NEOVASCULARIZATION AND FREE MICROSURGICAL TRANSFER OF IN VITRO CARTILAGE-ENGINEERED CONSTRUCTS NGUYEN THE HOANG, Ph.D., M.D., 1,2,3 * CHRISTOPH HOEHNKE, Ph.D., M.D., 2 PHAM THU HIEN, M.D., 3 VERONIKA MANDLIK, M.D. (student), 3 ACHIM FEUCHT, M.D. (student), 3 and RAINER STAUDENMAIER, Ph.D., M.D. 3 Cartilage tissue engineering shows to have tremendous potential for the reconstruction of three-dimensional cartilage defects. To ensure survival, shape, and function, in vitro cartilage-engineered constructs must be revascularized. This article presents an effective method for neovascularization and free microsurgical transfer of these in vitro constructs. Twelve female Chinchilla Bastard rabbits were used. Carti- lage-engineered constructs were created by isolating chondrocytes from auricular biopsies, amplifying in monolayer culture, and then seed- ing them onto polycaprolactone scaffolds. In each prefabricated skin flap, three in vitro cartilage-engineered constructs (2 3 2 3 0.5 cm) and one construct without cells (served as the control) were implanted beneath an 8 3 15 cm random-pattern skin flap, neovascularized by implantation of an arteriovenous vascular pedicle with maximal blood flow. Six weeks later, the neovascularized flaps with embedded cartilage-engineered constructs were completely removed based on the newly implanted vascular pedicle, and then freely retransferred into position using microsurgery. Macroscopic observation, selective microangiography, histology, and immunohistochemistry were per- formed to determine the construct vitality, neovascularization, and new cartilage formation. The results showed that all neovascularized skin flaps with embedded constructs were successfully free-transferred as free flaps. The implanted constructs were well integrated and protected within the flap. All constructs were well neovascularized and showed histologically stability in both size and form. Immunohistol- ogy showed the existence of cartilage-like tissue with extracellular matrix neosynthesis. V V C 2008 Wiley-Liss, Inc. Microsurgery 29:52–61, 2009. Tissue engineering can provide a promising method for repairing or replacing any tissue in the human body that is injured or damaged as a result of disease or trauma. In spite of technological advances and remarkable scientific progress in recent years, there are, however, very few clinical applications of tissue engineering reported in the literature. Challenges relating to the clinical use of tissue engineering are listed as follows: (a) problems associated with cell expansion, (b) challenges relating to cell sur- vival and function after seeding onto scaffolds, as well as necrosis of tissue-engineered constructs due to vascular disruption following implantation or transplantation, 1 and (c) difficulties associated with optimal scaffolds for cell seeding (e.g., biocompatibility and biodegradation, elas- ticity and mechanical stiffness, ability to allow nutrient diffusion, appropriate environment for cell adhesion, growth, differentiation and proliferation, etc.). 2 Although numerous publications were presented in the literature relating to the use of newly developed proce- dures for optimizing the cartilage tissue engineering method for future clinical applications (e.g., bioreactor systems, 3,4 cell type, 5,6 growth factors, 7–9 etc.), studies on revascularization of in vitro cartilage-engineered con- structs to ensure their in vivo survival, function, and shape—the ultimate goal of the procedure—were, how- ever, only rarely investigated and reported on. 10,11 Although cartilage is an avascular tissue consisting of only chondrocytes, which are embedded in a matrix com- posed of collagen and proteoglycan, 2,12 newly cartilage- engineered constructs with a large volume of expended cells usually require a hyperoxic environment for their growth and proliferation. 10 Disruption of blood and nutri- ent supply results in cell death and unavoidable necrosis of the cartilage-engineered construct with subsequent loss of shape and function. 1,11 In 2004, Staudenmaier et al. 10 reported preliminary experimental results of flap prefabrication and prelamina- tion with tissue-engineered cartilage using non-woven fleece scaffolds HYAFF 1 (hyaluronic-axid derivative, Biopolymers, Abano Terme, Italy), which were placed in different regions of the rabbit body including the prefab- ricated flap, subcutaneous abdominal wall, and in an intramuscular pocket of the thigh. Neovascularization and neocartilage formation in the constructs were analyzed by angiography, histology, and immunohistology. Despite the natural polymer fiber, HYAFF 1 has been identified by this study as an effective scaffold material based on excellent biocompatibility and shape-conforming proper- ties; however, it lacks the mechanical strength and ability 1 Department of Hand Surgery and Microsurgery, Institute of Trauma and Orthopedics, Central University Hospital 108, Hanoi, Vietnam 2 Department of Plastic Surgery, University Hospital ‘‘rechts der Isar’’, Techni- cal University of Munich, Germany 3 ENT Department, University Hospital ‘‘rechts der Isar’’, Technical University of Munich, Germany Grant sponsor: Bayerische Forschungsstiftung (FORTEPRO); Grant number: Az. 442/01. *Correspondence to: Nguyen The Hoang, Ph.D., M.D., Khoa B1-2, Vien Chan Thuong Chinh Hinh, Benh Vien 108, So 1-Tran Hung Dao, Hanoi, Vietnam. E-mail: [email protected] Received 2 May 2008; Accepted 31 July 2008 Published online 22 October 2008 in Wiley InterScience (www.interscience.wiley. com). DOI 10.1002/micr.20565 V V C 2008 Wiley-Liss, Inc.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

NEOVASCULARIZATION AND FREE MICROSURGICAL TRANSFEROF IN VITRO CARTILAGE-ENGINEERED CONSTRUCTS
NGUYEN THE HOANG, Ph.D., M.D.,1,2,3* CHRISTOPH HOEHNKE, Ph.D., M.D.,2 PHAM THU HIEN, M.D.,3
VERONIKA MANDLIK, M.D. (student),3 ACHIM FEUCHT, M.D. (student),3 and RAINER STAUDENMAIER, Ph.D., M.D.3
Cartilage tissue engineering shows to have tremendous potential for the reconstruction of three-dimensional cartilage defects. To ensuresurvival, shape, and function, in vitro cartilage-engineered constructs must be revascularized. This article presents an effective method forneovascularization and free microsurgical transfer of these in vitro constructs. Twelve female Chinchilla Bastard rabbits were used. Carti-lage-engineered constructs were created by isolating chondrocytes from auricular biopsies, amplifying in monolayer culture, and then seed-ing them onto polycaprolactone scaffolds. In each prefabricated skin flap, three in vitro cartilage-engineered constructs (2 3 2 3 0.5 cm)and one construct without cells (served as the control) were implanted beneath an 8 3 15 cm random-pattern skin flap, neovascularizedby implantation of an arteriovenous vascular pedicle with maximal blood flow. Six weeks later, the neovascularized flaps with embeddedcartilage-engineered constructs were completely removed based on the newly implanted vascular pedicle, and then freely retransferredinto position using microsurgery. Macroscopic observation, selective microangiography, histology, and immunohistochemistry were per-formed to determine the construct vitality, neovascularization, and new cartilage formation. The results showed that all neovascularizedskin flaps with embedded constructs were successfully free-transferred as free flaps. The implanted constructs were well integrated andprotected within the flap. All constructs were well neovascularized and showed histologically stability in both size and form. Immunohistol-ogy showed the existence of cartilage-like tissue with extracellular matrix neosynthesis. VVC 2008 Wiley-Liss, Inc. Microsurgery 29:52–61,2009.
Tissue engineering can provide a promising method for
repairing or replacing any tissue in the human body that
is injured or damaged as a result of disease or trauma. In
spite of technological advances and remarkable scientific
progress in recent years, there are, however, very few
clinical applications of tissue engineering reported in the
literature. Challenges relating to the clinical use of tissue
engineering are listed as follows: (a) problems associated
with cell expansion, (b) challenges relating to cell sur-
vival and function after seeding onto scaffolds, as well as
necrosis of tissue-engineered constructs due to vascular
disruption following implantation or transplantation,1 and
(c) difficulties associated with optimal scaffolds for cell
seeding (e.g., biocompatibility and biodegradation, elas-
ticity and mechanical stiffness, ability to allow nutrient
diffusion, appropriate environment for cell adhesion,
growth, differentiation and proliferation, etc.).2
Although numerous publications were presented in the
literature relating to the use of newly developed proce-
dures for optimizing the cartilage tissue engineering
method for future clinical applications (e.g., bioreactor
systems,3,4 cell type,5,6 growth factors,7–9 etc.), studies on
revascularization of in vitro cartilage-engineered con-
structs to ensure their in vivo survival, function, and
shape—the ultimate goal of the procedure—were, how-
ever, only rarely investigated and reported on.10,11
Although cartilage is an avascular tissue consisting of
only chondrocytes, which are embedded in a matrix com-
posed of collagen and proteoglycan,2,12 newly cartilage-
engineered constructs with a large volume of expended
cells usually require a hyperoxic environment for their
growth and proliferation.10 Disruption of blood and nutri-
ent supply results in cell death and unavoidable necrosis
of the cartilage-engineered construct with subsequent loss
of shape and function.1,11
In 2004, Staudenmaier et al.10 reported preliminary
experimental results of flap prefabrication and prelamina-
tion with tissue-engineered cartilage using non-woven
fleece scaffolds HYAFF1 (hyaluronic-axid derivative,
Biopolymers, Abano Terme, Italy), which were placed in
different regions of the rabbit body including the prefab-
ricated flap, subcutaneous abdominal wall, and in an
intramuscular pocket of the thigh. Neovascularization and
neocartilage formation in the constructs were analyzed by
angiography, histology, and immunohistology. Despite
the natural polymer fiber, HYAFF1 has been identified
by this study as an effective scaffold material based on
excellent biocompatibility and shape-conforming proper-
ties; however, it lacks the mechanical strength and ability
1Department of Hand Surgery and Microsurgery, Institute of Trauma andOrthopedics, Central University Hospital 108, Hanoi, Vietnam2Department of Plastic Surgery, University Hospital ‘‘rechts der Isar’’, Techni-cal University of Munich, Germany3ENT Department, University Hospital ‘‘rechts der Isar’’, Technical Universityof Munich, Germany
Grant sponsor: Bayerische Forschungsstiftung (FORTEPRO); Grant number:Az. 442/01.
*Correspondence to: Nguyen The Hoang, Ph.D., M.D., Khoa B1-2, VienChan Thuong Chinh Hinh, Benh Vien 108, So 1-Tran Hung Dao, Hanoi,Vietnam. E-mail: [email protected]
Received 2 May 2008; Accepted 31 July 2008
Published online 22 October 2008 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/micr.20565
VVC 2008 Wiley-Liss, Inc.

to withstand in vivo mechanical load-bearing, and there-
fore is not ideal for cartilage defect reconstruction.
Recently in a rat model, Neumeister et al.11 reported on
vascularized tissue-engineered ears by implantation of
in vitro cultured chondrocytes into molded fibrous capsu-
les appearing around an implanted human ear-shaped sili-
cone, neovascularized by transplantation of a femoral
vessel bundle onto the block. The development of new
cartilage tissue was determined by histology.
With respect to clinical applications, we hypothesized
that the survival and transplantation of tissue-engineered
constructs should be very easy and effective if they were
neovascularized and transferred as an axial free flap
based on a reliable vascular pedicle. This study was
designed to investigate the ability of combining flap pre-
fabrication and tissue engineering constructs as well as
neovascularization and free microsurgical transplantation
of combined skin-cartilage-construct-engineered flaps by
means of implanting cartilage-engineered constructs
within a prefabricated skin flap.
MATERIALS AND METHODS
Twelve adult female Chinchilla Bastard rabbits
weighing from 3 to 4 kg were investigated in this study.
They were housed in accordance with the European
Directive for the Care and Use of Lab Animals (Reg.
Obb. AZ 211-2531-38/95). Anesthesia was induced by in-
travenous infusions of a mixture of ketamin 40 mg/kg
and xylazin 4 mg/kg (i.v.). All operations were performed
under sterile conditions. Three procedures were per-
formed on each animal including: (1) in vitro fabrication
of cartilage-engineered constructs using polycaprolactone
(PCL)-based polyurethane scaffolds, (2) in vivo neovas-
cularization by mean of implantation within a prefabri-
cated flap, and (3) microsurgical transplantation of these
neovascularized cartilage-engineered constructs.
In Vitro Construct Fabrication
The auricular cartilage harvested from the left ear of
Chinchilla Bastard rabbits was used for the investigation.
The cartilage specimen was washed in saline and minced
into 1 3 1 mm pieces in a petri dish. The chondrocytes
were enzymatically isolated during 6 hours incubation at
378C in a collagenase solution (1,108 U/ml) and resus-
pended in Dulbecco’s modified Eagle medium (Sigma,
Berlin, Germany) containing 4.5 g/l glucose, 548 mg/l
glutamine, 10% fetal calf serum (Life Technologies,
Karlsruhe, Germany), 50 U/ml penicillin (Biochrom, Ber-
lin, Germany), 1 mM nonessential amino acids (Bio-
chrom, Berlin, Germany), and 0.4 mM proline (Sigma,
Berlin, Germany). For expansion, the chondrocytes were
cultured under conventional monolayer culture conditions
at 378C, 5% CO2 for 2 weeks. The cell suspension was
filtered using a 70 lm filter, pelleted by centrifuging at
1,500 rpm for 10 minutes, and washed three times with
phosphate buffered saline (PBS; Grosshadern, Munich,
Germany).
For cell-construct fabrication, cultured cells were sus-
pended in 20 ll fibrinogen solution and mixed with the
same volume of thrombin solution. Subsequently, the
cell-fibrin suspension was seeded onto 2 3 2 3 0.5 cm
samples of PCL-based polyurethane scaffolds (PolyMate-
rial AG, Kaufbeuren, Germany) at a concentration of
�20 3 106 cells per cm3. After an adhesion period of 5
hours the medium, supplemented with 50 lg/ml ascorbic
acid (Merck, Darmstadt, Germany), was renewed and
then subsequently replaced every 2–3 days. For each ani-
mal in this study, three cell-biomaterial constructs were
fabricated and further cultured for 1 week before in vivo
implantation. In addition, a construct without cells with
the same design and dimension served as control was
also prepared for in vivo implantation.
In Vivo Neovascularization and Free Transfer
of Cartilage-Engineered Constructs
Cartilage-engineered constructs and control constructs
were first neovascularized by means of implantation
within a prefabricated skin flap and next free-transferred
based on the newly axial implanted vascular pedicle
using microsurgical techniques.
Prefabrication of a neovascularized skin flap. On
the right abdomen of Chinchilla Bastard rabbits, a ran-
dom-pattern skin flap measuring 8 3 15 cm with lateral
pedicle was dissected and lifted up (Fig. 1A). After con-
trolling hemostasis throughout this area with a bipolar
electrocautery, a silicone sheet (LPI, Perouse, 60540 Bor-
nel, France) measuring 8 3 15 3 0.25 mm was placed
on the abdominal wall and anchored with Ethilon 3/0
(Fig. 1B). This silicone functioned as a barrier to prevent
neoangiogenesis from occurring between the underlying
vascular bed and the abdominal skin flap. An incision
extending from the inguinal ligament to immediately
above the calcaneous was made to harvest the femoral
and saphena magna vascular bundle. All branching ves-
sels were ligatured or closed using a bipolar coagulator.
In the next step, the artery and vein of the distal end of
the vascular bundle were freely dissected for 3 cm and
microanastomosed end-to-end using 10-0 Nylon monofila-
ment suture (Ethicon) to create maximal blood flow
within the vascular pedicle through the newly established
arteriovenous shunt. Next, the vascular bundle was turned
in the cranial position and anchored beneath the abdomi-
nal skin flap using Vicryl suture 8/0 (Fig. 1B).
Neovascularization of the cartilage-engineered
constructs. After pedicle implantation, three cartilage-
engineered constructs (�2 3 2 3 0.5 cm) were
In Vitro Cartilage-Engineered Constructs 53
Microsurgery DOI 10.1002/micr
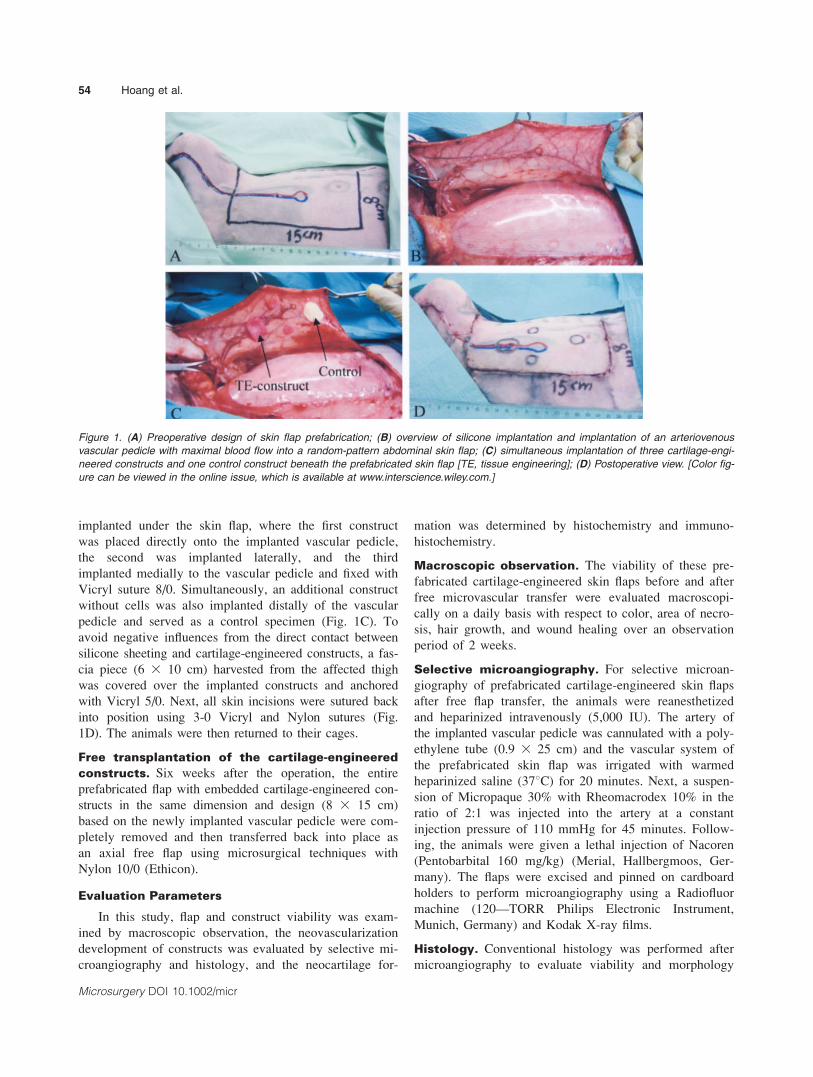
implanted under the skin flap, where the first construct
was placed directly onto the implanted vascular pedicle,
the second was implanted laterally, and the third
implanted medially to the vascular pedicle and fixed with
Vicryl suture 8/0. Simultaneously, an additional construct
without cells was also implanted distally of the vascular
pedicle and served as a control specimen (Fig. 1C). To
avoid negative influences from the direct contact between
silicone sheeting and cartilage-engineered constructs, a fas-
cia piece (6 3 10 cm) harvested from the affected thigh
was covered over the implanted constructs and anchored
with Vicryl 5/0. Next, all skin incisions were sutured back
into position using 3-0 Vicryl and Nylon sutures (Fig.
1D). The animals were then returned to their cages.
Free transplantation of the cartilage-engineered
constructs. Six weeks after the operation, the entire
prefabricated flap with embedded cartilage-engineered con-
structs in the same dimension and design (8 3 15 cm)
based on the newly implanted vascular pedicle were com-
pletely removed and then transferred back into place as
an axial free flap using microsurgical techniques with
Nylon 10/0 (Ethicon).
Evaluation Parameters
In this study, flap and construct viability was exam-
ined by macroscopic observation, the neovascularization
development of constructs was evaluated by selective mi-
croangiography and histology, and the neocartilage for-
mation was determined by histochemistry and immuno-
histochemistry.
Macroscopic observation. The viability of these pre-
fabricated cartilage-engineered skin flaps before and after
free microvascular transfer were evaluated macroscopi-
cally on a daily basis with respect to color, area of necro-
sis, hair growth, and wound healing over an observation
period of 2 weeks.
Selective microangiography. For selective microan-
giography of prefabricated cartilage-engineered skin flaps
after free flap transfer, the animals were reanesthetized
and heparinized intravenously (5,000 IU). The artery of
the implanted vascular pedicle was cannulated with a poly-
ethylene tube (0.9 3 25 cm) and the vascular system of
the prefabricated skin flap was irrigated with warmed
heparinized saline (378C) for 20 minutes. Next, a suspen-
sion of Micropaque 30% with Rheomacrodex 10% in the
ratio of 2:1 was injected into the artery at a constant
injection pressure of 110 mmHg for 45 minutes. Follow-
ing, the animals were given a lethal injection of Nacoren
(Pentobarbital 160 mg/kg) (Merial, Hallbergmoos, Ger-
many). The flaps were excised and pinned on cardboard
holders to perform microangiography using a Radiofluor
machine (120—TORR Philips Electronic Instrument,
Munich, Germany) and Kodak X-ray films.
Histology. Conventional histology was performed after
microangiography to evaluate viability and morphology
Figure 1. (A) Preoperative design of skin flap prefabrication; (B) overview of silicone implantation and implantation of an arteriovenous
vascular pedicle with maximal blood flow into a random-pattern abdominal skin flap; (C) simultaneous implantation of three cartilage-engi-
neered constructs and one control construct beneath the prefabricated skin flap [TE, tissue engineering]; (D) Postoperative view. [Color fig-
ure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
54 Hoang et al.
Microsurgery DOI 10.1002/micr

of the cartilage-engineered constructs and skin flap. Con-
structs with and without cells were marked and cut per-
pendicularly to the long axis of the vascular pedicle,
stained with Hematoxylin Eosin (HE) and Elastica van
Gieson (EvG).
Histochemistry. The cartilage-engineered constructs
were explanted and fixed for cryosectioning by immer-
sion in a 2% formaldehyde solution for 15 minutes. They
were stained for 60 minutes in an Alcian blue solution
(Chroma-Gesellschaft, Koengen, Germany), serially dehy-
drated with ethanol, and then embedded in Eukitt1 (Kindler,
Freiburg, Germany).
Immunohistochemistry. Immunohistochemistry to dete-
rmine type I and type II collagen was done on 7 lm cry-
osections. After fixation in ethanol for 10 minutes, three
washing steps in PBS were performed. For detection of
collagen type II, monoclonal anti-collagen type II anti-
body II-II6B3 was used (1:100 diluted in PBS), which
was provided by the Developmental Studies Hybridoma
Bank (Linsenmayer, IA). For collagen type I detection, a
polyclonal anti-collagen type I antibody (Cell Systems,
Remagen, Germany) (diluted 1:50 in PBS) was used.
RESULTS
Twelve rabbits were operated in this experimental
study; however, one rabbit died intraoperatively due to an
anesthetic overdose and one died postoperatively for
unknown reasons. In total, 10 rabbits were evaluated.
In Vitro Construct Fabrication
After cell isolation and expansion in monolayer cul-
ture, cell number was determined using stain with FDA
(fluorescin-diacetate) and PI (propidium iodine), and
counted using a hemocytometer. Living cells in these
constructs appeared as a green color, whereas dead cells
appeared as a red color (Fig. 2). On average, between
300,000 and 400,000 cells isolated from the biopsies
reached a total of �30 3 106 cells through three pas-
sages. In our study, cells were effectively distributed
throughout the entire construct and adhered well in the
pores of the scaffolds. Nearly 100% vital chondrocytes
were observed within the constructs.
In Vivo Study
Macroscopic observation. All neovascularized carti-
lage-engineered skin flaps in this study were successfully
free-transferred based on the newly implanted vascular
pedicle (Figs. 3A–3D). All free-transferred flaps showed
mild venous congestion in the first postoperative 3 days,
but this spontaneously regressed overtime. Over an obser-
vation period of 2 weeks, these cartilage-engineered skin
flaps showed inconspicuous wound healing with normal
hair growth and color similar to that seen in other
regions. Upon turning over the flap, a newly formed fi-
brous connective tissue capsule could be easily identified
underneath the flap. As a result of this capsule, the
implanted constructs, vascular pedicle, and the skin flap
became integrated together, such that the constructs were
well protected within the skin flap.
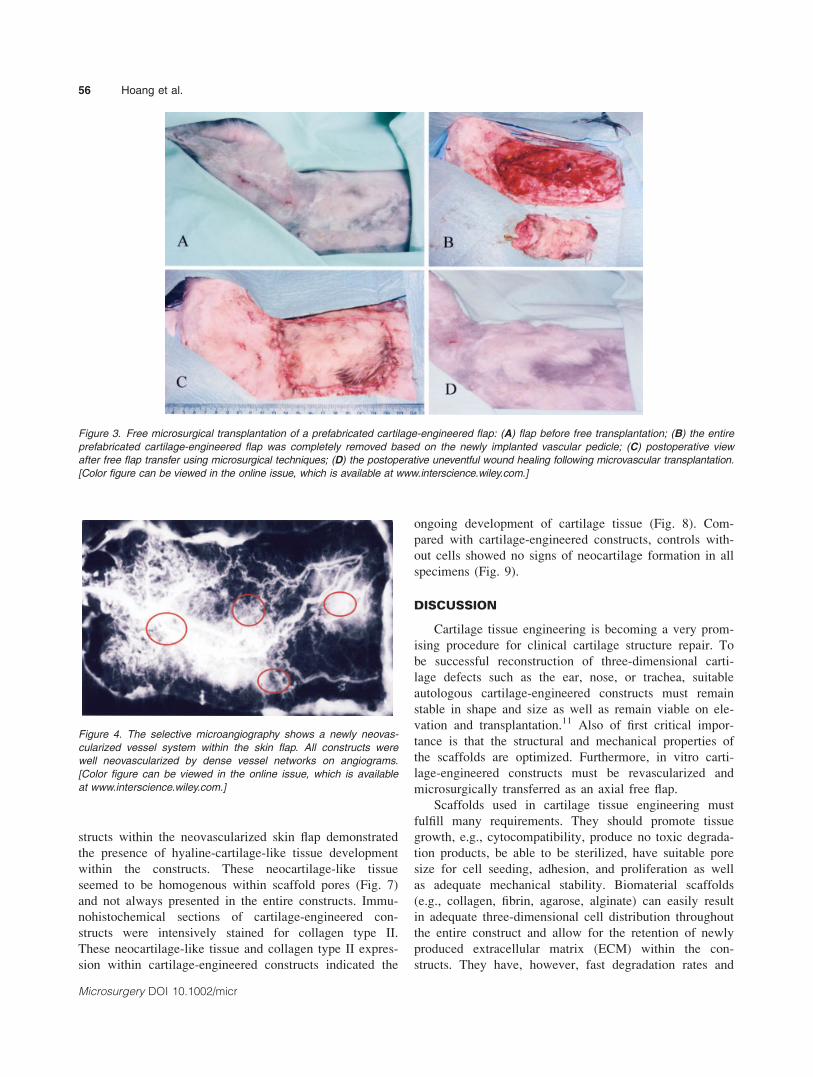
Selective microangiography. Selective microangiog-
raphy was supplied for all animals in this study. Microan-
giograms showed a newly neovascularized system in the
cartilage-engineered skin flap established from newly
formed vessels sprouting from the newly implanted vas-
cular pedicle and their innumerable vascular connections
with the originally available vasculature of the flap. All
implanted constructs (both cartilage-engineered and con-
trol constructs) were highly neovascularized with dense
vessel networks around and within the implanted con-
structs (Fig. 4).
Histology. All the neovascularized flaps were vital and
morphologically inconspicuous with normal epidermis,
hair follicles, connective tissue, and blood vessels. Both
implanted cartilage-engineered constructs (Fig. 5) and
control constructs (Fig. 6) were well integrated with the
skin flap, remaining mechanically stable in form and size,
and markedly infiltrated by various cell types and newly
formed vessels into the construct pores. There were no
signs of rejection reaction to the PCL-based polyurethane
scaffolds observed in all neovascularized skin flaps.
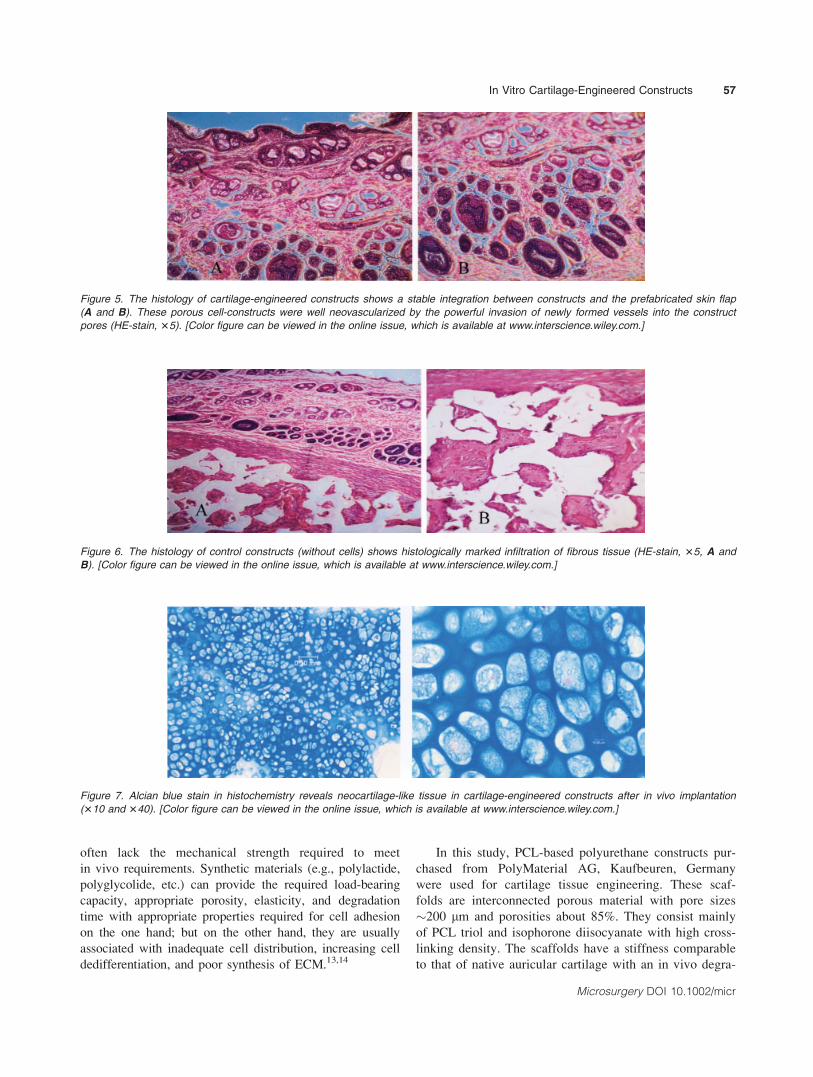
Histochemistry and immunohistochemistry. Histo-
chemical Alcian blue stain of cartilage-engineered con-
Figure 2. The result of in vitro cell seeding within scaffold pores
before in vivo implantation using FDA- and PI-stain, 380 (live cells
are green and dead cells are red). [Color figure can be viewed in
the online issue, which is available at www.interscience.wiley.com.]
In Vitro Cartilage-Engineered Constructs 55
Microsurgery DOI 10.1002/micr
structs within the neovascularized skin flap demonstrated
the presence of hyaline-cartilage-like tissue development
within the constructs. These neocartilage-like tissue
seemed to be homogenous within scaffold pores (Fig. 7)
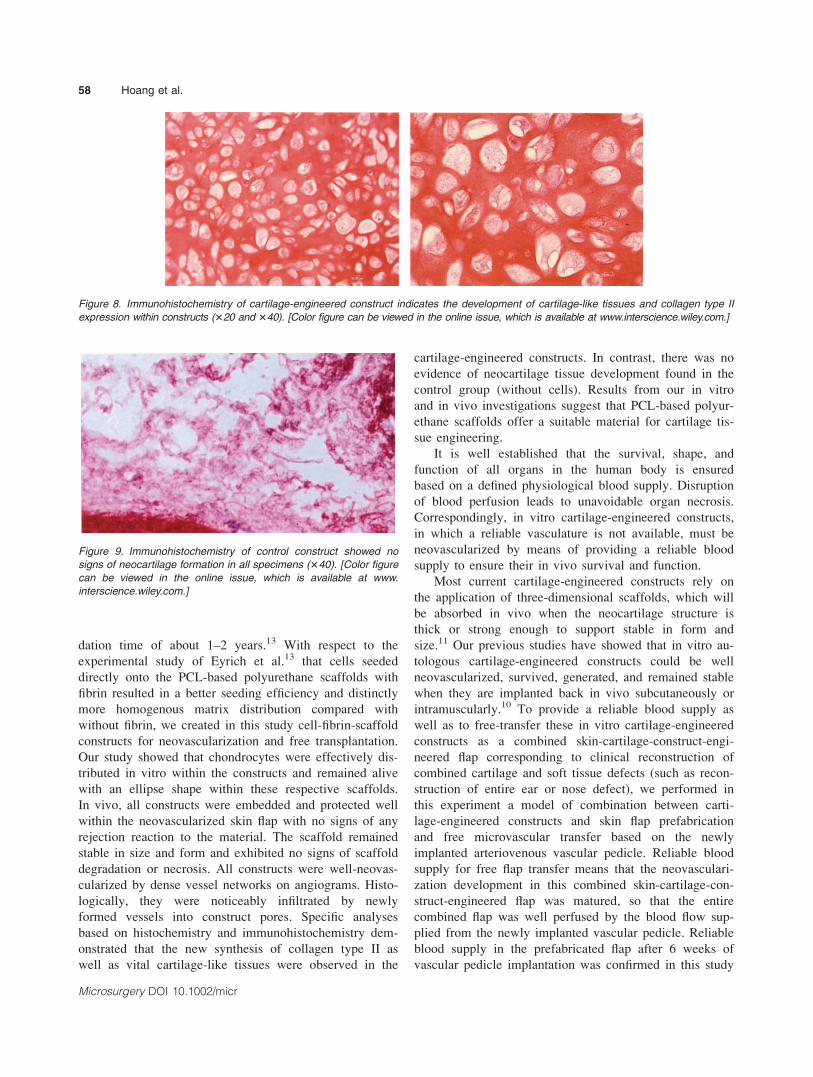
and not always presented in the entire constructs. Immu-
nohistochemical sections of cartilage-engineered con-
structs were intensively stained for collagen type II.
These neocartilage-like tissue and collagen type II expres-
sion within cartilage-engineered constructs indicated the
ongoing development of cartilage tissue (Fig. 8). Com-
pared with cartilage-engineered constructs, controls with-
out cells showed no signs of neocartilage formation in all
specimens (Fig. 9).
DISCUSSION
Cartilage tissue engineering is becoming a very prom-
ising procedure for clinical cartilage structure repair. To
be successful reconstruction of three-dimensional carti-
lage defects such as the ear, nose, or trachea, suitable
autologous cartilage-engineered constructs must remain
stable in shape and size as well as remain viable on ele-
vation and transplantation.11 Also of first critical impor-
tance is that the structural and mechanical properties of
the scaffolds are optimized. Furthermore, in vitro carti-
lage-engineered constructs must be revascularized and
microsurgically transferred as an axial free flap.
Scaffolds used in cartilage tissue engineering must
fulfill many requirements. They should promote tissue
growth, e.g., cytocompatibility, produce no toxic degrada-
tion products, be able to be sterilized, have suitable pore
size for cell seeding, adhesion, and proliferation as well
as adequate mechanical stability. Biomaterial scaffolds
(e.g., collagen, fibrin, agarose, alginate) can easily result
in adequate three-dimensional cell distribution throughout
the entire construct and allow for the retention of newly
produced extracellular matrix (ECM) within the con-
structs. They have, however, fast degradation rates and
Figure 3. Free microsurgical transplantation of a prefabricated cartilage-engineered flap: (A) flap before free transplantation; (B) the entire
prefabricated cartilage-engineered flap was completely removed based on the newly implanted vascular pedicle; (C) postoperative view
after free flap transfer using microsurgical techniques; (D) the postoperative uneventful wound healing following microvascular transplantation.
[Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
Figure 4. The selective microangiography shows a newly neovas-
cularized vessel system within the skin flap. All constructs were
well neovascularized by dense vessel networks on angiograms.
[Color figure can be viewed in the online issue, which is available
at www.interscience.wiley.com.]
56 Hoang et al.
Microsurgery DOI 10.1002/micr
often lack the mechanical strength required to meet
in vivo requirements. Synthetic materials (e.g., polylactide,
polyglycolide, etc.) can provide the required load-bearing
capacity, appropriate porosity, elasticity, and degradation
time with appropriate properties required for cell adhesion
on the one hand; but on the other hand, they are usually
associated with inadequate cell distribution, increasing cell
dedifferentiation, and poor synthesis of ECM.13,14
In this study, PCL-based polyurethane constructs pur-
chased from PolyMaterial AG, Kaufbeuren, Germany
were used for cartilage tissue engineering. These scaf-
folds are interconnected porous material with pore sizes
�200 lm and porosities about 85%. They consist mainly
of PCL triol and isophorone diisocyanate with high cross-
linking density. The scaffolds have a stiffness comparable
to that of native auricular cartilage with an in vivo degra-
Figure 5. The histology of cartilage-engineered constructs shows a stable integration between constructs and the prefabricated skin flap
(A and B). These porous cell-constructs were well neovascularized by the powerful invasion of newly formed vessels into the construct
pores (HE-stain, 35). [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
Figure 6. The histology of control constructs (without cells) shows histologically marked infiltration of fibrous tissue (HE-stain, 35, A and
B). [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
Figure 7. Alcian blue stain in histochemistry reveals neocartilage-like tissue in cartilage-engineered constructs after in vivo implantation
(310 and 340). [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
In Vitro Cartilage-Engineered Constructs 57
Microsurgery DOI 10.1002/micr
dation time of about 1–2 years.13 With respect to the
experimental study of Eyrich et al.13 that cells seeded
directly onto the PCL-based polyurethane scaffolds with
fibrin resulted in a better seeding efficiency and distinctly
more homogenous matrix distribution compared with
without fibrin, we created in this study cell-fibrin-scaffold
constructs for neovascularization and free transplantation.
Our study showed that chondrocytes were effectively dis-
tributed in vitro within the constructs and remained alive
with an ellipse shape within these respective scaffolds.
In vivo, all constructs were embedded and protected well
within the neovascularized skin flap with no signs of any
rejection reaction to the material. The scaffold remained
stable in size and form and exhibited no signs of scaffold
degradation or necrosis. All constructs were well-neovas-
cularized by dense vessel networks on angiograms. Histo-
logically, they were noticeably infiltrated by newly
formed vessels into construct pores. Specific analyses
based on histochemistry and immunohistochemistry dem-
onstrated that the new synthesis of collagen type II as
well as vital cartilage-like tissues were observed in the
cartilage-engineered constructs. In contrast, there was no
evidence of neocartilage tissue development found in the
control group (without cells). Results from our in vitro
and in vivo investigations suggest that PCL-based polyur-
ethane scaffolds offer a suitable material for cartilage tis-
sue engineering.
It is well established that the survival, shape, and
function of all organs in the human body is ensured
based on a defined physiological blood supply. Disruption
of blood perfusion leads to unavoidable organ necrosis.
Correspondingly, in vitro cartilage-engineered constructs,
in which a reliable vasculature is not available, must be
neovascularized by means of providing a reliable blood
supply to ensure their in vivo survival and function.
Most current cartilage-engineered constructs rely on
the application of three-dimensional scaffolds, which will
be absorbed in vivo when the neocartilage structure is
thick or strong enough to support stable in form and
size.11 Our previous studies have showed that in vitro au-
tologous cartilage-engineered constructs could be well
neovascularized, survived, generated, and remained stable
when they are implanted back in vivo subcutaneously or
intramuscularly.10 To provide a reliable blood supply as
well as to free-transfer these in vitro cartilage-engineered
constructs as a combined skin-cartilage-construct-engi-
neered flap corresponding to clinical reconstruction of
combined cartilage and soft tissue defects (such as recon-
struction of entire ear or nose defect), we performed in
this experiment a model of combination between carti-
lage-engineered constructs and skin flap prefabrication
and free microvascular transfer based on the newly
implanted arteriovenous vascular pedicle. Reliable blood
supply for free flap transfer means that the neovasculari-
zation development in this combined skin-cartilage-con-
struct-engineered flap was matured, so that the entire
combined flap was well perfused by the blood flow sup-
plied from the newly implanted vascular pedicle. Reliable
blood supply in the prefabricated flap after 6 weeks of
vascular pedicle implantation was confirmed in this study
Figure 8. Immunohistochemistry of cartilage-engineered construct indicates the development of cartilage-like tissues and collagen type II
expression within constructs (320 and 340). [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
Figure 9. Immunohistochemistry of control construct showed no
signs of neocartilage formation in all specimens (340). [Color figure
can be viewed in the online issue, which is available at www.
interscience.wiley.com.]
58 Hoang et al.
Microsurgery DOI 10.1002/micr

by selective microangiography, histology as well as by
various experimental investigations in the literature.15–19
Neovascularization of tissue engineering has been
reported on in the literature. In 2001, Tan et al.20
reported in a rat model on vascularizing acellular dermal
matrix (Integra1) with superficial inferiorepigastric ves-
sels and microsurgically transferring them as bioengi-
neered dermal flaps for 72 hours. Tanaka et al.21 wrapped
artificial dermis (1.5 3 2 cm) around a vascular pedicle
and implanted it beneath the rat inguinal skin for 4
weeks. Next, the volume of newly generated tissue within
the artificial dermis was measured or evaluated histologi-
cally. Recently, in 2004 Cronin et al.22 performed in rats
the insertion of a vascular pedicle and matrix material
into a very small closed chamber (0.6 3 0.3 cm), which
was buried subcutaneously. The results in this study
showed that there was evidence of migration into and
survival of native cells within the added matrix, generat-
ing a vascularized three-dimensional construct.
Most studies investigated tissue engineering only
in vitro23,24 or combined in vitro with in vivo implanta-
tion either on nude mice13,25,26 or in autologous animal
models14,27,28 without free microsurgical transplantation.
Moreover, investigation of neovascularization and free
transfer of cartilage-engineered constructs has, to our
knowledge, not appeared in the literature to date. To
allow for extrapolation from experimental investigations
to clinical applications, we implanted in vitro cartilage-
engineered constructs into large prefabricated flaps
(dimension of 8 3 15 cm). In addition, a construct with-
out cultured cells was also simultaneously implanted
within the flap to serve as the control. The experimental
results of this study showed that both cartilage-engineered
constructs and control constructs were macroscopically
well integrated and protected within the prefabricated
flap, which was established as a results of the newly
formed fibrovascular connective capsule underlying the
flap. All neovascularized skin flaps with embedded tissue
engineering constructs and control constructs were suc-
cessfully free-transferred after 6 weeks of prefabrication
using microsurgical techniques. The viability of these
free neovascularized skin flaps was macroscopically con-
firmed by uneventful postoperative wound healing over a
period of 2 weeks.
The effective neovascularization of skin flap as well
as implanted constructs (both cartilage-engineered and
control constructs) in this study was proven on angio-
grams by dense vessel networks within the constructs,
and through histology by good integration between con-
structs and skin flaps as well as a noticeable infiltration
of newly formed vessels into the construct pores. The
histochemistry and immunohistochemistry results showed
that cartilage-like tissue with amount of collagen II syn-
thesis were observed only in the scaffold pores of the
implanted cartilage-engineered constructs. In contrast,
there were no evidences of neocartilage development
detected in the control constructs.
An important question related to this experimental
study is to clarify the role of control constructs, which
were simultaneously implanted with cartilage-engineered
constructs beneath the prefabricated flap. Our experimen-
tal results demonstrated that after in vivo implantation,
porous PCL-based polyurethane constructs in both groups
(TE and control group) were well neovascularized by
newly formed vessels generated from the surrounding
vasculature. In principle, essential differences between
the study group (cartilage-engineered constructs) and the
control group (scaffolds) are that cartilage-engineered
constructs, depending on the newly developed neocarti-
lage cells, should maintain configured three-dimensional
structures stable in form and size when scaffolds were
completely in vivo absorbed. In contrast, three-dimen-
sional structure of scaffolds in the control group will be
totally absorbed and disappeared after 2 years of implan-
tation. Based on this reason, the control constructs used
in this study were served only to determine the existing
of no cartilage cell development within control constructs
following in vivo implantation. In this study, the compar-
ison of neocartilage formation between the study group
and the control group, of our opinion, should be opti-
mized depending on the same animal and the same pre-
fabricated flap.
Concerns regarding construct necrosis due to lack of
the blood supply in using in vitro fabricated tissue engi-
neering constructs were reported by many investiga-
tors.11,29 In this model, the cartilage-engineered construct
was well integrated within the skin flap and successfully
free-transferred based on its axial blood supply pedicle.
In our opinion, these results revealed that the diffusion of
nutrients from the surrounding area in the early phase, as
well as the blood supply from the neovascularization de-
velopment in the next phase, is enough to ensure con-
struct survival, function, and free transplantation.
From a clinical point of view, despite the fact that
cartilage tissue is often required in reconstructive surgery,
the supply of autologous cartilage is limited due to ana-
tomical constraints. In addition, in the clinical practice of
reconstruction of three-dimensional cartilage tissue defect
such as a total ear or nose defect appeared as a result of
burn injuries or tumor resection, there are however situa-
tions in which the appropriate matching local soft tissue
is not available. To optimize functional and esthetic final
results of such reconstructive procedures, prefabrication
of an axial well-vascularized three-dimensional and free-
transferable structures in desired regions by means of
combination between prefabricated flap and cartilage-
engineered configured constructs as a fully done structure
for free microsurgical transfer in the second stage of sur-
In Vitro Cartilage-Engineered Constructs 59
Microsurgery DOI 10.1002/micr

gery should be a valuable strategy. On the basis of this
method, we are in interest to hypothesis that appropriate
three-dimensional tissue-engineered constructs of ear,
nose, or trachea required in the clinical routine as well as
other human tissue organs should be performed (Fig. 10).
By using this method, the most important advantage is
that a new three-dimensional cartilage structure with suit-
able shape and form can be generated from a small bi-
opsy by seeding viable expanded cells onto appropriately
configured constructs.1 Subsequently, it is then neovascu-
larized in desired skin regions, regardless of the origin of
the natural vascular anatomy. These neovascularized, car-
tilage-engineered skin flaps can then be safely transferred
as axial free flaps for defect reconstruction. Based on
these advantages of the prefabrication procedure, esthetic
aspects are also markedly improved and donor site mor-
bidity can be significantly reduced.15–19,20–32
However, toward an effective clinical application, fur-
ther experimental investigations have to be underwent
using tissue-engineered constructs of different autologous
tissue such as cartilage, bone, fat, muscle, nerve, etc. to
assess in a relevant implantation. Furthermore, the
in vitro prefabrication of these constructs have to be per-
formed in combination with specific stimulating compo-
nents such as bioreactors, growth factors, serum-free
media, etc., to optimize the success of the procedure.
Nevertheless, the neovascularization and microsurgical
transplantation of in vitro tissue-engineered constructs by
mean of implantation within a prefabricated tissue flap
from this study, in our opinion, appears to be a promising
alternative in the clinical application of cartilage tissue
engineering.
CONCLUSIONS
In conclusion, this study demonstrated the reliable
ability of neovacularization and free microsurgical trans-
plantation of cartilage-engineered constructs using prefab-
ricated flap. In this experimental study, all constructs
6 weeks after implantation were well-protected within the
skin flaps, well neovascularized by blood flow supplied
from the newly implanted vascular pedicle and were suc-
cessfully free-transferred using microsurgical techniques.
Neocartilage development within the implanted cartilage-
engineered constructs was approved by the existence of
cartilage-like tissues and collagen II neosynthesis expres-
sion. With respect to effective clinical application, the
procedure should be a promising alternative for clinical
practice because of favorable esthetic outcomes with min-
imal donor site morbidity.
ACKNOWLEDGMENTS
The authors thank the Alexander von Humboldt Foun-
dation, Germany (AvH-Foundation) for their help in fi-
nancing the author’s research scholarship at the Univer-
sity Hospital ‘‘rechts der Isar’’ in Munich, Germany. The
authors also extend their appreciation to Ms. Christine
Cavanna at the University of Regensburg Medical Center
for her careful editing of this manuscript.
Figure 10. Perspective of clinical applications for reconstruction of three-dimensional cartilage tissue defect (such as an ear defect). [Color
figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
60 Hoang et al.
Microsurgery DOI 10.1002/micr

REFERENCES
1. Vacanti CA. The history of tissue engineering. J Cell Mol Med2006;10:569–576.
2. Mueller L, Mueller FA, Hofmann I, Greil P, Wenzel M, Staudenma-ier R. Cellulose-based scaffold materials for cartilage tissue engi-neering. Biomaterials 2006;27:3955–3963.
3. Bilgen B, Sucosky P, Neitzel GP, Barbino GA. Flow characteriza-tion of a wavy-walled bioreactor for cartilage tissue engineering.Biotechnol Bioeng 2006;95:1009–1022.
4. Abousleiman RI, Sikavitsas VI. Bioreactors for tissue of the muscu-loskeletal system. Adv Exp Med Biol 2006;585:243–259.
5. Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R,Mosca JD, Moorman MA, Simonetti DW, Craig S, Marshak DR.Multilineage potential of adult human mesenchymal stem cells. Sci-ence 1999;284:143–147.
6. Park DJ, Choi JH, Kim YJ, Kim KT. Nasal augmentation usinginjectable alginate and mesenchymal stem cells in the rabbit. Am JRhinol 2006;20:520–523.
7. Arevalo-Silva CA, Cao Y, Weng Y, Vacanti M, Rodrıguez A,Vacanti CA, Eavey RD. Influence of growth factors on tissue-engi-neered pediatric elastic cartilage. Arch Otolaryngol Head Neck Surg2000;126:1234–1238.
8. Sohier J, Hamann D, Koenders M, Cucchiarini M, Madry H, van Blit-terswijk C, Bezemer JM. Tailored release of TGF-b(1) from porousscaffolds for cartilage tissue engineering. Int J Pharm 2007;332:80–89.
9. Goessler UR, Bugert P, Bieback K, Sadick H, Baisch A, HormannK, Riedel F. In vitro analysis of differential expression of collagens,intergrins, and growth factors in cultured human chondrocytes. Oto-laryngol Head Neck Surg 2006;134:510–515.
10. Staudenmaier R, Hoang Nguyen T, Kleinsasser N, Schurr C, FrolichK, Wenzel MM, Aigner J. Flap prefabrication and prelamination withtissue-engineered cartilage. J Reconstr Microsurg 2004;20:555–564.
11. Neumeister MW, Wu T, Chambers C. Vascularized tissue-engi-neered ears. Plast Reconstr Surg 2006;117:116–122.
12. Wang YZ, Kim UJ, Blasioli DJ, Kim HJ, Kaplan DL. In vitro carti-lage tissue engineering with 3D porous aqueous-derived silk scaf-folds and mesenchymal stem cells. Biomaterials 2005;26:7082–7094.
13. Eyrich D, Wiese H, Maier G, Skodacek B, Appel H, Sarhan TessmarJ, Staudenmaier R, Wenzel MM, Goepferich A, Blunk T. In vitroand in vivo cartilage engineering using a combination of chondro-cyte-based polyurethane scaffolds. Tissue Eng 2007;13:2207–2218.
14. Hutmacher DW. Scaffolds in tissue engineering bone and cartilage.Biomaterials 2000;21:2529–2543.
15. Hoang NT, Kloeppel M, Staudenmaier R, Werner J, Biemer E. Pre-fabrication of large fasciocutaneous flaps using an isolated arterialisedvein as implanted vascular pedicle. Br J Plast Surg 2005;58: 632–639.
16. Hoang NT, Kloeppel M, Werner J, Staudenmaier R, Biemer E. Pro-posed new method for angiographically quantifying neovasculariza-tion in prefabricated flaps. Microsurgery 2005;25:220–226.
17. Hoang NT, Kloeppel M, Staudenmaier R, Werner J, Biemer E.Study of the neovascularisation process in flap prefabrication using asilicone sheet and an isolated arterial pedicle. Scand J Plast ReconstrHand Surg 2005;39:326–333.
18. Hoang NT, Kloeppel M, Staudenmaier R, Schweinbeck S, Biemer E.Neovascularization in prefabricated flaps using a tissue expander andan implanted arteriovenous pedicle. Microsurgery 2005;25:213–219.
19. Nguyen TH, Kloppel M, Staudenmaier R, Biemer E. [Experimentalinvestigation of neovascularisation in large prefabricated flaps afterarteriovenous pedicle implantation]. Handchir Mikrochir Plast Chir2004;36:212–217.
20. Tan BK, Chen HC, He TM, Song IC. Flap prefabrication—Thebridge between conventional flaps and tissue-engineered flaps. AnnAcad Med 2004;33:662–666.
21. Tanaka Y, Sung KC, Tsutsumi A, Ohba S, Ueda K, Morrison WA.Tissue engineering skin flaps: Which vascular carrier, arteriovenousshunt loop or arteriovenous bundle, has more potential for angio-genesis and tissue generation? Plast Reconstr Surg 2003;112:1626–1644.
22. Cronin KJ, Messina A, Knight KR, Cooper-White JJ, Stevens GW,Penington AJ, Morrison WA. New murine model of spontaneous tis-sue engineering, combining an arteriovenous pedicle with matrixmaterials. Plast Reconstr Surg 2004;113:260–269.
23. Kamil SH, Kojima K, Vacanti MP, Zaporojan V, Vacanti CA, EaveyRD. Tissue engineered cartilage: Utilization of autologous serum andserum-free media for chondrocyte culture. Int J Pediatr Otorhinolar-yngol 2007;71:71–75.
24. Yamamoto K, Tomita N, Fukuda Y, Suzuki S, Igarashi N, Suguro T,Tamada Y. Time-dependent changes in adhesive force betweenchondrocytes and silk fibroin subtrate. Biomaterials 2007;28:1838–1846.
25. Cao Y, Rodriguez A, Vacanti M, Ibarra C, Arevalo C, Vacanti CA.Comparative study of the use of poly(glycolic acid), calcium alginateand pluronics in the engineering of autologous porcine cartilage.J Biomater Sci Polym Ed 1998;9:475–487.
26. Baek CH, Ko YJ. Characteristics of tissue-engineered cartilage onmacroporous biodegradable PLGA scaffold. Laryngoscope 2006;116:1829–1834.
27. Osch van GJ, van der Veen SW, Burger EH, Verwoerd-Verhoef HL.Chondrogenic potential of in vitro multiplied rabbit perichondriumcells cultured in alginate beads in defined medium. Tissue Eng2000;6:321–330.
28. Chung C, Mesa J, Miller GJ, Randolph MA, Gill TJ, Burdick JA.Effects of auricular chondrocyte expansion on neocartilage formationin photocrosslinked hyaluronic acid networks. Tissue Eng 2006;12:2665–2673.
29. Britt JC, Park SS. Autogenous tissue-engineered cartilage: Evalua-tion as an implant. Arch Otolaryngol Head Neck Surg 1998;124:671–677.
30. Morrison WA, Dvir E, Doi K, Hurley JV, Hickey MJ, O’Brien BM.Prefabrication of thin transferable axial-pattern skin flaps: An experi-mental study in rabbits. Br J Plast Surg 1990;43:645–654.
31. Pribaz JJ, Fine N, Orgill DP. Flap prefabrication in the head andneck: A 10-year experience. Plast Reconstr Surg 1999;103:808–820.
32. Rotter N, Aigner J, Naumann A, Planck H, Hammer C, BurmeisterG, Sittinger M. Cartilage reconstruction in head and neck surgery:Comparison of reabsorbable polymer scaffolds for tissue engineer-ing of human septal cartilage. J Biomed Mater Res 1998;42:347–356.
In Vitro Cartilage-Engineered Constructs 61
Microsurgery DOI 10.1002/micr
Related Documents











