MAKING ABORTION SAFE Dr Sujoy Dasgupta MBBS (Gold Medalist, Hons) MS (OBGY- Gold Medalist) DNB (OBGY) MRCOG (London) FIAOG Consultant, Bavishi Pratiksha Fertility Institute, Kolkata Visiting Consultant, RSV Hospital, Kolkata Secretary, Website and Bulletin Committee, Bengal Obstetric and Gynaecological Society (BOGS)- 2017-18 Managing Committee Member, BOGS- 2017-18

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MAKING ABORTION SAFE
Dr Sujoy DasguptaMBBS (Gold Medalist, Hons)
MS (OBGY- Gold Medalist)
DNB (OBGY)
MRCOG (London)
FIAOG
Consultant, Bavishi Pratiksha Fertility Institute, Kolkata
Visiting Consultant, RSV Hospital, Kolkata
Secretary, Website and Bulletin Committee, Bengal Obstetric
and Gynaecological Society (BOGS)- 2017-18
Managing Committee Member, BOGS- 2017-18

• Do not perform abortion at all !!!!!

Why Safety is so important in Abortion
• It’s NOT Criminal Abortion
MTP ACT IN INDIA• Therapeutic Abortion Act by IPC 1860
• Code of Criminal Procedure 1898
• MTP Act 1971 – implemented on 01.4.1972- When and Where
• Revised in 1975
• Amended in 2002 ( MTP Amendment Act, 2002)
• MTP Rules ( amended in 2003)- Who can perform, approval of place- made by the
Central Government and passed by the parliament; notified in the official gazette
• MTP Regulations , 2003 ( applicable to all Union Territories)- Opinion, Consent,
Documentation, Record keeping- made by the state government and passed by the state
legislature

Are you a Doctor or a Lawyer?
• Over 100 million acts of Sexual Intercourse per day
• Result in over 900,000 pregnancies
50% are unplanned
25% are actually unwanted
• 150,000 pregnancies are terminated by induced abortions per day i.e. > 50 million per year worldwide
• WHO– at least 1/3rd are unsafe abortions
• 78000 women die/ year from complications of unsafe abortion
• Accounts for 13% of maternal mortality worldwide
• In India, 70 – 90 women /100,000 live birth die from unsafe abortions
GLOBAL SCENARIO OF ABORTION

• International Institute for
Population Sciences (IIPS),
Mumbai
• Population Council, New Delhi
• Guttmacher Institute, New York

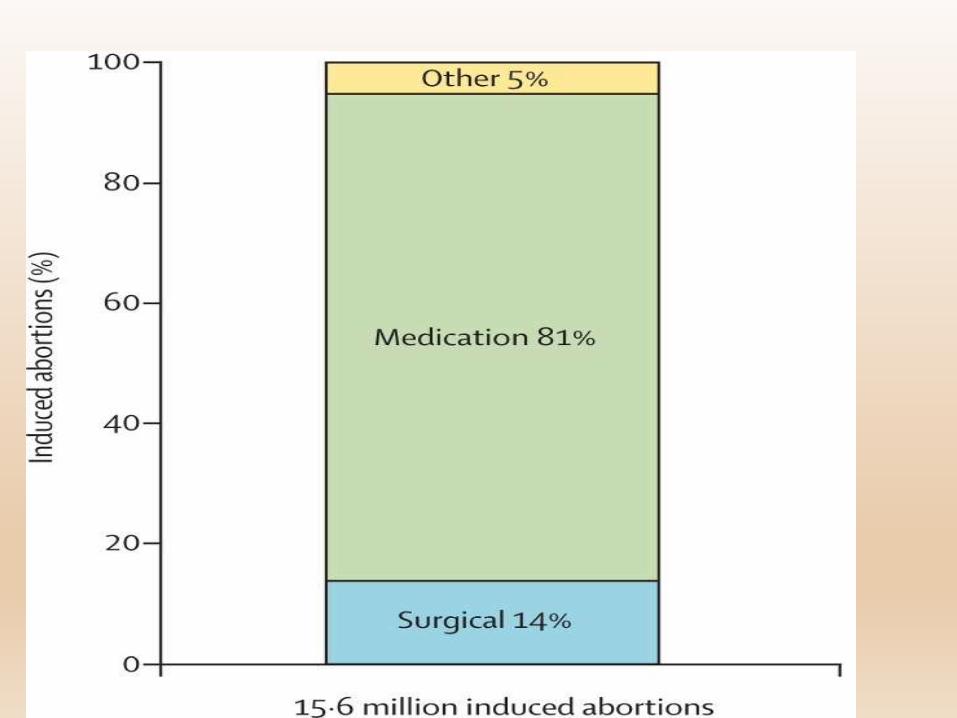
2015 Data• Total 48.1 million
pregnancies
• About half were unintended
• 15.6 million abortions
Per 1,000 woman aged 15-49
• Unintended pregnancy rate =70
• Abortion rate = 47
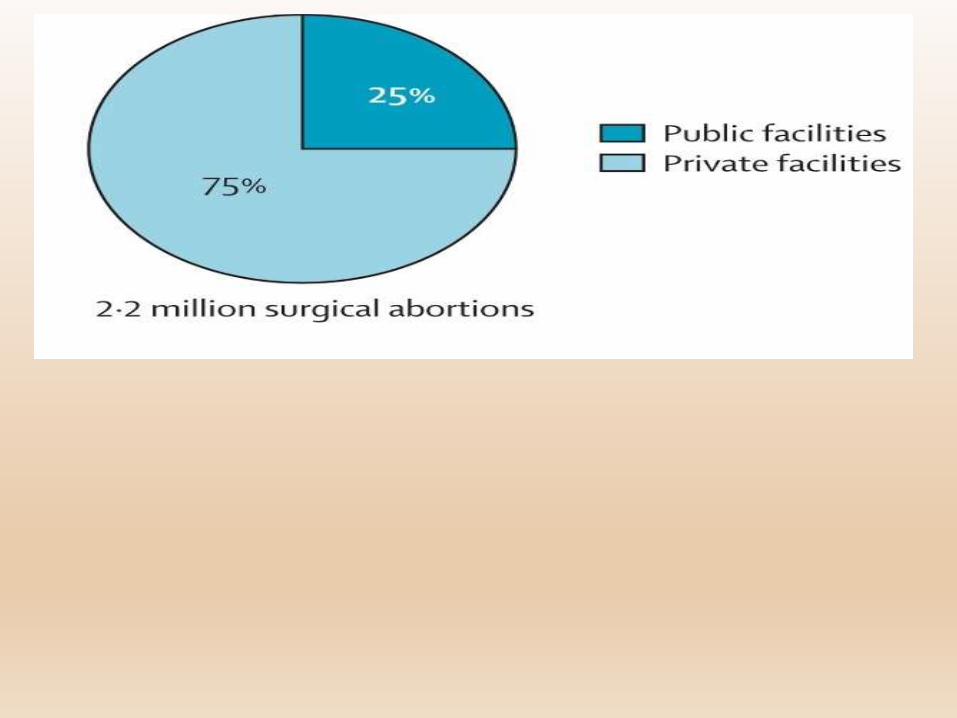
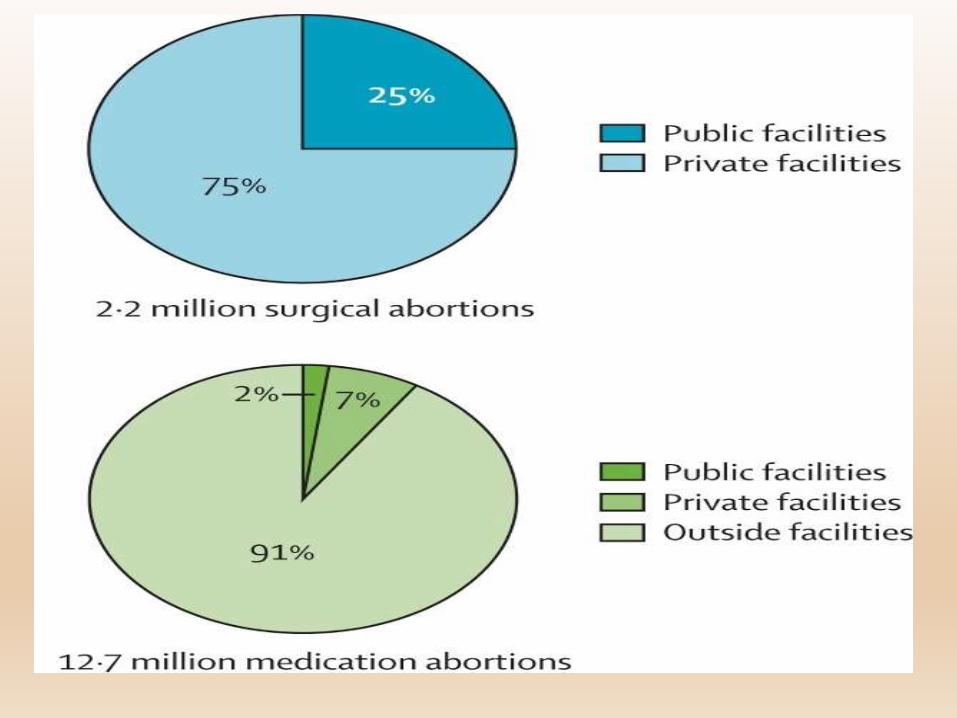

CONCERN !!!
• Currently, slightly fewer than 1 in 4
abortions are provided in health facilities.
HOW CAN WE ENSURE SAFETY
Patient
Place
Doctor
Patient Safety
Why Abortion?1. Continuation of pregnancy is a risk to the life of the
pregnant woman or can cause grave injury to her
physical or mental health (Therapeutic)
2. Substantial risk that the child, if born, would be
seriously handicapped due to physical or mental
abnormalities (Eugenic)
3. The pregnancy was caused by rape (Humanitarian)
4. Pregnancy was caused due to failure of contraception in
a married couple (Social)
Sex selection is NOT an indication for pregnancy termination
under the law
When Abortion?
• Up to 20+0 weeks of pregnancy
Up to 12 weeks, opinion of one RMP is required
From 12+1 to 20+0 weeks
• Opinion of 2 RMPs
When?
• ONLY in places specially approved for 2nd
trimester MTP
How Abortion?
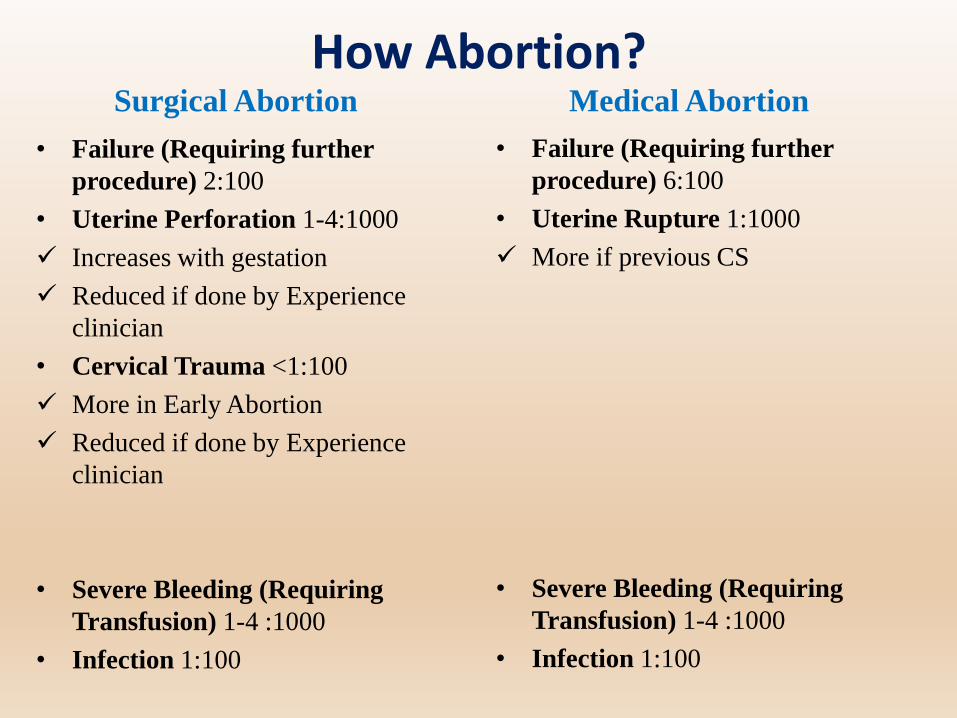
Surgical Abortion
• Failure (Requiring further
procedure) 2:100
• Uterine Perforation 1-4:1000
Increases with gestation
Reduced if done by Experience
clinician
• Cervical Trauma <1:100
More in Early Abortion
Reduced if done by Experience
clinician
• Severe Bleeding (Requiring
Transfusion) 1-4 :1000
• Infection 1:100
Medical Abortion
• Failure (Requiring further
procedure) 6:100
• Uterine Rupture 1:1000
More if previous CS
• Severe Bleeding (Requiring
Transfusion) 1-4 :1000
• Infection 1:100
How Abortion?
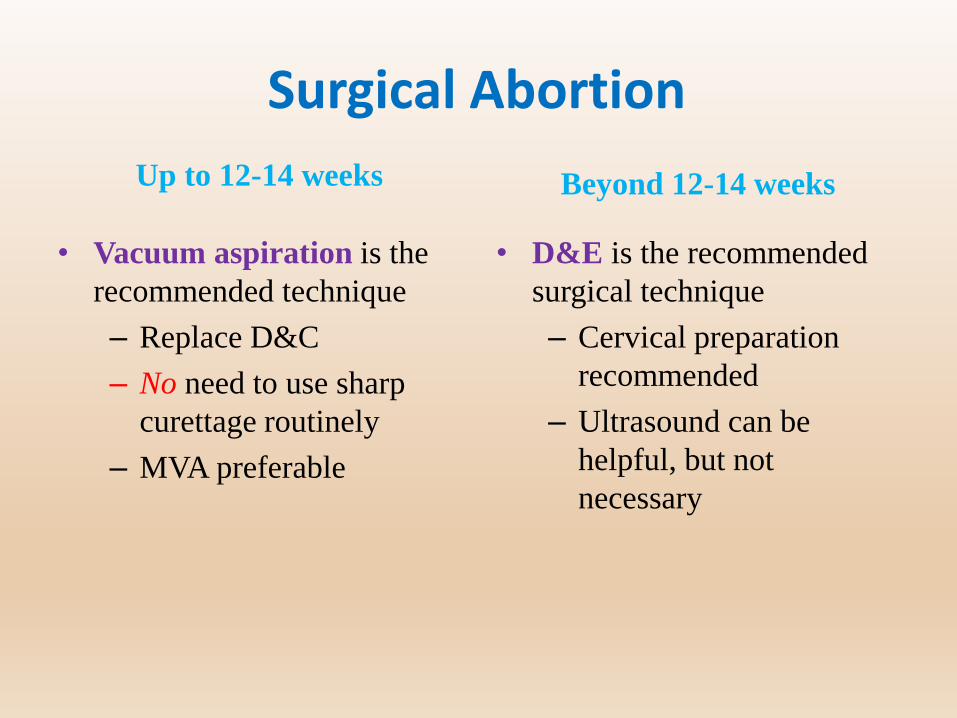
Surgical Abortion
Up to 12-14 weeks
• Vacuum aspiration is the
recommended technique
– Replace D&C
– No need to use sharp
curettage routinely
– MVA preferable
Beyond 12-14 weeks
• D&E is the recommended
surgical technique
– Cervical preparation
recommended
– Ultrasound can be
helpful, but not
necessary
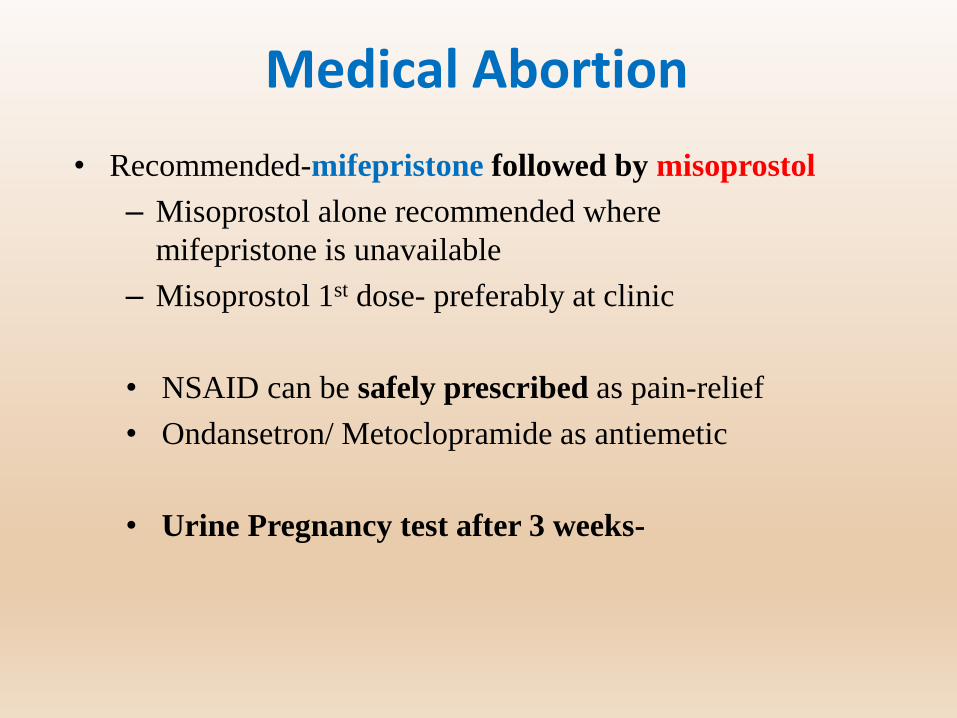
Medical Abortion
• Recommended-mifepristone followed by misoprostol
– Misoprostol alone recommended where
mifepristone is unavailable
– Misoprostol 1st dose- preferably at clinic
• NSAID can be safely prescribed as pain-relief
• Ondansetron/ Metoclopramide as antiemetic
• Urine Pregnancy test after 3 weeks-
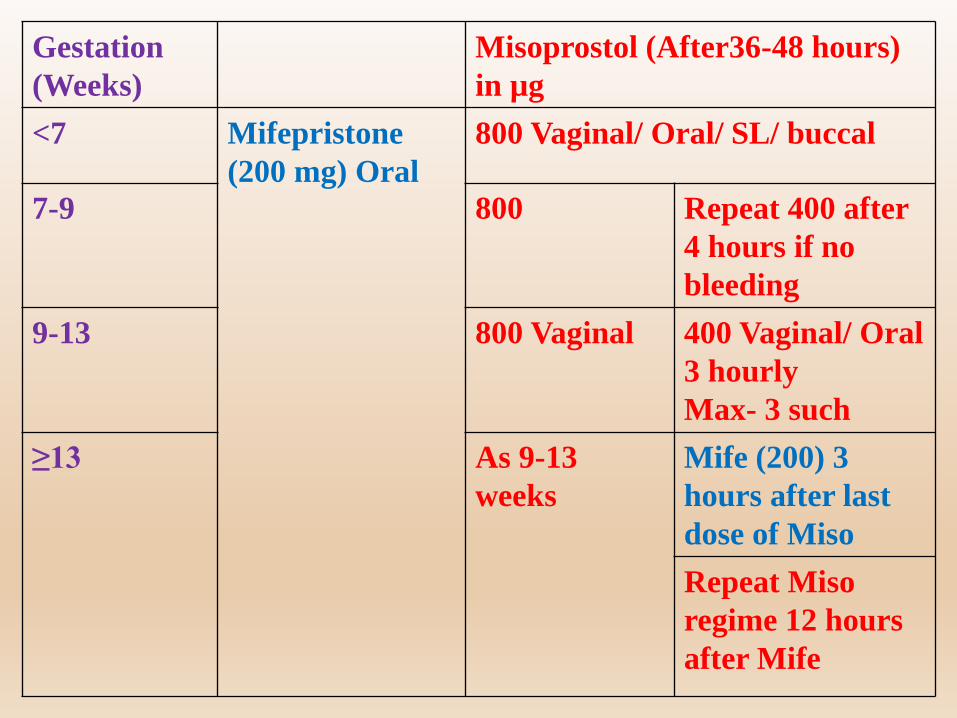
Gestation
(Weeks)
Misoprostol (After36-48 hours)
in µg
<7 Mifepristone
(200 mg) Oral
800 Vaginal/ Oral/ SL/ buccal
7-9 800 Repeat 400 after
4 hours if no
bleeding
9-13 800 Vaginal 400 Vaginal/ Oral
3 hourly
Max- 3 such
≥13 As 9-13
weeks
Mife (200) 3
hours after last
dose of Miso
Repeat Miso
regime 12 hours
after Mife
Your Safety
• Can you perform
abortion
• Do you know the law
• Record Keeping
• Can you handle the
complications
• Have you done
proper counseling

Can You Perform Abortion?
• A practitioner who
1. holds a post–graduate degree or diploma in O & G
2. has completed 6 months as House Surgeon in O & G
3. has at least 1 year experience in the practice of O & G at
any hospital that has all facilities
4. has assisted a RMP in 25 cases of MTP of which at least 5
have been performed independently in a hospital
established or maintained by the government or a training
institute approved for this purpose. Such a practitioner can
perform ONLY 1st trimester pregnancy termination

Know the Law
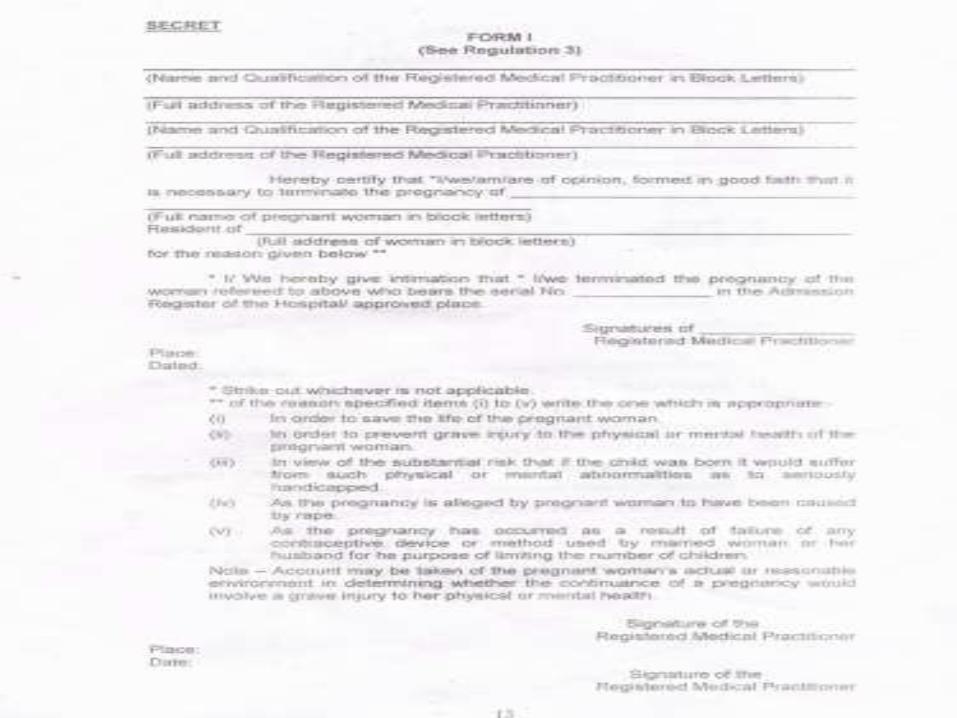
a) Form C: Consent Form
b) Form I (Opinion Form): RMP shall certify this form within
3 hours from the MTP
c) Form II: Head of the hospital or owner of the place shall
send a monthly statement of cases to the CMO of the district
in this form
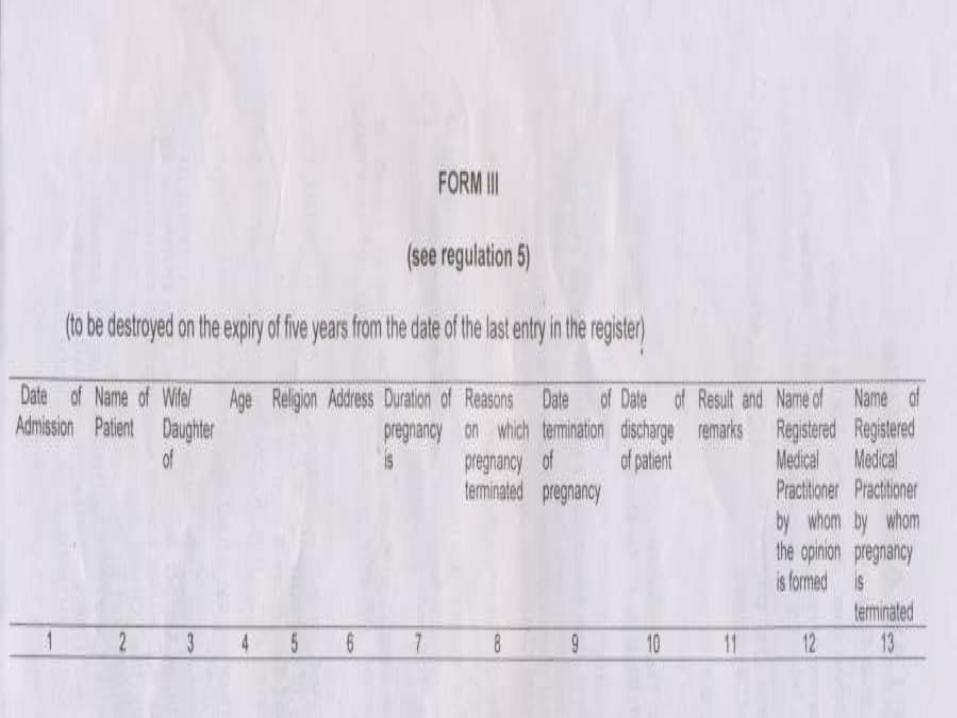
d) Form III (Admission Register): An approved site shall
maintain case records in Form III. This register is kept for a
period of 5 years from the date of last entry

Consent for Procedure
• Woman more than 18 years, only the consent of the woman
Unmarried?
Spouse Consent?
• If minor (<18 years) or a mentally ill person, consent of a
guardian
• Guardian = caretaker , responsible for the woman
• Age Proof?

Managing Complications
• Infection- Antibiotics, Repeat evacuation (selective cases)
• Bleeding- Oxytocics, Uterine Message, Transfusion, Laparotomy,
Hysterectomy
• Retained Product- based on clinical features
Routine ultrasound follow up NOT necessary
Repeat evacuation not decided on ultrasound findings
• GTN- 1:600- 1:2699
Routine H/P exam is NOT necessary

Managing Uterine Perforation
Shakir F, Diab Y. The perforated uterus. The Obstetrician & Gynaecologist 2013;15:256–61.
If anything goes wrong
• Maintain proper documentation
• Communicate
• Debrief
• Multidisciplinary Team Involvement
• Legal Advice
• The provider will get the protective cover of this
legislation only when he or she fulfills the medico-
legal requirements completely.
Counseling Before Abortion• Ensure eligibility
• Choose between abortion methods
• Possible outcomes
• Warning signs
• Complications- short term, long term
• Management of complications
• Offer tests- Hb%, Blood Group, Serology, STI Screening
• Future contraception

Safety Of The Place
• Approval
• Documentation

MTP Site Approval
Public Sites
• Hospital established or maintained by the Government
do not need separate
approval, provided they
have the required
infrastructure
Private Sites
• Approved by the Government or
a District Level Committee (DLC)
constituted by the Government
for the purpose
All private sites need approval
(Form B) before starting abortion
services
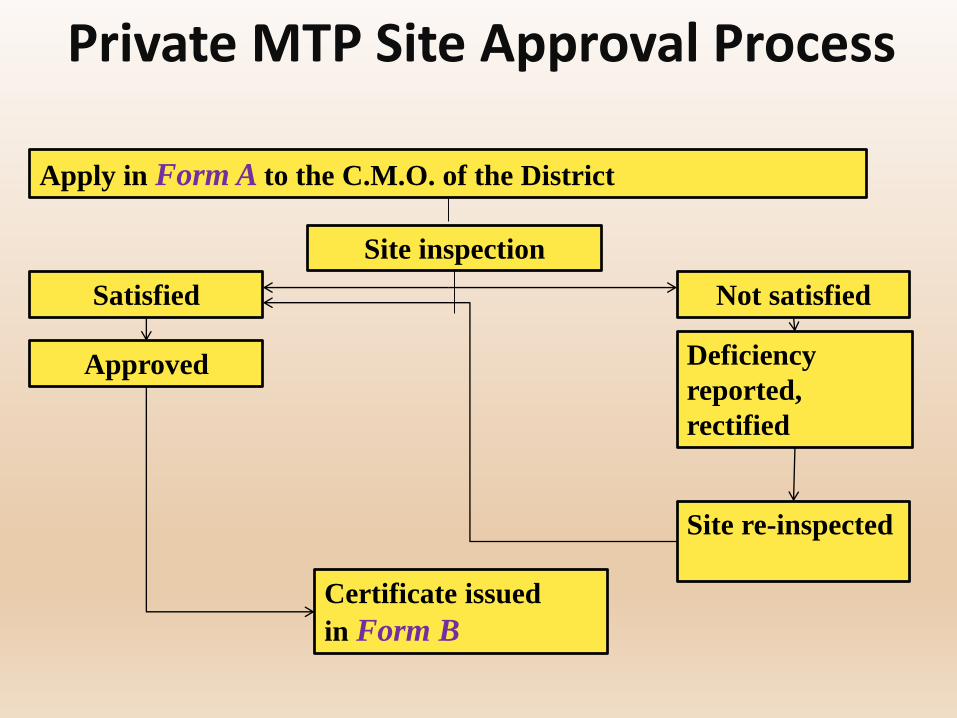
Private MTP Site Approval Process
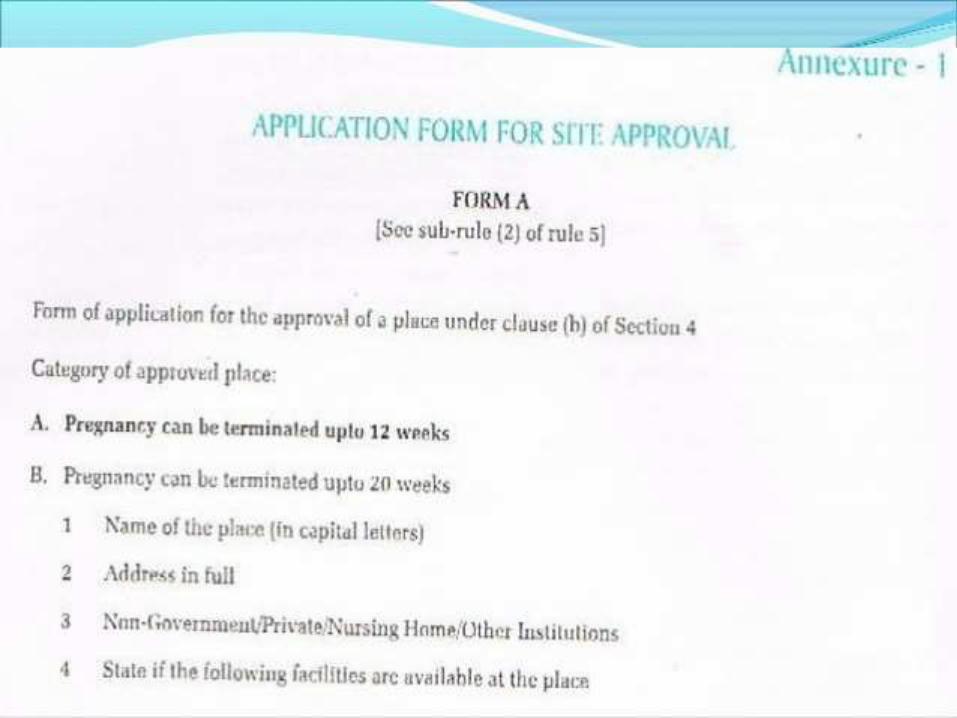
Apply in Form A to the C.M.O. of the District
Site inspection
Not satisfiedSatisfied
Approved Deficiency
reported,
rectified
Site re-inspected
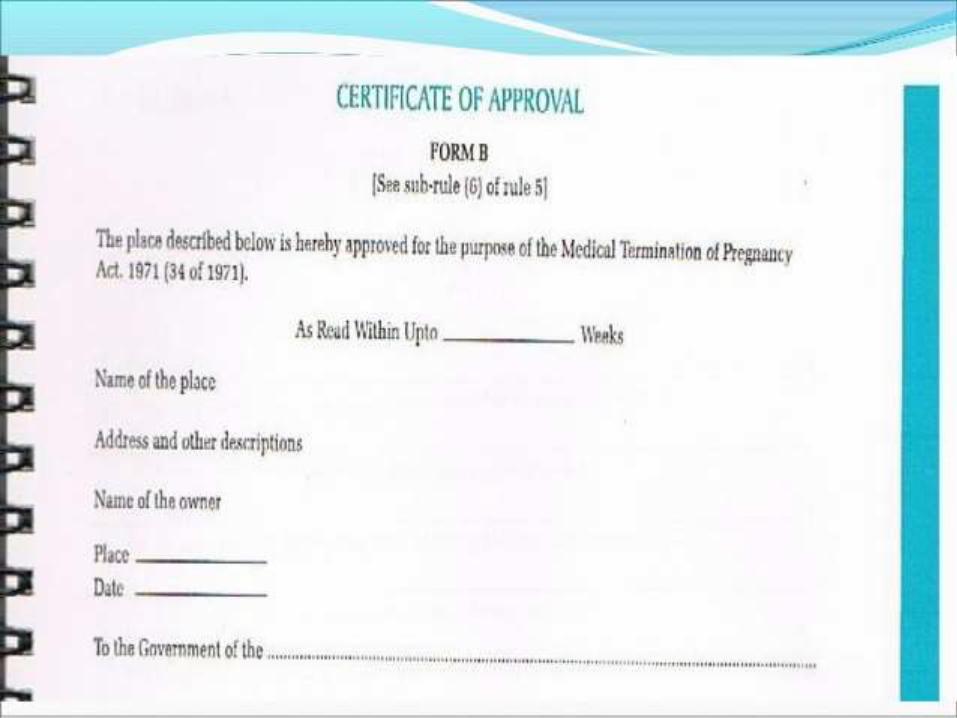
Certificate issued
in Form B

Infrastructure Requirement
1st Trimester Site
• Gynaecology examination/labour table
• Resuscitation and sterilization equipment
– Drugs and parenteral fluids for emergency use, notified by Government of India from time to time
• Back-up facilities for treatment of shock
• Facilities for transportation
2nd Trimester Site
• An operation table
• Instruments for performing
abdominal or gynecological
surgery
• Anaesthetic equipment
• Resuscitation and sterilization
equipment
• Back-up facilities for treatment
of shock
• Facilities for transportation
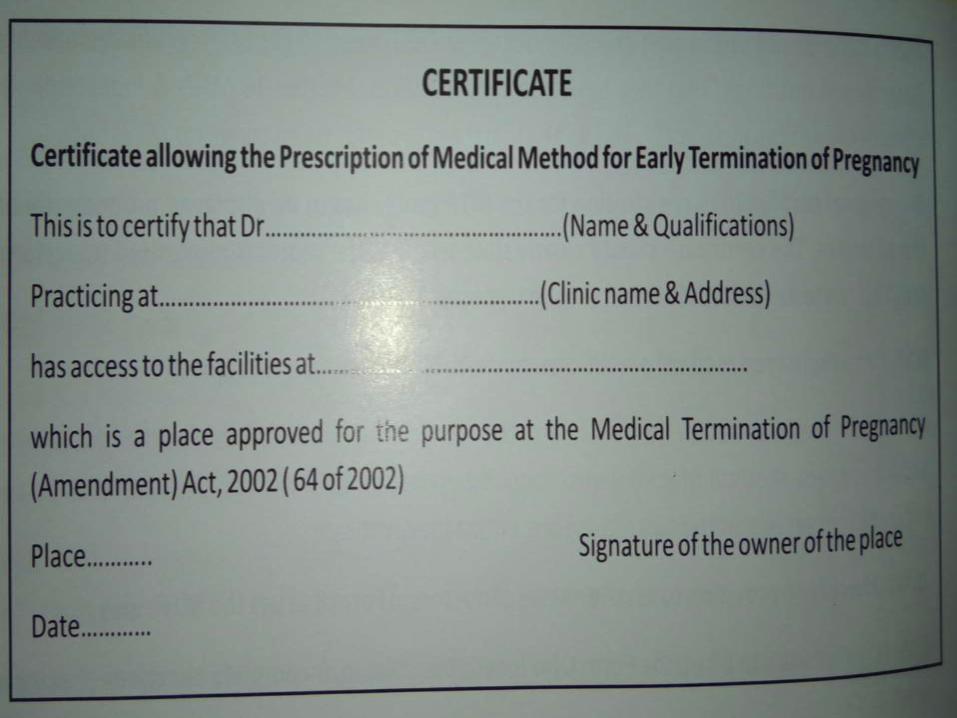
Medical Methods of Abortion (MMA)
• Only an RMP, as under the MTP Act, can prescribe MMA drugs
• Site eligibility: from an OPD clinic with established linkage to
an approved site
• A certificate to this effect by the owner of the approved site
has to be displayed at the OPD clinic
• Give Emergency Contact Number
• Up to 7 weeks
Up to 9 weeks- GOI Comprehensive Abortion care Guidelines
All the records of pregnancy termination have to be maintained
for MMA also (Consent Form, RMP Opinion Form, Admission
Register and Monthly Reporting Form)
Who Can Check Your Records
• Chief Secretary of the
Govt
• A Magistrate of the 1st
Class
• A District Judge
Some Case Scenarios
Case 1Consultant Gynaecologist was practicing at his own nursing
home that was registered for M.T.P.
Performed MTP of a patient at 10 weeks of pregnancy
2 hrs after patient died
P.M. report came as perforation of uterus involving uterine
vessels.
There was only OPD Paper
Indoor paper was BLANK
* Dean appointed a committee for this case.
* Committee gave a non committal opinion.
* Police referred the case to Government prosecutor.
* The prosecutor gave opinion that as per M.T.P. Act no procedure was followed , it was not an “M.T.P.” but a CRIMINAL ABORTION
Consultant was arrested. Got the bail after 3 months.
Case 225 Yr. married pt. was admitted by a consultant in a recognized
M.T.P. centre for termination of 18 wks pregnancy
Pt. was referred to him by a G.P. having qualification as
B.H.M.S.
Consultant took signature of G.P. with B.H.M.S. qualification
as second “ R. M. P.’’
Perforated the uterus, intestine. Pt. bled to death.
Husband complained. Police took charge of body & sent for P.M.
Police took possession of all case papers & consent forms.

M.O.H. lodged a police complaint.
Case was registered as “Criminal abortion”
Case 3• A recently passed post graduate in a Govt. PHC did a 2nd
trimester MTP.
• Patient bled to death before transfer
• The doctor was arrested & jailed

• 2nd Trimester MTP is NOT allowed at PHC

Case 4• Unmarried patient came for MMA
• Consultant Gynaecologist filled up all forms
• No ultrasound was done
• After 1 week, patient was brought to the emergency
• Diagnosed as ruptured ectopic pregnancy and died before any measures taken
• Ultrasound examination is NOT mandatory
before MMA, except in selected cases
Question 5
• Antibiotic Prophylaxis?
Both Medical and Surgical Abortion
1. Azithromycin 1 g + Metronidazole 800 mg
oral (At the time of Abortion)
2. Doxycycline 100 mg BD x 7 days (from the
day of Abortion) + Metronidazole 800 mg
oralRCOG Evidence-based Clinical Guideline Number 7, 2011. The Care of Women
Requesting Induced Abortion

Question 7
• Should Mife/Miso kits be available OTC?

Question 8
• Should AYUSH doctors be allowed to do
MTP?

Summary• In India, it is legal to terminate pregnancy up to 20 weeks, under
special circumstances.
• Only the consent of woman (more than 18 years) is required for
MTP
• For private sites: MTP site approval is done by District Level
Committee
• There are different experience / training and site requirements
for 1st and 2nd trimester MTPs
• Documentation of the MTP procedure includes filling up the
following forms: C (Consent Form); I (Opinion Form); II
(Monthly Reporting Form); III (Admission Register)

Acknowledgement

Acknowledgement
Dr Shyamal Sett
• Vice President , BOGS,
2017-18
• Chairperson, MTP
Committee of FOGSI,
2015 –2017

Related Documents