original writing, artwork and short films about safe abortion from young people around the world Cover Illustration: Yinkore (22, Nigeria)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
THE SAFEABORTION
WATCHDOG2020
original writing artwork and short filmsabout safe abortion from young people
around the world
Cover Illustration Yinkore (22 Nigeria)
LETTER FROMTHE EDITOR
I am very pleased to launch the Youth Coalition Safe Abortion Watchdog 2020 on International SafeAbortion Day to join the global movement for safe abortion on September 28th 2020 All throughSeptember the Youth Coalition has been running a digital advocacy campaign to spotlight the state ofabortion rights all over the world using the tools of digital media This has included startingconversations on AbortionAroundTheWorld how COVID-19 has affected the global access to abortionservices writing about abortion ethically and sensitively being trans inclusive in the abortion rightsdiscourse and of course self-managed abortions ndash the theme of International Safe Abortion Day 2020
COVID-19 brought sharply in focus what some abortion advocates have been saying for years ndash thatincreasing access to self-managed abortions is crucial in the fight for reproductive justice As COVID-19disrupted supply chains and widened the already considerable gaps in abortion and contraceptionaccess telemedical abortions emerged as the saving grace In our Safe Abortion campaign at YouthCoalition we hosted several conversations with experts to shed the misinformation and mythssurrounding self-managed abortions One of these conversations is even documented as a video here
With this Watchdog we wanted to encapsulate this current moment that young activists across the worldhave been thrown into by this pandemic We are living through a time of despair ndash tightened restrictionsincreased surveillance and exacerbated inequalities but also through a time of grit and resilience ndash offinding unlikely solutions and continuing to loudly champion the access to safe abortion as afundamental human right We were humbled by the volume of submissions we received from youngpeople all over the world and saddened at not being able to publish them all
In the following pages you will find articles painting poetry and films by young people from seventeendifferent countries ndash from Mauritius to Nicaragua to Philippines to Venezuela You will find analyticalpieces about the abortion access in different parts of the world after COVID-19 evocative illustrationscelebrating womanhood denouncing stigma and standing up fiercely for abortion access deeplypersonal accounts of having abortions of being an healthcare provider in a country with restrictiveaccess of leaving behind a conservative upbringing that denounced abortions as evil and so much more
These pages contain a snapshot of youth activists unceasing advocacy efforts to fight for reproductivejustice and access to safe abortions in these unprecedented times of crisis Of course even the act ofcreating these pieces of art and writing is an act of resistance in itself After all we live in a world thatstill hushes loudly and averts its eyes at the mention of the word abortion
I hope you enjoy reading this
In love rage and solidarity
Asmita GhoshYouth Coalition for Sexual and Reproductive Rights
TABLE OF CONTENTS
05
05
06
07
09
10
11
12
13
14
1 Untitled (Illustration)Aarushi Khanna 29 India
2 Abortion Law and Policies in Nigeria (Article)Oluwapelumi Alesinloye-King 23 Nigeria
3 Safe Abortion For All (Poem)Rukumani Tripathi 27 Nepal
4 Abortion in the LGBTQIA+ Community Identifying Gaps In OurMovements (Article)Carlos Acosta 26 Colombia
5 Pro-Choice Activism is My Community Care (Article)Laura OConnor 20 Canada
6 REFORM53 Abortion By Choice (Campaign Video)Nandini Tanya Lallmon 29 Mauritius
7 Global Gag Kills Women (Illustration)Jordan Stevenson 22 USA
8 The Global Gag Rule amp The Fight For Abortion Rights Globally (Article)Chandreyi Guharay 22 NicaraguaNetherlands
9 Not Sluts Not Saints Just Women (Illustration)Yinkore 22 Nigeria
10 Can Abortion Be Postponed In COVID-19 Absolutely Not (Article)Arshpreet Kaur 28India
1511 Abortion Stigma (Illustration)Diti Mistry 28 India
1612 COVID-19 Another Barrier To Safe Abortions In Colombia (Article)Catalina Calle Duraacuten 24 Colombia
17
18
18
21
22
23
24
25
26
27
13 Exorcism (Poem)Deepshikha Sharma 22 India
14 My Body My Choice (Illustration) Karren Barcita 22 Philippines
15 Sexual and Reproductive Rights In Uganda In The Global GagEra (Article amp Documentary)Ategeka Frank 30 Uganda
16 The Sound Of It Breaking (Poem)Tavleen Singh 22 India
17 The Frustration Of Being A Doctor In Honduras (Article)Marianela Martinez Buezo 26 Honduras
18 The Decision Is Mine (Animated Short Film)Karin Eckerling 27 Israel
19 Adolescent Girls and Young Womenrsquos Access To Abortion InSub-Saharan Africa (Article)Kerigo Odada 28 KenyaSouth Africa
20 A Letter of Gratitude To Non-Judgmental Abortion Providers (Letter)Anonymous 25 India
21 Untitled (Poem)Andrea Paolo Hernandez 24 Venezuela
22 COVID-19 And Its Implications For Sexual and ReproductiveHealth Services In Pakistan (Article)Neha Khan 25 Pakistan
2823 Addressing The Obstacle Of Safe Abortion In Nepal During COVID-19(Article)Lirisha Tuladhar 20 Nepal
2924 Self-Managed Abortions An Interview With Women On Web (Video)Youth Coalition For Sexual And Reproductive Rights
3025 Bodily Autonomy Is A Human Right (Illustration)Beatriz Rotoli 26 BrazilItaly
3126 Access to Abortion In Crisis And Humanitarian Settings (Article)Chelangat S Shema 25 Kenya
According to the Guttmacher Institute Nigeria hasone of the highest maternal mortality ratios in theworld with unsafe abortions being a majorcontributor In spite of restrictive abortion laws inNigeria abortions are still very common
Nigeria is a highly ldquoreligious and moralrdquo country thatdoes not allow for the free expression ofreproductive rights Sexuality education is avoidedlike a plague and the use of contraception is onlyreserved for married women It is believed thattalking about sexuality education will encouragepromiscuity
Many young women who have little or no knowledgeof pregnancy and contraception end up gettingpregnant and seek out the fastest most secretiveand easiest way to terminate their pregnancies
2 ABORTION LAW AND POLICIES INNIGERIA
Together we create new self-definitions that canvalidate our resistance our intersectional realitiesand pave the way for reproductive justice
Follow Aarushi on Twitter
AARUSHI KHANNA29 INDIA
1 UNTITLED
OLUWAPELUMI ALESINLOYE-KING 23 NIGERIA
The quacks that offer dangerous and unsafeabortions range from auxiliary nurses fake doctorslocal medicine vendors to traditional birthattendants
According to the World Health Organization ldquoUnsafeabortion is a procedure for terminating anunintended pregnancy carried out either by personslacking the necessary skills andor in an environmentthat does not conform to minimal medicalstandardsrdquo
Some methods of unsafe abortions include theinsertion of sharp objects into the vagina drinkingherbal concoctions a combination of drugs in largedoses such as painkillers and antibiotics drinkingdangerous chemicals such as bleach and dyeAccording to WHO the results of unsafe abortionsmm
Youth Coalition for Sexual and Reproductive Rights 05
range from infertility injury loss of blood uterineperforation incomplete abortion infections death
In order to drastically reduce deaths arising fromunsafe abortion cases in Nigeria organizations suchas Safe2choose work actively to provide safeabortions for women who need it But despite allefforts at this the word ldquoabortionrdquo is still met withstiff opposition from many religious organizationsand lawmakers (especially of the older generation)
An example of this opposition is the raid by theNigerian Police on the Marie Stopes Clinic in LagosOn the 21st of May 2019 officers of the NigerianPolice force raided the reproductive health clinic onthe basis of allegedly providing ldquoabortion and birthcontrolrdquo services for women This issue was highlycondemned by many individuals and womenrsquos rightsorganizations who were saddened by the constantinfringement on womenrsquos sexual and reproductivehealth rights
Sexual and reproductive health rights include freeunrestricted access to sexual and reproductivehealth care and information as well as autonomy in
sexual and reproductive decision-makingmdasharehuman rights they are universal indivisible andundeniable Until Nigerian abortion laws arereformed to respect fundamental human rightsmany women will keep dying in their numbers fromcomplications arising from unsafe abortions Inshort the question of womenrsquos rights is nothing elsethan a matter of human rights
At HowToUseAbortionPill we explain how medicalabortion works what you need to know in advancehow it is done safely and what to expect next Youcan read all this information on our website Ourchatbot is also available 247 to answer all yourmedical abortion-related questions
Follow Oluwapelumi on Facebook Twitter andLinkedIn
Until Nigerian abortion laws are
reformed to respect fundamental human
rights many women will keep dying from
complications arising from unsafe
abortions
3 SAFE ABORTION FOR ALL A POEMRUKUMANI TRIPATHI 27 NEPAL
I was a teenProbably sixteenThen one day I saw a boyWe hung out together we did enjoyI was in loveAnd thought of us as a pair of dovesNever did I know what is rightNever did we ever have a fightWith everything newAs fresh as dewI loved him even moreWe shared our heart we shared our soulWe had sex as we were deeply in loveBut then after a month my period stopped
I was worriedI was scaredI was in high school and I was not preparedI was very scared when I checkedOh my god I was pregnantI didnrsquot know what to doI didnrsquot know who to contactI told my boyfriend
And since then our relationship endedNo wonder I cried all night and smiled all dayI had to show the world that I am perfectly wellOne day I heard an advertisementSafe abortion for all
Youth Coalition for Sexual and Reproductive Rights 06
I went there and took counselling before I fallThank god I was just 8 weeks pregnantAnd they told me that I could abort it with my ownconsentI was relieved because I had given up hopeTo live any moreIf there wasnrsquot an abortion service at that timeI would have probably ended my lifeIt made me realize I should be careful and I shouldbe conscious
This incident taught me that I should be cautiousI have ambitionI have dreamsSafe abortion for all is a human rightBecause birth should bring joy not frightI will plan a baby when I am readyWith the promise to myself I will be capable for thatday
Follow Rukumani on Facebook
4 ABORTION IN THE LGBTQIA+COMMUNITY IDENTIFYING GAPS INOUR MOVEMENTS CARLOS ACOSTA 26 COLOMBIA
Abortion rights have largely been discussedworldwide and while progress has been made inmany countries the narrative of abortion serviceskeeps leaving certain vulnerable groups aside ndashtransgender men non-binary people lesbianwomen and other members of the LGBTQ+spectrum
Are these rights different
We can start the discussion with the most explicitdifference When talking about LGBTQ+ rights thereis little to no mention about abortion Over the yearscountries like Argentina have had progressivemoves in accepting marriage and even procreationfor same sex couples but somehow abortion stillseems to be out of the picture(1) This erasurebecomes an ethical question when we observe thatthe high rates of violence towards this populationcould easily result in unwanted pregnancies Onecannot help but wonder at the gap betweenabortion rights and the LGBTQ+ movementconsidering that both movements are built on thefoundation of bodily autonomy being a fundamentalright
Let us look at how LGBTQ+ and abortion discoursesare built Much of the conversation around LGBTQ+rights revolves around bodily autonomy marriageviolence and adoption These are in fact sexual andreproductive rights ndash however abortion is left outWhen looking to the abortion movement these havea natural focus on women and girls who are themost highly impacted by the lack of access to safeabortion However the abortion discourse oftenleaves out many individuals on the gender spectrumthat have female-assigned reproductive systemsAbortion is still a ldquosherdquo or ldquowomenrsquosrdquo topic andleaves out non-binary and transmasculine peopletrans men and other people who do not identify aswomen
This doesnrsquot necessarily mean that we haveeverything upside down We just need to drawattention to the fact that we must support abortionrights for everyone by amplifying our efforts todiversify who we think needs abortion and access tocontraceptive services In 2013 Chen etal evidencethat LGBTQ+ individuals suffer equal or moreintimate partner violence compared to non-LGBTQ+households(2) If we were to take this fact shouldnrsquot
Youth Coalition for Sexual and Reproductive Rights 07
we evaluate the consequences of intimate partnerviolence and correlate those facts to the potentialneed of abortion services to this population
I believe that unity and cross-sectoral conversationsamongst different movement can help us addressthese gaps
to mould comprehensive sexuality education (CSE)in accordance to current needs of the populationTailoring sexual education towards diversity is a keyfactor in preventing unwanted pregnancies inLGBTQ+ youth and also providing informationabout abortion to diverse youth The typical talkabout cucumbers and bananas doesnrsquot fit manyindividuals in the community and it is scientificallyoutdated There should not only be education aboutphysical relationships but also interpersonal onesand how to foster respect and tolerance for eachother With this we also prevent violence and otherviolations of human rights
In conclusion
Abortion advocacy should be a joint effort comingfrom diverse NGO governmental and civil societysectors Working collectively allows ourconversation to be intersectional However ouractions should follow the same trend Engaging withthe community helps to tailor our interventions to amore focused population This will help us see abetter and much larger impact Hopefully as a rippleeffect we can also see our projects convert intomeaningful reduction of harm and an increase inhealth benefits for millions of people This 28th ofSeptember stop for a moment to think how you caninclude more people in your beliefs surroundingabortion
What direction do we follow The short answerwould be the one where we leave no one behind
Follow Carlos on Instagram and LinkedIn
One cannot help but wonder at the gap
between abortion rights and the LGBTQ+
movement considering that both movements
are built on the foundation of bodily autonomy
Another aspect of why abortion services areimportant for diverse communities is because thereis a long history of treatment and care divergenciestowards the LGBTQ+ community
Abortion services in most countries come from thestudy of obstetrics and gynecology This area ofmedicine (study of specific organs and reproduction)has long been directed towards cis-gender peopleand their patterns of reproduction There are fewscientific focuses on different types of reproductionpatterns that lesbian women transgender men andother individuals in the community might haveleaving the needs of these populations unattendedCommon practices are still centred towards cis-women bodies and a larger attention on medicaleducation could ameliorate this situation (3)
Prevention should also be different We must attempt
1 Luna F (2018) From the Middle Ages to the 21st Century Abortion Assisted Reproduction Technologies and LGBT Rights in ArgentinaCanadian Journal of Bioethics Revue canadienne de bioeacutethique 1 (2) 26ndash36 httpsdoiorg1072021058266ar2 Chen PH Jacobs A Rovi SL Intimate partner violence IPV in the LGBT community FP Essentials 2013 Sep41228-353 Eckstrand KL Potter J Edmiston EK (2016) Obstetric and Gynecologic Care for Individuals Who Are LGBT In Eckstrand K Ehrenfeld J(eds) Lesbian Gay Bisexual and Transgender Healthcare Springer Cham httpsdoiorg101007978-3-319-19752-4_17
Youth Coalition for Sexual and Reproductive Rights 08
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
LETTER FROMTHE EDITOR
I am very pleased to launch the Youth Coalition Safe Abortion Watchdog 2020 on International SafeAbortion Day to join the global movement for safe abortion on September 28th 2020 All throughSeptember the Youth Coalition has been running a digital advocacy campaign to spotlight the state ofabortion rights all over the world using the tools of digital media This has included startingconversations on AbortionAroundTheWorld how COVID-19 has affected the global access to abortionservices writing about abortion ethically and sensitively being trans inclusive in the abortion rightsdiscourse and of course self-managed abortions ndash the theme of International Safe Abortion Day 2020
COVID-19 brought sharply in focus what some abortion advocates have been saying for years ndash thatincreasing access to self-managed abortions is crucial in the fight for reproductive justice As COVID-19disrupted supply chains and widened the already considerable gaps in abortion and contraceptionaccess telemedical abortions emerged as the saving grace In our Safe Abortion campaign at YouthCoalition we hosted several conversations with experts to shed the misinformation and mythssurrounding self-managed abortions One of these conversations is even documented as a video here
With this Watchdog we wanted to encapsulate this current moment that young activists across the worldhave been thrown into by this pandemic We are living through a time of despair ndash tightened restrictionsincreased surveillance and exacerbated inequalities but also through a time of grit and resilience ndash offinding unlikely solutions and continuing to loudly champion the access to safe abortion as afundamental human right We were humbled by the volume of submissions we received from youngpeople all over the world and saddened at not being able to publish them all
In the following pages you will find articles painting poetry and films by young people from seventeendifferent countries ndash from Mauritius to Nicaragua to Philippines to Venezuela You will find analyticalpieces about the abortion access in different parts of the world after COVID-19 evocative illustrationscelebrating womanhood denouncing stigma and standing up fiercely for abortion access deeplypersonal accounts of having abortions of being an healthcare provider in a country with restrictiveaccess of leaving behind a conservative upbringing that denounced abortions as evil and so much more
These pages contain a snapshot of youth activists unceasing advocacy efforts to fight for reproductivejustice and access to safe abortions in these unprecedented times of crisis Of course even the act ofcreating these pieces of art and writing is an act of resistance in itself After all we live in a world thatstill hushes loudly and averts its eyes at the mention of the word abortion
I hope you enjoy reading this
In love rage and solidarity
Asmita GhoshYouth Coalition for Sexual and Reproductive Rights
TABLE OF CONTENTS
05
05
06
07
09
10
11
12
13
14
1 Untitled (Illustration)Aarushi Khanna 29 India
2 Abortion Law and Policies in Nigeria (Article)Oluwapelumi Alesinloye-King 23 Nigeria
3 Safe Abortion For All (Poem)Rukumani Tripathi 27 Nepal
4 Abortion in the LGBTQIA+ Community Identifying Gaps In OurMovements (Article)Carlos Acosta 26 Colombia
5 Pro-Choice Activism is My Community Care (Article)Laura OConnor 20 Canada
6 REFORM53 Abortion By Choice (Campaign Video)Nandini Tanya Lallmon 29 Mauritius
7 Global Gag Kills Women (Illustration)Jordan Stevenson 22 USA
8 The Global Gag Rule amp The Fight For Abortion Rights Globally (Article)Chandreyi Guharay 22 NicaraguaNetherlands
9 Not Sluts Not Saints Just Women (Illustration)Yinkore 22 Nigeria
10 Can Abortion Be Postponed In COVID-19 Absolutely Not (Article)Arshpreet Kaur 28India
1511 Abortion Stigma (Illustration)Diti Mistry 28 India
1612 COVID-19 Another Barrier To Safe Abortions In Colombia (Article)Catalina Calle Duraacuten 24 Colombia
17
18
18
21
22
23
24
25
26
27
13 Exorcism (Poem)Deepshikha Sharma 22 India
14 My Body My Choice (Illustration) Karren Barcita 22 Philippines
15 Sexual and Reproductive Rights In Uganda In The Global GagEra (Article amp Documentary)Ategeka Frank 30 Uganda
16 The Sound Of It Breaking (Poem)Tavleen Singh 22 India
17 The Frustration Of Being A Doctor In Honduras (Article)Marianela Martinez Buezo 26 Honduras
18 The Decision Is Mine (Animated Short Film)Karin Eckerling 27 Israel
19 Adolescent Girls and Young Womenrsquos Access To Abortion InSub-Saharan Africa (Article)Kerigo Odada 28 KenyaSouth Africa
20 A Letter of Gratitude To Non-Judgmental Abortion Providers (Letter)Anonymous 25 India
21 Untitled (Poem)Andrea Paolo Hernandez 24 Venezuela
22 COVID-19 And Its Implications For Sexual and ReproductiveHealth Services In Pakistan (Article)Neha Khan 25 Pakistan
2823 Addressing The Obstacle Of Safe Abortion In Nepal During COVID-19(Article)Lirisha Tuladhar 20 Nepal
2924 Self-Managed Abortions An Interview With Women On Web (Video)Youth Coalition For Sexual And Reproductive Rights
3025 Bodily Autonomy Is A Human Right (Illustration)Beatriz Rotoli 26 BrazilItaly
3126 Access to Abortion In Crisis And Humanitarian Settings (Article)Chelangat S Shema 25 Kenya
According to the Guttmacher Institute Nigeria hasone of the highest maternal mortality ratios in theworld with unsafe abortions being a majorcontributor In spite of restrictive abortion laws inNigeria abortions are still very common
Nigeria is a highly ldquoreligious and moralrdquo country thatdoes not allow for the free expression ofreproductive rights Sexuality education is avoidedlike a plague and the use of contraception is onlyreserved for married women It is believed thattalking about sexuality education will encouragepromiscuity
Many young women who have little or no knowledgeof pregnancy and contraception end up gettingpregnant and seek out the fastest most secretiveand easiest way to terminate their pregnancies
2 ABORTION LAW AND POLICIES INNIGERIA
Together we create new self-definitions that canvalidate our resistance our intersectional realitiesand pave the way for reproductive justice
Follow Aarushi on Twitter
AARUSHI KHANNA29 INDIA
1 UNTITLED
OLUWAPELUMI ALESINLOYE-KING 23 NIGERIA
The quacks that offer dangerous and unsafeabortions range from auxiliary nurses fake doctorslocal medicine vendors to traditional birthattendants
According to the World Health Organization ldquoUnsafeabortion is a procedure for terminating anunintended pregnancy carried out either by personslacking the necessary skills andor in an environmentthat does not conform to minimal medicalstandardsrdquo
Some methods of unsafe abortions include theinsertion of sharp objects into the vagina drinkingherbal concoctions a combination of drugs in largedoses such as painkillers and antibiotics drinkingdangerous chemicals such as bleach and dyeAccording to WHO the results of unsafe abortionsmm
Youth Coalition for Sexual and Reproductive Rights 05
range from infertility injury loss of blood uterineperforation incomplete abortion infections death
In order to drastically reduce deaths arising fromunsafe abortion cases in Nigeria organizations suchas Safe2choose work actively to provide safeabortions for women who need it But despite allefforts at this the word ldquoabortionrdquo is still met withstiff opposition from many religious organizationsand lawmakers (especially of the older generation)
An example of this opposition is the raid by theNigerian Police on the Marie Stopes Clinic in LagosOn the 21st of May 2019 officers of the NigerianPolice force raided the reproductive health clinic onthe basis of allegedly providing ldquoabortion and birthcontrolrdquo services for women This issue was highlycondemned by many individuals and womenrsquos rightsorganizations who were saddened by the constantinfringement on womenrsquos sexual and reproductivehealth rights
Sexual and reproductive health rights include freeunrestricted access to sexual and reproductivehealth care and information as well as autonomy in
sexual and reproductive decision-makingmdasharehuman rights they are universal indivisible andundeniable Until Nigerian abortion laws arereformed to respect fundamental human rightsmany women will keep dying in their numbers fromcomplications arising from unsafe abortions Inshort the question of womenrsquos rights is nothing elsethan a matter of human rights
At HowToUseAbortionPill we explain how medicalabortion works what you need to know in advancehow it is done safely and what to expect next Youcan read all this information on our website Ourchatbot is also available 247 to answer all yourmedical abortion-related questions
Follow Oluwapelumi on Facebook Twitter andLinkedIn
Until Nigerian abortion laws are
reformed to respect fundamental human
rights many women will keep dying from
complications arising from unsafe
abortions
3 SAFE ABORTION FOR ALL A POEMRUKUMANI TRIPATHI 27 NEPAL
I was a teenProbably sixteenThen one day I saw a boyWe hung out together we did enjoyI was in loveAnd thought of us as a pair of dovesNever did I know what is rightNever did we ever have a fightWith everything newAs fresh as dewI loved him even moreWe shared our heart we shared our soulWe had sex as we were deeply in loveBut then after a month my period stopped
I was worriedI was scaredI was in high school and I was not preparedI was very scared when I checkedOh my god I was pregnantI didnrsquot know what to doI didnrsquot know who to contactI told my boyfriend
And since then our relationship endedNo wonder I cried all night and smiled all dayI had to show the world that I am perfectly wellOne day I heard an advertisementSafe abortion for all
Youth Coalition for Sexual and Reproductive Rights 06
I went there and took counselling before I fallThank god I was just 8 weeks pregnantAnd they told me that I could abort it with my ownconsentI was relieved because I had given up hopeTo live any moreIf there wasnrsquot an abortion service at that timeI would have probably ended my lifeIt made me realize I should be careful and I shouldbe conscious
This incident taught me that I should be cautiousI have ambitionI have dreamsSafe abortion for all is a human rightBecause birth should bring joy not frightI will plan a baby when I am readyWith the promise to myself I will be capable for thatday
Follow Rukumani on Facebook
4 ABORTION IN THE LGBTQIA+COMMUNITY IDENTIFYING GAPS INOUR MOVEMENTS CARLOS ACOSTA 26 COLOMBIA
Abortion rights have largely been discussedworldwide and while progress has been made inmany countries the narrative of abortion serviceskeeps leaving certain vulnerable groups aside ndashtransgender men non-binary people lesbianwomen and other members of the LGBTQ+spectrum
Are these rights different
We can start the discussion with the most explicitdifference When talking about LGBTQ+ rights thereis little to no mention about abortion Over the yearscountries like Argentina have had progressivemoves in accepting marriage and even procreationfor same sex couples but somehow abortion stillseems to be out of the picture(1) This erasurebecomes an ethical question when we observe thatthe high rates of violence towards this populationcould easily result in unwanted pregnancies Onecannot help but wonder at the gap betweenabortion rights and the LGBTQ+ movementconsidering that both movements are built on thefoundation of bodily autonomy being a fundamentalright
Let us look at how LGBTQ+ and abortion discoursesare built Much of the conversation around LGBTQ+rights revolves around bodily autonomy marriageviolence and adoption These are in fact sexual andreproductive rights ndash however abortion is left outWhen looking to the abortion movement these havea natural focus on women and girls who are themost highly impacted by the lack of access to safeabortion However the abortion discourse oftenleaves out many individuals on the gender spectrumthat have female-assigned reproductive systemsAbortion is still a ldquosherdquo or ldquowomenrsquosrdquo topic andleaves out non-binary and transmasculine peopletrans men and other people who do not identify aswomen
This doesnrsquot necessarily mean that we haveeverything upside down We just need to drawattention to the fact that we must support abortionrights for everyone by amplifying our efforts todiversify who we think needs abortion and access tocontraceptive services In 2013 Chen etal evidencethat LGBTQ+ individuals suffer equal or moreintimate partner violence compared to non-LGBTQ+households(2) If we were to take this fact shouldnrsquot
Youth Coalition for Sexual and Reproductive Rights 07
we evaluate the consequences of intimate partnerviolence and correlate those facts to the potentialneed of abortion services to this population
I believe that unity and cross-sectoral conversationsamongst different movement can help us addressthese gaps
to mould comprehensive sexuality education (CSE)in accordance to current needs of the populationTailoring sexual education towards diversity is a keyfactor in preventing unwanted pregnancies inLGBTQ+ youth and also providing informationabout abortion to diverse youth The typical talkabout cucumbers and bananas doesnrsquot fit manyindividuals in the community and it is scientificallyoutdated There should not only be education aboutphysical relationships but also interpersonal onesand how to foster respect and tolerance for eachother With this we also prevent violence and otherviolations of human rights
In conclusion
Abortion advocacy should be a joint effort comingfrom diverse NGO governmental and civil societysectors Working collectively allows ourconversation to be intersectional However ouractions should follow the same trend Engaging withthe community helps to tailor our interventions to amore focused population This will help us see abetter and much larger impact Hopefully as a rippleeffect we can also see our projects convert intomeaningful reduction of harm and an increase inhealth benefits for millions of people This 28th ofSeptember stop for a moment to think how you caninclude more people in your beliefs surroundingabortion
What direction do we follow The short answerwould be the one where we leave no one behind
Follow Carlos on Instagram and LinkedIn
One cannot help but wonder at the gap
between abortion rights and the LGBTQ+
movement considering that both movements
are built on the foundation of bodily autonomy
Another aspect of why abortion services areimportant for diverse communities is because thereis a long history of treatment and care divergenciestowards the LGBTQ+ community
Abortion services in most countries come from thestudy of obstetrics and gynecology This area ofmedicine (study of specific organs and reproduction)has long been directed towards cis-gender peopleand their patterns of reproduction There are fewscientific focuses on different types of reproductionpatterns that lesbian women transgender men andother individuals in the community might haveleaving the needs of these populations unattendedCommon practices are still centred towards cis-women bodies and a larger attention on medicaleducation could ameliorate this situation (3)
Prevention should also be different We must attempt
1 Luna F (2018) From the Middle Ages to the 21st Century Abortion Assisted Reproduction Technologies and LGBT Rights in ArgentinaCanadian Journal of Bioethics Revue canadienne de bioeacutethique 1 (2) 26ndash36 httpsdoiorg1072021058266ar2 Chen PH Jacobs A Rovi SL Intimate partner violence IPV in the LGBT community FP Essentials 2013 Sep41228-353 Eckstrand KL Potter J Edmiston EK (2016) Obstetric and Gynecologic Care for Individuals Who Are LGBT In Eckstrand K Ehrenfeld J(eds) Lesbian Gay Bisexual and Transgender Healthcare Springer Cham httpsdoiorg101007978-3-319-19752-4_17
Youth Coalition for Sexual and Reproductive Rights 08
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition

TABLE OF CONTENTS
05
05
06
07
09
10
11
12
13
14
1 Untitled (Illustration)Aarushi Khanna 29 India
2 Abortion Law and Policies in Nigeria (Article)Oluwapelumi Alesinloye-King 23 Nigeria
3 Safe Abortion For All (Poem)Rukumani Tripathi 27 Nepal
4 Abortion in the LGBTQIA+ Community Identifying Gaps In OurMovements (Article)Carlos Acosta 26 Colombia
5 Pro-Choice Activism is My Community Care (Article)Laura OConnor 20 Canada
6 REFORM53 Abortion By Choice (Campaign Video)Nandini Tanya Lallmon 29 Mauritius
7 Global Gag Kills Women (Illustration)Jordan Stevenson 22 USA
8 The Global Gag Rule amp The Fight For Abortion Rights Globally (Article)Chandreyi Guharay 22 NicaraguaNetherlands
9 Not Sluts Not Saints Just Women (Illustration)Yinkore 22 Nigeria
10 Can Abortion Be Postponed In COVID-19 Absolutely Not (Article)Arshpreet Kaur 28India
1511 Abortion Stigma (Illustration)Diti Mistry 28 India
1612 COVID-19 Another Barrier To Safe Abortions In Colombia (Article)Catalina Calle Duraacuten 24 Colombia
17
18
18
21
22
23
24
25
26
27
13 Exorcism (Poem)Deepshikha Sharma 22 India
14 My Body My Choice (Illustration) Karren Barcita 22 Philippines
15 Sexual and Reproductive Rights In Uganda In The Global GagEra (Article amp Documentary)Ategeka Frank 30 Uganda
16 The Sound Of It Breaking (Poem)Tavleen Singh 22 India
17 The Frustration Of Being A Doctor In Honduras (Article)Marianela Martinez Buezo 26 Honduras
18 The Decision Is Mine (Animated Short Film)Karin Eckerling 27 Israel
19 Adolescent Girls and Young Womenrsquos Access To Abortion InSub-Saharan Africa (Article)Kerigo Odada 28 KenyaSouth Africa
20 A Letter of Gratitude To Non-Judgmental Abortion Providers (Letter)Anonymous 25 India
21 Untitled (Poem)Andrea Paolo Hernandez 24 Venezuela
22 COVID-19 And Its Implications For Sexual and ReproductiveHealth Services In Pakistan (Article)Neha Khan 25 Pakistan
2823 Addressing The Obstacle Of Safe Abortion In Nepal During COVID-19(Article)Lirisha Tuladhar 20 Nepal
2924 Self-Managed Abortions An Interview With Women On Web (Video)Youth Coalition For Sexual And Reproductive Rights
3025 Bodily Autonomy Is A Human Right (Illustration)Beatriz Rotoli 26 BrazilItaly
3126 Access to Abortion In Crisis And Humanitarian Settings (Article)Chelangat S Shema 25 Kenya
According to the Guttmacher Institute Nigeria hasone of the highest maternal mortality ratios in theworld with unsafe abortions being a majorcontributor In spite of restrictive abortion laws inNigeria abortions are still very common
Nigeria is a highly ldquoreligious and moralrdquo country thatdoes not allow for the free expression ofreproductive rights Sexuality education is avoidedlike a plague and the use of contraception is onlyreserved for married women It is believed thattalking about sexuality education will encouragepromiscuity
Many young women who have little or no knowledgeof pregnancy and contraception end up gettingpregnant and seek out the fastest most secretiveand easiest way to terminate their pregnancies
2 ABORTION LAW AND POLICIES INNIGERIA
Together we create new self-definitions that canvalidate our resistance our intersectional realitiesand pave the way for reproductive justice
Follow Aarushi on Twitter
AARUSHI KHANNA29 INDIA
1 UNTITLED
OLUWAPELUMI ALESINLOYE-KING 23 NIGERIA
The quacks that offer dangerous and unsafeabortions range from auxiliary nurses fake doctorslocal medicine vendors to traditional birthattendants
According to the World Health Organization ldquoUnsafeabortion is a procedure for terminating anunintended pregnancy carried out either by personslacking the necessary skills andor in an environmentthat does not conform to minimal medicalstandardsrdquo
Some methods of unsafe abortions include theinsertion of sharp objects into the vagina drinkingherbal concoctions a combination of drugs in largedoses such as painkillers and antibiotics drinkingdangerous chemicals such as bleach and dyeAccording to WHO the results of unsafe abortionsmm
Youth Coalition for Sexual and Reproductive Rights 05
range from infertility injury loss of blood uterineperforation incomplete abortion infections death
In order to drastically reduce deaths arising fromunsafe abortion cases in Nigeria organizations suchas Safe2choose work actively to provide safeabortions for women who need it But despite allefforts at this the word ldquoabortionrdquo is still met withstiff opposition from many religious organizationsand lawmakers (especially of the older generation)
An example of this opposition is the raid by theNigerian Police on the Marie Stopes Clinic in LagosOn the 21st of May 2019 officers of the NigerianPolice force raided the reproductive health clinic onthe basis of allegedly providing ldquoabortion and birthcontrolrdquo services for women This issue was highlycondemned by many individuals and womenrsquos rightsorganizations who were saddened by the constantinfringement on womenrsquos sexual and reproductivehealth rights
Sexual and reproductive health rights include freeunrestricted access to sexual and reproductivehealth care and information as well as autonomy in
sexual and reproductive decision-makingmdasharehuman rights they are universal indivisible andundeniable Until Nigerian abortion laws arereformed to respect fundamental human rightsmany women will keep dying in their numbers fromcomplications arising from unsafe abortions Inshort the question of womenrsquos rights is nothing elsethan a matter of human rights
At HowToUseAbortionPill we explain how medicalabortion works what you need to know in advancehow it is done safely and what to expect next Youcan read all this information on our website Ourchatbot is also available 247 to answer all yourmedical abortion-related questions
Follow Oluwapelumi on Facebook Twitter andLinkedIn
Until Nigerian abortion laws are
reformed to respect fundamental human
rights many women will keep dying from
complications arising from unsafe
abortions
3 SAFE ABORTION FOR ALL A POEMRUKUMANI TRIPATHI 27 NEPAL
I was a teenProbably sixteenThen one day I saw a boyWe hung out together we did enjoyI was in loveAnd thought of us as a pair of dovesNever did I know what is rightNever did we ever have a fightWith everything newAs fresh as dewI loved him even moreWe shared our heart we shared our soulWe had sex as we were deeply in loveBut then after a month my period stopped
I was worriedI was scaredI was in high school and I was not preparedI was very scared when I checkedOh my god I was pregnantI didnrsquot know what to doI didnrsquot know who to contactI told my boyfriend
And since then our relationship endedNo wonder I cried all night and smiled all dayI had to show the world that I am perfectly wellOne day I heard an advertisementSafe abortion for all
Youth Coalition for Sexual and Reproductive Rights 06
I went there and took counselling before I fallThank god I was just 8 weeks pregnantAnd they told me that I could abort it with my ownconsentI was relieved because I had given up hopeTo live any moreIf there wasnrsquot an abortion service at that timeI would have probably ended my lifeIt made me realize I should be careful and I shouldbe conscious
This incident taught me that I should be cautiousI have ambitionI have dreamsSafe abortion for all is a human rightBecause birth should bring joy not frightI will plan a baby when I am readyWith the promise to myself I will be capable for thatday
Follow Rukumani on Facebook
4 ABORTION IN THE LGBTQIA+COMMUNITY IDENTIFYING GAPS INOUR MOVEMENTS CARLOS ACOSTA 26 COLOMBIA
Abortion rights have largely been discussedworldwide and while progress has been made inmany countries the narrative of abortion serviceskeeps leaving certain vulnerable groups aside ndashtransgender men non-binary people lesbianwomen and other members of the LGBTQ+spectrum
Are these rights different
We can start the discussion with the most explicitdifference When talking about LGBTQ+ rights thereis little to no mention about abortion Over the yearscountries like Argentina have had progressivemoves in accepting marriage and even procreationfor same sex couples but somehow abortion stillseems to be out of the picture(1) This erasurebecomes an ethical question when we observe thatthe high rates of violence towards this populationcould easily result in unwanted pregnancies Onecannot help but wonder at the gap betweenabortion rights and the LGBTQ+ movementconsidering that both movements are built on thefoundation of bodily autonomy being a fundamentalright
Let us look at how LGBTQ+ and abortion discoursesare built Much of the conversation around LGBTQ+rights revolves around bodily autonomy marriageviolence and adoption These are in fact sexual andreproductive rights ndash however abortion is left outWhen looking to the abortion movement these havea natural focus on women and girls who are themost highly impacted by the lack of access to safeabortion However the abortion discourse oftenleaves out many individuals on the gender spectrumthat have female-assigned reproductive systemsAbortion is still a ldquosherdquo or ldquowomenrsquosrdquo topic andleaves out non-binary and transmasculine peopletrans men and other people who do not identify aswomen
This doesnrsquot necessarily mean that we haveeverything upside down We just need to drawattention to the fact that we must support abortionrights for everyone by amplifying our efforts todiversify who we think needs abortion and access tocontraceptive services In 2013 Chen etal evidencethat LGBTQ+ individuals suffer equal or moreintimate partner violence compared to non-LGBTQ+households(2) If we were to take this fact shouldnrsquot
Youth Coalition for Sexual and Reproductive Rights 07
we evaluate the consequences of intimate partnerviolence and correlate those facts to the potentialneed of abortion services to this population
I believe that unity and cross-sectoral conversationsamongst different movement can help us addressthese gaps
to mould comprehensive sexuality education (CSE)in accordance to current needs of the populationTailoring sexual education towards diversity is a keyfactor in preventing unwanted pregnancies inLGBTQ+ youth and also providing informationabout abortion to diverse youth The typical talkabout cucumbers and bananas doesnrsquot fit manyindividuals in the community and it is scientificallyoutdated There should not only be education aboutphysical relationships but also interpersonal onesand how to foster respect and tolerance for eachother With this we also prevent violence and otherviolations of human rights
In conclusion
Abortion advocacy should be a joint effort comingfrom diverse NGO governmental and civil societysectors Working collectively allows ourconversation to be intersectional However ouractions should follow the same trend Engaging withthe community helps to tailor our interventions to amore focused population This will help us see abetter and much larger impact Hopefully as a rippleeffect we can also see our projects convert intomeaningful reduction of harm and an increase inhealth benefits for millions of people This 28th ofSeptember stop for a moment to think how you caninclude more people in your beliefs surroundingabortion
What direction do we follow The short answerwould be the one where we leave no one behind
Follow Carlos on Instagram and LinkedIn
One cannot help but wonder at the gap
between abortion rights and the LGBTQ+
movement considering that both movements
are built on the foundation of bodily autonomy
Another aspect of why abortion services areimportant for diverse communities is because thereis a long history of treatment and care divergenciestowards the LGBTQ+ community
Abortion services in most countries come from thestudy of obstetrics and gynecology This area ofmedicine (study of specific organs and reproduction)has long been directed towards cis-gender peopleand their patterns of reproduction There are fewscientific focuses on different types of reproductionpatterns that lesbian women transgender men andother individuals in the community might haveleaving the needs of these populations unattendedCommon practices are still centred towards cis-women bodies and a larger attention on medicaleducation could ameliorate this situation (3)
Prevention should also be different We must attempt
1 Luna F (2018) From the Middle Ages to the 21st Century Abortion Assisted Reproduction Technologies and LGBT Rights in ArgentinaCanadian Journal of Bioethics Revue canadienne de bioeacutethique 1 (2) 26ndash36 httpsdoiorg1072021058266ar2 Chen PH Jacobs A Rovi SL Intimate partner violence IPV in the LGBT community FP Essentials 2013 Sep41228-353 Eckstrand KL Potter J Edmiston EK (2016) Obstetric and Gynecologic Care for Individuals Who Are LGBT In Eckstrand K Ehrenfeld J(eds) Lesbian Gay Bisexual and Transgender Healthcare Springer Cham httpsdoiorg101007978-3-319-19752-4_17
Youth Coalition for Sexual and Reproductive Rights 08
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition

17
18
18
21
22
23
24
25
26
27
13 Exorcism (Poem)Deepshikha Sharma 22 India
14 My Body My Choice (Illustration) Karren Barcita 22 Philippines
15 Sexual and Reproductive Rights In Uganda In The Global GagEra (Article amp Documentary)Ategeka Frank 30 Uganda
16 The Sound Of It Breaking (Poem)Tavleen Singh 22 India
17 The Frustration Of Being A Doctor In Honduras (Article)Marianela Martinez Buezo 26 Honduras
18 The Decision Is Mine (Animated Short Film)Karin Eckerling 27 Israel
19 Adolescent Girls and Young Womenrsquos Access To Abortion InSub-Saharan Africa (Article)Kerigo Odada 28 KenyaSouth Africa
20 A Letter of Gratitude To Non-Judgmental Abortion Providers (Letter)Anonymous 25 India
21 Untitled (Poem)Andrea Paolo Hernandez 24 Venezuela
22 COVID-19 And Its Implications For Sexual and ReproductiveHealth Services In Pakistan (Article)Neha Khan 25 Pakistan
2823 Addressing The Obstacle Of Safe Abortion In Nepal During COVID-19(Article)Lirisha Tuladhar 20 Nepal
2924 Self-Managed Abortions An Interview With Women On Web (Video)Youth Coalition For Sexual And Reproductive Rights
3025 Bodily Autonomy Is A Human Right (Illustration)Beatriz Rotoli 26 BrazilItaly
3126 Access to Abortion In Crisis And Humanitarian Settings (Article)Chelangat S Shema 25 Kenya
According to the Guttmacher Institute Nigeria hasone of the highest maternal mortality ratios in theworld with unsafe abortions being a majorcontributor In spite of restrictive abortion laws inNigeria abortions are still very common
Nigeria is a highly ldquoreligious and moralrdquo country thatdoes not allow for the free expression ofreproductive rights Sexuality education is avoidedlike a plague and the use of contraception is onlyreserved for married women It is believed thattalking about sexuality education will encouragepromiscuity
Many young women who have little or no knowledgeof pregnancy and contraception end up gettingpregnant and seek out the fastest most secretiveand easiest way to terminate their pregnancies
2 ABORTION LAW AND POLICIES INNIGERIA
Together we create new self-definitions that canvalidate our resistance our intersectional realitiesand pave the way for reproductive justice
Follow Aarushi on Twitter
AARUSHI KHANNA29 INDIA
1 UNTITLED
OLUWAPELUMI ALESINLOYE-KING 23 NIGERIA
The quacks that offer dangerous and unsafeabortions range from auxiliary nurses fake doctorslocal medicine vendors to traditional birthattendants
According to the World Health Organization ldquoUnsafeabortion is a procedure for terminating anunintended pregnancy carried out either by personslacking the necessary skills andor in an environmentthat does not conform to minimal medicalstandardsrdquo
Some methods of unsafe abortions include theinsertion of sharp objects into the vagina drinkingherbal concoctions a combination of drugs in largedoses such as painkillers and antibiotics drinkingdangerous chemicals such as bleach and dyeAccording to WHO the results of unsafe abortionsmm
Youth Coalition for Sexual and Reproductive Rights 05
range from infertility injury loss of blood uterineperforation incomplete abortion infections death
In order to drastically reduce deaths arising fromunsafe abortion cases in Nigeria organizations suchas Safe2choose work actively to provide safeabortions for women who need it But despite allefforts at this the word ldquoabortionrdquo is still met withstiff opposition from many religious organizationsand lawmakers (especially of the older generation)
An example of this opposition is the raid by theNigerian Police on the Marie Stopes Clinic in LagosOn the 21st of May 2019 officers of the NigerianPolice force raided the reproductive health clinic onthe basis of allegedly providing ldquoabortion and birthcontrolrdquo services for women This issue was highlycondemned by many individuals and womenrsquos rightsorganizations who were saddened by the constantinfringement on womenrsquos sexual and reproductivehealth rights
Sexual and reproductive health rights include freeunrestricted access to sexual and reproductivehealth care and information as well as autonomy in
sexual and reproductive decision-makingmdasharehuman rights they are universal indivisible andundeniable Until Nigerian abortion laws arereformed to respect fundamental human rightsmany women will keep dying in their numbers fromcomplications arising from unsafe abortions Inshort the question of womenrsquos rights is nothing elsethan a matter of human rights
At HowToUseAbortionPill we explain how medicalabortion works what you need to know in advancehow it is done safely and what to expect next Youcan read all this information on our website Ourchatbot is also available 247 to answer all yourmedical abortion-related questions
Follow Oluwapelumi on Facebook Twitter andLinkedIn
Until Nigerian abortion laws are
reformed to respect fundamental human
rights many women will keep dying from
complications arising from unsafe
abortions
3 SAFE ABORTION FOR ALL A POEMRUKUMANI TRIPATHI 27 NEPAL
I was a teenProbably sixteenThen one day I saw a boyWe hung out together we did enjoyI was in loveAnd thought of us as a pair of dovesNever did I know what is rightNever did we ever have a fightWith everything newAs fresh as dewI loved him even moreWe shared our heart we shared our soulWe had sex as we were deeply in loveBut then after a month my period stopped
I was worriedI was scaredI was in high school and I was not preparedI was very scared when I checkedOh my god I was pregnantI didnrsquot know what to doI didnrsquot know who to contactI told my boyfriend
And since then our relationship endedNo wonder I cried all night and smiled all dayI had to show the world that I am perfectly wellOne day I heard an advertisementSafe abortion for all
Youth Coalition for Sexual and Reproductive Rights 06
I went there and took counselling before I fallThank god I was just 8 weeks pregnantAnd they told me that I could abort it with my ownconsentI was relieved because I had given up hopeTo live any moreIf there wasnrsquot an abortion service at that timeI would have probably ended my lifeIt made me realize I should be careful and I shouldbe conscious
This incident taught me that I should be cautiousI have ambitionI have dreamsSafe abortion for all is a human rightBecause birth should bring joy not frightI will plan a baby when I am readyWith the promise to myself I will be capable for thatday
Follow Rukumani on Facebook
4 ABORTION IN THE LGBTQIA+COMMUNITY IDENTIFYING GAPS INOUR MOVEMENTS CARLOS ACOSTA 26 COLOMBIA
Abortion rights have largely been discussedworldwide and while progress has been made inmany countries the narrative of abortion serviceskeeps leaving certain vulnerable groups aside ndashtransgender men non-binary people lesbianwomen and other members of the LGBTQ+spectrum
Are these rights different
We can start the discussion with the most explicitdifference When talking about LGBTQ+ rights thereis little to no mention about abortion Over the yearscountries like Argentina have had progressivemoves in accepting marriage and even procreationfor same sex couples but somehow abortion stillseems to be out of the picture(1) This erasurebecomes an ethical question when we observe thatthe high rates of violence towards this populationcould easily result in unwanted pregnancies Onecannot help but wonder at the gap betweenabortion rights and the LGBTQ+ movementconsidering that both movements are built on thefoundation of bodily autonomy being a fundamentalright
Let us look at how LGBTQ+ and abortion discoursesare built Much of the conversation around LGBTQ+rights revolves around bodily autonomy marriageviolence and adoption These are in fact sexual andreproductive rights ndash however abortion is left outWhen looking to the abortion movement these havea natural focus on women and girls who are themost highly impacted by the lack of access to safeabortion However the abortion discourse oftenleaves out many individuals on the gender spectrumthat have female-assigned reproductive systemsAbortion is still a ldquosherdquo or ldquowomenrsquosrdquo topic andleaves out non-binary and transmasculine peopletrans men and other people who do not identify aswomen
This doesnrsquot necessarily mean that we haveeverything upside down We just need to drawattention to the fact that we must support abortionrights for everyone by amplifying our efforts todiversify who we think needs abortion and access tocontraceptive services In 2013 Chen etal evidencethat LGBTQ+ individuals suffer equal or moreintimate partner violence compared to non-LGBTQ+households(2) If we were to take this fact shouldnrsquot
Youth Coalition for Sexual and Reproductive Rights 07
we evaluate the consequences of intimate partnerviolence and correlate those facts to the potentialneed of abortion services to this population
I believe that unity and cross-sectoral conversationsamongst different movement can help us addressthese gaps
to mould comprehensive sexuality education (CSE)in accordance to current needs of the populationTailoring sexual education towards diversity is a keyfactor in preventing unwanted pregnancies inLGBTQ+ youth and also providing informationabout abortion to diverse youth The typical talkabout cucumbers and bananas doesnrsquot fit manyindividuals in the community and it is scientificallyoutdated There should not only be education aboutphysical relationships but also interpersonal onesand how to foster respect and tolerance for eachother With this we also prevent violence and otherviolations of human rights
In conclusion
Abortion advocacy should be a joint effort comingfrom diverse NGO governmental and civil societysectors Working collectively allows ourconversation to be intersectional However ouractions should follow the same trend Engaging withthe community helps to tailor our interventions to amore focused population This will help us see abetter and much larger impact Hopefully as a rippleeffect we can also see our projects convert intomeaningful reduction of harm and an increase inhealth benefits for millions of people This 28th ofSeptember stop for a moment to think how you caninclude more people in your beliefs surroundingabortion
What direction do we follow The short answerwould be the one where we leave no one behind
Follow Carlos on Instagram and LinkedIn
One cannot help but wonder at the gap
between abortion rights and the LGBTQ+
movement considering that both movements
are built on the foundation of bodily autonomy
Another aspect of why abortion services areimportant for diverse communities is because thereis a long history of treatment and care divergenciestowards the LGBTQ+ community
Abortion services in most countries come from thestudy of obstetrics and gynecology This area ofmedicine (study of specific organs and reproduction)has long been directed towards cis-gender peopleand their patterns of reproduction There are fewscientific focuses on different types of reproductionpatterns that lesbian women transgender men andother individuals in the community might haveleaving the needs of these populations unattendedCommon practices are still centred towards cis-women bodies and a larger attention on medicaleducation could ameliorate this situation (3)
Prevention should also be different We must attempt
1 Luna F (2018) From the Middle Ages to the 21st Century Abortion Assisted Reproduction Technologies and LGBT Rights in ArgentinaCanadian Journal of Bioethics Revue canadienne de bioeacutethique 1 (2) 26ndash36 httpsdoiorg1072021058266ar2 Chen PH Jacobs A Rovi SL Intimate partner violence IPV in the LGBT community FP Essentials 2013 Sep41228-353 Eckstrand KL Potter J Edmiston EK (2016) Obstetric and Gynecologic Care for Individuals Who Are LGBT In Eckstrand K Ehrenfeld J(eds) Lesbian Gay Bisexual and Transgender Healthcare Springer Cham httpsdoiorg101007978-3-319-19752-4_17
Youth Coalition for Sexual and Reproductive Rights 08
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
According to the Guttmacher Institute Nigeria hasone of the highest maternal mortality ratios in theworld with unsafe abortions being a majorcontributor In spite of restrictive abortion laws inNigeria abortions are still very common
Nigeria is a highly ldquoreligious and moralrdquo country thatdoes not allow for the free expression ofreproductive rights Sexuality education is avoidedlike a plague and the use of contraception is onlyreserved for married women It is believed thattalking about sexuality education will encouragepromiscuity
Many young women who have little or no knowledgeof pregnancy and contraception end up gettingpregnant and seek out the fastest most secretiveand easiest way to terminate their pregnancies
2 ABORTION LAW AND POLICIES INNIGERIA
Together we create new self-definitions that canvalidate our resistance our intersectional realitiesand pave the way for reproductive justice
Follow Aarushi on Twitter
AARUSHI KHANNA29 INDIA
1 UNTITLED
OLUWAPELUMI ALESINLOYE-KING 23 NIGERIA
The quacks that offer dangerous and unsafeabortions range from auxiliary nurses fake doctorslocal medicine vendors to traditional birthattendants
According to the World Health Organization ldquoUnsafeabortion is a procedure for terminating anunintended pregnancy carried out either by personslacking the necessary skills andor in an environmentthat does not conform to minimal medicalstandardsrdquo
Some methods of unsafe abortions include theinsertion of sharp objects into the vagina drinkingherbal concoctions a combination of drugs in largedoses such as painkillers and antibiotics drinkingdangerous chemicals such as bleach and dyeAccording to WHO the results of unsafe abortionsmm
Youth Coalition for Sexual and Reproductive Rights 05
range from infertility injury loss of blood uterineperforation incomplete abortion infections death
In order to drastically reduce deaths arising fromunsafe abortion cases in Nigeria organizations suchas Safe2choose work actively to provide safeabortions for women who need it But despite allefforts at this the word ldquoabortionrdquo is still met withstiff opposition from many religious organizationsand lawmakers (especially of the older generation)
An example of this opposition is the raid by theNigerian Police on the Marie Stopes Clinic in LagosOn the 21st of May 2019 officers of the NigerianPolice force raided the reproductive health clinic onthe basis of allegedly providing ldquoabortion and birthcontrolrdquo services for women This issue was highlycondemned by many individuals and womenrsquos rightsorganizations who were saddened by the constantinfringement on womenrsquos sexual and reproductivehealth rights
Sexual and reproductive health rights include freeunrestricted access to sexual and reproductivehealth care and information as well as autonomy in
sexual and reproductive decision-makingmdasharehuman rights they are universal indivisible andundeniable Until Nigerian abortion laws arereformed to respect fundamental human rightsmany women will keep dying in their numbers fromcomplications arising from unsafe abortions Inshort the question of womenrsquos rights is nothing elsethan a matter of human rights
At HowToUseAbortionPill we explain how medicalabortion works what you need to know in advancehow it is done safely and what to expect next Youcan read all this information on our website Ourchatbot is also available 247 to answer all yourmedical abortion-related questions
Follow Oluwapelumi on Facebook Twitter andLinkedIn
Until Nigerian abortion laws are
reformed to respect fundamental human
rights many women will keep dying from
complications arising from unsafe
abortions
3 SAFE ABORTION FOR ALL A POEMRUKUMANI TRIPATHI 27 NEPAL
I was a teenProbably sixteenThen one day I saw a boyWe hung out together we did enjoyI was in loveAnd thought of us as a pair of dovesNever did I know what is rightNever did we ever have a fightWith everything newAs fresh as dewI loved him even moreWe shared our heart we shared our soulWe had sex as we were deeply in loveBut then after a month my period stopped
I was worriedI was scaredI was in high school and I was not preparedI was very scared when I checkedOh my god I was pregnantI didnrsquot know what to doI didnrsquot know who to contactI told my boyfriend
And since then our relationship endedNo wonder I cried all night and smiled all dayI had to show the world that I am perfectly wellOne day I heard an advertisementSafe abortion for all
Youth Coalition for Sexual and Reproductive Rights 06
I went there and took counselling before I fallThank god I was just 8 weeks pregnantAnd they told me that I could abort it with my ownconsentI was relieved because I had given up hopeTo live any moreIf there wasnrsquot an abortion service at that timeI would have probably ended my lifeIt made me realize I should be careful and I shouldbe conscious
This incident taught me that I should be cautiousI have ambitionI have dreamsSafe abortion for all is a human rightBecause birth should bring joy not frightI will plan a baby when I am readyWith the promise to myself I will be capable for thatday
Follow Rukumani on Facebook
4 ABORTION IN THE LGBTQIA+COMMUNITY IDENTIFYING GAPS INOUR MOVEMENTS CARLOS ACOSTA 26 COLOMBIA
Abortion rights have largely been discussedworldwide and while progress has been made inmany countries the narrative of abortion serviceskeeps leaving certain vulnerable groups aside ndashtransgender men non-binary people lesbianwomen and other members of the LGBTQ+spectrum
Are these rights different
We can start the discussion with the most explicitdifference When talking about LGBTQ+ rights thereis little to no mention about abortion Over the yearscountries like Argentina have had progressivemoves in accepting marriage and even procreationfor same sex couples but somehow abortion stillseems to be out of the picture(1) This erasurebecomes an ethical question when we observe thatthe high rates of violence towards this populationcould easily result in unwanted pregnancies Onecannot help but wonder at the gap betweenabortion rights and the LGBTQ+ movementconsidering that both movements are built on thefoundation of bodily autonomy being a fundamentalright
Let us look at how LGBTQ+ and abortion discoursesare built Much of the conversation around LGBTQ+rights revolves around bodily autonomy marriageviolence and adoption These are in fact sexual andreproductive rights ndash however abortion is left outWhen looking to the abortion movement these havea natural focus on women and girls who are themost highly impacted by the lack of access to safeabortion However the abortion discourse oftenleaves out many individuals on the gender spectrumthat have female-assigned reproductive systemsAbortion is still a ldquosherdquo or ldquowomenrsquosrdquo topic andleaves out non-binary and transmasculine peopletrans men and other people who do not identify aswomen
This doesnrsquot necessarily mean that we haveeverything upside down We just need to drawattention to the fact that we must support abortionrights for everyone by amplifying our efforts todiversify who we think needs abortion and access tocontraceptive services In 2013 Chen etal evidencethat LGBTQ+ individuals suffer equal or moreintimate partner violence compared to non-LGBTQ+households(2) If we were to take this fact shouldnrsquot
Youth Coalition for Sexual and Reproductive Rights 07
we evaluate the consequences of intimate partnerviolence and correlate those facts to the potentialneed of abortion services to this population
I believe that unity and cross-sectoral conversationsamongst different movement can help us addressthese gaps
to mould comprehensive sexuality education (CSE)in accordance to current needs of the populationTailoring sexual education towards diversity is a keyfactor in preventing unwanted pregnancies inLGBTQ+ youth and also providing informationabout abortion to diverse youth The typical talkabout cucumbers and bananas doesnrsquot fit manyindividuals in the community and it is scientificallyoutdated There should not only be education aboutphysical relationships but also interpersonal onesand how to foster respect and tolerance for eachother With this we also prevent violence and otherviolations of human rights
In conclusion
Abortion advocacy should be a joint effort comingfrom diverse NGO governmental and civil societysectors Working collectively allows ourconversation to be intersectional However ouractions should follow the same trend Engaging withthe community helps to tailor our interventions to amore focused population This will help us see abetter and much larger impact Hopefully as a rippleeffect we can also see our projects convert intomeaningful reduction of harm and an increase inhealth benefits for millions of people This 28th ofSeptember stop for a moment to think how you caninclude more people in your beliefs surroundingabortion
What direction do we follow The short answerwould be the one where we leave no one behind
Follow Carlos on Instagram and LinkedIn
One cannot help but wonder at the gap
between abortion rights and the LGBTQ+
movement considering that both movements
are built on the foundation of bodily autonomy
Another aspect of why abortion services areimportant for diverse communities is because thereis a long history of treatment and care divergenciestowards the LGBTQ+ community
Abortion services in most countries come from thestudy of obstetrics and gynecology This area ofmedicine (study of specific organs and reproduction)has long been directed towards cis-gender peopleand their patterns of reproduction There are fewscientific focuses on different types of reproductionpatterns that lesbian women transgender men andother individuals in the community might haveleaving the needs of these populations unattendedCommon practices are still centred towards cis-women bodies and a larger attention on medicaleducation could ameliorate this situation (3)
Prevention should also be different We must attempt
1 Luna F (2018) From the Middle Ages to the 21st Century Abortion Assisted Reproduction Technologies and LGBT Rights in ArgentinaCanadian Journal of Bioethics Revue canadienne de bioeacutethique 1 (2) 26ndash36 httpsdoiorg1072021058266ar2 Chen PH Jacobs A Rovi SL Intimate partner violence IPV in the LGBT community FP Essentials 2013 Sep41228-353 Eckstrand KL Potter J Edmiston EK (2016) Obstetric and Gynecologic Care for Individuals Who Are LGBT In Eckstrand K Ehrenfeld J(eds) Lesbian Gay Bisexual and Transgender Healthcare Springer Cham httpsdoiorg101007978-3-319-19752-4_17
Youth Coalition for Sexual and Reproductive Rights 08
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
range from infertility injury loss of blood uterineperforation incomplete abortion infections death
In order to drastically reduce deaths arising fromunsafe abortion cases in Nigeria organizations suchas Safe2choose work actively to provide safeabortions for women who need it But despite allefforts at this the word ldquoabortionrdquo is still met withstiff opposition from many religious organizationsand lawmakers (especially of the older generation)
An example of this opposition is the raid by theNigerian Police on the Marie Stopes Clinic in LagosOn the 21st of May 2019 officers of the NigerianPolice force raided the reproductive health clinic onthe basis of allegedly providing ldquoabortion and birthcontrolrdquo services for women This issue was highlycondemned by many individuals and womenrsquos rightsorganizations who were saddened by the constantinfringement on womenrsquos sexual and reproductivehealth rights
Sexual and reproductive health rights include freeunrestricted access to sexual and reproductivehealth care and information as well as autonomy in
sexual and reproductive decision-makingmdasharehuman rights they are universal indivisible andundeniable Until Nigerian abortion laws arereformed to respect fundamental human rightsmany women will keep dying in their numbers fromcomplications arising from unsafe abortions Inshort the question of womenrsquos rights is nothing elsethan a matter of human rights
At HowToUseAbortionPill we explain how medicalabortion works what you need to know in advancehow it is done safely and what to expect next Youcan read all this information on our website Ourchatbot is also available 247 to answer all yourmedical abortion-related questions
Follow Oluwapelumi on Facebook Twitter andLinkedIn
Until Nigerian abortion laws are
reformed to respect fundamental human
rights many women will keep dying from
complications arising from unsafe
abortions
3 SAFE ABORTION FOR ALL A POEMRUKUMANI TRIPATHI 27 NEPAL
I was a teenProbably sixteenThen one day I saw a boyWe hung out together we did enjoyI was in loveAnd thought of us as a pair of dovesNever did I know what is rightNever did we ever have a fightWith everything newAs fresh as dewI loved him even moreWe shared our heart we shared our soulWe had sex as we were deeply in loveBut then after a month my period stopped
I was worriedI was scaredI was in high school and I was not preparedI was very scared when I checkedOh my god I was pregnantI didnrsquot know what to doI didnrsquot know who to contactI told my boyfriend
And since then our relationship endedNo wonder I cried all night and smiled all dayI had to show the world that I am perfectly wellOne day I heard an advertisementSafe abortion for all
Youth Coalition for Sexual and Reproductive Rights 06
I went there and took counselling before I fallThank god I was just 8 weeks pregnantAnd they told me that I could abort it with my ownconsentI was relieved because I had given up hopeTo live any moreIf there wasnrsquot an abortion service at that timeI would have probably ended my lifeIt made me realize I should be careful and I shouldbe conscious
This incident taught me that I should be cautiousI have ambitionI have dreamsSafe abortion for all is a human rightBecause birth should bring joy not frightI will plan a baby when I am readyWith the promise to myself I will be capable for thatday
Follow Rukumani on Facebook
4 ABORTION IN THE LGBTQIA+COMMUNITY IDENTIFYING GAPS INOUR MOVEMENTS CARLOS ACOSTA 26 COLOMBIA
Abortion rights have largely been discussedworldwide and while progress has been made inmany countries the narrative of abortion serviceskeeps leaving certain vulnerable groups aside ndashtransgender men non-binary people lesbianwomen and other members of the LGBTQ+spectrum
Are these rights different
We can start the discussion with the most explicitdifference When talking about LGBTQ+ rights thereis little to no mention about abortion Over the yearscountries like Argentina have had progressivemoves in accepting marriage and even procreationfor same sex couples but somehow abortion stillseems to be out of the picture(1) This erasurebecomes an ethical question when we observe thatthe high rates of violence towards this populationcould easily result in unwanted pregnancies Onecannot help but wonder at the gap betweenabortion rights and the LGBTQ+ movementconsidering that both movements are built on thefoundation of bodily autonomy being a fundamentalright
Let us look at how LGBTQ+ and abortion discoursesare built Much of the conversation around LGBTQ+rights revolves around bodily autonomy marriageviolence and adoption These are in fact sexual andreproductive rights ndash however abortion is left outWhen looking to the abortion movement these havea natural focus on women and girls who are themost highly impacted by the lack of access to safeabortion However the abortion discourse oftenleaves out many individuals on the gender spectrumthat have female-assigned reproductive systemsAbortion is still a ldquosherdquo or ldquowomenrsquosrdquo topic andleaves out non-binary and transmasculine peopletrans men and other people who do not identify aswomen
This doesnrsquot necessarily mean that we haveeverything upside down We just need to drawattention to the fact that we must support abortionrights for everyone by amplifying our efforts todiversify who we think needs abortion and access tocontraceptive services In 2013 Chen etal evidencethat LGBTQ+ individuals suffer equal or moreintimate partner violence compared to non-LGBTQ+households(2) If we were to take this fact shouldnrsquot
Youth Coalition for Sexual and Reproductive Rights 07
we evaluate the consequences of intimate partnerviolence and correlate those facts to the potentialneed of abortion services to this population
I believe that unity and cross-sectoral conversationsamongst different movement can help us addressthese gaps
to mould comprehensive sexuality education (CSE)in accordance to current needs of the populationTailoring sexual education towards diversity is a keyfactor in preventing unwanted pregnancies inLGBTQ+ youth and also providing informationabout abortion to diverse youth The typical talkabout cucumbers and bananas doesnrsquot fit manyindividuals in the community and it is scientificallyoutdated There should not only be education aboutphysical relationships but also interpersonal onesand how to foster respect and tolerance for eachother With this we also prevent violence and otherviolations of human rights
In conclusion
Abortion advocacy should be a joint effort comingfrom diverse NGO governmental and civil societysectors Working collectively allows ourconversation to be intersectional However ouractions should follow the same trend Engaging withthe community helps to tailor our interventions to amore focused population This will help us see abetter and much larger impact Hopefully as a rippleeffect we can also see our projects convert intomeaningful reduction of harm and an increase inhealth benefits for millions of people This 28th ofSeptember stop for a moment to think how you caninclude more people in your beliefs surroundingabortion
What direction do we follow The short answerwould be the one where we leave no one behind
Follow Carlos on Instagram and LinkedIn
One cannot help but wonder at the gap
between abortion rights and the LGBTQ+
movement considering that both movements
are built on the foundation of bodily autonomy
Another aspect of why abortion services areimportant for diverse communities is because thereis a long history of treatment and care divergenciestowards the LGBTQ+ community
Abortion services in most countries come from thestudy of obstetrics and gynecology This area ofmedicine (study of specific organs and reproduction)has long been directed towards cis-gender peopleand their patterns of reproduction There are fewscientific focuses on different types of reproductionpatterns that lesbian women transgender men andother individuals in the community might haveleaving the needs of these populations unattendedCommon practices are still centred towards cis-women bodies and a larger attention on medicaleducation could ameliorate this situation (3)
Prevention should also be different We must attempt
1 Luna F (2018) From the Middle Ages to the 21st Century Abortion Assisted Reproduction Technologies and LGBT Rights in ArgentinaCanadian Journal of Bioethics Revue canadienne de bioeacutethique 1 (2) 26ndash36 httpsdoiorg1072021058266ar2 Chen PH Jacobs A Rovi SL Intimate partner violence IPV in the LGBT community FP Essentials 2013 Sep41228-353 Eckstrand KL Potter J Edmiston EK (2016) Obstetric and Gynecologic Care for Individuals Who Are LGBT In Eckstrand K Ehrenfeld J(eds) Lesbian Gay Bisexual and Transgender Healthcare Springer Cham httpsdoiorg101007978-3-319-19752-4_17
Youth Coalition for Sexual and Reproductive Rights 08
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
I went there and took counselling before I fallThank god I was just 8 weeks pregnantAnd they told me that I could abort it with my ownconsentI was relieved because I had given up hopeTo live any moreIf there wasnrsquot an abortion service at that timeI would have probably ended my lifeIt made me realize I should be careful and I shouldbe conscious
This incident taught me that I should be cautiousI have ambitionI have dreamsSafe abortion for all is a human rightBecause birth should bring joy not frightI will plan a baby when I am readyWith the promise to myself I will be capable for thatday
Follow Rukumani on Facebook
4 ABORTION IN THE LGBTQIA+COMMUNITY IDENTIFYING GAPS INOUR MOVEMENTS CARLOS ACOSTA 26 COLOMBIA
Abortion rights have largely been discussedworldwide and while progress has been made inmany countries the narrative of abortion serviceskeeps leaving certain vulnerable groups aside ndashtransgender men non-binary people lesbianwomen and other members of the LGBTQ+spectrum
Are these rights different
We can start the discussion with the most explicitdifference When talking about LGBTQ+ rights thereis little to no mention about abortion Over the yearscountries like Argentina have had progressivemoves in accepting marriage and even procreationfor same sex couples but somehow abortion stillseems to be out of the picture(1) This erasurebecomes an ethical question when we observe thatthe high rates of violence towards this populationcould easily result in unwanted pregnancies Onecannot help but wonder at the gap betweenabortion rights and the LGBTQ+ movementconsidering that both movements are built on thefoundation of bodily autonomy being a fundamentalright
Let us look at how LGBTQ+ and abortion discoursesare built Much of the conversation around LGBTQ+rights revolves around bodily autonomy marriageviolence and adoption These are in fact sexual andreproductive rights ndash however abortion is left outWhen looking to the abortion movement these havea natural focus on women and girls who are themost highly impacted by the lack of access to safeabortion However the abortion discourse oftenleaves out many individuals on the gender spectrumthat have female-assigned reproductive systemsAbortion is still a ldquosherdquo or ldquowomenrsquosrdquo topic andleaves out non-binary and transmasculine peopletrans men and other people who do not identify aswomen
This doesnrsquot necessarily mean that we haveeverything upside down We just need to drawattention to the fact that we must support abortionrights for everyone by amplifying our efforts todiversify who we think needs abortion and access tocontraceptive services In 2013 Chen etal evidencethat LGBTQ+ individuals suffer equal or moreintimate partner violence compared to non-LGBTQ+households(2) If we were to take this fact shouldnrsquot
Youth Coalition for Sexual and Reproductive Rights 07
we evaluate the consequences of intimate partnerviolence and correlate those facts to the potentialneed of abortion services to this population
I believe that unity and cross-sectoral conversationsamongst different movement can help us addressthese gaps
to mould comprehensive sexuality education (CSE)in accordance to current needs of the populationTailoring sexual education towards diversity is a keyfactor in preventing unwanted pregnancies inLGBTQ+ youth and also providing informationabout abortion to diverse youth The typical talkabout cucumbers and bananas doesnrsquot fit manyindividuals in the community and it is scientificallyoutdated There should not only be education aboutphysical relationships but also interpersonal onesand how to foster respect and tolerance for eachother With this we also prevent violence and otherviolations of human rights
In conclusion
Abortion advocacy should be a joint effort comingfrom diverse NGO governmental and civil societysectors Working collectively allows ourconversation to be intersectional However ouractions should follow the same trend Engaging withthe community helps to tailor our interventions to amore focused population This will help us see abetter and much larger impact Hopefully as a rippleeffect we can also see our projects convert intomeaningful reduction of harm and an increase inhealth benefits for millions of people This 28th ofSeptember stop for a moment to think how you caninclude more people in your beliefs surroundingabortion
What direction do we follow The short answerwould be the one where we leave no one behind
Follow Carlos on Instagram and LinkedIn
One cannot help but wonder at the gap
between abortion rights and the LGBTQ+
movement considering that both movements
are built on the foundation of bodily autonomy
Another aspect of why abortion services areimportant for diverse communities is because thereis a long history of treatment and care divergenciestowards the LGBTQ+ community
Abortion services in most countries come from thestudy of obstetrics and gynecology This area ofmedicine (study of specific organs and reproduction)has long been directed towards cis-gender peopleand their patterns of reproduction There are fewscientific focuses on different types of reproductionpatterns that lesbian women transgender men andother individuals in the community might haveleaving the needs of these populations unattendedCommon practices are still centred towards cis-women bodies and a larger attention on medicaleducation could ameliorate this situation (3)
Prevention should also be different We must attempt
1 Luna F (2018) From the Middle Ages to the 21st Century Abortion Assisted Reproduction Technologies and LGBT Rights in ArgentinaCanadian Journal of Bioethics Revue canadienne de bioeacutethique 1 (2) 26ndash36 httpsdoiorg1072021058266ar2 Chen PH Jacobs A Rovi SL Intimate partner violence IPV in the LGBT community FP Essentials 2013 Sep41228-353 Eckstrand KL Potter J Edmiston EK (2016) Obstetric and Gynecologic Care for Individuals Who Are LGBT In Eckstrand K Ehrenfeld J(eds) Lesbian Gay Bisexual and Transgender Healthcare Springer Cham httpsdoiorg101007978-3-319-19752-4_17
Youth Coalition for Sexual and Reproductive Rights 08
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition

we evaluate the consequences of intimate partnerviolence and correlate those facts to the potentialneed of abortion services to this population
I believe that unity and cross-sectoral conversationsamongst different movement can help us addressthese gaps
to mould comprehensive sexuality education (CSE)in accordance to current needs of the populationTailoring sexual education towards diversity is a keyfactor in preventing unwanted pregnancies inLGBTQ+ youth and also providing informationabout abortion to diverse youth The typical talkabout cucumbers and bananas doesnrsquot fit manyindividuals in the community and it is scientificallyoutdated There should not only be education aboutphysical relationships but also interpersonal onesand how to foster respect and tolerance for eachother With this we also prevent violence and otherviolations of human rights
In conclusion
Abortion advocacy should be a joint effort comingfrom diverse NGO governmental and civil societysectors Working collectively allows ourconversation to be intersectional However ouractions should follow the same trend Engaging withthe community helps to tailor our interventions to amore focused population This will help us see abetter and much larger impact Hopefully as a rippleeffect we can also see our projects convert intomeaningful reduction of harm and an increase inhealth benefits for millions of people This 28th ofSeptember stop for a moment to think how you caninclude more people in your beliefs surroundingabortion
What direction do we follow The short answerwould be the one where we leave no one behind
Follow Carlos on Instagram and LinkedIn
One cannot help but wonder at the gap
between abortion rights and the LGBTQ+
movement considering that both movements
are built on the foundation of bodily autonomy
Another aspect of why abortion services areimportant for diverse communities is because thereis a long history of treatment and care divergenciestowards the LGBTQ+ community
Abortion services in most countries come from thestudy of obstetrics and gynecology This area ofmedicine (study of specific organs and reproduction)has long been directed towards cis-gender peopleand their patterns of reproduction There are fewscientific focuses on different types of reproductionpatterns that lesbian women transgender men andother individuals in the community might haveleaving the needs of these populations unattendedCommon practices are still centred towards cis-women bodies and a larger attention on medicaleducation could ameliorate this situation (3)
Prevention should also be different We must attempt
1 Luna F (2018) From the Middle Ages to the 21st Century Abortion Assisted Reproduction Technologies and LGBT Rights in ArgentinaCanadian Journal of Bioethics Revue canadienne de bioeacutethique 1 (2) 26ndash36 httpsdoiorg1072021058266ar2 Chen PH Jacobs A Rovi SL Intimate partner violence IPV in the LGBT community FP Essentials 2013 Sep41228-353 Eckstrand KL Potter J Edmiston EK (2016) Obstetric and Gynecologic Care for Individuals Who Are LGBT In Eckstrand K Ehrenfeld J(eds) Lesbian Gay Bisexual and Transgender Healthcare Springer Cham httpsdoiorg101007978-3-319-19752-4_17
Youth Coalition for Sexual and Reproductive Rights 08
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
When I started to question the things
that I was being told about what someone
can and cannot do with their bodies I felt
alone and like I was turning my back on my
community
5 PRO-CHOICE ACTIVISM IS MYCOMMUNITY CARE LAURA O CONNOR 20 CANADA
I grew up in a highly homogeneous Catholiccommunity in Southeastern Ontario going to churchevery Sunday saying the rosary with my family on adaily basis and attending longstanding Catholicschools for the entirety of my primary and highschool years While I obviously love and care for myfamily and early childhood friends I canrsquot deny thatour paths diverged quite early in my life and havecontinued to go in polar opposite directions Forthose of us who grew up in these environmentsunlearning certain values can not only be difficult itcan be extremely painful One of the key principlesof the Catholic dogma that was taught to me was theldquovalue of the life of the unbornrdquo and the so-calledcommitment that each of us have in protecting anddefending these ldquolivesrdquo Phrases such as ldquothe unbornare the most innocentrdquo and highly anti-SemiticHolocaust comparisons were regularly heardthroughout my childhood and teenage years
world I felt euphoric that I was finding communityand making a new identity for myself but I also feltisolated from my hometown community and familyand afraid to share my views and how I was choosingto spend my time in Ottawa Unlearning the anti-choice views about abortion that I had been taughtto believe was liberating and terrifying at the sametime
That being said I gradually began leaning on mypro-choice activist community more and more andfelt my strongest links shifting from my hometowntowards Ottawa The reproductive justicecommunity is relatively small despite how impactfulit is Moreover the majority of pro-choice activistgroups and organizations operate from a grassrootsframework meaning that horizontal relationshipsand open dialogue are encouraged and fairlynormalized
Being in this new environment was wildly differentfrom the highly exclusive and hierarchical churchstructure I grew up in and the idea that I could freelyshare my views hardships and high points wasforeign to me In addition I felt shame that I hadgrown up in an environment that taught me ideasthat caused so much harm to the reproductivejustice movement However as my reprocommunity strengthened and I saw the sacrifices mypeers were making for me in addition to thegraciousness of my fellow community members forthe work I had done I began to unlearn the shame Ihad grown up to feel Once I began putting my trustinto my community the repro justice world becamemy source of community-care and where I began totruly become the woman I am today While I oncefelt isolated being able to lean on my activistcommunity was the key to feeling supported andtogether
In celebration of International Safe Abortion Day
Because of this when I started to question thethings that I was being told about what someonecan and cannot do with their bodies I felt alone andlike I was turning my back on my community What Iwas being told about abortion the life of a foetusand to what extent the state could interfere in onersquosbodily autonomy didnrsquot make sense to me as I heardmore about modern feminist movements and pro-choice activism While I still couldnrsquot tell you whythe more I questioned what I was being taught aboutabortion the more abortion became the issue Icared about the most After moving away foruniversity I delved head-first into the reproductivejustice community in Ottawa When I entered this
Youth Coalition for Sexual and Reproductive Rights 09
Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition

Watch on Youtube
In many countries the law says that abortion is not allowed However in practice people still perform the actbut with the use of crude tools which endangers their lives Young girls and women should be given access totheir sexual and reproductive health and rights Through the Reform53 anti-discriminatory laws campaignthe Commonwealth Youth Gender and Equality Network is lobbying to ensure provisions in the law for abortionby choice
Follow Nandini on Facebook Twitter and InstagramFollow Commonwealth Youth Gender and Equality Network on Facebook Twitter and Instagram
I thought sharing this little part of my pro-choiceactivist journey could help commemorate this dayThe community behind this movement behind SafeAbortion Day have been formative in shaping who Iam provided me with community when I most needit and continue to be my primary form ofcommunity care Not only this but I am confidentthat there are many people who are like me ndash who
6 REFORM53 ABORTION BYCHOICE NANDINI TANYA LALLMON 29 MAURITIUS
grew up in a difficult environment that didnrsquot accepttheir political activism and had to unlearn the self-stigma around abortion and shame of growing up inan anti-choice environment For myself and peoplelike me there could not be enough thanks given tothe reproductive justice community
Follow Laura on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 10
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
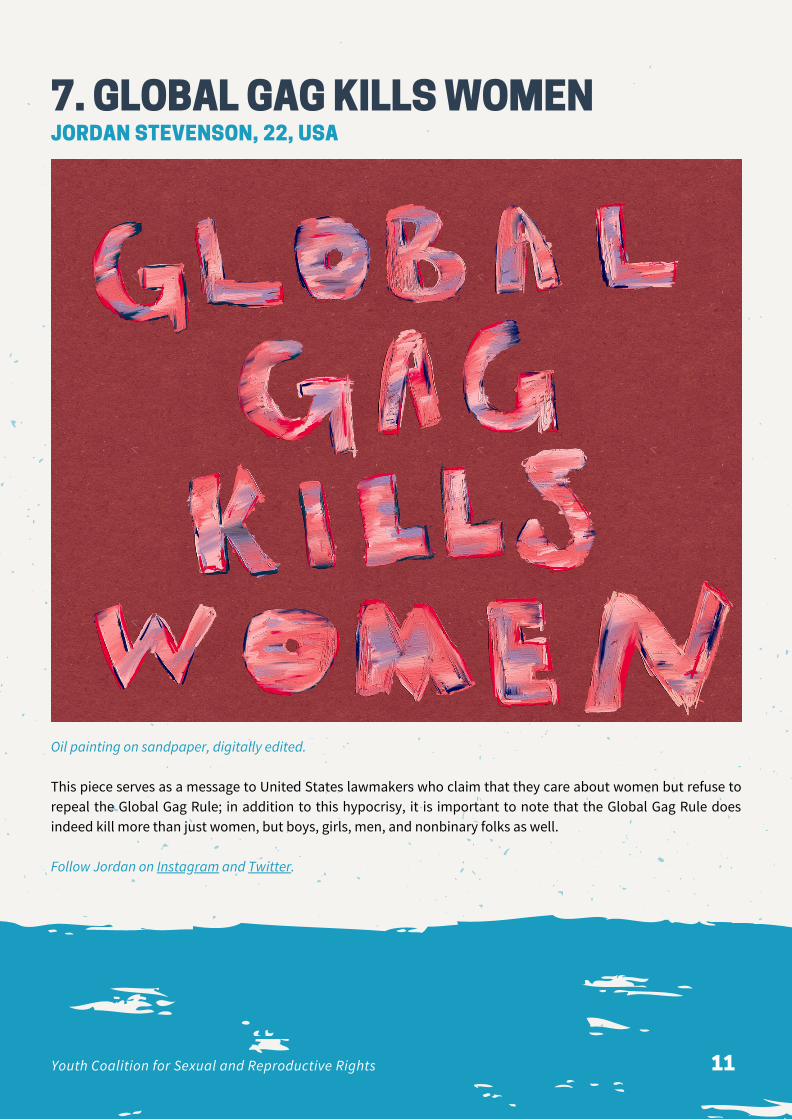
7 GLOBAL GAG KILLS WOMENJORDAN STEVENSON 22 USA
Oil painting on sandpaper digitally edited
This piece serves as a message to United States lawmakers who claim that they care about women but refuse torepeal the Global Gag Rule in addition to this hypocrisy it is important to note that the Global Gag Rule doesindeed kill more than just women but boys girls men and nonbinary folks as well
Follow Jordan on Instagram and Twitter
Youth Coalition for Sexual and Reproductive Rights 11
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
On January 23 2017 in his fourth day in officePresident Trump signed an executive order toreinstate the Mexico City Policy also known aslsquoGlobal Gag Rulersquo (GGR) In short the policy forbidsforeign NGOs from receiving US bilateral healthfunding if they provide information referralsadvocacy for access to safe abortion or services forlegal abortion in their country mdash even when usingtheir own non-US funds Due to these restrictions theGGR lsquogagsrsquo health providers counsellors advocatesand NGOs that provide abortion services
The latest GGR renamed as lsquoProtecting Life in GlobalHealth Assistance Policyrsquo (PLGHA) is an expandedversion of the previous iterations This time theTrump administration has gone further by placingunprecedented and radical restrictions that applynot only to family planning funding but also to all USglobal health assistance This includes assistancetowards HIV tuberculosis malaria Zika and watersanitation and hygiene among other programsWhile preceding versions of the GGR solely affectedfamily planning funding mdash averaging at $600 millionannuallymdash the PLGHA is estimated to affect between$85 to $1000 billion per year an amount 15 timesbigger
The effects of this dangerous anti-abortion policyare far-reaching and they disproportionately impactwomen girls and vulnerable populations mdash such asadolescents LGBTQI+ people and sex workers mdash inthe Global South The GGR puts ideology beforeevidence and rather than protecting life itendangers the right to health well-being and bodilyautonomy
In fact there is no evidence supporting theeffectiveness of the GGR in decreasing abortionrates Instead the limited but relevant studiesreviewing the policyrsquos impact suggest that the GGR
goes contrary to its stated purpose by reducingaccess to contraception and family planning servicesit then increases the number of unintendedpregnancies and (unsafe) abortions As a result thepolicy also has negative impacts on maternalnewborn and child health Besides the GGR has animperialistic nature by exporting the US domesticideological divide to the Global South wherewomenrsquos lives are risked for the political gain ofconservative and anti-abortion politicians andgroups
8 THE GLOBAL GAG RULE amp THE FIGHTFOR ABORTION RIGHTS GLOBALLYCHANDREYI GUHARAY 28 NICARAGUANETHERLANDS
The GGR goes contrary to its stated
purpose by reducing access to
contraception and family planning services
it then increases the number of unintended
pregnancies and (unsafe) abortions
Against the adversity and hostile environment thatthe GGR has created around access to safe abortionmultiple actors are devising creative and innovativeways to mitigate the policyrsquos harmful impact TheSheDecides movement emerged in 2017 as aninvigorating response to the current GGR SheDecideshas been supported by several country governmentsand has established itself as an internationalmovement that aims to raise awareness and unlockresources for contraception and abortion services forwomen and girls in the Global South In 2019 theGlobal Health Empowerment and Rights Act (GlobalHER Act) was introduced in the US Congress Ifpassed this bill would repeal the GGR and prevent itsfuture reinstatement
Other various organizations mdash such as PAI MarieStopes International and International PlannedParenthood Federation mdash have been fighting againstthe GGR since it was first instated by PresidentReagan in 1984 and are providing evidence of how
Youth Coalition for Sexual and Reproductive Rights 12
this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition

this harmful policy is endangering the health andhuman rights of people around the world It is yet tobe seen however whether these well-heartedefforts will be enough to mitigate the damage andthe social economic ethical and human costscaused by the current GGR
The Global Gag Rule is a direct attack on globalabortion rights and on the access to other essentiallife-saving health care putting the lives of millions indanger particularly the most marginalized In thesetrying times we must stand in solidarity and support
with organizations and movements who arestanding up against the GGR we must educate andraise awareness about the harmful impacts of thispolicy and most importantly we must keep fightingback regressive actors who threaten progress
Abortion is essential healthcare abortion is a humanright This should be the norm rather than theexception for every person in every corner of theworld
Follow Chandreyi on Twitter and Instagram
9
YINKORE 22 NIGERIA Follow Yinkore on Instagram and on her website
Youth Coalition for Sexual and Reproductive Rights 13
One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition

One of the most stringent lockdowns in the world inresponse to COVID-19 outbreak had an unforeseenconsequence ndash disruption of family planningservices in India It has grimly impacted the lives ofwomen due to lack of access to contraceptives andabortion services Hence therersquos been a surge inunintended pregnancies unsafe abortions andmaternal mortality
A recent study conducted by Marie StopesInternational revealed that 13 million women inIndia alone - out of two million women globally -missed out on sexual and reproductive health (SRH)services between January and June According todata released by UNFPA prolonged lockdown oversix months could keep 47 million women in low andmiddle-income countries from accessing and usingmodern contraceptives
Even though the Government of India listed safeabortion as an essential service during thenationwide lockdown pregnant people still found itdifficult to access this medical service As publichealth centres were converted to COVID-19 carecentres and ASHA workers (or Accredited SocialHealth Activists who distribute contraceptives atcommunity level) were diverted towardscoronavirus containment work it restricted theavailability of SRH services Many private healthcentres were also not operational due to lack ofpersonal protective equipment and mandatoryCOVID-19 testing facilities Medical supplies had alsobeen hit due to limitations on inter-state travel andtemporary shutdown of factories manufacturingfamily planning products
Clinicshospitals are not always located in onersquosneighbourhood Consequently many women wereunable to visit them due to suspension oftransportation Amidst the pandemic-led lockdown
they were concerned of being exposed to the virusPlus they also feared the inquiry by police regardingthe purpose of their visit The attitude towardsabortion in India has been ldquoWe are facing apandemic and you want to avail abortionrdquo Thewoman seeking an abortion does not look seriouslyill Therefore it is hard to explain to people why anormal and healthy looking woman needs medicalassistance
A girl who lives in my neighbourhood discovered herpregnancy just after the lockdown was announcedThe 23-year-old wanted an abortion immediatelyShe could not talk about it due to the stigmasurrounding abortion With clinics closed and wholecity at standstill she bought an abortion pill withoutconsulting a doctor (as per Indian law prescription ofpills is required by a licensed medical professional inIndia) Bleeding for hours and in extreme pain shecalled a gynaecologist who talked her throughtermination
Though lockdown restrictions are now easingexperts predict a spike in demand for abortion ndashespecially second-trimester abortions A recentreport by Foundation for Reproductive HealthServices India indicated that there could be anadditional 834042 unsafe abortions and 1743maternal deaths thanks to COVID-19 A delay inavailing medical intervention can lead to moresurgical abortions instead of medical ones Alsopregnancies over 20 weeks are not legally permittedto be terminated as per Indiarsquos abortion law
10 CAN ABORTION BE POSTPONED INCOVID-19 ABSOLUTELY NOTARSHPREET KAUR 28 INDIA
The attitude towards abortion in India
has been ldquoWe are facing a pandemic
and you want to avail abortionrdquo
Youth Coalition for Sexual and Reproductive Rights 14
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
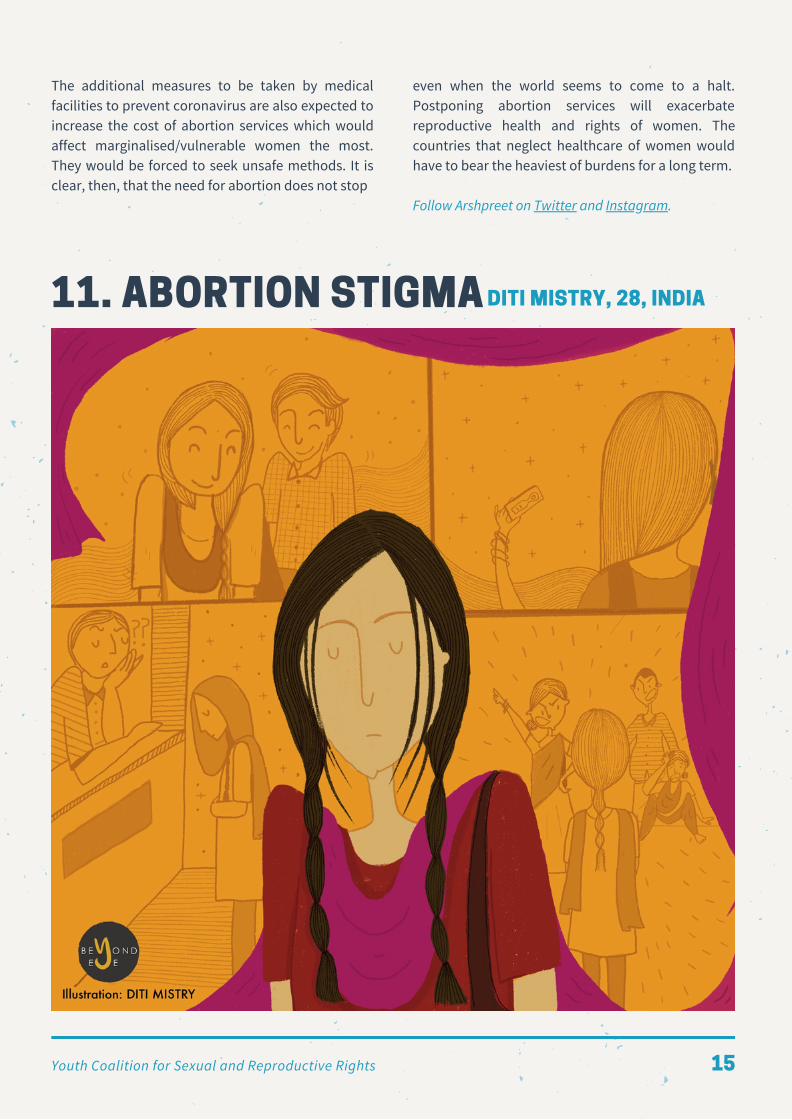
The additional measures to be taken by medicalfacilities to prevent coronavirus are also expected toincrease the cost of abortion services which wouldaffect marginalisedvulnerable women the mostThey would be forced to seek unsafe methods It isclear then that the need for abortion does not stop
11 ABORTION STIGMA DITI MISTRY 28 INDIA
even when the world seems to come to a haltPostponing abortion services will exacerbatereproductive health and rights of women Thecountries that neglect healthcare of women wouldhave to bear the heaviest of burdens for a long term
Follow Arshpreet on Twitter and Instagram
Youth Coalition for Sexual and Reproductive Rights 15
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
This illustration depicts the true story of anunmarried young girl from a marginalised socio-economic community in India and her struggles withaccessing abortion services without family support
Premarital sex is widely discouraged in our societyand pregnancy among unmarried women is soextremely stigmatized that it is perceived to ruin afamilys reputation In most cases young womenhave to face violence from their family members
Also health service providers with theirconservative nature discriminate against unmarriedwomen and dont allow them to access serviceswithout their parents These experiences result inyoung people spending cash to access undergroundunsafe abortion services and miss out on followinghealthy practices for post-abortion care
Follow Diti Mistryrsquos organisation Beyond Eye on theirwebsite Facebook Twitter and Instagram
12 COVID-19 ANOTHER BARRIER TOSAFE ABORTIONS IN COLOMBIACATALINA CALLE DURAacuteN 24 COLOMBIA
March 2nd 2020 ndash 14 years after the last decision bythe Colombian Constitutional Court that legalisedabortion on three specific grounds (if the health -mental or physical - of the pregnant person is indanger if the foetus presents a malformation thatmakes it incompatible with life or if the pregnancy isthe product of rape or incest) the Court ruled thatnothing changes The debate started last year whenthe Court received two lawsuits requesting acomplete ban on abortions arguing that life startsfrom gestation Taking advantage of the possibilityof changing the abortion laws of the country andfollowing the guidelines of international health andhuman rights organizations Magistrate AlejandroLinares sought to decriminalize abortion in the first12 weeks of gestation
The Court concluded that it was not legally feasibleto re-analyse the abortion laws of the country ndashmeaning that abortion in Colombia stayedconditional as it has been since 2006 The Courtitself has identified 14 barriers when accessing legalabortion services including delays in bureaucraticprocedures ignorance amp legal non-compliance fromhealth providers and economic amp cultural barriers
The conditionality and the obstacles to access safeabortions might be the reason for the low number ofthese procedures performed legally in the countryAccording to Profamilia an SRH provisioner in thecountry there are less than 17000 legal abortions ayear On the other hand according to theGuttmacher Institute there are around 400000clandestine abortions a year Unsafe abortionprocedures one of the leading causes of maternalmortality are accountable for 1 in 8 global maternaldeaths The data from the Health Ministry showsthat in Colombia an average of six women a monthdie from a complication from illegal abortions
The same day that the Court announced its decisionthe country increased from moderate to high risk ofthe Coronavirus entering the country Colombia stillhad zero cases but the LAC region already had a fewEven at that early stage international organizationslike International Planned Parenthood Federation(IPPF) had foreseen that this pandemic was going toput millions of additional women at risk of sexualviolence lack of access to contraception andunintended pregnancy Currently in Colombia Stateand private entities have already documented
Youth Coalition for Sexual and Reproductive Rights 16
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
that in the pandemic gender violence hasexploded
An increase in interpersonal violence can increaseunwanted pregnancies ndash especially with asinternational organizations that partnered with localsexual and reproductive health organizations likeIPPF and Meacutedecins Sans Frontiegraveres have reported ashortage of contraceptives in the LAC region In earlyApril IPPF published a survey with collectedevidence of how COVID-19 has affected the deliveryof sexual and reproductive health (SRH) services Inthe report data showed that Colombia was amongthe most affected countries by the closures of clinicsandor community-based service outlets reportingmore than 100 closures at the start of the pandemic
On April 24th the Ministry of Health issued astatement clarifying that SRH services includinglegal abortions had to continue to be accessible foreveryone At the same time the government-mandated social distancing and lack of PPE pushedlegal abortion clinics like Orientame to movetowards
towards telemedicine adding a barrier to accesslegal abortion services in Colombia
As of December 2019 Colombias Ministry ofInformation Technologies and Communicationsreported that nearly half the country lacks mobileinternet access People from lower-income groups inrural parts of the country encounter additionalobstacles when accessing safe abortion servicesIPPF Director-General stated that if governments donot address the increase in barriers to access safeabortion contraceptives and other SRH servicesldquothe consequences for women and girls will becatastrophic resulting in loss of health autonomyand liferdquo
Follow Catalina on Instagram Twitter and LinkedIn
An increase in interpersonal violence
can increase unwanted pregnancies ndash
especially with the shortage of
contraceptives in the LAC region
13 EXORCISM DEEPSHIKHA SHARMA 22 INDIA
A Faith inverse with the declaration of evil Two pink lines announce the possession Amidst plastic porcelain tears and urine I ready my corrupted soul to be chastised My body to be burntLegs spread apart on the altar Pitchforks in the hand of the priestA necessary evil for the cosmic good Does not pardon my masculine curiosity
By the pricking of my thumbs a warning by the gut Lunar incantations for the ldquogoodrdquo the society ina rut
ldquoA loose womanrdquo they say ldquobut it needs to be donerdquo
ldquoBlood split by the thornNeeds to be wiped
Youth Coalition for Sexual and Reproductive Rights 17
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Rotten fruits from the Devilrsquos rose Need to plucked Consorts of the typeNeed to be chastised Wombs of ringless women Need to be purifiedrdquo
As my shackles rattle and my body contorts I forget verbal stings about Devils and consort
Pain blinds my sight Screams numb my throat The soul holds unto my body Unwilling to partBall of flesh clot of blood Haunts the marrow in my bone As the sludge from the exorcism Slips into the cauldron Sight returns and jaw slackensI beg for the manacles to be taken The grass rustles underneath my feet The pain has set me freeAngst and guiltAre healed by the bruises in my thighs Stones are thrown pitchforks wave But nothing wicked comes my way Nothing I couldnrsquot nurture and grow Nothing I couldnrsquot provide for
Because I was right to choose about the when andwhere
KARREN BARCITA 22PHILIPPINES
14 MY BODYMY CHOICE
15 SEXUAL AND REPRODUCTIVE RIGHTSIN UGANDA IN THE GLOBAL GAG ERAATEGEKA FRANK 30 UGANDA
In January 2017 the Global Gag Rule (GGR) wassigned into law through an Executive Order by USPresident Donald Trump The GGR aims to block USfederal funding for non-governmental organizations(NGOs) and groups that provide abortioncounseling make referrals andor advocate to
decriminalize abortion or expand abortion servicesas a method of family planning This policy requiresnon-American NGOs to certify that they will notldquoperform or actively promote abortion as a methodof family planningrdquo with any of their funding(including non-US funds) as a condition for
Youth Coalition for Sexual and Reproductive Rights 18
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
receiving US global health assistance
Unlike previous versions the current version of thepolicy applies to recipients of family planningfunding and recipients of all global health assistanceunder US government departments or agenciesThis means that ldquoFor the first time everorganizations that provide counseling referrals orservices or advocate for safe abortion with their ownfunding will be banned from all global healthfunding from the US governmentrdquo The ban thusdirectly impacts funding for international healthprograms including HIVAIDS maternal and childhealth malaria family planning and global healthsecurity In earlier versions of the GGR PEPFAR oneof the biggest funders for HIVAIDs programs inmany countries including Uganda was excludedbut in the 2017 version it was ldquogaggedrsquorsquo since it isunder the Department of State in the PresidentrsquosCabinet
Implications of GGR on Sexual and ReproductiveHealth and Rights (SRHR) in Uganda
In Uganda the restrictive legal environment onabortion and the limited national health budgetdoes not guarantee SRH service delivery andabortion remains highly stigmatized Like in manyother countries in the world despite the legalrestrictions abortions occur in Uganda anywayoften in environments and with methods that putwomen and girls at higher risk In fact according toUgandarsquos New Vision 1500 women die annually dueto unsafe abortions more than 93000 women werehospitalized for complications from unsafe abortionin Uganda in 2013 and more than 10 of thecountryrsquos maternal deaths were due to unsafeabortion Rather than curbing abortion the GGR willinevitably increase these numbers
In the 2013ndash2014 Uganda Health Accounts NationalHealth Expenditure it was reported that 41 ofUgandarsquos current health expenditure is financed bydevelopment partners primarily bilateral donors Ofthe funding provided through health financing bydevelopment partners 49 of funds go topreventive care This is the scope of the impact of the
the GGR in Uganda mdash an entire 20 of the healthsectorrsquos preventative care will be lost
The report further indicates that the government ofUganda depends on $67 million (USD) in donorfunding for sexual and reproductive health (SRH)supplies According to the Ministry of Health thereremains an estimated gap of $9 million (USD) forfamily planning commodities overall Throughoutside funding many NGOs have been trying toclose this funding gap for SRH The statement of thecurrent GGR has delivered a huge blow to theseefforts causing many organizations to scale backservices or even close offices For example UgandaHealth Marketing Group (UHMG) accounts for 80 ofSRH supplies in Uganda and is funded by the USAIDproject AFFORD Because the SRH services providedby UHMG through their 256 clinics countrywide areldquogaggedrdquo by the GGR those accessing SRHcommodities there will not be counseled on optionsrelated to abortion even where abortion is legal
This is the scope of the impact of
the GGR in Uganda mdash an entire 20 of
the health sectorrsquos preventative care
will be lost
The Ugandan governmentrsquos project offering breastand cervical cancer screenings and promoting theuse of Sayana Press a new brand of injectablecontraceptives has been halted The GGR is alsolikely to further hinder advocacy efforts forprogressive health policies such as the sexualityeducation policy that would ultimately curbmaternal deaths caused by unsafe abortions inUganda Furthermore the policy is already adverselyaffecting Ugandarsquos commitments of providingaccess to family planning in line with thegovernmentrsquos National Family Planning Action Planand Family Planning 2020 Commitments because ofreduced or lost funding to NGOs that were theleading SRH service providers Ultimately the GGR isa major setback to Universal Health Coverage by2030 as most Ugandans will have to either pay forSRH services from private service providers or gowithout services if they cannot afford to do so
Youth Coalition for Sexual and Reproductive Rights 19
The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition

The Way Forward
Rural Aid Foundation the organization I co-lead withmy fellow Global Health Corps alumna CarolineAchola has been partnering with the Alert Fund forYouth to raise awareness about the GGR and itsimplications on access to SRH services for youngpeople in Uganda
We have already conducted a project inceptionmeeting with civil society and communityorganizations as well as adolescent girls and youngwomen and have begun documenting their healthchallenges as a result of the Global Gag Rule Using acommunity-led approach we supported them indeveloping and presenting a petition to protectyoung Ugandanrsquos access to sexual reproductivehealth services and rights The petition waspresented to the Vice-Chairperson of theParliamentary Health Committee requesting thatthe Ugandan government
Close the funding gap for reproductive healthservices for youths in Uganda by allocatingalternative local fundingConduct an impact assessment on theimplications of GGR on access to reproductivehealth service provision in Uganda and present asummary paper to the full Parliament
The Vice-Chairperson on the Health Committee ofParliament made a commitment to present thepetition to the health committee and also present iton the floor
The GGR poses a threat to sexual reproductivehealth service delivery and this will likely hinder therealization of Universal Health Coverage by 2030States must understand the implications and makeinformed decisions for SRHR policy change andfinancing to protect young people and othervulnerable populations to ensure no one is leftbehind
DOCUMENTARY ON IMPACT OF GLOBAL GAG RULE IN UGANDA BY FRANKATEGEKA AND RURAL AID FOUNDATION
Follow Franks organisation the Rural Aid Foundation Uganda on Facebook and Twitter
Youth Coalition for Sexual and Reproductive Rights 20
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Sometimes in the dead of the night I can still hear it in the silence
My phone beeps a little and lights up with your name I wonder what it is A link to a song A question about apending assignment A joke With half opened eyes I load the image oblivious to how this would change the course of our lives Slowly I seethe two lines on the white test stick Before I can reply you shoot me a screenshot It is with the lsquoboy you havebeen talking torsquo We refused to label him because we did not want to take him too seriously He has lsquoleft you on blue ticksrsquo a universal millennial acknowledgement of not taking you seriously either
Sometimes in the dead of the night I can still hear it in the silence We sit on your bathroom floor and Google tips because it is all we know Somehow you are calmer than I am I am looking up possibilities of false positives bated breath for some hope You are telling me that we need tolook up medicines that could help A few quick searches later we delete the histories on our phone No one canever know
Sometimes in the dead of the night I can still hear it in the silence Your mother drops the plate of curd rice she is carrying into the kitchen She prepared it because she wanted tocheer up her darling daughter wondering what had caused you to cry since morning but not daring to probe Itsplatters across the floor and I know now that even three years later when I visit there would still be stains onthe tiles She is shaking This is not her daughter But before the rest of the house can hear the noise thesimultaneous breaking of hearts and trust concealed by a clattering plate she must protect the baby Her babyShe tells you to not tell anyone and that she will lsquotake care of itrsquo
Sometimes in the dead of the night I can still hear it in the silence You donrsquot remind her she doesnrsquot say a word Two weeks later you are feeling sick every morning and yourfamily starts joking about how your mother had these signs when she was about to have you A tear escapesyour eye at this parallel She must lsquotake carersquo of things sooner A friend makes a prescription black clothing isbought and a trip is made to the local pharmacy She gives you the pills and as your family gets worried aboutyour deteriorating health she comes up with more excuses
Sometimes in the dead of the night I can still hear you whispering in pain Your cries get louder as the pain gets more unbearable You are clutching your stomach but you tell me it is yourheart you want to hold You ask me if the pills hurt to make you realize that you would always carry the burdenof this death You ask me if the weight of a secret could crush you Wrong names have been given at thedoctors school teachers have been allowed to gossip about what is happening They canrsquot come up withanything that is worse than the truth your mother has said You wonder what it would be like if you could justscream it Tell someone Anyone About the painful medication the refusal to let the doctor know the glancesfrom your mother But most of all the guilt in the relief of somehow still getting over with it
And so in the broad daylight I hear you You donrsquot have to be sorry for picking yourself You donrsquot have to be sorry because they did not stand up foryou You donrsquot have to be sorry because your body was never considered your own You donrsquot have to be sorryyou tell me and it might be a small start but I hear you
16 THE SOUND OF IT BREAKINGTAVLEEN SINGH 22 INDIA Follow Tavleen on Instagram
Youth Coalition for Sexual and Reproductive Rights 21
I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition

I work as a primary healthcare physician at a publicclinic at La Paz Honduras Everyday I haveconsultations related to sexual and reproductivehealth ndash usually prenatal care and providing birthcontrol In these last 10 months Irsquove seen 4 patientswho got pregnant after sexual violence One of themwas only 12 when she gave birth
The story of this girl is the one that has ripped meapart the most An older man raped her when shewas just 11 years old and she got pregnant Abortionis completely illegal in Honduras and she gave birthto a son She lived with her son at an orphanageunder the custody of the government of Honduras
The conditions at this place were unbearable for herand she decided to escape with her son and go backto her former house I met her when she visited theclinic with her one-year old son looking for medicalassistance She was terrified to go to a doctor as shebelieved she would be sent back to the orphanageShe was illiterate her child was malnourished andshe was living with family members who believedthat her abuser was her ldquohusbandrdquo
a country where the public health system does nothave a protocol to assist survivors of sexual violenceThey are mistreated and revictimized by the systemevery single time they mention their abuse
In 2009 Conservative groups pushed a motion at theCongress to prohibit the sale and distribution of theemergency contraceptive pill (ECP) as they wronglybelieve it causes abortions The ban of the ECP is yetanother obstacle for survivors
Every year more than 900 girls between 10 and 14years old get pregnant after sexual abuse inHonduras In 2017 2664 girls under 18 years wereevaluated by forensics after sexual abuse ndash thats atleast seven girls sexually assaulted every day
Honduras is one of the few countries in the worldwhere abortion is illegal and criminalized under anycircumstance Honduran law describes abortion asldquothe death of a human being in any moment of thepregnancy or during birthrdquo and though this definitionis not based on scientific facts women can besentenced to prison from 3 to 6 years for this ldquocrime
Each year between 50000 and 80000 self-inducedabortions are performed in Honduras Itrsquos beenrepeatedly proven that restrictive abortion laws andpenalization donrsquot stop unsafe abortions Impunity isalso a huge problem as rapists and abusers are rarelyheld accountable by the Honduran justice system
Working as a public healthcare provider in mycountry has made me see first-hand the huge gaps inour countryrsquos healthcare and justice systemHonduras is a conservative country with a distortednotion of morality Access to emergencycontraception and safe abortion and receivingqualified medical legal and psychological attentionare not allowed in a country that forces an 11-year-old child to give birth condemning her to becontrolled by her rapist for the rest of her life
Follow Marianela on Twitter
17 THE FRUSTRATION OF BEING ADOCTOR IN HONDURAS MARIANELA MARTINEZ
BUEZO 26 HONDURAS
In these last 10 months Irsquove
seen 4 patients who got pregnant
by sexual violence One of them
was only 12 when she gave birth
During the consultation she received a phone call Iasked her who it was and she told me it was hersons father This rapist had the nerve to contact thisyoung child when he is serving time in jail for rapingand impregnating her I reported this several timesto the police and Child Protective Services but theydid nothing This is not an isolated case ndash we havehundreds like this all over Honduras
The Honduran system has failed these girls Theyhave no immediate access to healthcare after sexualviolence and at La Paz there is not a singlepsychologist in the public system These girls live in
Youth Coalition for Sexual and Reproductive Rights 22
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Watch the animated short film on Youtube
Pregnancy termination is something everyone has heard about but do you really know what it entails In Israelcompleting an abortion without permission is considered a crime for which one may serve up to five years inprison The diagnosis treatment and process are outdated judgmental and humiliating based on patriarchalpolitical and religious normative values The shame that accompanies the process leads women to lose theirfreedom to choose what happens to their bodies during this futile and hurtful evaluation My final project for mydegree in visual communication at University delved into the abortion experience through my own personalstory My goal is to share my story support other girls and boys with their own abortion experience
Follow Karin on Instagram and Facebook
18 THE DECISION IS MINE KARIN ECKERLING27 ISRAEL
Youth Coalition for Sexual and Reproductive Rights 23
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
The right to safe abortion is not a single right It is acomposition of rights that includes the right tohealth the right to equality and non-discriminationthe right to self-determination dignity privacy theright to be free from cruel and inhumane treatmentamongst others Nonetheless the right to accesssafe abortion services still faces a lot of opposition inmany jurisdictions in Sub-Saharan Africa (SSA)whose laws and policies have their roots in WesternCustomary law that was influenced heavily byreligion Access to safe abortion services as wasstated in African Commission on Human andPeoplersquos Rights General Comment 2 on Article 14and United Nations Committee on Economic Socialand Cultural Rights General Comment 22 is animportant human right that every individualcapable of getting pregnant should be able toaccess without any form of discrimination orunnecessary barriers
With one-quarter of unsafe abortions occurringamongst adolescents aged 15-19 in Africa which isthe highest rate globally unsafe abortion is no longerjust a human rights concern but also a serious publichealth issue in SSA Restrictive laws and delayedaccess to abortion services have created anenvironment where AGYW are unable to access much-needed health care services which oftentimes resultsin adverse health outcomes According to the WorldHealth Organization unsafe abortion is lsquoa procedureof pregnancy termination either by persons lackingthe necessary skills or in an environment that doesnot conform to minimal medical standards or bothrsquoConsequently states in fulfilment of theirobligations under the various human rightsinstruments that safeguard rights that are violatedwhen access to safe abortion services is notguaranteed must take all appropriate measure toremedy the status quo
In SSA unsafe-abortion has been identified as one ofthe leading causes of maternal mortality andmorbidity It accounts for 520 deaths per 100 000 livebirths and this is caused by structural and legalbarriers and societal stigmatisation of abortionwhich ultimately prevent AGYW from accessingtimely safe abortion services The Maputo Protocolcalls upon governments to lsquoauthorise medicalabortion in cases of sexual assault rape incest andwhere the continued pregnancy endangers themental and physical health or life of the pregnantwoman or life of the foetusrsquo Further theInternational Conference on Population andDevelopment Programme of Action and the BeijingDeclaration and Platform for Action both of whichrevolutionised Sexual and Reproductive Health andRights call upon states to change how laws policiesand social programmes approach adolescentsexuality and their attendant health needsNevertheless in as much as this is the case 3 out of 4abortions that occur in Africa are still unsafe
19 ADOLESCENT GIRLS AND YOUNGWOMENrsquoS ACCESS TO ABORTION INAFRICA KERIGO ODADA 28 KENYASOUTH AFRICA
Accessing safe abortion services is
unfortunately a challenge that
disproportionately affects adolescent
girls and young women in SSA
Accessing safe abortion services is unfortunately achallenge that disproportionately affects adolescentgirls and young women (AGYW) in SSA Members ofthis social group are socially positioned toexperience intersecting forms of oppression due togender age class education status parity maritalstatus et al Therefore it is imperative that AGYWdeemed mature enough to comprehend andinternalise issues such as sex and its consequencesand be allowed to have access to confidential SRHservices including abortion States and other dutybearers must strike a balance between protectingadolescents from abuse and recognising theirsexual and bodily autonomy and evolvingcapacities
Youth Coalition for Sexual and Reproductive Rights 24
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
States have a duty to ensure all AGYW have access toquality services to manage abortion and thecomplications arising from unsafe abortion Theymust create an enabling environment for AGYW inSub-Saharan Africa to access abortion and post-abortion care services as and when they need soMembers of this social group in many parts of Africahave limited access to sexual and reproductivehealth information and services and are therefore ata heightened risk of unintended pregnancies due tosexual exploitation and abuse and the negativeoutcomes of early sexual debut At the momentAGYW make up the bulk of those who experienceproblems resulting from unsafe abortion althoughthis a health right recognised in regional andinternational human rights instruments
Additionally another significant barrier thatadolescents also face in accessing safe abortionservices is the service providers Medical serviceproviders may due to personal beliefs social-cultural norms of a society or ignorance denyabortion services to adolescents due to their ageirrespective of whether the law permits it or not
When health systems refuse or neglect to providehealth services that only women and girls need theyare guilty of discrimination Therefore structural andlegal barriers that many members of this social groupface while navigating health systems on their ownmust be eliminated because they violate the right toequality
In conclusion this article posits that laws thatprohibit abortion or restrict access to safe abortionservices must be repealed and where abortion isallowed like in South Africa more awareness must beraised States must ensure lsquodomestic abortion lawsand practice are transparent and accountable so thatany abortion rights that the state confers can bemeaningfully realised by all persons seeking anabortion Other factors include stigma refusal toprovide service by health care workers financialbarriers requirements for consent et cetera mustalso be eliminated because unsafe abortion ispreventable
Follow Kerigo on Twitter and LinkedIn
December 2019-January 2020
ldquoFunrsquos over kidsrdquo Dr Kumar said and laughed out loud
This was the first time he was speaking to my partner and me In no time we realised that he was not only thekindest but also the funniest doctor I had ever come across This morning appointment with him had resulted inus laughing out loud for the first time in the nine hours of knowing that I was pregnant
Ever since the abortion I have been looking forward to seeing him and thanking everyone at the hospital forbeing so kind to me in a difficult time in my life I remember the smallest and the biggest moments where DrKumar and his team ensured I was at ease throughout There was a moment when Dr Kumar showed me thehands that the foetus had started developing There was a brief pause followed by his words ldquoHey itrsquos not a bigdeal Donrsquot think much of itrdquo
20 A LETTER OF GRATITUDE TO NON-JUDGMENTAL ABORTION PROVIDERSANONYMOUS 25 INDIA
Youth Coalition for Sexual and Reproductive Rights 25
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Later when I was waiting for my surgery the nurses started chatting with me During those days I had beenfeeling utterly terrible about myself After months of therapy we realized that I had been going throughdepression This was even before I had even gotten to know that I was pregnant So when the nurses spoke tome I was still in a place where I did not think very highly of myself However just when I was drowning in mythoughts one of them said ldquoAapki awaaz kitni pyaari hai (You have such a lovely voice)rdquo And all of a sudden itfelt as though someone had pulled me out of the void of my self-deprecating thoughts At that very moment Ifelt good about myself I began to remember the feeling ndash almost like cycling after a long time
when I say death is inside meIrsquom really saying my flesh is just a raw woundI say veneration to the silenced painI say acid vomit gulps conquering my throat by knock outI say it hurts it hurts it hurtswhen I say dead insideI say I wish it was possiblenot to ooze fireto come back to my own eyesput on some shoeswalk a straight line
when I say death is inside meI mean I am inside deathI mean I wish I didnrsquot know the soundof organs melting away
Follow Andrea on Twitter and Instagram
21 UNTITLED ANDREA PAOLO HERNANDEZ 24 VENEZUELA
Through my abortion journey my brother partner friend therapist doctors and staffat Manna Hospital were all there for me and made sure that I didnt feel guilty forchoosing myself They supported me out and out Initially I didnrsquot expect any warmth from the hospital staff I expected to face judgement as a 25-year-oldunmarried pregnant woman But the empathy I received was so filling and warmTherefore this letter with the Tsunamika doll is dedicated to everybody at Manna Hospital who stood strongly by me and continue to stand strongly by every woman in their toughest times With strength and kindness
To everybody who stands by usThank you
names changed to protect authorrsquos anonymity
Youth Coalition for Sexual and Reproductive Rights 26
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
The Novel Corona Virus 2019 (COVID-19) outbreak inWuhan a province of China led to the spread ofinfectious virus across the world and afflictedaround 213 countries and territories In no timenumbers of corona cases surged in Pakistan forsharing porous borders with the two highly affectedstates of China and Iran Till date the confirmednumber of COVID cases in Pakistan are 309015 with6444 causalities
In Pakistan access and provision of safe abortionservices is already stigmatized which quadrupledduring COVID ndash like most countries A huge numberof COVID cases put an inordinate strain on thealready fragile healthcare system
The burden on the healthcare system resulted insocial unrest ndash shortage of personal protectiveequipment (PPEs) instigated protests amonghealthcare workers nationwide Several incidents ofviolence against healthcare providers (HCPs) werereported Moreover there were no proper SOPsdefined by Government for the protection ofhealthcare workers which led to the spontaneousspread of infection in health facilities and causalitiesof HCPs
As a result of the high numbers of Corona cases anemergency was declared nationally in all hospitals ndashonly emergency obstetric care was functional wherethe influx of patients recorded was significantlyreduced due to fear of spread which ultimatelylessened the approachability of women in need ofSexual Reproductive Health (SRH) servicesincluding Postabortion care (PAC) The number ofCOVID positive pregnant women also increasedalarmingly resulting in the spread of virus among
the gynaecologists Furthermore the closure ofmaternity wards of big hospitals like PakistanInstitute of Medical Sciences (PIMS) and Lady ReadingHospital (LRH) aggravated the situation
During COVID emergency PAC services were availableonly at tertiary care facilities but were compromiseddue to focus on COVID Providers have come forwardwith such emergency cases where womengirls havetaken abortion pills on their own and were brought tothe facility in a serious situation
Hence the lockdown has completely restricted SRHservices which has increased the risk of womengirlsentering the cycle of unsafe abortions Additionallydue to nationwide closure of Population WelfareDepartment provision of family planning andcounselling services halted and this will enormouslycontribute to the number of unwanted pregnanciespredicted to be reaching to 7 million in the middleand low-income countries during the pandemic
22 COVID-19 AND ITS IMPLICATIONSFOR SEXUAL AND REPRODUCTIVEHEALTH SERVICES IN PAKISTANNEHA KHAN 25 PAKISTAN
In Pakistan during COVID-19 the entire focus is ontreating Covid-positive patients and containing thevirus which reflects gaps in the existing approachtowards SRH and family planning NGOs and INGOssuch as Family Planning Association of Pakistan(FPAP) Ipas and UNFPA working on SRHR haveadopted new approaches to increase the access ofwomengirls to SRH services in emergency situations
In Pakistan access and provision of
safe abortion services is already
stigmatized which quadrupled
during COVID
Youth Coalition for Sexual and Reproductive Rights 27
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Rounds of Virtual Meetings have been held amongthe CSOs NGOs INGOs and the Ministry of Nationaland Provincial Health Services to review the SRHRsituation and refine and ease the service provision As a result of these efforts Ministry of NationalHealth Services Regulations amp Coordination(MoNHSRampC) has issued guidelines on ldquoContinuationof Sexual Reproductive and Maternal HealthServices during COVID-19rdquo which emphasizes on theavailability of SRH supplies and critical services asper Minimum Initial Service Package (MISP)telemedicine approaches for abortion care andcontraception self-care practices and interventionsfor medical management of abortions andpregnancies respectively The guidance has givensignificant emphasis on comprehensive abortioncare and contraception as an essential serviceavailable 247 at Health facilities MoNHSRampC hasalso
also endorsed the guidelines of Pakistan Alliance forPostabortion Care (PAPAC) calling out national levelpublicprivate facilities which are providing SRH careto remain open and continue providing theoutpatient servicescounselling during pandemic
The world is still struggling with the pandemicHowever cases are relatively decreasing in PakistanThe World Health Organization (WHO) has advisedstates to take all necessary preventive measureswhile moving towards normalization Thegovernment of Pakistan has started the gradualopening of offices and markets with stringentimplementation of standard operating procedures forpost-lockdown opening
Follow Neha on Facebook Instagram and LinkedIn
23 ADDRESSING THE OBSTACLE OFSAFE ABORTION IN NEPAL DURINGCOVID-19COVID-19 has given rise to a systemic crisis forhealth access and delivery for countries around theworld Sexual and reproductive health services anintegral necessity has been hugely impacted aswell The lockdown arising from the pandemic hasexacerbated inequalities especially for marginalizedgroups such as young women young migrants andrefugees youth living in rural areas young personswith disabilities and young people of differentsexual orientations Accessing sexual andreproductive health services is a major challenge forpeople living in developing countries like Nepal
Abortion in Nepal was legalized in 2002 under theNational Safe Abortion Policy which provided itsservices through a number of certified governmentnon-government and private health facilities Alongwith policy implementation Nepalrsquos governmentalso initiated the provision of safe abortion all overthe country including medical abortion services
Access to safe abortion is an essential service thedenial of which may lead to pregnant peoplereaching gestational thresholds seeking unsafemethods and putting their health and lives at riskTherefore it is crucial for the provision of safeabortion to be ensured at the right time and need Despite having one of the most liberal abortion lawsin Nepal an estimated 60 of all abortions that wereperformed in 2014 were unsafe Even before thepandemic Nepal saw many barriers in providingaccess to safe abortion services and care and COVID-19 has amplified the problem even more
According to IPPF the South Asia region includingNepal is found to have the largest numbers ofclosure of mobile clinics and community-based careoutlets due to the pandemic lockdowns It isimportant to find alternatives to address the problemof reduced access to safe abortion
LIRISHA TULADHAR 20 NEPAL
Youth Coalition for Sexual and Reproductive Rights 28
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Marie Stopes Nepal has been working to combat thisgulf with a mobile helpline called ldquoMeri Saathirdquo (MyFriend) It provides free and confidential counselingfor issues like contraception safe abortion safe sexpregnancy menstruation masturbation etcSimilarly Ipas is also working to ensure continuedaccess to abortion services via digital tools
The efforts from these organizations to provide thesafe abortion services however cannot be the onlysolution It is vital for Nepals telemedical healthservices to improve their reach Promotingtelemedical abortions enables women to self-manage their abortion in an environment that is safefrom COVID-19 confidential and relatively cheaper
Millions of the women self-manage their abortionsevery year with the use of medical abortion pillsrecommended by WHO It includes intake ofMifepristone and Misoprostol in the correct dosagewithout even needing to visit the clinicsPolicymakers government and health facilities mustincrease the potential of telemedicine in Nepal
The government should also provide support toorganizations like Marie Stopes UNFPA PSI etcwhich have been working extensively to ensure safeaccess to sexual and reproductive health servicesamidst this pandemic
Follow Lirisha on Facebook and Instagram
24 SELF-MANAGED ABORTIONS ANINTERVIEW WITH WOMEN ON WEB
Women on Web started in 2005 was the first ever organisation to provide telemedical counselling and abortionservices to pregnant people living in restrictive settings This year the theme for Interntional Safe Abortion Day isself-managed abortions and their work is finally being mainstreamed and recognised as a crucial weapon in thetoolkit for reproductive justice Catch Hazal Atay a member of Youth Coalition and Women on Web inconversation with her colleague Victoria Satchwell from Women in Web as they discuss the technical aspects ofself-managed abortions their experiences of being activists in this space and the impact of COVID-19
YOUTH COALITION FOR SEXUAL AND REPRODUCTIVE RIGHTS
Youth Coalition for Sexual and Reproductive Rights 29
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Youth Coalition for Sexual and Reproductive Rights 30
25 BODILY AUTONOMY IS A HUMANRIGHT BEATRIZ ROTOLI 26 BRAZILITALY
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Approximately 26 million women and girls ofreproductive age are in need of humanitarianassistance around the world Women and girls incrisis settings face tremendous obstacles to meetingtheir sexual and reproductive needs even when it isincredibly crucial In as much as this is afundamental right humanitarian laws policies andprotocols are yet to be meaningfully interpreted andadapted to respond to their specific needs includingtheir sexual and reproductive health and rights
In particular safe abortion services are routinelyomitted from sexual and reproductive healthservices in humanitarian settings for a variety ofreasons including an improper deference tonational law the disproportionate influence ofrestrictive funding policies like the Global Gag Ruleand the failure to treat abortion as medical care
Sexual and reproductive health is often invisiblecompared with the need for food water shelter andvaccines The prevalence of gender-based violenceagainst women and girls is well documented inhumanitarian settings Sexual violence is often usedas a weapon of war targeting civilian women andchildren In these crisis settings women facesignificant hardships trying to prevent pregnancyand end unwanted pregnancies The nature of life inthose setting make access to this right extremelydifficult Women living in those conditions suffergreatly because they are out of options Addressingthis need is an essential towards meeting their rightto health as prescribed by Article 14 of MaputoProtocol which guarantees respect and promotionof womens right to health including sexual andreproductive health (SRH) among other laws
Among the challenges that hamper the realization ofthis right in humanitarian settings is the fact thatthere is a lack of adequate funding towardsfacilitating this right in conflict areas Conflict-affected settings receive 57 less funding for repro-
The mistaken belief held by decision-makers thatabortion is illegal must be countered 93 of theworldrsquos population lives in a country where abortionis permitted under one or more circumstance Forinstance in Kenya abortion permitted only if in theopinion of a trained health professional there is needfor emergency treatment or the life or health of themother is in danger or if permitted by any other law
Finally we know safe abortion care reduces unsafeabortions and ultimately saves lives in any contextWe also know that sexual violence against women inhumanitarian settings is not only a risk during crisisbut continues during protracted emergencies whenwomen are supposed to be safe from coercion andassault Governments as duty bearers have anobligation to ensure sexual and reproductive healthfacilities information education goods and servicesare available accessible acceptable and of goodquality particularly for adolescents women inhumanitarian settings
26 ACCESS TO ABORTION IN CRISISAND HUMANITARIAN SETTINGSCHELANGAT S SHEMA 25 KENYA
ductive health care than countries without significantconflict Comprehensive sexual and reproductivehealth care including safe abortion andcontraception is neglected in emergency settings inlarge part because of misperceptions These mythsare the result of misinformation stigma and a lack ofcommitment to the basic human rights of womenThe myths result in organisations the donorcommunity and practitioners incorrectly assumingthat there is no demand for safe abortion care thedelivery of abortion is too complicated in fragilesettings donors will not fund abortion care in fragilesettings andor abortion is illegal
Conflict-affected settings receive
57 less funding for reproductive
health care than countries without
significant conflict
Youth Coalition for Sexual and Reproductive Rights 31
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Thank you for readingsharing andcontributing to the2020 Watchdog onSafe AbortionEditing compilation and design by Asmita Ghosh
Follow Youth CoalitionwwwyouthcoalitionorgfacebookcomYouthCoalitiontwittercomyouth_coalitioninstagramcomyouth_coalition
Related Documents











