Management of Paediatric SVT 1 of 8 1. Key Recommendations for operational use 1 Diagnosis of paediatric supra- ventricular tachycardia (SVT) SVT in a child usually is a narrow complex tachycardia. It can be difficult to distinguish from sinus tachycardia particularly in infants so consideration of other causes of tachycardia is important. Typical features usually include: Persistent heart rate >220bpm , can be lower Narrow complex regular tachycardia at a constant rate Patients may or may not present in a clinically shocked state 2 Access Early access is essential and can be gained by siting (ideally) two intra-venous cannulae or using the intra-osseous route early. 3 Management ABC approach Vagal manoeuvres Adenosine Amiodarone DC Cardioversion (As detailed on page 4-7) 4 Ongoing care If clinically stable and cardioverted the patient may be able to remain locally with ongoing joint care with the Scottish Paediatric Cardiac Service. If there are clinical concerns transfer to the Royal Hospital for Children may be required. 5 References See page 7

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Management of Paediatric SVT
1 of 8
1. Key Recommendations for operational use
1 Diagnosis of paediatric supra-ventricular tachycardia (SVT)
SVT in a child usually is a narrow complex tachycardia. It can be difficult to distinguish from sinus tachycardia particularly in infants so consideration of other causes of tachycardia is important. Typical features usually include:
Persistent heart rate >220bpm , can be lower Narrow complex regular tachycardia at a constant rate Patients may or may not present in a clinically shocked state
2 Access Early access is essential and can be gained by siting (ideally) two intra-venous cannulae or using the intra-osseous route early.
3 Management
ABC approach Vagal manoeuvres Adenosine Amiodarone DC Cardioversion
(As detailed on page 4-7)
4 Ongoing care
If clinically stable and cardioverted the patient may be able to remain locally with ongoing joint care with the Scottish Paediatric Cardiac Service. If there are clinical concerns transfer to the Royal Hospital for Children may be required.
5 References See page 7
Management of Paediatric SVT
2 of 8
2. Document History
Reference Number Version 1.0
Version 1
Writing group
(Chair in bold)
Mark Davidson Paediatric Intensivist ScotSTAR
Rebecca Goldman Consultant Pediatrician Ninewells
Karen McLeod Consultant Cardiologist RHC-Glasgow
Karen Pearson Consultant Anaesthetist Ninewells
Danni Seddon Consultant Anaesthetist RHC-Glasgow
Leanne Daly Retrieval Nurse ScotSTAR
Treasa Magee Retrieval Nurse ScotSTAR
Lauren Williams PICU Pharmacist RHC-Glasgow
Associate Medical Director Andrew Inglis
Date issued XX
Date for review XX
Distribution
BASICS Scotland X
Medic 1 X
Mountain rescue teams X
Referring centres via service websites ✓
Rural GPs Association of Scotland ✓
SAS
Air Ambulance for information
Specialist Services Desk for information
ScotSTAR
EMRS (West) ✓
EMRS (North) ✓
Paediatric ✓
Neonatal ✓
Management of Paediatric SVT
3 of 8
Tayside Trauma Team for information
3. Scope and purpose
• Overall objectives:
The aim of this guideline is to provide consistent guidance on the assessment and management of paediatric supra-
ventricular tachycardia (SVT).
The most common cause of paediatric tachyarrhythmia is a supra-ventricular tachycardia (SVT). These are common in
infancy and childhood with an incidence of between 1:250 and 1:1000. Most cases are due to re-entrant pathways and
occur in otherwise normal children. They can be very well tolerated for several hours meaning some children may not
present until hemodynamic compromise is evident. They can also present in patients with underlying congenital cardiac
conditions, cardiac conduction disorders or cardiac failure which may be secondary to the tachyarrhythmia. One should
remember to consider other causes of tachycardia including metabolic and electrolyte disturbance, sepsis, trauma and
poisoning.
• Statement of intent:
This guideline is not intended to be construed or to serve as a standard of care. Adherence to guideline recommendations
will not ensure a successful outcome in every case, nor should they be construed as including all proper methods of care
or excluding other acceptable methods of care aimed at the same results. The ultimate judgement must be made by the
appropriate healthcare professional(s) responsible for clinical decisions regarding a particular clinical procedure or
treatment plan. Clinicians using this guideline should work within their skill sets and usual scope of practice.
• Feedback:
Comments on this guideline can be sent to: [email protected]
• Equality Impact Assessment:
Applied to the ScotSTAR Clinical Standards group processes.
• Guideline process endorsed by the Scottish Trauma Network Prehospital, Transfer and Retrieval group,
as well as the Scottish Paediatric Cardiac Service Guidelines Group.
Management of Paediatric SVT
4 of 8
4. Diagnosis & Management of Paediatric SVT
4.1 Diagnosis of SVT Authors’
recommendation Level
[Reference]
This pathway is relevant to patients with broad or narrow complex tachycardia with input from a paediatric cardiology specialist. SVT in a child is usually but not always a narrow complex tachycardia. It can be difficult to distinguish from sinus tachycardia particularly in infants so consideration of other causes of tachycardia is important.
Typical features usually include: o Persistent heart rate >220bpm (can be lower) o Narrow complex regular tachycardia at a constant rate o If seen there are p waves after every QRS complex, at the onset of the T wave
Clinical assessment may show: o No signs of shock:
Poor feeding Dyspnoea, pallor, palpitations, tachypnea, chest discomfort
o Signs of cardiogenic shock: Low BP & prolonged capillary refill Hepatomegaly Agitation or confusion (though conscious state in infants and children
may be normal) 12 lead ECG assessment:
o Narrow complex tachycardia o P waves often difficult to see, if seen usually at onset of T wave
Strong 1-3
4.2 Access Authors’
recommendation Level
[Reference]
IV access is the preferred route for administration of drugs in these patients. If the patient is haemodynamically compromised, IO access is appropriate. In patients in whom peripheral IV access is difficult then sedation to obtain either peripheral or central access may be required. Ultrasound guided IV access may be useful in this instance, together with topical local anaesthesia. Sedation guidelines with doses may be found at on the GGC paediatric anaesthetic guideline website, choice of agent or agents will be guided by local familiarity with the drugs. Further advice can be found at: https://www.clinicalguidelines.scot.nhs.uk/nhsggc-paediatric-clinical-guidelines/nhsggc-guidelines/anaesthetics/premedication-guideline-for-paediatric-patients-prior-to-general-anaesthesia/
Strong 2-3
Management of Paediatric SVT
5 of 8
4.3 Management of SVT Authors’
recommendation Level
[Reference]
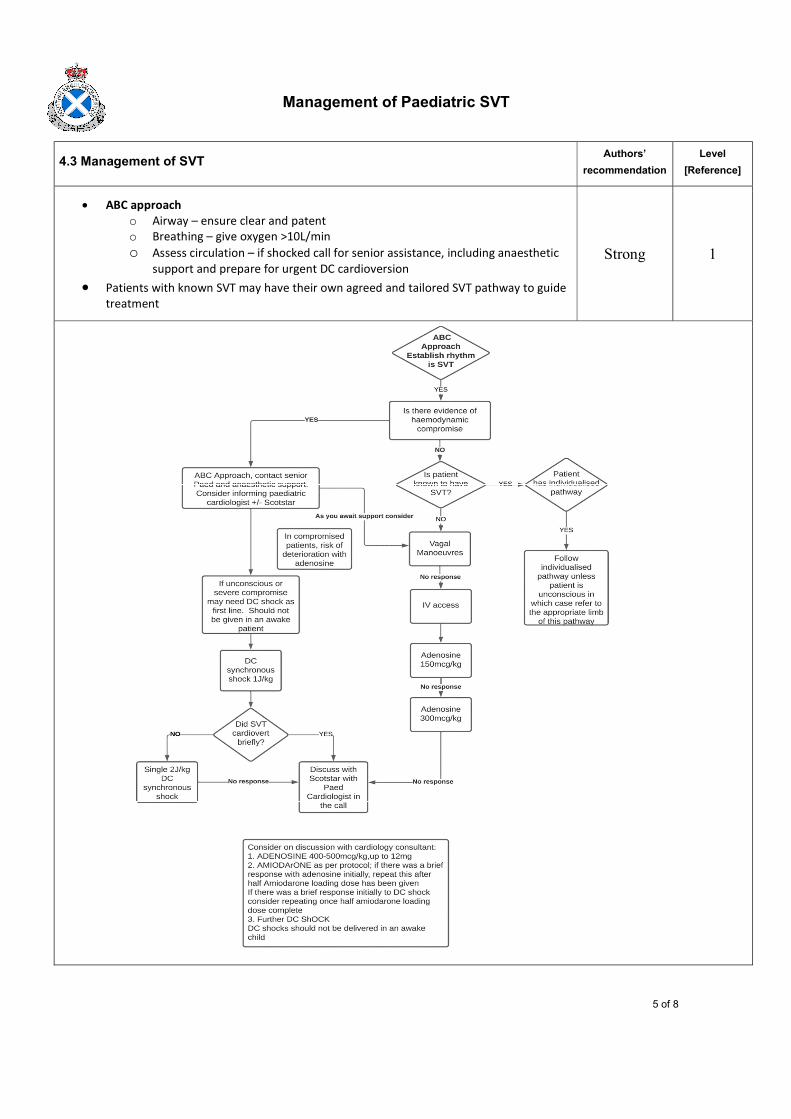
ABC approach o Airway – ensure clear and patent o Breathing – give oxygen >10L/min o Assess circulation – if shocked call for senior assistance, including anaesthetic
support and prepare for urgent DC cardioversion Patients with known SVT may have their own agreed and tailored SVT pathway to guide
treatment
Strong 1
Management of Paediatric SVT
6 of 8
Vagal manoeuvres (only if not clinically shocked) o Neonates & infants (ie < 1 year old) – facial immersion in iced water
Ensure monitoring (ECG, SpO2 & BP) in place on patient Explain to family Wrap patient and their arms in towel Immerse whole face in iced water for 5 seconds – do not need to
occlude airway – this will work in 90% cases o Toddlers
Apply facecloth soaked in ice cold water to face for 30 seconds Eyeball pressure is not recommended
o School aged children Valsalva technique
blow hard for 15 seconds on “thumb in mouth” after full inspiration or
blow as hard as possible through a syringe from the plunger end (with the plunger out obviously), if need be asking them to raise a suspended tissue as high as possible with the air jet.
Headstand Child can be helped, with appropriate adult support, to
perform a headstand
Strong 1
Adenosine o Administer preferably via large cannula in proximal vein with 3-way tap
attached o Ensure ECG attached and recording running o Remember adenosine can cause hypotension, chest tightness, flushing and can
cause bronchospasm, though is not contra-indicated in wheeze or asthma o Standard Adenosine vials are a solution of 6mg/2ml – do not reconstitute o Adenosine 150micrograms/kg (max 12mg) by fast injection followed rapidly
with 10ml flush of 0.9% NaCl (Sodium Chloride) o Wait 2 mins – if no return to sinus rhythm then give a second dose of
adenosine 300micrograms/kg (max 12mg) by fast injection followed rapidly with 10ml flush of 0.9% NaCl (Sodium Chloride)
o If there is no response at this stage contact ScotSTAR Pediatric Retrieval team who will dial in the Paediatric Cardiologist & Duty Cardiac Intensivist at the Royal Hospital for Children, Glasgow for further advice - further options include:
3rd dose of adenosine (400-500micrograms/kg (max 12mg)) IV amiodarone (see below) DC cardioversion (see below)
Strong 1-3
Management of Paediatric SVT
7 of 8
Amiodarone o Make up Amiodarone infusion as follows:
Concentration must be 100mg/50ml (2mg/ml) This concentration is safe to run via a peripheral or central line Calculate rates of infusion as per equations below (round rate to one
decimal place) 50mg/ml Ampoule already in solution – no reconstitution required Draw up required volume for concentration and add to glucose 5%
(volume of glucose = 50ml – volume drawn up from ampoule) Glucose 5% must be used (incompatible with saline) Standard dose delivery is as follows:
Loading dose 25micrograms/kg/min for 4 hours followed by a maintenance infusion of 15micrograms/kg/min as noted below.
Amiodarone loading dose infusion rate in ml/hr = (1.5 x patient weight in kg) / 2
Amiodarone maintenance infusion rate in ml/hr = 0.9 x patient weight (kg) / 2
o Example calculations: for a 5kg patient:
Loading dose infusion rate = (1.5 x 5)/2 = 3.8ml/hr Maintenance infusion rate = (0.9 x 5)/2 = 2.3ml/hr
for a 10kg patient Loading dose infusion rate = (1.5 x 10)/2 = 7.5ml/hr Maintenance infusion rate = (0.9 x 10)/2 = 4.5ml/hr
o Ideally amiodarone should be given via a dedicated point of access for this drug
alone. o Once amiodarone loading dose is completed a further dose of adenosine may
be given to return to sinus rhythm
Strong 2-3
DC cardioversion o If resistant to therapies noted above or if clinically shocked then DC
cardioversion may be required o Sedation is required for DC cardioversion unless the patient is unconscious
If sedation has been used to obtain intravenous (iv) access then this may be supplemented as required.
Sedative agents should be considered in terms of haemodynamic stability, and are at the discretion of the local anaesthetic team and advice from the ScotSTAR team who may advise 1-2mg/kg ketamine to be appropriate depending on the clinical condition of the patient and sedation already used. Patients may be haemodynamically unstable at the time of intubation and clear allocation of roles to plan for all eventualities, including the need for CPR, is recommended. Early intubation prior to further deterioration is encouraged.
Intubation – Ketamine 2mg/kg & Rocuronium 1mg/kg as per ScotSTAR intubation SOP
Maintenance of tube tolerance – Morphine 30micrograms/kg/min & Midazolam 0.05 mg/kg/min or if >5years old Propofol infusions
o Synchronised DC shock 1 J/kg If clinical deterioration into Polymorphic VT or VF then unsynchronised
shock as per APLS pathway
Strong 1-3
Management of Paediatric SVT
8 of 8
4.3 Ongoing care for paediatric patients with an episode of SVT Authors’
recommendation Level
[Reference]
If the patient is not being transferred their ongoing care needs and follow-up should be coordinated with the Duty Consultant Paediatric Cardiologist who can liaise with colleagues to coordinate local or tertiary follow-up.
Conditional N/A
5. References
1. https://www.jpeds.com/action/showPdf?pii=S0022-3476%2816%2931185-4
2. https://www.resus.org.uk/sites/default/files/2021-05/Paediatric%20Cardiac%20Arrhythmias%20Algorithm%202021.pdf
3. https://www.resus.org.uk/library/2021-resuscitation-guidelines/paediatric-advanced-life-support-guidelines
Related Documents











