New Hire Teacher Orientation Forms Name DOH: New Hire Forms: Received [J Application Form l-l Employment Eligibility Verification (l-9) l_l w-4 ll Request for Criminal Record Check Il Fingerprint Authorization Certificate (FAC) ll Agency of Human Services [ ] Request for Criminal Record-2nd Dissemination [J BSD FingerPrinting Procedure IJ EEO-s Lì Emergency Medical lnformation i l Direct DePosit (Mandatory) fl Medicaid PaYment Reassignment I Verification of Employment at prior schools Transcripts on file Teacher Certification on file HQT letter on file I nsurance/Benefit Material: ll BC/BS Enrollment Form (Coverage Date:J-J-\ ! Declaration of Health Care ll BC/BS Booklet il Cigna Dental Booklet n Enrollment Form lJ Life lnsurance Form lJ Add'l Life lnsurance Memo n +os(U) Retirement Savings Plan [] eSO Section L25 Plan U section 1-25 Plan Election of Benefits Form Policies/Procedure lnformation: fl B.E.A, Agreement ll Lateral Move Request {J Tuition Reimbursement Request tl Differentiated Teacher Supervision & Evaluation ! Key Policy l l School Calendar Orientation Date- Returned to HR X

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

New Hire Teacher Orientation Forms
NameDOH:
New Hire Forms:Received
[J Application Form
l-l Employment Eligibility Verification (l-9)
l_l w-4ll Request for Criminal Record Check
Il Fingerprint Authorization Certificate (FAC)
ll Agency of Human Services
[ ] Request for Criminal Record-2nd Dissemination
[J BSD FingerPrinting Procedure
IJ EEO-s
Lì Emergency Medical lnformation
i l Direct DePosit (Mandatory)
fl Medicaid PaYment Reassignment
I Verification of Employment at prior schools
Transcripts on fileTeacher Certification on file
HQT letter on file
I nsurance/Benefit Material:ll BC/BS Enrollment Form (Coverage Date:J-J-\
! Declaration of Health Care
ll BC/BS Booklet
il Cigna Dental Booklet
n Enrollment Form
lJ Life lnsurance Form
lJ Add'l Life lnsurance Memo
n +os(U) Retirement Savings Plan
[] eSO Section L25 Plan
U section 1-25 Plan Election of Benefits Form
Policies/Procedure lnformation:
fl B.E.A, Agreement
ll Lateral Move Request
{J Tuition Reimbursement Request
tl Differentiated Teacher Supervision & Evaluation
! Key Policy
l l School Calendar
Orientation Date-
Returned to HR
X

EMPLOYMENT APPLICATION
BURLINGTON SCHOOL DISTRICTt5o Colchester Avenue t Burlingtotl, Vermont o54'ol
- AN EQUAL OPPORTUNITY EMPLOYER -
Ap¡rlication Date
Personal DataPlease
Nam Social Security Number: -Last First M,I
Position Desired'
Mailing AddressCity State zipNurnber & Street
Day Tinre Pltone Nutu Evening Phone Number
f)ate of'Birth Email Address
o Can you provicle proof if hired, that you are legally eligible for employment in the united States without
sponsorship'Ì: (Tou will be reqttired. b2 law to d'o so upon olfer of etrptoyment) ! NO I YES
o Are you over the age of t s? [ NO ¡ YES
. Haue you appliecl to the Burlington School District within tlre last 6 months? [ NO n YES
¡ Have you ever been convicted of a crime other than a minor traflìc violation? ¡ NO ¡ YES
(so, please erpluin:
Responcling "Yes" cloes not automatically exclude the applicant frorn eligibility for emploYment
e Have you been placed on the ofïìce of the Inspector General's List of Excluded Individuals/Entities (LEIE)
or on the Excluded Parties List System (EPLS)? [ NO ¡ YES
o Has a complaint against you to the Department of Child and tramily services ever been substantiatedPINO IYES
¡ Have you ever been dischargecl or been requested to resign any position? [ No ¡ YES
If so, please etplain:
o In the employment setting, have you errer received greater discipline than an oral reprimandP ! NO ! YES
If so, please erþlain:
o As explainecl, can you perfbrnl the essential functions of the position for which you are applying with or
without reasonable acconlmoclations? ! NO I YES
If no, please etplain:
o If you are requirecl to have a professional licensure for the position you are applying for, has the professional
Iicensing agency ever disciplined you or revoked your license? [ NO ! YES
If so, þlease erplam:
¡ Have you ever been employed by the Burlington School DistrictP n NO ! YES
If so, give rÌates/position(s):
o Can you travel if'the job requires it'l I NO ! YES
EMP.Al)P #a ogt"¿"2otaPage t ofz
Statement of Understanding - Continued
AII qualifìed applicants receive consideration for ernployment in accordance r¡'ith the policy of the BSD. 1'he BSD is an
equai employmånt opportunity employer. Ernployrnãnt decisions are based ou merit and business needs, and tlot otl race,
"nln., url""riry, .eligio,'r, g"nä"., àgø -uritui oi civil union status, national oriqin, sexual orientation, place of birth,
citizenship, u"i"rurl Jtatus, or disability, as defìtred and required by state and federal laws.
Fìqual ernpl.yrnent opportunity r"rotices are posted on the rnain bulletin board in each building as required.by law' Tle.se
noti"", surnmarize tlie rights äf employees in equul opportunity in ernployrnent and-list the names and addresses of the
various governmerlt ug"i"i"s that måy be contacteà in the event that any employee believes he or she has been
disorininated against.
The BSD will comply with all the relevant and applicable provisions of the American Disabilities Act (ADA). We will not
discrirninate ugai.,ii any qualified ernployee n. job uppfi"unt with respect to any terms, privileges, o¡ conditions of
employrnent bà"uuse nf å pËrrn,",', physical-onneniul aiiáuitity. we will also rnalte a reasonable accomtnodation whenever
pnssibie fìrr ail "mplnyees
nr. ,ppìi"ä,.,ts with disabilities, piovided that the individual is otherwise qualified to safely
pe.fo'n the esse'tiål duties and assignments connected witlì the job, an{ provided that any accotnuodatious made do not
i,o¡rnr" au undue harctship on BSD on confirrrnance with state and fèderal laws'
I understancl that nothing contained in this application or in the interview process is intended to create an employment
contract between the tsSD and myself,
I understa'd that as part of rny employment application process, the BSD will conduct a review of existing s.tate and federal
crirninai records, Vermont state law indicates itrut "achlou
applicant to a school district be required to undergo a criminal
record chech, including an FBI fìngerprint record checli, una^ ì¡tut employment may be dependent upon the results of the
chech. (16 V.S.A. $ 255, et,al.)
Certain positions, because of physical requirements and/or legal requirements, may require me to pass a physical exam at
the expense of the BSD after á cónditional ofler of ernployment has been extended to me,
I understand this application will be retained for six months from the date of signature, after which I must reapply for any
position sought.
I u¡clersta¡d that this application, under no circumstances, represellts any obligation by the BSD to offer me employment
ofany type.
I' submitting this application I understand that should I be awarded this or arly other positions with Burlington School
District (BSD) t un, giuing consent to BSD to withhold frorn any payment^l reóeivecl from BSD the value of any and all
school p-p"riy I failio ..iu.n either upon request from BSD or at the end of my employnrent'
I understand that it is expected that I will comply with all Federal and State applicable laws and regulations,
I agree to comply with all policies, procedures, applicable laws and regulations. Failure to comply will result in
the appropriate action r-r""Ë.rury in keeping *itn in" gr.raranteed safety and privacy of the students, faculty and
stafT' of' the District, including aisciptinã up to anã including termination. I understand that it is my
responsibility to access and ,e"ad the Board Policies, (Board Policies are available on the District website,
bsdvt.org.)
f understand that BSD Ís a mandatory reportÌng agent and that ìf DÍstrÍct employees su,spect abuse or neglect ofchÌldren or students, they are requÍre7 ty taw tã rlport those suspÍcÍons to state authorÍties and |aw enforcement,
I irereby acknowledge that I have reacl each ofthe above statements and understand the same and consent thereto.
Signature of App
EMI).APP #6 ogteeot6
Da
Page z ol z

Employment Bligibility Verifìcation
Department of Homeland SecurityU.S. Citizenship and hnmigration Services
USCISForm I-9
OMII No. l6l5-0047ËxpiLes 08/3 l/2019
> START HERE: Read instructions carefully before completing this form, The instruct¡ons must be available, either in paper or electronically'
during completion of this form. Employers are liable for errors in the completion of this form'
ANTI-DISCRIMINATION NOTICE: lt is illegal to discriminate against work-authorized individuals. Employers cANNOT specify which
document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ
an individual because the documentation presented has a future expiration date may also constitute ìllegal discrimination.
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in
connection with the completion of this form.
I attest, under penalty of perjury, that I am (check one of the following boxes):
QR Code - Section 1
Do Not Write ln Ïhis SPace
1. Employee lnformation and AtteStatiOn (Emptoyees must complete and sign Secflon I of Form l-9 no later
than the first day of employment, but not before accepting a iob offer.)
Mìddle lnitìâl Other Last Names Used (if anY,lFirst Name (Given Name)Last Name (Family Name)
ZIP CodeApt. NumberAddress (Street Number and Name) City or Town
Emp¡oyee's Telephone Number
Stâte
Employee's Ë-mail AddressU.S. Social Security NumberDate of Birth (mm/dd/yyyy)
I l. n citizen of the United States
I Z. n noncitizen national of the United States lsee instructiotls)
I S,n lawful permanent resident (Alien Registration Number/USCIS Number):
f +. ,ln alien authorized to work until (expiration date, if applicable, mm/dd/yyyy):
Some aliens may wrìte "N/4" in the expiratìon date field, (See lnsfrucflons)
A¡iens authorizec! to work must provide onty one of the following clocument numbers to complete Form l-9:
An At¡en Registration Number/l/SClS Number OR Form !-94 Admission Number OR Foreign Passporl Number.
1. Alien Registration Number/USCIS Number:
OR
2, Form l-94 Admission Number:
OR3. Foreign Passport Number:
Country of lssuance:
Today's Dale (mm/dd/yyyy)Signature of Ëmployee
[] t oio not use å preparer or translator.
(Fields below must be completed andf-l A preparer(s) and/or translator(s) assisted the employee in completing Section 1,
signed when preparers and/or trans/afors asslsf an employee in completing Section 1')
Preparer and/or Trans Certification (check one):
I attest, under penalty of perjury, that I have assisted in the comp on of Section 1 of this form and that to the best of my
e the information is true and correct.Signature of Preparer or Translator Today's Dale (m m/dd/yyyy)
Last Name (Family Name) First Name (Given Name)
Address (Street Number and Name) City or Town State ZIP Code
Form l-9 I l/1412016 N
@r Employer Cornpletes Next Page @,
Page 1 of3
Employment Eligibility Verificatiort
Department of I-Iomeland SecurityU.S. Citizenship ar-rd Immigration Services
USCISIiorm l-9
OMII No. l6l5-0047Expires 08/3 I /20 I 9
ewRevi nddorizedoect¡ 2n Em ro RepreseployerYoutheof ,s first of2Secfion 3within business day employment.and days employeemusftheiror complete signauthorized representat¡ve(Employers"LlsfsLlstfrom asc thelisted onLrsffrom andB documentonecombinationa oneof documentdocumentone Lrsffrom ORAexamtnephysically
Acceptable Documents.M.t Citizenship/lmmigration StatusFirst Name (Given Name)Last Name (Family Name)
Employee lnfo from Section 1
ldentity and Employment Authorization ldent¡ty Employment Author¡zation
The employee's first day of employmenl (mm/dd/yyyy): (See instructions for exemptions)
I attest, under penalty of PerjurY, that to the best of my knowledge, this employee is authorized to work in the United States, and if
the employee prêsented document(s),
Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above'named employee,
(2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the
employee is authorized to work in the United States.
Document Title
lssulng Authorìty
Document Number
Êxpiration Dale (if any) (mm/dd/yyyy)
Document TitleDocument Title
lssuing Authority
Document Number
Expiration DaIe (if any) (mm/dd/yyyy)
lssuing Authority
Expiration Date (if any) (mm/dd/yyyy)
Document Number
Document Title
lssuing Authorìty
Document Number
Expiration Date (¡f any) (mm/dd/yyyy)
Document Title
lssuing Authority
Document Number
Additional lnformationQRCode-Sections2&3Do Not Write ln Ïh¡s SÞace
Expiration Date (if any)(mm/dd/yyyy)
S¡gnature of Employer or Authorized Representative Today's DaIe(mm/dd/YYYY) Title of Employer or Authorized Representative
Last Name of Employer or Authorized Representalive First Name of Employer or Authorized Represenlative Employer's Busìness or Organization Name
Employer's Business or Organtzation Address (Street Number and Name) City or Town Stale ZIP Code
Section 3. Reverification and (To completed signed by employer representative.)authorizedorandRehires beB. Date of RehireA. New Name (if
M¡ddle lnitial Date (mm/dd/yyyy)First Name (Given Name)Last Name (Family Nane)
establishesthefor thatordocumentthe nformation rece¡pthasauthorizationem ntta provideexpiredoftf the s employmentc ployee's previousbelowStn thecontinui e authorization providedpaceng mpl oyment
Expiration Dale (if any) (mm/dd/yyyy)Document NumberDocument Title
Form f-9 I l/141201ó N
the document(s) I have examined appear to be genuine and to relate to the individual
Page 2 of 3
Signature of Employer or Authorized Representative Today's Date (mm/dd/yYYY) Name of Employer or Authorized Representative
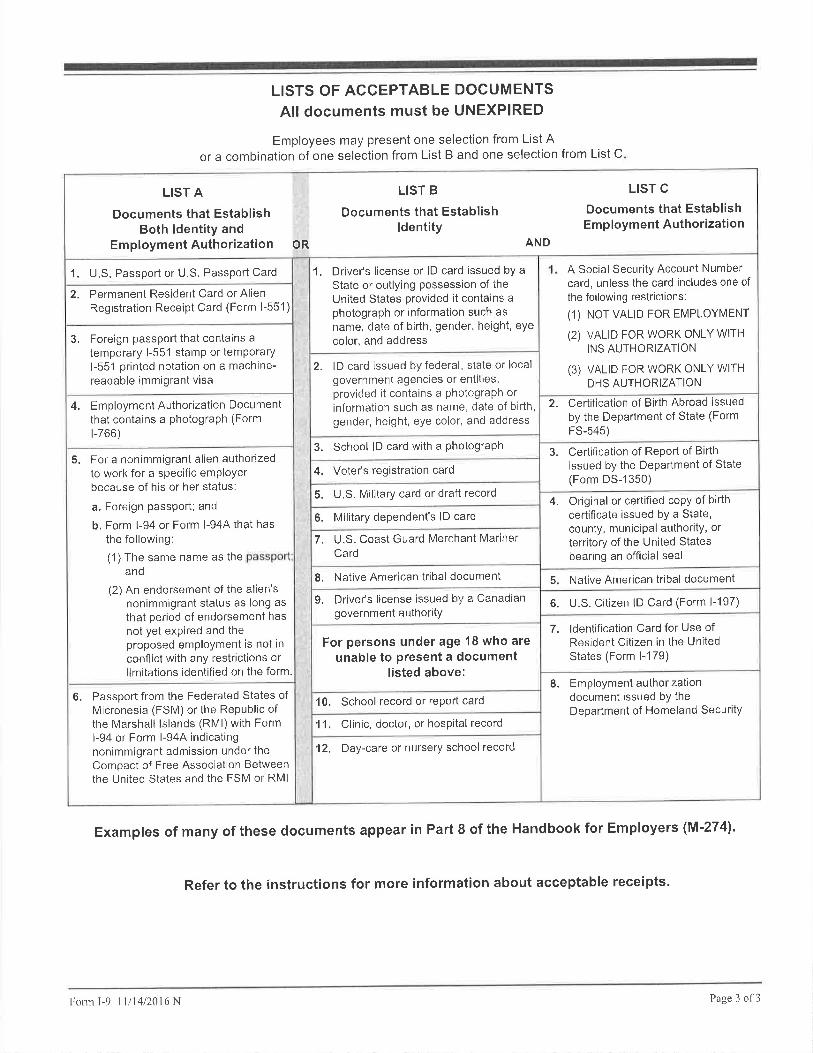
LISTS OF ACCEPTABLE DOCUMENTS
All documents must be UNEXPIRED
Employees may present one selection from List Aor a combination of one selection from List B and one selection from List C
Examples of many of these documents appear in Part I of the Handbook for Employers (M'274).
LIST A
Documents that EstablishBoth ldentity and
EmploymentAuthorization OR
LIST B
Documents that Establishldentity
LIST C
Documents that EstablishEmployment Authorization
AND
1. U.S. Passport or U.S. Passport Card
2. Permanent Resident Card or AlienRegistration Receipt Card (Form l-551)
1. Driver's license or lD card issued by a
State or outlying possession of theUnited States provided it contains a
photograph or information such asname, date of birth, gender, height, eye
color, and address
A Social Security Account Numbercard, unless the card includes one ofthe following restrictions:
(1) NOT VAL|D FOR EMPLOYMENT
(2) VALID FOR WORK ONLY WlrHINS AUTHORIZATION
(3) VALID FOR WORK ONLY WITH
DHS AUTHORIZATION
2. lD card issued by federal, state or localgovernment agencies or entities,provided it contains a photograph orinformation such as name, date of birth'gender, height, eye color, and address
2. Certification of Birth Abroad issuedby the Department of State (Form
FS-545)
3, Foreign passport that contains atemporary l-551 stamp or temporaryl-551 printed notation on a machine-readable immigrant visa
4. EmploymentAuthorization Documentthat contains a photograPh (Form
r-766)3. School lD card with a PhotograPh
4. Voter's registration card
3. Certification of Report of Birthissued by the DePartment of State(Form DS-1350)
5. U.S. Military card or draft record
6. Military dependent's lD card
7. U.S. Coast Guard Merchant MarinerCard
4. Original or certified copy of birthcertificate issued bY a State,county, municiPal authoritY, or
territory of the United Statesbearing an official seal
8. Native American tribal document 5. Native American tribal document
6. U.S. Citizen lD Card (Form l-197)9, Driver's license issued by a Canadiangovernment authoritY
7. ldentification Card for Use ofResident Citizen in the UnitedStates (Form l-179)
5. For a nonimmigrant alien authorizedto work for a specific emPloYerbecause of his or her status;
a. Foreign passport; and
b. Form l-94 or Form l-944 that hasthe following:
(1) The same name as theand
(2) An endorsement of the alien'snonimmigrant status as long asthat period of endorsement hasnot yet expired and theproposed employment is not in
conflict with any restrict¡ons orlimitations identified on the form.
For persons under age 18 who areunable to present a document
listed above:
10. School record or rePort card
11, Clinic, doctor, or hospital record
8. Employment authorizationdocument issued bY theDepartment of Homeland SecuritY
'12, Day-care or nursery school record
6. Passport from the Federated States ofMicronesia (FSM) or the Republic ofthe Marshall lslands (RMl) with Forml-94 or Form l-944 indicatingnonimmigrant admission under theCompact of Free Association Betweenthe United States and the FSM or RMI
Folnr I-9 l l/14/201ó N
Refer to the instructions for more information about acceptable rece¡pts.
Page 3 o1'3

Form W-4 (2OL7lPurpose, Complete Form W-4 so that youremolover can withhold the correct federal incometax frohr your pay. Consider completing a new FormW-4 each year and when your personal or financialsituation changes.
Exemption from w¡thholding. lf you are exempt,complete only lines 1, 2, 3, 4, and 7 and sign theform to validate it. Your exemption for 2017 expiresFebruary 15, 201 8. See Pub. 505, Tax Withholdingand Estimated Tax.
Note: lf anothor person can claim you as a dependenton his or her tax return, you can't claim exemptionfrom withholdino if vour total income exceeds $1,050and includes mõre ihan $350 of unearned income (forexample, interest and dividonds).
Except¡ons. An employee may be able to claimexemption from withholding even if the employee isa dependent, if the employee:. ls age 65 or older,
. ls blind, or
. Will claim adjustments to ìncome; tax credits; oritemized deductions, on his or her tax return.
The except¡ons don't apply to supplemental wagesgreater than $ 1,000,000.
Bas¡c ¡nstructions, lf you aren't exempt, complelethe Personal Allowances Worksheet below. Theworksheets on page 2 further adjust yourwithhold¡ng allowances based on itemizeddeductions, cenain credits, adjustments to ¡ncome,or two-earners/multiple jobs situations.
Complete all worksheels that apply, However, youmay claim fewer (or zero) allowances. For regularwages, withholding must be based on allowancesyou claimed and may not be a flat amount orpercentage of wages.
Head of household. Generally, you can claim headof household filing status on your tax return only ifVou ars unmarried and pay moro than 50% of theôosts of keepinq up a home for yourself and yourdepondent(s) orother qualifyrng indiv¡duals. SeePub. 50'1, Exemptions, Standard Deduction, andFiling lôformation, for information,
Tax cred¡ts. You can take projected tax credils intoaccount in figuring your allowable number ofw¡thholdinq ãllowãnces. Credits for child or dependentcare expeñses and the child tax credit may be claimedusing the Personal Allowances Workshect bclow.See Þub. 505 for information on converting your other
Nonwage income, lf you have a large amount ofnonwaoè income. such as ¡nterest or dividends,considðr making ôstimated tax paymenls using Form1040-ES, Estimated Tax for lnd¡viduals. Otherwise,vou mav owe additional tax. lf vou have Þension orännuitv'income, see Pub. 505 io find oui if you shouldadjust'your withholding on Form W-4 or W-4P.
Two earners or multiple jobs, lf you have aworking spouse or more than one iob, figure the
.
total nLlmber of allowances you are entitled lo claimon all jobs using worksheets from only one FormW-4. Your withholdino usuallv will be most accuratewhen ali allowances ãre claimed on the Form W-4for the highêst paying job and zero allowances areclaimed on the otherè. See Pub. 505 for details.
Nonresident alien, lf vou are a nonresident alien, seeNotice 1392, Supplem'ental Form W-4 lnstructions forNonresident Aliens, before complet¡ng this form.
Check your withholding. After your Form W-4 takeseffect, use Pub. 505 to see how the amount you arehavinó withheld compares to your projected total taxfor 2017 , See Pub. 505, especially if your earningsexceêd $130,000 (Single) or $180,000 (Married).
credils into allowances
Personal Allowances rksheetA Enter "1" for yourself if no one else can claim you as a dependent .
f ' You're single and have only one job; or IB Enter"l"if: {.You'remarried,haveonlyonejob,andyourspousedoesn'twork; or I
[ . your wages from a second job or your spouse's wages (or the total of both) are $1 ,500 or less' ,l
C Enter,,1', for your spouse. But, you may choose to enter "-0-" if you are married and have either a working spouse or more
than one job. (Entering ,,-0-" may help you avoid having too little tax withheld.)
D Enter number of dependents (other than your spouse or yourself) you will claim on your tax return .
E Enter ,,1" if you will file as head of household on your tax return (see conditions under Head of household above)
F Enter ,,1" if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit
(Note: Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.)
G Child Tax Credit (including additional child tax cred¡t). See Pub.972, Child Tax Credit, for more information.
. lf your total income will be less than $70,000 ($100,000 if married), enter "2" for each eligible child; then less "1" if you
have two to four eligible children or less "2" if you have five or more eligible children'
. lf your total income will be between $70,000 and $84,000 ($1oo,oo0 and $1 19,000 if manied), enter "1" for each eligible child.
H Add lines A through G and enter total here. (Note: This may be different from the number of exempt¡ons you claim on your tax return.) > H
. lf you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductionsand Adjustments Worksheet on page 2'
rA
B
cD
E
F
G
For accuracy,complete allworksheetsthat apply.
. lf you are single and have more than,one jo,b
earriings from a-ll jobs exceed $50,000 ($20,000to avoid having too little tax withheld.
or are married and you and your spouse both work and the combi ned
if married), see the Two-Earners/Multiple Jobs Worksheet on page 2
. lf neither of the above situat¡ons applies, stop here and enier the number from line H on line 5 of Form W-4 be¡ow
Last name
5
6
7
Separate here and give Form W-4 to your employer. Keep the top part for your records.
,.,. lllf-4 Employee's Withholding Allowance Certificate OlvlB No, 1545-0074
Þ Whether you are entitled to cla¡m a certainsubject to review by the lRS, Your employer
number of allowances or exemption from withholding is
may be required to send a copy of th¡s form to the lRS.2@17Department ol the Treasury
lnternal Revenue Sôrvice
name and social
Home address (number street or rural route) sn singte ! Married Married, but withhold at higher Single rate.
Note: ll married, but legally or is a nonresident alien, check lhe le" box.
City or town, state, and ZIP code 4 It your last name differs from that shown on your social security card,
check here. You must call 1-8OO-772-121glor a replacement card. Þ
S Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2)
6 Additional amount, if any, you want withheld from each paycheck
7 I claim exemption from withholding for 2017, and I certify that I meet both of the following conditions for exemption'
. Last year I had a right to a refund of all federal income tax withheld because I had no tax liabllity, and
r This year I expect a refund of all federal income tax withheld because I expect to have no tax liabil
meet both conditions, write "Exem here
Under penalties of I declare that I have examined certificate and, to the best of mY kn and belief, it is true, correct, complete.
Employee's signatureDate >form is not valid unless you sign ¡t.) >
8 Employer's name and address (Employer: Complete lines 8 and 10 only if sending to the I 1O Employer ¡dentification numbeÍ (ElN)
lf
I oflice code (optionâl)
For Privacy Act and Paperwork Reduction Act Notice, see page 2'
RS.)
cat. No. 10220Q Form (2017).
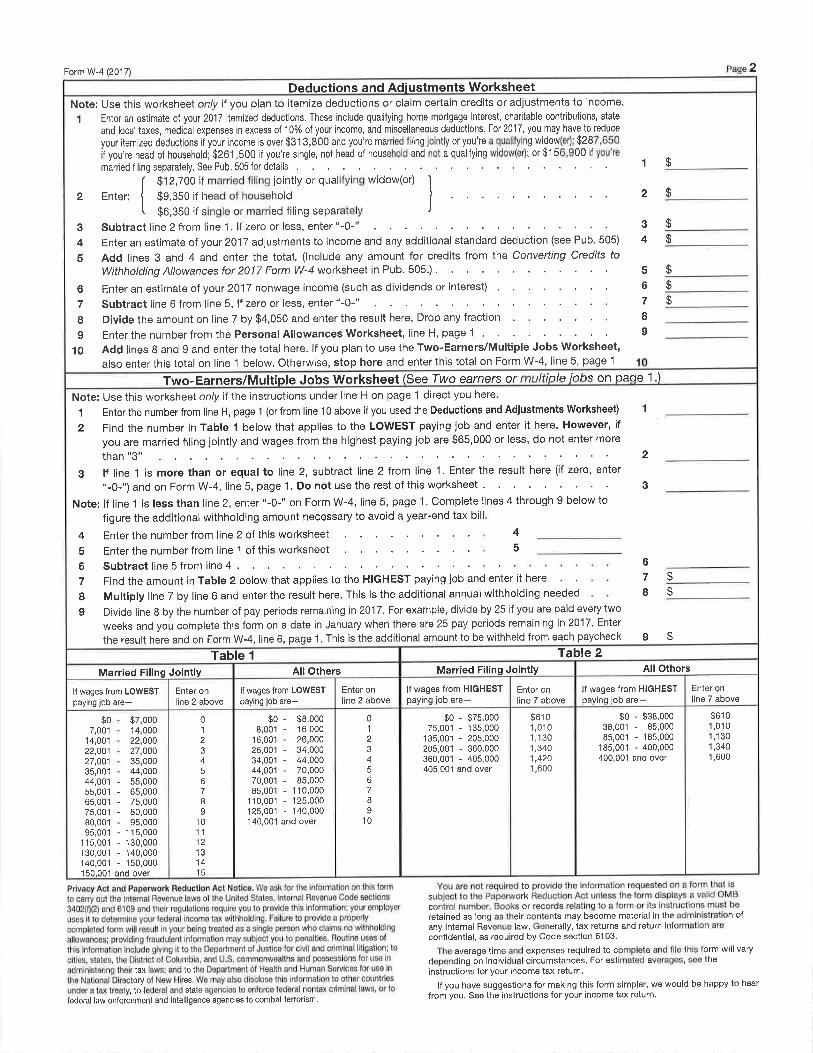
2Form W-4 (2017)
Deductions and Adiustments WorksheetNote: Use this worksheel only il you plan to itemize deductions or claim certain credits or adjustments to income.
1 Enter an estimate of your 2017 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state
and local taxes, mediðal expenses in excess of 10% of your income, and miscellaneous deductions. For 2017, you may have to reduce
your ¡emized deductions if your income is over $31 3,800 and you're married filing jointly or you're a qualifying widow(erl -$287,650
if you're head of household; $261 ,5OO if you're single, not head of household and not a qualifying widow(er); or $1 56,900 if you're
manied filing separately, See Pub. 505 for details
I $12,700 if married filing jointly or qualifying widow(er) ì2 Enter: { Ss,sso if head of household I .
[ $o,gso if single or manied filing separately )
3 Subtract line 2 from line 1. lf zero or less, enter "-0-"
4 Enter an estimate of your 2017 adjustments to income and any additional standard deduction (see Pub' 505)
S Add lines 3 and 4 and enter the total. (lnclude any amount for credits from the Convefting Credits to
Withholding Allowances for 2017 Form W-4 worksheet in Pub. 505.) .
6 Enter an estimate o'f your 2017 nonwage income (such as dividends or interest)
7 Subtract line 6 from line 5. lf zero or less, enter "-0-"
8 Þivide the amount on line 7 by $4,050 and enter the result here. Drop any fraction
9 Enter the number from the Personal Allowances Worksheet, line H' page 1
1O Add lines 8 and 9 and enter the total here. lf you plan to use the Two-Earners/Multíple Jobs Worksheet,
also enter this total on line 1 below, Otherw¡se, stop here and enter this total on Form W-4, line 5, page 1
2
3
4
5
67
8I
$
$
$
$
$
ü
1$
Two-Earners/Multiple .lohs Wo rksheet lSee Two tlfinlc iobs 1.1oâoeearners or on
Note: Use this worksheet onty if the instructions under line H on page 1 direct you
1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet)
2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if
you arê married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more
than "3"
3 lf line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter
"-0-") and on Form W-4, line 5, page 1' Do not use the rest of this worksheet '
Note:lf linel islessthanline2,enter FormW-4, line5,pagel.Completelines4through9belowtofigure the additional withholding amount necessary to avoid a year-end tax bill
Enter the number from line 2 of this worksheet
Enter the number from line 1 of this worksheet
Subtract line 5 from line 4 .
Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here
Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed
4
5
6
7
II
6
7
I
1
$
$
I $
2
3
here
Divide line B by the number of pay periods remai
weeks and you complete this form on a date in
the result here and on Form W-4, line 6, page 1.
ning in 2017. For example, divide by 25 if you are pald every two
January when there are 25 pay periods remaining in 2017' Enter
This is the additional amount to be withheld from each paycheck
4
:
Table 2Table 1
All OthersMarried Filing JointlyAll OthersMarried Filing JointlyEnter online 7 above
lf wages from HIGHESTpayinq job are-
lf wages from HIGHESTpaying job are-
Enter online 7 above
lf wages from LOWESTpaying iob are-
Enter online 2 above
lf wages from LoWESTpaying iob are-
Enter online 2 above
$61 o1,0101 ,1301,3401,600
$61 01 ,0101 ,1301,3401,4201,600
$0 - $38,00038,001 - 85,00085,001 - 185,000
185,001 - 400,000400,001 and over
01
4
678I
10
$0 - $75,00075,001 - 135,000
135,001 - 205,000205,001 - 360,000360,001 - 405,000405,001 and over
01
2e
45678o
1011
121314'15
$0 - $8,0008,001 - 16,000
16,001 - 26,00026,001 - 34,00034,001 - 44,00044,001 - 70,00070,001 - 85,00085,001 - 110,000
'1 1 0,001 - '1 25,000
'125,001 - 140,000140,00'1 and over
$o7,001
14,00122,00127,00135,00144,001s5,00165,00175,00180,00195,001
1 1s,001130,001140,001150.001
- 44,000- 55,000- 65,000- 75,000- 80,000- 95,000- 1 15,000- 130,000- 140,000- 150,000and over
$7,00014,00022,00027,00035,000
Privacy Act and Paperwork Reduction Act Notice. We ask for the jnformâtìon on this form
to carry out the lnlernal Rêvenue laws of the United States' lnternal Revonue Code sections
3402(f)(2) and 61 09 and their regulations requiro you to provide this informationl your employer
uses it 1o determine your federal income tax w¡thholding. Failure to provido a properly
completed form w¡ll resull in your being lroated as a single person who claims no withholding
allowancos; providing fraudulent information may subiect you to penalties. Routine uses of
this information includo giving it to the Departmont of Justice for c¡vil and crim¡nal litigation; to
cities, slates, the Districi of Columbia, and U.S. commonwealths and possessions for use in
adminìstsring thoir tax laws; and to the Depârtmênt of Health ând Humân Ssrvices for use in
the National Directory of New Hires. Wê may also disclose thìs information to othor countrios
under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to
federal law enforcement and intelligence agencies to combat terrorism,
You aro not rêquirod to provide thê information requestêd on a form that issubject to the Paperwork Reduction Act unless the form displays a valid OMBcontrol number, Books or records relating to a form or its instructions must beretained as long as theìr contents may become material in the admin¡stration ofany lnternal Revenue law. Gonerally, tax returns and return inlormation are
confldential, as required by Code section 61 03.
The average tims and expenses required to complete and file this form will vary
depending on individual circumstances. For estimated averages, soe thèinstruct¡ons for your income tax rêturn.
lf you have suggostions for making this form simplor, we would be happy to hêar
from you. See the instructions for your income tax return.

BURLINGTON SCHOOL DTSTRICT150 Colchester Avenue' Suite 2
Burtington' VT 05401(802) 8ó4-21s9
RJQUEST FOR CRIMINAL RECORI} CHECK
Initial Request Resubmission for FBI/Out of State Records
Applicant:Please Print Last Name First Middle
Maiden or Alias Names:
Gender:
Race:
Social S ecurity Number:
Place of Birth:City/Town State
Date of Birth:Month DaY Year
Telephone Number:A¡ea Code Number
following agencies:
XX Vermont Criminal Information Center (VCIC);
XX Federal Bureau of Investigatlons (FBÐ;
xx The followÍng states where I have resided or been employed:
Signature of Applicant:
Identity Verified by:
Country
Ir (Print Name)criminal record of criminal convictiooG p"r 13 VSA $ 13, which may be maintained by the
I understand the results of this check witt be made available to BurlÍngton school District' or
any affiliate thereof, for use in reviewing my suitability for employment and that my
employment is contingent upon a satisfactory criminal records check. Any routine costs
asrã.iát"o with the prõ".s tnitt u. ¡orne by me. I further understand that this process may
take some time to'complete, and although my employment may commence prlor to the
completion of this requirõd process, my continued employment is nonetheless contingent upon
a saiisfactory criminàl records cheek. I further understand that within thirty (30) days ofreceiving thä results of the record check, I have the right to appeal the fÏndings to the
Vermont Criminal Information Center, Department of Public Safety, 103 South Street'
Waterbury, VermonÇ 05671-21 01.
Date:
Date:
vcrc#3.03.03
Burlinglon School District
Position:

VERMONT CRIMINAL INFORMATION CENTERFING AUTHORIZATION RTIFICATE
*,,{<{.APPLICANT: You must bring this certificate with you to your fingerprinting appointment. Identification
Center staff lilLL NOT submit your fîngerprints to VCIC for processing without this form.***Agency Code: 0031 1-
REASON FINGERPRINTED:I Adoption f Education I NCPA-Employment I NCpA-Volunteer I Secretary of State
NAME:MiddleFirstLast
MAIDEN/OTHER NAMES
DOB SSN
PLACE OF BIRTH
Town State Country
TELEPHONE NUMBER:
In addition to Vennont I have resided or been employed in the following states: (If applicable, circle
appropriate states)
CO HI IL MA MS MT NB NH RI UT WY
Applicant Signature:
ffi I certify that the above applicant has appeared before me and paid his or her criminal record check fee. I
understand that the Department of Public Safety will bill my agency for this record check.
I Our agency is responsible for paying the record check fee. I understand that the Department of Public
Safety will bill my agency for this record check.
Agency Staff Signature: Date:
IDENTIFICATION CENTER USE ONLY:
TVT: Date Printed:
IDENT CENTER STAFF - Mail these fonns to:
VCIC - 103 South Main ST, Waterbury, VT 05671 Attn: Criminal Record Check Program
AW OBENG _ SUPERTNTENDEN]'
150 Colclrester Avenue, Burlington, Vermonr 05401 ' Phone: 802-864-8474' Website: www.bsclvt.org ' Twitter: @BTVSchools

BURLINGTON SCHOOL DISTRICT150 Colchester Avenue, Suite 2
Burlington, VT 05401(802) 864-21se
REQUEST FOR CRTMINAL RECORD CHECKSecondarY Dissemination
Applicant:Please Print Last Name First Middle
Maiden or Alias Names:
Gender:
Race:
Social Security Number:
Place of Birth:
Date of Birth:
Telephone Number:
following school(s);
Month DaY
City/Town State Country
Year
Area Code Number
I, (print Name) hereby acknowletlge and agree to a check of any
criminalrecordorffiperl3VSA$l3,whichmaybemaintainedbythe
Schoot that has your background check on file
Address
I understancl the results of this check will be made available to Burlington School District, or
any affiliate thereof, for use in reviewing my suitability for employment and that my
emptoyment is contingent upon a satisfactory criminal records check. Any routine costs
associated with the p.ã"us wiu be borne by me. I further understand that thÍs process may
take some time to complete, and although my employment may commence prior to the
completion of this requirãd process, my continued employment is nonetheless contingent upon
a saiisfactory criminãl records check. I further understand that within thirty (30) days ofreceiving the results of the record check, I have the right to appenl the fTndÍngs to the
Vermoni Criminal Information Center, Department of Public Safety, 103 South Street,
Waterbury, Vermont, 0567f -2101
Signature of Applicant: Date:
Identity Verified by: Date:
VCIC-Scl¡ool# L0l .03
Burlington School District
Position

,,^g-'Vglttr¡Onff Agency of Human Services
Adult protective Services, 103 S. Main Street, Ladd Hall, Waterbury, VT 05671'2309
Ch¡ld Abuse Regist ry Unit, 103 S. Main Street, Waterbury, VT 05671-@]-
FORM C
CONSENT FOR RELEASE OF REG¡STRY INFORMATION
This form is for use with the ON-LINE reoistrv checkino svstem ONLY
This consent form must be filled out completely and signed by the current
employee, prospective employee, contractor or volunteer and kept on file at the
requesting'organization. The-Agency of Human Services reserves the right toaudit these consent forms at any time.
Curent or prospective Employee. Contractor. or Voluntêer lnformâtion
Full Name: Gender: n Male nFemalet-il-rÞ r MrOOle lnlUalLAÞ I
Address
Last four digits of social security number XXX-XX-
Phone number: Birth Date Place of BitlhCity, State, CountrY
other FIRSInames I have used, if any (i.e. Nicknames, Aliases)(Type or Pr¡nt)
other LASInames I have used, if any (i.e. Maiden Names, Aliases)(Type or Print)
I hereby authorize release of any information of reports of abuse, neglect or exploitation
sJostañt¡ated against me and cóntained in the Vermont Adult Abuse Registry and/or the Vermont
Child Protection Registry to:
Burlington School District
(Print Organization Name)
(Prospective) Staff, Contractor, or Volunteer Signature Date
Last Modified: 9121/2010

Burlington School District Fingerprinting Procedure
lf,Ihere:
Hours: .A.t Burlington P.D.: By appointment only on Thursdays, l0am - 3:00pmSheriff's Office: By appointment only, Tues, Wed, & Thurs, lOam-3pm
Take with you the ¡TVERMONT CRIIVIINÃL INFORIIÃTION CENTERfINGERPRINT AUTHORIZ.II,TION CERTIFIC.H,TE" which you will get fromHuman Resources at the Schoot District.lldministrafion Office. You MUSThave this form with you in order to have your fingerprints taken. This formwilt be kept by the Police or Sheriffls office.
Burlingrton School District.ãdministration Office is at: t50 Golchester.ã,ve. It is on the western edgeof the IIVM Triníty campus. It is a low brick building set back from the road. I¡ook for the mustardyellow stripe around the roof.
Processing Fees: J. $12.00 payable to the BurlÍngrton School DÍstrict.Payments can be made by check or money order, or with cash. No credit cards'Payment must be made at the School District Ãdministration Office BEFORE you haveyour fingerprints taken.
Make checks payable to the Burlingrton School District.
2. $25.00 at the Bullington Police Department or Sheriff's OffÍcePayments must be made cash only. No checks or credit cards are accepted.
3. If you are a current U\IM student, you may have your fingerprintsdone at the [IVM security office on East Äve. at a cost of $ 10, payable with the CAT card only
They will require that you provide a regular No. l0 size business envelope with a $.48 stamp
ülhen you get your fingerprints taken, you must bring 2 forms of identification with you.
The primary form must be one of the fottowing current, valid, State approved photo ID's:Military ID, Photo Ðriver's lricense (any state)Photo Non-driver's ID (any state)
The second form of ID can be any of the following:Passport Social SecuritY CardBirth or Marriage Certificate Professional LicensesInsurance Cards Non-photo Driver's LicenseSchool or Employee ID
##.If you are a current UVM student, you may have your fingerprints done at the IIVM security office on East Äve' at a
cost of$10. See #3 above.
Burlingf on Police DepartmentI North ÃvenueBurlington, \If840-2246
Ghittenden County Sheriffls Office70 Ethan.AJlen DriveS. Burlington, \If863-4341
of
S:\FrontOffice\HR Specialist\Forms\ I Fingerprinting Procedure.doc October 13, 2016

rtF
EmployeeName:
Date of Birth:
Employee Signature:
RacelEthnic Backgtound :
Position: (círcle one)
Location: (circle one)
Ple¡se Print
MM/DD/YYYY
Teacher Paracducstor
Substitute Other:(Please
il;IBuilding e læaruing CommunitY
EEO-S EmPloYee RePort F'orm
ThlsformistobecompletedaflerlhecmployeehascompletedlhehìrÍngpracess,
Date:
trEIútrD
African-American (not of Hispanic origin)
American Indian or Alaskan Native
Asian or Pacific Islarrder
Caucasian (not of Hispanic origin)
HispanicOther : -
ti.", ot¡*"¿ tu""; *A*¡ origin not indicated abovc;)
Maintcnance FoodService,After-School
Barnes ChamPlain Edmunds Elem Flynn Smith r'lVheçler EMS Hunt
ãHl sfc Horizon OnTop District Maintenance Other:
Tþe Burlington School District is an Bqual Opportunity Employer'
Please retufü to Human Resources in a conftdential manner'
GTON SCHOOT DrsrructBunuN
EEO-5 fi4: 10,06
Frrll Name: -
FACULTY & STAFFEMERGENCY MEDICAL INFORMATION
BURLTNGTOI.{ SCHOOL D ISTRICTlS0 Colcltester Aventte I BLrllington, Vermont OS4'Ol
Worlt Location: Position:
Address;
I-Iome Phone Cell Phone:
EmergencY Contacts;
Name:
Address:
Home Phone:
Na{ne:
Address:
Home Phone:
Allergies:
Relationship:
Cell Phone: Work
Cell Phone: w
Medical Problems /Conditions :
Medications:
Doctor's Name;
Acldress: Phone:
Signature:Date
This information is strictly confrclentiaì ancl will tre maintainecÌ in the school oflìce and
the Centrai Offrce.
HR,EM ER(ìENCI'f I ^O I.(I9
In case of accident or illness, I have hereby authorized school personneì to seek
emergency medical ""r". f understand andïgree.that neither the School District
nor its employees *iU ¡" liable for injuries rãsulting from such medical care' If I
need to be taken to the emergency room, I hereby authorize the þhysician in
"trurg" to administe¡.whatever emergency treatment is necessary at my exPense'
I,
PROVIDER CERTIFICATION/REASSIGNMENT OF PAYMENTFOR PROViDERS OF SCHOOL-BASED I{EALTH SERVICES
Uncler Federal regulations, in order fur a supervisory union to bill Medicaid for services furnished by a
provider wiro is ondg contract oï agreement with the supervisory union, the provider must (1) meet
Meclicaicl provider qualifrcations, 1i) have a Provider Agreement with the State Medicaid Agency and (3)
r.eassign hfr/his right to Medicaid payment for such services to the supervisory union,
Provider QÈalificdions : (Please Print)
Provider Name Provider Title
certify tirat I am: (check all that apply)
Cunently enrolled as a Medicaid Provider (Provider #: .--.-)t Sign SECTION A on reverse
Licensed by the state of vetmont (Please attach a cop)' of license)
. Sign SECTION B on reverse
Licensed by the vermont Department of Education (Please attach a copy of license)
. Sign SECTION B on reverse
A graduate of a program of physical therapy approved 9tþlth the Committee on Allied
Health Education unã Aorrr.tiiation of the A*tti.un Medial Association and the American
Þhysical Therapy Association . (Please attach a copy of degree)
. Sign SECTION B on reverse
Have a certificate of clinical competence frorn the American speech and Hearing
Association or have the equivalent education and work experience to qualify for such
certification , (Please attach a copy of certif'cation or proo.f af qualifications)
. Sígn SECTION B on reverse
Registered by the American occupational Therapy Association , (Please attach a copy of
registration). Sign SECT(ON B an reverse
I{ave a Master,s Degree from an Accredited School of Social Work. (Please attach a copy
of degree)
" Sigru SECTION B on revetse
other Qualificatio ns,, (Please spectfu) sign SECTION B on reverse
HR MecJicaid Provider Form 02122009
(over)

NOTICE TO ALL PROVIDERS:The Vermon.t l)epørtment of Education will periodically be doing background checks on schooldistrict prctviders who work with school disÍrict that receive Federal funds. Burlington SchoolDistrict receives a large amount of Fecleralfunds, thereþre ot# providers are included in this
process.
I have read and understancl the above statement regarding background checks,
Provider's Signature Date
SECTION A - REASSIGNMENT OF PAYMENT:
i hereby voluntary reassign my right to payment from the Medícaid agency for services I provide
to students under my agreement with the Budington School District'
Signature of Provicler Title Date
S igrrature o f Supervisory Union Representative Ðate
SECTION B * THIS SECTION APPLIES TO PROVIDERS NOT OTHERWISEENROLLED IN MEDICAID PROGRAM.
As condition for provicling services to Medicaid eligible children, I agree to the following:
1. To conform to all applicable Federal and State laws and regulations,
Z, To offer services in accordance with Title VI of the 1964 Civil Rights Act and Section 504
of the Rehabilitation Act of 1973, as amended,
3, To keep such medical, case or business records as are necessary to fully document the
extent of services provided and to fumish these records to the State Medicaid Agency, the
U.S, Secretary of Health and Human Services and the Medicaid Provider Fraud Unit of the
Office of the Vermont Attorney General, if requested to do so.
I understancl that this Provider Agreement does not allow me to bill Medicaid directly for servioes I may
furnish to Medicaid recipients.
Signature of Provider Title Date
Si gnatLrre of Sup ervisory U nion Representative
HR Medicaid Providcr Form 07122009
Date

EMPLoYEEDIRECTDEPoSITAUTHoRIZATIoN
l, the undersigned, hereby authorize the Burlington school District to directly deposit my
paycheck to tÉe bank of my choice as listed below'
By signing this authorization, r hereby hord the Burríngton schoor District harmress from any and
all liability for act¡ons oi inaciions of ány party involviO.in thed¡rect deposit process as long as
the Burrington schoor-óisti¡ct nas compreted'its obrigations affecting the direct deposit'
ïhis authorization sharr remain in fuil force and effect untir such time as the contractual provisiQn
oroviding for the direct deposit has been altered by the Board and the Association in some
respect óther than the relevant dates'
BVO CH o AI
BANK NAME
Routing ccount #
DEPOSIT OPTIONS: (Select OnlY One)
DePosit ENTIRE Net PaY Amount
Deposit $
-
of Net Pay Each Pay Period
EMPLOYEEEMPLOYEE NAME:
DateEmploYee Signature
Account TYPe: Checking Savings
** Please complete one form for each Deposit Request

BURLINGTON PUBLIC SCHOOLSVERIFICATION OF EMPLOYMENT
Teacher's Name: Date:
Current Address:
TO: School
Address
I have been offered employment by the Burlington School District. Since my salary will be
determined by my y"uÅ oiu.rified teaching experience, I would appreciate your completing this
form and forwarding it to the following:
Burlington School DistrictHuman Resources150 Colchester Avenue
Burlington, VT 05401
Previous Name (if aPPlicable):* * {< *. i. * {< 't lk r,< {< rF i< * * ,t t * {< àl' ¡< l' * {< ¡l' * {' :t t * * * * * * * 'f tf * d< {' * * {< t( * *' * {< * ¡l"F {' {<:f t' t' t {< * :f X< t* tfi i' d( {< tk * * {' *< * {< :fi *
TO BE FILLED OUT BY PREVIOUS SCHOOL
Date of Hire
Signed
Date of Term
Leave of Absence (1 semester or more)?
Position held: Licensed Teacherunder contract
# days per school Year
-
Full-time
(from month / to month)
Administrator Other
Date
Part-time FTE ----.---.----.-
Print Name
Position
Signature
Telephone No
THANK YOU
RM
SECTION I . EMPLOYERiEMPLOYEE INFORMATION
PLEASE 5EE SECTION S ON PAGE 2 FOR SUBSCRIBER SIGNATURE
. = lnclu(lcs Party to ¿ C¡vil Union ar Darneslic p¿rlner
" = Aciditìonðl Dotumentatio. ßequìred
¡rlto nine
!.'rLmt2345ó50)
COMPsLUf.c^n€AÍ,I'LYING ÍON IvxrH5A SLUI [ ,unr ttso orurcnn,
No,
ÉfFEC'fIVE DAIÉ
N[wGnoup f]rnn¡lsrrnneo rRoM ANorHEfi Bc8svf PL^N rr¡ñsler'inq Írom certllì(¿lc l¡o
[rrnrH flaooelor'r [ *nRRtrce/ctvtL ut"'o''l florvoncE floeerrl
flcounr onoeRe o cnoNCr.. flnooraÛaove srous€/PAßTY rO Clvll UNION OR DIP€NпNI (Llst In StCrloN 5l
PAR I NEfìI'
I
oltoTMPLOYÊ8,/CHILDDA]E
5lN6LI r^MrtY\{rôôwED
f]¡clve Inerrneo Iconr'*umtoN
(Check.oñe, ¡hon go ro sEcflo¡f 5l. SECTION2-NÉw ENROLLMENT
I sloust tunr,*c act o:
SEçTIQN 3 . CHANGE (Çhe.ck,all that.rPPlYf
Ioruen (erpla¡n) -
REAsON TON CHAÑG6 TVÉNfDATE Of ¡VÊI'JT
IYPF
TO A CIVIL UNION
DtvoRc¿o
Ier.rt enlotscHttncÉ FßoM MILIIARY
I tunE cueruce [r'cl c"eNctflr-oss or covrnace"
! noo*tss ct n*ct
TMPLOYÊÉ ONIY
EMPLOYTÊ/CHILDFLN
I olrn etrnolrmtt'tr I colrlluarloN ot covtRAGÊ (cosÀ^/vlP!fi)
Inilvnrnt Int-xrne fllarotcot''lnsunrLÉMËNT" (At(àchcopvolMedìcarecôtd]
fl nrrusrt il
Sign¡tuæ fliquiredSECTIoN 4- P'oLlcY516N HENE
lsrhsc.iber or Group Bencfits M¡nager)
X
VOI,UNTARY CANCIL
iSubrcr¡ber 5ig¡,rlurc)
(ANCTL CON fINUATION COVÍNAGE
LEfT ÉMPLOYMENf
(6roup Bcnefill Mànaqer 5l9nÀtu'e)
El or¡r¡n, Éxpl¿¡n-------.--'----.{Subscriber Slgnèture}
SECTION
our of5o(lalcôlle(tlotìnr¡ndate¡t.lcll[rIMPOßTAM Fèiler¡l
ODEOORTO BE A
PRIMARY CÀRË PHYSICì¡r\N (t'Cf'Ì iNronMA-tloN(IF MANA6ED €ARE)
PCP of
^.e you ð <ulent
No.
NoYer
of
Arc you a culen( Pðt¡cnl? No
PCF ot
Are you ¿ curcrl Pat¡enl?No
ol
5SN""
MEMBÉR INFORMA]ION
FIR5f NAMÊ
Spouse/Party to ¿ Civ¡l Unlon
FIR5T NAMELAS T N^rv1E
lncðp¿(ìtated tlepende¡l 26loldcrIìÉMOVF- - Depêndcnt Child'
frÊsl ñAMËt-Â5T l'l^¡t1t
ln(¡pa(ilðlcd dependeol 26lolderoependcnì Ch¡ld
FINST NAMÉL^sÌ N^¡,1f
DOB
nEMOV€ - 5ub5(¡¡ber
f]r,rot"Ifemale
Iuot"Ir..otc
IAS-f NAME
ADD ssN""
DOB
s5N
DÔB
5SN
DO8
Ir,,lutu
flru^,te
Iruot"flrnmuto
Ir,roro
flro,.are
^re you à curcnl Pdlierrt? f] v"'
PCP l.låme
No
olN¿me
NoYe5
ola cureni P¡liènt?
Are you a currL{ìl P,llienll NoYe5
Ir,lul.,flt"*atc
DÔB
ln{¿p¿(ilàled dePendcnl 26loldcrLMOVI -Dcpe¡dcnt child
s5NFINST NAMELA5T NÀMI
lû(¿pâril¡ted dQpcndeñt 2ólolderlltMOVt OcPcilde'il ChrldssNÊIR5T Ñ^MTLASf N^tult
290 tc('(rtll 7) f'^6F I Ot 2
"' - Physi(ian A55ist¿nl5 & Nurse l)ra(titíoncr5 are not vôlid
,.. . SSí ,".i"¡,",i nge 45 ðnd older (terlerðl nìðrrdate requires the coliecl¡on of SSN)
lnsurancedèntôl Medlcarel?anotherwhh of (lncludingplånhealthbeent5 coveredwith wll ofUS, ofyour3ny dependlnsutanceAfter covelågê youheâlthobta¡nyouSECTIONtoNotf (Go 8)below)section trthe{tf applicablecompletepleascIves yes,
PAfif BPARI AfFfltßtrY NnNAMT
COMPAI.IY
ADÞR855
POLICY
fYPE
PSRSON fl, rtnson flrnr,r,rvOF
flzrtason flrmrttPERsON
Do you have exlitlng health care coverage thât you sre replðclng with thls covefðge? [Ves ElNo
Þ rrrr.r,rrr'r 'on^rr*,
X
or its designated agênl, anymy coverage. I understand
cafeheahh providerðuthotizetheto best anytfUêafe comand of my knowledge.furnlshed me pleteôlland lnformâtlon bythlsonthethôt stâtements pplicationcertfu thôtof olalc0fo trcat¡ncntwlth or futurcconnêctlon pârtln mylnformatlon acqulredofShleld Vormont,CrossBlue Êlueanddisclo¡eto t0 shallsame benottheand thatcleatedlrno whatsoevet appllcatlonby thlsthåtto rightorhe¡eln addedhereafternameddependentôny GOVERNEDAREMYTHAT BENEFITSVermont.of UNDEßSTANDBlueand 5hleldlssued CrossBluelscontÍðct byandunless the acluallYuntllconsldered acceptedOF COVERAGE.AND OUTLINEOF CERTIFICATEMYBY THÊ PROVISIONS
SIGN HERE
280 J0ó (6/12 ) PAG€ 2 Of 2
You can vlsit our website at wwlg--þgþSyl,EgllL
OFH H AR ERAGE - NUAL FO
Employer: you are required to maintain these documents together in a file in the event of an audit (for a minimum of three years)
I I certify the information provided is accurate and true to the best of my knowledge and belief
E 16-
Employer's Legal Name: BurtingtonSclrool Dístrict n 1 P n 2 P n Family Date of eligibility
PRINT YOUR Employee's Full Name:
Employee SS # I I DOB BSD POSITION-
EMPLOYEE TO COMPLETE: Ihe purpose of this form is to obtain information regarding your }URRENT health care
coverage. The information certified'on this form wittbe used sotely for fhe purposes of dete_rmining if your employer must
pay Hiatth Care Contributions andfor /RS ACA reporting, as required under 21 v's.A', Secfion 2003 & IRS regulations
M AM LE RE CO BY and
! I have elected to accept the health care coverage offered and provided by my employer
AM HEAL BY o BUT
N A co appropriate box):
! I have no health carc. (An employee must carry a current private group health in-surance, NoT a government
sponsored p lan, in order ta dectine our policy & be etigibte to receive a payback in lieu of enrollment)
! lhaveMedicaid, OR IlhaveGreenMountainCareOR IlhaveTri'Care 0R ! lamafull
iime employee and have health care as an individual on the Vermont Health Benefit Exchange DEcLtNtNG
BSD HEALTH CARE COVERAGE. PARTICIPATION IN A GOVERNMENT SPONSOR ED HEALTH CARE PLAN RUTES OUÏ
A PAYBACK IN LEIU OF DISTRICT HEALTH CARE COVERAGEPER 'RS
RUIES. EMPIOYEE INITIAL HERE:
IAM T ELIGIB FOR TH co GE BY EMPL appropriate box):
! I am a part-time employee who works less than 30 hours per week AND I have coverage from a source
other than Medicaid that offers hospital and physicians services,
n I am a seasonal employee who expects to work for BSD 20 or fewer weeks during this calendar year
AND I have coverage from a source other than Medicaid that offers hospital and physicians services'
n I have Health Caie Coverage that includes hospital and physicians services: LIST Carrier & provide
copy of insurance card:
n I have no health care.red by! am a part-ti me 0 r SC as0nal employee and do not have health care c0ve rage 0R am c0ve
Med cal d G reen Mou nta n Ca re Coverag e purchased 0n the H ealth nsura nce Exch ang e 0r Tn -Ca re
Employee Signature: Date
PLEASE RETURN THIS COMPLETED FORM TO HUMAN RESOURCES AT CENTRAL OFFICE
S:\Frontoffice\HR Specialist\Forms\DECLARATIoN oF HEALTH CARE FORM 1617'docx
Our dental carrier is CIGNA. Specific info on co-pays and deductibles is on a
summary handout sheet. Be sure to ask for this'
Your dentist will need your ss #, date of birth and the group number
CN001 3217048 to reference our plan. The customer service number for
CIGNA is 1 -800-ClGNA24 (1 -800-244-6224)
There is also a great website that can help you in determining what services
were performed and billed for all of your covered members. lt is free, and you
have io register but it is well worth the effort for the helpful reference and info it
provides.
The Link for signing up for your own individual account info is:
llm bl
There is helpful info on here as well as a place to print out a card facsimile for
dental.
The Burlington Board of School Commissioners account number is
CN001 g217048. Add that information to the "card" that you print for yourself.

CIGNA Traditionøl Benelit SummaryBurlington Boørd of Schools
Cigno
CIGNA Tradìtìonalß
'tooth nìissing priol ttl covclûgc llndcr
PrcÍsâtmcnt rcvicrv is availablc on a voluntary basis whcn cxtcnsivc
âre not
dcntal work in excess of $200 is proposcd
ncck canccr radiation. Thc progtam provides:
r 100%o covs¡ago lbr ccrtain dentål procedures
o guidancc on bchavioral issues relatecJ to rlrsl heaìth
. discoutrts on prcscription and non'prescription dcnlâl product$
For more information and to sec the comple te list of eligibl" coniitions, go to www.mxcien-a.cqm or call customer s crvicc24/7 at I '800'CICNA24'i+CICNA Dortal will ,"i,nuur." o""uiding to R.uson"ùle and custonrar! Atto*r,n"-t ¡,ii ttt" dcntist may balancc bill up to thcir usuol fces'
Cølendar Moxímun III exoenses)I, II and
$25 per person
90rh$7s
AllowanccsYou Pay
ofReasonable and
Plan Pays
.4nnual Deduclibleindividual
Reìmburcement
No100o/o
Oral DxamsRoutine CleaningsFull Mouth X-raysBitewing X-raysPanoramic X-rayPcriapical X-raysF'luorìde ApplicationSealantsSpace MaintainersErnergency Care to Relicvc Pain
F'illingsRoot Canal l'hcrapy/EndodonticsOssçous SurgeryPeriodontal Scaling and Root PlaningDcnture Adjustments ancl RePairs
Oral Surgery - Sirriple ExhactionsOral Surgcry - all except simple extractions
AnestheticsSurgical Extractions of Impacted Teeth
Cløss I - PrevenlÍve Díagnoslìc Care
Exams
II - Basic Rcstoralìve Care
Crowns a¡rd Ito
t,ifetime Maximum
III - Major Restoralìve Care
Class IV -
CrownsDcnturesBridgesInlays/OnlaysProsthcsis Over
¡*80o/o*
5IVo*50ù *
s0%
Dependcnt children to age 19
50%$1,000

CI6NA Tradilional Etcclusíons arul LimìlallonsProcedure Exclusions an¡l LinltationsI-âtt Tìntrants L¡trìit 500/o covcragc on Class lll an<l IV for l2 or 24 nltnlhsFlxanrs 'frvo pel Calcrrdar year
Pluplrylaris (Cìuarirrgs.¡ 'fwo pcr C{lcndût ycalFluoride I pcr Calendar ycar lbr pcoplc undct 19
llistopathologic Exurns Vorious iitnits per Calcndar ycar dcpcr:ding on spccific tost
X-tìays (routinc) Bitcrvings: 2 pcr Calendar ycar
X-Rays (non-routinc) Full nror¡thl I every 3 calenrJar ycars, Panorcx: 1 cvcry 3 calondar ycars
Mo<lcl Payublc only whcn in coniunction with Ortlìo workup attd cxtcnsive llcrio ncâtmcnt
Minor Pcrio (non-sLrLgical) Va¡ious limitations rlepcnding on thc sctvicc
Pclio Surgcry Various lirnitations depcnding on lhe scwice
Crorvns and Inlays Rcplacernent every 5 ycars
Bridgcs Rcpl{ìccmcnt evcry 5 YearsDcntllrcs and Partials Rcplaccmcnt cvory 5 ycors
Rclincs, Rcbases CoveretJ if rnore than 6 r¡onths afler installotion
Atijustrnents Covercd ilmorc than 6 months afìe¡ installation
Rcpoirs - Bridgcs Rcvicrvcd iftnotc tban once
Rcpairs - l)entt¡res Revicwcd ifmolc than oncc
sealants Limited to postcrior tooth. ono trcâtment pcr looth cvcly threc years
Space Maintaìners Linritcd to non-Orfhodontic trcahncnlProstlresis Ovcr Inrplant I pcr 5 yearu jfunserviceabÌc antl crnno( bc rcpaircd, tscnelÌts a¡c bascd on thc amorrnt paynhlc lhr nr.rn-
prcciolls mcltls. No porcelain orwhite/tooth 0olorcd ntalcrial on tnolat crowrs or bridgcs
Ältcrr¡atc Bcncfit Whcu .orc than one covered Dcntol Servicc coultt provide suitablc trcatnlent bascd on conìmon dcnlsl standar<ts, CIGNA
Hc11lthcarc will detcnninc thc covcrcd Dcntal Scn,ice orì which paynrcnt rvill bo b¡scd and tlrc cxpcnscs that will bc jnoiuded
ns Covcrcd Expcnses
Benefit Exclusions;o Scrvices porforntcd printarìly fot costnetic rcosot'ts
. Replaccmen( ofa lost or stoìcn appliancc
. Replaccnrcnt of rr bridge or dcnture within five ycurs lollowing thc dâtc ol its original inst¿rllation
. Itcplacenrent ol'ô bridge or denturc rvhich orn be madc uscable according k) accepted dcntal standards
pcrirxûlnølly involvcd tccth, or l'cstoro occlusioú. Ven"ers ofporcclnin or acrylic matcrials on crowns or pontics on or rr:placing thc upper antl lowor ärst, sccortd and third nlola¡s
n tsitc regishûtions; ptccision or scnti-preci.-ion fìltachnìcnls; splinting¡ A surgic¡l inrplant ofany rypet Instruction for pluque control, nral hygienc and tlict. Dental sorvices that <io ¡¡oi rncct conrnìon dcntal standards
c Scrviccs that arc deenrcd to be ntctlical serviccs¡ Sc¡viccs and supplics rcccivcd from a hospiml. Chargcs which thc pcrson is not legally rtquircd to pay
. ch¡rgcs rnade by ¿ hospitâl which pertìrrnrs serviccs for the u,s. Govemmcnr iflhc charges are dircctly rclatcd lo a condition corrcctcd !o a nrilitar servicc
. Expcrinronktl or investigational procedurcs älìd hcatnlenlfit Any injury resulting lÌom, or ¡n thc coursc of, any cnlploymcnt for rvagc or profit. ,{ny sir:kncss covcrcd under any workers' conlpcruûtion or sintiiar lawo Charges in excess of lhc ¡c¡sonablc and custonlsry allowonccsr To tlre cxtclì! that paynrent is unlawful whcre tlìe pcrson resitjcs wlten tltc cxpenses arc incuncd;
grandparcnts, and thc spttusc's siblings and parcnts);
. I-'or chsrgss rvhich rvould not hove bcen made lfihc pcrson had no insuranoc;
r Fo¡ charges fot unncccssary cûrc, ncatnlcnt ot sulgcryi
Mcdicaid;I To thc cxtent that bcncfìts arc paitl or payablc for thosc cxPcnscs uoder lhe nrândrlor part of any auto insurancù policy wittcn lo colrrply rvith a "no-fartlt"
of yor¡¡ Dcpendcnts.
for that sèrv;cc unrier this plan and ony mcrlicni cxpensc plan orprcpaid trcatmcnt progrâm sponsored or madc availablc by youL Employer.
Gener¡il Lik I nsurartt'e (hn4ttu.t'.
subsidiaries o.f CtGN.4 l{eultlt Cu'poration unù CIGN¿l Denlal Heal¡h, Inc.
BSÐ279-s0 o 2012 CIGNA

Horace Mann Life lnsurance Company1 Horace Mann PlazaSpringfield, lllinois 6271 5-0001
Group Life lnsurance enrollment form
Horace Mannþounded by Educators for Educators
Group #440111 Department / GrouP #
Note: you must meet the actively-at-work requirements set forth in the policy in order for coverage to become effective.
Basic Life/AD&D coverage amount ! $25,000 (paras and food service) OR tr $50,000 (all other grouPs)
(employer-paid)
check the box below and indicate the appticable coverage amount if optionat Life (employee'paid) insurance
is being elected:
n I wish to elect optional Life insurance - coverage amount: $37,500 (if applicable)
Foryourprotection,statelawrequiresthefollowingtoappearonthisform.
Any person who knowingly and with intentto defraud an insurer submits an application orfiles a claim containing false'
incåmplete, or misleadin! ltatements of material fact may be guilty of a crime.
Completion of this enrollment form does not ensure that coverage will be extended. Coverage is subject to the
plan terms.
By signing this form, I hereby authorize my employer to deduct from my paycheck any funds necessary to pay for
the coverage that I have eteóteo. I agree inat å pñotocopy of this authorization is as valid as the original'
Agent name Agent # Date
Date
This product is underwritten by Horace Mann Life Insurance company'
Employee signature
Name (last, first, m
Social Security #
r P.O. BoxStreet Address
City
Employment DateMo Day Year
Birth dateMo Day Year
Gender
¡M DFE-mail addressPhone #Area Gode
Job titleBurlington SchoolEmployer District
Primary beneficiary and relationship:
Secondary beneficiary and relationship
BURLINGTON.ENROLL

MEMORANDUM
TO: Administrators & Teachers Eligible for District LifeInsurance Benefits
FROM: Burlington School District Benefit Administration
RE: Life Insurance Coverage - Rate Effective L/ t/2OI5
The supplemental life insurance benefit of $37,500 is available in additíon to
the basic coverage of $50,000. The cost to you is $6'75 per biweekly payche-ck
($14.63 p., to'ith, or $175.50 per year) for the additional $37,500 worth of
life insurance coverage.
please indicate your name and the coverage desired below and return this form
to Maura Sawteile, Benefit Specialist at Central Office.
PLEASE CHECK ONE:
tr yes, I wish to elect to purchase the additional llfe insurance coverage
in the amount of $37,500 with $6.75 deducted from my biweekly pay
(teachers) ot $f+.OS deducted from my monthly pay' (administrators)
n No, I do not wish to elect to purchase the available additional life
insurance coverage of $37,500'
SIGNATURE: --
NAME: (PRINT)
s:\Frontoff¡ce\HR speclaligt\BENEFITs\LIFE HoRAcE MANN\Life lns Tchrs Adming addl.doc

Burlington School District403(b) Plan
SI]MMARY OF PROVISIONS
Provisions effective January l, 2016
Elisible Emnlovees:
. All employees except those who normally work less than twenty (20) hours per week'
Participation Date:
¡ For employee pre-tax salary defenal contributions: date of hire
Employee Salarv Deferral Contributions:
o Contributions are made with pre-tax compensation through payroll deduction; maximum
dollar amount may not exceed the amount indicated below.
- up to $18,000 îor 2016 (plus an additional $6,000 for a total of $24,000 if age 50 or
older by year-end)- may stop defenals or change your deferral amount on any pay period (a request for
change must be in writing ar-rd received by the payroll administrator at least seven days
prior to the effective date of the change)
Rollover contributions: amounts which participants received from a prior employer's plan
(including 401(k), p-ftî sharing, 403(b), -ott.y purchase, and defined benefit plans) may be
rolled over tax-free to this Plan'
vesting: - all contributions and earnings are 100% vested immediately
Hardship Withdrawals: permitted from cumulative salary deferrals (not the earnings) for
@idènce(partofthedownpayment),paymentofmedicaleXpenSeS'prevention of fo.arlorrre or eviction, college expenses, catastrophic loss to your home' or
funeral expenses. Employee must cease .onttibutions to the plan for 6 months following a
withdrawal. Hardship wiihdrawals are taxed as regular income plus a 10% excise tax penalty ifyou withdraw the money before age 59%.
Benefït vments:
o Timing: as soon as reasonable following the participant's termination of employment
o Form: any options available under the investment contract(s) you have selected
Ouestions: contact Nathan Lavery at the Superintendent's offîce for additional information
phone: (802) 540-0893 e-mail:nlaveryG?bsdvt'org
Forms: contact Erin Labonte at the Superintendent's office for Salary Deferral Election
Forms and supporting materials'phon.,(802)864-3458e-mail:elabonte@'bsdvt'org
1

Burlington School District403(b) Plan
DE S- SAI,ARY DUCTIO AGRE NT
Ernployee Name:
Provider Information
Name
Address
City State Zin
Check one: D New Agreement fl Change Í No Change
Salary deferral/reduction amount. This Agreement is effective immediately upon acceptance
UV tf-r. Plan Administrator, and I may modify the Agreement at any time' I authorize the
n*ptoy.l. to withhold from rny Compensatiôn (andtreat as my deferrals) the following amount:
Í currently enrolled in a Salary Reduction Agreement and I am electing to not change my
current payroll deduction amount'
r]$ per payroll
Authorization
X
Í Zero.I hereby elect not to participate or to terminate my prior Salary Reduction Agreement'
compensation to which Agreement applies. This election applies to all compensation'
Duty to review pay records. I understand I have a duty to review my pay records (pay stub'
etc.) to confirm the E-pl;;;;;{;p.ù hai implemgnleã my salarv reduction election.
Fufthermore, I have a duty to inform th.irl;'Ád;inistrator if I díscover any discrepancy
between my pay r..Jtðt ãnlthis Salary Reduction Agteement' I understand the Plan
Administrator will dgatmt failure to ..pott uny wrthñolding errors fo¡ flY payroll to which my
sarary Reduction Ag;;;;r-t'"ppii"s, uy ihe cut-off date foithe next following payroll, as my
affîrmative erection to defer the amount *itqut *ittth.ta lrn"ruding zero). However, I thereafter
;"y ñàìiimy Oéfeirat election prospectively, consistent with the Plan te1111s'
Signature of Pløn AdministratorNathatt Lavery, Director of Finance
DateSignature o.f' EtnPloYe e Dale
PLEASERETURNTHISFORMToTHEPLANADMINISTRATOR
2

Burlington School District403(b) Plan
ENROLLMENT PROCEDURES
The Burlington School District offers all eligible employees the opportunity to participate in a
tax sheltereã retirement plan for the benefit of its employees, It is intended that the plan comply
with the requirements of and qualify under Section 403(bX7) of the Internal Revenue Code' The
plan includås Annuity Contraóts and Custodial Agreements offered by vendors on the district's
provider list (Appendi* e of a03@) Plan Adoption Agreement: Funding Vehicles). The fact that
à particular conlract or custodial account may be available from a provider, does not constitute
an endorsement, recommendation, or approval of any kind'
General Information:
Each employee of the district is given an opportunity to participate in the district's 403(b) Plan
by entering Into a 403(b) Plan Salary Reduction Agreement except as limited below:
(a) Employees whose salary reduction would not exceed $200 per year'
(b) Employees who normally work less than2} hours per week'
Enrollment Procedures :
To participate in the 403(b) Plan, or to change salary reduction amounts from one provider on
thelist to ãnother provider.on the list, employees must follow the procedure below and submit
the completed forms to the school districiassistant payroll officer in the district business office,
telephone number 864-8458'
1) choose your 403(b) provider from the district's provider list
2) establish an account with this provider, and
:j thoro.rghly complete the 403(b) Plan Salary Reduction Agreement and forward to the
school district PaYroll officer.
All three steps must be completed before a Salary Reduction Agreement will become effective'
Termination/Suspension Procedures :
A written request must be submitted to the Assistant Payroll Officer in the Business Office at
150 Colchester Avenue, Burlington, VT 05401, telephone, 864-8458'
Contribution Limits:
According to IRS, employees can contribute up to the lesser of 518,000 or 100% of gross annual
salary foicalendar y"à, iOtO. In addition, if they are age 50 or over on December 3 1 , 20 I 6, they
can contribute an additional $6,000 for a potential total amount of 524,000'
J

Burlington School District403(b) Plan
VENDOR IN RMATION
Vendor (Company) NameI ING (Aetna Life Insurance & Annuity Co.)
One Orange Way, A3NWindsor, CT, 06095-47 7 4(860) s80-1649www.ing.gom
2 American Funds Service ComPanY
P.O. Box 2280Norfolk, VA 23501-2280(800) 421-ol 80
www. americanfunds. com
3 American General Life Insurance Group (AIG)P.O. Box 4373Houston, TX 77210(800) 231-365swww seneral.com
4 Ameriprise Financial1262 Ameriprise Financial CtrMinneapolis, MN 55474(800) 862-791ewww.ameliprise*com
5 Fidelity InvestmentsP,O. Box 770002Cincinnati, Ohio 4527 7 -0089(8oo) 868-1023www.fidelit)¿.com
6 Great American Life Insurance Co' GALIC525 Vine St., PO Box 5420Cincinnati, Ohio 45201(800) 6es-1471www.GAFRI.com
7 Horace Mann1 Horace Mann Plaza, P,O. Box 4657
Springfield, IL 627 08 -4 6 57(866) 999-r94swww.horacemann.com
4

Burlington School District403(b) Plan
Vendor (ComPanY) Name8 Metropolitan Life Insurance Company
400 Atrium Dr.Somerset, NJ 08873-4172(800) 638-s433www.metlife.com
9 National Life of Vermont1 National Life DriveMontpelier, VT 05604(800) 732-8939www.nat ionall ife.corn
10 New York Life Insurance & Annuity Corp'
463 Mountainview Dr.Colchester, VT 05446(802) 6s4-rt2rwww.new)¡orklife'com
11 Putnam InvestmentsP.O. Box 8383
Boston, MA 02266-8383(866) 201-7262www.putnaminv'com
12 Security Benefit (NEA ValuBuilder)P.O. Box 750497Topeka, KS 66675-0560(ssï) 724-7s26www' s ecuriî¡b ene fit' c om
13 T. Rowe PriceP.O.Box 17479Baltimore, MD 21297 -I47 9(800) 4e2-7670www.troweorice.com
14 The Vanguard GrouPP.O. Box 1106
Valley Forge, PA 19482-1106(800) 662-2003www.vanguard.com
15 Variable Annnuity Life Insurance VALIC (AIG)
P.O. Box 15648
Amarillo, TX 79i05(888) 478-7020www. ai cretireurent. com
5

Burlington School District403(b) Plan
Applicable Salary Deferral Limit & Age 50 Catch-up Table
Tax Year Deferral Limit Age 50 or Older Catch-up
2005 $14,000 $4,000
2006 $ 15,000 $5,000
2007 $ 15,500 s5,000
2008 $ 15,500 $5,000
2009 $ 16,500 $5,500
20r0 $16,500 $5,500
20r1 $ 16,500 $5,500
20r2 $ t 7,oo0 $5,500
2013 $ 17,500 $5,500
20t4 $17,500 $5,500
20r5 $18,000 $6,000
6

BUF. T'I"NTGîON SCTI OOL ÐIS TRJCTS.EC"JON 725 PLANrlsg!rylgstiÞles=---
City, State, ZiP Code
Plan Year
2015"20'16
Phone
ElecloN oF HEALTH C¡ne RetrvlauRseMENT
DateNarne (Last, First, Ml)
Mailing Address
Social SecuritY #
e-mail address
Employee's Signature:
I eleot to participatc in the Health care Reimbursement Account for the plan year' (see the
',Ílealth Care Reimbursement Worksheet" and list on "Qualiffing Expenses") NOTE: Ioør
contributian þ the Health Care Reimlturse¡ttent Account ís limited lo 62'550 per employee'
thc " Á.1'lo r rla h I e Ca r tt ,4 a t, " ()ve t"l' hc'C tn t ¡il e r benc.fils arc linr b l)oclors' Prcrcriqtiottt only!-1uc lo changes unrltr
Amount to be cleducted each pay period:
Number of pay periods in the Pla¡r Year:
Total for Plan Year (1 x 2):
n I elect NOTto Parltc ipate in ths Health Care Reimbursement Account'
WalveR oF PREMIUM CoNvenstotl
AlÌ emploYee-P aicl health ar¡d dental insttrance prenr iurns will automatically be paid through tlie
Burlingtorr School Dislrict Scctiorl 125 I)lan unloss you e Iect not to PaÉiciPate.
STOP: Can.tider Ylur resql nse. Checking thi,ç l:ctx rttay tlot do wl¿al )¡ou think it will do. Most
employees elecl trt pctrtici¡;ate ín thi.ç part of the Plan bY NOT checking the box, Check thís box onlY
you do nol wanl Your in'surance Prent iums deducted on a Pre-tax basis
n I clect NOT to ParticiPate ilr the I' remirtm PaYment Part of this Plan, This mearls all employee-paid
iurns will bc id with aller-tax do llir¡'s. thus rccs no rll tax sav
I have read and understand the "Other Terms and Conditio ns Statement" {found
onpage 2) before signing below'
1.aL:
3.
$x$
Date
I elect to participate in the Dependent care Assistance Account for the plan year' The maximum
amount which may be atlocated to the DepenJent Care Assistance Account is $5'000' (This limit
may be reduced if you are tnarriecl and you or your spouse are.not enr¡:loyed full timo or your
soouse is a fril_tirne stucient or your rpour""is-uräùl- tå care for rrirn/hcmerf. prease see ths Plnn
Ádrninirttutor for detai ls')
1
23
$X
$
Electlo¡¡ oF DEPENDENT Ceng Ass¡ste¡¡ce
I elect NOT to Partlc ipate in the Dependent Care Assistance Acoount'
Amount to be deducted each pay pcriod;
Number of pay periods in the Plan Year:
Total for Plau Ycar ( f x 2):
l of 3

TJ N milt llTf,\Tm\
TO;RE:
BSD Employees (who work 20 or more hours a week)
õ""t¡on ì zs pr-eru YEAR (July I , 2a16 - June 30' 2017)
open enroilment for the upcoming pran.year is Now rHRouGH June 17, 2010. lf you are interested in
participating in the Hàa[h'care añdlor the Dependent care Reimbursement accounts, you will need to
complete two forms to enroll: Election of denefit Form and Personal lnformation Form by June
17,20',16.
AFLAC, which allows you to privately purchase insurance for enhanced protection, is eligible through
Future pranning Associates, rnc. for premium Expense Account reimbursement. rf you are interested in
participating in the premium expense Ác"ornt, you win need to comprete the privatery Purchased
insurahc" pbtic¡es form by June 17, 20't6'
The sectio n 125 plan summary plan Description and section 125 Forms Kit information may be
found on the eso wá¡site undlr staff Forms (link under staff on the top right of website)' The
summary plan Description provides nelptul information to many basic questions regarding the
Section 125 Plan.
IMPORTANT PLAN FACTS
. The Plan Year will run from July 1,2016 - June 30' 2A17
. Your contribution to Health Care Reimbursement is limited to $2'550'00
. your contribution to the Dependent care Assistance Account is $5000,00 maximum per famíly
. once you make your benefit etections, they cannot be changed untll the next plan year' unless
you have a change in status, i.e.' Marriage, divorce, dependent status change, birth, adoption'
. Emptoye". jå noi ñave to párticipátä in irré BSD group health insurance plan to be eligible to
particiPate in this Plan. your election amolnt will be deducted on a pre{ax basis from each paycheck
When filling out your Election of Benefits Form,
July 1 ,2016.
PLEASE NOTE the number of pay periods you have after
Teachers _ 26 pay periods; paras & Liaisons -22 pay periods; personar services (year round) -26 pay
periods; personar s"*¡"år' (schoor year) - 22 payi: Maintenanc e - 26 pay periods; Admin Assts (yeat
round) - 26 pay p"riois; Áo*in nssts (school veár) - 26 pay periods; Administrators - 12 pay periods
Return your completed forms for enrollment to the Business office, Attention: Erin LaBonte by June
fi, 2A1A. lf you are not parlicipating, you do not need to do anything'
IìlìO: l'his nr¡te¡'iitl is'li) r'r{lttest a¡t tr:colnlltotlltt
YÀW OIIENG - Strpslttt'¡'l eNtltlx'r
150 ColcllEsrER AvL.. - BtJ¡ìLlN(ìloN VT 05'l'01
Pl¡olru: s0?-865-5332 - F¡x; 402_96,1.-8501 - Wtitlsl,f E: www.Ilsl)VT'()R(I
in alrr'¡tatc lì¡rnr¡ts {ì¡r Dct'sons rrith tlisr¡hilitics'
t:r¡ll :. stxl.'¿lill.0l0l ('l-lY) or I lt00,ri9()l{}5(\'()i(ìe)'¡rv¡ril¿lllc
ion, ¡rleasc

To: ParticiPant
From: Jaime Palmer, Future Planning Associates' lnc'
Date: APril L5, 20L6
Re: Health FSA (Health Flexible spending Accounts)- claim Reimbursement Requirements
At the beginning of each new Plan Yearwe need to have current documentation from your Doctor
or physicar rherapist stating your condition and treatment for the condition erigible for
reimbursement, e.g., swimming 3 times a week due to a specified condition' Expenses for your
generalwell being, such as "swimming is a good exercise, you would feel better if you swam three
times a week," would not be an eligible expense'
over-the-counter {oTc} prescriptions need to be updated each year as well'
Therapeutic massage must be a treatment for a medical condition, as with the swimming
example,ifthemassageisforyourgeneralwellbeing,itwouldnotbeaneligibleexpense'Proofof massage expenses must include a receipt or invoice that indicates the masseuse/masseur is
qualified as a massage theraPist'
This informat¡on must be updated each year, even if your condition has not changed, beginning
the first month of each new plan y.rr; ..g', the new Plan Year begins July L' 20L4' we need the
documentation from the Doctor or Rhysical Therapist dated in June, 20t4 or later'
Reimbursement requests for specific services or products will not be processed until we receive
the updated documentation'
TMPoRTANT: The documentation must be on the Doctors' or physicat rherapists' stationary,
prescription ,,pad,,and signed and dated by the Doctor or Physical Therapist.
we need this updated information since we are responsible for the legitimacy of all claims; we
must have the documentation to confirm that all reimbursements are paid from valid claims'
We thank You for Your helP'
Please contact your Plan Administrator with any questions'
Related Documents











