NTDs in Global Health Douglas Collins, MD University of Cincinnati Dept of Family and Community Medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
NTDs in Global Health
Douglas Collins, MD
University of Cincinnati Dept of Family and Community Medicine
Case: Malnutrition & Anemia
HPI: Jose is a 2 ½ yo Honduran boy brought in for a check up at a clinic in Honduras. Mom is concerned because Jose doesn’t seem hungry. He was hospitalized once at the age of 6 months for pneumonia. He had two episodes of diarrhea last year.
SH: Mom is raising Jose, as well as his 3 older brothers and sister alone. Their father went to the US to work, but they haven’t seen much money come back yet. There is sometimes not enough money to buy food.
PE: VS: Height: 86 cm, Weight 10 kg (Wt for Age z-score: -2.0). Temp 99.1. He is sitting on mom’s lap, alert; poor appearing, barefoot. His hair is thin but normal in color. His conjunctiva appear mild pale. His abdomen is distended, but nontender. Remainder of exam is unremarkable.
Case: Malnutrition & Anemia
• What do you think is the cause of Jose’s malnutrition and anemia?
• How would you treat Jose?
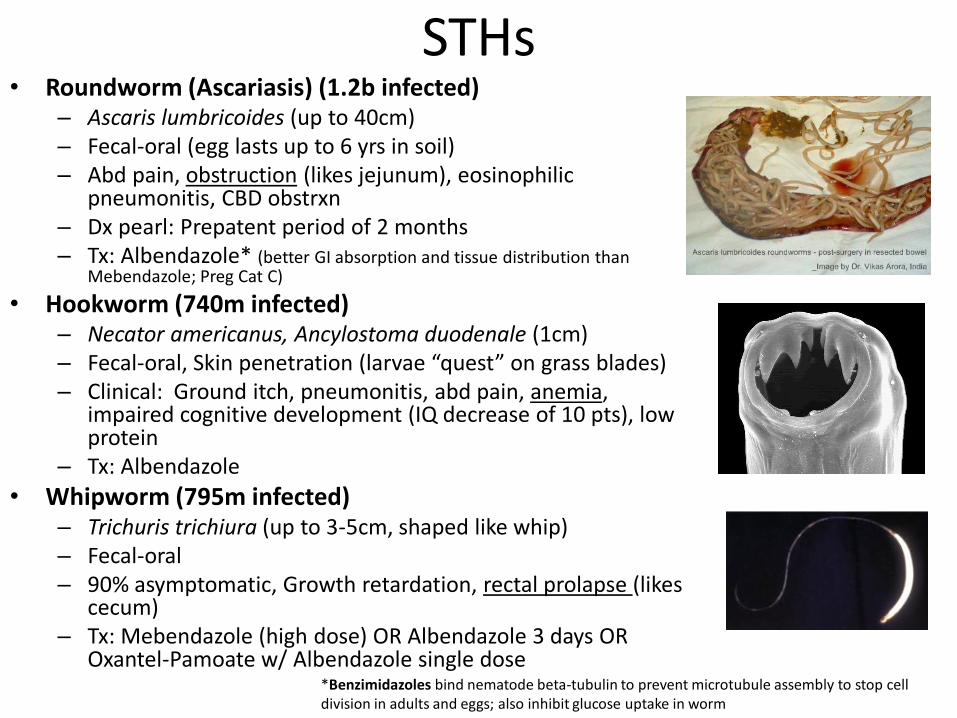
STHs• Roundworm (Ascariasis) (1.2b infected)
– Ascaris lumbricoides (up to 40cm)– Fecal-oral (egg lasts up to 6 yrs in soil)– Abd pain, obstruction (likes jejunum), eosinophilic
pneumonitis, CBD obstrxn– Dx pearl: Prepatent period of 2 months– Tx: Albendazole* (better GI absorption and tissue distribution than
Mebendazole; Preg Cat C)
• Hookworm (740m infected)– Necator americanus, Ancylostoma duodenale (1cm)– Fecal-oral, Skin penetration (larvae “quest” on grass blades)– Clinical: Ground itch, pneumonitis, abd pain, anemia,
impaired cognitive development (IQ decrease of 10 pts), low protein
– Tx: Albendazole
• Whipworm (795m infected)– Trichuris trichiura (up to 3-5cm, shaped like whip)– Fecal-oral– 90% asymptomatic, Growth retardation, rectal prolapse (likes
cecum)– Tx: Mebendazole (high dose) OR Albendazole 3 days OR
Oxantel-Pamoate w/ Albendazole single dose*Benzimidazoles bind nematode beta-tubulin to prevent microtubule assembly to stop cell division in adults and eggs; also inhibit glucose uptake in worm

The Helminths
• Nematodes– Intestinal
• Roundworm• Hookworm• Whipworm• Pinworm• Threadworm
– Filarial– Other Tissue
• Cestodes
• Trematodes
“Roundworms”Examples:
Ascaris lumbricoidesNecator americanus, Ancylostoma duodenaleTrichuris trichiuraEnterobius vermicularisStrongyloides stercolaris
Examples: Wuchereria bancrofti, Loa loa, Onchocerca volvulus
Examples: Dracunculus medinensis, Trichinella spp, Toxocara spp, Ancylostoma spp
“Tapeworms”Examples:
Taenia solium (and other Taenia spp)Echinococcus
“Flukes”Examples:
Schistosomiasis (hematobium)Intestinal Flukes: FasciolopsisLiver Flukes: Opisthorchis, ClonorchisLung Fluke: Paragonimus
Red = NTDs
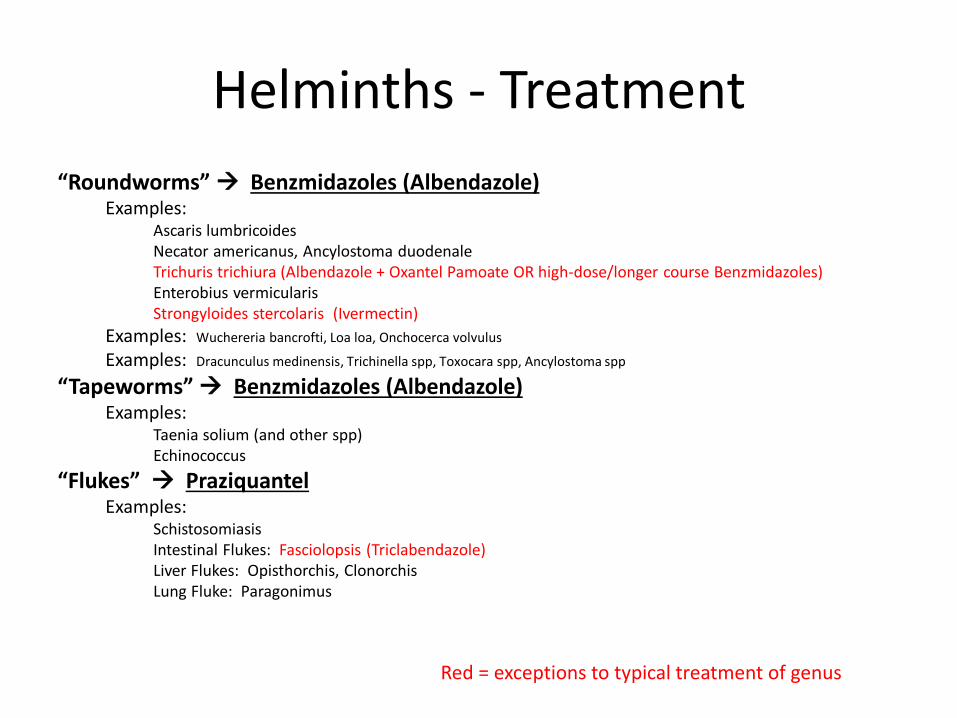
Helminths - Treatment
“Roundworms” Benzmidazoles (Albendazole)Examples:
Ascaris lumbricoidesNecator americanus, Ancylostoma duodenaleTrichuris trichiura (Albendazole + Oxantel Pamoate OR high-dose/longer course Benzmidazoles)Enterobius vermicularisStrongyloides stercolaris (Ivermectin)
Examples: Wuchereria bancrofti, Loa loa, Onchocerca volvulus
Examples: Dracunculus medinensis, Trichinella spp, Toxocara spp, Ancylostoma spp
“Tapeworms” Benzmidazoles (Albendazole)Examples:
Taenia solium (and other spp)Echinococcus
“Flukes” PraziquantelExamples:
SchistosomiasisIntestinal Flukes: Fasciolopsis (Triclabendazole)Liver Flukes: Opisthorchis, ClonorchisLung Fluke: Paragonimus
Red = exceptions to typical treatment of genus

Case: Leg wound
• A 38y man presents to you with a painful leg wound that started as a blister then ulcerated (pictured)
• What’s your DDX for ulcers in the tropics?
• What prevention interventions may be especially important in this region?
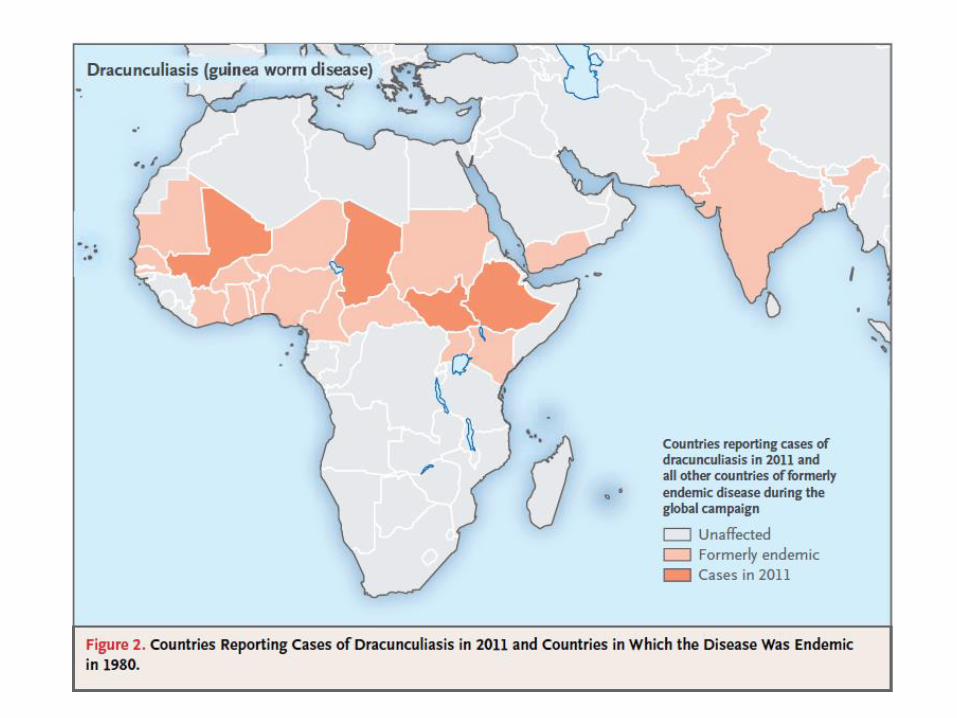
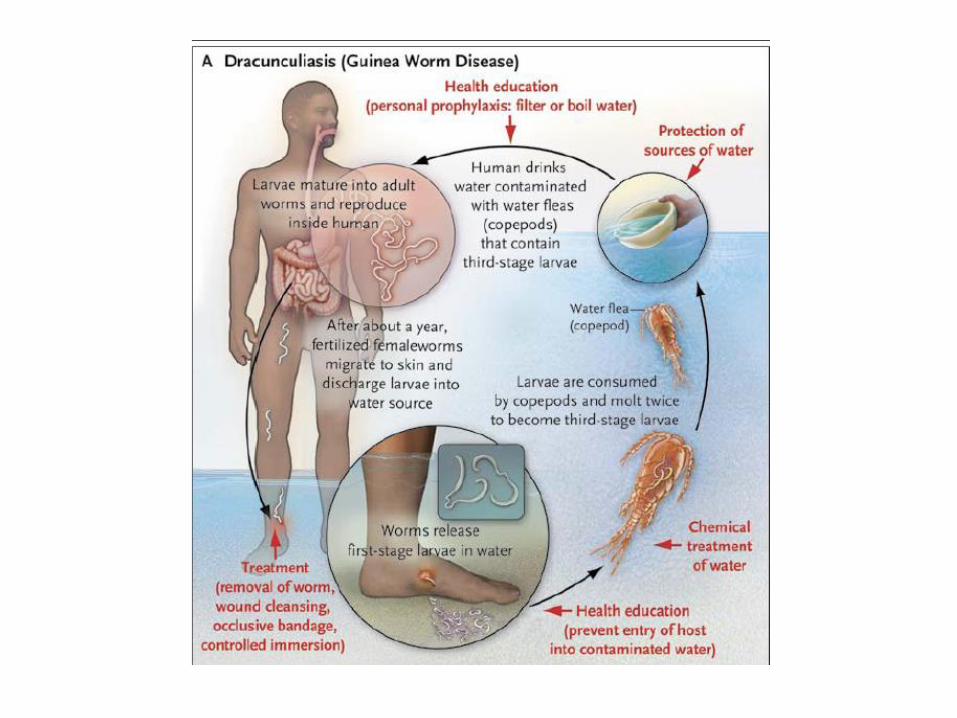
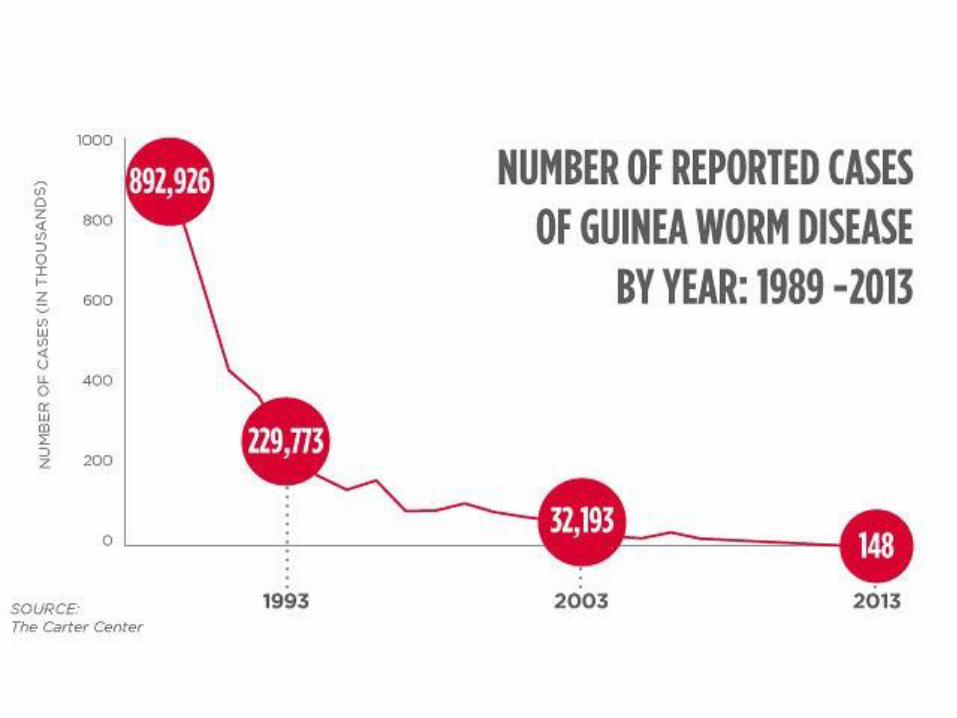
Dracunculiasis (Guinea Worm Disease)
• 16,000 infections (2007), now 126 (2014)
• Cause: Dracunculiasis medinensis
• SSA: Sudan, Mali, Ethiopia, Chad
• CLINICAL: Painful cutaneous blisters that ulcerate w/ emergence of worm as white filament
• GOAL: Targeted for Eradication. GWEP (Carter Center 1986): Community Health approach, keeping water sources clean, using boiled/filtered water
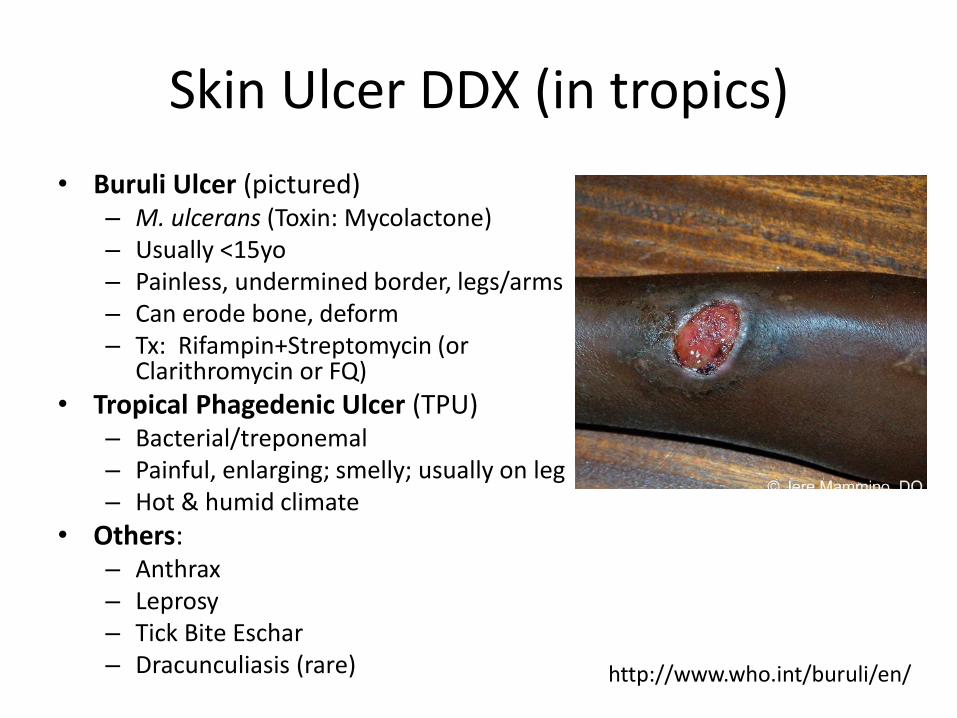
Skin Ulcer DDX (in tropics)
• Buruli Ulcer (pictured)– M. ulcerans (Toxin: Mycolactone) – Usually <15yo– Painless, undermined border, legs/arms– Can erode bone, deform– Tx: Rifampin+Streptomycin (or
Clarithromycin or FQ)
• Tropical Phagedenic Ulcer (TPU)– Bacterial/treponemal– Painful, enlarging; smelly; usually on leg– Hot & humid climate
• Others:– Anthrax– Leprosy– Tick Bite Eschar– Dracunculiasis (rare) http://www.who.int/buruli/en/
Case: Swollen Leg
HPI/PE: A 52 year old Rwandan man presents to the FMC for resettlement screening and is noted to have non-pitting edema of the right leg on physical exam. The remainder of your exam is normal. The patient states the problem has been present for >20 years with gradual worsening and is bothersome but not painful. He recalls an episode of acute swelling and pain in the leg as a teenager.
What is the likely diagnosis?What would you do?
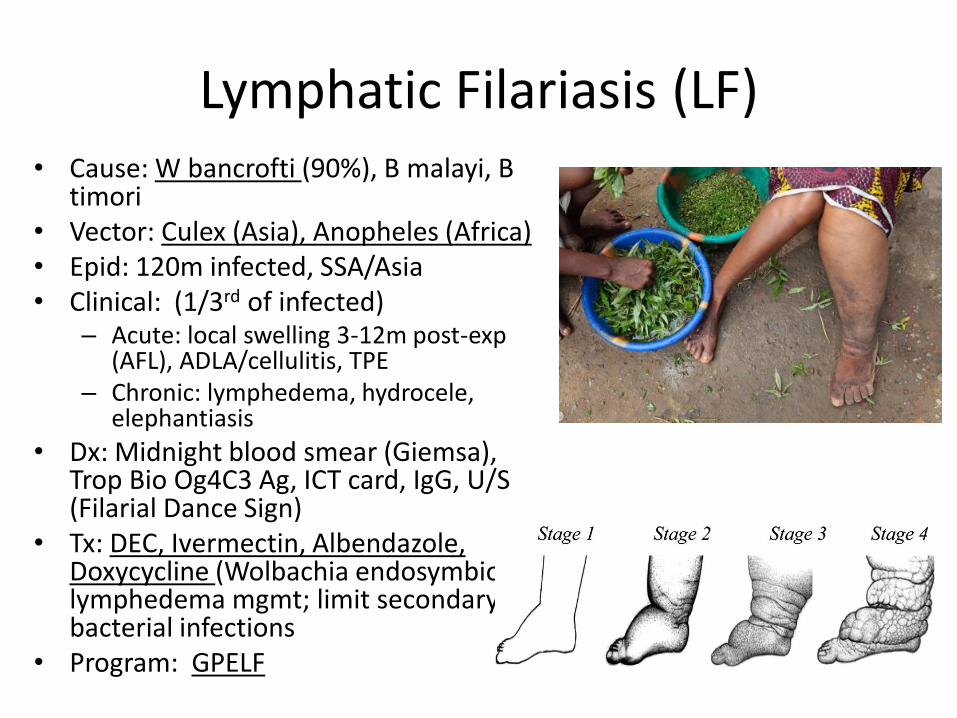
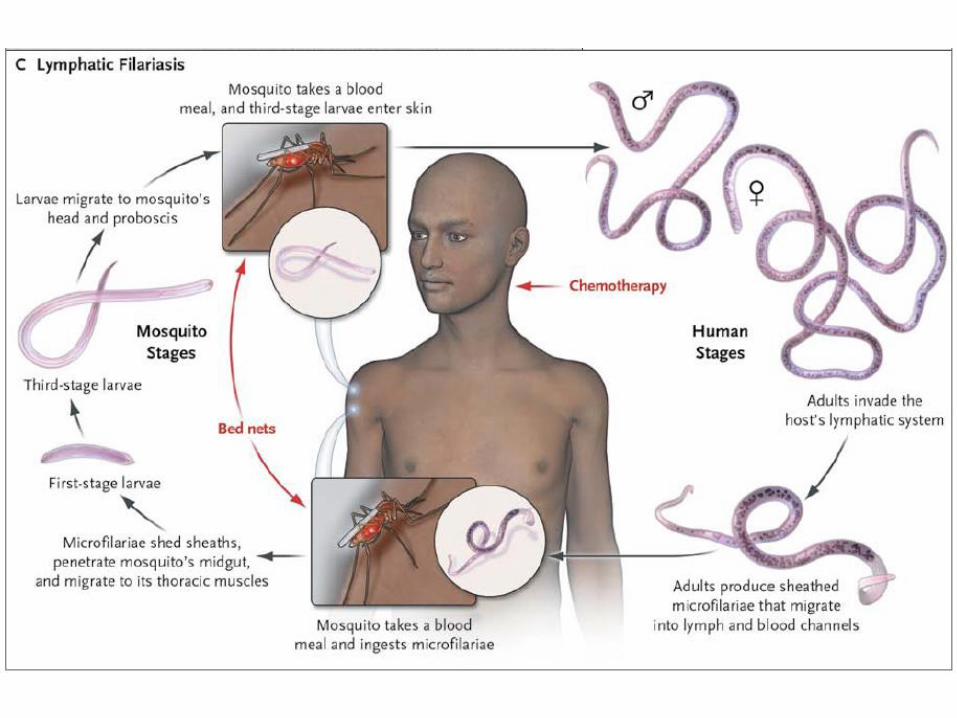
Lymphatic Filariasis (LF)• Cause: W bancrofti (90%), B malayi, B
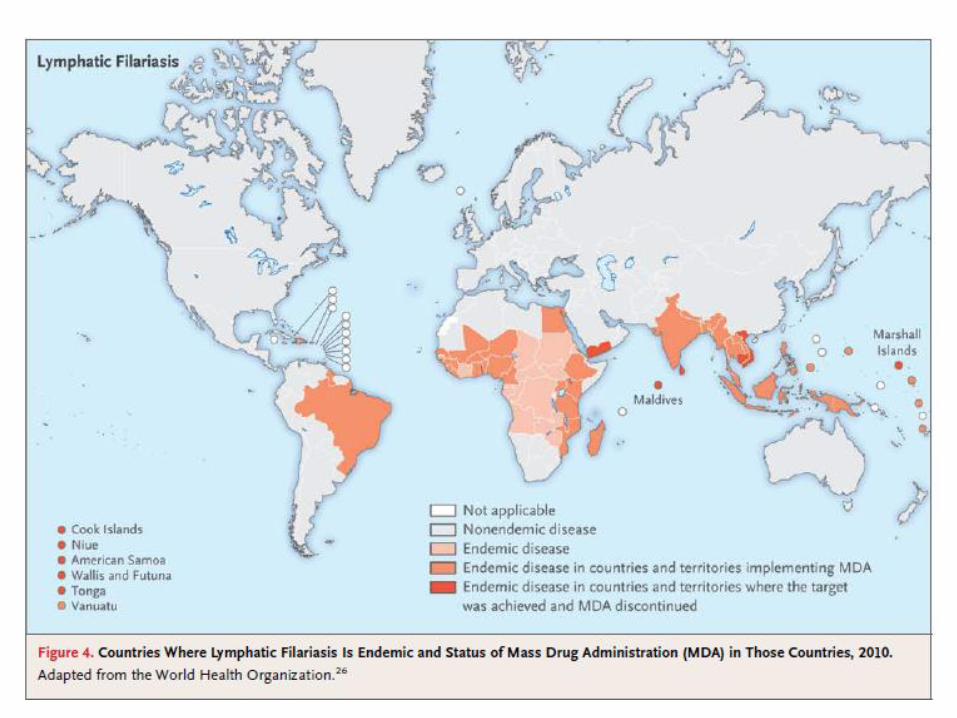
timori• Vector: Culex (Asia), Anopheles (Africa)• Epid: 120m infected, SSA/Asia• Clinical: (1/3rd of infected)
– Acute: local swelling 3-12m post-exp (AFL), ADLA/cellulitis, TPE
– Chronic: lymphedema, hydrocele, elephantiasis
• Dx: Midnight blood smear (Giemsa), Trop Bio Og4C3 Ag, ICT card, IgG, U/S (Filarial Dance Sign)
• Tx: DEC, Ivermectin, Albendazole, Doxycycline (Wolbachia endosymbiont); lymphedema mgmt; limit secondary bacterial infections
• Program: GPELF
Case: Hematuria & Hepatomegaly
HPI: A 10 year old boy from Yemen presents complaining of pain w/ urination for 6 months. He also noted some blood at the end of voiding. He described a “piece of meat” following the blood associated w/ lower abdominal pain.
PE: Normal VS. POS suprapubic tenderness. O/w negative exam.
What is the likely Diagnosis?
How would you diagnose and treat this?

Schistosomiasis
• Cause: Schistosoma haematobium (Fluke)• Vector: Snails (warm shallow fresh water)• Epidemiology: 207m people infected, most
in SSA• Clinical:
– Acute: dermatitis, pneumonitis, fever (+/-diarrhea) 4-6wks after infection (Katayama Fever)
– Chronic: GU tract disease including hematuria, SCC Bladder CA
• Dx:– Active: Ova on urine or rectal mucosa
scrapes/snips (Kato-Katz Smear)– Old: ELISA
• Tx:– Praziquantel (1d = 80-85% cure); re-treat 8
wks; f/u testing 3-6mo
Harries, JR, et al. Case 23, Clinical Problems in Tropical Medicine, WB Saunders, 1998.

Case: Blindness
• A 30y woman is brought to your clinic in Nigeria with decreased visual acuity and h/o of recurrent eye problems
• PE: bilateral conjunctivalscarring, eyelash entropion, and slight corneal scarring (pictured)
• What’s your DDX?• How would you manage
this case at a community health level?

Trachoma
• Cause: Chlamydia trachomatis
• 21m actively infected (2010)
• Cause of 3% of blindness worldwide
• Multiple re-infections in childhood results in conjunctival scarring, then trichiasis
• Tx: Azithromycin
www.trachomacoalition.org

Key Strategy for Elimination: SAFE
DDX for Blindness in Global Health
• Cataracts (46%)• Glaucoma (12.3%)• AMD (8.7%)• Corneal Opacities (5.1%)• Diabetic Retinopathy (4.8%)• Childhood Blindness/VAD (3.9%)• Trachoma (3.6%)• Onchocerciasis (0.8%)
– 37m infected (99% in Africa)– Cause: Onchocerca volvulus– Vector: Simulium damnosum– Migrate in skin/eye– Tx: Ivermectin– Programs:
• OEPA 1992 (L Am) Eliminated• OCP (Afr) Almost eliminated in 11 countries• APOC (Afr) Expanded OCP in 1995 (reduced from 46.5% 1995 to 28.5% in 2008)
% based on WHO 2002 data


Case: Syncope
HPI: 27y male admitted to hospital for syncope. Had been in excellent health, until day of admission, when he experienced palpitations and dizziness while playing soccer and then passed out. LOC x2-3min.
ROS: intermittent palpitations w/ CP over last 2 yrsPMH: o/w negSoc: Occas ETOH and MJ; POS h/o prostitute expPE: HR 56, o/w nl VS; athletic appearing; CV occas
premature beats, “forceful left ventricular lift”, S3; nl neuro exam
Scully, RE, et al. Case Records of the MGH, New Eng J Med, 8/12/1993; 329(7).

Case: Syncope
• What’s on your DDX?
• What more would you like to know?
• What further testing would you like to order?
Case: Syncope
• Pt is Latin-American born in El Salvador• DDX:
– Syncope: Cardiovascular vs Neurologic vs Other– Cardiac:
• Arrythmias (Long QT, WPW, PSVT, etc)• Valvular disease (AI from Syphilis)• CMP (HCOM, other)• Myocarditis (Viral, Syphilitic, Protozoal)
• Tests:– EKG: RBBB, LAD; Monitor: PVCs, 8b VT– CXR: LVH– Echo: Nl AV, Nl EF, POS LV dilation, hypokinesis of apex/septum– Cardiac Bx: multifocal fibrosis (neg stains for fungi, toxo,
trypanosomes, treponema, and mycobacterium)
Chagas Disease (American Trypanosomiasis)
• Epidemiology: >20m LAs infected; >300k USA, no txf screening before 2007, 50k deaths/yr, #1 cause of HF in LA
• Cause: Trypanosoma cruzi• Vector: Reduviid Bug (Triatomine)• Reservoir: Rodents, Armadillos, Opossums• Pathophysiology: Infection of autonomic ganglia, striated and
cardiac mm• Clinical:
– Acute: Rare (1%), Chagoma, Romana’s Sign, Giemsa Stain– Chronic: 30%, >20yrs after infection, Mega-esophagus, Mega-colon,
Cardiac disease (arrythmias, HF)
• Treatment:– Acute: Nifurtimox or Benznidazole– Chronic: Symptomatic (eg, anti-arrythmics)

Case: Fever & Headache
HPI: 30y Australian returned home after 4 wk trip to E Africa (Zambia) and 1 day later developed fever, severe headache, and rigors. Initial w/u was negative and pt worsened, developing nausea, vomiting and myalgia.
ROS/PMH o/w noncontributory
PE: T 39.5, HR>100, postural hypotn; enlarged spleen (1cm bcm), 5x6cm macular erythematouslesion on inner right thigh, no LA
Maddocks, S, O’Brien, R, New Eng J Med, 4/27/2000

Case: Fever & Headache
• What’s on your DDX?
• What more would you like to know?
• What further testing would you like to order?

Case: Fever & Headache
• DDX: (Fever+HA+Splenomegaly)– Malaria– Acute Schistosomiasis (Katayama Fever)– African Trypansomiasis– VL (Kala Azar, “Black Fever”)– ATBF
• Hx: Multiple insect bites while in Africa, none recalled as painful and did not recall being bitten at lesion site
• Tests:– CBC, CMP, Urine Cx normal/neg– Multiple malaria smears NEG, but POS for…
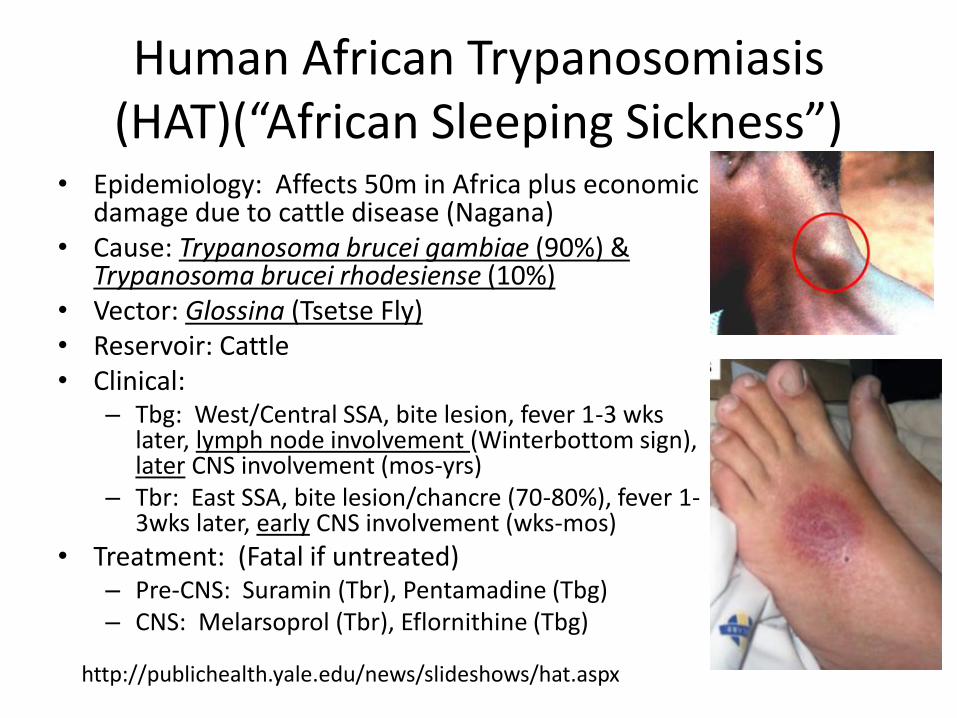
Human African Trypanosomiasis(HAT)(“African Sleeping Sickness”)
• Epidemiology: Affects 50m in Africa plus economic damage due to cattle disease (Nagana)
• Cause: Trypanosoma brucei gambiae (90%) & Trypanosoma brucei rhodesiense (10%)
• Vector: Glossina (Tsetse Fly)• Reservoir: Cattle• Clinical:
– Tbg: West/Central SSA, bite lesion, fever 1-3 wks later, lymph node involvement (Winterbottom sign), later CNS involvement (mos-yrs)
– Tbr: East SSA, bite lesion/chancre (70-80%), fever 1-3wks later, early CNS involvement (wks-mos)
• Treatment: (Fatal if untreated)– Pre-CNS: Suramin (Tbr), Pentamadine (Tbg)– CNS: Melarsoprol (Tbr), Eflornithine (Tbg)
http://publichealth.yale.edu/news/slideshows/hat.aspx

http://publichealth.yale.edu/news/slideshows/hat.aspx


Hotez, PJ, et al, Control of NTDs, NEJM, 2007
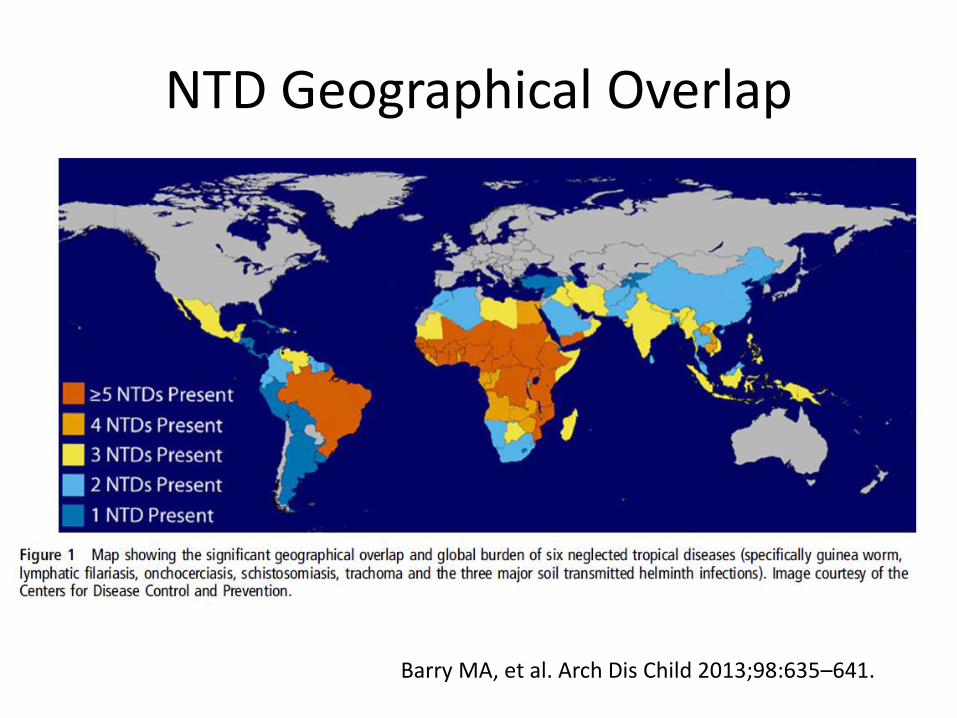
NTD Geographical Overlap
Barry MA, et al. Arch Dis Child 2013;98:635–641.
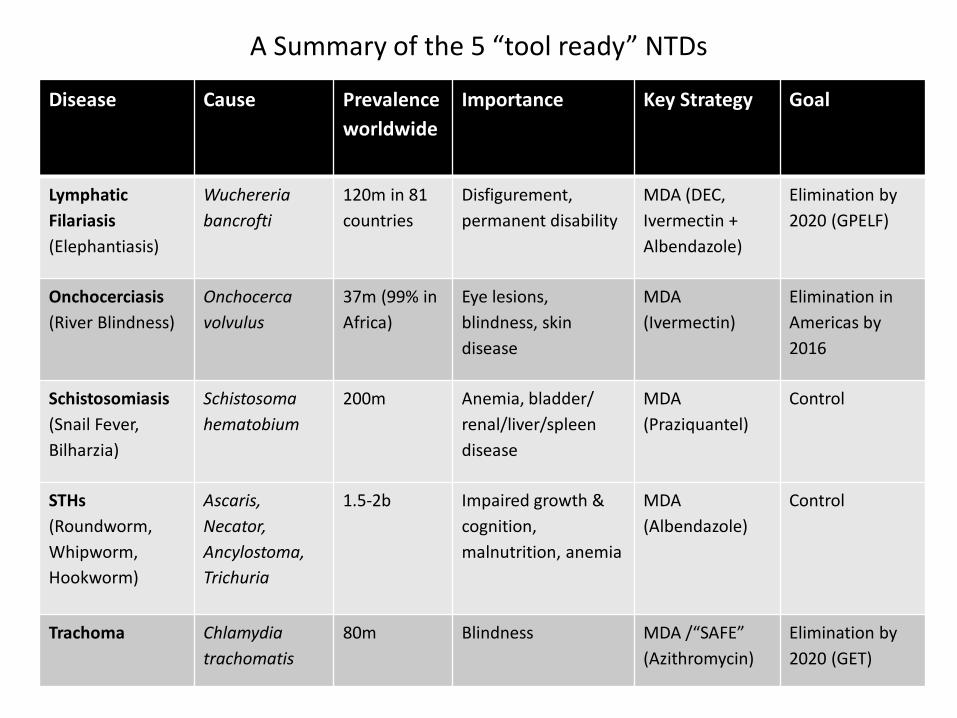
A Summary of the 5 “tool ready” NTDs
Disease Cause Prevalence
worldwide
Importance Key Strategy Goal
Lymphatic
Filariasis
(Elephantiasis)
Wuchereria
bancrofti
120m in 81
countries
Disfigurement,
permanent disability
MDA (DEC,
Ivermectin +
Albendazole)
Elimination by
2020 (GPELF)
Onchocerciasis
(River Blindness)
Onchocerca
volvulus
37m (99% in
Africa)
Eye lesions,
blindness, skin
disease
MDA
(Ivermectin)
Elimination in
Americas by
2016
Schistosomiasis
(Snail Fever,
Bilharzia)
Schistosoma
hematobium
200m Anemia, bladder/
renal/liver/spleen
disease
MDA
(Praziquantel)
Control
STHs
(Roundworm,
Whipworm,
Hookworm)
Ascaris,
Necator,
Ancylostoma,
Trichuria
1.5-2b Impaired growth &
cognition,
malnutrition, anemia
MDA
(Albendazole)
Control
Trachoma Chlamydia
trachomatis
80m Blindness MDA /“SAFE”
(Azithromycin)
Elimination by
2020 (GET)
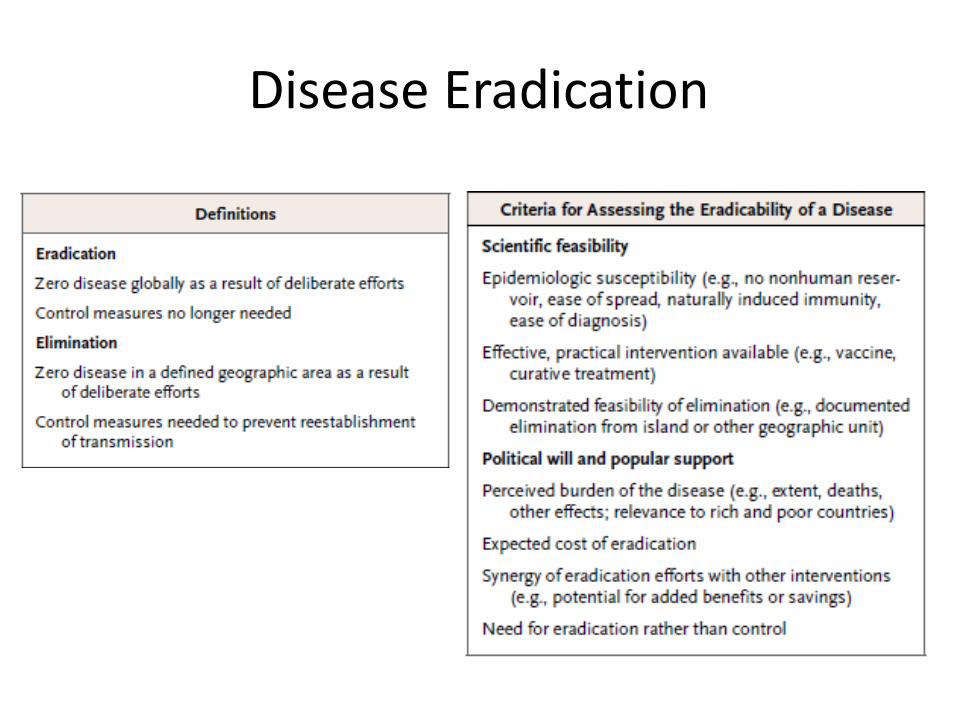
Disease Eradication
• Definitions (Dahlem Workshop, 1997)– Control – reduction to locally acceptable level w/
continued intervention– Elimination – reduction of incidence to zero in
defined area w/ continued intervention– Eradication – permanent reduction of worldwide
incidence to zero w/ continued intervention no longer needed
• History of Eradication– Success: Smallpox (1977)– Failure: Malaria, YF, Yaws
• Current Targets– Polio, Guinea Worm (Eradication)– LF, Oncho, Trachoma (Elimination)– STHs, Schistosomiasis (Control)

Mass Drug Administration (MDA)

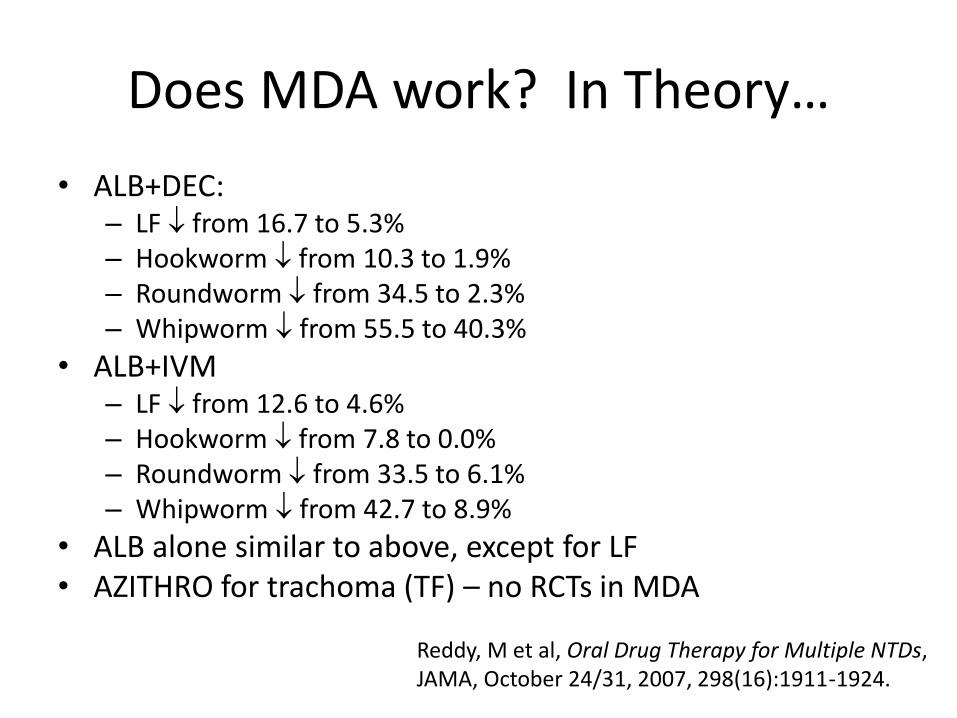
Does MDA work? In Theory…
• ALB+DEC:– LF from 16.7 to 5.3%– Hookworm from 10.3 to 1.9%– Roundworm from 34.5 to 2.3%– Whipworm from 55.5 to 40.3%
• ALB+IVM– LF from 12.6 to 4.6%– Hookworm from 7.8 to 0.0%– Roundworm from 33.5 to 6.1%– Whipworm from 42.7 to 8.9%
• ALB alone similar to above, except for LF• AZITHRO for trachoma (TF) – no RCTs in MDA
Reddy, M et al, Oral Drug Therapy for Multiple NTDs, JAMA, October 24/31, 2007, 298(16):1911-1924.
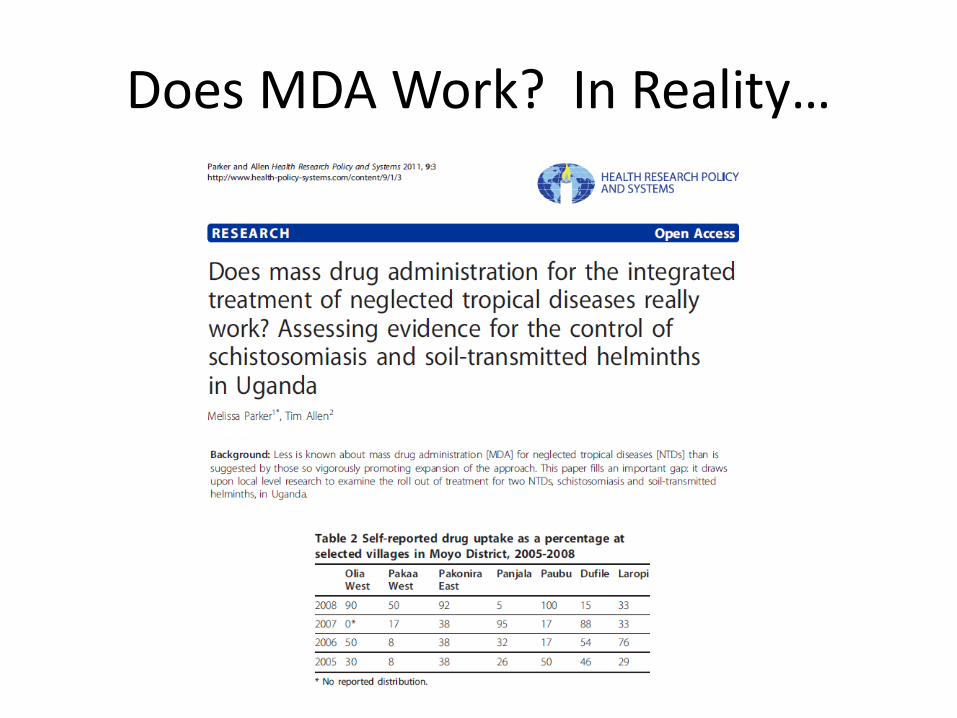
Does MDA Work? In Reality…

NTDs, MDA, & Child Health
Thank you!
Disease Eradication

History of Eradication, Elimination
• Eradication:– Smallpox has now been eradicated and programmes are
currently under way to eradicate poliomyelitis and guinea-worm disease.
– 1993: International Task Force for Disease Eradication evaluated over 80 potential infectious disease candidates and concluded that six were eradicable.
• Elimination:– 1997: World Health Assembly passed a res to eliminate LF– 1997: WHO listed leprosy, onchocerciasis, and Chagas
disease as being candidates for elimination
• With this background, the Dahlem Workshop on the Eradication of Infectious Diseases was held in March 1997
MMWR, December 31, 1999 / Vol. 48 / Supplement
Related Documents