Intravitreal Bevacizumab in Inflammatory Ocular Neovascularization AHMAD M. MANSOUR, FRIEDERIKE MACKENSEN, J. FERNANDO AREVALO, FOCKE ZIEMSSEN, PADMAMALINI MAHENDRADAS, ABLA MEHIO-SIBAI, NICHOLAS HRISOMALOS, TIMOTHY Y. Y. LAI, DAVID DODWELL, WAI-MAN CHAN, THOMAS NESS, ALAY S. BANKER, SIVAKAMI A. PAI, MARIA H. BERROCAL, RANIA TOHME, ARND HEILIGENHAUS, ZIAD F. BASHSHUR, MONCEF KHAIRALLAH, KHALIL M. SALEM, FRANK N. HRISOMALOS, MATTHEW H. WOOD, WILSON HERIOT, ALFREDO ADAN, ATUL KUMAR, LYNDELL LIM, ANTHONY HALL, AND MATTHIAS BECKER ● PURPOSE: To assess the role of bevacizumab in inflam- matory ocular neovascularization. ● DESIGN: Retrospective, multicenter, consecutive case series of inflammatory ocular neovascularization. ● METHODS: Patients with inflammatory ocular neovas- cularization of varying causes for whom standard therapy failed were treated with intravitreal injection of bevaci- zumab. Main outcome measures included improvement of best-corrected visual acuity (BCVA) expressed in logarithm of minimum angle of resolution units, response of inflammatory ocular neovascularization by funduscopy and angiography, and decrease in central foveal thickness as measured by optical coherence tomography at the three-month follow-up. ● RESULTS: At the three-month follow-up, 84 eyes of 79 patients had been treated with a mean of 1.3 injections (range, one to three). Thirty-four eyes showed juxtafo- veal choroidal neovascularization (CNV), 34 eyes showed subfoveal CNV, eight eyes showed peripapillary CNV, and 11 eyes showed neovascularization of the disc (NVD) or neovascularization elsewhere (NVE). BCVA improved 2.4 lines from 0.68 (6/28 or 20/94) to 0.44 (6/17 or 20/55) (P < .001). BCVA improved by one to three lines in 34.5% of the eyes, by four to six lines in 16.7% of the eyes, and by more than six lines in 14.2% of the eyes. Function was unchanged in 23.8% of the eyes. BCVA worsened in 10.7% (zero to three lines in 7.1%, more than four lines in 3.6%). Central foveal thickness decreased from baseline 346 to 252 m(P < .001). For CNV, 32 eyes (43.2%) had complete regres- sion after the injection, 27 (36.5%) had partial regres- sion, five (6.8%) had no response, and 10 eyes (13.5%) were not evaluated by the contributors. For NVD or NVE, seven eyes (63.6%) had complete regression of new vessels and four eyes (36.4%) had partial regression after the injection. ● CONCLUSIONS: Intravitreal bevacizumab led to short- term significant visual improvement and regression of inflammatory ocular neovascularization in a wide variety of inflammatory ocular diseases. (Am J Ophthalmol 2008;146:410 – 416. © 2008 by Elsevier Inc. All rights reserved.) I NFLAMMATORY CHOROIDAL NEOVASCULARIZATION (CNV) ranks third in the frequency of CNV after age-related macular degeneration (AMD) and patho- logic myopia. 1 Ocular neovascularization often responds to systemic 2 and periocular or intraocular corticosteroid ther- apy (CST). When this standard approach fails, additional therapies have included laser photocoagulation, 3–6 photo- dynamic therapy (PDT), 7–10 submacular surgery, 11,12 or macular translocation. 13 In this study, we analyzed the therapeutic role of intravitreal bevacizumab in inflamma- tory ocular neovascularization not responding to standard therapy in a multicenter, retrospective study. Accepted for publication May 16, 2008. From the Department of Ophthalmology (A.M.M., Z.F.B., K.M.S.), American University of Beirut and Rafic Hariri University Hospital, Beirut, Lebanon; the Interdisciplinary Uveitis Center, University of Heidelberg, Heidelberg, Germany (F.M., M.B.); the Clinica Oftalmo- logica Centro Caracas, University of Los Andes, Caracas, Venezuela (J.F.A.); the Department of Ophthalmology, University of Tuebingen, Tuebingen, Germany (F.Z.); the Tuebingen Bevacizumab Study Group, Departments of Uveitis and Retina, Narayana Nethralaya, Bangalore, India (P.M., S.A.P., R.T.); the Department of Epidemiology and Popu- lation Health, American University of Beirut and Rafic Hariri University Hospital, Beirut, Lebanon (A.M.-S.); the Department of Ophthalmology, University of Indiana, Indianapolis, Indiana (N.H., F.N.H.); the Depart- ment of Ophthalmology and Visual Sciences, Chinese University of Hong Kong, Hong Kong Eye Hospital, Kowloon, Hong Kong (T.Y.Y.L.); the Springfield Eye Clinic, Springfield, Illinois (D.D.); the Department of Ophthalmology, Chinese University of Hong Kong, Hong Kong Sanato- rium and Hospital, Happy Valley, Hong Kong (W.-M.C.); the University Eye Hospital, Freiburg, Germany (T.N.); the Banker’s Retina Clinic and Laser Center, Ahmedabad, Gujarat, India (A.S.B.); the Department of Ophthalmology, University of Puerto Rico, San Juan, Puerto Rico (M.H.B.); the Department of Ophthalmology, Uveitis Center, St Franziskus Hospital, Muenster, Germany (A.H.); the Department of Ophthalmology, Fattouma Bourguiba University Hospital, Monastir, Tunisia (M.K.); Eye Surgical Associates, Lincoln, Nebraska (M.H.W.); the Department of Surgery, Cabrini Medical Center, Malvern, Victoria, Australia (W.H., A.H.); the Department of Ophthalmology, Hospital Clinic de Barcelona, Universidad de Barcelona, Barcelona, Spain (A.A.); the DR Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India (A.K.); the Centre for Eye Research Australia, Department of Ophthalmology, University of Melbourne, Melbourne, Victoria, Australia (L.L.); and the Department of Ophthalmology, Alfred Hospital, Melbourne, Victoria, Australia (A.H.). Inquiries to Ahmad M. Mansour, Department of Ophthalmology, American University of Beirut, P. O. Box 113-6044, Beirut, Lebanon; e-mail: [email protected] © 2008 BY ELSEVIER INC.ALL RIGHTS RESERVED. 410 0002-9394/08/$34.00 doi:10.1016/j.ajo.2008.05.024

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

●
m●
s●
cfzoloaat
A
ABHl(TDIlHUmHtOrELO(FOTtACtIEMO
Ae
4
Intravitreal Bevacizumab in Inflammatory OcularNeovascularization
AHMAD M. MANSOUR, FRIEDERIKE MACKENSEN, J. FERNANDO AREVALO, FOCKE ZIEMSSEN,PADMAMALINI MAHENDRADAS, ABLA MEHIO-SIBAI, NICHOLAS HRISOMALOS, TIMOTHY Y. Y. LAI,
DAVID DODWELL, WAI-MAN CHAN, THOMAS NESS, ALAY S. BANKER, SIVAKAMI A. PAI,MARIA H. BERROCAL, RANIA TOHME, ARND HEILIGENHAUS, ZIAD F. BASHSHUR,
MONCEF KHAIRALLAH, KHALIL M. SALEM, FRANK N. HRISOMALOS, MATTHEW H. WOOD,WILSON HERIOT, ALFREDO ADAN, ATUL KUMAR, LYNDELL LIM, ANTHONY HALL, AND
MATTHIAS BECKER
●
p(vsC(i(t1oe7t.sswNna●
tio2r
Ilsatdmtt
PURPOSE: To assess the role of bevacizumab in inflam-atory ocular neovascularization.
DESIGN: Retrospective, multicenter, consecutive caseeries of inflammatory ocular neovascularization. METHODS: Patients with inflammatory ocular neovas-ularization of varying causes for whom standard therapyailed were treated with intravitreal injection of bevaci-umab. Main outcome measures included improvementf best-corrected visual acuity (BCVA) expressed inogarithm of minimum angle of resolution units, responsef inflammatory ocular neovascularization by funduscopynd angiography, and decrease in central foveal thicknesss measured by optical coherence tomography at thehree-month follow-up.
ccepted for publication May 16, 2008.From the Department of Ophthalmology (A.M.M., Z.F.B., K.M.S.),merican University of Beirut and Rafic Hariri University Hospital,eirut, Lebanon; the Interdisciplinary Uveitis Center, University ofeidelberg, Heidelberg, Germany (F.M., M.B.); the Clinica Oftalmo-
ogica Centro Caracas, University of Los Andes, Caracas, VenezuelaJ.F.A.); the Department of Ophthalmology, University of Tuebingen,uebingen, Germany (F.Z.); the Tuebingen Bevacizumab Study Group,epartments of Uveitis and Retina, Narayana Nethralaya, Bangalore,
ndia (P.M., S.A.P., R.T.); the Department of Epidemiology and Popu-ation Health, American University of Beirut and Rafic Hariri Universityospital, Beirut, Lebanon (A.M.-S.); the Department of Ophthalmology,niversity of Indiana, Indianapolis, Indiana (N.H., F.N.H.); the Depart-ent of Ophthalmology and Visual Sciences, Chinese University ofong Kong, Hong Kong Eye Hospital, Kowloon, Hong Kong (T.Y.Y.L.);
he Springfield Eye Clinic, Springfield, Illinois (D.D.); the Department ofphthalmology, Chinese University of Hong Kong, Hong Kong Sanato-
ium and Hospital, Happy Valley, Hong Kong (W.-M.C.); the Universityye Hospital, Freiburg, Germany (T.N.); the Banker’s Retina Clinic andaser Center, Ahmedabad, Gujarat, India (A.S.B.); the Department ofphthalmology, University of Puerto Rico, San Juan, Puerto Rico
M.H.B.); the Department of Ophthalmology, Uveitis Center, Stranziskus Hospital, Muenster, Germany (A.H.); the Department ofphthalmology, Fattouma Bourguiba University Hospital, Monastir,unisia (M.K.); Eye Surgical Associates, Lincoln, Nebraska (M.H.W.);
he Department of Surgery, Cabrini Medical Center, Malvern, Victoria,ustralia (W.H., A.H.); the Department of Ophthalmology, Hospitallinic de Barcelona, Universidad de Barcelona, Barcelona, Spain (A.A.);
he DR Rajendra Prasad Centre for Ophthalmic Sciences, All Indianstitute of Medical Sciences, New Delhi, India (A.K.); the Centre forye Research Australia, Department of Ophthalmology, University ofelbourne, Melbourne, Victoria, Australia (L.L.); and the Department ofphthalmology, Alfred Hospital, Melbourne, Victoria, Australia (A.H.).Inquiries to Ahmad M. Mansour, Department of Ophthalmology,
tmerican University of Beirut, P. O. Box 113-6044, Beirut, Lebanon;
-mail: [email protected]
© 2008 BY ELSEVIER INC. A10
RESULTS: At the three-month follow-up, 84 eyes of 79atients had been treated with a mean of 1.3 injectionsrange, one to three). Thirty-four eyes showed juxtafo-eal choroidal neovascularization (CNV), 34 eyeshowed subfoveal CNV, eight eyes showed peripapillaryNV, and 11 eyes showed neovascularization of the disc
NVD) or neovascularization elsewhere (NVE). BCVAmproved 2.4 lines from 0.68 (6/28 or 20/94) to 0.446/17 or 20/55) (P < .001). BCVA improved by one tohree lines in 34.5% of the eyes, by four to six lines in6.7% of the eyes, and by more than six lines in 14.2%f the eyes. Function was unchanged in 23.8% of theyes. BCVA worsened in 10.7% (zero to three lines in.1%, more than four lines in 3.6%). Central fovealhickness decreased from baseline 346 to 252 �m (P <001). For CNV, 32 eyes (43.2%) had complete regres-ion after the injection, 27 (36.5%) had partial regres-ion, five (6.8%) had no response, and 10 eyes (13.5%)ere not evaluated by the contributors. For NVD orVE, seven eyes (63.6%) had complete regression ofew vessels and four eyes (36.4%) had partial regressionfter the injection. CONCLUSIONS: Intravitreal bevacizumab led to short-erm significant visual improvement and regression ofnflammatory ocular neovascularization in a wide varietyf inflammatory ocular diseases. (Am J Ophthalmol008;146:410 – 416. © 2008 by Elsevier Inc. All rightseserved.)
NFLAMMATORY CHOROIDAL NEOVASCULARIZATION
(CNV) ranks third in the frequency of CNV afterage-related macular degeneration (AMD) and patho-
ogic myopia.1 Ocular neovascularization often responds toystemic2 and periocular or intraocular corticosteroid ther-py (CST). When this standard approach fails, additionalherapies have included laser photocoagulation,3–6 photo-ynamic therapy (PDT),7–10 submacular surgery,11,12 oracular translocation.13 In this study, we analyzed the
herapeutic role of intravitreal bevacizumab in inflamma-ory ocular neovascularization not responding to standard
herapy in a multicenter, retrospective study.LL RIGHTS RESERVED. 0002-9394/08/$34.00doi:10.1016/j.ajo.2008.05.024

M
iUctnAdeMfiafaebpc
np(Ucvshptuiarb
ecml(srvb
mbtrrzfi
is
fsBtsat
W
ca8g9opordtaaeblsspp
crpswosmtb(mvClisj
V
METHODS
EMBERS OF THE AMERICAN SOCIETY OF RETINAL SPECIAL-
sts, the American Uveitis Society, and the Internationalveitis Study Group were invited to contribute their
onsecutive cases of inflammatory ocular neovasculariza-ion not responding to standard therapy (CST or immu-osuppression) and treated with intravitreal bevacizumab.standardized spreadsheet was used to collect the clinical
ata. Cases with concomitant or prior cystoid maculardema (CME), diabetes mellitus, or AMD were excluded.ost of the patients initially had been treated in a stepwise
ashion with high doses of oral CST, with or withoutntraocular or sub-Tenon CST or immunosuppressive ther-py (as monitored by a rheumatologist). All patients optedor intravitreal bevacizumab after detailed informationbout the limited experience with, the potential sideffects of, and the off-label use of the drug. The risks andenefits of intravitreal therapy were discussed with theatients (or their guardians), who signed an informedonsent.
Intravitreal bevacizumab was injected using a 30-gaugeeedle in a sterile manner after topical anesthesia andovidone instillation in the lower cul de sac. BevacizumabAvastin; Genentech Inc, San Francisco, California,SA) was prepared in the hospital pharmacies of the
orresponding institution. The hospital pharmacies di-ided the 4-ml (100 mg) bevacizumab vial into 20 1-mlyringes using aseptic techniques under a laminar flowood with the syringes stored at 40 C. The intraocularressure (IOP) was controlled immediately after the injec-ion. Only in a few eyes was release of aqueous humorndertaken to lower the IOP. In pediatric cases, thenjection was given in the operating room under generalnesthesia. Bevacizumab therapy in young women wasestricted to those using adequate contraception and notreastfeeding.Best-corrected visual acuity (BCVA) was assessed using
ither Early Treatment of Diabetic Retinopathy or Snellenharts (half-and-half) and was listed as logarithm of theinimum angle of resolution (logMAR) equivalents. Fol-
ow-up examinations included fluorescein angiographyFA) and optical coherence tomography (OCT), withome patients also undergoing indocyanine green angiog-aphy. No attempt was made to measure the macularolume because of the use of different OCT machinesetween the centers.Retreatment varied between the collaborators, withost waiting for evidence of recurrent activity, evaluated
y funduscopy, FA (leakage, growth), or OCT examina-ion (increase in retinal thickness). The Chinese collabo-ators used three initial injections in monthly intervals,egardless of the clinical response. The response to bevaci-umab was classified by each contributor on angiographic
ndings as complete regression, partial regression (decrease sINFLAMMATORY NEOVOL. 146, NO. 3
n size with minimal leakage), or no response (increase inize or persistent leakage).
Descriptive statistics (mean � standard deviation andrequencies) were calculated and were stratified by diagno-is and location. Differences between final and initialCVA were tested using paired Wilcoxon nonparametric
ests. All statistical analyses were carried out using SPSSoftware version 13.0 (SPSS Inc, Chicago, Illinois, USA),nd a P value less than .01 was considered to be significanto adjust for multiple tests.
RESULTS
E TREATED 84 EYES OF 79 PATIENTS FROM 20 MEDICAL
enters. The study population was comprised of 49 womennd 30 men with a mean age of 40.0 years (range, eight to5 years). The youngest patients included an 8-year-oldirl with CNV resulting from idiopathic chorioretinitis, a-year-old girl with neovascularization of the disc (NVD)r neovascularization elsewhere (NVE) resulting from parslanitis, an 11-year-old girl with CNV resulting fromcular toxoplasmosis, and a 14-year-old girl with CNVesulting from ocular histoplasmosis. Mean duration of theisease before current therapy was 30.6 months (range, oneo 240 months). At the time of the injection, 23 eyes hadctive uveitis, whereas in 61 eyes, uveitis was inactive orbsent. The right eye was involved in 44 patients, the leftye was involved in 34 patients, and six patients hadilateral involvement. The inflammatory ocular neovascu-arization failed to regress with systemic immunosuppres-ive agents (14 patients), oral CST (41 patients),ub-Tenon CST (eight patients), and intraocular CST (11atients). A total of seven patients had undergone PDTreviously.The classified disease included 15 eyes with multifocal
horoiditis with panuveitis; 15 with punctate inner cho-oidopathy; 13 with ocular histoplasmosis; 10 with idio-athic uveitis; five eyes each with Vogt-Koyanagi-Harada,erpiginous choroiditis, and retinal vasculitis; four eyesith Eales disease; three eyes each with pars planitis andcular toxoplasmosis; two eyes each with tuberculosis andarcoidosis; and one eye with birdshot choroiditis. Theean number of intravitreal injections at the three-month
ime point was 1.3 (range, one to three). The volume ofevacizumab injected included 38 eyes receiving 0.1 ml2.5 mg) bevacizumab and 46 eyes receiving 0.05 ml (1.25g) bevacizumab. The type of inflammatory ocular neo-
ascularization was NVD or NVE (12 eyes), juxtafovealNV (34 eyes), subfoveal CNV (34 eyes), and peripapil-
ary CNV (eight eyes). Inflammatory ocular neovascular-zation was multifocal in four cases. Three eyes had twoeparate foci of CNV. One patient was found to haveuxtafoveal CNV in one eye and NVE in both eyes. CNV
ize had a mean of 1.3 disc diameters (range, 0.25 to 4 discASCULARIZATION 411
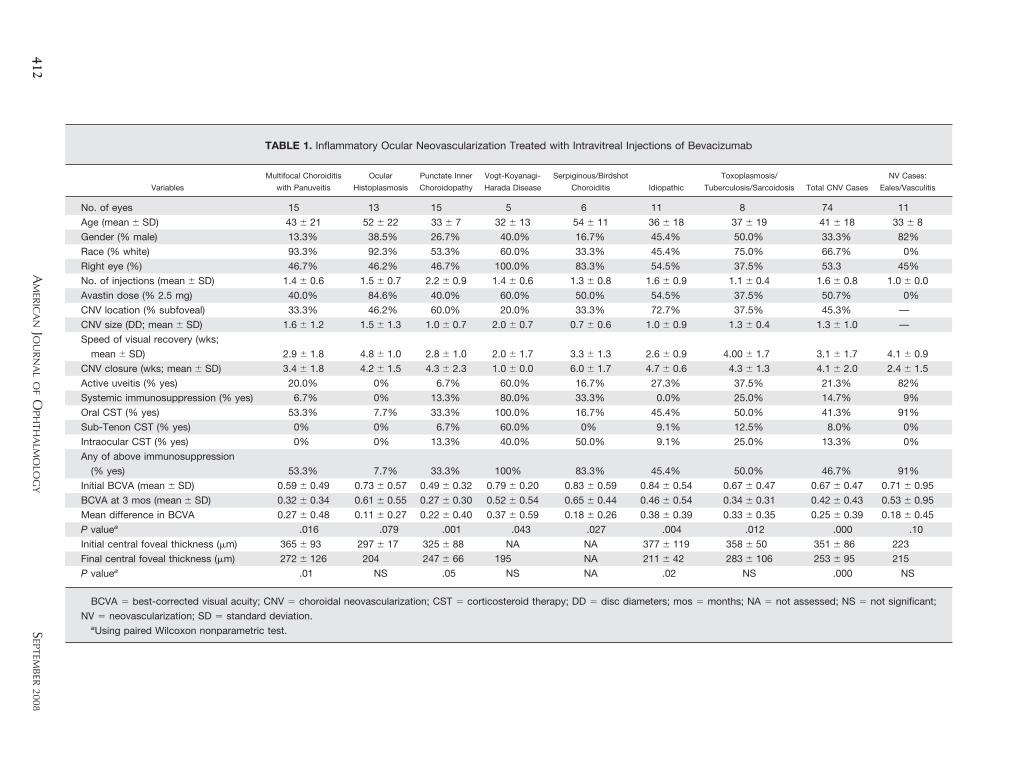
TABLE 1. Inflammatory Ocular Neovascularization Treated with Intravitreal Injections of Bevacizumab
Variables
Multifocal Choroiditis
with Panuveitis
Ocular
Histoplasmosis
Punctate Inner
Choroidopathy
Vogt-Koyanagi-
Harada Disease
Serpiginous/Birdshot
Choroiditis Idiopathic
Toxoplasmosis/
Tuberculosis/Sarcoidosis Total CNV Cases
NV Cases:
Eales/Vasculitis
No. of eyes 15 13 15 5 6 11 8 74 11
Age (mean � SD) 43 � 21 52 � 22 33 � 7 32 � 13 54 � 11 36 � 18 37 � 19 41 � 18 33 � 8
Gender (% male) 13.3% 38.5% 26.7% 40.0% 16.7% 45.4% 50.0% 33.3% 82%
Race (% white) 93.3% 92.3% 53.3% 60.0% 33.3% 45.4% 75.0% 66.7% 0%
Right eye (%) 46.7% 46.2% 46.7% 100.0% 83.3% 54.5% 37.5% 53.3 45%
No. of injections (mean � SD) 1.4 � 0.6 1.5 � 0.7 2.2 � 0.9 1.4 � 0.6 1.3 � 0.8 1.6 � 0.9 1.1 � 0.4 1.6 � 0.8 1.0 � 0.0
Avastin dose (% 2.5 mg) 40.0% 84.6% 40.0% 60.0% 50.0% 54.5% 37.5% 50.7% 0%
CNV location (% subfoveal) 33.3% 46.2% 60.0% 20.0% 33.3% 72.7% 37.5% 45.3% —
CNV size (DD; mean � SD) 1.6 � 1.2 1.5 � 1.3 1.0 � 0.7 2.0 � 0.7 0.7 � 0.6 1.0 � 0.9 1.3 � 0.4 1.3 � 1.0 —
Speed of visual recovery (wks;
mean � SD) 2.9 � 1.8 4.8 � 1.0 2.8 � 1.0 2.0 � 1.7 3.3 � 1.3 2.6 � 0.9 4.00 � 1.7 3.1 � 1.7 4.1 � 0.9
CNV closure (wks; mean � SD) 3.4 � 1.8 4.2 � 1.5 4.3 � 2.3 1.0 � 0.0 6.0 � 1.7 4.7 � 0.6 4.3 � 1.3 4.1 � 2.0 2.4 � 1.5
Active uveitis (% yes) 20.0% 0% 6.7% 60.0% 16.7% 27.3% 37.5% 21.3% 82%
Systemic immunosuppression (% yes) 6.7% 0% 13.3% 80.0% 33.3% 0.0% 25.0% 14.7% 9%
Oral CST (% yes) 53.3% 7.7% 33.3% 100.0% 16.7% 45.4% 50.0% 41.3% 91%
Sub-Tenon CST (% yes) 0% 0% 6.7% 60.0% 0% 9.1% 12.5% 8.0% 0%
Intraocular CST (% yes) 0% 0% 13.3% 40.0% 50.0% 9.1% 25.0% 13.3% 0%
Any of above immunosuppression
(% yes) 53.3% 7.7% 33.3% 100% 83.3% 45.4% 50.0% 46.7% 91%
Initial BCVA (mean � SD) 0.59 � 0.49 0.73 � 0.57 0.49 � 0.32 0.79 � 0.20 0.83 � 0.59 0.84 � 0.54 0.67 � 0.47 0.67 � 0.47 0.71 � 0.95
BCVA at 3 mos (mean � SD) 0.32 � 0.34 0.61 � 0.55 0.27 � 0.30 0.52 � 0.54 0.65 � 0.44 0.46 � 0.54 0.34 � 0.31 0.42 � 0.43 0.53 � 0.95
Mean difference in BCVA 0.27 � 0.48 0.11 � 0.27 0.22 � 0.40 0.37 � 0.59 0.18 � 0.26 0.38 � 0.39 0.33 � 0.35 0.25 � 0.39 0.18 � 0.45
P valuea .016 .079 .001 .043 .027 .004 .012 .000 .10
Initial central foveal thickness (�m) 365 � 93 297 � 17 325 � 88 NA NA 377 � 119 358 � 50 351 � 86 223
Final central foveal thickness (�m) 272 � 126 204 247 � 66 195 NA 211 � 42 283 � 106 253 � 95 215
P valuea .01 NS .05 NS NA .02 NS .000 NS
BCVA � best-corrected visual acuity; CNV � choroidal neovascularization; CST � corticosteroid therapy; DD � disc diameters; mos � months; NA � not assessed; NS � not significant;
NV � neovascularization; SD � standard deviation.aUsing paired Wilcoxon nonparametric test.
AM
ERIC
AN
JOU
RN
AL
OF
OPH
THA
LMO
LOG
Y412
SEPTEM
BER
2008
dird
0TgifiBmd
cov1l(isc
dCacmH43cT2hb
vsf2orsnm
V
iameters). Macular hemorrhage was noted after injectionn one eye. No other injection-related complications wereeported such as cataract, retinal detachment (RD), en-ophthalmitis, or exacerbation of uveitis.Best-corrected visual acuity improved 2.4 lines from
.68 (6/28 or 20/94) to 0.44 (6/17 or 20/55; P � .001).his visual improvement was significant independent ofender, age, dosage, size of CNV, and type of CNV. BCVAmproved from one to three lines in 34.5% of the eyes,rom four to six lines in 16.7%, and by more than six linesn 14.2%. Function was unchanged in 23.8% of the eyes.CVA worsened in 10.7% (zero to three lines in 7.1% andore than four lines in 3.6%). Central foveal thickness
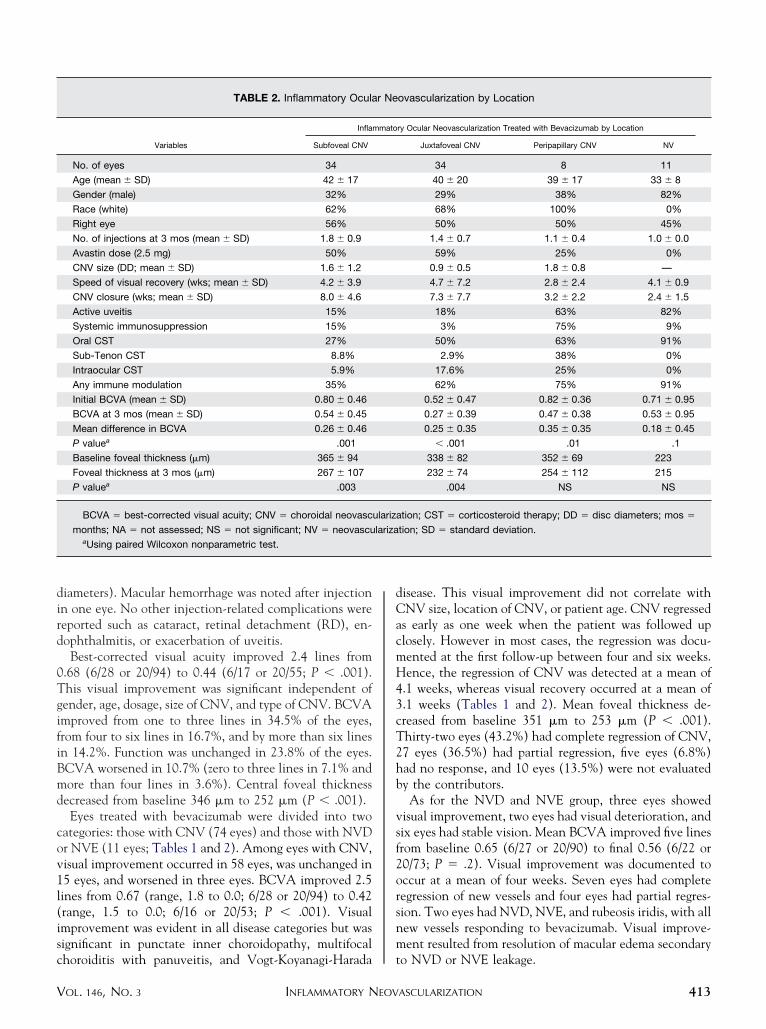
ecreased from baseline 346 �m to 252 �m (P � .001).Eyes treated with bevacizumab were divided into two
ategories: those with CNV (74 eyes) and those with NVDr NVE (11 eyes; Tables 1 and 2). Among eyes with CNV,isual improvement occurred in 58 eyes, was unchanged in5 eyes, and worsened in three eyes. BCVA improved 2.5ines from 0.67 (range, 1.8 to 0.0; 6/28 or 20/94) to 0.42range, 1.5 to 0.0; 6/16 or 20/53; P � .001). Visualmprovement was evident in all disease categories but wasignificant in punctate inner choroidopathy, multifocal
TABLE 2. Inflammatory Ocula
Variables
Infla
Subfoveal CNV
No. of eyes 34
Age (mean � SD) 42 � 17
Gender (male) 32%
Race (white) 62%
Right eye 56%
No. of injections at 3 mos (mean � SD) 1.8 � 0.9
Avastin dose (2.5 mg) 50%
CNV size (DD; mean � SD) 1.6 � 1.2
Speed of visual recovery (wks; mean � SD) 4.2 � 3.9
CNV closure (wks; mean � SD) 8.0 � 4.6
Active uveitis 15%
Systemic immunosuppression 15%
Oral CST 27%
Sub-Tenon CST 8.8%
Intraocular CST 5.9%
Any immune modulation 35%
Initial BCVA (mean � SD) 0.80 � 0.46
BCVA at 3 mos (mean � SD) 0.54 � 0.45
Mean difference in BCVA 0.26 � 0.46
P valuea .001
Baseline foveal thickness (�m) 365 � 94
Foveal thickness at 3 mos (�m) 267 � 107
P valuea .003
BCVA � best-corrected visual acuity; CNV � choroidal neovasc
months; NA � not assessed; NS � not significant; NV � neovascuaUsing paired Wilcoxon nonparametric test.
horoiditis with panuveitis, and Vogt-Koyanagi-Harada t
INFLAMMATORY NEOVOL. 146, NO. 3
isease. This visual improvement did not correlate withNV size, location of CNV, or patient age. CNV regressed
s early as one week when the patient was followed uplosely. However in most cases, the regression was docu-ented at the first follow-up between four and six weeks.ence, the regression of CNV was detected at a mean of
.1 weeks, whereas visual recovery occurred at a mean of
.1 weeks (Tables 1 and 2). Mean foveal thickness de-reased from baseline 351 �m to 253 �m (P � .001).hirty-two eyes (43.2%) had complete regression of CNV,7 eyes (36.5%) had partial regression, five eyes (6.8%)ad no response, and 10 eyes (13.5%) were not evaluatedy the contributors.As for the NVD and NVE group, three eyes showed
isual improvement, two eyes had visual deterioration, andix eyes had stable vision. Mean BCVA improved five linesrom baseline 0.65 (6/27 or 20/90) to final 0.56 (6/22 or0/73; P � .2). Visual improvement was documented toccur at a mean of four weeks. Seven eyes had completeegression of new vessels and four eyes had partial regres-ion. Two eyes had NVD, NVE, and rubeosis iridis, with allew vessels responding to bevacizumab. Visual improve-ent resulted from resolution of macular edema secondary
ovascularization by Location
ry Ocular Neovascularization Treated with Bevacizumab by Location
Juxtafoveal CNV Peripapillary CNV NV
34 8 11
40 � 20 39 � 17 33 � 8
29% 38% 82%
68% 100% 0%
50% 50% 45%
1.4 � 0.7 1.1 � 0.4 1.0 � 0.0
59% 25% 0%
0.9 � 0.5 1.8 � 0.8 —
4.7 � 7.2 2.8 � 2.4 4.1 � 0.9
7.3 � 7.7 3.2 � 2.2 2.4 � 1.5
18% 63% 82%
3% 75% 9%
50% 63% 91%
2.9% 38% 0%
17.6% 25% 0%
62% 75% 91%
0.52 � 0.47 0.82 � 0.36 0.71 � 0.95
0.27 � 0.39 0.47 � 0.38 0.53 � 0.95
0.25 � 0.35 0.35 � 0.35 0.18 � 0.45
� .001 .01 .1
338 � 82 352 � 69 223
232 � 74 254 � 112 215
.004 NS NS
tion; CST � corticosteroid therapy; DD � disc diameters; mos �
tion; SD � standard deviation.
r Ne
mmato
ulariza
lariza
o NVD or NVE leakage.
ASCULARIZATION 413

I
rpTmp7Ts(owfi(
owhMypmwlosmrvomo.R
Capsm0vadarn62ttmh(
ltCe
tiiivmpbcfrmtO1mi2ipTtsvBo
ssdos(tPsSMsvmiw
rarclw
4
DISCUSSION
NFLAMMATORY OCULAR NEOVASCULARIZATION IS FAIRLY
are1 in uveitis: CNV occurred in 12 (1.9%) of 648atients with uveitis. Still, it has a very poor prognosis.he natural history of subfoveal CNV in various inflam-atory chorioretinal disorders has been very guarded; of 74
atients with ocular histoplasmosis and subfoveal CNV,7% had 6/30 (20/100) or worse BCVA at 36 months.14
his was similar for 148 patients with juxtafoveal andubfoveal CNV resulting from ocular histoplasmosis69.6% had 6/30 or worse BCVA) followed up for a meanf 39 months.15 Brown and associates described 12 eyesith CNV related to punctate inner choroidopathy whereve of 12 eyes had final BCVA poorer than 6/6020/200).16
Pilot studies of photocoagulation of subfoveal CNV incular histoplasmosis3 were inconclusive. Laser therapyas found to be effective in juxtafoveal CNV in ocularistoplasmosis according to two randomized studies.4,5 Theacular Photocoagulation Study showed that after five
ears of follow-up, 12% of eyes with extrafoveal CNVhotocoagulated had severe visual loss (loss of six lines orore) compared with 42% of eyes that were observedithout treatment.4,5 However, the enlargement of the
aser scar with subsequent involvement of the fovea6 madephthalmologists try other options such as surgical exci-ion of CNV, macular translocation, and PDT. The Sub-acular Surgery Trials Research Group presented a
andomized comparison of surgery (112 patients) vs obser-ation (113 patients) for subfoveal CNV in eyes withcular histoplasmosis or idiopathic cause.12 At the 24-onth follow-up, median BCVA was 6/75 (20/250) in the
bservation arm and 6/48 (20/160) in the surgery arm (P �07). CNV recurred in 58% of surgically treated eyes andD occurred in 4%.12
Photodynamic therapy was shown to improve BCVA inNV in various inflammatory diseases. Parodi and associ-
tes treated 13 patients having multifocal choroiditis withanuveitis and subfoveal CNV with PDT (mean, 1.5essions) and reported stabilization of vision over a 12-onth follow-up (baseline BCVA, 0.55; final BCVA,
.52).7 Nowilaty and associates found that PDT stabilizedision in patients with CNV associated with Vogt-Koy-nagi-Harada disease.8 Subsequently, submacular fibrosiseveloped in half of the six patients. Mauget-Fays̈se andssociates treated eight patients with subfoveal CNVelated to toxoplasmic retinochoroiditis with PDT (meanumber of sessions, 1.75): BCVA improved 0.25 line from/67 (20/225) to 6/37 (20/123) over a mean follow-up of5 months.9 Wachtlin and associates used an average ofwo PDT sessions for subfoveal and juxtafoveal inflamma-ory CNV in 19 patients.17 Within the follow-up of 22.1onths, BCVA improved 1.63 lines: 63.2% (12/19) eyesad an improvement of two lines or more, whereas 26.3%
5/19) remained stable (within one line) and 10.5% (2/19) mAMERICAN JOURNAL OF14
ost two lines or more. The Verteporfin in Ocular His-oplasmosis Study treated 22 patients showing subfovealNV with 3.9 sessions of PDT.10 At the 24-month
xamination, the median improvement was 1.2 lines.Vascular endothelial growth factor (VEGF) is a cytokine
hat participates in multiple inflammatory processes and isncreased in eyes with uveitis, more so when uveitic CMEs present,18 and probably exhibits the highest levels innflammatory ocular neovascularization.19 So using intra-itreal injections with VEGF inhibitors is the first treat-ent approach actually influencing the pathogenic
athway of CNV formation. Chan and associates usedevacizumab to treat four patients with punctate innerhoroidopathy and CNV.20 The three patients with sub-oveal CNV and one patient with juxtafoveal CNVesponded over a six-month follow-up with visual improve-ent from a median of 6/19.5 (20/65) to 6/9.6 (20/32). At
he meeting of the Association for Research in Vision andphthalmology in 2007, Dodwell and associates presented
3 cases of ocular histoplasmosis with CNV treated withultiple intravitreal bevacizumab injections. Mean BCVA
mproved 2.1 lines from 0.58 (20/76) to 0.37 (20/49) at the5-week follow-up. Adán and associates described visualmprovement by a single bevacizumab injection in aatient with ocular histoplasmosis and juxtafoveal CNV.21
hese observations in small case series and the findings inhis largest case series of inflammatory CNV suggest thathort-term anti-VEGF treatment may be superior to pre-ious therapies, with an improvement of 2.5 lines inCVA. Long-term observation has yet to show frequencyf recurrences and long-term visual function.Similar effectiveness of anti-VEGF treatment can be
hown for NVE or NVD. Kumar and Sinha treated with aingle injection of bevacizumab one patient with Ealesisease with resolution of NVD and NVE over four monthsf follow-up.22 The similar sustained and complete re-ponse to therapy in Eales disease that we saw in our seriesone injection caused regression of NVD and NVE forhree months in three patients) may be explained byerentes and associates, who found massive VEGF expres-ion in Eales disease.19 During the American Uveitisociety at the American Academy of Ophthalmology 2006eeting (www.uveitissociety.org), Lew and associates pre-
ented the case of a 16-year-old female with lupus retinalasculitis who showed a dramatic regression of NVE in aatter of days after intravitreal bevacizumab. BCVA
mproved from counting fingers to 6/6 (20/20) over oneeek.Use of systemic bevacizumab in children has been
eported in malignancies,23 and use of intravitreal bev-cizumab has been reported in retinopathy of prematu-ity.24 –26 In the present study, bevacizumab was used inhildren with inflammatory ocular neovascularization. Theargest investigation of the safety of systemic bevacizumabas undertaken in 15 patients with solid pediatric tu-
ors.23 Bevacizumab was administered every two to threeOPHTHALMOLOGY SEPTEMBER 2008

wt(ssoRac
ploza
tstt
beawcmftatii
tiisbb
TcR(MTIr
V
eeks for 1.5 to 23 months. Systemic bevacizumab seemedo have a good acute safety profile with mild side effectshypertonia, proteinuria, hematuria, and epistaxis).23 Pro-pective clinical trials are underway to evaluate further theafety of bevacizumab in pediatric patients in the therapyf cancer or block retinopathy of prematurity (BLOCK-OP). Until then, investigational administration of bev-cizumab should be discussed carefully and monitoredlosely in children.
Women of childbearing age are counseled regarding therolonged exposure after intravitreal bevacizumab (half-ife, approximately 20 days) and the potential fatal effectsf bevacizumab on fetal development. Intravitreal bevaci-umab is avoided in pregnant women, women not usingdequate contraception, and in breastfeeding mothers.
As with any multicenter retrospective study, the limita-ions include relatively short follow-up, unmasked re-earchers, variations in the decision to initiate, repeat anderminate intravitreal therapy, variations in the accep-
ance of the visual outcome between patients of different atifocal choroiditis. Am J Ophthalmol 2004;138:263–269.
1
1
1
1
INFLAMMATORY NEOVOL. 146, NO. 3
ackgrounds, and the absence of a standardized OCTxamination algorithm. Moreover, some uveitic disordersssociated with inflammatory ocular neovascularizationere not included here, such as syphilis, Lyme disease,andidiasis, rubella, Behçet disease, sympathetic ophthal-ia, and others. In the absence of any proven treatment
or inflammatory ocular neovascularization, it is reasonableo suppress CNV growth, to reduce vascular permeability,nd to suppress the inflammatory response by a combina-ion of corticosteroids in various routes of administration,mmunosuppressive agents, and intravitreal bevacizumab,f necessary.
In summary, intravitreal bevacizumab led in the short-erm to significant visual improvement and regression ofnflammatory ocular neovascularization in a wide variety ofnflammatory ocular diseases. A long-term study of theafety and efficacy of intravitreal bevacizumab is warrantedecause the long-term visual prognosis may be jeopardizedy submacular fibrosis, CME, or spread of chorioretinal
trophy.HE AUTHORS INDICATE NO FINANCIAL SUPPORT OR FINANCIAL CONFLICT OF INTEREST. INVOLVED IN DESIGN ANDonduct of study (A.M.M.); data collection (A.M.M., F.M., J.F.A., F.Z., P.M., A.M.S., N.H., T.Y.Y.L., D.D., W.M.C., T.N., A.S.B., S.A.P., M.H.B.,.T., A.H., Z.F.B., M.K., K.M.S., F.N.H., M.H.W., W.H., A.A., A.K., L.L., A.H., M.B.); management, analysis, and interpretation the data
A.M.M., F.M., J.F.A., F.Z., P.M., A.M.S., N.H., T.Y.Y.L., D.D., W.M.C., T.N., A.S.B., S.A.P., M.H.B., R.T., A.H., Z.F.B., M.K., K.M.S., F.N.H.,.H.W., W.H., A.A., A.K., L.L., A.H., M.B.); and preparation, review, and approval of the manuscript (A.M.M., F.M., J.F.A., F.Z., P.M., A.M.S., N.H.,.Y.Y.L., D.D., W.M.C., T.N., A.S.B., S.A.P., M.H.B., R.T., A.H., Z.F.B., M.K., K.M.S., F.N.H., M.H.W., W.H., A.A., A.K., L.L., A.H., M.B.).
nstitutional review board approval was obtained for this research from the American University of Beirut Institutional Review Board. The study wasegistered in the National Clinical Trials (NCT 00645697).
The authors thank the Pan-American Collaborative Retina Study Group and Professor Howard Tessler for their contribution of cases.
REFERENCES
1. Perentes Y, van Tran T, Sickenberg M, Herbort CP. Sub-retinal neovascular membranes complicating uveitis: fre-quency, treatments, and visual outcome. Ocul ImmunolInflamm 2005;13:219–224.
2. Flaxel CJ, Owens SL, Mulholland B, Schwartz SD, GregorZJ. The use of corticosteroids for choroidal neovasculariza-tion in young patients. Eye 1998;12:266–272.
3. Fine SL, Wood WJ, Isernhagen RD, et al. Laser treatment forsubfoveal neovascular membranes in ocular histoplasmosissyndrome: results of a pilot randomized clinical trial. ArchOphthalmol 1993;111:19–20.
4. Macular Photocoagulation Study Group. Argon laser photo-coagulation for ocular histoplasmosis: results of a randomizedclinical trial. Arch Ophthalmol 1983;101:1347–1357.
5. Macular Photocoagulation Study Group. Krypton laser pho-tocoagulation for neovascular lesions of ocular histoplasmo-sis: results of a randomized clinical trial. Arch Ophthalmol1987;105:1499–1507.
6. Shah SS, Schachat AP, Murphy RP, Fine SL. The evolutionof argon laser photocoagulation scars in patients with theocular histoplasmosis syndrome. Arch Ophthalmol 1988;106:1533–1536.
7. Parodi MB, Di Crecchio L, Lanzetta P, Polito A, Bandello F,Ravalico G. Photodynamic therapy with verteporfin forsubfoveal choroidal neovascularization associated with mul-
8. Nowilaty SR, Bouhaimed M, Photodynamic Therapy StudyGroup. Photodynamic therapy for subfoveal choroidal neo-vascularization in Vogt-Koyanagi-Harada disease. Br J Oph-thalmol 2006;908:982–986.
9. Mauget-Fays̈se M, Mimoun G, Ruiz-Moreno JM, et al.Verteporfin photodynamic therapy for choroidal neovascu-larization associated with toxoplasmic retinochoroiditis. Ret-ina 2006;26:396–403.
0. Rosenfeld PJ, Saperstein DA, Bressler NM, et al, Verteporfinin Ocular Histoplasmosis Study Group. Photodynamic ther-apy with verteporfin in ocular histoplasmosis: uncontrolled,open-label 2-year study. Ophthalmology 2004;111:1725–1733.
1. Olsen TW, Capone A, Sternberg P, Grossniklaus HE, MartinDF, Aaberg TM. Subfoveal choroidal neovascularization inpunctate inner choroidopathy. Surgical management andpathologic findings. Ophthalmology 1996;103:2061–2069.
2. Hawkins BS, Bressler NM, Bressler SB, et al, SubmacularSurgery Trials Research Group. Surgical removal vs. obser-vation for subfoveal choroidal neovascularization, eitherassociated with the ocular histoplasmosis syndrome or idio-pathic: I. Ophthalmic findings from a randomized clinicaltrial: Submacular Surgery Trials (SST) Group H Trial: SSTReport No. 9. Arch Ophthalmol 2004;122:1597–1611.
3. Fujii GY, Humayun MS, Piemarici DJ, Schachat AP, AuEong KG, de Juan E Jr. Initial experience of inferior limited
macular translocation for subfoveal choroidal neovasculariza-ASCULARIZATION 415
1
1
1
1
1
1
2
2
2
2
2
2
2
4
tion resulting from causes other than age-related maculardegeneration. Am J Ophthalmol 2001;131:90–100.
4. Kleiner RC, Ratner CM, Enger C, Fine SL. Subfovealneovascularization in the ocular histoplasmosis syndrome. Anatural history study. Retina 1988;8:225–229.
5. Olk RJ, Burgess DB, McCormick PA. Subfoveal and juxtafo-veal subretinal neovascularization in the Presumed OcularHistoplasmosis syndrome: visual prognosis. Ophthalmology1984;91:1592–1602.
6. Brown J Jr, Folk JC, Reddy CV, Kimura AE. Visual prognosisof multifocal choroiditis, punctate inner choroidopathy, andthe diffuse subretinal fibrosis syndrome. Ophthalmology1996;103:1100–1105.
7. Wachtlin J, Heimann H, Behme T, Foerster MH. Long-termresults after photodynamic therapy with verteporfin forchoroidal neovascularizations secondary to inflammatorychorioretinal diseases. Graefe’s Arch Clin Exp Ophthalmol2003;241:899–906.
8. Fine HF, Baffi J, Reed GF, Csaky KG, Nussenblatt RB.Aqueous humor and plasma vascular endothelial growthfactor in uveitis-associated cystoid macular edema. Am JOphthalmol 2001;132:794–796.
9. Perentes Y, Chan CC, Bovey E, Uffer S, Herbort CP.Massive vascular endothelium growth factor (VEGF) expres-sion in Eales’ disease. Klin Monatsbl Augenheilkd 2002;219:311–314.
0. Chan WM, Lai TY, Liu DT, Lam DS. Intravitreal bevaci-
zumab (Avastin) for choroidal neovascularization second-AMERICAN JOURNAL OF16
ary to central serous chorioretinopathy, secondary topunctate inner choroidopathy, or of idiopathic origin.Am J Ophthalmol 2007;143:977–983.
1. Adán A, Navarro M, Casaroli-Marano RP, Ortiz S, MolinaJJ. Intravitreal bevacizumab as initial treatment for choroidalneovascularization associated with presumed ocular his-toplasmosis syndrome. Graefes Arch Clin Exp Ophthalmol2007;245:1873–1875.
2. Kumar A, Sinha S. Rapid regression of disc and retinalneovascularization in a case of Eales disease after intravitrealbevacizumab. Can J Ophthalmol 2007;42:335–336.
3. Benesch M, Windelberg M, Sauseng W, et al. Compassion-ate use of bevacizumab (Avastin) in children and youngadults with refractory or recurrent solid tumors. Ann Oncol2008;19:807–813.
4. Travassos A, Teixeira S, Ferreira P, et al. Intravitrealbevacizumab in aggressive posterior retinopathy of prema-turity. Ophthalmic Surg Lasers Imaging 2007;38:233–237.
5. Shah PK, Narendran V, Tawansy KA, Raghuram A, Naren-dran K. Intravitreal bevacizumab (Avastin) for post laseranterior segment ischemia in aggressive posterior retinopathyof prematurity. Indian J Ophthalmol 2007;55:75–76.
6. Chung EJ, Kim JH, Ahn HS, Koh HJ. Combination of laserphotocoagulation and intravitreal bevacizumab (Avastin) foraggressive zone I retinopathy of prematurity. Graefes Arch
Clin Exp Ophthalmol 2007;245:1727–1730.OPHTHALMOLOGY SEPTEMBER 2008
AOMAt
V
Biosketch
hmad M. Mansour, MD, has published over 100 peer-review articles, and is a Fellow of the American Board ofphthalmology, Honor awardee of both the Academy of Ophthalmology and American Society of Retina Specialists. Dransour was an Associate Professor at the University of Texas Medical Branch, and is currently a Professor at themerican University of Beirut and Chairman of the Ophthalmology Department at the Rafic Hariri University Hospital,
he largest medical facility in Lebanon.
INFLAMMATORY NEOVASCULARIZATIONOL. 146, NO. 3 416.e1
Related Documents

![Comparison of Intravitreal Ranibizumab and Bevacizumab ... · chroidal nevus, melanoma, choroidal rupture, polypoidal choroidal vasculopathy (PCV) and idiopathic causes [2,4]. Among](https://static.cupdf.com/doc/110x72/602950428aaed502c576bd94/comparison-of-intravitreal-ranibizumab-and-bevacizumab-chroidal-nevus-melanoma.jpg)









