Prof D.P S Gunasekera MBBS,MD, FRCP,FSLCP 10 th Annual Academic Sessions, USJP April 2015

Managing DHF in children: pitfalls & challenges
Jul 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Prof D.P S GunasekeraMBBS,MD, FRCP,FSLCP
10th Annual Academic Sessions, USJPApril 2015

What are the challenges?Is it viral fever OR Dengue fever?
Clinical features
High remittent fever
Severe arthralgia
Headache (retro-orbital)
Flushing of face

Pics –flushed face, petecahe
What are the challenges?In diagnosis
Is it viral fever OR Dengue fever?
Diagnostic tests help – Dengue Ag test(NS1)
Dengue Ab test
Dengue fever - simple Dengue fever?
OR DHF?

DF or DHF ?Clinical features
Warning signs
Ill looking – severe arthralgia
Headache (retro orbital)
Vomiting
RHC pain & tenderness (hepatomegally +)
Drowsy/ irritable/confused
Dizziness +
Bleeding from sites – petechae, gum bleeds, coffee ground vomitus
Deteriorates when fever settles
DF OR DHF?Warning signs
signs of circulatory compromise
Low volume pulse, colds peripheries
HR ↑
Pulse pressure ↓ (<20mmHg)
CRT > 2 sec
UOP ↓
Ix – HCT > 20% rise: pitfall- what is baseline HCT?
If DHF → SHOCK/ NON SHOCK ?
What is the baseline HCT?

DHF – what stage? Febrile phase – 2-7 days
Critical phase – 48 -72 hours (leaking +)
Convalescent phase
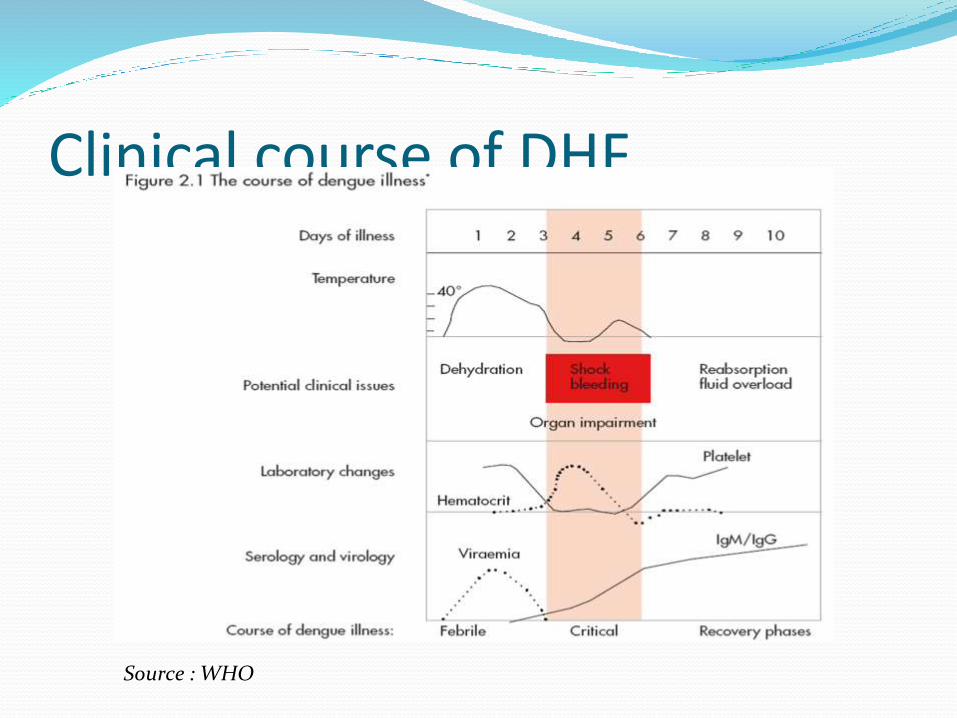
Clinical course of DHF
Source : WHO

In ManagementKey issues
Know clinical sequence of events
Meticulous monitoring in critical stage
replace lost fluid:
rapidly & adequately know when to stop!
*Do not overload*

Mx – critical phase Pitfalls – erratic rate of leakage
rapid leakage – in first 24 hours
extravasation of fluid –
into pleural &peritoneal cavities
Patient ay remain
conscious
Mx- critical phase (cont) METICULOUS monitoring
RAPID replacement with IV fluid
ADJUST IV fluid rates : (M + 5%) ↑↓
Give ISOTONIC solution (Normal saline)
Give colloids (Dextran 40) on time
CHALLENGE Too much fluid → more extravasation→
later→ pulmonary oedema
Too little fluid → shock

Challenges : critical phaseHaemorrhage Massive, concealed H’age
Pitfalls: hypovolemic changes already there
HCT already high → may not show classic ‘Low’
signs of H’age→ HR↑, systolic BP↓,M. acidosis +
Look for ‘drop’ in HCT
Replacement with Dextran - 40 bolus → reduces HCT by 10 (max)
Dengue Shock Syndrome(DSS)Management -
RAPID replacement of fluid:
10ml/kg IV bolus of N. saline
If no improvement → Dextran 40(10ml/Kg/hr)
If no improvement → LOOK for concealed H’age
Challenge
timely detection & Rx

Challenges in DSS early detection vital
Rapid replacement of fluid/blood
Prolonged shock → metabolic acidosis
organ dysfunction
liver failure, ARF, DIC
myocarditis
dengue encephalopathy

Convalescent Phase Clinical Improvement
Convalescent rash
Reabsorption of leaked fluid
Circ. Signs reversed -
HR↓
Pulse Pressure wide
CRT < 2 secs
UOP ↑

Challenges:Convalescent Phase
Risk of pulmonary oedema
Continue monitoring - HR↓, HCT↓, wide PP
Look for signs of pulmonary oedema -
Cough, RR↑, lungs – rhonchi & crepts
STOP IV fluid
Furosemide IV SOS only

ConclusionKey to success in Mx –
Know clinical sequence
Timely detection of leakage/shock
Meticulous monitoring – critical stage
Adequate replacement with IV fluid
Timely blood Txn
Rx associated problems – Met acidosis
hypocalcaemia
hypoglycaemia
Stop fluid at Convalescence
Thank You
Related Documents


![Top Legal Pitfalls When Managing Employees [Webcast Part 2: Employment Stage]](https://static.cupdf.com/doc/110x72/55cd43ebbb61ebaa0a8b45b6/top-legal-pitfalls-when-managing-employees-webcast-part-2-employment-stage.jpg)








