Management of Management of Asthma Exacerbations: Asthma Exacerbations: Key Points Key Points Early treatment is best. Important Early treatment is best. Important elements include: elements include: – A written action plan A written action plan Guides patient self-management of exacerbations Guides patient self-management of exacerbations at home at home Especially important for patients with moderate-to- Especially important for patients with moderate-to- severe persistent asthma and any patient with a severe persistent asthma and any patient with a history of severe exacerbations history of severe exacerbations – Recognition of early signs of worsening asthma Recognition of early signs of worsening asthma

Management of Asthma Exacerbations: Key Points n Early treatment is best. Important elements include: – A written action plan n Guides patient self-management.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Management of Management of Asthma Exacerbations:Asthma Exacerbations:
Key PointsKey Points Early treatment is best. Important elements Early treatment is best. Important elements
include:include:– A written action planA written action plan
Guides patient self-management of exacerbationsGuides patient self-management of exacerbationsat homeat home
Especially important for patients with moderate-to-Especially important for patients with moderate-to-severe persistent asthma and any patient with a severe persistent asthma and any patient with a history of severe exacerbationshistory of severe exacerbations
– Recognition of early signs of worsening asthmaRecognition of early signs of worsening asthma

Management of Management of Asthma Exacerbations:Asthma Exacerbations:
Key Points Key Points (continued)(continued)
– Appropriate intensification of therapyAppropriate intensification of therapy
– Prompt communication between patient and Prompt communication between patient and clinician about:clinician about: Serious deterioration in symptoms or peak flow, orSerious deterioration in symptoms or peak flow, or
Decreased responsiveness to inhaledDecreased responsiveness to inhaledbetabeta22-agonists, or-agonists, or
Decreased duration of betaDecreased duration of beta22-agonist effect-agonist effect

Management of Management of Asthma ExacerbationsAsthma Exacerbations
Inhaled betaInhaled beta22-agonist to provide prompt relief -agonist to provide prompt relief
of airflow obstructionof airflow obstruction
Systemic corticosteroids to suppress and Systemic corticosteroids to suppress and reverse airway inflammationreverse airway inflammation
– For moderate-to-severe exacerbations, orFor moderate-to-severe exacerbations, or
– For patients who fail to respond promptly and For patients who fail to respond promptly and completely to an inhaled betacompletely to an inhaled beta22-agonist -agonist
Management of Management of Asthma Exacerbations Asthma Exacerbations (continued)(continued)
Oxygen to relieve hypoxemia for moderate-Oxygen to relieve hypoxemia for moderate-to-severe exacerbationsto-severe exacerbations
Monitoring response to therapy with serial Monitoring response to therapy with serial measurements of lung functionmeasurements of lung function

Risk Factors for Risk Factors for Death From AsthmaDeath From Asthma
Past history of sudden severe exacerbationsPast history of sudden severe exacerbations Prior intubation or admission to ICUPrior intubation or admission to ICU
for asthmafor asthma Two or more hospitalizations for asthmaTwo or more hospitalizations for asthma
in the past yearin the past year Three or more ED visits for asthmaThree or more ED visits for asthma
in the past yearin the past year
Risk Factors for Risk Factors for Death From Asthma Death From Asthma (continued)(continued)
Hospitalization or an ED visit for asthmaHospitalization or an ED visit for asthmain the past monthin the past month
Use of >2 canisters per month of inhaled Use of >2 canisters per month of inhaled short-acting betashort-acting beta22-agonist-agonist
Current use of systemic corticosteroidsCurrent use of systemic corticosteroidsor recent withdrawal from systemic or recent withdrawal from systemic corticosteroidscorticosteroids
Risk Factors for Risk Factors for Death From Asthma Death From Asthma (continued)(continued)
Difficulty perceiving airflow obstructionDifficulty perceiving airflow obstructionor its severityor its severity
Comorbidity, as from cardiovascular diseases Comorbidity, as from cardiovascular diseases or chronic obstructive pulmonary diseaseor chronic obstructive pulmonary disease
Serious psychiatric disease or psychosocial Serious psychiatric disease or psychosocial problemsproblems
Risk Factors for Risk Factors for Death From Asthma Death From Asthma (continued)(continued)
Low socioeconomic status andLow socioeconomic status andurban residenceurban residence
Illicit drug useIllicit drug use
Sensitivity to Sensitivity to AlternariaAlternaria
Home ManagementHome Managementof Exacerbations:of Exacerbations:
Written Action PlanWritten Action Plan
Develop a written action plan with each Develop a written action plan with each patient, especially those with: patient, especially those with:
–Moderate-to-severe persistent asthma orModerate-to-severe persistent asthma or–History of severe exacerbationsHistory of severe exacerbations
Home ManagementHome Managementof Exacerbations:of Exacerbations:
Written Action Plan Written Action Plan (continued)(continued)
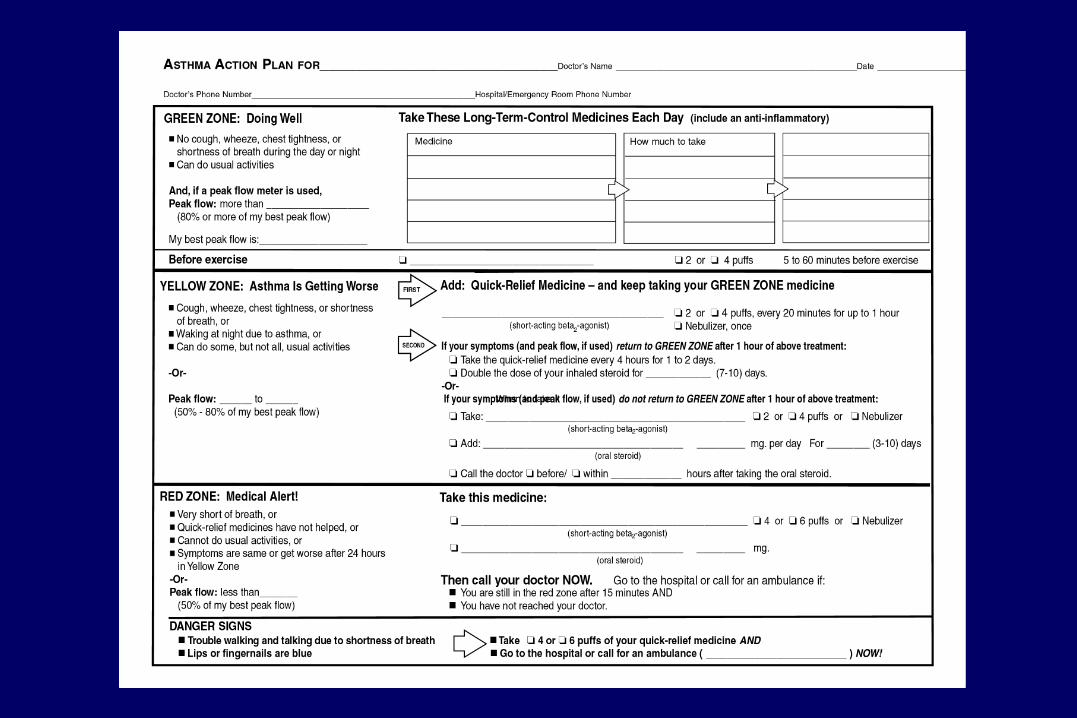
The plan should include:The plan should include:
–Signs, symptoms, and peak flow levels that indicateSigns, symptoms, and peak flow levels that indicate deteriorating asthmadeteriorating asthma
–How to adjust medications in response toHow to adjust medications in response todeteriorating asthmadeteriorating asthma
– When to seek medical helpWhen to seek medical help
–Emergency phone numbersEmergency phone numbers

Home Management Home Management of Exacerbations: What Toof Exacerbations: What To
Teach Patients and CaretakersTeach Patients and Caretakers Recognize symptoms and signsRecognize symptoms and signs
of deteriorationof deterioration
Monitor peak flow if patient has:Monitor peak flow if patient has:
– Moderate-to-severe persistent asthma orModerate-to-severe persistent asthma or
– History of severe exacerbationsHistory of severe exacerbations

Home Management Home Management of Exacerbations: What Toof Exacerbations: What To
Teach Patients and Caretakers Teach Patients and Caretakers (continued)(continued)
Seek medical help early if:Seek medical help early if:– Exacerbation is severeExacerbation is severe
– Therapy does not give rapid,Therapy does not give rapid,sustained improvement sustained improvement
– Condition worsensCondition worsens
Keep necessary medications and equipment at Keep necessary medications and equipment at home and take when travelinghome and take when traveling

Home Management Home Management of Exacerbations:of Exacerbations:
Instructions to Patient Instructions to Patient Use inhaled short-acting betaUse inhaled short-acting beta22-agonist:-agonist:
– Up to three treatments of 2 to 4 puffs by inhaler at Up to three treatments of 2 to 4 puffs by inhaler at 20-minute intervals 20-minute intervals
OROR– Single nebulizer treatmentSingle nebulizer treatment
Assess symptoms and/or peak flowAssess symptoms and/or peak flowafter 1 hourafter 1 hour
Home Management of Home Management of Exacerbations:Exacerbations:
Good Response (Mild Exacerbation)Good Response (Mild Exacerbation)
Peak flow >80% predicted or personal best Peak flow >80% predicted or personal best and/orand/or
No wheezing, shortness of breath, cough, or No wheezing, shortness of breath, cough, or chest tightness andchest tightness and
Response to betaResponse to beta22-agonist sustained for -agonist sustained for
4 hours4 hours
Home Management Home Management of Exacerbations:of Exacerbations:
Instructions for Good ResponseInstructions for Good Response
May continue 2 to 4 puffs betaMay continue 2 to 4 puffs beta22-agonist every 3 -agonist every 3
to 4 hours for 24 to 48 hours PRNto 4 hours for 24 to 48 hours PRN
For patients on inhaled corticosteroids, double For patients on inhaled corticosteroids, double dose for 7 to 10 daysdose for 7 to 10 days
Contact clinician within 48 hours for Contact clinician within 48 hours for instructionsinstructions

Home ManagementHome Managementof Exacerbations:of Exacerbations:
Incomplete Response (Moderate Exacerbation)Incomplete Response (Moderate Exacerbation)
Peak flow 50% to 80% predicted orPeak flow 50% to 80% predicted orpersonal best orpersonal best or
Persistent wheezing, shortness of breath, Persistent wheezing, shortness of breath, cough, or chest tightnesscough, or chest tightness

Home ManagementHome Managementof Exacerbations:of Exacerbations:
Instructions for Incomplete ResponseInstructions for Incomplete Response
Take 2 to 4 puffs betaTake 2 to 4 puffs beta22-agonist every-agonist every
2 to 4 hours for 24 to 48 hours PRN 2 to 4 hours for 24 to 48 hours PRN
Add oral corticosteroid for 3 to 10 days, at Add oral corticosteroid for 3 to 10 days, at least until symptoms and peak flow are stableleast until symptoms and peak flow are stable
Contact clinician urgently (same day) for Contact clinician urgently (same day) for instructionsinstructions
Home ManagementHome Managementof Exacerbations:of Exacerbations:
Poor Response (Severe Exacerbation)Poor Response (Severe Exacerbation)
• Peak flow <50% predicted or personalPeak flow <50% predicted or personalbest, orbest, or
• Marked wheezing, shortness of breath, Marked wheezing, shortness of breath, cough, or chest tightness, or cough, or chest tightness, or
• Distress is severe and nonresponsive, orDistress is severe and nonresponsive, or
• Response to betaResponse to beta22-agonist lasts <2 hours-agonist lasts <2 hours

Home Management of Home Management of Exacerbations:Exacerbations:
Instructions for Poor Response Instructions for Poor Response
IMMEDIATELYIMMEDIATELY Take up to three treatments of 4 to 6 puffs Take up to three treatments of 4 to 6 puffs
betabeta22-agonist every 20 minutes PRN-agonist every 20 minutes PRN Start oral corticosteroidStart oral corticosteroid Contact clinicianContact clinician Go to emergency department orGo to emergency department or
call ambulance or 9-1-1call ambulance or 9-1-1
Prehospital Ambulance Prehospital Ambulance ManagementManagement
Administer supplemental oxygenAdminister supplemental oxygen
Administer inhaled betaAdminister inhaled beta22-agonist-agonist
If inhaled therapy is not available, use If inhaled therapy is not available, use subcutaneous terbutaline or epinephrinesubcutaneous terbutaline or epinephrine

Emergency Department Emergency Department
and Hospital Managementand Hospital Management
Emergency DepartmentEmergency Department Functional Assessment Functional Assessment
Measure FEVMeasure FEV11 or PEF: or PEF: Upon presentation (begin treatment as soon as asthma Upon presentation (begin treatment as soon as asthma
exacerbation is recognized)exacerbation is recognized) After first betaAfter first beta22-agonist dose-agonist dose
After third betaAfter third beta22-agonist dose-agonist dose At intervals depending on response to therapyAt intervals depending on response to therapy Before dischargeBefore discharge
Monitor SaOMonitor SaO22 in patients with severe distress in patients with severe distress
or with FEVor with FEV11 or PEF <50% predicted or PEF <50% predicted
Emergency Department and Emergency Department and Hospital Management: Hospital Management:
Brief HistoryBrief History(after treatment is initiated)(after treatment is initiated)
Time of onset and cause of exacerbationTime of onset and cause of exacerbation
Severity of symptoms, especially compared Severity of symptoms, especially compared to previous attacksto previous attacks
All current medications and time of last doseAll current medications and time of last dose
Emergency Department and Emergency Department and Hospital Management: Hospital Management: Brief Brief
History (after treatment is History (after treatment is initiated)initiated) (continued)(continued)
Prior hospitalizations and ED visits, Prior hospitalizations and ED visits, especially in past yearespecially in past year
Prior episodes of respiratory failure or loss of Prior episodes of respiratory failure or loss of consciousness due to asthmaconsciousness due to asthma
Existence of comorbiditiesExistence of comorbidities

Emergency Department and Emergency Department and Hospital Management:Hospital Management:Brief Physical ExamBrief Physical Exam
Assess severity: Alertness, distress, accessory Assess severity: Alertness, distress, accessory muscle use, tachycardia, tachypnea, pulsus muscle use, tachycardia, tachypnea, pulsus paradoxus, cyanosisparadoxus, cyanosis
Identify complications (e.g., pneumonia, Identify complications (e.g., pneumonia, pneumothorax, pneumomediastinum)pneumothorax, pneumomediastinum)
Identify diseases that affect asthmaIdentify diseases that affect asthma(otitis, rhinitis, sinusitis)(otitis, rhinitis, sinusitis)
Rule out upper-airway obstructionRule out upper-airway obstruction
Emergency Department and Emergency Department and Hospital Management:Hospital Management:
Laboratory AssessmentLaboratory Assessment Consider ABG in patients with suspected Consider ABG in patients with suspected
hypoventilation, severe distress, or with FEVhypoventilation, severe distress, or with FEV11 or PEF or PEF
<30% predicted after initial treatment<30% predicted after initial treatment CBC may be appropriate in patients with fever or CBC may be appropriate in patients with fever or
purulent sputumpurulent sputum Serum theophylline concentrationSerum theophylline concentration Serum electrolytes, chest x-ray, ECG inSerum electrolytes, chest x-ray, ECG in
special circumstancesspecial circumstances
Emergency Department and Emergency Department and Hospital Management: GoalsHospital Management: Goals
Correction of significant hypoxemiaCorrection of significant hypoxemia
Rapid reversal of airflow obstructionRapid reversal of airflow obstruction
Reduction of likelihood of recurrenceReduction of likelihood of recurrence

Emergency Department Emergency Department and Hospital Management: and Hospital Management:
Initial TreatmentInitial Treatment
FEVFEV11 or PEF >50% or PEF >50% Oxygen to achieve OOxygen to achieve O22 saturation saturation >>90%90% Inhaled betaInhaled beta22-agonist by metered-dose inhaler or -agonist by metered-dose inhaler or
nebulizer, up to three treatments in first hournebulizer, up to three treatments in first hour Oral corticosteroids if no immediate response orOral corticosteroids if no immediate response or
if patient recently took oral corticosteroidsif patient recently took oral corticosteroids Repeat assessment (Sx, physical exam, PEF,Repeat assessment (Sx, physical exam, PEF,
OO2 2 saturation, other tests as needed)saturation, other tests as needed)
Emergency Department Emergency Department and Hospital Management:and Hospital Management:
Initial Treatment Initial Treatment (continued)(continued)
FEVFEV11 or PEF <50% or PEF <50% Oxygen to achieve OOxygen to achieve O2 2 saturation is saturation is >>90%90%
Inhaled high-dose betaInhaled high-dose beta22-agonist and anticholinergic by -agonist and anticholinergic by
nebulization every 20 minutes or continuouslynebulization every 20 minutes or continuouslyfor 1 hourfor 1 hour
Oral corticosteroidOral corticosteroid Repeat assessment (Sx, physical exam, PEF,Repeat assessment (Sx, physical exam, PEF,
OO2 2 saturation, other tests as needed)saturation, other tests as needed)
Emergency Department Emergency Department and Hospital Management:and Hospital Management:
Initial Treatment Initial Treatment (continued)(continued)
Impending or Actual Respiratory ArrestImpending or Actual Respiratory Arrest Intubation and mechanical ventilation with 100% OIntubation and mechanical ventilation with 100% O2 2
Nebulized betaNebulized beta22-agonist and anticholinergic-agonist and anticholinergic Intravenous corticosteroidIntravenous corticosteroid Admit to hospital intensive careAdmit to hospital intensive care
Emergency Department and Emergency Department and Hospital Management: Treatment Hospital Management: Treatment
After Repeat AssessmentAfter Repeat Assessment
• FEVFEV11 or PEF 50% to 80% predicted or or PEF 50% to 80% predicted or
personal best personal best • Physical exam: moderate symptomsPhysical exam: moderate symptoms
• Inhaled short-acting betaInhaled short-acting beta22-agonist every -agonist every
60 minutes60 minutes• Systemic corticosteroidSystemic corticosteroid• Continue treatment 1 to 3 hours, Continue treatment 1 to 3 hours,
provided there is improvementprovided there is improvement

Emergency Department and Emergency Department and Hospital Management: Treatment Hospital Management: Treatment After Repeat Assessment After Repeat Assessment (continued)(continued)
• FEVFEV11 or PEF <50% predicted or personal best or PEF <50% predicted or personal best• Physical exam: severe symptoms at rest, Physical exam: severe symptoms at rest,
accessory muscle use, chest retractionaccessory muscle use, chest retraction• History: high-risk patientHistory: high-risk patient• No improvement after initial treatmentNo improvement after initial treatment
• OxygenOxygen• Inhaled short-acting betaInhaled short-acting beta22-agonist hourly or -agonist hourly or
continuously + inhaled anticholinergiccontinuously + inhaled anticholinergic• Systemic corticosteroidSystemic corticosteroid

Emergency Department and Emergency Department and Hospital Management:Hospital Management:
Good ResponseGood Response• FEVFEV11 or PEF or PEF >>70%70%• Response sustained 60 minutes after last Response sustained 60 minutes after last
treatmenttreatment• No distressNo distress• Physical exam: normalPhysical exam: normal
• Discharge HomeDischarge Home

Emergency Department and Emergency Department and Hospital Management:Hospital Management:Incomplete ResponseIncomplete Response
• FEVFEV11 or PEF or PEF >>50% but <70%50% but <70%• Mild-to-moderate symptomsMild-to-moderate symptoms
• Individualized decision re: hospitalizationIndividualized decision re: hospitalization
Emergency Department and Emergency Department and Hospital Management:Hospital Management:
Poor ResponsePoor Response• FEVFEV11 or PEF <50% or PEF <50%• PCOPCO22 >>42 mm Hg42 mm Hg• Physical exam: symptoms severe, drowsiness, Physical exam: symptoms severe, drowsiness,
confusionconfusion
• Admit to hospital intensive careAdmit to hospital intensive care
Admit to Hospital Intensive CareAdmit to Hospital Intensive Care
• Inhaled betaInhaled beta22-agonist hourly or continuously + -agonist hourly or continuously +
inhaled anticholinergicinhaled anticholinergic• IV corticosteroidIV corticosteroid• OxygenOxygen• Possible intubation and mechanical ventilationPossible intubation and mechanical ventilation
• Admit to hospital wardAdmit to hospital ward
Emergency Department and Emergency Department and Hospital Management: Hospital Management:
HospitalizationHospitalization
Consider:Consider: Duration and severity of airflow obstructionDuration and severity of airflow obstruction Course and severity of prior attacksCourse and severity of prior attacks Medication useMedication use Access to careAccess to care Home conditions and supportHome conditions and support ComorbiditiesComorbidities

Emergency Department and Emergency Department and Hospital Management:Hospital Management:
HospitalizationHospitalization
Admit to Hospital WardAdmit to Hospital Ward Inhaled betaInhaled beta22-agonist + inhaled anticholinergic-agonist + inhaled anticholinergic Systemic corticosteroidSystemic corticosteroid OxygenOxygen
Monitor FEVMonitor FEV11 or PEF, O or PEF, O22 saturation saturation

Emergency Department and Emergency Department and Hospital ManagementHospital Management
Not generally recommended:Not generally recommended: MethylxanthinesMethylxanthines Antibiotics (except for patients with pneumonia, Antibiotics (except for patients with pneumonia,
bacterial sinusitis)bacterial sinusitis) ““Aggressive” hydrationAggressive” hydration Chest physical therapyChest physical therapy
Not recommended:Not recommended: MucolyticsMucolytics SedationSedation
Emergency Department Emergency Department Discharge CriteriaDischarge Criteria
If FEVIf FEV11 or PEF or PEF 70% predicted and symptoms70% predicted and symptoms
are minimal, dischargeare minimal, discharge
If FEVIf FEV11 or PEF or PEF >>50% but 50% but 70% predicted and 70% predicted and
symptoms are mild, decision is individualizedsymptoms are mild, decision is individualized If response is prompt, observe for If response is prompt, observe for
30 to 60 minutes before discharging30 to 60 minutes before discharging
Emergency Department and Emergency Department and Hospital Discharge ActionsHospital Discharge Actions
Prescribe sufficient medication and instructionsPrescribe sufficient medication and instructionsfor usefor use
– Short acting betaShort acting beta22-agonist-agonist
– Patients given systemic corticosteroids—continue oral Patients given systemic corticosteroids—continue oral corticosteroids for 3 to 10 dayscorticosteroids for 3 to 10 days
Schedule followup or referral visit within 3 to 5 daysSchedule followup or referral visit within 3 to 5 days– Consider referral to specialist if patient has history ofConsider referral to specialist if patient has history of
life-threatening exacerbations or multiple hospitalizationslife-threatening exacerbations or multiple hospitalizations
Emergency Department Emergency Department and Hospital Discharge Actions and Hospital Discharge Actions
(continued)(continued)
Instruct in simple action plan:Instruct in simple action plan:– How to recognize signs and symptoms of deteriorationHow to recognize signs and symptoms of deterioration– When to increase medications in response to When to increase medications in response to
deteriorationdeterioration Consider providing peak flow meterConsider providing peak flow meter When possible, teach correct inhaler use and When possible, teach correct inhaler use and
trigger avoidancetrigger avoidance
Hospital Discharge ActionsHospital Discharge Actions
Prior to discharge, adjust medication to an Prior to discharge, adjust medication to an oral and/or inhaled regimenoral and/or inhaled regimen
– This is generally done when:This is generally done when:• Patient is minimally symptomaticPatient is minimally symptomatic
• Patient has little wheezing on chest examinationPatient has little wheezing on chest examination
• PEF or FEVPEF or FEV11 >>70% predicted or personal best70% predicted or personal best
– Observe patient for 24 hours after adjustmentObserve patient for 24 hours after adjustment

Hospital Discharge Hospital Discharge Actions Actions (continued)(continued)
Discharge medications should include:Discharge medications should include:
– Short-acting betaShort-acting beta22-agonist-agonist
– Sufficient oral corticosteroid to complete course Sufficient oral corticosteroid to complete course of therapy or to continue therapy until followup of therapy or to continue therapy until followup appointmentappointment
– If inhaled corticosteroids are prescribed,If inhaled corticosteroids are prescribed,start before course of oral corticosteroidsstart before course of oral corticosteroidsis completedis completed
Management of Asthma Management of Asthma Exacerbations: Special Exacerbations: Special
Considerations for InfantsConsiderations for Infants Infants are at greater risk of respiratory failure.Infants are at greater risk of respiratory failure. Assessment depends on physical examination Assessment depends on physical examination
rather than objective measurements.rather than objective measurements. Use oral corticosteroids early in the episode.Use oral corticosteroids early in the episode. Antibiotics are generally not required. Acute Antibiotics are generally not required. Acute
wheezing generally results from viral infectionswheezing generally results from viral infectionsand may be accompanied by fever.and may be accompanied by fever.
Management of Asthma Management of Asthma Exacerbations: Signs of Exacerbations: Signs of
Serious Distress in InfantsSerious Distress in Infants
Use of accessory muscles, paradoxical Use of accessory muscles, paradoxical breathing, cyanosis, and a respiratory breathing, cyanosis, and a respiratory rate >60rate >60
Oxygen saturation <91%Oxygen saturation <91%
Lack of response to betaLack of response to beta22-agonist-agonist
Related Documents











