Midwall left ventricular systolic function in cardiac hypertrophy J Mayet, B Wasan, B Ariff, N Chapman, M Shahi, NR Poulter, PS Sever, RA Foale, SAMcG Thom Peart-Rose Clinic and Department of Cardiology St Mary’s Hospital, Imperial College, London

Midwall left ventricular systolic function in cardiac hypertrophy
Feb 08, 2016
Midwall left ventricular systolic function in cardiac hypertrophy. J Mayet, B Wasan, B Ariff, N Chapman, M Shahi, NR Poulter, PS Sever, RA Foale, SAMcG Thom Peart-Rose Clinic and Department of Cardiology St Mary’s Hospital, Imperial College, London. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Midwall left ventricular systolic function in cardiac hypertrophy
J Mayet, B Wasan, B Ariff, N Chapman, M Shahi, NR Poulter, PS Sever, RA Foale, SAMcG
Thom
Peart-Rose Clinic and Department of Cardiology St Mary’s Hospital, Imperial College, London

Is LV systolic function preserved in LVH?
• Discrepancy between experimental and human studies– Former suggest myocardial function depressed– Latter indicate it is preserved
• Experimental and human studies not strictly compatible– Experimental studies measure myocardial or
myofibril function– Human studies have assessed whole heart function
by utilising endocardial measurements

Midwall LV shortening
• It is often assumed that the inner and outer parts of the LV wall thicken equally in systole
• Myocardial shortening in subendocardial is greater than subepicardial layers
• Therefore a theoretical mid-point in the LV wall shows relative migration toward the epicardium throughout contraction

Epicardial migration of theoretical midwall fibre
during systole
......
Posterior wall
Theoretical midwall fibre

Midwall LV shortening
• Anatomic reasons why assessing shortening at the midwall may be preferable
• At the midwall circumferentially orientated fibres predominate while at the epicardium and endocardium fibres are longitudinally orientated
• When circumferential wall stress is considered to assess stress-shortening relations then correct anatomic plane is being addressed



What is the relationship between endocardial and
midwall shortening in normal subjects and those with LVH?
• 38 previously untreated hypertensives with LVH compared with normotensive controls (healthy volunteers)
• No patient had significant co-morbidity• Each underwent full two-dimensional
echocardiographic examination

How does regression of LVH effect midwall shortening?
• 32 hypertensive subjects with LVH– 24 previously untreated– 8 uncontrolled on existing medication
• Echocardiography at baseline• Treated with ramipril with addition of felodipine and
bendrofluazide if required• Echocardiography after BP control• Echocardiography after a further 6 months of BP
control

Calculations from echocardiographic data
• RWT = 2xPWTd / LVIDd• FS = 100 x (LVIDd - LVIDs) / LVIDd• End-diast volume = 7 x (LVIDd)3 / (2.4+LVIDd)• End-syst volume = 7 x (LVIDs)3 / (2.4+LVIDs)• CO = HR x SV = HR x (EDV- EDV)• EF = 100 x (EDV - ESV) / EDV• cESS =
SBPx1/2LVIDs2x{1+[(1/2LVIDs+PWTs)2/(1/2LVIDs+1/2PWTs)2]}/ [(1/2LVIDs+PWTs)2-1/2LVIDs2]

Calculations from echocardiographic data
• In order to calculate fractional shortening at the midwall, the position of a theoretical midwall fibre in systole needs to be known
• This can be calculated by using a cylindrical model of the LV with the assumption that volume remains constant through the cardiac cycle
(1/2LVID+1/2PWT)2 - (1/2LVID)2
End-diastolic volume = ___________________________________________
(1/2LVID+PWT)2 - (1/2LVID)2
(1/2LVIDs+a)2 -(1/2LVIDs)2 End-systolic volume = __________________________________________
(1/2LVID+PWT)2 - (1/2LVID)2
• Where “a” is the distance from the posterior wall endocardium of the theoretical midwall fibre at end-systole
• Because end-diastolic volume = end-systolic volume “a” can be calculated• From this: Midwall FS (%) = 100 x [(LVID+PWT)-(LVIDs+2a)] / (LVID+PWT)

Calculation of midwall fractional shortening
.
.
.
.
LVIDd LVIDs
a
a
a’
a’
Midwall fractional shortening %= [(LVIDd + 2a) - (LVIDs + 2a’)] / (LVIDd + 2a)

Patient characteristics and echo results of hypertensives with LVH and control
subjectsHypertensives with
LVHControl subjects
Age (years) 46+/-2.4* 40+/-1.7SBP (mmHg) 170+/-3.7* 124+/-2.3DBP (mmHg) 100+/-1.6* 77+/-7.6ECG voltage 39+/-3.3* 27+/-1.3IVS diastole (cm) 1.4+/-0.04* 1.1+/-0.02LVID diastole (cm) 4.7+/-0.08 4.8+/-0.08PWT diastole (cm) 1.3+/-0.05* 1.0+/-0.02LVID systole (cm) 3.1+/-0.11 3.0+/-0.07PWT systole (cm) 1.6+/-0.05* 1.2+/-0.02LVMI (g/m2) 140+/-3.6* 92+/-3.1RWT 0.55+/-0.02* 0.41+/-0.01CESS (kdyne/cm2) 166.4+/-9.6 150.6+/-6.7
*p<0.01 versus controls

Endocardial systolic function in patients with LVH and controls
0102030
40506070
LVH 62.5 34.5Control 66.4 37
EF (%) FS (%)

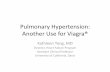
Cardiac output and midwall LV systolic function in patients with LVH and controls
0
5
10
15
20
25
LVH 4.32 17.9Control 4.55 21.6
CO (l/min) Midwall FS (%)
*
*p < 0.01 versus control group

Treatment study: hypertensives with LVH (males=28, females=4)
Baseline BP control 6 months postBP control
Age (years) 50+/-2.0 - -SBP (mmHg) 174+/-4.1 138+/-1.8* 143+/-2.8*DBP (mmHg) 103+/-1.9 84+/-1.2* 86+/-1.4*Heart rate (b/min) 66+/-2.0 66+/-2.1 65+/-1.9ECG voltage 39+/-2.4 - 36+/-2.4IVS diast (cm) 1.48+/-0.03 1.41+/-0.03 1.35+/-0.03*LVID diast(cm) 4.71+/-0.10 4.61+/-0.07 4.64+/-0.08PWT diast (cm) 1.30+/-0.03 1.28+/-0.02 1.26+/-0.02LVID syst (cm) 2.98+/-0.12 2.88+/-0.08 2.82+/-0.07PWT syst (cm) 1.62+/-0.04 1.54+/-0.05 1.51+/-0.04LVMI (g/m2) 145+/-3.8 133+/-3.5 124+/-3.4*RWT 0.56+/-0.02 0.56+/-0.02 0.55+/-0.02CESS (kdyne/cm2) 152.0+/-9.7 131.0+/-8.1 130.4+/-7.3
*p<0.01 versus controls

Changes in endocardial systolic function with treatment and LVH regression
0
20
40
60
80
Baseline 65.6 37BP control 67 386/12 BP control 69.3 39.5
EF (%) FS (%)

Changes in cardiac output and midwall LV systolic function with treatment and LVH
regression
0
5
10
15
20
25
Baseline 4.48 18.7BP control 4.37 206/12 BP control 4.34 21.9
CO (l/min) Midwall FS (%)
*
*p < 0.01 versus baseline

What is the relationship between endocardial and midwall shortening in normal subjects and those with
LVH?
• LVH group had a higher BP and a higher LVMI• Endocardial measures of LV systolic function were
similar between the 2 groups• Midwall systolic function was significantly depressed
in the LVH group

How does regression of LVH effect midwall shortening?
• Good BP control was achieved• There was significant regression of LVH• Endocardial fractional shortening was not
significantly changed• Midwall shortening improved with LVH regression

Discussion
• In spite of similar endocardial systolic function, midwall systolic function is significantly depressed in subjects with LVH secondary to hypertension
• Midwall shortening is improved with regression of LVH using an ACE inhibitor and calcium antagonist based treatment regime
• A reduced midwall shortening has been found to be associated with a lower exercise performance
• Depressed midwall shortening has been shown to be an independent predictor of an adverse outcome in hypertensive subjects, particularly in those subjects with additional LVH
Related Documents