What is colorectal cancer? Let us explain it to you. Colorectal Cancer ESMO/ACF Patient Guide Series based on the ESMO Clinical Practice Guidelines www.anticancerfund.org www.esmo.org

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

What is colorectal cancer?
Let us explain it to you.
Colorectal Cancer
ESMO/ACF Patient Guide Seriesbased on the ESMO Clinical Practice Guidelines
www.anticancerfund.org www.esmo.org
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page1ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
COLORECTALCANCER:AGUIDEFORPATIENTS
PATIENTINFORMATIONBASEDONESMOCLINICALPRACTICEGUIDELINESThisguide forpatientshasbeenpreparedby theAnticancerFundasa service topatients, tohelppatients and their relatives better understand the nature of colorectal cancer and appreciate thebesttreatmentchoicesavailableaccordingtothesubtypeofcolorectalcancer.Werecommendthatpatients ask their doctors aboutwhat tests or types of treatments are needed for their type andstageofdisease.ThemedicalinformationdescribedinthisdocumentisbasedontheclinicalpracticeguidelinesoftheEuropeanSocietyforMedicalOncology(ESMO)forthemanagementofcolorectalcancer.Thisguide forpatientshasbeenproduced incollaborationwithESMOand isdisseminatedwith the permission of ESMO. It has been written by a medical doctor and reviewed by twooncologists from ESMO including the leading author of the clinical practice guidelines forprofessionals. It has also been reviewed by patient representatives from ESMO’s Cancer PatientWorkingGroup.MoreinformationabouttheAnticancerFund:www.anticancerfund.orgMoreinformationabouttheEuropeanSocietyforMedicalOncology:www.esmo.orgForwordsmarkedwithanasterisk,adefinitionisprovidedattheendofthedocument.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page2ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Tableofcontents
Factsheetaboutcolorectalcancer...........................................................................................3
Definitionofcolorectalcancer..................................................................................................4
Iscolorectalcancerfrequent?...................................................................................................5
Whatcausescolorectalcancer?................................................................................................6
Howiscolorectalcancerdiagnosed?........................................................................................9
Screeningforcolorectalcancer...............................................................................................12
Whatisimportanttoknowtogettheoptimaltreatment?....................................................13
Whatarethetreatmentoptions?...........................................................................................17
Whatarethepossiblesideeffectsofthetreatment?.............................................................30
Whathappensafterthetreatment?.......................................................................................34
Definitionsofdifficultwords...................................................................................................36
ThistextwaswrittenbyDr.AnBilliau(CelsusMedicalWritingLLC,fortheAnticancerFund)andreviewedbyDr.GauthierBouche (theAnticancerFund),Dr. Svetlana Jezdic (ESMO),Prof.Roberto Labianca (ESMO),Prof.BengtGlimelius (ESMO),Prof.EricVanCutsem(ESMO),Prof.DirkArnold(ESMO)andProf.GabriellaKornek(ESMOCancerPatientWorkingGroup).This is the first update of this guide. Updates reflect changes in the successive version of the ESMO Clinical PracticeGuidelines.ThisfirstupdatewasdonebyDr.GauthierBouche(AnticancerFund),Dr.AnaUgarte(AnticancerFund)andwasreviewedbyDr.SvetlanaJezdic(ESMO).
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page3ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
FACTSHEETABOUTCOLORECTALCANCERDefinitionofcolorectalcancer• Cancerthatdevelopsinthelargeintestine.
Diagnosis• Colorectal cancer causes complaintsmore oftenwhen it is advanced. Common symptoms are
change inbowelhabits, abdominaldiscomfort, fatigue,weight loss.Blood in stools couldbeasignofalert.Itcouldbevisibletothenakedeyeorthroughalaboratoryanalysisofstools.
• Endoscopy is an examination in which a lighted tube is inserted through the anus into theintestine.Itallowsseeingtheinsideoftheintestine.Whenatumourisfoundwithin15cmfromtheanusitisconsideredrectaltumour,furtherawayitisconsideredcolontumour.
• Specialradiologicaltestsalsohelptovisualizethelocalisationandsizeofthetumour.• Bloodanalysislookingforcarcinoembryogenicantigen(CEA),atumourmarker,mightbeuseful
inselectedsituations,butdiagnosisshouldnotbereliedsolelyonit.• The confirmation of diagnosis is only given by laboratory analysis of the tumour and tissues
affected(histopathology).
TreatmentaccordingtotheextensionofthediseaseTreatmentofmalignantpolyps• Polyps foundtobecancerousshouldberemovedfromthecolon.Dependingonthedegreeof
theinvasionofmalignantcellsinthepolypawidersurgicalprocedurecouldberecommended.TreatmentaccordingtodiseasestageNote:Sometimesafterinitialtreatmentandanalysisofthetumourremoveditcouldbedeterminedthatthecancerismoreadvancedsothatthetreatmentprotocolhastobeadapted.• Instage0thecancer isconfinedtothemostsuperficial layerofthebowelwallofthemucosa.
Thetumourshouldberemovedsurgically.• StageIinvolvesonelayerdeeper,thesubmucosa,anditevenreachesthemuscleofthecolonor
rectum.Thetumourshouldbesurgicallyremovedaswellaslocallymphnodes.• Stage II involves the muscle of the intestine and invades surrounding organs. The treatment
consists of surgical removal of all affected tissues and for some patients additionalchemotherapy in case of colon cancer and radiotherapy or radiotherapy combined withchemotherapyforrectalcancerisnecessary.
• StageIIIinvolvesstructuresadjacenttothecolonbutalsoregionallymphnodes.Thetreatmentconsistsofsurgicalremovalofthetumoursandotheraffectedtissuesandadjuvanttherapyi.e.chemotherapyforcoloncancerandradiotherapyorchemotherapyplusradiotherapyforrectalcancer.
• Stage IV involvesdistantorgans,suchas liverand lungs.Chemotherapyandbiologicaltargetedtherapyaretreatmentoptions.Chemotherapyhelpsreducingthesizeofthemetastatictumourstomakethem,ifpossible,operable.
Follow-up• There is no follow-up protocol generally accepted. Your doctor will schedule visits after the
treatment completed with purpose of monitoring side effects of the treatment, possiblerecurrenceof thediseaseand toprovideyouwithsupport tobeback toyournormal life.Thefollow-upmaylastupto5years.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page4ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
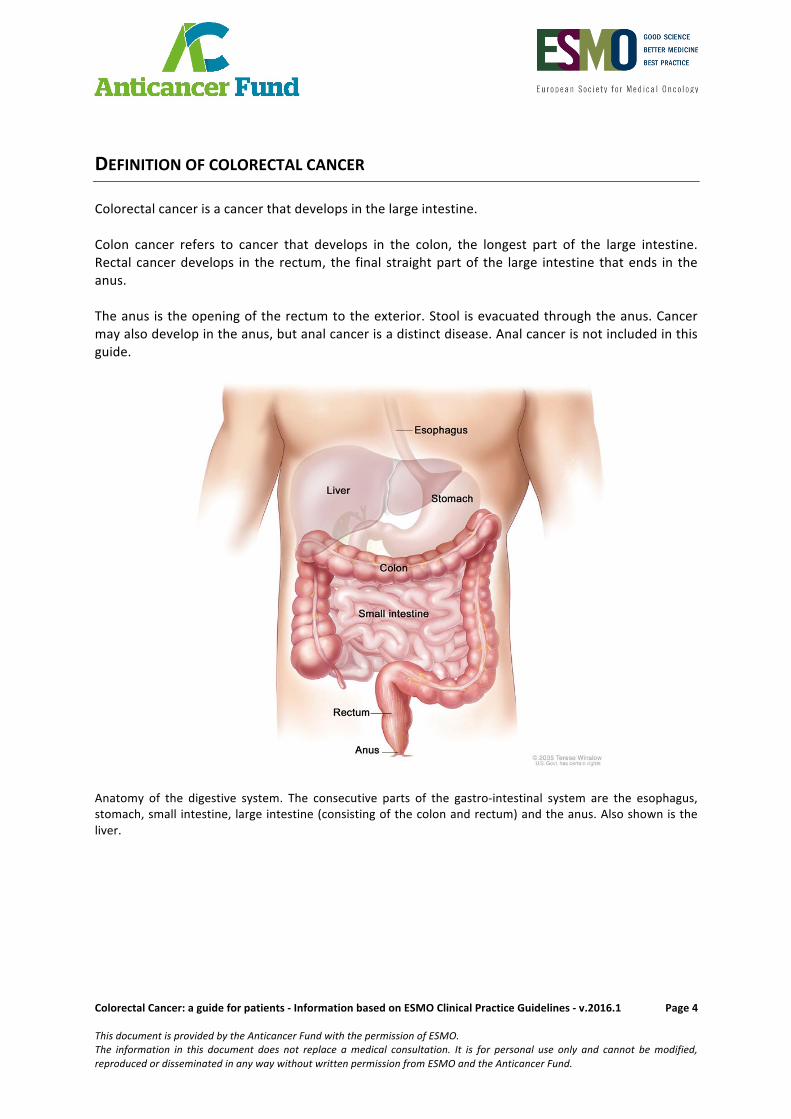
DEFINITIONOFCOLORECTALCANCERColorectalcancerisacancerthatdevelopsinthelargeintestine.Colon cancer refers to cancer that develops in the colon, the longest part of the large intestine.Rectal cancerdevelops in the rectum, the final straightpartof the large intestine thatends in theanus.Theanusistheopeningoftherectumtotheexterior.Stool isevacuatedthroughtheanus.Cancermayalsodevelopintheanus,butanalcancerisadistinctdisease.Analcancerisnotincludedinthisguide.
Anatomy of the digestive system. The consecutive parts of the gastro-intestinal system are the esophagus,stomach,small intestine,largeintestine(consistingofthecolonandrectum)andtheanus.Alsoshownistheliver.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page5ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
ISCOLORECTALCANCERFREQUENT?Colorectal cancer is the most common cancer in Europe and the third most common cancerworldwide. In 2012, approximately 447,000 patients were diagnosed with colorectal cancer inEurope.Thisaccountsforapproximately13%ofallcancersinthisregion.Themajorityofcolorectalcancersarelocatedinthecolon;thesearecalledcoloncancerandaccountfor9%ofallcancersinEurope.Approximatelyonethirdofcolorectalcancersarelocatedonlyintherectum,thesearecalledrectalcancer.Colorectalcancer ismorefrequent inmenthan inwomen. InEurope,aroundone inevery20menandaroundoneinevery35womenwilldevelopcolorectalcanceratsomepointintheirlifetime.Inotherwords, every year, inEurope, around35outof100,000menandaround25outof100,000womenarediagnosedwithcolorectalcancer.Overall,thefrequencyofcolorectalcancerishigherinmoreindustrializedandurbanizedregions.Mostpatientswithcolorectal canceraremore than60yearsoldat the timeof thediagnosis, andcolorectalcancerbelowtheageof40yearsisrare.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page6ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
WHATCAUSESCOLORECTALCANCER?Today, it is not entirely clear why colorectal cancer occurs. A number of risk factors* have beenidentified.Ariskfactor*increasestheriskofcanceroccurring,butisneithernecessarynorsufficienttocausecancer.Ariskfactor*isnotacauseinitself.Some people with these risk factors* will never develop colorectal cancer and some peoplewithoutanyoftheseriskfactors*maynonethelessdevelopcolorectalcancer.Colorectal cancermost commonly occurs as a sporadic disease*,meaning that it is not related toinheritedgenes*thatconveyariskforthistypeofcancer.Approximately20%ofcolorectalcancersoccurinafamilialcontext.Lessthanhalfoftheseariseasaresultofaknownhereditarycondition*.Intheremainderofthefamilialcasesthecauseisunknown.Thefamilialoccurrencemaynotonlybeduetosharedinheritedgenesbutalsotosharedfactorsintheenvironmentthatincreasetherisk.Themainriskfactors*ofcolorectalcancerare:
- Aging:theriskofcolorectalcancerincreasesasapersongetsolder.
- Lifestyle-relatedriskfactors*:o Diet: diet is the most important
environmental risk factor* forcolorectalcancer.Adietthatishighinred meat (beef, lamb, or pork) andprocessedmeat (hot dogs and someluncheonmeats), high in fat and/or low in fiber can increase theriskofdevelopingcolorectalcancer.Highconsumptionofalcoholisalsoariskfactor*forcolorectalcancer.
o Obesity:overweightincreasestheriskofdevelopingcolorectalcancer.o Sedentarylifestyle:individualswhoarenotveryphysicallyactiveareatahigherrisk
ofdevelopingcolorectalcancer.Thisisindependentoftheperson’sweight.o Diabetes mellitus type 2* increases the risk of developing a tumour in the large
intestine.Thisisindependentofwhetherthepersonisoverweightornot.o Smoking:smokingincreasestheriskofdevelopinglargecolorectalpolyps*,whichare
well-knownprecancerouslesions*.
- Previoushistoryofcolorectalpolyps:growthsinthebowel,called
polyps* or adenomas*, are not cancerous. However, thesegrowths can develop into cancer over a long period of time.Polyps* are therefore recognized as well-determined pre-cancerouslesions*.Whenpolyps*arefoundinthelargeintestine,for example during a screening investigation, they should beremovedtopreventthemfromturningintocancer.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page7ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
- Previous history of colorectal cancer: even if the tumour has been completely removedduringprevioustreatment,thereisanincreasedriskofdevelopinganewtumourinanotherpartofthelargeintestineorintherectum.
- Previous history of other types of cancer: a previous history of other tumours, likelymphoma*, testicular cancer* or endometrial cancer* enhances the risk of developingcolorectalcancer.
- Inflammatory bowel disease such as Crohn’s disease* or ulcerative colitis*. These areconditions inwhich the large intestine is inflamed over a long period of time. Aftermanyyears,thismaycausedysplasia*,adisorderedorganizationofthecellsoftheinnerliningofthe intestine. Dysplasia* can evolve into cancer over time. The risk increases with theduration of the inflammatory bowel disease and with the severity and extent of theinflammation. Colorectal cancer in patients with Crohn’s disease* or ulcerative colitisaccountsforapproximatelytwothirdsofallsporadic*colorectalcancers.
- Familyhistory:approximately20%ofcolorectalcancersoccurinafamilialcontext.Ifafirst-degreerelativehascolorectalcancer,theriskfordevelopingcolorectalcancerdoubles.Thiscanbeduetoinheritedgenesortosharedenvironmentalfactors*.Investigation into a possible family history of colorectal cancer is important. In selectedcases,screeningatayoungageand/orgeneticcounselling*shouldbeconsidered.
Knownhereditarysyndromes*thatpredisposesonetocolorectalcancerare:
o Familial Adenomatous Polyposis* (FAP). Individuals with this condition have amutation* or a loss of the FAP* gene, which causes hundreds or thousands ofpolyps*togrowinthelargeintestineatayoungage.Cancermaydevelopinoneormoreof thesepolyps*before theageof40,andsometimesasearlyasage20.Toprevent this from occurring, the large intestine should be surgically removed. AvariantistheAFAPsyndrome:AttenuatedFAP*syndromeinwhichpolyps*arelessfrequentandoccuratalaterage,comparedtoFAP*syndrome.
o Lynch syndrome*, also calledHereditaryNon-polyposisColorectalCancer (HNPCC).Individualswiththisconditionhavecertaingenemutations*thatcausefailureoftheDNArepairmechanisms*.Aconsequencehereof isthatabenigncolorectaltumourmaydevelopintocanceratafasterpace(onaverage2to3years)thaninindividualswho do not have Lynch syndrome*. When colorectal cancer occurs in Lynchsyndrome,theaverageageatdiagnosisis45years.Lynchsyndrome*alsocarriesanincreased risk for certain other types of cancer such as endometrial cancer* orovariancancer*.
Other, less frequent, hereditary syndromes include Turcot syndrome*, Peutz-Jegherssyndrome* and MYH-associated polyposis*. Individuals who have an Ashkenazi Jewishbackgroundareatahigherriskofdevelopingcolorectalcancerbecauseofcertaininheritedgeneticmutations*inthispopulationgroup.
Somefactorsmayhaveaprotectiveeffectagainstthedevelopmentofcolorectalcancer:
- Adiethighinvegetables,fruit,andwholegrainsdecreasetheriskofcolorectalcancer.
- Anincreaseinphysicalactivitymayhelptoreducethisriskofcolorectalcancer.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page8ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
- Long-termintakeofanti-inflammatorydrugssuchasaspirinhasbeensuggestedasawayofreducing the recurrence* of non-hereditary colorectal polyps. Aspirin has been shown toreduce the risk of colorectal cancer in people with Lynch syndrome*. It has also beensuggestedtosupportregressionofcolorectalpolyps*inFAP*patientsbut,moreresearchisnecessarytoobtaindefinitiveevidence.
- Intake of female hormones by postmenopausal women has been suggested as a way ofreducing the risk of colorectal cancer. However, more research is necessary to obtaindefinitiveevidence.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page9ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
HOWISCOLORECTALCANCERDIAGNOSED?Thesuspicionofcolorectalcancermayarise invariouscircumstances,butmostcommonlywhenapatientpresentscertaincomplaintsorsymptoms.Colorectalcancermayalsobedetectedasaresultofascreeningexamination.Manycountriesofferasystematicscreeningprogramtoindividualsover50 years old to detect colorectal polyps* and to detect colorectal cancer at an early stage. Thescreeningprocedureisexplainedinthenextchapter.SymptomsandsignsofcolorectalcancerSymptomsTheprincipalsymptomsofanearlycolorectal tumourareoftenvague.Moreover, thesesymptomscommonly occur in the context of other, non-malignantmedical conditions and are therefore notspecific for colorectal cancer. In a very early phase, most colorectal cancers do not cause anycomplaintsorsymptomsatall.SignsThepresenceofbloodinstoolscanbeasignofcolorectalcancerorofapolyp.Bloodinthestoolcanbe red,orblackwhen theblood isdigested.Darkblood in this context is calledmelenaandoftenresultsfromlesionsbleedingatalargerdistancefromtheanus.Thebloodlosscansometimesnotbevisiblewith the naked eye (microscopic). Blood lossmay lead to iron-deficiency and/or anaemia*(low red blood cell count* and low hemoglobin*) and lead to symptoms of fatigue, shortness ofbreathandpaleskin.DiagnosisAcombinationofthefollowingcomplaints,particularlyifpersistentoveralongerperiodoftime,shouldraisethesuspicionofcolorectalcancerandshouldwarrantfurtherinvestigation:
− achangeinbowelhabits− generalabdominaldiscomfort− unexplainedweightloss− prolongedfatigue
Thediagnosisofcolorectalcancerisbasedontheexaminationsdetailedbelow.Ofnote,inwomen,itisimportanttoruleoutpresenceofsynchronousbreast,ovarianandendometrialcancers*.
1. ClinicalexaminationThisincludesaphysicalexaminationoftheabdomenandarectalexamination. By palpating the abdomen the doctor determineswhetherthetumourhascausedthelivertoenlarge,andwhetherithascausedexcessfluidintheabdomen,calledascites.Duringarectalexamination,thedoctorwillusethefingerofaglovedhandto examine the interior of the anus and the rectum in order todetectabnormalswellingsortracesofblood.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page10ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
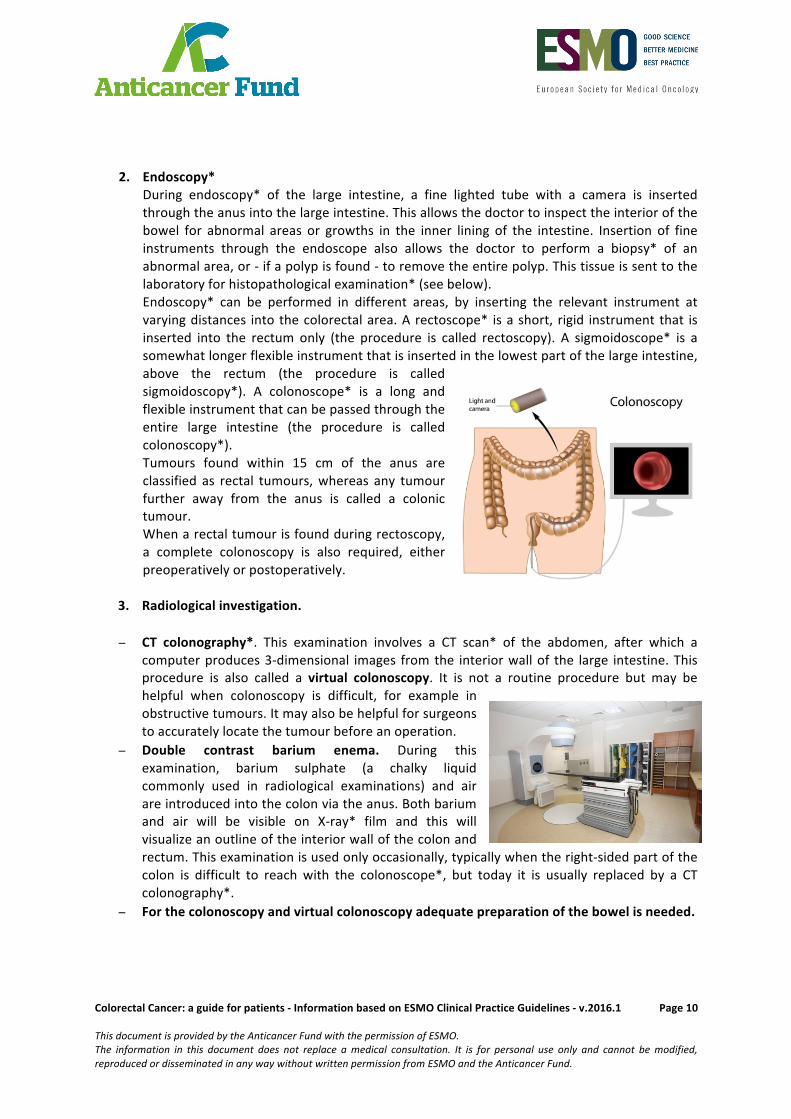
2. Endoscopy*
During endoscopy* of the large intestine, a fine lighted tube with a camera is insertedthroughtheanusintothelargeintestine.Thisallowsthedoctortoinspecttheinteriorofthebowel for abnormal areas or growths in the inner lining of the intestine. Insertion of fineinstruments through the endoscope also allows the doctor to perform a biopsy* of anabnormalarea,or-ifapolypisfound-toremovetheentirepolyp.Thistissueissenttothelaboratoryforhistopathologicalexamination*(seebelow).Endoscopy* can be performed in different areas, by inserting the relevant instrument atvaryingdistances intothecolorectalarea.Arectoscope* isashort, rigid instrumentthat isinserted into the rectum only (the procedure is called rectoscopy). A sigmoidoscope* is asomewhatlongerflexibleinstrumentthatisinsertedinthelowestpartofthelargeintestine,above the rectum (the procedure is calledsigmoidoscopy*). A colonoscope* is a long andflexibleinstrumentthatcanbepassedthroughtheentire large intestine (the procedure is calledcolonoscopy*).Tumours found within 15 cm of the anus areclassified as rectal tumours,whereas any tumourfurther away from the anus is called a colonictumour.Whenarectaltumourisfoundduringrectoscopy,a complete colonoscopy is also required, eitherpreoperativelyorpostoperatively.
3. Radiologicalinvestigation.
− CT colonography*. This examination involves a CT scan* of the abdomen, after which acomputerproduces3-dimensional images fromthe interiorwallof the large intestine.Thisprocedure is also called a virtual colonoscopy. It is not a routine procedure but may behelpful when colonoscopy is difficult, for example inobstructivetumours.Itmayalsobehelpfulforsurgeonstoaccuratelylocatethetumourbeforeanoperation.
− Double contrast barium enema. During thisexamination, barium sulphate (a chalky liquidcommonly used in radiological examinations) and airareintroducedintothecolonviatheanus.Bothbariumand air will be visible on X-ray* film and this willvisualizeanoutlineoftheinteriorwallofthecolonandrectum.Thisexaminationisusedonlyoccasionally,typicallywhentheright-sidedpartofthecolon is difficult to reach with the colonoscope*, but today it is usually replaced by a CTcolonography*.
− Forthecolonoscopyandvirtualcolonoscopyadequatepreparationofthebowelisneeded.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page11ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
4. Laboratoryinvestigations
- Routine blood tests are performed and include complete blood count, liver function andkidneyfunctiontests.
- Tumourmarkersarefactorsthatareproducedbytumoursandthatcanbemeasuredusing ablood test. Togetherwith results from the routineinvestigations, tumour markers may help to diagnose a recurrence* ofcancerafter initialtreatmentatanearlystageortofollowtheevolutionofcancerduringoraftertherapy.Agreatdealofresearcheffortisbeingspent in search of tumour markers for colorectal cancer. Except forcarcinoembryonic antigen (CEA, see below), which may be useful inselectedsituations,sofarnosuchtestisavailable.
- Carcinoembryonicantigen*(CEA).ColorectalcancercellsmayproducethefactorCEA*andthiscanbemeasuredusingabloodtest.However,notallcolorectalcancersproduceCEA*,andCEA*mayalsobeelevatedinothercancersandinnon-malignantconditions.Therefore,incolorectalcancer,CEA*isnotusefulasascreeningtest.InpatientswithcolorectalcancerwhohaveelevatedCEA*atdiagnosis,however,itmaybeusefulforevaluationofprognosis*andforfollow-upaftertreatment.
5. Histopathologicalexamination*.
Thisisthelaboratoryinvestigationofthetumourtissue.Itisperformedusingamicroscopeon the biopsy* or the polyp obtained via endoscopy*. The histopathological* informationwill confirm the diagnosis of colorectal cancer and reveals specific characteristics of thetumour.
If surgery is done, a histopathological examination* isperformed not only on the tumour tissue itself, but also onlymphnodes* that are routinely removed, andonorgans thathave been invaded by tumour and resected during surgery. Itmay also be necessary to perform a histopathologicalexamination* on metastases*. Histopathology* is part of adiagnostic process called staging*. Staging* means that thedoctor defines the extent towhich the colorectal tumour hasinvadedotherorgansorhascausedmetastases*.Staging*allows thedoctors todirect theoptimaltreatment.
The chapter ‘What is important to know to define the optimal treatment’ explains howhistopathological*informationisusedtodirecttreatment.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page12ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
SCREENINGFORCOLORECTALCANCERManycountriesoffera systematic screeningprogramto individualsover50yearsofage todetectcolorectalpolyps*andtodetectcolorectalcanceratanearlystage.Thereasonsforthisarefirstly,thatearlycolorectalcanceroftenproducesvagueornosymptoms,secondly, thatpolyps*arewelldeterminedprecancerouslesions*,andthird,thatagingisanimportantriskfactor*.ThescreeningprogramusuallyincludesaFaecalOccultBloodTest(FOBT)*,andacolonoscopy*forconfirmation. The FOBT* is used by doctors to examine the patient’s stool for traces of blood: acolorectaltumourmayshedsmallamountsofbloodthatmaynotbevisibletothenakedeye.Duringacolonoscopy,afinelightedtubewithacamerais insertedthroughtheanusintothelargeintestine: this allows the doctor to inspect the interior of the colon and rectum, and to detectpolyps*orothercolorectaltumours.InEurope,screeningisrecommendedtomenandwomenaged50orolder,withanintervalof1to2years, until the approximate age of 74 years. The screening programme considers a FOBT* and acolonoscopy*forindividualswhohaveapositiveFOBT*.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page13ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
WHATISIMPORTANTTOKNOWTOGETTHEOPTIMALTREATMENT?Doctorswillneedtoconsidermanyaspectsofboththepatientandthecancerinordertodecideonthebesttreatment.Relevantinformationaboutthepatient
• Gender• Age• Personalmedicalhistory,previousillnessesandtreatments• Familyhistoryofcolorectalcancer,colorectalpolyps*andotherforms
ofcancer• Generalwellbeingandgeneralperformancestatus• Specificphysicalcomplaints• Resultsoftheclinicalexamination• Resultsoflaboratorytestsonbloodcounts,kidneyandliverfunction,CEA*• Resultsofendoscopicandradiologicalinvestigations
Relevantinformationaboutthecancer
• Staging*
Whendoctorsdeterminethestageofthecancer,theyusedifferentmethodstoassesstheextenttowhichthecancerhasspreadlocallyandatadistanceinthebody.Thisprocessiscalledstaging*.The stage is fundamental inorder tomake the rightdecision about the treatment. The stage alsodeterminestheprognosis*ofthepatient:thelowerthestage,thebettertheprognosis*.Staging*isusuallyperformedtwice.Afterclinicalandradiologicalexaminationthedoctorsestimatethe stage of the cancer. If surgery is performed, staging* is influenced by the histopathologicalexamination* of the removed tumour, lymph nodes* and/or other organs that may have to besurgically removed. This process is called surgical staging*. The histopathological examination*shouldincludeexaminationofalltheresectionmarginsofthesurgicalspecimen,todetermineifthetumourhasspreadbeyondtheresectedtissue.Atleast12lymphnodes*shouldberemovedtoallowaccurate staging*. Also, the histopathological examination* should verifywhether the tumour hasinvadedbloodvesselsornerves.The TNM staging* system is commonly used. The combination size of the tumour and invasionofnearbytissue(T),involvementoflymphnodes*(N),andmetastasis*orspreadofthecancertootherorganof thebody (M),will classify thecancerasbeingatoneof thestagesexplained in the tablebelow. The definitions are somewhat technical and refer to the anatomy of the intestine and theabdominalcavity.Itisrecommendedtoaskdoctorsformoredetailedexplanations.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page14ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Stage Definition Category
Stage0 Carcinomainsitu:amalignanttumourthatisconfinedtothemucosa*,andthatdoesnotinvadethesubmucosa*
Localizedcolorectalcancer
StageI Thetumourinvadesthesubmucosa*orthemuscularispropria*StageIIA Thetumourinvadesthroughthemuscularispropria*intothesubserosa*or
intoneighboringtissuesintheintraperitonealspace*StageIIB The tumour penetrates the visceral peritoneum* and/or directly invades
organsorstructuresintheintraperitonealspace*StageIII Thetumourhasproducedmetastasis*inregionallymphnodes*.StageIIIis
divided into 3 different stages depending on the invasion of the localtumourandthenumberoflymphnodes*withmetastases*a• StageIIIA:Thetumourinvadesthesubmucosa*ormuscularispropria*
andhasspreadto1-3regionallymphnodes*• Stage IIIB: The tumour invades the subserosa*, visceralperitoneum*
orneighboringorgans,andhasspreadto1-3regionallymphnodes*• StageIIIC:Thetumour,irrespectiveofthedegreeoflocalinvasion,has
spreadto4ormoreregionallymphnodes*StageIV Thetumourhasspreadtodistantorgans,irrespectiveofthedegreeoflocal
invasionand/orspreadtoregionallymphnodes*Advancedcolorectalcancer
aduringsurgicalstaging*,atleast12lymphnodes*shouldberemovedtoaccuratelydeterminethenumberoflymphnodes*involved.
• RadiologicalinvestigationsRadiological investigationsmayhelptodeterminethelocalspreadofthetumourandthepresenceofmetastases*.Thesemayinclude:
− Computed tomography (CT)* of chest and abdomen areroutinelyperformedpreoperativelytodetectmetastaticspreadofthetumour.
− Intra-operative ultrasound* of the liver may help indetermining the presence of liver metastases* and indeterminingwhethertheyaresuitableforresection.
− Nuclear magnetic resonance imaging* (MRI) is useful toaccuratelyvisualize theextentof tumourspread,and todetectorconfirmthepresenceofmetastases*.MRI*oftherectumisaroutinestaging*procedureinrectalcancer.
− Endoscopicultrasound*canbeusedasanalternativeforMRI*inearlystagerectalcancertodeterminetheextensionofthetumour.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page15ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
− Positronemissiontomography*(PET) isnotperformedasaroutine investigation,butmaybeuseful to visualizemetastases*.PET* canhelp todeterminewhether adistant lesion ismalignantinnature,particularlyifitisusedincombinationwithcomputedtomography(CT).PET* also helps to accurately visualize livermetastases* thatmay be suitable for surgicalresection. PET* may also be useful to help visualize residual or recurring* tumours afterradiotherapy*and/orsurgery.
• Histopathologicalexamination*
Duringcolonoscopy,abiopsy*istakenfromsuspiciousareas,and–ifpossible–polyps*areentirelyremoved.Thesetissuesareexaminedinthe laboratory.Thisexaminationiscalledhistopathology*.Whensurgeryisindicated,asecondhistopathologicalexamination*involvestheexaminationofthetumourtissueandthelymphnodes*aftersurgicalremoval.Thisisveryimportanttoconfirmthefirsthistopathology*resultsandtoprovidemoreinformationonthecancer.Resultsofthehistopathologicalexamination*shouldinclude:
o HistologicaltypeofthelesionThehistologicaltypereferstothetypeofcellsthatcomposethelesion.Mostofthecolorectal cancers are adenocarcinomas* or subtypes of adenocarcinomas*(mucinousor signet-ring).Other rare typesof colorectal cancers include squamouscell carcinomas*, adenosquamous carcinomas*, undifferentiated carcinomas, andmedullarycarcinomas.Neuroendocrinecarcinomas*arecancersthatdevelopfromneuroendocrinecellsofthe colon or rectum. These cancers exhibit different behavior, making theirtreatment different. The information in this guide does not apply to this form ofcolorectalcancer.
o GradeThegradeisdeterminedonthebasisofhowdifferentthetumourcellslookfromthecellsnormallyfoundinthehealthycolorectal lining.Theabnormalfeaturesindicatetherateatwhichthecellsmultiplyandthedegreetowhichtheyareinvasive.In colorectal cancer, four grades are distinguished. In grade 1, the tumour tissuecloselyresemblesnormalcolorectaltissue,whereasingrade4,thetumourcellslookvery abnormal. Grades 2 and 3 are intermediate grades. The grade of colorectalcancerisoftenreferredtomoregenerally,as lowgrade(grade1-2)andhighgrade(grade3-4). Signet-ring cell carcinomas, small cell carcinomas,andundifferentiatedcarcinomasarealwaysclassifiedashighgrade.
o Levelofinvasioninmalignantcolorectalpolyps*Colorectalcancerusuallydevelopsfromabenigncolorectalpolyp.Whenacolorectalpolyp is removed and examined for the presence of invasive carcinoma, thepathologist*willspecificallylookforfeaturesthatmaypredicttheaggressivenessofthecancer.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page16ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Severalsystemshavebeenproposedtostagetheseso-called‘malignantpolyps*’todirect treatment. One of these is the ‘level of invasion’, referring to how far thecarcinomahasinvadedthestructureofthepolyp.Inpedunculatedpolyps*(polyps*attachedtothebowelliningbyanarrowelongatedstalk)fourlevelsofinvasionhavebeen defined. In sessile polyps* (polyps* that do not have a stalk) three levels ofinvasionhavebeendefined.Other histological findings that predict an aggressive outcome are the presence ofcancer cells in theexcisionmarginsof the resectedpolyp, invasionof thebloodorlymphaticvessels*bycancercells,andahighgradelesion.
• MolecularprofilingCancer develops when genes responsible for regulating cell growth and differentiation arealtered. Such gene alterations include for example a change in the DNA sequence of a gene(called a mutation*), a change in the number, or breakage, of chromosomes* (calledchromosomal instability*) and a change in the lengthof specific repeat sequences in theDNA(calledmicrosatelliteinstability*).Molecular profiling is a technique that reveals the entire set of genes expressed in a cell or atissue. This technique is increasingly being used to determine the profile of genes and genealterations expressed in cancers. By comparing these so-called molecular profiles amongstcancers,andbyrelatingthemtoclinicalinformation,ithelpsdoctorstounderstandtheoriginofthe cancer, its potential tometastasize, its responsiveness to treatment, and the likelihoodofrecurrence.Forcoloncancer,anumberofgenealternationshavebeendescribed,suchasRASmutations*,BRAFmutation*,MLH1mutation*,chromosomalinstability*andmicrosatelliteinstability*.Thepresenceorabsenceofthesemolecularprofileshelpstoclassifycolorectaltumoursandhelpstodetermine the optimal treatment. This is particularly true for RASmutations* (either KRAS orNRAS)whichwilldeterminewhethertwospecificdrugsmightbeeffectiveornot.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page17ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
WHATARETHETREATMENTOPTIONS?Planning of the treatment involves an interdisciplinary team* of medicalprofessionals. This usually implies a meeting of different specialists, calledmultidisciplinary opinion* or tumour board review*. In this meeting, theplanningoftreatmentwillbediscussedaccordingtotherelevantinformationmentionedbefore.Thetreatmentwillusuallycombinetherapiesthat:
• Actonthecancerlocally,suchassurgeryorradiotherapy*• Act on the cancer cells systemically (all over the body) such as
chemotherapy*andbiologicaltargetedtherapy*Theextentof the treatmentwill dependon the stageof the cancer,on thecharacteristicsofthetumourandontherisksforthepatient.Below, the general principlesof treatment in colorectal cancer are listed first. Colorectal cancer isusually foundwithinapolyp; thetreatmentofso-calledmalignantpolyps* isdescribedseparately.Thisisfollowedbyadescriptionofthetreatmentplansperstage.Coloncancerandrectalcanceraredescribedseparately.All treatmentshave theirbenefits, their risksand their contraindications*. It is recommended thatpatientsask theirdoctorsabout theexpectedbenefitsand risksofevery treatment inorder tobeinformed about the consequences of the treatment. For some patients, several possibilities areavailableandthechoiceshouldbediscussedaccordingtothebalancebetweenbenefitsandrisks.PRINCIPLESOFTREATMENT
SurgerySurgeryaimstoremovetheprimarytumour. Inpatientswithadvanceddisease,surgerymayalsobeperformedtoremovemetastaticlesions.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page18ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Theextentofsurgeryontheprimarytumourwilldependonthelocalspread of the tumour. In a simple excision, the tumour is removedlocallyfromsuperficialinnerlayerofthebowelwall.Whenthecancerdevelopsfromapolyp,theentirepolypisremoved,aprocedurecalledpolypectomy*. In a segmental resection, the bowel segment wherethe tumour is located is surgically removed and the bowel ends arereconnected.Standardized resections are now considered more appropriate thansegmentalresections inthetreatmentofcoloncancer.Dependingonthe location of the tumour, such standardized resection consists of removing either theascendingcolon(righthemicolectomy*)or thedescendingcolon(lefthemicolectomy)or thesigmoidcolon(sigmoidresection).Rightandlefthemicolectomy*aresometimesextendedtothe transverse colon and are then called extended (right or left) hemicolectomy*. Thecorrespondingsegmentofthebowelisremovedaswellastheregionallymphnodes*andanypartoftheadjacentorgansthatareinvadedbythetumour.Itisnecessarytoremoveatleast12regionallymphnodes*toperformaccuratestaging*.Thesurgeonwillalsoneedtotakethestructureofthebloodsupplyintoaccountandthemarginsmaythereforebewider.Wheninthe case of rectal cancer the entire rectum, along with the mesorectum* containing theregionallymphnode*isremoved,theprocedureiscalledtotalmesorectalexcision(TME).Usually, the healthy ends of the bowel are surgically reconnected during the initial operation(calledanastomosis*).Whenatotalmesorectalexcisionisperformedforrectalcancer,acolo-analanastomosis* is performed. However, in selected patients, the surgeon needs to create atemporaryconnectionbetweenthesmallorlargebowelandthewalloftheabdomen,calledanileostoma or colostoma, respectively (the procedure is called ileostomy and colostomy,respectively, see below). The stoma is usually temporary, but in some patients it may bepermanent,especiallyinpatientsoperatedonbecauseofacancerinthelowerpartoftherectum.Forrectalcancer,localexcisioncanbeperformedusingamagnifyingscopethatisinsertedviathe anus into the rectum. This procedure is called transanal endoscopicmicrosurgery*andrequires specific expertise. For colon tumours, simple excision and polypectomy* can beperformedusingacolonoscope*.Surgical resections can be performed by laparotomy, but also by laparoscopy. Laparotomyrefers toopen surgery,meaning that the surgeonmakesa large incision in theabdomen toperform the operation. During laparoscopy, fine lighted tubes and instruments are insertedthrough 3 or 4 small incisions in the abdomen. After laparoscopy, patients experience aquickerandeasierrecoverythenafterlaparotomy.Whenthecancerhascausedobstructionofthebowel,itmaybenecessaryforthesurgeontorelieve the obstruction and let the bowel heal by inserting a stent, or by performing acolostomy.Astentisatubethatisplacedinthebowelatthelevelofthetumourtoopenthenatural passage.When a colostomy is performed, the healthy bowel above the level of thetumour is connecteddirectly to the skinof theabdomenand the lowerendof thebowel isclosed; stoolcannow leave thebody throughthisnewpathand iscollected inaplasticbagattached to the skin. This new opening is called a stoma. Usually, the stoma is temporary,meaning that -when the tumour is resectedand thebowelhashad timetoheal -a secondoperation is performed to join the two ends of the bowel together (anastomosis*), and toclose the stoma. The stomamay be permanent in some patients (e.g. those with very lowpositionoftumourintherectum).

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page19ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Chemotherapy*
Chemotherapy* aims to kill or harm the tumour cells.Chemotherapy* is given orally or through a vein, and thereforeacts systemically. Themainstay of chemotherapy* for colorectalcancer is treatment with drugs called fluoropyrimidines*, giveneither as single therapy (calledmonotherapy), or in combinationwithotherdrugs(calledcombinationtherapy).The fluoropyrimidines* that are used are 5-fluorouracil* (5-FU),given intravenously*,andcapecitabine*ortegafur-uracil* (UFT),givenorally. Fluoropyrimidines* are usually given in combination withleucovorin*(LV),alsoknownas folinicacid*,adrugthatenhancestheefficiencyofthefluoropyrimidine*.Commonly,5-FU*isgivenwithLV*,abbreviated5-FU/LV.In combination chemotherapy*, fluoropyrimidines* are combinedwithotherchemotherapeuticdrugssuchasoxaliplatin*oririnotecan*.Biologicaltargetedtherapy*Biological targeted therapy* refers to the therapeuticuseof substances that are specificallydesignedtointerferewiththegrowthofcells.Bevacizumab* is amonoclonalantibody* thatbinds tovascular*endothelial growth factor*(VEGF), a growth factor for blood vessels. Colorectal cancer cells produce high amounts ofVEGF*,whichstimulatestheformationofnewbloodvessels inandaroundthetumour(thatfeed the tumour). Blocking VEGF* using bevacizumab* therefore may prevent this fromoccurring.Cetuximab* and panitumumab* are monoclonal antibodies* which act against epidermalgrowthfactorreceptor(EGFR*),astructureonthesurfaceofallnormalcellsthathelpsthemgrow.ColorectalcellscarryhighamountsofEGFR*ontheirsurface,andbindingofcetuximab*orpanitumumab*toEGFR*interfereswiththegrowthoftumourcellsandcausesthemtodie.Aflibercept* is a recombinant fusion protein that binds to circulating VEGF* and inhibitsactivity of different molecules belonging to VEGF* family. It inhibits the growth of bloodvesselsinthetumour.Regorafenib*isanoraltargetedtherapy*,amulti-kinaseinhibitor.Ittargetsreceptortyrosinekinases,highaffinitycellsurfacereceptorsthatarekeyregulatorsofnormalprocessesinthecell,butalsohaveacriticalroleindevelopmentandprogressionoftumours.Radiotherapy*Radiotherapy* aims to kill tumour cells through ionizing irradiation.Radiotherapy*isusedeitheraloneorincombinationwithchemotherapy*(chemoradiotherapy*),priortosurgeryinselectedstagesofrectalcancer.Surgery is usually performed 6-8 weeks after termination ofchemoradiotherapy*.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page20ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
In rectal cancer, radiotherapy* or chemoradiotherapy* is recommended to be givenpreoperatively whenever possible. Postoperative radiotherapy* or chemoradiotherapy* isreservedforselectedpatientswithrectalcancerwhohaveahighriskofrecurrence*andwhohadnotreceivedradiotherapy*preoperatively.In experienced centers, brachytherapy* or special contact techniques* can be used as analternativetolocalsurgery(withorwithoutadjuvantchemoradiotherapy*)forselectedformsofrectalcancer.
TREATMENTOFMALIGNANTPOLYPS*When a carcinoma is found in a colon or rectal polyp, it is known as a malignant polyp*. Thetreatmentofthislesiondependsontheextenttowhichthecarcinomahasinvadedthepolypitselforbeyond the polyp into the bowelwall, andwhether unfavourable histological features are present(see:Histopathologicalexamination*).
Malignantpolyps*inthecolon
Ifthecarcinomainthepolypshowsnoinvasionoralow/intermediatelevelofinvasion(level1-3inpedunculatedpolyps,level1-2insessilepolyps),apolypectomy*issufficient.Ifahighlevelofinvasion (level 4 in pedunculated polyps, level 2-3 in sessile polyps) or unfavorable histologicalfeaturesarepresent,asegmentalorstandardizedsurgicalresection,asdescribedintheprevioussection(andthereforeincludinglymphnodes*),isindicated.Malignantpolyps*intherectum
Ifthecarcinomainthepolyp*showsnoinvasionoralow/intermediatelevelofinvasion(level1-3in pedunculated polyps*, level 1-2 in sessile polyps*), a local excision procedure using thetransanalendoscopicmicrosurgery*techniqueissufficient.If the carcinoma in the resectedpolyp* showsahigh levelof invasion (level4 inpedunculatedpolyps*, level 2-3 in sessilepolyps*)orunfavorablehistological features, it is recommended toperformamoreextensivesurgicalresection,calledtotalmesorectalexcision(TME),inwhichtheentire rectum is removed as well as the regional lymph nodes* that are located in themesorectum*. In patients who are not fit for a more extensive surgical intervention,postoperativechemoradiotherapy*isrecommended.
If the invasive carcinoma is diagnosed on a biopsy* of the polyp* and if a local treatment isenvisagedusingthetransanalendoscopicmicrosurgery*approach,chemoradiotherapy*shouldbegivenpreoperatively.
In selected patients, doctors may consider to give local radiotherapy* (also calledbrachytherapy*) or local contact therapies* as an alternative to local surgery either with orwithoutchemoradiotherapy*.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page21ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
TREATMENTPLANSACCORDINGTODISEASESTAGETreatmentplanforStage0Atthisstage,thecancerisconfinedtothemucosa*anddoesnotinvadethesubmucosa*.Sincethetumourisconfinedtothemostsuperficiallayerofthebowelwall,themaingoalofthetreatmentistoremovethelocaltumourbysurgery,andadditionaltreatmentisnotneeded.A clinical stage is attributed to the cancer before surgery based on the clinical and radiologicalexaminations. Actually, the definitive stage is only known after examination of the tumour tissueresectedduringsurgery.Therefore,thetreatmentplanmaybemodifiedaftersurgery.
Thecolonorrectaltumourisremovedbysimplesurgicalexcision.Largerlesionsinthecolonaremoredifficult toexcise,and in thesecases, thebowelsegmentcontainingthetumour isremoved(calledsegmentalresection),followedbyanastomosis*.Forrectalcancerthedoctorwillusethetransanalendoscopicmicrosurgerytechnique*.
TreatmentplanforStageIAtthisstage,thecancerhasgrownintothesubmucosa*andmayhavegrownintothemusclelayerofthebowel.Sincethetumourhasgrowndeeperintothebowelwall,thetreatmentrequiresawidersurgicalresectionofboweltissue,aswellasresectionoftheregionallymphnodes*.However,sincethetumourisstillconsideredtobelocal,nofurthertreatmentisnecessary.A clinical stage is attributed to the cancer before surgery based on the clinical and radiologicalexaminations. The definitive stage is only known after examination of the tumour tissue resectedduringsurgery.Therefore,thetreatmentplanmaybemodifiedaftersurgery.
Forcoloncancerthedoctorperformsasurgicalresectionofthebowel,therebyremovingthesegmentofthecolonwherethecancerislocalized,aswellastheregionallymphnodes*.Forrectalcancertheprocedure isatotalmesorectalexcision,duringwhichtheentirerectumisremoved,aswellaswellastheregionallymphnodes*locatedinthemesorectum*.
TreatmentplanforStageIIAtthisstagethecancerhasgrownbeyondthemusclelayerofthebowelandmayhaveinvadedtheorgans surrounding the colonor rectum. Theprimary treatment consists of surgery,whichaims toremovethetumourandtheadjacentorgansinvadedbythetumour.However,forselectedpatients,additional treatment couldbe recommendedsince itdecreases the risk that the tumourmaycomeback.Forcoloncancerthisconsistsofchemotherapy*,forrectalcancerthisconsistsofradiotherapy*orchemoradiotherapy*.A clinical stage is attributed to the cancer before surgery based on the clinical and radiologicalexaminations. The definitive stage is only known after examination of the tumour tissue resectedduringsurgery.Therefore,thetreatmentplanmaybemodifiedaftersurgery.
ColonCancer
Thedoctorperformsasurgicalresectionofthebowel,therebyremovingthesegmentofthebowelwherethecancerislocalized,theregionallymphnodes*,aswellastheadjacentorgansthatareinvadedbythetumour.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page22ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Forpatientspresentinghigh-riskdisease,adjuvantchemotherapy*isrecommended.Itisgiveninaddition to primary, initial surgical treatment to prevent that tumour occurs again. In general,patientswithstageIIBareconsideredtobeathighrisk,aswellaspatientspresentingatleastoneof the following features: the tumour causes obstruction, the tumour penetrates the visceralperitoneum*and/orinvadesadjacentorgans,thesurgeoncouldnotremovesufficient(minimum12) regional lymph nodes* to determine lymph node* involvement, the tumour is poorlydifferentiated,orthetumourinvadesvascular*,lymphatic*orperineural*tissues*.
Chemotherapy*consistsofoxaliplatin*and5FU/LV,givenintravenously*.Thiscombinationisknown asFOLFOX. This can also be replacedby the combination of oral capecitabine*withintravenous*oxaliplatin*.Alternatively,aregimenwith5FU/LVbythe intravenous*routeorwithcapecitabine*bymouthcanbeconsidered.Chemotherapy*isgivenfor6months.In patients older than 70, one should be cautious in advising combination chemotherapy*drugssuchaswithoxaliplatin*.
Participation in clinical trials is encouraged so as to help develop the optimal treatment forpatientsinthiscategory.RectalCancer
In rectal cancer, anMRI* of the pelvis is fundamental to determine the local spread of thetumour before initiating treatment. In some selected cases, no pre-operative treatment isrequired since surgery alone is sufficient. For all other cases, it is recommended to giveradiotherapy*orchemoradiotherapy*beforesurgery.Therecommendedregimendependsonthe local spread of the tumour. If the tumour can be entirely removed by totalmesorectalexcisionandthetumourhasspreadonlytoorgansthatcanbereadilyresected,pre-operativeradiotherapy*orchemoradiotherapy*isindicated.Ifatotalmesorectalexcisiondoesnotallowremovingthetumourcompletely,and/or if thetumourhasspreadtoorgansthatcannotberesected,chemoradiotherapy*shouldbegiven.Theradiotherapy*regimenconsistsof25Gray*,givenin5fractionsof5Gray*,over1week,followedimmediatelybysurgery.Thechemoradiotherapy*regimenconsistsofradiotherapy*with46 -50.4Gray*given in fractionsof1.8 to2Gray*, togetherwithchemotherapy*with5FU*(intravenously*orbymouth),orcapecitabine*orUFT*(bymouth),followedbysurgery6-8 weeks later. In patients older than 80 or patients unfit for chemoradiotherapy*, theradiotherapy*regimenwith5fractionsof5Gray*maybeconsideredandsurgeryshouldbedelayedfor6-8weeksaftertheendoftheradiotherapy*.
Duringsurgery,thedoctorperformsatotalmesorectalexcision,therebyremovingtheentirerectum,theregionallymphnodes*locatedinthemesorectum*.Thesurgeonalsoremovestheadjacentorgansthatareinvadedbythetumour,ifthatispossible.
TreatmentplanforStageIIIAtthisstage, thecancerhasmetastasized*toregional lymphnodes*.Theprimary tumourmaybelimitedtothebowelormayhaveinvadedtheadjacentorgans.Sincethecancerhasspreadbeyondthebowel,thetreatmentnotonlyconsistsofsurgerytoremovealltumourtissuebutalsoofadjuvanttherapysinceitdecreasestheriskthatthetumourmaycomeback.Forcoloncancerthisconsistsofchemotherapy*,forrectalcanceritconsistsofradiotherapy*orchemoradiotherapy*.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page23ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
A clinical stage is attributed to the cancer before surgery based on the clinical and radiologicalexaminations. Actually, the definitive stage is only known after examination of the tumour tissueresectedduringsurgery.Therefore,thetreatmentplanmaybemodifiedaftersurgery.
ColonCancer
Thedoctorperformsasurgicalresection,therebyremovingthesegmentofthebowelwherethe cancer is localized, the regional lymph nodes*, as well as the adjacent organs that areinvadedbythetumour.The standard adjuvant chemotherapy* consists of oxaliplatin* and 5FU/LV, givenintravenously*. This combination is known as FOLFOX. A combination of capectabine andoxaliplatin* (a combination known as CAPOX) can also be proposed.Oxaliplatin* in somepatients iscontraindicated*: inthesecases, thestandardregimen is therapywith5FU/LVbytheintravenous*infusionorcapecitabine*bymouth.Chemotherapy*isgivenfor6months.
RectalCancer
In rectal cancer, anMRI* of the pelvis is fundamental to determine the local spread of thetumour before initiating treatment. Unfortunately, neither MRI* nor any other radiologicalexamcanaccuratelytellifthecancerhasspreadtoregionallymphnodes*.Inmostcases,itisrecommended to give radiotherapy* or chemoradiotherapy* before surgery. Therecommendedregimendependsonthelocalspreadofthetumour.Ifthetumourcanbeentirelyremovedbytotalmesorectalexcisionandthetumourhasspreadonly to organs that can be readily resected, pre-operative radiotherapy* orchemoradiotherapy*isindicated.
If a totalmesorectalexcisiondoesnotallow for complete removalof the tumour,and/or ifthe tumour has spread to organs that cannot be resected, chemoradiotherapy* should begiven.Theradiotherapy*regimenconsistsof25Gray*,givenin5fractionsof5Gray*,over1week,followedimmediatelybysurgery.Thechemoradiotherapy*regimenconsistsofradiotherapy*with46 -50.4Gray*given in fractionsof1.8 to2Gray*, togetherwithchemotherapy*with5FU* (intravenously* or orally), or capecitabine* or UFT* (orally), followed by surgery 6-8weeks later. In patients older than 80 or patients unfit for chemoradiotherapy*, theradiotherapy*regimenwith5fractionsof5Gray*maybeconsideredandsurgeryshouldbedelayedfor6-8weeksaftertheendoftheradiotherapy*.
Duringsurgery,thedoctorperformsatotalmesorectalexcision,therebyremovingtheentirerectumandtheregionallymphnodes*locatedinthemesorectum*.Thesurgeonalsoremovestheadjacentorgansthatareinvadedbythetumour,ifpossible.
Treatmentplanformetastaticcolorectalcancer:StageIVAtthisstage,thetumourhasspreadsignificantlyandcausedmetastasis* indistantorganssuchastheliverandlungs.Thetreatmentthereforenotonlyaimstoremovethetumourbysurgery,butalsototargetthetumourcellssystemicallywithchemotherapy*,orwithacombinationofchemotherapy*andbiologicaltargetedtherapy*.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page24ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Metastatic disease should be confirmed by adequate radiological investigations. Usually it isnecessarytoobtainhistopathological*confirmationofmetastases*beforechemotherapy*isstarted.The treatment plan should be individually optimized for each patient. It is determined by amultidisciplinary team* and should take several factors into account. Most patients presentunresectable metastases*. However, careful staging* allows doctors to identify metastases* thatmay become suitable for surgical removal when their volume is reduced by chemotherapy*. It isthereforecritical todeterminewhether thepatienthas resectabledisease,unresectabledisease,ordisease that is unresectable but may become amenable to resection after chemotherapy*.Furthermore, thepatient’sgeneral condition, thepatient’sorgan function, thepresenceofpossibleother illnessesandthepatient’spreferencealsodirectthedecision-makingindesigningtheoptimalindividualtreatment.
The principles of treatment are discussed below. Chemotherapy* and biological targeted therapy*arediscussedaccordingtowhetherornotthemetastases*areresectable.Surgeryincludesresectionoftheprimarytumour,butmayalsoincludeoperativeremovalofmetastases*.
Duringtreatment,follow-upisrecommendedinordertoevaluatetheresponsetochemotherapy*.Apossibleregimenrecommendsa2-to3-monthevaluationofhistory,generalcondition,sideeffectsofchemotherapy*, impact of chemotherapy* on quality of life, physical examination, laboratoryinvestigationoftheCEA*level(ifitwasinitiallyelevated),andCT*oftheinvolvedregions.
Treatmentoptions
Themain therapies used at this stage of the disease are briefly introduced in this section.Reading this section will help understanding the next section which describes the besttreatment strategy depending on the characteristics of the disease and the general healthstatusofthepatient.Surgery
SurgeryonprimarytumourThedoctorperformsasurgicalresection,therebyremovingthesegmentofthebowelwherethe cancer is localised, the regional lymph nodes*, as well as the adjacent organs that areinvadedbythetumour.Resectionofmetastases*The most frequent location of metastases* of colorectal cancer is in the liver. Surgicalresectionshouldbeconsideredforsolitaryorconfinedlivermetastases*,sinceitoffersthesepatients the best chance of long-term survival even if, in about 3 out of 4 patients, livermetastases* can come back after resection. Radiofrequency ablation*, in combination withsystemic treatment, is under investigation as an alternative, or a complement, to surgicalresectionoflivermetastases*incaseswherethisisnotpossibleorcomplete.Selectedmetastases* in the lungscanalsobe surgically removed.Thismaybeusefulonly iftherearenootherpoorprognosticsigns.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page25ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Ingeneral, resectionofmetastases*maybesuccessfulon thecondition that the locationofthemetastasis*doesnotcreateanoperativerisk,andontheconditionthatresectionwouldleavesufficientfunctionaltissue(forexampleatleast30%ofthelivertissue).Hencemultipleresections may be performed. Some metastases* may become resectable if they aredownsized during chemotherapy*; such patients should receive specific chemotherapeuticregimens(seeabove).
Chemotherapy*andbiologicaltargetedtherapy*ThelistofdrugsapprovedinthetreatmentofstageIVcolorectalcancerhasgrowngraduallyduringthepast10years.Inaddition,clinicaltrialshavebroughtuseful informationregardingseveralcombinationofdrugsandtheirrespectiveefficacy.Themaindrugsandcombinationsavailablearepresentedbelow.Individualchemotherapy*drugs
• 5-fluorouracil(abbreviated5-FU)*o 5-FU* is always used in combination with leucovorin (abbreviated LV)*.
Leucovorin* is reduced folinic acid*and increases theefficacyof5-FU*. Thecombinationofthetwoisabbreviated5-FU/LVorFOLF.
o 5-FU* is given in the veins and is either administered as a shot in a shortperiod of time (<60 min) or infused slowly over 24 hours. Slow infusionsshouldbepreferredastheyarebettertolerated.
• Capecitabine(abbreviatedCAP)*o Capecitabine*istransformedinto5-FU*inthebody.o Capecitabine*isgivenorally.
• Oxaliplatin(abbreviatedOX)*o Oxaliplatin*isusuallygivenincombinationwithotherdrugsinthetreatment
ofcolorectalcancer.o Oxaliplatin*isinfusedintoaveinusuallyover2hours.
• Irinotecan(abbreviatedIRI)*o Irinotecan*israrelygivenaloneinthetreatmentofcolorectalcancer.o Irinotecan*isinfusedintoaveinusuallyover90minutes.
Chemotherapy*combinationsforthetreatmentofcolorectalcancer
• FOLFOXisthecombinationof5-FU*,LV*andoxaliplatin*.• FOLFIRIisthecombinationof5FU*,LV*andirinotecan*.• FOLFOXIRIisthecombinationof5-FU*,LV*,oxaliplatin*andirinotecan*.• CAPOXisthecombinationofcapecitabine*andoxaliplatin*.
Biologicaltargetedtherapies*
• Aflibercept*o Aflibercept*isonlygivenincombinationwithFOLFIRIinpatientswhoalready
receivedoxaliplatin*-basedtherapy.o Aflibercept*isinfusedintoaveinusuallyover60minutes.
• Bevacizumab(abbreviatedBEV)*o Bevacizumab*canbegiventogetherwithanyofthechemotherapy*combinations.o Bevacizumab*isinfusedintoaveinusuallyover30to90minutes.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page26ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
• Cetuximab*o Cetuximab*canbegiveneitheraloneorincombinationwithchemotherapy*.o ItsuseislimitedtopatientswhosetumourdoesnotpresentaRASmutation*.
ARASmutation*isdetectedafteranalysisofatumoursampleinthelab.o Cetuximab*isinfusedintoaveinover1to2hours.
• Panitumumab*o Panitumumab* can be given either alone or in combination with
chemotherapy*.o ItsuseislimitedtopatientswhosetumourdoesnotpresentaRASmutation*.
ARASmutation*isdetectedafteranalysisofatumoursampleinthelab.o Panitumumab*isinfusedintoaveinover1hour.
• Regorafenib*o Regorafenib* is given as a single drug. It can be proposed to patients who
alreadyreceivedallothertreatmentoptions.o Regorafenib*isgivenorally.
Radiotherapy*
Radiotherapy* should be considered (possibly combined with chemotherapy*) for patientswithmetastaticrectalcancertoalleviatesymptomsfromtheprimarytumour.Radiotherapy*canalsobeusedtorelievesymptomscausedbymetastases*inthebones.Typesofradiationtherapythatuseradiationfromanexternalsource(radiotherapy*machine)arecalledexternalradiotherapy*.Selectiveinternalradiationtherapyinvolvesinjectingtinymicrospheresorradioactivematerialintoarteriesthatsupplythetumour.Thisradioembolisationcouldbeproposedwhenpatientshave metastases* in the liver only and received all available chemotherapeutic options.Radioembolisation using Yttrium 90 particles aims to embolize aswell as to bring radiationtherapy*veryclosetothetumour.Asmalltubeisplacedinthemainarterygoingtotheliver(hepaticartery), throughwhichmicroscopicballsare released.Theseballs reach the tumourthroughthebloodvesselsof the liverandcontaina radioactivesubstancecalledYttrium90.They block the supply of blood to the tumour, and at the same time emit radiation* thatdestroysthetumourcellssurroundingthem.Sincetheradiation*isdelivereddirectlyintotheblood vessels supplying the tumour, the radiation* is more potent than the usual externalradiationtherapy*.Theradioactivityoftheballsisgoneafter2weeks.
Treatmentstrategyorhowtodecidewhatthebesttreatmentis
Decisionabout thebest treatmenthasbecomecomplexas the listofdrugsapproved in thetreatmentofmetastaticcolorectalcancerhasbecomelonger.Insomecasesdirectcomparisonbetweentreatmentshavebeenperformedanditcanguidedecisions.Whenever possible, resection of the tumour(s) by surgery is recommended. Answering thequestionabout the“possibility”of removing the tumour(s)will actuallyguide the treatmentstrategybygroupingpatientsinseveralgroups.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page27ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
1- Patients for whom removing metastases* is deemed feasible by the multidisciplinaryteam*.Thesepatientshavewhatiscalledresectablemetastastic*disease.
Forpatientswhopresentliverand/orlungmetastases*thatcanbeoperativelyremoved,thetreatmentconsistsofsurgicalresectionofthemetastases*andcombinationchemotherapy*.Chemotherapy* consists of a 6-month regimen of 5-FU/LV with oxaliplatin* (FOLFOX).FOLFOXcanbegiveneitherperioperatively,meaningthatitisgivenfor3monthsbeforeandfor3monthsaftersurgeryor,aftertheoperation,for6months.
2- Patients for whom removingmetastases* is deemed not immediately feasible by the
multidisciplinary team*, but may become feasible if shrinkage of the metastases* isobtained. These patients have what is called unresectable disease that may becomeresectableafterchemotherapy*.
Selectedpatientsmaypresent livermetastases* that initially are unresectable, but that canbecome resectable when they are downsized by chemotherapy*. Such patients are treatedwithstandardcombinationchemotherapy*consistingof5-FU/LVandirinotecan*(FOLFIRI)or5-FU/LV and oxaliplatin* (FOLFOX). The addition of a third chemotherapeutic drug(FOLFOXIRI), or the biologic agents bevacizumab*, cetuximab* or panitimumab* increasesthe toxicity of the treatment but may be considered in selected patients. Cetuximab* andpanitumumab* seems toprovidebetter results thanbevacizumab* in this specific situation,butcannotbegiventopatientswhosetumourpresentsaRASmutation*.The patient is closelymonitored during chemotherapy*. Surgery is indicated as soon as themetastases* are considered to have become resectable.However, this needs to be delayedallowingatleast4weeksafterthelastcycleofcetuximab*,andatleast6weekafterthelastcycle of bevacizumab*, before surgery is undertaken. This delay reduces the risk ofcomplicationsofthesurgery.
3- Patients for whom removing metastases* is deemed never feasible by the
multidisciplinary team*. These patients have what is called disseminated diseasetechnicallyneverorunlikelyresectable.
Dependingonthegeneralhealthconditionofthepatients,amoreorlessintensivetreatmentwillbeproposed.Treatmentwillrelyonchemotherapy*andbiologicaltargetedtherapy*.Doctors are trying to continually improve the treatment forunresectablemetastatic diseaseand the optimal treatment is therefore rapidly evolving. The goal of the treatment and thedifferent options to reach this goal are tailored to the individual patient andmay thus varybetween patients. In case of symptomatic disease, combination therapy is the preferredchoice,andasequentialapproachremainsavalidoptioninselectedandfrailpatients.Severalfirst-linechemotherapeuticregimenscanbeproposed.Ifapatientfailstorespondtofirst-linechemotherapy*,and thegeneral conditionallows, further treatment in the formofsecond-linechemotherapy*shouldbeconsidered.Biological targeted therapy* shouldbeconsidered for selectedpatients.Theoptimal treatmentregimenistailoredtotheindividualpatientandthetypeoffirst-linetherapyreceived.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page28ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Thedurationofthetreatmentcanvarybetweenindividualpatients.Optionsareeitherafixedtreatment period of 3 to 6 months, or treatment until doctors document that the diseaseprogresses.Afteraninitialperiodofcombinationchemotherapy*,maintenancetreatmentcanimprove outcome in comparison to treatment break, and restart of combinationchemotherapy* is recommended if progression occurs. The principle behind amaintenancetreatmentistocontinueusingadrugthathasbeenwelltolerated.Thisusuallyconsistsof5-FUor capecitabine*, in combination with bevacizumab* can be considered. Combinationchemotherapy* may be discontinued or changed to a less intensive regimen if increasingtoxicityoccurs,whenthedisease iscontrolled,orwhenmetastases*havebecomesurgicallyresectable.
First-linechemotherapy*:Possibleregimensare:• Therapywith5-FU/LVgivenintravenously*,ormonotherapywithcapecitabine*given
orally.• Combination therapy of 5-FU/LV plus oxaliplatin* (FOLFOX) or 5-FU/LV plus
irinotecan* (FOLFIRI), given intravenously. This is the preferred treatment. Theseregimensaregivenas48-hourtreatmentinfusionseverytwoweeks.Bothareequallyeffectivebuthavedifferentsideeffects.An alternative regimen, based on a fluoropyrimidine* given orally (namelycapecitabine*), isthecombinationofcapecitabine*plusoxaliplatin*(CAPOX)whichisgiveninthreeweeksregimen.Thecombinationofcapecitabine*plusirinotecan*isless frequently used because of higher toxicity but it seems to be better supportedthanwaspreviouslythought.
• Combinationof3drugs(5-FU*,oxaliplatin*andirinotecan*calledFOLFOXIRI)hasnotbeenextensivelystudiedbutsuggestthat,eventhoughpatientsexperiencemoresideeffects,thiscombinationcouldprolongsurvivalofthepatients.Infrailpatientstheseagentsmay be given sequentially rather than as a combination, in order to reducetoxicity.
Second-linechemotherapy*The choice of second-line chemotherapy* depends on the regimen given as first-linetherapy:
• Ifa therapywith5-FU/LVorcapecitabine*wasadministered in first-line, it canbefollowed by 5-FU/LV plus oxaliplatin* (FOLFOX) or 5-FU/LV plus irinotecan*(FOLFIRI)
• If a combination therapywith5-FU/LVplusoxaliplatin* (FOLFOX)or capecitabine*plus oxaliplatin* (CAPOX) was administered in first-line, it can be followed bycombinationtherapywith5-FU/LVplusirinotecan*(FOLFIRI)
• Ifacombinationtherapywith5-FU/LVplus irinotecan*(FOLFIRI)wasadministeredin first-line, it can be followed by capecitabine* plus oxaliplatin* (CAPOX), or 5-FU/LVplusoxaliplatin*(FOLFOX)
Biologicaltargetedtherapy*Biological targeted therapy* should be considered in combination with selectedchemotherapy*regimens:

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page29ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
• Bevacizumab* should be considered in combinationwith first-line therapywith 5-FU*,capecitabine*,5-FU/LVplusoxaliplatin*(FOLFOX)and5-FU/LVplusirinotecan*(FOLFIRI). It can also be considered in combination with second-line 5-FU/LV plusoxaliplatin* (FOLFOX) or FOLFIRI therapy. Treatment with bevacizumab* can becontinued incombinationwithchemotherapy*untildiseaseprogression,toxicityormetastases*becomeresectable.
• Cetuximab* can be considered in combination with 5-FU/LV plus irinotecan*(FOLFIRI), 5-FU/LV plus oxaliplatin* (FOLFOX) and in combination with irinotecan.Panitumumab* can be considered in combination with 5-FU/LV plus oxaliplatin*(FOLFOX)andwith5-FU/LVplusirinotecan*(FOLFIRI).Molecular profiling of the tumour helps determining the appropriate choice ofcombination therapy. Approximately 50% of metastatic colorectal cancers have ageneticmutation*inRAS*and5-10%havetheBRAFmutation*.Thecombinationofcetuximab*andFOLFIRIistherecommendedtreatmentinmedicallyfitpatientswhohave a tumour without a RASmutation*. Cetuximab* and panitumumab* are notactiveagainstcolorectaltumourswiththeRASmutation*,anditisunclearwhetherthey are active against tumours with the BRAF mutation*. Cetuximab* andpanitumumab* should therefore only be used for tumours that do not have RASmutations*.If first- and second-line therapy has failed, cetuximab* with irinotecan* is thepreferredtreatment,althoughcetuximab*orpanitumumab*monotherapymayalsobeconsidered.
• Aflibercept* is given in combinationwith FOLFIRI in patientswhoalready receivedoxaliplatin-basedtherapy.
• Regorafenib*canbeconsideredafteralltheaboveoptionshavebeenused.Itisanoraldruggivenalone.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page30ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
WHATARETHEPOSSIBLESIDEEFFECTSOFTHETREATMENT?SurgeryGeneralrisksandsideeffects
Somerisksarecommonforeverysurgicalinterventionperformedundergeneralanesthesia*.Thesecomplications are unusual and include deep vein thrombosis*, heart or breathing problems,bleeding, infection or reaction to the anesthesia*. These are maximally prevented by thoroughmedicalevaluationbeforesurgery.
After a surgical intervention on the colon, it is frequent to experience problems of the intestinalmotility.This includescolickypain,diarrhoea,constipationandnausea. Intestinalobstructionisnotan uncommon complication that requires immediatemedical care. Vomiting or loss of any bowelmovement (no stool, no gas) may be signs of intestinal obstruction and should be immediatelyreported.
Rapidoralintakeoffoodaftersurgeryisrecommendedandcanbedonebyusinganasogastrictube*in somepatients.Nutritional advice shouldbe givenbyhealthprofessionals tominimize intestinaldiscomfort.
Thecolonislocatedintheabdomenandextendsthroughouttheentireabdomen.Itislocatedpartlyin the intraperitoneal space*, and partly in the retro- and infraperitoneal space*. The lower twothirdsoftherectumarelocatedintheinfraperitonealspace*.Thecolorectalbowelthereforeliesinclose proximity to several organs, lymph nodes* and major blood vessels. During the surgicalintervention,dependingontheextentoftumourspreadandtheextentofsurgicalresectionsneededtoobtain thebest results, someof these structuresmaybecomedamaged.Accuratepreoperativestaging*andimagingwillhelptominimizesuchrisk.
Colostomy
Ifthecancerhascausedobstructionofthebowel,itmaybenecessaryforthesurgeontorelievetheobstructionandletthebowelhealbyperformingacolostomy.Inthisprocedure,thehealthybowelabovethelevelofthetumourisconnecteddirectlytotheskinoftheabdomen,andthelowerendofthebowelisclosed.Stoolcannowleavethebodythroughthisnewpathandiscollectedinaplasticbag attached to the skin. This new opening is called a stoma. The stoma is usually temporary,meaningthat-whenthetumourisresectedandthebowelhashadtimetoheal-asecondoperationisperformedtosurgicallyjointhetwoendsoftheboweltogether(anastomosis*),andtoclosethestoma.Insomepatientsthestomamaybepermanent.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page31ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Chemotherapy*
Side effects of chemotherapy* are frequent, even if progress has beenmade in controlling themusing adequate supportivemeasures. Theywill dependon thedrug(s) administered, on thedosesandon individual factors. If apatienthas suffered fromothermedicalproblems in thepast, someprecautionsshouldbetakenand/oradaptationofthetreatmentshouldbemade.Listedbelowarethesideeffectsthatareknowntooccurwithoneorseveralofthechemotherapy*drugscurrentlyusedforcolorectalcancer.Thenature,frequencyandseverityofthesideeffectsvaryforeverychemotherapeuticdrugcombinationused.Themostfrequentgeneralsideeffectsofchemotherapy*are:
• Decreasedbloodcell counts,whichmay lead toanaemia*,bleeding,bruising,andinfections
• Fatigue,whichmaybeprolonged• Nauseaorvomiting• Diarrhea• Soremouthormouthulcers*
Listedbelowareothermore specific sideeffects thatmayoccurwith chemotherapeuticsused forcolorectalcancer.Forsomeofthesideeffectsitmaybenecessarytoadjusttreatment.
• Treatmentwith5-Fluorouracil*(5-FU)o Severe side effects may occur in individuals who have the inborn condition
dihydropyrimidine dehydrogenase (DPD) deficiency*: these individuals have low levels oftheenzymedihydropyrimidinedehydrogenaseneededbythebodytobreakdownthisdrug
o Skin sensitivity to sunlight: sun exposure should be avoided for at least one yearfollowingcompletionoftreatment
o Handandfootsyndrome(seebelow)
• Treatmentwithcapecitabine*:o Handandfootsyndrome(alsocalledpalmo-plantarerythema*):theskinofpalmsand
solesshowsreddeningandfeelssore;theskinmaypeel.Thesyndromeisusuallymild.o Dihydropyrimidinedehydrogenase(DPD)deficiency*(seeabove)maycausesevereside
effectso Capecitabine*mayinteractwithothertreatments, increasingtheriskofsideeffectsof
medications. All additionalmedications, especially folic acid*,warfarin* and St John’swort*shouldbedisclosedanddiscussedupfrontwiththedoctor.
• Treatmentwithtegafur-uracil*(UFT)o Skinrasheso Skinsensitivitytosunlight
• Treatmentwithirinotecan*o Sweatingo Wateryeyeso Increasedproductionofsalivao Crampingpainintheabdomeno Diarrhoeastartingthedayaftertreatmento Hairlossorhairthinning
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page32ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
• Treatmentwithoxaliplatin*o Numbnessofthelips,handsorfeeto Tinglingofhandsorfeeto Sensitivitytocoldo Thesespecificsideeffectsmaybepersistentaftertreatmentwithoxaliplatin*.
Biologicaltargetedtherapy*
Listed below are the most frequent side effects of the biologics used in colorectal cancer. Thecombination of biologic therapies with chemotherapy* increases the risk of chemotherapy* sideeffects,particularlywithcetuximab*andpanitumumab*.
• Treatmentwithcetuximab*andpanitumumabo Acneiformrashoccursinmostpatientso Hypomagnesaemiao Allergicreactions,slightlymorefrequentaftercetuximab*thanafterpanitumumab*.
• Treatmentwithbevacizumab*o Hypertension*andproteinuria*areratherfrequento Other rare but severe side effects include arterial thrombosis*, mucosal* bleeding
(mouth,nose,vagina,rectum),gastrointestinalperforation*andproblemswithwoundhealing.
• Treatmentwithaflibercept*o Headacheso Fatigueo Liverproblemswhichwillbemonitoredbylookingatthelevelofliverenzymeso Hypertension*andproteinuria*o Diarrhoeao Decreased blood cell counts, which may lead to anaemia*, bleeding, bruising, and
infectionso Bleeding
• Treatmentwithregorafenib*o Handandfootskinreaction:theskinofpalmsandsolesshowsreddeningandfeelssore,
verycharacteristicallylocalisedtoareasofpressureorfrictionontheskino Skinrasho Fatigueo Liverproblemswhichwillbemonitoredbylookingatthelevelofliverenzymeso Hypertension*andproteinuria*o Diarrhoeao Bleeding

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page33ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
Radiotherapy*
Duringradiotherapy*,sideeffectsmayoccurinorgansthataredirectlytargeted,butalsoinhealthyorgansthatlieclosetotheregionthatneedstobeirradiatedandthatcannotbeavoidedbytheX-rays*. Side effects are more intense when radiotherapy* is administered together withchemotherapy*. Use of radiotherapy* in addition to surgery also increases the risk of surgicalcomplications.Effectsofradiationonthe lowerdigestivetract includerectaldiscomfort,diarrhea,andmucusandbloodrectaldischarge.Effectsofradiationontheurinarytractarerarer.Theyincludepainfulurination,anurgentneedtourinate,presenceofblood in theurine,urinary tractobstruction*,andulceration*ornecrosis*ofthebladderlining.Inwomen,vaginalnarrowingisapossiblelateeffectofpelvicradiotherapy*.Strategies tomaximally prevent and relieve post-radiation reactions are providedby the radiationoncologist*.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page34ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
WHATHAPPENSAFTERTHETREATMENT?Itisnotunusualforcancerpatientstoexperiencetreatment-relatedsymptomsafterthetreatmenthasbeencompleted.
• Patientsmayexperienceanxiety,sleepingdifficultyordepression,andmayneedpsychologicalsupport.
• Duringandaftertreatment,nutritionmaybecomeproblematicduetoreducedappetite,nauseaandgeneralmalaise
• Difficulties inconcentratingandmemory lossarenotuncommonsideeffectsofsystemicchemotherapy*.
Follow-upwithdoctorsAftercompletionoftreatmentthedoctorwillproposeafollow-upaimingto:
• Detectandpreventadverseeffectsofthetreatment• Detectpossiblerecurrence*assoonaspossibleanddirectappropriatetreatment• Provide medical information, psychological support and referral to specialized support
providerstooptimizereturningtonormaldailylife.
The follow-up protocol will include regularly timed office visits and investigations. The protocoldepends on the staging* of the cancer that was treated, and on the type of treatment given. Ingeneral,follow-upvisitsmayincludeacombinationofthefollowinginvestigations:
• Questionsongeneralphysicalhealthandcolorectalcancer-relatedsymptoms• Physicalexamination• Laboratorytestforcarcinoembryonicantigen*(CEA)levelmayhelpindetectingrecurrence*• Colonoscopytodetectrecurrence*• Radiological investigations todetectprogressionor recurrence*of theprimary tumour,or
theappearanceofmetastasis*
Forpatientswhohavehadacolorectalpolypremoved,itisnecessarytofollow-upwithhistoryandcolonoscopy.
Patientstreatedforcolorectalcancershouldbefollowedupintensively.However,thereisnotonegenerallyacceptedfollow-upprotocol.
Thefollowingisapossiblefollow-upprotocolaftertreatmentforlocalisedcoloncancer.
• Historyandphysicalexaminationevery3to6monthsfor3years,andevery6to12monthsinyear4and5.
• Duringthesefollow-upvisits,CEA*couldbedetermined• Colonoscopyat1year,and thereafterevery3 to5years todetectnewcancerousornon-
malignanttumours. It is importanttonotethatwhencoloncancer isdiagnosed,theentirecolon should be visualised prior to surgery, so as to detect other simultaneous colontumours.
• Inpatientswhoareconsideredtobeathighriskofrecurrence*,aCTscan*ofthechestandabdomenevery6to12monthsforthefirst3yearscanbeconsidered
• AbdominalCTscan*canbereplacedbycontrastenhancedultrasound*
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page35ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
• In patients presenting specific symptoms that raise concern for recurring disease,appropriateadditionallaboratoryorradiologicalinvestigationsshouldbeperformed
In patients with rectal cancer, the follow-up protocol is similar to the one for colon cancerdescribedabove.
ReturningtonormallifeReturningtoanormaldailylifemaybedifficultknowingthatthecancermaycomeback.Ifanyoftheknownrisk factors* forcolorectalcancerarepresent, it isadvisedtoeliminatethesetoamaximalextent.
Follow-up visits with the doctor provide an opportunity for the patient to obtain medicalinformation, psychological support and referral to specialized support providers. Additional expertpsychologicaladvicemaybevaluable,andsomepatientsmay findsupport frompatientgroupsorpatient-targeted information media. Dieticians may provide advice on adequate nutrition. Socialworkersmayhelpinfindingresourcestoensuresuccessfulrehabilitation.
Whatifthecancercomesback?If the cancer returns, it is called ‘recurrence*’. The extent of the recurrence* will direct thetreatmentdecision,andthisshouldbecarefullydeterminedforeachindividualpatient.
Ifafterbeingtreatedforprimarycoloncancer,apatientpresentslocalordistantrecurringdisease,he/she will be treated according to the treatment plan for advanced disease (see ‘what are thetreatment options’). Patientswith advanced disease failing to respond to first-line treatmentwitheither chemotherapy* or chemotherapy* with biological targeted therapy* will be treated withsecond-linetreatment;ifsecond-linetherapyfails,treatmentwithbiologicaltargetedtherapy*(likeregorafenib*)isrecommended(see‘whatarethetreatmentoptions’).
Thetreatmentforpatientswhopresentlocalrecurrence*ofrectalcancerdependsonwhetherthepriortreatmentincludedradiotherapy*andwhethersalvagesurgeryispossible.
If radiotherapy*wasnot given in theprimary situation, radiotherapy* shouldbe given alongwithchemotherapy*. If theprevioustreatment includedradiotherapy*,additionalradiotherapy*canbeconsidered in the form of either external, intraoperative, or local radiotherapy*. However, ifradiotherapy* was already administered, additional radiotherapy* can rarely achieve appropriatecontrolofthecancergrowth.
Surgery is indicated 6-10 weeks after radiotherapy*. If salvage surgery is not an option,chemotherapy*shouldbeconsidered.
In colon cancer, the lung is the first site of recurrence* in approximately 20% of patients andpulmonaryresectioncouldbeconsidered if feasible.Lungmetastases*aremore frequent in rectalcancer.
Ifthecancerreturnsintheformofmetastasis*intheliver,surgicalresectionofthemetastases*canbe considered in selected patients, as described in the paragraph “Treatment plan for advancedcolorectalcancer:stageIV”.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page36ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
DEFINITIONSOFDIFFICULTWORDS5-fluorouracil(5-FU)Adrugusedtotreatsymptomsofcancerofthecolon,breast,stomach,andpancreas.Itisalsousedinacreamtotreatcertainskinconditions.5-fluorouracilstopscellsfrommakingDNAanditmaykillcancercells.Itisatypeofantimetabolite.Alsocalled5-FUandfluorouracil.Adenocarcinomas(mucinousorsignet-ring)Cancer that begins in cells that line certain internal organs and that have gland-like (secretory)properties.AdenomaBenigntumourofglandularorigin.Overtimethisbenigngrowthmaybecomemalignant,andevenwhilebenignitcanhavehealthconsequencesbycompressingotherstructures.AdenosquamouscarcinomasA typeof cancer that contains two typesof cells: squamous cells* (thin, flat cells that line certainorgans)andgland-likecells.AfliberceptAdrugusedtotreatcolorectalcancer. It isalsousedforthetreatmentofmaculardegeneration,amedicalconditionthatresultsinalossofvision.AfliberceptisaninhibitorofVEGF*.Structurallyitisa recombinant fusion protein that binds to circulating VEGF* and inhibits activity of differentmoleculesbelongingtoVEGF*family.Inthetumour,itinhibitsthegrowthofbloodvessels.AnastomosisAproceduretoconnecthealthysectionsoftubularstructuresinthebodyafterthediseasedportionhasbeensurgicallyremoved.AnaemiaConditioncharacterizedbytheshortageofredbloodcells*orhemoglobin*, the ironthatcontainsthehemoglobin*carriesoxygenfromthelungstothewholebody,thisprocessisdiminishedinthisconditionAnesthesiaReversiblestateoflossofawarenessinwhichthepatientfeelsnopain,hasnonormalreflexes,andresponds less to stress, induced artificially by the employment of certain substances known asanesthetics.Itcanbecompleteorpartialandallowspatientstoundergosurgery.ArterialthrombosisThepresenceofabloodclotinanartery.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page37ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
BevacizumabAdrugusedtotreatcertaintypesofcolorectalcancer,lungcancer,kidneycancerandglioblastoma(a type of brain cancer). It is also being studied in the treatment of other types of cancer.Bevacizumabbindstoaproteincalledvascularendothelialgrowthfactor*(VEGF).Thismaypreventthegrowthofnewbloodvessels thattumoursneedtogrow. It isa typeofantiangiogenesisagentandatypeofmonoclonalantibody*.BiopsyThe removal of cells or tissues for examinationby a pathologist*. Thepathologist*may study thetissue under amicroscopeor performother tests on the cells or tissue. There aremany differenttypesofbiopsyprocedures.Themostcommontypes include: (1) incisionalbiopsy, inwhichonlyasample of tissue is removed; (2) excisional biopsy, in which an entire lump or suspicious area isremoved;and(3)needlebiopsy,inwhichasampleoftissueorfluidisremovedwithaneedle.Whena wide needle is used, the procedure is called a core biopsy. When a thin needle is used, theprocedureiscalledafine-needleaspirationbiopsy.BrachytherapyAtypeofradiationtherapyinwhichradioactivematerialsealedinneedles,seeds,wires,orcathetersis placed directly into or near a tumour. Also called implant radiation therapy, internal radiationtherapy,andradiationbrachytherapy.BRAFmutationAspecificmutation* (change) in theBRAFgene,whichmakesaprotein that is involved insendingsignalsincellsandincellgrowth.ThisBRAFgenemutation*maybefoundinsometypesofcancer,includingmelanomaand colorectal cancer. Itmay increase the growth and spreadof cancer cells.CheckingforthisBRAFmutation*intumourtissuemayhelptoplancancertreatment.CapecitabineAdrugusedtotreatstageIIIcoloncancerinpatientswhohadsurgerytoremovethecancer.Itisalsoused to treat metastatic breast cancer that has not improved after treatment with certain otheranticancerdrugs.Capecitabineisbeingstudiedinthetreatmentofothertypesofcancer.Itistakenup by cancer cells and breaks down into 5-fluorouracil*, a substance that kills tumour cells.Capecitabineisatypeofantimetabolite.Carcinoembryonicantigen(CEA)Asubstancethatmaybefoundinthebloodofpeoplewhohavecoloncancer,othertypesofcanceror diseases, orwho smoke tobacco. Carcinoembryonic antigen levelsmay help keep track of howwellcancertreatmentsareworkingor ifcancerhascomeback. It isatypeoftumourmarker.AlsocalledCEA.CetuximabAdrugusedtotreatcertaintypesofheadandneckcancer,andacertaintypeofcolorectalcancerthathasspreadtootherpartsofthebody.Itisalsobeingstudiedinthetreatmentofothertypesofcancer.Cetuximabbindstoaproteincalledepidermalgrowthfactorreceptor (EGFR*),which isonthesurfaceofsometypesofcancercells.Thismaystopcancercells fromgrowing.Cetuximab isatypeofmonoclonalantibody*.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page38ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
ChemoradiotherapyTreatmentthatcombineschemotherapy*withradiationtherapy.Alsocalledchemoradiation.ChemotherapyAtypeofcancertreatmentusingdrugsthatkillcancercellsand/or limit theirgrowth.Thesedrugsare usually administered to the patient by slow infusion into a vein but can also be administeredorally,bydirectinfusiontothelimborbyinfusiontotheliver,accordingtocancerlocation.ChromosomalinstabilityAnincreasedtendencytoloseorgainwholechromosomes*orlargepartsofchromosomes*duringcelldivision,resultinginchromosomalaberrations.ChromosomesAnorganized structurewhichencodesgeneswhichare thebody's code for characteristics suchashaircolororgender.Humancellshave23pairsofchromosomes(totalof46chromosomes).Canceror leukemiacellsoftenhaveachromosomalabnormalitywhich isachangetotheirchromosomes,such as a chromosomal duplication or an extra chromosome (47 chromosomes) or have achromosomal deletion or a loss of a chromosome (45 chromosomes). A chromosomal or geneticinversioniswhennoextrachromosomesareaddedordeleted,butinsteadaportionisbackwards.ColonoscopeAthin,tube-likeinstrumentusedtoexaminetheinsideofthecolon.Acolonoscopehasalightandalensforviewingandmayhaveatooltoremovetissue.ContraindicationCondition or symptom that prevents the administration of a given treatment or procedure to thepatient. Contraindications are either absolute, meaning the treatment should never be given topatientswiththisconditionorsymptom,orrelative,meaningthattheriskcanbeoutweighedbythebenefitsinsomepatientswiththisconditionorsymptom.Crohn’sdiseaseChronic inflammation of the gastrointestinal tract,most commonly the small intestine and colon.Crohndiseaseincreasestheriskforcolorectalcancerandsmallintestinecancer.Alsocalledregionalenteritis.CTcolonographyAmethod to examine the insideof the colonby taking a seriesof X-rays*.A computer is used tomake 2-dimensional (2-D) and 3-D pictures of the colon from these X-rays*. The pictures can besaved, changed to givebetter viewingangles, and reviewedafter theprocedure, even years later.Also called computed tomographic colonography, computed tomography colonography, CTC, andvirtualcolonoscopy.CTscanAformofradiographyinwhichbodyorgansarescannedwithX-rays*andtheresultsaresynthesizedbyacomputertogenerateimagesofpartsofthebody.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page39ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
DeepveinthrombosisTheformationofabloodclotinadeepveinofthelegorlowerpelvis.Symptomsmayincludepain,swelling,warmth,andrednessintheaffectedarea.AlsocalledDVT.Diabetesmellitustype2Metabolic disease inwhich glucosebuilds up in theblood as consequenceof insulin deficiencyorresistanceofthebodycellstotheactionofinsulin.Insulinisahormonethattakesglucosefromthebloodintothebodycellssothattheycanuseitforenergy.Diabetesmellitustype2asopposedtodiabetesmellitustype1isnon-insulindependent,sincetheinsulindeficiencyisnotabsolute.Dihydropyrimidinedehydrogenase(DPD)deficiencyInherited metabolic disorder in which there is a decreased or absent activity of the enzymedihydropyrimidinedehydrogenase. This enzymenormallybreaksdown themolecules thymineanduracil incells.Thisdisordermayormaynotcausesymptomsandsigns.However,regardlessofanydiseasemanifestation,allindividualswiththisconditionareatriskoftoxicreactionstodrugscalledfluoropyrimidines*whichareusedincancertreatment.DNArepairmechanismsProcessesthathelpgenesmaintaintheirstabilityandintegrity.DysplasiaCellsthatlookabnormalunderthemicroscopebutarenotcancerous.EndometrialcancerCancerthatformsintissuesoftheuterus(thesmall,hollow,pear-shapedorganinawoman'spelvisinwhichafetusdevelops).Twotypesofuterinecancerareendometrialcanceranduterinesarcoma.Endometrialcancer iscancerthatbegins incells liningtheuterus.Uterinesarcomaisararecancerthatbeginsinmuscleorothertissuesintheuterus.EndoscopyAmedicalprocedurewhereadoctorputsatube-likeinstrumentintothebodytolookinsideit.Therearemanytypesofendoscopy,eachofwhichisdesignedforlookingatacertainpartofthebody.Epidermalgrowthfactorreceptor(EGFR)Theproteinfoundonthesurfaceofsomecellsandtowhichepidermalgrowthfactorbinds,causingthecellstodivide.Itisfoundatabnormallyhighlevelsonthesurfaceofmanytypesofcancercells,sothesecellsmaydivideexcessivelyinthepresenceofepidermalgrowthfactor.AlsocalledEGFR,ErbB1,andHER1.FaecalOccultBloodTest(FOBT)Atesttocheckforblood inthestool.Smallsamplesofstoolareplacedonspecialcardsandsenttoadoctororlaboratoryfortesting.Bloodinthestoolmaybeasignofcolorectalcancer.AlsocalledFOBT.FamilialAdenomatousPolyposis(FAP)Aninheritedconditioninwhichnumerouspolyps*(growthsthatprotrudefrommucousmembranes)formontheinsidewallsofthecolonandrectum.Itincreasestheriskofcolorectalcancer.AlsocalledfamilialpolyposisandFAP.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page40ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
FluoropyrimidineOneofagroupof substancesused to treat cancer.A fluoropyrimidine isa typeofantimetabolite.Examplesarecapecitabine*,floxuridine,andfluorouracil(5-FU*).FolicacidFolicacidisawatersolublevitaminknownasvitaminB9.Itisrequiredtoproducehealthyredbloodcells*.GastrointestinalperforationMedicalemergencyinwhichaholedevelopsthroughthewallofanypartofthedigestivetractfromtheesophagustotherectum,includingthegallbladder.GeneticcounsellingAcommunicationprocessbetweena specially trainedhealthprofessionalandapersonconcernedaboutthegeneticriskofdisease.Theperson'sfamilyandpersonalmedicalhistorymaybediscussed,andcounselingmayleadtogenetictesting.Gray(Gy)Unittomeasureenergy,generallyperkilogramoftissue.HemicolectomySurgery in which approximately half of the colon is removed. It could be right or left, dependingwhethertheascending(right)ordescending(left)colonisremoved.HemoglobinAproteininsideredbloodcells*thatcarriesoxygenfromthelungstotissuesandorgansinthebodyandcarriescarbondioxidebacktothe lungs.Testingfortheamountofhemoglobin inthebloodisusuallypartofacompletebloodcell(CBC)test.Itisusedtocheckforconditionssuchasanaemia*,dehydration,andmalnutrition.Histopathologicalexamination/histopathologyThestudyofdiseasedcellsandtissuesusingamicroscope.HypertensionA blood pressure of 140/90 or higher. Hypertension usually has no symptoms. It can harm thearteriesandcauseanincreaseintheriskofstroke,heartattack,kidneyfailure,andblindness.Alsocalledhighbloodpressure.InfraperitonealspaceAreawithintheabdominalcavitylocatedbelowtheintraperitonealspace*.IntraperitonealspaceAreawithintheabdominalcavitysurroundedbyamembranecalledperitoneum*.IntravenousIntoorwithinavein.Intravenoususuallyreferstoawayofgivingadrugorothersubstancethroughaneedleortubeinsertedintoavein.AlsocalledIV.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page41ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
IrinotecanIrinotecan isadrugused for the treatmentofcancer. IrinotecanpreventsDNA fromunwindingbyinhibitionoftopoisomeraseI.Inchemicalterms,itisasemisyntheticanalogueofthenaturalalkaloidcampthotecin.Itsmainuseisincoloncancer,inparticular,incombinationwithotherchemotherapyagents.ThisincludestheregimenFOLFIRI,whichconsistsofinfusional5-fluorouracil,leucovorin,andirinotecan.Leucovorin(LV)Theactiveingredientinadrugusedtolessenthetoxiceffectsofsubstancesthatblocktheactionoffolicacid*,especially theanticancerdrugmethotrexate. Leucovorin isused to treat some typesofanaemia*andisalsousedwithfluorouraciltotreatcolorectalcancer.Itisalsobeingstudiedinthetreatmentofother typesofcancerandotherconditions.Leucovorin isa formof folicacid*. It isatypeofchemoprotectiveagentandatypeofchemosensitizingagent.Alsocalledfolinicacid.LymphnodeA roundedmass of lymphatic tissue that is surrounded by a capsule of connective tissue. Lymphnodes filter lymph and they store lymphocytes. They are located along lymphatic vessels*. Alsocalledlymphgland.Lymphaticvessel/tissueThelymphatictissueisakindoftissueofwhichthetissuesandorgansofthelymphaticsystemaremade.Thelymphaticsystemproduces,stores,andcarrieswhitebloodcellsthatfightinfectionsandotherdiseases.Thissystemincludesthebonemarrow,spleen,thymus,lymphnodes*,andlymphaticvessels(anetworkofthintubesthatcarry lymphandwhitebloodcells).Lymphaticvesselsbranch,likebloodvessels, intoall the tissuesof thebody.Theyare thin tubes thatcarry lymph(lymphaticfluid)andwhitebloodcellsthroughthelymphaticsystem.Alsocalledlymphvessels.LymphomaCancerthatbeginsincellsoftheimmunesystem.Therearetwobasiccategoriesoflymphomas.OnekindisHodgkinlymphoma,whichismarkedbythepresenceofatypeofcellcalledReed-Sternbergcell.Theothercategoryinnon-Hodgkinlymphomas,whichincludesalarge,diversegroupofcancersof immunesystemcells.Non-Hodgkin lymphomascanbefurtherdivided intocancersthathaveanindolent (slow-growing) course and those that have an aggressive (fast-growing) course. Thesesubtypesbehaveandrespondtotreatmentdifferently.BothHodgkinandnon-Hodgkin lymphomascanoccurinchildrenandadults,andprognosis*andtreatmentdependonthestageandthetypeofcancer.LynchsyndromeAninheriteddisorderinwhichaffectedindividualshaveahigher-than-normalchanceofdevelopingcolorectalcancerandcertainothertypesofcancer,e.g.endometrialcancer*,oftenbeforetheageof50.AlsocalledhereditarynonpolyposiscoloncancerandHNPCC.MagneticResonanceImaging(MRI)An imaging technique that is used inmedicine. It usesmagnetic resonance. Sometimes, a fluid isinjected that enhances the contrast between different tissues to make structures more clearlyvisible.

ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page42ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
MesorectumThefoldofperitoneum*ormesenterythatsupportstherectum. Metastasis/metastasesThe spread of cancer from one part of the body to another. A tumour formed by cells that havespreadiscalledametastatictumourorametastasis.Themetastatictumourcontainscellsthatarelikethoseintheoriginaltumour.MicrosatelliteinstabilityA change that occurs in the DNA of certain cells (such as tumour cells) in which the number ofrepeatsofmicrosatellites(short,repeatedsequencesofDNA)isdifferenttothenumberofrepeatsthatwasintheDNAwhenitwasinherited.ThecauseofmicrosatelliteinstabilitymaybeadefectintheabilitytorepairmistakesmadewhenDNAiscopiedinthecell.AlsocalledMSI.MLH1mutationChangeinagenecalledMLH1,associatedwithhereditarynonpolyposiscoloncancer.MonoclonalantibodyMonoclonalantibodiesareantibodiesthatareexactlythesamebecausetheyareproducedbyclonesofthesameparentcell.MucosaThemoist, inner liningof someorgansandbodycavities.Glands in themucosamakemucus.Alsocalledmucousmembrane.MultidisciplinaryopinionAtreatmentplanningapproachinwhichanumberofdoctorswhoareexpertsindifferentspecialties(disciplines)reviewanddiscussthemedicalconditionandtreatmentoptionsofapatient.Incancertreatment, a multidisciplinary opinion may include that of a medical oncologist* (who providescancertreatmentwithdrugs),asurgicaloncologist*(whoprovidescancertreatmentwithsurgery),and a radiation oncologist* (who provides cancer treatment with radiation). Also called tumourboardreview.MuscularispropriaLayerofmuscleofmanyorgans.Itislocatednexttothesubmucosa*andisinvolvedinmovementssuchperistalsis.MutationAchangeinthesequenceofbasepairsintheDNAthatmakesupagene.Mutationsinagenedonotnecessarilychangethegenepermanently.MYH-associatedpolyposisHereditaryconditioninwhichthereisatendencytodevelopmultiplepolyps*inthecolonandhigherriskofcoloncancer.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page43ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
NasogastrictubeFlexibleplastictubeusedtoreachthestomach.Itisinsertedthroughthenose.NecrosisReferstothedeathoflivingtissues.Neuroendocrine(carcinomas/cells)Neuroendocrine cells are type of cells that bring integration between nervous and endocrinesystems.Inparticular,theyproduceandreleasehormonesintothebloodinresponsetostimulationof the nervous system. Neuroendocrine cells are found throughout the body. Therefore,neuroendocrinecarcinomascanstartinanumberoforgans,includingthelungsandgastrointestinaltract.Theyaresometimesslowgrowingbutbecausetheyarise fromcells thatproducehormones,neuroendocrinecancersproducehormonesaswellorhormone-likesubstanceswhichexcessivelevelmaycausesomesymptoms.OncologistAdoctorwhospecializesintreatingcancer.Someoncologistsspecializeinaparticulartypeofcancertreatment.Forexample,aradiationoncologistspecializesintreatingcancerwithradiation.OvariancancerCancerthatformsintissuesoftheovary.Anovaryisoneofapairoffemalereproductiveglandsinwhichtheova,oreggs,areformed.Mostovariancancersareeitherovarianepithelialcarcinomasormalignantgermcelltumours.Ovarianepithelialcarcinomasiscancerthatbeginsinthecellsonthesurfaceoftheovary.Malignantgermcelltumoursiscancerthatbeginsineggcells.OxaliplatinAdrugusedwithotherdrugstotreatcolorectalcancerthatisadvancedorhascomeback.Itisalsobeingstudiedinthetreatmentofothertypesofcancer.OxaliplatinattachestoDNAincellsandmaykillcancercells.Itisatypeofplatinumcompound.Palmo-plantarerythema(handandfootsyndrome)A condition marked by pain, swelling, numbness, tingling, or redness of the hands or feet. Itsometimes occurs as a side effect of certain anticancer drugs. Also called palmar-plantarerythrodysesthesia.PanitumumabPantimumabisamonoclonalantibody*.PanitumumabhasbeendesignedtoattachtoEGFR*,whichcan be found on the surface of certain cells, including cells in some tumours. As a result, thesetumourcellscannolongerreceivethemessagestransmittedviaEGFR*thattheyneedforgrowth,progressionandspreading.Pantimumabdoes not seem towork in tumour cells that containmutated KRAS*. This is becausetheirgrowthisnotcontrolledbysignalstransmittedviaEGFR*andtheycontinuetogrowevenwhentheEGFR*isblocked.PathologistAdoctorwhoidentifiesdiseasesbystudyingcellsandtissuesunderamicroscope.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page44ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
PerineuraltissueTissuearoundanerveorgroupofnerves.PeritoneumThetissuethatlinestheabdominalwallandcoversmostoftheorgansintheabdomen.Peutz-JegherssyndromeAgeneticdisorder inwhichpolyps*forminthe intestineanddarkspotsappearonthemouthandfingers.HavingPJSincreasestheriskofdevelopinggastrointestinalandmanyothertypesofcancer.AlsocalledPJS.PolypectomySurgerytoremoveapolyp.Polyps(pedunculatedorsessile)Growths that protrude from a mucous membrane. When they are attached to the mucousmembranebyathinstalktheyarecalledpendunculatedpolyps;ifnostalkispresenttheyaresessilepolyps.Positronemissiontomography(PET)A procedure inwhich a small amount of radioactive glucose (sugar) is injected into a vein, and ascannerisusedtomakedetailed,computerizedpicturesofareasinsidethebodywheretheglucoseistakenup.Becausecancercellsoftentakeupmoreglucosethannormalcells,thepicturescanbeusedtofindcancercellsinthebody.PrecancerouslesionsAbnormality in a tissue that does not indicate yetmalignancy, however it has signs that cancer islikelytodevelopinthefuture.PrognosisThelikelyoutcomeorcourseofadisease;thechanceofrecoveryorrecurrence*.ProteinuriaHigher-than-normalamountofproteinintheurine.RadiofrequencyablationA procedure that uses radio waves to heat and destroy abnormal cells. The radio waves travelthrough electrodes (small devices that carry electricity). Radiofrequency ablationmay be used totreatcancerandotherconditions.RadiotherapyAtherapyinwhichradiationisusedinthetreatmentofcanceralwaysorientedtothespecificareaofthecancer.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page45ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
RASgene(mutation*)Afamilyofgenesthatmaycausecancerwhentheyaremutated(changed).Theymakeproteinsthatareinvolvedincellsignalingpathways,cellgrowth,andapoptosis(celldeath).Agentsthatblocktheactionsof amutated ras geneor its proteinmay stop the growthof cancer.Membersof theRASgenefamilyincludeKRAS,HRAS,andNRAS.RectoscopeAthin,tube-likeinstrumentusedtolookinsidetheanusandrectum.Arectoscopehasalightandalensforviewing.Itmayalsohaveatooltoremovetissuetobecheckedunderamicroscopeforsignsofdisease.Ashorter instrumentconsistingofa thin tubewitha light source,used toexamine theinsideoftherectumiscalledproctoscope.RecurrenceCancerordisease (usuallyauto-immune) thathascomeback,usuallyafteraperiodof timeduringwhichthecancerordiseasewasnotpresentorcouldnotbedetected.Thismayhappenatthesamelocation as theoriginal (primary) tumouror to another location in thebody.Also called recurrentcancerordisease.Redbloodcell(count)Themostcommontypeofbloodcell.Itisthesubstancethatmakesthebloodappearred.Themainfunctionisthetransportofoxygen.RegorafenibAdrugused for the treatmentof colorectal cancer andgastrointestinal stromal tumours. It is oraltargeted therapy; amulti-kinase inhibitor that targets receptor tyrosine kinases withmechanismsinvolved in tumour growth and progression – angiogenesis, oncogenesis and the tumourmicroenvironment.ItinhibitsseveralVEGF*receptortyrosinekinasesthatplayaroleinthegrowthofnewbloodvesselsintumour.InadditiontoVEGFR1-3,italsoinhibitsotherkinasessuchasTIE-2,RAF-1,BRAF,KIT,RET,PDGFRandFGFR.
RiskfactorSomething that increases the chance of developing a disease. Some examples of risk factors forcancer are age, a family history of certain cancers, use of tobacco products, being exposed toradiationorcertainchemicals,infectionwithcertainvirusesorbacteria,andcertaingeneticchanges.Sigmoidoscope/sigmoidoscopyAthin,tube-likeinstrumentusedtoexaminetheinsideofthecolon.Asigmoidoscopehasalightandalensforviewingandmayhaveatooltoremovetissue.Specialcontacttechniques/LocalcontacttherapiesLocaltreatmentoptions,whetherradiotherapy*orsurgerytotreatsmalltumours.Sporadicdisease/sporadiccancerCancerthatoccursinpeoplewhodonothaveafamilyhistoryofthatcanceroraninheritedchangeintheirDNAthatwouldincreasetheirriskofdevelopingthattypeofcancer.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page46ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
SquamouscellcarcinomaCancerthatbeginsinsquamouscells.Squamouscellsarethin,flatcellsthatlooklikefishscales,andarefoundinthetissuethatformsthesurfaceoftheskin,theliningoftheholloworgansofthebody,and the lining of the respiratory and digestive tracts.Most cancers of the anus, cervix, head andneck,andvaginaaresquamouscellcarcinomas.Alsocalledepidermoidcarcinoma.StJohn’swortHypericum perforatum (St. John’s wort) is a popular anti-depressant agent which is also beingpromotedasanalternativecancertherapy.Eventhoughsomepreliminarypre-clinicalinvestigationshavegeneratedencouragingfindings,therearenoclinicalstudiestoshowthatSt.John’wortwouldchangethenaturalhistoryofanytypeofcancer.St.John’swortmayreducethebloodlevelsofmanyconventionaldrugs,includingsomecancerdrugs.StagingPerformingexamsandteststolearntheextentofthecancerwithinthebody,especiallywhetherthediseasehasspreadfromtheoriginalsitetootherpartsofthebody.Itisimportanttoknowthestageofthediseaseinordertoplanthebesttreatment.SubmucosaInthegastrointestinaltract,thesubmucosaisthelayerofdenseirregularconnectivetissueorlooseconnectivetissuethatsupportsthemucosa,aswellas joinsthemucosa*tothebulkofunderlyingsmoothmuscle(fibersrunningcircularlywithinlayersoflongitudinalmuscle).SubserosaThe subserosa is a layer of tissue between the muscularis* and serosa. The term is used inhistopathology*and is particularly associatedwith cancer staging* (for example, in staging* coloncancer).Surgicalstaging/pathologicalstagingAmethodusedtofindoutthestageofcancer(amountorspreadofcancerinthebody)byremovingtissuesamplesduringsurgery.Thepathologicalstageisbasedonhowdifferentfromnormalthecellsinthesampleslookunderamicroscope.(Biological)targetedtherapy/treatmentAtypeoftreatmentthatusesdrugsorothersubstances,suchasmonoclonalantibodies,toidentifyandattack specific cancer cells. Targeted therapymayhave fewer sideeffects thanother typesofcancertreatments.Tegafur-uracil(UFT)Asubstancebeingstudied inthetreatmentofsometypesofcancer. It isacombinationoftegafuranduracil.Thetegafuristakenupbythecancercellsandbreaksdowninto5-FU*,asubstancethatkills tumour cells. The uracil causes higher amounts of 5-FU to stay inside the cells and kill them.Tegafur-uracilisatypeofantimetabolite.
ColorectalCancer:aguideforpatients-InformationbasedonESMOClinicalPracticeGuidelines-v.2016.1 Page47ThisdocumentisprovidedbytheAnticancerFundwiththepermissionofESMO.The information in this document does not replace amedical consultation. It is for personal use only and cannot bemodified,reproducedordisseminatedinanywaywithoutwrittenpermissionfromESMOandtheAnticancerFund.
TesticularcancerCancer that forms in the tissues of the testicle. A testicle (or testis) is oneof the twoegg-shapedglands,containedinthescrotum,thatproducespermandmalesexhormones.ThrombosisTheformationorpresenceofathrombus(bloodclot)insideabloodvessel. TransanalendoscopicmicrosurgeryLocalexcisionofrectalcancer.Itisperformedusingaspecialmicroscopethatisinsertedviatheanusintotherectum.TurcotsyndromeCondition inwhich cells in the colon become abnormal and formmasses called polyps*. It is alsocharacterizedbynervoussystemtumours.UlcerationThedevelopmentofanulcerwhichisabreakontheskin,intheliningofanorgan,oronthesurfaceofatissue.UlcerativecolitisChronic inflammation of the colon that produces ulcers* in its lining. This condition ismarked byabdominalpain,cramps,andloosedischargesofpus,blood,andmucusfromthebowel.Ultrasound(intra-operativeandendoscopic)Aprocedureinwhichhigh-energysoundwavesarebouncedoffinternaltissuesororgansandmakeechoes.Theechopatternsareshownonthescreenofanultrasoundmachine,formingapictureofbodytissuescalledasonogram.Alsocalledultrasonography.Vascular(tissue)Relatingtothebloodvessels,e.g.thetissuefromwhichbloodvesselsaremadeofiscalledvasculartissue.Vascularendothelialgrowthfactor(VEGF)Asubstancemadebycellsthatstimulatesnewbloodvesselformation.AlsocalledVEGF.VisceralperitoneumThe layers of tissue that cover the outer surface of most organs in the abdomen, including theintestines.WarfarinAdrugthatpreventsbloodfromclotting.Itbelongstothefamilyofdrugscalledanticoagulants.X-raysX-raysarea formof radiationusedto take imagesof the insideofobjects. Inmedicine,X-raysarecommonlyusedtotakeimagesoftheinsideofthebody.
The ESMO / Anticancer Fund Guides for Patients are designed to assist patients, their relatives and caregivers to understand the nature of different types of cancer and evaluate the best available treatment choices. The medical information described in the Guides for Patients is based on the ESMO Clinical Practice Guidelines, which are designed to guide medical oncologists in the diagnosis, follow-up and treatment in different cancer types.These guides are produced by the Anticancer Fund in close collaboration with the ESMO Guidelines Working Group and the ESMO Cancer Patient Working Group.
For more information please visit www.esmo.org and www.anticancerfund.org
www.anticancerfund.org www.esmo.org
Related Documents











