RESEARCH POSTER PRESENTATION DESIGN © 2012 www.PosterPresentations.com INTRODUCTION RESULTS CONCLUSIONS REFERENCES Hughes C, Pain C, Braithwaite J, Hillman K. (2014) ‘Between the flags’: implementing a rapid response system at scale. BMJ Qual Saf. 23:714–717 Roland D, Oliver A, Edwards ED, Mason BW, Powell CVE. (2014). Use of paediatric early warning systems in Great Britain: has there been a change of practice in the last 7 years? Arch Dis Child 99:26-29 As part of the Deteriorating Child workstream at Evelina London Children’s Hospital (ELCH), aiming to improve recognition, escalation, and mitigation of safety risks for the deteriorating child, we are designing and implementing a new Paediatric Early Warning Score (PEWS) tool. There is no national or standardised Early Warning Score for children. ELCH is a regional children’s hospital housing multiple specialties, including cardiology, PICU, general paediatrics and high-dependency care, and a PEWS chart has been in use since 2010. Multidisciplinary PICU admission casenotes review identified problems with chart completion or calculation in 12.4% of cases in 2014, with a delay in recognition or escalation in 19.1% of cases. So far in 2015, casenotes review identified PEWS problems in 18.9% of cases and delay in recognition or escalation in 10.8% of cases. Paediatric Early Warning Score system: Experience from a tertiary children’s hospital The existing chart was noted to be difficult to score and interpret, and required a separate sheet to score the observations depending on the patient’s age. The creation of a new PEWS chart is a complex process that takes time and requires consensus from a multidiscplinary team across different specialties, as well as a pilot to identify issues with the chart that can only be detected with real-time use. An improved PEWS chart can facilitate earlier recognition of deteriorating child, allowing for earlier escalation and improved clinical outcomes. Ensuring a PEWS chart can be easily completed and quickly and reliably visually interpreted is therefore a clinical priority in paediatrics. OBJECTIVES & METHOD In response, the aim of this work was to create a new PEWS observation chart that could be easily and quickly filled in by the nursing staff looking after the patient, and also reliably interpreted by medical and senior nursing staff reviewing the patient, to enable: 1. Early recognition of the deteriorating child 2. Timely escalation 3. Appropriate mitigation of risk, preventing clinical problems for the child This would be better enabled by: • Colour-coded charts for quick visual recognition • Age-specific charts • Removing scores to avoid relying on adding up We used the Between the Flags (ref) system developed in Australia, which colour codes observations according to level of clinical concern, and adapted this for Evelina London Children’s Hospital, using 5 age groups: 0-3 months, 3-12 months, 1-4 years, 4-11 years, >12 years. The new chart was piloted for feasibility (usability with colour-blind members of staff) for three months in 2 settings: • general paediatric high dependency unit on Mountain ward, • paediatric orthopaedics on Savannah ward. New PEWS chart for age 1-4 years, in ABCDE format with colour-coded observation scoring. Case review of unplanned PICU admissions found that in 5 cases for which the new PEWS chart was used, there was early recognition in 100%, compared with 65.6% of 32 cases for which the old PEWS chart was used. Pilot data demonstrated high levels of user satisfaction. Some essential changes to the chart were identified, such as changes to ventilator observations for ventilated patients, and a need to colour code inhaled oxygen as this can indicate clinical deterioration. Collation of feedback and minor changes to the new charts are in progress. We are also designing a variation on the new chart specifically for cardiology patients who have different observation parameters, particularly for oxygen saturations. The aim is to introduce an updated new PEWS chart across Evelina London later in 2015. Escalation pathway for use with new colour coded observation chart to improve escalation of deteriorating child – not piloted; to be used when new PEWS chart is introduced across Evelina London. Rosanna Bevan 1 , Jeanette Braganza 1 , Alison Pienaar 1 , Ronny Cheung 1 1 Evelina London Children’s Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
RESEARCH POSTER PRESENTATION DESIGN © 2012
www.PosterPresentations.com
INTRODUCTION
RESULTS
CONCLUSIONS
REFERENCES Hughes C, Pain C, Braithwaite J, Hillman K. (2014) ‘Between the flags’: implementing a rapid response system at scale. BMJ Qual Saf. 23:714–717
Roland D, Oliver A, Edwards ED, Mason BW, Powell CVE. (2014). Use of paediatric early warning systems in Great Britain: has there been a change of practice in the last 7 years? Arch Dis Child 99:26-29
As part of the Deteriorating Child workstream at Evelina London Children’s Hospital (ELCH), aiming to improve recognition, escalation, and mitigation of safety risks for the deteriorating child, we are designing and implementing a new Paediatric Early Warning Score (PEWS) tool. There is no national or standardised Early Warning Score for children. ELCH is a regional children’s hospital housing multiple specialties, including cardiology, PICU, general paediatrics and high-dependency care, and a PEWS chart has been in use since 2010. Multidisciplinary PICU admission casenotes review identified problems with chart completion or calculation in 12.4% of cases in 2014, with a delay in recognition or escalation in 19.1% of cases. So far in 2015, casenotes review identified PEWS problems in 18.9% of cases and delay in recognition or escalation in 10.8% of cases.
Paediatric Early Warning Score system: Experience from a tertiary children’s hospital
The existing chart was noted to be difficult to score and interpret, and required a separate sheet to score the observations depending on the patient’s age.
The creation of a new PEWS chart is a complex process that takes time and requires consensus from a multidiscplinary team across different specialties, as well as a pilot to identify issues with the chart that can only be detected with real-time use.
An improved PEWS chart can facilitate earlier recognition of deteriorating child, allowing for earlier escalation and improved clinical outcomes. Ensuring a PEWS chart can be easily completed and quickly and reliably visually interpreted is therefore a clinical priority in paediatrics.
OBJECTIVES & METHOD In response, the aim of this work was to create a new PEWS observation chart that could be easily and quickly filled in by the nursing staff looking after the patient, and also reliably interpreted by medical and senior nursing staff reviewing the patient, to enable:
1. Early recognition of the deteriorating child
2. Timely escalation
3. Appropriate mitigation of risk, preventing clinical problems for the child
This would be better enabled by:
• Colour-coded charts for quick visual recognition
• Age-specific charts
• Removing scores to avoid relying on adding up
We used the Between the Flags (ref) system developed in Australia, which colour codes observations according to level of clinical concern, and adapted this for Evelina London Children’s Hospital, using 5 age groups: 0-3 months, 3-12 months, 1-4 years, 4-11 years, >12 years.
The new chart was piloted for feasibility (usability with colour-blind members of staff) for three months in 2 settings:
• general paediatric high dependency unit on Mountain ward,
• paediatric orthopaedics on Savannah ward.
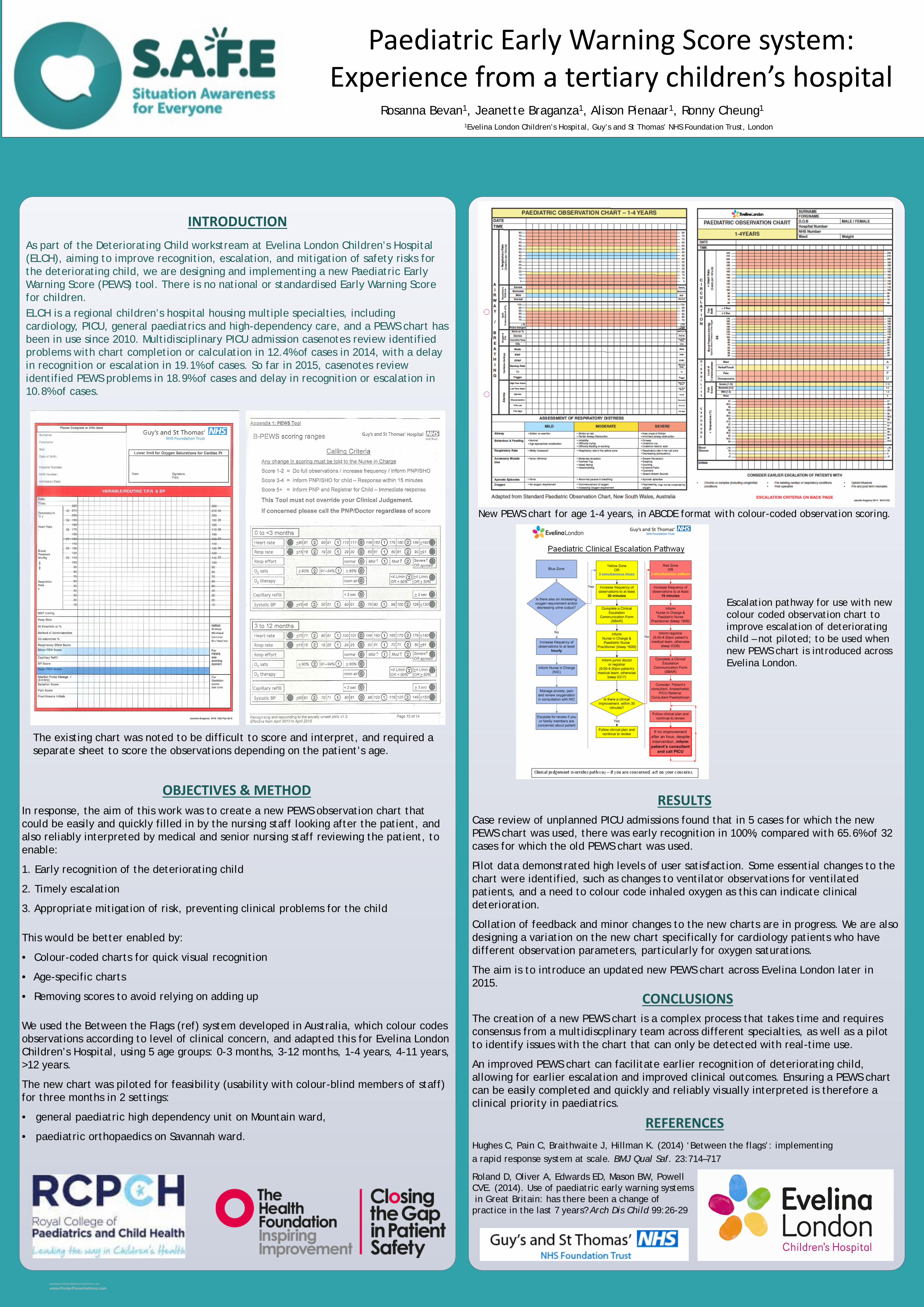
New PEWS chart for age 1-4 years, in ABCDE format with colour-coded observation scoring.
Case review of unplanned PICU admissions found that in 5 cases for which the new PEWS chart was used, there was early recognition in 100%, compared with 65.6% of 32 cases for which the old PEWS chart was used.
Pilot data demonstrated high levels of user satisfaction. Some essential changes to the chart were identified, such as changes to ventilator observations for ventilated patients, and a need to colour code inhaled oxygen as this can indicate clinical deterioration.
Collation of feedback and minor changes to the new charts are in progress. We are also designing a variation on the new chart specifically for cardiology patients who have different observation parameters, particularly for oxygen saturations.
The aim is to introduce an updated new PEWS chart across Evelina London later in 2015.
Escalation pathway for use with new colour coded observation chart to improve escalation of deteriorating child – not piloted; to be used when new PEWS chart is introduced across Evelina London.
Rosanna Bevan1, Jeanette Braganza1, Alison Pienaar1, Ronny Cheung1 1Evelina London Children’s Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London
Related Documents











