Spectrum Society for Healthcare Strategy and Market Development ® November/December 2013 MedStar Health: Sports Sponsorships as Part of the Brand Strategy Healthcare organizations can leverage sports sponsorships for philanthropic, employee engagement, and community relations opportunities. (Continued on next page) STRATEGY By Jean Hitchcock and Marc Bluestein In 2013 it is projected that $13.8 billion will be spent on sport sponsorships in North America, a 6 percent increase from 2012. 1 In fact, the amount spent on sports sponsor- ships is more than the total amount spent on all other forms of sponsorship combined, including entertainment, cause-related, arts, festivals, and membership organizations. Why Is Sponsorship Growing? ere are a number of reasons for the con- tinued increase in sponsorship spending: ● ● Decreasing efficiency of measured me- dia: Costs for traditional advertising continue to increase, while ratings and readership decline. ● ● Increasing need for two-way commu- nication: Organizations are looking for alternative methods to communicate, which allow them to deepen their rela- tionships with customers through live interactions, including sponsorship and social media. ● ● Favorable viewing by consumers: Con- sumers view it as a form of marketing that gives something back, benefit- ing another party in addition to the marketer. It implies a degree of altruism that is absent from more commercial types of marketing. Across the country, hospitals use sponsorships to: ● ● Promote general health and wellness messaging ● ● Showcase medical expertise in action ● ● Demonstrate community involvement ● ● Recruit and retain quality employees Where Do You Begin? Given the US sports culture, it can be difficult to understand the desire of some healthcare providers to enter into sponsorships with sports franchises. How- ever, not all sponsorships are created equal, and the first step in your evaluation of any sponsorship is how it complements your brand marketing strategy. Here are some key points to consider when evaluating a sports team sponsorship: ● ● What are your branding goals? Spon- sorships are tied into your brand—and should not be focused on revenue. When you consider the number of games multiplied by the number of sea- son ticket holders, you may find your target audience is greater than the TV- viewing audience. ● ● Advertising is about the number of eyes seeing your message. How can

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SpectrumSociety for Healthcare Strategy and Market Development® November/December 2013
MedStar Health: Sports Sponsorships as Part of the Brand StrategyHealthcare organizations can leverage sports sponsorships for philanthropic, employee engagement, and community relations opportunities.
(Continued on next page)
S T R A T E G Y
By Jean Hitchcock and Marc Bluestein
In 2013,� it is projected that $13.8 billion will be spent on sport sponsorships in North America, a 6 percent increase from 2012.1 In fact, the amount spent on sports sponsor-ships is more than the total amount spent on all other forms of sponsorship combined, including entertainment, cause-related, arts, festivals, and membership organizations.
Why Is Sponsorship Growing?There are a number of reasons for the con-tinued increase in sponsorship spending:
●● Decreasing efficiency of measured me-dia: Costs for traditional advertising continue to increase, while ratings and readership decline.
●● Increasing need for two-way commu-nication: Organizations are looking for alternative methods to communicate, which allow them to deepen their rela-tionships with customers through live interactions, including sponsorship and social media.
●● Favorable viewing by consumers: Con-sumers view it as a form of marketing that gives something back, benefit-ing another party in addition to the
marketer. It implies a degree of altruism that is absent from more commercial types of marketing.
Across the country, hospitals use sponsorships to:
●● Promote general health and wellness messaging
●● Showcase medical expertise in action
●● Demonstrate community involvement
●● Recruit and retain quality employees
Where Do You Begin?Given the US sports culture, it can be difficult to understand the desire of some healthcare providers to enter into
sponsorships with sports franchises. How-ever, not all sponsorships are created equal, and the first step in your evaluation of any sponsorship is how it complements your brand marketing strategy.
Here are some key points to consider when evaluating a sports team sponsorship:
●● What are your branding goals? Spon-sorships are tied into your brand—and should not be focused on revenue. When you consider the number of games multiplied by the number of sea-son ticket holders, you may find your target audience is greater than the TV-viewing audience.
●● Advertising is about the number of eyes seeing your message. How can

2 Spectrum | November-December 2013
Brand Strategy(continued from page 1)
you maximize your media buy? There is a reason the dasher boards in hockey and the rotating signs behind home plate are the highest priced: Television viewing is highest for both.
●● Are you doing this to drive business, brand, or both? It is difficult to deter-mine how much business you garner from sponsorships, and we recommend evaluating ROI on other metrics, like consumer perception.
●● How else could such a partnership help you? Sports sponsorships can aid your organization in community benefit, phi-lanthropy, and recruitment efforts.
●● Who will negotiate the team’s medi-cal care and advertising contracts? There should be no correlation between the team’s medical contract and a spon-sorship. The decision to select a medi-cal provider should be made, based on physician experience and quality outcomes. The level of sponsorship should not factor into this decision. You need to avoid any perception by the players or the public, that the team’s medical care is based on the value of the sponsorship.
Once you have decided that a sports spon-sorship fits within your business strategy, then you need to decide if you will negotiate directly with the team or bring in a sports marketing firm to evaluate the opportu-nity and negotiate the contract. If you are in a large sports market and negotiate with multiple leagues, we recommend bringing in a firm. It is too difficult to stay on top of all the rules regarding marketing assets, sports medicine, and the use of branding elements, like logos.
Official Medical Provider to the TeamConsider the following points when making your assessment of a sports sponsorship. The golden nugget in any sports sponsorship is the ability to use the designation “Official Medical Partner of the ____________.” If you are not, then it is difficult to justify sponsorship dollars when a competitor is making the claim. For MedStar Health, this is the go/no-go decision.
Relationship with Team OwnersThe relationship with the owners of a sports team is critical. You want a partner who will enhance your brand—which is different from a strictly paid advertising relationship. If you are a not-for-profit organization, you want to align with others who have strong community reputations. Sports sponsorships relate to co-branding; therefore, you must be selective about your partners.
Professional Versus Local TeamsThe difference between “professional sports” and “local sports” is cost. Most professional league sponsorships begin at the six-figure level and go up. However, with these spon-sorships, there are more media opportunities and a higher visibility. All things considered, you are part of a national organization. On the other hand, local teams may be your only option. If so, then maximize your invest-ment beyond signage.
Additionally, consider the amount of fan or audience participation as it relates to your local market. For example, marathons provide many sponsorship opportunities, but popular, large-scale marathons have high participation from out-of-town runners and spectators.
Maximizing the SponsorshipHealthcare organizations can maximize the sponsorship for a number of purposes: philanthropy, employee engagement, and community relations. Once you begin to negotiate a sponsorship, leverage it for your other business needs by:
●● Sponsoring free “Baseball Basics” clin-ics for 500 underserved kids to support community relations
●● Promoting player appearances for pa-tients, particularly children
●● Having access to tickets and suites for donors or key recruits
●● Ringing bases with cancer survivors to highlight breast and prostate cancer awareness
●● Being part of the NFL’s “A Crucial Catch” campaign on Monday Night Football for National Breast Cancer Awareness Month
●● Offering a bank of tickets to hospital lead-ership for employee recognition
●● Taking advantage of significant media relations opportunities
Society for HealthcareStrategy and Market Development®
PresidentHolli SallsPrincipal Salls GroupChicago, IL
President-electMark ParringtonVice President, Strategic Transactions and Development Catholic Health InitiativesEnglewood, CO
Immediate Past PresidentMaria RoyceSenior Vice President, Planning and Community DevelopmentWellSpan HealthYork, PA
Executive DirectorDiane Weber, RNSociety for Healthcare Strategy andMarket DevelopmentChicago, IL
EditorMary P. CampbellSociety for Healthcare Strategy andMarket DevelopmentChicago, IL
Design and Layout
Spectrum is the bimonthly newsletter of and a membership benefit for members of the Society for Healthcare Strategy and Market Development®. SHSMD welcomes unsolicited manuscripts, which will be used on a content and space-available basis. Preferred article length is from 1,200 to 1,500 words, and graphics (figures, tables, photos) and suggestions for sidebars are welcome. Please e-mail articles to [email protected].
The editorial office is located at:155 North Wacker, Suite 400 Chicago, IL 60606Phone: 312-422-3888Fax: 312-278-0883E-mail: [email protected] Website: www.shsmd.org
Opinions expressed in these articles are those of the authors and do not necessarily reflect the opinions of SHSMD or the American Hospital Association.
©2013, Society for Healthcare Strategy and Market Development. Reprinting or copying is prohibited without express consent from SHSMD.

November-December 2013 | Spectrum 3
Case Study: Professional Sports Sponsorships and MedStar HealthMedStar Health has a strong sports medicine program that has provided team and venue medical coverage for years. On a professional level, MedStar physicians provide medical care to the Washington Nationals and the Baltimore Ravens, as well as national sports associations, area college sports teams, and high school teams. Seminal concussion re-search among high school athletes, conduct-ed by MedStar Health Research Institute, helped ignite the national conversation on concussions.2 Community and media at-tention on this topic helped build MedStar Health’s strong sports medicine reputation, which is partly why so many sports teams approach us for sponsorships.
Market research in the Baltimore area consistently ranks MedStar as strong in orthopedics and sport medicine. This high level of awareness is a direct result of our longest sports sponsorship/relationship with the Baltimore Ravens. Through an exclusive relationship, MedStar’s sponsorship includes
television, radio, online, and print advertis-ing, as well as the injury report and high-profile in-stadium signage. The team has also collaborated with us on a concussion prevention program that is part of the NFL’s initiative in our market.
MedStar also has contracts for Ravens’ medical care and venue coverage that are kept separately for ethical reasons. That said, MedStar would not enter into a sports-team sponsorship if it did not include the medical contract.
In 2011, MedStar partnered with the Washington Nationals. MedStar physicians were already providing medical care for the team, and we wanted to expand our relation-ship and enhance our reputation in orthope-dics and sports medicine in the DC market. This sponsorship focuses heavily on televi-sion-camera-visible signage and digital as-sets because of the 81-home game schedule. MedStar Health now has relationships with two professional teams, in two different
sports leagues that cover both our markets, year-round. All aspects of these sponsorships are integrated into orthopedic marketing initiatives throughout the year.
Jean Hitchcock Vice President,� Public Affairs and Marketing
MedStar Health
Columbia,� MD
410-772-6557
Marc BluesteinPresident
Aquarius Sports and Entertainment
Gaithersburg,� MD
240-547-3498
[email protected] 1IEG. “2013 Sponsorship Outlook: Spending Increase Is Double-edged Sword,” IEG Sponsorship Report®, January 7, 2013, http://www.sponsorship.com/iegsr/2013/01/07/2013-Sponsorship-Outlook--Spending- Increase-Is-Dou.aspx.
2Andrew E. Lincoln, ScD, et al., “Trends in Concussion Incidence in High School Sports: A Prospective 11-Year Study,” The American Journal of Sports Medicine 39 (May 2011): 958–963.
4 Spectrum | November-December 2013
Here are six questions to gauge your hospital’s level of crisis communication preparedness.
A Crisis Communicator’s Self-Assessment
By Patrick Donohue and Christopher Lukach
We all have that dream. You know the one: You’re back in high school, and you forgot to study for the big test. You wake up in a sweat with the sensation of a dumbbell in the pit of your stomach. It is, thankfully, a fleeting sensation, when you realize it was only a dream.
Far less fleeting, but not entirely dissimi-lar, is the feeling communicators have when
C O M M U N I C A T I O N
they are unprepared to navigate a crisis. We subscribe to a simple precept: While
a crisis may be unexpected, it should never come as a surprise. At St. Mary Medical Center in Langhorne, PA, crisis communi-cation has earned priority status among the communication and leadership teams. The success of our crisis communication program exists because of a top-level commitment to preparedness, regular updating, rigorous testing, and unrelenting energy.
Moreover, we have high expectations. At St. Mary Medical Center, we periodically ask ourselves six fundamental crisis-pre-paredness questions. Some are tactical, and some are cultural. Some rest solely with the
communicators; others test the strength of our multidisciplinary response team.
1. Does your organization have a crisis communication plan? That’s step one, and it’s a biggie. A strong scenario-based crisis communication plan based on prob-ability and risk is the ultimate, versatile crisis communication resource. For guid-ance on constructing a strong, actionable crisis communication plan, see the sidebar “Does Your Crisis Communication Plan Make the Grade?”
2. Do you have reasonable approval processes that permit you to com-municate quickly? In today’s demand-ing 24/7 media landscape, “quickly” is an understatement. Communica-tion must be nearly instantaneous to be effective. And it’s the first response to a crisis that sets the tone. For many modern crises, “living down” the first

November-December 2013 | Spectrum 5
statement lasts well beyond the event’s actual resolution. Communicators need to act quickly and without the delay of a lengthy approval process. The crisis communication plan helps this process by providing pre-approved, pre-vetted statements that reinforce your values without speculating. But communi-cators also need a certain amount of leeway. This leads us to the next step.
3. Do you have the authority and con-fidence to act in a crisis? Earning a “seat at the table” status is a persistent cultural challenge for hospital and health-system communicators. But hav-ing the ear and respect for administration is a “must” for a successful program of crisis preparedness and response. The confidence of your leadership team can be a challenge to cultivate. You earn your seat routinely when you provide
Does Your Crisis Communication Plan Make the Grade? A crisis communication plan is an essential tool in the healthcare communicators’ toolbox. Unfortunately, not every organization that has a crisis communication plan has a useful crisis communication manual. With today’s demanding media and social media landscapes, we do not have the luxury of hours or even minutes to formulate our first response. And as myriad modern crises have demonstrated, if we’re not quick to fill the vacuum of information, someone else will do it for us.
First, be clear about what is considered a “crisis.” A no brainer, right? Not necessarily. For your planning purposes, a crisis is any event that has the potential to negatively impact your reputation or ability to operate. So while your crisis communication plan needs to consider the conventional crises, such as natural disasters, terrorism, and on-site acts of violence, it must also include those “lesser” crises and issues that carry the potential for great impact: a mismanaged merger or acquisition; sudden change in leadership; OSHA or regulatory violations; poor performance in a quality and safety rating; an inadvertent release of patient-identifiable information, etc. Any of these incidents has the potential to come on suddenly and to impact the organization’s reputation and, therefore, its ability to operate.
Second, make sure your crisis plan has actionable information. Too many crisis communication plans are policy repositories filled with complicated processes rather than actionable work
plans. Our crisis communication plan philosophy is simple: if it doesn’t offer the necessary information and communication framework to respond within 15 minutes, it isn’t prepared to do its job. Remove speed bumps by getting the plan’s contents pre-approved by legal and administrative teams.
Third, make sure it is accessible. A well-designed plan is worthless if you can’t find it precisely when you need it. Security and confidentiality are important, but not if they undercut the plan’s accessibility. Following a recent, innocuous bomb threat to our hospital, our response was impacted because the administrative first responders were not clear about location of the nearest plan. Now, at St. Mary, aside from a “hard” copy with each member of the leadership team, we keep multiple hard copies near the command center and key locations, and a copy with the hospital’s switchboard operators. Modifiable, interactive, intranet and thumb-drive versions are also available to the communication team.
Fourth, train your crisis response team in using the plan, then offer periodic refresher trainings. Spotlight the resources within the plan: the roles and responsibilities of the crisis communication team and how the plan can be accessed. And, most important, regularly test the contents using complex and difficult scenarios. Bend them. Stretch them. Break them. In the end, your plan will be stronger, and your hospital best prepared to weather a storm.
counseling on a myriad of issues, demon-strating your clear and reasoned thinking and your broad understanding of the healthcare “business.” Leaders also like to know that you have tested experience and have been through some battles.
4. Are your spokespersons trained and ready? In a crisis, it is ideal to have a single, primary spokesperson to keep the messaging consistent. But different situations require different backgrounds, skill sets, and levels of authority. At St. Mary Medical Center, we maintain a stable of spokespersons comprising ex-ecutives (CEO, COO, CMO, and, of course, the marketing and communica-tions director) and technical experts (di-rector of security, director of quality and patient safety, CNO, CIO, HR director, foundation director, and vice president of mission). Each is trained to focus on
key messages in answering questions, and we provide periodic refresher train-ing. Even those organizational leaders who may not be “spokespersons” in the microphone-and-camera sense are trained in the fundamentals, ensuring internal and external messages are con-sistent. We reinforce the process through practice.
5. Can you access key systems during an unusual event? As with many hospitals and health systems along the Eastern seaboard, Superstorm Sandy impacted St. Mary. While stranded at home with-out power, much of our communication team was unable to access our network and, therefore, put into action our crisis communication plan. Ensure your team has back-up processes to access the major communication vehicles in the event of a
(Continued on page 10)

6 Spectrum | November-December 2013
Aligning Strategic Vision to Consumer Education and Culture through BrandFind out how one health system created a common identity that supported the sum of its many parts.
M A R K E T I N G
By Erinne Kovi Dyer
In today’s healthcare environ-ment, there is a great deal of change. With change comes confusion, drastic shifts in priorities, and a general lack of clarity as to how to operate. For some, the unknown leaves them paralyzed. For others, it accel-erates the pace of change. Yet, regardless of the pace, the destination remains unclear.
So what do we still have within our con-trol? The answer is our fundamentals, our core values, our operational models, and our people. With these elements, we can create our future and define what it is we want our consumers to understand about who we are and the value that we provide.
Carolinas HealthCare SystemAt Carolinas HealthCare System, we have a unique story to share.
As one of the largest public, not-for-profit integrated healthcare delivery systems in the country, we are working every day to connect and transform care delivery in the Southeast. Our overarching goal is to provide seamless access to coordinated, high quality health-care—and to provide that care closer to where patients live.
With 41 hospitals and 900-plus care lo-cations in the Carolinas and Georgia, the depth and breadth of services we provide result in a full continuum of integrated care. It includes prevention and wellness, primary care at more than 180 locations, specialty care via several nationally recognized service lines, and one of the largest virtual programs in the nation. With more than 50 disease-specific certifications from The Joint Commission, we have one of the highest certification totals in the country among comparable systems.
As a system, we have more than 7,800 licensed beds, and in 2012 had more than
10.5 million patient encounters. We have more than 3,000 system-employed physi-cians, 14,000 nurses, and 60,000 employees. In 2012, we had more than $8 billion in annual revenue and generated $1.25 billion in community benefit.
Despite our depth, breadth, and clinical excellence, Carolinas HealthCare System has remained “one of the best kept secrets in healthcare.” Consequently, our senior leaders have made a strong commitment to better educate consumers as to who we are and how we can provide value to them.
To do this, we needed first to re-evaluate our corporate vision. At the same time, we knew that the organization needed a stronger sense of common identity, one that would have unifying power and enable us to move more quickly from good to great.
A New Day We embarked on a journey and emerged with a new strategic vision: “To be recog-nized nationally as a leader in the transfor-mation of healthcare delivery and chosen for the quality and value of services we provide.”
We have taken this vision to heart and have committed to achieve it through the development of a single unified enterprise. In every area of our business, we have fo-cused on developing enduring relationships with patients, based on superior personalized service and high quality outcomes—at every location, with every encounter, every time.
Seth Godin, author and entrepreneur, defines brand as “the set of expectations, memories, stories and relationships that, taken together, account for a consumer’s decision to choose one product or service over another.” In other words, brand = culture + experience.
The culture of an organization and the experiences of its employees and patients drive and define the brand.
There are several successful healthcare systems that have seen opportunity in uni-fying under one brand and one name as
they restructured their business model to enhance customer value. Cleveland Clinic, Mayo Clinic, and Dignity Health are just a few of these. The successes of these brands lies in their ability to transcend the parts of their organizations and build a unified belief or “impression” of their system among everyone it touches.
Carolinas HealthCare System is no dif-ferent. Like many systems that have “grown up” over the past 30 years, we have been built on a foundation of growth and integration both in the acute and ambulatory spaces. Although this growth lends itself naturally to better coordination and integration, we had not focused enough on understanding how complex this “house of brands” ap-peared to our patients and communities, especially in a time of extreme industry change and public confusion.
So we started with a new vision and began our brand journey.
Figure 1: Brand Manifesto
November-December 2013 | Spectrum 7
Defining the Brand: Getting to “One”There were several key differentiators that we knew we could take advantage of to meet our new vision. However, our most distinctive feature is our comprehensiveness and connectedness across a dense geogra-phy. Through a network of 900-plus care locations in three states, we knew we could provide access at every point of care across the continuum, with the highest level of quality, in a unique way.
Our Corporate Communications, Mar-keting and Outreach department was tasked
of confusion about who we were and what defined us and our value to our patients and the greater community.
What we uncovered was the widespread perception that Carolinas HealthCare System was everything but unified. We were seen as an amalgamation of many individual parts, many showcased with individual identities that had little connection to the master brand.
To become a nationally-recognized healthcare system, we had to (re)define what integrated care at Carolinas Health-Care System looked like.
Becoming “One” We created and evaluat-ed several concepts, and for the final campaign theme to introduce our master re-brand, we chose “One.”
To initiate the campaign design, we had to create a unify-ing and conceptual manifesto that helped define and position us as an integrated, connected organiza-tion working to im-prove the care of every patient (Figure 1).
We focused on four core principles: one sys-
tem, one team, one belief, and one mission.“One. Built for everyone, From the
knowledge of many, To bring health to all.” We then built a multi-channel strategy
to share this identity.
Measuring the BrandThe overall plan will roll out in many phases, and at this point we have only just begun. Nonetheless, through a strong initial launch in outdoor, broadcast, radio, and collateral media, we have laid a strong foundation.
To measure success, we were initially in-terested in “awareness” as a key indicator. And while awareness is important, we real-ized that in today’s competitive healthcare landscape, awareness alone is not enough. We knew we had to measure a deeper un-derstanding of brand attributes.
Taking a more innovative approach, we analyze our brand “health” in identified geographies and measure additional items,
such as an understanding of “connected-ness” and level of “trust” and belief in our ability to provide higher “quality.”
Only six months in, we have seen in-cremental lifts in both un-aided and aided brand awareness, as well as some key brand health attributes.
Internally, adoption has been nothing short of amazing. The message of “One” has clearly resonated through language, executive adoption of the concept, and its reiteration through all internal communica-tions channels (Figure 2).
Next StepsWhile we have been pleased with the ini-tial launch of the campaign, we have yet to fully transition our enterprise assets to the brand name, color, and signage require-ments. Healthcare is a complex industry, and there are many legal and regulatory requirements that directly impact the brand and its success.
For example, many of our facilities are not currently licensed under our formal name, and this affects our transition to uniform signage throughout the system. So while we would like to use the brand name, we are unable to do so until we formally re-file under the new name.
To summarize, the master re-branding and campaign launch provided an oppor-tunity for a “fresh” start—an opportunity to (re)define how our system provides care and to embed a new and important mindset into the corporate culture.
The campaign has also allowed us the opportunity to educate consumers and our own employees regarding complex concepts in healthcare, particularly during a time of rapid and profound change in our industry. And we are far from done. Over the next 18 months, we are going to continue refining our messages, focusing on what we do dif-ferently as a system, and earning the trust of our consumers, patients, and communities. Our future depends on it.
Erinne Kovi Dyer Corporate Vice President
Corporate Communications,�
Marketing & Outreach
Carolinas HealthCare System
Charlotte,� NC
704-631-0951
Figure 2: Internal Portal Screenshot
with helping to re-define the culture of the organization through a master re-branding effort and an accompanying campaign rollout. We had to get to know the orga-nization, and fast.
Together with our agency of record, Campbell Ewald, we embarked on a commu-nications evaluation, while gaining buy-in and support from key internal stakeholders. We performed interviews with more than 90 leaders throughout the system, administra-tive and clinical, to ensure we understood the full scope of the organization’s culture.
There was one major surprise—the many shared beliefs about the state of the system and its goals. So “unity of vision” was actu-ally the easy part.
We then had to understand how the external world understood and perceived Carolinas HealthCare System. This was the hard part, but findings validated our original suspicion: There was a great deal

8 Spectrum | November-December 2013
S T R A T E G Y
By Monica L. Carbajal and Daniel B. Walter
The Affordable Care Act,� accountable care organizations (ACOs), bundled payments, population health management, and all of the other major healthcare initiatives currently underway are clearly changing the way organizations pro-vide service. While many health systems are evaluating their IT systems, clinical service lines, and physician alignment strategies, one critical component that is often over-looked is the post-acute care continuum. Unfortu-nately, this may be a costly mistake. Although post-acute care is not as high profile as many other service offerings, the fact remains that effective post-acute programs will be needed more than ever to manage the highest acu-ity patients in any of the emerging shared-risk financial models.
What Is Post-acute Care?By definition, post-acute programs are those that patients may need to access following their discharge from acute care. These are usually patients that no longer meet con-tinuing stay criteria for acute care, but who are either not stable enough to return home or have ongoing clinical needs that are too great to be managed on an outpatient basis. Historically, Medicare has defined post-acute care as skilled nursing care (SNF), inpatient acute rehabilitation, long-term acute care (LTCH), and home health care. (Medicare does not include hospice in its traditional definition of post-acute care; however, many
Creating a Winning Post-acute Care Continuum for the FutureMemorial Hermann Health System demonstrates that creating the most effective post-acute continuum requires a thoughtful process that is no different than creating an integrated service line for any clinical service.
in the industry do include hospice in this definition because of the close link between home health and hospice.)
Although post-acute programs admit many patient types, because older popula-tions tend to recover more slowly and have more chronic conditions than younger populations, the most frequent users of all post-acute programs include Medicare and Medicare Advantage patients. In fact, Medi-care and Medicare Advantage patient popula-tions generally represent 60 to 65 percent of all post-acute admissions. The second largest group tends to be the high acuity (and high risk) catastrophic patients and/or patients with multiple systems failures. These patient populations generally incur long acute care lengths of stay and have multiple clinical or functional needs upon discharge that prevent them from achieving their desired level of independence.
Market SizeMany health systems consider post-acute care programs to be “one off,” since they are typically small compared to the marquee service lines of cardiology, orthopedics, or oncology. In fact, far more patients need to access post-acute programs than most health system executives realize. Figure 1 shows that about 40 percent of all Medicare acute care discharges will need to access some level of post-acute care upon discharge. Additionally, best practice referral patterns among those providers that have most effectively inte-grated their acute care and post-acute care continuums suggest that up to 50 percent of all Medicare acute care discharges will require post-acute care! This, of course, is in addition to patients from all other payer sources that may also require post-acute care.
While the data in Figure 1 estimate the demand for post-acute care under current fee-for-service (FFS) models, recent analy-ses of several local markets with high pen-etrations of Medicare Advantage programs
suggest that, as providers assume more finan-cial risk for patients, the utilization of post-acute programs will remain at approximately the same levels as the current national data. In these markets, while the use of higher cost services, such as long-term care and acute rehabilitation are less than current FFS use rates in Figure 1, the utilization of lower cost services (home care in particular) are substan-tively higher. The total use of post-acute care in these markets is between 40 to 50 percent of all Medicare Advantage discharges, indicat-ing that the demand for these programs will remain high, even as reimbursement models shift and providers assume greater risk.
The Burning Platform for Post-acute CareMany health systems are beginning to eval-uate their post-acute continuum today for several reasons. First, as previously discussed, the demand for post-acute care is high, and it is expected to remain high as the healthcare landscape evolves. Second, with an episode of care that extends 30–90 or more days beyond the acute care stay, health systems are able to measurably improve patient clinical and functional outcomes over a longer period of time with post-acute services. Finally, there is recognition that as health systems assume more financial risk for clinical performance over a longer period of time, owning or hav-ing some control over these programs will be critical to the success of the organiza-tion. Figure 2 provides a summary of the most recent Medicare operating margins for each level of care.
Pulling It TogetherCreating the most effective post-acute con-tinuum requires a thoughtful process that is no different than creating an integrated service line for any clinical service. It requires the input and support of the medical staff, the executive leadership, case management, financial services, and multiple clinical and ancillary services. The key steps in this pro-cess should include the following.
●● Market assessment. Since most post-acute patients originate from the acute care setting, it is important to know how many patients from the target health system require post-acute care today and what the demand is by diagnosis. Addi-tionally, providers must understand how this demand will shift under shared-risk

November-December 2013 | Spectrum 9
Discharge All Best Practices2
Disposition Medicare1 Low HighInpatient Rehab 3.2% 4.0% 6.0%
SNF 17.3% 12.0% 15.0%
HHA 16.0% 22.0% 24.0%
LTCH 1.0% 1.5% 2.0%
Hospice 2.1% 2.5% 3.0%
Total 39.6% 42.0% 50.0%
Level of Care Payment Basis Est. Margin
Inpatient Rehab • CMG• Per Discharge 8.0%
SNF • RUG Payment• Per Diem 14.6%2
HHA • HHRG• 60-day Episode 13.7%
LTCH • LTCH-DRG• Per Discharge 4.8%
Hospice • Per Diem 5.1%
1MedPAC June 2008 Annual Date Book.2Walter Consulting.
1MedPAC March 2013 Report to Congress.2Freestanding SNFs only; does not include HB-SNFs.
financial models, including population health management models.
●● Quality evaluation. A comprehensive assessment should consider the ability to improve the quality of patient care by implementing a plan of care that includes a potential referral to post-acute services. The impact on quality should then be measured through lower readmission rates, improved clinical and functional status, higher discharge rates to the com-munity, and other similar benchmarks.
●● Financial analysis. The financial analysis should assess both short-term and long-term financial impacts to the system. Pro-viders should understand the economic benefit of establishing or growing certain programs today, including the impact of reduced acute care length-of-stay. Providers should also assess the opportunity cost of not having these programs in the future, including increased utilization of acute care services if post-acute care is not available.
●● Build or buy. While the bias for many sys-tems is to own their post-acute programs, for many systems, the best solution may be to partner with existing community pro-viders. The correct approach will depend upon the critical mass of patients needing these services, the anticipated financial return, the capital cost required, potential Certificate-of-Need (CON) limitations, and other important factors.
●● Organizational structure. Too many organizations have failed in their imple-mentation due to less than effective orga-nizational structures. Although all parties may want the same outcome, without ac-countabilities for medical staff, post-acute
program managers, acute care case man-agers, and other staff, the risk of failure becomes far too great.
Creating the Foundation for SuccessMemorial Hermann Health System (MHHS) is a large 12-hospital system in Houston, Tex-as, that discharges approximately 125,000 patients annually. In addition to its acute care services, MHHS includes two acute rehabilitation hospitals, four hospital-based rehabilitation units, skilled care, and home health and hospice services.
In 2011, the leadership of MHHS decided to complete a post-acute strategic plan, to ensure that the organization was best posi-tioned for the new healthcare landscape for all of its programs and services. The key goals of the process were to:
●● Ensure through-put efficiencies for both acute care and post-acute care
●● Ensure patient placement in the most ap-propriate level of post-acute care
●● Capture all potential referrals available under current systems
●● Minimize outmigration
●● Understand network adequacy for these programs
The planning team included representa-tives from senior leadership, planning, fi-nance, case management, medical staff, and each of the post-acute programs. During the planning process, the team recognized that while today, under FFS reimbursement, the health system assumed little financial risk if patients did not stay within the system, or went to a post-acute program that might
be more intense than actually needed, these practice patterns would need to change as MHHS assumed greater financial risk under ACOs and other risk-sharing models.
As a result of this planning effort, MHHS changed its organization structure to ensure appropriate accountabilities for program development, referral manage-ment, clinical outcomes, and financial performance. Metrics have been established to monitor actual performance compared to the plan, with reviews conducted on a quarterly basis. While the health system envisions even tighter integration in the fu-ture, the foundation has been put in place to strengthen the post-acute continuum as the environment continues to change.
Like MHHS, many health systems are seeing a need to re-think their post-acute service offerings. While many systems will find significant opportunities in today’s en-vironment, the real opportunity is putting into place a post-acute continuum that can best serve the health system and its affiliates under any and all of the shared-risk finan-cial models that will dominate the future healthcare landscape.
Monica L. CarbajalDirector Strategic Planning
Memorial Hermann Health System
Houston,� TX
713-242-4791
Daniel B. WalterSenior Principal
Walter Consulting
Atlanta,� GA
404-636-9700
Figure 1: Medicare National Post-acute Utilization Rates
Figure 2: Estimated FY 2012 Medicare Post-acute Operating Margins1

10 Spectrum | November-December 2013
SHSMD DatebookJanuary 2014: Futurescan 2014 released
October 12–15, 2014: “Connections 2014,” SHSMD’s Annual Educational Conference and Exhibits, San Diego, CA
For more information on these and other professional development opportunities, go to www.shsmd.org.
The SHSMD AdvantageContinuing its commitment to providing members with practical, timely resources, SHSMD has just released the 2014 Calendar of Health Observances & Recognition Days. The easy-to-navigate online calendar—back in PDF format—gives you quick, convenient access to the dates and descriptions of more than 250 health-related observances. It’s perfect for planning 2014 health fairs, community outreach programs, and employee recognition events. Member login is all that’s required to access this great benefit of your SHSMD membership. 2014 will be here before you know it, so visit www.shsmd.org/calendar, and start planning today.
severe incident. This could mean any-thing from home generators, to mobile tethering software (to access the Internet from your mobile device), to a simple list of local libraries with internet access. Or, designate a representative to staff the hospital command center, where generator access to power should be uninterrupted. And, as if we needed it, here’s another way social media changes the game — your hospital’s Facebook and Twitter presence may be all you are able to access with limited power and mobile access. Use them.
6. Do you have the plans and policies to monitor and respond to social media? St. Mary and Anne Klein Communica-tions Group developed a proprietary and focused Social Media Crisis Communi-cation Plan to complement the hospital’s broader crisis plan. Beyond assigning team responsibilities, the plan takes the guesswork out of social media activity, assigning an “if-this-then-this” workflow strategy to evaluate influence and risk.
If you answered “yes” to these questions, you are ready. (Be sure you update your cri-sis preparedness plan at least yearly.) If you are in doubt regarding the answers to these questions, it’s time to take a hard look at your crisis preparedness strategy. And if you
answered, “no,” then it’s time to have a heart-to-heart talk with your CEO.
Patrick DonohueMarketing & Communications Director
St. Mary Medical Center
Langhorne,� PA
215-710-6908
Christopher Lukach, APRSenior Vice President and COO
Anne Klein Communications
Group,� LLC
Mount Laurel,� NJ
856-866-0411 ext. 15
A Crisis Communicator’s Self-Assessment(continued from page 5)

November-December 2013 | Spectrum 11
By Rick Wade
“Wade,� that is ab-solutely the goofiest thing I have ever read. If you’re going to write these so-called case studies, at least come up with stuff slightly in
the realm of reality!”The voice on the phone was an old
friend, a senior executive in marketing and communications for a major health system with a renowned academic medical center as its flagship. She was calling about one of the early “Tightrope Walker” columns … a story about a pile-up of conflicts of interest in a mid-size, Midwestern medical center.
“But it’s a true story,” I shot back before she could continue. “I masked the names and some details that might give the hos-pital away, but it actually happened.”
“No?” “Yes!”The following month I got a call from
the CEO of a rural hospital who accused me of having a “mole” inside his organiza-tion. It seems that a scenario about physi-cian recruitment gone awry mirrored a mess he had to clean up several months earlier.
The majority of “Tightrope Walker” col-umns over the past four years were rooted in events that I encountered during my 18 years as AHA’s senior communications officer. I was often directly involved as a counselor to the hospitals and health systems as they dealt with sticky situations in communications, patient privacy, community trust, mergers and acquisitions, screwy marketing, mis-leading advertising and, well, you name it. Some other column
Stranger than Fiction…T H E T I G H T R O P E W A L K E R
to everyone who sees it—about the com-passion, mission, and ethic of the people and place behind it.
Job One—earning and keeping the public’s trust and confidence is paramount.
Throughout the years I have watched many hospital and health systems’ pro-fessionals in communications, marketing, strategic planning, and similar disciplines be the leaders in ensuring their organiza-tions “did the right thing” when confront-ed with tough ethical and management decisions. Yes, they are part of the “team,” but their jobs compel them to probe, un-derstand, and respect the hospital’s singular role in the lives, hearts, and minds of its community in a way that others may not. They spoke as the conscience of the institu-tion and a steward of its reputation. They made the difference.
The pace and depth of change in health-care today is breathtaking. I suspect the fu-ture will bring clinical and corporate moral and ethical issues that will make some of the things I’ve written about seem simple.
You can be on the tightrope if you want to be, influencing the future of one of your community’s most impor-tant cornerstones—and ensuring that it keeps the promise symbolized by the blue and white “H.”
Stay on the tightrope … and thank you.
Editor’s note: On behalf of SHSMD, I thank Rick Wade for the wisdom, insight, and wit that he has shared with Spectrum readers over the last four years. Beginning with the January/February issue, Spectrum will feature select Q&A’s from the Society’s online communities. — Mary P. Campbell
cases came from professionals in the field who shared their experiences and the pain-ful choices that often came with them.
Spectrum will be changing over the next several months with new content and ap-proaches to the issues and challenges you face. It’s new editor, Mary Campbell, and I have agreed to retire the column. Good publications are like cities—they are not meant to stay the same. They change and rebuild with the times.
While I enjoyed writing the column, the real pleasure was the learning I gained from your responses, both directly and in the poll that accompanied each scenario. There never was unanimous agreement among the choices offered and respondents often checked the “other” box, indicating that another solution was possible even if they couldn’t quite articulate it.
AHA President Emeritus Dick David-son often reminded staff and members that “every failure of our society eventually ends up at the hospital door and every human trait, both good and bad, can be found inside.” Hospitals are the places that re-ceive and care for the victims of poverty, violence, substance abuse, and crime. They deal with our inability to care for our most vulnerable people, lack of basic health ser-vices in the community, and the illnesses and injuries that come with life itself.
Hospitals also are where a community’s most skilled and compassion-ate women and men work long
hours under emotionally and physically stressful conditions.
Everything they do has an impact on the lives around them. And every
hospital is a powerful economic and cul-tural influence on the area it serves. It generates jobs and supports dozens of businesses. What it says and how it behaves can make people deeply proud or ashamed.
The blue and white “H” sign along America’s
highways and streets holds out a host
of promises
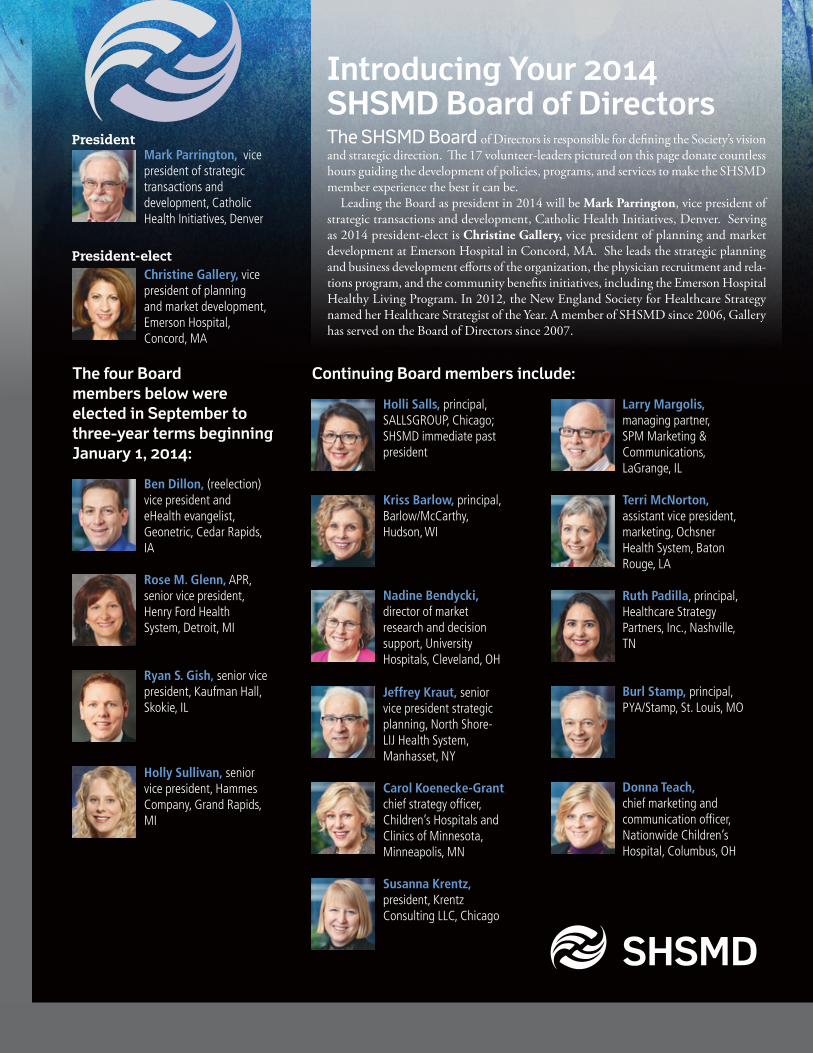
Introducing Your 2014 SHSMD Board of DirectorsThe SHSMD Board of Directors is responsible for defining the Society’s vision and strategic direction. The 17 volunteer-leaders pictured on this page donate countless hours guiding the development of policies, programs, and services to make the SHSMD member experience the best it can be.
Leading the Board as president in 2014 will be Mark Parrington, vice president of strategic transactions and development, Catholic Health Initiatives, Denver. Serving as 2014 president-elect is Christine Gallery, vice president of planning and market development at Emerson Hospital in Concord, MA. She leads the strategic planning and business development efforts of the organization, the physician recruitment and rela-tions program, and the community benefits initiatives, including the Emerson Hospital Healthy Living Program. In 2012, the New England Society for Healthcare Strategy named her Healthcare Strategist of the Year. A member of SHSMD since 2006, Gallery has served on the Board of Directors since 2007.
Continuing Board members include:
Ben Dillon, (reelection) vice president and eHealth evangelist, Geonetric, Cedar Rapids, IA
Rose M. Glenn, APR, senior vice president, Henry Ford Health System, Detroit, MI
Ryan S. Gish, senior vice president, Kaufman Hall, Skokie, IL
Holly Sullivan, senior vice president, Hammes Company, Grand Rapids, MI
SHSMD
Holli Salls, principal, SALLSGROUP, Chicago; SHSMD immediate past president
Kriss Barlow, principal, Barlow/McCarthy, Hudson, WI
Nadine Bendycki, director of market research and decision support, University Hospitals, Cleveland, OH
Jeffrey Kraut, senior vice president strategic planning, North Shore-LIJ Health System, Manhasset, NY
Carol Koenecke-Grant, chief strategy officer, Children’s Hospitals and Clinics of Minnesota, Minneapolis, MN
Susanna Krentz, president, Krentz Consulting LLC, Chicago
Larry Margolis, managing partner, SPM Marketing & Communications, LaGrange, IL
Terri McNorton, assistant vice president, marketing, Ochsner Health System, Baton Rouge, LA
Ruth Padilla, principal, Healthcare Strategy Partners, Inc., Nashville, TN
Burl Stamp, principal, PYA/Stamp, St. Louis, MO
Donna Teach, chief marketing and communication officer, Nationwide Children’s Hospital, Columbus, OH
The four Board members below were elected in September to three-year terms beginning January 1, 2014:
Mark Parrington, vice president of strategic transactions and development, Catholic Health Initiatives, Denver
Christine Gallery, vice president of planning and market development, Emerson Hospital, Concord, MA
President
President-elect
Related Documents











