Osteoporosis Clinical Updates www.nof.org Clinical Information for Healthcare Professionals Spring 2014 VITAMIN D AND BONE HEALTH Vitamin D is essential for attainment and maintenance of musculoskeletal health and key to calcium homeostasis and phosphorus balance. Chronic insufficiency leads to skeletal ab- normalities and fragility fracture and is linked to multiple extra-skeletal disorders includ- ing cancer, infection, and cardiovascular disease. Analysis of nutrient intake, through food and dietary supplements, has shown the majority of American adults fail to meet adequate intake recommendations for vitamin D established by the Institute of Medicine. 1,2 Many if not most of the patients seen in the typical primary care practice are vitamin D insufficient or deficient. Knowing who is most likely to be se- verely deficient will help practitioners identify those patients who should have targeted test- ing and therapy. Once a patient is found to be deficient, clinical management involves supplementation to raise and maintain serum vitamin D at levels necessary to support optimal bone and gener- al health.This issue of “Osteoporosis: Clinical Updates” will discuss the role of vitamin D in skeletal health, its sources, daily requirements, upper safe limits, and potential for building and maintaining strong bones throughout the lifespan. Editor-in-Chief, Angelo Licata, MD, PhD. National Osteoporosis Foundation 1150 17 th Street, NW • Washington, DC 20036 • 202/223-2226 • www.nof.org © National Osteoporosis Foundation. All rights reserved EDITORIAL BOARD Editor-in-Chief, Angelo Licata, MD, PhD Department of Endocrinology Cleveland Clinic Adrienne Berarducci, PhD, ARNP, BC University of South Florida Carolyn J. Bolognese, RN, CDE Bethesda Health Research Center JoAnn Caudill, RT, BD, CDT Carroll Arthritis, P.A. Peggy Doheny, PhD, RN, CNS, ONC Kent State University College of Nursing Patricia Graham, MD, PC Physical Medicine and Rehabilitation / Integrative Medicine Craig Langman, MD Northwestern University Barbara Messinger-Rapport, MD, PhD Cleveland Clinic Paul D. Miller, MD Colorado Center for Bone Research Jeri Nieves, PhD Columbia University, Helen Hayes Hospital Mary Beth O’Connell, PharmD, BCPS Eugene Applebaum College of Pharmacy and Health Sciences Rick Pope, MPAS, PA-C, DFAAPA Quinnipiac University Carol Sedlak, PhD, RN, CNS, ONC, CNE Kent State University College of Nursing Andrea Sikon, MD, FACP, CCD, NCMP Cleveland Clinic NOF Clincal Director, Andrea Singer, MD Georgetown University Medical School Guest Reviewer Taylor Wallace, PhD, Senior Director, Science Policy and Government Relations, National Osteoporosis Foundation Managing Editor, Kelly Trippe, MA National Osteoporosis Foundation Nurse CE Planner, Susan Randall, MSN National Osteoporosis Foundation Disclaimer: Osteoporosis: Clinical Updates is published by the National Osteoporosis Foundation (NOF).The views and observations presented in Osteoporosis: Clinical Updates are not those of the authors/editors and do not reflect those of the funders or producers of this publication. Readers are urged to consult current prescribing and clinical practice information on any drug, device, or procedure discussed in this publication. Contents Vitamin D Deficiency in the U.S. . .......................................... 2 e Role of Vitamin D in Bone Health 2 Vitamin D Synthesis and Activation 2 Factors that Affect Vitamin D Levels ....................................... 3 Sunlight Exposure 3 Dietary Intake 4 Absorption and Conversion Factors 4 Role of Vitamin D in Prevention of Falls and Fractures ....................... 6 How Much Vitamin D Is Needed and How to Get It 7 Current Daily Recommended Intakes for Vitamin D 7 Current RDAs & AIs for Vitamin D 8 Assessing Vitamin D Status 8 How Much Is too Much? 9 Ensuring Vitamin D Sufficiency 10 Nonskeletal Effects of Vitamin D 11 Patient Cases: Clinical Management of Vitamin D Deficiency ................ 11 Case 1: Eighty-Year-Old African American Man with Vertebral Fracture 11 Case 2: 77- Year-Old Caucasian Woman in Nursing Home 12 Summary 13 References 14

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Osteoporosis Clinical Updates
www.nof.org Clinical Information for Healthcare Professionals Spring 2014
Vitamin D anD Bone HealtH
Vitamin D is essential for attainment and maintenance of musculoskeletal health and key to calcium homeostasis and phosphorus balance. Chronic insufficiency leads to skeletal ab-normalities and fragility fracture and is linked to multiple extra-skeletal disorders includ-ing cancer, infection, and cardiovascular disease.
Analysis of nutrient intake, through food and dietary supplements, has shown the majority of American adults fail to meet adequate intake recommendations for vitamin D established by the Institute of Medicine.1,2 Many if not most of the patients seen in the typical primary care practice are vitamin D insufficient or deficient. Knowing who is most likely to be se-verely deficient will help practitioners identify those patients who should have targeted test-ing and therapy.
Once a patient is found to be deficient, clinical management involves supplementation to raise and maintain serum vitamin D at levels necessary to support optimal bone and gener-al health. This issue of “Osteoporosis: Clinical Updates” will discuss the role of vitamin D in skeletal health, its sources, daily requirements, upper safe limits, and potential for building and maintaining strong bones throughout the lifespan.
Editor-in-Chief, Angelo Licata, MD, PhD.
National Osteoporosis Foundation
1150 17th Street, NW • Washington, DC 20036 • 202/223-2226 • www.nof.org
© National Osteoporosis Foundation. All rights reserved
EDITORIAL BOARDEditor-in-Chief, Angelo Licata, MD, PhDDepartment of EndocrinologyCleveland ClinicAdrienne Berarducci, PhD, ARNP, BCUniversity of South Florida Carolyn J. Bolognese, RN, CDEBethesda Health Research CenterJoAnn Caudill, RT, BD, CDTCarroll Arthritis, P.A.Peggy Doheny, PhD, RN, CNS, ONCKent State University College of NursingPatricia Graham, MD, PCPhysical Medicine and Rehabilitation /Integrative MedicineCraig Langman, MDNorthwestern UniversityBarbara Messinger-Rapport, MD, PhDCleveland ClinicPaul D. Miller, MDColorado Center for Bone ResearchJeri Nieves, PhD Columbia University, Helen Hayes HospitalMary Beth O’Connell, PharmD, BCPSEugene Applebaum College of Pharmacy and Health SciencesRick Pope, MPAS, PA-C, DFAAPAQuinnipiac UniversityCarol Sedlak, PhD, RN, CNS, ONC, CNEKent State University College of NursingAndrea Sikon, MD, FACP, CCD, NCMPCleveland ClinicNOF Clincal Director, Andrea Singer, MDGeorgetown University Medical SchoolGuest ReviewerTaylor Wallace, PhD, Senior Director, Science Policy and Government Relations, National Osteoporosis FoundationManaging Editor, Kelly Trippe, MANational Osteoporosis FoundationNurse CE Planner, Susan Randall, MSN National Osteoporosis FoundationDisclaimer: Osteoporosis: Clinical Updates is published by the National Osteoporosis Foundation (NOF).The views and observations presented in Osteoporosis: Clinical Updates are not those of the authors/editors and do not reflect those of the funders or producers of this publication. Readers are urged to consult current prescribing and clinical practice information on any drug, device, or procedure discussed in this publication.
ContentsVitamin D Deficiency in the U.S. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
The Role of Vitamin D in Bone Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Vitamin D Synthesis and Activation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
Factors that Affect Vitamin D Levels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Sunlight Exposure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Dietary Intake . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4Absorption and Conversion Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Role of Vitamin D in Prevention of Falls and Fractures . . . . . . . . . . . . . . . . . . . . . . . 6How Much Vitamin D Is Needed and How to Get It . . . . . . . . . . . . . . . . . . . . . . . . . . . .7Current Daily Recommended Intakes for Vitamin D . . . . . . . . . . . . . . . . . . . . . . . . . . .7Current RDAs & AIs for Vitamin D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8Assessing Vitamin D Status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8How Much Is too Much? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9Ensuring Vitamin D Sufficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10Nonskeletal Effects of Vitamin D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
Patient Cases: Clinical Management of Vitamin D Deficiency . . . . . . . . . . . . . . . . 11Case 1: Eighty-Year-Old African American Man with Vertebral Fracture . . . . . . . . .11Case 2: 77- Year-Old Caucasian Woman in Nursing Home . . . . . . . . . . . . . . . . . . . . .12Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14

2
Vitamin D Deficiency in the U.S.Over the past decade, researchers and experts in the field have warned of a “silent epidemic” of vitamin D deficiency in the United States, citing prevalence data from the National Health and Nutrition Examination Survey (NHANES), which showed an increased preva-lence from 50% to 75% between 1988 and 2004.3 And yet, in 2010 the Institute of Medicine (IOM) reported that rather than an epidemic, vitamin D deficiency is not a problem for the majority of Americans. Authors writing for the National Center for Health Statistics (NCHS) supported this view, reporting that 67% of the U.S. population has sufficient serum vitamin D, about 25% is at risk of vitamin D inadequacy, and 8% is at risk of vitamin D deficiency.4
So, is vitamin D deficiency an epidemic or not? Put simply, it depends on how you define your terms: spe-cifically, what blood level constitutes vitamin D insuf-ficiency in an otherwise healthy population. IOM and NCHS conclusions rest on defining insufficiency as 25-hydroxyvitamin D (25[OH]D) blood levels below 20 ng/mL (<50 nmol/L), the level traditionally be-lieved adequate to protect bone health. However, due to increasing evidence that higher levels are needed to achieve skeletal and other health benefits, specialty so-cieties such as the Endocrine Society and the National Osteoporosis Foundation define insufficiency as 25(OH)D at or above 30 ng/mL (<75 nmol/L). This may seem like a small difference, but it has major pub-lic health ramifications, raising issues in primary care related to screening, treatment, and monitoring.
All sides of the debate agree that in certain populations, vitamin D insufficiency and deficiency are widespread.
Identifying patients at risk requires recognizing the factors that influence vitamin D synthesis, intake, and metabolism.
The Role of Vitamin D in Bone Health
Vitamin D is one of several fat-soluble steroids whose metabolization facilitates absorption and regulation of minerals such as calcium and phosphorus. There are two forms of vitamin D: D2 and D3. The vitamin D2 form (ergocalciferol) is found in small amounts in cer-tain plants and made commercially by UV irradiation of yeast. The more potent form, Vitamin D3 (chole-calciferol), is synthesized in the skin of vertebrates in response to exposure to UVB radiation either from the sun or from a synthetic light source. Vitamin D3 is the form commonly used in supplements and fortified foods. Vitamin D3 is available from animal foods such as fatty fish, egg yolks, and liver. It is produced com-mercially from cholesterol extracted from sheep wool that is exposed to UVB radiation.
Vitamin D Synthesis and Activation
Both vitamin D2 and D3 are biologically inactive, whether obtained through cutaneous UVB exposure, diet, or supplements. They go through a two-step pro-cess of hydroxylation, first in the liver, where the par-ent compound D is converted to 25-hydroxyvitamin D (25[OH]D), known as calcidiol, and second in the kidney, where it becomes the biologically active form 1,25 dihydroxyvitamin D (1,25[OH]2D), or calcitriol, which is involved in bone metabolism and absorption of dietary calcium, phosphorus and other minerals.
In the body, activated vitamin D regulates absorption of calcium from the gastrointestinal system and mobiliza-tion of calcium from bone. The activation of 25 OH vitamin D to 1,25(OH)2 vitamin D is stimulated by serum parathyroid (PTH) and low phosphorus. PTH is regulated by serum calcium and by the protein hor-mone FGF23, which is produced by bone.
Adequate calcium absorption depends on adequate lev-els of 25(OH)D being converted into activated 1,25 dihydroxyvitamin D. In a setting of optimal serum vita-min D, absorption of dietary calcium is approximately 30% to 40 percent.3 As vitamin D status declines, ab-sorption of dietary calcium declines to about 10% to 15 percent.3 Maximum absorption of dietary calcium
Activity Objectives
3
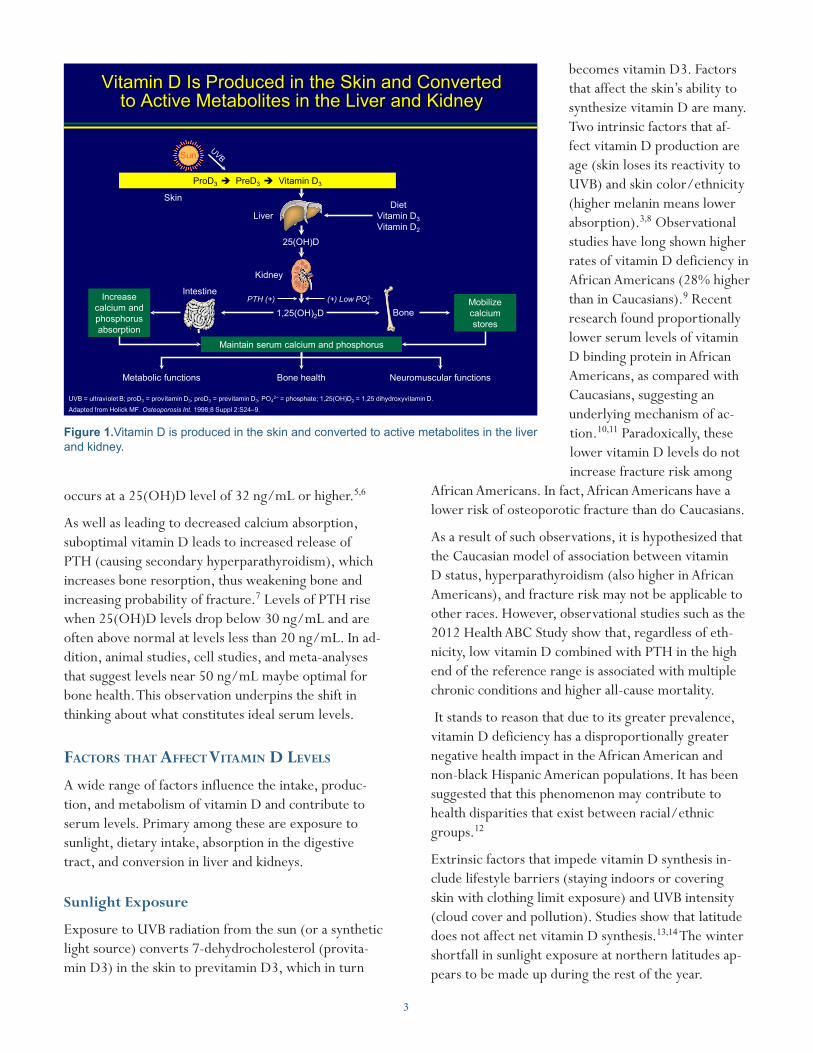
Vitamin D Is Produced in the Skin and Converted to Active Metabolites in the Liver and Kidney
Adapted from Holick MF. Osteoporosis Int. 1998;8 Suppl 2:S24–9.
Skin
Liver
Kidney
DietVitamin D3Vitamin D2
Intestine
Bone
ProD3 è PreD3 è Vitamin D3
25(OH)D
1,25(OH)2DPTH (+)
Sun
(+) Low PO2–4
Increase calcium and phosphorus absorption
Mobilize calcium stores
Maintain serum calcium and phosphorus
Metabolic functions Bone health Neuromuscular functions
UVB = ultraviolet B; proD3 = provitamin D3; preD3 = previtamin D3; PO42– = phosphate; 1,25(OH)D2 = 1,25 dihydroxyvitamin D.
occurs at a 25(OH)D level of 32 ng/mL or higher.5,6
As well as leading to decreased calcium absorption, suboptimal vitamin D leads to increased release of PTH (causing secondary hyperparathyroidism), which increases bone resorption, thus weakening bone and increasing probability of fracture.7 Levels of PTH rise when 25(OH)D levels drop below 30 ng/mL and are often above normal at levels less than 20 ng/mL. In ad-dition, animal studies, cell studies, and meta-analyses that suggest levels near 50 ng/mL maybe optimal for bone health. This observation underpins the shift in thinking about what constitutes ideal serum levels.
factorS that affect Vitamin D LeVeLS
A wide range of factors influence the intake, produc-tion, and metabolism of vitamin D and contribute to serum levels. Primary among these are exposure to sunlight, dietary intake, absorption in the digestive tract, and conversion in liver and kidneys.
Sunlight Exposure
Exposure to UVB radiation from the sun (or a synthetic light source) converts 7-dehydrocholesterol (provita-min D3) in the skin to previtamin D3, which in turn
becomes vitamin D3. Factors that affect the skin’s ability to synthesize vitamin D are many. Two intrinsic factors that af-fect vitamin D production are age (skin loses its reactivity to UVB) and skin color/ethnicity (higher melanin means lower absorption).3,8 Observational studies have long shown higher rates of vitamin D deficiency in African Americans (28% higher than in Caucasians).9 Recent research found proportionally lower serum levels of vitamin D binding protein in African Americans, as compared with Caucasians, suggesting an underlying mechanism of ac-tion.10,11 Paradoxically, these lower vitamin D levels do not increase fracture risk among
African Americans. In fact, African Americans have a lower risk of osteoporotic fracture than do Caucasians.
As a result of such observations, it is hypothesized that the Caucasian model of association between vitamin D status, hyperparathyroidism (also higher in African Americans), and fracture risk may not be applicable to other races. However, observational studies such as the 2012 Health ABC Study show that, regardless of eth-nicity, low vitamin D combined with PTH in the high end of the reference range is associated with multiple chronic conditions and higher all-cause mortality.
It stands to reason that due to its greater prevalence, vitamin D deficiency has a disproportionally greater negative health impact in the African American and non-black Hispanic American populations. It has been suggested that this phenomenon may contribute to health disparities that exist between racial/ethnic groups.12
Extrinsic factors that impede vitamin D synthesis in-clude lifestyle barriers (staying indoors or covering skin with clothing limit exposure) and UVB intensity (cloud cover and pollution). Studies show that latitude does not affect net vitamin D synthesis.13,14 The winter shortfall in sunlight exposure at northern latitudes ap-pears to be made up during the rest of the year.
Figure 1.Vitamin D is produced in the skin and converted to active metabolites in the liver and kidney.

4
not possible for most people. The better sources include fatty fish (herring, mackerel, catfish, salmon), fish liver oil, and to a lesser degree cheese, egg yolks, and beef liver. Mushrooms and lichen are the only known non-animal sources of vitamin D. Vitamin D available from mushrooms varies widely – from 3 IUs per 84-gram serving in raw crimini mushrooms to 943 IUs in raw maitake mushrooms. Exposure to UV light increases mush-room vitamin D content. The increase can be substantial. For example, unexposed portabella mushrooms contain approxi-mately 12 IUs per cup, while portabellas exposed to UVB light contain approximately 493 IUs per serving.20 In addi-
tion to these sources, dairy products, margarine, cere-al, and orange juice are regularly fortified with vitamin D in concentrations displayed on their packaging.
A listing of the vitamin D content of common foods is shown at the bottom of page 5. As is evident in this list, few foods contain high concentrations of vitamin D. Many people overestimate the amount of vitamin D in foods generally and even in fortified foods such as milk and breakfast cereal.
A diet chronically low in vitamin D, coupled with inad-equate sunlight exposure, over time can lead to vitamin D deficiency. Unless they get ample sun exposure, people with diets that restrict their intake of vitamin D rich foods, such as those with dairy allergies, lactose intolerance, or ovo-vegetarian and vegan diets, are at increased risk of vitamin D deficiency.
Absorption and Conversion Factors
Even with sufficient dietary intake, patients who have conditions that compromise the absorption or conver-sion of vitamin D may not benefit from the vitamin D in the foods they eat. Conditions such as cystic fibrosis, Crohn disease, or colitis can cause malabsorption of vitamin D and other nutrients in the digestive tract,
Vitamin D Intake Did Not Reach 400 IU/day for Women 50 Years and Older, Even With Supplementation
1. Calvo MS et al. Am J Clin Nutr. 2004;80(suppl):1710S–1716S.2. National Osteoporosis Foundation. National Osteoporosis Foundation’s Updated Recommendations for Calcium and Vitamin D3 Intake.
Available at: http://www.nof.org/prevention/calcium_and_VitmaminD.htm. Accessed April 24, 2007.3. Institute of Medicine of the National Academies. Dietary reference intakes (DRIs): recommended intakes for individuals.
Available at: http://www.iom.edu/?id=21381. Accessed April 24, 2007.
NHANES = National Health and Nutrition Examination Survey.
NHANES III Population1
187.2153.6 156.4
334.8
237.6 238.0
0
100
200
300
400
500
600
700
800
900
1000
Estim
ated
Mea
n Vi
tam
in D
In
take
, IU
/day
NOF recommended intake of vitamin D for individuals 50 years and older is 800 to 1000 IU/day2
Food only
Food + supplements
White African American
Mexican American
IOM recommended intake of vitamin D for individuals 51 to 70 years of age is 400 IU/day3
However, measurement of serum vitamin D levels of people living in northern regions such as Canada and Scandinavia show declines in vitamin D sufficiency dur-ing the winter and spring, which could result in miner-alization issues and other negative health effects during these periods.15
Theoretically, properly applied and replenished sun-screen would significantly reduce the skin’s exposure to UVB rays. However, research indicates that in practice most people don’t use enough sunscreen or reapply it often enough to completely block their exposure to UVB and production of vitamin D.16,17 A more likely culprit is the increasingly indoor lifestyle of Americans, who spend less time outdoors than at any time in the past.
Estimates for adequate UVB exposure range from 5 to 30 minutes of sunlight twice a week on the bare face, arms, legs, or back. Commercial tanning beds with an emission of 2% to 6% UVB used in moderation are roughly equivalent.18,19
Dietary Intake
As discussed earlier, dietary sources of vitamin D are limited. Getting enough vitamin D from diet alone is
Figure 2. In the NHANES III Population study, vitamin D Intake did not reach 400 IU/day for women 50 years and older, even with supplementation.
5
while kidney and liver disorders can disrupt the con-version of vitamin D into its active form.
Evidence regarding the effects of gastric bypass surgery on vitamin D absorption are inconclusive to date, with some data suggesting increase and some indicating at-tenuation in vitamin D levels following surgery.21,22,23 Because vitamin D is fat soluble, it is stored in subcu-taneous fat. As a result, body mass index (BMI) 30 or over is associated with lower serum 25(OH)D than BMI in the healthy range. In obese individuals, more vi-tamin D is sequestered in fat and less released into the bloodstream. Such individuals may need higher intake levels to compensate.24
Many medications and over-the-counter remedies can adversely interact with vitamin D. Some medications can interfere with vitamin D absorption and/or metab-olism. Others can have their absorption and/or effects intensified by combination with vitamin D. Potential interactions to be aware of include:• Most anticonvulsants, such as carbamazepine
(Tegretol®), phenobarbital (Luminal®), and phe-nytoin (Dilantin®), and gabapentin (Neurontin®) can cause reduced serum 25(OH)D and calcium absorption.25,26,27
• Antiretrovirals agents ritonavir (Norvir®), efavirenz (Sustiva® and Atripla®), and valproic acid (e.g. Depakene®) are associated with reduced 25(OH)D
levels.28
• Certain calcium channel blockers (brand names: Bosoptin®, Calan®, Covera-HS®, Isoptin®, Verapamil®, and Verelan®) may not be effective when taken with vitamin D.29
• Cimetidine: (brand names: Tagamet® and Tagamet HB®) cause disruption of vitamin D metabolism.30
• Cholesterol-lowering agent cholestyramine (brand names Questran®, LoCholest®, Prevalite®) can reduce absorption of vitamin D.31
• Digoxin (Lanoxin®), Digitalis (Crystodigin®) taken with vitamin D may increase effects of digoxin, caus-ing cardiac irregularities.32
• Oral corticosteroids/glucocorticoids (brand names include Aristocort®, Methylprednisolone®, Orasone®) impair vitamin D metabolism.33,34,35
• Psoriasis treatments calcipotriol/calcipotriene (brand names: Dovonex®/ Daivonex®), syn-thetic forms of vitamin D, suppress PTH and 1,25 dihydroxyvitamin D3 and increase absorption of calcium.36
• Statin drugs to lower cholesterol can increase serum vitamin D levels.37
• Weight loss drug orlistat (brand names Xenical® and Alli™) and food additive olestra (brand name and Olean®) have been shown to reduce absorption of vitamin D.38
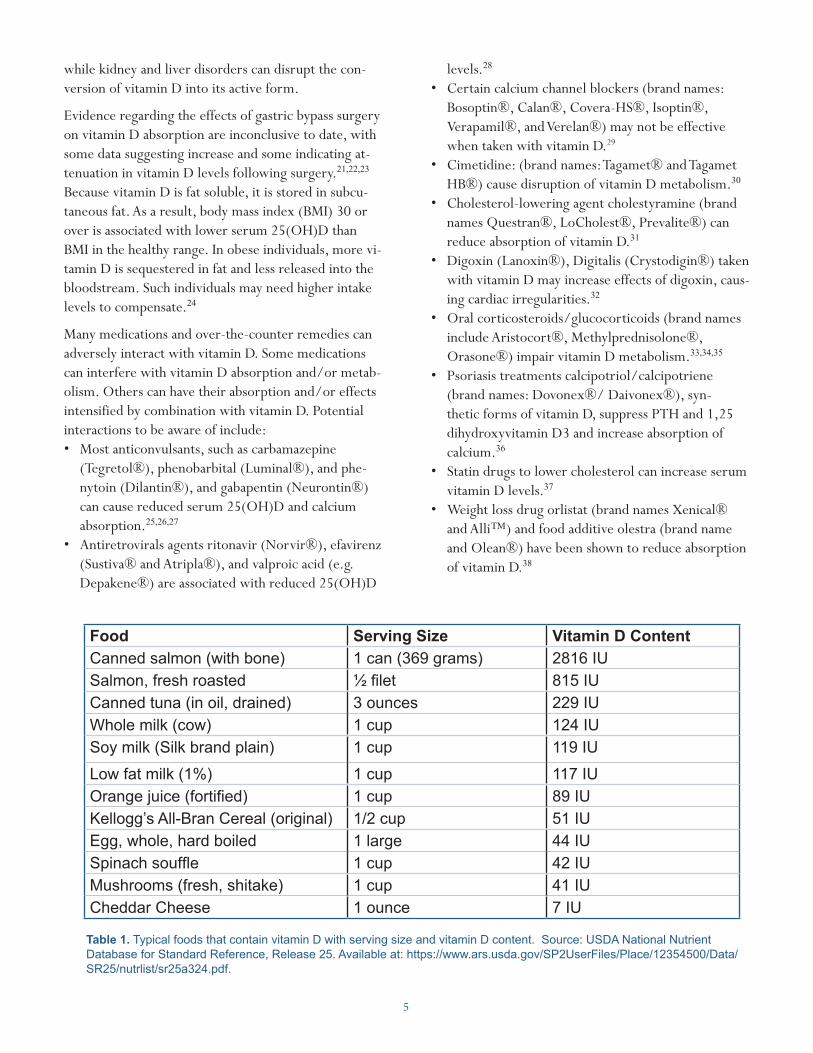
Food Serving Size Vitamin D ContentCanned salmon (with bone) 1 can (369 grams) 2816 IUSalmon, fresh roasted ½ filet 815 IUCanned tuna (in oil, drained) 3 ounces 229 IUWhole milk (cow) 1 cup 124 IUSoy milk (Silk brand plain) 1 cup 119 IU
Low fat milk (1%) 1 cup 117 IUOrange juice (fortified) 1 cup 89 IUKellogg’s All-Bran Cereal (original) 1/2 cup 51 IUEgg, whole, hard boiled 1 large 44 IUSpinach souffle 1 cup 42 IUMushrooms (fresh, shitake) 1 cup 41 IUCheddar Cheese 1 ounce 7 IU
Table 1. Typical foods that contain vitamin D with serving size and vitamin D content. Source: USDA National Nutrient Database for Standard Reference, Release 25. Available at: https://www.ars.usda.gov/SP2UserFiles/Place/12354500/Data/SR25/nutrlist/sr25a324.pdf.

6
Table 2. Individuals at Risk for Vitamin D Deficiency• Infantsfedonlybreastmilk• Homeboundandinstitutionalizedindividualsand
otherswithrestrictedsunexposure• Peoplewithdarkskin(e.g.,peopleofAfrican,
MiddleEastern,NativeAmerican,Hispanic,orSouthAsiandescent)
• Peoplewithconditionsthatcausefatmalabsorption,suchasCrohnsdisease,colitis,inflammatoryboweldisease,andcysticfibrosis
• Peoplewithliverorkidneydisease,includingkidneytransplant
• Peoplewhohaveundergonegastricbypass(conflictingresearch)
• Olderadults(overage60)• Obeseindividuals(BMI≥30)• Peoplewithdietaryrestrictions,suchasvegan,
milk-allergic,ovo-vegetarian,andlactose-intolerantindividuals
Osteoporosis: Clinical Updates
Osteoporosis Clinical Updates is a publication of the National Osteoporosis Foundation (NOF). Use and reproduction of this publication for educational purposes is permitted and encouraged without permission, with proper citation. This publication may not be used for commercial gain. NOF is a non-profit, 501(c)(3) educational organization. Suggested citation: National Osteoporosis Foundation. Osteoporosis Clinical Updates. Issue Title. Washington, DC; Year.
Please direct all inquiries to: National Osteoporosis Foundation 1150 17th Street NW Washington, DC 20037, USA Phone: 1 (202) 223-2226Fax: 1 (202) 223-1726 www.nof.org
Statement of Educational PurposeOsteoporosis Clinical Updates is published to improve osteoporosis patient care by providing clinicians with state-of-the-art information and pragmatic strategies on prevention, diagnosis, and treatment that they may apply in clinical practice.
Overall Objectives Despite the availability of effective prevention, diagnostic, and treatment protocols for osteoporosis, research indicates that it is significantly underdiagnosed and undertreated in the general population. Through this publication, NOF encourages participants to incorporate current evidence and expert recommendations into clinical practice to improve the bone health of their patients. Upon completion of each issue of Osteoporosis Clinical Updates, participants should be able to:• Recognize current concepts in osteoporosis research and
clinical practice • Identify implications of these concepts for osteoporosis
patient care• Adopt evidence-based strategies to study, prevent, and/
or treat osteoporosis• Improve patient care practices by integrating new data
and/or techniques
Intended AudienceThis continuing education activity is intended for health professionals who care for patients at risk for or suffering from osteoporosis practicing in primary care, endocrinology, geriatrics, gynecology, internal medicine, obstetrics, orthopedics, osteopathy, pediatrics, physiatry, radiology, rheumatology, and/or physical therapy.
This includes physicians, nurse practitioners, registered nurses, pharmacists, physician assistants, technologists, researchers, public health professionals and health educators with an interest in osteoporosis and bone health.
Before prescribing vitamin D supplementation, a care-ful medication review is necessary to avoid potentially harmful interactions.
roLe of Vitamin D in PreVention of faLLS anD fractUreS
Vitamin D protects the bones of older individuals through two mechanisms: maintaining bone mineral density (BMD) and preventing falls.39,40 It is well es-tablished that vitamin D sufficiency is required to absorb calcium and maintain bone density. Less well understood is the process by which vitamin D benefits muscle strength and function.
Possible mechanisms for this effect have been illumi-nated in recent animal research isolating vitamin D re-ceptors in specialized fast-twitch muscle fibers that are activated when a person starts to fall. In healthy young people, these muscles make it possible to catch oneself before losing one’s balance. Age weakens these muscle fibers, as does insufficient vitamin D. Animal studies have demonstrated vitamin D repletion to thicken and strengthen these specific fibers.
It is speculated that in humans this translates into fewer falls, fewer fractures, and lower rates of all-cause mor-tality.41,42 Recent data from a large population-based prospective observational study of elderly community-dwelling men showed a U-shaped association between
7
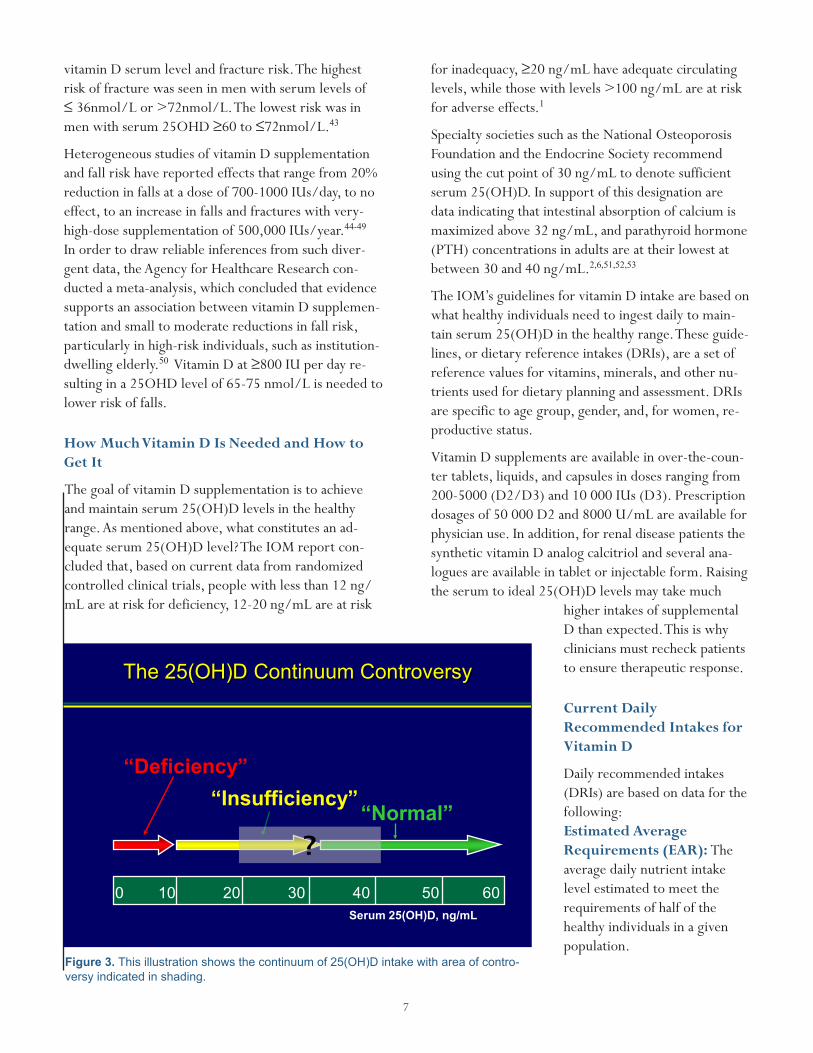
forinadequacy,≥20ng/mLhaveadequatecirculatinglevels, while those with levels >100 ng/mL are at risk for adverse effects.1
Specialty societies such as the National Osteoporosis Foundation and the Endocrine Society recommend using the cut point of 30 ng/mL to denote sufficient serum 25(OH)D. In support of this designation are data indicating that intestinal absorption of calcium is maximized above 32 ng/mL, and parathyroid hormone (PTH) concentrations in adults are at their lowest at between 30 and 40 ng/mL.2,6,51,52,53
The IOM’s guidelines for vitamin D intake are based on what healthy individuals need to ingest daily to main-tain serum 25(OH)D in the healthy range. These guide-lines, or dietary reference intakes (DRIs), are a set of reference values for vitamins, minerals, and other nu-trients used for dietary planning and assessment. DRIs are specific to age group, gender, and, for women, re-productive status.
Vitamin D supplements are available in over-the-coun-ter tablets, liquids, and capsules in doses ranging from 200-5000 (D2/D3) and 10 000 IUs (D3). Prescription dosages of 50 000 D2 and 8000 U/mL are available for physician use. In addition, for renal disease patients the synthetic vitamin D analog calcitriol and several ana-logues are available in tablet or injectable form. Raising the serum to ideal 25(OH)D levels may take much
higher intakes of supplemental D than expected. This is why clinicians must recheck patients to ensure therapeutic response.
Current Daily Recommended Intakes for Vitamin D
Daily recommended intakes (DRIs) are based on data for the following:Estimated Average Requirements (EAR): The average daily nutrient intake level estimated to meet the requirements of half of the healthy individuals in a given population.
vitamin D serum level and fracture risk. The highest risk of fracture was seen in men with serum levels of ≤36nmol/Lor>72nmol/L.Thelowestriskwasinmenwithserum25OHD≥60to≤72nmol/L.43
Heterogeneous studies of vitamin D supplementation and fall risk have reported effects that range from 20% reduction in falls at a dose of 700-1000 IUs/day, to no effect, to an increase in falls and fractures with very-high-dose supplementation of 500,000 IUs/year.44-49 In order to draw reliable inferences from such diver-gent data, the Agency for Healthcare Research con-ducted a meta-analysis, which concluded that evidence supports an association between vitamin D supplemen-tation and small to moderate reductions in fall risk, particularly in high-risk individuals, such as institution-dwelling elderly.50VitaminDat≥800IUperdayre-sulting in a 25OHD level of 65-75 nmol/L is needed to lower risk of falls.
How Much Vitamin D Is Needed and How to Get It
The goal of vitamin D supplementation is to achieve and maintain serum 25(OH)D levels in the healthy range. As mentioned above, what constitutes an ad-equate serum 25(OH)D level? The IOM report con-cluded that, based on current data from randomized controlled clinical trials, people with less than 12 ng/mL are at risk for deficiency, 12-20 ng/mL are at risk
Figure 3. This illustration shows the continuum of 25(OH)D intake with area of contro-versy indicated in shading.
0 10 20 30 40 50 60Serum 25(OH)D, ng/mL
The 25(OH)D Continuum Controversy
“Deficiency”“Insufficiency”
“Normal”?
Adapted from Heaney RP. Am J Clin Nutr. 2004;80(suppl):1706S-1709S. Reproduced with permission from The American Journal of Clinical Nutrition.

8
vitamin D deficiency would be suspected if laboratory findings showed normal serum calcium and normal to low phosphorus with high-normal to elevated levels of PTH and alkaline phosphatase.
Severe vitamin D deficiency obstructs calcium miner-alization in bone, causing osteomalacia (called rickets in children). Resulting bone is soft and prone to defor-mity and fracture. A red flag for osteomalacia is chronic musculoskeletal pain of unknown etiology. Studies have found very high prevalence of severe vitamin D defi-ciency in patients suffering from persistent nonspecific bone and muscle pain, headache, and fatigue. The ef-fect was seen in all ages and ethnicities, affecting men and women alike. Prevalence was most pronounced in African American, East African, Middle Eastern, South Asian, Hispanic, and American Indian patients with diffuse nonspecific pain, of whom 80% to 100% had levels at or below 20 ng/mL.54,55,56 D-deficient osteo-malacia resolves with vitamin D repletion.
Approximating a patient’s vitamin D status from their reported dietary and supplement intake can yield un-reliable results. Such estimates are confounded by sun exposure or lack thereof, absorption irregularities, vitamin D sequestration in body fat (in obese patients),
Recommended Dietary Allowances (RDA): The daily dietary intake level of a nutrient considered suf-ficient by the IOM Food and Nutrition Board to meet the requirements of nearly all (97–98%) healthy indi-viduals in each life-stage and gender group. Based on EARand≈20%higherthanEAR.
Adequate Intake (AI). Where not enough evi-dence exists to establish an RDA, an estimate of the amount sufficient to ensure health in a given healthy population.
Tolerable upper intake levels (UL): The highest level of consumption that current data have shown to be safe.
In its 2010 report, the IOM revised its recommenda-tions for vitamin D based on new research. The new recommendation for daily intake of vitamin D tripled the value previously considered adequate for children and adults from 200 IU to 600 IU/day, still considered too low by many experts.8
Current RDAs & AIs for Vitamin D
The following RDAs were established for children, teenagers, and adults by the recent IOM report: • Children 1-13 years: 15 micrograms (600 IU)/day• Teenagers 14-18 years: 15 micrograms (600 IU)/day• Adults 19-70 years: 15 micrograms (600 IU)/day• Adults above 70 years: 20 micrograms (800 IU)/day• Pregnant and lactating women: 15 micrograms (600
IU)/day• The following AIs were established for infants (RDAs
have not been developed for children under 1 year):• Infants 0-6 months: 10 micrograms (400 IU)/day• Infants 6-12 months: 10 micrograms (400 IU)/day
These recommendations may be adjusted upwards if research supports benefit and safety of higher doses.
Assessing Vitamin D Status
It is reasonable to assume that most if not all patients in an average primary care setting have less than optimal serum vitamin D and would benefit from supplementa-tion at recommended doses. Many patients, however, will be severely deficient and in need of more intensive intervention. These patients can be initially identi-fied on the basis of predictable patterns of routine biochemical indices associated with severe deficiency. For example, in a person with normal liver function,
Osteomalaciaandosteoporosishaveoverlappingclinicalindices.WithoutaccuratemeasurementofserumvitaminD,practitionerscaneasilymistakeosteomalaciaforosteoporosis.BothpresentwithlowBMDonDXAandfragilityfractures.However,theyaredifferentdisorderswithdifferenttreatments.
Osteomalaciaiscausedbypoordepositionofcalciuminbonematrices,leadingtosoft,fragilebones.Treatmentwithantiresorptivesintendedforosteoporosisamplifythispathologicalprocessbyslowingtheremodelingprocess.Antiresorptivesshouldneverbeusedinapatientwithosteomalacia.
Manypatientshavebothosteomalaciaandosteoporosis.Osteomalaciamustbecorrectedbeforeinitiationofosteoporosistherapy.OsteomalaciaiscorrectablewithvitaminDsupplementation(andcalciumifneeded),ofteninamatterofmonths.OnceserumvitaminDreachesoptimallevels,assessmentofBMDcanberepeated.OsteoporosismayneedtreatmentwiththeusualdrugsinthosewithdiagnosticT-scores,FRAXscores,and/orotherriskfactors.
Be Sure to Treat the Right Disease

9
and other factors. As a result, serum vitamin D mea-surement provides a more accurate picture of a given patient’s vitamin D status.
Serum vitamin D levels are assessed by measuring cir-culating calcidiol, 25(OH)D. Calcidiol is preferred over calcitriol because of its relatively long and stable con-centration in the blood. Calcitriol has a much shorter half-life than calcidiol (15 hours vs. 15 days) and is closely regulated by calcium, phosphorus, and para-thyroid hormone. Assays for measurement of serum calcidiol have been criticized by the IOM and others for lack of consistency and standardization. This has led many specialists to err on the side of caution and assume a slightly higher acceptable serum vitamin D levels.
How Much Is too Much?
The upper limit set by the Institute of Medicine’s Food and Nutrition Board is 4,000 IU/day. However, evi-dence supports the view of many experts that this level is too conservative and that higher doses can be safe and beneficial. It is instructive that the IOM set the “No Observed Adverse Effects Level,” or NOAE, at 10,000 IU/day, this being the dose at which there are no pub-lished studies showing any adverse effects.
Because increased vitamin D leads to higher serum cal-cium levels, it was once thought that prolonged expo-sure to doses over safe limits could lead to vascular and tissue calcification with damage to heart, vessels, and kidneys. Clinical trial data from multiple investigations into this question contradict this hypothesis, demon-strating calcium levels do not significantly increase in response to increases in vitamin D intake up to about the level of 10,000 IUs/day.57
While intakes of 700 to 800 IU per day lower fall risk by an average of 15% to 20%, higher vitamin D intake are associated with higher fall risk. Data from a large randomized trial of elderly women (aged >70) on high-dose vitamin D (500,000 units given in a single annual dose) showed increased risk of both falls and fractures.58
Chronic megadose supplementation (such as >50,000 IU/day) over an extended period has been demonstrat-ed to cause can lead to hypercalciuremia and hypercal-cemia, which can have life-threatening consequences. Symptoms of acute vitamin D toxicity range from mild (headaches, weight loss, increased urination) to severe
CME Program Eligibility Method of Participation in the Learning Process: Clinician learners will read and analyze the subject matter, conduct additional informal research through related internet searches on the subject matter, and complete a post-test assessment of knowledge and skills gained as a result of the activity.
After participating in this activity, the reader has the option of taking a post-test with a passing grade of 70% or better to qualify for continuing education credit for this activity. It is estimated it will take 1.0 hour(s) to complete the reading and take the post-test. Continuing education credit will be available for two years from the date of publication.
Accreditation The National Osteoporosis Foundation is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The National Osteoporosis Foundation designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)TM. Physicians should only claim credit commensurate with the extent of their participation in the activity.
The National Osteoporosis Foundation is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
The National Osteoporosis Foundation designates this educational activity for a maximum of 1.0 continuing nursing education credit(s).
Other healthcare providers will also be able to receive a certificate of completion; nurse practitioners and physician assistants may request an AMA PRA Category 1 Credit(s)™ certificate of participation.
Disclosure of Commercial SupportIt is the policy of the National Osteoporosis Foundation
(NOF) to ensure balance, independence, objectivity, and scientific rigor in all its sponsored publications and programs. NOF requires the disclosure of the existence of any significant financial interest or any other relationship the sponsor, editorial board, or guest contributors have with the manufacturer(s) of any commercial product(s) discussed in an educational presentation. All authors and contributors to this continuing education activity have disclosed any real or apparent interest that may have direct bearing on the subject matter of this program. NOF’s accreditation status with ACCME and ANCC does not imply endorsement by NOF, ACCME or ANCC of any commercial products displayed in conjunction with this activity or endorsement of any point of view.
Statement Regarding Off-Label Use Any publication of the Osteoporosis Clinical Updates that discusses off-label use of any medications or devices will be disclosed to the participant.

10
(kidney stones, cardiac arrhythmia).
Consistent blood levels of >200 ng/mL are considered toxic and potentially dangerous.59 Fortunately the body regulates conversion of 25(OH)D to 1,25(OH)2D, its potent biologically active form. This is why reports of vitamin D toxicity are so rare. Clinicians can be reas-sured that doses well over the current IOM recommen-dations are safe for most patients.
IOM 2010 Daily Vitamin D Tolerable Upper Intake Level • 0-6 months: 1000 IU (25 mcg)• 7-12 months: 1500 IU (38 mcg)• 1-3 years: 2500 IU (63 mcg)• 4-8 years: 3000 IU (75 mcg)• ≥9years,4000IU(100mcg)
These tolerable upper limits are meant as conservative guidelines. The level of 25(OH)D absorbed and circu-lated in the blood is what determines toxicity in a given individual.
Ensuring Vitamin D Sufficiency
How can a clinician determine the appropriate dose for a patient who is vitamin D deficient? IOM recommen-dations are based on what it takes to maintain adequate 25(OH)D levels in a population of healthy people.
In the elderly, infirm, or chronically ill, these recom-mendations may not apply. In these patients, vitamin D supplementation must be overseen on a case-by-case basis to ensure that healthy serum levels are reached and held steady over the long term. This means ex-perimenting with dosage and following up with serum measurement at regular intervals.
It may be difficult to estimate the dose that will be most effective for a specific patient. Serum response to supplementation is nonlinear, with greater propor-tional impact at low serum levels than at high. In other words, it takes a higher dose to raise circulating levels in a D-replete patient than in a D-deficient patient.
Data from NHANES III has been used to calculate the daily intake required to ensure that 97.5% of women over age 60 have 25(OH)D values at or above desirable levels (30 ng/mL).Theestimateis≈2600IUsofvita-min D per day. 60,61 This is way above recommended in-take levels, but well below the tolerable UL and could easily be accomplished through oral supplementation.62
Correction of vitamin D deficiency is commonly ac-complished by administering high initial doses for sev-eral weeks or months, followed by a maintenance dose once target levels have been reached. For example, a typical regimen could start with 50,000 IU once
weekly for 2 to 3 weeks. When follow-up testing shows adequa-cy, the dose could be reduced to 50,000 IU monthly or 2,000 daily for maintenance.
Retrospective analysis of multi-ple repletion regimens published by Pepper, et. al., observed that a minimum total dose of 600,000 IU administered over 40 to 60 days was needed to correct vi-tamin D insufficiency (reach 30 ng/mL) in the population of older men studied.63
Because vitamin D is fat soluble, it is best absorbed if eaten with a meal containing fat, ideally the largest meal of the day. Data suggest that this results in about a 50% increase in serum levels
Estimated Additional Vitamin D Intake (Up to 1886 IU/day) Needed to Correct Vitamin D Insufficiency
Weaver CM et al. Am J Clin Nutr. 2004;80(suppl):1735S–1739S [erratum].
25.8
18.8
23.6
0
10
20
30
40
White African American
Mexican American
32 ng/mL of 25(OH)D
Seru
m 2
5(O
H)D
, ng/
mL
Women 60 Years and Older (NHANES III Population) in Winter
886 IU/day
1886 IU/day
1211 IU/day
Additional daily vitamin D needed to achieve 25(OH)Dlevel of 32 ng/mL
NHANES = National Health and Nutrition Examination Survey; 25(OH)D = 25-hydroxyvitamin D.
Figure 4. Estimated additional vitamin D intake (up to 1886 IU/day) needed to correct vitamin D inadequacy.

11
D, history of gall bladder disease (potential fat malab-sorption), and lack of exposure to sunlight. It is likely that the patient is deficient in vitamin D, which may have contributed to low bone density and to his verte-bral fracture.
The patient is referred for bone density measurement by DXA. His spinal T-score is -5.0, and his hip T-score is -3.0.
Does this patient have osteoporosis?At first glance, one might say “Yes.” However, it is not as simple as that. The patient’s T-scores, history of fracture, lack of activity, and diet low in calcium and vitamin D all point to high future fracture risk. But does he have progressive remodeling-related bone loss (osteoporosis) or is his severe vitamin D deficiency re-sponsible for poor mineralization (osteomalacia)?
What can be done to refine his diagnosis?Running a series of lab tests can determine his levels of serum calcium, phosphorus, alkaline phosphatase, vita-min D, PTH, and urinary calcium excretion.
Lab results:• Calcium: 7.9 mg/dL (normal 8.5 –10.9 mg/dL )• Phosphorus: 2.2 mg/dL (normal 2.4 – 4.1 mg/dL)• Bone-specific alkaline phosphatase: 590 U/L (nor-
mal 20–140 IU/L)• Serum 25(OH) D: 10 ng/mL normal (30 – 80 ng/
mL)• Intact PTH: 565 pg/mL (normal 10 – 65 pg/mL)• Urine calcium: 23 mg/d (normal 100 – 300 mg/
day)
What is the diagnosis?Clearly, this patient is at risk for further fractures. His serum calcium is low, and his 25(OH)D and urine calcium are very low. His PTH is quite high. His low phosphorus is consistent with osteomalacia. When coupled with the patient’s low DXA T-score and his-tory of fracture, these lab values are sufficient to make a diagnosis of osteomalacia due to vitamin D deficiency and high fracture risk.
When can a diagnosis of osteoporosis be made?Until the vitamin D deficiency is corrected, we can-not know whether or not he actually has osteoporosis. Whereas osteomalacia is characterized by low bone mineralization as a result of vitamin D deficiency, os-teoporosis is characterized by progressive decline in
of 25(OH)D levels achieved.64 Compliance with daily supplementation is consistently low (about 50%) in reported studies. Simple reminder strategies can help patients stay on track, such as putting a note on the refrigerator door or keeping the vitamin bottle on the dining table.
Nonskeletal Effects of Vitamin D
Multiple large prospective studies have observed extra-skeletal benefits of vitamin D. Correlations have been reported between high intake of vitamin D and lower rates of chronic diseases such as colon, prostate, breast, and several other cancers, multiple sclerosis, rheuma-toid arthritis, and type 1 diabetes.65-70 Because these data came from observational studies, they were not included in the IOM’s analysis of vitamin D benefit, which restricted its analysis to data from placebo-con-trolled randomized clinical trials. Further research is needed to clarify the full spectrum of benefits and risks associated with vitamin D supplementation.
Patient caSeS: cLinicaL management of Vitamin D Deficiency
Case 1: Eighty-Year-Old African American Man with Vertebral Fracture
The first patient we will discuss is an 80-year-old re-tired teacher who has suffered a spinal fracture while golfing. He reports having severe pain in his back de-spite analgesics. A review of his medical history shows adeclineof4˝inheightsinceitwaslastmeasured(3years). The patient has lost about 20 pounds in that same time period. He had gall bladder cancer 25 years ago, underwent chemotherapy, and is currently in remission.
The patient is asked about his diet and activities.He reports having very little outdoor activity since his fracture due to pain. Since that time, he walks very little at home and cannot walk the golf course. He rou-tinely uses a wheelchair to ambulate.
The patient doesn’t have much of an appetite and avoids dairy, fish, and fatty foods because they make him feel queasy.
Is this patient at risk of vitamin D deficiency?Yes. His risk factors include his age, diet low in vitamin

12
bone density due to bone lost to unbalanced bone re-modeling. The treatment for osteomalacia is vitamin D; the treatment for osteoporosis is an antiresorptive or anabolic agent.
What are the options for treatment?First, the patient’s calcium and vitamin D deficiencies need to be corrected. He is prescribed 1200 mg cal-cium and 10,000 IUs vitamin D to be taken daily for 2 months. Next, because primary osteoporosis is rela-tively rare in men, the clinician looks for correctable secondary causes of bone loss.
Are there “red flags” in the patient’s history?Taken together, the patient’s history of weight loss and digestive discomfort strongly suggest the possibility of celiac disease. The patient is tested for celiac disease. Results are positive. The clinician refers him to a nutri-tionist for guidance on gluten-free eating.
What follow up should be done?To ensure that he is reaches optimal serum 25(OH)D and other chemical indices, follow-up blood chemistry should be done after 3 to 4 months.
The patient has bone specific chemistries run. His 25(OH)D is 56 ng/mL, PTH is normal, and serum cal-cium is 9.3 mg/d.
What further interventions should be made at this point?Correction of vitamin D deficiency has been demon-strated to increase bone mass in severely deficient cases such as this. However, it may not be enough to protect against fracture.
How can the clinician determine if the patient is still losing bone?The patient can have biochemical markers of bone turnover measured, such as bone-specific alkaline phos-phatase. Biomarkers above reference values in a setting of replete vitamin D point to elevated bone resorption and continued bone loss.
The patient’s bone specific alkaline phosphatase (BALP) is measured. His BALP level is lower than before vi-tamin D supplementation but is still high at 355 U/L, indicative of osteoporosis.
What are the patient’s therapeutic options to preserve bone and prevent fracture?
There are many FDA-approved medications avail-able for male patients with osteoporosis. Options range from daily oral alendronate to yearly inject-able zoledronic acid and the daily injectable anabolic, teriparatide.
The clinician discusses the options for treatment. The patient decides on yearly infusions of zoledronic acid and schedules his first infusion.
Are there additional measures that can be taken to help this patient avoid fracture?Yes. Falling is a significant risk for this patient due to his low activity level and fragile bones. The vast major-ity of fractures in patients with low bone density occur as the result of falls. Preventing falls means preventing fractures.
The clinician refers the patient to a physical therapist for muscle strengthening and weight-bearing program of exercise. Physical therapy that includes principles of safe movement and exercise to build muscle strength and improve balance will help him avoid falls and ad-ditional vertebral fractures in the course of daily activi-ties. The order for physical therapy includes a request for instruction on fall proofing the home environment. In addition to physical therapy, the patient is referred to an ophthalmologist to address any vision impairment, a known risk factor for falling.
Case 2: 77- Year-Old Caucasian Woman in Nursing Home
The second case we will discuss is a 77-year-old woman who has resided in an assisted living complex for five years since breaking a hip, which was surgically repairedwithnocomplications.Thepatientis5´2˝andweighs 190 pounds. Since her hip fracture, the patient has used a walker. At the time of her fracture, she was prescribed daily oral alendronate for osteoporosis. She reports having discontinued it after a few months due to gastric upset. She has now been referred for bone loss evaluation and potential treatment.
What risk factors does this patient have for vitamin D deficiency?The patient has several risk factors for compromised vitamin D: her age, her lack of sun exposure, and her obesity. She is tested for serum 25(OH)D, serum calcium, and PTH and found to have a low serum cal-cium (6.5 mg/dL) and very low circulating 25(OH)

13
D (8 ng/mL). Her PTH is high at 300 pg/mL and her phosphorus is low normal (2.8 mg/mL). Her spine and hip DXA measurements show T-scores of -3 and -3.5 respectively.
What impact could her 25(OH)D status have on osteoporosis therapy? Optimal vitamin D repletion is necessary to maximize response to antiresorptives in terms of BMD and anti-fracture efficacy. In studies, vitamin D deficient and vitamin D repleted subjects differed significantly for annualized spine and hip BMD changes adjusted for all available confounding factors (type of treatment, age, calcium intake, baseline BMD values, etc.).70
What treatment is recommended?Because the patient is obese, a higher dose of vitamin D will probably be required to raise her deficient circulat-ing 25(OH)D level to the optimal range. The patient is prescribed 50,000 IUs/day vitamin D and 1000 mg calcium (in split dose) for three months.
What follow-up would be recommended?The patient’s labs are rechecked in one month to as-sess her vitamin D and calcium status. If it is normal, she will be started on monthly oral risedronate and her vitamin D supplementation reduced to 2000 IU daily (with 1000 mg calcium).
If she tolerates the risedronate and her labs show im-provement in 25(OH)D (30ng/mL), her regimen will be maintained, with a planned follow-up twice yearly.
Are there any other interventions recommended?The patient is referred to the in-house exercise classes in her assisted living complex. She is encouraged to spend time outdoors and to improve her overall activ-ity level in a supervised setting. She is also referred to the in-house nutritionist for guidance on a healthy diet.
Summary
Vitamin D plays a complex role in calcium homeosta-sis, PTH regulation, and promotion of overall health. Maintenance of serum 25(OH)D levels is critical to skeletal health and is influenced by multiple factors, en-dogenous and exogenous to the individual.
Vitamin D deficiency is widespread in the U.S. The elderly and institutionalized are at particularly high risk for severe deficiency. Resulting low bone density
Support NOF . . . . . . . . . . . . . Join us in the fight against osteoporosis NOF depends on the generosity of individuals who recognize our important work educating the public and health professionals alike on how to prevent, diagnose and treat osteoporosis.
There are many ways to support NOF in its mission to defeat osteoporosis:
Individual GivingYour gift will help us provide better care and support for the most vulnerable – those who have suffered a fracture – and to protect future generations from this debilitating disease
Recurring GiftBy giving a little each month to sustain NOF throughout the year, you can make a big impact in our efforts to start conversations about bone health and family health history in order to elevate osteoporosis to an issue of national concern. Your support will help us reach our goals of better treating and ultimately preventing osteoporosis.
Memorial and Tribute GiftsGive a tribute or memorial gift honoring the memory of friends and loved ones. For all gifts made, NOF will send appropriate notification to the honoree or to the family of the deceased on your behalf and you will receive acknowledgment of your gift either online or through the mail.
Planned GivingNOF offers a variety of planned giving options. Planned giving allows supporters to leave gifts to NOF at death or to invest gifts during their lifetime. Investing during your lifetime allows you to receive the benefits while you are alive and bequest the remaining funds to NOF at the time of your death.
Visit www.nof.org today to make your tax-deductible donation.
The National Osteoporosis Foundation is a qualified 501(c)(3) tax-exempt organization and all donations to the orga-nization are tax deductible.

14
2010;140:817– 22 .2 Wallace TC, Reider C, Fulgoni VL 3rd . Calcium and vitamin D
disparities are related to gender, age, race, household income level, and weight classification but not vegetarian status in the United States: Analysis of the NHANES 2001-2008 data set . J Am Coll Nutr. 2013;32(5):321-30 .
3 Ginde AA, Liu MC, Camargo CA . Demographic Differences and Trends of vitamin D insufficiency in the US population, 1988-2004 . Arch Intern Med. 2009;169(6):626-32 .
4 Looker AC, Johnson CL, Lacher DA, et . al . Vitamin D status: United States, 2001–2006. NCHS data brief, no 59. Hyattsville, MD: National Center for Health Statistics . 2011 .
5 Heaney RP. The Vitamin D requirement in health and disease. J Steroid Biochem Mol Biol. 2005;97(1-2):13-9 .
6 Heaney RP, Dowell MS, Hale CA, Bendich A . Calcium absorption varies within the reference range for serum 25-hydroxyvitamin D . J Am Coll Nutr. 2003;22(2):142-6 .
7 Lips P . Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and thera-peutic implications . Endocr Rev. 2001 Aug;22(4):477-501 .
8 MacLaughlin J, Holick MF . Aging decreases the capacity of human skin to produce vitamin D3 . J Clin Invest. 1985;76:1536-8 .
9 Kritchevsky SB, Tooze JA, Neiberg RH, et . al; Health ABC Study . 25-hydroxyvitamin D, parathyroid hormone, and mortality in black and white older adults: the health ABC study . J Clin Endo-crinol Metab. 2012;97(11):4156-65 .
10 Guardia G, Parikh N, Eskridge T, et . al . Prevalence of vitamin D depletion among subjects seeking advice on osteoporosis: a five-year cross-sectional study with public health implications . Osteopo-ros Int. 2008;19:13–19 .
11 Aloia JF . African Americans, 25-hydroxyvitamin D, and osteoporo-sis: a paradox . Am J Clin Nutr. 2008;88(2):545S-50S .
12 Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care . Institute of Medicine . Unequal Treat-ment: Confronting Racial and Ethnic Disparities in Health Care . National Academy Press: Washington, DC: 2002 .
13 Björk A, Andersson Å, Johansson G, Björkegren K, Bardel A, Kristiansson P . Evaluation of sun holiday, diet habits, origin and other factors as determinants of vitamin D status in Swedish pri-mary health care patients: a cross-sectional study with regression analysis of ethnic Swedish and immigrant women . BMC Fam Pract. 2013;3;14:129 .
14 Institute of Medicine, Food and Nutrition Board . Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academy Press, 2010 .
15 Greene-Finestone LS, Berger C, de Groh M; CaMos Research Group . 25-Hydroxyvitamin D in Canadian adults: biologi-cal, environmental, and behavioral correlates . Osteoporos Int. 2011;22(5):1389-99 .
16 Neale R, Williams G, Green A . Application patterns among partici-pants randomized to daily sunscreen use in a skin cancer preven-tion trial . Arch Dermatol. 2002 Oct;138(10):1319-25 .
17 Lademann J, Schanzer S, Richter H, et . al . Sunscreen application at the beach . J Cosmet Dermatol. 2004;3(2):62-8 .
18 Holick MF . Vitamin D deficiency . N Engl J Med. 2007;357:266-81 .19 Holick MF . Vitamin D: the underappreciated D-lightful hormone
that is important for skeletal and cellular health . Curr Opin Endocri-nol Diabetes. 2002;9(1):87–98 .
20 U .S . Department of Agriculture, Agricultural Research Service, USDA Nutrient Data Laboratory. 2010. USDA National Nutrient Database for Standard Reference, Release 23. Available at www .ars .usda .gov/nutrientdata . Accessed March 2014 .
21 DiGiorgi M, Daud A, Inabnet WB, et . al . Markers of bone and calcium metabolism following gastric bypass and laparoscopic adjustable gastric banding . Obes Surg. 2008;18(9):1144-8 .
22 Clements RH, Yellumahanthi K, Wesley M, Ballem N, Bland KI . Hyperparathyroidism and vitamin D deficiency after laparoscopic gastric bypass . Am Surg. 2008;74(6):469-74 .
23 Goldner WS, Stoner JA, Lyden E, et . al . Finding the optimal dose
and fractures may indicate osteomalacia, osteoporosis, or both. Ensuring appropriate patient care requires accurate vitamin D measurement and correction of any D deficiency before diagnosis and treatment of osteoporosis.
Additional research is needed to clarify the many unan-swered questions about the full effects and function of vitamin D in human health.
References1 Bailey RL, Dodd KW, Goldman JA, et . al . Estimation of total
usual calcium and vitamin D intakes in the United States . J Nutr.
Join NOFNOFisthenation’sleading
resourceforup-to-date,medicallysoundinformation
andmaterialsonallaspectsofbonehealthandosteoporosisfor
cliniciansandtheirpatients.ProfessionalMembership—toconnectwithallthat
NOFhastooffer—isavailableatthreelevels: Professional Partners Network® (PPN) —IndividualForindividualphysiciansandadvancedpracticeclinicians(nursepractitionersandphysicianassistants)whoevaluateandinitiatethetreatmentofosteoporosispatientsoralliedhealthprofessionalswhowouldlikeaccesstotheadditionalbenefitsofferedforthismembershipcategory. Professional Partners Network® (PPN) —Group Formedicalpracticesandcenterswithindividualclinicians(nursepractitionersandphysicianassistants)whoevaluateandinitiatethetreatmentofosteoporosispatients.
Allied Health Professional Forallnon-prescribingindividualswhoworkinthehealthcare(orrelated)industriesorhaveapersonalorprofessionalinterestinosteoporosisorbonehealth.
Formoreinforamtion,[email protected]/223-2226.
FREE
CME f
or M
EMBER
S

15
NOF’s Support Group ProgramNOF sponsors osteoporosis support groups throughout the country. Patients can benefit in many ways from joining a support group:
• Learning more about the disease and treatment choices
• Receiving the most up-to-date information about osteoporosis
• Improving coping skills by learning how others handle the disease
• Exchanging information about community resources
• Helping identify healthcare providers who treat osteoporosis
• Improving mental and physical well-being• Finding hope and encouragement
Starting a Support GroupIf you are interested in starting your own support group, review and complete the NOF Support Group Application, available online at www.nof.org under Connect to Our Community
Support Group ResourcesNOF provides all support groups leaders with excellent resources including:
• Support group manual — A comprehensive guide to help you start, promote and conduct successful support group meetings.
• Free educational materials — NOF will provide brochures, information sheets, quarterly newsletters, PowerPoint presentations, posters and more.
• Networking opportunities — NOF will connect you with other support group leaders to help you network and exchange ideas.
• Topics and program ideas — NOF maintains a list of topics and program ideas.
• Referrals — NOF will direct all inquiries to join a support group in your area to you, helping you grow your membership.
For more information on joining a support group or to find a support group In your community, contact the National Osteoporosis Foundation at (202) 223-2226 or toll free at (800) 231-4222.
of vitamin D following Roux-en-Y gastric bypass: a prospective, randomized pilot clinical trial . Obes Surg. 2009;19(2):173-9 .
24 Blum M, Dallal GE, Dawson-Hughes B . Body size and serum 25 hydroxy-vitamin D response to oral supplements in healthy older adults . J Am Coll Nutr. 2008;27(2):274-9 .
25 Mintzer S, Boppana P, Toguri J, DeSantis A . Vitamin D levels and bone turnover in epilepsy patients taking carbamazepine or oxcar-bazepine . Epilepsia. 2006;47(3):510-5 .
26 Hoikka V, Savolainen K, Alhava EM, Sivenius J, Karjalainen P, Par-vianinen M . Anticonvulsant osteomalacia in epileptic outpatients . Ann Clin Res. 1982;14(3):129-32 .
27 Kulak CA, Borba VZ, Bilezikian JP, Silvado CE, Paola L, Bogusze-wski CL . Bone mineral density and serum levels of 25 OH vitamin D in chronic users of antiepileptic drugs . Arq Neuropsiquiatr. 2004;62(4):940-8 .
28 Brown TT, Qaqish RB . Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: a meta-analytic review . AIDS . 2006;20(17):2165-74 .
29 Fox J, Della-Santina CP . Oral verapamil and calcium and vita-min D metabolism in rats: effect of dietary calcium . Am J Physiol. 1989;257(5 Pt 1):E632-8 .
30 Odes HS, Fraser GM, Krugliak P, Lamprecht SA, Shany S . Effect of cimetidine on hepatic vitamin D metabolism in humans . Digestion. 1990;46(2):61-4 .
31 Compston JE, Horton LW . Oral 25-hydroxyvitamin D3 in treat-ment of osteomalacia associated with ileal resection and cholestyr-amine therapy . Gastroenterology. 1978;74(5 Pt 1):900-2 .
32 U .S . Department of Health and Human Services National Institutes of Health . Medline Plus . Vitamin D. Natural Medicines Comprehen-sive Database Consumer Version. U .S . National Library of Medicine 8600 Rockville Pike, Bethesda, MD Page last updated: 04 January 2011 . Available at: http://www .nlm .nih .gov/medlineplus/druginfo/natural/929 .html . Accessed March 2014 .
33 Buckley LM, Leib ES, Cartularo KS, Vacek PM, Cooper SM . Cal-cium and vitamin D3 supplementation prevents bone loss in spine secondary to low-dose corticosteroids in patients with rheumatoid arthritis . A randomized, placebo-controlled trial . Ann Intern Med. 1996;125(12):961-8 .
34 Lukert BP, Raisz LG . Gluococorticoid-induced osteoporosis: pathogenesis and management . Ann Intern Med. 1990;112:352-64 .
35 Skversky AL, Kumar J, Abramowitz MK, Kaskel FJ, Melamed ML . Association of glucocorticoid use and low 25-hydroxyvita-min D levels: results from the National Health and NutritionEx-amination Survey (NHANES): 2001-2006 . J Clin Endocrinol Metab. 2011 Dec;96(12):3838-45 .
36 Bourke JF, Mumford R, Whittaker P, et . al . The effects of topi-cal calcipotriol on systemic calcium homeostasis in patients with chronic plaque psoriasis . J Am Acad Dermatol. 1997;37(6):929-34 .
37 Aloia JF, Li-Ng M, Pollack S . Statins and Vitamin D . Am J Cardiol. 2007 October 15;100(8):1329 .
38 McDuffie JR, Calis KA, Booth SL, Uwaifo GI, Yanovski JA . Effects of orlistat on fat-soluable vitamins in obese adolescents . Pharmaco-therapy. 2002;22:814-22 .
39 Pfeifer M, Begerow B, Minne HW, et . al . Effects of a long-term vitamin D and calcium supplementation on falls and parameters of muscle function in community-dwelling older individuals . Osteopo-ros Int. 2009;20(2):315–22
40 Stockton KA, Mengersen K, Paratz JD, Kandiah D, Bennell KL . Ef-fect of vitamin D supplementation on muscle strength: a systematic review and meta-analysis . Osteoporos Int. 2011;59(12):859–71 .
41 Autier P, Gandini S . Vitamin D supplementation and total mortal-ity: a meta-analysis of randomized controlled trials . Arch Intern Med. 2007;167:1730–7 .
42 Zhu K, Austin N, Devine A, Bruce D, Prince RL . A randomized controlled trial of the effects of vitamin D on muscle strength and mobility in older women with vitamin D insufficiency . J Am Geriatr Soc. 2010;58:2063–8 .
43 Bleicher K, Cumming RG, Naganathan V, et . al . U-Shaped As-sociation Between Serum 25-Hydroxyvitamin D and Fracture Risk in Older Men: Results from the Prospective Population Based

16
CHAMP Study . J Bone Miner Res. 2014 Mar 27 . doi: 10 .1002/jbmr .2230 .
44 Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, et . al . Fall prevention with supplemental and active forms of vitamin D: a me-ta-analysis of randomised controlled trials . BMJ. 2009;339:b3692 .
45 Daksha P Trivedi DP, Doll R, Khaw KT . Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial . BMJ. 2003;326-469 .
46 Cranney A, Weiler HA, O’Donnell S, Puil L . Summary of evidence-based review on vitamin D efficacy and safety in relation to bone health . Am J Clin Nutr. 2008;88:513S-9S .
47 Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucci E, Di-etrich T, Dawson-Hughes B . Fracture prevention with vitamin D supplementation: a meta-analysis of randomized controlled trials . JAMA. 2005;293(18):2257-64 .
48 Bischoff-Ferrari HA, Willett WC, Wong JB, et . al . Prevention of nonvertebral fractures with oral vitamin D and dose dependency: a meta-analysis of randomized controlled trials . Arch Intern Med. 2009;169(6):551-61 .
49 Lyons RA, Johansen A, Brophy S, et . al . Preventing fractures among older people living in institutional care: a pragmatic randomised double blind placebo controlled trial of vitamin D supplementation . Osteoporos Int. 2007;18(6):811-8 .
50 Michael YL, Lin JS, Whitlock EP, et . al . Interventions to Prevent Falls in Older Adults: An Updated Systematic Review. Evidence Synthesis No. 80. AHRQ Publication No. 11-05150-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; December 2010 . Available at https://www .ncbi .nlm .nih .gov/books/NBK51685/ . Ac-cessed March 2014 .
51 Chapuy MC, Schott AM, Garnero P, Hans D, Delmas PD, Meunier J . Healthy elderly French women living at home have secondary hyperparathyroidism and high bone turnover in winter . J Clin Endocrinol Metab. 1996;81:1129–33 .
52 Holick MF, Siris ES, Binkley N, et . al . Prevalence of vitamin D in-adequacy among postmenopausal North American women receiv-ing osteoporosis therapy . J Clin Endocrinol Metab. 2005;90:3215–24 .
53 Thomas MK, Lloyd-Jones DM, Thadhani RI, et . al . Hypovitamino-sis D in medical inpatients . N Engl J Med. 1998;338:777–83 .
54 Plotnikoff GA, Quigley JM . Prevalence of severe hypovitamino-sis D in patients with persistent, nonspecific musculoskeletal pain . Mayo Clin Proc. 2003 Dec;78(12):1463-70 .
55 Knutsen KV, Brekke M, Gjelstad S, Lagerløv P . Vitamin D status in patients with musculoskeletal pain, fatigue and headache: a cross-sectional descriptive study in a multi-ethnic general practice in Norway . Scand J Prim Health Care. 2010;28(3):166-71
56 Prakash S, Kumar M, Belani P, Susvirkar A, Ahuja S . Interrela-tionships between chronic tension-type headache, musculoskel-etal pain, and vitamin D deficiency: Is osteomalacia responsible for both headache and musculoskeletal pain? Ann Indian Acad Neurol. 2013;16(4):650-8 .
57 Hathcock JN, Shoa A, Vieth R, Heaney R . Risk assessment for vitamin D1,2 . Am J Clin Nutr. 2007;85(1):6-18 .
58 Sanders KM, Stuart AL, Williamson EJ, Simpson JA, Kotowicz MA, Young D, Nicholson GC . Annual high-dose oral vitamin D and falls and fractures in older women: a randomized controlled trial . JAMA. 2010;303(18):1815-22 .
59 Jones G . Pharmacokinetics of vitamin D toxicity . Am J Clin Nutr. 2008;88:582S-6S .
60 Looker AC, Dawson-Hughes B, Calvo MS, Gunter EW, Sahy-oun NR . Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III . Bone. 2002;30:771–7 .
61 Heaney RP . Barriers to optimizing vitamin D3 intake for the elderly . J Nutr. 2006;136(4):1123-5 .
62 Kennel KA, Drake MT, Hurley DL . Vitamin D Deficiency in Adults: When to Test and How to Treat . Mayo Clin Proc. 2010;85(8):752-8 .
63 Pepper KJ, Judd SE, Nanes MS, Tangpricha V . Evaluation of
THE CLINICIAN’S GUIDE TO PREVENTION AND TREATMENT OF OSTEOPOROSIS
Download today to access the latest clinical decision making information right from your iPhone and iPad. Go to www.nof.org for more information.
vitamin D repletion regimens to correct vitamin D status in adults . Endocr Pract. 2009;15:95-103 .
64 Mulligan GB, Licata A . Taking vitamin D with the largest meal improves absorption and results in higher serum levels of 25-hy-droxyvitamin D . J Bone Miner Res. 2010;25(4):928-30 .
65 Munger KL, Zhang SM, O’Reilly E, et al . Vitamin D intake and incidence of multiple sclerosis . Neurology. 2004;62:60–5 .
66 Merlino LA, Curtis J, Mikuls TR, Cerhan JR, Criswell LA, Saag KG . Vitamin D intake is inversely associated with rheumatoid arthritis . Arthritis Rheum. 2004;50:72–7 .
67 Garland CF, Comstock GW, Garland FC, Helsing KJ, Shaw EK, Gorham ED . Serum 25-hydroxyvitamin D and colon cancer: eight-year prospective study . Lancet. 1989;2:1176–8 .
68 Garland CF, Garland FC, Gorham ED, et . al . The role of vitamin D in cancer prevention . Am J Public Health. 2006;96:252–61 .
69 Lappe JM, Travers-Gustafson D, Davies KM, Recker RR, Heaney RP . Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial . Am J Clin Nutr. 2007;85:1586–91 .
70 Hypponen E, Laara E, Jarvelin M-R, Virtanen SM . Intake of vitamin D and risk of type 1 diabetes: a birth-cohort study . Lancet. 2001;358:1500–3 .
71 Adami S, Giannini S, Bianchi G, et . al . Vitamin D status and

17
Osteoporosis InternationalOsteoporosis International is the leading scientific journal for clinical research in osteoporosis and related bone diseases. Published monthly, the journal is an international, multi-disciplinary joint initiative of NOF and the International Osteoporosis Foundation.
Free Subscription for NOF Professional Members
PRACTICE TOOLS & RESOURCES AVAILABLE AT WWW.NOF.ORG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
A Guide to Osteoporosis MedicinesThis brochure will help you better understand your osteoporosis treatment options. It provides information on the osteoporosis medicines approved by the U.S. Food and Drug Administration (FDA), discusses factors to consider when making a treatment decision and the issues you may face in staying with a treatment plan.
Boning up on Osteoporosis: A Guide to Prevention and TreatmentThis 100+ page patient care handbook offers up-to-date information on the prevention, diagnosis and treatment of osteoporosis.
Free printable downloads and discounts on print patient education publications for NOF Professional Members
How Strong Are Your Bones? This brochure helps people understand osteoporosis, their risk factors for the disease and the importance of bone healthy behaviors. It explains bone density testing and includes information on when to have a bone density test, what the results mean and when to consider treatment.
NOF STORE: Order Education Materials for Your Patients Member Discount on All Purchases
Related Documents











