Lymphoma and Multiple Myeloma Terry Hayes, M.D., Ph.D.

Lymphoma and Multiple Myeloma Terry Hayes, M.D., Ph.D.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Lymphoma and Multiple Myeloma
Terry Hayes, M.D., Ph.D.

Topics to be Covered
• Non-Hodgkin’s Lymphoma
• Hodgkin’s Disease
• Multiple Myeloma

Lymphoma and Multiple Myeloma2004 U.S. Predicted Values
Malignancy New Cases Deaths
All Cancer s 1,368,030 563,700Non-Hodgkin’s
Lymphoma 54,370 19,410
Hodgkin’s Disease 7,880 1,320
Multiple Myeloma 15,270 11,070
CA Cancer J Clin 2004; 54:8-29

Non-Hodgkin’s Lymphoma
Former First Lady
Jacqueline Kennedy Onassis

King Hussein of Jordan
Television star, The A-Team. Sylvester Stallone's adversary in "Rocky III.”
“Mr. T”(Lawrence Tureaud)

Non-Hodgkin’s Lymphoma
• 6th most common cause of cancer death in United States.
• Increasing in incidence and mortality.
• Since 1970, the incidence of lymphoma has almost doubled.

Overview• The types of non- Hodgkin’s lymphoma
reflect the developmental stages of lymphocytes.
• Each type of lymphoma can be viewed as a lymphocyte arrested at a certain stage of development and transformed into a malignant cell.
• 85% B cell origin, the rest T or null cell.

Precursor B Cell Leukemias
CLL, B Cell Lymphomas
Waldenström’s, Myeloma
B CELL DIFFERENTIATION
CD19CALLA (CD10)CD20CD38
Cell Surface Markers
sIgMsIgM,D
sIgM,G,A Ig

MATURATION IN LYMPHOID FOLLICLE
A B D EC
B lympho-
cyte
smallcleaved
largecleaved
smallnon-
cleaved
largenon-
cleaved
immunoblast
smalllymphocyte
plasmacell
F
G
H
Tlymphocyte

Chronic lymphocytic leukemiaSmall lymphocytic lymphomaWaldenström’s macroglobulinemia
Follicular lymphomaBurkitt’s lymphomaMantle zone
lymphoma
Sézary syndromeMycosis fungoidesPeripheral T cell lymphoma
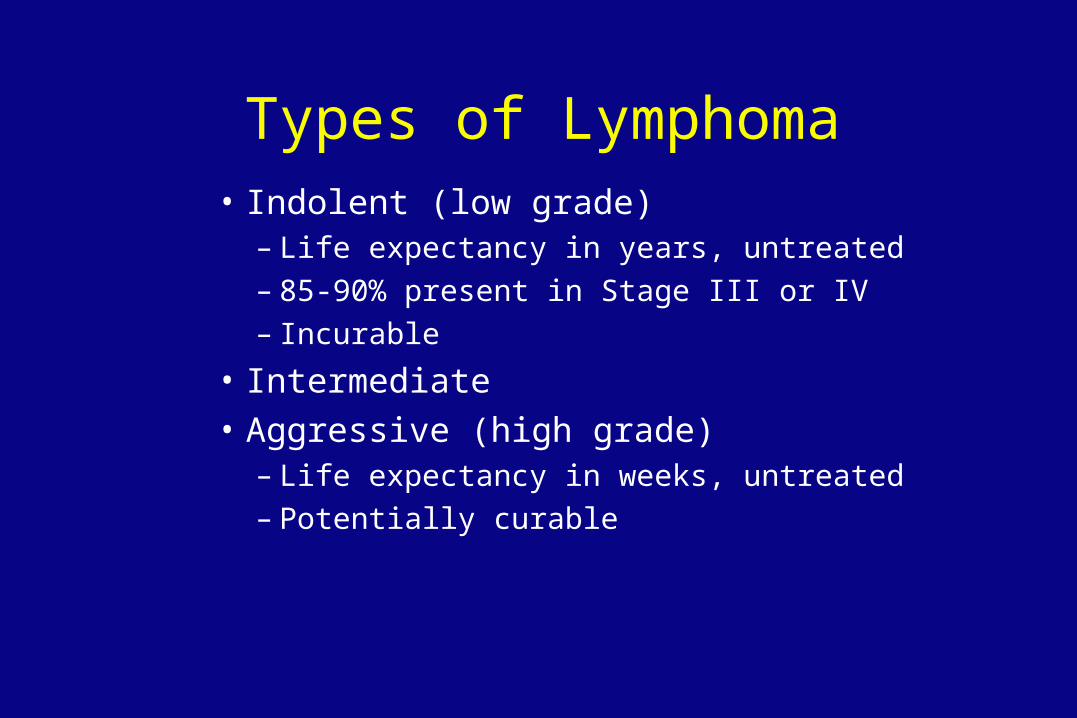
Types of Lymphoma• Indolent (low grade)
– Life expectancy in years, untreated– 85-90% present in Stage III or IV– Incurable
• Intermediate
• Aggressive (high grade)– Life expectancy in weeks, untreated– Potentially curable

Commonly Used Classifications Working Formulation
Low GradeLow Grade
Small lymphocytic
Follicular small cleaved
Follicular mixed
Rappaport
Diffuse well-differentiated lymphocytic (DWDL or WDLL)
Nodular poorly differentiated lymphocytic (NPDL)
Nodular mixed lymphocytic-histiocytic (NM)

Commonly Used Classifications Working Formulation
Intermediate GradeIntermediate Grade
Follicular large cell
Diffuse small cleaved cell
Diffuse mixed
Diffuse large cell
Rappaport
Nodular histiocytic (NH)
Diffuse poorly differentiated lymphocytic (DPDL)
Diffuse mixed lymphocytic-histiocytic (DM)
Diffuse histiocytic (DHL)

Commonly Used Classifications Working Formulation
High GradeHigh Grade
Large cell immunoblastic
Lymphoblastic lymphoma
Small noncleaved cell
• Burkitt’s
• Non-Burkitt’s
Rappaport
Diffuse histiocytic (DHL)
Diffuse lymphoblastic
Diffuse undifferentiated (DU)

Median Survival Histology (Years)
DWDL 8-12NPDL 5-8NM 5-8NH 1-3DPDL 2-4DM 1-3DHL .5-1.5DU .6- .7

Not Included inThese Classifications
• Mycosis fungoides
• Marginal zone B cell lymphoma– MALT lymphoma
• Mantle cell lymphoma
• Peripheral T cell lymphoma
• Angioimmunoblastic lymphoma
The REAL Classification (Revised European-American
Lymphoma Classification)September, 1994

REAL Classification
• Precursor B-lymphoblastic lymphoma/leukemia
• B cell CLL/prolymphocytic leukemia/small lymphocytic leukemia
• Lymphoplasmacytoid lymphoma
• Mantle cell lymphoma
• Follicular center lymphoma, follicular
• Follicular center lymphoma, diffuse

REAL Classification
• Extranodal marginal zone B cell lymphoma (MALT type)
• Nodal marginal zone B cell lymphoma
• Splenic marginal zone B-cell lymphoma
• Hairy cell leukemia
• Plasmacytoma/myeloma

REAL Classification
• Diffuse large B cell lymphoma
• Primary mediastinal large B cell lymphoma
• Burkitt’s lymphoma
• High grade B cell lymphoma, Burkitt-like
• Precursor T lymphoblastic lymphoma/leukemia
• T cell CLL/prolymphocytic leukemia

REAL Classification
• Large cell granular lymphocytic leukemia:
T cell type, NK cell type
• Mycosis fungoides/ Sézary syndrome
• Peripheral T cell lymphomas, unspecified
• Hepatosplenic T cell lymphoma
• Angioimmunoblastic T cell lymphoma

WHO ClassificationB-cell neoplasms T- and NK-cell neoplasmsPrecursor B-cell neoplasm Precursor T-cell neoplasmPrecursor B-lymphoblastic leukemia/lymphoma (precursor B-cell acute lymphoblastic leukemia)
Precursor T-lymphoblastic lymphoma/leukemia (precursor T- cell acute lymphoblastic leukemia)
Mature (peripheral) B-cell neoplasms Mature (peripheral) T-cell neoplasmsB-cell chronic lymphocytic leukemia/smalllymphocytic lymphoma
T-cell prolymphocytic leukemiaT-cell granular lymphocytic leukemia
B-cell prolymphocytic leukemia Aggressive NK-cell leukemiaLymphoplasmacytic lymphoma Adult T-cell lymphoma/leukemiaSplenic marginal zone B-cell lymphoma (with or w/o villous lymphocytes)
(human T-cell lymphotropic virus type I positive)Extranodal NK/T-cell lymphoma, nasal type
Hairy cell leukemia Enteropathy type T-cell lymphomaPlasma cell myeloma/plasmacytoma Hepatosplenic gammadelta T-cell lymphomaExtranodal marginal zone B-cell lymphoma of mucosa- associated lymphoid tissue type
Subcutaneous panniculitis-like T-cell lymphomaMycosis fungoides/Sezary syndrome
Nodal marginal zone B-cell lymphoma (with or w/o monocytoid B cells)
Anaplastic large cell lymphoma, T/null-cell, primary cutaneous type
Follicular lymphoma Peripheral T-cell lymphoma, not otherwiseMantle cell lymphomaDiffuse large B-cell lymphoma
characterizedAngioimmunoblastic T-cell lymphoma
Mediastinal large B-cell lymphomaPrimary effusion lymphoma
Anaplastic large cell lymphoma, T/null-cell, primary systemic type
Burkitt's lymphoma/Burkitt's cell leukemia

Small lymphocytic Immunoblastic
Mantle cell Large Cell
Types of Non-Hodgkin’s Lymphoma

Etiology of NHL
• Immune suppression– congenital (Wiskott-Aldrich)– organ transplant (cyclosporine)– AIDS– increasing age
• DNA repair defects– ataxia telangiectasia– xeroderma pigmentosum
Etiology of NHL
• Chronic inflammation and antigenic stimulation– Helicobacter pylori inflammation, stomach– Chlamydia psittaci inflammation, ocular adnexal tissues– Sjögren’s syndrome
• Viral causes– EBV and Burkitt’s lymphoma– HTLV-I and T cell leukemia-lymphoma– HTLV-V and cutaneous T cell lymphoma– Hepatitis C

Epidemiology
• Can occur at any age
• Overall incidence, and incidence of subtypes, varies with location:– Burkitt’s in tropical Africa– IPSID in Middle East– Adult T cell leukemia-lymphoma in Japan
and Caribbean
Epidemiology• Indolent lymphomas are rare in young people and
increase in incidence with age.
• Large cell lymphoma (DHL) is less age related, and is among most common cancers affecting the young.
• Burkitt’s and lymphoblastic lymphoma are common in adolescents.
• AIDS patients develop aggressive, high grade lymphomas.
Clinical Features
• Lymphadenopathy
• Cytopenias
• Systemic symptoms
• Hepatosplenomegaly
• Fever
• Night sweats



Clinical Features
• Lymphadenopathy may fluctuate or spontaneously remit, especially in low-grade lymphomas.
• B symptoms more common in high-grade lymphomas.
• Hematogenous spread of disease, with no predictable pattern.

Clinical Features
• Classic lymphoma: arises in lymph node or bone marrow.
• Extranodal primary more common in high-grade lymphoma.
• Waldeyer’s ring involvement frequent in GI lymphomas.
Diagnosis of NHL
• Excisional biopsy is preferred to show nodal architecture (follicular vs diffuse).
• Immunohistochemistry to confirm cells are lymphoid– LCA (leukocyte common antigen)– Monoclonal staining with Ig or Ig
• Flow cytometry:– CD 19, CD20 for B cell lymphomas– CD 3, CD 4, CD8 for T cell lymphomas

Diagnosis of NHL
• Chromosome changes– 14;18 translocation in follicular lymphoma
• bcl-2 oncogene
– t(8;14), t(2;8), t(8;22) in Burkitt’s lymphoma• c-myc oncogene
– t(11;14) in mantle cell lymphoma• cyclin D1 gene
Staging Workup
• CBC, chemistries, urinalysis
• CT scans of chest, abdomen and pelvis
• Bone marrow biopsy and aspirate
• (Lumbar puncture)– AIDS lymphoma– T cell lymphoblastic lymphoma– High grade lymphoma with positive marrow

Staging laparotomy and lymphangiogram
are not indicated in non-Hodgkin’s lymphoma.

Staging: Ann Arbor
I. 1 lymph node region or structure
II. >1 lymph node region or structure, same side of diaphragm
III. Both sides of diaphragm
IV. Extranodal sites beyond “E” designation
subscripts: A, B, E, S
Treatment Options:Indolent lymphomas
WDLL, NPDL
• 10-15% in Stage I or II– potentially curable– local radiotherapy
• 85-90% Stage III or IV– incurable– treatment does not prolong survival

Reasons to Treat in Advanced Indolent Lymphomas
• Constitutional symptoms
• Anatomic obstruction
• Organ dysfunction
• Cosmetic considerations
• Painful lymph nodes
• Cytopenias
Treatment Options inAdvanced Indolent Lymphomas
• Observation only.• Radiotherapy to site of problem.• Systemic chemotherapy
– oral agents: chlorambucil and prednisone– IV agents: CHOP, COP, fludarabine, 2-CDA.
• Antibody against CD20: Rituxan, Bexxar, Zevalin.
• Stem cell or bone marrow transplant.
CHOP Chemotherapy
• Cyclophosphamide (Cytoxan)
• Hydroxydaunorubicin (Adriamycin)
• Oncovin (vincristine)
• Prednisone

Treatment Options:Aggressive Lymphomas
Aggressive
• Diffuse large cell lymphoma, large cell anaplastic lymphoma, peripheral T cell lymphoma.
Very Aggressive
• Burkitt’s lymphoma and lymphoblastic lymphoma.
Treatment Options for Early Stage Aggressive Lymphomas
• Often in Stage I or II– potentially curable– disseminates through bloodstream early– must use systemic chemotherapy
• CHOP x 6 cycles
• CHOP x 3 cycles followed by radiotherapy

Treatment Options for Advanced Stage Aggressive Lymphomas
• Systemic chemotherapy– CHOP (± Rituxan for over 70 age group)
• ± Intrathecal chemotherapy – AIDS patients and CNS involvement
• ± Radiotherapy– Spinal cord compression, bulky disease

Lymphoblastic Lymphoma
• T cell malignancy.
• Male adolescents.
• Mediastinal mass.
• T cell variant of T cell acute lymphoblastic leukemia.
• Prognosis improving with intensive ALL regimens.

Burkitt’s Lymphoma• African variety: jaw tumor, strongly linked to
Epstein-Barr Virus infection.
• In U.S., about 50% EBV infection.
• May present as abdominal mass.
• Most rapidly growing human tumor.
• Typical chromosome abnormality: c-myc oncogene linked to one of the immunoglobulin genes.

Burkitt’s Lymphoma
• Treated with multidrug regimen similar to pediatric leukemia/lymphoma regimens.

Notable Subtypes of Lymphoma

Mycosis Fungoides
• Malignancy of helper T cells.
• Affinity for skin.
• Can be treated with electron beam radiation, ultraviolet light, or topical alkylating agents.

AIDS Lymphoma
• Aggressive lymphomas of B cell origin.
• Burkitt’s, Burkitt’s-like, and large cell immunoblastic.
• Treatment often limited by immune compromise of the patient.
• Prognosis improved with HAART therapy.
MALT Lymphoma
• Mucosa-Associated Lymphoid Tissue
• Chronic infection of the stomach by Helicobacter pylori.
• Localized to the stomach, indolent course.
• Can be cured in many cases by antibiotics against H. pylori.
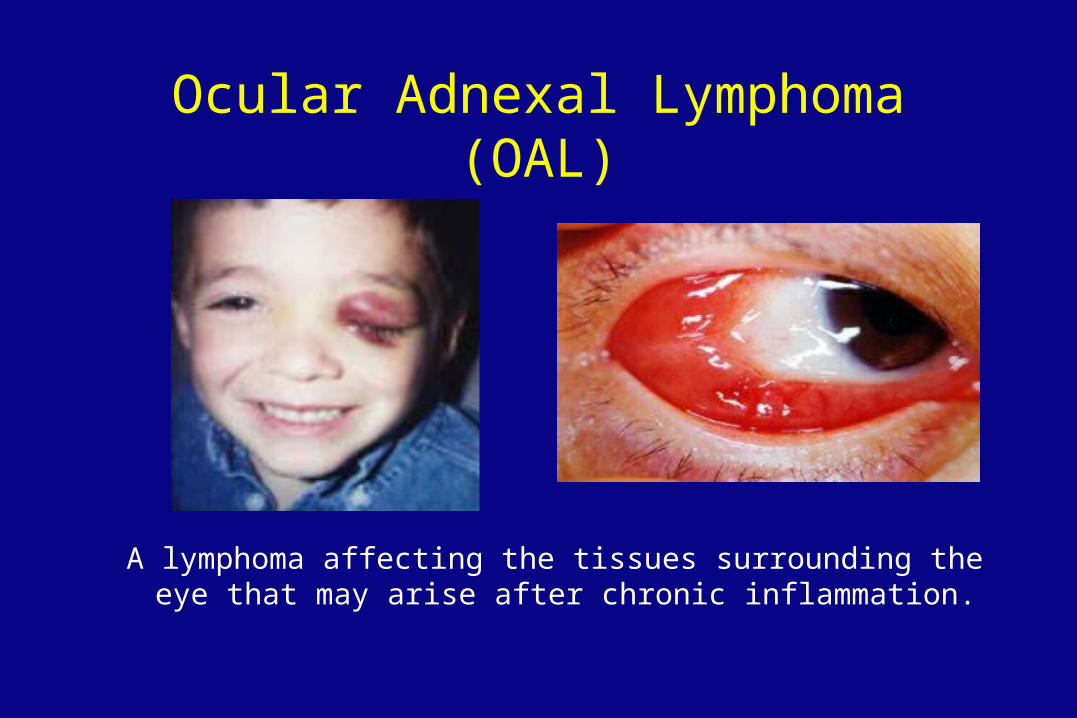
Ocular Adnexal Lymphoma (OAL)
A lymphoma affecting the tissues surrounding the eye that may arise after chronic inflammation.

Treatment
• May respond to antibiotic therapy against Chlamydia.
• One patient treated with doxycycline (100 mg bid for 3 weeks) had complete remission for more than 12 months, and another patient had minimal remission for more than 18 months.
ASCO 2003, Abstract 2273

Hodgkin’s Disease

Thomas Hodgkin
English pathologist, described the disease that bears his name in 1832.

Paul Allen
Cofounded Microsoft with Bill Gates

Mario Lemieux
Top player in the US National Hockey League

Brandon Tartikoff
Youngest US television network president(Cosby, Seinfeld)

Hodgkin’s Disease
• One-seventh as common a snon-Hodgkin’s lymphoma.
• Highly treatable and curable, even when disseminated.
• Presence of Reed-Sternberg cell is necessary to make diagnosis.
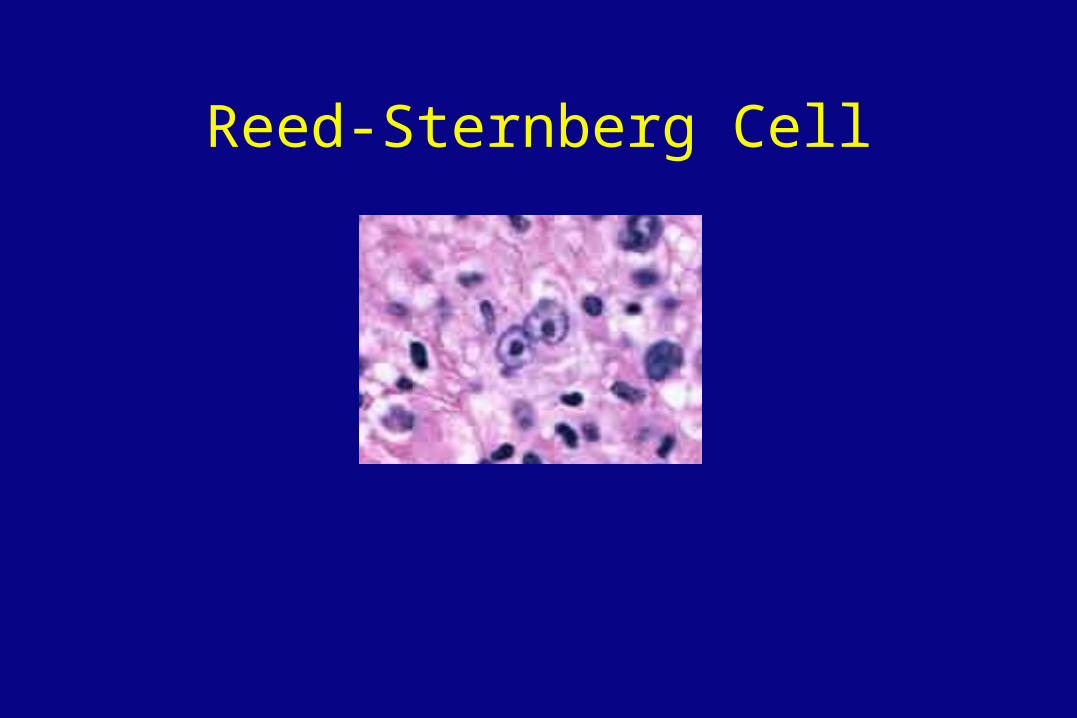
Reed-Sternberg Cell

Subtypes of Hodgkin’s Disease
• Lymphocyte predominant
• Nodular sclerosis
• Mixed cellularity
• Lymphocyte depleted
Unlike non-Hodgkin’s lymphoma, in Hodgkin’s Diseasethe histologic subtype does not determine how thedisease is treated.

Etiology ofHodgkin’s Disease
• Reed-Sternberg cells are the malignant cells.
• Minor population in the malignant tissues– many normal lymphocytes, eosinophils, other cells
• Cell of origin is unknown: T, B, both, neither.
• Some R-S cells contain EBV genomes.

Epidemiology
• In developed countries, bimodal distribution of patients.– young adulthood– after age 50
• More common in affluent families with few siblings.
• In developing countries, more common in young children.
Signs and Symptoms
• Lymph node enlargement, usually cervical or mediastinal.
• Systemic “B” symptoms common.
• Pel-Ebstein fever.– relapsing, high-grade fever that can reach 105-
106°F, periodicity of 7-10 days. Fever spikes abrupt in onset and resolution
• Pain on drinking alcohol.
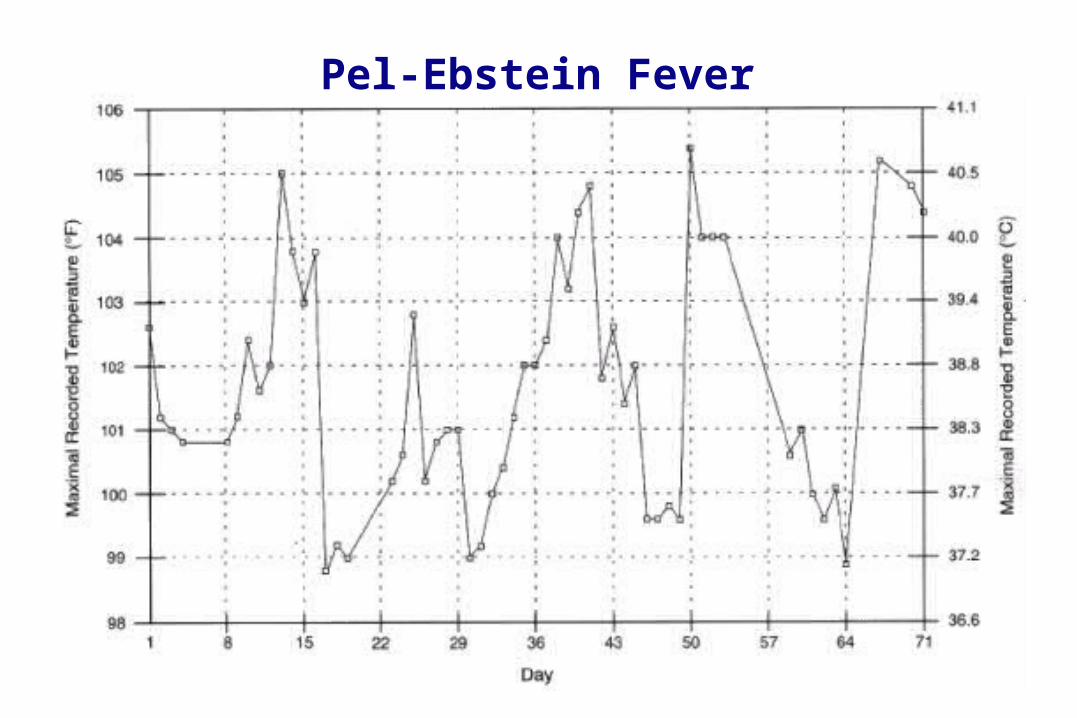
Pel-Ebstein Fever
Clinical Features
• T cell mediated immune deficiency, even in early stage disease. Prone to infections:– Herpes zoster (“shingles”) in one fourth of
patients– Fungal or mycobacterial infections
• Immune defect may persist even after lymphoma is cured.

Clinical Features
• Predictable contiguous spread of disease:– cervical nodes to mediastinum or axilla– mediastinum to periaortic nodes or spleen, etc.
• Basis for staging and treatment decisions.

Diagnosis
• Excisional biopsy of a lymph node.
Fine needle aspirate is not sufficient to make the diagnosis of Hodgkin’s disease.

Staging of Hodgkin’s Disease
Same as for non-Hodgkin’s:
• H + P, labs, CT scans, bone marrow biopsy
PLUS:
• Gallium scan
• Lymphangiogram or staging laparotomy ONLY if results would affect treatment decisions

Treatment by Stage
Stage Therapy % Cure
IA XRT 95
IIA XRT 85
IB, IIB XRT (Total Nodal) 70
IIIA XRT 70
IIIB, IV Combination Chemo 50

Chemotherapy Regimens
• MOPP
– Mechlorethamine, Oncovin, Procarbazine, Prednisone
• ABVD
– Adriamycin, Bleomycin, Vinblastine, Dacarbazine
• BEACOPP

Treatment Options
• Often, patients who relapse after radiotherapy can be cured by salvage chemotherapy.
• Combined chemotherapy and radiotherapy is given for bulky mediastinal masses.
• Chemotherapy now being tested for earlier stages of the disease.

Late Complications ofHodgkin’s Disease
• High incidence of second malignancies– leukemia first 10 years, solid tumors over time.
• Leukemia in patients receiving alkylating agents or combined chemo/XRT.
• Lung cancer and breast cancer in patients receiving XRT to chest. Lung cancer especially high in smokers.

Late Complications ofHodgkin’s Disease
• Hypothyroidism after irradiation of the neck.
• Constrictive pericarditis after radiotherapy to the mediastinum.
• Infertility after use of alkylating agents.
• Heart failure after Adriamycin treatment.
Multiple Myeloma

Ann Landers
Advice Columnist

Mark Lenard
Sarek (Spock’s father) on Star Trek

Overview of Multiple Myeloma
• Less common than non-Hodgkin’s lymphoma, more deadly.
• Average life expectancy 30 -36 months.
• Some patients develop a very indolent form and live for 10 years or more.
• Potentially curable with high dose chemotherapy (bone marrow or stem cell transplantation).

Overview of Multiple Myeloma
• Disease of malignant B-lymphocytes.
• Little similarity to lymphoma in presentation, age at diagnosis, treatment, or prognosis.
• Signs and symptoms of multiple myeloma are quite variable.
• Approximately 20% of patients have no symptoms.

Etiology of Multiple Myeloma
• Unknown. Suggested predisposing factors include:– Viral infection with Human Herpesvirus 8
(HHV-8).– MGUS (monoclonal gammopathy of
undetermined significance).

Epidemiology
• Average age at presentation is about 65.
• Males are affected more often than females.
• Incidence in blacks is twice that of whites.
• Five-year survival is approximately 25-30%.
• Median survival 30-36 months.

Multiple Myeloma
• More than 15% plasma cells in the bone marrow.
• Monoclonal immunoglobulin peak on SPEP – more than 3 gm/dL.
• Presence of Bence Jones protein in urine.
• Decreased levels of normal immunoglobulins.

Clinical Features
• Bone marrow failure- Anemia, thrombocytopenia, neutropenia
• Renal failure
• Bone disease with skeletal destruction
– lytic lesions
– generalized decrease in bone density
• Hypercalcemia
Clinical Features
• Hyperviscosity syndrome
• Recurrent infections
• Amyloidosis


Diagnosis and Staging Workup
• Bone marrow biopsy and aspirate
• Serum protein electrophoresis and immunofixation
• Skeletal survey– Plain x-rays are better than bone scan.– Lytic lesions do not show up well on bone scan.
• Quantitative immunoglobulins
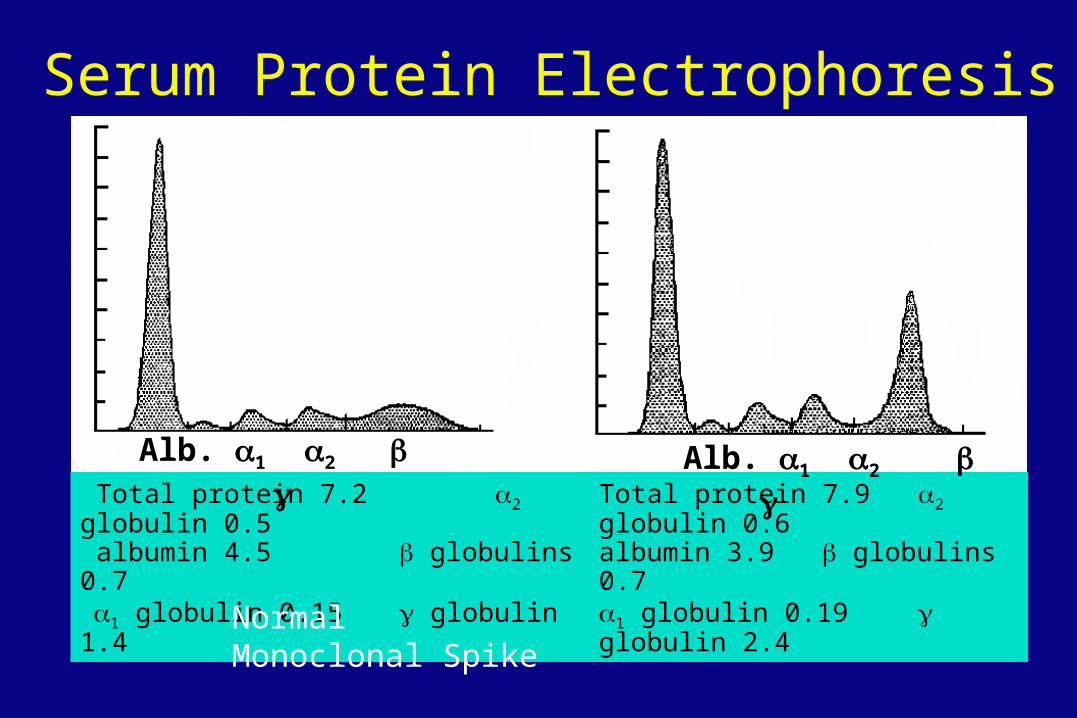
Serum Protein Electrophoresis
Total protein 7.2 2 globulin 0.5 albumin 4.5 globulins 0.71 globulin 0.15 globulin 1.4
Total protein 7.9 2 globulin 0.6albumin 3.9 globulins 0.71 globulin 0.19 globulin 2.4
Normal Monoclonal Spike
Alb. 1 2 Alb. 1 2
Monoclonal Immunoglobulin Spike on Serum Protein Electrophoresis (SPEP)
• Multiple myeloma
• Non-Hodgkin’s lymphoma
• Monoclonal gammopathy of undetermined significance (MGUS).
Not clinically significant unless present in high quantity (over 3 gm/dL).
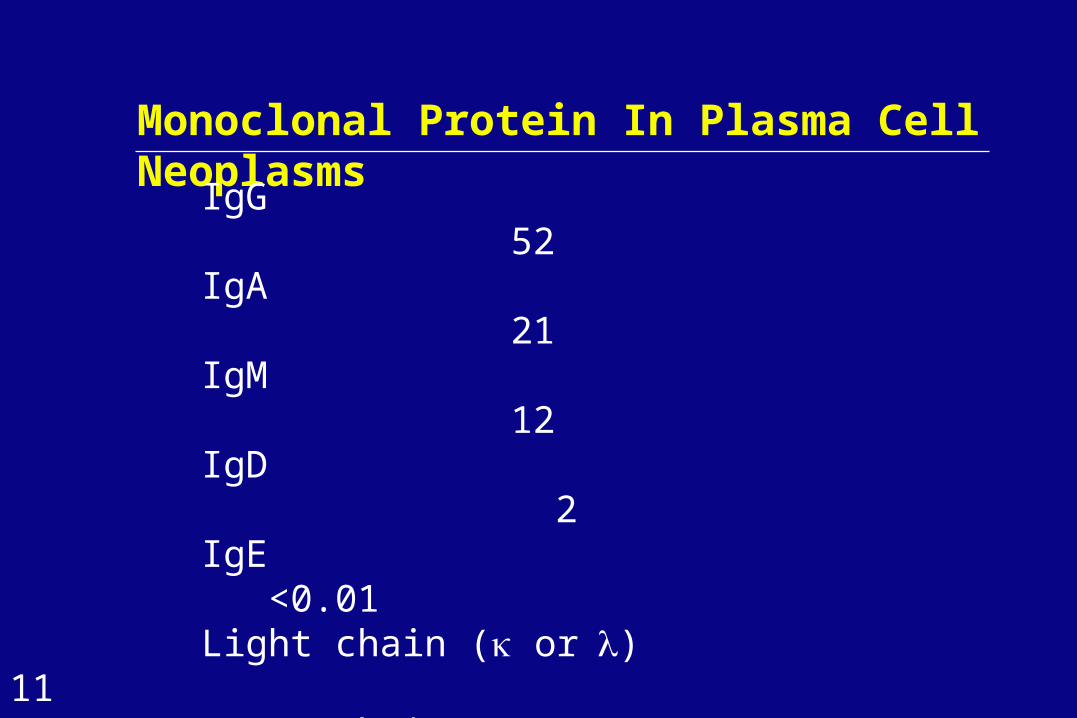
Monoclonal Protein In Plasma Cell Neoplasms
IgG 52
IgA 21
IgM 12
IgD 2
IgE <0.01Light chain ( or) 11Heavy chains (, or ) <1Two or more monoclonal proteins <1Nonsecretory myeloma 1

http://140.251.5.102/Pathology_Images/http://wheeless.orthoweb.be/o6/129.htm
Lytic Bone Lesions in Multiple Myeloma

Durie-Salmon Staging Systemfor Multiple Myeloma
Stage I Low myeloma cell mass
• Hemoglobin > 10 g/dL
• Normal bone, or solitary plasmacytoma
• Low immunoglobulin spike (M-component)– IgG < 5 g/dL, IgA < 3 g/dL– Bence-Jones protein < 4 g/24h
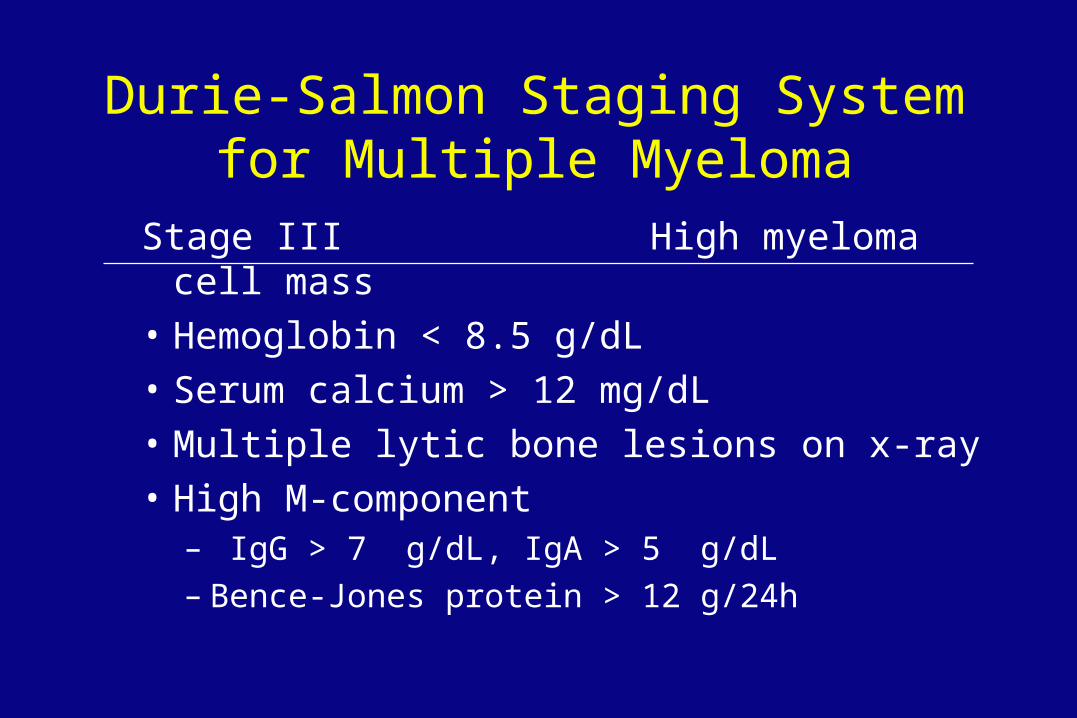
Durie-Salmon Staging Systemfor Multiple Myeloma
Stage III High myeloma cell mass
• Hemoglobin < 8.5 g/dL
• Serum calcium > 12 mg/dL
• Multiple lytic bone lesions on x-ray
• High M-component– IgG > 7 g/dL, IgA > 5 g/dL– Bence-Jones protein > 12 g/24h

Durie-Salmon Staging Systemfor Multiple Myeloma
Stage II Intermediate myeloma cell mass• In between Stages I and III
SubclassificationA: Normal renal function
- serum creatinine level < 2.0 mg/dLB: Abnormal renal function
- serum creatinine level 2.0 mg/dL

Treatment of Multiple Myeloma
Standard Chemotherapy• Melphalan and prednisone• VAD (vincristine, adriamycin, dexamethasone)
High Dose Chemotherapy• Bone marrow transplant• Peripheral stem cell transplant

Treatment of Multiple Myeloma
Other Modalities• Pulse dexamethasone• Interferon• Local radiotherapy to bony lesions• Pamidronate and other bisphosphonates• Thalidomide• Velcade (Bortezomib, PS-341)• Bendamustine


Prognostic Factors
Poor prognosis:
• Age > 65• High tumor mass• High 2 microglobulin• Renal failure, hypercalcemia

Conclusions:Lymphoma and Multiple Myeloma
• Malignancies of B cells.
• Sometimes preventable.
• Highly treatable and often curable.
• Study of these diseases have led to important advances in the understanding of the biology of lymphoid cells.
Related Documents











