One bird with two stones: Abnormal word length effects in pure alexia and semantic dementia T. B. Cumming and K. Patterson Q1 MRC Cognition and Brain Sciences Unit, Cambridge, UK M. Verfaellie Memory Disorders Research Centre, Boston VA Healthcare System and Boston University School of Medicine, Boston, MA, USA K. S. Graham MRC Cognition and Brain Sciences Unit, Cambridge, UK In pure alexia (PA)—an acquired reading disorder consequent on posterior left-hemisphere stroke— the hallmark is a pronounced and abnormal impact of word length on reading speed. Some patients with semantic dementia (SD)—a neurodegenerative condition affecting semantic memory—have also been reported to show an abnormal word length effect (AWLE) in reading, even though they are not thought to have the basic visual-processing deficits hypothesized to underlie this phenomenon in PA. In the current study, an AWLE in reading was consistently observed in both PA and SD patients, but further manipulations demonstrated marked differences between the groups in the conditions that produce the length effect, its specific manifestation, and the pattern of other deficits accompanying it. All of the results are compatible with the twin hypotheses that the AWLE in reading arises from a visual-processing deficit in PA but from reduced top-down lexical/semantic support for word identification in SD. In other words, the AWLE in the two patient groups appears to be a common symptom arising from different underlying deficits: one bird with two stones. INTRODUCTION The topic of the investigation Letter-by-letter (LBL) reading is a term that has, over the last few decades, come to be used synonymously with several older labels (e.g., alexia without agraphia, pure alexia, De ´jerine’s syndrome) for an acquired disorder of reading often observed following an infarct in the territory of the left posterior cerebral artery. Each of these labels has its own rationale. The syndrome was PCGN167386 TECHSET COMPOSITION LTD, SALISBURY, U.K. 4/3/2006 Correspondence should be addressed to Kim Graham, MRC Cognition and Brain Sciences Unit, 15 Chaucer Road, Cambridge, CB2 2EF, UK ([email protected]). We are indebted to the many patients and their families for their willingness to devote considerable time and effort to this experi- ment. We are also grateful to Dr B. Weekes, who allowed us to use his stimuli (Experiment 4) and to Professors J. R. Hodges, R. J. S Wise, and M. A. Lambon Ralph, and Dr E. Warburton for kindly granting us access to the patients. Our thanks go to Jo Drake, John Keane, and Jane Powis for help in data collection (Experiments 1 and 2), and to Anna Woollams for assistance with additional reading data for the patients with semantic dementia. TBC was funded by a Commonwealth Scholarship, and MV was supported by a Fogarty Senior International Fellowship and the Medical Research Service of the U.S. Department of Veterans Affairs. KSG and KP acknowledge the support of the Medical Research Council in the UK. # 0000 Psychology Press Ltd 1 http://www.psypress.com/cogneuropsychology DOI:10.1080/02643290600674143 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0), 1 – 32

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

One bird with two stones: Abnormal word lengtheffects in pure alexia and semantic dementia
T. B. Cumming and K. PattersonQ1MRC Cognition and Brain Sciences Unit, Cambridge, UK
M. VerfaellieMemory Disorders Research Centre, Boston VA Healthcare System and Boston University School of Medicine, Boston, MA, USA
K. S. GrahamMRC Cognition and Brain Sciences Unit, Cambridge, UK
In pure alexia (PA)—an acquired reading disorder consequent on posterior left-hemisphere stroke—the hallmark is a pronounced and abnormal impact of word length on reading speed. Some patientswith semantic dementia (SD)—a neurodegenerative condition affecting semantic memory—have alsobeen reported to show an abnormal word length effect (AWLE) in reading, even though they are notthought to have the basic visual-processing deficits hypothesized to underlie this phenomenon in PA.In the current study, an AWLE in reading was consistently observed in both PA and SD patients, butfurther manipulations demonstrated marked differences between the groups in the conditions thatproduce the length effect, its specific manifestation, and the pattern of other deficits accompanyingit. All of the results are compatible with the twin hypotheses that the AWLE in reading arisesfrom a visual-processing deficit in PA but from reduced top-down lexical/semantic support forword identification in SD. In other words, the AWLE in the two patient groups appears to be acommon symptom arising from different underlying deficits: one bird with two stones.
INTRODUCTION
The topic of the investigation
Letter-by-letter (LBL) reading is a term that has,over the last few decades, come to be used
synonymously with several older labels (e.g.,alexia without agraphia, pure alexia, Dejerine’ssyndrome) for an acquired disorder of readingoften observed following an infarct in the territoryof the left posterior cerebral artery. Each of theselabels has its own rationale. The syndrome was
PCGN167386 TECHSET COMPOSITION LTD, SALISBURY, U.K. 4/3/2006
Correspondence should be addressed to Kim Graham, MRC Cognition and Brain Sciences Unit, 15 Chaucer Road, Cambridge,
CB2 2EF, UK ([email protected]).
We are indebted to the many patients and their families for their willingness to devote considerable time and effort to this experi-
ment. We are also grateful to Dr B. Weekes, who allowed us to use his stimuli (Experiment 4) and to Professors J. R. Hodges, R. J. S
Wise, and M. A. Lambon Ralph, and Dr E. Warburton for kindly granting us access to the patients. Our thanks go to Jo Drake, John
Keane, and Jane Powis for help in data collection (Experiments 1 and 2), and to Anna Woollams for assistance with additional
reading data for the patients with semantic dementia. TBC was funded by a Commonwealth Scholarship, and MV was supported
by a Fogarty Senior International Fellowship and the Medical Research Service of the U.S. Department of Veterans Affairs. KSG
and KP acknowledge the support of the Medical Research Council in the UK.
# 0000 Psychology Press Ltd 1http://www.psypress.com/cogneuropsychology DOI:10.1080/02643290600674143
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0), 1–32

originally known as Dejerine’s syndrome because itwas he who first took a serious, or at least pub-lished, interest in this disorder (Dejerine, 1891).It was called alexia without agraphia because astriking feature of the disorder in its classicalform is that reading is disrupted but writing isnot, thus distinguishing this syndrome frommost language disorders in which writing/spellingis the most vulnerable of language abilities. Evenmore selectively, it has been labelled pure alexiabecause, again in its classical form, the disorderwas described as sparing not only writing butindeed all cognitive abilities other than reading.And most recently, it has changed its main desig-nation again because the cognitive neuropsycholo-gists who began to study this syndrome were moreinterested in the nature of the reading disorderitself than in who had discovered it or in theaccompanying pattern of other spared or affectedcognitive abilities.
This latest designation, LBL reading, has twolinked bases. First is the observation that thesepatients show a pronounced and abnormalimpact of word length on the speed and sometimesalso the accuracy of word reading. Second is theinference from this observation that such patientsread by identifying the letters of a word seriallyrather than in the parallel fashion that normalreaders are thought to do. Note that when we(and others) refer to word length effects inreading, this means the impact of the number ofconstituent letters in a word on the responsetime (RT) required for someone to read theword aloud correctly. To give a rough idea of thesize of the abnormal word length effect (AWLE)in LBL readers: For alphabetic words (in standardhorizontal format) varying in length from aboutthree to seven letters, normal readers show anessentially flat RT function, or perhaps an increaseof a few milliseconds per additional letter(Henderson, 1982). LBL patients, by contrast,have been reported to require an additional 1–3seconds for each extra letter in the stimulus(Hanley & Kay, 1996): three orders of magnitudemore impact of length than normal readers.
The take-off point of our study was the obser-vation, by our research group and others, that pure
alexia associated with left posterior-artery strokemay not be the only condition in which wordreading is characterized by an AWLE: Thisfeature of reading may also be observed in patientswith semantic dementia (e.g., Gold et al., 2005;Noble, Glosser, & Grossman, 2000; Patterson &Hodges, 1992). Both the lesion sites and the cog-nitive profiles differ markedly between pure alexia(PA) and semantic dementia (SD). The suggestionthat an AWLE—the hallmark of PA—might alsobe common in SD therefore raises the question ofwhether the source of the AWLE is the same ordifferent in the two disorders. As background toour experiments on reading by patients witheither PA or SD, the remainder of theIntroduction briefly reviews the major accountsof the AWLE in PA. The literature on thistopic is so large that we cannot review all of it,nor would it make sense to do so given thatmany of the issues cannot be resolved by findingsfrom the current study. While it is thereforenecessary to provide some theoretical backgroundto our study, we shall restrict it to the issues thatwill be germane to interpreting our results. SeeColtheart (1998) for a brief but excellentsummary of the main questions regarding PA.
Issues in pure alexia
One central question is whether “pure” alexia is aselective reading disorder or just one manifestationof a more general visual-processing impairment(Behrmann, Nelson, & Sekuler, 1998a; Farah,1997; Farah & Wallace, 1991; Patterson &Lambon Ralph, 1999). If, as traditionallyassumed, the disorder only affects reading andnot other cognitive abilities that require fine andrapid visual processing, then the AWLE andother aspects of abnormal reading in PA could inprinciple arise at a number of different loci in theprocess of written-word identification. Forexample, presented with words at a reducedexposure duration—but not all that reduced, forexample 250 ms in Coslett and Saffran (1994), oreven 500 ms in Chialant and Caramazza (1998):exposure durations that yield 100% correct identi-fication by normal readers—PA patients will
2 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

typically fail to identify many or most of them.This finding could be, and indeed has been, attri-buted to impairments at stages from early to late inthe reading process. By contrast, if limitedexposure and/or increased complexity of thevisual stimulus adversely affects PA patients’ pro-cessing of things other than words (e.g., abstractvisual patterns or faces or line drawings ofobjects), then it seems more likely that the deficitarises (a) somewhere other than the readingprocess and (b) probably at some relatively earlystage of perceptual processing that is common toa variety of visual stimuli. Recent years have seenan increasing trend toward reports of PA patientswho are impaired on nonreading tasks that makedemands on visual processing similar to those ofwritten-word identification (e.g., Behrmannet al., 1998a; Behrmann, Shomstein, Black, &Barton, 2001; Farah & Wallace, 1991); however,the only sensible comment at this point is thatthe jury is still out, because as yet relatively fewstudies of PA have included adequate assessmentof nonreading visual tasks. Furthermore, it mustbe remembered that even very consistent associ-ations of this kind do not prove common cause.Until research in this area can provide some wayin which to compare visual complexity in linguisticversus nonlinguistic stimuli, plus a more detailedpicture of how limited exposure duration affectsperformance on these different types of input, itwill not be possible to conclude definitively thatparallel deficits in reading and nonreading visualtasks have the same cause.
A second major difference between accounts ofPA is the model of reading to which the researchersubscribes. Choice of a reading model wouldobviously be critical to the interpretation of PAif the disorder were truly restricted to reading,but it is important even if PA is not pure. Thatis, even if PA patients are impaired in processingany complex visual input, we still want to under-stand the mechanisms by which they read, andthis requires a model. The two most explicit(because computationally implemented) classes ofreading model currently on offer are the DRCmodel of Coltheart and colleagues (e.g.,Coltheart, Rastle, Perry, Langdon, & Ziegler,
2001) and the triangle model of Plaut and collea-gues (e.g., Plaut, McClelland, Seidenberg, &Patterson, 1996). Suppose for the moment(though see the section below labelled LetterMisidentifications) that the AWLE hallmark ofPA does mean that the patients read letter byletter. What mechanism in each of these twomajor classes of reading model can account forreading via serial letter identification?
In the DRC model, which has separate mecha-nisms for lexical and nonlexical reading, the lexicalroute processes letter strings in parallel but thenonlexical grapheme-to-phoneme (GPC) routeprocesses letter strings serially, translating oneletter or grapheme to one phoneme at a time, ina left-to-right fashion. Reading by the GPCroute might therefore seem to offer a particularlyfelicitous account of an AWLE, but on its ownit could not explain the pattern of reading in PA.The GPC process produces regular, rule-governedpronunciations, resulting in the regularization ofwords with atypical spelling–sound correspon-dences (like pint or gone in English), but PApatients almost never make regularization errors.For example, when the slow and error-pronepatient C.H. (Patterson & Kay, 1982) was tryingto read the word gone, he started by misidentifyingthe initial letter, first as a d and then as a b, beforefinally settling on g (confusion within the class ofascender- and descender-letters is common insevere PA). In each case, however, his pronun-ciation of the whole word was lexically correct,even though the three words (done, bone, gone)have three different pronunciations of the vowel.The nonlexical route of the DRC model wouldread all three words to rhyme with “bone”. TheDRC model must therefore explain PA either interms of serial rather than parallel input to thelexical route or by interaction of the two routes.Reading solely by the GPC route is also ruledout by other documented features of PA reading,such as a normal or even augmented advantagefor reading words relative to nonwords andhigh- relative to low-imageability words(Behrmann, Plaut, & Nelson, 1998b; Howard,1991); these effects signal involvement of lexicaland/or semantic processing. The summary by
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 3
WORD LENGTH EFFECTS IN PA AND SD

Coltheart et al. (2001) of DRC explanations forvarious forms of acquired reading disordermerely says, with respect to PA, “future workwill be required . . .” (p. 244).
The triangle model, as exemplified, forexample, by Harm and Seidenberg (2004) andPlaut et al. (1996), does not yet offer a completeaccount of PA either. This approach could be saidto have two pathways from orthography (O) tophonology (P; neither corresponding to either ofthe two in the DRC model): one direct, O ! P,and one via semantics (S) or word meaning,O ! S ! P; however, in contrast to the DRCmodel, the fundamental nature of the processingis the same in the two pathways. The similarityof the principles on which the two pathwaysoperate includes the fact that, in both, theletters of a stimulus word are analysed and trans-lated to phonology in parallel. Plaut (1999),however, described an extension to the trianglemodel in which a recurrent network was trainedto generate the pronunciation for a letter stringas a sequence of phonemes. The network would,upon encountering any difficulty in its analysis ofa letter string, refixate at a new position in thestring, similar to a real reader making multiplefixations within a given word. As a simulation ofthe deficit in PA, the trained network was sub-jected to noise at the level of letter activations.This resulted in an increase in the averagenumber of fixations per word, which can betreated as an analogue of increased response timein oral reading. Furthermore, the “lesioned”network produced a significant interactionbetween word length and word frequency, asdemonstrated for real PA patients by Behrmannet al. (1998b). We acknowledge that Plaut’s(1999) damaged network is not a full simulationof the account of PA in Behrmann et al.(1998b), for two reasons. First, specifically, thisaccount relies substantially on top-down feedbackfrom lexical/semantic levels to orthographicprocessing, whereas Plaut’s refixation network isnot an interactive model. Second and moregenerally, there have been no further investi-gations of the extent to which the refixationnetwork can capture other aspects of normal and
impaired reading. Nevertheless, in principle, thecombination of an interactive triangle frameworkand the refixation network may—with futurework, as in the DRC—be able to simulate PA.
Although this is not a study explicitly designedto provide evidence for one model of reading overanother, we frequently refer to the way in whichthese two frameworks might interpret ourresults, including many references to the conceptof lexical/semantic support for reading aloud. Itmight be helpful to explain this concept moreexplicitly, as it is central to both theories but isimplemented differently in the two models. TheDRC theory assumes that reading aloud operatesonly on form-based O and P representations(either whole word in the lexical route orsubword in the nonlexical route); lexical support,therefore, means activation of word-specific,lexical, nonsemantic O and P representations. Incontrast, the triangle theory assumes—althoughit has not always instantiated this assumption inreal simulations—that semantic representationsof real words are always activated during readingand hence can provide additional feedback to Oand P; this is one kind of “lexical” support.Furthermore, although the triangle framework hasno lexicon (word-specific nodes) as such, it certainlyhas the equivalent of “lexical processing”. This takesthe form of (a) greater stability in familiar patternsof distributed representations, corresponding toreal words that have been encountered manytimes, at both O and P levels, and (b) additionalreinforcement that arises when the stablepattern on which the network settles at one level(e.g., over the O units) corresponds to the patternactivated at the other two levels (P and S).
Letter misidentifications
All of the above discussion has been based on thestandard assumption that PA patients are unableto identify words via the largely parallel processof letter identification that underlies normalreading. The corollary of this assumption is thatsuch a patient essentially always approaches aword with a letter-by-letter strategy (unlessprevented from doing so by some artificial
4 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

manipulation such as brief exposure duration:Saffran & Coslett, 1998). These twin assumptions,while typical, are not universal. Howard (1991)was perhaps the first to offer a persuasive argumentthat a PA patient might approach words with thesame parallel process that a normal reader does(and, of course, that the patient did premorbidly).If this process succeeded in identifying the word,the patient would produce a reasonably fastreading RT—perhaps still slow relative tonormal readers, but not too slow and, importantly,not incrementally slower for longer words, eventhough the likelihood of such fast readingresponses would be lower for longer words. Onmany occasions, however, the initial parallelapproach to identifying the word would fail, andthen the PA patient would be forced to resort toa sequential strategy. This is not dissimilar to theprinciple in Plaut’s (1999) network in which anydifficulty in identifying a word induces refixationsthat might, at the limit, involve serial fixation ofevery letter in the word. It also resonates withthe finding reported by Weekes (1997) of a signifi-cant effect of string length in normal subjects’ RTsto read nonwords but not words. This makes goodsense if the unfamiliar combinations of lettersin nonwords induce extra difficulty for parallelprocessing (Behrmann et al., 1998b).
In Howard’s (1991) proposal, difficulty, or evenfrank error, in identifying one or more of theletters in the string is the cause of the PAreader’s switch from normal parallel reading to aserial strategy. It is not completely clear how thereading system would always know that a letterhad been misidentified. In some cases (e.g., if thel in plan were misidentified as a different ascendersuch as t or f), it is not surprising that the “checker”might object and call for another opinion, sinceptan or pfan are not legal sequences in English.When patient C.H. (mentioned above) first readgone as done and then as bone, however, it is notso obvious why these responses were self-corrected(indeed many PA patients, especially the moresevere, do make a number of un-self-correctederrors that clearly result from letter misidentifica-tions). Setting that question aside, the importantidea here is the proposal that the fundamental
problem in PA is a deficit in recognizing theletters (or any visual symbols) in a string ratherthan a failure to process them in parallel. Andrecently, a related idea has burst upon the fieldin the form of a striking demonstration (Fiset,Arguin, Bub, Humphreys, & Riddoch, 2005; seealso Arguin & Bub, 2005; Arguin, Fiset, & Bub,2002) that the AWLE in PA patients disappearsif words of different lengths are equated forsummed letter confusability.
These issues regarding the most satisfactoryinterpretation of the AWLE in pure alexia arerevisited in the General Discussion, but now it istime to turn to our investigations. It is worth areminder that, under certain circumstances,normal readers also show an AWLE; these cir-cumstances include the reading of unfamiliarletter strings (i.e., nonwords; Mason, 1978;Weekes, 1997) or even of familiar words if theseare presented in an atypical format (such as mixedcase, e.g., pLaN) or viewed in the left visualfield at reduced exposure duration (Young &Ellis, 1985). For familiar words of no more thanabout 7–8 letters presented in undistortedformat and in central vision, however, an AWLEhas long been regarded as unique to patientswith pure alexia. The current study was promptedby the observation that a completely different sortof brain abnormality—the progressive anteriortemporal-lobe atrophy associated with semanticdementia (SD)—might also result in an AWLE(Gold et al., 2005). This raises at least twothought-provoking questions. First of all, with afew notable exceptions (e.g., Blazely, Coltheart,& Casey, 2005; Cipolotti & Warrington, 1995),the typical pattern of reading in SD—nowdocumented in many dozens of cases—is surfacedyslexia, the acquired reading disorder in whichaccuracy of word reading shows a dramaticFrequency � Regularity interaction. If anAWLE is the signature of a different kind ofreading disorder, should one then be thinkingthat SD patients often have two different formsof acquired dyslexia? Secondly, and of greaterinterest: Can the cause of the AWLE in PA beimported to explain the AWLE in SD? Or,given the almost complete lack of overlap in both
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 5
WORD LENGTH EFFECTS IN PA AND SD

lesion site and cognitive profile between PA andSD, should one now be thinking in terms of twodifferent causes of an AWLE? The centralfeature of SD is degraded semantic knowledge,and one main (though not universally accepted)story is that reduced semantic activation is respon-sible for the surface dyslexia in SD (Patterson et al.,2006). Might degraded semantic activation in theprocessing of written words also yield an AWLE?
The format of our study is as follows.Experiment 1, with SD patients only (N ¼ 8),had two purposes. First, it was intended to deter-mine whether all of the cases would reveal anAWLE in standard oral-reading tasks. Second,assuming a positive answer to the first question,and to begin the investigation of whether thesource of this effect in SD is similar to or distinctlydifferent from its cause in PA, we assessed the SDpatients’ performance on both (a) nonreadingvisual tasks on which PA patients are typicallyimpaired and (b) a nonvisual word identificationtask on which PA patients are typically unimpaired.This latter task requires the participant to identifywords from their oral spelling (e.g., “What doesP, L, A, N spell?”). Experiment 2 was a slight diver-sion from the comparison of SD with PA: It wasperformed to consider (and, we hoped, to ruleout) the possibility that the AWLE in SD is aconsequence of the general cognitive slowingassociated with normal ageing and then exacer-bated by organic brain disease. Experiment 2 there-fore tested the relationship between age, baselineword-reading response times, and word length inolder and younger groups of normal subjects. InExperiments 3 and 4, we directly contrasted theperformance of SD and PA patients (N ¼ 3each): in Experiment 3 on word reading, identifi-cation of words from oral spelling, and nonreadingvisual tasks, and in Experiment 4 on reading ofwords versus nonwords.
EXPERIMENT 1
This experiment aimed to build on the evidenceavailable at the time of the experiment’s design(Hodges et al., 1992; Noble et al., 2000;
Patterson & Hodges, 1992) reporting abnormalword length effects in reading by SD patients;since that time, Gold et al. (2005) have establishedthe phenomenon more persuasively. An analogousnonvisual task, identification of words from oralspelling, was employed to determine whether anylength effect in reading would also be present inword processing from a different modality. Threevisual matching tasks—one involving letters andtwo involving nonlinguistic materials—were usedto evaluate the status of visuoperceptual processingin SD.
Method
ParticipantsFor the word-reading task, the patient participantswere 8 cases with a clinical diagnosis of SD, basedon the cognitive and neuroradiological criteriaoutlined by Hodges et al. (1992). All wereidentified through the Memory and CognitiveDisorders Clinic or the Early Dementia Clinic atAddenbrooke’s Hospital, Cambridge, UK. Theiraverage age was 59.5 years, and average numberof years spent in education was 13.1. A total of24 controls were tested on the word-readingtask: 13 male and 11 female participants fromthe MRC Cognition and Brain Sciences Unit(MRC-CBU) volunteer panel, who werematched to the patients on age (mean ¼ 59.4years) and education (mean ¼ 13.2 years).Standard test scores are presented in Table 1(ordered for the patients by severity as reflectedby the ACE, an extended version of the Mini-Mental State Examination: Mathuranath,Nestor, Berrios, Rakowicz, & Hodges, 2000);the test scores shown for controls are meanstaken from a separate larger sample of 31 controls,also similar to the patients in age and education.
The pattern of results for SD patients wastypical: Scores were generally within the normalrange on copy and recall of the complex Reyfigure, subtests of the Visual Object and SpacePerception Battery (VOSP; Warrington &James, 1991), and digit span, but revealedvarying and often profound impairment (withthe exception of the mildest patient, A.N.) on
6 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

the three semantic tasks. The three tests employedto assess semantic function were taken from thesemantic battery used in our research programmein Cambridge (e.g., Bozeat, Lambon Ralph,Patterson, Garrard, & Hodges, 2000; Hodges &Patterson, 1995). Object Naming involves presen-tation of 64 line drawings of familiar objects fornaming. Word–Picture Matching (WPM;Hodges & Patterson, 1995) tests comprehensionof the same 64 concrete concepts: The patienthears the name of the object and is asked topoint to the corresponding picture in an array of10 line drawings from the same category. ThePyramids and Palm Trees test (PPT; Howard &Patterson, 1992) examines associative knowledgeof semantic concepts: Patients are presented with
one target and two response alternatives (wordsor pictures) and are asked to point to the alterna-tive that has a conceptual link with the target.Table 1 also reports the performance of all patients(at initial screening) plus control means in readinga list of words comprising high- and low-frequency regular and exception words (fromPatterson & Hodges, 1992). With the exceptionof W.M., every patient revealed the typicalsurface dyslexic pattern of a frequency-by-regularity interaction in reading accuracy. As thelowest control score for low-frequency irregularwords was 90%, W.M.’s reading at this stagecannot be designated abnormal, although she wasa well-educated woman whose reading of low-frequency irregular words would probably have
Table 1. Standard test scores for semantic dementia patientsa and mean scores for controls
SD patients
A.N. A.T. J.C. K.H. S.L. W.M. M.A. J.H. Controlsb
Agec 63 65 57 60 51 53 63 60 68.5 (7.1)
Educationc 9 19 10 16 12 16 13 10 11.2 (1.5)
MMSE 30 25 19 24 24 24 29 9 29 (1.0)
ACE 93 61 59 57 57 51 47 26 92.7 (3.0)
REY: Copy 36 36 31 36 30 36 36 36 34.2 (1.6)
Immediate 23 23 12.5 12 16 23 17.5 10.5 NT
Delayed 27 24 14.5 0 14 25 6.5 11 18.3 (5.2)
VOSP: Dots (10) 10 10 10 10 9 10 10 10 9.9 (0.3)
Position (20) 20 20 20 20 NT 20 20 19 19.8 (0.6)
Number location (10) 9 9 10 10 NT 10 10 10 8.9 (2.8)
Cubes (10) 10 10 10 9 10 10 10 10 9.3 (1.5)
Incomplete letters (20) 19 20 19 18 20 19 19 18 19.2 (0.8)
Object decision (20) 20 19 16 15 15 19 16 17 16.9 (2.3)
Digit span: Forward 7 8 7 4 5 8 6 6 7.1 (0.9)
Back 7 4 4 3 4 5 3 5 5.4 (1.4)
Naming (64) 64 10 41 30 18 26 13 6 62.3 (1.6)
WPM (64) 63 58 56 44 48 52 57 18 63.8 (0.4)
PPT: Pictures (52) 51 47 40 35 44 44 41 37 51.6 (1.1)
Reading: HF Regulard 100 93 93 100 100 100 100 100 99.8
LF regulard 98 90 74 88 95 98 95 91 99.5
HF exceptiond 98 100 88 95 100 93 98 91 99.5
LF exceptiond 67 74 57 64 67 90 79 60 95.4
Note: SD ¼ semantic dementia; MMSE ¼ Mini-Mental State Examination (Folstein, Folstein, & McHugh, 1975); ACE ¼
Addenbrooke’s Cognitive Examination (Mathuranath, Nestor, Berrios, Rakowicz, & Hodges, 2000); REY ¼ Rey–Osterreith
Complex Figure Test (Osterrieth, 1944); VOSP ¼ Visual Object and Space Perception Battery (Warrington & James, 1991);
WPM ¼ word–picture matching (Hodges & Patterson, 1995); PPT ¼ Pyramids and Palm Trees Test (Howard & Patterson,
1992); HF ¼ high frequency; LF ¼ low frequency; NT ¼ not tested.aStandard test scores for SD patients ordered by severity on the basis of the ACE. bStandard deviations in parentheses. cIn years.
dIn percentages.
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 7
WORD LENGTH EFFECTS IN PA AND SD

been perfect premorbidly (see Experiment 3 forevidence of W.M.’s subsequent decline intosevere surface dyslexia).
A.N. completed the standard tests and word-reading task but was not available for furthertesting. The remaining 7 SD patients agreed tobe tested on identification from oral spelling, butonly 4 of them—A.T., K.H., J.H. and W.M.—completed the task: The other three could notunderstand what they were meant to do. Datawere collected from all 7 SD patients (minusonly A.N.) on the visuospatial tasks and from 6patients on cross-case letter matching (M.A. wasunable to perform this task). A total of 8matched controls (mean age ¼ 58.4 years old,mean education ¼ 12.7 years) were tested onidentification from oral spelling and cross-caseletter matching.
MaterialsA set of 160 words that included 3-, 4-, 5-, and6-letter words was used to assess reading. Toincrease the likelihood that the SD patientswould read the target words correctly, all 160were regular words with pronunciations predict-able from their subword components. To avoidconfounding of RT measurements by differencesin initial phoneme, the 160 words consisted of 40quartets: Each quartet contained one word ateach of the four lengths matched precisely forinitial phoneme. The phonemic length of thewords, as expected, increased with letter length.Although the stimuli differed in written word fre-quency, with 3-letter words much more frequentthan those of the other lengths, the 4-, 5-, and6-letter stimuli were more comparable infrequency. According to the CELEX database(Baayen, Piepenbrock, & Gulikers, 1995),average frequencies were 172.5 for 3-letter words,11.7 for 4-letter words, 27.3 for 5-letter words,and 15.9 for 6-letter words. The set of wordsused in identification from oral spelling comprisedhalf of the stimuli from the reading set: 20 wordsfrom each of the 3-, 4-, 5-, and 6-letter word cat-egories. For the cross-case letter-matching task, aset of 12 letters was used (b, d, e, f, g, h, m, n, q,r, t, y) to construct 96 same-or-different trials.
Each target letter (e.g., f) was tested twice ineach of the four conditions: upper-case different(e.g., b-F), upper-case same (f-F), lower-casedifferent (D-f), and lower-case same (F-f). Theother two visuospatial tasks consisted of 16 smallmeaningless geometric figures (Frostig & Harne,1972) as targets and 16 small sketchy drawings ofobjects as targets (Kenkyukai, 1983); of the fourresponse alternatives that accompanied eachtarget, one was identical, and three were visuallyconfusable distractors.
ProcedureFor the reading task, target words were presented inthe centre of a computer screen. Participants wereinstructed to read each word aloud, and the onsetof a response triggered the microphone switch.Presentation order of the 160 words was random-ized. In identification from oral spelling, wordswere spelt out by the experimenter (at approxi-mately one letter per second), and participantswere asked to identify each word. Again, wordswere presented in random order. The cross-caseletter-matching task featured the brief presentationof a single letter, followed by a visual mask, followedby a second letter that differed in case to the firstletter. The exposure duration of the first letterwas lengthened if a patient could not perform thetask at the duration used for controls (33 ms).Participants were required to judge whether thefirst and second letters were the same or differentin letter identity. The other visual tests were alsomatching tasks and consisted of a single targetfigure or object and four response alternatives allpresented simultaneously. Participants were askedto circle the matching figure or object from thefour alternatives, and, although there was no timelimit, total time taken for the 16 trials was recorded.In all tasks, other than the self-explanatory readingaloud of single words, participants were given a setof practice items to ensure that they understoodwhat was required.
Results
Reading accuracy was relatively good: Across the 8SD patients, there were a total of 18 errors on
8 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

3-letter words (5.6%), 31 errors on 4-letter words(9.7%), 30 errors on 5-letter words (9.4%), and 52errors on 6-letter words (16.3%). For the RTanalysis, these incorrect responses were removed,and responses that were initiated before 200 msor after 4,000 ms were also excluded. Finally,responses with RTs that were further than 2 stan-dard deviations from the mean were removed.
SD patients exhibited a length effect in reading,with an average increase in RT of 112 ms peradditional letter. By contrast, controls showedonly a slight tendency for slower reading oflonger words; their average increase in RT was6 ms per letter increase. As there was considerablevariability amongst the SD patients, a median splitwas used to compare the 4 faster readers (A.N.,S.L., W.M., M.A.) and 4 slower readers (K.H.,A.T., J.H., J.C.), and data for these two groupsand controls are presented in Figure 1. Thefaster SD patients had, over all word lengths,mean word-reading RTs of about 700 ms; meanRTs of the 4 slower patients were approximatelytwice as long. Reading time increased by approxi-mately 20 ms for each additional letter in the wordfor the faster patients (cf. 4–5 ms for controls),and by about 150 ms for each added letter forthe slower patients. Individual patient data forreading and other tasks are provided in theAppendix.
The SD patients were treated as a single groupfor statistical analyses. A two-way repeatedmeasures analysis of variance (ANOVA; 2subject groups, 4 levels of letter length) revealedmain effects of group, F(1, 30) ¼ 20.2, p , .001,indicating that the SD patients were slower toread than controls, and of length, F(3, 90) ¼
22.1, p , .001, reflecting faster RTs to shorterwords. The highly significant interactionbetween group and length, F(3, 90) ¼ 17.5, p ,
.001, confirmed that the length effect was greaterin patients than in controls. Paired samples ttests were applied separately to each group todetermine whether the addition of a single letterresulted in significantly slower reading time. InSD patients, RT differences were identifiedbetween 3- and 4-letter words, t(7) ¼ 2.8, p ¼
.03, and between 5- and 6-letter words, t(7) ¼
2.3, p ¼ .05, but not between 4- and 5-letterwords, t(7) ¼ 1.1, ns. In controls, only the differ-ence between 5- and 6-letter words was reliable,t(7) ¼ 4.0, p ¼ .001.
To overcome differences between baselinereading RTs in patients and controls, z-scoreswere computed to determine the slope of thelength effects. The z-score transformation hasbeen proposed as a method for standardizingindividual differences in overall response latency(Faust, Balota, Spieler, & Ferraro, 1999).Z-scores were calculated for each participant bytaking his or her individual mean RT, subtractingthe group mean RT, and dividing by the standarddeviation of the group RT. Again, the figure(Figure 2) shows data for the two patient sub-groups and reveals that both SD subgroups exhib-ited a length effect that is greater than the effect oflength in controls. A two-way repeated measuresANOVA (2 levels of group, 4 levels of letterlength) on the z-scores identified a main effectof group, F(1, 30) ¼ 7.5, p ¼ .01, and a maineffect of length, F(3, 90) ¼ 15.4, p , .001. Theinteraction between group and length, F(3, 90) ¼4.0, p ¼ .01, was again significant, indicatingthat the patients’ greater length effect could notbe attributed solely to baseline slowing. InSD patients, paired t tests revealed differencesbetween 3- and 4-letter words, t(7) ¼ 11.1,
Figure 1. Mean reading response times for 3-, 4-, 5-, and 6-letter
words for 4 slower reading and 4 faster reading semantic dementia
(SD) patients and controls (standard error bars are shown).
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 9
WORD LENGTH EFFECTS IN PA AND SD
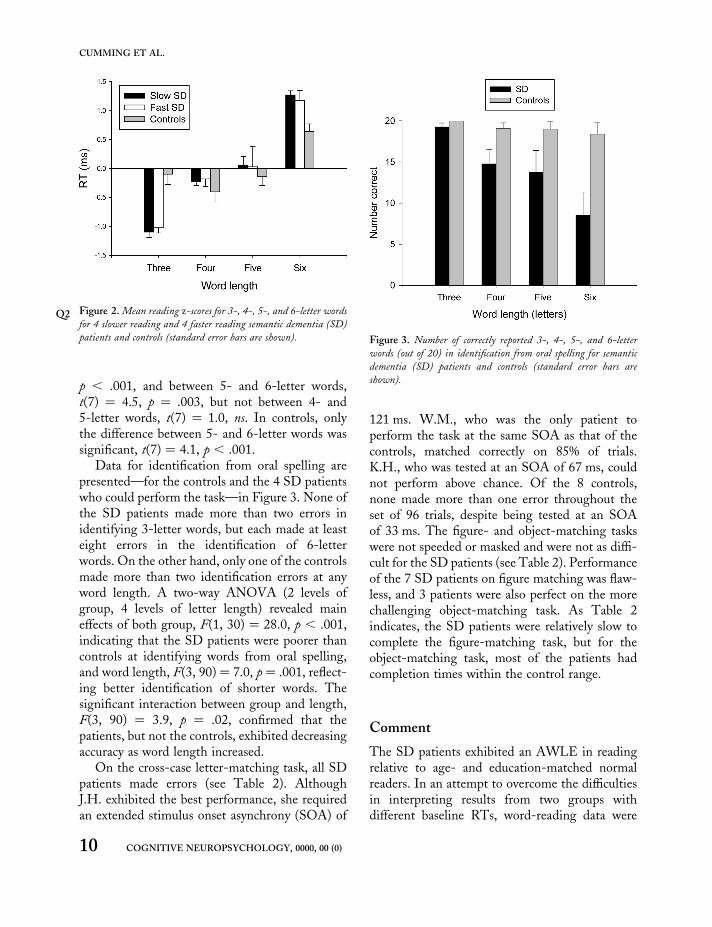
p , .001, and between 5- and 6-letter words,t(7) ¼ 4.5, p ¼ .003, but not between 4- and5-letter words, t(7) ¼ 1.0, ns. In controls, onlythe difference between 5- and 6-letter words wassignificant, t(7) ¼ 4.1, p , .001.
Data for identification from oral spelling arepresented—for the controls and the 4 SD patientswho could perform the task—in Figure 3. None ofthe SD patients made more than two errors inidentifying 3-letter words, but each made at leasteight errors in the identification of 6-letterwords. On the other hand, only one of the controlsmade more than two identification errors at anyword length. A two-way ANOVA (2 levels ofgroup, 4 levels of letter length) revealed maineffects of both group, F(1, 30) ¼ 28.0, p , .001,indicating that the SD patients were poorer thancontrols at identifying words from oral spelling,and word length, F(3, 90) ¼ 7.0, p ¼ .001, reflect-ing better identification of shorter words. Thesignificant interaction between group and length,F(3, 90) ¼ 3.9, p ¼ .02, confirmed that thepatients, but not the controls, exhibited decreasingaccuracy as word length increased.
On the cross-case letter-matching task, all SDpatients made errors (see Table 2). AlthoughJ.H. exhibited the best performance, she requiredan extended stimulus onset asynchrony (SOA) of
121 ms. W.M., who was the only patient toperform the task at the same SOA as that of thecontrols, matched correctly on 85% of trials.K.H., who was tested at an SOA of 67 ms, couldnot perform above chance. Of the 8 controls,none made more than one error throughout theset of 96 trials, despite being tested at an SOAof 33 ms. The figure- and object-matching taskswere not speeded or masked and were not as diffi-cult for the SD patients (see Table 2). Performanceof the 7 SD patients on figure matching was flaw-less, and 3 patients were also perfect on the morechallenging object-matching task. As Table 2indicates, the SD patients were relatively slow tocomplete the figure-matching task, but for theobject-matching task, most of the patients hadcompletion times within the control range.
Comment
The SD patients exhibited an AWLE in readingrelative to age- and education-matched normalreaders. In an attempt to overcome the difficultiesin interpreting results from two groups withdifferent baseline RTs, word-reading data were
Figure 2. MeanQ2 reading z-scores for 3-, 4-, 5-, and 6-letter words
for 4 slower reading and 4 faster reading semantic dementia (SD)
patients and controls (standard error bars are shown). Figure 3. Number of correctly reported 3-, 4-, 5-, and 6-letter
words (out of 20) in identification from oral spelling for semantic
dementia (SD) patients and controls (standard error bars are
shown).
10 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.
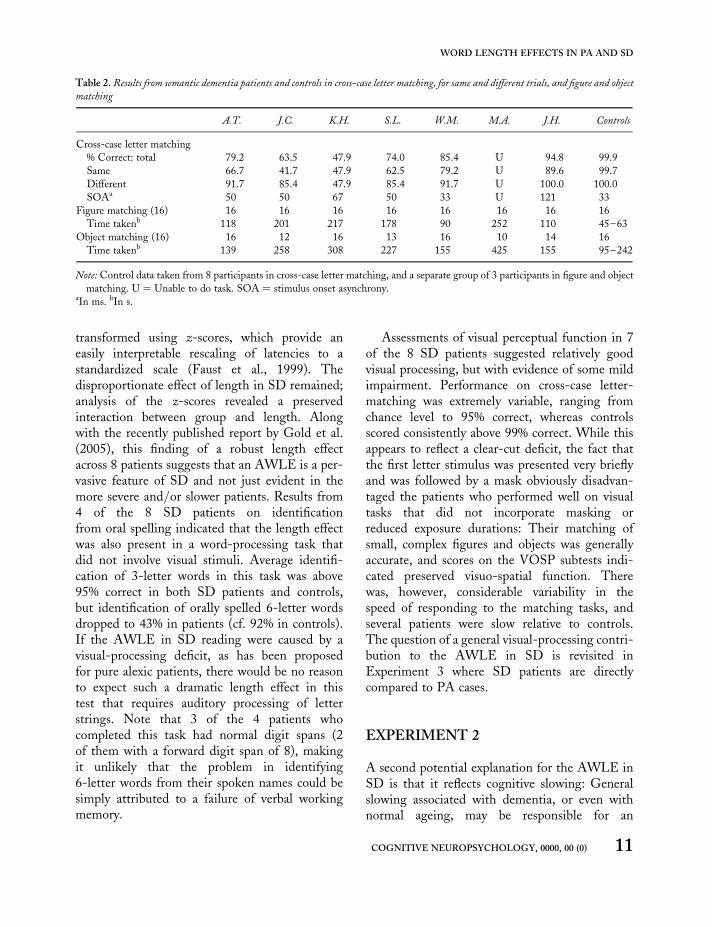
transformed using z-scores, which provide aneasily interpretable rescaling of latencies to astandardized scale (Faust et al., 1999). Thedisproportionate effect of length in SD remained;analysis of the z-scores revealed a preservedinteraction between group and length. Alongwith the recently published report by Gold et al.(2005), this finding of a robust length effectacross 8 patients suggests that an AWLE is a per-vasive feature of SD and not just evident in themore severe and/or slower patients. Results from4 of the 8 SD patients on identificationfrom oral spelling indicated that the length effectwas also present in a word-processing task thatdid not involve visual stimuli. Average identifi-cation of 3-letter words in this task was above95% correct in both SD patients and controls,but identification of orally spelled 6-letter wordsdropped to 43% in patients (cf. 92% in controls).If the AWLE in SD reading were caused by avisual-processing deficit, as has been proposedfor pure alexic patients, there would be no reasonto expect such a dramatic length effect in thistest that requires auditory processing of letterstrings. Note that 3 of the 4 patients whocompleted this task had normal digit spans (2of them with a forward digit span of 8), makingit unlikely that the problem in identifying6-letter words from their spoken names could besimply attributed to a failure of verbal workingmemory.
Assessments of visual perceptual function in 7of the 8 SD patients suggested relatively goodvisual processing, but with evidence of some mildimpairment. Performance on cross-case letter-matching was extremely variable, ranging fromchance level to 95% correct, whereas controlsscored consistently above 99% correct. While thisappears to reflect a clear-cut deficit, the fact thatthe first letter stimulus was presented very brieflyand was followed by a mask obviously disadvan-taged the patients who performed well on visualtasks that did not incorporate masking orreduced exposure durations: Their matching ofsmall, complex figures and objects was generallyaccurate, and scores on the VOSP subtests indi-cated preserved visuo-spatial function. Therewas, however, considerable variability in thespeed of responding to the matching tasks, andseveral patients were slow relative to controls.The question of a general visual-processing contri-bution to the AWLE in SD is revisited inExperiment 3 where SD patients are directlycompared to PA cases.
EXPERIMENT 2
A second potential explanation for the AWLE inSD is that it reflects cognitive slowing: Generalslowing associated with dementia, or even withnormal ageing, may be responsible for an
Table 2. Results from semantic dementia patients and controls in cross-case letter matching, for same and different trials, and figure and object
matching
A.T. J.C. K.H. S.L. W.M. M.A. J.H. Controls
Cross-case letter matching
% Correct: total 79.2 63.5 47.9 74.0 85.4 U 94.8 99.9
Same 66.7 41.7 47.9 62.5 79.2 U 89.6 99.7
Different 91.7 85.4 47.9 85.4 91.7 U 100.0 100.0
SOAa 50 50 67 50 33 U 121 33
Figure matching (16) 16 16 16 16 16 16 16 16
Time takenb 118 201 217 178 90 252 110 45–63
Object matching (16) 16 12 16 13 16 10 14 16
Time takenb 139 258 308 227 155 425 155 95–242
Note: Control data taken from 8 participants in cross-case letter matching, and a separate group of 3 participants in figure and object
matching. U ¼ Unable to do task. SOA ¼ stimulus onset asynchrony.aIn ms. bIn s.
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 11
WORD LENGTH EFFECTS IN PA AND SD
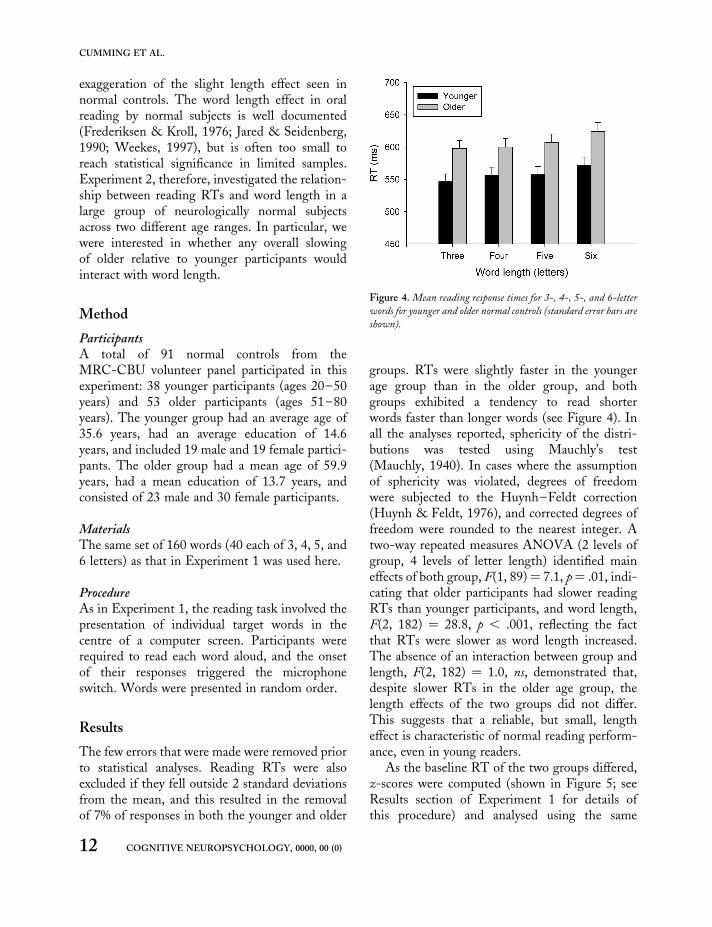
exaggeration of the slight length effect seen innormal controls. The word length effect in oralreading by normal subjects is well documented(Frederiksen & Kroll, 1976; Jared & Seidenberg,1990; Weekes, 1997), but is often too small toreach statistical significance in limited samples.Experiment 2, therefore, investigated the relation-ship between reading RTs and word length in alarge group of neurologically normal subjectsacross two different age ranges. In particular, wewere interested in whether any overall slowingof older relative to younger participants wouldinteract with word length.
Method
ParticipantsA total of 91 normal controls from theMRC-CBU volunteer panel participated in thisexperiment: 38 younger participants (ages 20–50years) and 53 older participants (ages 51–80years). The younger group had an average age of35.6 years, had an average education of 14.6years, and included 19 male and 19 female partici-pants. The older group had a mean age of 59.9years, had a mean education of 13.7 years, andconsisted of 23 male and 30 female participants.
MaterialsThe same set of 160 words (40 each of 3, 4, 5, and6 letters) as that in Experiment 1 was used here.
ProcedureAs in Experiment 1, the reading task involved thepresentation of individual target words in thecentre of a computer screen. Participants wererequired to read each word aloud, and the onsetof their responses triggered the microphoneswitch. Words were presented in random order.
Results
The few errors that were made were removed priorto statistical analyses. Reading RTs were alsoexcluded if they fell outside 2 standard deviationsfrom the mean, and this resulted in the removalof 7% of responses in both the younger and older
groups. RTs were slightly faster in the youngerage group than in the older group, and bothgroups exhibited a tendency to read shorterwords faster than longer words (see Figure 4). Inall the analyses reported, sphericity of the distri-butions was tested using Mauchly’s test(Mauchly, 1940). In cases where the assumptionof sphericity was violated, degrees of freedomwere subjected to the Huynh–Feldt correction(Huynh & Feldt, 1976), and corrected degrees offreedom were rounded to the nearest integer. Atwo-way repeated measures ANOVA (2 levels ofgroup, 4 levels of letter length) identified maineffects of both group, F(1, 89) ¼ 7.1, p¼ .01, indi-cating that older participants had slower readingRTs than younger participants, and word length,F(2, 182) ¼ 28.8, p , .001, reflecting the factthat RTs were slower as word length increased.The absence of an interaction between group andlength, F(2, 182) ¼ 1.0, ns, demonstrated that,despite slower RTs in the older age group, thelength effects of the two groups did not differ.This suggests that a reliable, but small, lengtheffect is characteristic of normal reading perform-ance, even in young readers.
As the baseline RT of the two groups differed,z-scores were computed (shown in Figure 5; seeResults section of Experiment 1 for details ofthis procedure) and analysed using the same
Figure 4. Mean reading response times for 3-, 4-, 5-, and 6-letter
words for younger and older normal controls (standard error bars are
shown).
12 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

two-way ANOVA that was applied to the raw RTdata. Results were unchanged: There was a maineffect of length, F(3, 267) ¼ 32.9, p , .001, butno interaction between group and length, F(3,267) ¼ 1.9, ns. If anything, the younger groupexhibited a larger length effect than the oldergroup posttransformation. No effect of group isreported, of course, as any difference is neutralizedby the z-score standardization.
Comment
A small but robust length effect in word readingwas consistent across both age groups: Anadditional 5–10 ms per additional letter wasrequired to name the target words. Older partici-pants exhibited slower reading RTs than didyounger participants, but this slowing did notresult in an exacerbation of the length effect inreading. On the basis of this result, there is noreason to suspect that overall word reading speedinteracts with the effect of word length. It isclear, however, from comparing word readingRTs of SD patients in Experiment 1 with thoseof older controls in the current experiment, thatcognitive slowing in dementia is noticeably morepronounced than slowing in normal ageing,which might still suggest that the length effect inSD is a product of profound slowing. Two findings
from Experiment 1 militate against this interpre-tation: (a) Z-score transformation did not diminishthe length effect in SD, and (b) the SD subgroupof 4 faster readers exhibited a z-transformedlength effect just as great as that shown by the 4slower readers. The failure to identify an inter-action between reading RTs and word length ina large sample of normal readers across differentage groups further demonstrates that slowerbaseline responses do not necessarily translate toexaggerated length effects. It is unlikely, therefore,that baseline differences alone can account for theAWLE observed in SD.
EXPERIMENT 3
The first two experiments yielded data concerningword length effects in the reading of SD patientsand normal controls, but the results do notpermit an unambiguous interpretation of theAWLE in SD, for several reasons. First, thewords in our reading test were not systematicallymatched for frequency between the four letterlength categories. Second, while we attempted totest most of the SD patients on all tasks inExperiment 1, this was not possible for variousreasons. Missing data were a particular problemfor the visual tasks, and, consequently, our hypo-thesis that visual impairments are not the principlecause of the AWLE in SD is less than secure.Third, the performance of SD patients inExperiment 1 was only contrasted with that ofcontrols. A more powerful test would bedirect comparison between patients with SD andcases with pure alexia (PA), for whom theAWLE in reading is a defining characteristic. InExperiment 3, therefore, we addressed theseissues by testing 3 SD and 3 PA patients on a setof tasks (word reading, identification from oralspelling, and visual matching) that used rigorouslymatched stimuli.
In the word-reading task, patients were askedto read aloud individually presented 3-, 5-, and7-letter words. In identification from oral spelling,the letters of the same 3-, 5-, and 7-letter wordswere spoken to the patients one letter at a time,
Figure 5. Mean reading z-scores for 3-, 4-, 5-, and 6-letter words
for younger and older normal controls (standard error bars are
shown).
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 13
WORD LENGTH EFFECTS IN PA AND SD

and again the task was to name the word. Wepredicted that the PA patients would exhibit anAWLE in the word-reading task, certainly forRT and possibly for accuracy as well, but thatthere would be no abnormal impact of wordlength on their performance in identificationfrom oral spelling as this task requires no identifi-cation of visual symbols. By contrast, we predictedthat the SD patients would demonstrate anAWLE in both word reading and identificationfrom oral spelling; by our hypothesis, this difficultyshould have nothing to do with visual or auditoryprocessing of the input but would be attributablein both tasks to reduced support from lexical/semantic knowledge about the stimulus words.In addition to the two word identification experi-ments, several tasks were employed to assess visualprocessing. Each of the visual tasks requiredsame-or-different judgements to pairs of stimulithat were either linguistic (within- or across-casesingle letters) or nonlinguistic (figures orobjects). We predicted that pure alexic patientswould show impairments for both linguistic andnonlinguistic stimuli, as a consequence of thegeneral visual processing deficit in PA identifiedby Behrmann et al. (1998a) and others. Moretentatively, we predicted normal visual matchingby the SD patients—tentative because, despiteevidence in SD of spared performance inunpaced visual tasks, reduced exposure durationor masking may yield a different outcome. Forthis reason, exposure duration was manipulatedin the visual tasks.
Method
ParticipantsA total of 12 individuals participated in this study:3 SD patients (2 from Experiment 1), 3 PApatients, and 6 controls (members of the MRC-CBU volunteer panel who were roughly age andeducation matched to the 6 patients: mean age ¼
63.2 years, mean education ¼ 11.3 years). Theaetiology of the PA cases was either stroke in theterritory of the left posterior cerebral artery (N ¼
2) or tumour (surgically removed) in the sameregion (N ¼ 1). The computed tomography
(CT) scan of M.P., one of the stroke patients,showed an area of infarction involving cortex andunderlying white matter of the left medialtemporal and left occipital region and also theposterior part of the left thalamus. The CT scanfor the other stroke patient, J.W., revealed hyper-densities involving the left parietal-occipitalregion, including the posterior limb of the internalcapsule and basal ganglia. No neuroradiologicalreport was available for the third case. A diagnosisof pure alexia was given on the basis of reading andwriting tests performed as part of a clinical assess-ment. Background information and standard testscores for the three groups are shown in Table 3.Values given for controls are means taken fromthe same control samples as those that appearedin Table 1, with the exception of the TrailMaking Test, where norms are presented. Inaddition to the standard tests—the Mini MentalState Examination (MMSE), Addenbrooke’sCognitive Examination (ACE), Rey figure,VOSP, and digit span—we included assessmentsof semantic knowledge (see the Methods sectionof Experiment 1 for a description of the threesemantic tasks), and motor speed and attention:the Trail Making Test (Reitan, 1958), whichinvolves joining, in a dot-to-dot fashion,numbered circles (in Part A) and numbered andlettered circles in alternating order (in Part B).
Scores on the MMSE and ACE indicate thatthe SD patients had more severe general cognitiveimpairment than the PA patients. Unsurprisingly,this was most striking in the semantic tests ofobject naming, WPM, and PPT. The PA patientsdemonstrated normal performance on the VOSPsubtests, which feature relatively simple visualarrangements, but a marked impairment incopying and recalling the visually complex Reyfigure. Performance on the Trail Making Testwas variable in both patient sets. On average,however, the SD patients managed this speededvisual task with more skill than did the PA cases:The slowest SD patient (A.T.) was comparablewith the fastest PA case (M.P.). All 3 SD patientsshowed a surface dyslexic pattern in the reading ofour standard “surface list” (the reading data in thetable are from the individual patient’s testing
14 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

session closest in time to his or her experimentaltesting). In the case of the 2 patients previouslyreported in Experiment 1, particularly A.T.,there had been a dramatic decline in theirreading ability over time. Both, however, stillrevealed the striking impairment on low-frequencyexception words characteristic of surface dyslexia,as did the new SD patient, D.V.
MaterialsThe experiment was carried out using the DMDXtachistoscopic software ( J. & K. Forster, Universityof Arizona). In all but two tasks, visual stimuliwere presented in the centre of the screen, andparticipants responded via a two-button responsebox interfaced with the computer. The exceptions
were the word-reading task, where a microphonerecorded auditory responses, and identificationfrom oral spelling, which involved auditory pres-entation of sequential letters and recording ofresponses by microphone. The same set of 75words (25 each of 3-, 5-, and 7-letter words)with regular spelling-to-sound correspondenceswas employed for reading and identification fromoral spelling. Words of different lengths werematched for frequency (3-letter mean ¼ 27.5,5-letter mean ¼ 27.3, 7-letter mean ¼ 27.4) andfor initial phoneme. For the letter-matchingtasks, the set of 12 letters employed inExperiment 1 was used to construct 96 same-or-different trials for cross-case letters and 48same-or-different trials for same-case letters.
Table 3. Standard test scores for semantic dementia and pure alexia patients, and mean scores for controls
SD patients PA patients
D.V. W.M. A.T. M.P. J.W. T.S. Controlsa
Ageb 65 56 68 66 53 51 68.5 (7.1)
Educationb 10 16 19 12 10 10 11.2 (1.5)
MMSE 25 21 15 26 26 23 29 (1.0)
ACE 59 37 33 78 75 64 92.7 (3.0)
REY: Copy 36 34 36 28.5 23 31.5 34.2 (1.6)
Immediate 16.5 12 16 8 2.5 1 NT
Delayed 16.5 14.5 8 3 1 1 18.3 (5.2)
VOSP: Dots (10) 10 10 10 10 9 10 9.9 (0.3)
Position (20) 20 20 20 20 20 20 19.8 (0.6)
Number location (10) 10 10 8 10 10 7 8.9 (2.8)
Cubes (10) 10 10 10 10 10 10 9.3 (1.5)
Digit span: Forward 8 5 7 7 7 8 7.1 (0.9)
Back 4 4 5 4 4 4 5.4 (1.4)
Naming (64) 13 6 0 53 52 40 62.3 (1.6)
WPM (64) 48 21 29 62 63 63 63.8 (0.4)
PPT: Pictures (52) 36 38 24 45 48 49 51.6 (1.1)
Reading: HF regularc 98 91 29 NT NT NT 99.8
LF regularc 76 88 10 NT NT NT 99.5
HF exceptionc 98 55 12 NT NT NT 99.5
LF exceptionc 55 21 2 NT NT NT 95.4
Trails: A 21s (0) 46s (0) 64s (0) 69s (0) 90s (0) 80s (0) 48s
B 53s (2) 113s (1) 179s (0) 133s (0) 192s (0) 309s (2) 119s
Note: SD ¼ semantic dementia; PA ¼ pure alexia; MMSE ¼ Mini-Mental State Examination (Folstein, Folstein, & McHugh,
1975); ACE ¼ Addenbrooke’s Cognitive Examination (Mathuranath, Nestor, Berrios, Rakowicz, & Hodges, 2000); REY ¼
Rey–Osterreith Complex Figure Test (Osterrieth, 1944); VOSP ¼ Visual Object and Space Perception Battery (Warrington
& James, 1991); WPM ¼ Word-picture matching (Hodges & Patterson, 1995); PPT ¼ Pyramids and Palm Trees Test
(Howard & Patterson, 1992); Trails ¼ Trail Making Test (Reitan, 1958), errors made in parentheses; HF ¼ high frequency;
LF ¼ low frequency; NT ¼ not tested.aStandard deviations in parentheses. bIn years. cIn percentages.
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 15
WORD LENGTH EFFECTS IN PA AND SD

For the figure- and object-matching tasks, thesame stimuli as those used in Experiment 1(Frostig & Harne, 1972; Kenkyukai, 1983) weretransferred onto the computer. Instead of provid-ing four response alternatives, a same-or-differentjudgement task was constructed by selecting twosimilar-looking distractors for each target. Asthere were 16 target figures, the figure-matchingtask consisted of 64 trials comprising 2 same and2 different trials for each target. The object-matching task had an identical format.
ProcedureTesting was carried out in two sessions, whichwere at least three weeks apart. Each task waspreceded by several practice items, and trialswere presented in random order (with the excep-tion of word reading, where words were blockedby letter length). The difficulty of the same–different matching tasks could be manipulated byaltering the exposure duration of the first stimulusand including or omitting a mask between the firstand second stimulus in a test pair. The letter-matching tasks began with a fixation cross pre-sented for 834 ms, followed by a blank screen for834 ms, then the first letter stimulus for either200 ms or 67 ms, then a hash mask (######) for834 ms, and finally the second letter stimulus,which remained on screen until a response wasmade. Participants were asked to press the rightbutton of the response box if the letters were thesame and the left button if the letters were differ-ent. In same-case matching, the first and secondletters were always the same case (either upper orlower case), whereas in cross-case matching thefirst and second letters were never the same case(one upper case, one lower case). Each of theletter-matching tasks was split into two versionsto minimize the effects of practice and fatigue.Each trial in the figure-matching tasks beganwith a blank screen for 1,667 ms, followed by thefirst figure for either 1,667 ms or 500 ms, then amask for 1,667 ms, and finally the second figure,which remained on screen until a response wasmade. Exposure duration was not manipulated inthe object-matching task, which is the most diffi-cult of the matching tasks because of the minimal
distinctions between targets and distractors. Here,trials consisted of a blank screen for 1,667 ms,followed by the first object for 1,667 ms, theneither a mask or blank screen for 1,667 ms, andfinally the second object.
In the word-reading task, a fixation cross waspresented for 834 ms, followed immediately bythe word to be read, which remained on thescreen until response. RT was measured from thepresentation of the word to the onset of the par-ticipant’s vocal response, and the next trial began5 s after the completion of the previous response.For identification from oral spelling, nothingappeared on the screen during the task. Thecomputer played soundfiles of each word beingspelt out one letter at a time, approximately asecond apart (recorded on DAT, then transferredto computer). RT was measured from the offsetof presentation of the final letter in the word tothe onset of the participant’s vocal response.Again, the next trial began 5 s after the completionof the previous trial. With only minimal variationto testing order, the first session includedsame-case letter matching with a 200-ms exposureduration of the first stimulus, cross-case lettermatching at 200 ms, figure matching at1,667 ms, object matching at 1,667 ms, and wordreading. The second session tested same-caseletter matching at 67 ms, cross-case lettermatching at 67 ms, figure matching at 500 ms,object matching at 1,667 ms (but with the inter-vening mask replaced by a blank screen), andidentification from oral spelling.
Results
ReadingErrors, including those that were self-corrected,were removed from the analysis of word-readingRT data. For the PA patients, this resulted inthe removal of 23% of responses to 3-letterwords, 21% of responses to 5-letter words, and39% of responses to 7-letter words. In SD patients,the corresponding error rates were 19% for 3-letterwords, 16% for 5-letter words, and 28% for7-letter words. Controls made errors on 1% of3-letter words, 2% of 5-letter words, and 3% of
16 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.
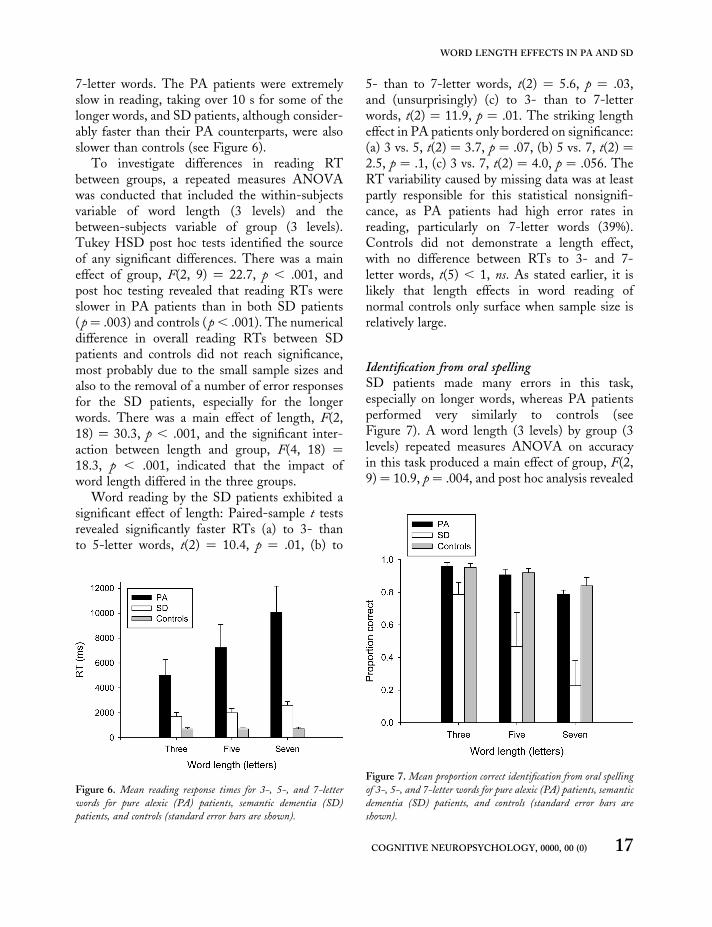
7-letter words. The PA patients were extremelyslow in reading, taking over 10 s for some of thelonger words, and SD patients, although consider-ably faster than their PA counterparts, were alsoslower than controls (see Figure 6).
To investigate differences in reading RTbetween groups, a repeated measures ANOVAwas conducted that included the within-subjectsvariable of word length (3 levels) and thebetween-subjects variable of group (3 levels).Tukey HSD post hoc tests identified the sourceof any significant differences. There was a maineffect of group, F(2, 9) ¼ 22.7, p , .001, andpost hoc testing revealed that reading RTs wereslower in PA patients than in both SD patients(p¼ .003) and controls (p, .001). The numericaldifference in overall reading RTs between SDpatients and controls did not reach significance,most probably due to the small sample sizes andalso to the removal of a number of error responsesfor the SD patients, especially for the longerwords. There was a main effect of length, F(2,18) ¼ 30.3, p , .001, and the significant inter-action between length and group, F(4, 18) ¼
18.3, p , .001, indicated that the impact ofword length differed in the three groups.
Word reading by the SD patients exhibited asignificant effect of length: Paired-sample t testsrevealed significantly faster RTs (a) to 3- thanto 5-letter words, t(2) ¼ 10.4, p ¼ .01, (b) to
5- than to 7-letter words, t(2) ¼ 5.6, p ¼ .03,and (unsurprisingly) (c) to 3- than to 7-letterwords, t(2) ¼ 11.9, p ¼ .01. The striking lengtheffect in PA patients only bordered on significance:(a) 3 vs. 5, t(2) ¼ 3.7, p ¼ .07, (b) 5 vs. 7, t(2) ¼2.5, p ¼ .1, (c) 3 vs. 7, t(2) ¼ 4.0, p ¼ .056. TheRT variability caused by missing data was at leastpartly responsible for this statistical nonsignifi-cance, as PA patients had high error rates inreading, particularly on 7-letter words (39%).Controls did not demonstrate a length effect,with no difference between RTs to 3- and 7-letter words, t(5) , 1, ns. As stated earlier, it islikely that length effects in word reading ofnormal controls only surface when sample size isrelatively large.
Identification from oral spellingSD patients made many errors in this task,especially on longer words, whereas PA patientsperformed very similarly to controls (seeFigure 7). A word length (3 levels) by group (3levels) repeated measures ANOVA on accuracyin this task produced a main effect of group, F(2,9) ¼ 10.9, p ¼ .004, and post hoc analysis revealed
Figure 6. Mean reading response times for 3-, 5-, and 7-letter
words for pure alexic (PA) patients, semantic dementia (SD)
patients, and controls (standard error bars are shown).
Figure 7. Mean proportion correct identification from oral spelling
of 3-, 5-, and 7-letter words for pure alexic (PA) patients, semantic
dementia (SD) patients, and controls (standard error bars are
shown).
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 17
WORD LENGTH EFFECTS IN PA AND SD

that SD patients made more identification errorsthan both PA patients (p ¼ .01) and controls(p ¼ .004). An effect of length was also identified,F(2, 18) ¼ 35.1, p , .001, and the significantinteraction between length and group, F(4, 18) ¼8.8, p , .001, indicated that the impact ofword length differed in the three groups. Bypaired-sample t tests, SD patients made signifi-cantly more errors to 7-letter words than to 3-letter words, t(2) ¼ 5.6, p ¼ .03. The differencebetween 3- and 7-letter words was also reliablein the PA group, t(2) ¼ 4.9, p ¼ .04. This effectwas not predicted, but perhaps is not surprisinggiven the difficulty of the task at longer wordlengths. Indeed, even normal controls mademore errors to 7- than to 3-letter words, t(5) ¼
2.6, p ¼ .047. Importantly, the impact of wordlength was greatest for the SD group.
Analysis of the RT data for this task wasclouded by the fact that some responses wereinitiated before the offset of the final stimulusletter and was further complicated by the largenumber of errors in the SD group. An indepen-dent t test revealed no significant differencebetween the RTs of PA patients and controls.
Errors in the two word identification tasksThe nature of errors as well as overall accuracy canbe informative about the underlying deficit, andthis experiment is no exception. Errors in bothreading and identification from oral spelling wereclassified in two different ways. First of all, eachfailure to respond with the correct target wordwas assigned to one of the following five categories(with real error examples given in parentheses): (a)no response (“I don’t know” or “I missed it”); (b)letter misidentification, which we restricted tocases where a single letter of the target word hadfairly obviously been identified as a differentletter (e.g., web ! “wed”, token ! “toker”); (c)LARC error—a term from Patterson, Suzuki,Wydell, and Sasanuma (1995) which stands forLegitimate Alternative Reading of Componentsand is a slightly more inclusive term for regulariz-ation errors (e.g., ski ! “sky” or ladle ! “laddle”);(d) letter omission or addition, restricted to caseswhere a single letter in the target word was
omitted or a single letter not in the target wordwas imported (e.g., dance ! “dace” or dance !
“dancer”); (e) other, which included a variety ofresponses not classifiable under one of the otherheadings, such as apparent replacement of morethan one letter in the target word (e.g., feather! “reacher”), or a degree of misordering ofletters present in the target word (e.g., housing! “singer”, faculty ! “face-tul”). Second, theresponse in each error of commission was classifiedas a real word or a nonword/neologism. Table 4presents the proportions for each of these twoforms of classification, for both patient groupsand both tasks.
The first striking difference between patientgroups is in the first type of classification for thereading task: The majority of the PA readingerrors were failures to give any response, whereasthere was not a single error of this type inreading for the SD patients. In the PA group,the only category of errors of commission withany appreciable number of occurrences was lettermisidentifications. SD patients also made anumber of letter misidentification errors, plus anumber of LARC errors (though not nearly asmany of these as they would do if presented withwords selected to have atypical spelling–sound
Table 4. Error analysis of reading and identification from oral
spelling for semantic dementia and pure alexia patients in
Experiment 3
Reading
ID from
oral spelling
SD PA SD PA
As proportion of all errors
No response .00 .74 .35 .46
Letter misidentification .42 .18 .15 .04
LARC .35 .05 .16 .11
Letter omission or addition .12 .02 .10 .07
Other .11 .02 .23 .32
As proportion of errors of
commission
Word responses .30 .83 .34 .81
Nonword responses .70 .17 .66 .19
Note: SD ¼ semantic dementia; PA ¼ pure alexia; LARC ¼
legitimate alternative reading of components.
18 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

correspondences) and also a few errors in theremaining two categories. The differencebetween patient groups in error types for recogniz-ing words from their oral spellings was lessstriking. Here, both groups were unable to giveany response on a fair proportion of trials, anddifficult-to-classify “other” errors were also morecommon for both groups in this task than inreading.
The second striking difference between patientgroups is in the second type of classification forboth tasks: Incorrect responses by the PA patientswere clearly and strongly biased towards realwords, whereas this was not true for the SDpatients, indeed au contraire. Task instructionsspecified, though perhaps did not make a fuss ofthe fact, that the stimuli were words, but thisinduced no word bias in the SD errors of commis-sion. Moreover, the majority of the SD patients’incorrect real-word responses occurred to 3-letterstimuli, which form an orthographic and phono-logical neighbourhood that is much more denselypopulated with real words than are 5- and 7-letter stimuli. In other words, some of the (few)real-word errors by SD patients may have beenreal words almost by accident.
Consistency across tasksThe use of the same stimuli for reading and identi-fication from oral spelling allows a direct compari-son between performance on these two tests.Recall that we predicted impairment in the PApatients for reading, given the visual nature of itsinput, but not in identification from oral spelling,given the nonvisual nature of its input. The corol-lary of this prediction is that any errors made byPA patients in identification from oral spellingshould bear no relationship to items yieldingerrors in the reading task. For the SD patients,on the other hand, we predicted impairment inboth tasks and for the same reason: degradedlexical/semantic support. And the corollary ofthis prediction is that the SD patients shouldshow a consistent pattern of responding acrossthe two tasks. More specifically, words incorrectlyread should also be more error prone in identifi-cation from oral spelling. To assess these
predictions, the items were categorized into fourcells, separately for the three word lengths (3, 5,and 7): correct on both tests; correct reading buterror on identification from oral spelling; viceversa; correct on neither test. These 2 by 2 tableswere analysed using either chi-squared analysisor Fisher’s Exact Test (if the expected cell frequen-cies were lower than five). For all word lengths, theSD patients showed a significant degree of associ-ation between the two tests (p , .05). Forexample, for 7-letter words, the patients made atotal of 28 reading errors, and 26 of those same28 words yielded errors in identification fromoral spelling. Similarly, of the 18 items of 7letters for which SD patients were correct onidentification from oral spelling, only 1 provokedan incorrect reading response. By contrast, thePA patients showed no such consistent patternof responding for 3- and 7-letter length words,although there was a hint of an association for 5-letter items (p , .05). This latter effect can beattributed to the fact that two of the patientsmade few (or no) reading errors for the 5-letterwords, so the cell for incorrect reading butcorrect identification from oral spelling—whichwould work against a significant association—had very few entries.
Visual tasksIn the letter-matching tasks, one of the SDpatients could not identify anything at 67 ms andso was assigned a chance value (.5) for thesetasks. Readers should be mindful of this wheninterpreting the average SD values for 67 ms.The other two SD patients performed well atthis SOA; indeed, despite one chance-level score,the average SD performance remained above theaverage for the three PA patients (see Figure 8).Repeated measures ANOVAs were performedseparately for same-case and cross-case letter-matching data. Although the PA patients werepoorer than the other two groups in same-caseletter-matching accuracy, there was no significanteffect of group, F(2, 9) ¼ 3.0, p ¼ .1. A maineffect of exposure duration, F(1, 9) ¼ 9.9, p ¼
.01, indicated more successful matching perform-ance when the first letter was presented for
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 19
WORD LENGTH EFFECTS IN PA AND SD
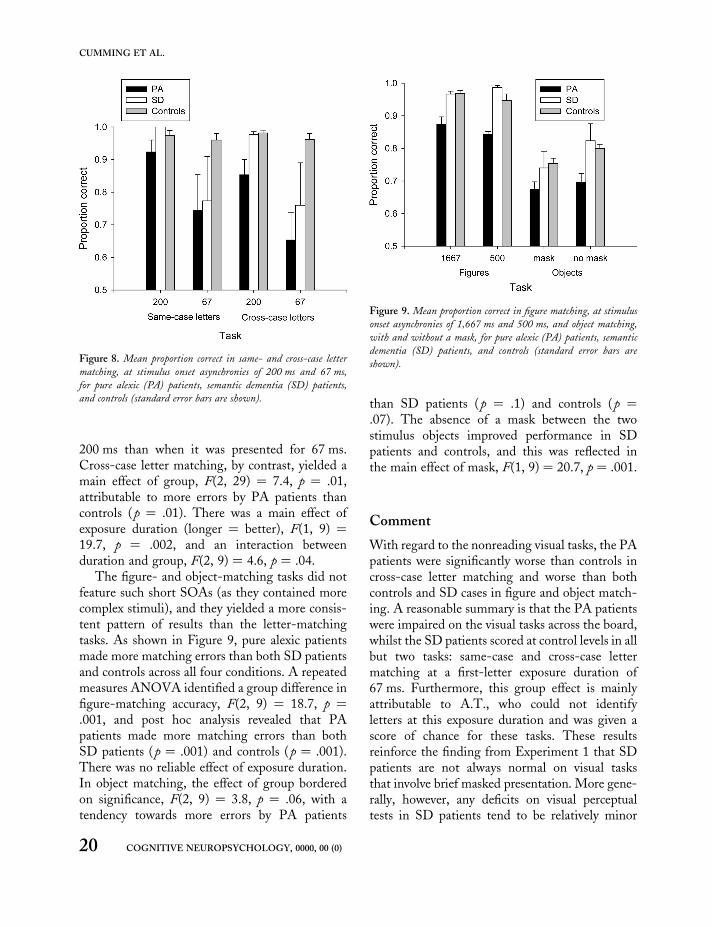
200 ms than when it was presented for 67 ms.Cross-case letter matching, by contrast, yielded amain effect of group, F(2, 29) ¼ 7.4, p ¼ .01,attributable to more errors by PA patients thancontrols (p ¼ .01). There was a main effect ofexposure duration (longer ¼ better), F(1, 9) ¼
19.7, p ¼ .002, and an interaction betweenduration and group, F(2, 9) ¼ 4.6, p ¼ .04.
The figure- and object-matching tasks did notfeature such short SOAs (as they contained morecomplex stimuli), and they yielded a more consis-tent pattern of results than the letter-matchingtasks. As shown in Figure 9, pure alexic patientsmade more matching errors than both SD patientsand controls across all four conditions. A repeatedmeasures ANOVA identified a group difference infigure-matching accuracy, F(2, 9) ¼ 18.7, p ¼
.001, and post hoc analysis revealed that PApatients made more matching errors than bothSD patients (p ¼ .001) and controls (p ¼ .001).There was no reliable effect of exposure duration.In object matching, the effect of group borderedon significance, F(2, 9) ¼ 3.8, p ¼ .06, with atendency towards more errors by PA patients
than SD patients (p ¼ .1) and controls (p ¼
.07). The absence of a mask between the twostimulus objects improved performance in SDpatients and controls, and this was reflected inthe main effect of mask, F(1, 9) ¼ 20.7, p ¼ .001.
Comment
With regard to the nonreading visual tasks, the PApatients were significantly worse than controls incross-case letter matching and worse than bothcontrols and SD cases in figure and object match-ing. A reasonable summary is that the PA patientswere impaired on the visual tasks across the board,whilst the SD patients scored at control levels in allbut two tasks: same-case and cross-case lettermatching at a first-letter exposure duration of67 ms. Furthermore, this group effect is mainlyattributable to A.T., who could not identifyletters at this exposure duration and was given ascore of chance for these tasks. These resultsreinforce the finding from Experiment 1 that SDpatients are not always normal on visual tasksthat involve brief masked presentation. More gene-rally, however, any deficits on visual perceptualtests in SD patients tend to be relatively minor
Figure 8. Mean proportion correct in same- and cross-case letter
matching, at stimulus onset asynchronies of 200 ms and 67 ms,
for pure alexic (PA) patients, semantic dementia (SD) patients,
and controls (standard error bars are shown).
Figure 9. Mean proportion correct in figure matching, at stimulus
onset asynchronies of 1,667 ms and 500 ms, and object matching,
with and without a mask, for pure alexic (PA) patients, semantic
dementia (SD) patients, and controls (standard error bars are
shown).
20 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

and/or variable (across tasks or patients) comparedwith the marked and consistent deficit that is afeature of PA.
Turning to the word-based tasks: Althoughdifferent, and frequency-matched, words wereused in Experiment 3, the AWLE exhibited bySD patients in reading was similar to that reportedin Experiment 1. Across the 3 SD patients,reading time increased by about 230 ms for eachadditional letter present in the word. RTs forreading by 6 age-matched controls demonstratedno reliable length effect, which was also consistentwith Experiment 1. PA patients’ reading wascharacterized by a pronounced length effect:about 1,260 ms, on average, for each added letterin the word. There were marked differencesbetween groups in average reading RTs,with controls taking about 0.7 s to respond, SDpatients approximately 2 s, and PA patients5–10 s depending on length.
The identification from the oral spelling taskused the same 3-, 5-, and 7-letter words. SDpatients found this task very difficult and exhibiteda remarkable effect of length on accuracy; indeed,one patient failed to identify any 7-letter wordscorrectly. The length effect in this task was morepronounced than its counterpart in Experiment1, probably due (a) to the inclusion of 7-letterwords in the current experiment, and (b) to themore advanced average stage of disease of thesmall SD group in this experiment. The perform-ance of the PA patients was very similar to thatof controls, with near-perfect identification of3-letter words, falling to about 80% correct for7-letter words.
Two striking findings emerged from the analy-sis of errors within and across the two wordidentification tasks. First, in both tasks, theerrors of commission by PA patients were almostentirely words. It seems clear that these patientsidentified whatever they could from encounteringa printed word or the spoken letter names of aword and that, in both tasks, this stimulusinformation interacted with lexical/semanticknowledge to produce either the correct responseor another real word with significant resemblanceto the target. For SD patients, whose errors of
commission were mainly nonwords, the firstcomponent of this process was presumably thesame as in PA—that is, identifying letters of aprinted word or combining the identities of letternames from their oral presentation—but thesecond component appears to be greatly diminished.What the SD patients produced were responsesbased mainly on stimulus information and largelyunconstrained by lexical/semantic knowledge.
The second striking finding was the similarityversus discrepancy of performance across the twotasks for the SD and PA cases, respectively. Thissimilarity or discrepancy applies to accuracy/errortypes, to the presence/absence of an AWLE, andto the item-specific consistency of success/failure. The PA patients were poor at thevisual-word reading task, presumably becausetheir reading problem is a manifestation of theirvisual-processing deficit, and most of theirreading errors were failures to respond at all. Forthe words that they could read, their RTs revealeda massive AWLE. Relative to reading, the PAcases were much more successful at identifyingwords from oral spelling (which is, for a normalreader, a much more taxing task) and showedonly a minimal (and normal) impact of wordlength. Moreover, there was essentially no consis-tency between the words on which they succeeded/failed in the two tasks. SD patients, by contrast,had difficulties in both tasks, had an AWLE inboth, and showed significant item-specific consis-tency between the two tasks. This difference inpattern strongly suggests different sources of theAWLE in reading for the two types of patient,and—especially when combined with the non-lexical nature of their errors of commission—also suggests that the SD patients’ AWLE inboth tasks reflects reduced feedback from whole-word knowledge.
EXPERIMENT 4
Results from the first three experiments are diffi-cult to reconcile with the notion that the AWLEin SD can be explained either by a visual deficitor by cognitive slowing. The error and consistency
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 21
WORD LENGTH EFFECTS IN PA AND SD

analyses from Experiment 3 suggest that thesource of this effect is a marked reduction in theextent to which perceptual analysis of a letterstring interacts with and is informed by wordknowledge. It would, however, be useful to havemore evidence to support this hypothesis, and afourth experiment was conducted for thispurpose. As mentioned in the Introduction,normal readers show an AWLE under some cir-cumstances, including the reading of unfamiliarletter strings—that is, nonwords. This suggeststhe possibility, as we have indeed been proposingfor SD patients, that an AWLE might be anatural consequence of reduced top-down feed-back in word identification. This is, of course,not the proposed reason for the AWLE in purealexia: PA patients show normal, or perhaps evenexaggerated, top-down effects in reading, such asa large advantage for high- versus low-frequencywords and high- versus low-imageability words(Behrmann et al., 1998b). To investigate readingunder conditions that do or do not provide anatural opportunity for interactive activationbetween letter and word levels, in Experiment 4we tested SD patients, PA patients, and normalcontrols on accuracy and RTs in reading 3-, 4-,5-, and 6-letter words and nonwords. On theassumption, based on much evidence, that wordknowledge is impoverished but not absent in SD,we predicted that they as well as normal and PAreaders would show an overall RT advantage inreading words relative to nonwords. More criti-cally, however, on the assumptions (a) thatneither patients nor normal readers can benefitmuch from lexical/semantic support in readingnonwords, and (b) that SD patients benefit signifi-cantly less than both normal readers and PApatients from lexical/semantic support in identify-ing real words, we predicted an interactionbetween lexicality and length in both control andPA participants but not for the SD patients.
Method
ParticipantsThe 6 patients—3 PA and 3 SD—who completedExperiment 3 also participated in this experiment.
For standard test scores and descriptions of thepatients, refer to the Participants section ofExperiment 3. A total of 9 normal adults fromthe MRC-CBU volunteer panel, who were ageand education matched to the 6 patients, weretested (mean age ¼ 61.1 years, and meaneducation ¼ 13.1 years) served as controls.
MaterialsThe equipment and software were the same asthose for the word-reading task in Experiment3. Stimuli were taken from the nonword andhigh-frequency word sets developed by Weekes(1997), N¼ 100 each. Each set contained 25 quar-tets of items, one at each of the four lengths of 3, 4,5, and 6 letters. Items within each quartet werematched for initial phoneme, and words werematched across length for written word frequency.At each letter length, words and nonwords werematched on number of phonemes, neighbourhoodsize, number of enemies, number of friends,bigram frequency, and grapheme frequency.
ProcedureThe reading task was preceded by 16 practiceitems, consisting of two words and two nonwordsat each letter length. The 200 trials were broken upinto five sections with a short break in betweensections. Target stimuli were presented in thecentre of the computer screen and appeared inrandom order. In each trial, a fixation cross waspresented for 834 ms, followed immediately bythe word or nonword to be read, which remainedon the screen until the response. RT was measuredfrom the presentation of the word to the onset ofthe participant’s vocal response, and the next trialbegan 2 s after completion of the previous trial.
Results
ANOVAs were performed individually for eachgroup, and degrees of freedom were subjected tothe Huynh–Feldt correction in cases where theassumption of sphericity was violated. Prior tothe RT analyses, errors—including those thatwere self-corrected—were first removed, andthen the data were further cleaned by the
22 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

removal of responses that were beyond 2 standarddeviations of the mean RT for that lexicality/length condition (means and standard deviationswere calculated individually for each patient butas a group for the controls given the homogeneityof control reading RTs). These two procedureshad the following impact for the three subjectgroups. For the SD patients, a total of 68 responsesto word stimuli were removed, 54 due to errors(18%) and 14 as outlier RTs (4.6%), and a totalof 87 responses to nonwords were likewiseremoved: 77 errors (25.7%) and 10 outliers(3.3%). For the PA patients, a total of 50 responsesto word stimuli were removed, 32 (10.7%) due toerrors and 18 (6.0%) as outlier RTs, and a totalof 62 responses to nonwords were likewiseremoved: 52 errors (17.3%) and 10 outliers(3.3%). The group of 9 controls made a total of3 (0.3%) errors on words and lost 32 word(3.6%) responses as RT outliers; for nonwords,they made 17 (1.9%) errors and had 34 (3.8%)outliers.
Average RTs to name words and nonwords forthe 3 SD patients, 3 PA patients, and 9 controlsubjects are shown in three separate panels inFigure 10. The SD patients exhibited a lengtheffect that was comparable for words and non-words, and this effect was consistent across thethree cases. The extra time taken to name atarget for every additional letter was, on average,161 ms for words and 131 ms for nonwords. Atwo-way repeated measures ANOVA (2 levels oflexicality, 4 levels of letter length) identified amain effect of lexicality, F(1, 2) ¼ 36.8, p ¼ .03,indicating faster responses to words than to non-words, and a main effect of length, F(3, 6) ¼
4.9, p ¼ .047, indicating faster responses toshorter items, but no interaction between lexicalityand length, F(3, 6) , 1, ns. The PA patientsdemonstrated a marked length effect for bothwords and nonwords. The extra time taken peradditional letter was, on average, 712 ms forwords and 1,229 ms for nonwords. A two-wayrepeated measures ANOVA revealed maineffects of both lexicality, F(1, 2) ¼ 22.7, p ¼ .04,and length, F(2, 5) ¼ 17.5, p¼ .005, plus a signifi-cant interaction, F(1, 2) ¼ 21.7, p ¼ .04,
demonstrating a greater effect of length onnaming time for nonwords than for words. Fornormal readers, the length effect amounted to anaverage naming-time increase of 5 ms per
Figure 10. Mean reading response times for semantic dementia
(SD) patients, pure alexic (PA) patients, and controls on 3-, 4-, 5-
, and 6-letter words and nonwords (standard error bars are shown).
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 23
WORD LENGTH EFFECTS IN PA AND SD

additional letter in words and 19 ms for eachadditional letter in nonwords. A two-way repeatedmeasures ANOVA identified main effects oflexicality, F(1, 8) ¼ 53.9, p , .001, and length,F(3, 24) ¼ 17.3, p , .001, and a reliable inter-action, F(2, 17) ¼ 8.1, p ¼ .003.
To allow a more appropriate comparison acrossgroups, z-scores were computed in an attempt toremove the influence of different baseline readingRTs (see Results section of Experiment 1). Z-scores were calculated for each participant indivi-dually at each letter length for both words andnonwords, and group means are presented inFigure 11, with words and nonwords in separatepanels. Analysis of the z-scores, again using two-way repeated measures ANOVA, confirmedresults of the basic RT analysis. Pure alexicpatients demonstrated a significant length effect,F(3, 6) ¼ 15.9, p ¼ .003, and the interactionwith lexicality indicated that this effect waslarger for nonwords than for words, F(3, 6) ¼
7.6, p ¼ .02. Controls showed an effect oflength, F(3, 24) ¼ 15.8, p , .001, that waslargely due to nonword reading, as evidenced bythe interaction between length and lexicality,F(2, 16) ¼ 5.8, p ¼ .01. SD patients exhibited alength effect, F(3, 6) ¼ 4.8, p ¼ .049, that wassimilar for words and nonwords, as illustratedby the lack of length by lexicality interaction,F(3, 6) , 1, ns.
Comment
The central, novel, and predicted finding in thisstudy was that PA patients and controls bothexhibited larger length effects for nonwords thanwords, whereas there was no difference in thenonword and word length effects in SD. Despite,or perhaps especially because of, impaired visualprocessing in PA, it appears that stimuli withfamiliar orthographic, phonological, and semanticrepresentations permit a greater degree of parallelidentification by PA patients. This phenomenon,which was highlighted by Behrmann et al.(1998b) and interpreted by them in a connectionistframework, could in fact be explained byany model incorporating interactive activation.
As expected, controls also showed strong evidenceof this kind of support in reading, with a lengtheffect only evident for reading of nonwords. Thesignificant impact of stimulus length on readingRT for SD patients, however, was no differentfor words and nonwords. The (expected) overallRT advantage for words demonstrates some top-down influence on reading, but the lexicality ofthe stimulus did not moderate reading speedaccording to letter length.
It was unlikely that these results could be attri-buted to differing baseline RTs, as the groupsthat had the fastest (controls) and slowest (PApatients) reading RTs both showed an interaction
Figure 11. Mean reading z-scores for 3-, 4-, 5-, and 6-letter
words and nonwords for pure alexic (PA) patients, semantic
dementia (SD) patients, and controls (standard error bars are
shown).
24 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

between length and lexicality. The reading speed ofSD patients was in between control and PA values,yet was not characterized by this interaction.Nevertheless, a z-score analysis was conducted toallow comparison of length effects on the samescale. Results confirmed the conclusions that weredrawn from the initial analyses. What becomesclear from the z-score analysis (see Figure 11) isthat the AWLE for nonwords was very similarfor SD patients and controls, and that theAWLE for words in SD patients was also similarto, if not a little larger than, these nonwordlength effects. In other words, it seems thatreduced top-down support for word identificationin SD yields an AWLE for words that is similarnot only to the patients’ own AWLE for nonwordsbut also to normal readers’ AWLE for nonwords.
GENERAL DISCUSSION
The results of this study, including some briefinterpretations, can be summarized as follows:
Normal reading1. A significant effect of length on time to read
aloud familiar words varying from 3–7 lettersin length can be demonstrated for normalreaders, but only with high “power” as achievedby large numbers of stimuli and participants(Experiment 2).
2. More generally, as reported previously byWeekes (1997), oral reading RTs of normalreaders reveal a reliable impact of length fornonwords, but a much smaller, and often insig-nificant, impact for real words (Experiments 1,3, 4).
Pure alexia (PA)1. An abnormal word length effect (AWLE) in
word reading is, as demonstrated by decadesof research and many different researchgroups, a pervasive and dramatic characteristicof patients with pure alexia (PA) consequenton lesions in the territory of the left posteriorcerebral artery (Experiments 3 and 4).
2. The AWLE in PA may be attributable to, or atleast is highly associated with, a visual-proces-sing deficit, given (a) that PA patients are con-sistently impaired on nonreading visual taskssuch as visual-pattern matching, and (b) thatthey have normal success (and no AWLE) inthe nonvisual “reading” task of identifyingwords from oral spelling (Experiment 3).
Semantic dementia (SD)1. As recently reported by Gold et al. (2005), an
AWLE in word reading also appears to be aconsistent finding in patients with semanticdementia (SD), though the additional timecost per added letter in SD is usually at thelower end of the range of dramatic AWLEsseen in PA (Experiments 1, 3, and 4).
2. As the reverse of (2) under Pure Alexia, theAWLE in SD is almost certainly not attribu-table to a visual-processing deficit, given (a)that SD patients are mostly unimpaired onnonreading visual tasks (though their successon these tends to be below control levels ifthe stimulus presentation is very brief and/ormasked) and (b) that they are severely impaired(and show a dramatic AWLE) in identifyingwords from oral spelling (Experiments 1 and 3).
3. The AWLE in SD is unlikely to result fromcognitive slowing due to ageing, because thereis no greater length effect in reading by olderthan younger participants (Experiment 2) andbecause the length effect in SD is unalteredby z-score transformations that control forbaseline differences (Experiment 1).
4. In contrast to PA patients, SD patients showeda significant degree of consistency betweenitems failed in the two word identificationtasks (reading and identification from oral spel-ling) at all word lengths, suggesting a morecentral deficit as the source of the SD patients’difficulty in both tasks (Experiment 3).
5. The predominantly nonlexical nature of the SDpatients’ error responses in both word identifi-cation tasks—unlike the errors of commissionby PA patients, which were almost exclusivelyreal words—suggests a significant reduction inthe lexical/semantic constraints on word
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 25
WORD LENGTH EFFECTS IN PA AND SD

identification that characterize both normaland PA performance (Experiment 3).
6. The absence of a length-by-lexicality inter-action in reading RTs for the SD patients—incontrast to the PA and control groups, bothof which showed a significant interaction—isalso compatible with the proposal that theAWLE in SD can be traced back to degradedlexical/semantic knowledge (Experiment 4).
We return now to some of the issues raised inthe Introduction. First of all, is pure alexia pure,or is the reading disorder in this condition justone manifestation of a visual-processing disorder?To some extent, the conclusion offered in theIntroduction, that the jury is still out on this judge-ment, must remain, in the sense that somewhere inthe world there may be one or more PA patientswho are impaired at reading but not at nonreadingvisual tasks, and also that association does not provecommon cause. All of the evidence currently avail-able, however, including that added by our study,suggests that PA is not a selective reading disorder.In Experiment 3, the PA patients were consistentlyimpaired on all visual tasks, whether they werereading words, identifying (matching) pairs ofsingle letters, or even matching visual stimulisuch as meaningless figures or small line drawingsof objects. They were notably impaired on thesematching tasks even in the easier versions, such asrelatively long or unmasked exposure duration ofthe initial item in a pair. At least three types ofobservation for PA cases (from our own study andothers) combine to suggest that their readingdeficit, of which an AWLE is perhaps the bestdocumented feature, reflects a letter identifi-cation deficit in word reading that is just one mani-festation of a visual-processing disorder: (a) Theyare impaired at nonreading visual tasks, (b) theyare completely normal at identifying words fromoral spelling, and (c) they have preserved wordprocessing at lexical/semantic levels. We concludethat the jury is, at the very least, beginning tostraggle in.
How would various models of reading interpretthe nature of PA reading? As noted previously byBehrmann et al. (1998b), the combination of a
massive AWLE with clear evidence of top-downinfluences in word identification seems todemand a process whereby letter identification isto some extent serial but is also interactivelyinformed by word representations. As noted inthe Introduction, both the DRC model ofColtheart et al. (2001) and the triangle model ofPlaut et al. (1996) if augmented with the refixationcomponent implemented by Plaut (1999) could inprinciple account for this combination of effects inPA, but neither has so far provided a full simu-lation of them.
Does the AWLE in SD have the same cause asthat in PA? Here, we suggest that the jury is in andhas delivered a negative verdict. The fact that atleast some SD patients are impaired at processingindividual letters with reduced or masked exposuredurations requires further investigation andexplanation, but for visual-processing tasks onnonlinguistic stimuli, even briefly presented ormasked, the SD patients’ performance was indis-tinguishable from that of control participants(Experiment 3, Figure 9). Furthermore, to theextent that there is comparable evidence in SDon the tasks where PA performance argues for avisual deficit, the evidence in SD all leads to theopposite conclusion. That is, SD patients areseverely impaired (and with an AWLE) in non-visual “reading” (identifying words from oralspelling) and have anything but preserved wordprocessing at lexical/semantic levels. We cannotcomment on the relationship of the AWLE inreading to letter confusability with respect to SDpatients: We did not know about the intriguingresults of Fiset et al. (2005) for PA at the timethat our study was conducted, and so we did notassess this factor in SD. In fact, one of the issuesthat remains unresolved in this and other reportsof an AWLE in SD concerns letter misidentifica-tions. As noted in the discussion of PA in theIntroduction, the earlier work of Howard (1991)as well as the recent reports by Fiset and Arguinand colleagues suggest that difficulty in identifyingletters in written words is at the root of the AWLEin PA. If SD patients do not have a basicvisual-processing deficit and indeed perform atceiling/control levels in same-case and cross-case
26 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

letter matching (at least with an exposure durationof 200 ms for the first letter of the pair; seeFigure 8), it is not yet clear why they make asignificant number of letter misidentificationerrors in reading words at unlimited exposureduration.
What is the source of the AWLE in SDpatients, and how does it relate to their “main”acquired reading disorder, surface dyslexia? TheDRC model offers one, indeed perhaps currentlythe most straightforward, account of both deficits:The patients have a frequency-modulated impair-ment to the lexical route for reading, and theirreading therefore proceeds largely by the non-lexical route whose operation will produce bothregularization errors for irregular words and asignificant word length effect for any type ofword or nonword. Whilst acknowledging thestrength of this account, we offer a somewhat(though not entirely) different interpretation. Itis similar to the DRC account in that we hypoth-esize that both the surface dyslexia and the AWLEin SD derive from the same source: The patients’reading is based mainly on analysing the individualcomponents of words and is lacking the normalinfluence of knowledge about whole words. Itdiffers from the DRC account in our claim,offered in several previous papers on this topic,that the patients’ surface dyslexia is meaningfully,causally related to their primary semantic degra-dation. For example, in a study of 14 SD patients(Patterson et al., 2006), every patient was impairedat reading words with an atypical spelling–soundcorrespondence, and the degree of this deficitcorrelated highly (r ¼ .81) with a compositescore from a variety of semantic tests (none invol-ving printed words). Blazely et al. (2005) claimthat this relationship is a spurious rather than aprincipled association of deficits, on the basis ofthe fact that a few reported SD patients have notmade errors in reading words with atypicalspelling–sound correspondences. Indeed, W.M.,one of the SD patients who participated inthis study, did not have a significant surface dys-lexia at presentation (Table 1). Like the seminalSD patient W.L.P. (Schwartz, Saffran, &Marin, 1980), however, W.M. developed a
surface-dyslexic pattern of reading with furthersemantic decline (Table 3). We acknowledge theneed for a much more precise account of suchindividual differences in the degree of semanticdegradation at which atypical words begin to beregularized in reading. What convinces us of theprincipled relationship between these two deficits,however, is this: The frequency-by-typicalityinteraction that was so prominent in the readingperformance of the 14 SD patients in Pattersonet al. (2006) was just as strong, and correlatedwith semantic impairment, in five other tasks: spel-ling, past-tense verb inflection, lexical decision,object decision, and delayed copy drawing. Wefail to see how a coincidental account of semanticdementia and surface dyslexia, with the latterattributed to a specifically lexical deficit and notrelated to the patients’ semantic degradation (asin Coltheart, 2004, and Blazely et al., 2005), canexplain these results. In our view, supported bythe fact that the patients’ performance in all ofthese tasks is characterized by the same strongfrequency-by-typicality interaction, the deficits inrecognition and production of words and objectsall arise from a reduction in semantic support.
What the current study adds to this picture isthe hypothesis that identifying printed wordsmainly on the basis of stimulus information, withlittle interaction with or support from higher levelknowledge, has not one but two consequences forreading. First, except for high-frequency wordswhose orthography-to-phonology relationship isoverlearned, it results in reliance on knowledge oftypical spelling–sound correspondences: hence thesurface dyslexia. Second, it appears to result inreliance on a more piecemeal identification of theletters in a word: hence the AWLE. A theoreticalaccount of this combination of reading deficits isprobably feasible in both DRC and triangleframeworks; progress in this regard will requiremore empirical evidence and especially moremodelling.
Manuscript received 5 October 2004
Revised manuscript received 25 October 2005
Revised manuscript accepted 6 March 2006
PrEview proof published online day month year
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 27
WORD LENGTH EFFECTS IN PA AND SD
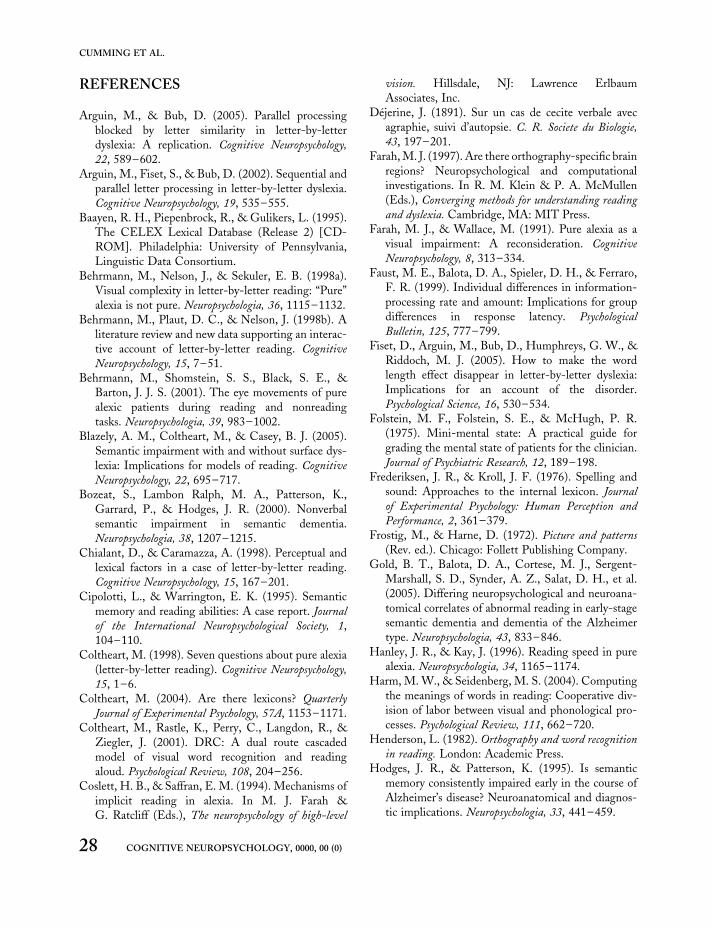
REFERENCES
Arguin, M., & Bub, D. (2005). Parallel processingblocked by letter similarity in letter-by-letterdyslexia: A replication. Cognitive Neuropsychology,
22, 589–602.Arguin, M., Fiset, S., & Bub, D. (2002). Sequential and
parallel letter processing in letter-by-letter dyslexia.Cognitive Neuropsychology, 19, 535–555.
Baayen, R. H., Piepenbrock, R., & Gulikers, L. (1995).The CELEX Lexical Database (Release 2) [CD-ROM]. Philadelphia: University of Pennsylvania,Linguistic Data Consortium.
Behrmann, M., Nelson, J., & Sekuler, E. B. (1998a).Visual complexity in letter-by-letter reading: “Pure”alexia is not pure. Neuropsychologia, 36, 1115–1132.
Behrmann, M., Plaut, D. C., & Nelson, J. (1998b). Aliterature review and new data supporting an interac-tive account of letter-by-letter reading. Cognitive
Neuropsychology, 15, 7–51.Behrmann, M., Shomstein, S. S., Black, S. E., &
Barton, J. J. S. (2001). The eye movements of purealexic patients during reading and nonreadingtasks. Neuropsychologia, 39, 983–1002.
Blazely, A. M., Coltheart, M., & Casey, B. J. (2005).Semantic impairment with and without surface dys-lexia: Implications for models of reading. CognitiveNeuropsychology, 22, 695–717.
Bozeat, S., Lambon Ralph, M. A., Patterson, K.,Garrard, P., & Hodges, J. R. (2000). Nonverbalsemantic impairment in semantic dementia.Neuropsychologia, 38, 1207–1215.
Chialant, D., & Caramazza, A. (1998). Perceptual andlexical factors in a case of letter-by-letter reading.Cognitive Neuropsychology, 15, 167–201.
Cipolotti, L., & Warrington, E. K. (1995). Semanticmemory and reading abilities: A case report. Journalof the International Neuropsychological Society, 1,104–110.
Coltheart, M. (1998). Seven questions about pure alexia(letter-by-letter reading). Cognitive Neuropsychology,
15, 1–6.Coltheart, M. (2004). Are there lexicons? Quarterly
Journal of Experimental Psychology, 57A, 1153–1171.Coltheart, M., Rastle, K., Perry, C., Langdon, R., &
Ziegler, J. (2001). DRC: A dual route cascadedmodel of visual word recognition and readingaloud. Psychological Review, 108, 204–256.
Coslett, H. B., & Saffran, E. M. (1994). Mechanisms ofimplicit reading in alexia. In M. J. Farah &G. Ratcliff (Eds.), The neuropsychology of high-level
vision. Hillsdale, NJ: Lawrence ErlbaumAssociates, Inc.
Dejerine, J. (1891). Sur un cas de cecite verbale avecagraphie, suivi d’autopsie. C. R. Societe du Biologie,
43, 197–201.Farah, M. J. (1997). Are there orthography-specific brain
regions? Neuropsychological and computationalinvestigations. In R. M. Klein & P. A. McMullen(Eds.), Converging methods for understanding readingand dyslexia. Cambridge, MA: MIT Press.
Farah, M. J., & Wallace, M. (1991). Pure alexia as avisual impairment: A reconsideration. Cognitive
Neuropsychology, 8, 313–334.Faust, M. E., Balota, D. A., Spieler, D. H., & Ferraro,
F. R. (1999). Individual differences in information-processing rate and amount: Implications for groupdifferences in response latency. Psychological
Bulletin, 125, 777–799.Fiset, D., Arguin, M., Bub, D., Humphreys, G. W., &
Riddoch, M. J. (2005). How to make the wordlength effect disappear in letter-by-letter dyslexia:Implications for an account of the disorder.Psychological Science, 16, 530–534.
Folstein, M. F., Folstein, S. E., & McHugh, P. R.(1975). Mini-mental state: A practical guide forgrading the mental state of patients for the clinician.Journal of Psychiatric Research, 12, 189–198.
Frederiksen, J. R., & Kroll, J. F. (1976). Spelling andsound: Approaches to the internal lexicon. Journalof Experimental Psychology: Human Perception and
Performance, 2, 361–379.Frostig, M., & Harne, D. (1972). Picture and patterns
(Rev. ed.). Chicago: Follett Publishing Company.Gold, B. T., Balota, D. A., Cortese, M. J., Sergent-
Marshall, S. D., Synder, A. Z., Salat, D. H., et al.(2005). Differing neuropsychological and neuroana-tomical correlates of abnormal reading in early-stagesemantic dementia and dementia of the Alzheimertype. Neuropsychologia, 43, 833–846.
Hanley, J. R., & Kay, J. (1996). Reading speed in purealexia. Neuropsychologia, 34, 1165–1174.
Harm, M. W., & Seidenberg, M. S. (2004). Computingthe meanings of words in reading: Cooperative div-ision of labor between visual and phonological pro-cesses. Psychological Review, 111, 662–720.
Henderson, L. (1982). Orthography and word recognitionin reading. London: Academic Press.
Hodges, J. R., & Patterson, K. (1995). Is semanticmemory consistently impaired early in the course ofAlzheimer’s disease? Neuroanatomical and diagnos-tic implications. Neuropsychologia, 33, 441–459.
28 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

Hodges, J. R., Patterson, K., Oxbury, S., & Funnell, E.(1992). Semantic dementia: Progressive fluentaphasia with temporal lobe atrophy. Brain, 115,1783–1806.
Howard, D. (1991). Letter-by-letter readers: Evidencefor parallel processing. In D. Besner & G. W.Humphreys (Eds.), Basic processes in reading: Visual
word recognition. Hillsdale, NJ: Lawrence ErlbaumAssociates, Inc.
Howard, D., & Patterson, K. (1992). Pyramids and PalmTrees. A test of semantic access from pictures and words.
Bury St Edmunds, UK: Thames Valley PublishingCompany.
Huynh, H., & Feldt, L. S. (1976). Estimation of the boxcorrection for degrees of freedom from sample datain randomized block and split-plot designs. Journalof Educational Statistics, 1, 69–82.
Jared, D., & Seidenberg, M. S. (1990). Namingmultisyllabic words. Journal of Experimental
Psychology: Human Perception and Performance,
16, 92–105.Kenkyukai (1983)Q3 . The General Vocational Aptitude Test
(Rev. ed.). Tokyo: Ministry of Labor.Mason, M. (1978). From print to sound in mature
readers as a function of reader ability and twoforms of orthographic regularity. Memory and
Cognition, 6, 568–581.Mathuranath, P. S., Nestor, P., Berrios, G. E.,
Rakowicz, W., & Hodges, J. R. (2000). A brief cog-nitive test battery to differentiate AD and FTD.Neurology, 55, 1613–1620.
Mauchly, J. W. (1940). Significance test for sphericity ofa normal n-variate distribution. Annals of
Mathematical Statistics, 11, 204–210.Noble, K., Glosser, G., & Grossman, M. (2000).
Reading in dementia. Brain and Language, 74,48–69.
Osterrieth, P. (1944). Le test de copie d’une figurecomplexe. Archives de Psychologie, 30, 205–220.
Patterson, K., & Hodges, J. R. (1992). Deterioration ofword meaning: Implications for reading.Neuropsychologia, 30, 1025–1040.
Patterson, K., & Kay, J. (1982). Letter by letter reading:Psychological descriptions of a neurological syn-drome. Quarterly Journal of Experimental Psychology,34A, 411–441.
Patterson, K., & Lambon Ralph, M. A. (1999).Selective disorders of reading? Current Opinion in
Neurobiology, 9, 235–239.Patterson, K., Lambon Ralph, M. A., Jeffries, E.,
Woollams, A., Jones, R., Hodges, J. R., et al.(2006). “Pre-semantic” cognition in semanticdementia: Six deficits in search of an explanation.Journal of Cognitive Neuroscience, 18, 169–183.
Patterson, K., Suzuki, T., Wydell, T., & Sasanuma,S. (1995). Progressive aphasia and surface alexia inJapanese. Neurocase, 1, 155–165.
Plaut, D. C. (1999). A connectionist approach to wordreading and acquired dyslexia: Extension to sequen-tial processing. Cognitive Science, 23, 543–568.
Plaut, D. C., McClelland, J. L., Seidenberg, M. S., &Patterson, K. (1996). Understanding normal andimpaired word reading: Computational principlesin quasi-regular domains. Psychological Review, 103,56–115.
Reitan, R. M. (1958). Validity of the Trail Making Testas an indicator of organic brain damage. PerceptualMotor Skills, 8, 271–276.
Saffran, E. M., & Coslett, H. B. (1998). Implicit vs.letter-by-letter reading in pure alexia: A tale of twosystems. Cognitive Neuropsychology, 15, 141–165.
Schwartz, M. F., Saffran, E. M., & Marin, O. S.M. (1980). Fractionating the reading process indementia: Evidence for word-specific print-to-sound associations. In M. Coltheart, K. Patterson,& J. C. Marshall (Eds.), Deep dyslexia (pp. 259–269). London: Routledge & Kegan Paul.
Warrington, E. K., & James, M. (1991). The Visual
Object and Space Perception Battery. Bury StEdmunds, UK: The Thames Valley Test Company.
Weekes, B. S. (1997). Differential effects of number ofletters on word and nonword naming latency.Quarterly Journal of Experimental Psychology, 50A,439–456.
Woollams, A., Lambon Ralph, M. A., Plaut, D. C., &Patterson, K. (2005) Q4. SD-squared: On the association
between semantic dementia and surface dyslexia.
Manuscript submitted for publication.Young, A. W., & Ellis, A. W. (1985). Different
methods of lexical access for words presented in theleft and right visual hemifields. Brain and
Language, 24, 326–358.
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 29
WORD LENGTH EFFECTS IN PA AND SD

APPENDIX
Individual data from the patients included inExperiment 1 and Experiment 3
Experiment 1
Wordreading
Word lengtha
3 4 5 6
Correct A.N. 1.0 1.0 1.0 .90A.T. .98 .83 .85 .70J.C. .98 .88 .85 .80K.H. .98 .95 .93 .88S.L. 1.0 1.0 1.0 1.0W.M. .98 .98 .98 .98M.A. 1.0 .98 1.0 .98J.H. .65 .63 .65 .48
RT A.N. 569 584 613 606A.T. 926 1,189 1,179 1,505J.C. 1,520 1,820 2,060 2,282K.H. 899 956 976 1,038S.L. 646 672 668 704W.M. 685 709 724 773M.A. 724 778 727 856J.H. 1,325 1,513 1,538 2,220
SD A.N. 454 503 364 538A.T. 455 536 363 630J.C. 428 588 799 619K.H. 358 295 415 628S.L. 69 122 125 109W.M. 84 133 126 204M.A. 209 224 227 217J.H. 321 498 454 861
RT ¼ mean reaction time in ms; SD ¼ standard deviation in
ms.aLetters, n ¼ 40 per length.
Experiment 1
Word lengtha
IDOS 3 4 5 6
Correct A.N. NT NT NT NTA.T. 1.0 .70 .90 .60J.C. TA TA TA TAK.H. .90 .50 .30 0S.L. TA TA TA TAW.M. 1.0 .85 .80 .55M.A. TA TA TA TAJ.H. .95 .90 .75 .55
IDOS ¼ identification from oral spelling; TA ¼ test
abandoned; NT ¼ not tested.aLetters, n ¼ 20 per length.
Experiment 1
Matchingtests
Cross-casematchinga
Figurematchingb
Objectmatchingb
Correct A.N. NT NT NTA.T. .79 1.0 1.0J.C. .64 1.0 .60K.H. .48 1.0 1.0S.L. .74 1.0 .81W.M. .85 1.0 1.0M.A. TA 1.0 .63J.H. .95 1.0 .88
Timetakenc
A.N. NM NT NT
A.T. NM 118 139J.C. NM 201 258K.H. NM 217 308S.L. NM 178 227W.M. NM 90 155M.A. NM 252 425J.H. NM 110 155
TA ¼ test abandoned; NT ¼ not tested; NM ¼ not measured.an ¼ 96. bn ¼ 16. c In s.
30 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.
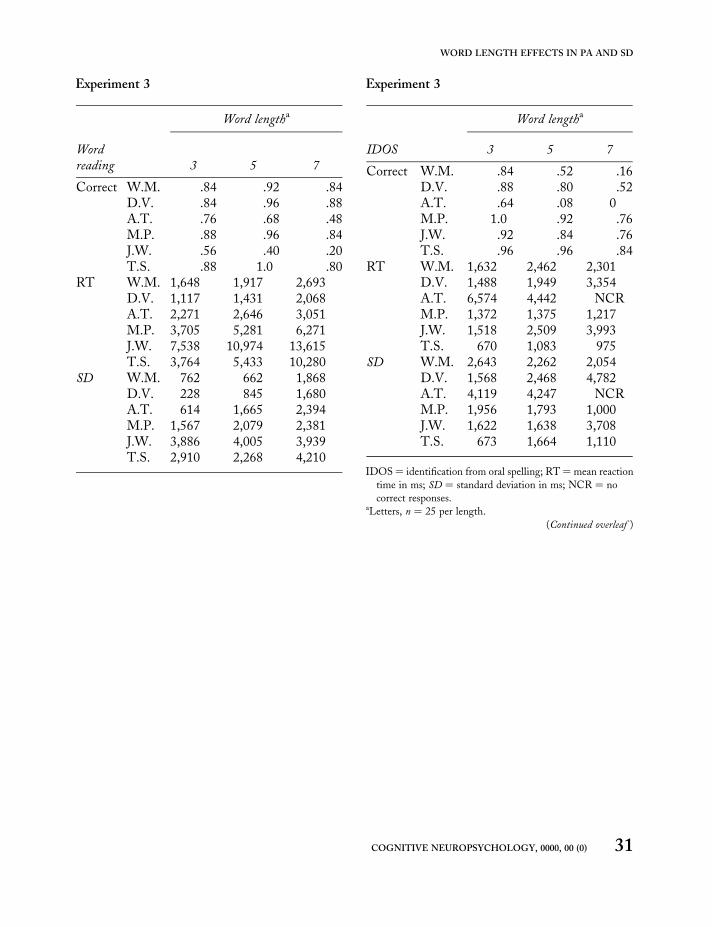
Experiment 3
Word lengtha
Wordreading 3 5 7
Correct W.M. .84 .92 .84D.V. .84 .96 .88A.T. .76 .68 .48M.P. .88 .96 .84J.W. .56 .40 .20T.S. .88 1.0 .80
RT W.M. 1,648 1,917 2,693D.V. 1,117 1,431 2,068A.T. 2,271 2,646 3,051M.P. 3,705 5,281 6,271J.W. 7,538 10,974 13,615T.S. 3,764 5,433 10,280
SD W.M. 762 662 1,868D.V. 228 845 1,680A.T. 614 1,665 2,394M.P. 1,567 2,079 2,381J.W. 3,886 4,005 3,939T.S. 2,910 2,268 4,210
Experiment 3
Word lengtha
IDOS 3 5 7
Correct W.M. .84 .52 .16D.V. .88 .80 .52A.T. .64 .08 0M.P. 1.0 .92 .76J.W. .92 .84 .76T.S. .96 .96 .84
RT W.M. 1,632 2,462 2,301D.V. 1,488 1,949 3,354A.T. 6,574 4,442 NCRM.P. 1,372 1,375 1,217J.W. 1,518 2,509 3,993T.S. 670 1,083 975
SD W.M. 2,643 2,262 2,054D.V. 1,568 2,468 4,782A.T. 4,119 4,247 NCRM.P. 1,956 1,793 1,000J.W. 1,622 1,638 3,708T.S. 673 1,664 1,110
IDOS ¼ identification from oral spelling; RT ¼ mean reaction
time in ms; SD ¼ standard deviation in ms; NCR ¼ no
correct responses.aLetters, n ¼ 25 per length.
(Continued overleaf )
COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0) 31
WORD LENGTH EFFECTS IN PA AND SD
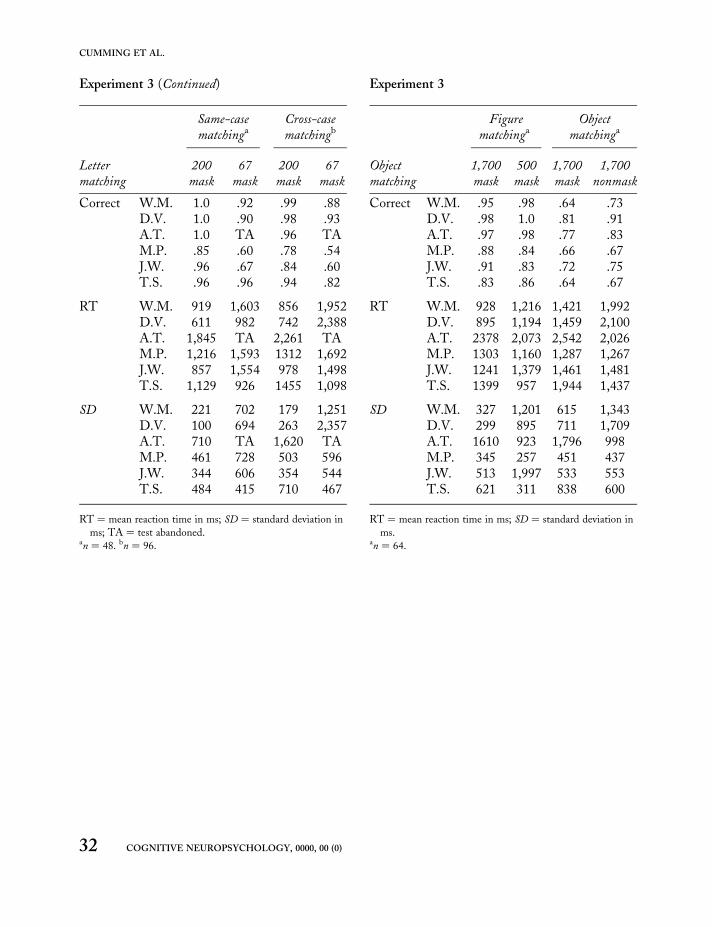
Experiment 3 (Continued)
Lettermatching
Same-casematchinga
Cross-casematchingb
200mask
67mask
200mask
67mask
Correct W.M. 1.0 .92 .99 .88D.V. 1.0 .90 .98 .93A.T. 1.0 TA .96 TAM.P. .85 .60 .78 .54J.W. .96 .67 .84 .60T.S. .96 .96 .94 .82
RT W.M. 919 1,603 856 1,952D.V. 611 982 742 2,388A.T. 1,845 TA 2,261 TAM.P. 1,216 1,593 1312 1,692J.W. 857 1,554 978 1,498T.S. 1,129 926 1455 1,098
SD W.M. 221 702 179 1,251D.V. 100 694 263 2,357A.T. 710 TA 1,620 TAM.P. 461 728 503 596J.W. 344 606 354 544T.S. 484 415 710 467
RT ¼ mean reaction time in ms; SD ¼ standard deviation in
ms; TA ¼ test abandoned.an ¼ 48. bn ¼ 96.
Experiment 3
Objectmatching
Figurematchinga
Objectmatchinga
1,700mask
500mask
1,700mask
1,700nonmask
Correct W.M. .95 .98 .64 .73D.V. .98 1.0 .81 .91A.T. .97 .98 .77 .83M.P. .88 .84 .66 .67J.W. .91 .83 .72 .75T.S. .83 .86 .64 .67
RT W.M. 928 1,216 1,421 1,992D.V. 895 1,194 1,459 2,100A.T. 2378 2,073 2,542 2,026M.P. 1303 1,160 1,287 1,267J.W. 1241 1,379 1,461 1,481T.S. 1399 957 1,944 1,437
SD W.M. 327 1,201 615 1,343D.V. 299 895 711 1,709A.T. 1610 923 1,796 998M.P. 345 257 451 437J.W. 513 1,997 533 553T.S. 621 311 838 600
RT ¼ mean reaction time in ms; SD ¼ standard deviation in
ms.an ¼ 64.
32 COGNITIVE NEUROPSYCHOLOGY, 0000, 00 (0)
CUMMING ET AL.

PCGN167386Queries
K. S. Graham
Q1 Replace initials with full names (as is usual in journal)?
Q2 Figure 2: y axis labelled RT not z-score.
Q3 Kenkyukai (1983). Author initial?
Q4 Woollams, Lambon Ralph, Plaut, & Patterson, submitted: 2005 OK for date read? [manuscriptsin preparation or submitted need date: “Use the year of the draft you read (not ‘in preparation’) inthe text citation”—APA5: 60, p. 264]Text citation?
Related Documents










![Alexia [reparado]](https://static.cupdf.com/doc/110x72/55ba47c7bb61eb65438b471e/alexia-reparado.jpg)
