MECHANISM AND PATTERNS OF BONE LOSS -DR. KAPIL ARORA

Mechanism of bone loss and patterns of bone loss
Aug 09, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MECHANISM AND PATTERNS OF BONE LOSS
-DR. KAPIL ARORA

INTRODUCTION

Bone Destruction Caused By Extension Of Gingival Inflammation

The extension of inflammation to the supporting structures of a tooth may be
modified by the pathogenic potential of plaque or the resistance of the host.
In a study Heijl et al , were able to convert a confined naturally occurring chronic gingivitis into a progressive periodontitis in experimental
animals by placing a silk ligature into the sulcus and tying it around the neck of the
tooth.
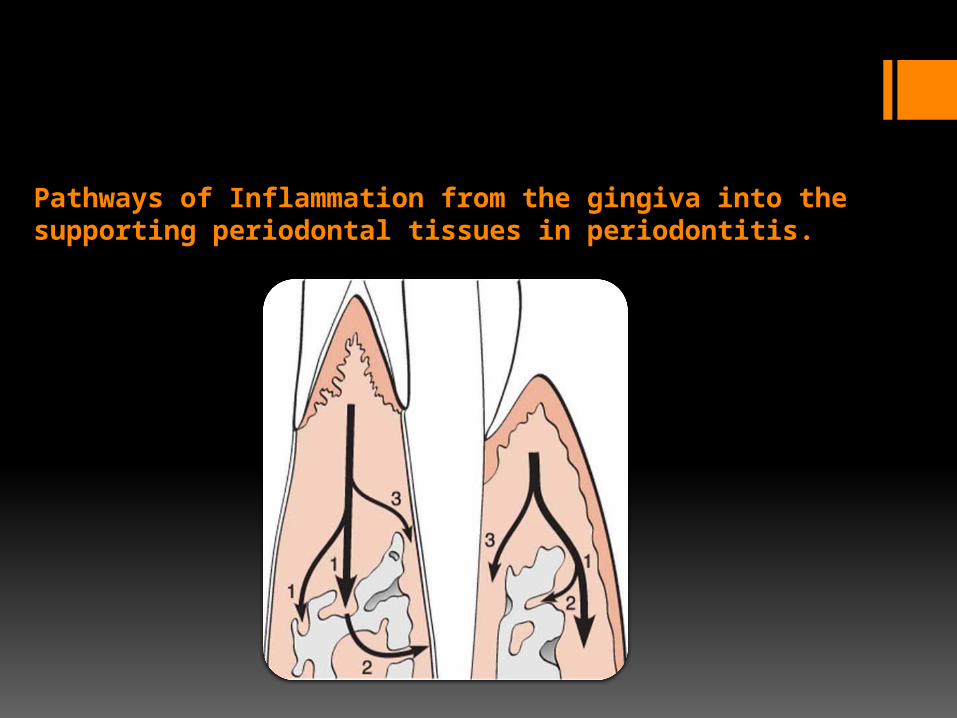
Pathways of Inflammation from the gingiva into the supporting periodontal tissues in periodontitis.
inflammationHistopathological changes during gingival inflammation
Gingival inflammation extends along the
collagen fiber bundle and follows the course of
blood vessels through the loosely arranged
tissue around them into the alveolar bone.
The inflammatory infiltrate is concentrated
in the marginal periodontium, the
reaction is a much more diffuse one, often
reaching the bone and eliciting a response before evidence of
crestal resorption or loss of attachment exists.

Area of inflammation extending from the
gingiva into the suprabony area.

INTERDENTAL BONE LOSS
Less frequently, the inflammation spreads from the
gingiva in the periodontal
ligament and from there in the
interdental septum.
Facially and Lingually,
inflammation from the gingiva
spreads along the outer periosteal
surface of the bone and penetrates into the marrow spaces
through vessel channels in the
outer cortex.

After inflammation reaches the bone, it spreads into the marrow spaces and replaces the marrow with a
leukocytic and fluid exudate, new blood vessels and proliferating fibroblasts.
Multinuclear osteoclasts and mononuclear phagocytes increase in number, and the bone surfaces appear, lined with Howship lacunae.
In the marrow spaces, resorption proceeds from within, causing a thinning of the surrounding bony trabeculae and enlargement of the marrow spaces, followed by destruction of the bone and a reduction
in bone height .

Local Factors Involved In Bone Destruction In Periodontal Disease
Plaque and its associated bacteria which populate the periodontal pocket, release lipopolysaccharide and other bacterial products into the sulcus, affecting both the immune cells in the connective tissue as well as the osteoblasts.
These products induce local factor production including IL-1α, IL-1β, IL-6, prostaglandin E2 and TNF-α.

These factors increase osteoclast formation and activation as well as inhibit osteoblast function.
The bacterial products also affect the osteoblasts directly, inhibiting their function and inducing factor production and release, eventually inducing pre - osteoclast differentiation and osteoblast activation.

Garant and Cho in 1979 suggested that locally produced bone resorption factors may need to be present in the
proximity of the bone surface to exert their action.
Page and Schroeder in 1982 , on the basis of Waerhaug’s measurement made an human autopsy, postulated a
range of effectiveness of about 1.5 – 2.5 mm within which bacterial plaque can induce loss of bone.
RADIUS OF ACTION

Beyond 2.5 mm there is no effect.
Interproximal angular defect can appear only in
spaces that are wider than 2.5 mm because
narrower spaces would be destroyed entirely.
Tal in 1984 corroborated this with measurements
in human patients.
(Tal H. Relationship between interproximal
distance of roots and the prevalence of intrabony pockets. J Periodontol
1984: 55: 604–607
Large defects greatly exceeding a distance of 2.5 mm
from the tooth surfaces (as described in aggressive types
of periodontitis) may be caused by the presence of bacteria in
the tissues.
(Carranza FA Jr , Cabrini RL : Histometric studies of
periodontal tissues ,Periodontics
5 :308 ,1967)

In a study of Sri lankan tea laborers with no oral hygiene , Loe et al in 1986 , found rate of bone loss to average about 0.2 mm a year for facial surfaces and
about 0.3 mm a year for proximal surfaces when periodontal disease was allowed to progress
untreated .
(Loe H, Anerud A , Boysen H : Natural history of periodontal disease in man; rapid , moderate ,and no loss of attachment in sri lankan laborers 14 to 46 yrs
of age ,J Periodontal 13 :432,1986)
RATE OF BONE LOSS
1. Approximately 8% of persons had rapid progression of periodontal disease, characterized by a yearly loss of attachment
of 0.1 to 1.0 mm .
2. Approximately 81% of individuals had moderately progressive periodontal disease, with a yearly loss of attachment of 0.05 to 0.5
mm
3. The remaining 11% of persons had minimal or no progression of destructive disease (0.05 - 0.09 mm yearly).
(Loe H, Anerud A , Boysen H : Natural history of periodontal disease in man; the rate of periodontal destruction before 40 yrs of
age, J Periodontal 49:607;1978
Loe et al in 1978 identified the following three subgroups of patients with periodontal disease based on interproximal loss of attachment and tooth mobility :

Periodontal destruction occurs in an episodic, intermittent manner, with periods of inactivity or
quiescence .
The destructive periods leads to loss of collagen and alveolar bone “ with deepening of the periodontal
pocket ’’.
PERIODS OF DESTRUCTION

Bursts of destructive activity are associated with sub gingival ulceration and an acute inflammatory reaction resulting in rapid loss of alveolar bone.
(Page RC, Schroeder HE, Lindhe J in 1982)
Bursts of destructive activity coincide with the conversion of predominantly t - lymphocytes to
lesion to one with a predominance of B –lymphocytes - plasma cell infiltration. (Seymour GJ, Powell RN, Davies WJR in 1979)

Periods of exacerbation are associated with an increase of the loose,
unattached, motile, gram negative flora with a tendency to
mineralize.
(Newman MG in 1979)
Tissue invasion by one or several bacterial
species is followed by an advanced local host defense that controls
the attack.
(Saglie RF, Renzende M, Pertuiser J, et al in
1987)

Mechanisms of alveolar bone destruction in periodontitis

Calcium blood levels
Release of PTH
Stimulates osteoblast
Release IL 1 & 6
Stimulates Monocytes
to migrate to bone
LIF+monocytes
Resorb bone

Release of Ca
PTH
Breakdown of
collagen
Release of
osteogenic
substrates
Stim & diff of
osteoblasts
Deposition of bone

Plaque products induce the
differentiation of bone progenitor cells into osteoclasts and
stimulate gingival cells to release
mediators that have the same effect.
(Hausmann E, Raisz LG , Miller WA ,1970)
They also act directly on
osteoblasts or their progenitors,
inhibiting their action and
reducing their numbers.

In addition, in rapidly progressing
periodontitis, bacterial micro colonies or
single bacterial cells may be present
between collagen fibers and over the bone
surface, suggesting a direct effect. (Schwartz Z , Goultschin J ,Dean
DD et al : Mechanism of alveolar bone destruction in periodontitis,
Periodontal 2000,14: 158 ,1997.)
Host factors released by inflammatory cells capable of inducing
bone resorption includes
prostaglandins and their precursors,
interleukin 1-α and β and TNF-α.

When injected intradermally, PGE2
induces the vascular changes seen in
inflammation ,when injected over bone
surface, it induces bone resorption in the
absence of inflammatory cell and
within few multinucleated
osteoclasts.
( Goodson JM , Haffajee AD ,
Socransky SS :1984 )
In addition non steroidal anti
inflammatory drugs, flurbiprofen or
ibuprofen, inhibit PGE2
production, slowing bone destruction in naturally occurring
periodontal diseases.
( Jeffcoat MK , William RC , Wachter WJ et al ,
1986)

HAUSMANN CONCEPTS OF BONE LOSS
Bone progenitor cells induces the differentiation of the cells into osteoclasts
Destroying bone through a non-cellular mechanism
Stimulates gingival cells, causing them to release mediators, which inturn induce bone progenitor cells to differentiate into osteoclasts
Cause gingival cells to release agents that can act as cofactors in bone resorption
Cause gingival cells to release agents tha destroy bone by direct chemical action without osteoclasts

PHARMACOLOGICAL AGENTS
Prostaglandins
Flurbiprofen
Lymphocytes (Horton & co—workers)
Proteolytic enzymes

OSTEOIMMUNOLOGY
INFLAMMATORY FORNT
CONCENTRATION OF MEDIATORS PENETRATE GINGIVAL TISSUES
INFLAMMATORY MEDIATORS AND BONE RESORPTION
cause inhibit
IL- 1,6,11,17, TNFα IL- 4,10,12,13,18, INF α / β

RECEPTOR ACTIVATOR OF NUCLEAR FACTOR-KAPPA B LIGAND RANKL
RANK/OPG 3.33:1.89 1.8:4.0
Crotti T, Smith MD, Hirsch R, et al. Receptor activator NF kappaB ligand (RANKL) and osteoprotegerin (OPG) protein expression in periodontitis. J Periodontal Res 2003;38:380-387.

The effect of occlusal forces on periodontium
MAGNITUDE
DURATION
FREQUENCY
DIRECTION

TFO in absence of inflammationpersistent trauma from occlusion results in “funnel-shaped widening” of the crestal portion of the periodontal ligament
"cushioning" When combined with inflammation, trauma from occlusion aggravates the bone destruction caused by the inflammation and results in bizarre bone patterns.

GLICKMAN’S CONCEPT (1965, 1967)
The pathway of the spread of a plaque-associated gingival lesion can change if
forces of an abnormal magnitude are acting
on teeth harboring subgingival plaque.
This would imply that the character of the progressive tissue destruction of the periodontium at a
"traumatized tooth" will be different from that characterizing a “non-
traumatized" tooth.

Based on this concept, the periodontal structures can be
divided into two zones:
Zone of irritation
Zone of co-destruction

It includes the marginal and interdental gingiva.
The soft tissues of this zone are bordered by hard tissue only on
side and this zone is not affected by forces
of occlusion.
Therefore, gingival inflammation is the
result of irritation from microbial deposits, not
from trauma from occlusion.
ZONE OF IRRITATION

This zone includes the PDL, the root cementum and the alveolar bone.
It is coronally demarcated by the transseptal and the
dentoalveolar collagen fiber bundles and is the seat of a lesion caused
by trauma from occlusion.
ZONE OF CO-DESTRUCTION

The fiber bundles which separate the zone of co-destruction from the zone of
irritation can be affected from two different directions:
from the inflammatory lesion maintained by plaque in the
zone of irritation.
from trauma induced changes in the zone of
co-destruction

WAERHAUG’S CONCEPT ( 1979 )
Waerhaug (1979) measured the distance
between the subgingival plaque and the periphery
of the associated inflammatory cell
infiltrate in the gingiva and the surface of the
adjacent alveolar bone.( in addition to Glickman
concept.)
He concluded that angular bony defects and infrabony pockets occur
equally often at periodontal sites of teeth which are not affected by
TFO as in traumatized teeth.

Loss of connective tissue attachment and the resorption of bone
around teeth are exclusively the result of
inflammatory lesions associated with
subgingival plaque.
Angular bony defects and infrabony pockets
occur when the subgingival plaque of tooth has reached a
more apical level than the microbiota of the
neighboring tooth and the volume of the
alveolar bone surrounding the roots is
comparatively large.

CLINICAL TRIALS
Several authors had conducted clinical trials in human patients and arrived at the following
conclusions:Rosling et al, 1976 : The infrabony pocket located at
hypermobile teeth exhibited the same degree of healing as those adjacent to firm teeth. (Rosling, B.,
Nyman, S. & Lindhe, J. (1976). The effect of systematic plaque control on bone regeneration in
infrabony pockets. Journal of Clinical Periodontology 3, 38-53.)

Fleszar et al, 1980 : Pockets of clinically mobile teeth do
not respond as well to periodontal treatment as
those of firm teeth exhibiting the same disease
activity.
(Fleszar, T.J., Knowles, J.W., Morrison, E.C., Burgett, F.G., Nissle, R.R. & Ramfjord, S.P.
(1980). Tooth mobility and periodontal therapy. Journal of Clinical Periodontology 7,
495-505.)
Pihlstrom et al, 1986 : teeth with increased mobility and widened PDL space had, in fact, deeper pockets, more attachment loss and less bone support than teeth
without these symptoms.
(Pihlstrom , B.L., Anderson K.A., Aeppli D. & Schaffer E.M. (1986). Association
between signs of trauma from occlusion and periodontitis.
Journal of Periodontology 57, 1-6.)

Burgett et al (1992) : Probing attachment
gain was on the average about 0.5mm larger in patients who received scaling and occlusal adjustment than in patients in whom the occlusal adjustment was not
included.
(Burgett F, Ramfjord S., Nissle R., Morrison E.,
Charbeneau T.& Caffesse R. (1992). A randomized trial of
occlusal adjustment in the treatment of
periodontitis patients. Journal of Clinical Periodontology 19,
381-387

Neiderud et al, 1992 : Tissue alterations which occur at mobile teeth with clinically healthy
gingiva may reduce the resistance offered by the periodontal tissues to probing.
Neiderud, A-M., Ericsson, I. & Lindhe, J. (1992). Probing pocket depth at mobile/ nonmobile teeth.
Journal of Clinical Periodontology 19, 754-759.

These studies involved the placement of high crowns or restorations on the teeth of dogs or
monkeys, resulting in a continuous or intermittent force in one direction.
When a tooth is exposed to unilateral forces of a magnitude , frequency or duration that its
periodontal tissues are unable to withstand and distribute while maintaining stability of the tooth,
certain well-defined reactions develop in the periodontal structures to the altered functional
demand.
ANIMAL EXPERIMENTS (Orthodontic Type Trauma)

When horizontally directed forces are
applied, the tooth tilts in direction of the
force resulting in the development of
pressure and tension zones within the
marginal and apical parts, the tooth
becomes hypermobile temporarily, moves to
a new position and healing takes place.
There is no gingival inflammation or loss of connective tissue
attachment in a healthy periodontium.

Radiographic signs of TFO may include the following:
Increased width of periodontal space, often with thickening of the lamina dura along the lateral aspect
of the root, in the apical region and in bifurcation areas.
These changes do not necessarily indicate destructive changes because they may result from
thickening and strengthening of the periodontal ligament and alveolar bone, constituting a favorable
response to increased occlusal forces.

A “vertical” rather than “horizontal”
destruction of the interdental septum.
Radioluscence and condensation of the
alveolar bone.
Root resorption

FACTORS DETERMINING BONE MORPHOLOGY IN PERIODONTAL
DISEASE
Normal Variation in Alveolar Bone
morphologic feature (which affects the osseous contours
produced by periodontal disease)
The anatomic features that substantially affect
the bone destructive pattern in periodontal disease include the
following:

The thickness, width and crestal angulation of the interdental septa .
The thickness of the facial and
lingual alveolar plates.
The presence of fenestrations
and dehiscence.
The alignment of the teeth .
Root and root trunk anatomy.
Root position within the
alveolar process.
Proximity with another
tooth surface.

Bone Deformities(Osseous Defects)

CLASSIFICATIONS
Goldman & Cohen (1958) classified angular defects as:-
Depending on number of walls present – Three osseous walls
Proximal, buccal and lingual walls Buccal, mesial and distal wall Lingual, mesial and distal walls

Two osseous walls Buccal and lingual walls (crater) Buccal and proximal wall Lingual and proximal walls
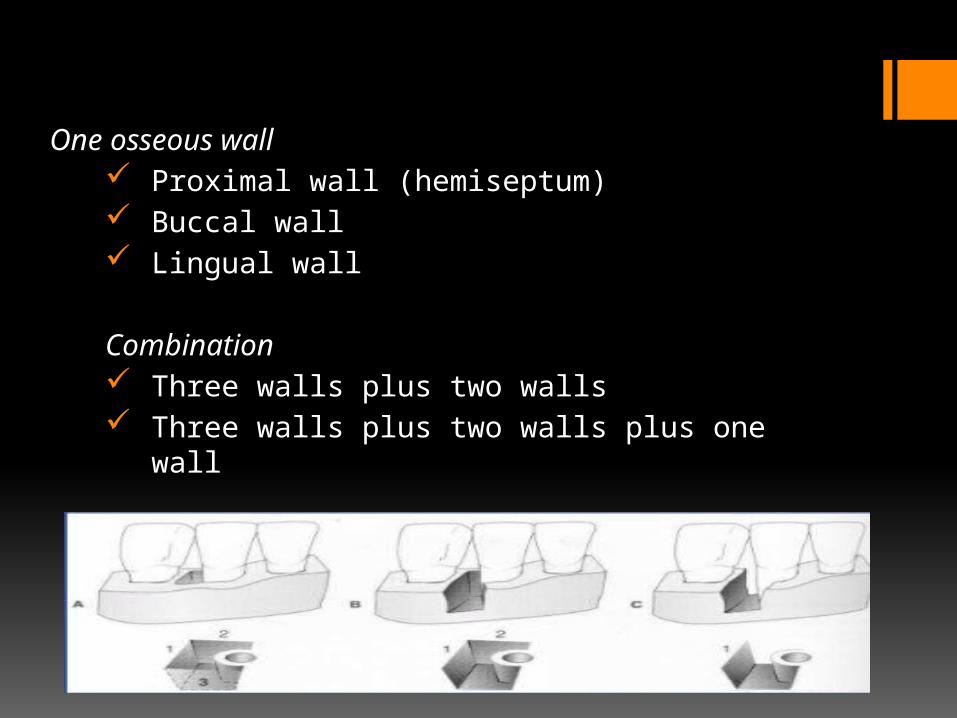
One osseous wall Proximal wall (hemiseptum) Buccal wall Lingual wall
Combination Three walls plus two walls Three walls plus two walls plus one wall

Glickman (1964) :
1) Vertical or angular defects 2) Osseous craters 3) Bulbous bone contours 4) Reverse architecture 5) Ledges 6) Furcation involvement

Karn et al (1983) :
1) Horizontal bone loss 2) Crater 3) Trench 4) Moat 5) Ramp 6) Cratered ramp 7) Ramp into a crater or trench

Prichards classification (1985):
• Interproximal craters• Inconsistent margins• Hemisepta• Furcation involvement • Intrabony defects• Combination of these defects
GRANTS CLASSIFICATION
A. Vestibular, lingual or palatal defects associated with
1) Normal anatomic structures External oblique ridge Retromolar triangle Mylohyoid ridge Zygomatic process
2) Exostoses or tori Mandibular lingual tori Buccal and posterior palatal exostoses
3) Dehiscence 4) Fenestration 5) Reverse osseous architecture

B. Vertical defects: i. Three wallii. Two walliii. One walliv. Combination
C. Furcation involvement

Panos & Toneiti (2000) classified osseous defects as
Suprabony defects Infrabony defects
Craters Intrabony defects
1 walled 2 walled 3 walled Combination
Interradicular defects (Furcation involvement)
Horizontal classificationClass IClass IIClass IIIVertical classification

According to the classification by Goldman & Cohen ( Goldman HM , Cohen WD. The infrabony pocket : classification and treatment .J Periodontal 1958 )
Suprabony defects are those where the base of the pocket is located coronal to the alveolar crest.
Infrabony defects, on the other hand, are defined by the apical location of the base of the pocket with respect to the residual alveolar crest.

HORIZONTAL BONE LOSS

VERTICAL OR ANGULAR DEFECTS:
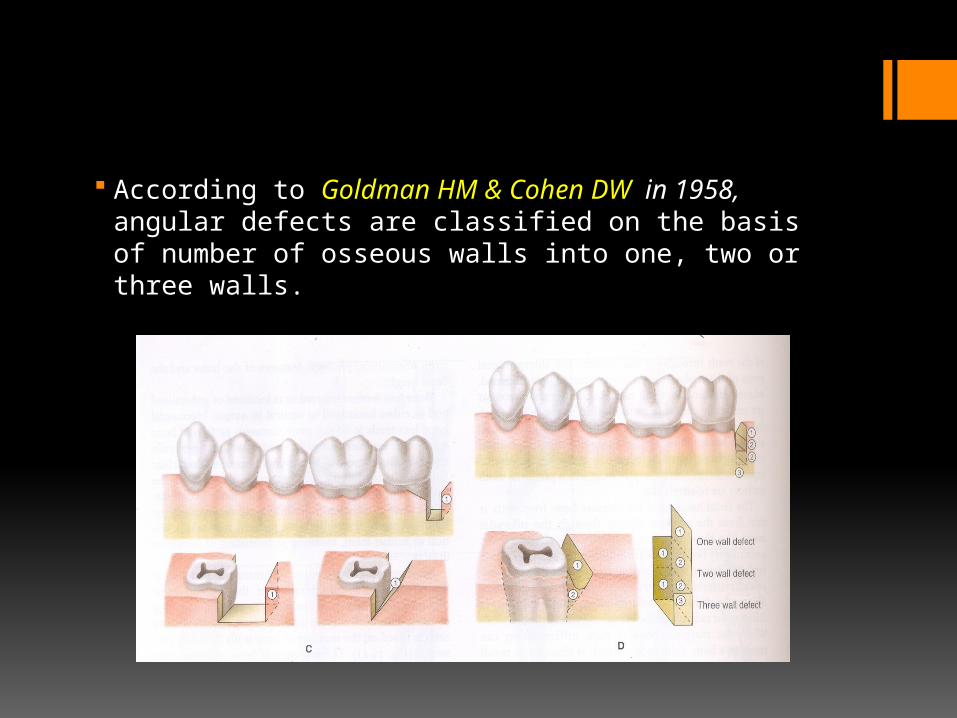
According to Goldman HM & Cohen DW in 1958, angular defects are classified on the basis of number of osseous walls into one, two or three walls.

Frequently, intrabony defects present a complex anatomy consisting of a three-wall component in the most apical portion of the defect, and two- and / or one-wall components in the more superficial portions. Such defects are frequently referred to as combination defects.

Hemiseptal defects, that is, vertical defects in the presence of adjacent roots and where half of a septum remains on one tooth, represent a special case of one wall defects.

However, most intrabony defects are of mixed types; eg, the entrance is one wall or two walls but the bottom is three walls.
A defect that extends to the tooth and surrounds the tooth continuously to two or more roots is called circumferential defect.

Vertical defects detected radiographically have been reported to appear most commonly on the distal surface
(Neilson JI, Glavind L, Karring T: J Clin Periodontol; 1980)
And mesial surfaces. (Papapanou, Wennstrom , Grondahl ; Journal of
clinical periodontology.1988; 15(7):469-78. Radiographic and clinical assessments of destructive periodontal disease.)
However three wall defects are more frequently found on the mesial surfaces of upper and lower molar.
(Larato DC in 1970)

OSSEOUS CRATERS
(Manson JD ,Nicholson K, The distribution of bone defects in chronic periodontitis , J Periodontal 1976)

Manson and Nicholson in 1974 reported that the interdental crater was found to represent one third ( 35.2 % ) of all maxillary defects and about two-thirds (62 %) of all mandibular defects.
Early to moderate interproximal craters often do not cause loss in papillary height.
They are seen as irregular areas of reduced radiopacity in the alveolar bone crest.
( Manson JD ,Nicholson K : The distribution of bone defects in chronic periodontitis, J Periodontal 54 : 88-92,1974.)

Ochsenbein divided bony craters into three basic types :
Crater type Dimension Shallow crater 1 -2 mm Medium crater 3 -4 mm Deep crater 5 mm or more
(Ochsenbein C :A Primer for osseous surgery, Int J Periodontics Restorative Dent 6(1):9,1986)

The heights of the facial and lingual crests of a crater have been found to be identical in 85% of cases, with the remaining 15% being almost equally divided between higher facial crests
and higher lingual crests.
The interdental area collects plaque and is difficult to clean.
The normal flat or even concave faciolingual shape of the interdental septum in lower molars may favor crater formation.
Vascular patterns from the gingiva to the center of the crest may provide a pathway for inflammation

EXOSTOSES
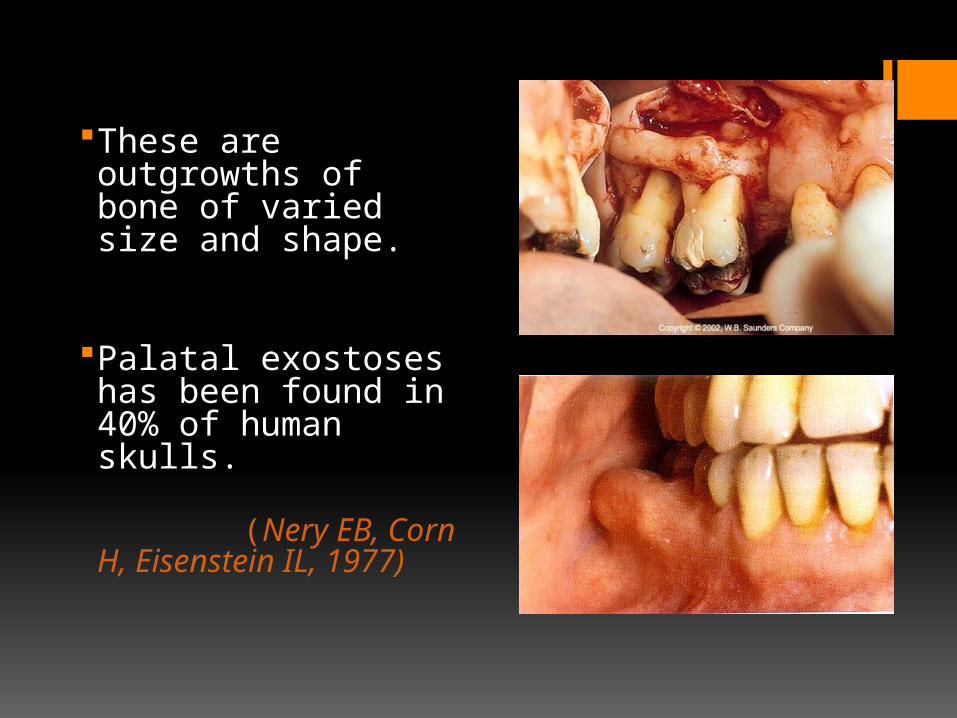
These are outgrowths of bone of varied size and shape.
Palatal exostoses has been found in 40% of human skulls.
(Nery EB, Corn H, Eisenstein IL, 1977)
Buccal exostoses : These are seen in about 25% of all teeth, and 77% of all individuals. They may be expressed as alveolar margin lippings(18 % of all teeth ) or as larger and more globular buccal exostoses (7% of all teeth).
Lingual Exostoses : this may be seen in 11% of all teeth, and in 50% of all individuals.
(Horning GM, Cohen ME, Neils TA, Buccal alveolar exostoses : prevalence ,characteristics and evidence for buttressing bone formation. J Periodontal 2000 ;71;1032 – 1042)
Several bony overgrowth occur on the vestibular alveolar bone and are called multiple exostoses.

A definitive female sex predilection is characteristic of this condition, which usually presents in the canine – premolar area of the mandible or maxilla.
EXOSTOSES IN THE FACIAL ASPECT OF SECOND PREMOLAR AND MOLARS
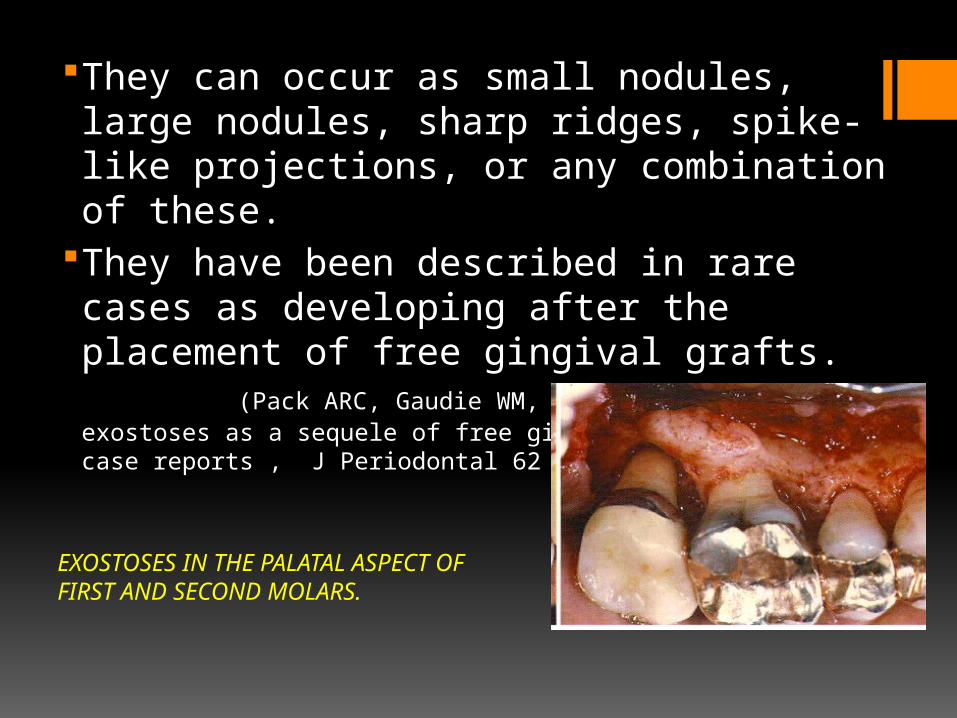
They can occur as small nodules, large nodules, sharp ridges, spike-like projections, or any combination of these.
They have been described in rare cases as developing after the placement of free gingival grafts. (Pack ARC, Gaudie WM, Jennings AM: Bony exostoses as a sequele of free gingival grafting : two case reports , J Periodontal 62 : 269,1991)
EXOSTOSES IN THE PALATAL ASPECT OF FIRST AND SECOND MOLARS.
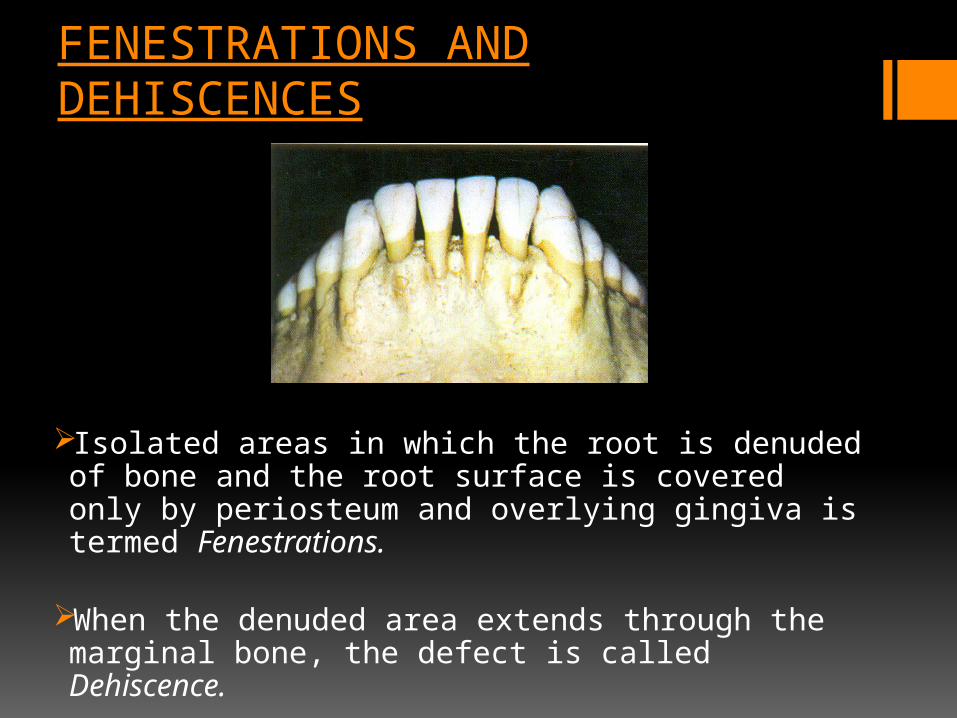
FENESTRATIONS AND DEHISCENCES
Isolated areas in which the root is denuded of bone and the root surface is covered only by periosteum and overlying gingiva is termed Fenestrations.
When the denuded area extends through the marginal bone, the defect is called Dehiscence.
They occur more often on the facial bone than on the lingual and more common in anterior teeth and frequently bilateral. These are important because they may complicate the outcome of periodontal surgery.
Approximately occurs on 20% of teeth.

Prominent root contours ,malposition and labial protrusion of the root combined with thin bony plate are predisposing factors. ( Elliot JR ,Bowers GM : Alveolar Dehiscence and fenestrations. Periodontics 1 : 245 ,1963 )

BUTTRESSING BONE FORMATION
Bone formation sometimes occurs in an attempt to buttress the bony trabeculae weakened by resorption.
When it occurs within the jaw, it is termed “central buttressing bone”
When it occurs on the external surface, it is referred to as “peripheral buttressing bone” formation.
This may cause bulging of bone contours, termed as “Lipping”
Buttressing bone formation in response to trauma from occlusion is a popular concept first proposed by Glickman and Smulow more than 35 yrs ago.
(Glickman I ,Smulow J: Buttressing bone formation in the periodontium, J Periodontal 36 : 365,1965 )

Buttressing bone formation has been described as the development of thickened or exostotic buccal alveolar bone in response to heavy occlusal forces.
In a study conducted by Horning GM ,Cohen, Neil's - Buccal alveolar bone enlargements were found in 25% of all teeth examined : 18% were expressed as marginal bony lippings and 7% as buccal exostoses.
(J Periodontal Jun 2000 ; Vol 71 (issue 6) : pg 1032-42 )

BULBOUS BONE CONTOUR :
( Manson JD ,Bone morphology and bone loss in periodontal disease ,JCP ,1976)

REVERSED ARCHITECTURE:

LEDGES

FURCATION INVOLVEMENT :
It refers to the invasion of the bifurcation and trifurcation of multirooted teeth by periodontal disease.
(Larato DC , J Periodontal ,1975) Mandibular first molar are the most common site
and maxillary premolar are the least common site.

CLASSIFICATION
One of the most widely used furcation classification systems was developed by Glickman (1958 ) .
In this system, furcation involvement is divided into four categories, primarily on the basis of the horizontal component of destruction

GRADE I Incipient bone loss
or early bone loss. The pocket is
suprabony and primarily affects the soft tissues.
Early furcation involvement just into the furcation is present.

GRADE II
Partial bone loss .
Distinct horizontal destruction of the furcation area is present. This lesion has been called a "cul de sac" because destruction may extend to any depth within the furcation, but does not extend all the way through the furcation to its other side.

The extent of horizontal probing determines whether the Grade II furcation is shallow or deep.
Vertical bone loss may or may not be present.
It can affect one or more furcations of the same tooth.

GRADE III
Total bone loss with through and through opening .
Bone is not attached to dome of furcation.
In early lesion, opening may be filled with soft tissue and may not be visible.
R/G found as a radiolucent area in the crotch of the tooth.

Destruction of bone and connective tissue all the way through the furcation such that an instrument can be passed from its opening to its exit.
The furcation defect is not visible to the eye because the gingival tissues cover the furcation entrance.

GRADE IV
Destruction of bone and connective tissue allthe way through the furcation.
Gingival recession hasoccurred to the point that the entire furcation invasion can be seen on visual examination.
PREVALENCE OF OSSEOUS DEFECTS
Nielsen et al conducted a study on 209 adult patients, osseous morphology was recorded in radiographs, the lesions with a depth and width of >= 2 mm were considered to be ‘‘periodontal intrabony defects”. (Nielsen IM, Glavind L, Karring T. Interproximal periodontal intrabony defects. Prevalence, localization and etiological factors. J Clin Periodontol 1980: 7: 187–198.)
18% of the subjects displayed >= 1 defects; higher prevalence was noted in older age groups;

Defects occurred equally frequently with respect to tooth type but more often at distal than mesial surfaces.
The presence of intrabony defects correlated with loss of attachment, increased tooth mobility, a wide interproximal space and open interdental mesiodistal contact relationships .

In a study by Papapanou et al - 531 dentate individuals aged 25–75 years angular defects were assessed in periapical or bite-wing radiographs.
(Papapanou PN, Wennstrom JL, Grondahl K. Periodontal status in relation to age and tooth type. A cross-sectional radiographic study. J Clin Periodontol 1988: 15: 469–478)
A defect was considered present if the ‘‘bottom of the oblique radiolucency was located >= 2 mm apical to the most coronal level of the interproximal alveolar bone and radiographic signs of bone resorption in the lateral boundary of the defect was evident.

Angular defects were registered at 8% of all teeth .
The frequency increased with age. It was higher at mesial than distal tooth surfaces (ratio 1.6 : 1)
Defects occurred most frequently adjacent to maxillary first premolars (14%) followed by mandibular second molars (12%) and second premolars (11%).

Wouters et al. studied 733 randomly selected dentate individuals aged > =20 years; presence of ‘‘intrabony’’ defects was recorded in x5-magnified periapical radiographs, defects were required to be >=1 mm wide and >=2 mm deep.
Defects were recorded in 32% of the subjects.
The number of defects per subject ranged from 1 to 15.
Prevalence increased with age and was higher in men than women and on mesial than distal tooth.
( Wouters FR, Salonen LE, Hellden LB, Frithiof L. Prevalence of interproximal periodontal intrabony defects in an adult population in Sweden. A radiographic study. J Clin Periodontol 1989: 16: 144–149.)

CONCLUSION
REFERENCESMichael G. Newman, Henry H. Takei, Fermin A. Carranza; Clinical periodontology,9th edition.Jan Lindhe, Clinical Periodontology and Implant dentistry.Panos n. Papapanou & Maurizio S. Tonetti ; Diagnosis and epidemiology of periodontal osseous lesions ; Periodontology 2000, Vol. 22, 2000, 8–21.Rose, Mealey, Genco, Cohen – Periodontics Medicine, Surgery and ImplantsMarcello Cattabriga, Vinicio Pedrazzoli & Thomas G. Wilson Jr ; The conservative approach in the treatment of furcation lesions ; Periodontology 2000, Vol. 22, 2000, 133–153

Molecular and cellular biology of alveolar bone- Jaro Sodek & Marc D. Mckee - Perio 2000, vol.24 , 99 -126 .Grant and Lisgarten, PeriodonticsBuccal Alveolar Exostoses : Prevalence, Characteristics ,and Evidence for Buttressing Bone Formation - Gregory M. Horning ,Mark E. Cohen and Todd A. Neils, J Periodontal ,Vol- 71,Jun 2000

Related Documents











