Socioeconomic Differentials in Mortality Risk among Men Screened for the Multiple Risk Factor Intervention Trial: II. Black Men George Davey Smith, MD, Deborah Wentworth, MPH, James D. Neaton, PhD, Rose Stamler, MA, and Jeremiah Stamler, MD Introduction Methods In the United States, health differ- ences between Black and White citizens have been extensively discussed.'6 The intended interpretation of racial/ethnic identity as an explanatory variable has sometimes been unclear. Black-White health differentials are often taken to be proxies for variations in health status related to socioeconomic position, a ten- dency that receives encouragement from the paucity of routine data regarding socioeconomic differentials in morbidity and mortality in the United States.7 This has meant that socioeconomic patterning of health status among African Ameri- cans has, to a degree, been neglected.6'8 The 1979 to 1985 follow-up of the National Longitudinal Mortality Study9 demonstrated substantial differentials in mortality for Black men and women according to family income. Only 965 deaths occurred among the 13 701 Black men with known family income who were 35 to 64 years of age at study entry, however. Because of this, mortality differ- entials for particular causes of death could not be examined in detail. In this paper, data are presented on the mortality experience, over a 16-year follow-up pe- riod, of the large cohort of Black men who were screened for the Multiple Risk Factor Intervention Trial.10'1' Analyses of the gradients of total and cause-specific mortality risk by median income of zip code area of residence were carried out. Availability of data regarding smoking behavior, blood pressure, cholesterol level, and preexisting disease allowed for assess- ment of the influence of these key risk factors on observed income-mortality gra- dients. A companion report gives findings for White men.'2 Methods used to recruit participants and a description of the men screened have been reported previously10"'1; full details of the specific procedures related to the analysis of income differentials are presented in the accompanying paper.'2 Of the men screened for the Multiple Risk Factor Intervention Trial, 23 490 indicated that they were Black; income data regarding families with Black heads of households (henceforth "income") were available for 20 224 (86.1%) of these men living in 1376 zip code areas. Fewer causes of death could be investigated for Black than for White men because the cohort was substantially smaller. For analyzing risk of total mortality, median zip code area family income was categorized into ten $2500- interval groups ranging from $7500 to $27 500. For analyses of particular causes, median zip code area family income was divided into three groups based on tertiles of income. The group of men from the zip code areas with the highest median family income was used as the reference group for calculation of relative risk estimates. Regres- sion coefficients from proportional hazards George Davey Smith is with the Department of Social Medicine, University of Bristol, Bristol, England. Deborah Wentworth and James D. Neaton are with the Division of Biostatistics, School of Public Health, University of Minne- sota, Minneapolis. Rose Stamler and Jeremiah Stamler are with the Department of Preventive Medicine, Northwestern University Medical School, Chicago, Ill. Requests for reprints should be sent to George Davey Smith, MD, Department of Social Medicine, University of Bristol, Canynge Hall, Whiteladies Rd, Bristol BS8 2PR, En- gland. This paper was accepted January 17, 1996. Editor's Note. See related editorial by Link and Phelan (p 471) in this issue. American Journal of Public Health 497

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Socioeconomic Differentials inMortality Risk among Men Screenedfor the Multiple Risk FactorIntervention Trial: II. Black Men
George Davey Smith, MD, Deborah Wentworth, MPH, James D. Neaton, PhD,Rose Stamler, MA, andJeremiah Stamler, MD
Introduction MethodsIn the United States, health differ-
ences between Black and White citizenshave been extensively discussed.'6 Theintended interpretation of racial/ethnicidentity as an explanatory variable hassometimes been unclear. Black-Whitehealth differentials are often taken to beproxies for variations in health statusrelated to socioeconomic position, a ten-dency that receives encouragement fromthe paucity of routine data regardingsocioeconomic differentials in morbidityand mortality in the United States.7 Thishas meant that socioeconomic patterningof health status among African Ameri-cans has, to a degree, been neglected.6'8
The 1979 to 1985 follow-up of theNational Longitudinal Mortality Study9demonstrated substantial differentials inmortality for Black men and womenaccording to family income. Only 965deaths occurred among the 13 701 Blackmen with known family income who were35 to 64 years of age at study entry,however. Because of this, mortality differ-entials for particular causes of deathcould not be examined in detail. In thispaper, data are presented on the mortalityexperience, over a 16-year follow-up pe-riod, of the large cohort of Black men whowere screened for the Multiple RiskFactor Intervention Trial.10'1' Analyses ofthe gradients of total and cause-specificmortality risk by median income of zipcode area of residence were carried out.Availability of data regarding smokingbehavior, blood pressure, cholesterol level,and preexisting disease allowed for assess-ment of the influence of these key riskfactors on observed income-mortality gra-dients. A companion report gives findingsfor White men.'2
Methods used to recruit participantsand a description of the men screenedhave been reported previously10"'1; fulldetails of the specific procedures relatedto the analysis of income differentials arepresented in the accompanying paper.'2Of the men screened for the MultipleRisk Factor Intervention Trial, 23 490indicated that they were Black; incomedata regarding families with Black headsof households (henceforth "income") wereavailable for 20 224 (86.1%) of these menliving in 1376 zip code areas. Fewer causesof death could be investigated for Blackthan for White men because the cohort wassubstantially smaller. For analyzing risk oftotal mortality, median zip code area familyincome was categorized into ten $2500-interval groups ranging from $7500 to$27 500. For analyses of particular causes,median zip code area family income wasdivided into three groups based on tertilesof income. The group of men from the zipcode areas with the highest median familyincome was used as the reference group forcalculation of relative risk estimates. Regres-sion coefficients from proportional hazards
George Davey Smith is with the Department ofSocial Medicine, University of Bristol, Bristol,England. Deborah Wentworth and James D.Neaton are with the Division of Biostatistics,School of Public Health, University of Minne-sota, Minneapolis. Rose Stamler and JeremiahStamler are with the Department of PreventiveMedicine, Northwestern University MedicalSchool, Chicago, Ill.
Requests for reprints should be sent toGeorge Davey Smith, MD, Department ofSocial Medicine, University of Bristol, CanyngeHall, Whiteladies Rd, Bristol BS8 2PR, En-gland.
This paper was accepted January 17,1996.
Editor's Note. See related editorial byLink and Phelan (p 471) in this issue.
American Journal of Public Health 497

Davey Smith et al.
TABLE 1-Baseline Data on BlackMen Screened between1973 and 1975, byAvailability of IncomeData for Zip Code Area:The Multiple RiskFactor Intervention Trial
IncomeIncome DataData Not
Available Available
No. men
Mean age, y
Cigarettesmokers, %
Mean systolicblood pres-sure, mm Hg
Mean diastolicblood pres-sure, mm Hg
Mean serum cho-lesterol, mg/dl
Prior hospitali-zation for heartattack, %
Medication fordiabetes, %
Age-adjusteddeath rate (per10 000 person-years)
20 224 3266
45.3 46.0
48.8 57.2
133.6 136.7
86.8 90.0
210.0 210.7
1.4 1.4
3.2 3.6
103.0 118.3
models were used to estimate the relativerisk associated with a $10 000 lower zipcode area median census tract income.Proportional hazards regression modelswith and without an interaction termbetween income and being Black or
White were compared to determine themagnitude and significance of any differ-ences in the regression coefficients associ-ated with income for Blacks and Whites.
ResultsTable 1 compares baseline and mortal-
ity data for the men for whom income datawere available with those for whom suchdata were not. The latter were more likelyto be smokers, had higher levels of bloodpressure, and had a higher all-cause mortal-ity rate than the former. The age-adjustedrelative risk of death for the men withoutincome data, in comparison with those withsuch data, was 1.12 (95% confidenceinterval [CI] = 1.02, 1.23). With adjustmentfor smoking, diastolic blood pressure, se-
rum cholesterol, previous heart attack, andmedication for diabetes, this relative risk
was reduced to 1.02 (95% CI = 0.93, 1.12).
The characteristics of the 20 224Black men for whom income data were
available are presented in Table 2 accord-ing to income tertile. The group in thehighest income tertile was lower in termsof mean age, blood pressure, prevalenceof cigarette smoking, and drug treatmentfor diabetes, and higher in terms of meanserum cholesterol level, than those in thetwo lower income tertiles. Stratificationbased on income was related to other
ecologically defined demographic charac-teristics in the zip code areas, includingpercentage unemployed, percentage be-low the poverty line, percentage in profes-sional or managerial occupations, andaverage years of schooling.
All-Cause MortalityDuring the 16 years of follow-up,
2937 deaths were identified among the
20 224 Black men in this cohort. Mortality
April 1996, Vol. 86, No. 4498 American Journal of Public Health
TABLE 2-Characteristics of Black Men Screened, by Level of Median FamilyIncome for Zip Code of Residence and Characteristics of Zip CodeAreas of Residence
Income, $ (Approximate Tertile)a
< 12 333 12 333-16 300 > 16 300(n = 6698) (n = 6744) (n = 6782)
Characteristics of men screenedMean age, y 45.9 45.4 44.7Mean systolic blood pressure, mm Hg 135.0 133.8 132.0Mean diastolic blood pressure, mm Hg 87.8 86.9 85.9Mean serum cholesterol, mg/dl 208.7 210.0 211.4Cigarette smokers, % 51.9 49.6 45.0Cigarettes per day for smokers, mean 18.4 18.3 19.0Prior hospitalization for heart attack, % 1.4 1.5 1.3Medication for diabetes, % 3.6 3.4 2.7
Population characteristics of zip code areasaUnemployment, % 5.2 4.9 4.3Average years of schooling 13.0 13.5 14.1Managerial or professional occupations, % 6.0 7.8 11.5Below the poverty line, % 21.6 13.6 6.6Median family income, $White households 16408 18686 23 838Black households 10 189 14 262 21 494
Note. Family income levels were based on data from the 1980 US census.aBased on data from the 1980 US census.
TABLE 3-All-Cause Mortality among Black Men Screened, by Level of MedianFamily Income for Zip Code of Residence
Age- Age-Adjusted Age- and RiskNo. No. Adjusted Relative Risk Factor-Adjusted
Income, $ Men Deaths Ratea (95% CI) Relative Risk (95% Cl)
< 7 500 423 84 137.2 2.09 (1.45, 3.00) 1.92 (1.34, 2.76)7 501-10 000 2245 393 120.5 1.97 (1.45, 2.67) 1.80 (1.33, 2.45)10 000-12 500 4255 720 116.9 1.88 (1.39, 2.53) 1.70 (1.26, 2.30)12501-15000 4787 740 107.8 1.71 (1.27,2.31) 1.59 (1.18,2.14)15 001-17 500 2615 326 89.9 1.43 (1.05, 1.94) 1.36 (1.00, 1.85)17501-20 000 2267 283 89.8 1.41 (1.03, 1.92) 1.34 (0.99,1.83)20 001-22 500 1900 228 86.8 1.40 (1.02,1.93) 1.34 (0.97, 1.84)22 501-25 000 757 83 86.5 1.38 (0.97,1.99) 1.34 (0.93,1.92)25 001-27 500 371 32 65.4 1.08 (0.69,1.70) 1.07 (0.68,1.68)27501+ 604 48 57.2 1.00 (Reference) 1.00 (Reference)
Note. Family income levels were based on data from the 1980 US census. Risk factors were diastolicblood pressure, serum cholesterol level, cigarettes per day, prior hospitalization for heart attack,and medication for diabetes. Cl = confidence interval.
aBy direct method to age distribution of all men screened per 10 000 person-years.

Mortality Rislk Black Men
rates and relative risk estimates accordingto income (categorized into 10 groups)are presented in Table 3. The associationwas continuous, with no evidence of a
threshold. The regression coefficient foreach $10 000 lower income increment,adjusted for age, translated into a relativerisk of mortality of 1.35 (95% CI = 1.24,1.46). Further adjustment for smokingbehavior, diastolic blood pressure, serum
cholesterol, history of heart attack, andmedication for diabetes reduced thisrelative risk to 1.29 (95% CI = 1.19, 1.40).
The relationship of income withall-cause mortality was examined sepa-
rately for smokers and nonsmokers andaccording to age at screening (those 35 to
44 years old vs those 45 to 57 years old).For the men who reported smokingcigarettes at the time of screening, theage-adjusted relative risk associated witha $10 000 lower income was 1.29 (95%CI = 1.16, 1.43). After adjustment forserum cholesterol, diastolic blood pres-
sure, cigarettes smoked per day, history ofheart attack, and medication for diabetes,this relative risk was 1.27 (95% CI = 1.14,1.41). For men who reported that theywere not currently smoking cigarettes, thecorresponding relative risks were 1.31(95% CI = 1.16, 1.49) in the age-adjustedanalysis and 1.29 (95% CI = 1.14, 1.47)after adjustment for the other risk factors.The inverse association between incomeand mortality risk was also similar for themen 35 to 44 years old at screening andthe men 45 to 57 years old. For theyounger men, the age-adjusted relativerisk of mortality for a $10 000 lowerincome was 1.33 (95% CI = 1.15, 1.54);for the older men, it was 1.36 (95%CI = 1.23, 1.49).
Cumulative mortality over the fol-low-up period revealed no tendency forthe rates of mortality to converge (Figure1). Cumulative mortality rates at 10 years
for men in the lower, middle, and upper
tertiles were 8.1%, 6.4%, and 5.0%.Corresponding percentages for 15 yearswere 15.9, 13.4, and 10.1.
Within each clinical center, men
were screened from a number of zip codeareas. Thus, there was a considerablerange in income among the Black men
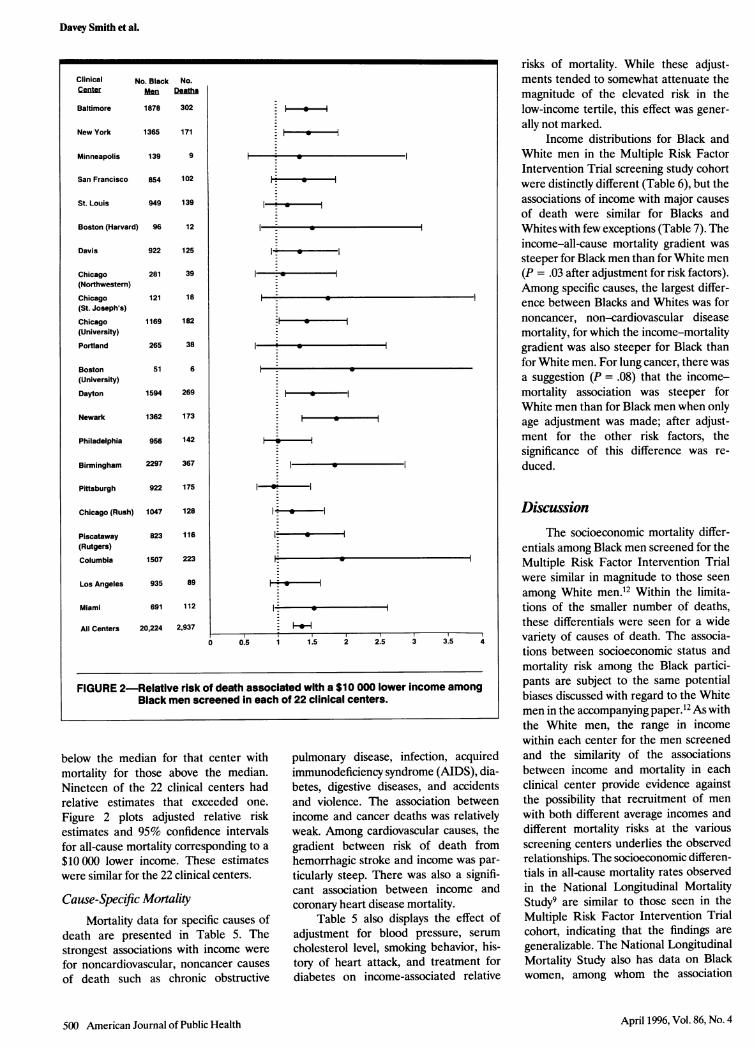
screened, not only between centers butwithin each center (Table 4). This permit-ted an estimate of the relationship be-tween income and mortality to be ob-tained for each center (Table 4 andFigure 2). In Table 4, adjusted relativerisk estimates of all-cause mortality are
given for each center. These estimatescompared mortality for those with income
American Journal of Public Health 499April 1996, Vol. 86, No. 4
25
20
0
0
10
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Years from Screening
Income < 12,333 ---- 12,333-16,300 ----- 16,301 +
FIGURE 1-Cumulative mortality among Black men screened, for three incomecategories.
TABLE 4-Income and All-Cause Mortality among Black Men Screened, byClinical Center
Range in Relative Risk of DeathbNo. No. Median Income for (Lower vs Higher
Clinical Black Zip Code Income, Zip Code Income Zip CodeCenter Men Areasa $ Areas, $ Areas) (95% Cl)
Baltimore 1878 83 15245 5000-40 101 1.48 (1.17,1.86)New York 1365 182 14 000 5000-50 000 1.47 (1.08,1.99)Minneapolis 139 20 20720 8629-40631 2.52(0.63,10.10)San Francisco 854 100 15 727 7451-50 000 1.53 (1.02, 2.28)St. Louis 949 55 14 061 6661 -35 926 1.27 (0.91,1.78)Boston 96 35 19 065 8552-50 000 3.02 (0.89,10.26)
(Harvard)Davis 922 39 14 686 6956-34 500 1.02 (0.71, 1.45)Chicago 281 50 15 956 5280-50 000 0.77 (0.41, 1.46)
(Northwestern)Chicago 121 44 15520 5280-50000 2.21 (0.83, 5.91)
(St. Joseph's)Chicago 1169 52 18 750 5280-37 781 1.33 (1.00,1.78)
(University)Portland 265 33 13 750 5000-39 625 1.51 (0.75, 3.04)Boston 51 16 18 158 5000-30 873 2.60 (0.47,14.30)
(University)Dayton 1594 59 13211 5000-38756 1.46(1.14,1.87)Newark 1362 147 15 813 7239-50 000 1.65 (1.23, 2.24)Philadelphia 956 119 14 971 5244-50 000 1.17 (0.84,1.63)Birmingham 2297 60 11 656 5491-36 239 1.26 (1.03,1.55)Pittsburgh 922 70 13 886 5000-27 652 0.81 (0.60,1.09)Chicago (Rush) 1047 83 18 750 5280-50 000 1.07 (0.76,1.52)Rutgers 823 162 17 893 7189-40 247 1.17 (0.82,1.69)Columbia 1507 64 13 000 7157-26 692 1.33 (1.02,1.73)Los Angeles 935 140 17 143 7409-50 000 0.98 (0.64,1.49)Miami 691 49 11 824 5000-42 500 1.05 (0.72,1.53)
aTotal adds to more than 1376 because some centers screened from the same zip code areas.
bRisk of death for those with income below median for clinical center vs those above median
adjusted for age. Cl = confidence interval.
Davey Smith et al.
below the median for that center withmortality for those above the median.Nineteen of the 22 clinical centers hadrelative estimates that exceeded one.
Figure 2 plots adjusted relative riskestimates and 95% confidence intervalsfor all-cause mortality corresponding to a
$10000 lower income. These estimateswere similar for the 22 clinical centers.
Cause-Specific Mortality
Mortality data for specific causes ofdeath are presented in Table 5. Thestrongest associations with income were
for noncardiovascular, noncancer causes
of death such as chronic obstructive
pulmonary disease, infection, acquiredimmunodeficiency syndrome (AIDS), dia-betes, digestive diseases, and accidentsand violence. The association betweenincome and cancer deaths was relativelyweak. Among cardiovascular causes, thegradient between risk of death fromhemorrhagic stroke and income was par-
ticularly steep. There was also a signifi-cant association between income andcoronary heart disease mortality.
Table 5 also displays the effect ofadjustment for blood pressure, serum
cholesterol level, smoking behavior, his-
tory of heart attack, and treatment fordiabetes on income-associated relative
risks of mortality. While these adjust-ments tended to somewhat attenuate themagnitude of the elevated risk in thelow-income tertile, this effect was gener-
ally not marked.Income distributions for Black and
White men in the Multiple Risk FactorIntervention Trial screening study cohortwere distinctly different (Table 6), but theassociations of income with major causes
of death were similar for Blacks andWhites with few exceptions (Table 7). Theincome-all-cause mortality gradient was
steeper for Black men than for White men(P = .03 after adjustment for risk factors).Among specific causes, the largest differ-ence between Blacks and Whites was fornoncancer, non-cardiovascular diseasemortality, for which the income-mortalitygradient was also steeper for Black thanfor White men. For lung cancer, there wasa suggestion (P = .08) that the income-mortality association was steeper forWhite men than for Black men when onlyage adjustment was made; after adjust-ment for the other risk factors, thesignificance of this difference was re-
duced.
DiscussionThe socioeconomic mortality differ-
entials among Black men screened for theMultiple Risk Factor Intervention Trialwere similar in magnitude to those seen
among White men.12 Within the limita-tions of the smaller number of deaths,these differentials were seen for a widevariety of causes of death. The associa-tions between socioeconomic status andmortality risk among the Black partici-pants are subject to the same potentialbiases discussed with regard to the Whitemen in the accompanying paper.12 As withthe White men, the range in incomewithin each center for the men screenedand the similarity of the associationsbetween income and mortality in eachclinical center provide evidence againstthe possibility that recruitment of men
with both different average incomes anddifferent mortality risks at the variousscreening centers underlies the observedrelationships. The socioeconomic differen-tials in all-cause mortality rates observedin the National Longitudinal MortalityStudy9 are similar to those seen in the
Multiple Risk Factor Intervention Trial
cohort, indicating that the findings are
generalizable. The National LongitudinalMortality Study also has data on Black
women, among whom the association
April 1996, Vol. 86, No. 4500 American Journal of Public Health
Clinical No. Black No.Center N[Mn Deatha
Baltimore 1878 302
New York 1365 171
Minneapolis 139 9
San Francisco 854 102
St. Louis 949 139
Boston (Harvard) 96 12
Davis 922 125
Chicago 281 39(Northwestern)
Chicago 121 18(St. Joseph's)
Chicago 1169 182 -(University)
Portland 265 38
Boston 51 6(University)
Dayton 1594 269
Newark 1362 173
Philadelphia 956 142
Birmingham 2297 367
Pittsburgh 922 175
Chicago (Rush) 1047 128
Piscataway 823 116 I *(Rutgers)Columbia 1507 223
Los Angeles 935 89
Miami 691 112 l_
All Centers 20,224 2,937
0 0.5 1 1.5 2 2.5 3 3.5 4
FIGURE 2-Relative risk of death associated with a $10 000 lower income amongBlack men screened in each of 22 clinical centers.

Mortality Risk:- BlackMen
-0c co to- LO I-
(D _LO CO)
0 0
_ _
0(0'-LO N1 0
LO 0) CY) OOOONO NOt CD v- 000000 00
. . . . . .
v
LO0 't Co0) co o, co
LO) 0
(000 0
V
0 CDLO LO(0 -0) C')0 C 0)
0t0t 0 uC o _ c') c LO
000oco0N- co C)0 Nto e)LC) O o0lt (0U)L -0 t Coo_'oo 66 66o o
00 00 0 0 0000 000000 00
0 0 000 0 90
00 0000 0 0000000000 00
00 00 0 0 0oo
oo oooI o ooo oooooIooI,I,I : 1
t (m0le CM co r-
4 _ c\i aD
0'T- 'tJ 0,, NM
'- 00'- I,,-0-N '-La)
O )OD Il a4) C) LO C14 (.0D Pv ~r_ r-0) o T- _N C N_ L
CM _ _
C') 0 C') D CD0)LO CD 0) oC) 000 0) rN CM c')0-oC_ )(co c) CM C') L
I-_ o:o o _ _N_N_c c c\ _ Cs _ _
000 0
000 0
000 0
N(0
N..
oooo-1-
CMooCY oI
r-
0)C')0
r11 co ltN.
0'-'_
co lt 0co aw0 CC C\l r co co T- C) LO LO 't CO _r-o0 (00 CM C\ () _ _ NC_ L L t c
.0 C'. C.(~~-~--'-NC')N'-C')c
LO CM r LO 't4 - c') V- N:0c')c')
v- cf) V- - ~-
C')N r- 0)mt 4 0
6 CM oc6C c C') N.CN
o LO 0)cn LO N NtCM co(CcONNCM C LOCM _-CN CM CNC') CN
T- - 0) LO LO ) C) C)C 'O0 r - CN Ooo lt _- CM _- _- a) t CD c\l _.- '4 o 0
'- )i '\ 0-
v- co 0)
C'C'N
r- CV) qt
O-Nil)
CD CD Il- CDC Ci cr 0 T- lt T- CDCO N c 'C o 0
0 't N\ CM CM CNJO Nt0 0 C CDO _- _.. _- _- _ CM CM qi CM CM qi CM _
CN0No (D 0)I'-t ItLO CO C L C) C')
(0 CN C') C') 0 0 c cN _c' c' 4 aC-C) -'- - C'
ONr - 0 CN C 0 0 It L-O - t CM )
coN C) 0 '.O ) 0) CN_ C (0 C') d-Cf) ___ CMJ
0Y)0 ,
O
-
1-C0
0
00C '
~°@~~~~~~~~E co CD m a CO)
m~~~~ C LO LO cc CO
2 ~~~~~~~~~~~IVt CM a% n -D 8 M
0 > CD C CC0~ ~ ~ ~ ~ ~ ~ ~
_oiU) NMT-- 0LO 0)4,' .6 o
(0 0I
0) C.)
0co
-
0)
LwO '
CO >
-0
L5O-0
)0co
,CDa c
Arnerican Journal of Public Health 501
Q..0 t0000
cN C) tNtc 0(0CM C) (0 LOcN cm cmN
co co
co co
CrI) _4
(0(0s
_x
a)
cr
CD
acc
a)
60)
0
E00
C
0
0
-
co
ca
<R.0
0
00
cn0
00
0n0
000U-
0
0
5o0Y)
0_*00
O:5'
00E0
w0
0
0
*13000
=E
._o
q._o00C
EjZu£
0
0
C')co
A
0
(0C')
CY)
cf)
C')
C')
C')C'MV-
V
C o43 0)
2 F<
)
Co(1 co, o
0)U
'0
)
co<
70
o) 6
Co,
0):3
6 °
70
0
o s
0 Co' U
0)M 0
< r X
0)
70 o
4-a
6) U
6):
Co
0
o
Cozcn
0)
-0 c,OrLUn a1) a) 13 0) = cts
< 0
0) <
63 "
'aeenz
6'a61
co
. r6 15
'ao
0
CD0)
0
0
co
0
LO)
C\)
cm
0
(0
c'
1-
C4c0'-
- cN
oi 6C') N
(0(0
co Lf
CMC41- 1-
lqt CY)
co 0)
't CM
6C'f)
0l
0-
0
'a
D
co
co
coC
a
..c
c
cn
75.2co
co, oLL-S N
0
*0
CL
.0
CD
CoVO
a)e
cE
0 v
-)
o
Co
o Co
°(D
DV
0
cDv
COo
Qi)
i3X
2
wU-J0I-
I
April 1996, Vol. 86, No. 4

Davey Smith et al.
between family income and mortality wassimilar to that seen in men.
The issues surrounding the use of anecological index of socioeconomic status,discussed with regard to White men in theaccompanying paper,12 are also germane
to consideration of the associations seen
among Black men. In the United States,there is substantial segregation of Whitesand Blacks, especially in metropolitanareas,13'4 but cutting across this segrega-
tion is a gradient of increasing medianfamily income of zip code area for bothgroups. Although the range of income issmaller for Blacks than for Whites, an
inverse association between mortality andincome is observed in both groups.
The association between mortalityrisk and income was not confined to thepoorest members of the cohort; instead, itpersisted over the full range of incomestudied. This was also seen among Whitemen in the study,12 for whom the average
level of income was considerably higher,in keeping with the situation in the UnitedStates generally.'5 The continuous associa-tion between socioeconomic status andmortality risk is a robust finding that hasbeen demonstrated for many populations,both historical and contemporary.'6-'9The existence of such a graded relation-ship requires explanations that go beyondattribution to serious absolute poverty.
The mortality differentials by incomegroup showed no sign of decline over a
16-year follow-up period. As discussed inthe accompanying paper, this arguesagainst an explanation based on the
postulate that poor health leads to declin-ing socioeconomic status. The absence ofan association between history of myocar-
dial infarction or use of medication fordiabetes at screening and income may
reflect selection occurring during recruit-ment to the cohort. Morbidity-includingoverall measures such as the rating ofgeneral health status as less than goodand the experience of limitation of activitydue to poor health-is more prevalentamong lower income Black men thanamong higher income Black men.20'21 Aswell as being related to a shorter expecta-tion of life, low income is accompanied bypoorer health status.
Cigarette smoking was strongly asso-
ciated with mortality risk and was more
common among the lower income men.
Similar gradients between income andall-cause mortality risk were found forsmokers and nonsmokers. Adjustment forsmoking behavior and the other cardiovas-cular disease risk factors measured atbaseline produced a moderate degree ofattenuation of the associations betweenincome and mortality from coronary heartdisease and cancer. The lack of dataregarding lifetime exposure to the mea-
sured factors, together with the absenceof any data regarding obesity, exercisepatterns, alcohol use, and diet, rendersquantification of the attribution of differ-entials to known risk factors problematic.However, the finding of socioeconomicdifferentials for causes of death that are
not the outcomes of such known riskfactors suggests that additional factorsneed to be invoked to account for the fullspectrum of income-mortality associa-tions.
The rate of noncoverage by healthinsurance is higher among those with low
household incomes20; therefore, access to
and availability of health care for lowerincome men will, on average, be inferiorto that of higher income men. It has beendemonstrated that lacking health insur-ance is a marker of increased mortalityrisk.22 In the Hypertension Detection andFollow-up Program, which enrolled a
large proportion of its White and Blackparticipants from relatively poor inner-city areas, higher mortality rates withlower levels of education were seen in thegroup randomized to receive usual medi-cal care in the community.23 Referral to
the specially established HypertensionDetection and Follow-up Program clinicalcenters led to a reduction in mortalityfrom cardiovascular disease, the target ofthe blood pressure-lowering intervention.A reduction in noncardiovascular disease(and consequently all-cause mortality)was also seen,24 however, suggesting thatthere may have been more general conse-
quences of rendering health care acces-
sible. Furthermore, in the group of partici-pants assigned to receive treatment at theclinical centers, the association betweensocioeconomic status and mortality riskwas markedly attenuated.
The lesser access to medical care thataccompanies lower income may explainsome of the socioeconomic differentials inmortality risk. Causes of death thatcannot be prevented by medical care showsimilar socioeconomic gradients to poten-tially preventable causes, however. Thisshould be considered together with theevidence that modifiable risk factors, suchas smoking, elevated blood pressure, andserum cholesterol, do not fully account forthe association between mortality andincome. This does not diminish the valueof efforts to expand access to health care
or to oppose the cynical targeting ofminority and poor populations in themarketing of health-damaging productssuch as cigarettes?25 It does, however,emphasize the conclusion of Adler andcolleagues that there is "no easy solu-tion"-in terms of the simple applicationof current knowledge of disease etiologyand health promotion practice-to thecontinued existence of socioeconomic in-
equalities in health?-6What is clear is that certain processes
that are intimately and robustly linked to
material well-being have a consistentimpact on health status. Comparison ofthe findings for Black men and White menscreened for the Multiple Risk FactorIntervention Trial demonstrates that, ingeneral, the association between income
and mortality risk is similar in the two
groups. The use of race as, in part at least,
April 1996, Vol. 86, No. 4502 American Journal of Public Health
TABLE 6-Distribution of Black and White Householder Median Family Incomefor Zip Code of Residence among Black and White Men Screened
Black Men White Men
Income, $ No. % No. %
< 10 000 2 628 13.0 397 0.110 000-12 499 4 278 21.2 892 0.312 500-14 999 4 799 23.7 4 480 1.515000-17499 2529 12.5 11 729 3.917 500-19 999 2 285 11.3 32 200 10.720 000-22 499 1 963 9.7 60 502 20.122500-24999 762 3.8 56458 18.825 000-27 499 376 1.9 45 311 15.127 500-29 999 221 1.1 36 580 12.230 000-32 499 146 0.7 25 265 8.432 500+ 237 1.2 26 871 8.9
Total 20 224 100.0 300 685 100.0
Note. Family income levels were based on data from the 1980 US census.

Mortality Risk: Black Men
TABLE 7-Relative Risks of Selected Causes of Death, Adjusted for Age and Other Risk Factors, Associated with a $10 000Lower Median Family Income of Zip Code of Residence for Black and White Men Screened
Black Men White MenP for Difference in P for Difference in
Age- and Risk Age- and Risk Income-Mortality Income-MortalityFactor- Factor- Association in Blacks Association in Blacks
Age-Adjusted Adjusted Age-Adjusted Adjusted and Whites after and Whites afterCause of Death Relative Risk Relative Risk Relative Risk Relative Risk Age Adjustmenta Risk Factor Adjustmenta
All causes 1.35 1.29 1.26 1.18 .12 .03Cardiovascular disease 1.31 1.25 1.26 1.17 .53 .38Coronary heart disease 1.32 1.26 1.25 1.16 .86 .65Stroke 1.40 1.31 1.26 1.17 .31 .89Cancer 1.15 1.10 1.21 1.15 .50 .81Lung cancer 1.13 1.05 1.40 1.27 .08 .30Noncancer, noncardio-
vascular disease 1.86 1.79 1.36 1.28 .001 .001Respiratory 1.70 1.61 1.56 1.44 .88 .71Suicide 0.93 0.87 1.17 1.11 .74 .79Homicide 2.29 2.23 2.10 2.00 .89 .87
Note. Risk factors were diastolic blood pressure, serum cholesterol level, medication for diabetes, prior hospitalization for a heart attack, andcigarettes per day.
ap value associated with an income and Black/White interaction term.
a proxy for socioeconomic position insome studies has tended to obscure thefact that the dependence of mortality riskon socioeconomic position among Blacksis at least as strong as that among Whitesin the United States. These Multiple RiskFactor Intervention Trial data, added tothe findings of other recent investiga-tions,3,8'2728 emphasize the importance offocusing on socioeconomic position as adeterminant of mortality among Blacks aswell as between Blacks and Whites. Theeconomic and social structure that pro-duces a marked gradation of income forBlack US citizens produces the same forWhites, but at higher average incomelevels. Explanations of two of the strikingdemographic mortality differentials in theUnited States (the higher mortality riskwith lower socioeconomic status and thehigher mortality rates for Blacks than forWhites) should focus on the commonunderlying factors (the lower levels ofwealth and the reduction in life chances)for the groups at higher levels of mortalityrisk. This does not, however, mean thatthe increased mortality experience ofBlacks can be simply and completelyexplained by lower average socioeco-nomic status.6'29 First, there needs to bedetailed consideration of the forces-including institutional and "everyday"racism6,29'30-that maintain the averagesocioeconomic status of Blacks well belowthat of Whites in the United States.Second, these same forces can ensurethat, even within a given socioeconomicstratum, the life circumstances for Blacks
in the United States can be unfavorable incomparison with those of Whites. O
AcknowledgmentsThe principal investigators and senior staff ofthe clinical, coordinating, and support centers;the National Heart, Lung and Blood Instituteproject office; and members of the MultipleRisk Factor Intervention Trial Policy AdvisoryBoard and Mortality Review Committee havebeen listed in a previous report (JAMA.1982;248:1465-1477). The mortality follow-upof the men screened for the Multiple RiskFactor Intervention Trial and data analysis forthis report were supported by a NationalInstitutes of Health research grant (ROlHL28715).
References1. Cooper R, Steinhauer M, Miller W, David
R, Schatzkin A. Racism, society anddisease: an exploration of the social andbiological mechanisms of differential mor-tality. IntJHealth Serv. 1981;11:389-414.
2. Otten MW, Teutsch SM, Williamson DF,Marks JS. The effects of known risk factorson the excess mortality of Black adults inthe United States. JAMA4. 1990;263:845-850.
3. Sorlie P, Rogot E, Anderson R, JohnsonNJ, Backlund E. Black-white mortalitydifferences by family income. Lancet. 1992;340:346-350.
4. Rogers RG. Living and dying in the U.S.A.:sociodemographic determinants of deathamong blacks and whites. Demography.1992;29:287-303.
5. Polednak AP. Poverty, residential segrega-tion, and black/white mortality ratios inurban areas. J Health Care Poor Under-served. 1993;4:363-373.
6. Krieger N, Rowley DL, Herman AA,Avery B, Phillips MT. Racism, sexism, andsocial class: implications for studies of
health, disease, and well-being. Am J PrevMed. 1993;9(suppl):82-122.
7. Krieger N. The making of public healthdata: paradigms, policies, and policy. JPublic Health Policy. 1992;13:412-427.
8. Cooper RS. Health and social status ofblacks in the United States.Ann Epidemiol.1993;3:137-144.
9. Rogot E, Sorlie PD, Johnson NJ, SchmittC.A Mortality Study of1.3 Million Persons byDemographic, Social, and Economic Fac-tors: 1979-1985 Follow-Up, U.S. NationalLongitudinal Mortality Study. Bethesda, Md:National Institutes of Health; 1993.
10. Neaton JD, Grimm RH, Cutler JA. Recruit-ment of participants for the Multiple RiskFactor Intervention Trial (MRFIT). Con-trolled Clin Tnals. 1987;8:41S-53S.
11. Neaton JD, Kuller LH, Wentworth D,Borhani NO. Total and cardiovascularmortality in relation to cigarette smoking,serum cholesterol concentration, and dia-stolic blood pressure among black andwhite males followed for up to five years.Am HeartJ. 1984;108:759-769.
12. Davey Smith G, Neaton JD, Wentworth D,Stamler R, Stamler J. Socioeconomic differ-entials in mortality risk among men in theMultiple Risk Factor Intervention Trial: I.White men. Am J Public Health. 1996;86:486-496.
13. Massey DS, Denton NA. Trends in residen-tial segregation of blacks, Hispanics, andAsians: 1970-1980.Am Sociol Rev. 1987;52:802-825.
14. Massey DS, Denton NA. Suburbanizationand segregation in the U.S. metropolitanareas.Am J Sociol. 1988;94:592-626.
15. Hacker A. Two Nations. Black and White,Separate, Hostile, Unequal. New York, NY:Ballantine Books; 1992.
16. Morrison AS, Kirshner J, Molho A. Lifecycle events in 15th century Florence:records of the Monte Delle Doti. Am JEpidemiol. 1977;106:487-492.
April 1996, Vol. 86, No. 4 American Journal of Public Health 503

Davey Smith et al.
17. Davey Smith G, Carroll D, Rankin S.Socio-economic differentials in mortality:evidence from Glasgow graveyards. BMJ.1992;305:1554-1557.
18. Goldblatt P. Mortality and alternativesocial classifications. In: Goldblatt P, ed.Longitudinal Study: Mortality and SocialOrganisation. London, England: Her Majes-ty's Stationery Office; 1990:163-192.
19. Davey Smith G, Shipley MJ, Rose G. Themagnitude and causes of socio-economicdifferentials in mortality: further evidencefrom the Whitehall study. J EpidemiolCommunity Health. 1990;44:265-270.
20. Health Status of the Disadvantaged: Chart-book 1990. Washington, DC: US Dept ofHealth and Human Services; 1990.
21. Ries P. Health of black and white Ameri-
cans, 1985-1987. Vital Health Stat [10].1990;171. DHHS no. PHS 90-1599.
22. Franks P, Clancy CM, Gold MR. Healthinsurance and mortality: evidence from anational cohort. JAMA. 1993;270:737-741.
23. Hypertension Detection and Follow-upProgram Cooperative Group. Educationlevel and 5-year all-cause mortality in theHDFP. Hypertension. 1987;9:641-646.
24. Hypertension Detection and Follow-upProgram Cooperative Group. Five-yearfindings of the HDFP. JAMA. 1979;242:2562-2577.
25. Davis RM. Current trends in cigaretteadvertising and marketing. N Engl J Med.1987;316:725-732.
26. Adler NE, Boyce WT, Chesney MA,Folkman S, Syme SL. Socioeconomic in-
equalities in health: no easy solution.JAMA. 1993;269:3140-3145.
27. Navarro V. Race or class versus race andclass: mortality differentials in the UnitedStates. Lancet. 1990;336:1238-1240.
28. Pappas G, Queen S, Hadden W, Fisher G.The increasing disparity in mortality be-tween socioeconomic groups in the U.S.,1960-1986. N Engl J Med. 1993;329:103-109.
29. Davey Smith G, Egger M. Socioeconomicdifferences in mortality in Britain and theUnited States.AmJPublic Health. 1992;82:1079-1081.
30. Essed P. Understanding Everyday Racism:An Interdisciplinary Theory. Newbury Park,Calif: Sage Publications; 1991.
Nominations Soughtfor 1996APHA Maternal andChild Health Section Awards
The Maternal and Child Health Section of the American Public Health Association is solicitingnominations for its two 1996 Section Awards:
* The Young Professional Award-This award is presented to an individual aged 40 or youngerwho has made a significant contribution to the field of maternal and child health through a specific,particularly creative endeavor or through outstanding achievement over a number of years.Contributions to administration, advocacy, clinical care, community service, education, and researchwill receive equal consideration. The award includes a plaque and participation in a special awardsession.
* The Herbert L. Needleman Medal and Award-This new award is presented to an individualwho has demonstrated outstanding scientific achievement and courageous advocacy on behalf ofchildren. The award includes a medal, a cash award of $2000, and participation in a special awardsession.
The award recipients will be announced at the APHA annual meeting. Nominations must besubmitted by May 1, 1996. Please specify for which award you are requesting a nomination form. Foradditional information please write or call Albert Chang, MD, MPH, GSPH-SDSU, 5500 CampanileDr, San Diego, CA 92182-4162; tel (619) 594-4493; fax (619) 594-6112.
504 American Journal of Public Health April 1996, Vol. 86, No.4
Related Documents