Optimization of Gold Nanoparticle Radiosensitizers for Cancer Therapy by Lei Cui A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Department of Pharmaceutical Sciences University of Toronto © Copyright by Lei Cui 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Optimization of Gold Nanoparticle Radiosensitizers
for Cancer Therapy
by
Lei Cui
A thesis submitted in conformity with the requirements for the degree of Doctor of
Philosophy
Department of Pharmaceutical Sciences
University of Toronto
© Copyright by Lei Cui 2016

ii
Optimization of Gold Nanoparticle Radiosensitizers
for Cancer Therapy
Lei Cui Doctor of Philosophy
Department of Pharmaceutical Sciences University of Toronto
2016
Abstract
Radiation therapy (RT) plays a pivotal role in cancer treatment [1], and
radiosensitizing agents are widely used to improve the outcome of RT [2]. There is keen
interest in the development of new tumor-specific radiosensitizing strategies given that
most of the commonly used radiosensitizers are inherently toxic [2]. In recent years, the
radosensitizing effects of gold nanoparticles (AuNPs) have been explored extensively
[3-5]. To further optimize radiosensitization by AuNPs, this thesis aims to (1) synthesize
and characterize AuNPs with varied physicochemical properties including size, surface
coating, and targeting moieties (2) investigate the cellular response (i.e., cell uptake and
toxicity) to AuNPs (3) assess the in vitro radiosensitizing effects of AuNPs and identify
the key parameters which determine the extent of radiosensitization by AuNPs and (4)
evaluate and compare the individual and combined radiation enhancement effects of
AuNPs and cisplatin both in vitro and in vivo. Overall, the current work demonstrated
that the cell response to AuNPs is highly dependent on a number of factors including
the physicochemical properties and concentration of the AuNPs, incubation time with
AuNPs, as well as the cell line employed. Importantly, cellular localization of AuNPs and
oxygen conditions were shown to be crucial in determining the radiosensitizing effect of
AuNPs. The highest level of radiosensitization was observed when AuNPs are
internalized, and in cells that are under oxia. In comparison to cisplatin at three doses of
IC25, AuNPs administered intratumorally demonstrated an equivalent radiation
enhancement effect without showing intrinsic toxicity or increasing the toxicity of IR, as
such AuNPs can be considered as a true radiosensitizer. The combination of AuNPs
iii
and cisplatin resulted in an additive and significant radiation enhancement effect with
fractionated RT, and is thus a promising strategy to be further considered. Future
research is warranted on the design of formulations that resulted in improved tumor
bioavailability of AuNPs and co-delivery of AuNPs and cisplatin to tumor sites, for the
achievement of tumor-specific radiosensitzation, minimal toxicity, and therefore a
greater therapeutic window for AuNP aided RT.

iv
References
1. Delaney G, Jacob S, Featherstone C, Barton M. The Role of Radiotherapy in Cancer Treatment: Estimating Optimal Utilization from a Review of Evidence-Based Clinical Guidelines. Cancer. 2005 Sep 15; 104:1129-37.
2. Seiwert TY, Salama JK, Vokes EE. The Concurrent Chemoradiation Paradigm--General Principles. Nat Clin Pract Oncol. 2007 Feb; 4:86-100.
3. Butterworth KT, McMahon SJ, Currell FJ, Prise KM. Physical Basis and Biological Mechanisms of Gold Nanoparticle Radiosensitization. Nanoscale. 2012 Aug 21; 4:4830-8.
4. Coulter JA, Hyland WB, Nicol J, Currell FJ. Radiosensitising Nanoparticles as Novel Cancer Therapeutics--Pipe Dream or Realistic Prospect? Clin Oncol (R Coll Radiol). 2013 Oct; 25:593-603.
5. Her S, Jaffray DA, Allen C. Gold Nanoparticles for Applications in Cancer Radiotherapy: Mechanisms and Recent Advancements. Adv Drug Deliv Rev. 2015 Dec 19.

v
Dedication
Emma Rongruo Chen & George Xiaotian Chen

vi
Acknowledgments
Completion of this doctoral dissertation was possible with the support of several
people, and I would like to extend my gratitude to all of them.
First I would like to express my extreme gratefulness to Prof. Christine Allen for
being a tremendous mentor over the past 6 years. This feat was possible only because
of the unconditional support from Dr. Allen. Firstly your valuable guidance, scholarly
inputs, and consistent inspiration throughout the research work allow me to grow as a
research scientist. Your constant encouragement guided me through the most difficult
moments in my life, and helped me to recognize the meaning and the value of effort I
have made in the past few years – words cannot express the importance of your
presence in my life.
Second I would like to thank my adversary committee professors, Dr. David
Jaffray, Dr. Robert Bristow, and Dr. Gang Zheng. Despite their tight schedule, they have
been constantly accessible. Their instruction and exceptional knowledge have made my
research progressing as efficient as possible.
I also would like to extend my thankfulness to Dr. Payam Zahedi and Dr. Raquel
De Souza, their help and support for this project, from experimental designing,
techniques, and scientific writing, have made this multitasking job feasible.
Furthermore I would like to thank Dr. Gaetano Zafarana and Dr. Gerben Borst,
their contribution and generous sharing of their expertise have made the project and this
doctorate much less challenging. I would also express my appreciation to Mike Dunne,
Drs. Changhai Lu, Andrew Mikhail, Jinzi Zheng, Kenneth Tse, and Shane Harding for
their help and guidance at various phases of the project.
My special gratitude is extended to Sohyoung Her, our mutual interest in
scientific research and friendship made us as great partners; I would have never come
even close to this result if it were not for her participation and help.

vii
Allen lab has provided a friendly and harmonious environment for me to work
with high efficiency. Yannan Dou and Huang Huang have been the best friends
provided a lot of help and beyond, making my memory of time in the lab filled with joy
and happiness. I would also like to thank my students Justin Saraceno, Kaitlynn
Almeida, Sarah Boetto, and Cathy Zhu, who all did outstanding experimental work.
My family has been incredibly supportive for me pursuing my dreams. My parents
have taught me to be firm and patient under all possible situations, and my brother told
me to always follow my heart. Especially, this work would not have been possible
without my husband George Xiaotian Chen, only his years of love and support has
provided me the liberty to make my dreams come true. I also would like to thank the
most important and precious person in my life, my little daughter Emma Rongruo Chen.
Her arrival in my life made me understand the meaning and beauty of life itself, and
made me stronger and kinder inside as a human being. With all the love and
appreciation, I would like to dedicate this doctorate to this beautiful and adorable little
person in my life.

viii
Table of Contents
Abstract .......................................................................................................................... ii
Dedication...................................................................................................................... v
Acknowledgments ......................................................................................................... vi
Table of Contents ........................................................................................................ viii
List of Tables ............................................................................................................... xiv
List of Figures ............................................................................................................... xv
List of Abbreviations ..................................................................................................... xx
Chapter 1 Introduction, Hypotheses, and Overview ...................................................... 1
1.1 Abstract ................................................................................................................ 2
1.2 Introduction ........................................................................................................... 3
1.3 Mechanisms of Radiosensitization by AuNPs ...................................................... 7
1.3.1 Physical Phase .......................................................................................... 9
1.3.2 Chemical Phase ....................................................................................... 11
1.3.3 Biological Phase ...................................................................................... 13
1.4 Previous Studies on Radiosensitization by AuNPs ............................................. 19
1.4.1 MC Studies .............................................................................................. 19
1.4.2 Radiosensitization in Plasmid DNA Models ............................................. 20
1.4.3 Radiosensitization in Cells ....................................................................... 20
1.4.4 Radiosensitization In Vivo ........................................................................ 21
1.5 Where Does the Therapeutic Window of AuNP-aided RT Lie? What Are the Key Parameters to be Considered? .................................................................... 25
1.5.1 Physicochemical Properties of AuNPs ..................................................... 26
1.5.2 Administration Route of AuNPs ............................................................... 30
1.5.3 Dosing Schedule of AuNPs and RT ......................................................... 31

ix
1.5.4 Type of RT ............................................................................................... 31
1.6 Conclusions and Future Directions ..................................................................... 34
1.7 Hypotheses and Objectives ................................................................................ 36
1.8 Overview of Thesis Chapters.............................................................................. 37
1.9 References ......................................................................................................... 39
Chapter 2 Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles ............ 55
2.1 Abstract .............................................................................................................. 56
2.2 Introduction ......................................................................................................... 57
2.3 Methods .............................................................................................................. 59
2.3.1 Quantitative Assessment of Cellular Accumulation of AuNP-TP .............. 59
2.3.2 Evaluation of Cytotoxicity of AuNP-TP ..................................................... 59
2.3.3 Measurement of Reactive Oxygen Species Production ........................... 60
2.4 Results ............................................................................................................... 61
2.4.1 Synthesis and Characterization of AuNP-TP ........................................... 61
2.4.2 Cellular Accumulation of AuNP-TP .......................................................... 63
2.4.3 Cytotoxicity of AuNP-TP .......................................................................... 67
2.4.4 Measurement of ROS Production ............................................................ 68
2.5 Discussion .......................................................................................................... 70
2.6 Conclusions ........................................................................................................ 77
2.7 Supporting Information ....................................................................................... 78
2.7.1 Preparation and Characterization of AuNP-TP ........................................ 78
2.7.2 Cell Culture .............................................................................................. 80
2.7.3 Qualitative Assessment of Cellular Accumulation of AuNP-TP ................ 80
2.7.4 Calculation of Number of AuNP-TP Accumulated in Cells ....................... 80
2.7.5 Statistical Analysis ................................................................................... 81

x
2.8 Acknowledgements ............................................................................................ 83
2.9 References ......................................................................................................... 84
Chapter 3 Hypoxia and Cellular Localization Influence the Radiosensitizing Effect of Gold Nanoparticles (AuNPs) in Breast Cancer Cells .............................. 88
3.1 Abstract .............................................................................................................. 89
3.2 Introduction ......................................................................................................... 90
3.3 Methods .............................................................................................................. 94
3.1.1 Preparation and Characterization of AuNPs ............................................ 94
3.1.2 Cell Culture and Hypoxia ......................................................................... 94
3.1.3 Quantitative Assessment of the Cellular Accumulation of AuNPs ............ 94
3.1.4 Qualitative Assessment of the Cellular Accumulation of AuNPs .............. 95
3.1.5 Radiation Source and Dose Calculations for Cell Irradiation Studies ...... 95
3.1.6 Clonogenic Survival Assays ..................................................................... 95
3.1.7 Cytotoxicity and Radiosensitizing Effects of AuNPs under Oxia .............. 96
3.1.8 Radiosensitizing Effects of AuNPs under Acute and Chronic Hypoxia .... 97
3.1.9 Western Blot Analysis .............................................................................. 98
3.1.10 Cell Cycle Analysis ................................................................................ 100
3.1.11 Immunofluorescence Assay ................................................................... 100
3.1.12 Statistical Analysis ................................................................................. 102
3.4 Results ............................................................................................................. 103
3.4.1 Cytotoxicity of the AuNPs ...................................................................... 103
3.4.2 Cellular Accumulation of the AuNPs ...................................................... 104
3.4.3 The Influence of Time, Concentration and Cellular Localization on the Radiosensitizing Effect of AuNPs .......................................................... 107
3.4.4 AuNPs Radiosensitization under Acute and Chronic Hypoxia ............... 110
3.4.5 Reduced Expression of Rad51 in Cells under Chronic Hypoxia ............ 113

xi
3.4.6 The Effect of AuNPs on Cell Cycle Distribution and Post Irradiation DNA Double Strand Breaks (DSBs) ....................................................... 113
3.5 Discussion ........................................................................................................ 116
3.6 Conclusions ...................................................................................................... 121
3.7 Acknowledgments ............................................................................................ 122
3.8 References ....................................................................................................... 123
Chapter 4 Triple Combination of Gold Nanoparticles, Cisplatin and Radiotherapy for Local Treatment of Triple Negatvie Breast Cancer .............................. 127
4.1 Abstract ............................................................................................................ 128
4.2 Introduction ....................................................................................................... 129
4.3 Methods ............................................................................................................ 131
4.3.1 Preparation of AuNPs ............................................................................ 131
4.3.2 Characterization of AuNPs ..................................................................... 131
4.3.3 Cell Culture: MDA-MB-231Luc+ ............................................................... 132
4.3.4 Qualitative Assessment of the Cellular Accumulation of AuNPs ............ 132
4.3.5 Quantitative Assessment of the Cellular Accumulation of AuNPs .......... 132
4.3.6 Radiation Source and Dose Calculations for Cell Irradiation Studies .... 133
4.3.7 In vitro Clonogenic Survival Assays ....................................................... 133
4.3.8 Evaluation of Cytotoxicity of AuNPs and Cisplatin ................................. 134
4.3.9 Radiosensitizing Effects of AuNPs and Cisplatin In Vitro – Individually and in Combination ................................................................................ 134
4.3.10 Animals and Tumor Model ..................................................................... 135
4.3.11 Intratumoral Infusion of AuNP-RME ....................................................... 135
4.3.12 Determination of Doses of AuNP-RME and Cisplatin to be Employed In Vivo .................................................................................................... 136
4.3.13 Work Flow for In Vivo Studies ................................................................ 136

xii
4.3.14 Intratumoral Distribution and Quantitative Measurement of AuNP-RME by TEM and CT ...................................................................................... 139
4.3.15 Localized X-ray Irradiation of Tumors .................................................... 139
4.3.16 Evaluation of Treatment Efficacy and Toxicity in Tumor-bearing Mice .. 140
4.3.17 Statistical Analysis ................................................................................. 140
4.4 Results ............................................................................................................. 141
4.4.1 Characterization of AuNPs and Cellular Uptake of AuNPs .................... 141
4.4.2 Cytotoxicity and Radiosensitization Effects of AuNPs and Cisplatin In Vitro ....................................................................................................... 143
4.4.3 Determination of Dose of AuNP-RME and Cisplatin In Vivo .................. 146
4.4.4 Cellular Uptake of AuNP-RME In Vivo by TEM ...................................... 146
4.4.5 Time Dependent Intratumoral Levels of Au as Determined by CT Scan 148
4.4.6 Treatment Efficacy and Toxicity In Vivo ................................................. 150
4.5 Discussion ........................................................................................................ 155
4.6 Conclusions ...................................................................................................... 159
4.7 Supporting Information ..................................................................................... 160
4.7.1 Cytotoxic of Cisplatin In Vitro ................................................................. 160
4.7.2 Bioluminescence Images (BLI) .............................................................. 160
4.7.3 Determination of Dose of Cisplatin and AuNPs for RT Study by Ex Vivo Clonogenic Assay .......................................................................... 161
4.7.4 Treatment Efficacy and Toxicity In Vivo – Single Dose of Cisplatin ....... 166
4.8 Acknowledgments ............................................................................................ 167
4.9 References ....................................................................................................... 168
Chapter 5 Conclusions and Future Directions ........................................................... 175
5.1 Summary of Findings ........................................................................................ 176
5.2 Conclusions and Future Directions ................................................................... 180

xiii
5.3 References ....................................................................................................... 187

xiv
List of Tables
Table 1-1: Properties of AuNPs and their biomedical applications. ................................ 5
Table 1-2: Summary of in vivo Studies ......................................................................... 23
Table 1-3: Physicochemical properties of AuNPs and their impact on biodistribution, pharmacokinetics, cellular uptake, and toxicity. ............................................................ 28
Table 1-4: Types of RT and radiobiological considerations for radiosensitization by AuNPs. .......................................................................................................................... 32
Table 3-1: Fitted parameters obtained using the LQ model, and DEF calculated at 0.1SF for on experimental data shown in Figure 3-5. .................................................. 109
Table 3-2: Fitted parameters obtained using the LQ model, and DEF calculated at 0.1SF for on experimental data shown in Figure 3-6. .................................................. 110
Table 3-3: SF ratio at 5 Gy ......................................................................................... 112
Table 3-4: Effect of oxygen on radiation cell kill .......................................................... 113
Table 4-1: Treatment groups for the assessment of efficacy and systemic toxicity: saline and cisplatin solutions were administered intraperitoneally (i.p.) 30 min prior to IR on days 1, 3, and 5. ............................................................................................ 138
Table 4-2: Radiation dose required to achieve 0.1 SF and DEF for each treatment. .. 144
Table 4-3: Statistical significance in the efficacy and toxicity data obtained for the different treatment groups. .......................................................................................... 152
Table 4-4: Treatment groups for ex vivo clonogenic assay. On day one, saline or cisplatin was administered intravenously 30 min prior to IR. ....................................... 162

xv
List of Figures
Figure 1-1: (A) Number of publications on AuNPs over the past two decades. (B) Number of publications on AuNPs in radiotherapy over the past two decades. Data show the number of publications compiled as of June 2016 using Scopus search engine with the following search words (A) gold nanoparticles and (B) gold nanoparticles radiation therapy. ...................................................................................... 6
Figure 1-2: Radiosensitization by AuNPs: mechanisms and key parameters. ............... 8
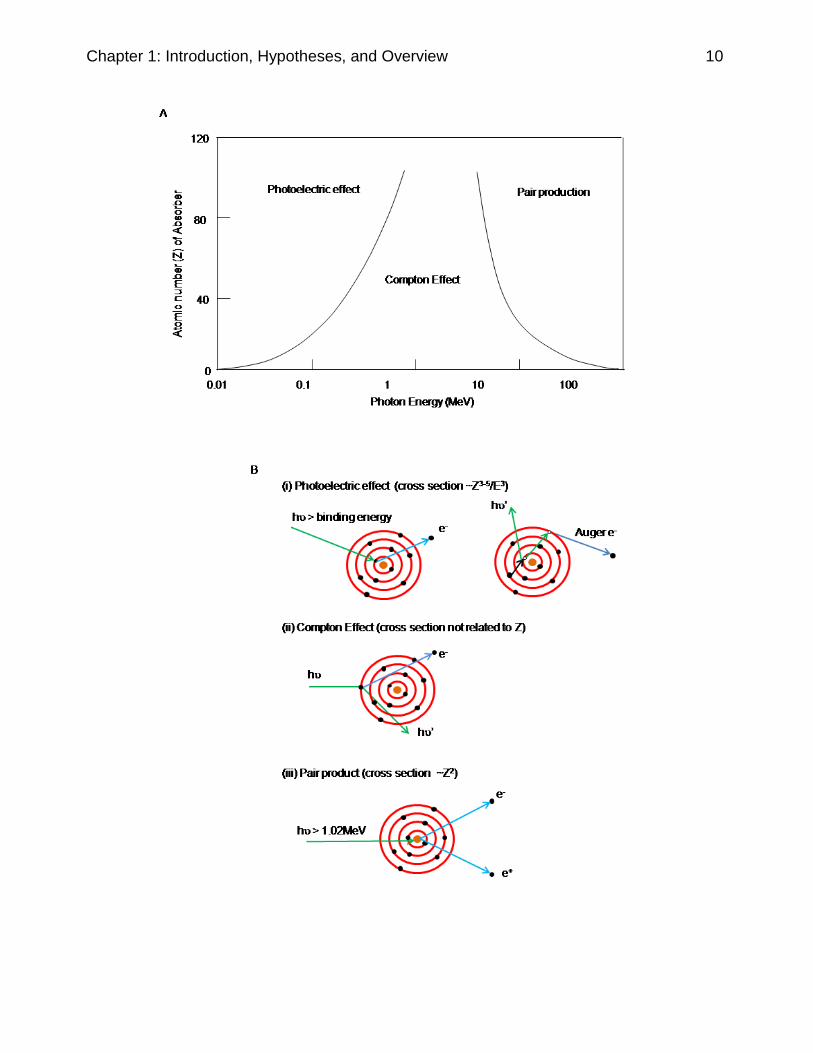
Figure 1-3: (A) Radiation energy and atomic number (Z) dependent interaction between radiation and materials. (B) Illustration of the Photoelectric effect, Compton Effect, and pair production. (i) In the photoelectric effect (10-500 keV): the energy of the incident photon (hʋ) is fully absorbed by an electron in the inner shell of an atom, and the electron is ejected from the atom. The vacant orbit is filled with an electron from an outer shell with high energy; extra energy is either released as photon or absorbed by another electron in an outer shell, which is ejected from the atom (Auger electron). This Auger effect occurs in cascade if there are multiple shells of electrons in the atom. (ii) In the Compton Effect (500 keV – 1.02 MeV): the energy of the incident photon is partially absorbed by an electron in the outer shell of an atom, and the extra energy is released as photons. (iii) In Pair product: when the energy of an incident photon is at least two fold larger than mec2 (> 1.02 MeV), and the energy is fully absorbed by the nucleus of an atom, a pair of electrons and positrons are generated from the nucleus [61, 64]. A “ ” represents incident or released photons; a “ " represents ejection of secondary or Auger electrons; electrons are
represented as “”, and a “ ” represents a vacancy in the electron orbit in an atom. ... 11
Figure 2-1: Preparation of AuNPs coated with a monolayer of tiopronin. ..................... 58
Figure 2-2: Characterization of the AuNP-TP. (A) A representative TEM image of the AuNP-TP. The scale bar represents 20 nm. (B) Core size distribution histogram calculated from over 1000 AuNP-TP. (C) 1H NMR spectrum of 0.5 mg/mL AuNP-TP suspension in D2O. (D) UV-vis spectrum of 1 mg/mL AuNP-TP in dd-H2O. (E) Percentage of Au that remains in the supernatant following incubation in cell culture
media at 37°C. Data represents mean SD (n=3). (F-H) TEM images of AuNP-TP in cell culture media following 24, 48, 72 h of incubation at 37°C. The scale bar represents 20 nm. ......................................................................................................... 63
Figure 2- 3: TEM images of AuNP-TP accumulation in MCF-7 (A, B), HeLa (C, D),
H520 (E, F), and L929 (G, H) cells. Scale bar represents 2 m in (A, C, E and G) and 100 nm in (B, D, F and H). As highlighted by the arrows in images (A) and (B) once the AuNP-TP enter cells they appear to sequester in large vacuoles such as endosomes and lysosomes, and mostly localize in the perinuclear region of cells. A similar trend was observed for all cell lines evaluated. .................................................. 65
Figure 2-4: In vitro cellular accumulation of AuNP-TP in (A) MCF-7, (B) HeLa, (C) H520, and (D) L929 cells quantified by ICP-AES with incubation at two different

xvi
concentrations (i.e., 0.05 and 0.25 mg/mL) of AuNP-TP. * Represents statistically significant difference between the two concentrations (p<0.05), and # Represents statistically significant difference in cell accumulation at different timepoints in
comparison to that at the 8 h timepoint. Data represents mean SD (n=3). ................. 66
Figure 2-5: Cell surviving fraction (SF) after 24 h of treatment with different concentrations of AuNP-TP. SF as determined by clonogenic assays is reported as plating efficiency compared to non-treated cells. * and # represent statistically significant differences between various concentrations for HeLa and MCF-7 cells,
respectively (p<0.05). Data represents mean SD (n=3). ............................................ 67
Figure 2-6: Amount of ROS produced relative to non-treated cells following treatment with AuNP-TP (0.5 mg/mL) in combination with antioxidants including NAC, reduced L cysteine, GSH or tiopronin (3mM) and the apoptotic inhibitor Z-VAD-fmk (50uM) in A) HeLa cells and B) L929 cells. The insets show relative ROS
produced in cells following treatment with 0.3% H2O2 or 10 M SIN for 1 h compared
to non-treated cells. Data represents mean SD (n=4). ............................................... 69
Figure 2-7: In vitro cellular level of AuNP-TP in (A) MCF-7, (B) HeLa, (C) H520, and (D) L929 cells quantified by ICP-AES with incubation at two different concentrations (i.e., 0.05 and 0.25 mg/mL) of AuNP-TP. * Represents statistically significant difference in cell accumulation at that timepoint in comparison to its previous
timepoint. Data represents mean SD (n=3). ............................................................... 82
Figure 3-1: AuNPs are involved as radiosensitizers in the physical, chemical, and biological phases of the effects of radiation on cells. (Timescale adapted from Joiner and van der Kogel, 2009. [1]) ........................................................................................ 92
Figure 3-2: Surviving fraction following 4, 8, or 24 h of treatment with different concentrations of AuNPs. * represents significant difference between groups. Data
represents mean SEM (n=3). ................................................................................... 104
Figure 3-3: (A) Cellular uptake of the AuNPs following incubation over 48 h. * represents statistically significant differences between the two concentrations (p<0.05). (B) The Cellular level of Au following a 4 h incubation period with seven different concentrations of AuNPs under oxia, chronic hypoxia and acute hypoxia. * represents statistically significant differences between oxia and hypoxia (p<0.05). # represents statistically significant differences between 0.5 mg/mL and other
concentrations under oxia (p<0.05). Data represents mean SEM (n=3). (C) TEM images of cells following a incubation with AuNPs under oxia 20 min (I and II); 1 hr (III and IV); 4 h (V and VI); 4 h under chronic hypoxia (VII and VIII); and, 4 h under acute hypoxia (IX and X). II, IV, VI, VIII and X represent high magnification images of
selected views in I, III, V, VII and IX. The scale bar represents 2 m in images I, III, V, VII and IX, and, 500 nm in images II, IV, VI, VIII and X. .......................................... 106
Figure 3-4: The radiosensitizing effect of AuNPs following a 4 h incubation period prior to irradiation (4Gy). The SF ratio is described by the following equation:
xvii
(SFIR+AuNPs/SFAuNPs)/SFIR. * represents statistically significant differences in the SF ratio at 0.5 mg/mL AuNPs and other concentrations. .................................................. 107
Figure 3-5: Radiation dose response curves for cells incubated with AuNPs for different periods of time (i.e. 20 min, 1, 4, 8, 16 or 24 h) and irradiated at 0, 2, 4, and
6 Gy. Data points represent mean SEM (n=3). ........................................................ 108
Figure 3-6: (A) Treatment groups to assess the dependence of the radiosensitizing effect of AuNPs on their localization with respect to cells. (B) Radiation dose response curves for cells with no AuNPs or intracellular and/or extracellular AuNPs.
Data points represent mean SEM (n=3). .................................................................. 109
Figure 3-7: (A) Survival of cells following irradiation and treatment with AuNPs under oxia or hypoxia as measure by clonogenic assay. “+” indicates cells receiving AuNPs or IR treatment, “-” indicates absence of the treatment. Blue squares “+” indicate
hypoxiahypoxia groups; red squares “+” indicate hypoxiaoxia groups. SF is reported as plating efficiency compared to the control group under oxia. Data
represents mean SEM (n=3). (B) Survival of cells with toxicity of hypoxia
normalized. Data represents mean SEM (n=3). (C) Protein expression levels of Ku70 and Rad51 in cells under oxia, chronic hypoxia and acute hypoxia. Numbers in parentheses indicate the relative amount of Rad51 in cells after normalization with the corresponding Ku70 level. ..................................................................................... 112
Figure 3-8: Cell cycle distribution in cells exposed to AuNPs (0.5 mg/mL) for 1, 4, 8, 16, 24, or 48 h. ............................................................................................................ 114
Figure 3-9: (A) Representative images from the immunofluorescence assay. (B)
Number of H2AX foci 30 mins or 24 h post irradiation (0, 2, 4 Gy). * represents statistically significant difference between the treatment groups. Data represents
mean SEM (n=3). ..................................................................................................... 115
Figure 4-1: Work flow for in vivo studies evaluating efficacy (measured by ex vivo clonogenic assay, tumor growth, and overall survival), as well as the toxicity (evaluated by body weight loss) of each treatment. .................................................... 137
Figure 4-2: (A) A representative TEM image of the AuNP-PEG formulation. The scale bar represents 100 nm. (B, C) UV spectra obtained for AuNP-PEG and AuNP-RME, respectively. The absence of a shift in the peak at 520 nm confirms that the AuNPs are stable without aggregation during the incubation period. (D) Cellular accumulation of AuNPs (0.50 mg/mL) in MDA-MB-231Luc+ cells quantified by ICP-AES following 4 h or 24 h of incubation. * represents statistically significant difference in cellular level of Au in cells treated with AuNP-RME in comparison to AuNP-PEG (p<). Cellular uptake of AuNP-RME was also found to be significantly
higher at 24h compared to 4h (p<0.05). Data represents mean SEM (n=3). (E, F) TEM images depicting cellular uptake of AuNPs (0.50 mg/mL) at 24h post-incubation with AuNP-PEG and AuNP-RME, respectively. Scale bars in E and F represent 2 µm

xviii
(left images) and 500 nm (right images). Following cell entry, AuNPs are clustered within endosomal and lysosomal vacuoles. ................................................................. 142
Figure 4-3: Radiation dose response of MDA-MB-231Luc+ cells fitted to a linear-quadratic model: SF = exp (-αD-βD2) of cells treated with IR (225 kVp, 13 mA, 0, 2, 4, or 6 Gy) in combination with pre-treatment with AuNPs (A), cisplatin (B) or AuNPs
and cisplatin (C). Data points represent meanSEM (n3). ........................................ 145
Figure 4-4: Representative TEM images of tumor sections obtained from mice 24 h post i.t. infusion of AuNP-RME. Scale bars represent 2 µm in panels A and D, 500 nm in panels B and E, and 100 nm in panels C and F. As indicated by arrows, AuNP-RME were internalized by cells at the tumor site and are present as single particles or clusters in vacuoles. ................................................................................................ 147
Figure 4-5: (A) Intratumoral levels of Au as measured by CT. The amount of Au in each tumor was calculated by converting Hounsfield Units (HU) to concentration of Au, using images acquired prior to AuNP infusion as baseline, and a standard curve established in a phantom. The amount of Au (mg) per tumor was calculated to be
0.48 at 5 min, 0.520.04 at 24 h, 0.520.06 at 72 h, and 0.49 at 120 h post i.t. infusion of AuNP-RME. There is no significant difference between Au levels obtained
at each time point. Data points represent meanSEM (n=7). (B) Percentage of tumor volume containing detectable levels of Au. (*) represents a significant difference in the percentage of tumor with Au at 120 h post-infusion compared to that at 5 min post-infusion. (C) Tumor volume over time. (*) represents a significant difference between the tumor volume at 120 h post-infusion compared to that at 5 min post-infusion. (D) Representative CT images of sections (~1.5 mm apart) of a tumor 5 min post-infusion. (E) Representative CT images of one section of a tumor pre-infusion and at 5 min, 24 h, 72 h, and 120 h post-infusion. Tumors are outlined in white in panels D and E. ........................................................................................................... 150
Figure 4-6: (A) Percent tumor volume change over time. The endpoint for each treatment group was reached when one mouse in the group had a tumor size greater than 1.5 cm in any dimension. Tumor size was measured by caliper and calculated using the formula: volume = (length x width2) x 0.5. Data represent mean±SEM (n=5–9). Within the legend, (*) indicates significant tumor growth delay compared to the no treatment control group, and (#) indicates significant tumor growth delay compared to IR alone. (B) Percent body weight change. Within the legend, (*) indicates significant body weight change compared to the no treatment control group, and a (#) indicates significant body weight change compared to IR alone. (C) Survival curves; median survival (days) for each treatment group is indicated in parentheses. Significantly prolonged survival was achieved with IR+AuNP-RME, IR+cisplatin, and IR+AuNP-RME+cisplatin, compared to the no treatment control, as represented by (*). In comparison to IR alone, significantly prolonged survival was achieved with IR+AuNP-RME+cisplatin, as represented by (#). ................................. 154
Figure 4-7: Cytotoxicity of cisplatin in MDA-MB-231Luc+ cells following 30 min or 48 h incubation periods. These plots were used to compute the IC25 values of cisplatin to
be used in subsequent IR experiments. Data represents mean SEM (n=3). ............ 160

xix
Figure 4-8: Bioluminescence images of mice after i.p. injection with D-luciferin, administered five min prior to BLI. (A) without metastases, (B) with metastases. ....... 161
Figure 4-9: Plating efficiency (PE) of cells evaluated using ex vivo clonogenic assay. A (*) indicates significantly lower PE for the treatment group in comparison to control. IC25 of cisplatin was determined to be 4 mg/kg and used in the subsequent stidies for the assessment of its radiation enhancement effects and toxicity. Based on this data, a dose of AuNP-RME at 0.50 mg Au per tumor, which was associated with no cytotoxicity and the highest level of cell kill in combination with IR, was employed in subsequent efficacy and toxicity studies in mice. ........................................................ 165
Figure 4-10: (A) Percent tumor volume change and (B) percent body weight change for mice in each treatment group. The endpoint for each treatment group was reached when one mouse in the group had a tumor size greater than 1.5 cm in any dimension. Tumor size was measured by caliper and calculated using the equation: volume = (length x width2) x 0.5. Data represent mean±SEM (n=5). (*) indicates significant tumor growth delay compared to the control group on day 7. IR+cisplatin did not show improvement in tumor growth delay compared to IR alone on day 9. There was no significant difference in body weight change amongst the groups. ....... 166
Figure 5-1: Schematic illustration of synthesis of peptide and cisplatin conjugated AuNPs. (A) Synthesis of AuNP-PEG. (B) Synthesis of cisplatin prodrug. (C) Conjugation of peptide and cisplatin to AuNPs. .......................................................... 181
Figure 5-2: TEM images of AuNP-(RME+cisplatin) accumulation in MDA-MB-231 (A,
B), and MDA-MB-436 (C, D) following 24 h of incubatiion. Scale bar represents 2 m in (A and C) and 100 nm in (C and D). Upon entering cells AuNP-(RME+cisplatin) are sequestered in endosomes and lysosomes. ......................................................... 183
Figure 5-3: In vitro cellular accumulation of AuNP-RME and AuNP-(RME+cisplatin) in MDA-MB-231 and MDA-MB-436 cells quantified by ICP-AES with incubation at the concentration of 0.5 mg/mL AuNPs. * Represents statistically significant differences between AuNP-RME and AuNP-(RME+cisplatin) in terms of cellular levels of Au
(p<0.05), Data represents mean SEM (n=3). ........................................................... 184
Figure 5-4: Cell surviving fraction (SF) following 24 h of treatment with different concentrations of AuNP-RME or AuNP-(RME+cisplatin) in MDA-MB-231 and MDA-MB-436 cells. SF as determined by clonogenic assays is reported as plating efficiency compared to non-treated cells. A (*) represents statistically significant differences between various concentrations for HeLa and MCF-7 cells, respectively
(p<0.05). Data represents mean SD (n=3). .............................................................. 185
Figure 5-5: Radiation dose response curves for cells pretreated with AuNP-RME or AuNP-(RME+cisplatin) (0.5 mg/mL, 24h). DEF values for AuNP-RME and AuNP-(RME+cisplatin) at 0.1 SF were 1.16 and 1.41 (MDA-MB-231), 1.25 and 1.91 (MDA-MB-436), respectively, using IR alone as control. ....................................................... 186

xx
List of Abbreviations
AgNPs Silver Nanoparticles
ANOVA Analysis of variance
ATP Adenosine Triphosphate
Au Gold
AuNPs Gold nanoparticles
AuNRs Gold Nanorods
BRCA1 Breast Cancer 1
BrdUrd Bromodeoxyuridine
BSA Bovine Serum Albumin
BW CBC
Body Weight Complete Blood Count
CDKs Cyclin-Dependent Kinases
COX-2 Cyclo-Oxygenase-2
DCF 2',7'-Dichlorofluorescein
DCFH-DA 2’,7’-Dichlorofluorescin Diacetate
DEF Dose Enhancement Factor
DLS Dynamic Lighter Scattering
DMEM Dulbecco's Modified Eagle Medium
DSB Double Strand Break
EDC 1-Ethyl-3-(3-dimethyl-aminopropyl)carbodiimide
EDTA Ethylenediaminetetraacetic Acid
EdU 5-Ethynyl-2'-deoxyuridine
EF5 2-Nitroimidazole
EGFR Epidermal Growth Factor Receptor
EPR Enhanced Permeability and Retention
FACS Fluorescence-activated Cell Sorting
FITC Fluorescein Isothiocyanate
GA Gum Arabicglycoprotein
GdNPs Gadolinium Nanoparticles
GSH Glutathione
HBSS Hank’s Balanced Salt Solution
HfO2NPs Hafnium Oxide Nanoparticles
HR Homologues Recombination
HUVEC Human Umbilical Vein Endothelial Cells
I.p. Intraperitoneal
I.t. Intratumoral
I.v. Intravenous
ICP-AES Inductively Coupled Plasma Atomic Emission Spectroscopy
IdUrd Iododeoxyuridine
IR Ionizing Radiation
LEEs Low Energy Electrons

xxi
LEM Local Effect Model
LET Linear Energy Transfer
MC Monte Carlo
MES 2-(N-morpholino)ethanesulfonic Acid
NAC N-Acetyl-Cysteine
NHEJ Non-homologous End Joining
NLS Nuclear Localization Signal
NMR Nuclear Magnetic Resonance
NP 40 Nonidet P40
NPs Nanoparticles
OER Oxygen Enhancement Ratio
PBS Phosphate-buffered Saline
PEG Polyethylene Glycol
PI Propidium Iodide
PtNPs Platinum Nanoparticles
RBE Relative Biological Effectiveness
RES Reticulo-Endothelial System
ROS Reactive Oxygen Species
RPMI Roswell Park Memorial Institute Medium
RT Radiation Therapy
S Sulphur
SBRT Stereotactic Body Radiation Therapy
SD Standard Deviation
SEM Standard Error of Mean
SF Surviving Fraction
SIN 3-Morpholino-Sydnonimine Hydrochloride
SOBP Spread-Out Bragg Peak
SRS Stereotactic Radiosurgery
SSB Single Strand Break
Sulfo-NHS Sulfo-N-Hydroxysulfosuccinimide
TBS Tris-buffered Saline
TEM Transmission Electron Microscope
TEMED Tetramethylethylenediamine
TNBC Triple Negative Breast Cancer
TP Tiopronin
UV-vis Ultraviolet-visible
VEGF Vascular Endothelial Growth Factor
Z Atomic Number Z-VAD-fmk Z-Val-Ala-Asp-Fluoromethylketone

Chapter 1: Introduction, Hypotheses, and Overview 1
Chapter 1
Introduction, Hypotheses, and Overview
Lei Cui, Sohyoung Her, Gerben R. Borst, Robert G. Bristow,
David A. Jaffray, and Christine Allen
Written by L.Cui & S. Her. Figures by L.Cui. Edited by C. Allen.

Chapter 1: Introduction, Hypotheses, and Overview 2
1.1 Abstract
The utilization of gold nanoparticles (AuNPs) as radiosensitizers has shown great
promise in pre-clinical research. In the current review, the physical, chemical, and
biological pathways via which AuNPs enhance the effects of radiation are presented
and discussed. In particular, the impact of AuNPs on the 5 R’s in radiobiology, namely
repair, reoxygenation, redistribution, repopulation, and intrinsic radiosensitivity, which
determine the extent of radiation enhancement effects are elucidated. Key findings from
previous studies are outlined, in addition, crucial parameters including the
physicochemical properties of AuNPs, route of administration, dosing schedule of
AuNPs and irradiation, as well as type of radiation therapy, are highlighted. The optimal
selection and combination of these parameters enable the achievement of a greater
therapeutic window for AuNP sensitized radiotherapy. Future directions are put forward
as a means to provide guidelines for successful translation of AuNPs to clinical
applications as radiosensitizers.

Chapter 1: Introduction, Hypotheses, and Overview 3
1.2 Introduction
Radiation therapy (RT) is commonly used as primary or adjuvant treatment in
over 50% of cancer patients [1-3]. In several types of cancer such as breast and
cancers of the central nervous system, the utilization rate of RT is as high as 80-90% [3,
4]. Despite its crucial role in cancer therapy, there are challenges associated with RT.
Firstly, toxicity to surrounding normal tissues often limits the maximum dose of
irradiation (IR) that can be delivered to tumors [5, 6]. In addition, tumor is a disease with
a high degree of heterogeneity in genotype, phenotype, and microenvironment, leading
to variability in radiation sensitivity and response in populations of tumor cells [7-9].
Recent advancements in physical targeting of RT, by techniques such as image
guidance and intensity modulation, allow the delivery of more accurate and nonuniform
radiation doses with greater conformality to tumor while avoiding healthy tissues [2, 10].
Meanwhile, multimodality cancer treatment is widely employed to improve the
therapeutic window of RT [6], wherein concomitant chemoradiotherapy is employed as
the standard treatment in most solid tumors, with the benefit of better local control,
eradication of distant metastases, down-staging of tumors, improved organ
preservation, increased rates of cure and overall survival [11].
As first defined by Steel and Peckham, there are four mechanisms via which an
enhanced therapeutic window can be achieved by concomitant chemoradiotherapy: (1)
spatial cooperation; (2) independent toxicity; (3) protection of normal tissue from
damage by IR; and (4) enhancement of tumor response to IR by radiosensitization [11,
12]. Specifically, radiosensitization is a process in which a radiosensitizer present at the
tumor site interacts with IR and/or the biological target(s) to optimize the outcome of RT
[11-13]. Radiosensitization plays a critical role in the management of most cancers and
is considered "the new dogma in cancer treatment" [14].
The effect of IR on biological systems can be divided into physical, chemical, and
biological phases [1, 15]. The physical phase is the period in which particles with high
energy (photons, electrons, protons, or heavy ions) travel through their biological targets
and cause ionization and/or excitation of the molecules, followed by breakage of

Chapter 1: Introduction, Hypotheses, and Overview 4
chemical bonds and generation of free radicals. The subsequent chemical phase
involves two types of competitive reactions - scavenging and fixation reactions - wherein
the highly reactive free radicals react instantly with other biological molecules to re-
establish “electronic charge equilibrium”. In particular, scavenging reactions refer to the
inactivation of free radicals by reducing agents such as thiol-containing molecules.
Fixation reactions result in permanent irreparable damage to biological components by
molecules with high electron affinity, such as oxygen. The biological phase is comprised
of the responses of the biological targets to IR at the molecular, cellular, and tissue
levels. In radiobiology, these responses are described as the 5 R's: repair,
reoxygenation, redistribution, repopulation, and intrinsic radiosensitivity, The 5 R's are
considered to be the key factors which determine the outcome of IR [16-18].
Radiosensitizers enhance the effects of RT via multiple mechanisms which are involved
in these three phases [1, 13, 15], leading to the elevated generation of toxic substances
such as radicals or electrons, consumption of radical scavengers, fixation of IR induced
damage, as well as modification of the 5 R’s which enhance the biological response to
IR [13, 16-18].
In recent years, AuNPs have provoked extensive interest in the biomedical field,
and there has been a rapid growth in the number of publications in this area (Figure 1-1
A). Due to their unique physical and chemical properties, AuNPs have been widely
explored for diagnostic and therapeutic purposes (Table 1-1) [19-22]. In particular,
AuNPs have been recognized as a potent radiosensitizing agent in the preclinical
setting (Figure 1-1 B). However, there's remains a significant gap between the current
status of the field and clinical implementation of AuNPs as radiosensitizers. As stated by
Coleman et al. and Wardman [13, 23], there are a number of key items that must be
examined for the clinical translation of a radiosensitizer including 1) identification of
targets of the radiosensitizer, 2) accessibility of radiosensitizer targets, 3) stability of the
targets and 4) toxicity of the radiosensitizer enhanced RT to tumor relative to normal
tissues. This review begins with an extensive discussion of the underlying mechanisms
and targets associated with radiosensitization by AuNPs (Figure 1-2). Moreover, the
dynamic nature of the biological targets (5 R's) is discussed, followed by a presentation
of the roles of several key parameters (i.e. physicochemical properties of AuNPs, route

Chapter 1: Introduction, Hypotheses, and Overview 5
of administration, dosing schedule of AuNPs and IR, as well as the type of RT) in
determining the bioavailability of AuNPs, efficacy, toxicity, and thereafter the therapeutic
window that can be achieved with AuNP sensitized RT. In addition, results from
previous research, from theoretical calculations and experimental observations, are
summarized. Conclusions and future directions are outlined to guide the advancement
of AuNP radiosensitizers to the clinic.
Table 1-1: Properties of AuNPs and their biomedical applications [19-22].
Properties of AuNPs Applications
Diagnostic Therapeutic
Surface Plasmon Resonance Optical imaging Phtotothermal therapy
Surface enhanced Raman Scattering
Fluorescence imaging
High atomic weight and contrast under electron
microscope
Immunostaining, phagokinetic tracks
imaging
High atomic number and elevated photoelectric
absorption
X-ray CT Sensitization of radiotherapy
Easy surface chemistry for functionalization and
bioconjugation
Delivery of gadolinium for MRI,
biosensing.
Drug delivery, tumor, cellular, and nuclear targeting

Chapter 1: Introduction, Hypotheses, and Overview 6
Figure 1-1: (A) Number of publications on AuNPs over the past two decades. (B)
Number of publications on AuNPs in radiotherapy over the past two decades. Data
show the number of publications compiled as of June 2016 using Scopus search engine
with the following search words (A) gold nanoparticles and (B) gold nanoparticles
radiation therapy.

Chapter 1: Introduction, Hypotheses, and Overview 7
1.3 Mechanisms of Radiosensitization by AuNPs
Elements with high atomic number, for instance iodine (I, Z=53) [24], gadolinium
(Gd, Z=64) [25], platinum (Pt, Z=78) [26], and gold (Au, Z=79) [27-60] were first
recognized as radiosensitizers due to their elevated photoelectric absorption of IR
energy in comparison to soft tissue (Section 1.3.1). However, experimentally measured
dose enhancement factor (DEF) values in biological systems have been substantially
greater than those predicted by the mass attenuation coefficients. These findings clearly
suggest the existence of other mechanisms via which NPs sensitize cells to IR. Indeed,
research has provided direct evidence of chemical (Section 1.3.2) and biologic al
(Section 1.3.3) pathways by which AuNPs enhance the effects of IR (Figure 1-2), which
explains the disparity between the biologically observed values of dose enhancemen
factors (DEF) and that predicted by physical dose enhancement alone.

Chapter 1: Introduction, Hypotheses, and Overview 8
Figure 1-2: Radiosensitization by AuNPs: mechanisms and key parameters.
(Timescale adapted from Joiner and van der Kogel, 2009 [1]

Chapter 1: Introduction, Hypotheses, and Overview 9
1.3.1 Physical Phase
There are three main types of physical interactions between photons and
materials: (1) the photoelectric effect which is usually followed by Auger cascades, (2)
Compton Effect, and (3) pair production; which of these interactions dominates is a
combined result of the energy of the incident photon and the atomic number (Z) of the
material (Figure 1-3 A) [61]. These various interactions between radiation and materials
are illustrated in Figure 1-3 B [61, 62]. At low radiation energy where photoelectric
effects dominate, the cross section is proportional to Z3-5, as a result, materials of high Z
have a much higher mass energy absorption coefficient in comparison to those with low
Z [61]. The absorbed radiation energy is released locally by the emission of photons
and numerous secondary electrons as well as Auger electrons. These low energy
electrons (LEEs) either cause direct damage to biological components in their close
proximity, or they interact with water molecules, which are the major component of
biological systems, to produce hydroxyl radicals (OH) and cause indirect damage to
biological molecules [63]. Therefore, by introducing high Z materials into soft tissue, the
local effect of radiation is significantly enhanced.
Chapter 1: Introduction, Hypotheses, and Overview 10

Chapter 1: Introduction, Hypotheses, and Overview 11
Figure 1-3: (A) Radiation energy and atomic number (Z) dependent interactionbetween
radiation and materials. (B) Illustration of the Photoelectric effect, Compton Effect, and
pair production. (i) In the photoelectric effect (10-500 keV): the energy of the incident
photon (hʋ) is fully absorbed by an electron in the inner shell of an atom, and the
electron is ejected from the atom. The vacant orbit is filled with an electron from an
outer shell with high energy; extra energy is either released as photon or absorbed by
another electron in an outer shell, which is ejected from the atom (Auger electron). This
Auger effect occurs in cascade if there are multiple shells of electrons in the atom. (ii) In
the Compton Effect (500 keV – 1.02 MeV): the energy of the incident photon is partially
absorbed by an electron in the outer shell of an atom, and the extra energy is released
as photons. (iii) In Pair product: when the energy of an incident photon is at least two
fold larger than mec2 (> 1.02 MeV), and the energy is fully absorbed by the nucleus of
an atom, a pair of electrons and positrons are generated from the nucleus [61, 64].
A “ ” represents incident or released photons; a “ ” represents ejection of
secondary or Auger electrons; electrons are represented as “”, and a “ ” represents a
vacancy in the electron orbit in an atom.
1.3.2 Chemical Phase
The existence of agents which are capable of interfering with radical scavenging
and fixation reactions has a great impact on the outcomes of the chemical phase.
Radical scavenging agents include reducing chemicals such as glutathione (GSH), the
depletion of which results in higher levels of IR induced damage in the biological
targets. The most important natural radical fixation agent involved in radiochemistry is
oxygen (O2); due to its high electron affinity, O2 reacts rapidly with free radicals (R) in
biomolecules to produce RO2, followed by the formation of stable ROOH. Therefore,
the IR induced damage is chemically fixed with a permanent change in the biological
components [1]. Inadequate supply of O2 (hypoxia) has long been recognized as the
cause of radioresistance - cells under hypoxia are usually 2-3 fold more resistant to
radiation (known as "the oxygen effect") [65-67].

Chapter 1: Introduction, Hypotheses, and Overview 12
A major difference between inorganic nanoparticles and their bulk counterpart is
their surface chemical properties. The highly curved surface of nanomaterials leads to
defects in their crystal structure. Therefore, the otherwise continuous electronic
configuration in the bulk material is disrupted, resulting in the generation of reactive
electron donating and accepting sites, which are capable of accommodating and
increasing the yield of the chemical reactions [68], as such nanoparticles (NPs) of many
materials are used as catalysts in chemistry [19, 69]. It has been recognized that the
radiosensitization by AuNPs is dependent on their surface chemistry. Misawa et al.,
observed that the amount of ROS generated by AuNPs under IR is not dependent on
their concentration by mass; yet, rather is inversely proportional to AuNP size [70]. More
recently, Cheng et al. reported “chemical enhancement” of X-rays in the presence of
AuNPs - the enhancement of radiation by AuNPs (measured by coumarin carboxylic
acid hydroxylation) was 2000 times higher than that predicted by enhanced physical
absorption. The authors proposed that superoxide generated under radiation bound to
the reactive sites on the surface of AuNPs to form AuNP-O2, this reactive molecule then
acted as a catalyst for subsequent reactions between radical intermediates and other
molecules, leading to the elevated generation of ROS including super oxide radical (O2-
), hydrogen peroxide (H2O2), and hydroxyl radical (OH) [62] [71]. Results from these
studies suggest that the radiosensitization effects of AuNPs will be oxygen dependent,
in that O2 plays a crucial role both as a substrate and an intermediate in ROS
generation. As a matter of fact, diminished radiosensitizing effects of AuNPs under
hypoxia have been demonstrated in one of our previous studies [42] and in other
research by Jain et al. [45]. These phenomena provide indirect evidence of chemical
mechanisms via which AuNPs enhance the effect of radiation.
Furthermore, measured in DNA-AuNPs complex, Sanche et al. reported a
chemical sensitization effect of AuNPs at low IR energy (electrons of 10eV), [72, 73] –
rather than generating significant numbers of secondary electrons, LEEs produced by
AuNPs under IR caused weakened bonds in DNA molecules by forming “transient
negative ions”, which ultimately lead to increased levels of DNA damage [74]. Full

Chapter 1: Introduction, Hypotheses, and Overview 13
exploitation of this chemical enhancement effect relies greatly on successful nuclear
targeting and binding of AuNPs to DNA molecules [74].
1.3.3 Biological Phase
Conventional RT is based on a fractionated regime (typically 1.8-2 Gy daily, 5
days per week for several weeks) [1], which allows effective recovery of normal tissues
to sublethal IR doses giving rise to an optimal therapeutic window [10, 75]. In
radiobiology, cellular and tissue response to fractionated IR are described by the 5 R’s,
namely repair, redistribution, reoxygenation, repopulation, and intrinsic radiosensitivity
[16-18]. The 5 R’s are considered to be the biological factors which determine the
"success or failure" of RT [16, 18, 76].
Radiosensitizers are designed to interact with biological targets such that they
alter their response to IR and consequently result in an enhanced effect of IR. At the
molecular and cellular levels, radiosensitizers can modify pathways involved in DNA
repair, cell cycle checkpoint and progression, as well as cellular death and proliferation,
to achieve higher levels of cell kill by IR. At the tissue level, radiosensitizers may
prevent tumor regrowth by specifically killing subpopulations of cancer cells that are
radioresistant (e.g., those under hypoxia or in S phase), inhibiting tumor angiogenesis,
or reducing tumor hypoxia prior to IR by regulating the function of tumor blood vessels,
as well as diminishing oxygen and nutrient supply by damaging tumor blood vessels
post IR. All these mechanisms converge to impact the 5 R’s and thereafter result in an
improved outcome for RT [11, 77]. Radiosensitization by AuNPs via biological pathways
has been recognized yet needs further investigation. Evidence obtained to date
suggests that ROS generation and oxidative stress contribute strongly to the biological
impact of AuNPs [44, 62, 68, 78-83]. In the following sections the influence of AuNPs on
the 5 R’s and in turn the effect of the 5 R’s on the radiosensitizating effects of AuNPs
are discussed.

Chapter 1: Introduction, Hypotheses, and Overview 14
Repair
It is widely recognized that DNA is the principal target of IR, the damage of which
has a direct correlation to cell death. When cells and organisms are exposed to internal
or external stress which causes damage to DNA, highly complex and coordinated
biological processes are initiated to maintain the structural integrity of DNA [1]. A
number of chemical agents sensitize radiation via interference with post-IR DNA repair
processes, such as halogenated pyrimidines (5-FU, BrdUrd, IdUrd), nucleoside analogs
(gemcitabine, fludarabine) [13], cytotoxic chemicals (cisplatin, doxorubicin), and DNA
topoisomerase I-targeted drugs (camptothecins, etoposide) [11, 13, 84].
To date there has been little direct evidence of DNA repair inhibition by AuNPs,
as exemplified recently by our group with tiopronin-coated AuNPs [42]. However,
inhibition of IR induced DNA damage repair by other inorganic nanoparticles has been
reported. Wojewodzka et al. showed that that silver nanoparticles (AgNPs) delay X-ray
induced DNA damage repair in HepG2 cells, and the authors ascribed this phenomenon
to ROS generation and oxidative stress caused by AgNPs [85], in that oxidatively
stressed cells are impaired in radical scavenging generated by IR [86]. The authors also
proposed another two possible mechanisms of DNA repair inhibition by AgNPs:
inadequate energy (ATP) supply due to malfunction of mitochondria under oxidative
stress, as well as depletion of GSH by ROS generated by the NPs, which disables
effective DNA single strand break (SSB) rejoining [85].
Reoxygenation
Oxygen plays both radiochemical and physiological roles in radiation therapy. Its
important role in radiochemistry for post IR radical fixation leads to the use of oxygen
mimic chemicals including nitrobenzenes, nitrofurans, and nitroimidazoles as effective
radiosensitizers [13]. On the other hand, prolonged lack of oxygen (chronic hypoxia)
decreases expression levels of homologues recombination (HR) related proteins, and
consequently lowers DNA damage repair capacity and enhances susceptibility of cells
to IR induced damage [87].

Chapter 1: Introduction, Hypotheses, and Overview 15
It is well known that tumors will be reoxygenized minutes to days following IR
exposure [1, 88]; in the clinic, the advantage of reoxygenzation is utilized in fractionated
RT [1], other strategies to elevate the oxygen level in tumors prior to IR include the use
of chemotherapy agents such as paclitaxel to debulk tumors [89], as well as anti-
angiogenic therapies which lead to momentary normalized function of tumor blood
vessels and better oxygen supply [11, 90].
Although significant inhibition of cell proliferation by AuNPs under both oxia and
hypoxia has been observed previously [42, 45], generally there has been no direct
evidence that AuNPs at the tumor site function to debulk or cause reoxygenation in
tumors prior to IR. It should be stressed that oxygen levels during IR have a great
impact on radiosensitization by AuNPs [42, 45]. Our previous research revealed that the
radiosensitization effect of AuNPs is greatest under oxia, followed by chronic hypoxia,
and lowest under acute hypoxia, suggesting the radiochemical role of oxygen on
radiosensitzation by AuNPs. Greater radiosensitization in cells under chronic hypoxia in
comparison to that under acute hypoxia is due to the diminished DNA repair capacity of
cells [42]. These results indicate that the reoxygenation that occurs between fractions of
RT may be utilized to enhance the radiosensitizing effects of AuNPs, yet a systemic
comparison of radiosensitization by AuNPs with large single dose or fractionated IR is
lacking.
Redistribution
Cells normally cycle through G1, S, G2, and M phases [91] and then upon
exposure to stress, which triggers DNA damage, checkpoints are activated which slow
down or block cell cycling [92]. Particularly, when cells are exposed to IR, G1, S, G2-
early, and G2-late checkpoints are activated, preventing cells from moving into S phase
or mitosis, prolonging cell progression through S phase, or accumulating cells in G2
phase [1]. Given that cells in G2/M phase are more radiosensitive compared to those in
G1/S phase, redistribution describes the phenomenon wherein cells in radioresistant
phases surviving one fraction of radiation progress in cell cycle to more sensitive

Chapter 1: Introduction, Hypotheses, and Overview 16
phases [18, 93]. A favored therapeutic window for fractionated RT stems in part to the
lack of checkpoints in many tumor cells in comparison to checkpoint competent normal
cells which cycle slowly [18, 94]. Several chemical agents sensitize cells to radiation via
cell cycle synchronization. As an example, taxanes arrest cells in the G2/M phase
through tubulin stabilization [11, 95].
The effects of AuNPs on cell cycle have been controversial. While it's been
reported in several studies that AuNPs do not affect cell cycle distribution [38, 42],
research by Roa et al. revealed that AuNPs enhance the effect of IR in human prostate
carcinoma cells by arresting them in the G2/M phase, which is associated with the
activation of cyclin-dependent kinases (CDK) as well as a lowered expression of p53
and cyclin A and increased expression of cyclin B1 and cyclin E [32]. In addition, Xu et
al. demonstrated that gold nanorods (AuNRs) induce significant accumulation of
melanoma cells in the G2/M phase [40]. Also, Pan’s study showed that treating cells
with AuNPs lead to down-regulation of cell cycle associated genes [80]. Similar
phenomena were observed in cells treated with other inorganic NPs such as silver [96]
and TiO2 [97] - in both cases it was concluded that ROS generation and oxidative stress
caused by nanoparticles led to DNA damage and consequently cell cycle
synchronization. Further research is needed to evaluate the impact of AuNPs on cell
cycle in animal models, and dosing schedule of AuNPs and IR should be taken into
consideration as a key parameter if cell cycle arrest is one of the mechanisms via which
AuNPs sensitize cells to radiation.
Repopulation
Repopulation of tumor cells between fractions of radiation has been considered
as the main cause of RT failure, especially accelerated regrowth of tumor following
exposure to sublethal doses of radiation [18, 75]. For this reason strategies have been
developed to kill subpopulations of cells that are radioresistant (e.g., those under
hypoxia or in S phase) to prevent tumor repopulation. Effective agents include
halopyrimidines (e.g., 5-FU, hydroxyurea) which are taken up by cells in the S phase,

Chapter 1: Introduction, Hypotheses, and Overview 17
or toxins which specifically kill cells under hypoxia (e.g., tirapazamine, mitomycin), or
receptor targeting molecules (e.g., cetuximab, trastuzumab) that inhibit active cellular
proliferation, as well as anti-angiogenic agents that diminish oxygen and nutrient supply
post IR and prevent tumor regrowth (e.g., mAb-VEGF, angiostatin, endostatin) [11, 13,
77, 84, 98].
The ability of AuNPs to inhibit cellular growth and proliferation has been shown in
several cell lines via integrin or receptor mediated pathways [40, 99-101]. Inhibition of
angiogenesis and tumor growth by AuNPs has been demonstrated in vivo. Mukkerjee et
al. reported "an intrinsic property" of AuNPs to inhibit VEGF-165 dependent permeability
and angiogenesis in mouse ovarian tumors, due to the strong semi-covalent bonds
between Au and thiols/amines, which cause direct binding of AuNPs to the cysteine
residues on growth factors [102]. More recently, Zhang et al. demonstrated an
observable tumor (s.c. cervical U 14) growth inhibition 24 days post i.p. injection of
PEGylated AuNPs [52]. These findings suggest the possibility of using AuNPs to inhibit
tumor growth.
On the other hand, it is worth noting that the local and cellular levels of AuNPs at
the tumor site are decreased during repopulation, which consequently leads to a
diminished DEF by AuNPs, in that radiosensitization by AuNPs is dependent on their
local and intracellular concentration [31, 42]. Kim et al. put forward that despite not
being exported from cells, the dose of AuNPs in cells is diluted during parent cell
division [103]. In agreement with this, previous kinetic studies in vitro have shown that
the cellular levels of AuNPs first increase with time, peak at a specific timepoint, and
then plateau or decrease[79, 104], due to the higher rate of proliferation relative to the
rate of cellular uptake of AuNPs [79]. Studies in animal models (MDA-MB-231
orthotopic) from our group revealed that following a single intratumoral (i.t.)
administration of AuNPs, the percentage of the tumor volume containing a certain level
of Au decreased over time (72 h post i.t. injection) due to ineffective penetration of
AuNPs and tumor growth. These observations suggest that the effect of repopulation on
local and cellular levels of AuNPs should be taken into account in terms of dosing

Chapter 1: Introduction, Hypotheses, and Overview 18
schedule of AuNPs and IR. Further the necessity for re-administration of AuNPs in
prolonged RT such as fractionated RT and brachytherapy should be considered.
Intrinsic radiosensitivity
Intrinsic radiosensitivity of cell lines, as measured by the surviving fraction (SF) of
cells at 2 Gy, is considered to be directly correlated with tumor radio-responsiveness,
and is an important prognostic factor that determines the outcome of RT [105-107].
Intrinsic radiosensitivity can be modified by radiosensitizers which inhibit cellular
synthesis of radioprotectors (e.g., L-S-buthionine sulphoximine), as well as agents that
are targeted to cellular receptors or pathways which enhance the response of cells to IR
via elevated cell death capacity (e.g., NS-398, SC-236) [13, 77, 108].
Induction of cell death via apoptosis and necrosis by AuNPs has been reported
consistently and is associated with upregulation of caspase, rupture and depolarization
of the mitochondrial membrane in cells followed by release of cytochrome c and Ca2+,
as well as overexpression of stress related genes [44, 80, 109-112]. Given that cells
that are capable of escaping programmed cell death are more radioresistant [113, 114],
enhanced apoptosis and necrosis of cells serves as a pathway by which AuNPs
sensitize IR.
Unfortunately, no research has been conducted to define the correlation between
radiosensitization by AuNPs and intrinsic radiosensitivity of cells. In recent research by
Marill et al., the radiosensitization effect of hafnium oxide NPs (HfO2NPs) was
evaluated. Hafnium has a high atomic number (Z=72) and in a similar manner to Au,
sensitizes cells to radiation via elevated absorption of radiation energy. Results from
this research suggested a positive correlation between the intrinsic radiosensitivity of
cells and their radiosensitization by HfO2NPs [115], with the underlying mechanisms
remaining unknown.

Chapter 1: Introduction, Hypotheses, and Overview 19
1.4 Previous Studies on Radiosensitization by AuNPs
The radiosensitization effects of AuNPs have been theoretically calculated using
Monte Carlo (MC) simulations [63, 116-132], and experimentally evaluated in vitro using
DNA plasmid [63, 133-136] and cell models [28-44], as well as in vivo in tumor bearing
animals [27, 47-59]. Results from these studies provide important guidelines for further
preclinical and clinical research. A detailed summary and comprehensive discussion of
these studies are available in several excellent review articles [41, 62, 64, 74, 137-142].
Table 1-2 presents an up-to-date summary of the published in vivo studies that examine
radiosensitization by AuNPs.
1.4.1 MC Studies
MC studies have been used to predict the macroscopic physical DEFs that can
be achieved using AuNPs based on their mass attenuation coefficients under different
radiation sources, as well as to evaluate the manner of deposition of microscopic
energy (effective range, deflection angle, energy deposition ratio, etc.) associated with
the secondary electrons and Auger electrons generated by AuNPs under IR [63, 116-
129]. MC studies define the fundamental physical parameters that determine the
radiation enhancement effects that can be achieved using AuNPs.
Optimal physical radiation enhancement by AuNPs is via photoelectric energy
absorption [121], and maximum enhancement effects are achieved with low energy
IR of X-rays (orthovoltage) and brachytherapy [130].
Due to the fact that AuNPs preferentially accumulate in tumor blood vessels post i.v.
injection, AuNPs can be employed as tumor vascular disrupting agents via local
dose spikes (elevate local dose from 2 Gy to > 15 Gy) in combination with
brachytherapy, proton therapy and large doses of external beam photon RT [122,
128, 129, 131].
A large proportion of LEEs generated by AuNPs under low energy IR are of short
effective range (i.e. nanoscale), therefore successful delivery of AuNPs to biological

Chapter 1: Introduction, Hypotheses, and Overview 20
targets is crucial to achieve maximum radiosensitization. On the contrary, electrons
produced by AuNPs under high radiation energy can reach far distances up to
hundreds of microns and cause cross fire effects spanning the distance of a few
cells. Thus, cellular localization of AuNPs may not have a profound effect on their
radiosensitization [124, 125].
1.4.2 Radiosensitization in Plasmid DNA Models
As the principal target of RT, DNA molecules are employed as an important
model in radiobiology [1, 143]. Advantages of the plasmid DNA model include easy
quantification of single strand breaks (SSBs) and double strand breaks (DSBs) using
gel electrophoresis, precise control over conditions such as location of AuNPs and
radical scavenging environment, as well as exclusion of complex biological processes
such as DNA damage repair [133, 137], which allow for an accurate characterization of
the LEEs produced by AuNPs under IR [137]. Studies in DNA models confirmed that in
the kVp radiation energy range most electrons ejected from AuNPs are LEEs with an
effective range on the nanoscale. Therefore, it is of important to deliver AuNPs to their
biological targets such as cells and DNA molecules [63].
1.4.3 Radiosensitization in Cells
A significant number of cell studies have examined the radiosensitization effects
of AuNPs [28-46]. However, important parameters including cell line, radiation energy,
physicochemical properties of the AuNPs (size, shape, and surfactant), concentration of
AuNPs, and incubation time with AuNPs, have varied greatly across these studies.
Therefore, it is near to impossible to make comparisons between these studies that lead
to meaningful conclusions [137, 138]. However, from these studies there have been
some consistent findings [28-46]:
Biologically observed DEFs by AuNPs have been substantially greater than that
estimated by physical calculation; in addition, AuNPs enhance the effects of high

Chapter 1: Introduction, Hypotheses, and Overview 21
energy photon RT where the Compton Effect dominates [28, 31, 35]. These results
indicated the possibility to utilize AuNPs as radiosensitizers for more clinically
relevant high radiation energy [83].
Due to the short effective range of LEEs produced by AuNPs under low radiation
energy, cellular localization has a great impact on their radiosensitization, with
intracellular AuNPs at close proximity to biological components exhibiting higher
levels of radiosensitization [42].
Rather than being uniformly distributed as single particles throughout the entire
volume of cells, AuNPs are found sequestered as clusters in endosomal and
lysosomal vacuoles following cell entry. The impact of the size of AuNPs on
radiosensitization is largely influential at the level of cellular uptake, rather than a
size dependent effect on the manner of energy deposition of electrons generated by
the AuNPs under IR [35, 104].
Hypoxia diminishes radiosensitization by AuNPs, due to the important roles of
oxygen in RT [42, 45].
1.4.4 Radiosensitization In Vivo
Table 1-2 summarizes previous in vivo studies on radiosensitization by AuNPs.
In these studies the many influential parameters including tumor model,
physicochemical properties of AuNPs, administration route, radiation type, energy and
dose, dosing schedule of AuNPs and IR, and endpoint to evaluate the efficacy, that are
varied across these studies, make it challenging to identify the optimal parameters that
lead to best outcomes. However, several of the critical findings are as follows:
Most of the previous in vivo studies evaluating the radiosensitization effects of
AuNPs under external beam radiation have employed one single high dose of IR (5-
30 Gy), with the rationale being the need to obtain an observable tumor response
[54, 144]. It should be noted that in several studies radiosensitization was observed
when tumors were irradiated with orthovoltage photon beam immediately or shortly
(20 min) following i.v. injection of AuNPs. Thus providing evidence that effective cell

Chapter 1: Introduction, Hypotheses, and Overview 22
uptake is not needed to achieve significant tumor cell kill and radiosensitization [27,
50, 52]. In comparison to conventional fractionated RT, single dose IR (>8-10 Gy) is
more effective at damaging vascular endothelial cells [145]. Given that AuNPs
preferably accumulate in the tumor vasculature following i.v. injection [128], it is
postulated that the AuNPs are functioning in these studies as vascular disrupting
agents [122, 131].
There has been evidence that the degree of cellular apoptosis that accumulates with
fractions of IR may exceed that achieved with a single large dose [48, 53, 146].
Given that the presence of AuNPs has been shown to elevate the level of apoptosis
under IR [48, 52], Chang et al. suggested that the combination of AuNPs and
fractionated IR may lead to a significant enhancement of RT [48].
AuNPs are also able to sensitize electron and proton beam IR [48, 53, 59]. The
dosing schedule of AuNPs and RT are critical to achieve effective cellular uptake of
AuNPs at the tumor site given that the effect of proton RT can only be enhanced
when AuNPs are located in the cell cytoplasm or nuclei [132].
Radionuclide therapy using 198AuNPs has been successful in tumor control [49, 51,
57]; utilization of AuNPs as delivery vehicles for other radioisotopes represents a
promising strategy with great potential.
The dose of AuNPs employed to date has varied widely with the tumor level ranging
from ~0.250 μg to 74.24 mg Au/g tumor, with significant tumor growth delay
observed in most cases, relative to IR alone.
Hebert et al. observed a radio-protective effect by AuNPs, which was attributed to
the radical scavenging property of the thiol-containing coating material (dithiolated
diethylenetriamine-pentaacetic acid, i.e., DTDTPA), suggesting the importance of
the choice of coating agents in the achievement of radiosensitization by AuNPs [50].

Chapter 1: Introduction, Hypotheses, and Overview 23
Table 1-2: Summary of in vivo Studies
Animal model, tumor model, & tumur size
AuNP (size and coating)
Administra-tion route and dose
Systemic toxicity
Tumor level of Au
IR (energy &
dose)
Timing for IR Radiation enhancement
Herold 2000 [47]
C.B17/lcr; s.c. mammary EMT-6
300-700 mm3
1.5–3.0 m microsphere
3 i.t. injections, 1mg/tumor
200 kVp, 8.0Gy
Immediately post injection
Ex vivo clonogenics IR: PE=0.248,
IR+AuNPs: PE=0.149
Hainfeld 2004 [27]
Balb/C s.c. mouse; mammary
EMT-6 50-90 mm3
1.9 nm i.v., 1.35g Au/Kg; 31 mg
Au/mouse
Cleared from kidney, nontoxic
7mg Au/g tumor
250kVp, 26Gy
2 min post injection
1 year survial: 20% IR vs. 50%
IR+AuNPs, and significant tumor
growth delay
Chang 2008 [48]
C57BL/6; Murine B16F10 melanoma;
50-90 mm3
13 nm citrate coated
i.v., 0.67 mg/mouse
AuNPs in spleen and
liver
74.24 mg Au/g tissue
Electron beam 6 MeV, 25 Gy
24 h post injection
Significant tumor growth delay, and
longer survival
Khan 2008 [49]
C57Bl/6J; s.c. melanoma cells
B16F10; 438-527 mm3
22 nm 198Au/den-
drimer nano-composites
i.t. injection No clinical toxicity
observed
74.4 μCi/mouse
99% β particles (βmax = 960 keV); γ-ray at
960 keV
>45% reduction of tumor growth
Hebert 2010 [50]
Balb/C, s.c. MC7-L1 mammary
ductal; 100 mm3
~5 nm AuNP-
DTDTPA:Gd
i.v. infusion No AuNPs in critical organs,
no toxicity
0.05 mg Au /g tumor
150 kVp, 10Gy
20 min post infusion
Slight radioprotective
effect from AuNPs
Chanda 2010 [51]
Female ICRSC-M SCID; s.c. human
prostate cancer PC-3; 100 mm3
85 nm Gum arabic glycoprotein
(GA)–198AuNPs
i.t. injection Transitory body weight
loss
GA-198AuNPs (408 μCi)/mouse
βmax = 960 keV,
70 Gy
Significant tumor volume control,
1000 mm3 (control) vs. 200mm3 (GA-
198AuNPs) 30 days post injection
Zhang 2012 [52]
Female Balb/C s.c. cervical U14,
50-100 mm3
12.1nm AuNP-PEG
i.p. injection, 4 mg/kg
High spleen index, & liver
damage
~0.250 μg Au/g tumor
γ-ray, 5 Gy
Immediately post injection
Significant tumor growth delay, and lower tumor weight
24 days post IR
Kim 2012 [53]
Balb/c mice s.c. mouse colon carcinoma CT26,
7-10mm
14 ± 1.2 nm AuNP-DTPA
i.v. injection, 300 mg/kg,
Inflammatory response at
tumor periphery; no sign of acute side effects
137.4 ± 50.2 μg Au/g
Proton beam 45 MeV, 31Gy
24 h post injection
100 % complete tumor regression vs. 33% proton alone; 96% 300 days survival vs. 11% proton alone

Chapter 1: Introduction, Hypotheses, and Overview 24
Chattopadhyay
2013 [54]
CD1 nu/nu; s.c. MDA-MB-361(EGFR+) 150-210 mm3
30 nm AuNP-HER-2
i.t. injection, 0.8mg
Au/tumor
No significant toxicity by BWI, CBC, and ALT
100 kVp, 11Gy
24 h post injection
Significant tumor growth delay
Hainfeld 2013 [55]
B5C3f1, Tu-2449 tumor
implantation into striatum 3-5 mm
11.2 ± 8.6 nm
i.v. injection, 4 g Au/kg
1.5 ± 0.2% w/w,
~15mg Au/g tumor
100 kVp, 30 Gy
15 h post injection
1 year survival: 50 % (IR+AuNPs) vs.
0 by IR alone
Joh 2013 [56]
Nude female; Orthotopic brain
glioblastoma 1x108 p/sec/cm2/sr by
BLI
12 nm AuNP-PEG
i.v. injection 0.4 g Au/kg
Minimum toxicity
measured by BW
175 kVp, 20 Gy
2-4 days post injection
Median survival of 28 days
(IR+AuNPs) vs. 14 days (IR)
Lin 2013 [57]
Male Nu/Nu; s.c. non-small lung
cancer H460; 200 mm3
60 nm 198AuNPs@ gum arbic
(198AuNPs@ GA)
i.t. injection
No significant toxicity
measured by BW
50% injected dose at tumor 2 weeks post
injection
103.00 ± 1.31 μCi/mouse; β particles
(βmax = 960 keV), γ-ray at
412 keV
>90% tumor volume control
compared to control and AuNPs@ GA
at day 17
Zaki 2014 [58]
Female nu/nu; s.c. human fibrosarcoma
250 mm3
1.9 nm AuNPs
encapsulated in block
copolymer
i.v. injection, 650 mg Au/Kg,
No toxicity (body weight (BW), activity,
and blood chemistry)
7% injected dose/g;
0.91mg Au/ g tumor
150 kVp, 6 Gy
24 h post injection
Significantly higher survival of 90 days
compared to IR alone
Wolfe 2014 [59]
Nude mice; s.c. human prostate
cancer PC3 8–10 mm
AuNP-goserelin
i.v. injection
0.2% Au w /w, 2mg Au/g
tumor; AuNPs are
internalized by tumor cells
Proton beam 180 MeV, 5Gy
24 h post injection
Significant tumor growth delay
compared to IR alone
Wolfe 2015 [60]
S.c. prostate cancer PC3
7-8 mm
AuNR-PEG-goserelin, length 31
nm, diameter 9 nm
i.v. injection, 300 μg Au per mouse
High level of Au
accumulation in liver and
spleen
1% injected Au, ~3 μg Au/
tumor
6 MV, 5 Gy 24 h post injection
Significant tumor growth delay at 17 ± 1 days compared to IR alone (total 36
days)

Chapter 1: Introduction, Hypotheses, and Overview 25
1.5 Where Does the Therapeutic Window of AuNP-aided RT Lie? What Are the Key Parameters to be Considered?
To achieve a favourable therapeutic window, an ideal radiosensitizer should have
additive or supra-additive effects with IR, while showing a minimum level of intrinsic
toxicity, as well as an insignificant and manageable increase, if any, in the toxicity of RT
[14, 77]. In reality very few agents have been recognized as true radiosensitizers with
negligible toxicity, one example is the hypoxic radiosensitizer nimorazole [11, 147]. In
contrast, the frequently used radiosensitizers are toxic and an improved therapeutic
window stems from greater toxicity to tumors relative to normal tissues [11, 77].
Cytotoxicity of AuNPs due to ROS generation and oxidative stress has been well
recognized [44, 62, 68, 78-83]. Following systemic administration, high levels of AuNPs
have been found in organs such as the liver, spleen, lung, and kidneys. In particular,,
several studies have reported that AuNPs (> 10 nm) accumulate and reside in the liver
for an extended period of time (i.e. days - months) [148-155]. Accumulation of AuNPs in
organs has been associated with adverse effects such as alterations in histology and
gene expression [150-152] and inflammatory immune responses [153-157].
Taken together, a favoured therapeutic window for AuNP sensitized RT lies in
successful delivery of AuNPs to the biological targets with minimal systemic exposure
and toxicity, and optimal in field cooperation between AuNPs and IR. To successfully
achieve these goals, several key parameters to be considered include 1)
physicochemical properties of AuNPs, 2) administration route of AuNPs, 3) dosing
schedule of AuNPs and IR, and 4) type of RT. The appropriate choice and combination
of these parameters should lead to improvements in the therapeutic window associated
with AuNP aided RT.

Chapter 1: Introduction, Hypotheses, and Overview 26
1.5.1 Physicochemical Properties of AuNPs
The effectiveness of AuNPs as radiosensitizers is largely governed by their
physicochemical properties (e.g. size, shape, coating, and functionalization) which
determines their in vitro and in vivo behavior [158]. Fine tuning the particle properties is
critical in enabling successful delivery of AuNPs to key biological targets, including the
tumor, blood vessels, cancer cells, and nuclei to exert radiosensitization. Table 1-3
summarizes the impact of the physicochemical properties of AuNPs on the
pharmacokinetics, biodistribution, tumor accumulation, intratumoral distribution, cellular
uptake, cytotoxicity, as well as effectiveness of ROS generation.
In order to achieve radiosensitization of cancer cells in vivo, AuNPs must
possess long circulating properties to achieve preferential accumulation in the tumor
upon i.v. injection via the enhanced permeability and retention (EPR) effect. Particle
size and surface coating have great impact on the pharmacokinetics of AuNPs - while
ultra-small AuNPs (i.e. < 10 nm) are rapidly eliminated via renal clearance [27], larger
AuNPs (i.e. > 50-100 nm) are readily recognized by the reticuloendothelial system
(RES) and removed from the circulation [159, 160]. As well, it is well established that
surface modification with PEG increases the circulation half-life of AuNPs by avoiding
RES uptake [161, 162].
Intratumoral distribution is another factor that greatly impacts the radiation
enhancement effects of AuNPs. Using imaging techniques such as microSPECT/CT,
TEM, and autoradiography, previous studies showed a high degree of heterogeneity in
distribution of AuNPs at tumor sites following different modes of administration [47, 51,
54, 58, 163-165]. The heterogeneity in distribution is attributed to particle aggregation
[166] and absorption of proteins onto the surface of AuNPs [167, 168] under
physiological conditions, which consequently leads to ineffective penetration of AuNPs
in the tumor. As such maintaining colloidal stability is essential to achieving
homogeneous intratumoral distribution of AuNPs.
One of the major determinants of AuNP radiosensitization at the cellular level is
the cellular uptake, especially under low radiation energy [28, 35, 42], which highlights

Chapter 1: Introduction, Hypotheses, and Overview 27
the need to optimize internalization of AuNPs. The size of NPs greatly influences their
cellular uptake via a balance between receptor diffusion kinetics and the thermodynamic
driving force to internalize the particles [169]. For example, Chithrani et al. compared
the uptake kinetics of 14, 50 and 74 nm citrate-AuNPs, and identified the 50 nm core
diameter as the "golden spot" to achieve the highest cell uptake [170]. Also, surface
charge has a great influence on the cell uptake kinetics: positively-charged AuNPs
promote cell uptake via electrostatic interactions with the negatively-charged
membrane, resulting in enhanced cell uptake [171, 172]. Further increase in the
intracellular concentration of AuNPs can be accomplished by introducing a targeting
moiety (e.g. peptides, antibodies), which enhances cancer cell-specific uptake of AuNPs
compared to their non-targeted counterparts [60, 173].
Within the cell, AuNPs sensitize cells to radiation through multiple mechanisms
as described in the previous section “Mechanisms of radiosensitization by AuNPs”.
While the impact of the physicochemical properties of AuNPs on radiosensitization
pathways has not been extensively studied, it has been shown that small AuNPs (< 10
nm) with large surface area to volume ratios generate more ROS compared to larger
AuNPs [68, 69, 80, 174]. To further impart damage to the DNA, nuclear localization of
AuNPs is desired [63, 72, 126, 175, 176] to fully exploit the effectiveness of LEEs and to
chemically sensitize DNA to IR induced damage [73, 177]. Ultra-small AuNPs (< 10 nm)
that are positively charged or labeled with peptides which contain a nuclear localization
signal (NLS) have been shown to successfully enter the nucleus [112, 178] yet have not
been evaluated for radiosensitization. AuNPs investigated for radiotherapeutic
applications to date have been limited to those that are enclosed in vesicles within the
cytoplasm, and have demonstrated that nuclear penetration is not necessary for
radiosensitization by AuNPs [35, 42].

Chapter 1: Introduction, Hypotheses, and Overview 28
Table 1-3: Physicochemical properties of AuNPs and their impact on biodistribution, pharmacokinetics, cellular uptake, and toxicity.
Physicochemical properties
In vitro, in vivo performance
Effects
Size Biodistribution AuNPs of all sizes are pre-dominantly found in the liver, spleen, and lung
Small (10-20 nm) AuNPs exhibit widespread organ distribution while large AuNPs (50-250 nm) were limited to liver, spleen, and lung [159, 179, 180]
Pharmacokinetics Longer circulation half-life for small (10-20 nm) AuNPs compared to large (~ 100 nm) AuNPs due to the rapid RES clearance of larger particles [159, 160] Rapid kidney filtration and urinary clearance of ultra-small AuNPs (< 10 nm) [27]
Cytotoxicity Greater cytotoxicity of ultra-small AuNPs (<10 nm) compared to larger AuNPs (>10 nm) [52, 80, 174] Greater ROS generation with ultra-small AuNPs (<10 nm) compared to larger AuNPs [68, 69, 80, 174]
Tumour accumulation and
retention
Higher tumour accumulation of small AuNPs (10-30 nm) compared to large AuNPs (50-100 nm) or ultra-small AuNPs (<10 nm) [52, 159] Longer tumour retention of small AuNPs (10-20 nm) compared to large AuNPs (30-100 nm) [160]
Tumour penetration Enhanced penetration of ultra-small and small AuNPs (<10 nm) in 3D multi-cellular tumour spheroids compared to large AuNPs (50-100 nm) [181, 182]
Cellular uptake Size-dependent cellular uptake of AuNPs is determined by the balance between thermodynamic driving force and receptor diffusion kinetics, as well as the degree of non-specific adsorption of proteins [169]
Highest uptake achieved with 50 nm citrate-AuNPs compared to 14 and 74 nm AuNPs [170]
Higher uptake of 30 and 50 nm PEG-AuNPs compared to 90 nm AuNPs [183]
Size-dependent uptake of ultra-small AuNPs (<10 nm) varied with charge: cell uptake increased with size for cationic AuNPs, whereas cell uptake decreased with size for anionic and neutral zwitterionic AuNPs in serum-free media [172]
Shape Pharmacokinetics Longer blood circulation of AuNRs compared to AuNSs as a result of lower clearance by liver and spleen [184]
Tumour accumulation
Higher tumour accumulation of AuNRs compared to AuNSs due to longer circulation half-life [184]
Cellular uptake No consistent data Lower cellular uptake of CTAB-AuNRs compared to citrate-AuNSs, possibly due to difference in surfactant [169]
Greater uptake of low aspect ratio (1:3) AuNRs compared to high aspect ratio (1:5) AuNRs Higher cellular uptake of PEG-AuNRs compared to PEG-AuNSs, possibly due to difference in zeta potential (positive for AuNRs, negative for AuNSs) [183] Lower macrophage uptake of Au nanords (10x45 nm) compared to nanospheres (50 nm) [184]

Chapter 1: Introduction, Hypotheses, and Overview 29
Surface charge Pharmacokinetics Longer circulation half-life of neutral and zwitterionic AuNPs compared to negatively or positively charged AuNPs following i.v. or i.p. injection [185]
Tumour accumulation
Higher tumour accumulation of neutral and zwitterionic AuNRs compared to the negatively or positively charged AuNPs due to longer circulation half-life [185]
Cytotoxicity Greater cytotoxicity of positively charged AuNPs compared to anionic or neutral AuNPs [186]
Cell uptake Greater cell uptake of positively charged AuNPs compared to anionic or neutral AuNPs [172] Nuclear localization achieved with positively charged AuNPs [187]
Surface coating Circulation half life Increase in circulation half-life with increase in PEG chain length [161, 162]
Cytotoxicity Reduced cytotoxicity with increase in PEG chain length [161]
Cell uptake Reduced cellular uptake with PEGylation compared to citrate-AuNPs [183, 188]
Targeting moiety Cellular uptake Increase in cell uptake with active targeting [60, 173]
Cellular localization Nuclear localization achieved with peptides containing NLS sequence [112, 178]

Chapter 1: Introduction, Hypotheses, and Overview 30
1.5.2 Administration Route of AuNPs
As shown in Table 1-2, the administration routes used in previous studies for
AuNPs as radiosensitizers include intravenous (i.v.), intraperitoneal (i.p.), and
intratumoral (i.t.).
I.v. administration is employed for conventional chemotherapy, with the
advantage of high systemic bioavailability, as well as potential for slow and sustained
delivery of medication over a prolonged treatment period when needed [189]. I.v.
injected AuNPs accumulate within the perivascular regions in tumors, making it a
competent vascular disrupting agent in combination with a single large dose of IR and
brachytherapy [122, 131]. One challenge associated with i.v. injection is that only a
small fraction of injected AuNPs (1-7%) is able to reach the tumor, due to clearance of
the particles from the circulation, as well as a high interstitial pressure at the tumor site
[190], creating the need for administration of high doses of AuNPs in order to achieve a
satisfactory radiosensitizing effect. Another disadvantage associated with i.v.
administration of AuNPs is systemic toxicity to organs such as the liver and spleen [156,
157].
Intraperitoneal (i.p.) administration is most often employed to achieve high
concentrations of therapeutic agents within the peritoneal cavity for local-regional
treatment of malignancies in this area such as ovarian [191, 192] and gastric cancers
[193, 194]. Clinical trials demonstrated a significant improvement in overall survival in
ovarian cancer patients following i.p. administration of radioactive colloidal 198Au [195-
197]. However, further clinical application ceased due to an undesirable heterogeneous
distribution of particles at the tumor sites [195]. Also, only a small portion (approximately
1% of the injected dose) of AuNPs was found at the tumor sites following i.p. injection
[185], with a significant amount of the AuNPs accumulating in organs such as the liver,
lungs, and heart [198, 199].
Intratumoral (i.t.) administration is an approach employed to achieve a high local
dose of therapeutic agent at the tumor site with minimal systemic toxicity [200]. In a
study by Lin et al. it was demonstrated that 50% of AuNPs remained at the tumor site 2
weeks post i.t. injection [57]. As well, a previous study by our group showed that almost

Chapter 1: Introduction, Hypotheses, and Overview 31
100% of i.t. infused AuNPs remained at the tumor site up to 120 h post administration.
As such i.t. injection is a suitable route of administration in well defined tumor models to
achieve high local concentrations of gold. Further research should aim to improve the
penetration and distribution of AuNPs within the tumor in order to maximize the
radiosensitizing effects.
1.5.3 Dosing Schedule of AuNPs and RT
The dosing schedule of AuNPs and RT is of crucial to achieve maximum
radiation enhancement effects, due to the dynamic nature of biological factors including
cell cycle, cell repopulation, tumor growth, as well as tumor microenvironment (e.g.
oxygen levels). Systematic studies in animal models are needed to unravel the
underlying roles of AuNPs as radiosensitizers (e.g., via cell cycle synchronization, tumor
cell eradication, or tumor vascular damaging), and to further define optimal timing for IR
(i.e. cells accumulated in the G2/M phase, efficient cellular uptake, or sufficient AuNPs
present in the systemic circulation). Similarly, the influence of the other factors such as
tumor and cellular bioavailability of AuNPs and oxygen level, should be investigated,
especially for long term conventional fractionated RT.
1.5.4 Type of RT
Different types of RT utilize altered radiation sources such as photons, electrons,
and protons with a spectrum of radiation energy, which are used to deliver a single large
dose or fractions of IR to tumor sites. Recent technical advancements in RT have been
exploited to increase the therapeutic window of RT by improving the quality of RT,
reducing toxicity in normal tissues, escalating radiation doses in tumor, and reducing
number of IR fractions [201]. These technical improvements provide a platform for
better in field cooperation between AuNPs and IR. Table 1-4 summarises the different
types of RT, their main advantages and applications in the clinic, as well as their
aspects for radiosensitization by AuNPs. It can be seen that the nature of RT
determines the physical interaction between IR and AuNPs, and thus the
radiosensitization by AuNPs.

Chapter 1: Introduction, Hypotheses, and Overview 32
Table 1- 4: Types of RT and radiobiological considerations for radiosensitization by AuNPs [1].
Types of RT Advantages & applications Radiosensitization by AuNPs
External beam of fractionated photon RT [1] (Superficial orthovoltage: 50-500 keV for cancers close to skin, megavoltage: 1-25 MeV for deep cancers). (1) Conventional fractionated RT: 1.8-2.0 Gy/day, 5 days/week, total dose 40-70 Gy. (2) Hyperfractionated RT: <1.8-2 Gy/fraction, 2 fractions/day, larger total dose compared to conventional RT. (3) Hypofractionated RT & or stereotactic RT: > 2 Gy/fraction, reduced total number of fractions. (4) Stereotactic radiosurgery (SRS) : one or more (8-30 Gy/fraction) extremely accurate high doses of IR [145, 202]. (5) Stereotactic body RT (SBRT): delivery of one or few fractions of RT (8-30Gy/fraction) [203, 204].
Allows efficient repair of normal tissues to get therapeutic benefit in large tumor. Total dose escalation to enhance tumor control with minimum increase in late toxicity, used in head and neck cancer. Improved therapeutic window in tumors with low α/β ratios; shorter period of treatment time; used for small tumors. Minimum damage to surrounding normal tissue, short treatment time, used in brain and spinal cancers. High degree of accuracy, short treatment time, used as adjuvant treatment with systemic cancer therapy for early stage small primary tumors in the lung, pelvis, liver, prostate, kidney, and pancreas.
Maximum radiosensitization by AuNPs was achieved at low IR energy (kVp), but not limited in high energy (MV) IR. Reoxygenation occurring between fractions of RT may benefit radiosensization effects of AuNPs. Elevated cellular apoptosis capacity in fractionated IR may further enhance radiosensitization by AuNPs. AuNPs preferentially accumulated in tumor vasculature post i.v. injection and acted as tumor vascular disrupting agents, which enhance the effects of hypofractionated RT, SRS, and SBRT, via local high dose spike [122, 131].
Intraoperative radiotherapy: delivery of single large dose of radiation during surgery, point source X-rays at 50 kVp, or electrons at 4-12 MeV [205].
Diminishes local recurrence, sparing healthy surrounding tissues, short treatment time [206]. Used in bile duct, brain , breast, cervical, colorectal, pancreatic, spinal cancers, and soft tissue sarcoma.
AuNPs enhanced the effect of electron RT both in vitro [31] and in vivo [48].
Proton therapy: [207] delivery of radiation by protons (70-230 MeV) [208].
Short distance of energy deposit within 0.5-1 cm (Bragg peak), complete of sparing surrounding tissues [207]. Employed in ocular, skull base, paraspinal tumors.
Cellular localization is crucial - only AuNPs in cell cytoplasm resulted in radiosensitization, AuNPs in nuclei showed highest radiosensitization [132].

Chapter 1: Introduction, Hypotheses, and Overview 33
Other charged particle (heavy ion) beam: delivery of radiation by ions such as carbon with energy up to 430 MeV/u [209, 210].
Sharp radiation dose deposition within Bragg peak. Applied to head and neck cancers, adeno-carcinoma, adenoid cystic acarcinoma, malignant melanoma, bone and soft tissue sarcomas, hepato-cellular, and prostate caricnomas etc.
No evidence up to date.
Internal RT (brachytherapy): placement of sealed radioactive materials inside or near tumor, for temporary or permanent delivery of IR at dose rate of 0.4->12 Gy/h [211].
Improved local delivery of radiation to small target volume. Employed in cervical, prostate, breast, and skin cancers.
High level of radiosensitization by AuNPs due to the low radiation energy of brachytherapy [117, 125, 130]. Safety of AuNPs need to be evaluated due to the prolonged treatment time [141].
Radioisotope therapy: systemic delivery (infusion or ingestion) of β-emitting radioisotope [212, 213].
Sparing healthy tissues due to short effective range of β particle. Used in thyroid cancer, bone metastases, cystic brain tumors [212].
Intratumoral injection of 198AuNPs showed significant tumor control [49, 51, 57]. Promising results in vascular targeting therapy by in vivo delivery of radioisotopes with AuNPs [214, 215].

Chapter 1: Introduction, Hypotheses, and Overview 34
1.6 Conclusions and Future Directions
To date the pre-clinical studies that have been conducted have taken a good first
step towards showing the promise of AuNPs as radiosensitizers. These studies have
provided insight into the physical, chemical, and biological pathways by which AuNPs
enhance the effects of IR. The numbers of groups working in this field is growing as
evidenced by the increasing number of publications in this area per year over the past
decade (Figure 1-1 B). To some extent each of these groups is working in silos with
their own “favourite” AuNP formulation with its unique size, shape, surface coating etc.
Unfortunately, in some cases the physicochemical properties of the AuNPs are not fully
examined and/or reported and each group is conducting their studies in their own cell
lines, animal models with distinct routes of administration, dosing schedules and RT
parameters. Therefore, it remains a significant challenge to build on and learn from
each other’s data. There is a dire need for some attempt at standardization in this field.
As a result we propose the following: (1) extensive characterization and meticulous
reporting on the synthetic procedure and physicochemical properties of AuNPs
employed in studies. This includes reporting on the size, shape, composition of surface
coating and functionalization as well as in vitro stability. (2) identification and use of at
least one cell line to be used by all groups to benchmark data. Herein we propose use
of the MDA-MB-231 cell line as it is available for purchase from ATCC and has been
used in many published studies on AuNPs as radiosensitizers [33, 38, 42, 44, 45, 216,
217]. (3) identification and use of at least one common in vivo model for conducting
benchmarking studies in vivo. For this we suggest MDA-MB-231 grown orthotopically in
the mammary fat pad of female mice. In each case the dose effects of AuNPs should be
examined with the lowest dose that results in efficacy and no toxicity employed. The
biodistribution (including tumor accumulation) of the AuNPs as a function of time should
be reported along with the efficacy and any observed toxicity. Evaluation of tumor
histopathology following treatment to assess impact on tumor cells versus the vascular
endothelium would be of value.
At least some extent of standardization in the in vitro and in vivo models used by
all groups will provide a means to compile the data and thus to draw meaningful

Chapter 1: Introduction, Hypotheses, and Overview 35
observations and conclusions on the various AuNP formulations. Beyond this, there is
also a need to identify the underlying mechanisms and biological targets associated
with AuNP-based radiosensitization. The challenge and opportunity here is that this
depends on effective multi-disciplinary collaboration between chemists, radiation
oncologists, radiation physicists and molecular biologists. This is a complex problem
with many variables that is worthy of solving given the recognized critical role for
radiosensitization in RT.

Chapter 1: Introduction, Hypotheses, and Overview 36
1.7 Hypotheses and Objectives
The work presented herein aims to improve the effectiveness of AuNP aided IR
by (1) developing formulations of AuNPs with strong potential for radiosensitization and
(2) identifying the key parameters that determine the extent of radiosensitization by
AuNPs. An additional goal of this research is to evaluate the individual and combined
radiation enhancement effects of AuNPs and cisplatin, given that (1) cisplatin is one of
the most widely used agents in chemoradiotherapy [1, 218] and (2) cisplatin and AuNPs
sensitize RT through distinct and overlapping mechanisms [42, 84, 219]. Therefore, the
combination of the two agents may represent a promising strategy for the achievement
of additive or synergistic radiation enhancement effects [135]. The two hypotheses and
specific objectives of the thesis are outlined below.
Hypothesis 1: Radiosensitization by AuNPs in in vitro cell culture is dependent
on the cellular localization of AuNPs and oxygen conditions.
Objective 1a: Synthesis and physicochemical characterization of AuNPs of
varied size, surface coatings, and +/- targeting moieties.
Objective 1b: Evaluation of the in vitro uptake and radiosensitizing effects of
AuNPs in established cell lines as a function of their physicochemical properties,
concentration, and incubation time, as well as oxygen conditions.
Hypothesis 2: The combination of AuNPs and cisplatin will result in an additive
or synergistic radiosensitization effect, in a human xenograft model of triple negative
breast cancer (TNBC) in mice, relative to the effect of AuNPs or cisplatin alone.
Objective 2a: Investigation and comparison of the radiosensitizing effects and
toxicity of AuNPs and cisplatin as individual agents both in vitro and in vivo.
Objective 2b: Evaluation of the in vivo radiation enhancement effect of the
combination of AuNPs and cisplatin in comparison to that of AuNPs or cisplatin alone.

Chapter 1: Introduction, Hypotheses, and Overview 37
1.8 Overview of Thesis Chapters
The thesis presented herein is divided into five chapters. The first chapter is an
introduction and the last chapter includes conclusions and a description of future
directions.
The first chapter provides an extensive overview of the utilization of AuNPs in RT
as a radiosensitizer. Detailed mechanisms (physical, chemical, and biological) via which
AuNPs sensitize IR are discussed; key findings from previous research are
summarized. Importantly, the roles of several key parameters (i.e., physicochemical
properties of AuNPs, route of administration, dosing schedule of AuNPs and IR, as well
as types of RT), in determining the therapeutic window of AuNP aided RT are
highlighted. This chapter also proposes guidelines to enable successful development
and translation of AuNPs to clinical applications as radiosensitizers.
The second chapter describes the synthesis of tiopronin coated AuNPs (AuNP-
TP) and characterization of these AuNPs in terms of size, coating efficiency, and
stability. Cellular uptake and survival following exposure to AuNP-TP were evaluated in
different cell lines including MCF-7, HeLa, H520, and L929. Overall, this study
demonstrated that cell response to AuNP-TP is dependent on AuNP concentration,
incubation time, as well as the cell line employed. Importantly this study enabled
identification of optimal conditions for the achievement of maximal cellular uptake of
AuNP-TP. Further, it was found that the cytotoxicity of AuNPs is due to their surface
chemistry and the production of ROS, which can be diminished by antioxidants such as
thiol-containing molecules
The third chapter applies the knowledge obtained in Chapter 2 to assess the
cellular response (cellular uptake and toxicity) and radiosensitizing effects of AuNP-TP
under varied conditions (incubation time, concentration, and oxygen levels), in a triple
negative breast cancer (TNBC) cell line MDA-MB-231. This study identified that cellular
localization (intracellular or extracellular) of AuNPs and oxygen conditions (oxia, acute
and chronic hypoxia, as well as reoxygenation) are two crucial parameters that
determine the extent of radiosensitization that can be achieved with AuNPs.

Chapter 1: Introduction, Hypotheses, and Overview 38
Furthermore, the possible mechanisms via which AuNP-TP enhance the effect of IR
were investigated, demonstrating that aside from physical and chemical enhancement,
AuNPs also sensitize IR via biological pathways such as inhibition of post IR DNA
repair.
The fourth chapter developed AuNP formulations to achieve improved stability
and cellular uptake by using PEG (AuNP-PEG) as the coating material and addition of a
cell targeting peptide (adenoviral receptor mediated endocytosis, AuNP-RME). The
toxicity and efficacy of AuNPs and/or cisplatin aided RT were evaluated in a TNBC
model of MDA-MB-231LUC+ both in vitro and in vivo. Results from this study in vitro
revealed that AuNP-RME at a non-cytotoxic concentration has a greater radiosensitizing
effect in comparison to that of cisplatin at IC25. Following i.t. administration, AuNPs
remained at the tumor site for up to 120 h (CT), with effective cellular uptake, as
evidenced by TEM, 24 h post administration. As measured by tumor growth control,
AuNPs administered i.t. resulted in an equivalent radiation enhancement effect to three
doses of cisplatin at IC25 (4 mg/kg), with the advantage of no intrinsic toxicity and no
increase in toxicity of IR. Therefore, AuNP-RME is the true radiosensitizer under these
conditions. Furthermore, the combination of AuNPs and cisplatin showed an additive
and significant radiation enhancement effect both in vitro and in vivo, and provides a
promising means to improve the therapeutic window of RT. Findings from this study
support future development of multifunctional formulations comprised of tumor targeting
AuNPs and cisplatin, for the achievement of tumor-selective radiosensitization, minimal
toxicity, and an improved therapeutic window for RT.

Chapter 1: Introduction, Hypotheses, and Overview 39
1.9 References
1. Joiner M, editor. Basic Clinical Radiobiology. London: Hodder Arnold; 2009.
2. Thariat J, Hannoun-Levi JM, Sun Myint A, Vuong T, Gerard JP. Past, Present, and Future of Radiotherapy for the Benefit of Patients. Nat Rev Clin Oncol. 2013 Jan; 10:52-60.
3. Delaney G, Jacob S, Featherstone C, Barton M. The Role of Radiotherapy in Cancer Treatment: Estimating Optimal Utilization from a Review of Evidence-Based Clinical Guidelines. Cancer. 2005 Sep 15; 104:1129-37.
4. Delaney G, Barton M, Jacob S. Estimation of an Optimal Radiotherapy Utilization Rate for Breast Carcinoma: A Review of the Evidence. Cancer. 2003 Nov 1; 98:1977-86.
5. Stone HB, Coleman CN, Anscher MS, McBride WH. Effects of Radiation on Normal Tissue: Consequences and Mechanisms. Lancet Oncol. 2003 Sep; 4:529-36.
6. Liauw SL, Connell PP, Weichselbaum RR. New Paradigms and Future Challenges in Radiation Oncology: An Update of Biological Targets and Technology. Sci Transl Med. 2013 Feb 20; 5:173sr2.
7. Meacham CE, Morrison SJ. Tumour Heterogeneity and Cancer Cell Plasticity. Nature. 2013 Sep 19; 501:328-37.
8. Burrell RA, McGranahan N, Bartek J, Swanton C. The Causes and Consequences of Genetic Heterogeneity in Cancer Evolution. Nature. 2013 Sep 19; 501:338-45.
9. Junttila MR, de Sauvage FJ. Influence of Tumour Micro-Environment Heterogeneity on Therapeutic Response. Nature. 2013 Sep 19; 501:346-54.
10. Baskar R, Lee KA, Yeo R, Yeoh KW. Cancer and Radiation Therapy: Current Advances and Future Directions. Int J Med Sci. 2012; 9:193-9.
11. Seiwert TY, Salama JK, Vokes EE. The Concurrent Chemoradiation Paradigm--General Principles. Nat Clin Pract Oncol. 2007 Feb; 4:86-100.
12. Steel GG, Peckham MJ. Exploitable Mechanisms in Combined Radiotherapy-Chemotherapy: The Concept of Additivity. Int J Radiat Oncol Biol Phys. 1979 Jan; 5:85-91.
13. Wardman P. Chemical Radiosensitizers for Use in Radiotherapy. Clinical Oncology. 2007 Aug; 19:397-417.
14. Bindhu J, Anupama, G. Radiosensitization: The New Dogma in Cancer Treatment. Austral - Asian Journal of Cancer. 2005; 4:241-50.
15. Boag J. The Time Scale in Radiobiology. 12th Failla memorial lecture. In: Nygaard OF, Adler HI, Sinclair WK (eds) Radiation research. , in Proceedings of the 5th international Congress of Radiation Research; New York1975.

Chapter 1: Introduction, Hypotheses, and Overview 40
16. Steel GG, McMillan TJ, Peacock JH. The 5rs of Radiobiology. Int J Radiat Biol. 1989 Dec; 56:1045-8.
17. Harrington K, Jankowska P, Hingorani M. Molecular Biology for the Radiation Oncologist: The 5rs of Radiobiology Meet the Hallmarks of Cancer. Clin Oncol (R Coll Radiol). 2007 Oct; 19:561-71.
18. Pajonk F, Vlashi E, McBride WH. Radiation Resistance of Cancer Stem Cells: The 4 R's of Radiobiology Revisited. Stem Cells. 2010 Apr; 28:639-48.
19. Daniel MC, Astruc D. Gold Nanoparticles: Assembly, Supramolecular Chemistry, Quantum-Size-Related Properties, and Applications toward Biology, Catalysis, and Nanotechnology. Chem Rev. 2004 Jan; 104:293-346.
20. Sperling RA, Rivera Gil P, Zhang F, Zanella M, Parak WJ. Biological Applications of Gold Nanoparticles. Chem Soc Rev. 2008 Sep; 37:1896-908.
21. Dykman LA, Khlebtsov NG. Gold Nanoparticles in Biology and Medicine: Recent Advances and Prospects. Acta Naturae. 2011 Apr; 3:34-55.
22. Matijevic E, editor. Fine Particles in Medicine and Pharmacy. 12 ed. New York: Springer; 2011.
23. Coleman CN, Mitchell JB. Clinical Radiosensitization: Why It Does and Does Not Work. J Clin Oncol. 1999 Jan; 17:1-3.
24. Matsudaira H, Ueno AM, Furuno I. Iodine Contrast Medium Sensitizes Cultured Mammalian Cells to X Rays but Not to Gamma Rays. Radiat Res. 1980 Oct; 84:144-8.
25. Taupin F, Flaender M, Delorme R, Brochard T, Mayol JF, Arnaud J, et al. Gadolinium Nanoparticles and Contrast Agent as Radiation Sensitizers. Phys Med Biol. 2015 Jun 7; 60:4449-64.
26. Biston MC, Joubert A, Adam JF, Elleaume H, Bohic S, Charvet AM, et al. Cure of Fisher Rats Bearing Radioresistant F98 Glioma Treated with Cis-Platinum and Irradiated with Monochromatic Synchrotron X-Rays. Cancer Res. 2004 Apr 1; 64:2317-23.
27. Hainfeld JF, Slatkin, D., Smilowitz, H.M. . The Use of Gold Nanoparticles to Enhance Radiotherapy in Mice. Phys Med Biol. 2004; 49:309-15.
28. Kong T, Zeng J, Wang X, Yang X, Yang J, McQuarrie S, et al. Enhancement of Radiation Cytotoxicity in Breast-Cancer Cells by Localized Attachment of Gold Nanoparticles. Small. 2008 Sep; 4:1537-43.
29. Liu CJ, Wang CH, Chien CC, Yang TY, Chen ST, Leng WH, et al. Enhanced X-Ray Irradiation-Induced Cancer Cell Damage by Gold Nanoparticles Treated by a New Synthesis Method of Polyethylene Glycol Modification. Nanotechnology. 2008 Jul 23; 19:295104.
30. Zhang X, Xing JZ, Chen J, Ko L, Amanie J, Gulavita S, et al. Enhanced Radiation Sensitivity in Prostate Cancer by Gold-Nanoparticles. Clin Invest Med. 2008; 31:E160-7.

Chapter 1: Introduction, Hypotheses, and Overview 41
31. Rahman WN, Bishara N, Ackerly T, He CF, Jackson P, Wong C, et al. Enhancement of Radiation Effects by Gold Nanoparticles for Superficial Radiation Therapy. Nanomedicine. 2009 Jun; 5:136-42.
32. Roa W, Zhang X, Guo L, Shaw A, Hu X, Xiong Y, et al. Gold Nanoparticle Sensitize Radiotherapy of Prostate Cancer Cells by Regulation of the Cell Cycle. Nanotechnology. 2009 Sep 16; 20:375101.
33. Butterworth KT, Coulter JA, Jain S, Forker J, McMahon SJ, Schettino G, et al. Evaluation of Cytotoxicity and Radiation Enhancement Using 1.9 Nm Gold Particles: Potential Application for Cancer Therapy. Nanotechnology. 2010 Jul 23; 21:295101.
34. Chattopadhyay N, Cai Z, Pignol JP, Keller B, Lechtman E, Bendayan R, et al. Design and Characterization of Her-2-Targeted Gold Nanoparticles for Enhanced X-Radiation Treatment of Locally Advanced Breast Cancer. Mol Pharm. 2010 Dec 6; 7:2194-206.
35. Chithrani BD, Jelveh, S., Jalai, F., van Prooijen, M., Allen, C., Bristow, R.G., Hill, R.P., Jaffray, D.A. Gold Nanoparticles as Radiation Sensitizers in Cancer Therapy. Radiation Research. 2010; 173:719-28.
36. Liu CJ, Wang CH, Chen ST, Chen HH, Leng WH, Chien CC, et al. Enhancement of Cell Radiation Sensitivity by Pegylated Gold Nanoparticles. Phys Med Biol. 2010 Feb 21; 55:931-45.
37. Geng F, Song K, Xing JZ, Yuan C, Yan S, Yang Q, et al. Thio-Glucose Bound Gold Nanoparticles Enhance Radio-Cytotoxic Targeting of Ovarian Cancer. Nanotechnology. 2011 Jul 15; 22:285101.
38. Jain S, Coulter JA, Hounsell AR, Butterworth KT, McMahon SJ, Hyland WB, et al. Cell-Specific Radiosensitization by Gold Nanoparticles at Megavoltage Radiation Energies. Int J Radiat Oncol Biol Phys. 2011 Feb 1; 79:531-9.
39. Ngwa W, Korideck H, Kassis AI, Kumar R, Sridhar S, Makrigiorgos GM, et al. In Vitro Radiosensitization by Gold Nanoparticles During Continuous Low-Dose-Rate Gamma Irradiation with I-125 Brachytherapy Seeds. Nanomedicine. 2013 Jan; 9:25-7.
40. Xu W, Luo T, Li P, Zhou C, Cui D, Pang B, et al. Rgd-Conjugated Gold Nanorods Induce Radiosensitization in Melanoma Cancer Cells by Downregulating Alpha(V)Beta(3) Expression. Int J Nanomedicine. 2012; 7:915-24.
41. Jeremic B, Aguerri AR, Filipovic N. Radiosensitization by Gold Nanoparticles. Clin Transl Oncol. 2013 Aug; 15:593-601.
42. Cui L, Tse K, Zahedi P, Harding SM, Zafarana G, Jaffray DA, et al. Hypoxia and Cellular Localization Influence the Radiosensitizing Effect of Gold Nanoparticles (Aunps) in Breast Cancer Cells. Radiat Res. 2014 Nov; 182:475-88.
43. Xu W, Luo, T., Pang, B., Li, P., Zhou C., Huang. P., Zhang C., Ren Q., Hu, W., Fu, S. The Radiosensitization of Melanoma Cells by Gold Nanorods Irradiated with Mv X-Ray. Nano Biomed Eng. 2012; 4:6-11.

Chapter 1: Introduction, Hypotheses, and Overview 42
44. Taggart LE, McMahon SJ, Currell FJ, Prise KM, Butterworth KT. The Role of Mitochondrial Function in Gold Nanoparticle Mediated Radiosensitisation. Cancer Nanotechnol. 2014; 5:5.
45. Jain S, Coulter JA, Butterworth KT, Hounsell AR, McMahon SJ, Hyland WB, et al. Gold Nanoparticle Cellular Uptake, Toxicity and Radiosensitisation in Hypoxic Conditions. Radiother Oncol. 2014 Feb; 110:342-7.
46. Polf JC, Bronk LF, Driessen WH, Arap W, Pasqualini R, Gillin M. Enhanced Relative Biological Effectiveness of Proton Radiotherapy in Tumor Cells with Internalized Gold Nanoparticles. Appl Phys Lett. 2011 May 9; 98:193702.
47. Herold DM, Das IJ, Stobbe CC, Iyer RV, Chapman JD. Gold Microspheres: A Selective Technique for Producing Biologically Effective Dose Enhancement. Int J Radiat Biol. 2000 Oct; 76:1357-64.
48. Chang MY, Shiau AL, Chen YH, Chang CJ, Chen HH, Wu CL. Increased Apoptotic Potential and Dose-Enhancing Effect of Gold Nanoparticles in Combination with Single-Dose Clinical Electron Beams on Tumor-Bearing Mice. Cancer Sci. 2008 Jul; 99:1479-84.
49. Khan MK, Minc LD, Nigavekar SS, Kariapper MS, Nair BM, Schipper M, et al. Fabrication of {198au0} Radioactive Composite Nanodevices and Their Use for Nanobrachytherapy. Nanomedicine. 2008 Mar; 4:57-69.
50. Hebert EM, Debouttiere PJ, Lepage M, Sanche L, Hunting DJ. Preferential Tumour Accumulation of Gold Nanoparticles, Visualised by Magnetic Resonance Imaging: Radiosensitisation Studies in Vivo and in Vitro. Int J Radiat Biol. 2010 Aug; 86:692-700.
51. Chanda N, Kan P, Watkinson LD, Shukla R, Zambre A, Carmack TL, et al. Radioactive Gold Nanoparticles in Cancer Therapy: Therapeutic Efficacy Studies of Ga-198aunp Nanoconstruct in Prostate Tumor-Bearing Mice. Nanomedicine. 2010 Apr; 6:201-9.
52. Zhang XD, Wu D, Shen X, Chen J, Sun YM, Liu PX, et al. Size-Dependent Radiosensitization of Peg-Coated Gold Nanoparticles for Cancer Radiation Therapy. Biomaterials. 2012 Sep; 33:6408-19.
53. Kim JK, Seo SJ, Kim HT, Kim KH, Chung MH, Kim KR, et al. Enhanced Proton Treatment in Mouse Tumors through Proton Irradiated Nanoradiator Effects on Metallic Nanoparticles. Phys Med Biol. 2012 Dec 21; 57:8309-23.
54. Chattopadhyay N, Cai Z, Kwon YL, Lechtman E, Pignol JP, Reilly RM. Molecularly Targeted Gold Nanoparticles Enhance the Radiation Response of Breast Cancer Cells and Tumor Xenografts to X-Radiation. Breast Cancer Res Treat. 2013 Jan; 137:81-91.
55. Hainfeld JF, Smilowitz HM, O'Connor MJ, Dilmanian FA, Slatkin DN. Gold Nanoparticle Imaging and Radiotherapy of Brain Tumors in Mice. Nanomedicine (Lond). 2013 Oct; 8:1601-9.

Chapter 1: Introduction, Hypotheses, and Overview 43
56. Joh DY, Sun L, Stangl M, Al Zaki A, Murty S, Santoiemma PP, et al. Selective Targeting of Brain Tumors with Gold Nanoparticle-Induced Radiosensitization. PLoS One. 2013; 8:e62425.
57. Lin FS, Chen CH, Tseng FG, Hwu Y, Chen JK, Lin SY, et al. Radiotherapy of the Excretable Radioactive Gold Nanocomposite with Intratumoral Injection. International Journal of Materials, Mechanics and Manufacturing. 2013; 1:265-8.
58. Al Zaki A, Joh D, Cheng Z, De Barros AL, Kao G, Dorsey J, et al. Gold-Loaded Polymeric Micelles for Computed Tomography-Guided Radiation Therapy Treatment and Radiosensitization. ACS Nano. 2014 Jan 28; 8:104-12.
59. Wolfe T, Grant J, Wolfe A, Gillin M, Krishnan S. Proton Therapy Enhanced by Tumor-Targeting Gold Nanoparticles: A Pilot in Vivo Experiment at the Proton Therapy Center at Md Anderson Cancer Center. Med Phys. 2014; 41:518.
60. Wolfe T, Chatterjee D, Lee J, Grant JD, Bhattarai S, Tailor R, et al. Targeted Gold Nanoparticles Enhance Sensitization of Prostate Tumors to Megavoltage Radiation Therapy in Vivo. Nanomedicine. 2015 Jul; 11:1277-83.
61. Attix FH, editor. Introduction to Radiological Physics and Radiation Dosimetry. New York: WILEY-VCH Verlag GmbH & Co. KGaA; 1986.
62. Butterworth KT, McMahon SJ, Currell FJ, Prise KM. Physical Basis and Biological Mechanisms of Gold Nanoparticle Radiosensitization. Nanoscale. 2012 Aug 21; 4:4830-8.
63. Carter JD, Cheng NN, Qu Y, Suarez GD, Guo T. Nanoscale Energy Deposition by X-Ray Absorbing Nanostructures. J Phys Chem B. 2007 Oct 11; 111:11622-5.
64. Mesbahi A. A Review on Gold Nanoparticles Radiosensitization Effect in Radiation Therapy of Cancer. Rep Pract Oncol Radiother. 2010; 15:176-80.
65. Hockel M, Vaupel P. Tumor Hypoxia: Definitions and Current Clinical, Biologic, and Molecular Aspects. J Natl Cancer Inst. 2001 Feb 21; 93:266-76.
66. Overgaard J. Hypoxic Radiosensitization: Adored and Ignored. J Clin Oncol. 2007 Sep 10; 25:4066-74.
67. Wilson WR, Hay MP. Targeting Hypoxia in Cancer Therapy. Nat Rev Cancer. 2011 Jun; 11:393-410.
68. Nel A, Xia T, Madler L, Li N. Toxic Potential of Materials at the Nanolevel. Science. 2006 Feb 3; 311:622-7.
69. Hvolbaek B, Janssens TVW, Clausen BS, Falsig H, Christensen CH, Norskov JK. Catalytic Activity of Au Nanoparticles. Nano Today. 2007 Aug; 2:14-8.
70. Misawa M, Takahashi J. Generation of Reactive Oxygen Species Induced by Gold Nanoparticles under X-Ray and Uv Irradiations. Nanomedicine. 2011 Oct; 7:604-14.
71. Cheng NN, Starkewolf Z, Davidson RA, Sharmah A, Lee C, Lien J, et al. Chemical Enhancement by Nanomaterials under X-Ray Irradiation. J Am Chem Soc. 2012 Feb 1; 134:1950-3.

Chapter 1: Introduction, Hypotheses, and Overview 44
72. Zheng Y, Hunting DJ, Ayotte P, Sanche L. Radiosensitization of DNA by Gold Nanoparticles Irradiated with High-Energy Electrons. Radiat Res. 2008 Jan; 169:19-27.
73. Yao X, Huang C, Chen X, Yi Z, Sanche L. Chemical Radiosensitivity of DNA Induced by Gold Nanoparticles. J Biomed Nanotechnol. 2015 Mar; 11:478-85.
74. Her S, Jaffray DA, Allen C. Gold Nanoparticles for Applications in Cancer Radiotherapy: Mechanisms and Recent Advancements. Adv Drug Deliv Rev. 2015 Dec 19.
75. Kim JJ, Tannock IF. Repopulation of Cancer Cells During Therapy: An Important Cause of Treatment Failure. Nat Rev Cancer. 2005 Jul; 5:516-25.
76. Brown JM, Carlson DJ, Brenner DJ. The Tumor Radiobiology of Srs and Sbrt: Are More Than the 5 Rs Involved? Int J Radiat Oncol Biol Phys. 2014 Feb 1; 88:254-62.
77. Ma BB, Bristow RG, Kim J, Siu LL. Combined-Modality Treatment of Solid Tumors Using Radiotherapy and Molecular Targeted Agents. J Clin Oncol. 2003 Jul 15; 21:2760-76.
78. Xia T, Kovochich M, Brant J, Hotze M, Sempf J, Oberley T, et al. Comparison of the Abilities of Ambient and Manufactured Nanoparticles to Induce Cellular Toxicity According to an Oxidative Stress Paradigm. Nano Lett. 2006 Aug; 6:1794-807.
79. Cui L, Zahedi P, Saraceno J, Bristow R, Jaffray D, Allen C. Neoplastic Cell Response to Tiopronin-Coated Gold Nanoparticles. Nanomedicine. 2013 Feb; 9:264-73.
80. Pan Y, Leifert A, Ruau D, Neuss S, Bornemann J, Schmid G, et al. Gold Nanoparticles of Diameter 1.4 Nm Trigger Necrosis by Oxidative Stress and Mitochondrial Damage. Small. 2009 Sep; 5:2067-76.
81. Mroz RM, Schins RP, Li H, Jimenez LA, Drost EM, Holownia A, et al. Nanoparticle-Driven DNA Damage Mimics Irradiation-Related Carcinogenesis Pathways. Eur Respir J. 2008 Feb; 31:241-51.
82. Rim KT, Song SW, Kim HY. Oxidative DNA Damage from Nanoparticle Exposure and Its Application to Workers' Health: A Literature Review. Saf Health Work. 2013 Dec; 4:177-86.
83. Berbeco RI, Korideck H, Ngwa W, Kumar R, Patel J, Sridhar S, et al. DNA Damage Enhancement from Gold Nanoparticles for Clinical Mv Photon Beams. Radiat Res. 2012 Dec; 178:604-8.
84. Kvols LK. Radiation Sensitizers: A Selective Review of Molecules Targeting DNA and Non-DNA Targets. J Nucl Med. 2005 Jan; 46 Suppl 1:187S-90S.
85. Wojewodzka M, Lankoff A, Dusinska M, Brunborg G, Czerwinska J, Iwanenko T, et al. Treatment with Silver Nanoparticlesdelays Repair of X-Ray Induced DNA Damage in Hepg2 Cells. NUKLEONIKA. 2011 May 23; 56:29-33.

Chapter 1: Introduction, Hypotheses, and Overview 45
86. Ogawa Y, Takahashi T, Kobayashi T, Kariya S, Nishioka A, Ohnishi T, et al. Apoptotic-Resistance of the Human Osteosarcoma Cell Line Hs-Os-1 to Irradiation Is Converted to Apoptotic-Susceptibility by Hydrogen Peroxide: A Potent Role of Hydrogen Peroxide as a New Radiosensitizer. Int J Mol Med. 2003 Dec; 12:845-50.
87. Chan N, Koritzinsky M, Zhao H, Bindra R, Glazer PM, Powell S, et al. Chronic Hypoxia Decreases Synthesis of Homologous Recombination Proteins to Offset Chemoresistance and Radioresistance. Cancer Res. 2008 Jan 15; 68:605-14.
88. Potiron VA, Abderrahmani R, Clement-Colmou K, Marionneau-Lambot S, Oullier T, Paris F, et al. Improved Functionality of the Vasculature During Conventionally Fractionated Radiation Therapy of Prostate Cancer. PLoS One. 2013; 8:e84076.
89. Milas L, Hunter N, Mason KA, Milross C, Peters LJ. Tumor Reoxygenation as a Mechanism of Taxol-Induced Enhancement of Tumor Radioresponse. Acta Oncol. 1995; 34:409-12.
90. Krause M, Ostermann G, Petersen C, Yaromina A, Hessel F, Harstrick A, et al. Decreased Repopulation as Well as Increased Reoxygenation Contribute to the Improvement in Local Control after Targeting of the Egfr by C225 During Fractionated Irradiation. Radiother Oncol. 2005 Aug; 76:162-7.
91. Grana X, Reddy EP. Cell Cycle Control in Mammalian Cells: Role of Cyclins, Cyclin Dependent Kinases (Cdks), Growth Suppressor Genes and Cyclin-Dependent Kinase Inhibitors (Ckis). Oncogene. 1995 Jul 20; 11:211-9.
92. Kastan MB, Bartek J. Cell-Cycle Checkpoints and Cancer. Nature. 2004 Nov 18; 432:316-23.
93. Pawlik TM, Keyomarsi K. Role of Cell Cycle in Mediating Sensitivity to Radiotherapy. Int J Radiat Oncol Biol Phys. 2004 Jul 15; 59:928-42.
94. Withers HR. Cell Cycle Redistribution as a Factor in Multifraction Irradiation. Radiology. 1975 Jan; 114:199-202.
95. Milas L, Milas MM, Mason KA. Combination of Taxanes with Radiation: Preclinical Studies. Semin Radiat Oncol. 1999 Apr; 9:12-26.
96. AshaRani PV, Low Kah Mun G, Hande MP, Valiyaveettil S. Cytotoxicity and Genotoxicity of Silver Nanoparticles in Human Cells. ACS Nano. 2009 Feb 24; 3:279-90.
97. Kansara K, Patel P, Shah D, Shukla RK, Singh S, Kumar A, et al. TiO2 Nanoparticles Induce DNA Double Strand Breaks and Cell Cycle Arrest in Human Alveolar Cells. Environ Mol Mutagen. 2015 Mar; 56:204-17.
98. Brown JM. The Hypoxic Cell: A Target for Selective Cancer Therapy--Eighteenth Bruce F. Cain Memorial Award Lecture. Cancer Res. 1999 Dec 1; 59:5863-70.
99. Kalishwaralal K, Sheikpranbabu S, BarathManiKanth S, Haribalaganesh R, Ramkumarpandian S, Gurunathan S. Gold Nanoparticles Inhibit Vascular Endothelial Growth Factor-Induced Angiogenesis and Vascular Permeability Via

Chapter 1: Introduction, Hypotheses, and Overview 46
Src Dependent Pathway in Retinal Endothelial Cells. Angiogenesis. 2011 Mar; 14:29-45.
100. Bhattacharya R, Mukherjee, P., Xiong, Z., Atala, A., Soker, S., Mukhopadhyay, D. Gold Nanoparticles Inhibit Vegf165-Induced Proliferation of Huvec Cells. Nano Letters. 2004; 4:2479-81.
101. Pan Y, Wu Q, Qin L, Cai J, Du B. Gold Nanoparticles Inhibit Vegf165-Induced Migration and Tube Formation of Endothelial Cells Via the Akt Pathway. Biomed Res Int. 2014; 2014:418624.
102. Mukherjee P, Bhattacharya R, Wang P, Wang L, Basu S, Nagy JA, et al. Antiangiogenic Properties of Gold Nanoparticles. Clin Cancer Res. 2005 May 1; 11:3530-4.
103. Kim JA, Aberg C, Salvati A, Dawson KA. Role of Cell Cycle on the Cellular Uptake and Dilution of Nanoparticles in a Cell Population. Nat Nanotechnol. 2012 Jan; 7:62-8.
104. Chithrani DB, Dunne M, Stewart J, Allen C, Jaffray DA. Cellular Uptake and Transport of Gold Nanoparticles Incorporated in a Liposomal Carrier. Nanomedicine. 2010 Feb; 6:161-9.
105. Fertil B, Malaise EP. Intrinsic Radiosensitivity of Human Cell Lines Is Correlated with Radioresponsiveness of Human Tumors: Analysis of 101 Published Survival Curves. Int J Radiat Oncol Biol Phys. 1985 Sep; 11:1699-707.
106. West CM, Davidson SE, Roberts SA, Hunter RD. Intrinsic Radiosensitivity and Prediction of Patient Response to Radiotherapy for Carcinoma of the Cervix. Br J Cancer. 1993 Oct; 68:819-23.
107. West CM, Davidson SE, Roberts SA, Hunter RD. The Independence of Intrinsic Radiosensitivity as a Prognostic Factor for Patient Response to Radiotherapy of Carcinoma of the Cervix. Br J Cancer. 1997; 76:1184-90.
108. Petersen C, Petersen S, Milas L, Lang FF, Tofilon PJ. Enhancement of Intrinsic Tumor Cell Radiosensitivity Induced by a Selective Cyclooxygenase-2 Inhibitor. Clin Cancer Res. 2000 Jun; 6:2513-20.
109. Mkandawire MM, Lakatos M, Springer A, Clemens A, Appelhans D, Krause-Buchholz U, et al. Induction of Apoptosis in Human Cancer Cells by Targeting Mitochondria with Gold Nanoparticles. Nanoscale. 2015 Jun 28; 7:10634-40.
110. Selim ME, Hendi AA. Gold Nanoparticles Induce Apoptosis in Mcf-7 Human Breast Cancer Cells. Asian Pac J Cancer Prev. 2012; 13:1617-20.
111. Lan MY, Hsu YB, Hsu CH, Ho CY, Lin JC, Lee SW. Induction of Apoptosis by High-Dose Gold Nanoparticles in Nasopharyngeal Carcinoma Cells. Auris Nasus Larynx. 2013 Dec; 40:563-8.
112. Kang B, Mackey MA, El-Sayed MA. Nuclear Targeting of Gold Nanoparticles in Cancer Cells Induces DNA Damage, Causing Cytokinesis Arrest and Apoptosis. J Am Chem Soc. 2010 Feb 10; 132:1517-9.

Chapter 1: Introduction, Hypotheses, and Overview 47
113. Zhivotovsky B, Joseph B, Orrenius S. Tumor Radiosensitivity and Apoptosis. Exp Cell Res. 1999 Apr 10; 248:10-7.
114. Brown JM, Wouters BG. Apoptosis, P53, and Tumor Cell Sensitivity to Anticancer Agents. Cancer Res. 1999 Apr 1; 59:1391-9.
115. Marill J, Anesary NM, Zhang P, Vivet S, Borghi E, Levy L, et al. Hafnium Oxide Nanoparticles: Toward an in Vitro Predictive Biological Effect? Radiat Oncol. 2014; 9:150.
116. Cho SH. Estimation of Tumour Dose Enhancement Due to Gold Nanoparticles During Typical Radiation Treatments: A Preliminary Monte Carlo Study. Phys Med Biol 2005:163-73.
117. Cho SH, Jones BL, Krishnan S. The Dosimetric Feasibility of Gold Nanoparticle-Aided Radiation Therapy (Gnrt) Via Brachytherapy Using Low-Energy Gamma-/X-Ray Sources. Phys Med Biol. 2009 Aug 21; 54:4889-905.
118. Ghasemi M, Shamsaei M, Ghannadi M, Raisali G. Dosimetric Studies of Micropencil X-Ray Beam Interacting with Labelled Tissues by Au and Gd Agents Using Geant4. Radiat Prot Dosimetry. 2009 Jan; 133:97-104.
119. Zhang SX, Gao J, Buchholz TA, Wang Z, Salehpour MR, Drezek RA, et al. Quantifying Tumor-Selective Radiation Dose Enhancements Using Gold Nanoparticles: A Monte Carlo Simulation Study. Biomed Microdevices. 2009 Aug; 11:925-33.
120. Jones BL, Krishnan S, Cho SH. Estimation of Microscopic Dose Enhancement Factor around Gold Nanoparticles by Monte Carlo Calculations. Med Phys. 2010 Jul; 37:3809-16.
121. Cho S, Jeong, J. H., Kim C. H. Monte Carlo Simulation Study on Dose Enhancement by Gold Nanoparticles in Brachytherapy. Journal of the Korean Physical Society. 2010; 56:1754-8.
122. Ngwa W, Makrigiorgos G.M., Berbeco R. I. Applying Gold Nanoparticles as Tumor-Vascular Disrupting Agents During Brachytherapy: Estimation of Endothelial Dose Enhancement. Phys Med Biol. 2010; 55:6533-48.
123. Chow JC, Leung MK, Jaffray DA. Monte Carlo Simulation on a Gold Nanoparticle Irradiated by Electron Beams. Phys Med Biol. 2012 Jun 7; 57:3323-31.
124. Lechtman E, Chattopadhyay N, Cai Z, Mashouf S, Reilly R, Pignol JP. Implications on Clinical Scenario of Gold Nanoparticle Radiosensitization in Regards to Photon Energy, Nanoparticle Size, Concentration and Location. Phys Med Biol. 2011 Aug 7; 56:4631-47.
125. Leung MK, Chow JC, Chithrani BD, Lee MJ, Oms B, Jaffray DA. Irradiation of Gold Nanoparticles by X-Rays: Monte Carlo Simulation of Dose Enhancements and the Spatial Properties of the Secondary Electrons Production. Med Phys. 2011 Feb; 38:624-31.

Chapter 1: Introduction, Hypotheses, and Overview 48
126. McMahon SJ, Hyland WB, Muir MF, Coulter JA, Jain S, Butterworth KT, et al. Nanodosimetric Effects of Gold Nanoparticles in Megavoltage Radiation Therapy. Radiother Oncol. 2011 Sep; 100:412-6.
127. Lechtman E, Mashouf S, Chattopadhyay N, Keller BM, Lai P, Cai Z, et al. A Monte Carlo-Based Model of Gold Nanoparticle Radiosensitization Accounting for Increased Radiobiological Effectiveness. Phys Med Biol. 2013 May 21; 58:3075-87.
128. Ngwa W, Makrigiorgos GM, Berbeco RI. Gold Nanoparticle-Aided Brachytherapy with Vascular Dose Painting: Estimation of Dose Enhancement to the Tumor Endothelial Cell Nucleus. Med Phys. 2012 Jan; 39:392-8.
129. Berbeco RI, Ngwa W, Makrigiorgos GM. Localized Dose Enhancement to Tumor Blood Vessel Endothelial Cells Via Megavoltage X-Rays and Targeted Gold Nanoparticles: New Potential for External Beam Radiotherapy. Int J Radiat Oncol Biol Phys. 2011 Sep 1; 81:270-6.
130. Roeske JC, Nunez L, Hoggarth M, Labay E, Weichselbaum RR. Characterization of the Theorectical Radiation Dose Enhancement from Nanoparticles. Technol Cancer Res Treat. 2007 Oct; 6:395-401.
131. Lin Y, Paganetti H, McMahon SJ, Schuemann J. Gold Nanoparticle Induced Vasculature Damage in Radiotherapy: Comparing Protons, Megavoltage Photons, and Kilovoltage Photons. Med Phys. 2015; 42:5890-902.
132. Lin Y, McMahon SJ, Paganetti H, Schuemann J. Biological Modeling of Gold Nanoparticle Enhanced Radiotherapy for Proton Therapy. Phys Med Biol. 2015 May 21; 60:4149-68.
133. Butterworth KT, Wyer JA, Brennan-Fournet M, Latimer CJ, Shah MB, Currell FJ, et al. Variation of Strand Break Yield for Plasmid DNA Irradiated with High-Z Metal Nanoparticles. Radiat Res. 2008 Sep; 170:381-7.
134. Brun E, Sanche L, Sicard-Roselli C. Parameters Governing Gold Nanoparticle X-Ray Radiosensitization of DNA in Solution. Colloids Surf B Biointerfaces. 2009 Aug 1; 72:128-34.
135. Zheng Y, Sanche L. Gold Nanoparticles Enhance DNA Damage Induced by Anti-Cancer Drugs and Radiation. Radiat Res. 2009 Jul; 172:114-9.
136. Foley EA, Carter JD, Shan F, Guo T. Enhanced Relaxation of Nanoparticle-Bound Supercoiled DNA in X-Ray Radiation. Chem Commun (Camb). 2005 Jul 7:3192-4.
137. Jain S, Hirst D.G., O'sullivan J.M. Gold Nanoparticles as Novel Agents for Cancer Therapy. The British Jounal of Radiology. 2012; 85:101-13.
138. Coulter JA, Hyland, W.B., Nicol, J., Currell F. J. Radiosensitising Nanoparticles as Novel Cancer Therapeutics - Pipe Dream or Realistic Prospect? Clinical Oncology. 2013; 25:593-603.

Chapter 1: Introduction, Hypotheses, and Overview 49
139. Su XY, Liu PD, Wu H, Gu N. Enhancement of Radiosensitization by Metal-Based Nanoparticles in Cancer Radiation Therapy. Cancer Biol Med. 2014 Jun; 11:86-91.
140. Pottier A, Borghi E, Levy L. New Use of Metals as Nanosized Radioenhancers. Anticancer Res. 2014 Jan; 34:443-53.
141. Ngwa W, Kumar R, Sridhar S, Korideck H, Zygmanski P, Cormack RA, et al. Targeted Radiotherapy with Gold Nanoparticles: Current Status and Future Perspectives. Nanomedicine (Lond). 2014 May; 9:1063-82.
142. kwatra D, Venugopal A, Anant S. Nanoparticles in Radiation Therapy: A Summary of Various Approaches to Enhance Radiosensitization in Cancer. Transl Cancer Res 2013; 2:330-42.
143. Warters RL, Hofer KG, Harris CR, Smith JM. Radionuclide Toxicity in Cultured Mammalian Cells: Elucidation of the Primary Site of Radiation Damage. Curr Top Radiat Res Q. 1978 Jan; 12:389-407.
144. Hainfeld JF, Dilmanian FA, Slatkin DN, Smilowitz HM. Radiotherapy Enhancement with Gold Nanoparticles. J Pharm Pharmacol. 2008 Aug; 60:977-85.
145. Fuks Z, Kolesnick R. Engaging the Vascular Component of the Tumor Response. Cancer Cell. 2005 Aug; 8:89-91.
146. Meyn RE, Stephens LC, Hunter NR, Ang KK, Milas L. Reemergence of Apoptotic Cells between Fractionated Doses in Irradiated Murine Tumors. Int J Radiat Oncol Biol Phys. 1994 Oct 15; 30:619-24.
147. Overgaard J, Hansen HS, Overgaard M, Bastholt L, Berthelsen A, Specht L, et al. A Randomized Double-Blind Phase Iii Study of Nimorazole as a Hypoxic Radiosensitizer of Primary Radiotherapy in Supraglottic Larynx and Pharynx Carcinoma. Results of the Danish Head and Neck Cancer Study (Dahanca) Protocol 5-85. Radiother Oncol. 1998 Feb; 46:135-46.
148. Fraga S, Brandao A, Soares ME, Morais T, Duarte JA, Pereira L, et al. Short- and Long-Term Distribution and Toxicity of Gold Nanoparticles in the Rat after a Single-Dose Intravenous Administration. Nanomedicine. 2014 Nov; 10:1757-66.
149. Sadauskas E, Danscher G, Stoltenberg M, Vogel U, Larsen A, Wallin H. Protracted Elimination of Gold Nanoparticles from Mouse Liver. Nanomedicine. 2009 Jun; 5:162-9.
150. Abdelhalim MA, Jarrar BM. Histological Alterations in the Liver of Rats Induced by Different Gold Nanoparticle Sizes, Doses and Exposure Duration. J Nanobiotechnology. 2012; 10:5.
151. Abdelhalim MA, Jarrar BM. Gold Nanoparticles Induced Cloudy Swelling to Hydropic Degeneration, Cytoplasmic Hyaline Vacuolation, Polymorphism, Binucleation, Karyopyknosis, Karyolysis, Karyorrhexis and Necrosis in the Liver. Lipids Health Dis. 2011; 10:166.

Chapter 1: Introduction, Hypotheses, and Overview 50
152. Balasubramanian SK, Jittiwat J, Manikandan J, Ong CN, Yu LE, Ong WY. Biodistribution of Gold Nanoparticles and Gene Expression Changes in the Liver and Spleen after Intravenous Administration in Rats. Biomaterials. 2010 Mar; 31:2034-42.
153. Cho WS, Cho M, Jeong J, Choi M, Cho HY, Han BS, et al. Acute Toxicity and Pharmacokinetics of 13 Nm-Sized Peg-Coated Gold Nanoparticles. Toxicol Appl Pharmacol. 2009 Apr 1; 236:16-24.
154. Zhang XD, Wu D, Shen X, Liu PX, Fan FY, Fan SJ. In Vivo Renal Clearance, Biodistribution, Toxicity of Gold Nanoclusters. Biomaterials. 2012 Jun; 33:4628-38.
155. Hwang JH, Kim SJ, Kim YH, Noh JR, Gang GT, Chung BH, et al. Susceptibility to Gold Nanoparticle-Induced Hepatotoxicity Is Enhanced in a Mouse Model of Nonalcoholic Steatohepatitis. Toxicology. 2012 Mar 29; 294:27-35.
156. Zhang XD, Wu HY, Wu D, Wang YY, Chang JH, Zhai ZB, et al. Toxicologic Effects of Gold Nanoparticles in Vivo by Different Administration Routes. Int J Nanomedicine. 2010; 5:771-81.
157. Chen YS, Hung YC, Liau I, Huang GS. Assessment of the in Vivo Toxicity of Gold Nanoparticles. Nanoscale Res Lett. 2009; 4:858-64.
158. Gerber A, Bundschuh M, Klingelhofer D, Groneberg DA. Gold Nanoparticles: Recent Aspects for Human Toxicology. J Occup Med Toxicol. 2013; 8:32.
159. Zhang G, Yang Z, Lu W, Zhang R, Huang Q, Tian M, et al. Influence of Anchoring Ligands and Particle Size on the Colloidal Stability and in Vivo Biodistribution of Polyethylene Glycol-Coated Gold Nanoparticles in Tumor-Xenografted Mice. Biomaterials. 2009 Apr; 30:1928-36.
160. Chou LY, Chan WC. Fluorescence-Tagged Gold Nanoparticles for Rapidly Characterizing the Size-Dependent Biodistribution in Tumor Models. Adv Healthc Mater. 2012 Nov; 1:714-21.
161. Simpson CA, Huffman BJ, Gerdon AE, Cliffel DE. Unexpected Toxicity of Mono Layer Protected Gold Clusters Eliminated by Peg-Thiol Place Exchange Reactions. Chemical Research in Toxicology 2010; 23:1608-16.
162. Perrault SD, Walkey C, Jennings T, Fischer HC, Chan WC. Mediating Tumor Targeting Efficiency of Nanoparticles through Design. Nano Lett. 2009 May; 9:1909-15.
163. Hainfeld JF, Slatkin DN, Focella TM, Smilowitz HM. Gold Nanoparticles: A New X-Ray Contrast Agent. Br J Radiol. 2006 Mar; 79:248-53.
164. Chattopadhyay N, Fonge H, Cai Z, Scollard D, Lechtman E, Done SJ, et al. Role of Antibody-Mediated Tumor Targeting and Route of Administration in Nanoparticle Tumor Accumulation in Vivo. Mol Pharm. 2012 Aug 6; 9:2168-79.
165. Chen CH, Lin FS, Liao WN, Liang SL, Chen MH, Chen YW, et al. Establishment of a Trimodality Analytical Platform for Tracing, Imaging and Quantification of

Chapter 1: Introduction, Hypotheses, and Overview 51
Gold Nanoparticles in Animals by Radiotracer Techniques. Anal Chem. 2015 Jan 6; 87:601-8.
166. Albanese A, Chan WC. Effect of Gold Nanoparticle Aggregation on Cell Uptake and Toxicity. ACS Nano. 2011 Jul 26; 5:5478-89.
167. Dobrovolskaia MA, Patri AK, Zheng J, Clogston JD, Ayub N, Aggarwal P, et al. Interaction of Colloidal Gold Nanoparticles with Human Blood: Effects on Particle Size and Analysis of Plasma Protein Binding Profiles. Nanomedicine. 2009 Jun; 5:106-17.
168. Boulos SP, Davis TA, Yang JA, Lohse SE, Alkilany AM, Holland LA, et al. Nanoparticle-Protein Interactions: A Thermodynamic and Kinetic Study of the Adsorption of Bovine Serum Albumin to Gold Nanoparticle Surfaces. Langmuir. 2013 Dec 3; 29:14984-96.
169. Chithrani BD, Chan WC. Elucidating the Mechanism of Cellular Uptake and Removal of Protein-Coated Gold Nanoparticles of Different Sizes and Shapes. Nano Lett. 2007 Jun; 7:1542-50.
170. Chithrani BD, Ghazani AA, Chan WC. Determining the Size and Shape Dependence of Gold Nanoparticle Uptake into Mammalian Cells. Nano Lett. 2006 Apr; 6:662-8.
171. Cho EC, Xie J, Wurm PA, Xia Y. Understanding the Role of Surface Charges in Cellular Adsorption Versus Internalization by Selectively Removing Gold Nanoparticles on the Cell Surface with a I2/Ki Etchant. Nano Lett. 2009 Mar; 9:1080-4.
172. Jiang Y, Huo S, Mizuhara T, Das R, Lee YW, Hou S, et al. The Interplay of Size and Surface Functionality on the Cellular Uptake of Sub-10 Nm Gold Nanoparticles. ACS Nano. 2015 Oct 27; 9:9986-93.
173. Khoshgard K, Hashemi B, Arbabi A, Rasaee MJ, Soleimani M. Radiosensitization Effect of Folate-Conjugated Gold Nanoparticles on Hela Cancer Cells under Orthovoltage Superficial Radiotherapy Techniques. Phys Med Biol. 2014 May 7; 59:2249-63.
174. Pan Y, Neuss S, Leifert A, Fischler M, Wen F, Simon U, et al. Size-Dependent Cytotoxicity of Gold Nanoparticles. Small. 2007 Nov; 3:1941-9.
175. Xiao F, Zheng Y, Cloutier P, He Y, Hunting D, Sanche L. On the Role of Low-Energy Electrons in the Radiosensitization of DNA by Gold Nanoparticles. Nanotechnology. 2011 Nov 18; 22:465101.
176. McMahon SJ, Hyland WB, Muir MF, Coulter JA, Jain S, Butterworth KT, et al. Biological Consequences of Nanoscale Energy Deposition near Irradiated Heavy Atom Nanoparticles. Sci Rep. 2011; 1:18.
177. Zheng Y CP, Hunting DJ, Sanche L, . . Radiosensitization by Gold Nanoparticles: Comparison of DNA Damage Induced by Low and High-Energy Electrons. ournal of Biomedical Nanotechnology 2008; 4:469-73.

Chapter 1: Introduction, Hypotheses, and Overview 52
178. Tkachenko AG, Xie H, Coleman D, Glomm W, Ryan J, Anderson MF, et al. Multifunctional Gold Nanoparticle-Peptide Complexes for Nuclear Targeting. J Am Chem Soc. 2003 Apr 23; 125:4700-1.
179. De Jong WH, Hagens WI, Krystek P, Burger MC, Sips AJ, Geertsma RE. Particle Size-Dependent Organ Distribution of Gold Nanoparticles after Intravenous Administration. Biomaterials. 2008 Apr; 29:1912-9.
180. Sonavane G, Tomoda K, Makino K. Biodistribution of Colloidal Gold Nanoparticles after Intravenous Administration: Effect of Particle Size. Colloids Surf B Biointerfaces. 2008 Oct 15; 66:274-80.
181. Huo S, Ma H, Huang K, Liu J, Wei T, Jin S, et al. Superior Penetration and Retention Behavior of 50 Nm Gold Nanoparticles in Tumors. Cancer Res. 2013 Jan 1; 73:319-30.
182. Huang K, Ma H, Liu J, Huo S, Kumar A, Wei T, et al. Size-Dependent Localization and Penetration of Ultrasmall Gold Nanoparticles in Cancer Cells, Multicellular Spheroids, and Tumors in Vivo. ACS Nano. 2012 May 22; 6:4483-93.
183. Malugin A, Ghandehari H. Cellular Uptake and Toxicity of Gold Nanoparticles in Prostate Cancer Cells: A Comparative Study of Rods and Spheres. J Appl Toxicol. 2010 Apr; 30:212-7.
184. Arnida J-AM, Ray A, Peterson CM, Ghandehari H, . Geometry and Surface Characteristics of Gold Nanoparticles Influence Their Biodistribution and Uptake by Macrophages. Eur J Pharm Biopharm. 2011; 77:417-23.
185. Arvizo RR, Miranda OR, Moyano DF, Walden CA, Giri K, Bhattacharya R, et al. Modulating Pharmacokinetics, Tumor Uptake and Biodistribution by Engineered Nanoparticles. PLoS One. 2011; 6:e24374.
186. Goodman CM, McCusker CD, Yilmaz T, Rotello VM. Toxicity of Gold Nanoparticles Functionalized with Cationic and Anionic Side Chains. Bioconjug Chem. 2004 Jul-Aug; 15:897-900.
187. Ojea-Jimenez I, Garcia-Fernandez L, Lorenzo J, Puntes VF. Facile Preparation of Cationic Gold Nanoparticle-Bioconjugates for Cell Penetration and Nuclear Targeting. ACS Nano. 2012 Sep 25; 6:7692-702.
188. Brandenberger C, Muhlfeld C, Ali Z, Lenz AG, Schmid O, Parak WJ, et al. Quantitative Evaluation of Cellular Uptake and Trafficking of Plain and Polyethylene Glycol-Coated Gold Nanoparticles. Small. 2010 Aug 2; 6:1669-78.
189. Vogelzang NJ. Continuous Infusion Chemotherapy: A Critical Review. J Clin Oncol. 1984 Nov; 2:1289-304.
190. Kudgus RA, Walden CA, McGovern RM, Reid JM, Robertson JD, Mukherjee P. Tuning Pharmacokinetics and Biodistribution of a Targeted Drug Delivery System through Incorporation of a Passive Targeting Component. Sci Rep. 2014; 4:5669.
191. Markman M. Intraperitoneal Chemotherapy in the Management of Ovarian Cancer: Focus on Carboplatin. Ther Clin Risk Manag. 2009 Feb; 5:161-8.

Chapter 1: Introduction, Hypotheses, and Overview 53
192. Markman M, Walker JL. Intraperitoneal Chemotherapy of Ovarian Cancer: A Review, with a Focus on Practical Aspects of Treatment. J Clin Oncol. 2006 Feb 20; 24:988-94.
193. de Bree E, Witkamp AJ, Zoetmulder FA. Intraperitoneal Chemotherapy for Colorectal Cancer. J Surg Oncol. 2002 Jan; 79:46-61.
194. Speyer JL. The Rationale Behind Intraperitoneal Chemotherapy in Gastrointestinal Malignancies. Semin Oncol. 1985 Sep; 12:23-8.
195. Cho SH, Krishnan S, editors. Cancer Nanotechnology: Principles and Applications in Radiation Oncology: CRC Press; 2013.
196. Muller JH. [the Treatment of Cancer of the Ovaries. Its Improvement by Intraperitoneal Administration of Radioactive Colloidal Gold]. Rev Fr Gynecol Obstet. 1963 Mar; 58:197-214.
197. Patyanik M, Mayer A, Polgar I. Results of Ovary Tumor Treatment with Abdominally Administered (198)Au Evaluated on the Basis of Long Term Follow Up. Pathol Oncol Res. 2002; 8:54-7.
198. Abdelhalim MA, Mady MM. Liver Uptake of Gold Nanoparticles after Intraperitoneal Administration in Vivo: A Fluorescence Study. Lipids Health Dis. 2011; 10:195.
199. Khan HA, Abdelhalim MA, Al-Ayed MS, Alhomida AS. Effect of Gold Nanoparticles on Glutathione and Malondialdehyde Levels in Liver, Lung and Heart of Rats. Saudi J Biol Sci. 2012 Oct; 19:461-4.
200. Celikoglu F, Celikoglu SI, Goldberg EP. Bronchoscopic Intratumoral Chemotherapy of Lung Cancer. Lung Cancer. 2008 Jul; 61:1-12.
201. Jaffray DA. Image-Guided Radiotherapy: From Current Concept to Future Perspectives. Nat Rev Clin Oncol. 2012 Dec; 9:688-99.
202. Flickinger JC, Kano H, Niranjan A, Kondziolka D, Lunsford LD. Dose Selection in Stereotactic Radiosurgery. Prog Neurol Surg. 2013; 27:49-57.
203. McGarry RC, Papiez L, Williams M, Whitford T, Timmerman RD. Stereotactic Body Radiation Therapy of Early-Stage Non-Small-Cell Lung Carcinoma: Phase I Study. Int J Radiat Oncol Biol Phys. 2005 Nov 15; 63:1010-5.
204. Timmerman R, McGarry R, Yiannoutsos C, Papiez L, Tudor K, DeLuca J, et al. Excessive Toxicity When Treating Central Tumors in a Phase Ii Study of Stereotactic Body Radiation Therapy for Medically Inoperable Early-Stage Lung Cancer. J Clin Oncol. 2006 Oct 20; 24:4833-9.
205. Vaidya JS, Tobias JS, Baum M, Wenz F, Kraus-Tiefenbacher U, D'Souza D, et al. Targeted Intraoperative Radiotherapy (Targit): An Innovative Approach to Partial-Breast Irradiation. Semin Radiat Oncol. 2005 Apr; 15:84-91.
206. Vaidya JS, Wenz F, Bulsara M, Tobias JS, Joseph DJ, Keshtgar M, et al. Risk-Adapted Targeted Intraoperative Radiotherapy Versus Whole-Breast

Chapter 1: Introduction, Hypotheses, and Overview 54
Radiotherapy for Breast Cancer: 5-Year Results for Local Control and Overall Survival from the Targit-a Randomised Trial. Lancet. 2014 Feb 15; 383:603-13.
207. MacDonald SM, DeLaney TF, Loeffler JS. Proton Beam Radiation Therapy. Cancer Invest. 2006 Mar; 24:199-208.
208. Paganetti H, Bortfeld T. Proton Beam Radiotherapy - the State of the Art. New Technologies in Radiation Oncology. 2005.
209. Jakel O, Kramer M, Karger CP, Debus J. Treatment Planning for Heavy Ion Radiotherapy: Clinical Implementation and Application. Phys Med Biol. 2001 Apr; 46:1101-16.
210. Kramer M, Jakel O, Haberer T, Kraft G, Schardt D, Weber U. Treatment Planning for Heavy-Ion Radiotherapy: Physical Beam Model and Dose Optimization. Phys Med Biol. 2000 Nov; 45:3299-317.
211. Benedict SH. Review of Radiation Oncology Physics: A Handbook for Teachers and Students,. Journal of Applied Clinical Medical Physics. 2004; 5:91-2.
212. Welsh JS. Beta Radiation. Oncologist. 2006 Feb; 11:181-3.
213. Olsen BB, Thisgaard H, Bolgel S, Thomassen M, Kruse TA, Needham D, et al. Novel Radioisotope-Based Nanomedical Approaches. Eur J Nanomed. 2013; 5:181-93.
214. Zhang L, Chen H, Wang L, Liu T, Yeh J, Lu G, et al. Delivery of Therapeutic Radioisotopes Using Nanoparticle Platforms: Potential Benefit in Systemic Radiation Therapy. Nanotechnol Sci Appl. 2010; 3:159-70.
215. Singh N, editor. Radioisotopes - Applications in Bio-Medical Science: InTech; 2011.
216. Coulter JA, Jain S, Butterworth KT, Taggart LE, Dickson GR, McMahon SJ, et al. Cell Type-Dependent Uptake, Localization, and Cytotoxicity of 1.9 Nm Gold Nanoparticles. Int J Nanomedicine. 2012; 7:2673-85.
217. Wang C, Jiang Y, Li X, Hu L. Thioglucose-Bound Gold Nanoparticles Increase the Radiosensitivity of a Triple-Negative Breast Cancer Cell Line (Mda-Mb-231). Breast Cancer. 2015 Jul; 22:413-20.
218. Chan AT, Leung SF, Ngan RK, Teo PM, Lau WH, Kwan WH, et al. Overall Survival after Concurrent Cisplatin-Radiotherapy Compared with Radiotherapy Alone in Locoregionally Advanced Nasopharyngeal Carcinoma. J Natl Cancer Inst. 2005 Apr 6; 97:536-9.
219. Lu QB, Kalantari S, Wang CR. Electron Transfer Reaction Mechanism of Cisplatin with DNA at the Molecular Level. Mol Pharm. 2007 Jul-Aug; 4:624-8.
Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 55
Chapter 2
Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles
Lei Cui, Payam Zahedi, Justin Saraceno, Robert G. Bristow,
David A. Jaffray, and Christine Allen
Reprint from Nanomedicine: Nanotechnology, Biology, and Medicine (2013)
DOI 10.1016/ j.nano.2012.05.016
Experiments by L.Cui. Written by L.Cui. Figures by L.Cui. Edited by C. Allen.
The copyright of this article belongs to Elsevier B.V., the publisher of Nanomedicine:
Nanotechnology, Biology, and Medicine. Permission had to be requested for publishing
the article as part of this dissertation, which was obtained.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 56
2.1 Abstract
The present study characterized the in vitro biological response of a
comprehensive set of cancer cell lines to gold nanoparticles (2.7 nm) coated with
tiopronin (AuNP-TP). Our findings suggest that upon entering cells, the AuNP-TP are
sequestered in vacuoles such as endosomes and lysosomes, and mostly localize in
perinuclear areas. Peak cell accumulation was achieved at 8 h after incubation. L929
and H520 cells showed more than 75% surviving fraction when treated with 0.5 mg/mL
of AuNP-TP for 24 h, whereas the surviving fractions were 60% in MCF-7 and 20% in
HeLa cells. Reactive oxygen species (ROS) production by the AuNP-TP was dependent
on cell line and exposure time. Antioxidants inhibited ROS generation to various
extents, with glutathione and tiopronin being most effective. Overall, exposure time,
concentration of the AuNP-TP, and cell line influenced neoplastic cell response.
Furthermore, the mechanism of cytotoxicity of the AuNP-TP was found to be ROS
generation.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 57
2.2 Introduction
The interest in nanotechnology for medical applications such as drug delivery,
imaging and tissue engineering has grown significantly [1]. In particular, gold
nanoparticles (AuNPs) have been heavily explored for their use in cancer diagnosis and
therapy [2, 3]. Several factors make gold attractive including its inert nature (i.e. stable
and non-metabolizable), biocompatibility, ease of nanoparticle size control, and well-
developed surface chemistry for functionalization [4]. Varying the size, shape and
surface properties of AuNPs allows for customized optical characteristics [5],
pharmacokinetics and biodistribution [6-8], and biocompatibility [9, 10].
The size of nanoparticles has been shown to influence their biodistribution in vivo
[11]. For instance, small sized nanoparticles (<5nm) have deeper tumour penetration
compared to larger particles (>10nm) [12]. As well in vitro, cellular uptake of
nanoparticles has been shown to be size dependent [8]. The surface properties of
nanoparticles, which are largely determined by the surfactants used during preparation
and for coating, is another crucial factor that can determine their in vitro and in vivo
performance [13, 14]. To date, one of the most commonly used surfactants for AuNPs
has been thiol-terminated polyethylene glycol (PEG-SH) [15]. Two limitations associated
with PEG-SH are its relatively large molecular weight and limitations with respect to
further functionalization.
The method of synthesizing small sized AuNPs coated with the hydrophilic
molecule tiopronin (AuNP-TP) was first developed by Templeton et al (Figure 2-1) [16],
and there are several advantages associated with the use of this surfactant. Firstly, the
core size of the AuNP-TP can be controlled by changing the molar ratio of gold to
tiopronin. As well, due to the hydrophilicity of tiopronin the AuNP-TP are water soluble,
which enables administration in vivo. Furthermore, the thiol group in tiopronin makes it
capable of tight conjugation to gold atoms through the strong sulphur-gold (S-Au) bond
[17]. Also, due to the small size of tiopronin there is less steric repulsion between the
stabilizing molecules, leading to greater coverage of the surface of AuNPs [16]. The
strong S-Au bond and high surface coverage make the AuNP-TP resistant to ligand

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 58
exchange reactions, reduce the possibility of absorption of other molecules such as
proteins onto their surface, and minimize aggregation. In addition, functional groups
such as fluorescent probes and active targeting peptides can be easily added to the
AuNP-TP through conjugation with the carboxyl group found on tiopronin [18, 19].
Although there are numerous advantages associated with AuNP-TP, their
biological properties have only been characterized to a limited extent [19, 20]. Herein, in
vitro studies were performed to evaluate and gain an improved understanding of cellular
response to AuNP-TP. Given that AuNPs have been mostly investigated for applications
in cancer diagnosis and therapy, three human cancer cell lines (MCF-7 breast cancer
cells, HeLa cervical cancer cells, H520 lung cancer cells) were selected for these
studies; and a murine fibroblast cell line (L929) was used as a control. Cellular
accumulation, intracellular distribution, cytotoxicity and reactive oxygen species (ROS)
production of the AuNP-TP were assessed. In addition, a series of antioxidants (N-
acetyl-cysteine, reduced L-cysteine, glutathione and tiopronin) were employed to
determine their influence on cellular ROS levels following co-treatment with the AuNP-
TP. A concentration range of 0.01-0.5 mg/mL AuNP-TP was used for these studies.
Similar concentration ranges have been investigated in vitro with AuNP systems [8, 10,
19].
Figure 2-1: Preparation of AuNPs coated with a monolayer of tiopronin.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 59
2.3 Methods
Detailed information on the materials and methods for preparation and
characterization of AuNPs, cell culture, qualitative assessment of cellular accumulation
of AuNP-TP, and statistical analysis is available in the Supplementary Materials online
at http://www.nanomedjournal.com.
2.3.1 Quantitative Assessment of Cellular Accumulation of AuNP-TP
For quantitative analysis of cellular accumulation, cells were seeded in 6-well
plates at a density of approximately 1x106 cells/well. Cells were treated with 2 different
concentrations of AuNP-TP (0.05 and 0.25 mg/mL) for 1, 4, 8, 24, 48 or 72 h. At each
timepoint cell media was removed, cells were washed 3 times with PBS and then
harvested with 0.25% Trypsin with EDTA (Gibco). Cells were counted using a
haemocytometer, centrifuged to a pellet, digested with HNO3 at 90°C for 60 min, and
diluted with dd-H2O. The amount of gold was measured by inductively coupled plasma
atomic emission spectroscopy (ICP-AES), and normalized to the number of cells in
each sample. The results were reported as the amount of Au (pg) per cells. The number
of AuNP-TP in cells was calculated as described in the Supplementary Materials.
2.3.2 Evaluation of Cytotoxicity of AuNP-TP
Clonogenic assays were performed as described previously [21, 22]. Cells were
seeded in 6-well plates at a density of 1x106 cells/well, and treated with various
concentrations of AuNP-TP (0.01-0.5 mg/mL). For the HeLa cells co-treatment with 0.5
mg/mL AuNP-TP and 3 mM glutathione (GSH) was also tested. After 24 h of incubation,
cells were washed twice with PBS and trypsinized. For each treatment, cells were
counted and added into 6-well plates at different cell densities (i.e. 300-1800 cells/well).
After 7-10 days, the colonies were washed with PBS, fixed with methanol and stained
with 1% crystal violet. The number of colonies, which consisted of at least 50 cells, was

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 60
counted on each plate. Cell surviving fraction (SF) was expressed as plating efficiency
compared to that of non-treated cells.
2.3.3 Measurement of Reactive Oxygen Species Production
The amount of reactive oxygen species (ROS) was measured using the 2’,7’-
dichlorofluorescin diacetate (DCFH-DA) assay as previously described [23]. Cells were
seeded into 96-well plates at a density of 20,000 cells/well. After recovery, cells were
washed twice with Hank’s Balanced Salt Solution (HBSS), and incubated with 100 M
DCFH-DA for 60 min. Cells were then washed with HBSS and exposed to different
treatments, with non-treated cells used as negative controls. Cells treated with 0.3%
H2O2 and 10 M 3-morpholino-sydnonimine hydrochloride (SIN) were employed as ROS
generating positive controls. The treatment groups included 0.5 mg/mL AuNP-TP; 0.5
mg/mL AuNP-TP + 3 mM N-acetyl-cysteine (NAC), reduced L-cysteine, glutathione
(GSH) or TP; and 0.5 mg/mL AuNP-TP + 50uM Z-VAD-fmk (BACHEM). At different
timepoints (1, 4, 8 and 24 h) post-treatment, fluorescent signal was measured with a
SpectraMax Gemini Plus (Molecular Devices Corporation) microplate reader (ex = 480
nm, em = 520 nm). The results were reported as relative ROS production compared to
non-treated cells.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 61
2.4 Results
2.4.1 Synthesis and Characterization of AuNP-TP
A representative TEM image of the AuNP-TP suspended in dd-H2O is shown in
Figure 2-2 A. The AuNP-TP had a mean core diameter of 2.7 nm as obtained from the
core size distribution histogram (Figure 2-2 B). It was determined that each 2.7 nm
AuNP-TP was composed of approximately 600 Au atoms. Au atoms composed 76.5 ±
0.3% of the mass of the AuNP-TP, and the coating efficiency of TP (i.e. the percentage
of gold atoms at the surface of the NPs that are coated with TP) was calculated to be
87.3 ± 0.3%. As seen from the 1H NMR spectrum (Figure 2-2 C), the final product was
spectroscoptically pure with the absence of signals due to unreacted thiol or disulfide
by-product [16]. As evidenced from the UV-vis spectrum (Figure 2-2 D), an absence of
absorbance at 520 nm demonstrated that the AuNP-TP were stable in dd-H2O with no
aggregation. However, it was found that upon incubation of AuNP-TP in cell culture
media a fraction of the nanoparticles aggregate and precipitate out of solution.
Following 24, 48, and 72 h of incubation in cell culture media 82 2 %, 78 2 %, and
76 2 % of the AuNP-TP, respectively, were found to remain in the supernatant. TEM
analysis revealed that the AuNP-TP that remain in the supernatant retain their size and
are well dispersed in the media (Figures 2-2 F-H).
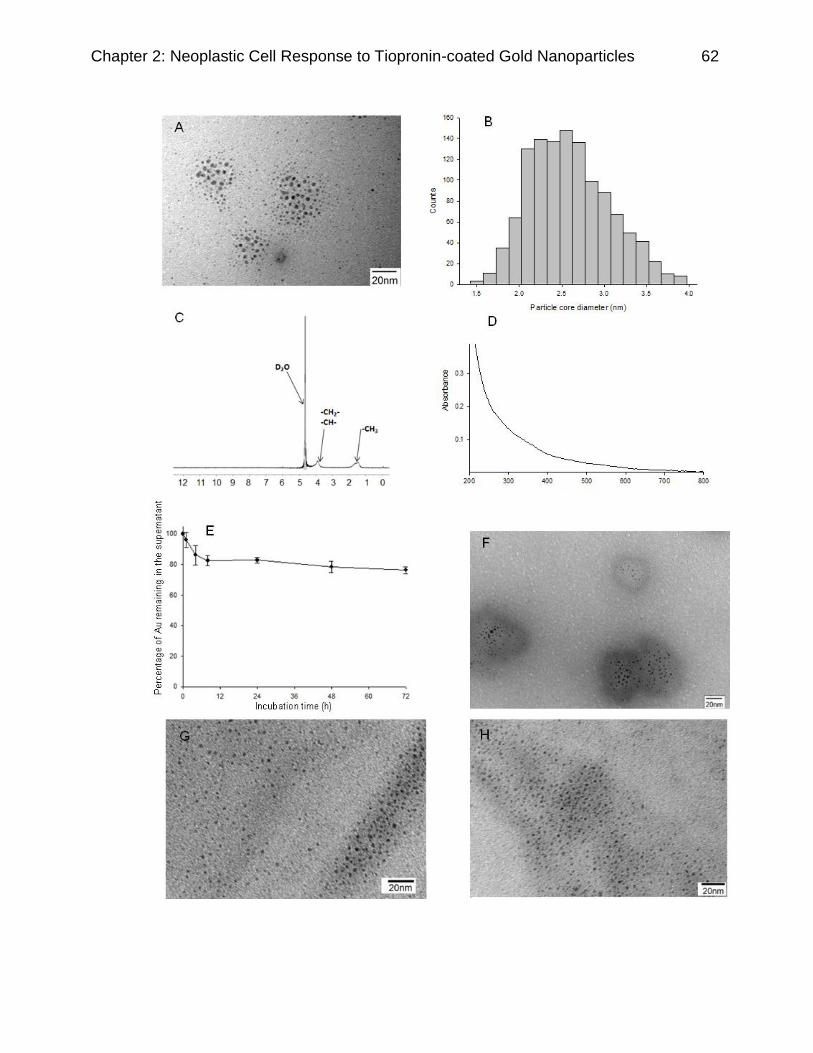
Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 62

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 63
Figure 2-2: Characterization of the AuNP-TP. (A) A representative TEM image of the
AuNP-TP. The scale bar represents 20 nm. (B) Core size distribution histogram
calculated from over 1000 AuNP-TP. (C) 1H NMR spectrum of 0.5 mg/mL AuNP-TP
suspension in D2O. (D) UV-vis spectrum of 1 mg/mL AuNP-TP in dd-H2O. (E)
Percentage of Au that remains in the supernatant following incubation in cell culture
media at 37°C. Data represents mean SD (n=3). (F-H) TEM images of AuNP-TP in
cell culture media following 24, 48, 72 h of incubation at 37°C. The scale bar represents
20 nm.
2.4.2 Cellular Accumulation of AuNP-TP
To study the intracellular fate of the AuNP-TP, cells were observed by TEM. TEM
images of four cell lines pre-treated with AuNP-TP are presented in Figure 2-3. From
these images, it can be seen that AuNP-TP mostly localized in the perinuclear areas of
cells. AuNP-TP in cytoplasm were sequestered in large clusters in vacuoles such as the
endosomes and lysosomes. The AuNP-TP did not localize in organelles such as the
nucleus or mitochondria.
Figure 2-4 summarizes the quantitative evaluation of cellular accumulation of
AuNP-TP. The total intracellular level of Au is presented in Figure 2-7 A-D. To assess
the effect of AuNP-TP concentration on cellular accumulation, cells were incubated with
two different concentrations (i.e., 0.05 mg/mL and 0.25 mg/mL). For all cell lines used,
the amount of cellular accumulation was dependent on AuNP-TP concentration.
Statistically significant differences (p<0.05) in cell accumulation were observed between
the two concentrations at all timepoints. Similar accumulation profiles were observed in
MCF-7 and HeLa cells. In the first 8 h of incubation there was an increase in Au
accumulation, the levels then decreased in the following 40 h, and reached a constant
level at 48 h. A similar profile was also observed in the L929 cells incubated with 0.25
mg/mL AuNP-TP. However, for the H520 cells the cellular accumulation profiles, for
both concentrations of AuNP-TP, reached a maximum at 8 h and this level remained
relatively constant up to 72 h. For the L929 cells incubated with 0.05 mg/mL AuNP-TP a

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 64
significant decrease was observed at 24 h compared to 8 h, after which the level
increased to a value similar to that achieved at the 8 h timepoint. Statistically significant
differences (p<0.05) in cell accumulation at different timepoints in comparison to the
uptake at the 8 h timepoint are shown in Figure 2-4.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 65
Figure 2-3: TEM images of AuNP-TP accumulation in MCF-7 (A, B), HeLa (C, D), H520
(E, F), and L929 (G, H) cells. As highlighted by the arrows in images (A) and (B) once
the AuNP-TP enter cells they appear to sequester in large vacuoles such as
endosomes and lysosomes, and mostly localize in the perinuclear region of cells. A
similar trend was observed for all cell lines evaluated. Scale bars represent 2 m in A,
C, E and G, and 100 nm in B, D, F and H.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 66
Figure 2-4: In vitro cellular accumulation of AuNP-TP in (A) MCF-7, (B) HeLa, (C)
H520, and (D) L929 cells quantified by ICP-AES with incubation at two different
concentrations (i.e., 0.05 and 0.25 mg/mL) of AuNP-TP. * Represents statistically
significant difference between the two concentrations (p<0.05), and # Represents
statistically significant difference in cell accumulation at different timepoints in
comparison to that at the 8 h timepoint. Data represents mean SD (n=3).
At the peak timepoint for accumulation (i.e. 8 h), HeLa and L929 cells showed
higher accumulation of AuNP-TP (42 pg/cell, 2.1x108 AuNP-TP/cell) compared to MCF-
7 (25 pg/cell, 1.3x108 AuNP-TP/cell) and H520 (15 pg/cell, 0.78x108 AuNP-TP/cell)
cells. Interestingly, despite the large differences seen in accumulation following the 8 h
incubation period, all cell lines showed a similar concentration of Au accumulation at 72
h. These concentrations were 15 pg/cell (0.78x108 AuNP-TP/cell) and 5 pg/cell

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 67
(0.26x108 AuNP-TP/cell) when incubated with 0.25 mg/mL and 0.05 mg/mL of the
AuNP-TP, respectively.
2.4.3 Cytotoxicity of AuNP-TP
The biocompatibility of the AuNP-TP was assessed by clonogenic assay.
Incubation of AuNP-TP with L929 and H520 cells resulted in more than 75% surviving
fraction (SF) even at the highest AuNP-TP concentration (i.e., 0.5 mg/mL). For HeLa
cells, the SF decreased significantly (p<0.05) when treated with 0.25 and 0.5 mg/mL of
the AuNP-TP. Specifically, HeLa cells showed only 20% SF at the highest concentration
tested. For MCF-7 cells, a significant decrease (p<0.05) in SF was observed at 0.5
mg/mL (Figure 2-5).
Figure 2-5: Cell surviving fraction (SF) after 24 h of treatment with different
concentrations of AuNP-TP. SF as determined by clonogenic assays is reported as
plating efficiency compared to non-treated cells. * and # represent statistically significant
differences between various concentrations for HeLa and MCF-7 cells, respectively
(p<0.05). Data represents mean SD (n=3).

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 68
2.4.4 Measurement of ROS Production
To determine if the cytotoxic effect of the AuNP-TP in HeLa and L929 cell lines
could be attributed to oxidative stress the ROS generated by the AuNP-TP was
measured using the DCFH-DA assay (Figure 2-6). Incubation of cells with 0.3% H2O2 or
10 M SIN for 1 h, as positive controls, resulted in high ROS levels compared to non-
treated cells. The amount of ROS produced following treatment with the AuNP-TP
increased with incubation time yet was lower than the positive controls. ROS production
following treatment with the AuNP-TP in combination with various antioxidants (i.e.
NAC, reduced L-cysteine, GSH or tiopronin) was also evaluated. The degree of ROS
inhibition depended on the antioxidant employed (Figure 2-6). GSH and tiopronin were
more effective in decreasing ROS compared to NAC and reduced L-cysteine. Co-
treatment of cells with Z-VAD-fmk and AuNP-TP resulted in ROS levels that were
similar to those achieved following treatment with AuNP-TP alone.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 69
Figure 2-6: Amount of ROS produced relative to non-treated cells following treatment
with AuNP-TP (0.5 mg/mL) in combination with antioxidants including NAC, reduced L
cysteine, GSH or tiopronin (3mM) and the apoptotic inhibitor Z-VAD-fmk (50uM) in A)
HeLa cells and B) L929 cells. The insets show relative ROS produced in cells following
treatment with 0.3% H2O2 or 10 M SIN for 1 h compared to non-treated cells. Data
represents mean SD (n=4).
The ability of GSH to rescue cells from AuNP-TP induced oxidative stress was
evaluated. Cell clonogenicity was compared between HeLa cells treated with AuNP-TP
alone and in combination with GSH. It was found that the cell SF was increased by 4
fold following combination treatment (i.e. SF = 19 0.45% (only AuNP-TP) vs 91 4.4%
(AuNP-TP + GSH)).

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 70
2.5 Discussion
With its unique physical and chemical characteristics, gold in the form of AuNPs
has been widely explored for biomedical applications such as drug delivery, imaging,
disease diagnosis and therapy [2, 3]. The size, shape and surface coating of AuNPs
can be modified to alter in vitro cellular response [7, 24]. Tiopronin has several
advantages over conventionally used PEG-based surfactants, however, little is known
about the biological performance of AuNP-TP. In this study, AuNP-TP were synthesized
and assessed in terms of size, purity, in vitro cell accumulation, and cytotoxicity. The
mechanism of cytotoxicity was also investigated.
A significant challenge in the chemical synthesis of AuNPs is achieving
monodispersity in size [25]. In this study, the mean core diameter of AuNP-TP
suspended in dd-H2O was 2.7 nm, and the size distribution histogram showed a
relatively narrow size distribution (1.5 to 3.9 nm). This relatively high monodispersity of
the AuNP-TP was achieved using the method described by Templeton et al., in which
synchronized growth and coating of the NPs are achieved with the thiol-containing
reducing reaction [16]. The stability of the AuNP-TP in dd-H2O was assessed based on
their optical properties (i.e. surface plasmon resonance). The UV spectrum of AuNPs
with diameters greater than 3 nm is known to include absorption at a wavelength of
approximately 520 nm. As well any change in the surface of the AuNP-TP such as
absorption of macromolecules or aggregation can lead to changes in the UV-vis
spectrum [26, 27]. The absence of peaks in the UV-vis spectra (i.e. in the 520 nm
range) of the AuNP-TP confirmed their stability and lack of aggregation in dd-H2O.
However, aggregation of AuNPs was observed upon incubation in cell culture media.
Aggregation occurs when NPs interact with cell culture media given that ions such as
Na+ and Cl- in the media neutralize the surface charge of the NPs [28]. This aggregation
is said to be an immediate and irreversible process. It is believed that absorption of
proteins onto the surface of some AuNPs can assist in stabilizing the particles and
preventing aggregation. However, absorption of proteins onto AuNP-TP is unlikely given
the high coating efficiency of TP (87.3 ± 0.3%) and the strong S-Au bond, which is
resistant to ligand exchange reactions.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 71
Cellular accumulation of the AuNP-TP was visualized in four different cell lines by
TEM. The AuNP-TP that entered the cells were sequestered in large clusters in
vacuoles in the perinuclear areas of the cytoplasm. Previous studies have made similar
observations [20, 29]. For applications such as drug delivery or radiosensitization it may
be important to target the AuNPs to specific subcellular organelles such as the nucleus.
This delivery to specific intracellular compartments may be achieved by conjugating
targeting moieties to the surface of the AuNP-TP. De la Fuente et al. conjugated the
TAT peptide onto the surface of AuNP-TP and demonstrated successful transport to the
cell nucleus [19].
Quantitative assessment of cellular accumulation of the AuNP-TP is of relevance
given that the cellular concentration determines potential toxicity and therapeutic effect.
There are many factors that contribute to the accumulation profile of nanoparticles in
cells including the physico-chemical properties of the nanoparticles (e.g. size,
morphology, surface properties), cell type, concentration of the nanoparticles, and
incubation conditions. These factors in turn determine the rate of cell proliferation (i.e.
doubling time), extent and rate of endocytosis of nanoparticles as well as extent and
rate of exocytosis. For instance, previous studies have shown that the size of AuNPs is
an important factor that influences the rate of endocytosis and exocytosis, and thus the
level of cellular accumulation [8, 29]. Chithrani et al. demonstrated that incubation of
HeLa cells with AuNPs of 50 nm in diameter resulted in the highest level of cell
accumulation following a 10 h incubation period, in comparison to AuNPs with
diameters of 14 nm and 74 nm [29]. Despite their small size, the AuNP-TP evaluated in
the current study showed a higher level of cellular accumulation (in HeLa cells) at 8 h
(42 pg/cell) than the 50 nm AuNPs (8 pg/cell) [8].
The time-dependent accumulation profiles of AuNP-TP revealed a peak at 8 h for
all cell lines incubated with AuNP-TP at a concentration of 0.25 mg/mL. A similar trend
was observed in previous studies, wherein peak AuNP accumulation was observed
following 6-10 h of incubation [8, 30]. The initial increase in the cellular level of AuNP-
TP that occurs at the early time point is largely attributed to endocytosis. There are
several factors that may contribute to the decrease in and constant cellular levels of

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 72
AuNP-TP that were achieved at later time points including: endocytosis and exocytosis
of the AuNP-TP that occur simultaneously, cell proliferation, saturation of uptake,
decrease in AuNP-TP dose due to cell uptake and nanoparticle aggregation, and state
of AuNP-TP in the cell culture media. Each of these factors has been considered below.
As shown in Supplementary Figures 2-7 A-D, the total amount of AuNP-TP that
is internalized into cells increases over the 72 h time period. This indicates that cellular
uptake of AuNP-TP occurs throughout the incubation period. In the current study
quantitative analysis of exocytosis was not conducted and therefore the contribution of
exocytosis to the cellular levels of AuNP-TP remains unknown. A previous study by
Chithrani et al. reported that following a 6 h incubation period and a subsequent 8 h
wash out period, approximately 8%, 20%, and 40% of the AuNPs that had been
endocytosed were exocytosed for AuNPs with diameters of 74, 50, and 14 nm,
respectively [29]. One drawback of this study is that exocytosis was only observed
under “washout” conditions, wherein cells are exposed to particle free media.
A recent study by Kim et al. indicates that cell proliferation is the major factor that
leads to dose reduction of NPs in cells [31, 32]. The authors demonstrated constant
levels of NPs throughout the cell cycle until cell division in A549 cells. Indeed in the
current study a comparison between the decrease in the number of AuNP-TP per cell
following the 8-h timepoint and the respective doubling time for each cell line indicates
that cell proliferation plays a significant role. The magnitude of the decrease in number
of AuNP-TP per cell decreased in the following order L929>HeLa>MCF-7>H520. The
doubling times for the cell lines are as follows: L929, 14 h; HeLa, 24 h; MCF-7, 29 h;
H520, 61 h. Therefore it can be seen that the decrease in number of AuNPs per cell is
related to the concomitant increase in cell number.
Given that the peak in the accumulation profile at 8 h is also observed, although
less prominently, for HeLa, MCF-7 and L929 cells incubated with the lower
concentration (0.05 mg/mL) of AuNP-TP, this peak cannot be attributed to saturation of
uptake. In addition at all timepoints it is only a fraction of the AuNP-TP present in
solution that are taken up into cells. Specifically, for L929 cells, which showed the

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 73
highest level of cell uptake following the 8 h incubation period, the amount of
intracellular gold was 54.8 2.7 g, which accounts for only 5.7 wt% of the total gold in
media containing 0.25 mg/mL AuNP-TP. This result suggests that there is always a
signficant excess of AuNP-TP available in the media. Furthermore, as shown in Figure
2-2, E there was no significant difference between the percentage of AuNP-TP that
remain dispersed in the supernatant following 8 and 24 h of incubation. Therefore the
decrease in the cellular level of AuNP-TP that occurs beyond the 8 h timepoint cannot
be attributed to a decrease in the total number of AuNPs available in solution due to
aggregation.
The state of AuNP-TP in the cell culture media could also influence the degree of
cellular uptake. TEM analysis of AuNP-TP following incubation in cell culture media for
24, 48 and 72 h revealed the AuNP-TP that remain in the supernatant retain their size
and are well dispersed in the media. However it is recognized that the size of particles
incubated in cell culture media alone (i.e. in the absence of cells) may not be
representative of their size in all regions of the cell culture wells in the presence of
cells. Based on the literature the relationship between the state of AuNPs in solution
and cell uptake is complex. For example, Cho et al. recently investigated the effects of
aggregation and consequent sedimentation of AuNPs on cell uptake. They
demonstrated that sedimentation leads to a higher concentration of AuNPs in the cell
uptake zone, as a result, a higher uptake was observed in cells in an upright
configuration compared to inverted cells [33]. This observation suggests that the actual
dose of AuNPs in the cell uptake zone is higher than that measured in the supernatant.
Furthermore a study by Albanese et al. demonstrated differential uptake patterns for
single and aggregated NPs in different cell lines. For example, HeLa and A549 cells
showed preferential uptake of single NPs, while uptake of aggregated NPs was
favoured in MDA-MB 435 cells. The authors ascribed this phenomenon to different
mechanisms of cellular uptake being operative in different cell lines. In addition to
receptor-mediated endocytosis, which is a major cell uptake pathway in cell lines such
as A549, receptor independent uptake also plays a significant role in cell lines such as
MDA-MB-435 [28].

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 74
Oxidative stress, which includes ROS generation, is the most established theory
for nanoparticle toxicity [34]. Oxidative stress has been shown to occur in cells following
exposure to nanoparticles of single composition such as silica [35], silver [36],
polystyrene [37], and gold [38]. The highly curved surface of nano-sized particles is said
to result in greater defects in crystal structure, therefore, disrupting the electronic
configuration in the bulk material [34]. These surface properties create reactive electron
donor and acceptor groups which can interact with molecules such as oxygen (O2). For
example, as reviewed by Nel et al. the transfer of an electron from a reactive donor
group at the surface of a nanoparticle to O2 results in the creation of superoxide radicals
[34]. Therefore despite the fact that bulk gold is considered to be chemically inert and
non toxic, AuNPs behave very differently than their bulk counterpart [39].
In this study the clonogenic assay was used to characterize the effect of the
AuNP-TP on cell proliferation. The results showed that cytotoxicity depended on both
the concentration of AuNP-TP and the type of cell line used. Using the MTT assay,
tiopronin was found to be non-toxic in HeLa and MCF-7 cells at a concentration
equivalent to that present on the surface of 0.5 mg/mL AuNP-TP (data not shown). As
well as shown in Figure 2-6 the presence of free tiopronin inhibited ROS generation by
AuNPs. This result confirms that the toxicity of the AuNP-TP cannot be attributed to
tiopronin.
The effect of various thiol-containing antioxidants (i.e. NAC, reduced L-cysteine,
GSH, tiopronin) on reducing ROS production due to AuNP-TP exposure was evaluated.
The intracellular levels of ROS were measured using the DCFH-DA assay [23]. Within
cells, DCFH-DA is hydrolyzed to DCFH by esterase, DCFH is then oxidized to
fluorescent DCF in the presence of ROS, and the fluorescent intensity produced is
proportional to the ROS concentration [40]. Results from the DCFH-DA assay
demonstrated that AuNP-TP induced high levels of ROS following a 24 h exposure, in
comparison to non-treated cells. The increase in ROS following AuNP-TP treatment
explains the toxicities observed for the AuNP-TP at high concentration.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 75
A comparison of relative ROS levels (3.69 0.30 for HeLa and 5.38 0.57 for
L929) and SF (19.0 0.45% for HeLa and 76.7 5.08% for L929) between the HeLa
and L929 cells reveals that the relative ROS level for a specific cell line cannot be used
to predict SF (i.e. a higher relative ROS level does not imply a lower SF). Cellular
response to ROS depends on the cell’s redox potential [41], which is mainly determined
by the intracellular amount of GSH [42]. A previous study has shown that the amount of
intracellular GSH varies between cell lines [43], and therefore the cellular response to
ROS can also vary.
The addition of antioxidants significantly decreased ROS production. There are
two proposed mechanisms that have been put forth for the inhibitory effects of thiol-
containing antioxidants on AuNP induced ROS production [38, 44]. Firstly, thiol
containing antioxidants are able to directly neutralize ROS due to their reducing nature.
Secondly, these agents bind to the AuNPs through Au-S bonds, shielding otherwise
exposed reactive sites, and thus, lowering the catalytic activity of the AuNPs. Findings
in a study by Pan et al. demonstrate that this second mechanism is likely more
important given that a non-thiol-containing antioxidant, ascorbic acid, was unable to
reduce the cytotoxicity of AuNPs while several thiol containing antioxidants were found
to significantly reduce their toxic effects [38].
Importantly, the amount of ROS produced in cells may be overestimated using
the DCFH-DA assay if apoptosis is induced. During apoptosis cytochrome c, a potent
catalyst for oxidation of DCFH [45], is released from mitochondria into the cytoplasm
[38]. In the current study, Z-VAD-fmk, a caspase inhibitor was employed in order to
determine if the observed ROS levels could be in part attributed to apoptosis [46]. The
inability of Z-VAD-fmk to reduce the level of DCF demonstrated that ROS was mainly
responsible for the oxidation of DCFH instead of cytochrome c. This also provides
indirect evidence that the main mechanism of cell death induced by the AuNP-TP is
necrosis and not apoptosis. Other research groups compared the surviving fraction of
cells treated with Z-VAD-fmk combined with AuNPs to that of AuNPs alone and showed
that Z-VAD-fmk did not increase the surviving fraction [38], this further supports that cell
death caused by AuNP exposure occurs by necrosis and not apoptosis.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 76
In this study GSH was found to be one of the most potent antioxidants resulting
in a significant decrease in ROS generation at all timepoints. GSH is an endogenous
antioxidant which protects cells from oxidative stress by lowering membrane lipid
peroxidation [47]. GSH depletion has been observed in cells exposed to nanoparticles
[38, 48-50]. Co-treatment of HeLa cells with GSH and AuNP-TP resulted in a fourfold
increase in the SF, in comparison to cells treated with AuNP-TP alone. These results
confirm that oxidative stress is the key cause of AuNP-TP cytotoxicity
.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 77
2.6 Conclusions
To sum up, gold in the form of nanoparticles can be customized for use in a
variety of applications by altering size, morphology and surface properties. In this study
AuNP-TP of 2.7 nm diameter were synthesized and characterized. To our knowledge,
this is the first time that the neoplastic cell response to AuNP-TP has been evaluated.
The mechanism of cytotoxicity of the AuNP-TP was found to be ROS generation.
Furthermore, antioxidants effectively inhibited ROS and reduced the cytotoxicity of the
AuNP-TP. Overall, the cellular accumulation; cytotoxicity and ROS production of the
AuNP-TP were shown to be time, concentration and cell line dependent. Future studies
will focus on evaluating the in vivo distribution of the AuNP-TP at the whole-body, tissue
and cellular levels.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 78
2.7 Supporting Information
2.7.1 Preparation and Characterization of AuNP-TP
All chemicals were purchased from Sigma-Aldrich (Oakville, Canada) and used
as received unless otherwise noted. AuNP-TP were synthesized through a reduction
reaction using tiopronin as the surfactant as previously described [16], and the product
was characterized in terms of size, purity, and stability. Briefly, 0.4 mmol of HAuCl4 ·
3H2O and 1.2 mmol of N-(2-mercaptopropionyl) glycine (i.e. tiopronin) were dissolved in
20 mL of 6:1 (v/v) mixture of methanol and acetic acid. Following this, 8.0 mmol of
NaBH4 dissolved in 7.5 mL of dd-H2O was added to the solution, and the reaction
mixture was left at room temperature for 30 minutes. The solvent was then removed
under vacuum at 40°C using a rotary evaporator. The final product was dissolved in 20
mL of dd-H2O with pH adjusted to 1 using concentrated HCl, then dialyzed against
excess dd-H2O for 72 h to remove unreacted reagents and finally lyophilized.
The purity of the AuNP-TP was verified using 1H NMR. 0.5 mg/mL of the AuNP-
TP dissolved in D2O was subjected to an Oxford 400 spectrometer (400 MHz). Chemical
shifts were reported in ppm relative to the residual signal of the solvent. The
morphology and size of AuNP-TP were assessed using TEM. Samples for TEM
analysis were prepared by suspending AuNP-TP in dd-H2O at a concentration of 0.01
mg/mL. 10 L of each sample was placed onto carbon-coated copper grids; air dried
and then imaged using a Hitachi H7000 TEM (Hitachi Corp., Tokyo, Japan) operated at
100 KeV. The core size distribution of the AuNP-TP was evaluated by analysis of 1200
particles using ImageJ software (NIH, Bethesda, USA).
The coating efficiency of tiopronin, i.e., the percentage of gold atoms at the
surface of the NPs that are coated with TP was evaluated using ICP-AES. Briefly, 5mL
of 0.1 mg/mL AuNP-TP in dd-H2O was evaluated by ICP-AES to determine the mass of
Au. The mass of TP was then calculated by subtracting the mass of Au from total mass
of AuNP-TP. The mass ratio of Au and TP was converted to molar ratio by dividing by

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 79
the molecular weight of Au and tiopronin, which are 197g/mol and 163 g/mol,
respectively.
The number of Au atoms (U) per AuNP was determined using the following
equation [8]:
U= 2/3 π (D/a)3
where D is the core diameter of the AuNP-TP and a is the edge of a unit cell
which has a value of 4.08 Å .
For AuNPs of 2.7 nm, U = 2/3 π (27/4.08) 3 = 600
The number of Au atoms at the surface (Ns) of the AuNP was calculated using
the following equation:
Ns = 4 U 2/3 = 4(600) 2/3 = 235
The number of TP per AuNP-TP was determined by the molar ratio of Au atoms
to TP and U. Finally, the coating efficiency was obtained by dividing Ns by the number of
TP per AuNP-TP.
The stability of the AuNP-TP in dd-H2O was assessed by incubation in the latter
for up to two weeks with analysis by ultraviolet–visible (UV-vis) spectroscopy (UltraSpec
2100 Pro UV/Visible spectrophotometer). The absorption spectrum of the AuNP-TP in
dd-H2O was recorded in the wavelength range of 200 to 800 nm.
To evaluate the stability of AuNP-TP in cell culture media, 0.25mg/mL AuNPs -TP
suspended in DMEM containing 10% (v/v) serum were incubated at 37ºC and after 1, 4,
8, 24, 48, and 72 h, samples of 0.5mL were collected from the supernatant. The sample
was digested in a 1:1 mixture of HCl and HNO3, and subjected to ICP-AES. The results
were reported as percentage of Au that remains in the supernatant versus incubation
time (Figure 2-2 E). As well, AuNP-TP remaining in the supernatant were analyzed
using a TEM. After 24, 48, and 72 h of incubation, 10 L samples were collected from

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 80
the supernatant, placed onto carbon-coated copper grids; air dried and then imaged
using a TEM operated at 100 KeV (Figures 2-2 F, 2-2 G, 2-2 H).
2.7.2 Cell Culture
MCF-7 breast cancer cells, HeLa cervical cancer cells, H520 lung cancer cells
and L929 mouse fibroblast cells were obtained from the American Type Culture
Collection (Rockville, USA). MCF-7 and HeLa cells were cultured in DMEM media and
H520 and L929 cells were cultured in RPMI 1640 media. Cell culture media was
supplemented with 10% fetal bovine serum and 1% penicillin-streptomycin. Cells were
grown as monolayers at 37°C in 5% CO2 and 90% relative humidity.
2.7.3 Qualitative Assessment of Cellular Accumulation of AuNP-TP
TEM analysis was employed for visualization of the cellular accumulation and
intracellular distribution of AuNP-TP as outlined elsewhere [51]. In brief, cells were
seeded in 6-well plates at a density of approximately 1x106 cells/well. Cells were treated
for 24 h with 0.25 mg/mL of AuNP-TP suspended in cell media. Following this, cells
were washed twice with PBS, fixed and sectioned. Each section was placed onto
copper grids, and visualized by TEM.
2.7.4 Calculation of Number of AuNP-TP Accumulated in Cells
The amount of Au per cell was measured by ICP-AES in terms of pg/cell, the
amount was converted to moles by dividing by the molecular weight of Au, which is
197g/mol. The total number of Au atoms per cell was then calculated by multiplying the
number of moles of Au atoms by Avogadro’s number. Finally, the number of AuNP-TP
(N) was calculated based on the total number of Au atoms (M) divided by the number of
Au atoms per AuNP (U):

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 81
N= M/U
For AuNPs of 2.7 nm, U = 600
2.7.5 Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social
Sciences V16.0 (SPSS Inc., USA). A two-sample t-test was used to measure statistical
significance between pairs of results. For statistical analyses among three or more
groups, one-way analysis of variance (ANOVA) was used and subsequent multiple
comparisons with Bonferroni correction was performed if any statistical significance was
detected by the ANOVA F-test. A p-value < 0.05 was considered to be significant.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 82
Figure 2-7: In vitro cellular level of AuNP-TP in (A) MCF-7, (B) HeLa, (C) H520, and (D)
L929 cells quantified by ICP-AES with incubation at two different concentrations (i.e.,
0.05 and 0.25 mg/mL) of AuNP-TP. * Represents statistically significant difference in
cell accumulation at that timepoint in comparison to its previous timepoint. Data
represents mean SD (n=3).

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 83
2.8 Acknowledgements
This research was funded by an operating grant from CIHR to D.A. Jaffray, R.
Bristow and C. Allen.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 84
2.9 References
1. Shi JJ, Votruba AR, Farokhzad OC, Langer R. Nanotechnology in Drug Delivery and Tissue Engineering: From Discovery to Applications. Nano Lett 2010;10:3223-3230.
2. Sperling RA, Rivera gil P, Zhang F, Zanella M, Parak WJ. Biological Applications of Gold Nanoparticles. Chem Soc Rev 2008;37:1896-1908.
3. Huang XH, Jain PK, El-Sayed IH, El-Sayed MA. Gold Nanoparticles: Interesting Optical Properties and Recent Applications in Cancer Diagnostic and Therapy. Nanomedicine 2007;2:681-693.
4. Hainfeld JF, Dilmanian FA, Slatkin DN, Smilowitz HM. Radiotherapy Enhancement with Gold Nanoparticles. Journal of Pharmacy and Pharmacology 2008;60:977-985.
5. Jain PK, Lee KS, El-Sayed IH, El-Sayed MA. Calculated Absorption and Scattering Properties of Gold Nanoparticles of Different Size, Shape, and Composition: Applications in Biological Imaging and Biomedicine. J Phys Chem B 2006;110:7238-7248.
6. Zhang G, Yang Z, Lu W, Zhang R, Huang Q, Tian M, et al. Influence of Anchoring Ligands and Particle Size on the Colloidal Stability and in Vivo Biodistribution of Polyethylene Glycol-Coated Gold Nanoparticles in Tumor-Xenografted Mice. Biomaterials 2009;30:1928-1936.
7. Hainfeld JF, Slatkin DN, Smilowitz HM. The Use of Gold Nanoparticles to Enhance Radiotherapy in Mice. Phys Med Biol 2004;49:N309-N315.
8. Chithrani BD, Ghazani AA, Chan WCW. Determining the Size and Shape Dependence of Gold Nanoparticle Uptake into Mammalian Cells. Nano Lett 2006;6:662-668.
9. Mironava T, Hadjiargyrou M, Simon M, Jurukovski V, Rafailovich MH. Gold Nanoparticles Cellular Toxicity and Recovery: Effect of Size, Concentration and Exposure Time. Nanotoxicology 2010;4:120-137.
10. Malugin A, Ghandehari H. Cellular Uptake and Toxicity of Gold Nanoparticles in Prostate Cancer Cells: A Comparative Study of Rods and Spheres. J Appl Toxicol 2010;30:212-217.
11. Li SD, Huang L. Pharmacokinetics and Biodistribution of Nanoparticles. Mol Pharm 2008;5:496-504.
12. Goodman TT, Chen JY, Matveev K, Pun SH. Spatio-Temporal Modeling of Nanoparticle Delivery to Multicellular Tumor Spheroids. Biotechnol Bioeng 2008;101:388-399.
13. Gupta AK, Gupta M. Synthesis and Surface Engineering of Iron Oxide Nanoparticles for Biomedical Applications. Biomaterials 2005;26:3995-4021.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 85
14. Otsuka H, Nagasaki Y, Kataoka K. Pegylated Nanoparticles for Biological and Pharmaceutical Applications. Adv Drug Deliv Rev 2003;55:403-419.
15. Johnston HJ, Hutchison G, Christensen FM, Peters S, Hankin S, Stone V. A Review of the in Vivo and in Vitro Toxicity of Silver and Gold Particulates: Particle Attributes and Biological Mechanisms Responsible for the Observed Toxicity. Crit Rev Toxicol 2010;40:328-346.
16. Templeton AC, Chen SW, Gross SM, Murray RW. Water-Soluble, Isolable Gold Clusters Protected by Tiopronin and Coenzyme a Monolayers. Langmuir 1999;15:66-76.
17. Rodriguez JA, Dvorak J, Jirsak T, Liu G, Hrbek J, Aray Y, et al. Coverage Effects and the Nature of the Metal-Sulfur Bond in S/Au(111): High-Resolution Photoemission and Density-Functional Studies. J Am Chem Soc 2003;125:276-285.
18. Templeton AC, Cliffel DE, R.W. M. Redox and Fluorophore Functionalization Pf Water-Soluble, Tiopronin-Protected Gold Clusters. J Am Chem Soc 1999;121:7081-7089.
19. de la Fuente JM, Berry CC. Tat Peptide as an Efficient Molecule to Translocate Gold Nanoparticles into the Cell Nucleus. Bioconjugate Chem 2005;16:1176-1180.
20. Cai X, Chen HH, Wang CL, Chen ST, Lai SF, Chien CC, et al. Imaging the Cellular Uptake of Tiopronin-Modified Gold Nanoparticles. Anal Bioanal Chem 2011;401:809-816.
21. De Souza R, Zahedi P, Moriyama EH, Allen CJ, Wilson BC, Piquette-Miller M. Continuous Docetaxel Chemotherapy Improves Therapeutic Efficacy in Murine Models of Ovarian Cancer. Mol Cancer Ther 2010;9:1820-1830.
22. Franken NA, Rodermond HM, Stap J, Haveman J, van Bree C. Clonogenic Assay of Cells in Vitro. Nat Protoc 2006;1:2315-2319.
23. Wang H, Joseph JA. Quantifying Cellular Oxidative Stress by Dichlorofluorescein Assay Using Microplate Reader. Free Radic Biol Med 1999;27:612-616.
24. Levy R, Shaheen U, Cesbron Y, See V. Gold Nanoparticles Delivery in Mammalian Live Cells: A Critical Review. Nano Rev 2010;1.
25. Hussain I, Graham S, Wang Z, Tan B, Sherrington DC, Rannard SP, et al. Size-Controlled Synthesis of near-Monodisperse Gold Nanoparticles in the 1-4 Nm Range Using Polymeric Stabilizers. J Am Chem Soc 2005;127:16398-16399.
26. Daniel MC, Astruc D. Gold Nanoparticles: Assembly, Supramolecular Chemistry, Quantum-Size-Related Properties, and Applications toward Biology, Catalysis, and Nanotechnology. Chem Rev 2004;104:293-346.
27. Haiss W, Thanh NT, Aveyard J, Fernig DG. Determination of Size and Concentration of Gold Nanoparticles from Uv-Vis Spectra. Anal Chem 2007;79:4215-4221.
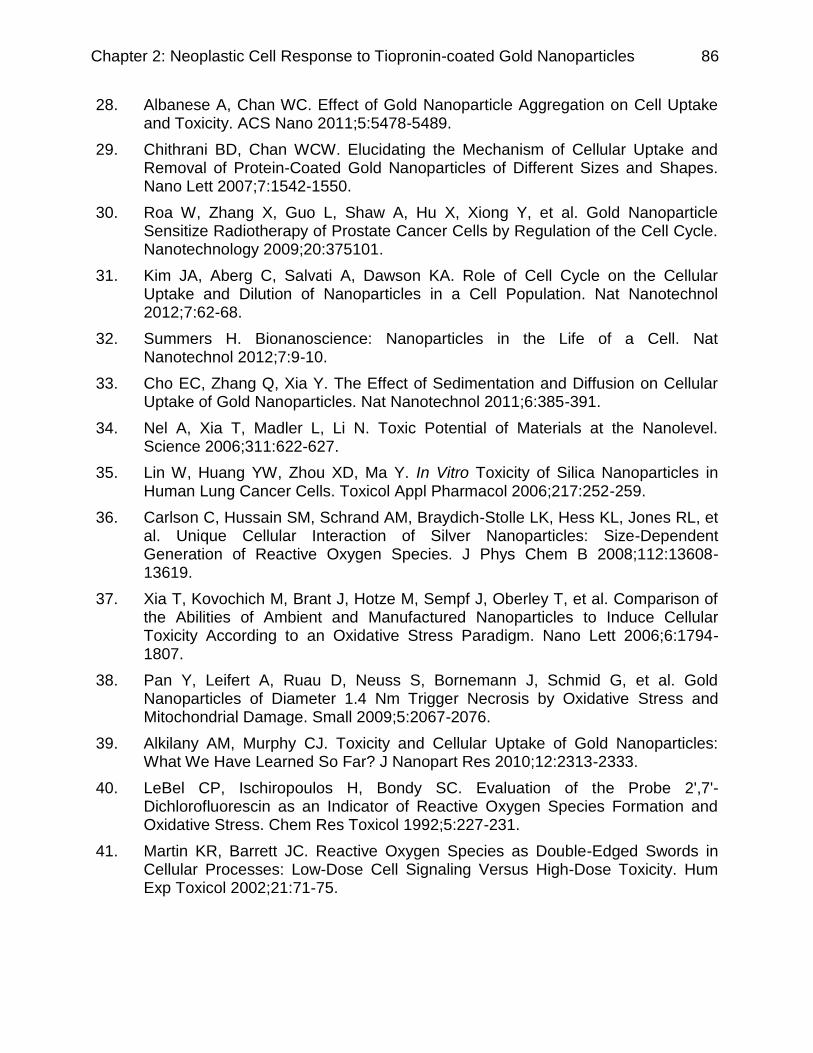
Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 86
28. Albanese A, Chan WC. Effect of Gold Nanoparticle Aggregation on Cell Uptake and Toxicity. ACS Nano 2011;5:5478-5489.
29. Chithrani BD, Chan WCW. Elucidating the Mechanism of Cellular Uptake and Removal of Protein-Coated Gold Nanoparticles of Different Sizes and Shapes. Nano Lett 2007;7:1542-1550.
30. Roa W, Zhang X, Guo L, Shaw A, Hu X, Xiong Y, et al. Gold Nanoparticle Sensitize Radiotherapy of Prostate Cancer Cells by Regulation of the Cell Cycle. Nanotechnology 2009;20:375101.
31. Kim JA, Aberg C, Salvati A, Dawson KA. Role of Cell Cycle on the Cellular Uptake and Dilution of Nanoparticles in a Cell Population. Nat Nanotechnol 2012;7:62-68.
32. Summers H. Bionanoscience: Nanoparticles in the Life of a Cell. Nat Nanotechnol 2012;7:9-10.
33. Cho EC, Zhang Q, Xia Y. The Effect of Sedimentation and Diffusion on Cellular Uptake of Gold Nanoparticles. Nat Nanotechnol 2011;6:385-391.
34. Nel A, Xia T, Madler L, Li N. Toxic Potential of Materials at the Nanolevel. Science 2006;311:622-627.
35. Lin W, Huang YW, Zhou XD, Ma Y. In Vitro Toxicity of Silica Nanoparticles in Human Lung Cancer Cells. Toxicol Appl Pharmacol 2006;217:252-259.
36. Carlson C, Hussain SM, Schrand AM, Braydich-Stolle LK, Hess KL, Jones RL, et al. Unique Cellular Interaction of Silver Nanoparticles: Size-Dependent Generation of Reactive Oxygen Species. J Phys Chem B 2008;112:13608-13619.
37. Xia T, Kovochich M, Brant J, Hotze M, Sempf J, Oberley T, et al. Comparison of the Abilities of Ambient and Manufactured Nanoparticles to Induce Cellular Toxicity According to an Oxidative Stress Paradigm. Nano Lett 2006;6:1794-1807.
38. Pan Y, Leifert A, Ruau D, Neuss S, Bornemann J, Schmid G, et al. Gold Nanoparticles of Diameter 1.4 Nm Trigger Necrosis by Oxidative Stress and Mitochondrial Damage. Small 2009;5:2067-2076.
39. Alkilany AM, Murphy CJ. Toxicity and Cellular Uptake of Gold Nanoparticles: What We Have Learned So Far? J Nanopart Res 2010;12:2313-2333.
40. LeBel CP, Ischiropoulos H, Bondy SC. Evaluation of the Probe 2',7'-Dichlorofluorescin as an Indicator of Reactive Oxygen Species Formation and Oxidative Stress. Chem Res Toxicol 1992;5:227-231.
41. Martin KR, Barrett JC. Reactive Oxygen Species as Double-Edged Swords in Cellular Processes: Low-Dose Cell Signaling Versus High-Dose Toxicity. Hum Exp Toxicol 2002;21:71-75.

Chapter 2: Neoplastic Cell Response to Tiopronin-coated Gold Nanoparticles 87
42. Schafer FQ, Buettner GR. Redox Environment of the Cell as Viewed through the Redox State of the Glutathione Disulfide/Glutathione Couple. Free Radic Biol Med 2001;30:1191-1212.
43. Parmentier C, Wellman M, Leroy P, Nicolas A. Measurement of Glutathione Redox Status and Related Enzyme Activities in Cultured Cells by Liquid Chromatography. Paris: John Libbey CIC; 1997.
44. Zhao Y. GX, Ma H., He X., Liu M., Ding Y. Association of Glutathione Level and Cytotoxicity of Gold Nanoparticles in Lung Cancer Cells. J Phys Chem 2011;115:12797-12802.
45. Burkitt MJ, Wardman P. Cytochrome C Is a Potent Catalyst of Dichlorofluorescin Oxidation: Implications for the Role of Reactive Oxygen Species in Apoptosis. Biochem Biophys Res Commun 2001;282:329-333.
46. Hirsch T, Marchetti P, Susin SA, Dallaporta B, Zamzami N, Marzo I, et al. The Apoptosis-Necrosis Paradox. Apoptogenic Proteases Activated after Mitochondrial Permeability Transition Determine the Mode of Cell Death. Oncogene 1997;15:1573-1581.
47. Kerksick C, Willoughby D. The Antioxidant Role of Glutathione and N-Acetyl-Cysteine Supplements and Exercise-Induced Oxidative Stress. J Int Soc Sports Nutr 2005;2:38-44.
48. Gao W, Xu K, Ji L, Tang B. Effect of Gold Nanoparticles on Glutathione Depletion-Induced Hydrogen Peroxide Generation and Apoptosis in Hl7702 Cells. Toxicol Lett 2011;205:86-95.
49. Hussain SM, Hess KL, Gearhart JM, Geiss KT, Schlager JJ. In Vitro Toxicity of Nanoparticles in Brl 3a Rat Liver Cells. Toxicol In Vitro 2005;19:975-983.
50. Radu M, Munteanu MC, Petrache S, Serban AI, Dinu D, Hermenean A, et al. Depletion of Intracellular Glutathione and Increased Lipid Peroxidation Mediate Cytotoxicity of Hematite Nanoparticles in Mrc-5 Cells. Acta Biochim Pol 2010;57:355-360.
51. Chithrani BD, Stewart J, Allen C, Jaffray DA. Intracellular Uptake, Transport, and Processing of Nanostructures in Cancer Cells. Nanomedicine 2009;5:118-127.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 88
Chapter 3
Hypoxia and Cellular Localization Influence the Radiosensitizing Effect of
Gold Nanoparticles (AuNPs) in Breast Cancer Cells
Lei Cui, Kenneth Tse, Payam Zahedi, Shane M. Harding, Gaetano Zafarana,
David A. Jaffray, Robert G. Bristow, and Christine Allen
Reprint from Radiation Research Society (2014)
DOI: 10.1667/RR13642.1
Experiments by L.Cui and K.Tse (Figure 3-7 C). Written by L.Cui. Figures by L.Cui.
Edited by D.A. Jaffray, R.G. Bristow, and C. Allen.
The copyright of this article belongs to Radiation Research Society, the publisher of
Radiation Research. Permission had to be requested for publishing the article as part of
this dissertation, which was obtained.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 89
3.1 Abstract
Hypoxia exists in all solid tumors and leads to clinical radioresistance and
adverse prognosis. We hypothesized that hypoxia and cellular localization of gold
nanoparticles (AuNPs) could be modifiers of AuNP-mediated radiosensitization. The
possible mechanistic effect of AuNPs on cell cycle distribution and DNA double-strand
break (DSB) repair post-irradiation were also studied. Clonogenic survival data revealed
that internalized and extracellular AuNPs at 0.5 mg/mL resulted in dose enhancement
factors of 1.39±0.07 and 1.09±0.01, respectively. Radiosensitization by AuNPs was
greatest in cells under oxia, followed by chronic and then acute hypoxia. The presence
of AuNPs inhibited post-irradiation DNA DSB repair, but did not lead to cell cycle
synchronization. The relative radiosensitivity of chronic hypoxic cells is attributed to
defective DSB repair (homologous recombination) due to decreased (RAD51)-
associated protein expression. Our results support further study of AuNPs for clinical
development in cancer therapy as their efficacy is not limited in chronic hypoxic cells.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 90
3.2 Introduction
Radiation therapy (RT) is a critical component in the management of over half of
all cancer patients [1, 2]. Two of the major challenges that limit the efficacy of RT
include (a) the need to limit dose to spare surrounding healthy tissue [3], and (b)
radiation resistance of hypoxic cells in solid tumors [4]. Recent physical targeting
advancements such as image guidance and intensity modulation have allowed higher
RT dose delivery to tumors while avoiding healthy tissues resulting in improvements in
the therapeutic ratio [5]. Radiosensitization is another promising strategy designed to
increase the biological effect of RT in a tumor through concurrent treatment with
chemical sensitizing agents (i.e. radiosensitizers) such as nitroimidazoles [6], cisplatin
[7], iodinated DNA targeting agents [6], and gold nanoparticles (AuNPs) [8].
As put forth originally by Boag, the effect of ionizing radiation (IR) on biological
systems can be divided into three phases: physical, chemical, and biological [1, 9]. The
physical phase is the period in which biological molecules are ionized or excited by
radiation to generate free radicals. In the chemical phase, these highly reactive free
radicals react with other molecules to “restore electronic charge equilibrium” [1]. The
biological phase refers to the stage in which the effects of radiation on cells lead to
events such as irreparable DNA damage, permanent cell cycle arrest, and finally, cell
death [1].
AuNPs were initially recognized as a potent radiosensitizer due to their significantly
larger x-ray cross section (i.e. probability of physical interaction with radiation) in
comparison to soft tissues [10]. The radiosensitizing effects of AuNPs have been
demonstrated both in vitro [11-21] and in vivo [8, 10, 22, 23]. However, the
experimentally determined radiation DEF values for AuNPs in biological systems have
been significantly higher than those predicted by consideration of physical interactions,
alone (i.e. calculations based on mass attenuation or Monte Carlo methods) [24]. As
more studies have been undertaken, it has been realized that as radiosensitizers,
AuNPs are also involved in the chemical phase of radiation [25]. As well, biological
pathways through which AuNPs sensitize radiation have been discovered [15]. These

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 91
additional mechanisms may start to explain the disparity between the experimental
measurements and theoretical predictions of DEF.
Low energy photoelectrons and Auger electrons produced during the physical
interaction between AuNPs and radiation have a short effective range that is on the
nanoscale [26-28]. Indeed, in a study by Kong et al. it was found that the
radiosensitization effect of intracellular AuNPs was more significant than that of AuNPs
associated with the cell membrane [11]. To date, the contribution of extracellular AuNPs
has not been quantitatively assessed. During the chemical phase, a recent study
showed that O2- produced by irradiation can bind to the reactive surface of AuNPs,
forming AuNP-O2- intermediates. These intermediates can then act as a catalyst to
further increase reactive oxygen species (ROS) generation [25], leading to greater cell
kill [19]. As oxygen acts both as a substrate and intermediate in ROS generation, lack of
intratumoral oxygen could theoretically diminish the radiosensitization effect of AuNPs.
Due to the radioresistance of cells under hypoxia it is important to understand the
radiosensitization effect of AuNPs under both oxic and hypoxic conditions. Biological
mechanisms have also been shown to be involved in the radiosensitization effects of
AuNPs [24]. For instance, Roa et al. demonstrated that cell cycle synchronization
caused by AuNPs was the mechanism underlying their radiosensitization, although this
phenomenon has not been observed widely [15]. To this point, the effects of hypoxia,
DNA repair and cell cycle on AuNP-associated radiosensitization have not
simultaneously been reported within a specific tumor cell model.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 92
Figure 3-1: AuNPs are involved as radiosensitizers in the physical, chemical, and
biological phases of the effects of radiation on cells. (Timescale adapted from Joiner
and van der Kogel, 2009. [1])
As shown in Figure 3-1 the aim of the present study was to evaluate aspects of
the three phases of the effects of radiation on cells with AuNPs as a radiosensitizer.
Due to the reported ease of penetration of small sized nanoparticles in the tumor
interstitium, relative to larger particles [29], AuNPs with an average diameter of 2.7nm
were employed. Their radiosensitizing effect was assessed in the human breast cancer
cell line MDA-MB-231, which has been used extensively in previous studies
investigating AuNPs as a radiosensitizer [16, 20]. Specifically, the influence of the
cellular localization of AuNPs on their radiosensitizing effect was determined. Given that
cell uptake of nanoparticles relies greatly on energy dependent endocytosis [30], which
can be impeded under hypoxia [31], uptake of AuNPs was evaluated under both oxic
and hypoxic conditions. In addition, the radiosensitization effect of AuNPs was

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 93
compared under these conditions. To the best of our knowledge, this is the first report of
the radiosensitization effects of AuNPs under oxia and hypoxia. Lastly, the effects of
these AuNPs on cell cycle distribution and irradiation induced DNA double strand
breaks (DSB) were evaluated.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 94
3.3 Methods
All chemicals were purchased from Sigma Aldrich (Oakville, Canada) and used
as received unless otherwise noted.
3.1.1 Preparation and Characterization of AuNPs
Materials and methods used for the preparation and characterization of the
AuNPs can be found in our previous report [32]. In brief, AuNPs with an average
diameter of 2.7nm were prepared by reducing Au3+ using NaBH4 as the reducing agent,
and tiopronin as the surfactant. The purity of the AuNPs was verified using 1H NMR and
the morphology and size were assessed by transmission electron microscope (TEM)
analysis. The stability of AuNPs in water and cell culture media were evaluated using
inductively coupled plasma atomic emission spectroscopy (ICP-AES) and TEM analysis
[32].
3.1.2 Cell Culture and Hypoxia
MDA-MB-231 breast cancer cells were obtained from the American Type Culture
Collection (Rockville, USA). Cells were cultured in DMEM/HAM F12 1:1 MIX media. The
cell culture media was supplemented with 10% fetal bovine serum and 1% penicillin-
streptomycin. Cells were grown as monolayers at 37°C in 5% CO2 and 90% relative
humidity. In order to achieve acute or chronic hypoxia, cells were plated under oxia and
incubated for 24 h prior to transfer to a hypoxia chamber with 0.2% O2 for 4 or 72 h
incubation, respectively [33].
3.1.3 Quantitative Assessment of the Cellular Accumulation of AuNPs
For quantitative analysis of cellular accumulation, cells (1x106 cells/well, 6 well
plates) were treated with two different concentrations of AuNPs (0.25 and 0.5 mg/mL,
which is equivalent to 1.61 and 3.21 M, respectively) for 1, 4, 8, 16, 24, or 48 h. At

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 95
each time point cell media was removed, cells were washed three times with PBS and
then harvested with 0.25% trypsin. Cells were counted using a haemocytometer,
centrifuged to a pellet, digested with HNO3 at 90°C for 60 mins, and diluted with dd-
H2O. The amount of Au was measured by ICP-AES, and normalized to the number of
cells in each sample. The results were reported as the amount of Au (pg) per cell. For
concentration dependent uptake, cells (under oxia, acute hypoxia and chronic hypoxia)
were treated with different concentrations of AuNPs (0.01 – 1mg/mL) for 4 h, and the
amount of Au was evaluated by ICP-AES analysis.
3.1.4 Qualitative Assessment of the Cellular Accumulation of AuNPs
TEM was employed for visualization of the cellular accumulation and intracellular
distribution of the AuNPs as outlined elsewhere [34]. In short, cells were plated into 6-
well plates at a density of 1x106 cells/plate. Following 24 h of incubation, cells were
treated with 0.5 mg/mL AuNPs in cell media. At different time points (20 min, 1 h or 4 h)
cells were washed twice with PBS, fixed and sectioned. Each section was placed onto a
copper grid, and imaged by TEM. Alternatively, cells were transferred to the hypoxia
chamber and incubated for 4 (acute hypoxia) or 72 h (chronic hypoxia), treated with a
0.5 mg/mL AuNP solution for 4 h, washed, fixed, and sectioned for TEM analysis.
3.1.5 Radiation Source and Dose Calculations for Cell Irradiation Studies
The energies used were obtained from a Gulmay D3225 orthovoltage unit at
dose rates of 3.47 Gy/min at 225 kVp, or 2.97 Gy/min at 225 kVp for experiments
investigating radiosensitization under hypoxia. Dose calculations for cell irradiation were
performed as previously described [34].
3.1.6 Clonogenic Survival Assays
Cell survival was evaluated by clonogenic assay as described previously [35]. In
brief, cells were plated in 6-well plates at a density of 1x106 (unless otherwise noted)

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 96
and incubated for 24 h prior to treatment. Following treatment (e.g. addition of AuNPs
and/or IR), cells were washed twice with PBS and trypsinized. For each treatment, cells
were counted and seeded into cell culture dishes at different cell densities to produce
an appropriate number of colonies. After 14 days, the colonies were fixed and stained
with 1% methylene blue in 50% ethanol. The number of colonies (at least 50 cells) was
counted. The cell surviving fraction (SF) was expressed as the plating efficiency
achieved with treatment in comparison to that for non-treated cells [1].
3.1.7 Cytotoxicity and Radiosensitizing Effects of AuNPs under Oxia
To evaluate the cytotoxicity of the AuNPs, cells were treated with various
concentrations of AuNPs (0 - 2.0 mg/mL) suspended in cell culture media. After 4, 8, or
24 h of incubation, cells were seeded for clonogenic assessment. SF of each treatment
group was reported.
To characterize the influence of the concentration of AuNPs on their
radiosensitizing effect, cells were treated with various concentrations of AuNPs (0-1.0
mg/mL). Following 4 h of incubation, cells were exposed to irradiation (4Gy) and seeded
for clonogenic assays. The results were plotted as SF ratio using the following equation:
(1)
where SFIR+AuNPs represents the SF of cells treated with AuNPs prior to irradiation,
SFAuNPs is the SF of cells treated with AuNPs alone, and SFIR represents the SF of cells
treated with irradiation alone. SFAuNPs was included in the equation to exclude the toxic
effect of AuNPs.
The impact of incubation time on the radiosensitizing effect of the AuNPs was
investigated. Following plating and incubation, the cell culture media was replaced with
fresh media containing 0 or 0.25 mg/mL of AuNPs. Cells were exposed to irradiation (0,
2, 4, 6 Gy) post 20 min, 1, 4, 8, 16, or 24 h of incubation with the AuNPs. Survival
curves were produced for each time point with or without pre-treatment with AuNPs.
IR+AuN AuNPsPsrati
R
o
I
/SFSFSF
SF

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 97
The data were fitted with a linear-quadratic model: SF = exp (-αD-βD2), as previously
reported [17]. The DEF of the AuNPs was calculated as the ratio of the radiation doses
which resulted in 0.1 SF with or without AuNPs [17].
For studies assessing the dependence of the radiosensitizing effect of AuNPs on
their localization with respect to cells (i.e. intracellular or extracellular; illustrated in
Figure 3-6 A), four treatment groups were used: (1) Control (no AuNPs); (2) AuNPs (0.5
mg/mL) added to cells immediately prior to irradiation; (3) cells pretreated with 0.5
mg/mL AuNPs for 4 h, washed twice with PBS, cell media replaced with fresh media
without AuNPs followed by irradiation; and (4), cells pretreated with 0.5 mg/mL AuNPs
for 4 h then exposed to irradiation with the AuNPs remaining in the cell media. For all
treatment groups, cells were kept on ice prior to addition or removal of AuNPs to avoid
energy-dependent endo- or exocytosis. Cells were then irradiated at 0, 2, 4 and 6 Gy
for colony formation and calculation of clonogenic survival. Final survival curve data was
fitted to the linear-quadratic model of cell kill.
3.1.8 Radiosensitizing Effects of AuNPs under Acute and Chronic Hypoxia
Hypoxia in solid tumors can exist as acute or “cycling” hypoxia due to altering
and dynamic flow in blood vessels (in which cells undergo cycles of hypoxia and re-
oxygenation over minutes to h) and chronic or diffusion-limited hypoxia as a function of
proliferation and increasing distance from blood vasculature (lasting h to days) [36, 37].
To evaluate the effect of different types of hypoxic conditions on the radiosensitizing
effect of the AuNPs, five different experimental conditions were used [38]: (1) incubation
and irradiation under oxia (oxiaoxia); (2) incubation under chronic hypoxia and
irradiation under hypoxia (chronic hypoxiahypoxia); (3) incubation under chronic
hypoxia followed by reoxygenation and irradiation under oxia (chronic hypoxiaoxia);
(4) incubation under acute hypoxia and irradiation under hypoxia (acute
hypoxiahypoxia); and (5), incubation under acute hypoxia followed by reoxygenation
and irradiation under oxia (acute hypoxiaoxia). Cells were seeded in 6-well plates at a
density of 0.3x106 or 1x106 cells/well, following 24 h of incubation under oxia, the plates
containing 1x106 cells were transferred to the hypoxia chamber. After 72 h, the plates

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 98
originally containing 0.3x106 cells were transferred into the same hypoxia chamber. For
both groups, cell culture media was replaced with fresh media (pre-degassed in the
hypoxia chamber) containing 0 or 0.5 mg/mL AuNPs, and the cells were further
incubated in the chamber for an additional 4 h. In parallel, another group of cells was
incubated with AuNPs under oxia. For the hypoxiahypoxia group, hypoxia was
maintained during irradiation by enclosing plates within a container degassed in the
hypoxia chamber that was completely sealed. For the hypoxiaoxia group, cells were
exposed to air for reoxygenation 10-15 min prior to irradiation [39, 40]. Following 5 Gy
irradiation, cell survival was evaluated by clonogenic assay. The radiosensitizing effects
were calculated as SF ratios, as described above in Equation (1).
The influence of oxygen on radiation was calculated in two different ways. In one
approach the SF of the hypoxiahypoxia treatment group was compared to that of the
oxiaoxia group. In another approach the SF of the hypoxiahypoxia treatment group
was compared to that of the hypoxiaoxia group. In the current study, Oxygen
enhancement ratios (O,E,R.) of Cell Kill 1 and 2 (i.e. OER-K1 and OER-K2) were used
to describe the effects of oxygen and hypoxia on radiation cell kill as follows:
hypoxia hypoxia
oxia oxia
SFOER-K1 =
SF
(2)
hypoxia hypoxia
hypoxia oxia
SFOER-K2 =
SF (3)
where SFhypoxiahypoxia, SFoxia oxia and SFhypoxiaoxia refer to the SF of cells following
irradiation for the hypoxiahypoxia, oxiaoxia, and hypoxiaoxia groups, respectively.
3.1.9 Western Blot Analysis
Cells were seeded in 15 cm tissue culture dishes at densities of 2x106 or 6x106
cells/dish. Following incubation under oxia, the dish with 6x106 cells was transferred to

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 99
the hypoxia chamber. After 72 h, the dish originally containing 2x106 cells were
transferred into the same hypoxia chamber. For the latter group, the cell culture media
was replaced with pre-degassed fresh media. Following an additional 4 h of incubation
under hypoxia, the cells were washed with degassed PBS, and collected using a cell
scraper. The cells were lysed using a lysis buffer (50 mM TRIS-HCl pH 7.5/150 mM
NaCl / 1mM EDTA/1% NP40 / 1unit/mL benzonase]) (Novagen, Billerica, US) containing
protease (1mM Benzamidine hydrochloride hydrate / 1μg/mL antipain / 5μg/mL aprotinin
/ 1μg/mL leupeptin / 1mM Phenylmethanesulfonyl fluoride) and phosphatase (10mM
sodium fluoride / 2 mM imidazole / 1.15 mM sodium molybdate / 4 mM sodium tartrate /
2 mM Sodium Pyrophosphate / 2mM β-Glycerophosphate / 2 mM sodium
orthovanadate) inhibitors [39]. For western blots, a 8% running gel was cast (8% 37.5:1
acrylamide bisacrylamide / 200 mM pH 7.0 TRIS-acetate buffer / 0.75 mg/mL-1
ammonium persulfate/0.125% TEMED), and overlayed with 6% stacking gel. 15 L of
sample in the sample buffer solution (6% glycerol/ 0.83% β-mercaptoethanol / 1.71%
SDS / 0.058M Tris-HCl pH 6.8 / 0.002% Bromophenol Blue) was loaded into each well.
Gels were run at 100 V in TRIS-acetate running buffer (50mM Tricine/50 mM Tris / 0.1%
SDS / 5mM sodium bisulfite). The proteins were then transferred onto a PVDF
membrane in transfer buffer (0.145% Tris / 0.72% glycine / 25% methanol) at 25 V and
100 mA in an ice packed bucket for 1 h. The membrane was blocked in Odyssey
blocking buffer for 1 h, and incubated in primary antibodies (Rad51 (H-92) sc-8349,
Rabbit polyclonal IgG; Ku70 (A-9) sc-5309, Mouse monoclonal IgG2a) (Santa Cruz
Biotechnology, Santa Cruz, CA) 1000 times diluted in TBS/ 0.1% Tween 20 overnight at
4°C. Following wash, the membrane was incubated in secondary antibodies (Donkey
anti-rabbit IR dye ® 800 CW 926-32213, Donkey anti-mouse IR dye ® 680 926-32222)
(LI-COR, Lincoln, US) which were diluted 20,000 fold in Odyssey Blocking Buffer
containing 0.1% Tween 20. After washing with 0.1% Tween 20 in TBS, blots were
imaged using the Odyssey scanner, and densitometry was conducted using an
Odyssey IRImaging System (LICORBioscience). The total amount of proteins in each
sample was normalized to 1 by the amount Ku70, and the amount of Rad51 was
normalized to the total amount of proteins.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 100
3.1.10 Cell Cycle Analysis
Cells were plated in 6-well plates at a density of 1x106 cells/well. Following 24 h
of incubation, the cell culture media was replaced with fresh media containing no or 0.5
mg/mL AuNPs. BrdU was added to the wells one h prior to fixation at a final
concentration of 50 M and following 1, 4, 8, 16, 24, or 48 h of incubation, cells were
harvested using trypsin. Cells were then centrifuged to a pellet and washed twice with
PBS. The pellet was resuspended in 100 L of PBS and fixed in 5 mL of 75% ethanol.
Fixed cells from early time points were kept at -20°C for storage. After all the samples
were collected, the cells were centrifuged to a pellet, the supernatant was removed and
the pellet was loosened by vortexing. The samples were then incubated in 1 mL of 2 N
HCl with 0.5% Triton X-100 for 30 mins to denature the DNA. The cells were centrifuged
again, and resuspended in 1 mL of 0.1 M Na2B4O7 to neutralize the acid. For each
sample, an aliquot of 106 cells was put into a new tube, centrifuged, and resuspended in
50 L of 0.5% Tween 20 (v/v) plus 1.0% BSA (Rockland antibodies and assays, PA,
USA) (w/v) in PBS. 20 L of anti-BrdU FITC (BD, Mississauga, CA) was added to each
sample and then all the samples were incubated at room temperature for 30 mins in the
dark. The cells were centrifuged, resuspended and incubated in 1 mL of 5 g/mL of PI
(Life Technologies Inc., Burlington, CA) and 10 M of RNAse A in PBS for 15-30 mins.
Cell cycle analysis was performed on a FACS Calibur flow cytometer (Canto II FCF,
BRV), and the data was analyzed using FlowJo software.
3.1.11 Immunofluorescence Assay
The immunofluorescence assay used was previously described [39]. Cells were
seeded onto 18X18 mm glass cover slips in 6-well plates. Following incubation, the cell
culture media was replaced with fresh media containing no or 0.50 mg/mL AuNPs and
incubated for 4 h. Cells were then exposed to irradiation (0, 2, or 4Gy), and further
incubated at 37°C for 30 min or 24 h before fixation. To exclude cells in the S phase,
which contain endogenous DSB, 5-ethynyl-2'-deoxyuridine (EdU) (Invitrogen, Burlington,
CA) was added to the cells at a final concentration of 10 M 1 h prior to fixation [39].

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 101
Cells were washed with PBS and fixed with 4% paraformaldehyde and 0.2% Triton X-
100 in pH 8.2 PBS at room temperature for 20 mins, and were then washed with PBS
and permeabilized with 0.5% Nonidet P40 (NP 40) in PBS. After another rinse with
PBS, cells with incorporated EdU were labeled using the Click-iT EdU Alexa Fluor 647
kit (Invitrogen, Burlington, CA) following the manufacturer’s protocol with slight
modification [39]. Coverslips were inverted onto parafilm containing 50 L of reaction
solution and incubated for 30 mins. The staining was followed by 3 washes with PBS.
Then cells were blocked with 1% normal donkey serum (Jackson Immunoresearch,
PA, USA), 2% BSA (Rockland antibodies and assays, PA, USA) in PBS for an h at
room temperature, and incubated on parafilm with primary antibodies in 3% BSA/PBS at
4°C overnight. The primary antibody used in this study was H2AX (mouse monoclonal,
JBW301 05-636 1:800, Millipore, Billerica, USA). After primary antibody incubation, the
coverslips were washed three times for 5 mins each with 0.175% Tween 20 and 0.5%
BSA in PBS, and then incubated in secondary antibodies, donkey anti-mouse Alexa 488
(Invitrogen, Burlington, CA), on parafilm for 45 mins at room temperature with light
shielding. The coverslips were washed again three times for 5 mins each with 0.175%
Tween 20 and 0.5% BSA in PBS, and incubated in 0.1 g/mL 4',6-diamidino-2-
phenylindole (DAPI, Invitrogen, Burlington, CA) for 10 mins at room temperature. After
rinse with PBS, the coverslips were mounted onto glass slides with Vectashield antifade
(Vector Laboratories, Burlingame, CA).
Cells were imaged as previously described using a 60x oil immersion objective
[41]. For each treatment group, at least 50 nuclei were analyzed using Image Pro Plus
software (Media Cybenetics). For foci counting, cells in their S phase (EdU positive
stain) were excluded, and manually adjusted thresholds were maintained for treatments
groups with or without AuNPs. For samples fixed 30 mins post 4 Gy irradiation, the “top
hat” filter was applied to increase the resolution of foci. Images for publication were
prepared using ImageJ software (NIH). Results are reported as number of foci per
nucleus (Figure 3-9 B) and SEM values represent experiment to experiment variability.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 102
3.1.12 Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social
Sciences V16.0 (SPSS Inc., USA). A two-sample t-test was used to measure statistical
significance between pairs of results. For statistical analyses among three or more
groups, one-way analysis of variance (ANOVA) was used and subsequent multiple
comparisons with Bonferroni correction was performed if any statistical significance was
detected by the ANOVA F-test. A p-value < 0.05 was considered to be significant.
(p<0.05).

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 103
3.4 Results
3.4.1 Cytotoxicity of the AuNPs
Cytotoxicity of AuNPs has been reported by several groups [20, 42, 43],
therefore, an initial study was conducted to identify an optimal concentration of AuNPs
that killed no more than 40 percent of cells to observe an additional effect by IR and
determine clonogenic cell radiosensitization based on combined agent studies. As
shown in Figure 3-2, a concomitant increase in the cytotoxicity of the AuNPs was
observed with both an increase in the concentration of particles and incubation time.
Given that a concentration of 0.5 mg/mL AuNPs showed significantly lower cytotoxicity
relative to higher concentrations (1.0 and 2.0 mg/mL), following a 4 h incubation period,
this concentration was selected for studies examining the influence of localization of
AuNPs on their radiosensitizing effect. A lower concentration of 0.25 mg/mL AuNPs was
selected to investigate time-dependent radiosensitization as it led to no more than 40%
clonogenic kill on its own.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 104
Figure 3-2: Surviving fraction following 4, 8, or 24 h of treatment with different
concentrations of AuNPs. * represents significant difference between groups. Data
represents mean SEM (n=3).
3.4.2 Cellular Accumulation of the AuNPs
The cellular uptake of AuNPs was both concentration- and time-dependent
(Figure 3-3 A). Statistically significant differences (p<0.05) in the cellular levels of
AuNPs were observed at all time points following incubation with the two different
concentrations of particles (0.25 and 0.5 mg/mL). The intracellular level of Au following
20 mins of incubation was below the detectable limit of the ICP method employed for
analysis (Figure 3-3 C). The cellular level of Au was found to increase in the first 8 h of
incubation with a decrease in the ensuing 40 h. Following a 4 h incubation period, the
amount of Au in cells was approximately 5% of the total amount of Au used for
treatment (i.e., 95% of Au remained in the cell culture media) for both concentrations
evaluated.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 105
Results from the concentration dependent uptake studies (Figure 3-3 B) revealed
that for cells under oxia, the level of AuNP cell uptake increased for concentrations up
to 0.5 mg/mL, then began to plateau at higher concentrations (i.e. 0.75 and 1.0 mg/mL).
For cells under hypoxia, uptake of AuNPs was much lower compared to cells under
oxia. Incubation of cells with 0.5 mg/mL AuNPs under oxia resulted in intracellular levels
of Au that were over 3-fold higher than levels achieved under chronic and acute hypoxia.
Cells under both chronic and acute hypoxia showed similar uptake patterns over a
broad concentration range of AuNPs (Figure 3-3 B).
The cellular localization of the AuNPs was visualized by TEM analysis (Figure 3-
3 C). From these images it can be seen that after 20 mins of incubation no cellular
uptake of AuNPs is evident. Upon entering the cells, following 1 h of incubation, the
AuNPs are mostly visible in the perinuclear region and are sequestered in large clusters
in vacuoles such as endosomes and/or lysosomes. No localization of the AuNPs in
organelles such as the nucleus or mitochondria is evident in the images. Similar
observations were made following TEM analysis of cells incubated with AuNPs for 4 h
under both oxia and hypoxia.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 106
Figure 3-3: (A) Cellular uptake of the AuNPs following incubation over 48 h. *
represents statistically significant differences between the two concentrations (p<0.05).
(B) The Cellular level of Au following a 4 h incubation period with seven different
concentrations of AuNPs under oxia, chronic hypoxia and acute hypoxia. * represents
statistically significant differences between oxia and hypoxia (p<0.05). # represents
statistically significant differences between 0.5 mg/mL and other concentrations under
oxia (p<0.05). Data represents mean SEM (n=3). (C) TEM images of cells following a
incubation with AuNPs under oxia 20 min (I and II); 1 h (III and IV); 4 h (V and VI); 4 h
under chronic hypoxia (VII and VIII); and, 4 h under acute hypoxia (IX and X). II, IV, VI,
VIII and X represent high magnification images of selected views in I, III, V, VII and IX.
The scale bar represents 2 m in images I, III, V, VII and IX, and, 500 nm in images II,
IV, VI, VIII and X.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 107
3.4.3 The Influence of Time, Concentration and Cellular Localization on the
Radiosensitizing Effect of AuNPs
Figure 3-4 shows the SF ratio ( ) as a function of the
concentration of AuNPs. The SF ratio reached a minimum at a concentration of 0.5
mg/mL AuNPs. The radiation dose response curves for cells following different
incubation times with AuNPs are shown in Figure 3-5. The fit parameters (α and β),
goodness of fit (R2) for the radiation dose response curves, and the values for DEF at
0.1 SF are are summarized in Table 3-1. The data show that an incubation time of 1 h
or longer results in similar values for DEF. The impact of cellular localization of AuNPs
on their radiosensitizing effect is illustrated in Figure 3-6 B. The fit parameters (α and β)
and goodness of fit (R2) for the radiation dose response curves, as well as the values
for DEF at 0.1 SF are summarized Table 3-2.
Figure 3-4: The radiosensitizing effect of AuNPs following a 4 h incubation period prior
to irradiation (4Gy). The SF ratio is described by the following equation:
(SFIR+AuNPs/SFAuNPs)/SFIR. * represents statistically significant differences in the SF ratio
at 0.5 mg/mL AuNPs and other concentrations.
IR+AuN AuNPsPsrati
R
o
I
/SFSFSF
SF

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 108
Figure 3-5: Radiation dose response curves for cells incubated with AuNPs for different
periods of time (i.e. 20 min, 1, 4, 8, 16 or 24 h) and irradiated at 0, 2, 4, and 6 Gy. Data
points represent mean SEM (n=3).

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 109
Table 3-1: Fitted parameters obtained using the LQ model, and DEF calculated at 0.1SF for on experimental data shown in Figure 3-5.
Incubation time
IR IR+AuNPs DEF at 0.1 SF α β R2 α β R2
20 min 0.59±0.06 0.049±0.010 0.984 0.62±0.06 0.055±0.011 0.982 1.04±0.02 1 h 0.66±0.07 0.033±0.012 0.978 0.99±0.08 1.35*10-16 0.915 1.31±0.05 4 h 0.73±0.08 0.022±0.014 0.971 1.03±0.08 4.07*10-14 0.869 1.26±0.01 8 h 0.50±0.10 0.047±0.018 0.939 0.90±0.12 0.023±0.022 0.945 1.44±0.02
16 h 0.47±0.06 0.056±0.010 0.981 0.69±0.07 0.068±0.013 0.980 1.33±0.08 24 h 0.33±0.09 0.073±0.017 0.942 0.58±0.06 0.082±0.010 0.984 1.31±0.06
Figure 3-6: (A) Treatment groups to assess the dependence of the radiosensitizing
effect of AuNPs on their localization with respect to cells. (B) Radiation dose response
curves for cells with no AuNPs or intracellular and/or extracellular AuNPs. Data points
represent mean SEM (n=3).

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 110
Table 3-2: Fitted parameters obtained using the LQ model, and DEF calculated at 0.1SF for on experimental data shown in Figure 3-6.
Treatment groups: 1. No AuNPs, 2. AuNPs added immediately prior to IR, 3. Removal of AuNPs in cell culture media following 4 h of pretreatment, 4 AuNPs remained in cell culture media following 4 h of pretreatment. “+” indicates the relative amount of AuNPs, “-” indicates absence of AuNPs.* represents statistically significant difference between the DEF values of treatment groups 2 and 3 (p<0.05).
3.4.4 AuNPs Radiosensitization under Acute and Chronic Hypoxia
The surviving fraction of cells treated with AuNPs and radiation under oxic and
hypoxic conditions is plotted in Figure 3-7A. Chronic hypoxia alone caused significant
cell death (SF = 0.470.04), while acute hypoxia was less damaging (SF = 0.930.04).
To exclude the effects of hypoxia, cell survival was re-plotted in Figure 3-7 B, with
normalization for the toxicity associated with each hypoxic condition. The
radiosensitizing effects of AuNPs were calculated as SF ratios as shown in Table 3-3.
Treatment Extracellular AuNPs
Intracellular AuNPs
α β R2 DEF at 0.1 SF
1 - - 0.69±0.02 0.012±0.004 0.997 1
2 +++ - 0.74±0.04 0.019±0.007 0.992 1.09±0.01*
3 - + 1.00±0.13 1.50e-16 0.940 1.39±0.07*
4 ++ + 1.02±0.17 1.57e-16 0.900 1.41±0.08

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 111

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 112
Figure 3-7: (A) Survival of cells following irradiation and treatment with AuNPs under
oxia or hypoxia as measure by clonogenic assay. “+” indicates cells receiving AuNPs or
IR treatment, “-” indicates absence of the treatment. Blue squares “+” indicate
hypoxiahypoxia groups; red squares “+” indicate hypoxiaoxia groups. SF is
reported as plating efficiency compared to the control group under oxia. Data represents
mean SEM (n=3). (B) Survival of cells with toxicity of hypoxia normalized. Data
represents mean SEM (n=3). (C) Protein expression levels of Ku70 and Rad51 in cells
under oxia, chronic hypoxia and acute hypoxia. Numbers in parentheses indicate the
relative amount of Rad51 in cells after normalization with the corresponding Ku70 level.
Table 3-3: SF ratio at 5 Gy
Treatment groups SF ratio
Oxia oxia 0.110.09
Chronic hypoxia hypoxia 0.220.08
Chronic hypoxia oxia 0.130.02
Acute hypoxia hypoxia 0.610.07
Acute hypoxia oxia 0.120.02

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 113
Table 3-4: Effect of oxygen on radiation cell kill
a Statistically significant difference between OER-K1 and OER-K2 for the chronic hypoxia group. b Statistically significant difference between the values of OER-K1 for the chronic and acute hypoxia group.
3.4.5 Reduced Expression of Rad51 in Cells under Chronic Hypoxia
Chronic hypoxia for up to 72 h has previously been shown by our labs to lead to
decreased translation of expression of RAD51, a master protein involved in the HR DSB
repair pathway. This led to a decreased OER when compared to acute hypoxic
treatments [37]. We therefore evaluated RAD51 expression relative to Ku70 (a protein
used in the non-homologous recombination pathway that is not affected by chronic
hypoxia) as a protein -expression control [37]. Consistent with our previous studies, we
observed reduced RAD51 expression in chronic hypoxia-treated cells in comparison to
oxic or acute hypoxia-treated cells (Figure 3-7 C). For chronic hypoxic cells the amount
of Rad51 decreased to 43%, while for cells exposed to acute hypoxia the value was
95%.
3.4.6 The Effect of AuNPs on Cell Cycle Distribution and Post Irradiation DNA Double
Strand Breaks (DSBs)
Figure 3-8 summarizes the cell cycle distribution of cells treated with AuNPs for
up to 48 h. Statistical analysis revealed that at each time point the percentage of cells in
the G2/M phase is similar for the control and the AuNPs treated groups. Figure 3-9 A
shows the representative images from the immunofluorescence assay. Cells in their S
phase containing endogenous DSB (EdU positive) were excluded from foci counting.
Treatment of cells with AuNPs alone for 24 h did not cause DSB. With the presence of
Chronic hypoxia Acute hypoxia
OER-K1 1.470.31a,b 4.360.70 OER-K2 3.380.24 4.351.34
Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 114
the AuNPs, there was no increase in the number of foci (H2AX) 30 mins post
irradiation. The residual breaks (24 h post irradiation) were increased from 10.410.66
to 13.980.37 when cells were irradiated with 2 Gy, and from 23.171.04 to 34.712.01
for 4 Gy irradiation (Figure 3-9 B).
Figure 3-8: Cell cycle distribution in cells exposed to AuNPs (0.5 mg/mL) for 1, 4, 8, 16,
24, or 48 h.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 115
Figure 3-9: (A) Representative images from the immunofluorescence assay. (B)
Number of H2AX foci 30 mins or 24 h post irradiation (0, 2, 4 Gy). * represents
statistically significant difference between the treatment groups. Data represents mean
SEM (n=3).

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 116
3.5 Discussion
As shown in the Introduction section and Figure 3-1, the effect of radiation on
biological systems can be divided into physical, chemical and biological phases. AuNPs
have become a radiosensitizer of significant, widespread interest and likely impact
these three phases. The physical interaction between AuNPs and radiation is known to
generate large numbers of electrons and photons [10]. The photoelectric effect and
subsequent Auger cascade occur at kVp radiation energies producing numerous
photoelectrons and Auger electrons. These electrons then interact with the biological
components of cells and transfer their energies to the latter by producing radicals and
ions, leading to increased cell damage and ultimately radiosensitization [24].
Using plasmid DNA as a model, previous studies have shown that most
electrons released from AuNPs irradiated by kVp X-rays are associated with low energy
that result in “localized energy deposition” at the nanoscale [26, 28]. In vitro studies
have further demonstrated that AuNPs in the cytoplasm of cells are more effective
radiosensitizers than those attached to the cell membrane, highlighting the role of short-
range electrons under kVp X-rays. These observations emphasize the importance of
targeting AuNPs to cellular components in order to achieve maximal radiosensitization
[11, 13]. The pioneering in vivo study by Hainfeld et al. showed the significant
radiosensitizing effect of AuNPs at two minutes post intravenous administration of the
formulation in mice using a 250 kVp X-ray source [8]. Although no information on the
intratumoral distribution of the AuNPs was provided, it is likely that the AuNPs were
localized primarily in the extracellular matrix of tumors at the time of irradiation. Thus,
these results indicate that extracellular AuNPs can significantly enhance the effect of
radiation. Pignol et al. have suggested that AuNPS outside cells may elicit a “cross fire
effect” in which longer range electrons released from AuNPs travel a distance of several
cell diameters to interact with cell nuclei, resulting in radiosensitization [44]. Further
investigation is needed to quantitatively verify the effect of long range electrons. Also, it
is worth noting that in several in vitro studies, radiation has been applied to cells without
prior removal of AuNPs from the cell culture media [12, 15-18, 20]. Although cellular
uptake of AuNPs was evaluated in some of these studies, the contribution of the AuNPs

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 117
outside the cells to radiosensitization was not quantitatively analyzed. Given that the
amount of AuNPs remaining in the cell culture media could be significantly higher than
that inside cells, it is important to delineate and understand the effect of AuNPs in cell
culture media versus that associated with AuNPs in cells.
In our study, cellular uptake of AuNPs was evaluated prior to quantitatively
analyzing the impact of the cellular localization of AuNPs on radiosensitization. The
kinetics of cellular uptake of AuNPs is a combined effect of endocytosis, exocytosis, and
cell proliferation [32]. Internalization of the AuNPs under oxia was found to be time and
concentration dependent (Figure 3-3 A). This is in agreement with our previous study
and findings by others [32, 45]. As shown in Figure 3-3 B, concentration dependent cell
uptake under oxia showed that uptake increased almost linearly with concentration of
AuNPs up to 0.5 mg/mL followed by a plateau. A similar trend was observed by
Chithrani et al. and was attributed to saturation of receptor-mediated endocytosis, given
that uptake of these AuNPs was shown to be mediated by nonspecific adsorption of
serum proteins onto the particles [45]. Interestingly, in our study at the same
concentration of AuNPs, the level of uptake was much lower for hypoxic cells compared
to oxic cells. This phenomenon can be attributed to decelerated endocytosis which has
been shown to result under hypoxia due to impeded fusion of early endosomes and the
prolonged half-life of receptor tyrosine kinases [31, 46].
Studies examining the radiosensitizing effect of AuNPs (Figure 3-4) revealed that
radiosensitiziation increased with concentrations of AuNPs up to 0.5 mg/mL. The lower
radiosensitizing effect seen at higher concentrations (0.75 and 1.0 mg/mL) is due to
saturated uptake, as well as, the higher toxicity of the AuNPs at these concentrations.
As summarized in Table 3-1, similar values of DEF were observed for incubation times
of 1 h or longer, but the DEF was much lower for 20 mins of incubation. Given that no
effective uptake was detected 20 mins post incubation, it can be concluded that
intracellular AuNPs play the most significant role in radiosensitization. A similar
observation was made by Zhang et al, in which a higher DEF was observed for
intracellular AuNPs compared to those attached to the cell membrane [13]. The key role
of AuNPs inside cells was further verified as shown in Figure 3-6. Although the AuNPs
in the cell culture media comprised about 95% of the total Au content, radiation

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 118
enhancement was not significant (DEF=1.09±0.01), while AuNPs inside cells led to a
significantly higher DEF of 1.39±0.07. These findings suggest that efficient delivery of
AuNPs into target cells is crucial for a full exploitation of their radiosensitization effects.
For future in vivo and clinical application, parameters such as administration route of
AuNPs, and timing sequence of AuNPs and IR, should be carefully considered to
achieve maximum level of cell uptake in the target tissue at the moment of IR.
Optimization in these parameters will help to decrease the dose of AuNPs needed and
potential systemic toxicity, and therefore the achievement of improved therapeutic ratio.
Aside from enhanced physical interaction with radiation, AuNPs are also involved
in the chemical phase of radiation via generation of elevated ROS levels [19, 47]. The
increase in ROS generation is partly due to the secondary electrons emitted from
AuNPs, which subsequently interact with molecules in their close proximity to produce
ROS [47]. Cheng et al. have demonstrated the concept of “chemical enhancement”
achieved by the reactive surface of AuNPs [25]. In this study, the enhanced
hydroxylation of coumarin carboxylic acid under radiation was attributed to the
“increased conversion of intermediates to the products”. It was proposed that
superoxide produced by radiation activates the slightly electronegative surface atoms of
the nanoparticles by forming AuNPs-O2-. These reactive molecules then catalyze the
reactions between radical intermediates and other molecules to produce more ROS
[25]. Due to the important role of oxygen in ROS generation as both substrate and
intermediate, lack of oxygen will lower the level of ROS generation and therefore the
radiosensitization effect of AuNPs. In the current study, the radiosensitizing effect of
AuNPs was investigated under hypoxia to confirm its oxygen dependence.
The role of oxygen to enhance the effects of irradiation by permanently “fixing”
damage onto DNA has been well established [48], and hypoxia has been long
recognized as the main reason for radioresistance in cancer cells [49]. In 2002, Zolzer
et al. showed that chronic hypoxia can increase the radiosensitivity of cells and reduce
the effect of oxygen [38]. In their study two different OER values were calculated by
using oxic and reoxygenated hypoxic cells as references to distinguish the effect of
oxygen on cell physiology and radiochemistry. A pure radiochemical oxygen effect was

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 119
obtained when the hypoxiahypoxia group was compared to the hypoxiaoxia group,
and the combination effects of oxygen on cell physiology and radiochemistry was
observed when oxicoxia group was used as the reference. As the chronic hypoxic
cells were observed to be less radioresistant, the value of combined OER was lower
than the pure radiochemical OER [38]. Herein, for chronic hypoxic cells, the combined
oxygen effect (OER-K1) was lower than the pure radiochemical effect (OER-K2)
(1.470.31 vs. 3.380.24), while for acute hypoxic cells, OER-K1 and OER-K2 had
similar values (4.360.70 vs. 4.351.34). These observations confirmed that chronic
hypoxia reduces radioresistance of cells. As expected, the values of OER-K2, which
represent the pure radiochemical OER, were statistically similar for chronic and acute
hypoxic cells (3.380.24 vs. 4.351.35).
The reduced radioresistance of cells under chronic hypoxia has been related to
the decreased capacity for HR due to decreased translation of HR-related proteins such
as RAD51 [37]. To confirm this, the level of RAD51 was evaluated for cells under oxia
and hypoxia. Ku70, a protein involved in non-homologous end-joining (NHEJ), was used
as a positive control given that levels of this protein should not be affected by hypoxia
[37]. The fact that the level of Rad51 was decreased to 43% in chronic hypoxic cells and
was relatively unchanged in acute hypoxic cells supports the observation that reduced
radioresistance of cells under chronic hypoxia is most likely due to a functional HR
deficiency as the latter has been observed in similarly-treated cells of varying histologic
background [37].
From Table 3-3, it can be seen that the radiosensitizing effects of AuNPs were
lowest for the hypoxiahypoxia group under acute hypoxia (SF ratio = 0.610.07),
while the value was greater for the hypoxiahypoxia group under chronic hypoxia (SF
ratio = 0.220.08). The greater radiosensitizing effect of AuNPs for cells under chronic
hypoxia was the consequence of HR deficiency. When cells were exposed to radiation
following reoxygenation (hypoxiaoxia), the radiosensitizing effects were similar for
both chronic and acute hypoxic groups (0.130.02 vs. 0.120.02). Unlike the
hypoxiahypoxia group, the effect of HR deficiency was not detected and this is likely

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 120
due to overkill by the presence of AuNPs which leads to more than a 7-fold increase in
cell death when irradiated under oxia.
There is growing evidence that biological interactions between AuNPs and cells
also contribute to their radiosensitizing effects [24]. Roa et al. observed accumulation of
cells in G2/M phase following 2 h of exposure to AuNPs, suggesting cell cycle
synchronization is an important biological pathway for radiosensitization [15]. In the
current study it was shown that cells treated with 2.7 nm AuNPs for up to 48 h do not
lead to cell cycle synchronization. Similarly, Butterworth et al. observed no change in
cell cycle distribution when cells were treated with 1.9 nm AuNPs for 24 or 48 h [16].
Another possible biological mechanism of radiosensitization is inhibition of DNA repair
[6]. Previous studies have reported different outcomes for the effect of AuNPs on DNA
damage post irradiation. Chithrani et al. showed 50 nm AuNPs lead to an increased
number of residual foci following 4 Gy irradiation in HeLa cells, however, initial DNA
DSBs were not evaluated [17]. Jain et al. observed that in MDA-MB-231 cells, there was
no increase in number of either initial (1 h post IR) or residual foci (24 h post IR) using
1.9 nm AuNPs at 1 Gy [20]. In our study, no increase in the number of initial foci was
observed in the presence of AuNPs; however, the number of residual foci increased
significantly. These results indicated that the 2.7 nm AuNPs inhibit DNA repair
processes post irradiation. Further studies are needed to elucidate the molecular
pathways involved in the inhibited DNA repair that results due to the presence of the
AuNPs. It is likely that the physico-chemical properties of AuNPs (i.e. size, surface
chemistry), cell line, incubation conditions and dose of radiation influence the biological
interactions between AuNPs and cellular components and thus may explain the different
results observed by various groups.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 121
3.6 Conclusions
Overall, the present study highlights the importance of cell uptake of AuNPs as a
means to fully exploit their radiosensitization effects. In addition, oxygen was shown to
play a critical role in determining the extent of radiosensitization by AuNPs. Cells under
acute hypoxia showed the greatest degree of radioresistance; but were still
radiosensitized by AuNPs and will not limit the use of AuNPs as a novel agent, in vivo.
Furthermore, the AuNPs inhibited post-irradiation DNA repair but did not lead to cell
cycle synchronization. Findings from these studies may be used to guide the design of
AuNPs as radiosensitizers and to assist with selection of parameters for further in vitro
and in vivo evaluation of their radiosensitization effects.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 122
3.7 Acknowledgments
This research was funded by an operating grant from CIHR to D.A. Jaffray, R.G.
Bristow and C. Allen and a Terry Fox New Frontiers Program grant. L. Cui has been
funded by the MDS Nordion Graduate Scholarship in Radiopharmaceutical Sciences,
Hoffmann-La Roche/Rosemarie Hager Graduate Fellowship, and an Ontario Graduate
Scholarship. Kenneth Tse has been funded by an Ontario Graduate Scholarship, the
Princess Margaret Hospital Foundation, and the Terry Fox Foundation Strategic
Training Initiative for Excellence in Radiation Research for the 21st Century, CIHR. S.
Harding has been funded by an Ontario Graduate Scholarship. L. Cui thanks summer
students, Kaiyin Zhu and Kaitlynn Almeida for assistance with cell studies. R.G. Bristow
is a Canadian Cancer Society Research Scientist.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 123
3.8 References
1. Joiner M, van der Kogel A, editors. Basic Clinical Radiobiology. 4th ed. London: Hodder Arnold; 2009.
2. Delaney G, Jacob S, Featherstone C, Barton M. The Role of Radiotherapy in Cancer Treatment: Estimating Optimal Utilization from a Review of Evidence-Based Clinical Guidelines. Cancer 2005;104:1129-1137.
3. Lacombe S, Le Sech C. Advances in Radiation Biology: Radiosensitization in DNA and Living Cells. Surface Science 2009;603:1953-1960.
4. Harrison LB, Chadha M, Hill RJ, Hu K, Shasha D. Impact of Tumor Hypoxia and Anemia on Radiation Therapy Outcomes. Oncologist 2002;7:492-508.
5. Bhide SA, Nutting CM. Recent Advances in Radiotherapy. BMC Med 2010;8:25.
6. Wardman P. Chemical Radiosensitizers for Use in Radiotherapy. Clinical Oncology 2007;19:397-417.
7. Boeckman HJ, Trego KS, Turchi JJ. Cisplatin Sensitizes Cancer Cells to Ionizing Radiation Via Inhibition of Nonhomologous End Joining. Mol Cancer Res 2005;3:277-285.
8. Hainfeld JF, Slatkin DN, Smilowitz HM. The Use of Gold Nanoparticles to Enhance Radiotherapy in Mice. Phys in Med and Biol 2004;49:N309-N315.
9. Boag J, editor. The Time Scale in Radiobiology. 12th Failla Memorial Lecture. In: Nygaard of, Adler Hi, Sinclair Wk (Eds) Radiation Research. Proceedings of the 5th International Congress of Radiation Research. New York: Academic Press, 9-29; 1975.
10. Hainfeld JF, Dilmanian FA, Slatkin DN, Smilowitz HM. Radiotherapy Enhancement with Gold Nanoparticles. J Pharm Pharmacol 2008;60:977-985.
11. Kong T, Zeng J, Wang X, Yang X, Yang J, McQuarrie S, et al. Enhancement of Radiation Cytotoxicity in Breast-Cancer Cells by Localized Attachment of Gold Nanoparticles. Small 2008;4:1537-1543.
12. Liu CJ, Wang CH, Chien CC, Yang TY, Chen ST, Leng WH, et al. Enhanced X-Ray Irradiation-Induced Cancer Cell Damage by Gold Nanoparticles Treated by a New Synthesis Method of Polyethylene Glycol Modification. Nanotechnology 2008;19.
13. Zhang X, Xing JZ, Chen J, Ko L, Amanie J, Gulavita S, et al. Enhanced Radiation Sensitivity in Prostate Cancer by Gold-Nanoparticles. Clin Invest Med 2008;31:E160-167.
14. Rahman WN, Bishara N, Ackerly T, He CF, Jackson P, Wong C, et al. Enhancement of Radiation Effects by Gold Nanoparticles for Superficial Radiation Therapy. Nanomedicine 2009;5:136-142.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 124
15. Roa W, Zhang X, Guo L, Shaw A, Hu X, Xiong Y, et al. Gold Nanoparticle Sensitize Radiotherapy of Prostate Cancer Cells by Regulation of the Cell Cycle. Nanotechnology 2009;20:375101.
16. Butterworth KT, Coulter JA, Jain S, Forker J, McMahon SJ, Schettino G, et al. Evaluation of Cytotoxicity and Radiation Enhancement Using 1.9 Nm Gold Particles: Potential Application for Cancer Therapy. Nanotechnology 2010;21:21-29.
17. Chithrani DB, Jelveh S, Jalali F, van Prooijen M, Allen C, Bristow RG, et al. Gold Nanoparticles as Radiation Sensitizers in Cancer Therapy. Radiat Res 2010;173:719-728.
18. Liu CJ, Wang CH, Chen ST, Chen HH, Leng WH, Chien CC, et al. Enhancement of Cell Radiation Sensitivity by Pegylated Gold Nanoparticles. Phys in Med and Biol 2010;55:931-945.
19. Geng F, Song K, Xing JZ, Yuan C, Yan S, Yang Q, et al. Thio-Glucose Bound Gold Nanoparticles Enhance Radio-Cytotoxic Targeting of Ovarian Cancer. Nanotechnology 2011;22:285101.
20. Jain S, Coulter JA, Hounsell AR, Butterworth KT, McMahon SJ, Hyland WB, et al. Cell-Specific Radiosensitization by Gold Nanoparticles at Megavoltage Radiation Energies. Int J Radiat Oncol 2011;79:531-539.
21. Xu WC, Luo T, Li P, Zhou CQ, Cui DX, Pang B, et al. Rgd-Conjugated Gold Nanorods Induce Radiosensitization in Melanoma Cancer Cells by Downregulating Alpha(V)Beta(3) Expression. Int J of Nanomedicine 2012;7:915-924.
22. Herold DM, Das IJ, Stobbe CC, Iyer RV, Chapman JD. Gold Microspheres: A Selective Technique for Producing Biologically Effective Dose Enhancement. Int J of Radiat Biol 2000;76:1357-1364.
23. Chang MY, Shiau AL, Chen YH, Chang CJ, Chen HH, Wu CL. Increased Apoptotic Potential and Dose-Enhancing Effect of Gold Nanoparticles in Combination with Single-Dose Clinical Electron Beams on Tumor-Bearing Mice. Cancer Sci 2008;99:1479-1484.
24. Butterworth KT, McMahon SJ, Currell FJ, Prise KM. Physical Basis and Biological Mechanisms of Gold Nanoparticle Radiosensitization. Nanoscale 2012;4:4830-4838.
25. Cheng NN, Starkewolf Z, Davidson RA, Sharmah A, Lee C, Lien J, et al. Chemical Enhancement by Nanomaterials under X-Ray Irradiation. J Am Chem Soc 2012;134:1950-1953.
26. Carter JD, Cheng NN, Qu Y, Suarez GD, Guo T. Nanoscale Energy Deposition by X-Ray Absorbing Nanostructures. J Phys Chem B 2007;111:11622-11625.
27. Jain S, Hirst DG, O'Sullivan JM. Gold Nanoparticles as Novel Agents for Cancer Therapy. Brit J Radiol 2012;85:101-113.

Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 125
28. Zheng Y, Hunting DJ, Ayotte P, Sanche L. Radiosensitization of DNA by Gold Nanoparticles Irradiated with High-Energy Electrons. Radiat Res 2008;169:19-27.
29. Dreher MR, Liu W, Michelich CR, Dewhirst MW, Yuan F, Chilkoti A. Tumor Vascular Permeability, Accumulation, and Penetration of Macromolecular Drug Carriers. J Natl Cancer Inst 2006;98:335-344.
30. Rejman J, Oberle V, Zuhorn IS, Hoekstra D. Size-Dependent Internalization of Particles Via the Pathways of Clathrin- and Caveolae-Mediated Endocytosis. Biochem J 2004;377:159-169.
31. Wang Y, Roche O, Yan MS, Finak G, Evans AJ, Metcalf JL, et al. Regulation of Endocytosis Via the Oxygen-Sensing Pathway. Nat Med 2009;15:319-324.
32. Cui L, Zahedi P, Saraceno J, Bristow R, Jaffray D, Allen C. Neoplastic Cell Response to Tiopronin-Coated Gold Nanoparticles. Nanomedicine 2013;9:264-273.
33. Bristow RG, Hill RP. Hypoxia and Metabolism. Hypoxia, DNA Repair and Genetic Instability. Nat Rev Cancer 2008;8:180-192.
34. Chithrani BD, Stewart J, Allen C, Jaffray DA. Intracellular Uptake, Transport, and Processing of Nanostructures in Cancer Cells. Nanomedicine 2009;5:118-127.
35. Franken NA, Rodermond HM, Stap J, Haveman J, van Bree C. Clonogenic Assay of Cells in Vitro. Nat Protoc 2006;1:2315-2319.
36. Hockel M, Vaupel P. Tumor Hypoxia: Definitions and Current Clinical, Biologic, and Molecular Aspects. J Natl Cancer Inst 2001;93:266-276.
37. Chan N, Koritzinsky M, Zhao H, Bindra R, Glazer PM, Powell S, et al. Chronic hypoxia decreases synthesis of homologous recombination proteins to offset chemoresistance and radioresistance. Cancer Res 2008; 68:605–14.
38. Zolzer F, Streffer C. Increased radiosensitivity with chronic hypoxia in four human tumor cell lines. Int J Radiat Oncol Biol Phys 2002; 54:910–20.
39. Young SD, Hill RP. Effects of reoxygenation on cells from hypoxic regions of solid tumors: analysis of transplanted murine tumors for evidence of DNA overreplication. Cancer Res 1990; 50:5031–8.
40. Iizuka M, Ando K, Aruga T, Furusawa Y, Itsukaichi H, Fukutsu K, et al. Effects of reoxygenation on repair of potentially lethal radiation damage in cultured MG-63 osteosarcoma cells. Radiat Res 1997; 147:179–84.
41. Harding SM, Bristow RG. Discordance between phosphorylation and recruitment of 53BP1 in response to DNA double-strand breaks. Cell Cycle 2012; 11:1432–44.
42. Pan Y, Neuss S, Leifert A, Fischler M, Wen F, Simon U, et al. Sizedependent cytotoxicity of gold nanoparticles. Small 2007; 3:1941–9.
Chapter 3: Hypoxia and Cellular Localization Influence Radiosensitization by AuNPs 126
43. Mironava T, Hadjiargyrou M, Simon M, Jurukovski V, Rafailovich MH. Gold nanoparticles cellular toxicity and recovery: effect of size, concentration and exposure time. Nanotoxicology 2010; 4:120–37.
44. Pignol JP, Lechtman E. Reply to Comment on ‘Implications on clinical scenario of gold nanoparticle radiosensitization in regards to photon energy, nanoparticle size, concentration and location’. Phys Med Biol 2012; 57:291–5.
45. Chithrani BD, Ghazani AA, Chan WC. Determining the size and shape dependence of gold nanoparticle uptake into mammalian cells. Nano Lett 2006; 6:662–8.
46. Abella JV, Park M. Breakdown of endocytosis in the oncogenic activation of receptor tyrosine kinases. Am J Physiol Endocrinol Metab 2009; 296:E973–84.
47. Misawa M, Takahashi J. Generation of reactive oxygen species induced by gold nanoparticles under x-ray and UV irradiations. Nanomedicine 2011; 7:604–14.
48. Brown JM. The hypoxic cell: a target for selective cancer therapy– eighteenth Bruce F. Cain Memorial Award lecture. Cancer Res 1999; 59:5863–70.
49. Gray LH, Conger AD, Ebert M, Hornsey S, Scott OCA. The Concentration of Oxygen Dissolved in Tissues at the Time of Irradiation as a Factor in Radiotherapy. Br J Radiol 1953; 26:638–48.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 127
Chapter 4
Triple Combination of Gold Nanoparticles, Cisplatin and Radiotherapy for
Local Treatment of Triple Negatvie Breast Cancer
Lei Cui, Sohyoung Her, Michael Dunne, Gerben R. Borst, Raquel De Souza,
Robert G. Bristow, David A. Jaffray, Christine Allen
Reprint from Radiation Research Society (under review)
Experiments by L.Cui and S.Her. Written by L.Cui. Figures by L.Cui. Edited by G.R.
Borst, R.G. Bristow, and C. Allen.
The copyright of this article will belong to Radiation Research Society, the publisher of
Radiation Research, if accepted. Permission has to be requested for publishing the
article as part of this dissertation, which will be obtained.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 128
4.1 Abstract
Gold nanoparticles (AuNPs) and cisplatin have been explored in concomitant
chemoradiotherapy, wherein they elicit their effects by distinct and overlapping
mechanisms. Herein their radiation enhancement effects, individually and in
combination, were investigated in in vitro and in vivo models of triple negative breast
cancer (MDA-MB-231Luc+). Cellular targeting AuNPs (AuNP-RME) at a non-cytotoxic
concentration (0.5 mg/mL) or cisplatin at IC25 (12 M) demonstrated dose enhancement
factors (DEF) of 1.25 and 1.14, respectively; combination of AuNP-RME and cisplatin
resulted in a significant DEF of 1.39 in vitro. Transmission electron microscopy (TEM)
images showed effective cellular uptake of AuNPs at tumor sites 24 h post intratumoral
infusion. Computed tomography (CT) images demonstrated a heterogeneous
intratumoral distribution of AuNPs, with Au levels remaining stable up to 120 h post-
infusion. The percentage of the tumor volume containing detectable levels of Au
decreased over time due to ineffective penetration of AuNPs and tumor growth. AuNPs
(0.5 mg Au per tumor) demonstrated an equivalent radiation enhancement effect to
three doses of cisplatin at IC25 (4 mg/kg), with the advantages of no intrinsic toxicity or
increased toxicity of irradiation. Results from this study suggest that AuNPs are the true
radiosensitizer in these settings. Importantly, AuNPs+cisplatin enhanced the effect of
irradiation (3x4 Gy) significantly, and provides a promising means to improve the
therapeutic window of fractionated radiotherapy.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 129
4.2 Introduction
Radiotherapy (RT) is utilized as primary or adjuvant treatment in over 50% of
cancer patients [1]. Multimodal treatment, for instance concomitant chemoradiotherapy
(CRT), has been employed in the clinic to improve the antitumor effects of RT [2-4]. As
an important mechanism of CRT, radiosensitization is the process in which a
radiosensitizer, present in the field of irradiation (IR), cooperates with IR and/or
biological targets to enhance the effects of RT [5, 6]. A true radiosensitizer is defined as
an agent which shows minimum intrinsic toxicity while demonstrating additive or supra-
additive effects with RT without causing a significant increase in the toxicity of RT [6-8].
Nevertheless, most agents currently used in the clinic for their radiosensitization effects,
as exemplified by cisplatin, are in fact toxic [9-13].
As one of the most widely used chemotherapeutic agents, cisplatin exerts its
cytotoxicity by producing intra- or inter-strand DNA crosslinks upon entering cell nuclei
[14]. As a radiosensitizer [15-26], cisplatin functions via the formation of toxic platinum
intermediates, inhibition of post-IR DNA damage repair, cell cycle arrest in the G2/M
phase, as well as radiation-induced increased cellular uptake of platinum [27]. It has
also been demonstrated that cisplatin is capable of capturing and transferring radicals
and low energy electrons (LEEs) generated under IR to guanine bases in DNA to
produce substantial DNA double strand breaks (DSBs) [28, 29]. Clinical applications of
cisplatin aided CRT have yielded significantly higher locoregional control and improved
overall progression-free survival in a variety of solid tumors [9-13]. However, the tumor
dose of such a CRT is limited by treatment induced toxicities to normal tissues, which
creates the need to develop novel tumor-selective radiosensitizing strategies [30].
Due to their unique physical and chemical properties, gold nanoparticles (AuNPs)
AuNPs are well established as potent radiosensitizers owing to their significantly higher
photoelectric absorption in comparison to soft tissues, which leads to the generation of
numerous LEEs and free radicals when irradiated [31, 32]. Recent research has also
revealed that the highly curved surface of AuNPs provides reactive electron donating
and accepting sites, which accommodate and catalyze chemical reactions to produce

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 130
elevated amount of radicals [32]. Furthermore, reactive oxygen species (ROS)
generated by AuNPs in the absence of IR imposes oxidative stress on cells, and may
enhance the effect of IR via biological pathways [31-33] such as cell cycle
synchronization in G2/M phase [34], inhibition of post-IR DNA damage repair [35],
mitochondrial malfunctioning, as well as an increase in cell death capacity and thus
intrinsic radiosensitivity [36, 37].
Since cisplatin and AuNPs enhance RT through a number of distinct and
overlapping mechanisms, the combination of the two agents to additively or
synergistically enhance the effects of IR is logical. For instance, Zheng et al. proposed
that in the proximate presence of cisplatin, LEEs and radicals produced by AuNPs
under IR can be captured and transferred to DNA molecules to induce greater damage.
The authors further demonstrated, in a DNA plasmid model, that the triple combination
of IR+AuNPs+cisplatin leads to a 2.95- and 3.22-fold increase in DNA (double strand
breaks) DSBs, respectively, in comparison to IR+cisplatin or IR+AuNPs [38]. It should
be noted that, in this DNA plasmid model, the location of the two agents is precisely
controlled, such that the DNA molecules and cisplatin are within the effective range of
the LEEs and radicals produced by AuNPs upon IR exposure. Moreover, complex
biological processes such as free radical scavenging and DNA damage repair are
excluded [39]. To further explore the potential of this triple combination, it is of crucial to
evaluate its efficacy and toxicity in biological systems.
This is the first study wherein the radiation enhancement effects of AuNPs and
cisplatin, individually and in combination, are examined and compared both in vitro and
in vivo. In addition, in vivo studies to date evaluating radiosensitization by AuNPs using
external beam RT have been limited to single large doses of IR (5 – 30 Gy) [31, 32].
Given that conventional RT is based on a fractionated scheme, it is critical to
understand the radiation enhancement effects of AuNPs in combination with
fractionated RT. To the best of our knowledge, this is also the first time the
radiosensitizing effect of AuNPs in combination with fractionated RT has been
evaluated in vivo. Findings from the current research suggest that AuNPs in
combination with cisplatin is a promising strategy to be applied in CRT.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 131
4.3 Methods
All chemicals were purchased from Sigma Aldrich (Oakville, Canada) and used
without further purification unless otherwise noted.
4.3.1 Preparation of AuNPs
AuNPs coated with polyethylene glycol (AuNP-PEG) were prepared following a
previously published method by Shimmin et al. [40] with minor modifications. 300 mg of
chlorauroric acid (HAuCl43H2O) were dissolved in a mixture of 60 mL of 2-propanol
and 10 mL of acetic acid. 320 mg of PEG 2-mercaptoethyl ether acetic acid (SH-
(PEG)22-COOH, Mn=3400, Laysan Bio) was added to the solution to achieve a molar
ratio of Au:PEG = 8:1, and stirred at room temperature for 15 minutes. 1 g NaBH4
dissolved in 10 mL of dd-H2O was then added to the solution, and the reaction mixture
was further stirred for 60 min at room temperature. The solvent was removed under
vacuum at 40°C using a rotary evaporator. The final product was resuspended in 20 mL
of dd-H2O and dialyzed against excess dd-H2O for 72 h to remove unreacted reagents,
and finally lyophilized. AuNP-PEG was further functionalized with an adenoviral receptor
mediated endocytosis (RME) peptide: CKKKKKKSEDEYPYVPN [41] custom-
synthesized by Genscript (US). 100 mg of AuNP-PEG was suspended in 10 mL of 2-(N-
morpholino) ethanesulfonic acid (MES) buffer (pH 7.5). 3.5 mg of 1-Ethyl-3-(3-dimethyl-
aminopropyl) carbodiimide (EDC) and 3.8 mg of sulfo-N-hydroxysulfosuccinimide (sulfo-
NHS) were added to the solution. After 15 min of stirring, peptide dissolved in 100 L of
MES buffer (pH 7.5) was added to the solution at a molar ratio of 1:10 to PEG.
Following 24 h of reaction, the mixture was dialyzed against excess dd-H2O for 72 h to
remove unreacted reagents followed by lyophilization.
4.3.2 Characterization of AuNPs
The morphology and core size of AuNPs were assessed using transmission
electron microscopy (TEM) [42, 43]. 10 L of AuNPs suspended in dd-H2O (0.01

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 132
mg/mL) was placed onto carbon-coated copper grids; air dried, and imaged using a
Hitachi H7000 TEM (Hitachi Corp., Tokyo, Japan) operated at 100 keV. The core size
distribution of AuNPs was evaluated using ImageJ software (NIH, Bethesda, USA).
Hydrodynamic diameters of AuNP samples were determined by dynamic light scattering
(DLS) using the Zetasizer Nano (Malvern Instruments, Malvern, UK). The in vitro
stability of AuNPs was evaluated in cell culture media (DMEM/HAM F-12 mixture (1:1))
supplemented with 10% fetal bovine serum (FBS) without phenol red (Tissue Culture
Media Facility, University Health Network, Toronto, Canada) at a concentration of 0.50
AuNPs mg/mL, with incubation at 37 °C for 48 h. At specific time points during the
incubation period aliquots of the solution were removed and the UV-Vis spectra were
obtained (Cary 50 UV-VIS spectrophotometer, Varian, Palo Alto, CA, USA).
4.3.3 Cell Culture: MDA-MB-231Luc+
Breast cancer cells were obtained from Cell Biolabs (San Diego, USA). Cells
were cultured in DMEM/HAM F12 1:1 mixture supplemented with 10% FBS and 1%
penicillin-streptomycin. Cells were grown as monolayers at 37°C in 5% CO2 and 90%
relative humidity.
4.3.4 Qualitative Assessment of the Cellular Accumulation of AuNPs
Cellular uptake and subcellular distribution of AuNPs were observed using TEM
[42]. Cells were plated onto 6-well plates at a density of 1x106 cells/plate and allowed to
recover for 24 h. Cell media was then replaced with fresh media containing 0.50 mg/mL
AuNPs. Following a 24 h incubation period, cells were washed with PBS and fixed for
TEM imaging, which was performed as described above in “Characterization of AuNPs”.
4.3.5 Quantitative Assessment of the Cellular Accumulation of AuNPs
Cells were plated onto 6-well plates (1x106 cells/plate) and allowed to recover for
24 h. Following a 4 or 24 h incubation period with AuNPs-containing media (0.50

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 133
mg/mL), cells were washed twice with PBS and harvested using 0.25% trypsin-EDTA
(Gibco, USA). The number of cells in each sample was counted using a
haemocytometer. Cells were centrifuged to a pellet, and then further digested with
HNO3 at 90°C for 10 mins, and diluted with dd-H2O. The amount of Au was measured
by inductively coupled plasma atomic emission spectroscopy (ICP-AES Optima
7300DV, PerkinElmer, Waltham, MA) as previously described [42], and the average
amount of Au accumulated in each cell was determined.
4.3.6 Radiation Source and Dose Calculations for Cell Irradiation Studies
Cell irradiation was performed using a small animal irradiator (X-RAD225Cx,
Precision X-ray, Inc. North Branford, CT, USA) at dose rates of 3.47 Gy min-1 at 225
kVp and 13 mA. Dose calculations for cell irradiation were performed as previously
described [44, 45].
4.3.7 In vitro Clonogenic Survival Assays
Cell survival was evaluated by clonogenic assay [35]. Cells were plated onto 6-
well plates at a density of 1x106 (unless otherwise noted) 24 h prior to treatment.
Following treatment with AuNPs, cisplatin, and/or IR, cells were washed twice with PBS
and trypsinized. For each treatment, cells were counted and seeded onto cell culture
dishes at various cell densities to achieve appropriate numbers of colonies. Following 9-
11 days of incubation, colonies were fixed and stained with 1% methylene blue in 50%
ethanol. The number of colonies was counted for each cell density. Colonies were
defined as structures containing ≥50 cells. The cell surviving fraction (SF) was
expressed as the plating efficiency of cells exposed to each treatment in comparison to
that for non-treated cells [46].

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 134
4.3.8 Evaluation of Cytotoxicity of AuNPs and Cisplatin
Quantitative analysis showed that prolonged incubation resulted in higher levels
of cellular accumulation AuNP-RME, the cytotoxicity of AuNPs at 0.50 mg/mL was
evaluated using clonogenic assay following 24 h of incubation. To choose an
appropriate concentration of cisplatin to evaluate its radiosensitization effects, the
cytotoxicity of cisplatin was assessed at two different incubation times (30 min and 48 h)
as described previously [19, 23]. Cells pre-treated with 0-40.00 M of cisplatin for 30
min, or 0-2.50 M of cisplatin for 48 h were seeded for clonogenic assessment. SF of
each treatment group was reported.
4.3.9 Radiosensitizing Effects of AuNPs and Cisplatin In Vitro – Individually and in
Combination
To obtain a sufficient and valid number of colonies for quantifiable assessment of
cisplatin radiosensitization, IC25 of cisplatin was chosen for radiation studies. For the
assessment of the individual radiosensitizing effect of the AuNPs and cisplatin, cells
were exposed to IR (0, 2, 4, 6 Gy) following incubation in cell culture media containing
AuNPs (0.50 mg/mL, 24 h), or cisplatin at IC25 (12 M for 30 min, 0.5 M for 48 h
incubation). To evaluate the radiosensitizing effect of AuNPs and cisplatin in
combination, cells were treated with AuNP-RME (0.50 mg/mL, 24 h), which showed
greater levels of cellular uptake and radiosensitzation in comparison to AuNP-PEG, and
cisplatin at IC25 (12 M for 30 min) prior to IR. Survival curves were produced for all
treatment groups with or without pre-treatment with AuNPs or cisplatin. The data were
fitted to a linear-quadratic model: SF = exp (-αD-βD2). For each AuNPs or cisplatin pre-
treated group, DEF values were calculated as the ratio of the IR dose required to yield
an SF of 0.1 in the presence of AuNPs to the IR dose required to yield the same SF in
the absence of the agents [35].

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 135
4.3.10 Animals and Tumor Model
All animal procedures were approved by the University Health Network Animal
Care Committee. As the current study aimed to evaluate the local treatment by AuNPs
and/or cisplatin aided RT, MDA-MB-231 cells transfected with luciferase vector (MDA-
MB-231Luc+) were employed, and BLI was used to monitor the appearance of metastatic
lesions during the course of the treatment [47]. 4x106 MDA-MB-231Luc+ cells suspended
in cell culture media with a total volume of 50 µL was injected using a 27 gauge needle
into the mammary fat pad of 6-8-week-old female NOD/SCID mice. Tumor size was
monitored by caliper measurement 2-3 times per week, and treatment was initiated
when tumor sizes reached 250 mm3 (approximately 2 weeks post inoculation). Tumor
size was calculated using the formula: volume = (length x width2) x 0.5 [45]. The
formation of metastatic lesions was monitored using BLI (detailed methods and results
included in Supporting Information). Mice with metastatic disease were excluded, since
the goal of the study was to evaluate the efficacy of locoregional control of the primary
tumor (Figure 4-8). Mice without metastases were randomized into groups based on the
tumor size, and treatments were initiated.
4.3.11 Intratumoral Infusion of AuNP-RME
Pilot studies by our group showed that leakage of agents is a common problem
with i.t. injection due to high interstitial pressure in solid tumors (data not shown) [48].
To minimize leakage, in the current study, AuNP-RME suspended in saline with a final
volume of 30 µL was administered via i.t. infusion at a rate of 2 µL/min [49], using a NE-
1010 high pressure programmable single syringe pump (PumpSystems Inc, USA), and
a Hamilton® syringe (800 series from Sigma).

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 136
4.3.12 Determination of Doses of AuNP-RME and Cisplatin to be Employed In Vivo
Three different doses (0.05, 0.25, and 0.5 mg Au per tumor) were administered
to assess the concentration-dependent radiosensitization effect of AuNP-RME by ex
vivo clonogenic assay (Supporting Information). IC25 (i.p.) of cisplatin for tumor cells was
determined by ex vivo clonogenic assay. Systemic toxicity, efficacy, and radiation
enhancement effect of single or three doses of cisplatin at IC25 were evaluated and
compared; the dose with observable radiation enhancement effect within the acceptable
limit defined in this study (i.e. <20% body weight loss) was employed for subsequent
efficacy and toxicity studies in vivo.
4.3.13 Work Flow for In Vivo Studies
The treatment schedule for in vivo studies is summarized in Figure 4-1. The
treatment groups for the assessment of efficacy (tumor growth delay and overall
survival) and systemic toxicity are shown in Table 4-1. To allow cellular internalization of
AuNP-RME the first fraction of localized IR was administered 24 h post intratumoral (i.t.)
infusion of AuNP-RME.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 137
Figure 4-1: Work flow for in vivo studies evaluating efficacy (measured by ex vivo clonogenic assay, tumor growth, and
overall survival), as well as the toxicity (evaluated by body weight loss) of each treatment.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 138
Table 4-1: Treatment groups for the assessment of efficacy and systemic toxicity: saline and cisplatin solutions were administered intraperitoneally (i.p.) 30 min prior to IR on days 1, 3, and 5.
Treatment groups Day 0 Day 1 Day 3 Day 5
No treatment control Saline, 30 µL ,i.t. Saline, 100 µL Saline, 100 µL Saline, 100 µL
Cisplatin Saline, 30 µL ,i.t. Cisplatin, 100 µL, 4 mg/kg
Cisplatin, 100 µL, 4 mg/kg
Cisplatin, 100 µL, 4 mg/kg
AuNP-RME AuNP-RME, 30mL, i.t., 0.5 mg Au per tumor
Saline, 100 µL Saline, 100 µL Saline, 100 µL
AuNP-RME+cisplatin AuNP-RME, 30mL, i.t., 0.5 mg Au per tumor
Cisplatin, 100 µL, 4 mg/kg
Cisplatin, 100 µL, 4 mg/kg
Cisplatin, 100 µL, 4 mg/kg
IR Saline, 30 µL ,i.t. Saline, 100 µL, IR 4Gy
Saline, 100 µL, IR 4Gy
Saline, 100 µL, IR 4Gy
IR+cisplatin Saline, 30 µL ,i.t. Cisplatin, 100 µL, 4 mg/kg, IR 4Gy
Cisplatin, 100 µL, 4 mg/kg, IR 4Gy
Cisplatin, 100 µL, 4 mg/kg, IR 4Gy
IR+AuNP-RME AuNP-RME, 30mL, i.t., 0.5 mg Au per tumor
Saline, 100 µL, IR 4Gy
Saline, 100 µL, IR 4Gy
Saline, 100 µL, IR 4Gy
IR+AuNP-RME+cisplatin AuNP-RME, 30mL, i.t., 0.5 mg Au per tumor
Cisplatin, 100 µL, 4 mg/kg, IR 4Gy
Cisplatin, 100 µL, 4 mg/kg, IR 4Gy
Cisplatin, 100 µL, 4 mg/kg, IR 4Gy

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 139
4.3.14 Intratumoral Distribution and Quantitative Measurement of AuNP-RME by TEM
and CT
For TEM imaging, mice were sacrificed 24 h post i.t. infusion of AuNP-RME, and
tumors were resected, sliced, and fixed. Samples were imaged using a Hitachi H7000
TEM (Hitachi Corp., Tokyo, Japan) operated at 100 keV. To monitor the intratumoral
level of Au over time, mice from the IR+AuNP-RME group were scanned by micro-CT at
80 kVp and 50 mA (GE Locus Ultra MicroCT, GE Healthcare, Waunakee, WI) prior to
AuNP infusion, and at 5 min, 24 h, 72 h, and 120 h post administration. Images
acquired prior to AuNP infusion were used as baseline for analysis. Voxels enhanced by
AuNP-RME were defined as those at each time point with HU greater than the average
voxel intensity plus two standard deviations for the tumor volume before AuNP infusion.
Average Au concentration in the tumor was determined by measuring the differences in
average HU in the tumor pre- and post-injection of AuNP-RME and relating the
difference in HU to a standard curve measured in a phantom that measured an increase
HU of 9.8 per 1 mg/mL of Au. Detailed imaging and analysis methods are available in a
previous paper from our group [50]. The radiation dose from CT imaging was less than
7 cGy, for which the biological effect is considered to be negligible [51].
4.3.15 Localized X-ray Irradiation of Tumors
Mice were anaesthetized with isoflurane (induced at 5% and maintained at 1-2%)
during IR. Tumors were locally irradiated using an image-guided small animal irradiator
(Xrad 225, Precision Xray, North Branford, CT, USA) at the Spatio-Temporal Targeting
and Amplification of Radiation Response (STTARR) Innovation Center at the University
Health Network, Toronto, Canada [45]. IR was conducted at 225 kVp and 13 mA with a
copper filter. The dose rates were 2.88 and 2.90 Gy/min with circular collimators with a
diameter of 1.0 or 1.5 cm, respectively. The irradiation regimen was either a single dose
of 4 Gy for ex vivo clonogenic assay or three fractions of 4 Gy 48 h apart for the
evaluation of treatment efficacy and toxicity. To minimize IR dose inhomogeneity in the

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 140
tumor, the irradiator was turned 180° midway during each session of IR, with 2 Gy of IR
delivered from the top and 2 Gy from the bottom to the tumor [52].
4.3.16 Evaluation of Treatment Efficacy and Toxicity in Tumor-bearing Mice
Tumor growth was monitored post treatment 2-3 times per week, and the ethical
endpoint was chosen to be a tumor size exceeding 1.5 cm in any dimension, at which
time mice were sacrificed. The endpoint for each treatment group was defined as the
time at which one of the mice reached the ethical endpoint. Along with the efficacy
study, systemic toxicity of these treatments was assessed by body weight change, as
well as kyphotic hunched posturing, lack of grooming, eating and drinking status, as well
as level of activity [53]. Statistical analyses of efficacy and toxicity data were done at the
endpoint dates of the control groups (no treatment control on day 7, and IR alone on
day 9).
4.3.17 Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social
Sciences V16.0 (SPSS Inc., USA). A two-sample t-test was used to measure statistical
significance between two groups. For comparisons between three or more groups, one-
way analysis of variance (ANOVA) was used. Subsequent multiple comparisons
analysis with Bonferroni correction was performed upon statistical significance as
detected by the ANOVA F-test. Significance was assigned at p<0.05. Statistic analysis
of general overall survival was performed using log rank test, further comparison was
conducted with p values adjusted by the Dunnett method, and a significant difference
was defined by p<0.05 after adjustment.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 141
4.4 Results
4.4.1 Characterization of AuNPs and Cellular Uptake of AuNPs
TEM images showed AuNP-PEG and AuNP-RME [41] have core diameters of
5.811.53 nm (Figure 4-2 A). Hydrodynamic diameters measured by dynamic light
scattering (DLS) were 20.873.32 and 23.892.23 nm for AuNP-PEG and AuNP-RME,
respectively. UV spectra (Figure 4-2 B, C) of AuNP-PEG and AuNP-RME following
incubation in complete cell culture media at 37°C demonstrated that these nanoparticles
remain stable over 48 h with a distinct and non-shifting peak at 520 nm.
TEM images of cellular accumulation of AuNP-PEG and AuNP-RME are
presented in Figures 4-2 E and F. It can be seen that AuNPs were clustered in
endosomes and lysosomes following cell entry. The quantitative analysis of AuNP
cellular accumulation is summarized in Figure 4-2 D. Actively targeted AuNP-RME
showed significantly higher levels of cell accumulation in comparison to non-targeted
AuNP-PEG at both 4 h and 24 h post-incubation. Prolonged incubation (24 h) with
AuNP-RME led to significantly higher cellular uptake compared to shorter incubation
times (4 h). There was no difference between the cellular level of Au when cells were
treated with AuNP-PEG for 4 h or 24 h.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 142
Figure 4-2: (A) A representative TEM image of the AuNP-PEG formulation. The scale
bar represents 100 nm. (B, C) UV spectra obtained for AuNP-PEG and AuNP-RME,
respectively. The absence of a shift in the peak at 520 nm confirms that the AuNPs are
stable without aggregation during the incubation period. (D) Cellular accumulation of
AuNPs (0.50 mg/mL) in MDA-MB-231Luc+ cells quantified by ICP-AES following 4 h or
24 h of incubation. * represents statistically significant difference in cellular level of Au in
cells treated with AuNP-RME in comparison to AuNP-PEG (p<0.05). Cellular uptake of

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 143
AuNP-RME was also found to be significantly higher at 24h compared to 4h (p<0.05).
Data represents mean SEM (n=3). (E, F) TEM images depicting cellular uptake of
AuNPs (0.50 mg/mL) at 24h post-incubation with AuNP-PEG and AuNP-RME,
respectively. Scale bars in E and F represent 2 µm (left images) and 500 nm (right
images). Following cell entry, AuNPs are clustered within endosomal and lysosomal
vacuoles.
4.4.2 Cytotoxicity and Radiosensitization Effects of AuNPs and Cisplatin In Vitro
In the absence of IR, AuNP-PEG and AuNP-RME showed no statistically
significant toxicity compared to control, with surviving fractions (SFs) of 0.850.02, and
0.840.07, respectively. IC25 values of cisplatin were identified to be 12 and 0.5 M for
30 min and 48 h of incubation, respectively (Figure 4-7, Supporting Information).
The cellular radiation dose responses following pre-treatment with AuNPs (24 h)
and/or cisplatin (30 min or 48 h) are presented in Figure 4-2. The radiation doses
required to achieve 0.1 SF, as well as the DEF values for each treatment, are
summarized in Table 4-2. Treatment with AuNP-RME, which showed higher cellular
uptake, led to a significant radiosensitization effect (measured by radiation dose
required to achieve 0.1 SF compared to IR alone), while radiosensitization was not
achieved with AuNP-PEG (Figure 4-3 A). The presence of cisplatin at IC25 did not result
in a significant radiosensitization effect (Figure 4-3 B). The combination of AuNP-RME
with cisplatin resulted in an additive effect, leading to a significant reduction in the IR
dose required to achieve 0.1 SF when compared to IR alone (2.700.13 Gy for
IR+AuNP-RME+cisplatin vs. 3.790.14 for IR alone) (Figure 4-3 C).

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 144
Table 4-2: Radiation dose required to achieve 0.1 SF and DEF for each treatment.
Treatment group Radiation dose for 0.1 SF DEF
IR 3.79 0.14 1.00
IR+AuNP-PEG (0.5 mg/mL) 3.30 0.09 1.14
IR+AuNP-RME (0.5 mg/mL) 3.01 0.08* 1.25
IR+cisplatin (0.50 M, 48 h) 3.41 0.05 1.11
IR+cisplatin (12.00 M, 30 min) 3.35 0.11 1.14
IR+AuNP-RME+ cisplatin (12.00 M, 30 min) 2.70 0.13* 1.39
Note: (*) represents a significant reduction in the radiation dose required to achieve a SF of 0.1 compared to IR alone. DEF values were calculated as the ratio of the IR dose required to yield an SF of 0.1 in the presence of AuNPs and/or cisplatin to the IR dose required to yield the same SF in the absence of the agents [35].

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 145
Figure 4-3: Radiation dose response of MDA-MB-231Luc+ cells fitted to a linear-
quadratic model: SF = exp (-αD-βD2) of cells treated with IR (225 kVp, 13 mA, 0, 2, 4, or
6 Gy) in combination with pre-treatment with AuNPs (A), cisplatin (B) or AuNPs and
cisplatin (C). Data points represent meanSEM (n3).

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 146
4.4.3 Determination of Dose of AuNP-RME and Cisplatin In Vivo
The highest level of radiosensitization was observed using 0.5 mg Au per tumor
(Supporting Information, Figure 4-9), and this dose was employed in subsequent
efficacy and toxicity studies.
The IC25 of cisplatin in tumor cells was determined to be 4 mg/kg. Ex vivo
clonogenic assays revealed that the combination of single dose cisplatin at IC25 with
one fraction of IR (4 Gy) did not show any improvements in tumor cell killing compared
to IR alone, with PE values of 0.042±0.006 and 0.039±0.002, for IR alone and
IR+cisplatin, respectively (Supporting Information, Figure 4-9). Single dose cisplatin at
IC25 (4 mg/kg) administered on day 1 did not show perceptible tumor growth delay
compared to the no treatment control. Further, the combination of single dose cisplatin
at IC25 on day 1 with three fractions of IR (4 Gy on days 1, 3 and 5) did not show
radiation enhancement effects as assessed by tumor growth delay (Supporting
information, Figure 4-10). In comparison, a significant tumor growth delay was achieved
when three doses of cisplatin at 4 mg/kg were administered alone (days 1, 3 and 5),
with the level of systemic toxicity ensued from this regimen within the acceptable limit
defined in this study (i.e. <20% body weight loss). Therefore, three doses of cisplatin at
4 mg/kg were employed for the subsequent in vivo efficacy and toxicity studies to
achieve an observable radiation enhancement effect.
4.4.4 Cellular Uptake of AuNP-RME In Vivo by TEM
Figure 4-4 presents TEM images of two tumor sections containing AuNP-RME 24
h post-infusion. It can be seen that AuNP-RME have been internalized by cells at the
tumor sites either as single particles or clusters in vacuoles.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 147
Figure 4-4: Representative TEM images of tumor sections obtained from mice 24 h
post i.t. infusion of AuNP-RME. Scale bars represent 2 µm in panels A and D, 500 nm in
panels B and E, and 100 nm in panels C and F. As indicated by arrows, AuNP-RME
were internalized by cells at the tumor site and are present as single particles or
clusters in vacuoles.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 148
4.4.5 Time Dependent Intratumoral Levels of Au as Determined by CT Scan
As shown in Figure 4-5 A, the intratumoral level of Au remains unchanged over
the 120 h period. However, the percentage of the total tumor volume that contains
detectable levels of Au decreased over time (Figure 4-5 B), with the level at 120 h being
significantly lower than that at 5 min post-infusion. This is likely due to rapid tumor
volume changes, as the tumor volumes at 72 and 120 h post-infusion were significantly
larger than those at 5 min. Figure 4-5 D includes CT images of four sections (~1.5 mm
apart) of one tumor obtained 5 min post-infusion. As shown, the distribution of AuNP-
RME throughout the tumor is highly heterogeneous. Figure 4-5 E shows CT images of
the same section of a tumor obtained pre-infusion, and 5 min, 24 h, 72 h, and 120 h
post-infusion. These images demonstrate that the AuNP-RME remain at the same
position without obvious diffusion over time.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 149

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 150
Figure 4-5: (A) Intratumoral levels of Au as measured by CT. The amount of Au in each
tumor was calculated by converting Hounsfield Units (HU) to concentration of Au, using
images acquired prior to AuNP infusion as baseline, and a standard curve established
in a phantom (details are included in “Methods: Intratumoral Distribution and
Quantitative Measurement of AuNP-RME by TEM and CT”). The amount of Au (mg) per
tumor was calculated to be 0.48 at 5 min, 0.520.04 at 24 h, 0.520.06 at 72 h, and
0.49 at 120 h post i.t. infusion of AuNP-RME. There is no significant difference
between Au levels obtained at each time point. Data points represent meanSEM (n=7).
(B) Percentage of tumor volume containing detectable levels of Au. (*) represents a
significant difference in the percentage of tumor with Au at 120 h post-infusion
compared to that at 5 min post-infusion. (C) Tumor volume over time. (*) represents a
significant difference between the tumor volume at 120 h post-infusion compared to that
at 5 min post-infusion. (D) Representative CT images of sections (~1.5 mm apart) of a
tumor 5 min post-infusion. (E) Representative CT images of one section of a tumor pre-
infusion and at 5 min, 24 h, 72 h, and 120 h post-infusion. Tumors are outlined in white
in panels D and E.
4.4.6 Treatment Efficacy and Toxicity In Vivo
Table 4-3 summarizes statistical analyses of the in vivo efficacy and toxicity data
associated with each treatment using no treatment and IR alone as controls. For
assessment of tumor growth and toxicity, statistical analyses were based on the data
collected when the control groups reached predetermined ethical endpoints (day 7 for
the no treatment control and day 9 for IR alone). Treatment efficacy as measured by
percent change in tumor volume is presented in Figure 4-6 A. With the exception of the
AuNP group, all treatment groups showed a significant tumor growth delay on day 7
compared to the no treatment control. Compared to IR alone on day 9, IR+AuNP-RME
and IR+cisplatin showed an equivalent trend in tumor growth delay (p=0.067 vs. 0.079).
IR+AuNP-RME+cisplatin resulted in significantly greater efficacy in comparison to IR
alone (p<0.05).

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 151
Evaluation of systemic toxicity (Figure 4-6 B), in terms of percent body weight
loss, revealed that all treatment groups containing cisplatin induced significant toxicity
relative to the no treatment control. The addition of cisplatin to IR (IR+cisplatin, and
IR+AuNP-RME+cisplatin) also showed significantly higher toxicity in comparison to IR
alone. Conversely, AuNP-RME did not induce systemic toxicity when used alone in
comparison to the no treatment control, as well as when used in combination with IR
(IR+AuNP-RME) as compared to IR alone. The more stringent independent t-test
confirmed that the addition of AuNP-RME to cisplatin in the AuNP-RME+cisplatin group
did not increase toxicity relative to that obtained with cisplatin alone. As well, toxicity of
IR+AuNP-RME+cisplatin was comparable to that of IR+cisplatin.
Survival analysis is shown in Figure 4-6 C, with median survival (days) indicated
in parentheses. An overall statistical test (log rank test) indicated significant survival
differences amongst the treatment groups (p<0.001). Further comparison with p values
adjusted by the Dunnett methods revealed that significant increases in survival were
achieved with IR+AuNP-RME, IR+cisplatin, and IR+AuNP-RME+cisplatin compared to
the no treatment control. In comparison to IR alone, a significant improvement in
survival was only achieved with IR+AuNP-RME+cisplatin.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 152
Table 4-3: Statistical significance in the efficacy and toxicity data obtained for the different treatment groups.
Control No treatment control IR
Treatment groups
Tumor growth
Toxicity Survival Tumor growth
Toxicity Survival
AuNP-RME
Cisplatin * *
AuNP-RME+cisplatin
* *
IR *
IR+AuNP-RME * *
IR+cisplatin * * * *
IR+AuNP-RME+cisplatin
* * * * * *
Note: (*) indicates a significant difference in terms of tumor growth delay, toxicity, or survival in comparison to that of the control groups (no treatment control, or IR alone). Statistical analyses were based on data collected when control groups reached predetermined ethical endpoints (day 7 for the no treatment control and day 9 for IR alone).

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 153

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 154
Figure 4-6: (A) Percent tumor volume change over time. The endpoint for each
treatment group was reached when one mouse in the group had a tumor size greater
than 1.5 cm in any dimension. Tumor size was measured by caliper and calculated
using the formula: volume = (length x width2) x 0.5. Data represent mean±SEM (n=5–9).
Within the legend, (*) indicates significant tumor growth delay compared to the no
treatment control group, and (#) indicates significant tumor growth delay compared to IR
alone. (B) Percent body weight change. Within the legend, (*) indicates significant body
weight change compared to the no treatment control group, and a (#) indicates
significant body weight change compared to IR alone. (C) Survival curves; median
survival (days) for each treatment group is indicated in parentheses. Significantly
prolonged survival was achieved with IR+AuNP-RME, IR+cisplatin, and IR+AuNP-
RME+cisplatin, compared to the no treatment control, as represented by (*). In
comparison to IR alone, significantly prolonged survival was achieved with IR+AuNP-
RME+cisplatin, as represented by (#).

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 155
4.5 Discussion
TNBC is an aggressive subtype of breast cancer that lacks the expression of
oestrogen, progesterone, and ERBB2 receptors (ER-, PR-, HER2-) [54, 55].
Consequently, endocrine and targeted systemic therapies are not applicable, and
treatment is limited to surgery in combination with chemo- and/or RT [56]. It is known
that TNBC cells exhibit radioresistance due to their slow cell cycle progression, which
allows efficient repair of DNA damage induced by IR [56]. The MDA-MB-231Luc+ cell line
used in this study is a TNBC cell line that is breast cancer gene 1 (BRCA1)-competent
with relatively low sensitivity to cisplatin [57]. As such, the CRT strategy
(IR+AuNPs+cisplatin) proposed here may be highly applicable in managing this
disease.
The AuNPs used in this work were coated with PEG to enhance the stability of
the nanoparticles [40, 58]. As shown previously, level of cellular uptake can greatly
impact radiosensitization effects of AuNPs [35, 59], since the LEEs generated by
AuNPs exposed to low energy IR of kilovoltage photons have a short effective range
that is typically on the nanoscale [31, 33, 39, 60, 61]. As such, AuNPs were further
functionalized using a cellular targeting adenoviral RME peptide with the sequence
CKKKKKKSEDEYPYVPN. The positive charge of the peptide promotes electrostatic
interactions with the negatively charged cell membrane, which is followed by NP
internalization [62]. In agreement with our previous work [35, 42] and other studies [63,
64], both AuNP-PEG and AuNP-RME were found to cluster inside vacuoles
(endosomes or lysosomes) upon entering the cells; more importantly, AuNP-RME were
internalized to a greater extent and resulted in a stronger radiosensitization effect than
the non-targeted AuNP-PEG [35, 59].
The radiosensitization effects of cisplatin have been evaluated in numerous in
vitro studies, with DEF values of 1.1-2.5 obtained in a variety of cancer cells treated with
2.50-30.00 M of cisplatin for 0.5-24 h prior to radiation [16-23]. Studies by Blommaert
et al. and Nel et al. have revealed that that while cisplatin-DNA adducts are formed
instantaneously upon addition of cisplatin with the levels of the adducts maintained 24 h

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 156
post-treatment [65, 66], other radiosensitization mechanisms such as cell cycle
synchronization require a relatively long time to occur [67]. Therefore, two different
treatment times (30 min and 48 h) were evaluated in the present study prior to
administration of IR. Cisplatin at IC25 did not show significant radiosensitizing effects in
vitro. These findings suggest that the AuNP-RME formulation employed in the current
study is more effective as a radiosensitizer compared to cisplatin in vitro, since it
demonstrated significant radiosensitizing effect with no observed cytotoxicity in the
absence of IR.
The combination of cisplatin and AuNP-RME yielded an additive and significant
radiosensitization effect in vitro. The absence of a synergistic effect for this combination
in the current study is in contrast to the synergy observed previously in a plasmid DNA
model [38] and is very likely due to the lack of nuclear co-localization of the two agents.
In the plasmid DNA model, both AuNPs and cisplatin are in close proximity to DNA,
allowing the effects of LEE produced by AuNPs to be maximally amplified by cisplatin;
however, AuNP-RME used in this study did not localize in the nucleus.
As an improved therapeutic window of CRT lies in minimizing systemic toxicity
while maximizing radiation enhancement effects, dosage and administration route of the
agents, as well as dosing schedule with RT are three key parameters to be considered
in in vivo studies. Previous in vivo studies have employed a wide range of doses of
AuNPs to evaluate their radiosensitizing effects, with intratumoral levels of Au varying
from 0.25 µg to 74 mg/g tumor [45, 68-77]. In the present study, a dose of 0.5 mg Au
per tumor (equivalent to 2 mg g-1 tumor with a tumor volume of 250 mm3) was
employed, which showed an observable level of clonogenic tumor cell killing in
combination with IR. Intravenously (i.v.) administered AuNPs were found to accumulate
in important organs such as liver and spleen, which may lead to systemic toxicity [78,
79]. In addition, only 0.2 – 7% of injected dose of AuNPs can reach tumor sites following
i.v. administration [76, 80]. As such, AuNP-RME were administered i.t. in the current
study to minimize organ exposure and potential systemic toxicity, and to achieve
maximum accumulation of AuNPs at tumor sites [45, 68, 81]. Given that the physical
interaction with IR is the primary mechanism of radiosensitization by AuNPs [31], it is

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 157
necessary that the AuNPs are present in the tumor at the time of irradiation. In addition,
as mentioned earlier, cellular localization of AuNPs has a great impact on their
radiosensitizing effects. Therefore, AuNP-RME were administered 24 h prior to IR to
allow cellular uptake. Effective cellular uptake as shown in TEM images (Figure 4-4)
suggested that AuNP-RME was an appropriate formulation to pursue radiosensitization
in vivo.
The usual dosage of cisplatin employed in previous in vivo studies to assess its
radiation enhancement effect was between 5-20 mg/kg [25, 52, 82-84]. Herein, three
doses of cisplatin with each administered at IC25 (4 mg/kg) were used to achieve an
observable radiation enhancement effect. In the clinic, cisplatin is administered
systemically [85], therefore, it was administered via i.p. injection in the current study.
Several previous in vivo studies have investigated the impact of cisplatin dosing
schedule on its radiation enhancement effect, with greater effects observed when
cisplatin was administered 15 min to 24 h prior to IR, depending on the tumor model
[25, 82-84, 86]. Based on these observations, as well as the fact that similar DEF values
were obtained in vitro when cells were treated with cisplatin 30 min or 48 h prior to IR,
cisplatin was administered in vivo 30 min prior to each fraction of IR.
In comparison to the no treatment control, both efficacious local tumor
management and prolonged survival of mice were achieved with CRT comprised of
IR+AuNP-RME, IR+cisplatin, and IR+AuNP-RME+cisplatin. These findings suggest that
CRT is more promising compared to IR alone, or chemotherapy (cisplatin) alone. Using
IR alone as a control, the presence of AuNP-RME individually showed a trend towards
enhancing the effects of IR as measured by tumor growth delay (p=0.067), without
showing tumor cell cytotoxicity or systemic toxicity. Failure to show statistically
significant (p<0.05) radiosensitization by AuNP-RME in the current study is likely due to
ineffective penetration and, consequently, a heterogeneous distribution of AuNP-RME
throughout the tumor volume. A heterogeneous intratumoral distribution of AuNP-RME
has been commonly observed following i.t. injection [45, 68]. Their limited penetration is
likely attributed to self-aggregation of AuNP-RME [87], and/or protein binding to the
particle surface [88, 89]. Furthermore, given that radiosensitizing effects of AuNP-RME

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 158
rely on their local concentration [90] and cellular localization [35], dilution of AuNP-RME
over the tumor volume and in tumor cells along the course of treatment, as a result of
repopulation of surviving cells during IR fractions [91], may be additional reasons for the
statistically insignificant radiation enhancement effect observed.
An observable yet not significant radiation enhancement effect measured by
tumor growth delay (p=0.079) was achieved with three doses of cisplatin at IC25. In the
absence of IR, this dose of cisplatin resulted in a significant tumor growth delay
compared to the no treatment control, and was also associated with significant systemic
toxicity. Consistent with our observations, a previous study by Begg et al. revealed that
a single dose of cisplatin (6 mg/kg) was not able to inhibit post-IR (250 kVp, 10 Gy, 15
mA) repair, irrespective of the fact that a significant tumor growth delay was achieved by
cisplatin alone [52]. These phenomena suggest that the observed additive effect of
cisplatin to IR occurs via its intrinsic toxicity as a chemotherapeutic agent rather than as
a radiosensitizer.
It should be stressed that AuNP-RME showed a higher radiation enhancement
effect (DEF =1.25) at a non-toxic concentration compared to cisplatin at IC25 (DEF =
1.14) in vitro. As measured by tumor growth in vivo, AuNP-RME demonstrated an
equivalent level of radiation enhancement as cisplatin (p=0.067 vs. 0.079), without
inducing cellular or systemic toxicity. Moreover, addition of AuNP-RME did not cause an
increase in the toxicity of IR. Therefore, the AuNP-RME formulation employed herein
can be categorized as a true radiosensitizer, as per the aforementioned definition [4, 6,
7].
More importantly, significant radiation enhancement was achieved by the
combination of AuNP-RME and cisplatin, evident by both tumor growth suppression and
overall survival, suggesting that the combination of AuNP with cisplatin is a potent
strategy to improve the outcome of RT. As its toxicity was within the threshold
measured by body weight loss (i.e. less than 20%), a favoured therapeutic window of
the CRT (triple combination of IR+AuNP-RME+cisplatin) lies in its greater toxicity to
tumors in comparison to normal tissues.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 159
4.6 Conclusions
For patients with TNBC, wherein the traditional endocrine and targeted systemic
therapies are not applicable, CRT has begun to play a critical role in improving clinical
outcomes. In the current study, we demonstrated that the combination of AuNPs and
cisplatin significantly enhanced the effects of fractionated IR, and is a promising
strategy to achieve an optimal therapeutic window with CRT for the treatment of chemo-
and radio- resistant TNBC. AuNP-RME was found to be equivalent to cisplatin in terms
of radiation enhancement effect, with the advantage of inducing no intrinsic toxicity or
an increase in the toxicity of IR. Therefore, AuNP-RME can be considered a true
radiosensitizer, while cisplatin functions via its intrinsic toxicity.
Future work will seek to achieve higher stability, homogeneous intratumoral
distribution, effective cellular uptake and nuclear localization of AuNPs by modifying
their physicochemical properties and addition of nuclear targeting moieties [32]. Since
co-delivery and spatial co-localization of AuNPs and cisplatin to biological targets such
as cell nuclei maximizes their IR dose enhancement potential, AuNPs should be utilized
as a cisplatin delivery vehicle, given their straightforward surface chemistry [92].
Furthermore, by conjugating cisplatin to AuNPs via a pH sensitive bond [93], local
release of cisplatin from the formulation can be successfully achieved by exploiting the
acidic tumor microenvironment and thereafter tumor-specific delivery of cisplatin [94]. A
full exploitation of the advantages of such a multimodal formulation will improve the
therapeutic window that can be achieved by CRT comprised of AuNPs and cisplatin.
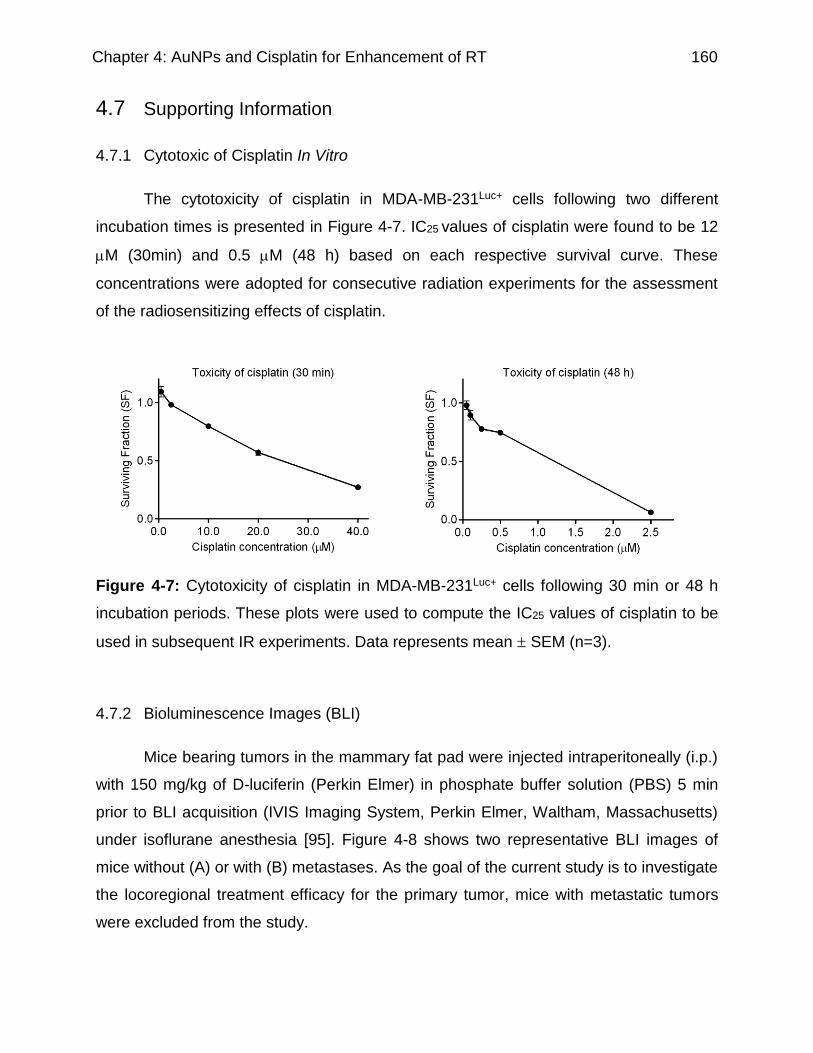
Chapter 4: AuNPs and Cisplatin for Enhancement of RT 160
4.7 Supporting Information
4.7.1 Cytotoxic of Cisplatin In Vitro
The cytotoxicity of cisplatin in MDA-MB-231Luc+ cells following two different
incubation times is presented in Figure 4-7. IC25 values of cisplatin were found to be 12
M (30min) and 0.5 M (48 h) based on each respective survival curve. These
concentrations were adopted for consecutive radiation experiments for the assessment
of the radiosensitizing effects of cisplatin.
Figure 4-7: Cytotoxicity of cisplatin in MDA-MB-231Luc+ cells following 30 min or 48 h
incubation periods. These plots were used to compute the IC25 values of cisplatin to be
used in subsequent IR experiments. Data represents mean SEM (n=3).
4.7.2 Bioluminescence Images (BLI)
Mice bearing tumors in the mammary fat pad were injected intraperitoneally (i.p.)
with 150 mg/kg of D-luciferin (Perkin Elmer) in phosphate buffer solution (PBS) 5 min
prior to BLI acquisition (IVIS Imaging System, Perkin Elmer, Waltham, Massachusetts)
under isoflurane anesthesia [95]. Figure 4-8 shows two representative BLI images of
mice without (A) or with (B) metastases. As the goal of the current study is to investigate
the locoregional treatment efficacy for the primary tumor, mice with metastatic tumors
were excluded from the study.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 161
Figure 4-8: Bioluminescence images of mice after i.p. injection with D-luciferin,
administered five min prior to BLI. (A) without metastases, (B) with metastases.
4.7.3 Determination of Dose of Cisplatin and AuNPs for RT Study by Ex Vivo
Clonogenic Assay
Ex vivo clonogenic assays were first used to determine the appropriate doses of
cisplatin and AuNP-RME for subsequent radiation studies (Table 4-4). The cytotoxicity
of cisplatin to tumor cells in the range of 2-10 mg/kg was evaluated. Previous in vivo
studies have employed a wide range of doses of AuNPs to evaluate their
radiosensitizing effects, with intratumoral levels of Au varying from 0.25 µg to 74 mg/g
tumor [45, 68-77]. In the current study, the radiosensitization effects of AuNPs at three
different doses (i.e., 0.05, 0.25, and 0.5 mg Au per tumor) were assessed and toxicity of
AuNPs at a dose of 0.5 mg Au per tumor was evaluated.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 162
Table 4-4: Treatment groups for ex vivo clonogenic assay. On day one, saline or cisplatin was administered intravenously 30 min prior to IR.
Treatment groups Day 0 Day 1 Day 2
No treatment control Saline, 30 µL ,i.t. Saline, 100 µL, i.p. Clonogenic assay Cisplatin Saline, 30 µL ,i.t. Cispatin, 100 µL,
2-10 mg/kg, i.p.
AuNP-RME AuNP-RME, 30 µL, i.t., 0.5 mg Au per tumor
Saline, 100 µL
AuNP-RME+cisplatin AuNP-RME, 30mL, i.t., 0.5 mg Au per tumor
Cispatin, 100 µL, 4 mg/kg, IR
IR Saline, 30 µL ,i.t. Saline, 100 µL, IR 4Gy
IR+cisplatin Saline, 30 µL ,i.t. Cispatin, 100 µL, 4 mg/kg, IR 4Gy
IR+AuNP-RME AuNP-RME, 30mL, i.t., 0.5 mg Au per tumor
Saline, 100 µL, IR 4Gy
IR+AuNP-RME+cisplatin
AuNP-RME, 30mL, i.t., 0.5 mg Au per tumor
Cispatin, 100 µL, 4 mg/kg, IR 4Gy
Mice were sacrificed and tumors were harvested 24 h post treatment on day two.
Tumors were minced aseptically, and digested in (25ml/tumor) a DMEM/HAM F12 1:1
MIX media supplemented with 2% FBS, 3 mg/mL of collagenase (type 1, BioShop), and
1% of HEPES buffer at 37°C on a shaking rocker for 2 h. Cells were centrifuged and the
digestive media was removed, 2 mL of 0.1% trypsin was added to the cells and
incubated at 37°C for 3 min, trypsin was then neutralized with 3 mL of DMEM/HAM F12
1:1 MIX media supplemented with 10% of FBS. Cells were resuspended in the media
and filtered through a 40-μm cell strainer. An aliquot of the cells was removed and 1:1
stained with trypan blue, and the cell number was counted. Two different cell densities
were seeded in 6-well plates to produce appropriate numbers of colonies. Following 9-
12 days of incubation, the colonies were fixed and stained with 1% methylene blue in
50% ethanol. The number of colonies containing at least 50 cells was counted, and the
results were reported as plating efficiency (number of colonies divided by the number of
cells seeded) for each treatment group [46].
The plating efficiency of each treatment group was plotted in Figure 4-9. A clear
trend of higher tumor cell toxicity was observed with higher doses of cisplatin, with 25%
of cell killing at 4 mg/kg. A pilot study in our group showed that three doses of 4 mg/kg,
48 h apart, was well tolerated in tumor bearing NOD/SCID mice (data not shown). The

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 163
radiosensitization effect of cisplatin was investigated at the dose of IC25, 4 mg/kg.
AuNPs of 0.5 mg Au per tumor showed a relatively greater radiation enhancement
effect in comparison to that of 0.05, or 0.25 mg Au per tumor, although not statistically
significant. As such, a dose of 0.5 mg Au per tumor was employed in subsequent
radiation studies. The presence of cisplatin (4 mg/kg) did not enhance the effect of IR
(PE=0.042±0.006, vs. 0.039±0.002). AuNPs individually (IR+AuNPs) or in combination
with cisplatin (IR+AuNPs+cisplatin) decreased the plating efficiency of IR alone from
0.042±0.006 to 0.031±0.007, and 0.026±0.003, yet not statistically significantly.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 164

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 165
Figure 4-9: Plating efficiency (PE) of cells evaluated using ex vivo clonogenic assay. A
(*) indicates significantly lower PE for the treatment group in comparison to control. IC25
of cisplatin was determined to be 4 mg/kg and used in the subsequent stidies for the
assessment of its radiation enhancement effects and toxicity. Based on this data, a
dose of AuNP-RME at 0.50 mg Au per tumor, which was associated with no cytotoxicity
and the highest level of cell kill in combination with IR, was employed in subsequent
efficacy and toxicity studies in mice.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 166
4.7.4 Treatment Efficacy and Toxicity In Vivo – Single Dose of Cisplatin
Figure 4-10: (A) Percent tumor volume change and (B) percent body weight change for
mice in each treatment group. The endpoint for each treatment group was reached
when one mouse in the group had a tumor size greater than 1.5 cm in any dimension.
Tumor size was measured by caliper and calculated using the equation: volume =
(length x width2) x 0.5. Data represent mean±SEM (n=5). (*) indicates significant tumor
growth delay compared to the control group on day 7. IR+cisplatin did not show
improvement in tumor growth delay compared to IR alone on day 9. There was no
significant difference in body weight change amongst the groups.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 167
4.8 Acknowledgments
This research was funded in part by a Canadian Institutes of Health Research
(CIHR) grant. L. Cui was funded in part by Ontario Graduate Scholarships (OGS), the
MDS Nordion Graduate Scholarship in Radiopharmaceutical Sciences, and the
Hoffmann-La Roche/Rosemarie Hager Graduate Fellowship. M. Dunne received OGS,
and a Dean’s Fund Scholarship. S. Her was funded by an NSERC Graduate
Scholarship. C. Allen is the GlaxoSmithKline Chair in Pharmaceutics and Drug Delivery.
R.G. Bristow is a Canadian Cancer Society Research Scientist. L. Cui thanks summer
student Kaitlynn Almeida for assistance with cell and animal studies.

Chapter 4: AuNPs and cisplatin for Enhancement of RT 168
4.9 References
1. Delaney G, Jacob S, Featherstone C, Barton M. The Role of Radiotherapy in Cancer Treatment: Estimating Optimal Utilization from a Review of Evidence-Based Clinical Guidelines. Cancer. 2005 Sep 15; 104:1129-37.
2. Liauw SL, Connell PP, Weichselbaum RR. New Paradigms and Future Challenges in Radiation Oncology: An Update of Biological Targets and Technology. Sci Transl Med. 2013 Feb 20; 5:173sr2.
3. Seiwert TY, Salama JK, Vokes EE. The Concurrent Chemoradiation Paradigm--General Principles. Nat Clin Pract Oncol. 2007 Feb; 4:86-100.
4. Steel GG, Peckham MJ. Exploitable Mechanisms in Combined Radiotherapy-Chemotherapy: The Concept of Additivity. Int J Radiat Oncol Biol Phys. 1979 Jan; 5:85-91.
5. Wardman P. Chemical Radiosensitizers for Use in Radiotherapy. Clin Oncol (R Coll Radiol). 2007 Aug; 19:397-417.
6. Bindhu J, Anupama, G. Radiosensitization: The New Dogma in Cancer Treatment. Austral - Asian Journal of Cancer. 2005; 4:241-50.
7. Ma BB, Bristow RG, Kim J, Siu LL. Combined-Modality Treatment of Solid Tumors Using Radiotherapy and Molecular Targeted Agents. J Clin Oncol. 2003 Jul 15; 21:2760-76.
8. Overgaard J, Hansen HS, Overgaard M, Bastholt L, Berthelsen A, Specht L, et al. A Randomized Double-Blind Phase Iii Study of Nimorazole as a Hypoxic Radiosensitizer of Primary Radiotherapy in Supraglottic Larynx and Pharynx Carcinoma. Results of the Danish Head and Neck Cancer Study (Dahanca) Protocol 5-85. Radiother Oncol. 1998 Feb; 46:135-46.
9. Rose PG, Bundy BN, Watkins EB, Thigpen JT, Deppe G, Maiman MA, et al. Concurrent Cisplatin-Based Radiotherapy and Chemotherapy for Locally Advanced Cervical Cancer. N Engl J Med. 1999 Apr 15; 340:1144-53.
10. Koutcher L, Sherman E, Fury M, Wolden S, Zhang Z, Mo Q, et al. Concurrent Cisplatin and Radiation Versus Cetuximab and Radiation for Locally Advanced Head-and-Neck Cancer. Int J Radiat Oncol Biol Phys. 2011 Nov 15; 81:915-22.
11. Duenas-Gonzalez A, Zarba JJ, Patel F, Alcedo JC, Beslija S, Casanova L, et al. Phase Iii, Open-Label, Randomized Study Comparing Concurrent Gemcitabine Plus Cisplatin and Radiation Followed by Adjuvant Gemcitabine and Cisplatin Versus Concurrent Cisplatin and Radiation in Patients with Stage Iib to Iva Carcinoma of the Cervix. Journal of Clinical Oncology. 2011 May 1; 29:1678-85.
12. Vokes EE, Senan S, Treat JA, Iscoe NA. Proclaim: A Phase Iii Study of Pemetrexed, Cisplatin, and Radiation Therapy Followed by Consolidation Pemetrexed Versus Etoposide, Cisplatin, and Radiation Therapy Followed by Consolidation Cytotoxic Chemotherapy of Choice in Locally Advanced Stage Iii

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 169
Non-Small-Cell Lung Cancer of Other Than Predominantly Squamous Cell Histology. Clin Lung Cancer. 2009 May; 10:193-8.
13. Dasari S, Tchounwou PB. Cisplatin in Cancer Therapy: Molecular Mechanisms of Action. Eur J Pharmacol. 2014 Oct 5; 740:364-78.
14. Jamieson ER, Lippard SJ. Structure, Recognition, and Processing of Cisplatin-DNA Adducts. Chem Rev. 1999 Sep 8; 99:2467-98.
15. Zak M, Drobnik, J. Effects of Cis-Dichlorodiammineplatinum (Ii) on the Post Irradiation Lethality in Mice after Irradiation with X Rays. Strahlentherapie, 142. 1971; 142:112-5.
16. Douple EB, Richmond RC. Platinum Complexes as Radiosensitizers of Hypoxic Mammalian Cells. Br J Cancer Suppl. 1978 Jun; 3:98-102.
17. Carde P, Laval F. Effect of Cis-Dichlorodiammine Platinum Ii and X Rays on Mammalian Cell Survival. Int J Radiat Oncol Biol Phys. 1981 Jul; 7:929-33.
18. Begg AC, van der Kolk PJ, Dewit L, Bartelink H. Radiosensitization by Cisplatin of Rif1 Tumour Cells in Vitro. Int J Radiat Biol Relat Stud Phys Chem Med. 1986 Nov; 50:871-84.
19. Melvik JE, Pettersen EO. Oxygen- and Temperature-Dependent Cytotoxic and Radiosensitizing Effects of Cis-Dichlorodiammineplatinum(Ii) on Human Nhik 3025 Cells in Vitro. Radiat Res. 1988 Jun; 114:489-99.
20. Wilkins DE, Ng CE, Raaphorst GP. Cisplatin and Low Dose Rate Irradiation in Cisplatin Resistant and Sensitive Human Glioma Cells. Int J Radiat Oncol Biol Phys. 1996 Aug 1; 36:105-11.
21. Raaphorst GP, Wang G, Stewart D, Ng CE. Concomitant Low Dose-Rate Irradiation and Cisplatin Treatment in Ovarian Carcinoma Cell Lines Sensitive and Resistant to Cisplatin Treatment. Int J Radiat Biol. 1996 May; 69:623-31.
22. Areberg J, Johnsson A, Wennerberg J. In Vitro Toxicity of (191)Pt-Labeled Cisplatin to a Human Cervical Carcinoma Cell Line (Me-180). Int J Radiat Oncol Biol Phys. 2000 Mar 15; 46:1275-80.
23. Boeckman HJ, Trego KS, Turchi JJ. Cisplatin Sensitizes Cancer Cells to Ionizing Radiation Via Inhibition of Nonhomologous End Joining. Mol Cancer Res. 2005 May; 3:277-85.
24. Julia AM, Canal P, Berg D, Bachaud JM, Daly NJ, Bugat R. Concomitant Evaluation of Efficiency, Acute and Delayed Toxicities of Combined Treatment of Radiation and Cddp on an in Vivo Model. Int J Radiat Oncol Biol Phys. 1991 Feb; 20:347-50.
25. Sun JR, Brown JM. Lack of Differential Radiosensitization of Hypoxic Cells in a Mouse Tumor at Low Radiation Doses Per Fraction by Cisplatin. Radiat Res. 1993 Feb; 133:252-6.
26. Rao BS, Devi PU. Response of Mouse Sarcoma-180 to Cis-Platin in Combination with Radiation & Hyperthermia. Indian J Med Res. 1996 Jun; 103:315-22.
Chapter 4: AuNPs and Cisplatin for Enhancement of RT 170
27. Kvols LK. Radiation Sensitizers: A Selective Review of Molecules Targeting DNA and Non-DNA Targets. J Nucl Med. 2005 Jan; 46 Suppl 1:187S-90S.
28. Lu QB. Molecular Reaction Mechanisms of Combination Treatments of Low-Dose Cisplatin with Radiotherapy and Photodynamic Therapy. J Med Chem. 2007 May 31; 50:2601-4.
29. Lu QB, Kalantari S, Wang CR. Electron Transfer Reaction Mechanism of Cisplatin with DNA at the Molecular Level. Mol Pharm. 2007 Jul-Aug; 4:624-8.
30. Stone HB, Coleman CN, Anscher MS, McBride WH. Effects of Radiation on Normal Tissue: Consequences and Mechanisms. Lancet Oncol. 2003 Sep; 4:529-36.
31. Butterworth KT, McMahon SJ, Currell FJ, Prise KM. Physical Basis and Biological Mechanisms of Gold Nanoparticle Radiosensitization. Nanoscale. 2012 Aug 21; 4:4830-8.
32. Her S, Jaffray DA, Allen C. Gold Nanoparticles for Applications in Cancer Radiotherapy: Mechanisms and Recent Advancements. Adv Drug Deliv Rev. 2015 Dec 19.
33. Coulter JA, Hyland WB, Nicol J, Currell FJ. Radiosensitising Nanoparticles as Novel Cancer Therapeutics--Pipe Dream or Realistic Prospect? Clin Oncol (R Coll Radiol). 2013 Oct; 25:593-603.
34. Roa W, Zhang X, Guo L, Shaw A, Hu X, Xiong Y, et al. Gold Nanoparticle Sensitize Radiotherapy of Prostate Cancer Cells by Regulation of the Cell Cycle. Nanotechnology. 2009 Sep 16; 20:375101.
35. Cui L, Tse K, Zahedi P, Harding SM, Zafarana G, Jaffray DA, et al. Hypoxia and Cellular Localization Influence the Radiosensitizing Effect of Gold Nanoparticles (Aunps) in Breast Cancer Cells. Radiat Res. 2014 Nov; 182:475-88.
36. Taggart LE, McMahon SJ, Currell FJ, Prise KM, Butterworth KT. The Role of Mitochondrial Function in Gold Nanoparticle Mediated Radiosensitisation. Cancer Nanotechnol. 2014; 5:5.
37. Pan Y, Leifert A, Ruau D, Neuss S, Bornemann J, Schmid G, et al. Gold Nanoparticles of Diameter 1.4 Nm Trigger Necrosis by Oxidative Stress and Mitochondrial Damage. Small. 2009 Sep; 5:2067-76.
38. Zheng Y, Sanche L. Gold Nanoparticles Enhance DNA Damage Induced by Anti-Cancer Drugs and Radiation. Radiat Res. 2009 Jul; 172:114-9.
39. Jain S, Hirst DG, O'Sullivan JM. Gold Nanoparticles as Novel Agents for Cancer Therapy. Br J Radiol. 2012 Feb; 85:101-13.
40. Shimmin RG, Schoch AB, Braun PV. Polymer Size and Concentration Effects on the Size of Gold Nanoparticles Capped by Polymeric Thiols. Langmuir. 2004 Jun 22; 20:5613-20.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 171
41. Liu Y, Shipton MK, Ryan J, Kaufman ED, Franzen S, Feldheim DL. Synthesis, Stability, and Cellular Internalization of Gold Nanoparticles Containing Mixed Peptide-Poly(Ethylene Glycol) Monolayers. Anal Chem. 2007 Mar 15; 79:2221-9.
42. Cui L, Zahedi P, Saraceno J, Bristow R, Jaffray D, Allen C. Neoplastic Cell Response to Tiopronin-Coated Gold Nanoparticles. Nanomedicine. 2013 Feb; 9:264-73.
43. Chithrani BD, Ghazani AA, Chan WC. Determining the Size and Shape Dependence of Gold Nanoparticle Uptake into Mammalian Cells. Nano Lett. 2006 Apr; 6:662-8.
44. Chithrani DB, Jelveh S, Jalali F, van Prooijen M, Allen C, Bristow RG, et al. Gold Nanoparticles as Radiation Sensitizers in Cancer Therapy. Radiat Res. 2010 Jun; 173:719-28.
45. Chattopadhyay N, Cai Z, Kwon YL, Lechtman E, Pignol JP, Reilly RM. Molecularly Targeted Gold Nanoparticles Enhance the Radiation Response of Breast Cancer Cells and Tumor Xenografts to X-Radiation. Breast Cancer Res Treat. 2013 Jan; 137:81-91.
46. Joiner M vdKA, editor. Basic Clinical Radiobiology. London: Hodder Arnold; 2009.
47. Sadikot RT, Blackwell TS. Bioluminescence Imaging. Proc Am Thorac Soc. 2005; 2:537-40, 11-2.
48. Heldin CH, Rubin K, Pietras K, Ostman A. High Interstitial Fluid Pressure - an Obstacle in Cancer Therapy. Nat Rev Cancer. 2004 Oct; 4:806-13.
49. Boucher Y, Brekken C, Netti PA, Baxter LT, Jain RK. Intratumoral Infusion of Fluid: Estimation of Hydraulic Conductivity and Implications for the Delivery of Therapeutic Agents. Br J Cancer. 1998 Dec; 78:1442-8.
50. Dunne M, Zheng J, Rosenblat J, Jaffray DA, Allen C. Apn/Cd13-Targeting as a Strategy to Alter the Tumor Accumulation of Liposomes. J Control Release. 2011 Sep 25; 154:298-305.
51. Du LY, Umoh J, Nikolov HN, Pollmann SI, Lee TY, Holdsworth DW. A Quality Assurance Phantom for the Performance Evaluation of Volumetric Micro-Ct Systems. Phys Med Biol. 2007 Dec 7; 52:7087-108.
52. Begg AC, Bohlken S, Bartelink H. The Effect of Cisplatin on the Repair of Radiation Damage in Rif1 Mouse Tumours in Vivo. Radiother Oncol. 1989 May; 15:79-91.
53. Dou YN, Zheng J, Foltz WD, Weersink R, Chaudary N, Jaffray DA, et al. Heat-Activated Thermosensitive Liposomal Cisplatin (Htlc) Results in Effective Growth Delay of Cervical Carcinoma in Mice. J Control Release. 2014 Mar 28; 178:69-78.
54. Cleator S, Heller W, Coombes RC. Triple-Negative Breast Cancer: Therapeutic Options. Lancet Oncol. 2007 Mar; 8:235-44.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 172
55. Anders CK, Zagar TM, Carey LA. The Management of Early-Stage and Metastatic Triple-Negative Breast Cancer: A Review. Hematol Oncol Clin North Am. 2013 Aug; 27:737-49, viii.
56. Eiermann W, Vallis KA. Locoregional Treatments for Triple-Negative Breast Cancer. Ann Oncol. 2012 Aug; 23 Suppl 6:vi30-4.
57. Tassone P, Tagliaferri P, Perricelli A, Blotta S, Quaresima B, Martelli ML, et al. Brca1 Expression Modulates Chemosensitivity of Brca1-Defective Hcc1937 Human Breast Cancer Cells. Br J Cancer. 2003 Apr 22; 88:1285-91.
58. De Jong WH, Borm PJ. Drug Delivery and Nanoparticles:Applications and Hazards. Int J Nanomedicine. 2008; 3:133-49.
59. Kong T, Zeng J, Wang X, Yang X, Yang J, McQuarrie S, et al. Enhancement of Radiation Cytotoxicity in Breast-Cancer Cells by Localized Attachment of Gold Nanoparticles. Small. 2008 Sep; 4:1537-43.
60. Mesbahi A. A Review on Gold Nanoparticles Radiosensitization Effect in Radiation Therapy of Cancer. Rep Pract Oncol Radiother. 2010; 15:176-80.
61. Jeremic B, Aguerri AR, Filipovic N. Radiosensitization by Gold Nanoparticles. Clin Transl Oncol. 2013 Aug; 15:593-601.
62. Nicol JR, Dixon D, Coulter JA. Gold Nanoparticle Surface Functionalization: A Necessary Requirement in the Development of Novel Nanotherapeutics. Nanomedicine (Lond). 2015 Apr; 10:1315-26.
63. Cai X, Chen HH, Wang CL, Chen ST, Lai SF, Chien CC, et al. Imaging the Cellular Uptake of Tiopronin-Modified Gold Nanoparticles. Anal Bioanal Chem. 2011 Aug; 401:809-16.
64. Levy R, Shaheen U, Cesbron Y, See V. Gold Nanoparticles Delivery in Mammalian Live Cells: A Critical Review. Nano Rev. 2010; 1.
65. Blommaert FA, Floot BG, van Dijk-Knijnenburg HC, Berends F, Baan RA, Schornagel JH, et al. The Formation and Repair of Cisplatin-DNA Adducts in Wild-Type and Cisplatin-Resistant L1210 Cells: Comparison of Immunocytochemical Determination with Detection in Isolated DNA. Chem Biol Interact. 1998 Jan 30; 108:209-25.
66. Nel I, Gauler TC, Eberhardt WE, Nickel AC, Schuler M, Thomale J, et al. Formation and Repair Kinetics of Pt-(Gpg) DNA Adducts in Extracted Circulating Tumour Cells and Response to Platinum Treatment. Br J Cancer. 2013 Sep 3; 109:1223-9.
67. Sorenson CM, Barry MA, Eastman A. Analysis of Events Associated with Cell Cycle Arrest at G2 Phase and Cell Death Induced by Cisplatin. J Natl Cancer Inst. 1990 May 2; 82:749-55.
68. Herold DM, Das IJ, Stobbe CC, Iyer RV, Chapman JD. Gold Microspheres: A Selective Technique for Producing Biologically Effective Dose Enhancement. Int J Radiat Biol. 2000 Oct; 76:1357-64.

Chapter 4: AuNPs and Cisplatin for Enhancement of RT 173
69. Hainfeld JF, Slatkin DN, Smilowitz HM. The Use of Gold Nanoparticles to Enhance Radiotherapy in Mice. Phys Med Biol. 2004 Sep 21; 49:N309-15.
70. Chang MY, Shiau AL, Chen YH, Chang CJ, Chen HH, Wu CL. Increased Apoptotic Potential and Dose-Enhancing Effect of Gold Nanoparticles in Combination with Single-Dose Clinical Electron Beams on Tumor-Bearing Mice. Cancer Sci. 2008 Jul; 99:1479-84.
71. Hebert EM, Debouttiere PJ, Lepage M, Sanche L, Hunting DJ. Preferential Tumour Accumulation of Gold Nanoparticles, Visualised by Magnetic Resonance Imaging: Radiosensitisation Studies in Vivo and in Vitro. Int J Radiat Biol. 2010 Aug; 86:692-700.
72. Zhang XD, Wu D, Shen X, Chen J, Sun YM, Liu PX, et al. Size-Dependent Radiosensitization of Peg-Coated Gold Nanoparticles for Cancer Radiation Therapy. Biomaterials. 2012 Sep; 33:6408-19.
73. Kim JK, Seo SJ, Kim HT, Kim KH, Chung MH, Kim KR, et al. Enhanced Proton Treatment in Mouse Tumors through Proton Irradiated Nanoradiator Effects on Metallic Nanoparticles. Phys Med Biol. 2012 Dec 21; 57:8309-23.
74. Hainfeld JF, Smilowitz HM, O'Connor MJ, Dilmanian FA, Slatkin DN. Gold Nanoparticle Imaging and Radiotherapy of Brain Tumors in Mice. Nanomedicine (Lond). 2013 Oct; 8:1601-9.
75. Joh DY, Sun L, Stangl M, Al Zaki A, Murty S, Santoiemma PP, et al. Selective Targeting of Brain Tumors with Gold Nanoparticle-Induced Radiosensitization. PLoS One. 2013; 8:e62425.
76. Al Zaki A, Joh D, Cheng Z, De Barros AL, Kao G, Dorsey J, et al. Gold-Loaded Polymeric Micelles for Computed Tomography-Guided Radiation Therapy Treatment and Radiosensitization. ACS Nano. 2014 Jan 28; 8:104-12.
77. Wolfe T, Chatterjee D, Lee J, Grant JD, Bhattarai S, Tailor R, et al. Targeted Gold Nanoparticles Enhance Sensitization of Prostate Tumors to Megavoltage Radiation Therapy in Vivo. Nanomedicine. 2015 Jul; 11:1277-83.
78. Zhang G, Yang Z, Lu W, Zhang R, Huang Q, Tian M, et al. Influence of Anchoring Ligands and Particle Size on the Colloidal Stability and in Vivo Biodistribution of Polyethylene Glycol-Coated Gold Nanoparticles in Tumor-Xenografted Mice. Biomaterials. 2009 Apr; 30:1928-36.
79. De Jong WH, Hagens WI, Krystek P, Burger MC, Sips AJ, Geertsma RE. Particle Size-Dependent Organ Distribution of Gold Nanoparticles after Intravenous Administration. Biomaterials. 2008 Apr; 29:1912-9.
80. Wolfe T. Proton Therapy Enhanced by Tumor-Targeting Gold Nanoparticles: A Pilot in Vivo Experiment at the Proton Therapy Center at Md Anderson Cancer Center. Med Phys. 2014; 41:518.
81. Lin FS. Radiotherapy of the Excretable Radioactive Gold Nanocomposite with Intratumoral Injection. International Journal of Materials, Mechanics and Manufacturing. 2013; 1:265-8.
Chapter 4: AuNPs and Cisplatin for Enhancement of RT 174
82. Douple EB. Treatment of an Intracerebral Rat Brain Tumor with Corynebacterium Parvum and Radiation. Natl Cancer Inst Monogr. 1977 Dec; 46:179-84.
83. Douple EB, Richmond RC. Enhancement of the Potentiation of Radiotherapy by Platinum Drugs in a Mouse Tumor. Int J Radiat Oncol Biol Phys. 1982 Mar-Apr; 8:501-3.
84. Kovacs CJ, Schenken LL, Burholt DR. Therapeutic Potentiation of Combined Cis-Dichlorodiammineplatinum (Ii) and Irradiation by Icrf-159. Int J Radiat Oncol Biol Phys. 1979 Aug; 5:1361-4.
85. Loehrer PJ, Einhorn LH. Drugs Five Years Later. Cisplatin. Ann Intern Med. 1984 May; 100:704-13.
86. Overgaard J, Khan AR. Selective Enhancement of Radiation Response in a C3h Mammary Carcinoma by Cisplatin. Cancer Trat Rep. 1981; 65:501-3.
87. Albanese A, Chan WC. Effect of Gold Nanoparticle Aggregation on Cell Uptake and Toxicity. ACS Nano. 2011 Jul 26; 5:5478-89.
88. Dobrovolskaia MA, Patri AK, Zheng J, Clogston JD, Ayub N, Aggarwal P, et al. Interaction of Colloidal Gold Nanoparticles with Human Blood: Effects on Particle Size and Analysis of Plasma Protein Binding Profiles. Nanomedicine. 2009 Jun; 5:106-17.
89. Boulos SP, Davis TA, Yang JA, Lohse SE, Alkilany AM, Holland LA, et al. Nanoparticle-Protein Interactions: A Thermodynamic and Kinetic Study of the Adsorption of Bovine Serum Albumin to Gold Nanoparticle Surfaces. Langmuir. 2013 Dec 3; 29:14984-96.
90. Liu Y, Liu X, Jin X, He P, Zheng X, Dai Z, et al. The Dependence of Radiation Enhancement Effect on the Concentration of Gold Nanoparticles Exposed to Low- and High-Let Radiations. Phys Med. 2015 May; 31:210-8.
91. Kim JA, Aberg C, Salvati A, Dawson KA. Role of Cell Cycle on the Cellular Uptake and Dilution of Nanoparticles in a Cell Population. Nat Nanotechnol. 2012 Jan; 7:62-8.
92. Daniel MC, Astruc D. Gold Nanoparticles: Assembly, Supramolecular Chemistry, Quantum-Size-Related Properties, and Applications toward Biology, Catalysis, and Nanotechnology. Chem Rev. 2004 Jan; 104:293-346.
93. Comenge J, Sotelo C, Romero F, Gallego O, Barnadas A, Parada TG, et al. Detoxifying Antitumoral Drugs Via Nanoconjugation: The Case of Gold Nanoparticles and Cisplatin. PLoS One. 2012; 7:e47562.
94. Estrella V, Chen T, Lloyd M, Wojtkowiak J, Cornnell HH, Ibrahim-Hashim A, et al. Acidity Generated by the Tumor Microenvironment Drives Local Invasion. Cancer Res. 2013 Mar 1; 73:1524-35.
95. Zheng J, Muhanna N, De Souza R, Wada H, Chan H, Akens MK, et al. A Multimodal Nano Agent for Image-Guided Cancer Surgery. Biomaterials. 2015 Oct; 67:160-8.

Chapter 5: Conclusions and Future Directions 175
Chapter 5
Conclusions and Future Directions
Lei Cui, Sohyoung Her, Christine Allen
Experiments by L.Cui and S.Her. Written by L.Cui. Figures by S.Her. Edited by C. Allen.

Chapter 5: Conclusions and Future Directions 176
5.1 Summary of Findings
The general goal of this thesis was to develop formulations of AuNPs and identify
parameters for the achievement of an improved radiosensiting effect by AuNPs. In
particular, it was hypothesized that cellular uptake of AuNPs and the level of oxygen
have great impacts on the radiosensitizing effect of AuNPs. Cellular uptake of AuNPs is
in turn determined by the physicochemical properties and concentration of AuNPs, as
well as the time of exposure of cells to AuNPs. An additional goal of this research was
to evaluate the radiation enhancement effect of AuNPs in combination to cisplatin as in
comparison to AuNPs or cisplatin alone.
The second chapter aimed to synthesize and characterize AuNP-TP, and further
to understand cell uptake and cytotoxicity of the nanoparticles in various cell lines. As
described in Chapter 2, AuNP-TP was synthesized by the reduction of Au3+ using
NaBH4 as the reducing agent, and tioprotin as the coating material. The average core
diameter of AuNP-TP synthesized (Figure 2-1) was found to be 2.7nm (Figure 2-2);
upon incubation in full cell culture medium a fraction of the nanoparticles aggregated
and precipitated out of the medium (with 76% ± 2% of the AuNPs remaining as single
particles in medium following 72 h of incubation). TEM images showed that upon
entering cells, AuNPs were sequestered as clusters in endosome and lysosome
vacuoles in the perinuclear region (Figure 2-3). Level of cellular uptake of AuNP-TP was
found to be dependent on incubation time, concentration of AuNPs, as well as the cell
line (Figure 2-4). A kinetic study revealed that the overall cellular uptake of AuNPs
increases with time and the decrease in the average amount of Au in a single cell at a
particular time point (8 h) is due to a faster rate of cell proliferation over cell uptake of
AuNPs. As well higher levels of uptake were achieved when cells were treated with
higher concentrations of particles. AuNP-TP exhibited a significant cytotoxicity in Hela
and MCF-7 as evaluated by the clonogenic assay (Figure 2-5), with ROS generation
being the underlying mechanism. Prolonged incubation of cells in AuNP-containing
media resulted in increased amounts of ROS (Figure 2-6). The toxicity of AuNPs were
found to be reduced by thiol-containing antioxidants such as GSH and tiopronin, which
function via ROS consumption, as well as shielding the reactive sites on the surface of

Chapter 5: Conclusions and Future Directions 177
AuNPs by binding to the nanoparticles through a strong, semi-covalent Au-S bond,
which consequently reduces the yield of ROS generation reactions.
In Chapter 3 it was found that a TNBC cell line’s response to AuNP-TP is
dependent on incubation time and concentration of AuNPs, furthermore,
radiosensitization by AuNP-TP was greatly influenced by cellular localization and
oxygen levels. Prolonged incubation of cells in media containing higher levels of AuNPs
resulted in diminished cell survival (Figure 3-2). Cellular uptake of AuNP-TP increased
with concentration (0.01-1.00 mg/mL) and began to plateau at 0.5 mg/mL (Figure 3-3 A
and B). In addition, hypoxia greatly decreased the amount of AuNPs internalized by
cells by three fold (Figure 3-3 B). Importantly, cellular localization showed a great
impact on the radiosensitizing effect of AuNPs - DEF values of 1.09, 1.37, and 1.41
were observed with AuNPs present in the extracellular, intracellular, or both
extracellular and intracellular regions (Figure 3-6, and Table 3-2). Thus, it can be
concluded that AuNPs that are internalized by cells are more effective enhancing the
effect of IR at 225 kVp. Furthermore, radiosensitization by AuNPs was found to be
oxygen dependent, which was highest under oxia, followed by chronic hypoxia, and
lowest under acute hypoxia (Figure 3-7 A, B, and Table 3-3). The relatively higher
radiosensitization effect of AuNPs under chronic hypoxia was attributed to the higher
radiosensitivity of these cells, which is due to their diminished capacity for homologous
recombination as a result of a lowered expression level of the HR related proteins such
as Rad51 (Figure 3-7 C). Mechanistic studies revealed that prolonged treatment of cells
with AuNP-TP, for up to 48 h, did not result in cell cycle arrest (Figure 3-8). However,
post IR DNA repair was inhibited by the AuNPs as higher numbers of residual foci of -
H2AX, but not the initial foci, was observed when cells were pretreated with AuNP-TP
(Figure 3-9). In general, results from this study highlighted that AuNPs employed here
were involved in all three phases (physical, chemical, and biological) of the effects of IR
on the biological targets, as such cellular localization of AuNPs and oxygen level are
critical in determining the level of radiosensitization that can be achieved by AuNPs.
In Chapter 4 non-targeted and cellular targeted AuNPs were synthesized and
characterized, their radiosensitizing effects were evaluated in the TNBC cells used in

Chapter 5: Conclusions and Future Directions 178
Chapter 3. In addition, the radiation enhancement effect of AuNPs and cisplatin,
individually or in combination, were examined both in vitro and in vivo. AuNP-PEG and
AuNP-RME synthesized in this chapter 4 have an average core diameter of 5.811.53
nm (Figure 4-2 A), and hydrodynamic diameters of 20.873.32 and 23.892.23 nm,
respectively. Both formulations were found to be stable when incubated in cell culture
media over 48 h. Significantly higher cellular uptake was achieved for AuNP-RME in
comparison to AuNP-PEG; prolonged incubation also led to higher intracellular levels of
AuNP-RME (Figure 4-2 D). TEM images revealed that both AuNP-PEG and AuNP-RME
were clustered in endosomal and lysosomal vacuoles upon entering cells. Both
formulations were found to be non-toxic (0.5 mg/mL, 24 h) (Figure 4-2 E, F). A
significant radiosensitization effect was achieved by AuNP-RME (DEF=1.25) but not
AuNP-PEG (DEF=1.14), indicating a positive correlation between level of intracellular
Au and the extent of radiosensitization by AuNPs (Figure 4-3 A). DEF values of 1.11
and 1.14 were achieved for cisplatin at IC25 with incubation periods of 48 h or 30 min,
respectively (Figure 4-3 B). The combination of AuNPs and cisplatin showed an additive
and significant DEF of 1.29 (Figure 4-3 C). TEM images revealed that AuNPs were
internalized by cells at tumor sites 24 h post intratumoral infusion at a dose of 0.5 mg
Au per tumor (Figure 4-4). The time dependent intratumoral levels of Au as measured
by CT suggest remained unchanged up to 120 h post i.t. administration (Figure 4-5 A).
The percentage of the tumor volume that contained detectable levels of Au decreased
(Figre 4-5 B) over time as a result of tumor growth (Figure 4-5 C) and ineffective
penetration of AuNPs in the tumor (Figure 4-5 D, E). Tumor growth assessment showed
that AuNPs at the dose of 0.5 mg Au per tumor or 3 doses of cisplatin at IC25
individually enhanced the effect of IR (3X4 Gy) equivalently yet not significantly
(p=0.067 vs. p=0.078) (Figure 4-6 A). A significant tumor growth delay compared to IR
alone was achieved by the triple combination of AuNPs+cisplatin+IR (Figure 4-6 A).
Also, significantly improved overall survival was achieved with IR+AuNPs+cisplatin in
comparison to IR alone (Figure 4-6 C). Toxicity (as measured by body weight loss)
revealed that the efficacy (tumor growth delay) of cisplatin were associated with
significant systemic toxicity (Figure 4-6 B). Overall, these observations suggest that
AuNP-RME is the true radiosensitizer with no intrinsic toxicity following i.t. infusion,

Chapter 5: Conclusions and Future Directions 179
while cisplatin enhances the effect of IR via its inherent toxicity. The combination of the
two agents was demonstrated as a promising strategy to enhance the effect of
fractionated IR.

Chapter 5: Conclusions and Future Directions 180
5.2 Conclusions and Future Directions
Results from this thesis suggest that better stability of AuNPs can be achieved by
choosing appropriate coating materials such as PEG. There is a positive correlation
between radiosensitization effects and the cellular uptake of AuNPs, which in turn is a
combined result of the physicochemical properties of the AuNPs (surface materials and
targeting modality) their concentration, incubation time, and the cell line employed. The
oxygen level at the time of IR greatly impacts radiosensitization by AuNPs. In
comparison to cisplatin, AuNP-RME administered intratumorally can be considered as a
true radiosensitizer due their negligible systemic toxicity. Findings from this thesis
warrant further optimization of formulations of AuNPs for the achievement of improved
bioavailability at tumor sites, in tumor cells, and further cell nuclei.
More importantly, with the observation of a significant radiation enhancement
effect for the combination of AuNPs and cisplatin in Chapter 4, using AuNPs as a
delivery vehicle for cisplatin to achieve co-delivery of the two agents to tumors may be a
valuable strategy. Advantages of such a formulation include 1) elevated tumor
accumulation and prolonged retention of cisplatin in tumors in comparison to cisplatin
alone, 2) diminished systemic toxicity of cisplatin [1, 2], and 3) local release of cisplatin
at tumor sites by conjugation of cisplatin to AuNPs via a pH sensitive bond [3], given the
acidic microenvironment in solid tumors [4, 5] and intracellular compartments [6].

Chapter 5: Conclusions and Future Directions 181
Figure 5-1: Schematic illustration of synthesis of peptide and cisplatin conjugated
AuNPs. (A) Synthesis of AuNP-PEG. (B) Synthesis of cisplatin prodrug. (C) Conjugation
of peptide and cisplatin to AuNPs.

Chapter 5: Conclusions and Future Directions 182
A preliminary study by our group developed a formulation of cisplatin and RME
conjugated AuNPs (AuNP-(RME+cisplatin) using a method described by Dhar et al. with
modifications [3] (Figure 5-1), with the final molar ratio of cisplatin to AuNPs being
330:1. The cellular response and radiosensitzation effect of this formulation was
evaluated in two TNBC cell lines MDA-MB-231 (BRCA-1 competent) and MDA-MB-436
(BRCA-1 deficient) using the same methods as described in the previous chapters. Cell
uptake studies revealed that AuNP-(RME+cisplatin) clustered in endosomes and
lysosomes following cell entry (Figure 5-2). Quantitative analysis by ICP-AES showed
that conjugation of cisplatin increased the cellular uptake of AuNPs. Further research
needs to be conducted to clarify whether this is due to a favorable electrostatic
interaction between AuNP-(RME+cisplatin) and the cell membrane, or a diminished rate
of cell proliferation given the cytotoxicity of cisplatin. The cytotoxicity of AuNP-RME and
AuNP-(RME+cisplatin) was evaluated by clonogenic assay at different concentrations of
AuNPs with a 24h incubation period. Significantly greater cytotoxicity was observed in
cells treated with AuNP-(RME+cisplatin) in comparison to those treated with AuNP-RME
alone (0.5 mg/mL, 24h), especially in BRCA-1 deficient and cisplatin sensitive MDA-MB-
436 cells. These findings suggest that the activity of cisplatin was retained following
conjugation to AuNPs, via the reduction of the prodrug in the form of Pt(IV) to its active
form Pt(II) in acidic cellular compartments such as lysosomes [3].

Chapter 5: Conclusions and Future Directions 183
Figure 5-2: TEM images of AuNP-(RME+cisplatin) accumulation in MDA-MB-231 (A,
B), and MDA-MB-436 (C, D) following 24 h of incubatiion. Scale bar represents 2 m in
(A and C) and 100 nm in (C and D). Upon entering cells AuNP-(RME+cisplatin) are
sequestered in endosomes and lysosomes.

Chapter 5: Conclusions and Future Directions 184
Figure 5-3: In vitro cellular accumulation of AuNP-RME and AuNP-(RME+cisplatin) in
MDA-MB-231 and MDA-MB-436 cells quantified by ICP-AES with incubation at the
concentration of 0.5 mg/mL AuNPs. * Represents statistically significant differences
between AuNP-RME and AuNP-(RME+cisplatin) in terms of cellular levels of Au
(p<0.05), Data represents mean SEM (n=3).

Chapter 5: Conclusions and Future Directions 185
Figure 5-4: Cell surviving fraction (SF) following 24 h of treatment with different
concentrations of AuNP-RME or AuNP-(RME+cisplatin) in MDA-MB-231 and MDA-MB-
436 cells. SF as determined by clonogenic assays is reported as plating efficiency
compared to non-treated cells. A (*) represents statistically significant differences
between various concentrations for HeLa and MCF-7 cells, respectively (p<0.05). Data
represents mean SD (n=3).
Furthermore, the radiosensitization effects of AuNP-RME and AuNP-
(RME+cisplatin) (0.5 mg/mL, 24h) were evaluated in MDA-MB-231 and MDA-MB-436.
Significantly higher DEF values were observed in cells pretreated with AuNP-
(RME+cisplatin) compared to those treated with AuNP-RME alone (1.16 vs. 1.41 in
MDA-MB-231, and 1.25 vs. 1.91 in MDA-MB-436) (Figure 5-5). These results revealed
that conjugation of cisplatin to AuNPs is a promising strategy to be utilized in CRT.
Following the successful proof of concept studies, further evaluation in the animal
xenograft model used in Chapter 4 is warranted. Especially, local release of cisplatin at
tumor sites may provide additional efficacy for this treatment given the acidic
microenvironment present in tumors [4], this may offset the heterogeneous intratumoral
distribution achieved with the AuNPs.

Chapter 5: Conclusions and Future Directions 186
Figure 5-5: Radiation dose response curves for cells pretreated with AuNP-RME or
AuNP-(RME+cisplatin) (0.5 mg/mL, 24h). DEF values for AuNP-RME and AuNP-
(RME+cisplatin) at 0.1 SF were 1.16 and 1.41 (MDA-MB-231), 1.25 and 1.91 (MDA-MB-
436), respectively, using IR alone as control.

Chapter 5: Conclusions and Future Directions 187
5.3 References
1. Comenge J, Sotelo C, Romero F, Gallego O, Barnadas A, Parada TG, et al. Detoxifying Antitumoral Drugs Via Nanoconjugation: The Case of Gold Nanoparticles and Cisplatin. PLoS One. 2012; 7:e47562.
2. Dhar S, Kolishetti N, Lippard SJ, Farokhzad OC. Targeted Delivery of a Cisplatin Prodrug for Safer and More Effective Prostate Cancer Therapy in Vivo. Proc Natl Acad Sci U S A. 2011 Feb 1; 108:1850-5.
3. Dhar S, Daniel WL, Giljohann DA, Mirkin CA, Lippard SJ. Polyvalent Oligonucleotide Gold Nanoparticle Conjugates as Delivery Vehicles for Platinum(Iv) Warheads. J Am Chem Soc. 2009 Oct 21; 131:14652-3.
4. Tredan O, Galmarini CM, Patel K, Tannock IF. Drug Resistance and the Solid Tumor Microenvironment. J Natl Cancer Inst. 2007 Oct 3; 99:1441-54.
5. Tannock IF, Rotin D. Acid Ph in Tumors and Its Potential for Therapeutic Exploitation. Cancer Res. 1989 Aug 15; 49:4373-84.
6. Anderson RG, Orci L. A View of Acidic Intracellular Compartments. J Cell Biol. 1988 Mar; 106:539-43.
Related Documents











