Joel E. Gray, PhD Colin G. Orton, PhD Index terms: Physics Radiology and radiologists, history Reflections Radiology 2000; 217:619 – 625 Abbreviations: AAPM 5 American Association of Physicists in Medicine ABR 5 American Board of Radiology ACR 5 American College of Radiology CAMPEP 5 Commission on Accreditation of Medical Physics Educational Programs MQSA 5 Mammography Quality Standards Act NCRP 5 National Council on Radiation Protection and Measurements RSNA 5 Radiological Society of North America 1 From the Department of Business and Clinical Development, Lorad, a Hologic Company, 36 Apple Ridge Rd, Danbury, CT 06810 (J.E.G.); and the Department of Radiation Oncology, Radiation Oncology Center, Harper Hospital, Detroit , Mich (C.G.O). Re- ceived November 30, 1999; revision requested January 24, 2000; revision received July 14; accepted July 26. Address correspondence to J.E.G. (e-mail: [email protected]). © RSNA, 2000 Medical Physics: Some Recollections in Diagnostic X-ray Imaging and Therapeutic Radiology 1 Medical physics has changed dramatically since 1895. There was a period of slow evolutionary change during the first 70 years after Roentgen’s discovery of x rays. With the advent of the computer, however, both diagnostic and therapeutic radi- ology have undergone rapid growth and changes. Technologic advances such as computed tomography and magnetic resonance imaging in diagnostic imaging and three-dimensional treatment planning systems, stereotactic radiosurgery, and in- tensity modulated radiation therapy in radiation oncology have resulted in substan- tial changes in medical physics. These advances have improved diagnostic imaging and radiation therapy while expanding the need for better educated and experi- enced medical physics staff. DIAGNOSTIC MEDICAL PHYSICS In 1895, Wilhelm Conrad Roentgen surprised the world with a revolutionary discovery that gave birth to the professions of diagnostic and therapeutic medical physics. Since then, physicists have worked avidly to develop new discoveries to advance the technology of medical imaging and radiation therapy. The first 70 years after Roentgen’s discovery witnessed the development of higher speed imaging systems, electronic amplification devices, scintillation cameras, ultrasonographic (US) devices, advanced high capacity x-ray tubes, and rapid film processors (1). However, maturation of the computer has accelerated even more and enabled technology such as computed tomography (CT), magnetic reso- nance (MR) imaging, and sophisticated interventional fluoroscopy. Medical physics in the United States was first recognized as a profession with the formation of the American Association of Physicists in Medicine (AAPM) in November 1958, during the annual meeting of the Radiological Society of North America (RSNA) (2). Many well-known medical physicists practicing in the 20th century made notable contri- butions to diagnostic medical physics (Table 1). In the early days of radiology, equipment was quite primitive with little or no shielding around the x-ray tube and bare metal high-voltage cables strung across the ceiling (Fig 1). Often the physician responsible for the “x-ray laboratory” served as the technologist, service engineer, and medical physicist to ensure that the equipment was functional. Major changes in the practice of medical physics started in the early 1970s with the introduction of the CT scanner. This author (J.E.G.) recalls being in the equipment exhibit hall shortly after the exhibits opened at the meeting of the RSNA at the Palmer House Hotel (Chicago, Ill) in 1972. The original EMI CT scanner was on display, and I quickly judged it to be something that the radiology community would not embrace because it produced images with checkerboard-sized pixels (Fig 2). I wondered why a radiologist would be interested in something that produced images with such poor spatial resolution? Since that time, medical physicists have learned that other image quality parameters, in addition to spatial resolution, are important in diagnostic imaging. CT made dramatic changes, first in neuroradiology and then in body imaging. It eliminated pneumoencephalography, performed in the dreaded “chair” in which a patient was positioned and, after a portion of the cerebrospinal fluid was removed and replaced with air, rotated around in various positions. The first (and, fortunately, last) pneumoen- Reflections 619

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Joel E. Gray, PhDColin G. Orton, PhD
Index terms:PhysicsRadiology and radiologists, historyReflections
Radiology 2000; 217:619–625
Abbreviations:AAPM 5 American Association of
Physicists in MedicineABR 5 American Board of RadiologyACR 5 American College of
RadiologyCAMPEP 5 Commission on
Accreditation of Medical PhysicsEducational Programs
MQSA 5 Mammography QualityStandards Act
NCRP 5 National Council onRadiation Protection andMeasurements
RSNA 5 Radiological Society ofNorth America
1 From the Department of Businessand Clinical Development, Lorad, aHologic Company, 36 Apple Ridge Rd,Danbury, CT 06810 (J.E.G.); and theDepartment of Radiation Oncology,Radiation Oncology Center, HarperHospital, Detroit , Mich (C.G.O). Re-ceived November 30, 1999; revisionrequested January 24, 2000; revisionreceived July 14; accepted July 26.Address correspondence to J.E.G.(e-mail: [email protected]).© RSNA, 2000
Medical Physics: SomeRecollections in DiagnosticX-ray Imaging andTherapeutic Radiology1
Medical physics has changed dramatically since 1895. There was a period of slowevolutionary change during the first 70 years after Roentgen’s discovery of x rays.With the advent of the computer, however, both diagnostic and therapeutic radi-ology have undergone rapid growth and changes. Technologic advances such ascomputed tomography and magnetic resonance imaging in diagnostic imaging andthree-dimensional treatment planning systems, stereotactic radiosurgery, and in-tensity modulated radiation therapy in radiation oncology have resulted in substan-tial changes in medical physics. These advances have improved diagnostic imagingand radiation therapy while expanding the need for better educated and experi-enced medical physics staff.
DIAGNOSTIC MEDICAL PHYSICS
In 1895, Wilhelm Conrad Roentgen surprised the world with a revolutionary discoverythat gave birth to the professions of diagnostic and therapeutic medical physics. Sincethen, physicists have worked avidly to develop new discoveries to advance the technologyof medical imaging and radiation therapy. The first 70 years after Roentgen’s discoverywitnessed the development of higher speed imaging systems, electronic amplificationdevices, scintillation cameras, ultrasonographic (US) devices, advanced high capacity x-raytubes, and rapid film processors (1). However, maturation of the computer has acceleratedeven more and enabled technology such as computed tomography (CT), magnetic reso-nance (MR) imaging, and sophisticated interventional fluoroscopy.
Medical physics in the United States was first recognized as a profession with theformation of the American Association of Physicists in Medicine (AAPM) in November1958, during the annual meeting of the Radiological Society of North America (RSNA) (2).Many well-known medical physicists practicing in the 20th century made notable contri-butions to diagnostic medical physics (Table 1).
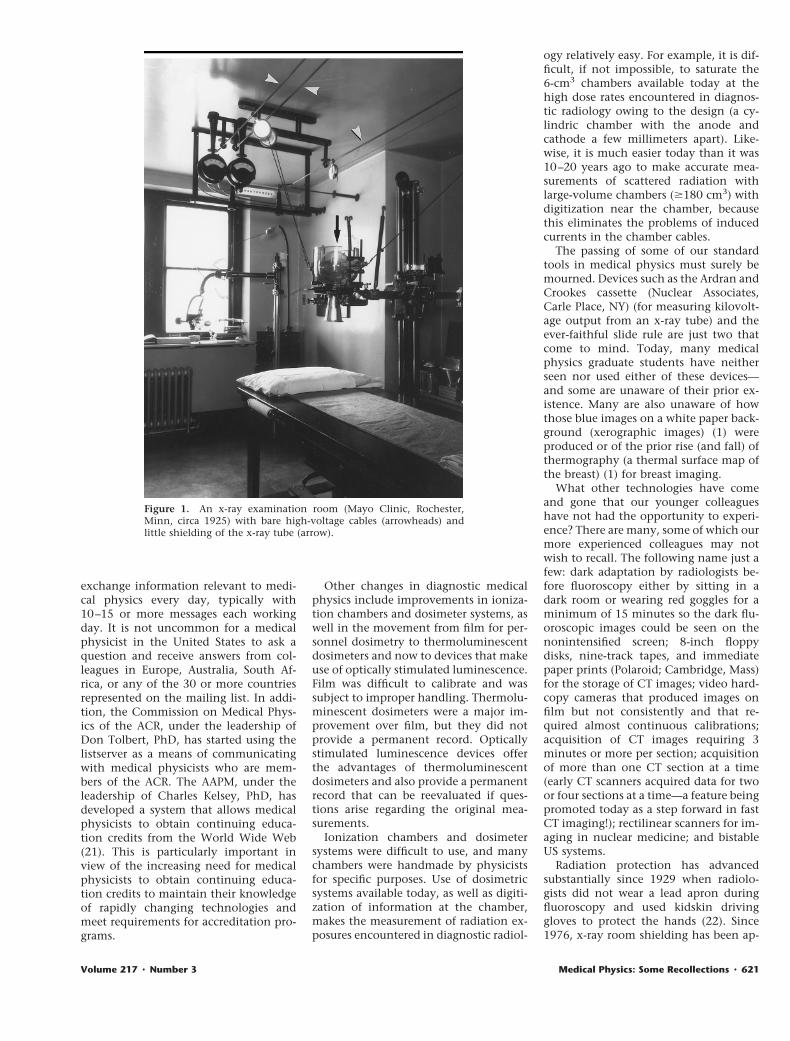
In the early days of radiology, equipment was quite primitive with little or no shieldingaround the x-ray tube and bare metal high-voltage cables strung across the ceiling (Fig 1).Often the physician responsible for the “x-ray laboratory” served as the technologist,service engineer, and medical physicist to ensure that the equipment was functional.
Major changes in the practice of medical physics started in the early 1970s with theintroduction of the CT scanner. This author (J.E.G.) recalls being in the equipment exhibithall shortly after the exhibits opened at the meeting of the RSNA at the Palmer HouseHotel (Chicago, Ill) in 1972. The original EMI CT scanner was on display, and I quicklyjudged it to be something that the radiology community would not embrace because itproduced images with checkerboard-sized pixels (Fig 2). I wondered why a radiologistwould be interested in something that produced images with such poor spatial resolution?Since that time, medical physicists have learned that other image quality parameters, inaddition to spatial resolution, are important in diagnostic imaging.
CT made dramatic changes, first in neuroradiology and then in body imaging. Iteliminated pneumoencephalography, performed in the dreaded “chair” in which a patientwas positioned and, after a portion of the cerebrospinal fluid was removed and replacedwith air, rotated around in various positions. The first (and, fortunately, last) pneumoen-
Reflections
619

cephalographic system that I (J.E.G.)evaluated had exceedingly low-contrastimages, primarily due to an excessiveamount of off-focus radiation and nomeans of reducing this unwanted radia-tion. With the x-ray imaging systemsavailable today, off-focus radiation is ad-dressed by means of better x-ray tube de-sign and lead apertures that eliminatemost of this problem. In fact, most med-ical physicists today do not attempt toquantify off-focus radiation.
Since the early 1970s, notable techno-logic changes in imaging have occurredon a rather frequent basis (Table 1). Thishas caused dramatic changes in the actualpractice of diagnostic medical physics, es-pecially because the medical physicistmust be up to date with the technologyand understand how it functions fromboth the technologic and clinical per-spectives. Furthermore, each time a newmodality is introduced, new techniquesmust be developed for acceptance testingand quality control of the modality toensure the optimum use of radiation,whether ionizing or nonionizing, andthe maximum quality of images. In addi-tion, information from each of the newmodalities must be incorporated into theradiology residency programs and intothe physics portion of the board exami-nations.
The application of intensifying screensto mammography was a major change indiagnostic imaging. The original use ofindustrial x-ray film resulted in low-con-trast images compared with those pro-duced today. In addition, the radiationexposures were much higher than thoseused today (eg, 0.1 Gy [10-rad entrancedose] with industrial x-ray film versus0.01 Gy [1-rad entrance dose] withscreen-film systems available today). Thefirst mammographic unit with otherthan a tungsten target was introducedwhile industrial x-ray film was beingused. The CGR Senographe (GE MedicalSystems, Milwaukee, Wis), introduced in1965, was the first dedicated mammogra-phy unit, and its molybdenum anodeand filter had many of the essential ele-ments found in modern equipment.
One of the major changes in the prac-tice of diagnostic medical physics was theintroduction by the American College ofRadiology (ACR) of their MammographyAccreditation Program in 1990 (12),which, by means of metamorphosis, be-came the core of the MammographyQuality Standards Act (MQSA) (13). Thisprogram has mandated medical physicssupport for all mammographic imagingfacilities throughout the United States.
The results clearly indicate dramatic im-provements in mammographic imaging,with improved image quality and opti-mized radiation doses.
The first publications about qualitycontrol in diagnostic imaging were pub-lished starting in 1968 (14–17). Beforethis, the term “quality control” was vir-tually unheard of in diagnostic radiology.The requirements by the ACR Mammog-raphy Accreditation Program and the MQSAprogram formally introduced quality con-trol into diagnostic radiology.
In the past, most staff in radiology de-partments were not aware of the expo-sures required for specific x-ray projec-tions. The Joint Commission on theAccreditation of Healthcare Organiza-tions attempted to address this lack ofawareness by requiring the posting of ra-diation exposure levels for typical x-rayexaminations. The levels were posted inmost departments, but, unfortunately,national benchmark data were seldomused to determine if the departmentalexposures were reasonable. The AAPMhas established reference values, similarto investigational levels, with which ra-diation exposure levels in individual de-partments can be compared (AAPM, writ-ten communication, 1999). The conceptof reference values was introduced by theInternational Commission on Radiologi-
cal Protection in 1991 with further infor-mation and recommendations in 1996(18,19). If the exposures used for exami-nations exceed the reference values, thenthe medical physicist must investigatethe reason for the higher exposure levels.If, after investigation, the radiologistsand medical physicist agree that thehigher levels are warranted, then thehigher exposures are justified and can beused. It should be stressed that the refer-ence values are not to be considered aslimits on exposures for examinations.The adoption of reference values has re-sulted in a major change in the way med-ical physicists will evaluate radiation ex-posures in the future. More attention willbe focused on patient exposures and aconcerted effort will be required to en-sure that radiation exposures are opti-mized in all medical imaging depart-ments.
The Internet has resulted in manychanges in our lives, and these includethe ability for medical physicists to inter-change information with their colleaguesin the United States and throughout theworld. The MEDPHYS Listserv (20) is agood example of the rapid interchange ofinformation among professionals to helpboth the professionals and their patients.More than 2,200 individuals throughoutthe world subscribe to the listserver and
TABLE 1A Few of the Technologic Advances in Diagnostic Imaging in the Past Century
Year Technologic Advance Prominent PioneersReferenceNumber
1895 Discovery of x rays W. C. Roentgen 11896 Calcium tungstate screens T. A. Edison 11896 Discovery of radioactivity H. Becquerel 11913 Hot-cathode x-ray tube W. D. Coolidge 11915 Bucky-Potter grid G. P. Bucky, H. E. Potter 11925 Dual-emulsion film on flexible base 11928 Pako mechanized film processor 11934 Conventional tomography A. Vallebona, G. Z. DesPlantes 11948 Westinghouse image intensifier* J. W. Coltman 11951 Rectilinear scanner B. Cassen 11951 Bistable US G. Ludwig, J. Wild, D. Howry 3–51956 Kodak X-Omat film processor† 11958 Scintillation camera H. Anger 11960 Xeroradiography 11962 Emission reconstruction
tomographyD. Kuhl 6
1962 Gray-scale US G. Kosoff 71965 Dedicated mammographic system 11972 CT G. N. Hounsfield 81973 Digital subtraction angiography C. Mistretta 91975 Positron emission tomography,
or PETM. Ter-Pogossian 10
1976 Single photon emission CT,or SPECT
J. Keyes 6
1980 MR imaging P. C. Lauterbur 11
* Pittsburgh, Pa.† Rochester, NY.
620 z Radiology z December 2000 Gray and Orton
exchange information relevant to medi-cal physics every day, typically with10–15 or more messages each workingday. It is not uncommon for a medicalphysicist in the United States to ask aquestion and receive answers from col-leagues in Europe, Australia, South Af-rica, or any of the 30 or more countriesrepresented on the mailing list. In addi-tion, the Commission on Medical Phys-ics of the ACR, under the leadership ofDon Tolbert, PhD, has started using thelistserver as a means of communicatingwith medical physicists who are mem-bers of the ACR. The AAPM, under theleadership of Charles Kelsey, PhD, hasdeveloped a system that allows medicalphysicists to obtain continuing educa-tion credits from the World Wide Web(21). This is particularly important inview of the increasing need for medicalphysicists to obtain continuing educa-tion credits to maintain their knowledgeof rapidly changing technologies andmeet requirements for accreditation pro-grams.
Other changes in diagnostic medicalphysics include improvements in ioniza-tion chambers and dosimeter systems, aswell in the movement from film for per-sonnel dosimetry to thermoluminescentdosimeters and now to devices that makeuse of optically stimulated luminescence.Film was difficult to calibrate and wassubject to improper handling. Thermolu-minescent dosimeters were a major im-provement over film, but they did notprovide a permanent record. Opticallystimulated luminescence devices offerthe advantages of thermoluminescentdosimeters and also provide a permanentrecord that can be reevaluated if ques-tions arise regarding the original mea-surements.
Ionization chambers and dosimetersystems were difficult to use, and manychambers were handmade by physicistsfor specific purposes. Use of dosimetricsystems available today, as well as digiti-zation of information at the chamber,makes the measurement of radiation ex-posures encountered in diagnostic radiol-
ogy relatively easy. For example, it is dif-ficult, if not impossible, to saturate the6-cm3 chambers available today at thehigh dose rates encountered in diagnos-tic radiology owing to the design (a cy-lindric chamber with the anode andcathode a few millimeters apart). Like-wise, it is much easier today than it was10–20 years ago to make accurate mea-surements of scattered radiation withlarge-volume chambers ($180 cm3) withdigitization near the chamber, becausethis eliminates the problems of inducedcurrents in the chamber cables.
The passing of some of our standardtools in medical physics must surely bemourned. Devices such as the Ardran andCrookes cassette (Nuclear Associates,Carle Place, NY) (for measuring kilovolt-age output from an x-ray tube) and theever-faithful slide rule are just two thatcome to mind. Today, many medicalphysics graduate students have neitherseen nor used either of these devices—and some are unaware of their prior ex-istence. Many are also unaware of howthose blue images on a white paper back-ground (xerographic images) (1) wereproduced or of the prior rise (and fall) ofthermography (a thermal surface map ofthe breast) (1) for breast imaging.
What other technologies have comeand gone that our younger colleagueshave not had the opportunity to experi-ence? There are many, some of which ourmore experienced colleagues may notwish to recall. The following name just afew: dark adaptation by radiologists be-fore fluoroscopy either by sitting in adark room or wearing red goggles for aminimum of 15 minutes so the dark flu-oroscopic images could be seen on thenonintensified screen; 8-inch floppydisks, nine-track tapes, and immediatepaper prints (Polaroid; Cambridge, Mass)for the storage of CT images; video hard-copy cameras that produced images onfilm but not consistently and that re-quired almost continuous calibrations;acquisition of CT images requiring 3minutes or more per section; acquisitionof more than one CT section at a time(early CT scanners acquired data for twoor four sections at a time—a feature beingpromoted today as a step forward in fastCT imaging!); rectilinear scanners for im-aging in nuclear medicine; and bistableUS systems.
Radiation protection has advancedsubstantially since 1929 when radiolo-gists did not wear a lead apron duringfluoroscopy and used kidskin drivinggloves to protect the hands (22). Since1976, x-ray room shielding has been ap-
Figure 1. An x-ray examination room (Mayo Clinic, Rochester,Minn, circa 1925) with bare high-voltage cables (arrowheads) andlittle shielding of the x-ray tube (arrow).
Volume 217 z Number 3 Medical Physics: Some Recollections z 621

plied on the basis of National Council onRadiation Protection and Measurements(NCRP) publication 49 (23). This docu-ment is being revised by a joint taskgroup formed by the AAPM and the
NCRP, which is important for two rea-sons. Not only will this new method becompletely different from that used inthe past, the recommendations producedby two of our professional organizations
working together will, no doubt, be bet-ter than those that either group couldproduce on their own. In this same light,we must not forget the long and symbi-otic relationship between the AAPM and
TABLE 2A Few of the Technologic Advances in Radiation Therapy in the Past Century
Year Technologic Advances Prominent PioneersReferenceNumber
1895 Discovery of x rays W. C. Roentgen 26,281896 Discovery of radioactivity H. Becquerel 26,291898 Discovery of radium M. and P. Curie 26,301913 Development of hot-cathode x-ray tube W. D. Coolidge 25,26,271914–1917 First radon plants established W. Duane, G. Failla 271921 First developments in radium dosimetry R. Sievert, E. Quimby 26,27,311928 Establishment of the roentgen as unit of “dose” 251933 First treatments with Van de Graaf generator J. Trump 251943–1948 First betatron treatments D. Kerst, G. Adams, J. Laughlin,
H. Johns25
1951 First cobalt 60 treatments H. Johns, L. Grimmett 251953 First linear accelerator treatments M. Day, F. Farmer 251958 Computerized treatment planning introduced J. Laughlin, T. D. Sterling,
K. C. Tsien, R. Wood25
1959 First remote afterloading units B. Proimos, K. Wright, J. Trump,W. Jennings, T. Davy, J. Brace,A. Green
25,32
1960 First remote afterloading units R. Walstam, U. Henschke 31,331962 Electronic portal imaging introduced S. Benner 341964 High-dose-rate remote afterloaders introduced U. Henschke, R. Walstam 31,331965 Conformal radiation therapy with multileaf collimation introduced S. Takahashi 32,351968 Gamma Knife introduced* Leksell 341968 Radiological Physics Center established† R. Shalek 21969 First commercial treatment planning systems R. Bentley, J. Cox, W. Powers 25,341980 First “modern” electronic portal imager N. A. Baily 341984 First “modern” multileaf collimator A. Brahme, J. Mantel, H. Perry 33,34
*AB Motala Verkstad, Motala, Sweden.† Houston, Tex.
Figure 2. (a) Original EMI CT head scanner (Mayo Clinic, Rochester, Minn, circa 1973) and (b) an 80 3 80-matrix head CT image obtained with it.
622 z Radiology z December 2000 Gray and Orton

the RSNA, including their cooperation inproviding a forum for medical physicsresearch papers, refresher courses, andscientific exhibits during the annualRSNA meeting. Such cooperation bene-fits our profession, medical physicists, ra-diologists, and technologists, as well asthe entire medical imaging community.
THERAPEUTIC MEDICALPHYSICS
The employment of physicists in radia-tion therapy dates back to soon afterx-rays were first used for treatment ofdiseases in the late 1890s and early 1900s(24,25). Physicists were needed becausethe early x-ray machines required con-stant nurturing to keep them runningreliably and with some consistency indose delivery. Many of the early develop-ments in dose specification and measure-ment were made by physicists, culminat-ing in the establishment of the first unitof “dose,” the roentgen, in 1928 (24,25).During this same period, a number ofhospitals began to employ physicists todeal with the handling and dosimetryassociated with radium and radon brachy-therapy. Two pioneers in the United Stateswhose names come to mind readily inthis context were Giaoacchino Failla,
DSc, and Edith Quimby, DSc, at the Me-morial Hospital in New York City (26).
The next several decades of advancesin radiation therapy were primarily con-cerned with development of treatmentmachines capable of higher and higherenergies, as shown in Table 2. Physicistspioneered the introduction into radia-tion therapy of the Van de Graaf genera-tor in the 1930s, the betatron in the1940s (Fig 3), and the linear acceleratorand the cobalt 60 unit in the 1950s. All ofthese machines required considerablesupport by medical physicists (24). Ofspecial concern in these early days wasthe unreliability of these treatment ma-chines. Many of the early linear acceler-ators were not operational more oftenthan they were operational, and somenever made it to the treatment of theirfirst patients. Even 60Co units were notimmune to major problems. For exam-ple, it was not uncommon for the 60Cosource to become fixed in the open posi-tion. This would mean that the techni-cians would have to rush into the roomto remove the patient from the couchwhile we physicists manually crankedthe source back into the off position. Oneof the major difficulties we faced in theseearly years of megavoltage radiation ther-apy was that the service engineers we hadavailable to correct these problems fre-
quently had little or no radiation therapyexperience. The servicemen for diagnos-tic x-ray machines worked on radiationtherapy machines in their spare time.Even though they were usually capable ofdiagnosing many of the problems by re-ferring to the schematics provided withthe machine, actual repair of the problemwas often impossible because it was notuncommon to find that the circuitry inthe machine did not match that in theschematic.
These problems were common duringthe early days of modern radiation ther-apy. We faced a new challenge every day.Almost all the equipment we physicistsused was primitive, if we had any at all.We calibrated our machines with Vic-toreen R-meters that we charged bymeans of friction. Our first attempts atcomputerized treatment planning in the1950s and 1960s often entailed use of themainframe computer at the hospital dur-ing off-peak hours, such as overnight.Calculation of only a single dose distri-bution typically took the entire night.The first commercial treatment planningcomputers were the RAD 8 and the Artro-nix PC-12 (Fig 4), with 8- and 12-kbytesof memory, respectively (24,35). Thesecomputers were slow and quite unreli-able, often needing a “kick-start” in themorning. To save time, we frequently re-sorted to hand calculations of isodosecurves.
One of our many “delights” was thefirst generation of isodose plotters, mostof which failed to meet specifications, ifthey could be made to work at all.
So what has happened in the past 30years to make things better today? A lot!Treatment machines are now far morereliable, deliver multiple high-energy x-ray and electron beams, and are availablewith computerized control of almost allparameters. With the aid of very fastthree-dimensional treatment planningcomputers and three-dimensional imag-ing, we can now make dose distributionsconform to the position and shape of thetumor far more accurately than ever be-fore (31,33). Some of the techniquesdeveloped by radiation therapy physi-cists to improve treatments include in-tensity modulated radiation therapy, ste-reotactic radiosurgery, electronic portalimaging, high-dose-rate brachytherapy,US-guided prostate brachytherapy, fastneutron and proton radiation therapy,three-dimensional planning, and CT sim-ulation (24,30–33). We now have numer-ous protocols for consistency in treat-ment delivery, calibration, and qualityassurance. Dosimetric equipment is now
Figure 3. Donald Kerst, PhD, (left) and Gail Adams, PhD, work on thefirst betatron (University of Illinois College of Medicine, Urbana, Ill, circa1971) to be used for radiation therapy. Later, Dr Adams became the firstPresident of the AAPM, the first Chairman of the American College ofMedical Physics, and the first Editor of Medical Physics.
Volume 217 z Number 3 Medical Physics: Some Recollections z 623

far more sophisticated and includes vari-ous solid state dosimeters and reliablebeam and film scanners. We now haveregional calibration laboratories to cali-brate our ionization chambers and ourbrachytherapy source calibrators.
Without question, these advances haveimproved radiation therapy, but havethey enhanced the job of the radiationtherapy physicist? They have certainlymade the job easier, but they have alsomade it more routine. I can well remem-ber when every day presented a new chal-lenge. Nothing was routine. It is betternow, but it is probably not as interesting,at least from my (C.G.O.) perspective.
EDUCATION, TRAINING, ANDBOARD CERTIFICATION OFMEDICAL PHYSICISTS
Learning how to become a medical phys-icist is much more organized today thanit used to be. Before the 1970s, the mostcommon way to enter the field was on-the-job training with little or no special-ized coursework after completion of agraduate degree in physics or a physicalscience. Alternatively, one might havebeen fortunate enough to attend one ofthe four formal medical physics educa-tional programs in North America: Me-morial Hospital in New York, NY; theM.D. Anderson Hospital in Houston, Tex;the University of Wisconsin in Madison;or the Princess Margaret Hospital inToronto, Ontario, Canada. Unfortunately,these were far too few programs to serveall of North America, so on-the-job train-ing had to be sufficient for the vast ma-jority of physicists. Gradually, however,throughout the 1970s and 1980s, gradu-ate medical physics programs began to beestablished and, in the middle 1980s, theAAPM formed a commission to accreditsuch educational programs, to be latercalled the Commission on Accreditationof Medical Physics Educational Programs(CAMPEP) (2,24). CAMPEP sets the stan-dards for good graduate programs and, todate, 10 graduate programs have achievedaccreditation in North America. Anothertype of training program, the ClinicalPhysics Residency, has recently begun toemerge and be eligible for CAMPEP ac-creditation (2). This is a program similarin concept to residency programs forphysician specialists. The intent is forstudents to first complete a master of sci-ence or doctor of philosophy program inmedical physics, in which they obtain alltheir didactic training, and then progressto a residency for 1–2 years to gain clin-
ical expertise before board certificationand independent clinical practice. This isa major step forward in formalization ofthe entire educational experience, but itcan only succeed if sufficient funding isavailable to support these residencies.
A major problem with all these effortsto formalize medical physics education isthe lack of a legal requirement to practicefor any accredited formal specialized ed-ucation. Consequently, less than 20% ofall graduate medical physics programs inNorth America are accredited (36). Nodoubt some of these nonaccredited pro-grams could meet the standards requiredby CAMPEP, but many might not. Untilthe profession mandates graduation froman accredited program to practice medi-cal physics, this regrettable situation willcontinue.
A somewhat analogous situation existswith board certification. Currently, med-ical physics can be practiced without cer-tification, although peer pressure and, ina few instances, state licensure may grad-ually correct this situation. Formal boardcertification began in 1949 when theAmerican Board of Radiology (ABR) ap-pointed three medical physicists to actas examiners, and the first five radiol-ogy physicists successfully completedthe examination (2,26). Since then, about1,500 such examinees have become ABRDiplomates (37). During the 1980s, thepetition of the AAPM to become a spon-sor of the ABR was denied; in response, asecond board for the examination of
medical physicists, the American Boardof Medical Physics, was established bythe American College of Medical Physicsin 1987 (38). This new board, directedentirely by medical physicists, began tooffer certification in 1990 (38). To date,about 550 medical physicists have beencertified by the American Board of Med-ical Physics. In the meantime, the ABRhas accepted the AAPM as sponsors, andthe AAPM became full sponsors of theABR with three trustees in 1994 (39). Re-cently, there have been movements onbehalf of the AAPM and the AmericanCollege of Medical Physics to try to unifythese two boards.
THE JOURNAL MEDICAL PHYSICS
In 1974, the AAPM formed its scientificjournal, Medical Physics. Before this, theonly journal of medical physics was Phys-ics in Medicine and Biology, published bythe Hospital Physicists’ Association inthe United Kingdom. Now, a quarter of acentury later, Medical Physics has becomean established international journal formedical physics, with a monthly circula-tion of more than 8,000 readers andmore than 300 new scientific articlespublished annually, more than 30% ofwhich originate outside North America.
In conclusion, it is clear that medicalphysics has changed dramatically andrapidly since the late 1800s, as have di-agnostic imaging and therapeutic radiol-
Figure 4. The Artronix PC-12 treatment-planning computer: rho-theta transducer (A), tapedeck(B), keyboard (C), hard-copy unit (D), storage scope (E), and digital plotter (F). (Reprinted, withpermission, from reference 35.)
624 z Radiology z December 2000 Gray and Orton

ogy. Most important, medical physicscontinues to change today, with the rateof change accelerating with time.
References1. Griggs ERN. The trail of the invisible
light. Springfield, Ill: Charles C. Thomas,1965.
2. Laughlin JS, Goodwin PN. History of theAmerican Association of Physicists inMedicine 1958–1998. Med Phys 1998; 25:1245–1248.
3. Ludwig GD. The velocity of soundthrough tissues and the acoustic imped-ance of tissues. J Acoust Soc Am 1950;22:862–866.
4. Wild JJ. The use of ultrasonic pulses forthe measurement of biological tissues andthe detection of tissue density changes.Surgery 1950; 27:183–188.
5. Howry DH. The ultrasonic visualization ofsoft tissue structures and disease pro-cesses. J Lab Clin Med 1952; 40:812–813.
6. Society of Nuclear Medicine. The historyof nuclear medicine. Available at: www.snm.org/nuclear/history.html. Accessed July7, 2000.
7. Kosoff G. An historical review of ultra-sonic investigations at the NationalAcoustics Laboratories. J Clin Ultrasound1975; 3:39–44.
8. Hounsfield GH. Computerized transverseaxial scanning (tomography). I. Descrip-tion of the system. Br J Radiol 1973; 68:166–172.
9. Mistretta CA, Ort MG, Kelcz F, CameronJR, Siedband MP, Crummy AB. Absorp-tion edge fluoroscopy using quasi-mo-noenergetic x-ray beams. Invest Radiol1973; 8:402–412.
10. Ter-Pogossian MM, Phelps ME, HoffmanEJ, Mullani NA. A positron-emissiontransaxial tomography for nuclear imag-ing (PETT). Radiology 1975; 114:89–98.
11. Lauterbur PC. Progress in NMR zeug-matography imaging. Philos Trans R SocLond B Biol Sci 1980; 289:483–487.
12. ACR Committee on Quality Assurance inMammography. 1999 mammographyquality control manual. Reston, Va:American College of Radiology, 1999.
13. Code of Federal Regulations 21 CFR parts16 and 900. Quality mammography stan-dards. Federal Register 1997; 62:60613–60632.
14. Poznanski AK, Smith LA. Practical prob-lems in processor control. Radiology1968; 90:135–138.
15. Lawrence DJ. A simple method of proces-sor control. Med Radiogr Photogr 1973;49:1–6.
16. Gray JE. Photographic quality assurancein diagnostic radiology, nuclear medi-cine, radiation therapy. In: The basicprinciples of daily photographic qualityassurance. Vol 1. HEW publication, FDA76-8043. Rockville, Md: Bureau of Radio-logical Health, 1976.
17. Gray JE. Photographic quality assurancein diagnostic radiology, nuclear medi-cine, radiation therapy. In: Photographicprocessing, quality assurance, and theevaluation of photographic materials.HEW publication, FDA 77-8018. Rock-ville, Md: Bureau of Radiological Health,1977.
18. International Commission on Radiologi-cal Protection. 1990 recommendations ofthe International Commission on Radio-logical Protection. New York, NY: Perga-mon, 1991.
19. International Commission on Radiologi-cal Protection. Radiological protectionand safety in medicine. New York, NY:Pergamon, 1996.
20. Wayne State University. Archives [email protected]. Availableat: lists.wayne.edu/archives/medphys.html.Accessed July 7, 2000.
21. American Association of Physicists in Med-icine. AAPM Online RDCE quiz. Availableat: www.aapm.org/educ/rdce.html. AccessedJuly 7, 2000.
22. Gray JE. The dangers of roentgenoscopyand methods of protection against them:state of the art, 1930s. Radiology 1995;196:24–26.
23. National Council on Radiation Protec-tion and Measurement (NCRP). Struc-tural shielding design and evaluation formedical use of x rays and gamma rays ofenergies up to 10 MeV. Washington, DC:NCRP, 1976.
24. Orton CG. Uses of therapeutic x rays inmedicine. Health Phys 1995; 69:662–676.
25. Cohen M, Trott NG. Radiology, physicalscience, and the emergence of medicalphysics. Med Phys 1995; 22:1889–1897.
26. Laughlin JS. AAPM and RAMPS: anteced-ents and perspectives. Med Phys 1983;10:387–394.
27. Rosenow U. Notes on the legacy of theRontgen rays. Med Phys 1995; 22:1855–1867.
28. Durteix J, Dutreix A. Henri Becquerel(1852–1908). Med Phys 1995; 22:1869–1875.
29. Chavaudra J. Pierre and Marie Curie-Sk-lodowska. Med Phys 1995; 22:1877–1887.
30. Walstam R. Therapeutic radiation phys-ics: a review of developments in Sweden.Acta Oncol 1995; 34:1041–1050.
31. Fraass BA. The development of conformalradiotherapy. Med Phys 1995; 22:1911–1921.
32. Orton CG. High and low dose-ratebrachytherapy for cervical carcinoma.Acta Oncol 1998; 37:117–125.
33. Webb S. The physics of three-dimen-sional radiation therapy. Philadelphia,Pa: Institute of Physics Publishing, 1993.
34. Takahashi S. Conformation radiotherapy:rotation techniques as applied to radiog-raphy and radiotherapy of cancer. ActaRadiol 1965; 242(suppl):1–142.
35. Mohan R, Holt JG, Laughlin JS, KrippnerK. Incorporation of a minicomputer as anintelligent terminal in a treatment plan-ning system. Radiology 1974; 110:183–190.
36. American Association of Physicists inMedicine. Education. Available at: www.aapm.org/educ/index.html. Accessed Au-gust 8, 2000.
37. American Board of Radiology. Radiologicphysics. Available at: www.theabr.org/physics.htm. Accessed August 8, 2000.
38. Suntharalingam N. The American Boardof Medical Physics. Med Phys 1995; 22:1961–1963.
39. Krohmer J. Certification of physicists bythe American Board of Radiology. MedPhys 1995; 22:1955–1960.
Volume 217 z Number 3 Medical Physics: Some Recollections z 625
Related Documents











