[CANCER RESEARCH (SUPPL.) 44, 4826s-4835s, October 1984] Pathological Effects of Hyperthermia in Normal Tissues1 Luis Felipe Fajardo L-G Department ol Pathology, Stanford University School of Medicine, Stanford, California 94305, and Veterans Administration Medical Center, Palo Alto, California 94304 Abstract This is a brief review of the major pathological alterations produced by hyperthermia in normal tissues of humans and other mammals. Whole-body hyperthermia, spontaneous or artificially induced, can produce severe lesions that have been best de scribed in humans: necropsies, of fatal cases of heatstroke or of individuals treated in the 1940s by hyperpyrexia, have demon strated important lesions in the central nervous system, liver, kidney, heart, adrenal, testis, and bone marrow. All cases have shown hemorrhagic diathesis affecting many tissues, and in some the hemorrhages may have directly contributed to death. The information on the pathology of localized hyperthermia comes mainly from experimental studies in mammals. Pathology descriptions are available mainly for skin, mesenchymal tissues (skeletal muscle and adipose tissue), liver, small intestine, brain, kidney, urinary bladder, prostate, and cartilage. In several of these tissues, however, the morphological data are incomplete, and very few have sequential observations. Thus, the ultimate (delayed) result of the acute lesions of focal hyperthermia is unknown for most tissues. Clearly, more information is needed in order to define the range of safety for clinical hyperthermia. Introduction Unquestionably, hyperthermia has an important role in cancer therapy today. Also, unquestionably, hyperthermia can affect the normal tissues adjacent to the treated tumor or, in the case of TBH,2 many normal tissues. Therefore, to apply this modality judiciously one must know, and weigh, these possible deleterious effects. In this article I describe the pathological effects of both whole- body (systemic), and localized hyperthermia on tissues of several mammals, including humans. The scope of this publication does not allow an extensive review of "thermal pathology." Therefore, I limit it to outlines of the morphological findings in selected tissues. The descriptions of organs and tissues are organized not along conventional organ systems but according to the quantity of pathology data available (Tables 1 and 2). Whole-Body Hyperthermia This was the initial form of therapeutic hyperthermia. It was based on reports of spontaneous cures of tumors following high (erysipelas-associated) fever, in the mid-19th century. Clinical TBH is used nowadays only in carefully controlled trials at a few institutions (8, 43). In such clinical trials, fluid loss, hemodynamic 1 Presented at the Workshop Conference on Hyperthermia in Cancer Treatment, March 19 to 21, 1984, Tucson, AZ. The experiments described here have been supported by Veterans Administration Research Funds (MRIS 2735-01), and USPHS Grants CA 04542, CA 19386, and CA 34686 of the National Cancer Institute, NIH. 2 The abbreviations used are: TBH, total-body hyperthermia; TER, thermal enhancement ratio; LDay,, 50% lethal dose at 7 days. alterations, serum enzyme abnormalities, and symptoms of var iable severity have been described (7, 44) [see also article by L. H. Cronau in this issue (11)]. It appears that, by the current methods used for TBH, fatalities directly attributed to the hyper thermia are rare; autospy descriptions are rather difficult to find. What we know about the pathology of systemic hyperthermia comes mostly from observations made in fatal cases of heat stroke (30, 36), or from deaths in patients treated by "hyperpy rexia" for conditions other than cancer (23) (see Table 1). These 2 situations are somewhat different from current TBH (because of the methodology, intensive care, and careful monitoring in TBH), but the pathology of the fatal cases is probably comparable and, at the present, is the best material available. One of the most informative morphological studies was made during the 1940s in patients subjected to "systemic hyperpyrexia." In their publication, Gore and Isaacson (23) described meticulously the findings in 17 necropsies of individuals who died of TBH induced (by the Kettering cabinet, by i.v. injection of typhoid vaccine, by hot baths, etc.) in an attempt to treat gonorrhea, nonsuppurative arthritis, etc. The temperatures (p.o. or rectal) reached were 40.5-43°, and the duration of hyperthermia was 3 to 11 hr (23). Unfortunately, the total number (the denominator) of patients treated by such a method was not stated, and probably was not available to the authors. Thus, although stated as low (23), one cannot decide from their paper the incidence of complications or fatalities of that unusual treatment. One other thorough and extensive clinicopathological study was made by Malamud et al. (36) on fatal cases of heatstroke.3 These pathologists described the findings in 125 necropsies of United States Army personnel who died between 1941 and 1944. In their series, the p.o. or rectal temperatures registered at admission to hospitals were 38-44°; in 107 of these patients the temperature range was 41.5-44° (36). In 70% of these cases death occurred in less than 24 hr, and in the rest between 1 and 12 days from initiation of illness (36). The following is a description of the alterations observed in the most affected organs or tissues (in order of severity), follow ing spontaneous (30, 36) or induced hyperthermia. Liver The most severe and consistent injuries observed in the Gore and Isaacson (23) series occurred in the liver: initially there was vacuolization of hepatocytes (8 to 16 hr after the end of therapy); then progressive necrosis of cells in the center of the lobules occurred, reaching a maximum ("60% of the central part of the lobule") by 60 hr. At 7 days necrotic debris was removed by macrophages. Regeneration from peripheral hepatocytes, and proliferation of bile ducts was active in those who died late; 3 Heatstroke must be distinguished from malignant hyperthermia, a genetically determined myopathy with fever. The latter is often accompanied by metabolic acidosis, hyperkalemia, muscle rigidity, etc. This condition may be precipitated by anesthesia and, if unrecognized, is often fatal. The pathology of malignant hyper thermia is not within the scope of this article. 4826s CANCER RESEARCH VOL. 44 on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
[CANCER RESEARCH (SUPPL.) 44, 4826s-4835s, October 1984]
Pathological Effects of Hyperthermia in Normal Tissues1
Luis Felipe Fajardo L-G
Department ol Pathology, Stanford University School of Medicine, Stanford, California 94305, and Veterans Administration Medical Center, Palo Alto, California 94304
Abstract
This is a brief review of the major pathological alterationsproduced by hyperthermia in normal tissues of humans and othermammals. Whole-body hyperthermia, spontaneous or artificially
induced, can produce severe lesions that have been best described in humans: necropsies, of fatal cases of heatstroke or ofindividuals treated in the 1940s by hyperpyrexia, have demonstrated important lesions in the central nervous system, liver,kidney, heart, adrenal, testis, and bone marrow. All cases haveshown hemorrhagic diathesis affecting many tissues, and insome the hemorrhages may have directly contributed to death.
The information on the pathology of localized hyperthermiacomes mainly from experimental studies in mammals. Pathologydescriptions are available mainly for skin, mesenchymal tissues(skeletal muscle and adipose tissue), liver, small intestine, brain,kidney, urinary bladder, prostate, and cartilage. In several ofthese tissues, however, the morphological data are incomplete,and very few have sequential observations. Thus, the ultimate(delayed) result of the acute lesions of focal hyperthermia isunknown for most tissues.
Clearly, more information is needed in order to define therange of safety for clinical hyperthermia.
Introduction
Unquestionably, hyperthermia has an important role in cancertherapy today. Also, unquestionably, hyperthermia can affect thenormal tissues adjacent to the treated tumor or, in the case ofTBH,2 many normal tissues. Therefore, to apply this modality
judiciously one must know, and weigh, these possible deleteriouseffects.
In this article I describe the pathological effects of both whole-
body (systemic), and localized hyperthermia on tissues of severalmammals, including humans. The scope of this publication doesnot allow an extensive review of "thermal pathology." Therefore,
I limit it to outlines of the morphological findings in selectedtissues. The descriptions of organs and tissues are organizednot along conventional organ systems but according to thequantity of pathology data available (Tables 1 and 2).
Whole-Body Hyperthermia
This was the initial form of therapeutic hyperthermia. It wasbased on reports of spontaneous cures of tumors following high(erysipelas-associated) fever, in the mid-19th century. Clinical
TBH is used nowadays only in carefully controlled trials at a fewinstitutions (8, 43). In such clinical trials, fluid loss, hemodynamic
1Presented at the Workshop Conference on Hyperthermia in Cancer Treatment,
March 19 to 21, 1984, Tucson, AZ. The experiments described here have beensupported by Veterans Administration Research Funds (MRIS 2735-01), andUSPHS Grants CA 04542, CA 19386, and CA 34686 of the National CancerInstitute, NIH.
2The abbreviations used are: TBH, total-body hyperthermia; TER, thermal
enhancement ratio; LDay,, 50% lethal dose at 7 days.
alterations, serum enzyme abnormalities, and symptoms of variable severity have been described (7, 44) [see also article by L.H. Cronau in this issue (11)]. It appears that, by the currentmethods used for TBH, fatalities directly attributed to the hyperthermia are rare; autospy descriptions are rather difficult to find.
What we know about the pathology of systemic hyperthermiacomes mostly from observations made in fatal cases of heatstroke (30, 36), or from deaths in patients treated by "hyperpyrexia" for conditions other than cancer (23) (see Table 1). These
2 situations are somewhat different from current TBH (becauseof the methodology, intensive care, and careful monitoring inTBH), but the pathology of the fatal cases is probably comparableand, at the present, is the best material available. One of themost informative morphological studies was made during the1940s in patients subjected to "systemic hyperpyrexia." In their
publication, Gore and Isaacson (23) described meticulously thefindings in 17 necropsies of individuals who died of TBH induced(by the Kettering cabinet, by i.v. injection of typhoid vaccine, byhot baths, etc.) in an attempt to treat gonorrhea, nonsuppurativearthritis, etc. The temperatures (p.o. or rectal) reached were40.5-43°, and the duration of hyperthermia was 3 to 11 hr (23).
Unfortunately, the total number (the denominator) of patientstreated by such a method was not stated, and probably was notavailable to the authors. Thus, although stated as low (23), onecannot decide from their paper the incidence of complications orfatalities of that unusual treatment.
One other thorough and extensive clinicopathological studywas made by Malamud et al. (36) on fatal cases of heatstroke.3
These pathologists described the findings in 125 necropsies ofUnited States Army personnel who died between 1941 and 1944.In their series, the p.o. or rectal temperatures registered atadmission to hospitals were 38-44°; in 107 of these patients thetemperature range was 41.5-44° (36). In 70% of these cases
death occurred in less than 24 hr, and in the rest between 1 and12 days from initiation of illness (36).
The following is a description of the alterations observed inthe most affected organs or tissues (in order of severity), following spontaneous (30, 36) or induced hyperthermia.
Liver
The most severe and consistent injuries observed in the Goreand Isaacson (23) series occurred in the liver: initially there wasvacuolization of hepatocytes (8 to 16 hr after the end of therapy);then progressive necrosis of cells in the center of the lobulesoccurred, reaching a maximum ("60% of the central part of thelobule") by 60 hr. At 7 days necrotic debris was removed by
macrophages. Regeneration from peripheral hepatocytes, andproliferation of bile ducts was active in those who died late;
3 Heatstroke must be distinguished from malignant hyperthermia, a genetically
determined myopathy with fever. The latter is often accompanied by metabolicacidosis, hyperkalemia, muscle rigidity, etc. This condition may be precipitated byanesthesia and, if unrecognized, is often fatal. The pathology of malignant hyperthermia is not within the scope of this article.
4826s CANCER RESEARCH VOL. 44
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Pathological Effects of Hyperthermia
Table 1Whole-body hyperthermia
Tissues most affected in fatal cases of heatstroke or therapeutic hyperpyrexia8
LiverCentral nervous systemKidneyHeart
AdrenalTestisBone marrow
* Hemorrhages in many tissues and cavities.
fibrosis, however, was not seen in the longest (14 days) survivor.Jaundice (interpreted as a sign of liver failure) was observed inall patients surviving more than 49 hr (23).
Similar but less striking liver alterations were described byMalamud ef al. (36). Additional information comes from Kew efal. (30), who studied 18 liver biopsies and 8 necropsies from 39Bantu miners afflicted by heatstroke. The biopsies showed usually mild lesions; 6 of the necropsies revealed structural alterations similar to those described above. Portal inflammatory infiltrate and fatty changes were also noted (30).
Pettigrew ef a/. (44) have described alterations of serum liverfunction tests in patients subjected to TBH by the paraffin bathmethod: patients who reached temperatures of 41.8-42.2°
showed elevation of lactic dehydrogenase (2-fold), aspartateaminotransferase (25-fold), alanine aminotransferase (8-fold),
and bilirubin (modest, to 1.56 mg/dl) (44). Higher levels of bilirubinhave been reported by Wills ef al. (54), up to 18.5 mg/dl 5 daysafter treatment of 42°for 8 hr. In vitro studies have indicated
that increase in ammonia production by liver tissue (accumulationin the medium) is a sensitive indicator of hyperthermic injury andbecomes detectable at 42°(9).
Central Nervous System
The entire brain was available for study in one-third of the
cases of Malamud ef al. (36). It showed strikingly severe lesions:congestion, edema (with increase in weight by several hundredg), extensive neuronal loss, and gliosis. The authors consideredthe neuronal damage to be a direct heat effect and the congestionand edema to be secondary to shock. Multiple hemorrhages, inthe cerebral parenchyma and meninges, were interpreted assecondary to thrombocytopenia (36).
Almost identical lesions were noted in the Gore and Isaacsondescription of 16 brains (23). They observed the most severealterations in the cerebellum, often with complete loss or damageof Purkinje cells (23).
Kidney
Renal lesions of variable severity were seen in 9 of 17 patientswho died following therapeutic hyperpyrexia (23). Three of thesepatients, who survived 4, 7, and 14 days, died of renal failure.The lesions observed were progressive necrosis of tubular cells,edema and lymphocytic, rather than granulocytic, infiltrate (23).
Following heatstroke, renal lesions are also frequent and important. These consist of edema and congestion, and tubularnecrosis (36). Of the 125 fatal cases reviewed in 1946, 19 hadenough tubular damage to be classified as "lower nephronnephrosis," the old term used to describe acute tubular necrosis.
The incidence of tubular necrosis increased with time of survivalin these series (36).
Heart
The most conspicuous lesions in spontaneous (36) or induced(23) hyperthermia have been hemorrhages: subepicardial, intramuscular, subendocardial, or even intravalvular. Some hemorrhages are massive (36), enough to produce ventricular failure.Various degrees of individual myocytolysis and myocyte necrosishave been described, from mild to extensive, but generally focal(23,36). Fragmentation and fatty degeneration of myocytes havebeen observed (36).
Adrenal
Both heatstroke and induced hyperthermia produce adrenallesions, limited to the cortex. Pericortical hemorrhage is common(36), but intraparenchymal hemorrhage is rare. Separation ofcortical cells (artifactual?) from their basement membrane andfrom each other results in a tubular-like arrangement (23, 36).
Focal necrosis is variable (23, 36). Gore and Isaacson (23)describe an early coalescence of lipid droplets in the zonafasciculata which results in large irregular vacuoles as early as 3hr after heat induction.
Interestingly enough, no alterations of other endocrine organsare described in whole-body hyperthermia.
7esf/s
As expected, the seminiferous tubules are affected, althoughonly in patients dying after 8 hr of induction of hyperthermia (23).
The lesions consist of severe decrease in spermatogenesis,with formation of multinucleated cells in the germinal layers,which desquamate into the lumen. Later there is loss of germinalcells. Interstitial cells are not affected and there is no inflammatory exúdate (23). These changes are similar to those seen afterradiation (17), or in starvation, or in deficiencies of vitamins A orE (23).
Bone Marrow
Malamud ef al. (36) studied 15 samples from their fatal casesof heatstroke. Depletion of granulocytes and erythrocytic precursors was present in patients surviving 35 hr or longer, butonly in one was there significant hypocellularity. The most consistent changes occurred in megakaryocytes: karyopyknosis,karyorrhexis, loss of nuclei, and reduction in number of megakaryocytes (in one-half of the cases). In 3 cases there was
evidence of regeneration, with many megakaryoblasts (36).These megakaryocyte alterations do not appear to be artifac
tual and were not seen in appropriate controls, including casesof anoxia (36). Furthermore, thrombocytopenia was present inthe majority of the patients having platelet counts (36), and it isknown to occur in induced hyperthermia (23).
Thrombocytopenia, therefore, could be explained by what maybe a selective effect of hyperthermia on megakaryocytes. This,however, does not explain the severe and widespread hemorrhages seen on multiple sites in fatal cases; the recorded plateletcounts were not below 22,000/ml and most were above 40.000/ml (36). Such levels ordinarily do not lead to hemorrhagic diathesis, unless other factors contribute to it. Such factors mayinclude deficiencies in soluble coagulation factors, especially if
OCTOBER 1984 4827s
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
L F. Fajardo L-G
there is severe liver injury. An important mechanism of hemorrhage may be injury to capillary endothelial cells by heat. Evidence for thermal sensitivity of endothelial cells has been foundrecently in our laboratory.4
Other Tissues
The striking alteration common to most organs and tissues,including serosal membranes, skin and mucosae, both in spontaneous (36) and induced (23) hyperthermia, is hemorrhage. Theimportance of this finding has been discussed for the individualorgans, and its possible mechanisms have been mentioned under"Bone Marrow."
Localized Hyperthermia
On the basis of human and experimental observations, onewould expect that local hyperthermia at 40-50°/30 min would
cause major injury in skin (42, 52), mesenchymal tissues (40),liver (23),5 intestine (28), testis (23), and tissues of the embryo.
In addition, important lesions may occur in tissues (organs) suchas kidney (36), endocrine glands (especially adrenal) (23, 36),lymphopoietic organs, and various structures of the eye. Thecentral nervous system and the bone marrow, which are affectedin systemic hyperpyrexia (see above), are less likely to sufferfrom local hyperthermia because of the poor heat conductivityof bone, unless the hyperthermia is designed to treat preciselysuch organs (see "Central Nervous System" below). The heart,
major blood vessels, and lung would be least affected by localhyperthermia because of very effective heat dissipation by convection.
Clearly, there is a need to study systematically the effects oftherapeutic hyperthermia in many of the tissues mentioned above(and in others not mentioned), as well as in normal cell lines.Radiobiologists have already begun this task. The thermal sensitivity and (conversely), the induced thermotolerance of severalnormal cell lines is already known (21).
The scope of this publication does not allow an extensivereview of "thermal pathology." Therefore, I limit it to brief descrip
tions of the morphological findings in selected tissues (see Table2). Some descriptions are based on studies performed in ourinstitution (38, 40).4~6 Many have been obtained from data of
other investigators. Notice that most morphological observationsof the effects of localized hyperthermia have been made inmammalian species other than humans. In some instances, onlygross pathology is available, and sequential observations arelacking for most tissues.
Skin
Although the skin has been perhaps the normal tissue mostoften studied in therapeutic hyperthermia (there are many morepublications than those listed here), relatively few clinical orexperimental protocols have included detailed morphological descriptions.
The careful sequential observations by Moritz and Henriquez(41) in 1947, in porcine and human skin, were aimed at studying
' L. f. Fajardo, A. Schreiber, N. Kelly and G. M. Hahn, unpublished observations.5S. D. Frionas, M. A. Taylor, L. F. Fajardo, N. I. Kelly, T. S. Nelson, and G. M.
Hahn. Thermal sensitivity of normal canine liver, submitted for publication.•L.F. Fajardo, S. Frionas, and N. I. Kelly, unpublished observations, 1983.
Table 2Effects of therapeutic localized hyperthermia'
SkinAdipose tissueSkeletal muscleLiverSmall intestineEmbryonal tissueCentral
nervous systemKidneyUrinary bladderProstateGrowing cartilage
* List of tissues for which information is most available
the effects of burns, and therefore included a range of temperatures (44-52°) and exposure times (e.g., 6 hr) not used in
therapeutic hyperthermia. They devised a grading system (hy-peremia, focal necrosis, and complete epidermal necrosis) basedon gross changes (41). They found similarities in the responsesof human and pig skin: complete epidermal necrosis occurred inboth at 45°for 180 min, but times were different for higher orlower temperatures (e.g., 30 versus 45 min, respectively, at 47°)
(24,41).One of the few studies including systematic histological ex
amination of the skin was performed by Thomson ef al. in swine(48). These authors compared the lesions produced by electricity(59 to 100,000 Hz) with those produced by heat, in sequentialbiopsies. They noted detachment of epidermis after heat, butnot after electrical injury, with fibrillary or granular cytoplasm inthe necrotic epidermocytes. Thomsen ef a/. (48) were successfulin distinguishing thermal burns from electric lesions (their aimwas to diagnose the effects of electrical torture), but unfortunately their findings are difficult to apply to the different levels ofheat used in clinical hyperthermia.
The skin of mice appears to be more thermosensitive thanhuman or porcine skin; in the latter, 45°for 1 hr does not seem
to cause permanent damage (24, 41 ). The mouse ear has beenused to quantitate thermal skin response (19, 31). From variousexperiments it appears that injury occurs after treatment at 44°
for 1 hr, or higher. Complete epidermal necrosis is seen in allanimals with doses of 45.5°for 45 min, and this occurs in 4 days
(19, 24). These lesions appear earlier than those produced by X-radiation (e.g., 3000 rads) (19). Recovery from this thermalnecrosis is slow or may not occur. Below 44°for 1 hr, lesions
are mild (mostly hyperemia), and recovery is usually completewithin 2 weeks. These time-dose data generally agree with the
observations of Okumura and Reinhold (42). Anderson ef a/. (1)have shown that the mouse ear lesions can be potentiated byexposure of the animals to ethanol.
A popular method for the study of hyperthermic injury hasbeen the immersion of a mouse foot in a water bath (52). Thesubsequent "foot reaction" has been quantitated by a scoring
system of gross changes that include edema, epilation, wetdesquamation, and may be as severe as complete loss of thefoot (52). This foot reaction includes, of course, damage toseveral tissues aside from skin, and hopefully it has been interpreted as such (49-51).
The mouse foot reaction has been quite useful in severalrespects. Urano ef a/. (51) have used it to demonstrate enhancement of the hyperthermia effect: Corynebacterium parvum givento the animals several days before hyperthermia enhanced theeffect of heat in tumors and, to a lesser degree, in the normaltissues. Glucose (i.p.) also enhanced the tumor response andproduced a lesser enhancement in the foot (50). The phenomenon of "step-down heating" (sensitization to low-temperature
heat by a prior shock of high temperature) was shown to occur
4828s CANCER RESEARCH VOL. 44
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Pathological Effects of Hyperthermia
in the mouse foot as well as in a transplanted tumor (49). Therewas no therapeutic advantage in this model (49).
The enhancement effect (TER) of hyperthermia on the effectof ionizing radiation has been studied in skin, as well as in othertissues. One of such studies (with ultrasound-induced hyperthermia and X-radiation), performed by Baker ef al. (2), has
shown that the TER was independent of the sequence of the 2treatments for intervals up to 1 hr in rodent skin.
Recently, a modified Fowler scale has been used to quantitatethe gross skin reaction in 80 patients treated by radiation (3395rads, mean total dose) and microwave hyperthermia (mean value,42.3°)(33); 17% of patients developed only desquamation; ery
thema occurred in 24%; blisters occurred in 7%; and ulcérationoccurred in 18% (33).
Perhaps the thermal sensitivity of skin is only of minor importance in clinical hyperthermia, especially when using electromagnetic sources; the skin can be effectively cooled during therapy,sparing it from any thermal damage (38, 40).
in the deep muscle layers; and fibrosis. The latter lesion was byfar the most important in severity (extent) and affected especiallythe adipose tissue; thick bands of collagen and fibroblasts replaced and deformed many of the normal adipocyte lobules (40).There was a clear dose response in these delayed lesions (38,40). Thermotolerance was demonstrated in both adipose tissueand muscle, and it was most remarkable in the former (38); inthe sites that received the initial conditioning dose, the scoreswere reduced by 76 to 86% at 45-48°. This induction of ther-motolerance in vivo provided an overall advantage of 2°for the
protection of these normal tissues (38).Although fibrosis and possibly deep abscesses are potentially
serious, chronic complications of therapeutic hyperthermia, theselesions were usually significant at 46°and above. Therefore, by
extrapolation, serious fibrosis and abscesses should not beexpected in treatment protocols using doses of 45°for 30 min
or less. Furthermore, the demonstration of thermotolerance invivo provides a possible therapeutic advantage.
Soft Tissues
Localized radio frequency-induced hyperthermia for superficialor deep-seated tumors often requires deposition of energy in
skin or in mesenchymal tissues. Damage to skin can be minimized by cooling of the electrodes (38). The mesenchymal (soft)tissues, such as skeletal muscle and adipose tissue, cannot beeffectively cooled by external means. The adipose tissue has arelatively high electrical resistivity which causes greater powerabsorption from radio frequency sources. The muscle hasgreater electrical conductivity and will absorb energy from microwave heating sources. Because of its low blood perfusion rate,adipose tissue removes heat poorly. Additionally, the fat-muscleinterface causes wave reflections leading to high-energy absorp
tion in the adipose tissue at some frequency ranges.All of the above, and other considerations (38), indicate that
damage to adipose tissue and skeletal muscle may be a limitingfactor in hyperthermia.
A systematic study of thermal injury has been performed inthe superficial skeletal muscle and adipose tissue of swine (38,40). Hyperthermia was induced by radio frequency currentspassed through electrodes placed symmetrically on the skin ofopposite sites of the flanks of pigs. Water circulating through thehollow electrodes cooled the skin. Fifteen sites were shamtreated (controls), while in 102 sites the temperature was increased, during 30 min, to levels of 40-48° (40). Some siteswere subjected to 43°for 30 min, 4 hr before the final, prese
lected treatment, testing for thermotolerance (40). Large samplesof the adipose and muscle layers were obtained 18 to 24 hr laterin some sites, and 28 to 31 days later in other sites (40). Thelesions were examined histologically, using a specially developedscoring system (40).
The early (acute) samples revealed edema, focal hemorrhage,necrosis, and granulocytic infiltrate. The latter 2 (particularlynecrosis) were more severe in muscle. In general (but not in allsamples), the severity of these acute lesions increased withdose, but it never reached the levels of the delayed lesions (40).Thermotolerance was not observed in these eaiiy samples (38).
The delayed samples revealed important lesions: chronic lym-
phohistiocytic infiltrate in both fat and muscle; evidence of fatnecrosis, with lipophages; persistent muscle necrosis and foci ofmuscle regeneration; abscesses (only at highest temperatures)
Liver
From the data of TBH (see above), the liver appears to be atrisk for significant injury from localized hyperthermia. Indeed,
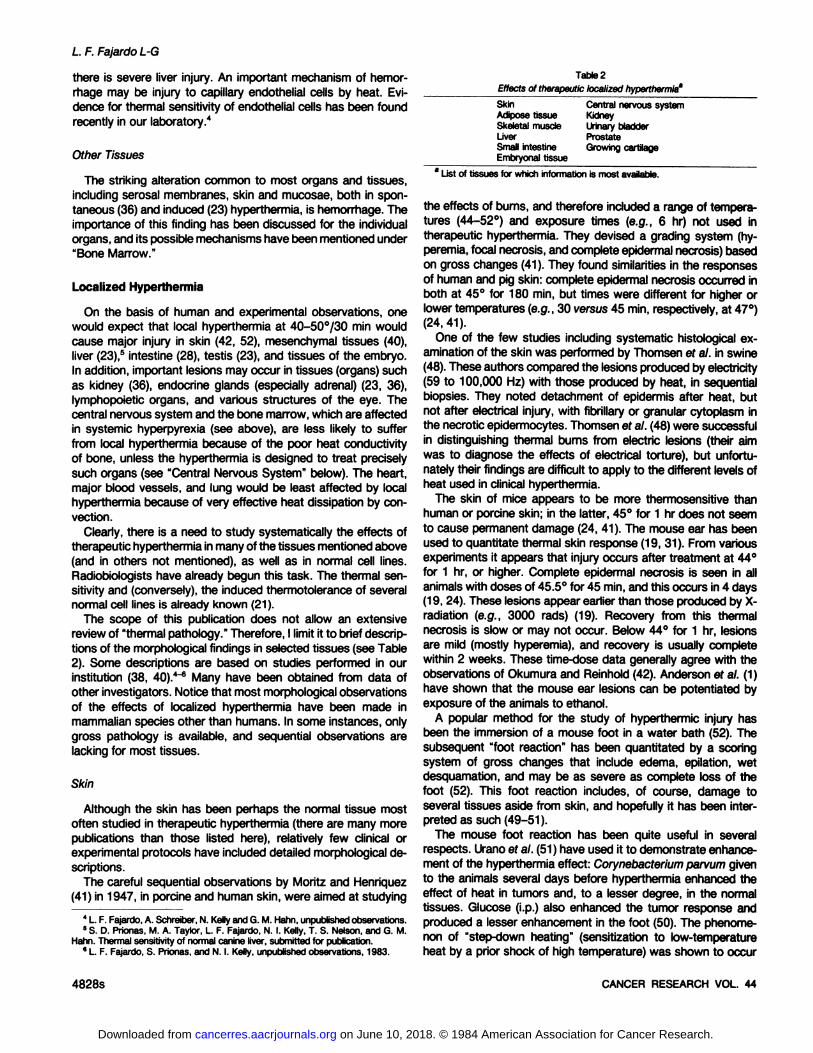
Fig. 1. Normal canine liver architecture, shown here for comparison with thesubsequent illustrations. A lobule occupies most of the central portion of thephotograph and is limited by 3 portal areas (arrows). Liver cell plates convergeradially toward the delicate central vein (clear oval in center). Human liver lobuleshave a similar structure. Gomori's trichrome, x 80.
OCTOBER 1984 4829s
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
L. F. Fajardo L-G
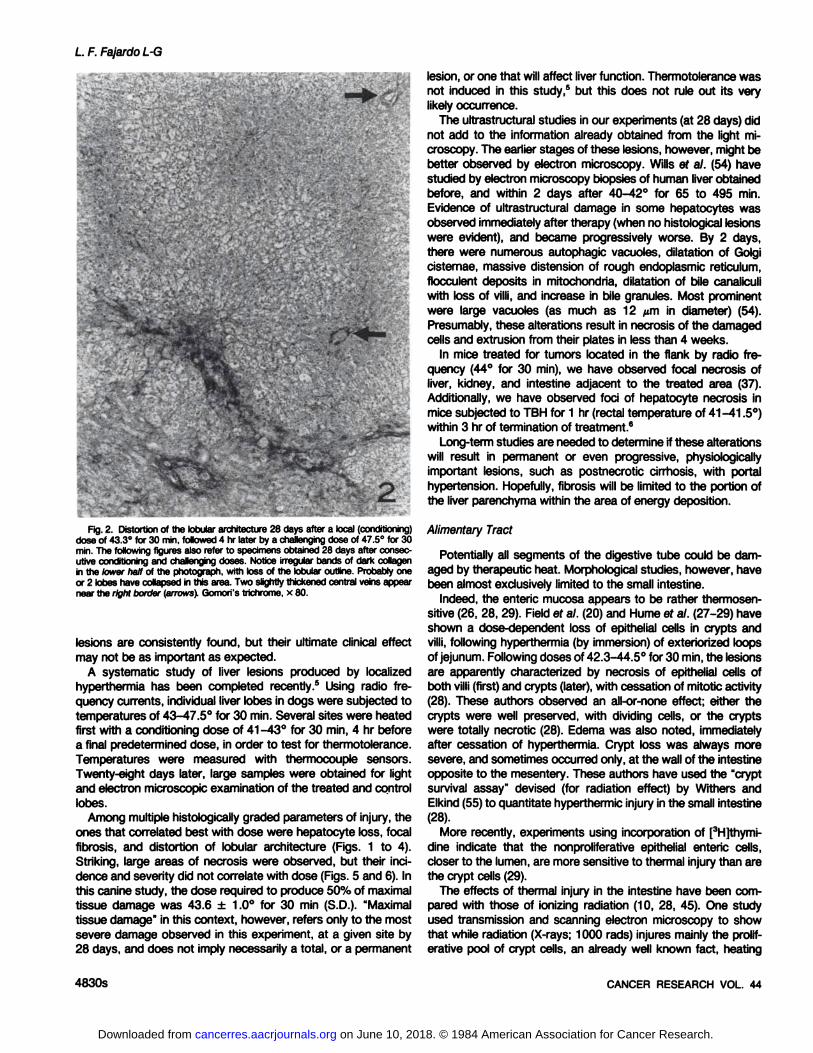
Flg. 2. Distortion of the lobular architecture 28 days after a local (conditioning)dose of 43.3°for 30 min, followed 4 hr later by a challenging dose of 47.5°for 30
min. The following figures also refer to specimens obtained 28 days after consecutive conditioning and challenging doses. Notice irregular bands of dark collagenin the lower half of the photograph, with loss of the lobular outline. Probably oneor 2 lobes have collapsed in this area. Two slightly thickened central veins appearnear the right border (arrows). Gomori's trichrome, x 80.
lesions are consistently found, but their ultimate clinical effectmay not be as important as expected.
A systematic study of liver lesions produced by localizedhyperthermia has been completed recently.5 Using radio fre
quency currents, individual liver lobes in dogs were subjected totemperatures of 43-47.5° for 30 min. Several sites were heatedfirst with a conditioning dose of 41-43° for 30 min, 4 hr before
a final predetermined dose, in order to test for thermotolerance.Temperatures were measured with thermocouple sensors.Twenty-eight days later, large samples were obtained for light
and electron microscopic examination of the treated and controllobes.
Among multiple histologically graded parameters of injury, theones that correlated best with dose were hepatocyte loss, focalfibrosis, and distortion of lobular architecture (Figs. 1 to 4).Striking, large areas of necrosis were observed, but their incidence and severity did not correlate with dose (Figs. 5 and 6). Inthis canine study, the dose required to produce 50% of maximaltissue damage was 43.6 ± 1.0° for 30 min (S.D.). "Maximaltissue damage" in this context, however, refers only to the most
severe damage observed in this experiment, at a given site by28 days, and does not imply necessarily a total, or a permanent
lesion, or one that will affect liver function. Thermotolerance wasnot induced in this study,5 but this does not rule out its very
likely occurrence.The ultrastructural studies in our experiments (at 28 days) did
not add to the information already obtained from the light microscopy. The earlier stages of these lesions, however, might bebetter observed by electron microscopy. Wills ef al. (54) havestudied by electron microscopy biopsies of human liver obtainedbefore, and within 2 days after 40-42° for 65 to 495 min.
Evidence of ultrastructural damage in some hepatocytes wasobserved immediately after therapy (when no histológica! lesionswere evident), and became progressively worse. By 2 days,there were numerous autophagic vacuoles, dilatation of Golgicisternae, massive distension of rough endoplasmic reticulum,flocculent deposits in mitochondria, dilatation of bile canaliculiwith loss of villi, and increase in bile granules. Most prominentwere large vacuoles (as much as 12 ¿¿min diameter) (54).Presumably, these alterations result in necrosis of the damagedcells and extrusion from their plates in less than 4 weeks.
In mice treated for tumors located in the flank by radio frequency (44°for 30 min), we have observed focal necrosis of
liver, kidney, and intestine adjacent to the treated area (37).Additionally, we have observed foci of hepatocyte necrosis inmice subjected to TBH for 1 hr (rectal temperature of 41 -41.5°)within 3 hr of termination of treatment.6
Long-term studies are needed to determine if these alterations
will result in permanent or even progressive, physiologicallyimportant lesions, such as postnecrotic cirrhosis, with portalhypertension. Hopefully, fibrosis will be limited to the portion ofthe liver parenchyma within the area of energy deposition.
Alimentary Tract
Potentially all segments of the digestive tube could be damaged by therapeutic heat. Morphological studies, however, havebeen almost exclusively limited to the small intestine.
Indeed, the enteric mucosa appears to be rather thermosen-sitive (26, 28, 29). Field ef al. (20) and Hume ef al. (27-29) haveshown a dose-dependent loss of epithelial cells in crypts and
villi, following hyperthermia (by immersion) of exteriorized loopsof jejunum. Following doses of 42.3-44.5° for 30 min, the lesions
are apparently characterized by necrosis of epithelial cells ofboth villi (first) and crypts (later), with cessation of mitotic activity(28). These authors observed an all-or-none effect; either the
crypts were well preserved, with dividing cells, or the cryptswere totally necrotic (28). Edema was also noted, immediatelyafter cessation of hyperthermia. Crypt loss was always moresevere, and sometimes occurred only, at the wall of the intestineopposite to the mesentery. These authors have used the "cryptsurvival assay" devised (for radiation effect) by Withers and
Elkind (55) to quantitate hyperthermic injury in the small intestine(28).
More recently, experiments using incorporation of [3H]thymi-
dine indicate that the nonproliferative epithelial enteric cells,closer to the lumen, are more sensitive to thermal injury than arethe crypt cells (29).
The effects of thermal injury in the intestine have been compared with those of ionizing radiation (10, 28, 45). One studyused transmission and scanning electron microscopy to showthat while radiation (X-rays; 1000 rads) injures mainly the prolif-
erative pool of crypt cells, an already well known fact, heating
4830s CANCER RESEARCH VOL. 44
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Pathological Effects of Hyperthermia
(43°for 20 min) affects mainly the villi (10). Both agents produced
conical villi (10).As could be suspected, hyperthermia enhances the effect of
radiation on the small intestinal mucosa (20). This has been welldemonstrated in the mouse by a study of Merino ef al. (39). Themaximum TER was quite significant, 4.7 for a dose of 44°for
30 min prior to radiation (total body single dose of 400 to 2000rads) (39).
Thermotolerance has been demonstrated in the mouse jejunum, both by crypt-survival assay (27), and by using death
(LDso/7) as the end point (26). Heating of exteriorized entericloops is often fatal to mice because septicemia develops, presumably due to penetration of bacteria through the denudedmucosa. The LDso/7is around 6 min of heating at 45°(26). This
LDso/7is independent of the length of the intestinal loop, priorfeeding of animals, and fluid replacement postheating (26). Gen-
tamicin administration increases the LDso/?to more than 9 min/45°(26).
The membrane labilizer retinol did not enhance gross damageto mouse small intestine, although it did enhance lysosomalmembrane permeability in the spleen, as measured by histo-
chemistry (45). These findings were interpreted by Rogers ef al.(45) as suggesting that lysosomal membrane injury is not aprimary event in hyperthermal cell killing. Our morphologicalstudy of a thermosensitive mouse neoplasm supports the sameview (18).
Since microwave heating is a more likely method than waterbath for abdominal neoplasms in clinical hyperthermia, oneshould also be concerned with the possible effects of microwaves on intestinal motility. A study of the effects of low-level
microwave irradiation (5 and 7.5 milliwatts/sq cm at 2.45 GHz)was made in the intestine of rats (47). Acceleration of slowwaves and inhibition of action potentials were shown in thismodel, using chronically implanted electrodes (47).
Most experiments have ignored the possibility of delayed injuryin the intestine. In one study, the rectum of rabbits was examinedhistologically up to 3 months following 43°for 30 min delivered
by a coaxial probe (56). In these experiments the authors foundno injury of the rectum in most of the animals (56).
Hahn (24) has suggested that intestinal heat lesions may bemore severe when there are lumenal masses of undigestedmaterial that may overheat and do not cool effectively. If so,colonie lesions would be worse in the presence of fecal masses,and these could be ameliorated by fasting (24).
We have not seen morphological descriptions of intestinallesions following therapeutic localized hyperthermia in humans.Considering the increasing clinical use of this modality, and theobvious sensitivity of the small intestine, we would not be surprised to find such lesions.
Central Nervous System
The possibility of treating cerebral neoplasms by local hyperthermia (either microwave or ultrasound induced) has greatpotential (4, 6, 34, 46). In preparation for clinical trials, studies ofthe thermal response of various normal brain structures havebeen made by several investigators (3,25), particularly the groupof Britt ef al. (4, 6, 34).
Ultrasound, applied to the exposed durai surface of cats during50 min, caused acute lesions detectable at temperatures above
42.5°(4). Such lesions were sharply demarcated and consisted
of edema of the white matter, pyknosis and loss of neurons(especially at 44-45°), and destruction of myelin. Coagulativenecrosis was observed at 47°(4).
Single or multiple intracerebral microwave antennas were usedto generate temperatures of 40-47° during 50 to 75 min in 3
groups of dogs: normal adults, normal growing animals (5 to 6weeks old) and dogs with SR-Rous sarcoma virus brain tumors
(34). The animals were terminated at the end of the thermalexposure. As in the cats, the acute lesions consisted of edemaof white matter, pyknosis of neurons, and damage of whitematter tracts. Neuronolysis was seen above 43°.Necrosis and
hemorrhage of tumor were noted (no control tumors were described) (34). It was concluded that the threshold of irreversibledamage occurred at 42.2°for 50 to 60 min.
Earlier observations of Harris ef al. (25) in regionally perfuseddogs also indicated absence of lesions below 42°and significantlesions above 44°,edema, focal hemorrhage, and infarcì.
A physiological study in cats subjected to TBH (5) (via cardi-opulmonary bypass) confirmed the above morphological observations: the critical temperature for evoked potential responseswas calculated, by Arrhenius equations, to be 42.2°per 1 hr (5).
Physiological observations in humans during TBH (electroencephalogram and somatosensory-evoked responses) suggestfunctional impairment at 41.8-42°, which is reversible (13). There
is concern about the combined effects of ionizing radiation andhyperthermia on the spinal cord (22). Sudden myelopathy occurred in 3 patients treated by spinal irradiation and TBH (12).Studies in mice suggest enhancement of the functional deficitwhen the 2 modalities are applied to the spinal cord within ashort time interval (22).
Hopefully, brain neoplasms may respond to hyperthermiadoses below the apparent threshold of 42°for 60 min.
Kidney
Because of its high blood flow rate the renal parenchyma hasnot been considered by some investigators as a likely site ofhyperthermic injury. Some studies, however, suggest that this isnot the case.
A well-described histological study in mice was published by
Elkon ef al. (15). After unilateral nephrectomy, the contralateralkidney was shielded from adjacent organs and heated intraoper-atively by ultrasound, reaching temperatures of 40.5, 42.5, and44.5°for 35 min, as measured by 4 thermocouples inserted in
the kidney. The kidneys were systematically examined by apathologist 1, 7, or 28 days later (15).
Sharply demarcated, subcapsular areas of necrosis occurred,involving only the tubules in minimal lesions, or tubules, glomeruli,and even vessels in large lesions. The extent of the necrosis didnot increase in time (i.e., it had reached maximum by 24 hr), butsegmented neutrophils were maximal at 7 days and had disappeared by 28 days. Calcium deposits increased with time. Evenat 28 days, there was no collapse of the framework of thetubules, although the epithelial cells had disappeared within thefirst day, and fibrosis was only minimal and peripheral (15).
In kidneys heated to 40.5°,lesions did not reach 5% of a given
section of the renal parenchyma; of those kidneys receiving thehigher doses (42.5°and 44.5°), one-third had lesions >5% of
the parenchyma. Based on these observations, the authors
OCTOBER 1984 4831s
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

L. F. Fajardo L-G
conclude that the mean renal temperature at which necrosisdeveloped was 43°for 20 min (15).
In a different study, exteriorized rabbit kidneys were treatedby brief (15 sec) exposures to ultrasound beam of total acousticpower of 30 watts (approximately 900 watts/sq cm at center)(14). The kidneys of 45 rabbits so treated were examined 10 minto 1 year later. The progression of the sharply defined histologicallesions ranged from acute injury at 10 min (lysis of erythrocytes,early necrosis of tubular cells, karyolysis, edema, etc.) to established, progressive necrosis between 1 and 10 days: tubulor-rhexis, glomerular necrosis, areas of coagulation necrosis, neu-
trophilic infiltrate, and later calcification. Between 1 week and 1year, there was removal of cell debris by macrophages andprogressive fibrosis which eventually resulted in a scar. Apparently some tubular regeneration occurred (14). Unfortunately, notemperature measurements were obtained in the kidneys, although the authors estimate that these exposures could haveresulted in temperatures of 60-70° (14). Such exposures are
difficult to compare with those used in clinical hyperthermia. Thehistological observations, however, serve to corroborate thefindings of sharply defined lesions observed later by Elkon ef al.(15). Furthermore, the long sequential study indicates that ultimately fibrous scars should be expected from early lesions, quitesimilar to those occurring at lower temperatures (15).
Lower Urinary Tract
Damage to these structures could occur in the course oftherapy, either to adjacent organs or to the urinary tract itself.
In rabbits, heating of the rectum at 43°for 30 min by means
of a coaxial probe did not produce gross or histological damageof the bladder examined sequentially at 16 time points, 1 day to3 months following exposure (56).
Hyperthermia of the bladder wall can be achieved by continuous irrigation with warm fluid. Using water, Linke ef al. (32)treated 20 dogs with exposures at 35-69° (measured by therm
istors) during 8 min. The urine was diverted and the animalswere killed 6 weeks later. Neither gross nor microscopic alterations were noted between 35 and 44.5°. Patchy destruction of
the mucosa, and focal necrosis of the muscularis were seenbetween 46.5 and 61.5°. The muscularis lesions were often
severe, of full thickness, and did not necessarily coincide withthe mucosa! lesions.
Complete destruction of the bladder wall occurred between59 and 69°;by 6 weeks the bladder was replaced by a fibrous
scar. Occasional thrombosis of small vessels was noted but nodamage was observed in the adjacent organs (32).
Thus, it appears that, at least in dogs and rabbits, the urinarybladder can tolerate temperatures of up to 44.5°for 8 min (and
perhaps longer) without significant damage.
Prostate
In 2 interesting experiments (35, 56), the thermal sensitivity ofthe normal prostate has been assayed histologically; by meansof a coaxial probe located in the rectum, microwave hyperthermiawas induced, reaching temperatures of 42.6-43° for 30 min in
the prostate, as measured by thermocouples (56). The 32 rabbitsthus treated were examined histologically at multiple times from1 day to 3 months after exposure(s). Only minimal alterations of
the rectum (focal karyopyknosis, edema, etc.) were observed ina few animals (56). The authors found no prostatic lesions afterone or two 43°/30-min exposures (56).
The above report contrasts sharply with (but does not necessarily contradict) that of Magin ef al. (35). These authors treatedintrasurgically the prostate of 8 dogs with microwaves (60°for
15 to 22 min, controlled by thermistor) after shielding the rectumand some of the adjacent muscles. At the end of this severetherapy, the prostate was edematous and dark; 1 week later (4dogs), although its volume was not decreased, there was coagulation necrosis of the entire organ with some foci of neutrophilicinfiltrate and/or liquefaction necrosis. Six months later (4 dogs)there was no recognizable prostate; the organ had been replacedby a fibrous scar. Minor lesions were seen in the bladder andthe vasa deferentia, but not in the (shielded) rectum (35).
These separate observations may, or may not, be pertinent tothe human prostate. If applicable, they would indicate a thresholdof thermal injury in the normal prostate, somewhere between43°for 30 min and 60°for 15 min. Hopefully, carcinomas will
respond at lower doses.As indicated above, the systemic temperatures reached by
these patients were not always documented, and obviously therenal temperatures were unknown (1).
Skeletal System
It is rather difficult to find studies of the osseous pathologyproduced by therapeutic hyperthermia. There seems to be moreinterest in the effects of high-speed drills and other surgical
instruments.An interesting device, designed for vital microscopic observa
tions during local bone heating, is the "thermal chamber" (16).
This titanium chamber is implanted for an indefinite time in abone, allowing multiple observations of various in vivo responses,especially vascular, to a thermal insult. Using this device in thetibia of rabbits, Eriksson ef al. (16) studied the effects of 53°for
1 min; blood flow became sluggish and stopped 2 days later.The original vessels gradually disappeared and were replaced bynew ones. Adipocytes decreased in number, and bone remodeling started 3 to 5 weeks postinjury (16). Although these dataare not too pertinent to clinical hyperthermia, the thermal chamber is potentially a very useful tool for the study of the effects oftherapeutic heat, ionizing radiation, etc.
The effect of hyperthermia on cartilage has been measured interms of its ability to inhibit the growth of the tail in baby ratsand mice (24). The tails are partially immersed in heated waterat 7 days of age. Several months later, the heated caudalvertebrae are compared radiographically with the unheated ones,and a quantitative index of stunting is obtained (24). In addition,necrosis occurs within a few days after exposures in the higherrange.
From these observations, Hahn ef al. (24) and Field ef al. (19)have shown a dose-related stunting effect; 43°for 1 hr resultedin 10% growth inhibition, but did not cause necrosis; 44°for 1hr caused necrosis in 50% of the animals; if the time at 44°was
reduced to 50 min or less, the necrosis was prevented (24).Thus, in this system the limit of tolerance for growth inhibition isbelow 43°for 1 hr, and the limit of tolerance for acute damagein the various soft tissues of the tail seems to be 44°for 1 hr.
4832s CANCER RESEARCH VOL. 44
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Pathological Effects of Hyperthermia
Embryo
Of great concern are the effects of temperature elevation onthe embryo. Retardation of brain growth has been documentedin guinea pig embryos exposed to maternal temperatures of41.8-43.9°for 1 hr (in an incubator) on the 21st day of gestation(53). Such exposures resulted in a dose-related microcephaly ofthe offspring (53). A comparison with 7-radiation in the sameexperimental system showed that an elevation of 1°produced a
deficit in brain weight equivalent to the effect caused by a doseincrement of 42.5 rad (53). Obviously, this information refers onlyto maternal temperatures; the embryonal temperatures are assumed to be equal, or at least to change parallel, to the maternalones, but this assumption may be wrong.
Other studies of the effects of systemic or local hyperthermiaon the embryo are available, but their review is beyond the scopeof this article. In any case, the possible teratogenic effects ofhyperthermia should be a consideration in the therapy of abdominal neoplasms, and even in the diagnostic use of ultrasound.
References
1. Anderson, R. L, Ahier, R. G., and Littleton, J. M. Observations on the cellulareffects of ethanol and hyperthermia in vivo. Radiât.Res., 94: 318-325,1983.
2. Baker, D. G., Sager, H., Constable, W., and Goodchild. N. The response ofpreviously irradiated skin to combinations of x-irradiation and ultrasound-induced hyperthermia. Radiât.Res., 96: 367-373, 1983.
3. Barnard, J. W., Fry, W. J., Fry, F. J., and Brennan, J. F. Small localizedultrasound lesions in the white and gray matter of the cat brain. Arch. Neural.Psychiatry, 75. 15-35, 1956.
4. Britt, R. H., Lyons, B. E., Pounds, D. W., and Prionas, S. D. Feasibility ofultrasound hyperthermia in the treatment of malignant brain tumors. Med.Instr, 77. 172-177, 1983.
5. Britt, R. H., Lyons, B. E., Ryan, T., Saxer, E., Obana, W., and Rossi, G. Effectof whole body hyperthermia on auditory brainstem, somatosensory and visualevoked potentials. In: J. R. S. Hates (ed.), Thermal Physiology, pp. 519-523.
New York: Raven Press, 1983.6. Britt, R. H., Pounds, D. W., and Lyons, B. E. Feasibility of treating malignant
brain tumors with focused ultrasound. Prog. Exp. Tumor Res., in press, 1984.7. Bull, J. M. Whole body hyperthermia as an anticancer agent. Cancer (Am.
Cancer See.), 32:123-128, 1982.8. Bull, J. M., Lees, D., Schuette, W., Whang-Peng, J., Smith, R., Bynum, G.,
Atkinson, E. R., Gottdiener, J. S., Gralnick, H. R., Shawker, T. H., and Devita,V. T., Jr. Whole body hyperthermia: a phase-l trial of a potential adjuvant tochemotherapy. Ann. Intern. Med., 90: 317-323, 1979.
9. Burger, F. J., and Fuhrman, A. Evidence of injury by heat in mammalian tissues.Am. J. Physiol., 206: 1057-1061, 1964.
10. Carr, K. E., Hume, S. P., Marigold, J. C., and Michalowski, A. Scanning andtransmission electron microscopy of the damage to small intestinal mucosafollowing x-radiation or hyperthermia. Scanning Electron Microsc., Part 1,393-
402, 1982.11. Cronau, L. H., Jr., Bourke, D. L., and Bull, J. M. General anesthesia for whole-
body hyperthermia. Cancer Res. (Suppl.), 44: 4873s-4877s, 1984.12. Douglas, M. A., Parks, L. C., and Bebin, J. Sudden myelopathy secondary to
therapeutic total-body hyperthermia after spinal cord irradiation. N. Engl. J.Med., 304: 583-585, 1981.
13. Dubois, M., Coppola, R., Buchsbaum, M. S., and Lees, D. E. Somatosensoryevoked potentials during whole body hyperthermia in humans. Etectroence-phalogr. Clin. Neurophysiol., 52:157-162,1981.
14. Elbadawi, A., Unke, C. A., Carstensen, E. L., and Fridd, C. W. Histomorpho-logic features of ultrasonic renal injury. Arch. Pathol. Lab. Med., 700: 199-
205, 1976.15. Elkon, D., Fechner, R. E., Homzie, M. J., Baker, D. J., and Constable, W. C.
Response of mouse kidney to hyperthermia. Pathology and temperature-dependence of injury. Arch. Pathol. Lab. Med., 704. 153-158,1980.
16. Eriksson, A., Albrektsson, T., Grane, B., and McQueen, D. Thermal injury tobone. A vital microscopic description of heat effects. Int. J. Oral Surg., 77:115-121, 1982.
17. Fajardo, L. F. Pathology of Radiation Injury. New York: Masson PublishingU.S.A., Inc., 1982.
18. Fajardo, L. F., Egbert, B., Marmor, J., and Hahn, G. M. Effects of hyperthermiain a malignant tumor. Cancer (Phila.), 45: 613-623, 1980.
19. Field, S. B., Hume, S., Law, M. P., Morris, C., and Meyers, R. Some effectsof combined hyperthermia and ionizing radiation on normal tissues. In: Proceedings of the International Symposium on Radiobiology Research Needed
for the Improvement of Radiotherapy. Vienna: International Atomic EnergyComission, 1976.
20. Field, S. B., Hume, S. P., Law, M. P., and Myers, R. The response of tissuesto combined hyperthermia and x-rays. Br. J. Radiol., 50: 129-134,1977.
21. Freeman, M. L., Raaphorst, G. P., Hopwcod, L. E., and Dewey, W. C. Theeffect of pH on cell lethality induced by hyperthermic treatment. Cancer (Phila.),45:2291-2300,1983.
22. Goffinet, D. R., Choi, K. Y., and Brown, J. M. The combined effects ofhyperthermia and ionizing radiation on the adult mouse spinal cord. Radiât.Res., 72:238-245, 1977.
23. Gore, I., and Isaacson, N. H. The pathology of hyperpyrexia. Am. J. Pathol.,25:1029-1060,1949.
24. Hahn, G. M. Hyperthermia and Cancer. New York: Plenum Press, 1982.25. Harris, A. B., Erickson, L., Kendig, J. H., Mingrino, S., and Goldring, S.
Observations on selective brain heating in dogs. J. Neurosurg., 79: 514-521,
1962.26. Hente, K. J. Thermotolerance in the murine jejunum. J. Nati. Cancer Inst., 68:
1033-1036,1982.
27. Hume, S. P., and Marigold, J. C. L. Transient, heat induced, thermal resistancein the small intestine of mouse. Radiât.Res., 82: 526-535, 1980.
28. Hume, S. P., Marigold, J. C. L., and Field, S. B. The effects of local hyperthermiaon the small intestine of mouse. Br. J. Radiol., 52: 657-662,1979.
29. Hume, S. P., Marigold, J. C., and Michalowski, A. The effect of local hyperthermia on nonproliferative, compared with proliferate, epithelial cells of themouse intestinal mucosa. Radiât.Res., 94: 252-262, 1983.
30. Kew, M., Bersohn, I., Seflel, H., and Kent, G. Liver damage in heatstroke. Am.J. Med., 49:192-202,1970.
31. Law, M. P., and Field, S. B. The response of the mouse ear to heat appliedalone or combined with x-rays. Br. J. Radiol., 57:132-138,1978.
32. Unke, C., Elbadawi, A., Netto, V., Roberts, A., and Russo, M. Effect of markedhyperthermia upon the canine bladder. J. Ural., 707: 599-602,1972.
33. Luk, K. H., Francis, M. E., Perez, C. A., and Johnson, R. J. Radiation therapyand hyperthermia in the treatment of superficial lesions: preliminary analysis:treatment efficacy and reaction of skin, subcutaneous tissues. Am. J. Clin.Oncol., 6:399-406,1983.
34. Lyons, B. E., Britt, R. H., and Strohbehn, J. W. Localized hyperthermia in thetreatment of malignant brain tumors using an interstitial microwave antennaassay. IEEE Trans. Biomed. Eng., 37: 53-62,1984.
35. Magin, R. L., Fridd, C. W., Bonfiglio, T. A., and Linke. C. A. Thermal destructionof the canine prostate by high intensity microwaves. J. Surg. Res., 29: 265-275, 1980.
36. Malamud, N., Haymaker, W., and Custer, R. P. Heat stroke. A clinico-patho-logic study of 125 fatal cases. Mil. Surg., 97: 397-449,1946.
37. Marmor, J. B., Hahn, N., and Hahn, G. M. Tumor cure and cell survival afterlocalized radtofrequency heating. Cancer Res., 37:879-883,1977.
38. Martinez, A. A., Meshorer, A., Meyer, J. L., Hahn, G. M., Fajardo, L. F., andPrionas, S. D. Thermal sensitivity and thermotolerance in normal porcinetissues. Cancer Res., 43: 2072-2075,1983.
39. Merino, 0. R., Peters, L. J., Mason, K. A., and Withers, H. R. Effect ofhyperthermia on the radiation response of the mouse jejunum. Int. J. Radiât.Oncol. Bicrf. Phys., 4: 407-414,1978.
40. Meshorer, A., Prionas, S. D., Fajardo, L. F., Meyer, J. L., Hahn, G. M., andMartinez, A. A. The effects of hyperthermia on normal mesenchymal tissues.Arch. Pathol. Lab. Med., 707: 328-334, 1983.
41. Moritz, A., and Henriquez, F. Studies of thermal injury. II. The relative importance of time and surface temperature in the causation of cutaneous bums.Am. J. Pathol., 23: 695-720,1947.
42. Okumura, Y., and Reinhold, H. Heat sensitivity of rat skin. Eur. J. Cancer, 74:1161-1166,1978.
43. Pettigrew, R. T., Galt, J. M., Ludgate, C. M., and Smith, A. N. Clinical effectsof whole-body hyperthermia in advanced malignancy. Br. Med. J., 4:679-682,
1974.44. Pettigrew, R. T., Galt, J. M., Ludgate, C. M., Horn, D. B., and Smith, A. N.
Circulatory and biochemical effects of whole body hyperthermia. Br. J. Surg.,6Õ:727-730,1974.
45. Rogers, M. A., Marigold, J. C., and Hume, S. P. The effect of retino! on thehyperthermal response of normal tissue in vivo. Radiât.Res., 95: 165-174,
1983.46. Salcman, M., and Samaras. G. M. Hyperthermia for brain tumors: biophysical
rationale. Neurosurgery, 9: 327-335, 1981.47. Santini, R., and Deschaux, P. Incidence of low-level microwave irradiation on
intestinal myelectrical activity in the rat. Health Phys., 45: 775-778,1983.48. Thomsen, H. K., Danielsen, L., Nielson, 0., Aalund, O., Nielsen, K. G., Karls
mark, T., Genefke, I. K., and Christoffersen, P. Epidermal changes in heat andelectrically injured pig skin. A light microscopic study of the influence of heatenergy intensity and electrical current frequency. Acta Pathol. Microbiol. Im-munol. Scand. (A), 97: 297-306,1983.
49. Urano, M., and Kahn, J. The effect of step-down heating on murine normaland tumor tissues. Radiât.Res., 94: 350-358,1983.
50. Urano, M., Montoya, V., and Booth, A. Effect of hyperglycemia on the thermalresponse of murine normal and tumor tissues. Cancer Res., 43: 453-455,
1983.51. Urano, M., Overgaard, M., Suit, H., Dunn, P., and Sedlacek, R. S. Enhancement
OCTOBER 1984 4833s
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

L. F. Fajardo L-G
by Corynebaeterium para/m of the normal skin and tumor tissue response to 54. Wills, E. J., Findlay, J. M., and McManus, J. P. A. Effects of hyperthermiahyperthermia. Cancer Res., 38: 862-864,1978. therapy on the liver. II. Morphological observations. J. Clin. Pathol. (Lond.), 29:
52. Urano, M., Rice, L., Kahn, J., and Sedlacek, R. S. Studies on fractionated 1-10,1976.hyperthermia ¡nexperimental animal systems. I. The foot reaction after equal 55. Withers, H. R., and Elkind, M. M. Microcolony survival assay for cells of mousedoses: heat resistance and repopulation. Int. J. Radiât.Oncol. Btol. Phys., 6: intestinal mucosa exposed to radiation. Int. J. Radiât.Btol. Relat. Stud. Phys.1519-1523,1980. Chem. Med., 17: 261-267,1970.
53. Wanner, R. A., and Edwards, M. J. Comparison of the effects of radiation and 56. Yerushalmi, A., Shpirer, Z., Hod, l., Gottesfeld, F., and Baos, D. D. Normalhyperthermia on prenatal retardation of brain growth of guinea pigs. Br. J. tissue response to localized deep microwave hyperthermia in the rabbit's
Radiol., 56: 33-39,1983. prostate: a preclinical study. Int. J. Radiât.Oncol. Biol. Phys., 9:77-82,1983.
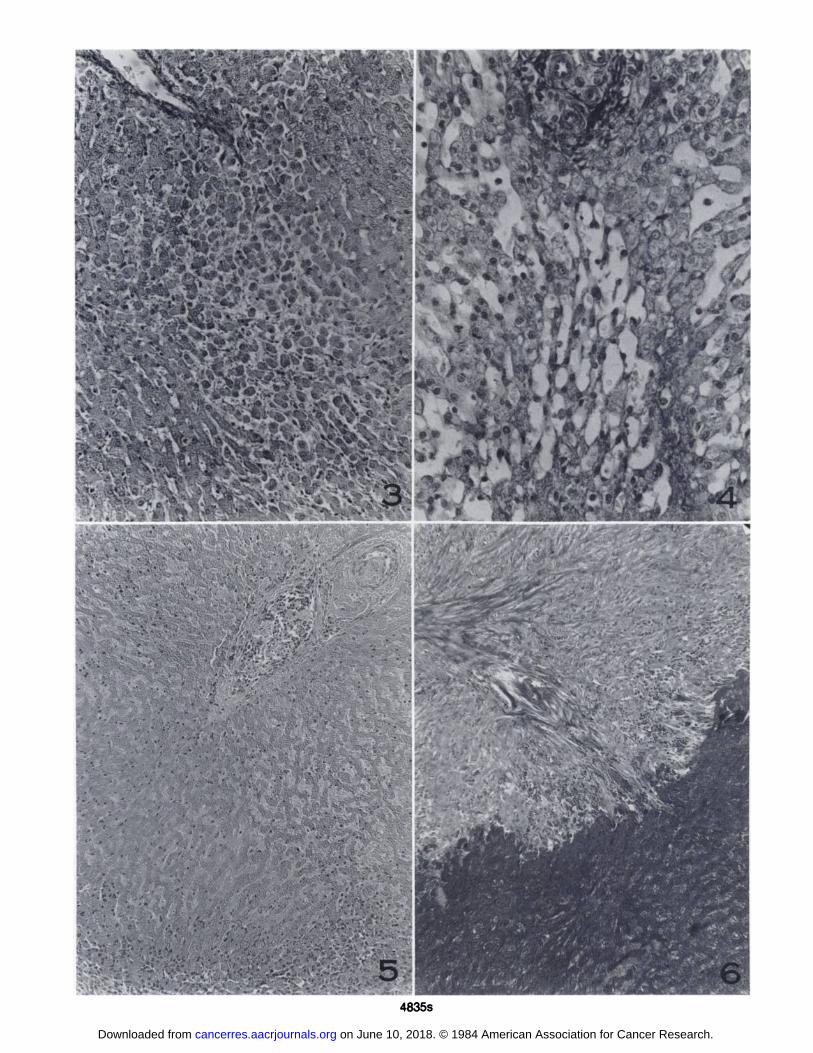
Fig. 3. Focal loss of hepatocytes is illustrated in the midzonal area of a lobule whose thickened central vein appears in the left upper corner. Normal, continuousplates of liver cells are present in the right upper and left lower areas, while in the center the hepatocytes do not form plates but are separate from each other, due tothe loss of multiple intervening liver cells. Treatments were at 43°for 30 min and 47.5°for 30 min. Gomori's trichrome, x 176.
Fig. 4. Focal toss of liver cells is shown in the center of this photograph from a canine liver treated at 43°for 30 min and 47.5°for 30 min. In the center, and below a
portal area, hepatocytes have disappeared, leaving delicate reticular-vascular framework. Compare with the normal hepatocytes plates and sinusoids in the right and leftportions of the field. Neither this nor Fig. 3 show cells in the process of necrosis, such as "acidophilic bodies." In this experiment, individual cell necrosis presumablyoccurred during the first weeks after hyperthermia, followed by removal of cell debris by macrophages. Gomori's trichrome, x 320.
Fig. 5. Massive area of liver necrosis (after 41.2" for 30 min and 45.3" for 30 min), involving more than one lobule. With this stain necrotic hepatocytes are pale and
devoid of nuclei, although the continuity of the plates is preserved. A large portal area, with thrombosis of the vein and artery, is present in the right upper corner. Amargin of inflammatory reaction (neutrophils) is seen at the lower edge. Unlike individual cell necrosis, massive necrosis did persist to 28 days. H & E, x 100.
Fig. 6. Early scar in area of massive necrosis, after 41 °for 30 min and 44.5°for 30 min. The persistent necrotic liver plates appear dark with this stain, at the bottom
of the figure. Invading collagen bands occupy the top. Although the ultimate result of these areas of fibrosis is unknown, probably localized hyperthermia affectingportions of the liver will not result in significant functional impairment of this organ. Gomori's trichrome, x 100.
4834s CANCER RESEARCH VOL. 44
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
*ï*"
El•W l* «»l I •*
.V V
»'
^
^"'.. à * ^ (jt<«.
4835s
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1984;44:4826s-4835s. Cancer Res Luis Felipe Fajardo L-G Pathological Effects of Hyperthermia in Normal Tissues
Updated version
http://cancerres.aacrjournals.org/content/44/10_Supplement/4826s
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/44/10_Supplement/4826sTo request permission to re-use all or part of this article, use this link
on June 10, 2018. © 1984 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Related Documents










![Effects of Hyperthermia on the Production and Activity of ... file[CANCER RESEARCH 38, 1120-1126, April 1978] Effects of Hyperthermia on the Production and Activity of Primary and](https://static.cupdf.com/doc/110x72/5d2cb83688c9936a308d8137/effects-of-hyperthermia-on-the-production-and-activity-of-cancer-research-38.jpg)