ONLINE ONLY S50.e1 Measuring the airway in 3 dimensions: A reliability and accuracy study Hakan El a and Juan Martin Palomo b Ankara, Turkey, and Cleveland, Ohio Introduction: The aim of the study was to compare the reliability and accuracy of 3 commercially avail- able digital imaging and communications in medicine (DICOM) viewers for measuring upper airway volumes. Methods: Thirty cone-beam computed tomography scans were randomly selected, and the upper airway volumes were calculated for both oropharynx and nasal passage. Dolphin3D (version 11, Dolphin Imaging & Management Solutions, Chatsworth, Calif), InVivoDental (version 4.0.70, Anatomage, San Jose, Calif), and OnDemand3D (version 1.0.1.8407, CyberMed, Seoul, Korea) were compared with a previously tested manual segmentation program called OrthoSegment (OS) (developed at the Department of Orthodontics at Case Western Reserve University, Cleveland, Ohio). The measurements were repeated after 2 weeks, and the intraclass correlation coefficient was used for the reliability tests. All commercially available programs were compared with the OS program by using regression analysis. The Pearson correlation was used to evaluate the correlation between the OS and the automatic segmentation programs. Results: The reliability was high for all programs. The highest correlation found was between the OS and Dolphin3D for the oropharynx, and between the OS and InVivoDental for nasal passage volume. A high correlation was found for all programs, but the results also showed statistically significant differences compared with the OS program. The programs also had inconsistencies among themselves. Conclusions: The 3 commercially available DICOM viewers are highly reliable in their airway volume calculations and showed high correlation of results but poor accuracy, suggesting systematic errors. (Am J Orthod Dentofacial Orthop 2010;137:S50.e1-S50.e9) T he upper airway has long been an area of in- terest in orthodontics, with topics such as the relationships between facial type and airway, airway shape and volume with growth and develop- ment, and the clinician’s potential to modify the air- way. 1-9 However, most studies evaluating the airway have been conducted with 2-dimensional (2D) ceph- alograms, providing limited data such as linear and angular measurements, for a complex 3-dimensional (3D) structure. With the introduction of cone-beam computed tomography (CBCT), the 3D diagnosis of the pa- tient became more accessible in dentistry. CBCT has become a well-accepted oral and maxillofacial diag- nostic imaging technique in a short time, and this was mainly due to lower radiation exposure and shorter scan acquisition times necessary to obtain an accept- able image compared with conventional computed tomography scans. 10-12 CBCT technology allows the segmentation and visualization of hollow structures such as the airway in 3 dimensions. Thus, with 3D im- aging, we are moving from lengths and angles toward volumes and surface areas. 13-17 To visualize a CBCT scan, digital imaging and communications in medi- cine (DICOM) viewer software is necessary. DICOM is the accepted file format for a medical image, and a DICOM viewer allows viewing, measuring, segment- ing, and complete analysis of a CBCT scan. To segment and structure the airway means to de- lineate and remove all other surrounding structures for a clearer analysis and visualization. The segmen- tation of the airway can be done either manually or automatically. Manual segmentation requires the op- erator to delineate the airway slice by slice and then render all data into a 3D volume for analysis. 13,14 Au- tomatic segmentation can be done by differentiating structures with different density values. This means that, because the airway is radiolucent, the density values for the airway are lower than the values for the surrounding soft tissues, allowing easy and automatic a Clinical instructor, Department of Orthodontics, School of Dental Medicine, Hacettepe University, Ankara, Turkey. b Associate professor and program director, Department of Orthodontics, and Director of the Craniofacial Imaging Center, School of Dental Medicine, Case Western Reserve University, Cleveland, Ohio. Partially funded by The Scientific and Technological Research Council of Turkey (TUBITAK). The authors report no commercial, proprietary, or financial interest in the prod- ucts or companies described in this article. Reprint requests to: Juan Martin Palomo, Case Western Reserve University, School of Dental Medicine, 10900 Euclid Ave, Cleveland, OH 44106; e-mail, [email protected]. Submitted, August 2009; revised and accepted, November 2009. 0889-5406/$36.00 Copyright © 2010 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2009.11.010

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Online Only
S50.e1
Measuring the airway in 3 dimensions: A reliability and accuracy studyHakan Ela and Juan Martin Palomob Ankara, Turkey, and Cleveland, Ohio
Introduction: The aim of the study was to compare the reliability and accuracy of 3 commercially avail-able digital imaging and communications in medicine (DICOM) viewers for measuring upper airway volumes. Methods: Thirty cone-beam computed tomography scans were randomly selected, and the upper airway volumes were calculated for both oropharynx and nasal passage. Dolphin3D (version 11, Dolphin Imaging & Management Solutions, Chatsworth, Calif), InVivoDental (version 4.0.70, Anatomage, San Jose, Calif), and OnDemand3D (version 1.0.1.8407, CyberMed, Seoul, Korea) were compared with a previously tested manual segmentation program called OrthoSegment (OS) (developed at the Department of Orthodontics at Case Western Reserve University, Cleveland, Ohio). The measurements were repeated after 2 weeks, and the intraclass correlation coefficient was used for the reliability tests. All commercially available programs were compared with the OS program by using regression analysis. The Pearson correlation was used to evaluate the correlation between the OS and the automatic segmentation programs. Results: The reliability was high for all programs. The highest correlation found was between the OS and Dolphin3D for the oropharynx, and between the OS and InVivoDental for nasal passage volume. A high correlation was found for all programs, but the results also showed statistically significant differences compared with the OS program. The programs also had inconsistencies among themselves. Conclusions: The 3 commercially available DICOM viewers are highly reliable in their airway volume calculations and showed high correlation of results but poor accuracy, suggesting systematic errors. (Am J Orthod Dentofacial Orthop 2010;137:S50.e1-S50.e9)
The upper airway has long been an area of in-terest in orthodontics, with topics such as the relationships between facial type and airway,
airway shape and volume with growth and develop-ment, and the clinician’s potential to modify the air-way.1-9 However, most studies evaluating the airway have been conducted with 2-dimensional (2D) ceph-alograms, providing limited data such as linear and angular measurements, for a complex 3-dimensional (3D) structure.
With the introduction of cone-beam computed tomography (CBCT), the 3D diagnosis of the pa-tient became more accessible in dentistry. CBCT has
become a well-accepted oral and maxillofacial diag-nostic imaging technique in a short time, and this was mainly due to lower radiation exposure and shorter scan acquisition times necessary to obtain an accept-able image compared with conventional computed tomography scans.10-12 CBCT technology allows the segmentation and visualization of hollow structures such as the airway in 3 dimensions. Thus, with 3D im-aging, we are moving from lengths and angles toward volumes and surface areas.13-17 To visualize a CBCT scan, digital imaging and communications in medi-cine (DiCOM) viewer software is necessary. DiCOM is the accepted file format for a medical image, and a DiCOM viewer allows viewing, measuring, segment-ing, and complete analysis of a CBCT scan.
To segment and structure the airway means to de-lineate and remove all other surrounding structures for a clearer analysis and visualization. The segmen-tation of the airway can be done either manually or automatically. Manual segmentation requires the op-erator to delineate the airway slice by slice and then render all data into a 3D volume for analysis.13,14 Au-tomatic segmentation can be done by differentiating structures with different density values. This means that, because the airway is radiolucent, the density values for the airway are lower than the values for the surrounding soft tissues, allowing easy and automatic
aClinical instructor, Department of Orthodontics, School of Dental Medicine, Hacettepe University, Ankara, Turkey.bAssociate professor and program director, Department of Orthodontics, and Director of the Craniofacial imaging Center, School of Dental Medicine, Case Western Reserve University, Cleveland, Ohio.Partially funded by The Scientific and Technological Research Council of Turkey (TUBiTAK).The authors report no commercial, proprietary, or financial interest in the prod-ucts or companies described in this article.Reprint requests to: Juan Martin Palomo, Case Western Reserve University, School of Dental Medicine, 10900 euclid Ave, Cleveland, OH 44106; e-mail, [email protected], August 2009; revised and accepted, november 2009.0889-5406/$36.00Copyright © 2010 by the American Association of Orthodontists.doi:10.1016/j.ajodo.2009.11.010
S50_AAOPRG_3044.indd 1 3/24/10 9:25 AM
S50.e2 and Palomo American Journal of Orthodontics and Dentofacial OrthopedicsApril 2010
was not clear or fully contained in the image and im-ages containing artifacts were excluded. each patient signed a consent form allowing the use of orthodontic records for research purposes.
The study sample consisted of 30 randomly se-lected patients. All DiCOM files were loaded to a computer with a Xeon (intel, Santa Clara, Calif) pro-cessor, running Windows XP Professional (Microsoft, Redmond, Wash) operating system. For the commer-cially available DiCOM viewers, the programs tested were Dolphin3D (version 11, Dolphin imaging & Management Solutions, Chatsworth, Calif), inVivo-Dental (version 4.0.70, Anatomage, San Jose, Calif), and OnDemand3D (version 1.0.1.8407, CyberMed, Seoul, Korea). Dolphin3D (D3D), inVivoDental (iVD), OnDemand3D (OD3D), and a custom-written program with Visual C++ (Micro soft) for the Depart-ment of Orthodontics, School of Dental Medicine, at Case Western Reserve University called OrthoSeg-ment (OS) were used to render the nP and OP airway volumes separately.
Amirlak et al18 used the OS program to test the reliability and accuracy of CBCT images. They used a water displacement technique for comparing the CBCT volumes with actual volumes and found that the manually segmented volumes of the OS program were highly accurate. Based on their results, we used the values from the OS program as the gold standard to which the other results were compared.
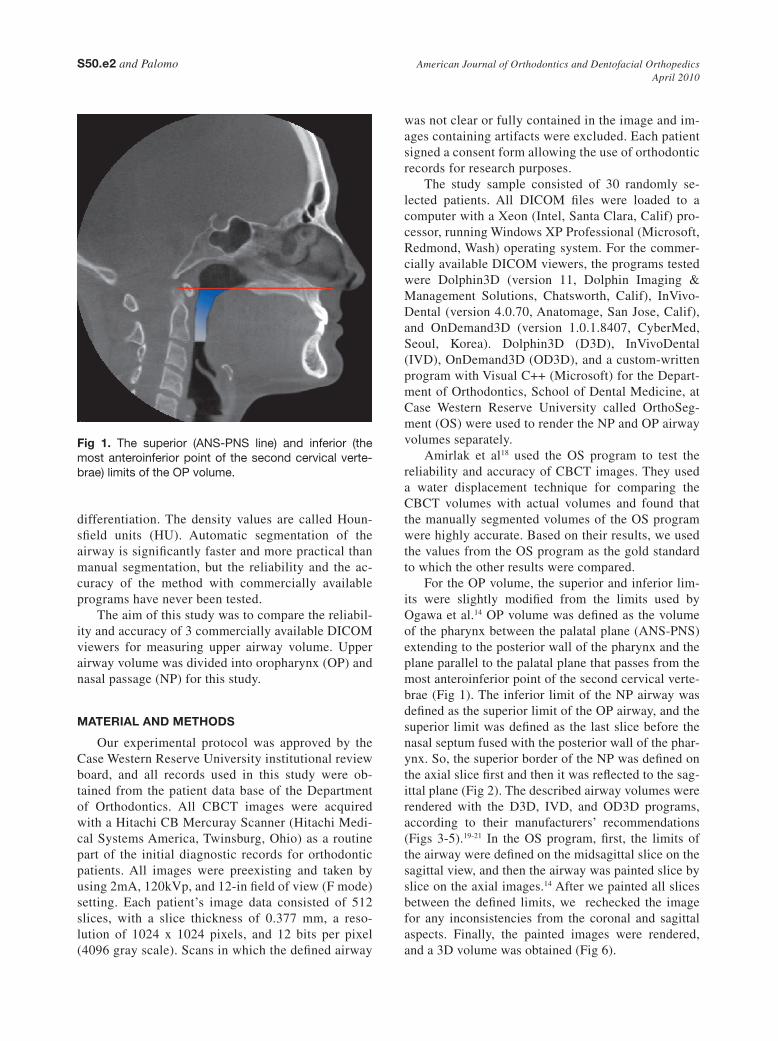
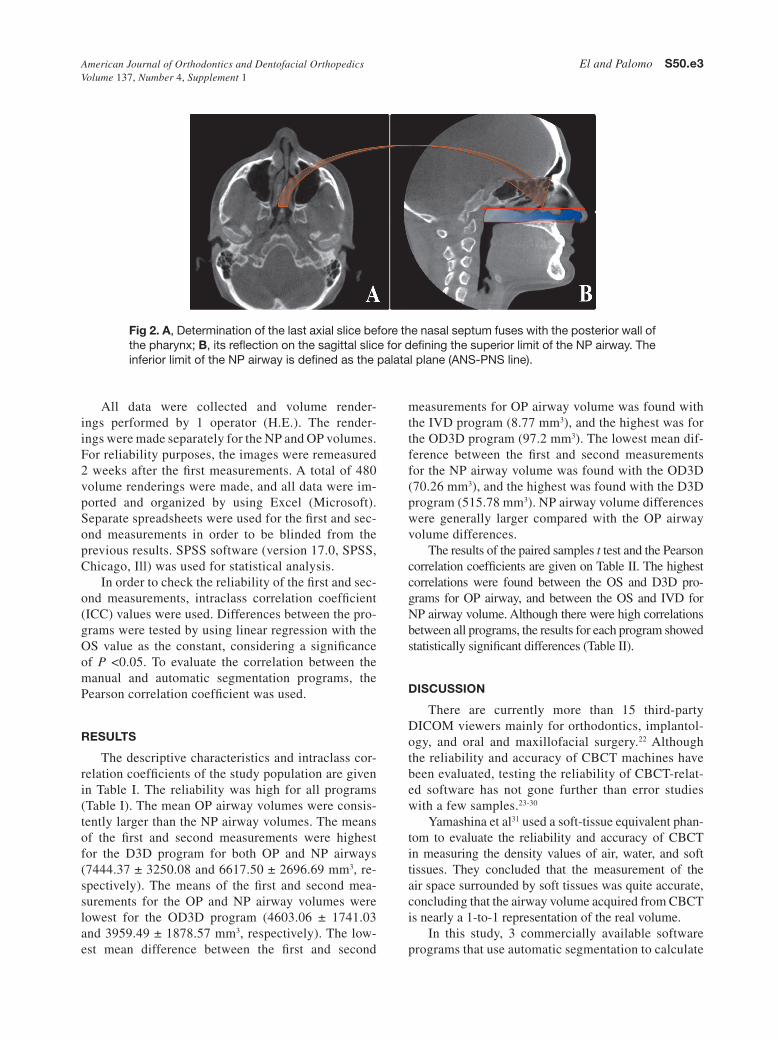
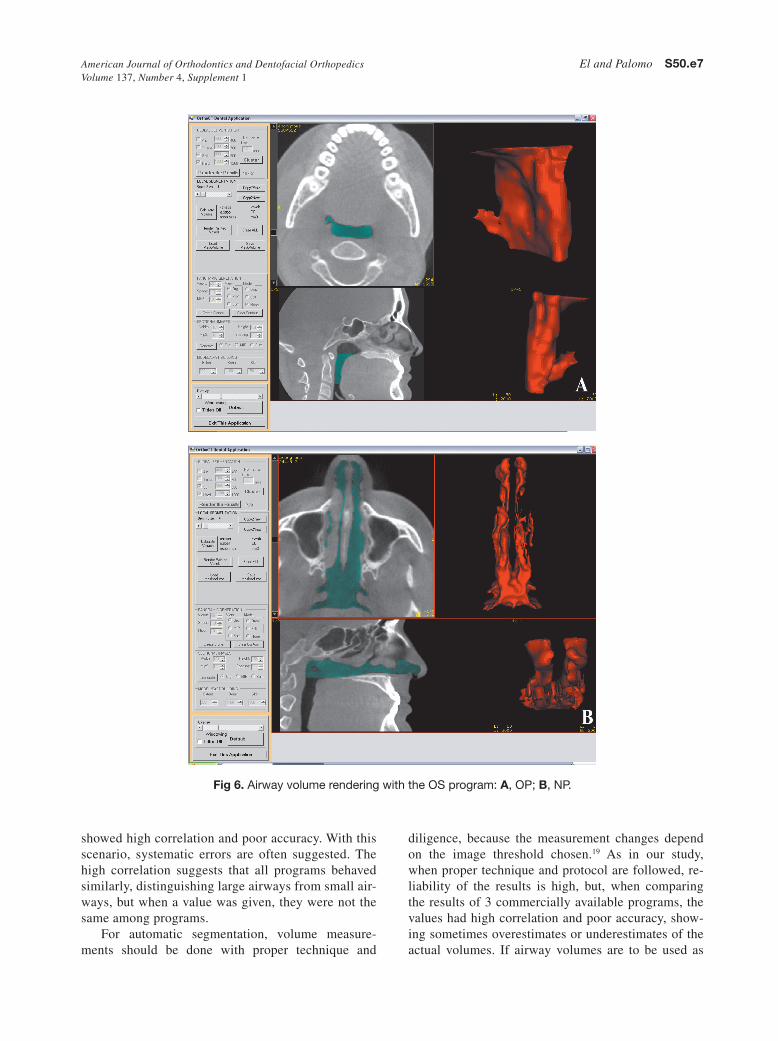
For the OP volume, the superior and inferior lim-its were slightly modified from the limits used by Ogawa et al.14 OP volume was defined as the volume of the pharynx between the palatal plane (AnS-PnS) extending to the posterior wall of the pharynx and the plane parallel to the palatal plane that passes from the most anteroinferior point of the second cervical verte-brae (Fig 1). The inferior limit of the nP airway was defined as the superior limit of the OP airway, and the superior limit was defined as the last slice before the nasal septum fused with the posterior wall of the phar-ynx. So, the superior border of the nP was defined on the axial slice first and then it was reflected to the sag-ittal plane (Fig 2). The described airway volumes were rendered with the D3D, iVD, and OD3D programs, according to their manufacturers’ recommendations (Figs 3-5).19-21 in the OS program, first, the limits of the airway were defined on the midsagittal slice on the sagittal view, and then the airway was painted slice by slice on the axial images.14 After we painted all slices between the defined limits, we rechecked the image for any inconsistencies from the coronal and sagittal aspects. Finally, the painted images were rendered, and a 3D volume was obtained (Fig 6).
differentiation. The density values are called Houn-sfield units (HU). Automatic segmentation of the airway is significantly faster and more practical than manual segmentation, but the reliability and the ac-curacy of the method with commercially available programs have never been tested.
The aim of this study was to compare the reliabil-ity and accuracy of 3 commercially available DiCOM viewers for measuring upper airway volume. Upper airway volume was divided into oropharynx (OP) and nasal passage (nP) for this study.
MatERIal and MEtHodS
Our experimental protocol was approved by the Case Western Reserve University institutional review board, and all records used in this study were ob-tained from the patient data base of the Department of Orthodontics. All CBCT images were acquired with a Hitachi CB Mercuray Scanner (Hitachi Medi-cal Systems America, Twinsburg, Ohio) as a routine part of the initial diagnostic records for orthodontic patients. All images were pre existing and taken by using 2mA, 120kVp, and 12-in field of view (F mode) setting. each patient’s image data consisted of 512 slices, with a slice thickness of 0.377 mm, a reso-lution of 1024 x 1024 pixels, and 12 bits per pixel (4096 gray scale). Scans in which the defined airway
Fig 1. The superior (ANS-PNS line) and inferior (the most anteroinferior point of the second cervical verte-brae) limits of the OP volume.
S50_AAOPRG_3044.indd 2 3/24/10 9:25 AM
American Journal of Orthodontics and Dentofacial Orthopedics El and Palomo S50.e3Volume 137, Number 4, Supplement 1
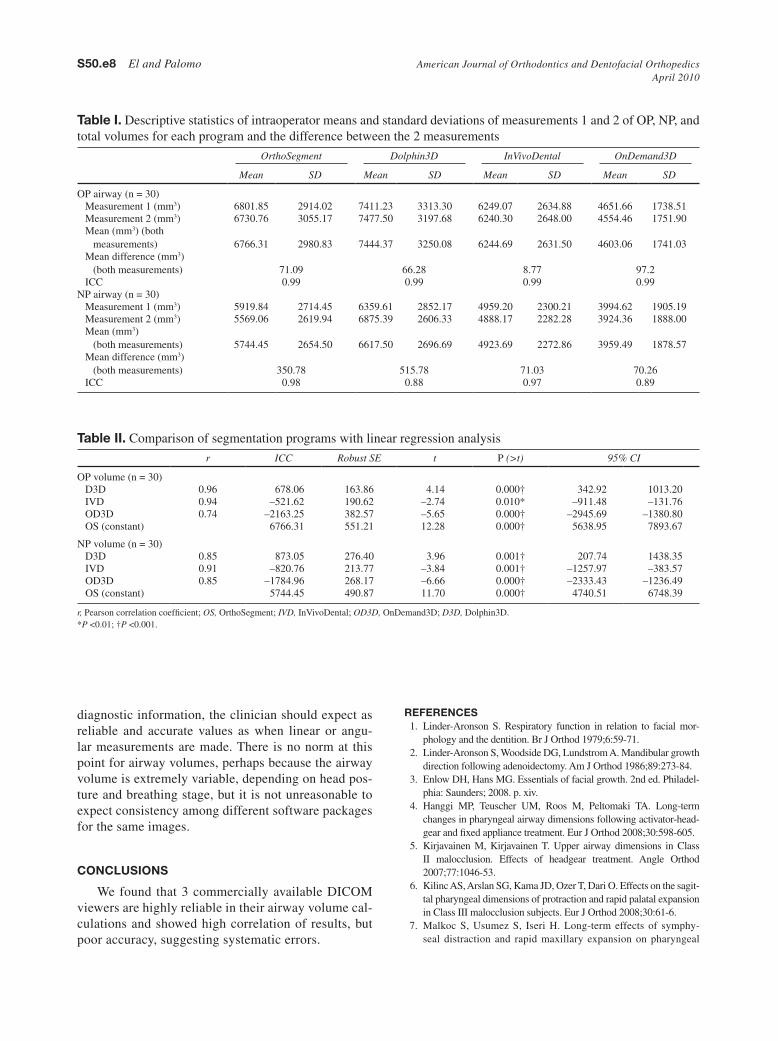
measurements for OP airway volume was found with the iVD program (8.77 mm3), and the highest was for the OD3D program (97.2 mm3). The lowest mean dif-ference between the first and second measurements for the nP airway volume was found with the OD3D (70.26 mm3), and the highest was found with the D3D program (515.78 mm3). nP airway volume differences were generally larger compared with the OP airway volume differences.
The results of the paired samples t test and the Pearson correlation coefficients are given on Table ii. The highest correlations were found between the OS and D3D pro-grams for OP airway, and between the OS and iVD for nP airway volume. Although there were high correlations between all programs, the results for each program showed statistically significant differences (Table ii).
dISCuSSIon
There are currently more than 15 third-party DiCOM viewers mainly for orthodontics, implantol-ogy, and oral and maxillofacial surgery.22 Although the reliability and accuracy of CBCT machines have been evaluated, testing the reliability of CBCT-relat-ed software has not gone further than error studies with a few samples.23-30
yamashina et al31 used a soft-tissue equivalent phan-tom to evaluate the reliability and accuracy of CBCT in measuring the density values of air, water, and soft tissues. They concluded that the measurement of the air space surrounded by soft tissues was quite accurate, concluding that the airway volume acquired from CBCT is nearly a 1-to-1 representation of the real volume.
in this study, 3 commercially available software programs that use automatic segmentation to calculate
All data were collected and volume render-ings performed by 1 operator (H.e.). The render-ings were made separately for the nP and OP volumes. For reliability purposes, the images were remeasured 2 weeks after the first measurements. A total of 480 volume renderings were made, and all data were im-ported and organized by using excel (Microsoft). Separate spreadsheets were used for the first and sec-ond measurements in order to be blinded from the previous results. SPSS software (version 17.0, SPSS, Chicago, ill) was used for statistical analysis.
in order to check the reliability of the first and sec-ond measurements, intraclass correlation coefficient (iCC) values were used. Differences between the pro-grams were tested by using linear regression with the OS value as the constant, considering a significance of P <0.05. To evaluate the correlation between the manual and automatic segmentation programs, the Pearson correlation coefficient was used.
RESultS
The descriptive characteristics and intraclass cor-relation coefficients of the study population are given in Table i. The reliability was high for all programs (Table i). The mean OP airway volumes were consis-tently larger than the nP airway volumes. The means of the first and second measurements were highest for the D3D program for both OP and nP airways (7444.37 ± 3250.08 and 6617.50 ± 2696.69 mm3, re-spectively). The means of the first and second mea-surements for the OP and nP airway volumes were lowest for the OD3D program (4603.06 ± 1741.03 and 3959.49 ± 1878.57 mm3, respectively). The low-est mean difference between the first and second
Fig 2. a, Determination of the last axial slice before the nasal septum fuses with the posterior wall of the pharynx; B, its reflection on the sagittal slice for defining the superior limit of the NP airway. The inferior limit of the NP airway is defined as the palatal plane (ANS-PNS line).
S50_AAOPRG_3044.indd 3 3/24/10 9:25 AM
S50.e4 El and Palomo American Journal of Orthodontics and Dentofacial OrthopedicsApril 2010
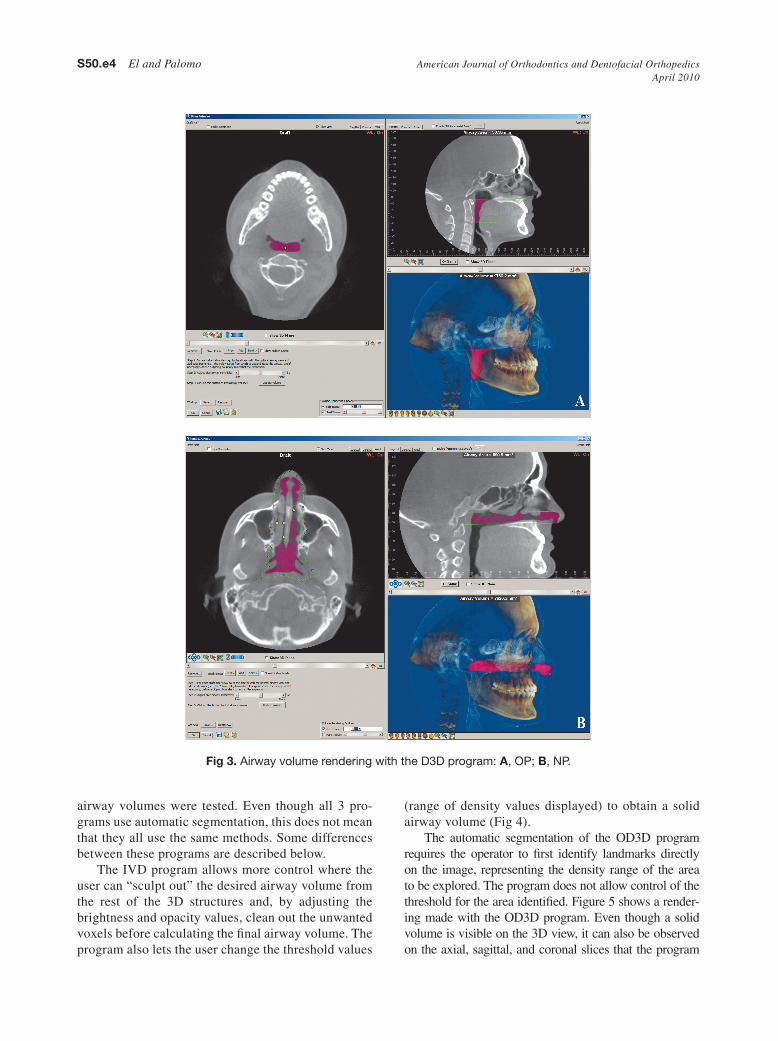
Fig 3. Airway volume rendering with the D3D program: a, OP; B, NP.
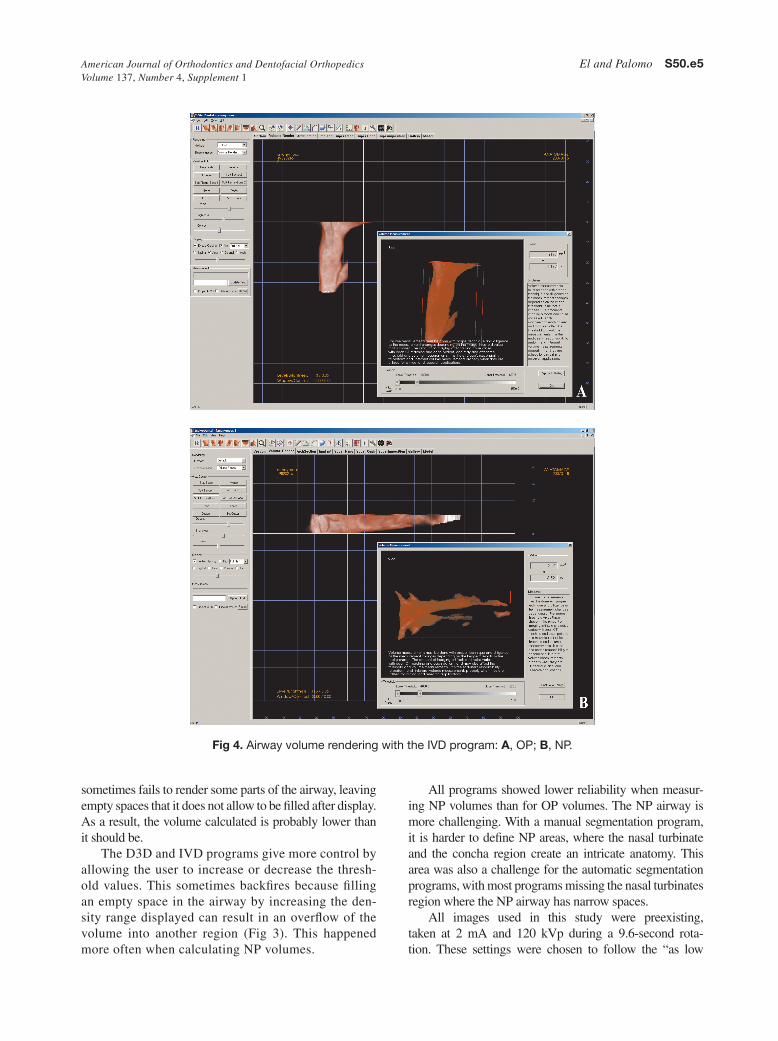
(range of density values displayed) to obtain a solid airway volume (Fig 4).
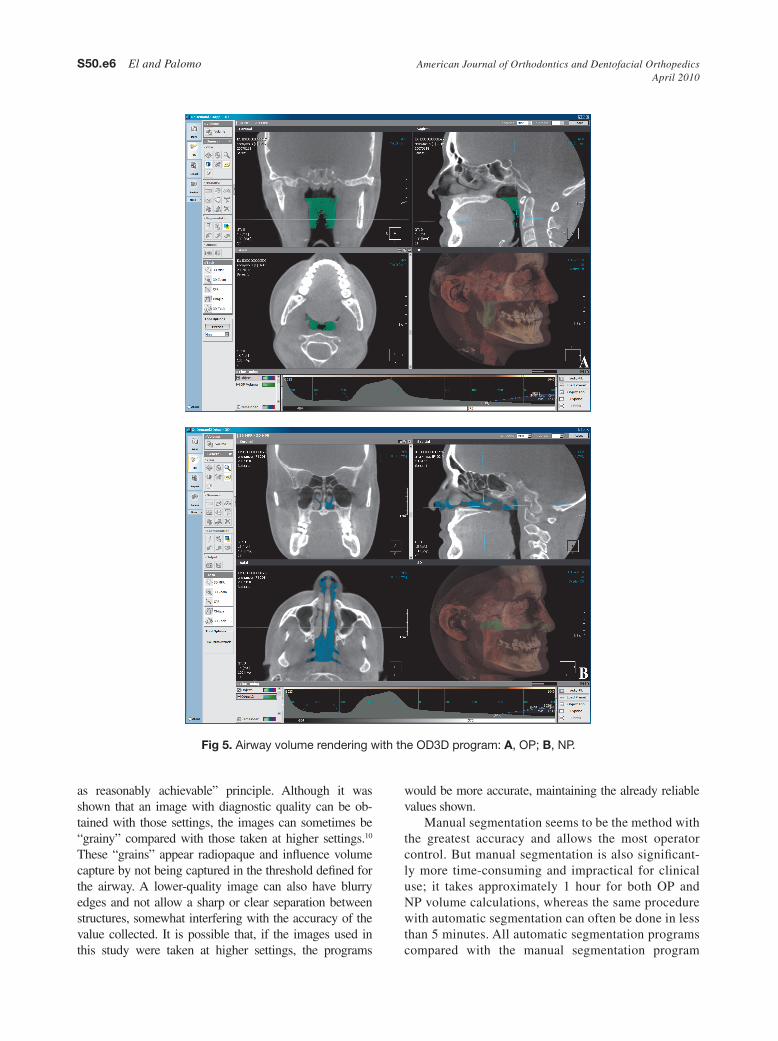
The automatic segmentation of the OD3D program requires the operator to first identify landmarks directly on the image, representing the density range of the area to be explored. The program does not allow control of the threshold for the area identified. Figure 5 shows a render-ing made with the OD3D program. even though a solid volume is visible on the 3D view, it can also be observed on the axial, sagittal, and coronal slices that the program
airway volumes were tested. even though all 3 pro-grams use automatic segmentation, this does not mean that they all use the same methods. Some differences between these programs are described below.
The iVD program allows more control where the user can “sculpt out” the desired airway volume from the rest of the 3D structures and, by adjusting the brightness and opacity values, clean out the unwanted voxels before calculating the final airway volume. The program also lets the user change the threshold values
S50_AAOPRG_3044.indd 4 3/24/10 9:25 AM
American Journal of Orthodontics and Dentofacial Orthopedics El and Palomo S50.e5Volume 137, Number 4, Supplement 1
Fig 4. Airway volume rendering with the IVD program: a, OP; B, NP.
All programs showed lower reliability when measur-ing nP volumes than for OP volumes. The nP airway is more challenging. With a manual segmentation program, it is harder to define nP areas, where the nasal turbinate and the concha region create an intricate anatomy. This area was also a challenge for the automatic segmentation programs, with most programs missing the nasal turbinates region where the nP airway has narrow spaces.
All images used in this study were preexisting, taken at 2 mA and 120 kVp during a 9.6-second rota-tion. These settings were chosen to follow the “as low
sometimes fails to render some parts of the airway, leaving empty spaces that it does not allow to be filled after display. As a result, the volume calculated is probably lower than it should be.
The D3D and iVD programs give more control by allowing the user to increase or decrease the thresh-old values. This sometimes backfires because filling an empty space in the airway by increasing the den-sity range displayed can result in an overflow of the volume into another region (Fig 3). This happened more often when calculating nP volumes.
S50_AAOPRG_3044.indd 5 3/24/10 9:25 AM
S50.e6 El and Palomo American Journal of Orthodontics and Dentofacial OrthopedicsApril 2010
Fig 5. Airway volume rendering with the OD3D program: a, OP; B, NP.
would be more accurate, maintaining the already reliable values shown.
Manual segmentation seems to be the method with the greatest accuracy and allows the most operator control. But manual segmentation is also significant-ly more time-consuming and impractical for clinical use; it takes approximately 1 hour for both OP and nP volume calculations, whereas the same procedure with automatic segmentation can often be done in less than 5 minutes. All automatic segmentation programs compared with the manual segmentation program
as reasonably achievable” principle. Although it was shown that an image with diagnostic quality can be ob-tained with those settings, the images can sometimes be “grainy” compared with those taken at higher settings.10 These “grains” appear radiopaque and influence volume capture by not being captured in the threshold defined for the airway. A lower-quality image can also have blurry edges and not allow a sharp or clear separation between structures, somewhat interfering with the accuracy of the value collected. it is possible that, if the images used in this study were taken at higher settings, the programs
S50_AAOPRG_3044.indd 6 3/24/10 9:25 AM
American Journal of Orthodontics and Dentofacial Orthopedics El and Palomo S50.e7Volume 137, Number 4, Supplement 1
diligence, because the measurement changes depend on the image threshold chosen.19 As in our study, when proper technique and protocol are followed, re-liability of the results is high, but, when comparing the results of 3 commercially available programs, the values had high correlation and poor accuracy, show-ing sometimes overestimates or underestimates of the actual volumes. if airway volumes are to be used as
showed high correlation and poor accuracy. With this scenario, systematic errors are often suggested. The high correlation suggests that all programs behaved similarly, distinguishing large airways from small air-ways, but when a value was given, they were not the same among programs.
For automatic segmentation, volume measure-ments should be done with proper technique and
Fig 6. Airway volume rendering with the OS program: a, OP; B, NP.
S50_AAOPRG_3044.indd 7 3/24/10 9:25 AM
S50.e8 El and Palomo American Journal of Orthodontics and Dentofacial OrthopedicsApril 2010
diagnostic information, the clinician should expect as reliable and accurate values as when linear or angu-lar measurements are made. There is no norm at this point for airway volumes, perhaps because the airway volume is extremely variable, depending on head pos-ture and breathing stage, but it is not unreasonable to expect consistency among different software packages for the same images.
ConCluSIonS
We found that 3 commercially available DiCOM viewers are highly reliable in their airway volume cal-culations and showed high correlation of results, but poor accuracy, suggesting systematic errors.
REFEREnCES 1. linder-Aronson S. Respiratory function in relation to facial mor-
phology and the dentition. Br J Orthod 1979;6:59-71. 2. linder-Aronson S, Woodside DG, lundstrom A. Mandibular growth
direction following adenoidectomy. Am J Orthod 1986;89:273-84. 3. enlow DH, Hans MG. essentials of facial growth. 2nd ed. Philadel-
phia: Saunders; 2008. p. xiv. 4. Hanggi MP, Teuscher UM, Roos M, Peltomaki TA. long-term
changes in pharyngeal airway dimensions following activator-head-gear and fixed appliance treatment. eur J Orthod 2008;30:598-605.
5. Kirjavainen M, Kirjavainen T. Upper airway dimensions in Class ii malocclusion. effects of headgear treatment. Angle Orthod 2007;77:1046-53.
6. Kilinc AS, Arslan SG, Kama JD, Ozer T, Dari O. effects on the sagit-tal pharyngeal dimensions of protraction and rapid palatal expansion in Class iii malocclusion subjects. eur J Orthod 2008;30:61-6.
7. Malkoc S, Usumez S, iseri H. long-term effects of symphy-seal distraction and rapid maxillary expansion on pharyngeal
table II. Comparison of segmentation programs with linear regression analysis
r ICC Robust SE t P (>t) 95% CI
OP volume (n = 30)D3D 0.96 678.06 163.86 4.14 0.000† 342.92 1013.20iVD 0.94 –521.62 190.62 –2.74 0.010* –911.48 –131.76OD3D 0.74 –2163.25 382.57 –5.65 0.000† –2945.69 –1380.80OS (constant) 6766.31 551.21 12.28 0.000† 5638.95 7893.67
nP volume (n = 30)D3D 0.85 873.05 276.40 3.96 0.001† 207.74 1438.35iVD 0.91 –820.76 213.77 –3.84 0.001† –1257.97 –383.57OD3D 0.85 –1784.96 268.17 –6.66 0.000† –2333.43 –1236.49OS (constant) 5744.45 490.87 11.70 0.000† 4740.51 6748.39
r, Pearson correlation coefficient; OS, OrthoSegment; IVD, inVivoDental; OD3D, OnDemand3D; D3D, Dolphin3D.*P <0.01; †P <0.001.
table I. Descriptive statistics of intraoperator means and standard deviations of measurements 1 and 2 of OP, nP, and total volumes for each program and the difference between the 2 measurements
OrthoSegment Dolphin3D InVivoDental OnDemand3D
Mean SD Mean SD Mean SD Mean SD
OP airway (n = 30)Measurement 1 (mm3) 6801.85 2914.02 7411.23 3313.30 6249.07 2634.88 4651.66 1738.51Measurement 2 (mm3) 6730.76 3055.17 7477.50 3197.68 6240.30 2648.00 4554.46 1751.90Mean (mm3) (both
measurements) 6766.31 2980.83 7444.37 3250.08 6244.69 2631.50 4603.06 1741.03Mean difference (mm3)
(both measurements) 71.09 66.28 8.77 97.2iCC 0.99 0.99 0.99 0.99
nP airway (n = 30)Measurement 1 (mm3) 5919.84 2714.45 6359.61 2852.17 4959.20 2300.21 3994.62 1905.19Measurement 2 (mm3) 5569.06 2619.94 6875.39 2606.33 4888.17 2282.28 3924.36 1888.00Mean (mm3)
(both measurements) 5744.45 2654.50 6617.50 2696.69 4923.69 2272.86 3959.49 1878.57Mean difference (mm3)
(both measurements) 350.78 515.78 71.03 70.26iCC 0.98 0.88 0.97 0.89
S50_AAOPRG_3044.indd 8 3/24/10 9:25 AM

American Journal of Orthodontics and Dentofacial Orthopedics El and Palomo S50.e9Volume 137, Number 4, Supplement 1
airway dimensions, tongue, and hyoid position. Am J Orthod Dentofacial Orthop 2007;132:769-75.
8. Marsan G, Vasfi Kuvat S, Oztas e, Cura n, Susal Z, emekli U. Oropharyngeal airway changes following bimaxillary surgery in Class iii female adults. J Craniomaxillofac Surg 2009;37:69-73.
9. Conley RS, legan Hl. Correction of severe obstructive sleep apnea with bimaxillary transverse distraction osteogenesis and maxillomandibular advancement. Am J Orthod Dentofacial Or-thop 2006;129:283-92.
10. Palomo JM, Rao PS, Hans MG. influence of CBCT exposure conditions on radiation dose. Oral Surg Oral Med Oral Pathol Oral Radiol endod 2008;105:773-82.
11. Mah JK, Danforth RA, Bumann A, Hatcher D. Radiation ab-sorbed in maxillofacial imaging with a new dental computed to-mography device. Oral Surg Oral Med Oral Pathol Oral Radiol endod 2003;96:508-13.
12. ludlow JB, Davies-ludlow le, Brooks Sl, Howerton WB. Do-simetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercuray, newTom 3G and i-CAT. Dentomaxillofac Radiol 2006;35:219-26.
13. Peters-Schuster BR, Hans MG, Strohl KP, Palomo JM. A 3D airway assessment of 12-13 year old subjects [thesis]. Cleve-land, Ohio: Case Western Reserve University; 2009.
14. Ogawa T, enciso R, Shintaku WH, Clark GT. evaluation of cross-section airway configuration of obstructive sleep ap-nea. Oral Surg Oral Med Oral Pathol Oral Radiol endod 2007;103:102-8.
15. Osorio F, Perilla M, Doyle DJ, Palomo JM. Cone beam com-puted tomography: an innovative tool for airway assessment. Anesth Analg 2008;106:1803-7.
16. Shigeta y, Ogawa T, Venturin J, nguyen M, Clark GT, enciso R. Gender- and age-based differences in computerized tomo-graphic measurements of the oropharynx. Oral Surg Oral Med Oral Pathol Oral Radiol endod 2008;106:563-70.
17. Alves PV, Zhao l, O’Gara M, Patel PK, Bolognese AM. Three-dimensional cephalometric study of upper airway space in skeletal Class ii and iii healthy patients. J Craniofac Surg 2008;19:1497-507.
18. Amirlak B, Tang C, Hans MG, Gosain AK, Palomo JM. Vol-ume calculation of alveolar cleft defects and bone grafts using CBCT: an experimental study [dissertation]. Cleveland, Ohio: Case Western Reserve University; 2008.
19. inVivoDental 4.0 reference manual. San Jose, Calif: Anatom-age; 2006.
20. OnDemand3D video tutorial index; 2006. Available at: http://demo.ondemand3d.com/video/3D_Segmentation_Airway/3D_Segmenta-tion_Airway.htm. Accessed April 15, 2009.
21. Dolphin3D user’s manual. Chatsworth, Calif: Dolphin imag-ing & Management Solutions; 2006.
22. The 3D orthodontist (updated in 2009). Available at: http://3dorthodontist.com/3D_Software.html. Accessed April 15, 2009.
23. Ballrick JW, Palomo JM, Ruch e, Amberman BD, Hans MG. image distortion and spatial resolution of a commercially available cone-beam computed tomography machine. Am J Orthod Dentofacial Orthop 2008;134:573-82.
24. Brown AA, Scarfe WC, Scheetz JP, Silveira AM, Farman AG. linear accuracy of cone beam CT derived 3D images. Angle Orthod 2009;79:150-7.
25. eggers G, Klein J, Welzel T, Muhling J. Geometric accuracy of digital volume tomography and conventional computed to-mography. Br J Oral Maxillofac Surg 2008;46:639-44.
26. lagravère MO, Carey J, Toogood RW, Major PW. Three-di-mensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Den-tofacial Orthop 2008;134:112-6.
27. ludlow JB, laster WS, See M, Bailey lJ, Hershey HG. Ac-curacy of measurements of mandibular anatomy in cone beam computed tomography images. Oral Surg Oral Med Oral Pathol Oral Radiol endod 2007;103:534-42.
28. Periago DR, Scarfe WC, Moshiri M, Scheetz JP, Silveira AM, Farman AG. linear accuracy and reliability of cone beam CT derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod 2008;78:387-95.
29. Pinsky HM, Dyda S, Pinsky RW, Misch KA, Sarment DP. Ac-curacy of three-dimensional measurements using cone-beam CT. Dentomaxillofac Radiol 2006;35:410-6.
30. Stratemann SA, Huang JC, Maki K, Miller AJ, Hatcher DC. Comparison of cone beam computed tomography imaging with physical measures. Dentomaxillofac Radiol 2008;37:80-93.
31. yamashina A, Tanimoto K, Sutthiprapaporn P, Hayakawa y. The reliability of computed tomography (CT) values and di-mensional measurements of the oropharyngeal region using cone beam CT: comparison with multidetector CT. Dentomax-illofac Radiol 2008;37:245-51.
S50_AAOPRG_3044.indd 9 3/24/10 9:25 AM
Related Documents



![Open Bite Sem [Recovered] / orthodontic courses by Indian dental academy](https://static.cupdf.com/doc/110x72/577cca0c1a28aba711a53b45/open-bite-sem-recovered-orthodontic-courses-by-indian-dental-academy.jpg)