Page 10 J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Appendicis Mimics, Thompson et al. Introducon Acute abdominal pain is the most common reason for an emergency department visit among paents age 15 and older, a large poron of them will complain of pain localizing to the right lower quadrant. 1 While appendicis is the most common cause of the surgical abdomen, a wide variety of acute gastrointesnal, genitourinary, and gynecological pathologic processes can present in similar fashion (Table 1). Acute gastrointesnal diseases, such as Crohn’s disease, infecous enterocolis, mesenteric adenis, cecal diverculis, Meckel’s diverculis, epiploic appendagis, and omental infarcts can present with right lower quadrant. In addion, acute genitourinary diseases, such as pyelonephris and ureterolithiasis, can present with similar symptoms. In a young woman, acute gynecological disease processes, such as ovarian torsion, hemorrhagic ovarian cyst, pelvic inflammatory disease, and ectopic pregnancy, should also be considered within the differenal diagnosis. Imaging modalies ulized in the emergency seng to evaluate right lower quadrant pain include computed tomography (CT), ultrasound (US), and magnec resonance imaging (MRI). These modalies may be value-added for paents with nonspecific symptoms, thus it is useful to triage surgical and non- surgical paents. It is important for the praccing radiologist to be familiar with the various acute disease enes which can cause right lower quadrant pain in order to determine the best approach or modality to make an accurate diagnosis. Imaging of the appendix The most common imaging modality for the evaluaon of the right lower quadrant pain is MDCT. MDCT has a sensivity of 97%, specificity of 98%, and accuracy of 98% in diagnosing acute appendicis, with the addional benefit of suggesng an alternave diagnosis for acute abdominal pain in up to two-thirds of paents. 2,3 The presence of intravenous and enteric contrast aids in idenficaon of the appendix. 3 The appendix arises from the cecum inferior to the ileocecal juncon (Fig. 1). MDCT signs of acute appendicis include appendiceal diameter > 7 mm with peri-appendiceal stranding of the mesenteric fat (Fig. 2A). 4 Both findings are present in up to 93% of appendicis cases idenfied on MDCT. 5 The diagnosis of appendicis should not be made using appendiceal diameter alone; wall thickening and increased enhancement should also be present. 6 Addional findings include the presence of an appendicolith, cecal apical thickening (“arrowhead sign”), mesenteric adenopathy, fluid in the paracolic guer, and the presence of phlegmon. 5 A focal wall defect, extraluminal air, or presence of an abscess are signs of perforaon. 5 While MDCT is currently the preferred imaging modality, in the pediatric and pregnant paent ultrasound as well as MRI has been shown to perform comparable to CT. 7 Ultrasound has a sensivity and specificity of 78% and 83%, respecvely. 8 The most common findings in appendicis are diameter > 6 mm, lack of compressibility, hyperemia of the appendiceal wall on Doppler imaging, peri-appendiceal inflammatory changes, and the presence of peritoneal fluid (Fig. 2B). Occasionally, a calcified appendicolith may be seen with posterior shadowing (Fig. 2C). However, ruling out appendiceal pathology is oſten difficult with US if the appendix cannot be visualized. One study reported posive ultrasound findings for appendicis in about 20% of cases, but equivocal findings in almost 50% of cases (i.e. inability to idenfy the appendix). 7 Evaluaon of the right lower quadrant is parcularly difficult in pregnant women due to distorted abdominal and pelvic anatomy (parcularly in the third trimester). MRI has been shown to be superior at localizing the appendix in comparison to ultrasound, with a sensivity and specificity of up to 89% and 99%. 8,9 Mimickers of Acute Appendicitis Joel P. Thompson, M.D., MPH, Dhana Selvaraj, M.D., Rey Nicola, D.O. Department of Imaging Sciences, University of Rochester Medical Center, Rochester, NY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Page 10 J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4
Appendicitis Mimics, Thompson et al.
Introduction
Acute abdominal pain is the most common reason for an emergency department visit among patients age 15 and older, a large portion of them will complain of pain localizing to the right lower quadrant.1 While appendicitis is the most common cause of the surgical abdomen, a wide variety of acute gastrointestinal, genitourinary, and gynecological pathologic processes can present in similar fashion (Table 1). Acute gastrointestinal diseases, such as Crohn’s disease, infectious enterocolitis, mesenteric adenitis, cecal diverticulitis, Meckel’s diverticulitis, epiploic appendagitis, and omental infarcts can present with right lower quadrant. In addition, acute genitourinary diseases, such as pyelonephritis and ureterolithiasis, can present with similar symptoms. In a young woman, acute gynecological disease processes, such as ovarian torsion, hemorrhagic ovarian cyst, pelvic inflammatory disease, and ectopic pregnancy, should also be considered within the differential diagnosis.
Imaging modalities utilized in the emergency setting to evaluate right lower quadrant pain include computed tomography (CT), ultrasound (US), and magnetic resonance imaging (MRI). These modalities may be value-added for patients with nonspecific symptoms, thus it is useful to triage surgical and non-surgical patients. It is important for the practicing radiologist to be familiar with the various acute disease entities which can cause right lower quadrant pain in order to determine the best approach or modality to make an accurate diagnosis.
Imaging of the appendix
The most common imaging modality for the evaluation of the right lower quadrant pain is MDCT. MDCT has a sensitivity of 97%, specificity of 98%, and accuracy of 98% in diagnosing acute appendicitis, with the additional benefit of suggesting an alternative diagnosis for acute abdominal pain in up to two-thirds
of patients.2,3 The presence of intravenous and enteric contrast aids in identification of the appendix.3
The appendix arises from the cecum inferior to the ileocecal junction (Fig. 1). MDCT signs of acute appendicitis include appendiceal diameter > 7 mm with peri-appendiceal stranding of the mesenteric fat (Fig. 2A).4 Both findings are present in up to 93% of appendicitis cases identified on MDCT.5 The diagnosis of appendicitis should not be made using appendiceal diameter alone; wall thickening and increased enhancement should also be present.6 Additional findings include the presence of an appendicolith, cecal apical thickening (“arrowhead sign”), mesenteric adenopathy, fluid in the paracolic gutter, and the presence of phlegmon.5 A focal wall defect, extraluminal air, or presence of an abscess are signs of perforation.5 While MDCT is currently the preferred imaging modality, in the pediatric and pregnant patient ultrasound as well as MRI has been shown to perform comparable to CT.7
Ultrasound has a sensitivity and specificity of 78% and 83%, respectively.8 The most common findings in appendicitis are diameter > 6 mm, lack of compressibility, hyperemia of the appendiceal wall on Doppler imaging, peri-appendiceal inflammatory changes, and the presence of peritoneal fluid (Fig. 2B). Occasionally, a calcified appendicolith may be seen with posterior shadowing (Fig. 2C). However, ruling out appendiceal pathology is often difficult with US if the appendix cannot be visualized. One study reported positive ultrasound findings for appendicitis in about 20% of cases, but equivocal findings in almost 50% of cases (i.e. inability to identify the appendix).7 Evaluation of the right lower quadrant is particularly difficult in pregnant women due to distorted abdominal and pelvic anatomy (particularly in the third trimester). MRI has been shown to be superior at localizing the appendix in comparison to ultrasound, with a sensitivity and specificity of up to 89% and 99%.8,9
Mimickers of Acute Appendicitis
Joel P. Thompson, M.D., MPH, Dhana Selvaraj, M.D., Refky Nicola, D.O.
Department of Imaging Sciences, University of Rochester Medical Center, Rochester, NY

J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 11
Appendicitis Mimics, Thompson et al.
Pathology Imaging Appearance Treatment Gastrointestinal
Crohn’s Disease Bowel wall thickening and mural stratification, most commonly involving
the terminal ileum. Chronic inflammation may result in fibrofatty
proliferation along the mesenteric side of the bowel wall. Fistulas and
abscesses may form.
Initially medical. Indications for surgery
include obstruction due to fibrotic stricture,
perforation, abscess formation, and fistulas
not able to be managed medically.
Diverticulitis Thick-walled diverticulum with adjacent infiltrative changes; short or long
-segment bowel wall thickening. Abscesses may form.
Medical. Surgical intervention may be
necessary for medically refractory cases,
large abscesses, and fistula formation.
Infectious
Enterocolitis
Long-segment circumferential wall thickening, usually without
mesenteric fat stranding.
Medical.
Mesenteric Adenitis Cluster of 3 or more right lower quadrant lymph nodes >5 mm in shortest
diameter, without identifiable cause.
Medical.
Neutropenic Colitis
(Typhlitis)
Distended and thick-walled cecum, infiltrative changes, pericolic fluid. Medical. High risk of bowel perforation; CT
may be used to monitor treatment response.
Meckel’s
Diverticulitis
Blind-ending tubular structure in the right lower quadrant arising from
the distal ileum; infiltrative changes, wall thickening, and
hyperenhancement may be seen.
Surgical resection.
Epiploic Appendagitis Pericolic fatty mass with surrounding inflammatory changes, most
commonly in the transverse and descending colon. A central thrombosed
vein may be identified.
Medical.
Omental Infarct Pericolic fatty mass with surrounding inflammatory changes, most
commonly in the right hemiabdomen between the colon and the anterior
abdominal wall.
Medical.
Genitourinary/Gynecological
Urolithiasis Obstructing calculus with hydronephrosis +/- hydroureter. Medical, unless calculus large.
Pyelonephritis Imaging most often normal. May see striated nephrogram or delayed
contrast excretion on CT. US may show loss of corticomedullary
differentiation.
Medical.
Ovarian Torsion US: Enlarged and heterogeneous ovary; may be midline. May see
reduced or absent venous flow.
Surgical detorsion.
Hemorrhagic Ovarian
Cyst
US: Finely septated “fishnet” pattern of fibrin bands; retractile clot or
avascular peripheral nodule non-acutely.
None.
Pelvic Inflammatory
Disease
Dilated tubular structures representing Fallopian tubes with wall
thickening. Ipsilateral ovary may be enlarged.
Medical.
Ectopic Pregnancy Non-visualization of an intrauterine pregnancy with positive beta-hCG.
US: May see yolk sac, detect fetal heartbeat, or see “ring of fire” sign of
peripheral hypervascularity around adnexal mass.
Medical but may require surgical
intervention.
Mittelschmerz Normal. May see physiologic fluid in the pelvis. None.
Table 1. Overview of gastrointestinal and genitourinary causes of right lower quadrant pain.

Page 12 J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4
Appendicitis Mimics, Thompson et al.
On MRI, the appearance of acute appendicitis includes an appendiceal diameter > 7 mm and adjacent fat stranding that is often best appreciated on T2 fat saturated sequences.10 An inflamed appendix demonstrates restricted diffusion.10 The appendix may be filled with high T2 fluid or edema, which decreases in signal intensity if the fluid is purulent (higher debris and protein content). Appendicoliths are low in T1 and T2 signal intensity, with blooming artifact on GRE images. A periappendiceal abscess is identified as a walled-off high T2 fluid collection with restricted diffusion. An appendix filled with high T2 fluid and diameter of 6-7 mm is indeterminate (if no adjacent fat stranding of fluid) and should be closely followed up.10
Differential Diagnosis
Crohn's Disease
Crohn's disease can involve any segment of the gastrointestinal tract, but the most common location is within the terminal ileum. Patients often present with abdominal cramps localized within right lower quadrant and bloody stools. The initial presentation typically occurs between 15 and 30 years of age.
The imaging features of Crohn's disease consist of bowel wall thickening (greater than 4 mm), mural stratification ("target" or stratified appearance of the bowel wall due to submucosal edema), and abnormal enhancement (Fig. 3).11 Active inflammation leads to engorgement of vasa recta (the "comb sign"). Chronic inflammation results in fibrofatty proliferation along the mesenteric side of the bowel wall, creating the "creeping fat" sign.12 Over time, the chronic
Figure 1. Normal appendix. Coronal MDCT with IV and enteric contrast (A) demonstrates a normal appendix (white arrow) arising from the cecum inferior to the ileocecal junction (yellow arrow). Longitudinal ultrasound image (B) shows a normal appearance of a blind-ending appendix, which measures 4 mm in diameter (caliper 2).
A B
Figure 2. Acute Appendicitis. Axial MDCT image with oral contrast (A) demonstrates an enlarged appendix, measuring up to 14 mm in diameter (white arrow), wall thickening, and adjacent inflammatory changes with phlegmon formation (yellow arrow). Surgical pathology demonstrated appendicitis. Longitudinal ultrasound images in a different patient (B) demonstrate an enlarged appendix, measuring up to 10 mm, that is noncompressible, consistent with appendicitis. Ultrasound image at a different level in the same patient demonstrates a hyperechoic focus with posterior shadowing, consistent with an appendicolith (C).
A B C

J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 13
Appendicitis Mimics, Thompson et al.
inflammatory process of Crohn's disease can result intramural or interloop abscesses. Fistulous anastomosis with the bowel, bladder, skin, and vagina can occur. This is best evaluated by MDCT or MRI enterography, which utilize IV contrast during the late arterial phase and low density oral contrast to facilitate evaluation of the small bowel mucosa.13 Bowel wall thickening (>3mm) and stratification, mucosal hyperenhancement, inflammatory changes in adjacent mesenteric fat, and engorged vasa recta ("comb sign") are all findings on enterography consistent with active inflammation.13 The initial management of Crohn’s disease is non-surgical. However, surgery may be necessary if fistulas or stricture formation develop.
Infectious Enterocolitis
Infectious enterocolitis can present clinically similar to appendicitis, particularly if caused by pathogens such as Yersinia, Campylobacter, or Salmonella, which may cause ileocecitis.12,14 The imaging findings on MDCT involve a long-segment circumferential wall thickening with homogenous enhancement, usually without stranding of the adjacent fat. In addition, mesenteric adenopathy and surrounding free fluid may be present.
Mesenteric Adenitis
Mesenteric adenitis, or right lower quadrant lymphadenopathy, is defined as a cluster of 3 or more lymph nodes greater than 5 mm in shortest diameter in the right lower quadrant mesentery (Fig. 4).15 Primary mesenteric adenitis is thought to be due to an underlying ileitis. Secondary mesenteric adenitis has an identifiable cause on MDCT, such as appendicitis or Crohn's disease. Patients present with abdominal pain, fever, and leukocytosis. This is an uncommon diagnosis, but may be considered in patients whose only imaging abnormality is focal mesenteric lymphadenopathy.
Figure 3. Crohn’s disease. 11-year-old boy with acute abdominal pain and history of Crohn's disease. Oblique axial MDCT enterography image (A) demonstrates signs of active inflammation in the terminal ileum (white arrow), including mucosal hyperenhancement, wall thickening, and adjacent inflammatory changes. The appendix is normal (yellow arrow). MR enterography in the same patient 2 years later (B) demonstrates wall thickening and fibrosis without adjacent inflammatory changes, consistent with sequela of multiple prior Crohn's flares.
A B
Figure 4. Mesenteric adenitis. Coronal MDCT with oral contrast shows a cluster of right lower quadrant mesenteric lymph nodes greater than 5 mm in shortest diameter without identifiable cause (circled), consistent with mesenteric adenitis. The appendix was normal (white arrow).
Page 14 J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4
Appendicitis Mimics, Thompson et al.
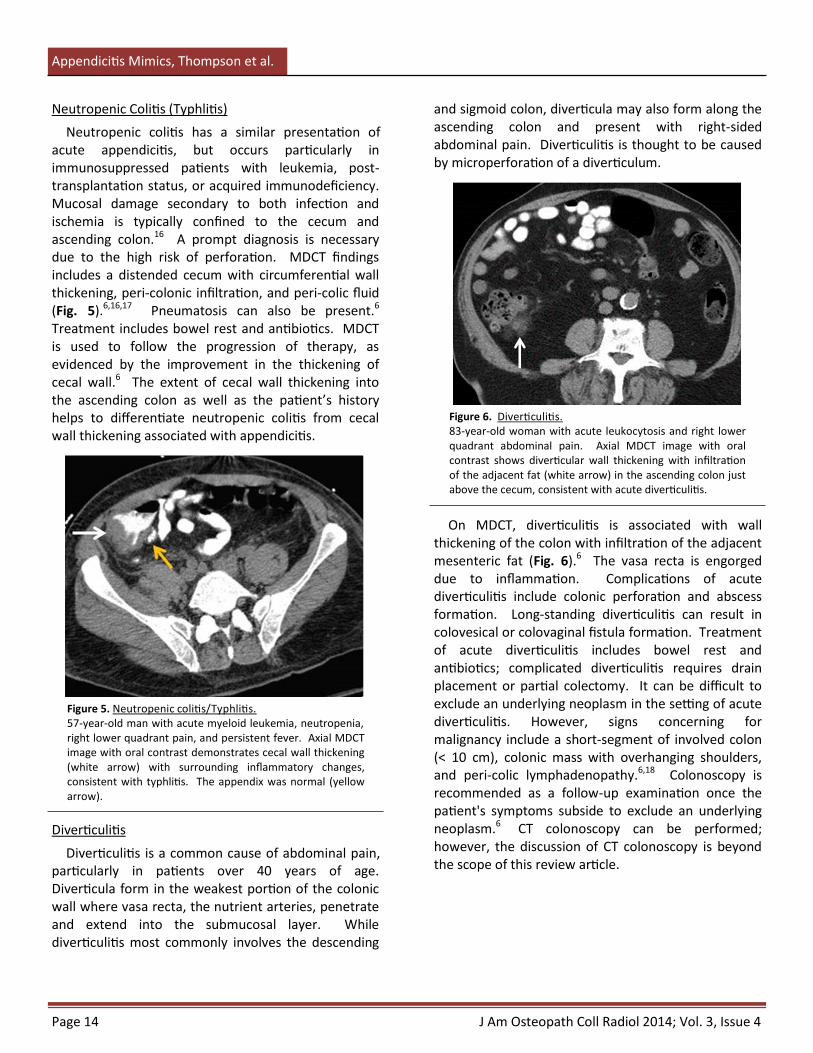
and sigmoid colon, diverticula may also form along the ascending colon and present with right-sided abdominal pain. Diverticulitis is thought to be caused by microperforation of a diverticulum.
On MDCT, diverticulitis is associated with wall thickening of the colon with infiltration of the adjacent mesenteric fat (Fig. 6).6 The vasa recta is engorged due to inflammation. Complications of acute diverticulitis include colonic perforation and abscess formation. Long-standing diverticulitis can result in colovesical or colovaginal fistula formation. Treatment of acute diverticulitis includes bowel rest and antibiotics; complicated diverticulitis requires drain placement or partial colectomy. It can be difficult to exclude an underlying neoplasm in the setting of acute diverticulitis. However, signs concerning for malignancy include a short-segment of involved colon (< 10 cm), colonic mass with overhanging shoulders, and peri-colic lymphadenopathy.6,18 Colonoscopy is recommended as a follow-up examination once the patient's symptoms subside to exclude an underlying neoplasm.6 CT colonoscopy can be performed; however, the discussion of CT colonoscopy is beyond the scope of this review article.
Neutropenic Colitis (Typhlitis)
Neutropenic colitis has a similar presentation of acute appendicitis, but occurs particularly in immunosuppressed patients with leukemia, post-transplantation status, or acquired immunodeficiency. Mucosal damage secondary to both infection and ischemia is typically confined to the cecum and ascending colon.16 A prompt diagnosis is necessary due to the high risk of perforation. MDCT findings includes a distended cecum with circumferential wall thickening, peri-colonic infiltration, and peri-colic fluid (Fig. 5).6,16,17 Pneumatosis can also be present.6 Treatment includes bowel rest and antibiotics. MDCT is used to follow the progression of therapy, as evidenced by the improvement in the thickening of cecal wall.6 The extent of cecal wall thickening into the ascending colon as well as the patient’s history helps to differentiate neutropenic colitis from cecal wall thickening associated with appendicitis.
Diverticulitis
Diverticulitis is a common cause of abdominal pain, particularly in patients over 40 years of age. Diverticula form in the weakest portion of the colonic wall where vasa recta, the nutrient arteries, penetrate and extend into the submucosal layer. While diverticulitis most commonly involves the descending
Figure 5. Neutropenic colitis/Typhlitis. 57-year-old man with acute myeloid leukemia, neutropenia, right lower quadrant pain, and persistent fever. Axial MDCT image with oral contrast demonstrates cecal wall thickening (white arrow) with surrounding inflammatory changes, consistent with typhlitis. The appendix was normal (yellow arrow).
Figure 6. Diverticulitis. 83-year-old woman with acute leukocytosis and right lower quadrant abdominal pain. Axial MDCT image with oral contrast shows diverticular wall thickening with infiltration of the adjacent fat (white arrow) in the ascending colon just above the cecum, consistent with acute diverticulitis.
J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 15
Appendicitis Mimics, Thompson et al.
Meckel’s Diverticulitis
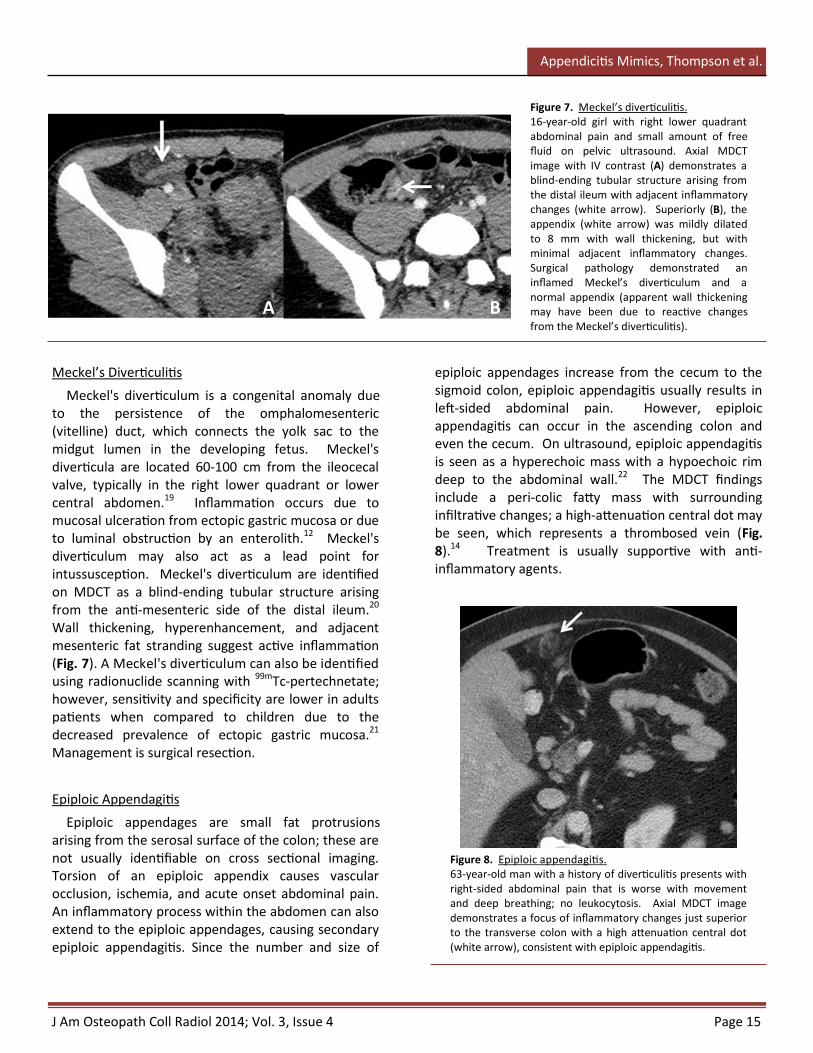
Meckel's diverticulum is a congenital anomaly due to the persistence of the omphalomesenteric (vitelline) duct, which connects the yolk sac to the midgut lumen in the developing fetus. Meckel's diverticula are located 60-100 cm from the ileocecal valve, typically in the right lower quadrant or lower central abdomen.19 Inflammation occurs due to mucosal ulceration from ectopic gastric mucosa or due to luminal obstruction by an enterolith.12 Meckel's diverticulum may also act as a lead point for intussusception. Meckel's diverticulum are identified on MDCT as a blind-ending tubular structure arising from the anti-mesenteric side of the distal ileum.20 Wall thickening, hyperenhancement, and adjacent mesenteric fat stranding suggest active inflammation (Fig. 7). A Meckel's diverticulum can also be identified using radionuclide scanning with 99mTc-pertechnetate; however, sensitivity and specificity are lower in adults patients when compared to children due to the decreased prevalence of ectopic gastric mucosa.21 Management is surgical resection.
Epiploic Appendagitis
Epiploic appendages are small fat protrusions arising from the serosal surface of the colon; these are not usually identifiable on cross sectional imaging. Torsion of an epiploic appendix causes vascular occlusion, ischemia, and acute onset abdominal pain. An inflammatory process within the abdomen can also extend to the epiploic appendages, causing secondary epiploic appendagitis. Since the number and size of
epiploic appendages increase from the cecum to the sigmoid colon, epiploic appendagitis usually results in left-sided abdominal pain. However, epiploic appendagitis can occur in the ascending colon and even the cecum. On ultrasound, epiploic appendagitis is seen as a hyperechoic mass with a hypoechoic rim deep to the abdominal wall.22 The MDCT findings include a peri-colic fatty mass with surrounding infiltrative changes; a high-attenuation central dot may be seen, which represents a thrombosed vein (Fig. 8).14 Treatment is usually supportive with anti-inflammatory agents.
Figure 7. Meckel’s diverticulitis. 16-year-old girl with right lower quadrant abdominal pain and small amount of free fluid on pelvic ultrasound. Axial MDCT image with IV contrast (A) demonstrates a blind-ending tubular structure arising from the distal ileum with adjacent inflammatory changes (white arrow). Superiorly (B), the appendix (white arrow) was mildly dilated to 8 mm with wall thickening, but with minimal adjacent inflammatory changes. Surgical pathology demonstrated an inflamed Meckel’s diverticulum and a normal appendix (apparent wall thickening may have been due to reactive changes from the Meckel’s diverticulitis).
Figure 8. Epiploic appendagitis. 63-year-old man with a history of diverticulitis presents with right-sided abdominal pain that is worse with movement and deep breathing; no leukocytosis. Axial MDCT image demonstrates a focus of inflammatory changes just superior to the transverse colon with a high attenuation central dot (white arrow), consistent with epiploic appendagitis.
A B

J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 16
Appendicitis Mimics, Thompson et al.
Omental Infarction
In contrast to epiploic appendagitis, omental infarction is most commonly a right-sided entity, perhaps due to longer length and mobility of the omentum in the right hemiabdomen compared to the left.17,23 Omental infarction is caused by torsion or vascular thrombosis secondary to postoperative omental adhesions, trauma, or increased intra-abdominal pressure (coughing, obesity, strenuous exercise).23 The most common presenting symptom is acute-onset abdominal pain. MDCT imaging findings vary from an ill-defined, heterogeneous fat-attenuation lesion to a well-defined heterogeneous fatty mass, classically located between the anterior abdominal wall and ascending or transverse colon (Fig. 9).12,23 Omental infarction may be differentiated from epiploic appendagitis by location (between the colon and anterior abdominal wall), larger size (often greater than 5 cm in diameter), absence of a peripheral rim, and absence of a central dot sign.17,23 Management is typically supportive; complications are rare.
Acute Genitourinary Diseases
Urolithiasis
Urolithiasis may present with right lower quadrant pain, particularly if an obstructing calculus is present in the right ureterovesicular junction. Ultrasound evaluation of the abdomen may demonstrate hydroureter, which can be differentiated from bowel due to the lack of bowel signature (alternating hyperechoic and hypoechoic tissue layers) (Fig. 10). If the bladder is distended, the obstructing calculus may be visualized as an echogenic focus in the region of the ureterovesicular junction. Identification is improved by creation of the twinkle artifact on Doppler images, which is rapidly changing red and blue colors behind the calcification due to "phase jitter" within the machine.24
CT images demonstrate a high attenuation calculus within the ureter, with or without proximal ureteral dilatation. Ureteral wall thickening and adjacent fat stranding may be present. Pelvic phleboliths may simulate distal ureteral calculi. If the ureter cannot be followed in its entirety and the calcification is indeterminate, the presence of a soft tissue rim ("rim sign" due to inflamed ureteral walls) and the absence of a soft tissue tail ("tail sign" due to thrombosed vein leading into the calcification) may help characterize urolithiasis.25,26 Treatment for ureteral calculi less than 4 mm in diameter is supportive.
Pyelonephritis
Pyelonephritis is most commonly associated with an ascending genitourinary tract infection and is a clinical diagnosis; often times, the sonographic and MDCT findings are normal.27 However, imaging is useful in excluding complications, such as abscess formation, emphysematous pyelonephritis (typically in diabetics and immunocompromised patients), or xanthogranulomatous pyelonephritis. Findings of pyelonephritis on CT include nephromegaly due to edema, a striated or delayed nephrogram, perinephric fat stranding, and wall-thickening and enhancement of the renal collecting system (Fig. 11).28 Delayed appearance of the calices may also be seen; however, since pyelonephritis is often bilateral, comparison between the two kidneys may not be helpful.
Figure 9. Omental infarct. 72-year-old man presents with 3 days of right lower quadrant pain. Axial MDCT demonstrates infiltrative changes with central fat density between the cecum and the anterior abdominal wall (white arrow), consistent with the appearance of omental infarct. The appendix was normal.
J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 17
Appendicitis Mimics, Thompson et al.
Ultrasound may show nephromegaly and loss of renal sinus fat due to inflammation, as well as loss of the corticomedullary junction. The kidneys may be abnormally hyperechoic or hypoechoic. In the absence of complications, treatment includes antibiotics and supportive measures.
Gynecologic Diseases
Gynecologic emergencies, especially those affecting the right adnexa, are important in the differential diagnosis of acute appendicitis in young women. Screening the right ovary is routinely performed along with ultrasound evaluation of the appendix in pediatric patients. Commonly encountered
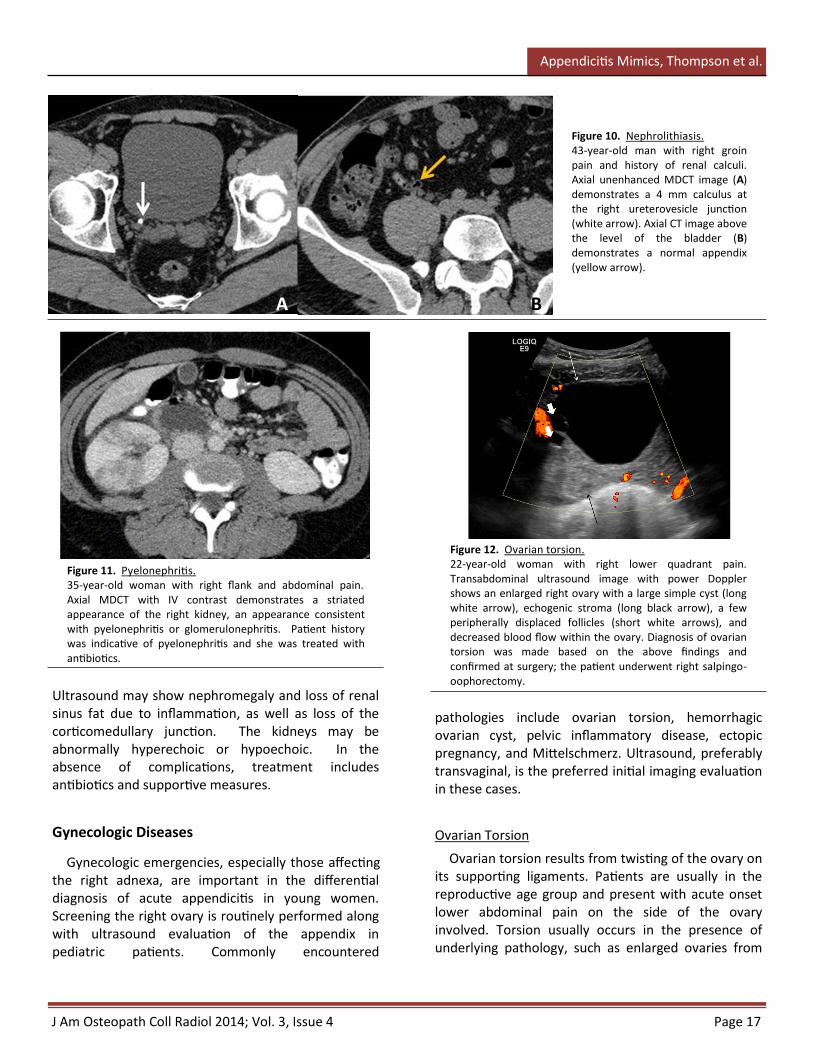
Figure 10. Nephrolithiasis. 43-year-old man with right groin pain and history of renal calculi. Axial unenhanced MDCT image (A) demonstrates a 4 mm calculus at the right ureterovesicle junction (white arrow). Axial CT image above the level of the bladder (B) demonstrates a normal appendix (yellow arrow).
pathologies include ovarian torsion, hemorrhagic ovarian cyst, pelvic inflammatory disease, ectopic pregnancy, and Mittelschmerz. Ultrasound, preferably transvaginal, is the preferred initial imaging evaluation in these cases.
Ovarian Torsion
Ovarian torsion results from twisting of the ovary on its supporting ligaments. Patients are usually in the reproductive age group and present with acute onset lower abdominal pain on the side of the ovary involved. Torsion usually occurs in the presence of underlying pathology, such as enlarged ovaries from
Figure 11. Pyelonephritis. 35-year-old woman with right flank and abdominal pain. Axial MDCT with IV contrast demonstrates a striated appearance of the right kidney, an appearance consistent with pyelonephritis or glomerulonephritis. Patient history was indicative of pyelonephritis and she was treated with antibiotics.
A B
Figure 12. Ovarian torsion. 22-year-old woman with right lower quadrant pain. Transabdominal ultrasound image with power Doppler shows an enlarged right ovary with a large simple cyst (long white arrow), echogenic stroma (long black arrow), a few peripherally displaced follicles (short white arrows), and decreased blood flow within the ovary. Diagnosis of ovarian torsion was made based on the above findings and confirmed at surgery; the patient underwent right salpingo-oophorectomy.
J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 18
Appendicitis Mimics, Thompson et al.
cysts, tumors, enlarged corpus luteum, or ovulation induction for infertility. Ultrasound is performed as the first line of imaging, demonstrating increased size (>4 cm in greatest diameter) and volume of the involved ovary, heterogeneous appearance from edema and hemorrhage, and typically an associated cyst or mass (Fig. 12). Multiple small follicles can be seen in the periphery of the enlarged ovary due to displacement from stromal edema, described as “string of pearls” sign.29 On Doppler, venous flow is often reduced or absent, but this is less sensitive than gray-scale findings. The arterial blood flow may be dampened or absent as well, but this finding is variable due to dual blood supply (ovarian artery and uterine branch artery). Comparison with the normal unaffected ovary is often helpful. Treatment is surgical detorsion and removal of necrotic tissue.
Hemorrhagic Ovarian Cyst
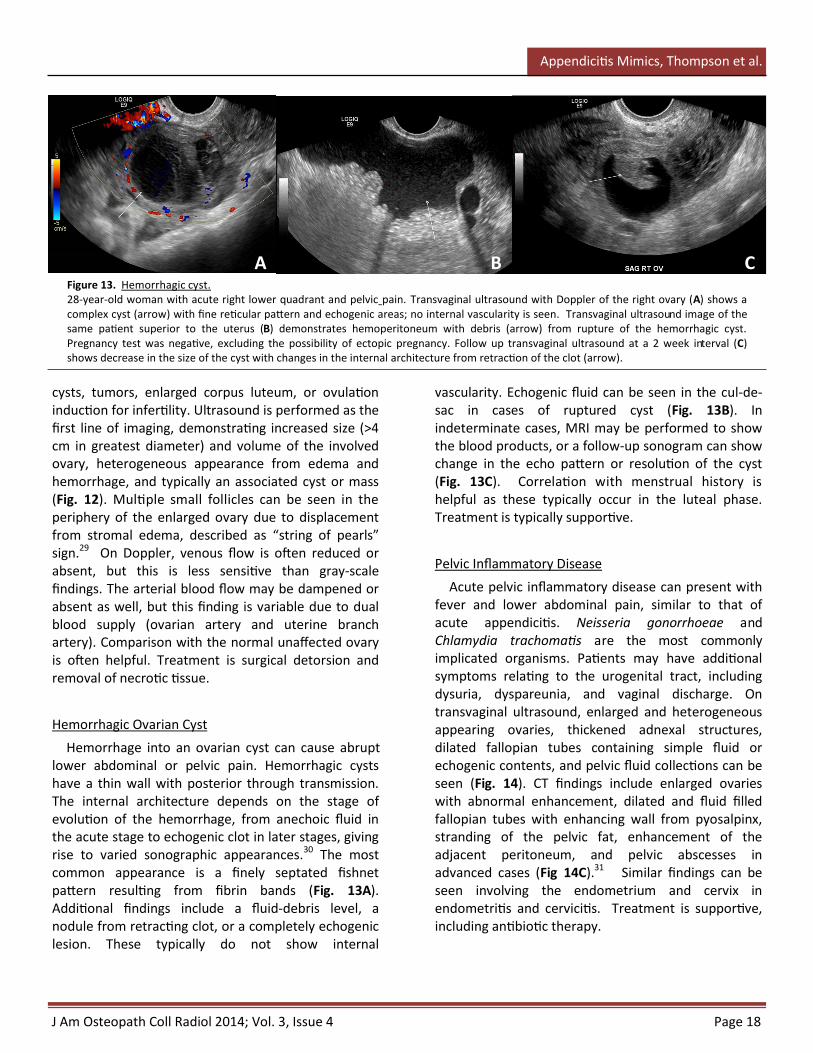
Hemorrhage into an ovarian cyst can cause abrupt lower abdominal or pelvic pain. Hemorrhagic cysts have a thin wall with posterior through transmission. The internal architecture depends on the stage of evolution of the hemorrhage, from anechoic fluid in the acute stage to echogenic clot in later stages, giving rise to varied sonographic appearances.30 The most common appearance is a finely septated fishnet pattern resulting from fibrin bands (Fig. 13A). Additional findings include a fluid-debris level, a nodule from retracting clot, or a completely echogenic lesion. These typically do not show internal
vascularity. Echogenic fluid can be seen in the cul-de-sac in cases of ruptured cyst (Fig. 13B). In indeterminate cases, MRI may be performed to show the blood products, or a follow-up sonogram can show change in the echo pattern or resolution of the cyst (Fig. 13C). Correlation with menstrual history is helpful as these typically occur in the luteal phase. Treatment is typically supportive.
Pelvic Inflammatory Disease
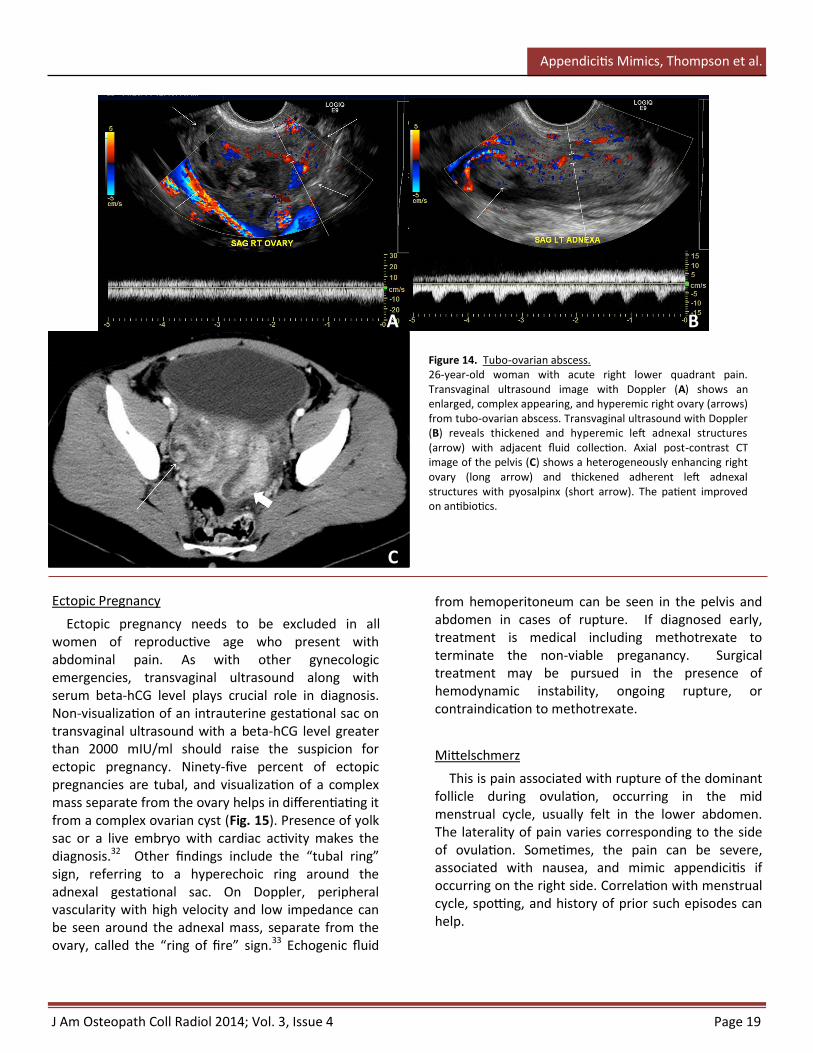
Acute pelvic inflammatory disease can present with fever and lower abdominal pain, similar to that of acute appendicitis. Neisseria gonorrhoeae and Chlamydia trachomatis are the most commonly implicated organisms. Patients may have additional symptoms relating to the urogenital tract, including dysuria, dyspareunia, and vaginal discharge. On transvaginal ultrasound, enlarged and heterogeneous appearing ovaries, thickened adnexal structures, dilated fallopian tubes containing simple fluid or echogenic contents, and pelvic fluid collections can be seen (Fig. 14). CT findings include enlarged ovaries with abnormal enhancement, dilated and fluid filled fallopian tubes with enhancing wall from pyosalpinx, stranding of the pelvic fat, enhancement of the adjacent peritoneum, and pelvic abscesses in advanced cases (Fig 14C).31 Similar findings can be seen involving the endometrium and cervix in endometritis and cervicitis. Treatment is supportive, including antibiotic therapy.
Figure 13. Hemorrhagic cyst. 28-year-old woman with acute right lower quadrant and pelvic pain. Transvaginal ultrasound with Doppler of the right ovary (A) shows a complex cyst (arrow) with fine reticular pattern and echogenic areas; no internal vascularity is seen. Transvaginal ultrasound image of the same patient superior to the uterus (B) demonstrates hemoperitoneum with debris (arrow) from rupture of the hemorrhagic cyst. Pregnancy test was negative, excluding the possibility of ectopic pregnancy. Follow up transvaginal ultrasound at a 2 week interval (C) shows decrease in the size of the cyst with changes in the internal architecture from retraction of the clot (arrow).
A B C
J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 19
Appendicitis Mimics, Thompson et al.
Ectopic Pregnancy
Ectopic pregnancy needs to be excluded in all women of reproductive age who present with abdominal pain. As with other gynecologic emergencies, transvaginal ultrasound along with serum beta-hCG level plays crucial role in diagnosis. Non-visualization of an intrauterine gestational sac on transvaginal ultrasound with a beta-hCG level greater than 2000 mIU/ml should raise the suspicion for ectopic pregnancy. Ninety-five percent of ectopic pregnancies are tubal, and visualization of a complex mass separate from the ovary helps in differentiating it from a complex ovarian cyst (Fig. 15). Presence of yolk sac or a live embryo with cardiac activity makes the diagnosis.32 Other findings include the “tubal ring” sign, referring to a hyperechoic ring around the adnexal gestational sac. On Doppler, peripheral vascularity with high velocity and low impedance can be seen around the adnexal mass, separate from the ovary, called the “ring of fire” sign.33 Echogenic fluid
from hemoperitoneum can be seen in the pelvis and abdomen in cases of rupture. If diagnosed early, treatment is medical including methotrexate to terminate the non-viable preganancy. Surgical treatment may be pursued in the presence of hemodynamic instability, ongoing rupture, or contraindication to methotrexate.
Mittelschmerz
This is pain associated with rupture of the dominant follicle during ovulation, occurring in the mid menstrual cycle, usually felt in the lower abdomen. The laterality of pain varies corresponding to the side of ovulation. Sometimes, the pain can be severe, associated with nausea, and mimic appendicitis if occurring on the right side. Correlation with menstrual cycle, spotting, and history of prior such episodes can help.
Figure 14. Tubo-ovarian abscess. 26-year-old woman with acute right lower quadrant pain. Transvaginal ultrasound image with Doppler (A) shows an enlarged, complex appearing, and hyperemic right ovary (arrows) from tubo-ovarian abscess. Transvaginal ultrasound with Doppler (B) reveals thickened and hyperemic left adnexal structures (arrow) with adjacent fluid collection. Axial post-contrast CT image of the pelvis (C) shows a heterogeneously enhancing right ovary (long arrow) and thickened adherent left adnexal structures with pyosalpinx (short arrow). The patient improved on antibiotics.
A B
C

J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 20
Appendicitis Mimics, Thompson et al.
Conclusion
A variety of acute gastrointestinal genitourinary, and gynecological pathologic processes are associated with clinical symptoms similar to that of appendicitis. Imaging with ultrasound, CT, and MRI is useful for identifying appendicitis and associated complications, as well as identifying alternative diagnoses for the patient’s symptoms. Familiarization with various processes causing right lower quadrant pain, such as those covered in this paper, will aid in providing timely and appropriate care to the patient.
References
1. National Hospital Ambulatory Medical Care Survey: 2010 Emergency Department Summary Tables. 2010. (Accessed Accessed May 9, 2014., at http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2010_ed_web_tables.pdf.)
2. Raman SS, Lu DS, Kadell BM, Vodopich DJ, Sayre J, Cryer H. Accuracy of nonfocused helical CT for the diagnosis of acute appendicitis: a 5-year review. AJR American journal of roentgenology 2002;178:1319-25.
3. Rao PM, Rhea JT, Novelline RA, et al. Helical CT technique for the diagnosis of appendicitis: prospective evaluation of a focused appendix CT examination. Radiology 1997;202:139-44.
4. Duda JB, Lynch ML, Bhatt S, Dogra VS. Computed tomography mimics of acute appendicitis: predictors of appendiceal disease confirmed at pathology. Journal of clinical imaging science 2012;2:73.
5. Rao PM, Rhea JT, Novelline RA. Sensitivity and specificity of the individual CT signs of appendicitis: experience with 200 helical appendiceal CT examinations. Journal of computer assisted tomography 1997;21:686-92.
6. Thoeni RF, Cello JP. CT imaging of colitis. Radiology 2006;240:623-38.
7. Aspelund G, Fingeret A, Gross E, et al. Ultrasonography/MRI Versus CT for Diagnosing Appendicitis. Pediatrics 2014;133:586-93.
8. Rosen MP, Ding A, Blake MA, et al. ACR Appropriateness Criteria(R) right lower quadrant pain--suspected appendicitis. Journal of the American College of Radiology : JACR 2011;8:749-55.
9. Rapp EJ, Naim F, Kadivar K, Davarpanah A, Cornfeld D. Integrating MR imaging into the clinical workup of pregnant patients suspected of having appendicitis is associated with a lower negative laparotomy rate: single-institution study. Radiology 2013;267:137-44.
10. Dewhurst C, Beddy P, Pedrosa I. MRI evaluation of acute appendicitis in pregnancy. Journal of magnetic resonance imaging : JMRI 2013;37:566-75.
11. Furukawa A, Saotome T, Yamasaki M, et al. Cross-sectional imaging in Crohn disease. Radiographics : a review publication of the Radiological Society of North America, Inc 2004;24:689-702.
12. Purysko AS, Remer EM, Filho HM, Bittencourt LK, Lima RV, Racy DJ. Beyond appendicitis: common and uncommon gastrointestinal causes of right lower quadrant abdominal pain at multidetector CT. Radiographics : a review publication of the Radiological Society of North America, Inc 2011;31:927-47.
13. Towbin AJ, Sullivan J, Denson LA, Wallihan DB, Podberesky DJ. CT and MR enterography in children and adolescents with inflammatory bowel disease. Radiographics : a review publication of the Radiological Society of North America, Inc 2013;33:1843-60.
14. van Breda Vriesman AC, Puylaert JB. Mimics of appendicitis: alternative nonsurgical diagnoses with sonography and CT. AJR American journal of roentgenology 2006;186:1103-12.
15. Macari M, Hines J, Balthazar E, Megibow A. Mesenteric adenitis: CT diagnosis of primary versus secondary causes, incidence, and clinical significance in pediatric and adult patients. AJR American journal of roentgenology 2002;178:853-8.
16. Horton KM, Corl FM, Fishman EK. CT evaluation of the colon: inflammatory disease. Radiographics : a review publication of the Radiological Society of North America, Inc 2000;20:399-418.
17. Lubner MG, Simard ML, Peterson CM, Bhalla S, Pickhardt PJ, Menias CO. Emergent and nonemergent nonbowel torsion: spectrum of imaging and clinical findings. Radiographics : a review publication of the Radiological Society of North America, Inc 2013;33:155-73.
Figure 15. Ectopic pregnancy. 30-year-old woman with severe lower abdominal pain. Patient’s last menstrual period was 7 weeks prior; urine pregnancy test was positive with a serum beta hCG of 62,157. Transabdominal ultrasound image shows a complex lesion with thick hyperechoic rim (long arrow) in the right adnexal location, seen separate from the right ovary (short arrow). The patient underwent salpingectomy and the diagnosis of ectopic pregnancy was confirmed.
J Am Osteopath Coll Radiol 2014; Vol. 3, Issue 4 Page 21
Appendicitis Mimics, Thompson et al.
18. Chintapalli KN, Esola CC, Chopra S, Ghiatas AA, Dodd GD, 3rd. Pericolic mesenteric lymph nodes: an aid in distinguishing diverticulitis from cancer of the colon. AJR American journal of roentgenology 1997;169:1253-5.
19. Levy AD, Hobbs CM. From the archives of the AFIP. Meckel diverticulum: radiologic features with pathologic Correlation. Radiographics : a review publication of the Radiological Society of North America, Inc 2004;24:565-87.
20. Hoeffel C, Crema MD, Belkacem A, et al. Multi-detector row CT: spectrum of diseases involving the ileocecal area. Radiographics : a review publication of the Radiological Society of North America, Inc 2006;26:1373-90.
21. Schwartz MJ, Lewis JH. Meckel's diverticulum: pitfalls in scintigraphic detection in the adult. The American journal of gastroenterology 1984;79:611-8.
22. Oztunali C, Kara T. Radiologic findings of epiploic appendagitis. Medical ultrasonography 2013;15:71-2.
23. Singh AK, Gervais DA, Lee P, et al. Omental infarct: CT imaging features. Abdominal imaging 2006;31:549-54.
24. Kielar AZ, Shabana W, Vakili M, Rubin J. Prospective evaluation of Doppler sonography to detect the twinkling artifact versus unenhanced computed tomography for identifying urinary tract calculi. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine 2012;31:1619-25.
25. Boridy IC, Nikolaidis P, Kawashima A, Goldman SM, Sandler CM. Ureterolithiasis: value of the tail sign in differentiating phleboliths from ureteral calculi at nonenhanced helical CT. Radiology 1999;211:619-21.
26. Heneghan JP, Dalrymple NC, Verga M, Rosenfield AT, Smith RC. Soft-tissue "rim" sign in the diagnosis of ureteral calculi with use of unenhanced helical CT. Radiology 1997;202:709-11.
27. Hammond NAN, P.; Miller, F.H. Infectious and inflammatory diseases of the kidney. Radiologic clinics of North America 2012;50:259-70.
28. Craig WD, Wagner BJ, Travis MD. Pyelonephritis: radiologic-pathologic review. Radiographics : a review publication of the Radiological Society of North America, Inc 2008;28:255-77; quiz 327-8.
29. Chang HC, Bhatt S, Dogra VS. Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics : a review publication of the Radiological Society of North America, Inc 2008;28:1355-68.
30. Jain KA. Sonographic spectrum of hemorrhagic ovarian cysts. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine 2002;21:879-86.
31. Sam JW, Jacobs JE, Birnbaum BA. Spectrum of CT findings in acute pyogenic pelvic inflammatory disease. Radiographics : a review publication of the Radiological Society of North America, Inc 2002;22:1327-34.
32. Lin EP, Bhatt S, Dogra VS. Diagnostic clues to ectopic pregnancy. Radiographics : a review publication of the Radiological Society of North America, Inc 2008;28:1661-71.
33. Pellerito JS, Taylor KJ, Quedens-Case C, et al. Ectopic pregnancy: evaluation with endovaginal color flow imaging. Radiology 1992;183:407-11
Related Documents










![9월 1월례집담회 토픽데이(IBD and mimickers) 새 케이스 추가[1].pptx](https://static.cupdf.com/doc/110x72/5695d3a21a28ab9b029ea633/9-1-ibd-and-mimickers-1pptx.jpg)