10.1192/bjp.167.2.202 Access the most recent version at doi: 1995 167: 202-210 The British Journal of Psychiatry Goodwin and KP Ebmeier SM Lawrie, GT Ingle, CG Santosh, AC Rogers, JE Rimmington, KP Naidu, JJ Best, Re O'Carroll, GM schizophrenia tomography in treatment-responsive and treatment-resistant Magnetic resonance imaging and single photon emission References http://bjp.rcpsych.org/cgi/content/abstract/167/2/202#otherarticles Article cited in: permissions Reprints/ [email protected] to To obtain reprints or permission to reproduce material from this paper, please write to this article at You can respond http://bjp.rcpsych.org/cgi/eletter-submit/167/2/202 service Email alerting click here top right corner of the article or Receive free email alerts when new articles cite this article - sign up in the box at the from Downloaded The Royal College of Psychiatrists Published by on July 15, 2011 bjp.rcpsych.org http://bjp.rcpsych.org/subscriptions/ go to: The British Journal of Psychiatry To subscribe to

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
10.1192/bjp.167.2.202Access the most recent version at doi: 1995 167: 202-210 The British Journal of Psychiatry
Goodwin and KP Ebmeier SM Lawrie, GT Ingle, CG Santosh, AC Rogers, JE Rimmington, KP Naidu, JJ Best, Re O'Carroll, GM
schizophreniatomography in treatment-responsive and treatment-resistant Magnetic resonance imaging and single photon emission
References
http://bjp.rcpsych.org/cgi/content/abstract/167/2/202#otherarticlesArticle cited in:
permissionsReprints/
[email protected] To obtain reprints or permission to reproduce material from this paper, please write
to this article atYou can respond http://bjp.rcpsych.org/cgi/eletter-submit/167/2/202
serviceEmail alerting
click heretop right corner of the article or Receive free email alerts when new articles cite this article - sign up in the box at the
fromDownloaded
The Royal College of PsychiatristsPublished by on July 15, 2011 bjp.rcpsych.org
http://bjp.rcpsych.org/subscriptions/ go to: The British Journal of PsychiatryTo subscribe to

British Journal of Psychiatry (1995), 167, 202—210
There is a consensus that patients with schizophreniashow a number of important differences fromcontrol subjects on a range of measures of brainstructure and function. Computerised tomography(CT) scanning has repeatedly identified enlargedlateral ventricles and reduced brain substance, bothin chronic cases and at initialpresentation(Johnstoneet a!, 1976; Daniel et a!, 1991). Magnetic resonanceimaging (MRI) has established that medial temporallobe structures are smaller in schizophrenic subjectsthan controls (Suddath et a!, 1990; Shenton et a!,1992). Functional brain-imaging methods i.e., singlephoton emission tomography (SPET) and positronemission tomography (PET), have found reductionsin regional cerebral blood flow or metabolism,particularly of the frontal lobes, in chronically ill andmedicated patients (Ebmeier, 1994). Severalresearchers have described cognitive deficits inpatients with schizophrenia, often in association withenlarged lateral ventricles (Johnstone et a!, 1976;Golden et a!, 1980).
It is less clear how these biological variables relateto clinically relevant features of the illness. Of these,response to treatment is of central importance. Whilemany patients make a virtually complete recoveryfrom a discrete episode, repeated trials have found
that up to 25% of patients derive relatively littlebenefit from typical neuroleptic drug therapy, and6—8%fail to respond to many months or years ofintensive antipsychotic treatment (May et a!, 1988).Optimal prediction of treatment response hasobvious relevance for the clinical management ofschizophrenia, and recent developments in brainimaging, along with renewed interest in neuropsychological measures of brain function, have increasedthe possibilities for investigations in this area. SeveralCT studies have examined the associations oftreatment response or illness outcome, but usuallyin post hoc differentiated patient groups, and resultshave both supported and refuted a relationshipbetween structural abnormality and worse response.There is a dearth of studies employing MRI,PET/SPET, or detailed neuropsychological testingto examine this issue. The purpose of this study wasto use such methods, in dichotomised patient groups,to identify the associations of treatment response.MRI, SPET, and a comprehensive neuropsychological test battery were employed to test thehypothesis that treatment-resistant patients showmore evidence of structural abnormality, functionalunderactivity, and cognitive deficit than treatmentresponsive patients.
202
Magnetic Resonance Imaging and Single Photon EmissionTomography in Treatment-Responsive and
Treatment-Resistant SchizophreniaSTEPHEN M. LAWRIE, GORDON T. INGLE, CELESTINE G. SANTOSH, ANDREW C. ROGERS,
J. EWEN RIMMINGTON, KALIPRASAD P. NAIDU, JONATHAN J. K. BEST, RONAN E. O'CARROLL,GUY M. GOODWIN, KLAUS P. EBMEIER and EVE C. JOHNSTONE
Background. Patients with schizophrenia differ from controls in several measures of brainstructureand function, but it is uncertainhow these relateto clinicalfeaturesof the illness.We dichotomisedpatientgroupsby treatmentresponseto test the hypothesisthat treatmentresistantpatients exhibit more marked biologicalabnormalitiesthan treatment-responsiveparients.Method. Twenty treatment-responsive and 20 treatment-resistant patients with schizophrenia,matchedfor sex, age, and illnessduration,were comparedby magneticresonanceimaging,singlephoton emissiontomography,and detailed neuropsychologicalassessment.Results.Brain-imagingvariableswere not statisticallyrelatedto treatmentresponse,althoughpoorly responsivepatients had lower volumes of most brain structures. Several highlysignificantdifferencesemergedbetweenpatientgroupsonneuropsychologicaltesting.Episodicmemoryfunctioningdistinguishedpatientgroupsevenafter we controlledfor globalcognitiveimpairment.Conclusions.Cerebralstructureand bloodflow have a limitedeffect on treatment responsein schizophrenia,but long-termepisodicmemory impairmentis associatedwith, and maypredict, poor prognosis.

MRI/SPET AND TREATMENT RESPONSE IN SCHIZOPHRENIA 203
Methods
Forty patients who satisfied DSM-III-R (AmericanPsychiatric Association, 1987) criteria forSchizophrenia or Schizophreniform disorder wererecruited for the study. Two dichotomous patientgroups were sought, treatment-responsive andtreatment-resistant, according to the criteriaproposed by May et a! (1988), which describe sixlevels of treatment resistance. The 20 treatmentresponsive patients “¿�respond[cdl well within onemonth being able to return to the same socialsituation as before with little if any residual scarring[level 2]―, or “¿�show[ed]a major reduction ofsymptoms withina month [butwith]reducedabilityto study or work [level 3]―. The 20 patientsdesignated as treatment-resistantall showed“¿�psychoticsymptoms or disturbed behaviour [that]does not remit such that they will remain for a longwhile in hospital or some alternative form of caringmilieu [level 5] “¿�.There were no patients at level 4.The two groups of 20 patients were matched for sex(10 male and 10 female in each group), age (withinsix years), and duration of illness (within six years).Patients were excluded if they suffered from anyneurological condition, current substance abuse, ormajor depression, or were pregnant.
Clinical assessments
All 40 subjects underwent a detailed clinicalexamination comprising a structured psychiatricinterview, the Present State Examination (Wing eta!, 1974);a standardised rating of current symptoms,the Manchester Symptom Scale (Krawiecka et a!,1977); and a brief neurological examination tocomplete the Abnormal Involuntary Movement Scale(AIMS) and the Targeting Abnormal Kinetic Effectsscale (TAKE; Wojcik et a!, 1980). This wassupplemented by information from the patients'psychiatric case-notes to complete the Schedule forAffective Disorders and Schizophrenia—LifetimeVersion, for Research Diagnostic Criteria (RDC;Spitzer & Endicott, 1978), and a modified versionof the DHSS Survey form (Johnstone, 1991). Illnessonset was defined as the age at first record ofsufficient features to satisfy DSM—III—Rdiagnosticcriteria for schizophrenia; the duration of illness wastaken from this date until the beginning of theinvestigation in January 1992. Additionalmeasurements of illness outcome were made frominterview and case-note information. Social outcome(self-care, employment history, acceptability ofbehaviour) was assessed on the rating scale devised
by Cooper (1961), and global outcome was measuredon the McGlashan cross-sectional and follow-upscales (McGlashan, 1984).
Magnetic resonance imaging (MRI)
All 40 patients underwent MRI scanning on a 1.0Tesla Siemens (Erlangen, Germany) scanner. Midlinesagittal localisation was followed by two sequencesto image the whole brain. A ‘¿�Turboflash'sequence,a 3-D-FLASH collection 500 ms after a spininversion (TI = 500 ms), produced an image thatcould be reconstructed in three dimensions. A spinecho (SE) dual-echo scan was also conducted, witha repetition time of 3656 ms, and echo times of 20 msfor a proton density-weighted image and 90 ms fora T2-weighted image (SE 3565/20—90).The 3-D-FLASH sequence was collected as 128 contiguous1.56 mm-thick coronal slices, with flip angle 10°,repetition time 10 ms, echo time 4 ms, field of view255 mm, and relaxation delay 1 s. The SE scangenerated 31 contiguous 5-mm-thick axial slices inthe Talairach plane, with flip angle 90°and field ofview 250 mm. Regular phantom measurements overthe 15 months of the study ensured that thesesequences remained reliable. A clinicalneuroradiologist (CGS) examined the MRI scans forstructural abnormalities and motion artefact —¿�one subject was rescanned because his first scan wasseverely degraded by movement.
Image processing was done on Sun Microsystemsworkstations with the software package ‘¿�Analyze'(Mayo Foundation, Rochester, MN, USA) to outlineand compute volumes of neuroanatomical structures.Structures were identified with the assistance of anMRI atlas, and volumes were calculated by summingvoxels on all slices included. Specific regions ofinterest selected a priori were prefrontal lobes (leftand right), temporal lobes (left and right),hippocampi (left and right), whole brain, intracranialcerebrospinalfluid(CSF),lateralventricles(leftandright), and third and fourth ventricles (combined).The prefrontal lobes were defined as by Suddath eta! (1990), the temporal lobes and hippocampi weredefined according to the method of Shenton et a!(1992), and the remaining regions of interest wereoutlined by naturalistic boundaries. The 3-D-FLASHscans were used for all measurements except thewhole-brain and intracranial CSF volumes, whichwere calculated from the SE 3565/20—90scans afterensuring that whole-brain volumes derived by bothmethods were similar (interscan correlation r= 0.96;mean difference 30.8 cc, standard deviation (s.d.)32.3). All three volume raters were blind to groupmembership. One (SML) calculated all ventricular
Subjects

204 LAWRIE ET AL
volumes,another(GTI)allwhole brainand intracranialCSF volumes,thethird(CGS)thehippocampi,and two raters (SML and GTI) estimated prefrontaland temporalvolumes.Allthreeratersexamined10prefrontal and temporal lobes to determine mterraterreliability (interrater correlation SML and GTIr = 0.93, mean difference 1.07 cc, s.d. 4.7; SML andCGS r= 0.90,mean difference1.95cc,s.d.3.7).
Single photon emission tomography (SPET)
SPET imagingwas doneon a dedicatedSME-MultiX8l0 Strichman brain scanner, @°‘Tc-Exametanime(HMPAO) being used to measure regional cerebralperfusion.Traceruptakewas measured as countdensity on slices at 5-mm intervals, extending the fulllengthofthebrain(14—18slicespersubject).Threeslices were used in this study: at the midventricularlevel (including the basal ganglia) 4cm above theorbitomeatalline(OML), and 6 and 8cm abovetheOML, to give 36 regions of interest (Table 2). Astandardised brain template, derived from an atlas,was symmetrically and linearly transformed to fit thebrain outline defined by 4001oof the image intensityspectrum, and regional reconstructed count densitieswere computed on SME 810 software2.61.
Neuropsychological testing battery
Comprehensive testing was undertaken with a widevariety of tasks, chosen because executive andmnemonic deficitshavebeenfrequentlyreportedinschizophrenic subjects and for ease of applicationinthispopulation.Theseincludedglobalmeasuresof premorbid intellectual ability, i.e. the NationalAdult ReadingTest(NART); currentIQ, i.e.theQuick Test; global intellectual functioning, i.e. theMini-Mental State Examination (MMSE);attention/working memory, i.e. the Digit Span(forward and backward) and psychomotor speed, i.e.Digit Symbol Substitution, from the Wechsler AdultIntelligence Scale—Revised(Wechsler, 1981). Testsofexecutivefunctioningincludedverbalfluency,orword production, for animals and for wordsbeginningwiththeletterA in60s;theStrooptest;and TrailsA and B. The Annettscalewas chosento measure handedness. The profile score of theRivermeadBehaviouralMemory Test(RBMT) wasused as an index of episodic memory. Selectedmeasuresfrom theCambridge NeuropsychologicalTesting Automated Battery (CANTAB) were alsoemployed. Finally,the testerratedthe patients'attention and cooperation on two five-point scales.The results from all these measures will be reportedindetailelsewhere(Rogerseta!,inpreparation),only
themain findingsand theirclinicaland biologicalassociations being given in this paper.
Timing of investigations and data analysis
The SPET scangenerallyfollowedMRI withinoneweek (median interval six days), and theneuropsychological and clinical assessments wereusuallycompletedintwo sittings,withina fewdaysof the SPET scan (median interval six days). Theresultswereanalysedby SPSS forMac 4.0.As age,sex, and duration of illness were matched betweengroups at the design stage, the effects of thesevariables were not examined. Multivariate analysisof variancewas conducted,the 11 MRI regionalvolumes and 36 SPET regional tracer uptake ratiosbeingtreatedasrepeatedmeasures.The MRI resultswereanalysedasbothabsolutevolumesand,aftercorrection for whole-brain volume, to control forvariationsinheadsize,whileSPET traceruptakewasanalysed after normalisation to both whole slice oroccipital uptake ratios. The effects of laterality andregion on structure volumes were examined with two‘¿�betweenfactors' (treatment-response groupmembership and sex) and two ‘¿�withinfactors'(laterality and region), followed by a t-test forindividual regions of interest. Effect sizes (asstandardised differences) were calculated forbetween-groupdifferencesin MRI volumes, bydividingthevolumedifferencebythelargerstandarddeviation.Neuropsychologicaltestresultswerecomparedbetweentheresponsegroupsby ANOVA,possibleconfounders being controlledfor byANCOVA. Associations between clinical and
outcome variables, with neuropsychological variablesand regional volumes, were explored by two-tailedSpearman rank correlationcoefficients.Thenumerous clinical/neuropsychologicalresultswerefactor analysed to allow correlations with the largenumber of SPET (and MRI) variables.
Results
Clinical characteristics
The DSM—III—Rdiagnosticcategorieswere asfollows:SchizophreniformPsychosis(n= 2) andSchizophrenia (n = 38), with subcategories ofParanoid (n = 19), Undifferentiated (n = 10),Disorganised (n = 8), and Catatonic (n = 1)Schizophrenia, and 36 patients suffered from DSMIII—RChronic Schizophrenia. Thirty-five patientsalso satisfied RDC criteria for Schizophrenia, theothers being Schizoaffective (n = 3) orSchizophreniform (n = 2). The patients were clinically

ResponsiveResistantEffectsizeWhole
brain1196.3 (113.7)1142.8(131.2)0.41IntracranialCSF218.8 (44.2)207.0(77.6)0.15Left
temporal lobe77.4 (8.2)73.4(10.8)0.37Righttemporal lobe80.3 (10.2)75.5(10.5)0.46Left
hippocampus5.3 (0.7)5.1(0.7)'0.29Righthippocampus5.5 (0.6)5.3(0.7)'0.29Left
prefrontal lobe61.0(8.3161.2(11.8)-0.02Rightprefrontal lobe63.7 (8.2)61.8(11.1)0.17Left
lateralventricle9.1 (4.5)8.5(3.5)0.17Rightlateral ventricle8.8 (4.0)8.0(3.2)0.25Thirdandfourthventricles4.1
(1.3)4.2(1.3)-0.08
MRI/SPET AND TREATMENT RESPONSE IN SCHIZOPHRENIA 205
versus5.6(2.1))and follow-up(15.4(2.0)versus6.0 (2.2)). Statistically significant differences werefound between the patient groups on the AIMS(mean score 1.0(1.7) versus 2.8(2.4), Mann-WhitneyU= 103.5,P= 0.006),butnottheTAKE (2.2(2.1)versus 3.4 (2.0), P=0.l).
Mifi and SPET scan results
MRI
The hippocampi could not be measured in twomale subjects because of movement artefact, butthe remaining structures were reliably identifiableinallscans.The mean heightoftheresistantpatients,at 167.8 cm, was lower but not significantly differentfrom that of the responsive patients, at 169.4cm(P= 0.6). Analysis between response groups byMANOVA found no significant differences inthe volumes of any measured structure, comparingeither raw volumes (F1,38= 1.1, P=0.3) or thosecorrected for whole-brain volume (F1,38=0.2,P= 0.9). Table 1 shows the absolute volumes ofthestructuresmeasured,togetherwitheffectsizesofthedifferencesbetweenresponsegroups.Almostall structures were smaller in the treatment-resistantgroup, with only the minor exceptionsof theleft prefrontal lobe and the third/fourth ventricles.There was no interaction between response andregion,but therewas a tendencyto one betweenresponse and side (F1,38= 3.0, P= 0.09). Post hocpaired t-tests, across all subjects, revealed smallerleft-thanright-sidedhippocampi(two-tailedt= 3.03,P= 0.004) and temporal lobes (two-tailed t = 1.93,P = 0.06). Analysis of the effects of sex revealedsignificantly smaller volumes of all structuresin women (F338= 7.44, P= 0.01), but no interactionwith response, region or side. Left-handed subjects(n = 4), had lower volumes of all structures thantheright-handers(ii= 35;one ambidextrous),butthis difference was statistically significant only inthe left temporal lobe (raw volumes 68.2 versus76.6 cc; two-tailed t = 3.26, P= 0.01).
SPET
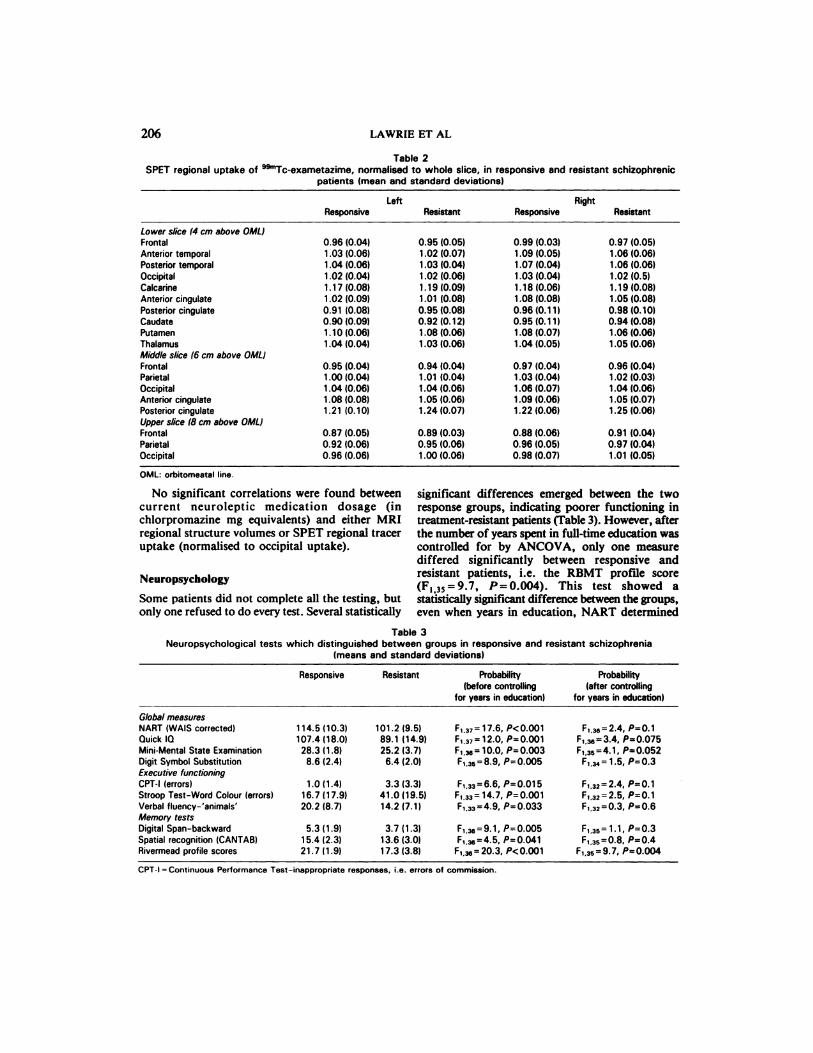
The overall effect of illness outcome on regionaluptakeratiosfailedtoreachstatisticalsignificanceby MANOVA, whetheruptakewas normalisedtothe whole slice(F1,38=0.98,P=0.5) or occipitaluptake (F1,38= 2.06,P= 0.3).Table 2 shows theuptake ratios, normalised to whole slice uptake, inthe 36 regions of interest from the three slicesanalysedinthisstudy.
stable at the time of the investigations, so that theeffectsofacuterelapse,largedosesofmedication,or both were minimised.The matchingofpatientsforsex(10maleand 10
female patientsin each group),age (responsivepatientsmean 36.5(s.d.9.9)years,resistantpatientsmean 34.7(10.3)years),and illnessduration(mean139.3 (105.05) months and 150.8 (106.0) months,respectively)was satisfactory,althoughtreatmentresistant patients were younger and yet had been illforlonger,indicatingan earlierageatonsetinthisgroup. As would be expected, the mean number ofadmissions (4.9 (4.7) versus 10.4 (6.5)), total timespent in hospital (6.6 (7.1) months versus 57.1(87.4))and current antipsychotic medication dosage (268(274) mg chlorpromazine equivalents versus 902(669) mg) were substantially higher in treatmentresistant patients. The mean current anticholinergicmedication dosage, in procyclidine equivalents, wassimilar in both groups (3.0 (6.4) versus 3.3 (4.7)).Paternal occupation (social class) was also similar(mean 2.6 (0.8)versus2.9 (0.5)),but the meannumber ofyearsspentineducationwas substantiallylower in treatment-resistant patients (14.0(2.8) versus10.9 (1.2)).
Several measures of the patients' clinical picture,at the time of testing, confirmed the desired betweengroupdifferences.The mean positivesymptom scoreon the Manchester scale was higher in treatmentresistant patients (0.4 (0.6) versus 1.8 (0.9)), as wasthe mean negative symptom score (0.5 (0.4) versus0.9(0.6)).Socialfunctioning,on Cooper'sscale,wasmuch betterintreatment-responsivepatients(meanscore4.8(0.8)versus1.8(0.5)),aswasglobaloutcomeon McGlashan's cross-sectional scales (15.4 (2.6)
Table 1Raw volumes (cc) on magnetic resonance imaging in
responsive and resistant schizophrenia (means and standarddeviations) and effect sizes (in standard deviation units)
= 18 as two male hippocampi were excluded for motion artefact.
LeftRightResponsiveResistantResponsiveResistantLower
slice(4cm aboveOML)Frontal0.96(0.04)0.95(0.05)0.99 (0.03)0.97(0.05)Anterior
temporal1.03 (0.06)1.02 (0.07)1.09 (0.05)1.06(0.06)Posteriortemporal1.04 (0.06)1.03 (0.04)1.07 (0.04)1.06(0.06)Occipital1.02
(0.04)1.02 (0.06)1.03(0.0411.02(0.5)Calcarine1.17(0.08)1.19 (0.09)1.18(0.06)1.19(0.08)Anterior
cingulate1.02 (0.09)1.01(0.08)1.08 (0.08)1.05(0.08)Posteriorcingulate0.91 (0.08)0.95 (0.08)0.96 (0.11)0.98(0.10)Caudate0.90(0.09)0.92
(0.12)0.95(0.11)0.94(0.08)Putamen1.10(0.06)1.08(0.06)1.08(0.07)1.06(0.06)Thalamus1.04
(0.04)1.03(0.06)1.04(0.05)1.05(0.06)Middleslice(6cm aboveOML)Frontal0.95
(0.04)0.94(0.04)0.97 (0.04)0.96(0.04)Parietal1.00(0.04)1.01(0.04)1.03 (0.04)1.02(0.03)Occipital1.04(0.06)1.04 (0.06)1.06 (0.07)1.04(0.06)Anterior
cingulate1.08 (0.08)1.05 (0.06)1.09(0.06)1.05(0.07)Posteriorcingulate1.21(0.10)1.24(0.07)1.22 (0.06)1.25(0.06)Upper
slice (8cm aboveOML)Frontal0.87(0.05)0.89 (0.03)0.88 (0.06)0.91(0.04)Parietal0.92(0.06)0.95(0.06)0.96(0.05)0.97(0.04)Occipital0.96(0.06)1.00(0.06)0.98(0.07)1.01(0.05)OML:
orbitomeatal line.
ResponsiveResistantProbability(beforecontrolling
for years in education)Probability(aftercontrolling
for years ineducation)Global
measuresNART(WAIScorrected)Quick 10Mini-MentalState ExaminationDigit Symbol SubstitutionExecutivefunctioningCPT-l (errors)Stroop Test-Word Colour (errors)Verbal fluency-'animals'Memory testsDigital Span-backwardSpatial recognition (CANTAB)Rivermead profile scores114.5
(10.3)107.4 (18.0)
28.3 (1.8)8.6 (2.4)
1.0(1.4)16.7 (17.9)20.2 (8.7)
5.3(1.9)15.4 (2.3)21.7 (1.9)101.2
(9.5)89.1 (14.9)25.2 (3.7)
6.4 (2.0)
3.3 (3.3)41.0 (19.5)14.2 (7.1)
3.7(1.3)13.6(3.0)17.3(3.8)F,37=
17.6, P<O.001F,37= 12.0, P=O.O01F,@= 10.0, P=O.003F,,35=8.9, P=O.005
F,33=6.6, P=O.O15F,33= 14.7, P=O.O01F,33=4.9, P=O.O33
F,3=9.1, P—O.O05F,@=4.5, P=O.041
F,@= 20.3, P<0.001F,36=2.4,
P=0.1F,.@e=3.4, P0.075F,35=4.1, P=0.052
F,3, 1.5, PO.3
F,32=2.4, P=O.1F,32=2.5, P=0.1F,32=0.3, P=0.6
F,351.1, PO.3F,35=O.8, P=O.4
F,35=9.7,P=0.004CPT-I
= Continuous PerformanceTest-inappropriateresponses, i.e. errorsofcommission.
206 LAWRIE ET AL
Table 2SPETregionaluptakeof @“¿�Tc-exametazime,normalisedto wholeslice,in responsiveandresistantschizophrenic
patients (mean and standard deviations)
No significantcorrelationswerefoundbetweencurrent neuroleptic medication dosage (inchlorpromazine mg equivalents) and either MRIregional structure volumes or SPET regional traceruptake (normalised to occipital uptake).
Neuropsychology
Some patients did not complete all the testing, butonly one refused to do every test. Several statistically
significant differences emerged between the tworesponse groups, indicating poorer functioning intreatment-resistant patients (Fable 3). However, afterthe number of years spent in full-time education wascontrolled for by ANCOVA, only one measurediffered significantly between responsive andresistantpatients,i.e.the RBMT profilescore(F1,35=9.7,P=0.004). This test showed astatistically significant difference between the groups,even when years in education, NART determined
Table 3Neuropsychological tests which distinguished between groups in responsive and resistant schizophrenia
(means and standard deviations)

NARTwQuick10MMSEDSSCPT-lStroopVFOS-BSpatialRPSWhole
brain0.41―0.45―0.48―0.33―—0.34―—0.300.34'0.41―0.160.28IntracranialCSF0.080.090.070.11—0.13—0.220.210.090.270.16Left
temporallobe0.48―0.57―0.52―0.34'—0.47―—0.52―0.39'0.68―0.300.32Righttemporallobe0.49―0.45―0.48―0.32—0.27—0.48―0.300.45―—0.020.31Left
hippocampus—0.080.130.090.03—0.06—0.060.11—0.090.110.02Righthippocampus—0.130.110.010.050.03—0.090.05—0.010.22—0.02Left
prefrontallobe0.34'0.39'0.34'0.28—0.31—0.290.250.36'0.34'0.28Rightprefrontallobe0.35'0.300.320.36'—0.22—0.260.200.170.110.32Left
lateralventricle0.180.060.290.29—0.25—0.020.130.32'0.15—0.00Rightlateralventricle0.12—0.020.140.32—0.24—0.050.160.210.27—0.02Thirdandfourthventncles—0.16—0.150.040.13—0.290.05—0.18—0.01—0.05—0.12
MRI/SPET AND TREATMENT RESPONSE IN SCHIZOPHRENIA 207
premorbid IQ, paternal social class, currentantipsychotic medication, and lifetime exposure toanticholinergicswere takenintoaccount.Table3shows the between-group differences both before andafter controlling for years spent in education to allowthe reader to examine the magnitude of the effect.
ainical and biologicalcorrelationsAs shown inTable4,Spearman rankcorrelationswere fairly strong among the MRI whole-brain,temporal,andprefrontallobevolumes(particularlythe left side) and many neuropsychological testresults,particularlythe globalmeasures.MRIvolumes correlated less strongly with the clinicalmeasures, but the left and right temporal lobevolumes consistently correlated with the outcomemeasures (0.28 <r<0.40). The only significantcorrelationbetweenMRI and Manchestersyndromescores was for the right temporal lobe and positivesymptoms (r= —¿�0.35,P<0.01).The differentiatingneuropsychological tests were also consistentlycorrelated with the outcome measures(0.23 <r<0.65). Several significant correlations werefound between the neuropsychology results andpositive syndrome scores (NART r = —¿�0.46,P<0.0l; Quick IQ r= —¿�0.45, P<0.01; Stroop
Word Colour r=0.41, P<0.05, Digit Span-backwardr= —¿�0.40,P<0.05; RBMT profile scorer= —¿�0.50,P<0.01), but none with the negativesyndromescores. The correlation between RBMT profile scoreand negative syndrome score was —¿�0.19(P= 0.2).
Factor analysis of the symptom ratings and thedistinguishing neuropsychological tests identified fivefactors within eight iterations. Spearman rank
correlations between SPET tracer uptake werenormalised to occipital uptake, and these five factorsrevealed only seven, relatively weak correlations outof 140 comparisons. However, some strongcorrelations were found with MRI volumes betweenfactor 1 (composed of hallucinations, delusions, andall the distinguishing neuropsychological tests) andthe left (r=0.68, P<zO.001) and right (r=0.55,P<0.001) temporal lobe volumes, and betweenfactor 2 (flat affect, poverty of speech, psychomotorretardation, and Rivermead profile scores) and thevolumes of the left (r=0.40, P=0.017) and right(r= 0.49, P= 0.003) lateral ventricles. Factor 1 wasalso strongly correlated with whole-brain volume(r=0.41, P=0.015).
Discussion
The principal finding of this study is that treatmentresistant schizophrenic patients in comparison withtreatment-responsive patients, have neither astatisticallysignificantlower volume of brainstructures with MRI nor reduced tracer uptake withSPET. However, several differences were found
between the groups on neuropsychological testing,and the most discriminating test, the RBMT,remained significant after controlling for severalpossibleconfounders.Therearea number ofpossiblereasons for the negative findings on the brain scans,including insufficient dichotomisation of the patientgroups, inadequate statistical power, and lack ofbiological differences between such patient groupsand/or the masking of any differences betweensubtypes by the heterogeneity inherent inschizophrenia.
Table 4SpearmancorrelationsbetweenMRI structurevolumesandneuropsychologicaltests(distinguishingtwo groups)
in responsive and resistant schizophrenia
NARTw= NationalAdultReadingTest (WAIScorrected); MMSE= Mini-MentalState Examination;DSS = DigitSymbol Substitution;CPTI= ContinuousPerformanceTest-inappropriateresponses (errors);Stroop= StroopWordColourTest (errors);VF= VerbalFluency-'Animals';DS-B= DigitSpan-backward; Spatial= Spatial Recognition Test (CANTAB);RPS= Riverrnead Behavioural Memory Test-profile score000.Significant correlations shown in bold; ‘¿�P<0.05;*‘¿�P<O.O1;“¿�‘¿�P<0.001.

208 LAWRIE ET AL
Itisclearfrom theavailableclinicalinformationon the patientgroups thatthey were markedlydifferentintermsofmedicationresponse,symptomseverity, abnormal movements, social and globaloutcomes, and cognitive performance. Althoughthere was no consistent relationship between SPETtracer uptake and treatment response, it isnoteworthythatalmostallstructureson MRI weresmallerinresistantpatients.Thisiscompatiblewiththe neurodevelopmental model of schizophrenia,where themore profoundthecerebralaberration,thegreatertheeffecton brainsize,ageatonset,andclinical outcome (Weinberger, 1987). If this modelisaccurate,themain problem indetectingsubtledifferences between patients and controls, and evensmaller differences between patient subgroups, is instudy power.
The largest effect size of MRI variables betweenresponse groups in this study was 0.46 for the righttemporallobevolume difference;80% power todetecta statisticallysignificantdifferencein thisvariablewould demand two groupsof 75 patients.The patientgroupsinthisstudydifferedmarkedlyin terms of ‘¿�positivesymptoms' but less so in thelevels of ‘¿�negativesymptoms'. Positive symptoms,particularlydelusionsand hallucinations,havebeenlinkedto pathologicalprocessespredominantlyaffecting neuronal networks in temporolimbicstructures (Liddle et a!, 1992; Ebmeier, 1994), andMRI studies have demonstrated reduced superiortemporal gyral volume in schizophrenic subjects ascompared with controls (Barta et a!, 1990; Shentoneta!1992),althoughtheseabnormalitiesaregenerallythoughtto be more marked intheleftthan righthemisphere. These results are supported by therelativelystrong correlationsbetween temporalvolumes and the clinical/neuropsychological resultsfound here. The lessmarked between-groupdifferenceinnegativesymptoms couldaccountforthe failure to find larger differences in the volumesofotherstructures,particularlythelateralventricles,whichwerequitestronglycorrelatedwiththefactorcomposed of threenegativesymptoms (factor2).
The results from CT studies examining therelationship between structural abnormalities,usuallylateralventricularenlargment,and pooroutcomehavebeenconflicting.Inthestudiesdirectlyexamining this issue, two main approaches have beenused. Schizophrenic patients have been selectedfora particularlyhighventriclebrainratio(VBR)(usually two standard deviations above a controlgroup mean) or not, before treatment, thosewith large ventricles generally (Weinberger et a!,1980; Schulz et a!, 1983; Luchins et a!, 1984), butnot always (Nasrallah et a!, 1983), showing less
symptomatic improvement. Alternatively, individualpatients assigned to relatively good or bad outcomeon a post hoc basis have had their symptomimprovement scores correlated with the VBR; thisapproach has shown a strong negative correlation(Kolakowska et a!, 1985; Schroder et a!, 1993), norelationship (Williams eta!, 1985; Nimgaonkar eta!,1988), or a positive association between a high VBRand better neuroleptic response (Smith et a!, 1985;Losonczy et a!, 1986; Wilms et a!, 1992). Clearly,thereisno consistentrelationshipbetweenventricularenlargementand treatmentresponse,atleastwiththe relatively insensitive VBR in CT.
A volumetric rather than area approach, usingMRI rather than CT, in specifically selected patients,should more powerfully determine the relationshipbetweenneuroanatomyand outcome or treatmentresponse. Certainly, previous MRI studies suggestan association between increased ventricular size andpoor outcome (Johnstoneeta!,1989;DeLisieta!,1992), or more negative symptoms (Young et a!,1991; Gur et a!, 1994), and between reducedmesiotemporal volumes and more severe positivesymptoms (Bogerts et a!, 1993). Few other relevantMRI studies have been conducted. A group of outpatients have been dichotomised on a scale ofdeficit (negative) symptoms and studied withMRI (Buchanan et a!, 1993), but the patient groupwith more symptoms had larger volumes ofall structures measured, approximating thoseof a normal comparison group. Similarly,noconsistent morphological differences were foundbetween schizophrenic patients with favourable,intermediate,or poor outcomes in anotherMRIstudy (Harvey et a!, 1993).These resultsareconsistent with the findings of this study that thereisonlya weak relationshipbetweenbrainstructureand clinical outcome in most patients withschizophrenia.
The possibility remains that a subgroup ofschizophrenicpatientswithmarked structuralbrainchanges could be delineated. This would becompatible with the great variability in MRI volumeswithinpatientgroupsinthisstudy,whichwas moremarked inthetreatment-resistantgroup.Previousstudiesofpatientswithparticularlylargeventricularareashavegenerallyfoundthattheyrespondpoorlyto treatment (see above), but patients withschizophrenia do not have a bimodal distribution ofVBR on CT (Daniel et a!, 1991), suggesting thatventricularenlargementisnota markerfora specificsubtypeof schizophrenia.Inthisstudy,althoughimagingvariablesdidnot
distinguish the patient groups, cognitive testing,particularlyof long-termmemory functioning

MRI/SPET AND I REATMENT RESPONSE IN SCHIZOPHRENIA 209
(RBMT), diddo so.Severalpreviousstudieshaveshown that schizophrenic subjects have cognitivedeficits, primarily of memory, learning, and conceptformation,ascompared withcontrols(Goldbergeta!, 1990;Frith eta!, 1991;Saykin eta!, 1991). Indeed,further evidence suggests that schizophrenic patientsexhibit a relatively specific pattern of neuropsychological abnormality —¿�primarily that ofimpaired long-term memory —¿�akin to a dysmnesicsyndrome, and thatthesedeficitsare relatedtooutcome measures (Goldberg et a!, 1990; Tamlynet a!, 1992; Goldberg et a!, 1993). However, therearealsoreportsofspecificimpairmentsinexecutivetasks(Shalliceeta!,1991).The resultsfromthisstudyconfirm findings of particular deficits in memory,and suggestthatthesemay even be a relativelyspecific marker for poor outcome. For example,memory impairment may adversely affect treatmentcompliance or hinder abilities on several everydaytasks. Although the RBMT profile score correlatedmore stronglywithpositivethannegativesyndromescores, the loading onto both factors 1 and 2 suggeststhat this may simply reflect that these measures bestdistinguished the patient groups. The correlationsbetweentheneuropsychologicalresultsand severalregional volumes are compatible with evidence thatneuropsychological deficits reflect generalisedcerebral dysfunction, but that this is most pronounced in temporal areas and memory functions(Goldberg et a!, 1990).
In conclusion, the ability of episodic memory teststo distinguishsubgroups of patients withschizophreniasuggeststhatmemory functioningisan important determinant of outcome inschizophrenia. Morphological differences aredetectable between treatment-responsive andtreatment-resistantpatientgroups,but relativelylarge study groups would be required to differentiatethem by neuroimaging methods. Neuropsychologicaltesting might be better able to delineate prognosticand even aetiological subtypes of schizophrenia. Thepossibility that there is a subtype of schizophreniaassociated with clearly abnormal cerebral structureand poor outcome cannot be excluded, but thefindings of this and other studies suggest that illnessoutcome - or even treatment response - is confoundedby toomany variablestobe predictedby currentlyavailable imaging methods. The variability in otherillness factors in schizophrenia appears to be greaterthanthatrelatedtooutcomeortreatmentresponse.
Acknowledgements
for supervising the patients during SPET scanning, to Annette Blancand Jill Rollo for conducting the MRI scans, and to Nadine Dougallfor technical assistance in developing the SPET scan templates andfitting the images to them. Finally, we thank the patients and staffof the Royal Edinburgh Hospital for their help in conducting thisstudy.
References
AMERICAN PSYCHIATRIC ASSOCIATION (1987) Diagnostic andStatistical Manual of Mental Disorders (3rd edn, revised)(DSM-IIl-R). Washington, DC: APA.
BARTA, P. E., PEARLSON, G. D., POWERS, R. E., et a! (1990)Auditory hallucinations and smaller superior temporal gyralvolume in schizophrenia. American Journal of Psychiatry, 147,1457—1462.
BOGERTS, B., LIEBERMAN, J. A., ASHTARI, M., et al (1993)
Hippocampus-amygdala volumes and psychopathology inchronic schizophrenia. Biological Psychiatry, 33, 236—246.
BUCHANAN, R. W., BREIER, A., KIRKPATRICK, B., et al (1993)
Structural abnormalities in deficit and nondeficit schizophrenia.American Journal of Psychiatry, 150, 59-65.
COOPER, B. (1961) Social class and prognosis in schizophrenia. Iand 11. British Journal of Preventative and Social Medicine, 15,17—41.
DANIEL, D. G., GOLDBERG, T. E., GIBBONS, R. D., ci a! (1991) Lack
of a bimodal distribution of ventricular size in schizophrenia:a Gaussian mixture analysis of 1056 cases and controls.Biological Psychiatry, 30, 887—903.
DELISI, L. E., STRITZKE, P., RIORDAN, H., et al (1992) The timingof brain morphological changes in schizophrenia and theirrelationship to clinical outcome. Biological Psychiatry, 31,241—254.
EBMEIER, K. P. (1994) Brain imaging and schizophrenia. In
Advancesin theNeurobiologyof Schizophrenia(edsJ. A. DenBoer,H.G.M. Westenberg& H. M. vonPraag),pp.131-155.New York: Wiley.
FRITH, C. D., LEARY, J., CAHILL, C. & JOHNSTONE, E. C. (1991)
Disabilities and circumstances of schizophrenic patients. IV.Performance on psychological tests. British Journal ofPsychiatry, 159 (suppl. 13), 26—29.
GOLDBERG, T. E., RAGLAND, J. D., TORREY, E. F., et al (1990)
Neuropsychologicalassessmentof monozygotic twins discordantforschizophrenia.ArchivesofGeneralPsychiatry,47,1066-1072.
TORREY, E. F., GoLD, J. M., et al (1993) Learning andmemory in monozygotic twins discordant for schizophrenia.PsychologicalMedicine, 23, 71—85.
GOLDEN, C. J., MOSRS, J. A., ZELAZOWSKI, R., et a! (1980) Cerebral
ventricular size and neuropsychological impairment in youngchronic schizophrenics: measurement by the standardised LuriaNebraska Neuropsychological Battery. Archives of GeneralPsychiatry, 37, 619—623.
GUR, R. E., MOZLEY, P. D., SHATSEL, D. L., et al (1994) Clinicalsubtypes of schizophrenia: differences in brain and CSF volume.American Journal of Psychiatry, 151, 343-350.
HARVEY, I., RON, M. A., Du BOULAY, G., ci al (1993) Reductionof cortical volume in schizophrenia on magnetic resonanceimaging. Psychological Medicine, 23, 591—604.
JoHNs-roNE, E. C. (ed.) (1991) Disabilities and circumstances of
schizophrenic patients —¿�a follow-up study. British Journal ofPsychiatry, 159 (suppl. 13).
CROW, T. J., FRITH, C. D., ci al (1976) Cerebralventricular size and cognitive impairment in chronicschizophrenia. Lancet, ii, 924—926.
OWENS, D. G. C., CROW, T. J., ci al (1989) Temporal lobe
structure as determined by nuclear magnetic resonance inschizophrenia and bipolar affective disorder. Journal ofNeurology, Neurosurgery and Psychiatry, 52, 736-741.
This work was supported by the Wellcome Trust; S.M.L. was aWellcome ResearchRegistrar.We aregreatfulto CatherineMurray

210
KOLAKOWSKA, T., WILLIAMS, A. 0., ARDERN, M., et a!(1985) Schizophrenia with good and poor outcome. 1. Earlyclinical features, response to neuroleptics and signs oforganic dysfunctions. British Journal of Psychiatry, 146,229—246.
KRAWIECKA, M., GOLDBERG, D. & VAUGHN, M. (1977) Astandardised psychiatric assessment scale for ratingchronic psychotic patients. Acta Psychiatrica Scandinavica, 55,299-308.
LIDDLE, P. F., FRISTON, K. J., FRITH, C. D., et a! (1992) Patterns
of cerebral blood flow in schizophrenia. British Journal ofPsychiatry, 160, 179—186.
LOSONCZY, M. F., So@, IS., MoHs, R. C., ci al (1986) Correlates
of lateral ventricular size in chronic schizophrenia. I. Behavioraland treatment response measures. American Journal ofPsychiatry, 143, 976—981.
LUCHINS, D. J., LEWINE, R. R. J. & MELTZER, H. Y. (1984) Lateral
ventricular size, psychopathology, and medication response inthe psychoses. Biological Psychiatry, 19, 29—44.
MCGLASHAN, T. H. (1984) The Chestnut Lodge follow-up study.
II: long-term outcome of schizophrenia and the affectivedisorders. Archives of General Psychiatry, 41, 586—601.
MAY, P. R. A., DENCKER, S. J., HUBBARD, J. W., ci a! (1988) A
systematic approach to treatment resistance in schizophrenicdisorders. In TreatmentResistance in Schizophrenia (eds S. J.Dencker & F. Kulhanek), pp. 22—33.Braunschweig/Wiesbaden:Viewag Verlag.
NASRALLAH, H. Y., KUPERMAN, S., HAMRA, B. J., et a! (1983)Clinical differences between schizophrenic patients with andwithout large cerebral ventricles. Journal of Clinical Psychiatry,44,407—409.
NIMGAONKAR, V. L., WESSELY, S., TUr'm, L. E., et al (1988)Response to drugs in schizophrenia: the influence of familyhistory, obstetric complications and ventricular enlargement.PsychologicalMedicine, 18, 583—592.
SAYKIN, A. J., GUR, R. C., OUR, R. E., et a! (1991)
Neuropsychological function in schizophrenia: selectiveimpairment in memory and learning. Archives of GeneralPsychiatry, 48, 618—624.
SCHRODER, J., GEIDER, F. J. & SAUER, H. (1993) Can computerised
tomography be used to predict early treatment response inschizophrenia? British Journal of Psychiatry, 163 (suppl. 21),13—15.
SCHULZ, S. C., SINICROPE, P. S., KISHORE, P., et at (1983)
Treatment response and ventricularbrainenlargementin youngschizophrenic patients. Psychopharmacology Bulletin, 19,510—512.
SHALLICE, T., BURGESS, P. W. & FRJTH, C. D. (1991) Can theneuropsychological case-study approach be applied toschizophrenia? Psychological Medicine, 21, 661-673.
SHEWr0N, M. E., KIKIM5, R., Joissz, F. A., et a! (1992)Abnormalities of the left temporal lobe and thought disorderin schizophrenia: a quantitative magnetic resonance imagingstudy. New England Journal of Medicine, 327, 604—612.
SMITh, R. C., BAUMGARTNER, R., RAVICHANDRAM, G. K., et a!(1985) Lateral ventricularenlargement and clinical response inschizophrenia. Psychiatry Research, 14, 241—253.
SPITZER, R. L. & ENDICOTr, J. (1978) Schedule for Affective
Disorders and Schizophrenia - Lifetime Version. New York:New York State Psychiatric Institute.
SUDDATH, R. L., CHRISTISON, G. W., TORREY, E. F., et a! (1990)Anatomical abnormalities in the brains of monozygotic twinsdiscordantforschizophrenia.New EnglandJournalofMedicine,322, 789—794.
TAMLYN, D., MCKENNA, P. J., MORTIMER, A. M., et a! (1992)
Memory impairment in schizophrenia: its extent, affiliations andneuropsychologicalcharacter. Psychological Medicine,22, 101-115.
WECHSLER, D. (1981) Wechsler Adult Intelligence Scale —¿�Revised(WAIS-R). New York: Psychological Corporation.
WEINBERGER, D. R. (1987) Implications of normal braindevelopment for the pathogenesis of schizophrenia.Archives ofGeneral Psychiatry, 44, 660-669.
BIGELOW, L. B., KLEINMAN, J. E., ci a! (1980) Cerebralventricularenlargementinchronicschizophrenia:anassociationwith poor responseto treatment.Archivesof GeneralPsychiatry,37, 11—13.
WILLIAMS, A. 0., REVELEY, M. A., KOLAKOWSKA, T. A., ci a!(1985) Schizophreniawith good and poor outcome. II. Cerebralventricular size and its clinical significance. British Journal ofPsychiatry, 146, 239—246.
WILM5, 0., VAN ONGEVAL, C., BAERT, A. L., ci at (1992)Ventricular enlargement, clinical correlates and treatmentoutcome in chronic schizophrenic inpatients. Ada PsychiatricaScandinavica, 85, 306—312.
WIBO, J. K., Cooean, J. & [email protected], N. (1974) The Measurementand Ctassjficationof PsychiatricSymptoms. Cambridge:Cambridge University Press.
W0JCIK, J. D., GELENBERG, A. J., LABRIE, R. A., ci a! (1980)Prevalence of tardive dyskinesia in an outpatient population.
Comprehensive Psychiatry, 21, 370—380.YOUNG, A. H., BLACKWOOD, D. H. R., ROXBOROUGH, H., ci a!
(1991) A magnetic resonance imaging study of schizophrenia:brain structure and clinical symptoms. British Journal ofPsychiatry, 158, 158-164.
(First received 20 June 1994, final revision 29 November 1994, accepted 20 January 1995)
LAWRIE ET AL
Stephen M. Lawne, MPhil, MRCPsych,Gordon T. Ingle, BSC, Edinburgh University Department ofPsychiatry; Celestine G. Santosh, MD, MRCR,Magnetic Resonance Imaging Unit, Edinburgh UniversityDepartment of Medical Radiology; Andrew C. Rogers, BSC, Edinburgh University Department ofPsychiatry; J. Ewen Rimmington, BSc, DPhil, Kaliprasad P. Naldu, MBA, MSc, Jonathan J. K. Best, MSc,FRCR, Magnetic Resonance Imaging Unit, Edinburgh University Department of Medical Radiology; RonanE. O'Carroll, BSc, PhD, Guy M. Goodwin, DPhil, MRCP,MRCPsych,Klaus P. Ebmeier, MD, MRCPsych,MRCBrain Metabolism Unit, Royal Edinburgh Hospital; Eve C. Johnstone, MD, FRCP, FRCPsych,EdinburghUniversity Department of Psychiatry
Correspondence: Dr Stephen M. Lawrie, Edinburgh University Department of Psychiatry, Kennedy Tower, RoyalEdinburghHospital,MorningsidePark,EdinburghEH1O 5HF
Related Documents











