schizophrenia.

Treatment resistant schizophrenia
Aug 09, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Treatment resistant schizophrenia.
History
19 th century till now.
Divide into 2 groups – pre and post chlorpromazine.
Post neuroleptic era studies -60-70% improve
20-30% are resistant to treatment.
Kane J, Hognifeld G, Singer J, et al.1988
Miller A, McEvoy J, Jeste D,etal.2006
Hasan A, Falkai P, Wobrock T, et al.2012

Chronicity
vs
Refractoriness
vs
TRS
1] INCOMPLETE RECOVERY
VS
TREATMENT REFRACTORY
RESPONSE TO TREATMENT
2] REMISSION
VS
RECOVERY
Epidemiology Prevalence:
20% doesn’t respond after one year of treatment.
Generally assumed to be around 20-30%.
Some authors report upto 60%.
Meltzer H, Kostacoglu A.2001.
Age of onset: 17 yrs compared to 20 [ non TRS]
Male predominance.
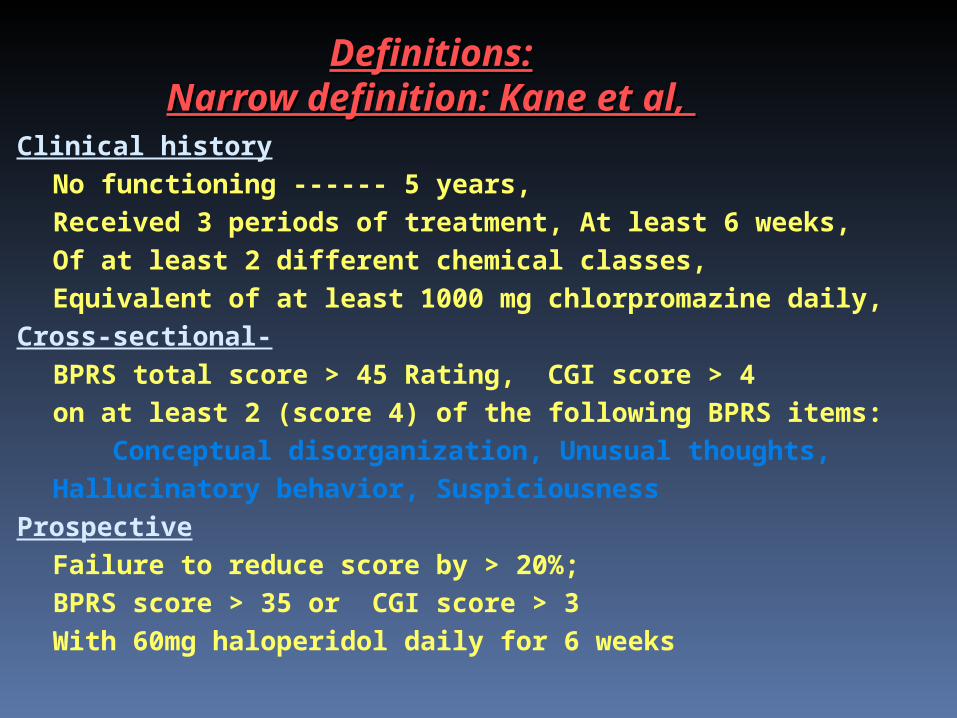
Definitions:Definitions:Narrow definition: Kane et al, Narrow definition: Kane et al,
Clinical history
No functioning ------ 5 years,
Received 3 periods of treatment, At least 6 weeks,
Of at least 2 different chemical classes,
Equivalent of at least 1000 mg chlorpromazine daily,
Cross-sectional-
BPRS total score > 45 Rating, CGI score > 4
on at least 2 (score 4) of the following BPRS items:
Conceptual disorganization, Unusual thoughts,
Hallucinatory behavior, Suspiciousness
Prospective
Failure to reduce score by > 20%;
BPRS score > 35 or CGI score > 3
With 60mg haloperidol daily for 6 weeks
Present definition :
“ TRS is suggested by a lack of a satisfactory clinical improvement despite the sequential use of the recommended doses for 6 to 8 weeks of at least two antipsychotics at least one of which should be an atypical ”
(NICE, 2002)
30% of patients fall under this category.

EARLY OPERATIONAL DEFINITIONS:

American Psychiatric Association guidelines and the Schizophrenia Patient Outcomes ResearchTeam guidelines, or algorithms, such as theTexas Medication Algorithm Project state that:
“ A patient who has not responded to two or three treatments using atypical antipsychotics for a duration of at least 4 to 6 weeks can be considered as having TRS and is eligible for treatment with clozapine.”
APA-2004

International Pharmacological Algorithm Project:
“who has not responded to two trials of 4 to 6 weeks’ duration using monotherapy with two different SGAs (or two trials with an FGA, if SGAs are not available) is considered to have TRS and is eligible for treatment with clozapine, for a six month trial with doses up to 900 mg/d.”
IPAP-2006
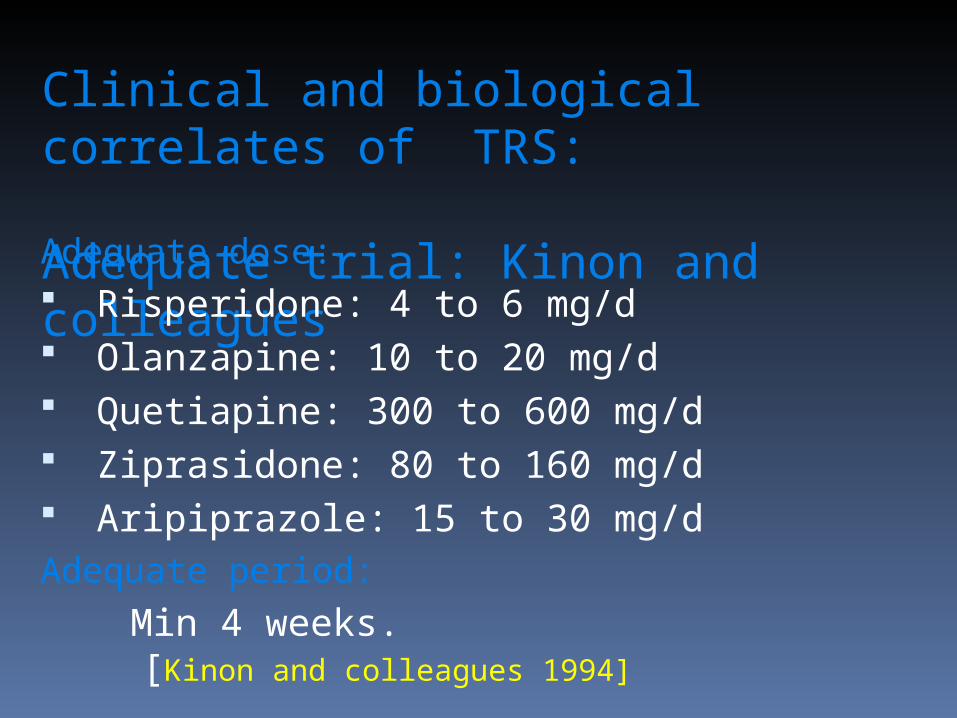
Clinical and biological correlates of TRS:
Adequate trial: Kinon and colleaguesAdequate dose: Risperidone: 4 to 6 mg/d Olanzapine: 10 to 20 mg/d Quetiapine: 300 to 600 mg/d Ziprasidone: 80 to 160 mg/d Aripiprazole: 15 to 30 mg/dAdequate period:
Min 4 weeks. [Kinon and colleagues 1994]
Apparent treatment resistance or Incomplete recovery.
Poor compliance Lack of family support Substance abuse Physical comorbidity Intolerable side effects Incorrect dose schedule Poor therapeutic alliance
Elkis H, Treatment resistant schizophrenia, Psychiatr Clin N Am 30; 2007
Neuroimagimg correlates of TRS TRS develops accoring to 3 stages:
Childhood : cortical pathology and deficient neuro modulatory capacity resulting from genetic/epigenetic etiologic factors.
Adolescence: neuro chemical sensitization leading to dopamine release and development
Of psychotic episodes.
Adulthood: neurotoxicity with consequent development of structural neuronal changes .
Sheitman and lieberman :1988
Neuroimagimg correlates of TRS Ventricular enlargement- non remitters.
Liebermann1996
[Prospective 18 months study]
Retrospective study: ventricular enlargement-poor outcome
Crosthwaite CG, London 2000 Prospective studies:
Ventricular enlargement: response to typicals
Cortical atrophy: response to atypicals Staal WG , AJP: 2001

other neurobiological correlates: HVA levels higher among responders in 1st episode Liberman J and colleagues,1994.
Altered ‘T’cell response.
Altered inflammatory response due to interleukins.
Altamura AC, Bassetti R, Cattaneo E, etal,2004 .
REASONS FOR FAILURE TO RESPOND: PATIENT FACTORS: Dual diagnosis. Organic factors. Poor adherence. Familial factors. Poor psychosocial support . Cultural backgrounds and expectations. Premorbid factors.
REASONS FOR FAILURE TO RESPOND: Illness factors Negative symptoms Early onset Lack of early response Delay in 1st treatment Type 1 v/s type 2 schizophrenia “Neurodevelopment” v/s “adult” type Cognitive impairment
REASONS FOR FAILURE TO RESPOND: Treatment factors Improper dosage Inappropriate drug treatment Aberrant metabolism (necessary to monitor drug levels)

MANAGEMENT STRATERGIES
Pharmacological
Non pharmacological

Pharmacological methods:
Increasing the dose Swtching the drug Combination Augmentation

Treatment guidelines: [NICE]
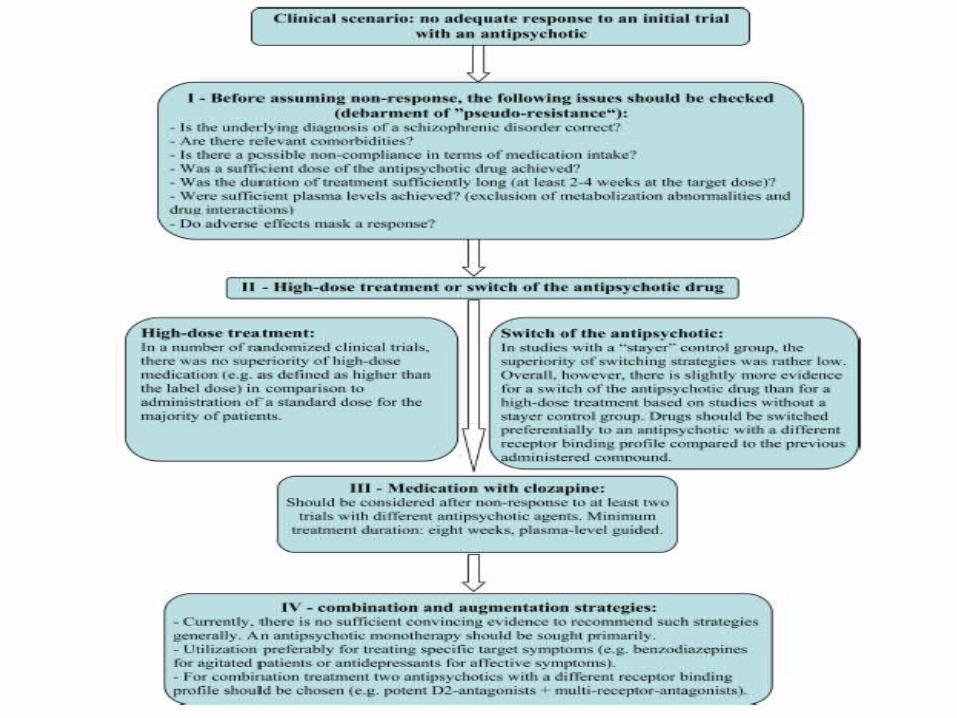
Algorithm for the pharmacological treatment of patients with treatment-resistant schizophrenia (modified from refs 3 and 4).
Markus Dold, and Stefan Leucht Evid Based Mental Health 2014;17:33-37
Copyright © by the BMJ Publishing Group Ltd, Royal College of Psychiatrists & British Psychological Society. All rights reserved.
Step 1:
Establish that therapy has failed to adequate trials of antipsychotic drugs:
In terms of dosage, duration and adherence.
Other causes Of non-response as:
co-morbid substance misuse
concurrent use of other prescribed medicines and
physical illness.
NICE-2002
Step 2:
Clozapine should be introduced at the earliest opportunity.
The prescribing clinician and service user may
wish to consider an atypical antipsychotic in advance of a
trial of clozapine. in such cases, olanzapine or risperidone
may be worth considering.
Service users should be informed:
evidence for improvement is more limited than for clozapine.
NICE-2002
Combination therapy: Definition This refers to the concurrent administration of more than one
antipsychotic.
The efficacy of combining two or more conventional antipsychotics, or two or more atypical antipsychotics has not been established.
There is limited evidence that adding a conventional antipsychotic to clozapine may produce benefits compared to clozapine alone.
Combining one antipsychotic with another antipsychotic may increase the risk of adverse effects and pharmacokinetic interactions
NICE-2002
Summary: There is no convincing evidence to support the routine use of
combined antipsychotics .
Doing so may increase the likelihood of adverse events and high doses of drugs.
There is some limited evidence to support the use of combined antipsychotics for people TRS.
NICE-2002

CLINICAL PRACTICE RECOMMENDATIONS
More than one antipsychotic drug, whether atypical or typical, should not be prescribed concurrently, except for short periods to cover changeover.
However, the addition of a second antipsychotic to clozapine may be a supportable intervention in people with treatment resistant schizophrenia for whom clozapine alone has proved insufficiently effective.
NICE-2002
AUGMENTATION WITH CLOZAPINE: ANTIPSYCHOTICS:
OLANZEPINE
SULPIRIDE
AMISULPIRIDE
LOXEPINE
ZIPRAZIDONE ANTIDEPRESSANTS:
FLUOXETINE
MIRTAZEPINE
NICE-2002

Augmentation stratergies: MOOD STABLEZIRES:
LITHIUM
VALPROATE
CARBAMAZEPINE
LAMOTREGINE BENZODIAZEPINES OTHER AGENTS:
GLYCINE,SERINE, CYCLOSERINE
NICE-2002
Non pharmacological augmenters: ECT TMS
Combination and augmentation strategies are only empirical and are based on case reports and open label trials.
Not enough data to support any of these strategies
Needs further RCT to support these strategies.
NICE-2002
APA DEFINITION:
“Treatment resistance is defined as little or no symptomatic response to multiple (at least two) antipsychotic trials of an adequate duration (at least 6 weeks) and dose (therapeutic range).”
APA-2004
APA GUIDELINES: Evaluate for adequacy of trial
Establishing therapeutic alliance
Improving treatment adherence
APA-2004
Because of clozapine’s superior efficacy, a trial of clozapine should be considered for a patient with a clinically inadequate response to antipsychotic treatment or for a patient with suicidal ideation or behavior .
Besides clozapine very limited options for individuals who have significant residual symptoms.
Various augmentation strategies with limited or no evidence are tried.
APA-2004
AUGMENTATION STRATERGIES: Depending on the type of residual symptom (eg.Positive, negative,
cognitive, or mood symptoms, aggressive behavior): Antipsychotic Anticonvulsants Benzodiazepine. NMDA receptor allosteric agonists.[D-serine] Glycine D- cycloserine Cholinergic agonists ECT CBT positive symptoms. Cognitive remediation- to reduce severity of cognitive deficits.
APA-2004
IPS GUIDELINES:
Although there is some suggestion of efficacy of risperidone and olanzapine in this condition, and despite recent doubts about the effectiveness of clozapine, it still is the drug of choice in these situations (Sartorius et al., 2002).
INDIAN DATA: Solanki and colleagues in a review concluded that :
“clozapine exhibits superiority over typical antipsychotics in terms of both efficacy (as shown by an improvement in overall psychopathology) and safety. However the magnitude of its effect is not consistent. Efficacy data for other SGA’s in the
treatment of refractory schizophrenics were inconclusive.”
Solanki et al, IJP, NOV-DEC: 2009
Canadian guidelines:2005 To confirm diagnosis: To rule out schizoaffective disorder Bipolar disorder: mania Depression
TREATMENT GUIDELINES FOR NON RESPONDERS: Optimization, Substitution, Augmentation And combination.
Canadian guidelines: 2005
If a trial of clozapine is not effective, the next steps are augmentation,followed by combination strategies.
Augmentation : data available are case series only
Except for lamotrigene. Combination stratergies:
Limited evidence
Higher chances of side effects.
ECT: There was limited evidence to support
its use as adjunctive treatment with antipsychotics for
those who show limited response to medication alone.
STUDIES WITH CLOZAPINE. STUDIES WITH CLOZAPINE.
John Kane 1992
Multicenter trial
Clozapine was compared with chlorpromazine.
30 percent of patients improved ---------- 6-week trial.
60 percent of patients improved ---------- 6 months.
Schooler et al 1993
60% with clozapine, but only 12% with haloperidol;
Rodriguez et al (1998)
Factors Clozapine responders
Cognitive disorganization ----- non-responders
Behavioral disorganization-----partial responders.
Jalenques et al (1992),
Improvement
Positive symptoms by 1 month
Negative symptoms by 3 months
Improvement in social functions by 4-6 months
Meltzer and Okayli (1995)
Clozapine treatment of 6 months to 7 years duration
Reported decrease in suicidality
Lieberman et al (1994)
Optimal trial of Clozapine ------------12 -24 weeks.
STUDIES OF CLOZAPINE WITH ECT: STUDIES OF CLOZAPINE WITH ECT:
Kales et al (1999)
Supplementing clozapine with ECTs
Effective in treatment resistant schizophrenia.
Its beneficial effects were short-lived.
Bhatia et al (1998)
Clozapine was combined with ECT.
Both the reports opined that such a combination is safe.
ADJUVANT MEDICATIONS . ADJUVANT MEDICATIONS .
Newer neuroleptic ECT’s Lithium Benzodiazepines Propranlol Carbamazepine Valproate Glycine (30gm/day)
Christinson et al (1991)
Schizophrenia Patient Outcomes Research Team (PORT)
A Trial of Adjunctive Pharmacotherapy With
BENZODIAZEPINES,
CARBAMAZEPINE,
PROPRANOLOL,
LITHIUM.

COGNITIVE REMEDIATION AND THERAPY COGNITIVE REMEDIATION AND THERAPY
Two approaches to cognitive work
1. Cognitive retraining
2. Cognitive therapy
Comprehensive textbook ofpsychiatry,9th edition.
Psychosocial intervention
Family therapy Social skills and communication training Cognitive Behavior therapy Behavioral intervention Vocational training Anxiety management
Family therapy
Reduces burden Better coping skills and problem solving abilities Reduces relapse rates by 50% Better compliance in the 1st two years post discharge
Cochrane Meta-analysis






Cognitive Deficits :Cognitive Deficits :
Decreased attention,
Attention shifting tasks,
Working memory,
Scanning(Vigilance),
Executive function,
Language processing(Verbal fluency,
Poor Abstract ability,
Fine motor skills,
General intelligence
Comprehensive textbook ofpsychiatry,9th edition.

NEURO COGNITIVE DEFICITS
Before the onset of illness.
Family studies-
Children of schizophrenia
First degree relatives
Shizotaxia
Comprehensive textbook ofpsychiatry,9th edition.

Cognitive retraining. Cognitive retraining.
- Assessment
- InterventionsAttention enhancing tasks
Word fluency
Vigilance tasks
Card sorting
Picture completion
Memory recall retraining
Computer assisted training
Comprehensive textbook of psychiatry,9th edition.
Cognitive therapy. Cognitive therapy. Delusions Rapport building Psychopathology to be elicited and documented Empathizing Asking for evidence Asking for alternative explanations Reinforcing the alternative explanations Confrontation
Hallucinations Distraction techniques Sub vocalisation CBT-----Reattribution Comprehensive textbook ofpsychiatry,9th edition.
SOCIAL SKILLS TRAININGSOCIAL SKILLS TRAINING
Social skills training involves behavioral techniques or learning activities that enable patients to acquire instrumental and affiliative skills in domains required to meet the interpersonal, self-care, and coping demands of community living.
Comprehensive textbook ofpsychiatry,9th edition.

Social skills:Social skills:
Verbal:
Voice tone and pitch, affect, loudness, speech fluency, amount of
speech, Latency of response, content.
Nonverbal:
Eye contact, facial expression, gestures, interpersonal distance,
body posture, body orientation etc.
Comprehensive textbook ofpsychiatry,9th edition.
Core skills:
Expressing positive feelings,
Making positive request,
Expressing negative feelings.
Supplementary skills:
Active listening,
Compromise and negotiation,
Requesting time out.
Comprehensive textbook ofpsychiatry,9th edition.
Steps. Steps.
Done in treatment settings Providing rationale Live modeling, video , role play, drama etc (Communication skill training) Rehearsals of skills, Coaching and feed back Problem solving techniques Group therapy Self help groupDone in natural environment In vivo exercise Home work assignment Booster sessions Comprehensive textbook ofpsychiatry,9th edition.
Treatment refractoriness:Treatment refractoriness:
Refractoriness may be defined as Persisting positive and negative psychotic symptomsDeficits in social functioning and bizarre behaviorsthat interfere with community adaptation.
(Brenner et al 1999)

Brenner et al 1999 proposed Brenner et al 1999 proposed criteria for refractoriness. criteria for refractoriness.
ICD 10 diagnosis of schizophrenia Continuous hospitalization in the past 2 years Psychosocial functioning on GAS less than 40% Severe or moderate on at least 3 of the below items
Flattened affect
Psychomotor retardation
Delusions
Hallucinations
Poverty of speech
Incoherent speech
Vocational rehab
Sheltered workshops
Long-term hospitalization
5 -10 % requires institutional care
Comprehensive textbook ofpsychiatry,9th edition.

REFERENCES
Sadock BJ, Sadock VA, Ruiz P. Comprehensive textbook of Psychiatry,Schizophrenia. 9th Edition,VOL1:Lippincott Williams ltd; 2009.
IPS guidelines for management of schizophrenia.
NICE guidelines: core interventions in treatment and management of schizophrenia ,2002.
APA guidelines: practice guidelines for treatment of patients with schizophrenia,2004.

REFERENCES
Canadian clinical practice guidelines: Treatment of schizophrenia, canadian journal of psychiatry, vol50, no2, supplement 1,Nov, 2005.
Elkis H, Treatment resistant schizophrenia, Psychiatr Clin N Am 30; 2007.
Dold M,Leucht S. Evid Based Mental Health, Vol 17: No 2,May2014.

THANK YOU
Treatment resistant schizophrenia
Treatment resistant schizophrenia
Treatment resistant schizophrenia
Treatment resistant schizophrenia



THANK YOU

Related Documents











