Pediatric Depression and Suicide: An Update for School Nurses W. Burleson Daviss, MD Dept. of Psychiatry University of Texas Health Science Center at San Antonio

Pediatric Depression and Suicide: An Update for School Nurses W. Burleson Daviss, MD Dept. of Psychiatry University of Texas Health Science Center at San.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pediatric Depression and Suicide: An Update for School Nurses
W. Burleson Daviss, MDDept. of Psychiatry
University of Texas Health Science Center at San Antonio
Objectives Learn about burdens associated with
pediatric depression and suicide Learn about strategies for assessing pediatric
depression Genetic and social risk factors Clinical signs, comorbidity, differential diagnosis Assessment strategies in a school-based setting.
Discuss treatment options for pediatric depression (providing essential information for school nurses).

Symptoms of Depression--SIGECAPS:
Sleep problems Interests decreased Guilty, worthlessness Energy problems Concentration problems Appetite problems Psychomotor activity problems: agitation or
slowing Suicidal thoughts or behaviors

Types of Pediatric Depression
Major Depression: sad-irritable moods or decreased interests, + 4 other symptoms, 2 weeks duration, impairing
Minor Depressions: Dysthymia: 2+ symptoms, 1 year duration Adjustment disorder with depression: fewer sxs
and shorter duration, response to stress Depressive disorder not otherwise specified
Bipolar depression
Mania Mnemonic Markedly elevated or irritable moods and 3-4 GR:RAPID symptoms:
Grandiosity Racing thoughts Reckless pleasure-seeking behavior Activity increased (goal-directed) Pressured speech Insomnia: decreased need for sleep Distractibility

Bipolar Disorders Must have had at least 1 manic or near-
manic (hypomanic) episode Manic episodes must last 4+ days with
markedly irritable or elated moods Depressed symptoms often last longer than
manic symptoms
Bipolar Disorders in Children
Rapid cycles Mixed episodes Often occur with psychotic symptoms Positive family history of bipolar disorder

Prevalence in Youths
MDD: 2% in children, 8% in adolescents 20% by the end of adolescents have had at
least one MDD episode Bipolar disorder: 1-2% 20-40% of patients with MDD become
bipolar
Morbidity/Mortality of Unipolar and Bipolar Mood Disorders Bipolar more severe risk than unipolar Both typically recur, with worsening severity Both have serious long-term impact:
Scholastic Interpersonal Occupational Substance abuse Legal problems Suicide
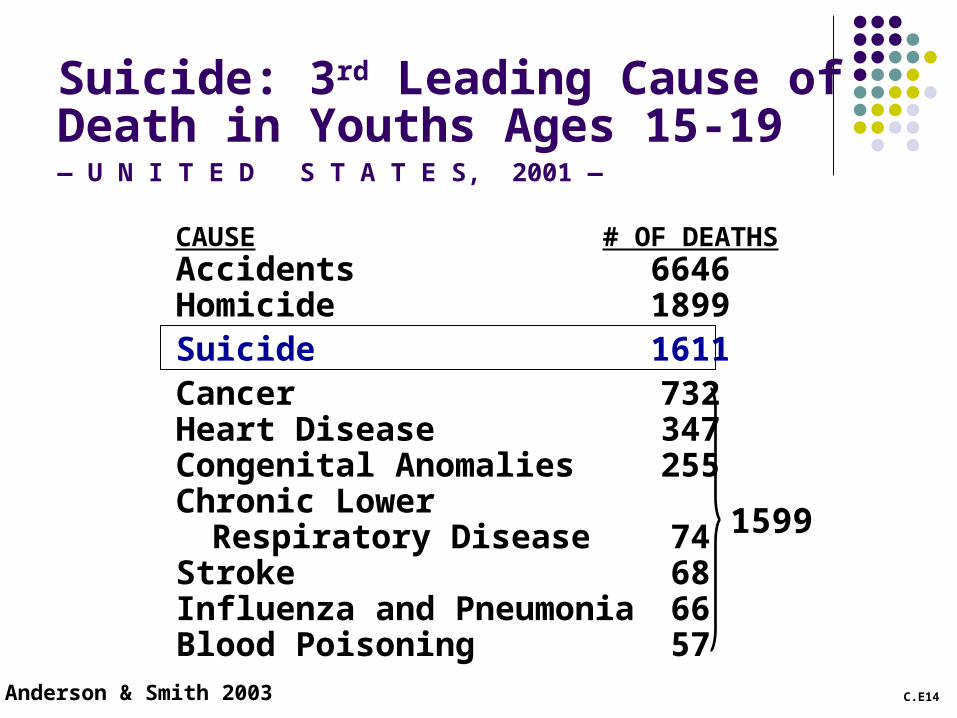
CAUSE # OF DEATHSAccidents 6646Homicide 1899Suicide 1611Cancer 732Heart Disease 347Congenital Anomalies 255Chronic Lower
Respiratory Disease 74Stroke 68Influenza and Pneumonia 66Blood Poisoning 57
Anderson & Smith 2003
1599
C.E14
Suicide: 3rd Leading Cause of Death in Youths Ages 15-19— U N I T E D S T A T E S, 2001 —
Environmental factors Traumatic exposure and other adverse life
events Family conflicts Parental stress Peer problems School problems Are these a cause or an effect?
Heritability
How much of the disorder is due to inherited, genetic factors (Nature) as opposed to environmental factors (Nurture)?
Genetic Factors Depressive disorders: 40% heritability
3X higher risk of depression in immediate family Bipolar disorders: 75% heritability
8X higher risk of bipolar disorder in immediate family
3X higher risk of depression in immediate family Family members of bipolar patients more
likely to have unipolar than bipolar moods.

Pediatric Depression:Challenges of Assessment

Differential diagnoses: Anxiety Disorders
Separation anxiety: child fearful anticipating separation from parent, clingy, school avoidant
Social phobia: reluctant to interact with peers or perform because of fear of embarrassment
Differential diagnoses: Anxiety Disorders, continued
Obsessive compulsive disorder: repetitive thoughts or behaviors, anxious/agitated when not able to do these, distressing and time consuming
Panic disorder: intense panic attacks, brief and must sometimes occur without a specific trigger
Generalized anxiety disorder: pervasive worries multiple things, physical complaints (insomnia, muscle tension, restlessness), irritability

Differential Diagnoses: Disruptive Disorders
Irritability limited to specific situations involving authority figure
Oppositional disorders: child angry, irritable & defiant with adults’ limit-setting, deliberately breaks rules, avoids accepting blame
Conduct disorder: more severe DBD, lying, stealing, vandalism, aggression to animals or people

Differential Diagnosis: ADHD
Problems in 1+ domains of symptoms Inattention: distractibility, disorganization,
trouble listening Hyperactivity/impulsivity: restlessness, and
the “butt-in-skies”Best discriminators: depressive
cognitions > somatic/vegetative sxs
Comorbid Disorders
Most mood disorders co-occur with some other disorders (comorbidity)
Comorbid disorders occur first Complicate recognition of mood disorder Reduce effectiveness of treatments Worsen psychosocial outcomes

Assessment Strategies for Pediatric Depression
Diagnostic Work Up: History
Review history of psychiatric symptoms Review medical problems Review family’s mental health history Assess child’s function at school, with peers,
and at home Review stressors that may be contributing
Rating Scales
Allow collection of data from multiple raters (child, parent, teachers)
Screen for depressive symptoms and other diagnoses
Help to monitor course of mood disorder and response to treatment

Rating Scales: General Scales
Child Behavior Checklist, Teacher’s Report Form, Youth Self Report
Child and Adolescent Symptoms Inventory, Adolescent Symptom Inventory
Vanderbilt Parent and Teacher Rating Scales (see handout) Simple, easy to use and score Good screen for disruptive behaviors Spanish version available Available free on the web:
http://devbehavpeds.ouhsc.edu/rokplay.asp
Vanderbilt Scales: Scoring
Scoring guide on handout Count the number of symptoms rated 2 or 3 in
various sections Symptoms clumped by disorders
ADHD: #1-18 ODD: #19-26 CD: #27-40 Anxious/depressed: 41-47
Functional assessment section: #48-55, count the performance items rated 4 or 5

Rating Scales for Depression
Beck Depression Inventory Children’s Depression Inventory Mood and Feelings Questionnaire (see
handout) Parent- and child- versions, long and short forms Simple wording and structure Available free on web: http://devepi.mc.duke.edu Spanish version for parents developed by our
group
Mood and Feelings Questionnaire: Scoring
Useful to combine both parent and child ratings to see if there are at least 5 symptoms of depression reported as “True”
Scores suggestive of possible major depression) Scores on long version > 24 Scores on short version > 7
Diagnostic Work Up: Mental Status Exam (MSE) Activity level Spontaneity Eye contact Affect Mood How do you feel talking to this kid?
MSE: Thought Content
Self esteem Hopelessness Helplessness Delusions Hallucinations Suicidal thoughts or behaviors
Assessing for Suicide Ask about suicide, and document you did Use matter of fact questions:
“Sometimes kids with these sorts of problems may feel like they’d be better off if they were dead. Do you ever feel that way?”
“Have you ever thought about killing yourself?” “Have you thought of ways you could do it?” “What would make you more (or less) likely to
do it?”
Assessing Suicide Risk
Current mental health problems? Positive and negative environmental factors? Past history of suicide attempts? Does the child have current intentions to
suicide? Lethality of methods considered? Availability of methods considered? Are there guns at home?

Treatment

Two Main Treatment OptionsPsychosocialPharmacological
Psychosocial Treatments Supportive therapy
Educate child and family, address contributing stressors, refer for assessment and treatment
Cognitive behavioral therapy Depression result from cognitive distortions that
can be corrected with training and practice Interpersonal therapy
Uses the issues that come up in relationship with therapist to help child to cope more effectively

Antidepressants: Selective Serotoninergic Reuptake Inhibitors (SSRIs) Fluoxetine (Prozac): FDA-approved pedi dep, well
tolerated, slow onset of effects, good for noncompliant patients
Sertraline (Zoloft): approved for pedi OCD, wider dose range, some GI side effects and activation
Citalopram (Celexa), Escitalopram (Lexapro): often well-tolerated and effective; faster acting?
Fluvoxamine (Luvox): approved for pedi OCD, more drug interactions, less well tolerated
Paroxetine (Paxil): No longer recommended in pediatric age range, withdrawal problems
Treatment of Adolescents with Depression Study (TADS) NIH-sponsored study of adolescents with
major depression Compared fluoxetine, cognitive behavioral
therapy, and combination treatments versus placebo
Antidepressants were more effective than therapy, especially for severe depression
Combination therapy more effective and safe

CDRS: Adjusted Means (ITT)
30
40
50
60
Baseline Week 6 Week 12
Stage I Assessments
Me
an
CD
RS
Sc
ore
- A
dju
ste
d
COMB
FLX
CBT
PBO
TADS Team (2004), JAMA 292: 807-820

Non-SSRI Antidepressants: Bupropion (Wellbutrin): noradrenergic &
dopaminergic, help pedi ADHD; risk of seizures Mirtazapine (Remeron): Useful for insomnia Duloxetine (Cymbalta): serotonin & noradrenergic
effects Venlafaxine (Effexor): no longer recommended
because of withdrawal symptoms Tricyclics: desipramine, imipramine, nortriptyline;
helpful for insomnia and enuresis but not pedi depression; cardiovascular risks require ECG & plasma levels, fatal in overdoses
DepresseDepresseddChild or Child or Teen?Teen?
At the University of Texas Health Science Center at San Antonio, we are conducting a clinical research study using an investigational medication bupropion for depression in adolescents ages 11-18 weighing at least 66lbs.Symptoms include:
• Sad or irritable mood
• Lack of concentration in school
•Loss of interest or pleasure •Changes in appetite or weight
• Fatigue or loss of energy
• Feelings of worthlessness
• Feelings of hopelessness
•Sleep Problems
Those who qualify will receive: Interview and Assessment Physical Exams Comprehensive Lab Analysis Medication Resource ReferralCompensation availableContinued care if applicableCall us at 210-562-5400 for more information
FDA “black box” warning for Antidepressants, October 2004
Higher suicidality in first weeks on antidepressants: 4% on antidepressant medication vs. 2% on placebo
Applies to all antidepressants in all age groups
Need close follow-up early for emerging suicidal thoughts, worsening mood or other intolerable side effects

C.E16.XX
Why Use Antidepressants At All? US Epidemiological Studies, Ages 15-24
Rat
e p
er10
0,00
0
Anderson 2002, CDC Wonder 2003, USDHEW 1956, Vital Statistics U.S. 1954–1978
0
2
4
6
8
10
12
14
16
18
20
22
24
26
Females
Males
2-Years After Black Box…
~10% drop in antidepressant prescriptions to adolescents from 2004 to 2005
~20% increase in adolescent suicide rates in the US (from 7.3 to 8.2 per 100K)
Hamilton et al. (2007), Annual summary of vital statistics: 2005. Pediatrics 119(2):345-359
David Brent, MD:“The risk of emergent suicidality in
children and adolescents receiving SSRIs is real-- but small.”
Antidepressants help many more people than they hurt
Brent DA (2004), N Engl J Medicine 351(16), p 1601
School Nurse’s Potential Role in Monitoring Weekly assessments, especially early in
treatment for new or worsening symptoms: Suicidal thoughts or behaviors Insomnia Agitation or irritability Depressed moods or mania
Communication with the prescribing physician if there are any concerns
Dr. Brent: “The Risk of Doing Nothing”
“Families and clinicians must find the right balance between the risk of suicidality and [the] greater risk …that lies in doing nothing.”
Brent DA (2004), N Engl J Medicine 351(16), p 1601

Summary Pediatric depression a potentially devastating
problem, if undiagnosed or untreated We’ve reviewed risk factors, signs and
symptoms of pediatric depression and suicide We’ve discussed strategies for assessment
and treatment, especially in school setting

School Nurses’ Key Role
Identification of children at risk for depression and/or suicide
Offering education and support to children, parents, and staff at schools
Helping families to weigh risks/benefits of various treatments and to follow through
Helping clinicians to monitor children’s response to treatment

Potential Resources
Web-pages for parents: www.aacap.org www.nami.org www.moodykids.org www.wpic.pitt.edu/research/CARENET/
Web pages for clinicians www.moodykids.org www.wpic.pitt.edu/research/CARENET/

Thanks!!!

Appendices:
Vanderbilt Teacher’s Rating Scale Vanderbilt Parent’s Rating Scale Vanderbilt Parent’s Rating Scale– Spanish
Version Child Mood and Feelings Questionnaire Parent Mood and Feelings Questionnaire Parent Mood and Feelings Questionnaire--
Spanish Version Study flyer for UTHSCSA Depression Trial
Related Documents











