Imaging the liver and biliary tract Tom L Kaye J Ashley Guthrie Abstract A variety of modalities is available to image the liver and biliary tract, many offering complementary information, with a combination of tech- niques often being required to make the diagnosis or determine optimal patient management. Ultrasound is commonly used as the primary inves- tigation as it is safe, cheap and widely available. Computed tomography has a central role for emergency imaging, cancer diagnosis and staging, and assessment of treatment response. Magnetic resonance imaging is excellent for interrogating the liver parenchyma, and is the modality of choice for characterizing a focal liver lesion and non-invasive investiga- tion of the biliary tree. The addition of hepatobiliary contrast agents and diffusion-weighted imaging has further improved accuracy. This article describes the role of each of these modalities, highlighting several common, benign and malignant hepatobiliary disease processes. Other less commonly used modalities such as PET/CT and cholescintigraphy are described and various hepatobiliary interventional techniques are summarized. Keywords Bile ducts; biliary tract diseases; cholangiography; computed tomography; liver; liver diseases; magnetic resonance imaging; positron- emission tomography; ultrasonography Ultrasonography Ultrasonography (US) remains the most widely performed pri- mary investigation for suspected hepatobiliary disease, owing to its wide availability and avoidance of ionizing radiation. Biliary disease In the fasted state, the gallbladder appears on US as an oval hypo-echoic structure with a smooth thin wall. Gallstones usually appear as mobile echogenic foci with posterior acoustic shadowing, and are identified with >95% accuracy in the gallbladder, but less so in the common bile duct due to adjacent bowel gas. 1 The US findings in acute cholecystitis include mural thickening (>3 mm), pericholecystic fluid and a positive sonographic Murphy’s sign (Figure 1). 2 Gallbladder polyps appear as fixed luminal defects without acoustic shadowing. Adenomyomatosis and chronic cholecystitis are other common benign causes of mural thickening demon- strated on US. Carcinoma of the gallbladder can present as a polypoid luminal tumour or as diffuse wall thickening and is often difficult to differentiate from benign conditions. Gall- bladders containing polyps >1 cm are generally resected due to such difficulties. US has a major role in identifying biliary dilatation in the context of jaundice or right upper quadrant pain, which may be caused by obstructive pathology (duct stones, benign or malig- nant strictures), but dilatation is also found after cholecystec- tomy, prolonged fasting or with sphincter of Oddi dysfunction. The common hepatic duct (CHD) normally measures up to 6 mm until age 60, with a further allowance of 1 mm per decade thereafter. 3 The double duct sign refers to dilatation of the pancreatic (>4 mm) and common duct, which is suggestive of a pancreatic head or ampullary tumour and is usually further investigated by multiphasic computed tomography (CT). Liver disease The normal liver has a uniform and homogenous echotexture. Fatty infiltration gives a diffusely echogenic liver, with attenua- tion of the US beam as it passes deep into the organ. With the recognition of non-alcoholic fatty liver disease as a cause of chronic liver disease there is interest in using US attenuation parameters to quantify steatosis, although this is not established as a clinical tool at present. In cirrhosis the liver usually appears coarse and echogenic. Common features include surface nodularity, atrophy of the right lobe, hypertrophy of the caudate lobe and enlargement of the gallbladder fossa and umbilical fissure. Associated findings related to portal hypertension include reduced, reversed or ab- sent portal vein flow, varices, splenomegaly and ascites. 4 Changes in stiffness correlate with fibrosis, currently assessed by invasive liver biopsy, and can now be quantified using US (or magnetic resonance imaging; MRI) via techniques such as tran- sient elastography (FibroScan Ò ), performed without generating images, or shear-wave elastography, where stiffness is measured in a region of interest while imaging the liver. 5 What’s new? C Non-invasive quantitative US and MRI techniques are playing an increasing role in the assessment of fibrosis, fat and iron in parenchymal liver disease C The combination of liver-specific contrast agents, diffusion- weighted imaging, and improved MRI technology has increased the accuracy of focal liver lesion detection and characterization, in many cases avoiding the need for biopsy C CT dose-reduction techniques such as iterative reconstruction have been introduced, which can substantially reduce patient dose in multi-phase hepatobiliary examinations C Image-guided ablative and endovascular treatments such as RFA now have an established role in the treatment of hepato- cellular carcinoma and unresectable hepatic malignancy Tom L Kaye BMBS BMedSci MSc(Edin) FRCR is a Radiology Registrar at St James’s University Hospital, Leeds, UK. Competing interests: none declared. J Ashley Guthrie MB BChir FRCR is a Consultant Radiologist at St James’s University Hospital, Leeds, UK. Competing interests: Dr Guthrie has received honoraria for lecturing and chairing sessions for Bayer HealthCare. ASSESSMENT OF LIVER DISEASE MEDICINE 43:10 562 Ó 2015 Elsevier Ltd. All rights reserved.

Pencitraan Hepar dan Traktus Biliaris
Feb 17, 2016
radiologi
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

What’s new?
C Non-invasive quantitative US and MRI techniques are playing an
increasing role in the assessment of fibrosis, fat and iron in
parenchymal liver disease
C The combination of liver-specific contrast agents, diffusion-
ASSESSMENT OF LIVER DISEASE
Imaging the liver and biliarytractTom L Kaye
J Ashley Guthrie
weighted imaging, and improved MRI technology has
increased the accuracy of focal liver lesion detection and
Abstract characterization, in many cases avoiding the need for biopsyC CT dose-reduction techniques such as iterative reconstruction
have been introduced, which can substantially reduce patient
dose in multi-phase hepatobiliary examinations
C Image-guided ablative and endovascular treatments such as
RFA now have an established role in the treatment of hepato-
cellular carcinoma and unresectable hepatic malignancy
A variety of modalities is available to image the liver and biliary tract,
many offering complementary information, with a combination of tech-
niques often being required to make the diagnosis or determine optimal
patient management. Ultrasound is commonly used as the primary inves-
tigation as it is safe, cheap and widely available. Computed tomography
has a central role for emergency imaging, cancer diagnosis and staging,
and assessment of treatment response. Magnetic resonance imaging is
excellent for interrogating the liver parenchyma, and is the modality of
choice for characterizing a focal liver lesion and non-invasive investiga-
tion of the biliary tree. The addition of hepatobiliary contrast agents
and diffusion-weighted imaging has further improved accuracy. This
article describes the role of each of these modalities, highlighting several
common, benign and malignant hepatobiliary disease processes. Other
less commonly used modalities such as PET/CT and cholescintigraphy
are described and various hepatobiliary interventional techniques are
summarized.
Keywords Bile ducts; biliary tract diseases; cholangiography; computed
tomography; liver; liver diseases; magnetic resonance imaging; positron-
emission tomography; ultrasonography
Ultrasonography
Ultrasonography (US) remains the most widely performed pri-
mary investigation for suspected hepatobiliary disease, owing to
its wide availability and avoidance of ionizing radiation.
Biliary disease
In the fasted state, the gallbladder appears on US as an oval
hypo-echoic structure with a smooth thin wall. Gallstones
usually appear as mobile echogenic foci with posterior
acoustic shadowing, and are identified with >95% accuracy in
the gallbladder, but less so in the common bile duct due
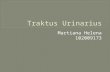
to adjacent bowel gas.1 The US findings in acute cholecystitis
include mural thickening (>3 mm), pericholecystic fluid and
a positive sonographic Murphy’s sign (Figure 1).2 Gallbladder
polyps appear as fixed luminal defects without acoustic
Tom L Kaye BMBS BMedSci MSc(Edin) FRCR is a Radiology Registrar at St
James’s University Hospital, Leeds, UK. Competing interests: none
declared.
J Ashley Guthrie MB BChir FRCR is a Consultant Radiologist at St James’s
University Hospital, Leeds, UK. Competing interests: Dr Guthrie has
received honoraria for lecturing and chairing sessions for Bayer
HealthCare.
MEDICINE 43:10 562
shadowing. Adenomyomatosis and chronic cholecystitis are
other common benign causes of mural thickening demon-
strated on US. Carcinoma of the gallbladder can present as a
polypoid luminal tumour or as diffuse wall thickening and is
often difficult to differentiate from benign conditions. Gall-
bladders containing polyps >1 cm are generally resected due
to such difficulties.
US has a major role in identifying biliary dilatation in the
context of jaundice or right upper quadrant pain, which may be
caused by obstructive pathology (duct stones, benign or malig-
nant strictures), but dilatation is also found after cholecystec-
tomy, prolonged fasting or with sphincter of Oddi dysfunction.
The common hepatic duct (CHD) normally measures up to 6 mm
until age 60, with a further allowance of 1 mm per decade
thereafter.3 The double duct sign refers to dilatation of the
pancreatic (>4 mm) and common duct, which is suggestive of a
pancreatic head or ampullary tumour and is usually further
investigated by multiphasic computed tomography (CT).
Liver disease
The normal liver has a uniform and homogenous echotexture.
Fatty infiltration gives a diffusely echogenic liver, with attenua-
tion of the US beam as it passes deep into the organ. With the
recognition of non-alcoholic fatty liver disease as a cause of
chronic liver disease there is interest in using US attenuation
parameters to quantify steatosis, although this is not established
as a clinical tool at present.
In cirrhosis the liver usually appears coarse and echogenic.
Common features include surface nodularity, atrophy of the right
lobe, hypertrophy of the caudate lobe and enlargement of the
gallbladder fossa and umbilical fissure. Associated findings
related to portal hypertension include reduced, reversed or ab-
sent portal vein flow, varices, splenomegaly and ascites.4
Changes in stiffness correlate with fibrosis, currently assessed
by invasive liver biopsy, and can now be quantified using US (or
magnetic resonance imaging; MRI) via techniques such as tran-
sient elastography (FibroScan�), performed without generating
images, or shear-wave elastography, where stiffness is measured
in a region of interest while imaging the liver.5
� 2015 Elsevier Ltd. All rights reserved.

Figure 1 (a) US image showing normal thin walled gallbladder. (b) acute calculous cholecystitis. The gallbladder wall is diffusely thickened (dashed white
arrows) and contains echogenic bile, with a gallstone impacted in the neck (solid white arrows).
ASSESSMENT OF LIVER DISEASE
Doppler ultrasound
The frequency shift of an ultrasonic wave (Doppler effect) that
occurs when it is reflected from a moving target (such as blood)
can be used to create a colour map of blood flow and direction
(colour Doppler) or a targeted waveform of blood flow (spectral
Doppler). This is commonly used to interrogate the major hepatic
vessels in chronic liver disease and after liver transplantation.
Contrast-enhanced ultrasound (CEUS)
Grey-scale US has modest sensitivity (50e65%) for metastatic
disease and hepatocellular carcinoma (HCC).6,7 It can differen-
tiate simple cysts reliably but is limited in the characterization of
solid focal lesions. CEUS improves both lesion detection and
characterization.8 It involves the intravenous injection of
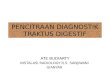
microbubble contrast media. Benign lesions are usually iso- or
hyper-echoic to background liver in the late phase of enhance-
ment (Figure 2). Although comparable to CT and MRI for lesion
detection and characterization in ideal circumstances,9 multiple
lesions and lesions near the diaphragm or obscured by bowel gas
are difficult to evaluate.
Computed tomography
Modern multi-detector CT is widely used and versatile, allowing
rapid imaging of a large volume with high spatial resolution,
facilitating accurate multi-phase imaging of the liver and biliary
tree. Iodinated contrast is used for most examinations; it is
contra-indicated in those with severe renal impairment or a
history of anaphylactic reaction. The high-radiation dose of CT
should be considered (especially with multiphase imaging), but
can be reduced by decreasing scanning dose parameters, peak
kVp and mA. Increased computing power has enabled iterative
reconstruction techniques to further reduce dose.10
Imaging the acute abdomen
CT retains an important role for imaging in the emergency
situation. In major trauma, dual phase imaging or a military
protocol with a single biphasic contrast injection has a high ac-
curacy for traumatic liver injuries and active arterial
MEDICINE 43:10 563
bleeding.11,12 High-quality 3D reformats of hepatobiliary
vascular anatomy are useful for planning endovascular inter-
vention in cases of vascular injury.
CT demonstrates complications of cholecystitis such as ne-
crosis, perforation, or pericholecystic abscess (Figure 3). Intra-
hepatic or perihepatic fluid collections and abscesses are
accurately depicted and CT can facilitate drainage. In severe
acute pancreatitis CT is widely used for identifying complications
such as necrosis, collections or bleeding.
Hepatobiliary oncology imaging
Metastases are by far the most common malignant liver lesions,
exceeding primary liver tumours by a factor of at least twenty. CT
is used for staging and to assess response to treatment for the
majority of malignancies that metastasize to the liver and pri-
mary tumours arising from the liver, pancreas and biliary tree.
The blood supply to the liver is via the hepatic artery (25%) and
portal vein (75%), with most tumours taking their blood supply
from the hepatic artery and displaying a varying degree of
vascularity. Hypervascular tumours such as hepatocellular car-
cinoma (HCC) or neuroendocrine malignancy should be imaged
in the arterial phase to maximize contrast enhancement between
tumour and background liver.
The majority of metastases from other sources (such as
colorectal cancer) are hypovascular and best depicted on the
portal venous phase scan. Triple-phase CT (unenhanced, arterial
and portal venous phase) is used to clarify the cause of biliary
obstruction identified on US (when stones are not suspected) and
to stage pancreatic malignancy.13
Characterization of liver lesions
In cases where MRI is contraindicated or unsuitable, multi-phase
CT may be used to characterize liver lesions. European and
American Liver Associations allow multiphasic CT to be used as
a non-invasive means of diagnosing HCC in patients with
cirrhosis. Key diagnostic criteria include arterial hypervascularity
with ‘washout’ demonstrated on a portal venous or 3-
minute delayed acquisition.14,15 Benign lesions, such as
� 2015 Elsevier Ltd. All rights reserved.

Figure 2 (a) Grey scale US image in a 24-year-old female shows a well-defined isoechoic mass adjacent to the gallbladder fossa. (b) CEUS images shows
avid homogenous arterial enhancement within the lesion, (c) which is near isointense in the delayed phase with a faint central scar visible. (d) Sub-
sequent coronal hepatobiliary phase MRI image shows persisting uptake of contrast with a central scar, confirming focal nodular hyperplasia (FNH).
ASSESSMENT OF LIVER DISEASE
haemangiomas, focal nodular hyperplasia (FNH) and adenomas,
can be identified although contrast resolution is inferior to MRI
and characterization of lesions smaller than 1 cm is poor.16
Magnetic resonance imaging
MRI is a versatile imaging technique, allowing manipulation of
sequence parameters to vary soft tissue contrast or obtain
structural data. It is the examination of choice for imaging
complex biliary disease and characterizing liver lesions in both
the normal and cirrhotic liver. MRI has excellent liver-to-lesion
contrast resolution and incurs no ionizing radiation. The addi-
tion of hepatocyte-specific contrast agents and diffusion-
weighted images (DWI) has further improved sensitivity and
specificity.17 Limitations include cost, length of examination
(particularly for unwell patients who cannot lie still), and con-
traindications such as pacemakers and implants.
Biliary disease
Magnetic resonance cholangiopancreatography (MRCP) uses
heavily weighted T2 sequences to display static or slow-moving
fluid within the biliary tree and pancreatic duct. MRCP can
identify ductal stones as small as 2 mm with comparable accu-
racy to endoscopic retrograde cholangiopancreatography
(ERCP)18 (Figure 4a). Flow artefacts, intra-ductal gas and adja-
cent pulsatile vascular compression can lead to false-positive
MEDICINE 43:10 564
interpretation. Both benign (iatrogenic, post-inflammatory or
secondary to primary sclerosing cholangitis (PSC)) and malig-
nant strictures can be identified (Figure 4b). Malignant biliary
strictures tend to be longer, with wall thickening and an irregular
margin.19
Variant biliary anatomy is well demonstrated and MRCP can
identify the relationship between the pancreatic duct and cystic
pancreatic tumours. More recently, functional assessment of
biliary excretion and pancreatic exocrine function has become
possible using hepatobiliary contrast media and secretin-
stimulated MRCP, respectively. Direct cholangiography (ERCP)
has now been largely replaced as a diagnostic test, being reserved
for tissue biopsy, stone extraction or stent insertion.
Diffuse and focal liver disease
MRI can characterize both diffuse liver disease and focal liver
lesions, in certain cases obviating the need for biopsy. A standard
liver protocol usually includes T2-weighted sequences that pro-
vide an overview of anatomy and can help identify simple cysts
or haemangiomas. In- and out-of-phase T1 imaging is used to
identify cellular fat within a lesion (such as in adenomas, HCC or
areas of focal fatty infiltration), or to detect iron deposition in
haemochromatosis or haemosiderosis. Various contrast agents
can be used to achieve imaging in the arterial, portal venous and
delayed phases. MRI can be used accurately to quantify fat and
� 2015 Elsevier Ltd. All rights reserved.

Figure 3 Perforated cholecystitis with hepatic abscess. Coronal (a) and axial (b) contrast enhanced CT images show irregular thick walled gallbladder
containing a large stone (solid white arrows), with extensive multi-loculated hepatic abscess (dashed white arrows).
ASSESSMENT OF LIVER DISEASE
iron, and MR elastography is under evaluation as a means of
measuring fibrosis.
Gadolinium chelates are commonly used and are confined to
the extracellular space, behaving in a similar way to iodinated
contrast used in CT. Hepatocyte-specific contrast agents (such as
gadobenate dimeglamine and gadoxetic acid) show a degree of
active uptake by lesions with hepatocyte function and are
excreted into the bile, providing additional information about the
cellular constituents of a focal lesion.
The use of DWI gives unique information about the move-
ment of water molecules at the cellular level. Malignant lesions
have a significantly lower apparent diffusion co-efficient (ADC)
and display greater diffusion restriction than benign lesions
(Figure 5).20 DWI is particularly useful in the detection of ma-
lignant lesions in the non-cirrhotic liver.
MRI allows accurate characterization of benign liver lesions,
such as haemangiomas, adenomas and FNH, differentiating them
Figure 4 (a) Reconstructed MRCP maximum intensity projection (MIP) showing
(solid white arrow). (b) Reconstructed MRCP MIP showing the classic findings
diverticula affecting the intrahepatic ducts. A dominant CBD stricture (dashed w
inflammatory.
MEDICINE 43:10 565
from primary and secondary malignant lesions. In both the
cirrhotic and non-cirrhotic liver, MRI is the investigation choice
for demonstrating the anatomical distribution of disease with
high accuracy before liver resection and transplantation.
Positron emission tomography e CT
FDG (2-[fluorine-18]fluoro-2-deoxy-D-glucose) positron emission
tomography with CT (PET/CT) is a functional imaging technique
using a glucose analogue that is taken up by metabolically active
tissues and tumour cells. PET/CT is frequently used for demon-
strating disseminated malignant disease and may identify occult
primary tumours in patients with metastatic liver disease from an
unknown primary. It is unreliable for the identification of HCC
(although a high standardized uptake value (SUV) correlates
with poor differentiation21) and is inferior to MRI for identifica-
tion of liver metastases. It may improve the detection rate of
proximal biliary dilatation with a 9 mm calculus in the common bile duct
of primary sclerosing cholangitis (PSC) with beading, stricturing and
hite arrow) was investigated for cholangiocarcinoma but was found to be
� 2015 Elsevier Ltd. All rights reserved.

Figure 5 Typical MRI appearances of a HCC. (a) T2 axial image shows mildly hyperintense lesion in the left lobe. (b)e(d) Arterial, hepatobiliary phase and
DWI axial images after gadoxetate disodium show arterial enhancement, reduced uptake of hepatobiliary contrast and diffusion restriction.
ASSESSMENT OF LIVER DISEASE
occult metastatic disease in HCC (as these tend to be less well
differentiated tumours), cholangiocarcinoma and gallbladder
cancer but is not in widespread use for detecting these tumours.
It can differentiate benign from malignant liver lesions, the latter
usually having an SUV of greater than 3.5.21 PET/CT is
commonly used to identify occult metastatic disease in patients
with colorectal liver metastases being assessed for liver resec-
tion. Limitations include cost, low spatial resolution, large radi-
ation burden and lack of specificity.
Cholescintigraphy
This technique involves an intravenous injection of a
technetium-99 labelled hepatobiliary iminodiacetic acid (99m Tc-
HIDA), which is taken up by the liver and excreted in the bile.
The technique retains an important role in the paediatric setting,
differentiating between biliary atresia and neonatal hepatitis. In
biliary atresia there is good hepatic uptake but no excretion into
the bowel 24 hours after injection. It is rarely used as a first-line
investigation in the diagnosis of acute cholecystitis, although it is
highly accurate. Absence of activity in the gallbladder after
4 hours is diagnostic as HIDA cannot enter through an inflamed
and oedematous cystic duct. False positives can occur due to
underlying liver disease or after a prolonged fast.
Endoscopic US (EUS)
EUS is an invasive technique in which a high-frequency trans-
ducer is attached to the tip of an endoscope. The left lobe of the
liver, pancreas, biliary tree, and associated nodal chains can be
MEDICINE 43:10 566
evaluated. EUS is more sensitive than US or CT for detecting
early chronic pancreatitis, biliary microlithiasis and small
pancreatic or ampullary masses. Fine-needle aspiration of lymph
nodes and solid and cystic pancreatic lesions can be performed.22
Hepatic interventional oncology
Percutaneous radio-frequency ablation (RFA) is an accepted
treatment modality for unresectable HCC and liver metastases.
A needle is introduced into the tumour under US or CT guid-
ance and rapidly alternating current produces frictional heat
leading to liquefactive necrosis. Local disease control is ach-
ieved in up to 98% of patients with colorectal liver metastases
<3e4 cm and for HCC <5 cm 4-year survival is comparable to
surgery.23 Alternative ablative therapies include cryotherapy,
microwave and laser therapy and high-intensity focused US.
These may be combined with endovascular treatments such as
trans-arterial chemoembolization (TACE) or Yttrium-90 radio-
embolization in which microspheres are delivered to the
tumour and emit beta radiation. Successfully ablated lesions
followed up with CT show no residual internal enhancement,
sometimes with intra-lesional air bubbles and a surrounding
hypervascular rim.24 A
REFERENCES
1 Cronan JJ. US diagnosis of choledocolithiasis: a re-appraisal. Radi-
ology 1986; 161: 133e4.
2 Trowbridge RL, Rutkowski NK, Shojania KG. Does this patient have
acute cholecystitis. JAMA 2009; 289: 80e6.
� 2015 Elsevier Ltd. All rights reserved.

ASSESSMENT OF LIVER DISEASE
3 Wu CC, Ho YH, Chen CY. Effect of aging on common bile duct diam-
eter: a real-time ultrasonographic study. J Clin Ultrasound 1984; 12:
473e8.
4 Murakami T, Mochizuki K, Nakamura H. Imaging evaluation of the
cirrhotic liver. Semin Liver Dis 2001; 21: 213e24.
5 Frulio N, Trillaud H. Ultrasound elastography in liver. Diagn Interv
Imaging 2013; 94: 515e34.
6 Schima W, Kulinna C, Langenberger H, et al. Liver metastases of
colorectal cancer: US, CT or MR. Cancer Imaging 2005; 5: 149e56.
7 Memon WA, Haider Z, Beg MA, et al. Diagnosis of hepatoma using
greyscale and Doppler ultrasound in patients with chronic liver dis-
ease. Int J Gen Med 2011; 4: 751e4.
8 National Institute for Health and Care Excellence. SonoVue ( sulphur
hexafluoride microbubbles) contrast agent for contrast-enhanced
ultrasound imaging of the liver. London (UK): NICE diagnostics
guidance (DG5), 2012.
9 Ryu SW, Bok GH, Jang JY, et al. Clinically useful diagnostic tool of
contrast enhanced ultrasonography for focal liver masses: compari-
son to computed tomography and magnetic resonance imaging. Gut
Liver 2014; 8: 292e7.
10 Silva AC, Lawder HJ, Hara A, et al. Innovations in CT dose reduction
strategy: application of the adaptive statistical iterative reconstruc-
tion algorithm. AJR Am J Roentgenol 2010; 194: 191e9.
11 Yoon W, Jeong YY, Kim JK, et al. CT in blunt liver trauma. Radio-
graphics 2005; 25: 87e104.
12 Graham RNJ. Battlefield radiology. Br J Radiol 2012; 85: 1556e65.
13 Guthrie AJ, Sheridan MB. Investigation of abdominal pain to detect
pancreatic cancer. BMJ 2008; 336: 1067e9.
14 European Association For The Study Of The Liver, European Organi-
sation For Research And Treatment Of Cancer. EASL-EORTC clinical
practice guidelines: management of hepatocellular carcinoma.
J Hepatol 2012; 56: 908e43.
MEDICINE 43:10 567
15 Bruix J, Sherman M, American Association for the Study of Liver
Diseases. Management of hepatocellular carcinoma: an update.
Hepatology 2011; 53: 1020e2.
16 Semelka RC, Martin DR, Balci C, et al. Focal liver lesions: comparison
of dual-phase CT and multisequence multiplanar MR imaging
including dynamic gadolinium enhancement. J Magn Reson Imaging
2001; 13: 397e401.
17 Frydrychowicz A, Lubner MG, Brown JJ, et al. Hepatobiliary MR im-
aging with gadolinium-based contrast agents. J Magn Reson Imaging
2012; 35: 492e511.
18 Griffin N, Charles-Edwards G, Grant LA. Magnetic resonance chol-
angiopancreatography: the ABC or MRCP. Insights Imaging 2012; 3:
11e21.
19 Shanbhogue AKP, Tirumani SH, Prasad SR, et al. Benign biliary
strictures: a current comprehensive clinical and imaging review. AJR
2011; 197: 295e306.
20 Parikh T, Drew SJ, Lee VS, et al. Focal liver lesion detection and
characterization with diffusion-weighted MR imaging: comparison
with standard breath-hold T2-weighted imaging. Radiology 2008;
246: 812e22.
21 Sacks A, Peller PJ, Surasi DS, et al. Value of PET/CT in the manage-
ment of primary hepatobiliary tumors, part 2. AJR 2011; 197: 260e5.
22 Schwartz DA, Wiersema MJ. The role of endoscopic ultrasound in
hepatobiliary disease. Curr Gastroenterol Rep 2002; 4: 72e8.
23 Gervais DA, Goldberg SN, Brown DB, et al. Society of interventional
radiology position statement on percutaneous radiofrequency abla-
tion for the treatment of liver tumors. J Vasc Interv Radiol 2009; 20:
342e7.
24 Park MH, Rhim H, Kim YS. Spectrum of CT findings after radio-
frequency ablation of hepatic tumors. Radiographics 2008; 28:
379e90.
� 2015 Elsevier Ltd. All rights reserved.
Related Documents