Meduri et all Chest 2007;131;954-963

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Meduri et allChest 2007;131;954-963

Background
Inflammation in the first week of MV determines resolving vs un-resolving
Un-resolving ARDS LIS by day 7PEEPPaO2/FIO2Static Lung ComplianceCXR
Dysregulated systemic inflammation

Methylprednisolone (2 mg/kg/d) non-improvers after 9 days ofSustained reductions in plasma and BAL
inflammatory Improvement in lung injury and MODS scores.Reduction in duration of MV and ICU mortality
Background
Meduri GU, Headley S, Golden E, et al. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA 1998; 280:159 –165

Background
These results do not support the routine use of methylprednisolone for persistent ARDS despite the improvement in cardiopulmonary physiology. In addition, starting methylprednisolone therapy more than two weeks after the onset of ARDS may increase the risk of death
Hypothesis
Prolonged administration of low-dose methylprednisolone (1 mg/kg/d) initiated in early ARDS (within 72 h of diagnosis) downregulates systemic inflammation and leads to earlier resolution of pulmonary organ dysfunction and a reduction in duration of mechanical ventilation and ICU

Design April 1997 to April 2002 in 5 ICU’s 2:1 methylprednisolone: placebo randomization Loading dose of 1 mg/kg
1 mg/kg/d from day 1 to day 14,0.5 mg/kg/d from day 15 to day 21, 0.25 mg/kg/d from day 22 to day 25, 0.125 mg/kg/d from day 26 to day 28.
240 mL of normal saline solution and administered daily as an infusion at 10 mL/h

MV ARDSnet
Bronch + bl BAL was per- formed prior to study entry, and then every 5 to 7 days
Day 7 and 9, un-blinded methylpred- nisolone therapy (2 mg/kg/d) for un-resolving ARDS
Infection surveillance and avoidance of neuromuscular blocking agents
Design

The primary outcome variable was
Improvement in LIS by study day 7
For patients remaining intubated on study day 7
a reduction in LIS 1 point day 7 LIS ≤ 2.0 (for study entry LIS ≤
2.9) or 2.5 (for study entry LIS ≥ 3.0)
Design

Statistical Analysis The study was analyzed as
intention-to- treat. “Per protocol” analysis is
recommended to reflect scientific methods of the protocol.
All statistical calculations were preformed using the SAS System for Windows
Significance was defined as a 2-tailed test with an alpha of .05.

Results

Baseline Characteristics

Baseline Characteristics

Results
Among patients with and without shock, improvement in the primary variable was observed: methylprednisolone vs placebo, 67% vs 23% (p 0.03) and 71% vs 47%(p 0.09)

Results

Results
Results
Results ICU mortality
Pts catecholamine-dependent shock was 73% vs 46% (p 0.24)
Pts w/o shock was 81% vs 67% (p 0.29).In per-protocol analysis with catecholamine-dependent
shock was 90% vs 71% (p 0.07)
Between day 7 - 9, 14 patients failed to meet criteria for improvement in LIS (8% vs 36%; p 0.002) and received open-label.
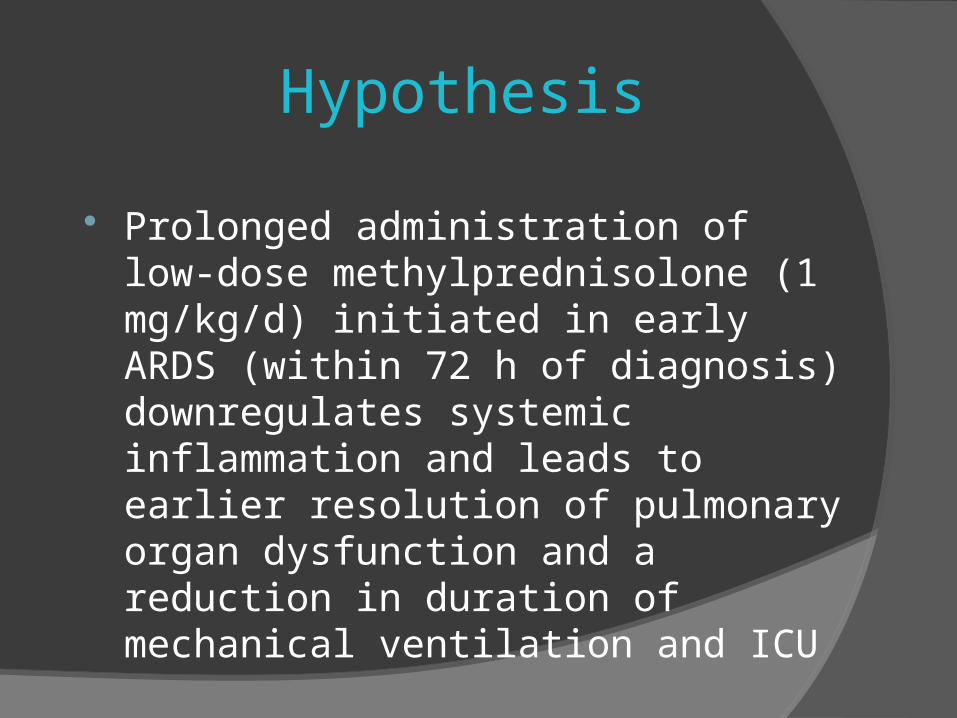
Day 14, 3 pts (5%) in the Rx group and 10 pts (36%) in the control group remained on MV (p 0.0001).
Results
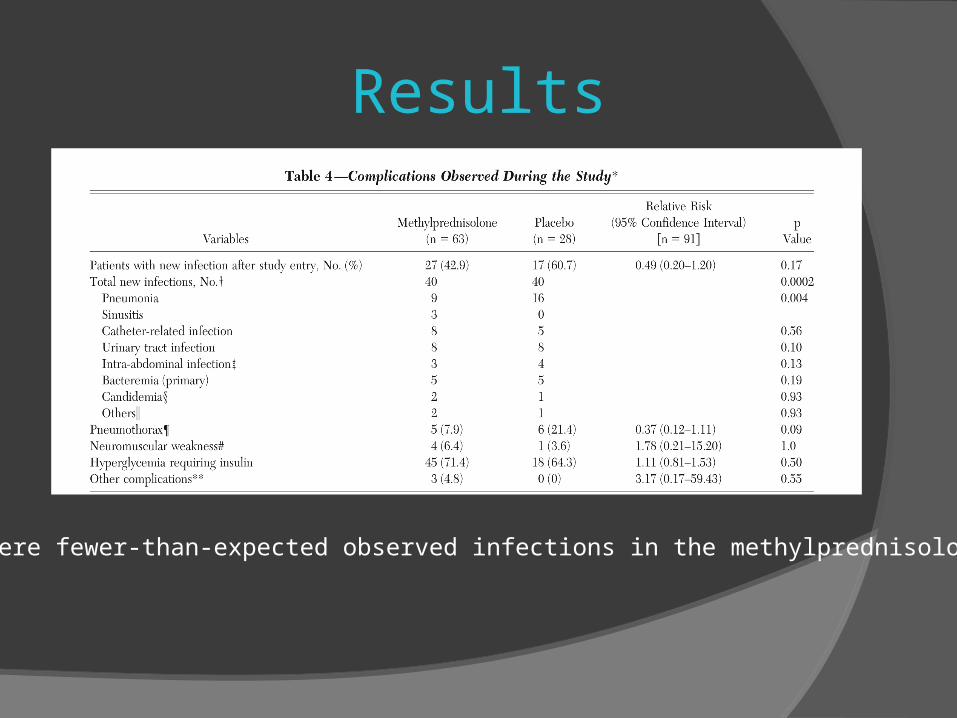
• There were fewer-than-expected observed infections in the methylprednisolone group

Discussion The surrogate marker for pulmonary
inflammation was LIS; the markers for systemic inflammation were CRP
By study day 7 twice the proportion of patients randomized to Rx achieving a 1-point reduction in LIS
Improvement was not significantly affected by the baseline imbalance in the proportion of patients with catecholamine-dependent shock
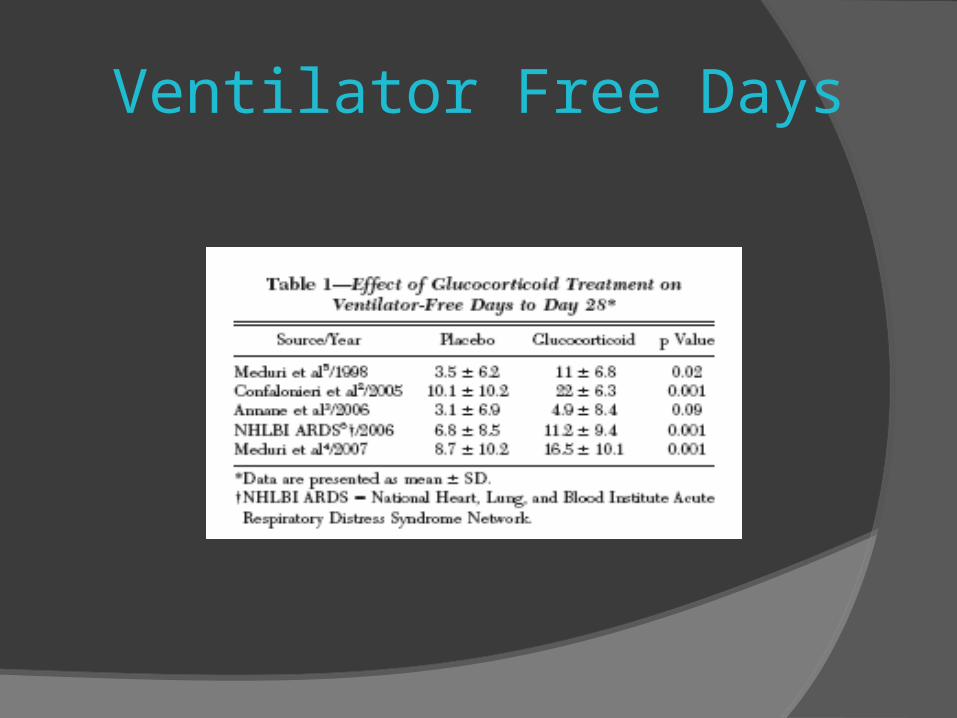
Ventilator Free Days

In patients with un-resolving ARDS, premature discontinuation of methylpred-nisolone administration was associated with physiologic deterioration
In the recent ARDS network study, the large benefits observed during methylprednisolone treatment were partially lost after premature discontinuation of study drug
Discussion

Limitations
Small Sample size Imbalances pts with catecholamine-
dependent shock that may have biased the estimate of the treatment effect on mortality
Surviving sepsis Ventilator protocol Open label cross over
Related Documents