112 INTRODUCTION Diabetes mellitus (DM) is a group of metabolic diseases characterized by hyperglycaemia resulting from defects in insulin secretion, insulin action, or both. 1 The chronic hyperglycaemia of diabetes affects the vascular system directly or indirectly and is the main cause of morbidity and mortality seen in these patients. 2 These injurious effects are broadly classified into the macrovascular and the microvascular complications. 2 Macrovascular complications mainly involve the large vessels such as arteries and veins clinically manifesting as cardiovascular disease, peripheral artery disease and cerebrovascular disease. 2 Cardiovascular disease (CVD) is the leading cause of death (~70%) in patients with type 2 DM (T2DM). 3,4 Although, CVD risk factors like age, obesity, dyslipidaemia, hypertension are more common in these patients, diabetes itself is an independent risk factor for CVD. 5 Similarly, diabetes is an independent risk factor for stroke across all ages. 6 Presence of DM adversely affects the cerebrovascular circulation by increasing the risk of intracranial and extra- cranial (e.g., carotid artery) atherosclerosis. 3,7 Review Article: Molecular mechanisms underlying microvascular complications in diabetes mellitus Aparna R. Bitla, N. Harini Devi, V.S. Kiranmayi Department of Biochemistry, Sri Venkateswara Institute of Medical Sciences, Tirupati ABSTRACT Vascular complications are a major cause of morbidity and mortality in patients with diabetes mellitus. Diabetic microvascular complications include diabetic retinopathy, neuropathy and nephropathy. Hyperglycaemia-induced activation of metabolic pathways, hyperglycaemia-induced growth factors, components of metabolic syndrome and hyperglycaemia-induced epigenetic changes act through a common platform i.e endothelial dysfunction. Hyperglycaemia, is the initiating cause of diabetic tissue damage. Under conditions of hyperglycaemia, four important pathways are activated which shuttle glucose and its intermediates through alternate pathways especially the polyol pathway forming sorbitol which exerts an osmotic effect; advanced glycation end products which modify biomolecules and alter their functions; protein kinase C activation causing altered signal transduction and hexosamine pathway which forms uridine diphosphate) N-acetyl glucosamine which glycosylates transcription factors and increases expression of procoagulant molecules. Hyperglycaemia is thought to activate these four pathways through increased generation of superoxide anions. Though hyperglycaemia is thought to be essential to cause clinically important microangiopathy, there are other factors which predispose an individual to these complications. Hyperglycaemia- induced epigenetic changes i.e., changes in the deoxyribonucleic acid (DNA) molecule due to causes outside the DNA molecule are currently being probed for their role in development and progression of vascular complications. The ultimate purpose of understanding these mechanisms is to devise therapeutic measures which will target these mechanisms and will help in preventing the development as well as delaying the progression of diabetic vascular complications and improve the quality of life in these patients. Key words: Diabetes mellitus, Endothelial dysfunction, Microvascular; Hyperglycaemia, Epigenetics Bitla AR, Harini Devi N, Kiranmayi VS, Molecular mechanisms underlying microvascular complications in diabetes mellitus. J Clin Sci Res 2016;5:112-23. DOI: http://dx.doi.org/10.15380/2277-5706.JCSR.16.01.003. Corresponding author Dr Aparna R Bitla, Associate Professor, Department of Biochemistry, Venkateswara Institute of Medical Sciences, Tirupati, India. e-mail: [email protected] Received: January 12, 2016; Accepted: February 29, 2016. Online access http://svimstpt.ap.nic.in/jcsr/apr-jun16_files/ra16.pdf DOI: http://dx.doi.org/10.15380/2277-5706.JCSR.16.01.003 Mechanisms of microvascular complications in diabetes mellitus Bitla et al

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

112
INTRODUCTION
Diabetes mellitus (DM) is a group of metabolicdiseases characterized by hyperglycaemiaresulting from defects in insulin secretion,insulin act ion, or both.1 The chronichyperglycaemia of diabetes affects the vascularsystem directly or indirectly and is the maincause of morbidity and mortality seen in thesepatients.2 These injurious effects are broadlyclassified into the macrovascular and themicrovascular complications.2
Macrovascular complications mainly involvethe large vessels such as arteries and veins
clinically manifesting as cardiovasculardisease, peripheral artery disease andcerebrovascular disease.2 Cardiovasculardisease (CVD) is the leading cause of death(~70%) in patients with type 2 DM (T2DM).3,4
Although, CVD risk factors like age, obesity,dyslipidaemia, hypertension are more commonin these patients, diabetes it self is anindependent risk factor for CVD.5 Similarly,diabetes is an independent risk factor for strokeacross all ages.6 Presence of DM adverselyaffects the cerebrovascular circulation byincreasing the risk of intracranial and extra-cranial (e.g., carotid artery) atherosclerosis.3,7
Review Article:Molecular mechanisms underlying microvascular complications in diabetes
mellitusAparna R. Bitla, N. Harini Devi, V.S. Kiranmayi
Department of Biochemistry, Sri Venkateswara Institute of Medical Sciences, Tirupati
ABSTRACTVascular complications are a major cause of morbidity and mortality in patients with diabetes mellitus. Diabeticmicrovascular complications include diabetic retinopathy, neuropathy and nephropathy. Hyperglycaemia-inducedactivation of metabolic pathways, hyperglycaemia-induced growth factors, components of metabolic syndrome andhyperglycaemia-induced epigenetic changes act through a common platform i.e endothelial dysfunction.Hyperglycaemia, is the initiating cause of diabetic tissue damage. Under conditions of hyperglycaemia, four importantpathways are activated which shuttle glucose and its intermediates through alternate pathways especially the polyolpathway forming sorbitol which exerts an osmotic effect; advanced glycation end products which modify biomoleculesand alter their functions; protein kinase C activation causing altered signal transduction and hexosamine pathwaywhich forms uridine diphosphate) N-acetyl glucosamine which glycosylates transcription factors and increasesexpression of procoagulant molecules. Hyperglycaemia is thought to activate these four pathways through increasedgeneration of superoxide anions. Though hyperglycaemia is thought to be essential to cause clinically importantmicroangiopathy, there are other factors which predispose an individual to these complications. Hyperglycaemia-induced epigenetic changes i.e., changes in the deoxyribonucleic acid (DNA) molecule due to causes outside the DNAmolecule are currently being probed for their role in development and progression of vascular complications. Theultimate purpose of understanding these mechanisms is to devise therapeutic measures which will target thesemechanisms and will help in preventing the development as well as delaying the progression of diabetic vascularcomplications and improve the quality of life in these patients.
Key words: Diabetes mellitus, Endothelial dysfunction, Microvascular; Hyperglycaemia, EpigeneticsBitla AR, Harini Devi N, Kiranmayi VS, Molecular mechanisms underlying microvascular complications in diabetes mellitus.J Clin Sci Res 2016;5:112-23. DOI: http://dx.doi.org/10.15380/2277-5706.JCSR.16.01.003.
Corresponding author Dr Aparna R Bitla,Associate Professor, Department ofBiochemistry, Venkateswara Institute ofMedical Sciences, Tirupati, India.e-mail: [email protected]
Received: January 12, 2016; Accepted: February 29, 2016.
Online accesshttp://svimstpt.ap.nic.in/jcsr/apr-jun16_files/ra16.pdf
DOI: http://dx.doi.org/10.15380/2277-5706.JCSR.16.01.003
Mechanisms of microvascular complications in diabetes mellitus Bitla et al

113
Peripheral artery disease characterized byocclusion of the lower extremity arteries,8 canresult in functional impairment and disability,and is related to the duration and severity ofdiabetes.9
Microvascular complications involve the smallvessels such as the capillaries and includediabet ic retinopathy, neuropathy andnephropathy affecting the vessels of the retina,nerves and the kidneys respectively. Diabeticretinopathy (DR) is a complication affecting theperipheral retina, the macula, or both and is aleading cause of visual disability and blindnessin people with diabetes. The severity of DRranges from the less severe nonproliferative andpreproliferative to the more severe proliferativeDR, characterized by abnormal growth of newvessels.10 About 50% of patients with DM candevelop either autonomic or peripheralneuropathy. Autonomic neuropathy manifestsas abnormal heart rate and vascular control.11
Characteristic features of peripheral neuropathyinclude axonal thickening with progression toaxonal loss, basement membrane thickening,pericyte loss, loss of microfilaments (actin andmyosin), and decreased capillary blood flowto C fibers, leading to decreased nerveperfusion and endoneurial hypoxia.3 Diabeticnephropathy (DN) is a serious and progressivecomplication which typically manifests asmicroalbuminuria. Other characteristic featuresof DN include thickening of glomerularbasement membranes and glomerularhyperfiltration, leading to mesangialextracellular matrix expansion. This leads tofurther increase in urinary albumin excretionand progression to glomerular and tubularsclerosis and renal failure.3
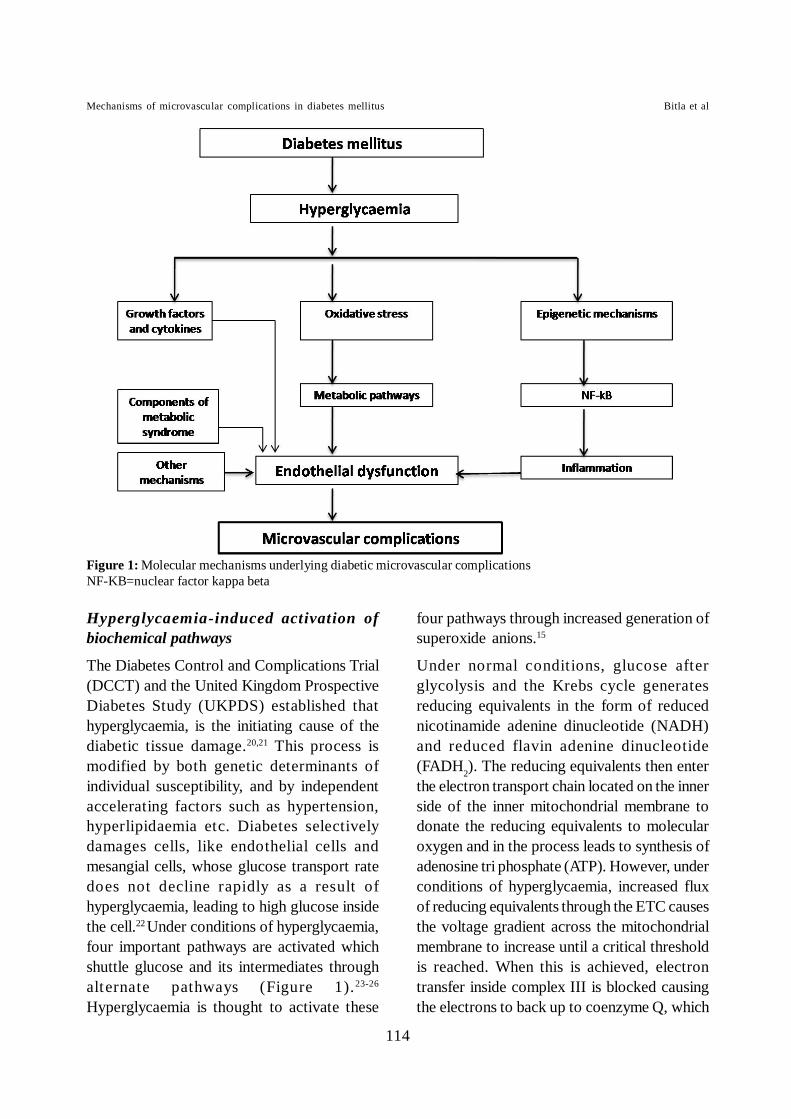
The principle biochemical mechanismsinvolved in these complications include thehyperglycaemia induced activation of themetabolic pathways12-14, oxidative stress15 andgrowth factors (Figure 1). Endothelialdysfunction is being increasingly recognized as
the principle mediator of both micro-andmacrovascular complications in diabetes.16
Dysfunction of the vascular endothelium isregarded as an important factor in thepathogenesis of micro- and macro-angiopathy.Endothelial dysfunction is an early reversiblestep in the process of atherosclerosis.17 Undernormal conditions, the vascular endotheliumreleases vasoprotective factors like nitric oxide(NO) also called the endothelium-derivedrelaxing factor, prostacyclin, bradykinin, andendothelium-derived hyperpolarizing factor(EDHF) and harmful vasoconstrictorsubstances like endothelin (ET), reactiveoxygen species (ROS), endothelium-derivedcyclooxygenase (COX)-dependent vasocon-stricting factor (EDCF), and angiotensin II (AngII) to maintain vascular homeostasis with aanticoagulant, antithrombotic and fibrinolyticphenotype. Nitric oxide is synthesized byendothelial nitric oxide synthase (eNOS) andis the chief vasodilator. Damage to theendothelial layer upsets the balance betweenvasoconstriction and vasodilation, initiating anumber of events/processes that promote orexacerbate atherosclerosis18 via increasedendothelial permeabilization, plateletaggregation, leukocyte adhesion, and cytokineproduction.
MICROVASCULAR COMPLICATIONSMECHANISMS
The present review discusses the mechanismsinvolved in diabetic microvascular compli-cations and its clinical implications.
Endothelial dysfunction in diabetic micro-vascular Complications has been attributed tothe following hyperglycaemia linked mecha-nisms.19 (i) hyperglycaemia-induced activationof biochemical pathways; (ii) hyperglycaemia-induced synthesis of growth factors andvasoact ive agents; (iii) components ofmetabolic syndrome and (iv) hyperglycaemia-induced epigenetic changes.
Mechanisms of microvascular complications in diabetes mellitus Bitla et al
114
Hyperglycaemia-induced activation ofbiochemical pathways
The Diabetes Control and Complications Trial(DCCT) and the United Kingdom ProspectiveDiabetes Study (UKPDS) established thathyperglycaemia, is the initiating cause of thediabetic tissue damage.20,21 This process ismodified by both genetic determinants ofindividual susceptibility, and by independentaccelerating factors such as hypertension,hyperlipidaemia etc. Diabetes selectivelydamages cells, like endothelial cells andmesangial cells, whose glucose transport ratedoes not decline rapidly as a result ofhyperglycaemia, leading to high glucose insidethe cell.22 Under conditions of hyperglycaemia,four important pathways are activated whichshuttle glucose and its intermediates throughalternate pathways (Figure 1).23-26
Hyperglycaemia is thought to activate these
four pathways through increased generation ofsuperoxide anions.15
Under normal conditions, glucose afterglycolysis and the Krebs cycle generatesreducing equivalents in the form of reducednicotinamide adenine dinucleotide (NADH)and reduced flavin adenine dinucleotide(FADH2). The reducing equivalents then enterthe electron transport chain located on the innerside of the inner mitochondrial membrane todonate the reducing equivalents to molecularoxygen and in the process leads to synthesis ofadenosine tri phosphate (ATP). However, underconditions of hyperglycaemia, increased fluxof reducing equivalents through the ETC causesthe voltage gradient across the mitochondrialmembrane to increase until a critical thresholdis reached. When this is achieved, electrontransfer inside complex III is blocked causingthe electrons to back up to coenzyme Q, which
Figure 1: Molecular mechanisms underlying diabetic microvascular complicationsNF-KB=nuclear factor kappa beta
Mechanisms of microvascular complications in diabetes mellitus Bitla et al
115
donates electrons one at a time to molecularoxygen, thereby generating superoxide.27 It hasbeen proposed that hyperglycaemia-inducedmitochondrial superoxide production activatesthe four damaging pathways by inhibitingglyceraldehydes-3 phosphate dehydrogenase(GAPDH) through the activation of polyadenosine diphosphate (ADP) ribosepolymerase.15 The four pathways are the polyolpathway, glyoxylation pathway, protein kinaseC pathway and the hexosamine pathway.
Polyol pathway
The first pathway proposed was the polyolpathway. Under normal conditions, aldosereductase (AR) reduces toxic aldehydes in thecell to inactive alcohols, but under conditions
of hyperglycaemia, AR also reduces glucose tosorbitol. This sorbitol exerts osmotic effect andthereby causes damage to cells. Sorbitol is lateroxidized to fructose in a reaction consumingthe cofactor reduced nicotinamide adeninedinucleotide phosphate (NADPH). NADPH isan essential cofactor for regenerating reducedglutathione, an important int racellularantioxidant protecting cell against reactiveoxygen species (ROS). Glutathione exists inthe oxidized glutathione (GSSG) (inactive)form and the reduced (GSH)(active)form.Depletion of NADPH in the polyol pathwaythus increases the susceptibility of cells tointracellular oxidative stress.28
Studies have shown that AR catalyzes thereduction of a large number of aldehydes
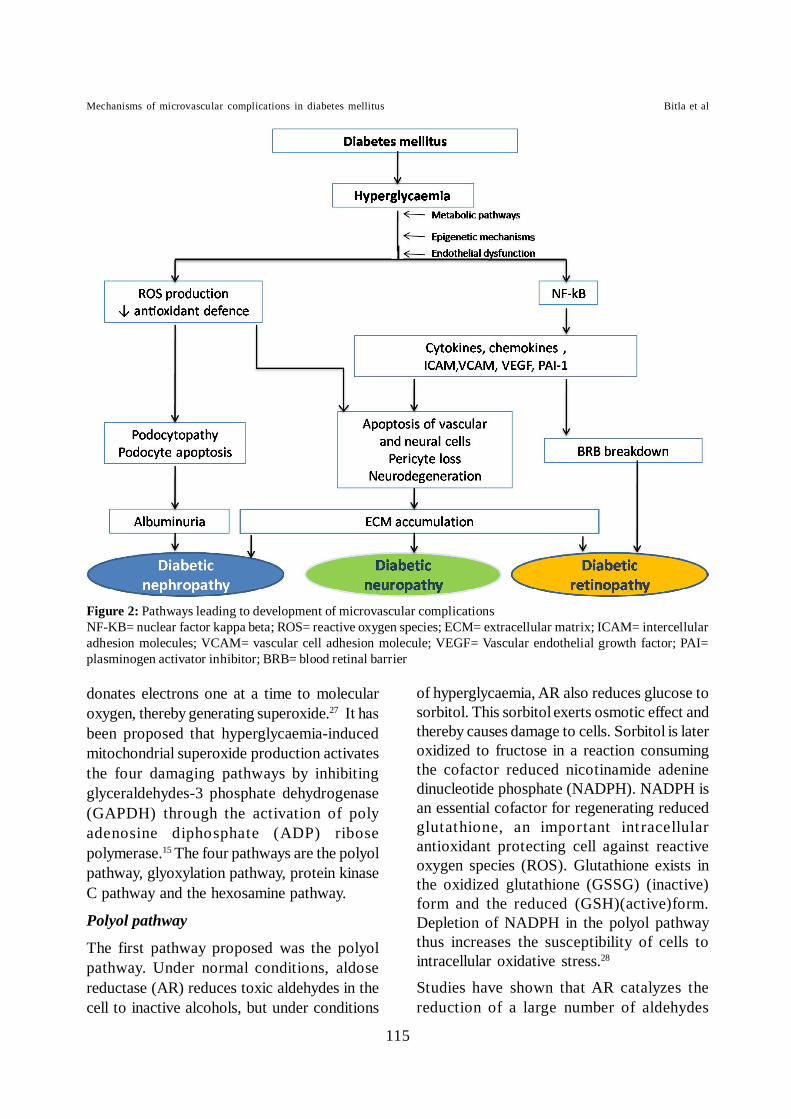
Figure 2: Pathways leading to development of microvascular complicationsNF-KB= nuclear factor kappa beta; ROS= reactive oxygen species; ECM= extracellular matrix; ICAM= intercellularadhesion molecules; VCAM= vascular cell adhesion molecule; VEGF= Vascular endothelial growth factor; PAI=plasminogen activator inhibitor; BRB= blood retinal barrier
Mechanisms of microvascular complications in diabetes mellitus Bitla et al
s

116
generated from lipid peroxidation with 103 to104 fold higher efficiency than glucose and thatglucose may be an incidental substrate of AR.29
AR is susceptible to oxidants such as hydrogenperoxide (H2O2) and NO owing to the presenceof a highly reactive cysteine (Cys-298) residueat its active site. These oxidants can causeinactivation of AR. The enzyme also catalyzesthe reduction of the glutathione conjugates ofunsaturated aldehydes, which is considered tobe a protective mechanism in minimizing thereactivity of the aldehyde function unquenchedby glutathiolation. AR can be inactivated byundergoing glutathiolation of the Cys- 298residue.30
NO has been shown to regulate intracellularAR activity.31 AR is either S-thiolated(inactivated enzyme) or S-nitrosated (activatedenzyme) depending on the conditions of thereaction and the nature of the NO donor used.NO secreted by endothelial cells can undergoS-glutathionylation and form GSNO withglutathione that is abundant in vascular smoothmuscle cells (VSMC). The GSNO formed canin turn S-glutathiolate AR at Cys-298 32 S-glutathiolation inactivates AR and thus undernormoglycaemic conditions, much of the ARis in the inactive form, whereas inhyperglycaemia a decrease in NADPH/NADP+ratio and other factors decrease NO and the ARwould be in the active form. S-glutathiolationof AR in vascular smooth muscle cells (VSMC)by NO donors such as GSNO, which inactivatesthe enzyme, is reversible.
AR can thus be a therapeutic target forpreventing or treating diabetic complicationsthrough increasing NO levels.33,34 AR is also acritical component of intracellular signaling,and inhibition of the enzyme prevents highglucose-, cytokine-, or growth factor-inducedactivation of protein kinase C and nuclearfactor-kappa beta (NF-Kβ)-binding protein.35
Glyoxylation pathway
The second pathway is the glyoxylationpathway which increases the intracellularconcentration of advanced glycation endproducts (AGEs).36 AGEs are heterogeneousgroup of molecules formed from the nonenzymatic reaction of reducing sugars with thefree amino groups of proteins, lipids and nucleicacids. AGE precursors diffuse out of the celland bind covalently with proteins formingcrosslink’s thus modifying circulating proteinsin the blood37 such as albumin. These modifiedcirculating proteins can then bind to AGEreceptors (RAGEs)38 and are taken up byendocytosis.
Endocytosed AGEs activate the cells causingthe production of inflammatory cytokines andgrowth factors, which in turn have beenimplicated in vascular pathology.39,40 AGEsalso directly affect the vascular endothelium.Diabetic patients have been shown to haveimpaired endothelial-dependent andendothelium-independent vasodilatation whichcorrelated with serum AGEs concentration.41
Depletion of endothelial NO production wasaugmented by AGEs42 thus showing the directeffects of AGEs on endothelial cells apart fromcausing the inflammatory response.
Protein kinase C pathway
The third pathway proposed is the activationof protein kinase C (PKC) pathway.43 PKCphosphorylates a number of proteins andregulates their activity. Hyperglycaemia insidethe cell increases the synthesis diacylglycerol,a critical activating cofactor for the classicisoforms of PKC, β, δ, and α. High glucose,via PKC signaling affects gene expression of anumber of important molecules thereby leadingto decreased synthesis of endothelial nitricoxide (NO) synthase (eNOS).44 It also inducesoxidative stress and up-regulation of COX-2,resulting in reduced NO availability and alteredprostanoid profile.45 PKC activation has been
Mechanisms of microvascular complications in diabetes mellitus Bitla et al

117
shown to produce endothelium-dependentvasodilator dysfunction by altering thebioavailability of nitric oxide (NO), andincreasing the production of thromboxane,other COX-dependent vasoconstrictors andendothelin-1 (ET-1),46 causing an imbalance inthe vasodilating nitric oxide and thevasoconstricting endothelin-1.
Hexosamine pathway
The fourth pathway activated in the presenceof hyperglycaemia is the hexoamine pathway.In glycolysis, glucose is first converted toglucose-6 phosphate and then fructose-6phosphate followed by the further reactions thatlead to the formation of pyruvate under aerobicconditions. However, under conditions ofhyperglycaemia, some of the fructose-6-phosphate gets diverted into a signallingpathway in which an enzyme glutamine:fructose-6 phosphate amidotransferase (GFAT)converts fructose-6 phosphate to glucosamine-6 phosphate and finally to uridine diphosphate(UDP) N-acetyl glucosamine (UDP-GlcNAC).47
UDP-GlcNAC the product of activation of thehexosamine pathway glycosylates transcriptionfactors on the serine and threonine residuesleading to altered gene expression. Eg.modification of transcription factor Stimulatoryprotein (Sp1) results in increased expressionof transforming growth factor-β andplasminogen activator inhibitor-1 (PAI-1)which leads to a procoagulant state,modification of eNOS leading to decreased NOsynthesis. O-GlcNAcylation also impairs theactivation of the insulin receptor signallingpathway, resulting in deregulation of eNOSactivity and decreased NO production.48
Hyperglycaemia-induced synthesis ofgrowth factors and vasoactive agents
Hyperglycaemia-induced synthesis of growthfactors, cytokines and vasoactive agents indifferent cells can indirectly affect endothelial
cell functioning.49 Vascular endothelial growthfactor (VEGF) and the angiopoietins are twofamilies of growth factors that act on vascularendothelial cells and are involved inangiogenesis.50 During angiogenesis, VEGFinteracts with several other angiogenic factors,playing an important role in cell proliferation,differentiation, migration, cell survival, NOproduction, release of other growth factors, andsympathetic innervation.51 Diabetic patientshave been shown to have elevated circulatinglevels of VEGF.52 Under normal physiologicalconditions VEGF-A is constitutively expressedin the glomerular podocytes. Up-regulation ofVEGF-A in early diabetic nephropathy has beenreported.52 This leads to glomerular capillarypathology and increased vascular permeability.Experimental studies have shown that up-regulation of VEGF leads to activation oftransforming growth factor (TGF)-β1, andstimulates extracellular matrix production andaccumulation leading to glomerular basementmembrane thickening.53 A complex interactionexists between VEGF-A, NO and endothelialdysfunction in diabetic nephropathy. VEGF isbeneficial for endothelial cells when NO issynthesized normally. Conditions which leadto decrease in NO synthesis/bioavailabilitycause the deleterious effects of VEGF topredominate.54 Interaction of VEGF withendothelium leads to alteration in retinalmicrovasculature and increased vascularpermeability contributing to diabet icretinopathy.55 VEGF is thus an importanttherapeutic target in diabetic retinopathy.56
The inflammatory cytokine tumour necrosisfactor- α (TNF-α), produces endothelialdysfunction directly or through the productionof interleukin-6 (IL-6) and the downstream C-reactive protein (CRP) by the liver. Thesefactors independently or in combination canlead to endothelial dysfunction.49
Hyperglycaemia and TNF- α also causeactivation of NF-KB which leads to activationof a number of genes involved in acute
Mechanisms of microvascular complications in diabetes mellitus Bitla et al

118
inflammatory response.57,58 NF-KB regulatesthe expression of a number of genes, includingthe expression of adhesion moleculesintracellular adhesion molecule-1 (ICAM-1),vascular cell adhesion molecule-1 (VCAM-1),E-selectin, interleukin (IL-1), interleukin-6 (IL-6) and interleukin-8) (IL-8) tissue factor, PAI-1 and inducible NOS (Figure 2).49,58 Thesemarkers were found to be elevated even innormoalbuminuric patients, indicating the earlyoccurrence of vascular dysfunction even beforeit manifests clinically as microalbuminuria.59
Apart from causing endothelial dysfunctionthey also produce other effects like increasingthe vascular permeability, alterat ion ofvasoregulatory responses, increasing leucocyteadhesion to endothelium and facilitatethrombus formation by inducing pro-coagulantactivity and by inhibiting anti-coagulantpathways by impairing fibrinolysis viastimulation of PAI-1.49,58
Components of metabolic syndrome
Metabolic syndrome is a clustering of severalrisk factors including diabetes and raised fastingplasma glucose, abdominal obesity, highcholesterol and high blood pressure.60 Allelements of the syndrome share twopathophysiological features i.e insulinresistance and endothelial dysfunction.61
Hyperglycaemia and elevated free fatty acidsseen in diabetes have been shown to up-regulateBone morphogenic protein 4 (BMP4) inendothelial cells.62 BMP4 has been shown toinduce an inflammatory response followingoscillatory shear stress leading to increasedexpression of intracellular adhesion molecule-1 (ICAM-1) and monocyte adhesion.63 BMP4infusion was shown to impair endothelium-dependent dilatation of mouse arteries andincrease the vascular NADPH oxidases activity.BMP4 was also reported to impairendothelium-dependent vasodilatation throughoxidative stress–dependent and COX-2–
dependent mechanisms.64,65 BMP4 may thusserve as one of common initiators of endothelialdysfunction in hypertension and diabetesthrough increasing oxidative stress within thevascular wall.
Obesity contributes to endothelial dysfunctionthrough insulin resistance as well as the effectsof adipose tissue derived hormones i.eadipokines and pro-inflammatory cytokineswhich can induce oxidative stress and thusreduce the bio-availability of NO.65 Obeseindividuals also have elevated levels ofendothelins and PAI.66
Hyperglycaemia-induced epigenetic changes
Another aspect of diabetic vascularcomplications which is currently being probedis the epigenetic mechanisms which deal withchanges in the DNA molecule due to causesoutside the DNA molecule i.e changes in thecellular environment. An individual’s risk ofdeveloping microvascular complications is alsodependent on the complex interaction betweengenetic factors and environmental interactions,especially dietary habits and lifestyle, whichaccelerate or slow down the diseaseprogression. These environmental factorsmainly trigger an inflammatory responsethereby promoting inflammation-mediatedinsulin resistance and endothelial dysfunction.67 I t has been shown that transienthyperglycemia induces the so called ‘metabolicmemory’68 which promotes gene-activatingepigenetic changes and signalling events whichare critical in development and progression ofvascular complications. Mitochondrial ROSproduction as a result of hyperglycaemia is saidto be the most relevant nuclear epigeneticmechanism. These nuclear epigenetic changesinclude, DNA methylation and post-translational histone modifications (PTHMs)thereby affecting the chromatin structure. ThePTHM changes in diabetes include acetylationof lysine and arginine residues by histoneacetyltransferases (HATs), favouring the
Mechanisms of microvascular complications in diabetes mellitus Bitla et al

119
euchromatin st ructure and thus genetranscription to occur.69 These can becomeirreversible overtime and thus explain the long-term effects of metabolic memory on vascularcomplications despite an improvement inglycaemic control.67
Cellular events involved in metabolic memoryinclude increased production of AGEs,RAGEoverexpression, increased anion superoxideformation, mitochondrial (mt) proteinglycation, mt DNA damage, PKC activation,polyol pathway and hexosamine fluxalterat ions.70 Pro-inflammatory st imuli,including hyperglycaemia, oxidative stress, andother inflammatory mediators, can affectepigenetic mechanisms, altering the expressionof specific genes in target cells.67
The role of non-coding ribonucleic acids(RNAs) in modulating metabolic memory andthus the risk of developing microvascularcomplications is emerging. These micro-RNAs(miRs) are a family of small, non-coding RNAsabout 21-25 nucleotides in length, that regulategene expression in a sequence-specific manner.They belong to a novel class of endogenousinterfering RNAs that play a crucial role in posttranscriptional gene silencing throughmessenger RNA (mRNA) targeting and are thusinvolved in many biological processes likeapoptosis, cell cycle control, cell proliferation,DNA repair, immunity, metabolism etc.70
Although most miRs are involved in genesilencing, a few can also cause geneactivation.71 miRNAs are released into thecirculation from cells and can thus serve asbiomarkers. Dysregulation of miR expressionhas been shown in patients in many diseasesincluding T2DM. Abnormal miR levels miR-25 and miR21 have been shown in pre-clinicalmodels of diabetic nephropathy.72,73 The miR-25 was shown to negatively regulate NOX4expression, a major catalytic subunit ofNADPH oxidase under hyperglycaemia.
Recently miR-15a expression levels wereshown to be significantly lower in patients withT2DM and impaired fasting glucose /impairedglucose tolerance and could thus serve as apotential biomarker for T2DM and pre-diabetes.74 In an experimental model, elevatedglucose concentration (25 mmol/L) decreasedthe miR-146a expression and increasedexpression of extracellular matrix protein,fibronectin; a characteristic of diabetic vascularcomplications.75
Thus, multiple mechanisms act in consertthrough a common platform i.e., by causingendothelial dysfunction, the basic mechanismtriggering microvascular complications. Theultimate purpose of understanding thesemechanisms is to devise therapeutic measureswhich will target these mechanisms and willhelp in preventing the development as well asdelaying the progression of diabetic vascularcomplications and improve the quality of lifein these patients.
REFERENCES1. American Diabetes Association. Diagnosis and
classification of diabetes mellitus. DiabetesCare 2004;27 Suppl 1:S5-S10.
2. Fowler MJ. Microvascular and MacrovascularComplications of Diabetes. ClinicalDiabetes 2008;26:277-82.
3. Cade WT. Diabetes-Related Microvascular andMacrovascular Diseases in the Physical TherapySetting. Phys Ther 2008; 88:1322-35.
4. Laakso M. Hyperglycemia and cardiovascular di-sease in type 2 diabetes. Diabetes. 1999;48:937-42.
5. Buyken AE, von Eckardstein A, Schulte H, CullenP, Assmann G . Type 2 diabetes mellitus and riskof coronary heart disease: results of the 10-yearfollow-up of the PROCAM study. Eur JCardiovasc Prev Rehabil 2007;14:230-6.
6. Abbott RD, Curb JD, Rodriguez BL, Masaki KH,Popper JS, Ross GW, Petrovitch H. Age-relatedchanges in risk factor effects on the incidence ofthromboembolic and hemorrhagic stroke. J ClinEpidemiol 2003; 56:479-86.
7. Friedlander AH, Maeder LA. The prevalence ofcalcified carotid artery atheromas on the
Mechanisms of microvascular complications in diabetes mellitus Bitla et al

120
panoramic radiographs of patients with type 2diabetes mellitus. Oral Surg Oral Med Oral PatholOral Radiol Endod 2000;89:420-4.
8. Kullo IJ, Bailey KR, Kardia SL, Mosley TH Jr,Boerwinkle E, Turner ST. Ethnic differences inperipheral arterial disease in the NHLBI GeneticEpidemiology Network of Arteriopathy (GENOA)study. Vasc Med 2003;8:237-42.
9. Jude EB, Oyibo SO, Chalmers N, Boulton AJ.Peripheral arterial disease in diabetic andnondiabetic patients: a comparison of severity andoutcome. Diabetes Care 2001; 24:1433-7.
10. Harding S. Extracts from “concise clinicalevidence”. Diabetic retinopathy. BMJ 2003;326:1023-5.
11. Vinik AI, Maser RE, Mitchell BD, Freeman R.Diabetic autonomic neuropathy Diabetes Care2003; 26:1553-79.
12. Pirart J. Diabetes mellitus and its degenerativecomplications: a prospective study of 4,400patients observed between 1947 and 1973.Diabetes Care 1978,1:168-88.
13. Diabetes Control and Complications Trial: Arecontinuing studies of metabolic control andmicrovascular complications in insulin-dependentdiabetes mellitus justified? The Diabetes Controland Complications Trial. N Engl J Med1988;318:246-50.
14. Merimee TJ. Diabetic retinopathy. N Engl J Med1990;322:978-83.
15. Giacco F, Brownlee M. Oxidative stress and diabe-tic complications. Circ Res 2010;107:1058-70.
16. De Vriese AS, Verbeuren TJ, Van de Voorde J,Lameire NH, Vanhoutte PM. Endothelialdysfunction in diabetes. Br J Pharmacol.2000;130:963-74.
17. Brunner H, Cockcroft JR, Deanfield J, Donald A,Ferrannini E, Halcox J, et al. Endothelial functionand dysfunction, part II: association withcardiovascular risk factors and diseases: astatement by the Working Group on Endothelinsand Endothelial Factors of the European Societyof Hypertension. J Hypertens 2005;23:23-46.
18. Davignon J, Ganz P. Role of endothelialdysfunction in atherosclerosis. Circulation 2004;109:III27-32.
19. Schalkwijk CG, Stehouwer CD. Vascularcomplications in diabetes mellitus: the role of
endothelial dysfunction. Clin Sci; 2005;109:143-59.
20. The Diabetes Control and Complications TrialResearch Group: The effect of intensive treatmentof diabetes on the development and progressionof long-term complications in insulin-dependentdiabetes mellitus. N Engl J Med1993;329:977-86.
21. UK Prospective Diabetes Study (UKPDS) Group:Intensive blood-glucose control withsulphonylureas or insulin compared withconventional treatment and risk of complicationsin patients with type 2 diabetes (UKPDS 33).Lancet 1998;352:837-53.
22. Brownlee M. The pathobiology of diabeticcomplications:a unifying mechanism. Diabetes2005;54;1615-25.
23. Brownlee M, Cerami A, Vlassara H. Advancedglycosylation end products in tissue and thebiochemical basis of diabetic complications. NEngl J Med 1988;318:1315-21.
24. Wolf BA, Williamson JR, Easom RA, Chang K,Sherman WR, Turk J. Diacylglycerol accumulationand microvascular abnormalities induced by ele-vated glucose levels. J Clin Invest 1991;87:31-8.
25. Greene DA, Lattimer SA, Sima AA. Sorbitol,phosphoinositides, and sodium-potassium-ATPasein the pathogenesis of diabetic complications. NEngl J Med1987; 316:599-606.
26. King GL, Johnson S, Wu G. Possible growthmodulators involved in the pathogenesis ofdiabetic proliferative retinopathy. In: Growthfactors in health and disease. New York: ExcerptaMed; 1990.p.303-17.
27. Trumpower BL. The proton motive Q cycle:energy transduction by coupling of protontranslocation to electron transfer by thecytochrome bc1 complex. J BiolChem 1990;265:11409-12.
28. Lee AY, Chung SS: Contributions of polyolpathway to oxidative stress in diabetic cataract.FASEB J 1999;13:23-30.
29. Srivastava S, Watowich SJ, Petrash JM, SrivastavaSK, Bhatnagar A. Structural and kineticdeterminants of aldehyde reduction by aldosereductase. Biochemistry 1999;38:42-54.
30. Petrash JM, Harter TM, Devine CS, Olins PO,Bhatnagar A, Liu S, et al. Involvement of cysteine
Mechanisms of microvascular complications in diabetes mellitus Bitla et al
121
residues in catalysis and inhibition of human aldosereductase. Site-directed mutagenesis of Cys-80, -298, and -303. J Biol Chem 1992;267:24833-40.
31. Chandra D, Jackson EB, Ramana KV, Kelley R,Srivastava SK, Bhatnagar A. Nitric oxide preventsaldose reductase activation and sorbitolaccumulation during diabetes. Diabetes2002;51:3095-101.
32. Chandra A, Srivastava S, Petrash JM, BhatnagarA, Srivastava SK. Active site modification ofaldose reductase by nitric oxidedonors. BiochimBiophys Acta 1997;1341:217-22.
33. Srivastava SK, Ramana KV, Chandra D, SrivastavaS, Bhatnagar A. Regulation of aldose reductaseand the polyol pathway activity by nitric oxide.Chem Biol Interact 2003;143-144:333-40.
34. Ramana KV, Chandra D, Srivastava S, BhatnagarA, Srivastava SK. Nitric oxide regulates the polyolpathway of glucose metabolism in vascular smoothmuscle cells. FASEB J 2003;17:417-25.
35. Srivastava SK, Ramana KV, Bhatnagar A. Role ofaldose reductase and oxidative damage in diabetesand the consequent potential for therapeutic options. Endocrine Reviews 26:380-92.
36. Giardino I, Edelstein D, Brownlee M:Nonenzymatic glycosylation in vitro and in bovineendothelial cells alters basic fibroblast growthfactor activity: a model for intracellularglycosylation in diabetes. J Clin Invest1994;94:110-1.
37. McLellan AC, Thornalley PJ, Benn J, Sonksen PH.Glyoxalase system in clinical diabetes mellitus andcorrelation with diabetic complications. Clin Sci(Lond) 1994;87:21-9.
38. Neeper M, Schmidt AM, Brett J, Yan SD, Wang F,Pan YC, et al. Cloning and expression of a cellsurface receptor for advanced glycosylation endproducts of proteins. J Biol Chem1992;267:14998-15004.
39. Doi T, Vlassara H, Kirstein M, Yamada Y, StrikerGE, Striker LJ. Receptor specific increase inextracellular matrix production in mousemesangial cells by advanced glycosylation endproducts is mediated via platelet derived growthfactor. Proc Natl Acad Sci USA1992;89:2873-77.
40. Schmidt AM, Hori O, Chen JX, Li JF, Crandall J,Zhang J, Cao R, Yan SD, Brett J, Stern D:Advanced glycation endproducts interacting with
their endothelial receptor induce expression ofvascular cell adhesion molecule- 1 (VCAM-1) incultured human endothelial cells and in mice: apotential mechanism for the acceleratedvasculopathy of diabetes. J Clin Invest1995;96:1395-1403.
41. Tan KC, Chow WS, Ai VH, Metz C, BucalaR, Lam KS. Advanced glycation end products andendothelial dysfunction in type 2 diabetes.Diabetes Care 2002;25:1055-9
42. Soro-Paavonen A, Zhang WZ, VenardosK, Coughlan MT, Harris E, Tong DC, et al.Advanced glycation end-products induce vasculardysfunction via resistance to nitric oxide andsuppression of endothelial nitric oxide synthase. JHypertens 2010;28:780-8.
43. Koya D, King GL: Protein kinase C activation andthe development of diabetic complications.Diabetes 1998;47:859-66.
44. Kuboki K, Jiang ZY, Takahara N, Ha SW, IgarashiM, Yamauchi T, et al. Regulation of endothelialconstitutive nitric oxide synthase gene expressionin endothelial cells and in vivo : a specific vascularaction of insulin. Circulation 2000;101:676-81.
45. Cosentino F, Eto M, De Paolis P, van der LooB, Bachschmid M, Ullrich V, et al. High glucosecauses upregulation of cyclooxygenase-2 andalters prostanoid profile in human endothelialcells: role of protein kinase C and reactive oxygenspecies. Circulation 2003; 107:1017-23.
46. Cardillo C, Campia U, Bryant MB, Panza JA.Increased activity of endogenous endothelin inpatients with type 2 diabetes mellitus.Circulation 2002;106:1783-87.
47. Nerlich AG, Sauer U, Kolm-Litty V, Wagner E,Koch M, Schleicher ED. Expression ofglutamine:fructose-6-phosphate amidotransferasein human tissues: evidence for high variability anddistinct regulation in diabetes. Diabetes1998;47:170-8.
48. Federici M, Menghini R, Mauriello A, HribalML, Ferrelli F, Lauro D, et al. Insulin-dependentactivation of endothelial nitric oxide synthase isimpaired by O-linked glycosylation modificationof signaling proteins in human coronaryendothelial cells. Circulation 2002;106:466-72.
49. Schalkwijk CG, Stehouwer CD. Vascularcomplications in diabetes mellitus: the role of en-dothelial dysfunction. Clin Sci; 2005;109:143-59.
Mechanisms of microvascular complications in diabetes mellitus Bitla et al
122
50. Lim HS, Blann AD, Chong AY, Freestone B, LipGY. Plasma vascular endothelial growth factor,angiopoietin-1, and angiopoietin-2 in diabetes:implications for cardiovascular risk and effects ofmultifactorial intervention. Diabetes Care 2004;27:2918-24.
51. Jeong IK, King GL. New perspectives on diabeticvascular complications: the loss of endo-genous protective factors induced by hyper-glycemia. Diabetes Metab J 2011;35:8-11.
52. Chen S, Ziyadeh FN. Vascular endothelial growthfactor and diabetic nephropathy. Curr Diab Rep2008;8:470-76.
53. Ku CH, White KE, Dei Cas A, Hayward A,Webster Z, Bilous R, et al. Inducibleoverexpression of sFlt-1 in podocytes amelioratesglomerulopathy in diabetic mice. Diabetes2008;57:2824-33.
54. Nakagawa T. Uncoupling of the VEGF endothelialnitric oxide axis in diabetic nephropathy: anexplanation for the paradoxical effects of VEGFin renal disease. Am J Physiol Renal Physiol2007;292:F1665–F1672.
55. Fong D S, Aiello LP, Ferris III FL,Klein R. Diabetic retinopathy. Diabetes Care2004;27:2540-53.
56. Simó R, Sundstrom JM, Antonetti DA. OcularAnti-VEGF therapy for diabetic retinopathy: therole of VEGF in the pathogenesisof diabetic retinopathy. Diabetes Care2014;37:893-9.
57. Blann AD, Belgore FM, McCollum CN, SilvermanS, Lip PL, Lip GY. Vascular endothelial growthfactor and its receptor, Flt-1, in the plasma ofpatients with coronary or peripheralatherosclerosis, or type II diabetes. Clin Sci (Lond)2002;102:187-94.
58. Karatzis EM. The role of inflammatory agents inendothelial function and their contribution toatherosclerosis. Hellenic J Cardiol 2005;46:232-9.
59. Monaco C, Paleolog E. Nuclear factor κB: apotential therapeutic target in atherosclerosis andthrombosis. Cardiovasc Res 2004;61:671-82.
60. Lim SC, Caballero AE, Smakowski P, LoGerfoFW, Horton ES, Veves A. Soluble intercellularadhesion molecule, vascular cell adhesion
molecule, and impaired microvascular reactivityare early markers of vasculopathy in type 2 diabeticindividuals without microalbuminuria. DiabetesCare 1999;22:1865-70.
61. Grundy SM, Brewer HB Jr, Cleeman JI, Smith SCJr, Lenfant C; American Heart Association;National Heart, Lung, and Blood Institute.Definition of Metabolic Syndrome: Report of theNational Heart, Lung, and Blood Institute/American Heart Association Conference onScientific Issues Related to Definition. Circulation2004;109:433-8.
62. Bostrom KI, Jumabay M, Matveyenko A, NicholasSB, Yao Y. Activation of vascular bonemorphogenetic protein signaling in diabetesmellitus. Circ Res 2011;108:446-57.
63. Sorescu GP, Song H, Tressel SL, Hwang J, DikalovS, Smith DA, et al. Bone morphogenic protein 4produced in endothelial cells by oscillatory shearstress induces monocyte adhesion by stimulatingreactive oxygen species production from a NOX1-based NADPH oxidase. Circ Res 2004;95:773-9.
64. Youn JY, Zhou J, Cai H. Bone MorphogenicProtein 4 Mediates NOX1-Dependent eNOSUncoupling, Endothelial Dysfunction, and COX2Induction in Type 2 Diabetes Mellitus. MolEndocrinol 2015;29:1123-33.
65. Taddei S, Ghiadoni L, Salvetti G, Virdis A, SalvettiA. Obesity and endothelial dysfunction. G ItalCardiol (Rome) 2006;7:715-23.
66. Calles-Escandon J, Cipolla M. Diabetes andendothelial dysfunction: a clinical perspec-tive. Endocr Rev 2001;22:36-52.
67. Prattichizzo F, Giuliani A, Ceka A, RippoMR, Bonfigli AR, Testa R, et al. Epigeneticmechanisms of endothelial dysfunction in type 2diabetes. Clin Epigenetics 2015;7:56.
68. Roy S, Sala R, Cagliero E, Lorenzi M.Overexpression of fibronectin induced by diabetesor high glucose: phenomenon with a memory. ProcNatl Acad Sci USA 1990;87:404-8.
69. Wegner M, Neddermann D, Piorunska-stolzmannM, Jagodzinski PP. Role of epigenetic mechanismsin the development of chronic complications ofdiabetes. Diabetes Res Clin Pract 2014;105:164-75.
Mechanisms of microvascular complications in diabetes mellitus Bitla et al
123
70. Ceriello A. The emerging challenge in diabetes:the “metabolic memory”. Vascul Pharmacol2012;57:133-8.
71. Bartel DP. MicroRNAs: genomics, biogenesis,mechanism, and function. Cell 2004;116:281-97.
72. Vasudevan S, Tong Y, Steitz JA. Switching fromrepression to activation: microRNAs can up-regulate translation. Science 2007;318:1931-4.
73. Fu Y, Zhang Y, Wang Z, Wang L, Wei X, ZhangB, et al. Regulation of NADPH oxidase activityis associated with miRNA-25-mediated NOX4
expression in experimental diabetic nephropathy.Am J Nephrol 2010;32:581-9.
74. Al-Kafaji G, Al-Mahroos G, Alsayed NA, HasanZA, Nawaz S, Bakhiet M. Peripheral bloodmicroRNA-15a is a potential biomarker for type2 diabetes mellitus and pre-diabetes. Mol Med Rep2015;12:7485-90.
75. Feng B, Chen S, McArthur K, Wu Y, Sen S, DingQ, et al. miR-146a-Mediated extracellular matrixprotein production in chronic diabetescomplications. Diabetes 2011;60:2975-84.
Mechanisms of microvascular complications in diabetes mellitus Bitla et al
Related Documents











