MacGyver Jobs in Dermatology Ümit Türsen, * MD Address: * Mersin University, School of Medicine, Department of Dermatology, Mersin E-mail: [email protected] Corresponding Author: Dr. Ümit Türsen. Mersin University, School of Medicine, Department of Dermatology, Mersin. Review DOI: 10.6003/jtad.19131r2 Published: J Turk Acad Dermatol 2019; 13 (1): 19131r2. This article is available from: http://www.jtad.org/2019/1/jtad191314r2.pdf Keywords: MacGyver, Dermatology, Aesthetic, Dermatosurgery Abstract Background: Hair loss is a common clinical presentation in any medical clinic. Telogen effluvium is considered among the most prevalent causes of hair loss particularly in female patients. Telogen effluvium may associate with significant psychosocial comorbidities and the medical treatment may be challenging. In this article we will review the recent literatures about epidemiology, etiopathogenesis, clinical presentation and management of telogen effluvium. Method: An electronic literature search was performed using the PubMed and Google Scholar to identify relevant articles published between 1993 and 2017. Search keywords included “telogen effluvium” and “hair loss”. We included studies published in English. Editorials, brief notes, conference proceedings, and letters to editors were excluded. Introduction The Oxford Dictionaries state that to “MacGy- ver” is to make or repair (an object) in an im- provised or inventive way, making use of whatever items are at hand. Origin comes from Angus MacGyver, the lead character in the television series MacGyver (1985–1992), who often made or repaired objects in an im- provised way. Main character of show by the same name. Full name Angus Macgyver. Part secret agent for government and phoenix fo- undation, part handyman, part mad scien- tist, part community service volunteer. He might refuse to use guns, but nobody could ever call him a pussy. Macgyver can battle Soviet supersoldiers and serve soup at a ho- meless shelter all in one episode. Macgyver was the epitome of 1980s era optimism. Beats the commies, fixes the environment, cures aids, and can make a helicopter out of garbage bags and bamboo. Most importantly, he's the only guy who ever looked cool in a mullet and is probably the only guy who could get away with it now [1,2]. In dermato- logy, we can solve different problems in a creative, resourceful, typically “jury-rigged” fashion as Macgyverism (Table 1). MacGyver Jobs with Skin Biopsy Punches Punch instrument is a circular hollow blade attached to a pencil-like handle ranging in size from 0.5 mm to 10 mm available as a dis- posable, reusable, and automated instru- ment. Punch biopsy is an apparently simple procedure include the relative easiness to perform, minimal complications, and provi- sion of a full-thickness sample. The skin punch is an instrument which is used almost exclusively by dermatologists. The skin bi- opsy is a relatively simple, but essential pro- Page 1 of 39 (page number not for citation purposes)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MacGyver Jobs in Dermatology
Ümit Türsen,* MD
Address: *Mersin University, School of Medicine, Department of Dermatology, MersinE-mail: [email protected] Author: Dr. Ümit Türsen. Mersin University, School of Medicine, Department of Dermatology, Mersin.
Review DOI: 10.6003/jtad.19131r2
Published:J Turk Acad Dermatol 2019; 13 (1): 19131r2.This article is available from: http://www.jtad.org/2019/1/jtad191314r2.pdf Keywords: MacGyver, Dermatology, Aesthetic, Dermatosurgery
Abstract
Background: Hair loss is a common clinical presentation in any medical clinic. Telogen effluvium isconsidered among the most prevalent causes of hair loss particularly in female patients. Telogeneffluvium may associate with significant psychosocial comorbidities and the medical treatment maybe challenging. In this article we will review the recent literatures about epidemiology,etiopathogenesis, clinical presentation and management of telogen effluvium.
Method: An electronic literature search was performed using the PubMed and Google Scholar toidentify relevant articles published between 1993 and 2017. Search keywords included “telogeneffluvium” and “hair loss”. We included studies published in English. Editorials, brief notes, conferenceproceedings, and letters to editors were excluded.
Introduction
The Oxford Dictionaries state that to “MacGy-ver” is to make or repair (an object) in an im-provised or inventive way, making use ofwhatever items are at hand. Origin comesfrom Angus MacGyver, the lead character inthe television series MacGyver (1985–1992),who often made or repaired objects in an im-provised way. Main character of show by thesame name. Full name Angus Macgyver. Partsecret agent for government and phoenix fo-undation, part handyman, part mad scien-tist, part community service volunteer. Hemight refuse to use guns, but nobody couldever call him a pussy. Macgyver can battleSoviet supersoldiers and serve soup at a ho-meless shelter all in one episode. Macgyverwas the epitome of 1980s era optimism.Beats the commies, fixes the environment,cures aids, and can make a helicopter out of
garbage bags and bamboo. Most importantly,he's the only guy who ever looked cool in amullet and is probably the only guy whocould get away with it now [1,2]. In dermato-logy, we can solve different problems in acreative, resourceful, typically “jury-rigged”fashion as Macgyverism (Table 1).
MacGyver Jobs with Skin Biopsy Punches
Punch instrument is a circular hollow bladeattached to a pencil-like handle ranging insize from 0.5 mm to 10 mm available as a dis-posable, reusable, and automated instru-ment. Punch biopsy is an apparently simpleprocedure include the relative easiness toperform, minimal complications, and provi-sion of a full-thickness sample. The skinpunch is an instrument which is used almostexclusively by dermatologists. The skin bi-opsy is a relatively simple, but essential pro-
Page 1 of 39(page number not for citation purposes)

cedure in the management of skin disorders.Properly performed, it may confirm a diagno-sis, remove cosmetically unacceptable lesi-ons, and provide definitive treatment for anumber of skin conditions. Variants of handheld punches are characterised by metallicpunches with tapering or cylindrical tip; me-tallic handle with attachable tips; disposable,plastic handle punches; available in sizesfrom 0.5 to 10 mm in diameter. Power punc-hes, here the shaft of the punch is mountedonto a hand machine with adjustable rotatio-nal speed varying from 2000 to 10,000 rpm.It is available in various sizes of 0.5-1.3 mm.It is a circular hollow blade attached to a pen-cil-like handle ranging in size from 1 to 8 mm.It is available as a disposable, reusable, andautomated instrument. Disposable puncheshave the advantages of being presterilized,readily available, always sharp, and requiringno maintenance. Reusable steel punches aremore expensive, require sterilization betweenprocedures, get dull with repeated use, andmust be maintained by proper, skilled shar-pening [3,4].
Uses of Punches Can Be Classified İntoThree Categories
A-Diagnostic purposes: Skin biopsy for di-agnosis of dermatological diseases. Punch bi-opsies are simple to perform, have fewcomplications, and if small, can heal withoutsuturing. For non-facial lesions, a 4-mmpunch is sufficient; however, in granuloma-tous conditions or conditions with atypicalfeatures, biopsies of 5 mm or more are prefe-rable[3].
Basic punch: Punch surgery tray should in-clude alcohol pads, local anesthetic, a punchinstrument of the desired size, forceps, scis-sors and gauze. After preparation of the site,the fingers of the nondominant hand are usedto stretch the skin perpendicular to the direc-tion of relaxed skin tension lines to producean oval defect that is easier to close. Thepunch is withdrawn, and the specimen is ret-rieved by piercing it with the needle from thesyringe used for anesthesia or by handling itwith the forceps. If needed, scissors can beused to transect the subcutaneous tissue atits deepest portion. The advantages of punchbiopsy include the relative easiness to per-form, minimal complications, and provisionof a full-thickness sample; because of that, it
is preferred over shave biopsy. Punch biopsyhas some disadvantages. First, its small sizeand variable depth lead to difficulty in histo-pathologic interpretation in conditions invol-ving adipose tissue such as morphea andpanniculitis. Because of that, a modificationcalled the double-trephine punch biopsytechnique was proposed. Second, the shea-ring effect of the punch may cause loss of theblister roof. In such cases, a topical refrige-rant such as ethyl chloride spray can be usedto freeze the blister in place when a punch bi-opsy is taken [4,5].
Modified diagnostic punch surgery: Punchbiopsy is an apparently simple procedure, butit has some pitfalls. Being aware of the pitfallsand ways to work around them helps in subs-tantially improving the outcome of this diag-nostic procedure. Most important is choosingthe most representative lesion for the biopsy,which will yield a better diagnostic outcome.Always take a fully evolved, untreated lesionand avoid excoriated or ulcerated lesions un-less there is no option. Avoid taking a biopsyover bony prominences or pressure-bearingareas as a sparse, nonspecific, lymphocyticinfiltrate present over frictional sites cancomplicate its interpretation. Punch surgerydoes have certain risks, including possibledisturbance of deeper underlying structuressuch as nerves and arteries. Therefore, physi-cians must be familiar with the underlyinganatomy and the danger zones. Punch sur-gery in critical areas such as the digits or theeyelid overlying the globe are generally to beavoided. Caution should also be exercisedover areas where there is little soft tissue bet-ween skin and bone because the punch cancut through the underlying bone [4].
Split-punch biopsy technique: This techni-que is used to obtain two tissue samples fordifferent studies from one punch biopsy. Thesplit-punch biopsy technique is used to ob-tain two tissue samples for different studiesfrom one punch biopsy. It is done by advan-cing the punch just into the papillary dermis.This is followed by using a no. 11 blade heldnearly perpendicular to the skin surface; thespecimen is bisected to the subcutis. Thenthe punch is reintroduced and advanced tothe subcutis. On removal of the punch, thebisected specimen is held in place only by abit of subcutaneous tissue, which must beundercut to complete the procedure, resul-
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
(page number not for citation purposes)Page 2 of 39
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
(page number not for citation purposes)Page 3 of 39
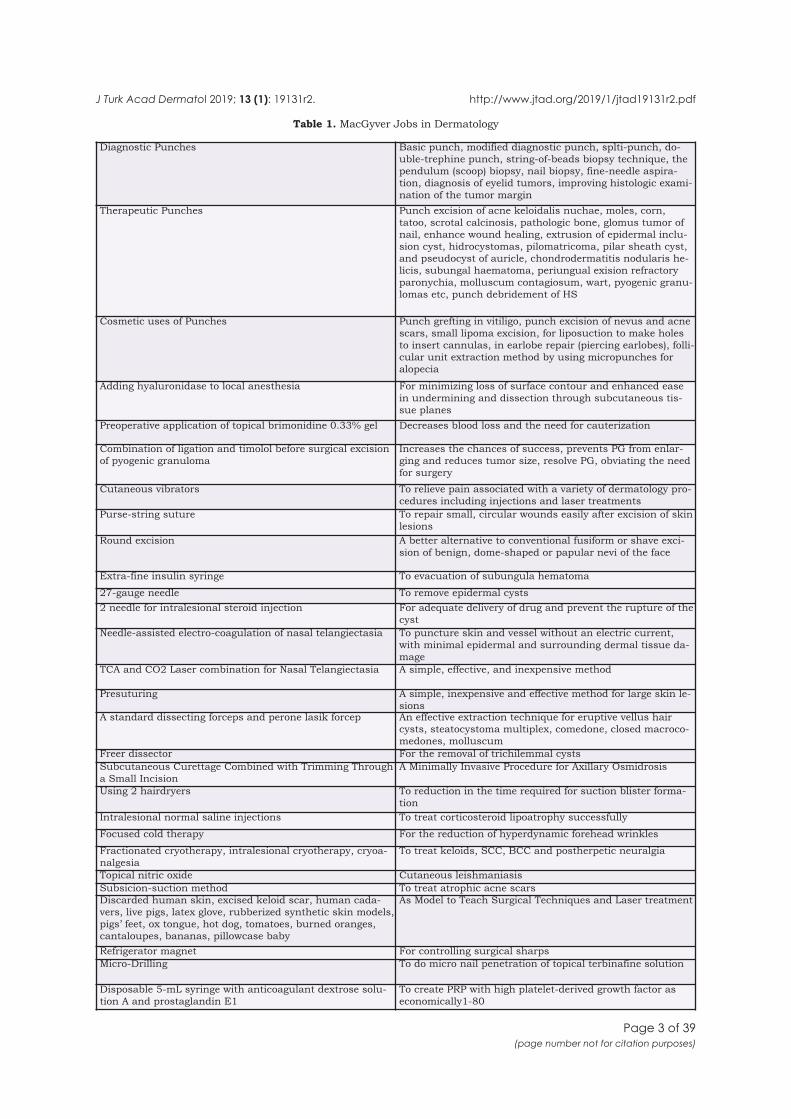
Table 1. MacGyver Jobs in Dermatology
Diagnostic Punches Basic punch, modified diagnostic punch, splti-punch, do-uble-trephine punch, string-of-beads biopsy technique, thependulum (scoop) biopsy, nail biopsy, fine-needle aspira-tion, diagnosis of eyelid tumors, improving histologic exami-nation of the tumor margin
Therapeutic Punches Punch excision of acne keloidalis nuchae, moles, corn,tatoo, scrotal calcinosis, pathologic bone, glomus tumor ofnail, enhance wound healing, extrusion of epidermal inclu-sion cyst, hidrocystomas, pilomatricoma, pilar sheath cyst,and pseudocyst of auricle, chondrodermatitis nodularis he-licis, subungal haematoma, periungual exision refractoryparonychia, molluscum contagiosum, wart, pyogenic granu-lomas etc, punch debridement of HS
Cosmetic uses of Punches Punch grefting in vitiligo, punch excision of nevus and acnescars, small lipoma excision, for liposuction to make holesto insert cannulas, in earlobe repair (piercing earlobes), folli-cular unit extraction method by using micropunches foralopecia
Adding hyaluronidase to local anesthesia For minimizing loss of surface contour and enhanced easein undermining and dissection through subcutaneous tis-sue planes
Preoperative application of topical brimonidine 0.33% gel Decreases blood loss and the need for cauterization
Combination of ligation and timolol before surgical excisionof pyogenic granuloma
Increases the chances of success, prevents PG from enlar-ging and reduces tumor size, resolve PG, obviating the needfor surgery
Cutaneous vibrators To relieve pain associated with a variety of dermatology pro-cedures including injections and laser treatments
Purse-string suture To repair small, circular wounds easily after excision of skinlesions
Round excision A better alternative to conventional fusiform or shave exci-sion of benign, dome-shaped or papular nevi of the face
Extra-fine insulin syringe To evacuation of subungula hematoma
27-gauge needle To remove epidermal cysts2 needle for intralesional steroid injection For adequate delivery of drug and prevent the rupture of the
cystNeedle-assisted electro-coagulation of nasal telangiectasia To puncture skin and vessel without an electric current,
with minimal epidermal and surrounding dermal tissue da-mage
TCA and CO2 Laser combination for Nasal Telangiectasia A simple, effective, and inexpensive method
Presuturing A simple, inexpensive and effective method for large skin le-sions
A standard dissecting forceps and perone lasik forcep An effective extraction technique for eruptive vellus haircysts, steatocystoma multiplex, comedone, closed macroco-medones, molluscum
Freer dissector For the removal of trichilemmal cystsSubcutaneous Curettage Combined with Trimming Througha Small Incision
A Minimally Invasive Procedure for Axillary Osmidrosis
Using 2 hairdryers To reduction in the time required for suction blister forma-tion
Intralesional normal saline injections To treat corticosteroid lipoatrophy successfully
Focused cold therapy For the reduction of hyperdynamic forehead wrinkles
Fractionated cryotherapy, intralesional cryotherapy, cryoa-nalgesia
To treat keloids, SCC, BCC and postherpetic neuralgia
Topical nitric oxide Cutaneous leishmaniasisSubsicion-suction method To treat atrophic acne scarsDiscarded human skin, excised keloid scar, human cada-vers, live pigs, latex glove, rubberized synthetic skin models,pigs’ feet, ox tongue, hot dog, tomatoes, burned oranges,cantaloupes, bananas, pillowcase baby
As Model to Teach Surgical Techniques and Laser treatment
Refrigerator magnet For controlling surgical sharpsMicro-Drilling To do micro nail penetration of topical terbinafine solution
Disposable 5-mL syringe with anticoagulant dextrose solu-tion A and prostaglandin E1
To create PRP with high platelet-derived growth factor aseconomically1-80

ting in a clean, bisected tissue split. Thistechnique can be used to avoid taking two bi-opsies or splitting a single specimen, whichmight distort or crush the tissue [3].
Double-trephine punch biopsy: This tech-nique is used to obtain tissue samples for di-agnosis of dermatoses that affect the subcutaneous tissue. A 6 to 8 mm punch is inser-ted to obtain the initial sample. A 6 to 8 mmpunch tool is inserted to the hilt of the ins-trument to obtain the initial sample. Oncethe superficial core is removed, a 4 mmpunch is subsequently used within the cen-ter of the 8 mm defect to obtain the subcu-taneous tissue [4,6].
String-of-beads biopsy technique: Diag-nostic challenges often require a significantamount of tissue for a complete evaluation,which is done either by 6 to 8 mm punch bi-opsy or incisional biopsy followed by dividingthe tissue sample into several pieces for mul-tiple studies. These methods are time consu-ming, with associated risks of crush artifacton the specimen and a possible sharps in-jury to the physician. The string-of-beads bi-opsy technique is done by performing smaller, adjacent 4 mm punch biopsies in arow, and the individual biopsy defects maybe closed in a linear or multiple O-to-Z/Wdesign with nonabsorbable sutures placedusing the simple interrupted suture techni-que. This method obviates the need for dis-section of tissue in pieces [3].
The pendulum or scoop biopsy: The poten-tial disadvantage of shaving a flat lesion orplaque is the inability to achieve a suffici-ently deep or representative sample. Thescoop ensures that adequate tissue samplingis achieved, thus making a histopathologicdiagnosis readily available. The scoop alsoresults in a smooth biopsy edge which re-sults in less trauma and more rapid healingwithout scar. The scoop has the additionalbenefit of providing enough depth so as tomake prognostication more accurate in casesof suspected malignancy. Observing stan-dard surgical techniques, the lesion is clean-sed and locally anesthetized. Countertraction is applied with the nondominanthand, and the biopsy-pen is inserted into theskin in a pendulous manner. The punch toolscoops the skin like a pendulum. Once thetissue is removed, the subcutaneous tissue
is visualized and a procoagulant, such asMonsel's solution or Drysol may be appliedfor hemostasis [4].
Nail biopsy: 2 to 3 mm punch biopsy is ade-quate for nail plate, nail bed, and nail matrixin most instances. For a biopsy of the nailbed, a two-punch method may be used. Inthis technique, a larger size punch is used toremove the overlying nail plate and then asmaller punch is used to sample the bed.Dermatologists have traditionally taken thenail matrix tissue by exposing the nail matrixafter incising the proximal nail fold. Althoughthis has offered much more histopathologicalinformation to dermatologists and shown ahigh success rate in achieving a diagnosis, ithas many disadvantages. First, the methodis a complex one which needs expert skills ofthe operator because it needs several stepsuntil exposure of the nail matrix, so calledcul-de-sac. Second, because of the anesthe-sia which needs much amount of local anest-hetic, the patients surely suffer from harshpain during injection. Third, the traditionalnail matrix biopsy leads to decrease in thesize of the nail plate, eventually. Therefore,the patient may undergo cosmetic problems.Finally, a long period of wound healing is ne-cessary and a postoperative scar may result.Hence, some authors introduced a simplebut informative method for patients with nailmatrix disorders. After achieving local anest-hesia that does not need lots of anesthetic ascompared to the conventional method, theyperformed two 2-mm punch biopsies on theproximal nail fold for taking proximal nailmatrix tissue. Considering the individual dif-ference of the location of the nail matrix, theychosed two different punch biopsy sites fromthe proximal nail fold. The 2-mm punch wasadvanced down to the nail matrix until thephysician got the feeling of touching bone.Then, they punched through the nail plate oflunula to the underlying tissue using a 2-mm punch to obtain the distal nail matrix.Without suturing, a simple dressing with to-pical antibiotics was needed for three to fivedays. The advantages of their technique are:it is less painful, has a rapid healing time,there is almost no risk of scarring and morp-hological change. They adapted this simpletechnique for 18 patients which yielded thesatisfactory results without exposing nailmatrix. As a result they found that 17 out of
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 4 of 39(page number not for citation purposes)

18 nail specimens contained the nail matrix.Almost histological findings were consistentwith clinical diagnoses. The method especiallybenefited to classify twenty-nail dys trophyinto several histological types. It showed a re-latively high success rate in achieving a diag-nosis, considering that 2-mm specimens areprone to crush injury during handling andare hard to interpret. However, matrix tissuewas sometimes missing in tissue specimensbecause of its fragility and size. Thus theywere developing an advanced technique to re-duce the loss of tissue. Another limitation wasthat it was not suitable to be applied to a ma-lignancy such as acral lentiginous melanomabecause blind technique may not capture theatypical area of the lesion, correctly. In gene-ral, malignant lesions may be clinically dis-tinguish from other benign lesions by usingother devices such as dermoscopy, clinicianscan choose more invasive and conventionaltechnique to the doubtful cases. Therefore,this less invasive tec hnique could be widelyapplicable to various benign nail disorders es-pecially involving the nail matrix, like twenty-nail dystrophy and median nail dystrophy,and it can provide histopathologic informa-tion of whole nail tissues. The dorsal portionof the proximal nail fold, ventral part of theproximal nail fold, and the proximal nail mat-rix were sequentially shown in the specimenfrom the proximal nail fold. The specimenfrom the lunula shows the distal nail matrixjust beneath the nail plate3,4. Since early2009, they had got useful histopathologic fin-dings from patients with various nail disor-ders through this technique. So far, nocomplications concerning the procedure haveoccurred and the physicians and the patientsare all satisfied. In summary, the proximalnail fold-lunula double punch technique isboth, a physician- and patient-friendly diag-nostic tool. This enables the ph ysician totake nail biopsies more easily and to detectmore histopathologic findings of inflammatorynail disorders in the future. There are manytypes of nail unit biopsy, including biopsy ofthe nail matrix, which is done by retraction ofthe proximal nail fold; then a punch is intro-duced through the newly formed nail plate ex-tending down to the periosteum of theterminal phalanx. In most ins tances, theplate will be avulsed first and the proximalfold retracted for complete visualization. Indi-cations for nail biopsy include a pigmented
streak in the nail plate; suspicion of skin can-cer, either melanoma or nonmelanoma; andspace-occupying lesions, either benign or ma-lignant tumors. Biopsy of the nail matrix isnot to be taken lightly because of the real pos-sibility of scarring, a permanent nail split, orother longitudinal dystrophy. The patientshould be fully aware of these potential con-sequences [3].
Saw-toothed power punch for effortlessnail biopsy: A nail biopsy is an important di-agnostic procedure for many nail diseases in-volving the nail bed and the nail matrix. The3 methods commonly used for nailbed biop-sies include excision biopsy, longitudinal bi-opsy, and punch biopsy using skin biopsypunches. The punch method is the least in-vasive method and conserves tissue, there-fore, is more popular. A nail plate consists ofa densely packed tough keratinized tissue;therefore, skin biopsy punches are unsuitableand often require excessive physical force lea-ding to damage to the biopsy specimen andthe surrounding tissue. Furthermore, it is dif-ficult to insert a punch to the desired depthin one attempt because of the resistance pro-duced by the tough nail plate. To overcomethis, a 2-punch method has been proposed.In this method, a larger punch is used to re-move the nail plate and then a smaller punchis used to take the nail bed or matrix biopsy.In such biopsies, the absence of the attachednail plate leads to loss of orientation of the bi-opsy specimen. All these factors sometimeslead to inconclusive histology reports. If thenail plate is thick, such as in patients withpincer nails, obtaining a nail bed or nail mat-rix biopsy specimen requires removal of thecomplete nail plate first; this causes unduetrauma and delayed healing. To overcomethese problems, the authors introduce use ofsaw-toothed motorized punches of 3 mm ormore in diameter for obtaining a nail biopsy.The dimensions of these punches have beenmade to fit in the hand piece of the micromo-tor dermabrader machine, which is usuallyavailable in dermatology operating rooms.These motorized saw-toothed punches penet-rate even the toughest of the nail plates at2000 to 3000 rotations per minute withoutexcessive manual force and easily reach to thelevel of the periosteum. The specimen so ob-tained has an attached nail plate so that tis-sue orientation is not lost. Moreover, the nailplate removal is not needed for nail bed or
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 5 of 39(page number not for citation purposes)

matrix biopsy even in the presence of a verythick nail plate, and healing is faster. Thecurrently available micromotor dermabraderhand pieces have very good hand control, sothere is a minimal risk of going too deep. Theyneed to stop when they feel the ‘‘give’’ on re-aching the nail bed to avoid trauma to thedeeper structures [7].
Window Nail Plate Avulsion: Nail problemslimited to a confined portion of the nail bedcan be accessed using a window plate avul-sion. This technique is helpful when removinga localized foreignbody in the nail bed, explo-ring the nail bed for a welldemarcated neo-plasm, evacuating a subungual hematoma, ordraining an acute paronychia. It is performedusing a 5mm, 6 mm, or larger punch to drillthrough the localized area of nail plate. Thena no. 11 blade is used to pry open and lift thecircular porthole window of the nail plate, ex-posing the underlying bed. Then a smallerpunch can be used to biopsy the appropriateunderlying tissue, if necessary. If these win-dows of nail plate do not require processingfor pathology or microbiology, they can bereplaced and secured with a single suture orSteril-Strips. The procedure can be faster ifthe punch is heated [8].
Skin punch as an adjunct to fine-needle as-piration: Use of the punch is helpful in diag-nosing solid organ tumors that are close tothe skin surface, such as lymph nodes, thebreast, and the thyroid, especially if the FNAyielded a non-diagnostic result. Fine-needleaspiration (FNA) is a percutaneous procedurethat uses a fine-gauge needle and a syringe tosample fluid from a cyst or remove clusters ofcells from a solid mass. The advantages ofFNA are that it is a fast, easy method for bi-opsy, the results are rapidly available, it doesnot require stitches, and patients are usuallyable to resume normal activity almost imme-diately after the procedure. An important di-sadvantage of FNA is that the procedureobtains only very small samples of tissue orcells from the lesion. If the sample is benignfluid, then the procedure is ideal. However, ifthe tissue is solid or if a sample of cloudy,suspicious-looking fluid is obtained, the smallnumber of cells removed by FNA allow only fora cytologic diagnosis. This can be an incom-plete assessment because the cells cannot beevaluated in relation to the surrounding tis-sue. Moreover, it is difficult to use the FNA to
aspirate lesions that are small, ill-defined, fib-rotic, or dermal in location. Consequently,use of the punch might be very helpful in di-agnosing solid organ tumors that are close tothe skin surface, such as lymph nodes, thebreast, and the thyroid, especially if the FNAyielded a nondiagnostic result. In one study,the use of a punch gave a diagnosis in 17 of21 breast tumor cases in which FNA was non-diagnostic because of scant cellularity[9].
Diagnosis of Eyelid Tumors: The manage-ment of eyelid tumors requires histologic di-agnosis, which is usually obtained by biopsy.Although incisional biopsy is consistently re-cognized as the gold standard, a certain deg-ree of surgical skill is necessary, and theprocedure is time consuming. In a retrospec-tive analysis of 20 consecutive incisional bi-opsies and 20 consecutive punch biopsiesdone by Rice and colleagues, the histology ob-tained by both biopsy methods was comparedto that identified at the time of tumor exci-sion. The accuracy rates were 95 and 85% forincisional and punch biopsy, respectively.Punch biopsy has the advantage of being aquick technique requiring minimum equip-ment. In addition, the operator requires nospecific surgical skills. The biopsy specimencan easily be taken at the patient’s initial cli-nic visit, allowing a more rapid diagnosis andfacilitating more efficient tumor managementand fewer visits to hospital [10].
Improving Histologic Examination of theTumor Margin: Histologic examination of thesurgical margins of skin tumors removed bystandard surgical excision is not alwaysaccu-rate. Vertical sections of surgical specimensrepresent check points of the margin only 7microns thick. This means that most of thesurgical margin is not checked microscopi-cally, allowing small tumor islands at themargin to remain undetected. To avoid thisand be more accurate, a new punch with con-centric cutting edges separated by 2 mm hasbeen made to obtain a 2 mm strip of tissuerepresenting the entire lateral border of theexcision. This specimen is easily mounted asa flat section for frozen or paraffin processing.These sections will be cut to show the entirelateral excision margin to be checked fortumor. It requires little additional skill on thepart of the surgeon and is easily handled bythe pathology laboratory [3].
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 6 of 39(page number not for citation purposes)

B-Therapeutic uses: Punch excision of themole can be done for therapeutic reasons. Apunch size is chosen that is 0.5 mm largerthan the maximum diameter of the mole toensure its complete removal. The depth of theexcised tissue should be adequate to includeall pigmented tissue. The procedure can bestopped here and the defect sutured or follo-wed by grafting from the postauricular area askin punch graft that is 0.5 mm larger thanthe recipient area to allow contraction of thegraft and expansion of the recipient socket.The recipient site is dressed with nonadhe-rent tulle. Alternatively, it can be dressed withlubricating jelly. If the lesion is large and ovalin shape, it can still be excised with a punch,as described by Warino and Brodell, where apunch is held at a 45µ angle with the cuttingedge of the punch touching the skin at onepole of the lesion. An oval mole is then squee-zed into the opening of the punch as the han-dle is reoriented perpendicular to the skin, sothat the cutting edge is flush with the skinsurface; then the punch is rolled and excisionis followed by suture closure. The use ofpunch for excision can be performed for otherconditions, such as Spitz nevi and small tat-toos [3,4].
Punch excision of acne keloidalis nuchae:The punch should extend deep into the sub-cutaneous tissue so that the entire hair fol-licle is excised. After excision is performed,the wound edges can be injected with 10-40mg/mL of triamcinolone acetonide to reduceinflammation. Silk sutures may be used to re-approximate the skin [4].
Punch excision of corn: The hyperkeratotictissue surrounding and over the corn area ispared using number 20-24 sterile surgicalblade which makes the central core or kernelclearly visible. According to the size of the ker-nel punch with slow gradual rotatory half cir-cular motion is pushed into the tissue. Thepunched out tissue is gradually pulled wit-hout cutting and pressure bandage is applied.Hard corns are firm, small, dome-shaped pa-pules with translucent central cores, whichoccur on the palmoplantar region of toes andhands due to repeated trauma. Medical ma-nagement of hard corns is difficult and some-times requires surgical excision. Punchincision is a technique which is performedusing a circular blade or trephine attached toa pencil-like handle. It might serve as an al-ternative method to surgical excision in the
treatment of recalcitrant corns. Punch inci-sion is a simple and effective technique for thetreatment of small corns on the palms andsoles. Punch incision is a technique perfor-med using a circular blade or trephine 2-6mm in diameter and 1 cm in length, attachedto a pencil-like handle. The advantages of thistechnique versus classical elliptical excisionare that it facilitates obtaining deeper andnarrower tissue, causes less damage to perip-heral tissue, is associated with more rapidhealing and less scarring and is simpler andeasier to perform. The authors recommendedthe use of a punch tool that is the same sizeor larger than the corn. Based on the abovestudy it can be concluded that punch incisionis a simple and effective technique for the tre-atment of small corns on the palms and soles[11].
Pinch punch excision of scrotal calcinosis:Scrotal skin is pinched to highlight the sub-cutaneous nodules and using appropriatesize of punch, nodules/cysts are excised. So-metimes scrotal calcinosis requires excision ifthe subcutaneous nodules are symptomatic,draining chalky white material, or causing de-formity to the scrotum. This can be done witha pinch-punch excision, using tumescentanesthesia, 1:10,000 epinephrine and 0.1%lidocaineneutralized with sodium bicarbo-nate. Use of a tumescent anesthetic exerts ahydrodissecting effect, thereby separating thecysts from surrounding connective tissue andthe superficial scrotal fascia. Then you canpinch scrotal skin to highlight the subcuta-neous nodules; after that, incise the skin withan appropriate-sized punch. Suture closureis not necessary because of the small-sizedwounds, the hemostatic effect of the tumes-cent agent, and the contractile nature of thescrotal skin [12].
Pathologic Bone Excision: Osteoid osteomais a benign skeletal neoplasm of unknownetiology that is composed of osteoid andwoven bone. The tumor is usually smallerthan 1.5 cm in diameter. It causes focal bonepain at the site of the tumor. The lesion canbe completely excised with a skin punch. Thismethod has proven to be both minimally in-vasive and effective in the management of pa-tellar osteoid osteoma [3].
Punch excision of glomus tumor of nail: Awindow is created in nail plate by using 5-6mm punch and tumor in nail bed is excised
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 7 of 39(page number not for citation purposes)

by taking a smaller punch incision (3-4 mm)and sutured [4].
Use of the punch to enhance wound hea-ling: The full thickness punch grafts (3 mm)are harvested from the buttocks or thigh.Punch holes (2-2.5 mm) are made in the floorof the granulating ulcer 5 mm from eachother, and grafts are pushed into these reci-pient holes. To increase granulation tissue,the punch is used in nonhealing ulcers andcentral ear lobe defects. Nonhealing ulcerscreate a great therapeutic challenge to the cli-nician. Large ulcers that fail to epithelializewith local dressings for 3 to 4 weeks despitehealthy granulation tissue are usually takenup for grafting. Moreover, use of skin punchbiopsy to provide an autologous full-thicknessskin substitute for healing chronic wounds isreported to have a high success rate. Externalear defect can be healed with secondary in-tention if the surrounding intact cartilage hasits perichondrium. Granulation and reepithe-lialization will proceed somewhat more slowlythan when the perichondrium is intact, but ifthe denuded cartilage is more than 10 mm indiameter, trephining with 2 mm punches toexpose the perichondrium and dermis of theposterior aspect of the ear may facilitate de-velopment of granulation tissue in the woundbed and speed healing [3].
Punch can be used for extrusion of: epider-mal inclusion cyst, hidrocystomas, pilomatri-coma, pilar sheath cyst, and pseudocyst ofauricle with a punch hole technique and thecontents of cyst are drained and pressurebandage is applied. Pseudocyst of the auricleis a benign, asymptomatic, noninflammatorypseudocyst that contains yellow, viscous fluidresembling olive oil. If left untreated, a per-manent deformity may occur. It can be trea-ted by a small, superficial punch incision onthe lower part of the cyst to allow for opendrainage, avoiding cartilage injury, until anoily viscous fluid is drained from the punchbiopsy opening. Then taped with a pressurebolster as dental roll for 2 weeks, with dailycleaning and reapplication of the bolster. Ext-rusion with a punch hole has been used withgood outcome in other cutaneous conditions,such as small, isolated epidermal cysts orhidrocystomas, drainage of infected or infla-med cysts, and epidermal inclusion cysts. Re-moval of pilar cysts can also be achievedusing the standard punch incision technique.First, inject 1% lidocaine with epinephrine
overlying the cyst; then use a 4 mm punch toincise the lesion. After that, the contents ofthe cyst are expressed with lateral pressure[3,4].
The punch and graft technique in chondro-dermatitis nodularis helicis: A punch bi-opsy is applied perpendicular to the skinsurface and advanced until a deep punch ofunderlying cartilage is cut. Then the same-sized punch of a full-thickness skin graft fromthe postauricular area donor site is harvestedand fixed in place with 6-0 interrupted sutu-res. Chondrodermatitis nodularis helicis is apainful inflammatory condition that affectsthe helix of the ear. A punch biopsy, of a dia-meter similar to that of the lesion, is appliedperpendicular to the skin surface and advan-ced until a deep punch of underlying cartilageis cut. Then the same-sized punch of a full-thickness skin graft from the postauriculararea donor site can be harvested along withunderlying fat. The graft is fixed in place with6-0 interrupted sutures, such that the con-tour of the helical rim is preserved [13].
Subungal haematoma: Hematoma is drainedby making an opening through the nail platewith either number 11 blade, electrocauteryor punch of size 1.5 or 2 mm or larger. Punchis preferred as it remains patent after decom-pression and allows further drainage withoutthe opening getting sealed. The procedurewas easily undertaken in the accident andemergency treatment room. No infiltration oflocal anaesthetic or ring block was requiredin our series and none of the adults or child-ren complained of pain during trephination.All patients had an uneventful outcome at the1 week hand clinic follow-up. This techniquecan be easily learnt by junior doctors as wellas accident and emergency nursing staff, em-ploys a portable, cheap, sterile and easilyavailable instrument and also avoids re-accu-mulation of the haematoma. Additionallythere is no danger of electrical or thermalburns which may occur with diathermy orheated needles [14,15].
Periungual Exision: The excision of inflamedtissue on chronic, refractory-totreatment pa-ronychia can be done with nail-fold punch bi-opsy as described earlier [4].
Punch is used to remove: molluscum conta-giosum, wart, pyogenic granulomas, etc [4].
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 8 of 39(page number not for citation purposes)

Punch can be held like a pencil or apen:which can mimic the cutting angle of astandard curette. With alternating flexion andextension of the wrist one can use the punchas a curette when curette is not available.Punch can be used as an alternative to othersurgical tools, such as curettage. Curettagewith a punch has the advantages of low costand easy availability, which makes it a goodalternative when a curet is not available. Itcan be used for debulking tumor before exci-sion, curettage and desiccation, and treat-ment of benign conditions such as warts,molluscum, or syringomas after light electro-desiccation. The punch has a sharp circularcutting edge similar to that of the disposablecuret. It can be held like a pencil or a pen,which can mimic the cutting angle of a stan-dard curet. With alternating flexion and ex-tension of the wrist, one can use the punchas a curet [3].
Punch debridement of hidradenitis suppu-rativa: Punch debridement (mini-unroofing)is perfect for the management of early orsmall acute or subacute inflammatory lesi-ons, often involving only 1 folliculopiloseba-ceous unit (FPSU). This is a simple procedureperformed in the office, clinic, or emergencyroom setting. Use a 5- to 8-mm circular dis-posable biopsy punch. Center the excisionover the acutely inflamed FPSU nodule, in-clude a small amount of surrounding tissue,and ensure that a deep specimen is obtainedby using a firm twisting action. Remove theplug, submit for histology, and obtain bacte-rial cultures if purulent. Aggressive debride-ment involves digital pressure to removepurulent elements and then curettage and/orsimple grattage (scrubbing) with gauze wrap-ped around a cotton swab. The specimen willcontain the fractured FPSU with its associa-ted sebaceous glands and more importantly,the ‘‘bulge’’ area of the pilar unit of the FPSUthat contains the stem cells, which are hypot-hesized to be responsible for growth of theIPGM and the sinus tracts. For hemostasis,ferric chloride 3.8 molal (37.5%) is appliedwith a cotton swab, and the excess is wipedaway. A thick layer of petrolatum is applieddirectly to the wound, held in place with agauze pad or simple bandage. No drain isused. Healing is by secondary intention. Painrelief and healing are swift. Recurrences donot occur, but additional FPSUs in the treated
area are at risk until preventive measures areeffective [16].
Cosmetic uses
Miniature punch grafting in vitiligo: Punchgrafting can be used on many depigmenteddiseases, such as vitiligo, chemical leuko-derma, lichen sclerosus, and postburn leuko-derma. Punch grafting is also used on hairtransplant procedures. Refractory and stablevitiligo can be treated with surgical replenish-ment ofmelanocytes by variousmethods. Oneof these methods is punch skin grafting.Punch grafts of 1 to 2 mm may be used toyield better cosmetic results. Sockets arecreated in the recipient area at a distance of5 to 10 mm, and harvested grafts are placedin these sockets. The cosmetic result andcobblestoning problem depend on the punchsize. The smaller the punch size, the betterthe cosmetic result and the lesser the cobb-lestoning. This method consists of taking mi-niature punch grafts of sizes varying from 1to 3 mm in diameter from donor site, graftingthem in appropriate punched out areas spa-ced 2 to 5 mm apart at the recipient site andfurther securing them by firm pressure.Punch grafting is used in different parts of theworld, variable success for the surgical treat-ment of vitiligo. Flip-top transplantation (FTT)is a relatively new procedure for the treatmentof vitiligo and has been tried in many patientswith various skin types. In a study done byFalabella and colleagues, 59.1% of patientsshowed excellent repigmentation with MiniPunch Grafting (MPG). In an Indian studydone by Pasricha and colleagues, 75.2% ofpatients showed excellent repigmentationwith MPG. Similarily Savant and colleagues,in their study of MPG in stable vitiligo, foundthat 91.9% of patients had excellent repig-mentation, and 8.0% did not show repigmen-tation with MPG. In a study done by Malakarand colleagues, 74.5% of patients showed ex-cellent repigmentation with MPG, and 10.6%did not show repigmentation. In the studydone by McGovern and colleagues on FTT,75% of patients showed excellent repigmen-tation. The authors felt that high graft uptakerate in FTT was due to the flap that covers theunderlying graft, which works as a biologicaldressing and retains the graft in place. Thereasons for nonsurvival of punch grafts couldbe excessive exudation of serum, thicker der-miş that may favor infection, or inadvertentcrushing during handling. The reason could
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 9 of 39(page number not for citation purposes)

be that grafts used in FTT are superficial, un-like the grafts used in MPG, so there is lessexudation of serum under the graft and grea-ter possibility of survival of the graft. Flapnecrosis could also induce infection, reducingthe chance of graft survival. In this study,maximum pigment spread with FTT was 8.1mm in the head and neck area, and minimumpigment spread was 1.2 mm, also in the headand neck area. In MPG, maximum pigmentspread was 4.5 mm in head and neck area,and minimum pigment spread was 2.8 mm,on the trunk. The differences in pigmentspread between the two techniques were sta-tistically significant. In a study conducted bySavant and colleagues, maximum pigmentspread was 5 to 10 mm, in the head and neckarea, with MPG, whereas McGovern and col-leagues found maximum pigment spread tobe 6 to 8 mm, in the head and neck area, withFTT. The greater pigment spread with FTT isbecause of preservation of follicular reservoirsand melanocytes in depigmented lesion be-cause we do not remove skin from recipientsite, whereas in punch grafting we removeskin and thus melanocytes reservoir from re-cipient site. Nevertheless, more surgical der-mal manipulation may result in morescarring, cobblestoning, infection, and othercomplications. When minigrafts or epidermalgrafts or epidermal suspensions are used,fewer side effects will also occur. An excellentoutcome means not only a high repigmenta-tion rate, but minimizing unsightly side ef-fects also is equally or even more important.In the study done by Malakar and colleagues,onset of repigmentation ranged from 15 to 20days, and completion of repigmentation wasseen in 16 to 20 weeks in MPG, whereas inthe study done by McGovern and colleagues,onset of repigmentation ranged from 15 to 20days, and completion of repigmentation wasseen in 16 to 20 weeks in FTT. This studyconcluded that treatment variables that affec-ted the development of cobblestoning weredonor and recipient punch sizes; the smallerthe donor and recipient punch sizes, thelower the incidence of cobblestoning. Fongersand colleagues also advised smaller punchsizes to minimize cobblestoning. Cobblesto-ning is slightly more common in MPG thanFTT, but it was seen in both procedures inthis study. Variegated appearance is mainlyseen with FTT and usually does not occur inMPG. More cobblestoning is seen in PG, be-cause fitting a 4-mm punch graft into a 3-mm
recipient site may result in two effects: redu-cing the radius by 1 mm may decrease mela-nocyte and pigment spread and becausepunch grafts are definitely thicker than thinshaved grafts. Furthermore, retraction of a 3-mm recipient site during healing may force a4-mm graft upward, enhancing cobblestoningin spite of an apparent appropriate recipientsite at the moment of grafting. Variegated ap-pearance is mainly seen with FTT because ofinability to regulate depth while attempting toobtain ultrathin grafts. Hyperpigmentation isseen with both techniques, but this is regar-ded as a temporary phenomenon that decrea-ses spontaneously over time. The cost of arazor blade, the main surgical instrumentused in FTT, is 1.0 Indi,an Rupee (US$0.02),versus 80 to 90 Indian Rupee (US$1.79–2.01)for the punches used in MPG. So FTT is moreeconomical. Although this difference in costis large, in practical terms, both are inexpen-sive, and for repigmentation purposes, it ismore important to avoid cobblestoning orhyperpigmentation and to achieve approp-riate repigmentation than to worry aboutsuch small costs. FTT was equally effective asPG for treating stable vitiligo. In FTT, the graftuptake rate was higher, there was greater pig-ment spread, and the cost of the procedurewas lower than with PG [17].
Smashed skin grafting or smash grafting:A number of new therapeutic options for viti-ligo have become available over the last de-cade or so both on the medical as well assurgical side. One among them is the smas-hed skin grafting or simply smash grafting,which is a modification of split-thickness graf-ting. In this method, the graft undergoes‘‘smashing’’ before being applied to the recipi-ent site. Though a simple and effective proce-dure, very few people are doing the procedureeither due to lack of awareness or due to lackof published data. Smashed skin grafting is asimple procedure with fewer side effects, bet-ter outcome, and high patient satisfaction or,in simple words, it can be considered as analternative to various conventional surgicalmodalities like punch grafting and mela-nocyte cell culture methods. Various surgicalmodalities for vitiligo available now includeautologous suction blister grafting, split-thickness grafting, punch grafting, mini-punch grafting, single follicular unit grafting,smash grafting, cultured epidermal suspensi-ons, flip-flop pigment transplantation, and
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 10 of 39(page number not for citation purposes)

autologous melanocyte culture grafting. Someof these procedures have been combined withphototherapy to achieve optimal results. Onemajor issue with surgical therapy is compli-cations like scarring and incomplete pigmen-tation. Though a lot of alternatives, for example covering up the lesion with cosmetic ca-mouflage or tattooing the lesion, are available,they are not longstanding and not suitable forall areas and many times need expert surge-ons. Common surgical modality like punchgrafting is easy to perform and does not re-quire any sophisticated instruments, but itcarries a high risk of scarring on the patientin the form of cobblestoning, which is a majorproblem for people coming for cosmetic treat-ment. Recently, a new technique known assmashed skin grafting or smash grafting isbeing popularized in India by certain derma-tologists and plastic surgeons and is quite analternative for all the conventional surgeriesand is giving results similar to melanocyte celltransfer techniques. The biggest advantage ofthis new method is the simplicity of the sur-gery in itself and the high rate of repigmenta-tion with this method. Even the beginners inthe field of dermatosurgery can perform theprocedure without much difficulty and get avery satisfying result. Though the journal se-arch for smashed skin grafting or smash graf-ting yields very few results, some dermatologysurgeons in India have reported, in variousconferences held in our country, a very pro-mising result with this new method. Thoughit is very effective, very few people are doingthis surgery, and especially in poor countriesit is sad to know that this new technique hasnot been embraced with the same enthusiasmshown to other methods. This is mainly be-cause of the lack of awareness about the method among the dermatologists and non-availability of the published data. So far theliterature search yielded only two articlesmentioning this technique. Another impor-tant factor is the advancements made in themelanocyte cell culture method that moredermatologists prefer this method over smas-hed skin grafting. Though cell culture techni-ques are giving good results, the procedureneeds costly equipment, its time consuming,and cost to the patient is very high. Smashedskin grafting on the other hand hardly needsspecialized equipment and is cost effective tothe patient. Most comparison studies on graf-ting techniques in vitiligo have shown thatmaximum repigmentation is achieved with
either suction blister grafting or splitthick-ness grafting. Smashed skin grafting is a va-riant of the split-thickness graft with a slightmodification. In this method, the split-thick-ness graft obtained from the donor site un-dergoes a process of ‘‘smashing’’ before beingapplied onto the donor site. Smashing of thedonor tissue can be performed using a simplesterile scissor. The amount of graft needed inthe case of smashed skin grafting comparedwith the conventional split-thickness grafts ismuch less. The amount of donor tissue nee-ded is roughly 1/10th the size of the recipientarea. This technique also gives an excellentcolor and texture matching after repigmenta-tion, and it has been observed that the inci-dence of repigmentation with this techniqueis quite high. Surgical therapy for vitiligo hasundergone a lot of advances in the past de-cade. But the accessibility of the patient tothem has been limited by the high cost of theprocedure. Moreover, many of the proceduresare complicated and time consuming. Cellculture and melanocyte transfer methodsneed sophisticated workplaces unlike smashgrafting, which can be performed in a minoroperation theatre under local anesthesia.Smashed skin grafting has evolved into a sim-ple and effective method for the treatment ofvitiligo. Advantages of smash grafting overother surgical modalities can be summarizedas follows: Need simple instruments, cost ef-fective to the patient, minimal residual chan-ges at the donor and recipient sites, unlikesuction blister and thin split-thickness graftwhere the graft needs to be applied with thedermal side coming into contact with the re-cipient area, smash graft can be applied wit-hout any side consideration, easy to masterwith training and expertise. A few modificati-ons have been added to this technique by va-rious dermatologic surgeons, for example:Kocher’s forceps can be used for holding therazor blade, hand dermatome, Humby’s knifeor Silver’s knife can be used, instead of vase-line or antibiotic gauze, we can use a thinlinen that is moistened with normal saline tocover the recipient area, collagen sheets arebetter dressing agents, assuming that the pa-tient can afford them, erbium-YAG laser ab-lation for the donor area is also a goodalternative for dermabrasion. Large-scale stu-dies have to be undertaken to fully evaluatesmash grafting, including the long-term com-plications, if any. Because smashed skin graf-ting is a simple procedure, it is necessary that
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 11 of 39(page number not for citation purposes)

it should be popularized as it is a very cost-effective method for the patient [18].
Chinese Cupping: A Simple Method to Ob-tain Epithelial Grafts for the Managementof Resistant Localized Vitiligo: The intro-duction of surgical techniques provided amajor development in the management of re-sistant vitiligo and replaced other conventio-nal unsuccessful therapies. Most of theseprocedures require special devices and expe-rience that prevent many dermatologists fromutilizing them. The aim of this work is to eva-luate the introduction of a new simple tech-nique that can be used in epithelial graftingfor recalcitrant patches of vitiligo. Twenty vi-tiligo patients, nonresponding to classic pho-totherapy, were candidates in this study. Asimple Chinese cupping device was used toinduce blisters on the inner aspect of thethighs of the patients and the resulting blisterroofs were used for grafting on dermabradedvitiliginous patches. The patients were follo-wed up for 1 year. Blister roofs induced byChinese cupping were able to repigment viti-liginous patches in 80% of the patients withadmirable coloring match, and the donorareas did not show any cosmetic disfigure-ment at the end of the study. Chinese cup-ping is a simple and easy-to-use method toobtain epithelial grafts for vitiligo manage-ment [19].
A simple office-based procedure for pati-ents with extensive vitiligo: The setup re-quired for various grafting techniques forvitiligo is difficult, and specialized reagentsalong with expertise are requisites to performthem. The color matching and repigmentationmay not be uniform in all cases, particularlyat the margins. To surpass these drawbacks,the authors tried simple microneedling with adermaroller device as an inexpensive andquick office-based procedure; it can also beused as transdermal drug delivery modalityfor large-molecular-weight drugs such as tac-rolimus. Microdermaroller-mediated drug de-livery can substantially increase effectivenessby passing the stratum corneum barrier anddelivering this drug in adequate concentra-tion to the melanocytes and keratinocytes.The site was anesthetized with topical lido-caine cream. A Dermaroller with needlelength selected according to skin thicknessand site of vitiligo was used to cause pin-pointbleeding by rolling it for 15 to 20 minutes withparallel pressure strokes in a crisscross pat-
tern. A thin layer of tacrolimus ointment 0.1%was applied during the final pressure strokes.Avoidance of harsh chemical applications, to-pical antibiotics, and sunscreens was advisedto the patient in the immediate postoperativeperiod. There was mild discomfort to the pa-tient for 1 to 2 days. This procedure was doneat an interval of 7 to 10 days for a period of 2to 3 months. Vitiligo Area Scoring Index(VASI) scoring was done before and after pro-cedure. After approximately 7 to 8 sittings ofthe procedure over a period of 3 months therewas 70% to 80% repigmentation withoutscarring. Wood’s lamp examination confirmedthe results. Dermaroller with tacrolimus is asimple, effective, office-based procedure withmuch less downtime that can be used for pa-tients with extensive vitiligo [20].
Punch excision of melanocytic nevus:Round excision may be a better alternative toconventional fusiform or shave excision of be-nign papular or dome-shape nevus (<5 mm)of the face because it leaves an almost imper-ceptible scar [21].
Punch excision techniques in acne scars:
-Punch excision and closure: If the scar is>3.5 mm in size, it is excised and suturedafter undermining.
-Punch incision and elevation: If the depres-sed scar has a normal surface texture, it is in-cised up to the subcutaneous tissue andelevated to the level of the surrounding skin.
-Punch excision and grafting: Depressed pit-ted ice pick scars up to 4 mm in diameter areexcised and replaced with an autologous, full-thickness punch graft.
There are two types of acne scars; atrophicdeep dermal scars and hyperplastic scars. At-rophic scars include icepick, rolling, and box-car scars. The icepick scars are usuallysmaller in diameter and deep with tracts tothe dermis or subcutaneous tissue. Boxcarscars are deep and are often 1.5-4 mm in dia-meter. They have sharply defined edges withsteep, almost vertical walls. Soft, rolling scarscan be circular or linear, are often greaterthan 4 mm in diameter, and have gently slo-ped edges that merge with normal-appearingskin. Examples of hyperplastic acne scars arehypertrophic scars and keloids. Punch biopsyis a treatment option for deep dermal scarsthrough different techniques such as punchexcision, punch elevation, and punch repla-
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 12 of 39(page number not for citation purposes)

cement grafting. Punch excision, done forscars less than 3.5 mm, removes a pitted scarwith a straight wall by a punch that is slightlylarger than the scar being addressed. The sitemay then be allowed to heal by second inten-tion, or sutures may be placed to close thewound. This technique is preferred for icepickscars. A scar requiring a punch larger than3.5 mm is repaired by elliptical excision orpunch elevation because these larger defectslead to ‘‘dog ear’’ formation on the face. Punchelevation is similar to punch excision exceptthat the scar that is punched out is not dis-carded. It is useful if the scar is 3 mm in dia-meter or greater with a good color match andstraight walls. The tissue cylinder is inciseddown to the level of the subcutaneous fat. Thescar is allowed to float up until it is the samelevel as the surrounding skin. If it does notrise easily, it may be transected free at thelevel of the fat. The cylinder of tissue will befixed in place by the patient’s serum and sitsas a graft, held in position by some surgicaltape. Punch elevation is a method of treat-ment for boxcar scars. Punch replacementgrafting is useful for deep fibrotic scarring.The scar is excised as with the basic punchexcision technique. The scar is discarded andis replaced with a slightly larger full-thicknesspunch graft, usually from the postauriculararea. It is critical to allow each anestheticwheal to flatten completely to prevent distor-tion of scars. Unless the graft is traumatized,it will usually survive well. Some of the graftswill heal with the same skin surface level andsome will be elevated. Donor holes should beapproximately 0.5 mm larger than the recipi-ent holes. These seal in 5 to 7 days with a fib-rin clot. Dermal graft for atrophic scar, 3-5mm punch biopsy up to deep dermis is donein covered parts of the body. The epidermispart is excised and only dermal part is preser-ved. Subcision of the scar is done 1 weekprior to the dermal graft. Depending on thesize of the atrophic scar, appropriate size ofdermal graft is inserted to the atrophic scarafter making the pockets below the scar with18-G needle. Seal the entry point with Steri-strip [22].
Small lipoma excision through narrow holeextrusion technique (NHET): In NHET, asmall, circular punch defect is created in theskin and then the lipoma is extruded throughthe hole by applying lateral pressure. A cur-ved hemostat can be inserted in the defect to
separate the lipoma from the surrounding tis-sue. Lipomas of subcutaneous fat are amongthe most common benign neoplasms obser-ved in humans. Patients often come to theirdermatologist for evaluation and removal ofthese tumors. Standard treatment commonlyincludes incision with extrication or ellipticalexcision. Unfortunately, these treatmentsoften elicit a large scar. Many persons havemultiple lipomatous lesions. For patients withmultiple lipomas or angiolipomas, such con-ventional surgical treatments may be exces-sively scarring and cost prohibitive. Thecommon cutaneous punch may regularly beapplied to remove most lipomas in a variety oflocations. The cutaneous punch is customa-rily used to perform biopsies. Extended usesof the punch previously published include re-moval of epithelial cysts, dermabrasion Loo-punch excision technique for removal ofacne-induced osteoma cutis, and trephinepunch for diagnosis of panniculitis. Briefmention of the biopsy punch to remove a va-riety of lesions including lipomas was repor-ted earlier, as was instruction on the use ofthe punch for treatment of lipomas. The li-poma is identified by palpation and visualinspection. The area overlying the center ofthe tumor is marked with gentian violet. Thearea is subsequently anesthetized with 1% li-docaine with epinephrine at the subcuta-neous level and the incision site. A 4-mmpunch is inserted into the marked center ofthe epidermis overlying the lipoma. Thepunch should be inserted to the hub of itscutting surface. The lipoma is then firmlygrasped between the thumb and the other di-gits. Firm pressure and squeezing are appliedat the base of the lipoma in an upward fas-hion. The force is directed towards the inci-sion site. This will usually result in theextrication of the lipoma. Larger tumors mayrequire both hands to accomplish this remo-val. A deeper blunt probe or dissection withinthe incision site may be required to loosen thelipoma. Often, small clumps of fatty fibroustissue will appear at the opening just beforeexpulsion of the entire tumor. When the fib-rous capsule of the lipoma appears at theopening, the tumor can often be expressed intoto with additional pressure. If the lipomaappears fibrosed and is difficult to extricate,then a semidestructive step may be required.The 4-mm punch is held in one hand and afirm upward grasp of the lipoma is held in theother. One performs a repetitive up-and-down
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 13 of 39(page number not for citation purposes)

chopping motion with the cutaneous punchwithin the previous punch incision site to loo-sen the upper fibrous portions of the lipoma.The lipoma is then expressed piecemeal thro-ugh the punch incision site via firm lateroin-ferior pressure. Continued deep pinching andupward pressure in a kneading motion maybe required to remove all of the portions of thelipoma. Once the lipoma is completely remo-ved, exploration of the defect for residual li-poma should be performed. This can beperformed with curved hemostats. The inci-sion site usually heals well by either secondintention or the placement of 1 to 2 interrup-ted cutaneous sutures. The postoperativewound requires care similar to that of anypunch biopsy procedure. The incision site willgenerally heal with minimal scarring, especi-ally in comparison to conventional excisionscars. Excellent locations for the punch ex-pulsion of lipomas are the extremities andface. Appropriately, these are areas of greatestcosmetic consequence for any surgical proce-dure. Because it is important to be able togain a firm grip under the lipoma, areas of thebody with thickened dermis or minimal skinpliability are difficult areas for this technique.Thus removal of lipomas on the torso by thismethod is variably successful because of thethickened cutis. Nevertheless, most caseswarrant a trial removal attempt with thistechnique. If no success at removal is attai-ned, other conventional surgical methodsmay be attempted. This technique often re-quires moderate manual physical effort toexpel the lipoma, especially in areas of thic-kened integument. However, there are manyobvious benefits to this removal method. Riskof hemorrhage and infection may be minimi-zed secondary to the decreased degree of in-vasion. In cosmetically sensitive areas, thistechnique is an effective and aestheticallypleasing method for removal of single lipomasand tender angiolipomas. It is especially app-licable to the patient with multiple lesions, inthat many tumors may be easily removed ata single office visit. NHET is widely used. Inthis technique, the lipoma is removed thro-ugh a narrow punch hole done by punch bi-opsy, and the site is left to heal secondarily orone to two interrupted cutaneous sutures areplaced. Modification of the NHET, called thepot-lid technique, aiming to improve the aest-hetic outcome, was described recently. Afterdoing a punch, the punched-out piece of skin
is kept in normal saline. Then you proceedwith extrusion of lipoma, as in the NHET, andthen the punched-out piece of skin is reposi-tioned to cover the defect and sutured intoplace [23].
‘Pot-lid” technique for aesthetic removal ofsmall lipoma on the face: A 5-mm punch in-serted deep into the center of the lesion tocreate a circular hole. The punched-out pieceof skin kept in normal saline. The lipoma isextruded with the help of a hemostat and bysqueezing pressure. After achieving hemosta-sis, two absorbable buried subcutaneous su-tures are placed to create support for thegraft. The punched-out piece of skin is thenpositioned to cover the defect, like a “lid on apot” and dressed. Patients presenting with anasymptomatic subcutaneous facial lipoma de-sire its removal in order to restore the contourof the face. The standard treatment for lipomais excision, with the size of the incision beingabout one-half of that of the tumor itself. Thelong linear scar resulting from simple excisionmay fail to improve the appearance of the pa-tient. The removal of the lipoma through asmall incision or a punch hole decreases thesize of the resulting scar, but does not elimi-nate it completely. They improved the aesthe-tic outcome of the commonly used techniquefor lipoma removal, known as the narrow holeextrusion technique (NHET), by modification.Four patients (three men and one woman)with small lipomas on the face (three on theforehead and one on the cheek) were selectedfor the procedure. A 5-mm punch was inser-ted deep into the center of the lesion to createa circular hole. The punched-out piece of skinwas kept in normal saline. The lipoma wasextruded with the help of a hemostat and bysqueezing pressure. This resulted in the for-mation of a subcutaneous cavity. After achi-eving hemostasis, two absorbable buriedsubcutaneous sutures were placed to createsupport for the graft. The punched-out pieceof skin was then positioned to cover the de-fect, like a ``lid on a pot'' and dressed. Thecolor and texture match of the graft with thesurrounding skin were excellent in three ofthe four patients by the end of 6 months. Thegraft, which was depressed in the fourth pa-tient, improved through spot dermabrasion.The proposed modification of the NHET for li-poma removal improves the cosmetic out-come.
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 14 of 39(page number not for citation purposes)

NHET is probably the most widely used tech-nique; it is simple and gives a good cosmeticoutcome. In this technique, the lipoma is re-moved through a narrow punch hole and thesite is left to heal or one or two interruptedcutaneous sutures are placed. This results ina circular scar of healing or a linear scar withtissue protrusion (``dog ear''), respectively.Even though the size of the scar is small, thismay not be acceptable when the lipoma is lo-cated at cosmetically prominent sites. Punchexcision and grafting has been in use forsome time for the management of a variety ofskin conditions of the face, such as the remo-val of moles, small skin cancers, and trauma-tic and ice-pick acne scars. The commonlyused donor site for grafts in these conditionsis the retroauricular area. Although it is agood match for facial skin, some mismatch incolor, texture, thickness, degree of actinic da-mage, and sebaceous quality is expected. Thismay result in a conspicuous graft. Therefore,they decided to remove the lipoma through anarrow punch hole and to place the punched-out piece of skin back to cover the defect, likea ``lid on a pot.'' This gave us an excellent cos-metic result with no conspicuous scar, as itwas a small, full thickness grafting procedurein which the donor and recipient sites werethe same. There were two procedural prob-lems in this technique. First, after the remo-val of the lipoma, a dead space was createdand no recipient bed was left for the graft. Se-cond, due to the effect of the elasticity of theskin, the punchedout piece of skin tended toshrink and the defect expanded, which resul-ted in a mismatch in the size of the hole andthe graft. This was more pronounced in youn-ger patients. To overcome these problems,they placed two buried subcutaneous sutu-res. The lightly tightened sutures reduced thesize of the defect to match it with the size ofthe graft. The sutures also supported the graftand prevented the sinking of the graft into thedead space. Although the artificially createdsupport does not fulfill the essential require-ments for an ideal recipient bed (i.e. rich vas-cularity for capillary ingrowth and fibroblaststo support collagen18), the graft survives bythe ``phenomenon of bridging.'' In this pheno-menon, the requirements of a small-sizedgraft are fulfilled satisfactorily from the wallsof the defect and the survival of the graft isnot jeopardized. Rather, it helps to preventelevation of the graft (cobblestone formation)a common complication of punch grafting), as
the excessive growth of fibroblasts and depo-sition of collagen do not occur. Hypo/hyper-pigmentation at the grafted site, if it occurs,disappears with the passage of time and thegrafted site becomes almost imperceptible 3±4months later. The potential complications ofthe procedure include hematoma formation,which can be avoided by achieving hemosta-sis and applying a firm pressure bandage.Another potential complication is failure ofthe graft to take hold due to mobility of thepart or necrosis. In this case, the final out-come will be no worse than that seen inNHET. In conclusion, the described techniquehas excellent potential for the removal ofsmall lipomas located at cosmetically sensi-tive sites [23].
Liposuction: Punch is used to make holes toinsert cannulas. A micro-adit used in tumes-cent liposuction is a small circular hole madeby a tiny skin biopsy punch facilitate and pro-mote the drainage of residual blood-tingedanesthetic solution associated with tumes-cent liposuction [24].
In earlobe repair: Using a punch biopsy ins-tead of the scalpel blade to excise the partialcleft in an elliptical fashion. The opposingmargins are sutured together in a straightline. Piercing earlobes is a common practiceall over the world. Several methods have beendescribed for repair of an unwanted lengthe-ned earring hole. One of these methods isusing a punch technique that removes thepreexisting hole and then subsequently sutu-ring the newly created nonepithelialized tract[25].
Tattoo removal: Very tiny tattoos, in parti-cular remnant of post traumatic tattoos orfirst attempts at self-tattooing (traditionalgreen tattoo on forehead), may be removed bya punch biopsy closed by a single suture [26].
Follicular unit extraction (FUE) method byusing micropunches for: Androgenitic alope-cia, eyebrow transplant, eye lash implanta-tion, vitiligo surgeries for poliosis etc. In FUE,the extraction of intact follicular unit is de-pendent on the principle that the area of at-tachment of arrector muscle to the follicularunit is the tightest zone. Once this is madeloose and separated from the surroundingdermis, the inferior segment can be extractedeasily. Because the follicular unit is narrowestat the surface, one needs to use special mic-ropunches of size 0.6-1.0 mm and therefore
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 15 of 39(page number not for citation purposes)

the resulting scar is too small to be recogni-zed. Uses of the punch to diagnose and treatmany medical and surgical conditions makeit important to many other specialties besidedermatology. We can propose a punch tech-nique as a novel method for dermatosurgicaltreatment of various lesions with curative andgood cosmetic results when compared withother existing surgical methods. A simple andan inexpensive skin biopsy punch have vastapplications in dermatology. It is not onlyused to confirm a diagnosis, but used to re-move cosmetically unacceptable lesions, andprovide definitive treatment for a number ofskin conditions. The use of skin biopsy punchis not only limited to the field of dermatologybut also extended to the other specialties.Punch surgery is a simple, readily available,cheap tool that has many advantages, suchas easiness to perform and no need for gene-ral anesthesia. Punch surgery also has a lowrisk of infection and bleeding and can be donein an outpatient setting. Uses of the punch todiagnose and treat many medical and surgicalconditions make it important to many otherspecialties beside dermatology [27].
The use of hyaluronidase as an adjunct tosurgical procedures: Although the use ofhyaluronidase as an adjunct to anesthesia isfrequently described for plastic surgery andophthalmologic procedures, its use in derma-tologic surgery has not been well investigated.They reviewed the advantages and disadvan-tages of using hyaluronidase in dermatologicprocedures. The effect of adding hyaluroni-dase to local anesthesia was evaluated in 72operations performed over a 1-year period.Although the duration of anesthesia wasslightly decreased, the addition of hyaluroni-dase to local anesthesia offers the benefits ofminimizing loss of surface contour and en-hanced ease in undermining and dissectionthrough subcutaneous tissue planes. Theonset of anesthesia using hyaluronidase wasimmediate and the area of anesthesia appearsincreased over anesthesia without hyaluroni-dase. They recommended the adjunct of hya-luronidase to local anesthesia as a usefuladvancement in surgical technique [28].
Topical brimonidine for hemostasis: Chenet al evaluated the use of topical brimonidinefor hemostasis during Mohs micrographicsurgery. Although topical brimonidine hadbeen previously reported as a hemostaticagent in ophthalmologic surgery and oto-
laryngology, this case report was, to ourknowledge, the first describing its use in der-matologic surgery. This pilot study by Chenet al analyzed the use of brimonidine 0.33%gel (1 g) applied topically approximately 15minutes before beginning MMS in patients ta-king anticoagulant and/or antiplateletagents. The results demonstrated that preo-perative application of brimonidine decreasedblood loss and the need for cauterization. Thesafety of topical brimonidine gel has been stu-died for its US Food and Drug Administra-tione approved indication, rosacea; however,it has yet to be studied for its use as a topicalhemostatic agent. However, 2 cases of centralnervous system depression with topical bri-monidine gel when used for hemostasis havebeen reported. Both patients experienced re-versible but serious central nervous systemdepression requiring hospitalization. In thesecases, larger quantities (10 g) of brimonidine0.33% gel were used under occlusion in acti-vely oozing open surgical wounds on the face.Brimonidine should not be used for hemosta-sis in open surgical wounds, particularly inthe head and neck. Although safety outcomeswere not directly reported by Chen et al, thepreoperative topical application of a smallamount of brimonidine 0.33% gel to the sur-gical site can be reasonably assumed to yieldexposures and risks similar to those with itsuse in rosacea [29,30].
Tripod vibration anesthesia: Cutaneous vib-rators have been introduced to relieve painassociated with a variety of dermatology pro-cedures including injections and laser treat-ments. The simple tripod massager describedin this report is effective and acceptable to pa-tients for cutaneous injection anesthesia.Most pain associated with cutaneous proce-dures results from injection of the local anest-hetic. Smith et al. have described vibrationanesthesia in this journal as an adjunct toany injection procedure, eliminating the needfor local anesthesia for some procedures. Theauthors recommend several units includingthe Acu Vibe Softouch™, the Hitachi MagicWand™, and Conair™ double headed massa-ger. They had used the technique they des-cribe, and found it quite helpful for minimizing the pain of injections. These rather largemassagers can be intimidating to some pati-ents. Two of the three vibrators (the Acu VibeSoftouch™ and Hitachi Magic Wand™), haveelectric cords and therefore take a little extra
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 16 of 39(page number not for citation purposes)

time to use. Some of the vibration units re-commended by Smith et al. are apparentlysold for sexual stimulation and may be recog-nized as such by some patients. They foundthe inexpensive Homedics Mini Massage-On-The-Go™ massager to be useful for reducingthe pain of injections. The unit is cordless andcan be managed by a single operator. Theycover each "foot" of the unit with a small sheetof Allrap All Purpose Adhesive Covering as abarrier for antisepsis. The injection is donewithin the triangular region formed by the 3feet of the unit. One of the feet should be po-sitioned so that it is proximal to the injectionsite. The unit has a toy-like appearance andmay contribute to reduction of anxiety in pe-diatric patients. The arch allows placement ofice, if desired, followed by injection withoutneeding to move the unit. The tripod techni-que is limited to broad surface areas such asthe trunk and proximal extremities. For othersites such as fingers, two of the feet may beplaced along the finger, one foot proximal tothe injection site [31,32].
Purse-string suture: Purse-string sutureenabled us to repair small, circular woundseasily after excision of skin lesions. It is an ex-cellent alternative to other reconstructionsand a rapid, simple method to close skin de-fects with minimal scarring, achieving an ex-cellent long-term cosmetic and functionaloutcome. Round and oval skin lesions, like fa-cial pigmented nevi, are common and are tra-ditionally sutured linearly for closure afterexcision, leaving scars longer than the nevithemselves, which greatly influences their ap-pearance. The purse-string suture enabled usto repair small, circular wounds easily afterexcision of skin lesions, especially in the fa-ciocervical region, and is suitable for peoplewith different skin characteristics. Based onthe principle that tensile force converges to-ward a central point when the purse-stringsuture is employed after incision of circularlesions, tension placed on the suture uni-formly advances the skin from the entire pe-riphery of the wound, resulting in a significant reduction of the defect size by the grea-test extent, making it much easier for cells atthe wound edge to sprawl to repair the wo-unds. Also, because the suture compressesboth the larger vessels in the reticular dermişand the smaller vessels in the papillary der-mis, enhanced hemostasis is achieved. So thewounds heal in the slightest tensile force, re-
ducing the possibility of scar hyperplasia. Thetransition of the wounds from circles to pointsby this method, in our point of view, is a kindof leap geometrically. It is an excellent alter-native to other reconstructions and a simplemethod to close skin defects with minimalscarring, achieving an optimal long-term cos-metic and functional outcome [33].
Round excision: Round excision may be abetter alternative to conventional fusiform orshave excision of benign, dome-shaped or pa-pular nevi of the face. Round or circumferen-tial excision is carried out just outside theperimeter of the lesion. This technique maybe chosen when the region involved overliescartilage (i.e. nasal tip or ear rim) or when thebest repair orientation or approach is not ap-parent before the excision. Round excisionhas been recommended for the excision ofnevi, but as round excision and primary clo-sure may cause tissue protrusions or dog-ears, many dermatologists avoid thisprocedure. The possibility of dog-ear forma-tion is related to skin elasticity as well as thelength of the incision. In areas of the bodysuch as the face, the skin is quite elastic andeasily movable and dog-ear formation is rarelyobserved. Although the defects left after remo-val of nevi by this technique are circular,stretching the skin perpendicular to the linesofrelaxed skin tension whilst performing theprocedure often results in an elliptical defect.These elliptical defects were easy to under-mine and close with interrupted sutures orburied and interrupted sutures in combina-tion. The use of the round excision techniqueresults in an elliptical defect with a shorterlong axis when compared to that created bythe conventional elliptical excision technique.Less skin is excised in the round excisiontechnique (approximately half that removedusing a fusiform excision) and therefore a sig-nificant amount of skin is preserved. Under-mining is usually not necessary and theround defect quickly assumes an oval shapewhich is ready for closure, usually with oneor two buried, absorbable sutures and thentwo or three superficial sutures. The resultingwound is shorter than that expected with el-liptical excision. As is usual for certain siteson the face that have a concave surface (e.g.temple, inner canthus, nose), there is a riskof a surgical scar spreading with time, but,again, it is usually a much smaller scar thanwould have been accomplished with elliptical
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 17 of 39(page number not for citation purposes)

excision. In our experience, round excisionmay be a better alternative to conventional fu-siform or shave excision of benign, papularand dome-shaped nevi of the face, because itleaves an imperceptible scar, gives cosmeti-cally superior results, and requires a smallerincision, minimizing tissue trauma [34].
Extra-Fine Insulin Syringe Needle: An Ex-cellent Instrument for the Evacuation ofSubungual Hematoma: The most commonlyused treatment method for subungual hema-toma is nail trephining, which has some di-sadvantages. We introduced a very simpleand well-tolerated treatment technique forthis common problem. We used an extra-fine,29-gauge insulin syringe for evacuation. Weinserted the needle very close to the nail platetominimize pain. We drained the blood fromthe hyponychium under the nail plate usingthis extra-fine needle. The technique descri-bed herein is very fast and simple, and thepatients tolerate it well. It is particularly suc-cessful for the treatment of smaller subun-gual hematomas of the second, third, andfourth toenails, in which the trephining isharder. For these reasons, we suggest thistechnique as a practical alternative to the tra-ditional nail trephining methods. Trauma tothe nail and systemic pathology, medicationand drug reactions, and aging usually causesubungual hematoma. Hematoma formationoccurs because of the disruption of the highlyvascular nail bed. A sudden, blunt, externalforce or repeated microtrauma causes blee-ding beneath the nail plate. The collection ofblood produces intense pain that is caused bypressure and a bluish discoloration. The mostcommon method of treatment has been thenail trephining. For decades physicians haveused a heated paper clip for this purpose. Inaddition to a heated paper clip, a heated ne-edle, a dental bur, a fine-point scalpel blade,a drill, a cautery device, and carbon dioxidelaser have been used for trephining, and nailavulsion, proximal incision or distal incisionbeneath the nail tip, pressure dressings, andobservation have been employed in the treat-ment of subungual hematoma. However, thethrobbing pain is relieved only when the bloodis evacuated. Nail bed lacerations and fractu-res of the distal phalanx require further tre-atment. However, nail plate removal and nailbed exploration are not required for subun-gual hematomas as long as the nail and thenail margin are intact. Regardless of size, only
simple trephining for symptomatic relief is re-quired for simple subungual hematomas, andaggressive surgical treatment, as suggested inprevious studies, is unnecessary. Prompt de-compression will significantly alleviate painand decrease the likelihood of delay in theregrowth of the nail plate and secondarydystrophy that might result from pressure onthe matrix caused by accumulated bloodunder the nail and allows nail bed healing.Therefore, evacuation should be done no laterthan 6 to 12 hours after injury. We used anextra-fine, 29-gauge insulin syringe for eva-cuation. We drained the blood from thehyponychium under the nail plate using thisextra-fine needle. Nails should be trimmedbefore the procedure. The toenail is cleanedand prepared with alcohol and allowed to dry.The area of blood pooling under the nail is vi-sualized under a good light. The most distalpart of the hematoma is selected for evacua-tion. If the distal part of the hematoma is onone level, the lateral side is preferred for eva-cuation. The patient grasps the affected toebetween index finger and the thumb and fixesit. Grasping the toe also gives the patient apressure feeling and reduces the pain, andthe patient feels more confident. The sterile,disposable, extra-fine insulin syringe with a29-gauge mounted needle is held between thethumb and index finger of the dominanthand. It is inserted to hyponychium, parallelto the nail plate. We keep the needle veryclose to the nail plate, avoiding contact withthe nail bed as much as we can to reducepain. While slowly progressing to the hema-toma with a gentle push, we give a back andforward drilling movement to the needle. Nosudden movement is necessary. If the patientfeels pain, we stop moving for 3 to 5 secondsand start to progress again closer to the nailplate. Once the hematoma is penetrated, theneedle is withdrawn. The trapped blood isevacuated rapidly because of the pressurethrough the small hole. Total evacuation ofthe hematoma is achieved with light pressureto the nail. The drained blood is removed withsterile gauze. If evacuation is incomplete, thismay be due to a septum between hematomas,and in this case, the procedure is repeatedfrom the other side. The drainage is usuallycompleted in seconds. The treatment of a sim-ple subungual hematoma requires subungualdecompression, which is usually achieved bycreating small holes in the nail plate.3 Howe-ver, there are several disadvantages of nail
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 18 of 39(page number not for citation purposes)

trephining. A heated paper clip can sear theblood and plug the hole, and the metal mayhave to be reheated several times. Drilling thenail can be quite painful because of the pres-sure needed to puncture the nail plate, and adigital nerve block may be required. However,draining the blood with an insulin syringe ne-edle from the hyponychium is significantlyless painful than one injection of digital nailblock. It is well tolerated by the patients; the-refore, there is no need for anesthesia. Be-cause we insert the needle adjacent to the nailplate, where the tissue is not viable, it doesnot cause significant pain. As this tissue isnot as hard as the nail plate and does notshow resistance while progressing the needle,the procedure is very simple and fast. In ad-ditional, our technique is very successful inthe treatment of smaller hematomas of se-cond, third, and fourth toenails, which havevery small nails that are hard to trephine. Inearly cases, as in our patient, the hematomasof second, third, and fourth toenails are in avery small space with very high pressure; the-refore, they always appear very obscure atfirst. In late cases, they become more wides-pread because of progression of the blood pe-ripherally between nail plate and nail bedbecause of the pressure. Thus, the late lesi-ons appear larger and can be observed easily.However, in late cases, this progression maycause secondary dystrophy if it reaches to thematrix. Therefore, early treatment is very im-portant. We do not suggest performing thisevacuation technique with thick syringe ne-edles because they may cause significantpain, especially if the hematoma is locatedproximally. Because the needle is sterile, therisk of infection is minimal. It is cosmeticallysuperior to nail trephination because the nailplate is left intact. We also performed thistechnique successfully to the older hemato-mas. However, we did not have a chance toperform this technique to the patients withsignificant onychogryphosis and in patientswith significant subungual keratinaceousdebris as tinea unguium. We have been per-forming this technique for 3 years and havenot observed any complications such as in-fection and cosmetic or functional deficits yet.According to our experience, even in promptlytreated cases, once the detachment occurs,the nail plate could not attach to the nail bedagain. After the evacuation of hematomas, anail can be broken or shed in the following
months, as the attached distal part of the nailplate becomes smaller as it grows out. Insummary, this is a very fast, simple, and well-tolerated technique and is particularly suc-cessful for the treatment of subungualhematomas of the second, third, and fourthtoenails. For these reasons, we suggest thistechnique as an alternative to the traditionalnail trephining methods [35].
Eruptive vellus hair cysts: an effective ext-raction technique for treatment and diag-nosis: We treated the lesions by using cauteryand a standard dissecting forceps under topi-cal anaesthesia. After puncturing the overl-ying skin in the centre using the sharp-tippedcautery point, we grasped the base of the cystusing a standard dissecting forceps and weextracted the cysts out. Over 150 cysts wereextracted with this technique in two patients.The technique was simple, quick and tolera-ted well. No lesion recurrence was observedafter 4 months. On histopathological exami-nation, extracted cysts were observed to havecyst walls. In patient 2, the diagnosis wasmade within minutes by microscopic exami-nation of the potassium hydroxide preparati-ons of the extracted material. Our extractiontechnique is a simple and effective treatmentoption for these cysts. It can be regarded ascurative since the cyst walls were also extrac-ted. Microscopic examination of the potas-sium hydroxide preparation of the extractedcysts suggests that this technique can also beused as a simple diagnostic procedure [36].
A simple open comedone extraction tech-nique for Favre–Racouchot disease: Favre–Racouchot disease (FRD) is a common diseasecharacterized by solar elastosis and largeopen comedones and cysts. This disorder ma-inly affects elderly Caucasian men who havehad a great deal of exposure to the sun. Pati-ents having FRD continuously develop nume-rous large open comedones that could causea cosmetic problem. We performed a simpleand effective extraction technique for theseopen comedones using a standard dissectingforceps. This technique is well tolerated andno complications were observed. We suggestthis comedone extraction technique as a sim-ple alternative treatment for this commoncosmetic problem [37].
The use of the freer dissector for the remo-val of trichilemmal cysts: Trichilemmalcysts are keratin-containing cysts, usually si-
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 19 of 39(page number not for citation purposes)

tuated on the scalp. They often show an au-tosomal dominant inheritance pattern. Exci-sion is the treatment of choice. We describeeda practical surgical technique that eases theremoval of these cysts. A 24-year-old womanpresented with a 5-year history of cystic lesi-ons on her scalp, clinically diagnosed as tric-hilemmal cysts. She was treated with the newtechnique. After making a small incisionunder local anesthesia, a freer dissector (Aes-culap OL 165 R) was used as a blunt dissec-tor. The freer dissector was inserted throughthe incision. A blunt dissection was made todissect the cyst free from the surroundingdermis and, by using the dissector as a lever,gentle pressure was applied to the oppositeside to ease the cyst from the dermis. Fourcysts were removed with this technique. Thetreatment was well tolerated by the patient.No complications developed during or afterthe procedure. This modified technique issimple and practical. The slight curve at eachend of the freer dissector makes it easy tograsp the cyst and, functioning like forceps,the cyst can be eased from the dermis. We be-lieve that the use of the freer dissector in thesurgical excision of trichilemmal cysts aidsand speeds up the procedure [38].
Multiple epidermal inclusion cysts of theeyelid: a simple technique for removal:More extensive cyst removal with skin exci-sion followed by skin grafting would have ledto an unsightly end result, as there was nodonor skin of like consistency available. The27-gauge needle technique is simple and re-peatable and is associated with little recoverytime and rapid healing [39].
A simple surgical technique for the treat-ment of steatocystoma multiplex: Sincesteatocystoma multiplex is an uncommon di-sorder, its treatment has not been discussedin detail in the textbooks and surgical exci-sion is the most commonly mentioned met-hod. We described a very simple surgicaltechnique, which was developed by modifyingprevious reports. A 29-year-old woman, diag-nosed clinically and histologically as stea-tocystoma multiplex, was treated with thismodified technique. We punctured the cystsunder local anesthesia with a sharp-tippedcautery point and evacuated the contents bysqueezing the cyst with a fine forceps. Then,the cyst wall was grasped by the forceps andthe sacs were extracted through small holes.More than 50 cysts were treated. The treat-
ment was well tolerated by the patient. Nocomplications developed during or after theprocedure. After 14 months follow up no re-currences were observed and the results werecosmetically excellent. This modi®ed techni-que is very simple and time saving. Its cosme-tic and longterm results are successful. Webelieve that it must be considered as the tre-atment of choice for steatocystoma multiplex[40].
A Minimally Invasive Procedure for Axil-lary Osmidrosis: Subcutaneous CurettageCombined with Trimming Through a SmallIncision: Though minimally invasive proce-dures often yield excellent esthetic results foraxillary osmidrosis, the high recurrence ratesof malodor limit its further application. In-complete removal of the apocrine glandswould lead to recurrence of the axillary brom-hidrosis, while excessive resection of theapocrine glands firmly attached to the dermiswould easily result in local skin necrosis. The-refore, accurate management of the apocrineglands is extraordinarily important, particu-larly with a limited access. Herein, we wouldlike to introduce an effective and minimallyinvasive procedure combining subcutaneouscurettage and trimming for the treatment ofaxillary osmidrosis. A 5-mm incision wasmarked at the inferior pole of the central axil-lary crease. Subcutaneous undermining wasdone clinging to the axillary superficial fascia.The whole procedure was performed in thefollowing sequence of ‘‘scraping–trimming–scraping’’ against the undermined skin flapuntil the remaining hairs were easily pulledout. All the wounds healed primarily withoutsignificant complications. Out of 300 axillae,294 (98 %) showed good to excellent resultsfor malodor elimination. Scars were invisiblein 280 axillae (93.3 %) and slightly visible in18 axillae (6 %). The dermatology life qualityindex score decreased significantly after theoperation. The procedure is an efficacious andminimally invasive method for the treatmentof axillary osmidrosis. Level of evidence wasIV of this article [41].
Faster suction blister formation using 2hair dryers: Suction blisters are importantfor surgical treatment of vitiligo. One of themain limitations of suction blisters is the timerequired to create them. Several methodshave been described in the literature to shor-ten the duration needed for the developmentof suction blisters. All described methods aim
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 20 of 39(page number not for citation purposes)

to increase the local temperature to facilitateblister formation. One recently described met-hod is the use of a hair dryer. The time requi-red for blister formation was reduced from120 minutes to 70 minutes. This is still con-sidered a long duration and additional met-hods to shorten the duration would beappreciated. Using 2 hair dryers from oppo-site directions would further reduce the du-ration required for blister formation. Twosuction (5-mL and 3-mL) syringes were used.The syringe plunger was removed and theproximal part of the syringe was placed on theskin. The distal part of the syringe was attac-hed to a 3-way valve. A 10-mL syringe wasused to apply suction through the other endof the 3-way valve. A hair dryer operating atlow heat was then directed towards the suc-tion area from an; 20-cm distance. At this dis-tance, there is mild to no pain associated withthe procedure. When using 2 hair dryers fromopposite directions, there is an; 10-minute re-duction in the time required for blister forma-tion. Some blisters form in a multilocularfashion. Applying gentle lateral pressure al-lows formation of a unilocular blister [42,43].
Perone LASIK forcep for molluscum: Mol-luscum contagiosum, a common viral infec-tion, is a self resolving condition. However,intervention in the form of ablation or curet-tage is desired in a number of cases. Mollus-cum lesions pose a challenge when they arepresent around eyelid margins. Patients, aswell as the dermatologists, are apprehensiveregarding the use of available modalities forthe removal of eyelid margin molluscum. Mec-hanical treatment modalities and chemicaltreatment modalities might not be advisablebecause of the proximity to the eye. We ca-nuse of the Perone LASIK forcep for easy ext-raction of eyelid margin molluscum. ThePerone LASIK forcep is commonly used inLASIK (laser in situ keratomileusis) surgeryfor holding the corneal flap. This forcep isavailable for purchase through surgical ins-trument vendors or through online shopping.This forcep has a circular ring on both tips,which enables a firmhold on molluscum lesi-ons. Molluscum can be held between the cir-cular rings and then extracted with gentlepressure. The procedure is painless and thedegree of damage to the skin is less extensive[44].
Combination of ligation and timolol beforesurgical excision of pyogenic granuloma:Pyogenic granuloma (PG) is a benign vascular
tumor that commonly grows on fingers andthe orofacial region. While many therapeuticoptions exist, surgical excision is associatedwith the lowest probability of recurrence. Ho-wever, surgical excision leaves a linear scar,which can be a cosmetic or functional chal-lenge, especially in the digits and orofacialarea. Immediate surgery is not always feasibledue to either the patient’s or surgeon’s sche-dule, and a delay of the procedure is inevi-table. For PGs that cannot be removedimmediately, it can be ligated the base with4-0 black silk followed by application with ti-molol maleate ophthalmic 0.5% solution (2dropsx4/daily). A previous study showedthat ligation of PG base with suture materialleads to necrosis. Recently, timolol, a nonse-lective b-blocker, was introduced for PG tre-atment. However, these methods frequentlyfail to involute PG. The combination of liga-tion and timolol strangulation increases thechances of success. This preoperative combi-natorial approach has a few advantages.First, it prevents PG from enlarging and fre-quently reduces the tumor size before theplanned surgery. In addition, this proceduremight completely resolve PG, obviating theneed for surgery. Therefore, the combinationof ligation and timolol represents an accep-table therapeutic strategy for PG before sur-gery [45].
Successful treatment of lipoatrophy withnormal saline: Margulies and Morris presen-ted a case of lipoatrophy treated successfullywith intralesional normal saline injections.Localized lipodystrophy, or lipoatrophy, pre-sents as focal loss of subcutaneous fat withvariable overlying skin changes and depth de-pending on the cause. Lipoatrophy could re-sult from both oral and local intralesionalcorticosteroid use, with the buttocks and pro-ximal extremities being the most commonlyaffected sites with oral use. Minimal literatureexists about corticosteroid-induced lipoat-rophy. Localized reactions to injected corti-costeroids are thought to occur in less than0.5% of cases, which primarily include he-morrhage, atrophy, secondary infection,changes in pigment, hypersensitivity reacti-ons, and panniculitis. The observed lipoat-rophy typically begins 2 to 3 months afterinjection and can resolve spontaneously. Herethe authors reported a case of acquired loca-lized lipodystrophy, which results mostly incosmetic concerns but has limited treatmentoptions to offer patients. They described the
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 21 of 39(page number not for citation purposes)

technique for intralesional saline injections toassist clinicians in use of this treatment. Suc-cess of this technique has been previouslydescribed, and their case report confirms thisprevious report but uses different time inter-vals between injections. Corticosteroids arecommonly used intralesionally for hypertrop-hic scars, alopecia, and other skin conditions.Glucocorticoids suppress leukocytes from ad-hering to endothelial cells, which limits theability of leukocytes to enter the nearby tis-sues and decreases inflammation. In addi-tion, corticosteroids are potent vasoconstrictors, reducing both oxygen delivery to thewound and reepithelialization. Collagen synthesis is also slowed by the steroid’s antimito-tic effects. Decreasing inflammatory molecu-les with intralesional corticosteroid injectionscan improve scar pliability, shrink scar size,and reduce pain. Although steroids such astriamcinolone are efficacious in this scenario,side effects can include subcutaneous tissueatrophy, capillary dilation, and hypopigmen-tation. Many articles cite known side effectsof the drug. However, it is difficult to find howmany patients experience corticosteroid-indu-ced lipoatrophy. One study found that lipoat-rophy was preceded by an injection in 62% ofpatients. Histologically, it has been found thatafter corticosteroid injections, adipocytes dec-rease in size and number and are surroundedby hyaline. The fat cells were noted to resem-ble embryonic fat cells because of prominenceof vessels, termed involutional fat. Macropha-ges, some with yellow-gray and mucin-posi-tive granules have been found in the area ofinterest as well. In some instances, macrop-hages were shown to engulf adipose tissue,thereby becoming lipophages. As the micros-copic findings of the substance engulfed bymacrophages disappeared, the lipoatrophyfaded as well Serial saline injections on a we-ekly basis are found to completely resolve thecosmetic effect of lipoatrophy within 4 to 8weeks of the initial saline injection. In onecase report, autologous fat injection was usedto treat atrophy with results noted 6 monthsafter treatment began. Intralesional poly-L-lactic acid acts to induce fibroblast and colla-gen formation, has been used for treatment ofhuman immunodeficiency virus associatedfacial lipoatrophy, and was recently reportedin a case of corticosteroid-induced lipoat-rophy. Maximal improvement of the lipoat-rophy was noted in 3 to 5 months. Theirpatient was followed over a 9-month period.
The alternative treatments mentioned aboveare expensive and inconvenient, potentiallyprohibiting patients from following throughwith experimental treatment. On the otherhand, monthly intralesional bacteriostatic sa-line can be a convenient and affordable treat-ment for lipoatrophy attributed to intralesional or intra-articular steroids. Their pati-ent had improvement in the appearance ofher skin lesions while undergoing monthly in-jections and had no significant side effects.There may have been faster improvement ifshe had undergone weekly injections as des-cribed previously. However, further studiesmay help determine if a synergistic effect bet-ween time and saline injection is possible,further delineating the need for injections ona monthly versus weekly basis. It is hypothe-sized that injecting saline where steroidcrystals lie would put them back into suspen-sion, where the crystals could then be recog-nized as foreign bodies and naturally removedfrom the body. The pathogenesis of post-in-jection induced localised lipoatrophy remainsunclear. Several reports identified the clusterof differentiation 68(+) macrophages in theirpatients’ specimen and suggested that theyplayed an important role in the developmentof the lesions. Iftikhar Ahmed postulated thatmacrophages may be activated through non-immunologic means and was a natural res-ponse of the body to eliminate those injectedforeign materials. The post-injection localisedlipoatrophy occurred in various medicationsand seemed to affect women predominantly.The exact causes for this gender difference re-mained speculative. Presumably, there arehormone-related differences in resistance ofadipose tissue or it is a result from the hete-rogeneous receptor status of human adiposetissue. There is no specific treatment for cor-ticosteroid injection induced localised involu-tional lipoatrophy but the majority of thelesions resolve spontaneously within 1–2years. Shumaker et al. performed localised in-tralesional normal saline infiltration in fourpatients with persistent cutaneous atrophyfollowing the corticosteroid injection and gai-ned satisfactory results after 5–8 weeks, res-pectively. Saline is a non-allergenic, inexpensive and readily available material andthey suggested the saline was capable of re-suspension and redistribution of poorly so-luble corticosteroid crystals [46,47,48].
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 22 of 39(page number not for citation purposes)
Cold Therapy: Palmer at al assessed the cli-nical safety and effectiveness of focused coldtherapy (FCT) for the reduction of hyperdyna-mic forehead wrinkles. Subjects treated for fo-rehead wrinkles showed significant clinicalimprovement with high subject satisfactionand no serious adverse events. Focused coldtherapy seems to be an effective, safe nonto-xic alternative to popular wrinkle-reducingtreatments. Second-degree nerve injury invol-ving Wallerian degeneration of the axon oc-curs at temperatures of -20 to -100 ˚C.Treatment in this range results in a reversibledegeneration of the axon and myelin sheath.However, the structural elements of the nervebundle remain intact; therefore, the axon isable to regenerate along the previously estab-lished path to reinnervate the muscle at a rateof approximately 1 mm/d. Focused cold the-rapy (FCT) uses the well-established princip-les of cryotherapy to induce a second-degreenerve injury, resulting in reduced muscle ac-tivity. When applied to temporal nerve branc-hes of the facial nerve, the result is temporaryreduction in forehead animation and a corres-ponding reduction in hyperdynamic wrinkles.This study demonstrates that the applicationof low temperatures to the temporal branchesof the facial nerve results in a temporary in-terruption of target muscle function and rela-xation of hyperdynamic forehead wrinkles.Treatment with FCT resulted in an effectivereduction in forehead wrinkles. Less dramaticresults occurred for the treatment of glabellabecause of the FCT treating 1 (corrugator) ofthe 3 muscles (corrugator, depressor, andprocerus) involved in glabellar furrowing.Most subjects (91%) appreciate continuing ef-fectiveness at 1 month after treatment withthe majority noting an improvement in the fo-rehead wrinkle after the treatment. The dura-tion of effect due to treatment with FCT ismost comparable with that of neurotoxins. Incomparison with the duration of effect, 16 to32 units of botulinum toxin Type A for fore-head wrinkles and 25 units of abobotulinumtoxin A for glabellar wrinkles retained its ef-fect in 40% of the subjects after 12 weeks, alt-hough another study showed that 40% of thesubjects may retain effects to 180 days afterthe treatment. Given that the nerve regene-rates at a rate of approximately 1 mm per day,future treatments will be placed at sites furt-her from the innervation site (2–3 cm) to pro-long the effect. Focused cold therapy resultsin an immediate effect, whereas in other met-
hods, particularly neurotoxins, the effect isdelayed. An immediate effect can be in partdue to the effects of a lidocaine block, howe-ver care was taken to inject lidocaine superfi-cially to avoid any interactions with the nerve.The 7-day results for the horizontal foreheadlines indicate that a small percentage of sub-ject (6%) results did not carry over from theirimmediate experience. This percentage ofsubjects was larger for the glabellar region(21%), although this may be because of thesuperficial nerve branch innervating the cor-rugator muscle where the lidocaine was injec-ted. The side effects reported were mild,transient, and consistent for a needle-basedtreatment, and the reporting rate of 10% forheadaches is lower than 30% for injectableneurotoxins for the treatment of hyperdyna-mic wrinkles. Although the incidence of epi-dermal cold injury was somewhat high (22%),recent device improvements have shown pro-mise for the reduction or elimination of thisside effect. It is believed that hyperpigmenta-tion and dimpling are secondary to epidermalcold injury development and will be reducedwith device improvement. It is estimated that25% of patients exploring treatments forhyperdynamic wrinkle reduction have reser-vations about toxins. The results demonstratethat FCT is a safe, effective minimally invasivenonsurgical treatment option for reducinghyperdynamic forehead lines. Focused coldtherapy may appeal to patients who areaverse to the use of toxins and fillers but re-main interested in the reduction of foreheadrhytides. This study demonstrates that theapplication of FCT to temporal branches ofthe facial nerve can induce a temporary nerveinjury, leading to reduced muscle contractionand a corresponding reduction inhyperdyna-mic forehead wrinkles. Focused cold therapycould fill an, as of yet, unmet clinical need foran effective, safe, and toxin-free alternative fortemporary dynamic wrinkle reduction [49].
Fractionated cryotherapy: Cryotherapy is acommonly performed procedure in dermato-logy outpatient departments for destructionof pathologic tissue. It is an easy-to-perform,inexpensive, and sutureless technique andcarries a minimal risk of infection. However,the procedure is associated with many com-plications and sequelae such as blistering, ul-ceration, necrosis, and permanent orlongstanding pigmentary alterations. This li-mits its use on cosmetically sensitive sites
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 23 of 39(page number not for citation purposes)

and for indications like facial rejuvenation,particularly in people with pigmented skin.Fractionated cryotherapy can reduce thecomplication rates and expand its indicationsin rejuvenation and aesthetics. For this, thinplywood or transparent plastic plates (poorconductors of heat) have been taken andcreated multiple uniform holes using a drillmachine. The size and distance between holescan be customized depending on the site andindication for which fractionated cryosurgeryis planned. Closely placed larger holes aresuited for indications for more aggressivecryotherapy such as thick keloids on thechest and shoulders. Templates with closelyplaced smaller holes and sparsely placedsmaller holes with alternate rows are suitedfor less aggressive cryotherapy on cosmeti-cally sensitive sites such as post herpes zosterhypertrophic scars on the face. Sparsely pla-ced smaller holes are well-suited for resurfa-cing, like cold slush peels and rejuvenation.The plate was firmly placed on the area ofskin to be treated and liquid nitrogen wassprayed by the spiral or paint brush methodover the entire plate. The duration of freezingis generally longer than that for conventionalcontinuous freezing. Two to three 30-40 se-cond freezethaw cycles (after repositioning ofthe template) may be used for thick nonfacialkeloids, and one or two 15-20 second freeze-thaw cycles may be used for facial scars. Thisleads to fractionated freezing and a rapid tha-wing of the frozen tissue resulting from thedispersion of thermal energy from intermit-tent areas of unfrozen tissue. After treatment,improvement might be seen without pigmen-tary changes. The procedure is much less pa-inful as compared with conventional uniformfreezing. Using this technique multiple timescan be safely done in 1 session, and the pro-cedure can be repeated at frequent intervals.For curved surfaces, mouldable plastic mate-rial can be used. Transparent plastic templa-tes allow better visualization of the area to betreated under the template. Fractionating hasthe potential to expand the indications forcryotherapy in aesthetics and rejuvenation[50].
Safety and Efficacy of Imiquimod 3.75%Cream When Used After Cryotherapy in theTreatment of Hypertrophic Actinic Kera-tose: Cryotherapy plus imiquimod 3.75%cream resulted in a statistically significantimprovement in the reduction of hypertrophic
actinic keratoses (HAKs) than cryotherapyalone at 14 weeks. In this study, the authorsshow a benefit of using imiquimod 3.75% im-mediately after cryotherapy for the treatmentof HAKs. For patients with HAKs, combina-tion treatment of cryotherapy plus imiquimodis superior to cryotherapy alone in reducinglesion count [51].
Intralesional cryosurgery for Keloids: In1993, Weshahy described his new techniquefor applying cryosurgery in depth, i.e., intra-lesional cryosurgery (ILC), by using Wes-hahy’s cryoneedles in order to achieve ahigher degree of effectiveness and avoid manyof the disadvantages of the conventional sur-face techniques. Some trials have been pub-lished using the ILC for treatment of keloidsand hypertrophic scars. Cryosurgery hasbeen successfully used to treat keloids andhypertrophic scars. Better results may beexplained by the more timewe gave until theice cylinder formed extended 2 mm outsidethe clinical borders of the lesions, and by thedeep insertion of cryoneedles at or immedia-tely under the base of the lesions, targetingthe blood supply of the lesion, others mightdo the procedure more superficially. The the-rapeutic effects of cryosurgery depend on di-rect cell damage and changes in themicrocirculation provoked by freezing thatcause vascular damage and blood stasis wit-hin the keloid tissue leading to cell anoxia,the keloid is composed mainly of fibrous tis-sue that resists the freezing process. The con-tact and spray techniques are the two mostlypracticed methods for cryosurgery. However,the depth of freezing attained by these twotechniques is not enough to complete the ope-ration in one or two sessions, and can’t reachthe base of the lesion effectively leading tohigh rates of recurrence. Surface cryotherapyalso produces an open, oozing wound whichis considerably larger than the size of the le-sion due to the lateral extension of cryodes-truction that usually takes several weeks toheal. In addition, a certain degree of skin at-rophy and longer hypopigmentation is also in-evitable with this approach because ofmelanocyte sensitivity to low temperatures.Therefore, this characteristic probably ren-ders surface cryotherapy in dark-skinned pa-tients less than optimal. It destroys the coreof the keloid immediately due to destructionof the cellular element and blood vessels atthe base which are more sensitive to the
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 24 of 39(page number not for citation purposes)
cryoprocess than the fibrous core causing itsnecrosis, with a minimal limited damage tothe superficial tissue and melanocytes. Incontrast, the lethal zone, which is created bythe contact probe, includes the epidermis,melanocytes, upper dermis, and to a lesserextent, the deeper dermis due to the counte-racting heating effect produced by the bloodvessels so the efficacy is minimal and the rateof recurrence is high. This technique cantransfer the maximum intensity of cold di-rectly to the base avoiding that counteractingheating effect of the blood vessels [52].
Successful treatment of cutaneous squa-mous cell carcinoma and basal cell carci-noma with intralesional cryosurgery: Wideexcision or Mohs surgery is the standard tre-atment of skin squamous cell carcinoma(SCC). Superficial SCC or tumor smaller than1 cm has been treated successfully with openspray cryosurgery. Larger tumor may not beas effective because tissue destruction is usu-ally superficial. Intralesional cryosurgery (IC)may provide a deeper and better cell killing ef-fect in larger tumors. Lee et al investigated thesafety and efficacy of treating nodular SCC in4 patients with IC. Complete remission wasnoted in all tumors (100%) in 2 months. Norecurrence was noted during follow-up. Allpatients were satisfied with the results. Thisobservation suggests that IC could be simpleand effective alternative treatment for SCCpatients whose condition is not suitable for orwho refused operation [53]. A single intrale-sional cryosurgery session can also comple-tely eradicate BCC on the lower extremities inelderly patients. This technique is associatedwith relatively minor complications, is well to-lerated, and represents a safe and effectivetherapeutic modality for BCC of the lowerlimbs [54].
Cryoanalgesia for post-herpetic neuralgia:The existent therapeutic options for post-her-petic neuralgia (PHN) are varied, albeit notsufficiently effective. The aim of this studywas to try a new treatment modality for PHN.A spray of liquid nitrogen (LN) was used in 47patients suffering from PHN as a stimulatorof a mechanism not yet completely unders-tood. The LN spray was carefully applied (soas not to freeze the skin surface) along the di-seased sensory nerve dermatome, at weeklysessions lasting for 30 seconds each, with amean of three applications per patient. Thearea corresponding to the dermatomes affec-
ted by the herpes zoster satisfactorily atte-nuated the herpetic neuralgia in all patients.Before the sixth treatment session, good orexcellent improvement was obtained in 94%of the study patients. Pain was eliminatedwith one session in nine patients (19%), andwith two sessions in eight patients (17%).They concluded that this non-freezing techni-que is absolutely safe and injury-free, and isvery efficient in calming PHN [55].
Is topical nitric oxide and cryotherapymore effective than cryotherapy inthe tre-atment of oldworld cutaneous leishmania-sis? Current systemic treatments forcutaneous leishmaniasis (CL) are limited bytheir toxicity, high cost, side effects and theemergence of drug resistance. New approac-hes, including topical therapies, are urgentlynee ded. Nitric oxide (NO) produced by humanand canine macrophages has long been de-monstrated to be involved in the intracellularkilling of Leishmania. There is evidence fromseveral experiments that NO is involved in themicrobicidal activity of macrophages againsta number of intracellular pathogens includingLeishmania major, Trypanosoma cruzi andToxoplasma gondii. However, the cellular andmolecular mechanisms whereby NO exerts itscytotoxic activity are not yet well described.Recent studies found that apoptotic processesand several targets in organisms may be af-fected by NO. The leishmanicidal effect of NOseemed to be the consequence of induction ofa programmed cell death-like process. Howe-ver, both in vitro and in vivo immunologicalstudies indicate that NO radicals within Le-ishmania lesions could reduce the parasitenumber. Application of NO donors/inducerscould mediate the leishmanicidal activity ofmacrophages and may prevent progression ofinfectious diseases. Delivery of supplemen-tary NO to target areas where the protectiveeffects of endogenous NO have been lost is anattractive therapeutic option. Topical treat-ment for CL, in which the parasites are foundin the dermis up to a depth of 5 mm or more,is problematic because of the very limited pe-netration of drugs through the skin. BecauseNO is so freely diffusible, we reasoned that itmay be possible to apply an acidified nitritecream over the lesions of CL and thereby ge-nerate enough NO exogenously to kill Leish-mania without causing damage to host tissue.In one study, 16 Ecuadorean patients weretreated with a SNAP (NO-donor, S-nitroso-N-acetylpenicillamine) cream administered on
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 25 of 39(page number not for citation purposes)

lesions for 10 days. All lesions were parasito-logically cured and clinically healed by day30. In another study, a different NO-produ-cing cream was employed to treat 40 Syrianpatients. Only 11 (28%) of 40 patients showedimprovement and only five (12%) of 40 werecured at 2 months. This study was designedto determine the clinical responses and effec-tiveness of NO plus cryotherapy for the treat-ment of old world CL. A double-blind,randomized, placebocontrolled clinical trialwas performed for the evaluation of therapywith topical nitric oxide 3% and cryotherapyin 63 Iranian patients with CL in the south ofIran. Thirty of 36 participants (83.3%) hadcomplete improvement in the treatment groupas did 20 of 27 (74.1%) from the control group(p = 0.627). This study could not show anymore effectiveness from combining a 12-weekcourse of treatment with 3% nitric oxidecream and a once-weekly treatment withcryotherapy in comparison with cryotherapyand placebo in patients with CL [56].
Local anesthesia injection technique foraesthetic removal of dermal nevi: Derma-tologists should be aware of the surgical tech-niques that reduce the level of skin distortionfollowing biopsy procedures. (1) a dilution oflidocaine with bacteriostatic 0.9% sodiumchloride and (2) injection of the solution di-rectly into the nevus. The nevus balloons insize and shape and becomes tenser resultingin a change in the skin level permitting foreasy shave. Good injection technique ofanesthesia may represent a simple, but im-portant means to improve postoperative cos-metic outcomes. Zaiac et al found goodcosmetic result with (1) a dilution of lidocainewith bacteriostatic 0.9% sodium chloride and(2) subcutaneous injection of the solution di-rectly into the nevus. Our solution consists of3 mL of 1% lidocaine in 30 mL of bacteriosta-tic 0.9% sodium chloride in a 1:10 ratio, inwhich each mL contained 9 mg of sodiumchloride and 9 mg of benzyl alcohol. Using a30-gauge needle, this solution is directly in-jected into the nevus. The nevus balloons insize and shape and becomes tenser resultingin a change in the skin level permitting foreasy shave. This technique results in a smo-oth-surfaced area devoid of stitches that healsin an aesthetically pleasing manner [57].
A Simple Elastomer-Pad Vibratory Dampe-ner to Maximize Pain Control of Injectionsin Patients' Undergoing DermatologicalSurgery: For many dermatology patients,
pain associated with procedures is a frequentcomplaint and may be a reason that theyavoid the treatment for both medical and cos-metic dermatology issues. According to infor-mation cited by these authors, almost 3quarters of surgery patients have inadequatepain control. Although the advent of safe andeffective local anesthetics made much of der-matologic surgerymore comfortable, the injec-tion of these anesthetics is a source ofdiscomfort. Clearly, there is ample room forimprovement, and this article suggests moda-lity that seems to be simple and effective.Using the gate theory of pain control, theseauthors have proposed an “anodyne” devicemade from a few cotton balls, a disposableglove, and a vibrating massager. Placed on thesite before injection, it inhibits transmissionof pain in a manner that minimizes discom-fort. The authors further postulate that thistype of vibratory stimulus can be comfortingto patients. It is always important for physi-cians to try to improve the experiences of thepatients. This modification of readily avai-lable, inexpensive products is 1 potentialmeans of doing so. Given its simplicity andminimal risk, it is likely that it will be tried bymany of our colleagues [58].
A simple and effective treatment for nasaltelangiectasia; Needle-assisted electrocoa-gulation: Nasal telangiectasia is a commonphenomenon and can cause significant cos-metic and psychological problems. Althoughthere exist various lasers and chemical treat-ments for nasal telangiectasia, insufficient ef-fect and side effects such as purpura andpostinflammatory hyperpigmentation arecommon. They used needleassisted electro-coagulation as treatment for nasal telangiec-tasia with success. Electrocoagulation hasbeen reported to be safe and effective in here-ditary hemorrhagic telangiectasia, especiallywith epistaxis. The authors used Surgitron®for needle-assisted electrocoagulation. After30 minutes of local anesthesia with lido-caine/prilocaine cream and applying groun-ding plate underneath the patient, a 30Gneedle tip was placed in the telangiectatic ves-sel lumen through the skin overlying the ves-sel. Then an electric current with a powerintensity of 30 W was delivered through it for1 second. With an electric current, the bloodvessel disappeared, instantly. The same pro-cedure was repeated along the vessel at about1 to 2 mm distance between needle punctu-res. The total procedure time was approxima-
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 26 of 39(page number not for citation purposes)

tely 10 minutes. There may be a slight stin-ging sensation during the procedure, madetolerable with just the EMLA cream. Conven-tional electrosurgery tips, even the finest one,cannot easily puncture skin by itself. Using aneedle tip enabled us to puncture skin andvessel without an electric current. Then anelectric current was delivered directly into thevessel lumen. Because the electrical resis-tance of blood is much lower than that of epi-dermis or surrounding dermis, selectivecoagulation of the vessel walls with minimalepidermal and surrounding dermal tissue da-mage can be achieved. Immediately after theprocedure, only needle marks exist, whichheal well without dressing. Patients can seethe improvement of telangiectasis immedia-tely after the procedure. There was no pur-pura with a minimal risk forpostinflammatory hyperpigmentation. Theyused Surgitron®, but they think this methodmay be applicable with other bipolar devices.A patient with nasal telangiectasia showeddramatic improvement after 1 session. After4 sessions, almost complete clearance wasobtained and there was no recurrence duringthe 2 years after last treatment [59].
Presuturing: A simple technique for exci-sion of large skin lesions: Excisions of largeskin lesions, for example, congenital mela-nocytic nevi, often require staged excisions ormore sophisticated reconstructive procedu-res. A simple and reliable way to reduce thenumber of staged excisions and risk of wounddehiscence is the so-called presuturing tech-nique. Under local anesthesia, multiple non-resorbable sutures are placed across thelesion, pulling the edges and folding the adja-cent skin over the area that is to be excised.The sutures should be placed at least 24hours up to 5 days before excision. The prin-ciple behind this technique is the stretchingof adjacent skin beyond its inherent extensi-bility to reach sufficient skin laxity. Thus, re-duction of the number of staged excisions ora complete 1-stage excision of the lesion witha standard primary closure technique can beachieved. The amount of undermining can bereduced or even eliminated, maintaining abetter vascularity. For the subsequent pri-mary closure, we suggest the use of pulleystitches and butterfly sutures with a slowlyabsorbable material. Although tissue expan-ders are also an long-proven alternative forskin expansion, the described presuturing
technique has several advantages. The tech-nique is simpler and faster with less morbi-dity and an improved cost-benefit ratiocompared with tissue expanders, which re-quires the insertion of a prosthesis. Althoughfor defects localized on the forehead or tem-ple, presuturing can be considered, it shouldbe noted that in localizations with less skinlaxity, for example, lesions on the scalp, thepresuturing technique is not suitable. Inthese cases, tissue expanders are a goodchoice for skin expansion. If appropriate re-garding defect size and localization, the pre-suturing technique can be used beforeexcision of congenital nevi and benign lesionsand correction of scar tissue. Presuturingenables primary wound closure for defectsthat would normally necessitate staged exci-sions or reconstruction with a more sophisti-cated technique, such as local flaps or skingrafts. It is a reliable, inexpensive techniquewith a low complication rate that provides anexcellent cosmetic outcome and is especiallysuitable in an outpatient setting [60].
Ligation of the base of pyogenic granu-loma—An atraumatic, simple, and cost-ef-fective procedure: Pyogenic granuloma (PG)is a common, benign, acquired vasculartumor mostly presenting as a rapidly growingred and sometimes pedunculated papule.Commonly described treatment options arecomplete surgical excision, shave excision, orcurettage followed by electrodesiccation, vari-ous forms of laser operation, cryotherapy, orinjection of sclerosing agents. The authorsdescribed an atraumatic, simple, fast, andcost-effective alternative treatment option.The PG is ligated as closely as possible to itsbase using soft surgical suture material. Thismaneuver can be facilitated by lifting the PGwith forceps. The tumor is then ligated withknots that are as tight as possible and the su-ture material is snipped so short that it willnot irritate the surrounding skin. The ligatedtumor can be covered by a wound dressing.The tumor will become necrotic and fall off inseveral days. Patients, parents, or both needto be advised that bleeding could occur fromthe nurturing blood vessel. This unusualevent can be controlled by self-applied simplecompression of the lesion for several minutes.Only clinically obvious cases of PG should betreated by this technique because no histolo-gic examination will be available. This proce-dure is very simple, fast, and can be
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 27 of 39(page number not for citation purposes)

performed even in small children. No anest-hesia is required because it is atraumatic.This smaller lesion can be easily treated, eg,by laser operation or light electrodesiccation.A persisting vessel can also cause recurrencesas described after shave excision or curettagefollowed by electrodesiccation. It is so simpleand fast that it can be performed in any der-matologist’s office, and it is less expensivethan most alternatives. In case of persistenceor recurrence of the PG, complete excisioncan still be performed [61].
A Simple Technique for Treatment of NasalTelangiectasia Using Trichloroacetic Acidand CO2 Laser: Nasal telangiectasia is acommon disfiguring condition and may causesignificant psychological distress. Althoughlasers are effective in treating such lesions,there are many disadvantages, such as pur-pura, scarring, and cost. objective. Twentypatients with nasal telangiectasia were trea-ted with CO2 laser 2 weeks after modifiedsclerotherapy using 80% TCA. After one tre-atment session, all patients had excellent re-sults with more than 75% vessel clearance.There were mild side effects, such as transi-ent erythema and fine frosting. After follow-up of 1 year, there were no relapses. Theyconcluded that CO2 laser after modified scle-rotherapy using 80% TCA appears to be asimple, effective, and inexpensive method forthe treatment of nasal telangiectasia [62].
Intralesional drainage injection of triamci-nolone acetonide for epidermal cyst: Infla-med but noninfectious epidermal inclusioncysts are often injected with intralesional tri-amcinolone acetonide before surgical exci-sion. This method helps reduce inflammation.However, giving an excessive amount of fluidduring the injection has the potential to rup-ture the cyst, further aggravating the inflam-mation and potentially causing a secondaryinfection. Hence, it is of utmost importancethat an optimum amount of steroid is injectedinto the cyst cavity. Two needles can be inser-ted into the cavity of the cyst. Sudden loss ofresistance while inserting the needle indicatesthat the needle is in the cavity. One needle isattached to a syringe and used for injectingthe steroid and the other needle is not attac-hed to a syringe and preferably positioned inthe punctum, if present. As the steroid fills upthe entire cyst cavity, the excess steroid overf-lows into the other needle. This indicates thecavity is full. Both needles may be pulled out,
and the breaks in the skin can be securedwith gauze. This ensures an adequate deliveryof drug, preventing the rupture of the cyst[63].
Medical Student Preference for SimulationModels: The pig foot model is preferred for te-aching dermatologic surgical skills. These re-sults re-affirm that the pig foot model is aneffective, low-cost solution for training. The IlDuomo Basic – With Tumor is the first appa-ratus on the market designed for dermatolo-gic surgery with respect to tissue planes(epidermis, dermis, and fat), underlying ana-tomy, and simulated tumors with margin in-dicators. This mannequin is anatomicallysophisticated and provides a more-robusttraining experience for dermatology residentsthan others on the market, but it is expen-sive. With it, trainees can perform local anest-hetic administration, nerve blocks, suturingtechniques, punch biopsy, elliptical closure,random axial and interpolation flaps, skingrafts, botulinum toxin injections, tumor ex-cision with realistic margins, and scar revi-sion. The layers simulated are skin,subcutaneous fat, facial muscles and nerves,blood vessels, parotid glands and ducts, su-perficial muscular aponeurotic system, nasalcartilage, skull, and auricular cartilage. Thecost is more than $1,500 per mannequin.Despite its sophistication, the medical stu-dents in the surgical skills laboratory leastpreferred the Il Duomo mannequin. It scoredpoorly in epidermal and dermal quality be-cause they felt that it did not resemble the feelof human skin. Its highest average scorescame in the underlying anatomy and reusa-bility sections. One disadvantage of the IlDuomo simulator for medical students is thatthe platform is designed to teach moresophis-ticated skills such as large lesion excision rat-her than simple surgical skills such as apunch biopsy and suturing. In contrast, a re-cent study by Nicholas and colleagues usingthe Il Duomo mannequin found that derma-tology residents rated the Il Duomo platformfor initial training of advanced procedures indermatologic surgery as very beneficial. TheSynDaver Basic Surgical Pad was chosen torepresent the nonfoam skin simulator groupbecause its tissue planes, moisture content,and feel are similar to those of human skin.Uses for this platform include subcuticularand subcutaneous suturing, subcutaneousinjections, fine dissection, and surgical stap-
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 28 of 39(page number not for citation purposes)

les and adhesives. Layers simulated are epi-dermis, dermis, hypodermis, subcutaneousfascia, and fat. Unique features of this modelare realistic puncture resistance and compa-tibility with electrocautery, laser scalpel, radiofrequency ablation devices, harmonic blades,monopolar and bipolar devices, gamma kni-ves, ultrasound equipment, computed tomog-raphy, and magnetic resonance imaging. Thisproduct represents the two classes of more-typical “bench model” simulators in the stu-dent skills laboratory. It is more limited thanthe Il Duomo mannequin but represents aclass of models within reach of many prog-rams’ budgets. Anastakis and colleagues, ina study comparing efficacy of different simu-lators, found that bench models have trainingcapabilities equivalent to that of cadavers andemphasized that underlying anatomy is notessential for learning some procedural skills.Data from the student surveys reveal that theskin pad was the second most preferred of thethree groups. It scored poorly in underlyinganatomy, because this product group doesnot recreate underlying anatomy beneath thesubcutaneous fat. This model’s highest scoreswere in movement, pliability, and reusability.Students felt that this model moved and feltlike human skin and survey results demons-trate that this model is a viable option forbasic dermatologic surgical skills laborato-ries. Olson and colleagues recently publishedtheir experience with the use of hydrophilicfoam pads as a suturing model. This inexpen-sive simulation platform suffers from the li-mitation that it does not reproduceunderlying anatomy, although it provides anexcellent model to practice wound eversion,demonstrating “step off” deformities createdby uneven height of everting dermal sutures,and running subcuticular closure. Medicalstudent preference data from this study de-monstrate that the pig foot model is an effec-tive, low-cost solution for teaching basicdermatologic surgery skills. The major limita-tions of the pig foot model is that it is best forteaching basic procedural skills and is poten-tially less useful for training of more-sophis-ticated dermatologic techniques such asflaps, grafts, and curettage. Preference datashould continue to be collected to fully assessthe Il Duomo mannequin and other morecom-plex synthetic lesion simulator platforms, alt-hough we found that the tried-and-true pigfoot platform is still a preferred platform for
teaching basic dermatology surgical skills tomedical students [64].
Banana: A New Simulation Model to TeachSurgical Techniques for Treating IngrownToenails: Ingrown toenails, when recurrentand painful, are often treated surgically. Sur-gical treatment has traditionally been perfor-med as matricectomy involving sharp excisionof the matrix; another option is chemical era-dication of the matrix with phenol, which hasbecome more popular and is more effective atpreventing symptomatic recurrence. Thereare no animal models on which to teach andpractice these techniques. Surgical modelscan be used to improve depth perception andsurgical skills. The authors sought to developan economical simulation model to teach thedifferent phases and surgical techniques usedto treat ingrown toenails to dermatology resi-dents. The authors selected large, ripe bana-nas without imperfections on the peel tosimulate toes. The banana peel was incised tocreate a nail bed. They used flexible acetateplates to create the nail plate and matrix. Theplates were fixed into the banana’s core,slightly oblique to the peel, and were ade-quate for delicate manipulation. The platemust be cut larger than the nail bed so thatit is inserted and fixed. No glue or external fi-xation was used. The acetate plate remainsfixed during the peel incision, but becausethere are no ligaments created with the bed,it is necessary to hold this plate using thecontralateral hand. They used conventionalsurgical materials to demonstrate and prac-tice the techniques. Acetate plates are com-monly used as document covers. The bananaand acetate plate were adequate to create amodel for the composition of the nail unit.This model allows good representation of theproportions and anatomic structures involvedin surgery for ingrown toenails. Each bananamodel was used only once for each technique.They demonstrated to undergraduate stu-dents and residents the main techniques forsurgical treatment of ingrown toenails, suchas digital block anesthesia, tourniquet or rub-ber band around the toe, classic matricec-tomy, avulsion of the nail plate. Afterward,the residents may practice these procedures.No major difficulties were faced in the processof teaching these techniques for surgical tre-atment of ingrown toenails using this model.Simulation is increasingly recognized as aneffective means of team training, the acquisi-
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 29 of 39(page number not for citation purposes)

tion and maintenance of technical and profes-sional skills, and reliable performance assessment. In addition, a simulated surgical model encourages active participation and canenhance the retention and transfer of lear-ning. Surgical models using fruit have beenpreviously reported: tomatoes for shave biop-sies, burned oranges for necrotic ulcer debri-dement, cantaloupes for sigmoidoscopy techniques, and bananas as a training model torefine blade control for Mohs layer removaland skin incisions. In the case of partial avul-sion of the nail plate with chemical matricec-tomy, it is possible to discuss the differentprotocols. There are protocols using 80% to88% phenol applied directly to the nail mat-rix, including two cycles of 1 minute andthree cycles of 1 minute, as well as protocolsusing 10% sodium hydroxide for 1 minuteand 100% trichloroacetic acid. The pros andcons of each protocol can also be discussed.This simulation model for teaching techni-ques to treat ingrown toenails is easy to useand allows performance and visualization ofall surgical phases. This model also allows de-velopment of new surgical techniques for trea-ting nail problems [65].
Pillowcase Baby: A Laser Teaching Tool forDermatology Residents: Pigs’ feet are widelyused as a teaching tool for suturing and bi-opsying and have served as a traditional met-hod to help dermatology residents becomeacquainted with these procedures before per-forming them on live patients, but there hasnot been an equivalently effective teachingmodality for lasers. Because dermatologistsperform more laser procedures than anyother specialtists, it is important that derma-tology residents receive proper training inlaser surgery during their residency, for pati-ent safety and for upholding high standardsof care as experts of procedural dermatology.It has been reported that the resident role inlaser procedures varies greatly, raising con-cerns about adequate training during resi-dency. Practicing the proper use of a laserdevice before performing the procedure on apatient is especially important in pediatricdermatology, where patients may be less coo-perative than their adult counterparts, addingto the technical complexity of the procedure.To introduce dermatology residents to lasers,the authors used a pillowcase on which a dra-wing of a target is made using a red perma-nent marker. The drawing serves as an
imaginary patient with a red vascular lesionon which residents can learn firsthand howto properly hold the laser, activate approp-riate buttons, and aim at the target. With thistechnique, residents are also readily able tosee the effect of the pulsed dye laser (PDL) onthe target. The drawn and colored in targetserves well as an imaginary vascular targetthat allows learners to immediately visualizethe outcome of their PDL treatment. PDL, inparticular, is an ideal device for application ofthis teaching tool since it is the laser that der-matology residents use most frequently. Pil-lowcase Baby can be adapted in various waysto practice the use of other lasers on differenttypes of targets. For example, we drew and co-lored in a black circular target that could beused as a model for a nevus of Ota, tattoo, orother pigmented lesion for practicing quality-switched alexandrite (and other Q-switched)lasers. Again, the marker target allows forgood visualization of the target, guide light,and treatment effect. It is important to notethat this teaching technique is safe and clean.To minimize the risk of fire or injury to theunderlying pillow or examining table, the pil-lowcasewas placed on a folded sheet moiste-ned with saline before starting the trainingsession. The marker pigments do not penet-rate through the pillowcase even after nume-rous passes of the different lasers thatresidents practice with. As with actual lasertreatment sessions, residents should be ins-tructed to check their surroundings and en-sure that there is nothing flammable aroundbefore treating their Pillowcase Babies. Othervariables that increase the risk of fire includean oxygen-rich environment, which is especi-ally relevant in real-life cases in which inha-lation anesthesia is used or when the laserprocedure is performed in the oxygenenrichedatmosphere of the operating room. Certaintypes of lasers such as carbon dioxide laserand certain types of materials such as polyes-ter also increase the risk of fire, and caremust be taken to minimize the risk of fire inaccordance with the safety protocol of the in-dividual institution. In summary, PillowcaseBaby can serve as an effective teaching toolfor dermatology residents during laser proce-dure training. The teaching session also in-corporates other aspects of laser surgery,such as wearing proper protective goggles andsetting laser parameters, which further helpslearners become familiar with the overall pro-cess of laser treatments. Performing laser the-
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 30 of 39(page number not for citation purposes)

rapy on a Pillowcase Baby as their first lasercase is not only safe, but it is also a fun met-hod for introducing dermatology residents tothe exciting field of cutaneous laser surgery[66].
Short-contact topical tretinoin therapy tostimulate granulation tissue in chronic wo-unds: The use of retinoids in wound healingis increasing. It has been shown that retinoicacid reverses the inhibitory effects of gluco-corticoids on wound healing and acceleratesthe formation of healthy granulation tissue.Pretreatment with tretinoin before epidermalinjury such as chemical peeling and dermab-rasion has shown accelerated wound healing.Enhanced healing of full-thickness skin wo-unds has also been demonstrated in earlywound healing studies. However, tretinointherapy can be quite irritating. The authorsobserved the clinical and histologic effects oftopical tretinoin solution 0.05% applied di-rectly to the wound beds of chronic leg ulce-rations. All were treated with topical tretinoinsolution 0.05% applied directly to the woundbed. The tretinoin solution was left in contactwith the ulcer bed for a maximum of 10 mi-nutes daily and then rinsed with normal sa-line. Punch biopsy specimens were obtainedfrom the wound beds at baseline and mid the-rapy. Standard wound care was continuedthroughout the study. They founded that asearly as 1 week after treatment with topicaltretinoin solution 0.05%, there was increasedgranulation tissue first noted at the wound’sedge. After 4 weeks of therapy with tretinoin,there was further stimulation of granulationtissue, new vascular tissue, and new collagenformation. Short-contact tretinoin therapycan be a novel modality in which to treatchronic ulcers and stimulate the formation ofgranulation tissue [67].
A simple means of disarming the “lockedand loaded” needle: Surgery, in any setting,has several inherent risks not only to the pa-tient, but the physician and his assistants aswell. Safe handling and management of thesharps to prevent inoculation injuries is oneof these risks, in particular: 1) instrumenthand-off of the needle and needle driver bet-ween the physician and his assistants; 2) ret-rieval of instruments from the surgical tray.The authors’ review a simple means of disar-ming the needle loaded in the needle driver toreduce sharps injury. Before the needle andneedle driver are either handed off to the as-
sistant or returned to the surgical tray, pivotthe needle 90 degrees toward the instrumentjoint. The needle’s point should be directed to-ward and touching the needle driver, and the-reby, disarming the needle. To avoid dullingthe needle, the point should not be graspedby the needle driver. Disarming the loaded ne-edle may reduce the chance of sharps injuryduring instrument hand off and retrievinginstruments from the surgical tray. Ninety-nine percent of surgical residents incur atleast one needlestick injury during their trai-ning. The Center for Disease Control and Pre-vention estimates that there are over 1000needlestick injuries per day. Percutaneous in-juries represent both an infection and conta-mination risk, as well as a major cost:follow-up after a single needlestick injury cancost up to $3000 even when no infection oc-curs. Needlestick injuries can occur manytimes during surgery. The following methodaddresses sharps exposure during instru-ment hand-off between the physician and as-sistant, and during the retrieval of from thesurgical tray [68].
Simple method for controlling surgicalsharps: During surgical procedures, controlof sharps is important for both infection con-trol and for minimizing contamination. Infact, there has recently been a push to in-crease the awareness of the risks of sharp in-juries and development of new devices tominimize said risks. In dermatologic surgery,the main culprits for sharp injuries are scal-pels, hooks, and needles. Attempts to mini-mize sharps injuries include the use of‘‘neutral zones’’ for hands-free transfer ofsharps, and placement of potentially injuri-ous devices under drapes and into dentalrolls. Although the number of sharp injuriesamong health care workers has declined, thenumber is still not zero. As a result, any de-vice or technique that can help to decreasethis hazard to health care workers is invalu-able. As curved needle injury is the most com-mon type of sharp injury, and the mostcommonly used needle in dermatologic sur-gery, our focus is on decreasing the risk of in-jury from this type of instrument. The authorsdescribed a simple device for eliminating therisk of suture needle injury. During packingof our surgical trays, they include a thin smallsection of a refrigerator magnet, similar tothose found on, for instance, many notepadsand advertisements for pharmaceuticals. The
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 31 of 39(page number not for citation purposes)

magnet is sterilized along with the entire sur-gical pack before the first use. During the sur-gical procedure, the needle can be placed onthe magnet, which is kept in a corner of thesurgical tray. During placement of the needle,the magnet will attract the needle to it, furt-her aiding in placement in the desired loca-tion. Furthermore, the magnet will serve tohold the needle in place, and allows for easyretrieval with the needle driver when suturingis initiated. During breaks in suturing, theneedle is simply replaced onto the magnet,thus, safely isolating it from the rest of thetray and, thereby, minimizing the risk for ac-cidental injury. Although this technique doesnot prevent injury during suturing, it is asimple and novel approach to minimizing therisk in the surgical tray area. It also serves todeclutter the surgical tray when multiple ne-edles are used. This is done without the po-tentially dangerous method of placing theneedle into a dental roll, which on occasioncan lead to needle-stick injury. These mag-nets are generally easy to find at little to nocost. At the end of the procedure, these mag-nets can be sterilized along with the othersurgical instruments in the tray. As a resultof this simple device, needle-stick injuries canbe reduced with no cost to provider and pati-ent [69].
Rapid treatment of subungual onychomy-cosis using controlled micro nail penetra-tion and terbinafine solution: Onychomycosis continues to be a common and intractableproblem in adults, often responding poorly todrug treatment. Toenails are most frequentlyaffected by the infection, particularly the hal-lux.1 Studies suggest its prevalence to be aro-und 29% across Europe, showing an increasein prevalence with age and in countries withlonger winters. The causative agents are typi-cally the dermatophyte species of fungi whichspread from plantar skin over many monthsto invade the nails through a distal and late-ral subungual route producing the characte-ristic discolouration of the nail plate.4 Overmany months, complete invasion of the nailmay lead to total dystrophy. Onychomycosisis often trivialised as a cosmetic condition butstudies have confirmed its effect on the pati-ent’s wellbeing and quality of life. Moreover,the presence of fungus on the foot is a riskfactor for the development of lower limb cel-lulitis – a particular risk for patients with pe-ripheral vascular disease and diabetes who
have an increased propensity for the disease.Management of the condition to date has pro-ved challenging. Oral systemic agents such asterbinafine and itraconazole have shown goodmycological cure rates when taken over anumber of months. However, potential sideeffects, drug interactions and reluctance fromsome patients to oral medications remains alimitation. Exploring new techniques, the useof lasers has been suggested and reported asa less invasive and safer technology to destroythe subungual infection by rapid heating ofthe infected area. However, results have sug-gested that it has little evidence to date tosupport their widespread use in onychomyco-sis. Topical treatments, applied directly to thenail plate, have also been used widely butconsistently have been shown to be less effec-tive than the systemic drug regimes. The nailplate is naturally a barrier to drug penetra-tion, effectively shielding the subungual areaso the underlying infection remains protected.In addition, patients are expected to apply themedicament to the nail for many months.Studies of topical medicament usage haveshown that compliance decreases the longerthe treatment continues, which may result ina treatment failure. Measures designed to en-hance topical drug delivery have been trialledwith some success. Chemical penetration en-hancers have been developed and incorpora-ted into many topical drugs to boost deliveryof the active ingredient through the nail.Combination therapy has also been shown toimprove overall cure rates. Topically, nail re-duction by mechanical thinning of the nailhas shown to modestly improve the clinicalresponse to antifungal agents. Recently, rese-archers have employed the use of fractionallasers to penetrate the full thickness of nailplate to create a porous structure, thus allo-wing the easier passage of any applied anti-fungal. Fractional lasers concentrate power toa very small area, thus reducing the risks ofthermal damage to peripheral tissue. Thiswork is ongoing, with potential promise, butthe expense of such systems is still prohibi-tive for general podiatric use. In addition, aswith most “hot” lasers, pain appears to be acommonly reported side effect of the treat-ment with a risk of damage to the delicate su-bungual tissues. For the last few years therehave been few significant advances in the on-going struggle to treat onychomycosis morequickly and effectively. As reported by Podi-
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 32 of 39(page number not for citation purposes)

atry Today in November of 2007, the novelidea of drug delivery to the nail using trephi-nation or “mesoscissioning” was first introdu-ced using Pathformer, a handheld device, thatuses a microscopic cutter to penetrate thenail plate but not the nail bed. The principalof this device is based on electrical impe-dance, effectively decreasing the inherentelectrical potential of the epidermis, a knowninsulator. This idea allows drugs to enter the“stratum corneum-free” nailbed painlessly. APhase 1 study conducted at Bringham andWomen’s Hospi tal found the procedure to bepainless, offering both depth control and amycological cure in a diverse patient popula-tion. Of interest, a terbinafine 1% cream wasapplied to the nails, in direct contrast to to-day’s standard of care with low molecular we-ight, hydrophilic solutions widely preferred. Arecent study from Shemer and Gupta AK, inIsrael presents a noteworthy exception. Thework reveals an open comparative study ofnail drilling by trephine, as an adjunctive tre-atment for toenail onychomycosis. Presentedas a parallel three-arm trial the study inves-tigates the effects, outcome and safety of tre-atment using trephine technology. The studyconcludes that both groups managed concur-rently with trephined holes in the nails had asignificantly higher percentage of clear nailcompared with topical terbinafine alone. Inte-restingly, the addition of oral terbinafine pro-vided no significant advantage withcomparable out comes. Treatment of fungalnails with holes plus topical terbinafine pro-duces greater improvement in the appearanceof the toenail and a higher, and significantlyearlier, mycological cure rate. For nail trephi-nation, the Israeli study used an ingeniousapparatus, an automatic device manufactu-red by Ex-It Medical Devices Ltd. This is usedto drill two horizontal lines of holes just pro-ximal to the border between the diseased andhealthy segment of the nail. Holes are of a 1.8mm diameter, spaced 2mm apart. Grossly,the nail plate consists of a superficially drycompartment and a deeper humid depart-ment. This trephine technology is designed todetect when the drill has reached the morehumid department. When a pre-definedhumid level is reached the drill aborts, to pro-tect against pain and nail bed injury. Nailtrephination is required one time only. Afterthis work, data analysis confirms that no caseof bleeding or pain was reported. It was alsoreported further treatment success in 3 case
studies of onychomycosis, using controlledmicro-nail penetration delivered by a U.K. de-vice known as Clearanail. The authors furtherhypothesize that a “subungual mass of der-matophyte hyphae which are not attached tothe nail bed or nail plate remain shielded bythe overlying nail plate.” This presence of adermatophytoma slows the passage of low-tension anti-fungal solution without the ad-junct of micro-drilling. It is a safe andpainless, turbo-charged drug-delivery systemto the affected nail and nail bed, via ‘micro-pores’. Trephination as a concept, it seems,would certainly provide a podiatrist with avery useful and welcome addition to the tool-box [70].
Knot Technique: A New Treatment of In-grown Nails: Ingrown nails are a painfulproblem that affects all ages, particularly theyoung, and it may become chronic if not trea-ted. A new technique was used to treat pati-ents with Stages 2 and 3 ingrown nails inwhom conservative and surgical methodswere attempted. A total of 30 patients presen-ting with Stages 2 and 3 ingrown nails to theclinic between 2010 and 2012 were included.A wedge excision of the upper and lower softtissues of the nail was performed. The woundmargins were simply sutured with 2/0 polyp-ropylene. Approximately 8 to 10 knots weretied without cutting the stitches under thenail. These knots were used to push the softtissue down and to raise the nail. This wasachieved by placing a knot under the nailafter the needle had been passed inside thenail, without cutting the suture before anot-her knot was tied above the nail. Therefore,the ingrown part of the nail was raised. Pati-ents were followed up for 20 months (range,10–24 months). Relapse was observed in only1 patient. No infection was observed, andnone of the patients required additional sur-gery. Stages 2 and 3 ingrown nails can alsobe safely treated with this technique. Thisstudy demonstrated that ingrown nails can besuccessfully treated using a simple surgicaltechnique with low rates of recurrence [71].
Treatment of ingrown nail with a specialdevice composed of shape-memory alloy:Ingrown nail is a common nail problem resul-ting in pain and disability in daily life. Re-cently, a new treatment modality for aningrown nail was reported that used a devicecomposed of shape-memory alloy, K-D. Theaim of the present study was to determine the
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 33 of 39(page number not for citation purposes)

efficacy, recurrence rate and complications ofK-D. The majority of patients were very satis-fied. There were no side-effects in most pati-ents except loss of nail in one patient. K-Dhas some advantages such as simple applica-tion steps, no deformity after the procedure,high patient satisfaction and obvious effectcompared to other non-invasive and invasivemethods [72].
A Simple, Pain-Free Treatment for IngrownToenails Complicated with GranulationTissue: Gulru decided to apply a small appa-ratus made of 0.4 mm-thick stainless dentalwire with two hook-like pieces attached toeach side of the nail, which were connectedby a dental string in the middle. The granula-tion tissue was cauterized by silver nitrate,and they were advised to have foot baths withone tablet of 250 mg potassium permanga-nate diluted in 2 L of warm water twice daily,for 10 minutes each time. Patients were calledback 1 and 6 months after the cessation ofthe treatment, and none had any complaintwith their toenails. Applying a special nail ap-paratus together with silver nitrate and potas-sium permanganate foot baths may be aninexpensive, easy, and patient-friendly treat-ment alternative to surgical interventions foringrown toenails complicated with granula-tion tissue [73].
The Effectiveness of Matrix CauterizationWith Bichloracetic Acid in the Treatmentof Ingrown Toenails: Partial nail avulsion fol-lowed by BCA matricectomy is a safe, simple,and effective method with low rates of posto-perative morbidity and high rates of success.Therefore, partial nail avulsion and BCA mat-ricectomy can be used as an alternative tre-atment method for the treatment of ingrowntoenails. This is the first study to use BCA forthe treatment of ingrown toenail. In ourstudy, side effects such as postoperative painand drainage were at a minimal level in themajority of the patients. None of the patientshad postoperative infection. The success rateof treatment was found to be 96.6%. One pa-tient who underwent matricectomy had re-currence at the 12th month of the follow-up.In this study, 90% BCA matricectomy showstreatment success comparable with those ofphenol, TCA and sodium hydroxide matricec-tomy. Partial nail avulsion followed by BCAmatricectomy is a safe, simple, and effectivemethod with low rates of postoperative mor-
bidity and high rates of success. Therefore,partial nail avulsion and BCA matricectomycan be used as an alternative treatment met-hod for the treatment of ingrowing toenails.Bichloracetic acid is a viable alternative toother modalities in the management of ungiusincarinatus. Advantages include simplicity,cost-effectiveness, speed, safety, and effica cy[74].
The effectiveness of matrix cauterizationwith trichloroacetic acid in the treatmentof ingrown toenails: Ingrown toenail is anoften painful clinical condition that usuallyaffects the big toe. Chemical matricectomywith phenol has a low recurrence rate andgood cosmetic results. However, it producesextensive tissue destruction that can result indrainage and delayed healing. Alternativessuch as sodium hydroxide and trichloroaceticacid (TCA) have therefore come into vogue. Atotal of 39 patients with 56 ingrown toenailedges underwent chemical matricectomy with90% TCA after partial nail avulsion. In mostof the patients, adverse effects such as posto-perative pain and drainage were minimal.One patient who underwent matricectomyhad recurrence in a single nail edge (1.8%) at12 months follow‑up. No recurrence was ob-served among 38 patients during the meanfollow‑up period. This was considered to bestatistically significant (P < 0.001). Partial nailavulsion followed by TCA matricectomy is asafe, simple, and effective method with lowrates of postoperative morbidity and highrates of success [75].
Resin splint as a new conservative treat-ment for ingrown toenails: Several conser-vative as well as surgical methods are usedfor the treatment of ingrown toenails untildate. The conservative methods are eitherbased on nail splinting or on orthonyxia, butno methods employing both principles havebeen reported thus far. Moreover, surgicalmethods usually involve postoperative pain,prolonged wound healing and restricted acti-vities of daily living. Therefore, consideringthe need of a simplified, non-invasive method,in this study, we applied a novel splint to treatpatients with ingrown toenails and estimatedthe clinical efficacy as well as rate of recur-rence following treatment. The splint is aplate made of resin that is attached to the la-teral edge of the nail using a bandage. Theauthors studied 61 patients with an average
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 34 of 39(page number not for citation purposes)

application duration of 9.3 months and anaverage follow-up period of 10 months in allpatients. All patients experienced pain reliefwithin a week of splint application and a dec-rease in the degree of nail deformity. Moreo-ver, follow-up revealed a recurrence rate of8.2%. Therefore, the authors believe that thisnew device is an excellent conservative treat-ment method for patients with ingrown toe-nails [76].
Nail-splinting method with flexible plastictubes for ingrown toenails: Ingrown toenailis a common disorder in the great toe. Manytreatments have been described for ingrownnails. But they have many disadvantages,such as a prolonged wound-healing period,the production of an unsightly nail, or therestriction of normal activities. The authorsperformed a modified method of lateral nailmanipulation with placement of splints on 6patients who gained instant relief from painand resumed normal activities immediately.Most patients experienced no recurrence 20months after the treatment77. Nazari also en-countered 32 cases ingrown toenails in thisclinical trial. All of the patients were treatedusing the plastic nail tube insertion techniquefor 7 to 15 days. Patients were examined dailyfor the first 3 days of treatment and were eva-luated 3 and 6 months after treatment. All pa-tients were followed up by a single observer.Recurrence was seen in only two patientsafter 6 months of treatment. The low recur-rence rate using the nail splinting techniquein the treatment of ingrown toenail, as well asits simple application, shows that this treat-ment constitutes an effective, non-invasivemethod. It appears that this technique cansubstitute other more invasive surgical met-hods, particularly in the early stages of thisdisease [77].
A ConservativeMethod to Gutter Splint In-grown Toenails: In conservative approachesfor treating ingrown toenails, lifting the nailplate out of the ulcer bed using the guttertechnique improves wound healing. There isno need to free the side of the nail plate all theway to the proximalnail fold or matrix. Pus-hing a plastic gutter between the nail edgeand the ulcer bed is all that is necessary andusually does not require anesthesia. Cyano-acrylate glue offers more security and stabilitythan suturing or other methods for attachingthe gutter. This approach is more effective,easy to perform, more acceptable to patients,
and less traumatic than classical gutter tech-nique. It can be considered an initial treat-ment for most patients with mild ingrowntoenail. However, this conservative methodmay not be the first choice for cases with soft-tissue overgrowth or extensive granulationtissue. Acrylic treatment with gutter splintand sculptured nail was found to be vastlysuperior to the other methods described, es-pecially in the ability to firmly affix the guttersplint and sculptured nail for the extendedperiod required for treatment. The treatmentleads to a complete remission with almostinstant alleviation of pain, with no disfigure-ment, while allowing for the resumption ofdaily activities. Conservative methods utili-zing formable acrylics are highly beneficial inthe treatment of an ingrowing nail and shouldbe viewed as the first treatment option [78].
A New Economic Method for Preparing Pla-telet-rich Plasma: Although platelet-richplasma (PRP) is nowadays a common methodin various medical fields, including cosmeticsurgery or dermatology, the expensiveness ofthe kit for processing is still a hurdle. A newunique economic method for preparing PRPwas reported. The method consists in a sim-ple modification of a disposable 5-mL syringethat allows insertion into a common centri-fuge and positioning of the syringe on the cen-trifuge so the PRP separates next to the tip ofthe syringe. Platelet-derived growth factor BBin PRP was measured under anticoagulantdextrose solution A (ACD-A) or heparin as an-ticoagulant and with or without prostaglandinE1 (PGE1) as a platelet aggregation suppres-sant. The new method successfully createdPRP with high platelet-derived growth factorBB in all conditions, and the highest valuewas obtained by using ACD-A and PGE1. Thenew method is useful, and the use of ACD-Aand PGE1 is the most recommended. Thewhole blood of 60 mL was taken from eachhealthy volunteer. Thirty milliliters was underexistence of ACD-A solution, and the rest 30mL was under heparin. The mixing rate was9:1 in volume. Sixteen pieces of disposable 5-mL syringes were prepared for the first cen-trifugation with their finger-holders cut byscissors. Four milliliters of the whole bloodwas put into each syringe and centrifuged asit stands. The rotation speed and time was3000 rpm × 3 minutes, which was the mini-mum for separating red blood cells (RBCs)from plasma empirically by KOKUSAN H-19α
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 35 of 39(page number not for citation purposes)

centrifuge with RF-109 rotor and MA-109Kbuckets. The centrifugal force was calculatedwith the corrected real radius to be 704g. Thesyringes were then taken out from the centri-fuge and arranged on a special handmadeholder. A 3-way cock and an extension tube(both are common medical disposables) wereconnected, and the other end of the extensiontube was attached to the syringe after centri-fugation. Eight syringes for the second centri-fugation were prepared as the same way asthe syringes used for the first centrifugation.One microgram of PGE1 diluted in 0.05 mL ofsaline was added to each of 4 syringes befo-rehand. The syringe was connected to the 3-way cock and the plasma was aspirated. Thesecond centrifugation was performed at 4000rpm (1252g) for 15 minutes, which is the fas-test speed of the machine and considered tobe the realistic time as a daily practice. Thesupernatant was discarded leaving 0.65 mLin each group (namely, ACD-A PGE1+, ACD-A PGE1−, Heparin PGE1+, and HeparinPGE1−), and the sediment was mixed with itusing a vortex mixer (Vortex V-1 plus, BIO-SAN). Finally, 0.65 mL of PRP solution wasprepared from 16 mL of the whole blood ineach group. PRP in each group was dividedinto 3 pieces of 0.2 mL. Twenty microliters of0.5% Triton X in saline was added to 1 of the3 and 20 μL of 8.5% calcium glucuronate toanother. Triton-X is a kind of detergent thatdestroys cell membrane and let α-granulesdischarge nonspecifically. Calcium glucuro-nate neutralizes the anticoagulant effect ofACD-A while it has no effect to heparin. Pla-telet count of the 4 groups was performed byusing disposable counting chambers. ThePRP solutions were stored at 22–29°C4 over-night for the delivery to a laboratory. PDGF-BB was measured there using HumanPDGF-BB immunoassay microplate (R&Dsystems). Ten microliters of the specimen wastaken from each whole blood or PRP solutionafter mingling, diluted to 190 mL buffer andmeasured. The rest 190 μL of the sampleswere centrifuged at 10,000 rpm for 10 minu-tes, and the supernatants were also measu-red. This new method is useful and ethical inclinical practice. The use of ACD-A and PGE1is recommended for preparing PRP with densePDGF-BB [79].
A single injection technique for midfacerejuvenation: The correction of volume losshas become an important part of facial reju-
venation treatments, particularly in the mid-face region. Techniques to date have largelyrelied on multiple injections, fanning techni-ques and deep placement of product undermuscle or on periosteum. A new technique toenhance volume in the midface using a singleinjection of cross-linked hyaluronic acid atthe subdermal level and above the muscle hasbeen described. The technique approachesmidface rejuvenation with reference to boththe bony skeleton and the medial malar fatcompartment. After appropriately markingthe skin, the filler is placed using a blunt can-nula. The treatment achieves satisfactory vo-lume correction, enhancing the sharp cheekbones and malar fullness typical of an attrac-tive adult face. The approach is simple, quick,and well tolerated by the patient and may re-sult in less bruising than deeper techniques.The attractive adult midface has clean, sharpcheekbones accentuated by a shadow bene-ath them formed by a concavity in the cheekand a smooth transition between differentareas of the face. With aging, there is a lossof projection in the midface as fullness andvolume reduces. In particular, reduction infat over the upper maxilla flattens the malararea. Malar fat has been shown to consist ofthree separate compartments; medial, middle,and lateral temporal cheek fat. A change ofvolume in the medial compartment in parti-cular, lateral to the nasolabial fold, has beensuggested as the main cause of the loss ofmidface projection, exaggeration of the naso-labial fat compartment and, therefore, loss ofthe smooth transition typical of the youthfulface. Restoration of facial shape by sculpturalmanipulation of facial soft tissues has beendeemed the highest priority in midface reju-venation. Volumetric replacement at the mid-face region can restore a more youthful andfuller facial appearance and may also softenthe nasolabial folds by elevating loose skinabove the folds. This technique approachesmidface rejuvenation with reference to boththe bony skeleton and the medial malar fatcompartment. Fullness of the malar regionconveys a youthful appearance and promi-nent malar eminences are typically conside-red aesthetic. The area posterior and superiorto the crossing of Hinderer’s lines is used toindicate the location of the most prominentpart of the malar eminence. Newer hyaluronicacid fillers provide an effective option for vo-lume enhancement in the midface region. To
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 36 of 39(page number not for citation purposes)

date, these have typically been applied usingeither multiple ‘‘bolus’’ injections or a fanningtechnique to place product deeply either inthe muscle layer or just above the perios-teum. This method achieves adequate volumecorrection but can result in plump, ‘‘babyface’’ cheeks with little shape. The single in-jection technique described enhances thesharp cheek bones and malar fullness typicalof the attractive adult face. Reference to thebony skeleton in injection placement assistsin achieving this. The limited resistance tomovement of the cannula assists to establishthat the cannula is in the subdermal level andabove the muscle. By contrast, vigorous back-ward and forward cannula motion would beneeded to penetrate the muscle. Using thedegree of resistance against the cannula toestablish cannula position in the midface isdescribed by Berros and Taieb. Additionally,the overlying tissue can be tented with thecannula tip to ensure the correct injectiondepth as recommended by Wu et al. Becausethe cannula is confined to the subdermal leveland remains above the muscle, the single in-jection technique reduces the bruising andswelling often associated with deeper injecti-ons and reduces the potential for nerve da-mage. The latter can mean that the techniqueis more feasible for less experienced injectors,for whom deeper cannula techniques are notadvisable. The injector may draw back theplunger after advancing the cannula to con-firm the cannula is not positioned in a bloodvessel. Effective rejuvenation of the midfacecan be achieved using this safe and simpletechnique. The use of a single injection oneach side of the face yields highly satisfyingresults with reduced patient discomfort com-pared to currently favored, deeper injectiontechniques [80].
References 1. https://en.oxforddictionaries.com/definition/macgy
ver
2. https://www.imdb.com/title/tt0088559/?ref_=tt_rec_tti.
3. Hurkudli DS, Sarvajnamurthy S, Suryanarayan S,Chugh VS. Novel Uses of Skin Biopsy Punches inDermatosurgery. Indian J Dermatol 2015; 60: 170–175. PMID: 25814706
4. AlGhamdi KM, AlEnazi MM. Versatile punch surgery.J Cutan Med Surg 2011; 15: 87-96. PMID: 21477556
5. Kim JE, Ahn HS, Cheon MS, Lee KJ, Cho BK, ParkHJ. Proximal nail fold-lunula double punchtechnique: A less invasive method for sampling nailmatrix without nail avulsion. Indian J DermatolVenereol Leprol 2011; 77: 346-348. PMID: 21508584
6. Christenson L, Patterson J, Davis D. Surgical pearl:use of the cutaneous punch for the removal oflipomas. J Am Acad Dermatol. 2000; 42: 675-676.PMID: 10727317
7. Gupta S, Jangra RS, Gupta S, Mahendra A, Singla R.Saw-toothed power punch for effortless nail biopsy. JAm Acad Dermatol 2016; 75: 109-111. PMID:27543233
8. Collins SC, Cordova K, Jellinek NJ. Alternatives tocomplete nail plate avulsion. J Am Acad Dermatol.2008; 59: 619-626. PMID: 18793936
9. Shin HJ, Sneige N, Staerkel GA. Utility of punchbiopsy for lesions that are hard to aspirate byconventional fine-needle aspiration.Cancer. 1999;87:149-154. PMID: 10385446
10. Rice JC, Zaragoza P, Waheed K, Schofield J, JonesCA.Efficacy of incisional vs punch biopsy in thehistological diagnosis of periocular skin tumours. Eye(Lond). 2003;17: 478-481. PMID: 12802346
11. Güngör Ş, Bahçetepe N, Topal I. Removal of corns bypunch incision: A retrospective analysis of 15patients. Indian J Dermatol Venereol Leprol 2014;80:41-43. PMID: 24448122
12. Chang CH, Yang CH, Hong HS. Surgical Pearl: Pinch-punch excisions for scrotal calcinosis. J Am AcadDermatol. 2004; 50: 780-781. PMID: 15097965
13. Rajan N, Langtry JA. The punch and graft technique:a novel method of surgical treatment for chondrodermatitisnodularis helicis. Br J Dermatol. 2007; 157:744-747. PMID: 17672876
14. Kain N, Koshy O. Evacuation of subungualhaematomas using punch biopsy. J Plast ReconstrAesthet Surg. 2010; 63: 1932-1933. PMID: 20359972
15. Khan MA, West E, Tyler M.Two millimetre biopsypunch: A painless and practical instrument forevacuation of subungual haematomas in adults andchildren. J Hand Surg Eur Vol 2011; 36: 615-617.PMID: 21724686
16. Danby FW, Hazen PG, Boer J. New and traditionalsurgical approaches to hidradenitis suppurativa. JAm Acad Dermatol 2015; 73: S62-65. PMID:26470619
17. Sharma S, Garg VK, Sarkar R, Relhan V.Comparative study of flip-top transplantation andpunch grafting in stable vitiligo. Dermatol Surg 2013;39: 1376-1384. PMID: 23898910
18. Krishnan A, Kar S. Smashed skin grafting or smashgrafting a novel method of vitiligo surgery. Int JDermatol. 2012; 51: 1242-1247. PMID: 22994670
19. Awad SS. Chinese cupping: a simple method toobtain epithelial grafts for the management ofresistantlocalized vitiligo. Dermatol Surg. 2008; 34:1186-1192. PMID: 18537996
20. Malik N, Singh Y, Goyal T. A simple office-basedprocedure for patients with extensive vitiligo. J AmAcad Dermatol 2016; 75: e195-e197. PMID: 27745651
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 37 of 39(page number not for citation purposes)
21. Gupta S, Handa S, Kumar B, Rai R.Surgical pearl:punch excision and grafting for removal of mole. J AmAcad Dermatol 1999; 41: 635-637.PMID: 10495387
22. Grevelink JM, White VR. Concurrent use of laser skinresurfacing and punch excision in the treatment offacial acne scarring. Dermatol Surg 1998; 24: 527-530. PMID: 9598006
23. Gupta S, Pandhi R, Kumar B.Pot-lid technique foraesthetic removal of small lipoma on the face. Int JDermatol. 2001; 40: 420-424. PMID: 11589751
24. Netri G, Tambasco D. Punch biopsy to optimise thehealing of liposuction incisional wounds. Int WoundJ 2016; 13: 148. PMID: 24618278
25. Dessy LA, Buccheri EM, Anniboletti T. Modifiedpunch technique for incomplete earlobe cleftrepair.Aesthetic Plast Surg. 2006; 30: 731-732.PMID:17077953
26. Bregnhøj A, Haedersdal M.Q-switched YAG laser vs.punch biopsy excision for iatrogenic radiation tattoomarkers--a randomized controlled trial. J Eur AcadDermatol Venereol. 2010; 24: 1183-1186. PMID:20236380
27. Rassman WR, Bernstein RM, McClellan R, Jones R,Worton E, Uyttendaele H. Follicular unit extraction:minimally invasive surgery for hair transplantation.Dermatol Surg. 2002; 28: 720-728. PMID: 12174065
28. Clark LE, Mellette JR Jr. The use of hyaluronidase asan adjunct to surgical procedures. J Dermatol SurgOncol 1994; 20: 842-844.PMID: 7798421
29. Chen E, Patel RA, Kwak YJ, Huang CC. Randomizedcontrolled pilot study of the preoperative use ofbrimonidine 0.33% topical gel for hemostasis in Mohsmicrographic surgery. J Am Acad Dermatol 2017;n77: 1114-1118. PMID: 29031658
30. Shagalov DR, Taylor D, Schleichert R, Weiss J, WeissE. Association of central nervous system depressionwith topical brimonidine when used for hemostasis:a serious adverse event. JAMA Dermatol 2017; 153:575-577. PMID: 28403392
31.Stoecker WV, Malters JM, Xu J, Pikka J. Tripodvibration anesthesia. Dermatol Online J 2008; 14: 20.PMID: 18319037
32. Smith KC, Comite SL, Balasubramanian S, Carver A,Liu JF. Vibration anesthesia: a noninvasive methodof reducing discomfort prior to dermatologicprocedures. Dermatol Online J 2004; 10: 1. PMID:15530291
33. Zhu JW, Wu XJ, Lu ZF, Cai SQ, Zheng M. Purse-String Suture for Round and Oval Defects: A UsefulTechnique in Dermatologic Surgery. J Cut Med Surg2012: 16: 11-17. PMID: 22417990
34. Tursen U, Kaya TI, Ikizoglu G. Round excision ofsmall, benign, papular and dome-shaped melanocyticnevi on the face. Int J Dermatol 2004: 43: 844 –846.PMID: 15533071
35. Kaya TI, Tursen U, Baz K, Ikizoglu G. Extra fineinsulin syringe needle: an excellent instrument forthe evacuation of subungualhematoma. DermatolSurg 2003;29: 1141-1143.PMID: 14641342
36. Kaya TI, Tataroglu C, Tursen U, Ikizoglu G. Eruptivevellus hair cysts: an effective extraction technique fortreatment and diagnosis. J Eur Acad DermatolVenereol 2006; 20: 264-268. PMID: 16503884
37. Kaya TI, Tursen U, Yazici AC, Ikizoglu G.A simpleopen comedone extraction technique for Favre-Racouchot disease. Photodermatol PhotoimmunolPhotomed 2005; 21: 275-277. PMID: 16149941
38. Ikizoglu G, Kaya TI, Tursen U, Baz K. The use of thefreer dissector for the removal of trichilemmal cysts.Int J Dermatol 2003; 42: 405-407. PMID: 12755985
39. Jordan DR. Multiple epidermal inclusion cysts of theeyelid: a simple technique for removal. Can J Ophthalmol 2002; 37: 39-40. PMID: 11865958
40. Kaya TI, Ikizoglu G, Kokturk A, Tursen U. A simplesurgical technique for the treatment of steatocystomamultiplex. Int J Dermatol 2001; 40: 785-788. PMID:11903679
41. Wang R, Yang J, Sun J. A Minimally InvasiveProcedure for Axillary Osmidrosis: SubcutaneousCurettage Combined with Trimming Through a SmallIncision. Aesthetic Plast Surg 2015; 39: 106-113.PMID: 25476603
42. Arora S, Kar BR. Reduction of blister formation timein suction blister epidermal grafting in vitiligopatients using a household hair dryer. J CutanAesthet Surg 2016; 9: 232-235. PMID: 28163453
43. AlJasser MI.n Faster suction blister formation using2 hair dryers. J Am Acad Dermatol 2018; 78: e153-154. PMID: 29274347
44. Khare S, Dubey S, Nagar R. New method for removalof eyelid margin molluscum. J Am Acad Dermatol2018; 78: e151-152. PMID: 29274346
45. Baek YS, Kwon SH, Jeon J. Combination of ligationand timolol before surgical excision of pyogenicgranuloma. J Am Acad Dermatol 2018; 78: e141-142.PMID: 29307642
46. Margulies SL, Morris A. Successful treatment oflipoatrophy with normal saline. JAAD Case Rep 2015;1: 415-417. PMID: 27051796
47. Shumaker PR, Rao J, Goldman MP. Treatment oflocal, persistent cutaneous atrophy following corticosteroid injection with normal saline infiltration.Dermatol Surg 2005; 31: 1340-1343.
48. Lo LK, Hung CM, Tsai TF. Successful treatment oftwo cases of localised involutional lipoatrophy withintralesional normal saline. J Paediatr Child Health.2008; 44: 749-751. PMID: 19166537
49. Munyon T, Day D, Karnik J, Tatsutani K. Safety andEffectiveness of Focused Cold Therapy for theTreatment of Hyperdynamic Forehead Wrinkles.Dermatol Surg 2015; 41: 232–241. PMID: 25654195
50. Gupta S, Yadav S, Patra S, Gupta S. Fractionatedcryotherapy. J Am Acad Dermatol 2017;77:e69-71.PMID: 28807122
51. Goldenberg G, Linkner RV, Singer G, Frankel A. AnInvestigator-initiated Study to Assess the Safety andEfficacy of Imiquimod 3.75% Cream When Used AfterCryotherapy in the Treatment of Hypertrophic ActinicKeratoses on Dorsal Hands and Forearms. J ClinAesthet Dermatol 2013; 6: 36–43. PMID: 23441239
52. Weshahy AH, Abdel Hay R. Intralesional cryosurgeryand intralesional steroid injection: a good combination therapy for treatment of keloids and hypertrophic scars. Dermatol Ther 2012; 25: 273-276.PMID: 22913446
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 38 of 39(page number not for citation purposes)
53. Lee CN, Pan SC, Lee JY, Wong TW. Successfultreatment of cutaneous squamous cell carcinomawith intralesional cryosurgery: Case report. Medicine(Baltimore) 2016; 95: e4991. PMID: 27684856
54. Har-Shai Y, Sommer A, Gil T, Krausz J, Gal-Or N,Mettanes I, Lavi I, Eyal N, Brizgalin L, Taran A, Har-Shai L, Elmalach I. Intralesional cryosurgery for thetreatment of basal cell carcinoma of the lowerextremities in elderly subjects: a feasibility study. IntJ Dermatol 2016; 55: 342-350. PMID: 26749491
55. Calandria L.Cryoanalgesia for post-herpeticneuralgia: a new treatment.Int J Dermatol 2011; 50:746-750. PMID: 21595675
56. Jowkar F, Dehghani F, Jamshidzadeh A. Is topicalnitric oxide and cryotherapy more effective thancryotherapy inthe treatment of oldworld cutaneousleishmaniasis? J Dermatolog Treat 2012; 23: 131-135. PMID: 20964568
57. Zaiac M, Shah VV, Mlacker S, Bray FN, Alsaidan M.Local anesthesia injection technique for aestheticremoval of dermal nevi. J Cosmet Dermatol 2016; 15:559-560. PMID: 27329072
58. Beer KR. Commentary on a Simple Elastomer-PadVibratory Dampener to Maximize Pain Control ofInjections in Patients' Undergoing DermatologicalSurgery. Dermatol Surg 2016; 42: 790. PMID:27045748
59. Byun SY, Kim BR, Park JT, Chae JB, Na JI. A simpleand effective treatment for nasal telangiectasia:Needle-assisted electrocoagulation. J Am AcadDermatol 2016; 74: e49-50. PMID: 26892666
60. Valavanis K, Hessam S, Meier N, Scholl L, BecharaFG. Presuturing: A simple technique for excision oflarge skin lesions. J Am Acad Dermatol 2016; 74:e33-34. PMID: 26775792
61. Hölbe HC, Frosch PJ, Herbst RA.Surgical pearl:ligation of the base of pyogenic granuloma-anatraumatic, simple, and cost-effective procedure. JAm Acad Dermatol 2003; 49: 509-510. PMID:12963919
62. Kim YJ, Shin BS, Chung BS, Cho SH.A simpletechnique for treatment of nasal telangiectasia usingtrichloroacetic acid and CO2 laser. Dermatol Surg2002; 28: 729-731. PMID: 12174066
63. Jakhar D, Kaur I. Intralesional drainage injection oftriamcinolone acetonide for epidermal cyst. J AmAcad Dermatol 2018; 78: e149-e150. PMID:29229576
64. Adams CC, Marquart JD, Nicholas LL, Sperling LC,Meyerle JH. Survey of medical student preference forsimulation models for basic dermatologic surgeryskills: simulation platforms in medical education.Dermatol Surg 2014; 40: 427-435. PMID: 24460761
65. Abbade LP, Silva F, Guiotoku MM, Miot HA. Banana:a new simulation model to teach surgical techniquesfor treating ingrown toenails. Dermatol Surg 2013;39: 1274-1276. PMID: 23631629
66. Jeon H, Grossberg AL, Cohen B. Pillowcase Baby: ALaser Teaching Tool for Dermatology Residents.Pediatr Dermatol 2016; 33: 112-114. PMID:26647223
67. Paquette D, Badiavas E, Falanga V. Short-contacttopical tretinoin therapy to stimulate granulationtissue in chronic wounds. J Am Acad Dermatol 2001;45: 382-386.PMID: 11511834
68. Kunishige J, Wanitphakdeedecha R, Nguyen TH,Chen TM. Surgical pearl: a simple means ofdisarming the"locked and loaded" needle. Int JDermatol 2008; 47: 848-849. PMID: 18717870
69. Ali SO, Vogel PS.Surgical pearl: simple method forcontrolling surgical sharps. J Am Acad Dermatol2006; 54: 878-879. PMID: 16635672
70. Bristow I, Baran R, Score M. Rapid Treatment ofSubungual Onychomycosis Using Controlled MicroNail Penetration and Terbinafi-ne Solution. J DrugsDermatol 2016; 15: 974-978. PMID: 27537998
71. Ince B, Dadaci M, Altuntas Z. Knot technique: a newtreatment of ingrown nails. Dermatol Surg 2015; 41:250-254. PMID: 25627634
72. Park SW, Park JH, Lee JH, Lee DY, Lee JH, Yang JM.Treatment of ingrown nail witha special devicecomposed of shape-memory alloy. J Dermatol 2014;41: 292-295. PMID: 24612270
73. Erdogan FG, Erdogan G.Long-term results of nailbrace application in diabetic patients with ingrownnails.Dermatol Surg 2008; 34: 84-86
74. Terzi E, Guvenc U, Tursen B, Tursen U, Kaya TI. TheEffectiveness of Matrix Cauterization WithBichloracetic Acid in the Treatment of IngrownToenails. Dermatol Surg 2017; 43: 728–733. PMID:18053045
75. Terzi E, Guvenc U, Türsen B, Kaya Tİ, Erdem T,Türsen Ü. The effectiveness of matrix cauterizationwith trichloroacetic acid in the treatment of ingrowntoenails. Indian Dermatol Online J 2015; 6: 4-8.PMID: 25657908
76. Matsumoto K, Hashimoto I, Nakanishi H, Kubo Y,Murao K, Arase S. Resin splint as a new conservativetreatment for ingrown toenails. J Med Invest 2010;57: 321-325. PMID: 20847533
77. Nazari S. A simple and practical method in treatmentof ingrown nails: splinting by flexible tube. J EurAcad Dermatol Venereol 2006; 20: 1302-1306. PMID:17062049
78. Taheri A, Mansoori P, Alinia H, Lewallen R, FeldmanSR. A conservative method to gutter splint ingrowntoenails. JAMA Dermatol 2014; 150: 1359-1360.PMID: 25188750
79. Fukaya M, Ito A. A New Economic Method forPreparing Platelet-rich Plasma. Plast Reconstr SurgGlob Open 2014; 2: e162. PMID: 25289355
80. Cattin TA. A single injection technique for midfacerejuvenation. J Cosmet Dermatol 2010; 9: 256-259.PMID: 20883303
J Turk Acad Dermatol 2019; 13 (1): 19131r2. http://www.jtad.org/2019/1/jtad19131r2.pdf
Page 39 of 39(page number not for citation purposes)
Related Documents











