Non-Communicable Diseases: Malaysia in Global Public Health Feisul Idzwan Mustapha MBBS, MPH, AM(M) Public Health Physician, NCD Section, Disease Control Division Ministry of Health, Malaysia NIH Research Week 2014, CME Session 26 November 2014 Kuala Lumpur [email protected] Ministry of Health Malaysia

Non-Communicable Diseases: Malaysia in Global Public Health
Jul 13, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Non-Communicable Diseases:Malaysia in Global Public
Health
Feisul Idzwan Mustapha MBBS, MPH, AM(M)
Public Health Physician, NCD Section, Disease Control DivisionMinistry of Health, Malaysia
NIH Research Week 2014, CME Session26 November 2014
Kuala Lumpur
Ministry of Health
Malaysia

Engagement of Non-State Actors
2
Photos courtesy of PublicAffairsAsia
SharingValueAsia Summit, 9 October 2014, Singapore:“Unlocking the Value of
Government: New Approaches
for Policymakers”

Engagement of Non-State Actors
3
Photos courtesy of PublicAffairsAsia
• What considerations should government abide by when collaborating with businesses?
• How do I expect multi-stakeholder collaborations to change the role of government in coming decades?
• How should collaborative mechanisms best be insulated from changes of government that may affect policy? • Can Malaysia play an active role
in global public health in the context of WHO’s work in engagement of non-State actors?
• What can the private sector do if governments are not receptive to collaborative work?
4
Source of icons: World Heart Federation Champion Advocates Programme
Global NCD
Targets

Proportional mortality, Malaysia (% of total deaths, all ages, both sexes)
5

Premature mortality due to NCDs, Malaysia
6
The probability of dying between ages 30 and 70 years from the 4 main NCDs is 20%

DALYs attributable to risk factors
7
10.8%
10.7%
9.0%
8.3%
5.2%
4.3%
3.1%
0.7%
0.1%
10.8%
0.7%
11.4%
12.1%
5.1%
0.9%
4.3%
0.7%
0.1%
15.0% 10.0% 5.0% 0.0% 5.0% 10.0% 15.0%
High BP
Tobacco
Diabetes Mellitus
High BMI
High Cholesterol
Alcohol
Physical Inactivity
Underweight
Poor Water & Sanitation
Male Female
Burden of Disease Study Malaysia 2008, slide courtesy of Dr Mohd. Azahadi Omar, Institute for Public Health
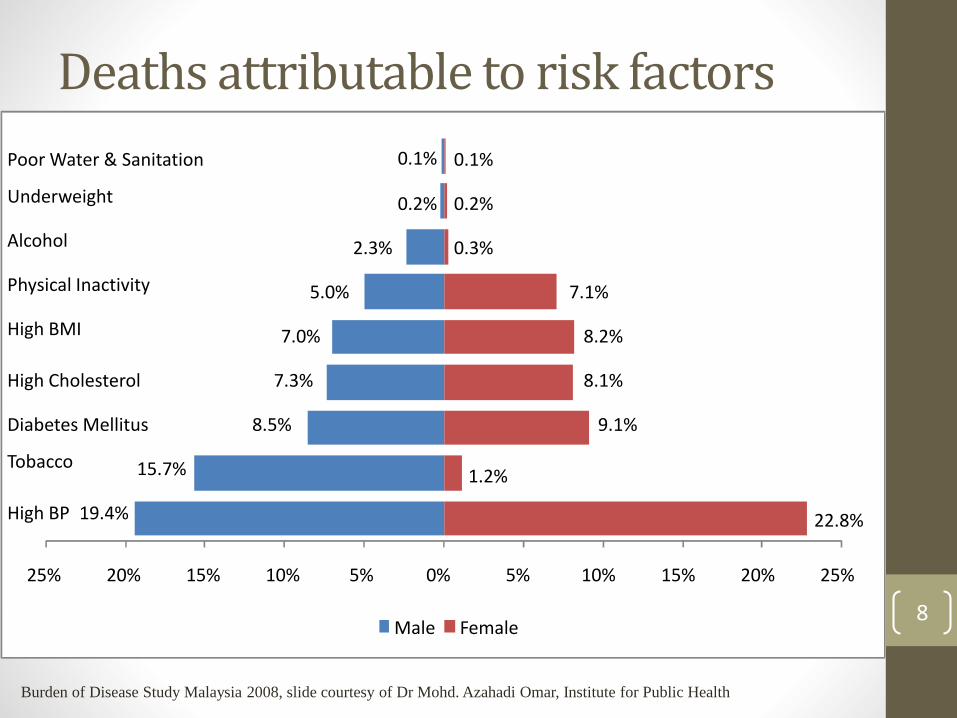
19.4%
15.7%
8.5%
7.3%
7.0%
5.0%
2.3%
0.2%
0.1%
22.8%
1.2%
9.1%
8.1%
8.2%
7.1%
0.3%
0.2%
0.1%
25% 20% 15% 10% 5% 0% 5% 10% 15% 20% 25%
High BP
Tobacco
Diabetes Mellitus
High Cholesterol
High BMI
Physical Inactivity
Alcohol
Underweight
Poor Water & Sanitation
Male Female
Deaths attributable to risk factors
Burden of Disease Study Malaysia 2008, slide courtesy of Dr Mohd. Azahadi Omar, Institute for Public Health
8
9
Source of icons: World Heart Federation Champion Advocates Programme
Global NCD
Targets
10
65th World Health
Assembly (May 2012):
Decided to adopt a global target of a 25% reduction in premature mortality from NCD by 2025.
66th World Health Assembly (May 2013):
Adoption of the Global Action plan for the Prevention and Control of NCDs (2013-2020), including 25 NCD indicators with 9 voluntary global targets.
11

First High-level Meeting on NCDs (New York, 19-20 September 2011)
2011
Second high-level Meeting on NCDs (New York, 10-11 July 2014) to take stock of the progress made since 2011
2014
Third High-level Meeting on NCDs to report on progress achieved since 2014
2018
Outcome Document of the 2014 UN General Assembly High-level Meeting on NCDs
12
Slide courtesy of Dr Shin Hai-rim, WHO Western Pacific Region Office

2014 UN Outcome Document on NCDs(resolution A/RES/68/300)
• Bottom line: Governments committed themselves to intensify their efforts towards a world free of the avoidable burden of NCDs
• Moving forward: Maps out a set of concrete national commitments to be implemented between 2014 and 2018, and provides 3 new global assignments
• Towards the world we want: Next milestone in 2018
13
Slide courtesy of Dr Shin Hai-rim, WHO Western Pacific Region Office

National commitments included in the 2014 UN Outcome Document on NCDs
By 2015, consider setting national targets for NCDs
By 2015, consider developing national multisectoral policies and plans
Integrate NCDs into health-planning and national development plans
By 2016, implement "best buys" to reduce risk factors for NCDs
By 2016, implement "best buys" to enable health systems to respond
Strengthen national surveillance systems
14
Slide courtesy of Dr Shin Hai-rim, WHO Western Pacific Region Office

Global assignments included in the 2014 UN Outcome Document on NCDs
By 2015, WHO to develop an approach to register and publish contributions of non-State actors towards the 9 global NCD targets
WHA68: Framework for country action to mobilize sectors beyond health
OECD/DAC: Purpose code to track development assistance for NCDs
By 2017, WHO to submit a progress report to UN General Assembly
By 2018, UN General Assembly to convene a third High-level Meeting
15
Slide courtesy of Dr Shin Hai-rim, WHO Western Pacific Region Office
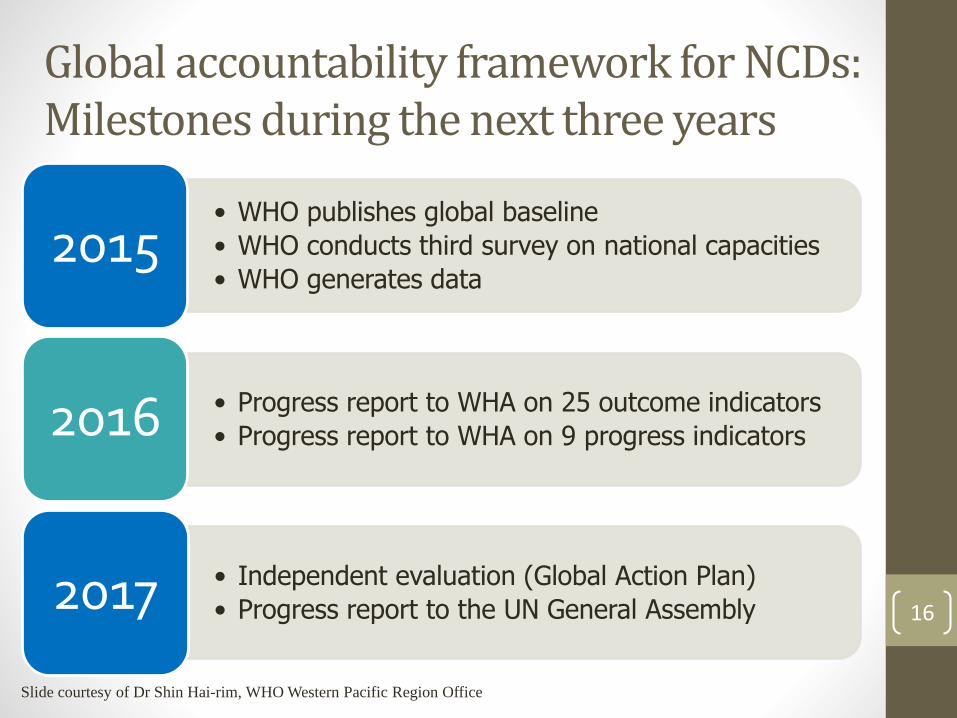
Global accountability framework for NCDs:Milestones during the next three years
• WHO publishes global baseline
• WHO conducts third survey on national capacities
• WHO generates data2015
• Progress report to WHA on 25 outcome indicators
• Progress report to WHA on 9 progress indicators2016
• Independent evaluation (Global Action Plan)
• Progress report to the UN General Assembly2017 16
Slide courtesy of Dr Shin Hai-rim, WHO Western Pacific Region Office
NCDs in the post-2015 development agenda: Towards the world we want
• 10 September 2014: Member States welcomed the report of the Open Working Group of the UN General Assembly on Sustainable Development Goals
• Next 12 months: Proposal shall be the main basis for integrating sustainable development goals into the post-2015 development agenda
• Target 3.4: By 2030 reduce by one-third pre-mature mortality from NCDs through prevention and treatment, and promote mental health and well-being
17
Slide courtesy of Dr Shin Hai-rim, WHO Western Pacific Region Office
18
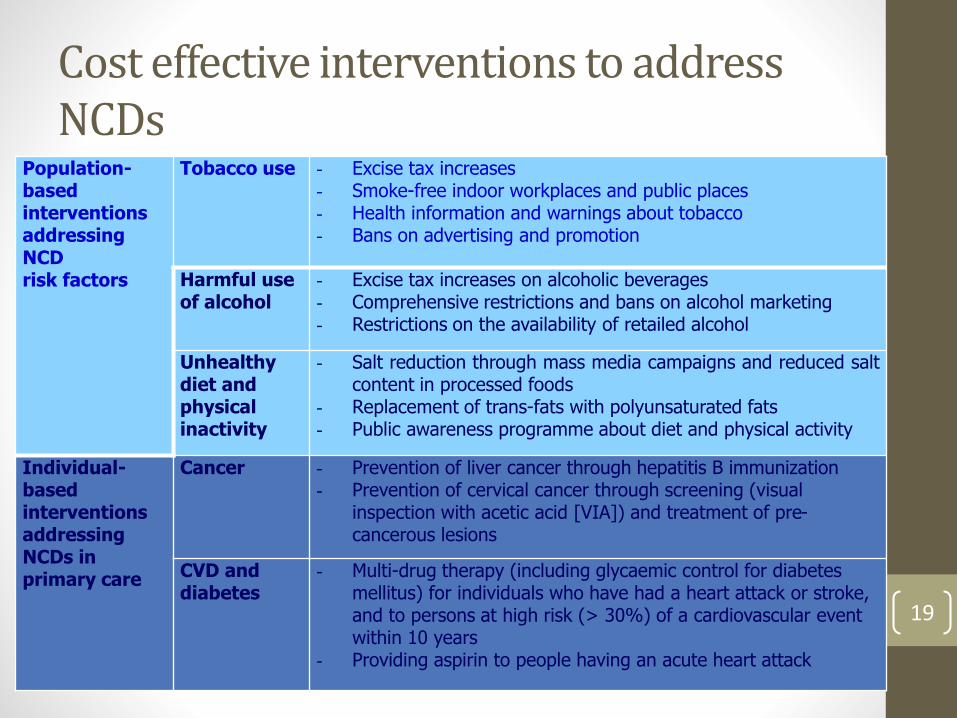
Cost effective interventions to address NCDs
Population-based interventions addressing NCD risk factors
Tobacco use - Excise tax increases- Smoke-free indoor workplaces and public places- Health information and warnings about tobacco- Bans on advertising and promotion
Harmful use of alcohol
- Excise tax increases on alcoholic beverages- Comprehensive restrictions and bans on alcohol marketing- Restrictions on the availability of retailed alcohol
Unhealthy diet and physical inactivity
- Salt reduction through mass media campaigns and reduced saltcontent in processed foods
- Replacement of trans-fats with polyunsaturated fats- Public awareness programme about diet and physical activity
Individual-based interventionsaddressing NCDs in primary care
Cancer - Prevention of liver cancer through hepatitis B immunization- Prevention of cervical cancer through screening (visual
inspection with acetic acid [VIA]) and treatment of pre-cancerous lesions
CVD and diabetes
- Multi-drug therapy (including glycaemic control for diabetes mellitus) for individuals who have had a heart attack or stroke, and to persons at high risk (> 30%) of a cardiovascular event within 10 years
- Providing aspirin to people having an acute heart attack
19

Cost effective NCD interventions…
• What works, what can we afford, and what should we adopt?
• The challenge? Identify interventions that:• are effective;• can lead to measurable declines in NCD death rates
quickly (e.g. over 10 years);• are affordable; and• can easily be implemented and sustained.
The Lancet. December 8, 2007 Volume 370:Gaziano T, Galea G and Reddy K. Scaling up interventions for chronic disease prevention: the evidence. pp 1939-1946.
The Lancet. December 15, 2007. Volume 370:Asaria P, Crisholm D, Mathers C, Ezzati M, Beaglehole R. Chronic disease prevention: health effects and financial costs of strategies to reduce salt intake and control tobacco use. pp 2044-2053.Lim S, et. al. Prevention of cardiovascular disease in high-risk individuals in low-income and middle-income countries: health effects and costs. pp 2054-2061.
20

2000
2001-03
2004-06
2008
2009-11
Healthy Islands Initiative WPDD Call for Action on Obesity ControlRegional plan for integrated CVD and Diabetes Prevention 1998-2003
Regional Tobacco action plan FCTC implementationRegional NCD STEP Surveys
Healthy Cities Initiatives addressing NCD and tobaccoNCD & Poverty: Pro-Poor Strategy 2006
Regional Action plans for NCD Regional Strategy to ReduceAlcohol related harm
Regional Initiative on multi-sectoralintervention for NCD prevention: Obesity Strategy & programme: Breast/cervical cancer control
2012National multisectoral plansMarketing of foods/ NCD and PHC/Surveillance
2013 Cancer Leadership and LeAd-NCDRegional action plan (2014-2020)
2014NCD knowledge net work2nd Lead NCDNCD surveillance
WHO Regional Response
21
Slide courtesy of Dr Shin Hai-rim, WHO Western Pacific Region Office

National Strategic Plan for
Non-Communicable Diseases
(NSP-NCD) 2010-2014
• Presented and approved by the Cabinet on 17
December 2010.
• Provides the framework for strengthening NCD
prevention & control program in Malaysia.
• Adopts the “whole-of-government” and
“whole-of-society approach”.
• Diabetes & obesity are used as the entry
points.
Seven Strategies:1. Prevention and
Promotion
2. Clinical Management
3. Increasing Patient
Compliance
4. Action with NGOs,
Professional Bodies &
Other Stakeholders
5. Monitoring, Research
and Surveillance
6. Capacity Building
7. Policy and Regulatory
interventions
22

Strategy 7 NSP-NCD: Policy & Regulatory Interventions• Main thrust of NSP-NCD
• Health promotion and education will increase awareness and knowledge
• However changes in behaviour is strongly influenced by our living environment
Awareness KnowledgeBehavioural
Change
Supportive living environment
Health promotion & educations
Policies & regulations23

The Great Prevention Debate
Personal choice
versus
government responsibility
24

Personal Choice is Important
25

BUT … If we want people to make healthy choices we have to make healthy choices available, accessible and affordable
26
Prevention is BOTH a personal and
government responsibility
27
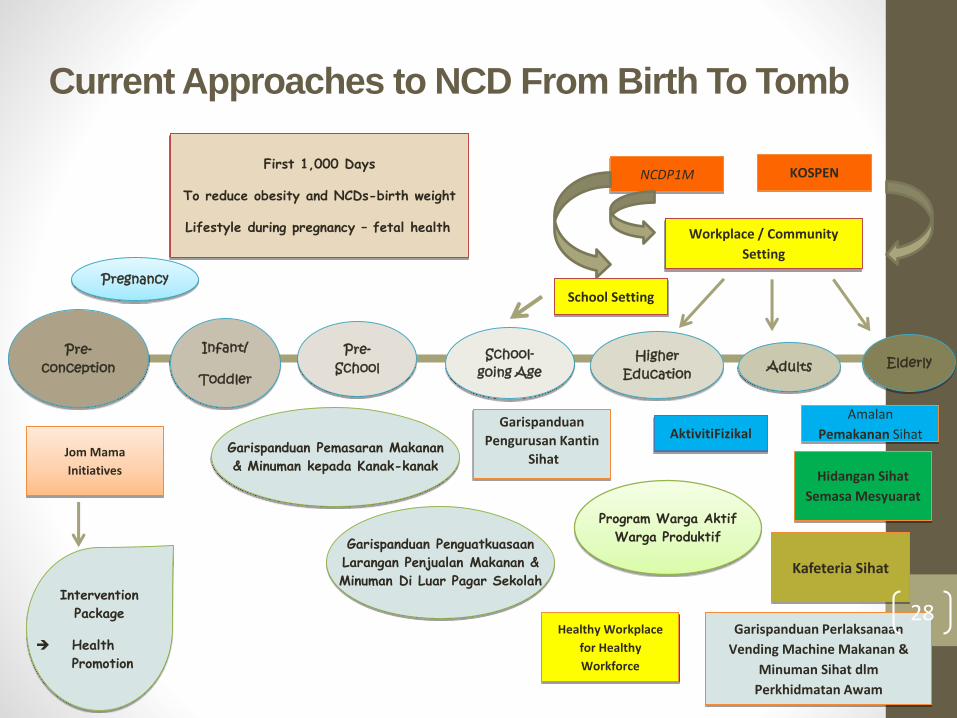
Current Approaches to NCD From Birth To Tomb
Intervention
Package
Health
Promotion
Pregnancy
Pre-conception
Infant/
Toddler
First 1,000 Days
To reduce obesity and NCDs-birth weight
Lifestyle during pregnancy – fetal health
Pre-School
School-going Age
Garispanduan Pemasaran Makanan
& Minuman kepada Kanak-kanak
Garispanduan Penguatkuasaan
Larangan Penjualan Makanan &
Minuman Di Luar Pagar Sekolah
Higher Education Adults Elderly
School Setting
NCDP1M
Workplace / Community
Setting
KOSPEN
AktivitiFizikal
Program Warga Aktif
Warga Produktif
Healthy Workplace
for Healthy
Workforce
Garispanduan
Pengurusan Kantin
Sihat
Garispanduan Perlaksanaan
Vending Machine Makanan &
Minuman Sihat dlm
Perkhidmatan Awam
Kafeteria Sihat
Hidangan Sihat
Semasa Mesyuarat
Amalan
Pemakanan SihatJom Mama
Initiatives
28
Strategy 7 NSP-NCD: Policy & Regulatory Interventions, Progress thus far…
• Guideline on marketing of foods and non-alcoholic beverages to children (Self-regulatory, August 2013).
• Strengthening implementation of the Framework Convention for Tobacco Control (FCTC).
• Guideline on food and beverages sold in school canteens (revised guideline, January 2012).
• Banning of sale of food & beverages by mobile vendors outside of school perimeters (2012)
• Health-promoting workplaces in the public sector
• Healthy menus during meetings
• Healthy vending machines
• Healthy cafeterias
29
There is still much that needs to be done….
Other strategies under NSP-NCD, Progress thus far…
• Continue to work with food and beverage industries to reduce the content of salt, sugar and fat in processed food.
• Development of Salt Reduction Strategy
• Prioritising interventions to fight obesity
• “Komuniti Sihat, Perkasa Negara” initiative
• Involvement of PIBG to support implementation of health-related programs in schools
30
There is still much that needs to be done….

National Systems Response to NCDs –ASEAN Countries
BR
N
CA
M
IND
LAO
MA
L
MY
N
PH
I
SIN
THA
VIE
T
Has an operational NCD unit/branch or department within MOH ✓ ✓ ✓ ✗ ✓ ✗ ✓ ✓ ✓ ✗
Has an operational multisectoral & integrated national policy, strategy or action plan ✗ ✗ ✓ ✗ ✓ ✓ ✗ ✗ ✗ ✗
Has an operational policy, strategy or action plan to reduce the harmful use of alcohol ✓ ✓ ✓ ✗ ✗ ✓ ✓ ✗ ✓ ✗
Has an operational policy, strategy or action plan to reduce physical inactivity ✗ ✓ ✓ ✗ ✓ ✓ ✓ ✓ ✓ ✗
Has an operational policy, strategy or action plan to reduce the burden of tobacco use ✗ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓
Has an operational policy, strategy or action plan to reduce unhealthy diet and/or promote healthy diets ✗ ✓ ✓ ✗ ✓ ✓ ✓ ✓ ✓ ✓
Has evidence-based national guidelines for the Mx of major NCDs through a primary care approach ✓ ✗ ✓ ✗ ✓ ✓ ✗ ✓ ✓ ✗
Has an NCD surveillance and monitoring system in place to enable reporting for the GMF ✗ ✓ ✗ ✗ ✓ ✗ ✗ ✓ ✓ ✓
Has a national, population-based cancer registry ✓ ✗ ✗ ✗ ✗ ✗ ✗ ✓ ✗ ✗
31

ASEAN Task Force for Non-Communicable Diseases (ATFNCD)• STRATEGY I: Revitalise and implement ‘ASEAN Healthy Life Style
2002
• Engage in advocacy opportunities at regional/international platforms
• Policy advocacy on NCD concerns that includes but not limited to:• Labeling and standards for healthy low salt food
• Ethical advertising of food products for children
• Alcohol consumption reduction
• Strategy II: Facilitating enabling environment for ensuring promotion of healthy lifestyle for the people of ASEAN
• Networking among ASEAN Cancer Data and Registry Information System
• Key indicators on Healthy Lifestyle especially on 4 selected NCDs
• Regional Workshop to harmonize guidelines on physical activity in collaboration with WHO
• Regional framework for NCD screening and management 32
Consultation on Overweight, Obesity, Diabetes and Law in the Western Pacific Region, April 2014
• Co-organised by the International Development Law Organisation (IDLO), University of Sydney (Faculty of Law and Boden Institute of Obesity, Nutrition and Exercise) and WHO WPRO.
• Several themes and areas for action were identified :• Generating and sharing evidence for action
• Capacity-building: Strengthen the linkages between health and the law, building the capacity of each profession to understand and work with one another. Suggestions for achieving this included:• Training the legal and health workforces through changes to
academic curricula;
• Conducting workshops and forums to encourage greater dialogue between government and civil society, and
• Developing a multidisciplinary group of public health law experts. 33

Consultation on Overweight, Obesity, Diabetes and Law in the Western Pacific Region, April 2014
• Promising interventions: In-depth technical advice on specific promising interventions, including • Regulation and taxation of sugar-sweetened beverages;
• Restriction of marketing unhealthy food products and beverages to children;
• Requirements for interpretative front-of-pack labelling on packaged foods; and
• Legislation to facilitate environments that are conducive to physical activity.
• Social mobilization: The support and participation of civil society is crucial to the development, implementation and enforcement of innovative legal approaches to overweight, obesity and diabetes.
• Actions to address industry interference: Clear guidelines are needed to avoid conflicts of interest and to ensure that government interactions with the food industry are transparent and constructive, and do not jeopardise public health goals. 34

65th Regional Committee Meeting for the Western Pacific, 13-17 Oct 2014
• One of the main agenda items is Tobacco free initiative: Regional Action Plan 2015–2019
• Malaysia made a strong statement on this issue
35
“I think it will be fool hardy for us to expect that the tobacco industry will not interfere. By virtue of being the Tobacco industry itself it is their duty to interfere and they will continue to interfere”
65th Regional Committee Meeting for the Western Pacific, 13-17 Oct 2014
Malaysia’s stand:
• We cannot handle the issue of tobacco without looking at the trade and economical aspects of tobacco
• Malaysia is quite consistent in this idea that we should try to exclude tobacco in all forms of trade agreements e.g. in TPPA.
• Must address issue of illicit tobacco and transboundarysmuggling – need multisectoral involvement.
• Increasing excise duty.
• Need to gather further evidence to support policy implementation.
36

6th Session of the Conference of Parties (COP) to the WHO Framework Convention on Tobacco Control (FCTC) – 13-18 Oct 2014
37
• Malaysia continues to fight for carving out tobacco from trade agreements and hosted a drafting group.
• Met with strong opposition from several countries.

Commission on Ending Childhood Obesity
38
• Announced by Dr Margaret Chan at the 67th World Health Assembly 2014• The Commission has been tasked with producing a report specifying
which approaches and combinations of interventions are likely to be most effective in tackling childhood and adolescent obesity in different contexts around the world.
• The Commission will deliver its report to the WHO Director-General so that she can convey its recommendations to the World Health Assembly.
http://www.who.int/entity/end-childhood-obesity/about/en/
National Strategic Plan for
Non-Communicable Diseases
(NSP-NCD) 2010-2014
• Presented and approved by the Cabinet on 17
December 2010.
• Provides the framework for strengthening NCD
prevention & control program in Malaysia.
• Adopts the “whole-of-government” and
“whole-of-society approach”.
• Diabetes & obesity are used as the entry
points.
Seven Strategies:1. Prevention and
Promotion
2. Clinical Management
3. Increasing Patient
Compliance
4. Action with NGOs,
Professional Bodies &
Other Stakeholders
5. Monitoring, Research
and Surveillance
6. Capacity Building
7. Policy and Regulatory
interventions
39
MyBFF@school MyBFF@home MyBFF@work
“My Body is Fit
and Fabulous”
INTERVENTION PROGRAMMES
TO COMBAT OBESITY IN MALAYSIA
An Implementation Research (qualitative + quantitative approaches)
Slide courtesy of Dr Wan Nazaimoon, IMR; [email protected]
40

JOM MAMA: Focus on pre-pregnancy for prevention
41
Public-private partnership Implementation
Nurul (25) & Khairil (27)
Academia/Partners
Evidence base Pre-conception / young couples Malaysia
Phase 1
Co-creatIon
Phase 2
Programme development
Phase 3
Evaluation and Evaluation
Slide courtesy of Priya Matzen, Novo Nordisk; [email protected]

JOM MAMA: Objective
42
What we want to do
To investigate if pre-pregnancy interventions improves young couples
health literacy and women’s health
To assess if the intervention improves
delivery and birth outcomes.
Prevent/reduce risk
of NCDs
Slide courtesy of Priya Matzen, Novo Nordisk; [email protected]

HOPE-4 Study
• Intervening the epidemiologic transition through innovative means of controlling hypertension
• Collaboration between UiTM, NCD MOH, McMaster University, Toronto University and London School of Hygiene & Tropical Medicine
• Grand Alliance for Chronic Diseases, supported by Grand Challenges Canada.
• 50 communities in Malaysia, Columbia, India and Sub-Sahara Africa.
• Task shifting – non-physician healthcare workers under supervision of doctors.
• Use of polypill.43
Information courtesy of Prof. Dato’ Dr Khalid Yusoff, [email protected]

v
South East Asia Community Observatory
SEACO: Research for a healthy community
D.D. Reidpath & P. Allotey
44

DHSS: A Research PlatformSEACO: A research platform
• A community-based sentinel surveillance system that captures longitudinally, a fully enumerated population within circumscribed geographical location.
• The data collection process explicitly captures information on demography, morbidity and mortality from the individual, within the context of the household, and the household within the context of the community, as well as the physical, social, geographical relationships between these.
Slide courtesy of Prof. Pascale Allotey, Monash University Sunway Campus; [email protected]
45

Lessons learned from the past and current attempts to work with other sectors
• Go for the path of least resistance.• Perhaps less impact, but at least establish the link and develop
trust.
• Compromise, find the “middle path”• You cannot force the other sectors to go 100% your way.
• Be creative – think “out-of-the-box”• Use other existing mechanisms not previously used to move the
NCD prevention and control agenda forward.
• Be sensitive to current global/national trends.• Use any opportunity to move the NCD prevention agenda
forward.46

threeste
ps
mutuality of interest
specificity of purpose
identification of specific resources
sir g
eorg
e
alle
yne
47

Related Documents











