1521-0103/347/1/91–99$25.00 http://dx.doi.org/10.1124/jpet.113.204313 THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS J Pharmacol Exp Ther 347:91–99, October 2013 Copyright ª 2013 by The American Society for Pharmacology and Experimental Therapeutics Mechanisms That Underlie m-Opioid Receptor Agonist–Induced Constipation: Differential Involvement of m-Opioid Receptor Sites and Responsible Regions Tomohisa Mori, Yumiko Shibasaki, Kenjiro Matsumoto, Masahiro Shibasaki, Minami Hasegawa, Erika Wang, Daiki Masukawa, Kazumi Yoshizawa, Syunji Horie, and Tsutomu Suzuki Department of Toxicology, Hoshi University School of Pharmacy and Pharmaceutical Sciences, Tokyo, Japan (T.M., Y.S., K.M., M.S., M.H., E.W., D.M., K.Y., T.S.); Laboratory of Pharmacology, Faculty of Pharmaceutical Sciences, Josai International University, Chiba, Japan (K.M., S.H.); and Department of Pharmacology and Therapeutics, Faculty of Pharmaceutical Sciences, Tokyo University of Science, Chiba, Japan (K.Y.) Received April 3, 2013; accepted July 24, 2013 ABSTRACT Reducing the side effects of pain treatment is one of the most important strategies for improving the quality of life of cancer patients. However, little is known about the mechanisms that underlie these side effects, especially constipation induced by opioid receptor agonists; i.e., do they involve naloxonazine- sensitive versus -insensitive sites or central-versus-peripheral m-opioid receptors? The present study was designed to in- vestigate the mechanisms of m-opioid receptor agonist-induced constipation (i.e., the inhibition of gastrointestinal transit and colonic expulsion) that are antagonized by the peripherally re- stricted opioid receptor antagonist naloxone methiodide and naloxonazine in mice. Naloxonazine attenuated the fentanyl- induced inhibition of gastrointestinal transit more potently than the inhibition induced by morphine or oxycodone. Naloxone methiodide suppressed the oxycodone-induced inhibition of gastrointestinal transit more potently than the inhibition induced by morphine, indicating that m-opioid receptor agonists induce the inhibition of gastrointestinal transit through different mech- anisms. Furthermore, we found that the route of administration (intracerebroventricular, intrathecally, and/or intraperitoneally) of naloxone methiodide differentially influenced the suppressive effect on the inhibition of colorectal transit induced by morphine, oxycodone, and fentanyl. These results suggest that morphine, oxycodone, and fentanyl induce constipation through different mech- anisms (naloxonazine-sensitive versus naloxonazine-insensitive sites and central versus peripheral opioid receptors), and these findings may help us to understand the characteristics of the constipation induced by each m-opioid receptor agonist and improve the quality of life by reducing constipation in patients being treated for pain. Introduction Pain is a common medical problem, and the relief of pain is an important goal in pain management. m-Opioid receptor agonists, especially morphine, have been considered to be the “gold standard” for the treatment of patients who are experiencing moderate to severe cancer pain (WHO, 1996) or noncancer pain such as chronic inflammatory and postoperative pain. Reducing the side effects of m-opioid receptor agonists, such as emesis, constipation, drowsiness, hallucination, and delirium, is an important strategy for improving the quality of life (QOL) of patients suffering from pain. Constipation is an especially distressing side effect of opioids used to manage pain that occurs in 40–95% of patients treated with opioids (Swegle and Logemann, 2006). Further- more, severe constipation, caused by the activation of m-opioid receptors in the central nervous system (through the autonomic system) and gastrointestinal tract (through direct stimulation of the enteric nervous system) that are responsi- ble for gut motility (Shook et al., 1987), reduces the amount of opioid that can be obtained from a given dose, which in turn decreases the antinociceptive effects of opioids. The QOL of patients suffering from cancer pain is complicated by tolerance, which involves the loss of analgesic potency that in turn leads to an increase in the required dose and hence an increase in possible side effects (Finkel et al., 2007). Opioid rotation (switching) and the use of peripherally restricted opioid-receptor antagonists, such as methylnaltrex- one, which has a limited ability to cross the blood-brain barrier, or oral naloxone administered in a prolonged-release manner, have been shown to reverse opioid-induced re- fractory constipation (Holzer et al., 2009; Leppert, 2010), which indicates that the stimulation of peripheral opioid receptors is important for the expression of m-opioid receptor agonist-induced constipation. In fact, peripheral m-opioid receptors contribute to intestinal function (Gmerek et al., 1986; Radbruch and Elsner, 2004; Ross et al., 2008; Kang et al., 2012). Animal studies have shown that both the i.c.v. dx.doi.org/10.1124/jpet.113.204313. ABBREVIATIONS: b-FNA, b-funaltrexamine; GIT, gastrointestinal transit; NM, naloxone methiodide; QOL, quality of life. 91 at ASPET Journals on June 19, 2018 jpet.aspetjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1521-0103/347/1/91–99$25.00 http://dx.doi.org/10.1124/jpet.113.204313THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS J Pharmacol Exp Ther 347:91–99, October 2013Copyright ª 2013 by The American Society for Pharmacology and Experimental Therapeutics
Mechanisms That Underlie m-Opioid Receptor Agonist–InducedConstipation: Differential Involvement of m-Opioid Receptor Sitesand Responsible Regions
Tomohisa Mori, Yumiko Shibasaki, Kenjiro Matsumoto, Masahiro Shibasaki,Minami Hasegawa, Erika Wang, Daiki Masukawa, Kazumi Yoshizawa, Syunji Horie,and Tsutomu SuzukiDepartment of Toxicology, Hoshi University School of Pharmacy and Pharmaceutical Sciences, Tokyo, Japan (T.M., Y.S.,K.M., M.S., M.H., E.W., D.M., K.Y., T.S.); Laboratory of Pharmacology, Faculty of Pharmaceutical Sciences, Josai InternationalUniversity, Chiba, Japan (K.M., S.H.); and Department of Pharmacology and Therapeutics, Faculty of Pharmaceutical Sciences,Tokyo University of Science, Chiba, Japan (K.Y.)
Received April 3, 2013; accepted July 24, 2013
ABSTRACTReducing the side effects of pain treatment is one of the mostimportant strategies for improving the quality of life of cancerpatients. However, little is known about the mechanisms thatunderlie these side effects, especially constipation induced byopioid receptor agonists; i.e., do they involve naloxonazine-sensitive versus -insensitive sites or central-versus-peripheralm-opioid receptors? The present study was designed to in-vestigate the mechanisms of m-opioid receptor agonist-inducedconstipation (i.e., the inhibition of gastrointestinal transit andcolonic expulsion) that are antagonized by the peripherally re-stricted opioid receptor antagonist naloxone methiodide andnaloxonazine in mice. Naloxonazine attenuated the fentanyl-induced inhibition of gastrointestinal transit more potently thanthe inhibition induced by morphine or oxycodone. Naloxonemethiodide suppressed the oxycodone-induced inhibition of
gastrointestinal transit more potently than the inhibition inducedby morphine, indicating that m-opioid receptor agonists inducethe inhibition of gastrointestinal transit through different mech-anisms. Furthermore, we found that the route of administration(intracerebroventricular, intrathecally, and/or intraperitoneally) ofnaloxone methiodide differentially influenced the suppressiveeffect on the inhibition of colorectal transit induced by morphine,oxycodone, and fentanyl. These results suggest that morphine,oxycodone, and fentanyl induceconstipation throughdifferentmech-anisms (naloxonazine-sensitive versus naloxonazine-insensitivesites and central versus peripheral opioid receptors), and thesefindings may help us to understand the characteristics of theconstipation induced by each m-opioid receptor agonist andimprove the quality of life by reducing constipation in patientsbeing treated for pain.
IntroductionPain is a common medical problem, and the relief of pain is
an important goal in pain management. m-Opioid receptoragonists, especially morphine, have been considered to bethe “gold standard” for the treatment of patients who areexperiencing moderate to severe cancer pain (WHO, 1996)or noncancer pain such as chronic inflammatory andpostoperative pain. Reducing the side effects of m-opioidreceptor agonists, such as emesis, constipation, drowsiness,hallucination, and delirium, is an important strategy forimproving the quality of life (QOL) of patients suffering frompain. Constipation is an especially distressing side effect ofopioids used to manage pain that occurs in 40–95% of patientstreated with opioids (Swegle and Logemann, 2006). Further-more, severe constipation, caused by the activation of m-opioidreceptors in the central nervous system (through theautonomic system) and gastrointestinal tract (through direct
stimulation of the enteric nervous system) that are responsi-ble for gut motility (Shook et al., 1987), reduces the amount ofopioid that can be obtained from a given dose, which in turndecreases the antinociceptive effects of opioids.The QOL of patients suffering from cancer pain is
complicated by tolerance, which involves the loss of analgesicpotency that in turn leads to an increase in the required doseand hence an increase in possible side effects (Finkel et al.,2007). Opioid rotation (switching) and the use of peripherallyrestricted opioid-receptor antagonists, such as methylnaltrex-one, which has a limited ability to cross the blood-brainbarrier, or oral naloxone administered in a prolonged-releasemanner, have been shown to reverse opioid-induced re-fractory constipation (Holzer et al., 2009; Leppert, 2010),which indicates that the stimulation of peripheral opioidreceptors is important for the expression of m-opioid receptoragonist-induced constipation. In fact, peripheral m-opioidreceptors contribute to intestinal function (Gmerek et al.,1986; Radbruch and Elsner, 2004; Ross et al., 2008; Kanget al., 2012). Animal studies have shown that both the i.c.v.dx.doi.org/10.1124/jpet.113.204313.
ABBREVIATIONS: b-FNA, b-funaltrexamine; GIT, gastrointestinal transit; NM, naloxone methiodide; QOL, quality of life.
91
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from

and i.t. administration of opioid receptor agonists can inducethe delay of intestinal movement (Koslo et al., 1986; Raffaet al., 1987; Heyman et al., 1988). On the other hand,pharmacological findings have suggested that there are at leasttwo m-opioid-receptor sites indicated as follows: naloxonazine-sensitive (m1-opioid receptors) and naloxonazine-insensitive(m2-opioid receptors) (Pasternak, 1993; Elliott et al., 1994; Cadet,2004). Naloxonazine, a so-called m1-opioid receptor antagonist, isfrequently used to discriminate the pharmacological actions ofm-opioid receptor subtypes. However, the mechanisms by whichopioid receptor agonists induce constipation are not yet clear;i.e., do they involve naloxonazine-sensitive or -insensitive sitesand central (spinal or supraspinal) or peripheral receptors?Morphine, oxycodone, and fentanyl are clinically prescribed
opioids that have prominent antinociceptive effects. Eachm-opioid receptor agonist has a distinct pharmacological profileby which it exerts its antinociceptive effects (Minami et al.,2009; Nakamura et al., 2011). These different pharmaco-logical effects can be explained by differences in patterns ofplasma concentrations (Nakamura et al., 2011), blood-brainbarrier transport (Dagenais et al., 2004; Bostrom et al., 2008),receptor subtypes (Cadet, 2004), and intracellular signal trans-duction. However, limited information is available regardingthe different pharmacological mechanisms of opioid receptoragonist-induced constipation. Therefore, the present study wasdesigned to investigate the adverse effects of opioid receptoragonists, especially those that target bowel function, using theperipherally restricted opioid receptor antagonists naloxonemethiodide and naloxonazine.
Materials and MethodsAnimals. In the present study, male imprinting control region
(ICR) mice (20–25 g) (Tokyo Laboratory Animals Science Co. Ltd.,Tokyo, Japan) were used. Food and water were available ad libitumfor mice in their individual home cages. Mice were housed in a roommaintained at 22 6 1°C with a 12-hour light-dark cycle (light on 8:00AM to 8:00 PM). The present study was conducted in accordance withthe Guiding Principles for the Care and Use of Laboratory Animals atHoshi University, as adopted by the Committee on Animal Researchof Hoshi University. Every effort was made to minimize the numbersand any suffering of animals used in the following experiments.
Hot-Plate Test. The antinociceptve response was evaluated byrecording the latency to paw licking or tapping in the hot-plate test(55 6 0.5°C; Muromachi Kikai Co., Ltd., Tokyo, Japan) as describedpreviously (Narita et al., 2005). To prevent tissue damage, weestablished a 30-second cut-off time. Antinociceptive effects weremeasured at 30 minutes after the administration of morphine (1–10mg/kg s.c.), and 10 minutes after the administration of oxycodone(1–10mg/kg s.c.) and fentanyl (10–300 mg/kg s.c.). Each animal servedas its own control, and the latency to a response was measured bothbefore and after drug administration. Antinociception was calculatedas a percentage of the maximum possible effect (% antinociception)according to the following formula: % antinociception5 (test latency2predrug latency)/(cut-off time 2 predrug latency) � 100. The anti-nociceptive response represents the mean 6 S.E.M. of the %antinociception.
Gastrointestinal Transit. In the study of gastrointestinal transit(Torigoe et al., 2012), mice were fasted for 12 hours before theexperiments. At 30 minutes after the administration of morphine(0.3–10 mg/kg s.c.), 10 minutes after the administration of oxycodone(0.3–10 mg/kg s.c.), or 10 minutes after the administration of fentanyl(10–300 mg/kg s.c.), blue ink (0.3 ml/mouse; Pilot Co. Ltd., Tokyo,Japan) was administered orally. Thirty minutes after the administra-tion of blue ink, the animal was killed by cervical dislocation and the
small intestine was removed. The percentage inhibition of gastrointes-tinal transit was calculated as follows: (distance traveled by the ink/length from the pylorus to the cecum) � 100. In antagonism tests,naxolonazine (35 mg/kg i.p., 24-hour pretreatment), naloxone methio-dide (10mg/kg i.p.; 4mM i.c.v. or i.t., 10-minute pretreatment), or salinewas administered before the injection of morphine, fentanyl, oroxycodone.
Effect on Colonic Expulsion. The effects of morphine, oxycodone,and fentanyl on colonic propulsion were evaluated as described pre-viously (Yamada and Onoda, 1992). In brief, 30 minutes after theadministration of morphine (1–10 mg/kg s.c.) and 10 minutes afterthe administration of oxycodone (0.3–10 mg/kg s.c.), fentanyl (10–300mg/kg s.c.), or saline, a glass bead (approximately 3 mm in diameter;BZ-3 Ikeda Rika, Tokyo, Japan) was inserted into the distal colon toa depth of 2 cm from the anus with a silicone tube (approximately 2 mmin diameter). In the antagonism tests, naloxonazine (35 mg/kg i.p.) orsaline was administered 24 hours before treatment with morphine,fentanyl, or oxycodone. Naloxone methiodide (10 mg/kg i.p., or 4 mMi.c.v. and i.t.) was administered 10 minutes before treatment withmorphine, fentanyl, or oxycodone. The time required to expel the beadwas measured up to 120 minutes.
Intracerebroventricular and Intrathecal Injection. Intra-cerebroventricular administration was given as described previously(Haley, 1957). The injection was made with a 2-mm double-needle(Natsume Seisakusho, Co., Ltd., Tokyo, Japan) attached to a 25-mlHamilton microsyringe. Solution was injected in a volume of 4 ml permouse. Administration was done intrathecally as described pre-viously (Hylden and Wilcox, 1980), using a 25-ml Hamilton syringewith a 30-gauge needle. Solution was injected in a volume of 4 ml permouse. Three days before intracerebroventricular administration,a hole was made under ether analgesia, for ethical reasons, to reducethe stress in mice.
Electrical Stimulation of the Mouse Small and LargeIntestine. Approximately 2 cm of the small intestine (ileum) andlarge intestine (rectum to distal colon) were dissected and placed inKrebs-Henseleit solution (in mM: NaCl, 112.08; KCl, 5.90; CaCl2,1.97; MgCl2, 1.18; NaH2PO4, 1.22; NaHCO3, 25.00, and glucose,11.49). The small or large intestine was placed under 0.5 g of tensionin a 20-ml organ bath containing the nutrient solution. The bath wasmaintained at 37°C and continuously bubbled with a mixture of 95%O2 and 5% CO2. Tissues were stimulated by a platinum needle–ringelectrode. After equilibration, the intestine was transmurally stimu-lated with monophasic pulses (50 V, 5 Hz, 1 millisecond duration)every 1 minute by a stimulator (SEN-7203; Nihon Kohden, Tokyo,Japan). Contractions were isotonically recorded by using a displace-ment transducer (NEC Type 45347; San-ei Instruments Ltd., Tokyo,Japan). The effects of drug treatment on the twitch contractionsevoked by transmural stimulation elicited through the ring electrodeswere examined. The height of the twitch response to transmuralstimulation was measured before and after drug challenge. Theresponses are expressed as a percentage, where the twitch response totransmural stimulation before drug challenge was considered to be100%. b-Funaltrexamine (b-FNA; 40 mg/kg i.p.), naloxonazine (35 mg/kgi.p.), or saline was administered 24 hours prior to isolation of thesegment. As previously reported, the irreversible m-opioid receptorantagonist b-FNA and the irreversible m1-opioid antagonist nalox-onazine reversed the effect of the peripheral opioid agonist loper-amide in mice (Baker and Meert, 2002). These antagonistic effectsof b-FNA and naloxonazine were substantially maintained underextensive washout in motility experiments using mouse isolatedcolon (Yu et al., 2007). Thus, we used these protocols to investigate theinvolvement of m-opioid subtypes in the inhibitory effects of morphine,oxycodone, and fentanyl on electrically stimulated contraction.
Drugs. The drugs used in the present study were morphinehydrochloride, oxycodone hydrochloride (Shionogi PharmaceuticalCo., Inc., Osaka, Japan), and fentanyl citrate (Hisamitsu Pharma-ceutical Co. Inc., Tokyo, Japan). Naloxonazine and naloxone methio-dide were synthesized at Toray Industries (Kanagawa, Japan). All
92 Mori et al.
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from
drugs were dissolved in saline and administered in a volume of 10 ml/kg.The pretreatment times and doses of naloxone, naloxone methiodide,and naloxonazine were based on our previous reports (Suzuki et al.,1995; Matsuzawa et al., 2000).
Statistical Analysis. Data are expressed as the mean 6 S.E.M.The statistical significance of differences between groups was assessedby theMann–Whitney test. The 50% effective dose (ED50) values weredetermined using an analysis of variance and linear regression tech-niques. Where appropriate, a one-way analysis of variance (ANOVA)followed by the Bonferroni multiple comparisons test was used forstatistical analysis. All statistical analyses were performed usingPrism software (Version 5.0a; GraphPad Software, Inc., La Jolla, CA).A P value of , 0.05 was considered to reflect significance.
ResultsPharmacological Differences between m-Opioid Re-
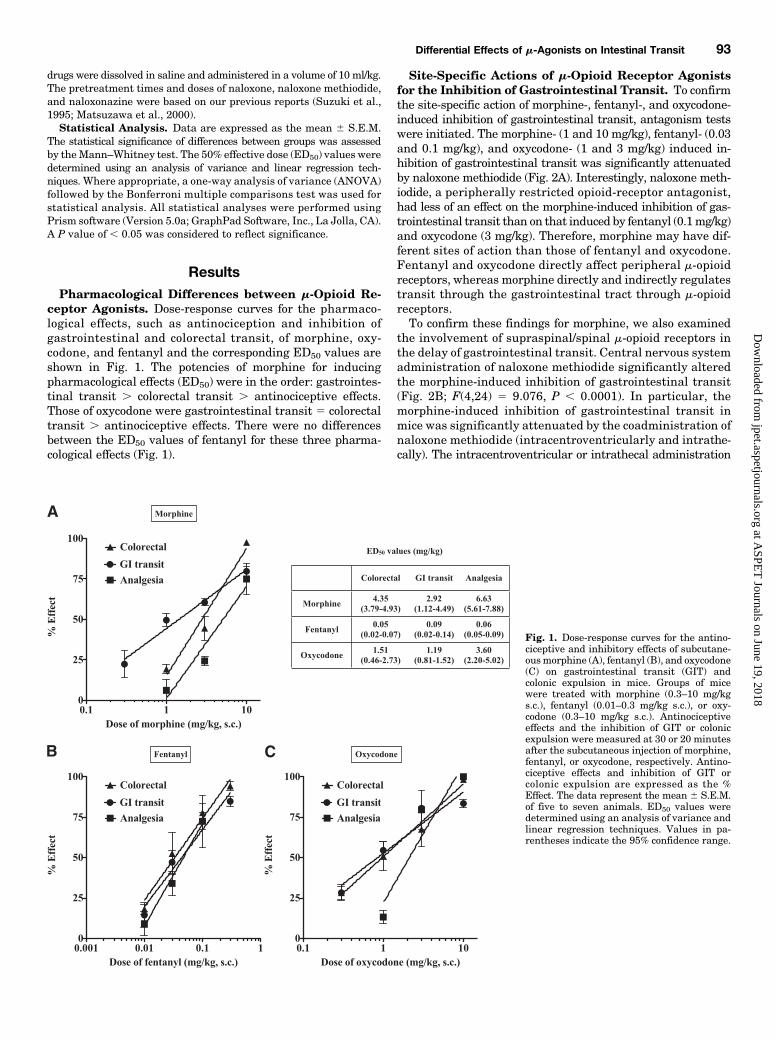
ceptor Agonists. Dose-response curves for the pharmaco-logical effects, such as antinociception and inhibition ofgastrointestinal and colorectal transit, of morphine, oxy-codone, and fentanyl and the corresponding ED50 values areshown in Fig. 1. The potencies of morphine for inducingpharmacological effects (ED50) were in the order: gastrointes-tinal transit . colorectal transit . antinociceptive effects.Those of oxycodone were gastrointestinal transit 5 colorectaltransit . antinociceptive effects. There were no differencesbetween the ED50 values of fentanyl for these three pharma-cological effects (Fig. 1).
Site-Specific Actions of m-Opioid Receptor Agonistsfor the Inhibition of Gastrointestinal Transit. To confirmthe site-specific action of morphine-, fentanyl-, and oxycodone-induced inhibition of gastrointestinal transit, antagonism testswere initiated. The morphine- (1 and 10 mg/kg), fentanyl- (0.03and 0.1 mg/kg), and oxycodone- (1 and 3 mg/kg) induced in-hibition of gastrointestinal transit was significantly attenuatedby naloxone methiodide (Fig. 2A). Interestingly, naloxone meth-iodide, a peripherally restricted opioid-receptor antagonist,had less of an effect on the morphine-induced inhibition of gas-trointestinal transit than on that induced by fentanyl (0.1mg/kg)and oxycodone (3 mg/kg). Therefore, morphine may have dif-ferent sites of action than those of fentanyl and oxycodone.Fentanyl and oxycodone directly affect peripheral m-opioidreceptors, whereas morphine directly and indirectly regulatestransit through the gastrointestinal tract through m-opioidreceptors.To confirm these findings for morphine, we also examined
the involvement of supraspinal/spinal m-opioid receptors inthe delay of gastrointestinal transit. Central nervous systemadministration of naloxone methiodide significantly alteredthe morphine-induced inhibition of gastrointestinal transit(Fig. 2B; F(4,24) 5 9.076, P , 0.0001). In particular, themorphine-induced inhibition of gastrointestinal transit inmice was significantly attenuated by the coadministration ofnaloxone methiodide (intracentroventricularly and intrathe-cally). The intracentroventricular or intrathecal administration
Fig. 1. Dose-response curves for the antino-ciceptive and inhibitory effects of subcutane-ousmorphine (A), fentanyl (B), and oxycodone(C) on gastrointestinal transit (GIT) andcolonic expulsion in mice. Groups of micewere treated with morphine (0.3–10 mg/kgs.c.), fentanyl (0.01–0.3 mg/kg s.c.), or oxy-codone (0.3–10 mg/kg s.c.). Antinociceptiveeffects and the inhibition of GIT or colonicexpulsion were measured at 30 or 20 minutesafter the subcutaneous injection of morphine,fentanyl, or oxycodone, respectively. Antino-ciceptive effects and inhibition of GIT orcolonic expulsion are expressed as the %Effect. The data represent the mean 6 S.E.M.of five to seven animals. ED50 values weredetermined using an analysis of variance andlinear regression techniques. Values in pa-rentheses indicate the 95% confidence range.
Differential Effects of m-Agonists on Intestinal Transit 93
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from
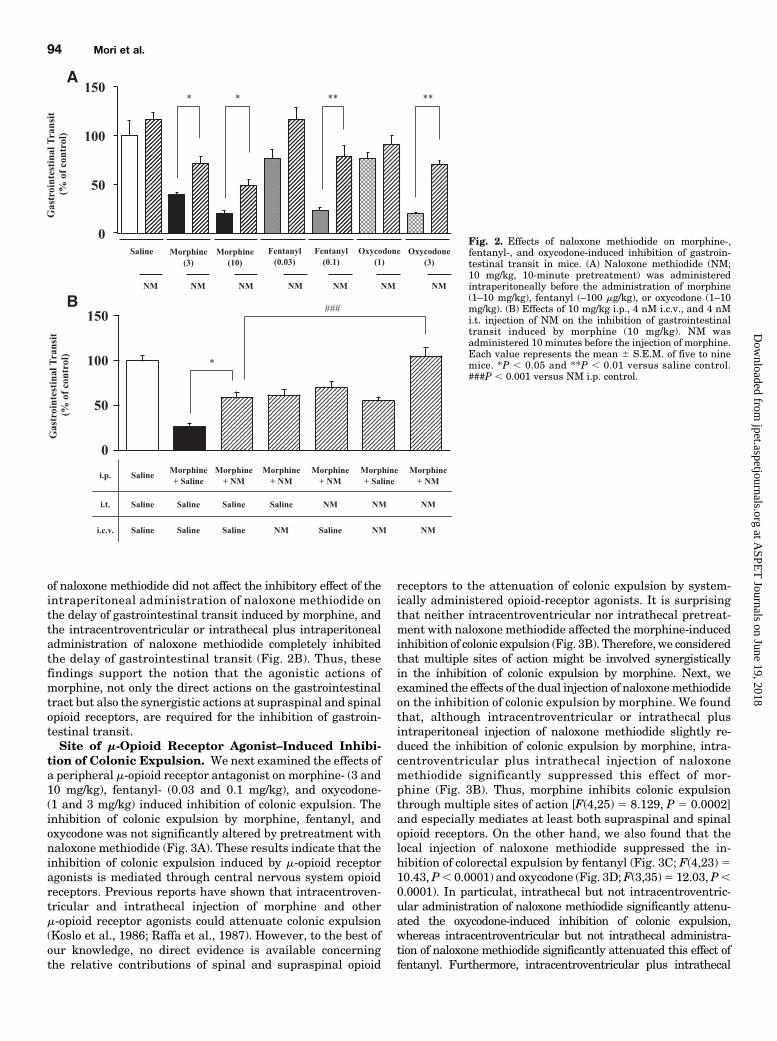
of naloxone methiodide did not affect the inhibitory effect of theintraperitoneal administration of naloxone methiodide onthe delay of gastrointestinal transit induced by morphine, andthe intracentroventricular or intrathecal plus intraperitonealadministration of naloxone methiodide completely inhibitedthe delay of gastrointestinal transit (Fig. 2B). Thus, thesefindings support the notion that the agonistic actions ofmorphine, not only the direct actions on the gastrointestinaltract but also the synergistic actions at supraspinal and spinalopioid receptors, are required for the inhibition of gastroin-testinal transit.Site of m-Opioid Receptor Agonist–Induced Inhibi-
tion of Colonic Expulsion. We next examined the effects ofa peripheral m-opioid receptor antagonist on morphine- (3 and10 mg/kg), fentanyl- (0.03 and 0.1 mg/kg), and oxycodone-(1 and 3 mg/kg) induced inhibition of colonic expulsion. Theinhibition of colonic expulsion by morphine, fentanyl, andoxycodone was not significantly altered by pretreatment withnaloxone methiodide (Fig. 3A). These results indicate that theinhibition of colonic expulsion induced by m-opioid receptoragonists is mediated through central nervous system opioidreceptors. Previous reports have shown that intracentroven-tricular and intrathecal injection of morphine and otherm-opioid receptor agonists could attenuate colonic expulsion(Koslo et al., 1986; Raffa et al., 1987). However, to the best ofour knowledge, no direct evidence is available concerningthe relative contributions of spinal and supraspinal opioid
receptors to the attenuation of colonic expulsion by system-ically administered opioid-receptor agonists. It is surprisingthat neither intracentroventricular nor intrathecal pretreat-ment with naloxone methiodide affected the morphine-inducedinhibition of colonic expulsion (Fig. 3B). Therefore, we consideredthat multiple sites of action might be involved synergisticallyin the inhibition of colonic expulsion by morphine. Next, weexamined the effects of the dual injection of naloxonemethiodideon the inhibition of colonic expulsion by morphine. We foundthat, although intracentroventricular or intrathecal plusintraperitoneal injection of naloxone methiodide slightly re-duced the inhibition of colonic expulsion by morphine, intra-centroventricular plus intrathecal injection of naloxonemethiodide significantly suppressed this effect of mor-phine (Fig. 3B). Thus, morphine inhibits colonic expulsionthrough multiple sites of action [F(4,25) 5 8.129, P 5 0.0002]and especially mediates at least both supraspinal and spinalopioid receptors. On the other hand, we also found that thelocal injection of naloxone methiodide suppressed the in-hibition of colorectal expulsion by fentanyl (Fig. 3C; F(4,23) 510.43, P, 0.0001) and oxycodone (Fig. 3D;F(3,35)5 12.03, P,0.0001). In particulat, intrathecal but not intracentroventric-ular administration of naloxone methiodide significantly attenu-ated the oxycodone-induced inhibition of colonic expulsion,whereas intracentroventricular but not intrathecal administra-tion of naloxone methiodide significantly attenuated this effect offentanyl. Furthermore, intracentroventricular plus intrathecal
Fig. 2. Effects of naloxone methiodide on morphine-,fentanyl-, and oxycodone-induced inhibition of gastroin-testinal transit in mice. (A) Naloxone methiodide (NM;10 mg/kg, 10-minute pretreatment) was administeredintraperitoneally before the administration of morphine(1–10 mg/kg), fentanyl (–100 mg/kg), or oxycodone (1–10mg/kg). (B) Effects of 10 mg/kg i.p., 4 nM i.c.v., and 4 nMi.t. injection of NM on the inhibition of gastrointestinaltransit induced by morphine (10 mg/kg). NM wasadministered 10 minutes before the injection of morphine.Each value represents the mean 6 S.E.M. of five to ninemice. *P , 0.05 and **P , 0.01 versus saline control.###P , 0.001 versus NM i.p. control.
94 Mori et al.
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from
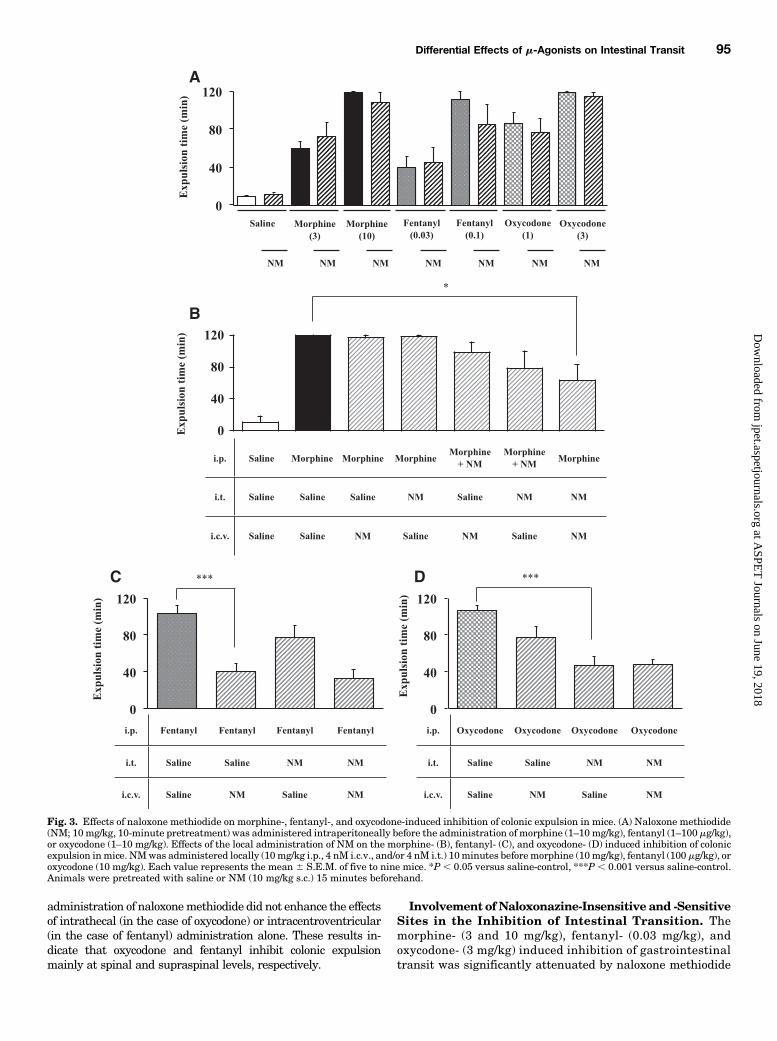
administration of naloxonemethiodide did not enhance the effectsof intrathecal (in the case of oxycodone) or intracentroventricular(in the case of fentanyl) administration alone. These results in-dicate that oxycodone and fentanyl inhibit colonic expulsionmainly at spinal and supraspinal levels, respectively.
Involvement of Naloxonazine-Insensitive and -SensitiveSites in the Inhibition of Intestinal Transition. Themorphine- (3 and 10 mg/kg), fentanyl- (0.03 mg/kg), andoxycodone- (3 mg/kg) induced inhibition of gastrointestinaltransit was significantly attenuated by naloxone methiodide
Fig. 3. Effects of naloxone methiodide on morphine-, fentanyl-, and oxycodone-induced inhibition of colonic expulsion in mice. (A) Naloxone methiodide(NM; 10mg/kg, 10-minute pretreatment) was administered intraperitoneally before the administration of morphine (1–10 mg/kg), fentanyl (1–100 mg/kg),or oxycodone (1–10 mg/kg). Effects of the local administration of NM on the morphine- (B), fentanyl- (C), and oxycodone- (D) induced inhibition of colonicexpulsion inmice. NMwas administered locally (10mg/kg i.p., 4 nM i.c.v., and/or 4 nM i.t.) 10minutes beforemorphine (10mg/kg), fentanyl (100 mg/kg), oroxycodone (10 mg/kg). Each value represents the mean 6 S.E.M. of five to nine mice. *P , 0.05 versus saline-control, ***P , 0.001 versus saline-control.Animals were pretreated with saline or NM (10 mg/kg s.c.) 15 minutes beforehand.
Differential Effects of m-Agonists on Intestinal Transit 95
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from
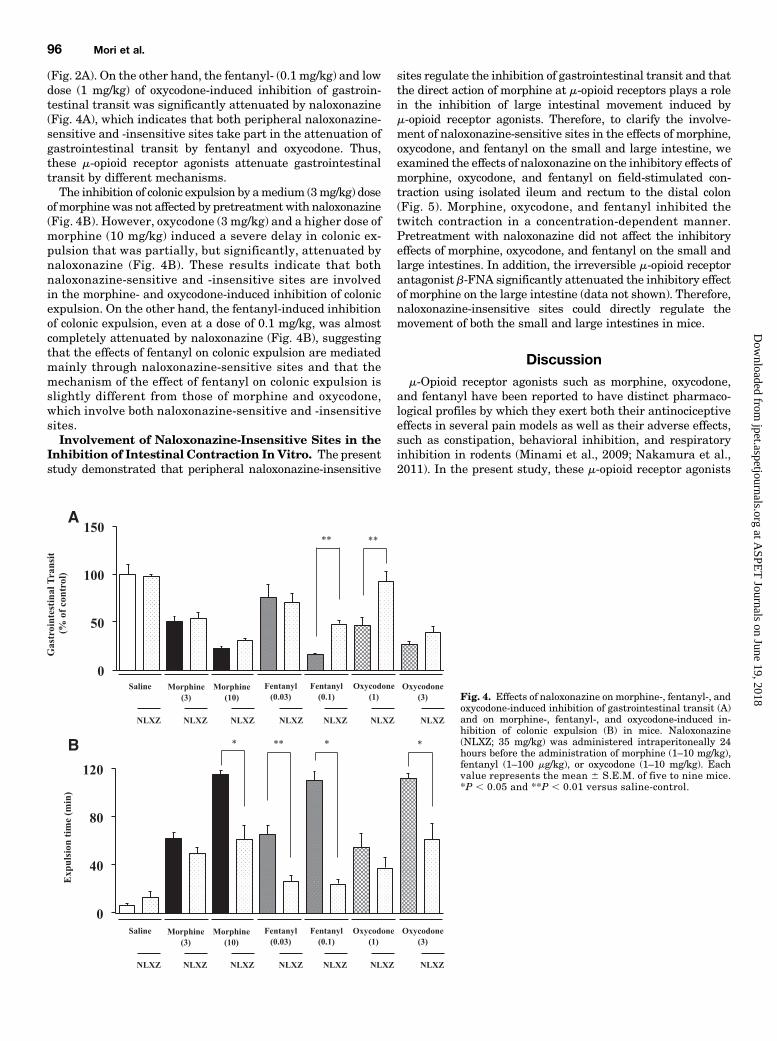
(Fig. 2A). On the other hand, the fentanyl- (0.1 mg/kg) and lowdose (1 mg/kg) of oxycodone-induced inhibition of gastroin-testinal transit was significantly attenuated by naloxonazine(Fig. 4A), which indicates that both peripheral naloxonazine-sensitive and -insensitive sites take part in the attenuation ofgastrointestinal transit by fentanyl and oxycodone. Thus,these m-opioid receptor agonists attenuate gastrointestinaltransit by different mechanisms.The inhibition of colonic expulsion by amedium (3mg/kg) dose
of morphinewas not affected by pretreatment with naloxonazine(Fig. 4B). However, oxycodone (3 mg/kg) and a higher dose ofmorphine (10 mg/kg) induced a severe delay in colonic ex-pulsion that was partially, but significantly, attenuated bynaloxonazine (Fig. 4B). These results indicate that bothnaloxonazine-sensitive and -insensitive sites are involvedin the morphine- and oxycodone-induced inhibition of colonicexpulsion. On the other hand, the fentanyl-induced inhibitionof colonic expulsion, even at a dose of 0.1 mg/kg, was almostcompletely attenuated by naloxonazine (Fig. 4B), suggestingthat the effects of fentanyl on colonic expulsion are mediatedmainly through naloxonazine-sensitive sites and that themechanism of the effect of fentanyl on colonic expulsion isslightly different from those of morphine and oxycodone,which involve both naloxonazine-sensitive and -insensitivesites.Involvement of Naloxonazine-Insensitive Sites in the
Inhibition of Intestinal Contraction In Vitro. The presentstudy demonstrated that peripheral naloxonazine-insensitive
sites regulate the inhibition of gastrointestinal transit and thatthe direct action of morphine at m-opioid receptors plays a rolein the inhibition of large intestinal movement induced bym-opioid receptor agonists. Therefore, to clarify the involve-ment of naloxonazine-sensitive sites in the effects of morphine,oxycodone, and fentanyl on the small and large intestine, weexamined the effects of naloxonazine on the inhibitory effects ofmorphine, oxycodone, and fentanyl on field-stimulated con-traction using isolated ileum and rectum to the distal colon(Fig. 5). Morphine, oxycodone, and fentanyl inhibited thetwitch contraction in a concentration-dependent manner.Pretreatment with naloxonazine did not affect the inhibitoryeffects of morphine, oxycodone, and fentanyl on the small andlarge intestines. In addition, the irreversible m-opioid receptorantagonist b-FNA significantly attenuated the inhibitory effectof morphine on the large intestine (data not shown). Therefore,naloxonazine-insensitive sites could directly regulate themovement of both the small and large intestines in mice.
Discussionm-Opioid receptor agonists such as morphine, oxycodone,
and fentanyl have been reported to have distinct pharmaco-logical profiles by which they exert both their antinociceptiveeffects in several pain models as well as their adverse effects,such as constipation, behavioral inhibition, and respiratoryinhibition in rodents (Minami et al., 2009; Nakamura et al.,2011). In the present study, these m-opioid receptor agonists
Fig. 4. Effects of naloxonazine on morphine-, fentanyl-, andoxycodone-induced inhibition of gastrointestinal transit (A)and on morphine-, fentanyl-, and oxycodone-induced in-hibition of colonic expulsion (B) in mice. Naloxonazine(NLXZ; 35 mg/kg) was administered intraperitoneally 24hours before the administration of morphine (1–10 mg/kg),fentanyl (1–100 mg/kg), or oxycodone (1–10 mg/kg). Eachvalue represents the mean 6 S.E.M. of five to nine mice.*P , 0.05 and **P , 0.01 versus saline-control.
96 Mori et al.
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from

exerted different pharmacological profiles to inhibit gastroin-testinal transit and colorectal expulsion in comparison withtheir antinociceptive effects. Previous studies have demon-strated that intracentroventricular and intrathecal adminis-tration of morphine inhibits gastrointestinal and colonicfunction (Koslo et al., 1986; Heyman et al., 1988; Pol et al.,1999), whereas peripheral m-opioid receptors also contributeto morphine-induced intestinal movement in rodents (Gmereket al., 1986; Pol et al., 1999; Ross et al., 2008). On the other
hand, naloxonazine could not reverse the morphine-inducedinhibition of gastrointestinal transit, even though it reversedthe morphine-induced (intrathecally) inhibition of gastrointes-tinal transit (Heyman et al., 1988), and partially reversed themorphine-induced inhibition of colonic transit (Koslo et al.,1986). Thus, the mechanism by which opioid receptor agonistsinduce constipation throughnaloxonazine-sensitive or -insensitivesites and supraspinal, spinal, or peripheral receptors remainsunclear. Furthermore, little information is available regarding
Fig. 5. Effects of naloxonazine on the inhibitory effects of morphine, oxycodone, and fentanyl on field-stimulated contraction using isolated smallintestine (ileum) and large intestine (rectum to distal colon). Naloxonazine (NLXZ; 35mg/kg i.p.) was administered 24 hours before the administration ofmorphine (1 mM–1 mM), fentanyl (1 nM–1 mM), or oxycodone (1 mM–1 mM). Each value represents the mean 6 S.E.M. of four to six mice.
Differential Effects of m-Agonists on Intestinal Transit 97
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from
the differential pharmacological profiles of morphine, oxy-codone, and fentanyl with regard to intestinal transit (Gmereket al., 1986).Similar to the results in previous studies (Koslo et al., 1986;
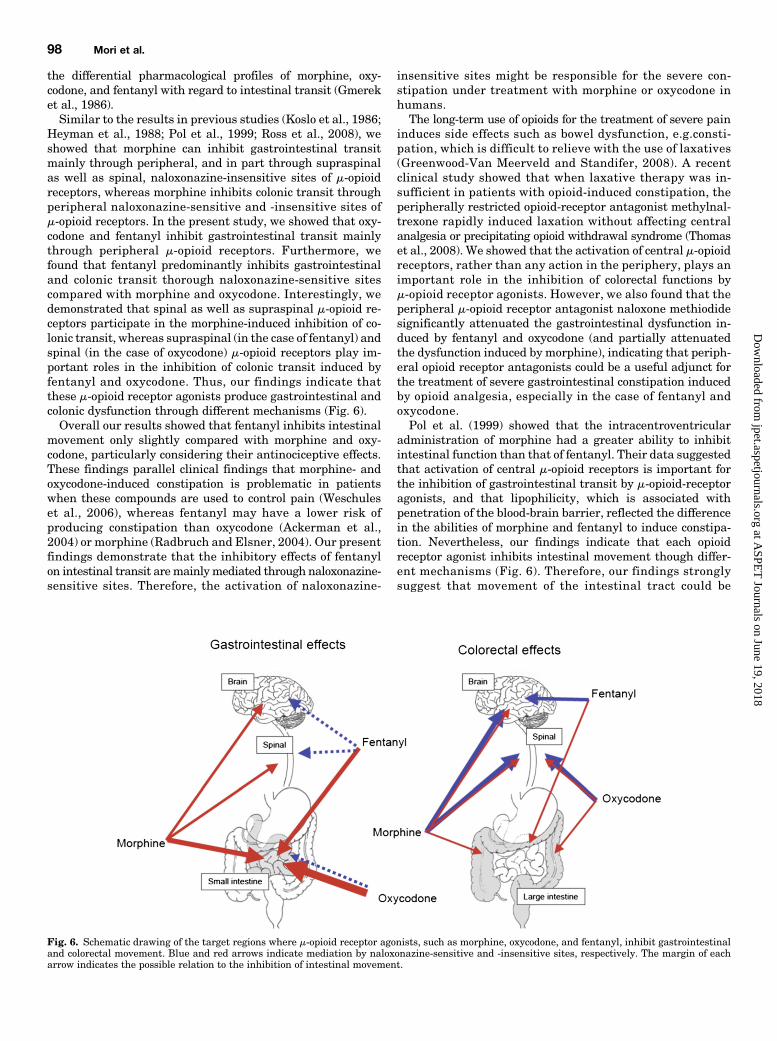
Heyman et al., 1988; Pol et al., 1999; Ross et al., 2008), weshowed that morphine can inhibit gastrointestinal transitmainly through peripheral, and in part through supraspinalas well as spinal, naloxonazine-insensitive sites of m-opioidreceptors, whereas morphine inhibits colonic transit throughperipheral naloxonazine-sensitive and -insensitive sites ofm-opioid receptors. In the present study, we showed that oxy-codone and fentanyl inhibit gastrointestinal transit mainlythrough peripheral m-opioid receptors. Furthermore, wefound that fentanyl predominantly inhibits gastrointestinaland colonic transit thorough naloxonazine-sensitive sitescompared with morphine and oxycodone. Interestingly, wedemonstrated that spinal as well as supraspinal m-opioid re-ceptors participate in the morphine-induced inhibition of co-lonic transit, whereas supraspinal (in the case of fentanyl) andspinal (in the case of oxycodone) m-opioid receptors play im-portant roles in the inhibition of colonic transit induced byfentanyl and oxycodone. Thus, our findings indicate thatthese m-opioid receptor agonists produce gastrointestinal andcolonic dysfunction through different mechanisms (Fig. 6).Overall our results showed that fentanyl inhibits intestinal
movement only slightly compared with morphine and oxy-codone, particularly considering their antinociceptive effects.These findings parallel clinical findings that morphine- andoxycodone-induced constipation is problematic in patientswhen these compounds are used to control pain (Weschuleset al., 2006), whereas fentanyl may have a lower risk ofproducing constipation than oxycodone (Ackerman et al.,2004) or morphine (Radbruch and Elsner, 2004). Our presentfindings demonstrate that the inhibitory effects of fentanylon intestinal transit aremainlymediated through naloxonazine-sensitive sites. Therefore, the activation of naloxonazine-
insensitive sites might be responsible for the severe con-stipation under treatment with morphine or oxycodone inhumans.The long-term use of opioids for the treatment of severe pain
induces side effects such as bowel dysfunction, e.g.consti-pation, which is difficult to relieve with the use of laxatives(Greenwood-Van Meerveld and Standifer, 2008). A recentclinical study showed that when laxative therapy was in-sufficient in patients with opioid-induced constipation, theperipherally restricted opioid-receptor antagonist methylnal-trexone rapidly induced laxation without affecting centralanalgesia or precipitating opioid withdrawal syndrome (Thomaset al., 2008). We showed that the activation of central m-opioidreceptors, rather than any action in the periphery, plays animportant role in the inhibition of colorectal functions bym-opioid receptor agonists. However, we also found that theperipheral m-opioid receptor antagonist naloxone methiodidesignificantly attenuated the gastrointestinal dysfunction in-duced by fentanyl and oxycodone (and partially attenuatedthe dysfunction induced by morphine), indicating that periph-eral opioid receptor antagonists could be a useful adjunct forthe treatment of severe gastrointestinal constipation inducedby opioid analgesia, especially in the case of fentanyl andoxycodone.Pol et al. (1999) showed that the intracentroventricular
administration of morphine had a greater ability to inhibitintestinal function than that of fentanyl. Their data suggestedthat activation of central m-opioid receptors is important forthe inhibition of gastrointestinal transit by m-opioid-receptoragonists, and that lipophilicity, which is associated withpenetration of the blood-brain barrier, reflected the differencein the abilities of morphine and fentanyl to induce constipa-tion. Nevertheless, our findings indicate that each opioidreceptor agonist inhibits intestinal movement though differ-ent mechanisms (Fig. 6). Therefore, our findings stronglysuggest that movement of the intestinal tract could be
Fig. 6. Schematic drawing of the target regions where m-opioid receptor agonists, such as morphine, oxycodone, and fentanyl, inhibit gastrointestinaland colorectal movement. Blue and red arrows indicate mediation by naloxonazine-sensitive and -insensitive sites, respectively. The margin of eacharrow indicates the possible relation to the inhibition of intestinal movement.
98 Mori et al.
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from

governed by m-opioid receptor agonists through severalmechanisms, and these inhibitory effects of m-opioid receptoragonists on the gastrointestinal tract depend on the partic-ular characteristics of each opioid.In conclusion, morphine, oxycodone, and fentanyl were shown
to induce constipation though different mechanisms that in-volved naloxonazine-sensitive versus -insensitive sites andsupraspinal/spinal-versus-peripheral opioid receptors. Ourfindings suggest that peripherally acting m-receptor antag-onists, such as methylnaltrexone and alvimopan, would bebeneficial for gastrointestinally originated constipation in-duced by opioid receptor agonists without compromising painrelief (Becker and Blum, 2009). Other laxatives that targetcolorectal-originated constipation could be useful as a cotreat-ment along with peripherally acting m-receptor antagoniststo suppress opioid receptor agonist–induced constipation. Webelieve that our findings provide some insight into the re-ceptor agonists studied as well as information that couldcontribute to the application of peripherally restricted opioidreceptor antagonists in addition to future drug design forimproving the QOL of patients under pain control.
Authorship Contributions
Participated in research design: Mori, Shibasaki Y., Shibasaki M.,Horie, Suzuki.
Conducted experiments:Matsumoto, Hasegawa, Wang, Masukawa.Performed data analysis: Mori, Yoshizawa.Wrote or contributed to the writing of the manuscript: Mori,
Shibasaki Y., Yoshizawa, Suzuki.
References
Ackerman SJ, Knight T, Schein J, Carter C, and Staats P (2004) Risk of constipationin patients prescribed fentanyl transdermal system or oxycodone hydrochloridecontrolled-release in a California Medicaid population. Consult Pharm 19:118–132.
Becker G and Blum HE (2009) Novel opioid antagonists for opioid-induced boweldysfunction and postoperative ileus. Lancet 373:1198–1206.
Baker AK and Meert TF (2002) Functional effects of systemically administeredagonists and antagonists of mu, delta, and kappa opioid receptor subtypes on bodytemperature in mice. J Pharmacol Exp Ther 302:1253–1264.
Boström E, Hammarlund-Udenaes M, and Simonsson US (2008) Blood-brain barriertransport helps to explain discrepancies in in vivo potency between oxycodone andmorphine. Anesthesiology 108:495–505.
Cadet P (2004) Mu opiate receptor subtypes. Med Sci Monit 10:MS28–MS32.Dagenais C, Graff CL, and Pollack GM (2004) Variable modulation of opioid brainuptake by P-glycoprotein in mice. Biochem Pharmacol 67:269–276.
Elliott J, Smart D, Lambert DG, and Traynor JR (1994) Characterisation of mu-opioid receptors on SH-SY5Y cells using naloxonazine and beta-funaltrexamine.Eur J Pharmacol 268:447–450.
Finkel JC, Pestieau SR, and Quezado ZM (2007) Ketamine as an adjuvant fortreatment of cancer pain in children and adolescents. J Pain 8:515–521.
Gmerek DE, Cowan A, and Woods JH (1986) Independent central and peripheralmediation of morphine-induced inhibition of gastrointestinal transit in rats.J Pharmacol Exp Ther 236:8–13.
Greenwood-Van Meerveld B and Standifer KM (2008) Methylnaltrexone in thetreatment of opioid-induced constipation. Clin Exp Gastroenterol 1:49–58.
Haley TJ (1957) 5-Hydroxytryptamine antagonism by lysergic acid diethylamideafter intracerebral injection in conscious mice. J Am Pharm Assoc Am Pharm Assoc(Baltim) 46:428–430.
Heyman JS, Williams CL, Burks TF, Mosberg HI, and Porreca F (1988) Dissociationof opioid antinociception and central gastrointestinal propulsion in the mouse:studies with naloxonazine. J Pharmacol Exp Ther 245:238–243.
Holzer P, Ahmedzai SH, Niederle N, Leyendecker P, Hopp M, Bosse B, Spohr I,and Reimer K (2009) Opioid-induced bowel dysfunction in cancer-related pain:causes, consequences, and a novel approach for its management. J Opioid Manag5:145–151.
Hylden JL and Wilcox GL (1980) Intrathecal morphine in mice: a new technique. EurJ Pharmacol 67:313–316.
Kang M, Maguma HT, Smith TH, Ross GR, Dewey WL, and Akbarali HI (2012) Therole of b-arrestin2 in the mechanism of morphine tolerance in the mouse andguinea pig gastrointestinal tract. J Pharmacol Exp Ther 340:567–576.
Koslo RJ, Burks TF, and Porreca F (1986) Centrally administered bombesin affectsgastrointestinal transit and colonic bead expulsion through supraspinal mecha-nisms. J Pharmacol Exp Ther 238:62–67.
Leppert W (2010) The role of opioid receptor antagonists in the treatment of opioid-induced constipation: a review. Adv Ther 27:714–730.
Matsuzawa S, Suzuki T, and Misawa M (2000) Involvement of mu-opioid receptor inthe salsolinol-associated place preference in rats exposed to conditioned fear stress.Alcohol Clin Exp Res 24:366–372.
Minami K, Hasegawa M, Ito H, Nakamura A, Tomii T, Matsumoto M, Orita S,Matsushima S, Miyoshi T, and Masuno K, et al. (2009) Morphine, oxycodone, andfentanyl exhibit different analgesic profiles in mouse pain models. J Pharmacol Sci111:60–72.
Nakamura A, Hasegawa M, Ito H, Minami K, Koike K, Habu-Tomita N, Nanba K,Hamaguchi K, Noshi E, and Hashimoto H, et al. (2011) Distinct relations amongplasma concentrations required for different pharmacological effects in oxycodone,morphine, and fentanyl. J Pain Palliat Care Pharmacother 25:318–334.
Narita M, Kishimoto Y, Ise Y, Yajima Y, Misawa K, and Suzuki T (2005) Directevidence for the involvement of the mesolimbic kappa-opioid system in themorphine-induced rewarding effect under an inflammatory pain-like state. Neu-ropsychopharmacology 30:111–118.
Pasternak GW (1993) Pharmacological mechanisms of opioid analgesics. Clin Neu-ropharmacol 16:1–18.
Pol O, Valle L, Sánchez-Blázquez P, Garzón J, and Puig MM (1999) Antibodies andantisense oligodeoxynucleotides to mu-opioid receptors, selectively block the effectsof mu-opioid agonists on intestinal transit and permeability in mice. Br J Phar-macol 127:397–404.
Radbruch L and Elsner F (2004) Clinical experience with transdermal fentanyl forthe treatment of cancer pain in Germany. Keio J Med 53:23–29.
Raffa RB, Mathiasen JR, and Jacoby HI (1987) Colonic bead expulsion time in nor-mal and mu-opioid receptor deficient (CXBK) mice following central (ICV) ad-ministration of mu- and delta-opioid agonists. Life Sci 41:2229–2234.
Ross GR, Gabra BH, Dewey WL, and Akbarali HI (2008) Morphine tolerance in themouse ileum and colon. J Pharmacol Exp Ther 327:561–572.
Shook JE, Pelton JT, Hruby VJ, and Burks TF (1987) Peptide opioid antagonistseparates peripheral and central opioid antitransit effects. J Pharmacol Exp Ther243:492–500.
Suzuki T, Mori T, Tsuji M, Misawa M, and Nagase H (1995) Discriminative stimulusproperties of morphine mediated by mu 1-opioid receptors. Eur J Pharmacol 284:195–198.
Swegle JM and Logemann C (2006) Management of common opioid-induced adverseeffects. Am Fam Physician 74:1347–1354.
Thomas J, Karver S, Cooney GA, Chamberlain BH, Watt CK, Slatkin NE, StamblerN, Kremer AB, and Israel RJ (2008) Methylnaltrexone for opioid-induced con-stipation in advanced illness. N Engl J Med 358:2332–2343.
Torigoe K, Nakahara K, Rahmadi M, Yoshizawa K, Horiuchi H, Hirayama S, Imai S,Kuzumaki N, Itoh T, and Yamashita A, et al. (2012) Usefulness of olanzapine as anadjunct to opioid treatment and for the treatment of neuropathic pain. Anesthesi-ology 116:159–169.
WHO (1996) Cancer Pain Relief, World Health Organization, Geneva.Weschules DJ, Bain KT, Reifsnyder J, McMath JA, Kupperman DE, Gallagher RM,Hauck WW, and Knowlton CH (2006) Toward evidence-based prescribing at end oflife: a comparative analysis of sustained-release morphine, oxycodone, and trans-dermal fentanyl, with pain, constipation, and caregiver interaction outcomes inhospice patients. Pain Med 7:320–329.
Yamada K and Onoda Y (1992) Effects of trimebutine on colonic propulsion in mice.J Smooth Muscle Res 28:87–93.
Yu Y, Cui Y, Wang X, Lai LH, Wang CL, Fan YZ, Liu J, and Wang R (2007) In vitrocharacterization of the effects of endomorphin 1 and 2, endogenous ligands for mu-opioid receptors, on mouse colonic motility. Biochem Pharmacol 73:1384–1393.
Address correspondence to: Dr. Tsutomu Suzuki, Department of Toxicology,School of Pharmacy, Hoshi University School of Pharmacy and Pharmaceu-tical Sciences, 2-4-41 Ebara, Shinagawa-ku, Tokyo 142-8501, Japan. E-mail:[email protected]
Differential Effects of m-Agonists on Intestinal Transit 99
at ASPE
T Journals on June 19, 2018
jpet.aspetjournals.orgD
ownloaded from
Related Documents











