Perceptions and Practices of Cardiovascular Health A population perspective from a peri-urban Nepalese community Abhinav Vaidya Institute of Medicine at Sahlgrenska Academy University of Gothenburg

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Ab
hinav Vaidya
P
erceptio
ns and P
ractices of C
ardio
vascular Health – A
po
pulatio
n persp
ective from
a peri-urb
an Nep
alese com
munity
Perceptions and Practices of Cardiovascular Health
A population perspective from a peri-urban Nepalese community
2014
Abhinav Vaidya
Institute of Medicineat Sahlgrenska AcademyUniversity of Gothenburg
ISBN 978-91-628-8946-3Printed by Ale Tryckteam AB, Bohus

Doctoral thesis for the degree of Doctor of Philosophy (PhD) in Medical Science
PERCEPTIONS AND PRACTICES OF
CARDIOVASCULAR HEALTH: A population perspective from a peri-urban Nepalese community
Abhinav Vaidya
Institute of Medicine
Sahlgrenska Academy at University of Gothenburg
Göteborg, Sweden
2014
iii
A doctoral thesis at a university in Sweden is produced either as a monograph or as a collection of papers. In the latter case, the introductory part constitutes the formal thesis, which summarizes the accompanying papers. These have either been published or are manuscripts at various stages (in press, submitted, or in manuscript). Abhinav Vaidya Department of Internal Medicine and Clinical Nutrition, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Authors hold the rights to the published articles
ISBN 978-91-628-8946-3
Printed at Ale Tryckteam AB, Bohus, Sweden
iv
This work is dedicated to those who are doing
their bit to preserve and promote cardiovascular health
and prevent cardiovascular diseases.

iii
A doctoral thesis at a university in Sweden is produced either as a monograph or as a collection of papers. In the latter case, the introductory part constitutes the formal thesis, which summarizes the accompanying papers. These have either been published or are manuscripts at various stages (in press, submitted, or in manuscript). Abhinav Vaidya Department of Internal Medicine and Clinical Nutrition, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Authors hold the rights to the published articles
ISBN 978-91-628-8946-3
Printed at Ale Tryckteam AB, Bohus, Sweden
iv
This work is dedicated to those who are doing
their bit to preserve and promote cardiovascular health
and prevent cardiovascular diseases.
v
ABSTRACT Background Global phenomena such as urbanization and individual traits such as health literacy affect people’s exposure and vulnerability to cardiovascular risk factors. Nepal, a low-income South Asian country undergoing epidemiological transition, has limited data and understanding of cardiovascular health issues, particularly regarding cardiovascular health literacy, perception and practice on the community level. Aims This Thesis investigated issues of cardiovascular health from a population perspective. Specifically, it first aimed to establish a Health Demographic Surveillance Site in a peri-urban Nepalese setting; then, assess knowledge, attitude, and practice (KAP)/behavior regarding cardiovascular risk factors, manifestations, and preventability; understand behavioral and life-style risk factors such as physical activity and diet in terms of their sociodemographic correlates; and finally, explore the perceptions of cardiovascular health and disease among those already affected. Methods A health demographic surveillance site was established in Jhaukhel and Duwakot, two peri-urban villages near Kathmandu. A mixed methods research approach was then used. Quantitative studies assessed cardiovascular health literacy, knowledge and attitude in a sample population. Cardiovascular health behaviour, particularly physical inactivity and fruit and vegetable intake, were studied. Additionally, a qualitative study to explore perceptions and experiences of patients with cardiometabolic diseases was conducted. Results Forty four percent of the study population had poor knowledge of cardiovascular health. Moreover, only 14.7% and 13.9% of respondents with highly satisfactory knowledge also had highly satisfactory attitude and practices, respectively. Behavioral cardiovascular risk factors were high (low physical activity: 43.3%, inadequate fruit and vegetable consumption: 97.9%) and varied by sociodemographic correlates. Furthermore, patients understood the importance of lifestyle modification only after diagnosis. Conclusions The studies presented in this Thesis demonstrate the current inadequacy of health literacy in Nepal. In addition, gaps exist between cardiovascular health knowledge, attitude, and practice/behavior, even among those already affected. The coupling of high behavioral risk burden with low cardiovascular health literacy implies need for multi-sector health promotional strategies in the country. Keywords Attitude, behavior, cardiovascular diseases, cardiovascular health, fruit and vegetable intake, health literacy, knowledge, practice, physical activity, urbanization
vi
LIST OF PAPERS
This Thesis is based on the following papers, which are referred to in the text by their Roman numerals. Paper I Aryal UR*, Vaidya A*, Shakya-Vaidya S, Petzold M, Krettek A. Establishing a health demographic surveillance site in Bhaktapur district, Nepal: initial experiences and findings. (*Equal contribution) BMC Research Notes 2012;5(1):489. Paper II Vaidya A, Aryal UR, Krettek A. Cardiovascular health knowledge, attitude, and practice/behaviour in an urbanising community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot Health Demographic Surveillance Site. BMJ Open 2013; 3:e002976. Paper III Vaidya A, Krettek A. Physical activity level and its sociodemographic correlates in a peri-urban Nepalese population: a cross-sectional study from the Jhaukhel-Duwakot health demographic surveillance site. International Journal of Behavioural Nutrition and Physical Activity 2014;11:39. Paper IV Vaidya A, Oli N, Aryal UR, Karki DB, Krettek A. Disparities in fruit and vegetable intake by socio-demographic characteristics in peri-urban Nepalese adults: findings from the Heart-Health Associated Research and Dissemination in the Community (HARDIC) Study, Bhaktapur, Nepal. Journal of Kathmandu Medical College 2013;2(1):3-11. Paper V Oli N*, Vaidya A*, Subedi M, Krettek A. Experiences and perceptions about cause and prevention of cardiovascular disease among people with cardiometabolic conditions: findings of in-depth interviews from a peri-urban Nepalese community. (*Equal contribution) Global Health Action 2014; 7:24023
v
ABSTRACT Background Global phenomena such as urbanization and individual traits such as health literacy affect people’s exposure and vulnerability to cardiovascular risk factors. Nepal, a low-income South Asian country undergoing epidemiological transition, has limited data and understanding of cardiovascular health issues, particularly regarding cardiovascular health literacy, perception and practice on the community level. Aims This Thesis investigated issues of cardiovascular health from a population perspective. Specifically, it first aimed to establish a Health Demographic Surveillance Site in a peri-urban Nepalese setting; then, assess knowledge, attitude, and practice (KAP)/behavior regarding cardiovascular risk factors, manifestations, and preventability; understand behavioral and life-style risk factors such as physical activity and diet in terms of their sociodemographic correlates; and finally, explore the perceptions of cardiovascular health and disease among those already affected. Methods A health demographic surveillance site was established in Jhaukhel and Duwakot, two peri-urban villages near Kathmandu. A mixed methods research approach was then used. Quantitative studies assessed cardiovascular health literacy, knowledge and attitude in a sample population. Cardiovascular health behaviour, particularly physical inactivity and fruit and vegetable intake, were studied. Additionally, a qualitative study to explore perceptions and experiences of patients with cardiometabolic diseases was conducted. Results Forty four percent of the study population had poor knowledge of cardiovascular health. Moreover, only 14.7% and 13.9% of respondents with highly satisfactory knowledge also had highly satisfactory attitude and practices, respectively. Behavioral cardiovascular risk factors were high (low physical activity: 43.3%, inadequate fruit and vegetable consumption: 97.9%) and varied by sociodemographic correlates. Furthermore, patients understood the importance of lifestyle modification only after diagnosis. Conclusions The studies presented in this Thesis demonstrate the current inadequacy of health literacy in Nepal. In addition, gaps exist between cardiovascular health knowledge, attitude, and practice/behavior, even among those already affected. The coupling of high behavioral risk burden with low cardiovascular health literacy implies need for multi-sector health promotional strategies in the country. Keywords Attitude, behavior, cardiovascular diseases, cardiovascular health, fruit and vegetable intake, health literacy, knowledge, practice, physical activity, urbanization
vi
LIST OF PAPERS
This Thesis is based on the following papers, which are referred to in the text by their Roman numerals. Paper I Aryal UR*, Vaidya A*, Shakya-Vaidya S, Petzold M, Krettek A. Establishing a health demographic surveillance site in Bhaktapur district, Nepal: initial experiences and findings. (*Equal contribution) BMC Research Notes 2012;5(1):489. Paper II Vaidya A, Aryal UR, Krettek A. Cardiovascular health knowledge, attitude, and practice/behaviour in an urbanising community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot Health Demographic Surveillance Site. BMJ Open 2013; 3:e002976. Paper III Vaidya A, Krettek A. Physical activity level and its sociodemographic correlates in a peri-urban Nepalese population: a cross-sectional study from the Jhaukhel-Duwakot health demographic surveillance site. International Journal of Behavioural Nutrition and Physical Activity 2014;11:39. Paper IV Vaidya A, Oli N, Aryal UR, Karki DB, Krettek A. Disparities in fruit and vegetable intake by socio-demographic characteristics in peri-urban Nepalese adults: findings from the Heart-Health Associated Research and Dissemination in the Community (HARDIC) Study, Bhaktapur, Nepal. Journal of Kathmandu Medical College 2013;2(1):3-11. Paper V Oli N*, Vaidya A*, Subedi M, Krettek A. Experiences and perceptions about cause and prevention of cardiovascular disease among people with cardiometabolic conditions: findings of in-depth interviews from a peri-urban Nepalese community. (*Equal contribution) Global Health Action 2014; 7:24023

vii
Additionally, this Thesis incorporates the following articles published during the study period. They are attached as Appendix. 1. Vaidya A. Tackling cardiovascular health and disease in Nepal:
epidemiology, strategies and implementation. BMJ Heart Asia 2011;3:87-91.
2. Vaidya A*, Shakya S*, Krettek A. Obesity Prevalence in Nepal: Public Health Challenges in a Low-Income Nation during an Alarming Worldwide Trend. (*Equal contribution) Int. J. Environ. Res. Public Health 2010;7:2726-2744.
3. Vaidya A, Krettek A. Is health promotion the starting point of primary cardiovascular care in low- and middle-income countries like Nepal? Health Promot. Pract. 2012;13:3 412-415.
viii
ABBREVIATIONS
CVD cardiovascular disease
GPAQ Global Physical Activity Questionnaire
HARDIC Heart-Health Associated Research and Dissemination In the Community
HDSS health-demographic surveillance site
KMC Kathmandu Medical College
LPA low physical activity
LMIC low- and middle- income country
MDG Millennium Development Goal
NCD non-communicable disease
NMC Nepal Medical College
RF/RHD rheumatic fever/rheumatic heart disease
TPA total physical activity
VDC village development committee
WHO World Health Organization
vii
Additionally, this Thesis incorporates the following articles published during the study period. They are attached as Appendix. 1. Vaidya A. Tackling cardiovascular health and disease in Nepal:
epidemiology, strategies and implementation. BMJ Heart Asia 2011;3:87-91.
2. Vaidya A*, Shakya S*, Krettek A. Obesity Prevalence in Nepal: Public Health Challenges in a Low-Income Nation during an Alarming Worldwide Trend. (*Equal contribution) Int. J. Environ. Res. Public Health 2010;7:2726-2744.
3. Vaidya A, Krettek A. Is health promotion the starting point of primary cardiovascular care in low- and middle-income countries like Nepal? Health Promot. Pract. 2012;13:3 412-415.
viii
ABBREVIATIONS
CVD cardiovascular disease
GPAQ Global Physical Activity Questionnaire
HARDIC Heart-Health Associated Research and Dissemination In the Community
HDSS health-demographic surveillance site
KMC Kathmandu Medical College
LPA low physical activity
LMIC low- and middle- income country
MDG Millennium Development Goal
NCD non-communicable disease
NMC Nepal Medical College
RF/RHD rheumatic fever/rheumatic heart disease
TPA total physical activity
VDC village development committee
WHO World Health Organization
ix
PRELUDE
I have been interested in the epidemiological and preventive aspects of
cardiovascular disease since I graduated in medicine in 2000. Apart from the
clinical work I did as a doctor, I had pursued cardiovascular research in various
capacities since the beginning of my career. During 2002–2003, I participated as
a research officer in the multicentric INTERHEART study. During my MD
training, I was principal investigator of the first and only community-based
prevalence study of coronary heart disease in Nepal. To pursue further training
in cardiovascular epidemiology and prevention, I went to England in August
2008 to attend a 10-day teaching seminar that was organized by The
International Society of Cardiovascular Disease Epidemiology and Prevention.
Thirty participants from different Asian, African, European, and South
American countries had gathered at Oxford. Among them was Alexandra
Krettek, who would become my future supervisor. During one of those 10 days,
I was chatting with Alexandra about Nepal and what both of us were doing. I
discovered that her institute, the Nordic School of Public Health NHV, had
shown some interest in Nepal in the past but somehow the collaboration process
had remained incomplete. On the other hand, I was seeking an opportunity to
pursue cardiovascular health issues. Soon our discussion turned out to be
productive for both of us. On the last evening of the seminar, Alexandra and I
bade each other goodbye and said we would stay in touch about our common
interest. Six months later, I was a PhD student at the Nordic School of Public
Health NHV.
That was the beginning of my journey into the PhD world, a journey that
began with mixed feelings of enthusiasm, confusion, and uncertainty. A detour
quickly appeared in the form of a major change in the research plan. Instead of
plunging directly into my area of work in cardiovascular health, financial
x
circumstance required me to first establish a health demographic surveillance
site in the study area. At the time, it felt like an unnecessary deviation, but the
establishment of a surveillance site turned out to be a blessing in disguise
because it would provide us with detailed otherwise unavailable social and
health-related information about the population of the study site.
However, the major blow was yet to come. During the penultimate year of
my planned PhD defense, the Nordic Council of Ministers decided unexpectedly
to close the Nordic School of Public Health NHV by the end of 2014. Weeks of
despair and desperation followed. Attempts to acquire academic asylum at the
University of Gothenburg became a long administrative struggle that was
gallantly spearheaded by my supervisor, Alexandra. Finally, an auspicious
morning in August 2013 brought the good news that the University of
Gothenburg had officially confirmed my acceptance into its PhD program. The
storm was over. It was time for some science again!
Speaking of science, the most fulfilling part of my PhD has been the
opportunity to work on cardiovascular health in the community. Indeed, my area
of work not only fulfills my personal interest, but also answers an urgent need in
Nepal. I am happy that I have been able to contribute something toward that
effort. However, much work remains, and this is just the beginning of my
journey.
ix
PRELUDE
I have been interested in the epidemiological and preventive aspects of
cardiovascular disease since I graduated in medicine in 2000. Apart from the
clinical work I did as a doctor, I had pursued cardiovascular research in various
capacities since the beginning of my career. During 2002–2003, I participated as
a research officer in the multicentric INTERHEART study. During my MD
training, I was principal investigator of the first and only community-based
prevalence study of coronary heart disease in Nepal. To pursue further training
in cardiovascular epidemiology and prevention, I went to England in August
2008 to attend a 10-day teaching seminar that was organized by The
International Society of Cardiovascular Disease Epidemiology and Prevention.
Thirty participants from different Asian, African, European, and South
American countries had gathered at Oxford. Among them was Alexandra
Krettek, who would become my future supervisor. During one of those 10 days,
I was chatting with Alexandra about Nepal and what both of us were doing. I
discovered that her institute, the Nordic School of Public Health NHV, had
shown some interest in Nepal in the past but somehow the collaboration process
had remained incomplete. On the other hand, I was seeking an opportunity to
pursue cardiovascular health issues. Soon our discussion turned out to be
productive for both of us. On the last evening of the seminar, Alexandra and I
bade each other goodbye and said we would stay in touch about our common
interest. Six months later, I was a PhD student at the Nordic School of Public
Health NHV.
That was the beginning of my journey into the PhD world, a journey that
began with mixed feelings of enthusiasm, confusion, and uncertainty. A detour
quickly appeared in the form of a major change in the research plan. Instead of
plunging directly into my area of work in cardiovascular health, financial
x
circumstance required me to first establish a health demographic surveillance
site in the study area. At the time, it felt like an unnecessary deviation, but the
establishment of a surveillance site turned out to be a blessing in disguise
because it would provide us with detailed otherwise unavailable social and
health-related information about the population of the study site.
However, the major blow was yet to come. During the penultimate year of
my planned PhD defense, the Nordic Council of Ministers decided unexpectedly
to close the Nordic School of Public Health NHV by the end of 2014. Weeks of
despair and desperation followed. Attempts to acquire academic asylum at the
University of Gothenburg became a long administrative struggle that was
gallantly spearheaded by my supervisor, Alexandra. Finally, an auspicious
morning in August 2013 brought the good news that the University of
Gothenburg had officially confirmed my acceptance into its PhD program. The
storm was over. It was time for some science again!
Speaking of science, the most fulfilling part of my PhD has been the
opportunity to work on cardiovascular health in the community. Indeed, my area
of work not only fulfills my personal interest, but also answers an urgent need in
Nepal. I am happy that I have been able to contribute something toward that
effort. However, much work remains, and this is just the beginning of my
journey.
xi
TABLE OF CONTENTS
BACKGROUND ................................................................................................................................ 1 Cardiovascular diseases: a growing epidemic of non-communicable disease ............................. 1
Epidemiological transition: a contributing factor to the cardiovascular disease epidemic .......... 1
Behavioral risk factors underlie the non-communicable disease epidemic .................................. 2
Increased physical inactivity as a reflection of changing lifestyle ............................................... 3
Inadequate intake of fruit and vegetables ..................................................................................... 4
Health literacy as a factor influencing cardiovascular health behavior ........................................ 4
Nepal: a country with geo-ethnic diversity ................................................................................... 5
Sociodemographic transition in Nepal .......................................................................................... 5
Healthcare system of Nepal .......................................................................................................... 6
Burden of cardiovascular disease and its risk factors in Nepal .................................................... 6
Current focus of cardiovascular disease prevention and control strategies in Nepal ................... 9
Cardiovascular health literacy/health knowledge research in Nepal .......................................... 10
Health demographic surveillance site as a setting for studies on non-communicable diseases . 10
RESEARCH AIMS .......................................................................................................................... 12 THEORETICAL FRAMEWORK ................................................................................................... 13 CONCEPTUAL FRAMEWORK..................................................................................................... 15 METHODOLOGICAL CONSIDERATIONS ................................................................................. 16
Study site and population ............................................................................................................ 16
Research design .......................................................................................................................... 18
Sampling ..................................................................................................................................... 18
Data collection ............................................................................................................................ 23
Tools and definitions .................................................................................................................. 23
Data management ....................................................................................................................... 28
Data analysis ............................................................................................................................... 29
Ethical considerations ................................................................................................................. 35
xii
RESULTS ......................................................................................................................................... 37 Paper I: Establishing a health demographic surveillance site in Bhaktapur district, Nepal: initial experiences and findings .................................................................................................. 37
Paper II: Cardiovascular health knowledge, attitude, and practice/behaviour in an urbanizing community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot health demographic surveillance site .......................................................................... 39
Paper III: Physical activity level and its sociodemographic correlates in a peri-urban Nepalese population: a cross-sectional study from the Jhaukhel-Duwakot health demographic surveillance site. .................................................................................................... 47
Paper IV: Disparities in fruit and vegetable intake by socio-demographic characteristics in peri-urban Nepalese adults: findings from the Heart-Health Associated Research and Dissemination in the Community (HARDIC) Study, Bhaktapur, Nepal .................................... 51
Paper V: Experiences and perceptions about cause and prevention of cardiovascular disease among people with cardiometabolic conditions: findings of in-depth interviews from a peri-urban Nepalese community ........................................................................................................ 52
DISCUSSION .................................................................................................................................. 55
Epidemiological perspectives ..................................................................................................... 55
Learning points for cardiovascular health promotion in Nepal .................................................. 60
Implications for health policy in Nepal ...................................................................................... 65
Relevance of the study findings to other low- and middle-income countries ............................ 67
CONCLUSIONS .............................................................................................................................. 68 FUTURE PERSPECTIVES ............................................................................................................. 70 ACKNOWLEDGMENTS ................................................................................................................ 71 REFERENCES ................................................................................................................................. 76 PAPERS I-V
APPENDIX
xi
TABLE OF CONTENTS
BACKGROUND ................................................................................................................................ 1 Cardiovascular diseases: a growing epidemic of non-communicable disease ............................. 1
Epidemiological transition: a contributing factor to the cardiovascular disease epidemic .......... 1
Behavioral risk factors underlie the non-communicable disease epidemic .................................. 2
Increased physical inactivity as a reflection of changing lifestyle ............................................... 3
Inadequate intake of fruit and vegetables ..................................................................................... 4
Health literacy as a factor influencing cardiovascular health behavior ........................................ 4
Nepal: a country with geo-ethnic diversity ................................................................................... 5
Sociodemographic transition in Nepal .......................................................................................... 5
Healthcare system of Nepal .......................................................................................................... 6
Burden of cardiovascular disease and its risk factors in Nepal .................................................... 6
Current focus of cardiovascular disease prevention and control strategies in Nepal ................... 9
Cardiovascular health literacy/health knowledge research in Nepal .......................................... 10
Health demographic surveillance site as a setting for studies on non-communicable diseases . 10
RESEARCH AIMS .......................................................................................................................... 12 THEORETICAL FRAMEWORK ................................................................................................... 13 CONCEPTUAL FRAMEWORK..................................................................................................... 15 METHODOLOGICAL CONSIDERATIONS ................................................................................. 16
Study site and population ............................................................................................................ 16
Research design .......................................................................................................................... 18
Sampling ..................................................................................................................................... 18
Data collection ............................................................................................................................ 23
Tools and definitions .................................................................................................................. 23
Data management ....................................................................................................................... 28
Data analysis ............................................................................................................................... 29
Ethical considerations ................................................................................................................. 35
xii
RESULTS ......................................................................................................................................... 37 Paper I: Establishing a health demographic surveillance site in Bhaktapur district, Nepal: initial experiences and findings .................................................................................................. 37
Paper II: Cardiovascular health knowledge, attitude, and practice/behaviour in an urbanizing community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot health demographic surveillance site .......................................................................... 39
Paper III: Physical activity level and its sociodemographic correlates in a peri-urban Nepalese population: a cross-sectional study from the Jhaukhel-Duwakot health demographic surveillance site. .................................................................................................... 47
Paper IV: Disparities in fruit and vegetable intake by socio-demographic characteristics in peri-urban Nepalese adults: findings from the Heart-Health Associated Research and Dissemination in the Community (HARDIC) Study, Bhaktapur, Nepal .................................... 51
Paper V: Experiences and perceptions about cause and prevention of cardiovascular disease among people with cardiometabolic conditions: findings of in-depth interviews from a peri-urban Nepalese community ........................................................................................................ 52
DISCUSSION .................................................................................................................................. 55
Epidemiological perspectives ..................................................................................................... 55
Learning points for cardiovascular health promotion in Nepal .................................................. 60
Implications for health policy in Nepal ...................................................................................... 65
Relevance of the study findings to other low- and middle-income countries ............................ 67
CONCLUSIONS .............................................................................................................................. 68 FUTURE PERSPECTIVES ............................................................................................................. 70 ACKNOWLEDGMENTS ................................................................................................................ 71 REFERENCES ................................................................................................................................. 76 PAPERS I-V
APPENDIX

1
BACKGROUND
Cardiovascular diseases: a growing epidemic of non-communicable disease
Non-communicable, or chronic, diseases (NCDs) have long duration and
generally progress slowly (1). Based on disease burden, cardiovascular disease
(CVD), cancer, chronic respiratory disease, and diabetes mellitus comprise the
four main NCDs (1). Other NCDs include mental disease, sensory disorders
such as blindness and hearing loss, digestive disorders such as liver cirrhosis,
and musculo-skeletal diseases such as arthritis (2). NCDs are the major causes of
adult mortality and morbidity (3). In 2010, NCDs killed 34.5 million people
worldwide (i.e., two thirds of 52.8 million deaths) (3). Projections suggest that
the impact of NCDs will continue to rise worldwide, particularly in low- and
middle-income countries (LMICs) where 80% of NCD deaths currently occur
(4).
CVDs, which represent the single largest cause of death worldwide,
include a group of diseases that involve the heart, blood vessels, or the sequelae
of poor blood supply resulting from diseased vascular supply (2). Globally,
CVDs account for 30% of all deaths and 50% of NCD deaths (4). Among CVDs,
the leading cause of death is ischemic heart disease (IHD) (4).
Epidemiological transition: a contributing factor to the cardiovascular
disease epidemic
In developed countries, NCDs, particularly CVDs, were once termed diseases of
the rich (5). However, over the past two decades CVD deaths have declined in
high-income countries and significantly increased in LMICs (6). One reason for
this increase is epidemiological transition such as that currently occurring in the
South Asia region (7).
Epidemiological transition refers to a shift from the predominance of
infectious diseases and nutritional disorders toward degenerative or chronic
1
BACKGROUND
Cardiovascular diseases: a growing epidemic of non-communicable disease
Non-communicable, or chronic, diseases (NCDs) have long duration and
generally progress slowly (1). Based on disease burden, cardiovascular disease
(CVD), cancer, chronic respiratory disease, and diabetes mellitus comprise the
four main NCDs (1). Other NCDs include mental disease, sensory disorders
such as blindness and hearing loss, digestive disorders such as liver cirrhosis,
and musculo-skeletal diseases such as arthritis (2). NCDs are the major causes of
adult mortality and morbidity (3). In 2010, NCDs killed 34.5 million people
worldwide (i.e., two thirds of 52.8 million deaths) (3). Projections suggest that
the impact of NCDs will continue to rise worldwide, particularly in low- and
middle-income countries (LMICs) where 80% of NCD deaths currently occur
(4).
CVDs, which represent the single largest cause of death worldwide,
include a group of diseases that involve the heart, blood vessels, or the sequelae
of poor blood supply resulting from diseased vascular supply (2). Globally,
CVDs account for 30% of all deaths and 50% of NCD deaths (4). Among CVDs,
the leading cause of death is ischemic heart disease (IHD) (4).
Epidemiological transition: a contributing factor to the cardiovascular
disease epidemic
In developed countries, NCDs, particularly CVDs, were once termed diseases of
the rich (5). However, over the past two decades CVD deaths have declined in
high-income countries and significantly increased in LMICs (6). One reason for
this increase is epidemiological transition such as that currently occurring in the
South Asia region (7).
Epidemiological transition refers to a shift from the predominance of
infectious diseases and nutritional disorders toward degenerative or chronic
2
diseases (8). Five stages of epidemiological transition have been described (9).
Every country, or different regions within a country, is in one stage or another
(9). As countries move through the stages, NCDs dominate communicable,
nutritional, and maternal causes of diseases. Drivers of transition include
industrialization and urbanization. Urbanization, which involves the transition
from rural to more urban society, currently occurs mainly in LMICs in Asia and
Africa. In the next two decades, LMICs will comprise more than 80% of the
world’s urban population (10). The increasing trend toward urbanization
presents large health challenges, including pollution, communicable diseases,
and NCDs (11). The urbanization process precipitates lifestyle-related risk
factors such as increased prevalence of sedentary habits and higher consumption
of calories and fat (12). Changing dietary habits and reduced physical mobility
can shift a society’s disease pattern from previously predominant infectious and
communicable diseases toward a double disease burden and increased
prevalence of NCDs, including CVDs (13). For this reason, NCDs have been
called diseases of urbanization. Indeed, risk factors of NCDs are found more
commonly among urban communities compared to rural communities in LMICs
(14).
Behavioral risk factors underlie the non-communicable disease epidemic
Risk factors that underlie most NCDs, including CVDs, are largely preventable
and stem from behaviors such as tobacco consumption, harmful use of alcohol,
inadequate physical activity, and unhealthy diet (4). Eliminating these common
risk factors could prevent up to 80% of heart disease, stroke, and type 2 diabetes
and over one third of cancers (15). Recently, the prevalence of such behavioral
risk factors has accelerated due to the impact of global drivers such as
globalization and urbanization (11).
3
Increased physical inactivity as a reflection of changing lifestyle
Reflecting the growing impact of globalization and urbanization, almost one
third of the world’s population now exhibits physical inactivity (4). Low
physical activity (LPA) is the fourth leading cause of mortality worldwide and
accounts for 6% of CHD and 7% of type 2 diabetes mellitus (16). Following
recognition as an independent risk factor in the 1990s (17), physical inactivity
received global attention with the Global Strategy on Diet, Physical Activity and
Health of the World Health Organization (WHO) (15). Since then,
epidemiological studies on physical inactivity have evolved in various aspects.
First, researchers are increasingly using pedometers and other devices to conduct
objective assessments. However, despite improved accuracy, such devices are
difficult and impractical to use in many settings, particularly in low-income
countries (18). On the other hand, subjective assessments based on
questionnaires and recall methods, such as the International Physical Activity
Questionnaire (IPAQ) and Global Physical Activity Questionnaire (GPAQ),
remain the only way to measure physical activity in settings with limited
resources despite a high level of recall and other biases (19).
Second, there have been recent attempts to study the determinants and
correlates of physical inactivity, many of which are demographic, psychosocial,
behavioral, and environmental in origin (20). Such determinants include
urbanization and its impact, especially regarding more sedentary behavior and
the increased use of automated vehicles. Third, different domains of physical
activity in everyday life (i.e., work, household, travel, and leisure) are gaining
increased interest, particularly regarding their associations with cardiovascular
health (21). Fourth, scientists now advocate physical activity in the form of
“exercise on prescription” for the prevention and treatment of cardiometabolic
diseases (22).
2
diseases (8). Five stages of epidemiological transition have been described (9).
Every country, or different regions within a country, is in one stage or another
(9). As countries move through the stages, NCDs dominate communicable,
nutritional, and maternal causes of diseases. Drivers of transition include
industrialization and urbanization. Urbanization, which involves the transition
from rural to more urban society, currently occurs mainly in LMICs in Asia and
Africa. In the next two decades, LMICs will comprise more than 80% of the
world’s urban population (10). The increasing trend toward urbanization
presents large health challenges, including pollution, communicable diseases,
and NCDs (11). The urbanization process precipitates lifestyle-related risk
factors such as increased prevalence of sedentary habits and higher consumption
of calories and fat (12). Changing dietary habits and reduced physical mobility
can shift a society’s disease pattern from previously predominant infectious and
communicable diseases toward a double disease burden and increased
prevalence of NCDs, including CVDs (13). For this reason, NCDs have been
called diseases of urbanization. Indeed, risk factors of NCDs are found more
commonly among urban communities compared to rural communities in LMICs
(14).
Behavioral risk factors underlie the non-communicable disease epidemic
Risk factors that underlie most NCDs, including CVDs, are largely preventable
and stem from behaviors such as tobacco consumption, harmful use of alcohol,
inadequate physical activity, and unhealthy diet (4). Eliminating these common
risk factors could prevent up to 80% of heart disease, stroke, and type 2 diabetes
and over one third of cancers (15). Recently, the prevalence of such behavioral
risk factors has accelerated due to the impact of global drivers such as
globalization and urbanization (11).
3
Increased physical inactivity as a reflection of changing lifestyle
Reflecting the growing impact of globalization and urbanization, almost one
third of the world’s population now exhibits physical inactivity (4). Low
physical activity (LPA) is the fourth leading cause of mortality worldwide and
accounts for 6% of CHD and 7% of type 2 diabetes mellitus (16). Following
recognition as an independent risk factor in the 1990s (17), physical inactivity
received global attention with the Global Strategy on Diet, Physical Activity and
Health of the World Health Organization (WHO) (15). Since then,
epidemiological studies on physical inactivity have evolved in various aspects.
First, researchers are increasingly using pedometers and other devices to conduct
objective assessments. However, despite improved accuracy, such devices are
difficult and impractical to use in many settings, particularly in low-income
countries (18). On the other hand, subjective assessments based on
questionnaires and recall methods, such as the International Physical Activity
Questionnaire (IPAQ) and Global Physical Activity Questionnaire (GPAQ),
remain the only way to measure physical activity in settings with limited
resources despite a high level of recall and other biases (19).
Second, there have been recent attempts to study the determinants and
correlates of physical inactivity, many of which are demographic, psychosocial,
behavioral, and environmental in origin (20). Such determinants include
urbanization and its impact, especially regarding more sedentary behavior and
the increased use of automated vehicles. Third, different domains of physical
activity in everyday life (i.e., work, household, travel, and leisure) are gaining
increased interest, particularly regarding their associations with cardiovascular
health (21). Fourth, scientists now advocate physical activity in the form of
“exercise on prescription” for the prevention and treatment of cardiometabolic
diseases (22).
4
Inadequate intake of fruit and vegetables
Low intake of fruits and vegetables accounts for 11% of IHD (4). WHO
recommends a daily minimum of five servings (400g) of fruits and vegetables
(23). Underscoring the importance and health potential of fruits and vegetables,
increased intake (up to 600g) could reduce the burden of IHD and ischemic
stroke by 31% and 19%, respectively (24). In the context of WHO’s
recommendation, fruit and vegetable intake varies extensively worldwide. (25).
Health literacy as a factor influencing cardiovascular health behavior
Health literacy, which is a key concept for health promotion and health
education, was used originally in the United States to describe a patient’s
decision-making ability, compliance with prescription medication, and capacity
to self-manage chronic diseases (26). From this narrow healthcare perspective,
health literacy has evolved to a much broader interpretation that defines public
health literacy as an outcome of health education and health promotion (27, 28).
Another dimension of health literacy focuses mainly on the link between health
and education (29). Although these different perspectives have spawned many
definitions of health literacy, this Thesis uses the WHO-endorsed definition,
which states that health literacy implies “cognitive and social skills which
determine the motivation and ability of individuals to gain access to, understand,
and use information in ways which promote and maintain good health” (30).
Limited health literacy associates with increased occurrence and poor
management of NCDs (31) as well as poor knowledge of the disease condition
(32). Evidence on the effectiveness of interventions to improve health literacy
has been limited, variable, and mixed. For example, interventions in Canada and
the United States that aimed only at cardiovascular knowledge through health
education did not yield better health behavior (33, 34). Although scarce in
LMICs, research on health literacy is definitely needed due to the growing
epidemic of CVDs in countries with limited resources (35).
5
Nepal: a country with geo-ethnic diversity
Nepal, a federal democratic republic with approximately 26.6 million
inhabitants, is a landlocked low-income country in South Asia, located between
China and India. Its geography, culture, and religions are highly diverse and
rich. Nepal comprises three distinct geographical areas: the southern plain belt,
called terai; the middle hills and valleys, including the capital region of
Kathmandu, Bhaktapur, and Lalitpur; and the northern Himalayan Mountains.
For administrative purposes, Nepal is divided into five developmental
regions, from east to west. The country consists of 14 zones and 75 districts.
Each district contains mostly rural areas (i.e., village development committees
[VDCs]) and several townships, or municipalities. According to the 2011
census, Nepal has 125 castes and ethnic groups and 123 different languages and
dialects (36). The largest caste/ethnic group is Chhetri, followed by Brahmin,
Magar, Tharu, Tamang, Newar, Kami, Musalman, Yadav, and Rai. Broadly, the
different ethnic groups derive from two main ethno-origins: Tibeto-Burman and
Indo-Aryan (37). The people of the Tibeto-Burman group originated through
large-scale migrations of Mongoloid groups from Tibet and include ethnic
groups such as Tamang, Rai, Limbu, Sherpa, and Newar. Indo-Aryan people hail
from northern India and participated in the early settlement of Nepal. They
include the Brahmins and the Chhetris, the people of the terai, and the Tharus.
The Tibeto-Burman group has a higher prevalence of hypertension compared to
the Indo-Aryan group (25.3% vs. 14.0%) (38).
Sociodemographic transition in Nepal
Nepal is currently experiencing significant lifestyle changes that spring from
various social and demographic changes. This epidemiological transition
includes urbanization and migration. High unemployment and underemployment
force people to choose between remaining in a vicious circle of poverty or
migrating to seek better livelihood opportunities both within and outside Nepal.
4
Inadequate intake of fruit and vegetables
Low intake of fruits and vegetables accounts for 11% of IHD (4). WHO
recommends a daily minimum of five servings (400g) of fruits and vegetables
(23). Underscoring the importance and health potential of fruits and vegetables,
increased intake (up to 600g) could reduce the burden of IHD and ischemic
stroke by 31% and 19%, respectively (24). In the context of WHO’s
recommendation, fruit and vegetable intake varies extensively worldwide. (25).
Health literacy as a factor influencing cardiovascular health behavior
Health literacy, which is a key concept for health promotion and health
education, was used originally in the United States to describe a patient’s
decision-making ability, compliance with prescription medication, and capacity
to self-manage chronic diseases (26). From this narrow healthcare perspective,
health literacy has evolved to a much broader interpretation that defines public
health literacy as an outcome of health education and health promotion (27, 28).
Another dimension of health literacy focuses mainly on the link between health
and education (29). Although these different perspectives have spawned many
definitions of health literacy, this Thesis uses the WHO-endorsed definition,
which states that health literacy implies “cognitive and social skills which
determine the motivation and ability of individuals to gain access to, understand,
and use information in ways which promote and maintain good health” (30).
Limited health literacy associates with increased occurrence and poor
management of NCDs (31) as well as poor knowledge of the disease condition
(32). Evidence on the effectiveness of interventions to improve health literacy
has been limited, variable, and mixed. For example, interventions in Canada and
the United States that aimed only at cardiovascular knowledge through health
education did not yield better health behavior (33, 34). Although scarce in
LMICs, research on health literacy is definitely needed due to the growing
epidemic of CVDs in countries with limited resources (35).
5
Nepal: a country with geo-ethnic diversity
Nepal, a federal democratic republic with approximately 26.6 million
inhabitants, is a landlocked low-income country in South Asia, located between
China and India. Its geography, culture, and religions are highly diverse and
rich. Nepal comprises three distinct geographical areas: the southern plain belt,
called terai; the middle hills and valleys, including the capital region of
Kathmandu, Bhaktapur, and Lalitpur; and the northern Himalayan Mountains.
For administrative purposes, Nepal is divided into five developmental
regions, from east to west. The country consists of 14 zones and 75 districts.
Each district contains mostly rural areas (i.e., village development committees
[VDCs]) and several townships, or municipalities. According to the 2011
census, Nepal has 125 castes and ethnic groups and 123 different languages and
dialects (36). The largest caste/ethnic group is Chhetri, followed by Brahmin,
Magar, Tharu, Tamang, Newar, Kami, Musalman, Yadav, and Rai. Broadly, the
different ethnic groups derive from two main ethno-origins: Tibeto-Burman and
Indo-Aryan (37). The people of the Tibeto-Burman group originated through
large-scale migrations of Mongoloid groups from Tibet and include ethnic
groups such as Tamang, Rai, Limbu, Sherpa, and Newar. Indo-Aryan people hail
from northern India and participated in the early settlement of Nepal. They
include the Brahmins and the Chhetris, the people of the terai, and the Tharus.
The Tibeto-Burman group has a higher prevalence of hypertension compared to
the Indo-Aryan group (25.3% vs. 14.0%) (38).
Sociodemographic transition in Nepal
Nepal is currently experiencing significant lifestyle changes that spring from
various social and demographic changes. This epidemiological transition
includes urbanization and migration. High unemployment and underemployment
force people to choose between remaining in a vicious circle of poverty or
migrating to seek better livelihood opportunities both within and outside Nepal.
6
According to the 2011 national census, about 17% of the total Nepalese
population lives in urban areas (36). Most of the urban population is
concentrated in Kathmandu, Nepal’s capital city.
Healthcare system of Nepal
Like many other nations, Nepal’s public health system is based on the principles
of primary health care and deals mostly with infectious diseases and maternal
and child health. Although Nepal is on track to achieve the Millennium
Development Goals (MDGs) for maternal and child health, its infant and
maternal mortality rates are still high (46 per 1,000 live births and 281 per
1,00,000 live births respectively) (39).
Nepal’s healthcare system is both public (governmental) and private. In
the governmental health system, the Ministry of Health and Population occupies
the central position (40), and decentralization occurs at each level of the
hierarchical organogram. The five Regional Health Directorates are responsible
for health in each of the five regions, and District Public Health Offices/District
Health Offices monitor each of the 75 districts. Successively smaller
geographical areas are served by primary health care centers, health posts, and
sub-health posts (41). Although workers in the public health system are spread
throughout the country, including rural areas, those who work in the private
sector, especially doctors, mostly cluster in urban areas.
Burden of cardiovascular disease and its risk factors in Nepal
CVDs are a major public health issue in Nepal and now account, along with
other major NCDs, for 60% of the disease burden (42). Nepal displays an
abundance of harmful risk factors that lead to CVDs and lacks a system to
maintain cardiovascular health (Figure 1) (43, 44). Major reasons for such weak
preparedness to tackle NCDs include the concomitant challenges of poverty,
7
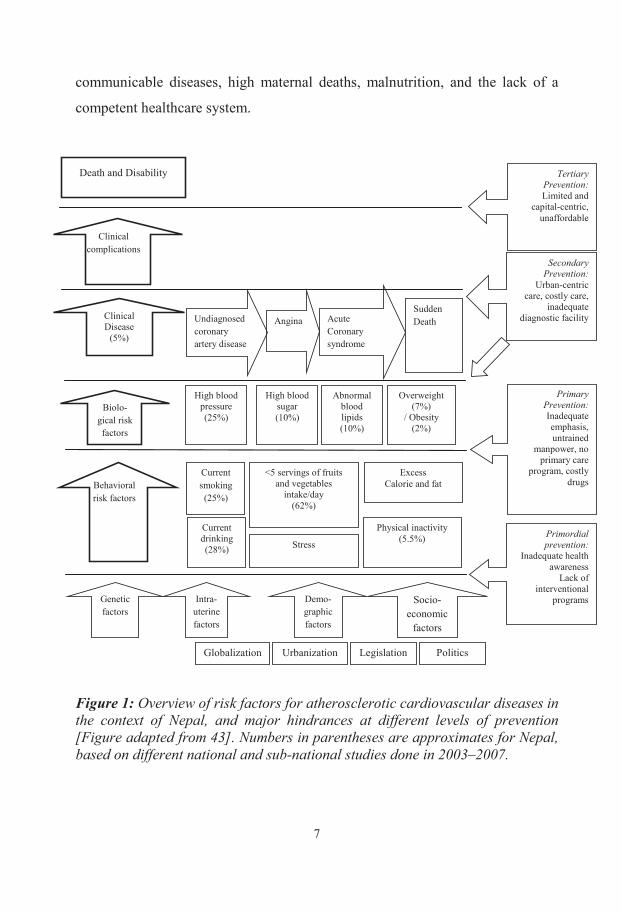
communicable diseases, high maternal deaths, malnutrition, and the lack of a
competent healthcare system.
Figure 1: Overview of risk factors for atherosclerotic cardiovascular diseases in the context of Nepal, and major hindrances at different levels of prevention [Figure adapted from 43]. Numbers in parentheses are approximates for Nepal, based on different national and sub-national studies done in 2003–2007.
Legislation
Tertiary Prevention: Limited and
capital-centric, unaffordable
Clinical Disease
(5%)
Clinical complications
Death and Disability
Undiagnosed coronary artery disease
Angina Acute Coronary syndrome
Sudden Death
Genetic factors
Intra-uterine factors
Demo-graphic factors
Primordial prevention:
Inadequate health awareness
Lack of interventional
programs
Secondary Prevention:
Urban-centric care, costly care,
inadequate diagnostic facility
Primary Prevention: Inadequate emphasis, untrained
manpower, no primary care
program, costly drugs
Socio-economic
factors
Politics Globalization Urbanization
Biolo-gical risk factors
High blood pressure (25%)
High blood sugar (10%)
Abnormal blood lipids (10%)
Overweight (7%)
/ Obesity (2%)
Behavioral risk factors
Current smoking (25%)
Current drinking (28%)
Physical inactivity (5.5%)
<5 servings of fruits and vegetables
intake/day (62%)
Stress
Excess Calorie and fat
6
According to the 2011 national census, about 17% of the total Nepalese
population lives in urban areas (36). Most of the urban population is
concentrated in Kathmandu, Nepal’s capital city.
Healthcare system of Nepal
Like many other nations, Nepal’s public health system is based on the principles
of primary health care and deals mostly with infectious diseases and maternal
and child health. Although Nepal is on track to achieve the Millennium
Development Goals (MDGs) for maternal and child health, its infant and
maternal mortality rates are still high (46 per 1,000 live births and 281 per
1,00,000 live births respectively) (39).
Nepal’s healthcare system is both public (governmental) and private. In
the governmental health system, the Ministry of Health and Population occupies
the central position (40), and decentralization occurs at each level of the
hierarchical organogram. The five Regional Health Directorates are responsible
for health in each of the five regions, and District Public Health Offices/District
Health Offices monitor each of the 75 districts. Successively smaller
geographical areas are served by primary health care centers, health posts, and
sub-health posts (41). Although workers in the public health system are spread
throughout the country, including rural areas, those who work in the private
sector, especially doctors, mostly cluster in urban areas.
Burden of cardiovascular disease and its risk factors in Nepal
CVDs are a major public health issue in Nepal and now account, along with
other major NCDs, for 60% of the disease burden (42). Nepal displays an
abundance of harmful risk factors that lead to CVDs and lacks a system to
maintain cardiovascular health (Figure 1) (43, 44). Major reasons for such weak
preparedness to tackle NCDs include the concomitant challenges of poverty,
7
communicable diseases, high maternal deaths, malnutrition, and the lack of a
competent healthcare system.
Figure 1: Overview of risk factors for atherosclerotic cardiovascular diseases in the context of Nepal, and major hindrances at different levels of prevention [Figure adapted from 43]. Numbers in parentheses are approximates for Nepal, based on different national and sub-national studies done in 2003–2007.
Legislation
Tertiary Prevention: Limited and
capital-centric, unaffordable
Clinical Disease
(5%)
Clinical complications
Death and Disability
Undiagnosed coronary artery disease
Angina Acute Coronary syndrome
Sudden Death
Genetic factors
Intra-uterine factors
Demo-graphic factors
Primordial prevention:
Inadequate health awareness
Lack of interventional
programs
Secondary Prevention:
Urban-centric care, costly care,
inadequate diagnostic facility
Primary Prevention: Inadequate emphasis, untrained
manpower, no primary care
program, costly drugs
Socio-economic
factors
Politics Globalization Urbanization
Biolo-gical risk factors
High blood pressure (25%)
High blood sugar (10%)
Abnormal blood lipids (10%)
Overweight (7%)
/ Obesity (2%)
Behavioral risk factors
Current smoking (25%)
Current drinking (28%)
Physical inactivity (5.5%)
<5 servings of fruits and vegetables
intake/day (62%)
Stress
Excess Calorie and fat
8
The actual burden and trend of CVDs in Nepal is unknown. However,
data from various sources indicate that the problem is common and could be
increasing (43). Common cardiovascular problems include hypertension,
coronary artery disease, stroke, rheumatic fever/rheumatic heart disease
(RF/RHD), congenital heart disease, and congestive heart failure (43).
Prevalence of hypertension affects 20%–33% of the adult population (44–48),
and coronary heart disease affects around 6% of adults in urban areas (49).
RF/RHD is common in Nepal: approximately 1–2 per 1,000 school-age children
suffer from this disease (50, 51). Congenital heart diseases account for most
cardiac surgeries in the National Heart Center in Kathmandu (52).
WHO recognizes four major modifiable behavioral risk factors for CVDs:
tobacco use, unhealthy diet, insufficient physical activity, and harmful use of
alcohol. All four are prevalent in Nepal (44). These risk factors lead to four
major metabolic conditions: overweight/obesity, high blood pressure, elevated
blood sugar, and elevated lipids. In turn, these conditions cause increased
incidence of coronary artery disease, stroke, congestive heart failure, and
chronic kidney disease.
Although data in Nepal has been inconsistent, physical inactivity ranges
from moderate (18%) to a staggering 92% (20). Once an agro-based country,
Nepal is in the midst of an epidemiological transition, and a majority of its
people now lives an urban or urbanizing lifestyle. Therefore, this Thesis
measures physical inactivity to show how ongoing urbanization affects the
Nepalese community, and studies the possible sociodemographic variations
within the population. Importantly, information on such variations helps to tailor
future interventions to improve physical activity in the population.
In Nepal, fruit and vegetable intake is consistently low. For example, the
2007–2008 WHO-STEPS Non-Communicable Diseases Risk Factors Survey
showed that both men and women do not consume the recommended amount of
fruit and vegetables (60.5% and 63.5%, respectively) (25). Therefore, this Thesis
9
explored possible sociodemographic disparities in fruit and vegetable intake
within a community. Apart from the national NCD survey that studied this risk
factor gender-wise (44), no previous study in Nepal has investigated the
relationship between fruit and vegetable intake and sociodemographic factors
such as educational level and occupation.
Current focus of cardiovascular disease prevention and control strategies in
Nepal
In tackling CVDs, the Government of Nepal mainly invests in strengthening
therapeutic services (e.g., establishing tertiary care centers) and providing
financial assistance for the treatment of poor patients. Although this approach is
important and should be continued, preventive services still lack adequate
attention (53). Even therapeutic services are very limited and available only in
urban areas. Privately operated hospitals provide most treatment services in
Nepal’s major cities.
The availability of interventional cardiology and cardiothoracic surgery
services increased dramatically in the last decade. Among about 80 registered
cardiologists in Nepal, 90% are located in Kathmandu. However, most of the
country consists of villages. Health care in these often remote areas is provided
mainly by auxiliary health manpower (about 7,000) and community health
volunteers (about 50,000) who are neither trained nor expected to manage CVD
in the primary healthcare services that they provide.
Regarding health promotional activities, Nepal has at least a dozen
patient-centric societies, clubs, associations, and volunteer groups that operate
different awareness and screening programs for both patients and the general
public. Although their motives are noble, inadequate networking, manpower,
and funding limit their outreach to urban areas and to the observation of special
days (e.g., World Heart Day) (53).
8
The actual burden and trend of CVDs in Nepal is unknown. However,
data from various sources indicate that the problem is common and could be
increasing (43). Common cardiovascular problems include hypertension,
coronary artery disease, stroke, rheumatic fever/rheumatic heart disease
(RF/RHD), congenital heart disease, and congestive heart failure (43).
Prevalence of hypertension affects 20%–33% of the adult population (44–48),
and coronary heart disease affects around 6% of adults in urban areas (49).
RF/RHD is common in Nepal: approximately 1–2 per 1,000 school-age children
suffer from this disease (50, 51). Congenital heart diseases account for most
cardiac surgeries in the National Heart Center in Kathmandu (52).
WHO recognizes four major modifiable behavioral risk factors for CVDs:
tobacco use, unhealthy diet, insufficient physical activity, and harmful use of
alcohol. All four are prevalent in Nepal (44). These risk factors lead to four
major metabolic conditions: overweight/obesity, high blood pressure, elevated
blood sugar, and elevated lipids. In turn, these conditions cause increased
incidence of coronary artery disease, stroke, congestive heart failure, and
chronic kidney disease.
Although data in Nepal has been inconsistent, physical inactivity ranges
from moderate (18%) to a staggering 92% (20). Once an agro-based country,
Nepal is in the midst of an epidemiological transition, and a majority of its
people now lives an urban or urbanizing lifestyle. Therefore, this Thesis
measures physical inactivity to show how ongoing urbanization affects the
Nepalese community, and studies the possible sociodemographic variations
within the population. Importantly, information on such variations helps to tailor
future interventions to improve physical activity in the population.
In Nepal, fruit and vegetable intake is consistently low. For example, the
2007–2008 WHO-STEPS Non-Communicable Diseases Risk Factors Survey
showed that both men and women do not consume the recommended amount of
fruit and vegetables (60.5% and 63.5%, respectively) (25). Therefore, this Thesis
9
explored possible sociodemographic disparities in fruit and vegetable intake
within a community. Apart from the national NCD survey that studied this risk
factor gender-wise (44), no previous study in Nepal has investigated the
relationship between fruit and vegetable intake and sociodemographic factors
such as educational level and occupation.
Current focus of cardiovascular disease prevention and control strategies in
Nepal
In tackling CVDs, the Government of Nepal mainly invests in strengthening
therapeutic services (e.g., establishing tertiary care centers) and providing
financial assistance for the treatment of poor patients. Although this approach is
important and should be continued, preventive services still lack adequate
attention (53). Even therapeutic services are very limited and available only in
urban areas. Privately operated hospitals provide most treatment services in
Nepal’s major cities.
The availability of interventional cardiology and cardiothoracic surgery
services increased dramatically in the last decade. Among about 80 registered
cardiologists in Nepal, 90% are located in Kathmandu. However, most of the
country consists of villages. Health care in these often remote areas is provided
mainly by auxiliary health manpower (about 7,000) and community health
volunteers (about 50,000) who are neither trained nor expected to manage CVD
in the primary healthcare services that they provide.
Regarding health promotional activities, Nepal has at least a dozen
patient-centric societies, clubs, associations, and volunteer groups that operate
different awareness and screening programs for both patients and the general
public. Although their motives are noble, inadequate networking, manpower,
and funding limit their outreach to urban areas and to the observation of special
days (e.g., World Heart Day) (53).
10
On the policy front, recent national and international attention on CVD
resulted in formulation of a NCD policy draft, but it has not yet gained
government endorsement (54). However, the ongoing global effort to include
NCDs in the MDG agenda has stirred renewed interest among the stakeholders.
Cardiovascular health literacy/health knowledge research in Nepal
Public health literacy regarding underlying risk factors and symptoms of heart
disease or possible ways to prevent them is an important issue in tackling CVDs
(32, 55, 56). Studies in Nepal report low knowledge about heart attack
symptoms in the general population and about diabetes even among diabetes
patients (57, 58). Our pilot study in Duwakot Village in the Bhaktapur district
also shows lack of understanding and inability to apply knowledge (13). Hence,
this Thesis aimed to further explore the concept of cardiovascular health literacy
in the Nepalese context.
Health demographic surveillance site as a setting for studies on non-
communicable diseases
There are many sources of health information in Nepal including the Health
Management Information System, which pools data from the grass roots to the
central level and publishes it in an annual report (59). However, Nepal currently
lacks a mechanism that regularly generates relevant information on CVDs. The
WHO-STEPS Non-Communicable Disease Risk Factors Survey, which was
conducted nationwide for the first time in 2007, focuses mainly on risk factors
(44). On the other hand, population-based surveys such as the National Health
Demographic Surveys, which collect health information every 5 years, do not
include CVD-related questions. At the community level, these surveys are too
widely spaced and often do not cover the same population. Therefore, most
available CVD data comes from two sources: (i) sporadic and often one-time
cross-sectional studies, and (ii) publications based on hospital records that
11
inherently cannot represent the whole population. Further, hospital data are
usually incomplete, not maintained digitally, and lack a system that can pool
data from different hospitals. Thus, there is a gap in the information system for
regularly providing population-based data on CVDs. Health and demographic
surveillance systems (HDSS) somewhat fill that gap.
A HDSS is a longitudinal, population-based health and vital registration
system that monitors demographic (e.g., birth, deaths, and migration) and health
(e.g., clinical attendance and hospital admissions) events in a geographically
defined population and also produces timely data (60). Moreover, HDSSs can be
used as a surveillance system to monitor disease trends over time. They also
serve as a platform for evaluating specific interventions (61). However, the
concept of HDSS is not entirely free of criticism. For example, a debate favoring
investment in the vital registration system rather than HDSS as a source of data
has recently ensued. The basis of the argument is that HDSSs are usually small
in size and not representative beyond a certain socio-geographic locale (62).
Nonetheless, recent studies demonstrate that HDSS data can be nationally
representative (63).
HDSSs are especially important where the quality and accessibility of
health services are poor and recording systems are poorly developed (64). To
study NCDs in Nepal, HDSSs become even more important because information
on NCDs is not available through routine sources. Indeed, HDSSs have been
used as an epidemiological resource to study clusters of NCD risk factors in
other countries (65).
10
On the policy front, recent national and international attention on CVD
resulted in formulation of a NCD policy draft, but it has not yet gained
government endorsement (54). However, the ongoing global effort to include
NCDs in the MDG agenda has stirred renewed interest among the stakeholders.
Cardiovascular health literacy/health knowledge research in Nepal
Public health literacy regarding underlying risk factors and symptoms of heart
disease or possible ways to prevent them is an important issue in tackling CVDs
(32, 55, 56). Studies in Nepal report low knowledge about heart attack
symptoms in the general population and about diabetes even among diabetes
patients (57, 58). Our pilot study in Duwakot Village in the Bhaktapur district
also shows lack of understanding and inability to apply knowledge (13). Hence,
this Thesis aimed to further explore the concept of cardiovascular health literacy
in the Nepalese context.
Health demographic surveillance site as a setting for studies on non-
communicable diseases
There are many sources of health information in Nepal including the Health
Management Information System, which pools data from the grass roots to the
central level and publishes it in an annual report (59). However, Nepal currently
lacks a mechanism that regularly generates relevant information on CVDs. The
WHO-STEPS Non-Communicable Disease Risk Factors Survey, which was
conducted nationwide for the first time in 2007, focuses mainly on risk factors
(44). On the other hand, population-based surveys such as the National Health
Demographic Surveys, which collect health information every 5 years, do not
include CVD-related questions. At the community level, these surveys are too
widely spaced and often do not cover the same population. Therefore, most
available CVD data comes from two sources: (i) sporadic and often one-time
cross-sectional studies, and (ii) publications based on hospital records that
11
inherently cannot represent the whole population. Further, hospital data are
usually incomplete, not maintained digitally, and lack a system that can pool
data from different hospitals. Thus, there is a gap in the information system for
regularly providing population-based data on CVDs. Health and demographic
surveillance systems (HDSS) somewhat fill that gap.
A HDSS is a longitudinal, population-based health and vital registration
system that monitors demographic (e.g., birth, deaths, and migration) and health
(e.g., clinical attendance and hospital admissions) events in a geographically
defined population and also produces timely data (60). Moreover, HDSSs can be
used as a surveillance system to monitor disease trends over time. They also
serve as a platform for evaluating specific interventions (61). However, the
concept of HDSS is not entirely free of criticism. For example, a debate favoring
investment in the vital registration system rather than HDSS as a source of data
has recently ensued. The basis of the argument is that HDSSs are usually small
in size and not representative beyond a certain socio-geographic locale (62).
Nonetheless, recent studies demonstrate that HDSS data can be nationally
representative (63).
HDSSs are especially important where the quality and accessibility of
health services are poor and recording systems are poorly developed (64). To
study NCDs in Nepal, HDSSs become even more important because information
on NCDs is not available through routine sources. Indeed, HDSSs have been
used as an epidemiological resource to study clusters of NCD risk factors in
other countries (65).
12
RESEARCH AIMS
The overall aim of this Thesis is to understand cardiovascular health issues from
a population perspective, especially in terms of perceptions about cardiovascular
risk factors, cardiovascular disease manifestation, and preventability. Further,
this Thesis focuses on behavioral and life-style related risk factors, mainly diet
and physical activity, and intends to provide a foundation for future
cardiovascular health promotional interventions in Nepal.
Specifically, I wanted to
• establish an HDSS in Bhaktapur, Nepal, to conduct specific studies on
cardiovascular health (Paper I);
• assess knowledge, attitude, and practice (KAP)/behavior regarding
cardiovascular risk factors, manifestations, and preventability of
cardiovascular disease among the general population (Paper II);
• understand behavioral and life-style risk factors such as physical
activity (Paper III) and diet (Paper IV) in terms of their
sociodemographic correlates, particularly in the context of
urbanization; and
• explore perception and practice of cardiovascular health and disease
among those already affected (Paper V).
13
THEORETICAL FRAMEWORK
The central theme of this Thesis is studying cardiovascular health behavior in
Nepal through the lens of health literacy. The Thesis incorporates constructs of
three different health behavior theories to explain the cardiovascular health
behavior of the study population and, in combination, help to identify the
potential foci of intervention (Figure 2, next page).
Health belief model
The health belief model (HBM) explains health behavior through better
understanding of individuals’ health beliefs (66). HBM explains whether they
perceive themselves at risk, if they think there will be serious consequences if
they develop disease, whether they believe that there are ways to reduce their
susceptibility, and if the benefits of actions outweigh costs and barriers (67).
Social cognitive theory
Social cognitive theory (SCT) proposes that behavior can be explained in terms
of triadic reciprocity between three key concepts that operate as determinants of
each other: the person, the environment, and the behavior (68). SCT has been
widely applied to health behavior with respect to prevention and health
promotion (66).
Theory of reasoned action The theory of reasoned action (TRA) assumes that intention to act is the most
immediate determinant of behavior and that all other factors that influence
behavior will do so through behavioral intention (66). In TRA, intentions are
grounded in values and expectations (69). Intentions are also affected by
subjective norms (i.e., a person’s beliefs about what other people think he/she
should do) (67).
12
RESEARCH AIMS
The overall aim of this Thesis is to understand cardiovascular health issues from
a population perspective, especially in terms of perceptions about cardiovascular
risk factors, cardiovascular disease manifestation, and preventability. Further,
this Thesis focuses on behavioral and life-style related risk factors, mainly diet
and physical activity, and intends to provide a foundation for future
cardiovascular health promotional interventions in Nepal.
Specifically, I wanted to
• establish an HDSS in Bhaktapur, Nepal, to conduct specific studies on
cardiovascular health (Paper I);
• assess knowledge, attitude, and practice (KAP)/behavior regarding
cardiovascular risk factors, manifestations, and preventability of
cardiovascular disease among the general population (Paper II);
• understand behavioral and life-style risk factors such as physical
activity (Paper III) and diet (Paper IV) in terms of their
sociodemographic correlates, particularly in the context of
urbanization; and
• explore perception and practice of cardiovascular health and disease
among those already affected (Paper V).
13
THEORETICAL FRAMEWORK
The central theme of this Thesis is studying cardiovascular health behavior in
Nepal through the lens of health literacy. The Thesis incorporates constructs of
three different health behavior theories to explain the cardiovascular health
behavior of the study population and, in combination, help to identify the
potential foci of intervention (Figure 2, next page).
Health belief model
The health belief model (HBM) explains health behavior through better
understanding of individuals’ health beliefs (66). HBM explains whether they
perceive themselves at risk, if they think there will be serious consequences if
they develop disease, whether they believe that there are ways to reduce their
susceptibility, and if the benefits of actions outweigh costs and barriers (67).
Social cognitive theory
Social cognitive theory (SCT) proposes that behavior can be explained in terms
of triadic reciprocity between three key concepts that operate as determinants of
each other: the person, the environment, and the behavior (68). SCT has been
widely applied to health behavior with respect to prevention and health
promotion (66).
Theory of reasoned action The theory of reasoned action (TRA) assumes that intention to act is the most
immediate determinant of behavior and that all other factors that influence
behavior will do so through behavioral intention (66). In TRA, intentions are
grounded in values and expectations (69). Intentions are also affected by
subjective norms (i.e., a person’s beliefs about what other people think he/she
should do) (67).
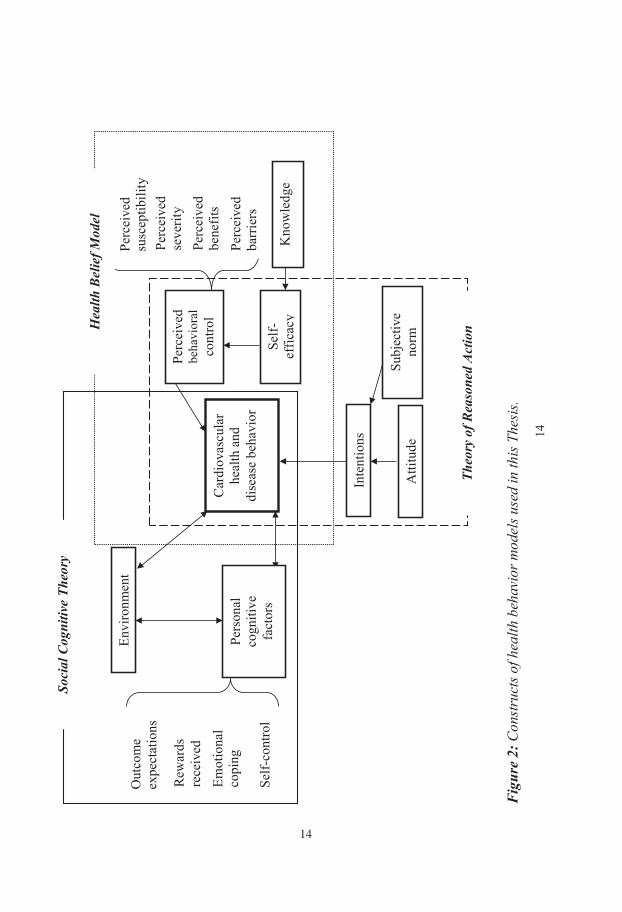
15
CONCEPTUAL FRAMEWORK
The central concept of this Thesis is health literacy and practice regarding
cardiovascular health and diseases (Figure 3). This Thesis discusses
KAP/behavior regarding cardiovascular health in an urbanizing Nepalese society
by first establishing an HDSS in the study area. In particular, I have studied two
behavioral risk factors (i.e., physical activity and fruit and vegetable
consumption) in the context of urbanization and other sociodemographic
correlates. Visualizing the cardiovascular health issues through the lens of health
literacy, this Thesis further explores the perception and experience of individuals
who already have cardiometabolic disease.
CVD, cardiovascular disease; HDSS, health demographic surveillance site
Figure 3: Conceptual framework of the Thesis and the areas of study covered by Papers I–V.
Paper V
Paper IV
Perception and impact of CVD on the diseased
Fruit and vegetable consumption
Physical activity and its correlates
Knowledge, attitude, and practice of cardiovascular health in the general population
Paper III
Paper II
Behavioral Risk Factors
Cardiovascular Diseases
Health Literacy
Urbanization Paper I HDSS as a setting in an urbanizing community to study cardiovascular health
14
14
Fig
ure
2: C
onst
ruct
s of h
ealth
beh
avio
r mod
els u
sed
in th
is T
hesi
s.
Subj
ectiv
e no
rm
Emot
iona
l co
ping
Out
com
e ex
pect
atio
ns
Rew
ards
re
ceiv
ed
Self-
cont
rol
Hea
lth B
elie
f Mod
el
Perc
eive
d se
verit
y Pe
rcei
ved
bene
fits
Perc
eive
d ba
rrie
rs
Perc
eive
d su
scep
tibili
ty
Envi
ronm
ent
Pers
onal
co
gniti
ve
fact
ors
Car
diov
ascu
lar
heal
th a
nd
dise
ase
beha
vior
Inte
ntio
ns
Atti
tude
Perc
eive
d be
havi
oral
co
ntro
l
Self-
ef
ficac
y K
now
ledg
e
Soci
al C
ogni
tive
Theo
ry
Theo
ry o
f Rea
sone
d A
ctio
n
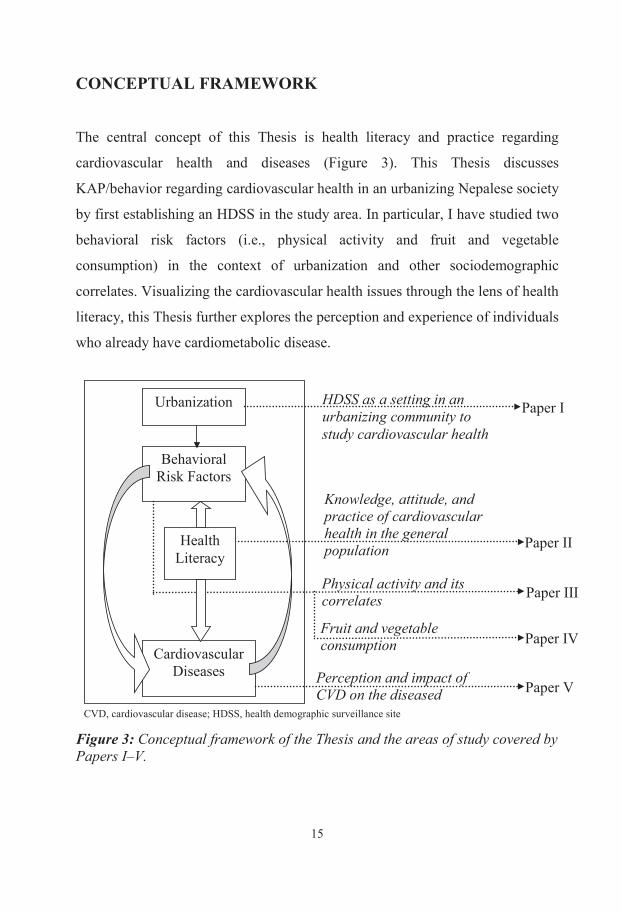
15
CONCEPTUAL FRAMEWORK
The central concept of this Thesis is health literacy and practice regarding
cardiovascular health and diseases (Figure 3). This Thesis discusses
KAP/behavior regarding cardiovascular health in an urbanizing Nepalese society
by first establishing an HDSS in the study area. In particular, I have studied two
behavioral risk factors (i.e., physical activity and fruit and vegetable
consumption) in the context of urbanization and other sociodemographic
correlates. Visualizing the cardiovascular health issues through the lens of health
literacy, this Thesis further explores the perception and experience of individuals
who already have cardiometabolic disease.
CVD, cardiovascular disease; HDSS, health demographic surveillance site
Figure 3: Conceptual framework of the Thesis and the areas of study covered by Papers I–V.
Paper V
Paper IV
Perception and impact of CVD on the diseased
Fruit and vegetable consumption
Physical activity and its correlates
Knowledge, attitude, and practice of cardiovascular health in the general population
Paper III
Paper II
Behavioral Risk Factors
Cardiovascular Diseases
Health Literacy
Urbanization Paper I HDSS as a setting in an urbanizing community to study cardiovascular health
14
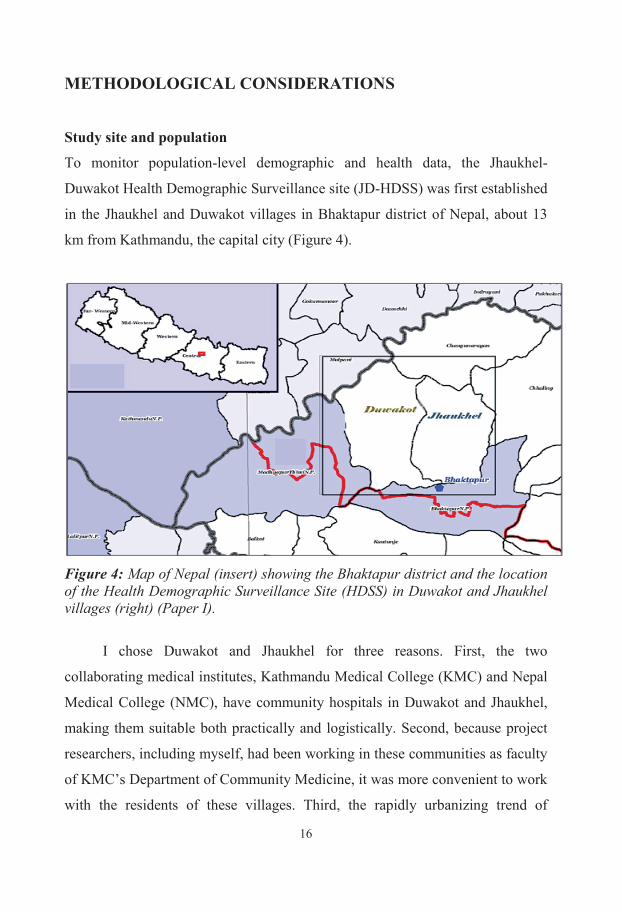
16
METHODOLOGICAL CONSIDERATIONS
Study site and population
To monitor population-level demographic and health data, the Jhaukhel-
Duwakot Health Demographic Surveillance site (JD-HDSS) was first established
in the Jhaukhel and Duwakot villages in Bhaktapur district of Nepal, about 13
km from Kathmandu, the capital city (Figure 4).
Figure 4: Map of Nepal (insert) showing the Bhaktapur district and the location of the Health Demographic Surveillance Site (HDSS) in Duwakot and Jhaukhel villages (right) (Paper I).
I chose Duwakot and Jhaukhel for three reasons. First, the two
collaborating medical institutes, Kathmandu Medical College (KMC) and Nepal
Medical College (NMC), have community hospitals in Duwakot and Jhaukhel,
making them suitable both practically and logistically. Second, because project
researchers, including myself, had been working in these communities as faculty
of KMC’s Department of Community Medicine, it was more convenient to work
with the residents of these villages. Third, the rapidly urbanizing trend of
17
Duwakot and Jhaukhel and their proximity to Kathmandu provided a good
platform to study the lifestyle-related conditions I was interested in.
After its establishment, JD-HDSS became a setting for different studies,
including research on community-based cardiovascular health literacy and
behavior issues. This cardiovascular health component of JD-HDSS has been
termed HARDIC (Heart-Health Associated Research and Dissemination In the
Community). Interestingly, HARDIC translates to “heartily” in the Nepalese
language. Other ongoing research in JD-HDSS includes studies on smoking,
neonatal health, and uterine prolapse.
The overall objectives of JD-HDSS were to develop an epidemiological
surveillance system in Nepal to produce basic population-based health data;
serve as a background and sampling frame for specific studies, especially
longitudinal studies; create formal training capabilities, particularly for
epidemiological training of research students; and provide evidence to
policymakers for better policies/health care interventions.
Although listed as villages for administrative purposes, Jhaukhel and
Duwakot are quickly transforming into peri-urban areas. Hence, the Papers used
the terms peri-urban, semi-urban, and urbanizing, along with villages or VDCs,
to describe these fast-changing areas. Situated 1,401 m above sea level and
covering 5.41 km2, Jhaukhel has a health post operated by the governmental
health system and headed by a health assistant. NMC operates a community
hospital in Jhaukhel. In addition, JD-HDSS office is located on the premises of
the NMC Community Hospital. Duwakot is situated 1,367 m above sea level and
covers 6.42 km2. Apart from a governmental health post, the locality is served
by Kathmandu Medical College Community Hospital, which provides general
and specialist services.
16
METHODOLOGICAL CONSIDERATIONS
Study site and population
To monitor population-level demographic and health data, the Jhaukhel-
Duwakot Health Demographic Surveillance site (JD-HDSS) was first established
in the Jhaukhel and Duwakot villages in Bhaktapur district of Nepal, about 13
km from Kathmandu, the capital city (Figure 4).
Figure 4: Map of Nepal (insert) showing the Bhaktapur district and the location of the Health Demographic Surveillance Site (HDSS) in Duwakot and Jhaukhel villages (right) (Paper I).
I chose Duwakot and Jhaukhel for three reasons. First, the two
collaborating medical institutes, Kathmandu Medical College (KMC) and Nepal
Medical College (NMC), have community hospitals in Duwakot and Jhaukhel,
making them suitable both practically and logistically. Second, because project
researchers, including myself, had been working in these communities as faculty
of KMC’s Department of Community Medicine, it was more convenient to work
with the residents of these villages. Third, the rapidly urbanizing trend of
17
Duwakot and Jhaukhel and their proximity to Kathmandu provided a good
platform to study the lifestyle-related conditions I was interested in.
After its establishment, JD-HDSS became a setting for different studies,
including research on community-based cardiovascular health literacy and
behavior issues. This cardiovascular health component of JD-HDSS has been
termed HARDIC (Heart-Health Associated Research and Dissemination In the
Community). Interestingly, HARDIC translates to “heartily” in the Nepalese
language. Other ongoing research in JD-HDSS includes studies on smoking,
neonatal health, and uterine prolapse.
The overall objectives of JD-HDSS were to develop an epidemiological
surveillance system in Nepal to produce basic population-based health data;
serve as a background and sampling frame for specific studies, especially
longitudinal studies; create formal training capabilities, particularly for
epidemiological training of research students; and provide evidence to
policymakers for better policies/health care interventions.
Although listed as villages for administrative purposes, Jhaukhel and
Duwakot are quickly transforming into peri-urban areas. Hence, the Papers used
the terms peri-urban, semi-urban, and urbanizing, along with villages or VDCs,
to describe these fast-changing areas. Situated 1,401 m above sea level and
covering 5.41 km2, Jhaukhel has a health post operated by the governmental
health system and headed by a health assistant. NMC operates a community
hospital in Jhaukhel. In addition, JD-HDSS office is located on the premises of
the NMC Community Hospital. Duwakot is situated 1,367 m above sea level and
covers 6.42 km2. Apart from a governmental health post, the locality is served
by Kathmandu Medical College Community Hospital, which provides general
and specialist services.
18
Research design
The mixed methods design of this Thesis combines four quantitative studies and
one qualitative study, a strategy often termed “multiple-study” mixed methods
(70). I conducted the studies separately and completed the quantitative studies
first. Papers I–IV used quantitative methods to report the baseline findings of
JD-HDSS (Paper I); assess the cardiovascular KAP/behavior status of the
community (Paper II); and estimate physical activity level (Paper III) and fruit
and vegetable consumption (Paper IV). In Paper V, I conducted in-depth
interviews to explore the experiences and perceptions of heart diseases among
individuals already affected by cardiometabolic diseases.
The point of interface (71) between the qualitative studies (Papers II–IV)
and the qualitative study (Paper V) is triangulation at the level of interpretation
(72). I used the health behavior theories to enhance and enrich the
cardiovascular health issues from a community perspective. Indeed, inclusion of
both quantitative and qualitative methods in this Thesis provided an opportunity
to do a more comprehensive research on Nepal’s cardiovascular health issues
(73). Furthermore, in-depth interviews further validated quantitative data on the
community’s perceptions about lifestyle-related factors, such as physical
activity. Similarly, the qualitative findings allowed retrospective reflection on
the results of the quantitative data through the lens of health behavior models.
Sampling
Table 1 outlines the sampling details. For baseline JD-HDSS data (Paper I), all
households in the nine administrative units or wards of Jhaukhel and Duwakot
were enlisted and a detailed survey of each household was carried out.
19
Table 1: Sampling details of the quantitative and the qualitative studies.
Paper Sampling
unit
Sampling
method
Sample
size
Response
rate, N (%)
Complete
data, N (%)
I
Households Census 2,825
2,712/2,825 (96)
2,712/2,712 (100)
II Primary (6 of 18 wards in Jhaukhel and Duwakot)
Simple random sampling
6 - -
Secondary (households in the 6 wards)
All
840 - -
Tertiary (one 25–59-year-old adult from each household)
Kish technique
840 789/840 (93.9)
777/789 (98.5)
III As in II As in II 840 789/840 (93.9)
640/789 (81.1)
IV As in II As in II 840 789/840 (93.9)
777/789 (98.5)
V Patients with heart disease, hypertension, or diabetes
13 13/13 (100)
13/13 (100)
For Papers II-IV, three of the nine wards from both Jhaukhel and Duwakot (n=6)
were randomly selected (Table 2).
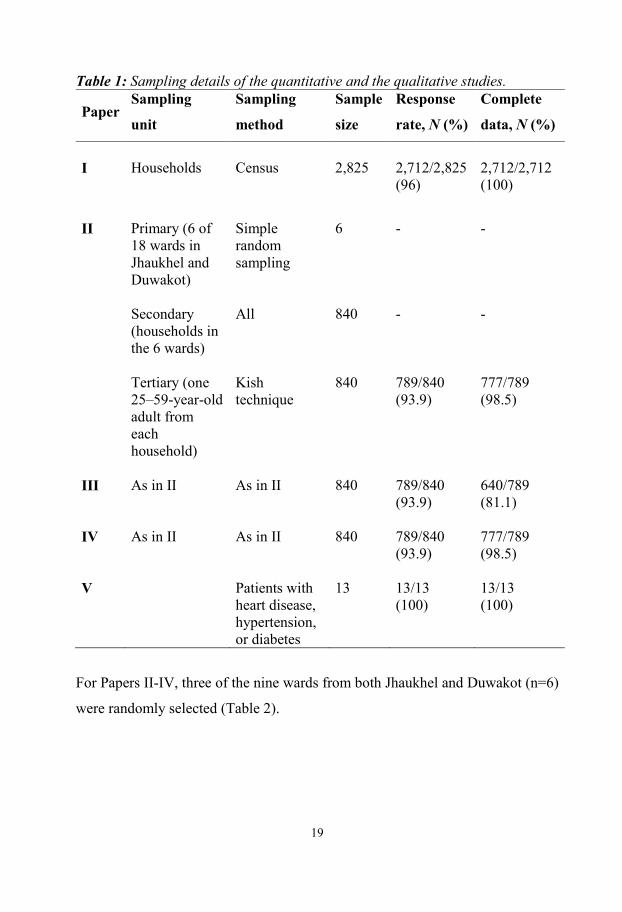
18
Research design
The mixed methods design of this Thesis combines four quantitative studies and
one qualitative study, a strategy often termed “multiple-study” mixed methods
(70). I conducted the studies separately and completed the quantitative studies
first. Papers I–IV used quantitative methods to report the baseline findings of
JD-HDSS (Paper I); assess the cardiovascular KAP/behavior status of the
community (Paper II); and estimate physical activity level (Paper III) and fruit
and vegetable consumption (Paper IV). In Paper V, I conducted in-depth
interviews to explore the experiences and perceptions of heart diseases among
individuals already affected by cardiometabolic diseases.
The point of interface (71) between the qualitative studies (Papers II–IV)
and the qualitative study (Paper V) is triangulation at the level of interpretation
(72). I used the health behavior theories to enhance and enrich the
cardiovascular health issues from a community perspective. Indeed, inclusion of
both quantitative and qualitative methods in this Thesis provided an opportunity
to do a more comprehensive research on Nepal’s cardiovascular health issues
(73). Furthermore, in-depth interviews further validated quantitative data on the
community’s perceptions about lifestyle-related factors, such as physical
activity. Similarly, the qualitative findings allowed retrospective reflection on
the results of the quantitative data through the lens of health behavior models.
Sampling
Table 1 outlines the sampling details. For baseline JD-HDSS data (Paper I), all
households in the nine administrative units or wards of Jhaukhel and Duwakot
were enlisted and a detailed survey of each household was carried out.
19
Table 1: Sampling details of the quantitative and the qualitative studies.
Paper Sampling
unit
Sampling
method
Sample
size
Response
rate, N (%)
Complete
data, N (%)
I
Households Census 2,825
2,712/2,825 (96)
2,712/2,712 (100)
II Primary (6 of 18 wards in Jhaukhel and Duwakot)
Simple random sampling
6 - -
Secondary (households in the 6 wards)
All
840 - -
Tertiary (one 25–59-year-old adult from each household)
Kish technique
840 789/840 (93.9)
777/789 (98.5)
III As in II As in II 840 789/840 (93.9)
640/789 (81.1)
IV As in II As in II 840 789/840 (93.9)
777/789 (98.5)
V Patients with heart disease, hypertension, or diabetes
13 13/13 (100)
13/13 (100)
For Papers II-IV, three of the nine wards from both Jhaukhel and Duwakot (n=6)
were randomly selected (Table 2).
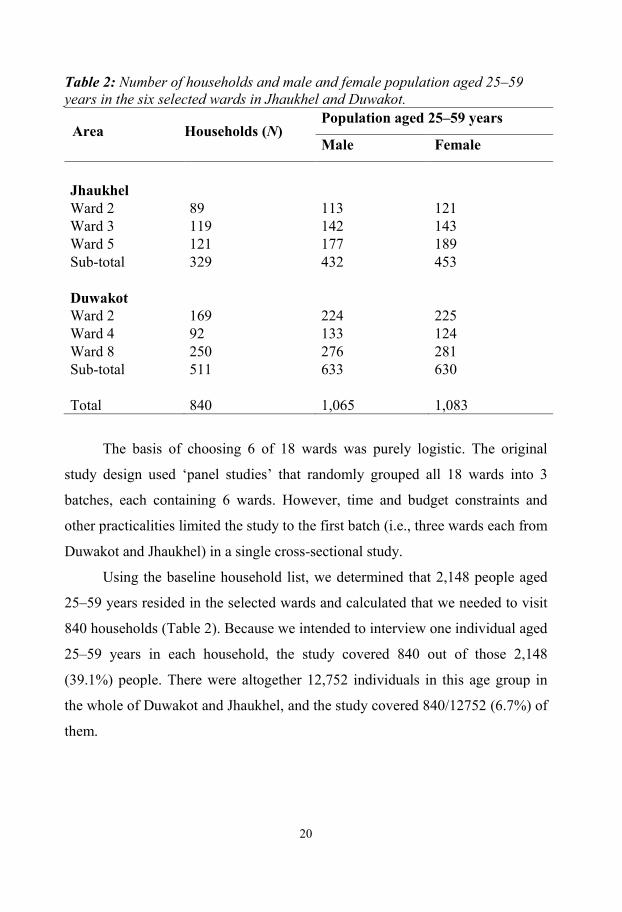
20
Table 2: Number of households and male and female population aged 25–59 years in the six selected wards in Jhaukhel and Duwakot.
Area Households (N) Population aged 25–59 years
Male Female
Jhaukhel Ward 2 89 113 121 Ward 3 119 142 143 Ward 5 121 177 189 Sub-total 329 432 453
Duwakot Ward 2 169 224 225
Ward 4 92 133 124 Ward 8 250 276 281 Sub-total 511 633 630
Total 840 1,065 1,083
The basis of choosing 6 of 18 wards was purely logistic. The original
study design used ‘panel studies’ that randomly grouped all 18 wards into 3
batches, each containing 6 wards. However, time and budget constraints and
other practicalities limited the study to the first batch (i.e., three wards each from
Duwakot and Jhaukhel) in a single cross-sectional study.
Using the baseline household list, we determined that 2,148 people aged
25–59 years resided in the selected wards and calculated that we needed to visit
840 households (Table 2). Because we intended to interview one individual aged
25–59 years in each household, the study covered 840 out of those 2,148
(39.1%) people. There were altogether 12,752 individuals in this age group in
the whole of Duwakot and Jhaukhel, and the study covered 840/12752 (6.7%) of
them.
21
Oversampling of female respondents
The data collection process unintentionally oversampled women for Papers II–
IV. First, the overrepresentation of women would have been expected if the
population itself contained more women than men. However, the baseline census
in the study site (Paper I) showed a male to female ratio of 1.010. Second,
enumerators had applied the Kish technique when selecting a single respondent
from households with more than one eligible candidate (74). The Kish
technique, which is based on probability sampling theory, is widely used
because every adult in a population has equal probability of selection, and the
selected sample closely represents the demographic characteristics of the
surveyed population (75). In terms of equal probability of selection, the Kish
technique outscores not only quasi-probability techniques such as the next or last
birthday method but also non-probability sampling techniques such as the
Troldahl-Carter or quota methods (76). However, the Kish technique has
oversampled women in other settings (77), particularly in populations that differ
drastically in age-sex composition from the 1950s’ American population on
whom the technique was originally based. However, many enumerators in my
study may not have applied the Kish technique due to lengthy administrative
time requirements and also due to the intrusiveness of the questions (76), a trait
reported in other settings (77). Consequently, the enumerators simply may have
interviewed the first contact available, usually a woman because women were
more available during daytime hours and also were more likely to participate.
Besides, most of the enumerators were women who, for social reasons, were
more likely to interview women than men. Nevertheless, I addressed this
important issue of disproportionate sampling at the analysis level by stratifying
the results according to gender, particularly when findings differed markedly
among men and women.
20
Table 2: Number of households and male and female population aged 25–59 years in the six selected wards in Jhaukhel and Duwakot.
Area Households (N) Population aged 25–59 years
Male Female
Jhaukhel Ward 2 89 113 121 Ward 3 119 142 143 Ward 5 121 177 189 Sub-total 329 432 453
Duwakot Ward 2 169 224 225
Ward 4 92 133 124 Ward 8 250 276 281 Sub-total 511 633 630
Total 840 1,065 1,083
The basis of choosing 6 of 18 wards was purely logistic. The original
study design used ‘panel studies’ that randomly grouped all 18 wards into 3
batches, each containing 6 wards. However, time and budget constraints and
other practicalities limited the study to the first batch (i.e., three wards each from
Duwakot and Jhaukhel) in a single cross-sectional study.
Using the baseline household list, we determined that 2,148 people aged
25–59 years resided in the selected wards and calculated that we needed to visit
840 households (Table 2). Because we intended to interview one individual aged
25–59 years in each household, the study covered 840 out of those 2,148
(39.1%) people. There were altogether 12,752 individuals in this age group in
the whole of Duwakot and Jhaukhel, and the study covered 840/12752 (6.7%) of
them.
21
Oversampling of female respondents
The data collection process unintentionally oversampled women for Papers II–
IV. First, the overrepresentation of women would have been expected if the
population itself contained more women than men. However, the baseline census
in the study site (Paper I) showed a male to female ratio of 1.010. Second,
enumerators had applied the Kish technique when selecting a single respondent
from households with more than one eligible candidate (74). The Kish
technique, which is based on probability sampling theory, is widely used
because every adult in a population has equal probability of selection, and the
selected sample closely represents the demographic characteristics of the
surveyed population (75). In terms of equal probability of selection, the Kish
technique outscores not only quasi-probability techniques such as the next or last
birthday method but also non-probability sampling techniques such as the
Troldahl-Carter or quota methods (76). However, the Kish technique has
oversampled women in other settings (77), particularly in populations that differ
drastically in age-sex composition from the 1950s’ American population on
whom the technique was originally based. However, many enumerators in my
study may not have applied the Kish technique due to lengthy administrative
time requirements and also due to the intrusiveness of the questions (76), a trait
reported in other settings (77). Consequently, the enumerators simply may have
interviewed the first contact available, usually a woman because women were
more available during daytime hours and also were more likely to participate.
Besides, most of the enumerators were women who, for social reasons, were
more likely to interview women than men. Nevertheless, I addressed this
important issue of disproportionate sampling at the analysis level by stratifying
the results according to gender, particularly when findings differed markedly
among men and women.
22
High response rate
Another data collection issue involved respondent cooperation. For the most
part, respondents were cooperative, as reflected by the high response rates: 96%
for Paper I; 93.9% for Papers II–IV, which were all based on the same data set;
and 100% for Paper V. Several reasons may account for the high response rates.
First, Nepalese society considers it impolite to turn somebody away when he/she
is at the doorstep; this is especially true in more rural settings. Second, the
enumerators were from the same locality and most of them were women, which
can positively influence respondent participation. Third, enumerators visited
households as many as three times when they were not able to access the
potential candidate. Fourth, it is possible that the high response rate could have
resulted from enumerators interviewing any available adult in the household,
particularly if the Kish-selected candidate did not agree to participate, resulting
in a selection bias that favored more cooperative respondents.
Despite the high response rate, many respondents hesitated to answer
some questions (e.g., questions related to migration) (Paper I). Several
respondents refused to undergo anthropometric measurement or all three blood
pressure readings (Paper III). Such refusals can lead to information bias.
Other possible biases
Paper V, in which I interviewed patients, includes a possibility of recall bias
regarding questions that explored feelings at the time of diagnosis because some
interviewees had been ill for several decades. Additionally, most interviewees
could have had a positive opinion about healthcare facilities and personnel
because my colleague and I (both doctors) conducted the interviews in a
hospital, even though we were not the treating doctors. Additionally, the study
sample may be considered heterogeneous because it consisted of patients with
hypertension, diabetes, ischemic heart disease, arrhythmia, and valvular heart
disease.
23
Data collection
Details of data collection process are summarized in Table 3.
Table 3: Characteristics of data collection. Paper Year Data type Interviewers (N) Interview type
I 2010 Primary Enumerators (18) Face-to-face
II 2011 Primary Enumerators (12) Face-to-face
III 2011 Primary Enumerators (12) Face-to-face
IV 2011 Primary Enumerators (12) Face-to-face
V 2013 Primary PhD students (2) Face-to-face, in-depth
Enumerators collected quantitative data during face-to-face interviews and also
recorded anthropometric and blood pressure measurements. The enumerators
lived in the area and had completed schooling through at least Grade 10. Most
enumerators were women. Before each phase of data collection, all enumerators
received five days of training from the research team, including myself.
Enumerators pre-tested the questionnaire in nearby Changunarayan Village.
Qualitative data collection was conducted by me and a colleague (Natalia Oli, a
fellow PhD student at University of Gothenburg). We conducted in-depth
interviews with patients having manifest CVD, hypertension, or diabetes. We
recorded these interviews on a tape-recorder (Sony Digital Voice Recorder
ICDUX523B).
Tools and definitions
Table 4 provides a brief overview of the structure of questionnaires used and the
main variables studied in the individual papers, followed by details about the
tools and definitions used in Papers I–V.
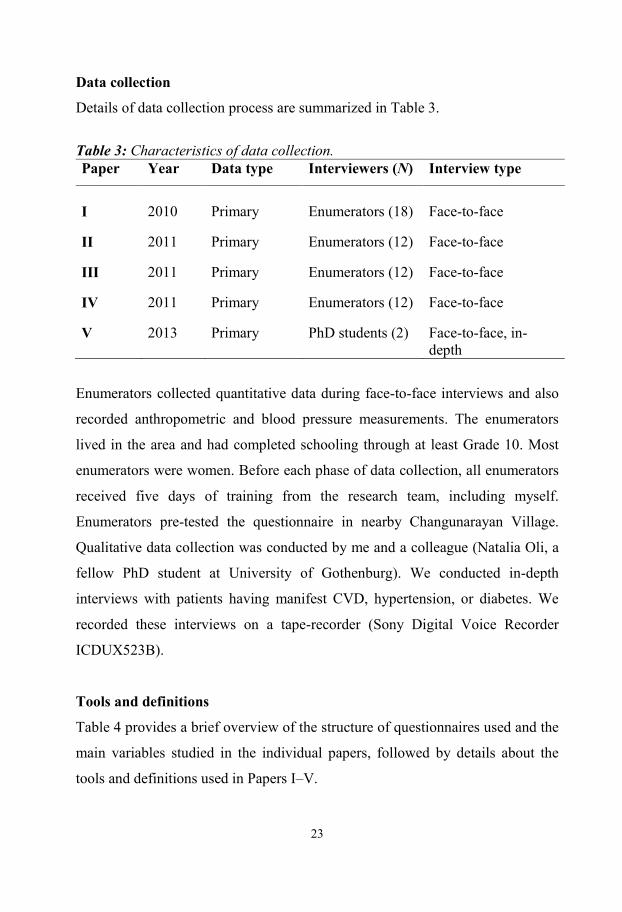
22
High response rate
Another data collection issue involved respondent cooperation. For the most
part, respondents were cooperative, as reflected by the high response rates: 96%
for Paper I; 93.9% for Papers II–IV, which were all based on the same data set;
and 100% for Paper V. Several reasons may account for the high response rates.
First, Nepalese society considers it impolite to turn somebody away when he/she
is at the doorstep; this is especially true in more rural settings. Second, the
enumerators were from the same locality and most of them were women, which
can positively influence respondent participation. Third, enumerators visited
households as many as three times when they were not able to access the
potential candidate. Fourth, it is possible that the high response rate could have
resulted from enumerators interviewing any available adult in the household,
particularly if the Kish-selected candidate did not agree to participate, resulting
in a selection bias that favored more cooperative respondents.
Despite the high response rate, many respondents hesitated to answer
some questions (e.g., questions related to migration) (Paper I). Several
respondents refused to undergo anthropometric measurement or all three blood
pressure readings (Paper III). Such refusals can lead to information bias.
Other possible biases
Paper V, in which I interviewed patients, includes a possibility of recall bias
regarding questions that explored feelings at the time of diagnosis because some
interviewees had been ill for several decades. Additionally, most interviewees
could have had a positive opinion about healthcare facilities and personnel
because my colleague and I (both doctors) conducted the interviews in a
hospital, even though we were not the treating doctors. Additionally, the study
sample may be considered heterogeneous because it consisted of patients with
hypertension, diabetes, ischemic heart disease, arrhythmia, and valvular heart
disease.
23
Data collection
Details of data collection process are summarized in Table 3.
Table 3: Characteristics of data collection. Paper Year Data type Interviewers (N) Interview type
I 2010 Primary Enumerators (18) Face-to-face
II 2011 Primary Enumerators (12) Face-to-face
III 2011 Primary Enumerators (12) Face-to-face
IV 2011 Primary Enumerators (12) Face-to-face
V 2013 Primary PhD students (2) Face-to-face, in-depth
Enumerators collected quantitative data during face-to-face interviews and also
recorded anthropometric and blood pressure measurements. The enumerators
lived in the area and had completed schooling through at least Grade 10. Most
enumerators were women. Before each phase of data collection, all enumerators
received five days of training from the research team, including myself.
Enumerators pre-tested the questionnaire in nearby Changunarayan Village.
Qualitative data collection was conducted by me and a colleague (Natalia Oli, a
fellow PhD student at University of Gothenburg). We conducted in-depth
interviews with patients having manifest CVD, hypertension, or diabetes. We
recorded these interviews on a tape-recorder (Sony Digital Voice Recorder
ICDUX523B).
Tools and definitions
Table 4 provides a brief overview of the structure of questionnaires used and the
main variables studied in the individual papers, followed by details about the
tools and definitions used in Papers I–V.
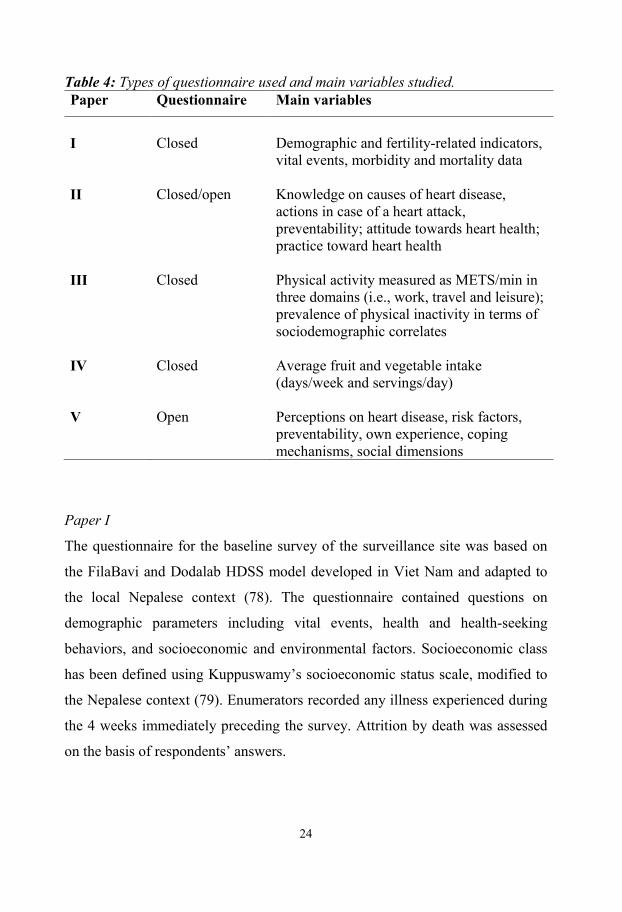
24
Table 4: Types of questionnaire used and main variables studied. Paper Questionnaire Main variables
I Closed Demographic and fertility-related indicators,
vital events, morbidity and mortality data
II Closed/open Knowledge on causes of heart disease, actions in case of a heart attack, preventability; attitude towards heart health; practice toward heart health
III Closed Physical activity measured as METS/min in three domains (i.e., work, travel and leisure); prevalence of physical inactivity in terms of sociodemographic correlates
IV Closed Average fruit and vegetable intake (days/week and servings/day)
V Open Perceptions on heart disease, risk factors, preventability, own experience, coping mechanisms, social dimensions
Paper I
The questionnaire for the baseline survey of the surveillance site was based on
the FilaBavi and Dodalab HDSS model developed in Viet Nam and adapted to
the local Nepalese context (78). The questionnaire contained questions on
demographic parameters including vital events, health and health-seeking
behaviors, and socioeconomic and environmental factors. Socioeconomic class
has been defined using Kuppuswamy’s socioeconomic status scale, modified to
the Nepalese context (79). Enumerators recorded any illness experienced during
the 4 weeks immediately preceding the survey. Attrition by death was assessed
on the basis of respondents’ answers.
25
Paper II
Demographic information and behavioral and physical measurements were
based on the instruction manual of the WHO-STEPS Instrument (80). Current
smokers were defined as those who responded “yes” to “Do you smoke?” Past
smokers were defined as those who replied “yes” to “Did you ever smoke in the
past?” Ever drinkers indicated they had “consumed a drink that contained
alcohol ever in their lifetime,” and current drinkers indicated that they had
consumed alcohol within the previous month. Increased waist circumference
referred to waist measurements ≥80 cm (females) and ≥90 cm (males). Waist/hip
ratio ≥0.85 in females and ≥0.90 in males was considered high. Hypertension
included those with known history of hypertension (diagnosed cases) and those
diagnosed during the study according to the criteria established by the Joint
National Committee VII (81).
Questions on KAP/behavior were based on various resources (32, 55, 82–
97). In some parts of the knowledge section, we used unprompted (open-ended)
questions followed by prompted (closed-ended) questions for the same topic.
Prompted-response questions showed sharply increased acknowledgment of
given options as risk factors, even for incorrect options. This elicited a debate on
whether unprompted or prompted questions are a true measure of one’s
knowledge (98, 99). Response to prompted questions is easier because the
respondent simply needs to recognize the options, and he/she may do some
“guess-work” even without actually knowing the options. On the other hand,
unprompted questions require the respondent to mentally retrieve and synthesize
the answers (98, 99).
Although I assert that unprompted responses are superior measures of
knowledge, I had to use the prompted responses to calculate knowledge scores
because I needed a denominator (i.e., “full marks”) to calculate percentages. I
also scored cardiovascular health attitude and practice/behavior responses, all
24
Table 4: Types of questionnaire used and main variables studied. Paper Questionnaire Main variables
I Closed Demographic and fertility-related indicators,
vital events, morbidity and mortality data
II Closed/open Knowledge on causes of heart disease, actions in case of a heart attack, preventability; attitude towards heart health; practice toward heart health
III Closed Physical activity measured as METS/min in three domains (i.e., work, travel and leisure); prevalence of physical inactivity in terms of sociodemographic correlates
IV Closed Average fruit and vegetable intake (days/week and servings/day)
V Open Perceptions on heart disease, risk factors, preventability, own experience, coping mechanisms, social dimensions
Paper I
The questionnaire for the baseline survey of the surveillance site was based on
the FilaBavi and Dodalab HDSS model developed in Viet Nam and adapted to
the local Nepalese context (78). The questionnaire contained questions on
demographic parameters including vital events, health and health-seeking
behaviors, and socioeconomic and environmental factors. Socioeconomic class
has been defined using Kuppuswamy’s socioeconomic status scale, modified to
the Nepalese context (79). Enumerators recorded any illness experienced during
the 4 weeks immediately preceding the survey. Attrition by death was assessed
on the basis of respondents’ answers.
25
Paper II
Demographic information and behavioral and physical measurements were
based on the instruction manual of the WHO-STEPS Instrument (80). Current
smokers were defined as those who responded “yes” to “Do you smoke?” Past
smokers were defined as those who replied “yes” to “Did you ever smoke in the
past?” Ever drinkers indicated they had “consumed a drink that contained
alcohol ever in their lifetime,” and current drinkers indicated that they had
consumed alcohol within the previous month. Increased waist circumference
referred to waist measurements ≥80 cm (females) and ≥90 cm (males). Waist/hip
ratio ≥0.85 in females and ≥0.90 in males was considered high. Hypertension
included those with known history of hypertension (diagnosed cases) and those
diagnosed during the study according to the criteria established by the Joint
National Committee VII (81).
Questions on KAP/behavior were based on various resources (32, 55, 82–
97). In some parts of the knowledge section, we used unprompted (open-ended)
questions followed by prompted (closed-ended) questions for the same topic.
Prompted-response questions showed sharply increased acknowledgment of
given options as risk factors, even for incorrect options. This elicited a debate on
whether unprompted or prompted questions are a true measure of one’s
knowledge (98, 99). Response to prompted questions is easier because the
respondent simply needs to recognize the options, and he/she may do some
“guess-work” even without actually knowing the options. On the other hand,
unprompted questions require the respondent to mentally retrieve and synthesize
the answers (98, 99).
Although I assert that unprompted responses are superior measures of
knowledge, I had to use the prompted responses to calculate knowledge scores
because I needed a denominator (i.e., “full marks”) to calculate percentages. I
also scored cardiovascular health attitude and practice/behavior responses, all
26
based on closed-ended questions. Maximum scores possible for the three
domains were 53, 56, and 25.
Paper III
Demographic information and behavioral and physical measurements were
based on the instruction manual of the WHO-STEPS Instrument (80). Level of
physical activity was assessed according to the Global Physical Activity
Questionnaire (GPAQ) version 2 (100, 101) and included questions on physical
activity at work, during travel to and from places, and during leisure.
Respondents were asked about days per week and time per day they spent doing
vigorous (e.g., heavy load lifting) and moderate (e.g., carrying light loads)
activities at work; continuous walking or cycling for ≥10 minutes during
commute to work, market, etc; and vigorous (e.g., intense sports) and moderate
activity (e.g., swimming) during leisure.
Metabolic equivalents (METs) are commonly used to express the intensity
of physical activity (101). MET is the ratio of a person’s working metabolic rate
relative to the resting metabolic rate. One MET is defined as the energy cost of
sitting quietly and is equivalent to a caloric consumption of 1 kcal/kg per hour.
As outlined in the instruction manual, all durations of physical activities were
first converted to MET-minutes/week by multiplying time (minutes per day) by
the number of days on which that activity was done per week, and further
multiplying the product by eight for vigorous activity and by four for moderate
activity (e.g., cycling or walking for transport) (101). Compared to sitting
quietly, estimates suggest that a person's caloric consumption increases four-fold
during moderate activity and eight-fold during vigorous activity.
Total physical activity (TPA) was calculated by adding together MET-
minutes of all the activities. Depending on their total MET-minutes/week or
other combination criteria, the respondents’ physical activity was categorized as
high, moderate, and low. “High activity” indicates a person who engages in
27
vigorous-intensity activity at least 3 days/week and achieves at least 1,500 MET-
minutes/week, or who completes any combination of walking or moderate or
vigorous activities on 7 or more days and achieves at least 3,000 MET-
minutes/week.“Moderate activity” identifies a person who does not meet the
criteria for “high activity,” but completes either 3 or more days of vigorous-
intensity activity for at least 20 minutes/day, or 5 or more days of moderate
intensity activity (i.e., at least 30 minutes/day, or 5 or more days of any
combination of walking or moderate- or vigorous-intensity activities), achieving
a minimum of at least 600 MET-minutes/week. “Low activity” describes a
person who did not meet any of the above criteria. In addition, we classified
respondents according to the WHO-recommended minimum, i.e., 150 or 75
minutes of moderate or vigorous aerobic physical activity, respectively or an
equivalent combination of moderate- and vigorous-intensity activity throughout
the week (102).
Paper III measured the sociodemographic correlates of physical activity
and used the self-reported questionnaire. Classifying population on the basis of
self-reported physical activity suffers from an innate weakness of recall bias,
which is reported mainly for moderate-level activities (19). Nevertheless, the
self-reported questionnaire provides data for comparison with methodologically
similar national and international data. In addition, more accurate objective
measurements using accelerometers were not feasible in my study setting.
Further, although important in understanding the ecology of physical activity, I
did not venture into studying the built environment of the study setting and its
relation with physical activity of the study population. Indeed, a full picture of
the epidemiology of physical activity can be understood only by including
physical and built environment and the psychosocial correlates of physical
activity (103, 104).
26
based on closed-ended questions. Maximum scores possible for the three
domains were 53, 56, and 25.
Paper III
Demographic information and behavioral and physical measurements were
based on the instruction manual of the WHO-STEPS Instrument (80). Level of
physical activity was assessed according to the Global Physical Activity
Questionnaire (GPAQ) version 2 (100, 101) and included questions on physical
activity at work, during travel to and from places, and during leisure.
Respondents were asked about days per week and time per day they spent doing
vigorous (e.g., heavy load lifting) and moderate (e.g., carrying light loads)
activities at work; continuous walking or cycling for ≥10 minutes during
commute to work, market, etc; and vigorous (e.g., intense sports) and moderate
activity (e.g., swimming) during leisure.
Metabolic equivalents (METs) are commonly used to express the intensity
of physical activity (101). MET is the ratio of a person’s working metabolic rate
relative to the resting metabolic rate. One MET is defined as the energy cost of
sitting quietly and is equivalent to a caloric consumption of 1 kcal/kg per hour.
As outlined in the instruction manual, all durations of physical activities were
first converted to MET-minutes/week by multiplying time (minutes per day) by
the number of days on which that activity was done per week, and further
multiplying the product by eight for vigorous activity and by four for moderate
activity (e.g., cycling or walking for transport) (101). Compared to sitting
quietly, estimates suggest that a person's caloric consumption increases four-fold
during moderate activity and eight-fold during vigorous activity.
Total physical activity (TPA) was calculated by adding together MET-
minutes of all the activities. Depending on their total MET-minutes/week or
other combination criteria, the respondents’ physical activity was categorized as
high, moderate, and low. “High activity” indicates a person who engages in
27
vigorous-intensity activity at least 3 days/week and achieves at least 1,500 MET-
minutes/week, or who completes any combination of walking or moderate or
vigorous activities on 7 or more days and achieves at least 3,000 MET-
minutes/week.“Moderate activity” identifies a person who does not meet the
criteria for “high activity,” but completes either 3 or more days of vigorous-
intensity activity for at least 20 minutes/day, or 5 or more days of moderate
intensity activity (i.e., at least 30 minutes/day, or 5 or more days of any
combination of walking or moderate- or vigorous-intensity activities), achieving
a minimum of at least 600 MET-minutes/week. “Low activity” describes a
person who did not meet any of the above criteria. In addition, we classified
respondents according to the WHO-recommended minimum, i.e., 150 or 75
minutes of moderate or vigorous aerobic physical activity, respectively or an
equivalent combination of moderate- and vigorous-intensity activity throughout
the week (102).
Paper III measured the sociodemographic correlates of physical activity
and used the self-reported questionnaire. Classifying population on the basis of
self-reported physical activity suffers from an innate weakness of recall bias,
which is reported mainly for moderate-level activities (19). Nevertheless, the
self-reported questionnaire provides data for comparison with methodologically
similar national and international data. In addition, more accurate objective
measurements using accelerometers were not feasible in my study setting.
Further, although important in understanding the ecology of physical activity, I
did not venture into studying the built environment of the study setting and its
relation with physical activity of the study population. Indeed, a full picture of
the epidemiology of physical activity can be understood only by including
physical and built environment and the psychosocial correlates of physical
activity (103, 104).
28
Paper IV
Demographic information for Paper IV was based on the instruction manual of
the WHO-STEPs Instrument (80). To assess fruit and vegetable intake, we asked
respondents to report the number of days/week and servings/day that they
consumed fruit and vegetables. “Low fruit and vegetable intake” was defined as
consuming less than the five WHO-recommended servings of fruit and
vegetables.
The study largely focused on quantifying fruit and vegetable intake. It did
not explore different factors in the study community that might influence intake.
Ecology of the terrain, availability, and affordability are known determinants of
fruit and vegetable intake (105–108). Likewise, habits (including those of
parents), attitudes, motivation, knowledge, and taste preferences influence fruit
and vegetable consumption (105).
Paper V
Data were collected through open-ended questions using an in-depth interview
guide. The guide was developed using relevant literature (109–116) and by
consulting researchers with experience in qualitative studies. Pre-testing was
done with two hypertensive patients (i.e., one 74-year-old male and one 39-year-
old female). I participated in all aspects of the study. For the data collection
process, I functioned as an interviewer along with my colleague. I have previous
research experience in community-based cardiovascular health.
Data management
For Papers I–IV, enumerators collected data on questionnaire sheets, which they
carried in shoulder bags. At the end of each day, all enumerators met with field
supervisors in the JD-HDSS office. The supervisors checked the completed
questionnaires and instructed the enumerators to revisit households and collect
any missing information. On a weekly basis, enumerators securely deposited
29
completed questionnaires at the JD-HDSS office at NMC Community Hospital,
Jhaukhel. These filled forms were stacked in steel racks according to codes
developed for the purpose.
Under close supervision, a team of public health graduates entered data
into Epidata software version 3.1. I and other colleagues checked for any
inconsistency. We held regular meetings and presentations to update the data
entry progress. For the qualitative study (Paper V), data was present in two
formats (i.e., tape recordings and interview notes). Both formats were securely
kept in my office. Only those involved in the research had access to the data.
Data analysis
Because this Thesis contains both quantitative and qualitative data, I analyzed
the data accordingly (Table 5). I used statistical analyses packages, such as
Statistical Package for Social Sciences (SPSS) and STATA, for quantitative
analysis and also applied relevant tests of significance. I considered p<0.05 as
statistically significant. Analyses for risk factors, such as hypertension, physical
activity, and fruit and vegetable intake, follow the guidelines provided in the
manual of the WHO-STEPS Non-Communicable Disease Risk Factors Survey
(80). We used qualitative content analysis to analyze qualitative data (117). Data
from quantitative and qualitative studies were not triangulated during data
analysis, but rather at the interpretation level. Table 5 provides details of the data
analysis procedure for each paper.
28
Paper IV
Demographic information for Paper IV was based on the instruction manual of
the WHO-STEPs Instrument (80). To assess fruit and vegetable intake, we asked
respondents to report the number of days/week and servings/day that they
consumed fruit and vegetables. “Low fruit and vegetable intake” was defined as
consuming less than the five WHO-recommended servings of fruit and
vegetables.
The study largely focused on quantifying fruit and vegetable intake. It did
not explore different factors in the study community that might influence intake.
Ecology of the terrain, availability, and affordability are known determinants of
fruit and vegetable intake (105–108). Likewise, habits (including those of
parents), attitudes, motivation, knowledge, and taste preferences influence fruit
and vegetable consumption (105).
Paper V
Data were collected through open-ended questions using an in-depth interview
guide. The guide was developed using relevant literature (109–116) and by
consulting researchers with experience in qualitative studies. Pre-testing was
done with two hypertensive patients (i.e., one 74-year-old male and one 39-year-
old female). I participated in all aspects of the study. For the data collection
process, I functioned as an interviewer along with my colleague. I have previous
research experience in community-based cardiovascular health.
Data management
For Papers I–IV, enumerators collected data on questionnaire sheets, which they
carried in shoulder bags. At the end of each day, all enumerators met with field
supervisors in the JD-HDSS office. The supervisors checked the completed
questionnaires and instructed the enumerators to revisit households and collect
any missing information. On a weekly basis, enumerators securely deposited
29
completed questionnaires at the JD-HDSS office at NMC Community Hospital,
Jhaukhel. These filled forms were stacked in steel racks according to codes
developed for the purpose.
Under close supervision, a team of public health graduates entered data
into Epidata software version 3.1. I and other colleagues checked for any
inconsistency. We held regular meetings and presentations to update the data
entry progress. For the qualitative study (Paper V), data was present in two
formats (i.e., tape recordings and interview notes). Both formats were securely
kept in my office. Only those involved in the research had access to the data.
Data analysis
Because this Thesis contains both quantitative and qualitative data, I analyzed
the data accordingly (Table 5). I used statistical analyses packages, such as
Statistical Package for Social Sciences (SPSS) and STATA, for quantitative
analysis and also applied relevant tests of significance. I considered p<0.05 as
statistically significant. Analyses for risk factors, such as hypertension, physical
activity, and fruit and vegetable intake, follow the guidelines provided in the
manual of the WHO-STEPS Non-Communicable Disease Risk Factors Survey
(80). We used qualitative content analysis to analyze qualitative data (117). Data
from quantitative and qualitative studies were not triangulated during data
analysis, but rather at the interpretation level. Table 5 provides details of the data
analysis procedure for each paper.
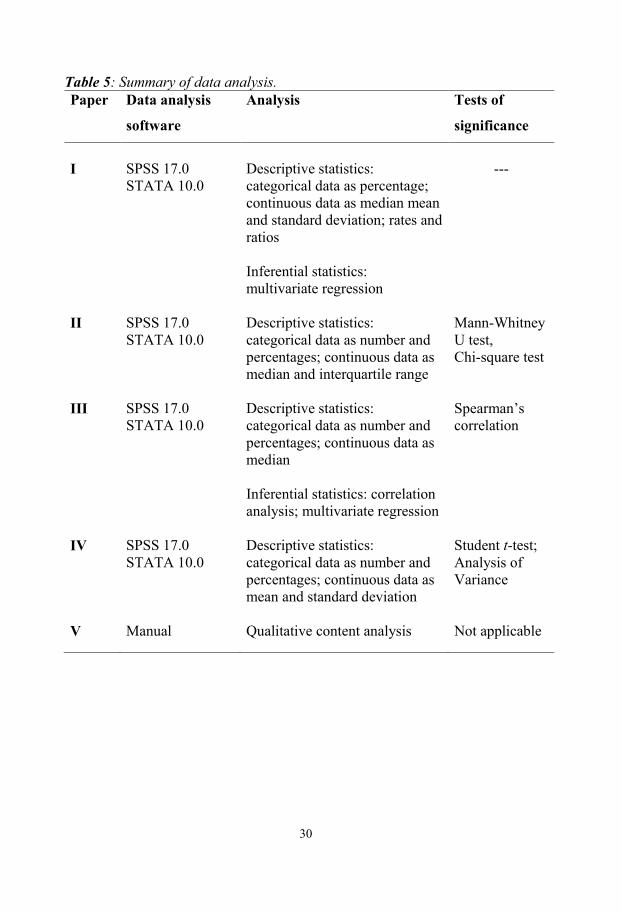
30
Table 5: Summary of data analysis. Paper Data analysis
software
Analysis Tests of
significance
I
SPSS 17.0 STATA 10.0
Descriptive statistics: categorical data as percentage; continuous data as median mean and standard deviation; rates and ratios Inferential statistics: multivariate regression
---
II SPSS 17.0 STATA 10.0
Descriptive statistics: categorical data as number and percentages; continuous data as median and interquartile range
Mann-Whitney U test, Chi-square test
III SPSS 17.0 STATA 10.0
Descriptive statistics: categorical data as number and percentages; continuous data as median Inferential statistics: correlation analysis; multivariate regression
Spearman’s correlation
IV SPSS 17.0 STATA 10.0
Descriptive statistics: categorical data as number and percentages; continuous data as mean and standard deviation
Student t-test; Analysis of Variance
V Manual Qualitative content analysis Not applicable
31
Paper I
Nominal data are presented as percentages. Continuous variables are expressed
as mean and standard deviations. Various crude and specific rates and ratios
were calculated for fertility, morbidity, and mortality. Further, I conducted age-
adjusted multivariate analysis of composite self-reported prevalence of the
NCDs (CVDs including hypertension, cancer, and diabetes).
Paper II
The KAP/behavior components of the questionnaire were given scores, and
higher score indicated better KAP/behavior. Maximum possible scores were 53,
56, and 25 for knowledge, attitude and practice/behavior, respectively. I
converted the individual score into percent of maximum score, and calculated
median percent scores for each subset of the study population (e.g., median
percent score of knowledge among men). Also, the percent scores were
classified into five categories based on the quintile values: highly insufficient
(≤20%), insufficient (20%–40%), sufficient (41%–60%), satisfactory (61%–
80%), and highly satisfactory (>80%) (97).
Descriptive statistical analysis was performed. Categorical data were
presented as numbers and percentages, and continuous data were presented as
median and interquartile range (IQR). Chi-square and Mann-Whitney U tests
were applied to compare proportions and medians, respectively.
Paper III
The questionnaire on physical activity and its analysis and interpretation are
based on the GPAQ and the WHO-STEPS manual (80, 101). MET-minutes per
week is considered the basic unit of physical activity, and its median values were
calculated for work, travel, and leisure. LPA is defined as those individuals not
meeting the GPAQ criteria for high or moderate physical activity. To calculate
the odds of having LPA, high and moderate physical activity was arbitrarily
combined into one group: moderate to vigorous physical activity. Using
30
Table 5: Summary of data analysis. Paper Data analysis
software
Analysis Tests of
significance
I
SPSS 17.0 STATA 10.0
Descriptive statistics: categorical data as percentage; continuous data as median mean and standard deviation; rates and ratios Inferential statistics: multivariate regression
---
II SPSS 17.0 STATA 10.0
Descriptive statistics: categorical data as number and percentages; continuous data as median and interquartile range
Mann-Whitney U test, Chi-square test
III SPSS 17.0 STATA 10.0
Descriptive statistics: categorical data as number and percentages; continuous data as median Inferential statistics: correlation analysis; multivariate regression
Spearman’s correlation
IV SPSS 17.0 STATA 10.0
Descriptive statistics: categorical data as number and percentages; continuous data as mean and standard deviation
Student t-test; Analysis of Variance
V Manual Qualitative content analysis Not applicable
31
Paper I
Nominal data are presented as percentages. Continuous variables are expressed
as mean and standard deviations. Various crude and specific rates and ratios
were calculated for fertility, morbidity, and mortality. Further, I conducted age-
adjusted multivariate analysis of composite self-reported prevalence of the
NCDs (CVDs including hypertension, cancer, and diabetes).
Paper II
The KAP/behavior components of the questionnaire were given scores, and
higher score indicated better KAP/behavior. Maximum possible scores were 53,
56, and 25 for knowledge, attitude and practice/behavior, respectively. I
converted the individual score into percent of maximum score, and calculated
median percent scores for each subset of the study population (e.g., median
percent score of knowledge among men). Also, the percent scores were
classified into five categories based on the quintile values: highly insufficient
(≤20%), insufficient (20%–40%), sufficient (41%–60%), satisfactory (61%–
80%), and highly satisfactory (>80%) (97).
Descriptive statistical analysis was performed. Categorical data were
presented as numbers and percentages, and continuous data were presented as
median and interquartile range (IQR). Chi-square and Mann-Whitney U tests
were applied to compare proportions and medians, respectively.
Paper III
The questionnaire on physical activity and its analysis and interpretation are
based on the GPAQ and the WHO-STEPS manual (80, 101). MET-minutes per
week is considered the basic unit of physical activity, and its median values were
calculated for work, travel, and leisure. LPA is defined as those individuals not
meeting the GPAQ criteria for high or moderate physical activity. To calculate
the odds of having LPA, high and moderate physical activity was arbitrarily
combined into one group: moderate to vigorous physical activity. Using
32
multivariate analysis, we calculated odds ratios and 95% CI for having LPA for
the various sociodemographic and risk factor substrata. Spearman’s correlation
coefficient was calculated to test the correlation between non-normal continuous
variables. I also computed the percentage of study population meeting the WHO
recommendations for physical activity (102).
The analysis excluded 137 of the 777 respondents because mandatory data
on 3 blood pressure readings or anthropometric measurements were missing.
This resulted in an 18% reduction in the final sample, but improved the internal
validity of the study.
Paper IV
Demographic parameters were measured as nominal variables and expressed in
numbers and percentages. Fruit and vegetable intakes are presented as means
and standard deviations. Student t-test and analysis of variance (ANOVA) were
applied to compare the average values across each sociodemographic variable.
Results are presented separately for men and women.
Paper V
The data was analyzed manually applying qualitative content analysis. The
analysis focused on manifest content (i.e., visible and obvious components).
First, the data from the tape recordings, complemented by the field notes, were
transcribed verbatim and translated from Nepalese language into English.
Meaningful units were extracted from the transcripts and condensed, and codes
were generated (Table 6).
33
Table 6: Example of meaningful units: condensation and abstraction.
Respon
dent
Meanin
gful
Units
Condense
d
Meaningf
ul Units
Codes
Sub-
sub
categories
Sub-
categori
es
Catego
ries
R7
Causes of heart disease include smoking and excessive alcohol
Smoking and excessive alcohol cause heart disease
Smoking Smoking
Risk factors
Heart disease linked to diet and other health behaviors
Alcohol
Excess Alcohol
R13
Festivals affect health and heart due to greater consumption of alcohol and high-content fats, spices, oily foods.
Festivals affect heart due to high consumption of alcohol, spices, and fat.
Festivals Effect of tradition and culture
Socio-demographic environment
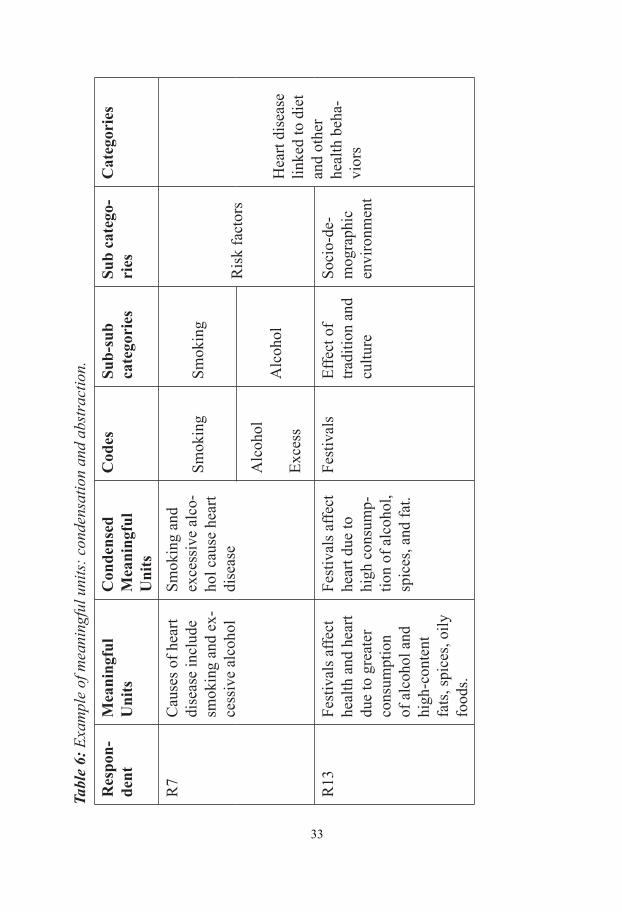
32
multivariate analysis, we calculated odds ratios and 95% CI for having LPA for
the various sociodemographic and risk factor substrata. Spearman’s correlation
coefficient was calculated to test the correlation between non-normal continuous
variables. I also computed the percentage of study population meeting the WHO
recommendations for physical activity (102).
The analysis excluded 137 of the 777 respondents because mandatory data
on 3 blood pressure readings or anthropometric measurements were missing.
This resulted in an 18% reduction in the final sample, but improved the internal
validity of the study.
Paper IV
Demographic parameters were measured as nominal variables and expressed in
numbers and percentages. Fruit and vegetable intakes are presented as means
and standard deviations. Student t-test and analysis of variance (ANOVA) were
applied to compare the average values across each sociodemographic variable.
Results are presented separately for men and women.
Paper V
The data was analyzed manually applying qualitative content analysis. The
analysis focused on manifest content (i.e., visible and obvious components).
First, the data from the tape recordings, complemented by the field notes, were
transcribed verbatim and translated from Nepalese language into English.
Meaningful units were extracted from the transcripts and condensed, and codes
were generated (Table 6).
33
Table 6: Example of meaningful units: condensation and abstraction.
Respon
dent
Meanin
gful
Units
Condense
d
Meaningf
ul Units
Codes
Sub-
sub
categories
Sub-
categori
es
Catego
ries
R7
Causes of heart disease include smoking and excessive alcohol
Smoking and excessive alcohol cause heart disease
Smoking Smoking
Risk factors
Heart disease linked to diet and other health behaviors
Alcohol
Excess Alcohol
R13
Festivals affect health and heart due to greater consumption of alcohol and high-content fats, spices, oily foods.
Festivals affect heart due to high consumption of alcohol, spices, and fat.
Festivals Effect of tradition and culture
Socio-demographic environment
Tabl
e 6:
Exa
mpl
e of
mea
ning
ful u
nits
: con
dens
atio
n an
d ab
stra
ctio
n.
Res
pon-
dent
Mea
ning
ful
Uni
tsC
onde
nsed
M
eani
ngfu
l U
nits
Cod
esSu
b-su
b ca
tego
ries
Sub
cate
go-
ries
Cat
egor
ies
R7
Cau
ses o
f hea
rt di
seas
e in
clud
e sm
okin
g an
d ex
-ce
ssiv
e al
coho
l
Smok
ing
and
exce
ssiv
e al
co-
hol c
ause
hea
rt di
seas
e
Smok
ing
Smok
ing
Ris
k fa
ctor
s
Hea
rt di
seas
e lin
ked
to d
iet
and
othe
r he
alth
beh
a-vi
ors
Alc
ohol
Exce
ssA
lcoh
ol
R13
Fest
ival
s affe
ct
heal
th a
nd h
eart
due
to g
reat
er
cons
umpt
ion
of a
lcoh
ol a
nd
high
-con
tent
fa
ts, s
pice
s, oi
ly
food
s.
Fest
ival
s affe
ct
hear
t due
to
high
con
sum
p-tio
n of
alc
ohol
, sp
ices
, and
fat.
Fest
ival
sEf
fect
of
tradi
tion
and
cultu
re
Soci
o-de
-m
ogra
phic
en
viro
nmen
t
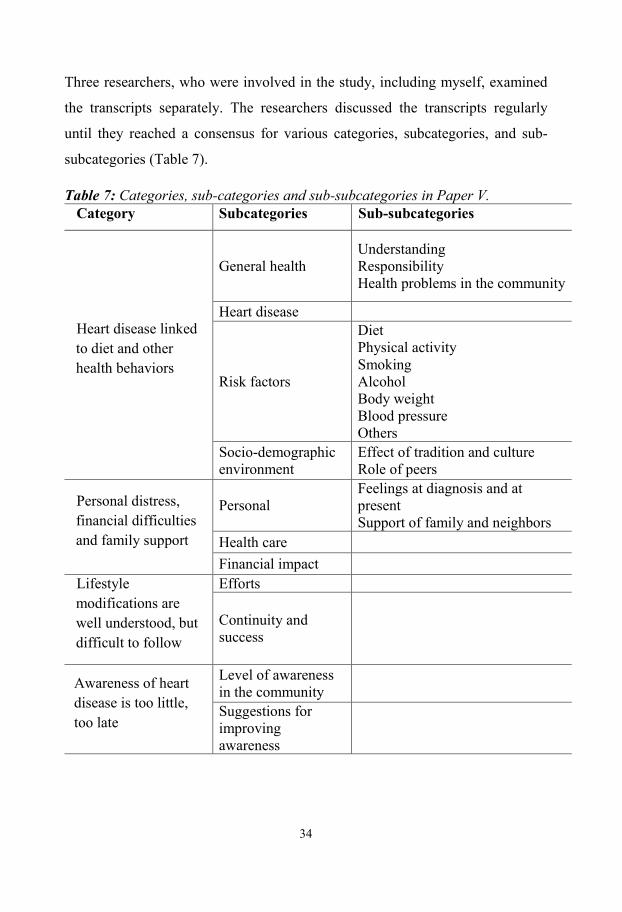
34
Three researchers, who were involved in the study, including myself, examined
the transcripts separately. The researchers discussed the transcripts regularly
until they reached a consensus for various categories, subcategories, and sub-
subcategories (Table 7).
Table 7: Categories, sub-categories and sub-subcategories in Paper V. Category Subcategories Sub-subcategories
Heart disease linked to diet and other health behaviors
General health Understanding Responsibility Health problems in the community
Heart disease
Risk factors
Diet Physical activity Smoking Alcohol Body weight Blood pressure Others
Socio-demographic environment
Effect of tradition and culture Role of peers
Personal distress, financial difficulties and family support
Personal Feelings at diagnosis and at present Support of family and neighbors
Health care Financial impact
Lifestyle modifications are well understood, but difficult to follow
Efforts
Continuity and success
Awareness of heart disease is too little, too late
Level of awareness in the community
Suggestions for improving awareness
35
Ethical considerations
Permission to operate a surveillance site in Duwakot and Jhaukhel villages
materialized through formal and informal discussions at different levels. At the
authority level, I met with personnel of the Ministry of Health and Population,
who confirmed the Ministry’s support. Official permission to conduct the studies
was obtained from the Nepal Health Research Council, which is the research
wing of the Ministry and the main authority of health-related research in Nepal. I
also obtained ethical clearance from the Institutional Review Board of
Kathmandu Medical College. At the local level, I initially and regularly
consulted local political and health leaders regarding any pertinent issue and
periodically briefed them regarding progress. Although often unwritten, their
support remained critical to the studies.
At the household level, the enumerators explained the objectives of the
study to the respondents and sought their written consent. Because people
generally hesitate to sign documents for they fear misuse, enumerators asked for
verbal consent if a respondent wanted to participate in the study but did not want
to give written consent. This process was implemented in all five studies (Papers
I–V). Further, we obtained additional permission from respondents for tape
recording and note taking during in-depth interviews (Paper V).
Before beginning an interview, enumerators told respondents for the
quantitative (Papers I–IV) and qualitative studies (Paper V) that they were free
to terminate the interview at anytime. We also told them that they could skip any
question or a particular section of the questionnaire if they were not comfortable
with that question or section. For example, a few respondents answered the
questions but did not want to have their anthropometric measurements taken.
All interviews for the quantitative studies (Papers I–IV) were conducted
in the households of the respondents. Of the 13 in-depth interviews in the
qualitative study (Paper V), all but 1 interview was conducted in the community
hospital of Kathmandu Medical College at Duwakot. Confidentiality of the
34
Three researchers, who were involved in the study, including myself, examined
the transcripts separately. The researchers discussed the transcripts regularly
until they reached a consensus for various categories, subcategories, and sub-
subcategories (Table 7).
Table 7: Categories, sub-categories and sub-subcategories in Paper V. Category Subcategories Sub-subcategories
Heart disease linked to diet and other health behaviors
General health Understanding Responsibility Health problems in the community
Heart disease
Risk factors
Diet Physical activity Smoking Alcohol Body weight Blood pressure Others
Socio-demographic environment
Effect of tradition and culture Role of peers
Personal distress, financial difficulties and family support
Personal Feelings at diagnosis and at present Support of family and neighbors
Health care Financial impact
Lifestyle modifications are well understood, but difficult to follow
Efforts
Continuity and success
Awareness of heart disease is too little, too late
Level of awareness in the community
Suggestions for improving awareness
35
Ethical considerations
Permission to operate a surveillance site in Duwakot and Jhaukhel villages
materialized through formal and informal discussions at different levels. At the
authority level, I met with personnel of the Ministry of Health and Population,
who confirmed the Ministry’s support. Official permission to conduct the studies
was obtained from the Nepal Health Research Council, which is the research
wing of the Ministry and the main authority of health-related research in Nepal. I
also obtained ethical clearance from the Institutional Review Board of
Kathmandu Medical College. At the local level, I initially and regularly
consulted local political and health leaders regarding any pertinent issue and
periodically briefed them regarding progress. Although often unwritten, their
support remained critical to the studies.
At the household level, the enumerators explained the objectives of the
study to the respondents and sought their written consent. Because people
generally hesitate to sign documents for they fear misuse, enumerators asked for
verbal consent if a respondent wanted to participate in the study but did not want
to give written consent. This process was implemented in all five studies (Papers
I–V). Further, we obtained additional permission from respondents for tape
recording and note taking during in-depth interviews (Paper V).
Before beginning an interview, enumerators told respondents for the
quantitative (Papers I–IV) and qualitative studies (Paper V) that they were free
to terminate the interview at anytime. We also told them that they could skip any
question or a particular section of the questionnaire if they were not comfortable
with that question or section. For example, a few respondents answered the
questions but did not want to have their anthropometric measurements taken.
All interviews for the quantitative studies (Papers I–IV) were conducted
in the households of the respondents. Of the 13 in-depth interviews in the
qualitative study (Paper V), all but 1 interview was conducted in the community
hospital of Kathmandu Medical College at Duwakot. Confidentiality of the
36
interviews was maintained by avoiding potential onlookers, usually by
conducting the interviews indoors or separately.
Data security was rigorously maintained. Completed forms were securely
kept in the HDSS office at the community hospital of Nepal Medical College at
Jhaukhel. Only the research team had access to the digital data. No name of any
individual respondent, including the interviewees of the qualitative study,
appears in the published papers or the thesis.
Study participants were exposed to no apparent risk, physical or
psychological. However, some participants (e.g., Brahmin women) may have
considered a few questions offensive, such as those on alcohol consumption.
Inquiry about intake of fruits and vegetables might be embarrassing for some
because it may reflect their purchasing capacity. Enumerators were told to
handle such situations sensibly. Additionally, the in-depth interviews (Paper V)
explored the experiences of patients with cardiovascular conditions, which
potentially could touch upon both sensitive and emotional aspects.
Study respondents received no monetary benefit, either directly or in the
form of a gift. Respondents identified as needing health services, including those
with newly diagnosed hypertension, were referred to the community hospitals of
either KMC or NMC with a provision for discounted consultation fees.
37
RESULTS Paper I: Establishing a health demographic surveillance site in Bhaktapur
district, Nepal: initial experiences and findings
Paper I presents two aspects of the HDSS establishment in Duwakot and
Jhaukhel villages in the Bhaktapur district of Nepal: experience of the initiation
of the HDSS itself, and findings of the baseline study conducted in 2010. The
main objectives of establishing JD-HDSS were to (i) collect baseline data on
sociodemographic and vital events; (ii) identify the prevalent health problems,
with a focus on NCDs; and (iii) provide appropriate sampling frames for future
studies.
Eighteen enumerators surveyed 2,712 households (1,155 in Jhaukhel and
1,557 in Duwakot) during 3 months in 2010 and collected information on 13,669
individuals (6,057 in Jhaukhel and 7,612 in Duwakot). The median age for both
sexes was 27 years, and adults comprised 69.9% of the total population. Males
accounted for 51% of the total population. The major three ethnic groups were
Brahmin, Chhetri, and Newar. The illiteracy rate for individuals >6 years of age
was 18.2%. More than two thirds of the population was economically active, and
about 2% of the population had migrated from other parts of Nepal.
The crude birth rate in the JD-HDSS population was 9.7/1,000; about 10%
of all births occurred at home. The crude death rate was 3.9/1,000 per year and
we recorded no deaths among infants or children younger than 5 years. Two
thirds of all deaths were registered. About one third of deaths were premature
(<65 years of age). NCDs such as CVDs, hypertension, diabetes, and cancer
were the leading causes of mortality. Along with respiratory problems, NCDs
were also the main causes of morbidity in the community (Figure 5). Thus,
Paper I justified further studies of CVDs in the community. In addition, Paper I
36
interviews was maintained by avoiding potential onlookers, usually by
conducting the interviews indoors or separately.
Data security was rigorously maintained. Completed forms were securely
kept in the HDSS office at the community hospital of Nepal Medical College at
Jhaukhel. Only the research team had access to the digital data. No name of any
individual respondent, including the interviewees of the qualitative study,
appears in the published papers or the thesis.
Study participants were exposed to no apparent risk, physical or
psychological. However, some participants (e.g., Brahmin women) may have
considered a few questions offensive, such as those on alcohol consumption.
Inquiry about intake of fruits and vegetables might be embarrassing for some
because it may reflect their purchasing capacity. Enumerators were told to
handle such situations sensibly. Additionally, the in-depth interviews (Paper V)
explored the experiences of patients with cardiovascular conditions, which
potentially could touch upon both sensitive and emotional aspects.
Study respondents received no monetary benefit, either directly or in the
form of a gift. Respondents identified as needing health services, including those
with newly diagnosed hypertension, were referred to the community hospitals of
either KMC or NMC with a provision for discounted consultation fees.
37
RESULTS Paper I: Establishing a health demographic surveillance site in Bhaktapur
district, Nepal: initial experiences and findings
Paper I presents two aspects of the HDSS establishment in Duwakot and
Jhaukhel villages in the Bhaktapur district of Nepal: experience of the initiation
of the HDSS itself, and findings of the baseline study conducted in 2010. The
main objectives of establishing JD-HDSS were to (i) collect baseline data on
sociodemographic and vital events; (ii) identify the prevalent health problems,
with a focus on NCDs; and (iii) provide appropriate sampling frames for future
studies.
Eighteen enumerators surveyed 2,712 households (1,155 in Jhaukhel and
1,557 in Duwakot) during 3 months in 2010 and collected information on 13,669
individuals (6,057 in Jhaukhel and 7,612 in Duwakot). The median age for both
sexes was 27 years, and adults comprised 69.9% of the total population. Males
accounted for 51% of the total population. The major three ethnic groups were
Brahmin, Chhetri, and Newar. The illiteracy rate for individuals >6 years of age
was 18.2%. More than two thirds of the population was economically active, and
about 2% of the population had migrated from other parts of Nepal.
The crude birth rate in the JD-HDSS population was 9.7/1,000; about 10%
of all births occurred at home. The crude death rate was 3.9/1,000 per year and
we recorded no deaths among infants or children younger than 5 years. Two
thirds of all deaths were registered. About one third of deaths were premature
(<65 years of age). NCDs such as CVDs, hypertension, diabetes, and cancer
were the leading causes of mortality. Along with respiratory problems, NCDs
were also the main causes of morbidity in the community (Figure 5). Thus,
Paper I justified further studies of CVDs in the community. In addition, Paper I
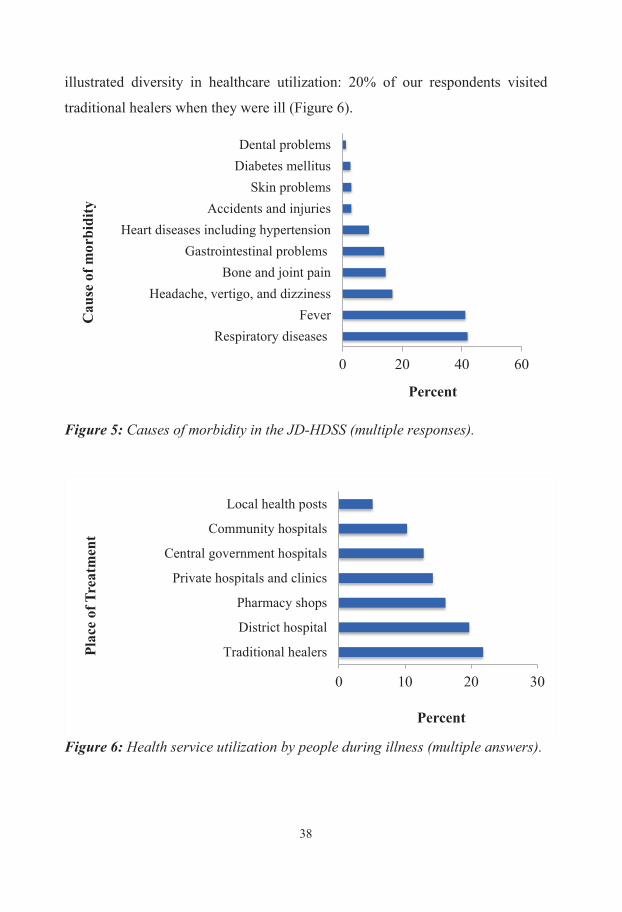
38
illustrated diversity in healthcare utilization: 20% of our respondents visited
traditional healers when they were ill (Figure 6).
Figure 5: Causes of morbidity in the JD-HDSS (multiple responses).
Figure 6: Health service utilization by people during illness (multiple answers).
0 20 40 60
Respiratory diseasesFever
Headache, vertigo, and dizzinessBone and joint pain
Gastrointestinal problemsHeart diseases including hypertension
Accidents and injuriesSkin problems
Diabetes mellitusDental problems
Percent
Cau
se o
f mor
bidi
ty
0 10 20 30
Traditional healers
District hospital
Pharmacy shops
Private hospitals and clinics
Central government hospitals
Community hospitals
Local health posts
Percent
Plac
e of
Tre
atm
ent
39
Paper II: Cardiovascular health knowledge, attitude, and practice/
behaviour in an urbanizing community of Nepal: a population-based cross-
sectional study from Jhaukhel-Duwakot health demographic surveillance
site
Paper II assessed the status of cardiovascular health KAP/behavior in a sample
population in JD-HDSS. We aimed to interview one adult aged 25–59 years
from each of the 840 households in the randomly selected six clusters
(administrative units, or wards).
Study population
Seventy percent of the respondents were female; one third lacked formal
education and two thirds were housewives. Among 229 male respondents, about
20% worked in agriculture and one third was either into service or self-
employed. Of the 777 respondents with complete information, approximately
one third belonged to each of the three age-group intervals (25–34, 35–44, and
45–59 years).
Risk factors
Tobacco and alcohol consumption was higher in males than females (current
smoking [33.5% vs. 14.7%], smokeless tobacco [20.2% vs. 3.3%], and current
drinking [34.5% vs. 12.6%], respectively). On the other hand, metabolism-
related risk factors were more prevalent in females than males (low physical
activity [45.2% vs. 38.3%], overweight [31.6% vs. 25.0%], obesity by body
mass index [11.2% vs. 5.4%], and increased waist circumference [56.6% vs.
21.6%], respectively).
Knowledge about causes of heart diseases
When asked to spontaneously name the reasons why people suffer from heart
disease, respondents showed low overall knowledge, ranging from 1.0% for high
blood sugar to 29.2% for smoking (Table 8). Generally, males, younger
38
illustrated diversity in healthcare utilization: 20% of our respondents visited
traditional healers when they were ill (Figure 6).
Figure 5: Causes of morbidity in the JD-HDSS (multiple responses).
Figure 6: Health service utilization by people during illness (multiple answers).
0 20 40 60
Respiratory diseasesFever
Headache, vertigo, and dizzinessBone and joint pain
Gastrointestinal problemsHeart diseases including hypertension
Accidents and injuriesSkin problems
Diabetes mellitusDental problems
Percent
Cau
se o
f mor
bidi
ty
0 10 20 30
Traditional healers
District hospital
Pharmacy shops
Private hospitals and clinics
Central government hospitals
Community hospitals
Local health posts
Percent
Plac
e of
Tre
atm
ent
39
Paper II: Cardiovascular health knowledge, attitude, and practice/
behaviour in an urbanizing community of Nepal: a population-based cross-
sectional study from Jhaukhel-Duwakot health demographic surveillance
site
Paper II assessed the status of cardiovascular health KAP/behavior in a sample
population in JD-HDSS. We aimed to interview one adult aged 25–59 years
from each of the 840 households in the randomly selected six clusters
(administrative units, or wards).
Study population
Seventy percent of the respondents were female; one third lacked formal
education and two thirds were housewives. Among 229 male respondents, about
20% worked in agriculture and one third was either into service or self-
employed. Of the 777 respondents with complete information, approximately
one third belonged to each of the three age-group intervals (25–34, 35–44, and
45–59 years).
Risk factors
Tobacco and alcohol consumption was higher in males than females (current
smoking [33.5% vs. 14.7%], smokeless tobacco [20.2% vs. 3.3%], and current
drinking [34.5% vs. 12.6%], respectively). On the other hand, metabolism-
related risk factors were more prevalent in females than males (low physical
activity [45.2% vs. 38.3%], overweight [31.6% vs. 25.0%], obesity by body
mass index [11.2% vs. 5.4%], and increased waist circumference [56.6% vs.
21.6%], respectively).
Knowledge about causes of heart diseases
When asked to spontaneously name the reasons why people suffer from heart
disease, respondents showed low overall knowledge, ranging from 1.0% for high
blood sugar to 29.2% for smoking (Table 8). Generally, males, younger
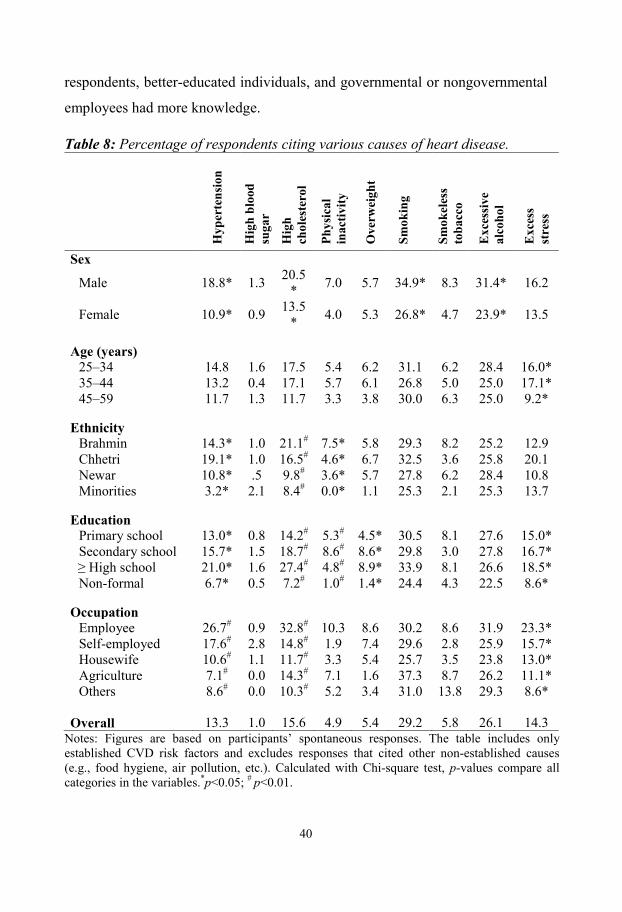
40
respondents, better-educated individuals, and governmental or nongovernmental
employees had more knowledge.
Table 8: Percentage of respondents citing various causes of heart disease.
H
yper
tens
ion
Hig
h bl
ood
suga
r
Hig
h ch
oles
tero
l
Phys
ical
in
activ
ity
Ove
rwei
ght
Smok
ing
Smok
eles
s to
bacc
o
Exc
essi
ve
alco
hol
Exc
ess
stre
ss
Sex
Male 18.8* 1.3 20.5* 7.0 5.7 34.9* 8.3 31.4* 16.2
Female 10.9* 0.9 13.5* 4.0 5.3 26.8* 4.7 23.9* 13.5
Age (years) 25–34 14.8 1.6 17.5 5.4 6.2 31.1 6.2 28.4 16.0* 35–44 13.2 0.4 17.1 5.7 6.1 26.8 5.0 25.0 17.1* 45–59 11.7 1.3 11.7 3.3 3.8 30.0 6.3 25.0 9.2*
Ethnicity Brahmin 14.3* 1.0 21.1# 7.5* 5.8 29.3 8.2 25.2 12.9 Chhetri 19.1* 1.0 16.5# 4.6* 6.7 32.5 3.6 25.8 20.1 Newar 10.8* .5 9.8# 3.6* 5.7 27.8 6.2 28.4 10.8 Minorities 3.2* 2.1 8.4# 0.0* 1.1 25.3 2.1 25.3 13.7
Education Primary school 13.0* 0.8 14.2# 5.3# 4.5* 30.5 8.1 27.6 15.0* Secondary school 15.7* 1.5 18.7# 8.6# 8.6* 29.8 3.0 27.8 16.7* ≥ High school 21.0* 1.6 27.4# 4.8# 8.9* 33.9 8.1 26.6 18.5* Non-formal 6.7* 0.5 7.2# 1.0# 1.4* 24.4 4.3 22.5 8.6*
Occupation Employee 26.7# 0.9 32.8# 10.3 8.6 30.2 8.6 31.9 23.3* Self-employed 17.6# 2.8 14.8# 1.9 7.4 29.6 2.8 25.9 15.7* Housewife 10.6# 1.1 11.7# 3.3 5.4 25.7 3.5 23.8 13.0* Agriculture 7.1# 0.0 14.3# 7.1 1.6 37.3 8.7 26.2 11.1* Others 8.6# 0.0 10.3# 5.2 3.4 31.0 13.8 29.3 8.6*
Overall 13.3 1.0 15.6 4.9 5.4 29.2 5.8 26.1 14.3 Notes: Figures are based on participants’ spontaneous responses. The table includes only established CVD risk factors and excludes responses that cited other non-established causes (e.g., food hygiene, air pollution, etc.). Calculated with Chi-square test, p-values compare all categories in the variables.*p<0.05; # p<0.01.
41
Questions on causes of heart disease were repeated in a closed-ended manner
that stated the risk factors and provided “yes/no” options. When asked in this
manner, respondents appeared to have greater knowledge about the causes of
heart disease compared to the earlier spontaneous responses; the percentage of
respondents saying “yes” to the risk factors increased considerably (Figure 7).
Figure 7: Comparison of spontaneous and prompted responses (%) given for cause of heart disease.
Knowledge about heart attack: signs and management
Almost 60% of respondents did not know any sign of a heart attack, 20% knew
one sign, and 20% mentioned 2–4 signs. These percentages were true across all
demographic subsets and showed no significant differences in terms of gender
(p>0.05), age (p=0.49), caste/ethnicity (p=0.40), and education (p=0.53). Loss of
consciousness (23.7%) was the most common sign mentioned, followed by chest
0 50 100
High blood sugarOld age
Physical inactivityHereditary
OverweightSmokeless tobacco
High blood pressureExcess stress
High cholesterolExcessive alcohol
Smoking
Percent
Cau
se o
f hea
rt d
isea
se
Spontaneous (%) Prompted (%)
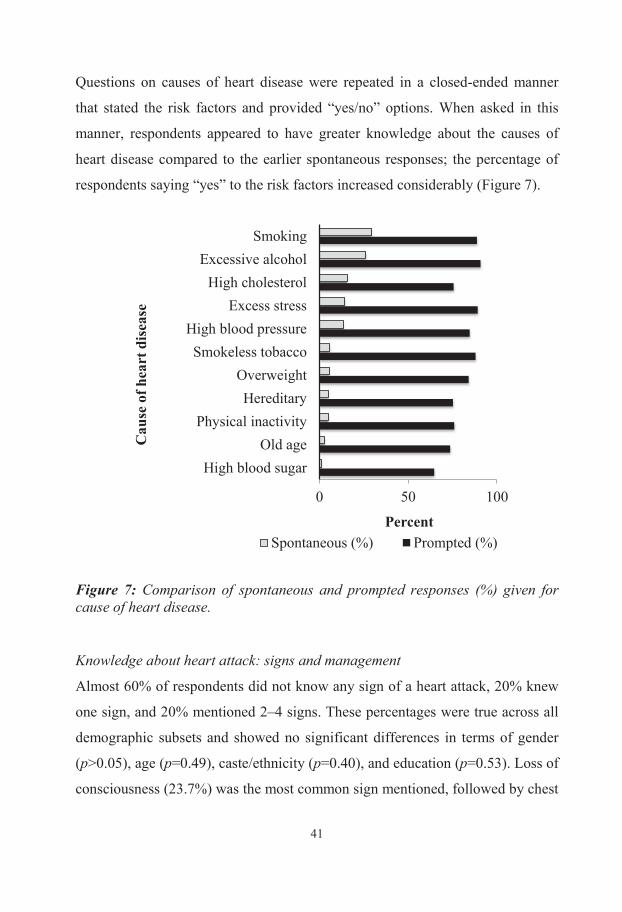
40
respondents, better-educated individuals, and governmental or nongovernmental
employees had more knowledge.
Table 8: Percentage of respondents citing various causes of heart disease.
Hyp
erte
nsio
n
Hig
h bl
ood
suga
r
Hig
h ch
oles
tero
l
Phys
ical
in
activ
ity
Ove
rwei
ght
Smok
ing
Smok
eles
s to
bacc
o
Exc
essi
ve
alco
hol
Exc
ess
stre
ss
Sex
Male 18.8* 1.3 20.5* 7.0 5.7 34.9* 8.3 31.4* 16.2
Female 10.9* 0.9 13.5* 4.0 5.3 26.8* 4.7 23.9* 13.5
Age (years) 25–34 14.8 1.6 17.5 5.4 6.2 31.1 6.2 28.4 16.0* 35–44 13.2 0.4 17.1 5.7 6.1 26.8 5.0 25.0 17.1* 45–59 11.7 1.3 11.7 3.3 3.8 30.0 6.3 25.0 9.2*
Ethnicity Brahmin 14.3* 1.0 21.1# 7.5* 5.8 29.3 8.2 25.2 12.9 Chhetri 19.1* 1.0 16.5# 4.6* 6.7 32.5 3.6 25.8 20.1 Newar 10.8* .5 9.8# 3.6* 5.7 27.8 6.2 28.4 10.8 Minorities 3.2* 2.1 8.4# 0.0* 1.1 25.3 2.1 25.3 13.7
Education Primary school 13.0* 0.8 14.2# 5.3# 4.5* 30.5 8.1 27.6 15.0* Secondary school 15.7* 1.5 18.7# 8.6# 8.6* 29.8 3.0 27.8 16.7* ≥ High school 21.0* 1.6 27.4# 4.8# 8.9* 33.9 8.1 26.6 18.5* Non-formal 6.7* 0.5 7.2# 1.0# 1.4* 24.4 4.3 22.5 8.6*
Occupation Employee 26.7# 0.9 32.8# 10.3 8.6 30.2 8.6 31.9 23.3* Self-employed 17.6# 2.8 14.8# 1.9 7.4 29.6 2.8 25.9 15.7* Housewife 10.6# 1.1 11.7# 3.3 5.4 25.7 3.5 23.8 13.0* Agriculture 7.1# 0.0 14.3# 7.1 1.6 37.3 8.7 26.2 11.1* Others 8.6# 0.0 10.3# 5.2 3.4 31.0 13.8 29.3 8.6*
Overall 13.3 1.0 15.6 4.9 5.4 29.2 5.8 26.1 14.3 Notes: Figures are based on participants’ spontaneous responses. The table includes only established CVD risk factors and excludes responses that cited other non-established causes (e.g., food hygiene, air pollution, etc.). Calculated with Chi-square test, p-values compare all categories in the variables.*p<0.05; # p<0.01.
41
Questions on causes of heart disease were repeated in a closed-ended manner
that stated the risk factors and provided “yes/no” options. When asked in this
manner, respondents appeared to have greater knowledge about the causes of
heart disease compared to the earlier spontaneous responses; the percentage of
respondents saying “yes” to the risk factors increased considerably (Figure 7).
Figure 7: Comparison of spontaneous and prompted responses (%) given for cause of heart disease.
Knowledge about heart attack: signs and management
Almost 60% of respondents did not know any sign of a heart attack, 20% knew
one sign, and 20% mentioned 2–4 signs. These percentages were true across all
demographic subsets and showed no significant differences in terms of gender
(p>0.05), age (p=0.49), caste/ethnicity (p=0.40), and education (p=0.53). Loss of
consciousness (23.7%) was the most common sign mentioned, followed by chest
0 50 100
High blood sugarOld age
Physical inactivityHereditary
OverweightSmokeless tobacco
High blood pressureExcess stress
High cholesterolExcessive alcohol
Smoking
Percent
Cau
se o
f hea
rt d
isea
se
Spontaneous (%) Prompted (%)
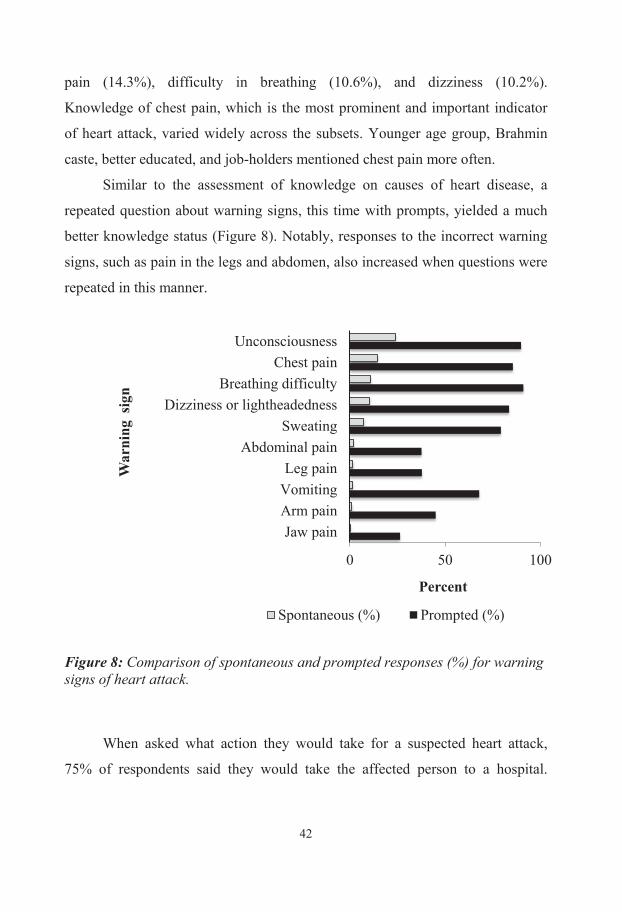
42
pain (14.3%), difficulty in breathing (10.6%), and dizziness (10.2%).
Knowledge of chest pain, which is the most prominent and important indicator
of heart attack, varied widely across the subsets. Younger age group, Brahmin
caste, better educated, and job-holders mentioned chest pain more often.
Similar to the assessment of knowledge on causes of heart disease, a
repeated question about warning signs, this time with prompts, yielded a much
better knowledge status (Figure 8). Notably, responses to the incorrect warning
signs, such as pain in the legs and abdomen, also increased when questions were
repeated in this manner.
Figure 8: Comparison of spontaneous and prompted responses (%) for warning signs of heart attack.
When asked what action they would take for a suspected heart attack,
75% of respondents said they would take the affected person to a hospital.
0 50 100
Jaw painArm painVomitingLeg pain
Abdominal painSweating
Dizziness or lightheadednessBreathing difficulty
Chest painUnconsciousness
Percent
War
ning
sig
n
Spontaneous (%) Prompted (%)
43
However, 20% of respondents gave no response, and the remaining 5% said they
would try home therapy or consult a traditional healer.
Knowledge about heart-healthy food
Overall knowledge about heart-healthy food was good, particularly regarding
green vegetables and fruit, which 94.6% and 92.1% of respondents believed to
be healthy, respectively. High fat-containing foods like ghee (clarified butter)
and traditional sweets were considered healthy by 6.7% and 13.3% of
respondents, respectively. Similarly, 7.6% and 8.4% of respondents considered
fried and processed foods heart-healthy, respectively. Regarding animal
products, 12.2% of respondents perceived red meat as a heart-friendly food and
24.5% thought that eggs are healthy. However, only one quarter of the
respondents considered fish as healthy, and 21.8% thought that salty food items
(e.g., pickles) are healthy. Knowledge of heart-healthy food associated with
neither socioeconomic variables (age, sex, ethnicity, educational status, and
occupation) nor diagnosed health status, such as hypertension and diabetes.
Knowledge about preventability of heart disease
A large majority (86.1%) of respondents thought that it was possible to prevent
heart disease by changing their lifestyle. Percentages of affirmative responses to
specific actions that reduce the risk of heart disease were as follows: reducing fat
intake (93.7%), reducing stress (93.6%), quitting smoking (92.5%), maintaining
a healthy blood pressure (92.3%), getting adequate physical activity (89.1%),
reducing salt in the diet (88.8%), and losing weight (86.1%). In general,
respondents aged 25–34 years, those with post-graduate education, and students
were 5%–20% more knowledgeable about preventive actions for heart disease
than their counterparts.
Locus of control
More than half (52.4%) of the male respondents either strongly (27.1%) or
somewhat (25.3%) agreed with the notion that the locus of control of their health
42
pain (14.3%), difficulty in breathing (10.6%), and dizziness (10.2%).
Knowledge of chest pain, which is the most prominent and important indicator
of heart attack, varied widely across the subsets. Younger age group, Brahmin
caste, better educated, and job-holders mentioned chest pain more often.
Similar to the assessment of knowledge on causes of heart disease, a
repeated question about warning signs, this time with prompts, yielded a much
better knowledge status (Figure 8). Notably, responses to the incorrect warning
signs, such as pain in the legs and abdomen, also increased when questions were
repeated in this manner.
Figure 8: Comparison of spontaneous and prompted responses (%) for warning signs of heart attack.
When asked what action they would take for a suspected heart attack,
75% of respondents said they would take the affected person to a hospital.
0 50 100
Jaw painArm painVomitingLeg pain
Abdominal painSweating
Dizziness or lightheadednessBreathing difficulty
Chest painUnconsciousness
Percent
War
ning
sig
n
Spontaneous (%) Prompted (%)
43
However, 20% of respondents gave no response, and the remaining 5% said they
would try home therapy or consult a traditional healer.
Knowledge about heart-healthy food
Overall knowledge about heart-healthy food was good, particularly regarding
green vegetables and fruit, which 94.6% and 92.1% of respondents believed to
be healthy, respectively. High fat-containing foods like ghee (clarified butter)
and traditional sweets were considered healthy by 6.7% and 13.3% of
respondents, respectively. Similarly, 7.6% and 8.4% of respondents considered
fried and processed foods heart-healthy, respectively. Regarding animal
products, 12.2% of respondents perceived red meat as a heart-friendly food and
24.5% thought that eggs are healthy. However, only one quarter of the
respondents considered fish as healthy, and 21.8% thought that salty food items
(e.g., pickles) are healthy. Knowledge of heart-healthy food associated with
neither socioeconomic variables (age, sex, ethnicity, educational status, and
occupation) nor diagnosed health status, such as hypertension and diabetes.
Knowledge about preventability of heart disease
A large majority (86.1%) of respondents thought that it was possible to prevent
heart disease by changing their lifestyle. Percentages of affirmative responses to
specific actions that reduce the risk of heart disease were as follows: reducing fat
intake (93.7%), reducing stress (93.6%), quitting smoking (92.5%), maintaining
a healthy blood pressure (92.3%), getting adequate physical activity (89.1%),
reducing salt in the diet (88.8%), and losing weight (86.1%). In general,
respondents aged 25–34 years, those with post-graduate education, and students
were 5%–20% more knowledgeable about preventive actions for heart disease
than their counterparts.
Locus of control
More than half (52.4%) of the male respondents either strongly (27.1%) or
somewhat (25.3%) agreed with the notion that the locus of control of their health
44
was God or a higher power. The proportion was higher (60.8%) among females
(strongly agreed, 38.5%; somewhat agreed, 22.3%).
Attitude towards heart-health and prevention of heart diseases
One quarter of respondents did not perceive themselves to be at risk for heart
disease. Collaterally, a majority of respondents and more men (64.6%) than
women (54.4%) did not want to improve their present lifestyle because they
thought that changing their behavior would not reduce their risk. This finding is
ironic because most respondents understood the benefits of preventive and
promotive measures such as increasing their intake of fruit and vegetables,
accessibility to recreational facilities, and banning smoking.
Although almost all respondents agreed that additional awareness
programs and healthcare facilities would be useful, fewer males (82.1%) than
females (98.5%) believed that local health volunteers could change adverse
health behavior in the general population.
Cardiovascular health practice
Despite the above-mentioned resistance to changing health behavior, many
respondents had participated in some heart friendly behavior in the past year,
from getting a diagnostic test for heart disease (10%) to reducing their
consumption of unhealthy foods (59.6%). Such actions were undertaken mostly
by more educated respondents or those working as employees in government or
nongovernment jobs. The reasons for respondents’ heart-healthy actions are
shown in Figure 9.
45
Figure 9: Number of respondents citing reasons for initiation of heart-friendly behavior (multiple responses).
It is evident from these responses that most actions were initiated after
respondents had been diagnosed with a disease condition. Four of five known
hypertensives and three fourths of the diabetics had their blood pressure and
blood sugar measured in the previous year. One third of overweight respondents
attempted to reduce their weight or improve their physical activity.
Unfortunately, the mere presence of a risk factor (e.g., smoking, alcohol
consumption, or inadequate physical activity) did not lead to better health-
seeking behavior (e.g., blood pressure measurement or blood sugar examination)
or a change in health practice. For example, only 12% of smokers attempted to
quit smoking.
0 20 40 60 80
Wanted to feel better
I saw, heard, or read information
I did it for my family
My healthcare professional encouragedme
A family member or relativeencouraged me
A friend encouraged me to take action
Wanted to avoid taking medications
A relative or a friend developed heartdisease, got sick, or passed away
Experienced symptom
Percent
Rea
son
for
initi
atin
g a
hear
t-fr
iend
ly
actio
n
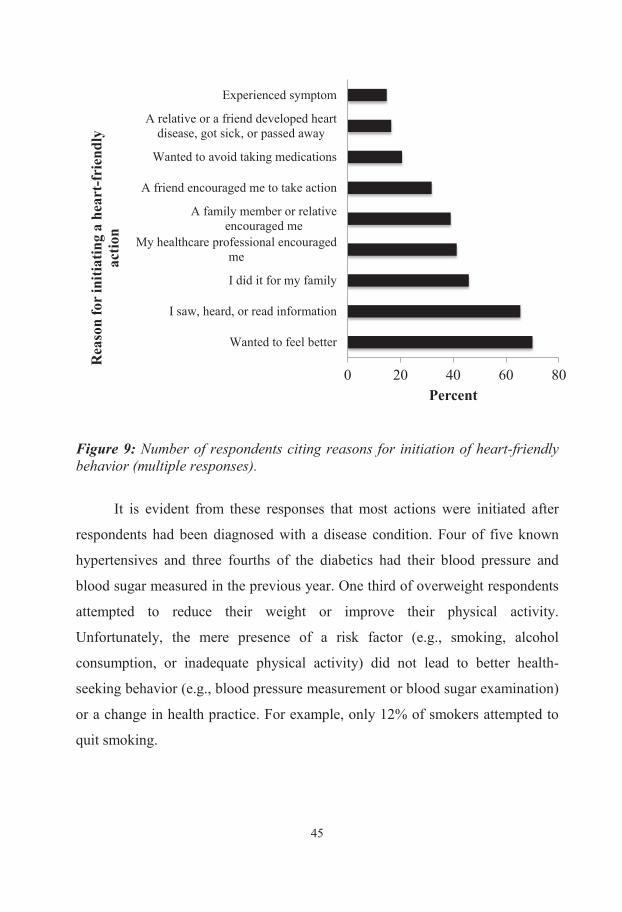
44
was God or a higher power. The proportion was higher (60.8%) among females
(strongly agreed, 38.5%; somewhat agreed, 22.3%).
Attitude towards heart-health and prevention of heart diseases
One quarter of respondents did not perceive themselves to be at risk for heart
disease. Collaterally, a majority of respondents and more men (64.6%) than
women (54.4%) did not want to improve their present lifestyle because they
thought that changing their behavior would not reduce their risk. This finding is
ironic because most respondents understood the benefits of preventive and
promotive measures such as increasing their intake of fruit and vegetables,
accessibility to recreational facilities, and banning smoking.
Although almost all respondents agreed that additional awareness
programs and healthcare facilities would be useful, fewer males (82.1%) than
females (98.5%) believed that local health volunteers could change adverse
health behavior in the general population.
Cardiovascular health practice
Despite the above-mentioned resistance to changing health behavior, many
respondents had participated in some heart friendly behavior in the past year,
from getting a diagnostic test for heart disease (10%) to reducing their
consumption of unhealthy foods (59.6%). Such actions were undertaken mostly
by more educated respondents or those working as employees in government or
nongovernment jobs. The reasons for respondents’ heart-healthy actions are
shown in Figure 9.
45
Figure 9: Number of respondents citing reasons for initiation of heart-friendly behavior (multiple responses).
It is evident from these responses that most actions were initiated after
respondents had been diagnosed with a disease condition. Four of five known
hypertensives and three fourths of the diabetics had their blood pressure and
blood sugar measured in the previous year. One third of overweight respondents
attempted to reduce their weight or improve their physical activity.
Unfortunately, the mere presence of a risk factor (e.g., smoking, alcohol
consumption, or inadequate physical activity) did not lead to better health-
seeking behavior (e.g., blood pressure measurement or blood sugar examination)
or a change in health practice. For example, only 12% of smokers attempted to
quit smoking.
0 20 40 60 80
Wanted to feel better
I saw, heard, or read information
I did it for my family
My healthcare professional encouragedme
A family member or relativeencouraged me
A friend encouraged me to take action
Wanted to avoid taking medications
A relative or a friend developed heartdisease, got sick, or passed away
Experienced symptom
Percent
Rea
son
for
initi
atin
g a
hear
t-fr
iend
ly
actio
n
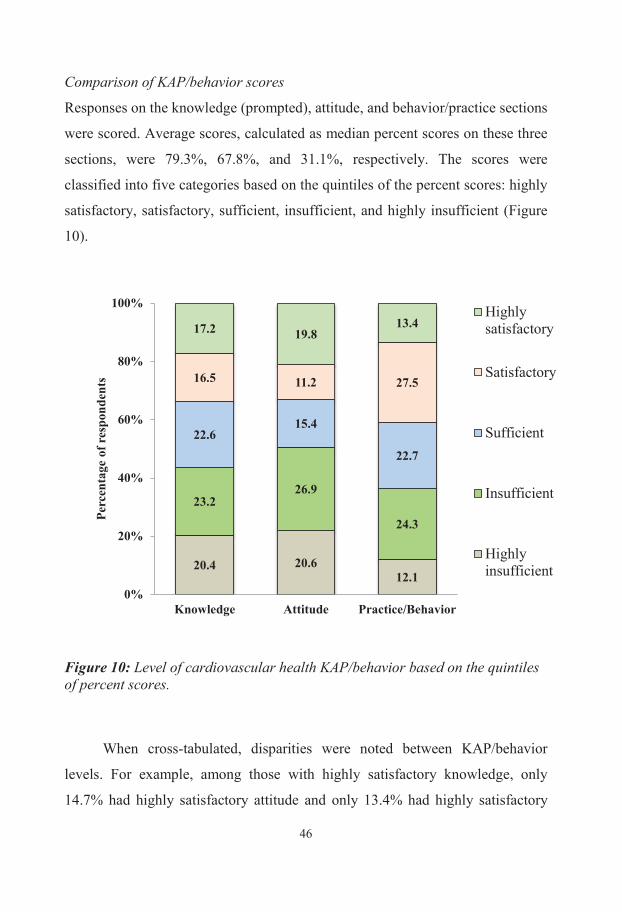
46
Comparison of KAP/behavior scores
Responses on the knowledge (prompted), attitude, and behavior/practice sections
were scored. Average scores, calculated as median percent scores on these three
sections, were 79.3%, 67.8%, and 31.1%, respectively. The scores were
classified into five categories based on the quintiles of the percent scores: highly
satisfactory, satisfactory, sufficient, insufficient, and highly insufficient (Figure
10).
Figure 10: Level of cardiovascular health KAP/behavior based on the quintiles of percent scores.
When cross-tabulated, disparities were noted between KAP/behavior
levels. For example, among those with highly satisfactory knowledge, only
14.7% had highly satisfactory attitude and only 13.4% had highly satisfactory
20.4 20.6 12.1
23.2 26.9
24.3
22.6 15.4
22.7
16.5 11.2 27.5
17.2 19.8 13.4
0%
20%
40%
60%
80%
100%
Knowledge Attitude Practice/Behavior
Perc
enta
ge o
f res
pond
ents
Highlysatisfactory
Satisfactory
Sufficient
Insufficient
Highlyinsufficient
47
behavior. Likewise, among those with highly insufficient knowledge, 26% had
highly insufficient attitude and 16.4% had highly insufficient behavior. Similar
mismatches were also observed between attitude and behavior: only 11% of
those with highly satisfactory attitude also possessed highly satisfactory
behavior.
Sociodemographic variations in KAP/behavior scores
The KAP/behavior scores showed no significant gender differences. On the
other hand, I observed statistically significant differences for age,
caste/ethnicity, and education level on knowledge and practice scores, but not
for attitude.
Paper III: Physical activity level and its sociodemographic correlates in a
peri-urban Nepalese population: a cross-sectional study from the Jhaukhel-
Duwakot health demographic surveillance site.
Paper III describes in detail the physical activity level of an urbanizing
population of Nepal. Using the standard GPAQ questionnaire, I first determined
the level of physical activity in the population, and then explored physical
activity in relation to different sociodemographic correlates.
Physical activity across the sociodemographic subgroups
Among the three domains of physical activity studied, work-related activities
accounted for the highest level of physical activity, not travel or leisure-time
physical activities (Figures 11–15). Physical activity during work was higher
among females (Figure 11), respondents aged 35–44 years (Figure 12), Newars
and ethnic minorities (Figure 13), those with informal education (Figure 14), and
those doing agriculture-related work (Figure 15). On the other hand, physical
activity during travel was lower among housewives, government employees, and
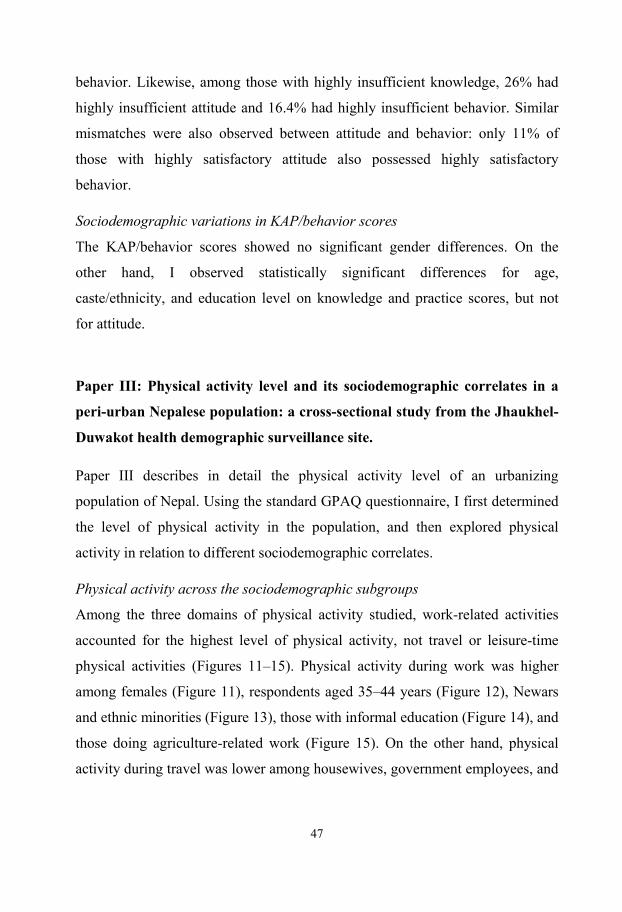
46
Comparison of KAP/behavior scores
Responses on the knowledge (prompted), attitude, and behavior/practice sections
were scored. Average scores, calculated as median percent scores on these three
sections, were 79.3%, 67.8%, and 31.1%, respectively. The scores were
classified into five categories based on the quintiles of the percent scores: highly
satisfactory, satisfactory, sufficient, insufficient, and highly insufficient (Figure
10).
Figure 10: Level of cardiovascular health KAP/behavior based on the quintiles of percent scores.
When cross-tabulated, disparities were noted between KAP/behavior
levels. For example, among those with highly satisfactory knowledge, only
14.7% had highly satisfactory attitude and only 13.4% had highly satisfactory
20.4 20.6 12.1
23.2 26.9
24.3
22.6 15.4
22.7
16.5 11.2 27.5
17.2 19.8 13.4
0%
20%
40%
60%
80%
100%
Knowledge Attitude Practice/Behavior
Perc
enta
ge o
f res
pond
ents
Highlysatisfactory
Satisfactory
Sufficient
Insufficient
Highlyinsufficient
47
behavior. Likewise, among those with highly insufficient knowledge, 26% had
highly insufficient attitude and 16.4% had highly insufficient behavior. Similar
mismatches were also observed between attitude and behavior: only 11% of
those with highly satisfactory attitude also possessed highly satisfactory
behavior.
Sociodemographic variations in KAP/behavior scores
The KAP/behavior scores showed no significant gender differences. On the
other hand, I observed statistically significant differences for age,
caste/ethnicity, and education level on knowledge and practice scores, but not
for attitude.
Paper III: Physical activity level and its sociodemographic correlates in a
peri-urban Nepalese population: a cross-sectional study from the Jhaukhel-
Duwakot health demographic surveillance site.
Paper III describes in detail the physical activity level of an urbanizing
population of Nepal. Using the standard GPAQ questionnaire, I first determined
the level of physical activity in the population, and then explored physical
activity in relation to different sociodemographic correlates.
Physical activity across the sociodemographic subgroups
Among the three domains of physical activity studied, work-related activities
accounted for the highest level of physical activity, not travel or leisure-time
physical activities (Figures 11–15). Physical activity during work was higher
among females (Figure 11), respondents aged 35–44 years (Figure 12), Newars
and ethnic minorities (Figure 13), those with informal education (Figure 14), and
those doing agriculture-related work (Figure 15). On the other hand, physical
activity during travel was lower among housewives, government employees, and
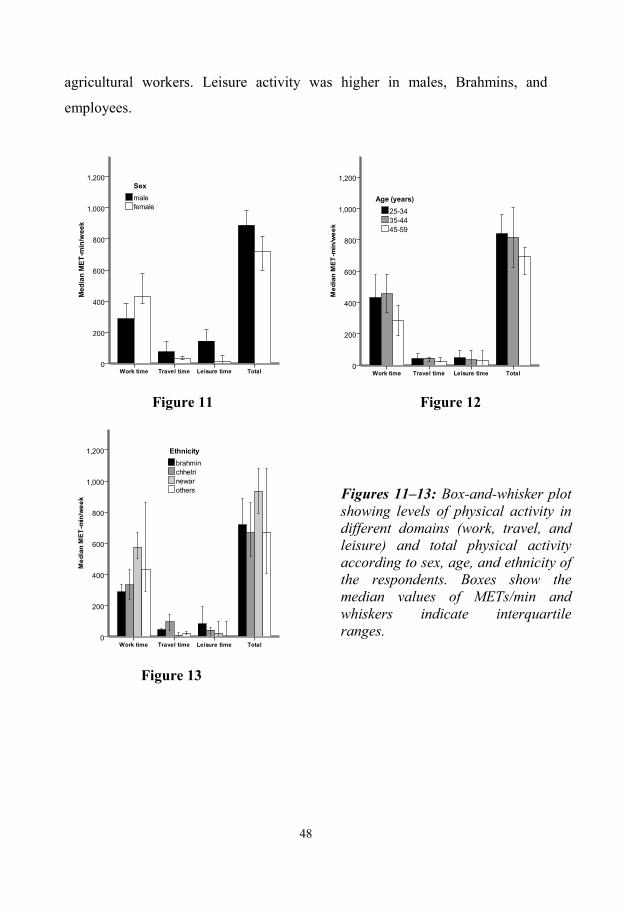
48
agricultural workers. Leisure activity was higher in males, Brahmins, and
employees.
Figure 11 Figure 12
Figure 13
Figures 11–13: Box-and-whisker plot showing levels of physical activity in different domains (work, travel, and leisure) and total physical activity according to sex, age, and ethnicity of the respondents. Boxes show the median values of METs/min and whiskers indicate interquartile ranges.
49
Figure 14
Figure 15
Figures 14–15: Box-and-whisker plots showing levels of physical activity in different domains (work, travel, and leisure) and total physical activity according to education and occupation of the respondents. Boxes show the median values of METs/min and whiskers indicate the interquartile ranges.
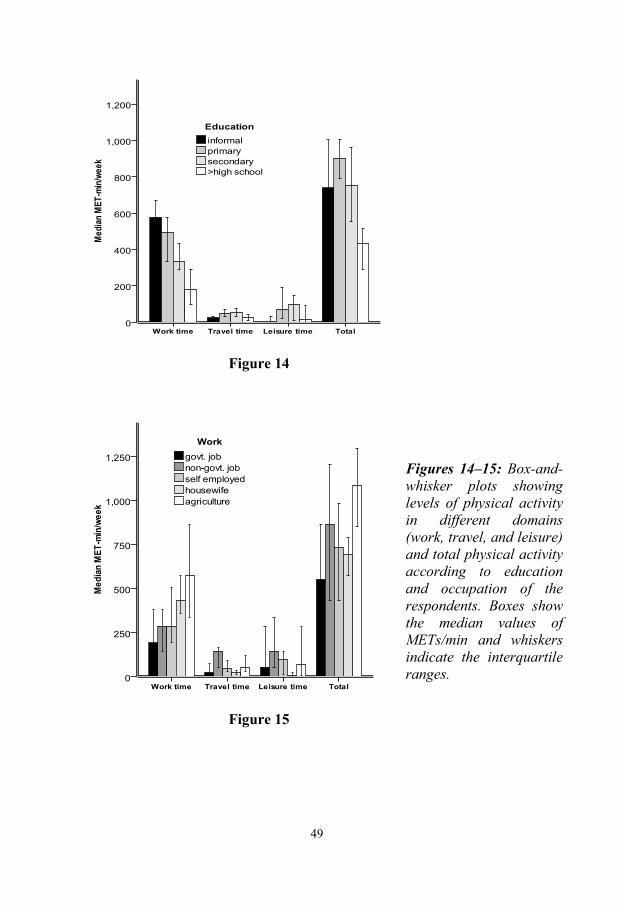
48
agricultural workers. Leisure activity was higher in males, Brahmins, and
employees.
Figure 11 Figure 12
Figure 13
Figures 11–13: Box-and-whisker plot showing levels of physical activity in different domains (work, travel, and leisure) and total physical activity according to sex, age, and ethnicity of the respondents. Boxes show the median values of METs/min and whiskers indicate interquartile ranges.
49
Figure 14
Figure 15
Figures 14–15: Box-and-whisker plots showing levels of physical activity in different domains (work, travel, and leisure) and total physical activity according to education and occupation of the respondents. Boxes show the median values of METs/min and whiskers indicate the interquartile ranges.
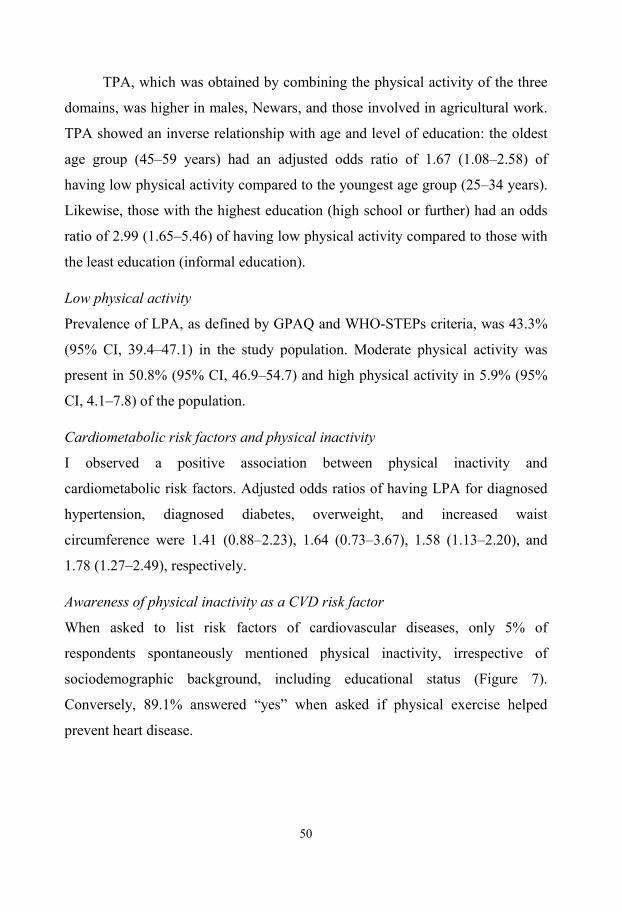
50
TPA, which was obtained by combining the physical activity of the three
domains, was higher in males, Newars, and those involved in agricultural work.
TPA showed an inverse relationship with age and level of education: the oldest
age group (45–59 years) had an adjusted odds ratio of 1.67 (1.08–2.58) of
having low physical activity compared to the youngest age group (25–34 years).
Likewise, those with the highest education (high school or further) had an odds
ratio of 2.99 (1.65–5.46) of having low physical activity compared to those with
the least education (informal education).
Low physical activity
Prevalence of LPA, as defined by GPAQ and WHO-STEPs criteria, was 43.3%
(95% CI, 39.4–47.1) in the study population. Moderate physical activity was
present in 50.8% (95% CI, 46.9–54.7) and high physical activity in 5.9% (95%
CI, 4.1–7.8) of the population.
Cardiometabolic risk factors and physical inactivity
I observed a positive association between physical inactivity and
cardiometabolic risk factors. Adjusted odds ratios of having LPA for diagnosed
hypertension, diagnosed diabetes, overweight, and increased waist
circumference were 1.41 (0.88–2.23), 1.64 (0.73–3.67), 1.58 (1.13–2.20), and
1.78 (1.27–2.49), respectively.
Awareness of physical inactivity as a CVD risk factor
When asked to list risk factors of cardiovascular diseases, only 5% of
respondents spontaneously mentioned physical inactivity, irrespective of
sociodemographic background, including educational status (Figure 7).
Conversely, 89.1% answered “yes” when asked if physical exercise helped
prevent heart disease.
51
Paper IV: Disparities in fruit and vegetable intake by socio-demographic
characteristics in peri-urban Nepalese adults: findings from the Heart-
Health Associated Research and Dissemination in the Community
(HARDIC) Study, Bhaktapur, Nepal
Paper IV investigated the overall intake of fruit and vegetable in a sample
population of JD-HDSS (Table 9).
Table 9: Average fruit and vegetable intake in men and women.
Mean (SD)
P Males Females Fruit Days/week 2.63 (1.97) 3.34 (2.17) <0.001 Servings/day 0.92 (0.63) 0.99 (0.64) 0.184 Vegetable Days/week 5.33 (1.69) 5.64 (1.55) 0.016 Servings/day 1.42 (0.57) 1.48 (0.62) 0.210 Fruit and vegetable combined Servings/day 2.34 (0.88) 2.49 (0.93) 0.056
SD: standard deviation
Fruit intake
Fruit intake was particularly less than vegetable intake, both in terms of days of
intake per week and number of servings. During a week, males ate fruit on 2.63
(±1.97) days compared to 3.34 (±2.17) days for women. Average number of
servings per day was higher for females (0.99±0.64) compared to males
(0.92±0.63). Fruit intake did not differ significantly in males and females.
Ethnicity-wise, Brahmin males and females had higher fruit intake compared to
other ethnicity or castes. Consumption of fruit increased with level of education
for females; the association was similar for males, except for post-graduates. In
terms of occupation, retired females, but not retired males, had the highest
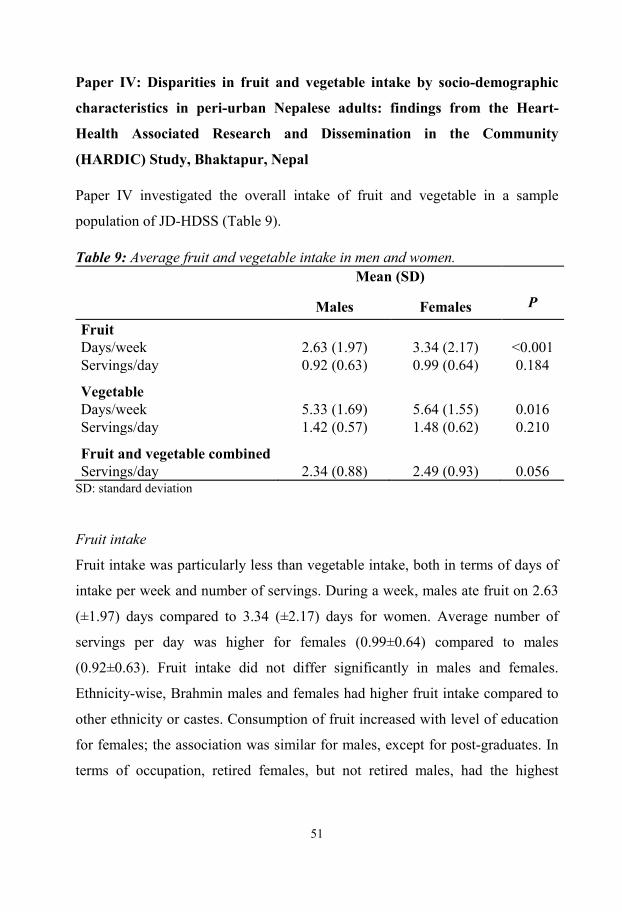
50
TPA, which was obtained by combining the physical activity of the three
domains, was higher in males, Newars, and those involved in agricultural work.
TPA showed an inverse relationship with age and level of education: the oldest
age group (45–59 years) had an adjusted odds ratio of 1.67 (1.08–2.58) of
having low physical activity compared to the youngest age group (25–34 years).
Likewise, those with the highest education (high school or further) had an odds
ratio of 2.99 (1.65–5.46) of having low physical activity compared to those with
the least education (informal education).
Low physical activity
Prevalence of LPA, as defined by GPAQ and WHO-STEPs criteria, was 43.3%
(95% CI, 39.4–47.1) in the study population. Moderate physical activity was
present in 50.8% (95% CI, 46.9–54.7) and high physical activity in 5.9% (95%
CI, 4.1–7.8) of the population.
Cardiometabolic risk factors and physical inactivity
I observed a positive association between physical inactivity and
cardiometabolic risk factors. Adjusted odds ratios of having LPA for diagnosed
hypertension, diagnosed diabetes, overweight, and increased waist
circumference were 1.41 (0.88–2.23), 1.64 (0.73–3.67), 1.58 (1.13–2.20), and
1.78 (1.27–2.49), respectively.
Awareness of physical inactivity as a CVD risk factor
When asked to list risk factors of cardiovascular diseases, only 5% of
respondents spontaneously mentioned physical inactivity, irrespective of
sociodemographic background, including educational status (Figure 7).
Conversely, 89.1% answered “yes” when asked if physical exercise helped
prevent heart disease.
51
Paper IV: Disparities in fruit and vegetable intake by socio-demographic
characteristics in peri-urban Nepalese adults: findings from the Heart-
Health Associated Research and Dissemination in the Community
(HARDIC) Study, Bhaktapur, Nepal
Paper IV investigated the overall intake of fruit and vegetable in a sample
population of JD-HDSS (Table 9).
Table 9: Average fruit and vegetable intake in men and women.
Mean (SD)
P Males Females Fruit Days/week 2.63 (1.97) 3.34 (2.17) <0.001 Servings/day 0.92 (0.63) 0.99 (0.64) 0.184 Vegetable Days/week 5.33 (1.69) 5.64 (1.55) 0.016 Servings/day 1.42 (0.57) 1.48 (0.62) 0.210 Fruit and vegetable combined Servings/day 2.34 (0.88) 2.49 (0.93) 0.056
SD: standard deviation
Fruit intake
Fruit intake was particularly less than vegetable intake, both in terms of days of
intake per week and number of servings. During a week, males ate fruit on 2.63
(±1.97) days compared to 3.34 (±2.17) days for women. Average number of
servings per day was higher for females (0.99±0.64) compared to males
(0.92±0.63). Fruit intake did not differ significantly in males and females.
Ethnicity-wise, Brahmin males and females had higher fruit intake compared to
other ethnicity or castes. Consumption of fruit increased with level of education
for females; the association was similar for males, except for post-graduates. In
terms of occupation, retired females, but not retired males, had the highest
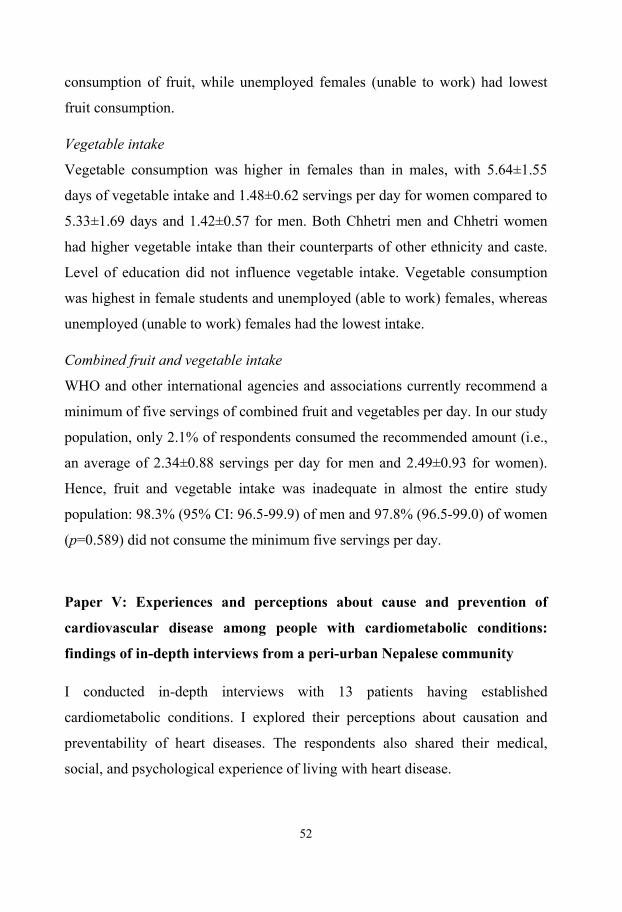
52
consumption of fruit, while unemployed females (unable to work) had lowest
fruit consumption.
Vegetable intake
Vegetable consumption was higher in females than in males, with 5.64±1.55
days of vegetable intake and 1.48±0.62 servings per day for women compared to
5.33±1.69 days and 1.42±0.57 for men. Both Chhetri men and Chhetri women
had higher vegetable intake than their counterparts of other ethnicity and caste.
Level of education did not influence vegetable intake. Vegetable consumption
was highest in female students and unemployed (able to work) females, whereas
unemployed (unable to work) females had the lowest intake.
Combined fruit and vegetable intake
WHO and other international agencies and associations currently recommend a
minimum of five servings of combined fruit and vegetables per day. In our study
population, only 2.1% of respondents consumed the recommended amount (i.e.,
an average of 2.34±0.88 servings per day for men and 2.49±0.93 for women).
Hence, fruit and vegetable intake was inadequate in almost the entire study
population: 98.3% (95% CI: 96.5-99.9) of men and 97.8% (96.5-99.0) of women
(p=0.589) did not consume the minimum five servings per day.
Paper V: Experiences and perceptions about cause and prevention of
cardiovascular disease among people with cardiometabolic conditions:
findings of in-depth interviews from a peri-urban Nepalese community
I conducted in-depth interviews with 13 patients having established
cardiometabolic conditions. I explored their perceptions about causation and
preventability of heart diseases. The respondents also shared their medical,
social, and psychological experience of living with heart disease.
53
Perceptions of heart diseases, risk factors, and sociocultural environment
Respondents placed a high value on health, and linked being “healthy” to ability
to do everyday work without difficulty. Most respondents thought that their
health was their own responsibility. They opined that “sugar” (diabetes mellitus)
and “pressure” (hypertension) were prevalent conditions in their neighborhood.
The term “heart disease” meant different conditions to the respondents,
ranging from pain in the heart to formation of a hole in the heart. Some
respondents immediately associated heart disease with underlying causative
factors such as smoking and heredity. Dietary factors, particularly consumption
of fatty and oily food, were universally and repeatedly mentioned as the main
reason why people suffer from heart disease. Similarly, respondents
unanimously linked smoking, alcohol intake, and high blood pressure to cardiac
ailments. However, they had varying opinions regarding the relationship of body
weight and physical inactivity with heart disease.
Most respondents felt that traditional and cultural practices in Nepal
contribute to heart disease. They particularly incriminated festivals, because
people engage in binge eating of fatty and spicy food during such occasions, and
many ethnic groups tend toward more alcohol drinking.
Experience of living with the disease: psychosocial and financial burden
All respondents reported having depressive symptoms and psychological stress
when they were diagnosed with a cardiometabolic condition, but they were able
to handle the situation better in the due course of time. All of them reported
receiving good healthcare support from their family. However, the financial
burden of managing their illness was a major issue in the family.
Lifestyle modification after diagnosis
All respondents understood the importance of lifestyle modification, such as
reducing salt intake or fat consumption and cutting down on smoking and
52
consumption of fruit, while unemployed females (unable to work) had lowest
fruit consumption.
Vegetable intake
Vegetable consumption was higher in females than in males, with 5.64±1.55
days of vegetable intake and 1.48±0.62 servings per day for women compared to
5.33±1.69 days and 1.42±0.57 for men. Both Chhetri men and Chhetri women
had higher vegetable intake than their counterparts of other ethnicity and caste.
Level of education did not influence vegetable intake. Vegetable consumption
was highest in female students and unemployed (able to work) females, whereas
unemployed (unable to work) females had the lowest intake.
Combined fruit and vegetable intake
WHO and other international agencies and associations currently recommend a
minimum of five servings of combined fruit and vegetables per day. In our study
population, only 2.1% of respondents consumed the recommended amount (i.e.,
an average of 2.34±0.88 servings per day for men and 2.49±0.93 for women).
Hence, fruit and vegetable intake was inadequate in almost the entire study
population: 98.3% (95% CI: 96.5-99.9) of men and 97.8% (96.5-99.0) of women
(p=0.589) did not consume the minimum five servings per day.
Paper V: Experiences and perceptions about cause and prevention of
cardiovascular disease among people with cardiometabolic conditions:
findings of in-depth interviews from a peri-urban Nepalese community
I conducted in-depth interviews with 13 patients having established
cardiometabolic conditions. I explored their perceptions about causation and
preventability of heart diseases. The respondents also shared their medical,
social, and psychological experience of living with heart disease.
53
Perceptions of heart diseases, risk factors, and sociocultural environment
Respondents placed a high value on health, and linked being “healthy” to ability
to do everyday work without difficulty. Most respondents thought that their
health was their own responsibility. They opined that “sugar” (diabetes mellitus)
and “pressure” (hypertension) were prevalent conditions in their neighborhood.
The term “heart disease” meant different conditions to the respondents,
ranging from pain in the heart to formation of a hole in the heart. Some
respondents immediately associated heart disease with underlying causative
factors such as smoking and heredity. Dietary factors, particularly consumption
of fatty and oily food, were universally and repeatedly mentioned as the main
reason why people suffer from heart disease. Similarly, respondents
unanimously linked smoking, alcohol intake, and high blood pressure to cardiac
ailments. However, they had varying opinions regarding the relationship of body
weight and physical inactivity with heart disease.
Most respondents felt that traditional and cultural practices in Nepal
contribute to heart disease. They particularly incriminated festivals, because
people engage in binge eating of fatty and spicy food during such occasions, and
many ethnic groups tend toward more alcohol drinking.
Experience of living with the disease: psychosocial and financial burden
All respondents reported having depressive symptoms and psychological stress
when they were diagnosed with a cardiometabolic condition, but they were able
to handle the situation better in the due course of time. All of them reported
receiving good healthcare support from their family. However, the financial
burden of managing their illness was a major issue in the family.
Lifestyle modification after diagnosis
All respondents understood the importance of lifestyle modification, such as
reducing salt intake or fat consumption and cutting down on smoking and
54
alcohol intake, although half of them acknowledged that it was difficult to
continue those behavioral modifications.
Prevention and awareness
All participants remarked that the community’s awareness of cardiovascular
diseases was inadequate, and that medical doctors or trained local people should
spread awareness in the community to increase people’s knowledge about the
causes and effects of heart diseases and encourage them to seek medical care if
necessary.
55
DISCUSSION
This Thesis contributes to the understanding of cardiovascular health literacy
and practice issues in the Nepalese context. To conduct studies included in the
Thesis, a HDSS was established in a peri-urban community near Kathmandu, the
capital city (Paper I). Next, I explored KAP/behavior components of
cardiovascular health in the community through a population-based survey
(Paper II). Physical inactivity (Paper III) and low fruit and vegetable intake
(Paper IV) were assessed as two examples of lifestyle-related behavioral risk
factors. Finally, I explored cardiovascular health issues from patients’
perspectives through in-depth interviews (Paper V).
Epidemiological perspectives
By studying the burden of risk factors in a peri-urban community, this Thesis
documents Nepal’s cardiovascular health status during a rural-to-urban
transition. With particular emphasis on behavioral risk factors such as physical
activity, my Thesis explores the distribution of cardiovascular risk according to
different sociodemographic correlates in the study population. In addition, it
investigates psychosocial determinants of cardiovascular health behavior in the
community, paving the way for future health promotional and other
interventional studies.
Urbanization as a driving force behind behavioral changes
Although urbanization is a central theme of this Thesis, I made no attempt to
study urbanization as a separate variable or to quantify its level (118). Similar to
studies from Pakistan, Egypt, and Iran, this Thesis simply acknowledges the
urbanization process as an overarching theme that has been postulated as a
driver of NCD in the community (119). Because of its absence as a tangible
variable in my Thesis, I cannot claim epidemiologically that urbanization is
54
alcohol intake, although half of them acknowledged that it was difficult to
continue those behavioral modifications.
Prevention and awareness
All participants remarked that the community’s awareness of cardiovascular
diseases was inadequate, and that medical doctors or trained local people should
spread awareness in the community to increase people’s knowledge about the
causes and effects of heart diseases and encourage them to seek medical care if
necessary.
55
DISCUSSION
This Thesis contributes to the understanding of cardiovascular health literacy
and practice issues in the Nepalese context. To conduct studies included in the
Thesis, a HDSS was established in a peri-urban community near Kathmandu, the
capital city (Paper I). Next, I explored KAP/behavior components of
cardiovascular health in the community through a population-based survey
(Paper II). Physical inactivity (Paper III) and low fruit and vegetable intake
(Paper IV) were assessed as two examples of lifestyle-related behavioral risk
factors. Finally, I explored cardiovascular health issues from patients’
perspectives through in-depth interviews (Paper V).
Epidemiological perspectives
By studying the burden of risk factors in a peri-urban community, this Thesis
documents Nepal’s cardiovascular health status during a rural-to-urban
transition. With particular emphasis on behavioral risk factors such as physical
activity, my Thesis explores the distribution of cardiovascular risk according to
different sociodemographic correlates in the study population. In addition, it
investigates psychosocial determinants of cardiovascular health behavior in the
community, paving the way for future health promotional and other
interventional studies.
Urbanization as a driving force behind behavioral changes
Although urbanization is a central theme of this Thesis, I made no attempt to
study urbanization as a separate variable or to quantify its level (118). Similar to
studies from Pakistan, Egypt, and Iran, this Thesis simply acknowledges the
urbanization process as an overarching theme that has been postulated as a
driver of NCD in the community (119). Because of its absence as a tangible
variable in my Thesis, I cannot claim epidemiologically that urbanization is
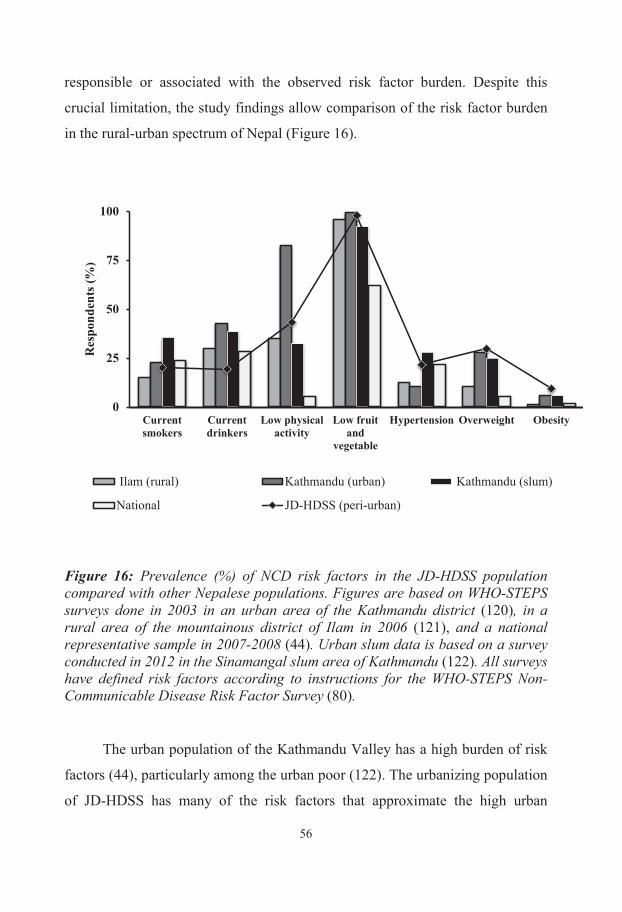
56
responsible or associated with the observed risk factor burden. Despite this
crucial limitation, the study findings allow comparison of the risk factor burden
in the rural-urban spectrum of Nepal (Figure 16).
Figure 16: Prevalence (%) of NCD risk factors in the JD-HDSS population compared with other Nepalese populations. Figures are based on WHO-STEPS surveys done in 2003 in an urban area of the Kathmandu district (120), in a rural area of the mountainous district of Ilam in 2006 (121), and a national representative sample in 2007-2008 (44). Urban slum data is based on a survey conducted in 2012 in the Sinamangal slum area of Kathmandu (122). All surveys have defined risk factors according to instructions for the WHO-STEPS Non-Communicable Disease Risk Factor Survey (80).
The urban population of the Kathmandu Valley has a high burden of risk
factors (44), particularly among the urban poor (122). The urbanizing population
of JD-HDSS has many of the risk factors that approximate the high urban
0
25
50
75
100
Currentsmokers
Currentdrinkers
Low physicalactivity
Low fruitand
vegetable
Hypertension Overweight Obesity
R
espo
nden
ts (%
)
Ilam (rural) Kathmandu (urban) Kathmandu (slum)
National JD-HDSS (peri-urban)
57
figures, particularly biological risk factors such as increased blood pressure and
body weight. However, the urban Kathmandu study was conducted about eight
years before the present study in peri-urban JD-HDSS. Therefore, the proximity
of prevalence rates of the risk factors in the two areas may be considered an
overestimation as the current urban prevalences are likely to be even higher.
Although data like these demonstrate ongoing efforts to obtain regular
data on risk factors at national and sub-national levels, data on urbanization
trends in Nepal is also available. At the national level, Nepal is urbanizing at an
annual rate of 3.62% (123); however, there are intra-country disparities (124).
For example, the capital Kathmandu, which contained 82% of Nepal’s urban
population in 1950s, had only 31% of that share by 2001 (124). Also, the rate of
urbanization is accelerating in newer areas. For example, while urbanization in
Kathmandu rose from 55% to 65% between 1981 and 2001, the corresponding
increase almost doubled (from 30% to 53%) in the neighboring Bhaktapur
district, where JD-HDSS is located (124). Therefore, while some data describe
the ongoing urbanization process in Nepal, there is a need for studies that couple
urbanization trends with the changing status of behavioral risk factors to provide
a better estimate of their association (118, 125, 126).
Physical inactivity and obesity as outcomes of changing population lifestyle
Physical inactivity in JD-HDSS (43%), a peri-urban area in Kathmandu Valley,
is higher than the mountainous rural area of Ilam (35%), but currently less than
prevalence in urban Kathmandu (82.3%) (Figure 16). Although this Thesis lacks
a stringent measure of association, the comparative data does hint at a positive
relationship between urbanization and physical inactivity, an association that has
been observed in different settings, including China (127) and Israel (128). Also,
the finding that most physical activity currently derives from work activities is a
matter of concern (Paper III) because this domain of physical activity will
invariably decrease in the future as more and more jobs become sedentary or
56
responsible or associated with the observed risk factor burden. Despite this
crucial limitation, the study findings allow comparison of the risk factor burden
in the rural-urban spectrum of Nepal (Figure 16).
Figure 16: Prevalence (%) of NCD risk factors in the JD-HDSS population compared with other Nepalese populations. Figures are based on WHO-STEPS surveys done in 2003 in an urban area of the Kathmandu district (120), in a rural area of the mountainous district of Ilam in 2006 (121), and a national representative sample in 2007-2008 (44). Urban slum data is based on a survey conducted in 2012 in the Sinamangal slum area of Kathmandu (122). All surveys have defined risk factors according to instructions for the WHO-STEPS Non-Communicable Disease Risk Factor Survey (80).
The urban population of the Kathmandu Valley has a high burden of risk
factors (44), particularly among the urban poor (122). The urbanizing population
of JD-HDSS has many of the risk factors that approximate the high urban
0
25
50
75
100
Currentsmokers
Currentdrinkers
Low physicalactivity
Low fruitand
vegetable
Hypertension Overweight Obesity
R
espo
nden
ts (%
)
Ilam (rural) Kathmandu (urban) Kathmandu (slum)
National JD-HDSS (peri-urban)
57
figures, particularly biological risk factors such as increased blood pressure and
body weight. However, the urban Kathmandu study was conducted about eight
years before the present study in peri-urban JD-HDSS. Therefore, the proximity
of prevalence rates of the risk factors in the two areas may be considered an
overestimation as the current urban prevalences are likely to be even higher.
Although data like these demonstrate ongoing efforts to obtain regular
data on risk factors at national and sub-national levels, data on urbanization
trends in Nepal is also available. At the national level, Nepal is urbanizing at an
annual rate of 3.62% (123); however, there are intra-country disparities (124).
For example, the capital Kathmandu, which contained 82% of Nepal’s urban
population in 1950s, had only 31% of that share by 2001 (124). Also, the rate of
urbanization is accelerating in newer areas. For example, while urbanization in
Kathmandu rose from 55% to 65% between 1981 and 2001, the corresponding
increase almost doubled (from 30% to 53%) in the neighboring Bhaktapur
district, where JD-HDSS is located (124). Therefore, while some data describe
the ongoing urbanization process in Nepal, there is a need for studies that couple
urbanization trends with the changing status of behavioral risk factors to provide
a better estimate of their association (118, 125, 126).
Physical inactivity and obesity as outcomes of changing population lifestyle
Physical inactivity in JD-HDSS (43%), a peri-urban area in Kathmandu Valley,
is higher than the mountainous rural area of Ilam (35%), but currently less than
prevalence in urban Kathmandu (82.3%) (Figure 16). Although this Thesis lacks
a stringent measure of association, the comparative data does hint at a positive
relationship between urbanization and physical inactivity, an association that has
been observed in different settings, including China (127) and Israel (128). Also,
the finding that most physical activity currently derives from work activities is a
matter of concern (Paper III) because this domain of physical activity will
invariably decrease in the future as more and more jobs become sedentary or
58
mechanized (127, 129). For example, the percent of people involved in farming
in Nepal has decreased (from 94% to 65%) in the last three decades (130).
Unless adequate physical activity is compensated through leisure and travel
activities, the overall level of physical activity in the Nepalese population will
drop significantly in the future.
Possibly in parallel to the level of low physical activity mentioned above,
increased body mass index also follows the urbanization trend in Nepal (13).
The relationship between overweight/obesity and physical activity is complex,
often forming a vicious cycle of reduced physical activity that leads to increased
body weight and vice versa (131).
Sociodemographic disparities in risk factor prevalence
This Thesis explored cardiovascular risk factors through the lens of various
sociodemographic subsets of the study population. Although males’ lower
prevalence of physical inactivity and obesity is similar to nationally
representative data (44), they showed a higher prevalence of tobacco and alcohol
consumption (Paper II). Females consumed more fruits and vegetables than
males, but most did not attain the WHO recommendations (Paper IV). In terms
of age, elderly people had lower cardiovascular health knowledge and physical
activity, but increasing age did not affect fruit and vegetable intake (Papers II
and IV). Ethnicity had no influence on perception or practice about heart
disease. On the other hand, higher level of education associated with decreased
prevalence of tobacco and alcohol consumption and improved fruit and
vegetable intake, but concurrently with higher prevalence of physical inactivity
and hypertension. These findings are important from epidemiological viewpoint
because they help identify individuals who are at higher risk for any given risk
factor.
59
HDSS as a setting for studying cardiovascular health
Similar to other HDSSs in various LMICs (65,132,133), JD-HDSS provided an
appropriate platform for cardiovascular health studies in Nepal. Conducted in
2010, my initial survey provided up-to-date data about the study population as
well as sampling frames for subsequent studies (Paper I). It also determined that
CVDs are major causes of morbidity and mortality, validating the public health
importance of cardiovascular studies in the community. Because the community
is undergoing rapid urbanization, JD-HDSS provided an excellent opportunity to
capture various sociodemographic aspects of CVDs in the changing Nepalese
context. Establishment of the HDSS itself, however, was a challenge in terms of
administrative hurdles, undue political influences, and other logistic difficulties
(Paper I). Endorsement of the surveillance site by local collaborators, including
the local administration and the partnering medical institutes, is another key
issue for its long-term sustainability.
With the data of this Thesis as a baseline, longitudinal studies using the
WHO-STEPS Non-Communicable Disease Risk Factors Survey can provide
trends of risk factors in the population (134). However, there are many potential
operational challenges (e.g., field monitoring) (135) and issues (e.g., incomplete
data) (136). In addition, JD-HDSS has the necessary infrastructure and
manpower to conduct community-based interventions that target single or
multiple risk factors in its population sub-sets (137). It will be interesting to see
whether such interventions can be generalized to a wider population base in
other parts of Nepal. Although observational or interventional studies from an
HDSS can provide useful epidemiological data, they cannot replace the need for
routine monitoring and a surveillance system of cardiovascular health indicators,
including morbidity and mortality data (138).
58
mechanized (127, 129). For example, the percent of people involved in farming
in Nepal has decreased (from 94% to 65%) in the last three decades (130).
Unless adequate physical activity is compensated through leisure and travel
activities, the overall level of physical activity in the Nepalese population will
drop significantly in the future.
Possibly in parallel to the level of low physical activity mentioned above,
increased body mass index also follows the urbanization trend in Nepal (13).
The relationship between overweight/obesity and physical activity is complex,
often forming a vicious cycle of reduced physical activity that leads to increased
body weight and vice versa (131).
Sociodemographic disparities in risk factor prevalence
This Thesis explored cardiovascular risk factors through the lens of various
sociodemographic subsets of the study population. Although males’ lower
prevalence of physical inactivity and obesity is similar to nationally
representative data (44), they showed a higher prevalence of tobacco and alcohol
consumption (Paper II). Females consumed more fruits and vegetables than
males, but most did not attain the WHO recommendations (Paper IV). In terms
of age, elderly people had lower cardiovascular health knowledge and physical
activity, but increasing age did not affect fruit and vegetable intake (Papers II
and IV). Ethnicity had no influence on perception or practice about heart
disease. On the other hand, higher level of education associated with decreased
prevalence of tobacco and alcohol consumption and improved fruit and
vegetable intake, but concurrently with higher prevalence of physical inactivity
and hypertension. These findings are important from epidemiological viewpoint
because they help identify individuals who are at higher risk for any given risk
factor.
59
HDSS as a setting for studying cardiovascular health
Similar to other HDSSs in various LMICs (65,132,133), JD-HDSS provided an
appropriate platform for cardiovascular health studies in Nepal. Conducted in
2010, my initial survey provided up-to-date data about the study population as
well as sampling frames for subsequent studies (Paper I). It also determined that
CVDs are major causes of morbidity and mortality, validating the public health
importance of cardiovascular studies in the community. Because the community
is undergoing rapid urbanization, JD-HDSS provided an excellent opportunity to
capture various sociodemographic aspects of CVDs in the changing Nepalese
context. Establishment of the HDSS itself, however, was a challenge in terms of
administrative hurdles, undue political influences, and other logistic difficulties
(Paper I). Endorsement of the surveillance site by local collaborators, including
the local administration and the partnering medical institutes, is another key
issue for its long-term sustainability.
With the data of this Thesis as a baseline, longitudinal studies using the
WHO-STEPS Non-Communicable Disease Risk Factors Survey can provide
trends of risk factors in the population (134). However, there are many potential
operational challenges (e.g., field monitoring) (135) and issues (e.g., incomplete
data) (136). In addition, JD-HDSS has the necessary infrastructure and
manpower to conduct community-based interventions that target single or
multiple risk factors in its population sub-sets (137). It will be interesting to see
whether such interventions can be generalized to a wider population base in
other parts of Nepal. Although observational or interventional studies from an
HDSS can provide useful epidemiological data, they cannot replace the need for
routine monitoring and a surveillance system of cardiovascular health indicators,
including morbidity and mortality data (138).
60
Learning points for cardiovascular health promotion in Nepal
Findings of this Thesis provide important learning points to better understand
the cardiovascular health behavior of the study population. Because all
stakeholders in a population aim to achieve healthy behavior (139), the factors
that affect and influence health behavior are vital information for health
promotion activities (140). Health promotion aims to invent, introduce, or
improvise practices that improve public health (139). Particularly for NCDs,
where many causes and solutions lie outside the walls of clinical medicine and
often in human behavior, health promotion, with its emphasis on social action, is
undoubtedly a logical partner to disease-oriented specialists (140). In resource-
constrained settings like Nepal, health promotion is even more relevant and
rational (53, 141).
The health promotion implications of this Thesis can be better
comprehended by first considering its basic constructs, knowledge and attitude,
and behavior/practice. This facilitates discussion of the findings through the lens
of health literacy. A brief account of the different approaches of health
promotion provides the premise to argue in support of health promotional
activities in Nepal.
Limited health knowledge
Most often, knowledge alone is viewed as the most important determinant of
health behavior. However, health promotional activities based solely on this
assumption do not always lead to encouraging outcomes (142, 143).
Despite the high burden of risk factors, the study population’s
cardiovascular health knowledge was limited regarding heart diseases, even
among diseased individuals (Papers II and V). Cigarette smoking and excessive
alcohol consumption were spontaneously linked to heart diseases by the general
population and patients alike, a finding that has been reported in other settings as
61
well (91, 95). However, physical inactivity and inadequate fruit and vegetable
intake were not usually seen as important determinants of heart disease.
Attitude including perceived locus of control is a key factor
Like knowledge, attitude is an often-explored construct (144, 145). A majority
of our respondents underestimated their cardiovascular risk and did not want to
modify their adverse lifestyles despite having adequate knowledge about risk
factors (Paper II). Hence, this Thesis incriminates the attitude of the study
population as an important bottleneck toward heart-healthy behavior.
Another attitude-related finding of this Thesis is about locus of control.
Health locus of control is the expectation of individuals regarding the effects of
their behavior on their health (146, 147). Due to a strong conviction among
respondents that their health is determined by a higher power (i.e., “chance
externality”), the locus is external in our study population. When respondents
become ill, the locus shifts toward doctors or medical professionals (i.e.,
“powerful others externality”). In fact, previous studies have shown that
individuals who believe that their health status depends on their personal
decisions and behaviors (i.e., “internality”) show better mastery of their health
situation (148).
Delayed attempts at modifying cardiovascular health behavior
Because health behavior is not a linear phenomenon (149), it cannot be
explained with knowledge and attitude perspectives alone (150). Hence,
although this Thesis begins by exploring both of these constructs in relation to
cardiovascular health behavior and practice in the community (Paper II), it
quickly expands to include other constructs of health behavior, especially after
triangulation at the interpretation level described in the qualitative study (Paper
V).
Lifestyle modification is an important health behavioral act (151, 152),
and many respondents changed their lifestyles after they developed disease
60
Learning points for cardiovascular health promotion in Nepal
Findings of this Thesis provide important learning points to better understand
the cardiovascular health behavior of the study population. Because all
stakeholders in a population aim to achieve healthy behavior (139), the factors
that affect and influence health behavior are vital information for health
promotion activities (140). Health promotion aims to invent, introduce, or
improvise practices that improve public health (139). Particularly for NCDs,
where many causes and solutions lie outside the walls of clinical medicine and
often in human behavior, health promotion, with its emphasis on social action, is
undoubtedly a logical partner to disease-oriented specialists (140). In resource-
constrained settings like Nepal, health promotion is even more relevant and
rational (53, 141).
The health promotion implications of this Thesis can be better
comprehended by first considering its basic constructs, knowledge and attitude,
and behavior/practice. This facilitates discussion of the findings through the lens
of health literacy. A brief account of the different approaches of health
promotion provides the premise to argue in support of health promotional
activities in Nepal.
Limited health knowledge
Most often, knowledge alone is viewed as the most important determinant of
health behavior. However, health promotional activities based solely on this
assumption do not always lead to encouraging outcomes (142, 143).
Despite the high burden of risk factors, the study population’s
cardiovascular health knowledge was limited regarding heart diseases, even
among diseased individuals (Papers II and V). Cigarette smoking and excessive
alcohol consumption were spontaneously linked to heart diseases by the general
population and patients alike, a finding that has been reported in other settings as
61
well (91, 95). However, physical inactivity and inadequate fruit and vegetable
intake were not usually seen as important determinants of heart disease.
Attitude including perceived locus of control is a key factor
Like knowledge, attitude is an often-explored construct (144, 145). A majority
of our respondents underestimated their cardiovascular risk and did not want to
modify their adverse lifestyles despite having adequate knowledge about risk
factors (Paper II). Hence, this Thesis incriminates the attitude of the study
population as an important bottleneck toward heart-healthy behavior.
Another attitude-related finding of this Thesis is about locus of control.
Health locus of control is the expectation of individuals regarding the effects of
their behavior on their health (146, 147). Due to a strong conviction among
respondents that their health is determined by a higher power (i.e., “chance
externality”), the locus is external in our study population. When respondents
become ill, the locus shifts toward doctors or medical professionals (i.e.,
“powerful others externality”). In fact, previous studies have shown that
individuals who believe that their health status depends on their personal
decisions and behaviors (i.e., “internality”) show better mastery of their health
situation (148).
Delayed attempts at modifying cardiovascular health behavior
Because health behavior is not a linear phenomenon (149), it cannot be
explained with knowledge and attitude perspectives alone (150). Hence,
although this Thesis begins by exploring both of these constructs in relation to
cardiovascular health behavior and practice in the community (Paper II), it
quickly expands to include other constructs of health behavior, especially after
triangulation at the interpretation level described in the qualitative study (Paper
V).
Lifestyle modification is an important health behavioral act (151, 152),
and many respondents changed their lifestyles after they developed disease
62
(Paper V). Because they did not consider themselves at risk before the overt
manifestation of disease, they had been reluctant to make any behavioral
modification. Different theories of health behavior help explain a situation like
this (66). For example, perceived susceptibility (as explained in the health belief
model) and attitude that leads to intention toward heart-healthy behavior (as
explained by the Theory of Reasoned Action) are important determinants of
cardiovascular health behavior in the study population (66). In addition, personal
cognitive factors such as outcome expectations, rewards received and emotional
coping (as explained by Social Cognitive Theory), also affect practice and
behavior (68). However, respondents did not emphasize the third component of
the triad (i.e., environment). For example, they did not link inadequate physical
activity with unavailability of walkable pavements, playgrounds, and parks in
their community (20). This may be due to less emphasis on physical inactivity
and ignorance about the effect of environmental factors on physical activity.
Inadequate health literacy
Often labeled as a repackaging of health education and health promotion
strategies, health literacy is commonly viewed as a bridging concept between
knowledge and practice (140). Basically, it has been conceptualized as the skills
that an individual possesses to translate his/her health knowledge into health
practice (153). Three levels of health literacy have been described: functional
(basic reading and writing skills to understand and follow simple health
messages); interactive (cognitive and interpersonal skills to manage health in
partnership with professionals); and critical (ability to analyze information
critically, increase awareness, and participate in action to address barriers) (154).
Secondary and tertiary care settings often evaluate patients’ health literacy
with tools that assess reading fluency regarding health-related print and oral
literacy (153). In a primary or preventive care facility, the assessment of health
literacy is less well-defined and still evolving (28, 154). Hence, this Thesis did
63
not assess health literacy with any particular tool, but rather used the concept
broadly to describe a person’s ability to utilize the health knowledge that he/she
has.
If lifestyle modification is a crucial outcome of health behavior, the
community lacks adequate health literacy at all three levels. The first level (i.e.,
functional health literacy) may be lacking due not only to the community’s
inability to comprehend heart-healthy messages but also because the community
lacks suitable resources for such messages (153). In fact, when asked to rate how
well they were informed about cardiovascular health issues, 43% of the
respondents acknowledged that they were not informed at all (unpublished data).
Among those who said they were informed, media was the source of information
for half of them; only 14% had ever received any cardiovascular health
information from a health worker. Similarly, the community’s sub-optimal
interactive health literacy is exemplified by patients’ complete dependency on
doctors for disease management (Papers II and V). Further, lack of any regular
health promotional programs and cardiovascular primary care virtually rules out
the scope to even assess critical health literacy. Thus, improving the
cardiovascular health literacy of this community requires attempts not only to
improve an individual’s psychosocial factors that increase functional and
interactive health literacy, but also to encourage an environment that fosters
critical health literacy (155).
Dominance of the medical approach to health promotion in Nepal
There are five different approaches to health promotion (156, 157). The medical,
or preventive, approach targets entire populations or high-risk groups. It has
three levels of intervention (primary, secondary, and tertiary) and is popular
because it is expert-driven. The behavior change approach, which encourages
individuals to adopt healthy behaviors, is considered the bedrock of health
promotional activities. It is complex due to the multi-dimensional interactions of
62
(Paper V). Because they did not consider themselves at risk before the overt
manifestation of disease, they had been reluctant to make any behavioral
modification. Different theories of health behavior help explain a situation like
this (66). For example, perceived susceptibility (as explained in the health belief
model) and attitude that leads to intention toward heart-healthy behavior (as
explained by the Theory of Reasoned Action) are important determinants of
cardiovascular health behavior in the study population (66). In addition, personal
cognitive factors such as outcome expectations, rewards received and emotional
coping (as explained by Social Cognitive Theory), also affect practice and
behavior (68). However, respondents did not emphasize the third component of
the triad (i.e., environment). For example, they did not link inadequate physical
activity with unavailability of walkable pavements, playgrounds, and parks in
their community (20). This may be due to less emphasis on physical inactivity
and ignorance about the effect of environmental factors on physical activity.
Inadequate health literacy
Often labeled as a repackaging of health education and health promotion
strategies, health literacy is commonly viewed as a bridging concept between
knowledge and practice (140). Basically, it has been conceptualized as the skills
that an individual possesses to translate his/her health knowledge into health
practice (153). Three levels of health literacy have been described: functional
(basic reading and writing skills to understand and follow simple health
messages); interactive (cognitive and interpersonal skills to manage health in
partnership with professionals); and critical (ability to analyze information
critically, increase awareness, and participate in action to address barriers) (154).
Secondary and tertiary care settings often evaluate patients’ health literacy
with tools that assess reading fluency regarding health-related print and oral
literacy (153). In a primary or preventive care facility, the assessment of health
literacy is less well-defined and still evolving (28, 154). Hence, this Thesis did
63
not assess health literacy with any particular tool, but rather used the concept
broadly to describe a person’s ability to utilize the health knowledge that he/she
has.
If lifestyle modification is a crucial outcome of health behavior, the
community lacks adequate health literacy at all three levels. The first level (i.e.,
functional health literacy) may be lacking due not only to the community’s
inability to comprehend heart-healthy messages but also because the community
lacks suitable resources for such messages (153). In fact, when asked to rate how
well they were informed about cardiovascular health issues, 43% of the
respondents acknowledged that they were not informed at all (unpublished data).
Among those who said they were informed, media was the source of information
for half of them; only 14% had ever received any cardiovascular health
information from a health worker. Similarly, the community’s sub-optimal
interactive health literacy is exemplified by patients’ complete dependency on
doctors for disease management (Papers II and V). Further, lack of any regular
health promotional programs and cardiovascular primary care virtually rules out
the scope to even assess critical health literacy. Thus, improving the
cardiovascular health literacy of this community requires attempts not only to
improve an individual’s psychosocial factors that increase functional and
interactive health literacy, but also to encourage an environment that fosters
critical health literacy (155).
Dominance of the medical approach to health promotion in Nepal
There are five different approaches to health promotion (156, 157). The medical,
or preventive, approach targets entire populations or high-risk groups. It has
three levels of intervention (primary, secondary, and tertiary) and is popular
because it is expert-driven. The behavior change approach, which encourages
individuals to adopt healthy behaviors, is considered the bedrock of health
promotional activities. It is complex due to the multi-dimensional interactions of
64
human behavior with social and environmental factors. The third method is the
educational approach, which provides knowledge and information that enable
people to make informed choices about their health behavior but does not aim to
persuade or motivate change in a particular way. This approach assumes that
increased knowledge will automatically lead to positive changes in attitude that
will, in turn, promote healthy behavior. On the other hand, the empowerment
approach is client-centric and requires practitioners to use their own power to
help clients get power. The fifth approach, called the social change approach, is
more radical, and encompasses policy and environmental dimensions of health
promotion.
Nepal’s current strategy for tackling NCDs is based largely on the medical
model (i.e., treatment), which receives much greater attention, investment, and
importance than other forms of health promotion (43). This approach is entirely
top-down, and the patient-healer equation is diametrically opposite to what one
expects in the empowerment approach. Such equations are better explored with
explanatory models that look at both patient and provider perspectives (158).
Although this Thesis did not use explanatory models, information based on
patients’ perspectives does illustrate the aforementioned remarks that
cardiovascular health promotion occurs mostly through a provider-centric
medical approach, focused disproportionately on curative strategies and
practiced more often at secondary and tertiary levels.
Health promotion as a starting point of primary cardiovascular care in Nepal
The findings in this Thesis reinforce my earlier viewpoint that the practice of
health promotion in Nepal should expand beyond the hospital walls and focus
instead on primary care settings (141). Inadequate health knowledge and
literacy, adverse attitudes, and the high burden of behavioral and biological risk
factors in the community all point toward a need for community-oriented
activities for cardiovascular health promotion. Thus, cardiovascular health and
65
other NCDs should be part of primary health care in Nepal. Nepal has a well-
established primary healthcare system (41) that practices varying degrees of
different health promotional approaches, mainly for maternal and children’s
health problems (159–161) but also for newer areas like oral health (162). The
feasibility of broadening such community-level health promotional activities to
include cardiovascular and other NCD components requires exploration.
Additionally, primary health care must be upgraded at the grass roots level, and
primary care health workers must be re-oriented to NCD-related health
promotion activities (23). Nonetheless, in addition to the general
recommendations for all major risk factors, health promotion activities must
consider the local risk factor burden and behavior gaps. For example, the JD-
HDSS community must prioritize physical activity, tobacco consumption, and
fruit and vegetable intake. Similarly, strategies that improve attitude would add
an important component to health promotion in this population (163).
Implications for health policy in Nepal
Nepal’s current National Health Policy dates to 1991 (164). Riding the
aspirations of newly achieved democracy, this landmark document provided a
framework to guide health sector development in Nepal and emphasized rural
health. It focused mainly on issues pertaining to maternal and child health and
communicable diseases.
Nepal’s National Health Policy 1991 stood on a tripod of preventive,
promotive, and curative health services (164). In retrospect, preventive services
did remarkably well, particularly in reducing childhood mortality. The success
of curative services was moderate, but with influx of private sector and urban-
centric treatment facilities, health inequity has actually widened in the last
decade or so (165). However, the promotive component, which aimed to
motivate healthy behavior in the population, was not really successful, mainly
due to lower priority (166).
64
human behavior with social and environmental factors. The third method is the
educational approach, which provides knowledge and information that enable
people to make informed choices about their health behavior but does not aim to
persuade or motivate change in a particular way. This approach assumes that
increased knowledge will automatically lead to positive changes in attitude that
will, in turn, promote healthy behavior. On the other hand, the empowerment
approach is client-centric and requires practitioners to use their own power to
help clients get power. The fifth approach, called the social change approach, is
more radical, and encompasses policy and environmental dimensions of health
promotion.
Nepal’s current strategy for tackling NCDs is based largely on the medical
model (i.e., treatment), which receives much greater attention, investment, and
importance than other forms of health promotion (43). This approach is entirely
top-down, and the patient-healer equation is diametrically opposite to what one
expects in the empowerment approach. Such equations are better explored with
explanatory models that look at both patient and provider perspectives (158).
Although this Thesis did not use explanatory models, information based on
patients’ perspectives does illustrate the aforementioned remarks that
cardiovascular health promotion occurs mostly through a provider-centric
medical approach, focused disproportionately on curative strategies and
practiced more often at secondary and tertiary levels.
Health promotion as a starting point of primary cardiovascular care in Nepal
The findings in this Thesis reinforce my earlier viewpoint that the practice of
health promotion in Nepal should expand beyond the hospital walls and focus
instead on primary care settings (141). Inadequate health knowledge and
literacy, adverse attitudes, and the high burden of behavioral and biological risk
factors in the community all point toward a need for community-oriented
activities for cardiovascular health promotion. Thus, cardiovascular health and
65
other NCDs should be part of primary health care in Nepal. Nepal has a well-
established primary healthcare system (41) that practices varying degrees of
different health promotional approaches, mainly for maternal and children’s
health problems (159–161) but also for newer areas like oral health (162). The
feasibility of broadening such community-level health promotional activities to
include cardiovascular and other NCD components requires exploration.
Additionally, primary health care must be upgraded at the grass roots level, and
primary care health workers must be re-oriented to NCD-related health
promotion activities (23). Nonetheless, in addition to the general
recommendations for all major risk factors, health promotion activities must
consider the local risk factor burden and behavior gaps. For example, the JD-
HDSS community must prioritize physical activity, tobacco consumption, and
fruit and vegetable intake. Similarly, strategies that improve attitude would add
an important component to health promotion in this population (163).
Implications for health policy in Nepal
Nepal’s current National Health Policy dates to 1991 (164). Riding the
aspirations of newly achieved democracy, this landmark document provided a
framework to guide health sector development in Nepal and emphasized rural
health. It focused mainly on issues pertaining to maternal and child health and
communicable diseases.
Nepal’s National Health Policy 1991 stood on a tripod of preventive,
promotive, and curative health services (164). In retrospect, preventive services
did remarkably well, particularly in reducing childhood mortality. The success
of curative services was moderate, but with influx of private sector and urban-
centric treatment facilities, health inequity has actually widened in the last
decade or so (165). However, the promotive component, which aimed to
motivate healthy behavior in the population, was not really successful, mainly
due to lower priority (166).
66
Since 1991, Nepal has witnessed further political upheaval,
sociodemographic transformations, and a changing mosaic of health problems
(42). The existing health policy could not address newer health issues (e.g.,
urban health, NCDs, international and global health), and recent efforts have
sought to revise the policy (167). Currently, NCDs are an important addition in
the ongoing revised health policy draft (168).
This Thesis was not based on health policy research and did not
investigate health policy issues pertaining to cardiovascular health. However,
some of its findings are relevant to health policy. First, the NCD section of the
draft health policy gives adequate importance to health promotion (168), and the
study findings described in this Thesis reaffirm that emphasis. Second, the draft
policy aims to ensure that NCD services trickle down from super-specialty to
primary care outlets such as health posts. This Thesis also indicates the need and
relevancy of that strategy. For example, only 20% of respondents with
cardiometabolic diseases visited nearby health posts. While 35% had to visit
hospitals and private clinics in the city and another 20% received medicines
directly from pharmacy shops, 14% and 11% did home-based therapies or
consulted traditional healers, respectively (unpublished data). Third, the draft
policy underscores the necessity of population-based monitoring and
surveillance of NCD-related indicators, including risk factor trends. Using an
HDSS setting, this Thesis demonstrates the possibility and potential of obtaining
quality data on risk factor trends and other sociomedical aspects of CVDs,
including cardiovascular health literacy, practice, and behavior.
Lack of an appropriate health policy that addresses cardiovascular health
issues is a known barrier to achieving cardiovascular health goals (169, 170).
Further, health policy should be evidence-based (171). Hence, in the context of
Nepal, swift enactment of the revised health policy is crucial, as is fair
evaluation of its implementation.
67
Relevance of the study findings to other low- and middle-income countries
Although generalization of the Thesis findings should be done with caution, the
epidemiological situation in Nepal is in many ways typical of that in many other
LMICs (172, 173). The common threads in most LMICs are high burden of
NCD morbidity and mortality (174); inadequate local research and data on the
NCD burden (172), including intervention trials (171); and lack of financial,
technical, and manpower resources to tackle NCDs (175, 176). Compared to the
earlier epidemiological transition in high-income nations, the ongoing transition
in Nepal and other LMICs differ sociodemographically in terms of a rapidly
aging population, urbanization patterns, and rural out-migrations (171). In
addition, unlike high-income nations, NCD-related risk estimation in LMICs
goes beyond clinical (175) and biochemical risk factor profiling, and the social
and cultural context of health behavioral patterns is more important (171).
Nevertheless, even among the LMICs, differences are inevitable in terms of
sociodemographic structures, differential prevalence of risk factors, and health
systems (171, 175).
Despite inter-country variations, contextual similarities allow the
usefulness of research findings across LMICs (176). For example, studies from
other LMICs echo the findings of low cardiovascular health literacy presented in
this Thesis (177). Likewise, the qualitative study findings of patients’
perceptions presented here would be relevant in other similar settings. On the
other hand, findings of interventional studies from other LMICs will provide
useful learning lessons for JD-HDSS and Nepal (177–179).
66
Since 1991, Nepal has witnessed further political upheaval,
sociodemographic transformations, and a changing mosaic of health problems
(42). The existing health policy could not address newer health issues (e.g.,
urban health, NCDs, international and global health), and recent efforts have
sought to revise the policy (167). Currently, NCDs are an important addition in
the ongoing revised health policy draft (168).
This Thesis was not based on health policy research and did not
investigate health policy issues pertaining to cardiovascular health. However,
some of its findings are relevant to health policy. First, the NCD section of the
draft health policy gives adequate importance to health promotion (168), and the
study findings described in this Thesis reaffirm that emphasis. Second, the draft
policy aims to ensure that NCD services trickle down from super-specialty to
primary care outlets such as health posts. This Thesis also indicates the need and
relevancy of that strategy. For example, only 20% of respondents with
cardiometabolic diseases visited nearby health posts. While 35% had to visit
hospitals and private clinics in the city and another 20% received medicines
directly from pharmacy shops, 14% and 11% did home-based therapies or
consulted traditional healers, respectively (unpublished data). Third, the draft
policy underscores the necessity of population-based monitoring and
surveillance of NCD-related indicators, including risk factor trends. Using an
HDSS setting, this Thesis demonstrates the possibility and potential of obtaining
quality data on risk factor trends and other sociomedical aspects of CVDs,
including cardiovascular health literacy, practice, and behavior.
Lack of an appropriate health policy that addresses cardiovascular health
issues is a known barrier to achieving cardiovascular health goals (169, 170).
Further, health policy should be evidence-based (171). Hence, in the context of
Nepal, swift enactment of the revised health policy is crucial, as is fair
evaluation of its implementation.
67
Relevance of the study findings to other low- and middle-income countries
Although generalization of the Thesis findings should be done with caution, the
epidemiological situation in Nepal is in many ways typical of that in many other
LMICs (172, 173). The common threads in most LMICs are high burden of
NCD morbidity and mortality (174); inadequate local research and data on the
NCD burden (172), including intervention trials (171); and lack of financial,
technical, and manpower resources to tackle NCDs (175, 176). Compared to the
earlier epidemiological transition in high-income nations, the ongoing transition
in Nepal and other LMICs differ sociodemographically in terms of a rapidly
aging population, urbanization patterns, and rural out-migrations (171). In
addition, unlike high-income nations, NCD-related risk estimation in LMICs
goes beyond clinical (175) and biochemical risk factor profiling, and the social
and cultural context of health behavioral patterns is more important (171).
Nevertheless, even among the LMICs, differences are inevitable in terms of
sociodemographic structures, differential prevalence of risk factors, and health
systems (171, 175).
Despite inter-country variations, contextual similarities allow the
usefulness of research findings across LMICs (176). For example, studies from
other LMICs echo the findings of low cardiovascular health literacy presented in
this Thesis (177). Likewise, the qualitative study findings of patients’
perceptions presented here would be relevant in other similar settings. On the
other hand, findings of interventional studies from other LMICs will provide
useful learning lessons for JD-HDSS and Nepal (177–179).
68
CONCLUSIONS
This Thesis adds new dimensions to population-based cardiovascular health
research in Nepal. In a setting where cardiovascular health research has
traditionally been limited to the estimation of risk factor burden, the findings
presented here widen the research arena by encompassing psychosocial aspects
of cardiovascular health and investigating links between cardiovascular health
knowledge, attitude, literacy, and behavior. Similarly, this Thesis provides a
deeper exploration of the sociodemographic aspects of behavioral risk factors
(e.g., physical activity and fruit and vegetable consumption).
Study findings reconfirm the rising burden of CVD risk factors in a low-
income country like Nepal, and also expose population-level barriers for
achieving better cardiovascular health status. For example, lack of adequate
cardiovascular health literacy in the study population potentially hinders
implementation of any public health effort. Indeed, the major bottlenecks in
achieving better cardiovascular health literacy in this population include
insufficient knowledge, adverse attitudinal attributes, and lack of application of
evidence-based health promotional activities at all levels of care.
This Thesis highlights the major challenges for cardiovascular health at
the population level, and also provides useful information for public health
practice. First, although the findings reported here pertain to the Nepalese
context, the inference from the studies can be relevant for similar communities,
both in Nepal and in other LMICs. Second, although the studies employ
internationally validated questionnaires and guidelines, they also include local
anthropological and cultural constructs. Thus, the study findings present a
holistic situational analysis of cardiovascular health in Nepal from the
population perspective. Therefore, solutions based on these local findings are
more likely to work. Third, the use of health behavior theories helps untangle the
69
most important determinants of cardiovascular health behavior, thus offering
opportunities to formulate locally tailored health promotion strategies. Finally,
the patients’ narrations of their experiences and dilemmas surrounding lifestyle
modifications demonstrate the potential of better cardiovascular health care at
the community level.
68
CONCLUSIONS
This Thesis adds new dimensions to population-based cardiovascular health
research in Nepal. In a setting where cardiovascular health research has
traditionally been limited to the estimation of risk factor burden, the findings
presented here widen the research arena by encompassing psychosocial aspects
of cardiovascular health and investigating links between cardiovascular health
knowledge, attitude, literacy, and behavior. Similarly, this Thesis provides a
deeper exploration of the sociodemographic aspects of behavioral risk factors
(e.g., physical activity and fruit and vegetable consumption).
Study findings reconfirm the rising burden of CVD risk factors in a low-
income country like Nepal, and also expose population-level barriers for
achieving better cardiovascular health status. For example, lack of adequate
cardiovascular health literacy in the study population potentially hinders
implementation of any public health effort. Indeed, the major bottlenecks in
achieving better cardiovascular health literacy in this population include
insufficient knowledge, adverse attitudinal attributes, and lack of application of
evidence-based health promotional activities at all levels of care.
This Thesis highlights the major challenges for cardiovascular health at
the population level, and also provides useful information for public health
practice. First, although the findings reported here pertain to the Nepalese
context, the inference from the studies can be relevant for similar communities,
both in Nepal and in other LMICs. Second, although the studies employ
internationally validated questionnaires and guidelines, they also include local
anthropological and cultural constructs. Thus, the study findings present a
holistic situational analysis of cardiovascular health in Nepal from the
population perspective. Therefore, solutions based on these local findings are
more likely to work. Third, the use of health behavior theories helps untangle the
69
most important determinants of cardiovascular health behavior, thus offering
opportunities to formulate locally tailored health promotion strategies. Finally,
the patients’ narrations of their experiences and dilemmas surrounding lifestyle
modifications demonstrate the potential of better cardiovascular health care at
the community level.
70
FUTURE PERSPECTIVES
By uncovering the gaps in cardiovascular health literacy and practice, this Thesis
underscores the need for cardiovascular health promotion at the community
level. Instead of a one-size-fits-all strategy, health promotional activities should
target different subgroups of population with appropriate strategies. For this,
future studies should also explore cardiovascular health issues in specific groups
(e.g., children and adolescents).
Further studies on behavioral risk factors (e.g., physical activity) should
incorporate ecological and environmental attributes. Controlling diet-related risk
factors will require greater in-depth analysis of psychosocial characteristics such
as eating habits. Ethnographic approaches will increase our ability to explore
cultural and other social aspects of cardiovascular health behavior.
Appropriate study designs, such as longitudinal studies in the current JD-
HDSS setting, should document how urbanization affects risk factor trends.
Finally, research that investigates the perspectives of healthcare providers,
policy-makers, and other stakeholders can form a more comprehensive picture
of the current cardiovascular health situation of Nepal.
71
ACKNOWLEDGMENTS Professor Alexandra Krettek: my supervisor. I did not know that the term
SUPERvisor was coined for her! I have now known Alexandra for five years
and seven months, and ironically, I have never felt that she is like is a
supervisor. Instead, she has been a friend, philosopher and guide, and more.
With a brilliant blend of scientific knowledge, management skills, and
superlative humanity, she has been an inspiring person, a motherly figure, a
strict teacher, and an exceptional host. In fact, her home is my address in
Sweden. With her around, I feel nothing is impossible. She makes things
happen. I must have been born lucky to have a supervisor like her. Thank you,
Alexandra, for everything. This work would not have been possible without you.
Period. I shall miss you in this role, but I know that we still have a long way to
go together as we pursue our common endeavors.
As an endless source of inspiration, I owe a lot to Professor Emeritus Bo
Eriksson, Nordic School of Public Health NHV. I still remember him saying this
to me regarding implementation of my research plan: “You have thought about
this for too long, Abhinav. Now, it’s time to actually do it.” In addition, I
acknowledge the historic contribution of Professor Göran Bondjers in
establishing academic ties between Sweden and Nepal. I also thank Professor
Max Petzold for his contribution for the JD-HDSS project in Nepal, and for
being there whenever we needed his guidance and support. I am also absolutely
indebted to my co-supervisor, Professor Göran Bergström, for coming into the
picture at a very critical juncture of my PhD.
Professor Dambar Bahadur Karki, who is Head of the Department of
Internal Medicine, Kathmandu Medical College, and my mentor, has been a
father figure to me. He often conveyed his unwavering faith in me and my work
through his gentle eyes, firm handshakes, and tender pats on the back. I thank
you, sir. Aside from Professor Karki, two other prominent cardiologists who are
equally devoted to cardiovascular epidemiology and cardiovascular health
70
FUTURE PERSPECTIVES
By uncovering the gaps in cardiovascular health literacy and practice, this Thesis
underscores the need for cardiovascular health promotion at the community
level. Instead of a one-size-fits-all strategy, health promotional activities should
target different subgroups of population with appropriate strategies. For this,
future studies should also explore cardiovascular health issues in specific groups
(e.g., children and adolescents).
Further studies on behavioral risk factors (e.g., physical activity) should
incorporate ecological and environmental attributes. Controlling diet-related risk
factors will require greater in-depth analysis of psychosocial characteristics such
as eating habits. Ethnographic approaches will increase our ability to explore
cultural and other social aspects of cardiovascular health behavior.
Appropriate study designs, such as longitudinal studies in the current JD-
HDSS setting, should document how urbanization affects risk factor trends.
Finally, research that investigates the perspectives of healthcare providers,
policy-makers, and other stakeholders can form a more comprehensive picture
of the current cardiovascular health situation of Nepal.
71
ACKNOWLEDGMENTS Professor Alexandra Krettek: my supervisor. I did not know that the term
SUPERvisor was coined for her! I have now known Alexandra for five years
and seven months, and ironically, I have never felt that she is like is a
supervisor. Instead, she has been a friend, philosopher and guide, and more.
With a brilliant blend of scientific knowledge, management skills, and
superlative humanity, she has been an inspiring person, a motherly figure, a
strict teacher, and an exceptional host. In fact, her home is my address in
Sweden. With her around, I feel nothing is impossible. She makes things
happen. I must have been born lucky to have a supervisor like her. Thank you,
Alexandra, for everything. This work would not have been possible without you.
Period. I shall miss you in this role, but I know that we still have a long way to
go together as we pursue our common endeavors.
As an endless source of inspiration, I owe a lot to Professor Emeritus Bo
Eriksson, Nordic School of Public Health NHV. I still remember him saying this
to me regarding implementation of my research plan: “You have thought about
this for too long, Abhinav. Now, it’s time to actually do it.” In addition, I
acknowledge the historic contribution of Professor Göran Bondjers in
establishing academic ties between Sweden and Nepal. I also thank Professor
Max Petzold for his contribution for the JD-HDSS project in Nepal, and for
being there whenever we needed his guidance and support. I am also absolutely
indebted to my co-supervisor, Professor Göran Bergström, for coming into the
picture at a very critical juncture of my PhD.
Professor Dambar Bahadur Karki, who is Head of the Department of
Internal Medicine, Kathmandu Medical College, and my mentor, has been a
father figure to me. He often conveyed his unwavering faith in me and my work
through his gentle eyes, firm handshakes, and tender pats on the back. I thank
you, sir. Aside from Professor Karki, two other prominent cardiologists who are
equally devoted to cardiovascular epidemiology and cardiovascular health
72
promotion in Nepal, and with whom I have the good fortune of working closely,
have substantially influenced my career path. I thank you, Dr. Bharat Rawat and
Dr. Mrigendra Raj Pandey, for your wit, words of wisdom, and good wishes.
It was the quartet of Suraj Shakya Vaidya, Umesh Raj Aryal, Muni Raj
Chhetri, and me that worked as a local managing committee to establish the JD-
HDSS in Nepal and carry out further studies. Pooling together our individual
strengths and skills, our teamwork could weather the plethora of challenges,
including those encountered during fieldwork, and achieve our research goals. I
thank you all for being there for the project and for me. Special thanks to Umesh
for being my research partner and for standing by me, particularly during
difficult times. And now I am happy to welcome Natalia Oli to our JD-HDSS
team, and I thank her for her thoughtful insights. Her passion to do something
good for cardiovascular health issues of children has always been infectious and
inspirational.
Many people have worked hard behind the scenes to ensure quality data. I
thank my field supervisors, Vishal Bhandari, Ranjan Kapali, Rachana Shrestha,
Chandra Shova Khaitu, and Shova Poudel, for their untiring enthusiasm. Face-
to-face interviewing is not an easy job, particularly when you have to walk for
miles on uneven terrains to cover widely separated houses. This daunting task
was well-handled by our spirited team of enumerators. I also thank Mirak
Angdembe and his team for managing the data entry procedure in a most
professional way. Similarly, Amit and Bhavana Mishra were incredible during
the qualitative study. But above all, I thank all the study participants for their
contribution in making the studies possible. Additionally, I acknowledge the
cooperation extended by community leaders, health post in-charges Mr. Dil
Kumar Duwal and Mr. Yam Bahadur Darlami, and the staff of Duwakot and
Jhaukhel.
Two Nepalese medical institutes, Kathmandu Medical College and Nepal
Medical College, collaborated on the JD-HDSS project. I thank Professor
73
Shekhar Babu Rizyal, Dr. Shyam Prasad Bhattarai, Dr. Aparna Rizyal, and the
management of Nepal Medical College for their support, including sheltering the
JD-HDSS office on the premises of Nepal Medical College Community Hospital
at Jhaukhel. I must thank Staff Nurse Bishnu Subedi and other staff there for
their warm and welcoming hospitality during the training sessions. I am also
thankful to Muna Aryal for going out of her way to extend logistic support every
time we needed her.
My institute, Kathmandu Medical College, has stood behind me
throughout my PhD work. I am grateful to my CEO Professor Govind Prasad
Sharma, former Principal Professor Hemang Dixit, former Campus Chief
Professor Bisharad Man Shrestha, and Principal Professor Chanda Karki for
their support and words of encouragement. I also thank Dr. Binita Pradhan and
the staff of Kathmandu Medical College Community Hospital, Duwakot, for
their cooperation. My department of Community Medicine, Kathmandu Medical
College has borne the brunt of my PhD work, which seemed never-ending (five
years, to be precise). I heartily thank my department head Professor Indur
Dudani and other faculty members, and my post-graduate students for their
cooperation and tolerance with my periodic absences and, worse still, my
demands, tantrums, and irritability. At Kathmandu Medical College, I also thank
my friends and senior faculty in the clinical departments for taking care of my
endless health issues. Here, I also thank everyone at Norvic International
Hospital for ensuring that my heart went on!
Qualitative study was never my cup of tea. In fact, I never even thought of
it as a cup or as tea! I thank Associate Professor Lene Povlsen of the Nordic
School of Public Health NHV for changing me and helping me understand the
importance of qualitative studies in health sciences. And, thank you Associate
Professor Madhusudan Subedi, Patan Academy of Health Sciences, for
reaffirming that the change had indeed taken place.
72
promotion in Nepal, and with whom I have the good fortune of working closely,
have substantially influenced my career path. I thank you, Dr. Bharat Rawat and
Dr. Mrigendra Raj Pandey, for your wit, words of wisdom, and good wishes.
It was the quartet of Suraj Shakya Vaidya, Umesh Raj Aryal, Muni Raj
Chhetri, and me that worked as a local managing committee to establish the JD-
HDSS in Nepal and carry out further studies. Pooling together our individual
strengths and skills, our teamwork could weather the plethora of challenges,
including those encountered during fieldwork, and achieve our research goals. I
thank you all for being there for the project and for me. Special thanks to Umesh
for being my research partner and for standing by me, particularly during
difficult times. And now I am happy to welcome Natalia Oli to our JD-HDSS
team, and I thank her for her thoughtful insights. Her passion to do something
good for cardiovascular health issues of children has always been infectious and
inspirational.
Many people have worked hard behind the scenes to ensure quality data. I
thank my field supervisors, Vishal Bhandari, Ranjan Kapali, Rachana Shrestha,
Chandra Shova Khaitu, and Shova Poudel, for their untiring enthusiasm. Face-
to-face interviewing is not an easy job, particularly when you have to walk for
miles on uneven terrains to cover widely separated houses. This daunting task
was well-handled by our spirited team of enumerators. I also thank Mirak
Angdembe and his team for managing the data entry procedure in a most
professional way. Similarly, Amit and Bhavana Mishra were incredible during
the qualitative study. But above all, I thank all the study participants for their
contribution in making the studies possible. Additionally, I acknowledge the
cooperation extended by community leaders, health post in-charges Mr. Dil
Kumar Duwal and Mr. Yam Bahadur Darlami, and the staff of Duwakot and
Jhaukhel.
Two Nepalese medical institutes, Kathmandu Medical College and Nepal
Medical College, collaborated on the JD-HDSS project. I thank Professor
73
Shekhar Babu Rizyal, Dr. Shyam Prasad Bhattarai, Dr. Aparna Rizyal, and the
management of Nepal Medical College for their support, including sheltering the
JD-HDSS office on the premises of Nepal Medical College Community Hospital
at Jhaukhel. I must thank Staff Nurse Bishnu Subedi and other staff there for
their warm and welcoming hospitality during the training sessions. I am also
thankful to Muna Aryal for going out of her way to extend logistic support every
time we needed her.
My institute, Kathmandu Medical College, has stood behind me
throughout my PhD work. I am grateful to my CEO Professor Govind Prasad
Sharma, former Principal Professor Hemang Dixit, former Campus Chief
Professor Bisharad Man Shrestha, and Principal Professor Chanda Karki for
their support and words of encouragement. I also thank Dr. Binita Pradhan and
the staff of Kathmandu Medical College Community Hospital, Duwakot, for
their cooperation. My department of Community Medicine, Kathmandu Medical
College has borne the brunt of my PhD work, which seemed never-ending (five
years, to be precise). I heartily thank my department head Professor Indur
Dudani and other faculty members, and my post-graduate students for their
cooperation and tolerance with my periodic absences and, worse still, my
demands, tantrums, and irritability. At Kathmandu Medical College, I also thank
my friends and senior faculty in the clinical departments for taking care of my
endless health issues. Here, I also thank everyone at Norvic International
Hospital for ensuring that my heart went on!
Qualitative study was never my cup of tea. In fact, I never even thought of
it as a cup or as tea! I thank Associate Professor Lene Povlsen of the Nordic
School of Public Health NHV for changing me and helping me understand the
importance of qualitative studies in health sciences. And, thank you Associate
Professor Madhusudan Subedi, Patan Academy of Health Sciences, for
reaffirming that the change had indeed taken place.
74
Speaking of the Nordic School of Public Health NHV, I absolutely thank
the school for everything: for all the courses and training it has given and for all
the funds it has provided to facilitate my travel and other costs. Nordic School of
Public Health NHV shall always remain special to me. I thank all the staff and
faculty there, especially Josefin Bergenholtz, Susanne Tidblom-Kjellberger,
Tanja Johansson, and Associate Professor Karolina Andersson Sundell, for their
cooperation. I thank my fellow PhD students and friends Toan Tran Khanh,
Nguyen Thu Huong, Ylva Bjereld, Susann Regber, Hildur Gunnarsdottir, Hanna
Gyllensten, Katja Hakkarainen, Kristine Crondahl and Ruth Montgomery-
Andersen, and not to forget, Suraj Shakya Vaidya and Umesh Raj Aryal.
Besides the Nordic School of Public Health NHV, I acknowledge the
financial support provided by the Swedish Society of Medicine, Wilhelm and
Martina Lundgren Foundation, Johan & Jacob Söderberg Foundation, and the
“Global University” grant from the University of Gothenburg, Sweden. Further,
I express my gratitude to everyone who helped enhance the scientific quality of
my work, including my examiners, the journal editors and reviewers of my
papers, and most importantly, the person who has been extremely supportive in
editing my manuscripts, Karen Williams. Thank you, Karen, for making my
English look so good!
All my love to my wife Prarthana who has seen me only studying, and
that too often well into the wee hours, for eight of our ten years of married life,
first, during my Masters, and then, during my PhD. Thank you, dear. Also, big
‘thank you’ hugs to my eight-year-old son Abhipraaya for being the most
understanding son. Some three years ago, on seeing me working at home all the
time, he once quipped, “I want to be a doctor like you when I grow up, so that I
also get to work ... on a laptop!”
Speaking of family, I fondly remember my Swedish family members, who
are absolutely wonderful human beings. Sven-Olof Jönsson, thank you for all
the support, smiles, and, not to forget, your engineering skills that I often had to
75
put into use. And for always making me feel at home away from home, I express
my gratitude, love, and respect to the Krettek family, Detlef and Evaline and
their daughter Alexandra!
Abhinav Vaidya, Kathmandu, Nepal April 5, 2014

74
Speaking of the Nordic School of Public Health NHV, I absolutely thank
the school for everything: for all the courses and training it has given and for all
the funds it has provided to facilitate my travel and other costs. Nordic School of
Public Health NHV shall always remain special to me. I thank all the staff and
faculty there, especially Josefin Bergenholtz, Susanne Tidblom-Kjellberger,
Tanja Johansson, and Associate Professor Karolina Andersson Sundell, for their
cooperation. I thank my fellow PhD students and friends Toan Tran Khanh,
Nguyen Thu Huong, Ylva Bjereld, Susann Regber, Hildur Gunnarsdottir, Hanna
Gyllensten, Katja Hakkarainen, Kristine Crondahl and Ruth Montgomery-
Andersen, and not to forget, Suraj Shakya Vaidya and Umesh Raj Aryal.
Besides the Nordic School of Public Health NHV, I acknowledge the
financial support provided by the Swedish Society of Medicine, Wilhelm and
Martina Lundgren Foundation, Johan & Jacob Söderberg Foundation, and the
“Global University” grant from the University of Gothenburg, Sweden. Further,
I express my gratitude to everyone who helped enhance the scientific quality of
my work, including my examiners, the journal editors and reviewers of my
papers, and most importantly, the person who has been extremely supportive in
editing my manuscripts, Karen Williams. Thank you, Karen, for making my
English look so good!
All my love to my wife Prarthana who has seen me only studying, and
that too often well into the wee hours, for eight of our ten years of married life,
first, during my Masters, and then, during my PhD. Thank you, dear. Also, big
‘thank you’ hugs to my eight-year-old son Abhipraaya for being the most
understanding son. Some three years ago, on seeing me working at home all the
time, he once quipped, “I want to be a doctor like you when I grow up, so that I
also get to work ... on a laptop!”
Speaking of family, I fondly remember my Swedish family members, who
are absolutely wonderful human beings. Sven-Olof Jönsson, thank you for all
the support, smiles, and, not to forget, your engineering skills that I often had to
75
put into use. And for always making me feel at home away from home, I express
my gratitude, love, and respect to the Krettek family, Detlef and Evaline and
their daughter Alexandra!
Abhinav Vaidya, Kathmandu, Nepal April 5, 2014
76
REFERENCES
(1) Non-communicable diseases fact sheet 2013. Available at: http://www.who.int/mediacentre/factsheets/fs355/en/. Accessed on January 12, 2014.
(2) Bloom D, Cafiero E, Jané-Llopis E, Abrahams-Gessel S, Bloom L, Fathima S. The global economic burden of non-communicable diseases: A report by the World Economic Forum and the Harvard School of Public Health.Geneva: World Economic Forum; 2011.
(3) Lozano R, Naghavi M, Foreman K, AlMazroa MA, Memish ZA. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2095–2128.
(4) Alwan A. Global status report on noncommunicable diseases 2010. Geneva: World Health Organization; 2011.
(5) Yach D, Hawkes C. Chronic Diseases and Risks. In: Merson M, Black RE, Mills AJ, editors. International Public Health. Burlington, MA: Jones & Bartlett Publishers; 2006. p. 273-313.
(6) World Health Organization. Global atlas on cardiovascular disease prevention and control.Mendis S, Puska P, Norrving B, editors. Geneva: World Health Organization; 2011.
(7) Engelgau MM, El-Saharty S, Kudesia P, Rajan V, Rosenhouse S, Okamoto K. Capitalizing on the demographic transition: tackling noncommunicable diseases in South Asia. Washington, DC: World Bank Publications; 2011.
(8) Omran AR. The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem Fund Q 1971;49(4):509-538.
(9) Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: Part II: variations in cardiovascular disease by specific ethnic groups and geographic regions and prevention strategies. Circulation 2001;104(23):2855-2864.
(10) Martine G, Marshall A. State of world population 2007: unleashing the potential of urban growth. New York; UNFPA; 2007.
77
(11) Patel RB, Burke TF. Urbanization—an emerging humanitarian disaster. N Engl J Med 2009;361(8):741-743.
(12) Ezzati M, Vander Hoorn S, Lawes CM, Leach R, James WPT, Lopez AD, et al. Rethinking the “diseases of affluence” paradigm: global patterns of nutritional risks in relation to economic development. PLoS Med2005;2(5):e133.
(13) Vaidya A, Shakya S, Krettek A. Obesity prevalence in Nepal: public health challenges in a low-income nation during an alarming worldwide trend. Int J Environ Res Public Health 2010;7(6):2726-2744.
(14) Anand K, Shah B, Yadav K, Singh R, Mathur P, Paul E, et al. Are the urban poor vulnerable to non-communicable diseases? A survey of risk factors for non-communicable diseases in urban slums of Faridabad. Natl Med J India 2007;20(3):115.
(15) World Health Organization. 2008-2013 action plan for the global strategy for the prevention and control of non-communicable diseases. 2000. Geneva: World Health Organization; 2010.
(16) Lee I, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. The Lancet 2012;380(9838):219-229.
(17) Fletcher GF, Blair SN, Blumenthal J, Caspersen C, Chaitman B, Epstein S, et al. Statement on exercise. Benefits and recommendations for physical activity programs for all Americans. A statement for health professionals by the Committee on Exercise and Cardiac Rehabilitation of the Council on Clinical Cardiology, American Heart association. Circulation 1992;86(1):340-344.
(18) Ainsworth BE. How do I measure physical activity in my patients? Questionnaires and objective methods. Br J Sports Med 2009;43(1):6-9.
(19) Shephard R. Limits to the measurement of habitual physical activity by questionnaires. Br J Sports Med 2003;37(3):197-206.
(20) Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? The Lancet 2012;380(9838):258-271.
(21) Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. The Lancet 2012;380(9838):247-257.
76
REFERENCES
(1) Non-communicable diseases fact sheet 2013. Available at: http://www.who.int/mediacentre/factsheets/fs355/en/. Accessed on January 12, 2014.
(2) Bloom D, Cafiero E, Jané-Llopis E, Abrahams-Gessel S, Bloom L, Fathima S. The global economic burden of non-communicable diseases: A report by the World Economic Forum and the Harvard School of Public Health.Geneva: World Economic Forum; 2011.
(3) Lozano R, Naghavi M, Foreman K, AlMazroa MA, Memish ZA. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2095–2128.
(4) Alwan A. Global status report on noncommunicable diseases 2010. Geneva: World Health Organization; 2011.
(5) Yach D, Hawkes C. Chronic Diseases and Risks. In: Merson M, Black RE, Mills AJ, editors. International Public Health. Burlington, MA: Jones & Bartlett Publishers; 2006. p. 273-313.
(6) World Health Organization. Global atlas on cardiovascular disease prevention and control.Mendis S, Puska P, Norrving B, editors. Geneva: World Health Organization; 2011.
(7) Engelgau MM, El-Saharty S, Kudesia P, Rajan V, Rosenhouse S, Okamoto K. Capitalizing on the demographic transition: tackling noncommunicable diseases in South Asia. Washington, DC: World Bank Publications; 2011.
(8) Omran AR. The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem Fund Q 1971;49(4):509-538.
(9) Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: Part II: variations in cardiovascular disease by specific ethnic groups and geographic regions and prevention strategies. Circulation 2001;104(23):2855-2864.
(10) Martine G, Marshall A. State of world population 2007: unleashing the potential of urban growth. New York; UNFPA; 2007.
77
(11) Patel RB, Burke TF. Urbanization—an emerging humanitarian disaster. N Engl J Med 2009;361(8):741-743.
(12) Ezzati M, Vander Hoorn S, Lawes CM, Leach R, James WPT, Lopez AD, et al. Rethinking the “diseases of affluence” paradigm: global patterns of nutritional risks in relation to economic development. PLoS Med2005;2(5):e133.
(13) Vaidya A, Shakya S, Krettek A. Obesity prevalence in Nepal: public health challenges in a low-income nation during an alarming worldwide trend. Int J Environ Res Public Health 2010;7(6):2726-2744.
(14) Anand K, Shah B, Yadav K, Singh R, Mathur P, Paul E, et al. Are the urban poor vulnerable to non-communicable diseases? A survey of risk factors for non-communicable diseases in urban slums of Faridabad. Natl Med J India 2007;20(3):115.
(15) World Health Organization. 2008-2013 action plan for the global strategy for the prevention and control of non-communicable diseases. 2000. Geneva: World Health Organization; 2010.
(16) Lee I, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. The Lancet 2012;380(9838):219-229.
(17) Fletcher GF, Blair SN, Blumenthal J, Caspersen C, Chaitman B, Epstein S, et al. Statement on exercise. Benefits and recommendations for physical activity programs for all Americans. A statement for health professionals by the Committee on Exercise and Cardiac Rehabilitation of the Council on Clinical Cardiology, American Heart association. Circulation 1992;86(1):340-344.
(18) Ainsworth BE. How do I measure physical activity in my patients? Questionnaires and objective methods. Br J Sports Med 2009;43(1):6-9.
(19) Shephard R. Limits to the measurement of habitual physical activity by questionnaires. Br J Sports Med 2003;37(3):197-206.
(20) Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? The Lancet 2012;380(9838):258-271.
(21) Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. The Lancet 2012;380(9838):247-257.
78
(22) Hellénius M, Sundberg CJ. Physical activity as medicine: time to translate evidence into clinical practice. Br J Sports Med 2011;45(3):158.
(23) World Health Organization. Package of essential noncommunicable (PEN) disease interventions for primary health care in low-resource settings. Geneva: World Health Organization; 2010.
(24) Lock K, Pomerleau J, Causer L, Altmann DR, McKee M. The global burden of disease attributable to low consumption of fruit and vegetables: implications for the global strategy on diet. Bull World Health Organ 2005;83(2):100-108.
(25) Hall JN, Moore S, Harper SB, Lynch JW. Global variability in fruit and vegetable consumption. Am J Prev Med 2009;36(5):402-409. e5.
(26) Nutbeam D. The evolving concept of health literacy. Soc Sci Med 2008;67(12):2072-2078.
(27) Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Internation 2000;15(3):259-267.
(28) Freedman DA, Bess KD, Tucker HA, Boyd DL, Tuchman AM, Wallston KA. Public health literacy defined. Am J Prev Med 2009;36(5):446-451.
(29) Ratzan SC. Health literacy: communication for the public good. Health Promot Internation 2001;16(2):207-214.
(30) Nutbeam D. Health promotion glossary. Health Promot Internation 1998;13(4):349.
(31) Williams MV, Baker DW, Parker RM, Nurss JR. Relationship of functional health literacy to patients' knowledge of their chronic disease: a study of patients with hypertension and diabetes. Arch Intern Med 1998;158(2):166.
(32) Gazmararian JA, Williams MV, Peel J, Baker DW. Health literacy and knowledge of chronic disease. Patient Educ Couns 2003;51(3):267-275.
(33) Kaczorowski J, Chambers LW, Karwalajtys T, Dolovich L, Farrell B, McDonough B, et al. Cardiovascular Health Awareness Program (CHAP): a community cluster-randomised trial among elderly Canadians. Prev Med 2008;46(6):537-544.
79
(34) Young DR, Haskell WL, Taylor CB, Fortmann SP. Effect of Community Health Education on Physical Activity Knowledge, Attitudes, and Behavior The Stanford Five-City Project. Am J Epidemiol 1996;144(3):264-274.
(35) Mendis S, Alwan A. Prioritized research agenda for prevention and control of noncommunicable diseases. Geneva: World Health Organization; 2011.
(36) Central Bureau of Statistics. National Population and Housing Census 2011. Kathmandu: National Planning Commission Secretariat; 2012.
(37) Bista DB. People of Nepal. Kathmandu:Ratna Pustak Bhandar; 1972.
(38) Vaidya A. Is ethnicity an important determinant of high blood pressure in nepalese population? A community-based cross sectional study in duwakot, Nepal. Kathmandu Univ Med J 2012;10(37):20-23.
(39) New Era, Ministry of Health and Population, ICF International Inc. Nepal demographic and health survey, 2011. Calverton, Maryland: Ministry of Health and Population, New ERA, and ICF International; 2012.
(40) Ministry of Health and Population, Nepal . Available at: http://www.mohp.gov.np/english/home/index.php. Accessed on February 13, 2014.
(41) Department of Health Services, Ministry of Health and Population, Nepal. Annual Report 2011-2012. Kathmandu: Ministry of Health and Population, Nepal; 2013.
(42) World Health Organization. Disease and country estimates 2013. Available at: http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html. Accessed on February 15, 2014.
(43) Vaidya A. Tackling cardiovascular health and disease in Nepal: epidemiology, strategies and implementation. Heart Asia 2011;3(1):87-91.
(44) Ministry of Health and Population, Nepal. Nepal non-communicable diseases risk factors survey 2007. Kathmandu: Ministry of Health and Population, Nepal; 2008.
(45) Vaidya A, Pokharel P, Karki P, Nagesh S. Exploring the iceberg of hypertension: a community based study in an eastern Nepal town. Kathmandu Univ Med J 2007;5(3):349-359.
78
(22) Hellénius M, Sundberg CJ. Physical activity as medicine: time to translate evidence into clinical practice. Br J Sports Med 2011;45(3):158.
(23) World Health Organization. Package of essential noncommunicable (PEN) disease interventions for primary health care in low-resource settings. Geneva: World Health Organization; 2010.
(24) Lock K, Pomerleau J, Causer L, Altmann DR, McKee M. The global burden of disease attributable to low consumption of fruit and vegetables: implications for the global strategy on diet. Bull World Health Organ 2005;83(2):100-108.
(25) Hall JN, Moore S, Harper SB, Lynch JW. Global variability in fruit and vegetable consumption. Am J Prev Med 2009;36(5):402-409. e5.
(26) Nutbeam D. The evolving concept of health literacy. Soc Sci Med 2008;67(12):2072-2078.
(27) Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Internation 2000;15(3):259-267.
(28) Freedman DA, Bess KD, Tucker HA, Boyd DL, Tuchman AM, Wallston KA. Public health literacy defined. Am J Prev Med 2009;36(5):446-451.
(29) Ratzan SC. Health literacy: communication for the public good. Health Promot Internation 2001;16(2):207-214.
(30) Nutbeam D. Health promotion glossary. Health Promot Internation 1998;13(4):349.
(31) Williams MV, Baker DW, Parker RM, Nurss JR. Relationship of functional health literacy to patients' knowledge of their chronic disease: a study of patients with hypertension and diabetes. Arch Intern Med 1998;158(2):166.
(32) Gazmararian JA, Williams MV, Peel J, Baker DW. Health literacy and knowledge of chronic disease. Patient Educ Couns 2003;51(3):267-275.
(33) Kaczorowski J, Chambers LW, Karwalajtys T, Dolovich L, Farrell B, McDonough B, et al. Cardiovascular Health Awareness Program (CHAP): a community cluster-randomised trial among elderly Canadians. Prev Med 2008;46(6):537-544.
79
(34) Young DR, Haskell WL, Taylor CB, Fortmann SP. Effect of Community Health Education on Physical Activity Knowledge, Attitudes, and Behavior The Stanford Five-City Project. Am J Epidemiol 1996;144(3):264-274.
(35) Mendis S, Alwan A. Prioritized research agenda for prevention and control of noncommunicable diseases. Geneva: World Health Organization; 2011.
(36) Central Bureau of Statistics. National Population and Housing Census 2011. Kathmandu: National Planning Commission Secretariat; 2012.
(37) Bista DB. People of Nepal. Kathmandu:Ratna Pustak Bhandar; 1972.
(38) Vaidya A. Is ethnicity an important determinant of high blood pressure in nepalese population? A community-based cross sectional study in duwakot, Nepal. Kathmandu Univ Med J 2012;10(37):20-23.
(39) New Era, Ministry of Health and Population, ICF International Inc. Nepal demographic and health survey, 2011. Calverton, Maryland: Ministry of Health and Population, New ERA, and ICF International; 2012.
(40) Ministry of Health and Population, Nepal . Available at: http://www.mohp.gov.np/english/home/index.php. Accessed on February 13, 2014.
(41) Department of Health Services, Ministry of Health and Population, Nepal. Annual Report 2011-2012. Kathmandu: Ministry of Health and Population, Nepal; 2013.
(42) World Health Organization. Disease and country estimates 2013. Available at: http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html. Accessed on February 15, 2014.
(43) Vaidya A. Tackling cardiovascular health and disease in Nepal: epidemiology, strategies and implementation. Heart Asia 2011;3(1):87-91.
(44) Ministry of Health and Population, Nepal. Nepal non-communicable diseases risk factors survey 2007. Kathmandu: Ministry of Health and Population, Nepal; 2008.
(45) Vaidya A, Pokharel P, Karki P, Nagesh S. Exploring the iceberg of hypertension: a community based study in an eastern Nepal town. Kathmandu Univ Med J 2007;5(3):349-359.
80
(46) Sharma SK, Ghimire A, Radhakrishnan J, Thapa L, Shrestha NR, Paudel N, et al. Prevalence of hypertension, obesity, diabetes, and metabolic syndrome in Nepal. Int J Hypertens 2011. doi:10.4061/2011/821971.
(47) Sharma D, KC MB, Rajbhandari S, Raut R, Baidya SG, Kafle PM, et al. Study of prevalence, awareness,and control of hypertension in a suburban area of Kathmandu, Nepal. Indian Heart J 2006;58(1):34-37.
(48) Vaidya A, Pathak RP, Pandey MR. Prevalence of hypertension in Nepalese community triples in 25 years: a repeat cross-sectional study in rural Kathmandu. Indian Heart J 2012;64(2):128-131.
(49) Vaidya A, Pokharel PK, Nagesh S, Karki P, Kumar S, Majhi S. Prevalence of coronary heart disease in the urban adult males of eastern Nepal: A population-based analytical cross-sectional study. Indian Heart J 2009;61:341-347.
(50) KC MB, Sharma D, Shrestha MP, Gurung S, Rajbhandari S, Malla R, et al. Prevalence of rheumatic and congenital heart disease in schoolchildren of Kathmandu valley in Nepal. Indian Heart J 2003;55(6):615-618.
(51) Shrestha UK, Bhattarai TN, Pandey MR. Prevalence of rheumatic fever and rheumatic heart disease in school children in a rural community of the hill region of Nepal. Indian Heart J 1991;43(1):39-41.
(52) Shahid Gangalal national heart centre annual report 2007. Available at: http://www.sgnhc.org.np/publication-2007.htm. Accessed on December 24, 2010.
(53) Vaidya A. Need for community-based primary prevention of coronary heart disease in Nepal. Kathmandu Univ Med J 2008;6(24):435-436.
(54) Ministry of Health and Population, Nepal. Nepal national policy, strategy and plan of action for prevention and control of Non-Communicable Diseases. Kathmandu: Ministry of Health and Population, Nepal; 2009.
(55) Khan MS, Jafary FH, Faruqui AM, Rasool SI, Hatcher J, Chaturvedi N, et al. High prevalence of lack of knowledge of symptoms of acute myocardial infarction in Pakistan and its contribution to delayed presentationto the hospital. BMC Public Health 2007;7(1):284.
81
(56) Pearson TA, Bazzarre TL, Daniels SR, Fair JM, Fortmann SP, Franklin BA, et al. American Heart Association guide for improving cardiovascular health at the community level: a statement for public health practitioners, healthcare providers, and health policy makers from the American Heart Association Expert Panel on Population and Prevention Science. Circulation 2003;107(4):645-651.
(57) Limbu YR, Malla R, Regmi SR, Dahal R, Nakarmi HL, Yonzan G, et al. Public knowledge of heart attack in a Nepalese population survey. Heart Lung 2006;35(3):164-169.
(58) Upadhyay DK, Palaian S, Shankar PR, Mishra P, Pokhara N. Knowledge, attitude and practice about diabetes among diabetes patients in Western Nepal. Rawal Med J 2008;33(1):8-11.
(59) Department of Health Services, Ministry of Health and Population, Nepal. Annual Report 2002-2003. Kathmandu: Ministry of Health and Population, Nepal; 2004.
(60) INDEPTH Network. Population and health in developing countries: Population, health and survival at INDEPTH Sites, Volume I. Canada: International Development Research Centre; 2002.
(61) Adazu K, Lindblade KA, Rosen DH, Odhiambo F, Ofware P, Kwach J, et al. Health and demographic surveillance in rural western Kenya: a platform for evaluating interventions to reduce morbidity and mortality from infectious diseases. Am J Trop Med Hyg 2005;73(6):1151.
(62) Chandramohan D, Shibuya K, Setel P, Cairncross S, Lopez AD, Murray CJL, et al. Should data from demographic surveillance systems be made more widely available to researchers? PLoS Med 2008;5(2):e57.
(63) Byass P, Sankoh O, Tollman SM, Högberg U, Wall S. Lessons from history for designing and validating epidemiological surveillance in uncounted populations. PloS One 2011;6(8):e22897.
(64) Pronyk PM, Kahn K, Tollman SM. Using health and demographic surveillance to understand the burden of disease in populations: The case of tuberculosis in rural South Africa. Scand J Public Health 2007;35:45-51.
(65) Ahmed SM, Hadi A, Razzaque A, Ashraf A, Juvekar S, Ng N, et al. Clustering of chronic non-communicable disease risk factors among selected Asian populations: levels and determinants. Glob Health Action 2009;2.
80
(46) Sharma SK, Ghimire A, Radhakrishnan J, Thapa L, Shrestha NR, Paudel N, et al. Prevalence of hypertension, obesity, diabetes, and metabolic syndrome in Nepal. Int J Hypertens 2011. doi:10.4061/2011/821971.
(47) Sharma D, KC MB, Rajbhandari S, Raut R, Baidya SG, Kafle PM, et al. Study of prevalence, awareness,and control of hypertension in a suburban area of Kathmandu, Nepal. Indian Heart J 2006;58(1):34-37.
(48) Vaidya A, Pathak RP, Pandey MR. Prevalence of hypertension in Nepalese community triples in 25 years: a repeat cross-sectional study in rural Kathmandu. Indian Heart J 2012;64(2):128-131.
(49) Vaidya A, Pokharel PK, Nagesh S, Karki P, Kumar S, Majhi S. Prevalence of coronary heart disease in the urban adult males of eastern Nepal: A population-based analytical cross-sectional study. Indian Heart J 2009;61:341-347.
(50) KC MB, Sharma D, Shrestha MP, Gurung S, Rajbhandari S, Malla R, et al. Prevalence of rheumatic and congenital heart disease in schoolchildren of Kathmandu valley in Nepal. Indian Heart J 2003;55(6):615-618.
(51) Shrestha UK, Bhattarai TN, Pandey MR. Prevalence of rheumatic fever and rheumatic heart disease in school children in a rural community of the hill region of Nepal. Indian Heart J 1991;43(1):39-41.
(52) Shahid Gangalal national heart centre annual report 2007. Available at: http://www.sgnhc.org.np/publication-2007.htm. Accessed on December 24, 2010.
(53) Vaidya A. Need for community-based primary prevention of coronary heart disease in Nepal. Kathmandu Univ Med J 2008;6(24):435-436.
(54) Ministry of Health and Population, Nepal. Nepal national policy, strategy and plan of action for prevention and control of Non-Communicable Diseases. Kathmandu: Ministry of Health and Population, Nepal; 2009.
(55) Khan MS, Jafary FH, Faruqui AM, Rasool SI, Hatcher J, Chaturvedi N, et al. High prevalence of lack of knowledge of symptoms of acute myocardial infarction in Pakistan and its contribution to delayed presentationto the hospital. BMC Public Health 2007;7(1):284.
81
(56) Pearson TA, Bazzarre TL, Daniels SR, Fair JM, Fortmann SP, Franklin BA, et al. American Heart Association guide for improving cardiovascular health at the community level: a statement for public health practitioners, healthcare providers, and health policy makers from the American Heart Association Expert Panel on Population and Prevention Science. Circulation 2003;107(4):645-651.
(57) Limbu YR, Malla R, Regmi SR, Dahal R, Nakarmi HL, Yonzan G, et al. Public knowledge of heart attack in a Nepalese population survey. Heart Lung 2006;35(3):164-169.
(58) Upadhyay DK, Palaian S, Shankar PR, Mishra P, Pokhara N. Knowledge, attitude and practice about diabetes among diabetes patients in Western Nepal. Rawal Med J 2008;33(1):8-11.
(59) Department of Health Services, Ministry of Health and Population, Nepal. Annual Report 2002-2003. Kathmandu: Ministry of Health and Population, Nepal; 2004.
(60) INDEPTH Network. Population and health in developing countries: Population, health and survival at INDEPTH Sites, Volume I. Canada: International Development Research Centre; 2002.
(61) Adazu K, Lindblade KA, Rosen DH, Odhiambo F, Ofware P, Kwach J, et al. Health and demographic surveillance in rural western Kenya: a platform for evaluating interventions to reduce morbidity and mortality from infectious diseases. Am J Trop Med Hyg 2005;73(6):1151.
(62) Chandramohan D, Shibuya K, Setel P, Cairncross S, Lopez AD, Murray CJL, et al. Should data from demographic surveillance systems be made more widely available to researchers? PLoS Med 2008;5(2):e57.
(63) Byass P, Sankoh O, Tollman SM, Högberg U, Wall S. Lessons from history for designing and validating epidemiological surveillance in uncounted populations. PloS One 2011;6(8):e22897.
(64) Pronyk PM, Kahn K, Tollman SM. Using health and demographic surveillance to understand the burden of disease in populations: The case of tuberculosis in rural South Africa. Scand J Public Health 2007;35:45-51.
(65) Ahmed SM, Hadi A, Razzaque A, Ashraf A, Juvekar S, Ng N, et al. Clustering of chronic non-communicable disease risk factors among selected Asian populations: levels and determinants. Glob Health Action 2009;2.
82
(66) Redding CA, Rossi S, Rossi R, Velicer WF, Prochaska O. Health behavior models. The International Electronic Journal of Health Education 2000;3:180-193.
(67) Nutbeam D, Harris E, Harris E. Theory in a nutshell: a guide to health promotion theory. McGraw-Hill Sydney, Australia; 1999.
(68) Bandura A. Health promotion by social cognitive means. Health Educ Behav 2004;31(2):143-164.
(69) Lowenstein A, Foord-May L, Romano J. Teaching strategies for health education and health promotion: working with patients, families, and communities. Burlington: Jones & Bartlett Publishers; 2009.
(70) Creswell JW. Designing and conducting mixed methods research. Wiley Online Library; 2007.
(71) Creswell JW, Klassen AC, Plano Clark VL, Smith KC. Best practices for mixed methods research in the health sciences. Bethesda (Maryland): National Institutes of Health; 2011.
(72) O'Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ 2010;341:c4587.
(73) Curry LA, Nembhard IM, Bradley EH. Qualitative and mixed methods provide unique contributions to outcomes research. Circulation 2009;119(10):1442-1452.
(74) Kish L. Sampling organizations and groups of unequal sizes. Am Sociol Rev 1965;30:564-572.
(75) Bryant BE. Respondent selection in a time of changing household composition. Journal of Marketing Research 1975;12(2):129-135.
(76) Gaziano C. Comparative analysis of within-household respondent selection techniques. Public Opin Q 2005;69(1):124-157.
(77) Nemeth R. Respondent selection within the household-A modification of the Kish grid. In: Meeting of Young Statisticians, p. 51; 2002.
(78) Chuc NT, Diwan V. FilaBavi, a demographic surveillance site, an epidemiological field laboratory in Vietnam. Scand J Public Health Suppl 2003;62:3-7.
83
(79) Ghosh A, Ghosh T. Modification of Kuppuswamy's socioeconomic status scale in context to Nepal. Indian Pediatr 2009;46(12):1104-1105.
(80) World Health Organization. WHO STEPS Instrument (Core and Expanded): The WHO STEPwise approach to chronic disease risk factor surveillance (STEPS). 2008; Available at: http://www.who.int/chp/steps/STEPS_Instrument_v2.1.pdf. Accessed on March 24, 2010.
(81) Lenfant C, Chobanian AV, Jones DW, Roccella EJ. Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Circulation 2003;107(24):2993-2994.
(82) Lin W, Yang H, Hang C, Pan W. Nutrition knowledge, attitude, and behavior of Taiwanese elementary school children. Asia Pac J Clin Nutr 2007;16:534.
(83) Torabi MR, Yang J, Li J. Comparison of tobacco use knowledge, attitude and practice among college students in China and the United States. Health Promot Internation 2002;17(3):247-253.
(84) Kosaryan M, Vahidshahi K, Siami R, Nazari M, Karami H, Ehteshami S. Knowledge, attitude, and practice of reproductive behavior in Iranian minor thalassemia couples. Saudi Med J 2009;30(6):835-839.
(85) Neamatollahi H, Ebrahimi M, Talebi M, Ardabili MH, Kondori K. Major differences in oral health knowledge and behavior in a group of Iranian pre-university students: a cross-sectional study. J Oral Sci 2011;53(2):177-184.
(86) Sharda AJ, Shetty S. A comparative study of oral health knowledge, attitude and behavior of first and final year dental students of Udaipur city, Rajasthan, India. International journal of dental hygiene 2008;6(4):347-353.
(87) Yap J, Lee V, Yau T, Ng T, Tor P. Knowledge, attitudes and practices towards pandemic influenza among cases, close contacts, and healthcare workers in tropical Singapore: a cross-sectional survey. BMC Public Health 2010;10(1):442.
(88) Maimaiti N, Shamsuddin K, Abdurahim A, Tohti N, Memet R. Knowledge, attitude and practice regarding HIV/AIDS among University students in Xinjiang. Glob J Health Sci 2010;2(2):51.
82
(66) Redding CA, Rossi S, Rossi R, Velicer WF, Prochaska O. Health behavior models. The International Electronic Journal of Health Education 2000;3:180-193.
(67) Nutbeam D, Harris E, Harris E. Theory in a nutshell: a guide to health promotion theory. McGraw-Hill Sydney, Australia; 1999.
(68) Bandura A. Health promotion by social cognitive means. Health Educ Behav 2004;31(2):143-164.
(69) Lowenstein A, Foord-May L, Romano J. Teaching strategies for health education and health promotion: working with patients, families, and communities. Burlington: Jones & Bartlett Publishers; 2009.
(70) Creswell JW. Designing and conducting mixed methods research. Wiley Online Library; 2007.
(71) Creswell JW, Klassen AC, Plano Clark VL, Smith KC. Best practices for mixed methods research in the health sciences. Bethesda (Maryland): National Institutes of Health; 2011.
(72) O'Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ 2010;341:c4587.
(73) Curry LA, Nembhard IM, Bradley EH. Qualitative and mixed methods provide unique contributions to outcomes research. Circulation 2009;119(10):1442-1452.
(74) Kish L. Sampling organizations and groups of unequal sizes. Am Sociol Rev 1965;30:564-572.
(75) Bryant BE. Respondent selection in a time of changing household composition. Journal of Marketing Research 1975;12(2):129-135.
(76) Gaziano C. Comparative analysis of within-household respondent selection techniques. Public Opin Q 2005;69(1):124-157.
(77) Nemeth R. Respondent selection within the household-A modification of the Kish grid. In: Meeting of Young Statisticians, p. 51; 2002.
(78) Chuc NT, Diwan V. FilaBavi, a demographic surveillance site, an epidemiological field laboratory in Vietnam. Scand J Public Health Suppl 2003;62:3-7.
83
(79) Ghosh A, Ghosh T. Modification of Kuppuswamy's socioeconomic status scale in context to Nepal. Indian Pediatr 2009;46(12):1104-1105.
(80) World Health Organization. WHO STEPS Instrument (Core and Expanded): The WHO STEPwise approach to chronic disease risk factor surveillance (STEPS). 2008; Available at: http://www.who.int/chp/steps/STEPS_Instrument_v2.1.pdf. Accessed on March 24, 2010.
(81) Lenfant C, Chobanian AV, Jones DW, Roccella EJ. Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Circulation 2003;107(24):2993-2994.
(82) Lin W, Yang H, Hang C, Pan W. Nutrition knowledge, attitude, and behavior of Taiwanese elementary school children. Asia Pac J Clin Nutr 2007;16:534.
(83) Torabi MR, Yang J, Li J. Comparison of tobacco use knowledge, attitude and practice among college students in China and the United States. Health Promot Internation 2002;17(3):247-253.
(84) Kosaryan M, Vahidshahi K, Siami R, Nazari M, Karami H, Ehteshami S. Knowledge, attitude, and practice of reproductive behavior in Iranian minor thalassemia couples. Saudi Med J 2009;30(6):835-839.
(85) Neamatollahi H, Ebrahimi M, Talebi M, Ardabili MH, Kondori K. Major differences in oral health knowledge and behavior in a group of Iranian pre-university students: a cross-sectional study. J Oral Sci 2011;53(2):177-184.
(86) Sharda AJ, Shetty S. A comparative study of oral health knowledge, attitude and behavior of first and final year dental students of Udaipur city, Rajasthan, India. International journal of dental hygiene 2008;6(4):347-353.
(87) Yap J, Lee V, Yau T, Ng T, Tor P. Knowledge, attitudes and practices towards pandemic influenza among cases, close contacts, and healthcare workers in tropical Singapore: a cross-sectional survey. BMC Public Health 2010;10(1):442.
(88) Maimaiti N, Shamsuddin K, Abdurahim A, Tohti N, Memet R. Knowledge, attitude and practice regarding HIV/AIDS among University students in Xinjiang. Glob J Health Sci 2010;2(2):51.
84
(89) Chen W-C, Yu Y-C, Glaser K. The knowledge and attitudes of coronary heart disease prevention among middle and older aged people in a community in Taipei. Taiwan Geriatrics & Gerontology 2009;4(4):251-262.
(90) Dodani S, Mistry R, Khwaja A, Farooqi M, Qureshi R, Kazmi K. Prevalence and awareness of risk factors and behaviours of coronary heart disease in an urban population of Karachi, the largest city of Pakistan: a community survey. J Public Health 2004;26(3):245-249.
(91) Saeed O, Gupta V, Dhawan N, Streja L, Shin JS, Ku M, et al. Knowledge of modifiable risk factors of Coronary Atherosclerotic Heart Disease (CASHD) among a sample in India. BMC Int Health Hum Rights 2009;9(1):2.
(92) Mosca L, Jones WK, King KB, Ouyang P, Redberg RF, Hill MN. Awareness, perception, and knowledge of heart disease risk and prevention among women in the United States. Arch Fam Med 2000;9(6):506.
(93) Potvin L, Richard L, Edwards AC. Knowledge of cardiovascular disease risk factors among the Canadian population: relationships with indicators of socioeconomic status. Can Med Assoc J 2000;162(9 suppl):S5-S11.
(94) Lim K, Sumarni M, Amal N, Hanjeet K, Wan Rozita W, Norhamimah A. Tobacco use, knowledge and attitude among Malaysians age 18 and above. Trop Biomed 2009;26:92-99.
(95) Wong BM, Garcia Y, Barr A, Glazier RH, Abramson BL. Cardiovascular risk factor awareness in a disadvantaged inner-city population–implications for preventive strategies. Can J Cardiol 2008;24(9):677-682.
(96) Schweigman K, Eichner J, Welty TK, Zhang Y. Cardiovascular disease risk factor awareness in American Indian communities: The Strong Heart Study. Ethn Dis 2006;16(3):647.
(97) United Nations Children Fund. Baseline Survey of the Knowledge, Attitude and Practice (KAP) of Parents/Guardians on Early Childhood Development and Primary Education in Nepal. Pulchowk, Lalipur: UNICEF; 2009.
(98) Waller J, McCaffery K, Wardle J. Measuring cancer knowledge: comparing prompted and unprompted recall. Br J Psychol 2004;95(2):219-234.
(99) Glass AL, Holyoak KJ. Cognition . Second ed. New York: McGraw-Hill; 1986.
85
(100) Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health 2006;14(2):66-70.
(101) World Health Organization. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. Geneva: World Health Organization; 2012.
(102) World Health Organization. Global recommendations on physical activity for health. Geneva: World Health Organization; 2010. p. 8-10.
(103) Humphrey NP. Does the built environment influence physical activity? TR NEWS 2005;237:32.
(104) Sallis JF, Floyd MF, Rodriguez DA, Saelens BE. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation 2012;125(5):729-737.
(105) Guillaumie L, Godin G, Vézina-Im L. Psychosocial determinants of fruit and vegetable intake in adult population: a systematic review. Int J Behav Nutr Phys Act 2010;7(1):12.
(106) Johnson JS, Nobmann ED, Asay E. Factors related to fruit, vegetable and traditional food consumption which may affect health among Alaska Native People in Western Alaska. Int J Circumpolar Health 2012;71.
(107) Rose D, Richards R. Food store access and household fruit and vegetable use among participants in the US Food Stamp Program. Public Health Nutr 2004;7(08):1081-1088.
(108) Pearson N, Timperio A, Salmon J, Crawford D, Biddle SJ. Family influences on children's physical activity and fruit and vegetable consumption. Int J Behav Nutr Phys Act2009;6:34.
(109) Davidson PM, Daly J, Leung D, Ang E, Paull G, DiGiacomo M, et al. Health-seeking beliefs of cardiovascular patients: A qualitative study. Int J Nurs Stud 2011;48(11):1367-1375.
(110) Awah PK, Kengne AP, Fezeu LL, Mbanya J. Perceived risk factors of cardiovascular diseases and diabetes in Cameroon. Health Educ Res 2008;23(4):612-620.
(111) Jolles EP, Padwal RS, Clark AM, Braam B. A qualitative study of patient perspectives about hypertension. Stress 2013;46(27):19.
84
(89) Chen W-C, Yu Y-C, Glaser K. The knowledge and attitudes of coronary heart disease prevention among middle and older aged people in a community in Taipei. Taiwan Geriatrics & Gerontology 2009;4(4):251-262.
(90) Dodani S, Mistry R, Khwaja A, Farooqi M, Qureshi R, Kazmi K. Prevalence and awareness of risk factors and behaviours of coronary heart disease in an urban population of Karachi, the largest city of Pakistan: a community survey. J Public Health 2004;26(3):245-249.
(91) Saeed O, Gupta V, Dhawan N, Streja L, Shin JS, Ku M, et al. Knowledge of modifiable risk factors of Coronary Atherosclerotic Heart Disease (CASHD) among a sample in India. BMC Int Health Hum Rights 2009;9(1):2.
(92) Mosca L, Jones WK, King KB, Ouyang P, Redberg RF, Hill MN. Awareness, perception, and knowledge of heart disease risk and prevention among women in the United States. Arch Fam Med 2000;9(6):506.
(93) Potvin L, Richard L, Edwards AC. Knowledge of cardiovascular disease risk factors among the Canadian population: relationships with indicators of socioeconomic status. Can Med Assoc J 2000;162(9 suppl):S5-S11.
(94) Lim K, Sumarni M, Amal N, Hanjeet K, Wan Rozita W, Norhamimah A. Tobacco use, knowledge and attitude among Malaysians age 18 and above. Trop Biomed 2009;26:92-99.
(95) Wong BM, Garcia Y, Barr A, Glazier RH, Abramson BL. Cardiovascular risk factor awareness in a disadvantaged inner-city population–implications for preventive strategies. Can J Cardiol 2008;24(9):677-682.
(96) Schweigman K, Eichner J, Welty TK, Zhang Y. Cardiovascular disease risk factor awareness in American Indian communities: The Strong Heart Study. Ethn Dis 2006;16(3):647.
(97) United Nations Children Fund. Baseline Survey of the Knowledge, Attitude and Practice (KAP) of Parents/Guardians on Early Childhood Development and Primary Education in Nepal. Pulchowk, Lalipur: UNICEF; 2009.
(98) Waller J, McCaffery K, Wardle J. Measuring cancer knowledge: comparing prompted and unprompted recall. Br J Psychol 2004;95(2):219-234.
(99) Glass AL, Holyoak KJ. Cognition . Second ed. New York: McGraw-Hill; 1986.
85
(100) Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health 2006;14(2):66-70.
(101) World Health Organization. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. Geneva: World Health Organization; 2012.
(102) World Health Organization. Global recommendations on physical activity for health. Geneva: World Health Organization; 2010. p. 8-10.
(103) Humphrey NP. Does the built environment influence physical activity? TR NEWS 2005;237:32.
(104) Sallis JF, Floyd MF, Rodriguez DA, Saelens BE. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation 2012;125(5):729-737.
(105) Guillaumie L, Godin G, Vézina-Im L. Psychosocial determinants of fruit and vegetable intake in adult population: a systematic review. Int J Behav Nutr Phys Act 2010;7(1):12.
(106) Johnson JS, Nobmann ED, Asay E. Factors related to fruit, vegetable and traditional food consumption which may affect health among Alaska Native People in Western Alaska. Int J Circumpolar Health 2012;71.
(107) Rose D, Richards R. Food store access and household fruit and vegetable use among participants in the US Food Stamp Program. Public Health Nutr 2004;7(08):1081-1088.
(108) Pearson N, Timperio A, Salmon J, Crawford D, Biddle SJ. Family influences on children's physical activity and fruit and vegetable consumption. Int J Behav Nutr Phys Act2009;6:34.
(109) Davidson PM, Daly J, Leung D, Ang E, Paull G, DiGiacomo M, et al. Health-seeking beliefs of cardiovascular patients: A qualitative study. Int J Nurs Stud 2011;48(11):1367-1375.
(110) Awah PK, Kengne AP, Fezeu LL, Mbanya J. Perceived risk factors of cardiovascular diseases and diabetes in Cameroon. Health Educ Res 2008;23(4):612-620.
(111) Jolles EP, Padwal RS, Clark AM, Braam B. A qualitative study of patient perspectives about hypertension. Stress 2013;46(27):19.
86
(112) van Steenkiste B, van der Weijden T, Timmermans D, Vaes J, Stoffers J, Grol R. Patients’ ideas, fears and expectations of their coronary risk: barriers for primary prevention. Patient Educ Couns 2004;55(2):301-307.
(113) Higgins M, Dunn S, Theobald K. The patients’ perception of recovery after coronary angioplasty. Aust Crit Care 2000;13(3):83-88.
(114) Bryant LL, Chin NP, Fernandez ID, Cottrell LA, Duckles JM, Garces DM, et al. Perceptions of cardiovascular health in underserved communities. Prev Chronic Dis 2010;7(2):A30.
(115) Montano CM, Estrada K, Chávez A, Ramírez-Zea M. Perceptions, knowledge and beliefs about prevention of cardiovascular diseases in Villa Nueva, Guatemala. Prev Control 2008;3(1):1-9.
(116) Beya M. Lay beliefs of hypertensive patients attending Katleho District Hospital (KDH) in Virginia in Free State regarding their disease. Lay beliefs of hypertensive patients attending Katleho District Hospital (KDH) in Virginia in Free State regarding their disease (Master's thesis, University of Limpopo, 2010).
(117) Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today 2004;24(2):105-112.
(118) Allender S, Foster C, Hutchinson L, Arambepola C. Quantification of urbanization in relation to chronic diseases in developing countries: a systematic review. J Urban Health 2008;85(6):938-951.
(119) World Health Organization Regional Office for the Eastern Mediterranean. Effects of urbanization on incidence of noncommunicable diseases. Cairo: World Health Organization; 2012.
(120) Research report on NCD risk factors surveillance in Nepal 2003. Available at: http://www.who.int/chp/steps/NepalSTEPSReport2003Kathmandu.pdf. Accessed on June 21, 2013.
(121) Surveillance of risk factors for non-communicable diseases in Nepal 2006: Report of Survey in Ilam, Lalitpur and Tanahun. 2013; Available at: http://www.who.int/chp/steps/NepalSTEPSReport2005_3districts.pdf.Accessed on June 21, 2013.
87
(122) Oli N, Vaidya A, Thapa G. Behavioural risk factors of non-communicable diseases among Nepalese urban poor: a descriptive study from a slum area of Kathmandu. Epidemiol Res Int 2013. doi.org/10.1155/2013/329156.
(123) Central Bureau of Statistics. Nepal demographics profile 2013. Available at: http://www.indexmundi.com/nepal/demographics_profile.html. Accessed on January 15, 2010.
(124) Sharma P. Urbanization and development. Available at: http://cbs.gov.np/wp-content/uploads/2012/Population/Monograph/Chapter%2010%20%20Urbanization%20and%20Development.pdf. Accessed on December 12, 2013.
(125) Allender S, Lacey B, Webster P, Rayner M, Deepa M, Scarborough P, et al. Level of urbanization and noncommunicable disease risk factors in Tamil Nadu, India. Bull World Health Organ 2010;88(4):297-304.
(126) Das M, Pal S, Ghosh A. Rural urban differences of cardiovascular disease risk factors in adult Asian Indians. Am J Hum Biol 2008;20(4):440-445.
(127) Monda KL, Gordon-Larsen P, Stevens J, Popkin BM. China's transition: the effect of rapid urbanization on adult occupational physical activity. Soc Sci Med 2007;64(4):858-870.
(128) Merom D, Sinnreich R, Aboudi V, Kark JD, Nassar H. Lifestyle physical activity among urban Palestinians and Israelis: a cross-sectional comparison in the Palestinian-Israeli Jerusalem risk factor study. BMC Public Health 2012;12(1):90.
(129) Katzmarzyk PT, Mason C. The physical activity transition. JPhys Act Health 2009;6(3):269-280.
(130) International Labour Organization. Labour and Social Trends in Nepal 2010. 2010. Available at: http://www.ilo.org/wcmsp5/groups/public/---asia/---ro-bangkok/---ilo-kathmandu/documents/publication/wcms_151322.pdf. Accessed on January 11, 2014.
(131) Stankov I, Olds T, Cargo M. Overweight and obese adolescents: what turns them off physical activity? Int J Behav Nutr Phys Act 2012;9(1):53.
(132) Ng N, Van Minh H, Juvekar S, Razzaque A, Bich TH, Kanungsukkasem U, et al. Using the INDEPTH HDSS to build capacity for chronic non-communicable disease risk factor surveillance in low and middle-income countries. Glob Health Action 2009;2.
86
(112) van Steenkiste B, van der Weijden T, Timmermans D, Vaes J, Stoffers J, Grol R. Patients’ ideas, fears and expectations of their coronary risk: barriers for primary prevention. Patient Educ Couns 2004;55(2):301-307.
(113) Higgins M, Dunn S, Theobald K. The patients’ perception of recovery after coronary angioplasty. Aust Crit Care 2000;13(3):83-88.
(114) Bryant LL, Chin NP, Fernandez ID, Cottrell LA, Duckles JM, Garces DM, et al. Perceptions of cardiovascular health in underserved communities. Prev Chronic Dis 2010;7(2):A30.
(115) Montano CM, Estrada K, Chávez A, Ramírez-Zea M. Perceptions, knowledge and beliefs about prevention of cardiovascular diseases in Villa Nueva, Guatemala. Prev Control 2008;3(1):1-9.
(116) Beya M. Lay beliefs of hypertensive patients attending Katleho District Hospital (KDH) in Virginia in Free State regarding their disease. Lay beliefs of hypertensive patients attending Katleho District Hospital (KDH) in Virginia in Free State regarding their disease (Master's thesis, University of Limpopo, 2010).
(117) Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today 2004;24(2):105-112.
(118) Allender S, Foster C, Hutchinson L, Arambepola C. Quantification of urbanization in relation to chronic diseases in developing countries: a systematic review. J Urban Health 2008;85(6):938-951.
(119) World Health Organization Regional Office for the Eastern Mediterranean. Effects of urbanization on incidence of noncommunicable diseases. Cairo: World Health Organization; 2012.
(120) Research report on NCD risk factors surveillance in Nepal 2003. Available at: http://www.who.int/chp/steps/NepalSTEPSReport2003Kathmandu.pdf. Accessed on June 21, 2013.
(121) Surveillance of risk factors for non-communicable diseases in Nepal 2006: Report of Survey in Ilam, Lalitpur and Tanahun. 2013; Available at: http://www.who.int/chp/steps/NepalSTEPSReport2005_3districts.pdf.Accessed on June 21, 2013.
87
(122) Oli N, Vaidya A, Thapa G. Behavioural risk factors of non-communicable diseases among Nepalese urban poor: a descriptive study from a slum area of Kathmandu. Epidemiol Res Int 2013. doi.org/10.1155/2013/329156.
(123) Central Bureau of Statistics. Nepal demographics profile 2013. Available at: http://www.indexmundi.com/nepal/demographics_profile.html. Accessed on January 15, 2010.
(124) Sharma P. Urbanization and development. Available at: http://cbs.gov.np/wp-content/uploads/2012/Population/Monograph/Chapter%2010%20%20Urbanization%20and%20Development.pdf. Accessed on December 12, 2013.
(125) Allender S, Lacey B, Webster P, Rayner M, Deepa M, Scarborough P, et al. Level of urbanization and noncommunicable disease risk factors in Tamil Nadu, India. Bull World Health Organ 2010;88(4):297-304.
(126) Das M, Pal S, Ghosh A. Rural urban differences of cardiovascular disease risk factors in adult Asian Indians. Am J Hum Biol 2008;20(4):440-445.
(127) Monda KL, Gordon-Larsen P, Stevens J, Popkin BM. China's transition: the effect of rapid urbanization on adult occupational physical activity. Soc Sci Med 2007;64(4):858-870.
(128) Merom D, Sinnreich R, Aboudi V, Kark JD, Nassar H. Lifestyle physical activity among urban Palestinians and Israelis: a cross-sectional comparison in the Palestinian-Israeli Jerusalem risk factor study. BMC Public Health 2012;12(1):90.
(129) Katzmarzyk PT, Mason C. The physical activity transition. JPhys Act Health 2009;6(3):269-280.
(130) International Labour Organization. Labour and Social Trends in Nepal 2010. 2010. Available at: http://www.ilo.org/wcmsp5/groups/public/---asia/---ro-bangkok/---ilo-kathmandu/documents/publication/wcms_151322.pdf. Accessed on January 11, 2014.
(131) Stankov I, Olds T, Cargo M. Overweight and obese adolescents: what turns them off physical activity? Int J Behav Nutr Phys Act 2012;9(1):53.
(132) Ng N, Van Minh H, Juvekar S, Razzaque A, Bich TH, Kanungsukkasem U, et al. Using the INDEPTH HDSS to build capacity for chronic non-communicable disease risk factor surveillance in low and middle-income countries. Glob Health Action 2009;2.
88
(133) Bloomfield GS, Mwangi A, Chege P, Simiyu CJ, Aswa DF, Odhiambo D, et al. Multiple cardiovascular risk factors in Kenya: evidence from a health and demographic surveillance system using the WHO STEPwise approach to chronic disease risk factor surveillance. Heart 2013;99(18):1323-1329.
(134) Ng N, Van Minh H, Tesfaye F, Bonita R, Byass P, Stenlund H, et al. Combining risk factors and demographic surveillance: potentials of WHO STEPS and INDEPTH methodologies for assessing epidemiological transition. Scand J Public Health 2006;34(2):199-208.
(135) Deepa M, Pradeepa R, Anjana R, Mohan V. Noncommunicable diseases risk factor surveillance: experience and challenge from India. Indian J Community Med 2011 Dec;36(Suppl 1):S50-56.
(136) Raban MZ, Dandona R, Dandona L. Availability of data for monitoring noncommunicable disease risk factors in India. Bull World Health Organ 2012;90(1):20-29.
(137) Nissinen A, Berrios X, Puska P. Community-based noncommunicable disease interventions: lessons from developed countries for developing ones. Bull World Health Organ 2001;79:963-970.
(138) Centers for Disease Control and Prevention, Division for Heart Disease and Stroke Prevention: Data trends and maps. Available at: http://apps.nccd.cdc.gov/NCVDSS_DTM/. Accessed on January 6, 2014.
(139) DiClemente RJ, Crosby RA, Kegler M. Emerging theories in health promotion practice and research. San Francisco: Jossey-Bass; 2009.
(140) McQueen DV. Global Handbook on Noncommunicable Diseases and Health Promotion. New York: Springer; 2013.
(141) Vaidya A, Krettek A. Is health promotion the starting point of primary cardiovascular care in low-and middle-income countries like Nepal? Health Promot Pract 2012;13(3):412-415.
(142) Rutherford L, Reid S. Knowledge, attitudes and motivations to health: A module of the Scottish Health Survey 2008-11. Edinburgh: NHS Health Scotland; 2013.
(143) Murray J, Fenton G, Honey S, Bara AC, Hill KM, House A. A qualitative synthesis of factors influencing maintenance of lifestyle behaviour change in individuals with high cardiovascular risk. BMC Cardiovasc Disord 2013;13(1):48.
89
(144) Cleland J. A critique of KAP studies and some suggestions for their improvement. Stud Fam Plann 1973;4(2):42-47.
(145) Kaliyaperumal K. Guideline for conducting a knowledge, attitude and practice (KAP) study. AECS Illumination 2004;4(1):7-9.
(146) Rotter JB. Generalized expectancies for internal versus external control of reinforcement. Psychol Monogr1966;80(1):1.
(147) Rotter JB. Some problems and misconceptions related to the construct of internal versus external control of reinforcement. J Consult Clin Psychol 1975;43(1):56.
(148) Younger J, Marsh KJ, Grap MJ. The relationship of health locus of control and cardiac rehabilitation to mastery of illness‐related stress. J Adv Nurs 1995;22(2):294-299.
(149) Valente TW, Paredes P, Poppe PR. Matching the message to the process- the relative ordering of knowledge, attitudes, and practices in behavior change research. Human Commun Res1998;24(3):366-385.
(150) Patel M, Phillips-Caesar E, Boutin-Foster C. Barriers to lifestyle behavioral change in migrant South Asian populations. J Immigr Minor Health 2012;14(5):774-785.
(151) Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M, Evans PH, et al. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011;11(1):119.
(152) Janssen V, De Gucht V, Dusseldorp E, Maes S. Lifestyle modification programmes for patients with coronary heart disease: a systematic review and meta-analysis of randomized controlled trials. Eur J Prev Cardiol 2013;20(4):620-640.
(153) Baker DW. The meaning and the measure of health literacy. J Gen Intern Med 2006;21(8):878-883.
(154) Keleher H, Hagger V. Health literacy in primary health care. Australian J Prim Health 2007;13(2):24-30.
(155) Pignone M, DeWalt DA, Sheridan S, Berkman N, Lohr KN. Interventions to improve health outcomes for patients with low literacy. JGen Intern Med 2005;20(2):185-192.
88
(133) Bloomfield GS, Mwangi A, Chege P, Simiyu CJ, Aswa DF, Odhiambo D, et al. Multiple cardiovascular risk factors in Kenya: evidence from a health and demographic surveillance system using the WHO STEPwise approach to chronic disease risk factor surveillance. Heart 2013;99(18):1323-1329.
(134) Ng N, Van Minh H, Tesfaye F, Bonita R, Byass P, Stenlund H, et al. Combining risk factors and demographic surveillance: potentials of WHO STEPS and INDEPTH methodologies for assessing epidemiological transition. Scand J Public Health 2006;34(2):199-208.
(135) Deepa M, Pradeepa R, Anjana R, Mohan V. Noncommunicable diseases risk factor surveillance: experience and challenge from India. Indian J Community Med 2011 Dec;36(Suppl 1):S50-56.
(136) Raban MZ, Dandona R, Dandona L. Availability of data for monitoring noncommunicable disease risk factors in India. Bull World Health Organ 2012;90(1):20-29.
(137) Nissinen A, Berrios X, Puska P. Community-based noncommunicable disease interventions: lessons from developed countries for developing ones. Bull World Health Organ 2001;79:963-970.
(138) Centers for Disease Control and Prevention, Division for Heart Disease and Stroke Prevention: Data trends and maps. Available at: http://apps.nccd.cdc.gov/NCVDSS_DTM/. Accessed on January 6, 2014.
(139) DiClemente RJ, Crosby RA, Kegler M. Emerging theories in health promotion practice and research. San Francisco: Jossey-Bass; 2009.
(140) McQueen DV. Global Handbook on Noncommunicable Diseases and Health Promotion. New York: Springer; 2013.
(141) Vaidya A, Krettek A. Is health promotion the starting point of primary cardiovascular care in low-and middle-income countries like Nepal? Health Promot Pract 2012;13(3):412-415.
(142) Rutherford L, Reid S. Knowledge, attitudes and motivations to health: A module of the Scottish Health Survey 2008-11. Edinburgh: NHS Health Scotland; 2013.
(143) Murray J, Fenton G, Honey S, Bara AC, Hill KM, House A. A qualitative synthesis of factors influencing maintenance of lifestyle behaviour change in individuals with high cardiovascular risk. BMC Cardiovasc Disord 2013;13(1):48.
89
(144) Cleland J. A critique of KAP studies and some suggestions for their improvement. Stud Fam Plann 1973;4(2):42-47.
(145) Kaliyaperumal K. Guideline for conducting a knowledge, attitude and practice (KAP) study. AECS Illumination 2004;4(1):7-9.
(146) Rotter JB. Generalized expectancies for internal versus external control of reinforcement. Psychol Monogr1966;80(1):1.
(147) Rotter JB. Some problems and misconceptions related to the construct of internal versus external control of reinforcement. J Consult Clin Psychol 1975;43(1):56.
(148) Younger J, Marsh KJ, Grap MJ. The relationship of health locus of control and cardiac rehabilitation to mastery of illness‐related stress. J Adv Nurs 1995;22(2):294-299.
(149) Valente TW, Paredes P, Poppe PR. Matching the message to the process- the relative ordering of knowledge, attitudes, and practices in behavior change research. Human Commun Res1998;24(3):366-385.
(150) Patel M, Phillips-Caesar E, Boutin-Foster C. Barriers to lifestyle behavioral change in migrant South Asian populations. J Immigr Minor Health 2012;14(5):774-785.
(151) Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M, Evans PH, et al. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011;11(1):119.
(152) Janssen V, De Gucht V, Dusseldorp E, Maes S. Lifestyle modification programmes for patients with coronary heart disease: a systematic review and meta-analysis of randomized controlled trials. Eur J Prev Cardiol 2013;20(4):620-640.
(153) Baker DW. The meaning and the measure of health literacy. J Gen Intern Med 2006;21(8):878-883.
(154) Keleher H, Hagger V. Health literacy in primary health care. Australian J Prim Health 2007;13(2):24-30.
(155) Pignone M, DeWalt DA, Sheridan S, Berkman N, Lohr KN. Interventions to improve health outcomes for patients with low literacy. JGen Intern Med 2005;20(2):185-192.
90
(156) Naidoo J, Wills J. Health promotion: foundations for practice. 3rd edition. Oxford: Bailliere Tindall; 2009.
(157) Tones K, Tilford S. Health promotion: effectiveness, efficiency and equity. Cheltenham : Nelson Thornes; 2001.
(158) Kleinman A. Patients and healers in the context of culture: an exploration of the borderland between anthropology, medicine and psychiatry. Oakland: University of California Press; 1980.
(159) Manandhar DS, Osrin D, Shrestha BP, Mesko N, Morrison J, Tumbahangphe KM, et al. Effect of a participatory intervention with women's groups on birth outcomes in Nepal: cluster-randomised controlled trial. The Lancet 2004;364(9438):970-979.
(160) Mullany BC, Becker S, Hindin MJ. The impact of including husbands in antenatal health education services on maternal health practices in urban Nepal: results from a randomized controlled trial. Health Educ Res 2007;22(2):166-176.
(161) Hodgins S, McPherson R, Suvedi B, Shrestha R, Silwal R, Ban B, et al. Testing a scalable community-based approach to improve maternal and neonatal health in rural Nepal. J Perinatol 2010;30(6):388-395.
(162) Knevel R. Training rural women to improve access to oral health awareness programmes in remote villages in Nepal. Int JDentHyg 2010;8(4):286-293.
(163) Communication for Governance and Accountability Program (CommGAP): Theories of behavior change. Available at: http://siteresources.worldbank.org/EXTGOVACC/Resources/BehaviorChangeweb.pdf. Accessed on December 12, 2013.
(164) Ministry of Health & Population, Government of Nepal: National Health Policy, 1991. 2009; Available at: http://www.mohp.gov.np/english/publication/national_health_policy_1991.php. Accessed on Janaury 3, 2014.
(165) Magar A. National Health Policy of Nepal-Time to Revisit and Reform. J Nepal Med Assoc 2013;52(190): I-II.
(166) Ministry of Health and Population, Nepal. National Health Communication Policy 2012. Kathmandu: Ministry of Health and Population, Nepal; 2013.
91
(167) Shrestha I B, Pathak LR. Review of National Health Policy 1991.Kathmandu: Ministry of Health and Population, Nepal; 2012.
(168) Miinstry of Health and Population, Nepal: Integrated Non-Communicable Diseases (NCDs) Prevention and Control Policy of Nepal. Kathmandu: Ministry of Health and Population, Nepal; 2012.
(169) Fuster V, Kelly BB, Vedanthan R. Promoting global cardiovascular health: moving forward. Circulation 2011;123(15):1671-1678.
(170) Fuster V, Kelly BB. Promoting cardiovascular health in the developing world: a critical challenge to achieve global health. Washington, DC: National Academies Press (US); 2010.
(171) Miranda J, Kinra S, Casas J, Davey Smith G, Ebrahim S. Non‐communicable diseases in low‐and middle‐income countries: context, determinants and health policy. Trop Med Int Health 2008;13(10):1225-1234.
(172) Ebrahim S, Pearce N, Smeeth L, Casas JP, Jaffar S, Piot P. Tackling non-communicable diseases in low-and middle-income countries: is the evidence from high-income countries all we need? PLoS Med 2013;10(1):e1001377.
(173) Labarthe DR, Dunbar SB. Global cardiovascular health promotion and disease prevention: 2011 and beyond. Circulation 2012;125(21):2667-2676.
(174) Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and costs of chronic diseases in low-income and middle-income countries. The Lancet 2007;370(9603):1929-1938.
(175) Gaziano TA, Bitton A, Anand S, Abrahams-Gessel S, Murphy A. Growing epidemic of coronary heart disease in low-and middle-income countries. Curr Probl Cardiol 2010;35(2):72-115.
(176) Kishore SP, Vedanthan R, Fuster V. Promoting global cardiovascular healthensuring access to essential cardiovascular medicines in low-and middle-income countries. J Am Coll Cardiol 2011;57(20):1980-1987.
(177) Joshi R, Chow CK, Raju PK, Raju KR, Gottumukkala AK, Reddy KS, et al. The Rural Andhra Pradesh Cardiovascular Prevention Study (RAPCAPS)- a cluster randomized trial. J Am Coll Cardiol 2012;59(13):1188-1196.
(178) Pandey RM, Agrawal A, Misra A, Vikram NK, Misra P, Dey S, et al. Population-based intervention for cardiovascular diseases related knowledge and behaviours in Asian Indian women. Indian Heart J 2013:65(1):40-47.
90
(156) Naidoo J, Wills J. Health promotion: foundations for practice. 3rd edition. Oxford: Bailliere Tindall; 2009.
(157) Tones K, Tilford S. Health promotion: effectiveness, efficiency and equity. Cheltenham : Nelson Thornes; 2001.
(158) Kleinman A. Patients and healers in the context of culture: an exploration of the borderland between anthropology, medicine and psychiatry. Oakland: University of California Press; 1980.
(159) Manandhar DS, Osrin D, Shrestha BP, Mesko N, Morrison J, Tumbahangphe KM, et al. Effect of a participatory intervention with women's groups on birth outcomes in Nepal: cluster-randomised controlled trial. The Lancet 2004;364(9438):970-979.
(160) Mullany BC, Becker S, Hindin MJ. The impact of including husbands in antenatal health education services on maternal health practices in urban Nepal: results from a randomized controlled trial. Health Educ Res 2007;22(2):166-176.
(161) Hodgins S, McPherson R, Suvedi B, Shrestha R, Silwal R, Ban B, et al. Testing a scalable community-based approach to improve maternal and neonatal health in rural Nepal. J Perinatol 2010;30(6):388-395.
(162) Knevel R. Training rural women to improve access to oral health awareness programmes in remote villages in Nepal. Int JDentHyg 2010;8(4):286-293.
(163) Communication for Governance and Accountability Program (CommGAP): Theories of behavior change. Available at: http://siteresources.worldbank.org/EXTGOVACC/Resources/BehaviorChangeweb.pdf. Accessed on December 12, 2013.
(164) Ministry of Health & Population, Government of Nepal: National Health Policy, 1991. 2009; Available at: http://www.mohp.gov.np/english/publication/national_health_policy_1991.php. Accessed on Janaury 3, 2014.
(165) Magar A. National Health Policy of Nepal-Time to Revisit and Reform. J Nepal Med Assoc 2013;52(190): I-II.
(166) Ministry of Health and Population, Nepal. National Health Communication Policy 2012. Kathmandu: Ministry of Health and Population, Nepal; 2013.
91
(167) Shrestha I B, Pathak LR. Review of National Health Policy 1991.Kathmandu: Ministry of Health and Population, Nepal; 2012.
(168) Miinstry of Health and Population, Nepal: Integrated Non-Communicable Diseases (NCDs) Prevention and Control Policy of Nepal. Kathmandu: Ministry of Health and Population, Nepal; 2012.
(169) Fuster V, Kelly BB, Vedanthan R. Promoting global cardiovascular health: moving forward. Circulation 2011;123(15):1671-1678.
(170) Fuster V, Kelly BB. Promoting cardiovascular health in the developing world: a critical challenge to achieve global health. Washington, DC: National Academies Press (US); 2010.
(171) Miranda J, Kinra S, Casas J, Davey Smith G, Ebrahim S. Non‐communicable diseases in low‐and middle‐income countries: context, determinants and health policy. Trop Med Int Health 2008;13(10):1225-1234.
(172) Ebrahim S, Pearce N, Smeeth L, Casas JP, Jaffar S, Piot P. Tackling non-communicable diseases in low-and middle-income countries: is the evidence from high-income countries all we need? PLoS Med 2013;10(1):e1001377.
(173) Labarthe DR, Dunbar SB. Global cardiovascular health promotion and disease prevention: 2011 and beyond. Circulation 2012;125(21):2667-2676.
(174) Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and costs of chronic diseases in low-income and middle-income countries. The Lancet 2007;370(9603):1929-1938.
(175) Gaziano TA, Bitton A, Anand S, Abrahams-Gessel S, Murphy A. Growing epidemic of coronary heart disease in low-and middle-income countries. Curr Probl Cardiol 2010;35(2):72-115.
(176) Kishore SP, Vedanthan R, Fuster V. Promoting global cardiovascular healthensuring access to essential cardiovascular medicines in low-and middle-income countries. J Am Coll Cardiol 2011;57(20):1980-1987.
(177) Joshi R, Chow CK, Raju PK, Raju KR, Gottumukkala AK, Reddy KS, et al. The Rural Andhra Pradesh Cardiovascular Prevention Study (RAPCAPS)- a cluster randomized trial. J Am Coll Cardiol 2012;59(13):1188-1196.
(178) Pandey RM, Agrawal A, Misra A, Vikram NK, Misra P, Dey S, et al. Population-based intervention for cardiovascular diseases related knowledge and behaviours in Asian Indian women. Indian Heart J 2013:65(1):40-47.

92
(179) World Health Organization. Preventing chronic diseases: a vital investment. Geneva: World Health Organization; 2005.


Ab
hinav Vaidya
P
erceptio
ns and P
ractices of C
ardio
vascular Health – A
po
pulatio
n persp
ective from
a peri-urb
an Nep
alese com
munity
Perceptions and Practices of Cardiovascular Health
A population perspective from a peri-urban Nepalese community
2014
Abhinav Vaidya
Institute of Medicineat Sahlgrenska AcademyUniversity of Gothenburg
ISBN 978-91-628-8946-3Printed by Ale Tryckteam AB, Bohus
Related Documents