
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MIDDLE EAST JOURNAL OF ANESTHESIOLOGY
Department of Anesthesiology
American University of Beirut Medical Center
P.O. Box 11-0236. Beirut 1107-2020, Lebanon
Editorial Executive Board Consultant Editors
Editor-In-Chief: Bikhazi George
Executive Editors Mohamad El-Khatib
Editors Chakib Ayoub
Marie Aouad
Ghassan Kanazi
Sahar Siddik-Sayyid
Managing Editor Mohamad El-Khatib
Founding Editor Bernard Brandstater
Emeritus Editor-In-Chief Anis Baraka
Honorary Editors Nicholas Greene
Musa Muallem
Managing Editor Assistant Iman Jaafar
Webmaster Rabi Moukalled
Secretary Alice Demirdjian
Assem Abdel-Razik (Egypt)
Bassam Barzangi (Iraq)
Izdiyad Bedran (Jordan)
Dhafir AI-Khudhairi (Saudi Arabia)
Mohammad Seraj (Saudi Arabia)
Abdul-Hamid Samarkandi (Saudi Arabia)
Mohamad Takrouri (Saudi Arabia)
Bourhan E. Abed (Syria)
Mohamed Salah Ben Ammar (Tunis)
M. Ramez Salem (USA)
Elizabeth A.M. Frost (USA)
Halim Habr (USA)
The Middle East Journal of Anesthesiology is a publication of the Department of Anesthesiology of the American
University of Beirut, founded in 1966 by Dr. Bernard Brandstater who coined its famous motto:
"For some must watch, while some must sleep" (Hamlet-Act. III, Sc. ii).
and gave it the symbol of the poppy flower (Papaver somniferum), it being the first cultivated flower in the
Middle East which has given unique service to the suffering humanity for thousands of years. The Journal's cover
design depicts The Lebanese Cedar Tree, with's Lebanon unique geographical location between East and West.
Graphic designer Rabi Moukalled
The Journal is published three times a year (February, June and October) The volume consists of a two year indexed
six issues. The Journal has also an electronic issue accessed at www.aub.edu.lb/meja
The Journal is indexed in the Index Medicus and MEDLARS SYSTEM. E-mail: [email protected]
Fax: +961 - (0)1-754249

“For some must watch, while some must sleep”
(Hamlet-Act. III, Sc. ii)

B. Braun Melsungen AG | Hospital Care | 34209 Melsungen | GermanyTel. +49 5661 71-0 | www.bbraun.com
Thanks to AirStop in the drip chamber - the sight of a container running empty is no longer cause for alarm and no reason for energy and time to be wasted rushing around because the patient gets upset.
When the container is empty, AirStop maintains a constant � uid level. No air can get through to the patient.
Thanks to the PrimeStop at the patient connector - you can now prepare several infusions at once, quicker and more hygienic than ever before. Right away your hands are free to prepare the next infusion.
Intra� x® SafeSet The � rst IV administration set with AirStop and PrimeStop
Gives every ward that extra measure of safety while providing higher e� ciency.
Prime Stop
AirStop
Prime Stop
AirStop
www.safeinfusiontherapy.com
For more information about Intrafix® SafeSet and Safe Infusion Therapy:
Risk Prevention in Infusion TherapyParticulate Contamination
www.safeinfusiontherapy.com
Chemical Contamination
Risk Prevention in Infusion Therapy
www.safeinfusiontherapy.com
Risk Prevention in Infusion TherapyAir Embolism
www.safeinfusiontherapy.com
Risk Prevention in Infusion TherapyMedication Error
www.safeinfusiontherapy.com
www.safeinfusiontherapy.com
Risk Prevention in Infusion TherapyDrug Incompatibility
www.safeinfusiontherapy.com
www.safeinfusiontherapy.comwww.safeinfusiontherapy.com
www.safeinfusiontherapy.com
Risk Prevention in Infusion TherapyMicrobiological Contamination
www.safeinfusiontherapy.com
.
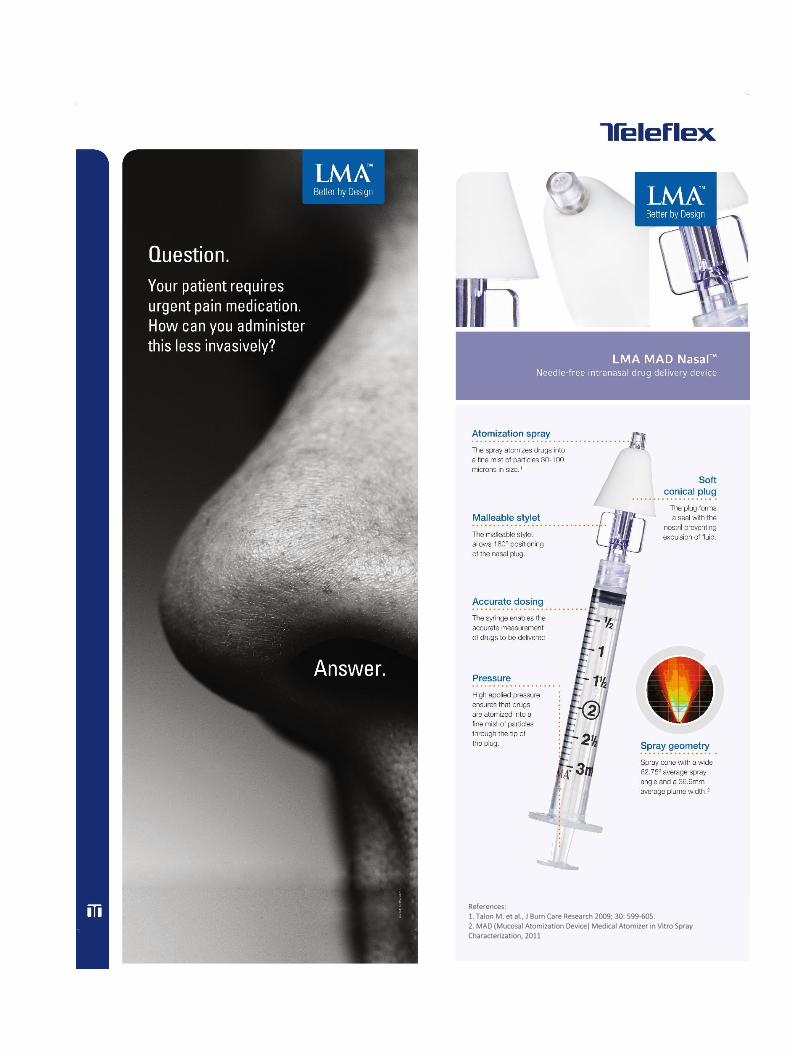
References: 1. Talon M. et al., J Burn Care Research 2009; 30: 599-605. 2. MAD (Mucosal Atomization Device) Medical Atomizer in Vitro Spray Characterization, 2011

127 M.E.J. ANESTH 23 (2), 2015
Middle East Journal of Anesthesiology
Vol. 23, No. 2, June 2015
CONTENTS
editorialCOmpliCaTiONS FOllOwiNg DiFFErENT TEChNiquES OF ONE-luNg VENTilaTiON -TraChEal TubE VErSuS
uNiVENT, Or DOublE-lumEN TubE- .................................................................................................................................. Anis Baraka 129
reView articleaNESThETiC maNagEmENT FOr Drug iNDuCED SlEEp ENDOSCOpy
................................................................................................................................. Nabil Shallik 131pEriOpEraTiVE paiN CONTrOl iN gaSTrOiNTESTiNal SurgEry
................................................... Lee Hingula, Benjamin Maslin, Sirisha Rao, Stephanie Wood, Kurt Roberts, Gopal Kodumudi, Erika Schermer, Nalini Vadivelu 137
scieNtific articlesrESiDENT implEmENTaTiON OF ThE 2007 aCC/aha guiDEliNES ON prEOpEraTiVE CarDiaC EValuaTiON
iN NON-CarDiaC SurgEry paTiENTS: iS CliNiCal ExpEriENCE ENOugh? ............................................... Hassan H. Amhaz, Ruth Kuo, Elie J. Chidiac, Vinay Pallekonda,
Samir F. Fuleihan, George McKelvey , Romeo N. Kaddoum 147pSEuDOChOliNESTEraSE DEFiCiENCy iN a OCTOgENariaN uNDErgOiNg TOTal iNTraVENOuS aNESThESia;
impliCaTiONS FOr NEurOmONiTOriNg
....................................................................................Matthew Wecksell, Demetri Koutsospyros 157aN auDiT OF ThE CurrENT praCTiCES OF airway maNagEmENT iN paTiENTS uNDErgOiNg SurgEry FOr
aTlaNTO-axial DiSlOCaTiON iN a SiNglE iNSTiTuTiON
.........................................................ShrutiRedhu, M. Radhakrishnan ,GSU mamaheswara Rao 163ulTraSOuND-guiDED SCiaTiC pOliTEal NErVE blOCk: a COmpariSON OF SEparaTE Tibial aND COmmON
pErONEal NErVE iNjECTiONS VErSuS iNjECTiNg prOximal TO ThE biFurCaTiON
..........................................................................................Magdy H. Eldegwy, Sami M. Ibrahim, Samy Hnora, Elsayed Elkarta, Ayman S. Elsily 171
iNTraVENOuS DExamEThaSONE iN COmbiNaTiON wiTh CauDal blOCk prOlONgS pOSTOpEraTiVE aNalgESia iN paEDiaTriC DayCarE SurgEry
...................................................Murnisari Ahmad Arbi, Azarinah Izaham, Esa Kamaruzaman, Khairulamir Zainudin, Hamidah Ismail, Norsidah Abdul Manap 177
COmparaTiVE STuDy bETwEEN ulTraSOuND aND NErVE STimulaTOr guiDED SCiaTiC NErVE blOCk ThrOugh ThE aNTEriOr apprOaCh" .....................................................Wafik A. Amin, M. Osama Abou Seada, Mansour M. Elkersh,
Abraham Mathai, Sona Medekova, Tafazzul Husain 185wOuND iNSTillaTiON OF lOCal aNESThETiC bupiVaCaiNE FOr pOSTOpEraTiVE aNalgESia FOllOwiNg
lumbar lamiNECTOmy
............................................... Nirmala Jonnavithula, Sandeep Garre, Sailakshman Pasupuleti, Padmaja Durga, Dilip Kumar Kulkarni, Gopinath Ramachandran 193

128
ThE EFFECTS OF iNTraThECal NEOSTigmiNE aDDED TO bupiVaCaiNE ON pOSTOpEraTiVE aNalgESiC rEquirEmENT iN paTiENTS uNDErgOiNg lOwEr limb OrThOpEDiC SurgEry
...........................................................Hamid Kayalha, Zinat Sadat Mousavi, Ameneh Barikani, Siamak Yaghoobi,Marzieh Beigom Khezri 199
ThE bENEFiCial ValuES OF TraNSOESOphagEal DOpplEr iN iNTraOpEraTiVE FluiD guiDaNCE VErSuS STaNDarD CliNiCal mONiTOriNg paramETErS iN iNFaNTS uNDErgOiNg kaSai OpEraTiON
...................................................................................... Eman Sayed Ibrahim, Taha Aid Yassein, Wesam Saber Morad 205
DESFluraNE COmparED TO SEVOFluraNE FOr CirrhOTiC paTiENTS uNDErgOiNg majOr liVEr rESECTiON. a raNDOmizED CONTrOl STuDy
....................................................................................Abou Hussein M, Mahmoud F, Beltagy R, Hasanin A, Yassen K, Attar A 213
myOCarDial OxygENaTiON DuriNg aCuTE NOrmOVOlEmiC hEmODiluTiON: impaCT OF hypOCapNiC alkalOSiS
..................................................................................... Edward A. Czinn, M. Ramez Salem, MD, George J. Crystal, PhD 225
aSSESSmENT OF prEOpEraTiVE aND pOSTOpEraTiVE aNxiETy amONg ElECTiVE majOr SurgEry paTiENTS iN a TErTiary hOSpiTal iN NigEria
............................................................................Adesanmi Akinsulore, Afolabi M. Owojuyigbe, Aramide F. Faponle, Femi O. Fatoye 235
ThE EFFECTS OF liSTENiNg TO ThE mOThEr’S hEarTbEaT ON ThE DEpTh OF aNESThESia iN ChilDrEN
....................................................................... Senem Yildirim, Başak Akça, Aysun Ankay Yilbaş, Ayşe Heves Karagöz, Özgür Canbay, Nalan Çelebi, Turgay Öcal 241
lEarNiNg by SimulaTiON
.........................................................................................................Ghaleb Okla, Douglas Eden 247
CaSE rEpOrTSulTraSOuND guiDED DOrSal ramuS NErVE blOCk FOr rEDuCTiON OF pOSTOpEraTiVE paiN iN paTiENTS
uNDErgOiNg lumbar SpiNE SurgEry: a CaSE SEriES imagiNg STuDy
..................................................................... Achir Al-alami, Ashraf Abou El Ezz, Farid Kassab 251a SharED OpEraTiVE FiElD aND ThE DiSpuTE - iS ThErE a way OuT?
........................................................................................... M-Irfan Suleman, Anita N Akbar Ali, Saif Siddiqui, William F Alfonso 257
letter to tHe editorrESiDual NEurOmuSCular blOCkaDE (rNmb): rOCurONium'S DEFaSCiCulaTiNg DOSE, NEOSTigmiNE-
iNDuCED wEakNESS, aND awarENESS DuriNg rECOVEry
............................................................................................................................... Deepak Gupta 261
129 M.E.J. ANESTH 23 (2), 2015
EDITORIAL
COMPLICATIONS FOLLOWING DIFFERENT TECHNIQUES OF ONE-LUNG VENTILATION
-Tracheal tube versus univent, or double-lumen tube-
One-lung ventilation (OLV) is recommended in patients undergoing thoracoscopy or thoracotomy. This can be achieved by contralateral ventilation of the non-operated lung using the traditional single-lumen tracheal tube, the univent tube, or the double-lumen tube. The present Editorial reports serious complications which may follow the three techniques of one-lung ventilation.
Using a single-lumen tracheal tube, collapse of the nonventilated lung can be achieved by carbon dioxide insufflation into the contralateral closed intrapleural chest cavity to a pressure as low as 5 mmHg. However, this technique may create a physiological response very similar to that of a unilateral tension pneumothorax, with a consequent hemodynamic instability secondary to decreased venous return, and/or mediastinal shift1.
Another technique of achieving OLV is using the univent tube, while collapsing the nonventilated lung by applying suction via the bronchial blocker before thoracotomy. However, applying suction, with the chest closed, can result in a marked negative intrathoracic pressure that diverts blood from the ventilated lung to the nonventilated lung with a consequent decrease of cardiac output and development of hypoxemia2.
Our present anesthetic technique for one-lung ventilation during thoracotomy or video-assisted thoracoscopy depends on double-lumen intubation which provides selective ventilation of the contralateral lung, while allowing collapse of the ipsilateral lung without the need of intrapleural carbon dioxide insufflation3.
Partial collapse of the lung on the thoracoscoped side occurs when the air enters the pleural cavity. To augment collapse, the lumen of the double-lumen tube on thoracoscoped side is opened to room air, while suction is applied intermittently as indicated. The technique provides a quiet field on the thoracoscoped side, without the need for carbon dioxide insufflation into the ipsilateral pleural space, or direct tracheal suctioning, and hence will not be complicated by inadvertent tension pneumothorax or negative pressure pulmonary edema3.
During one-lung ventilation, it is advisable to use the double-lumen tracheal tube. The right upper lobe bronchus arises near the carina as an offshoot from the right main stem bronchus, while the left upper lobe bronchus arises further away from the carina as a bifurcation of the main trunk. In addition, the right main bronchus is only 2cm long or may be shorter, and occasionally, the right upper lobe bronchus arises from the lower end of the trachea. That is why, right bronchial intubation can occlude the opening to the right upper lobe bronchus, with a consequent decrease of PaO2. In contrast, the left main stem bronchus is longer than the right main stem bronchus, and hence right bronchial intubation should be only used if left bronchial intubation is contraindicated. The use of a small double-lumen tube can facilitate overinflation of the bronchial cuff and/or down displacement of the tube which results in obstruction of the right or left upper lobe bronchus4.

130 ANIS BARAkA
Owing to the greater length of the left main stem bronchus, it is always advisable to use left bronchial intubation unless contraindicated by certain procedures such as left pneumonectomy, and to select the largest possible sized tube in order to avoid placing the bronchial limb too far into the bronchus.
Adequate fixation of the double-lumen tube and repeated checking by chest auscultation and fiberoptic bronchoscopy are required to detect malposition. Despite all these precautions, we came across two cases of left upper lobe bronchus blocking following left bronchial intubation, with a consequent ventilation limited to one lobe, resulting in severe hypoxemia in one patient, and in lung rupture with a consequent tension pneumothorax in the second patient4,5.
To optimize oxygenation during OLV, the original proposed ventilation strategy was based on maintaining a large tidal volume of 10 ml.kg, while applying continuous positive airway pressure (CPAP) using 100% oxygen to the non-ventilated lung.
However, applying CPAP to the non-ventilated lung on the operative side disturbed the surgeon during video-assisted thoracoscopy.
Also, recent studies have shown that ventilation with large tidal volume can result in lung injury. So, a revision of these guidelines has been necessary. The present recommended ventilation strategy during OLV is to use normal tidal volume, associated with PEEP. The use of PEEP is associated with an increase of oxygenation, without any other change of ventilation strategy. Thus, a normal tidal volume, associated with PEEP should be considered as a prevention strategy against both hypoxemia and lung injury. The present strategy during OLV is to use a normal tidal volume, associated with a low level PEEP.
Anis Baraka, MD, FRCA (Hon)
Emeritus Professor of Anesthesiology
American University of Beirut
References
1. Baraka a: Hazards of carbon dioxide insufflation during thoracoscopy. Br J Anaesth; 81, 100, 1998.
2. anis Baraka, Maud nawfal, nadine kawkaBani: Severe hypoxemia after suction of the nonventilated lung via the bronchial blocker lumen of the Univent tube. J Cardiothoracic & Vascular Anesthesia; 10:5, 694-695, 1996.
3. Baraka a: The technique of single-lumen versus double-lumen tube during thoracoscopy. MEJ Anesth; 15(3):215-216, 1999.
4. anis Baraka, Claude aBu Jaude, MauriCe Baroody et al: Right upper lobe collapse following right bronchial intubation. MEJ Anesth; 255-258, 1985.
5. anis Baraka, Joseph Maalouli, MohaMed Jazzar: Severe hypoxemia secondary to inadvertent left lower bronchial intubation. MEJ Anesth; 17(2):295-298, 2003.
6. Capan lM, turndorf h, patel C: Optimization of arterial oxygenation during one-lung anesthesia. Anesth Analg; 59:847-851, 1980.
7. Baraka a, siBai an, MualleM M.et al: CPAP oxygenation during one-lung ventilation using an underwater seal assembly. Anesthesiology; 65:102-103, 1986.
8. senturk M: Protective ventilation during one-lung ventilation. Anesthesiology; 107:176-177, 2007.
131 M.E.J. ANESTH 23 (2), 2015
REVIEW ARTICLE
Anesthetic MAnAgeMent for Drug inDuceD sleep enDoscopy
Nabil Shallik*
Keywords: sleep endoscopy, Dise, nasoendoscopy, sne and propofol infusion.
Introduction
sleep endoscopy, also known as sleep nasoendoscopy (sne) or drug-induced sleep endoscopy (Dise), is a powerful tool for studying the dynamic airway in a sleeping patient with obstructive sleep apnea (osA). using the knowledge gained from sleep endoscopy, the surgeon can tailor the operative procedure to the patient's specific condition.
Based on the level and pattern of airway obstruction in a patient with osA, sleep endoscopy allows the physician to tailor the treatment plan to each patient. this can improve the results of surgical intervention and/or minimize the scope of intervention. sleep endoscopy may also provide information that erases the need for surgery altogether. 70% of patients surveyed in an outpatient setting by hewitt et al were determined to have a palatal cause of obstruction and were surgical intervention. however, after undergoing sleep endoscopy the number of patients deemed to need surgical procedures decreased to 54%1.
The diagnosis and treatment of OSA is a complex and multidimensional due to the difficulty in establishing the site of obstruction in the awake patient who carries a diagnosis of obstructive Sleep Apnea Hypopnea Syndrome (OSAHS). Croft and Pringle first proposed sleep endoscopy in 19912. Using midazolam as a sedating agent, they demonstrated the utility of passing a fiberoptic endoscope through a sleeping patient’s nasal cavity to assess pharyngeal structures for evidence of obstruction and were able to induce the preexisting snoring in 95% of their patients2.
other investigators used propofol because it is a hypnotic drug with a very short half-life (approximately three minutes), and its eventual adverse effects are rapidly recovered as soon as administration is discontinued. Moreover, its effect on respiratory depression is lower than that observed with benzodiazepines, and it leads to a low incidence of side effects,( e.g. nausea, headache) and is considered to be a very safe drug for sedation3.
in 1993, croft and pringle developed a grading scale that utilized sleep endoscopy to categorize snoring and obstruction. grading was based on whether the obstruction was palatal, multilevel, or tongue-based4. sleep endoscopy, in combination with the grading scale, allows the physician to directly observe and record pharyngeal structures in the sedated patient with osA and categorize the obstruction.
* MD, Assistant professor of clinical Anesthesia, Weill cornell Medical college Doha, Qatar. Assistant professor of Anesthesia and intensive care, tanta university, egypt. consultant in Department of Anesthesia, intensive care, pain Management and peri-operative Medicine Department,
hamad Medical corporation, Doha, Qatar. correspondence should be addressed to: [email protected]

132 nABil shAllik
Also, sleep endoscopy is enormously useful as a tool for teaching all levels of staff about airway management, and it is useful for anesthesiology and otolaryngology residents who are learning about airway anatomy and physiology.
the main indications of sleep endoscopy reported in the literature are: severe osAhs, surgical failure, mismatch between awake endoscopic assessment and clinical features and suspected central nervous system diseases.
the aim of this review is to help anesthesiologists and ent surgeons in management of Dise before, during and after Dise techniques.
Technique of DISE
All sleep endoscopies are carried out in an operation theater setting. the patients is placed in the supine position on their ward beds or operating theatre beds in comfortable ambient temperatures, dimmed lighting, with their eyes covered by a paper face mask and they are encouraged to sleep.
Prior to DISE, flexible nasal endoscopy is performed on the patient whilst awake, using the Müller maneuver (forced inspiratory suction with mouth and nose closed) that allows an estimation of different patterns of pharyngeal collapse. endoscopic examination in both awake and asleep patients is performed using flexible nasopharyngoscope5.
following this upper airway evaluation, further clinical assessment of the patients includes review of the sleep study report and preoperative medical clearance. sedatives and narcotics are avoided before the procedure, and heart rate (hr), non-invasive blood pressure (niBp), oxygen saturation (spo2), and bispectral index (Bis) are monitored, together with continuous monitoring Bis ( a scale derived from cerebral electrical activity and that measures the effect of specific anesthetic drugs on the brain. the recommended range in anesthesia guided by Bis is 40–60)6.
Pharmacological regimen in adults
the ‘ideal’ drug for Dise, should have a short half-life and be available for iV and infusion with
minimal impact on respiratory drive, muscle tone and rapid eye movement (reM) sleep (kezirian 2006)7. In addition, it should have a specific, rapidly acting antidote. there is no ideal agent but propofol is currently the drug of choice for Dise.
Propofol manual infusion for DISE
sleep endoscopy is manually performed using a 20 ml syringe containing 1% or 2% propofol. An induction bolus of 1 mg/kg propofol is followed by 20 mg boluses every two minutes until the start of the so-called snoring-apnea cycle (sAc), through wide bore cannula in a large vein to prevent pain during injection5.
Propofol target-controlled infusion (TCI) for DISE- TCI
sleep endoscopy is performed by a target-controlled infusion (tci) system using schnider model in effect-site (cerebral) targeted infusion 50 ml prefilled syringe of 1% propofol. The Schnider system is a complex pharmacokinetic/pharmacodynamic (pk/pD) model that allows obtaining different rates of drug from the values of age, height, weight, and lean body mass of the patient8. the initial target for propofol is 1.5 mcg/ml and increasing in increments of 0.2 mcg/ml every 2 minutes until the start of snoring-apnea cycle (sAc). the propofol rate will continue by last rate of infusion till the end of examination. and this is known as the ‘slow’ technique5. for ‘rapid’ technique, the initial target of propofol is 2.5 mcg/ml and increasing in increments of 0.2 mcg/ml every two minutes until the start sAc. the propofol rate will continue by last rate of infusion till the end of examination. During either procedure, the above mentioned vital parameters shall be monitored every two minutes together with any observed alterations in upper airways’ (uA) opening or snoring-apneas events before the next injection of propofol.
During the Dise, the onset of the so-called cAs should be identified and reported in a specific data sheet. Moreover it is important to mark the different sites and patterns of uA collapses. Different endoscopic classification systems could be used for this purpose,

M.E.J. ANESTH 23 (2), 2015
133Drug inDuceD sleep enDoscopy
such as the nose, oropharynx, hypopharynx and larynx (NOHL) classification9 or the velum, oropharyngeal lateral wall, tongue base and epiglottis (Vote) classification10.
Other techniques
iV midazolam (3–5 mg) iV and propofol (30–50 mg) can be titrated individually by an anaesthetist, with additional 20-mg boluses of propofol every two minutes to maintain a satisfactory level of sedation. however, benzodiazepines reduce muscle tone and respiratory drive and flumazenil may be needed for reversal of these side effects11.
Dexmedetomidine may be useful for outpatient anesthesia, sleep nasendoscopy and sleep studies. it can be given as 1mcg/kg loading infusion over 10 min., followed by continuous iV infusion between 0.2-0.7 mcg/kg/h12 which still under clinical trials.
Pharmacological regimen in pediatrics
the induction in children is performed by mask inhalational of sevoflurane. An IV cannula is then inserted, and anesthesia is maintained with an infusion of dexmedetomidine at 1-2 mcg/kg/hr without a loading dose, with additional ketamine (10mg/kg). previously, a propofol infusion was used to maintain anesthesia. however, Aaron and peter have found that, with this propofol technique in pediatrics, the muscle relaxation is less marked resulting in more prolonged expiratory effort. they also vasoconstrict and anesthetize the nose with a half and half mixture of oxymetazoline and 1% xylocaine delivered on a 1cm × 4cm cottonoid pledget. spontaneous respiration is supported by oxygen (2l/min) delivered via nasal cannula. the child should be positioned in the supine position without a shoulder roll, mimicking the position of natural sleep as much as possible13.
once a rhythmic pattern of respiration is established, a flexible fiberoptic laryngoscope is passed directly into the child’s nose, passing posteriorly toward the nasopharynx. for visualization and documentation, a digital video camera is used with the endoscope.
At the nasopharynx, the adenoids are examined as a potential site of obstruction. the position of the
palate and uvula in relation to the posterior pharyngeal is identified. The scope is then passed into the oropharynx lingual tonsils, and pharyngeal tonsils (if still present) are examined. the position of the base of tongue, vallecula, and epiglottis in relation to the posterior pharyngeal wall are noted. in some cases, the tongue base can be seen collapsed against the posterior pharyngeal wall. in such cases, visualizing the improvement in airway patency by lifting the tongue base with jaw thrust can be quite dramatic. the dynamics of lateral pharyngeal wall motion can be seen. the scope is then passed under the epiglottis where the dynamics of the supraglottic soft tissues, as well as the motion of the vocal cords, are observed. At the completion of the sleep endoscopy, the scope is removed. Direct laryngoscopy and bronchoscopy can then be performed to complete the airway evaluation13.
Post procedure Management
the American society of Anesthesiologist (AsA) guidelines states that, all patients should be monitored for three hours longer than non-obstructive sleep apnea patients. oxygen saturation on room air should return to its preoperative baseline. patients should not be hypoxemic or have signs of developing airway obstruction when left alone. As there is no pain during or after the technique there is no need for analgesia. the patients are usually drowsy after the procedure, so they must not drive, operate heavy machinery or work on the same day14.
Advantages of DISE: versus Polysomnography
Dynamic assessment of the effects of sleep on the airway.
Directly visualization of the source of obstruction and related structures
Precise identification of the relevant structures which enables the surgeon to define surgical treatment.
Complication of DISE
complications associated with sleep endoscopy include the following:
Nasal bleeding induced by the flexible fiberscope
134 nABil shAllik
laryngospasmpulmonary aspirationhypercapnea, desaturation and loss of the airwayneed for intubation or a surgical airwaycardiac dysrhythmiassystemic hypertensionSo, all resuscitation equipments, difficult airway
trolley and trained personnel should be ready to manage these complications.
Contraindications of DISE
relative contraindications include patients who are pregnant or who have a known history of propofol allergy or allergies to propofol components such as egg, lecithin, or soybean oil. other contraindications are significant nasal obstruction that impedes passage of the flexible fiberoptic laryngoscope (FFL), an “unsafe” airway, a frank aspiration history, and patients are not fasting.
Challenges of DISE for Anesthesiologist
no o2 supplementno guedel’s airway allowedAnti-cholinergic not allowedrisk of aspirationsedation for patients who are by nature sensitive for sedativesAll patients are done as day care
Discussion
propofol is an ‘ideal’ agent because it is a hypnotic drug with a very short half-life (approximately three minutes), and any adverse effects are rapidly reversed immediately after administration is discontinued. Moreover, its effect on respiratory depression is lower than that observed with benzodiazepines, and associated with a low incidence of side effects such as nausea and headache15-17.
Berry et al performed propofol sedation in two different groups, those with and those without history of snoring and apnea. they observed that no asymptomatic subject presented snoring during
sedation, whereas snoring occurred in all patients in the “snoring and apnea” group. The authors concluded that propofol sedation does not induce snoring or apneas in patients without snoring or apneas during regular sleep18.
similarly, fábio et al. did not observe snoring in asymptomatic patients, compared with 100 percent of osA patients w/w did snore20. such consistency was also observed by croft and pringle2 Berry et al18, and llatas et al19.
fábio et al. were the first investigators to observe that, for these procedures, propofol distorts the eeg structure, and reM sleep is replaced by n3 sleep in every sedated patient20. the mechanism(s) of action of propofol have not been fully clarified, although it is known that the drug interacts with the gamma-aminobutyric acid (gABA) A–benzodiazepine receptor complex18. this interaction would consequently reduce the firing rate of cholinergic neurons in the frontal cortex and hippocampus, which are important during wakefulness and reM sleep21.
nasoendoscopy under propofol sedation using an infusion pump has been reported, but the plasma levels of the drug vary in literature from 2 to 8 ug/ml22 -24. in 2005, Jones et al21 reported that the minimal plasma concentration of propofol for the patient to tolerate this examination was 1.5 ug/ml.
Conclusion
in osAhs patients, the observation of apneic events is mandatory for diagnostic accuracy, especially for patients undergoing surgical therapy. sleep endoscopy represents a remarkable diagnostic tool, but all efforts to increase the accuracy, stability and safety of the technique applied should be implemented.
Acknowledgments
We would like to acknowledge the support of prof. Claudio Vicini, Dr. Nicholas Scott, Dr. Ahmed El jazery, and Dr. Vanni Agnoletti for their revision assistance and their great help.

M.E.J. ANESTH 23 (2), 2015
135Drug inDuceD sleep enDoscopy
References
1. hewitt RJ, DaSgupta a, SiNgh a, Dutta C, koteCha bt: is sleep nasendoscopy a valuable adjunct to clinical examination in the evaluation of upper airway obstruction? Eur Arch Otorhinolaryngol; May, 266(5):691-697, 2009.
2. CRoft Cb, pRiNgle M: sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin Otolaryngol Allied Sci; oct, 16(5):504-409, 1991.
3. CoNNoly aap, MaRtiN J, white p: sedation with target-controlled propofol infusion system during assessment of upper airway in snorers. J Laryngol Otol; oct, 108(10):865-867, 1994.
4. pRiNgle Mb, CRoft Cb: A grading system for patients with obstructive sleep apnoea-based on sleep nasendoscopy. Clin Otolaryngol Allied Sci; Dec, 18(6):480-484, 1993.
5. De Vito a, agNoletti V, beRRettiNi S, piRaCCiNi e, CRiSCuolo a, CoRSo R, CaMpaNiNi a, gaMbale g, ViCiNi C: Drug-induced sleep endoscopy: conventional versus target controlled infusion techniques-a randomized controlled study. Eur Arch Otorhinolaryngol; Mar, 268(3):457-462, 2011.
6. puNJaSawaDwoNg y, booNJeuNgMoNkol N, phoNgChiewbooN a: Bispectral index for improving anaesthetic delivery and postoperative recovery. Cochrane Database Syst Rev; oct, 17 (4):cD003843, 2007.
7. keziRiaN eJ: Drug-induced sleep endoscopy. Oper Tech Otolaryngol; 17:230-232, 2006.
8. abSaloM a, StRuyS MMRf: An overview of tci & tiVA. 2nd edn, Academia press, ghent, 2007.
9. ViCiNi C, De Vito a, beNazzo M, fRaSSiNeti S, CaMpaNiNi a, fRaSCoNi p, MiRa e: nose, oropharynx, hypopharynx and larynx (NOHL) classification: a new system of diagnostic standardized examination for osAhs patients. Eur Arch Otorhinolaryngol; Apr, 269(4):1297-1300, 2012.
10. keziRiaN eJ, hoheNhoRSt w, De VRieS N: Drug-induced sleep endoscopy: the VOTE classification: Eur Arch Otorhinolaryngol; Aug, 268(8):1233-1236, 2011.
11. aMa Johal, JoaNNa M, battagel aND bhik t: kotecha eur orthod J. sleep nasendoscopy: a diagnostic tool for predicting treatment success with mandibular advancement splints in obstructive sleep apnoea. Eur J Orthod; Dec, 27(6):607-614, 2005.
12. geRlaCh at, DaSta Jf: Dexmedetomidine: An updated review. Ann Pharmacother; feb, 41(2):245-252, 2007.
13. aaRoN C, peteR J: sleep endoscopy in the evaluation of pediatric
obstructive sleep Apnea. International Journal of Pediatrics; Volume 2012, Article iD 576719, 6 pages doi:10.1155/2012/576719, 2012.
14. practice guidelines for perioperative Management of patients with obstructive sleep Apnea. A report by the American society of Anesthesiologists task force on the perioperative Management of patients with obstructive sleep Apnea. Anesthesiology; May, 104(5):1081-1093, 2006.
15. gueRiN ph, leSeNeCal l: pharyngeal and bronchial endoscopic study in the diagnoses and treatment of sleep apnea syndrome. Presse Med; feb, 21(6):249-252, 1992.
16. CoNNoly aap, MaRtiN J, white p: sedation with target-controlled propofol infusion system during assessment of upper airway in snorers. J Laryngol Otol; oct, 108(10):865-867, 1994.
17. QuiN SJ, huaNg l, elliS pD: observation of the mechanism of snoring using sleep nasoendoscopy. Clin Otolaryngol; Aug, 20(4):360-374, 1995.
18. beRRy S, RobliN g, williaMS a: Validity of sleep nasendoscopy in the investigation of sleep related breathing disorders. Laryngoscope; Mar, 115(3):538-540, 2005.
19. llataS MC, galofRe JD, MaRtNez Rl, CaRRaSCo l M J, lópez R: Our findings in the sleep endoscopy exams. Acta Otorrinolaringolol Esp; Jan, 56(1):17-21, 2005.
20. fábio a.w. Rabelo, aDRiaNo bRaga, DaNiel S. küppeR, JoSé a.a. De oliVeiRa, feRNaNDo M. lopeS, peDRo luiz Vaz De liMa MattoS, ShiRley g. baRReto, heiDi h. SaNDeR, RegiNa M.f. feRNaNDeS aND fabiaNa C.p, ValeRa f.C: propofol-induced sleep: polysomnographic evaluation of patients with obstructive sleep apnea and controls. Otolaryngol Head Neck Surg; feb, 142(2):218-224, 2010.
21. Jones Be: in: opp M, editor. Basics of sleep guide. 1st ed. Westchester (il): sleep research society, p. 57-64, 2005.
22. MaRaiS J: the value of sleep nasoendoscopy: a comparison between snoring and non-snoring patients. Clin Tolaryngol; feb, 23(1):74-76, 1998.
23. RobliN g, williMS a, whittet hb: target controlled infusion in sleep endoscopy. Laryngoscope; Jan, 111(1):175-176, 2001.
24. JoNeS tM, ho MS, eaRiS Je, Swift aC, ChaRteRS p: Acoustic parameters of snoring sound to compare natural snores during “steady-state” propofol sedation. Clin Otolaringol; feb, 31(1):46-52, 2006.


137 M.E.J. ANESTH 23 (2), 2015
PerioPerative Pain Control in Gastrointestinal surGery
Lee HinguLa*, Benjamin masLin*, sirisHa rao*, stepHanie Wood**, Kurt roBerts**, gopaL Kodumudi***,
eriKa scHermer**** and naLini VadiVeLu*
Abstract:
Perioperative pain control in the setting of gastrointestinal surgery presents unique challenges for the clinician, including the incidence of ileus and its potential exacerbation by analgesics, large incisions, patient characteristics and a wide variety of other factors. at the same time, optimizing postoperative pain control is of key significance in this patient population and has implications for both medical and surgical outcomes, length of hospital stay and associated costs and risks of developing chronic postsurgical pain. Data from recent clinical trials and other studies have highlighted the impact of specific surgical and anesthetic techniques on post-operative pain for several types of abdominal surgeries, including pancreatoduodenectomy, hepatectomy, gastric bypass, cholecystectomy, colectomy, and appendectomy. the management of pain may be optimized through the multidisciplinary and concerted efforts between clinicians involved in the perioperative care of patients undergoing gastrointestinal surgery.
Introduction
the incidence of gastrointestinal surgery in both the inpatient and outpatient settings has been increasing steadily in recent years, likely due to the increasing aging population of the united states. large abdominal procedures, such as pancreatic, liver, and bariatric procedures, continue to comprise a large proportion of the clinical case volume in academic medical centers. effective management of perioperative pain in gastrointestinal surgery is a primary consideration in terms of improving patient recovery time, length of hospital stay and patient satisfaction.
Postoperative pain continues to be a barrier to successful recovery and rehabilitation after surgery. one study estimates that roughly 75% of postoperative patients experience moderate to severe postoperative pain, often due suboptimal analgesic therapy1. in addition to problems discovered while the patients remain in the hospital, such as delayed wound healing and respiratory distress, acute-postsurgical pain is widely accepted today as a risk factor for the development of long term psychological distress and chronic postsurgical pain2.
Gastrointestinal surgery has a particularly high incidence of both postoperative pain and gastrointestinal symptoms, such as nausea, vomiting and the development of ileus. these
* MD, Department of anesthesiology, yale university school of Medicine, new Haven, Ct, usa.** MD, Department of surgery, yale university school of Medicine, new Haven, Ct, usa.*** Bs, Department of structural and Cellular Biology, tulane university, new orleans, la, usa.**** Bs, yale College, yale university, new Haven, Ct, usa.

138 BenjaMin Maslin et. al
gastrointestinal symptoms are frequently related to the preoperative diagnosis or surgical interventions; however, some analgesic medical therapies, such as commonly used opiates, are also known to contribute to nausea and vomiting. For this reason, optimizing perioperative pain control in the setting of gastrointestinal surgery presents unique challenges for the clinician in this particular subset of surgical patients.
Several studies and meta-analyses have looked at variable surgical techniques in order to investigate whether factors such as laparoscopic port size and number, insufflation pressures, use of local anesthetics, and various other surgical variables have any significant impact on postoperative pain and recovery. in addition, many recent studies have investigated different modalities of pain control, including epidural and intrathecal administration routes, and their role in improving postoperative pain compared to more traditional, intravenous medications.
Much attention in the literature has recently focused on the importance of perioperative pain control, in particular the concept of preventative analgesia. Preventive analgesia encompasses the use of various modalities before, during and after surgery to minimize postoperative pain3. analgesic therapy can be started before surgical incision, for example, preoperative epidural administration of local anesthetics and opioids or the performance of a nerve block to provide anesthesia in the anatomical distribution of the surgical procedure. In fact, such pre-incision therapies have been shown to help prevent the development of altered processing of afferent neuronal pain input, which would otherwise heighten postoperative pain4. this is one of the concepts supporting the practice of multimodal analgesia, utilizing different types and routes of analgesic therapy in order to manage postsurgical pain.
this review article summarizes the literature detailing the impact of different surgical and anesthetic techniques on post-operative pain for several types of gastrointestinal surgeries, including pancreatoduodenectomy, hepatectomy, gastric bypass, cholecystectomy, colectomy, and appendectomy. in addition, this review also highlights the need for increased attention and comparative outcome studies
addressing perioperative pain management after gastrointestinal surgery.
Pancreatoduodenectomy
Pancreatoduodenectomy, or Whipple procedure, is performed to treat cancerous tumors located in the pancreas, bile ducts, and duodenum. By removing portions of the stomach, gallbladder, pancreas, and duodenum, the surgeon reattaches the pancreas to the jejunum to allow food and gastrointestinal juices to empty. although there is wide variation among centers and particular surgeons, the procedure typically involves a moderate to large size abdominal incision which contributes to significant post-operative pain. numerous recent studied have focused on the effects of intravenous (iv) versus epidural analgesia. epidural catheters have been found to provide better pain relief than iv analgesic medications. they have been associated with a significantly decreased risk of postoperative pneumonia and insulin resistance, while improving pulmonary function and arterial oxygenation5, and decreased hospital time6.
in particular, thoracic epidural anesthesia has been demonstrated to improve post-operative pain in major abdominal surgeries and has also been associated with decreased rates of post-operative pneumonia7 and even insulin resistance8. as such, it has become a standard approach to post-operative pain control in patients undergoing pancreatic and other major abdominal surgery. However, there are instances in which the procedure is contraindicated, for example, in the setting of coagulopathy. other studies have suggested that it may increase the risk of hemodynamic instability and compromise to enteric anastomoses, intestinal perfusion and recovery of bowel function6.
a number of gastrointestinal complications, including ileus, biliary leakage, and bleeding, have been shown to increase with epidural use9. The fluid shifts that occur during epidural use can lead to an increased risk of intensive care unit admission. Likewise, up to one-third of epidurals may not function satisfactorily due to poor insertion levels, insufficient local anesthetic/opioid dosages, or pump failure. since, the use of epidural analgesics seem to decrease hospitalization time and control pain effectively,

M.E.J. ANESTH 23 (2), 2015
139Pain Control in Gastrointestinal surGery
more evidence has been building in favor for its use6. additional studies on epidural use in laparoscopic pancreatic resections are necessary, as not all situations allow for its use.
The most common alternative to post-operative pain control is patient controlled analgesia (PCa), in which intravenous opioid therapy may be administered in increments based on patient preferences. another alternative is intravenous infusion of lidocaine. in a systemic review of 8 trials, there was a decrease in the duration of ileus, length of hospital stay, post-operative pain and post-operative nausea and vomiting with intravenous lidocaine infusion compared to PCa morphine10.
Further, ultrasound guided transversus abdominis plane (taP) block has been shown to provide anesthesia to the anterolateral abdominal wall. although there are no studies comparing taP blocks to epidurals and other modalities of post-operative pain control, a recent meta-analysis of randomized controlled trials found the procedure to reduce opioid requirements and opioid-associated side effects, in addition to improving pain relief compared to patients who did not receive a taP block as part of the perioperative pain management plan11.
the surgical techniques utilized in pancreatic surgery have also been found to impact postoperative pain. Minimally invasive surgery has been the desired method of surgery in recent years, as it tends to reduce postoperative pain, increase patient mobility, increase recovery rates, and provide a better cosmetic appearance12. a recent retrospective analysis compared outcomes between patients undergoing hybrid laparoscopy-assisted pancreaticoduodenectomy (HlaPD), in which pancreaticoduodenal resection is performed laparoscopically while reconstruction is completed via a small upper midline minilaparotomy, and open pancreaticoduodenectomy (oPD). the HLAPD demonstrated not only a significantly lower estimated intraoperative blood loss and a shorter length of hospital stay, but also the HlaPD tended to have lower analgesic requirements. twelve (92%) patients in the HlaPD group used an epidural for postoperative pain control compared with 19 (95%) patients in the OPD group. Mean 7-day analgesic requirements were lower in patients who underwent HlaPD than those
who underwent oPD (174 mg v. 288 mg), though this trend did not achieve significance (p = 0.08)13. therefore, in addition to medical and anesthetic variables contributing to improved postoperative pain, novel and less-invasive surgical techniques also may impact postoperative pain in patients undergoing pancreatoduodenectomy. However, further research is warranted, particularly larger and multi-centered comparative randomized trials evaluating postoperative pain between open versus minimally invasive techniques may help further define its role in improving postoperative pain outcomes.
Hepatectomy
a partial hepatectomy can refer to the resection of hepatic tissue from a diseased liver, either due to benign or malignant neoplasms, metastases, gallstones or parasitic cysts. as in the case of pancreatoduodenectomy, hepatectomies can frequently involve wide upper abdominal incisions, contributing to post-operative pain control and affecting recovery time.
the risk of coagulopathy after liver resection surgery has made the placement of epidurals controversial. although no cases of epidural hematoma formation have been linked to liver resection14, catheters are often not removed before coagulation studies return to normal postoperatively. even at 7 days postoperatively, the prothrombin time (Pt) may be as prolonged as long as 22%. Further, 7-8% of catheters can be expected to spontaneously dislodge during use15, and 50% of epidural hematomas occur as a result of catheter removal16. Previously, an inr of 1.4 was considered the highest safe value for removal of an epidural catheter. a large prospective study in patients with epidurals and demonstrated that epidural removal with inrs higher than 1.4 did not result in any epidural hematoma formation of over 4,000 patients17. this may not be generalizable to all liver procedures. in the study, patients were on warfarin, which selectively inhibits the vitamin K-dependent coagulation factors. therefore, the use of epidurals has been demonstrated to be safe with a certain degree of coagulopathy, and it has been studied extensively in its role on postoperative pain after liver surgery.

140 BenjaMin Maslin et. al
a working epidural provides excellent pain control for liver resection. However, one study found that 20% of epidurals in one study did not function or functioned poorly18. intrathecal morphine has been used as a substitute for epidural analgesia with mixed results. some studies have demonstrated a higher rate of rescue parenteral opioid analgesia with intrathecal morphine19. others have attempted to demonstrate adequate pain relief with intrathecal morphine and gabapentin compared with epidural analgesia. However, use of other analgesic modalities such as nsaiDs and systemic opioids has made the results unclear20. interestingly, patients treated with their regimen of intrathecal morphine and gabapentin pre- and postoperatively ate 4 hours earlier on average and were discharged 1.9 days earlier than patients in the epidural group.
Another modality utilized for post-operative pain control after hepatic surgery is infusion of local anesthetic via the On-Q Pain Buster, which can continuously deliver local anesthetics for up to five days. In one study involving forty-eight patients scheduled for elective liver surgery, the treatment group received ropivacaine 0.25% infusion at 4 ml/hr for 68 hours via two multi-orifice indwelling catheters placed within the musculo-fascial layer before skin closure along with morphine PCa. Compared to the control group receiving saline infusion, the ropivacaine group had decreased morphine requirements and improved post-operative pain relief21. an infusion of no more than 0.25% ropivacaine or duration of infusion of less than 2 days is recommended due to concerns of increased plasma levels post hepatectomy22. in a recent prospective, randomized study forty adult living liver donors were assigned to receive either intrathecal morphine along with intravenous fentanyl or 0.5% ropivacaine via a multi-orifice catheter (On-Q Pain Buster) placed at the wound. While analgesia was less effective in the first twelve hours after surgery in the Pain Buster group and comparable in later hours, patients in the Pain Buster group had shorter bowel recovery time23. local anesthetic infusions through the Pain Buster, therefore, represent an appealing alternative to epidural, intravenous and intrathecal methods of post-operative pain control after liver surgery.
recently, several surgical approaches have evolved for liver resections, including totally laparoscopic, hand-assisted, and laparoscopic-assisted open “hybrid” techniques. these surgically techniques, which are less invasive than standard open approaches, tend to be associated with less operative blood loss, less postoperative pain and analgesic requirements, and a shorter length of hospital stay, with comparable postoperative morbidity and mortality to open liver resection24. therefore, surgical technique along with anesthetic approaches, have significant impacts on perioperative pain control in liver surgery.
Gastric Bypass Surgery:
there are approximately 9 million morbidly obese (BMi of 40 or above) individuals in the united states. obesity predisposes individuals to a variety of health factors throughout their lives. Cases of morbid obesity are rising in the united states, with an estimated 300,000 deaths attributed to complications of the disease snnually in the united states25. Gastric bypass, a type of bariatric surgery to treat obese, morbidly obese, or super-obese patients, typically divides the stomach into an upper and lower pouch that, when reconnected to the small intestine, reduces the functional volume of the stomach and amount of food stored. in this particular type of surgery, the effects of surgical technique and multimodal pain management interventionas on postoperative pain have been studied extensively.
obesity presents unique challenges to the clinician with regard to controlling pain and respiratory and hemodynamic stability perioperatively when bariatric surgery is performed. obese patients may be more sensitive to the respiratory depressant effect of opioid analgesic drugs and are more likely to require postoperative ventilation to avoid hypoxic episodes. Patients that were placed on continuous low dose ketamine infusion (1lg/kg/min) with remifentanil and propofol infusion (TIVA) for laparoscopic Roux-en-Y gastric bypass (lryGB) had decreased pain scores, morphine PCa consumption, and better hemodynamic stability than a combination of remifentanil-propofol alone26. this may be due to ketamine’s activation of descending pain inhibitory mono-aminergic pathways

M.E.J. ANESTH 23 (2), 2015
141Pain Control in Gastrointestinal surGery
to produce anti-nociception. Likewise, the use of 0.5% iP bupivacaine during lryGB compared to saline alone reduced overall postoperative opioid consumption. However, other outcome variables, including length of stay and vas scores, showed no significant difference27.
Laparoscopic procedures require insufflation of the abdomen with carbon dioxide in order to enhance the visual field and facilitate instrumentation. One study looked at whether different values of intra-abdominal pressures had an impact on postoperative visceral type pain. Patients were randomized into low pressure (8 mmHg), standard pressure (12 mmHg), and high pressure (14 mmHg) groups. However, when comparing these groups based on age, weight, and analgesic consumption, no statistically significant difference was found, suggesting that insufflation pressures did not have a major impact on postoperative visceral pain28.
several recent studies have investigated the role of multimodal approaches to the management of perioperative pain in patient scheduled for obesity related surgery, such as gastric bypass. in a study of 114 patients undergoing gastric bypass surgery, patients were randomized to incisional local anesthetic infiltration plus post-operative PCA (Group a), epidural anesthesia and analgesia (Group B) or post-operative PCA (Group C). The authors demonstrated lower pain scores in Group a than in Groups B or C when measured 0, 12 and 36 hours in the post-operative period, thereby demonstrating that a multimodal approach—incorporating incisional local anesthetic to more conventional modalities such as PCA—can result in optimized post-operative pain control29. a recent retrospective analysis attempted to compare traditional approaches to pain management in obese patients undergoing various bariatric surgeries, including laparoscopic Roux-en-Y gastric bypass and laparoscopic adjustable banding to a multidisciplinary approach. Karlnoski and colleagues demonstrated that compared to standard ketolorac and morphine PCa for pain control, an interdisciplinary approach with ketorolac, hydromorphone PCa and bariatric team consisting of a psychologist, exercise physiologist and nutritionist, significantly improved pain control in post-operative days one through five30. thus, bariatric
surgery is one area of gastrointestinal surgery that has been studied that demonstrates the benefits of both multimodal therapy and multidisciplinary approaches to post-operative pain management.
Cholecystectomy
Cholecystectomies, of which more than 750,000 are performed annually in the united states, are performed for a wide variety of reasons, most commonly as treatment for cholecystitis, biliary colic and cancer of the gallbladder. although most commonly performed laparoscopically, pain continues to be a significant barrier to discharge during the postoperative course.
epidural analgesia is seldom used for the treatment of post-cholecystectomy pain, but it is a feasible option. one group investigated the feasibility of epidural analgesia for laparo-endoscopic single-site cholecystectomy (LESS) in a 20-patient cohort31. Patients receiving epidural analgesia had lower pain scores on a visual analogue scale (vas) score than patients receiving general anesthesia and were able to be discharged on the day of surgery. Patients in the epidural group had higher rates of shoulder pain but less nausea and vomiting. These findings were not statistically significant. Interestingly, patients remained spontaneously breathing during epidural anesthesia, and did not have adverse respiratory outcomes or impaired respiration as evidenced by arterial blood gas analysis. another study found that open cholecystectomy pain was better managed with epidural analgesia than iv analgesia. although both groups had similar numbers of patients discharged within 36 hours, only 4.1% of epidural patients required additional analgesia, compared with 29.4% in the iv group. nausea was also significantly lower in the epidural group than in the iv group32. These findings, however, are in contrast to a group that investigated epidural versus general anesthesia for laparoscopic cholecystectomy in elderly patients at a single hospital33. they found that analgesia was that same in both groups, but that patient satisfaction was higher in the general anesthesia group, which was attributed to the discomfort associated with the epidural placement.
in the united states, most cholecystectomies are

142 BenjaMin Maslin et. al
performed laparoscopically with small incisions, and for this reason epidural analgesia has played a smaller role in management of postoperative pain. However, when an open cholecystectomy must be performed, or if the cholecystectomy is a component of a larger abdominal surgery, epidural analgesia is more often considered. in these cases, epidural analgesia is considered, as it has been found to be associated with fewer pulmonary and cardiac complications compared with patient-controlled opioid analgesia in patients undergoing laparotomy. Based on a meta-analysis of patients undergoing thoracic and abdominal surgery, those who received an epidural had an odds ratio of 0.54 of developing pneumonia when compared with patients receiving parenteral, oral, or intramuscular opioids7. epidurals also decreased the odds of prolonged ventilation and reintubation. in addition, the odds of myocardial infarction were decreased in their study, odds ratio 0.55, nnt 48. they also determined that as pulmonary complications of surgery decreased with time, this difference had become smaller in subsequent trials.
several recent studies have demonstrated improved post-operative pain control after cholecystectomy utilizing agents that function to modulate GaBa, a neurotransmitter whose activation has been linked to dampening of the response to painful stimuli. one such medication is pregabalin, a GaBa analogue used as an anticonvulsant and treatment for neuropathic pain. in a randomized controlled trial involving patients undergoing laparoscopic cholecystectomy, administration of pregabalin 600 mg orally, divided in two preoperative doses, significantly reduced post-operative pain and opioid requirements, however did lead to greater incidence of dizziness34. Gabapentin, a GaBa analogue used widely in the treatment of neuropathic pain, is another medication which has recently been shown to improve post-operative pain specifically in patients undergoing laparoscopic cholecystectomy. in a randomized controlled study, patients receiving Gabapentin 300 mg two hours before laparoscopic cholecystectomy were found to have significantly lower postoperative pain and fentanyl requirements when compared to subjects receiving tramadol 100 mg or placebo35.
surgical technique has also been studied with
regard to its effects on postoperative pain after cholecystectomy. one study investigated whether active aspiration of subdiaphragmatic gas verses simple evacuation reduced pain after laparoscopic cholecystectomy. study outcomes were based on postoperative analgesic requirement and level of abdominal and shoulder pain after 24 hours. investigators found that the simple evacuation group had higher use of analgesics and experienced more abdominal and shoulder pain than the active aspiration group36. Additionally, the use of warm, humidified insufflation was found to reduce pain after laparoscopy. these conclusions were drawn from seven randomized controlled studies on adults undergoing elective laparoscopic cholecystectomies in which the exposure groups had warm, humidified insufflation and the control groups had standard, cold dry carbon dioxide. The group exposed to warm, humidified insufflation had lower pain scores on the vas and decreased morphine usage37. all of these studies suggest that modification of the surgical technique with respect to insufflation can significantly impact postoperative analgesia.
another study investigating surgical technique and postoperative pain in cholecystectomies demonstrated that the number of ports had a significant impact on postoperative pain and analgesic requirements. in the prospective trial, patients were randomized to undergo elective surgery with either the conventional 4-port laparoscopic cholecystectomy or a single-port cholecystectomy. after surgery, postoperative pain on a visual analogue scale and analgesic use were measured, and the single port group had significantly lower pain scores and analgesic use (9 of 24 in single port group versus 19 of 25 in the four-port group; P = 0.007)38. similar conclusions were found in another study that compared a new surgical technique of a single incision laparoscopic colectomy with a conventional multiple incision colectomy. Patients in the single incision group had lower pains scores, shorter hospital stays, and improved cosmetic outcomes39.
Furthermore, another study examined whether the port location that was used for gallbladder removal had any impact on postoperative pain scores. over a six-month period, adult patients who were scheduled to undergo elective laparoscopic cholecystectomies

M.E.J. ANESTH 23 (2), 2015
143Pain Control in Gastrointestinal surGery
were randomized into two groups: those who had gallbladder retrieval through the epigastric port and those who had it through the umbilical port. those who had gallbladder removal from the umbilical port were found to have less pain after 24 hours40.
Finally, another modality of surgical technique that has been studied with regard to postoperative pain outcomes is intraperitoneal administration of local anesthesia (IP-LA) either during or after laparoscopic cholecystectomy. A meta-analysis of IP-LA on postoperative abdominal pain outcomes in laparoscopic cholecystectomies reports a significant improvement in 50% of the cases and a quicker hospital discharge. local anesthesia resulted in a smaller reduction in pain when a PCa was also used41. Perioperative pain control during cholecystectomy, therefore, appears to have the potential to be optimized by a wide variety of analgesic and surgical techniques.
Colectomy
More than 250,000 colorectal resections are performed annually in the united states, and up to 35% of these will develop a complication. Colorectal surgeries encompass vein inflammation (hemorrhoids), fissures, fistulas, cancers, and inflammatory bowel disease. Postoperative pain is a major contributor to increased hospitalization, morbidity and patient satisfaction after colorectal surgery.
as in other gastrointestinal surgeries, the effect of epidural analgesia on postoperative pain after colorectal surgery is a subject of several recent studies. A recent meta-analysis of colorectal surgery patients demonstrated that epidural placement was associated with improved analgesia as judged on a visual analogue scale when compared with parenteral opioid analgesia42. Postoperative ileus was 36 hours shorter on average in the epidural groups with the exception of one study included in the analysis. However, the primary outcome of the study was length of hospital stay, which was not different between the two groups. not surprisingly, higher rates of urinary retention, arterial hypotension, and pruritus were found in the epidural group. The study did not find a difference in anastomotic leakage rates regardless of the type of postoperative analgesia43.
the utilization of epidural analgesia in colorectal surgery, however, is controversial due to possible effects on postoperative bowel function. epidural analgesia invariably leads to increased fluid loading due to the associated hypotension, which appears to have an impact in bowel procedures. one study demonstrated an increased length of stay in patients that received higher amounts of fluid during elective colon surgery. Gastric emptying was delayed for solid and liquids 56 and 52 minutes, respectively, in the group who received liberal amounts of fluid versus a group who had their fluids restricted44. However, in one study, when patients received intrathecal pain management (which acts neuraxially like epidural analgesia), hypotension developed but was not managed with fluid administration. These patients were compared to those not receiving intrathecal therapy and there was no observed difference in return of bowel function or postoperative complications45. Another meta-analysis came to the conclusion that epidural local anesthetics led to improved pain control as well as faster return of bowel function than opioids, whether administered systemically or epidurally46. Postoperative ileus was shorter in patients receiving epidural analgesia; however, prolonged ileus, defined as first bowel movement after postoperative day 7, occurred with equal frequency47. Patients with prolonged ileus were more likely to have multiple comorbidities. in this study, as well as others, time to hospital discharge was not decreased in patients receiving epidural analgesia.
surgical technique has also been studied with respect to effects on postoperative pain after colorectal surgery. studies have found that colonic motility and patient condition improve more rapidly following laparoscopic assisted sigmoid colectomy (lasC) compared to an open procedure, although there were no differences in nausea, bowel sounds, or abdominal pain48. another study compared a new surgical technique of a single incision laparoscopic colectomy with a conventional multiple incision colectomy. Patients in the single incision group had lower pains scores, shorter hospital stays, and improved cosmetic outcomes39. Perioperative pain control during colectomy, therefore, appears to have the potential to be optimized by a wide variety of analgesic and surgical techniques.

144 BenjaMin Maslin et. al
Appendectomy
the laparoscopic appendectomy is one of the most common procedures performed in the united states, for acute appendicitis and on an emergent basis in the setting of abscess or peritonitis. With over 270,000 appendectomies performed annually in the united states, postoperative pain control represents a significant barrier to discharge and patient satisfaction.
as in other gastrointestinal surgeries, surgical technique may impact postoperative pain. Conventional laparoscopic appendectomies are performed using 10-mm sized ports; however, there has been a recent increase in use of smaller laparoscopic scopes, including 5- and 2-mm sizes. While smaller ports may lead to less postoperative pain, there are significant limitations to their use. these ports can limit the Co2 flow rate and lessen the ability to coagulate during instances of bleeding. studies have demonstrated that those patients of increasing age or with a history of abdominal surgeries may be predisposed to requiring larger ports49.
a surgical technique being studied is the use of a single-port laparoscopic approach. The primary advantage of single-port laparoscopic appendectomy (sPla) is that it requires only a single incision at the umbilicus, which reduces incisional pain and creates better cosmetic effects without the need for open and invasive techniques. Conventional laparoscopy, which uses 3 ports, tends to have longer operative times and less desirable perioperative outcomes compared to sPla50,51.
since the vast majority of appendectomies performed in the united states are done laparoscopically with small incisions, the use of epidural analgesia is very rate. interestingly, Bupivacaine, which is often administered via an epidural injection to reduce postoperative pain in surgical procedures, was studied in the form of wound infiltration to reduce postoperative pain after appendectomies. the use of preincisional 0.5% bupivacaine infiltration in single-incision laparoscopic appendectomy (SILS-A) was found to reduce postoperative pain compared to the conventional laparoscopic approach52. therefore, variables in surgical technique and analgesic modalities have impacts on the optimization of perioperative pain control for appendectomy.
Conclusion
Postoperative pain is widely considered a significant public health concern in the United States and abroad and its under-treatment impacts morbidity, patient satisfaction and hospital costs significantly. Poorly managed perioperative pain can lead not only to suffering in the immediate postoperative period, but has also been shown to contribute to the development of long term psychological distress and even chronic, postsurgical pain requiring medical attention well beyond the perioperative period [Cohen 2013].
surgeries of the gastrointestinal tract present unique challenges to the clinician in both preventing and managing post-operative pain. Surgical techniques, the necessity of larger incisions and the possibility of surgically related ileus complicate both the prevention and management of pain. in addition, there exists great variability in the timing and types of analgesic therapies that may be utilized to help manage pain throughout the entire perioperative period. though much research has been devoted in the past several years to addressing possible surgical, medical and anesthetic techniques to improve postoperative pain in general, there is a dearth of literature on pain management addressing the specific challenges encountered in gastrointestinal surgery.
Given the high prevalence of gastrointestinal surgeries, and the potential for increased incidence along with the aging of the united states population, further outcomes and comparative research studies in perioperative pain control specifically addressing these procedures are warranted. Based on available evidence, it is clear that both surgical and analgesic variables may impact pain control. in particular, there is consistent evidence supporting the practice of less invasive surgical manipulation and the utilization of epidural analgesia for certain types of gastrointestinal procedures. the role of multimodal analgesia, with medications and interventions used together, also appears to optimize perioperative pain control in certain types of gastrointestinal surgeries. nevertheless, large randomized controlled studies are warranted to help further elucidate the role of novel multimodal approaches to perioperative pain control in gastrointestinal surgery to benefit patients well beyond the immediate postoperative period.
M.E.J. ANESTH 23 (2), 2015
145Pain Control in Gastrointestinal surGery
References
1. FiLos Ks, LeHmann Ka: Current concepts and practice in postoperative pain management: need for a change? Eur Surg Res; 31:997-107, 1999.
2. coHen p, raja sn: Prevention of chronic postsurgical pain. the ongoing search for the holy grail of anesthesiology. Anesthesiology; 118:241-243, 2013.
3. VadiVeLu n, mitra s, scHermer e, Kodumudi V, Kaye ad, urman rd: Preventive analgesia for postoperative pain control: a broader concept. Local Reg Anesth; May, 29, 7:17-22, 2014.
4. Kissin i: Pre-emptive analgesia. Anesthesiology; 93:1138-1143, 2000.
5. Lassen K, cooLsen mm, sLim K, et aL: Guidelines for perioperative care for pancreaticoduodenectomy: enhanced recovery after surgery (eras) society recommendations. Clinical Nutrition; 31:817-30, 2012.
6. pratt WB., steinBrooK ra, maitHeL sK, Vanounou t, caLLery mp, VoLLmer cm: epidural analgesia for pancreatoduodenectomy: a critical appraisal. Journal of Gastrointestinal Surgery; 12(7):1207-20, 2008.
7. pöpping dm, eLia n, marret e, remy c, tramèr mr: Protective effects of epidural analgesia on pulmonary complications after abdominal and thoracic surgery: a meta-analysis. Archives of Surgery; 143(10):990-9, 2008.
8. ucHida i, asoH t, sHirasaKa c, tsuji H: effect of epidural analgesia on post-operative insulin resistance as evaluated by insulin clamp technique. Br J Surg; 75:557-62, 1988.
9. cHoi dX, scHoeniger Lo: For patients undergoing pancreatoduodenectomy, epidural anesthesia and analgesia improves pain but increases rates of intensive care unit admissions and alterations in analgesics. Pancreas; 39(4):492-7, 2010.
10. marrett e, roLin m, Beaussier m, Bonnet F: Meta-analysis of intravenous lidocaine and postoperative recovery after abdominal surgery. Br J Surg; 95:1331-8, 2008.
11. siddiqui mr, sajid ms, uncLes dr, cHeeK L, Baig mK: A meta-analysis on the clinical effectiveness of transversus abdominis plane block. J Clin Anesth; 23:7e14, 2011.
12. nigri g, petrucciani n, La torre m, magistri p, VaLaBrega s, aureLLo p, et aL: Duodenopancreatectomy: open or minimally invasive approach? The Surgeon; 1-8, 2014.
13. Wang y, Bergman s, piedimonte s, Vanounou t: Bridging the gap between open and minimally invasive pancreaticoduodenectomy: the hybrid approach. Can J Surg; august, vol. 57, no. 4, 2014.
14. stamenKoVic dm, janKoVic ZB, toogood gj, Lodge jp, BeLLamy mc: epidural analgesia and liver resection: postoperative coagulation disorders and epidural catheter removal. Minerva Anestesiologica; 77(7):671-9, 2011.
15. tsui sL, yong BH, ng KF, yuen ts, Li cc, cHui Ky: Delayed epidural catheter removal: the impact of postoperative coagulopathy. Anaesthesia and Intensive Care; 32:630-6, 2004.
16. VandermeuLen ep, Van aKen H, VermyLen j: anticoagulants and spinal-epidural anesthesia. Anesthesia and Analgesia; 79:1165-77, 1994.
17. Liu ss, BuVanendran a, Viscusi er, et aL: uncomplicated removal of epidural catheters in 4365 patients with international normalized ratio greater than 1.4 during initiation of warfarin therapy. Reg Anesth Pain Med; 36(3):231-5, 2011.
18. reVie ej, massie Lj, mcnaLLy sj, mcKeoWn dW, garden oj,
Wigmore sj: effectiveness of epidural analgesia following open liver resection. HPB; (Oxford), 13:206-11, 2011.
19. de pietri L, siniscaLcHi a, reggian a, et aL: the use of intrathecal morphine for postoperative pain relief after liver resection: a comparison with epidural analgesia. Anesthesia and Analgesia; 102(4):1157-63, 2006.
20. Koea jB., young y, gunn K: Fast track liver resection: the effect of a comprehensive care package and analgesia with single dose intrathecal morphine with gabapentin or continuous epidural analgesia. HPB; 2009.
21. cHan sK, Lai pB, Li pt, et aL: The analgesic efficacy of continuous wound instillation with ropivacaine after open hepatic surgery. Anaesthesia; Dec, (65)12:1180-6, 2010.
22. WrigHton Lj, o’BosKy Kr, namm jp, sentHiL m: Postoperative management after hepatic resection. J Gastrointest Oncol; Mar, 3(1):41-7, 2012.
23. Lee sH, gWaK ms, cHoi sj, et aL: Prospective, randomized study of ropivacaine wound infusion versus intrathecal morphine with intravenous fentanyl for analgesia in living donors for liver transplantation. Liver Transpl; Sep, 19(9):1036-45, 2013.
24. reddy sK, tsung a, geLLer da: laparoscopic liver resection. World J Surg; Jul, 35(7):1478-86, 2011.
25. aLLison dB, Fontaine Kr, manson je, steVens j, VanLtaLLie tB: annual deaths attributable to obesity in the united states. JAMA; 282:1530-1538, 1999.
26. Hasanein r, eL-sayed W, naBiL n, eLsayed g: the effect of combined remifentanil and low dose ketamine infusion in patients undergoing laparoscopic gastric bypass. Egyptian Journal of Anesthesia; 27:255-60, 2011.
27. symons jL, Kemmeter pr, daVis at, et aL: A Double-Blinded, Prospective randomized Controlled trial of intraperitoneal Bupivacaine in Laparoscopic Roux-en-Y Gastric Bypass. J Am Coll Surg; 204:392-8, 2007.
28. ceLiK as, Frat n, ceLeBi F, et aL: laparoscopic Cholecystectomy and Postoperative Pain: Is it Affected by Intra-Abdominal Pressure? Surgical laparoscopy endoscopy & percutaneous techniques; aug, 20(4):220-2, 2010.
29. scHumann r, sHiKora s, Weiss jm, Wurm H, strasseLs s, carr dB: a comparison of multimodal perioperative analgesia to epidural pain management after gastric bypass surgery. Anesth Analg; Feb, 96(2):469-74, 2003.
30. KarLnosKi ra, sprenKer c, suViKram p, et aL: reduced Postoperative Pain and Complications after a Modified Multidisciplinary approach for Bariatric surgery. The Open Obesity Journal; 5:60-64, 2013.
31. ross sB, mangar d, KarLnosKi r, et aL: Laparo-endoscopic single-site (less) cholecystectomy with epidural vs. general anesthesia. Surgical Endoscopy; 27(5):1810-9, 2013.
32. ZaHoor mu, masroor r, KHursHid t, aZHar r, amjad yasin mm: thoracic epidural anaesthesia for open cholecystectomy. Journal of the College of Physicians and Surgeons; 21(11):654-8, 2011.
33. nisHiKaWa K, Kimura s, sHimodate y, igarasHi m, namiKi a: a comparison of intravenous-based and epidural-based techniques for anesthesia and postoperative analgesia in elderly patients undergoing laparoscopic cholecystectomy. Journal of Anesthesia; 21(1):1-6, 2007.
34. saraKatsianou c, tHeodorou e, georgopouLou s, stamatiou g,

146 BenjaMin Maslin et. al
tZoVaras g: Effect of pre-emptive pregabalin on pain intensity and postoperative morphine consumption after laparoscopic cholecystectomy. Surg Endosc; Jul, 27(7):2504-11, 2013.
35. pandey cK, priye s, singH s, singH u, singH rB, singH pK: Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscpic cholecystectomy. Can J Anaesth; Apr, 5(4):358-63, 2004.
36. ataK i, oZBagriaciK m, aKinci oF, et aL: active Gas aspiration to reduce Pain after laparoscopic Cholecystectomy. Surgical laparoscopy endoscopy & percutaneous techniques; Apr, 21(2): 98-100, 2011.
37. asaKuma m, HayasHi m, Komeda K, et aL: Impact of Single-Port Cholecystectomy on Postoperative Pain. British journal of surgery, Jul, 98(7):991-5, 2011.
38. sammour t, KaHoKeHr a, HiLL ag: Meta-Analysis of the Effect of Warm Humidified Insufflation on Pain After Laparoscopy. British Journal of Surgery; Aug, 95(8):950-6, 2008.
39. poon jt, cHeung cW, Fan jK, Lo os, LaW WL: Single-Incision versus Conventional laparoscopic Colectomy for Colonic neoplasm: a randomized, Controlled trial. Surgical endoscopy; Oct, 26(10):2729-34, 2012.
40. siddiqui na, aZami r, murtaZa g, nasim s: Postoperative Port-site Pain after Gall Bladder retrieval from epigastric vs. umbilical Port in laparoscopic Cholecystectomy: a randomized Controlled trial. International Journal Of Surgery; 10(4):213-6, 2012.
41. Boddy ap, meHta s, rHodes m: the effect of intraperitoneal local anesthesia in laparoscopic Cholecystectomy: a systematic review and Meta-Analysis. Anesth Analg;103:682-8, 2006.
42. marret e, remy c, Bonnet F: Meta-analysis of epidural analgesia versus parenteral opioid analgesia after colorectal surgery. British Journal of Surgery; 94(6):665-673, 2007.
43. micHeLet p, d'journo XB, rocH a, et aL: Perioperative risk factors for anastomotic leakage after esophagectomy: influence of thoracic epidural analgesia. Chest; 128:3461-346, 2005.
44. LoBo dn, BostocK Ka, neaL Kr, perKins ac, roWLands Bj, aLLison sp: effect of salt and water balance on recovery of
gastrointestinal function after electvie colonoic resection: a randomized controlled trial. The Lancet; 359(9320):1812-1818, 2002.
45. HuBner m, LoVeLy jK, HueBner m, sLettedaHL sW, jacoB aK, Larson dW: intrathecal analgesia and restrictive Perioperative Fluid Management within enhanced recovery Pathway: Hemodynamic implications. Journal of the American College of Surgeons; 216(6):1124-1134, 2013.
46. jorgensen H, WettersLeV j, moinicHe s, daHL jB: epidural local anesthetics versus opioid-based analgesic regimens for postoperative gastrointestinal paralysis, Ponv and pain after abdominal surgery. Cochrane Database of Systematic Reviews; (4), 2000.
47. KuruBa r, Fayard n, snyder d: epidural analgesia and laparoscopic technique do not reduce incidence of prolonged ileus in elective colon resections. The American Journal of Surgery; 204(5):613-618, 2012.
48. KaspareK ms, muLLer mH, gLatZLe, et aL: Postoperative Colonic Motility in Patients Following Laparoscopic-Assisted and Open sigmoid Colectomy. J Gastrointest Surg;7:1073-81, 2003.
49. eL-dHuWaiB y, Hamade am, issa me, BaLBisi Bm, aBid g, ammori Bj: An “All 5-mm Ports” Selective Approach to Laparoscopic Cholecystectomy, Appendectomy, and Anti-Reflux Surgery. Surg Laparosc Endosc Percutan Tech; 14:141-4, 2004.
50. qiu j, yuan H, cHen s, He Z, Wu H: Single-port Laparoscopic appendectomy versus Conventional laparoscopic appendectomy: evidence From randomized Controlled trials and nonrandomized Comparative studies. Surg Laparosc Endosc Percutan Tech; 24:12-21, 2014.
51. ding j, Xia y, ZHang Zm, et aL: Single-incision versus conventional three-incision laparoscopic appendicetomy for appendicitis: a systematic review and meta-analysis. Journal of Pediatric Surgery; 48:1088-98, 2013.
52. aHn sr, Kang dB, Lee c, parK Wc, Lee jK: Postoperative Pain Relief Using Wound Infiltration With 0.5% Bupivacaine in Single-Incision Laparoscopic Surgery for an Appendectomy. Ann Coloproctol; 29(6):238-42, 2013.

147 M.E.J. ANESTH 23 (2), 2015
SCIENTIFIC ARTICLES
Resident implementation of the 2007 aCC/aha Guidelines on pReopeRative CaRdiaC
evaluation in non-CaRdiaC suRGeRy patients: is CliniCal expeRienCe enouGh?
Hassan H. amHaz*, RutH Kuo**, EliE J. CHidiaC**, Vinay PallEKonda**, samiR F. FulEiHan**, GEoRGE mCKElVEy***
and RomEo n. Kaddoum**
Abstract
Background: preoperative evaluation of surgical patients is important, as perioperative complications are associated with increased mortality. specialties including anesthesiology, internal medicine, cardiology, and surgery are involved in the evaluation and management of these patients. this institutional study investigated the residents’ knowledge of the 2007 american College of Cardiology/american heart association (aCC/aha) guidelines on perioperative evaluation of patients undergoing non-cardiac surgery.
Methods: this pilot study used a web-based survey questionnaire to assess resident’s knowledge of the 2007 aCC/aha guidelines through individual steps and corresponding branch point(s) in twelve clinical scenarios. additionally, residents were asked if they were aware of, or if they had received lectures on aCC/aha guidelines. staff anesthesiologists with training in cardiac and intensive care medicine validated the scenarios.
Results: a total of 104 resident participants were surveyed including 35 anesthesiology residents, 41 internal medicine residents, 20 surgery residents, and 8 cardiology fellows. awareness of the 2007 aCC/aha guidelines by specialty was: anesthesiology (85%), internal medicine (97.6%), cardiology (100%), and surgery (70%). only 54.3% of anesthesiology, 31.7% of internal medicine, 100% of cardiology, and 10% of surgery residents stated they received lectures. the overall mean score achieved on the eleven scenarios was 50.4% for anesthesiology, 47.0% for internal medicine, 55.7% for cardiology, and 42.3% for surgery.
Conclusions: although the majority of residents were aware of the 2007 aCC/aha guidelines, fewer received lectures and regardless of specialty, implementation of these guidelines was poor. There exists significant room for improvement in the understanding of preoperative assessment of non-cardiac surgery patients.
* md, ms.** md.*** phd. Affiliation: Department of Anesthesiology, Wayne State University, Detroit Medical Center; Detroit, Michigan, United
states. Corresponding author: Romeo N. Kaddoum, MD Assistant Professor; Wayne State University, Detroit Medical Center;
3990 John R, Rm 2901; 2-Hudson, Detroit, MI 48201, United States. Office: 1-313-745-7233, Fax: 1-313-993-3889. Email: [email protected]

148 Romeo n. Kaddoum et. al
Introduction
preoperative evaluation of surgical patients is critically important as perioperative complications are associated with increased costs and mortality1,2. the american College of Cardiology (aCC) and american heart association (aha), beginning in 1980, jointly established evidence-based guidelines to systematically facilitate cardiac evaluation in non-cardiac surgery patients. numerous specialties including anesthesiology, cardiology, internal medicine and surgery are involved in the evaluation and management of patients undergoing surgery and thus should have facile and comprehensive knowledge of these guidelines. for this reason, we decided to investigate the residents’ knowledge, amongst the aforementioned specialties at our institution, of the 2007 aCC/aha guidelines on perioperative cardiac management for patients undergoing non-cardiac surgery.
Methods
after institutional iRB approval (iRB#036612B3x) was obtained, we developed a pilot study at our institution using a web-based survey questionnaire to assess residents’ knowledge of the 2007 aCC/aha guidelines on preoperative cardiac evaluation of patients undergoing non-cardiac surgery. Residents from anesthesiology, cardiology, internal medicine and general surgery were asked to complete this questionnaire (appendix). each resident was asked to identify which specialty they belonged to and level of training they were at, whether they were aware of the 2007 aCC/aha guidelines and if they had lectures on these guidelines. additionally, they were asked to answer twelve clinical scenarios developed to test their knowledge of each possible step and its corresponding branch point(s) of the 2007 aCC/aha algorithm.
AppendixQuestions:1. What is your area of specialization?
a. Anesthesiologyb. Internal Medicinec. Cardiologyd. General Surgery
2. Which year of training are you in?e. If selected Anesthesiology – will have the
following choicesi. PGY-1ii. CA1iii. CA2iv. CA3v. Fellowvi. Other:f. If selected Internal Medicinei. PGY-1ii. PGY-2iii. PGY-3g. If selected Cardiologyi. Fellow – first yearii. Fellow – second yeariii. Fellow – third yeariv. Other:h. If selected Surgeryi. PGY-1ii. PGY-2iii. PGY-3iv. PGY-4v. PGY-5vi. PGY-6vii. Other:
3. Are you aware that there are guidelines for the preoperative evaluation of noncardiac surgery patients (e.g. 2007 ACC/AHA guidelines)?
i. Yesj. No
4. Have you had any formal lectures or teaching that reviewed these guidelines?
k. Yesl. No
5. Scenario 1:a 58-year-old man with uncontrolled hypertension, CKd stage iii, and insulin-dependent diabetes mellitus with a hgba1c of 10.7, who recently went to his primary care physician for complaints of worsening chest pain presents after being involved in a motor vehicle accident and is found to be hypotensive with significant abdominal ecchymoses with positive peritoneal lavage.the most appropriate next step would be to:
1. patient should undergo cardiac stress testing prior to surgery2. start patient on a β-blocker for heart rate control and proceed with surgery3. patient should go immediately to surgery4. patient needs cardiac catheterization prior to surgery5. patient needs a 2-d echocardiogram
6. Scenario 2:a 71-year-old woman with hypertension, diabetes, right
M.E.J. ANESTH 23 (2), 2015
149Resident implementation of the aCC/aha pReopeRative Guidelines
upper extremity weakness with cervical stenosis, and renal insufficiency with Cr = 2.4 mg/dL comes for pre-operative evaluation for anterior cervical discectomy and fusion. she reports that she has been experiencing worsening chest pain and shortness of breath over the past week while gardening outside.the most appropriate next step would be to:
1. allow patient to proceed with surgery2. patient can proceed with surgery if her pre-operative eKG is normal3. start patient on a β-blocker for heart rate control and proceed with surgery4. patient should have cardiac stress testing prior to surgery5. patient should get cardiac catheterization prior to surgery
7. Scenario 3:a 59-year-old man with hypertension, diabetes, and Chf presents for pre-operative evaluation for inguinal hernia repair.he reports having light-headedness and palpitations. physical exam reveals irregular pulse and crackles on lung auscultation.the most appropriate next step would be to:
1. allow patient to proceed with surgery2. patient can proceed with surgery if his pre-operative eKG is normal3. patient should undergo additional medical testing prior to surgery4. start patient on a β-blocker for heart rate control and proceed with surgery5. patient should get cardiac catheterization prior to surgery
8. Scenario 4:a 69-year-old man with hypertension, diabetes and osteoarthritis presents for pre-operative evaluation for total left knee replacement. he complains of worsening shortness of breath on exertion and has been awaking at night gasping for air. on exam, there is a diastolic murmur at the left sternal border and head nodding synchronous with the heartbeat.the most appropriate next step would be to:
1. allow patient to proceed with surgery2. patient can proceed with surgery if her pre-operative eKG is normal3. start patient on a b-blocker for heart rate control and proceed with surgery4. patient should have echocardiography testing prior to surgery5. patient should get cardiac catheterization before pre-operative evaluation can be completed
9. Scenario 5:a 78-year-old man with poorly controlled hypertension and diabetes, hyperlipidemia, and osteoarthritis is scheduled for a lipoma excision. he takes morning walks and works in his
garage without any difficulty.the most appropriate next step would be to:
1. allow patient to proceed with surgery2. patient can proceed with surgery if her pre-operative eKG is normal3. start patient on a b-blocker for heart rate control and proceed with surgery4. patient should undergo cardiac stress testing prior to surgery5. patient needs medical management of hypertension and diabetes prior to surgery
10. Scenario 6:a 51-year-old man with history of smoking, gastroesophageal reflux, poorly controlled diabetes, and prior MI 3 months ago comes to the pre-operative clinic in preparation for a hiatal hernia repair. in the mornings, he walks with his wife for 30 minutes several times around the block without any difficulty.the most appropriate next step would be to:
1. patient can proceed with surgery if his pre-operative eKG is normal2. start patient on a b-blocker for heart rate control and proceed with surgery3. allow patient to proceed with surgery4. patient should undergo cardiac stress testing prior to surgery5. patient needs medical management of diabetes prior to surgery
11. Scenario 7:a 69-year-old woman with long-standing diabetes, prior transient ischemic attack without residual deficits, and chronic renal insufficiency with Cr = 2.2 mg/dL presents for pre-operative evaluation for subtotal colectomy and ileostomy secondary to recurrent bleeding from diverticulosis. she is able to go up stairs to her bedroom; however, she must take short breaks to catch her breath.the most appropriate next step would be to:
1. patient can proceed with surgery if her pre-operative eKG is normal2. start patient on a b-blocker for heart rate control and proceed with surgery3. allow patient to proceed with surgery4. patient must undergo cardiac stress testing prior to surgery5. patient needs medical management of diabetes prior to surgery
12. Scenario 8:a 53-year-old obese man with osteoarthritis and 35-pack year smoking history is scheduled for left knee replacement. he has a family history of stroke and his father died of an mi at 49 years of age. pre-operatively his Bp is 160/87 mm hg.the most appropriate next step would be to:
150 Romeo n. Kaddoum et. al
1. patient can proceed with surgery if his pre-operative eKG is normal2. start patient on a b-blocker for heart rate control and proceed with surgery3. patient should undergo cardiac stress testing prior to surgery4. patient needs medical management of hypertension prior to surgery5. allow patient to proceed with surgery
13. Scenario 9:
a 79-year-old woman with uncontrolled diabetes, CKd stage ii, nyha class iii Chf, and peripheral artery disease who is scheduled for a femoral to popliteal bypass due to worsening claudication. patient’s pre-operative Bp is 144/78 mm hg and hR is 82 bpm.
the most appropriate next step would be to:1. patient can proceed with surgery if his pre-operative eKG is normal2. start patient on a b-blocker for heart rate control and proceed with surgery3. patient needs medical management of diabetes prior to surgery4. patient must undergo additional cardiac testing prior to surgery5. allow patient to proceed with surgery
14. Scenario 10:a 86-year-old man with 30-pack-year smoking history, mi 3 years ago, poorly controlled diabetes, and claudications resulting from peripheral vascular disease is found to have a pulsatile abdominal mass. Ct imaging shows a 6.7-cm abdominal aortic aneurysm. patient’s pre-operative Bp is 132/84 mm hg and hR is 82 bpm.the most appropriate next step would be to:
1. patient can proceed with surgery if his pre-operative eKG is normal2. start patient on a b-blocker for heart rate control and proceed with surgery3. patient needs medical management of diabetes prior to surgery4. patient must undergo additional cardiac testing prior to surgery5. allow patient to proceed with surgery
15. Scenario 11:a 63-year-old man with history osteoarthritis, 30-pack-year smoking history, and claudications from advanced peripheral vascular disease is scheduled for a Whipple secondary to pancreatic carcinoma.the most appropriate next step would be to:
1. patient can proceed with surgery if his pre-operative eKG is normal
2. start patient on a b-blocker for heart rate control and proceed with surgery3. surgery should be cancelled if patient continues to smoke4. patient should undergo additional cardiac testing prior to surgery5. allow patient to proceed with surgery
We believe that to fully evaluate knowledge of these guidelines, each step should be evaluated, including patients requiring emergency surgery. additionally, we presented several case scenarios in which residents had to identify several conditions considered as “active” as well as how functional capacity and clinical risk factors influenced medical management of patients undergoing intermediate and high-risk vascular surgeries. in addition to anesthesiologists, internists, cardiologists, we chose to include surgical residents, since they are also involved in the preoperative assessment of patients.
a formal cover letter describing the study’s goals along with the web-based survey link was sent to the program coordinator of each respective department. this was forwarded to the residents for their participation. the cover letter stated that participation was completely voluntary and that lack of participation would have no influence on their residency status. Each residency program director was met with in person to discuss the details of the study and we asked for them to follow up with the residents during afternoon conferences and through reminder emails asking for increased resident participation.
the creation of the clinical scenarios was a collaborative effort amongst several anesthesiologists including our residency program director (eJC), chief of anesthesia services (sff), a fellowship-trained critical care medicine and heart failure anesthesiologists (vp) and a fellowship-trained cardiac anesthesiologist (RnK). the clinical scenarios were considered accurate in their presentation of a patient requiring emergency surgery, inclusion of appropriate clinical risk factors and active conditions as defined by the 2007 aCC/aha guidelines, functional capacity and risk of surgery. each clinical scenario corresponded one of the five steps and its branch point(s) in the 2007 aCC/aha algorithm (figure 1).
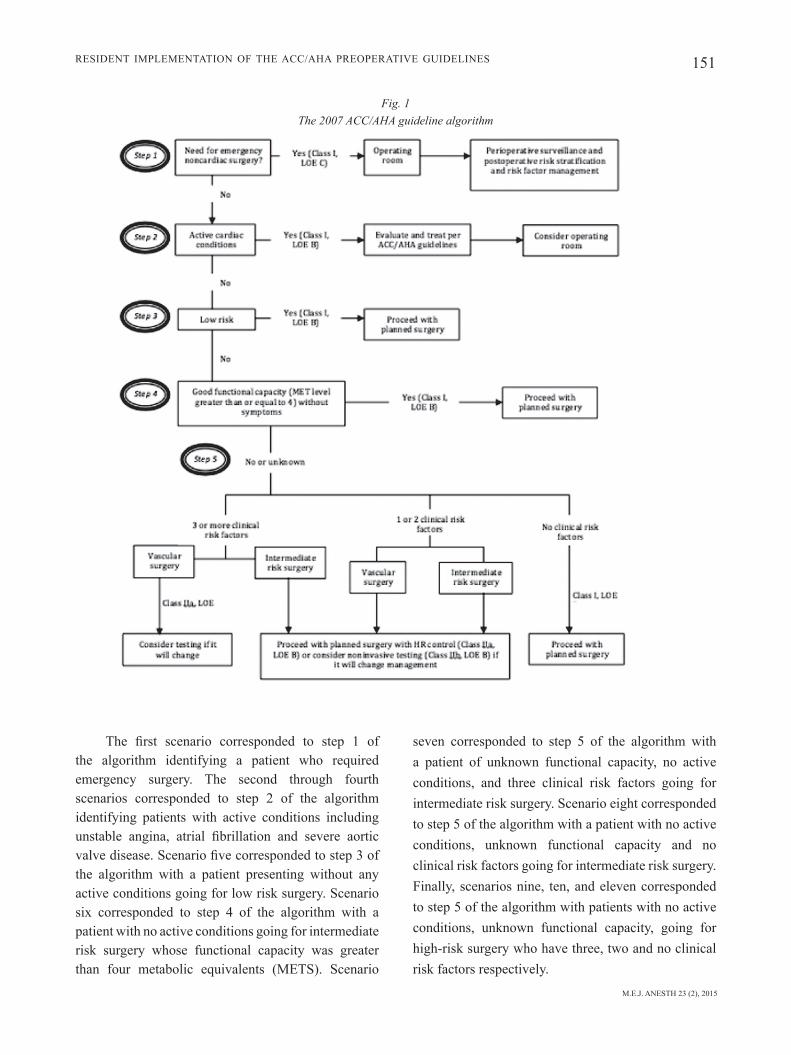
M.E.J. ANESTH 23 (2), 2015
151
seven corresponded to step 5 of the algorithm with a patient of unknown functional capacity, no active conditions, and three clinical risk factors going for intermediate risk surgery. scenario eight corresponded to step 5 of the algorithm with a patient with no active conditions, unknown functional capacity and no clinical risk factors going for intermediate risk surgery. finally, scenarios nine, ten, and eleven corresponded to step 5 of the algorithm with patients with no active conditions, unknown functional capacity, going for high-risk surgery who have three, two and no clinical risk factors respectively.
The first scenario corresponded to step 1 of the algorithm identifying a patient who required emergency surgery. the second through fourth scenarios corresponded to step 2 of the algorithm identifying patients with active conditions including unstable angina, atrial fibrillation and severe aortic valve disease. Scenario five corresponded to step 3 of the algorithm with a patient presenting without any active conditions going for low risk surgery. scenario six corresponded to step 4 of the algorithm with a patient with no active conditions going for intermediate risk surgery whose functional capacity was greater than four metabolic equivalents (mets). scenario
Resident implementation of the aCC/aha pReopeRative Guidelines
Fig. 1 The 2007 ACC/AHA guideline algorithm
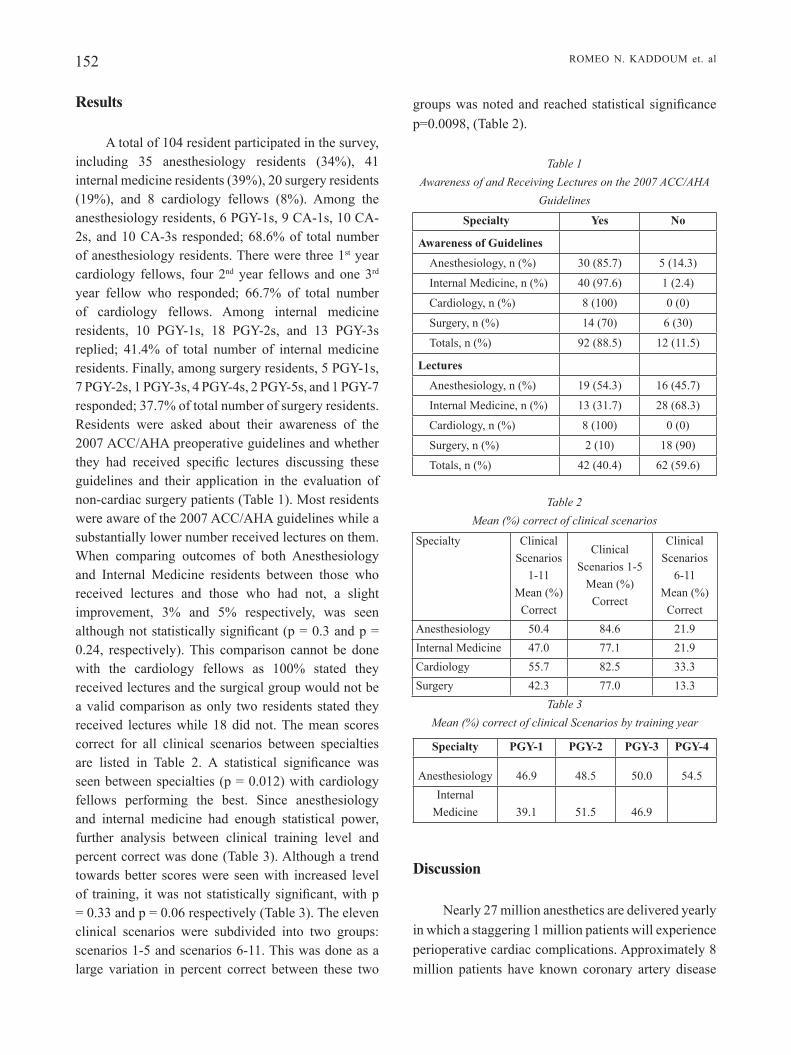
152 Romeo n. Kaddoum et. al
Results
a total of 104 resident participated in the survey, including 35 anesthesiology residents (34%), 41 internal medicine residents (39%), 20 surgery residents (19%), and 8 cardiology fellows (8%). among the anesthesiology residents, 6 pGy-1s, 9 Ca-1s, 10 Ca-2s, and 10 CA-3s responded; 68.6% of total number of anesthesiology residents. there were three 1st year cardiology fellows, four 2nd year fellows and one 3rd year fellow who responded; 66.7% of total number of cardiology fellows. among internal medicine residents, 10 pGy-1s, 18 pGy-2s, and 13 pGy-3s replied; 41.4% of total number of internal medicine residents. finally, among surgery residents, 5 pGy-1s, 7 pGy-2s, 1 pGy-3s, 4 pGy-4s, 2 pGy-5s, and 1 pGy-7 responded; 37.7% of total number of surgery residents. Residents were asked about their awareness of the 2007 aCC/aha preoperative guidelines and whether they had received specific lectures discussing these guidelines and their application in the evaluation of non-cardiac surgery patients (table 1). most residents were aware of the 2007 aCC/aha guidelines while a substantially lower number received lectures on them. When comparing outcomes of both Anesthesiology and internal medicine residents between those who received lectures and those who had not, a slight improvement, 3% and 5% respectively, was seen although not statistically significant (p = 0.3 and p = 0.24, respectively). this comparison cannot be done with the cardiology fellows as 100% stated they received lectures and the surgical group would not be a valid comparison as only two residents stated they received lectures while 18 did not. the mean scores correct for all clinical scenarios between specialties are listed in Table 2. A statistical significance was seen between specialties (p = 0.012) with cardiology fellows performing the best. since anesthesiology and internal medicine had enough statistical power, further analysis between clinical training level and percent correct was done (table 3). although a trend towards better scores were seen with increased level of training, it was not statistically significant, with p = 0.33 and p = 0.06 respectively (Table 3). The eleven clinical scenarios were subdivided into two groups: scenarios 1-5 and scenarios 6-11. this was done as a large variation in percent correct between these two
groups was noted and reached statistical significance p=0.0098, (Table 2).
Table 1 Awareness of and Receiving Lectures on the 2007 ACC/AHA
Guidelines
Specialty Yes No
Awareness of Guidelines
anesthesiology, n (%) 30 (85.7) 5 (14.3)
internal medicine, n (%) 40 (97.6) 1 (2.4)
Cardiology, n (%) 8 (100) 0 (0)
surgery, n (%) 14 (70) 6 (30)
totals, n (%) 92 (88.5) 12 (11.5)
Lectures
anesthesiology, n (%) 19 (54.3) 16 (45.7)
internal medicine, n (%) 13 (31.7) 28 (68.3)
Cardiology, n (%) 8 (100) 0 (0)
surgery, n (%) 2 (10) 18 (90)
totals, n (%) 42 (40.4) 62 (59.6)
Table 2 Mean (%) correct of clinical scenarios
specialty Clinical scenarios
1-11 mean (%)
Correct
Clinical scenarios 1-5
mean (%) Correct
Clinical scenarios
6-11 mean (%)
Correctanesthesiology 50.4 84.6 21.9internal medicine 47.0 77.1 21.9Cardiology 55.7 82.5 33.3surgery 42.3 77.0 13.3
Table 3 Mean (%) correct of clinical Scenarios by training year
Specialty PGY-1 PGY-2 PGY-3 PGY-4
anesthesiology 46.9 48.5 50.0 54.5internal
medicine 39.1 51.5 46.9
Discussion
nearly 27 million anesthetics are delivered yearly in which a staggering 1 million patients will experience perioperative cardiac complications. approximately 8 million patients have known coronary artery disease

M.E.J. ANESTH 23 (2), 2015
153Resident implementation of the aCC/aha pReopeRative Guidelines
or cardiac risk factors and 50,000 patients will suffer a perioperative myocardial infarction. These figures equate to 20 billion dollars in increased costs3-7. preoperative evaluation of surgical patients is critically important and relies upon close collaboration amongst physicians from multiple specialties8. evaluation is not done to provide clearance for surgery but rather to provide further clarification of a patient’s current medical condition, assess cardiac risk to guide peri-operative care and provide optimal medical management such that cardiac risk may be reduced2-7. there are clear associations between surgical procedures and adverse perioperative outcomes which is why a command of perioperative cardiac guidelines by physicians involved in the care of surgical patients, regardless of their specialty, is so vitally important8.
An internist or surgeon is typically the first to encounter patients requiring surgical management. the role of the surgeon goes beyond devising a surgical plan for the patient but to also ensure that proper preoperative planning and consultation takes place such that perioperative risks are identified and minimized. in the inpatient setting, surgical patients are typically seen by either cardiology or internal medicine consultants who are expected to optimize and “clear” a patient prior to surgery. typically, the anesthesiologist will encounter their patients the morning of surgery and within a very brief period of time are responsible for synthesizing all the medical information and testing and have to make a decision regarding whether the patient may proceed safely with surgery. it is not uncommon that patients are improperly evaluated and present with either poorly controlled chronic medical problems or acute pathology which either went unrecognized, typically by midlevel providers, or whose perioperative significance is unknown. this leaves the anesthesiologist in a highly undesirable situation where the pressures to proceed with surgery conflict with that of patient safety. This undoubtedly creates further stress on the patient as they wait for a decision to be made whether it is safe for them to proceed with surgery, resulting in poor patient care.
due to increased healthcare costs, there is trend by hospitals to rely on phone interviews conducted by midlevel providers for preoperative patient
evaluation9. thorough patient evaluation cannot be conducted in this manner as there are often gaps in patients’ understanding of their own medical problems and a disconnect between what constitutes relevant signs or symptoms by a patient and the health care provider conducting the interview. this further emphasizes the importance of directly conducting a detailed history and physical examination and medical evaluation. additionally, evaluation of a patient’s functional capacity is an important step in the aCC/aha guidelines. providers who lack a more comprehensive understanding of the relationship between functional capacity and clinical risk factors may not be able to delineate reduced functional capacity due to, for example, osteoarthritis from that of poorly controlled cardiopulmonary disease. it is unclear if this trend shows any cost benefits or whether higher surgical cancellation rates are seen, however several studies have shown that preoperative patient evaluation does indeed reduce costs and the number of cancellations9-11.
medical guidelines are ubiquitous amongst all specialties. they provide a framework for which physicians can approach medical illnesses and in most instances are evidence-based. lack of knowledge of guidelines amongst residents is not just a problem in anesthesiology but spans the entire medical profession12-14. Karakousis et al., conduced a survey of u.s. medical resident familiarity with tuberculosis guidelines. they found that the median percent of questions answered correctly was 55% and most importantly there was not a significant increase in knowledge with increasing post-graduate years of training. furthermore, agrawal et al. conducted a survey of internal medicine residents to evaluate their knowledge of chronic kidney disease (CKd) and its management. they found that over 33% of residents did not know how to stage CKd and aside from traditional risk factors like hypertension and diabetes, a significantly lower percentage of residents knew that obesity, age and african american race were also risks factors. like Karakousis et al, this study found that additional post-graduate experience did not result in meaningful improvement in knowledge5. a study by hoeks et al., applied the aCC/aha guidelines retrospectively to patients undergoing peripheral vascular surgery. they found that patients in whom

154 Romeo n. Kaddoum et. al
the guidelines were inappropriately applied received the same amount of evaluation as those patients undergoing low-risk surgery. hence, lack of guideline knowledge resulted in less use of cardioprotective medications like b-blockers8. these studies along with ours demonstrate that clinical experience is indeed not enough on its own to provide a comprehensive knowledge of specialty specific guidelines.
in our study, there was a large variation in awareness of the 2007 aCC/aha preoperative guidelines for patients undergoing non-cardiac surgery. although 100% of cardiology fellows were aware of these guidelines only 70% of surgery residents were (table 1). although all cardiology fellows stated they had lectures specifically discussing the 2007 aCC/aha guidelines, 54.3% of anesthesiology residents, 31.7% of internal medicine residents, and only 10% of surgery residents stated they received such lectures (table 1). as mentioned earlier, only a slight, non-statistically significant improvement (3-5%) in questions correctly answered was seen among the anesthesiology and internal medicine residents who stated they received lectures. the eleven clinical scenarios were divided into two groups, scenarios 1-5 (steps 1-3 of algorithm) and scenarios 6-11 (steps 4-5). The first five scenarios focused on whether residents could identify that: patients requiring emergency surgery should proceed to the operating room without delay and that patients with active conditions including unstable angina, severe valvular disease or arrhythmias should not proceed with surgery but rather undergo a thorough medical evaluation. among all specialties, the residents correctly answered the first group of scenarios with a mean score of 80.3%. the residents answered the second group of scenarios with a mean score of 22.6% (table 2). this can be explained as the second group of clinical scenarios required residents to have a deeper understanding of the 2007 aCC/aha guidelines and how functional capacity, risk of surgical procedures, and clinical risk factors govern the level of preoperative workup required before surgery should take place. it is safe to say that even without the knowledge of the 2007 aCC/aha guidelines, residents can appreciate both the need to proceed with emergency surgery and that patients who are acutely decompensated require further medical evaluation.
Concerns about cancellations and surgical delay, medico-legal liabilities and beliefs that “other” physicians want certain tests or evaluations to be completed has lead to increased waste, costs, utilization of resources, morbidity, and lack of proper preoperative evaluation15. hence, guidelines provide for a more systematic approach to patient evaluation; however poor adherence is multifactorial and is attributed to lack of awareness, perpetuation of old practice habits, personal preferences, and administrative constraints8,15.
although much effort was made by all programs and their coordinators, resident participation was less than desirable, which significantly limited the power of our study. another limitation was given that our study was conducted via a web-based survey; residents could theoretically collaborate in answering the questions. We felt however that if this occurred, it would be amongst a minimal number of residents. additionally, the honor code should act as a sufficient reminder that accurate results were desired so that the assessment of the deficiencies in resident knowledge could take place and appropriate modifications in resident education could be made. despite these limitations, it is clear that much improvement needs to be made in educating residents about preoperative management of non-cardiac surgery patients. even though residents receiving lectures did slightly better overall, it is likely that the number, depth and application of the 2007 aCC/aha guidelines in the form of problem-based learning could improve overall performance. Clinical training by itself arguably increases a resident’s ability to evaluate and manage patients but as our study and others have shown2,16-24, it is neither a substitute or sufficient in producing physicians with comprehensive skills in preoperative patient management.
Conclusions
although the majority of residents were aware of the 2007 aCC/aha guidelines, implementation of these guidelines was poor. despite increased training there was no significant difference in residents’ ability to apply the 2007 aCC/aha guidelines appropriately. There exists significant room for improvement in the understanding of preoperative assessment of non-cardiac surgery patients amongst all specialties involved in the care of these patients.

M.E.J. ANESTH 23 (2), 2015
155
ambulatory surgery patient. Curr Opin Anaesthesiol; 22:705-711.12. loGiE Ci, smitH sE, naGy P: evaluation of resident familiarity
and utilization of the aCR musculoskeletal study appropriateness criteria in the context of medical decision support. Acad Radiol; 17:251-4.
13. KaRaKousis PC, siFaKis FG, dE oCa Rm, amoRosa VC, PaGE KR, manabE yC, CamPbEll Jd: u.s. medical resident familiarity with national tuberculosis guidelines. BMC Infect Dis; 7:89.
14. bRown sR, bRown J: Why do physicians order unnecessary preoperative tests? a qualitative study. Fam Med; 43:338-343.
15. baHaziq w, CRosby E: physician professional behaviour affects outcomes: a framework for teaching professionalism during anesthesia residency. Can J Anaesth; 58:1039-50.
16. baKER K: determining Resident Clinical performance: Getting Beyond the noise. Anesthesiology; 115:862-78.
17. KoPP sl, smitH Hm: developing effective web-based regional anesthesia education: a randomized study evaluating case-based versus non-case-based module design. Reg Anesth Pain Med; 36:336-42.
18. sCaVonE bm, tolEdo P, HiGGins n, woJCiECHowsKi K, mCCaRtHy RJ: a randomized controlled trial of the impact of simulation-based training on resident performance during a simulated obstetric anesthesia emergency; 5:320-4.
19. boEt s, bould md, bRuPPaCHER HR, dEsJaRdins F, CHandRa db, naiK Vn: Looking in the mirror: self-debriefing versus instructor debriefing for simulated crises. Crit Care Med; 39:1377-81.
20. baKER K: Clinical teaching improves with resident evaluation and feedback. Anesthesiology; 113:693-703.
21. CHu lF, younG C, zamoRa a, KuRuP V, maCaRio a: anesthesia 2.0: internet-based information resources and Web 2.0 applications in anesthesia education. Curr Opin Anaesthesiol; 23:218-27.
22. FaHy bG, CHau dF, bEnsalEm-owEn m: evaluating the requirements of electroencephalograph instruction for anesthesiology residents. Anesth Analg; 109:535-8.
23. JoHnson Kb, syRoid nd, dREws Fa, oGdEn ll, stRayER dl, PaCE nl, tylER dl, wHitE Jl, wEstEnsKow dR: part task and variable priority training in first-year anesthesia resident education: a combined didactic and simulation-based approach to improve management of adverse airway and respiratory events. Anesthesiology; 108:831-40.
Resident implementation of the aCC/aha pReopeRative Guidelines
References
1. la FlEisHER, Ja bECKman and Ka bRown, Et al: aCC/aha guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the american College of Cardiology/american heart association task force on practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular evaluation for noncardiac surgery). J Am Coll Cardiol; 50:151-241, 2007.
2. ViGoda mm, swEitzER b, milJKoViC n, aRHEaRt Kl, mEssinGER s, Candiotti K, lubaRsKy d: american College of Cardiology/american heart association (aCC/aha) Guidelines on perioperative cardiac evaluation are usually incorrectly applied by anesthesiology residents evaluating simulated patients. Anesth Analg; 112:940-9, 2007.
3. wolF Jm, atHwal Gs, HoanG bH, mEHta s, williams aE, owEns bd: Knowledge of levels of evidence criteria in orthopedic residents. Orthopedics; 32:494.
4. lEa JP, mCClEllan wm, mElCHER C, GladstonE E, HostEttER t: CKd risk factors reported by primary care physicians: do guidelines make a difference? Am J Kidney Dis; 47:72-7.
5. aGRawal V, GHosH aK, baRnEs ma, mCCullouGH Pa: awareness and knowledge of clinical practice guidelines for CKd among internal medicine residents: a national online survey. Am J Kidney Dis; 52:1061-9.
6. auERbaCH ad, Goldman l: Beta-Blockers and reduction of cardiac events in noncardiac surgery: scientific review. JAMA; 287:1435-44.
7. lawREnCE Va, HilsEnbECK sG, mulRow Cd, dHanda R, saPP J, PaGE CP: incidence and hospital stay for cardiac and pulmonary complications after abdominal surgery. J Gen Intern Med; 10:671-8.
8. HoEKs sE, sCHoltE oP REimER wJ, lEnzEn mJ, Van uRK H, JöRninG PJ, boERsma E, simoons ml, bax JJ, PoldERmans d: Guidelines for cardiac management in noncardiac surgery are poorly implemented in clinical practice: results from a peripheral vascular survey in the netherlands. Anesthesiology; 107:537-44.
9. PatEl Ri, HannallaH Rs: preoperative screening for pediatric ambulatory surgery: evaluation of a telephone questionnaire method. Anesth Analg; 75:258-261.
10. issa mR, isoni nF, soaREs am, FERnandEs ml: preanesthesia evaluation and reduction of preoperative care costs. Rev Bras Anestesio; 61:60-71.
11. GuPta a: preoperative screening and risk assessment in the


157 M.E.J. ANESTH 23 (2), 2015
Pseudocholinesterase deficiency in a octogenarian undergoing total intravenous
anesthesia; imPlications for neuromonitoring
Matthew wecksell* and deMetri koutsospyros**
Abstract
Pseudocholinesterase deficiency manifests as prolonged motor blockade after the administration of succinylcholine. A previously unknown homozygous form of the disease, became apparent during a lumbar laminectomy seriously limiting the ability to monitor motor evoked potentials and perform electromyelography (EMG). Moreover, concerns were raised as to how the enzyme deficiency would affect the metabolism of remifentanil and other esters during a total intravenous anesthetic. We present the perioperative management of the patient and a literature review of the syndrome.
The patient provided written permission for the authors to publish this report. At our institution, IRB review and approval is not required for a single case report.
Introduction
A major anesthetic concern in caring for patients undergoing spine surgery with pedicle screw placement is the ability to obtain optimal motor, sensory, and EMG evoked potentials. Our patient was diagnosed intraoperatively with a pseudocholinesterase deficiency, which, due to the administration of succinylcholine, prevented both the monitoring of motor, and EMG evoked potentials, and which precluded an immediate postoperative neurologic assessment of the patient.
Case Presentation
An 89 year old female presented with chronic back pain and spinal stenosis for an L2 – S1 laminectomy and fusion. She gave a history of elevated serum cholesterol, type II diabetes, and hypertension. In recent years, she had undergone surgeries on her right thumb and breast which were both uneventful and likely performed without muscle relaxation with succinylcholine. A half-century prior she had two other surgeries: a total abdominal hysterectomy and an appendectomy,
* MD, Assistant Professor, New York Medical College. E-mail: [email protected], Matthew Wecksell reported no conflicts of interest, Matthew Wecksell approved the final manuscript.
** MD, resident, New York Medical College. E-mail: [email protected], Demetri Koutsospyros reported no conflicts of interest, Demetri Koutsospyros approved the final manuscript.
Corresponding author: Matthew Wecksell, MD, New York Medical College, Dept of Anesthesiology, 100 Woods Road, Valhalla NY 10595. Phone: 9144937693, Fax: 9144937693. E-mail: [email protected]<mailto:[email protected]>

158 MATThEW WECKSELL et. al
after both of which she described being “sleepy and hard to wake up.” Owing to the ensuing 50 year time interval, the patient was unable to provide any further detail or records about those procedures.. She had stated allergies to aspirin and penicillin.
The patient was brought to the operating room, and after sedation with fentanyl and midazolam, anesthesia was induced with propofol and succinylcholine. her trachea was easily intubated, and infusions of propofol and remifentanil were immediately started for the maintenance of anesthesia. She was soon placed in the prone position, at which time multiple electrodes were placed to enable neurophysiologic monitoring of somatosensory, motor and EMG evoked potentials.
After the surgeons prepped and draped the surgical field, the neurophysiologist obtained baseline measurements. At this point, approximately forty minutes after induction, we were made aware that the patient had no peripheral motor twitches. We independently verified this finding with a peripheral nerve stimulator, and notified the surgeon that we had a presumptive diagnosis of pseudocholinesterase deficiency, which would preclude intraoperative motor and EMG evoked potential monitoring. As the patient was already anesthetized and we were able to obtain good baseline sensory evoked potentials, the surgeon made the decision to proceed with the planned operation.
Approximately one hour and forty five minutes after succinylcholine administration, we were able to obtain one twitch on a train of four, which is consistent with a diagnosis of homozygous pseudocholinesterase deficiency, and helped to comfirm our diagnosis. The procedure was concluded five hours after administration of succinylcholine at which time the patient had four ulnar twitches, with significant fade in twitch intensity from the first to the fourth twitch. We opted to bring the patient to our recovery room still sedated and intubated, with a plan to extubate upon the complete recovery of motor function.
Eight hours after our initial dose of paralytic, the patient had sustained tetany for longer than 5 seconds in response to a 100 hz stimulation, good spontaneous ventilatory function. her tracheawas uneventfully
extubated. Examination at this time revealed intact motor and sensory function in all four extremities. She was discharged to a rehabilitation facility as planed several days postoperatively.
Discussion
Pseudocholinesterase, also known as butyrylcholinesterase, is one of many esterases in man. While its native purpose is unclear, it does interact with several exogenous esters. The two most commonly explored and publicized are succinylcholine and mivacurium, both of which are rapidly broken down by pseudocholinesterase. As such, they have been used for several years in the field of anesthesiology to provide neuromuscular blockade with a rapid onset and short lived effect. In our patient, succinylcholine was used at induction with the expectation that it would wear off swiftly so that monitoring of motor and EMG evoked potentials could proceed unhindered.
The gene which codes for pseudocholinesterase is the BChE gene, located on chromosome site 3q261. Any mutation to this gene can lead to decreased enzyme function and a clinical pseudocholinesterase deficiency. Several documented mutations have been found to lead to varying levels of pseudocholinesterase activity. At least 5 alleles are known to cause an easily identifiable decrease in enzyme activity2, with 65 named variants causing minimal to extreme post succinylcholine paralysis3. New alleles are discovered frequently, including two in 20084. While heterozygous mutations of this allele lead to mildly decreased pseudocholiesterase effect, patients who carry homozygous mutations show severely decreased pseudocholinesterase function.
In the general population approximately 4% of people carry at least one mutated allele of the BChE gene, and approximately 1:3000 are homozygous for abnormal alleles5. however, the incidence of pseudocholinesterase deficiency can vary widely in different populations. For example, the Vysya community in India has been found to have a homozygous mutation incidence of 2-4%5,6. Our patient was clearly homozygous for abnormal alleles clinically

M.E.J. ANESTH 23 (2), 2015
159intraoPerative diagnosis of Pseudocholinesterase deficiency
although we were unable to confirm the diagnosis by genotyping we followed her motor function, with one twitch returning two hours after dosing and full power returning after approximately eight hours.
In a patient with a known pseudocholinesterase deficiency, the administration of agents dependent on pseudocholinesterase for metabolism can be avoided, thus sidestepping any potential problems. Unfortunately, despite reaching the age of 89 and having had several prior surgeries, our patient had not previously been diagnosed. While the surgeon expressed amazement at this apparent lapse, our lack of understanding of the native function of pseudocholinesterase implies that, in the absence of the administration of an ester drug, a person carrying a mutation in this gene may never receive a diagnosis. had we known about her condition, our initial muscle relaxation could have been achieved with other non depolarizing agents, in doses titrated to wear off prior to the initiation of monitoring.
Of note, is her prior anesthetic history. While it is impossible to know exactly which agents she received in the early 1960s, the description of post operative “sleepiness” is different from one of actual muscle relaxation, although lacking further narrative, delayed awakening might be consistent with some degree of continued paralysis. It is possible at that time that she was anesthetized with ether and succinylcholine was almost universally used for intubation. The recommended treatment for prolonged paralysis secondary to pseudocholinesterase deficiency is supportive. Patients remain apneic secondary to paralysis of the diaphragm, and therefore mechanical ventilation must be maintained until spontaneous respiration resumes. Given the rarity of the condition, there are few treatment options. however, a literature search provides a few possible choices, some theoretical, and others clinically proven.
Difficulty arises in diagnosing pseudocholinesterase deficiency, as our current screening tests are both imperfect, and seldom administered. Several mutations can cause clinical pseudocholinesterase deficiency. The mainstay of detection is the dibucaine number, but this is only effective in certain genotypes6. With genetic testing
becoming more affordable and widespread, it is likely that it will completely replace the dibucaine number as the preferred means of detection of any pseudocholinesterase deficiency; at this point it is too expensive to consider genetic testing on everyone who may possibly require succinylcholine use.
Pseudocholisesterase exists in circulating plasma. This sparked the idea that perhaps it may still be present and active in stored blood or fresh frozen plasma. Epstein et al tested the activity of pseudocholinesterase in bank blood7. By measuring pre-donation pseudocholinesterase activity, then measuring its activity in that same blood after storage for 21 days in acid-citrate-dextrose-anticoagulant solution, the authors found that it only lost about 15% of its activity. While this was statistically significant, it was found not to be clinically significant, as it led to an increase in apneic time after succinylcholine administration from three minutes to 3.6 minutes8. No reason was found for the decreased activity, but Calloway et al theorized that it was due to the fact that red blood cells were present in the whole blood9. The data from Epstein et al shows that indeed, when red blood cells and plasma were immediately separated after donation, pseudocholinesterase activity remained stable6. The results of these studies indicate that transfusion of whole blood or FFP are likely viable options in treating prolonged paralysis secondary to pseudocholinesterase deficiency as such transfusions would provide the patient with sufficient pseudocholinesterase activity to metabolize the succinylcholine and end the prolonged paralysis.
Another logical course of action is isolating and administering pseudocholinesterase itself. Several human enzymes are commercially available and have been successful in treating a number of enzyme deficiencies. Behringwerke, a Greman pharmaceutical company, created a purified, injectable form of human psuedocholinesterase. In two separate studies, injection of 90-135mg of this preparation led to a return of spontaneous ventilation in 10 minutes10,11. This dose was found to have equivalent pseudocholinesterase activity to 500ml of fresh human plasma in vitro. Other pharmaceutical companies are attempting to find more cost efficient

160 MATThEW WECKSELL et. al
ways to make recombinant pseudocholinesterase for general medical use. In 2007, one such company, Pharmathene, began using genetically modified goats to create pseudocholinesterase in large quantities12. By genetically modifying the animals, they were able to make them excrete large quantities of pseudocholinesterase in their milk: approximately 2-3 grams per liter of milk.
As mentioned earlier, pseudocholinesterase is also responsible for the breakdown of ester local anesthetics including procaine, chloroprocaine, and, to a lesser extent, cocaine. As such, pseudocholinesterase deficiency is a relative contraindication to the use of these drugs. At least two case reports describe situations where epidural administration of chloroprocaine was prolonged, and its effects enhanced, in patients with low/abnormal pseudocholinesterase activity13,14. It is clear that pseudocholinesterase is responsible also for the metabolism of cocaine:, however, it has a much lower catalytic activity towards cocaine than it does towards succinylcholine15. As such, there are several studies on modifying pseudocholinesterase to have a more profound breakdown of cocaine; thus making it useful in treating cocaine overdoses or preventing cocaine’s effects proactively. One such study by Xue et al found that a modified pseudocholinesterase mutant with a high catalytic activity towards cocaine could, in fact, be used as described above14. Extending this to its theoretical conclusion, it is likely that different forms of synthetic pseudocholinesterase mutants could be created to rapidly metabolize any kind of ester.
In cases where neurophysiologic monitoring with motor, sensory, and EMG evoked potentials is necessary, it is important that the anesthetic agents do not interfere with said monitoring. As such, it is preferable that any neuromuscular blocker used is short acting, and will have worn off prior to incision so that accurate baseline neurophysiologic signals can be obtained. Such monitoring certainly requires the absence of any paralytic effect by the time the surgeon has finished his dissection and is ready for instrumentation. Similarly, it is important the use of volatile anesthetics are minimized as they may interfere with the monitoring. As such, the most commonly used method for these cases is a total intravenous anesthetic16
consisting of hypnotic and analgesic infusions. One common regimen, used in our case, is an infusion of propofol and remifentanil. Propofol has a predictable effect on neurophysiologic monitoring; as such it does not significantly affect the results and interpretation of those results. Remifentanil has no effect on monitoring and provides excellent intraoperative analgesia. Most importantly, remifentanil has a very short context sensitive half time in contrast to most other opioids17. These properties are due to the fact that remifentanil is an ester and as such is broken down rapidly by several plasma esterases. Nelson et al described a case of prolonged emergence from anesthesia with remifentanil18. It is known that extremes of age, liver function, and kidney function have minimal effects on its metabolism19, however, it is possible that this delayed emergence was secondary to an esterase deficiency. As mentioned earlier, it is nonspecific esterases that are responsible for breaking down remifentanil; as such there are no tests for measuring their function. Similarly, there are no reports of a deficiency of one or more of these esterases in conjunction with deficiency of pseudocholinesterase. Perhaps as more case reports of delayed emergence from remifentanil arise, more research will be done on the esterases responsible for its breakdown, as well as deficiencies of those esterases.
Conclusion
At this time in the United States there are not many options for quick onset, short term paralysis apart from succinylcholine. In several countries rocuronium has replaced succinylcholine as it has a similar rate of onset and is completely, readily reversible with sugammadex. however, sugammadex is not currently available in the US.. Similarly, in other countries mivacurium can be used as it also has a fairly rapid rate of onset and offset. Again, mivacurium is no longer available in the US.. Thus, as the only short acting agent, the use of succinylcholine is inevitable in certain situations. As such, it is important that the possibility of undiagnosed pseudocholinesterase deficiency is entertained.. More studies should be done on the use of FFP or whole blood in treating prolonged

M.E.J. ANESTH 23 (2), 2015
161intraoPerative diagnosis of Pseudocholinesterase deficiency
paralysis after succinylcholine administration due to pseudocholinesterase deficiency.
With the growing use of neurophysiologic monitoring, it is important that anesthesiologists take into account the need for accurate measurements and the effects different medications have on monitoring. It is equally important to take into account the possibility of conditions such as pseudocholinesterase deficiency..
The loss of motor potentials in a case such as the one presented can be catastrophic. The surgeon may be unable to confidently perform the surgery and ensure proper placement of the pedicle screws While SSEP monitoring can help approximate damage to the motor tract, there have been numerous reports of damage to motor tracts with no change in SSEP20.

162 MATThEW WECKSELL et. al
References
1. allderdice pw, Gardner ha, Galutira d, lockridGe o, ladu Bn, Mcalpine pJ: "The cloned butyrylcholinesterase (BChE) gene maps to a single chromosome site, 3q26". Genomics, 11(2):452-4, 1991.
2. Geyer Bc: "Reversal of Succinylcholine Induced Apnea with an Organophosphate Scavenging Recombinant Butyrylcholinesterase". PloS one; 8.3:e59159, 2013.
3. soliday Fk, conley yp, henker r: "Pseudocholinesterase deficiency: a comprehensive review of genetic, acquired, and drug influences". J Am Assoc Nurse Anesth;78:313-320, 2010.
4. Jensen Fs, ViBy-MoGensen J: "Plasma cholinesterase and abnormal reaction to succinylcholine: twenty years' experience with the Danish Cholinesterase Research Unit". Acta Anaesthesiologica Scandinavica; 39:150-156, 2008.
5. putnaM l: “Pseudocholinesterase Deficiency: An Additional Preoperative Consideration in Outpatient Diagnos-tic Procedures”, Southern Medical Journal, 70(7):831-833, 1977.
6. aBdallah B, udoMtecha d: "Pseudocholinesterase activity: determination and interpretation in pediatric anesthesia". MEJ Anesth; 19:423-8, 2007.
7. epstein hM, JarzeMsky d, zuckerMan l, VaGher p: "Plasma cholinesterase activity in bank blood". Anesth Analg; 59(21):1-21, 1980.
8. Foldes FF, rendell-Baker l, Birch Jh: "Causes and prevention of prolonged apnea with succinylcholine. Anesth Analg; 35:609, 1956.
9. callaway s, daVies dr, rutland Jp: "Blood cholinesterase levels and range of personal variation in a healthy adult population". Brit Med J; II:812-816, 1951.
10. scholler kl, Goedde hw, BenkMann hG: "The use of serum cholinesterase in succinylcholine apnoea". Can Anaesth SOC J; 24, 396-400, 1977.
11. stoVner J, stadsklieV k: "Suxamethonium apnea terminated with commerial serum cholinesterase". Acta Anesthesiol Scand; 20:211-215, 1976.
12. huanG yJ, huanG y, Baldassarre h, wanG B, lazaris a, leduc M, Bilodeau as, BelleMare a, côté M, herskoVits p, touati M, turcotte c, Valeanu l, leMée n, wilGus h, BéGin i, Bhatia B, rao k, neVeu n, Brochu e, pierson J, hockley dk, cerasoli dM, lenz de, karatzas cn, lanGerMann s: "Recombinant human butyrylcholinesterase from milk of transgenic animals to protect against organophosphate poisoning". Proc Natl Acad Sci USA; 104(34):13603-8, 2007.
13. kuhnert Br, philipson eh, piMental r, kuhnert pM: "A Prolonged Chloroprocaine Epidural Block in a Postpartum Patient with Abnormal Pseudocholinesterase". Anesthesiology; 56(6):477, 1982.
14. Monedero p, hess p: "high epidural block with chloroprocaine in a parturient with low pseudo-cholinesterase activity". Canadian Journal of Anesthesia; 48(3):318-319, 2001.
15. Xue l, hou s, tonG M, FanG l, chen X, Jin z, tai hh, zhenG F, zhan cG: "Preparation and in vivo characterization of a cocaine hydrolase engineered from human butyrylcholinesterase for metabolizing cocaine". Biochem J; Aug 1, 453(3):447-54, 2013.
16. Gonzalez aa, JeyanandaraJan d, hansen c, zada G, hsieh pc: "Intraoperative neurophysiological monitoring during spine surgery: a review". Neurosurg Focus; 27(4):E6, 2009.
17. eGan td: "Remifentanil Pharmacokinetics and Pharmacodynamics: A Preliminary Appraisal". Clinical Pharmacokinetics; 29(2):80-94, 1995.
18. nelson ry: "Prolonged apnea after remifentanil". J Clin Anesth, 19(1):60-3, 2007.
19. Beers r, caMporesi e: "Remifentanil update: clinical science and utility". CNS Drugs; 18(15):1085-104, 2004.
20. Macdonald dB, skinner s, shils J, yinGlinG c: "Intraoperative motor evoked potential monitoring - A position statement by the American Society of Neurophysiological Monitoring". Clinical Neurophysiology; 124(12):2291-2316, 2013.

163 M.E.J. ANESTH 23 (2), 2015
An Audit of the current prActices of AirwAy mAnAgement in pAtients undergoing
surgery for AtlAnto-AxiAl dislocAtion in A single institution
Shruti redhu*, M. radhakriShnan** and GS uMaMaheSwara rao***
Abstract
Background: patients with atlanto axial dislocation (AAd) undergo stabilisation procedures under general anesthesia. Airway management in these patients is difficult as cervical spine movements during laryngoscopy can worsen spinal cord damage. Though multiple airway devices are used to intubate the trachea of these patients, there is no evidence of superiority of one technique over another. This retrospective study was designed to audit the practice of airway management during surgery for AAD over a 5 year period, starting from 2006 till 2011.
Methods: Patients’ demographics, airway intervention techniques, types of surgical procedures, postoperative neurological and respiratory deterioration were recorded from the case files. Association between the types of airway interventions and the postoperative neurological and respiratory deterioration were analysed.
Results: one hundred and six patients underwent surgery for AAd during the study period. Sixty one percent of the patients were intubated with the help of a fiberoptic bronchoscope (FOB) and among them 15% received general anesthesia to facilitate FOB. Eighteen patients developed neurological deterioration and 15 patients developed respiratory weakness requiring ventilation postoperatively. Congenital AAD patients had higher chances for extubation at the end of surgery when intubated using FOB (p=0.007). Among the AAD patients, female gender had significantly higher incidence of neurological deterioration compared to males.
Conclusion: In the current audit, there was no correlation between the perioperative variables and postoperative respiratory and neurological deterioration. Most of the respiratory problems occurred between 2-5 postoperative days stressing the need for extended intensive postoperative monitoring of these patients.
Keywords: airway, atlanto-axial dislocation, complication, cervical spine surgery, fiberoptic bronchoscopy.
* senior resident m.d., pdcc.** Additional professor md, dm.*** senior professor md. Department of Neuroanesthesia, National Institute of Mental Health and Neuro Sciences, Bangalore - 560029, India. Address for correspondence: Dr. M. Radhakrishnan, Additional Professor, Department of Neuroanesthesia, National
Institute of Mental Health and Neuro Sciences, Bangalore - 560029, India. Tel: +91-80-26995415, E-mail ID: [email protected].

164 rAdhAKrishnAn .m et. al
Introduction
Atlanto axial dislocation (AAd) is characterized by excessive movement and displacement at the junction between the atlas (C1) and axis (C2) of cervical spine, leading to instability. the causes of AAd are varied and include congenital anomalies, syndromes like Klippel-Fleil and Down's syndrome, metabolic diseases, tuberculosis, trauma and rheumatoid arthritis. Depending on the extent of cervical spinal cord compression, the patients’ symptoms vary from isolated neck pain to complete quadriparesis with respiratory difficulty1,2. to stabilise the spine, these patients undergo transoral odontoidectomy with or without posterior cervical fusion. When these patients, with unstable cervical spine undergo surgery, several techniques are adopted to secure the airway with an endotracheal tube. Airway management in these patients presents a challenge to the anesthesiologist because movement of the upper cervical spine during intubation could exaggerate the dislocation, resulting in spinal cord injury3. Currently, various airway equipment are used to secure the airway in these patients, but there is no evidence to prove the superiority of one technique over another. There is no reliable literature on the frequency with which different alternative techniques of airway management are used over the conventional laryngoscopy and intubation. Also, there is no evidence to show that one particular technique is associated with greater degree of injury to the spinal cord over other. Choice of airway equipment used during anesthesia depends on the availability, expertise and the patient characteristics. the present retrospective study was designed to audit the current practices of securing airway using different airway equipments in patients undergoing surgery for AAD in our centre over the last five years.
Materials and Methods
The study was approved by the Institutional ethics committee. Anesthesia register maintained in the operation theatre was screened for identifying patients operated upon for AAD from January 2006 till December 2011. The anesthesia charts and the progress notes maintained in the case files of these
patients were reviewed for the following data – age, gender, etiology of AAD, results of pre-operative pulmonary function tests, surgical approach (anterior, posterior or combined), method of securing the airway (direct laryngoscopy, fibreoptic intubation, McCoy blade), anesthesia for intubation (awake vs general anesthesia with muscle relaxants), intraoperative management (duration of surgery, intake of fluids, urinary output, blood transfusion), early vs delayed extubation, postoperative course, any deterioration in the neurological status (decrease in muscle power by one grade compared to preoperative value and respiratory muscle weakness requiring intervention) or any other complications.
Statistical Analysis
the patients’ demographics, type of surgery, incidence of complications and airway techniques are expressed as numbers and percentages and volume of perioperative fluids and blood are expressed as mean and standard deviation. Association of the airway interventions, etiology of AAD, and surgical approach with postoperative neurological and respiratory deterioration was analysed by chi square tests and association of perioperative fluid management with postoperative deterioration was analysed by using an independent samples t-test. A p value of <0.05 was considered significant. SPSS 15 software (SPSS®, chicago, il, usA) was used for statistical analysis.
Results:
one hundred and six patients underwent surgery for AAD during the study period of five years. The patient characteristics, etiology and surgical approach are detailed in table 1. Of the 106 patients, 61% were intubated with the help of FOB, while the remaining were intubated using direct laryngoscopy (mc coy blade was used in two patients); one patient had tracheostomy in situ prior to the surgical procedure. nylon reinforced latex endotracheal tubes were used in 88% of the patients. The details of airway management techniques are given in table 2. Of the 64 patients who underwent FOB intubation, general anesthesia with muscle relaxants was used in 9 (15%) patients and the
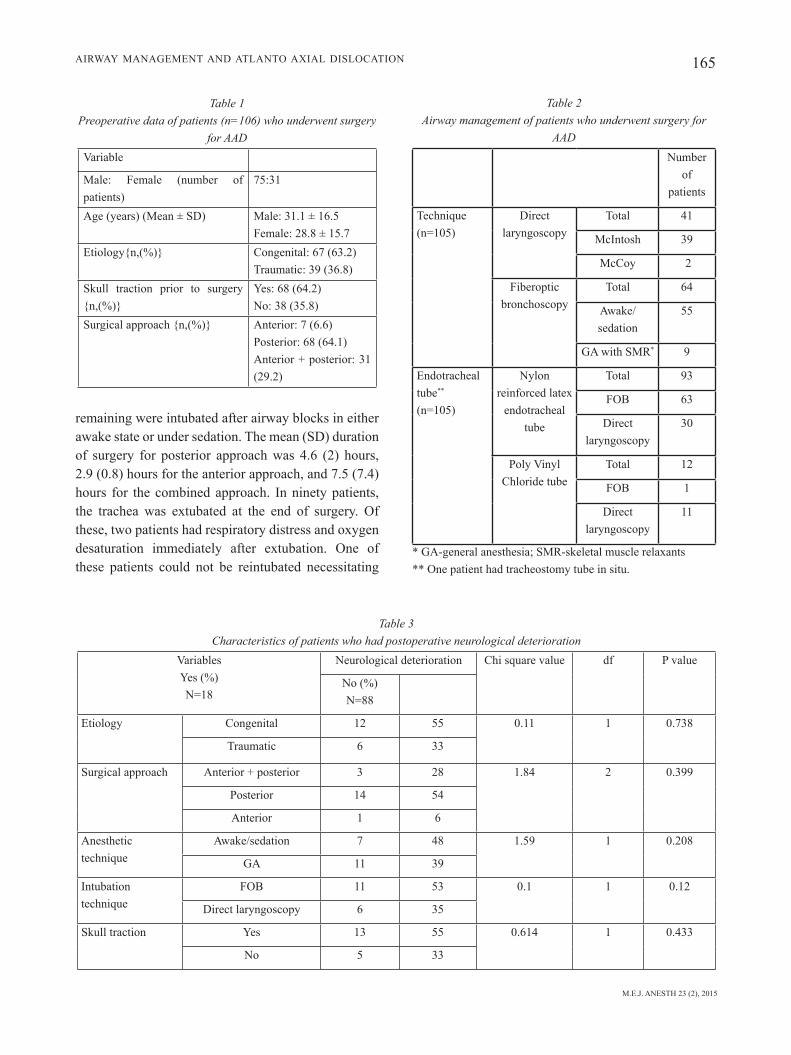
M.E.J. ANESTH 23 (2), 2015
165AirwAy mAnAgement And AtlAnto AxiAl dislocAtion
remaining were intubated after airway blocks in either awake state or under sedation. The mean (SD) duration of surgery for posterior approach was 4.6 (2) hours, 2.9 (0.8) hours for the anterior approach, and 7.5 (7.4) hours for the combined approach. in ninety patients, the trachea was extubated at the end of surgery. of these, two patients had respiratory distress and oxygen desaturation immediately after extubation. one of these patients could not be reintubated necessitating
Table 1 Preoperative data of patients (n=106) who underwent surgery
for AADVariable
Male: Female (number of patients)
75:31
Age (years) (mean ± sd) Male: 31.1 ± 16.5Female: 28.8 ± 15.7
Etiology{n,(%)} Congenital: 67 (63.2)Traumatic: 39 (36.8)
Skull traction prior to surgery {n,(%)}
Yes: 68 (64.2)No: 38 (35.8)
Surgical approach {n,(%)} Anterior: 7 (6.6)Posterior: 68 (64.1)Anterior + posterior: 31 (29.2)
Table 2 Airway management of patients who underwent surgery for
AADnumber
of patients
Technique(n=105)
direct laryngoscopy
total 41
mcintosh 39
mccoy 2
fiberoptic bronchoscopy
total 64
Awake/sedation
55
gA with smr* 9
endotracheal tube**
(n=105)
nylon reinforced latex
endotracheal tube
total 93
FOB 63
direct laryngoscopy
30
poly Vinyl chloride tube
total 12
FOB 1
direct laryngoscopy
11
* GA-general anesthesia; SMR-skeletal muscle relaxants** one patient had tracheostomy tube in situ.
Table 3 Characteristics of patients who had postoperative neurological deterioration
VariablesYes (%)N=18
neurological deterioration Chi square value df P value
No (%)N=88
etiology congenital 12 55 0.11 1 0.738
traumatic 6 33
surgical approach Anterior + posterior 3 28 1.84 2 0.399
posterior 14 54
Anterior 1 6
Anesthetic technique
Awake/sedation 7 48 1.59 1 0.208
gA 11 39
intubation technique
FOB 11 53 0.1 1 0.12
direct laryngoscopy 6 35
Skull traction yes 13 55 0.614 1 0.433
no 5 33
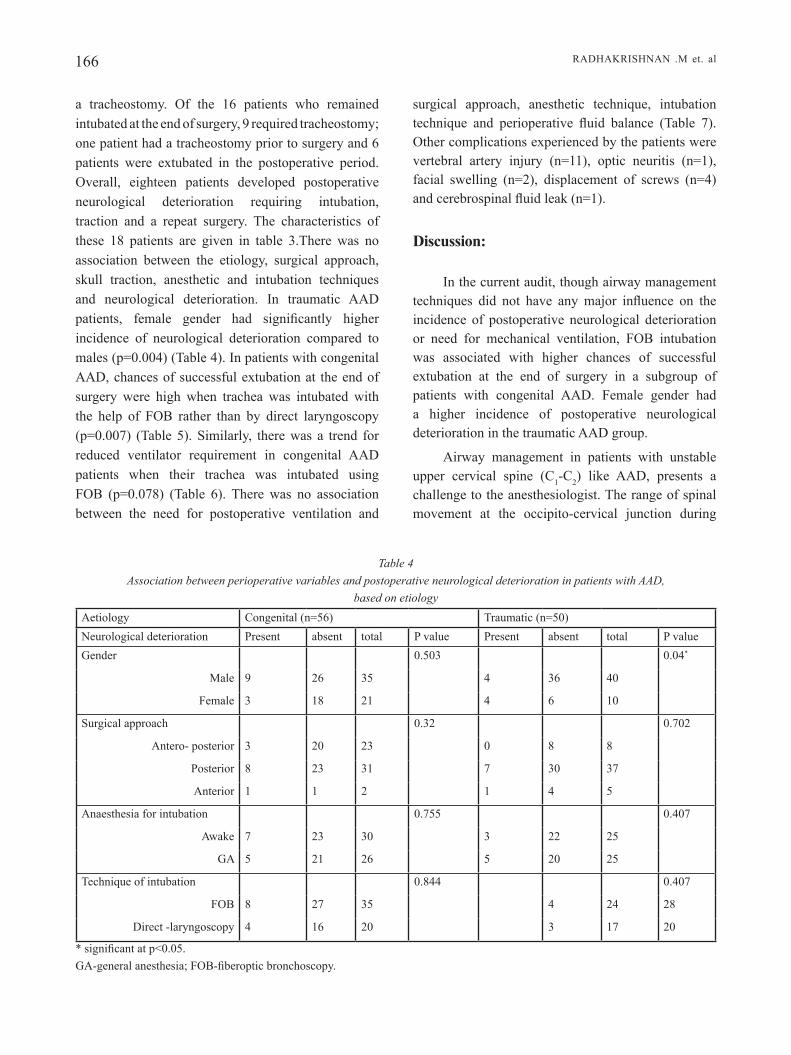
166 rAdhAKrishnAn .m et. al
a tracheostomy. of the 16 patients who remained intubated at the end of surgery, 9 required tracheostomy; one patient had a tracheostomy prior to surgery and 6 patients were extubated in the postoperative period. Overall, eighteen patients developed postoperative neurological deterioration requiring intubation, traction and a repeat surgery. the characteristics of these 18 patients are given in table 3.There was no association between the etiology, surgical approach, skull traction, anesthetic and intubation techniques and neurological deterioration. in traumatic AAd patients, female gender had significantly higher incidence of neurological deterioration compared to males (p=0.004) (Table 4). In patients with congenital AAd, chances of successful extubation at the end of surgery were high when trachea was intubated with the help of FOB rather than by direct laryngoscopy (p=0.007) (Table 5). Similarly, there was a trend for reduced ventilator requirement in congenital AAD patients when their trachea was intubated using FOB (p=0.078) (Table 6). There was no association between the need for postoperative ventilation and
surgical approach, anesthetic technique, intubation technique and perioperative fluid balance (Table 7). other complications experienced by the patients were vertebral artery injury (n=11), optic neuritis (n=1), facial swelling (n=2), displacement of screws (n=4) and cerebrospinal fluid leak (n=1).
Discussion:
in the current audit, though airway management techniques did not have any major influence on the incidence of postoperative neurological deterioration or need for mechanical ventilation, FOB intubation was associated with higher chances of successful extubation at the end of surgery in a subgroup of patients with congenital AAd. female gender had a higher incidence of postoperative neurological deterioration in the traumatic AAd group.
Airway management in patients with unstable upper cervical spine (C1-c2) like AAD, presents a challenge to the anesthesiologist. the range of spinal movement at the occipito-cervical junction during
Table 4 Association between perioperative variables and postoperative neurological deterioration in patients with AAD,
based on etiologyAetiology Congenital (n=56) Traumatic (n=50)neurological deterioration present absent total P value present absent total P valuegender 0.503 0.04*
male 9 26 35 4 36 40
female 3 18 21 4 6 10
surgical approach 0.32 0.702
Antero- posterior 3 20 23 0 8 8
posterior 8 23 31 7 30 37
Anterior 1 1 2 1 4 5
Anaesthesia for intubation 0.755 0.407
Awake 7 23 30 3 22 25
gA 5 21 26 5 20 25
Technique of intubation 0.844 0.407
FOB 8 27 35 4 24 28
direct -laryngoscopy 4 16 20 3 17 20
* significant at p<0.05.GA-general anesthesia; FOB-fiberoptic bronchoscopy.

M.E.J. ANESTH 23 (2), 2015
167AirwAy mAnAgement And AtlAnto AxiAl dislocAtion
Table 5 Association between perioperative variables and successful extubation in OT in patients with AAD, based on their etiology.
Aetiology Congenital (n=56) Traumatic (n=50)extubation in ot yes no total P value yes no total P value
gender 1.000 0.360
male 30 5 35 34 6 40
female 18 3 21 7 3 10
surgical approach 0.384 0.350
Antero- posterior 18 5 23 8 0 8
posterior 28 3 31 29 8 37
Anterior 2 0 2 4 1 5
Anaesthesia for intubation 0.127 0.463
Awake 28 2 30 22 3 25
gA 20 6 26 19 6 25
Technique of intubation 0.007* 0.470
FOB 33 2 35 23 5 28
direct-laryngoscopy 15 5 20 17 3 20* significant at p<0.05.GA-general anesthesia; FOB-fiberoptic bronchoscopy.
Table 6 Association between perioperative variables and postoperative ventilator requirement
in patients with AAD, based on their etiology
Aetiology Congenital (n=56) Traumatic (n=50)Post operative ventilation
Required not required
total P value Required not required
total P value
gender 1 0.188
male 7 28 35 5 35 40
female 4 17 21 3 7 10
surgical approach 0.513 0.403
Antero- posterior 6 17 23 0 8 8
posterior 5 26 31 7 30 37
Anterior 0 2 2 1 4 5
Anaesthesia for intubation
0.313 0.7
Awake 4 26 30 3 22 25
gA 7 19 26 5 20 25
Technique of intubation
0.078 0.312
FOB 5 30 35 5 23 28
direct-laryngoscopy
5 15 20 2 18 20
GA-general anesthesia; FOB-fiberoptic bronchoscopy.
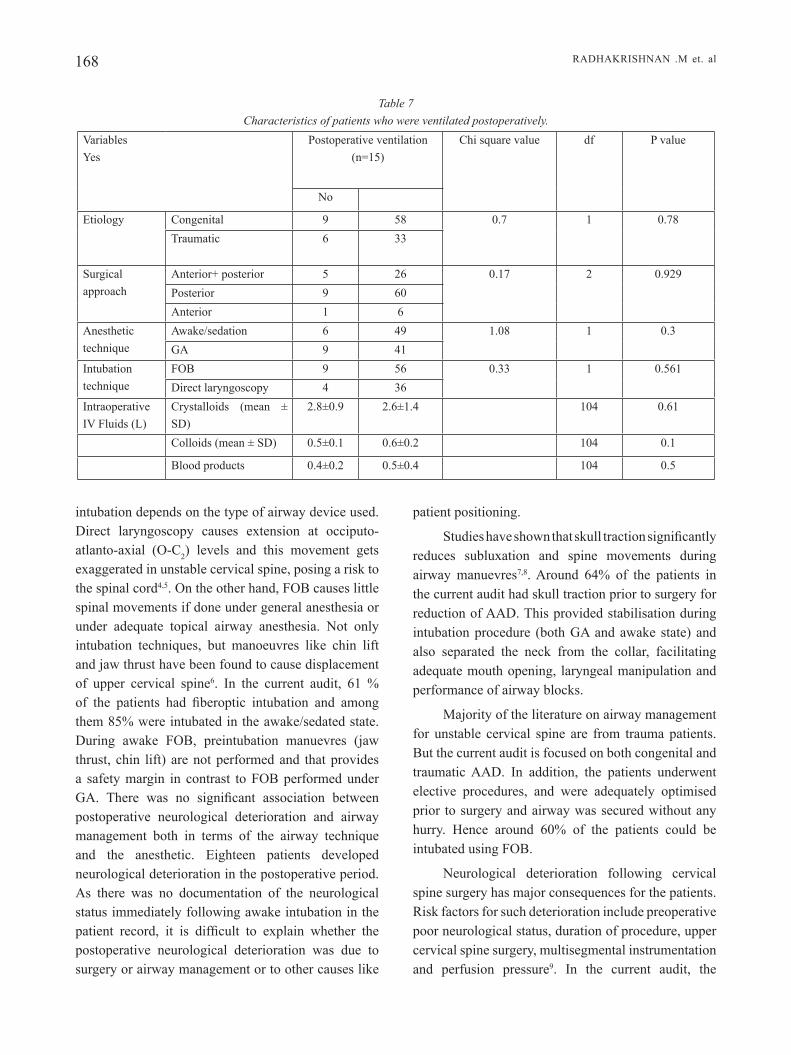
168 rAdhAKrishnAn .m et. al
intubation depends on the type of airway device used. direct laryngoscopy causes extension at occiputo-atlanto-axial (o-c2) levels and this movement gets exaggerated in unstable cervical spine, posing a risk to the spinal cord4,5. On the other hand, FOB causes little spinal movements if done under general anesthesia or under adequate topical airway anesthesia. Not only intubation techniques, but manoeuvres like chin lift and jaw thrust have been found to cause displacement of upper cervical spine6. In the current audit, 61 % of the patients had fiberoptic intubation and among them 85% were intubated in the awake/sedated state. During awake FOB, preintubation manuevres (jaw thrust, chin lift) are not performed and that provides a safety margin in contrast to FOB performed under GA. There was no significant association between postoperative neurological deterioration and airway management both in terms of the airway technique and the anesthetic. Eighteen patients developed neurological deterioration in the postoperative period. As there was no documentation of the neurological status immediately following awake intubation in the patient record, it is difficult to explain whether the postoperative neurological deterioration was due to surgery or airway management or to other causes like
patient positioning.
Studies have shown that skull traction significantly reduces subluxation and spine movements during airway manuevres7,8. Around 64% of the patients in the current audit had skull traction prior to surgery for reduction of AAD. This provided stabilisation during intubation procedure (both GA and awake state) and also separated the neck from the collar, facilitating adequate mouth opening, laryngeal manipulation and performance of airway blocks.
majority of the literature on airway management for unstable cervical spine are from trauma patients. But the current audit is focused on both congenital and traumatic AAd. in addition, the patients underwent elective procedures, and were adequately optimised prior to surgery and airway was secured without any hurry. Hence around 60% of the patients could be intubated using FOB.
Neurological deterioration following cervical spine surgery has major consequences for the patients. Risk factors for such deterioration include preoperative poor neurological status, duration of procedure, upper cervical spine surgery, multisegmental instrumentation and perfusion pressure9. in the current audit, the
Table 7 Characteristics of patients who were ventilated postoperatively.
Variablesyes
Postoperative ventilation (n=15)
Chi square value df P value
no
etiology congenital 9 58 0.7 1 0.78traumatic 6 33
surgical approach
Anterior+ posterior 5 26 0.17 2 0.929posterior 9 60Anterior 1 6
Anesthetic technique
Awake/sedation 6 49 1.08 1 0.3gA 9 41
intubation technique
FOB 9 56 0.33 1 0.561direct laryngoscopy 4 36
Intraoperative iV fluids (l)
crystalloids (mean ± sd)
2.8±0.9 2.6±1.4 104 0.61
colloids (mean ± sd) 0.5±0.1 0.6±0.2 104 0.1
Blood products 0.4±0.2 0.5±0.4 104 0.5

M.E.J. ANESTH 23 (2), 2015
169AirwAy mAnAgement And AtlAnto AxiAl dislocAtion
duration of procedure did not predict postoperative neurological deterioration. Involvement of autonomic nervous system in these patients has been described and the resultant blood pressure variations in the perioperative period, theoretically could aggravate spinal cord ischemia10,11. Awake positioning does not always assure intact neurological status at the end of procedure as hemodynamic changes, surgical manipulation of spinal structures and spinal instrumentation in the intraoperative period can result in neurological deterioration and can be detected only by neurophysiologic monitoring throughout the surgical procedure. in the current audit, it was noticed that female gender in the traumatic group (n=4) experienced higher incidence of neurological deterioration as compared to females in the congenital group. Though the difference is statistically significant, the total number of female traumatic patients were only 10. It is likely that the data is not adequately powered to detect the actual significance.
In a study on combined approaches for cervical spine surgery, patients who underwent combined anterior and posterior surgery had higher chances of postoperative airway problems12. But in the current audit, surgical approach had no influence on the postoperative airway problems. Acute postoperative airway obstruction occurred in 4 (1.2%) patients requiring reintubation but it was not related to the technique of airway management. In a study on rheumatoid arthritis patients undergoing posterior stabilisation procedures, FOB resulted in fewer postoperative airway complications and the authors recommended FOB for all cervical spine procedures13. in the current audit, patients with congenital AAd had higher chances for successful extubation at the end of surgery when their trachea was intubated using FOB and this benefit was not seen in traumatic AAD and the reasons are not clear. one possible explanation could be minimal movement of the cervical spine associated with FOB. In the congenital subgroup, the disease process is slower and the lung parenchyma is normal which is in contrast with the traumatic group where the clinical presentation is acute and chances for respiratory muscle dysfunction and low functional residual capacity are high. The audit did not have enough information on the preoperative pulmonary function tests, preoperative respiratory muscle activity,
power of individual muscle groups and hence difficult to compare the baseline respiratory activity of the congenital and the traumatic patients groups.
the respiratory complications were seen on the second to third postoperative day stressing the need for extending the intensive postoperative monitoring for a longer period. Reddy, et al found that significant deterioration of pulmonary function tests (pft) persisted even at 1 week after surgery for congenital AAd14.
Being retrospective in nature, missing data is the main limitation of this study. The data on perioperative hemodynamics were not collected and hence whether hypotension had an adverse impact on postoperative neurological deterioration, could not be ascertained. Also, other methods of intubation like the intubating LMA or Airtraq were seldom used for intubation.
in conclusion, in the current audit, there are several significant observations though there was no overall correlation between the technique of intubation and neurological deterioration or postoperative ventilatory requirement. In AAD patients, female gender had significantly higher incidence of neurological deterioration compared to males. in patients with congenital AAd, chances of successful extubation at the end of surgery were high when trachea was intubated with the help of FOB rather than by direct laryngoscopy (p=0.007). Similarly, there was a trend for reduced ventilator requirement in congenital AAd patients when their trachea was intubated using FOB (p=0.078). Minimal cervical spine movement associated with FOB seems to favour better outcome at least in small subsets of patients. there was no association between the need for postoperative ventilation and surgical approach, anesthetic technique, intubation technique and perioperative fluid balance. high incidence of respiratory complications on day 2-3 postoperatively, stresses the need for extending the intensive postoperative monitoring for a longer period. future studies with larger samples should identify the subgroups where specific airway techniques could considerably decrease the incidence of postoperative neurological deterioration.

170 rAdhAKrishnAn .m et. al
References
1. Pandya Sk: Atlanto axial dislocation (review). Neurol India; 20:13-48, 1972.
2. wadia nh: Chronic progressive myelopathy complicating atlanto axial dislocation due to congenital abnormality. Neurolindia; 8:81-94, 1960.
3. haStinGS rh, kelley Sd: Neurologic deterioration associated with airway management in a cervical spine-injured patient. Anesthesiology; 78:580-583, 1993.
4. horton wa, Fahy l, CharterS P: Disposition of the cervical vertebrae, atlanto-axial joint, hyoid and mandible during x-ray laryngoscopy. Br J Anaesth; 63:435-8, 1989.
5. Sawin Pd, todd MM, trayneliS VC, et al: Cervical spine motion with direct laryngoscopy and orotracheal intubation: an in vivo cinefluroscopic study of subjects without cervical abnormality. Anesthesiology; 85:26-32, 1996.
6. donaldSon wF iii, heil BV, donaldSon VP, et al. the effect of airway maneuvers on the unstable C1-C2 segment: A cadaver study. Spine; 22:1215-8, 1997.
7. lennarSon PJ, SMith dw, Sawin Pd, et al: Cervical spinal motion during intubation: efficacy of stabilization maneuvers in the setting of complete segmental instability. J Neurosurg; 94:265-7, 2001.
8. lennarSon PJ, SMith d, todd MM, et al: Segmental cervical spine
motion during orotracheal intubation of the intact and injured spine with and without external stabilization. J Neurosurg; 92:201-6, 2000.
9. Calder i: Anesthesia for spinal surgery. Baillere's Clinical anesthesiology; 13:629-42, 1999.
10. MoGuel Gd, kinSella lJ: Reversal of sympathetic failure due to cervical myelopathy in a patient with Down’s syndrome. Clin Auton Res; 13:224-6, 2003.
11. VaCCaro ar, SChwartz dM: Neurophysiologic monitoring during cervical spine surgery. In: Clark CR, editor. The cervical spine. Phildadelphia: Lippincott Williams Wilkins; p. 239-44, 2005.
12. terao y, MatSuMoto S, yaMaShita k, et al: increased incidence of emergency airway management after combined anterior-posterior cervical spine surgery. J Neurosurg Anesthesiol; 16:282-6, 2004.
13. wattenMaker i, ConCePCion M, hiBBerd P, et al: Upper-airway obstruction and perioperative management of the airway in patients managed with posterior operations on the cervical spine for rheumatoid arthritis. J Bone Joint Surg Am; 76:360-5, 1994.
14. reddy kr, rao GS, deVi Bi, et al: pulmonary function After surgery for congenital Atlantoaxial dislocation, A comparison with Surgery for Compressive Cervical Myelopathy and Craniotomy. J Neurosurg Anesthesiol; 21:196-201, 2009.

171 M.E.J. ANESTH 23 (2), 2015
UltrasoUnd-gUided sciatic Politeal nerve Block: a comParison of seParate tiBial
and common Peroneal nerve injections versUs injecting Proximal to the BifUrcation
Magdy H. EldEgwy*, SaMi M. ibraHiM**, SaMy Hanora*, ElSayEd Elkarta*, ayMan S. ElSily*
Abstract
Objective: Block of the sciatic nerve at the popliteal fossa can be performed using the ultrasound machine; it may be proximally or distally to the bifurcation of the sciatic nerve using lateral, medial, or posterior approaches. it is frequently used for surgeries below the knee specially the foot and ankle operations.
Purpose: this study compares one and two injections of the sciatic nerve in the popliteal fossa with ultrasound-guided block in foot or ankle surgeries.
Methods: forty patients received ultrasound-guided sciatic nerve block with the nerve stimulator, using the posterior approach. the patients were enrolled into two groups (20 patients each), group 1: received one injection at 2 cm cephalad to the bifurcation of the sciatic nerve, and group 2: received two injections caudate to the sciatic bifurcation; one for tibial nerve and the other for common peroneal nerve. all patients received 20 ml of levobupivacaine 0.5%. the block performance time, block efficacy, success rate, complications and patient’s satisfaction were evaluated.
Results: Block the tibial and common peroneal nerves separately (two injections) distal to the point of bifurcation of the sciatic nerve has a significantly (P<0.05) faster time to complete sensory block of tibial and common peroneal nerves compared to a pre-bifurcation sciatic nerve block (one injection). The complete motor block, block time performance, success rate and patient’s satisfaction were not significantly different between groups (P>0.05).
Conclusion: the block of tibial and common peroneal nerves separately distal to the sciatic nerve bifurcation is superior to single injection block of sciatic nerve above the bifurcation in the popliteal fossa as regard complete sensory block time.
Keywords: sciatic nerve block; popliteal fossa; ultrasound-guided.
* md, department of anesthesiology and icU, faculty of medicine, al-azhar University, egypt.** md, department of anesthesia & icU ,faculty of medicine , Zagazig University, egypt.

172 magdy h. eldegwy et. al
Introduction
Ultrasound guidance for peripheral nerve blocks reduces the number of complications and improves the quality of regional blockade in adults, compared with blind techniques or nerve stimulator guidance1. Ultrasound guidance may, theoretically, offer an advantage over conventional technique since it allows direct visualization of nerve structures, needle pathway and local anesthetic spread in real time2. foot surgery is often associated with severe and long standing postoperative pain requiring large amounts of parenteral opioids3. the sciatic nerve block at popliteal fossa is frequently used for surgeries below the knee; it may be used alone or in combination with other peripheral nerve blocks for orthopedic procedures involving the lower limb.
several approaches to block the sciatic nervehave been described3-6.
there are some approaches for popliteal sciatic nerve block have been described as posterior, lateral and medial. the classical posterior approach to the sciatic nerve in the popliteal fossa requires placement of the patient in the prone position, which may be contraindicated in pregnant women or impossible in trauma patients8. the medial approach did not need elevation of the limb or change the position9.
a sciatic nerve block via a lateral approach is an especially useful technique for foot surgery, because it provides prolonged anesthesia rapidly and effectively below the knee especially in patients in whom the supine position is impossible or extremely uncomfortable (pregnancy, trauma)10. the lower limb must be sufficiently elevated to enable adequate space around the knee joint for transducer application11.
the multiple twitch technique is based on searching and identifying the targeted nerve by eliciting each nerve’s motor component with nerve stimulation13. it has been associated with a reduction in sensory and motor block onset and a greater efficacy than a single injection technique14. recently, ultrasound guidance has been introduced in order to improve the efficacy of peripheral nerve blocks, to shorten procedural time, to reduce the minimum local anesthetic volume required for a successful block and to lower the incidence of complications and side-
effects15,16. Ultrasound guidance may, theoretically, offer an advantage over conventional technique (anatomical landmarks and nerve stimulation) since it allows direct visualization of nerve structures, needle pathway and local anesthetic spread in real time17,18.
levobupivacaine is the latest local anesthetic introduced into clinical practice. levobupivacaine is a s(-) -enantiomer of the racemic formulation of bupivacaine. while both the r- and s-enantiomers of bupivacaine show anesthetic activity, preclinical studies suggested that levobupivacaine might be less cardiotoxic than the racemic bupivacaine19.
aim of this study was to compare ultrasound-guided one injection; cephalad 2 cm to the bifurcation, of the popliteal sciatic nerve versus two injections of tn and cPn separately, caudate to the bifurcation as regard the performance time and efficacy of the block.
Patients and Methods
after obtaining approval from the regional ethics committee and written informed consent had been obtained from patients, forty adult patients (asa i, ii or iii), undergoing ankle or foot surgery, were enrolled and randomized into two groups (20 patients each). group 1: the patients received a popliteal sciatic nerve block cephalad to its bifurcation with single injection. group 2: the patients received a popliteal sciatic nerve block caudate to the bifurcation with separate injection of tn and cPn. all patients received 20 ml of levobupivacaine 0.5%. exclusive criteria were patients with allergy to local anesthetics, blood coagulopathy, pregnancy and neurologic or neuromuscular disease. all patients received i.v. 2 mg of midazolam and 50 mcg fentanyl pre-block. Before the nerve block, continuous electrocardiogram, spo2, and non-invasive blood pressure were monitored during the nerve blockade and throughout the operation. we used the posterior approach at the popliteal fossa in the supine position with ultrasound guidance and the use of nerve stimulator. Patients in group 1, the sciatic nerve was traced cephalad to the bifurcation at least 2 cm and a seesaw sign visualized6, then levobupivacaine 0.5% was injected around the nerve in 5 ml increments, after negative aspiration test for blood, to a total volume of 20 ml. Patients in
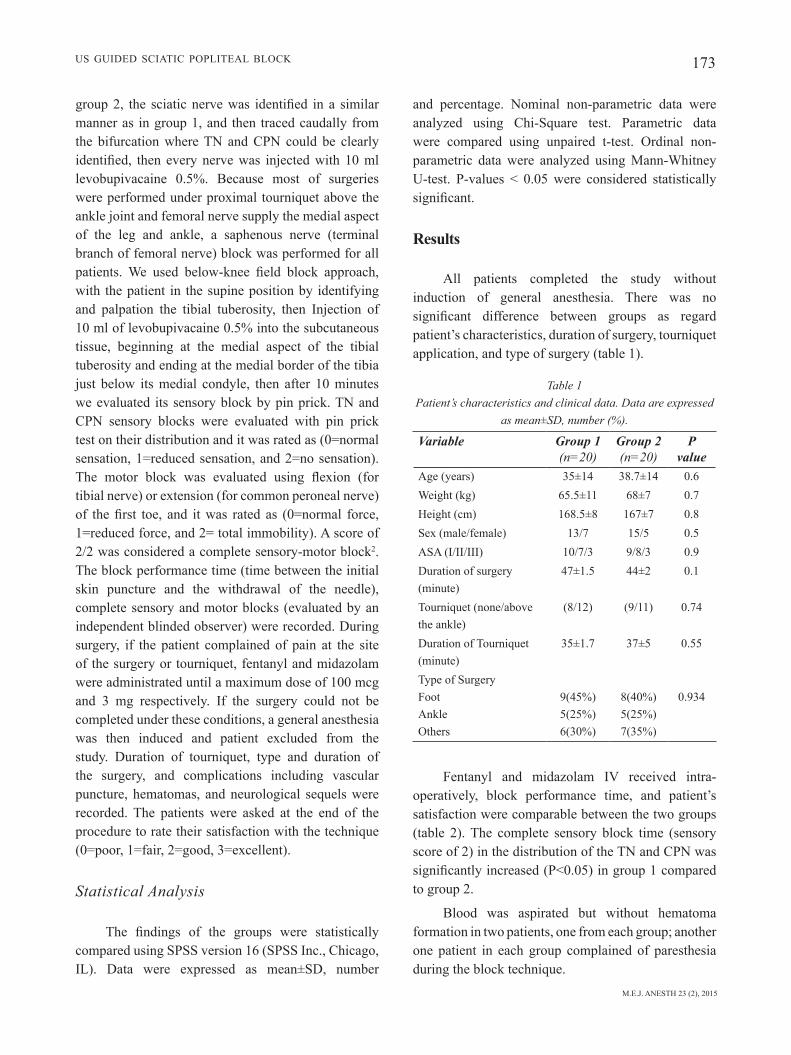
M.E.J. ANESTH 23 (2), 2015
173Us gUided sciatic PoPliteal Block
group 2, the sciatic nerve was identified in a similar manner as in group 1, and then traced caudally from the bifurcation where tn and cPn could be clearly identified, then every nerve was injected with 10 ml levobupivacaine 0.5%. Because most of surgeries were performed under proximal tourniquet above the ankle joint and femoral nerve supply the medial aspect of the leg and ankle, a saphenous nerve (terminal branch of femoral nerve) block was performed for all patients. We used below-knee field block approach, with the patient in the supine position by identifying and palpation the tibial tuberosity, then injection of 10 ml of levobupivacaine 0.5% into the subcutaneous tissue, beginning at the medial aspect of the tibial tuberosity and ending at the medial border of the tibia just below its medial condyle, then after 10 minutes we evaluated its sensory block by pin prick. tn and cPn sensory blocks were evaluated with pin prick test on their distribution and it was rated as (0=normal sensation, 1=reduced sensation, and 2=no sensation). The motor block was evaluated using flexion (for tibial nerve) or extension (for common peroneal nerve) of the first toe, and it was rated as (0=normal force, 1=reduced force, and 2= total immobility). a score of 2/2 was considered a complete sensory-motor block2. the block performance time (time between the initial skin puncture and the withdrawal of the needle), complete sensory and motor blocks (evaluated by an independent blinded observer) were recorded. during surgery, if the patient complained of pain at the site of the surgery or tourniquet, fentanyl and midazolam were administrated until a maximum dose of 100 mcg and 3 mg respectively. if the surgery could not be completed under these conditions, a general anesthesia was then induced and patient excluded from the study. duration of tourniquet, type and duration of the surgery, and complications including vascular puncture, hematomas, and neurological sequels were recorded. the patients were asked at the end of the procedure to rate their satisfaction with the technique (0=poor, 1=fair, 2=good, 3=excellent).
Statistical Analysis
The findings of the groups were statistically compared using sPss version 16 (sPss inc., chicago, il). data were expressed as mean±sd, number
and percentage. nominal non-parametric data were analyzed using chi-square test. Parametric data were compared using unpaired t-test. ordinal non-parametric data were analyzed using mann-whitney U-test. P-values < 0.05 were considered statistically significant.
Results
all patients completed the study without induction of general anesthesia. there was no significant difference between groups as regard patient’s characteristics, duration of surgery, tourniquet application, and type of surgery (table 1).
Table 1 Patient’s characteristics and clinical data. Data are expressed
as mean±SD, number (%).
Variable Group 1(n=20)
Group 2(n=20)
P value
age (years) 35±14 38.7±14 0.6weight (kg) 65.5±11 68±7 0.7height (cm) 168.5±8 167±7 0.8sex (male/female) 13/7 15/5 0.5asa (i/ii/iii) 10/7/3 9/8/3 0.9duration of surgery (minute)
47±1.5 44±2 0.1
tourniquet (none/above the ankle)
(8/12) (9/11) 0.74
duration of tourniquet (minute)
35±1.7 37±5 0.55
type of surgeryfootankleothers
9(45%)5(25%)6(30%)
8(40%)5(25%)7(35%)
0.934
fentanyl and midazolam iv received intra-operatively, block performance time, and patient’s satisfaction were comparable between the two groups (table 2). the complete sensory block time (sensory score of 2) in the distribution of the tn and cPn was significantly increased (P<0.05) in group 1 compared to group 2.
Blood was aspirated but without hematoma formation in two patients, one from each group; another one patient in each group complained of paresthesia during the block technique.
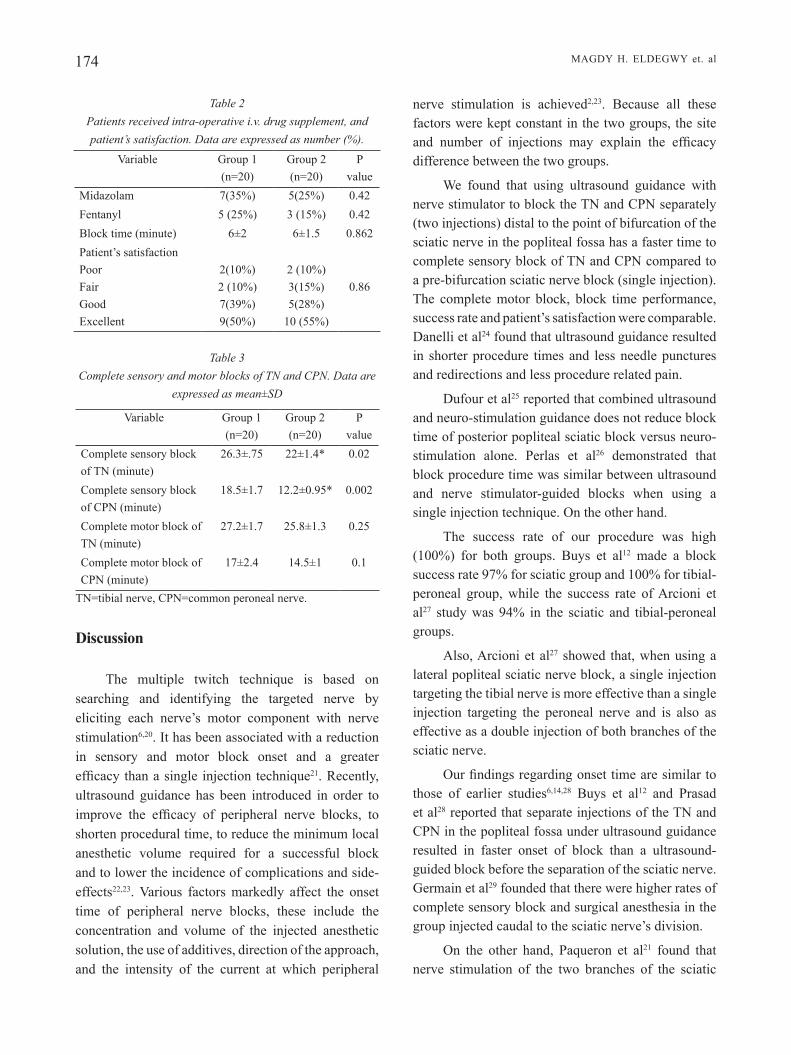
174 magdy h. eldegwy et. al
Table 2 Patients received intra-operative i.v. drug supplement, and patient’s satisfaction. Data are expressed as number (%).
variable group 1(n=20)
group 2(n=20)
P value
midazolam 7(35%) 5(25%) 0.42fentanyl 5 (25%) 3 (15%) 0.42Block time (minute) 6±2 6±1.5 0.862Patient’s satisfactionPoorfairgoodexcellent
2(10%)2 (10%)7(39%)9(50%)
2 (10%)3(15%)5(28%)
10 (55%)
0.86
Table 3 Complete sensory and motor blocks of TN and CPN. Data are
expressed as mean±SD
variable group 1(n=20)
group 2(n=20)
P value
complete sensory block of tn (minute)
26.3±.75 22±1.4* 0.02
complete sensory block of cPn (minute)
18.5±1.7 12.2±0.95* 0.002
complete motor block of tn (minute)
27.2±1.7 25.8±1.3 0.25
complete motor block of cPn (minute)
17±2.4 14.5±1 0.1
tn=tibial nerve, cPn=common peroneal nerve.
Discussion
the multiple twitch technique is based on searching and identifying the targeted nerve by eliciting each nerve’s motor component with nerve stimulation6,20. it has been associated with a reduction in sensory and motor block onset and a greater efficacy than a single injection technique21. recently, ultrasound guidance has been introduced in order to improve the efficacy of peripheral nerve blocks, to shorten procedural time, to reduce the minimum local anesthetic volume required for a successful block and to lower the incidence of complications and side-effects22,23. various factors markedly affect the onset time of peripheral nerve blocks, these include the concentration and volume of the injected anesthetic solution, the use of additives, direction of the approach, and the intensity of the current at which peripheral
nerve stimulation is achieved2,23. Because all these factors were kept constant in the two groups, the site and number of injections may explain the efficacy difference between the two groups.
we found that using ultrasound guidance with nerve stimulator to block the tn and cPn separately (two injections) distal to the point of bifurcation of the sciatic nerve in the popliteal fossa has a faster time to complete sensory block of tn and cPn compared to a pre-bifurcation sciatic nerve block (single injection). the complete motor block, block time performance, success rate and patient’s satisfaction were comparable. danelli et al24 found that ultrasound guidance resulted in shorter procedure times and less needle punctures and redirections and less procedure related pain.
dufour et al25 reported that combined ultrasound and neuro-stimulation guidance does not reduce block time of posterior popliteal sciatic block versus neuro-stimulation alone. Perlas et al26 demonstrated that block procedure time was similar between ultrasound and nerve stimulator-guided blocks when using a single injection technique. on the other hand.
the success rate of our procedure was high (100%) for both groups. Buys et al12 made a block success rate 97% for sciatic group and 100% for tibial-peroneal group, while the success rate of arcioni et al27 study was 94% in the sciatic and tibial-peroneal groups.
also, arcioni et al27 showed that, when using a lateral popliteal sciatic nerve block, a single injection targeting the tibial nerve is more effective than a single injection targeting the peroneal nerve and is also as effective as a double injection of both branches of the sciatic nerve.
Our findings regarding onset time are similar to those of earlier studies6,14,28 Buys et al12 and Prasad et al28 reported that separate injections of the tn and cPn in the popliteal fossa under ultrasound guidance resulted in faster onset of block than a ultrasound-guided block before the separation of the sciatic nerve. germain et al29 founded that there were higher rates of complete sensory block and surgical anesthesia in the group injected caudal to the sciatic nerve’s division.
on the other hand, Paqueron et al21 found that nerve stimulation of the two branches of the sciatic

M.E.J. ANESTH 23 (2), 2015
175Us gUided sciatic PoPliteal Block
nerve at the popliteal level with a posterior approach, at 10 cm from the popliteal skin crease, did not result in a reduced complete onset time or improved success rate when compared with that obtained with single stimulation. march et al6 found that only the superficial peroneal nerve was blocked earlier in group of double injections than in group of single injection.
also, the higher rates of complete sensory block in separately block of tn and cPn in our study in accordance with 3 recent studies demonstrating enhanced effectiveness of the double injection technique for tn and cPn12,28.
In our study there were no significant differences
as regard fentanyl and midazolam received intra-operatively in all patients, also adverse effects were minimal and comparable which was in agreement of other studies24,25.
Conclusion
double injections of tn and cPn distal to bifurcation of the sciatic nerve gives faster sensory block onset time compared to single injection of the sciatic nerve proximal to the bifurcation in the popliteal fossa.

176 magdy h. eldegwy et. al
References
1. MarHofEr P, ScHrogEndorfEr k, koinig H, Et al: Ultrasonographic guidance improves sensory block and onset time of three in-one blocks. Anesth Analg; 85:854-7, 1997.
2. caSati a, danElli g, baciarEllo M, Et al: a prospective randomized comparison between ultrasound and nerve stimulation guidance for multiple injection axillary brachial plexus block. Anesthesiology; 106:992-6, 2007.
3. roriE dk, byEr dE, nElSon do, Et al: assessment of block of the sciatic nerve in the popliteal fossa. Anesth Analg; 59:371-6,1980.
4. MclEod dH, wong dHw, claridgE rJ, MErrick PM: lateral popliteal sciatic nerve block compared with subcutaneous infiltration for analgesia following foot surgery. Can J Anaesth; 41:673-6, 1994.
5. Vloka Jd, Hadzic a, lESSEr Jb, Et al: a common epineural sheath for the nerves in the popliteal fossa and its possible implications for sciatic nerve block. Anesth Analg; 84:387-90, 1997. MarcH X, PinEda o, garcia MM, Et al: the posterior approach 6. to the sciatic nerve in the popliteal fossa: a comparison of single-versus double-injection technique. Anesth Analg; 103:1571-3, 2006.
7. roriE dk, byEr dE, nElSon do, Et al: assessment of block of the sciatic nerve in the popliteal fossa. Anesth Analg; 59:371-376, 1980.
8. Sala-blancH X, riVa nd, carrEra a, Et al: Ultrasound-guided popliteal sciatic block with a single injection at the sciatic division results in faster block onset than the classical nerve stimulator technique. Anesth Analg; 114:1121-1127, 2012.
9. yanaru t, SHigEMatSu k, Higa k, Et al: medial approach to the sciatic nerve at the popliteal fossa in the supine position with ultrasound guidance and nerve stimulator. ISRN Anesthesiology; volume article id 676823, 3 pages, 2012.
10. SingElyn fJ: single-injection applications for foot and ankle surgery. Best Pract Res Clin Anaenesthesoil; 16:247-254, 2002.
11. MccartnEy cJl, braunE i and cHan VwS: Ultrasound guidance for a lateral approach to the sciatic nerve in the popliteal fossa. Anaesthesia; 59:1023-1025, 2004.
12. buyS MJ, arndt cd, VagH f, Hoard a and gErStEin n: Ultrasound-guided sciatic nerve block in the popliteal fossa using a lateral approach: onset time comparing separate tibial and common peroneal nerve injections versus injecting proximal to the bifurcation. Anesth Analg; 110:635-637, 2010.
13. Handoll HH, koSciElniak-niElSEn zJ: single, double or multiple injection techniques for axillary brachial plexus block for hand, wrist or forearm surgery. Cochrane Database Systematic Review; 25:cd003842, 2006.
14. PaquEron X, bouaziz H, Macalou d, Et al: the lateral approach to the sciatic nerve at the popliteal fossa: one or two injections? Anesth Analg; 89:1221-5, 1999.
15. orEbaugH Sl, williaMS ba, kEntor Ml: Ultrasound guidance with nerve stimulation reduces the time necessary for with nerve stimulation reduces the time necessary for resident peripheral nerve blockade. Regional Pain Medicine; 32: 448-54, 2007.
16. caSati a, baciarEllo M, di cianni S, Et al: effects of ultrasound guidance on the minimum effective anesthetic volume required to block the femoral nerve. British Journal of Anesthesia; 98:823-7, 2007.
17. caSati a, danElli g, baciarEllo M, Et al: a prospective randomized comparison between ultrasound and nerve stimulation guidance for multiple injection axillary brachial plexus block. Anesthesiology; 106:992-6, 2007.
18. MarHofEr P, grEHEr M, kaPral S: Ultrasound guidance in regional anesthesia. British Journal of Anaesthesia; 94:7-17, 2005.
19. foStEr rH, MarkHaM a: levobupivacaine: a review of its pharmacology and use as a local anesthetic. Drugs; 59:551-79, 2000.
20. Handoll HH, koSciElniak-niElSEn zJ: single, double or multiple injection techniques for axillary brachial plexus block for hand, wrist or forearm surgery. Cochrane Database Systematic Review; 25:cd003842, 2006.
21. PaquEron X, bouaziz H, Macalou d, Et al: the lateral approach to the sciatic nerve at the popliteal fossa: one or two injections? Anesth Analg; 89:1221-5, 1999.
22. orEbaugH Sl, williaMS ba, kEntor Ml: Ultrasound guidance with nerve stimulation reduces the time necessary for resident peripheral nerve blockade. Reg Anesth Pain Med; 32:448-54, 2007.
23. caSati a, baciarEllo M, di cianni S, Et al: effects of ultrasound guidance on the minimum effective anaesthetic volume required to block the femoral nerve. British Journal of Anaesthesia; 98:823-7, 2007.
24. danElli g, fanElli a, gHiSi d, Et al: Ultrasound vs nerve stimulation multiple injection technique for posterior popliteal sciatic nerve block. Anaesthesia; 64:638-642, 2009.
25. dufour E, quEnnESSon P, Van robaiS al, Et al: combined ultrasound and neuro-stimulation guidance for popliteal sciatic nerve block: a prospective, randomized comparison with neuro-stimulation alone. Regional Anesthesia; 106:1553-8, 2008.
26. PErlaS a, brull r, cHan VwS, nuica a, abbas s: Ultrasound guidance improves the success of sciatic nerve block at the popliteal fossa. Reg Anesth Pain Med; 33:259-65, 2008.
27. arcioni r, PalMaSani S, Et al: lateral popliteal sciatic nerve block: a single injection targeting the tibial branch of the sciatic nerve is as effective as a double-injection technique. Acta Anaesthesiol Scand; 51:115-121, 2007.
28. PraSad a, PErlaS a, raMlogan r, brull r, cHan V: Ultrasound-guided popliteal block distal to sciatic nerve bifurcation shortens onset time: a prospective randomized double-blind study. Reg Anesth Pain Med; 35:267-71, 2010.
29. gErMain g, lE´VESquE S, dion n, Et al: a comparison of an injection cephalad or caudad to the division of the sciatic nerve for Ultrasound-guided Popliteal Block: a Prospective randomized study. Anesth Analg; 114:233-5, 2012.

177 M.E.J. ANESTH 23 (2), 2015
Intravenous Dexamethasone In CombInatIon wIth CauDal bloCk Prolongs PostoPeratIve
analgesIa In PeDIatrIC DayCare surgery
Murni Sari ahMad arbi*, azarinah izahaM**, ESa KaMaruzaMan*, KhairulaMir zainuddin***,
haMidah iSMail** and norSidah abdul Manap****
Abstract
Background: this study was conducted to determine if intravenous dexamethasone combined with caudal block was able to prolong post-operative analgesia in pediatric daycare surgeries.
Methods: sixty four asa I or II children aged 3 to 10 year old scheduled for daycare open unilateral herniotomy received general anesthesia and caudal block using 0.25% levobupivacaine 0.75 mg.kg-1 with suppository paracetamol 30 mg.kg-1. after anesthesia induction, they were randomized to receive either intravenous dexamethasone 0.5 mg.kg-1 (group I) or same volume intravenous normal saline (group II). Postoperatively, pain scores were assessed using wong-Baker faces scale. At home, their parents assessed and recorded the pain scores, time to first oral paracetamol served and frequency of paracetamol given in two consecutive days post surgery. on the third postoperative day, these information were gathered from the parents via a phone call.
Results: There were statistically significant differences between Group I and Group II in the median time to first paracetamol (800 vs 520 min, p = 0.01), mean pain scores postoperative day 1 (1.9 ± 2.0 vs 3.5 ± 2.2, p = 0.05), mean pain score postoperative day 2 (0.8 ± 1.6 vs 2.3 ± 2.0, p = 0.03) and mean frequencies of paracetamol given on postoperative day 2 (0.3 ± 0.8 vs 1.1 ± 1.0, p = 0.02).
Conclusion: a single intravenous dexamethasone dose when combined with caudal block reduces postoperative pain, decreases paracetamol requirement and prolongs analgesic duration in children after open herniotomy.
Keywords: dexamethasone, postoperative, analgesia, pediatric, daycare.
* mD (usm), mmed (anaesth) ukm.** mD (ukm), mmed (anaesth) ukm.*** mbChb (otago), mmed (anaesth) ukm.*** mbbs (sydney), mmed (anaesth) ukm. Department of anaesthesiology& Intensive Care, universiti kebangsaan malaysia (ukm) medical Centre, kuala lumpur,
malaysia. Department of anaesthesiology& Intensive Care, hospital kuala lumpur, kuala lumpur, malaysia. Address for correspondence:azarinah Izaham, Department of anaesthesiology& Intensive Care, universiti kebangsaan
Malaysia Medical Centre, JalanYaacob Latif, Bandar Tun Razak, 56000 Cheras, Kuala Lumpur, Malaysia. Tel: +603 91455797, Fax: +603 91456585, E-mail: [email protected]

178 azarInah Izaham et. al
Introduction
Pediatric daycare surgeries now form alarge part of pediatric anesthetic practice. In the united states of america, 2.3 millions pediatric surgeries were performed on a daycare basis in 20061. Children are candidates for daycare surgeries as they are usually healthy, free of systemic disease and typically require straightforward, minor or intermediate surgical procedures2,3.
an audit of pediatric daycare surgeries in a district general hospital in the uk by Jolliffe et al (1997) found that postoperatively, pain was more of a problem than nausea and vomiting4. most studies of analgesia in pediatric daycare surgeries have focused on the immediate postoperative course, and largely ignored the potential for moderate or severe pain after discharge home, when it then becomes the responsibility of the parents5.
Studies have been conducted to find the appropriate method to improve postoperative pain in pediatric daycare setting. the use of local anesthetic infiltration, oral non-steroidal anti-inflammatory drugs or tramadol, intravenous or caudal clonidine and ketamine have been shown to improve the postoperative analgesia and to reduce the postoperative pain. however, the use of these drugs has been limited by unacceptable adverse effects in children undergoing daycare surgery6-10.
Dexamethasone is a potent synthetic glucocor-ticoid which has a powerful anti-inflammatory action. Preoperative administration of dexamethasone has been shown to reduce pain and swelling after oral, spinal and laparoscopic surgeries. Despite the exact mechanism by which dexamethasone exerts its analgesic effect is not fully understood, a reduction in pain by steroids has been supported by many studies11.
this study was conducted to determine if a single intravenous dexamethasone dose when combined with caudal block was able to reduce post-operative pain and prolong post-operative analgesia in pediatric daycare herniotomies.
Methods
this was a prospective, randomized, controlled and double blind study conducted at hospital kuala lumpur, malaysia following approval from the medical research Committee of universiti kebangsaan malaysia medical Centre and the national medical research and ethics Committee malaysia. a total of 64 ASA I or II children aged between 3 to 10 years old, scheduled for daycare open unilateral herniotomy were included in the study.
Children who have contraindication to caudal block, have allergy to any drugs used in the study, who developed complications intraoperatively and required admission postoperatively were excluded from the study.
In the morning of surgery, parents were informed regarding the study at the daycare ward and written informed consents were obtained. both parents and their children were taught regarding the usage of wong-baker faces scale for pain scoring after discharge. they were given a diary to record the pain score when their children complaint of pain and frequency of paracetamol given at home. the children were kept fasting according to the daycare protocol. they were randomized using computer generated random number into two groups, group I received intravenous dexamethasone 0.5 mg.kg-1 (maximum of 10 mg) and group II who were given the same volume of intravenous saline after induction of anesthesia.
In the operating theatre, the children were induced by inhalational technique with sevoflurane 8% in 100% oxygen. Standard monitoring of non-invasive blood pressure, electrocardiogram and pulse oximeter were applied. after securing intravenous access, the children received intravenous fentanyl 1 µg.kg-1. an appropriate sized Proseal laryngeal mask airway (lma) was inserted accordingly. the end tidal concentration of sevoflurane was adjusted to deliver a minimum alveolar anesthetic concentration (maC) of 1.0. the patients then received either intravenous dexamethasone or normal saline according to their group allocation.
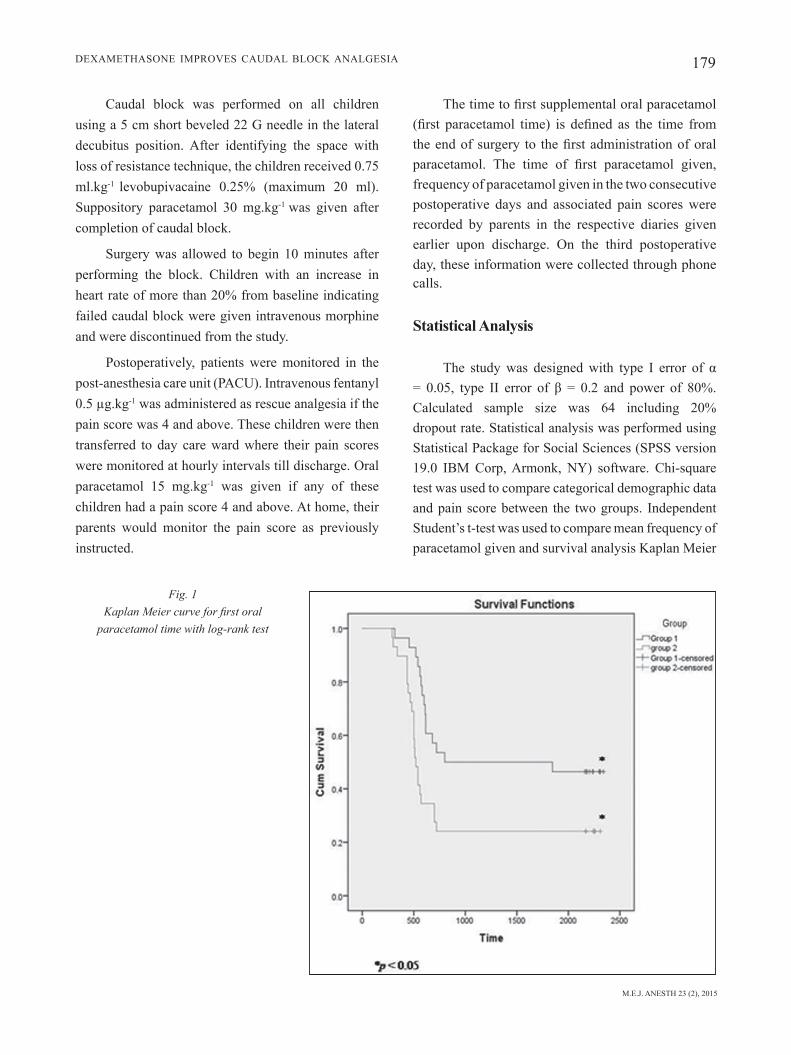
M.E.J. ANESTH 23 (2), 2015
179Dexamethasone ImProves CauDal bloCk analgesIa
Caudal block was performed on all children using a 5 cm short beveled 22 g needle in the lateral decubitus position. after identifying the space with loss of resistance technique, the children received 0.75 ml.kg-1 levobupivacaine 0.25% (maximum 20 ml). suppository paracetamol 30 mg.kg-1 was given after completion of caudal block.
surgery was allowed to begin 10 minutes after performing the block. Children with an increase in heart rate of more than 20% from baseline indicating failed caudal block were given intravenous morphine and were discontinued from the study.
Postoperatively, patients were monitored in the post-anesthesia care unit (PaCu). Intravenous fentanyl 0.5 µg.kg-1 was administered as rescue analgesia if the pain score was 4 and above. these children were then transferred to day care ward where their pain scores were monitored at hourly intervals till discharge. oral paracetamol 15 mg.kg-1 was given if any of these children had a pain score 4 and above. at home, their parents would monitor the pain score as previously instructed.
The time to first supplemental oral paracetamol (first paracetamol time) is defined as the time from the end of surgery to the first administration of oral paracetamol. The time of first paracetamol given, frequency of paracetamol given in the two consecutive postoperative days and associated pain scores were recorded by parents in the respective diaries given earlier upon discharge. on the third postoperative day, these information were collected through phone calls.
Statistical Analysis
The study was designed with type I error of α = 0.05, type II error of β = 0.2 and power of 80%. Calculated sample size was 64 including 20% dropout rate. statistical analysis was performed using statistical Package for social sciences (sPss version 19.0 Ibm Corp, armonk, ny) software. Chi-square test was used to compare categorical demographic data and pain score between the two groups. Independent student’s t-test was used to compare mean frequency of paracetamol given and survival analysis kaplan meier
Fig. 1 Kaplan Meier curve for first oral
paracetamol time with log-rank test
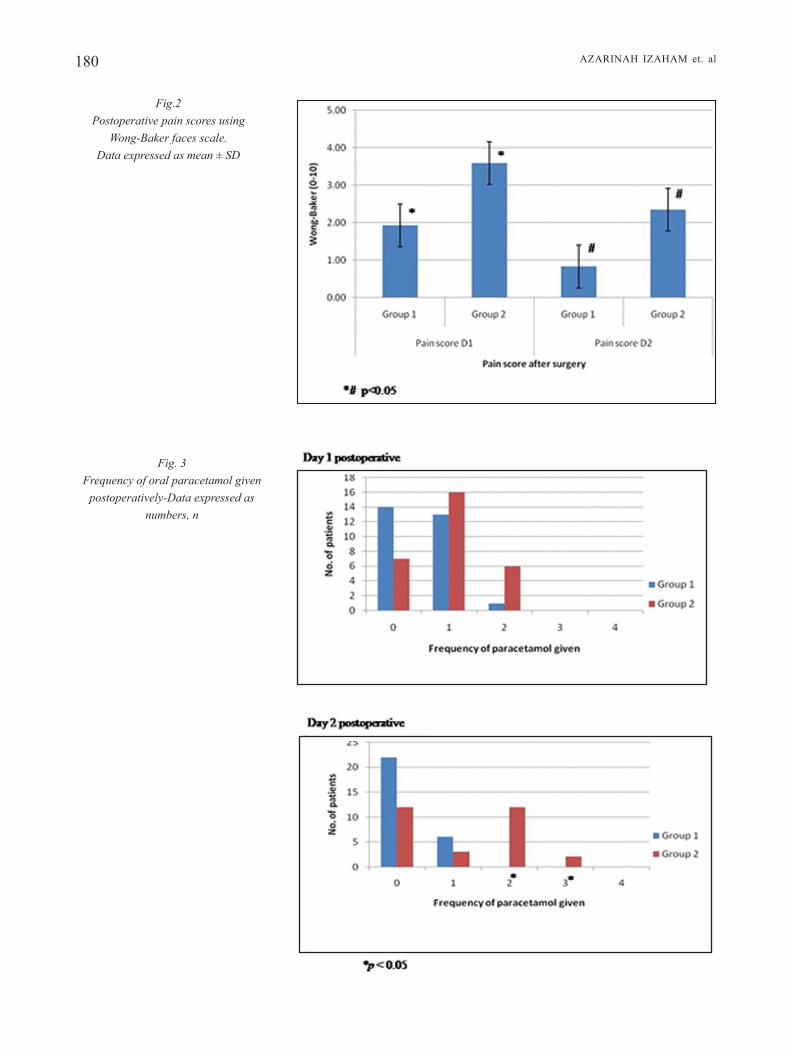
180 azarInah Izaham et. al
Fig. 3 Frequency of oral paracetamol given
postoperatively-Data expressed as numbers, n
Fig.2 Postoperative pain scores using
Wong-Baker faces scale. Data expressed as mean ± SD

M.E.J. ANESTH 23 (2), 2015
181Dexamethasone ImProves CauDal bloCk analgesIa
was used to demonstrate the time to first paracetamol between groups. a p value of < 0.05 was considered statistically significant.
Results
a total of sixty four patients were recruited to the study but only 57 patients had reliable data. seven patients were excluded from the study: 2 parents were uncontactable after discharge, 3 patients were readmitted to the ward on postoperative day 1 due to surgical complications and 2 mothers had violated the protocol postoperatively. there were no statistically significant difference between the two groups with regard to their age, weight, gender and races (table I). there was no failure of caudal blocks in any patients.
none of the children in both groups required rescue fentanyl in the PaCu or rescue oral paracetamol in the daycare ward. The time to first oral paracetamol administration was significantly longer in Group I (800 minutes) compared with group II (520 minutes), (p = 0.011) (Figure 1).
Pain scores assessed using wong-baker faces scale showed that the pain was less in group I compared to Group II in the first (1.9 ± 2.0 vs 3.5 ± 2.2, p ˂0.05) and second postoperative days (0.8 ± 1.6 vs 2.3 ± 2.0, p ˂0.05) as shown in Figure 2. None of these children experienced pain in PaCu or daycare ward.
There was no statistically significant difference in paracetamol administration during day 1 postoperatively although 14 children in group I did not require any paracetamol as compared to 7 children in Group II. There was, however, significant difference in paracetamol administration on day 2 postoperatively where the frequency of paracetamol administration was less in group I compared to Group II (0.3 ± 0.8 vs 1.1 ± 1.0, p = 0.022). It was noted that on day 2, 22 children in group I did not require paracetamol for pain relief compared to only 12 children in group II. this reduction in paracetamol requirement reflected an improved quality of pain relief in group I (Figure 3).
Discussion
Daycare surgery is a modern, effective and economical way to treat patients while maintaining the same level of quality of patient care. Daycare surgery has been reported to be safe and effective for a large proportion of infants and children requiring operation in many pediatric hospitals. It is gaining considerable acceptance and many parents have expressed satisfaction with this approach18. Inguinal hernia repair is one of the frequently performed surgical procedures in children whereby it is frequently performed as daycare surgery19. a study by obalum et al (2008) reported that postoperative pain was the most common complication of daycare inguinal herniotomy and herniorrhaphy20. adequate postoperative pain relief is one of the most fundamental issues for successful pediatric outpatient surgery, but unfortunately this is not always the case despite the various analgesic treatment options that are available21.
we demonstrated that a single dose of intravenous dexamethasone in combination with a caudal block prolongs the postoperative pain relief significantly. This finding is comparable to a study done by Hong et al (2010) which reported that a single dose of intravenous dexamethasone 0.5 mg.kg-1 combined with caudal block prolongs postoperative pain relief in pediatric orchidopexy23. these results may be due to the onset of dexamethasone which has been shown to have a long duration of action of 36 to 54 hours11. the exact mechanism by which dexamethasone may exert an analgesic effect is not fully understood. It has been postulated that systemic administration of steroids has been found to suppress tissue levels of bradykinin and the release of neuropeptides from nerve endings, both of which can enhance nociception in inflamed tissue. the established reduction in prostaglandin production may further contribute to analgesia by inhibiting the synthesis of cyclooxygenase isoform-2 in peripheral tissues and in the central nervous system. they also inhibit other mediators of inflammatory hyperalgesia, for example, tumour necrosis factor-α, interleukin-17β and interleukin-623.
this study also showed that dexamethasone improved the quality of pain relief. this may be due to the action of dexamethasone as an anti-inflammatory

182 azarInah Izaham et. al
agent which reduces local edema and swelling24.
The above finding is comparable to a study done by mohamed et al (2009) where the combination of both intravenous dexamethasone 0.5 mg.kg-1 and bilateral glossopharyngeal nerve block reduces visual analogue score significantly at 8 and 12 hours postoperatively compared to either intravenous dexamethasone or glossopharyngeal nerve block alone25.
we demonstrated in this study that there was no significant difference in paracetamol administration on day 1 post-operation. however on day 2 post-operation, there was significantly less frequency of paracetamol administration when caudal block combine with intravenous dexamethasone. This finding correlates with its prolong duration of action and is comparable to a study done by gomez-hernandez et al (2010) which reported that postoperative ketorolac were required more in patients of the control group than in the dexamethasone group in breast cancer patients undergoing mastectomy14.
In our study, none of the children experienced any postoperative nausea and vomiting. all the children were able to tolerate oral intake well before being discharged home. this may be due to minimal usage of intraoperative opioids, good pain relief by caudal block and effect of dexamethasone. the exact
mechanism of action is unknown but dexamethasone may exert an antiemetic action via prostaglandin antagonism, serotonin inhibition in the gut and release of endorphins21. this is similar to a study done by samarkandi et al (2004) which demonstrated intravenous dexamethasone reduces postoperative vomiting and pain in pediatric tonsillectomy procedures16.
there were several limitations to this study. we did not study the side effects of dexamethasone such as aggression, agitation, anxiety and blurred vision. Furthermore, there was no report of adverse effects in a single dose of dexamethasone in pediatric or adult surgery in previous studies12-17,23,25,26. our study is limited to only two postoperative days as the parents needed to resume back to their daily activities. the pain score was assessed by the parents at home and this may be subjected to bias as the parents were the sole assessors.
Acknowledgements
we would like to thank Dr. azrin azidin for his help in the data collections and manuscript for this study.
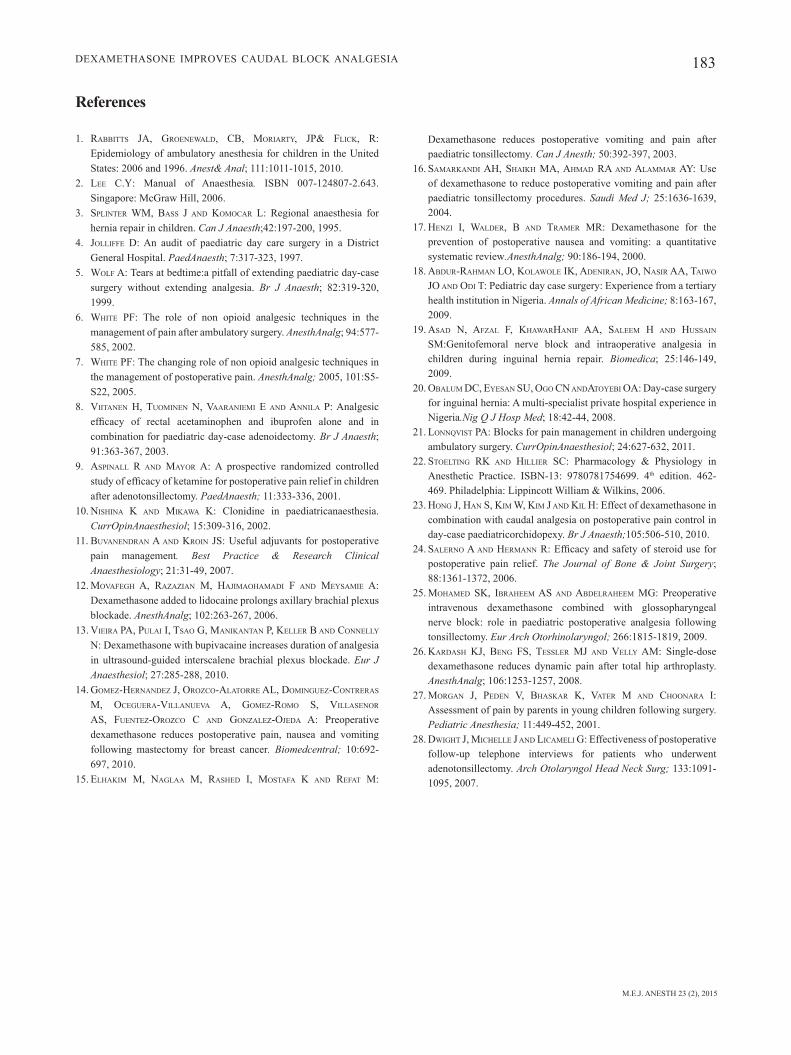
M.E.J. ANESTH 23 (2), 2015
183Dexamethasone ImProves CauDal bloCk analgesIa
References
1. rabbittS Ja, GroEnEwald, Cb, Moriarty, Jp& FliCK, r: epidemiology of ambulatory anesthesia for children in the united States: 2006 and 1996. Anest& Anal; 111:1011-1015, 2010.
2. lEE C.y: manual of anaesthesia. ISBN 007-124807-2.643. Singapore: McGraw Hill, 2006.
3. SplintEr wM, baSS J and KoMoCar l: regional anaesthesia for hernia repair in children. Can J Anaesth;42:197-200, 1995.
4. JolliFFE d: an audit of paediatric day care surgery in a District general hospital. PaedAnaesth; 7:317-323, 1997.
5. wolF a: tears at bedtime:a pitfall of extending paediatric day-case surgery without extending analgesia. Br J Anaesth; 82:319-320, 1999.
6. whitE pF: the role of non opioid analgesic techniques in the management of pain after ambulatory surgery. AnesthAnalg; 94:577-585, 2002.
7. whitE pF: the changing role of non opioid analgesic techniques in the management of postoperative pain. AnesthAnalg; 2005, 101:s5-s22, 2005.
8. ViitanEn h, tuoMinEn n, VaaraniEMi E and annila p: analgesic efficacy of rectal acetaminophen and ibuprofen alone and in combination for paediatric day-case adenoidectomy. Br J Anaesth; 91:363-367, 2003.
9. aSpinall r and Mayor a: a prospective randomized controlled study of efficacy of ketamine for postoperative pain relief in children after adenotonsillectomy. PaedAnaesth; 11:333-336, 2001.
10. niShina K and MiKawa K: Clonidine in paediatricanaesthesia. CurrOpinAnaesthesiol; 15:309-316, 2002.
11. buVanEndran a and Kroin JS: Useful adjuvants for postoperative pain management. Best Practice & Research Clinical Anaesthesiology; 21:31-49, 2007.
12. MoVaFEGh a, razazian M, haJiMaohaMadi F and MEySaMiE a: Dexamethasone added to lidocaine prolongs axillary brachial plexus blockade. AnesthAnalg; 102:263-267, 2006.
13. ViEira pa, pulai i, tSao G, ManiKantan p, KEllEr b and ConnElly n: Dexamethasone with bupivacaine increases duration of analgesia in ultrasound-guided interscalene brachial plexus blockade. Eur J Anaesthesiol; 27:285-288, 2010.
14. GoMEz-hErnandEz J, orozCo-alatorrE al, doMinGuEz-ContrEraS M, oCEGuEra-VillanuEVa a, GoMEz-roMo S, VillaSEnor aS, FuEntEz-orozCo C and GonzalEz-oJEda a: Preoperative dexamethasone reduces postoperative pain, nausea and vomiting following mastectomy for breast cancer. Biomedcentral; 10:692-697, 2010.
15. ElhaKiM M, naGlaa M, raShEd i, MoStaFa K and rEFat M:
Dexamethasone reduces postoperative vomiting and pain after paediatric tonsillectomy. Can J Anesth; 50:392-397, 2003.
16. SaMarKandi ah, ShaiKh Ma, ahMad ra and alaMMar ay: use of dexamethasone to reduce postoperative vomiting and pain after paediatric tonsillectomy procedures. Saudi Med J; 25:1636-1639, 2004.
17. hEnzi i, waldEr, b and traMEr Mr: Dexamethasone for the prevention of postoperative nausea and vomiting: a quantitative systematic review.AnesthAnalg; 90:186-194, 2000.
18. abdur-rahMan lo, KolawolE iK, adEniran, Jo, naSir aa, taiwo Jo and odi t: Pediatric day case surgery: experience from a tertiary health institution in nigeria. Annals of African Medicine; 8:163-167, 2009.
19. aSad n, aFzal F, KhawarhaniF aa, SalEEM h and huSSain SM:genitofemoral nerve block and intraoperative analgesia in children during inguinal hernia repair. Biomedica; 25:146-149, 2009.
20. obaluM dC, EyESan Su, oGo Cn andatoyEbi oa: Day-case surgery for inguinal hernia: a multi-specialist private hospital experience in nigeria.Nig Q J Hosp Med; 18:42-44, 2008.
21. lonnqViSt pa: blocks for pain management in children undergoing ambulatory surgery. CurrOpinAnaesthesiol; 24:627-632, 2011.
22. StoEltinG rK and hilliEr SC: Pharmacology & Physiology in Anesthetic Practice. ISBN-13: 9780781754699. 4th edition. 462-469. Philadelphia: Lippincott William & Wilkins, 2006.
23. honG J, han S, KiM w, KiM J and Kil h: effect of dexamethasone in combination with caudal analgesia on postoperative pain control in day-case paediatricorchidopexy. Br J Anaesth;105:506-510, 2010.
24. SalErno a and hErMann r: Efficacy and safety of steroid use for postoperative pain relief. The Journal of Bone & Joint Surgery; 88:1361-1372, 2006.
25. MohaMEd SK, ibrahEEM aS and abdElrahEEM MG: Preoperative intravenous dexamethasone combined with glossopharyngeal nerve block: role in paediatric postoperative analgesia following tonsillectomy. Eur Arch Otorhinolaryngol; 266:1815-1819, 2009.
26. KardaSh KJ, bEnG FS, tESSlEr MJ and VElly aM: single-dose dexamethasone reduces dynamic pain after total hip arthroplasty. AnesthAnalg; 106:1253-1257, 2008.
27. MorGan J, pEdEn V, bhaSKar K, VatEr M and Choonara i: assessment of pain by parents in young children following surgery. Pediatric Anesthesia; 11:449-452, 2001.
28. dwiGht J, MiChEllE J and liCaMEli G: effectiveness of postoperative follow-up telephone interviews for patients who underwent adenotonsillectomy. Arch Otolaryngol Head Neck Surg; 133:1091-1095, 2007.


185 M.E.J. ANESTH 23 (2), 2015
COMPARATIVE STUDY BETWEEN ULTRASOUND AND NERVE STIMULATOR GUIDED SCIATIC
NERVE BLOCK THROUGH THE ANTERIOR APPROACH
Wafik a. amin*, m. Osama abOu seada*, mansOur m. elkersh**, abraham mathai***,
sOna medekOva**** and tafazzul husain***
Abstract
Introduction: The aim of the current study was to compare block of the sciatic nerve through the anterior approach by two methods, namely, the nerve-stimulator guided and ultrasound-guided, with or without nerve stimulation, with regard to the ease of performance, reliability and safety of this approach.
Patients and Methods: 36 adult patients were randomly allocated equally into one of 2 main groups: “Nerve Stimulator-Guided Group (NSG)” where the nerve was located by nerve stimulator only and “Ultrasound guided group (USG)” where the sciatic nerves were blocked by a stimulated needle under guidance of the ultrasound. Assessment of performing each technique, sensory and motor blockades, occurrence of acute systemic toxicity and haematoma formation were compared.
Results: Only one-third of the sciatic nerves could be visualized by US. This did not affect the block execution time but caused less number of needle passes in a statistically significant value. Sensory and motor block showed significant differences between the 2 groups. Criteria of acute systemic toxicity and occurrence of hematoma were not reported in both groups.
Conclusion: Results of the current study showed that the addition of ultrasound to nerve stimulator in the anterior approach to the sciatic nerve block added only little to the ease of performance, reliability and safety. This was because only one-third of the nerves could be seen. More practice, better machines and new blocking techniques may be needed to overcome the problem of anisotropy of the nerve.
Keywords: Sciatic nerve, anterior approach, ultrasound, nerve stimulator, reliability.
* MD, Professor of Anesthesia and ICU, Al-Azhar Faculty of Medicine, Egypt, Senior consultant of Anesthesia and ICU Hamad Medical Corporation (HMC), Qatar.
** MD, Lecturer in Anesthesiology DPT, Al-Azhar Faculty of Medicine, Egypt and Specialist of Anesthesia, (HMC), Qatar.*** MD, Specialist of Anesthesia and ICU, (HMC), Qatar.**** MD, Consultant of Anesthesia and ICU, Hamad (HMC), Qatar.

186 WAFIK A. AMIN et. al
Introduction
Every pass made with the stimulator needle that does not produce a twitch represents a possible pass through the sciatic nerve and since there is no reliable relationship between the current producing the twitch and the proximity of the needle to the nerve, any needle position which does not produce a twitch could be within the body of the nerve i.e., intraneural. One of the major concerns with nerve stimulation is that up to 70% of the patients have no motor response with stimulating currents of up to 1mA despite patients experiencing parasthesia with positive verification of nerve proximity with ultrasound1.
The use of the ultrasound with or without nerve stimulation may cause the anterior approach to block the sciatic nerve to be safer and easier and consequently more popular as it needs high experience specially in obese patients2. The aim of the current study was to compare block of the sciatic nerve through the anterior approach by two methods, namely, the nerve-stimulator guided and ultrasound-guided, with nerve stimulation, with regard to the ease of performance, reliability and safety of this approach.
Patients and Methods
The current work is a prospective and controlled open clinical trial. After approval of the Local Ethical Committee and obtaining the informed written consent from patients, 36 adult patients of different ages, both genders, and ASA class I-III were enrolled in the study. Patients had received a successful femoral nerve block as well to complete the analgesia for knee and leg surgeries.
Patients refusing the procedure, uncooperative, have allergy to any of the drugs used in the study, with diabetic peripheral neuropathy or have a history of stroke with lesion affecting the side to surgery were excluded form the study. Patients with bleeding disorders or receiving an anticoagulant and those with infection at the site of injection were also excluded.
Patients were randomly allocated into one of two main groups, 18 patients each. Patients received either general anesthesia or spinal anesthesia for the operation. When patient became completely oriented
or was able to move his legs, femoral nerve block (with 10 ml of bupivacaine) and sciatic nerve block through the anterior approach were performed for the postoperative pain relief.
Nerve Stimulator-Guided Group (NSG)
Landmarks of the approach included a line drawn between the inferior border of the anterior superior iliac spine (ASIS) and superior angle of the pubic tubercle. Next, a perpendicular line bisecting the initial line was drawn and extended 8 cm caudad. The needle was inserted perpendicular to the skin. Stimuplex HNS11 machine was adjusted at pulse duration of 0.1 ms and a frequency of 2 Hz and a current of 0.7 - 1 mA. After disinfection and local infiltration, a Stimuplex® D Set (120 mm) (B. Braun Melsungen AG) was advanced with a strictly sagittal orientation, with the leg internally rotated from 10-15 degrees3, until stimulation of the sciatic nerve in the form of planter and dorsiflexion of the foot was triggered. Stimulation current was lowered until a current of 0.2 mA did not stimulate the nerve. The needle length at this level was recorded and the number of times the needle was proceeded farther than this depth was considered as a pass in the nerve. After negative aspiration test, 20 ml of bupivacaine 0.5% (Marcaine, Astra, Sweden), was injected slowly. The ultrasound probe was later on used to detect any hematoma formed.
Ultrasound-Guided Group (USG)
Patients in this group had their sciatic nerves blocked by a stimulated needle under guidance of the ultrasound. The upper thigh is widely prepared from the inguinal crease to about mid-thigh. Either General Electric Healthcare (Logiq e BT12) or Toshiba (Viamo SSA-640A) ultrasound machines were used in the examinations. A low frequency ultrasound curved probe (2-5 MHz) was applied, transversely, 10 cm distal and 5 cm medial to the position of the femoral nerve at the inguinal ligament. After establishing right/left orientation of the ultrasound probe, the scan depth would be adjusted to about 13-15cm.The needle entry point was lateral to the femoral vessels and medial to the femur. If the sciatic nerve could be seen by

M.E.J. ANESTH 23 (2), 2015
187US. VS NERVE STIMULATOR GUIDED SCIATIC BLOCK
the ultrasound, the stimulator was set in the sentinel mode (0.2 mA). The needle (Stimuplex, D plus Set or Stimuplex Ultra, 120 mm) was visually guided until the nerve was reached. When the nerve was stimulated, the needle should be withdrawn by fine adjustments until stimulation stops. This was also considered as a needle pass. After negative aspiration, 20 ml of 0.5% bupivacaine was injected to get a “Dough nut” sign of the nerve. If the nerve could not be seen, we proceeded with the needle to a point just beneath the posterior border of the adductors and straight down from the femoral vessels. This point is marked by the hyperechoic deep layer of the adductor group and also by the fact that the adductor stimulation (flashing) stopped. The Stimulator was adjusted and the number of needle passes was determined by the same way followed in the Nerve Stimulator - Guided Group (NSG). In either case the needle was advanced in out of plane fashion.
Assessment
I- Block Technique:
� Block execution time: defined as time from skin puncture to the end of injection.
� Needle depth.
� Number of needle passes.
� Vascular puncture: defined as blood coming in the side way tube or aspirated during the procedure and/or a hematoma collection thereafter diagnosed by the ultrasound.
II- Block Assessment:
Sensory Block:
� Onset of sensory block: from time of injection to the start of sensory changes elicited by cold test.
� Duration of sensory block: measured from the time of injection to the time patient had a VAS of 5/10 or higher.
� Quality of sensory block: measured using Visual Analogue Scale1-10.
Motor Block:
� Onset of motor block: from time of injection to time of motor changes in any of the sciatic branches.
� Duration: from time of motor changes to the time patient can planter flex fully.
III- Neurological and Hemodynamic Assessment:
� Monitor any agitation or convulsions.
� Electrocardiogram (ECG), heart rate (HR), oxygen saturation (SpO2), were monitored continuously, and systolic arterial pressure (SBP) every 2.5 min during and after injection. Patients were assessed for occurrence of any hemodynamic changes e.g., bradycardia and/or hypotension and treated accordingly.
Statistical Analysis
Categorical data were expressed as frequency along with percentage and continuous data values presented in mean ± SD. Descriptive statistics were used to summarize all demographic anthropometric, anthropometric measures and other characteristics of the participants. Quantitative variables means between the two groups (NS and US) were analyzed using unpaired t test. Associations between two or more qualitative variables were assessed using chi-square test. For small cell frequencies, chi-square test with continuity correction factor or Fisher exact test was applied. Pearson’s correlation coefficient was used to assess the strength of linear relationship between two or more quantitative variables. Pictorial presentations of the key results were made using appropriate statistical graphs. A two-sided P value <0.05 was considered to be statistically significant. All statistical analyses were done using the statistical package SPSS 19.0 (SPSS Inc. Chicago, IL).
Results
Demographic and Anthropometric Data:
Demographic data showed no significant difference between the 2 groups of patients (p>0.05) (Table 1).
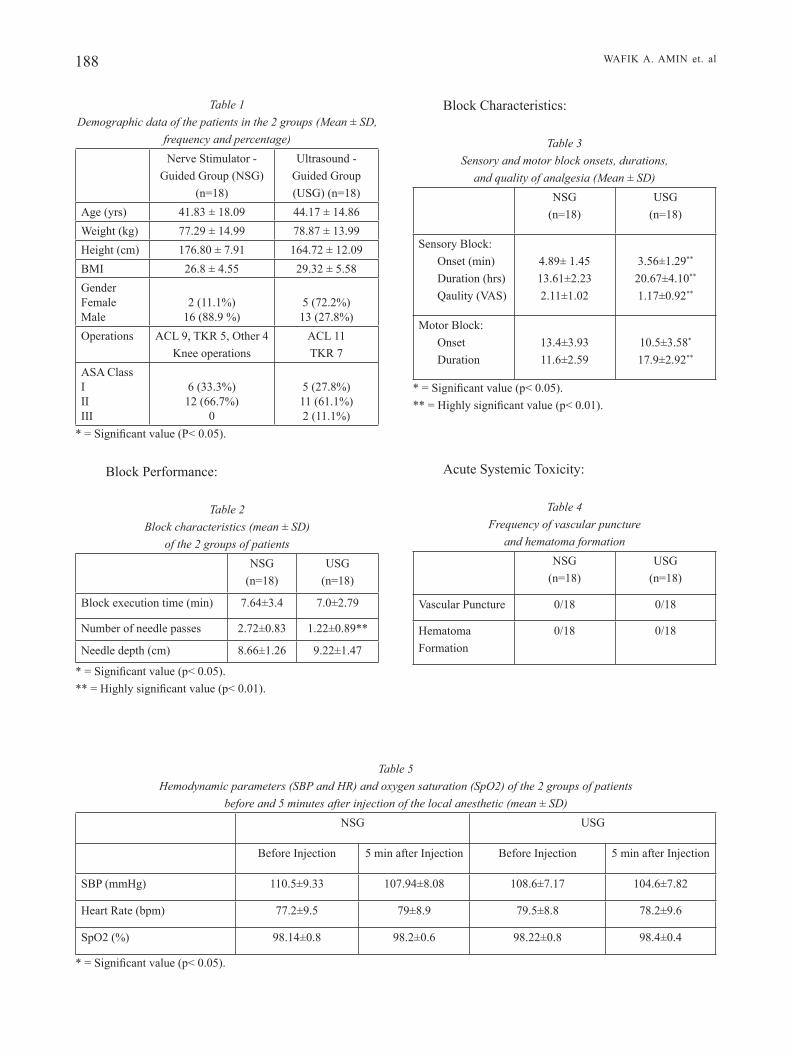
188 WAFIK A. AMIN et. al
Table 1 Demographic data of the patients in the 2 groups (Mean ± SD,
frequency and percentage)Nerve Stimulator -
Guided Group (NSG) (n=18)
Ultrasound - Guided Group (USG) (n=18)
Age (yrs) 41.83 ± 18.09 44.17 ± 14.86Weight (kg) 77.29 ± 14.99 78.87 ± 13.99Height (cm) 176.80 ± 7.91 164.72 ± 12.09BMI 26.8 ± 4.55 29.32 ± 5.58GenderFemaleMale
2 (11.1%)16 (88.9 %)
5 (72.2%)13 (27.8%)
Operations ACL 9, TKR 5, Other 4 Knee operations
ACL 11TKR 7
ASA ClassIIIIII
6 (33.3%)12 (66.7%)
0
5 (27.8%)11 (61.1%)2 (11.1%)
* = Significant value (P< 0.05).
Block Performance:
Table 2 Block characteristics (mean ± SD)
of the 2 groups of patientsNSG
(n=18)USG
(n=18)
Block execution time (min) 7.64±3.4 7.0±2.79
Number of needle passes 2.72±0.83 1.22±0.89**
Needle depth (cm) 8.66±1.26 9.22±1.47
* = Significant value (p< 0.05).** = Highly significant value (p< 0.01).
Block Characteristics:
Table 3 Sensory and motor block onsets, durations,
and quality of analgesia (Mean ± SD)NSG
(n=18)USG
(n=18)
Sensory Block:Onset (min)Duration (hrs)Qaulity (VAS)
4.89± 1.4513.61±2.232.11±1.02
3.56±1.29**
20.67±4.10**
1.17±0.92**
Motor Block:OnsetDuration
13.4±3.9311.6±2.59
10.5±3.58*
17.9±2.92**
* = Significant value (p< 0.05).** = Highly significant value (p< 0.01).
Acute Systemic Toxicity:
Table 4 Frequency of vascular puncture
and hematoma formationNSG
(n=18)USG
(n=18)
Vascular Puncture 0/18 0/18
Hematoma Formation
0/18 0/18
Table 5 Hemodynamic parameters (SBP and HR) and oxygen saturation (SpO2) of the 2 groups of patients
before and 5 minutes after injection of the local anesthetic (mean ± SD)NSG USG
Before Injection 5 min after Injection Before Injection 5 min after Injection
SBP (mmHg) 110.5±9.33 107.94±8.08 108.6±7.17 104.6±7.82
Heart Rate (bpm) 77.2±9.5 79±8.9 79.5±8.8 78.2±9.6
SpO2 (%) 98.14±0.8 98.2±0.6 98.22±0.8 98.4±0.4
* = Significant value (p< 0.05).
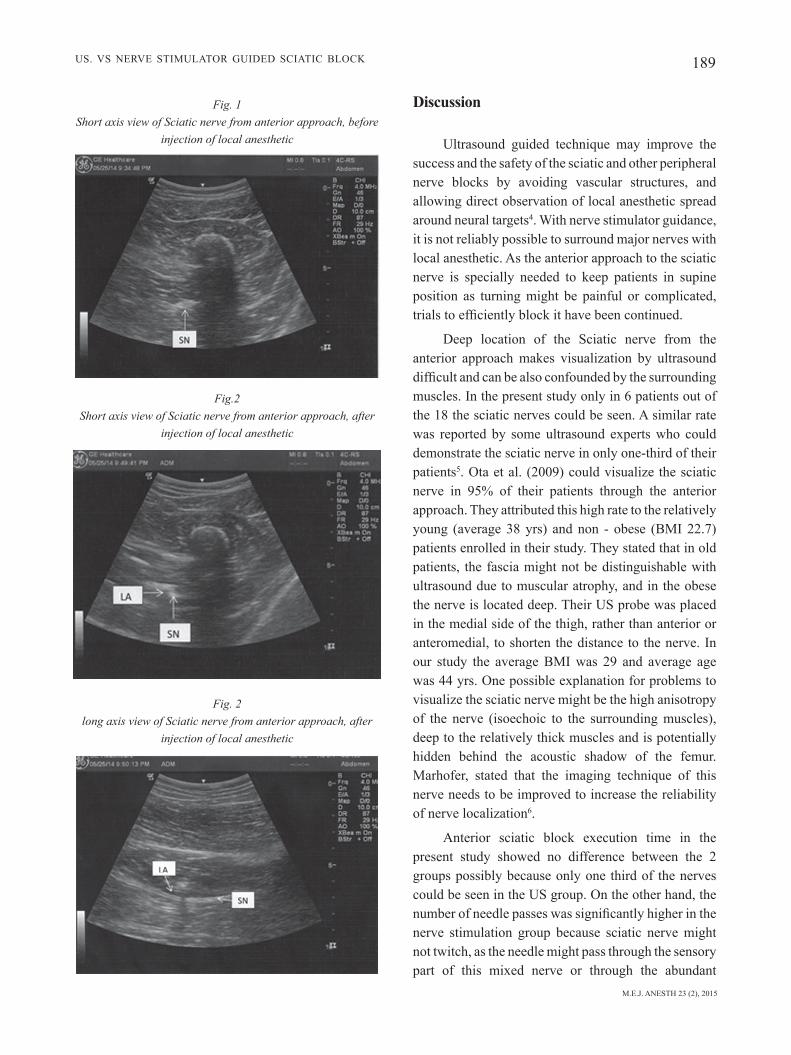
M.E.J. ANESTH 23 (2), 2015
189US. VS NERVE STIMULATOR GUIDED SCIATIC BLOCK
Discussion
Ultrasound guided technique may improve the success and the safety of the sciatic and other peripheral nerve blocks by avoiding vascular structures, and allowing direct observation of local anesthetic spread around neural targets4. With nerve stimulator guidance, it is not reliably possible to surround major nerves with local anesthetic. As the anterior approach to the sciatic nerve is specially needed to keep patients in supine position as turning might be painful or complicated, trials to efficiently block it have been continued.
Deep location of the Sciatic nerve from the anterior approach makes visualization by ultrasound difficult and can be also confounded by the surrounding muscles. In the present study only in 6 patients out of the 18 the sciatic nerves could be seen. A similar rate was reported by some ultrasound experts who could demonstrate the sciatic nerve in only one-third of their patients5. Ota et al. (2009) could visualize the sciatic nerve in 95% of their patients through the anterior approach. They attributed this high rate to the relatively young (average 38 yrs) and non - obese (BMI 22.7) patients enrolled in their study. They stated that in old patients, the fascia might not be distinguishable with ultrasound due to muscular atrophy, and in the obese the nerve is located deep. Their US probe was placed in the medial side of the thigh, rather than anterior or anteromedial, to shorten the distance to the nerve. In our study the average BMI was 29 and average age was 44 yrs. One possible explanation for problems to visualize the sciatic nerve might be the high anisotropy of the nerve (isoechoic to the surrounding muscles), deep to the relatively thick muscles and is potentially hidden behind the acoustic shadow of the femur. Marhofer, stated that the imaging technique of this nerve needs to be improved to increase the reliability of nerve localization6.
Anterior sciatic block execution time in the present study showed no difference between the 2 groups possibly because only one third of the nerves could be seen in the US group. On the other hand, the number of needle passes was significantly higher in the nerve stimulation group because sciatic nerve might not twitch, as the needle might pass through the sensory part of this mixed nerve or through the abundant
Fig. 1 Short axis view of Sciatic nerve from anterior approach, before
injection of local anesthetic
Fig.2 Short axis view of Sciatic nerve from anterior approach, after
injection of local anesthetic
Fig. 2 long axis view of Sciatic nerve from anterior approach, after
injection of local anesthetic

190 WAFIK A. AMIN et. al
connective tissue in that thick nerve. Visualization of this one third with US made the difference to decrease the number of needle passes. Similar results were obtained by Orebaugh and coworkers7. The ultrasound helps to locate the sciatic nerve either by visualization or by defining its location anatomically as it lies just beneath the deep fascia of the adductor group at the level of the lesser trochanter. This was in agreement with Ban, who stated that nerve stimulation is a variable and blind technique, and one of the major concerns with it is that up to 70% of patients had no motor response with stimulating currents of up to 1mA despite patient experiencing parasthesias with positive verification of nerve proximity with ultrasound. While intraneural injection does not always produce a clinically demonstrable nerve injury, it is a situation that should be avoided if possible8.
The current study showed that the onset time, duration and quality of sensory block (VAS) were highly significant in the US group compared to the NS Group. Also the onset of motor block was shorter and duration was longer in the US group. This can be attributed to injection in the nearest vicinity of the nerve documented by the US. Abrahams et al., suggested that US guidance of peripheral nerve block produced a higher rate of block success, shorter procedure times, faster onset time, and longer block duration and reduce the risk of inadvertent vascular puncture during block performance. So, US can improve block success rates, especially for the anesthetist who does not frequently perform peripheral nerve blocks9.
Ultrasound guidance may reduce the frequency
of vascular puncture, but there are no RCTs that confirm or refute an actual reduction of LAST (Local Anesthetic Systemic Toxicity)10. In the present study, LAST was not a problem in either of the 2 groups as seen from the hemodynamic stability and absence of central nervous system toxicity (agitation and/or seizures). Inadvertent vascular puncture seemed to be absent in the used approach, as no blood was aspirated and no occurrence of hematoma looked at by US in both groups.
Safety of the sciatic nerve and the consequences of the multiple passes through it e.g., neuralgia were not sought. This is one of the limitations of the study. It also seems better to classify patients, for the frequency to visualize the sciatic nerve by US, according to thigh circumference rather than the body weight or BMI.
Results of the current study showed that the addition of ultrasound to nerve stimulator in the anterior approach to the sciatic nerve added only little to the ease of performance, reliability and safety. This was because only one-third of the nerves could be seen. More practice, better machines and new blocking techniques may be needed to overcome the problem of anisotropy of the nerve.
Acknowledgment
The authors would like to thank Dr. Prem Chandra, PhD, for performing the statistics of the study. We would also like to thank all the staff of the Medical Research Center for their kind help and support.

M.E.J. ANESTH 23 (2), 2015
191US. VS NERVE STIMULATOR GUIDED SCIATIC BLOCK
References
1. urmey Wf, stntOn J: Inability to consistently elicit a motor response following sensory parasthesia during interscalene block. Anesthesiology; 202, 96:552-554.
2. Wafik amin, abOu seada m, saeed m, farag s, abd elhaleem t, shaaban e: Continuous sciatic nerve block: Comparative study between the parasacral, lateral and anterior approaches for lower limb surgery. MEJ Anesth; 20(5), 2010.
3. vlOka J, hadzic a, april e, thys d: Anterior approach to the sciatic nerve block: effects of leg rotation. Anesth Analg; Feb, 92(2):460-2, 2001.
4. gray at, cOllins ab, schafhalter-zOppOth i: Sciatic nerve block in a child: a sonographic approach. Anesth Analg; 97:1300-2, 2003.
5. Neuroaxion.com. Ultrasound guided regional nerve blocks: the anterior approach to the sciatic nerve block. Oct., 2008.
6. marhOfer p: Peripheral blocks. What’s new in regional anesthesia
and pain therapy? Esra.org.7. Orebaugh sl, Williams ba, kentOr ml: Ultrasound guidance with
nerve stimulation reduces the time necessary for resident peripheral nerve blockade. Reg Anesth Pain Med; 32:448-454, 2007.
8. ban ch tsui: Electrical Nerve Stimulation. In: Atlas of Ultrasound and Nerve Stimulation-Guided Regional Anesthesia. Ch. 2, p. 9-18. Springer 2007. Eds. V. Chan; B.T. Fin cane, Th. Grau, A. Walji.
9. abrahams ms, aziz mf, hOrn Jl: Ultrasound guidance compared with electrical neurostimulation for peripheral nerve block: a systematic review and meta-analysis of randomized controlled trials. Br J Anaesth; 102(3):408-17, 2009.
10. neal Jm: Ultrasound-guided regional anesthesia and patient safety: an evidence-based analysis. Reg Anesth Pain Med; 35(suppl 1):S59-S67, 2010.


193 M.E.J. ANESTH 23 (2), 2015
Wound InstIllatIon of local anesthetIc BupIvacaIne for postoperatIve analgesIa
folloWIng lumBar lamInectomy
Dr. Nirmala JoNNavithula*, Dr. SaNDeep Garre**, Dr. SailakShmaN paSupuleti***, Dr. paDmaJa DurGa****,
Dr. Dilip kumar kulkarNi***** aND Dr. GopiNath ramachaNDraN
Abstract
Purpose: lumbar laminectomy is a commonly performed procedure in neurosurgical and orthopedic practice. postoperative pain relief helps in early mobilization, initiation of physiotherapy, provides satisfaction to the patients and plays an important role in reducing the morbidity and mortality. this prospective study investigated the simple technique of instillation of wound with bupivacaine and leaving a contact time of 60 seconds on postoperative pain following lumbar laminectomy.
Methods: 32 asa I and II patients scheduled for laminectomy were randomly allocated to receive either20 ml of normal saline (group I) or 0.25% of bupivacaine (group II) into the wound after securing hemostasis. after a dwell time of 60sec the wound was closed in layers without mopping or suctioning. after extubation, the pain scores were evaluated by visual analog scale at every 4 hrs. for 24hrs and also the time for first demand of analgesia, number of analgesic demands and the total amount of analgesia consumed were noted by an independent observer..
Results: the median duration of analgesia in group I was 8.8 [5-11] and in group II 13 [8.5-16] hrs. with a p=0.04. the number of demands and the amount of analgesia consumed was also statistically significant.
Conclusion: Wound instillation technique is simple, safe and effective in management of acute pain management after lumbar laminectomy and can be used as one among the multimodal armamentarium in pain management.
Keywords: lumbar laminectomy, bupivacaine, postoperative pain, wound instillation.
* md, additional professor, dept. of anesthesiology and Intensive care, nizam’s Institute of medical sciences, e-mail Id: [email protected]** md, Junior resident, dept. of anesthesiology and Intensive care, nizam’s Institute of medical sciences. e-mail Id: [email protected]*** md, Junior resident, dept. of anesthesiology and Intensive care, nizam’s Institute of medical sciences. e-mail Id: [email protected]**** md, professor, dept. of anesthesiology and Intensive care, nizam’s Institute of medical sciences. e-mail com: [email protected]***** md, professor, dept. of anesthesiology and Intensive care, nizam’s Institute of medical sciences. e-mail: [email protected]****** md, ffarcs I, professor and hod, dept. of anesthesiology and Intensive care, nizam’s Institute of medical sciences.
e-mail Id: [email protected] address for correspondence: dr. nirmala Jonnavithula md, additional professor, dept. of anesthesiology and Intensive
care, nizam’s Institute of medical sciences, panjagutta, hyderabad 82, India. telangana, e-mail Id: [email protected] contact: 040 23304466, mobile: 09849422749, fax: 4023323016.

194 nIrmala JonnavIthula et. al
Introduction
lumbar laminectomy is a commonly performed procedure in neurosurgical and orthopedic practice. Patients usually suffer significant pain after lumbar laminectomy. postoperative pain relief helps in early mobilization, initiation of physiotherapy, provides satisfaction to the patients and plays an important role in reducing the morbidity and mortality1. there has been an increased attention in the understanding of the pathophysiology of acute pain and development in newer modalities of analgesic treatment. currently several postoperative analgesic options are available. Intravenous opioids, nsaIds, intrathecal administration of opioids and local anesthetics have been evaluated. epidural or paravertebral administration of drugs using catheter for continuous infusions have also been studied. regional techniques offer many advantages: pain is cured at /close to damaged tissue and when local anesthetics are used, they provide analgesia and substantially reduce the need for opioids2-4. most of these techniques may be limited by potentially high failure rates, high cost, technically challenging, and labor intensive, adverse /toxic effects, and procedure-related complications. Wound site infiltration5,6 is an efficient method in acute post-operative pain management, but has a potential theoretical risk of wound site infection. Instillation of local anesthetic drug into the wound was found to provide postoperative analgesia in certain surgical procedures like hernia repair and laparoscopic cholecystecytomy7-9. the role of wound instillation with local anesthetic has not been studied. simple technique of instillation of wound with bupivacaine and leaving a contact time of 60 seconds may alleviate postoperative pain following lumbar laminectomy aims and objectives:
the aim of the current study is to evaluate the duration and analgesic efficacy of 0.25% bupivacaine on wound instillation following lumbar laminectomy.
Methods
Institutional ethics committee approval and informed consent from the patient was taken for this prospective randomized double blind study. this study
was undertaken in 32 patients of asa physical status I and II scheduled for lumbar laminectomy who were planned to have single level lumbar disc surgery. patients with instrumentation due to spondylolisthesis or spinal stenosis, and are planned to have multiple distance or double site laminectomy, patients who underwent prior lumbar disc surgery, have asa III-Iv status, prior neurological deficits, preoperative opioid use or any history of substance abuse or on steroids, infection, have known local anesthetics allergy were excluded from the study. patients with bleeding, cerebrospinal fluid leak, or requiring placement of drain were excluded after initial recruitment.
patients were randomized into two groups of 16 each by computer generated random numbers (figure1). All patients received standard general anesthesia with endotracheal tube of appropriate size. paracetamol 1 gram Iv was administered after induction of anesthesia for intraoperative analgesia. once the surgical procedure was completed and hemostasis was secured-patients in group I received 20ml of normal saline instillation which remained in the wound for a dwell time of 60 seconds and patients in group II received 20ml of 0.25% bupivacaine for the same contact period and the wound was closed in layers without mopping or suctioning.
patients were assessed for postoperative pain score by visual analog scale, a 10 point scale ranging from “0” minimum or no pain to “10” the maximum pain score perceived by the patient. postoperative pain was assessed by an independent observer blinded to the study first at 0 hours i.e., immediately after extubation and then at every 4 hours intervals for 24 hours. the duration of analgesia was considered from the time the study drug was instilled to the time for first demand of analgesia. When the pain score exceeded 3 rescue analgesia (diclofenac 75mg deep Im) was given with a lock-out period of 8 hr and maximum dose of 225mg in 24hrs. the number of analgesic demands and the amount of analgesia administered were also noted.
Statistical Analysis
sample size was based on a pilot study of 20 patients with 10 in each group. a group sample size of 12 each achieves 86% power to detect a difference
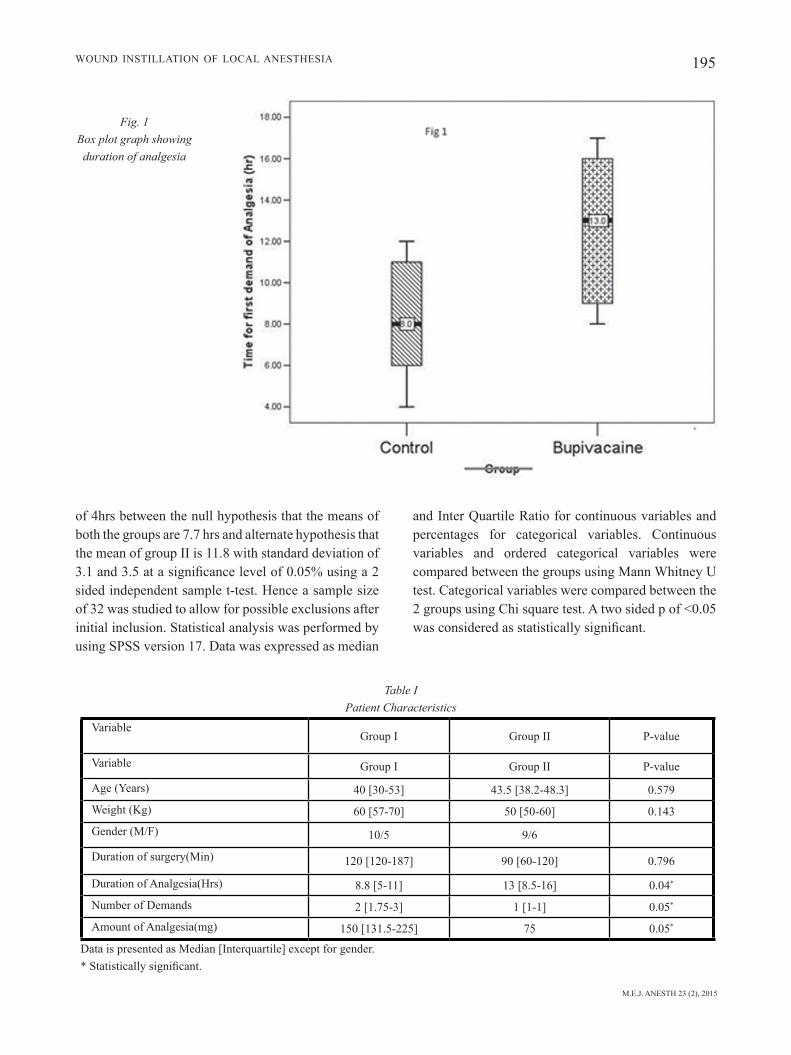
M.E.J. ANESTH 23 (2), 2015
195Wound InstIllatIon of local anesthesIa
of 4hrs between the null hypothesis that the means of both the groups are 7.7 hrs and alternate hypothesis that the mean of group II is 11.8 with standard deviation of 3.1 and 3.5 at a significance level of 0.05% using a 2 sided independent sample t-test. hence a sample size of 32 was studied to allow for possible exclusions after initial inclusion. statistical analysis was performed by using spss version 17. data was expressed as median
and Inter Quartile ratio for continuous variables and percentages for categorical variables. continuous variables and ordered categorical variables were compared between the groups using mann Whitney u test. categorical variables were compared between the 2 groups using chi square test. a two sided p of <0.05 was considered as statistically significant.
Fig. 1 Box plot graph showing duration of analgesia
Table I Patient Characteristics
variablegroup I group II p-value
variable group I group II p-value
age (years) 40 [30-53] 43.5 [38.2-48.3] 0.579
Weight (Kg) 60 [57-70] 50 [50-60] 0.143
gender (m/f) 10/5 9/6
duration of surgery(min) 120 [120-187] 90 [60-120] 0.796
duration of analgesia(hrs) 8.8 [5-11] 13 [8.5-16] 0.04*
number of demands 2 [1.75-3] 1 [1-1] 0.05*
amount of analgesia(mg) 150 [131.5-225] 75 0.05*
data is presented as median [Interquartile] except for gender.* Statistically significant.
196 nIrmala JonnavIthula et. al
Results
demographic data was comparable between the groups. (table I). two patients (one from each group) were excluded due to surgical complications. the median duration of analgesia in group I was 8.8 [5-11] hrs. and in group II 13 [8.5-16] hrs. which was statistically significant with a p 0.04. (Fig. 1) the number of demands and the amount of analgesia consumed was also significantly lower in the group II as compared to group 1 (p=0.05). the pain scores were significantly lower in group II at all-time intervals (figure 2).
Discussion
In this prospective study, the results showed that patients who received wound instillation with 20ml of 0.25% bupivacaine experienced better post-operative analgesia as compared with patients who received saline. In the current study, the study drug was instilled and allowed a dwell time of 60 seconds; the probable mechanism of pain relief could be due to the anesthetic effect of bupivacaine acting on the pain receptors distributed in the soft tissues and the
nerve endings exposed in the wound right from the skin to the dura meninge10 (skin, paraspinal muscle, posterior longitudinal ligament, dorsal annulus, facet joint capsule, nerve root which was under compression and the spinal meninges the dura supplied by recurrent nerve of von luschka). the pain scores were low at all points of time in the study group. the time to first demand of analgesia was prolonged in the study group. cumulative rescue analgesic consumption and number of demands for analgesia in the first 24 h was significantly lower in the bupivacaine group.
Wound infiltration with local anesthetics with or without adjuvant drugs has for long been known to produce efficient postoperative analgesia.11 cherian and co authors12 in their study evaluating the efficacy of wound infiltration with bupivacaine after lumbar laminectomy found significant analgesia compared to placebo group. the mean time before administration of the first dose of analgesic postoperatively in the bupivacaine and placebo recipients was 807.7 (567.6) minutes and 181.4 (110.1) minutes. In another study by milligan et al13 where patients received injection of 10 ml of 0.5% bupivacaine into the wound found less pain scores and longer duration of analgesia following lumbar discectomy. hernández-palazón and colleagues14 studied wound infusion of 0.25%
Fig. 2 Box plot showing VAS pain scores

M.E.J. ANESTH 23 (2), 2015
197Wound InstIllatIon of local anesthesIa
bupivacaine and 0.25% ropivacaine into the paraspinal muscle and skin before closure of wound following lumbar laminectomy and found mean time until the first request for analgesia was significantly longer in bupivacaine group than in ropivacaine or control group (164 +/- 53 min versus 68 +/- 31 and 38 +/- 14 min, respectively). continuous wound infusion with ropivacaine was found to be effective following spinal instrumentation, iliac crest bone graft and shoulder surgery15-17. a single time instillation of local anesthetic into the laminectomy wound has not been evaluated earlier. unlike the present study; all these studies involved injection, infiltration or infusion of the study drug bupivacaine or ropivacaine for analgesia. But the present study is different, here it involved only instillation of the study drug and allowing it for a dwell time of 60 seconds and the analgesia was unremarkable.
local tissue instillation of local anesthetic bupivacaine is a simple, safe and low cost technique. Whenever a peripheral tissue injury occurs it results in two kinds of responsiveness in the cns: a peripheral and a central sensitization. the central sensitization leads to an increased excitability of spinal cord neurons that is triggered by nociceptive afferent inputs which results in an increase in the response to pain.
The local infiltration of anesthetic blocks C-fiber input to the dorsal horn and may thereby inhibit central sensitization18. It can also have potential benefits such as inhibition of both the early inflammatory response (edema, fibrin formation, capillary dilatation, leukocyte aggregation) and the late effects of this process (proliferation of capillaries and fibroblasts, collagen formation and scarring)19,20. It has been shown that adequate relief of acute postoperative pain can result in improved long term outcomes.
In the present study the median duration of analgesia was 13hrs with instillation of local anesthetic bupivacaine with good quality of analgesia was good. none of our patients developed side effects typically associated with spread of local anesthetic to nerve roots or intrathecal space with resultant problem with mobility and differences in wound infection rates. however the concentration of bupivacaine used was 0.25% where it can mostly cause sensory blockade.
Wound instillation technique is simple, safe and effective in management of acute pain management after lumbar laminectomy and can be used as one among the multimodal armamentarium in pain management.

198 nIrmala JonnavIthula et. al
References
1. BallaNtyNe Jc: does epidural analgesia improve surgical outcome? Br J Anaesth; 92:4-6, 2004.
2. viNtar N: operation-site local anesthetic techniques for postoperative analgesia: Wound Infiltration techniques. Period boil; 3(2):227-30, 2003.
3. Block Bm, liu SS, rowliNGSoN aJ, cowaN ar, cowaN Ja Jr, wu cl: Efficacy of postoperative epidural analgesia a meta analysis. JAM Med Assoc; 290:2455-63, 2003.
4. elDor J: postoperative wound analgesia. a renewed modality? Journal NYSORA; 13:9-1, 2009.
5. thorNtoN pc, BuGGy J: Local anesthetic wound infiltration for acute postoperative pain: a viable option? Br J Anesth; 107:656-8, 2011.
6. moiNiche S, mikkelSeN S, wetterSlev J, Dahl JB: a qualitative systematic review of incisional local anaesthesia for postoperative pain relief after abdominal operations. Br J Anaesthesia; 81:377-83, 1998.
7. peterSSoN N, BerGGreN p, larSSoN m, weStmaN B, hahN rG: Pain relief by wound infiltration with bupivacaine or high-dose ropivacaine after inguinal hernia repair. Reg Anesth Pain Med; 24(6):569-75, 1999.
8. mraovic B, JuriSic t, koGler-maJeric v, SuStic a: Intraperitoneal bupivacaine for analgesia after laparoscopic cholecystectomy. Acta Anaesthesiol Scand; 41:193-6, 1997.
9. BiSGaarD t, klarSkov B, roSeNBerG J, kehlet h: characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain; 90:261-9, 2001.
10. JuerGeN kraemer: Intervertebral disk diseases causes, diagnosis, treatment and prophylaxis 3rd ed. thieme ltd. 64, 2010.
11. GurBet a, Bekar a, BilGiN h, korfali G, yilmazlar S, tercaN m: Pre-emptive infiltration of levobupivacaine is superior to at-closure administration in lumbar laminectomy patients. Eur Spine J; 17(9):1237-1241, 2008.
12. cheriaN mN, mathewS mp, chaNDy mJ: Local wound infiltration with bupivacaine in lumbar laminectomy. Surg Neur; 47(2):120-2, 1997.
13. milliGaN kr, macafee al, foGarty DJ, wallace rG, ramSey p: Intraoperative bupivacaine diminishes pain after lumbar discectomy. a randomised double-blind study. J Bone Joint Surg Br; 75(5):769-71, 1993.
14. herNáNDez-palazóN J, tortoSa SerraNo Ja, BurGuilloS lópez S, molero molero e: Infiltration of the surgical wound with local anesthetic for postoperative analgesia in patients operated on for lumbar disc herniation. comparative study of ropivacaine and bupivacaine. Rev Esp Anestesiol Reanim; Jan, 48(1):17-20, 2001.
15. BiaNcoNi m, ferraro l, ricci r, zaNoli G, aNtoNelli t, Giulia B, GuBerti a, maSSari l: The pharmacokinetics and efficacy of ropivacaine continuous wound instillation after spine fusion surgery. Anesth Analg; 98(1):166-72, 2004.
16. BlumeNthal S, DulleNkopf a, reNtSch k, BorGeat a: continuous infusion of ropivacaine for pain relief after iliac crest bone grafting for shoulder surgery. Anesthesiology; 102:392-7, 2005.
17. GottSchalk a, BurmeiSter ma, raDtke p, krieG m, farokhzaD f, kreiSSl S, StrauSS m, StaNDl t: Continuous wound infiltration with ropivacaine reduces pain and analgesic requirement after shoulder surgery. Anesth Analg; 97(4):1086-91, 2003.
18. woolf c, choNG wS: preemptive analgesia-treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg; 77:362-379, 1993.
19. craSteiN BN, kimmel Sc, leviN ri, et al: a mechanism for the anti-inflammatory effects of corticosteroids: the glucocorticoid receptor regulates leukocyte adhesion to endothelial cells and expression of endothelialleukocyte adhesion molecule-1 and intercellular adhesion molecule-I Proc Natl Acad Sci USA; 89:9991-9995, 1992.
20. morGaN Ge, mikhail mS, murray mJ: clinical anesthesiology, 3rd edn. london: lange medical; local anesthetics; pp. 233-241, 2002.

199 M.E.J. ANESTH 23 (2), 2015
The effecTs of inTraThecal neosTigmine added To bupivacaine on posToperaTive
analgesic requiremenT in paTienTs undergoing lower limb orThopedic surgery
Hamid KayalHa*, Zinat Sadat mouSavi**, ameneH BariKani***, SiamaK yagHooBi**** and marZieH Beigom KHeZri*****
Abstract
Background: several additives have been suggested to enhance analgesic effect of local anesthetic agents to decrease the adverse effects of them and increase the degree of satisfaction. we designed this randomized double-blind controlled study to evaluate the analgesic efficacy of the neostigmine added to bupivacaine using spinal anesthesia in patients undergoing lower limb orthopedic surgery.
Methods: sixty patients 18-80 yr old american society of anesthesiologists (asa) physical status i or ii, scheduled for femur surgery under spinal anesthesia, were recruited in a prospective, double-blinded, randomized way. The patients were randomly allocated to one of two groups of 30 each. The neostigmine group (group n) received bupivacaine 20 mg combined with 25 µg neostigmine, and the placebo group (group c) received bupivacaine 20 mg combined with 0.5ml distilled water (intrathecally) 5 minutes prior to surgery. The time to the first analgesic request, analgesic requirement in the first 12 hours after surgery, the duration of sensory and motor blockade, the incidence of adverse effects such as nausea,vomiting,hypotension, ephedrine requirements, bradycardia, and hypoxemia were recorded.
Results: Patients receiving neostigmine had a significantly prolonged duration of motor block (c95%ci 30.27 to 87.65; p <0.001) and sensory block (c95%ci 101.04 to 224.64; p <0.001) compared to the control group. The difference of the mean time to the first analgesic request was also significantly longer in neostigmine group (C95%CI 83.139 to 208.526; P <0.001). The total analgesic consumption during the first 12 hours after surgery was devoid of any significant difference between groups N and C (p = 0.41).The two groups were not significantly different in terms of intraoperative and postoperative side effects.
Conclusion: intrathecal neostigmine 25 µg with bupivacaine caused a prolonged time to the first analgesic request and its use was not associated with any side effects.
Keywords: spinal anesthesia, bupivacaine, neostigmine, sensory block, motor block, pain.
* assistant professor of qazvin university medical science, department of anesthesiology, faculty of medicine. [email protected]
** resident of anestheia, qazvin university medical science, department of anesthesiology, qazvin, iran.*** associate professor, social medicine specialist and faculty members of qazvin university of medical science, faculty of
medicine. [email protected]**** assistant professor of qazvin university medical science, department of anesthesiology, faculty of medicine. siamak.
[email protected]***** marzieh beigom Khezri.
Corresponding author: associate professor of qazvin university medical science, department of anesthesiology, faculty of medicine. shahid bahonar blvd, p.o. box: 3419759811, qazvin, iran. phone: +98-912-3811009, fax: +98-28-32236378. e-mail: [email protected]. alternative email: [email protected]

200 marzieh Khezri et. al
Introduction
postoperative pain is associated with catecholamine release, and the central sensitization is supposed to be among the mechanisms concerned with the persistence of postoperative pain1.
neuraxial blocks have been introduced to produce superior analgesia and decrease the blood loss and the incidence of deep venous thrombosis (dvT), pulmonary embolism, and to minimize the adverse effects of general anesthesia and improve the patients outcomes2.
There are many additives to be used to enhance analgesic effect of neuraxial blocks such as clonidine, magnesium, ketamine, opioids, vasoconstrictor agents and steroids, and neostigmine3-5.
it is reported that the inhibition of spinal cholinesterase by neostigmine produces great enhancement of endogenous acetylcholine, which is most likely released from intrinsic cholinergic neurons within the dorsal horn of the spinal cord6. an action at nicotinic receptors at the dorsal horn ganglion7 and at the spinal meninges8 has also been demonstrated9. muscarinic receptor antagonists have been shown to reverse the analgesic effects of intrathecal neostigmine10.
we hypothesized that neostigmine may provide a better pain relief after orthopedic surgery under spinal anesthesia compared to conventional agents. in addition, unlike opioids, neostigmine does not produce pruritus, respiratory depression or hyperalgesia. To test our hypothesis, we designed this randomized-double-blind, placebo-controlled study to evaluate the postoperative analgesic effect of intratechal neostigmine added to bupivacaine in patients undergoing lower limb surgery.
Method
This study was a placebo-controlled, randomized, double-blind clinical trial in which the patients, investigators and anesthesiologists were blinded to the given treatment. patients were fully informed about the study protocol and provided written informed consent. The study was approved by the institutional ethics committee and performed during July 2011 to
February 2012. Exclusion criteria included significant coexisting complications such as hepatorenal and cardiovascular diseases, any contraindication to regional anesthesia such as local infection or bleeding disorders, allergy to neostigmine, long-term opioid use, or a history of chronic pain, pregnancy and menstruation, digestive problems with nausea or vomiting, and asthma. using a computer-generated randomization schedule, sixty patients 18-80 yr old asa physical status i or ii, scheduled for lower limb orthopedic surgery under spinal anesthesia, were randomly allocated to one of the two groups of 30 members each. The consolidated standards of reporting Trials (consorT) recommendations for reporting randomized, controlled clinical trials were followed (fig. 1)11. blinding was achieved through the use of equal amounts of drugs (4.5 ml) while the syringes used were labeled as a and b according to their content. identical coded syringe prepared by the operating room personnel, not involved in the study, were randomly handed to the anesthetist, who was unaware of the identities of the drugs. The neostigmine group (group n) received bupivacaine 20 mg combined with 25 µg neostigmin (Trittau, germany), and the control group (group c) received bupivacaine (mylan s.a.s france) 20 mg combined with 0.5ml distilled water intrathecally. all patients received an intravenous preload of 5-7 ml/kg lactated ringer’s solution before a subarachnoid block. after, using an aseptic technique, a 25-gauge quincke needle was inserted intrathecally via a midline approach into the l4-5 interspaces by the anesthetist who was unaware of patient assignment while the patient in sitting position. following a successful dural puncture, the anesthetic solution was injected. The primary outcomes were to evaluate the time to the first requirement of analgesic supplement and the total analgesic consumption in the first 12h postoperative. in this study, postoperative analgesia was defined as the time to the first requirement of analgesic supplement from the time of the intrathecal anesthetic solution injection. no additional analgesic was administered unless requested by the patient. patients were elucidated preoperatively for the use of the verbal rating scale (vrs) from 0 to 10 (0 no pain, 10 maximum imaginable pain) for pain assessment. if the vrs exceeded four and the patient requested a supplement analgesic, pethidine 25 mg iv was
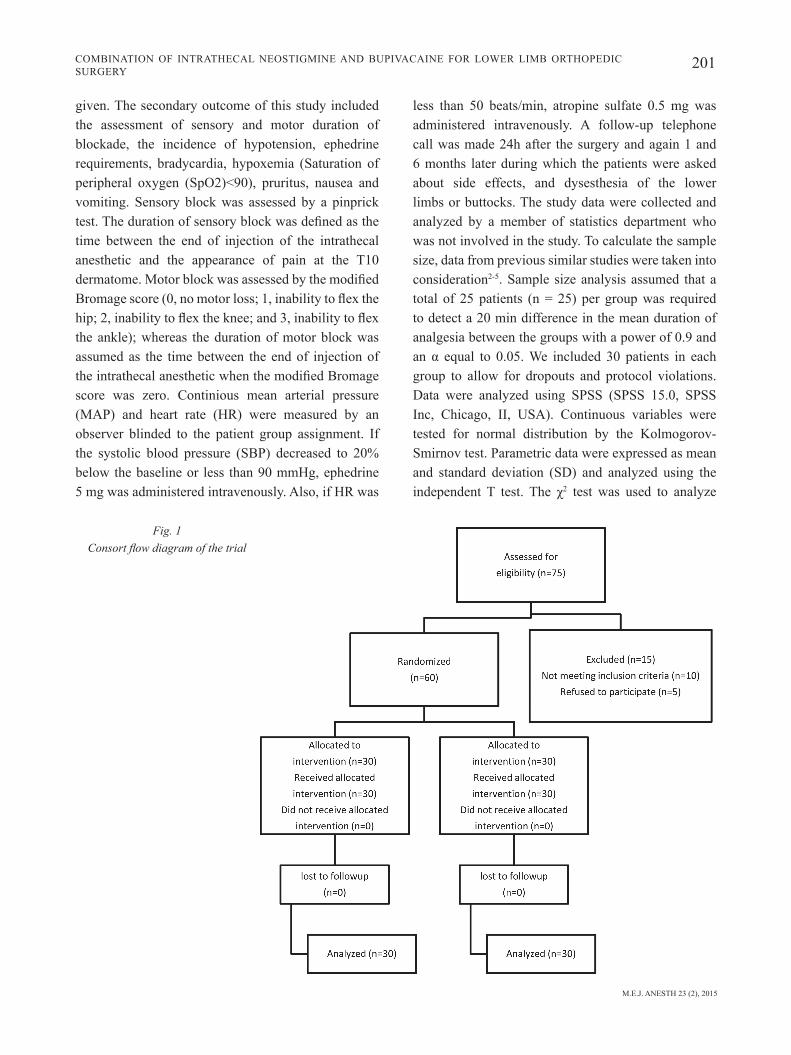
M.E.J. ANESTH 23 (2), 2015
201combinaTion of inTraThecal neosTigmine and bupivacaine for lower limb orThopedic surgery
given. The secondary outcome of this study included the assessment of sensory and motor duration of blockade, the incidence of hypotension, ephedrine requirements, bradycardia, hypoxemia (saturation of peripheral oxygen (spo2)<90), pruritus, nausea and vomiting. sensory block was assessed by a pinprick test. The duration of sensory block was defined as the time between the end of injection of the intrathecal anesthetic and the appearance of pain at the T10 dermatome. Motor block was assessed by the modified Bromage score (0, no motor loss; 1, inability to flex the hip; 2, inability to flex the knee; and 3, inability to flex the ankle); whereas the duration of motor block was assumed as the time between the end of injection of the intrathecal anesthetic when the modified Bromage score was zero. continious mean arterial pressure (map) and heart rate (hr) were measured by an observer blinded to the patient group assignment. if the systolic blood pressure (sbp) decreased to 20% below the baseline or less than 90 mmhg, ephedrine 5 mg was administered intravenously. also, if hr was
less than 50 beats/min, atropine sulfate 0.5 mg was administered intravenously. a follow-up telephone call was made 24h after the surgery and again 1 and 6 months later during which the patients were asked about side effects, and dysesthesia of the lower limbs or buttocks. The study data were collected and analyzed by a member of statistics department who was not involved in the study. To calculate the sample size, data from previous similar studies were taken into consideration2-5. sample size analysis assumed that a total of 25 patients (n = 25) per group was required to detect a 20 min difference in the mean duration of analgesia between the groups with a power of 0.9 and an α equal to 0.05. We included 30 patients in each group to allow for dropouts and protocol violations. data were analyzed using spss (spss 15.0, spss inc, chicago, ii, usa). continuous variables were tested for normal distribution by the Kolmogorov-smirnov test. parametric data were expressed as mean and standard deviation (sd) and analyzed using the independent T test. The χ2 test was used to analyze
Fig. 1 Consort flow diagram of the trial
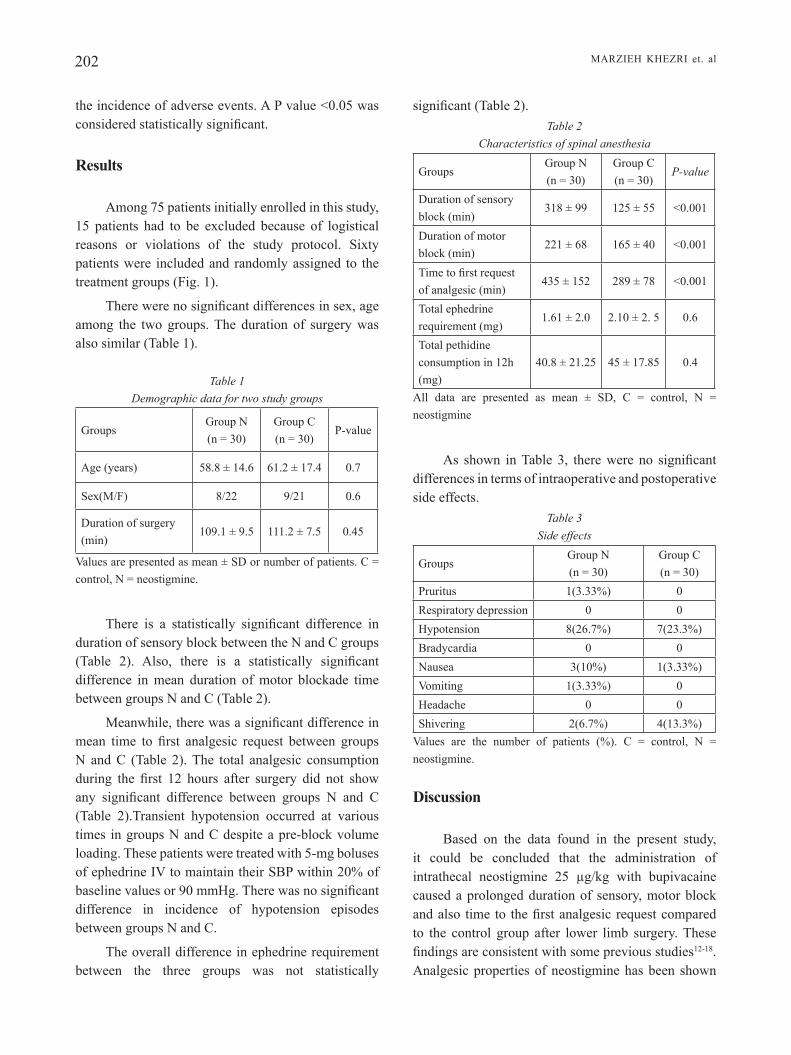
202 marzieh Khezri et. al
the incidence of adverse events. a p value <0.05 was considered statistically significant.
Results
among 75 patients initially enrolled in this study, 15 patients had to be excluded because of logistical reasons or violations of the study protocol. sixty patients were included and randomly assigned to the treatment groups (fig. 1).
There were no significant differences in sex, age among the two groups. The duration of surgery was also similar (Table 1).
Table 1 Demographic data for two study groups
groupsgroup n(n = 30)
group c(n = 30)
p-value
age (years) 58.8 ± 14.6 61.2 ± 17.4 0.7
sex(m/f) 8/22 9/21 0.6
duration of surgery (min)
109.1 ± 9.5 111.2 ± 7.5 0.45
values are presented as mean ± sd or number of patients. c = control, n = neostigmine.
There is a statistically significant difference in duration of sensory block between the n and c groups (Table 2). Also, there is a statistically significant difference in mean duration of motor blockade time between groups n and c (Table 2).
Meanwhile, there was a significant difference in mean time to first analgesic request between groups n and c (Table 2). The total analgesic consumption during the first 12 hours after surgery did not show any significant difference between groups N and C (Table 2).Transient hypotension occurred at various times in groups n and c despite a pre-block volume loading. These patients were treated with 5-mg boluses of ephedrine iv to maintain their sbp within 20% of baseline values or 90 mmHg. There was no significant difference in incidence of hypotension episodes between groups n and c.
The overall difference in ephedrine requirement between the three groups was not statistically
significant (Table 2).Table 2
Characteristics of spinal anesthesia
P-valuegroup c(n = 30)
group n(n = 30)
groups
<0.001125 ± 55318 ± 99 duration of sensoryblock (min)
<0.001165 ± 40221 ± 68 duration of motorblock (min)
<0.001289 ± 78435 ± 152 Time to first requestof analgesic (min)
0.62.10 ± 2. 51.61 ± 2.0 Total ephedrinerequirement (mg)
0.445 ± 17.8540.8 ± 21.25 Total pethidine consumption in 12h(mg)
all data are presented as mean ± sd, c = control, n = neostigmine
As shown in Table 3, there were no significant differences in terms of intraoperative and postoperative side effects.
Table 3 Side effects
groupsgroup n(n = 30)
group c(n = 30)
pruritus 1(3.33%) 0respiratory depression 0 0hypotension 8(26.7%) 7(23.3%)bradycardia 0 0nausea 3(10%) 1(3.33%)vomiting 1(3.33%) 0headache 0 0shivering 2(6.7%) 4(13.3%)
values are the number of patients (%). c = control, n = neostigmine.
Discussion
based on the data found in the present study, it could be concluded that the administration of intrathecal neostigmine 25 µg/kg with bupivacaine caused a prolonged duration of sensory, motor block and also time to the first analgesic request compared to the control group after lower limb surgery. These findings are consistent with some previous studies12-18. analgesic properties of neostigmine has been shown

M.E.J. ANESTH 23 (2), 2015
203combinaTion of inTraThecal neosTigmine and bupivacaine for lower limb orThopedic surgery
to depend on the release of no in spinal cord and increasing acetylcholine in the spinal synapses which leads to the further stimulation of nicotinic and muscarinic receptors6-10,19. The selection dose of intrathecal neostigmine was based on the fact that several previous studies showed that the 25 µg/kg of neostigmine adding to bupivacaine could prolong the duration of spinal analgesia without additional side effects12-14,15.
The second observation which should be noted is that the transient hypotension episodes and ephedrine requirement between the two groups was statistically insignificant.. The overall results of our study is in consistency with studies by hye ma13, who declared that the use of intrathecal neostigmine was associated with minimal hemodynamic fluctuations. However in gupta s study, hypotension in the group receiving neostigmine 75 µg was more than the other group receiving 50µg of neostigmine12. These apparently controversial results may be due to either different dosage of neostigmine or population variation.
The third finding which should be taken into account is that, the incidence of nausea and vomiting between the two groups was statistically insignificant. This finding is in contrast with the result obtained in the Klamt study16 in which a significant difference in nausea and vomiting episodes in patients who received 100µg of neostigmine and bupivacaine was reported. The authors of the present study speculate that the lower dose of neostigmine was not associated with high
incidence of nausea vomiting. This idea is supported by the result of guptas12 and lauretti18 studies in which observed that the incidence of nausea and vomiting increased with larger dose of neostigmine.
The another observation which should be emphasized is that neostigmine prolonged the time to first analgesic requirement but it failed to decreased total opioids consumption in the first 12 hours postoperatively as compared with the control group. The possible explanation for this finding is that the analgesic effect of neostigmine follows a dose-dependent manner. This result is harmony with the findings by Gupta S study12 who reported that total of analgesic consumption after surgery in the patients receiving 75 mg of neostigmine and bupivacaine was lower than the other patients receiving 50 mg neostigmine and bupivacaine; and both groups used less drugs comparing to the bupivacaine group.
we concluded that intrathecal neostigmine 25 µg with bupivacaine prolonged sensory, motor block and the time to first analgesic request compared to control group, and its use was not associated with any serious side effects. however, the total analgesic consumption in the first 12h postoperative was similar in bupivacaine and neostigmine groups following surgery. further studies are needed to evaluate the analgesic efficacy of neostigmine with other neuraxial drug combinations such as epinephrine, ketamine, and magnesium to provide better analgesia and reduce the incidence and severity of side effects.
204 marzieh Khezri et. al
References
1. FaiZ SH, raHimZadeH P, imani F, BaKHtiari a: intrathecal injection of magnesium sulfate shivering prevention during cesarean section: a randomized, double-blinded, controlled study. Korean J Anesthesiol; 65(4):293-8, 2013.
2. KHeZri mB, reZaei m, delKHoSH reiHany m, Haji Seid javadi e: comparison of postoperative analgesic effect of intrathecal clonidine and fentanyl added to bupivacaine in patients undergoing cesarean section: a prospective randomized double-blind study. Pain Res Treat; 2014: 513628, 2014.
3. KHeZri mB, gHaSemi j, moHammadi n: evaluation of the analgesic effect of ketamine as an additive to intrathecal bupivacaine in patients undergoing cesarean section. Acta Anaesthesiol Taiwan; 51(4):155-60, 2013.
4. yagHooBi S, SeddigHi m, yaZdi Z, gHaFouri r, KHeZri mB: comparison of postoperative analgesic effect of dexamethasone and fentanyl added to lidocaine through axillary block in forearm fracture. Pain Res Treat; 2013:761583, 2013.
5. jain a, jain K, BHardawaj n: Analgesic efficacy of low-dose intrathecal neostigmine in combination with fentanyl and bupivacaine for total knee replacement surgery. J Anaesthesiol Clin Pharmacol; 28(4):486-90, 2012.
6. riBeiro da Silva a, Cuello aC: choline acetyltransferase-immunoreactive profiles are presynaptic to primary sensory fibers in the rat superficial dorsal horn. J Comp Neurol; 295(3):370-84, 1990.
7. genZen jr, van Cleve w, mCgeHee dS: dorsal root ganglion neurons express multiple nicotinic acetylcholine receptor subtypes. J Neuro physiol; 86:1773-82, 2001.
8. ummenHoFer wC, Brown Sm, BernardS Cm: acetylcholinesterase and butyrylcholinesterase are expressed in the spinal meninges of monkeys and pigs. Anesthesiology; 88:1259-65, 1998. ZHuo m, geBHart gF: Tonic cholinergic inhibition of spinal 9.
mechanical transmission. Pain; 46:211-22, 1991.10. naguiB m, yaKSH tl: characterization of muscarinic receptor
subtypes that mediate antinociception in the rat spinal cord. AnesthAnalg; 85:847-53, 1997.
11. moHer d, SCHulZ KF, altman dg: The consorT statement: revised recommendations for improving the quality of reports of parallel group randomized trial. BMC Med Res Methodol; 1:2, 2001.
12. guPta S: post operative analgesia with intrathecal neostegmin. The internet journal of Anesthesiology; 25:10-13, 2010.
13. Hye ma, maSud Km, BaniK d, Haqe mF, aKHtaruZZaman Km: intrathecalneostegmin for postoperative analgesia in caesarean section. Mymensingh Med J; 19(4):586-93, 2012. yegin a, yilmaZ m, KarSli B, erman m: analagesic effect 14. of intrathecalneostegmin in perianal surgery. Ear J Anesthesiol;
20(5):404-8, 2003.15. Klamtj g, Slullitel a, garCiaH v: post operativeanalagesia effect
of intrathecalneostegmin and its influence on spinal anesthesia. Anesthesia; 52:547-551, 2002.
16. joSHi-KHadKe Sl, KHadKe vv, Patel Sj, BorSe ym, KelKar Kv, digHe jP, SuBHedar rd: Efficacy of spinal additives neostigmine and magnesium sulfate on characteristics of subarachnoid block, hemodynamic stability and postoperative pain relief: a randomized clinical trial. Anesth Essays Res; Jan-apr, 9(1):63-71, 2015.
17. yoganaraSimHa n, ragHavendra t, amitHa S, SHridHar K, radHa ma: comparative study between intrathecal clonidine and neostigmine with intrathecal bupivacaine for lower abdominal surgeries. Indian J Anaesth; Jan, 58(1):43-7, 2014.
18. lauretti gr, mattoS al, reiS mP: intrathecal neostegmin for postoperative analgesia after orthopedic surgery. Jclinanesth; 9(6):437-7, 1997.
19. larry m, jordan jr, mCvagH Br, noga am, CaBaj H, majczyński urSZula Sławińska j, ProvenCHer H, leBlond Serge roSSignol: cholinergic mechanisms in spinal locomotion-potential target for rehabilitation approaches. Front Neural Circuits; 8:132, 2014.

205 M.E.J. ANESTH 23 (2), 2015
The beneficial values of Transoesophageal Doppler in inTraoperaTive fluiD guiDance versus
sTanDarD clinical moniToring parameTers in infanTs unDergoing Kasai operaTion
Eman SayEd IbrahIm*, Taha aId yaSSEIn** and WESam SabEr morad***
Abstract
Background: fluid overload in infants can result from inappropriate volume expansion (VE). The aim of this work was to evaluate the beneficial values of Transoesophageal Doppler TED in intraoperative fluid guidance versus standard clinical monitoring parameters in infants undergoing Kasai operation.
Methods: forty infants scheduled for Kasai procedure were randomly allocated into two groups (Doppler and clinical group). In Doppler group decided to provide VE (10-30 ml/kg of Hydroxyethyl starches HES) when the index stroke volume decreased by ≥15% from the baseline value, in clinical group, hemodynamic variables triggering colloid administration mean arterial blood pressure (MAP) less than 20% below baseline or central venous pressure (CVP) <5 cmH2o in both groups: Ringer's acetate was infused at constant rate (6 m l/kg/h). Standard and TED-derived data were recorded before and after ve. follow up the postoperative outcome and hospital stay.
Results: There were significantly lower mean volume of HES (42.85 ± 3.93 versus 84 ± 14.29 ml) and percent of infants required it (30% versus 90%) associated with earlier tolerance to oral feeding (2 ± 0.66 versus 3.4 ± 0.51), shorter hospital stay (5.30 ± 0.47 versus 6.7 ± 0.92 days) and lower rate of chest infection (15% versus 30%) in Doppler group than clinical group. There was no difference between the two studied groups regarding heart rate, MAP.
Conclusions: TED guided intraoperative fluid intake in infants undergoing Kasai operation optimize fluid consumption and improve outcome associated with shorter hospital stay.
Keywords: Infants, Kasai operation, Transoesophageal Doppler, volume expansion.
* MD, Lecturer of anesthesia (National Liver Institute)-Menofeya University.** MD, lecturer of hepatobilliary surgery (National Liver Institute) Menofeya university.*** mD, lecturer of public health (national liver institute) menofeya university. Corresponding author: Eman Sayed Ibrahim MD, Lecturer of anesthesia (National Liver Institute)-Menofeya University.
Phone: 01282271464 - 0123548537. E-mail: [email protected]. Address: 18 Hassan Abdel Latif, Maleka, Fesal, Giza, Egypt.

206 eman sayeD ibrahim et. al
Introduction
extrahepatic biliary atresia (ehba) is an inflammatory, progressive, fibrosclerosing cholan-giopathy of infancy, affecting both the extrahepatic and intrahepatic bile ducts to a variable extent that results in destruction and obstruction of the biliary tract1. Without medical and surgical intervention, disease progression leads to hepatic fibrosis, cirrhosis with portal hypertension, liver failure, and death within 2 to 3 years. It classically presents in 1 in 8,000 to 1 in 18,000 live births, during the neonatal period, with cholestatic jaundice, acholic stools, and hepatomegaly, in an otherwise apparently healthy infant2. current treatment of EHBA is surgical hepatoportoenterostomy (Kasai procedure) for the relief of biliary obstruction in these infants3.
Perioperative fluid optimization is essential in Kasai procedures for reducing morbidity. Hypovolemia is associated in particular with improper organ perfusion and increased length of hospital stay, while excessive fluid administration produces the clinical picture of pulmonary peripheral and gut edema with associated morbidity and mortality4.The assessment of perioperative hypovolemia and the trigger for volume expansion (ve) in pediatric anesthesia are based on the interpretation of multiple variables and clinical endpoints such as arterial pressure, heart rate (hr), pulse pressure, urine output, type of surgery, surgical events (e.g. bleeding), and laboratory findings (e.g. hematocrit, lactate). fluid requirements when based only according to these variables can be inappropriate5. minimally invasive tools that could predict patient responsiveness to ve would be extremely useful. Transoesophageal Doppler (TED) has been shown to effectively measure co in newborns and children and therefore, could allow for better assessment of the efficacy of VE6.
We therefore designed a prospective, randomized, controlled trial to evaluate the effectiveness of TeD on intraoperative fluid optimization versus standard clinical monitoring parameters in infants undergoing Kasai operation.
Methods
After receiving approval from Ethical Committee and informed consent from patient's parents, this prospective cohort study enrolled 40 infants who were randomly assigned into two groups using a random number generator in sealed envelopes of 20 each: the Doppler group and the clinical group. Infants aged ≤3 months, weighing <10 kg, without myocardial dysfunction, American Society of Anaesthesiologists (ASA) grade I/II, who required general anesthesia and tracheal intubation for hepatoportoenterostomy for biliary atresia (ba) were included in the study. exclusion criteria were asa class >ii, preoperative hemodynamic instability or catecholamine infusion, known congenital heart disease with hemodynamic consequences and esophageal malformation, any patient with history of bleeding tendency, and no written informed consent.all infants received an oral intake of 15 ml/kg of 10% glucose 2 h before surgery. Patients were optimized before operation and deemed hemodynamically stable and clinically euvolemic before the induction of anesthesia. after denitrogenation, general anesthesia was induced by inhalation of 100% oxygen and 8% sevoflurane until the patient lost consciousness and then the sevoflurane concentration was decreased to 4%. An IV cannula was inserted and fentanyl (1 µg/kg) and atracurium (0.5 mg/kg) were administered to facilitate tracheal intubation. anesthesia was then maintained with 50% oxygen, air and sevoflurane (1 MAC end-tidal concentration). mechanical ventilation was performed in all patients using a semi closed system adjusted to keep sao2>95% and end tidal CO2 between 25 mmHg and 35 mmHg (GE Datex Ohmeda S/5 Anesthetic Delivery unit system). arterial pressure was measured using a standard non-invasive cuff applied to the upper limb. Nasopharyngeal temperature was monitored and maintained in a normal range with a forced-air warmer (Bair Hugger Temperature Management Unit, arizant, USA). Following induction of anesthesia, data of patients in the Doppler group (age, weight, and height) were registered in the Doppler monitor. A 4 MHz, flexible TED probe specific for single-patient pediatric use (KDP n-Kinder Doppler Probe®) was greased with a lubricating gel and passed orally into the mid esophagus until aortic blood flow signals were

M.E.J. ANESTH 23 (2), 2015
207Transoesophageal Doppler in Kasai operaTion
best identified. The optimal position of the probe was suggested by an audible, maximal pitch and a sharply defined velocity waveform with minimal spectral dispersion. The monitoring system used (Cardio QpTm, Deltex medical Tm, chichester, uK) which shows all the needed hemodynamic variables both in numerical and graphical forms... The probe was rotated to display the best aortic blood flow signal before each measurement. cardiac index (ci), index stroke volume (ISV), corrected flow time (CFT) (length of time of systolic blood flow adjusted for HR, that is, divided by the square root of the heart cycle time), peak velocity (PV) (maximal velocity during systole), of the descending aorta velocity waveform were recorded. TED measurements pre- and post-VE were completed and averaged In the clinical group (A 4- to 5.5-Fr central venous catheter AMECATH single lumen central venous catheter) was placed through the right internal jugular vein by ultrasound guided method (sonosite-nano max ultrasound system-usa).
In Doppler group. Boluses of colloid were administered, guided by an algorithm depending on the Doppler estimations of isv, when the isv decreased by ≥15% from the baseline value.VE consisted of an infusion of 10-30 ml/ kg of colloid (Voluven hydroxyethyl starch 130/0.4 6%). Over a period of 20-40 min, repeated by other boluses only if isv is not increased by ≥15% this algorithm was similar to that used by roux et al.7, In clinical group, hemodynamic variables triggering colloid administration based on clinical appreciation and standard monitoring data that involves either a decrease in mean arterial blood pressure less than 20% below baseline or CVP<5 mmHg.VE was the same of that used in TED group. In both groups, Ringer's acetate solution was infused intraoperative at approximately constant rate (6 m l/kg/h) via an infusion pump (Fresenius Kabi, Germany) to cover fluid deficit and basal fluid requirements. Four sets of data were recorded and each set included: heart rate (hr), mean arterial pressure (map), end tidal co2 (eTco2), isv, cfT, pv and cardiac output (CO). The measurements were obtained at 10 min after induction of anesthesia when hemodynamicaly stable with controlled ventilation established, (To) before VE(T1), T2: after VE(T2) and at the end of surgery(T3).
The primary out-come was to evaluate the beneficial values of TED in intraoperative fluid guidance versus standard clinical monitoring parameters in infants undergoing Kasai operation regarding volume of colloid administered. Secondary outcomes included evaluation of complications such as vomiting, post-operative pulmonary complications, return of bowel function and the length of intensive care and hospital stay.
20 patients in arm 1 (Doppler group) and 20 patients in arm 2 (clinical group) were recruited based on the following assumptions: with the power of 80 %, α = 0.05 and the ratio of cases to controls = 1:1. The required sample size was determined using (power and sample size calculation) software.
The sample size was determined as regard patients attending our institute meeting the inclusion and exclusion criteria which are 40/year. Normally distributed data were analyzed using t-test, and categorical data were analyzed using the Chi-square test. continuous data are presented as mean and standard deviation, whereas categorical data are presented as number of patients and percentage. Data were analyzed using IBM SPSS statistics 20.0 software. P <0.05 was considered statistically significant.
Results
Data is presented at baseline, before and after VE (Table 1). There were no differences in the demographic data between Doppler and clinical groups (Table 1). The percentage of patients who required volume expansion was significantly lower in the Doppler group (Table 1). Furthermore, the volume of HES needed was also significantly smaller I the Doppler group (Table 1). There was no statistically significant difference between both groups regarding Ringer's acetate requirements (Table 1). There were no differences between the two studied groups regarding heart rate, mean blood pressure (map) (Table 2). The TED group demonstrated significant hemodynamic changes in post fluid boluses, increase of ISV and cardiac output associated with an increase in cfT and PV (Table 4). There was statistically significant decreased in mean heart rate post vs. pre- VE (123 ± 6.548 versus 136.8 ± 10.04 beat /min; p <0.05) and
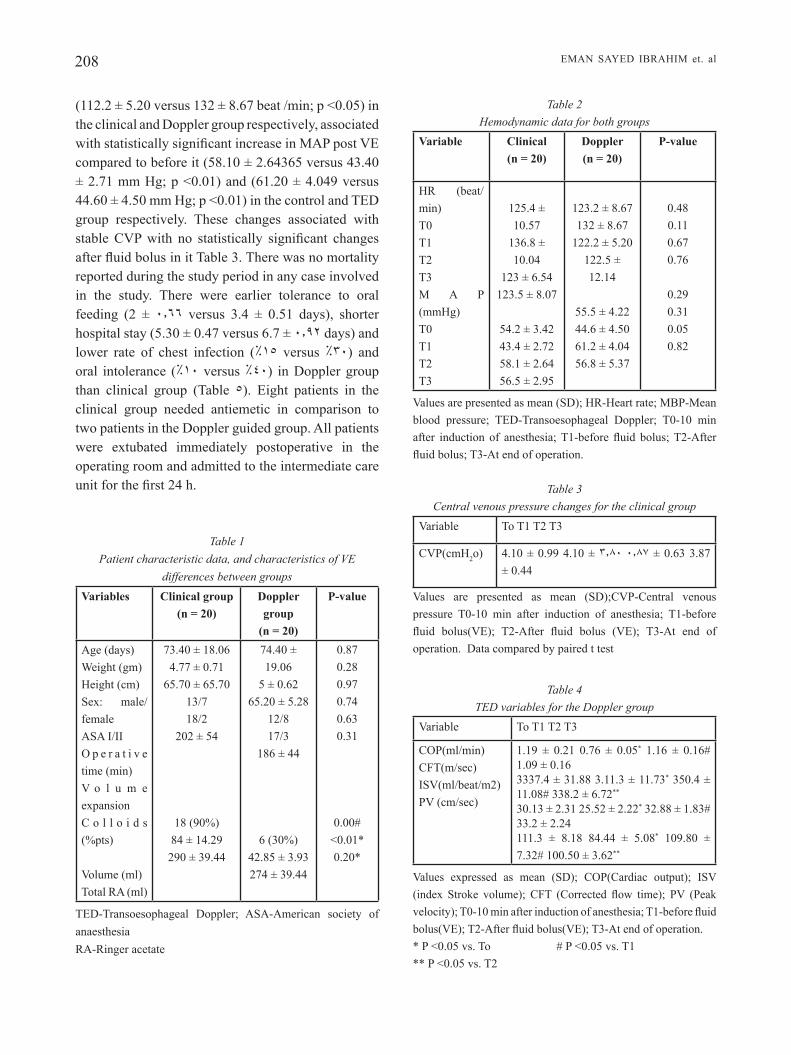
208 eman sayeD ibrahim et. al
(112.2 ± 5.20 versus 132 ± 8.67 beat /min; p <0.05) in the clinical and Doppler group respectively, associated with statistically significant increase in MAP post VE compared to before it (58.10 ± 2.64365 versus 43.40 ± 2.71 mm Hg; p <0.01) and (61.20 ± 4.049 versus 44.60 ± 4.50 mm Hg; p <0.01) in the control and TED group respectively. These changes associated with stable CVP with no statistically significant changes after fluid bolus in it Table 3. There was no mortality reported during the study period in any case involved in the study. There were earlier tolerance to oral feeding (2 ± 0.66 versus 3.4 ± 0.51 days), shorter hospital stay (5.30 ± 0.47 versus 6.7 ± 0.92 days) and lower rate of chest infection (%15 versus %30) and oral intolerance (%10 versus %40) in Doppler group than clinical group (Table 5). Eight patients in the clinical group needed antiemetic in comparison to two patients in the Doppler guided group. All patients were extubated immediately postoperative in the operating room and admitted to the intermediate care unit for the first 24 h.
Table 1 Patient characteristic data, and characteristics of VE
differences between groupsVariables Clinical group
(n = 20)Doppler group
(n = 20)
P-value
Age (days)Weight (gm)Height (cm)Sex: male/femaleASA I/IIo p e r a t i v e time (min)v o l u m e expansionc o l l o i d s (%pts)
volume (ml)Total ra (ml)
73.40 ± 18.064.77 ± 0.71
65.70 ± 65.7013/718/2
202 ± 54
18 (90%)84 ± 14.29290 ± 39.44
74.40 ± 19.06
5 ± 0.6265.20 ± 5.28
12/817/3
186 ± 44
6 (30%)42.85 ± 3.93274 ± 39.44
0.870.280.970.740.630.31
0.00#<0.01*0.20*
TED-Transoesophageal Doppler; ASA-American society of anaesthesiaRA-Ringer acetate
Table 2 Hemodynamic data for both groups
Variable Clinical(n = 20)
Doppler(n = 20)
P-value
HR (beat/min)T0T1T2 T3m a p (mmHg)T0T1 T2 T3
125.4 ± 10.57
136.8 ± 10.04
123 ± 6.54123.5 ± 8.07
54.2 ± 3.4243.4 ± 2.7258.1 ± 2.6456.5 ± 2.95
123.2 ± 8.67132 ± 8.67
122.2 ± 5.20122.5 ± 12.14
55.5 ± 4.2244.6 ± 4.5061.2 ± 4.0456.8 ± 5.37
0.480.110.670.76
0.290.310.050.82
Values are presented as mean (SD); HR-Heart rate; MBP-Mean blood pressure; TED-Transoesophageal Doppler; T0-10 min after induction of anesthesia; T1-before fluid bolus; T2-After fluid bolus; T3-At end of operation.
Table 3 Central venous pressure changes for the clinical group
variable To T1 T2 T3
cvp(cmh2o) 4.10 ± 0.99 4.10 ± 3.80 0.87 ± 0.63 3.87 ± 0.44
Values are presented as mean (SD);CVP-Central venous pressure T0-10 min after induction of anesthesia; T1-before fluid bolus(VE); T2-After fluid bolus (VE); T3-At end of operation. Data compared by paired t test
Table 4 TED variables for the Doppler group
variable To T1 T2 T3
COP(ml/min)CFT(m/sec)ISV(ml/beat/m2)PV (cm/sec)
1.19 ± 0.21 0.76 ± 0.05* 1.16 ± 0.16# 1.09 ± 0.163337.4 ± 31.88 3.11.3 ± 11.73* 350.4 ± 11.08# 338.2 ± 6.72**
30.13 ± 2.31 25.52 ± 2.22* 32.88 ± 1.83# 33.2 ± 2.24111.3 ± 8.18 84.44 ± 5.08* 109.80 ± 7.32# 100.50 ± 3.62**
Values expressed as mean (SD); COP(Cardiac output); ISV (index Stroke volume); CFT (Corrected flow time); PV (Peak velocity); T0-10 min after induction of anesthesia; T1-before fluid bolus(VE); T2-After fluid bolus(VE); T3-At end of operation.* P ˂0.05 vs. To # P ˂0.05 vs. T1** P ˂0.05 vs. T2

M.E.J. ANESTH 23 (2), 2015
209Transoesophageal Doppler in Kasai operaTion
Table 5 Postoperative outcome
Variable Doppler Clinical P-value
(n = 20) (n = 20)
Chest infection n (%) 3(15%) 6 (30%) 0.26
Oral intolerance 2(10%) 8(40%) 0.03
Hospital stays (days) 5.30 ± 0.47 6.7 ± 0.92 <0.01
Day of oral feeding (days) 2 ± 0.66 3.4 ± 0.51 <0.01
Discussion
The results of this study demonstrate that TeD was able to predict responsiveness to fluid and optimize intraoperative fluid consumption, as indicated by significant lower mean volume of colloid (HES) received and percent of infants requiring volume expanders.. in a study by lee, et al.8, fTc and ppv (pulse pressure variation) of Doppler were found to be better than cvp and lveDai (left ventricular end end-diastolic area index) in predicting fluid responsiveness and that changes in the stroke volume index caused by fluid loading correlated significantly with the fTc values. estimation of intravascular volume status in critically ill infants and neonates is a particular challenge as traditional indices, such as blood pressure and heart rate, may not reflect mild to moderate blood loss and because, in the majority of cases, invasive monitoring is not used9. in our study, fluid boluses based on standard clinical monitoring data was shown to be inappropriate in the patients as CVP was stable after fluid boluses in spite of significant changes in heart rate and MAP. MAP and HR did not reliably reflect CO in anesthetized pediatric patients10,11. Kumar et al and marik et al. found that CVP is not able to indicate changes in intravascular volume and fluid responsiveness accurately12,13. Value of CVP is influenced by the diastolic compliance of the right ventricle, intra-abdominal pressure, positive end expiratory pressure, and forced expiration. indeed, cvp does not predict fluid responsiveness and only poorly reflects preload in adults, children, and pediatric animal models14. The hypotensive effect of sevoflurane is well described and is especially significant in the youngest pediatric patients15.This effect, mostly attributable to a decrease in systemic vascular resistance, may explain the
arterial hypotension among our patients before fluid bolus. The increase in map observed in control patient's post-fluid bolus, without an improvement in cvp may be explained by other factors such as the subsequent reduction in sevoflurane during the period of arterial hypotension. our study was able to demonstrate the ability of minimally invasive TED to reduce fluid therapy when compared to standard clinical monitor parameter guided fluid management associated with earlier tolerance to oral feeding, shorter hospital stay and lower rate of chest infection and oral intolerance. recent randomized trials and meta-analyses have confirmed that intraoperative fluid optimization using TED improve outcome8,16 absi et al.17 reported that the application of esophageal Doppler guided fluid management has produced a similar improvement in outcome for patients undergoing cardiac surgery. Roche et al.18 studied Goal-directed fluid management with trans-esophageal Doppler and found a significant reduction in hospital stay. in the current study, chest infection and post-operative vomiting and intolerance to oral feeding were significantly less reported in the Doppler guided fluid group. This was also supported by mythen and Webb study, which demonstrated that the esophageal Doppler guided plasma volume optimization significantly reduced the incidence of gastric mucosal hypoperfusion leading to a significant reduction in complication rates and length of hospital stay following cardiac surgery19. increase extravascular lung water from excessive intravascular volume may predispose patients to pneumonia and respiratory failure. It can lead to edema of the gut, which may inhibit gastrointestinal motility and prolong postoperative ileus and intolerance for enteric alimentation. The potential for bacterial translocation and development of sepsis and multiorgan failure is also increased. increase cutaneous edema may decrease tissue oxygenation,which can lead to delayed wound healing20. Previous literatures suggest that perioperative goal-directed therapy (GDT) based on flow-related hemodynamic parameters improve patient outcome21,22. clinical studies have mostly shown outcome benefits only within postoperative nausea and vomiting, ileus, morbidity, and hospital stay23,24. However, only limited pathophysiological data are available to explain this benefit. Lopes et al.25,

210 eman sayeD ibrahim et. al
in their work revealed that there is reduced morbidity and hospital stay by gDT and this also associated with a reduced interleukin-6 response. Other studies on perioperative changes of the vascular barrier suggest that the endothelial gly-cocalyx plays a key role26,27.
The limited number of cases enrolled in our study was related to the limited number of cases of
biliary atresia selected for kasai surgery in our national liver institute. The use of TED for intraoperative fluid guidance in infants undergoing Kasai operation need to be studied in further planned research work.
In conclusion: TED guided intraoperative fluid management in infants undergoing Kasai operation optimizes fluid consumption and improve outcome associated with shorter hospital stay.

M.E.J. ANESTH 23 (2), 2015
211Transoesophageal Doppler in Kasai operaTion
Respiratory variation in aortic blood flow velocity as a predictor of fluid responsiveness in children after repair of ventricular septal
defect. Pediatr Cardiol; 31(8):1166-1170, 2010. LErman J, SIkIch n, kLEInman S and yEnTIS S: The pharmacology 15. of sevoflurane in infants and children. Anesthesiology; 80:814-24,
1994. WakELIng hg, mcFaLL mr, JEnkInS cS, WoodS Wg, mILES WF, 16. barcLay gr and FLEmIng Sc: Intraoperative oesophageal Doppler guided fluid management shortens postoperative hospital stay after
major bowel surgery. Br J Anaesth; 95:634-42, 2005.17. abSI ma, LuTTErman J and WETzEL gT: Noninvasive cardiac output
monitoring in the pediatric cardiac intensive care unit. Current Opinion in Cardiology; 25:77-79, 2010.
18. rochE am, mILLEr TE and gan TJ: Goal-directed fluid management with trans-oesophageal Doppler. Best Practice & Research Clinical Anaesthesiology; 23:327-334, 2009.
19. myThEn mg and WEbb ar: Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery. Arch Surg; 130:4239, 1995.
20. hoLTE k, Sharrock E and kEhLET h: Pathophysiology and clinical implication of perioperative fluid excess. Br J Anaesth; 89:622-32, 2002.
21. PEarSE r, daWSon d, FaWcETT J, rhodES a, groundS rm and bEnnET Ed: Early goal-directed therapy after major surgery reduces complications and hospital stay.a randomized, controlled trial. Crit Care; 9:687-93, 2005.
22. bundgaard-nIELSEn m, hoLTE k, SEchEr nh and kEhLET h: Monitoring of perioperative fluid administration by Individualized goal-directed therapy. Acta Anaesthesiol Scand; 132:1817-24, 2007. abbaS Sm and hILL ag: Systematic review of the literature for 23. the use of oesophageal Doppler monitor for fluid replacement in
major abdominal surgery. Anaesthesia; 63:44-51, 2008.24. buETTnEr m, SchummEr W, huETTEmann E, SchEnkE S, vanhouT
n and Sakka Sg: Influence of systolic-pressure-variation-guided intraoperative fluid management on organ function and oxygen transport. Br J Anaesth; 101:194-9, 2008. LoPES mr, oLIvEIra ma, PErEIra vo, LEmoS IP, auLEr Jr and 25. mIchar F: Goal-directed fluid management based on pulse Pressure variation monitoring during high-risk surgery: a pilot randomized
controlled trial. Crit Care; 11:100-9, 2007. nobLETT SE, SnoWdEn cP, ShEnTon bk, horgan aF: 26. Randomized clinical trial assessing the effect of Doppler Optimized fluid management on outcome after elective colorectal resection. Br
J Surg; 93:1069-76, 2006.27. Jacob m, bruEggEr d, rEhm m, WELSch u, conzEn P and bEckEr
bF: Contrasting effects of colloid and crystalloid resuscitation fluids on cardiac vascular permeability. Anesthesiology; 104:1223-31, 2006.
References
1. kahn E: biliary atresia revisited. Pediatr Dev Pathol; 7: 109-124, 2004.
2. PErLmuTTEr dh and ShEPhErd rW: Extrahepatic biliary atresia: a disease or a phenotype? Hepatology; 35:1297-1304, 2002.
3. kaSaI m: Treatment of biliary atresia with special reference to hepatic porto-enterostomy and its modifications. Prog Pediatr Surg; 6:5-52, 1974.
4. brandSTruP b, TonnESEn h, bEIEr-hoLgErSEn r, hJorTSo E, ordIng h, LIndorFF-LarSEn k, raSmuSSEn mS, Lanng c, WaLLIn L, IvErSEn Lh, gramkoW cS, okhoLm m, bLEmmEr T, SvEndSEn PE, roTTEnSTEn hh, ThagE b, rIIS J, JEPPESEn IS, TEILum d, chrISTEnSEn am, graungaard b and PoTT F: Effects of intravenous fluid restriction on postoperative complications comparison of two perioperative fluid regimens. Ann Surg; 238:641-8, 2003.
5. TIbby Sm, haThErILL m, marSh mJ, murdoch Ia: Clinicians’ abilities to estimate cardiac index in ventilated children and infants. Arch Dis Child; 77:516-8, 1997. Archives of Disease in childhoodadc.bmj.com
6. TIbby Sm, haThErILL m, murdoch Ia: Use of transesophageal Doppler ultrasonography in ventilated pediatric patients: derivation of cardiac output. Crit Care Med; 28:2045-50, 2000.
7. raux o, SPEncEr a, FESSEau r, mErcIEr g, rochETTE a, brInguIEr S, LakhaL k, caPdEvILa x and dadurE c: Intraoperative use of transoesophageal Doppler to predict response to volume expansion in infants and neonates. Br J Anaesth; 108(1):100-7, 2012.
8. LEE Jh, kIm JT, yoon Sz, LIm yJ, JEon y, bahk Jh and kIm cS: Evaluation of corrected Flow time in oesophageal Doppler as a predictor of fluid responsiveness. Br J Anaesth; 99:343-8, 2007. rIchardSon Jr, FErguSon J, hIScox J and raWLES J: Noninvasive 9. assessment of cardiac output in children. J Accid Emerg Med;
15(5):304-307, 1998.10. oSThauS Wa, hubEr d, bEck c, roEhLEr a, marx g, hEckEr h
and SümPELmann r: Correlation of oxygen delivery with central venous oxygen saturation, mean arterial pressure and heart rate in piglets. Paediatr Anaesth; 16(9):944-7, 2006.
11. kLuckoW m and EvanS n: Relationship between blood pressure and cardiac output in preterm infants requiring mechanical ventilation. J Pediatr; 129(4):506-12, 1996.
12. kumar a, anEL r, bunnELL E, habET k, zanoTTI S, marShaLL S, nEumann a, aLI a, chEang m, kavInSky c and ParrILLo JE: pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Crit Care Med; 32(3):691-9, 2004.
13. marIk PE, baram m and vahId b: Does central venous pressure predict fluid responsiveness? A systematic review of the literature. Chest; 134(1):172-8, 2008. choI dy, kWak hJ, Park hy, kIm yb, choI ch and LEE Jy: 14.


213 M.E.J. ANESTH 23 (2), 2015
Desflurane compareD to sevoflurane for cirrhotic patients unDergoing major liver
resection. a ranDomizeD control stuDy
Abou Hussein M*, MAHMoud F**, beltAgyR*, HAsAnin A**, yAssen K** And AttAR A*
Abstract
Background: major liver resection is associated with haemodynamic, hepatic and renal changes as a result of the procedure.
Aim: To compare Desflurane (D) versus Sevoflurane (S) on hepatic, renal functions, haemodynamics and perioperative course for cirrhotic patients undergoing major liver resection.
Patients and Methods: A prospective randomized control study with 50 patients (Child A) (D, n=25 and S, n=25). End tidal D or S adjusted with Entropy (40-60). Haemodynamics monitored with invasive blood pressure and trans-oesophageal Doppler (TED). Liver and kidney function tests, blood Glutathione-S-transferase (GST), urinary microalbuminuria (Microalb) were assayed. extubation time and anaesthetic consumption were recorded.
Results: Systemic vascular resistance (SVR) post-resection and stroke volume of D vs S were 835.04±12.02vs778.16±11.97dyn.sec.cm-5, P<0.01, and 85.72±2.95vs76.16±6.52 ml, P<0.01 respectively. Doppler corrected flow time (FTc) between groups were comparable (P>0.05). No difference post-operatively regarding hepatic and renal functions, and urine Microalb (14.76±3.95vs14.24±8.65 µg/ml, P=0.78), but a statistically difference was foundwith GST (0.046±0.003vs0.043±0.002 IU/ml, P<0.01).Despite a higher D consumption (73±17 vs 64±22 ml, P=0.102), cost in Egyptian pounds (LE) was lower with D (141.14 ± 32.90 vs 320.60 ± 114.01, le, P<0.01). Extubation time and ICU stay with D vS (4.52±2 vs 7.72±2 min, P <0.01) and (1.40 ± 0.50 vs 1.64 ± 0.48, days P=0.09) respectively.
Conclusion: neither D nor s were clinically superior to the other with respect to liver and kidneys functions, but D was found to preserve better the haemodynamic parameters and enhance recovery at a lower cost.
Keywords: Desflurane, Sevoflurane, Cirrhosis, Liver resection.
* anaesthesia Department, faculty of medicine, alexandria university, egypt.** Anaesthesia Department, National Liver Institute, Menoufiya University, Egypt. Corresponding author: Prof. Khaled Yassen, Anaesthesia Department, Liver Institute, Menoufiya University, Egypt. Tel:
+2010 6 30 80 170. E-mail: [email protected]

214 yassen K et. al
Introduction
Egypt has a high Hepatitis C virus (HCV) prevalence and accordinglya high morbidity and mortality from chronic liver disease, cirrhosis, and hepatocellular carcinoma1,2. this increases the incidence of cirrhotic patients undergoing liver related and unrelated surgeries3. liver resection improves overall survival in patients with small hepatocellular carcinoma, non-invasive and non-metastatic4,5; however this surgery may be followed by clinical or subclinical hepatocellular derangements, metabolic abnormalities, hemodynamic changes due to temporary liver dysfunction frequently encountered in the immediate postoperative period6-9. the anaesthetic technique and the choice of inhalational agent used during liver resection surgeries are very crucial to minimize the unwanted effects of anesthesia on different organs especially the liver and the kidneys.
the aim of the current study is to compare Desflurane to Sevoflurane based anesthesia for cirrhotic patients undergoing major liver resection in regards to hepatic and renal functions, hemodynamic parameters, and inhalational agentconsumption and cost.
Patients and Methods
In this double-blinded prospective randomized controlled study, written informed consent and local institutional research and ethics committee approval (12/2013) were obtained. The study was registered at the cochrane research data base of south africa (PACTR201404000804408) (www.pactr.org).
Fifty three adult cirrhotic (Child A) patients were presented for major liver resection. three patients did not meet the inclusion criteria and only fifty were randomized and equally divided into two groups using the closed envelope technique; the desflurance group(group D) and the seroflurance group (Group S).
included patients were those with written informed consent, age 25 years or older, scheduled for elective major liver resection surgery and classified as Child A and ASA II or III according to the Child-Pugh classification and American Society of Anesthesia classification, respectively. Patients with a history of esophageal disease, or contraindication for esophageal
Doppler insertion (esophageal or nasopharyngeal pathology, coarctation of the aorta), any patient with pre-operative arrhythmia (frequent ectopic beats) or history of bleeding tendency, recent anesthesia (within 7 days before the resection surgery), re-operation and patients with preoperative renal dysfunction Were excluded from the study.
Both groups received entropy guided general anesthesia induction (Anesthesia Depth monitor, General Electric, Helsinki, Finland) with fentanyl (1-2 µg/kg), propofol (1-1.5 mg/kg) and rocuronium (1 mg/kg). Two large peripheral venous lines (16 gauge or larger), multi-lumen central venous catheter in the right internal jugular vein (ultrasound guided) and an arterial catheter in the non dominant hand were inserted. End-tidal inhalational concentration during the induction was limited to 1 mac. general anesthesia was maintained with a 50% mixture of air and oxygen with either desflurane or sevofluraneat a fresh gas flow of 2 litres/min. Inhalational agent concentrations were adjusted according to an entropy between 40 and 60. Ventilation was controlled to maintain etco2 between 32 and 36 mmHg. If mean arterial blood pressure (MAP) or heart rate (HR) remained elevated after 5 minutes, supplemental doses of fentanyl (0.5 µg/ kg) were given. Atropine 0.5 mg was given intravenously if HR drops below 45 beats/ min. A trancesophageal Doppler(TED) probe (Cardio QP) for cardiac output (CO) monitoring (EDM™; Deltex Medical, Chichester, UK) was inserted orally into the mid-oesophagus till the aortic blood flow signals were identified during hepatic dissection and after insertion of the surgical abdominal retractors. preoperative prothrombin activity and platelet count were checked prior to insertion of the probe. Replacement of intraoperative fluid loss was guided with the teD parameters.
the parameters obtained by the teD include: the corrected flow time (FTc) which is the systolic flow time corrected for heart rate, the stroke volume (SV), the cardiac output (CO) and thesystemic vascular resistance (SVR).
In both groups, boluses of colloid (6% HES 130/0.4 Voluven; Fresenius-Kabi, Bad Homburg, Germany) were administered, guided by an algorithm depending on the Doppler estimations of stroke volume
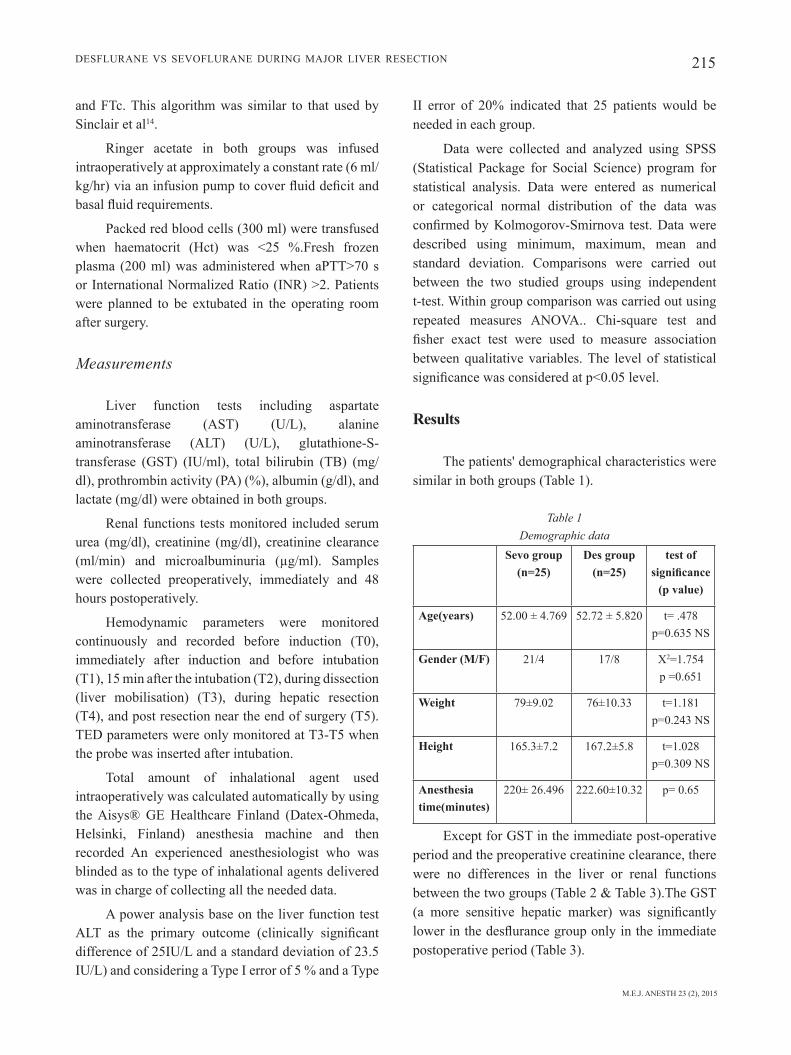
M.E.J. ANESTH 23 (2), 2015
215Desflurane vs sevoflurane During major liver resection
and ftc. this algorithm was similar to that used by sinclair et al14.
ringer acetate in both groups was infused intraoperatively at approximately a constant rate (6 ml/kg/hr) via an infusion pump to cover fluid deficit and basal fluid requirements.
Packed red blood cells (300 ml) were transfused when haematocrit (Hct) was <25 %.Fresh frozen plasma (200 ml) was administered when aPTT>70 s or International Normalized Ratio (INR) >2. Patients were planned to be extubated in the operating room after surgery.
Measurements
liver function tests including aspartate aminotransferase (AST) (U/L), alanine aminotransferase (ALT) (U/L), glutathione-S-transferase (GST) (IU/ml), total bilirubin (TB) (mg/dl), prothrombin activity (PA) (%), albumin (g/dl), and lactate (mg/dl) were obtained in both groups.
renal functions tests monitored included serum urea (mg/dl), creatinine (mg/dl), creatinine clearance (ml/min) and microalbuminuria (µg/ml). Samples were collected preoperatively, immediately and 48 hours postoperatively.
hemodynamic parameters were monitored continuously and recorded before induction (T0), immediately after induction and before intubation (T1), 15 min after the intubation (T2), during dissection (liver mobilisation) (T3), during hepatic resection (T4), and post resection near the end of surgery (T5). TED parameters were only monitored at T3-T5 when the probe was inserted after intubation.
total amount of inhalational agent used intraoperatively was calculated automatically by using the Aisys® GE Healthcare Finland (Datex-Ohmeda, Helsinki, Finland) anesthesia machine and then recorded an experienced anesthesiologist who was blinded as to the type of inhalational agents delivered was in charge of collecting all the needed data.
a power analysis base on the liver function test ALT as the primary outcome (clinically significant difference of 25IU/L and a standard deviation of 23.5 IU/L) and considering a Type I error of 5 % and a Type
ii error of 20% indicated that 25 patients would be needed in each group.
Data were collected and analyzed using spss (Statistical Package for Social Science) program for statistical analysis. Data were entered as numerical or categorical normal distribution of the data was confirmed by Kolmogorov-Smirnova test. Data were described using minimum, maximum, mean and standard deviation. comparisons were carried out between the two studied groups using independent t-test. Within group comparison was carried out using repeated measures ANOVA.. Chi-square test and fisher exact test were used to measure association between qualitative variables. the level of statistical significance was considered at p˂0.05 level.
Results
the patients' demographical characteristics were similar in both groups (Table 1).
Table 1 Demographic data
Sevo group(n=25)
Des group(n=25)
test of significance
(p value)
Age(years) 52.00 ± 4.769 52.72 ± 5.820 t= .478p=0.635 NS
Gender (M/F) 21/4 17/8 X2=1.754p =0.651
Weight 79±9.02 76±10.33 t=1.181p=0.243 NS
Height 165.3±7.2 167.2±5.8 t=1.028p=0.309 NS
Anesthesia time(minutes)
220± 26.496 222.60±10.32 p= 0.65
Except for GST in the immediate post-operative period and the preoperative creatinine clearance, there were no differences in the liver or renal functions between the two groups (Table 2 & Table 3).The GST (a more sensitive hepatic marker) was significantly lower in the desflurance group only in the immediate postoperative period (Table 3).
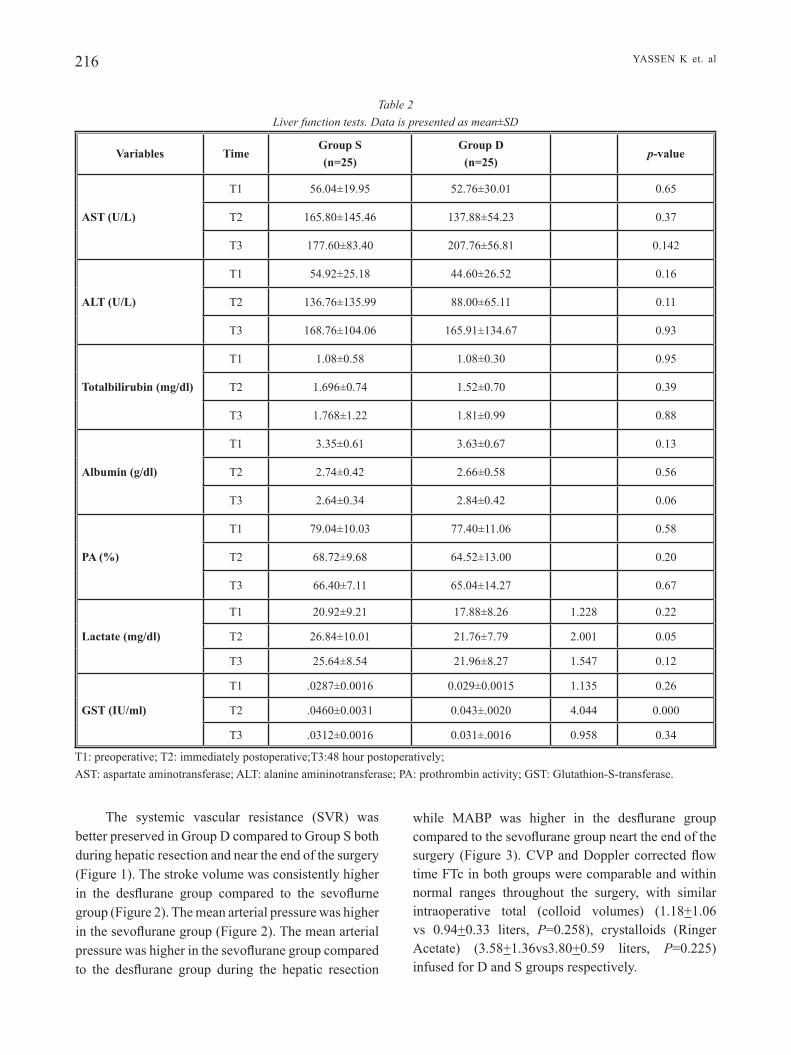
216
while MABP was higher in the desflurane group compared to the sevoflurane group neart the end of the surgery (Figure 3). CVP and Doppler corrected flow time ftc in both groups were comparable and within normal ranges throughout the surgery, with similar intraoperative total (colloid volumes) (1.18+1.06 vs 0.94+0.33 liters, P=0.258), crystalloids (Ringer Acetate) (3.58+1.36vs3.80+0.59 liters, P=0.225) infused for D and s groups respectively.
The systemic vascular resistance (SVR) was better preserved in group D compared to group s both during hepatic resection and near the end of the surgery (Figure 1). The stroke volume was consistently higher in the desflurane group compared to the sevoflurne group (Figure 2). The mean arterial pressure was higher in the sevoflurane group (Figure 2). The mean arterial pressure was higher in the sevoflurane group compared to the desflurane group during the hepatic resection
yassen K et. al
Table 2 Liver function tests. Data is presented as mean±SD
Variables TimeGroup S(n=25)
Group D(n=25)
p-value
AST (U/L)
t1 56.04±19.95 52.76±30.01 0.65
t2 165.80±145.46 137.88±54.23 0.37
t3 177.60±83.40 207.76±56.81 0.142
ALT (U/L)
t1 54.92±25.18 44.60±26.52 0.16
t2 136.76±135.99 88.00±65.11 0.11
t3 168.76±104.06 165.91±134.67 0.93
Totalbilirubin (mg/dl)
t1 1.08±0.58 1.08±0.30 0.95
t2 1.696±0.74 1.52±0.70 0.39
t3 1.768±1.22 1.81±0.99 0.88
Albumin (g/dl)
t1 3.35±0.61 3.63±0.67 0.13
t2 2.74±0.42 2.66±0.58 0.56
t3 2.64±0.34 2.84±0.42 0.06
PA (%)
t1 79.04±10.03 77.40±11.06 0.58
t2 68.72±9.68 64.52±13.00 0.20
t3 66.40±7.11 65.04±14.27 0.67
Lactate (mg/dl)
t1 20.92±9.21 17.88±8.26 1.228 0.22
t2 26.84±10.01 21.76±7.79 2.001 0.05
t3 25.64±8.54 21.96±8.27 1.547 0.12
GST (IU/ml)
t1 .0287±0.0016 0.029±0.0015 1.135 0.26
t2 .0460±0.0031 0.043±.0020 4.044 0.000
t3 .0312±0.0016 0.031±.0016 0.958 0.34
T1: preoperative; T2: immediately postoperative;T3:48 hour postoperatively;AST: aspartate aminotransferase; ALT: alanine amininotransferase; PA: prothrombin activity; GST: Glutathion-S-transferase.
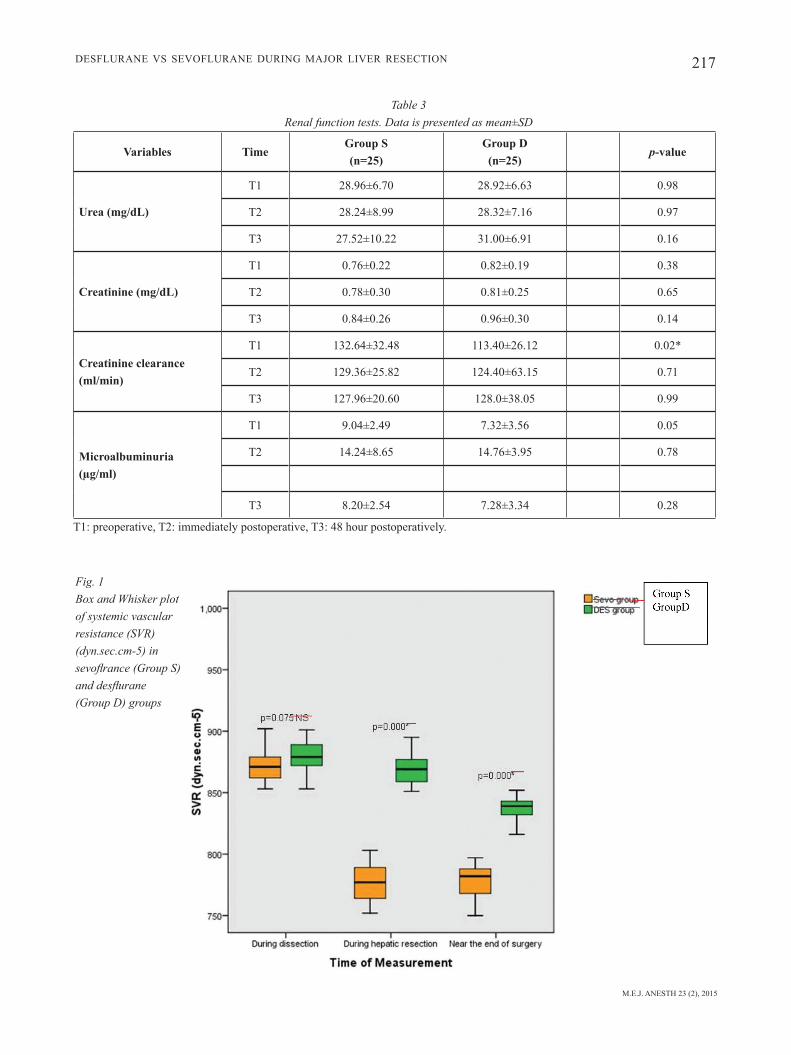
M.E.J. ANESTH 23 (2), 2015
217Desflurane vs sevoflurane During major liver resection
Table 3 Renal function tests. Data is presented as mean±SD
Variables TimeGroup S(n=25)
Group D(n=25)
p-value
Urea (mg/dL)
t1 28.96±6.70 28.92±6.63 0.98
t2 28.24±8.99 28.32±7.16 0.97
t3 27.52±10.22 31.00±6.91 0.16
Creatinine (mg/dL)
t1 0.76±0.22 0.82±0.19 0.38
t2 0.78±0.30 0.81±0.25 0.65
t3 0.84±0.26 0.96±0.30 0.14
Creatinine clearance(ml/min)
t1 132.64±32.48 113.40±26.12 0.02*
t2 129.36±25.82 124.40±63.15 0.71
t3 127.96±20.60 128.0±38.05 0.99
Microalbuminuria(µg/ml)
t1 9.04±2.49 7.32±3.56 0.05
t2 14.24±8.65 14.76±3.95 0.78
t3 8.20±2.54 7.28±3.34 0.28
T1: preoperative, T2: immediately postoperative, T3: 48 hour postoperatively.
Fig. 1 Box and Whisker plot of systemic vascular resistance (SVR) (dyn.sec.cm-5) in sevoflrance (Group S) and desflurane (Group D) groups
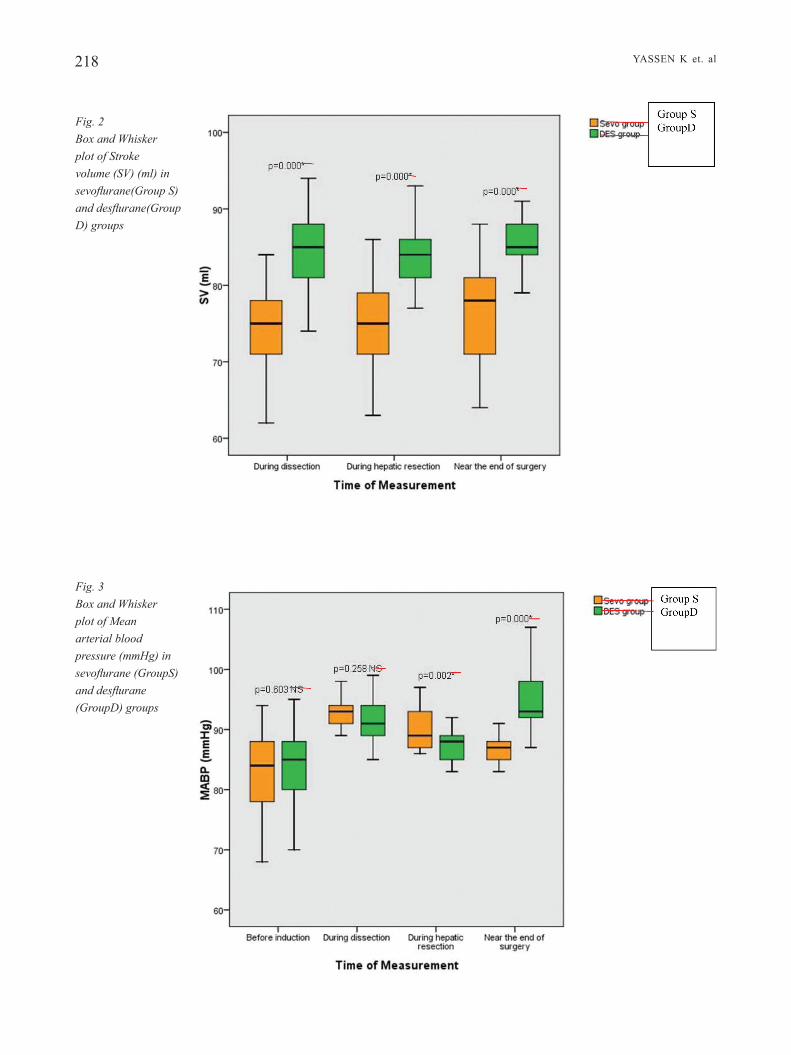
218 yassen K et. al
Fig. 3 Box and Whisker plot of Mean arterial blood pressure (mmHg) in sevoflurane (GroupS) and desflurane (GroupD) groups
Fig. 2 Box and Whisker plot of Stroke volume (SV) (ml) in sevoflurane(Group S) and desflurane(Group D) groups
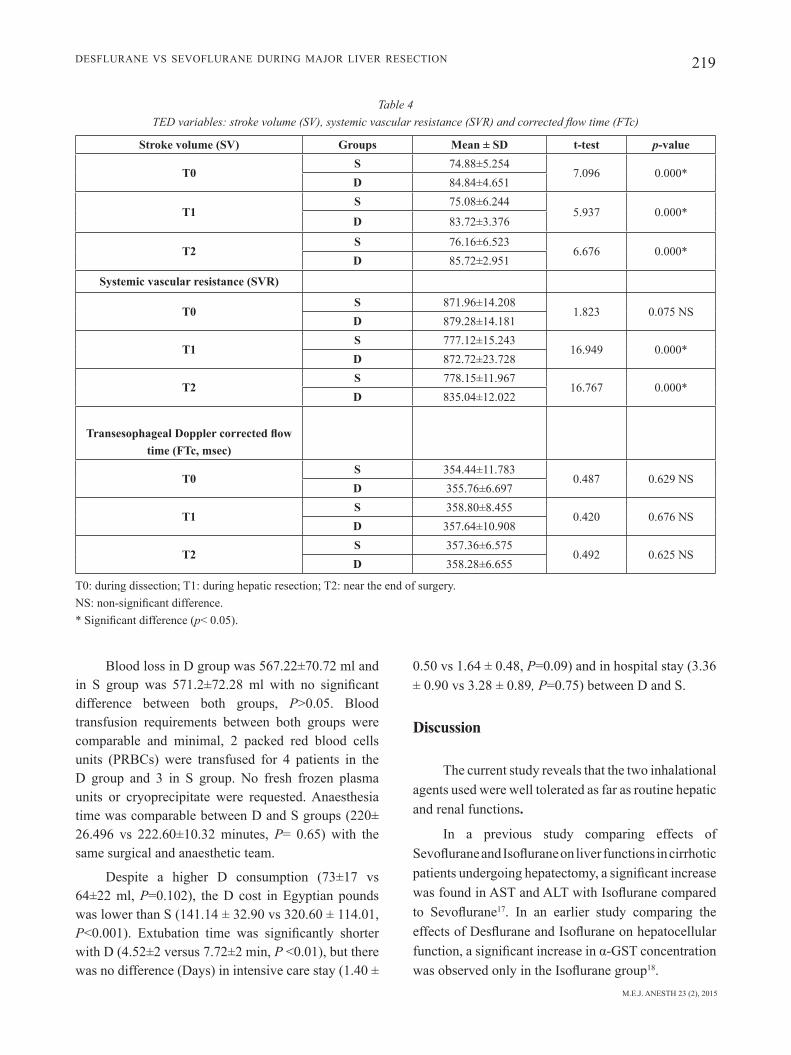
M.E.J. ANESTH 23 (2), 2015
219Desflurane vs sevoflurane During major liver resection
Blood loss in D group was 567.22±70.72 ml and in S group was 571.2±72.28 ml with no significant difference between both groups, P>0.05. Blood transfusion requirements between both groups were comparable and minimal, 2 packed red blood cells units (PRBCs) were transfused for 4 patients in the D group and 3 in s group. no fresh frozen plasma units or cryoprecipitate were requested. anaesthesia time was comparable between D and S groups (220± 26.496 vs 222.60±10.32 minutes, P= 0.65) with the same surgical and anaesthetic team.
Despite a higher D consumption (73±17 vs 64±22 ml, P=0.102), the D cost in Egyptian pounds was lower than S (141.14 ± 32.90 vs 320.60 ± 114.01, P<0.001). Extubation time was significantly shorter with D (4.52±2 versus 7.72±2 min, P <0.01), but there was no difference (Days) in intensive care stay (1.40 ±
0.50 vs 1.64 ± 0.48, P=0.09) and in hospital stay (3.36 ± 0.90 vs 3.28 ± 0.89, P=0.75) between D and S.
Discussion
the current study reveals that the two inhalational agents used were well tolerated as far as routine hepatic and renal functions.
in a previous study comparing effects of Sevoflurane and Isoflurane on liver functions in cirrhotic patients undergoing hepatectomy, a significant increase was found in AST and ALT with Isoflurane compared to Sevoflurane17. in an earlier study comparing the effects of Desflurane and Isoflurane on hepatocellular function, a significant increase in α-GST concentration was observed only in the Isoflurane group18.
Table 4 TED variables: stroke volume (SV), systemic vascular resistance (SVR) and corrected flow time (FTc)
Stroke volume (SV) Groups Mean ± SD t-test p-value
T0S 74.88±5.254
7.096 0.000*D 84.84±4.651
T1S 75.08±6.244
5.937 0.000*D 83.72±3.376
T2S 76.16±6.523
6.676 0.000*D 85.72±2.951
Systemic vascular resistance (SVR)
T0S 871.96±14.208
1.823 0.075 NSD 879.28±14.181
T1S 777.12±15.243
16.949 0.000*D 872.72±23.728
T2S 778.15±11.967
16.767 0.000*D 835.04±12.022
Transesophageal Doppler corrected flow time (FTc, msec)
T0S 354.44±11.783
0.487 0.629 NSD 355.76±6.697
T1S 358.80±8.455
0.420 0.676 NSD 357.64±10.908
T2S 357.36±6.575
0.492 0.625 NSD 358.28±6.655
t0: during dissection; t1: during hepatic resection; t2: near the end of surgery.NS: non-significant difference.* Significant difference (p< 0.05).

220 yassen K et. al
Desflurane, in particular, was expected to have the least effect due to its very little degradation and minimal excretion of organic or inorganic fluoride19,20, in contrast to Sevoflurane which is known to be biotransformed and metabolized by the liver into compound a that requires the kidneys for excretion; however in the present study the effects of Sevoflurane compared to Desflurane on perioperative renal and hepatic functions appear to be relatively similar as reflected by both routine renal and liver functions, including the more specific renal tubular monitor microalbuminuria provided that hemodynamic stability is maintained. this is in agreement with several earlier studies21,22.
gst is one of the most sensitive tests for detecting early hepatocellular damage. It offers significant clinical advantages over conventional aminotransferases for monitoring hepatocellular integrity. It has a short half-life of about 60 min, much shorter than the standard enzyme markers ALT (about 48 h) and AST (about 20 h). It is also predominantly found in the liver where it is uniformly distributed into the lobule in contrast with alt and ast that are found mainly within the periportal area. thus, substantial centrilobular necrosis can be accompanied by an increase in α-GST without a concomitant increase in serum aminotransferases23,24. in many studies, a disruption in the hepatocellular integrity with inhalation anaesthetic agents was observed only when the more specific hepatic marker, gst, was used25,26.
the changes in gst concentrations observed in our study in both groups was in agreement with the above two studies reflecting a derangement of the hepatocellular integrity from the combined effects of anaesthesia and surgical stress, together with injury to the liver cells during the surgical excision of the tumor. It also showed a more significant affection with Sevoflurane than Desflurane immediately postoperative. this will need further extensive studies with more patients.
AST and ALT present in hepatocytes can leak into the blood during the resection process. Unlike the present study, suttner sW et al27 and Kojs et al15 were able to demonstrate minimal effects when patients in both studies were exposed to Desflurane. in suttner s et al study the patients were elderly patients undergoing non-hepatic surgery and in the
second study by Kojs et al, the patients enrolled in his study where healthy donors undergo liver resection for living liver transplantation donation. few studies monitored the effect of Desflurane in cirrhotic patients undergoing liver resection. tao Km et al study28 is one of these studies among cirrhotic patients, they stated that hepatic inflow occlusion during the liver surgery may result in a transient ischemia period followed by reperfusion, and may initiate liver injury. in cirrhotic patients, the tolerance time to ischemia is much shorter and the outcome would hence be worse. in our study and in contrast to tao Km et al study, we were able to perform all the liver resections with no occlusion of the hepatic and portal blood flow (Pringle Maneuver) which could explain in part why there was no difference between both groups in our study as they were able to sustain the hepatic blood flow to the liver cells by maintaining a haemodynamic status of stability throughout the procedure. it is not only the anaesthetic choice that plays an important role in reducing the liver dysfunction but the surgical technique adopted by the surgeons also plays an important role together with haemodynmic stability. our results support the importance of a combined and mutual understanding between the anaesthesia management and the adopted surgical technique to achieve the appropriate level of protection to both the liver and kidneys. Avoiding the Pringle maneuver during the surgical procedure (no ischaemic reperfusion injury) and the preservation of the middle hepatic vein in all the patients contributed to a minimal perioperative blood transfusion requirements, this lead to no haemodynamic supportive therapy used and allowed for the use of less invasive techniques for monitoring as the trans-oesophageal doppler adopted in the current study. selective vascular occlusion of hepatic inflow was not adopted by the surgeons in our study, but instead the anterior parenchymal resection was used and this technique did not require significant reduction in the cvp6,29,30.
the haemodynamic changes demonstrated in the results section were found to be in favour with Desflurane compared to Sevoflurane based anaesthesia, this could be due to the better preservation of the systemic vascular resistance with desflurane when used to maintain the general anaesthetic status in contrast to Sevoflurane. Cirrhotic patients are known to be peripherally vasodilated as a result of their liver

M.E.J. ANESTH 23 (2), 2015
221Desflurane vs sevoflurane During major liver resection
disease, which necessitates the use of an anaesthetic technique with the least effect on their vascular tone. Sevoflurane resulted in a sustained decrease in SVR and this was associated with a decrease in maBp.
In a previous study by El Sharkawy O et al6 designed to monitor the haemodynamic changes among cirrhotic patients undergoing liver resection with teD, the authors were able to present data demonstrating significant haemodynamic changes that associate liver resection procedure itself, particularly in the immediate post-resection. Reporting an increase in sv and cardiac output as monitored by teD, together with an associated decrease in calculated svr despite stable and normal readings of both central venous pressure (CVP) and corrected flow time (FTc).
the present study demonstrated similar changes in svr and sv in both groups but with cardiac output increase only demonstrated with Desflurane. Similar changes were previously described also by niemann et al31 in patients with healthy livers undergoing the same procedure (major hepatic resection) for living donor liver transplantation with inhalation anaesthetic agent. in niemann et al study they had to inject indocyanine green and measure plasma levels with a pulse dye densitometry, not usually available in the operating theaters and which is still considered as a research tool. in contrast, the teD was used in our current study and was found to be easy to use and less invasive with the possible availability in operating suites.
the haemodynamic changes observed in this current study after hepatotomy could be due to the possible reduction in portal blood flow32 or to the release of various splanchnic mediators such as endotoxin, during liver surgery33 and changes in the levels of nitric oxide, a potent vasodilator, which could be elevated in response to endotoxin and cytokine release34. Boermeester, et al., found that these haemodynamic changes improved after the administration of endotoxin-neutralizing protein35.
the extubation time in this current study was enhanced by Desflurane as demonstrated by other similar studies, this may be due to the to the peculiar nature of Desflurane which enjoys a low blood/gas solubility coefficient and low metabolic rate which can reach to 0.02% of administered Desflurane that will
definitely shorten and enhance recovery36,37.
one of the limitations of this study was the small number of the patients included, this may be attributed to the restricted inclusion of only major liver resection procedures performed for cirrhotic patients of child a.
another limitation observed when the liver was mobilized during resection of hepatic tumors was the frequent requirement to reposition the Doppler probe. This can be considered as an important weak point in the teD monitoring system which needs frequent attention from the anaesthetist.
the inability to continue monitoring in this study with the TED post-extubation as it needs to be left nasally which is uncomfortable with a nasogatric tube in place in the other nostril and finally TED traces were also affected during the periods of diathermy application from temporary interferences.
In conclusion, Desflurane was found to offer better haemodynamic parameters, shorter and enhanced recovery at a lower cost when compared to Sevoflurane, but neither is clinically superior to the other with respect to their effects on liver and kidneys. Both Desflurane and Sevoflurane can be used safely during liver surgery in cirrhotic patients. the statistical difference in gst between both groups remains to be investigated further on a larger scale for more evidence based support and may be at different clinical scenarios as in association with major blood loss in cirrhotic patients when a difference could be of clinical importance. teD was able to present significant hemodynamic changes in association with the major liver resection procedure; however the use of the less invasive teD monitoring and the development of TED guided fluid management protocols for this population need to be further studied, particularly in comparison to the routinely used standard central venous catheter monitoring and fluid management protocols with special emphasis during and after major liver surgery.
Acknowledgement
I would like to express my thanks to Dr. El-sayed amr for his assistance in statistics.

222
References
1. MoHAMoud yA, MuMtAz gR, RioMe s, MilleR dW, Abu-RAddAd lJ: the epidemiology of hepatitis c virus in egypt: a systematic review and data synthesis. BMC Infectious Diseases; 13:288, 2013.
2. MeMon Mi, MeMon MA, HepAtitis C: an epidemiological review. Journal of Viral Hepatology; 9:84-100, 2002.
3. FRAnK C, MoHAMed MK, stRiCKlAnd gt, lAvAnCHy d, ARtHuR RR, MAgdeR ls, et Al: the role of parenteral antischistosomal therapy in the spread of hepatitis c virus in egypt. Lancet; 355:887-91, 2000.
4. HAssAn MM, zAgHloul As, el-seRAgg Hb, soliMAn o, pAtt yz, CHAppell Cl, beAsley Rp, HWAng ly: the role of hepatitis c in hepatocellular carcinoma: a case control study among egyptian patients. J Clin Gastroenterol; 33:123-126, 2001.
5. el-zAyAdi AR, bAdRAn HM, bARAKAt eM, AttiA Mel-d, sHAWKy s, MoHAMed MK, seliM o, sAeid A: hepatocellular carcinoma in egypt: a single center study over a decade. World J Gastroenterol; 11:5193-8, 2005.
6. el sHARKAWy o, ReFAAt e, ibRAHeeM A, et Al: transoesophageal Doppler compared to central venous pressure for perioperative hemodynamic monitoring and fluid guidance in liver resection. Saudi J Anaesth; 7(4):54-62, 2013.
7. Clus u, nieMunn, JoHn p, RobeRts, nunCy l, AsCbeR, und C, spenCeR y: Intraoperative hemodynamic and liver function in adult-to-adult living liver donors. Liver Transplantation; 8:1126-33, 2002.
8. bedAWy A, FAyed n, MoRAd W, MAdAny s, neMAtAlAH F, yAssen K: rotational thrombo elastometry and standard coagulation tests for hepatic patients undergoing major liver resection. J Anesth and Clin Research; 3(9):1-5, 2012.
9. AyAnoglu Ho, uluKAyA s, yuzeR y, toKAt y: anesthetic management and complications in living donor hepatectomy. Transplant Proc; 35:2970-3, 2003.
10. sHARMA J, bHise M, singH A, MeHtA y, tReHAn n: hemodynamic measurements after cardiac surgery: transesophageal Doppler versus pulmonary artery catheter. J Cardiothorac Vasc Anesth; 19:746-50, 2005.
11. KinCAid eH, Fly Mg, CHAng MC: noninvasive measurements of preload using esophageal Doppler are superior to pressure-based estimates in critically injured patients. Crit Care Med; 27:100, 1999.
12. tuRneR MA: Doppler-based hemodynamic monitoring: A minimally invasive alternative. AACN Clin Issues; 14:220-31, 2003.
13. singeR M, Allen MJ, Webb AR, bennett ed: effects of alterations in left ventricular filling, contractility and systemic vascular resistance on the ascending aortic blood velocity waveform of normal subjects. Crit Care Med; 19:1138-45, 1991.
14. sinClAiR s, JAMes s, singeR M: intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. BMJ; 315:909-12, 1997.
15. Ko Js, gWAK Ms, CHoi sJ, yAng M, KiM MJ, lee Jy, KiM gs, KWon CHd And JoH JW: The effects of desflurane and sevoflurane on hepatic and renal functions after right hepatectomy in living donors. Transplant International; 23:736-744, 2010.
16. Field A: sample size calculation. in: field a, editor. Discovering statistics using spss. 2 ed. london, california, new Delhi: sage Publications Ltd; p. 143-217, 2006.
17. nisHiyAMA t, FuJiMoto t, HAnAoKA K: a comparison of liver function after hepatectomy in cirrhotic patients Between Sevoflurane and Isoflurane in Anesthesia with Nitrous Oxide and
yassen K et. al
Epidural Block. Anesthesia & Analgesia; April, 98(4):990-3, 2004.18. sCHMidt CC, suttneR sW, pipeR sn, nAgel d, boldt J. comparison
of the effects of desflurane and isoflurane anaesthesia on hepatocellular function assessed by alpha glutathione S-transferase. Anaesthesia; Dec, 54(12):1207-11, 1999.
19. KAti i, teKin M, tAs A, RAgbetti C, ugRAs s: histopathological Effects of Desflurane on the Liver and the Kidney Using Light microscopy. Animal and Veterinary Advances; 9:1940-2, 2010.
20. Koblin dd: Characteristics and implications of desflurane metabolism and toxicity. Anesth Analg; 75:10-6, 1992.
21. Ko Js, gWAK Ms, CHoi sJ, KiM gs, KiM JA, yAng M, lee sM, CHo Hs, CHung is And KiM MH: The effects of desflurane and propofol-remifentanil on postoperative hepatic and renal functions after right hepatectomy in liver donors. Liver Transplantation; 14:1150-1158, 2008.
22. obAtA R, bito H, oHMuRA M, MoRiWAKi g, iKeuCHi y, KAtoH t, sAto s: The effects of prolonged low-flow sevoflurane anesthesia on renal and hepatic function. Anesth Analg; Nov, 91(5):1262-8, 2000.
23. beCKett gJ, HAyes Jd: Glutathione S-transferases: biomedical applications. Adv Clin Chem; 30:281-380, 1993.
24. HAyes pC, bouCHieR iA, beCKett gJ: Glutathione S-transferase in humans in health and disease. Gut; 32:813-818, 1991.
25. sCHMidt CC, suttneR sW, pipeR sn, nAgel d, boldt J: comparison of the effects of desflurane and isoflurane anaesthesia on hepatocellular function assessed by alpha glutathione S-transferase. Anaesthesia; Dec, 54(12):1207-11, 1999.
26. tiAnen p, lindgRen l, RosenbeRg pH: changes in hepatocellular integrity during and after desflurane or isofluraneanaesthesia in patients undergoing breast surgery. Br J Anaesth; Jan, 80(1):87-9, 1998.
27. suttneR sW, sCHMidt CC, boldt J, HüttneR i, KuMle b, pipeR sn: Low-flow desflurane and sevoflurane anesthesia minimally affect hepatic integrity and function in elderly patients. Anesth Analg; jul, 91(1):206-12, 2000.
28. tAo KM, yAng lQ, liu yt, tAo y, song JC, Wu FX, et Al: volatile anesthetics might be more beneficial than propofol for postoperative liver function in cirrhotic patients receiving hepatectomy. Med Hypotheses; Dec, 75(6):555-7, 2010.
29. RedAi i, eMond J, bRentJens t: anesthetic considerations during liver surgery. Surg Clin North Am; Apr, 84(2):401-11, 2004.
30. CHen Cl, CHen ys, de villA vH, WAng CC, lin Cl, goto s, et Al: minimal blood loss living donor hepatectomy. Transplantation; jun 27, 69(12):2580-6, 2000.
31. nieMAnn Cu, RobeRts Jp, AsCHeR nl, yost Cs: intraoperative hemodynamics and liver function in adult-to-adult living liver donors. Liver Transpl; Dec, 8(12):1126-32, 2002.
32. KAWAsAKi t, MoRiyAsu F, KiMuRA t, soMedA H, FuKudA y, ozAWA K: Changes in portal blood flow consequent to partial hepatectomy: Doppler estimation. Radiology; Aug, 180(2):373-7, 1991.
33. boeRMeesteR MA, stRAAtsbuRg iH, HoudiJK Ap, MeyeR C, FRedeRiKs WM, WesdoRp Ri, et Al: Endotoxin and interleukin-1 related hepatic inflammatory response promotes liver failure after partial hepatectomy. Hepatology; Nov, 22(5):1499-506, 1995.
34. pAlMeR RM: the discovery of nitric oxide in the vessel wall. a unifying concept in the pathogenesis of sepsis. Arch Surg; apr, 128(4):396-401, 1993.
35. boeRMeesteR MA, HoudiJK Ap, stRAAtsbuRg iH, vAn nooRden CJ,

M.E.J. ANESTH 23 (2), 2015
223Desflurane vs sevoflurane During major liver resection
recovery characteristics. The Internet Journal of Anesthesiology; (9)(1), 2005.
37. KAuR A, JAin AK, seHgAl R, sood J: hemodynamics and early recovery characteristics of desflurane versus sevoflurane in bariatric surgery. J Anaesthesiol Clin Pharmacol; 29:36-40, 2013.
vAn leeuWen pA: Organ blood flow after partial hepatectomy in rats: modification by endotoxin-neutralizing bactericidal/permeability-increasing protein (rBPI23). J Hepatol; Nov, 31(5):905-12, 1999.
36. geRgin s, CeviK b, yildiRiM g, CiplAKligil e, ColAKoglu s: SevofluraneVs Desflurane: Haemodynamic Parameters And


225 M.E.J. ANESTH 23 (2), 2015
Myocardial oxygenation during acute norMovoleMic HeModilution: iMpact
of Hypocapnic alkalosis
Edward a. Czinn*, M. raMEz SalEM** and GEorGE J. CryStal***
Abstract
Background: Increases in myocardial blood flow preserve myocardial oxygenation during moderate acute normovolemic hemodilution. Hypocapnic alkalosis (HA) is known to cause coronary vasoconstriction and increase hemoglobin-oxygen affinity. We evaluated whether these effects would compromise myocardial oxygenation during hemodilution.
Methods: Eighteen anesthetized dogs were studied. Myocardial blood flow (MBF) was measured with radioactive microspheres. Arterial and coronary sinus samples were analyzed for oxygen content and plasma lactate. Myocardial oxygen supply, oxygen uptake, and lactate uptake were calculated. HA (PaCO2, 23±2 (SD); pHa, 7.56±0.03) was induced by removal of dead space tubing at baseline (n=8) and during hemodilution (n = 10), with hematocrit at 43 ± 4% and 19 ± 2 %, respectively.
Results: Hemodilution during normocapnia caused decreases in arterial oxygen content (19.9 ± 2.4 to 9.3 ± 1.2 ml/100; P < 0.05) and the coronary arteriovenous O2 difference (13.0 ± 3.0 to 6.4 ± 0.9 ml/100ml; P < 0.05). MBF increased (52 ± 12 to 111 ± 36 ml/min/100g; P < 0.05) to maintain myocardial oxygen supply and oxygen uptake. Myocardial lactate uptake increased (31 ± 19 to 68 ± 35 µeq/min/100g; P < 0.05). At normal hematocrit, HA decreased MBF (57 ± 18 to 45 ± 10 ml/min/100; P < 0.05), implying vasoconstriction, accompanied by decreased myocardial oxygen supply. These myocardial effects of HA were not apparent during hemodilution. HA did not alter myocardial lactate uptake during hemodilution.
Conclusion: When HA was induced during hemodilution, its ability to cause coronary vasoconstriction was lost, and myocardial oxygenation remained well preserved.
Keywords: anemia; carbon dioxide; coronary circulation; dog; myocardial blood flow: myocardial oxygen uptake; radioactive microspheres.
* MD, Medical Director, Department of Anesthesiology, Broward Health Medical Center, Fort Lauderdale, FL; Clinical Assistant Professor of Anesthesiology, Florida International University-Herbert Wertheim College of Medicine, Miami, FL.
** MD, Emeritus Chairman, Department of Anesthesiology, Advocate Illinois Masonic Medical, Center; Clinical Professor, Department of Anesthesiology, University of Illinois College of Medicine, Chicago, IL.
*** PhD, Professor, Department of Anesthesiology, Advocate Illinois Masonic Medical Center, and Departments of Anesthesiology and of Physiology and Biophysics, University of Illinois College of Medicine, Chicago, IL.
Department of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL; Departments of Anesthesiology and of Physiology and Biophysics, University of Illinois College of Medicine, Chicago, IL, Department of Anesthesiology, Broward Health Medical Center, Fort Lauderdale, Fl.
Corresponding author: George J. Crystal, PhD, Department of Anesthesiology, Advocate Illinois Masonic Medical Center, 836 West Wellington Avenue, Chicago, Illinois 60657 USA. Tel: (773) 296-5375; Fax: (773) 296-5362. E-mail: [email protected]

226 GEOrGE J. CrySTAL et. al
Introduction
The increased frequency of complex surgical procedures with extensive blood loss, the risk of transmission of blood-borne antigens during donor blood transfusion, the high cost of transfusion therapy, and shortages at blood banks have led to the implementation of more restrictive transfusion triggers1,2. This has increased the number of hemodiluted patients in the perioperative period.
Under baseline conditions, the left ventricle extracts approximately 70-75% of delivered oxygen, resulting in a limited oxygen extraction reserve3. Consequently, in situations of low hemoglobin, the myocardium must rely primarily on increases in blood flow to offset the induced decreases in arterial oxygen content. Experimentally, this compensatory mechanism is adequate for maintaining myocardial oxygenation as long as hematocrit ≥ 10%, as evidenced by stable indices of global cardiac performance, e.g., aortic pressure and pulmonary capillary wedge pressure, an unchanged value for coronary sinus PO2 (an estimate of myocardial PO2
4), and continued lactate extraction suggesting absence of anaerobic metabolism and of myocardial ischemia5,6.
Intentional (i.e., to reduce intracranial pressure in head trauma) or unintentional (e.g., excessive mechanical ventilation) hypocapnic alkalosis is common perioperatively and in critically ill patients7,8. Studies in anesthetized dogs9-12 and conscious humans13,14 have demonstrated that hypocapnic alkalosis can cause coronary vasoconstriction and a decrease in myocardial blood flow. This decrease in myocardial blood flow was accompanied by an increase in oxygen extraction, suggesting that it is due, at least in part, to direct coronary vasoconstriction15. Hypocapnic alkalosis also causes a leftward shift of the oxyhemoglobin dissociation curve, increasing hemoglobin oxygen affinity, and thus impairing diffusion of oxygen into the tissue16.
Although compensatory coronary vascular responses may maintain myocardial oxygenation during hemodilution under normocapnic conditions, these responses could be compromised when hypocapnic alkalosis is co-existent. The current canine study tested the hypothesis that hypocapnic alkalosis
impairs the maintenance of myocardial oxygenation under hemodiluted conditions.
Methods
The study was conducted after approval from the Institutional Animal research Committee of the University of Illinois at Chicago. Experiments were performed on 18 adult, healthy, mongrel dogs of either sex (weight range 21-24 kg). Anesthesia was induced with an intravenous bolus injection of thiopental (30 mg/kg). After tracheal intubation, anesthesia was maintained by controlled ventilation with 0.9 % (1 MAC) halothane in oxygen using a semi-closed circular system. Initially, dead space tubing (volume of 300 ml) was added to the endotracheal tube with tidal volume and ventilator rate adjusted to establish PaCO2 at a physiological value (approximately 40 mmHg). This volume of dead space was demonstrated in preliminary studies to reduce arterial PCO2 by approximately 50 % when removed. Values for PO2, PCO2, and pH in arterial blood samples were obtained electrometrically (model 413, Instrumentation Laboratories, Lexington, MA). Sodium bicarbonate solution was given as necessary to correct metabolic acidosis. Hematocrit of blood samples was determined volumetrically. Core body temperature was monitored and maintained at 38° C with a heating pad, warmed intravenous fluids, and warming lights.
Polyethylene cannulas were inserted into 1) the thoracic aorta for monitoring arterial blood pressure and for obtaining samples of arterial blood for analysis, 2) the right femoral vein for IV injections, and 3) the left femoral vein and left femoral artery for isovolemic exchange of whole blood with 5 % dextran solution. A left thoracotomy was performed in the fourth intercostal space and the pericardium was incised to expose the heart. A small polyethylene catheter was inserted into the left atrium via the left atrial appendage for injecting radioactive microspheres. Heparin, 300 U/kg, was administered IV post-surgically to prevent coagulation in exchange circuits. Arterial pressure was measured with a Statham transducer (model P23ID, Gould, Cleveland, Ohio), averaged electronically, and recorded (model 2800S, Gould, Cleveland, Ohio). A non-cannulating electromagnetic flow transducer was

M.E.J. ANESTH 23 (2), 2015
227Myocardial oxygenation in Hypocapnia and HeModilution
placed around the ascending aorta to measure cardiac output (less coronary blood flow).
Hypocapnic alkalosis was demonstrated in our preliminary studies and in previously published reports9,10 to cause a decrease in arterial pressure. Hypotension can influence myocardial blood flow by reducing perfusion pressure and by altering determinants of cardiac work demand, i.e., afterload and heart rate15. To avoid this potentially confounding variable, a controlled pressure reservoir was used17. Translocation of blood from the reservoir to the animal’s circulation stabilized arterial pressure during hypocapnic alkalosis.
Experimental Measurements
Regional myocardial blood flow. regional myocardial blood flow was measured with the radioactive microsphere technique, as described in detail previously6. This technique is based on the principle that microspheres injected into the left atrium are well mixed in the left ventricular output, that they distribute to body tissues in proportion to flow rate, and that they remain permanently entrapped18. After the final injection of microspheres, the heart was stopped with potassium chloride and excised, and full thickness myocardial samples were obtained from the left and right ventricular free walls. The samples from the left ventricular wall were cut into thirds transmurally and those from the right ventricular wall into halves to yield regional myocardial samples. A value for regional myocardial blood flow (ml/min/100g) was determined for each tissue sample by comparing its radioactivity, assessed with a gamma scintillation counter, to that in a reference arterial blood sample withdrawn at a known rate at the time of microsphere injection. A value for mean transmural blood flow was calculated in each ventricular wall by averaging the values for regional myocardial blood flow. An endocardial-to-epicardial flow ratio was calculated by dividing the value for myocardial blood flow in the subendocardial sample by that in the subepicardial sample.
Myocardial oxygen uptake. A polyethylene cannula was positioned in the coronary sinus through the right jugular vein and the right atrium for collecting samples of venous effluent from the left
ventricle. One milliliter blood samples were collected anaerobically from the aorta and the coronary sinus to determine the left coronary arteriovenous oxygen difference. Myocardial oxygen extraction (EO2; %) was determined by dividing the arteriovenous oxygen difference by the oxygen content of the aortic blood.
Myocardial oxygen uptake (MVO2; ml/min/100g) for the left ventricle was calculated from the Fick equation: MVO2 = MBF x [(a - v) O2 difference/100], where MBF is mean transmural myocardial blood flow for the left ventricle (ml/min/100g) and the (a-v) O2 difference is the coronary arteriovenous oxygen difference (ml/100 ml). Oxygen supply to the left and right ventricles was calculated by multiplying the values for arterial oxygen content and the respective myocardial blood flow. Systemic oxygen supply was calculated by multiplying the values for arterial oxygen content and cardiac output.
Myocardial lactate extraction and uptake. paired 1-ml blood samples were obtained from the aorta and coronary sinus and analyzed for plasma lactate concentration using an enzymatic method (Paramax Analytical System, Baxter, Irvine, CA). These values were used to calculate percent myocardial lactate extraction for the left ventricle. Myocardial lactate uptake for the left ventricle was calculated by substituting the coronary arteriovenous difference for plasma lactate concentration and the plasma flow (determined from blood flow and hematocrit) into the Fick equation.
Experimental Protocol
The dogs were divided into two groups. In the Control Group (n = 8), after baseline hemodynamic measurements were obtained, hypocapnic alkalosis was induced by removal of the dead space tubing. This approach avoided the hemodynamic instabilities, e.g., reductions in cardiac output and systemic arterial pressure, which characterize increases in mechanical ventilation19. After approximately 30 min, when paco2 stabilized at a minimal level (approximately 20 mmHg), hemodynamic measurements were repeated. In the Hemodilution Group (n = 10), after baseline measurements, isovolemic hemodilution was produced by removing blood from the left femoral artery at a
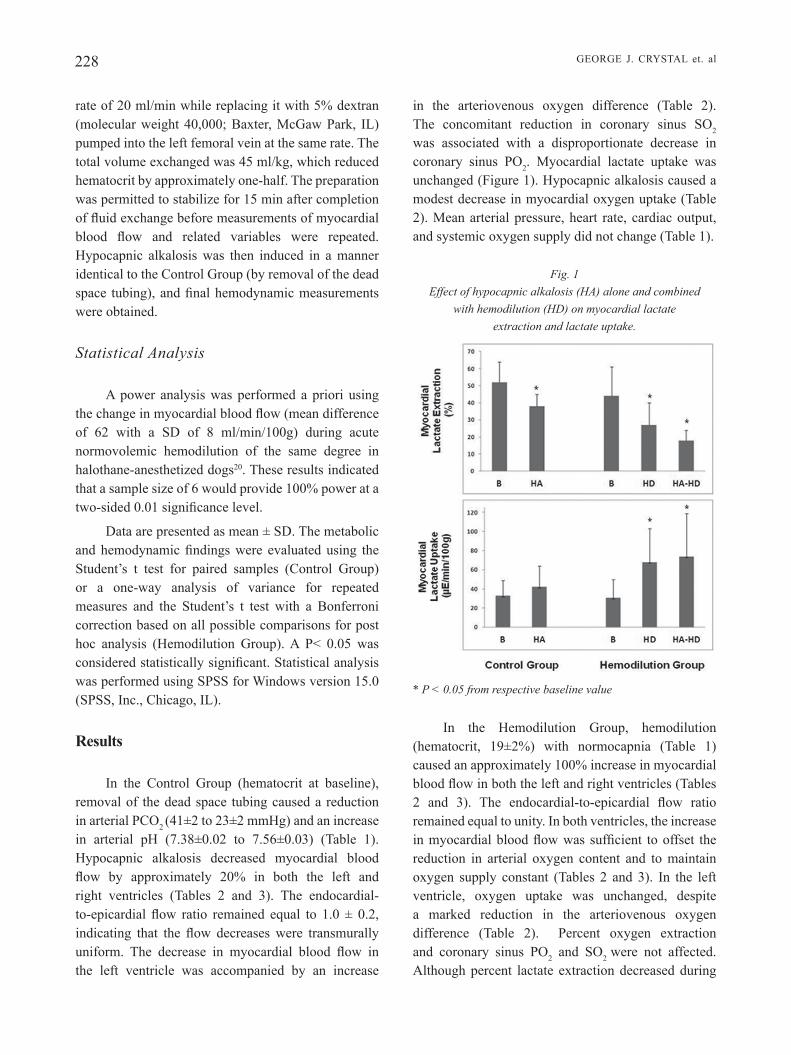
228 GEOrGE J. CrySTAL et. al
rate of 20 ml/min while replacing it with 5% dextran (molecular weight 40,000; Baxter, McGaw Park, IL) pumped into the left femoral vein at the same rate. The total volume exchanged was 45 ml/kg, which reduced hematocrit by approximately one-half. The preparation was permitted to stabilize for 15 min after completion of fluid exchange before measurements of myocardial blood flow and related variables were repeated. Hypocapnic alkalosis was then induced in a manner identical to the Control Group (by removal of the dead space tubing), and final hemodynamic measurements were obtained.
Statistical Analysis
A power analysis was performed a priori using the change in myocardial blood flow (mean difference of 62 with a SD of 8 ml/min/100g) during acute normovolemic hemodilution of the same degree in halothane-anesthetized dogs20. These results indicated that a sample size of 6 would provide 100% power at a two-sided 0.01 significance level.
Data are presented as mean ± SD. The metabolic and hemodynamic findings were evaluated using the Student’s t test for paired samples (Control Group) or a one-way analysis of variance for repeated measures and the Student’s t test with a Bonferroni correction based on all possible comparisons for post hoc analysis (Hemodilution Group). A P< 0.05 was considered statistically significant. Statistical analysis was performed using SPSS for Windows version 15.0 (SPSS, Inc., Chicago, IL).
Results
In the Control Group (hematocrit at baseline), removal of the dead space tubing caused a reduction in arterial PCO2 (41±2 to 23±2 mmHg) and an increase in arterial pH (7.38±0.02 to 7.56±0.03) (Table 1). Hypocapnic alkalosis decreased myocardial blood flow by approximately 20% in both the left and right ventricles (Tables 2 and 3). The endocardial-to-epicardial flow ratio remained equal to 1.0 ± 0.2, indicating that the flow decreases were transmurally uniform. The decrease in myocardial blood flow in the left ventricle was accompanied by an increase
in the arteriovenous oxygen difference (Table 2). The concomitant reduction in coronary sinus SO2
was associated with a disproportionate decrease in coronary sinus PO2. Myocardial lactate uptake was unchanged (Figure 1). Hypocapnic alkalosis caused a modest decrease in myocardial oxygen uptake (Table 2). Mean arterial pressure, heart rate, cardiac output, and systemic oxygen supply did not change (Table 1).
Fig. 1 Effect of hypocapnic alkalosis (HA) alone and combined
with hemodilution (HD) on myocardial lactate extraction and lactate uptake.
* P < 0.05 from respective baseline value
In the Hemodilution Group, hemodilution (hematocrit, 19±2%) with normocapnia (Table 1) caused an approximately 100% increase in myocardial blood flow in both the left and right ventricles (Tables 2 and 3). The endocardial-to-epicardial flow ratio remained equal to unity. In both ventricles, the increase in myocardial blood flow was sufficient to offset the reduction in arterial oxygen content and to maintain oxygen supply constant (Tables 2 and 3). In the left ventricle, oxygen uptake was unchanged, despite a marked reduction in the arteriovenous oxygen difference (Table 2). Percent oxygen extraction and coronary sinus PO2 and so2 were not affected. Although percent lactate extraction decreased during
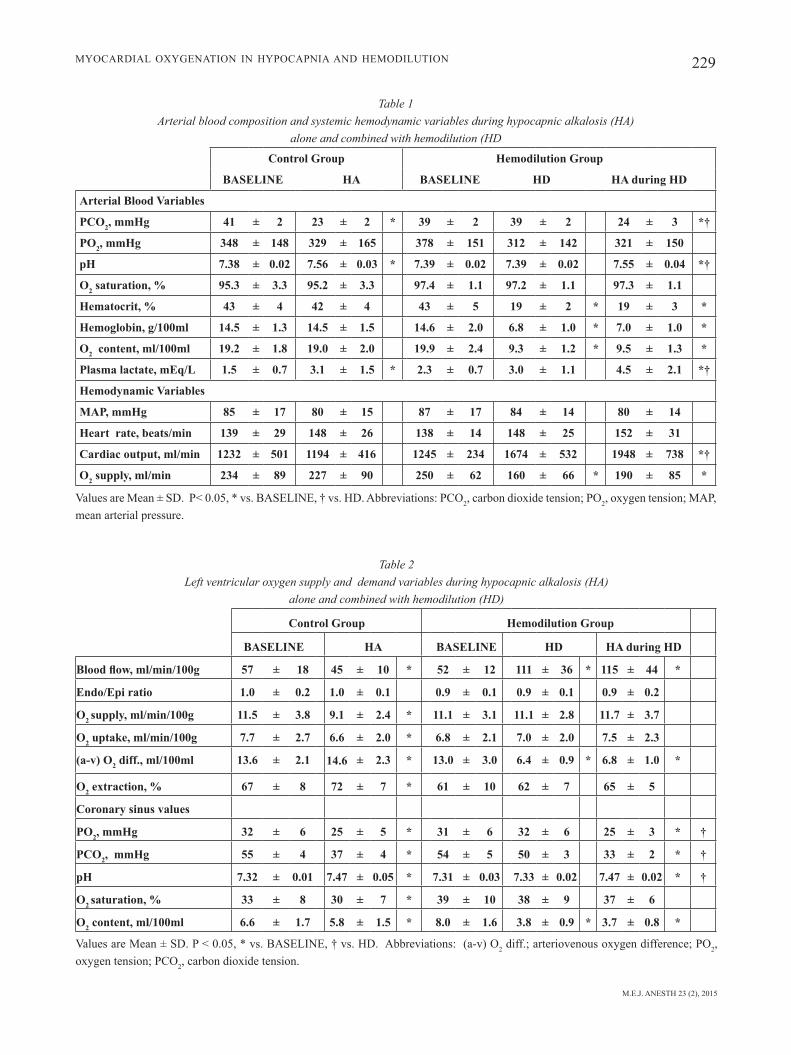
M.E.J. ANESTH 23 (2), 2015
229Myocardial oxygenation in Hypocapnia and HeModilution
Table 1 Arterial blood composition and systemic hemodynamic variables during hypocapnic alkalosis (HA)
alone and combined with hemodilution (HD
Control Group Hemodilution Group
BASELINE HA BASELINE HD HA during HD
Arterial Blood Variables
PCO2, mmHg 41 ± 2 23 ± 2 * 39 ± 2 39 ± 2 24 ± 3 *†
PO2, mmHg 348 ± 148 329 ± 165 378 ± 151 312 ± 142 321 ± 150
pH 7.38 ± 0.02 7.56 ± 0.03 * 7.39 ± 0.02 7.39 ± 0.02 7.55 ± 0.04 *†
O2 saturation, % 95.3 ± 3.3 95.2 ± 3.3 97.4 ± 1.1 97.2 ± 1.1 97.3 ± 1.1
Hematocrit, % 43 ± 4 42 ± 4 43 ± 5 19 ± 2 * 19 ± 3 *
Hemoglobin, g/100ml 14.5 ± 1.3 14.5 ± 1.5 14.6 ± 2.0 6.8 ± 1.0 * 7.0 ± 1.0 *
O2 content, ml/100ml 19.2 ± 1.8 19.0 ± 2.0 19.9 ± 2.4 9.3 ± 1.2 * 9.5 ± 1.3 *
Plasma lactate, mEq/L 1.5 ± 0.7 3.1 ± 1.5 * 2.3 ± 0.7 3.0 ± 1.1 4.5 ± 2.1 *†
Hemodynamic Variables
MAP, mmHg 85 ± 17 80 ± 15 87 ± 17 84 ± 14 80 ± 14
Heart rate, beats/min 139 ± 29 148 ± 26 138 ± 14 148 ± 25 152 ± 31
Cardiac output, ml/min 1232 ± 501 1194 ± 416 1245 ± 234 1674 ± 532 1948 ± 738 *†
O2 supply, ml/min 234 ± 89 227 ± 90 250 ± 62 160 ± 66 * 190 ± 85 *
Values are Mean ± SD. P< 0.05, * vs. BASELINE, † vs. HD. Abbreviations: PCO2, carbon dioxide tension; PO2, oxygen tension; MAP, mean arterial pressure.
Table 2 Left ventricular oxygen supply and demand variables during hypocapnic alkalosis (HA)
alone and combined with hemodilution (HD)
Control Group Hemodilution Group
BASELINE HA BASELINE HD HA during HD
Blood flow, ml/min/100g 57 ± 18 45 ± 10 * 52 ± 12 111 ± 36 * 115 ± 44 *
Endo/Epi ratio 1.0 ± 0.2 1.0 ± 0.1 0.9 ± 0.1 0.9 ± 0.1 0.9 ± 0.2
O2 supply, ml/min/100g 11.5 ± 3.8 9.1 ± 2.4 * 11.1 ± 3.1 11.1 ± 2.8 11.7 ± 3.7
O2 uptake, ml/min/100g 7.7 ± 2.7 6.6 ± 2.0 * 6.8 ± 2.1 7.0 ± 2.0 7.5 ± 2.3
(a-v) O2 diff., ml/100ml 13.6 ± 2.1 14.6 ± 2.3 * 13.0 ± 3.0 6.4 ± 0.9 * 6.8 ± 1.0 *
O2 extraction, % 67 ± 8 72 ± 7 * 61 ± 10 62 ± 7 65 ± 5
Coronary sinus values
PO2, mmHg 32 ± 6 25 ± 5 * 31 ± 6 32 ± 6 25 ± 3 * †
PCO2, mmHg 55 ± 4 37 ± 4 * 54 ± 5 50 ± 3 33 ± 2 * †
pH 7.32 ± 0.01 7.47 ± 0.05 * 7.31 ± 0.03 7.33 ± 0.02 7.47 ± 0.02 * †
O2 saturation, % 33 ± 8 30 ± 7 * 39 ± 10 38 ± 9 37 ± 6
O2 content, ml/100ml 6.6 ± 1.7 5.8 ± 1.5 * 8.0 ± 1.6 3.8 ± 0.9 * 3.7 ± 0.8 *
Values are Mean ± SD. P < 0.05, * vs. BASELINE, † vs. HD. Abbreviations: (a-v) O2 diff.; arteriovenous oxygen difference; PO2, oxygen tension; PCO2, carbon dioxide tension.

230
constant, the increase in myocardial blood flow was the result of a decrease in coronary vascular resistance. Two factors can theoretically account for the decrease in coronary vascular resistance: 1) coronary vasodilation in response to reduced arterial oxygen content, and 2) reduced blood viscosity21. Hemodilution has been demonstrated to cause a reduction in the coronary vasodilator reserve in both the left and right ventricles, as indicated by diminished reactive hyperemic responses5,6. These findings provided evidence that coronary vasodilation was integral to the hemodilution-related decrease in coronary vascular resistance. The inability of hemodilution to raise peak reactive hyperemic flow argued against an influence for reduced blood viscosity as an explanation for this response5,6.
The increases in myocardial blood flow were proportional to the induced decreases in hemoglobin concentration (and thus arterial oxygen content), which maintained oxygen supply in both ventricles at the baseline level. In the left ventricle (where samples of venous effluent were available), the increases in myocardial blood flow during hemodilution completely offset the decreases in the arteriovenous oxygen difference, and thus maintained oxygen uptake, percent oxygen extraction, coronary sinus oxygen saturation, and coronary sinus PO2 constant. These findings were evidence that local metabolic control mechanisms were effective in matching the extent of coronary vasodilation to the prevailing myocardial oxygen demands15. The continued, and, in fact, increased uptake of lactate, was an indication
hemodilution, presumably due to the increased flow rate, myocardial lactate uptake increased (Figure 1). The mean value for cardiac output was greater during hemodilution compared with baseline, but this did not quite achieve statistical significance (P = 0.07; Table 1). Because the increase in cardiac output during hemodilution was much less than proportional to the reduction in arterial oxygen content, systemic oxygen supply decreased (Table 1).
In contrast to findings with hematocrit at baseline, hypocapnic alkalosis during hemodilution did not alter myocardial blood flow, myocardial oxygen supply, the coronary arteriovenous oxygen difference, or coronary sinus SO2; however, coronary sinus PO2 again decreased (all Table 2). Myocardial lactate uptake remained at the increased level observed during hemodilution prior to hypocapnic alkalosis (Figure 1). Hypocapnic alkalosis during hemodilution caused an increase in cardiac output, which was associated with visible movement of blood from the controlled pressure reservoir into the animal’s circulation (Table 1). Mean arterial pressure was constant during hemodilution alone and combined with hypocapnic alkalosis.
Discussion
In this study, we observed that hemodilution caused a transmurally-uniform increase in myocardial blood flow in both ventricular walls, a finding in agreement with previous investigations5. Since perfusion pressure (arterial pressure) was maintained
GEOrGE J. CrySTAL et. al
Table 3 Right ventricular blood flow and oxygen supply (both in ml/min/100g) during hypocapnic alkalosis alone (HA)
and combined with hemodilution (HD) .
Control Group Hemodilution Group
BASELINE HA BASELINE HD HA during HD
Blood flow 40 ± 8 33 ± 6 * 38 ± 17 82 ± 30 * 90 ± 44 *
Endo/Epi ratio 1.0 ± 0.2 1.0 ± 0.1 1.0 ± 0.1 0.9 ± 0.2 1.0 ± 0.2
O2 Supply 8.2 ± 2.0 6.7 ± 1.5 * 8.0 ± 3.9 8.2 ± 2.5 9.0 ± 3.4
Values are Mean ± SD. * P < 0.05 from BASELINE.

M.E.J. ANESTH 23 (2), 2015
231Myocardial oxygenation in Hypocapnia and HeModilution
that myocardial oxygenation remained adequate at the mitochondrial level3,22. The increase in lactate uptake during hemodilution presumably reflected its increased delivery at a higher flow rate and the preference of the myocardium for lactate as a substrate for energy metabolism23.
In contrast to findings obtained in the myocardium, the increases in blood flow in the systemic circulation, i.e., cardiac output, during hemodilution were small and insufficient to avert a decline in systemic oxygen supply. Nevertheless, previous studies have demonstrated that systemic oxygen uptake is maintained because of the recruitment of an oxygen extraction reserve, which results in decreases in both mixed venous oxygen saturation and PO2
5. The reduced values for mixed venous PO2 during hemodilution reflected decreases in the aggregate PO2 of the body tissues4. However, arterial lactate concentration remained unchanged, which suggested absence of widespread anaerobic metabolism.
Hypocapnic alkalosis with hematocrit normal caused an approximate 20%, transmurally-uniform, decrease in myocardial blood flow in both the left and right ventricles, which, in the presence of controlled perfusion pressure, reflected coronary vasoconstriction. These findings are in keeping with data obtained in the dog9-12 and conscious man13,14. In the left ventricle the coronary vasoconstriction could be attributed, in part, to the action of local metabolic mechanisms responding to a decrease, albeit modest, in myocardial oxygen uptake15. The latter effect was presumably the result of a decrease in myocardial contractility due to chemoreflex-mediated reduction in sympathetic drive24,25. The predominant coronary vasoconstrictor mechanism operating during hypocapnic alkalosis was a directly induced increase in vasomotor tone. The magnitude of this vasoconstriction was reflected in the degree to which hypocapnic alkalosis caused an imbalance between myocardial oxygen supply and demand, that is, in the increases in oxygen extraction and the resultant decreases in coronary sinus oxygen saturation and PO2
15. The increased oxygen extraction during hypocapnic alkalosis required a disproportionate reduction in coronary PO2, reflecting a leftward shift of the oxyhemoglobin dissociation curve. However, it is important to note that hypocapnic alkalosis did
not reduce myocardial lactate uptake or convert it to production, which suggested that intramyocardial po2 remained adequate for unimpaired oxidative metabolism3,22.
We observed that the coronary vasoconstrictor effect of hypocapnic alkalosis disappeared during hemodilution. The increase in myocardial blood flow during hemodilution remained intact and able to compensate fully for the reduction in the arteriovenous oxygen difference, and thus to maintain myocardial oxygen uptake. Adequate tissue oxygenation was implied by continued and undiminished lactate uptake. Apparently the local metabolic vasodilating factors operating during hemodilution were sufficiently potent to prevent the coronary vasoconstriction by hypocapnic alkalosis. In contrast to findings during normal hematocrit, a decrease in myocardial uptake (and the accompanying metabolic coronary vasoconstriction) during hypocapnic alkalosis was not observed in the presence of hemodilution. This may be due to the inability of hypocapnic alkalosis to reduce cardiac sympathetic tone when it was at a heightened state during hemodilution26.
Case et al.12 showed in anesthetized dogs that extreme hyperventilation (PaCO2, 11±1; pHa, 7.74± 0.01 mmHg) with hematocrit normal caused severe coronary vasoconstriction, as reflected in coronary sinus PO2 values of less than 9 mmHg with a corresponding myocardial oxygen extraction of nearly 90%. reductions in coronary sinus PO2 of this magnitude are associated with insufficient myocardial oxygenation and lactate production22. The findings from Case et al. indicate that extreme hyperventilation may be risky in any patient, regardless of hematocrit.
Several methodological issues warrant address. Since anesthetic drugs may have different effects on baseline vascular tone, vascular reactivity, and the determinants of myocardial oxygen demand, it is conceivable that the responses to hemodilution and/or hypocapnic alkalosis would differ if an anesthetic other than halothane were used. An Fio2 equal to 1.0 was used to ensure that arterial PO2 was sufficient to fully saturate hemoglobin. The large variation in the arterial PO2 values within each condition reflects differences in the physiological status of the lungs of the dogs and the difference in their ability to tolerate

232 GEOrGE J. CrySTAL et. al
general anesthesia, a thoracotomy, and invasive surgery. However, the average arterial PO2 values were comparable across all treatment conditions. Previous canine studies have demonstrated that hyperoxia can be a coronary vasoconstrictor15, which in conscious dogs has been shown to cause an 18% decrease in myocardial blood flow27. The influence of this factor should be less in the current study because the increases in arterial PO2 were smaller (approximately 300 vs. 500 mmHg). The induced reduction in hematocrit was to a value equivalent to the suggested “transfusion trigger” of 7g/100 ml and thus approximated the most severe degree of hemodilution likely to be encountered clinically. It is possible that the level of hypocapnic alkalosis that we tested would have been detrimental to myocardial oxygenation if hematocrit were reduced further.
In conclusion, we demonstrated that moderate hypocapnic alkalosis did not compromise myocardial oxygenation either in the absence or presence of hemodilution. The current findings pertain strictly to the specific conditions of this study. An extrapolation to human patients should be made only with caution. It would be inappropriate to apply our findings in the normal canine coronary circulation to the patient who presents with conditions, such as coronary atherosclerosis, which may alter the responsiveness of the coronary circulation to hypocapnic alkalosis and hemodilution.
Acknowledgment
The authors thank Dana Villines, MA, for her expert statistical assistance.

M.E.J. ANESTH 23 (2), 2015
233Myocardial oxygenation in Hypocapnia and HeModilution
References
1. CarSon Jl, Hill S, CarlESS P, HEbErt P, HEnry d: Transfusion triggers: a systematic review of the literature. Transfus Med Rev; 16:187-99, 2002.
2. VaMVakaS EC, blaJCHMan Ma: Transfusion-related mortality: the ongoing risks of allogeneic blood transfusion and the available strategies for their prevention. Blood; 113:3406-17, 2009.
3. wEbEr kt, JaniCki JS: The metabolic demand and oxygen supply of the heart: physiologic and clinical considerations. Am J Cardiol; 44:722-9, 1979.
4. tEnnEy SM: A theoretical analysis of the relationship between venous blood and mean tissue oxygen pressures. Respir Physiol; 20:283-96, 1974.
5. CryStal GJ, kiM SJ, SalEM Mr: right and left ventricular O2 uptake during hemodilution and beta-adrenergic stimulation. Am J Physiol; 265:H1769-77, 1993.
6. lEVy PS, kiM SJ, ECkEl Pk, CHaVEz r, iSMail EF, Gould Sa, SalEM Mr, CryStal GJ: Limit to cardiac compensation during acute isovolemic hemodilution: influence of coronary stenosis. Am J Physiol; 265:H340-9, 1993.
7. CurlEy G, laFFEy JG, kaVanaGH bP: Bench-to-bedside review: carbon dioxide. Crit Care; 14:220, 2010.
8. laFFEy JG, kaVanaGH bP: Hypocapnia. N Engl J Med; 347:43-53, 2002.
9. alExandEr CS, liu SM: Effect of hypercapnia and hypocapnia on myocardial blood flow and performance in anaesthetized dogs. Cardiovasc Res; 10:341-8, 1976.
10. kittlE CF, aoki H, brown Eb, Jr: The role of pH and CO2 in the distribution of blood flow. Surgery; 57:139-54, 1965.
11. VanCE JP, brown dM, SMitH G: The effects of hypocapnia on myocardial blood flow and metabolism. Br J Anaesth; 45:455-63, 1973.
12. CaSE rb, GrEEnbErG H, MoSkowitz r: Alterations in coronary sinus pO2 and o2 saturation resulting from pCO2 changes. Cardiovasc Res; 9:167-77, 1975.
13. rowE GG, CaStillo Ca, CruMPton Cw: Effects of hyperventilation on systemic and coronary hemodynamics. Am Heart J; 63:67-77, 1962.
14. nEill wa, HattEnHauEr M: Impairment of myocardial O2 supply due to hyperventilation. Circulation; 52:854-8, 1975.
15. FEiGl Eo: Coronary physiology. Physiol Rev; 63:1-205, 1983.16. wEibEl Er: The Pathway for Oxygen. Structure and Function in
the Mammalian respiratory System. Harvard University Press, Cambridge, MA, 1984.
17. CryStal GJ, kiM SJ, SalEM Mr, abdEl-latiF M: Myocardial oxygen supply/demand relations during phenylephrine infusions in dogs. Anesth Analg; 73:283-8, 1991.
18. doMEnECH rJ, HoFFMan Ji, noblE Mi, SaundErS kb, HEnSon Jr, SubiJanto S: Total and regional coronary blood flow measured by radioactive microspheres in conscious and anesthetized dogs. Circ Res; 25:581-96, 1969.
19. kontoS Ha, Jr MauCk HP, riCHardSon dw, Jr PattErSon Jl: Circulatory responses to hypocapnia in the anesthetized dog. Am J Physiol; 208:139-43, 1965.
20. CryStal GJ, SalEM Mr: Myocardial and systemic hemodynamics during isovolemic hemodilution alone and combined with nitroprusside-induced controlled hypotension. Anesth Analg; 72:227-37, 1991.
21. Fan FC, CHEn ry, SCHuESSlEr Gb, CHiEn S: Effects of hematocrit variations on regional hemodynamics and oxygen transport in the dog. Am J Physiol; 238:H545-52, 1980.
22. SHEa tM, watSon rM, PiotrowSki SF, dErMkSian G, CaSE rb: Anaerobic myocardial metabolism. Am J Physiol; 203:463-9, 1962.
23. drakE aJ, HainES Jr, noblE Mi: Preferential uptake of lactate by the normal myocardium in dogs. Cardiovasc Res; 14:65-72, 1980.
24. MarSHall JM: Peripheral chemoreceptors and cardiovascular regulation. Physiol Rev; 74:543-94, 1994.
25. GuyEnEt PG, StornEtta rl, abbott Sb, dEPuy Sd, Fortuna MG, kanbar r: Central CO2 chemoreception and integrated neural mechanisms of cardiovascular and respiratory control. J Appl Physiol; 108:995-1002, 2010.
26. HablEr oP, klEEn MS, PodtSCHaSkE aH, HuttEr Jw, tiEdE M, kEMMinG Gi, wEltE MV, CorSo Co, MESSMEr kF: The effect of acute normovolemic hemodilution (ANH) on myocardial contractility in anesthetized dogs. Anesth Analg; 83:451-8, 1996.
27. riVaS F, rEMbErt JC, baCHE rJ, Cobb Fr, Jr GrEEnFiEld JC: Effect of hyperoxia on regional blood flow after coronary occlusion in awake dogs. Am J Physiol; 238:H244-8, 1980.


235 M.E.J. ANESTH 23 (2), 2015
ASSESSMENT OF PREOPERATIVE AND POSTOPERATIVE ANXIETY AMONG ELECTIVE MAJOR SURGERY
PATIENTS IN A TERTIARY HOSPITAL IN NIGERIA
AdesAnmi Akinsulore, AfolAbi m. owojuyigbe, ArAmide f. fAponle And femi o. fAtoye
Abstract
Background: Anxiety is an unpleasant emotional experience that involves feelings of tension, apprehension, nervousness and high autonomic activity. Few studies have been conducted in Nigeria on anxiety levels among patient undergoing surgical operation. The aim of this study is to assess preoperative and postoperative anxiety level of patients and identify factors that may influence patient’s preoperative anxiety level.
Methods: Fifty one adult patients scheduled for elective surgery in a tertiary public hospital in Nigeria were assessed a day before and after their surgery using a questionnaire with socio-demographic and clinical details. Anxiety was assessed with the state portion of the State-Trait Anxiety Inventory (STAI) and different factors responsible for their anxiety were selected from a list. Statistical analysis was done using SPSS version 17.
Result: Twenty-six patients (51.0%) had significant preoperative anxiety while 8 (15.7%) had significant postoperative anxiety. The patients preoperative mean anxiety score of STAI (42.72 ± 9.84) was statistically significantly higher than their postoperative mean anxiety score (37.73 ± 8.44; p =.001). In10 items of STAI, there were significant differences between the preoperative and postoperative mean STAI scores. Fear of complications and result of operation were the most common factors responsible for preoperative anxiety while few patients were anxious about nil per mouth, getting stuck with needle and harm from doctor/nurse mistake.
Conclusion: The prevalence of preoperative anxiety is high in Nigerian surgical patients. Psychological preparation and provision of correct information that addresses identified factors may help in reducing preoperative anxiety.
Keywords: Anxiety; Surgery; Preoperative; Postoperative; Nigeria.

236 ADESANMI AkINSULORE et. al
Introduction
Anxiety is an unpleasant emotional experience which may cause patients undergoing planned surgical operation to avoid such procedures1. Anxiety can be defined as feelings of tension, apprehension, nervousness, fear and high autonomic activity that varies in intensity and degree of fluctuation over time2. Extreme form of anxiety prior to surgical operation has been shown to lead to cardiovascular disturbances such as tachycardia, hypertension, arrhythmias and increase in postoperative pain3. Patients with high levels of anxiety require higher doses of anesthetic induction agents and recover poorly1,4. Therefore, efforts at assessing and reducing preoperative anxiety should include timely preoperative visit by the anesthesiologist, and appropriate premedication and psychological preparation of the patient.
Various instruments have been used in the assessment of levels of anxiety in adult surgical patients in the developed countries. The commonly used scales include the Depression, Anxiety and Stress Scale (DASS)5, the State-Trait Anxiety Inventory questionnaire (STAI)6 and the Visual Analogue Scale of Anxiety (VAS)1. The STAI has been validated and used in the Nigerian general adult population7,8. Among adult patients, prevalence rates of preoperative anxiety have been reported to vary from 11% to 80%9,10.
In Nigeria, few studies have been conducted on anxiety levels among patient undergoing surgical operation11. In a recent study conducted in Port Harcourt, Niger Delta region of Nigeria, a prevalence of 34.4% was reported using a visual analogue scale12. However, there is the need to assess preoperative anxiety with a standardized questionnaire.
Patients undergoing surgical procedure or operation experience fear and anxiety prior to surgery at one point in time or the other12,13. However, a high level of anxiety is very deleterious to patients’ health. Therefore, it is important to identify factors associated with high anxiety in our local population so as to develop appropriate management plan. Anxiety as a contributing factor for peri-operative complications has been poorly explored by Nigerian researchers. Identifying factors that may influence patient’s anxiety level will help anaesthesiologist/surgeon in preventing
or minimizing associated complications.
The aim of this study is to assess pre and post operative anxiety level of patients and identify factors that may influence patient’s preoperative anxiety level.
Methods
Subjects
Patients scheduled for elective surgery between July and September 2013 participated in the study. The study was conducted at the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria, which is a tertiary care public hospital. Inclusion criteria included patients aged 18years and above with American Society of Anesthesiology (ASA) classification I and II, and ability to give informed consent. Exclusion criteria were inability to give informed consent, ASA classification of III-V, cognitive impairment, and patients with previous diagnosis of anxiety or depression with psychiatric treatment. For the selection of individuals, we used a convenient sampling of consecutive patients who attended a pre-anesthetic consultation and met the selection criteria.
Procedure and Assessments
The study protocol was approved by Ethics and Research Committee of the OAUTHC. Written informed consent was taken from all the patients after the objectives of the study had been explained to them. Socio-demographic characteristics (such as age, sex, level of education) and clinical details (such as surgical procedure, past history of surgery, duration of illness) of patients were collected. From a prepared list, patients were asked to select different factors responsible for their anxiety. Anxiety was assessed using the state portion of the State-Trait Anxiety Inventory (STAI) questionnaire the day before and the day after surgery. The STAI is a self-report measure consisting of a 20-item state portion which assesses how one feels right now and a 20-item trait portion on how one generally feels6. In the state portion of STAI, ten statements express anxiety (item number 3, 4, 6, 7, 9, 12, 13, 14, 17 and 18) while the remaining 10 statements (item number 1, 2, 5, 8, 10, 11, 15, 16,
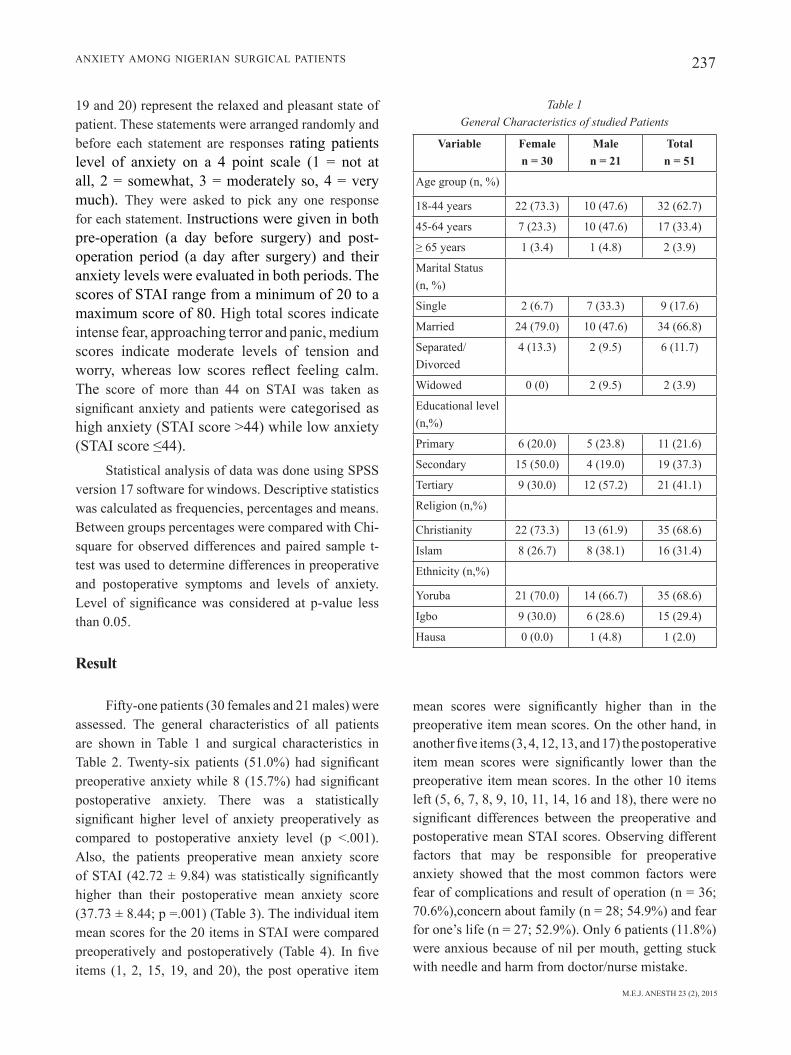
M.E.J. ANESTH 23 (2), 2015
237ANXIETY AMONG NIGERIAN SURGICAL PATIENTS
19 and 20) represent the relaxed and pleasant state of patient. These statements were arranged randomly and before each statement are responses rating patients level of anxiety on a 4 point scale (1 = not at all, 2 = somewhat, 3 = moderately so, 4 = very much). They were asked to pick any one response for each statement. Instructions were given in both pre-operation (a day before surgery) and post-operation period (a day after surgery) and their anxiety levels were evaluated in both periods. The scores of STAI range from a minimum of 20 to a maximum score of 80. High total scores indicate intense fear, approaching terror and panic, medium scores indicate moderate levels of tension and worry, whereas low scores reflect feeling calm. The score of more than 44 on STAI was taken as significant anxiety and patients were categorised as high anxiety (STAI score >44) while low anxiety (STAI score ≤44).
Statistical analysis of data was done using SPSS version 17 software for windows. Descriptive statistics was calculated as frequencies, percentages and means. Between groups percentages were compared with Chi-square for observed differences and paired sample t- test was used to determine differences in preoperative and postoperative symptoms and levels of anxiety. Level of significance was considered at p-value less than 0.05.
Result
Fifty-one patients (30 females and 21 males) were assessed. The general characteristics of all patients are shown in Table 1 and surgical characteristics in Table 2. Twenty-six patients (51.0%) had significant preoperative anxiety while 8 (15.7%) had significant postoperative anxiety. There was a statistically significant higher level of anxiety preoperatively as compared to postoperative anxiety level (p <.001). Also, the patients preoperative mean anxiety score of STAI (42.72 ± 9.84) was statistically significantly higher than their postoperative mean anxiety score (37.73 ± 8.44; p =.001) (Table 3). The individual item mean scores for the 20 items in STAI were compared preoperatively and postoperatively (Table 4). In five items (1, 2, 15, 19, and 20), the post operative item
Table 1 General Characteristics of studied Patients
Variable Femalen = 30
Malen = 21
Totaln = 51
Age group (n, %)
18-44 years 22 (73.3) 10 (47.6) 32 (62.7)
45-64 years 7 (23.3) 10 (47.6) 17 (33.4)
≥ 65 years 1 (3.4) 1 (4.8) 2 (3.9)
Marital Status (n, %)
Single 2 (6.7) 7 (33.3) 9 (17.6)
Married 24 (79.0) 10 (47.6) 34 (66.8)
Separated/Divorced
4 (13.3) 2 (9.5) 6 (11.7)
Widowed 0 (0) 2 (9.5) 2 (3.9)
Educational level (n,%)
Primary 6 (20.0) 5 (23.8) 11 (21.6)
Secondary 15 (50.0) 4 (19.0) 19 (37.3)
Tertiary 9 (30.0) 12 (57.2) 21 (41.1)
Religion (n,%)
Christianity 22 (73.3) 13 (61.9) 35 (68.6)
Islam 8 (26.7) 8 (38.1) 16 (31.4)
Ethnicity (n,%)
Yoruba 21 (70.0) 14 (66.7) 35 (68.6)
Igbo 9 (30.0) 6 (28.6) 15 (29.4)
Hausa 0 (0.0) 1 (4.8) 1 (2.0)
mean scores were significantly higher than in the preoperative item mean scores. On the other hand, in another five items (3, 4, 12, 13, and 17) the postoperative item mean scores were significantly lower than the preoperative item mean scores. In the other 10 items left (5, 6, 7, 8, 9, 10, 11, 14, 16 and 18), there were no significant differences between the preoperative and postoperative mean STAI scores. Observing different factors that may be responsible for preoperative anxiety showed that the most common factors were fear of complications and result of operation (n = 36; 70.6%),concern about family (n = 28; 54.9%) and fear for one’s life (n = 27; 52.9%). Only 6 patients (11.8%) were anxious because of nil per mouth, getting stuck with needle and harm from doctor/nurse mistake.
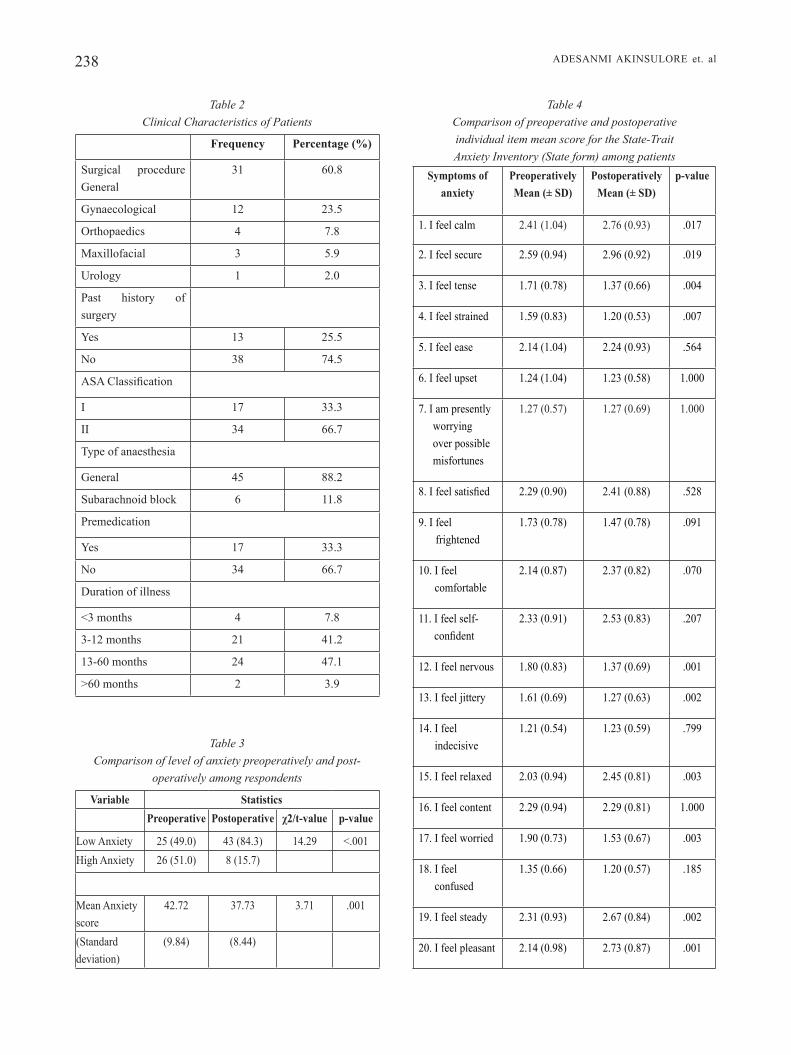
238 ADESANMI AkINSULORE et. al
Table 3 Comparison of level of anxiety preoperatively and post-
operatively among respondents
Variable StatisticsPreoperative Postoperative χ2/t-value p-value
Low Anxiety 25 (49.0) 43 (84.3) 14.29 <.001High Anxiety 26 (51.0) 8 (15.7)
Mean Anxiety score
42.72 37.73 3.71 .001
(Standard deviation)
(9.84) (8.44)
Table 4 Comparison of preoperative and postoperative individual item mean score for the State-Trait Anxiety Inventory (State form) among patients
Symptoms of anxiety
PreoperativelyMean (± SD)
PostoperativelyMean (± SD)
p-value
1. I feel calm 2.41 (1.04) 2.76 (0.93) .017
2. I feel secure 2.59 (0.94) 2.96 (0.92) .019
3. I feel tense 1.71 (0.78) 1.37 (0.66) .004
4. I feel strained 1.59 (0.83) 1.20 (0.53) .007
5. I feel ease 2.14 (1.04) 2.24 (0.93) .564
6. I feel upset 1.24 (1.04) 1.23 (0.58) 1.000
7. I am presently worrying over possible misfortunes
1.27 (0.57) 1.27 (0.69) 1.000
8. I feel satisfied 2.29 (0.90) 2.41 (0.88) .528
9. I feel frightened
1.73 (0.78) 1.47 (0.78) .091
10. I feel comfortable
2.14 (0.87) 2.37 (0.82) .070
11. I feel self- confident
2.33 (0.91) 2.53 (0.83) .207
12. I feel nervous 1.80 (0.83) 1.37 (0.69) .001
13. I feel jittery 1.61 (0.69) 1.27 (0.63) .002
14. I feel indecisive
1.21 (0.54) 1.23 (0.59) .799
15. I feel relaxed 2.03 (0.94) 2.45 (0.81) .003
16. I feel content 2.29 (0.94) 2.29 (0.81) 1.000
17. I feel worried 1.90 (0.73) 1.53 (0.67) .003
18. I feel confused
1.35 (0.66) 1.20 (0.57) .185
19. I feel steady 2.31 (0.93) 2.67 (0.84) .002
20. I feel pleasant 2.14 (0.98) 2.73 (0.87) .001
Table 2 Clinical Characteristics of Patients
Frequency Percentage (%)
Surgical procedure General
31 60.8
Gynaecological 12 23.5
Orthopaedics 4 7.8
Maxillofacial 3 5.9
Urology 1 2.0
Past history of surgery
Yes 13 25.5
No 38 74.5
ASA Classification
I 17 33.3
II 34 66.7
Type of anaesthesia
General 45 88.2
Subarachnoid block 6 11.8
Premedication
Yes 17 33.3
No 34 66.7
Duration of illness
<3 months 4 7.8
3-12 months 21 41.2
13-60 months 24 47.1
>60 months 2 3.9
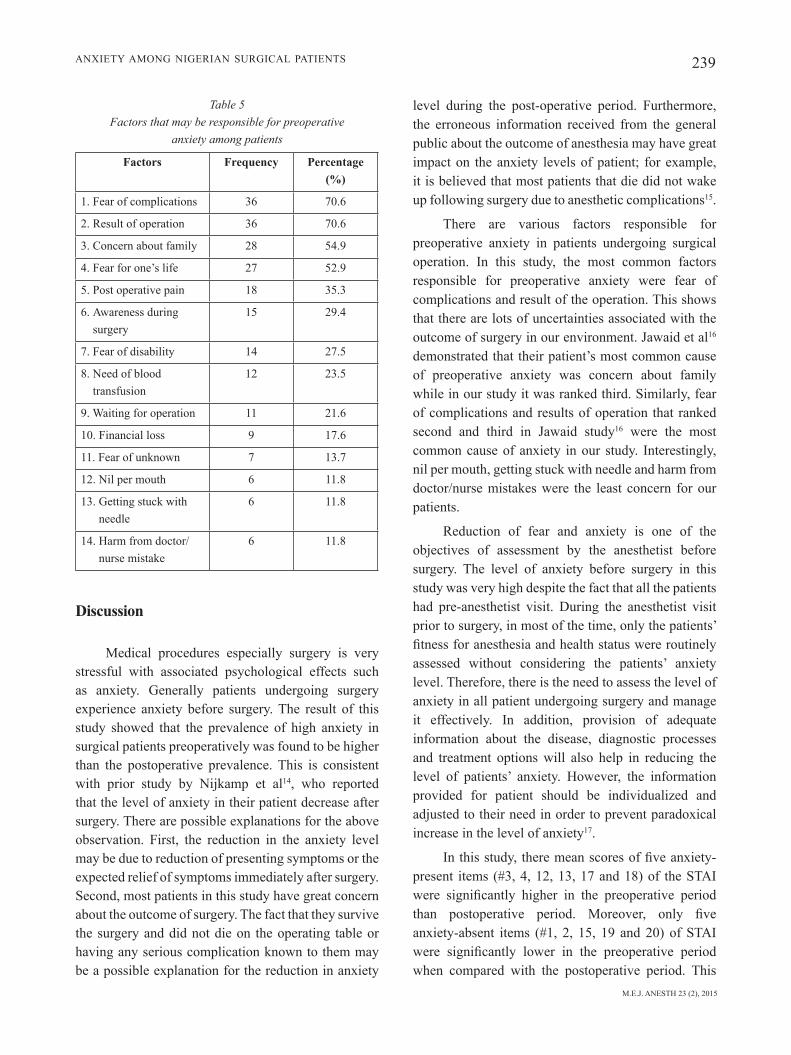
M.E.J. ANESTH 23 (2), 2015
239ANXIETY AMONG NIGERIAN SURGICAL PATIENTS
Discussion
Medical procedures especially surgery is very stressful with associated psychological effects such as anxiety. Generally patients undergoing surgery experience anxiety before surgery. The result of this study showed that the prevalence of high anxiety in surgical patients preoperatively was found to be higher than the postoperative prevalence. This is consistent with prior study by Nijkamp et al14, who reported that the level of anxiety in their patient decrease after surgery. There are possible explanations for the above observation. First, the reduction in the anxiety level may be due to reduction of presenting symptoms or the expected relief of symptoms immediately after surgery. Second, most patients in this study have great concern about the outcome of surgery. The fact that they survive the surgery and did not die on the operating table or having any serious complication known to them may be a possible explanation for the reduction in anxiety
level during the post-operative period. Furthermore, the erroneous information received from the general public about the outcome of anesthesia may have great impact on the anxiety levels of patient; for example, it is believed that most patients that die did not wake up following surgery due to anesthetic complications15.
There are various factors responsible for preoperative anxiety in patients undergoing surgical operation. In this study, the most common factors responsible for preoperative anxiety were fear of complications and result of the operation. This shows that there are lots of uncertainties associated with the outcome of surgery in our environment. Jawaid et al16 demonstrated that their patient’s most common cause of preoperative anxiety was concern about family while in our study it was ranked third. Similarly, fear of complications and results of operation that ranked second and third in Jawaid study16 were the most common cause of anxiety in our study. Interestingly, nil per mouth, getting stuck with needle and harm from doctor/nurse mistakes were the least concern for our patients.
Reduction of fear and anxiety is one of the objectives of assessment by the anesthetist before surgery. The level of anxiety before surgery in this study was very high despite the fact that all the patients had pre-anesthetist visit. During the anesthetist visit prior to surgery, in most of the time, only the patients’ fitness for anesthesia and health status were routinely assessed without considering the patients’ anxiety level. Therefore, there is the need to assess the level of anxiety in all patient undergoing surgery and manage it effectively. In addition, provision of adequate information about the disease, diagnostic processes and treatment options will also help in reducing the level of patients’ anxiety. However, the information provided for patient should be individualized and adjusted to their need in order to prevent paradoxical increase in the level of anxiety17.
In this study, there mean scores of five anxiety-present items (#3, 4, 12, 13, 17 and 18) of the STAI were significantly higher in the preoperative period than postoperative period. Moreover, only five anxiety-absent items (#1, 2, 15, 19 and 20) of STAI were significantly lower in the preoperative period when compared with the postoperative period. This
Table 5 Factors that may be responsible for preoperative
anxiety among patients
Factors Frequency Percentage (%)
1. Fear of complications 36 70.6
2. Result of operation 36 70.6
3. Concern about family 28 54.9
4. Fear for one’s life 27 52.9
5. Post operative pain 18 35.3
6. Awareness during surgery
15 29.4
7. Fear of disability 14 27.5
8. Need of blood transfusion
12 23.5
9. Waiting for operation 11 21.6
10. Financial loss 9 17.6
11. Fear of unknown 7 13.7
12. Nil per mouth 6 11.8
13. Getting stuck with needle
6 11.8
14. Harm from doctor/nurse mistake
6 11.8

240
bAndeirA d: Risk factors for preoperative anxiety in adults. Acta Anaesthesiologica Scandinavica; 45(3):298-307, 2001.
10. kAin Zn, severino f, AlexAnder gm, pincus s, mAyes lc: Preoperative anxiety and postoperative pain in women undergoing hysterectomy. A repeated-measures design. J Psychosom Res; 49:417-422, 2000.
11. ukpong di, AdesunkAnmi Ark: Psychiatric symptoms in surgical patients: An assessment of the course of anxiety. The Nigerian Postgraduate Medical Journal; 2:75-78, 2004.
12. ebirim l, tobin m: Factors responsible for pre-operative anxiety in elective surgical patients at a University Teaching Hospital: A pilot study. The Internet Journal of Anesthesiology; 29(2):1, 2010.
13. moosA myH, cHAit l, coHen A, et Al: Anxiety associated with colposcopy at Chris Hani Baragwanath Hospital, Johannesburg. South African Journal of Psychiatry, 15(2):48-52, 2009.
14. nijkAmp m, kenens c, dijker A, ruiter r, HiddemA f, nuijts r: Determinants of surgery related anxiety in cataract patients. The British Journal of Ophthamology; 88(10):1310-1314, 2004.
15. mcgAw cd, HAnnA wj: knowledge and fears of anesthesia and surgery. The Jamaican perspective. West Indian Med J; 47:64-67, 1998.
16. jAwAid m, musHtAq A, mukHtAr s, kHAn Z: Preoperative anxiety before elective surgery. Neurosciences; 12(2):145-148, 2007.
17. romAnik w, kański A, solucH p, szymańska o: Preoperative anxiety assessed by questionnaires and patient declarations. Anaesthesiology Intensive Therapy; 41(2):80-84, 2009.
ADESANMI AkINSULORE et. al
finding suggests that there is a need to further study the usefulness of the 20-item version of STAI in this environment and such study might also look at the possibility of creating a shorter item version of STAI (e.g. 10-item version of STAI).
Although our study has provided valuable information regarding the prevalence of preoperative and post-operative anxiety among surgical patients, there is the need to acknowledge that there were some limitations that could be addressed in future research.
First, the study was conducted in a single centre and this might not be representative of all the surgical patients in Nigeria. Second, our cut-off point for high anxiety was based on studies done among non patient population and this may not be fully applicable to surgical patient group. Finally, this study did not assess patients’ anxiety level prior to admission and this may affect the prevalence of anxiety level of
surgical patients. Therefore, future research may focus on preadmission anxiety level among surgical patient and the use of medication among those at higher risk of anxiety.
In conclusion, the prevalence of preoperative anxiety is high in Nigerian surgical patients.
Fear of complications and the result of operation were the most common factors responsible for preoperative anxiety. Provision of correct and adequate information on identified factors may help in reducing preoperative anxiety. Such information should be patient specific and tailored towards patients need. This study has demonstrated the importance psychological preparation of surgical patients and the need for psychological intervention when indicated. Therefore psychological assessment should be incorporated as part of routine assessment for patient that is being worked up for elective surgery.
References
1. kindler cH, HArms c, Amsler f, iHde-scHoll t, scHeidegger d: The Visual Analogue Scale allows effective measurement of preoperative anxiety and detection of patients’anaesthetic concerns. Anaesthesia and analgesia; 90:706-12, 2000.
2. vAlenZuelA-millán j, bArrerA-serrAno jr, ornelAs-Aguirre jm: Anxiety in preoperative anesthetic procedures. Cirugia Y Cirujanos; 78:147-151, 2010.
3. boker A, brownell l, donen n: The Amsterdam Preoperative anxiety and information scale provides a simple and reliable measure of preoperative anxiety. Canaadian Journal of Anaestheasia; 49:792-98, 2002.
4. mArAnets i, kAin Zn: Preoperative anxiety and intraoperative anesthetic requirements. Anesth Analg; 89:1346-1351, 1999.
5. sukAntArAt kt, williAmson rc, brett sj: Psychological assessment of ICU survivors: a comparison between the Hospital Anxiety and Depression Scale and the Depression, Anxiety and Stress Scale. Anaesthesia; 62:239-243, 2007.
6. spielberger c: Manual for the State-trait Anxiety Inventory (Form Y). Palo Alto, Calif. Consulting Psychologists Press; 121, 1983.
7. AwAritefe AA, kAdiri Au: Validation of the STAI in Nigerian subjects. IRCS Medical Science: Psychology and psychiatry. Social and Occupational Medicine; 9:419-420, 1981.
8. fAtoye fo, Adeyemi Ab, olAdimeji by: Emotional distress and its correlates among Nigerian women in late pregnancy. Journal of Obstetrics and Gynaecology; 24(5):504-509, 2004.
9. cAumo w, scHmidt A, scHneider c, petry s, brAtHwAit o,

241 M.E.J. ANESTH 23 (2), 2015
THE EFFECTS OF LISTENING TO THE MOTHER’S HEARTBEAT ON THE DEPTH OF ANAESTHESIA
IN CHILDREN
Senem Yildirim*, Başak Akça*, AYSun Ankay Yilbaş*, Ayşe HeveS kArAgöz*, özgür CAnBAY**,
nAlAn çeleBi** And TurgAY öCAl**
Abstract
Background: The present study aimed to evaluate the effects of listening to the mother’s heartbeat and womb sounds on the depth of anaesthesia in children.
Methods: The present study included 40 children scheduled for minor surgery under general anaesthesia, with an American Society of Anaesthesiologists (ASA) status of 1 to 2. Anaesthesia was induced with sevoflurane, and maintained with sevoflurane and oxygen in nitrous oxide. Patients were randomly divided into two groups. The children in Group I were made to listen to recordings of their mothers’ heartbeat and womb sounds via earphones during anaesthesia induction, while those in Group II were made to listen to ambient noise via earphones. The music was turned off when the inhalational anaesthetics were discontinued. Intraoperative monitoring included electrocardiogram (ECG) recordings, heart rate (HR), oxygen saturation, non-invasive systolic blood pressure (SBP) and diastolic blood pressure (DBP), bispectral index system (BIS), end-tidal (ET) sevoflurane, ET N2O, ET CO2, and SaO2.
Results: In Group I, there was a significant decrease in bispectral index (BIS) values over time (p <0.05). Although blood pressure and heart rate were lower in Group I, no significant differences between the groups were detected. While the duration of extubation was shorter in Group I, overall, there was no significant difference between the groups.
Conclusion: We found that children exposed to recordings of their mothers’ heartbeat and womb sounds in addition to music had lower BIS values under anaesthesia, which indicates deeper anaesthesia levels.
Keywords: child, age, audit, depth of anaesthesia.
* Specialist, Hacettepe University Faculty of Medicine, Department of Anesthesiology.** Professor, Hacettepe University Faculty of Medicine, Department of Anaesthesiology. Corresponding author: Başak AKÇA. Hacettepe University Faculty of Medicine Department of Anaesthesiology, Sıhhiye,
Ankara, 06100, Turkey. Phone: 00903123051255, Fax: 00903123109600. E-mail: [email protected]

242 BAşAK AKÇA et. al
Introduction
Music is an essential part of human life, and its multifaceted aspects have revived interest in its use in the medical field. Although not curative alone, music has been shown to help in relieving pain, in allowing individuals to express themselves, and in alleviating stress1-3. The use of music during the anaesthesia phase of surgery could potentially serve as an adjunctive therapy across patient populations, including children.
When treating children, induction of anaesthesia should be carefully monitored, both medically and psychologically. Anaesthesia should prevent the child from experiencing the trauma of the surgical procedure, and not lead to additional trauma. To that end, we considered whether it would be beneficial for patients to listen to music he/she chose during the perioperative period, as a simple, cheap, and non-invasive method in addition to pharmacological methods. (Listening to white noise, which masks ambient noise, has also been found to decrease anxiety and worry, although to a lesser extent than music). Porcaro et al demonstrated that a foetus can respond to a mother’s heart beat and external auditory stimuli4. Further, in a study evaluating the effects of music on the bispectral index system (BIS) and the sedation levels during the preoperative period, Ganidagli et al found that listening to music during midazolam premedication increased the level of sedation and decreased the BIS values during the preoperative period5.
The aim of our study was to evaluate the effects of listening to music along with the sound of their mother’s heartbeat and womb sounds on the depth of anaesthesia in children.
Methods
After approval was obtained from the hospital ethics committee, 40 children, aged 0 to18 months, scheduled for minor surgery and having an American Society of Anaesthesiologists (ASA) status of 1 to 2, were included in the study. Children with hearing problems were excluded. Written informed consent was obtained from the children’s parents, and each child was evaluated preoperatively. Children older than 6 months were premedicated with 0.8 mg/kg intranasal midazolam
20 minutes before the surgery. The BIS monitoring was initiated with the induction of anaesthesia. After anaesthesia was induced with oxygen and sevoflurane, intravenous catheterization was performed. Normal saline (1/3) at a dose of 5-10 ml/h was started, and after muscle relaxation had been achieved with 0.6 mg/kg of rocuronium, anaesthesia was maintained with sevoflurane and 50% O2 in 50% N2O. After induction, patients were given 20 mg/kg of rectal or intravenous paracetamol for postoperative pain relief. During the procedures, the minimal alveolar concentration (MAC) of sevoflurane was maintained at 1.5. After the surgery, atropine (0.01 mg/kg) and neostigmine (0.05 mg/kg) were administered to all children to reverse the action of the muscle relaxant. Patients were randomly assigned to two groups: the children in the first group (Group I) listened to their mothers’ heartbeat and womb sounds in addition to music, and the children in the second group (Group II) listened to recorded ambient noise via earphones. During anaesthesia induction, the children in Group I listened to a CD recording of their mothers’ heartbeat and womb sounds via earphones; the music was turned off when the inhalational anaesthetics were discontinued.
Patients’ age, gender, ASA status, and type of surgery were recorded. The time from the beginning to the end of anaesthesia was defined as “duration of anaesthesia”, and the time from the beginning to the end of surgery was recorded as “duration of surgery”. Extubation time was recorded, and the time interval between the discontinuation of anaesthetic gases and extubation was recorded as “duration of extubation”. In addition, BIS, systolic blood pressure (SBP) and diastolic blood pressure (DBP), end-tidal (ET) sevoflurane, ET N2O, ET CO2, and SaO2 values were recorded before anaesthesia induction (baseline), at 10-minute intervals during anaesthesia, and immediately after the inhalational anaesthetics were discontinued (recorded as “end of procedure”).
Statistical Analysis
Data were analysed with the statistical package for the social sciences (SPSS Inc., Chicago, IL) version 15.0 software. Repeated measures analysis of variance (ANOVA) was used for the analysis of data.
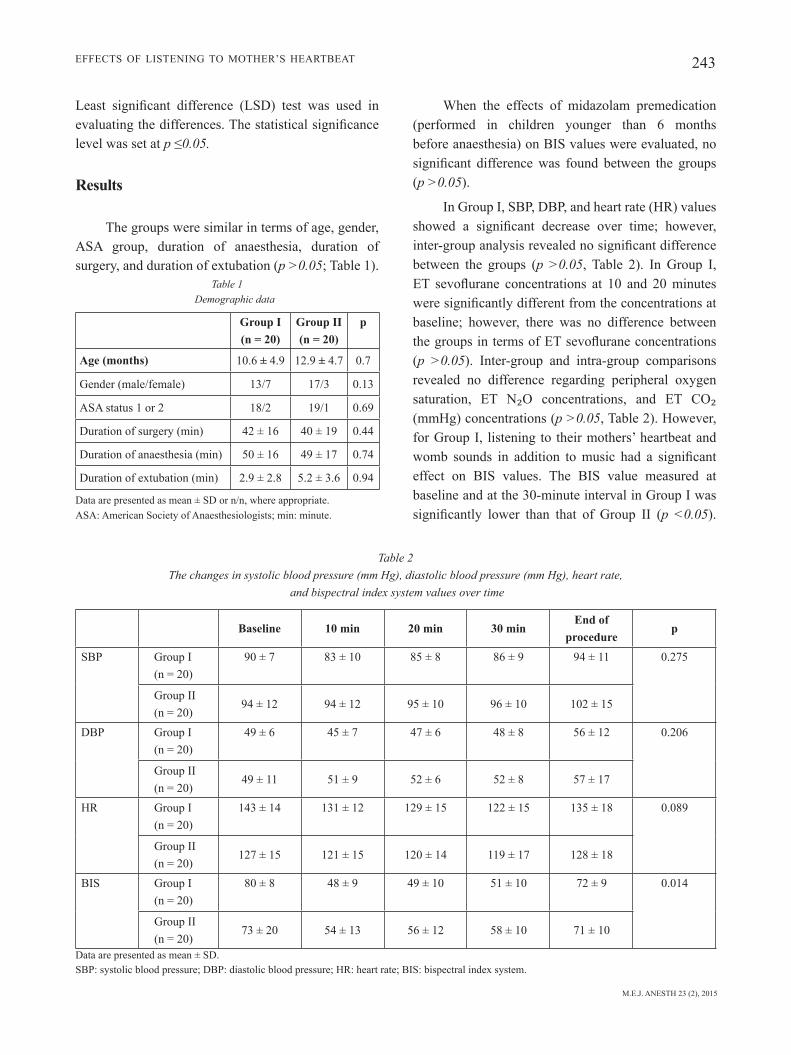
M.E.J. ANESTH 23 (2), 2015
243EFFECTS OF LISTENING TO MOTHER’S HEARTBEAT
Least significant difference (LSD) test was used in evaluating the differences. The statistical significance level was set at p ≤0.05.
Results
The groups were similar in terms of age, gender, ASA group, duration of anaesthesia, duration of surgery, and duration of extubation (p >0.05; Table 1).
Table 1 Demographic data
Group I (n = 20)
Group II (n = 20)
p
Age (months) 10.6 ± 4.9 12.9 ± 4.7 0.7
Gender (male/female) 13/7 17/3 0.13
ASA status 1 or 2 18/2 19/1 0.69
Duration of surgery (min) 42 ± 16 40 ± 19 0.44
Duration of anaesthesia (min) 50 ± 16 49 ± 17 0.74
Duration of extubation (min) 2.9 ± 2.8 5.2 ± 3.6 0.94
Data are presented as mean ± SD or n/n, where appropriate.ASA: American Society of Anaesthesiologists; min: minute.
When the effects of midazolam premedication (performed in children younger than 6 months before anaesthesia) on BIS values were evaluated, no significant difference was found between the groups (p >0.05).
In Group I, SBP, DBP, and heart rate (HR) values showed a significant decrease over time; however, inter-group analysis revealed no significant difference between the groups (p >0.05, Table 2). In Group I, ET sevoflurane concentrations at 10 and 20 minutes were significantly different from the concentrations at baseline; however, there was no difference between the groups in terms of ET sevoflurane concentrations (p >0.05). Inter-group and intra-group comparisons revealed no difference regarding peripheral oxygen saturation, ET N₂O concentrations, and ET CO₂ (mmHg) concentrations (p >0.05, Table 2). However, for Group I, listening to their mothers’ heartbeat and womb sounds in addition to music had a significant effect on BIS values. The BIS value measured at baseline and at the 30-minute interval in Group I was significantly lower than that of Group II (p <0.05).
Table 2 The changes in systolic blood pressure (mm Hg), diastolic blood pressure (mm Hg), heart rate,
and bispectral index system values over time
Baseline 10 min 20 min 30 minEnd of
procedurep
SBP Group I (n = 20)
90 ± 7 83 ± 10 85 ± 8 86 ± 9 94 ± 11 0.275
Group II (n = 20)
94 ± 12 94 ± 12 95 ± 10 96 ± 10 102 ± 15
DBP Group I (n = 20)
49 ± 6 45 ± 7 47 ± 6 48 ± 8 56 ± 12 0.206
Group II (n = 20)
49 ± 11 51 ± 9 52 ± 6 52 ± 8 57 ± 17
HR Group I (n = 20)
143 ± 14 131 ± 12 129 ± 15 122 ± 15 135 ± 18 0.089
Group II (n = 20)
127 ± 15 121 ± 15 120 ± 14 119 ± 17 128 ± 18
BIS Group I (n = 20)
80 ± 8 48 ± 9 49 ± 10 51 ± 10 72 ± 9 0.014
Group II (n = 20)
73 ± 20 54 ± 13 56 ± 12 58 ± 10 71 ± 10
Data are presented as mean ± SD.SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; BIS: bispectral index system.

244 BAşAK AKÇA et. al
Intra-group analysis revealed that the change in BIS values over time was significant at all time points in Group I, while there was a significant difference between the BIS values measured at 10, 20, and 30 minutes in Group II (Table 2).
Discussion
At present, the use of pharmacological agents in outpatient practice is limited because of their prolonged effects, and thus researchers continue their efforts to find alternative non-pharmacological methods to prevent patient anxiety. In anaesthesia practice, listening to music during the preoperative period has been found to have an anxiolytic effect6-8. Individuals are mostly affected by music of their own culture, as that can often better express their emotions, although the choice of music varies according to the social and cultural structure of the population they live in and their education level. Therefore, in our study, infants between the age of 0 and 18 months were made to listen to their mother’s heartbeat and womb sounds (as the most known, familiar, and best-recognized noise) along with music, and its effect on the depth of anaesthesia levels was evaluated using BIS monitoring. Our study demonstrated that listening to the mother’s heartbeat and womb sounds during surgical intervention increased the depth of anaesthesia, as could be seen from the BIS values of the groups (<50 in Group I and >50 in Group II). This finding is consistent with those of Ovayolu et al9, who reported that listening to Turkish classical music decreased anxiety, pain, and dissatisfaction in patients and reduced the dose of sedative drugs used during colonoscopy.
We found that induction of anaesthesia while maintaining the BIS between 45 and 60 decreased propofol use and allowed rapid awakening. Bannister et al also found that the use of sevoflurane, desflurane, and isoflurane led to rapid awakening and a decrease in the use of anaesthetic drugs10. Another study revealed that BIS monitoring decreased the dose of anaesthetic drugs, shortened the duration of extubation, and eased awakening11. Bannister et al10 carried out a study on children between the ages of 0 and 3 years and the ages of 3 and 18 years, who received sevoflurane and 60%
N2O/O2 as anaesthetics. They created a BIS-controlled group and compared the data of this group with that of a control group given a standard anaesthesia protocol. They found that when the BIS values of children between the ages of 0 and 6 months, who were given combined general/regional anaesthesia, were maintained between 45 and 60, the use of anaesthetic drugs decreased with no effect on awakening and recovery period. These same researchers found that in children aged 6 months to 3 years, who were anaesthetized with BIS-controlled combined general/regional anaesthesia, the requirement for anaesthetic drugs did not decrease and the recovery time was not affected. BIS-controlled anaesthesia decreased anaesthetic use, and provided early awakening and rapid recovery in older children. Zhang et al12 evaluated the effects of music on the requirement for target-controlled infusion of propofol and demonstrated the beneficial sedative effects of music during combined spinal-epidural anaesthesia. Further, a study evaluating the efficacy of music in providing preoperative sedation by observer's assessment of alertness/sedation (OAA/SS) and BIS measurements showed that the level of sedation was significantly decreased in the group that listened to music5.
In our study, we found that the duration of extubation was shorter in children who listened to their mothers’ womb sounds (2.9 minutes vs 5.2 minutes for the control group). In addition, they experienced early awakening and rapid recovery; however, there was no significant difference between the two groups.
Besides being used to measure the depth of general anaesthesia, the BIS index is also used to monitor the level of sedation13. The fact that awareness incidence can be as high as 0.8% clearly shows the importance of monitoring the depth of anaesthesia in paediatric patients14. As the use of BIS monitoring in children is still being debated, we used traditional monitoring methods along with BIS in this study. In our study, intra-group analysis performed in both groups showed a significant decrease in HR, SBP, and DBP compared to baseline values. However, although the decrease in Group I was higher than that of Group II, there was no significant difference between the groups.
Denman et al15 found that BIS measurements of awake and anaesthetized children between the ages of 1

M.E.J. ANESTH 23 (2), 2015
245EFFECTS OF LISTENING TO MOTHER’S HEARTBEAT
month and 12 years correlated with the data from adults used as the control group; in other words, BIS values do provide correct clinical information for children. It has also been demonstrated that BIS could be used in controlling the depth of anaesthesia in children other than infants, as well as decreasing medication consumption and speeding awakening in children older than 3 years16,17. Rodriguez et al18 evaluated the relationship between BIS measurements and simple clinical findings in children between the ages of 4 months and 14 years, and found that BIS values during inhalation induction correlated with several levels of hypnosis. On the other hand, Davidson et al16 found a relationship between BIS values and ET sevoflurane in children undergoing circumcision, but this relationship was not present in infants. They pointed out that, similar to adults, BIS values in children increased with the decrease in ET sevoflurane concentrations during arousal; however, they stressed that BIS values should be carefully interpreted in infants. They stated that BIS values in infants vary across a broad spectrum; in their study, BIS values were low immediately before arousal, and again during arousal, indicating no correlation between ET sevoflurane and BIS values.
In our study, while ET sevoflurane, ET N₂O, and ET CO₂ concentrations were similar in both groups, BIS values in the children who listened to music were
lower. Although there were no significant differences between the groups, ET sevoflurane and ET N₂O concentrations were higher in Group II. The fact that there was no difference between the groups indicates that we maintained MAC at the same level in all patients.
In the children who were premedicated with midazolam (0.08 mg/kg IM), perioperative music was associated with higher sedation levels and decreased BIS values5. We also found that premedication with midazolam before anaesthesia had similar effects on the BIS values of both groups. While children younger than 6 months had lower BIS values than those older than 6 months, the mean BIS values of the groups were similar. In Group I, there was a significant decrease in the BIS values of over time (p <0.05). While there was no significant difference between the groups in terms of mean SBP, DBP, and HR, these parameters were lower in Group I versus Group II. Duration of extubation was shorter in Group I than in Group II; however, the difference between the groups did not reach statistical significance. Our findings do indicate that listening to their mother’s heartbeat and womb sounds along with music decreased the BIS values and increased the depth of anaesthesia in children undergoing minor surgery.

246 BAşAK AKÇA et. al
References
1. SmiTH JC, JoYCe CA: Mozart versus new age music: relaxation states, stress, and ABC relaxation theory. J Music Ther; 41:215-224, 2004.
2. SAlAmon e, BernSTein SR, kim Sa, kim m, STefAno gB: The effects of auditory perception and musical preference on anxiety in naive human subjects. Med Sci Monit; 9:CR396-CR399, 2003.
3. BurnS SJ, HArBuz mS, HucklebRidge f, BunT l: A pilot study into the therapeutic effects of music therapy at a cancer help center. Altern Ther Health Med; 7:48-56, 2001.
4. PorCAro C, zAPPASodi f, BArBATi g, eT Al: Fetal auditory responses to external sounds and mother's heart beat: detection improved by Independent Component Analysis. Brain Res; 1101:51-58, 2006.
5. gAnidAgli S, Cengiz m, Yanik m, BeceRik C, unAl B: The effect of music on preoperative sedation and the bispectral index. Anesth Analg; 101:103-106, 2005.
6. CunningHAm mf, monSon B, BookbindeR m: Introducing a music program in the perioperative area. AORN J; 66:674-682, 1997.
7. updike PA, CHArleS dm: Music Rx: physiological and emotional responses to taped music programs of preoperative patients awaiting plastic surgery. Ann Plast Surg; 19:29-33, 1987.
8. THomPSon JF, KAm PC: Music in the operating theatre. Br J Surg; 82:1586-1587, 1995.
9. ovAYolu n, uCAn o, PeHlivAn S, eT Al: Listening to Turkish classical music decreases patients' anxiety, pain, dissatisfaction and the dose of sedative and analgesic drugs during colonoscopy: a prospective randomized controlled trial. World J Gastroenterol; 12:7532-7536, 2006.
10. BAnniSTer Cf, BroSiuS kk, Sigl JC, meYer BJ, SeBel PS: The effect of bispectral index monitoring on anesthetic use and recovery in children anesthetized with sevoflurane in nitrous oxide. Anesth Analg; 92:877-881, 2001.
11. SAmmArTino m, volPe B, SBArAgliA f, gArrA r, d'AddeSSi A: Capnography and the bispectral index-their role in pediatric sedation: a brief review. Int J Pediatr; 2010, doi: http://dx.doi.org/10.1155/2010/828347.
12. zHAng XW, fAn Y, mAnYAnde A, TiAn yk, yin P: Effects of music on target-controlled infusion of propofol requirements during combined spinal-epidural anesthesia. Anesthesia; 60:990-994, 2005.
13. ozkan-SeYHAn T, Sungur mo, SentuRk e, eT Al: BIS guided sedation with propofol during spinal anesthesia: influence of anaesthetic level on sedation requirement. Br J Anaesth; 96:645-649, 2006.
14. dAvidSon AJ, HuAng gH, CzaRnecki C, eT Al: Awareness during anesthesia in children: a prospective cohort study. Anesth Analg; 100:653-661, 2005.
15. denmAn WT, SWAnSon el, roSoW d, ezbicki k, connorS Pd, roSoW Ce: Pediatric evaluation of the bispectral index (BIS) monitor and correlation of BIS with end-tidal sevoflurane concentration in infants and children. Anesth Analg; 90:872-877, 2000.
16. dAvidSon AJ, mCCAnn me, devAvArAm P, eT Al: The differences in the bispectral index between infants and children during emergence from anesthesia after circumcision surgery. Anesth Analg; 93:326-330, 2001.
17. degouTe CS, mACABeo C, duBreuil C, duClAuX r, BAnSSillon v: EEG bispectral index and hypnotic component of anesthesia induced by sevoflurane: comparison between children and adults. Br J Anaesth; 86:209-212, 2001.
18. rodriguez rA, HAll le, duggAn S, SPlinTer Wm: The bispectral index does not correlate with clinical signs of inhalational anesthesia during sevoflurane induction and arousal in children. Can J Anaesth; 51:472-480, 2004.

247 M.E.J. ANESTH 23 (2), 2015
Learning By SimuLation
Ghaleb Okla* and dOuGlas eden**
in this article, the authors will discuss the general history of simulation-based medical education (SBme)1 including what simulation is, why simulation should be used and clinical simulation lab evaluation. With simulation labs emerging internationally and across multiple disciplines, the article will shed light on the positive impact of simulation in education and the high return on the investment that simulation requires to be most effective. additionally, the article will address the question of whether or not the use of simulation as an education technique is a “passing trend”.
as early as 1910.simulation was used in aviation as a training method and skills improvement of pilots in World War i2. the standard training for pilots developed simultaneously with pilot simulation training. aviation continues to remain on the forefront of simulation use and development into the 21st century. Simulation has played a key role in the advancement of aviation training over the last hundred years.
though aviation was on the cutting edge of simulation during WWii, troopers were also utilizing simulation for learning horse riding2. mechanical horses aided in training members of the military who had no previous experience riding horses and mechanical horses are still used in training today3. the military continues to be one of the leading users of simulation for multitude of training objectives, evaluation, and improvements. although simulation in the military involves a long history of gaming4 to predict outcomes and prepare for battle, contemporary military simulation includes medical training along with combat training5.
a wide variety of disciplines are also utilizing simulation training. these disciplines include but are not limited to:
• Aerospace industry:anaturalextensionof theaviation industry,utilizingsimulation insimilar ways.
• Nuclear Industry: has achieved reasonably safe records over the second half of thetwentieth century due to an intensive use of simulation training8.
• LawEnforcement: use of simulations to prepare officers for nearly any scenario theymight face on the streets.
Themedical profession has been a relatively recent newcomer to the use of high-fidelitysimulation9. one author referred to the growth of simulation in medicine as a “prolonged gestation”9. medicine has long used low-tech mannequins for CPr training. By the end of the 20th century, hi-fidelitysimulationmannequinsanddedicatedlaboratorieswerebecomingthenewstandardformedical schools, hospitals and nursing and allied health training programs. medical simulation mannequins are now available in 3D for advanced medical training in trauma, anesthesia, obstetrics, neonatology, respiratory care and numerous other specialties10.Thefirst useof a computerizedsimulator for SBme was established at the university of miami medical School in the 1960’s11. medical students and residents were trained in cardiology using the simulator nicknamed “Harvey”,
* PhD, rrt, rCP, FHCa, Fama. Dr. okla is the President and Ceo of Health Care resources LLC, and Program Director of the respiratory Care Program at Carrington College in Pleasant Hill, California. no gratuities were accepted for this article andtherearenoethicalconflictsofinterest.
** edD(c), rrt, rCP. mr. eden is a faculty member in the respiratory Care Program a Carrington College in Pleasant Hill, Californiaandadoctoralcandidate.Nogratuitieswereacceptedforthisarticleandtherearenoethicalconflictsofinterest.

248 gHaLeB okLa et. al
and those practitioners outperformed their traditionally trained peers12. Ziv referred to SBme as an ethical imperative13 suggesting that simulation is an essential component of the medical training curriculum.
the rationale for simulation use in medicine has long been based on improving patient outcomes. the number that continues to drive the use of simulation for medical training in the united States is the widely quoted 98,000 accidental hospital deaths annually. this alarming number has remained constant for over a decade14. the actual number of accidental hospital deaths may be higher and closer to 400,000 deaths15. to provide some perspective, these numbers exceed the total sum of deaths in the united States from automobile accidents, breast cancer and aiDS. two studies looked at the adverse effects in hospitalized patients and the percentage of adverse effects that lead to death16,17. one study reported that in Colorado and utah adverse events occurred in 2.9 percent of patients and that death was the outcome in 6.6 percent of those adverse events16. another study in new york reported adverse events in 3.7% of hospitalizations with death as the outcome in 13.6% of those cases17.
the question that naturally follows the simulation conversation in medicine is “does simulation increase patient safety”? There appears to be no definitivestatistical link at this time between simulation use and positive outcomes though further studies are encouraged17. over the last decade, research from around the world indicates that simulation helps in improving safely by training users on high-end technologies associated with anesthesia and surgical procedures. SBme has been linked to clinical improvement in laparoscopic surgery outcomes and adherence to aCLS protocol17. as a stand-alone training method with direct impact to patient safety, the data on use of medical simulation is still lacking though supporters maintain that it is better to train on simulators and move to live patients than to train directly on live patients. mcgaghie claimed that SBme with deliberate practice was superior in achieving clinical skills to the traditional medical education of “see one, do one, teach one”18. Morestudiesareneededtoconfirmapermanentroleformedical simulation training in improving patient safety.
in 2005 the position of the Joint Commission on the accreditation of Healthcare organizations (JCaHo)
on simulation use in medicine was supportive. JCaHo issued a statement that recommends the adoption of simulation technology and the establishment of evidenced-based research to prove impact on patient safety. JCaHo went on to propose that those seeking to implement simulation technology pursue proposals to offset the cost19 of constructing Sim-Center labs.
medical simulation has become state of the art and extremely valuable in the early phases of all medical training20,21. For instance, simulation training has become a routine part of training for respiratory therapists in the united Sates22. respiratory therapists are frequently involved in resuscitations, trauma, and ventilator care as a daily part of their duties. Low-tech simulation laboratories have become less common in respiratory training programs and high-tech simulation laboratories are slowly becoming more common22. in colleges that share space with registered nurse training programs the cost may be more justifiable. High-Fidelity simulators are available in the form of Sim-man, Sim-Baby, Sim-mom, and various a la carte add-ons for trauma and respiratory diseases11. the cost of onehigh-fidelitysimulatorwithassociatedequipmentcan reach $uS200,000.0023. the cost of building a high-tech simulation lab, or converting space, can be in excess of $uS1,000,000.00 and prohibitive for some budgets.
the development of medical education, at any level, fits into a general framework ofclinical assessment using a simple pyramid model from bottom-to-top: knowledge, competencies, performance, and action24. all levels of simulation facilitate critical thinking skills needed in the learning process. in terms of evidenced-based research that lends legitimacy to the claims that patient safety is improved by use of simulation the literature is slowly piling up. Berkenstadt called SBme a “mistake-forgiving” environment25. there are numerous other benefits from the use of simulation inmedicaleducation and they all fit into the universalmissionof improving patient outcomes. teamwork within disciplines and interdisciplinary teams is established through the use of simulation as well as collaborative strategies. Bearman referred to SBme as linked to a “new professionalism” that supports a patient-centered and team-based approach to healthcare26. a

M.E.J. ANESTH 23 (2), 2015
249Learning By SimuLation
range of technologies are available via simulation and frequent practice assists users in developing a wide range of skills. For instance, simulation allows for the development of clinical judgment and the process of acclimation to accountability for patient outcomes.
the most valuable phase of simulation may take place during the evaluation process that is often associated with a debriefing session27. Debriefingsessions are held immediately after a simulation experience with participants and evaluators sitting around a table. these sessions are designed to be a time when participants can speak freely about the simulation, watch video of the simulation, and generallyandspecificallydiscusswhatwentwellandwhatneededimprovement.TheDebriefingAssessmentfor Simulation in Healthcare (DaSH) program at HarvardMedicalSimulationCenterisafineexampleofhowdebriefingcanbeutilizedtoenhancemedicaltraining28.Atraineddebriefingguidesetsafriendlytonebut typically does little of the talking unless problems arise. a common technique is to write down on a board lists of how the participants critique themselves (what wentwellandwhatdidnotgowell).Debriefingguideswithhold their view of what transpired during the simulation until the conclusion and only state minimal, objective facts shared in a positive light.
the simulation experience is enhanced when participants have had a live set of clinical experiences to create a framework. often students will say that they appreciated their simulation experience more after they went to a live clinical experience. Students are allowed to makes errors in the simulation environment both minor and major without fear of a penalty and they are pre-briefed about this criterion ahead of time. the simulation experience becomes more rich and valuable when students understand the philosophy of simulation and feel free to fully immerse themselves in the role-playing model. at the conclusion of the simulation and debrief there should be a positive feeling of satisfaction among students, mentors, and faculty. there is an axiom in simulation that strongly discourages anyone leaving the simulation and debriefing session withnegative feelings.
Simulation always provides hands-on training that students universally desire and that builds skills andconfidence.Frommeasuringabloodpressure to
placing eCg leads, interpreting cardiac rhythms to manipulating mechanical ventilators, auscultating breath sounds to physical assessment, simulations allow students to develop through role playing as respiratory therapists, doctors, nurses and even family members of the patient. Students will often receive clinical contact hours for their experience in the simulation lab.
Simulation is not always expensive, offering less costly options such as the use of “standardized patients”. a standardized patient is a real person who volunteers or is paid to play the role of a hospital patient. Cases and scripts are selected and developed ahead of time and the standardized patient stays in character through the simulation. Some patients with actual disease processes such as pulmonary or cardiac volunteer can be members of a standardized patient pool available to some simulation programs. the added value of having simulation training with a live person able to interact authentically with participants is one way to substitute a high-value simulation experience without having a high-fidelity simulation lab. Oftenthe value-added phase of standardized patient use occurs during debriefing when the actor providesdetailed feedback about their perception of the event. obvious limitations with standardized patients exist such as inability to simulate trauma and resuscitation scenarios and that some receive reimbursement.
Summary
the future appears bright for the use of simulation in medical education. medical, nursing, and allied healthcare students trained through simulation have opportunities to practice hands on techniques, teamwork, and communication through trial and error in a safe environment before working with live patients. The cost of high-fidelity simulationwill continue tomake its use prohibitive and challenging for some programs though the use of low-fidelity simulation,standardized patients, and role-playing continues to have measureable qualitative value. Cost center sharing is one way for programs on a tight budget who desirehigh-fidelitysimulationtoaccessthisvaluableskills-building, outcome-improving medical education adjunct tool.

250 gHaLeB okLa et. al
References
1. McGaGhie Wc, issenburG sb, Petrusa er, scalesek rJ: a Critical review of simulation-based education research: 2003-2009. Medical Education; 44(1):50-63, 2010.
2. www.simulationinformation.com, 2015. 3. www.theatlantic.com/technology/archive/2012/09/a-brief-history-
of-mechanical-horses/262942/. 2015.4. www.racewood.com/dressage.php, 2015.5. www.army.mil/article/11936/History_of_military_gaming/, 2015.6. www.simulatorsystems.com. 2015.7. www.pub.iaea.org/books/iaeaBooks/6670/application-of-
Simulation-techniques-for-accident-management-training-in-nuclear-Power-Plants. 2015.
8. bradley, P: the History of simulation in medical education and possible future directions. Medical Education; march, 40(3):254-62, 2006.
9. www.laerdal.com/us/nav/207/Patient-Simulators. 2015.10. www.gcrme.miami.edu/harvey_features.php. 2015.11. Ziv a, WOlPe Pr, sMall sd, Glick s: Simulation-based medical
education: an ethical imperative. Academic Medicine; 78(8):783-88, 2003.
12. aGGarWal r, MyttOn Ot, derbreW M, et al: training and simulation for patient safety. BMJ Quality & Safety: 19(2):34-43, 2010.
13. www.propublica.org/article/how-many-die-from-medical-mistakes-in-us-hospitals. 2015.
14. www.iom.edu/~/media/Files/report%20Files/1999/to-err-is-Human/to%20err%20is%20Human%201999%20%20report%20brief.pdf. 2015.
15. Okuda y, brysOn eO, deMaria s, et al: the utility of simulation in medical education: What is the evidence? The Mount Sinai Journal of Medicine; new york, 78(4):330-43, 2009.
16. McGaGhie Wc, issenberG sb, cOhen er, barsuk Jh, Wayne db: Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? a meta-analytic comparative review of the evidence. Academic Medicine; June, 86(6):706-11, 2011.
17. www.jointcommission.org/assets/1/18/medical_Liability.pdf. 2015.18. www.medicalsim.org/dawson.htm. 2015
www.cimit.org/about.html. 2015. 19.20. h t tp: / /www.r tmagazine.com/2012/05/educat ing-heal th-
professionals-with-simulation-programs-implications-for-respiratory-therapists/. 2015.
21. www.ncbi.nlm.nih.gov/pmc/articles/PmC3195067/. 2015.22. harris ib, Miller WJ: Feedback in an objective structured clinical
examination by medical students serving as patients, examiners, and teachers. Academic Medicine: Journal of the Association of American Medical Colleges; July, 65(7), 427-96, 1990.
23. berkenstadt h, ereZ d, MunZ y, siMOn d, Ziv a: training assessment of trauma management: the role of simulation-based medical education. Anesthesiology Clinics, 25(1):65-74, 2007.
24. bearMan M, nestel d, andreatta P: Simulation-Based medical education. Oxford Textbook of Medical Education; 186-97, 2013.
25. www.ncbi.nlm.nih.gov/pubmed/22902606. 2015.26.www.harvardmedsim.org/debriefing-assesment-simulation-
healthcare.php. 2015.

251 M.E.J. ANESTH 23 (2), 2015
CASE REPORTS
UltrasoUnd gUided dorsal ramUs nerve block for redUction of postoperative
pain in patients Undergoing lUmbar spine sUrgery: a case series imaging stUdy
Achir Al-AlAmi*, AshrAf Abou El Ezz** And fArid KAssAb***
Abstract
in patients undergoing spine surgery postoperative pain management can often be complicated with side effects associated with high dose narcotic such as respiratory depression and those associated with non-steroidal anti-inflammatory drugs such as interference with bone healing process. local anesthetics can help in both decreasing postoperative pain and minimizing side effects associated with systematically administered analgesics. this report describes the use of preoperative ultrasound guided dorsal ramus nerve block to reduce postoperative pain in six patients undergoing lumbar spine surgery under general anesthesia.
Introduction
patients undergoing spine surgery usually experience severe postoperative pain1-3. in the literature there are many reports describing different techniques of pain relief ranging from systemically administered analgesia to acute pain procedures such as neuraxial analgesia, paravertebral block and local anesthesia infiltration. Intrachecal morphine showed good results in postoperative analgesia for multilevel spine surgery. epidural opioids in form of either single shot extended-release morphine or catheter placement had better safety margin in terms of respiratory depression and urinary retention. Ultrasound- guided bilateral paravertebral catheters recently have been described for postoperative analgesia in patients undergoing lumbar and thoracic laminectomy. Finally intraoperative infiltrations of local anesthesia into the wound, onto the neural root sheath or at the facet joint have also been described4-10.
* MD, Title: Associate Consultant, Affiliation: Anesthesia, International Medical Center, Jeddah, Saudi Arabia. E-mail: [email protected]
Conflicts of Interest: none** md, Consultant & chairman, Affiliation: Anesthesia, International Medical Center, Jeddah, Saudi Arabia. E-mail:elezzay@
aol.com Conflicts of Interest: None*** Consultant & Chairman, Affiliation: Musculoskeletal Center, International Medical Center, Jeddah, Saudi Arabia. E-mail:
[email protected] Conflicts of Interest: None Anesthesia and musculoskeletal departments, International Medical Center, Jeddah, Saudi Arabia Corresponding author: name achir al-alami, department of anesthesia, institution international medical center, mailing
address, 9414 crestwood dr parma Heights, oH 44130. tel: 2672105822. e-mail [email protected]

252 acHir al-alami et. al
Case Description
after obtaining irb approval we collected six patients undergoing spine surgery under general anesthesia to receive dorsal ramus nerveblock for postoperative analgesia (table 1). asa standard monitoring was applied and oxygen was supplemented using face mask at 5 l/min. moderate sedation with intravenous midazolam and propofol infusion was provided. all patients were lying prone with two pillows one under their pelvis and one under their head. the lumbar and lower thoracic areas of spine were prepped with iodine and 75 % alcohol. Us curved probe covered with sterile sheath oscillating at 3.3 or 5 Hz and 6-7 cm depth was used. the levels were identified and labeled by marking pen by longitudinal scanning over transverse process (tp) of lumbo-thoracic vertebra by counting from the sacrum upward.
block method: longitudinal paramedian scanning of tp of thoraco-lumbar spine was obtained. bilateral Us guided block of corresponding drn using in-plane approach with hydrodissection technique was performed. two injections were done: for t11-l4 drn, injections were made at the postero-superior edge of tp just lateral to the zygapophesal (Zp) joint of t and l tp. for l5 drn, injections were made at tp of l5 and at the sacroiliac (si) groove midway between l5 tp and sacral ala (sa) (fig. 1, 2, 3, 4).
Discussion
the sensation of back pain originating from different structures is divided into two types: segmental type is mediated by nociceptors and mechanoreceptors originating from vertebrae, intervertebral disk, dura, nerve root sleeves, facet joint capsules, muscles, ligaments, fascia and skin. non-segmental type of sensation is mediated through sympathetic and parasympathetic innervation reaching vertebral structures via rami communicants. both types of innervation come from drn travelling through spinal nerve roots to reach the spinal cord3,11,12.
drn block using various imaging modalities has been described in relieving chronic low back pain. fluoroscopy-guided drn block appears to be a useful and safe treatment option for chronic back pain. the target point would be at the junction of tp and sap of the sub-adjacent vertebra, midway between the
superior border of the tp and the mamillo-accessory notch12,13. ct-guidance has been described in l5 drn block where the needle just rests between the sa and sap of the sacrum14. finally, Usg has also been described in l5 drn block using initially longitudinal scanning over the tp of l5 than rotating the probe to perform transverse scanning of the sa and sap of the sacrum junction to perform l5/s1 injection15. to our knowledge this is the first report describing USG-guided t12-l5 drn block for postoperative pain relief in patients undergoing lumbar spine surgery.
in cadaver dissection, the l 1-4 drn project almost perpendicular to spinal nerves and run dorsocaudally through the intertransverse space where each divides into 3 branches: lateral and inter-mediate and medial. the lateral branches innervate iliocostalis lumborum then pierce the dorsal layer of thoracolumbar fascia and become cutaneous. the intermediate branches run dorsally and caudally from the intertransverse spaces forming intersegmental communicating branches that innervate longissimus thoracis muscle. each medial branch passes dorsally and caudally through the intertransverse space towards the superior border of the root of the sub-adjacent tp. from there it continues dorsally and caudally, lying against the groove formed by the junction of the root of the tp with that of the sap16.
Having arisen from the spinal nerve it arches over the rostral and dorsal aspect of the sa, lying in the groove formed by the junction of the sa with the root of the sap of the sacrum. along this course it divides into two branches: medial and an intermediate. The intermediate branch innervates those fibers of longissimus thoracis which arose from the medial aspect of the dorsal segment of the iliac crest. the medial branch curves medially around the caudal aspect of the lumbosacral Zp joint, which it innervates ending in multifidus16.
in ultrasound anatomy, as the spinal nerves emerge from their respective intervertebral foramina they branch mainly into ventral and dorsal rami. the ventral rami continue anteriorly into the psoas muscle and terminate as thoraco-abdominal nerves. Whereas drn emerge posteriorly through the neural foramen and divide into medial and lateral branches at the junction of the Zp joints and the upper margin of the tp at which they divide to medial, intermediate and
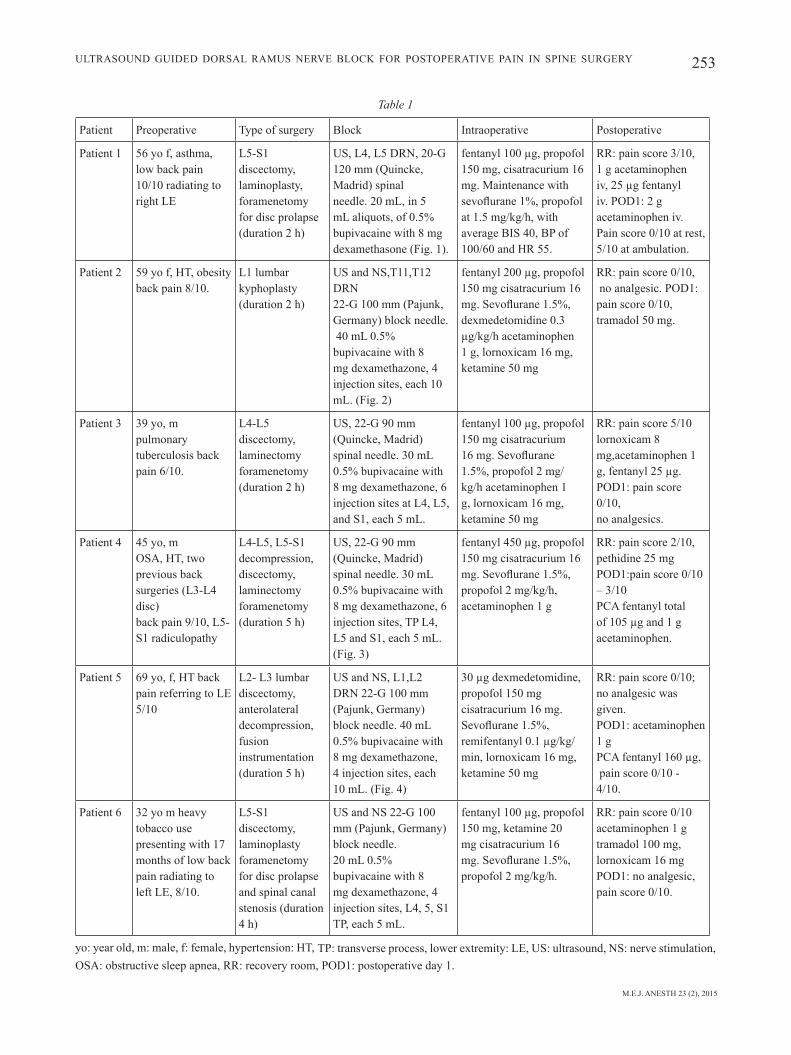
M.E.J. ANESTH 23 (2), 2015
253UltrasoUnd gUided dorsal ramUs nerve block for postoperative pain in spine sUrgery
Table 1
patient preoperative type of surgery block intraoperative postoperative
patient 1 56 yo f, asthma, low back pain 10/10 radiating to right le
l5-s1 discectomy, laminoplasty, foramenetomy for disc prolapse (duration 2 h)
Us, l4, l5 drn, 20-g 120 mm (Quincke, madrid) spinal needle. 20 ml, in 5 ml aliquots, of 0.5% bupivacaine with 8 mg dexamethasone (fig. 1).
fentanyl 100 µg, propofol 150 mg, cisatracurium 16 mg. maintenance with sevoflurane 1%, propofol at 1.5 mg/kg/h, with average bis 40, bp of 100/60 and Hr 55.
rr: pain score 3/10, 1 g acetaminophen iv, 25 µg fentanyl iv. pod1: 2 g acetaminophen iv. pain score 0/10 at rest, 5/10 at ambulation.
patient 2 59 yo f, Ht, obesityback pain 8/10.
l1 lumbar kyphoplasty (duration 2 h)
Us and ns,t11,t12 drn22-g 100 mm (pajunk, germany) block needle. 40 ml 0.5% bupivacaine with 8 mg dexamethazone, 4 injection sites, each 10 ml. (fig. 2)
fentanyl 200 µg, propofol 150 mg cisatracurium 16 mg. Sevoflurane 1.5%, dexmedetomidine 0.3 µg/kg/h acetaminophen 1 g, lornoxicam 16 mg, ketamine 50 mg
rr: pain score 0/10, no analgesic. pod1:pain score 0/10, tramadol 50 mg.
patient 3 39 yo, mpulmonary tuberculosis back pain 6/10.
l4-l5 discectomy, laminectomy foramenetomy (duration 2 h)
Us, 22-g 90 mm (Quincke, madrid) spinal needle. 30 ml 0.5% bupivacaine with 8 mg dexamethazone, 6 injection sites at l4, l5, and s1, each 5 ml.
fentanyl 100 µg, propofol 150 mg cisatracurium 16 mg. Sevoflurane 1.5%, propofol 2 mg/kg/h acetaminophen 1 g, lornoxicam 16 mg, ketamine 50 mg
rr: pain score 5/10 lornoxicam 8 mg,acetaminophen 1 g, fentanyl 25 µg.pod1: pain score 0/10,no analgesics.
patient 4 45 yo, mosa, Ht, two previous back surgeries (l3-l4 disc)back pain 9/10, l5-s1 radiculopathy
l4-l5, l5-s1 decompression, discectomy, laminectomy foramenetomy (duration 5 h)
Us, 22-g 90 mm (Quincke, madrid) spinal needle. 30 ml 0.5% bupivacaine with 8 mg dexamethazone, 6 injection sites, tp l4, l5 and s1, each 5 ml. (fig. 3)
fentanyl 450 µg, propofol 150 mg cisatracurium 16 mg. Sevoflurane 1.5%, propofol 2 mg/kg/h, acetaminophen 1 g
rr: pain score 2/10, pethidine 25 mg pod1:pain score 0/10 – 3/10 pca fentanyl total of 105 µg and 1 g acetaminophen.
patient 5 69 yo, f, Ht back pain referring to le 5/10
l2- l3 lumbar discectomy, anterolateral decompression, fusion instrumentation (duration 5 h)
Us and ns, l1,l2 drn 22-g 100 mm (pajunk, germany) block needle. 40 ml 0.5% bupivacaine with 8 mg dexamethazone, 4 injection sites, each 10 ml. (fig. 4)
30 µg dexmedetomidine, propofol 150 mg cisatracurium 16 mg. Sevoflurane 1.5%, remifentanyl 0.1 µg/kg/min, lornoxicam 16 mg, ketamine 50 mg
rr: pain score 0/10; no analgesic was given. pod1: acetaminophen 1 g pca fentanyl 160 µg, pain score 0/10 - 4/10.
patient 6 32 yo m heavy tobacco use presenting with 17 months of low back pain radiating to left le, 8/10.
l5-s1 discectomy, laminoplasty foramenetomy for disc prolapse and spinal canal stenosis (duration 4 h)
Us and ns 22-g 100 mm (pajunk, germany) block needle.20 ml 0.5% bupivacaine with 8 mg dexamethazone, 4 injection sites, l4, 5, s1 tp, each 5 ml.
fentanyl 100 µg, propofol 150 mg, ketamine 20 mg cisatracurium 16 mg. Sevoflurane 1.5%, propofol 2 mg/kg/h.
rr: pain score 0/10 acetaminophen 1 gtramadol 100 mg, lornoxicam 16 mg pod1: no analgesic, pain score 0/10.
yo: year old, m: male, f: female, hypertension: Ht, tp: transverse process, lower extremity: le, Us: ultrasound, ns: nerve stimulation, osa: obstructive sleep apnea, rr: recovery room, pod1: postoperative day 1.
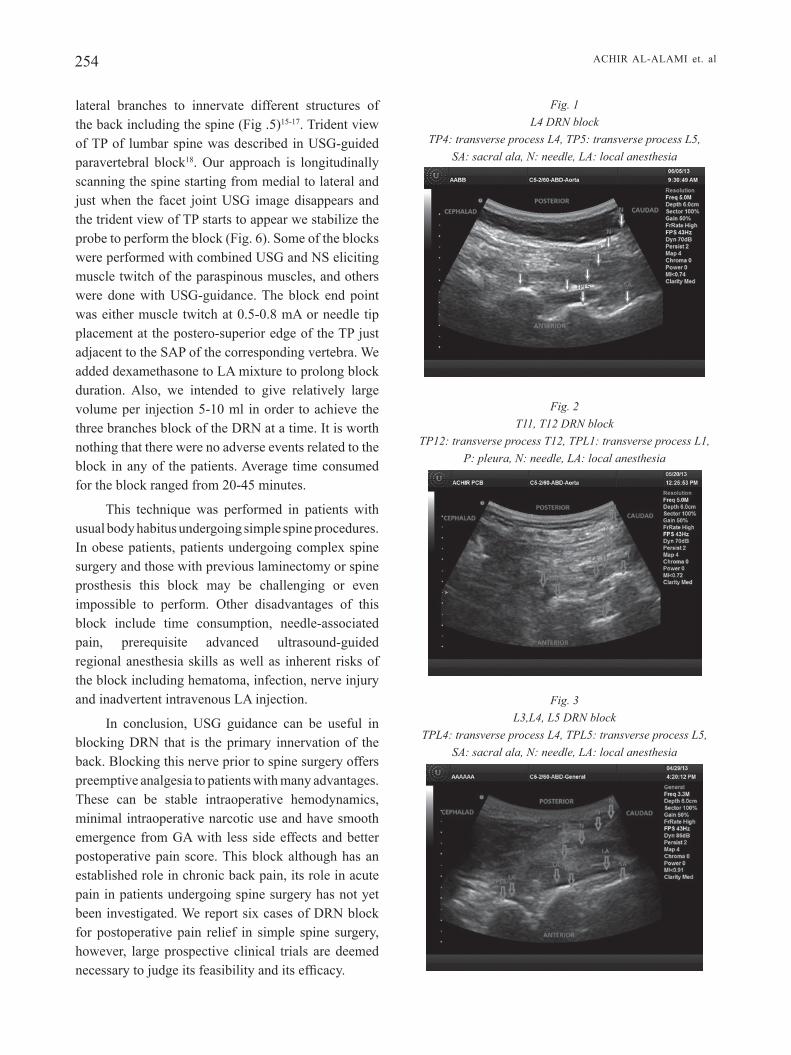
254 acHir al-alami et. al
lateral branches to innervate different structures of the back including the spine (fig .5)15-17. trident view of tp of lumbar spine was described in Usg-guided paravertebral block18. our approach is longitudinally scanning the spine starting from medial to lateral and just when the facet joint Usg image disappears and the trident view of tp starts to appear we stabilize the probe to perform the block (fig. 6). some of the blocks were performed with combined Usg and ns eliciting muscle twitch of the paraspinous muscles, and others were done with Usg-guidance. the block end point was either muscle twitch at 0.5-0.8 ma or needle tip placement at the postero-superior edge of the tp just adjacent to the sap of the corresponding vertebra. We added dexamethasone to la mixture to prolong block duration. also, we intended to give relatively large volume per injection 5-10 ml in order to achieve the three branches block of the drn at a time. it is worth nothing that there were no adverse events related to the block in any of the patients. average time consumed for the block ranged from 20-45 minutes.
this technique was performed in patients with usual body habitus undergoing simple spine procedures. in obese patients, patients undergoing complex spine surgery and those with previous laminectomy or spine prosthesis this block may be challenging or even impossible to perform. other disadvantages of this block include time consumption, needle-associated pain, prerequisite advanced ultrasound-guided regional anesthesia skills as well as inherent risks of the block including hematoma, infection, nerve injury and inadvertent intravenous la injection.
in conclusion, Usg guidance can be useful in blocking drn that is the primary innervation of the back. blocking this nerve prior to spine surgery offers preemptive analgesia to patients with many advantages. these can be stable intraoperative hemodynamics, minimal intraoperative narcotic use and have smooth emergence from ga with less side effects and better postoperative pain score. this block although has an established role in chronic back pain, its role in acute pain in patients undergoing spine surgery has not yet been investigated. We report six cases of drn block for postoperative pain relief in simple spine surgery, however, large prospective clinical trials are deemed necessary to judge its feasibility and its efficacy.
Fig. 1 L4 DRN block
TP4: transverse process L4, TP5: transverse process L5, SA: sacral ala, N: needle, LA: local anesthesia
Fig. 2 T11, T12 DRN block
TP12: transverse process T12, TPL1: transverse process L1, P: pleura, N: needle, LA: local anesthesia
Fig. 3 L3,L4, L5 DRN block
TPL4: transverse process L4, TPL5: transverse process L5, SA: sacral ala, N: needle, LA: local anesthesia
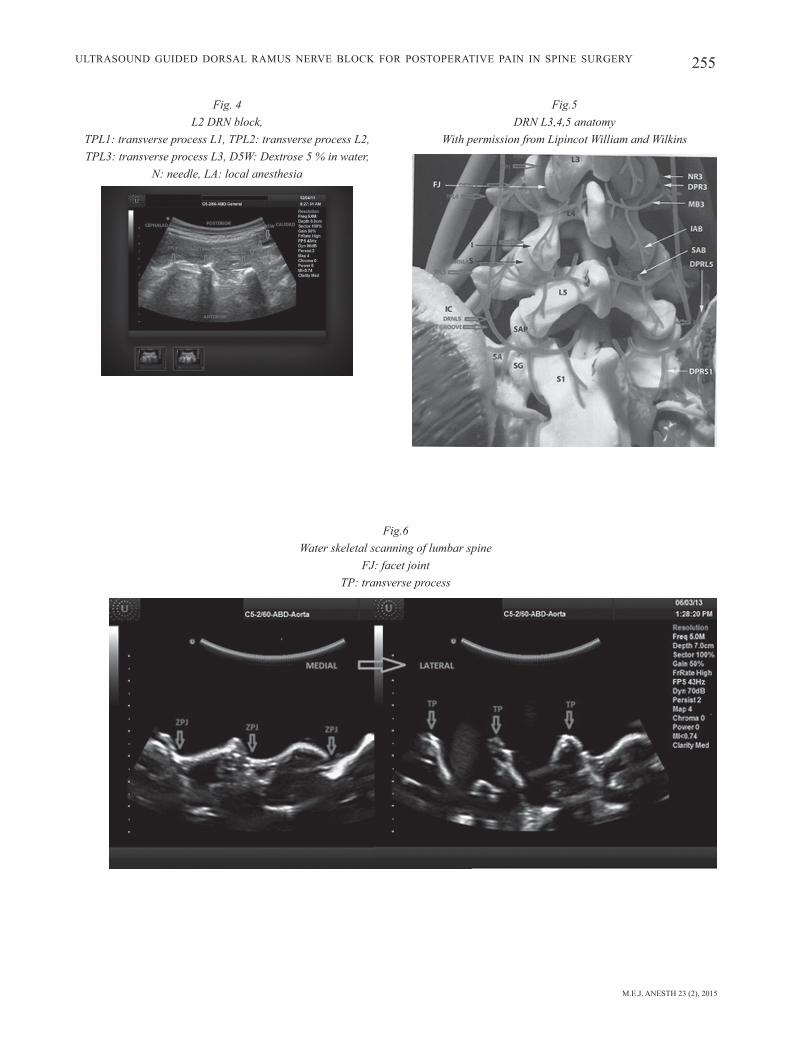
M.E.J. ANESTH 23 (2), 2015
255
Fig.5DRN L3,4,5 anatomy
With permission from Lipincot William and Wilkins
UltrasoUnd gUided dorsal ramUs nerve block for postoperative pain in spine sUrgery
Fig. 4L2 DRN block,
TPL1: transverse process L1, TPL2: transverse process L2,TPL3: transverse process L3, D5W: Dextrose 5 % in water,
N: needle, LA: local anesthesia
Fig.6Water skeletal scanning of lumbar spine
FJ: facet jointTP: transverse process

256 acHir al-alami et. al
References
1. biAnconi m, fErrAro l, ricci r, zAnoli G, AntonElli t, GiuliA b, GubErti A, mAssAri l, Et Al: The pharmacokinetics and efficacy of ropivacaine continuous wound installation after spine fusion surgery. Anesth Analg; 98:166-72, 2004.
2. cohEn bE, hArtmAn mb, WAdE Jt, millEr Js, GilbErt r, chApmAn tm: postoperative pain control after lumbar spine fusion: patient-controlled analgesia versus continuous epidural analgesia. Spine; 22:1892-7, 1997.
3. lAi lt, ortiz-cArdonA Jr, bEndo AA: perioperative pain management in the neurosurgical patient. Anesthesiol Clin; 30:347-67, 2012.
4. schEnK mr, putziEr m, KuGlEr b, tohtz s, VoiGt K, schinK t, Kox WJ, spiEs c, VolK t: postoperative analgesia after major spine surgery: patient-controlled analgesia versus patient-controlled intravenous analgesia. Anesth analg; 103:1311-7, 2006.
5. KlubA t, hofmAnn f, brEdAnGEr s, blumEnstocK G, niEmEyEr t: Efficacy of postoperative analgesia after posterior lumbar instrumented fusion for degenerative disc disease: a prospective randomized comparison of epidural catheter and intravenous administration of analgesics. Orthop Rev; 20:2(1), 2010.
6. pAndin p, rEttAb s, lubAnsu A: Ultrasound guidance is Helpful for paravertebral block performance and catheter placement in patients with laminectomy after thoracotomy or lumbotomy: a case series imaging study. Open Journal of Anesthesiology; 3:67-73, 2013.
7. GurbEt A, bEKAr A, bilGin h, KorfAli G, yilmAzlAr s, tErcAn m: Pre-emptive infiltration of levobupivacaine is superior to at closure administration in lumbar laminectomy patients. Eur Spine J; 17:1237-41, 2008.
8. bAhAri s, El-dAhAb m, clEAry m, spArKEd J: Efficacy of triamcinolone acetonide and bupivacaine for pain after lumbar discectomy. Eur Spine J; 19:1099-103, 2010.
9. bAdEmci G, bAsAr h, sAhin s, ozcAKir s, AnbArci h, EVliyAoGlu c, KEsKil s: Can facet joint infiltrative analgesia reduce postoperative pain in degenerative lumbar disc surgery? Neurocirugia; 19:45-9, 2008.
10. hiGuchi K, sAto t: anatomical study of lumbar spine innervation. Folia Morphol; 61:71-9, 2002.
11. ohtori s, yAmAshitA m, inouE G, yAmAuchi K, suzuKi m, oritA s, EGuchi y, ochiAi n, KishidA s, tAKAso m, tAKAhAshi K: the l2 spinal verve block effects on acute low back pain from osteoporotic vertebral fracture. Journal of Pain; 10:870-875, 2009.
12. miyAKoshi n, shimAdA y, KAsuKAWA y, sAito h, KodAmA h, itoi E: total dorsal ramus block for the treatment of chronic low back pain: a preliminary study. Joint Bone Spine; 74:270-4, 2007.
13. KyounG-tAE K, sEunG-Won p, tAEK-Kyun n: lumbar dorsal ramus block for low back pain. J Kor Neurotraumatol Soc; 3:82-86, 2007.
14. stoJAnoVic mp: basic pain management interventions using fluoroscopy: targets and optimal imaging of lumbar spine. Techniques in Regional Anesthesia and Pain Management; 11:55-62, 2007.
15. biGElEisEn p, orEbAuGh s: Ultrasound-guided regional anesthesia and pain medicine. 1st ed. baltimore, Wolters kluwer, lippincott Williams &Wilkins, 2010.
16. boGduK n, Wilson As, tynAn W: the human lumbar dorsal rami. J Anat; 2:383-397, 1982.
17. zhou l, schnEcK cd, shAo z: the anatomy of dorsal ramus nerves and its implications in lower back pain. Neuroscience & Medicine; 3:192-201, 2012.
18. KArmAKAr mK, ho Am, li x, KWoKWh, tsAnG K, nGAn KEE Wd: Ultrasound-guided lumbar plexus block through the acoustic window of the lumbar ultrasound trident. Br J Anaesth; 100:533-7, 2008.

257 M.E.J. ANESTH 23 (2), 2015
A ShAred OperAtive Field And the diSpute – iS there A WAy Out?
M-Irfan SuleMan*, anIta n. akbaralI*, M. SaIf SIddIquI* and WIllIaM f alfonSo*
Abstract
Submental intubation is an alternative to tracheostomy in patients requiring surgical access to both oral and nasal cavities. it is relatively safe, simple, and low morbidity procedure and requires only basic surgical equipment to perform. We successfully performed a submental intubation in a young patient with maxillofacial hypoplasia undergoing le Fort i maxillary advancement without any intra- and post-operative complications.
Keywords: Submental intubation, maxillofacial procedure, facial trauma, and airway.
Introduction
Maxillofacial procedures can create an exhaustive drill for an anesthesiologist to acquire a secure airway, which necessitates a substantial amount of cooperation between the surgeon and the anesthesiologist when the operative field is a constant threat to the airway. Alternative options like tracheostomy, retromolar, and submental intubation are techniques that can be utilized in such scenarios. Of these, submental intubation has shown to be simple, safe, and cost effective with no major post-operative complications1,2. due to the rapidity of access, submental intubation has also been utilized in establishing airway in patients with maxillofacial trauma3,4. here we describe our experience in a patient undergoing submental intubation for maxillary advancement who previously had multiple surgeries as a child to correct dysplasia.
Case description
A 22-year-old female patient with severe maxillary hypoplasia and frontonasal dysplasia (Mallampati score, Mpii) was scheduled for le Fort i maxillary advancement. After application of standard monitors and preoxygenation, slow inhalational induction was performed. initially, we used inhalation induction to keep the patient spontaneously breathing under anesthesia. Bilateral nares were prepared using oxymetazoline nasal spray in anticipation of nasal intubation. A trial of inserting a 14 French catheter through the bilateral nares was unsuccessful. Fiber optic visualization revealed distorted anatomy probably secondary to previous surgical procedures. Alternatively, after controlled intravenous induction, a direct laryngoscopy with a Macintosh laryngoscope size 3 blade was performed and a grade III view, as classified by Cormack and Lehane5, was observed. A 6.0mm reinforced endotracheal tube was inserted and secured temporarily. A small
* Md. Corresponding author: M-irfan Suleman, Md, Assistant professor of Anesthesiology, division of pediatric Anesthesia and
Pain Medicine, Arkansas Children’s Hospital and University of Arkansas for Medical Sciences, 1 Children's Way Slot #203, Little Rock, AR 72202 USA. Office phone: 502-386-2444. E-mail: [email protected]

258 M- irFAn SuleMAn et. al
incision was placed through the skin in the submental region by the surgeon (Fig 1). A curved hemostat was inserted through the skin incision to gain access to the floor of the mouth (Fig 2). Access was established on the lingual surface of the mandible in order to avoid injury to the lingual nerve and artery, and Wharton’s duct. the proximal endotracheal tube connector was removed and the tube was pulled through the skin incision using a hemostat. the proximal connector was then reattached to the endotracheal tube and it was sutured and secured. Once the airway was secure, general anesthesia maintained it by using a sevoflurane inhalation agent along with oxygen and an opioid for pain control with pressure control ventilation. Throughout the procedure, an adequate surgical field was available to the surgeon with no compromise on respiratory parameters. After completion of the procedure, the endotracheal tube was pulled back into the oral cavity and submental incision was sutured. the patient was extubated awake. no complications were noted in post-operative period.
Discussion
Maxillofacial anomalies and trauma has been a challenging scenario for anesthesiologists. establishing a secure airway and sharing the narrow field with surgeons was not without major complication until 1986 when the submental route of intubation was
introduced. It was first described by Hernandez6. it not only revolutionized the approach to surgical airway management but also showed prominent advantages over other surgical airway techniques like tracheostomy and retromolar intubation2,7,8. Although tracheostomy is an efficient and time-tested option, it has major post-operative complications like infections, prolonged hospital admission, and tracheostomy care expense9-11. By decreasing the number of emergent and controlled tracheostomies, considerable decrease in post-operative complications and management cost have been shown12. On the other hand, retromolar intubation might not be the option in many patients due to inadequate retromolar space.
Submental intubation is a simple and quick technique that can be incorporated with a majority of maxillofacial surgical procedures without a major increase in procedure time. the technique allows easy and unobstructed access to the maxillofacial anatomy and prevents the need for a tracheotomy for airway maintenance during surgery. if there is a contraindication to a nasal tube, this technique allows the work to proceed. Since its introduction, modifications have been described and several institutional reviews have been published demonstrating its safety and efficacy1,2,8. Submental intubation is a surgical airway management technique that has shown to be a better procedure than others, is largely accepted by surgeons and patients, and does not involve substantial morbidity1,8.
Fig. 2
Fig. 1

M.E.J. ANESTH 23 (2), 2015
259SuBMentAl intuBAtiOn
References
1. Meyer C, Valfrey J, kJartanSdottIr t, WIlk a, barrIère P: Indication for and technical refinements of submental intubation in oral and maxillofacial surgery. J Craniomaxillofac Surg; 31(6):383-388, 2003.
2. Gadre kS, WaknIS PP: transmylohyoid/submental intubation: review, analysis, and refinements. J Craniofac Surg; 21(2):516-519, 2010.
3. lIMa SM Jr, aSPrIno l, MoreIra rW, de MoraeS M: A retrospective analysis of submental intubation in maxillofacial trauma patients. J Oral Maxillofac Surg; 69(7):2001-2005, 2011.
4. JunIor JM, kluPPel le, PereIra StabIle Cl, VIttI StabIle Ga: Submental endotracheal intubation as an alternative to tracheostomy in selected cases of facial fracture: literature review and technique report. Ulus Travma Acil Cerrahi Derg; 18(6):545-548, 2012.
5. CorMaCk rS, lehane J: Difficult tracheal intubation on obstetrics. Anaesthesia; 39:1105-1111, 1984.
6. hernandez, af: the submental route for endotracheal intubation. A new technique. J Maxillofac Surg; 14(1):64-65, 1986.
7. adeyeMo Wl, oGunleWe Mo, deSalu I, akanMu on, ladeInde al: Submental / transmylohyoid intubation in maxillofacial surgery: report of two cases. Niger J Clin Pract; 14(1):98-101, 2011.
8. o'Connell Je, kearnS GJ: Submental intubation: a retrospective review of 45 cases. Ir J Med Sci 182(3):309-313, 2012.
9. Carr MM, Poje CP, Kingston L, Leilma D, Heard C. Complications in pediatric tracheostomies. Laryngoscope; 111(Pt 1):1925-1928, 2001.
10. butnaru CS, ColreaVy MP, ayarI S, froehlICh P: tracheotomy in children: evolution in indications. Int J Pediatr Otorhinolaryngol 70(1):115-119, 2006.
11. ItaMoto Ch, lIMa bt, Sato J, fuJIta rr: indications and complications of tracheostomy in children. Braz J Otorhinolaryngol; 76(3):326-331, 2010.
12. klotz da, henGerer aS: Safety of pediatric bedside tracheostomy in the intensive care unit. Arch Otolaryngol Head Neck Surg; 127:950-955, 2001.


261 M.E.J. ANESTH 23 (2), 2015
LETTER TO THE EDITOR
Residual NeuRomusculaR Blockade (RNmB): RocuRoNium's defasciculatiNg dose, NeostigmiNe-
iNduced WeakNess, aNd aWaReNess duRiNg RecoveRy
Deepak Gupta*
Residual neuromuscular blockade (RNmB) is always a potential concern for anesthesiologists. However, there is no uniformity and/or universal protocol (because it constantly keeps evolving) in regards to neuromuscular blocking drugs (NmBds) administrations based on peri-operative neuromuscular monitoring as well as tracheal extubations guided by neuromuscular monitoring. moreover, neuromuscular monitors are either qualitative that is subjective visual assessment by providers for presence of twitches for train-of-four (tof) stimulations, or quantitative wherein numerical values for tof ratios are ascertained by either acceleromyographic (amg) monitoring or electromyographic (emg) monitoring. to avoid the tof ratios' overestimation by amg monitoring1 that can cause more false-positives in regards to preparedness for extubations and more false-negatives in regards to RNmB as gold standardized by emg monitoring, recent intra-departmental implementation of quantitative emg monitoring by todd et al.2 appears as commendable tool against RNmB. However, as many as 37% patients had been reported to not receive neostigmine despite receiving intraoperative rocuronium (most commonly used non-depolarizing NmBds) presumably secondary to assumed spontaneous reversal. it is interesting to note that post-extubation tof ratios can give insight into assumed spontaneous reversal's etiologies and the patterns they follow such as time elapsed since rocuronium's last dose and rocuronium's total dose, or exclusive use of depolarizing NmBds (succinylcholine). moreover, in future research it remains to be seen if a pre-quantified duration since last dose of rocuronium matters in the currently followed definition for RNMB (TOF ratio<0.9 by EMG monitoring1) for the patients who receive only one-time defasciculating doses or one-time intubating doses of rocuronium without any additional dose supplementations. these future investigations will give insight into variable frequencies of spontaneous reversals (without neostigmine administration) and potential for suboptimal recovery-room tof ratios because (a) rocuronium's defasciculating doses (despite prevalent variable defasciculating doses3 and variable lag periods for succinylcholine administration after rocuronium affecting tof ratios) may or may not require neostigmine, and (b) intubation-induced parasympathetic surge-related acetylcholine release (although primarily implicated in intubation-induced bronchospasm4) may or may not hasten spontaneous reversal by decreasing rocuronium's intubating doses' duration of action5-6. moreover, as neostigmine-administration can (a) itself depress tof ratio in upto 13% patients for variable time-periods after 40mcg/kg neostigmine dose7 or (b) be avoided for the potential risk of post-reversal weakness in spontaneously reversed patients with TOF ratio >0.92 or (c) cause weakness in patients who had not received prior non-depolarizing NmBds8, an appropriate sequential-emg monitoring should include pre-reversal (neostigmine/spontaneous) tof ratio followed by pre-extubation tof
* md, department of anesthesiology, Wayne state university/detroit medical center, detroit, michigan, united states. Corresponding author: Dr. Deepak Gupta, Box No. 162, 3990 John R, Detroit, MI 48201, United States. Ph: 1-313-745-
7233, Fax: 1-313-993-3889. E-mail: [email protected]

262 deepak gupta
ratio followed by post-extubation tof ratio followed by recovery-room tof ratio. an enhanced form of intra-departmental implementation should also ensure standardized protocol for sedation among patients with clinically-underdiagnosed but emg-exposed RNmB because in-vivo muscle relaxants (although not specifically studied during residual paralysis stages)9 may increase the risk for awareness under anesthesia10 with subsequent long-term psychological sequelae11 when patient is recovering from intraoperative neuromuscular blockade through intermediary transient postoperative RNmB. the standardization of sedation protocol for RNmB primarily needs to address indications and timeline when to initiate sedation in "paralyzed" patients recovering from general anesthetics (whether end-expiratory inhalational gas concentrations vs. tof ratios needs to be used as sedation-initiation triggers) and what medications needs to be administered for recovery-
room intravenous sedation (amnestics vs. anesthetics). finally, universal quantitative emg monitoring needs to account for how to manage emg-overdiagnosed "paralyzed" patients' awareness risks despite these patients (sometimes) undergoing otherwise uneventful post-anesthesia cardio-respiratory recoveries even when their recovery room tof ratios are well below 0.92. in summary, skeptics can always question the universal use of emg-monitoring based reversals, extubations and recoveries of patients receiving peri-operative non-depolarizing NmBds; however they can never deny the fact that in the face of risks for RNmB-complicated recovery room cardio-respiratory events and still-non-quantified incidence of RNMB-related awareness of “paralysis” and its sequelae, emg-based tof ratios as quantitative neuromuscular monitoring can never be found guilty for being overused by anesthesiologists.
References
1. LianG SS, Stewart pa, phiLLipS S: an ipsilateral comparison of acceleromyography and electromyography during recovery from nondepolarizing neuromuscular block under general anesthesia in humans. Anesth Analg; 117:373-379, 2013.
2. toDD MM, hinDMan BJ, kinG BJ: the implementation of quantitative electromyographic neuromuscular monitoring in an academic anesthesia department. Anesth Analg; 119:323-331, 2014.
3. kiM kn, kiM kS, Choi hi, JeonG JS, Lee hJ: optimal precurarizing dose of rocuronium to decrease fasciculation and myalgia following succinylcholine administration. Korean J Anesthesiol; 66:451-456, 2014.
4. JooSte e, kLafter f, hirShMan Ca, eMaLa Cw: a mechanism for rapacuronium-induced bronchospasm: m2 muscarinic receptor antagonism. Anesthesiology; 98:906-911, 2003.
5. roBertSon en, DrieSSen JJ, BooiJ Lh: suxamethonium administration prolongs the duration of action of subsequent
rocuronium. Eur J Anaesthesiol; 21:734-737, 2004.6. DuBoiS MY, Lea De, kataria B, GaDDe pL, tran DQ, Shearrow
t: Pharmacodynamics of rocuronium with and without prior administration of succinylcholine. J Clin Anesth; 7:44-48, 1995.
7. CaLDweLL Je: Reversal of residual neuromuscular block with neostigmine at one to four hours after a single intubating dose of vecuronium. Anesth Analg; 80:1168-1174, 1995.
8. paYne Jp, huGheS r, aL azawi S: Neuromuscular blockade by neostigmine in anaesthetized man. Br J Anaesth; 52:69-76, 1980.
9. SiGaLovSkY n: awareness under general anesthesia. AANA J; 71:373-379, 2003.
10. SanDin rh, enLunD G, SaMueLSSon p, LennMarken C: awareness during anaesthesia: a prospective case study. Lancet; 355:707-711, 2000.
11. LennMarken C, BiLDforS k, enLunD G, SaMueLSSon p, SanDin r: victims of awareness. Acta Anaesthesiol Scand; 46: 229-231, 2002.
M.E.J. ANESTH 22 (6), 2014
Clinical or laboratory investigations:The following structured format is required:
1. Cover Letter 7. Discussion
2. Title page 8. Acknowledgements
3. Abstract 9. References
4. Introduction 10. Tables
5. Methods 11. Figures
6. Results
1. Cover LetterManuscripts must be accompanied by a cover letter, signed by all authors and stating that:
- All authors have contributed intellectually to the manuscript and the manuscript has been read and approved by all the authors.
- The manuscript has not been published, simultaneously submitted or accepted for publication elsewhere.
2. Title PageStarts at page 1 and includes:
- A concise and informative title (preferably less than 15 words). Authors should include all information in the title that will make electronic retrieval of the article both sensitive and specific.
- Authors listing: first name, middle initial and last name with a superscript denoting the academic degrees as footprints.
- The name of the department(s) and institutions(s) to which the work should be attributed.
- The name, address, telephone, fax numbers and e-mail address of the corresponding author.
- Disclose sources of financial support (grants, equipment, drug etc…).
- Conflict of interest: disclosure of any financial relationships between authors and commercial interests with a vested interest in the outcome of the study.
- A running head, around 40 characters.- Word count of the text only (excluding abstract,
acknowledgements, figure legends and references).
3. AbstractAbstract should follow the title page. It should be
structured with background, methods, results and conclusion.
The Middle East of Anesthesiology publishes original work in the fields of anesthesiology, intensive care, pain, and emergency medicine. This includes clinical or laboratory investigations, review articles, case reports and letters to the Editor.
Submission of manuscripts:The Middle East Journal of Anesthesiology accepts
electronic submission of manuscripts as an e-mail attachment only.
Manuscripts must be submitted via email attachment to:
Editor-In-Chief,
Department of Anesthesiology,
American University of Beirut Medical Center
Beirut, Lebanon
E-mail: [email protected]
Human SubjectsManuscripts describing investigations performed in
humans must state that the study was approved by the appropriate Institutional Review Board and written informed consent was obtained from all patients or parents of minors.
Language:Articles are published in English.
Manuscript PreparationManuscript format required:
Double-spaced lines
Wide margins (1.5 inches or 3.8 cm)
Page numbers start on title page
Word count should reflect text only (excluding abstract, references, figures and tables).
Editorial 1500
Abstract 250 (General articles)100 (Case Reports)
Review article 4000
Original article 3000
Case Reports 800
Letter to Editor 500
GUIDELINES FOR AUTHORS
8. AcknowledgementsThey should be brief. Individuals named must be given
the opportunity to read the paper and approve their inclusion in the acknowledgments.
9. References- References should be indicated by Arabic numerals in
the text in the form of superscript and listed at the end of the paper in the order of their appearance. Please be accurate, giving the names of all authors and initials, the exact title, the correct abbreviation of the journal, year of publication, volume number and page numbers.
- The titles of journals should be abbreviated according to the style used in the list of Journals Indexed for MEDLINE.
Example: (1) from a journal (2) from a book.1. SHAWW: AND ROOT B: Brachial plexus anesthesia
Comparatives study of agents and techniques. Am. J. Surg.; 1951, 81:407.
2. ROBINSON JS: Modern Trends in Anaesthesia, Evans and Gray Ch. 8, Butterworth Pub. Co., London 1967.
10. TablesTables capture information concisely and display it
efficiently: They also provide information at any desired level of details and precision. Including data in tables rather than text frequently makes it possible to reduce the length of the text.
- Type or print each table with double spacing on a separate sheet of paper.
- Number tables consecutively in the order of their first citation in the text.
- Supply a brief title for each.- Place explanatory matter in footnotes, not in the
heading.- Explain all nonstandard abbreviations in footnotes.- Identify statistical measures of variations, such as
standard deviation and standard error of the mean.
11. Figures- Figures should be submitted in JPEG or TIFF format
with a minimum of 150 DPI in resolution.- Colored data if requested by author is chargeable.- If a figure has been published previously, acknowledge
the original source and submit written permission from the copyrights holder to produce the figure.
Abbreviations and symbols:- Use only standard abbreviations.- Avoid abbreviations in the title of the manuscript.- The spelled-out abbreviations followed by the
abbreviation in parenthesis should be used in first mention.
It should state, the specific purpose of the research or hypotheses tested by the study, basic procedures, main findings and principal conclusions.
Provide separate word count for the abstract.
4. IntroductionProvide the nature of the problem and its significance.
State the specific purpose or research objectives or hypothesis tested. Provide only directly pertinent references and do not include data or conclusions from the work being reported.
5. MethodsA. Selection and description of participants:
- Describe selection of participants (including controls) clearly, including eligibility and exclusion criteria.
B. Technical information:- Identify the methods, apparatus (give the
manufacturer’s name and address in parentheses), and procedure in sufficient detail to allow others to reproduce the results. Give references to established methods. Provide references and brief descriptions for methods that have been published. Identify precisely all drugs and chemicals used, including generic names(s), dose(s) ands routes(s) of administration.
C. Statistics-describe statistical methods with enough detail to enable a knowledgeable reader with access to the original date to verify the reported results. Define statistical terms, abbreviations and most symbols. Specify the computer software used. Provide a power analysis for the study.
6. ResultsPresent your results in logical sequence in the text, tables
and illustrations, giving the main or most important findings first. Do not repeat all the data in the tables or illustrations in the text: emphasize or summarize only the most important observations. Extra or supplementary materials and technical details can be placed in an appendix.
7. DiscussionEmphasize the new and important findings of the study
and the conclusions that may be drawn.
Do not repeat in details data or other information given in the Introduction or the Results sections. For experimental studies, it is useful to begin the discussion by summarizing briefly the main findings, then explore possible mechanisms or explanations for these findings, compare and contrast the results with other relevant studies. State the limitations of the study, and explore the implications of the findings for future research and for clinical practice. Link the conclusions with the goals of the study, but avoid unjustified statements and conclusions not adequately supported by the data.

Related Documents











