Malaria 101 Malaria 101 What wasn't declared at customs... What wasn't declared at customs... Manitoba 9 th Annual Travel Health Conference April 14/15, 2011 Dr. Sergio Fanella FRCPC, FAAP, DTM&H Assistant Professor, Pediatrics & Child Health University of Manitoba

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Malaria 101Malaria 101
What wasn't declared at customs...What wasn't declared at customs...
Manitoba 9th
Annual Travel Health ConferenceApril 14/15, 2011
Dr. Sergio Fanella FRCPC, FAAP, DTM&HAssistant Professor, Pediatrics & Child Health
University of Manitoba

ObjectivesObjectives
Discuss basic aspects of malaria lifecycle, epidemiology, clinical presentations, diagnostics, and therapy.Describe available malaria chemoprophylaxisReview research on pediatric malaria at Winnipeg Children's Hospital

No Conflicts of InterestNo Conflicts of Interest


Malaria Malaria ––
An Age Old ProblemAn Age Old Problem
Ancient Chinese medical writingsAncient Greece, 4th century B.C.Established in Colonial America◦
Florida →
Ohio
Malaria parasites identified, 1880◦
A. Laveran
Differentiation of species of malaria, 1886◦
Camillo Golgi
http://www.cdc.gov/malaria/about/history/, Accessed March 24, 2011

Malaria Malaria ––
An Age Old ProblemAn Age Old Problem
Mosquitoes transmit malaria, 1897◦
Ronald Ross◦
Nobel Prize 1902
Influence on Panama Canal◦
French failure, 1881-1889◦
22, 000 deaths◦
Landslides, poor equipment◦
Malaria, yellow fever

Malaria and the Panama CanalMalaria and the Panama Canal
U.S. Construction, 1904-1914◦
Isthmian Canal Commission◦
Col. W.C. Gorgas◦
Cuban experience
Military Efficiency!!!◦
Drainage, Brush & Grass cutting◦
Oiling & larviciding◦
Screening◦
Prophylactic Quinine

Malaria and the Panama CanalMalaria and the Panama Canal

Malaria and the Panama CanalMalaria and the Panama Canal
Death Rate from malaria;◦
Nov 1906 –
11.6 per 1,000 workers
◦
Nov 1909 –
1.3 per 1, 000 workers
Death Rate in total population:◦
July 1906 –
16. 2 per 1,000
◦
Dec 1909 –
2.6 per 1,000

Malaria is in the DDx of any patient Malaria is in the DDx of any patient with fever who could have been with fever who could have been exposed to malaria...exposed to malaria...
Could this be malaria???

Falciparum malaria is a medical Falciparum malaria is a medical emergency!!!emergency!!!
Early treatment is curativeEarly diagnosis is imperativeSevere malaria has 20% mortality even with optimal treatment

Basic BiologyBasic Biology5 major spp* of Plasmodium◦
P. falciparum
◦
P. vivax
◦
P. ovale, P. malariae
◦
P. knowlesi
Anopheles mosquitoes, ♀Reservoir, IH - ManDefinitive Host – mosquito2 types asexual multiplication◦
Sporozoites (mosquito)
◦
Schizonts (man)
LiverRBCs

UpToDate, Pathogenesis of Malaria, Accessed March 15, 2011

P. vivax P. falciparum
Hypnozoite Yes No
Sequestration No?? Yes
RBC preference Reticulocytes All RBCs
Infected RBC membrane
Caveolae-vesicle complexes
Knobs

Liver SchizontLiver Schizont
30-70 um diameterMerozoites released into blood 6-7days2 liver schizontal drugs:◦
Atovaquone/proguanil◦
primaquine

N Engl J Med 2008;359:603-12

Malaria Relapse Malaria Relapse --
HypnozoiteHypnozoitePv & PoSporozoites from mosquito → liver (minutes)Schizont vs hypnozoite◦
Factors unknown◦
Greatly delayed prepatency (bite to blood stages)
Weeks, months
◦
Triggers? Stress? Geography/Mosquito cycles?
Within heptocytesClonal with each relapse

NEJM 2008;359:603
2.5 billion live in at2.5 billion live in at--risk areasrisk areas 300300--500 million clinical cases/year500 million clinical cases/year
1.5 1.5 ––
2.7 millions deaths/year (kids in SSA)2.7 millions deaths/year (kids in SSA)

Malaria EpidemiologyMalaria EpidemiologyDifferences in host susceptibility◦
Exposure frequency◦
Development of immunity
Premunition◦
Partial immunity◦
Stable malaria, continuous exposure◦
Controlled, not prevented◦
Young kids who survive → premunition
Asymptomatic parasitemia in up to 75% of schoolchildren.
◦
Loss of exposure → Loss of immunity

ReRe--emergence of Malariaemergence of MalariaDrug resistant P. falciparum in Africa◦
CLQ, Fansidar◦
Artemisin drugs $2-3 per dose
Korea – 1st cases in decadesAmazon – narco trafficJamaica No recent resurgence in travellers◦
Effective prophylaxis

Not all bad newsNot all bad news…… Decline of Malaria in the GambiaDecline of Malaria in the Gambia
PLoS One 2010;5(8)e12242PLoS One 2010;5(8)e12242

Malaria Risk by RegionMalaria Risk by Region CID 2004:39; 1104CID 2004:39; 1104--11121112



N = 1140 malaria cases in travellers60% Pf = 90% SSA (33 severe – 3 deaths)24% Pv = 30% in SSA !!5% of cases in trips < 1week97% develop SSx after travelIllness onset < 4 weeks in 80% for Pf◦
40% for Pv
Leder et al. CID 2004; 39:1104

Pretravel Advice & VFRsPretravel Advice & VFRs

Who dies from malaria?Who dies from malaria? Tan KR et al. ASTMH 2009Tan KR et al. ASTMH 2009
VFRs – 33%, Missionaries - 27%, Tourists – 13%USA, 2003 – 2008, N = 34 deathsNo or wrong chemoproph 100%Missed by MD 62%Lab misDx/delays 44%Inappropriate therapy 41%Diagnosis at autopsy 27%

P. vivax P. vivax ––
Presents LaterPresents Later

P. vivaxP. vivax80-300 million cases/year◦
Not well studied
◦
South & SE Asia
◦
Often overlaps with Pf, except:
Temperate areas (Korea)Much of SSA, except West Africa???
“Neglected Tropical Disease”◦
Severe febrile illness, significant morbidity◦
Economic impact
Control issues◦
Hyponozoites
Lancet Infect Dis 2009;9:555

Global Distribution of Pf and Pv in 2005Global Distribution of Pf and Pv in 2005 Trends in Parasitology 2005;22:353Trends in Parasitology 2005;22:353--358358
Pf
Pv


Malaria Malaria ––
Patient HistoryPatient History
Geographically possible?Actual risk of exposure◦
Travel pattern◦
Vector intensity
Nature/compliance with prophylaxisRR of other infections

Malaria Malaria ––
Patient HistoryPatient History
FeverHeadacheChillsMalaiseSweatsNauseaVomitingDiarrheaAbdominal PainCough

Extensive Differential DxExtensive Differential DxTyphoidMeningococcal diseaseArboviral disease (Dengue, etc...)Hemorrhagic feversLeptospirosisAcute SchistosomiasisTyphus/Rickettsial DiseaseAcute HIVSyphilis

Malaria Malaria ––
Patient HistoryPatient History
Returning Traveler often misdiagnosed:◦
Pneumonia◦
Gastroenteritis
When it isn’t malaria◦
Dermatologic findings◦
Joint involvement

Malaria Malaria ––
Patient HistoryPatient History SyndromesSyndromes
Asymptomatic infectionAcute, uncomplicated febrile illnessSevere or complicated malariaDeathInfluence of:◦
Immune status (Endemic exp vs traveller)◦
Prior chemoprophylaxis

Clinical Presentation with Effective Clinical Presentation with Effective ChemoprophylaxisChemoprophylaxis……
Is different◦
Sub-acute, insidious onset◦
Atypical symptoms◦
Afebrile◦
Low parasitemias
Effect of other drugs:◦
Azithromycin◦
Clindamycin◦
Tetracyclines, TMP-SMX

Acute Uncomplicated MalariaAcute Uncomplicated Malaria
Acute, uncomplicated febrile illness◦
Pf, Pv, Po, Pm, Pk◦
Objective:
cure infection, prevent severe d/s
Severe/complicated malaria◦
= end organ involvement = P. falciparum *◦
Brain, renal, pulmonary edema/ARDS◦
Severe anemia/hyperparasitemia ◦
Objective:
prevent death

Uncomplicated vs Complicated PfUncomplicated vs Complicated Pf Staging the PatientStaging the Patient
Is malaria (Pf) possible?Any signs of EOD?◦
Abnormal VS, CNS, lungs, kidneys
Parasitologic DiagnosisAre IV drugs needed?Specific drug therapy◦
Consider resistance & geography◦
Can you use CLQ?

Why is Why is P. falciparum P. falciparum so dangerous?so dangerous?
Pf infects all stages of RBCsHigher multiplication capacitySequestration◦
Cytoadherance
Capillary leak syndromesEnd organ failure

Severe or Complicated MalariaSevere or Complicated Malaria
Symptomatic malaria ◦
Parasitemia ≥
5 %
OR
Evidence of End Organ Dysfunction or Complications


P. vivax P. vivax --
ClinicalClinical
Maybe not be as benign as once thoughtProdromal stage for 1-2 days◦
HA, chills, LG fever, myalgias
Paroxysms, profuse sweatingGI & Respiratory complaints (cough) very commonInitial fever pattern often hectic◦
Multiple broods of parasites

Severe Pv malariaSevere Pv malaria?similar spectrum to Pf?Splenic rupture more likely with Pv than PfCase reports, retrospective/prospective studiesNo longitudinal studies with PCR, R/O other DDx◦
AJTMH 2009 80(2);194-198
40 cases severe Pv, IndiaPCR, RDT, smears◦
Testing for typhoid, lepto, HIV, dengue, HBV/HCV◦
+/-
BC, CT-scans, LP, etc…
◦
Excluded mixed infections

Severe Pv malariaSevere Pv malaria635 with Pf, 456 with PvMean age ~ 30 years

Malaria Malaria --
DiagnosisDiagnosisMicroscopy◦
Thick & Thin smears
False +◦
Slide artifacts◦
Experience of lab
False –◦
Low parasitemias◦
Misdiagnosis (is Pf but called Pv)
Most pts will be smear (+) on 1st sample◦
**prior drugs, VFRs

1% parasitemia = 1 iRBC/100 RBCs !1% parasitemia = 1 iRBC/100 RBCs !

RDT PerformanceRDT Performance
Clin Infect Dis. 2009 Sept 15;49(6):908-13

Clin Infect Dis. 2009 Sept 15;49(6):908-13

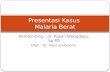
Cerebral MalariaCerebral Malaria (Any impairment of LOC or convulsions in a patient (Any impairment of LOC or convulsions in a patient
exposed to malaria)exposed to malaria)
Cerebral microvasculature obstruction◦
Level of sequestration = level of impairment
oxygen spp, cytokine releaseBreakdown of BBB → vascular permeabilityGradual impairment, comaSeizure (~80%)Immobile vs tossing about*Retinal Pathology in CM◦
Microvascular obstruction

Figure 1.
Fundus photograph displaying malarial retinopathy consisting of
multiple white centered hemorrhages, macular whitening (arrowheads) and orange discoloration of vessels (arrow). PLOS One 2009;4(1)

DDx of Cerebral MalariaDDx of Cerebral Malaria
MeningitisSepsisHypoglycemiaEncephalitis
Therapy – NEVER give steroids (harmful)

Initial ManagementInitial ManagementLabs◦
Malaria smear◦
Rapid glucose◦
CBC, electrolytes, BUN, Cr, glucose, lactate◦
Liver functions◦
Blood cultures, serologies◦
Blood gas
All pts should be considered for admission (esp kids) ORInitial therapy & observation in ER

CATMAT 2009 Malaria Guidelines

Uncomplicated Uncomplicated PfPfProgressive if not treated1st line = oral combo with artemesinin cmpd (WHO)◦
Not in Canada
CLQ- resistant area◦
Atovaquone/proguanil (Malarone®)◦
Quinine + 2nd
agent (clindamycin or doxycycline)
If can’t tolerate PO meds → IV antimalarials

Complicated Complicated PfPfHospitalization, ICUMonitoring◦
VS, respiratory pattern, LOC, U/O◦
Rapid glucose q4h*
Treat seizures as neededBe careful with over-aggressive IVFs ID, ICU consultationsIV antimalarialsExchange transfusion?

Complicated Complicated PfPfEither IV quinine or IV artesunateBUT, should be IV artesunate if available**◦
Why?
Both stored at St Boniface Pharmacy◦
Sent by cab
Should be started within 1 hour of malaria DxIf stuck – PO quinine via NGIV quinine – loading dose◦
Exc if quinine within last 24 hrs, MFQ within last 2 weeks




ArtesunateArtesunate
Most rapidly acting antimalarial◦
Fever◦
parasitemia
No stage specificityNeeds 2nd agent to “protect” it

Why Do We See Bad Outcomes?Why Do We See Bad Outcomes?
Delay!◦
Onset of SSx until presentation (Pt Delay)◦
1st
contact until consideration of Dx (MD
Delay)◦
Consideration of diagnosis until microscopic confirmation (Diagnostic Delay)◦
Consideration of Dx until start of appropriate therapy (Management Delay)

Pyramid of Malaria PreventionPyramid of Malaria Prevention
D – Diagnosis: Prompt Dx & early Rx
C – Compliance with chemoprophylaxis
B – Bites: Personal Protection Measures
A – Awareness: know the risks

Chemoprophylaxis Choices 2011Chemoprophylaxis Choices 2011
MefloquineAtovaquone/proguanilChloroquineDoxycyclinePrimaquine

Chemoprophylaxis can work in 1 of Chemoprophylaxis can work in 1 of 2 ways2 ways
1. Killing parasites as they develop in the liver◦
Tissue schizonticidal drugs◦
Causal prophylaxis
2. Killing parasites as they differentiate in RBCs◦
Blood schizonticidal drugs◦
Suppressive prophylaxis

N Engl J Med 2008;359:603-12

N Engl J Med 2008;359:603-12

Does your traveler need Does your traveler need prophylaxis?prophylaxis?
Yes or NoConsider several different “guidelines”:◦
CATMAT/PHAC◦
CDC Yellow Book◦
WHO “green book”◦
Commercial (ex.. Travax)
May differ

MefloquineMefloquine
EfficaciousNot tolerated by all…Neurotoxicity concernsScreen patients◦
Used before without issues?◦
Education ++, other options?
Benefits vs. Risks

NeuroNeuro--psychiatric AEs with MQpsychiatric AEs with MQ
MOA unknownHigher risk: low BMI; womenVivid dreams in 15-25%Severe AEs – seizures, psychosis◦
1 in 6500-10,600 users
Less severe AEs – insomnia, nightmares…◦
1 in 200-500 users
~95% of users complete their course

MQ MQ ––
OthersOthers
MQ-resistant Pf on Thai-Cambodian & Thai-Burmese bordersPediatrics◦
Approved for > 5 kg◦
Considered for all kids at HR for malaria
Used safely through most of pregnancy◦
Limited data before T#2◦
Use when unavoidable exp to CQ-R Pf in T#1

DoxycyclineDoxycycline
Positives:◦
“Broad-spectrum”
activity
◦
Lepto, Rickettsia, Mycoplasma, Chlamydia◦
No reported resistance◦
Inexpensive◦
No dose change with renal failure

DoxycyclineDoxycycline
Negatives:◦
Daily dosing◦
Not causal –
28 days after leaving
◦
Enamel discoloration (kids <8y, BF, pregy)◦
GI upset◦
Photosensitivity◦
Vaginal yeast infections◦
Drug interaction

DoxycyclineDoxycyclineMeds that ↓ serum doxy levels:◦
Antacids with Ca, Al, Mg◦
Oral Fe, bismuth, laxatives (Mg)◦
Phenobarb, phenytoin, carbamazepine ↑hepatic metabolism
Meds that ↑ serum doxy levels:◦
Warfarin
OCPs – nil interactions* Is monohydrate salt better vs. hyclate salt??◦
Reported lower rates of GI SEs◦
No comparative studies

Doxycycline Doxycycline ––
Best ApproachBest Approach
Take in AMUprightFull glass of waterTake with foodSunblockAnti-yeast self Rx course pre-travel for all women

AtovaquoneAtovaquone--ProguanilProguanilVery well tolerated & efficaciousCausal activity (7 days after leaving)No geographic considerations for resistance (yet)Optimal choice for ST travel (2-3 weeks)AEs: both parts have good safety records◦
GI most common◦
Occasional derm SAEs (SJS)
Better tolerated vs. MQ, doxy in RDBPC

AtovaquoneAtovaquone--ProguanilProguanilSignificant AE – bankruptcy ($$)OD dosing not best for someDoesn't prevent hypnozoite relapse◦
Pv, Po
For use in children, >5 kgInsufficient data for use in pregnancy◦
May be considered after careful discussion in T#1 for unavoidable exposure in MQ-R areas

PrimaquinePrimaquine
Not willing or able to take doxy, Malarone, or MQ in CLQ-R areasCheck G6PD statusOK in all agesNOT in pregnancyCausal (for 7 days after leaving area)Post-travel terminal prophylaxis ◦
If had PV, Po while abroad

Chemoprophylaxis SummaryChemoprophylaxis SummaryAll are equally efficacious, give all optionsPick a drug least likely to exacerbate underlying problemDoesn’t prevent initial infectionNo plan is 100%!!!>90% of malaria in travellers◦
Inappropriate or no prophylaxis
Death associated with no chemoprophylaxisGin & tonic would be a lot of work!

Pediatric Malaria at WCH, 1989Pediatric Malaria at WCH, 1989-- 20082008
38 cases8.4 ± 4.6 years, 50% males
11 cases born in malaria non-endemic areas
10 born in Canada; 1 born in UK and moved to Canada
10 /11 were cases of VFRs (visiting friends and relatives)
6 VFRs in India
4 VFRs in SSA

27 cases were immigrants/refugees, born in malaria endemic areas
23 from Sub-Saharan Africa, 4 from India/Pakistan


Country of Origin or Visited
Number of Cases
Nigeria 8Mozambique 7
India 7Uganda 3Pakistan 3Uganda 3Zambia 2
Sudan, Burundi, Sierra Leone,
Guinea, Tanzania, Congo, Ghana
1 each



20 cases were seen by an offsite MD before presentation to WCH
11/20 (55%)had a smear at an outside facility or clinic.16/20 (80%) had >24 hour delay before presentation to WCH ER or clinicsThere were no significant differences for delayed presentation/diagnostics for those < 6 or ≥ 6 years of age.
Nineteen (50%) cases were admitted to hospital, for a mean of 2.6 ± 1.9 days.

ConclusionsConclusionsCommon & serious infection, many at riskShould be considered in anyone with fever who could have been exposed to malaria (1st, 2nd, 3rd
Dx)Falciparum malaria is a medical emergencyPrompt Dx and therapy are keys to good outcomesIV artesunate is best therapy for severe PfPick the chemoprophylaxis best suited to your patient

Thank YouThank YouTime to put more insecticide on my net.......
Related Documents