NAMI News September 2013 Issue
Mar 14, 2016
Â
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Awakening to Wellness
NewsSeptember, 2013
NAMI YakimaFirst Edition - Volume One Issue Two
Produced and Distributed By:
Welcome!We hope you enjoy the September 2013 issue ofNAMI News.
From Suicide Prevention Awareness Month ... To our upcoming NAMI Yakima Reunion and Annual Meeting Event ... To NAMI Basics ... To Wellness Recovery Action Planning training ... TTo NAMI Smarts ... To Mental Illness AwarenessWeek ....
There is so much to know, share and do to make sure that all families impacted by mental health disorders find resources and recovery. And NAMIYakima is here to help lead those vital efforts.
We exist to help families find help and hope. WWe believe that there is no true health without good mental health. We know that wellness and recovery are possible.
Contact us anytime to learn more or get involved. We’ll look forward to hearing from you soon!
In this issue ...
Book Reviews
Program News
Community Partners
NAMI Yakima Reunion
State & National News
Suicide PreventionSuicide PreventionAwareness Month
Membership Info
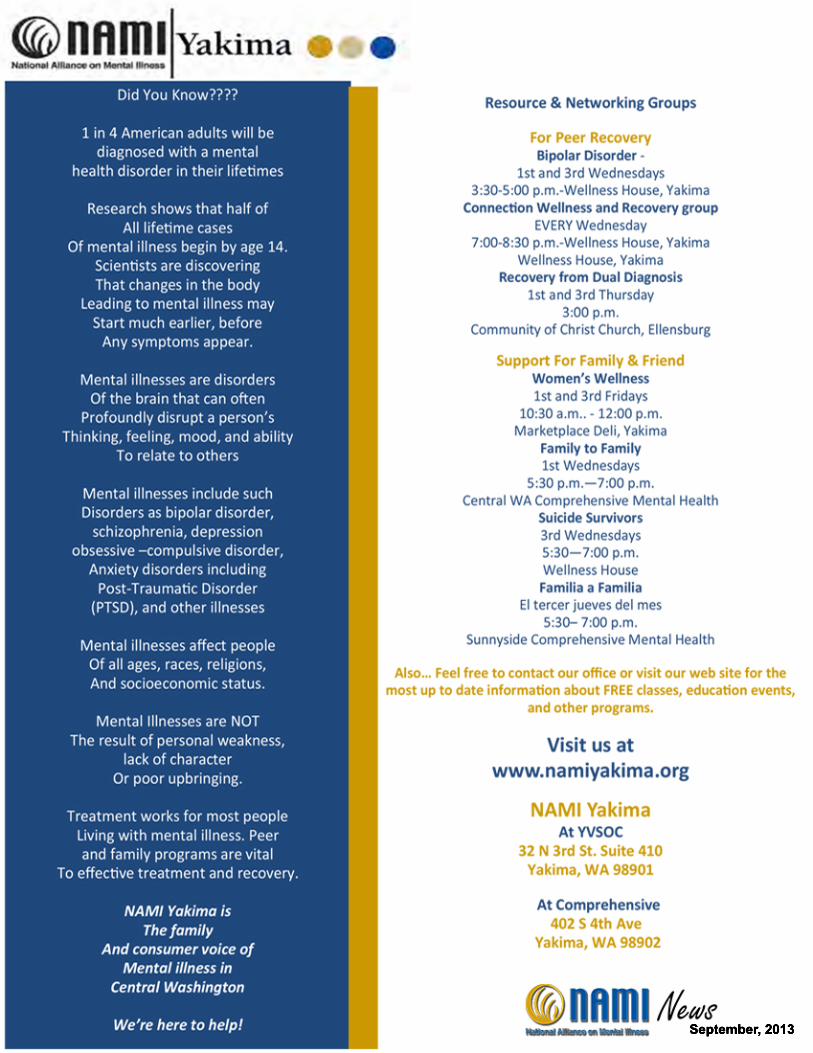
Group Schedules
Mental Illness Awareness Week
Class Updates
And so much more!And so much more!
September, 2013
SuicideSuicide is one of the greatest tragedies imaginable for a victim and their loved ones. Each year suicide claims approximately 30,000 lives in America which makes it responsible for slightly more than 1 percent of deaths in the United States. Suicidal thoughts and behaviors are a psychiatric emergency requiring immediate intervention to prevent this disastrous event. It is the most common psychiatric emergency with close to 1 million Americans receiving treatment for suicidal thoughts, behaviors or attempts on a yearly basis.
Who is at risk for suicide? Who is at risk for suicide? Take a look at some facts.The single biggest risk factor for suicide is a prior history of suicidal behaviors or attempts.
Over 90 percent of people who commit suicide have been diagnosed with mental illness. Some of the mental illnesses most commonly associated with suicide include depression, bipolar disorder, schizophrenia, personality disorders (including borderline personality disorder), anxiety disorders (including post traumatic stress disorder and panic attacks) and eating disorders (including bulimia nervosa and anorexia nervosa).
Substance abuse and addiction - often the presence of a co-occurring or otherwise dually diagnosed set ofdisorders - are also associated with an increased risk of suicide. More than one in three people who die from disorders - are also associated with an increased risk of suicide. More than one in three people who die from suicide are intoxicated, most commonly with alcohol or opiates (e.g., heroin, Percocet [oxycodone]). The majority of completed suicides in America involve firearms and access to firearms is associated with a significantly increased risk of suicide. Among youth aged 15 to 24 suicide is the third leading cause of death. Older age is also associated with increased risk of suicide; people above the age of 65 are at the greatest risk for death by suicide.
In addition, chronic medical illness (including chronic pain) is associated with increased risk of suicide. While women are more likely to attempt suicide, men are approximately 4 times more likely to die by suicide While women are more likely to attempt suicide, men are approximately 4 times more likely to die by suicide People of all races and ethnicities are at risk for suicide. People who feel socially-isolated (e.g., divorced, widowed) are at increased risk of suicide compared with people who have responsibility for family members (cont)
From the author of the best-selling memoir An Unquiet Mind, Night Falls Fast is tragically timely: suicide has become one of the most common killers of Americans between the ages of fifteen and forty-five.
An internationally acknowledged authority on depressive illnesses, Dr. Jamison has also known suicide firsthand: after years of struggling with manic-depression (now known as bipolar disorder), she tried at age twenty-eight to kill herself. to kill herself. Weaving together a historical and scientific exploration of the subject with personal essays on individual suicides, she brings not only her remarkable compassion and literary skill but also all of her knowledge and research to bear on this devastating problem. This is a book that helps us to understand the suicidal mind, to recognize and come to the aid of those at risk, and to comprehend the profound effects on those left behind. It is critical reading for parents, educators, and anyone wanting to understand this tragic epidemic.tragic epidemic.
“The most authentic thing about us is our capacity to create, to overcome, to endure, to transform, to love and to
be greater than our suffering.”Ben Okri, Nigerian Activist
September, 2013
September, 2013
(Suicide, cont.)
(e.g., people who are married or people with children)
While scientists have not discovered one specific gene that causes suicide, it is known that people with a family history of suicide are at increased risk. People with a history of trauma (e.g., childhood abuse or combat experience) are also at increased risk of suicide. For many, involvement in community or religious organizations may decrease the risk of suicide.
How can suicide be prevented?How can suicide be prevented?As suicidal thoughts or behaviors are a psychiatric emergency, the involvement of properly-trained mental health professionals is necessary. For some people, this means making an appointment to see a therapist or a psychiatrist; for other people, it may mean calling 911 or going to the nearest emergency room. After they are evaluated by a mental health professional, some people may be able to continue outpatient treatment; others may require inpatient psychiatric hospitalization to manage their symptoms.
Ongoing psychiatric treatment is helpful for most people with suicidal thoughts and behaviors. Some forms of psychotherapy—including cognitive behavioral therapy (CBT) and dialectical behavior therapy (DBT)—of psychotherapy—including cognitive behavioral therapy (CBT) and dialectical behavior therapy (DBT)—are useful in treatment of suicidal thoughts and behaviors. Psychotherapy can also be a helpful part in the ongoing treatment of people mental illness, something which further decreases the risk of suicide.
Alcohol and drugs are very dangerous for people at risk of suicide. Addiction—also called alcohol or drug dependency—puts people at increased risk of suicide and can also worsen other mental illnesses which further increases this risk. Additionally, people who are intoxicated or withdrawing from drugs and alcohol are more impulsive.are more impulsive. This impulsiveness can make people more likely to attempt suicide and perhaps less likely to ask for help with their troubling symptoms.
Some medications may be helpful in reducing the risk of suicide in certain patients with mental illness. While antidepressants carry a “Black Box Warning” from the US-FDA regarding the risk of increased suicide, most people with depression or anxiety will be less likely to hurt themselves if they are taking an antidepressant medication. Most scientific studies of people with depression suggest that antidepressants save lives by preventing suicide because untreated depression is such a significant risk factor for suicide. Other medications may also be useful: for some people with symptoms of depression, lithium can be Other medications may also be useful: for some people with symptoms of depression, lithium can be helpful in decreasing the risk of suicide. For some individuals with schizophrenia, Clozaril (clozapine) can reduce the risk of suicide. As with any other medical illness, a thorough evaluation by one’s physician—either a primary care doctor or a psychiatrist—is appropriate prior to starting most medications.
What can friends and family members do?If they have concerns that someone close to them is suicidal, family and friends can be most helpful in encouraging their loved one to seek treatment. Some people may be afraid that they could worsen the situation if they bring up the topic of suicide with their loved one. While this is a common concern, scientific situation if they bring up the topic of suicide with their loved one. While this is a common concern, scientific studies show that asking about suicide—and encouraging their loved one to get help—does not increase the risk of suicide. Rather, addressing concerns about suicide is helpful in preventing suicide.
Adapted from www.nami.org Reviewed by Ken Duckworth, M.D., and Jacob L. Freedman, M.D., January 2013The authors would like to thank Jane Pearson, Ph.D., who was responsible for an earlier version of this review.
September, 2013
September, 2013

September, 2013
When Someone You Love Has a Mental Illness ... Boundary BattlesBeing in a situation where caring and supporting a loved one who has a brain illness can bring about stressful life conditions that can add to the family’s problems. When we frequently are in a position where we feel we have to take as much as we can, give as much as we can, and please others without giving consideration to ourselves, we can lose our self-esteem while our own welfare and good health slowly but surely fall apart.surely fall apart. This is an all-too-common condition in families dealing with the challenges presented when one of its members has been diagnosed with a mood disorder.
Personal health professionals often caution companions, family members and caregivers to someone battling the symptoms of a mood disorder with the need to be sure to have well-established and well-defined guidelines to protect their physical, mental and emotional boundaries. These therapists, social workers, nurses and physicians advise that reasonable and clear rules with limits are imperative to have in place if we hope to maintain a strong self-image and adequately meet our own physical, mental, emotional and spiritual needs.emotional and spiritual needs.
Establishing clear and safe boundaries usually involve the following areas:• Our personal and physical space which must always be respected.• Our beliefs, thoughts, decisions and choices which we have a right to.• The emotional boundaries that are necessary to maintain our self-esteem, positive feelings and mutual trust.• Established clear lines of responsibility.• How we will respond when someone steps over or beyond our limits.• How we will respond when someone steps over or beyond our limits.
When establishing boundaries it is believed to be important to avoid having the limits too soft or blurred so as to be susceptible to manipulation or readily giving in to unhelpful codependency. Yes should mean yes and no should mean no. It is also recommended to avoid being too rigid in setting up guidelines and limits to where we become walled-off from appropriate closeness or important and necessary suggestions. Some openness to flexibility is usually considered the wiser path.
Professionals are usually very experienced in helping to set up healthy and realistic boundaries. Why not give one a try?give one a try?
Find a caregivers support group. Join it…Sooner rather than later. Reprinted from: http://surfcitypress.org/
NAMI Yakima Family and Friends Groups
September, 2013


September, 2013

September, 2013
September, 2013

September, 2013
A Community of Partners
NAMI Yakima will be hosting all of these great NAMI signatureprograms in coming months ... To learn more, get in touch withus today! 509.453.8229 [email protected] www.namiyakima.org
Catholic Family & Child ServiceCentral Office
5301 Tieton Drive, Suite CYakima, WA 98908-3478
509.965.7100800.246.2962
Catholic Family and Child Services network of 7 offices services 60,000 persons annually. Whether supporting families through early learning services, strengthening families through specialized mental health services, or assisting seniors so they can remain living independently, CFCS is an essential resource for scores of people each year.
CFCS envisions communities where people are treated with dignity and respect, their basic needs are met,and they are empowered to enhance the quality of their own lives.
September, 2013

September, 2013

September, 2013

September, 2013
Wellness
RecoveryActionPlanThe Wellness Recovery Action Plan®, or WRAP®, is an evidence-based system that is used world-wide by people who are dealing with mental health and other kinds of health challenges. It was developed by a group of people who have a lived experience of mental health difficulties; people who were searching for ways to resolve issues that had been troubling them for a long time. resolve issues that had been troubling them for a long time.
WRAP® is universal ― it is for anyone, any time, and for any of life's challenges.
WRAP is a self-designed plan for staying well and for helping you to feel better when you are not feeling well, to increase personal responsibility, and to improve your quality of life.
FREE WRA
P Classes S
tart
Tuesday, Se
ptember 24t
h
1 - 3:30 p.m
.
32 N 3rd Str
eet, Suite 4
10
Contact NA
MI to regis
ter!
509.453.82
29
ininfo@namiya
kima.org
It’s Autumn Movie Night!
Join usto supportNNAMI &celebrateMentalIllnessAwarenessWeek
Friday, Oct 116:00 p.m.Perry TechAuditorium
Tickets $10(group discountsonline)online)
Buy tickets atwww.namiyakima.orgor contact us [email protected]
See you there!
September, 2013
September, 2013
For Help
1-800-SUICIDE (1-800-784-2433)1-800-273-TALK (1-800-273-8255)
September, 2013
September, 2013

The biological basis for addiction is the reason to have new hope for eradicating stigma, implementing evidence-based treatments that work and helping people with these brain disorders to work toward a commitment to recovery and advocacy throughout their lives.
This is the message Christopher Lawford Kennedy effectively shares in his informative and comprehensive book, Recover to Live: Kick Any Habit, Manage Any Addiction (BenBella Books, Inc., 2013).
Kennedy Lawford, who is in recovery from drug addiction for more than 26 years, Kennedy Lawford, who is in recovery from drug addiction for more than 26 years, interviewed the top experts in addiction from around the world to present the most up to date scientific findings on the cause and effect of the most prevalent addictions and the evidence-based treatments that show the most promise for sobriety and abstinence. He also examines the effectiveness of 12-step programs and delves into the complex dynamics of codependency in families and other relationships.
But the author is most passionate when he calls for a global movement that encourages
people in recovery from addiction to step out of the shadows of shame and become active participants in an effort to make these brain disorders a public health priority and not a cause for marginalization, criminalization or denial.Kennedy Lawford does all of this in a text that is honest, nonjudgmental and free of pity. Instead, he educates readers and gives them the tools to objectively examine their own unhealthy tendencies or those of loved ones to make informed decisions about how to stop the pain and lead a purposeful life.
"The disease lives in the mind," Kennedy Lawford writes early in the book. Dr. Drew Pinsky, addiction medicine specialist and clinical professor of psychiatry at the University of South California School of Medicine, states in an interview that and clinical professor of psychiatry at the University of South California School of Medicine, states in an interview that addiction "is a biological disorder with a genetic basis. … Addiction is a biological switch having been thrown in deep regions of the brain."
Kennedy Lawford writes that in late 2011, the American Society of Addiction Medicine changed its long-held definition of addiction to now call it "a primary, chronic disease of brain reward, motivation, memory and related circuitry."Pamela Hyde, administrator of the Substance Abuse and Mental Health Service Administration, states that "almost half of the people with an identifiable addictive disorder also have an identifiable mental illness or anxiety disordethe people with an identifiable addictive disorder also have an identifiable mental illness or anxiety disorder." She also states that "20 percent of people suffering anxiety or mental problems have some sort of addiction."
Once the foundation for the biological basis of addiction is laid, Kennedy Lawford presents a chapter to each of the seven "toxic compulsions" that are known as addictions – alcohol abuse, drug abuse, eating disorders, gambling dependence, hoarding, sex and pornography and nicotine dependence. Each chapter details the latest scientific findings on the biological cause of the compulsion and its consequences. The chapter also includes a questionnaire to help readers determine if the compulsion is a problem for them. readers determine if the compulsion is a problem for them.
Kennedy Lawford then takes a look at the scientific evidence for treatment methods such as cognitive behavorial therapy, 12-step programs, mindfulness, meditation, nutrition and exercise, body work (acupuncture) and journaling. He devotes an entire chapter to 12-step programs and lets the experts talk about their effectiveness and reasons why some people may shy away from them.
In a final chapter, Kennedy Lawford writes about recovery and what it means. Early on he establishes that although people may not be responsible for inheriting a brain disorder that leads to an addiction, they are responsible for their treatment and recovertreatment and recovery. As a person who has walked the path of recovery for more than 25 years, Kennedy Lawford makes it clear that recovery is a lifelong process and that it is about "maintaining a life worth living." It is up to each person to determine what that means.
But once that commitment is made, people in recovery should be able to share their experiences with others without public ridicule and make a positive impact on the lives of others and public health policy.
Kennedy Lawford is moving forward with this concept through his book and The Global Recovery Initiative he has launched, along with its website wwlaunched, along with its website www.Recover2Live.com. His goal is to disseminate information to give people "the tools to enable them to have a full and productive life." He writes "we must never stop our efforts until addiction is treated with the same level of resources, and recovery from addiction becomes celebrated with the same openness."
Recover to Live is a definitive step in a new direction toward hope and healing for people with toxic compulsions and mental illnesses.Lisa R. Rhodes is a journalist and a member of NAMI Prince George's County in Maryland. September, 2013

Sunday, September 29th11:00 - 4:00Franklin Park, YakimaRotary Park Pavilion
Everyone is welcome ...
For fun, food, our annual
“business” and so much more.
See you there!
BBQ Friends
GamesMemories
Jumper
Please [email protected]
September, 2013

September, 2013
September, 2013
September, 2013

Have Quesons?? Find Answers!NAMI’s “Ask the Psychiatric Pharmacist”Find us at: hp://www.nami.org/Template.cfm?Secon=Ask_the_Pharmacist&Template=/TaggedPage/TaggedPageDisplay.cfm&TPLID=61&ContentID=28925
September, 2013

September, 2013
September, 2013
September, 2013
September, 2013

September, 2013PO Box 10918Yakima, WA [email protected] First Edition - Volume One Issue One
Produced and Distributed By:
Related Documents