Bone Pathology Oral Pathology I Disease Def’n/Mode of Inheritance (KNOW!) Clinical Features Radiographic Features Oral Features Histo- pathological Features Treatment and Prognosis Extra Information Osteogenesis Imperfecta -AD, AR, spontaneous mutations -all affect collagen maturation -fragile bones, blue sclera, hypoacusis, bone deformities, joint hyperextensibility -osteopenia -bowing, angulation & deformity of long bones -multiple fx -Wormian bones in skull -clinically & radiographically identical to dentinogenesis imperfecta; termed opalescent teeth (1&2 dentitions involved; blue to brown translucence, pulpal obliteration) -often class III malocclusion -florid osseous dysplasia -attenuated bone -minimal matrix -immature woven bone -bone fracture management -teeth often show attrition -overall disability depends on severity of disease -there are 4 types of Osteogenesis Imperfecta (we don’t need to know specifics for each type) Osteopetrosis -rare disease of osteoclastic defect -Infantile osteopetrosis has AR inheritance -really is a BONE disease, not a tooth disease Infantile: -increased skeletal density (delayed tooth eruption) -Infantile ranges from malignant to intermediate to transient -Adult usually is benign -Osteosclerosis is NOT = osteopetrosis! sclerosis is more of an inflammatory dz Cleidocranial Dysplasia -AD and spontaneous mutation -defect of osteoblastic differentiation -hypoplasia, malformation or absence of clavicles -short stature, large heads, frontal bossing, ocular hypertelorism, depressed nasal bridge -open skull sutures, Wormian bones -increased prevalence of cleft palate -retained deciduous teeth -unerupted permanent & supernumerary teeth (lack secondary cementum) -narrow ascending mandibular ramus (may develop class III malocclusion) -IS significant dentally

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 1/16
Bone Pathology Oral Pathology I
Disease Def’n/Mode of Inheritance(KNOW!)
Clinical Features RadiographicFeatures
Oral Features Histo-pathologicalFeatures
Treatment andPrognosis
Extra Information
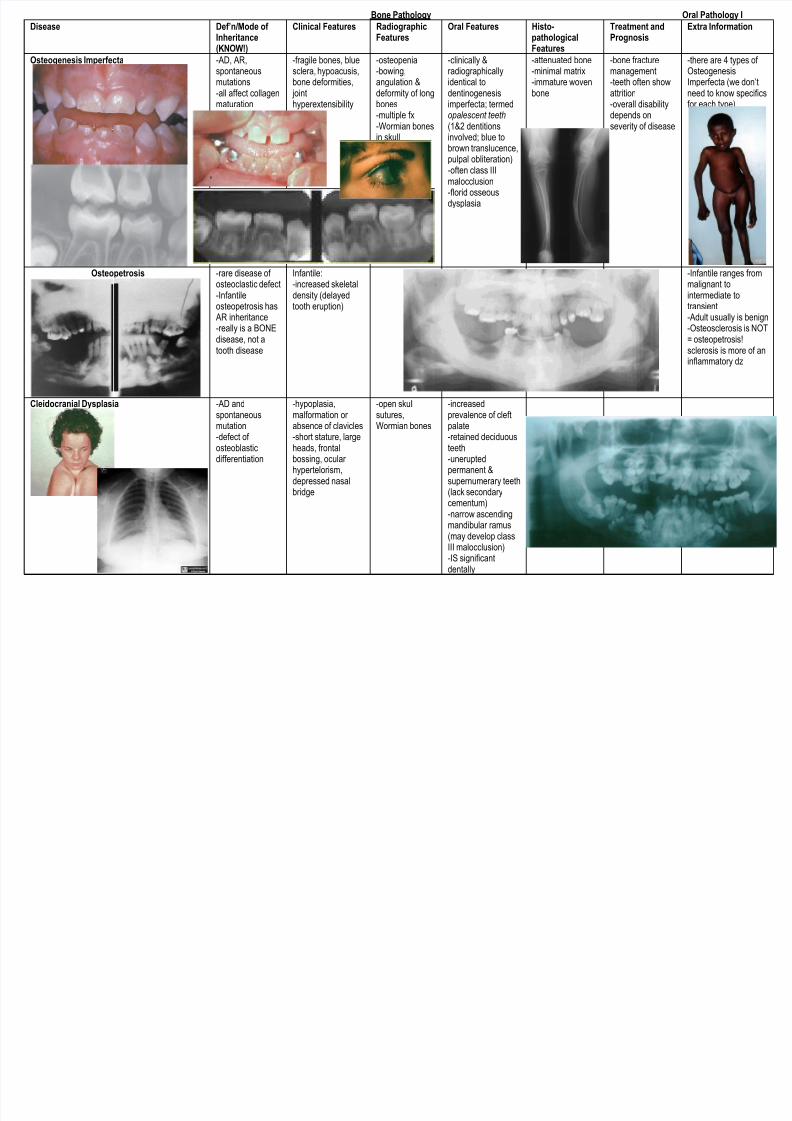
Osteogenesis Imperfecta -AD, AR,spontaneousmutations-all affect collagenmaturation
-fragile bones, bluesclera, hypoacusis,bone deformities, jointhyperextensibility
-osteopenia-bowing,angulation &deformity of longbones-multiple fx-Wormian bones
in skull
-clinically &radiographicallyidentical todentinogenesisimperfecta; termedopalescent teeth(1&2 dentitions
involved; blue tobrown translucence,pulpal obliteration)-often class IIImalocclusion-florid osseousdysplasia
-attenuated bone-minimal matrix-immature wovenbone
-bone fracturemanagement-teeth often showattrition-overall disabilitydepends onseverity of disease
-there are 4 types of OsteogenesisImperfecta (we don’tneed to know specificsfor each type)
Osteopetrosis -rare disease of osteoclastic defect-Infantileosteopetrosis has AR inheritance-really is a BONEdisease, not atooth disease
Infantile:-increased skeletaldensity (delayedtooth eruption)
-Infantile ranges frommalignant tointermediate totransient-Adult usually is benign-Osteosclerosis is NOT= osteopetrosis!sclerosis is more of aninflammatory dz
Cleidocranial Dysplasia -AD andspontaneousmutation-defect of osteoblasticdifferentiation
-hypoplasia,malformation or absence of clavicles-short stature, largeheads, frontalbossing, ocular hypertelorism,depressed nasalbridge
-open skullsutures,Wormian bones
-increasedprevalence of cleftpalate-retained deciduousteeth-uneruptedpermanent &supernumerary teeth(lack secondarycementum)-narrow ascendingmandibular ramus
(may develop classIII malocclusion)-IS significantdentally
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 2/16
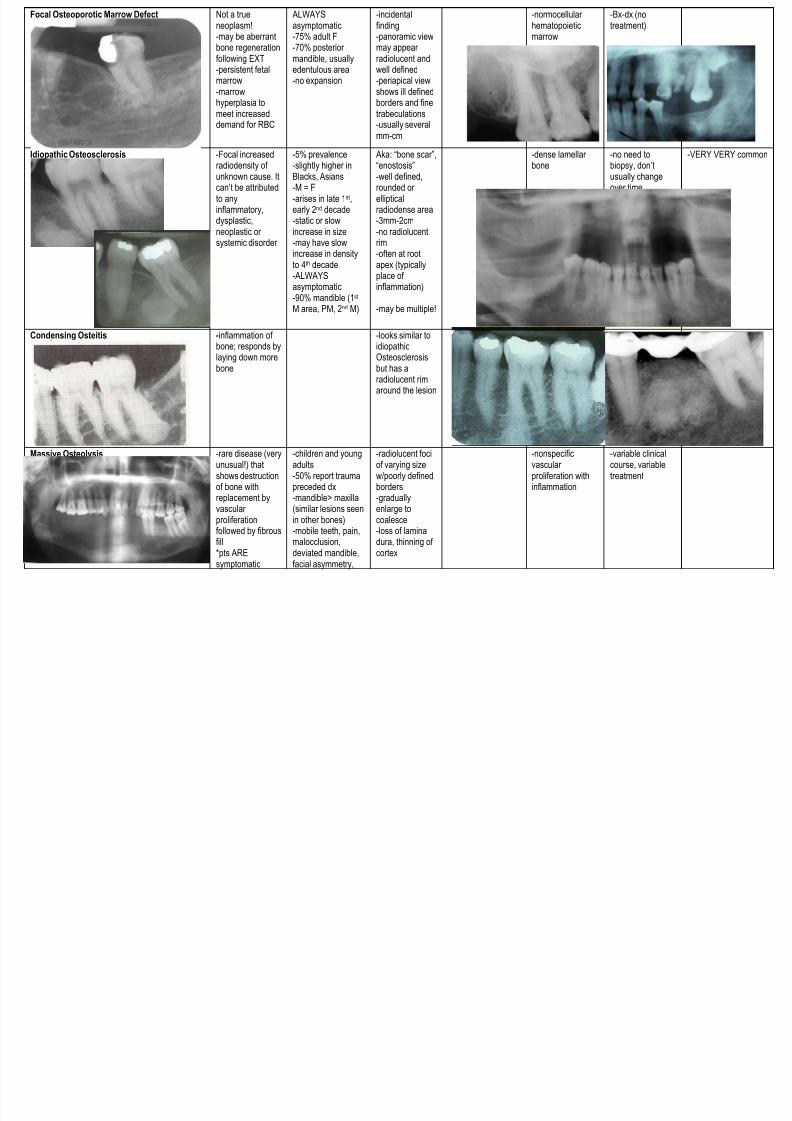
Focal Osteoporotic Marrow Defect Not a trueneoplasm!-may be aberrantbone regenerationfollowing EXT-persistent fetalmarrow-marrowhyperplasia tomeet increaseddemand for RBC
ALWAYSasymptomatic-75% adult F-70% posterior mandible, usuallyedentulous area-no expansion
-incidentalfinding-panoramic viewmay appear radiolucent andwell defined-periapical viewshows ill definedborders and finetrabeculations-usually several
mm-cm
-normocellular hematopoieticmarrow
-Bx-dx (notreatment)
Idiopathic Osteosclerosis -Focal increasedradiodensity of unknown cause. Itcan’t be attributedto anyinflammatory,dysplastic,neoplastic or systemic disorder
-5% prevalence-slightly higher inBlacks, Asians-M = F-arises in late 1st,early 2nd decade-static or slowincrease in size-may have slowincrease in density
to 4th
decade-ALWAYSasymptomatic-90% mandible (1st M area, PM, 2nd M)
Aka: “bone scar”,“enostosis” -well defined,rounded or ellipticalradiodense area-3mm-2cm-no radiolucentrim-often at root
apex (typicallyplace of inflammation)
-may be multiple!
-dense lamellar bone
-no need tobiopsy, don’tusually changeover time.
-VERY VERY common
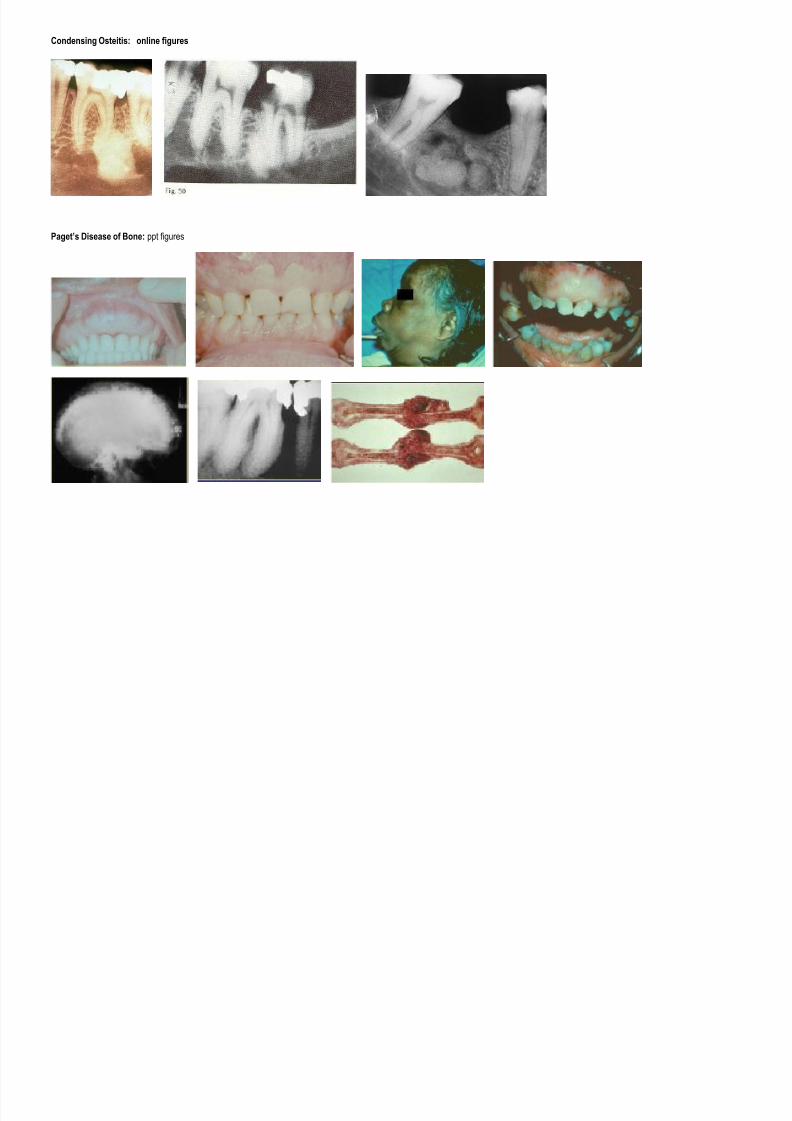
Condensing Osteitis -inflammation of bone; responds bylaying down morebone
-looks similar toidiopathicOsteosclerosisbut has aradiolucent rimaround the lesion
Massive Osteolysis -rare disease (veryunusual!) thatshows destructionof bone withreplacement byvascular proliferation
followed by fibrousfill*pts AREsymptomatic
-children and youngadults-50% report traumapreceded dx-mandible> maxilla(similar lesions seenin other bones)
-mobile teeth, pain,malocclusion,deviated mandible,facial asymmetry,
-radiolucent fociof varying sizew/poorly definedborders-graduallyenlarge tocoalesce
-loss of laminadura, thinning of cortex
-nonspecificvascular proliferation withinflammation
-variable clinicalcourse, variabletreatment
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 3/16
sleep apnea,pathologic fx
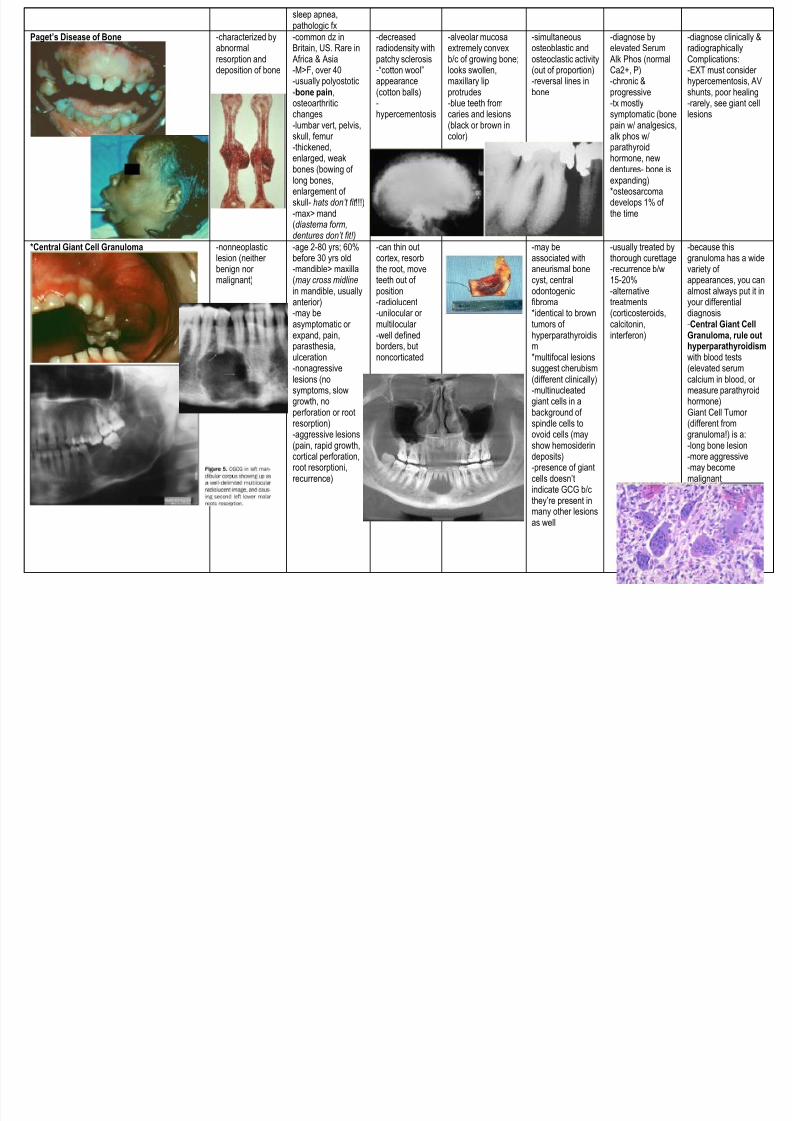
Paget’s Disease of Bone
-characterized byabnormalresorption anddeposition of bone
-common dz inBritain, US. Rare in Africa & Asia-M>F, over 40-usually polyostotic-bone pain,osteoarthriticchanges-lumbar vert, pelvis,
skull, femur -thickened,enlarged, weakbones (bowing of long bones,enlargement of skull- hats don’t fit !!!)-max> mand(diastema form,dentures don’t fit!)
-decreasedradiodensity withpatchy sclerosis-“cotton wool”appearance(cotton balls)-hypercementosis
-alveolar mucosaextremely convexb/c of growing bone;looks swollen,maxillary lipprotrudes-blue teeth fromcaries and lesions(black or brown in
color)
-simultaneousosteoblastic andosteoclastic activity(out of proportion)-reversal lines inbone
-diagnose byelevated Serum Alk Phos (normalCa2+, P)-chronic &progressive-tx mostlysymptomatic (bonepain w/ analgesics,
alk phos w/parathyroidhormone, newdentures- bone isexpanding)*osteosarcomadevelops 1% of the time
-diagnose clinically &radiographicallyComplications:-EXT must consider hypercementosis, AVshunts, poor healing-rarely, see giant celllesions
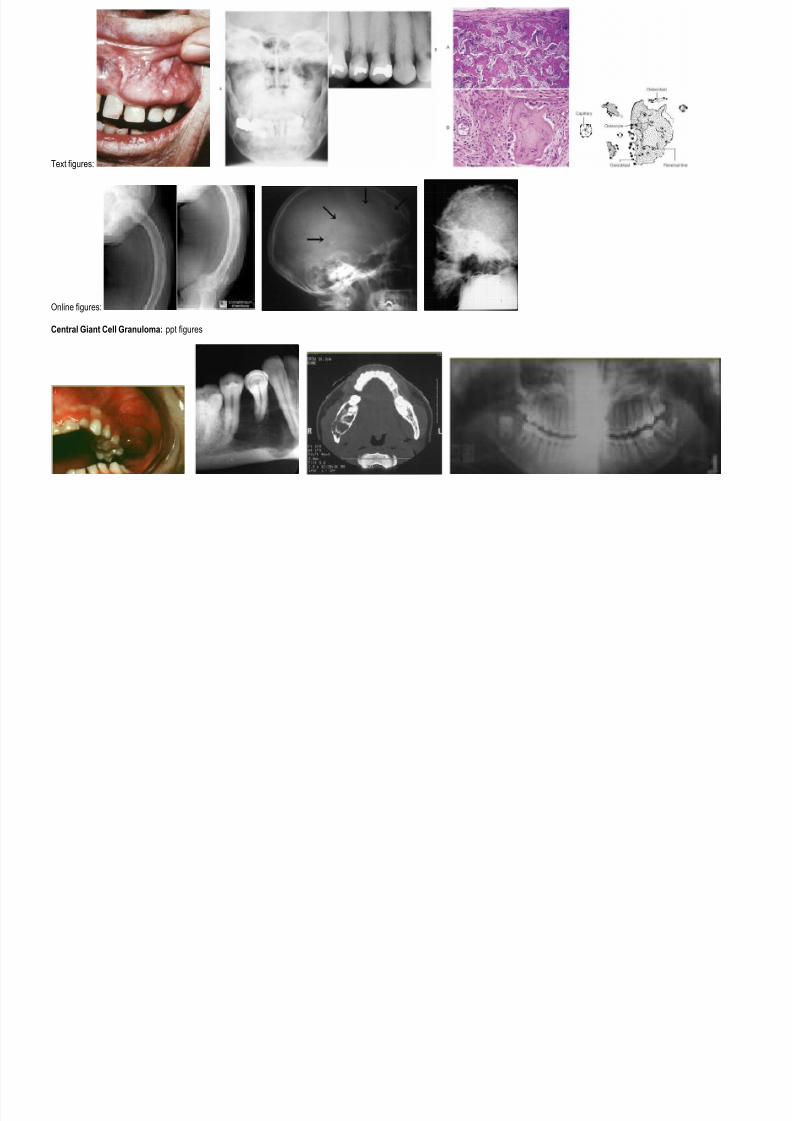
*Central Giant Cell Granuloma -nonneoplasticlesion (neither
benign nor malignant)
-age 2-80 yrs; 60%before 30 yrs old
-mandible> maxilla(may cross midline in mandible, usuallyanterior)-may beasymptomatic or expand, pain,parasthesia,ulceration-nonagressivelesions (nosymptoms, slow
growth, noperforation or rootresorption)-aggressive lesions(pain, rapid growth,cortical perforation,root resorptioni,recurrence)
-can thin outcortex, resorb
the root, moveteeth out of position-radiolucent-unilocular or multilocular -well definedborders, butnoncorticated
-may beassociated with
aneurismal bonecyst, centralodontogenicfibroma*identical to browntumors of hyperparathyroidism*multifocal lesionssuggest cherubism(different clinically)-multinucleated
giant cells in abackground of spindle cells toovoid cells (mayshow hemosiderindeposits)-presence of giantcells doesn’tindicate GCG b/cthey’re present inmany other lesionsas well
-usually treated bythorough curettage
-recurrence b/w15-20%-alternativetreatments(corticosteroids,calcitonin,interferon)
-because thisgranuloma has a wide
variety of appearances, you canalmost always put it inyour differentialdiagnosis-Central Giant CellGranuloma, rule outhyperparathyroidism with blood tests(elevated serumcalcium in blood, or measure parathyroid
hormone)Giant Cell Tumor (different fromgranuloma!) is a:-long bone lesion-more aggressive-may becomemalignant
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 4/16
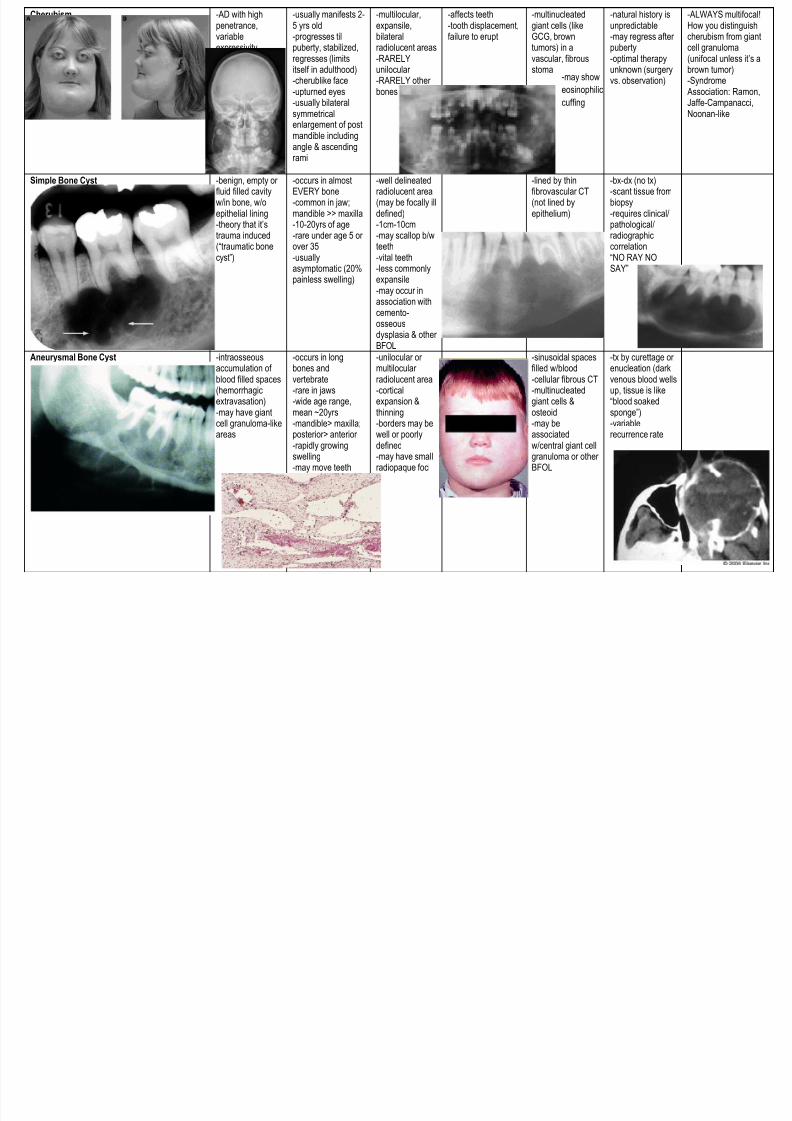
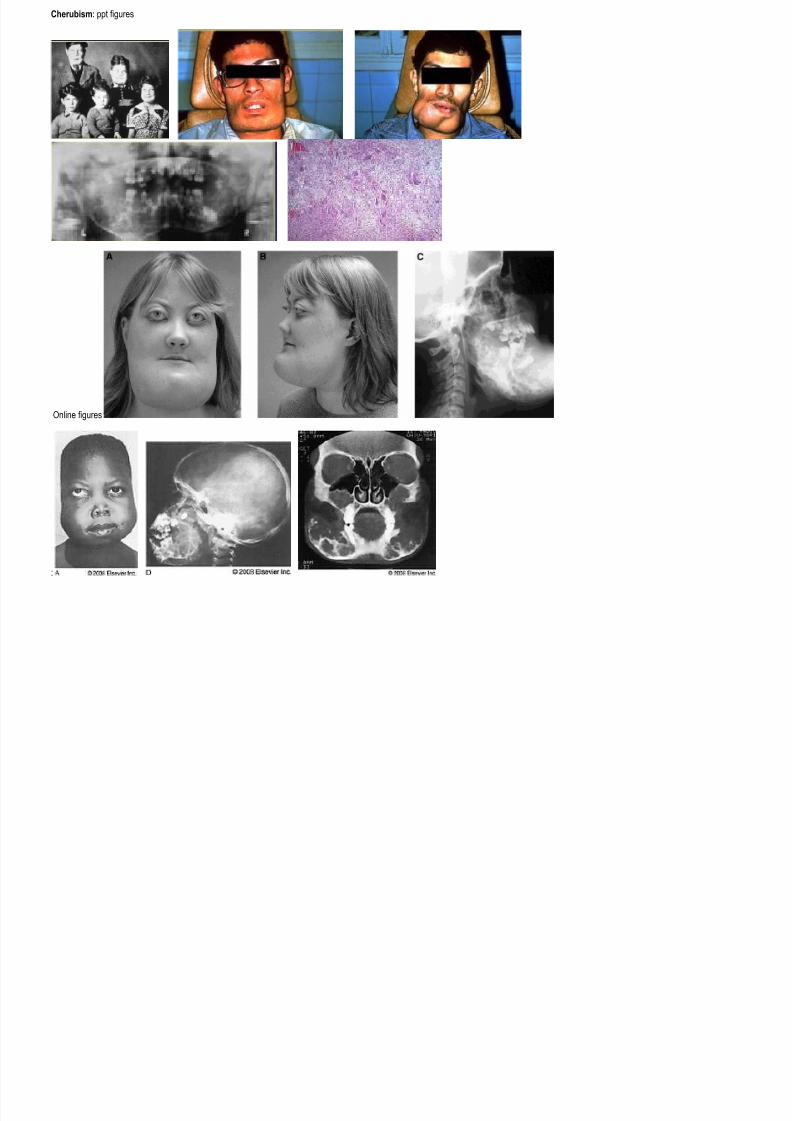
Cherubism -AD with highpenetrance,variableexpressivity
-usually manifests 2-5 yrs old-progresses tilpuberty, stabilized,regresses (limitsitself in adulthood)-cherublike face-upturned eyes-usually bilateralsymmetricalenlargement of post
mandible includingangle & ascendingrami
-multilocular,expansile,bilateralradiolucent areas-RARELYunilocular -RARELY other bones
-affects teeth-tooth displacement,failure to erupt
-multinucleatedgiant cells (likeGCG, browntumors) in avascular, fibrousstoma
-natural history isunpredictable-may regress after puberty-optimal therapyunknown (surgeryvs. observation)
-ALWAYS multifocal!How you distinguishcherubism from giantcell granuloma(unifocal unless it’s abrown tumor)-Syndrome Association: Ramon,Jaffe-Campanacci,Noonan-like
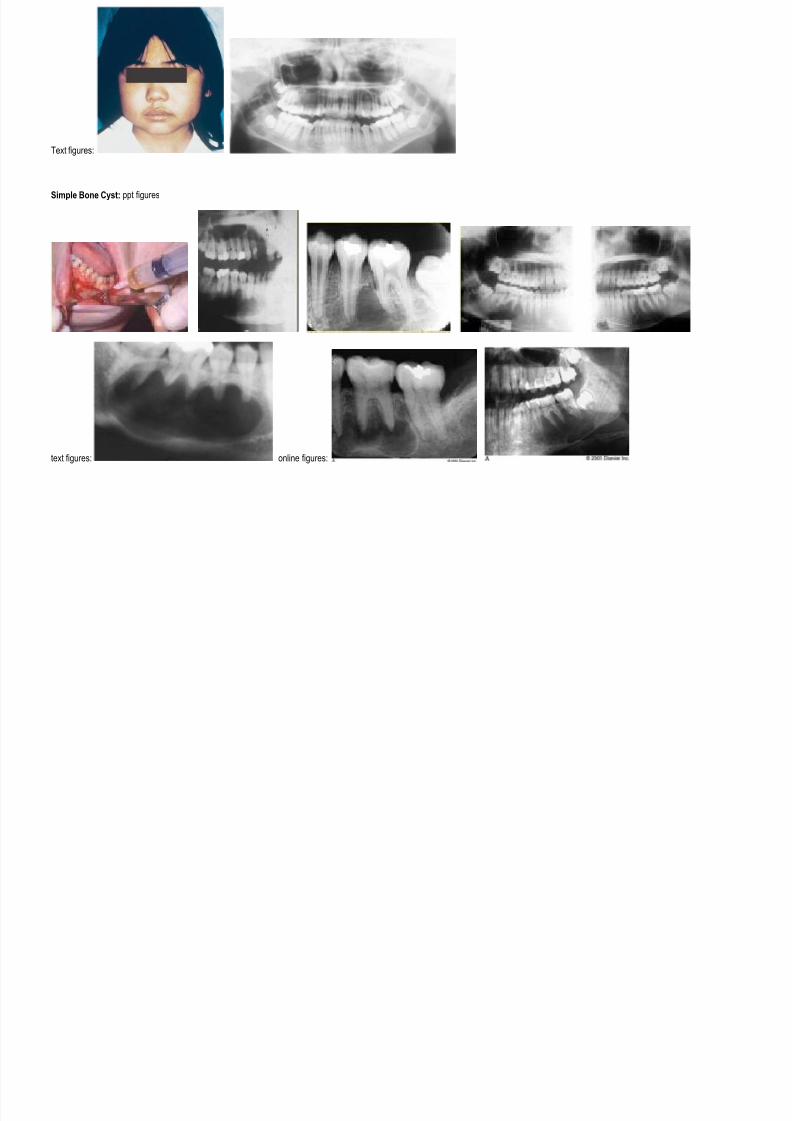
Simple Bone Cyst -benign, empty or fluid filled cavityw/in bone, w/oepithelial lining-theory that it’strauma induced(“traumatic bonecyst”)
-occurs in almostEVERY bone-common in jaw;mandible >> maxilla-10-20yrs of age-rare under age 5 or over 35-usually
asymptomatic (20%painless swelling)
-well delineatedradiolucent area(may be focally illdefined)-1cm-10cm-may scallop b/wteeth-vital teeth
-less commonlyexpansile-may occur inassociation withcemento-osseousdysplasia & other BFOL
-lined by thinfibrovascular CT(not lined byepithelium)
-bx-dx (no tx)-scant tissue frombiopsy-requires clinical/pathological/radiographiccorrelation“NO RAY NO
SAY”
Aneurysmal Bone Cyst -intraosseousaccumulation of blood filled spaces(hemorrhagic
extravasation)-may have giantcell granuloma-likeareas
-occurs in longbones andvertebrate-rare in jaws
-wide age range,mean ~20yrs-mandible> maxilla;posterior> anterior -rapidly growingswelling-may move teeth
-unilocular or multilocular radiolucent area-cortical
expansion &thinning-borders may bewell or poorlydefined-may have smallradiopaque foci
-sinusoidal spacesfilled w/blood-cellular fibrous CT-multinucleated
giant cells &osteoid-may beassociatedw/central giant cellgranuloma or other BFOL
-tx by curettage or enucleation (darkvenous blood wellsup, tissue is like
“blood soakedsponge”) -variablerecurrence rate
-may show
eosinophilic
cuffing
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 5/16
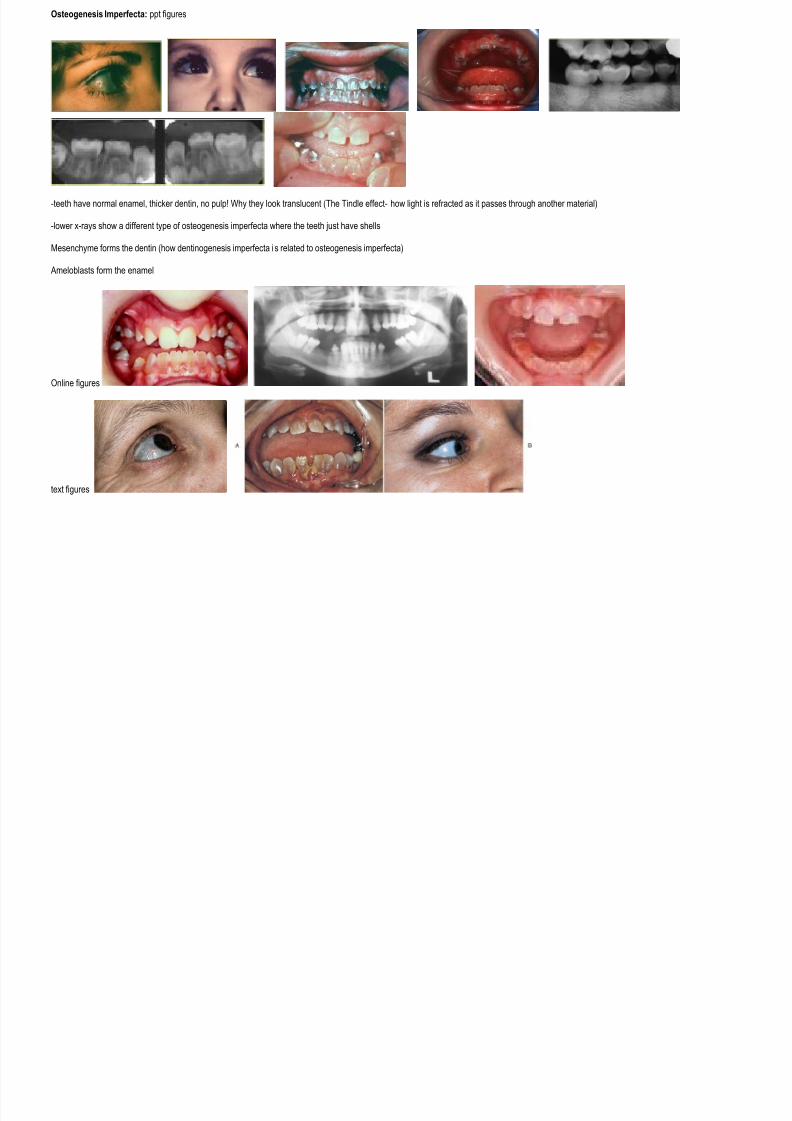
Osteogenesis Imperfecta: ppt figures
-teeth have normal enamel, thicker dentin, no pulp! Why they look translucent (The Tindle effect- how light is refracted as it passes through another material)
-lower x-rays show a different type of osteogenesis imperfecta where the teeth just have shells
Mesenchyme forms the dentin (how dentinogenesis imperfecta is related to osteogenesis imperfecta)
Ameloblasts form the enamel
Online figures
text figures

7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 6/16
Osteopetrosis: text figures FIGURE 4-20Osteopetrosis. A, Ribs, humerus, and clavicles exhibit increased bone density. B, Increase in bone density of cranial and base-of-skull bones.
FIGURE 4-21Osteopetrosis. Panoramic radiograph demonstrating unerupted teeth and areas of increased bone density of the mandible and maxilla.
Online figures
Cleidocranial Dysplasia: ppt figures:
(no clavicles in x-ray)
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 7/16
Online figures:
Text figures:
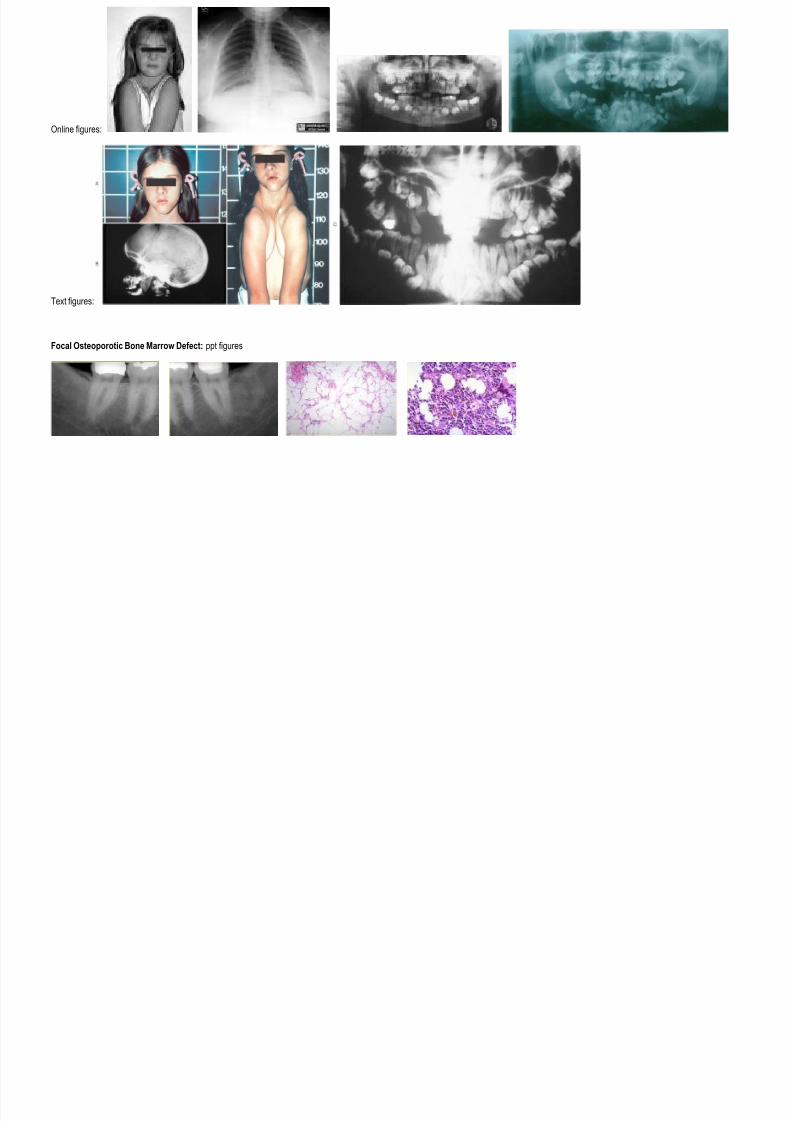
Focal Osteoporotic Bone Marrow Defect: ppt figures
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 8/16
Online figures: text figures:
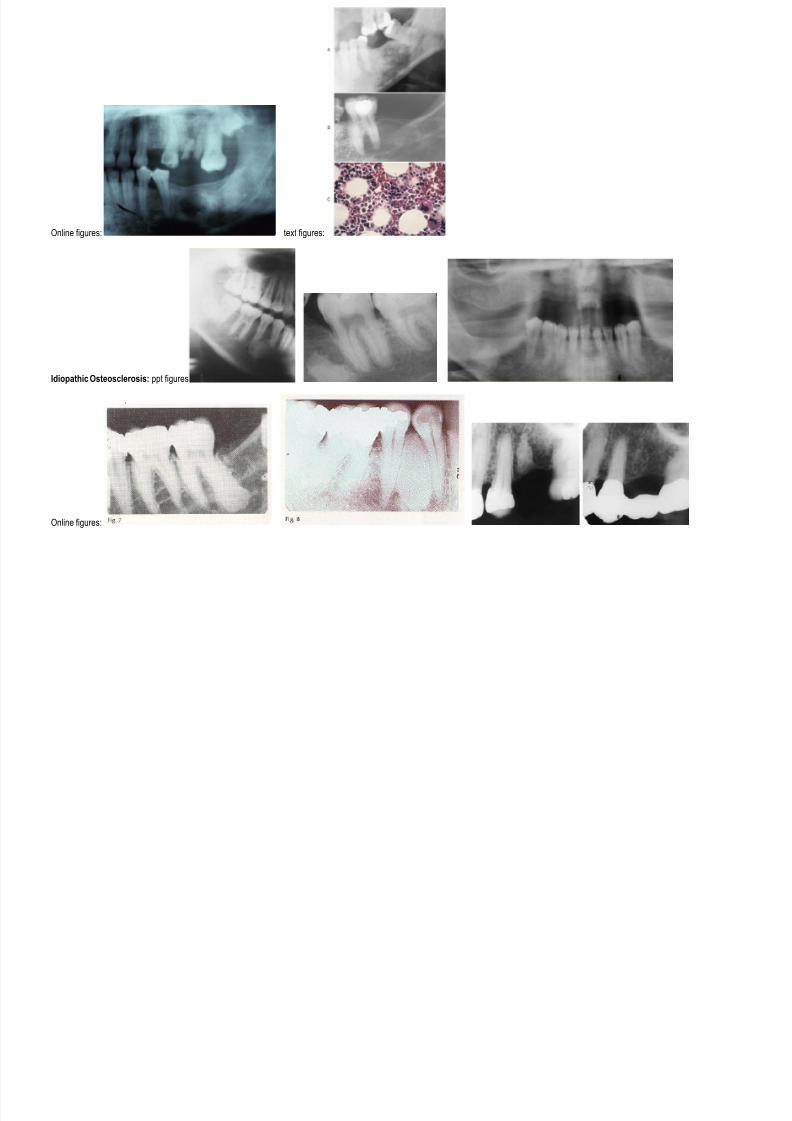
Idiopathic Osteosclerosis: ppt figures
Online figures:
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 9/16
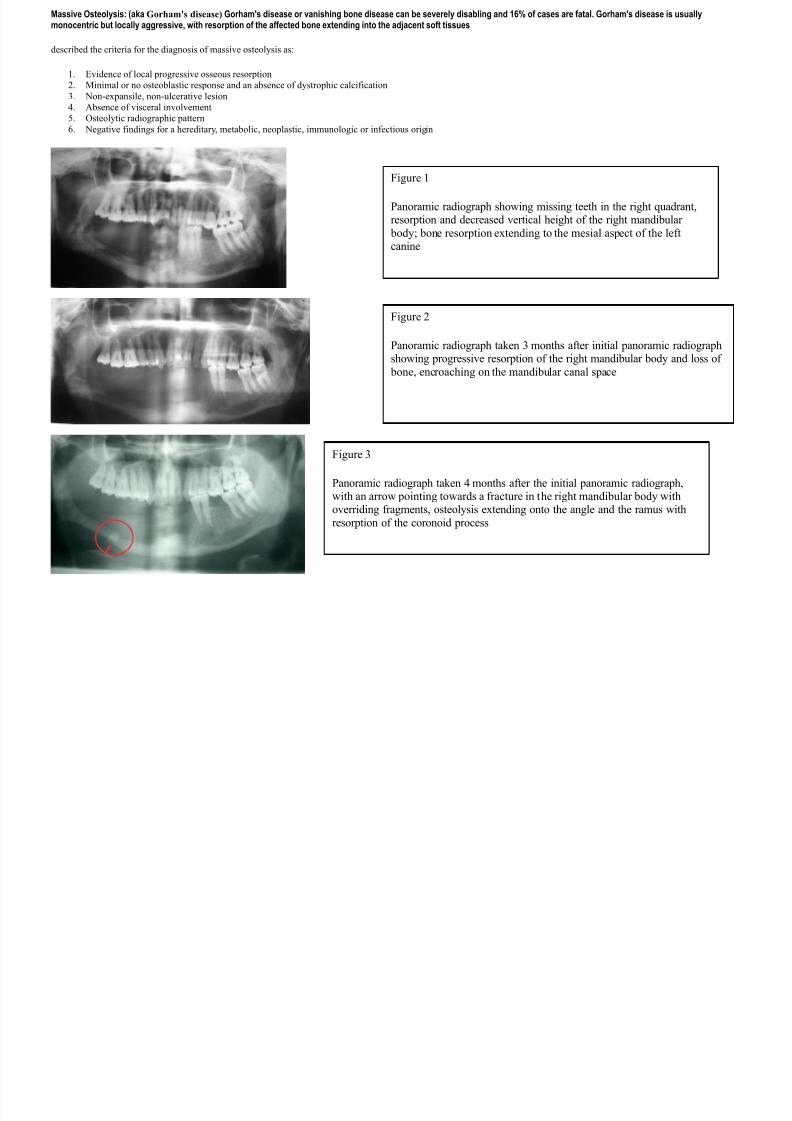
Massive Osteolysis: (aka Gorham's disease) Gorham's disease or vanishing bone disease can be severely disabling and 16% of cases are fatal. Gorham's disease is usuallymonocentric but locally aggressive, with resorption of the affected bone extending into the adjacent soft tissues
described the criteria for the diagnosis of massive osteolysis as:
1. Evidence of local progressive osseous resorption
2. Minimal or no osteoblastic response and an absence of dystrophic calcification
3. Non-expansile, non-ulcerative lesion
4. Absence of visceral involvement
5. Osteolytic radiographic pattern
6. Negative findings for a hereditary, metabolic, neoplastic, immunologic or infectious origin
Figure 1
Panoramic radiograph showing missing teeth in the right quadrant,resorption and decreased vertical height of the right mandibular
body; bone resorption extending to the mesial aspect of the leftcanine
Figure 2
Panoramic radiograph taken 3 months after initial panoramic radiographshowing progressive resorption of the right mandibular body and loss of
bone, encroaching on the mandibular canal space
Figure 3
Panoramic radiograph taken 4 months after the initial panoramic radiograph,with an arrow pointing towards a fracture in the right mandibular body withoverriding fragments, osteolysis extending onto the angle and the ramus with
resorption of the coronoid process
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 10/16
Condensing Osteitis: online figures
Paget’s Disease of Bone: ppt figures
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 11/16
Text figures:
Online figures:
Central Giant Cell Granuloma: ppt figures

7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 12/16
Online figures:
Text figures:
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 13/16
Cherubism: ppt figures
Online figures
:
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 14/16
Text figures:
Simple Bone Cyst: ppt figures
text figures: online figures:

7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 15/16
Aneurysmal Bone Cyst: ppt figures
online figures:
text figures:
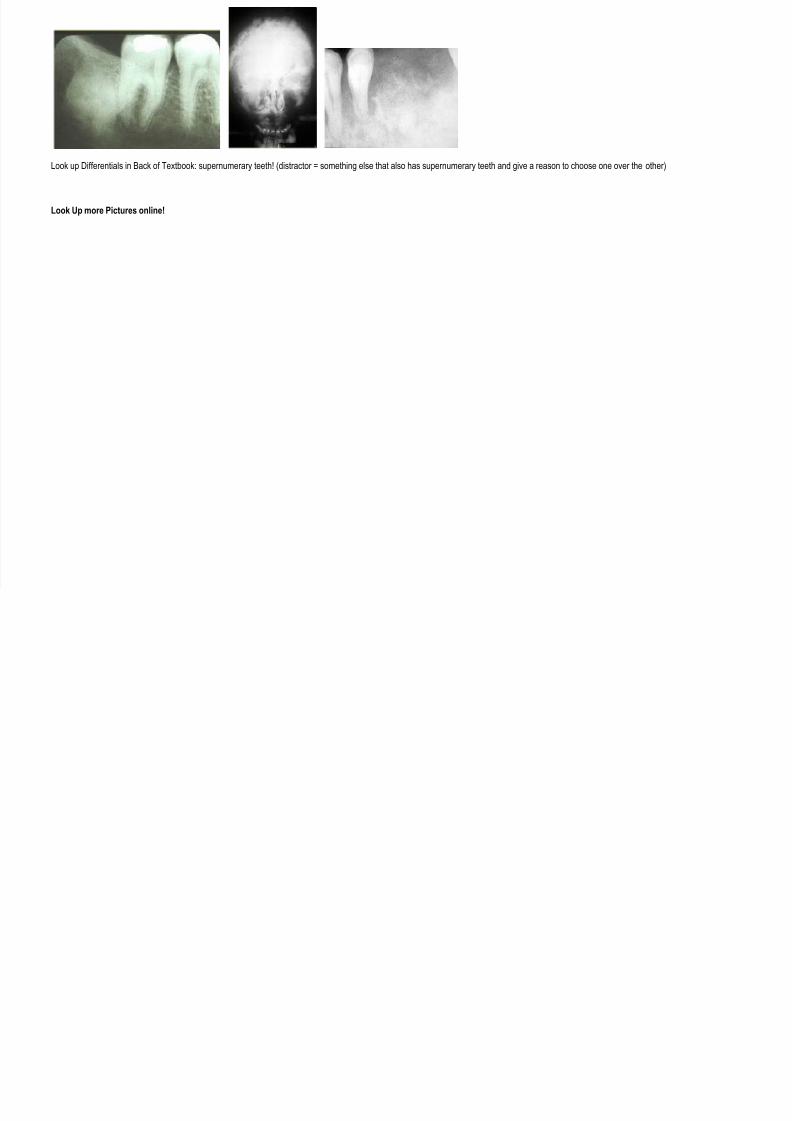
Diagnose These Pictures? (I assume that’s what we’re supposed to do with these!):
7/27/2019 Oral Path Bone Lesions
http://slidepdf.com/reader/full/oral-path-bone-lesions 16/16
Look up Differentials in Back of Textbook: supernumerary teeth! (distractor = something else that also has supernumerary teeth and give a reason to choose one over the other)
Look Up more Pictures online!
Related Documents











