NEURODIAGNOSTICS Wynne Bird, BSN, RN, CPN, CNRN Epilepsy Program Coordinator Children's Hospital Colorado 720-777-6895 OBJECTIVES 0 Recognize different types of seizures 0 Describe common epilepsy syndromes 0 Apply practical skills and interventions related to seizures 0 Understand medications used for seizure types Seizure vs Epilepsy b Anyone can have a seizure under certain circumstances. For instance, a fever, lack of oxygen, head trauma, or illness could bring on a seizure. 0 Diagnosed with epilepsy when they have seizures that occur more than twice without a specific cause. s In most cases — about 1:10 — the cause is unknown. This type of seizure is called "idiopathic" or "cryptogenic," meaning that we don't know what causes them. Whether to treat after one seizure? 0 Everyone is allowed 2 seizures in their lifetime since many seizures occur only once and don't recur 0 Side effect of chronic medication treatment weighed against benefit 0 If someone has > 2 seizures or if acute reason for seizures (tumor, stroke, etc.), most physicians will treat with medications WHAT IS EPILEPSY ? 0 Characterizes by at least 2 or more unprovoked, recurring seizures. It's also called a seizure disorder. h Caused by an uncontrolled electrical discharge from nerve cells in the cerebral cortex - this is part of the brain that integrates higher mental functions, general movement, perception, and behavioral reactions. 0 Can affect all or part of the brain. What does intractable epilepsy mean? a Seizures that are not controlled with medications. 0 Failure of 3 or more epilepsy medications 0 A number of different terms may be used: "uncontrolled," "intractable," "refractory," or "drug resistant." 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
NEURODIAGNOSTICS
Wynne Bird, BSN, RN, CPN, CNRN Epilepsy Program Coordinator Children's Hospital Colorado
720-777-6895
OBJECTIVES
0 Recognize different types of seizures 0 Describe common epilepsy syndromes 0 Apply practical skills and interventions
related to seizures 0 Understand medications used for seizure
types
Seizure vs Epilepsy
b Anyone can have a seizure under certain circumstances. For instance, a fever, lack of oxygen, head trauma, or illness could bring on a seizure.
0 Diagnosed with epilepsy when they have seizures that occur more than twice without a specific cause.
s In most cases — about 1:10 — the cause is unknown. This type of seizure is called "idiopathic" or "cryptogenic," meaning that we don't know what causes them.
Whether to treat after one seizure?
0 Everyone is allowed 2 seizures in their lifetime since many seizures occur only once and don't recur
0 Side effect of chronic medication treatment weighed against benefit
0 If someone has > 2 seizures or if acute reason for seizures (tumor, stroke, etc.), most physicians will treat with medications
WHAT IS EPILEPSY ?
0 Characterizes by at least 2 or more unprovoked, recurring seizures. It's also called a seizure disorder.
h Caused by an uncontrolled electrical discharge from nerve cells in the cerebral cortex - this is part of the brain that integrates higher mental functions, general movement, perception, and behavioral reactions.
0 Can affect all or part of the brain.
What does intractable epilepsy mean?
a Seizures that are not controlled with medications.
0 Failure of 3 or more epilepsy medications 0 A number of different terms may be used:
"uncontrolled," "intractable," "refractory," or "drug resistant."
1
Etiology
• genetic factors • metabolic or
chemical imbalances- Glut-1 deficiency
• fever/infection • birth trauma • head/brain trauma • progressive brain
disease
Stroke Brain tumors Cortical dysplasia Mesial temporal Sclerosis Congenital defect -hemimegalencephaly Maternal drug usage/medications unknown reasons
Types of Seizures
• Partial seizures - also called focal or localized
E Generalized Seizures
B Myoclonic
B Status Epilepticus
S Non-epileptic Events (NES)- pseudoseizures
S Febrile Seizures
Partial Seizures
0 More common than generalized 0 Occur in one or more specific locations 0 Can spread to wide regions of the brain 0 2 types of partial seizures
• Simple • Complex
Simple Partial Seizure
b No loss of consciousness, but no control a May experience confusion a Unilateral uncontrolled movements
• Motor - blinking, tongue movement, facial twitching, jerky movements
• Emotional - fearful feeling, d6jci vu, feeling something bad is going to happen
• Sensations- buzzing in ears, voices that aren't there, unpleasant smells, visual distortions, sudden nausea or odd feeling rising in the stomach, tingling, numbness
• Usually has temporaiy weakness of certain muscles after seizure
s May present with aura B May be able to recall event after it is over
Complex Partial Seizure (CPS) s Majority of childhood epilepsy e Post-ictal confusion h Used to be called psychomotor seizures. 0 80% originate in temporal lobe s Staring occurs - but longer than absence seizures and includes
movements a Can have loss of judgment, involuntary or uncontrolled behavior,
or loss of consciousness • "Oroalimentary" Automatisms - Chewing, lip smacking,
repetitive movements of tongue/lips/jaw • Hand Automatisms - picking at objects, aimless walking, blank
stare, removing clothing, repeating phrases, rolling, grasping, searching movements
• Other behaviors : screaming, kicking, disrobing, sexual-like movements.
Partial seizures -Brain Localization
0 Temporal E Frontal a Occipital s Parietal
2
Partial seizures - Localization
a Temporal Lobe • Most common • 40-80% have automatisms of hands/mouth - lip
smacking, rubbing hands • Gradual recovery, several minutes of confusion • Amnesic for seizure but may recall aura • Language and memory • aura- feeling deep down/gut feeling, rising up
from the abdomen/chest, emotional feelings -fear, anxiety
« Can secondarily generalize
Partial seizures - Localization
s Frontal Lobe • Motor seizure - tonic extension of limb - abrupt,
bilateral or asymmetric, Todd's paralysis • Inability to talk - muscle of tongue, mouth • Motor automatisms - pedaling, sexual movement,
vocalizations • "Somatosensory" aura - touch aura - pressure,
temp- warm sensation, pain, sensation of muscle movement, facial expression - (also seen in parietal)
• Can occur in clusters • Minimal post-ictal confusion • Can be mistaken as pseudoseizures
Partial seizures - Localization
s Occipital Lobe • Visual aura, tunnel vision, image repetition • Ictal blindness • Rapid blinking, eyelid fluttering • Version of head/eyes to opposite side -
involuntary eye movements, nystagmus • flashing lights • Can be mistaken as a migraine
Partial seizures - Localization 0 Parietal lobe - rare
• Vestibular hallucinations (vertigo) • Feeling physical sensations of numbness, tingling,
heat, pressure, and/or pain. • Distortion of visual perception: objects seem too
close, too far, too large, too small, • Language dysfunction- difficulty understanding
spoken words or language, difficulty reading or performing simple math.
• "Somatosensory" aura - touch aura - epigastric sensations, pressure, temp, pain, sensation of muscle movement, facial expression - frontal/parietal
• Panic attacks • Spreads to temporal lobe quickly
Generalized Seizures
s Typically occur in both sides of the brain, or may start in one area and spread quickly
s Patient safety a priority - airway, injury a 3 types
• Tonic-clonic (grand mal) • Absence (petit mal) • Atonic - "drop attack"
Generalized Tonic/Clonic Seizures (Grand Mal)
s Tonic phase « First stage • Loss of consciousness • Muscles contract/extension and stiffening of extremities • Loss of balance • Stridor due to muscle contacting in throat - lasts about 30 sec • May have aura
• Clonic Phase • Muscles alternate between relaxation and rigidity • Rhythmic movement without stiffening • Sometimes loss of bowel and bladder
• Post-ictal phase - fatigue., memory loss, headache, confusion, can be minutes- hours
E Can be scary to watch
3
Absence Seizures (petit mal)
0 Brief losses of consciousness - usually lasting no longer than 30 sec, can have up to 100/day
a Abrupt onset, no aura s Staring, unresponsive h Automatisms - chewing, rapid eye blinking, lip
smacking - (atypical absence) o Mild increase or decrease in muscle tone h No post-ictal phase 0 Can be provoked by hyperventilation
Atonic or "drop attacks"
0 Abrupt, Complete or partial loss of muscle tone a Eyelids may droop, head may nod, may drop
things, body will get limp - may fall or slump over.
a May need protective headgear and sometimes a face mask to prevent injury.
0 Beware of the difference- seizures that cause them to fall rigidly (like a tree trunk) often have tonic seizures (involving sudden muscle contraction) rather than atonic seizures
Myoclonic Seizures
b Sudden, Brief, involuntary jerk of a muscle or a group of muscles.
e "Myo" means muscle and "clonus" means rapidly alternating contraction and relaxation — jerking or twitching —of a muscle,
a Lasts only a second or two. 0 Can be one or a cluster a No loss of consciousness 0 Mild: only affects one part of body 0 Severe: may cause child to abruptly fall
Status Epilepticus
s Seizure activity (either a single event or several consecutive events) lasting longer than 30 minutes
• Tapering/ Adjusting of medications can increase this risk
a 4 types • Convulsive Status - easy to recognize • Non-convulsive or Non-Clinical - difficult to recognize • Complex Partial Status - confusion, lack of
responsiveness, but not loss of awareness, personality changes, emotional disturbances (fear, anxiety)
* Absence Status - clouding of consciousness, slowed speech, decreased attention, "stupor", expressionless, ' trance like state"
Non- Epileptic Events
a No single presentation s Usually occur in kids older than 8 yrs old 0 Frequently seen in kids that have seizures 0 Only happens when kids are awake, never in
sleep 0 Strong emotional content s Pelvic thrusting, non-rhythmic jerking 0 Eyes closed
Febrile Seizures
0 Onset from 3 months- 6 years
0 Temperature rises rapidly to 102 or higher
0 Not the same as epilepsy as a fever provokes the seizure and the child is not having recurrent unprovoked seizures
4
Epilepsy Syndromes
• Defined by a group of features usually occurring together. These may include: • Types of seizures • Age the seizures begin • Causes of the seizures - genetics • Part of the brain involved • Factors that provoke seizures • How severe and how frequent the seizures are • A pattern of seizures by lime of day
• Certain patterns on the EEC, during and between seizures • Brain imaging findings- MRI, CT scan, PET » Other disorders/problems in addition to seizures • Prospects for recovery or worsening
Common Epilepsy Syndromes
a LGS - Lennox-Gastaut Syndrome a Landau -Kleffner Syndrome a Dravet a Doose - Myoclonic Astatic Epilepsy s Infantile (West Syndrome) or Epileptic Spasms s ESES a Childhood Absence Epilepsy s Juvenile Myoclonic Epilepsy 0 Sturge - Weber 0 Glut-1 deficiency
Lennox-Gastaut Syndrome (LGS)
a 2 to 5% of childhood epilepsies. a Caused by brain malformations, perinatal asphyxia, severe
head injury, central nervous system infection and inherited degenerative or metabolic conditions or unknown
a Typically begins before 4 yr. old a Intellectual development is usually impaired, a Multiple different types of seizures- particularly tonic
(stiffening), atonic (drop), atypical absence, and myoclonic seizures.
a EEG shows a classic pattern of background slowing and spike-wave bursts at frequencies less than 2.5 per second,
a Seizures are hard to control - partial relief of seizures may be obtained by medications, VNS, Dietary, Corpus Callosotomy
Landau -Kleffner Syndrome
0 Rare disorder
a Usually begins 3-7 years old.
s Experiences language problems
0 Simple partial seizures, generalized tonic-clonic and atypical absence seizures.
0 The EEG is often the key. A normal EEG, especially one done when the child is awake, does not rule out this disorder. Sleep activates the epilepsy waves in these children, so sleep recordings are extremely important. The stage of sleep most affected is called slow-wave sleep.
0 After age 10, only 20% of patients still have seizures.
0 Associated with autism - intense ST helps
Dravet 0 Rare genetic disorder
B The most common gene mutation is SCN1A.
s It begins in the first year of life
s Most develop some level of developmental disability
0 The first seizure is often associated with a fever and may be a tonic clonic seizure or a clonic (jerking) seizure on one side of the body.Myoclonic seizures appear between 1 and 5 years in 85% of children
s Children are very sensitive to infections, slight changes in body temperature, bright lights, emotional stress or excitement.
a Usually 2 or more seizure medications are needed to treat the multiple seizure types.
Doose - Myoclonic Astatic Epilepsy (MAE)
a Rare syndrome - Possible genetic link but cause unknown s Onset in first 5 years of life. s Children who previously developed normally, and boys are twice as
likely as girls. a Characterized by difficult-to-control generalized seizures - can be daily, a GTC seizures usually occur during the daytime in this disorder, at least
in the early stages. Failure to suppress the "EEG abnormalities (4- to 7-Hz rhythms and spike-wave discharges) during therapy and absence of occipital alpha-rhythm with therapy suggest a poor prognosis
s Unfavorable Signs for poor prognosis: • Nocturnal GTC seizures
b Complete seizure control can be achieved in about half of the cases with medications
G Medicines and/or ketogenic diet
5
Infantile (West syndrome) or Epileptic Spasms
0 Typically begins 3 -12 months of age and usually stop by 4 years s Consists of a sudden jerk followed by stiffening, a Seizure lasts only a second or two but can occurs in clusters. • Many later develop other kinds of epilepsy. E EEG - unusual pattern called hypsarrhythmia when the
seizures are not occurring. Chaotic, hign-voltage pattern is often helpful in confirming diagnosis.
e Primary approved treatments for children with infantile spasms include: » Steroid therapy - adrenocorticotropic hormone [ACTH by
injection] or prednisone • Sabril (vigabatrin) - associated with damage to the retina of the
eye which can result in permanent loss of peripheral vision when the drug is used for many months.
Electrical Status Epilepticus In Sleep (ESES)
a Usually appears in mid-childhood 0 First sign is the rate of a child's learning appears to
slow or regress significantly. 0 EEG - continuous spike and wave epileptic activity
during sleep (>85% of time) - and especially during part of the sleep called 'slow wave' sleep.
0 EEG is often abnormal when the child is awake but may also be normal.
0 Medications - high dose Valium, IVIG, steroids and clobazam.
a Some children do not respond to any medication.
Childhood Absence Epilepsy
h Account for 2-8 % with epilepsy, a Predominantly genetic. 0 Ages 4-8 years, normal neurologic function. 0 Staring spells - not aware or responsive. 0 Lasts about 10 seconds and ends abruptly. 0 Can occur 1 to 50 times per day.
Juvenile Myoclonic Epilepsy (JME)
a Most common generalized genetic epilepsy 0 First seizure (absence) starts between 5-16 years
followed by myoclonic jerks about 1-9 years later. GTC can also appear.
0 The EEG is the most important test in making a diagnosis. The EEG is typically abnormal with a 36 Hz generalized polyspike and wave discharge.
0 Myoclonic jerks that occur on awakening. Typically clusters.
b Common precipitating factors include: stress, emotions, flickering light, missed medications.
Sturge - Weber b Presence of a birthmark ('port wine' stain), usually on
one side of the face, associated with an abnormality of the brain. Caused by abnormal blood vessels on the surface of the brain.
q Start at birth or in first year of life, a Usually partial motor seizures involving jerks of one
side of the body only. May become generalized and evolve into other types of seizures.
0 Learning disabilities are typically present. 0 Seizures are frequent and prolonged. 0 Prognosis depends on the extent to which the brain is
affected. This seems to be closely linked with the frequency and the severity of the seizures.
Glut-1 deficiency
0 Frequent seizures beginning in the first months. 0 SLC2A1 gene - provides instructions for producing a
protein called the glucose transporter protein type 1 (GLUT1). GLUT1 protein is involved in moving glucose, which is the brain's main energy source, across the blood-brain barrier. The GLUT1 protein also moves glucose between cells in the brain called glia, which protect and maintain nerve cells.
0 SLC2A1 gene mutations reduce/eliminate the function of the GLUT1 protein. Having less functional GLUT1 grotein reduces the amount of glucose available to
rain cells, which affects brain development and function.
0 Only treatment to date is the ketogenic diet
6
Seizure Management
0 Seizure Safety
0 Rescue medications and administration
0 Risks of epilepsy
1st Step to Seizure Safety
• Know type of seizures
• Know developmental status of patient
• Know triggers for seizures
• Know basic first aid
• Know rescue meds
• Know medications and if meds are being adjusted
Triggers
• Stress 0 Sleep - lack of 0 Lights 0 Sounds 0 Fever/illness S Menstrual cycle 0 Foods- caffeine, sugar, food coloring 0 Missed medications 0 OTC or other medication interactions
Seizure Safety
0 Always stay with the child 0 Safety and comfort 0 Do not hold the person down 0 Do not put anything in the mouth 0 Airway management 0 Time the seizure 0 Stay calm 0 Seizure Action Plan
Airway Management
a Seizures can alter the perception of respiration and fullness of breath (shortness of breath), respiratory rate and pattern (tachypnea, hypopnea, apnea), reflexes (coughing), quality (stridor), and secretions.
• Apnea and cyanosis are common during tonic-clonic seizures and prolonged tonic seizures. Brief apnea occurs during many complex partial seizures.
e After the seizure make sure respirations return to normal
Rescue Medications
a Know the medication and dosage
0 Know when to give it
0 Know how to administer it correctly
0 Know how quickly it works
a Know side effects of medication
Rescue Medications • Rectal diazepam (Diastat)
• Typically if GTC over 5 min or CPS or cluster >10 min or 6 seizures in an hour
• Rectal administration » Dialed down and locked by pharmacy - set dosage » Most seizures controlled within 5-15 min
e Intranasal Midazolam • Typically Older Children • Caregiver has to draw it up - Partial dosage • IV product (5mg/mL) administered nasally • Need atomizer and teaching • Most seizures controlled within 3 minutes
Rescue Medications
s Buccal midazolam • IV product administered buccally/orally • Most seizures controlled within 5 minutes
h Clonazepam or Valium-Oral/GT • Typically with aura • Works better with certain types of seizures
• VNS • Swipe magnet at onset of seizures • Helps stop or shorter seizure
Seizure Safety
a Get Emergency Help: • If longer than 5-10 minutes (after giving
rescue medications) « If one seizure after another (except for known
cluster seizure). • If injured or injury is suspected. • If the person isn't returning to their baseline.
After Seizure Safety
• Don't leave anyone alone after a seizure until: • They are breathing normally. • They can talk/communicate per baseline • Able to answer the four W's: who, what, when, and
where - developmentally appropriate. • Able to wake them up if they fall asleep • They are in a safe environment
a Document seizure • Date/Time • Length of seizure • Description of seizure • Interventions/Medications given
Risks due to Epilepsy
s Can lead to brain damage or death 0 Developmental delays E Progressive loss of abilities /Regression • Injury • Loss of hope for independence 0 Strong association to depression, psychiatric
disorders, autism, ADHD a 50,000 annual deaths from status or SUDEP
What is SUDEP? Sudden Unexpected Death in Epilepsy (SUDEP) Person with epilepsy dies unexpectedly and was previously in their usual state of health. Occurs most often at night or during sleep, leaving many questions unanswered. No one knows what causes SUDEP. Possible causes of SUDEP focuses on problems with breathing, heart rhythm and brain function that occur with a seizure. • Breathing: A seizure typically may cause a person to briefly stop
breathing (apnea). If these breathing pauses last too long, tney can reduce tne amount of oxygen that gets to the heart and tne brain. Also, a person's airway may sometimes get blocked during a convulsive seizure, leading to suffocation.
• Heart Rhythm: A seizure may cause a dangerous heart rhythm or cardiac arrest.
• Brain Function: Seizures may suppress or interfere with the function of vital areas in the brainstem.
8
Treatment Options
b Medications
s Diet • Ketogenic • MAD
0 Surgery • "curative" • palliative
Choosing the Right Medicine
0 The type of seizure/syndrome 0 The person's age and gender
• Pill/liquid • Female - childbearing age
a Other medical problems a Possible side effects from the medicine a Other medications child is on (interactions)
Picking a Medication ta Base it on type of seizure
• Generalized vs. partial: broad spectrum vs. partial • Syndromes (some medications worsen some
seizures) • Base it on side effect profile
• Age of patient and sex: D no valproic acid for teenage girls due to polycystic
ovary disease and potential fetal issues ° No valproic acid for children <2 years old
• If child has liver, kidney issues: avoiding meds worsening it
• If child has acidosis: no topiramate or zonisamide
Response to Anticonvulsants
0 60% of patients will respond to first or second medication chosen • 47% responded to first AED • 13% responded to second • 1% to third • 3% controlled with two AED's
b About a third will not respond to any medication - diet, surgery, palliative care
Treatment Challenges
s Same challenges for all « Mixed seizure types • Partial responders • Efficacy vs. tolerability • Drug interactions • Monitoring blood levels
Treatment Challenges Why Are Kids So Different?
a Additional challenges in pediatrics • Lack of research • Metabolism and clearance « Dosing formulations • Ketogenic diet • Rescue meds for school
Off-Label Treatment/Dosing
• Lack of evidence in pediatrics a Pharmacoresistant epilepsy syndromes
• Have to move to 3rd and 4th line options
a Examples: • IV levetiracetam is not FDA-approved for use in
patients <16 yo • Zonisamide not approved for <16 yo or for
infantile spasms
Super-Metabolizers
Kids may need higher doses on a mg/kg basis compared to adults - Lamotrigine (esp. 2-6 year old, <30kg) - Oxcarbazepine (esp. 2-4 year old) - Phenobarbital (esp. 1-5 year old) - Phenytoin ("infants and_young children") - Diastat
Dosing Formulations
a Not all are kid-friendly • Extemporaneous suspensions
0 Clonazepam Q Lamotrigine n Topiramate 0 Zonisamide
• Enteral tubes 0 Sprinkle caps (divalproex, topiramate) clog tubes ° DR/ER tabs shouldn't be crushed or broken
Rational for Polytherapy
s Failure of 2 medications
a Target different MOAs
0 Aim for different adverse effect profiles
b Watch drug interactions
a Consider compliance
28+ Anticonvulsant Choices a ACTH a Au'taz-oinmidi' (Di.uncix) a Benzodiazepine (Valium) a Bromides a Carbamazepine
{T egretal,Carbatrol) B Clonazepam (Kionopin) s Clobazam (Onfi) a Eslicarbiizepint' a Ethosuximide (Zaronlin) 0 Elholoin a Ezogabino (Poliga) a Felbamatc (Felbatrol) a Gabapenlin (Nourontin) a Lacosamide (Vimpat) a Lamotrigine (Lamictal)
B Levetiracetam (Keppra) a Mi'thsuximidi' a Oxcarbazepine (Trileptal,
Oxtellar XR) a Pcrampaiwl s Phtmyliun (Dilantin) a Phenobarbital (Luminal) a Progabalin (Lyrira) a Primidone (Mysolino) 0 Rufinamide (Banzel) a Stiripentol a Tiagabine (Babilri!) 0 Topiramate (Topamax) a Valproic acid (Depakene,
Depakote) a Vigabatrin (sabril) a Zonisamide (Zonegnm)
Broad Spectrum Medications
• Traditional • Acetazolamide » Benzodiazepines -
Valium, Clonazepam • Bromides • Carbamazepine • Ethosuxamide (absence) • Ethotoin • Methsuximide (absence) • Phenobarbital • Phenytoin • Valproic Acid
E Newer • Clobazam • Felbamate (LGS) • Lamotrigine • Levetiracetam • Neurontin • Primidone • Rufinamide • Topiramate • Zonisamide

Partial Medications
E Traditional • Carbamazepine • Eslicarbazepine • Phenytoin • Pregabalin
e Newer • Clobazam • Ezogabine • Oxcarbazepine • Perampanel » Tiagabine • Vigabatrin
Newest Medications Out Since 2008
a Lacosamide s Rufinamide s Vigabatrin 0 Clobazam 0 Ezogabine
Lacosamide (Vimpat)
0 Approved October 2008 • MOA: Inactivation of slow sodium channels to
stabilize hyperexcitable neuronal membranes a Use: partial onset seizures >17 years old • Dose: start l-5mg/kg/day in divided doses;
titrate to 10-20mg/kg/day, max 400-600mg/day
s AE: dizziness, ataxia, diplopia, nausea E Availability: tablets, oral suspension, IV
• Schedule V controlled substance
Rufinamide (Banzel)
0 Approved November 2008 0 MOA: unknown, triazole derivative,
possibly prevents sodium-chartnel-dependent neuronal firing
h Use: broad spectrum (generalized), LGS(>4 years old)
0 Dose: 5mg/kg BID up to 22.5mg/kg BID (max 3200mg/ day)
0 AE: dose-dependent QT-shortening, dizziness, HA, somnolence, vomiting
0 Availability: tablet, suspension h Other: take with food
Vigabatrin (Sabril)
a Approved August 2009 a MOA: irreversible GABA-transaminase inhibitor
(increases circulating GABA) a Use: infantile spasms or complex partial seizures a Dose: 25mg/kg to 75mg/kg BID; max 3g/day 0 AE: Vision loss (permanent, progressive, increases
w/ cumulative close); anemia, somnolence, infection, HA, white matter changes
0 SHARE program • Consent form • Registered provider/patient/pharmacy
• Availability: 500 mg packets and tablets
Clobazam (Onfi) a Approved October 2011 a MOA: binds to BZD site (receptor site 5 compared to
other BZDs) on GABA receptors 0 Use: LGS (>2 y.o.), ESES 0 Dose: 5 mg daily up to 10-20 mg BID or
0.5 -1 mg/kg/day q day or BID a AE: somnolence, infection, constipation, aggression,
tolerance • Less than other BZD - less drooling and sedation. • Thought to be more effective seizure control
a Availability: tablet (ok to crush) • Schedule IV controlled substance
11
Ezogabine (Potiga)
a Approved in 2010 E MOA: potassium channel opener s Use: partial-onset seizures a Dosage: 200 mg - 400 mg TID B AE: blue skin discoloration, eye abnormalities
characterized by pigment changes in the retina, urinary retention
0 Availability: tablets • Schedule V controlled substance
Specialty Medications
a ACTH - infantile spasms
a High Dose Oral Valium - ESES
a Stiripentol- Dravet syndrome
a CBD or Cannabidiol - medical marijuana
ACTH
0 Infantile spasms
0 Ordered from ACTHAR Support - sent via mail
0 Given IM - parents to give
0 High dose Steroid
0 Given daily and weaned every 5-7 days over a month
0 Suggest immunizations be held during treatment as well as keeping patient away as much as possible from other children due to potential for immunosuppression
0 Good Hand washing
0 Requires weekly: weight check, blood pressure check, occult stool lest and dextrosticks due to side effects from ACTH
High Dose Valium
b Given for ESES - Electrical Status Epilepticus during Sleep
a ESES can cause learning regression/ delays, behavior problems, sleep problems
s Given orally at bedtime h First dose given in hospital to monitor EEG
changes (25% improvement) and respiratory/other side effects
0 Initial dose 1 mg/kg/ dose then 0.5 mg/kg/dose 0 Weaned off over time (1-3 months plus) 0 Side effects; respiratory depression, irritability,
sleepiness, hyperactivity
Stiripentol 0 DravetSyndrome- documented SCNla mutation 0 Not available in US - FDA approved provider for compassionate
use a Shipped to home 0 Failed 2 or more medications 0 Must be on Clobazam 0 Clinic visit every 3 months mandatory a Capsule or "sachet" form a AE: loss of appetite, weight loss, difficulty sleeping, sleepiness,
unsteady gait, and low muscle tone, dizziness, low VVBC, liver problems.
h In addition, this medication will likely cause problems with the levels of other seizure medications requiring adjustments and more frequent blood draws for levels of these medications.
0 Labs need to be obtained at baseline and every 6 months (CBC and LFT)
CBD a Little objective data about effective treatment
with MCBD - Safety and efficacy of these products have not yet been determined,
a As of April 30, 2014, over 307 patients under the age of 18 had registered as users of MCBD
a Children's Hospital Colorado are not registered providers for medicinal cannabis and therefore are not able to prescribe these products.
s Other names/strains: CBD, THCa, THC, charlotte's web
0 Forms: liquid, edibles, patches, lotions
Resources a www.epilepsv.com - This website is a nice resource for information on
epilepsy and its treatments
s www,epilepsy foundation.org - This is an advocacy organization that has a chapter in Colorado that can be a useful resource for answering questions about epilepsy.
a www.seiiairetracker.com - Provides a way to track seizures using on-line tools. Also has an iPlume Application.
• http://wvvw.cdc.i'ov/epilcpsv - CDC information regarding seizures and seizure disorders
E Children's Hospital Colorado Neurology Department
g Lots of foundations and websites out there * Dravetfoundation.org * Hemifoundalion.org * Charliefoundalion.org - keto diet
QUESTIONS?
THANK YOU FOR YOUR TIME
13
Diastaf (diazepam rectal gel)
DiasfafAcuDiar (diazepam rectal gel)
Confirme que la tlosis y la banda verde "ready" esten vlsibles. Ventana del visor de la dosis / Banda verde
"READY"
INSTRUCCIONES DE ADMINISTRACION A NINOS Y DESECHO
Lea antes de usar Para el encargado de la atencion que usa DIASTAT®: No administre DIASTAT® hasta: 1. Que haya lei'do cuidadosamente estas instrucciones 2. Que haya revisado los pasos de administration con el medico 3. Comprenda las indicaciones Para el encargado de la atencion que usa DIASTAT® AcuDiaP: No administre DIASTAT® AcuDial™ hasta: 1. Que haya confirmado que:
• La dosis recetada esta a la vista y, si la conoce, es correcta • La banda verde "ready" esta visible
2. Que haya lei'do cuidadosamente estas instrucciones 3. Que haya revisado los pasos de administration con el medico 4. Comprenda las indicaciones Por favor no administre DIASTAT® hasta que se sienta comodo con el uso de DIASTAT®. El medico le dira exactamente cuando usar DIASTAT®. Cuando use DIASTAT® en forma correcta y segura ayudara a controlar las convulsiones. Asegurese de discutir todos los aspectos de su funcion con el medico. Si no se siente comodo, discuta su funcion nuevamente con el medico. Para ayudar a la persona que tiene convulsiones: • Usted debera ser capaz de distinguir entre
convulsiones ordinarias y en accesos. • Debe sentirse comodo y satisfecho de ser capaz
de administrar DIASTAT®. Debe ponerse de acuerdo con el medico sobre las condiciones exactas de cuando tratar con DIASTAT®.
y/ Debe saber como y por cuanto tiempo tiene que vigilar a la persona despues de administrar DIASTAT®.
Saber que respuestas esperar: • Debe saber que tan pronto deben parar las convulsiones o
disminuir en frecuencia despues de administrar DIASTAT®. • Necesita saber que hacer si las convulsiones no paran
o si hay cambios en la respiration, la conducta o la condition de la persona que lo alarmen.
Si tiene dudas o se siente inseguro acerca de usar el tratamiento, LLAME AL MfeDICO antes de usar DIASTAT®.
iDonde puede encontrar mas information y apoyo? Para obtener informaci6n sobre DIASTAT®
y DIASTAT® AcuDial™: Llame al 1-877-361-2719 o visite www.diastat.com
Recursos adicionales: Epilepsy Foundation (EF). Puede comunicarse con EF
llamando al 1-800-EFA-1000 o en www.efa.org.
^ V A L E A N T " . © 2008 Valeant Pharmaceuticals North America Impreso en E.U.A, 4/08
Cuando tratar. Segun las indicaciones o receta del medico
Consideraciones especiales DIASTAT® se debe usar con precaution: • En personas con dificultades respiratorias (por ejemplo, asma o neumonia) • En ancianos • En mujeres en edad reproductiva, durante el embarazo o la lactancia Discuta previamente con el medico los pasos adicionales que puede tener que seguir si hay una perdida de DIASTAT® o defecation. La dosis de DIASTAT® del paciente es: mg Frecuencia respiratoria del paciente en reposo Peso actual del paciente Confirme que el peso actual sea el mismo que cuando se receto DIASTAT® Verifique la fecha de caducidad y siempre retire la tapa antes de usar. Asegurese de retirar el perno del sello con la tapa.
T R A T A M I E N T O 1 Cosas importantes para decirle al medico
Fecha:
Convulsiones antes de DIASTAT® Hora Tipo de Niim. de
convulsiones convulsiones
Convulsiones despues de DIASTAT* Hora Tipo de Num. de
convulsiones convulsiones
Cosas que se deben hacer despues del tratamiento con DIASTAT® AcuDial™ Permanezca con la persona durante 4 horas y tome nota de lo siguiente: • Cambios de la frecuencia respiratoria en reposo • Cambios en el color
Posibles efectos secundarios del tratamiento .
T R A T A M I E N T O 2 Cosas importantes para decirle al medico
Fecha:
Convulsiones antes de DIASTAT* Hora Tipo de Num. de
convulsiones convulsiones
Convulsiones despues de DIASTAT Hora Tipo de Num. de
convulsiones convulsiones
Cosas que se deben hacer despues del tratamiento con DIASTAT® AcuDial™ Permanezca con la persona durante 4 horas y tome nota de lo siguiente: • Cambios de la frecuencia respiratoria en reposo • Cambios en el color
1 Posibles efectos secundarios del tratamiento.
INSTRUCCIONES DE DESECHO PARA DIASTAT' AcuDial"
£mbolo -
' Tire del 6mbolo hasta retirarlo por completo de la jeringa
' Dirija la punta al lavabo o al Inodoro
1 Vuelva a colocar el £mbolodentrodela jeringa empuj3ndolo suavemente hasta que sedetenga
1 Halelabombadel inodoro o enjuague el lavabo con agua hasta queya no se vea el gel
LAVABO 0 INODORO I Este paso es sdlo para usuados de DIASTAT® AcuDial™
Alterminarelpaso 14a: 8 Deseche todos los materlales
usados en el bote de la basura
* Noreutiiice
* Deseche en un lugar seguro, fuera del alcance de los nlnos
DESECHO PARA DIASTAT® 2.5 mg
Alterminarelpaso 13:
* Deseche todos los materiates usados en el bote de la basura
* Deseche en un lugar seguro, fuera del alcance de los nihos
Instrucciones de administration en adultos disponibles para descargar en diastat.com
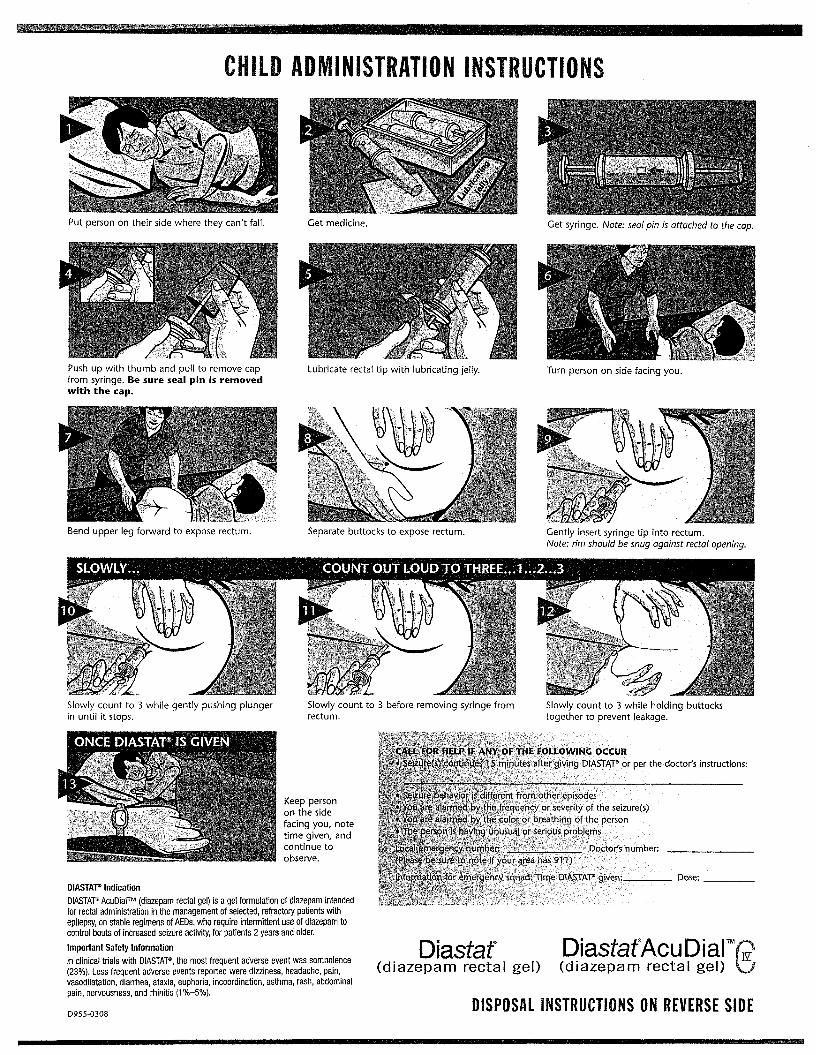
CHILD ADMINISTRATION INSTRUCTIONS
Put person on their side where they can't fall. Get medicine.
:• Wr- i . . I • II ''«»
* • i v * • * ,*\'j, y . s? *•ft>
Get syringe. Note: seal pin is attached to the cap.
Push up with thumb and pull to remove cap from syringe. Be sure seal pin is removed with the cap.
Lubricate rectal tip with lubricating jelly. Turn person on side facing you.
W&mm
Bend upper leg forward to expose rectum.
SLOWLY...
Separate buttocks to expose rectum. Gently insert syringe tip into rectum. Note: rim should be snug against rectal opening.
COUNT OUT LOUD TO THREE...1...2...3
Slowly count to 3 while gently pushing plunger in until it stops.
1MB—
• < *i'i
Slowly count to 3 before removing syringe from rectum.
Slowly count to 3 while holding buttocks together to prevent leakage.
w.-
Keep person on the side facing you, note time given, and continue to observe.
DIASTAT® Indication DIASTAT® AcuDial™ (diazepam rectal gel) is a gel formulation of diazepam intended for rectal administration in the management of selected, refractory patients with epilepsy, on stable regimens of AEDs, who require intermittent use of diazepam to control bouts of increased seizure activity, for patients 2 years and older. Important Safety Information In clinical trials with DIASTAT®, the most frequent adverse event was somnolence (23%). Less frequent adverse events reported were dizziness, headache, pain, vasodilatation, diarrhea, ataxia, euphoria, incoordination, asthma, rash, abdominal pain, nervousness, and rhinitis (1 %—5%).
D955-0308
CALL FOR HELP IF ANV OF THE FOLLOWING OCCUR Seizure(s).continues ! 5 minutes after giving D|ASTA"P or per the doctor's instructions:
• . v • — • Seizurt behavior is different from other episodes
' ,{i You are alarmed by :the frequency or severity of the seizure(s) ;.'t •,YouVre alarmed by the color or breathing qf the person
'? The person is having unusual or serious problems . • ^ • v
}/•Local'epnergency number: • • ••••v - Doctor's number: .' _ JPIease be sure to note if your area has 911)
V-'V .jhformation'fdr emergency squad; Time DIASTAT® given:
Dia staf DiasfafAcuDiaf (diazepam rectal gel) (diazepam rectal gel)
Dose:.
DISPOSAL INSTRUCTIONS ON REVERSE SIDE

I Children's Hospital Colorado
IN CARE OF KIDS Home Therapy for Seizures
Using Intranasal Midazolam Therapy What is intranasal Midazolam therapy and when is ,.v, it used? ' This therapy is for treating seizures by spraying the medicine on the skin inside the nose (intranasal injection). The medicine is injected (sprayed) into the nose using a needleless syringe.
What you need to know before using midazolam: Before you need to use this medicine be sure you know how much medicine you will give your child.
It is a good idea to keep this handout with the medicine.
Medicine: Midazolam
Dose (amount):
How given: Inject into nose using needleless syringe
Amount in each nostril:
Questions or problems Children's Hospital Colorado Neurology Dept. 720-777-6895
• Always store all the supplies in one place so they can be easily used when you need them.
• Supplies needed: syringes or needless vial adapter, atomizer tips, bottle with medicine.
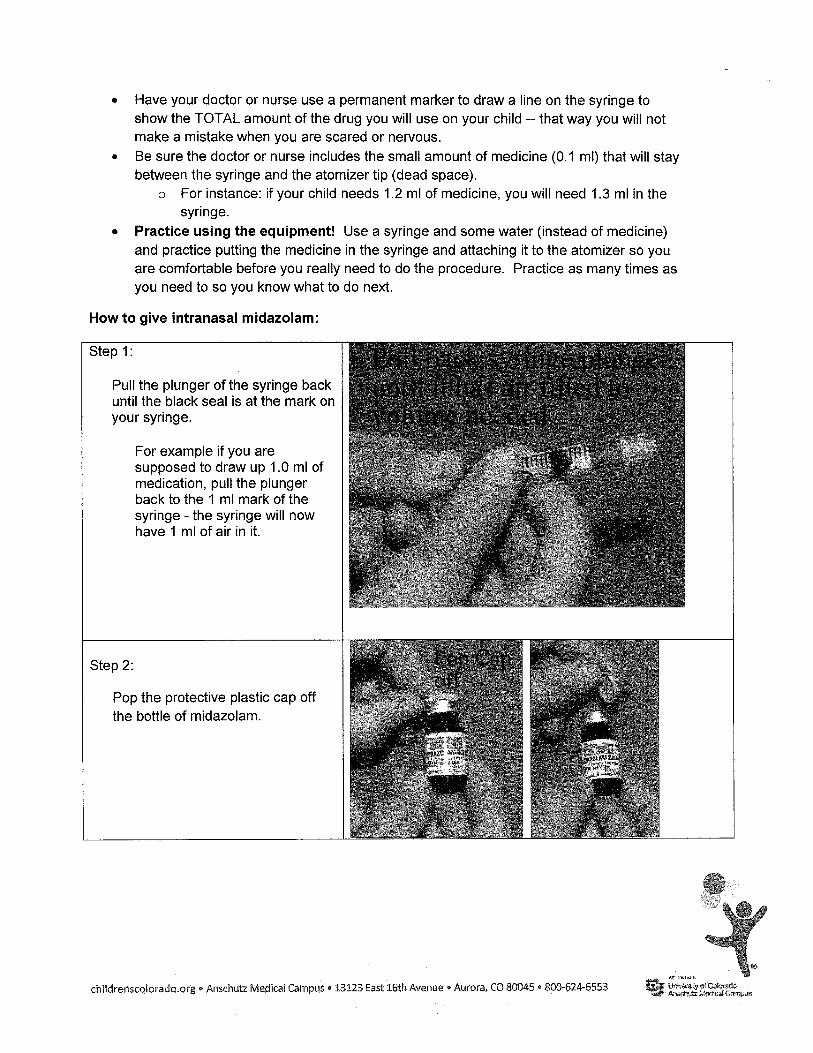
• Have your doctor or nurse use a permanent marker to draw a line on the syringe to show the TOTAL amount of the drug you will use on your child - that way you will not make a mistake when you are scared or nervous.
• Be sure the doctor or nurse includes the small amount of medicine (0.1 ml) that will stay between the syringe and the atomizer tip (dead space).
o For instance: if your child needs 1.2 ml of medicine, you will need 1.3 ml in the syringe.
• Practice using the equipment! Use a syringe and some water (instead of medicine) and practice putting the medicine in the syringe and attaching it to the atomizer so you are comfortable before you really need to do the procedure. Practice as many times as you need to so you know what to do next.
How to give intranasal midazolam:
Step 1:
Pull the plunger of the syringe back until the black seal is at the mark on your syringe.
For example if you are supposed to draw up 1.0 ml of medication, pull the plunger back to the 1 ml mark of the syringe - the syringe will now have 1 ml of air in it.
plungesB '.irjfeisai.r fifow- to ,. %\
jf '-
Step 1:
Pull the plunger of the syringe back until the black seal is at the mark on your syringe.
For example if you are supposed to draw up 1.0 ml of medication, pull the plunger back to the 1 ml mark of the syringe - the syringe will now have 1 ml of air in it.
Step 2:
Pop the protective plastic cap off the bottle of midazolam.
Pop Cai Pk Otr
m
•< 1
\i
childrenscolorado.org • Anschutz Medical Campus • 13123 East 16th Avenue • Aurora, CO 80045 • 800-624-6553 if v
Unto^otCoEoracio Anschutz MzcMcM Oa-ftpus

Step 3:
Connect the syringe or needleless access device by twisting or slipping. Poke the access device into the rubber seal of the medicine bottle.
Step 4:
Tip the bottle up-side down so the syringe is on the bottom and the bottle rubber seal faces down.
Push the syringe plunger towards the bottle - injecting (pushing) air into the bottle.
Step 5:
Pull the plunger back and let the syringe fill with medicine. (Look inside the bottle to check that the tip of the needle is in the liquid drug, otherwise you will just draw the air into the syringe). Pull the plunger back so the medicine fills the syringe to the black line.
childrenscolorado.org • Arischutz Medical Campus • 13123 East 16th Avenue • Aurora, CO 80045 • 800-624-6553 University d Cokirgcfo Anschutz Campus
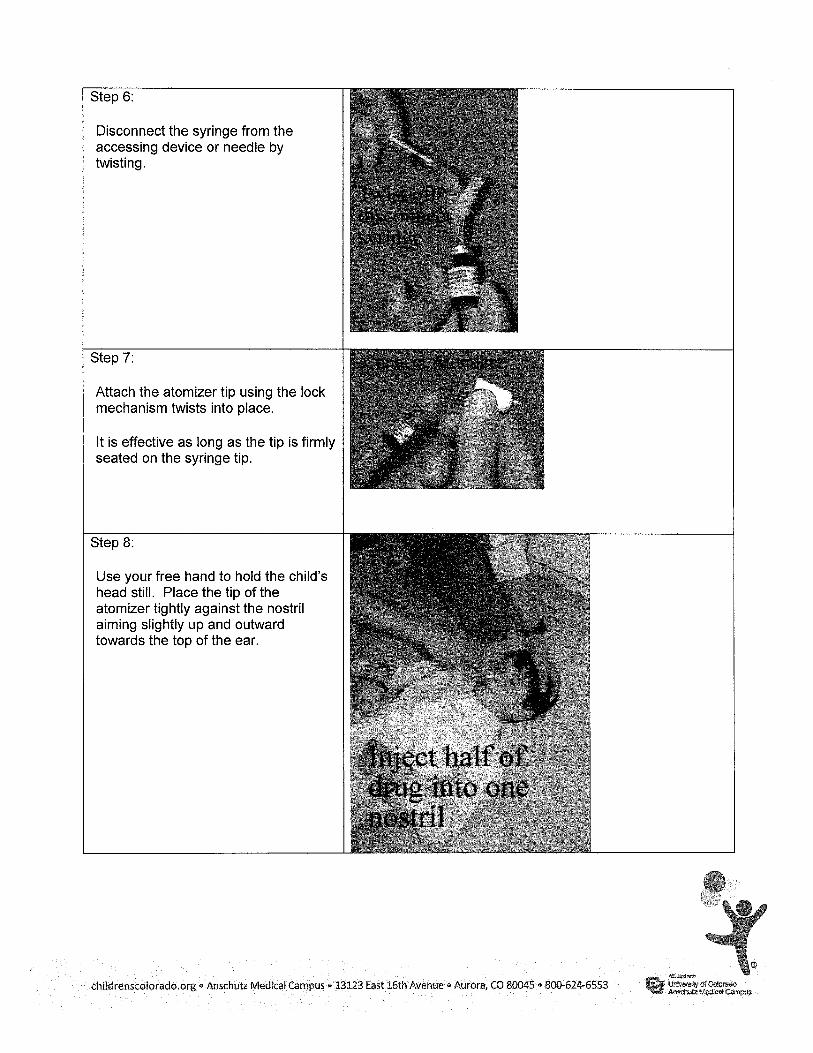
Step 6:
Disconnect the syringe from the accessing device or needle by twisting.
Step 7:
Attach the atomizer tip using the lock mechanism twists into place.
It is effective as long as the tip is firmly seated on the syringe tip.
Step 8:
Use your free hand to hold the child's head still. Place the tip of the atomizer tightly against the nostril aiming slightly up and outward towards the top of the ear.
•V Z "Xt*
Twist o i f f discovmeci \vun*ie
; . . v y r \
t>rmccr Atomizer
Inject half of drug imo one nostril
childrenscolorado.org • Anschutz Medical Campus • 13123 East 16th Avenue • Aurora, CO 80045 • 800-624-6553
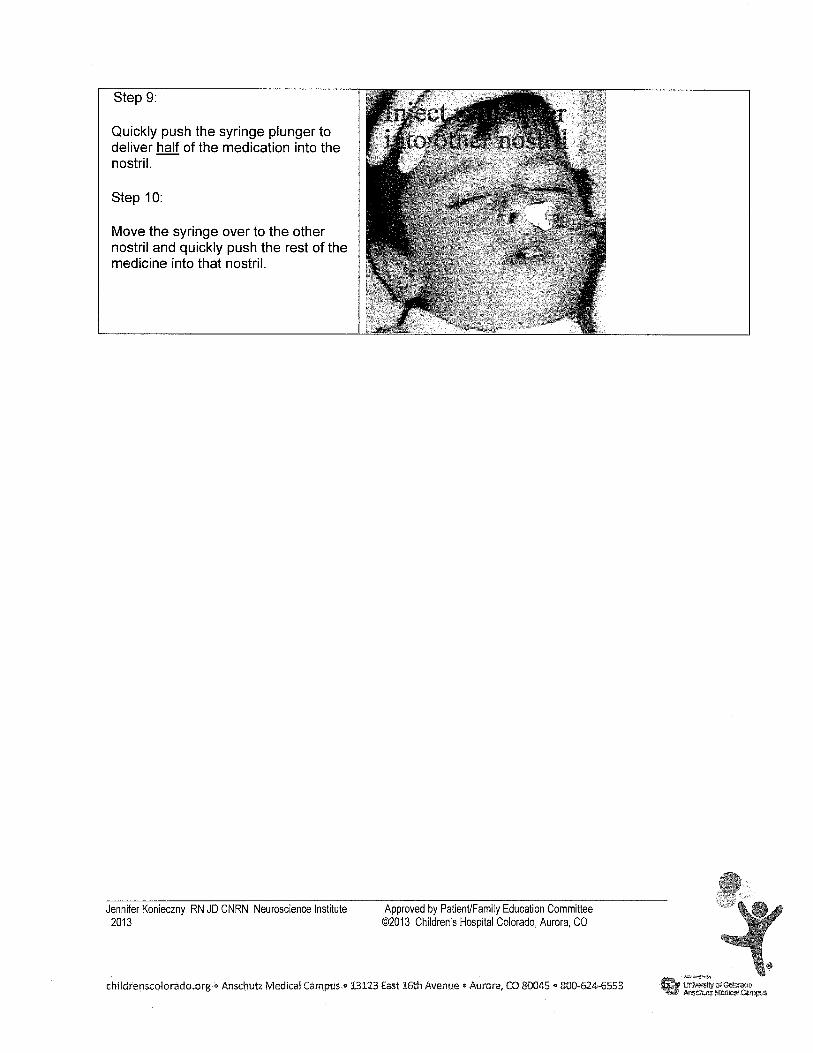
Step 9: / -Quickly push the syringe plunger to deliver hajf of the medication into the nostril. U Step 10: W Move the syringe over to the other nostril and quickly push the rest of the medicine into that nostril. 1. V4
Jennifer Konieczny RN JD CNRN Neuroscience Institute Approved by Patient/Family Education Committee 2013 ©2013 Children's Hospital Colorado, Aurora, CO
5
* childrenscolorado.org • Anschutz Medical Campus « 13123 East 16th Avenue • Aurora, CO 80045 • 800-624-6553 Gt iw»«<«troico(waro
is# Arsschute Mfjwcaf Campus
Related Documents











