i National Five-Year Safe Surgery Strategic Plan Saving Lives Through Safe Surgery (SaLTS) Strategic Plan 2016-2020 Addis Ababa, 2016 Ministry of Health of Ethiopia National Safe Surgery Strategic Plan Ministry of Health

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

iNational Five-Year Safe Surgery Strategic Plan
Saving Lives Through Safe Surgery (SaLTS)Strategic Plan 2016-2020
Addis Ababa, 2016
Ministry of Health of EthiopiaNational Safe Surgery Strategic Plan
Ministry of Health
This document was developed and printed with funding from the GE Foundation through the Safe Surgery 2020 Initiative. The contents are the responsibility of the Ministry of Heath of Ethiopia and do not necessarily reflect the views of the GE Foundation and Safe Surgery 2020 Initiative.

National Five-Year Safe Surgery Strategic Plan
Ministry of Health of Ethiopia
National Safe Surgery Strategic Plan
Saving Lives Through Safe Surgery (SaLTS) Strategic Plan 2016–2020
Ministry of Health
i

National Five-Year Safe Surgery Strategic Plan
Table of ContentsTable of Contents .........................................................................................................................................ii
Abbreviations .............................................................................................................................................iv
Foreword ......................................................................................................................................................v
Acknowledgments ..................................................................................................................................... vi
Background ..................................................................................................................................................1
Introduction .................................................................................................................................................2
Rationale for Saving Lives through Safe surgery .....................................................................................................2
Country Surgical and Anesthesia Care Assessment ..............................................................................3
Strengths and Weaknesses ............................................................................................................................................4
Stakeholders’ Analysis ...................................................................................................................................................8
Saving Lives Through Safe Surgery Aim and Objectives .......................................................................................9
Strategic Pillars and Strategic Results ........................................................................................................................9
Strategic Pillar One: Leadership, Management and Governance ...................................................10
Strategic Objectives .....................................................................................................................................................10
Strategic Results ...........................................................................................................................................................11
Structure ........................................................................................................................................................................11
Strategic Pillar Two: Infrastructure Development ...........................................................................14
Strategic Objectives .....................................................................................................................................................14
Strategic Pillar Three: Equipment and Supplies Management ......................................................15
Strategic Objectives 1 ...................................................................................................................................................15
Strategic Pillar Four: Excellence in Human Resource Development ...........................................16
Strategic Objectives .....................................................................................................................................................16
Strategic Pillar Five: Excellence in Advocacy and Partnership .................................................... 26
Strategic Objectives .....................................................................................................................................................26
Components ..................................................................................................................................................................26
Structure ........................................................................................................................................................................26
Identified Interventions ..............................................................................................................................................27
ii

National Five-Year Safe Surgery Strategic Plan
Measurement/Indicators ............................................................................................................................................27
Strategic Pillar Six: Excellence in Quality and Safety .................................................................... 30
Objective 1: Improve efficiency in surgical and anesthesia care. .........................................................................30
Objective 2: Improve effectiveness of surgical and anesthetic care using evidence-based clinical care. ...............................................................................................................31
Objective 3: Establish a culture of patient-centered care in the surgical system ..............................................31
Objective 4: Improve safety in surgical and anesthesia care. ...............................................................................32
Objective 5: Ensure the provision of timely surgical and anesthesia care for emergency conditions and elective procedures. ..............................................................................32
Objective 6: Ensure equity in surgical and anesthesia care. .................................................................................33
Strategic Pillar Seven: Excellence in Innovations ........................................................................... 34
Strategic Objective .......................................................................................................................................................34
Component ...................................................................................................................................................................34
Strategic Pillar Eight: Excellence in Monitoring and Evaluation ................................................ 38
References ...................................................................................................................................................45
Annex A. Tool for Situational Analysis to Assess Emergency and Essential ................................ 46
Surgical Care in Ethiopia ................................................................................................................................................
Annex B: Safe surgery checklist ............................................................................................................ 77
Surgical and Anesthesia Care Audit Tool ................................................................................................................79
Annex C. Procedure Lists .......................................................................................................................91
iii
National Five-Year Safe Surgery Strategic Plan
AbbreviationsCOSECSA College of Surgeons of East, Central, and Southern Africa
CPD Continuous professional development
CRC Compassionate, respectful and caring
CRCP Curative and rehabilitative core process
CRCPT Curative and rehabilitative core process team
EHAQ Ethiopian Hospitals Alliance for Quality
FMOH Federal Ministry of Health
HEI Higher education institution
HMIS Health management information system
HSTP Health Sector Transformation Plan
IESO Integrated Emergency Surgical Officer
IST In-service training
KPI Key Performance Indicators
M&E Monitoring and evaluation
MOF Ministry of Finance
OR Operating room
RHB Regional health bureau
SaLTS Saving Lives Through Safe Surgery
TWG Technical working group
WHO World Health Organization
iv
National Five-Year Safe Surgery Strategic Plan
Foreword The Ethiopia Federal Ministry of Health (FMOH) has launched the Health Sector Transformation Plan (HSTP) as part of the second Growth and Transformation Plan of the Ethiopian government. The HSTP has set ambitious targets toward realizing the sustainable development goals and identified four transfor-mation agendas: Quality and Equity, Woreda Transformation, Information Revolution and Compassionate, Respectful and Caring (CRC) health workforce.
In line with the quality and equity transformation agenda and as part of recognizing the key roles essen-tial and emergency surgical care plays in achieving universal health coverage, the FMOH has prioritized surgical and anesthesia care by launching the national flagship initiative-Saving Lives through Safe Surgery (SaLTS).
The SaLTS initiative was launched in response to the World Health Assembly resolution-68/15 and aims to make essential and emergency surgical and anesthesia care accessible and affordable as part of the univer-sal health coverage. It is expected that the SaLTS initiative will streamline all efforts toward defining a package of essential and emergency surgical care for Ethiopia: to be available at all levels of the health care delivery system so that they will be accessed equitably by all segments of the population.
The FMOH extends its firm commitment to improving the situation of surgical and anesthesia care in Ethiopia by launching this strategic plan. As a flagship initiative, SaLTS will receive the highest level of attention by the leadership of the health sector.
I would like to take this opportunity to extend our profound appreciation to all individuals and organiza-tions who have actively participated in the development of the SaLTS strategic plan.
Daniel Gebremichael Burssa (MD, MPH)
Director General, Medical Services General Directorate
v
National Five-Year Safe Surgery Strategic Plan
Acknowledgments The Federal Ministry of Health would like to acknowledge the following individuals and their institutions for serving as core team members of the SaLTS plan development team:
Dr Daniel Gebremichael, FMOH
Mr. Esayas Melese FMOH
Dr Atlibachew Teshome FMOH
Dr Samuel Zemenfeskidus FMOH
Dr Andualem Deneke Surgical Society of Ethiopia
Dr Rediet Shimelis Ethiopian Society of Anesthesiologists
Dr Abebe Bekele Addis Ababa University/FMOH
Dr Abraham Endeshaw Jhpiego
Dr Samson Esseye Jhpiego/FMOH
Kaya Garringer PGSSC
Olivia Ahearn PGSSC
Additionally, the following individuals have provided various technical inputs to the development of the SaLTS strategic plan:
Alemayehu Berhanu CHAI
Dr Dereje Gulilat Surgical Society of Ethiopia
Professor Milliard Derebew COSECSA
Dr Tigistu Ashengo Jhpiego
Sr Teruwork Kebede Jhpiego
Alena Skeels Jhpiego
Erin Barringer Dalberg
Asha Varghese GE Foundation
Ashley Eberhart Dalberg
Cheri Reynolds Assist International
The Federal Ministry of Health is very grateful to the following organizations for actively supporting the SaLTS plan development process:
Safe Surgery 2020 and GE Foundation
PFSA: Pharmaceutical Fund and Supply Agency
Surgical Society of Ethiopia
Ethiopian Society of Anesthesiologists
Ethiopian Society of Anesthetists
Ethiopian Society of Obstetricians and Gynecologists
USAID/HFG (HEALTH FINANCE AND GOVERNACE)
SCMS: Supply Chain Management System
CHAI: Clinton Health Access Initiative
World Health Organization
AMREF Health Africa
St Paul Hospital Millennium CollegeAddis Ababa University School of Medicine
vi

1National Five-Year Safe Surgery Strategic Plan
BackgroundSafe surgery has been an essential component of health care for years. However, the increasing incidence of traumatic injuries, cancers and cardiovascular diseases continue to raise the impact of surgical interven-tion in public health systems. In fact, safe surgery is the second global patients’ safety challenge next to health care associated infections. Surgical safety is a concern because most institutions do not implement the standard World Health Organization (WHO) surgical checklist.
Disorders that could be managed by surgery constitute a significant portion of the global disease burden (Debas et al. 2015). Annually, injuries kill nearly 5 million people, and about 270,000 women die from complications of pregnancy. Many of these injury-related and obstetric-related deaths, as well as deaths from other causes (e.g., abdominal emergencies and congenital anomalies), could be prevented by im-proved access to surgical care (Debas et al. 2015).
An estimated 234 million major surgeries are performed around the world each year, corresponding to one surgery for every 30 people alive. Yet, surgical services are unevenly distributed with 30% of the world’s population receiving 75% of major operations. Lack of access to high quality surgical care remains a sig-nificant problem in much of the world despite the fact that surgical interventions can be cost effective in terms of lives saved and disability averted. Despite this large burden, surgical services are not being deliv-ered to many of the individuals who need them most. An estimated 2 billion people lack access to even the most basic of surgical care (WHO 2008).
This need has not been widely acknowledged, and, therefore, priorities for investment in health sys-tems’ surgical capacities have only recently been investigated. Indeed, until the 1990s, health policy in resource-constrained settings focused sharply on infectious diseases and under nutrition, especially in children. Surgical capacity was developing in urban areas, but was often viewed as a secondary priority that mainly served socio-economically advantaged people.
The number of surgeries done in Ethiopia is not more than 200,000 a year with 250 general surgeons, 300 gynecologists, 50 orthopedic surgeons, and 100 ophthalmologists, which is inadequate to reach the unmet need of 5,000,000 surgeries per year. The waiting time for surgery extends up to four years, especially in referral hospitals.
Surgical site infections remain one of the most common causes of serious surgical complications. Evidenc-es show that proven measures, such as antibiotic prophylaxis within the hour before incision and effective sterilization of instruments, are inconsistently followed often not because of cost or lack of resources but because of poor systematization. Antibiotics, for example, are given perioperative in both developed and developing countries, but they are often administered too early, too late or simply erratically, making them ineffective in reducing patient harm.
Mortality from general anesthesia alone is reported to be as high as 1 in 150 in parts of sub-Saharan Africa. Three decades ago, a patient undergoing general anesthesia had an estimated 1 in 5,000 chance of death. With improvements in knowledge and basic standards of care, the risk has dropped to 1 in 200,000 in the developed world—a 40-fold improvement. Unfortunately, the rate of anesthesia-associated mortality in developing countries appears to be 100–1000 times higher, indicating a serious, sustained lack of safe anesthesia for surgery in these settings. In addition, anesthetic complications remain a substantial cause of surgical death globally, despite safety and monitoring standards that have significantly reduced unnecessary deaths and disability in developed countries.
2 National Five-Year Safe Surgery Strategic Plan
IntroductionThe Ethiopian Federal Ministry of Health (FMOH) implemented the Health Sector Development Pro-gram 1–4 successfully that helped reform the nation’s health system in the last 20 years. Currently, the FMOH launched the fifth strategic plan, called the Health Sector Transformation Plan (HSTP), which is aligned with country’s second growth and transformation plan. The HSTP has identified quality and equi-ty as a cornerstone of the transformation agenda focusing mainly on essential and emergency safe surgical and anesthesia care, in addition to maternal, neonatal and child health; nutrition; chronic non-communica-ble diseases and infectious diseases.
Saving Lives Through Safe Surgery (SaLTS) is the FMOH’s flagship initiative that is designed to respond to the World Health Assembly resolution of A68/15 in making emergency and essential surgical and anesthesia care accessible and affordable as part of the universal health coverage. The SaLTS initiative was developed with the objective to ensure the delivery of quality, safe, essential and emergency surgery throughout the country to alleviate the national burden of diseases, disability and death that are prevent-able throughout safe surgery.
The development of the SaLTS initiative was informed by input from various stakeholders and it aims to build on the experiences of existing reform agendas including but not limited to the Ethiopian Hospitals Reform initiative and utilizes the Ethiopian Hospitals Alliance for Quality (EHAQ) as a platform for rapid scale up. As a flagship initiative of the HSTP under the quality and equity transformation agenda, it will be integrated into the newly revised the Ethiopian hospitals reform implementation guideline for rapid imple-mentation and scale up in all health centers, primary hospitals and tertiary hospitals.
Rationale for Saving Lives through Safe surgery The provision of essential surgical procedures ranks among the most cost effective of all health interventions and would avert about 1.5 million deaths a year, or 6%–7% of all avertable deaths in low-income and middle-income countries (Debas et al. 2015; Mock et al. 2015).
In general, the large burden of surgical disorders, cost-effectiveness of essential surgery, and strong public demand for surgical services suggest that universal coverage of essential surgery should be financed early on the path to universal health coverage. Full coverage of universal coverage of essential surgery applicable to first-level hospitals would require over an estimated US $3 billion annually of additional spending and yield a benefit–cost ratio of more than 10:1. It would efficiently and equitably provide health benefits, financial protection, and contributions to stronger health systems (Mock et al. 2015).

3National Five-Year Safe Surgery Strategic Plan
Country Surgical and Anesthesia Care Assessment
A situational analysis was conducted on selected health centers, primary hospitals and tertiary hospitals using the WHO surgical and anesthesia needs and status assessment tool.
According to WHO, properly equipped primary hospitals in low-income countries such as Ethiopia are able to perform emergency surgery for a number of conditions, including obstetric complications; abdom-inal emergencies and basic surgeries and injuries; simple orthopedic care for extremity fractures, dislo-cations, and amputations; burn care and uncomplicated general surgery for hernias; and treatment and control of surgical infections (Debas et al. 2006). However, many primary hospitals in rural Ethiopia are not in a position to provide the mentioned services due to lack of appropriate human resources, supporting staff, equipment and supplies.
A total of 44 essential surgical procedures that have been recommended in the Disease Control Priorities will provide a reasonable starting point for an essential surgical package, although there will be coun-try-specific variations (Debas et al. 2015). Safe anesthesia and perioperative care are necessary components of all of these procedures.
The surgical platform of the first-level hospital delivers 28 of the 44 essential procedures. Investing in this platform is also highly cost effective for the long term to expand access to surgery. Task sharing by health officers through short-term training has been shown to be safe and effective while the country made long-term investments in building the surgical and anesthesia workforces.
SaLTS focuses on availing a package of essential and emergency surgical and anesthesia care at all levels of the Ethiopian health care delivery system with special emphasis in strengthening primary care to provide essential surgical care. Feasible measures, such as WHO’s Surgical Safety Checklist, have led to improve-ments in safety and quality. (Debas et al. 2006).

4 National Five-Year Safe Surgery Strategic Plan
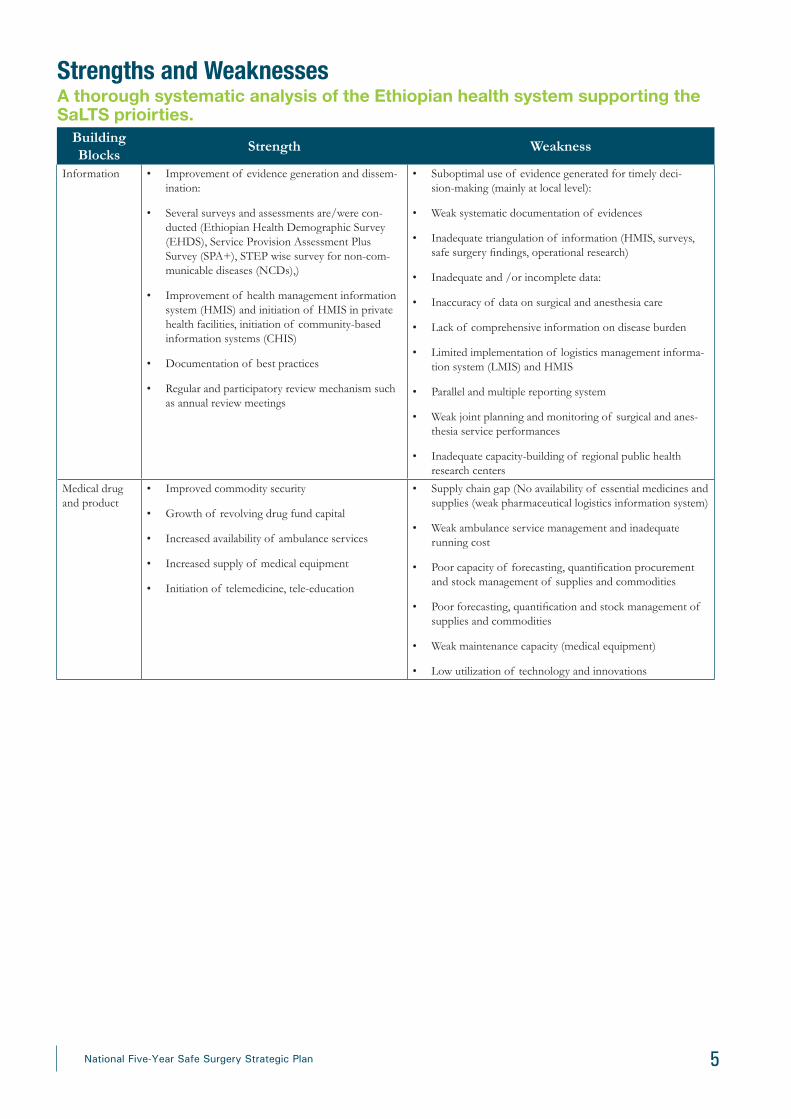
Strengths and WeaknessesA thorough systematic analysis of the Ethiopian health system supporting the SaLTS prioirties.
Building Blocks
Strength Weakness
Leadership and governance
Leading and coordinating
• Use of technical working groups (TWGs)
• Establishment of partner’s forum at subnational level
• Health Extension Program (HEP) and Health Development Army (HAD) as a demand creation, improving access and community empowerment tool
• Improved integrated supportive supervision practice
• Institutionalization of service improvement ap-proaches like Balanced Score Card (BSC), EHAQ.
Controlling and monitoring
• Strengthening of regulatory system
• Actions for standardization and regulation (facility standard, licensing)
• Establishment of quality control of lab
• Essential surgical and anesthesia care were not classified as primary health care
• Donor dependent program designing, resource and funding allocation
• Inadequate focus for streamlined planning and implemen-tation among the directorates and agencies of FMOH, partners and regions.
• Low involvement of patients in decision-making/leadership level
• Inequity across regional capacity in leading and implemen-tation capacity among regions and health facilities
• Weak implementation capacities among agencies, FMOH and regional health bureaus (RHBs).
• Lack of structural review and adjustment along with stra-tegic plan
Human resources and infrastructure
• Rapid increase in the availability of human re-sources for health IESOs, surgeons
• New initiatives such as CPD, leadership programs, by Ethiopian Food Medicine Health Care Admin-istration and Control Authority (FMHACA) under FMOH
• Rapid expansion of health institutions with prima-ry health care to 100%
• Procurement of medical equipment including op-erating room (OR) tables and anesthesia machines
• Wide gap in the global indicator of surgical capacity per population
• Lack of clarity in implementation of national guidelines in big cities, including health center and primary hospital reforms
• Limited capacity to own and lead some program areas at national level
• Poor provider attitude and low commitment of various stakeholders
• High attrition rate and absence of human resources motiva-tion and retention strategy
• Weak institutional knowledge management
• Weak knowledge generation and utilization at national level
• Inequity in the distribution of skilled manpower
• Lack of motivation and retention strategy
5National Five-Year Safe Surgery Strategic Plan
Building Blocks
Strength Weakness
Information • Improvement of evidence generation and dissem-ination:
• Several surveys and assessments are/were con-ducted (Ethiopian Health Demographic Survey (EHDS), Service Provision Assessment Plus Survey (SPA+), STEP wise survey for non-com-municable diseases (NCDs),)
• Improvement of health management information system (HMIS) and initiation of HMIS in private health facilities, initiation of community-based information systems (CHIS)
• Documentation of best practices
• Regular and participatory review mechanism such as annual review meetings
• Suboptimal use of evidence generated for timely deci-sion-making (mainly at local level):
• Weak systematic documentation of evidences
• Inadequate triangulation of information (HMIS, surveys, safe surgery findings, operational research)
• Inadequate and /or incomplete data:
• Inaccuracy of data on surgical and anesthesia care
• Lack of comprehensive information on disease burden
• Limited implementation of logistics management informa-tion system (LMIS) and HMIS
• Parallel and multiple reporting system
• Weak joint planning and monitoring of surgical and anes-thesia service performances
• Inadequate capacity-building of regional public health research centers
Medical drug and product
• Improved commodity security
• Growth of revolving drug fund capital
• Increased availability of ambulance services
• Increased supply of medical equipment
• Initiation of telemedicine, tele-education
• Supply chain gap (No availability of essential medicines and supplies (weak pharmaceutical logistics information system)
• Weak ambulance service management and inadequate running cost
• Poor capacity of forecasting, quantification procurement and stock management of supplies and commodities
• Poor forecasting, quantification and stock management of supplies and commodities
• Weak maintenance capacity (medical equipment)
• Low utilization of technology and innovations
Strengths and WeaknessesA thorough systematic analysis of the Ethiopian health system supporting the SaLTS prioirties.

6 National Five-Year Safe Surgery Strategic Plan
Building Blocks
Strength Weakness
Service delivery • Increase in construction of hospitals and health centers
• Steady increase in key diagnostic and radiological intervention coverage
• Health facility expansion particularly to primary health care facilities
• Increase in availability of ambulance services
• Storage and distribution capacity of pharmaceuti-cal supplies and services
• Experience in implementing large scale successful programs
• Efforts for preparation of minimum service standards
• Decentralized lab services
• Sub-optimal functionality of health facilities
• Sub-optimal service availability and readiness at health facilities
• Missed opportunities for essential health interventions due to limited focus on integrated service delivery
• Inadequacy in continuum of care:
• Potential tertiary care gaps - limited surgeons, gynecolo-gists, IESOs, anesthesia professionals, trained OR nurses/managers access to hospital care, with negative influence on the continuum of care
• Inequitable distribution of human resources
• Socioeconomic situations (gender, education, income)
• Service points are not user-friendly particularly for disabled people and women
• Sub-optimal quality of care
• Inadequate availability of clinical service protocols for health facilities
• Absence of surgical and anesthesia care standard operating procedures, clinical auditing guidelines, standardized service assessment tools/checklists, indicators
• Inadequate follow-up on implementation of strategies, guidelines and standard operating procedures
• Weak referral and feedback system
Laboratory and imaging
• Presence of national strategic plan for laboratory services and designated unit
• Decentralized laboratory services
• Presence of national laboratory services with referral network
• Presence of national quality assurance and accred-itation system
• Initiation of backup laboratory system in Addis Ababa
• Increasing investment in high tech imaging ser-vices
• Improving national blood transfusion services accessibility
• Frequent interruption of important laboratory services
• Lack of supplies and consumables
• Inadequate human resources for laboratory and imaging services
• Lack of safe blood in some parts of the country
• Poor medical equipment management
• Lack of strategic plan for imaging services
Health financ-ing
• Implementation of health care financing reform (such as fee retention, private wing, service fee revision, etc.)
• Establishment of health insurance
• Resource mobilization (Millenium Development Goals Pool Fund (MDG PF); Revolving drug fund capital is improving
• Encouraging multi-sectorial collaborative efforts National Nutrition Program (NNP), water and sanitation, non-communicable diseases, s, MoE-Ministry of Education)
• Gaps in mobilizing local resources
• Low utilization and liquidation at all levels
• Poor resource mapping capacity especially at sub-national level
• Weak financial utilization and timely liquidation
Strengths and WeaknessesA thorough systematic analysis of the Ethiopian health system supporting the SaLTS prioirties.
7National Five-Year Safe Surgery Strategic Plan
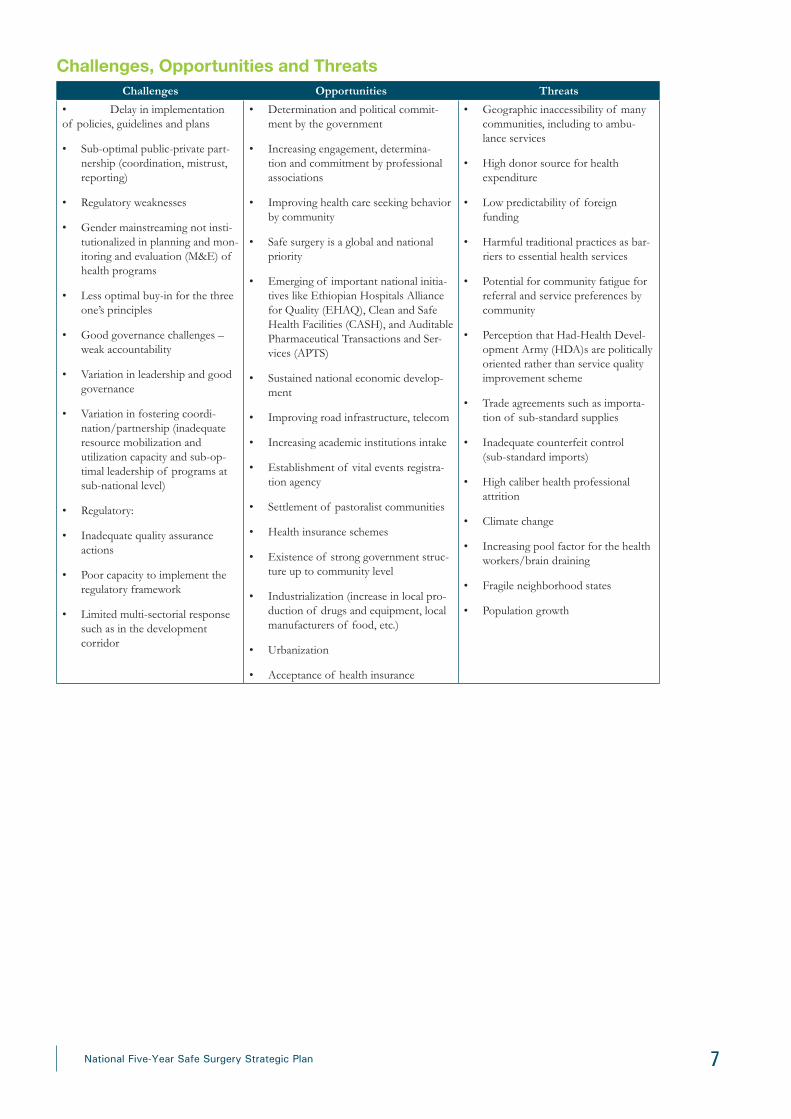
Challenges, Opportunities and ThreatsChallenges Opportunities Threats
• Delay in implementation of policies, guidelines and plans
• Sub-optimal public-private part-nership (coordination, mistrust, reporting)
• Regulatory weaknesses
• Gender mainstreaming not insti-tutionalized in planning and mon-itoring and evaluation (M&E) of health programs
• Less optimal buy-in for the three one’s principles
• Good governance challenges – weak accountability
• Variation in leadership and good governance
• Variation in fostering coordi-nation/partnership (inadequate resource mobilization and utilization capacity and sub-op-timal leadership of programs at sub-national level)
• Regulatory:
• Inadequate quality assurance actions
• Poor capacity to implement the regulatory framework
• Limited multi-sectorial response such as in the development corridor
• Determination and political commit-ment by the government
• Increasing engagement, determina-tion and commitment by professional associations
• Improving health care seeking behavior by community
• Safe surgery is a global and national priority
• Emerging of important national initia-tives like Ethiopian Hospitals Alliance for Quality (EHAQ), Clean and Safe Health Facilities (CASH), and Auditable Pharmaceutical Transactions and Ser-vices (APTS)
• Sustained national economic develop-ment
• Improving road infrastructure, telecom
• Increasing academic institutions intake
• Establishment of vital events registra-tion agency
• Settlement of pastoralist communities
• Health insurance schemes
• Existence of strong government struc-ture up to community level
• Industrialization (increase in local pro-duction of drugs and equipment, local manufacturers of food, etc.)
• Urbanization
• Acceptance of health insurance
• Geographic inaccessibility of many communities, including to ambu-lance services
• High donor source for health expenditure
• Low predictability of foreign funding
• Harmful traditional practices as bar-riers to essential health services
• Potential for community fatigue for referral and service preferences by community
• Perception that Had-Health Devel-opment Army (HDA)s are politically oriented rather than service quality improvement scheme
• Trade agreements such as importa-tion of sub-standard supplies
• Inadequate counterfeit control (sub-standard imports)
• High caliber health professional attrition
• Climate change
• Increasing pool factor for the health workers/brain draining
• Fragile neighborhood states
• Population growth

8 National Five-Year Safe Surgery Strategic Plan
Stak
ehol
ders
’ Ana
lysi
sSt
akeh
olde
rsB
ehav
iors
the
SaL
TS
Init
iativ
e de
sire
sSt
akeh
olde
r ne
eds
Ant
icip
ated
Cha
lleng
esL
evel
of
Impa
ctIn
stit
utio
nal r
espo
nse
• C
omm
unity
• Pa
rtic
ipat
ion,
eng
agem
ent O
wne
rshi
p an
d
• H
ealth
y lif
e st
yle
• A
cces
s to
hea
lth in
form
atio
n an
d se
rvic
e E
mpo
wer
men
t,
• Q
ualit
y of
sur
gica
l and
ane
sthe
-si
a ca
re
• D
issa
tisfa
ctio
n
• O
ptin
g fo
r uns
afe
alte
rnat
ives
• U
nder
utili
zatio
n
Hig
h•
Com
mun
ity m
obili
zatio
n, e
nsur
e pa
rtic
ipat
ion
• Q
ualit
y an
d eq
uita
ble
serv
ice
and
info
rmat
ion
• Pa
rliam
ents
, Prim
e M
inis
ter’s
Offi
ce,
Cou
ncil
of M
inis
ters
,
• ag
enci
es, r
egio
nal
gove
rnm
ents
• R
atifi
catio
n of
Pol
icy
proc
lam
atio
ns,
polic
es, e
tc.
• R
esou
rces
allo
catio
n
• Im
plem
enta
tion
of p
rocl
ama-
tions
, Pol
icy,
etc.
• E
quity
& q
ualit
y
• Pl
ans
& R
epor
ts
• A
dmin
istr
ativ
e m
easu
res
• O
rgan
izat
iona
l res
truc
turin
g
• In
fluen
ce o
n bu
dget
allo
catio
n
Hig
h•
Put i
n pl
ace
stro
ng M
&E
sys
tem
&
com
preh
ensiv
e ca
paci
ty-b
uild
-in
g m
echa
nism
s
• Li
ne M
inis
trie
s (W
a-te
r, el
ectr
icity
, fina
nce,
la
bor,
wom
en’s
affa
irs,
agric
ultu
re, e
tc.)
• In
ter-
sect
oria
l col
labo
ratio
n
• C
onsi
der h
ealth
in a
ll po
licie
s an
d st
rate
gies
• E
vide
nce-
base
d pl
ans;
Rep
orts
• E
ffec
tive
& e
ffici
ent u
se o
f re
sour
ces
& c
oord
inat
ion
• Te
chni
cal s
uppo
rt
• Fr
agm
enta
tion
• D
issa
tisfa
ctio
n
• C
onsi
derin
g he
alth
as
low
pr
iorit
y
Med
ium
• C
olla
bora
tion
• Tr
ansp
aren
cy
• A
dvoc
acy
• H
ealth
pro
fess
iona
l as
soci
atio
ns a
nd
univ
ersi
ties
• K
now
ledg
eabl
e, s
kille
d an
d et
hica
l su
rgic
al a
nd a
nest
hesi
a pr
ofes
sion
als
prod
uced
• Pa
rtic
ipat
e in
lice
nsin
g an
d ac
cred
i-ta
tion
• Pr
omot
e pr
ofes
sion
al c
ode
of c
ondu
ct
• Te
chni
cal,
polic
y su
ppor
t, gu
idan
ce
• In
volv
ed in
pla
nnin
g, im
ple-
men
tatio
n &
M&
E
• C
urric
ulum
revi
sion
• D
issa
tisfa
ctio
n
• Fr
agm
enta
tion
• Sc
ale
dow
n
• W
ithdr
awal
Hig
h •
Polic
y, fin
anci
al a
nd le
ader
ship
su
ppor
t
• C
apac
ity-b
uild
ing
• D
evel
opm
ent p
art-
ners
• H
arm
oniz
ed &
alig
ned
• Pa
rtic
ipat
ion
• M
ore
finan
cing
• Te
chni
cal s
uppo
rt
• H
arm
oniz
atio
n &
alig
nmen
t
• Fi
nanc
ial s
yste
m a
ccou
ntab
le &
tr
ansp
aren
t •
Frag
men
tatio
n
• H
igh
tran
sact
ion
cost
• In
effic
ienc
y &
inef
fect
ive
Med
ium
• G
over
nmen
t lea
ders
hip
• Tr
ansp
aren
cy
• E
ffici
ent r
esou
rce
use
• B
uild
fina
ncia
l man
agem
ent
capa
city
• D
iasp
ora
and
priv
ate
for p
rofit
)•
Qua
lity
of c
are;
Clie
nt o
rient
ed;
• K
now
ledg
e an
d te
chno
logy
tran
sfer
• E
nabl
ing
envi
ronm
ent f
or th
eir
enga
gem
ent
• M
istr
ust
• R
ent s
eeki
ng
Med
ium
•
Tran
spar
ency
• A
ccou
ntab
ility
• D
ialo
gue
• C
ivil
serv
ants
• C
omm
itmen
t,
• Pa
rtic
ipat
ion
• C
PD
• C
ondu
cive
env
ironm
ent
• Tr
ansp
aren
cy
• In
cent
ive
• D
issa
tisfa
ctio
n
• U
npro
duct
ive
• A
ttriti
on
Hig
h•
Mot
ivat
ion,
Inv
olve
men
t
9National Five-Year Safe Surgery Strategic Plan
Saving Lives Through Safe Surgery Aim and Objectives AimTo improve equitable access to high-quality and safe essential and emergency surgical and anesthesia care as part of the universal health coverage.
Objectives
¡ To implement a nationally coordinated national plan on surgical care.
¡ To define and implement essential surgery package for all levels of the Ethiopian health care delivery system.
¡ To create better awareness on surgical and anesthesia care with different stakeholders.
¡ To improve the safety of surgical care by implementing the surgical safety checklist and improving the safety culture.
¡ To implement a quality improvement and audit tool in surgical care.
¡ To proactively identify best practices and scale up rapidly through EHAQ.
Core Values:
¡ Accountability
¡ Transparency
¡ Compassion
¡ Respect
¡ Care
¡ Patient centeredness
¡ Quality focused
¡ Innovation
¡ Partnership
Strategic Pillars and Strategic ResultsA high-level professional workshop was conducted to develop the strategic pillars and plan documents on the pil-lars of essential and emergency surgical care based on mapping the development and the existing capacity, commit-ment and funding.
The SaLTS initiative has identified key strategic objectives in line with the commitment of approaching the initia-tive through the health system building blocks. Considering the vast undertakings in making essential surgical care available and accessible, innovative approaches and wider partnerships will be solicited. Accordingly, the following key strategic pillars were identified.
1. Leadership, management and governance
2. Infrastructure development
3. Equipment and supplies management
4. Human resources development
5. Partnership and advocacy
6. Quality and Safety
7. Innovation
8. Monitoring and evaluation
10 National Five-Year Safe Surgery Strategic Plan
Strategic Pillar One: Leadership, Management and GovernanceEffective leadership and governance are key to the successful implementation of such an ambitious program. Accordingly, functional structures will be established at all levels of the health system to oversee the program. The initiative will be led at the national level by the Minister of Health. Regionally, the program implementations will be integrated within the Medical Services General Directorateand the Health Services Quality Directorate and curative and rehabilitative core process (CRCP)/health care quality process. Similarly, the SaLTS leadership and management structure extends below the RHBs in zones, woredas and health facilities.
Existing structures and staff have limited experience in safe surgery leadership and management to effectively address essential and emergency surgical issues in the country, so the executive leadership will be supported by a TWG at the national level and a technical advisory group at the regional level. Day-to-day activities will be led and managed by respective government structures (project management team) at all levels. Additionally, the initiative will be incorporated with the existing EHAQ structure.
Current budget allocation for safe surgery is inadequate to address specific problems such as medical equipment, supplies, surgical workforce availability, capacity-building, improvement of operational quality capabilities and infrastructural development. Therefore, the FMOH will work in partnership with professional societies, partners, senior service providers and universities that have responsibilities for overall SaLTS program implementation and management in the country.
Strategic Objectives1. Establish effective leadership and management system across all levels of the health system.
¡ Establish leadership and management structure at all levels.
• Identify potential members. • Invite participants.• Conduct regular meetings
¡ Develop guidelines/manual for leadership and management structure.
• Develop a draft guideline. • Incorporate feedback from national TWG. • Finalize the guidelines/manual. • Circulate the manual for RHBs and facilities.
¡ Preparation of tool kits (assessment tool, SaLTS leadership guidelines, and standard operating procedures).
¡ Designate individual champions and institutions for SaLTS.
¡ Monitor, report and evaluate leadership and management activities.
2. Strengthen leadership and management capabilities at all levels.
¡ Provide short-term trainings on leadership and management skills.
• Develop training packages. • Identify trainees. • Conduct the training.• Conduct supportive supervisions, mentorship and coaching (on team building, communication).• Identify mentors.• Develop mentorship guide.• Conduct mentorship.
11National Five-Year Safe Surgery Strategic Plan
¡ Seconded expertise to build the capacity of government.
• Identify and communicate partners. • Develop Terms of Reference (ToR).• Identify and assign the expert.
¡ International and local experience sharing
• Identify areas that have best practices. • Secure budget. • Conduct the experience sharing.
¡ Establish knowledge management center.
Strategic ResultsImproved leadership and management system, measured by the following components:
¡ Establishing safe surgery leadership structure at all levels including their respective ToR.
¡ Identifying major leadership gaps at all levels in leading safe surgery program.
¡ Designing leadership support/training package based on identifying gaps.
¡ Implementing leadership support/training package.
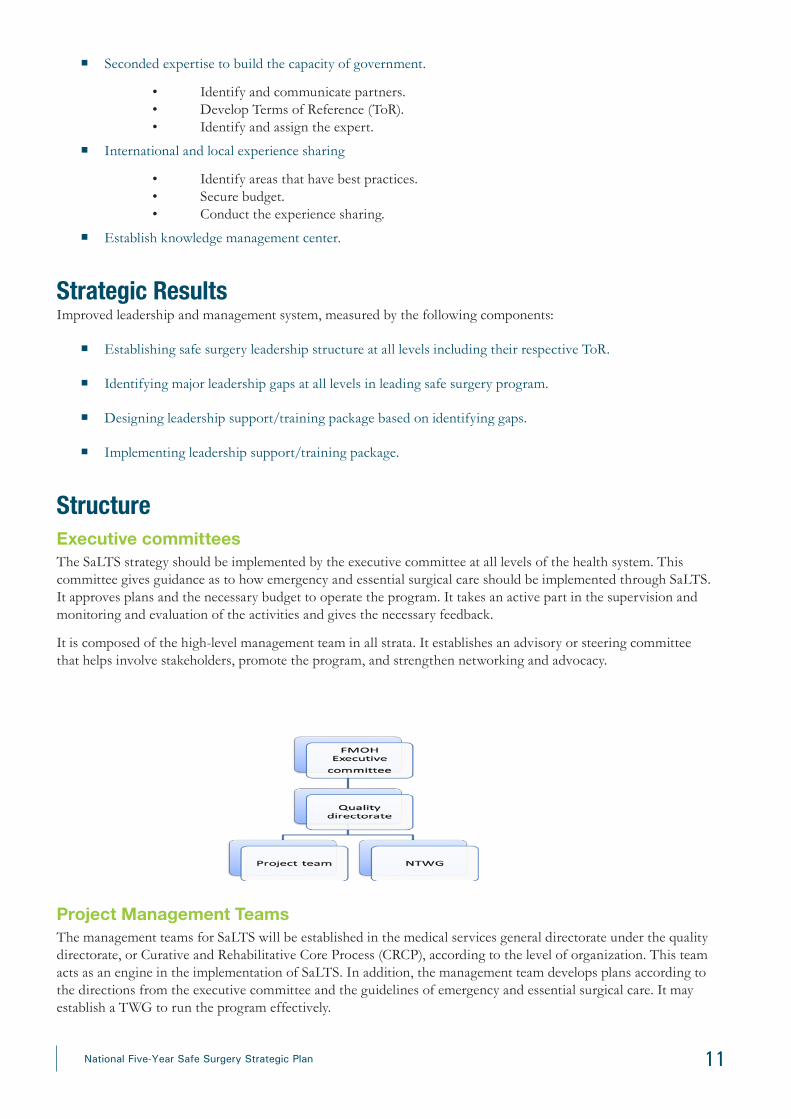
Structure Executive committeesThe SaLTS strategy should be implemented by the executive committee at all levels of the health system. This committee gives guidance as to how emergency and essential surgical care should be implemented through SaLTS. It approves plans and the necessary budget to operate the program. It takes an active part in the supervision and monitoring and evaluation of the activities and gives the necessary feedback.
It is composed of the high-level management team in all strata. It establishes an advisory or steering committee that helps involve stakeholders, promote the program, and strengthen networking and advocacy.
Project Management TeamsThe management teams for SaLTS will be established in the medical services general directorate under the quality directorate, or Curative and Rehabilitative Core Process (CRCP), according to the level of organization. This team acts as an engine in the implementation of SaLTS. In addition, the management team develops plans according to the directions from the executive committee and the guidelines of emergency and essential surgical care. It may establish a TWG to run the program effectively.

12 National Five-Year Safe Surgery Strategic Plan
Technical Working Groups The Medical Services General Directorate or CRCP of the health structure will create the TWG, which will be comprised of management teams, various professional societies, and partners relevant to SaLTS.
Health Facility Structure Roles and responsibilities
Hospital/health center CEO/clinical director/Se-nior Management Team (SMT)
• Supervise overall SaLTS activities
• Conduct baseline and ongoing assessment
• Assign necessary surgical team and OR manager
• Engage senior professionals in leadership
• Allocate and mobilize resources
• Evaluate the progress of implementation
• Assess and reward champion provider
• Ensure availability of necessary supplies
• Ensure the availability and utilization of WHO safe surgery essential checklists
• Establish facility level taskforce that follows the implementation of SaLTS strategy by delegating authority
SaLTS program coordinating teams (surgical team) • Develop SaLTS specific action plan
• Support the implementation of the facility SaLTS plan
• Conduct ongoing assessment to advise SMT and provide feedback to service units
• Provide training to clinical and non-clinical surgical staff
• Plan and supervise the activity of respective unit
• Discuss with team to improve the quality of surgical activities
• Organize hospital wide advocacy and communications
• Involve in all surgical team meetings
• Document all activities and submit the report
Full-time OR manager • Act as a secretary of SaLTS implementing team
• Oversee day to day activity of OR
• Conduct daily supervision to key function units and give information to SaLTS coordinating team
• Participate on senior management team representing surgical team
13National Five-Year Safe Surgery Strategic Plan
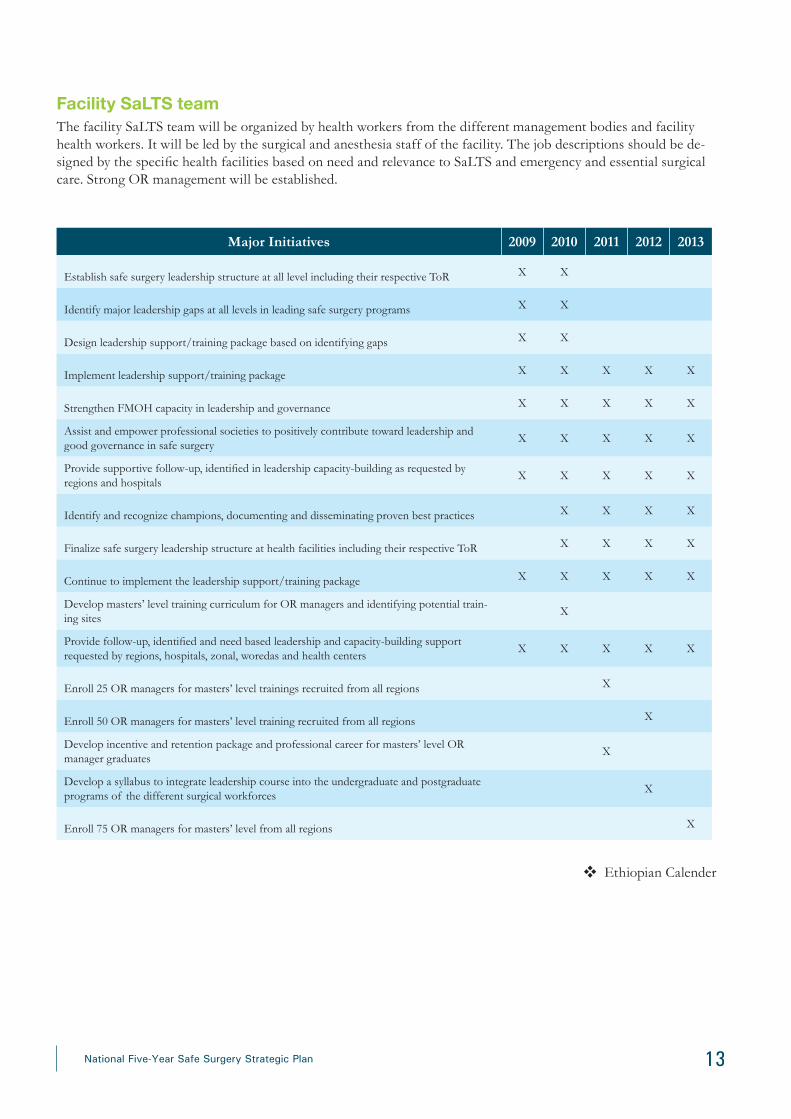
Facility SaLTS teamThe facility SaLTS team will be organized by health workers from the different management bodies and facility health workers. It will be led by the surgical and anesthesia staff of the facility. The job descriptions should be de-signed by the specific health facilities based on need and relevance to SaLTS and emergency and essential surgical care. Strong OR management will be established.
Major Initiatives 2009 2010 2011 2012 2013
Establish safe surgery leadership structure at all level including their respective ToR X X
Identify major leadership gaps at all levels in leading safe surgery programs X X
Design leadership support/training package based on identifying gaps X X
Implement leadership support/training package X X X X X
Strengthen FMOH capacity in leadership and governance X X X X X
Assist and empower professional societies to positively contribute toward leadership and good governance in safe surgery
X X X X X
Provide supportive follow-up, identified in leadership capacity-building as requested by regions and hospitals
X X X X X
Identify and recognize champions, documenting and disseminating proven best practices X X X X
Finalize safe surgery leadership structure at health facilities including their respective ToR X X X X
Continue to implement the leadership support/training package X X X X X
Develop masters’ level training curriculum for OR managers and identifying potential train-ing sites
X
Provide follow-up, identified and need based leadership and capacity-building support requested by regions, hospitals, zonal, woredas and health centers
X X X X X
Enroll 25 OR managers for masters’ level trainings recruited from all regions X
Enroll 50 OR managers for masters’ level training recruited from all regions X
Develop incentive and retention package and professional career for masters’ level OR manager graduates
X
Develop a syllabus to integrate leadership course into the undergraduate and postgraduate programs of the different surgical workforces
X
Enroll 75 OR managers for masters’ level from all regions X
Ethiopian Calender
14 National Five-Year Safe Surgery Strategic Plan
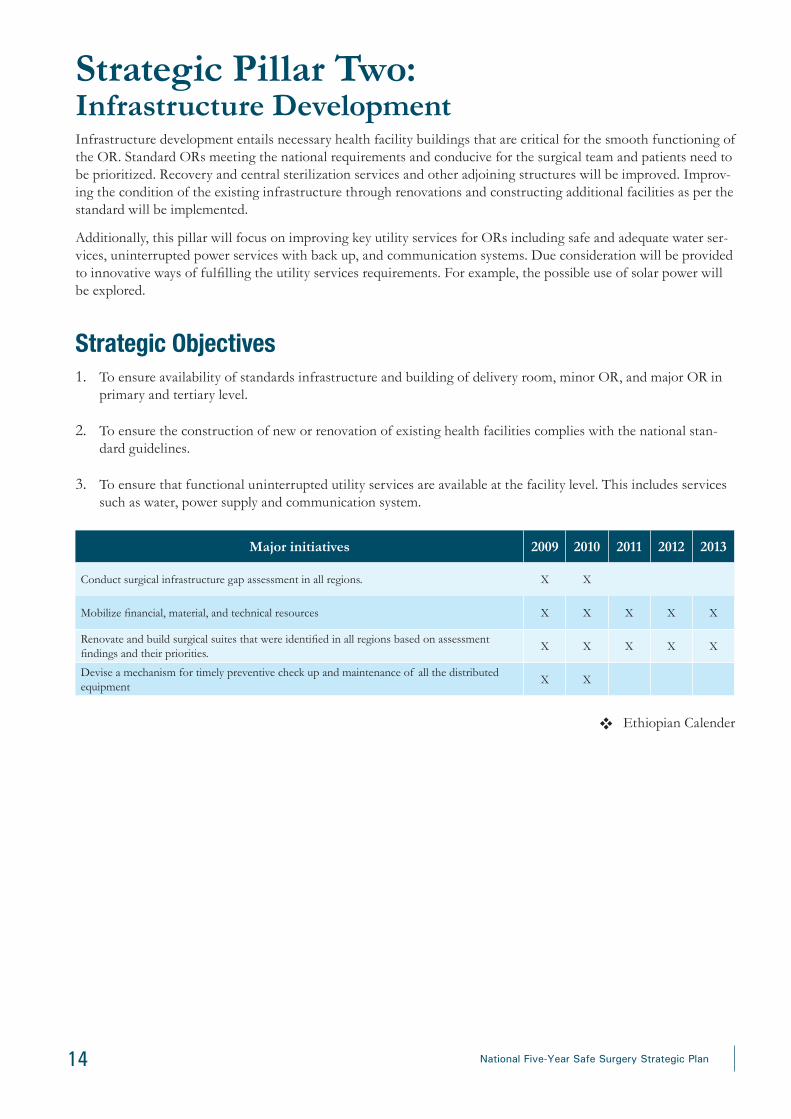
Strategic Pillar Two: Infrastructure DevelopmentInfrastructure development entails necessary health facility buildings that are critical for the smooth functioning of the OR. Standard ORs meeting the national requirements and conducive for the surgical team and patients need to be prioritized. Recovery and central sterilization services and other adjoining structures will be improved. Improv-ing the condition of the existing infrastructure through renovations and constructing additional facilities as per the standard will be implemented.
Additionally, this pillar will focus on improving key utility services for ORs including safe and adequate water ser-vices, uninterrupted power services with back up, and communication systems. Due consideration will be provided to innovative ways of fulfilling the utility services requirements. For example, the possible use of solar power will be explored.
Strategic Objectives1. To ensure availability of standards infrastructure and building of delivery room, minor OR, and major OR in
primary and tertiary level.
2. To ensure the construction of new or renovation of existing health facilities complies with the national stan-dard guidelines.
3. To ensure that functional uninterrupted utility services are available at the facility level. This includes services such as water, power supply and communication system.
Major initiatives 2009 2010 2011 2012 2013
Conduct surgical infrastructure gap assessment in all regions. X X
Mobilize financial, material, and technical resources X X X X X
Renovate and build surgical suites that were identified in all regions based on assessment findings and their priorities.
X X X X X
Devise a mechanism for timely preventive check up and maintenance of all the distributed equipment
X X
Ethiopian Calender

15National Five-Year Safe Surgery Strategic Plan
Strategic Pillar Three: Equipment and Supplies ManagementAvailability of essential equipment, supplies, and consumables are key for the provision of surgical and anesthe-sia care. The SaLTS initiative will identify a national package of essential surgical and anesthesia procedures, and standard lists of national supplies and consumables will be prepared. Similarly, essential medical equipment and package of surgical instruments will be developed in accordance with the nationally identified essential surgical ser-vices package. Using a standardized inventory checklist, an assessment will be conducted to estimate the capacity and identify the gaps in supplies and equipment.
Evidence-based quantification of the supplies and equipment will be used to procure these essential items. A close follow-up system will be established for procurement and distribution of these items. Appraisal of existing anesthe-sia drugs for safety and effectiveness will be performed and, as necessary, newer and safer anesthesia drugs will be introduced into the system. A number of standardized tools will be introduced to assist health facilities to conduct regular inventories of the critical supplies and medical equipment.
Strategic Objectives1. To ensure that health centers and hospitals are equipped with the standard list of surgical and anesthesia equip-
ment according to the SaLTS equipment list and standard operating procedures and protocols to enable the provision of essential and emergency anesthesia care.
2. To ensure that required consumables are available in a timely way at each level and that supply chain manage-ment for pharmaceuticals is in place for essential and emergency surgical and anesthetic care the standard for health centers and hospitals.
3. To ensure there are centers for medical equipment maintenance and innovation.
4. To ensure that safe anesthesia drugs and consumables are available in the health care delivery system.
5. To ensure that a standard audit tool and monitoring guidelines for quality SaLTS are used across the entire region.
Major initiatives 2009 2010 2011 2012 2013
Develop comprehensive package of equipment, medicine and consumables for national essential and safe surgery package.
X
Procure and distribute essential OR and related infrastructure and supplies to the already established and newly constructed hospitals.
X X X X X
Quantify, forecast and procure comprehensive package of equipment, medicine and consumables for national essential and safe surgery package.
X X X X
Establish national safe surgery and anesthesia procurement and supply technical advisory committee inclusive of all stakeholders including professional societies.
X
Provide need based capacity-building training for all regions on pharmaceutical chain management.
X X X
Mobilize financial, material, and technical resources. X X X X X
Encourage and support local investors to produce surgical and anesthetic supplies that can be manufactured in country.
X X X X X
Distribute procured pharmaceutical items in a timely manner. X X X X X
Conduct mid-project review meeting with stakeholders. X X
Conduct supportive supervision in the hospitals to audit the newly distributed equipment and gadgets
X X X X X
Ethiopian Calender

16 National Five-Year Safe Surgery Strategic Plan
Strategic Pillar Four: Excellence in Human Resource DevelopmentThe surgical workforce is the most important component of the SaLTS strategy. The availability of a motivated and competent surgical workforce is key to the success of the SaLTS initiative. A rapid analysis of the existing work-force, including identifying opportunities and potential challenges, needs to be conducted.
To ensure equitable distribution of competent health workers, innovative approaches will be introduced. Strategies for maximizing the efficiency of the existing workforce will be developed and implemented.
Evidence-based approaches such as task sharing and task shifting will be utilized meticulously. Leveraging high-level hospitals to support lower-level health facilities under them will be structured and highly encouraged. There will also be frequent capacity-building trainings at all levels based on the gaps identified.
The concept of compassionate, respectful and caring health professionals will be the main agenda and, as such, mechanisms for continuous engagement with the surgical workforce at all levels will be designed, and a motivation and recognition system will be implemented. In areas where there is an acute shortage of a skilled surgical work-force, strategies such as medical campaigns and surgical missions will be strengthened in the interim.
Strategic Objectives1. To ensure availability of surgical team in all primary, general and tertiary hospitals.
2. To ensure the motivation and retention of workforce for SaLTS through effective and efficient mechanism of surgical taskforce.
3. To ensure that qualified and certified health care providers deliver essential and emergency surgical and anes-thetic care.
4. To ensure and support all efforts toward capacity-building for productivity of surgical team.
5. To ensure compassionate, respectful and caring surgical health workforce (CRC).
6. To ensure bottlenecks are adequately managed
Strategies for Objectives
1. Increase availability of essential surgical team (focusing on anesthesia, IESO and OR nursing professionals).
¡ Implement strategies to increase surgical specialties:
• Partner with the College of Surgeons of East, Central, and Southern Africa (COSECSA).• Support medical schools to increase trainee pool.• Explore the establishment of additional specialty training centers.• Pair institutions.
¡ Implement task shifting.
• IESO are trained in emergency obstetric and surgical conditions at the primary care level• Anesthesia technician/Level 5 will fill the significant anesthesia professionals gap• Clinical nurses - Perioperative nursing technical and non-technical update trainings
¡ Implement task sharing
• Integrate leadership competencies into existing curricula of key forces.
17National Five-Year Safe Surgery Strategic Plan
• Conduct induction training on NTS (inter-professional collaboration) before deployment.• Review OR nurses curriculum to integrate post-anesthesia care unit and central sterilization room (CSR) competencies –• Select OR managers short term training.
¡ Maximize current enrollment of key surgical taskforce through innovative solutions:
• Introduce simulation laboratory. • Encourage cognitive apprenticeship (expanding clinical practice site).• Improve partnership with private sector. • Avail required infrastructure and teaching and learning materials • Promote and advocate new cadre.
¡ Create new essential surgical cadre.
• Emergency surgery physician • OR managers (post-grad)• Anesthesia technicians• OR/perioperative nurse (post-grad)• IESO future career structure • OR technician
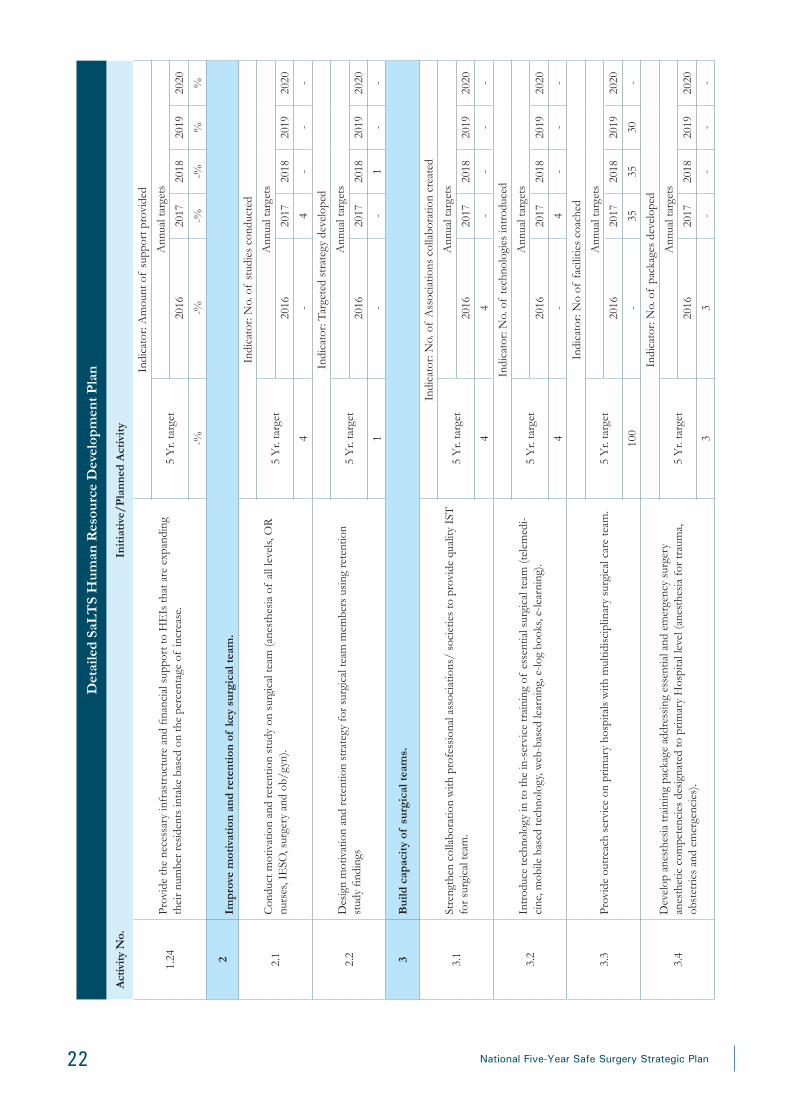
2. Improve motivation and retention of key surgical team.
• Conduct professional development activities.
• Conduct motivation and retention study.
• Design motivation and retention strategies for key SaLTS surgical teams
• Establish career and incentive packages for new cadres.
• Link the human resources motivation strategy with the CRC movement
• Support the accreditation of surgical workforce.
3. Build capacity of surgical task force.
• Provide short-term training, including OR leadership and management.
• Use technology for learning (online training, telemedicine)
• Conduct on-the-job training
• Establish a system of mentorship and coaching.
• Provide long-term training to advance the technical and managerial skills of the surgical team.
• Work collaboratively with professional associations to provide quality in-service training (IST) – sustain-ability.
• Ensure quality of IST-training package.
4. Increase productivity of surgical team.
• Conduct technical update trainings and experience sharing, including NTS.
• Implement day care surgery.
• Explore and implement multiple shift surgery.
• Utilize the private wing initiative to benefit the surgical team
• Conduct surgical campaigns
• Identify, officially recognize and award champions.
• Prepare and implement benefit and incentive packages.

18 National Five-Year Safe Surgery Strategic Plan
5. Balance deployment by offering privileges and incentives for those assigned to remote areas.
6. Improve quality of surgical care.
• Create a simulation lab in lead hospitals.
• Establish educational standards for pre-service education.
• Develop and implement practice standards.
• Create a licensure examination.
• Use a facility quality improvement tool.
• Review anesthetist competencies addressed in the pre-service education curriculum.
• Implement an organized coaching and mentorship system at all levels
Bottlenecks• Critical shortage of key surgical team (IESO, anesthesia provider and OR nurses).
• Inadequate skill mix of existing professionals.
• Lack of systemic human resources management system.
• Flexibility in including additional cadres of health workers in to the surgical system for e.g. - OR manager
• Challenges in developing career structure.

19National Five-Year Safe Surgery Strategic Plan
Det
aile
d Sa
LT
S H
uman
Res
ourc
e D
evel
opm
ent P
lan
Act
ivity
No.
Init
iativ
e/P
lann
ed A
ctiv
ity
1In
crea
se a
vaila
bilit
y of
ess
enti
al s
urgi
cal t
eam
(fo
cusi
ng o
n an
esth
esia
, IE
SO a
nd O
R n
ursi
ng p
rofe
ssio
nals
).
1.1
In p
artn
ersh
ip w
ith th
e M
inis
try
of E
duca
tion
, hig
her e
duca
tion
inst
itutio
ns (H
EIs
) an
d so
ciet
ies,
enco
urag
e re
view
of
surg
ical
team
cur
ricul
a to
inte
grat
e no
n-te
chni
cal
skill
s co
mpe
tenc
ies
incl
udin
g et
hics
, med
ical
law
in E
thio
pia,
rese
arch
met
hodo
logy
, ta
rget
ed le
ader
ship
and
man
agem
ent (
anes
thes
ia a
ll le
vels,
IE
SO, O
R n
urse
, sur
gery
and
ob
/gyn
spe
cial
ties)
.
Indi
cato
r: N
umbe
r of
curr
icul
a re
view
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
70
43
00
1.2
Det
erm
ine
surg
ical
wor
kfor
ce re
quire
d fo
r nex
t 10
year
s (a
nest
hesi
olog
ists
, ane
sthe
tists
, su
rgeo
ns, o
bste
tric
ians
, OR
nur
ses
and
othe
rs).
Indi
cato
r: W
orkf
orce
dev
elop
men
t doc
umen
t pre
pare
d
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
1-
--
--
1.3
Des
ign
indu
ctio
n tr
aini
ng o
n no
n-te
chni
cal s
kills
, saf
e su
rger
y, C
RC
, and
eth
ical
car
e fo
r ne
wly
gra
duat
ing
surg
ical
team
bef
ore
depl
oym
ent (
all t
eam
s m
embe
rs a
s on
e).
Indi
cato
r: N
o. o
f gr
adua
tes
trai
ned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
1,50
030
030
030
030
0
1.4
Rev
iew
OR
nur
ses
(BSc
or M
Sc) c
urric
ulum
to in
tegr
ate
Post
-Ane
sthe
sia
Car
e U
nit a
nd
(CSR
) com
pete
ncie
s.
Indi
cato
r: C
urric
ulum
revi
ewed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
22
--
--
1.5
Des
ign
and
prov
ide
shor
t-te
rm tr
aini
ng o
n O
R m
anag
emen
t for
iden
tified
sur
gica
l tea
m
mem
bers
from
diff
eren
t hos
pita
ls (n
atio
nally
).
Indi
cato
r: N
o. o
f H
ospi
tals
hav
ing
trai
ned
staf
f
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
500
-10
010
010
010
0
1.6
Stre
ngth
en s
kill
deve
lopm
ent l
abs
of (H
ighe
r Edu
catio
n In
stitu
tions
) HE
Is to
pro
vide
.
Indi
cato
r: N
o. o
f la
bs s
tren
gthe
ned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
14-
33
44
1.7
Prov
ide
shor
t-ter
m te
chni
cal u
pdat
e tra
inin
g (o
n pr
e-op
pre
para
tion,
pos
t-ane
sthe
sia c
are
unit,
CSR
(Cen
tral S
teril
izat
ion
Serv
ices
) and
scru
b) fo
r clin
ical
nur
ses w
orki
ng in
OR
.
Indi
cato
r: N
o. o
f nu
rses
trai
ned
from
3 a
reas
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
1,00
0-
200
200
200
200

20 National Five-Year Safe Surgery Strategic Plan
Det
aile
d Sa
LT
S H
uman
Res
ourc
e D
evel
opm
ent P
lan
Act
ivity
No.
Init
iativ
e/P
lann
ed A
ctiv
ity
1.8
Prom
ote
pre-
serv
ice
educ
atio
n ho
spita
l-bas
ed tr
aini
ng (c
ogni
tive
appr
entic
eshi
p) a
mon
g tr
aini
ng in
stitu
tions
to in
crea
se e
nrol
lmen
t.
Indi
cato
r: N
o. o
f H
EIs
impl
emen
ting
the
stra
tegy
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
14-
14-
--
1.9
Prov
ide
finan
cial
sup
port
for H
EIs
to im
plem
ent h
ospi
tal-b
ased
pre
-ser
vice
edu
catio
n tr
aini
ng (c
ogni
tive
appr
entic
eshi
p).
Indi
cato
r: N
o. o
f H
EIs
sup
port
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
5-
-2
3-
1.10
Supp
ort H
EIs
to s
ign
mem
oran
dum
of
unde
rsta
ndin
g w
ith p
rivat
e se
ctor
s to
cre
ate
addi
tiona
l tra
inin
g si
tes
for s
urge
ons,
obst
etric
ians
, ane
sthe
sia,
OR
nur
se a
nd I
ESO
st
uden
ts.
Indi
cato
r: N
o. o
f m
emor
anda
of
unde
rsta
ndin
g si
gned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
30-
1515
--
1.11
Con
duct
pro
mot
ion
of s
urgi
cal t
eam
mem
bers
(ane
sthe
siol
ogy,
OR
nur
sing
, Lev
el 5
an
esth
esia
and
IE
SO).
Indi
cato
r: N
o. o
f pr
omot
ions
con
duct
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
20-
55
55
1.12
Ava
il re
quire
d in
fras
truc
ture
and
teac
hing
and
lear
ning
mat
eria
ls in
HE
Is p
rovi
ding
su
rgic
al te
am tr
aini
ng.
Indi
cato
r: N
o. o
f te
achi
ng in
stitu
tions
sup
port
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
144
44
2
1.13
Enc
oura
ge a
nd a
ssis
t 10
univ
ersi
ties
to s
tart
BSc
pro
gram
in a
nest
hesi
a.
Indi
cato
r: N
o of
new
BSc
pro
gram
s st
arte
d
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
10-
43
3-
1.14
Supp
ort H
EIs
to s
tart
ane
sthe
siol
ogy
resi
denc
y pr
ogra
m.
Indi
cato
r: N
o. o
f H
EIs
sta
rtin
g pr
ogra
m
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
51
22
-
1.15
Dev
elop
an
MSc
pro
gram
cur
ricul
um in
OR
man
agem
ent t
o tr
ain
OR
man
ager
s.
Indi
cato
r: Ta
rget
ed c
urric
ulum
dev
elop
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
11
--
--

21National Five-Year Safe Surgery Strategic Plan
Det
aile
d Sa
LT
S H
uman
Res
ourc
e D
evel
opm
ent P
lan
Act
ivity
No.
Init
iativ
e/P
lann
ed A
ctiv
ity
1.16
Supp
ort H
EIs
to s
tart
MSc
pro
gram
in O
R m
anag
emen
t.
Indi
cato
r: N
o. o
f gr
adua
tes
trai
ned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
150
-25
5050
50
1.17
Dev
elop
an
MSc
pro
gram
cur
ricul
um in
OR
and
per
iope
rativ
e nu
rsin
g to
trai
n O
R
nurs
es in
per
iope
rativ
e/O
R n
ursi
ng.
Indi
cato
r: Ta
rget
ed c
urric
ulum
dev
elop
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
1-
1-
--
1.18
Trai
n O
R n
urse
s in
MSc
in O
R n
ursi
ng/p
erio
pera
tive
nurs
ing.
Indi
cato
r: N
o. o
f gr
adua
tes
trai
ned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
500
100
100
100
100
100
1.19
Enc
oura
ge th
e ex
istin
g an
esth
esio
logy
resi
denc
y pr
ogra
m fo
r int
ake.
Indi
cato
r: N
umbe
r of
trai
nees
enr
olle
d
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
3-
--
--
1.20
Dev
elop
a s
trat
egic
pla
n fo
r IE
SO fu
ture
car
eer.
Indi
cato
r: Ta
rget
ed c
urric
ulum
dev
elop
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
1-
-1
--
1.21
Exp
and
the
CO
SEC
SA b
ased
trai
ning
of
gene
ral s
urge
ons
in th
e co
untr
y.
Indi
cato
r: N
o. n
ew p
rogr
ams
open
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
152
33
34
1.22
Enc
oura
ge e
xist
ing
surg
ery
and
obst
etric
resi
denc
y pr
ogra
ms
to in
crea
se th
eir a
nnua
l in
take
.
Indi
cato
r: Pe
rcen
tage
of
incr
ease
in u
ptak
e
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
100%
20%
20%
20%
20%
20%
1.23
Enc
oura
ge n
ew H
EIs
to c
omm
ence
resi
denc
y pr
ogra
ms
in s
urge
ry a
nd o
bste
tric
s.
Indi
cato
r: N
umbe
r of
new
pro
gram
s op
ened
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
10-%
22 National Five-Year Safe Surgery Strategic Plan
Det
aile
d Sa
LT
S H
uman
Res
ourc
e D
evel
opm
ent P
lan
Act
ivity
No.
Init
iativ
e/P
lann
ed A
ctiv
ity
1.24
Prov
ide
the
nece
ssar
y in
fras
truc
ture
and
fina
ncia
l sup
port
to H
EIs
that
are
exp
andi
ng
thei
r num
ber r
esid
ents
inta
ke b
ased
on
the
perc
enta
ge o
f in
crea
se.
Indi
cato
r: A
mou
nt o
f su
ppor
t pro
vide
d
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
-%-%
-%-%
%%
2Im
prov
e m
otiv
atio
n an
d re
tent
ion
of k
ey s
urgi
cal t
eam
.
2.1
Con
duct
mot
ivat
ion
and
rete
ntio
n st
udy
on s
urgi
cal t
eam
(ane
sthe
sia
of a
ll le
vels,
OR
nu
rses
, IE
SO, s
urge
ry a
nd o
b/gy
n).
Indi
cato
r: N
o. o
f st
udie
s co
nduc
ted
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
4-
4-
--
2.2
Des
ign
mot
ivat
ion
and
rete
ntio
n st
rate
gy fo
r sur
gica
l tea
m m
embe
rs u
sing
rete
ntio
n st
udy
findi
ngs
Indi
cato
r: Ta
rget
ed s
trat
egy
deve
lope
d
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
1-
-1
--
3B
uild
cap
acit
y of
sur
gica
l tea
ms.
3.1
Stre
ngth
en c
olla
bora
tion
with
pro
fess
iona
l ass
ocia
tions
/ so
ciet
ies
to p
rovi
de q
ualit
y IS
T
for s
urgi
cal t
eam
.
Indi
cato
r: N
o. o
f A
ssoc
iatio
ns c
olla
bora
tion
crea
ted
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
44
--
--
3.2
Intr
oduc
e te
chno
logy
in to
the
in-s
ervi
ce tr
aini
ng o
f es
sent
ial s
urgi
cal t
eam
(tel
emed
i-ci
ne, m
obile
bas
ed te
chno
logy
, web
-bas
ed le
arni
ng, e
-log
book
s, e-
lear
ning
).
Indi
cato
r: N
o. o
f te
chno
logi
es in
trod
uced
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
4-
4-
--
3.3
Prov
ide
outr
each
ser
vice
on
prim
ary
hosp
itals
with
mul
tidis
cipl
inar
y su
rgic
al c
are
team
.
Indi
cato
r: N
o of
faci
litie
s co
ache
d
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
100
-35
3530
-
3.4
Dev
elop
ane
sthe
sia
trai
ning
pac
kage
add
ress
ing
esse
ntia
l and
em
erge
ncy
surg
ery
anes
thet
ic c
ompe
tenc
ies
desi
gnat
ed to
prim
ary
Hos
pita
l lev
el (a
nest
hesi
a fo
r tra
uma,
ob
stet
rics
and
emer
genc
ies)
.
Indi
cato
r: N
o. o
f pa
ckag
es d
evel
oped
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
33
--
--

23National Five-Year Safe Surgery Strategic Plan
Det
aile
d Sa
LT
S H
uman
Res
ourc
e D
evel
opm
ent P
lan
Act
ivity
No.
Init
iativ
e/P
lann
ed A
ctiv
ity
3.5
Prov
ide
tech
nica
l upd
ate
trai
ning
on
anes
thes
ia fo
r tra
uma,
obs
tetr
ics
and
emer
genc
y pr
oced
ures
at p
rimar
y ho
spita
l lev
el.
Indi
cato
r: N
o. o
f an
esth
etis
ts tr
aine
d
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
200
-10
010
0-
-
3.6
Prov
ide
trai
ning
of
trai
ners
trai
ning
in m
ento
ring
and
coac
hing
for s
enio
r sur
gica
l tea
m
that
will
pro
vide
coa
chin
g an
d m
ento
ring
visi
ts (e
qual
pro
port
ion
of a
nest
hesi
a pr
ofes
-si
onal
s, su
rgeo
ns a
nd o
b/gy
n).
Indi
cato
r: N
o. o
f pr
ofes
sion
als
trai
ned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
360
-12
012
012
0-
3.7
Prov
ide
coac
hing
and
men
torin
g tr
aini
ng fo
r sen
ior s
urgi
cal t
eam
pla
nned
to b
e in
volv
ed
in c
oach
ing
and
men
torin
g vi
sits
.
Indi
cato
r: N
o. o
f st
affs
ass
igne
d as
coa
ch
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
360
-12
012
012
0-
3.8
Prov
ide
SaLT
S le
ader
ship
and
man
agem
ent t
rain
ing
for n
atio
nal a
nd re
gion
al T
WG
m
embe
rs.
Indi
cato
r: N
o. o
f pr
ofes
sion
als
trai
ned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
155
33
31
3.9
Prov
ide
SaLT
S le
ader
ship
and
man
agem
ent t
rain
ing
for n
atio
nal a
nd re
gion
al p
roje
ct
team
mem
bers
.
Indi
cato
r: N
o. o
f pr
ofes
sion
als
trai
ned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
5010
1010
1010
4In
crea
se p
rodu
ctiv
ity
of s
urgi
cal t
eam
.
4.1
Perf
orm
ance
-bas
ed re
cogn
ition
for s
urgi
cal t
eam
mem
bers
exc
eedi
ng s
et ta
rget
pro
ce-
dure
num
ber.
Indi
cato
r: N
o. o
f te
ams
reco
gniz
ed e
xcee
ding
targ
et
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
160
-40
4040
40
4.4
Perf
orm
ance
-bas
ed re
cogn
ition
for b
est f
acili
ty in
impl
emen
ting
SALT
initi
ativ
e.
Indi
cato
r: N
o. F
acili
ty re
cogn
ized
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
4010
1010
10

24 National Five-Year Safe Surgery Strategic Plan
Det
aile
d Sa
LT
S H
uman
Res
ourc
e D
evel
opm
ent P
lan
Act
ivity
No.
Init
iativ
e/P
lann
ed A
ctiv
ity
4.5
Dev
elop
com
preh
ensiv
e tr
aini
ng p
acka
ge o
n da
y ca
re s
urge
ry a
nd a
nest
hesi
a.
Indi
cato
r: Ta
rget
ed p
acka
ge d
evel
oped
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
11
--
--
4.6
Bas
ed o
n de
velo
ped
trai
ning
pac
kage
, pro
vide
trai
ning
for m
ulti-
disc
iplin
ary
surg
ical
te
am m
embe
rs o
n da
y ca
re s
urge
ry a
nd a
nest
hesi
a.
Indi
cato
r: N
o. o
f Pr
ofes
sion
als
trai
ned
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
500
-80
140
140
140
4.7
Supp
ort l
ead
hosp
itals
to in
itiat
e da
y ca
re s
urge
ry.
Indi
cato
r: N
o. o
f H
ospi
tals
pro
vidi
ng d
ayca
re s
urge
ry p
er s
tand
ard
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
103
34
-
5Im
prov
e qu
alit
y of
sur
gica
l car
e.
5.1
Ass
ist H
EIs
to d
evel
op s
imul
atio
n la
b in
lead
hos
pita
ls.
Indi
cato
r: N
o. o
f si
mul
atio
ns d
evel
oped
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
10-
43
3-
5.2
Supp
ort t
he S
SE in
dev
elop
ing
a B
oard
of
Surg
ical
Spe
cial
ties
unde
r the
FM
OH
.
Indi
cato
r: B
oard
est
ablis
hed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
1-
1-
--
5.3
Supp
ort a
nest
hesi
olog
y so
ciet
y in
sta
ndar
dizi
ng th
e tr
aini
ng o
f an
esth
esio
logi
sts
in th
e co
untr
y.
Indi
cato
r: St
anda
rd c
urric
ulum
dev
elop
ed
5 Y
r. ta
rget
Ann
ual t
arge
ts
2016
2017
2018
2019
2020
1-
1-
--

25National Five-Year Safe Surgery Strategic Plan
Planned number health professionals to be trained
Activity No. Initiative/Planned Activity 5 Year targetAnnual target
2016 2017 2018 2019 2020
1 General surgeon 750 150 150 150 150 150
2 OB/GYN specialist 750 150 150 150 150 150
3 Anesthesiologist 100 20 20 20 20 20
4 Anesthetist 2,000 400 400 400 400 400
5 Scrub nurse 2,000 400 400 400 400 400
6 Recovery room nurse 2,000 400 400 400 400 400
7 OR manager 200 40 40 40 40 40
8 IESO 500 100 100 100 100 100
9 Dental surgeon 100 20 20 20 20 20
10 Ophthalmologist 200 40 40 40 40 40
11 Ophthalmology nurse 1,000 200 200 200 200 200
12 Orthopedists 150 30 30 30 30 30
15 Chest surgeon 15 3 3 3 3 3
16 Pediatric surgeon 20 5 5 5 5 5
17 Neurosurgeon 50 10 10 10 10 10
18 ENT Surgeon 50 10 10 10 10 10
19 Urologist 50 10 10 10 10 10
20 Plastic surgeon 25 5 5 5 5 5
21 OR technician 250 50 50 50 50 50
26 National Five-Year Safe Surgery Strategic Plan
Strategic Pillar Five: Excellence in Advocacy and PartnershipExcellence in advocacy and partnership signifies that all stakeholders, including leaders at the FMOH and MOF, health care professionals (via training centers, universities, professional societies, etc.), partners, and the public (via health workers and the media), are aware of SaLTS and the national priority around improving safe surgery, and that SaLTS has sufficient partner engagement for implementation alongside the FMOH.
Strategic Objectives1. To ensure increased awareness of SaLTS among FMOH and MOF staff, health care professionals (both inside
and outside of surgery) and the general public.
2. To mobilize the surgical workforce as part of this movement, with every surgical professional (including sur-geons, OBGYNS, anesthetists, and nurses).
3. To increase the number of partners as well as investment by each partner in surgery in Ethiopia.
ComponentsAwareness
• Promote advocacy to key stakeholders within the FMOH and Ministry of Finance (MOF) as well as to health care management to inform them of SaLTS.
• Build awareness through a campaign to target health care professionals both directly working in surgery as well as more broadly working on maternal, newborn and child health issues (i.e., health service managers, surgeons, health workers, health trainees, and professional associations)
• Conduct a mass media campaign to target broader public (i.e., communities, patients).
Partner Engagement
• Divide responsibilities across core partners to ensure appropriate support for each SaLTS pillar.
• Cultivate additional partners to ensure necessary support for SaLTS strategy.
• Establish institutional arrangement for partner engagement .e.g. strengthening of Technical Working Groups for SaLTS at national and regional levels.
Structure • Awareness: The project team at the FMOH will take ownership over executing the awareness building
campaign and mass media campaign. They will design these campaigns in close collaboration with the SaLTS TWG and with approval from the executive team. The campaigns will then be rolled out with key partners, including the professional societies, universities and the mass media, as well as via quarterly pub-lic forums.
Partner engagement: The SaLTS TWG will be the primary means of engagement for core safe surgery partners in Ethiopia. On an ongoing basis, this group will monitor levels of partner support relative to strategic priorities across the eight SaLTS pillars and determine if additional support is necessary in any
27National Five-Year Safe Surgery Strategic Plan
particular area. When significant gaps in support for SaLTS become apparent, members of the TWG alongside the executive team will seek additional funders or partners to fill the identified gaps.
Identified InterventionsAdvocacy to create and increase awareness on SaLTSThe FMOH will develop standard SaLTS communication materials to update people on the importance of safe surgery in Ethiopia, as well as SaLTS objectives, pillars and activities. This effort will be completed as soon as possible in 2016. These communication materials should include: a two-page overview document, a key message document for surgical leaders and the full strategy document.
• The FMOH, in collaboration with key disseminating bodies like the RHBs, societies, and universities, will disseminate communication materials via key channels, including but not limited to, RHBs, professional society networks and meetings (including societies for surgeons, anesthetists, emergency surgical officers, ob/gyn, ophthalmologists, plastic surgeons and nurses), and university teaching facilities, among others. This dissemination will be completed within the first six months of strategy in 2016.
• The FMOH in collaboration with societies and media, will identify key public meetings where SaLTS should be shared, most likely the Annual Review Meeting, regional public forums, and larger health meet-ings in the country and seek media coverage at these forums to ensure that articles are written and news coverage is televised. This activity will be completed as soon as possible in 2016 but then carried out as events occur.
Partner Engagement• The FMOH will convene partners regularly (i.e., monthly in the first six months of SaLTS, and then quar-
terly) as part of the TWG to discuss progress against the SaLTS strategy, and identify any gaps or areas for further work. The TWG is recommended to be composed of at least 1-2 partners from each level of work (e.g., global/regional, national and local), but likely should not include all partners given the large group. Partners that are investing the most amount of time and resources to SaLTS should be prioritized for for-mal representation on the TWG while other partners should be asked for input on an ongoing basis.
• The FMOH will convey through the TWG meetings the most important areas for additional partner sup-port based on shifting priorities and gaps and then helps attract partners to core areas.
• As of early 2016, the core partners working with the FMOH on SaLTS include: at the global/regional level, the GE Foundation, Safe Surgery 2020, the Lancet Commission for Safe Surgery, the Harvard Program for Global Surgery and Social Change, G4 Alliance, the World Health Organization, and COSECSA; at the national level, Jhpiego, CHAI, AMREF, MSH, the World Health Organization, and a number of relevant professional societies and associations (i.e., Ethiopian Surgical Society, Anesthesia Society, etc.); and, at the local level, RHBs and local universities. Many of the global and national partners are also engaging deeply at the regional level. The table below shows in more detail which partners will be working to support which pillars.
Measurement/IndicatorsMeasuring awareness and partner engagement is inherently more challenging than measuring other aspects of this SaLTS strategy. Thus, the indicators outlined below should be considered a starting point to understand relative progress in these areas, but other signals of increased awareness and partner engagement may also become relevant over time.
• Awareness: FMOH will track annually the number of SaLTS overview materials distributed; number of in-bound requests regarding SaLTS that come to the FMOH; number of public media mentions (in articles/TV shows).

28 National Five-Year Safe Surgery Strategic Plan
• Partner engagement: FMOH will track the total resources committed across partners; number of new partners that join SaLTS TWG.
Monitoring and EvaluationThis area of the strategy only requires light monitoring and evaluation. It is recommended that the above indicators are tracked on a more continual basis. Once a year, when the broader SaLTS strategy is reviewed, progress on these indicators should also be reviewed.
Strategic Result • Federal: Increased awareness of SaLTS program and increased investment from partners to support the
program and to improve surgical outcomes more broadly across Ethiopia.
• Regional, Zonal and Woreda: Increased awareness of SaLTS program and increased investment from re-gions / zones / woreda as well as other partners to support the program and to improve surgical outcomes more broadly in the regions
• University: Increased awareness of SaLTS and increased investment by universities to train surgical profes-sionals
• Health facilities: Increased awareness of SaLTS and increased investment by facility leadership in surgical infrastructure and equipment

29National Five-Year Safe Surgery Strategic Plan
Maj
or I
niti
ativ
es20
0920
1020
1120
1220
13
Iden
tify
and
enga
ge k
ey lo
cal a
nd in
tern
atio
nal p
artn
ers
that
will
sup
port
the
safe
sur
gery
and
ane
sthe
sia
care
pro
gram
.X
XX
XX
Dev
elop
nat
iona
l adv
ocac
y an
d pa
rtne
rshi
p m
anag
emen
t gui
delin
es.
XX
XX
X
Supp
ort a
nd p
rom
ote
activ
e en
gage
men
t of
loca
l sur
gica
l and
ane
sthe
sia
prof
essi
onal
soc
ietie
s in
SaL
TS
impl
emen
tatio
n at
all
leve
ls.X
XX
XX
Rec
ogni
ze a
nd a
war
d be
st p
erfo
rmin
g lo
cal p
rofe
ssio
nal s
ocie
ties.
XX
XX
X
Mak
e “S
afe
surg
ical
and
ane
sthe
sia
care
dis
cuss
ion”
a s
tand
ing
agen
da it
em b
oth
in n
atio
nal a
nd re
gion
al p
erfo
rman
ce m
eetin
gs.
XX
XX
X
Est
ablis
h na
tiona
l and
regi
onal
par
tner
s fo
rum
that
will
sup
port
the
safe
sur
gery
and
ane
sthe
sia
care
pro
gram
. X
XX
XX
Stre
ngth
en in
tern
atio
nal p
artn
ersh
ips
with
sur
gica
l and
ane
sthe
sia
prof
essi
onal
soc
ietie
s, co
llege
s an
d do
nors
. X
XX
XX
Stre
ngth
en a
nd e
xpan
d th
e C
OSE
CSA
bas
ed tr
aini
ng o
f su
rgeo
ns.
XX
XX
X
Inte
grat
e a
natio
nal a
dvoc
acy
live
TV
and
radi
o pr
ogra
ms
XX
XX
X
Impl
emen
t the
nat
iona
l adv
ocac
y an
d pa
rtne
rshi
p gu
idel
ine
acro
ss th
e co
untr
y X
XX
XX
Supp
ort a
nd m
onito
r act
ive
enga
gem
ent a
nd fu
nctio
nalit
y of
pro
fess
iona
l soc
ietie
s an
d fo
rum
s X
XX
XX
Con
duct
qua
rter
ly n
atio
nal a
nd re
gion
al p
artn
er fo
rum
s X
XX
XX
Supp
ort a
nd e
ncou
rage
act
ive
enga
gem
ent o
f lo
cal p
rofe
ssio
nal s
ocie
ties
thro
ugh
build
ing
thei
r fina
ncia
l, m
ater
ial,
lead
ersh
ip a
nd m
anag
emen
t cap
aciti
es
XX
XX
X
Part
ner w
ith lo
cal p
rofe
ssio
nal s
ocie
ties
and
part
ners
for e
ffec
tive
and
effic
ient
impl
emen
tatio
nX
XX
XX
Part
icip
ate
in in
tern
atio
nal p
rofe
ssio
nal s
ocie
ties
conf
eren
ce/m
eetin
g an
d sh
arin
g E
thio
pian
exp
erie
nces
of
safe
sur
gica
l and
ane
sthe
sia
care
pro
gram
impl
e-
men
tatio
n an
d br
ing
new
inte
rnat
iona
l exp
erie
nces
X
XX
XX
Stre
ngth
en in
tern
atio
nal p
artn
ersh
ips
with
sur
gica
l and
ane
sthe
sia
prof
essi
onal
soc
ietie
s, co
llege
s an
d do
nors
X
XX
XX
Org
aniz
e na
tiona
l ann
ual s
umm
it on
“E
thio
pian
Saf
e Su
rgic
al a
nd A
nest
hesi
a C
are
Prog
ram
”X
XX
XX
Eth
iopi
an C
alen
der

30 National Five-Year Safe Surgery Strategic Plan
Strategic Pillar Six: Excellence in Quality and SafetyQuality and safety are essential components of the provision of surgical and anesthesia care.
Patient safety issues in Ethiopia include: death, disability (uncontrolled disability, seizure,) infection, fall injury, wrong site, wrong limb, and wrong person surgery, theft of personal materials during death care, psychological trauma, wrong medication. Of all medical errors reported, the largest proportion happened in in OR. Safety of surgical team (PEP, Hepatitis, physical protection) is also an important issue.
The national health care quality strategy has identified six dimensions of quality. These include Safety, efficiency, effectiveness, person-centered care, timeliness of care and equity .Relevant activities will be implemented in accor-dance with the dimensions of quality in health care. SaLTS will implement interventions to improve quality and safety outcomes.
Objective 1: Improve efficiency in surgical and anesthesia care.Major Activities:1. Plan surgical intervention for each procedure (cost, supplies, time of surgery, duration of stay and potential discharge time)
2. Prepare package of consumables for each procedure.
3. Establish and ensure adherence of national standards:
a. Set incision time in the morning.
b. Set first case start time-anesthesia.
c. Set time between two patients: turn over time.
d. Decision-to-incision time.
4. Implement a patient scheduling management system.
5. Establish interdepartmental and inter-specialty consultation and coordination mechanism.
6. Introduce shift work in surgery.
7. Improve OR management between departments.
8. Expand OR structure in tertiary hospitals.
9. Implement strategies to enhance productivity of surgical team: plan number of surgeries per surgeon and surgical team considering the case mix.
10. Expand day care surgery.
11. Implement consumption audit for each patient after procedure-checklist.
12. Establish preoperative evaluation clinic-joint evaluation by clinician and anesthetist before admission.
13. Set duration of validity for investigations and laboratory test (e.g., after how long should we order additional tests?).
14. Improve discharge management:
a. Introduce discharge lounge.
b. Set 24/7 discharge and set time after discharge decision within 2 hours.

31National Five-Year Safe Surgery Strategic Plan
Objective 2: Improve effectiveness of surgical and anesthetic care using evidence-based clinical care.
Major Activities 1. Develop and implement standard operating procedures for all surgeries.
2. Establish CPD systems.
3. Establish skill laboratory in major and lead hospitals.
4. Establish a system of clinical mentorship and coaching.
5. Conduct clinical auditing and quality improvement.
6. Develop and implement perioperative guidelines.
7. Develop and implement preoperative assessment guidelines, anesthesia care management
guidelines.
8. Improve patient information, procedure/data documentation.
9. Conduct operational research in surgical care at all levels.
Objective 3: Establish a culture of patient-centered care in the surgical system
Major Activities1. Improve health literacy in surgical and anesthesia care.
2. Strengthen public forums prioritizing surgical care; champions, training.
3. Enhance capacity-building on team building.
4. Implement interventions to improve communication.
a. Between the surgical team and the patient
b. Between the surgical team during difficult scenarios
c. Among colleagues
d. With management and other bodies
5. Develop and implement standard counseling guideline for informed consent and decision.
6. Develop and implement guidelines for person centered surgical care in Ethiopia to address issues like: facility improvement, confidentiality, and student-patient ratio.
7. Establish conflict management of surgical team prioritizing patient.
8. Conduct training on CRC in surgery: attitudinal training.
9. Establish immediate post-surgical briefing system for family and attendants
10. Develop Model of care for multidisciplinary cases: (grand round, clinical board, multidisciplinary specialty outpatient clinic so that patient patients will get all relevant professionals in the same clinic.)
11. Ensure presence of birth companion for cesarean section and consider having mothers close to babies for pediatric surgeries.
32 National Five-Year Safe Surgery Strategic Plan
12. Develop patient transport policy: (who, how on what procedure: nurse to transport assisted by a trained porter.)
13. Implement national pain management guideline for all surgical patients.
14. Assign anesthesia professional and start anesthesia care starting in the outpatient department, inpatient department, preoperative and postoperative care.
15. Ensure clinical governance: authority with responsibility in the medical hierarchy.
16. Ensure the adherence to scope of practice by different professionals.
Objective 4: Improve safety in surgical and anesthesia care.Major Activities:
Improve communication between members of the surgical team
1. Implement safety checklist.
2. Introduce system safe design: transport stretcher improved, site marking, patient identification-name tag; time out: standard operating procedures for each surgery.
3. Introduce safe anesthesia drugs.
4. Use technology that reduces medical error: disposable drape, better transporting.
5. Introduce a system of independent check: verification.
6. Improve teamwork: training and HDA.
7. Establish a safety culture: Just culture establishment through awareness and training.
8. Conduct a clinical audit/death audit.
9. Develop and implement guidelines for medical error disclosure.
10. Capacity-building on medical error management-regular yearly patient safety forums.
11. Compile medical error-database and share with all professionals.
Objective 5: Ensure the provision of timely surgical and anesthesia care for emergency conditions and elective procedures.
Emergencies:
¡ Triage and prioritize cases and standard operating procedure for each case.
¡ Increase awareness on golden hour for injury.
¡ Strengthen pre-hospital care.
¡ Strengthen consultation process.
¡ Strengthen referral process.
¡ Designate ER table-back up.
¡ Set standard decision-to-incision for emergency conditions.
¡ Create a major incidence plan.

33National Five-Year Safe Surgery Strategic Plan
¡ Define critical pathway for each serious condition.
¡ Establish ER waiting list monitoring system.
Elective procedures:¡ Establish waiting list registration and management.
¡ Set time for each procedure-standards.
¡ Plan appropriate human resources, supplies, or tables.
¡ Conduct campaigns and weekend surgeries.
¡ Build capacity of lower facilities: networking and back referral and continuous support, clinical mentoring.
Set national time target for elective surgical procedure.
Objective 6: Ensure equity in surgical and anesthesia care.1. Establish social worker services.
2. Strengthen liaison services.
3. Avail interpretation service where necessary.
4. Improve labeling and sign posts.
5. Establish a system to prioritize people with disabilities.
6. Collect and utilize data on equity dimensions.
7. Develop and implement standards on what kind of cases to be seen by what level of physicians especially in referral cases in teaching facilities.
8. Conduct surgical campaigns.
Major Initiatives 2009 2010 2011 2012 2013
Develop locally adoptable treatment guideline for the essential surgical and anesthesia pro-cedures included in the surgical and anesthesia care package.
X X X X X
Develop and standardize a nationally endorsed quality assurance and audit system in surgi-cal and anesthesia care.
X X X X X
Identify EHAQ LEAD hospitals and establish new hospital clusters. X
Conduct continuous onsite technical capacity-building and clinical mentorship for regional clinical support teams/committees and EHAQ LEAD hospitals and health centers on surgical and anesthesia care.
X X X X X
Develop support package for EHAQ LEAD hospitals and other surgical care facilities on surgical and anesthesia care.
X
Establish clinical support teams/committee on surgical and anesthesia care in all regions. X X
Identify and recognize champions, document and disseminate proven best practices/devel-opment of change package.
X X X X X
Strengthen and promote the national ethical practice guideline for surgical care providers. X X
Implement an adoptable WHO safe surgery checklist at hospitals. X X X
Provide continuous training regarding the ethical practice guideline and the rules and regu-lations regarding ethical and legal surgical and anesthesia care practice.
X X X X
Conduct clinical auditing and death reviews in selected hospitals and health centers. X X X X
Ethiopian Calender
34 National Five-Year Safe Surgery Strategic Plan
Strategic Pillar Seven: Excellence in InnovationsEthiopia is seeking to develop new tools and processes or bring existing tools and processes that are not yet in Ethiopia to address some of the largest identified gaps to improve access to safe surgery in the country. Innovation in this context is defined quite broadly to include any product or tool, process, or item that is new to a particular setting and can help transform the way in which care is delivered in that setting.
Strategic ObjectiveTo increase use of innovations in Ethiopia related to improving safe surgery, either by locally developing these innovations or bringing them to Ethiopia from elsewhere.
ComponentsBased on existing data from hospitals performing surgery, input from a team drafting the SaLTS strategy, as well as extensive baseline assessments of five hospitals in the Tigray region conducted by the Harvard Program in Global Surgery & Social Change, the areas have been identified as priorities for innovation to improve surgical outcomes in Ethiopia. The partner that will be most closely overseeing each priority area is noted in brackets, with certain priority areas still in need of a specific overseeing partner. The table shows the year in which each innovation will be initiated, but these innovations are likely to carry across multiple years.
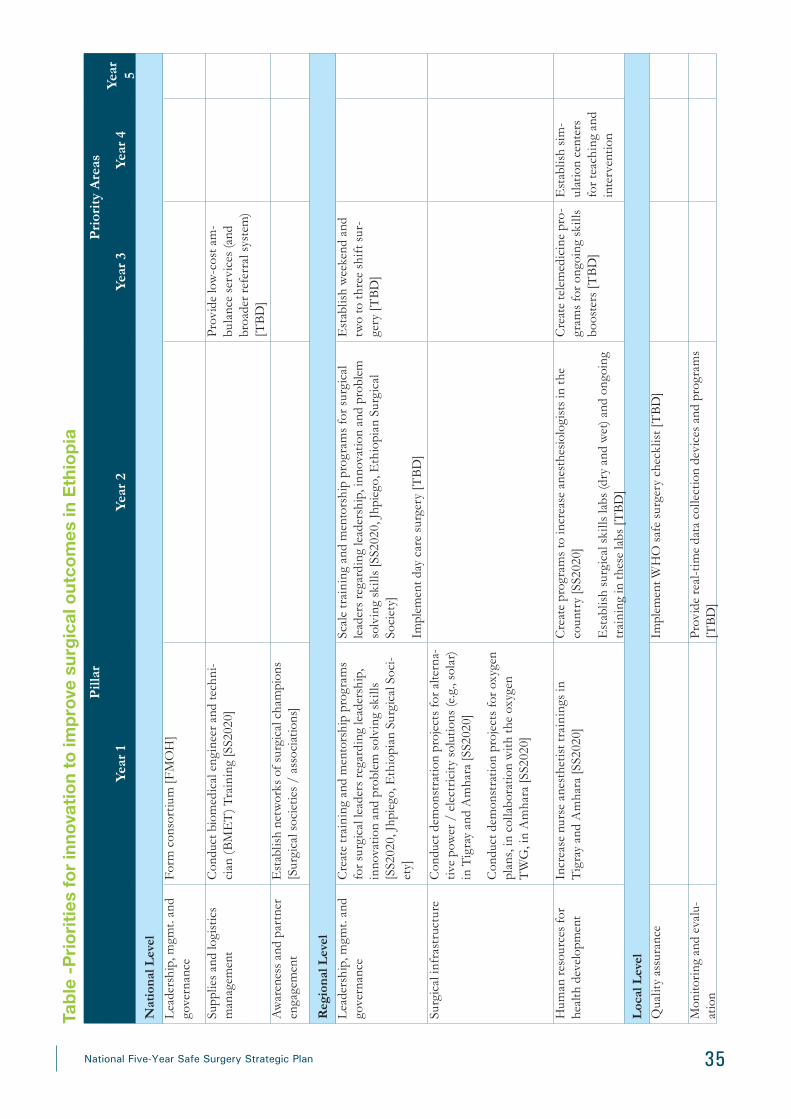
35National Five-Year Safe Surgery Strategic Plan
Tabl
e -P
riorit
ies
for i
nnov
atio
n to
impr
ove
surg
ical
out
com
es in
Eth
iopi
aP
illar
Pri
orit
y A
reas
Year
1Ye
ar 2
Year
3Ye
ar 4
Year
5
Nat
iona
l Lev
el
Lea
ders
hip,
mgm
t. an
d go
vern
ance
Form
con
sort
ium
[FM
OH
]
Supp
lies
and
logi
stic
s m
anag
emen
tC
ondu
ct b
iom
edic
al e
ngin
eer a
nd te
chni
-ci
an (
BM
ET
) Tra
inin
g [S
S202
0]Pr
ovid
e lo
w-c
ost a
m-
bula
nce
serv
ices
(and
br
oade
r ref
erra
l sys
tem
) [T
BD
]A
war
enes
s an
d pa
rtne
r en
gage
men
tE
stab
lish
netw
orks
of s
urgi
cal c
ham
pion
s [S
urgi
cal s
ocie
ties
/ as
soci
atio
ns]
Reg
iona
l Lev
elL
eade
rshi
p, m
gmt.
and
gove
rnan
ceC
reat
e tr
aini
ng a
nd m
ento
rshi
p pr
ogra
ms
for s
urgi
cal l
eade
rs re
gard
ing
lead
ersh
ip,
inno
vatio
n an
d pr
oble
m s
olvi
ng s
kills
[S
S202
0, J
hpie
go, E
thio
pian
Sur
gica
l Soc
i-et
y]
Scal
e tr
aini
ng a
nd m
ento
rshi
p pr
ogra
ms
for s
urgi
cal
lead
ers
rega
rdin
g le
ader
ship
, inn
ovat
ion
and
prob
lem
so
lvin
g sk
ills
[SS2
020,
Jhp
iego
, Eth
iopi
an S
urgi
cal
Soci
ety]
Impl
emen
t day
car
e su
rger
y [T
BD
]
Est
ablis
h w
eeke
nd a
nd
two
to th
ree
shif
t sur
-ge
ry [T
BD
]
Surg
ical
infr
astr
uctu
reC
ondu
ct d
emon
stra
tion
proj
ects
for a
ltern
a-tiv
e po
wer
/ e
lect
rici
ty s
olut
ions
(e.g
., so
lar)
in
Tig
ray
and
Am
hara
[SS2
020]
Con
duct
dem
onst
ratio
n pr
ojec
ts fo
r oxy
gen
plan
s, in
col
labo
ratio
n w
ith th
e ox
ygen
T
WG
, in
Am
hara
[SS2
020]
Hum
an re
sour
ces
for
heal
th d
evel
opm
ent
Incr
ease
nur
se a
nest
hetis
t tra
inin
gs in
T
igra
y an
d A
mha
ra [S
S202
0]C
reat
e pr
ogra
ms
to in
crea
se a
nest
hesi
olog
ists
in th
e co
untr
y [S
S202
0]
Est
ablis
h su
rgic
al s
kills
labs
(dry
and
wet
) and
ong
oing
tr
aini
ng in
thes
e la
bs [T
BD
]
Cre
ate
tele
med
icin
e pr
o-gr
ams
for o
ngoi
ng s
kills
bo
oste
rs [T
BD
]
Est
ablis
h si
m-
ulat
ion
cent
ers
for t
each
ing
and
inte
rven
tion
Loc
al L
evel
Qua
lity
assu
ranc
eIm
plem
ent W
HO
saf
e su
rger
y ch
eckl
ist [
TB
D]
Mon
itori
ng a
nd e
valu
-at
ion
Prov
ide
real
-tim
e da
ta c
olle
ctio
n de
vice
s an
d pr
ogra
ms
[TB
D]

36 National Five-Year Safe Surgery Strategic Plan
Structure
The FMOH will oversee all work within innovation and will source innovation needs from the FMOH data, the TWG, as well as other core surgery partners on a semi-annual basis, which will allow the innovation priority areas listed in Table XX to be updated on an ongoing basis. As the list of innovation priorities is updated, the FMOH will identify appropriate partners to take responsibility for pursuing those innovations.
Identified InterventionFor each of the prioritized areas of innovation above, the FMOH will identify one or two core partners to begin to pursue the innovation and develop a specific plan. Innovations that already have selected partners are listed in the table next to the innovation. The first TWG will work to identify partners to carry forward innovations prioritized for year 1 for those that do not already have a clear owner. After a partner is identified to lead the activity on a specific intervention, they will manage their process in close collaboration with the FMOH and will report back to the TWG every six months.
Measurement/IndicatorsIndicators will be specific to the innovation itself. For example, an innovation that supports leadership training for surgical teams to improve their problem-solving, innovation and communication skills will have very different in-dicators than an innovation to support power and electricity solutions at specific hospitals. Thus, it is recommend-ed that each partner that is implementing a specific innovation intervention should determine their own metrics, in collaboration with the FMOH, at the beginning of implementation and track those metrics over the course of implementation.
Monitoring and EvaluationA specific monitoring and evaluation plan will need to be developed for each innovation intervention to account for variability in the target metrics, method for data collection and frequency of reporting.
Strategic Results ¡ Federal: Improved leadership, management and governance of surgery at a national level; strong asso-
ciations or networks of surgical resources; fewer broken machines (as a result of increased number of BMETs); and strengthened referral process.
¡ Regional, Zonal and Woreda: Improved leadership, management and governance at the regional level, as well as among surgical teams at the hospital level; increased volumes of surgeries being delivered (as a result of day surgeries and weekend shifts); uptake of power and oxygen solutions by government and local public-private partnerships; improved surgical outcomes (as a result of increased numbers and quality of nurse anesthetists and anesthesiologists, increased skills labs, increased simulation centers and uptake of telemedicine).
¡ University: Improved training capacity, including leadership training, nurse anesthetist training, anesthesi-ologist training, and hard skills training.
¡ Health facilities: Improved surgical volumes and outcomes as noted above.

37National Five-Year Safe Surgery Strategic Plan
Major Initiatives 2009 2010 2011 2012 2013
Promote solar panel electric supply to improve electric supply to operating facilities.
X x x x x
Dig local water wells for hospitals. X x x x x
Develop a postoperative patient tracking system. X x
Assist teaching institutions in graduate tracking system. X x
Promote day care surgery in the country. X x x x x
Develop lists of day surgery and their management. X x x x x
Promote advanced anesthesia consultation throughout the coun-try (tele-anesthesia).
X x x x x
Utilize innovative ways of increasing the surgical workforce training capacity.
X x x x x
Establish continuous oxygen supply to selected hospitals. X x x x x
Support and promote day surgery and post-operative patient tracking system.
X x x x x
Support and monitor implementation of surgical and anesthesia graduates tracking system.
x x x
Support and promote effective networks of surgical champions. X x x x x
Low-cost ambulance services for broader referral system. X x x x x
Support and promote effective simulation centers for teaching and intervention.
X x x x x
Ethiopian Calender
Major intiatives for innovation pillar

38 National Five-Year Safe Surgery Strategic Plan
Strategic Pillar Eight: Excellence in Monitoring and Evaluation
SaLTS project M&E FrameworkAim: To improve equitable access to quality and safe essential and emergency surgical and anesthesia care as part of the universal health coverage.
Objectives:
• Implement a nationally coordinated national plan on surgical care
• To define and implement essential surgery package for all levels of the Ethiopian health care delivery system.
• To create better awareness on surgical and anesthesia care with different stakeholders
• To improve the safety of surgical care by implementing the surgical safety check list and improving the safety culture
• Implement quality improvement and audit tool in surgical care
• Proactively identify best practices and scale up rapidly through EHAQ
Major contents of SaLTS M&E frameworkThe SaLTS M&E framework is developed as part and parcel of the national Framework for Hospital Performance
Monitoring and Improvement. The framework have four major components described in table 1 below.
1) The establishment, reporting and review of a core set of hospital KPIs on SaLTS.
2) The facilities will monitor additional site level indicators that are not part of KPI but necessary
for site level decision making
3) Supportive supervision site visits to surgical units of hospitals, led by the respective mentors at
each cluster hospitals and including other bodies such as RHB, MSD or partners as necessary; and
4) Review meetings:
• Regional (or cluster) review meetings between each RHB and all hospitals in the respective Region (or
cluster); and
• MSD and all Regional Curative and Rehabilitative Core Process Teams (CRCPTs) review meet-
ings.

39National Five-Year Safe Surgery Strategic Plan
Table. Key elements of the Hospital Performance Monitoring and Improvement Framework
Element Description
KPIs on SaLTS • A set of core hospital KPIs on SaLTS that meets the needs of Governing Boards, CRCPTs, MSD and the public will streamline reporting processes and prevent dupli-cation of efforts by the different stakeholders. The burden on hospitals will be mini-mized.
• A common set of KPIs on SaLTS will allow hospital performance on surgery to be tracked over time, and comparisons between hospitals and regions can be made
• The KPIs on SaLTS can be used by Governing Boards to monitor hospital perfor-mance. Problems will be identified at an early stage, allowing the Governing Board to take remedial action where necessary.
• KPIs on SaLTS should be reported by each hospital to the RHB CRCPT every month. Comparisons between hospitals can be made, identifying best practice as well as areas where improvement is needed.
• The SaLTS team at MSD can review cluster, regional and hospital performance and identify areas where additional support is needed
Supportive supervision site visits
• Supportive supervision site visits to hospitals should be conducted in order to check (validate) hospital performance in relation to the KPIs on SaLTS, to identify good practice, and to provide supervision and guidance to help surgical units of hospitals to improve areas that require strengthening
• Supervision should be conducted by a team of supervisors. The supervisors could in-clude cluster mentors, RHB CRCPT staff, MSD staff, staff from other hospitals (e.g. CEOs) and other partners such as SSE. It would not be necessary for all stakeholders to attend every supervision visit, rather the team for each visit can be drawn from the different stakeholders.
• All supervision should be under the direction of the respective CRCPT. No stakehold-er should conduct supervision without the approval?/awareness of the CRCPT.
Review meetings Regional
Review meetings between the CRCPT and hospitals (either region wide or in clusters) will allow for benchmarking and the dissemination of good practices At each review meeting hospitals should present a performance report based on their KPIs on SaLTS. Hospitals will have the opportunity to share successes and challenges in order to learn from each other.
Regional “all hospital” review meetings can also be used to discuss other relevant topics
National
Review meetings between MSD and all regional CRCPTs will allow for benchmarking and the dissemination of good practice between regions.
At each review meeting CRCPTs should present a regional performance report based on their KPIs. Regional CRCPTs will have the opportunity to share successes and challenges in order to learn from each other.
MSD/CRCPT meetings can also be used to discuss other relevant topics.

40 National Five-Year Safe Surgery Strategic Plan
Logi
c mod
el fo
r SaL
TS p
rojec
t
• Su
rgic
al te
ams
of h
ospi
-ta
ls•
MO
H a
nd R
HB
sup
er-
viso
rs•
Part
ners
like
SSA
• Su
rgic
al th
eatr
es a
nd
othe
r inf
rast
ruct
ures
• E
ssen
tial e
quip
men
t, su
pplie
s an
d co
nsum
-ab
les
• Fu
ndin
g fr
om lo
cal a
nd
inte
rnat
iona
l sou
rces
• G
uide
lines
and
pol
icie
s on
sur
gery
and
hos
pita
l qu
ality
impr
ovem
ent
• C
ondu
ct S
ite re
adin
ess
asse
ssm
ent
• C
ondu
ct le
ader
ship
de
velo
pmen
t tra
inin
g •
Con
duct
men
tori
ng
visit
s at
clu
ster
leve
l•
Con
duct
sup
ervi
sory
vi
sit a
t eac
h ho
spita
l•
Con
duct
clu
ster
/reg
iona
l re
view
mee
ting
• C
ondu
ct in
tegr
ated
sup
-po
rtiv
e su
perv
isio
n•
Faci
litat
e b
ench
mar
k-in
g vi
sit b
etw
een
hoso
i-ta
ls
• D
evel
op o
r ada
pt fa
cilit
y de
velo
pmen
t che
cklis
t•
Con
duct
clin
ical
aud
it
• Im
plem
enta
tion
perf
orm
ance
gap
s id
entifi
ed a
nd p
ossi
ble
solu
tions
pro
vide
d•
Clin
icia
ns tr
aine
d,
supp
orte
d to
be
lead
-er
s in
saf
e su
rger
y•
Exp
erie
nce
of b
est
impl
emen
ting
hosp
i-ta
ls s
hare
d w
ith o
ther
ho
spita
ls•
Use
of s
tand
ard
prac
tices
and
tool
s in
trod
uced
• R
educ
tion
in p
erio
p-er
ativ
e m
orta
lity
• Im
prov
ed v
olum
e an
d qu
ality
of b
ellw
ethe
r su
rgic
al p
roce
dure
s•
Ens
ured
Saf
ety
in
surg
ery
• D
ecre
ased
in
mor
bidi
ty
and
mor
talit
y fr
om s
urgi
cal
cond
ition
s in
E
thio
pia
Inpu
t
Act
ivit
ies
Out
put
Out
com
eIm
pact
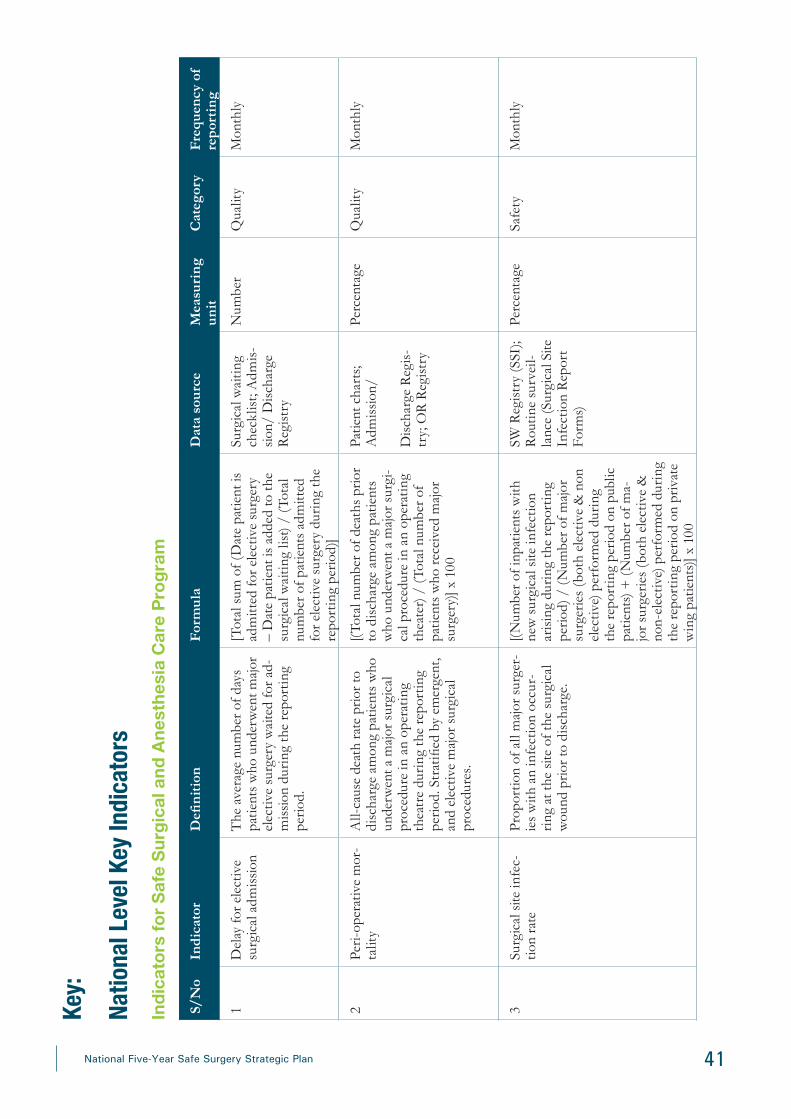
41National Five-Year Safe Surgery Strategic Plan
Key:
Natio
nal L
evel
Key I
ndica
tors
Indi
cato
rs fo
r Saf
e Su
rgic
al a
nd A
nest
hesi
a C
are
Prog
ram
S/N
oIn
dica
tor
Defi
niti
onF
orm
ula
Dat
a so
urce
Mea
suri
ng
unit
Cat
egor
yF
requ
ency
of
repo
rtin
g
1D
elay
for e
lect
ive
surg
ical
adm
issi
onT
he a
vera
ge n
umbe
r of d
ays
patie
nts
who
und
erw
ent m
ajor
el
ectiv
e su
rger
y w
aite
d fo
r ad-
mis
sion
dur
ing
the
repo
rtin
g pe
riod.
[Tot
al s
um o
f (D
ate
patie
nt is
ad
mitt
ed fo
r ele
ctiv
e su
rger
y –
Dat
e pa
tient
is a
dded
to th
e su
rgic
al w
aitin
g lis
t) /
(Tot
al
num
ber o
f pat
ient
s ad
mitt
ed
for e
lect
ive
surg
ery
duri
ng th
e re
port
ing
perio
d)]
Surg
ical
wai
ting
chec
klis
t; A
dmis
-si
on/
Dis
char
ge
Reg
istr
y
Num
ber
Qua
lity
Mon
thly
2Pe
ri-o
pera
tive
mor
-ta
lity
All-
caus
e de
ath
rate
prio
r to
disc
harg
e am
ong
patie
nts
who
un
derw
ent a
maj
or s
urgi
cal
proc
edur
e in
an
oper
atin
g th
eatr
e du
ring
the
repo
rtin
g pe
riod.
Str
atifi
ed b
y em
erge
nt,
and
elec
tive
maj
or s
urgi
cal
proc
edur
es.
[(Tot
al n
umbe
r of d
eath
s pr
ior
to d
isch
arge
am
ong
patie
nts
who
und
erw
ent a
maj
or s
urgi
-ca
l pro
cedu
re in
an
oper
atin
g th
eate
r) /
(Tot
al n
umbe
r of
patie
nts
who
rece
ived
maj
or
surg
ery)
] x 1
00
Patie
nt c
hart
s; A
dmis
sion
/
Dis
char
ge R
egis
-tr
y; O
R R
egis
try
Perc
enta
geQ
ualit
yM
onth
ly
3Su
rgic
al s
ite in
fec-
tion
rate
Prop
ortio
n of
all
maj
or s
urge
r-ie
s w
ith a
n in
fect
ion
occu
r-ri
ng a
t the
site
of t
he s
urgi
cal
wou
nd p
rior t
o di
scha
rge.
[(Num
ber o
f inp
atie
nts
with
ne
w s
urgi
cal s
ite in
fect
ion
aris
ing
duri
ng th
e re
port
ing
perio
d) /
(N
umbe
r of m
ajor
su
rger
ies
(bot
h el
ectiv
e &
non
el
ectiv
e) p
erfo
rmed
dur
ing
the
repo
rtin
g pe
riod
on p
ublic
pa
tient
s) +
(N
umbe
r of m
a-jo
r sur
gerie
s (b
oth
elec
tive
&
non-
elec
tive)
per
form
ed d
urin
g th
e re
port
ing
perio
d on
pri
vate
w
ing
patie
nts)]
x 1
00
SW R
egis
try
(SSI
); R
outin
e su
rvei
l-la
nce
(Sur
gica
l Site
In
fect
ion
Rep
ort
Form
s)
Perc
enta
geSa
fety
Mon
thly
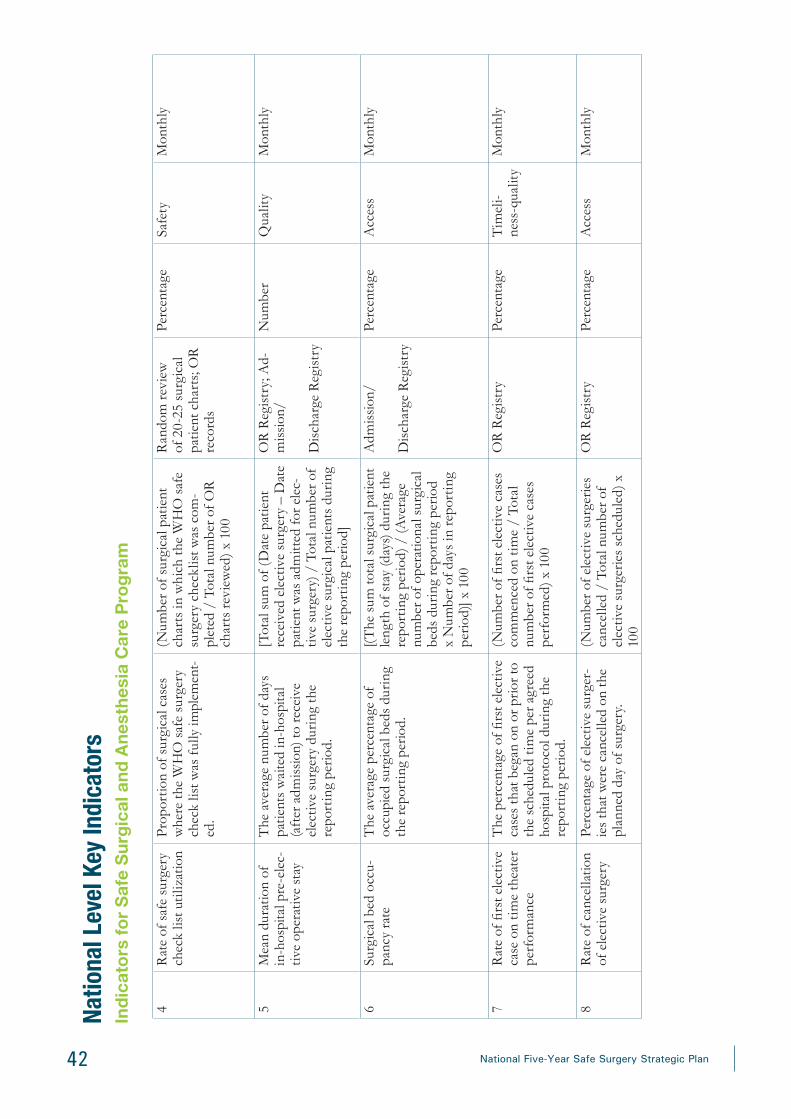
42 National Five-Year Safe Surgery Strategic Plan
4R
ate
of s
afe
surg
ery
chec
k lis
t uti
lizat
ion
Prop
ortio
n of
sur
gica
l cas
es
whe
re th
e W
HO
saf
e su
rger
y ch
eck
list w
as f
ully
impl
emen
t-ed
.
(Num
ber o
f sur
gica
l pat
ient
ch
arts
in w
hich
the
WH
O s
afe
surg
ery
chec
klis
t was
com
-pl
eted
/ T
otal
num
ber o
f OR
ch
arts
revi
ewed
) x 1
00
Ran
dom
revi
ew
of 2
0-25
sur
gica
l pa
tient
cha
rts;
OR
re
cord
s
Perc
enta
geSa
fety
Mon
thly
5M
ean
dura
tion
of
in-h
ospi
tal p
re-e
lec-
tive
oper
ativ
e st
ay
The
ave
rage
num
ber o
f day
s pa
tient
s w
aite
d in
-hos
pita
l (a
fter
adm
issi
on) t
o re
ceiv
e el
ectiv
e su
rger
y du
ring
the
repo
rtin
g pe
riod.
[Tot
al s
um o
f (D
ate
patie
nt
rece
ived
ele
ctiv
e su
rger
y –
Dat
e pa
tient
was
adm
itted
for e
lec-
tive
surg
ery)
/ T
otal
num
ber o
f el
ectiv
e su
rgic
al p
atie
nts
duri
ng
the
repo
rtin
g pe
riod]
OR
Reg
istr
y; A
d-m
issi
on/
Dis
char
ge R
egis
try
Num
ber
Qua
lity
Mon
thly
6Su
rgic
al b
ed o
ccu-
panc
y ra
teT
he a
vera
ge p
erce
ntag
e of
oc
cupi
ed s
urgi
cal b
eds
duri
ng
the
repo
rtin
g pe
riod.
[(The
sum
tota
l sur
gica
l pat
ient
le
ngth
of s
tay
(day
s) d
urin
g th
e re
port
ing
perio
d) /
(Ave
rage
nu
mbe
r of o
pera
tiona
l sur
gica
l be
ds d
urin
g re
port
ing
perio
d x
Num
ber o
f day
s in
repo
rtin
g pe
riod)
] x 1
00
Adm
issi
on/
Dis
char
ge R
egis
try
Perc
enta
geA
cces
sM
onth
ly
7R
ate
of fi
rst e
lect
ive
case
on
time
thea
ter
perf
orm
ance
The
per
cent
age
of fi
rst e
lect
ive
case
s th
at b
egan
on
or p
rior t
o th
e sc
hedu
led
time
per a
gree
d ho
spita
l pro
toco
l dur
ing
the
repo
rtin
g pe
riod.
(Num
ber o
f firs
t ele
ctiv
e ca
ses
com
men
ced
on ti
me
/ To
tal
num
ber o
f firs
t ele
ctiv
e ca
ses
perf
orm
ed) x
100
OR
Reg
istr
yPe
rcen
tage
Tim
eli-
ness
-qua
lity
Mon
thly
8R
ate
of c
ance
llatio
n of
ele
ctiv
e su
rger
yPe
rcen
tage
of e
lect
ive
surg
er-
ies
that
wer
e ca
ncel
led
on th
e pl
anne
d da
y of
sur
gery
.
(Num
ber o
f ele
ctiv
e su
rger
ies
canc
elle
d /
Tota
l num
ber o
f el
ectiv
e su
rger
ies
sche
dule
d) x
10
0
OR
Reg
istr
yPe
rcen
tage
Acc
ess
Mon
thly
Natio
nal L
evel
Key I
ndica
tors
Indi
cato
rs fo
r Saf
e Su
rgic
al a
nd A
nest
hesi
a C
are
Prog
ram

43National Five-Year Safe Surgery Strategic Plan
Natio
nal L
evel
Key I
ndica
tors
Indi
cato
rs fo
r Saf
e Su
rgic
al a
nd A
nest
hesi
a C
are
Prog
ram
9E
mer
genc
y su
rgic
al
acce
ssT
he p
ropo
rtio
n of
pat
ient
s w
hose
trav
el ti
me
from
whe
n th
ey fi
rst s
eek
care
to th
eir
arri
val a
t a fa
cilit
y pr
ovid
ing
AN
Y o
f the
sel
ecte
d B
ellw
eth-
er p
roce
dure
s (C
-sec
tions
, la
paro
tom
ies,
or o
pen
frac
ture
re
pair
s) is
less
than
or e
qual
to
2 ho
urs.
Stra
tified
by
each
of
the
thre
e pr
oced
ures
.
(Num
ber o
f em
erge
ncy
surg
ical
pa
tient
s w
hose
trav
el ti
me
from
w
hen
they
firs
t see
k ca
re to
th
eir a
rriv
al a
t a fa
cilit
y pr
ovid
-in
g ei
ther
C-s
ectio
ns, l
apar
oto-
mie
s, o
r ope
n fr
actu
re re
pair
s is
less
than
or e
qual
to 2
hou
rs
/ To
tal n
umbe
r of e
mer
genc
y su
rgic
al p
atie
nts)
x 1
00
Patie
nt s
urve
y; O
R
regi
stry
Perc
enta
geA
cces
sQ
uart
erly
10Su
rgic
al v
olum
eTo
tal n
umbe
r of m
ajor
sur
gica
l pr
oced
ures
per
form
ed in
op
erat
ing
thea
tre
per 1
00,0
00
popu
latio
n pe
r yea
r.
(Tot
al n
umbe
r of m
ajor
sur
gica
l pr
oced
ures
per
form
ed in
OT
pe
r yea
r / T
otal
pop
ulat
ion
of
catc
hmen
t are
a) x
100
,000
OR
Reg
istr
yN
umbe
rA
cces
sA
nnua
l
11Pr
opor
tion
of
budg
et s
pent
on
surg
ical
ser
vice
s
Prop
ortio
n of
recu
rren
t bud
-ge
t tha
t is
spen
t on
surg
ical
se
rvic
es.
(Am
ount
of r
ecur
rent
bud
get
spen
t on
surg
ical
ser
vice
s /
To-
tal h
ealth
faci
lity
budg
et) x
100
Hos
pita
l fina
nces
re
cord
Perc
enta
geFi
nanc
ing
Ann
ual
12B
lood
una
vaila
bilit
y ra
tioT
he p
erce
ntag
e of
maj
or s
urgi
-ca
l cas
es fo
r whi
ch b
lood
was
un
avai
labl
e up
on re
ques
t.
(Tot
al n
umbe
r of m
ajor
sur
gica
l ca
ses
for w
hich
blo
od w
as u
n-av
aila
ble
upon
requ
est)
/ (T
otal
nu
mbe
r of m
ajor
sur
gica
l cas
es
for w
hich
blo
od w
as re
ques
ted)
x
100
Lab
orat
ory
bloo
d re
cord
sPe
rcen
tage
Qua
lity
Mon
thly
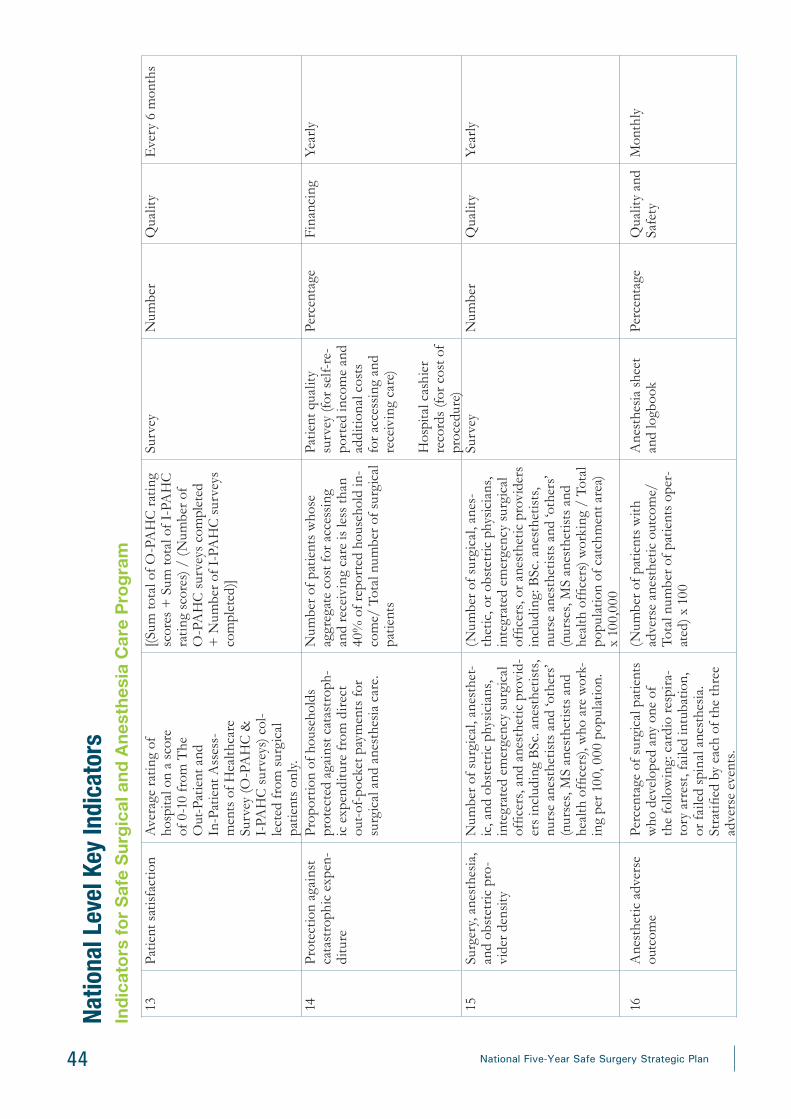
44 National Five-Year Safe Surgery Strategic Plan
13Pa
tient
sat
isfac
tion
Ave
rage
rat
ing
of
hosp
ital o
n a
scor
e of
0-1
0 fr
om T
he
Out
-Pat
ient
and
In
-Pat
ient
Ass
ess-
men
ts o
f Hea
lthca
re
Surv
ey (O
-PA
HC
&
I-PA
HC
sur
veys
) col
-le
cted
from
sur
gica
l pa
tient
s on
ly.
[(Sum
tota
l of O
-PA
HC
rat
ing
scor
es +
Sum
tota
l of I
-PA
HC
ra
ting
scor
es) /
(N
umbe
r of
O-P
AH
C s
urve
ys c
ompl
eted
+
Num
ber o
f I-P
AH
C s
urve
ys
com
plet
ed)]
Surv
eyN
umbe
rQ
ualit
yE
very
6 m
onth
s
14Pr
otec
tion
agai
nst
cata
stro
phic
exp
en-
ditu
re
Prop
ortio
n of
hou
seho
lds
prot
ecte
d ag
ains
t cat
astr
oph-
ic e
xpen
ditu
re fr
om d
irect
ou
t-of
-poc
ket p
aym
ents
for
surg
ical
and
ane
sthe
sia
care
.
Num
ber o
f pat
ient
s w
hose
ag
greg
ate
cost
for a
cces
sing
an
d re
ceiv
ing
care
is le
ss th
an
40%
of r
epor
ted
hous
ehol
d in
-co
me/
Tot
al n
umbe
r of s
urgi
cal
patie
nts
Patie
nt q
ualit
y su
rvey
(for
sel
f-re
-po
rted
inco
me
and
addi
tiona
l cos
ts
for a
cces
sing
and
re
ceiv
ing
care
)
Hos
pita
l cas
hier
re
cord
s (fo
r cos
t of
proc
edur
e)
Perc
enta
geFi
nanc
ing
Year
ly
15Su
rger
y, a
nest
hesi
a,
and
obst
etric
pro
-vi
der d
ensit
y
Num
ber o
f sur
gica
l, an
esth
et-
ic, a
nd o
bste
tric
phy
sici
ans,
in
tegr
ated
em
erge
ncy
surg
ical
of
ficer
s, a
nd a
nest
hetic
pro
vid-
ers
incl
udin
g B
Sc. a
nest
hetis
ts,
nurs
e an
esth
etis
ts a
nd ‘o
ther
s’ (n
urse
s, M
S an
esth
etis
ts a
nd
heal
th o
ffice
rs),
who
are
wor
k-in
g pe
r 100
, 000
pop
ulat
ion.
(Num
ber o
f sur
gica
l, an
es-
thet
ic, o
r obs
tetr
ic p
hysi
cian
s,
inte
grat
ed e
mer
genc
y su
rgic
al
offic
ers,
or a
nest
hetic
pro
vide
rs
incl
udin
g: B
Sc. a
nest
hetis
ts,
nurs
e an
esth
etis
ts a
nd ‘o
ther
s’ (n
urse
s, M
S an
esth
etis
ts a
nd
heal
th o
ffice
rs) w
orki
ng /
Tot
al
popu
latio
n of
cat
chm
ent a
rea)
x
100,
000
Surv
eyN
umbe
rQ
ualit
yYe
arly
16A
nest
hetic
adv
erse
ou
tcom
ePe
rcen
tage
of s
urgi
cal p
atie
nts
who
dev
elop
ed a
ny o
ne o
f th
e fo
llow
ing:
car
dio
resp
ira-
tory
arr
est,
faile
d in
tuba
tion,
or
faile
d sp
inal
ane
sthe
sia.
St
ratifi
ed b
y ea
ch o
f the
thre
e ad
vers
e ev
ents
.
(Num
ber o
f pat
ient
s w
ith
adve
rse
anes
thet
ic o
utco
me/
To
tal n
umbe
r of p
atie
nts
oper
-at
ed) x
100
Ane
sthe
sia
shee
t an
d lo
gboo
k Pe
rcen
tage
Qua
lity
and
Safe
ty
Mon
thly
Natio
nal L
evel
Key I
ndica
tors
Indi
cato
rs fo
r Saf
e Su
rgic
al a
nd A
nest
hesi
a C
are
Prog
ram

45National Five-Year Safe Surgery Strategic Plan
ReferencesDebas HT, Donkor P, Gawande A, Jamison DT, Kruk ME, Mock CN, eds. 2015. Disease Control Priorities: Es-sential Surgery. 3rd ed. Washington, DC: World Bank Group.
Debas H, Gosselin R, McCord C, Thind A. 2006. Surgery. In: Jamison DT, Breman JG, Measham AR, et al., eds. Disease Control Priorities in Developing Countries. 2nd ed. New York: Oxford University Press; 1245–1259.
Mock CN, Donkor P, Gawande A, et al. 2015. Essential surgery: key messages from Disease Control Priorities, 3rd edition. Lancet. 385(9983): 2209-2219.
World Health Organization. 2008. The Second Global Patient Safety Challenge: Safe Surgery Saves Lives. Geneva: WHO.

46 National Five-Year Safe Surgery Strategic Plan
Annex A. Tool for Situational Analysis to Assess Emergency and Essential Surgical Care in Ethiopia Objective: To assess the gaps in the availability of Emergency and Essential Surgical Care (EESC) at hospitals in Ethiopia.
Key Category of Data
General Information
Infrastructure
Human Resources
Interventions
Emergency and Essential Surgical Care Equipment and Supplies
Financing
Information Management
Surgical Sets
Involvement of following providers is required to complete assessment:
1. Hospital Director or CEO
2. Surgeon/IESO
3. OB/GYN (Surgeon/IESO if not available)
4. Anesthetist/Nurse
If any of the providers listed above are not available, please direct all questions (where applicable ) to Hospital Director or CEO.

47National Five-Year Safe Surgery Strategic Plan
Facility Information
Fields marked with an asterisk (*) are mandatory REGION*
DATE OF DATA COLLECTION* (dd/mm/yyyy) NAME of person(s) filling out form*
PHONE NUMBER of person(s) filling out form*
EMAIL*
NAME and ADDRESS of health care facili-ty*
(include city, woreda or zone and region) Phone number of health care facility*
Data Collector
Type of health care facility be-ing evaluated
Primary
Hospital
General
Hospital
Specialized
Hospital
Private Hos-pital
NGO Hospital Mission Hos-pital

48 National Five-Year Safe Surgery Strategic Plan
Hospital DirectorInfrastructure
Insert number.
1. Total population served by this health care facility #
2. Total number of hospital beds #
3. Total number of surgical beds (ENT, Trauma, GS, orthopedics and others) #
4. Total number of obstetric and gynecologic beds #
5. Total number of post-op recovery beds #
6. Total number of advanced care/ICU beds #
7. Total number of emergency area beds #
8. Total number of admissions in a year #
9. Total number of total surgical admissions in one year (ENT and orthope-dics included) #
10. Total number of obstetric and gynecologic admissions #
11. Total number of outpatients seen in one year #
12. What percentage of your patients can reach the hospital within 2 hours of travel?
* 0 (None) * 1-25% * 26-50%
* 51-75% * 76-99% * 100% (All)
13. Who is acting as OT manager?
OT Manager: defined as the person(s) responsible for the surgical and OB/GYN operating theatres
14. What is the average number of peri-operative, in-hospital deaths per month? #
Fill in with percentages.
15. Over the past month, how often do you have running water?
* 0 (Never) * 1-25% * 26-50% * 51-75% * 76-99% * 100% (Always)
16. Over the past month, how often do you have a regular, 24/7 electricity source?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
17. Over the past month, how often do you have a generator/back-up elec-tricity source?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
18. Over the past month, how often do you have internet?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
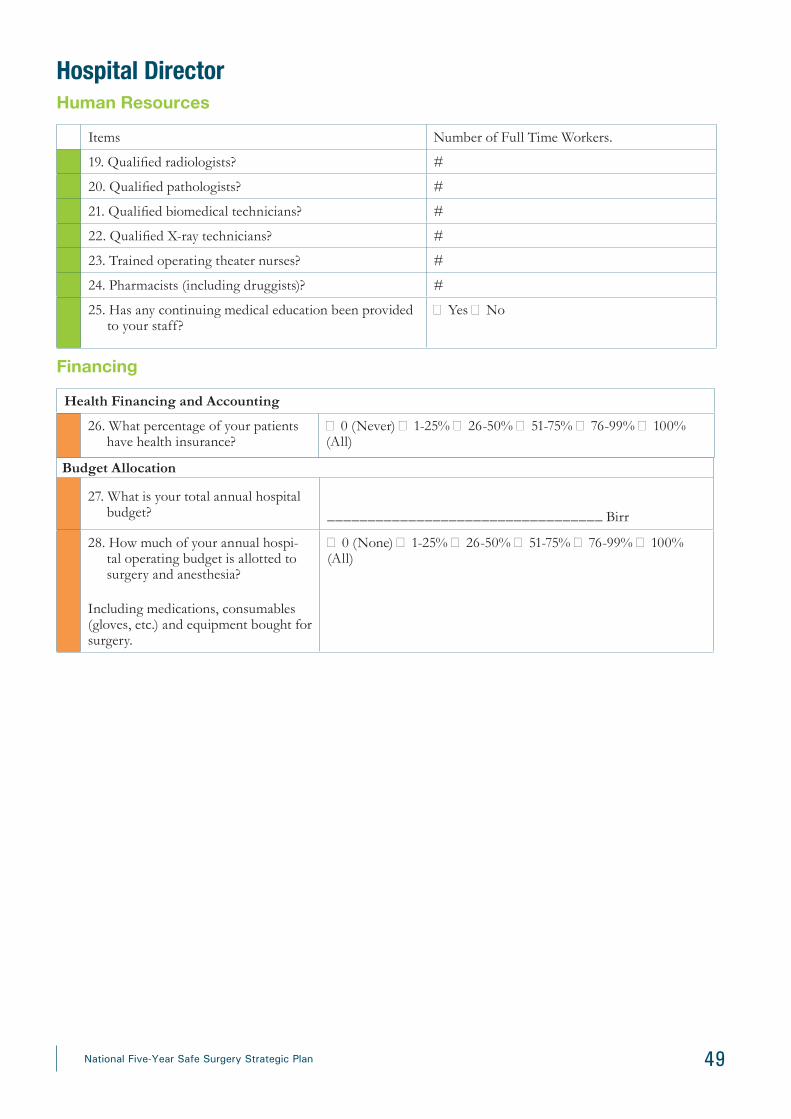
49National Five-Year Safe Surgery Strategic Plan
Hospital DirectorHuman Resources
Items Number of Full Time Workers.
19. Qualified radiologists? #
20. Qualified pathologists? #
21. Qualified biomedical technicians? #
22. Qualified X-ray technicians? #
23. Trained operating theater nurses? #
24. Pharmacists (including druggists)? #
25. Has any continuing medical education been provided to your staff?
� Yes � No
Financing
Health Financing and Accounting
26. What percentage of your patients have health insurance?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (All)
Budget Allocation
27. What is your total annual hospital budget? __________________________________ Birr
28. How much of your annual hospi-tal operating budget is allotted to surgery and anesthesia?
Including medications, consumables (gloves, etc.) and equipment bought for surgery.
� 0 (None) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (All)
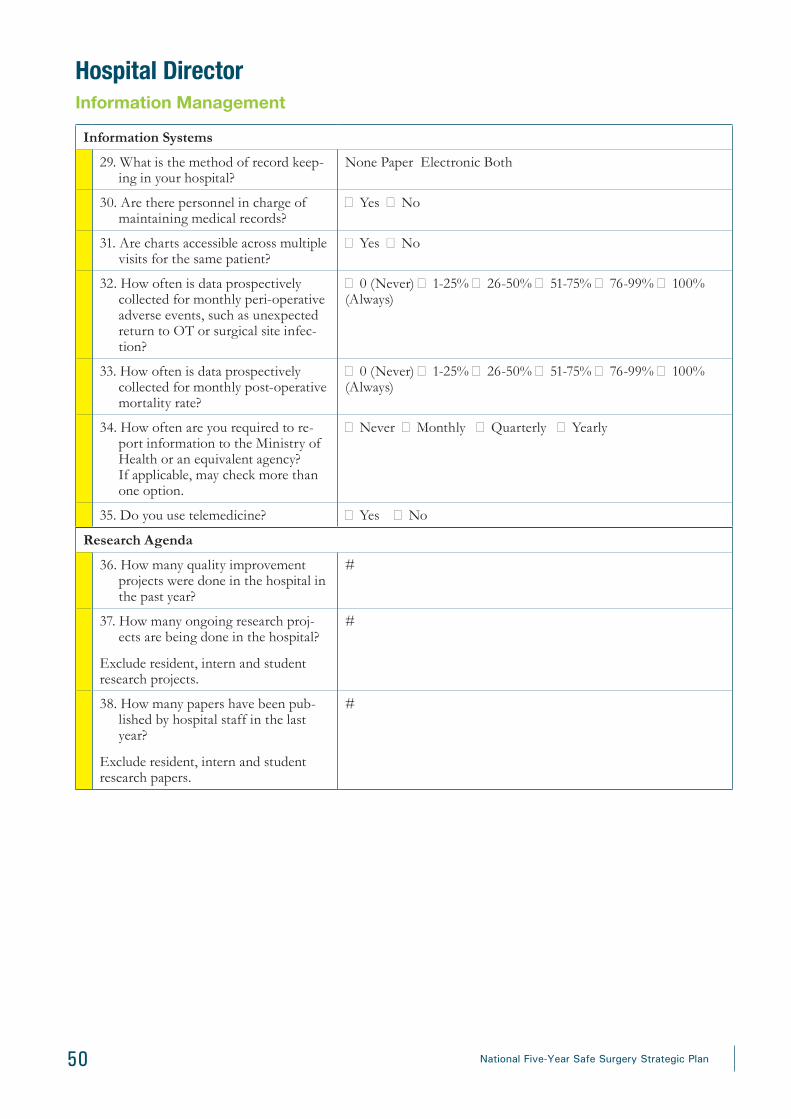
50 National Five-Year Safe Surgery Strategic Plan
Hospital DirectorInformation Management
Information Systems
29. What is the method of record keep-ing in your hospital?
None Paper Electronic Both
30. Are there personnel in charge of maintaining medical records?
� Yes � No
31. Are charts accessible across multiple visits for the same patient?
� Yes � No
32. How often is data prospectively collected for monthly peri-operative adverse events, such as unexpected return to OT or surgical site infec-tion?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
33. How often is data prospectively collected for monthly post-operative mortality rate?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
34. How often are you required to re-port information to the Ministry of Health or an equivalent agency? If applicable, may check more than one option.
� Never � Monthly � Quarterly � Yearly
35. Do you use telemedicine? � Yes � No
Research Agenda
36. How many quality improvement projects were done in the hospital in the past year?
#
37. How many ongoing research proj-ects are being done in the hospital?
Exclude resident, intern and student research projects.
#
38. How many papers have been pub-lished by hospital staff in the last year?
Exclude resident, intern and student research papers.
#
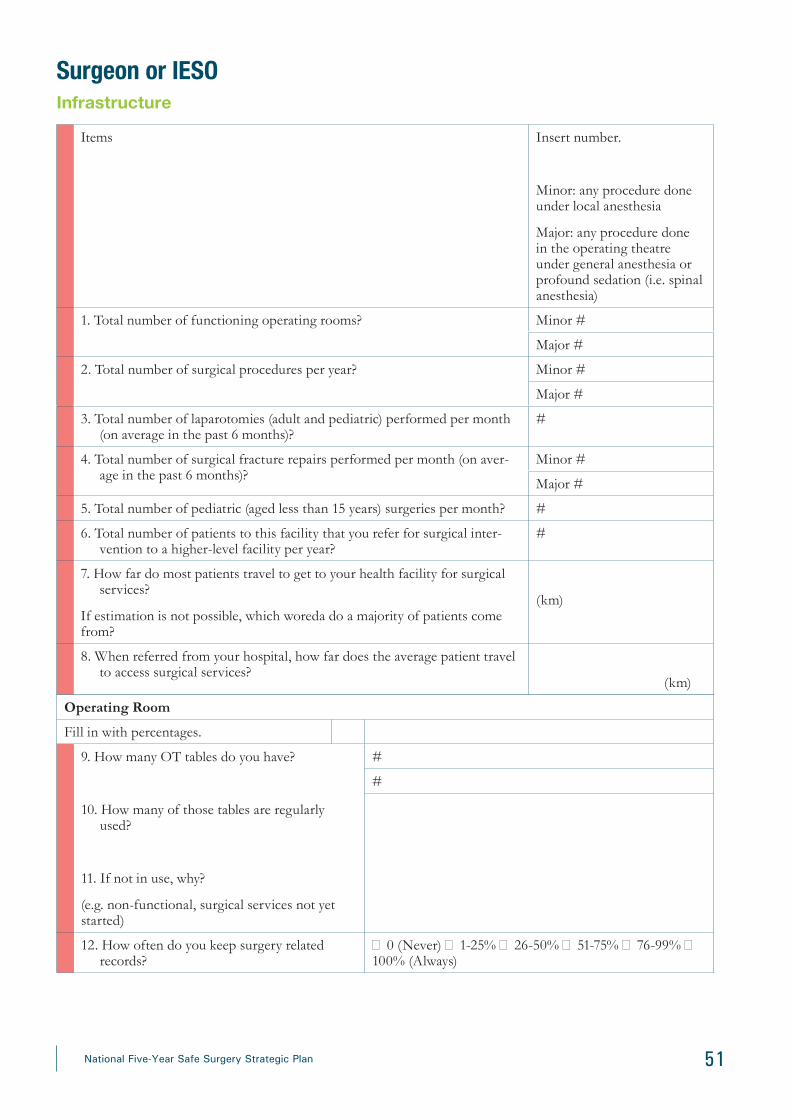
51National Five-Year Safe Surgery Strategic Plan
Surgeon or IESOInfrastructure
Items Insert number.
Minor: any procedure done under local anesthesia
Major: any procedure done in the operating theatre under general anesthesia or profound sedation (i.e. spinal anesthesia)
1. Total number of functioning operating rooms? Minor #
Major #
2. Total number of surgical procedures per year? Minor #
Major #
3. Total number of laparotomies (adult and pediatric) performed per month (on average in the past 6 months)?
#
4. Total number of surgical fracture repairs performed per month (on aver-age in the past 6 months)?
Minor #
Major #
5. Total number of pediatric (aged less than 15 years) surgeries per month? #
6. Total number of patients to this facility that you refer for surgical inter-vention to a higher-level facility per year?
#
7. How far do most patients travel to get to your health facility for surgical services?
If estimation is not possible, which woreda do a majority of patients come from?
(km)
8. When referred from your hospital, how far does the average patient travel to access surgical services?
(km)
Operating Room
Fill in with percentages.
9. How many OT tables do you have?
10. How many of those tables are regularly used?
11. If not in use, why?
(e.g. non-functional, surgical services not yet started)
#
#
12. How often do you keep surgery related records?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)

52 National Five-Year Safe Surgery Strategic Plan
Surgeon or IESOManagement Guidelines
Fill in with percentages.
13. Do you have management guidelines available for emergency care?
*Yes *No
14. Do you have management guidelines available for surgery?
*Yes *No
Laboratory
15. How often do you have access for blood?
16. How long does it take to get blood that is in stock after you place an order?
17. How long does it take to get blood that is not in stock after you place an order?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
18. How often is a Complete Blood Count available (including hemoglobin, hematocrit, WBCs, platelets)?
19. What do you have available often?
20. What do you not have available often?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
21. How often a full chemistry panel available (including BUN, creatinine, Na, K, etc.)?
22. What do you have available often?
23. What do you not have available often?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
24. How often is the lab able to run all coagulation studies (including PT, PTT, BT, INR)?
25. What do you have available often?
26. What do you not have available often?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
27. How often are you able to screen for an infectious panel (HIV, hepatitis virus, syphilis)?
28. What do you have available often?
29. What do you not have available often?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
30. How often is the lab able to do a urinalysis? � 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)

53National Five-Year Safe Surgery Strategic Plan
Surgeon or IESORadiology
31. How many X-ray machines do you have?
32. How many of those machines are reg-ularly used?
33. If not in use, why?
(e.g. non-functional, surgical services not yet started)
#
#
34. How many ultrasound machines do you have?
35. How many of those machines are regu-larly used?
35. If not in use, why?
(e.g. non-functional, surgical services not yet started)
#
#
36. How many CT scanners do you have?
37. How many of those machines are regu-larly used?
38. If not in use, why?
(e.g. non-functional, surgical services not yet started)
#
#
39. How many MRI scanners do you have?
40. How many of those machines are reg-ularly used?
41. If not in use, why?
(e.g. non-functional, surgical services not yet started)
#
#
42. How often do you have 24-hour access to radiology imaging services?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
Supplies43. How many CSR machines do you
have?
44. How many of those machines are reg-ularly used?
45. If not in use, why?
(e.g. non-functional, surgical services not yet started)
#
#
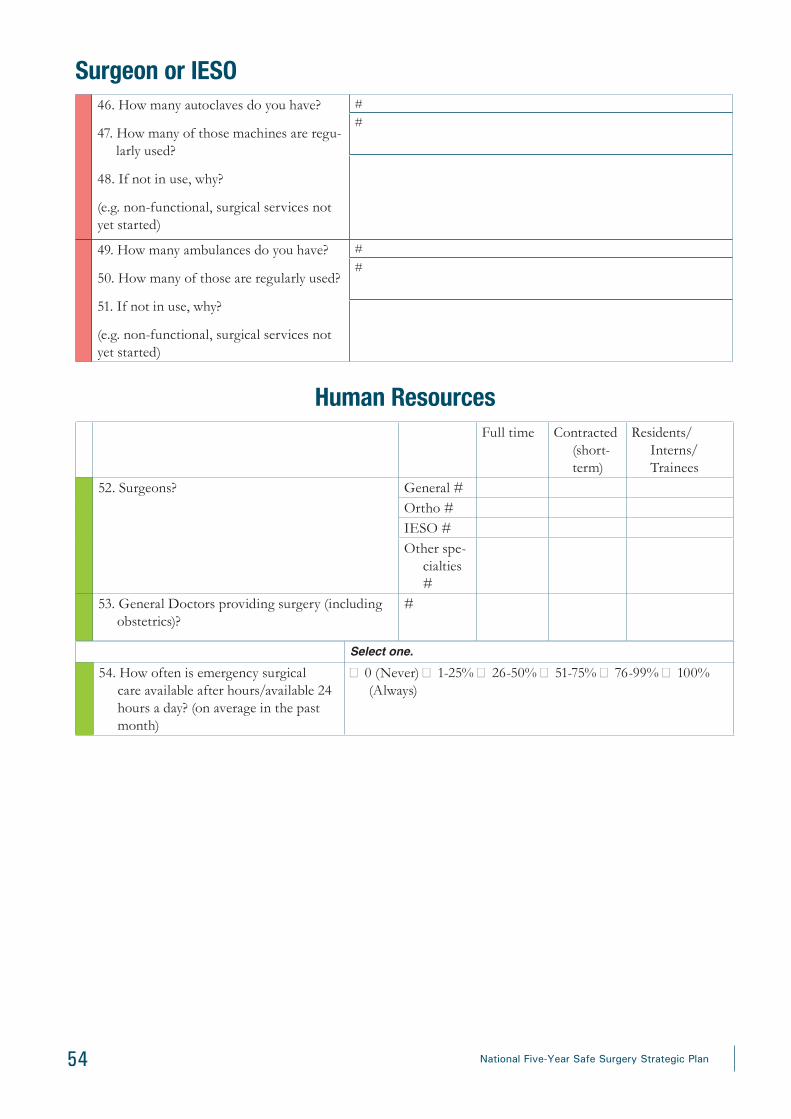
54 National Five-Year Safe Surgery Strategic Plan
46. How many autoclaves do you have?
47. How many of those machines are regu-larly used?
48. If not in use, why?
(e.g. non-functional, surgical services not yet started)
#
#
49. How many ambulances do you have?
50. How many of those are regularly used?
51. If not in use, why?
(e.g. non-functional, surgical services not yet started)
#
#
Human ResourcesFull time Contracted
(short-term)
Residents/Interns/ Trainees
52. Surgeons? General #Ortho #IESO #Other spe-
cialties #
53. General Doctors providing surgery (including obstetrics)?
#
Surgeon or IESO
Select one.
54. How often is emergency surgical care available after hours/available 24 hours a day? (on average in the past month)
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
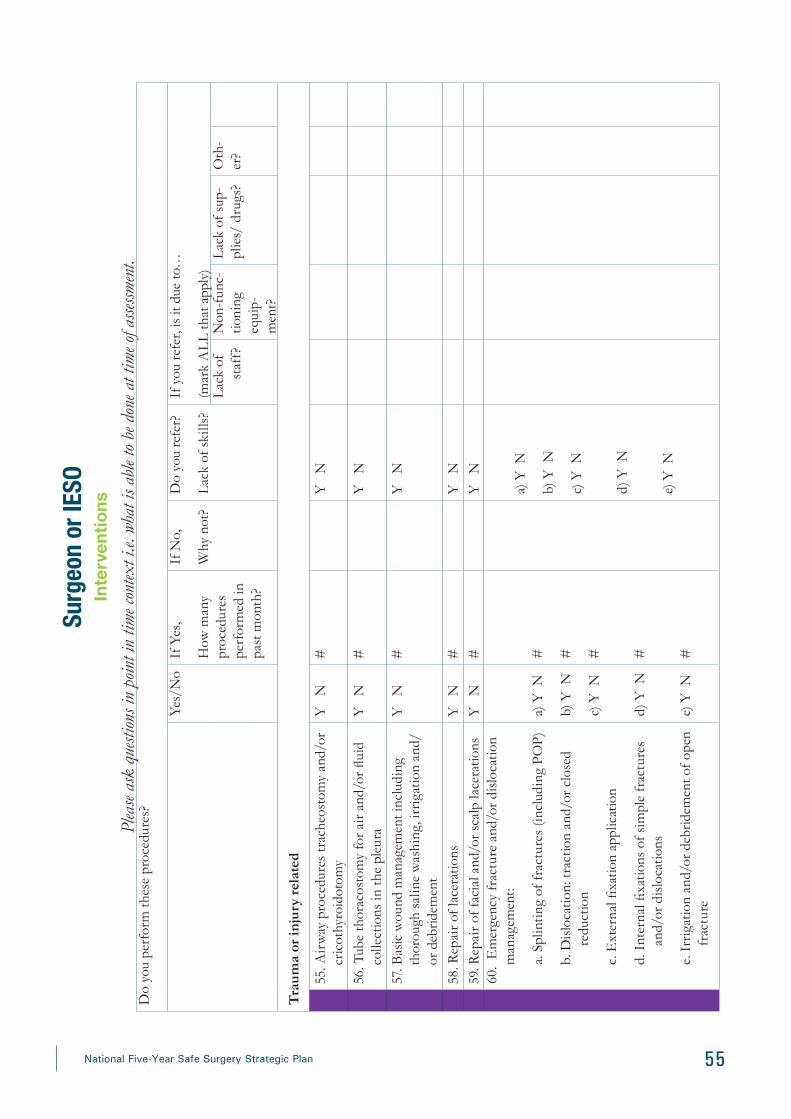
55National Five-Year Safe Surgery Strategic Plan
Surg
eon
or IE
SOIn
terv
entio
nsPl
ease
ask
quest
ions i
n po
int i
n tim
e con
text i
.e. w
hat i
s abl
e to
be d
one a
t tim
e of a
ssessm
ent.
Do
you
perf
orm
thes
e pr
oced
ures
?
Yes/
No
If Y
es,
How
man
y pr
oced
ures
pe
rfor
med
in
past
mon
th?
If N
o,
Why
not
?
Do
you
refe
r?
Lac
k of
ski
lls?
If y
ou re
fer,
is it
due
to…
(mar
k A
LL
that
app
ly)
Lac
k of
st
aff?
Non
-fun
c-tio
ning
eq
uip-
men
t?
Lac
k of
sup
-pl
ies/
dru
gs?
Oth
-er
?
Tra
uma
or in
jury
rel
ated
55. A
irw
ay p
roce
dure
s tr
ache
osto
my
and/
or
cric
othy
roid
otom
yY
N
#Y
N
56. T
ube
thor
acos
tom
y fo
r air
and/
or fl
uid
colle
ctio
ns in
the
pleu
raY
N
#Y
N
57. B
asic
wou
nd m
anag
emen
t inc
ludi
ng
thor
ough
sal
ine
was
hing
, irr
igat
ion
and/
or d
ebrid
emen
t
Y
N#
Y
N
58. R
epai
r of l
acer
atio
nsY
N
#Y
N
59. R
epai
r of f
acia
l and
/or s
calp
lace
ratio
nsY
N
#Y
N
60.
Em
erge
ncy
frac
ture
and
/or d
islo
catio
n m
anag
emen
t:
a. S
plin
ting
of fr
actu
res
(incl
udin
g PO
P)
b. D
islo
catio
n: tr
actio
n an
d/or
clo
sed
redu
ctio
n
c. E
xter
nal fi
xatio
n ap
plic
atio
n
d. I
nter
nal fi
xatio
ns o
f sim
ple
frac
ture
s an
d/or
dis
loca
tions
e. I
rrig
atio
n an
d/or
deb
ridem
ent o
f ope
n fr
actu
re
a) Y
N
b) Y
N
c) Y
N
d) Y
N
e) Y
N
# # # # #
a) Y
N
b) Y
N
c) Y
N
d) Y
N
e) Y
N
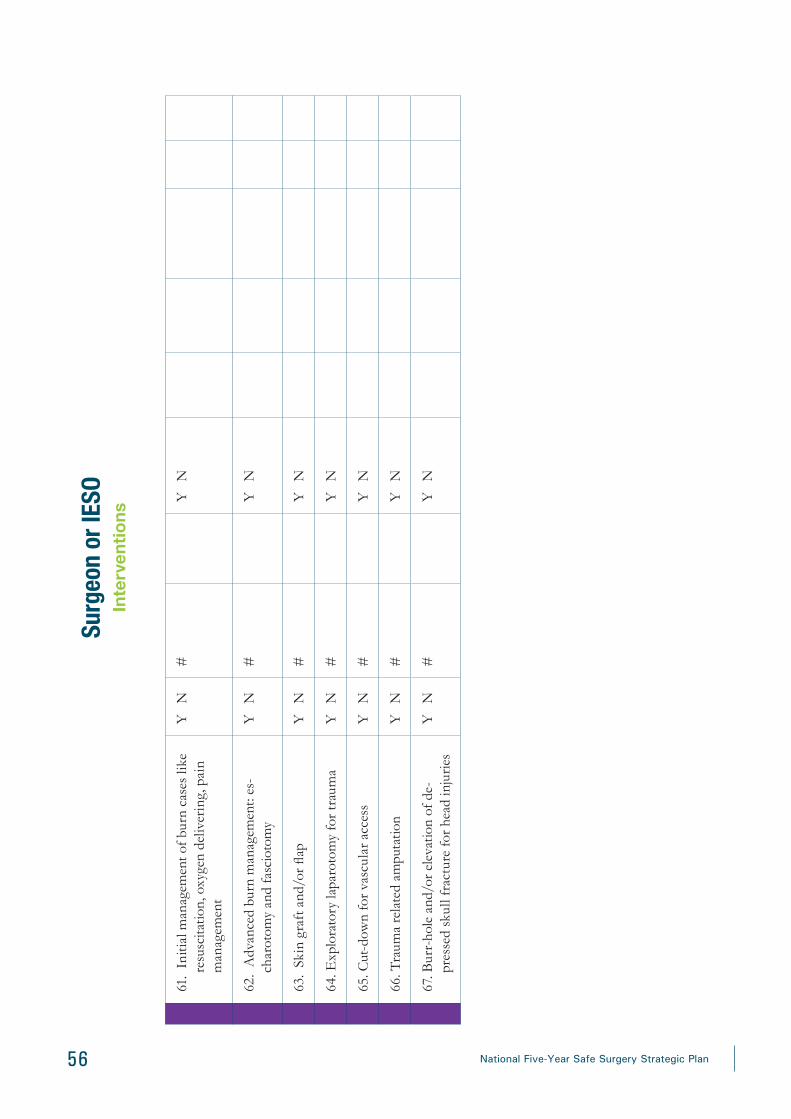
56 National Five-Year Safe Surgery Strategic Plan
Surg
eon
or IE
SOIn
terv
entio
ns
61.
Initi
al m
anag
emen
t of b
urn
case
s lik
e re
susc
itatio
n, o
xyge
n de
liver
ing,
pai
n m
anag
emen
t
Y
N#
Y
N
62.
Adv
ance
d bu
rn m
anag
emen
t: es
-ch
arot
omy
and
fasc
ioto
my
Y
N#
Y
N
63.
Skin
gra
ft a
nd/o
r flap
Y
N#
Y
N
64. E
xplo
rato
ry la
paro
tom
y fo
r tra
uma
Y
N#
Y
N
65. C
ut-d
own
for v
ascu
lar a
cces
sY
N
#Y
N
66. T
raum
a re
late
d am
puta
tion
Y
N#
Y
N
67. B
urr-
hole
and
/or e
leva
tion
of d
e-pr
esse
d sk
ull f
ract
ure
for h
ead
inju
ries
Y
N#
Y
N

57National Five-Year Safe Surgery Strategic Plan
Do
you
perf
orm
thes
e pr
oced
ures
?
Yes/
No
If Y
es,
How
man
y pr
oced
ures
pe
rfor
med
in
past
mon
th?
If N
o,
Why
not
?
Do
you
refe
r?
Lac
k of
sk
ills?
If y
ou re
fer,
is it
due
to…
(mar
k A
LL
that
app
ly)
Lac
k of
st
aff?
Non
-fun
c-tio
ning
eq
uip-
men
t?
Lac
k of
su
pplie
s/
drug
s?
Oth
er?
68. V
ascu
lar e
xplo
ratio
n an
d/or
repa
ir/an
asto
-m
osis
for t
raum
a Y
N
#Y
N
69. N
eck
expl
orat
ion
for s
ever
e ne
ck in
jurie
sY
N
#Y
N
70. E
mer
genc
y th
orac
otom
y fo
r sev
ere
ches
t in
jury
Y
N#
Y
N
71. M
anag
emen
t of a
cute
han
d tr
aum
a (te
n-do
n an
d ne
urov
ascu
lar)
Y
N
#Y
N
72. M
anag
emen
t of m
uscu
losk
elet
al m
ulti-
ple
trau
ma
and
com
plex
frac
ture
s (e
.g. h
emi
arth
ropl
asty
, int
ra-a
rtic
ular
, spi
ne a
nd p
elvi
c fr
actu
re)
Y
N#
Y
N
Surg
eon
or IE
SOIn
terv
entio
ns

58 National Five-Year Safe Surgery Strategic Plan
Non
-tra
uma
emer
genc
y an
d es
sent
ial g
ener
al s
urgi
cal c
ondi
tion
s
73. D
rain
ing
supe
rfici
al a
bsce
sses
Y
N#
Y
N
74. M
ale
circ
umci
sion
Y
N#
Y
N75
. Vas
ecto
my
Y
N#
Y
N76
. Exc
isio
n of
sm
all s
oft t
issu
e tu
mor
s lik
e lip
oma,
ga
nglio
nY
N
#Y
N
77. R
elie
ving
acu
te u
rina
ry re
tent
ion:
a) C
athe
teri
zatio
n
b) C
lose
d su
prap
ubic
cys
tost
omy
Y
N
Y
N
# #
Y
N
Y
N78
. Hyd
roce
lect
omy
Y
N#
Y
N79
. Rec
tal t
ube
defla
tion
for s
igm
oid
volv
ulus
Y
N#
Y
N
80. E
xplo
rativ
e la
paro
tom
y fo
r acu
te a
bdom
en
a. A
cute
app
endi
citis
b. A
cute
per
fora
tion
c. B
owel
Obs
truc
tion
a) Y
N
b) Y
N
c) Y
N
# # #
a) Y
N
b) Y
N
c) Y
N
Surg
eon
or IE
SOIn
terv
entio
ns

59National Five-Year Safe Surgery Strategic Plan
Do
you
perf
orm
thes
e pr
oced
ures
?Ye
s/N
oIf
Yes
,
How
man
y pr
oced
ures
pe
rfor
med
in
pas
t m
onth
?
If N
o,
Why
not
?
Do
you
refe
r?
Lac
k of
sk
ills?
If y
ou re
fer,
is it
due
to…
(mar
k A
LL
that
app
ly)
Lac
k of
st
aff?
Non
-fun
c-tio
ning
eq
uipm
ent?
Lac
k of
sup
-pl
ies/
dru
gs?
Oth
er?
81. M
anag
emen
t of G
allb
ladd
er P
atho
logi
es
a. C
hole
cyst
ecto
my
b. C
hole
cyst
osto
my
a) Y
N
b) Y
N
# #
a) Y
N
b) Y
N82
. Rep
air o
f her
nias
Y
N#
Y
N83
. Ana
l Pat
holo
gy M
anag
emen
t:
• H
aem
orrh
oide
ctom
y
• Fi
stul
otom
ies
and/
or d
rain
age
of p
eria
nal
absc
esse
s
Y
N#
Y
N
84. C
ompl
ex s
urgi
cal i
nfec
tion
man
age-
men
t:
a. S
eptic
art
hriti
s, o
steo
mye
litis
b. P
yom
yosit
is
c. S
urgi
cal m
anag
emen
t of h
and
infe
ctio
n
a) Y
N
b) Y
N
c) Y
N
# # #
a) Y
N
b) Y
N
c) Y
N
85. T
rans
vesi
cal-p
rost
atec
tom
y (T
VP)
Y
N#
Y
N
Surg
eon
or IE
SOIn
terv
entio
ns
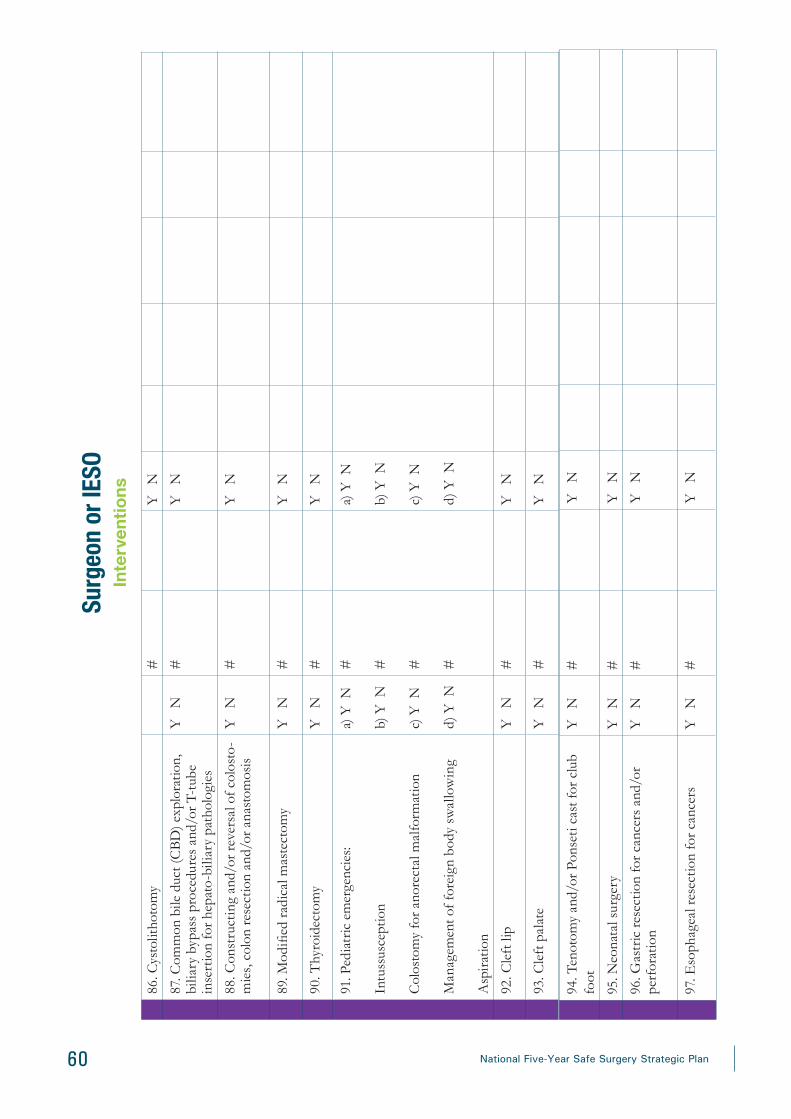
60 National Five-Year Safe Surgery Strategic Plan
86. C
ysto
litho
tom
y#
Y
N
87. C
omm
on b
ile d
uct (
CB
D) e
xplo
ratio
n,
bilia
ry b
ypas
s pr
oced
ures
and
/or T
-tub
e in
sert
ion
for h
epat
o-bi
liary
pat
holo
gies
Y
N#
Y
N
88. C
onst
ruct
ing
and/
or re
vers
al o
f col
osto
-m
ies,
col
on re
sect
ion
and/
or a
nast
omos
isY
N
#Y
N
89. M
odifi
ed r
adic
al m
aste
ctom
y Y
N
#Y
N
90. T
hyro
idec
tom
yY
N
#Y
N
91. P
edia
tric
em
erge
ncie
s:
Intu
ssus
cept
ion
Col
osto
my
for a
nore
ctal
mal
form
atio
n
Man
agem
ent o
f for
eign
bod
y sw
allo
win
g
Asp
irat
ion
a) Y
N
b) Y
N
c) Y
N
d) Y
N
# # # #
a) Y
N
b) Y
N
c) Y
N
d) Y
N
92. C
left
lip
Y
N#
Y
N
93. C
left
pal
ate
Y
N#
Y
N
Surg
eon
or IE
SOIn
terv
entio
ns
94. T
enot
omy
and/
or P
onse
ti ca
st fo
r clu
b fo
otY
N
#Y
N
95. N
eona
tal s
urge
ryY
N
#Y
N
96. G
astr
ic re
sect
ion
for c
ance
rs a
nd/o
r pe
rfor
atio
nY
N
#Y
N
97. E
soph
agea
l res
ectio
n fo
r can
cers
Y
N#
Y
N

61National Five-Year Safe Surgery Strategic Plan
98. E
soph
agea
l res
ectio
n fo
r per
fora
tion
Y
N#
Y
N
99. P
ulm
onar
y re
sect
ions
and
/or m
edia
sti-
nal p
roce
dure
s fo
r che
st p
atho
logi
esY
N
#Y
N
Oph
thal
mic
, Ora
l, D
enta
l Pro
cedu
res
100.
Ext
ract
ion
of p
rim
ary
and
perm
anen
t to
oth
Y
N#
Y
N
101.
Inc
isio
n an
d/or
dra
inag
e (p
erio
dont
al a
nd
dent
al a
bsce
ss)
Y
N#
Y
N
102.
Den
tal c
arie
s tr
eatm
ents
and
/or s
calin
g Y
N
#Y
N
103.
Rep
lant
atio
n of
avu
lsed
teet
hY
N
#Y
N
104.
Dis
impa
ctio
n Y
N
#Y
N
105.
For
eign
bod
y re
mov
al fr
om n
ose,
ear
s,
thro
atY
N
#Y
N
106.
Ear
and
/or e
ye ir
riga
tion
Y
N#
Y
N
107.
Red
uctio
n of
acu
te T
MJ d
islo
catio
nY
N
#Y
N
108.
Oro
faci
al in
fect
ion
man
agem
ent
Y
N#
Y
N
109.
Cat
arac
t sur
gery
Y
N#
Y
N
110.
Tar
soto
my
(upp
er e
yelid
)Y
N
#Y
N
111.
Eye
enu
clea
tion
Y
N#
Y
N
Surg
eon
or IE
SOIn
terv
entio
ns

62 National Five-Year Safe Surgery Strategic Plan
112.
Man
agem
ent o
f fac
ial b
one
frac
ture
s an
d/or
inju
ry to
den
titio
n (in
terd
enta
l wir
ing,
ar
ch b
ar, I
MF
and
open
redu
ctio
n)
Y
N#
Y
N
113.
Myr
ingo
tom
y fo
r otit
is m
edia
Y
N#
Y
N
114.
Ton
sille
ctom
yY
N
#Y
N
115.
Sur
gica
l man
agem
ent o
f com
mon
ben
ign
and/
or m
alig
nant
tum
ors
and
cyst
of o
ral
& m
axill
ofac
ial r
egio
ns
Y
N#
Y
N
Surg
eon
or IE
SOIn
terv
entio
ns

63National Five-Year Safe Surgery Strategic Plan
Emergency and Essential Surgical Care Equipment and SuppliesPlease ask questions in point in time context i.e. what is able to be done at time of assessment.Capital Outlays
0
absent
1
available with
shortages or difficulties
2
fully available for
all patients all the time
Remark
116. Suction pump (manual or electric) with catheter117. Blood pressure measuring equip-ment118. Scalpel with blades119. Retractors120. Scissors121. Tissue forceps122. Gloves (sterile)123. Gloves (examination)124. Needle holder125. Sterilizing skin prep
Renewable Items
126. Nasogastric tubes127. Light source (lamp & flash light)128. Intravenous fluid infusion set129. Intravenous cannulas/scalp vein infusion set130. Syringes with needles (disposable)131. Sharps disposal container132. Tourniquet
133. Needles & sutures134. Splints for arm, leg135. Waste disposal container136. Face masks137. Eye protection138. Protective gowns/aprons139. Soap140 Electrocautery
Supplementary Equipment for use by skilled health professionals141. Adult Mcgill forceps
142. Pediatric Mcgill forceps
143. Chest tubes insertion equipment
144. Tracheostomy set

64 National Five-Year Safe Surgery Strategic Plan
Surgeon or IESOFinancing
Cost145. What is the average out-of-pocket cost to a patient
for an open fracture repair (procedure only)? #
146. What is the average out-of-pocket cost to a patient for a laparotomy (procedure only)?
#
147. What is the average out-of-pocket cost to a patient for a CBC?
#
148. What is the average out-of-pocket cost to a patient for a chest X-ray?
#
149. What is the average out-of-pocket cost to a patient for surgery-associated lodging (e.g. bed, overnight stays) per visit?
Surgery-associated lodging: defined as in a single visit, before returning home (include lodging for patient and lodging for the caretaker)
#
150. What do the most patients pay out-of-pocket for patient and family transportation per visit?
a. Emergency visitsb. Elective visits
#
#
151. What is the average out-of-pocket cost to a patient for surgery-associated medication per visit (e.g. perfo-rated appendix)?
#
152. What is the average out-of-pocket cost to a patient for other necessities (e.g. laundry/food) per visit?
#
Information Management
Research Agenda153. How many ongoing research projects does the de-
partment of surgery have?
Exclude resident, intern and student research papers.
#

65National Five-Year Safe Surgery Strategic Plan
Surgeon or IESOSurgical Sets
154. How many surgical sets are available for treatment of open fractures?
Missing: defined as any part of a surgical set that is absent or non-functional
a) Complete #
b) Incomplete #
c) If incomplete, what is missing?
155. How many surgical sets are available for laparoto-my?
Missing: defined as any part of a surgical set that is absent or non-functional
a) Complete #
b) Incomplete #
c) If incomplete, what is missing?

66 National Five-Year Safe Surgery Strategic Plan
OB/GYN (Surgeon/IESO if not available)Infrastructure
Items Insert number.
1. Total number of surgical OB/GYN procedures per month (on average in the past 6 months)?
Minor #
Major #
Management Guidelines
Fill in with percentages.
2. How often do you have management guidelines available for obstetrics?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
3. How often do you have management guidelines available for maternal delivery?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
Human ResourcesFull time Contracted
(short-term)
Residents/trainees
4. OB/GYNs? #
5. Midwives? #
6. How often are OB/GYN services available for 24 hours a day? (on average in the past month)
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)

67National Five-Year Safe Surgery Strategic Plan
OB/G
YN (S
urge
on/IE
SO if
not
avail
able)
Inte
rven
tion
sPl
ease
ask
que
stio
ns in
poi
nt in
tim
e co
ntex
t i.e
. wha
t is
able
to b
e do
ne a
t tim
e of
ass
essm
ent.
Do
you
perf
orm
thes
e pr
oced
ures
?
Yes/
No
If Y
es,
How
man
y pr
oced
ures
pe
rfor
med
in
past
mon
th?
If N
o,
Why
not
?
Do
you
refe
r?
Lac
k of
sk
ills?
If y
ou re
fer,
is it
due
to…
(mar
k A
LL
that
app
ly)
Lac
k of
st
aff?
Non
-fun
c-tio
ning
eq
uipm
ent?
Lac
k of
su
pplie
s/
drug
s?
Oth
er?
Obs
tetr
ics
7. C
aesa
rean
Sec
tion
Y
N#
Y
N
8. A
bdom
inal
Hys
tere
ctom
yY
N
#Y
N
9. R
epai
r of U
teri
ne p
erfo
ratio
n or
rup
ture
(in
trac
tabl
e PP
H)
Y
N#
Y
N
10. N
orm
al d
eliv
ery
Y
N#
Y
N
11. M
anua
l rem
oval
of t
he p
lace
nta
Y
N#
Y
N
12. V
acuu
m-a
ssis
ted
deliv
ery
Y
N#
Y
N
13. R
epai
r of G
enita
l Lac
erat
ion/
Inju
ryY
N
#Y
N
14. C
ompr
ehen
sive
abo
rtio
n ca
re
Y
N#
Y
N
15. S
urge
ry fo
r ect
opic
pre
gnan
cyY
N
#Y
N

68 National Five-Year Safe Surgery Strategic Plan
16. V
IAY
N
#Y
N
17. C
ryot
hera
py fo
r pre
canc
erou
s ce
rvic
al
lesi
ons
Y
N#
Y
N
18. C
ervi
cal b
iops
yY
N
#Y
N
19. E
ndom
etri
al b
iops
yY
N
#Y
N
20. T
ubal
liga
tion
Y
N#
Y
N
21. I
ncis
ion
of H
ymen
for i
mpe
rfor
ate
hym
en
with
hem
atoc
olpo
s an
d/or
hem
atom
ata
Y
N#
Y
N
22. S
urgi
cal m
anag
emen
t of p
elvi
c or
gan
prol
apse
Y
N#
Y
N
23. S
urgi
cal m
anag
emen
t of m
ajor
ben
ign
and/
or m
alig
nant
gyn
ecol
ogic
con
ditio
ns
Y
N#
Y
N
24. R
epai
r of o
bste
tric
fist
ula
Y
N#
Y
N
OB/G
YN (S
urge
on/IE
SO if
not
avail
able)
Inte
rven
tion
s
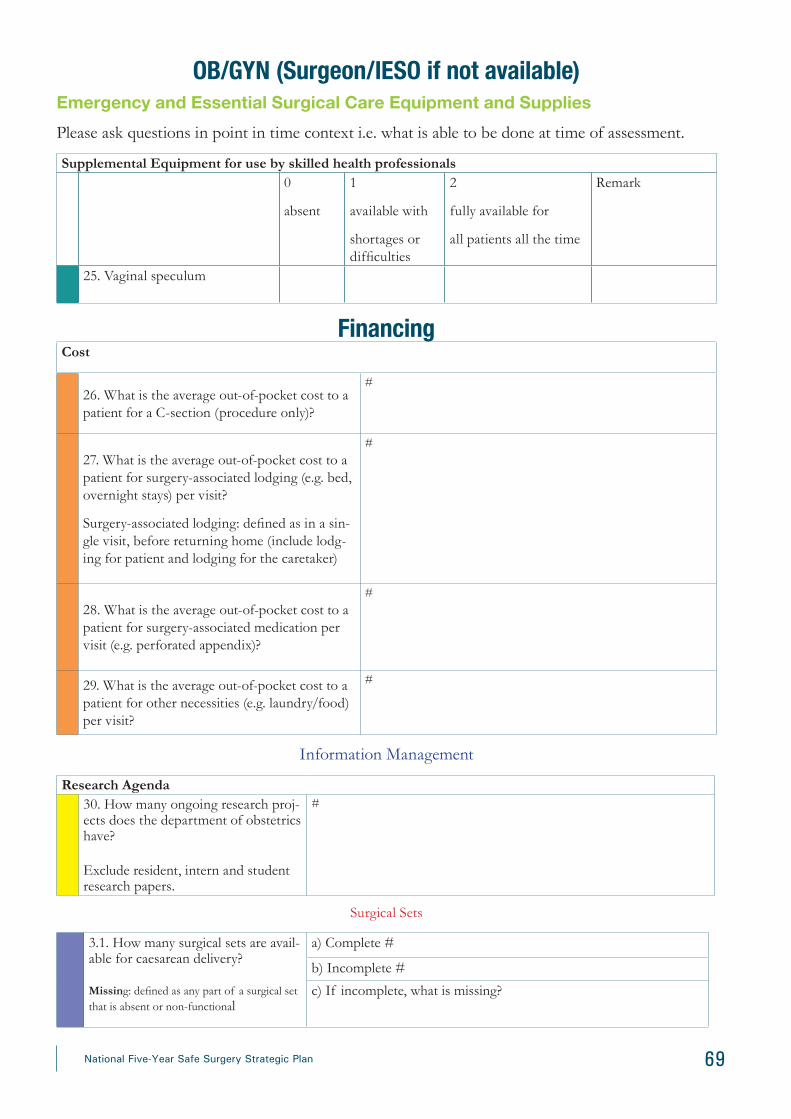
69National Five-Year Safe Surgery Strategic Plan
OB/GYN (Surgeon/IESO if not available)Emergency and Essential Surgical Care Equipment and SuppliesPlease ask questions in point in time context i.e. what is able to be done at time of assessment.
Supplemental Equipment for use by skilled health professionals0
absent
1
available with
shortages or difficulties
2
fully available for
all patients all the time
Remark
25. Vaginal speculum
FinancingCost
26. What is the average out-of-pocket cost to a patient for a C-section (procedure only)?
#
27. What is the average out-of-pocket cost to a patient for surgery-associated lodging (e.g. bed, overnight stays) per visit?
Surgery-associated lodging: defined as in a sin-gle visit, before returning home (include lodg-ing for patient and lodging for the caretaker)
#
28. What is the average out-of-pocket cost to a patient for surgery-associated medication per visit (e.g. perforated appendix)?
#
29. What is the average out-of-pocket cost to a patient for other necessities (e.g. laundry/food) per visit?
#
Information Management
Research Agenda30. How many ongoing research proj-ects does the department of obstetrics have?
Exclude resident, intern and student research papers.
#
Surgical Sets
3.1. How many surgical sets are avail-able for caesarean delivery?
Missing: defined as any part of a surgical set that is absent or non-functional
a) Complete #
b) Incomplete #
c) If incomplete, what is missing?

70 National Five-Year Safe Surgery Strategic Plan
OB/GYN (Surgeon/IESO if not available)
InfrastructureQuality and Safety
1. For Anesthetist/Nurse to answer:
How often is the WHO surgical safety check-list utilized in the operating rooms?
2. For Data Collector (if able):
Calculate # of times the checklist is used in a random selection of 20 charts:
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
#
Operating RoomFill in with percentages.3. How many anesthesia machines do you have for the OT?
4. How many of those machines are regular-ly used?
5. If not in use, why? (e.g. machines not functional, surgical ser-vices not yet started)
#
#
6, How often do you have oxygen cylin-der or concentrator supply with mask and tubing?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
7. How often is a pulse oximetry used in the operating theater?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
8. How often do you keep anesthesia related records?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
Management Guidelines
Fill in with percentages.
9. How often do you have management guidelines available for anesthesia?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
10. How often do you have management guidelines available for pain relief?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
Supplies11. How often do you have a functioning adult pulse oximeter available?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
12. How often do you have a functioning pediatric pulse oximeter available?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
13. How often do you have adult blood pres-sure monitoring available?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
14. How often do you have pediatric blood pressure monitoring available?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
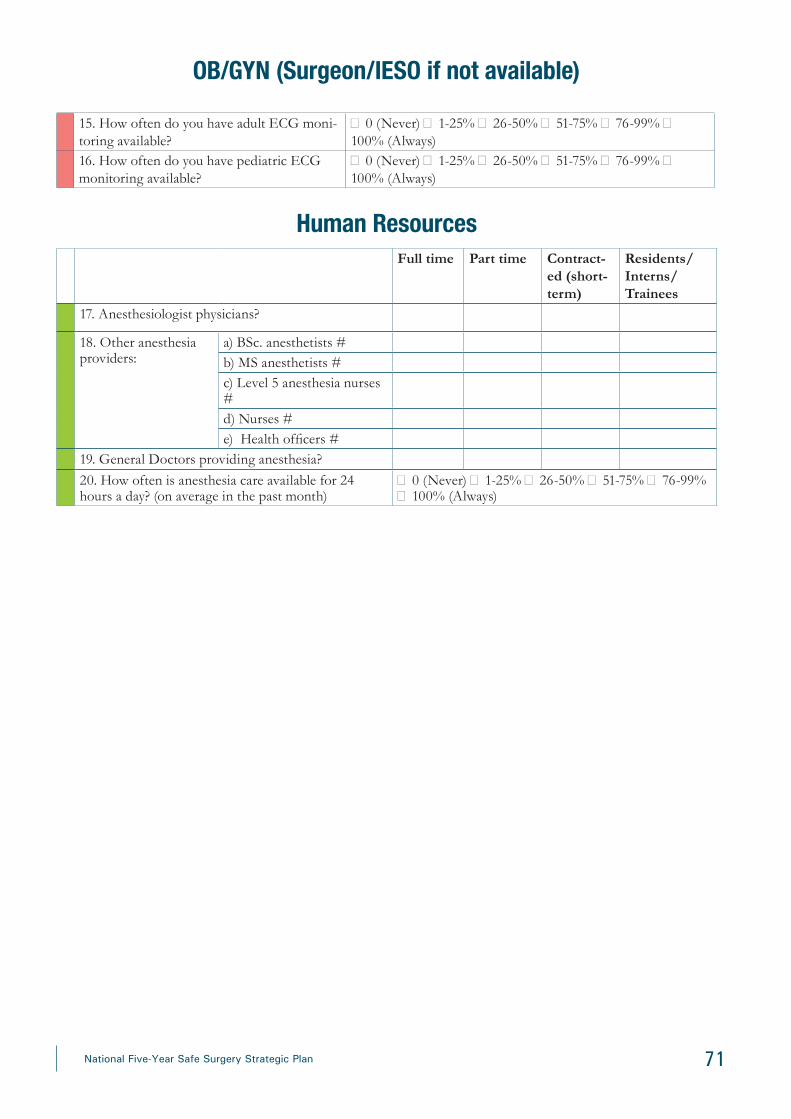
71National Five-Year Safe Surgery Strategic Plan
15. How often do you have adult ECG moni-toring available?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
16. How often do you have pediatric ECG monitoring available?
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
Human ResourcesFull time Part time Contract-
ed (short-term)
Residents/Interns/ Trainees
17. Anesthesiologist physicians?
18. Other anesthesia providers:
a) BSc. anesthetists #b) MS anesthetists #c) Level 5 anesthesia nurses #d) Nurses #e) Health officers #
19. General Doctors providing anesthesia?20. How often is anesthesia care available for 24 hours a day? (on average in the past month)
� 0 (Never) � 1-25% � 26-50% � 51-75% � 76-99% � 100% (Always)
OB/GYN (Surgeon/IESO if not available)
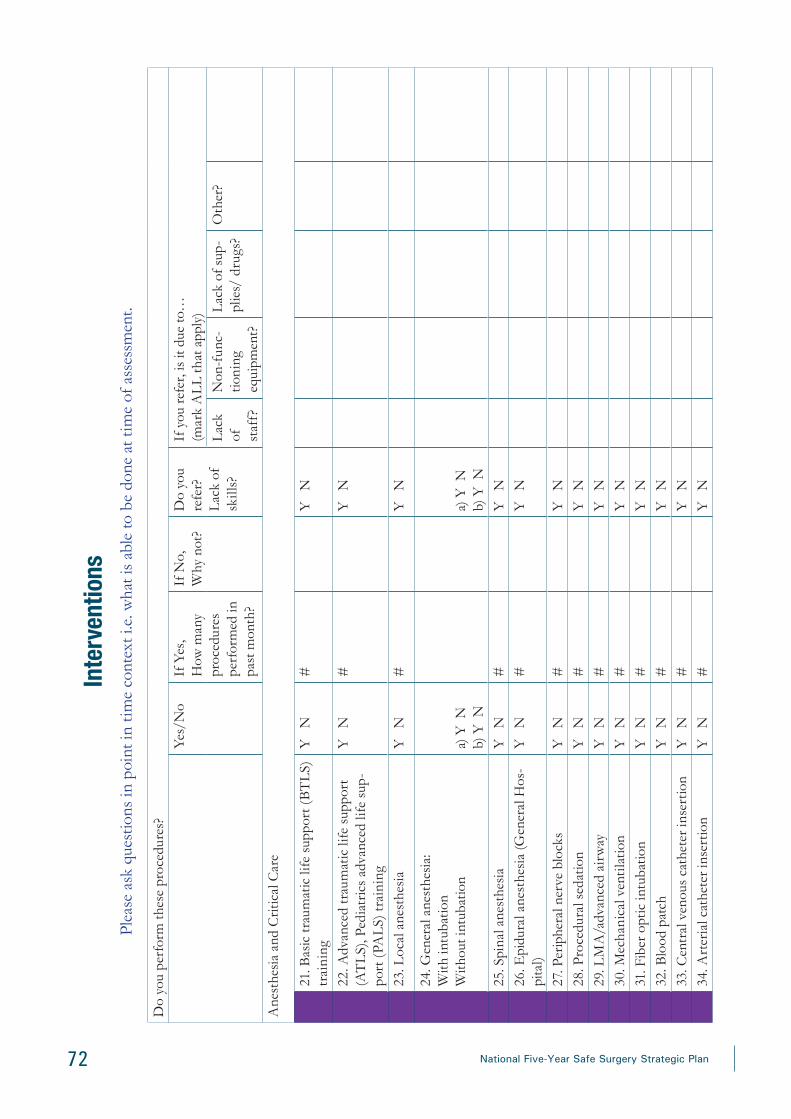
72 National Five-Year Safe Surgery Strategic Plan
Inte
rven
tions
Plea
se a
sk q
uest
ions
in p
oint
in ti
me
cont
ext i
.e. w
hat i
s ab
le to
be
done
at t
ime
of a
sses
smen
t.
Do
you
perf
orm
thes
e pr
oced
ures
?Ye
s/N
oIf
Yes
, H
ow m
any
proc
edur
es
perf
orm
ed in
pa
st m
onth
?
If N
o,
Why
not
?D
o yo
u re
fer?
Lac
k of
sk
ills?
If y
ou re
fer,
is it
due
to…
(mar
k A
LL
that
app
ly)
Lac
k of
st
aff?
Non
-fun
c-tio
ning
eq
uipm
ent?
Lac
k of
sup
-pl
ies/
dru
gs?
Oth
er?
Ane
sthe
sia
and
Crit
ical
Car
e
21. B
asic
trau
mat
ic li
fe s
uppo
rt (
BT
LS)
tr
aini
ng
Y
N#
Y
N
22. A
dvan
ced
trau
mat
ic li
fe s
uppo
rt
(AT
LS)
, Ped
iatr
ics
adva
nced
life
sup
-po
rt (
PAL
S) tr
aini
ng
Y
N#
Y
N
23. L
ocal
ane
sthe
sia
Y
N#
Y
N
24. G
ener
al a
nest
hesi
a:W
ith in
tuba
tion
With
out i
ntub
atio
na)
Y N
b) Y
Na)
Y N
b) Y
N25
. Spi
nal a
nest
hesi
aY
N
#Y
N
26. E
pidu
ral a
nest
hesi
a (G
ener
al H
os-
pita
l)Y
N
#Y
N
27. P
erip
hera
l ner
ve b
lock
sY
N
#Y
N
28. P
roce
dura
l sed
atio
nY
N
#Y
N
29. L
MA
/adv
ance
d ai
rway
Y
N#
Y
N30
. Mec
hani
cal v
enti
latio
nY
N
#Y
N
31. F
iber
opt
ic in
tuba
tion
Y
N#
Y
N32
. Blo
od p
atch
Y
N#
Y
N33
. Cen
tral
ven
ous
cath
eter
inse
rtio
nY
N
#Y
N
34. A
rter
ial c
athe
ter i
nser
tion
Y
N#
Y
N

73National Five-Year Safe Surgery Strategic Plan
Emergency and Essential Surgical Care Equipment and SuppliesPlease ask questions in point in time context i.e. what is able to be done at time of assessment.
Capital Outlays0absent
1available with shortages or difficulties
2fully available forall patients all the time
Remark
35. Resuscitator bag valve & mask (adult)
36. Resuscitator bag valve & mask (pediatric)
37. Stethoscope
38. Thermometer
39. Oropharyngeal airway (adult size)
40. Oropharyngeal airway (pediatric size)
Supplementary equipment for use by skilled health professionals
41. Endotracheal tubes (adult)
42. Endotracheal tubes (pediatric)
43. IV infuser bags
44. Laryngoscope Macintosh blades with bulbs & batteries (adult) 45. Laryngoscope Macintosh blades with bulbs & batteries (pediatric)
Please check availability of following items.Items Yes No Remark 46. Functional Anesthesia Machine47. Anesthesia machine48. Ambu bag 49. Oral airways 50. Nasal airways51. Perfuser52. Patient monitor53. Patient monitor for transport54. Esophageal stethoscope55. Blood or Fluid pumper56. Warming blanket57. Mechanical ventilator for transport58. Suction machine 59. Capnogram60. Portable pulse oximeter61. Blood warmer62. Stethoscope

74 National Five-Year Safe Surgery Strategic Plan
63. Manual BP apparatus64. Oxygen gauge65. Oxygen cylinder66. Bougie (Adult)67. Bougie (Pediatric)68. Stylet (Adult)69. Stylet (Pediatric)70. Anesthesia trolley71. Oxygen concentrator72. Double lumen tube 35- 4273. Suction tip74. Urinary Catheter75. Spinal needle 22-2676. Epidural set77. Tegaderm78. Insulated nerve block needles79. Central venous catheterization set80. Arterial line set with module81. Defibrillator
Items Yes No Remark
Emergency and Essential Surgical Care Equipment and Supplies
PharmaceuticalsLocal Anesthetics
82. Lidocaine 1% with adrenaline83. Lidocaine 2% with adrenaline84. Lidocaine 1% without adrenaline85. Lidocaine 2% without adrenaline86. Bupivacaine 0.5%
General Anesthetics87. Halothane 88. Isoflurane89. Sevoflurane
Paralytics90. Succinylcholine91. Rocuronium92. Vecuronium93. Pancuronium94. Atracurium95. Cisatricurium
Sedatives96. Thiopental

75National Five-Year Safe Surgery Strategic Plan
Items Yes No Remark
97. Ketamine98. Propofol99. Etomidate
Analgesic 100. Pethidine101. Fentanyl102. Sufentanil 103. Morphine10.4. Alfentanil
Benzodiazepines 105. Diazepam106. Midazolam
Diuretics107. Furosemide IV
Vasopressors108. Noradrenaline109. Dopamine 110. Dobutamine111. Phenylephrine112. Adrenaline113. Ephedrine
Beta-blockers114. Labetolol115. Metoprolol116. Propranolol117. Esmolol
Steroids118. Hydrocortisone119. Dexamethasone
Anti-emetics120. Ondansetrone121. Metaclopramide
IV Fluids122. Normal Saline123. Dextrose in Normal Saline124. 5% Dextrose125. Ringer’s Lactate
Miscellaneous
Emergency and Essential Surgical Care Equipment and Supplies

76 National Five-Year Safe Surgery Strategic Plan
126. Naloxone127. Salbutamol inhaler128. Dantrolene129. Atropine130. Glycopyrrolate131. Neostigmine 132. Aminophylline133. Lidocaine IV134. Hydralazine 135. Amiodarone136. Intralipid137. 40% glucose
Information ManagementResearch Agenda
138. How many ongoing research projects does the department of anesthesia have?
Exclude resident, intern and student research papers.
#
Items Yes No Remark
Emergency and Essential Surgical Care Equipment and Supplies

77National Five-Year Safe Surgery Strategic Plan
Ann
ex B
: Sa
fe s
urge
ry c
heck
list
Patie
nt N
ame:
___
____
____
____
____
____
____
____
__
Med
ical
Rec
ord
Num
ber:
____
____
____
__
Bef
ore
indu
ctio
n of
ane
sthe
sia
Bef
ore
skin
inci
sion
Bef
ore
pati
ent l
eave
s O
R
Patie
nt h
as c
onfir
med
Con
firm
all
team
mem
bers
hav
e in
trod
uced
them
-se
lves
by
nam
e an
d ro
leN
urse
ver
bally
con
firm
s w
ith th
e te
am:
Iden
tity
Surg
eon,
ane
sthe
sia
prof
essi
onal
and
nur
se v
erba
l-ly
con
firm
The
nam
e of
the
proc
edur
e re
cord
ed
Site
Patie
ntT
hat i
nstr
umen
t, sp
onge
and
nee
dle
Proc
edur
eSi
teC
ount
s ar
e co
rrec
t (or
not
app
licab
le)
Con
sent
Proc
edur
eSp
ecim
en is
labe
lled
(incl
udin
g pa
tient
na
me)
Site
mar
ked/
not a
pplic
able
Ant
icip
ated
crit
ical
eve
nts
Any
equ
ipm
ent p
robl
ems
to b
e ad
dres
sed
Ane
sthe
sia
safe
ty c
heck
com
plet
edSu
rgeo
n re
view
s: cr
itica
l or u
nexp
ecte
d st
eps,
op
erat
ive
dura
tion,
ant
icip
ated
blo
od lo
ss?
Surg
eon,
ana
esth
esia
pro
fess
iona
l and
nur
se
revi
ew th
e ke
y co
ncer
ns fo
r rec
over
y an
d m
anag
emen
t of t
his
patie
nt
Puls
e ox
imet
er o
n pa
tient
and
fun
ctio
ning
Ane
sthe
sia
team
revi
ews:
any
patie
nt-s
peci
fic
conc
erns
?D
oes
patie
nt h
ave
know
n al
lerg
y?
•
No
•
Yes
Nur
sing
team
revi
ews:
has
ster
ility
(Inc
ludi
ng in
dica
tor r
esul
ts) b
een
confi
rmed
? ar
e th
ere
equi
pmen
t iss
ues
or a
ny c
once
rns?

78 National Five-Year Safe Surgery Strategic Plan
Bef
ore
indu
ctio
n of
ane
sthe
sia
Bef
ore
skin
inci
sion
Bef
ore
pati
ent l
eave
s O
R
Diffi
cult
airw
ay/a
spir
atio
n ri
sk?
•
No
Ant
ibio
tic p
roph
ylax
is g
iven
with
in la
st 6
0 m
in-
utes
?
yes
•
Yes,
and
equ
ipm
ent/
assi
stan
ce a
vaila
ble
Not
app
licab
leR
isk o
f >50
0ml b
lood
loss
(7m
l/kg
in c
hild
ren)
?
Is e
ssen
tial i
mag
ing
disp
laye
d?
yes
•
No
Not
app
licab
le•
Ye
s, a
nd a
dequ
ate
intr
aven
ous
acce
ss
and
fluid
s pl
anne
d
Safe
sur
gery
che
cklis
t

79National Five-Year Safe Surgery Strategic Plan
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
olSu
rgic
al a
nd A
nest
hesi
a C
are
Aud
it T
ool
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
Surg
ical
Ser
vice
Sta
ndar
d 1:
The
hea
lth fa
cilit
y ha
s an
app
ropr
iate
wor
king
sys
tem
AN
D p
hysi
cal e
nviro
nmen
t with
ade
quat
e w
orki
ng g
uide
lines
, uti
litie
s, m
edi-
cine
s, s
uppl
ies
and
equi
pmen
t for
pro
vidi
ng q
ualit
y su
rgic
al s
ervi
ces.
SS 1
.1 W
ater
, ene
rgy,
san
itatio
n, h
andw
ash-
ing
and
was
te d
ispo
sal f
acili
ties
are
func
-tio
nal,
relia
ble,
saf
e an
d su
ffici
ent t
o m
eet
the
need
s of
sta
ff, c
lient
s an
d th
eir f
amili
es
(as
per n
atio
nal s
tand
ard)
.
Con
tinu
ous
elec
tric
sup
ply
with
bac
kup
gene
rato
r is
avai
labl
e.
1
In c
ase
of p
ower
cut
, gen
erat
or is
aut
omat
ic o
r can
be
star
ted
with
in 5
m
inut
es.
1
Con
tinu
ous
wat
er s
uppl
y is
ava
ilabl
e.
1
Ade
quat
e ba
ckup
wat
er s
ourc
e is
ava
ilabl
e w
hen
ther
e is
inte
rrup
tion
from
the
mai
n so
urce
. 1
Tank
ers,
roto
s
Func
tiona
l tel
epho
ne is
ava
ilabl
e in
liai
son
offic
e.
1
Tele
phon
e se
rvic
e is
ava
ilabl
e fo
r int
erna
l com
mun
icat
ion
(fixe
d or
m
obile
).1
Cen
tral
ope
rato
r or s
epar
ate
lines
in
labo
rato
ry, p
harm
acy
etc.
Lea
kpro
of c
over
ed a
nd la
bele
d w
aste
bin
s an
d im
perm
eabl
e sh
arps
co
ntai
ners
ava
ilabl
e to
seg
rega
te w
aste
into
3 c
ateg
orie
s.1
Ver
ify
in a
ll w
ards
/roo
ms
used
for
surg
ical
ser
vice
0 if
mis
sed/
non
func
tiona
l eve
n in
one
ro
om
At l
east
one
fun
ctio
ning
han
d hy
gien
e st
atio
n pe
r 10
beds
with
soa
p an
d w
ater
or a
lcoh
ol b
ased
han
d ru
bs in
all
surg
ical
war
ds (1
:6).
3
Ver
ify
in a
ll w
ards
/roo
ms
used
for
surg
ical
ser
vice
0 if
mis
sed/
nonf
unct
iona
l eve
n in
one
ro
om
Hea
lth c
are
staf
f dem
onst
rate
cle
anin
g th
eir h
ands
cor
rect
ly a
s pe
r the
W
HO
5 m
omen
ts fo
r han
d hy
gien
e (a
udit
tool
exi
sts)
.8
Staf
f Int
ervi
ew
Che
ck th
e sk
ills
of fo
ur h
ealth
car
e w
orke
rs

80 National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
Writ
ten,
up-
to-d
ate
prot
ocol
s an
d aw
aren
ess
rais
ing
mat
eria
ls (
post
ers)
on
cle
anin
g an
d di
sinf
ectio
n, h
and
hygi
ene,
ope
rati
ng a
nd m
aint
aini
ng
wat
er, s
anita
tion
and
hygi
ene
faci
litie
s, s
afe
was
te m
anag
emen
t are
ava
il-ab
le a
t all
area
s an
d ar
e vi
sibl
y po
sted
. 1
Ver
ify
in a
ll w
ards
/roo
ms
used
for
surg
ical
ser
vice
0 if
mis
sed/
nonf
unct
iona
l eve
n in
one
ro
om
Sani
tatio
n fa
cilit
ies
are
appr
opri
atel
y ill
umin
ated
at n
ight
, acc
essi
ble
to
peop
le w
ith li
mite
d m
obili
ty, g
ende
r sep
arat
ed fo
r sta
ff a
nd p
atie
nts,
in
clud
e at
leas
t one
toile
t tha
t mee
ts m
enst
rual
hyg
iene
man
agem
ent
need
s, h
andw
ashi
ng s
tatio
ns w
ith s
oap
and
wat
er a
dequ
ate
num
ber (
at
leas
t 1 la
trin
e pe
r 20
user
s fo
r inp
atie
nt s
etti
ngs)
.
6
1 fo
r eac
h bu
llet
Suffi
cien
t fun
ds a
re a
lloca
ted
to s
uppo
rt re
habi
litat
ion,
impr
ovem
ents
an
d on
goin
g op
erat
ion
and
mai
nten
ance
of w
ater
, san
itatio
n, h
ygie
ne
and
heal
th c
are
was
te s
ervi
ces.
3D
ocum
ent r
evie
w
Cur
ativ
e an
d pr
even
tativ
e ri
sk-m
anag
emen
t pla
n ex
ists
for m
anag
ing
and
impr
ovin
g w
ater
, san
itatio
n an
d hy
gien
e se
rvic
es.
1
Sugg
estio
n bo
x, re
gist
er, c
ompl
aint
han
dlin
g of
fice
is a
vaila
ble
for h
an-
dlin
g co
mpl
iant
of c
lient
s an
d th
eir f
amili
es.
1
Sugg
estio
ns a
nd c
ompl
aint
s ar
e re
view
ed in
the
day
to d
ay H
DA
and
ap
prop
riat
e m
easu
res
are
take
n w
hen
need
ed.
5
Clie
nts
and
fam
ilies
att
endi
ng th
e he
alth
faci
lity
wer
e sa
tisfie
d w
ith th
e w
ater
, san
itatio
n an
d en
ergy
ser
vice
s an
d w
ould
reco
mm
end
the
heal
th
faci
lity
to f
rien
ds a
nd fa
mily
.10
Clie
nt I
nter
view
All
heal
th c
are
staf
f are
sat
isfie
d w
ith th
e w
ater
, san
itatio
n an
d en
ergy
se
rvic
es a
nd b
elie
ved
that
suc
h se
rvic
es c
ontr
ibut
e po
sitiv
ely
to p
rovi
d-in
g qu
ality
car
e.8
Staf
f Int
ervi
ew
2 he
alth
car
e w
orke
rs a
nd 2
sup
port
st
affs
Clie
nts
and
thei
r fam
ilies
att
endi
ng th
e he
alth
faci
lity
wer
e sa
tisfie
d w
ith
the
pow
er a
nd li
ghti
ng s
ourc
e an
d w
ould
reco
mm
end
the
heal
th fa
cilit
y to
fri
ends
and
fam
ily.
10C
lient
Int
ervi
ew
Roo
ms
are
wel
l ven
tila
ted,
illu
min
ated
, reg
ular
ly c
lean
ed a
nd m
ain-
tain
ed.
1
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol
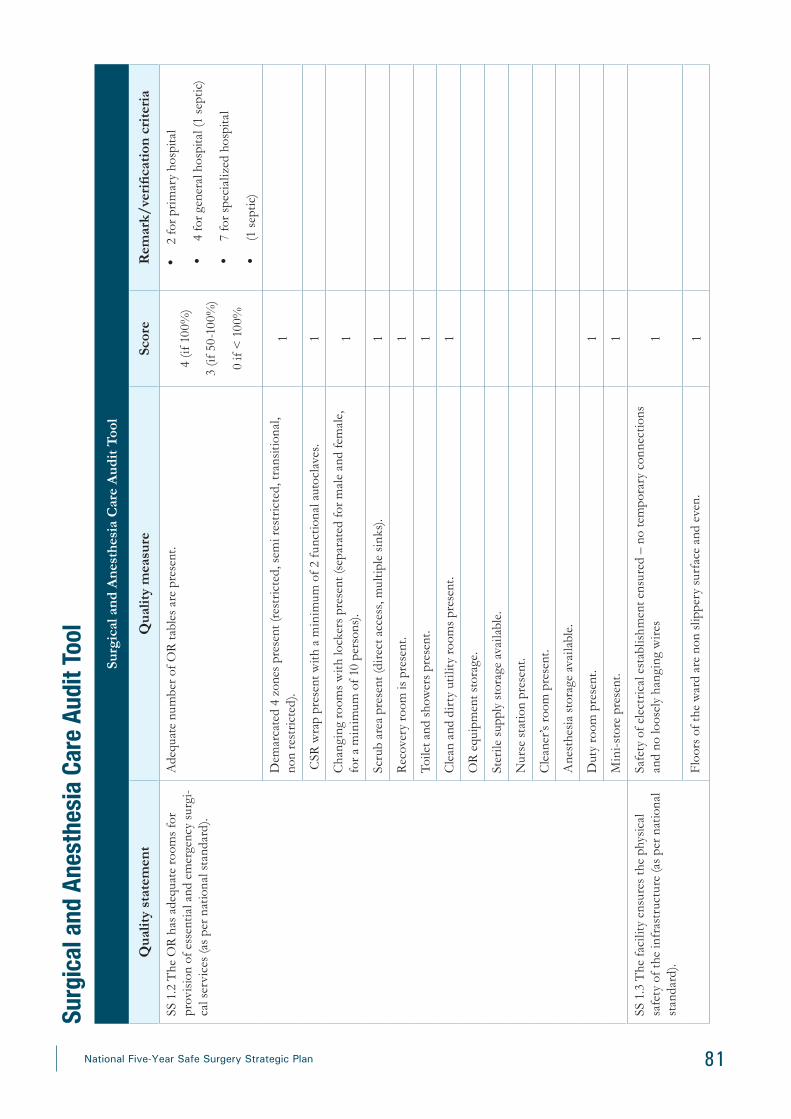
81National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
SS 1
.2 T
he O
R h
as a
dequ
ate
room
s fo
r pr
ovis
ion
of e
ssen
tial a
nd e
mer
genc
y su
rgi-
cal s
ervi
ces
(as
per n
atio
nal s
tand
ard)
.
Ade
quat
e nu
mbe
r of O
R ta
bles
are
pre
sent
. 4
(if 1
00%
)
3 (if
50-
100%
)
0 if
< 1
00%
•
2 fo
r pri
mar
y ho
spita
l
•
4 fo
r gen
eral
hos
pita
l (1
sept
ic)
•
7 fo
r spe
cial
ized
hos
pita
l
•
(1 s
eptic
)
Dem
arca
ted
4 zo
nes
pres
ent (
rest
rict
ed, s
emi r
estr
icte
d, tr
ansi
tiona
l, no
n re
stri
cted
).1
CSR
wra
p pr
esen
t with
a m
inim
um o
f 2 f
unct
iona
l aut
ocla
ves.
1
Cha
ngin
g ro
oms
with
lock
ers
pres
ent (
sepa
rate
d fo
r mal
e an
d fe
mal
e,
for a
min
imum
of 1
0 pe
rson
s).
1
Scru
b ar
ea p
rese
nt (d
irec
t acc
ess,
mul
tiple
sin
ks).
1
Rec
over
y ro
om is
pre
sent
. 1
Toile
t and
sho
wer
s pr
esen
t. 1
Cle
an a
nd d
irty
uti
lity
room
s pr
esen
t. 1
OR
equ
ipm
ent s
tora
ge.
Ster
ile s
uppl
y st
orag
e av
aila
ble.
Nur
se s
tatio
n pr
esen
t.
Cle
aner
’s ro
om p
rese
nt.
Ane
sthe
sia
stor
age
avai
labl
e.
Dut
y ro
om p
rese
nt.
1
Min
i-sto
re p
rese
nt.
1
SS 1
.3 T
he fa
cilit
y en
sure
s th
e ph
ysic
al
safe
ty o
f the
infr
astr
uctu
re (a
s pe
r nat
iona
l st
anda
rd).
Safe
ty o
f ele
ctri
cal e
stab
lishm
ent e
nsur
ed –
no
tem
pora
ry c
onne
ctio
ns
and
no lo
osel
y ha
ngin
g w
ires
1
Floo
rs o
f the
war
d ar
e no
n sl
ippe
ry s
urfa
ce a
nd e
ven.
1
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

82 National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
Win
dow
s/ v
enti
lato
rs if
any
in th
e O
R a
re in
tact
and
sea
led.
1
SS 1
.4 F
inan
cial
pro
tect
ion
give
n fr
om c
ost
of c
are.
Ove
rall
cost
of c
are
is n
ot e
xpen
sive
. 10
Clie
nt I
nter
view
Pres
crib
ed in
vest
igat
ions
are
ava
ilabl
e at
the
faci
lity.
10C
hart
Rev
iew
The
faci
lity
ensu
res
that
dru
gs p
resc
ribe
d ar
e av
aila
ble
at p
harm
acy
and
war
ds.
10C
hart
Rev
iew
Surg
ical
Ser
vice
Sta
ndar
d 2:
For
eve
ry s
urgi
cal p
atie
nt, c
ompe
tent
and
mot
ivat
ed s
taff
are
con
sist
ently
ava
ilabl
e to
pro
vide
rout
ine
care
and
man
age
com
plic
atio
ns.
SS 2
.1 E
very
sur
gica
l pat
ient
has
acc
ess
at
all t
imes
to a
t lea
st o
ne s
kille
d pr
ovid
er (a
s pe
r nat
iona
l sta
ndar
d).
Ade
quat
e nu
mbe
r of s
urge
ons
are
avai
labl
e ba
sed
on le
vel o
f hos
pita
l.•
5
•
5 if
100%
•
3 if
50-
100%
•
2 if
25-
50%
•
0 if
<
25%
•
Prim
ary
hosp
ital –
1 I
ESO
•
Gen
eral
hos
pita
l – 2
Gen
eral
su
rgeo
n, 2
OB
-GY
N a
nd 1
or
thop
edis
t
•
Spec
ializ
ed h
ospi
tal –
3 G
en-
eral
sur
geon
(1 s
ubsp
ecia
list),
2
orth
oped
ic s
urge
on, 3
obs
te-
tric
ians
, 1 a
nest
hesi
olog
ist,
10
anes
thet
ists
.
A c
lear
com
mun
icat
ion
chan
nel i
s pr
esen
t to
reac
h st
aff o
n du
ty a
t all
tim
es.
1
A ro
ster
is u
sed
whi
ch is
acc
essi
bly
disp
laye
d in
all
area
s, d
etai
ling
the
nam
es o
f sta
ff o
n du
ty, t
he ti
mes
of t
heir
shi
ft a
nd th
eir s
peci
fic ro
les
and
resp
onsi
bilit
ies.
1
All
surg
ical
pat
ient
s w
ere
satis
fied
with
the
heal
th c
are
rece
ived
.10
Clie
nt I
nter
view
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

83National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
SS 2
.2 S
urgi
cal s
taff
wor
king
in O
R a
nd
surg
ical
war
d ha
ve a
ppro
pria
te c
ompe
ten-
cies
and
ski
lls m
ix to
mee
t nee
ds d
urin
g la
bor,
child
birt
h an
d th
e ea
rly p
ostn
atal
pe
riod
(as
per n
atio
nal s
tand
ard)
.
Hea
lth p
rofe
ssio
nals
kno
w h
ow to
pre
pare
0.5
% c
hlor
ine
solu
tion
(spe
c-if
y pr
ofes
sion
)8
Staf
f Int
ervi
ew
Sele
ct 4
hea
lth c
are
wor
kers
ran
dom
ly
and
veri
fy if
they
hav
e th
e kn
owle
dge
Hea
lth p
rofe
ssio
nals
kno
w h
ow to
pro
cess
use
d in
stru
men
ts (i
nstr
u-m
enta
l pro
cess
ing)
.8
Staf
f Int
ervi
ew
Sele
ct 4
hea
lth c
are
wor
kers
ran
dom
ly
and
veri
fy if
they
hav
e th
e kn
owle
dge
All
surg
ical
pat
ient
s w
ere
satis
fied
with
the
care
and
sup
port
fro
m th
e fa
cilit
y st
aff.
10C
lient
Int
ervi
ew
Mor
e th
an 8
0% o
f OR
and
sur
gica
l war
d st
aff h
ad a
sat
isfac
tory
per
for-
man
ce a
ppra
isal
on
the
prev
ious
mon
th a
ppra
isal
.5
All
OR
and
sur
gica
l war
d st
affs
repo
rted
to b
e “h
ighl
y sa
tisfie
d” w
ith
thei
r job
in re
latio
n to
the
wor
king
env
iron
men
t and
sup
port
of h
ospi
tal
man
agem
ent.
8
Staf
f Int
ervi
ew
Sele
ct 4
hea
lth c
are
wor
kers
ran
dom
ly
and
veri
fy
No
staf
f in
OR
and
sur
gica
l war
d is
act
ivel
y co
nsid
erin
g lo
okin
g fo
r a
new
job
beca
use
of p
oor w
orki
ng e
nvir
onm
ent a
nd p
oor h
ospi
tal m
an-
agem
ent s
uppo
rt.
8
Staf
f Int
ervi
ew
Sele
ct 4
hea
lth c
are
wor
kers
ran
dom
ly
and
veri
fy
A w
ritte
n, u
p-to
-dat
e qu
ality
-of-
care
impr
ovem
ent p
lan
and
pa-
tient
-saf
ety
prog
ram
is p
rese
nt in
OR
and
sur
gica
l war
d.
1
A w
ritte
n, u
p-to
-dat
e, le
ader
ship
str
uctu
re, i
ndic
atin
g ro
les
and
resp
on-
sibi
litie
s w
ith re
port
ing
lines
of a
ccou
ntab
ility
is p
rese
nt in
OR
and
su
rgic
al w
ard.
1
A m
echa
nism
is in
pla
ce fo
r reg
ular
col
lect
ion
of in
form
atio
n on
pat
ient
sa
tisfa
ctio
n (m
onth
ly) a
nd p
rovi
der s
atisf
actio
n (q
uart
erly
) in
OR
and
su
rgic
al w
ard.
1
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

84 National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
Surg
ical
sta
ff e
ffici
ency
is m
onito
red.
M
ajor
sur
geri
es p
er f
ull-t
ime
surg
eon
in th
e fa
cilit
y (la
st m
onth
)
10
•
10 if
mor
e th
an 4
5 or
less
than
45
but
0 s
urgi
cal w
aiti
ng li
st
•
7 if
30–4
5•
5
if 20
–30
•
2 if
10–2
0
•
0 if
less
than
10
Del
ay fo
r ele
ctiv
e su
rger
y (la
st m
onth
)
10
•
10 if
less
than
1 m
onth
•
7 if
b/n
1–3
mon
th•
5
if b/
n 3–
6 m
onth
•
2 if
b/n
6–9m
onth
•
0 if
mor
e th
an 9
mon
th
SS 2
.3 E
very
hea
lth fa
cilit
y ha
s m
anag
eria
l an
d cl
inic
al le
ader
ship
that
is c
olle
ctiv
ely
resp
onsi
ble
for c
reat
ing
and
impl
emen
t-in
g ap
prop
riat
e po
licie
s an
d fo
ster
s an
en
viro
nmen
t tha
t sup
port
s fa
cilit
y st
aff t
o un
dert
ake
cont
inuo
us q
ualit
y im
prov
emen
t (m
anag
eria
l and
clin
ical
lead
ersh
ip s
houl
d be
don
e by
the
righ
t pro
fess
iona
l as
per t
he
natio
nal s
tand
ard)
.
Mon
thly
mee
ting
is c
ondu
cted
to re
view
dat
a, m
onito
r qua
lity
impr
ove-
men
t per
form
ance
and
mak
e re
com
men
datio
ns to
add
ress
pro
blem
s id
entifi
ed, a
nd to
cel
ebra
te th
ose
who
hav
e pe
rfor
med
and
enc
oura
ge
staf
f who
are
str
uggl
ing
to im
prov
e.5
Ver
ify
if it
was
don
e in
the
prev
ious
m
onth
All
OR
and
sur
gica
l war
d le
ader
s ar
e tr
aine
d in
qua
lity
impr
ovem
ent
and
lead
ing
chan
ge (u
se o
f inf
orm
atio
n, e
nabl
ing
beha
vior
, con
tinu
ous
lear
ning
).5
Act
ion
plan
is d
evel
oped
and
impl
emen
ted
/ im
plem
enta
tion
in p
rog-
ress
for t
he g
aps
iden
tified
fro
m c
lient
s fe
edba
cks,
sta
ff fe
edba
cks,
dat
a re
view
, clin
ical
aud
it fe
edba
ck, e
tc.
10
Hea
lth fa
cilit
y le
ader
s an
d fr
ont l
ine
wor
kers
are
com
mun
icat
ed th
roug
h es
tabl
ishe
d m
echa
nism
s (e
.g.,
a da
shbo
ard
of k
ey m
etri
cs) t
hat t
rack
the
perf
orm
ance
of t
he d
epar
tmen
t. 5
See
last
mon
th’s
repo
rt a
nd m
anag
e-m
ent m
eeti
ng m
inut
e
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

85National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
Surg
ical
Ser
vice
Sta
ndar
d 3:
Evi
denc
e-ba
sed
care
is p
rovi
ded
for a
ll su
rgic
al p
atie
nts.
SS 3
.1 T
he fa
cilit
y ha
s de
fined
and
est
ab-
lishe
d pr
oced
ures
for c
linic
al a
sses
smen
t an
d re
asse
ssm
ent o
f the
pat
ient
s.
Preo
pera
tive
asse
ssm
ent i
s do
ne fo
r all
surg
ical
pat
ient
s (P
/E, r
esul
ts o
f la
b in
vest
igat
ion,
dia
gnos
is a
nd p
ropo
sed
surg
ery)
. 10
Cha
rt R
evie
w
Min
imum
pre
oper
ativ
ely
need
ed la
b te
sts
are
done
.10
Cha
rt R
evie
w
All
lab
test
s w
ere
done
in th
e sa
me
faci
lity.
10
Cha
rt R
evie
w
SS 3
.2 F
acili
ty h
as d
efine
d an
d es
tabl
ishe
d pr
oced
ures
for c
onti
nuity
of c
are
of p
atie
nt
and
refe
rral
.
Prot
ocol
for t
rans
ferr
ing
and
cons
ulta
tion
mec
hani
sms
are
pres
ent.
1
Est
ablis
hed
proc
edur
e of
han
ding
ove
r is
pres
ent w
hile
rece
ivin
g pa
tient
fr
om O
R to
war
ds a
nd in
tens
ive
care
uni
t (tr
ansf
er fo
rm d
ocum
ente
d).
10C
hart
Rev
iew
Inte
rdep
artm
enta
l or i
nter
prof
essi
onal
con
sulta
tions
are
eff
ecte
d no
t m
ore
than
2 h
ours
. 10
Cha
rt R
evie
w
SS 3
.3 R
atio
nal u
se o
f dru
gs is
pra
ctic
ed.
Ant
ibio
tics
used
for s
urgi
cal p
roph
ylax
is a
re a
s pe
r sta
ndar
d tr
eatm
ent
guid
elin
es (S
TG
) rec
omm
enda
tion.
10
Cha
rt R
evie
w
Dru
gs a
re p
resc
ribe
d un
der g
ener
ic n
ame
only
10C
hart
and
Pre
scri
ptio
n R
evie
w
Ant
ibio
tics
used
for s
urgi
cal p
roph
ylax
is: d
ose,
fre
quen
cy, r
oute
and
nu
mbe
r of d
oses
, tim
ing
of a
dmin
istr
atio
n ar
e as
per
sta
ndar
d tr
eatm
ent
guid
elin
es (S
TG
) rec
omm
enda
tions
. 10
Cha
rt R
evie
w
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

86 National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
SS 3
.4 A
ll th
e ne
cess
ary
preo
pera
tive
prep
arat
ions
are
don
e be
fore
sur
gery
. A
nest
hetic
eva
luat
ion
was
don
e.
10C
hart
Rev
iew
Cro
ss m
atch
ed b
lood
pre
pare
d.
10C
hart
Rev
iew
Writ
ten
cons
ent t
aken
.10
Cha
rt R
evie
w
Patie
nt in
form
ed o
f the
clin
ical
con
ditio
n, tr
eatm
ent p
lan
and
poss
ible
ou
tcom
es.
10C
hart
Rev
iew
and
Clie
nt I
ntev
iew
Dat
e of
sur
gery
was
pre
plan
ned
at a
dmis
sion
and
info
rmed
to th
e pa
tient
. 10
Clie
nt I
ntev
iew
No
dela
y fr
om th
e pr
epla
nned
pro
cedu
re d
ay.
10C
lient
Int
evie
w
Surg
ical
saf
ety
chec
klis
t is
used
. 10
Cha
rt R
evie
w
SS 3
.5 F
acili
ty h
as d
efine
d an
d es
tabl
ishe
d pr
oced
ures
of s
urgi
cal s
ervi
ces.
The
re is
pro
cedu
re O
T s
ched
ulin
g.1
Surg
ical
site
is m
arke
d be
fore
ent
erin
g in
to O
R to
pre
vent
wro
ng s
ite
and
wro
ng s
urge
ry.
10C
lient
Int
evie
w
Spon
ge a
nd in
stru
men
t cou
nt p
ract
ice
is im
plem
ente
d.10
Cha
rt R
evie
w
Post
oper
ativ
e m
onito
ring
is d
one
befo
re d
isch
argi
ng to
war
d.10
Cha
rt R
evie
w
SS 3
.6 F
acili
ty h
as e
stab
lishe
d pr
oced
ures
fo
r mon
itori
ng d
urin
g an
esth
esia
.A
nest
hesi
a pl
an is
doc
umen
ted
befo
re e
nter
ing
into
OR
.10
Cha
rt R
evie
w
Food
inta
ke s
tatu
s of
pat
ient
is c
heck
ed.
10C
hart
Rev
iew
Patie
nts’
vita
ls a
re re
cord
ed d
urin
g an
esth
esia
.10
Cha
rt R
evie
w
Post
-ane
sthe
sia
stat
us is
mon
itore
d an
d do
cum
ente
d.10
Cha
rt R
evie
w
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

87National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
Surg
ical
Ser
vice
Sta
ndar
d 4:
The
hea
lth in
form
atio
n sy
stem
ena
bles
the
use
of d
ata
for e
arly
and
app
ropr
iate
act
ion
to im
prov
e ca
re fo
r sur
gica
l pat
ient
s.
SS 4
.1 A
ll su
rgic
al p
atie
nts
have
a c
ompl
ete
and
accu
rate
sta
ndar
dize
d m
edic
al re
cord
. T
he h
ealth
faci
lity
has
regi
ster
s, d
ata-
colle
ctio
n fo
rms,
clin
ical
and
ob
serv
atio
n ch
arts
in p
lace
at a
ll ti
mes
, des
igne
d to
rout
inel
y re
cord
and
tr
ack
all k
ey c
are
proc
esse
s fo
r sur
gica
l pat
ient
s (s
ee a
nnex
). 1
Obs
erva
tion
All
surg
ical
pat
ient
s ha
ve c
ompl
ete
reco
rd o
f all
info
rmat
ion
in th
e cl
ient
cha
rt a
nd re
gist
ered
on
the
HM
IS re
gist
er in
alig
nmen
t with
IC
D
code
. 10
Cha
rt R
evie
w
•
Ver
ify
if al
l inf
orm
atio
n is
re
cord
ed in
the
clie
nt c
hart
and
if
the
diag
nosi
s is
regi
ster
ed o
n th
e H
MIS
regi
ster
in a
lignm
ent
with
IC
D c
ode
The
hea
lth fa
cilit
y ha
s a
syst
em to
cla
ssif
y di
seas
es in
alig
nmen
t with
IC
D c
odes
at a
ll ti
mes
.
10
Cha
rt R
evie
w
•
Ver
ify
if th
e di
agno
sis
writ
ten
in th
e cl
ient
cha
rt is
doc
umen
t-ed
in th
e H
MIS
regi
ster
in
alig
nmen
t with
the
ICD
cod
es
SS 4
.2 F
acili
ty h
as d
efine
d an
d es
tabl
ishe
d pr
oced
ures
for m
aint
aini
ng, u
pdat
ing
pa-
tient
s’ cl
inic
al re
cord
s an
d th
eir s
tora
ge.
Rec
ords
of i
ntra
oper
ativ
e m
onito
ring
mai
ntai
ned.
10
Cha
rt R
evie
w
Ope
rativ
e no
tes
are
reco
rded
(dat
e, id
entifi
catio
n of
pat
ient
incl
udin
g M
RN
num
ber,
surg
ical
and
ane
sthe
sia
team
, pre
oper
ativ
e an
d po
stop
er-
ativ
e di
agno
sis,
type
and
des
crip
tion
of p
roce
dure
, typ
e of
inci
sion
s an
d us
ed s
utur
e m
ater
ials
, pos
tope
rativ
e pl
an).
10
Cha
rt R
evie
w
Ane
sthe
sia
note
s ar
e re
cord
ed.
Reg
iste
rs a
nd re
cord
s ar
e m
aint
aine
d.
10R
egis
ter R
evie
w
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

88 National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
SS 4
.3 E
very
hea
lth fa
cilit
y ha
s a
mec
ha-
nism
in p
lace
for d
ata
colle
ctio
n, a
naly
sis
and
feed
back
, as
part
of i
ts m
onito
ring
and
pe
rfor
man
ce im
prov
emen
t act
iviti
es.
OR
and
sur
gica
l war
d w
orki
ng h
ealth
car
e w
orke
rs re
gula
rly c
ondu
cts
revi
ews
of s
urgi
cal c
are
and
thei
r dat
a ev
ery
mon
th A
ND
dev
elop
s an
d im
plem
ents
a q
ualit
y im
prov
emen
t pro
ject
for a
ll th
e ga
ps id
entifi
ed.
40
40 (1
0 fo
r eac
h bu
llete
d cr
iteri
a’s) i
f the
fo
llow
ing
wer
e do
ne in
the
prev
ious
m
onth •
Surg
ical
car
e as
sess
men
t was
do
ne th
e pr
evio
us m
onth
•
G
aps
wer
e id
entifi
ed
•
Qua
lity
Plan
ning
(act
ion
plan
) fo
r the
gap
•
Impl
emen
tatio
n an
d fo
llow
up
in p
rogr
ess
The
hea
lth fa
cilit
y im
plem
ents
sta
ndar
d op
erat
ing
proc
edur
es a
nd p
ro-
toco
ls in
pla
ce a
t all
tim
es fo
r che
ckin
g, v
alid
atin
g an
d re
port
ing
data
5C
heck
pre
viou
s m
onth
min
utes
if th
e O
R a
nd s
urgi
cal w
ard
staf
f eva
luat
ed
thei
r dat
a be
fore
repo
rtin
g
Surg
ical
Ser
vice
Sta
ndar
d 5:
Com
mun
icat
ion
with
sur
gica
l pat
ient
s an
d th
eir f
amili
es is
eff
ectiv
e an
d in
resp
onse
to th
eir n
eeds
and
pre
fere
nces
.
SS 5
.1 A
ll su
rgic
al p
atie
nts
and
thei
r fam
-ili
es re
ceiv
e in
form
atio
n ab
out t
heir
car
e an
d ex
peri
ence
eff
ectiv
e in
tera
ctio
ns w
ith
staf
f.
Surg
ical
pat
ient
s ar
e gi
ven
the
oppo
rtun
ity to
dis
cuss
thei
r con
cern
s an
d pr
efer
ence
s.10
Clie
nt I
ntev
iew
Hea
lth c
are
staf
f dem
onst
rate
the
follo
win
g sk
ills:
activ
e lis
teni
ng,
aski
ng q
uest
ions
, res
pond
ing
to q
uest
ions
, ver
ifyi
ng c
lient
’s an
d th
eir
fam
ilies
und
erst
andi
ng, a
nd s
uppo
rtin
g cl
ient
’s in
pro
blem
- sol
ving
.10
Clie
nt I
ntev
iew
Surg
ical
pat
ient
s an
d th
eir f
amili
es c
ared
in th
e fa
cilit
y fe
lt th
ey w
ere
adeq
uate
ly in
form
ed b
y th
e at
tend
ing
care
pro
vide
r(s)
rega
rdin
g ex
am-
inat
ions
, any
act
ions
and
dec
isio
ns ta
ken
abou
t the
ir c
are.
10C
lient
Int
evie
w
Surg
ical
pat
ient
s an
d th
eir f
amili
es c
ared
in th
e fa
cilit
y ex
pres
sed
over
all
satis
fact
ion
with
the
heal
th s
ervi
ces.
10C
lient
Int
evie
w
Surg
ical
pat
ient
s an
d th
eir f
amili
es c
ared
in th
e fa
cilit
y re
port
ed th
at
they
wer
e sa
tisfie
d w
ith th
e he
alth
edu
catio
n an
d in
form
atio
n th
ey
rece
ived
fro
m th
e ca
re p
rovi
ders
.10
Clie
nt I
ntev
iew
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol
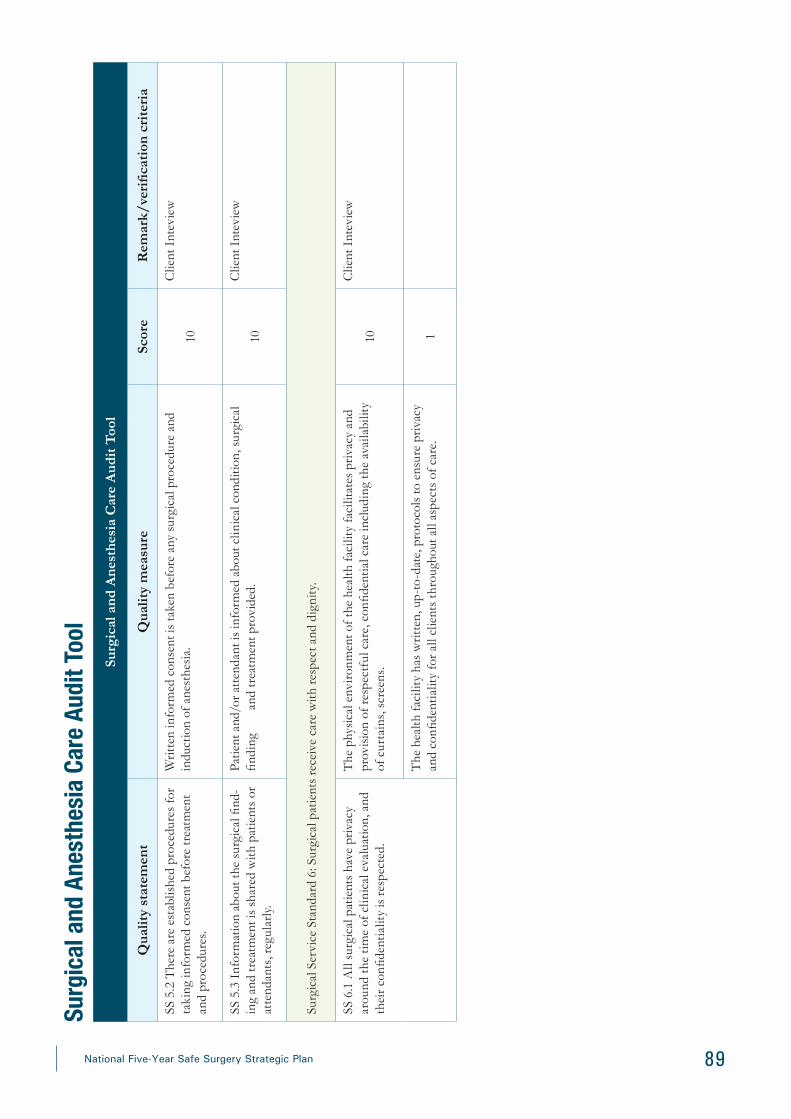
89National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
SS 5
.2 T
here
are
est
ablis
hed
proc
edur
es fo
r ta
king
info
rmed
con
sent
bef
ore
trea
tmen
t an
d pr
oced
ures
.
Writ
ten
info
rmed
con
sent
is ta
ken
befo
re a
ny s
urgi
cal p
roce
dure
and
in
duct
ion
of a
nest
hesi
a.
10
Clie
nt I
ntev
iew
SS 5
.3 I
nfor
mat
ion
abou
t the
sur
gica
l find
-in
g an
d tr
eatm
ent i
s sh
ared
with
pat
ient
s or
at
tend
ants
, reg
ular
ly.
Patie
nt a
nd/o
r att
enda
nt is
info
rmed
abo
ut c
linic
al c
ondi
tion,
sur
gica
l fin
ding
and
trea
tmen
t pro
vide
d.10
Clie
nt I
ntev
iew
Surg
ical
Ser
vice
Sta
ndar
d 6:
Sur
gica
l pat
ient
s re
ceiv
e ca
re w
ith re
spec
t and
dig
nity
.
SS 6
.1 A
ll su
rgic
al p
atie
nts
have
pri
vacy
ar
ound
the
tim
e of
clin
ical
eva
luat
ion,
and
th
eir c
onfid
entia
lity
is re
spec
ted.
The
phy
sica
l env
iron
men
t of t
he h
ealth
faci
lity
faci
litat
es p
riva
cy a
nd
prov
isio
n of
resp
ectf
ul c
are,
con
fiden
tial c
are
incl
udin
g th
e av
aila
bilit
y of
cur
tain
s, s
cree
ns.
10
Clie
nt I
ntev
iew
The
hea
lth fa
cilit
y ha
s w
ritte
n, u
p-to
-dat
e, p
roto
cols
to e
nsur
e pr
ivac
y an
d co
nfide
ntia
lity
for a
ll cl
ient
s th
roug
hout
all
aspe
cts
of c
are.
1
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

90 National Five-Year Safe Surgery Strategic Plan
Surg
ical
and
Ane
sthe
sia
Car
e A
udit
Too
l
Qua
lity
stat
emen
tQ
ualit
y m
easu
reSc
ore
Rem
ark/
veri
ficat
ion
crit
eria
SS 6
.2 N
o su
rgic
al p
atie
nt is
sub
ject
ed to
m
istr
eatm
ent s
uch
as p
hysi
cal,
sexu
al o
r ve
rbal
abu
se, d
iscr
imin
atio
n, n
egle
ct, d
e-ta
inm
ent,
exto
rtio
n or
den
ial o
f ser
vice
s.
The
hea
lth fa
cilit
y ha
s ac
coun
tabi
lity
mec
hani
sms
for r
edre
ss in
the
even
t of v
iola
tions
of p
riva
cy, c
onfid
entia
lity
and
cons
ent.
1
The
hea
lth fa
cilit
y ha
s w
ritte
n, u
p-to
-dat
e, z
ero-
tole
ranc
e, n
on-d
iscr
imi-
nato
ry p
olic
ies
rela
ting
to th
e m
istr
eatm
ent o
f clie
nts.
1
Any
clie
nt w
ho re
port
ed p
hysi
cal,
verb
al o
r sex
ual a
buse
, to
them
selv
es
or th
eir f
amili
es d
urin
g cl
inic
al e
valu
atio
n.
20
•
Sele
ct a
nd v
erif
y 5
clie
nts
exiti
ng
from
the
OR
regi
ster
•
4
for e
ach
clie
nt if
they
are
pr
otec
ted
•
0 fo
r eac
h cl
ient
if re
port
of
abus
e (s
ampl
ing
met
hod)
The
hea
lth fa
cilit
y ha
s w
ritte
n ac
coun
tabi
lity
mec
hani
sms
for r
edre
ss in
an
eve
nt o
f mis
trea
tmen
t.1
The
hea
lth fa
cilit
y ha
s a
writ
ten,
up-
to-d
ate
polic
y an
d pr
otoc
ols
out-
linin
g cl
ient
s ri
ght t
o m
ake
a co
mpl
aint
abo
ut th
e ca
re re
ceiv
ed a
nd h
as
an e
asily
acc
essi
ble
mec
hani
sm (
box)
for h
andi
ng in
com
plai
nts
and
is
perio
dica
lly e
mpt
ied
and
revi
ewed
.
4
•
4 if
pres
ent A
ND
per
iodi
cally
em
ptie
d an
d re
view
ed
•
1 if
only
pre
sent
All
clie
nts
wer
e sa
tisfie
d w
ith th
e fa
cilit
y m
eeti
ng th
eir r
elig
ious
and
cu
ltura
l nee
ds.
10C
lient
Int
evie
w
SS 6
.3 A
ll cl
ient
s ha
ve in
form
ed c
hoic
es in
th
e se
rvic
es th
ey re
ceiv
e, a
nd th
e re
ason
s fo
r int
erve
ntio
n or
out
com
es a
re c
lear
ly
expl
aine
d
All
clie
nts
repo
rted
to b
e tr
eate
d w
ith re
spec
t and
dig
nity
.10
Clie
nt I
ntev
iew
The
hea
lth fa
cilit
y ha
s a
writ
ten,
up-
to-d
ate,
pol
icy
in p
lace
to p
rom
ote
for o
btai
ning
info
rmed
con
sent
fro
m c
lient
s pr
ior t
o ex
amin
atio
ns a
nd
proc
edur
es.
1D
ocum
ent r
evie
w
Surg
ical a
nd A
nest
hesia
Car
e Aud
it To
ol

91National Five-Year Safe Surgery Strategic Plan
Ann
ex C
. P
roce
dure
Lis
ts Eth
iopi
an N
atio
nal L
ists
of
Ess
enti
al a
nd E
mer
genc
y Su
rgic
al a
nd A
nest
hesi
a C
are
Pro
cedu
res
S/ No
Spec
ialit
yPr
oced
ures
Ava
ilabi
lity
of P
roce
dure
s B
ased
on
Hea
lth
Faci
lity
Typ
es
Hea
lth
Cen
ter
Pri
mar
y H
ospi
tal
Gen
eral
H
ospi
tal
Spec
ializ
ed
Hos
pita
l
1G
ynec
olog
y an
d O
bste
tric
s C
aesa
rean
Sec
tion
2A
bdom
inal
Hys
tere
ctom
y or
Rep
air o
f U
teri
ne p
erfo
ratio
n fo
r rup
ture
(ass
ocia
ted
with
in
trac
tabl
e PP
H
3N
orm
al d
eliv
ery,
Man
ual r
emov
al o
f the
pla
cent
a, V
acuu
m D
eliv
ery
and
Rep
air o
f Gen
i-ta
l Inj
ury/
Lac
erat
ion
4C
ompr
ehen
sive
Abo
rtio
n C
are
5M
anag
emen
t of p
elvi
c or
gan
prol
apse
(Thi
s is
not
an
esse
ntia
l sur
gery
)
6R
epai
r of O
bste
tric
Fis
tula
7V
IA a
nd c
ryot
hera
py fo
r pre
canc
erou
s ce
rvic
al le
sion
s
8M
anag
emen
t of M
ajor
Ben
ign
and
Mal
igna
nt G
ynec
olog
ic C
ondi
tions
9Tu
bal l
igat
ion/
Vas
ecto
my
10Tr
aum
a an
d In
jury
R
elat
ed
Trac
heos
tom
y an
d cr
ico-
thyr
oide
otom
y
11Tu
be th
orac
osto
my
for a
ir or
flui
d co
llect
ion
in th
e pl
eura
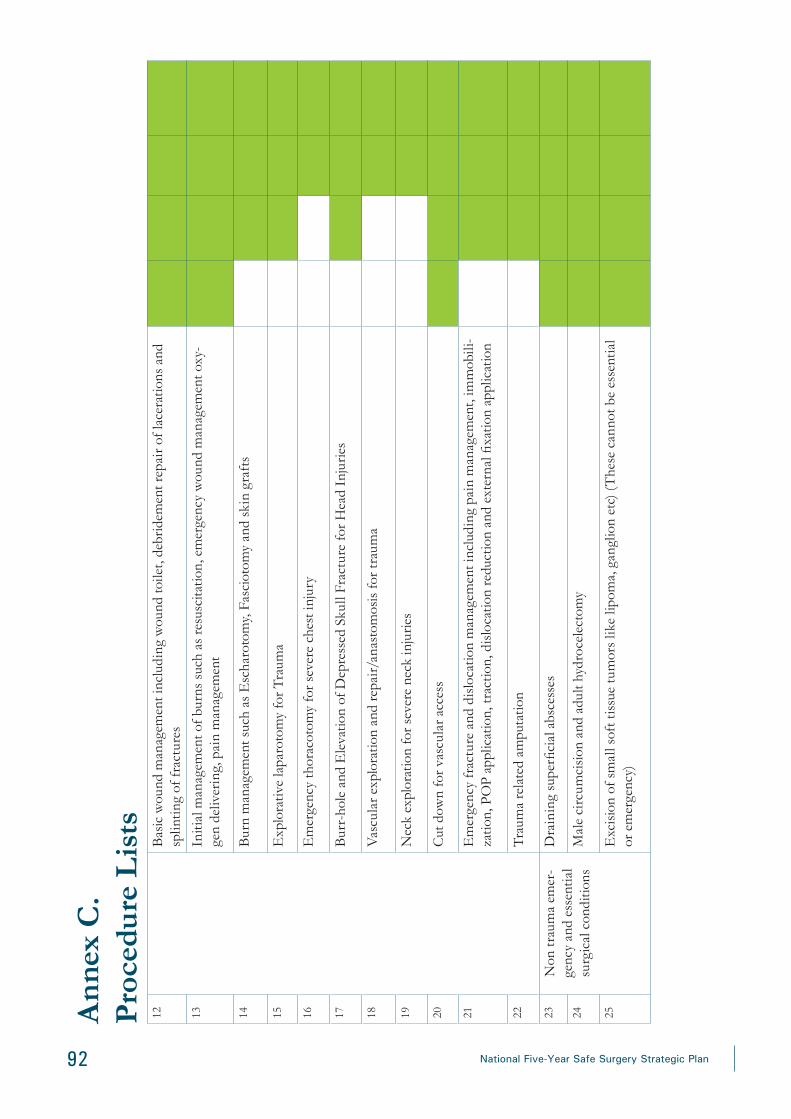
92 National Five-Year Safe Surgery Strategic Plan
12B
asic
wou
nd m
anag
emen
t inc
ludi
ng w
ound
toile
t, de
brid
emen
t rep
air o
f lac
erat
ions
and
sp
lintin
g of
frac
ture
s
13In
itial
man
agem
ent o
f bur
ns s
uch
as re
susc
itatio
n, e
mer
genc
y w
ound
man
agem
ent o
xy-
gen
deliv
erin
g, p
ain
man
agem
ent
14B
urn
man
agem
ent s
uch
as E
scha
roto
my,
Fas
ciot
omy
and
skin
gra
fts
15E
xplo
rativ
e la
paro
tom
y fo
r Tra
uma
16E
mer
genc
y th
orac
otom
y fo
r sev
ere
ches
t inj
ury
17B
urr-
hole
and
Ele
vatio
n of
Dep
ress
ed S
kull
Frac
ture
for H
ead
Inju
ries
18V
ascu
lar e
xplo
ratio
n an
d re
pair/
anas
tom
osis
for t
raum
a
19N
eck
expl
orat
ion
for s
ever
e ne
ck in
jurie
s
20C
ut d
own
for v
ascu
lar a
cces
s
21E
mer
genc
y fr
actu
re a
nd d
islo
catio
n m
anag
emen
t inc
ludi
ng p
ain
man
agem
ent,
imm
obili
-za
tion,
PO
P ap
plic
atio
n, tr
actio
n, d
islo
catio
n re
duct
ion
and
exte
rnal
fixa
tion
appl
icat
ion
22Tr
aum
a re
late
d am
puta
tion
23N
on tr
aum
a em
er-
genc
y an
d es
sent
ial
surg
ical
con
ditio
ns
Dra
inin
g su
perfi
cial
abs
cess
es
24M
ale
circ
umci
sion
and
adu
lt hy
droc
elec
tom
y
25E
xcis
ion
of s
mal
l sof
t tis
sue
tum
ors
like
lipom
a, g
angl
ion
etc)
(The
se c
anno
t be
esse
ntia
l or
em
erge
ncy)
Ann
ex C
. P
roce
dure
Lis
ts

93National Five-Year Safe Surgery Strategic Plan
Ann
ex C
. P
roce
dure
Lis
ts26
Rel
ievi
ng a
cute
uri
nary
rete
ntio
n by
cat
hete
riza
tion,
clo
sed
supr
a-pu
bic
cyst
osto
my
27Tr
ans
vesi
cal p
rost
atec
tom
y (T
VP)
, Cys
to-li
thot
omy
28R
ecta
l tub
e de
flatio
n fo
r sig
moi
d vo
lvul
us
29Pe
diat
ric e
mer
genc
ies
incl
udin
g in
tuss
usce
ptio
n, c
olos
tom
y fo
r ano
-rec
tal m
alfo
rmat
ion
and
fore
ign
body
sw
allo
win
g/as
pira
tion
man
agem
ent
30E
xplo
rativ
e la
paro
tom
y fo
r acu
te a
bdom
en (a
cute
app
endi
citis
, ect
opic
pre
gnan
cy, o
vari
an
tors
ion,
hol
low
vis
cus
perf
orat
ion
and
trau
ma)
31C
hole
cyst
ecto
my,
cho
lecy
stos
tom
y, C
BD
exp
lora
tion,
bili
ary
bypa
ss p
roce
dure
s an
d T-
tube
inse
rtio
n fo
r hep
ato-
bilia
ry p
atho
logi
es
32R
epai
r of a
bdom
inal
wal
l her
nias
33
Con
stru
ctin
g an
d re
vers
al o
f col
osto
mie
s, c
olon
ic re
sect
ion
and
anas
tom
osis
, Hae
mor
-rh
oide
ctom
ies,
Fis
tulo
tom
ies,
fiss
ure
surg
ery
and
drai
nage
of p
eria
nal a
bsce
sses
34M
odifi
ed r
adic
al m
aste
ctom
y an
d th
yroi
dect
omy
(all
form
s)
35G
astr
ic a
nd e
soph
agea
l res
ectio
n fo
r can
cers
and
per
fora
tion
36O
pera
tive
and
non
oper
ativ
e m
anag
emen
t of c
lub
foot
37M
anag
emen
t of S
eptic
Art
hriti
s, O
steo
mye
litis
, Pyo
myo
sitis
, and
han
d in
fect
ion
38
Com
plex
ort
hope
dic
trau
ma
care
incl
udin
g h
emi a
rthr
opla
sty,
intr
a-ar
ticul
ar fr
actu
res,
sp
ine
and
pelv
ic fr
actu
re m
anag
emen
t)
39A
nest
hesi
a an
d C
riti-
cal C
are
Gen
eral
ane
sthe
sia
40Sp
inal
ane
sthe
sia
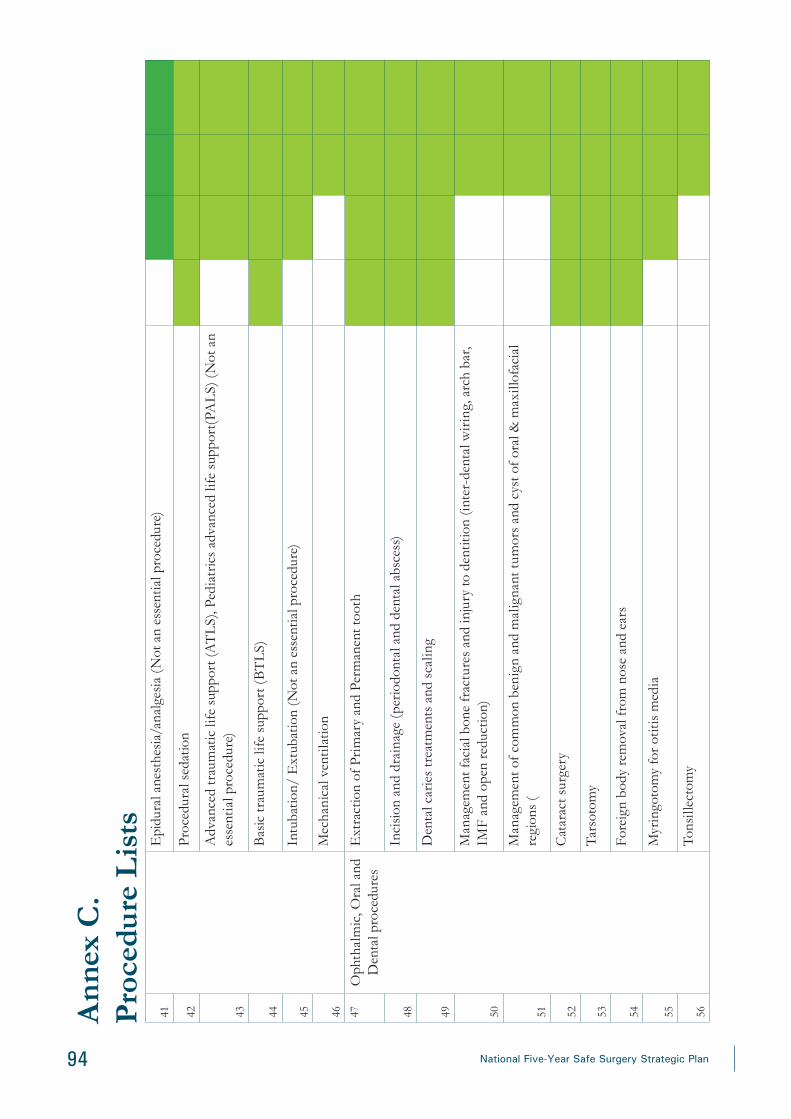
94 National Five-Year Safe Surgery Strategic Plan
41E
pidu
ral a
nest
hesi
a/an
alge
sia
(Not
an
esse
ntia
l pro
cedu
re)
42Pr
oced
ural
sed
atio
n
43
Adv
ance
d tr
aum
atic
life
sup
port
(AT
LS)
, Ped
iatr
ics
adva
nced
life
sup
port
(PA
LS)
(N
ot a
n es
sent
ial p
roce
dure
)
44B
asic
trau
mat
ic li
fe s
uppo
rt (
BT
LS)
45In
tuba
tion/
Ext
ubat
ion
(Not
an
esse
ntia
l pro
cedu
re)
46M
echa
nica
l ven
tila
tion
47O
phth
alm
ic, O
ral a
nd
Den
tal p
roce
dure
s E
xtra
ctio
n of
Pri
mar
y an
d Pe
rman
ent t
ooth
48In
cisi
on a
nd d
rain
age
(per
iodo
ntal
and
den
tal a
bsce
ss)
49D
enta
l car
ies
trea
tmen
ts a
nd s
calin
g
50
Man
agem
ent f
acia
l bon
e fr
actu
res
and
inju
ry to
den
titio
n (in
ter-
dent
al w
irin
g, a
rch
bar,
IMF
and
open
redu
ctio
n)
51
Man
agem
ent o
f com
mon
ben
ign
and
mal
igna
nt tu
mor
s an
d cy
st o
f ora
l & m
axill
ofac
ial
regi
ons
(
52C
atar
act s
urge
ry
53Ta
rsot
omy
54Fo
reig
n bo
dy re
mov
al fr
om n
ose
and
ears
55M
yrin
goto
my
for o
titis
med
ia
56To
nsill
ecto
my
Ann
ex C
. P
roce
dure
Lis
ts


Related Documents











