Clinical and Experimental Pharmacology and Physiology (2005) 32, 871–881 OPERATIVE CONTRACTILITY: A FUNCTIONAL CONCEPT OF THE INOTROPIC STATE Roberto Curiel,* Juan Perez-Gonzalez, † Edwar Torres, ‡ Ruben Landaeta ‡ and Miguel Cerrolaza ‡ *Centro Medico Docente La Trinidad, † Instituto de Medicina Experimental, Facultad de Medicina and ‡ Centro de Bioingeniería, Facultad de Ingeniería, Universidad Central de Venezuela, Caracas, Venezuela SUMMARY 1. Initial unsuccessful attempts to evaluate ventricular function in terms of the ‘heart as a pump’ led to focusing on the ‘heart as a muscle’ and to the concept of myocardial contractility. However, no clinically ideal index exists to assess the contractile state. The aim of the present study was to develop a mathematical model to assess cardiac contractility. 2. A tri-axial system was conceived for preload (PL), after- load (AL) and contractility, where stroke volume (SV) was represented as the volume of the tetrahedron. Based on this model, ‘operative’ contractility (‘OperCon’) was calculated from the readily measured values of PL, AL and SV. The model was tested retrospectively under a variety of different experimental and clinical conditions, in 71 studies in humans and 29 studies in dogs. A prospective echocardiographic study was performed in 143 consecutive subjects to evaluate the ability of the model to assess contractility when SV and PL were measured volumetrically (mL) or dimensionally (cm). 3. With inotropic interventions, OperCon changes were comparable to those of ejection fraction (EF), velocity of short- ening (Vcf) and dP/dt-max. Only with positive inotropic interventions did elastance (Ees) show significantly larger changes. With load manipulations, OperCon showed signifi- cantly smaller changes than EF and Ees and comparable changes to Vcf and dP/dt-max. Values of OperCon were similar when AL was represented by systolic blood pressure or wall stress and when volumetric or dimensional values were used. 4. Operative contractility is a reliable, simple and versatile method to assess cardiac contractility. Key words: computer modelling, contractile function, haemodynamic, heart failure, ventricular function. INTRODUCTION Classically, heart function has been assessed in terms of pump performance by directly relating stroke volume (SV) and ventric- ular filling (Frank–Starling law). Starling, working with a heart- lung preparation, found that SV was directly related to the increase in venous inflow. 1 Later, in better-controlled experiments with isolated papillary muscle as well as in intact heart preparations, an inverse relationship between SV and arterial pressure became evident. 2 Furthermore, Sarnoff and his collaborators constructed a family of ventricular stroke-work/end-diastolic pressure curves attributable to diverse contractile states. 3 Thus, the relevance of preload (PL) in the control of ventricular function drifted out of focus, because reflex and humoral changes in heart rate, venous return, afterload (AL) and contractility affect the Frank–Starling mechanism and conceptual emphasis was shifted from the ‘heart as a pump’ to the ‘heart as a muscle’. In this context, the original force–velocity relationship from striated muscle mechanics and its extrapolation to a maximal velocity of shortening (Vmax) became useful 4 and was later extended for the myocardium, as pioneered by Abbot and Mommaerts 5 and Sonnenblick. 6 It is well recognized that neural and humoral influences, as well as muscle mechanisms (myofilament, energetic and molecular), are constantly modulating the inotropic state. In addition, it is hard to define an isolated parameter of cardiac contractility owing to this variable’s incomplete intrinsic independence of PL, AL and heart rate. 7 Apart from these theoretical considerations, most contractil- ity parameters have serious methodological limitations. The most reliable indices usually require sophisticated equipment, pharma- cological interventions or theoretical manipulations of the results. This makes them expensive, time consuming and requires special training, limiting their application in routine clinical practice. A novel approach to the assessment of cardiac contractility can be constructed from the physiological outcome of the mechanical processes occurring in the intact ventricle. For the ventricular chamber, myocardial shortening is expressed by SV. Because the performance of the left ventricle as a pump depends on contrac- tility as well as the loading conditions, the interactions of these factors are reflected in changes of SV. 3,6–8 Under these conditions, PL is adequately represented by end-diastolic volume (EDV) 9 and AL may be represented by aortic impedance, 10 systemic vascular resistance, 11 systolic wall stress 12 or systolic blood pressure (SBP). 13,14 Only cardiac contractility remains elusive. Therefore, it should be possible to approach a measurement of contractility from the interaction of the other, easily quantifiable variables. The present study represents an attempt to test this hypothesis and validate the resulting calculation as an operative contractility index (‘OperCon’). METHODS Development of the model Under experimental conditions with controlled variables, changes in PL or AL produce significant and opposite changes in SV (Table 1). 15–21 (Note, Correspondence: Dr Roberto Curiel, c/o Manuel Perez, Apartado Postal 80929, Caracas 1080-A, Venezuela. Email: [email protected] Received 30 August 2004; revision 27 March 2005; accepted 6 June 2005.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical and Experimental Pharmacology and Physiology
(2005)
32
,
871–881
OPERATIVE CONTRACTILITY: A FUNCTIONAL CONCEPT OF THE INOTROPIC STATE
Roberto Curiel,* Juan Perez-Gonzalez,
†
Edwar Torres,
‡
Ruben Landaeta
‡
and Miguel Cerrolaza
‡
*
Centro Medico Docente La Trinidad,
†
Instituto de Medicina Experimental, Facultad de Medicina and
‡
Centro de Bioingeniería, Facultad de Ingeniería, Universidad Central de Venezuela, Caracas, Venezuela
SUMMARY
1. Initial unsuccessful attempts to evaluate ventricularfunction in terms of the ‘heart as a pump’ led to focusing onthe ‘heart as a muscle’ and to the concept of myocardialcontractility. However, no clinically ideal index exists to assessthe contractile state. The aim of the present study was todevelop a mathematical model to assess cardiac contractility.
2. A tri-axial system was conceived for preload (PL), after-load (AL) and contractility, where stroke volume (SV) wasrepresented as the volume of the tetrahedron. Based on thismodel, ‘operative’ contractility (‘OperCon’) was calculatedfrom the readily measured values of PL, AL and SV. Themodel was tested retrospectively under a variety of differentexperimental and clinical conditions, in 71 studies in humansand 29 studies in dogs. A prospective echocardiographic studywas performed in 143 consecutive subjects to evaluate theability of the model to assess contractility when SV and PLwere measured volumetrically (mL) or dimensionally (cm).
3. With inotropic interventions, OperCon changes werecomparable to those of ejection fraction (EF), velocity of short-ening (Vcf) and dP/dt-max. Only with positive inotropicinterventions did elastance (Ees) show significantly largerchanges. With load manipulations, OperCon showed signifi-cantly smaller changes than EF and Ees and comparablechanges to Vcf and dP/dt-max. Values of OperCon were similarwhen AL was represented by systolic blood pressure or wallstress and when volumetric or dimensional values were used.
4. Operative contractility is a reliable, simple and versatilemethod to assess cardiac contractility.
Key words: computer modelling, contractile function,haemodynamic, heart failure, ventricular function.
INTRODUCTION
Classically, heart function has been assessed in terms of pumpperformance by directly relating stroke volume (SV) and ventric-ular filling (Frank–Starling law). Starling, working with a heart-lung preparation, found that SV was directly related to the increasein venous inflow.
1
Later, in better-controlled experiments with
isolated papillary muscle as well as in intact heart preparations, aninverse relationship between SV and arterial pressure becameevident.
2
Furthermore, Sarnoff and his collaborators constructed afamily of ventricular stroke-work/end-diastolic pressure curvesattributable to diverse contractile states.
3
Thus, the relevance ofpreload (PL) in the control of ventricular function drifted out offocus, because reflex and humoral changes in heart rate, venousreturn, afterload (AL) and contractility affect the Frank–Starlingmechanism and conceptual emphasis was shifted from the ‘heartas a pump’ to the ‘heart as a muscle’. In this context, the originalforce–velocity relationship from striated muscle mechanics and itsextrapolation to a maximal velocity of shortening (V
max
) becameuseful
4
and was later extended for the myocardium, as pioneeredby Abbot and Mommaerts
5
and Sonnenblick.
6
It is well recognized that neural and humoral influences, as wellas muscle mechanisms (myofilament, energetic and molecular), areconstantly modulating the inotropic state. In addition, it is hard todefine an isolated parameter of cardiac contractility owing to thisvariable’s incomplete intrinsic independence of PL, AL and heartrate.
7
Apart from these theoretical considerations, most contractil-ity parameters have serious methodological limitations. The mostreliable indices usually require sophisticated equipment, pharma-cological interventions or theoretical manipulations of the results.This makes them expensive, time consuming and requires specialtraining, limiting their application in routine clinical practice.
A novel approach to the assessment of cardiac contractility canbe constructed from the physiological outcome of the mechanicalprocesses occurring in the intact ventricle. For the ventricularchamber, myocardial shortening is expressed by SV. Because theperformance of the left ventricle as a pump depends on contrac-tility as well as the loading conditions, the interactions of thesefactors are reflected in changes of SV.
3,6–8
Under these conditions,PL is adequately represented by end-diastolic volume (EDV)
9
andAL may be represented by aortic impedance,
10
systemic vascularresistance,
11
systolic wall stress
12
or systolic blood pressure(SBP).
13,14
Only cardiac contractility remains elusive. Therefore, itshould be possible to approach a measurement of contractility fromthe interaction of the other, easily quantifiable variables. Thepresent study represents an attempt to test this hypothesis andvalidate the resulting calculation as an operative contractility index(‘OperCon’).
METHODS
Development of the model
Under experimental conditions with controlled variables, changes in PL orAL produce significant and opposite changes in SV (Table 1).
15–21
(Note,
Correspondence: Dr Roberto Curiel, c/o Manuel Perez, Apartado Postal80929, Caracas 1080-A, Venezuela. Email: [email protected]
Received 30 August 2004; revision 27 March 2005; accepted 6 June2005.

872
R Curiel
et al.
the references used to develop and test the model described herein havebeen provided to enable the verification of the data by any reader.
15–124
) Incontrast, with an intact circulation, a primary change in PL elicits corres-ponding secondary variations of AL, and vice versa, and SV changes resultfrom the interaction of these variables. Consequently, under any givencondition, increases in EDV are significantly correlated with changes in SV,whereas rises in SBP are not adequately correlated with changes in SV orend-systolic volume (cf. Table 1),
22–42
because the latter is determined byboth the inotropic state and AL.
13,14
It follows that, under physiologicalconditions, SV cannot be adequately predicted solely by the interaction ofPL and AL and requires the introduction of a third variable, contractility(C). This concept can be used to develop a mathematical model to assess Cbecause, if the values of PL, AL and C at a given moment are representedalong each axis of a three axial system, the volume of the resultingtetrahedron represents the value of SV (Fig. 1). In this representation, avalue of zero SV corresponds to the vertex of the set of axes. In order toattain this while respecting physiological relationships, PL and C must bezero at that point and AL at the vertex must correspond to the isometricvalue in an inverted scale. For example, if AL is represented as systolicpressure, its value at the vertex must correspond to the left ventricularisovolumic pressure.
The volume of a tetrahedron may be obtained by means of an integralequation or by analytical geometry. The last approach was chosen becauseit best fitted a broad range of haemodynamic values. It is known that thevolume of the tetrahedron can be calculated as follows:
Volume
= (
AreaBase
�
Height
)/3
In our model, ‘
Volume’
is SV and ‘
Height’
is C. The area of the base triangle(
AreaBase
) is given by the following equation:
AreaBase
= (
b
�
h
)/2
Substituting ‘
b
’ with PL and ‘
h
’ with AL gives:
AreaBase
= (PL
�
AL)/2
Therefore:
SV = 1/3
�
((PL
�
AL
�
C)/2)
Tabl
e 1
Eff
ect o
f in
crea
ses
in p
relo
ad a
nd a
fter
load
on
stro
ke v
olum
e
HR
SBP
ED
VE
SVSV
SV/E
DV
(
�
%)
SV/S
BP
(
�
%)
ESV
/SB
P (
�
%)
�
b.p.
m.
�
%
�
mm
Hg
�
%
�
mL
�
%
�
mL
�
%
�
mL
�
%
Con
trol
led
vari
able
sIn
crea
se P
L
15–1
7
00
00
10.3
39.3
0.7
2.6
9.7
221
y
= 1
0.2
x
–
177.
8
r =
0.9
3–
–
Incr
ease
AL
16,1
8–21
00
41.6
143
00
1.9
42.2
–
12
–
68–
y
=
–
0.12
x
–
50.8
r =
0.6
5
y
= 0
.15
x
+ 2
3.4
r =
0.9
6In
tact
cir
cula
tion
Incr
ease
PL
22–2
9
6.1
5.5
11.9
9.6
16.1
21.3
6.9
19.9
9.2
24.3
y
= 0
.87
x
+ 5
.8
r =
0.9
0
y
= 0
.032
x
+ 2
3.9
r =
0.0
2
y
= 0
.19
x
+ 1
8
r =
0.1
1In
crea
se A
L
24,2
5,30
–42
–
2
–
144
.738
13.3
18.4
10.3
32.8
2.5
5
y
= 0
.78
x
–
9.4
r =
0.7
6
y
= 0
.64
x
+ 2
9.4
r =
0.4
6
y
= 0
.007
x
+ 3
7.7
r =
0.0
2
AL
, aft
erlo
ad; P
L, p
relo
ad; E
DV
, end
-dia
stol
ic v
olum
e; E
SV, e
nd-s
ysto
lic v
olum
e; S
V, s
trok
e vo
lum
e; H
R, h
eart
rat
e; S
BP,
sys
tolic
blo
od p
ress
ure.
In e
ach
colu
mn,
y
and
x
rep
rese
nt th
e pa
ram
eter
s of
the
corr
espo
ndin
g ra
tio.
Fig. 1
Preload, afterload and contractility are represented along each axisand the volume of the resulting tetrahedron represents the value of strokevolume. In accordance with physiological relationships, the isometric valueof afterload is represented at the vertex, in an inverted scale, whereaspreload and contractility have a value of zero at that point.

Operative contractility: A new index
873
That is:
SV = (PL
�
AL
�
C)/6
Finally:
C = (SV
�
6)/(PL
�
AL)
Because the relevant point here is the proportional relationship between thevariables, a more genaral expression could be:
C =
K
(SV/(PL
�
AL))
where
K
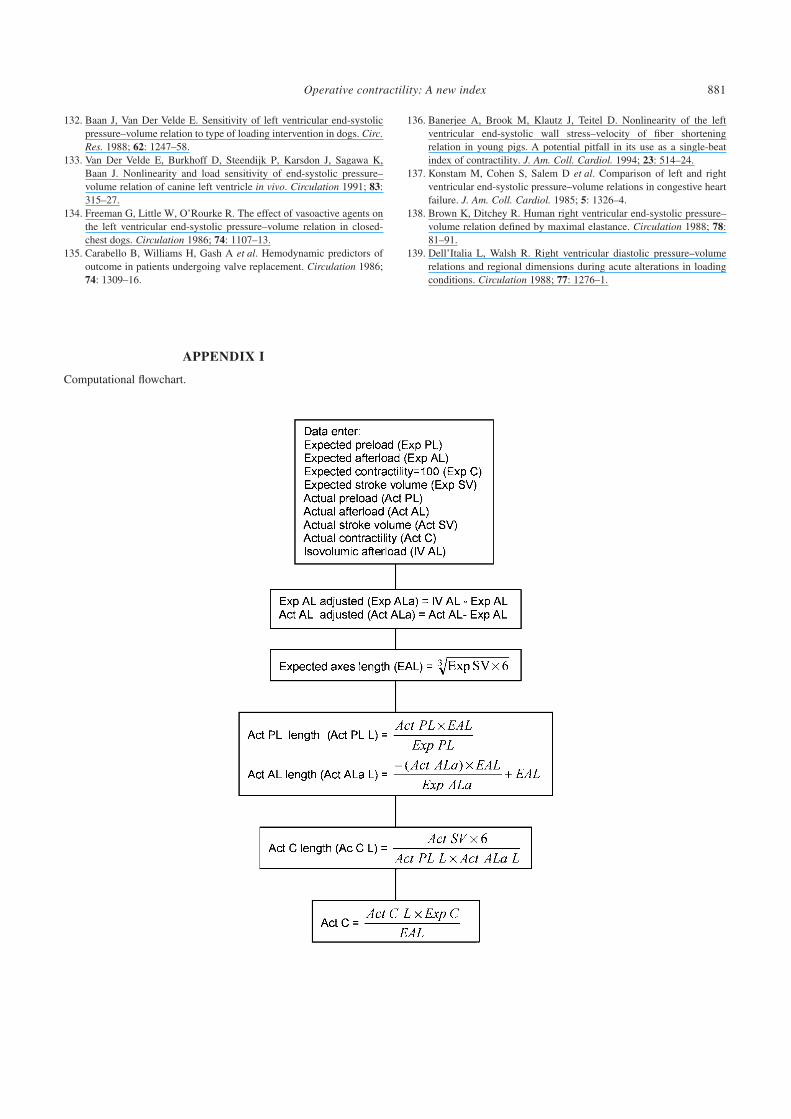
is a dispensable constant.In order to accomplish these calculations, the equivalence between these
variables must be established. To this end, from known volumetric (cm
3
)SV values, the dimensional (cm) values of PL, AL and C were determined.This procedure was programmed in a computer (see Appendix i) andcalibrated with reference or expected values. Values used for calibrationmay be those obtained for SV, PL and AL by any of the standard techniques,in normal subjects under basal conditions, or may be ‘control’ values in anygiven experiment. At this reference level, C is assigned a value of 100 units.Thereafter, for any set of actual values introduced for SV, PL and AL, thesoftware calculates the level of C (units) that fits the volume of thetetrahedron (SV) with the given values for PL and AL in the remaining axes.The computational program to obtain OperCon values is available athttp://www.cardiac-contractility.org/
Testing the model
Retrospective data
The ability of the model to assess cardiac contractility was evaluated byusing data from various experiments published in the literature. Our originalbibliography relating to ventricular function was reviewed. In addition, asystematic review was performed of seven cardiology journals (
AmericanHeart Journal
,
American Journal of Cardiology
,
British Heart Journal
,
Cardiovascular Research
,
Circulation
,
Circulation Research
and
Journal ofthe American College of Cardiology
), of which a complete collectionbetween 1980 and 2000 was available in our libraries. From this database,articles were selected according to three criteria: (i) that they provided data(in humans or dogs) for all the variables required to run the model (i.e. SV,PL and AL), PL was represented by EDV and echocardiographicdimensions were converted into volumes by means of the Teichholzformula
43
and AL was represented by its simplest expression, namely SBP;(ii) that the articles included a measurement of contractility using ejectionfraction (EF), velocity of shortening (Vcf), dP/dt-max and/or elastance asend-systolic pressure/volume relationship (Ees), but the end-systolicpressure/end-systolic volume (ESP/ESV) ratio was not included; (iii) inarticles referring to inotropic manipulations, it was required that dP/dt-maxand/or Ees were included in addition to EF or Vcf. Eighty-three articlesfulfilled all these criteria, but 16 were excluded owing to: (i) methodologicallimitations (i.e. without a control group;
n
= 7); and (ii) ambiguous orlimited haemodynamic modifications (i.e. long-term effects of beta-blockers or calcium blockers in patients with coronary artery disease,etc.;
n
= 9). After exclusion of these articles, 67 studies were analysed,which contained data from load
22–42,44–56
and inotropic manipu-lations,
24,25,30,37,40,41,53,57–89
38 in humans (
n
= 687 subjects) and 29 in dogs(
n
= 302 animals). All these articles reported their findings as mean valuesand 12
34–37,40,46,52,64,68,75,83,84
further provided individual values for therelevant variables (11 in humans, one in dogs).
To test the model, a value of 500 mmHg (66 661 Pa) was always used forisovolumic pressure and represented the vertex in the AL scale. This valuewas obtained from reported and calculated isovolumic pressure values fromthe studies reviewed. In studies reporting Ees, isovolumic pressure valueswere calculated by using this slope to find the SBP level corresponding toan EDV 20% above the highest EDV reported. Isovolumic pressure valueswere averaged and a range was constructed in steps of 100 mmHg aboveand below this average. The model was then run with each isovolumicpressure and the corresponding sets of variables and the ‘optimum’isovolumic pressure was selected as that which optimized the performance
of the model. Finally, the mean of optimum isovolumic pressure values,rounded to the nearest 100, resulted in a value of 500 mmHg that wasthereafter used as isovolumic pressure for all the tests reported in thepresent study. Approximation to the nearest 100 was warranted by the factthat C values varied by only 2% when tested within a range of
�
100 mmHg (13 332.2 Pa) around 500.In a further series of tests, the model was evaluated using wall end-
systolic stress instead of SBP as the AL parameter. In this regard, a Medlinesearch of ‘ventricular wall stress’ was performed from 1967 to January2000. Of 2229 articles cited, 188 were considered as potentially useful onthe basis of the abstract. Of those, 132 (71%) were obtained as full text andevaluated according to the criteria described above and 33 were selected assuitable (80 experiments and 2397 subjects).
63,76,90–120
Circumferentialand/or meridional end-systolic stress (ESCWS and ESMWS, respectively;39 and 41 experiments, respectively), were chosen for analysis because theywere the types of stress most frequently reported. Nine articles wereexcluded for using wall stress other that ESCWS or ESMWS (
n
= 7) or forsignificant primary mitral regurgitation (
n
= 2). For our purposes, stressvalues were all expressed as kdyn/cm
2
. Values of 600 kdyn/cm
2
forESMWS and 1.100 kdyn/cm
2
for ESCWS were established for isovolumicstress in a similar manner as described above for isovolumic pressure andused for testing the model in all cases.
Prospective data
A prospective echocardiographic assessment of left ventricular functionwas performed in 176 consecutive patients by a single operator andinterpreted by a single observer (RC). Variability of the measurements inour hands has been reported previously.42 The investigation conformed tothe principles of the Declaration of Helsinki. The inclusion criteria werefulfilled by 143 of these patients, who were separated into four groups asfollows.
1. Group 1: Normal left ventricle, with normal dimensions,121 mass121 andEF (� 50%), 58 patients, mean (�SD) age 41.0 � 16.6 years.2. Group 2: Ventricular hypertrophy, increased ventricular mass (> 95%percentile) and normal EF, 48 patients, mean age 62.3 � 11.1 years.3. Group 3: Ventricular systolic dysfunction (EF < 50%), 26 patients,mean age 63.1 � 14.0 years.4. Group 4: Valvular aortic stenosis with normal ventricular systolicfunction, peak systolic gradient > 15 mmHg, 11 patients, mean age66.8 � 14.0 years.
Thirty-three patients were excluded owing to other heart diseases(n = 26), inadequate echocardiographic window (n = 4) or pregnancy(n = 3).
Preload and SV were obtained from M-mode echocardiographicmeasurements (guided by two-dimensional echo) of left ventriculardimensions according to the standards of the American Society ofEchocardiography.122 Volumes were calculated by the Teichholz formula.43
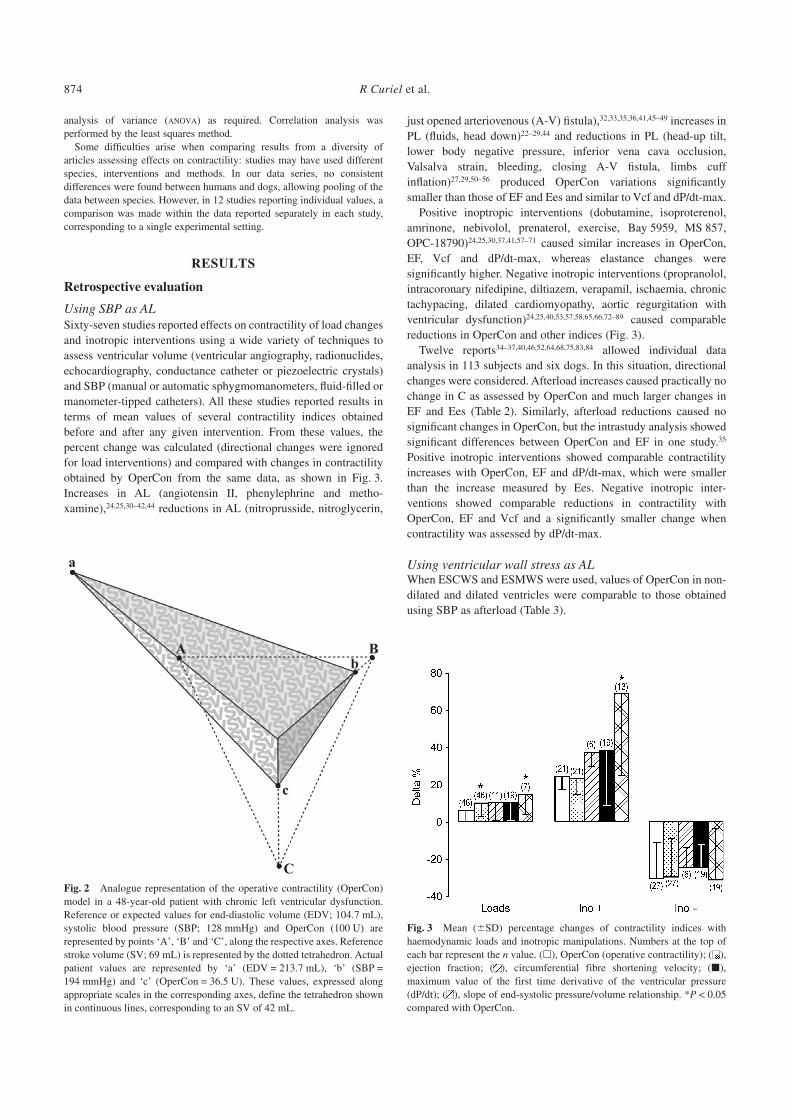
Afterload was assessed by sphygmomanometric quantification of SBP. Inpatients with aortic stenosis, AL was estimated by SBP + systolic gradient,as calculated by Doppler. Left ventricular contractility was assessed byOperCon with both the calculated volumes (EDV and ESV) and ventriculardimensions (left ventricular diastolic and systolic dimension) and volu-metric (EDV – ESV) or dimensional (left ventricular diastolic minussystolic dimension) SV. Reference values for all parameters were used tocalibrate the model. Reference left ventricular dimensions were setaccording to criteria of Henry et al.123 and the reference SBP according tocriteria of Schettini et al.124 Figure 2 illustrates the appearance of thegraphic expression of the model when run with data from a patient withsevere LV dysfunction.
Data analysis
With the retrospective data, the performance of the model was evaluated bycomparing percent changes in contractility from basal levels (�%) reportedin each original article with those obtained from the computer software byrunning the model with the same SV, PL and AL data. Means of �%calculated from both sets of data were compared by t-test or one-way
874 R Curiel et al.
analysis of variance (ANOVA) as required. Correlation analysis wasperformed by the least squares method.
Some difficulties arise when comparing results from a diversity ofarticles assessing effects on contractility: studies may have used differentspecies, interventions and methods. In our data series, no consistentdifferences were found between humans and dogs, allowing pooling of thedata between species. However, in 12 studies reporting individual values, acomparison was made within the data reported separately in each study,corresponding to a single experimental setting.
RESULTS
Retrospective evaluation
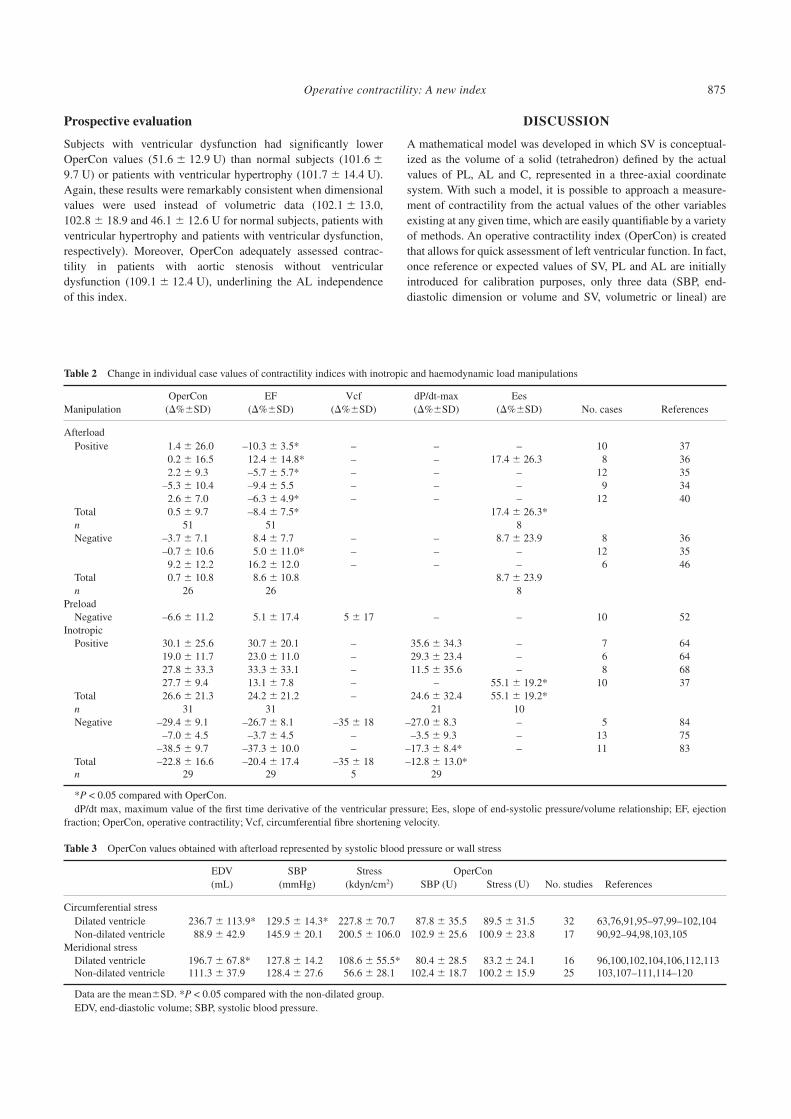
Using SBP as ALSixty-seven studies reported effects on contractility of load changesand inotropic interventions using a wide variety of techniques toassess ventricular volume (ventricular angiography, radionuclides,echocardiography, conductance catheter or piezoelectric crystals)and SBP (manual or automatic sphygmomanometers, fluid-filled ormanometer-tipped catheters). All these studies reported results interms of mean values of several contractility indices obtainedbefore and after any given intervention. From these values, thepercent change was calculated (directional changes were ignoredfor load interventions) and compared with changes in contractilityobtained by OperCon from the same data, as shown in Fig. 3.Increases in AL (angiotensin II, phenylephrine and metho-xamine),24,25,30–42,44 reductions in AL (nitroprusside, nitroglycerin,
just opened arteriovenous (A-V) fistula),32,33,35,36,41,45–49 increases inPL (fluids, head down)22–29,44 and reductions in PL (head-up tilt,lower body negative pressure, inferior vena cava occlusion,Valsalva strain, bleeding, closing A-V fistula, limbs cuffinflation)27,29,50–56 produced OperCon variations significantlysmaller than those of EF and Ees and similar to Vcf and dP/dt-max.
Positive inoptropic interventions (dobutamine, isoproterenol,amrinone, nebivolol, prenaterol, exercise, Bay 5959, MS 857,OPC-18790)24,25,30,37,41,57–71 caused similar increases in OperCon,EF, Vcf and dP/dt-max, whereas elastance changes weresignificantly higher. Negative inotropic interventions (propranolol,intracoronary nifedipine, diltiazem, verapamil, ischaemia, chronictachypacing, dilated cardiomyopathy, aortic regurgitation withventricular dysfunction)24,25,40,53,57,58,65,66,72–89 caused comparablereductions in OperCon and other indices (Fig. 3).
Twelve reports34–37,40,46,52,64,68,75,83,84 allowed individual dataanalysis in 113 subjects and six dogs. In this situation, directionalchanges were considered. Afterload increases caused practically nochange in C as assessed by OperCon and much larger changes inEF and Ees (Table 2). Similarly, afterload reductions caused nosignificant changes in OperCon, but the intrastudy analysis showedsignificant differences between OperCon and EF in one study.35
Positive inotropic interventions showed comparable contractilityincreases with OperCon, EF and dP/dt-max, which were smallerthan the increase measured by Ees. Negative inotropic inter-ventions showed comparable reductions in contractility withOperCon, EF and Vcf and a significantly smaller change whencontractility was assessed by dP/dt-max.
Using ventricular wall stress as ALWhen ESCWS and ESMWS were used, values of OperCon in non-dilated and dilated ventricles were comparable to those obtainedusing SBP as afterload (Table 3).
Fig. 2 Analogue representation of the operative contractility (OperCon)model in a 48-year-old patient with chronic left ventricular dysfunction.Reference or expected values for end-diastolic volume (EDV; 104.7 mL),systolic blood pressure (SBP; 128 mmHg) and OperCon (100 U) arerepresented by points ‘A’, ‘B’ and ‘C’, along the respective axes. Referencestroke volume (SV; 69 mL) is represented by the dotted tetrahedron. Actualpatient values are represented by ‘a’ (EDV = 213.7 mL), ‘b’ (SBP =194 mmHg) and ‘c’ (OperCon = 36.5 U). These values, expressed alongappropriate scales in the corresponding axes, define the tetrahedron shownin continuous lines, corresponding to an SV of 42 mL.
Fig. 3 Mean (�SD) percentage changes of contractility indices withhaemodynamic loads and inotropic manipulations. Numbers at the top ofeach bar represent the n value. (�), OperCon (operative contractility); ( ),ejection fraction; ( ), circumferential fibre shortening velocity; (�),maximum value of the first time derivative of the ventricular pressure(dP/dt); ( ), slope of end-systolic pressure/volume relationship. *P < 0.05compared with OperCon.
Operative contractility: A new index 875
Prospective evaluation
Subjects with ventricular dysfunction had significantly lowerOperCon values (51.6 � 12.9 U) than normal subjects (101.6 �9.7 U) or patients with ventricular hypertrophy (101.7 � 14.4 U).Again, these results were remarkably consistent when dimensionalvalues were used instead of volumetric data (102.1 � 13.0,102.8 � 18.9 and 46.1 � 12.6 U for normal subjects, patients withventricular hypertrophy and patients with ventricular dysfunction,respectively). Moreover, OperCon adequately assessed contrac-tility in patients with aortic stenosis without ventriculardysfunction (109.1 � 12.4 U), underlining the AL independenceof this index.
DISCUSSION
A mathematical model was developed in which SV is conceptual-ized as the volume of a solid (tetrahedron) defined by the actualvalues of PL, AL and C, represented in a three-axial coordinatesystem. With such a model, it is possible to approach a measure-ment of contractility from the actual values of the other variablesexisting at any given time, which are easily quantifiable by a varietyof methods. An operative contractility index (OperCon) is createdthat allows for quick assessment of left ventricular function. In fact,once reference or expected values of SV, PL and AL are initiallyintroduced for calibration purposes, only three data (SBP, end-diastolic dimension or volume and SV, volumetric or lineal) are
Table 2 Change in individual case values of contractility indices with inotropic and haemodynamic load manipulations
ManipulationOperCon
(�%�SD)EF
(�%�SD)Vcf
(�%�SD)dP/dt-max(�%�SD)
Ees(�%�SD) No. cases References
AfterloadPositive 1.4 � 26.0 –10.3 � 3.5* – – – 10 37
0.2 � 16.5 12.4 � 14.8* – – 17.4 � 26.30 8 362.2 � 9.3 –5.7 � 5.7* – – – 12 35
–5.3 � 10.4 –9.4 � 5.5 – – – 9 342.6 � 7.0 –6.3 � 4.9* – – – 12 40
Total 0.5 � 9.7 –8.4 � 7.5* 17.4 � 26.3*n 51 51 8Negative –3.7 � 7.10 8.4 � 7.7 – – 8.7 � 23.9 8 36
–0.7 � 10.6 5.0 � 11.0* – – – 12 359.2 � 12.2 16.2 � 12.0 – – – 6 46
Total 0.7 � 10.8 8.6 � 10.8 8.7 � 23.9n 26 26 8
PreloadNegative –6.6 � 11.2 5.1 � 17.4 5 � 17 – – 10 52
InotropicPositive 30.1 � 25.6 30.7 � 20.1 – 35.6 � 34.3 – 7 64
19.0 � 11.7 23.0 � 11.0 – 29.3 � 23.4 – 6 6427.8 � 33.3 33.3 � 33.1 – 11.5 � 35.6 – 8 6827.7 � 9.40 13.1 � 7.8 – – 55.1 � 19.2* 10 37
Total 26.6 � 21.3 24.2 � 21.2 – 24.6 � 32.4 55.1 � 19.2*n 31 31 21 10Negative –29.4 � 9.100 –26.7 � 8.10 –35 � 18 –27.0 � 8.300 – 5 84
–7.0 � 4.50 –3.7 � 4.5 – –3.5 � 9.30 – 13 75–38.5 � 9.700 –37.3 � 10.0 – –17.3 � 8.4*0 – 11 83
Total –22.8 � 16.60 –20.4 � 17.4 –35 � 18 –12.8 � 13.0*n 29 29 5 29
*P < 0.05 compared with OperCon.dP/dt max, maximum value of the first time derivative of the ventricular pressure; Ees, slope of end-systolic pressure/volume relationship; EF, ejection
fraction; OperCon, operative contractility; Vcf, circumferential fibre shortening velocity.
Table 3 OperCon values obtained with afterload represented by systolic blood pressure or wall stress
EDV(mL)
SBP(mmHg)
Stress(kdyn/cm2)
OperConNo. studies ReferencesSBP (U) Stress (U)
Circumferential stressDilated ventricle 236.7 � 113.9* 129.5 � 14.3* 227.8 � 70.70 87.8 � 35.5 89.5 � 31.5 32 63,76,91,95–97,99–102,104Non-dilated ventricle 88.9 � 42.90 145.9 � 20.10 200.5 � 106.0 102.9 � 25.6 100.9 � 23.8 17 90,92–94,98,103,105
Meridional stressDilated ventricle 196.7 � 67.8*0 127.8 � 14.20 108.6 � 55.5* 80.4 � 28.5 83.2 � 24.1 16 96,100,102,104,106,112,113Non-dilated ventricle 111.3 � 37.900 128.4 � 27.60 56.6 � 28.1 102.4 � 18.7 100.2 � 15.9 25 103,107–111,114–120
Data are the mean�SD. *P < 0.05 compared with the non-dilated group.EDV, end-diastolic volume; SBP, systolic blood pressure.

876 R Curiel et al.
required to immediately calculate OperCon. If this assumption isvalid, the model and its derived index should be applicable to avariety of different experimental and clinical conditions.
Inotropic interventions
OperCon values were comparable to EF, Vcf and dP/dt-max in theability to detect the effects of inotropic interventions, both positiveand negative. Only with positive interventions were Ees changesmore marked than changes in OperCon and in all other indices.This observation, arising from the pooled results of a significantproportion of experimental data with an intact circulation, contrastswith the results of carefully controlled experiments in canineisolated, supported ventricles, in which Ees has been shown to bethe least sensitive contractility index.18 In our pooled review data,Ees showed considerable variability in range (1.1–150 mmHg/mL)and standard deviation (� 46.6). OperCon values obtained fromthe same data showed less variation (range 11.7–39 U; SD � 7.2).The behaviour of Ees may be attributed to the non-linearity of theend-systolic pressure/volume relationship. In fact, of five articlesreporting Ees changes above the mean for all studies,30,41,57,66,67
four30,57,66,67 reported a shift to the right of V0, which was attributedto non-linearity. This implies that important changes in the slope ofthe end-systolic pressure/volume relationship (Ees) may occurwithout adequate correspondence with concurrent changes in SV, afact that could suggest an apparent dissociation between theincrement in contractility and its effect on pump function. Incontrast, when the same data were used with OperCon, the modelallowed the measurement, within a single beat and, therefore,without AL manipulation, of the amount of contractility respon-sible for generating a given SV under the prevailing conditions ofPL and AL.
We have shown that OperCon behaves as well as or even betterthan the traditional indices in the face of varying load conditionsand inotropic interventions and we suggest that it represents thecontractility of the ventricle chamber; that is, the contractility of thewhole left ventricular myocardium, which is not necessarily thesame as the inotropic state of each individual muscle fibre. Thisconceptual difference could be of particular importance in patho-logical conditions were one may expect heterogeneity in theinotropic state of individual fibres. Under such conditions, globalfunctional or ‘operative’ contractility could be normal in thepresence of an abnormal inotropic state of muscle fibres, which iscompensated for by an increase in the total amount of muscletissue. In these situations, OperCon should be corrected by leftventricular mass, thus allowing evaluation of the intrinsiccontractility of the muscle fibre (IntriCon). Preliminary data fromour laboratory in patients with high blood pressure and compen-sated left ventricular hypertrophy in whom we compare IntriConvalues with mid-wall fractional shortening is encouraging.125
Although a considerable variety of cardiac contractility indiceshas been proposed, only four (EF, Vcf, dP/dt and Ees) were chosenfor the present study because they have been the most widelyevaluated under a considerable variety of haemodynamicconditions, thus allowing statistical comparison with OperCon.Newer contractility indices have recently been introduced, derivedfrom the method of single-beat estimation of Ees.36,126 However, acloser analysis has shown that these methods lack the accuracyrequired for in vivo use.127 In a further approach to simplify Ees, by
obviating the need for recording of P-V loops, maximal ventricularpower (Wmax) has been used as a cardiac contractility index.128 Inorder to correct its PL dependency, this value is divided by thesquared end-diastolic volume, thus originating an index known aspreload-adjusted maximal power (Wmax/V2ed). Although clinicalusefulness has been suggested for this index,129 it, too, has beenreported to be sensitive to changes in loads.130,131
Haemodynamic load manipulations
Contractility indices are sensitive to changes in haemodynamicloads. Ejective phase and isovolumic indices are modified bychanges in AL and PL7 and, although initially Ees was consideredinsensitive to changes in load,13,14,57 it was later shown that this isnot the case.25,32,132,133 Moreover, Ees has also been shown to besensitive to the nature of the load manipulation intervention,whether mechanical or pharmacological.134 In our reviewed data,changes in measured contractility during manipulations of haemo-dynamic loads resulted in OperCon changes that were significantlylower than those of EF and Ees and not significantly different toVcf and dP/dt-max, in spite of the similar magnitude of change inthese indices to EF, probably because of the small number ofobservations involved. A similar trend was observed in the intra-study, as well in the pooled data analysis performed on 12 reportsthat allowed individual case assessment. In almost all types ofanalysis and independently of the nature and direction of loadmanipulation, OperCon never showed greater changes than anyother contractility index with which it was compared.
Ejection fraction has been established as a standard formeasuring LV function. However, this parameter is far from theproposed ideal contractility index because it is markedly modifiedby AL. This is particularly relevant under clinical conditions, whereAL is high (i.e. aortic stenosis) or contractility is depressed and,therefore, SV is affected by small changes in AL.60 In an attempt toovercome this dependence, myocardial shortening indices (EF andVcf) have been corrected by wall stress.135 However, the effect ofAL on ejection phase indices is not constant and, therefore,abnormal single-point measurement may not necessarily reflectchanges in contractility.136 In contrast, as mentioned above, wehave shown OperCon to be little affected by haemodynamic loadsand this feature is clearly shown in Table 2 and Fig. 3.
Limitations
First, an overestimation of contractility may be expected when theAL determining a given ventricular SV (EDV – ESV) is notadequately represented by SBP or systolic wall stress, as is the casein significant primary mitral regurgitation or ventricular septaldefect. In order to correct for this limitation, we are initiating astudy in which the regurgitant fraction or shunt ratio will be usedto adjust AL according to the proportional distribution of flows.Thus, the model would run with the total SV (EDV – ESV) and aweighted mean of AL. This limitation notwithstanding, dataobtained from the literature and from our own prospective patientstudies showed that patients with left ventricular dysfunction, whomay have had varying degrees of secondary mitral regurgitation,exhibited no difference in the qualitative behaviour of the index.
Second, in the intact circulation, changes in either PL or AL areaccompanied by corresponding changes in the other variable,

Operative contractility: A new index 877
causing an attenuation of any effects on SV. In contrast, in experi-ments with controlled PL or AL, any change in the uncontrolledvariable will result in significant changes in SV because the othervariable remains constant. Because it is based on the free inter-action of all variables involved, OperCon, as described above, wasnot designed for controlled-variable conditions. However, themodel may be modified to be suitable under these conditions byreducing the scale in the corresponding variable’s axis. Thus, forexample, in the experimental studies presented in Table 1, anadequate performance of the model with increases in PL or AL maybe achieved by reducing the scale by 47 or 64% on the respectiveaxis.
Third, another situation demanding an adjustment of the modelwould be its application to experimental animals with levels of SBPthat would render an isovolumic pressure of 500 mmHg unsuitable,such as the guinea-pig (SBP = 60 mmHg) or the giraffe(SBP = 300 mmHg.).
Afterload represented by SBP or end-systolic stress
A comparative analysis of the behaviour of the model when AL wasrepresented by SBP or wall stress showed that either parameter isequally adequate for evaluation of the inotropic state withOperCon, both in normal and dilated ventricles. Because theisovolumic value of AL in the corresponding scale is fitted to thevariable used (SBP or wall stress), changes in AL are representedin comparable proportions along the axis. In fact, when the basallevels of these variables in our data were normalized with respectto their isovolumic level and percent changes obtained in theexperiments were compared, no significant differences were foundbetween mean �SBP and mean �ESCWS (�SBP = 2.1 � 2.7% vs�ESCWS = 3.1 � 2.7%) or between mean �SBP and mean�ESMWS (�SBP = 1.2 � 3.3% vs �ESMWS = 1.9 � 6.6%).However, for practical purposes it is preferable to use SBP as theexpression of AL in the model.
Volumetric versus dimensional measurements
In our prospective study, we found that contractility valuesobtained with the model were comparable when PL and SV wereexpressed either in volume or dimension units in normal, hyper-trophic or ventricular dysfunctional hearts. Under all conditions,the model adequately identified the patients with impairedventricular function. Therefore, in the absence of abnormalregional wall motion, OperCon can be used properly to assesscontractility using ventricular dimensions (i.e. piezoelectriccrystals or M-mode echocardiography).
Versatility and applicability of the model
The model is based on a ‘normal’ level of OperCon of 100 units,resulting from ‘normal’ levels of SBP (or wall stress), EDV (ordimension) and SV, as defined by several authors.7,43,123,124 The‘normal’ OperCon level is absolute and constant and is calibratedfor the specific methods used to measure PL, AL and SV in eachinstance. This feature of the model allowed it to be appliedsuccessfully to the diversity of methods used in the studies selectedfor our retrospective evaluation and considerably simplifies the useof OperCon by avoiding the corrections required when different
methods are used. The reference to a ‘normal’ level is important forclinical use because it allows an adequate assessment of ventricularfunction in any given patient by a single, simple procedure. Interms of the features described, OperCon surpasses Ees, which hasno basal values (because it is determined by changes in AL) orknown normal values and is mainly useful for comparisonsbetween conditions. In clinical practice, OperCon would beparticularly useful during acute management, where a prompt andcomplete comprehension of LV function alterations is required toensure precise therapeutic decisions. In this setting, the modelallows a quick integration of all ventricular function variables usingonly three easily quantifiable variables. The result of thisintegration may be recorded numerically or analogically, asillustrated in Fig. 2. In either manner, it can be available ‘on-line’or sampled periodically.
Right ventricular evaluation
OperCon may be adequate for the assessment of right ventricularcontractility if AL is represented by pulmonary artery systolicpressure and PL by right ventricular EDV. Preliminary data fromhuman studies in the literature measuring right ventricular volumeswith angiography or radionuclides show adequate assessment ofcontractility by OperCon under experimental conditions involvingchanges in the inotropic state137,138 or haemodynamic loads.139
In conclusion, we have described a model by which ventricularcontractility may be readily assessed from the interaction of SV, PLand AL. The resulting operative contractility index (OperCon) wasshown to be sensitive to changes in the inotropic state and littleaffected by haemodynamic loads. In addition, OperCon is versatile,because it maintains normal values independently of the techniqueused to quantify ventricular volumes and AL. We have shownOperCon to be applicable to a variety of experimental and clinicalconditions. Further investigation is required to evaluate its fullpotential.
REFERENCES
1. Patterson S, Piper H, Starling E. The regulation of the heart beat.J. Physiol. 1914; 48: 465–513.
2. Sonnenblick E, Downing E. Afterload as primary determinant ofventricular performance. Am. J. Physiol. 1963; 204: 604–10.
3. Sarnoff J, Berglund E. Ventricular function: I. Starling’s law of theheart studied by means of simultaneous right end left ventricularfunction curves in the dog. Circulation 1954; 9: 706–18.
4. Hill A. The heat of shortening and the dynamic constants of muscle.Proc. R. Soc. Lond. B Biol. Sci. 1938; 126: 136–95.
5. Abbot B, Mommaerts WE. A study of inotropic mechanisms in thepapillary muscle preparation. J. Gen. Physiol. 1959; 42: 533–51.
6. Sonnenblick E. Force–velocity relations in mammalian heart muscle.Am. J. Physiol. 1962; 202: 931–9.
7. Little WC. Assessment of normal and abnormal cardiac function. In:Braunwald E, Zipes D, Libby P (eds). Heart Disease: A Textbook ofCardiovascular Medicine, 6th edn. WB Saunders, Philadelphia. 2001;479–502.
8. Brutsaert D, Sonnenblick E. Cardiac muscle mechanism in theevaluation of myocardial contractility and pump function: Problems,concepts and directions. Prog. Cardiovasc. Dis. 1973; 16: 337–61.
9. Sonnenblick E, Skelton C. Reconsideration of ultrastructural basis ofcardiac length–tension relations. Circ. Res. 1974; 35: 517–26.
10. Nichols W, Conti C, Walker W, Milnor W. Input impedance of thesystemic circulation in man. Circ. Res. 1977; 40: 451–8.
878 R Curiel et al.
11. Imperial E, Levy M, Zieske H. Outflow resistance as anindependent determinant of cardiac performance. Circ. Res. 1961;9: 1148–55.
12. Yin F. Ventricular wall stress. Circ. Res. 1981; 49: 829–42.13. Suga H, Sagawa K. Instantaneous pressure–volume relationships and
their ratio in the excised, supported canine left ventricle. Circ. Res.1974; 35: 117–26.
14. Sagawa K. The ventricular pressure–volume diagram revisited. Circ.Res. 1978; 43: 677–87.
15. Taylor R, Cingolani H, McDonald R. Relationship between left ven-tricular volume, ejected fraction, and wall stress. Am. J. Physiol. 1966;211: 674–780.
16. Burns J, Covell J, Ross Jr J. Mechanics of isotonic left ventricularcontractions. Am. J. Physiol. 1973; 224: 725–32.
17. Suga H, Sagawa K, Shoukas A. Load independence of the instan-taneous pressure–volume ratio of the canine left ventricle andeffects of epinephrine and heart rate on the ratio. Circ. Res. 1973;32: 314–22.
18. Kass D, Maughan L, Guo Z, Kono A, Sunagawa K, Sagawa K.Comparative influence of load versus inotropic states on indexes ofventricular contractility: Experimental and theoretical analysisbased on pressure–volume relationships. Circulation 1987; 76:1422–36.
19. Weber K, Janicki J, Reeves R, Hefner L, Reeves J. Determinants ofstroke volume in isolated canine heart. J. Appl. Physiol. 1974; 37:742–7.
20. MacGregor D, Covell J, Mahler F, Dilley R, Ross Jr J. Relationsbetween afterload, stroke volume, and descending limb of Starling’scurve. Am. J. Physiol. 1974; 227: 884–90.
21. Suga H. Time course of left ventricular pressure–volume relationshipunder various extents of aortic occlusion. Jpn. Heart J. 1970; 11:373–8.
22. Hoit B, Shao Y, Gabel M, Walsh M. Influence of loading conditionsand contractile state on pulmonary venous flow. Circulation 1992; 86:651–9.
23. Courtois M, Mecem C, Barzilai B, Gutierrez F, Ludbrook P. Deline-ation of determinants of left ventricular early filling. Circulation 1994;90: 2041–50.
24. Mahler F, Ross Jr J, O’Rourke R, Covell J. Effects of change inpreload, afterload and inotropic state on ejection and isovolumic phasemeasures of contractility in the conscious dog. Am. J. Cardiol. 1975;35: 626–34.
25. Sodums M, Badke F, Starling M, Little W, O’Rourke R.Evaluation of left ventricular contractile performance utilizing end-systolic pressure–volume relationships in conscious dogs. Circ. Res.1984; 54: 731–9.
26. Miller C, Daughters G, Derby G et al. Effect of early postoperativevolume loading on left ventricular systoilic function (including leftventricular ejection fraction determined by myocardial marker)after myocardial revascularization. Circulation 1985; 72 (Suppl. II):II–207–15.
27. Nixon J, Murray G, Leonard P, Mitchell J, Blomqvist G. Effect oflarge variations in preload on left ventricular performance character-istics in normal subjects. Circulation 1982; 65: 698–703.
28. Burggraf G, Parker J. Effects of dextran infusion on left ventricularvolume and pressure in man. Cathet. Cardiovasc. Diagn. 1978; 4:383–90.
29. Szwarc R, Mickleborough L, Mizuno S, Wilson G, Liu P, MohamedS. Conductance catheter measurements of left ventricular volume inthe intact dog: Parallel conductance is independent of left ventricularsize. Cardiovasc. Res. 1994; 28: 252–8.
30. Little W, Cheng C, Mumma M, Igarashi Y, Vinten-Johansen J,Johnston W. Comparison of measures of left ventricular contractileperformance derived from pressure–volume loops in conscious dogs.Circulation 1989; 80: 1378–87.
31. Shen W, Roubin G, Choong C et al. Evaluation of relationshipbetween myocardial contractile state and lef ventricular function inpatients with aortic regurgitation. Circulation 1985; 71: 31–8.
32. Crottogini A, Willshaw P, Barra J, Pichel R. Left ventricular end-systolic elastance is incorrectly estimated by the use of stepwiseafterload variations in conscious, unsedated, autonomically intactdogs. Circulation 1994; 90: 1431–40.
33. Starling M, Walsh R, Dell’Italia L, Mancini G, Lasher J, Lancaster J.The relationship of various measures of end-systole to left ventricularmaximum time-varying elastance in man. Circulation 1987; 76:32–43.
34. Branzi A, Lolli C, Piovaccari G et al. Echocardiographic evaluation ofthe response to afterload stress test in young asymptomatic patientswith chronic severe aortic regurgitation: Sensitivity of left ventricularend-systolic pressure–volume relationship. Circulation 1984; 70:561–9.
35. Mehmel H, Stockins B, Ruffmann K, Olshausen K, Schuler G, KublerW. The linearity of the end-systolic pressure–volume relationship inman and its sensitivity for assessment of left ventricular function.Circulation 1981; 63: 1216–22.
36. Takeuchi M, Igarashi Y, Tomimoto S et al. Single-beat estimation ofthe slope of the end-systolic pressure–volume relation in the humanleft ventricle. Circulation 1991; 83: 202–12.
37. Borow K, Neumann A, Wynne J. Sensitivity of end-systolic pressure-dimension and pressure–volume relations to the inotropic state inhumans. Circulation 1982; 65: 988–97.
38. Asanoi H, Kameyama T, Ishizaka S, Nozawa T, Inoue H. Ener-getically optimal left ventricular pressure for the failing human heart.Circulation 1996; 93: 67–73.
39. O’Rourke R, Horwitz L. Effects of chronic oral quinidine on leftventricular performance. Am. Heart J. 1981; 101: 769–73.
40. Watkins J, Slutsky R, Tubau J, Karliner J. Scintigraphic study ofrelation between left ventricular peak systolic pressure and end-systolic volume in patients with coronary artery disease and normalsubjects. Br. Heart J. 1982; 48: 39–47.
41. Starling M. Left ventricular–arterial coupling relations in the normalhuman heart. Am. Heart J. 1993; 125: 1659–66.
42. Curiel R, Perez-Gonzalez J, Brito N et al. Positive inotropic effectsmediated by alpha-1 adrenoceptors in intact humans subjects.J. Cardiovasc. Pharmacol. 1989; 14: 603–15.
43. Teichholz L, Kreulen T, Herman M, Gorlin R. Problems in echo-cardiographic volume determinations: Echocardiographic–angio-graphic correlation in the presence or absence of asynergy. Am. J.Cardiol. 1976; 37: 7–11.
44. Morgan D, Tomlinson C, Qayumi A, Toleikis P, McConville B,Jamieson W. Evaluation of contractility indexes in the dog with leftventricular dysfunction induced by rapid atrial pacing. J. Am. Coll.Cardiol. 1989; 14: 489–95.
45. Herrmann H, Ruddy T, Dec W, Srauss H, Boucher C, Fifer M.Inotropic effect of enoximone in patients with severe heart failure:Demonstration by left ventricular end-systolic pressure–volumeanalysis. J. Am. Coll. Cardiol. 1987; 9: 1117–23.
46. Bhargava V, Shabetai R, Ross Jr J, Shirato K, Pavelec R, Mason P.Influence of the pericardium on left ventricular diastolic pressure–volume curves in dogs with sustained volume overload. Am. Heart J.1983; 105: 995–1001.
47. Fujisawa A, Sasayama S, Takahashi M et al. Enhancement of leftventricular contractility after opening of an arteriovenous fistula indogs. Cardiovasc. Res. 1984; 18: 51–9.
48. Capomolla S, Pozzoli M, Opasich C et al. Dobutamine and nitro-prusside infusion in patients with severe congestive heart failure:Hemodynamic improvement by discordant effects on mitral regurgi-tation, left atrial function, and ventricular function. Am. Heart J. 1997;134: 1089–98.
49. Konstan M, Cohen S, Weiland D et al. Relative contribution ofinotropic and vasodilator effects to amrinone-induced hemodynamicimprovement in congestive heart failure. Am. J. Cardiol. 1986; 57:242–8.
50. Crozatier B, Bical O, Belot J, Caillet D. End-systolic left ventricularpressure–dimension shift during acute relief of volume overload in theconscious dog. Am. J. Cardiol. 1985; 55: 1102–6.
Operative contractility: A new index 879
51. Nutter D, Hurst V, Murray R. Ventricular performance during gradedhypovolemia induced by lower body negative pressure. J. Appl.Physiol. 1969; 26: 23–30.
52. Rankin L. Alterations in preload and ejection phase indexes of leftventricular performance. Circulation 1975; 51: 910–15.
53. Ishizaka S, Asanoi H, ada O, Kameyama T, Inoue H. Loadingsequence plys an important role in enhanced sensitivity of leftventricular relaxation in conscious dogs with tachycardia-inducedcardiomyopathy. Circulation 1995; 92: 3560–7.
54. Hoshino P, Blaustein A, Gaasch W. Effect of propranolol on the leftventricular response to the Valsalva maneuver in normal subjects. Am.J. Cardiol. 1988; 61: 400–4.
55. Castini D, Mangiarotti E, Vitolo E, Conconi B, Triulzi M. Effects ofvenous return reduction in hypertensive patients: Is there a Dopplerdiastolic dysfunction index independent of preload reduction? Am.Heart J. 1992; 123: 1299–306.
56. Nwosu E, Rahko P, Hanson P, Grogan E. Hemodynamic andvolumetric response of the normal left ventricle to upright tilttesting. Am. Heart J. 1994; 128: 106–13.
57. Lee J, Tajimi T, Widmann T, Ross Jr J. Application of end-systolicpressure–volume and pressure-wall thickness relations in consciousdogs. J. Am. Coll. Cardiol. 1987; 9: 136–46.
58. Ohyagi A, Sasayama S, Nakamura Y, Lee J, Kihara Y, Kawai C.Effect of ICI 118 587 on left ventricular function during gradedtreadmill exercise in conscious dogs. Am. J. Cardiol. 1984; 54:1108–13.
59. Wisenbaugh T, Katz I, Davis J et al. Long-term (3-month) effects of anew beta-blocker (Nebivolol) on cardiac performance in dilatedcardiomyopathy. J. Am. Coll. Cardiol. 1993; 21: 1094–100.
60. Borow K, Neumann A, Marcus R, Sareli P, Lang R. Effects ofsimultaneous alterations in preload and afterload on measurements ofleft ventricular contractility in patients with dilated cardiomyopathy:Comparisons of ejection phase, isovolumetric and end-systolic force–velocity indexes. J. Am. Coll. Cardiol. 1992; 20: 787–95.
61. Kass D, Grayson R, Marino P. Pressure–volume analysis as a methodfor quantifying simultaneous drug (amrinone) effects on arterial loadand contractile state in vivo. J. Am. Coll. Cardiol. 1990; 16: 726–32.
62. Rousseau M, Massart P, vanEyll C et al. Dose-related hemodynamicand electrocardiographic effects of the calcium promoter BAY y 5959in the presence or absence of congestive heart failure. J. Am. Coll.Cardiol. 1997; 30: 1751–7.
63. Nagata K, Iwase M, Sobue T, Yokota M. Differential effects ofdobutamine and a phosphodiesterase inhibitor on early diastolic fillingin patients with congestive heart failure. J. Am. Coll. Cardiol. 1995;25: 295–304.
64. Erbel R, Meyer J, Lambertz H et al. Hemodynamic effects ofprenalterol in patients with ischemic heart disease and congestivecardiomyopathy. Circulation 1982; 66: 361–9.
65. Crottogini A, Willshaw P, Barra J, Armentano R, Cabrera E, Pichel R.Inconsistency of the slope and the volume intercept of the end-systolicpressure–volume relationship as individual indexes of inotropic statein conscious dogs: Presentation of an index combining both variables.Circulation 1987; 76: 1115–26.
66. Little W, Cheng C, Peterson P, Vinten-Johansen J. Response of the leftventricular end-systolic pressure–volume relation in conscious dogs toa wide range of contractile states. Circulation 1988; 78: 736–45.
67. Feldman M, Pak P, Wu C et al. Acute cardiovascular effects of OPC-18790 in patients with congestive heart failure. Circulation 1996; 93:474–83.
68. Wilmshurst P, Thompson D, Coltart D, Weeb-Peploe M. Haemo-dynamic effects of intravenous amrinone in patients with impairedventricular function. Br. Heart J. 1983; 49: 77–82.
69. Mori M, Takeuchi M, Takaoka H, Yokoyama M. Lusitropic effects ofa Ca2+ sensitization with a new cardiotonic agent, MCI-154, ondiseased human hearts. Cardiovasc. Res. 1995; 30: 915–22.
70. Miura T, Miyazaki S, Guth B, Kambayashi M, Ross Jr J. Influence ofthe the force–frequency relation on left ventricular function duringexercise in conscious dogs. Circulation 1992; 86: 563–71.
71. Goldman S, Hager D, Olajos M, Perrier D, Mayersohn M. Effect ofthe ouabain–quinidine interaction on left ventricular and left atrialfunction in conscious dogs. Circulation 1983; 67: 1054–8.
72. Asanoi H, Ishizaka S, Joho S, Kameyama T, Inoue H, Sasayama S.Altered inotropic and lusitropic responses to heart rate in consciousdogs with tachycardia-induced heart failure. J. Am. Coll. Cardiol.1996; 27: 728–35.
73. Starling M, Kirsh M, Montgomery D, Gross M. Mechanisms for leftventricular systolic dysfunction in aortic regurgitation: Importance forpredicting the functional response to aortic valve replacement. J. Am.Coll. Cardiol. 1991; 17: 887–97.
74. Lavine S, Prcevski P, Held C, Johnson V. Experimental model ofchronic global left ventricular dysfunction secondary to left coronarymicroembolization. J. Am. Coll. Cardiol. 1991; 18: 1794–803.
75. Murakami T, Hess O, Krayenbuehl H. Left ventricular function beforeand after diltiazem in patients with coronary artery disease. J. Am.Coll. Cardiol. 1985; 5: 723–30.
76. Applegate R. Load dependence of left ventricular diastolic pressure–volume relations during short-term coronary artery occlusion.Circulation 1991; 83: 661–73.
77. Merillon J, Chaster P, Gourgon W. Left ventricular function andhyperthyroidism. Br. Heart. J. 1981; 46: 137–43.
78. Kato R, Yokota M, Ishihara H, Sobue T. Correlation between leftventricular contractility and relaxation in patients with dilatedcardiomyopathy. Clin. Cardiol. 1996; 19: 413–18.
79. Rahko P. Comparative efficacy of three indexes of left ventricularperformance derived from pressure–volume loops in heart failureinduced by tachypacing. J. Am. Coll. Cardiol. 1994; 23: 209–18.
80. Little W, O’Rourke R. Effect of regional ischemia on left ventricularend-systolic pressure–volume relation in chronically instrumenteddogs. J. Am. Coll. Cardiol. 1985; 5: 297–302.
81. Lawrence W, Maughan L, Kass D. Mechanism of global functionalrecovery despite sustained postischemic regional stunning. Circulation1992; 85: 816–27.
82. Asanoi H, Sasayama S, Kameyama T. Ventriculoarterial coupling innormal and failing heart in humans. Circ. Res. 1989; 65: 483–93.
83. De Bruyne B, Bronzwaer J, Heyndrickx G, Paulus E. Comparativeeffects of ischemia and hypoxemia on left ventricular systolic anddiastolic function in humans. Circulation 1993; 88: 461–71.
84. Serruys P, Hooghoudt T, Reiber J, Slager C, Brower R, Hugenholtz P.Influence of intracoronary nifedipine on left ventricular function,coronary vasomotility, and myocardial oxygen consumption. Br. HeartJ. 1983; 49: 427–41.
85. Prabhu S. Load sensitivity of left ventricular relaxation in normal andfailing hearts: Evidence of a nonlinear response. Cardiovasc. Res.1999; 43: 354–63.
86. Victory J, Foëx P, Leone B. End systolic pressure–length relations inhalothane anaesthetised dogs: Effects of regional ischaemia andinotropic agents. Cardiovasc. Res. 1991; 25: 110–17.
87. Takaoka H, Takeuchi M, Odake M et al. Depressed contractile stateand increased myocardial consumption for non-mechanical work inpatients with heart failure due to old myocardial infarction.Cardiovasc. Res. 1994; 28: 1251–7.
88. Bhargava V, Shabetai R, Mathiäsen R, Dalton N, Hunter J, Ross Jr J.Loss of adrenergic control of the force–frequency relation in heartfailure secondary to idiopathic or ischemic cardiomyopathy. Am. J.Cardiol. 1998; 81: 1130–7.
89. Merino A, Alegría E, Castelló R, Martínez-Caro D. Influence ofage on left ventricular contractility. Am. J. Cardiol. 1988; 62:1103–8.
90. Aurigemma G, Silver K, McLaughlin M, Mauser J, Gaasch W. Impactof chamber geometry and gender on left ventricular systolic functionin patients > 60 years of age with aortic stenosis. Am. J. Cardiol. 1994;74: 794–8.
91. Alpert M, Terry B, Mulekar M et al. Cardiac morphology and leftventricular function in normotensive morbidly obese patients with andwithout congestive heart failure, and effect of weight loss. Am. J.Cardiol. 1997; 80: 736–40.
880 R Curiel et al.
92. Scognamiglio R, Avogaro A, Casara D et al. Myocardial dysfunctionand adrenergic cardiac innervation i patients with insulin-dependentdiabetes mellitus. J. Am. Coll. Cardiol. 1998; 31: 104–12.
93. Foster R, Johnson D, Barilla F et al. Changes in left ventricular massand volumes in patients receiving angiotensin-converting enzymeinhibitor therapy for left ventricular dysfunction after Q-wavemyocardial infarction. Am. Heart J. 1998; 136: 269–75.
94. Shimizu G, Hirota Y, Kawamura K. Empiric determination of thetransition from concentric hipertrophy heart failure in essential hyper-tension. J. Am. Coll. Cardiol. 1995; 25: 888–94.
95. Taniguchi K, Nakano S, Kawashima Y et al. Left ventricular ejectionperformance, wall stress, and contractile state in aortic regurgitationbefore and after aortic valve replacement. Circulation 1990; 82:798–807.
96. Douglas P, Morrow R, Ioli A, Reichek N. Left ventricular shape,afterload and survival in idiopathic dilated cardiomyopathy. J. Am.Coll. Cardiol. 1989; 13: 311–15.
97. Taniguchi K, Nakano S, Hirose H et al. Preoperative left ventricularfunction: Minimal requirement for successful late results of valvereplacement for aortic regurgitation. J. Am. Coll. Cardiol. 1987; 10:510–18.
98. Donner R, Black I, Spann J, Carabello B. Left ventricular wall stressand function in childhood coarctation of the aorta. J. Am. Coll.Cardiol. 1985; 5: 1161–7.
99. Hasenfuss G, Holubarsch C, Heiss W, Just H. Influence of UDCG-115on hemodynamics and myocardial energetics in patients withidiopathic dilated cardiomyopathy. Am. Heart J. 1989; 118:512–19.
100. Sutton M, Plappert T, Hirshfeld J, Reichek N. Assessment of leftventricular mechanics in patients with asymptomatic aortic regurgi-tation: A two-dimensional echocardiographic study. Circulation 1984;69: 259–68.
101. Kumpuris A, Quinones M, Waggoner A, Kanon D, Nelson J, Miller R.Importance of preoperative hypertrophy, wall stress and end-systolicdimension as echocardiographic predictors of normalization of leftventricular dilatation after valve replacement in chronic aorticinsufficiency. Am. J. Cardiol. 1982; 49: 1091–100.
102. Koilpillai C, Quiñones M, Greenberg B et al. Relation of ventricularsize and function to heart failure status and ventricular dysrhythmia inpatients with severe left ventricular dysfunction. Am. J. Cardiol. 1996;77: 606–11.
103. Smart S, Knickelbine T, Malik F, Sagar K. Dobutamine–atropinestress echocardiography for the detection of coronary artery disease inpatients with left ventricular hypertrophy. Circulation 2000; 101:258–63.
104. Borow K, Lang R, Neumann A, Carroll J, Rajfer S. Physiologicmechanisms governing hemodynamic responses to positive inotropictherapy in patients with dilated cardiomyopathy. Circulation 1988; 77:625–37.
105. Aurigemma G, Gaasch W, McLaughlin M, McGinn R, Sweeney A,Meyer T. Reduced left ventricular systolic pump performance anddepressed myocardial contractile function in patients > 65 years of agewith normal ejection fraction and high relative wall thickness. Am. J.Cardiol. 1995; 76: 702–5.
106. Semelka R, Tomei E, Wagner S et al. Interstudy reproducibility ofdimensional and functional measurements between cine magneticresonance studies in the morphologically abnormal left ventricle. Am.Heart J. 1990; 119: 1367–73.
107. Zabalgoitia M, Rahman N, Haley H et al. Comparison in systemichypertension of left ventricular mass and geometry with systolic anddiastolic function in patients < 65 to > 65 years of age. Am. J. Cardiol.1998; 82: 604–8.
108. Scheidt W, Neuder J, Erdmann D, Kemkes B, Gokel M, Autenrieth G.Contractility of the transplanted, denervated human heart. Am. HeartJ. 1991; 121: 1480–8.
109. Goertz A, Mehl T, Lindner K et al. Effect of 7.2% hypertonic saline/6% hetastarch on left ventricular contractility in anesthetized humans.Anesthesiology 1995; 82: 1389–95.
110. Schmidt C, Roosens C, Struys M et al. Contractility in human aftercoronary artery surgery. Anesthesiology 1999; 91: 58–70.
111. Fontanet H, Pérez J, Dávila-Román V. Diminished contractilityreserve in patients with left ventricular hypertrophy and increased end-systolic stress during dobutamine stress echocardiography. Am. J.Cardiol. 1996; 78: 1029–35.
112. Greenberg B, Massie B, Thomas D et al. Association between theexercise ejection fraction response and systolic wall stress in patientswith chronic aortic insufficiency. Circulation 1985; 71: 458–65.
113. Kleaveland J, Reichek N, McCarthy D et al. Effects of six-monthafterload reduction therapy with hydralazine in chronic aorticregurgitation. Am. J. Cardiol. 1986; 57: 1109–16.
114. Kitzman D, Sheikh K, Beere P, Philips J, Higginbotham M. Age-related alteration of Doppler left ventricular filling indexes innormal subjects are independent of left ventricular mass, heart rate,contractility and loading conditions. J. Am. Coll. Cardiol. 1991; 18:1243–50.
115. Mone S, Sanders S, Colan S. Control mechanisms for physiologicalhypertrophy of pregnancy. Circulation 1996; 94: 667–72.
116. Igarashi H, Shiraishi H, Endoh H. Left ventricular contractile state inpreterm infants: Relation between wall stress and velocity of circum-ferential fiber shortening. Am. Heart J. 1994; 127: 1336–40.
117. Mier C, Turner M, Ehsani A, Spina R. Cardiovascular adaptations to10 days of cycle exercise. J. Appl. Physiol. 1997; 83: 1900–6.
118. Spina R, Turner M, Ehsani A. Beta-adrenergic-mediated improvementin left ventricular function by exercise training in older men. Am. J.Physiol. 1998; 274: H397–404.
119. Borow K, Come P, Neumann A, Baim D, Braunwald E, Grossman W.Physiologic assessment of the inotropic, vasodilator and afterloadreducing effects of milrinone in subjects without cardiac disease. Am.J. Cardiol. 1985; 55: 1204–9.
120. Borow K, Neumann A, Lang R. Milrinone versus dobutamine:Contribution of altered myocardial mechanics and augmentedinotropic state to improved left ventricular performance. Circulation1986; 73 (Suppl. 3): III–153–61.
121. Vasan R, Larson M, Levy D, Evans J, Benjamin E. Distribution andcategorization of echocardiographic measurements in relation toreference limits. Circulation 1997; 96: 1863–73.
122. Sahn D, De Maria A, Kisslo J, Weyman A. Recommendationsregarding quantitation in M-mode echocardiography: Results of asurvey of echocardiographic measurements. Circulation 1978; 58:1072–83.
123. Henry W, Gardin J, Ware J. Echocardiographic measurements innormal subjects from infancy to old age. Circulation 1980; 62:1054–61.
124. Schettini C, Bianchi M, Nieto F, Sandoya E, Senra H. Ambulatoryblood pressure. Normality and comparison with other measurements.Hypertension 1999; 34: 818–25.
125. Curiel R, Octavio J, Perez-Gonzalez J. Nuevo índice para evaluar lafunción contráctil en la cardiopatía hipertensiva compensada. AvancesCardiológicos 2003; 23 (Suppl. 1): S23 (Abstract).
126. Senzaki H, Chen CH, Kass DA. Single-beat estimation of end-systolicpressure–volume relation in humans. A new method with the potentialfor noninvasive application. Circulation 1996; 94: 2497–506.
127. Kjorstad K, Korvald C, Myrmel T. Pressure–volume-based single-beatestimations cannot predict left ventricular contractility in vivo. Am. J.Physiol. Heart Circ. Physiol. 2002; 282: H1739–50.
128. Kass D, Beyar R. Evaluation of contractile state by maximalventricular power divided by the square of end-diastolic volume.Circulation 1991; 84: 1698–708.
129. Cotter C, Simon W, Vered Z, Tan L. Role of cardiac power in heartfailure. Curr. Opin. Cardiol. 2003; 18: 215–22.
130. Leather H, Segers P, Sun Y, De Ruyter H, Vandermeersch E, WoutersP. The limitations of preload-adjusted maximal power as an index ofright ventricular contractility. Anesth. Analg. 2002; 95: 798–804.
131. Lester S, Shin H, Lambert A et al. Is PA-PWRmax truly a preload-independent index of myocardial contractility in anaesthetizedhumans? Cardiology 2004; 102: 77–81.
Operative contractility: A new index 881
132. Baan J, Van Der Velde E. Sensitivity of left ventricular end-systolicpressure–volume relation to type of loading intervention in dogs. Circ.Res. 1988; 62: 1247–58.
133. Van Der Velde E, Burkhoff D, Steendijk P, Karsdon J, Sagawa K,Baan J. Nonlinearity and load sensitivity of end-systolic pressure–volume relation of canine left ventricle in vivo. Circulation 1991; 83:315–27.
134. Freeman G, Little W, O’Rourke R. The effect of vasoactive agents onthe left ventricular end-systolic pressure–volume relation in closed-chest dogs. Circulation 1986; 74: 1107–13.
135. Carabello B, Williams H, Gash A et al. Hemodynamic predictors ofoutcome in patients undergoing valve replacement. Circulation 1986;74: 1309–16.
136. Banerjee A, Brook M, Klautz J, Teitel D. Nonlinearity of the leftventricular end-systolic wall stress–velocity of fiber shorteningrelation in young pigs. A potential pitfall in its use as a single-beatindex of contractility. J. Am. Coll. Cardiol. 1994; 23: 514–24.
137. Konstam M, Cohen S, Salem D et al. Comparison of left and rightventricular end-systolic pressure–volume relations in congestive heartfailure. J. Am. Coll. Cardiol. 1985; 5: 1326–4.
138. Brown K, Ditchey R. Human right ventricular end-systolic pressure–volume relation defined by maximal elastance. Circulation 1988; 78:81–91.
139. Dell’Italia L, Walsh R. Right ventricular diastolic pressure–volumerelations and regional dimensions during acute alterations in loadingconditions. Circulation 1988; 77: 1276–1.
APPENDIX I
Computational flowchart.
Related Documents











