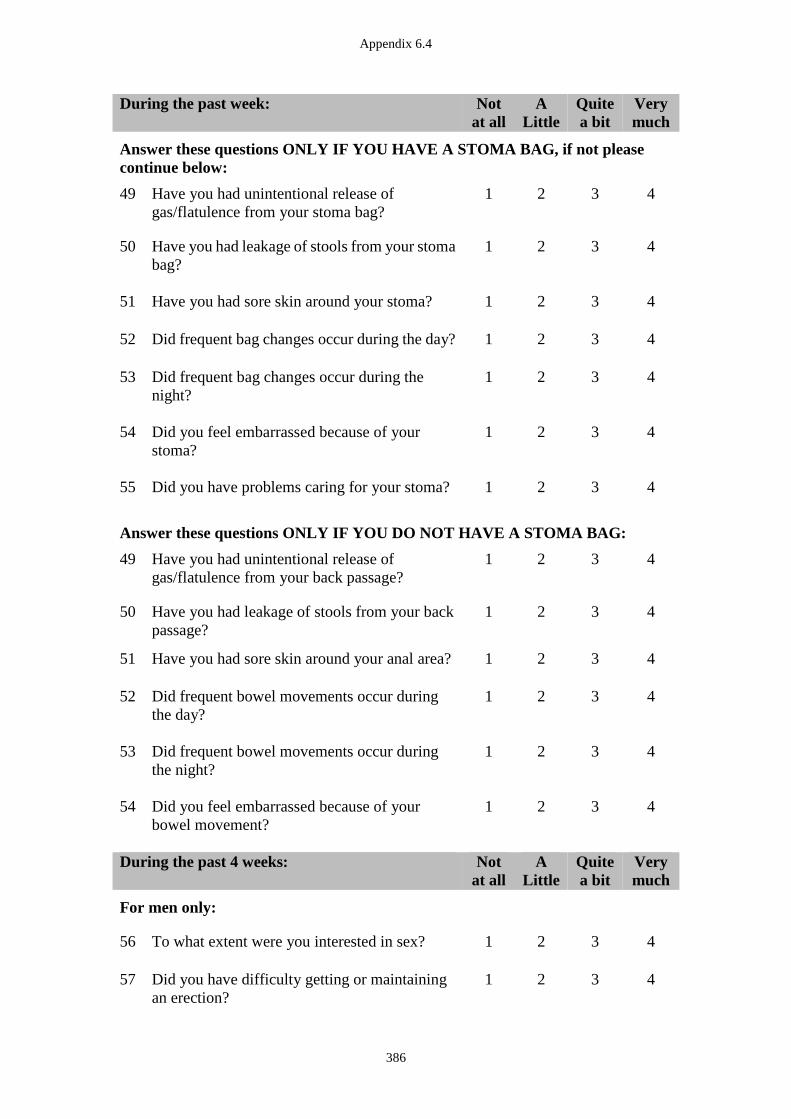
Appendix 6.4
386
During the past week: Not
at all
A
Little
Quite
a bit
Very
much
Answer these questions ONLY IF YOU HAVE A STOMA BAG, if not please
continue below:
49 Have you had unintentional release of
gas/flatulence from your stoma bag?
1 2 3 4
50 Have you had leakage of stools from your stoma
bag?
1 2 3 4
51 Have you had sore skin around your stoma?
1 2 3 4
52 Did frequent bag changes occur during the day?
1 2 3 4
53 Did frequent bag changes occur during the
night?
1 2 3 4
54 Did you feel embarrassed because of your
stoma?
1 2 3 4
55 Did you have problems caring for your stoma?
1 2 3 4
Answer these questions ONLY IF YOU DO NOT HAVE A STOMA BAG:
49 Have you had unintentional release of
gas/flatulence from your back passage?
1 2 3 4
50 Have you had leakage of stools from your back
passage?
1 2 3 4
51 Have you had sore skin around your anal area?
1 2 3 4
52 Did frequent bowel movements occur during
the day?
1 2 3 4
53 Did frequent bowel movements occur during
the night?
1 2 3 4
54 Did you feel embarrassed because of your
bowel movement?
1 2 3 4
During the past 4 weeks: Not
at all
A
Little
Quite
a bit
Very
much
For men only:
56 To what extent were you interested in sex? 1 2 3 4
57 Did you have difficulty getting or maintaining
an erection?
1 2 3 4
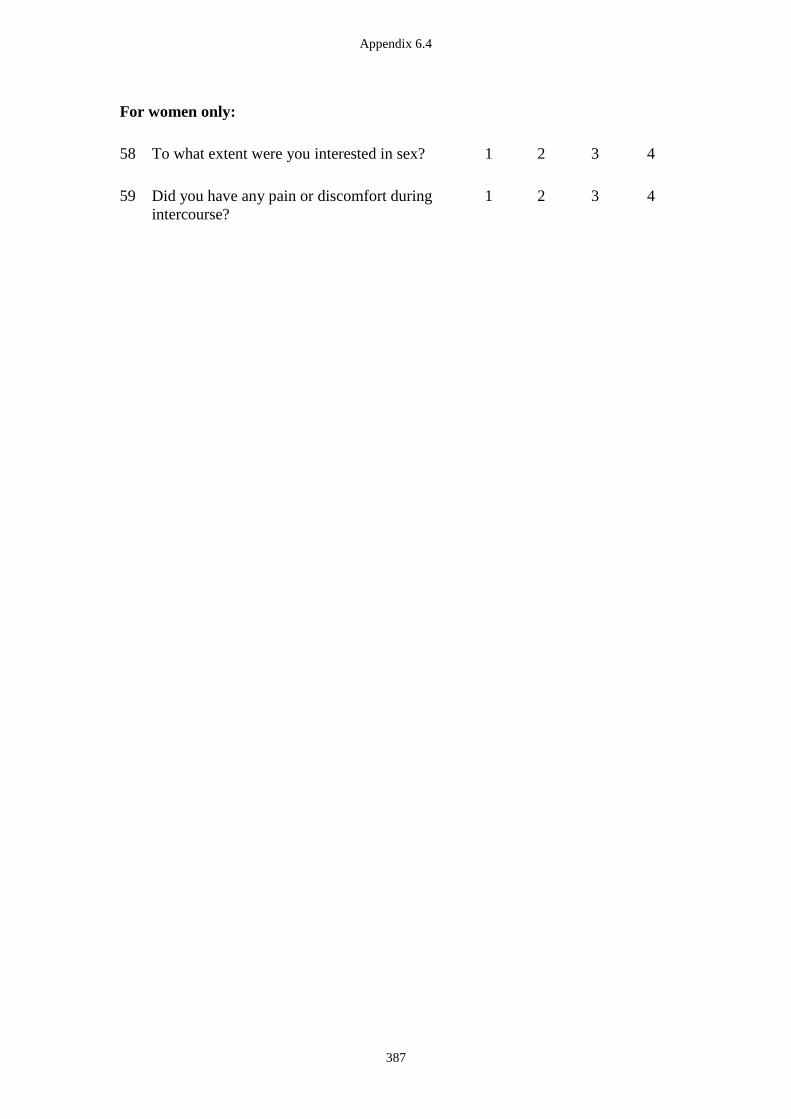
Appendix 6.4
387
For women only:
58 To what extent were you interested in sex? 1 2 3 4
59 Did you have any pain or discomfort during
intercourse?
1 2 3 4

Appendix 6.4
388
SELF-EFFICACY SCALES
Self-efficacy is a measure of your personal belief, or confidence to succeed with your
goals to adopt and maintain a healthy lifestyle.
Please answer by circling the number that best applies to you.
1. The Nutrition Self-Efficacy Scale
“How certain are you that you could overcome the following barriers”
I can manage to stick to healthy foods, … Very
uncertain
Rather
uncertain
Rather
certain
Very
certain
1 …even if I need a long time to develop
the necessary routines.
1 2 3 4
2 …even if I have to try several times until
it works.
1 2 3 4
3 …even if I have to rethink my entire way
of nutrition.
1 2 3 4
4 …even if I do not receive a great deal of
support from others when making my
first attempts.
1 2 3 4
5 …even if I have to make a detailed plan. 1 2 3 4
2. The Physical Exercise Self-Efficacy Scale
“How certain are you that you could overcome the following barriers”
I can manage to carry out my exercise
intentions, …
Very
uncertain
Rather
uncertain
Rather
certain
Very
certain
1 …even when I have worries and
problems.
1 2 3 4
2 …even if I feel depressed. 1 2 3 4
3 …even when I feel tense. 1 2 3 4
4 …even when I am tired. 1 2 3 4
5 …even when I am busy. 1 2 3 4
Schwarzer, R. and B. Renner. Health-specific self-efficacy scales. 2005; Available from:
http://userpage.fu-berlin.de/health/healself.pdf.
Appendix 6.4
389
GLOBAL RATING OF CHANGE
Please circle the number/response that best applies to you, for each question.
1: “How does your fitness now, compare to your fitness at the start of the study?”
1 2 3 4 5 6 7
Much
better
Better A little
better
No change A little
worse
Worse Much
worse
2: “How do your pelvic floor symptoms / control now, compare to your pelvic floor
symptoms / control at the start of the study?”
1 2 3 4 5 6 7
Much
better
Better A little
better
No change A little
worse
Worse Much
worse
This is the end of the questionnaire booklet, thank you for very much for answering
these questions.
PLEASE BRING THIS QUESTIONNAIRE BOOKLET TO YOUR ASSESSMENT
APPOINTMENT.

Appendix 7.1
390
Appendix 7.1 Ethics Approval Documentation (Study 5)
Appendix 7.1
391
Appendix 7.1
392
Appendix 7.1
393
Appendix 7.1
394

Appendix 7.2
395
Appendix 7.2 Data Collection Sheets (Study 5)
Time Point (please tick the box):
� Baseline (T1)
� Immediately post-Physiotherapy intervention (T2)
� Follow up at 6 months after baseline (T3)
DIGITAL ASSESSMENT
Latex allergy �1.Yes �2. No
Gel allergy �1.Yes �2. No
Verbal consent �1.Yes �2. No
1. OBSERVATION
a. Perianal condition 1. soiling �2. scarring �3.tags
�4.haemorrhoids
�5. prolapse 6. fissure � 7. excoriation 8.
other_____
b. Voluntary pelvic floor muscle contraction �1. Absent �2. Present
If absent, anorectal reflex 1. Absent �2. Present
If incorrect, correct after � 1st try � 2nd try � 3rd try
�still incorrect after 3 tries
2. DIGITAL PALPATION
Appropriate to perform digital palpation: �1.Yes � 2. No.
If No: �1. Recent anal surgery or trauma (< 6 weeks)
�2. Recent radiotherapy
�3. Acute pain related to active haemorrhoids/fissures etc
�4. Active inflammatory conditions
�5. Obvious bleeding
�6. Current infection
�7. other________________________________
a. IAS Resting Pressure �1. Increased �2. Normal �3. Reduced
b. Pain: �1.Yes �2. No
3. MUSCLE TESTING (3 x 3 sec reps, only 1 is MVC)
a. EAS
ICS Grade �1. Absent �2. Weak �3. Mod �4. Strong
b. Puborectalis
ICS Grade �1. Absent �2. Weak �3. Mod �4. Strong
c. Relaxation �1. Absent �2. Partial �3. Full
ANORECTAL AND PELVIC FLOOR MUSCLE TEST

Appendix 7.2
396
MANOMETRY
Appropriate to perform manometry: �1.Yes � 2. No.
If No: �1. current infection / pain
�2. swollen and painful haemorrhoid
�3. fissure
�4. excoriation / rash / erythema
�5. wound
�6. no voluntary squeeze observed
�7. other________________________________
Verbal consent �1.Yes �2. No
1. a. 1 x 30 SEC MVC.
Resting pressure upon insertion (cm H2O)
Peak
Average
Gradient
Area under curve
b. Decision to discontinue due to poor technique
If yes, how many seconds:_______________
Reasons:
�1. Altered respiratory pattern
�2. Excessive use of external obliques
�3. Rectus abdominus activity
�4. Gluteal/adductor activity
�5. Other______________
TRANSPERINEAL ULTRASOUND
Verbal consent �1.Yes �2. No
Variable
condition
Variable description Value
1. Rest a. distance levator hiatus (sagittal plane) A-P
direction (cm)
b. AR angle (degree)
c. distance AR angle to horizontal (cm)
2. Voluntary
contraction
1. 3 sec MVC
a. distance levator hiatus (sagittal plane) A-P
direction (cm)
b. AR angle (degree)
c. distance AR angle to horizontal (cm)
2. attempted 60 sec sustained contraction at
maximum: time to start of decay (from maximum
elevation) (seconds)
� If symptomatic, refer to the surgeon: date________________
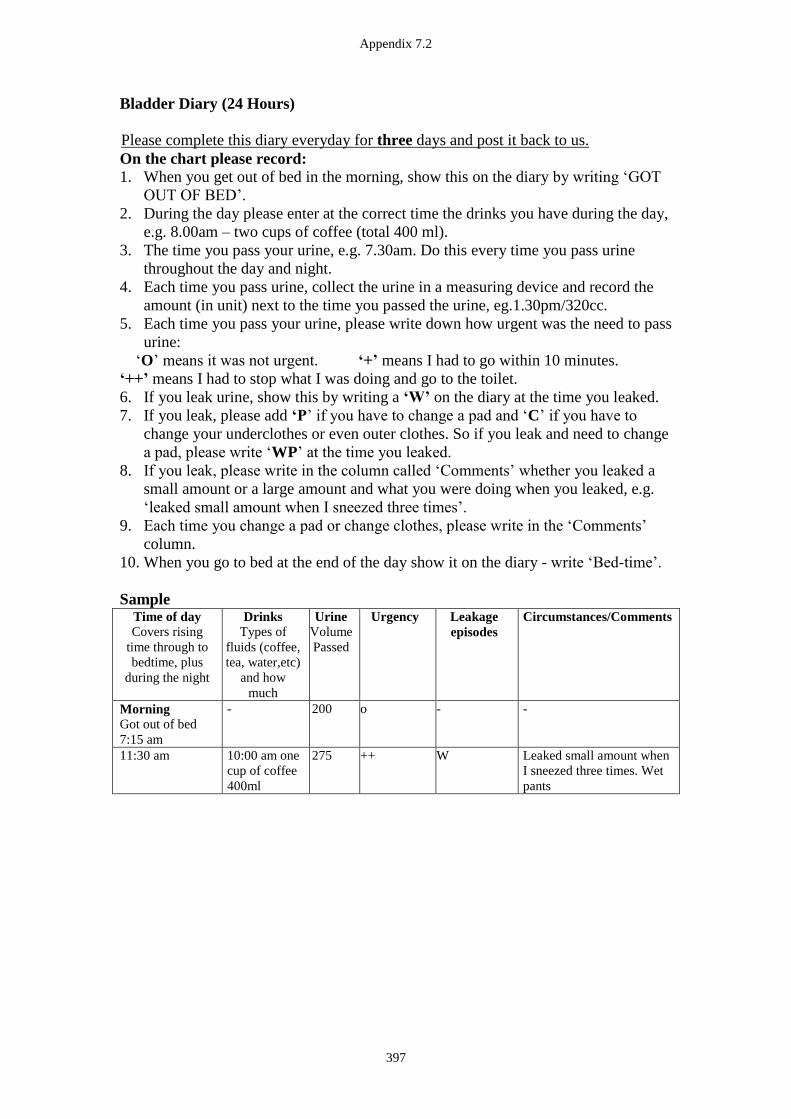
Appendix 7.2
397
Bladder Diary (24 Hours)
Please complete this diary everyday for three days and post it back to us.
On the chart please record:
1. When you get out of bed in the morning, show this on the diary by writing ‘GOT
OUT OF BED’.
2. During the day please enter at the correct time the drinks you have during the day,
e.g. 8.00am – two cups of coffee (total 400 ml).
3. The time you pass your urine, e.g. 7.30am. Do this every time you pass urine
throughout the day and night.
4. Each time you pass urine, collect the urine in a measuring device and record the
amount (in unit) next to the time you passed the urine, eg.1.30pm/320cc.
5. Each time you pass your urine, please write down how urgent was the need to pass
urine:
‘O’ means it was not urgent. ‘+’ means I had to go within 10 minutes.
‘++’ means I had to stop what I was doing and go to the toilet.
6. If you leak urine, show this by writing a ‘W’ on the diary at the time you leaked.
7. If you leak, please add ‘P’ if you have to change a pad and ‘C’ if you have to
change your underclothes or even outer clothes. So if you leak and need to change
a pad, please write ‘WP’ at the time you leaked.
8. If you leak, please write in the column called ‘Comments’ whether you leaked a
small amount or a large amount and what you were doing when you leaked, e.g.
‘leaked small amount when I sneezed three times’.
9. Each time you change a pad or change clothes, please write in the ‘Comments’
column.
10. When you go to bed at the end of the day show it on the diary - write ‘Bed-time’.
Sample Time of day
Covers rising
time through to
bedtime, plus
during the night
Drinks
Types of
fluids (coffee,
tea, water,etc)
and how
much
Urine
Volume
Passed
Urgency Leakage
episodes
Circumstances/Comments
Morning
Got out of bed
7:15 am
- 200 o - -
11:30 am 10:00 am one
cup of coffee
400ml
275 ++ W Leaked small amount when
I sneezed three times. Wet
pants
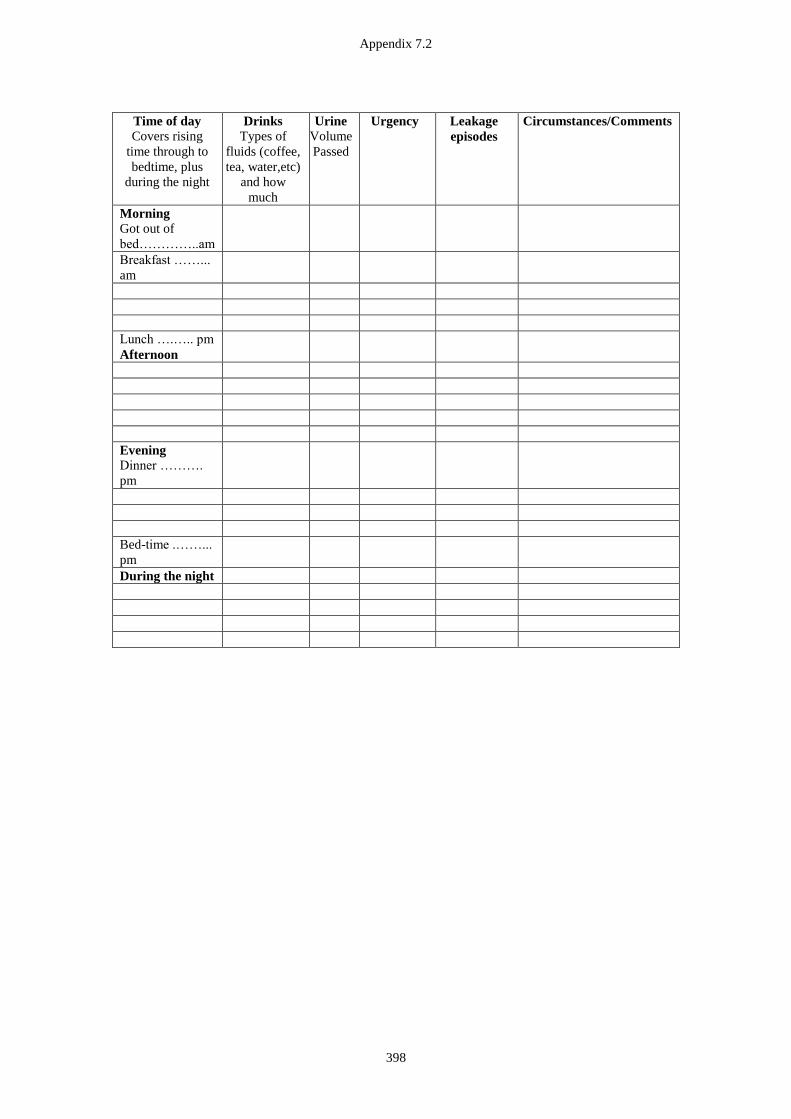
Appendix 7.2
398
Time of day
Covers rising
time through to
bedtime, plus
during the night
Drinks
Types of
fluids (coffee,
tea, water,etc)
and how
much
Urine
Volume
Passed
Urgency Leakage
episodes
Circumstances/Comments
Morning
Got out of
bed…………..am
Breakfast ……...
am
Lunch ….….. pm
Afternoon
Evening
Dinner ……….
pm
Bed-time .……...
pm
During the night
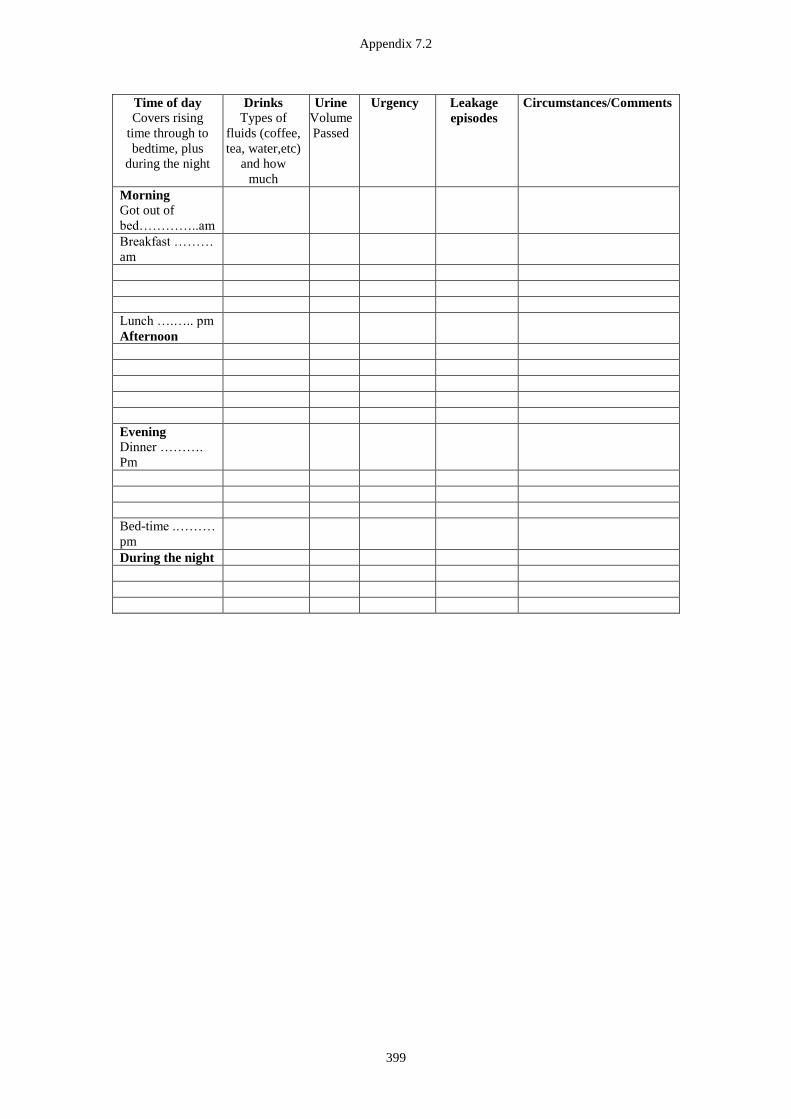
Appendix 7.2
399
Time of day
Covers rising
time through to
bedtime, plus
during the night
Drinks
Types of
fluids (coffee,
tea, water,etc)
and how
much
Urine
Volume
Passed
Urgency Leakage
episodes
Circumstances/Comments
Morning
Got out of
bed…………..am
Breakfast ………
am
Lunch ….….. pm
Afternoon
Evening
Dinner ……….
Pm
Bed-time .………
pm
During the night
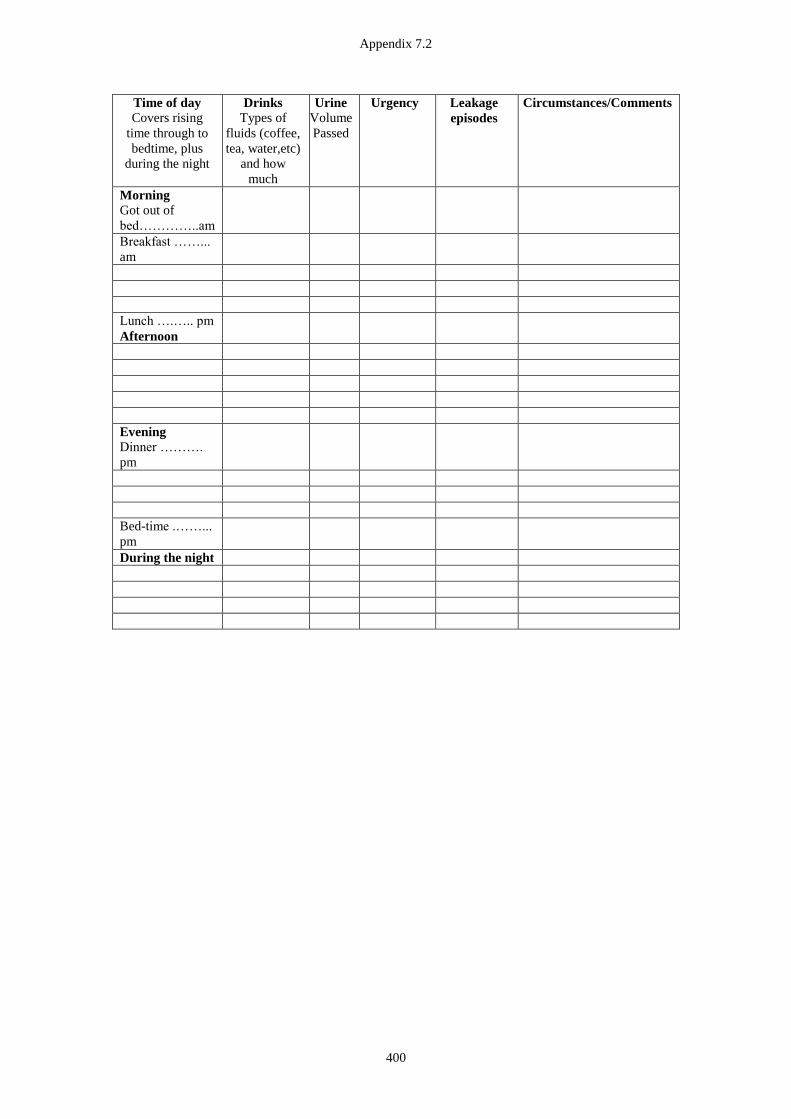
Appendix 7.2
400
Time of day
Covers rising
time through to
bedtime, plus
during the night
Drinks
Types of
fluids (coffee,
tea, water,etc)
and how
much
Urine
Volume
Passed
Urgency Leakage
episodes
Circumstances/Comments
Morning
Got out of
bed…………..am
Breakfast ……...
am
Lunch ….….. pm
Afternoon
Evening
Dinner ……….
pm
Bed-time .……...
pm
During the night
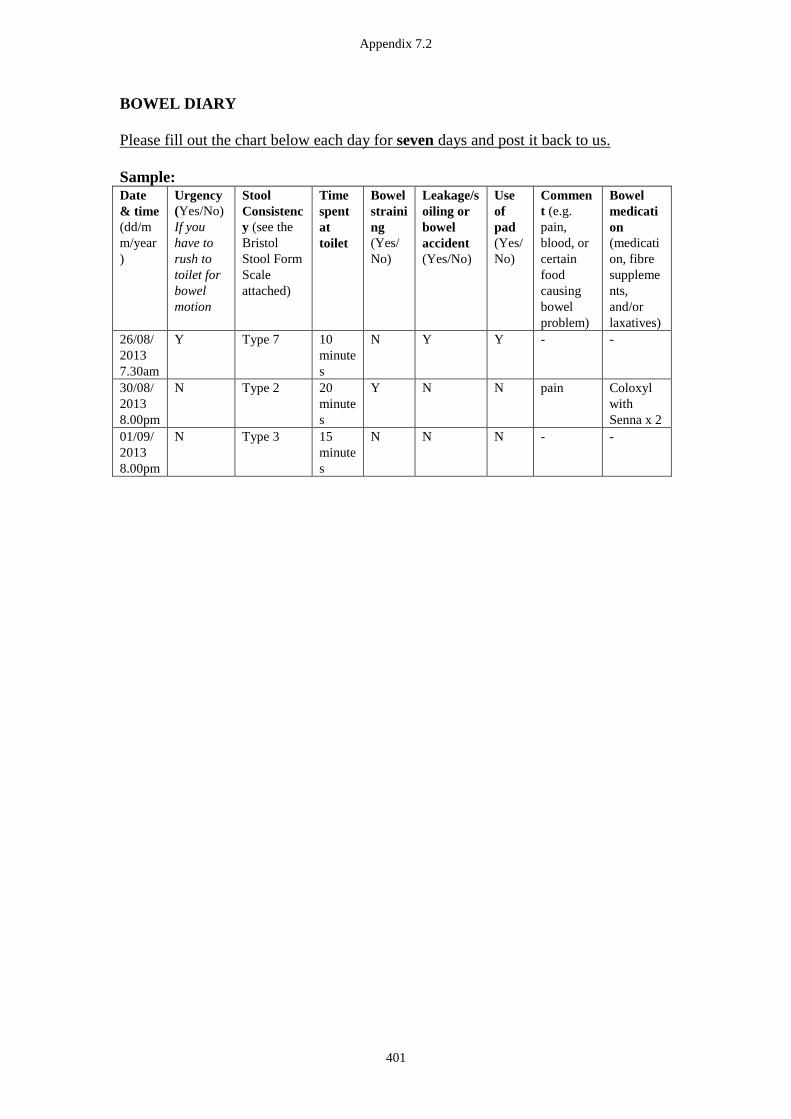
Appendix 7.2
401
BOWEL DIARY
Please fill out the chart below each day for seven days and post it back to us.
Sample: Date
& time
(dd/m
m/year
)
Urgency
(Yes/No)
If you
have to
rush to
toilet for
bowel
motion
Stool
Consistenc
y (see the
Bristol
Stool Form
Scale
attached)
Time
spent
at
toilet
Bowel
straini
ng
(Yes/
No)
Leakage/s
oiling or
bowel
accident
(Yes/No)
Use
of
pad
(Yes/
No)
Commen
t (e.g.
pain,
blood, or
certain
food
causing
bowel
problem)
Bowel
medicati
on
(medicati
on, fibre
suppleme
nts,
and/or
laxatives)
26/08/
2013
7.30am
Y Type 7 10
minute
s
N Y Y - -
30/08/
2013
8.00pm
N Type 2 20
minute
s
Y N N pain Coloxyl
with
Senna x 2
01/09/
2013
8.00pm
N Type 3 15
minute
s
N N N - -

Appendix 7.2
402
Reference: Heaton, K W & Lewis, S J 1997, 'Stool form scale as a useful guide to intestinal transit time'. Scandinavian Journal of
Gastroenterology, vol.32, no.9, pp.920 - 924. Retrieved on 2/3/2007.
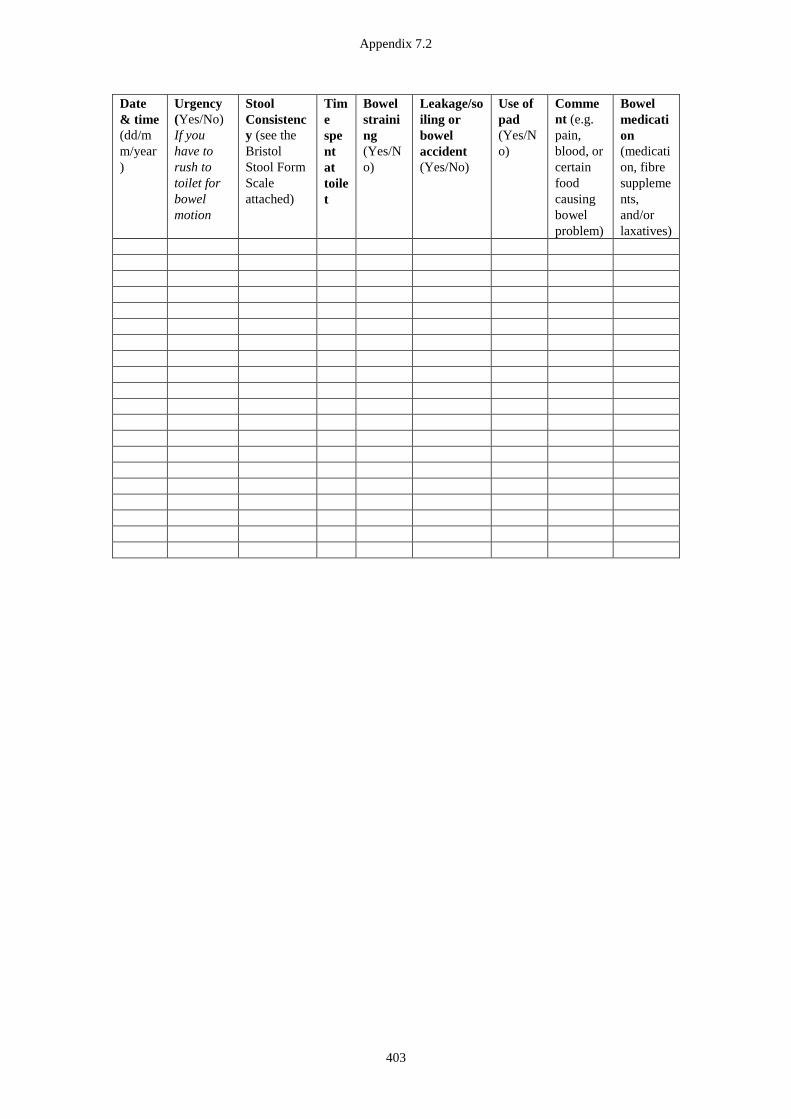
Appendix 7.2
403
Date
& time
(dd/m
m/year
)
Urgency
(Yes/No)
If you
have to
rush to
toilet for
bowel
motion
Stool
Consistenc
y (see the
Bristol
Stool Form
Scale
attached)
Tim
e
spe
nt
at
toile
t
Bowel
straini
ng
(Yes/N
o)
Leakage/so
iling or
bowel
accident
(Yes/No)
Use of
pad
(Yes/N
o)
Comme
nt (e.g.
pain,
blood, or
certain
food
causing
bowel
problem)
Bowel
medicati
on
(medicati
on, fibre
suppleme
nts,
and/or
laxatives)

Appendix 8.1
404
Appendix 8.1 Systematic review article
Appendix 8.1
405

Appendix 8.1
406
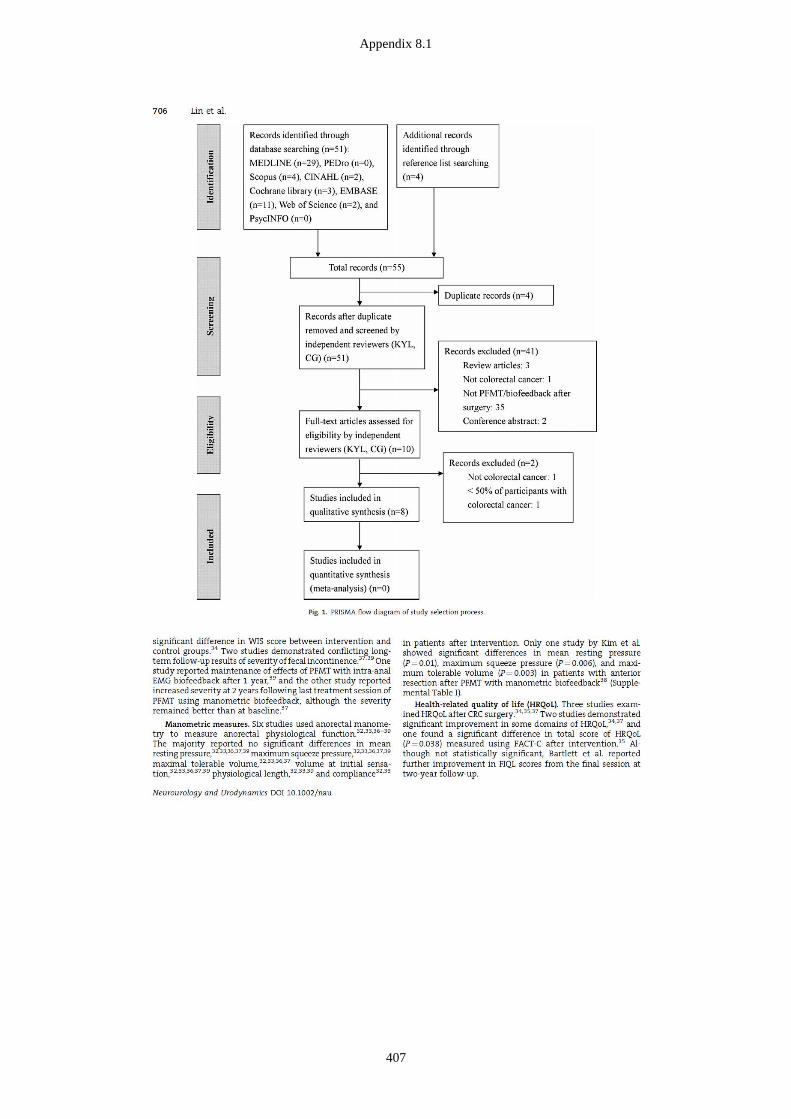
Appendix 8.1
407
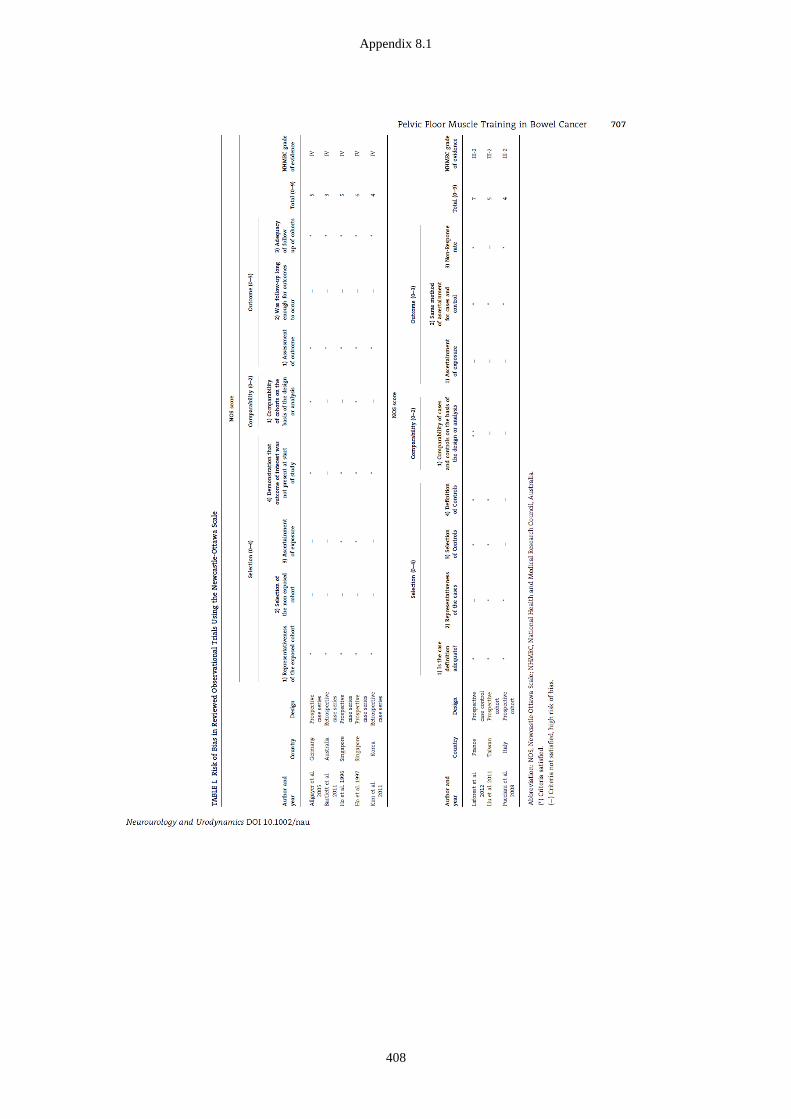
Appendix 8.1
408
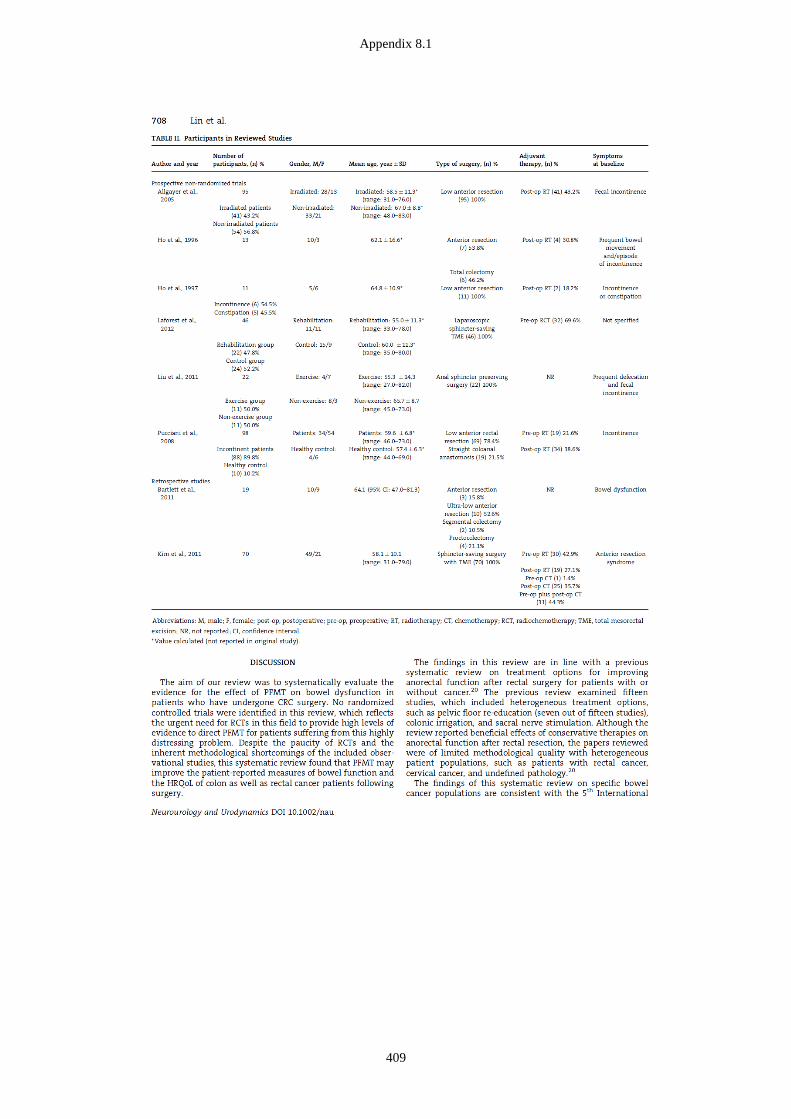
Appendix 8.1
409
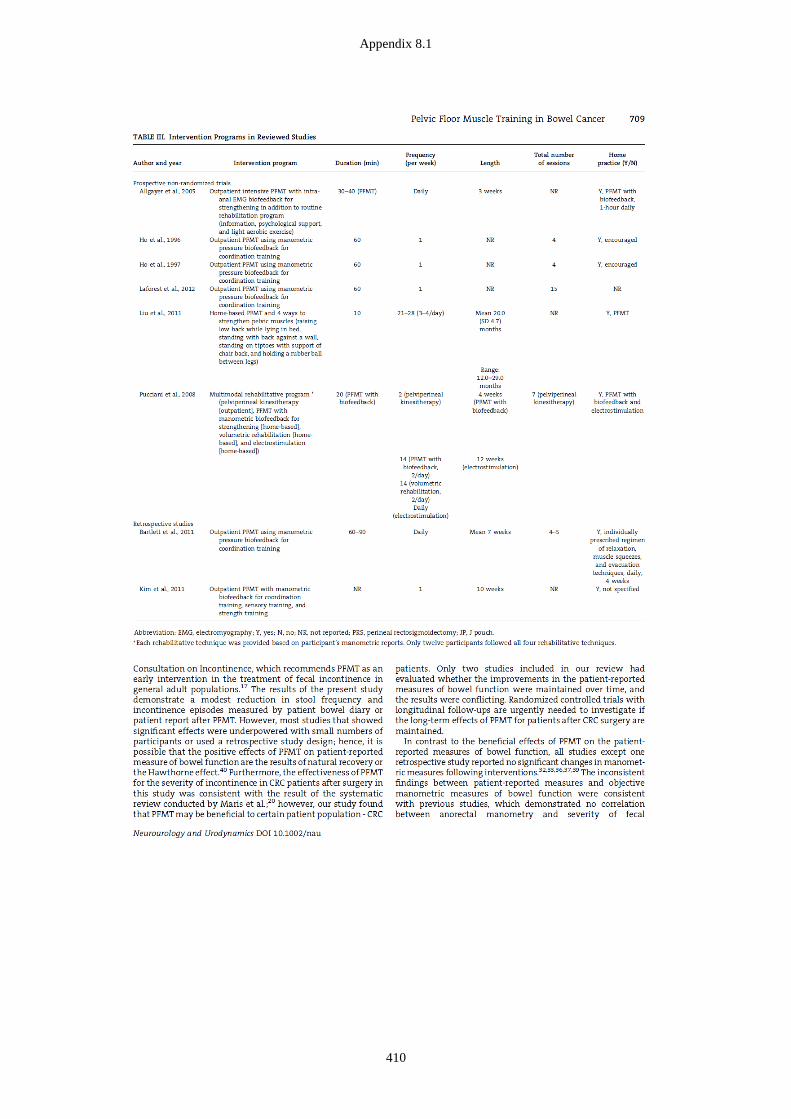
Appendix 8.1
410
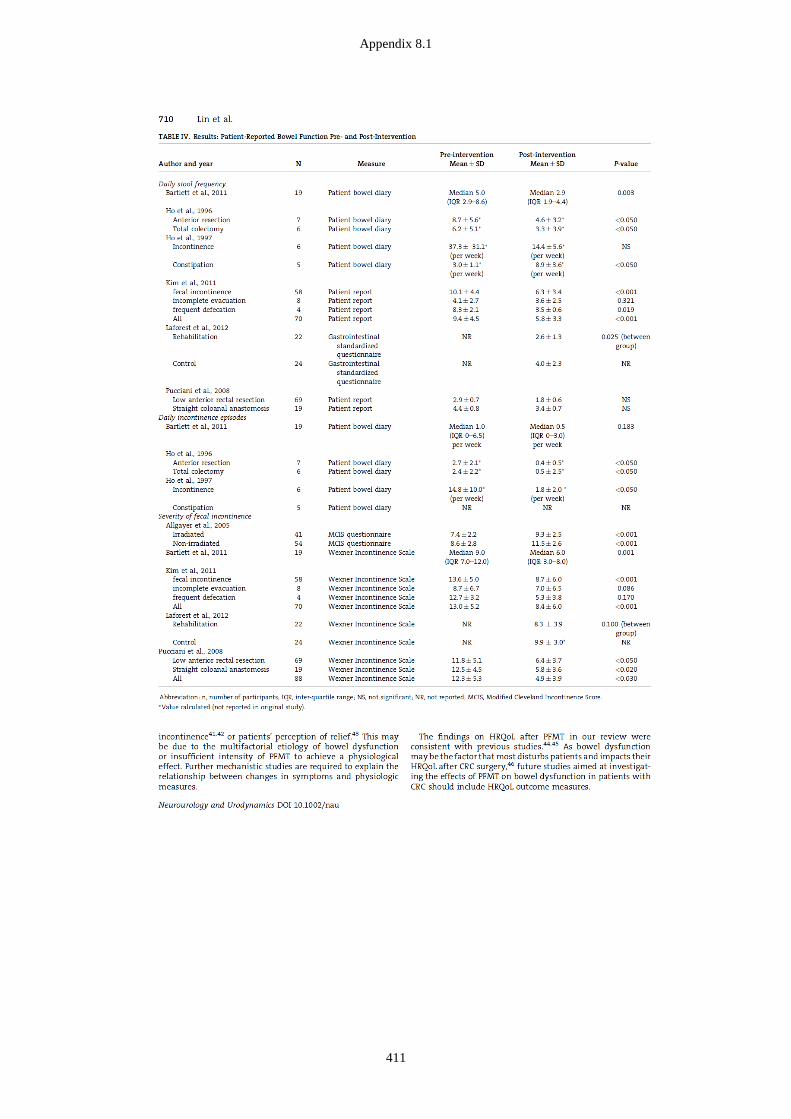
Appendix 8.1
411
Appendix 8.1
412
Appendix 8.1
413
Appendix 8.2
414
Appendix 8.2 Example of search strategy
MEDLINE was searched using the Web of Knowledge interface on 10/03/2014 for
the period 1950 to March 2014
1. MeSH Heading:exp=(Rehabilitation) (141786)
2. MeSH Heading:exp=(Physical Therapy Modalities) (119321)
3. MeSH Heading=(Biofeedback Psychology) (6093)
4. Topic=(pelvic floor muscle training) (628)
5. Topic=(pelvic floor exercise) (1123)
6. Topic=(kegel) (122)
7. Topic=(biofeedback) (7821)
8. MeSH Heading:exp=(Defecation) (5501)
9. MeSH Heading:exp=(Fecal Incontinence) (7570)
10. Topic=(bowel function) (10987)
11. Topic=(gastrointestinal function) (21721)
12. Topic=(total mesorectal excision) (1477)
13. Topic=(sphincter-saving surgery) (516)
14. Topic=(anterior resection) (10805)
15. Topic=(Abdominoperineal resection) (2345)
16. MeSH Heading:exp=(Colectomy) (14382)
17. MeSH Heading:exp=(Colorectal Surgery) (1907)
18. Topic=(sphincter-preserving surgery) (465)
19. MeSH Heading:exp=(Colorectal Neoplasms) (141,110)
20. MeSH Heading:exp=(Rectal Neoplasms) (36,511)
21. MeSH Heading:exp=(Colonic Neoplasms) (65,271)
Appendix 8.2
415
22. 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 (235,136)
23. 8 OR 9 OR 10 OR 11 (41,226)
24. 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 (29,296)
25. 19 OR 20 OR 21 (141,110)
26. 22 AND 23 AND 24 AND 25 (35)
Refined by English (29)
Minerva Access is the Institutional Repository of The University of Melbourne
Author/s:Lin, Kuan-Yin
Title:Physical function in patients following surgery for colorectal cancer
Date:2016
Persistent Link:http://hdl.handle.net/11343/123734
Terms and Conditions:Terms and Conditions: Copyright in works deposited in Minerva Access is retained by thecopyright owner. The work may not be altered without permission from the copyright owner.Readers may only download, print and save electronic copies of whole works for their ownpersonal non-commercial use. Any use that exceeds these limits requires permission fromthe copyright owner. Attribution is essential when quoting or paraphrasing from these works.
Related Documents











