Neurobiology of consciousness and its disorders Dr Parag Moon Senior resident, Dept. of Neurology, GMC Kota.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Neurobiology of consciousness and its
disordersDr Parag Moon
Senior resident, Dept. of Neurology,
GMC Kota.

William James (1890) defined consciousness as awareness of oneself (or one's own cognitive experience) and environment.
Consciousness encompasses two main components: wakefulness and awareness.
Wakefulness-state in which eyes are open and have degree of motor arousal.
Awareness-ability to have and having of experience of any kind
Bedside, wakefullness observed by looking at presence of eye opening.
Bedside, awareness mostly inferred by command following.

Dependent on ascending reticular activating system in upper brainstem tegmentum and midline and intralaminar nuclei of thalamus.
Extends through to cerebral cortex Thalamic reticular nucleus-responsible for
"gating" specific reticular information that is transmitted to cerebral cortex
Also provides feedback to brainstem centers that play a role in arousal and alertness.
Alertness
Neurotransmitter systems relevant to arousal are cholinergic, monoaminergic, and γ-aminoburtyric acid–ergic.
Neuropeptides (thyrotropin-releasing hormone, vasopressin corticotropin-releasing hormone, somatostatin, substance P, and neuropeptide Y)-modulating cortical activity and influencing cognitive processes.
Requires cerebral cortical activity that is intimately connected to subcortical structures
On EEG gamma or 40-Hz rhythm-produced by thalamocortical circuits during attention and sensory processing tasks.
Require binding of processed sensory information with memory, attention, and motor responses.
Synchronous across various regions, linking thalamocortical networks as well as the hippocampus and neocortex.
Awareness
Necessary for conscious appreciation. Involves awareness, on part of individual, of something
happening as a result of stimulus acting on sensory receptor.
Have discrete (modular) primary cerebral cortical–receiving regions and association areas for processing.
Primary sensory modalities include visual, auditory, somatosensory, olfactory, gustatory, vestibular, and visceral sensations.
Have temporal and spatial characteristics and are modality specific.
Are linked with memory and affect.
Sensation

Involves processing of sensory information, allowing a symbolic concept of what is happening in the external world.
Perception overrides sensation when both are present.
Conscious vision involves object recognition, process involving primary visual cortex, visual association areas and reciprocal connections with memory stores.
Prefrontal regions-plays role in choosing information to be consciously perceived with processing and linkage to other modalities including memory, motivational and motor areas.
Perception

Control process that enables individual to select, from a number of alternatives, task he will perform or stimulus he will process, and cognitive strategy he will adopt to carry out these operations.
Prerequisite, he must be awake and alert. Main features include directivity and
selectivity of mental processes.
Attention

Anterior cingulate gyrus, dorsolateral prefrontal cortex, inferior parietal lobule, centromedian and parafasicular thalamic nuclei, thalamic reticular nucleus, reticular formation of midbrain tegmentum and superior colliculus.
Dopaminergic and noradrenergic systems are important in attentional responses.
When axon of cell A is near enough to excite cell B and repeatedly and persistently takes part in firing it, some growth process or metabolic change takes place in one or both cells such that A's efficiency, as one of cells firing B, is increased.
Anterograde memory: hippocampus, parahippocampal gyrus, subiculum, entorhinal and perirhinal cortex, mammillary bodies, dorsomedial thalamic nucleus, cingulate cortex, fornix and tracts connecting these structures.
Memory

Amnestic individual, without ability to store conscious, explicit memories, cannot be considered unconscious as alertness is preserved and can interacts with environment.
Explicit, but not implicit, memories are accompanied by consciousness.
Explicit-hippocampus and related structures. Short-term retention of limited number of
items held in consciousness for immediate use.

Motivational drives help to determine behavior after person has attended to stimulus and assessed its significance relevant to competing internal or external factors.
Closely allied to crude consciousness, perception, goal-directed activity, and emotions.
Emotional cognition, including motivation-limbic and nonlimbic system.
Motivation-amygdala, hypothalamus, and associated limbic structures.
Motivational system

Hippocampus and amygdala on each side receive parallel-convergent projections from various sensory systems.
Hippocampus consolidates information into memory and accesses stores of recent memory in neocortex.
Amygdala-gives sensory information affective, experiential tone and expression of emotion.

Hypothalamus-role in outward expressions of emotion—autonomic phenomena and behaviors.
Receives afferents from various parts of brain including amygdala-diencephalon and hippocampal-forniceal-mammillary subdivision, cerebral cortex and reticular formation.
Hypothalamus- responsible for maintaining homeostasis through endocrine, autonomical, and behavioral inputs and outputs.
Involves network of numerous interconnected modular processors across vast regions of cerebral cortex (with reciprocal connections with subcortical structures) that provide parallel processing of information.
Executive function of frontal lobes-impact on conscious experience.
Frontal lobes-organize input, devise retrieval strategies, verify output, and place it in proper historic context.
Prefrontal-use this information to direct and plan further action.
Cognition and focusing of awareness

Language-left tempero-parietal region Cognitive awareness- frontal, inferior
parietal and superior temporal regions

Alertness-ascending reticular formation's activating role Awareness depends on an infrastructure of attention. Awareness of outside world (for all but olfaction) requires
parietal cortex for sensory processing and interpretation, after initial reception in primary sensory areas.
Sensory information channeled into limbic system through temporal lobes, especially amygdala.
Memory stores allow for appreciation of relevance or importance of contemporary experiences.
Motivation, self-awareness, and communications with the motor system relate to widespread integration of various cortical and subcortical regions.
Frontal lobes-executive role in directing and maintaining attention and in planning behavior.


Disorders of conciousness
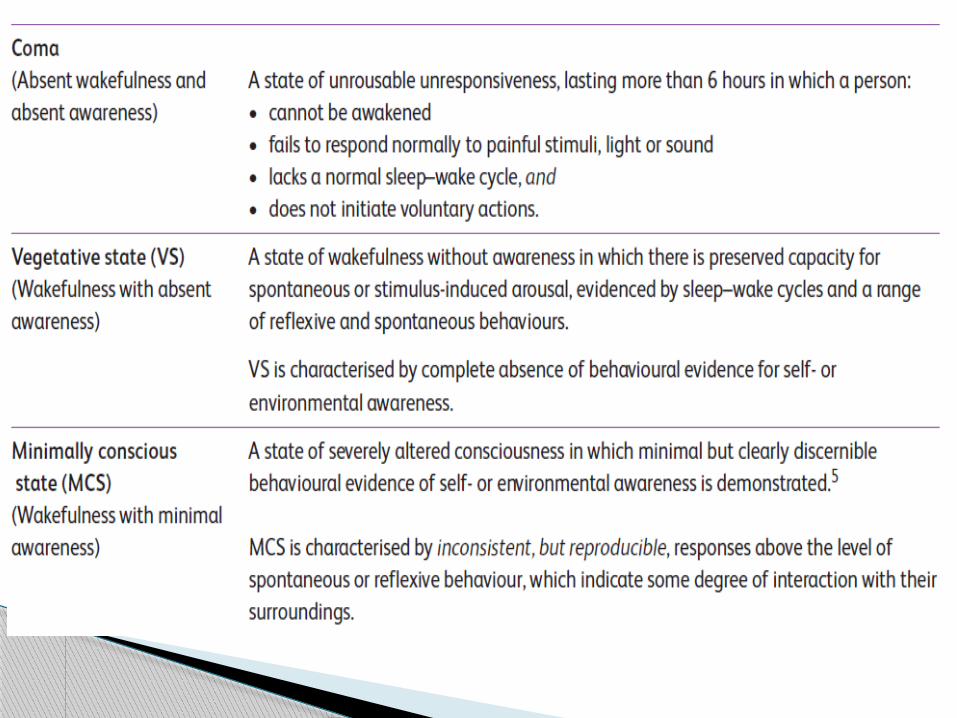

State of non-responsiveness to external as well as internal need
No awareness of self or of environment Patients lie with eyes closed and cannot be
awakened even when intensively stimulated. Lack of sleep–wake cycles No verbal production nor response to
command Can present reflexive responses to painful
stimulation.
Coma

Autonomous functions and thermoregulation reduced.
May require respiratory assistance Global brain metabolism diminished by 50–70%
of normal Caused by diffuse cortical or white matter
damage or brainstem lesion Coma must last at least 1 h to be distinguished
from states of transient unconsciousness. Prognosis made within 3 days. Can last 2–5 weeks.
Unresponsive wakefulness syndrome Defined by eyes opening, either spontaneously or
after stimulation. Sleep–wake cycles characterized by alternating
phases of eye opening. Autonomous functions are preserved Breathing occurs usually without assistance. No intelligible verbalization No voluntary response No signs of awareness of self or environment Awake but not aware.
Vegetative State

Brainstem functions are preserved Cortical and thalamic injuries are present. Brain metabolism diminished by 40–50% of
normal values. Able to perform a variety of movements such as
grinding teeth, blinking and moving eyes, swallowing, chewing, yawning, crying, smiling, grunting or groaning.
Motor behavior is reduced to a few stereotyped or reflexive movements
Do not track a moving object or their image in mirror.
Persistent vegetative state >1month. Permanent vegetative state >3month
non traumatic etiology and >1 year traumatic etiology.
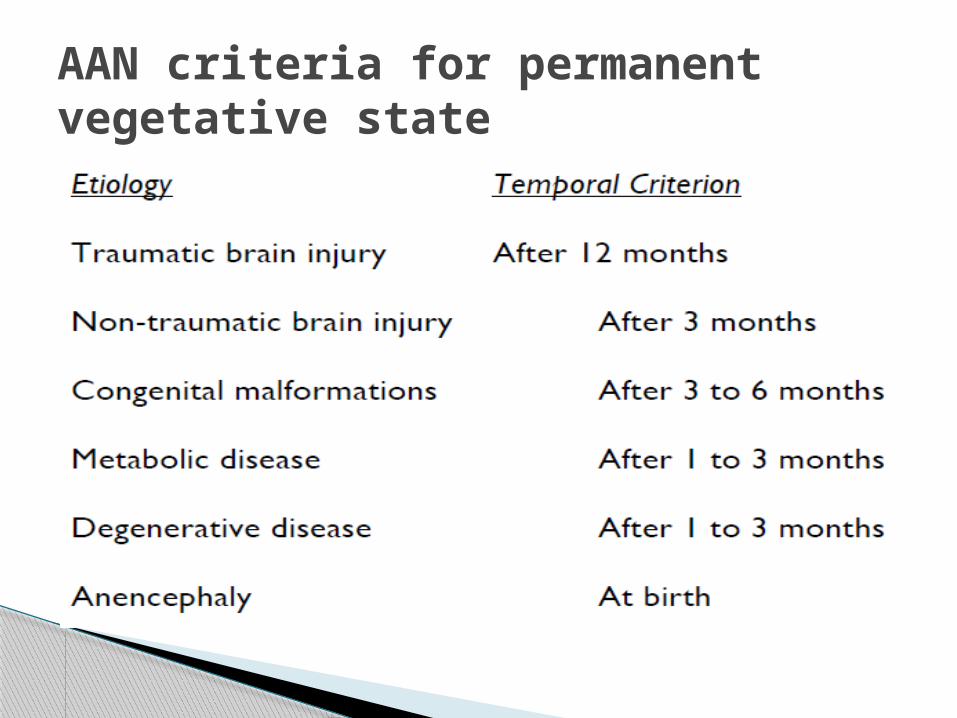
AAN criteria for permanent vegetative state

Characterized by primary and inconsistent signs of consciousness of self and environment.
Pts. are unable to communicate functionally Can sometimes respond adequately to
verbal commands and make understandable verbalizations.
Emotional behaviors, such as smiles, laughter or tears may be observed.
May track a moving object, mirror or person.
Minimally Conscious State

Responses must be reproducible in order to conclude that action is intentional.
Cerebral metabolic activity is reduced by 20–40%
Autonomous functions are preserved Thalamocortical and corticocortical
connections are partly restored. State may be transitory, chronic or
permanent.

MCS-plus patients-show more complex behaviours such as command following.
MCS-minus patients-show only non-reflexive movements such as orientation to noxious stimuli, pursuit eye movements, etc
Continuing MCS >4 weeks. Permanent MCS >5 years.
Functional interactive communication (verbalization, writing, signaling or augmentative communication devices)- answer 6 out of 6 basic yes/no questions on 2 separate occasions regarding personal or environmental orientation
Functional use of objects-demonstrating the ability to appropriately use 2 different objects on 2 consecutive evaluations.
Emergence from MCS

Atleast one consistent response1. Functional use of objects-at least 2
different objects on 2 consecutive evaluations(with or without instruction)
2. Consistent discriminatory choice-making-correct choice from 2 pictures or matches paired objects on 6/6 trials on 2 consecutive evaluations.
Operational parameters

3. Evidence of awareness of self-Gives correct yes/no responses to 6/6 autobiographical questions on 2 occasion
4. Evidence of awareness of their environment-Correct yes/no responses to 6/6 basic situational questions on 2 evaluations

Irreversible loss of all reflexes of brainstem Demonstration of continuing cessation of
brain function and respiration in persistently comatose patient.
Absence of electrical brain activity EEG Absence of cerebral blood flow
Brain death

Pseudocoma Complete paralysis of body from lesion in brainstem Oral and gestural communications are impossible Able to blink and move the eyes. Fully aware of their environment and themselves Communication skill (E-T-A-O-I-N-S-R-H-L-D-C-U-M-F-
P-G-W-Y-B-V-K-X-J-Q-Z) where patient blinks when pronounces desired letter.
Brain computer interface developed. 90% vascular etiology Cognitive functions are fully preserved.
Locked-In Syndrome

1 Detailed clinical history, examination and general investigation
• To identify cause of brain injury and any complications arising from it.
• To exclude other conditions (eg metabolic/infective disorders, hydrocephalus)
2 Review of medication• To identify and, if possible, withdraw or reduce any drugs which
could affect arousal.3 Standard imaging (computed tomography or magnetic
resonance imaging scan of the brain)• To exclude specific structural, operable causes (such as
hydrocephalus) and localise areas of injurywithin the brain.4 Standard EEGs or trial of anticonvulsant, if subclinical
seizure activity is suspected.
Approach to patient of PDOC
5 Detailed neurological evaluation to include assessment of:
• primary visual pathways:– pupillary light reflex, response to visual threat, or
evidence of visual tracking.• primary auditory pathways:– startle or blink reflexes in response to sudden loud
noises, or any evidence of localisation towards sound.• primary somatosensory pathways:– stretch reflexes, response to touch or pain.• primary motor output pathways:– any spontaneous or reflexive movements• spinal pathways
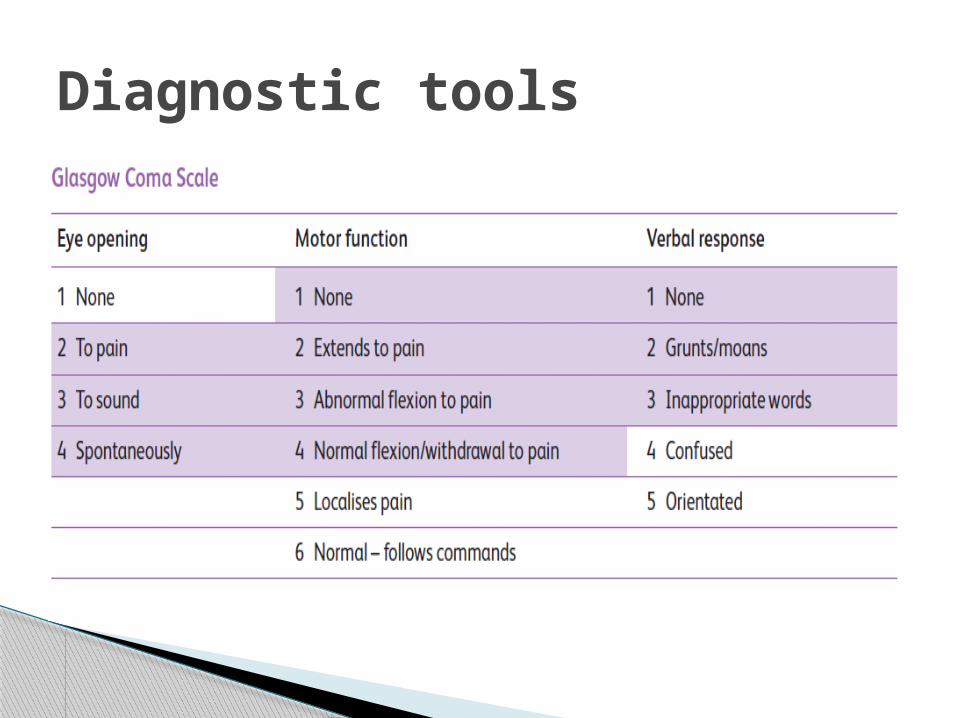
Diagnostic tools

A screening tool to identify patients with PDOC
Not a valid diagnostic tool for VS and MCS. Patients with locked-in syndrome may score
lower than PDOC
GCS

Behaviour assessment scale 62-item hierarchical scale Developed to monitor changes from coma
through to emergence from post-traumatic amnesia.
Paid manual.
Wessex Head Injury Matrix (WHIM)

Developed to detect awareness, functional and communicative capacity in VS and MCS
Used where there no consistent or reliable responses elicited and where the pts. potential function has not yet been fully explored
Family perspectives recorded Takes significantly longer(10-12hrs) than
other tools(3hrs). Training mandatory.
Sensory Modality Assessment and Rehabilitation Technique (SMART)

Informal component (Smart-informs)-information from family and carers-observed behaviours and pre-morbid interests, likes and dislikes.
Formal component-10 sessions within a 3-week period:◦ SMART Behavioural Observation Assessment – a
10-minute quiet period observes any reflexive, spontaneous and purposeful behaviours
◦ SMART Sensory Assessment◦ sensory modalities (visual, auditory, tactile, olfactory,
gustatory)◦ motor function, functional communication, wakefulness.

Assessed on 5-point hierarchical scale:1. No response – to any stimulus2. Reflexive and generalised responses-startle,
flexor or extensor patterns3. Withdrawal-turning head or eyes away or
withdrawing limbs from a stimulus4. Localising – turning head or moving upper
limbs towards a stimulus5. Discriminating responses-following visual or
auditory commands or using object appropriately.

25 hierarchically arranged items with 6 subscales (auditory, visual, motor, oromotor, communication and arousal)
JFK Coma Recovery Scale – Revised (CRS-R)

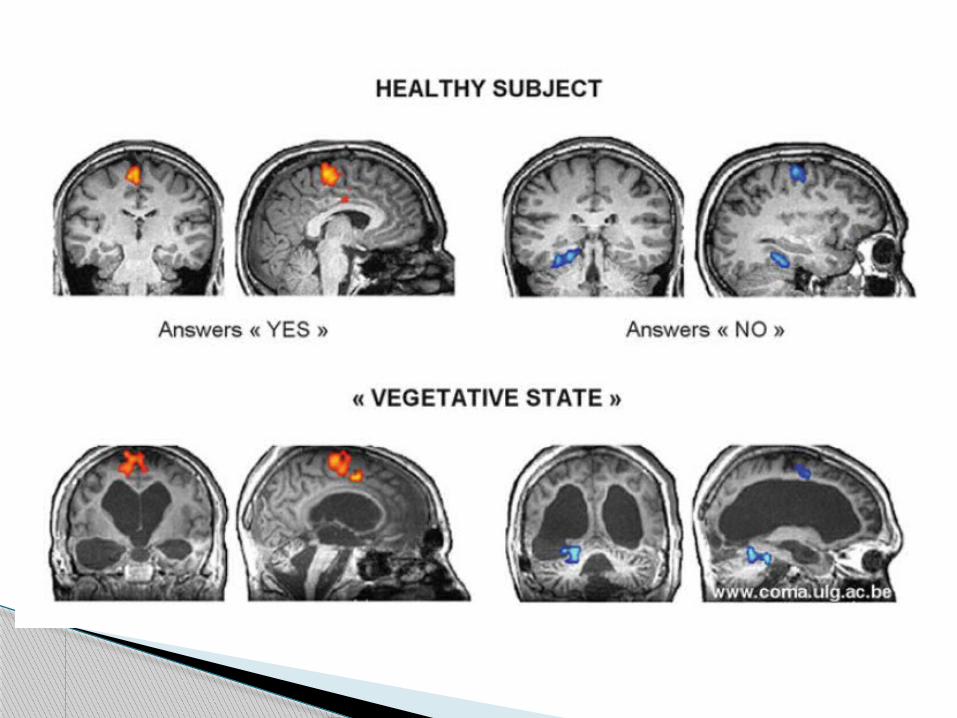
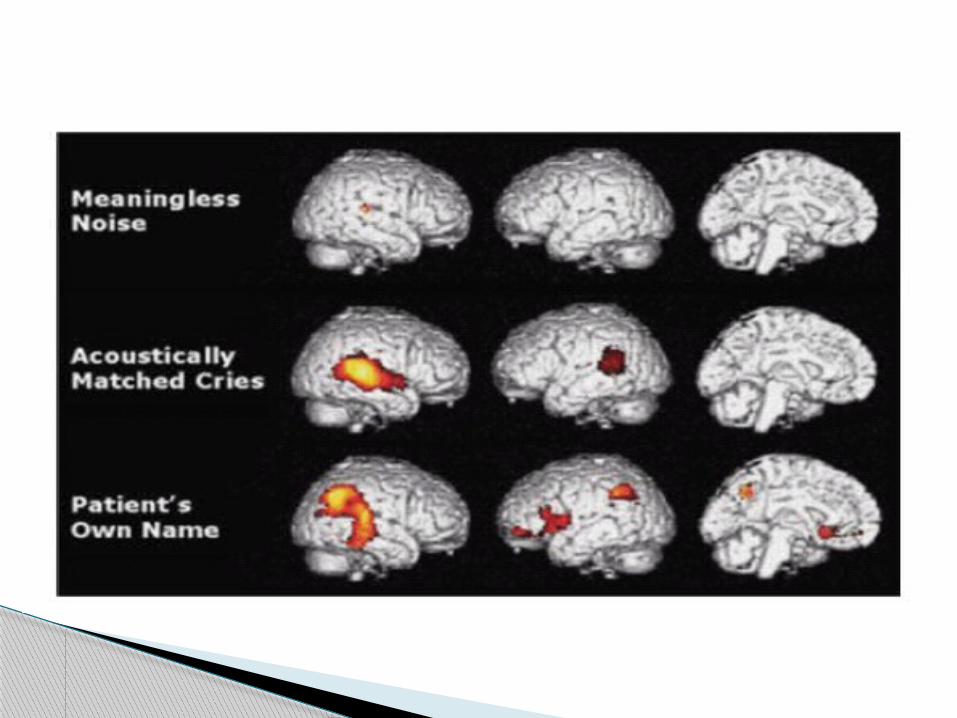
Conventional imaging(CT,MRI) Functional MRI-indirectly measures regional
increases in blood flow by analyzing magnetic resonance properties of hemoglobin
PET scan-measure changes in brain’s metabolism using radioactive tracer labeled glucose
EEG Sensory evoked potentials Cognitive evoked potentials
Imaging
Dopaminergic drugs (levodopa, amantadine,bromocriptine)
Gabanergic drugs (zolpidem) Serotonin/adrenaline reuptake inhibitor
(methylphenidate, SSRI)
Treatment

Deep brain stimulation Dorsal column stimulation Transcranial magnetic stimulation Multimodal sensory stimulation
Neurostimulation

Young age Traumatic etiology Short duration MCS
Prognosis


Thank You

The neurology of consciousness:cognitive neuroscience and neuropathology; steven Laureys and Giulio Tononi; Elsevier Ltd. 2009
Disorders of Consciousness: Coma, Vegetative and Minimally Conscious States. States of Consciousness; Olivia Gosseries et al;Springer-Verlag Berlin Heidelberg 2011
Neurobiological Basis of Consciousness;G. Bryan Young, MD; Susan E. Pigott; Arch Neurol. 1999;56(2):153-157.
Prolonged disorders of consciousness: National clinical guidelines 2013; Royal college of physicians
References
Related Documents











