Lymphadenopathy Author: Vikramjit S Kanwar, MD, MBA, MRCP(UK), FAAP, Associate Professor of Pediatric Hematology and Oncology, Department of Pediatrics, Albany Medical Center; Faculty, Alden March Bioethics Institute Coauthor(s): Richard H Sills, MD, Professor of Pediatrics, Upstate Medical University Contributor Information and Disclosures Updated: Mar 4, 2010 Lymphadenopathy is a swelling, or enlargement, of the lymph nodes. Swollen lymph nodes may be brought on by a variety of reasons. Some occur due to local infections, while others can appear due to systemic conditions or diseases. A similar term is lymphadenitis, which refers to inflammation of the nodes. There is often nothing distinguishing the way the two terms are used. Causes Lymphadenopathy causes are numerous. A doctor should determine whether the swollen lymph nodes have anything to do with a particular condition. Remember that what you find on this page is not an exhaustive list, and it is possible that enlarged nodes could be caused by another condition. Some of the many potential causes include: Cat scratch disease Hairy cell leukemia HIV/AIDS Hodgkin lymphoma Human African trypanosomiasis Infectious mononucleosis Neuroblastoma Non-Hodgkin lymphoma Parasitic disease Systemic lupus erythematosus (SLE) Toxoplasmosis Tuberculous lymphadenitis Tumors and their metastasis Virchow's node More causes information. Classifications 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Lymphadenopathy
Author: Vikramjit S Kanwar, MD, MBA, MRCP(UK), FAAP, Associate Professor of Pediatric Hematology and Oncology, Department of Pediatrics, Albany Medical Center; Faculty, Alden March Bioethics InstituteCoauthor(s): Richard H Sills, MD, Professor of Pediatrics, Upstate Medical UniversityContributor Information and Disclosures
Updated: Mar 4, 2010
Lymphadenopathy is a swelling, or enlargement, of the lymph nodes. Swollen lymph nodes may be brought on by a variety of reasons. Some occur due to local infections, while others can appear due to systemic conditions or diseases. A similar term is lymphadenitis, which refers to inflammation of the nodes. There is often nothing distinguishing the way the two terms are used.
Causes
Lymphadenopathy causes are numerous. A doctor should determine whether the swollen lymph nodes have anything to do with a particular condition. Remember that what you find on this page is not an exhaustive list, and it is possible that enlarged nodes could be caused by another condition. Some of the many potential causes include:
Cat scratch diseaseHairy cell leukemiaHIV/AIDSHodgkin lymphomaHuman African trypanosomiasisInfectious mononucleosisNeuroblastomaNon-Hodgkin lymphomaParasitic diseaseSystemic lupus erythematosus (SLE)ToxoplasmosisTuberculous lymphadenitisTumors and their metastasisVirchow's node
More causes information.
Classifications
Lymphadenopathy can be localized, generalized, or dermatopathic. The first type refers to enlargement that occurs in a particular spot. The second means a type that happens at various places throughout the body. The third form describes this condition when it is associated with a case of skin disease.
Symptoms
Lymphadenopathy symptoms vary depending upon the case, patient, underlying cause, and other circumstances. Some potential symptoms may include:
Enlarged lymph nodesFeverTender nodes
1

Warmth or redness over nodes
More symptoms information.
Diagnosis
Lymphadenopathy diagnosis is to be made by a doctor or medical professional. The presence of a possible underlying cause, like particular infections, may assist in diagnosing the case. Physical examinations and medical history may also be used. A lymph node biopsy is one possible diagnostic tool. Additional tests may be taken in order to discover whether any particular diseases or infections are present. Details such as the size, location, length of time of the swelling, and whether there is pain may also be beneficial when attempting to determine the cause.
Treatment
Lymphadenopathy treatment varies based upon the case, underlying cause, the individual patient, and other factors. Possible treatment methods may include:
Antibiotics (bacterial infections)MedicationsFurther evaluationSymptomatic treatment
http://www.lymphadenopathy.net/
2

Introduction
Background
Lymph nodes, in conjunction with the spleen, tonsils, adenoids, and Peyer patches, are highly organized centers of immune cells that filter antigen from the extracellular fluid. Directly interior to the fibrous capsule is the subcapsular sinus. This allows lymph, an ultrafiltrate of blood, to traverse from the afferent lymph vessels, through the sinuses, and out the efferent vessels. The sinuses are studded with macrophages, which remove 99% of all delivered antigens.
Interior to the subcapsular sinus is the cortex, which contains primary follicles, secondary follicles, and the interfollicular zone. Follicles within the cortex are major sites of B-cell proliferation, whereas the interfollicular zone is the site of antigen-dependent T-cell differentiation and proliferation. The deepest structure within the lymph node is the medulla, consisting of cords of plasma cells and small B lymphocytes that facilitate immunoglobulin secretion into the exiting lymph.
The lymph node, with its high concentration of lymphocytes and antigen-presenting cells, is an ideal organ for receiving antigens that gain access through the skin or gastrointestinal tract. Nodes have considerable capacity for growth and change. Lymph node size depends on the person's age, the location of the lymph node in the body, and antecedent immunological events. In neonates, lymph nodes are barely perceptible, but a progressive increase in total lymph node mass is observed until later childhood. Lymph node atrophy begins during adolescence and continues through later life.
Pathophysiology
Most lymphadenopathy in children is due to benign self-limited disease such as viral infections, and adenopathy is secondary to an increase in normal lymphocytes and macrophages in response to an antigen. Other less common mechanisms responsible for adenopathy include nodal accumulation of inflammatory cells in response to an infection in the node (lymphadenitis), neoplastic lymphocytes or macrophages (lymphoma), or metabolite-laden macrophages in storage diseases (Gaucher disease).
Frequency
United States
The precise incidence of lymphadenopathy is not known, but estimates of palpable adenopathy in childhood vary from 38-45%,1 and lymphadenopathy is one of the most common clinical problems encountered in pediatrics.2
Determining whether adenopathy is simply a normal response to frequent viral infections within an age group or if it is significant enough to consider more serious underlying disease is often difficult.
In the United States, common viral and bacterial infections are overwhelmingly the most common cause of adenopathy. Infectious mononucleosis and cytomegalovirus (CMV) are important etiologies, but adenopathy is usually caused by common viral upper respiratory tract infections. Localized lymphadenitis is most often caused by staphylococci and beta-hemolytic streptococci.
Other infections, such as human immunodeficiency virus (HIV), malignancies, and autoimmune diseases, are less common causes of adenopathy.
International
3

Infections that are rarely observed in the United States, such as tuberculosis, typhoid fever, leishmaniasis, trypanosomiasis, schistosomiasis, filariasis, and fungal infections, are common causes of lymphadenopathy in developing nations.3 HIV infections must be strongly considered in areas of high incidence.
Mortality/Morbidity
In the United States, mortality and serious morbidity caused by adenopathy are unusual given the common infectious etiologies.
Malignancies, such as leukemia, lymphomas, and neuroblastoma, are the primary causes of mortality in the United States.4
Significant morbidity and mortality are also associated with autoimmune disorders (eg, juvenile rheumatoid arthritis, systemic lupus erythematosus), histiocytoses, and storage diseases.
HIV is an uncommon cause of adenopathy in the United States, but its associated mortality requires consideration.
Race
Race is not a factor in most lymphadenopathy. Rare causes may be associated with particular ethnic groups (eg, sarcoidosis in Africans, Kikuchi-Fujimori disease in Asians).
Sex
Sex does not influence childhood lymphadenopathy.
Age
Adenopathy is most common in young children whose immune systems are responding to newly encountered infections. Adenopathy may be seen in one third of neonates and infants, usually in nodes that drain areas with mild skin irritation. Generalized adenopathy is rare in the neonate and suggests congenital infections, such as CMV. Adenopathy related to malignancy is rare at all ages. If diagnosed, it is often secondary to leukemia or neuroblastoma in younger children, and to Hodgkin lymphoma in adolescents.5
Clinical
History
The differential diagnosis of lymphadenopathy is broad. A patient's medical history and review of systems is important in narrowing this differential. Upon examination, recognizing the pattern of lymph drainage aids in seeking an infectious focus.6
Although the underlying etiology is often self-limited infection, more serious underlying etiologies must be quickly recognized. Serious infections and malignancies are important considerations, as discussed in Outline - Etiologies of Lymphadenopathy.
In adolescents, screening for intravenous drug use and sexual activity is important.
Physical
Assess the size, location, and character of the adenopathy, along with any associated physical findings. Erythema, tenderness, warmth, and fluctuance suggests lymphadenitis, and nodes that are matted together, firm, and nontender suggest malignancy, although this distinction is not invariable.
4

Recognize that most children have palpable lymph nodes in the anterior cervical, inguinal, and axillary regions that, if evaluated by adult standards, would qualify as lymphadenopathy. Lymphoid mass steadily increases after birth until age 8-12 years, and undergoes progressive atrophy during puberty.7
In young children, anterior cervical lymph nodes as large as 2 cm, axillary nodes as large as 1 cm, and inguinal nodes as large as 1.5 cm in diameter are normal, and further evaluation is usually not indicated. In a series of 457 children, malignancy was usually associated with nodes larger than 3 cm in diameter.8
However, the presence of even shotty (<0.5 cm) supraclavicular or epitrochlear adenopathy may be associated with malignancy and warrants further evaluation. Newborns usually have small adenopathy (<0.5 cm), and larger nodes not associated with a focus of inflammation are an indication for further evaluation.
Seek a focus of infection or inflammation in the territory drained by the lymph nodes. For example, the classic manifestation of group A streptococcal pharyngitis is sore throat, fever, and anterior cervical lymphadenopathy (tonsillar node). When examining the oropharynx, pay special attention to the dentition. Similarly, impetigo of the buttock area is associated with inguinal adenopathy. Scalp lesions, such as seborrheic dermatitis (cradle cap), can cause newborn occipital adenopathy.
Consider the possibility that palpable "lymph nodes" may in fact be other masses; for example, branchial cysts and other benign tumors can mimic cervical adenopathy.9
A careful history and physical examination, with a consideration of the factors listed above, help determine whether an enlarged lymph node merits further investigation.
Causes
Generalized lymphadenopathy is defined as enlargement of more than 2 noncontiguous lymph node groups. A thorough history and physical examination are critical in establishing a diagnosis. Causes of generalized lymphadenopathy include infections, autoimmune diseases, malignancies, histiocytoses, storage diseases, benign hyperplasia, and drug reactions.
Infectionso Generalized lymphadenopathy is most often associated with systemic viral infections.o Infectious mononucleosis results in widespread adenopathy.o Roseola infantum (caused by human herpes virus 6), cytomegalovirus (CMV), varicella, and
adenovirus all cause generalized lymphadenopathy.o Human immunodeficiency virus (HIV) is often associated with generalized adenopathy, which
may be the presenting sign. Children with HIV are at increased risk for tuberculosis, as well.10
o Although usually associated with localized node enlargement, some bacterial infections present with generalized adenopathy. Examples include typhoid fever caused by Salmonella typhi, syphilis, plague, and tuberculosis. Less common bacteremias, including those caused by endocarditis, result in generalized lymphadenopathies.
Malignant etiologieso Concern about malignant etiologies often drives further diagnostic testing in children with
adenopathy. Malignancy is often associated with constitutional signs, such as fever, anorexia, nonspecific aches and pains, weight loss, and night sweats. The acute leukemias and lymphomas often present with these nonspecific findings.
o Generalized lymphadenopathy is present at diagnosis in two thirds of children with acute lymphoblastic leukemia (ALL) and in one third of children with acute myeloblastic leukemia (AML). Abnormalities of peripheral blood counts usually lead to the correct diagnosis. The lymphomas more often present with regional lymphadenopathy, but generalized lymphadenopathy occurs.
o Constitutional signs and symptoms observed in the leukemias are less reliable findings in the lymphomas. Only one third of children with Hodgkin disease and 10% with non-Hodgkin lymphoma display them. Malignancies usually present with nodes that tend to be firmer and less mobile or matted; however, this finding can be misleading. Benign reactive lymph nodes may be associated with fibrotic reactions that make them firm.
5

Storage diseases: Generalized lymphadenopathy is an important manifestation of the lipid storage diseases. In Niemann-Pick disease, sphingomyelin and other lipids accumulate in the spleen, liver, lymph nodes, and CNS. In Gaucher disease, the accumulation of the glucosylceramide leads to the engorgement of the spleen, lymph nodes, and the bone marrow. Although widespread lymphadenopathy is common, additional findings, such as hepatosplenomegaly and developmental delay in Niemann-Pick disease and blood dyscrasias in Gaucher disease, are usually present. These diagnoses are established by leukocyte assay.
Drug reactions: Adverse drug reactions can cause generalized lymphadenopathy. Within a couple of weeks of initiating phenytoin, some patients experience a syndrome of regional or generalized lymph node enlargement, followed by a severe maculopapular rash, fever, hepatosplenomegaly, jaundice, and anemia. These symptoms abate 2-3 months after discontinuation of the drug. Several other drugs are implicated in similar symptomatology, including mephenytoin, pyrimethamine, phenylbutazone, allopurinol, and isoniazid.
Other nonneoplastic etiologies: Rare nonneoplastic causes of generalized lymphadenopathy include Langerhans cell histiocytosis and Epstein-Barr virus (EBV)-associated lymphoproliferative disease. Autoimmune etiologies include juvenile rheumatoid arthritis, which often presents with adenopathy, especially during the acute phases of the disease. Sarcoidosis and graft verses host disease also merit consideration.
Regional lymphadenopathy involves enlargement of a single node or multiple contiguous nodal regions. Lymph nodes are clustered in groups throughout the body and are concentrated in the head and neck, axillae, mediastinum, abdomen, and along the vascular trunks of the extremities. Each group drains lymph from a particular region of the body. Knowledge of the pattern of lymph drainage aids in determining the etiology.
Cervical lymphadenopathy: Cervical lymphadenopathy is a common problem in children.11 Cervical nodes drain the tongue, external ear, parotid gland, and deeper structures of the neck, including the larynx, thyroid, and trachea. Inflammation or direct infection of these areas causes subsequent engorgement and hyperplasia of their respective node groups. Adenopathy is most common in cervical nodes in children and is usually related to infectious etiologies. Lymphadenopathy posterior to the sternocleidomastoid is typically a more ominous finding, with a higher risk of serious underlying disease.
o Infectious etiologies Cervical adenopathy is a common feature of many viral infections. Infectious
mononucleosis often manifests with posterior and anterior cervical adenopathy. Firm tender nodes that are not warm or erythematous characterize this lymph node enlargement. Other viral causes of cervical lymphadenopathy include adenovirus, herpesvirus, coxsackievirus, and CMV. In herpes gingivostomatitis, impressive submandibular and submental adenopathy reflects the amount of oral involvement.
Bacterial infections cause cervical adenopathy by causing the draining nodes to respond to local infection or by the infection localizing within the node itself as a lymphadenitis. Bacterial infection often results in enlarged lymph nodes that are warm, erythematous, and tender. Localized cervical lymphadenitis typically begins as enlarged, tender, and then fluctuant nodes. The appropriate management of a suppurative lymph node includes both antibiotics and incision and drainage. Antibiotic therapy should always include coverage for Staphylococcus aureus and Streptococcus pyogenes.
In patients with cervical adenopathy, determine whether the patient has had recent or ongoing sore throat or ear pain. Examine the oropharynx, paying special attention to the posterior pharynx and the dentition. The classic manifestation of group A streptococcal pharyngitis is sore throat, fever, and anterior cervical lymphadenopathy. Other streptococcal infections causing cervical adenopathy include otitis media, impetigo, and cellulitis.
Atypical mycobacteria cause subacute cervical lymphadenitis, with nodes that are large and indurated but not tender. The only definitive cure is removal of the infected node.12
Mycobacterium tuberculosis may manifest with a suppurative lymph node identical to that of atypical mycobacterium. Intradermal skin testing may be equivocal. A biopsy may be necessary to establish the diagnosis.
6
Catscratch disease , caused by Bartonella henselae, presents with subacute lymphadenopathy often in the cervical region. The disease develops after the infected pet (usually a kitten) inoculates the host, usually through a scratch. Approximately 30 days later, fever, headache, and malaise develop, along with adenopathy that is often tender. Several lymph node chains may be involved. Suppurative adenopathy occurs in 10-35% of patients. Antibiotic therapy has not been shown to shorten the course.
o Noninfectious etiologies Malignant childhood tumors develop in the head and neck region in one quarter of cases.
In the first 6 years of life, neuroblastoma, leukemia, non-Hodgkin lymphoma, and rhabdomyosarcoma (in order of decreasing frequency) are most common in the head and neck region. In children older than 6 years, Hodgkin disease and non-Hodgkin lymphoma both predominate. Children with Hodgkin disease present with cervical adenopathy in 80-90% of cases as opposed to 40% of those with non-Hodgkin lymphoma.
Kawasaki disease is an important cause of cervical adenopathy. These children have fever for at least 5 days, and cervical lymphadenopathy is one of the 5 diagnostic criteria (of which 4 are necessary to establish the diagnosis).
Submaxillary and submental lymphadenopathy: These nodes drain the teeth, tongue, gums, and buccal mucosa. Their enlargement is usually the result of localized infection, such as pharyngitis, herpetic gingivostomatitis, and dental abscess.
Occipital lymphadenopathy: Occipital nodes drain the posterior scalp. These nodes are palpable in 5% of healthy children. Common etiologies of occipital lymphadenopathy include tinea capitis, seborrheic dermatitis, insect bites, orbital cellulitis, and pediculosis. Viral etiologies include rubella and roseola infantum. Rarely, occipital lymphadenopathy may be noted after enucleation of the eye for retinoblastoma.
Preauricular lymphadenopathy: Preauricular nodes drain the conjunctivae, skin of the cheek, eyelids, and temporal region of the scalp and rarely are palpable in healthy children. The oculoglandular syndrome consists of severe conjunctivitis, corneal ulceration, eyelid edema, and ipsilateral preauricular lymphadenopathy. Chlamydia trachomatis and adenovirus can cause this syndrome.
Mediastinal lymphadenopathyo Mediastinal nodes drain the thoracic viscera, including the lungs, heart, thymus, and thoracic
esophagus. Because these nodes are not directly demonstrable upon physical examination, their enlargement must be indirectly assessed. Supraclavicular adenopathy is often associated with mediastinal adenopathy. Mediastinal nodes may cause cough, wheezing, dysphagia, airway erosion with hemoptysis, atelectasis, and the obstruction of the great vessels, which constitutes superior vena cava syndrome. Airway compromise may be life threatening.
o Mediastinal lymphadenopathy is usually a sign of serious underlying disease. More than 95% of mediastinal masses are caused by tumors or cysts. Lymphomas and acute lymphoblastic leukemia are the most common etiologies and usually involve the anterior mediastinum. These malignancies are associated with a high risk of superior vena cava syndrome and are associated with several potentially life-threatening complications, as follows:
The danger of sedation of patients, especially in the supine position for scans and procedures (The prone position actually may be safer.)
The risk during intubation of these patients, usually at the time of biopsy or placement of a central venous catheter
The risk of cardiovascular collapse during general anesthesia because of compression of venous return or because of previously undiagnosed pleural effusions
The risk of losing the ability to establish a pathologic diagnosis because of the use of steroids or radiation therapy
o Unlike most other adenopathies, mediastinal lymphadenopathy is less frequently a result of infection. Infections frequently involve the hilar region and include histoplasmosis, coccidioidomycosis, and tuberculosis.
o Nonlymphoid mediastinal tumors may be confused with adenopathy. These include neurogenic tumors (usually found in the posterior mediastinum), germ cell tumors, and teratomas.
o Nonneoplastic conditions may also be confused with mediastinal adenopathy. These include the typically large thymus of a child, substernal thyroid glands, bronchogenic cysts, and abnormalities of the great vessels.
7

Supraclavicular lymphadenopathyo Supraclavicular nodes drain the head, neck, arms, superficial thorax, lungs, mediastinum, and
abdomen. Left supraclavicular nodes also reflect intra-abdominal drainage and enlarge in response to malignancies in that region. This is particularly true when adenopathy in this region occurs in the absence of other cervical adenopathy.
o Right supraclavicular nodes drain the lung and mediastinum and are typically enlarged with intrathoracic lesions.
o Serious underlying disease is frequent in children with supraclavicular adenopathy and always merits further evaluation. The potential for malignancy necessitates peripheral blood counts, skin testing for tuberculosis, and chemical studies, including uric acid, lactate dehydrogenase, calcium (Ca), phosphorus (P), and renal and hepatic function studies. Chest radiography and possibly CT scanning are indicated.
o Several important infections may occur with supraclavicular adenopathy, including tuberculosis, histoplasmosis, and coccidioidomycosis.
o Early lymph node biopsy should be considered in children with supraclavicular adenopathy. Axillary lymphadenopathy
o Axillary nodes drain the hand, arm, lateral chest, abdominal walls, and the lateral portion of the breast.
o A common cause of axillary lymphadenopathy is catscratch disease. Local axillary skin infection and irritation commonly are associated with local adenopathy. Other etiologies include recent immunizations in the arm (particularly with bacille Calmette-Guerin vaccine), brucellosis, juvenile rheumatoid arthritis, and non-Hodgkin lymphoma.
o Hidradenitis suppurativa is a condition of enlarged tender lymph nodes that typically affects children with obesity and is caused by recurrent abscesses of lymph nodes in the axillary chain. The etiology is unknown, and treatment may include antibiotics. Many patients require incision and drainage.
Abdominal lymphadenopathyo Abdominal nodes drain the lower extremities, pelvis, and abdominal organs. Although abdominal
adenopathy is not usually demonstrable upon physical examination, abdominal pain, backache, increased urinary frequency, constipation, and intestinal obstruction secondary to intussusception are possible presentations.
o Mesenteric adenitis is thought to be viral in etiology and is characterized by right lower quadrant abdominal pain caused by nodal enlargement near the ileocecal valve. Differentiating mesenteric adenitis from appendicitis may be difficult.
o Mesenteric adenopathy may be caused by non-Hodgkin lymphoma or Hodgkin disease.o Typhoid fever and ulcerative colitis are other etiologies of mesenteric adenopathy.
Iliac and inguinal lymphadenopathy: The lower extremities, perineum, buttocks, genitalia, and lower abdominal wall drain to these nodes. They are typically palpable in healthy children, although they are usually no larger than 1-1.5 cm in diameter. Regional lymphadenopathy is typically caused by infection; however, insect bites and diaper dermatitis are also frequent. Nonlymphoid masses that may be confused with adenopathy include hernias, ectopic testes, and lipomas.
Outline - Etiologies of Lymphadenopathy
I. Generalized lymphadenopathy
1. Infections1. Viral
Common upper respiratory infections Infectious mononucleosis CMV Acquired immunodeficiency syndrome Rubella Varicella
8
Measles 2. Bacterial
Septicemia Typhoid fever Tuberculosis Syphilis Plague
3. Protozoal - Toxoplasmosis4. Fungal - Coccidioidomycosis
2. Autoimmune disorders and hypersensitivity states1. Juvenile rheumatoid arthritis2. Systemic lupus erythematosus3. Drug reactions (eg, phenytoin, allopurinol)4. Serum sickness
3. Storage Diseases1. Gaucher disease2. Niemann-Pick disease
4. Neoplastic and proliferative disorders1. Acute leukemias2. Lymphomas (Hodgkin, non-Hodgkin)3. Neuroblastoma4. Histiocytoses
II. Regional lymphadenopathy
1. Cervical1. Viral upper respiratory infection2. Infectious mononucleosis3. Rubella4. Catscratch disease5. Streptococcal pharyngitis6. Acute bacterial lymphadenitis7. Toxoplasmosis 8. Tuberculosis/atypical mycobacterial infection9. Acute leukemia10. Lymphoma11. Neuroblastoma12. Rhabdomyosarcoma 13. Kawasaki disease
2. Submaxillary and submental1. Oral and dental infections2. Acute lymphadenitis
3. Occipital1. Pediculosis capitis2. Tinea capitis3. Secondary to local skin infection4. Rubella5. Roseola
4. Preauricular1. Local skin infection2. Chronic ophthalmic infection3. Catscratch disease
5. Mediastinal1. Acute lymphoblastic leukemia2. Lymphoma
9

3. Sarcoidosis 4. Cystic fibrosis 5. Tuberculosis6. Histoplasmosis7. Coccidioidomycosis
6. Supraclavicular1. Lymphoma2. Tuberculosis3. Histoplasmosis4. Coccidioidomycosis
7. Axillary1. Local infection2. Catscratch disease3. Brucellosis4. Reactions to immunizations5. Lymphoma6. Juvenile rheumatoid arthritis
8. Abdominal1. Acute mesenteric adenitis2. Lymphoma
9. Inguinal1. Local infection2. Diaper dermatitis3. Insect bites4. Syphilis5. Lymphogranuloma venereum
http://emedicine.medscape.com/article/956340-overview
Differential Diagnoses
Acute Lymphoblastic Leukemia Non-Hodgkin LymphomaAcute Myelocytic Leukemia Pediculosis (Lice)Brucellosis PlagueCoccidioidomycosis RhabdomyosarcomaCystic Fibrosis RubellaDiaper Dermatitis SarcoidosisGaucher Disease Serum SicknessHistiocytosis Streptococcal Infection, Group
AHistoplasmosis SyphilisHodgkin Disease Systemic Lupus ErythematosusHuman Immunodeficiency Virus Infection Taenia InfectionJuvenile Rheumatoid Arthritis ToxoplasmosisKawasaki Disease TuberculosisMeasles VaricellaMononucleosis and Epstein-Barr Virus InfectionNeuroblastomaNiemann-Pick Disease
Other Problems to Be Considered
Insect bitesRoseola
10

Oral and dental infectionsTyphoid feverUpper respiratory infectionAcquired immunodeficiency syndrome (AIDS)
Workup
Laboratory Studies
The laboratory evaluation of lymphadenopathy must be directed by the history and physical examination and is based on the size and other characteristics of the nodes and the overall clinical assessment of the patient. When a laboratory evaluation is indicated, it must be driven by the clinical evaluation.13 The following studies are typically included:
CBC count, including a careful evaluation of the peripheral blood smear. An erythrocyte sedimentation rate is nonspecific but may be helpful.
Evaluation of hepatic and renal function and a urine analysis are useful to identify underlying systemic disorders that may be associated with lymphadenopathy. Additional studies, such as lactate dehydrogenase (LDH), uric acid, calcium, and phosphate, may be indicated if malignancy is suspected. Skin testing for tuberculosis is usually indicated.
In evaluating specific regional adenopathy, lymph node aspirate for culture may be important if lymphadenitis is clinically suspected.
Titers for specific microorganisms may be indicated, particularly if generalized adenopathy is present. These may include Epstein-Barr virus, cytomegalovirus (CMV), B henselae, Toxoplasma species, and human immunodeficiency virus (HIV).
Imaging Studies
Imaging studies may include the following:
Chest radiography is usually the primary screening imaging study. Additional imaging studies are usually based on abnormal chest radiograph findings. Chest radiography is often helpful in elucidating mediastinal adenopathy and underlying diseases affecting the lungs, including tuberculosis, coccidioidomycosis, lymphomas, neuroblastoma, histiocytoses, and Gaucher disease.
Supraclavicular adenopathy, with its high associated rate of serious underlying disease, may be an indication for other studies, including CT scanning of the chest, abdomen, or both.
Nuclear medicine scanning is helpful in the evaluation of lymphomas. Ultrasonography may be helpful in evaluating the changes in the lymph nodes and in evaluating the extent
of lymph node involvement in patients with lymphadenopathy.14
In children with inguinal adenopathy or abdominal complaints, ultrasonography of the abdomen, CT scanning of the abdomen, or both may be indicated.15
Procedures
The critical question is often whether or not to perform a lymph node biopsy; this requires an overall assessment of the history and physical examination as described above.
Images taken during and after a lymph node biopsy are shown below.
A lymph node biopsy is performed. Note that a marking pen has been used to outline the node before removal and that a silk suture has been used to provide traction to assist the removal.
11

A lymph node biopsy is performed. Note that a marking pen has been used to outline the node before removal and that a silk suture has been used to provide traction to assist the removal.
A lymph node after removal by means of biopsy, which was performed completely under a local anesthetic technique.
A lymph node after removal by means of biopsy, which was performed completely under a local anesthetic technique.
A gross image of a node following excision. The cut surface of the node shows the typical fish-flesh appearance seen with lymphoma.
A gross image of a node following excision. The cut surface of the node shows the typical fish-flesh appearance seen with lymphoma.
Treatment with antibiotics (covering the bacterial pathogens frequently implicated in lymphadenitis) followed by reevaluation in 2-4 weeks is reasonable if clinical findings suggest lymphadenitis. Benign reactive adenopathy may be safely observed for months.6
If the size, location, or character of the lymphadenopathy suggests malignancy, the need for laboratory studies and biopsy is more urgent. If laboratory testing is inconclusive, a lymph node biopsy is immediately indicated.
Fine needle aspiration and core needle biopsy yield small samples with limited ability to perform flow cytometry and chromosomal analysis; most pediatric hematologists and pathologists prefer excisional biopsy.
Excisional biopsy also has limitations and may yield a definitive diagnosis in only 40-60% of patients because of inadequate specimen size, improper handling, or node-sampling error.
Hodgkin disease may be associated with reactive changes in surrounding nodes, and sampling more accessible nodes may miss the underlying malignancy.
Sampling inguinal nodes may yield specimens with an architecture distorted by chronic inflammatory changes.
The surgeon should perform a biopsy on larger, firmer, and most recently enlarging nodes, even if it is technically difficult, with appropriate preparation and handling of the specimen. If an excisional biopsy does not reveal the diagnosis despite appropriate sampling practice, a second biopsy may be indicated if symptoms persist or worsen.
Histologic Findings
Histiologic findings depend on the underlying etiology of the lymphadenopathy. Nonspecific changes consistent with reactive adenopathy are often the only findings. This is helpful in ruling out malignancy, histiocytoses, granulomatous disorders, and storage diseases. Specific infections can be diagnosed if tissues are appropriately stained.
When examining the tissue, histiologic findings are often inadequate. Flow cytometric and chromosomal analysis may provide critical information to permit a diagnosis to be established.
Staging
Staging is relevant only when a specific malignancy is diagnosed as the etiology of lymphadenopathy.
Treatment
Medical Care
12

Treatment is determined by the specific underlying etiology of lymphadenopathy.
Most clinicians treat children with cervical lymphadenopathy conservatively. Antibiotics should be given only if a bacterial infection is suspected. This treatment is often given before biopsy or aspiration is performed. This practice may result in unnecessary prescription of antimicrobials. However, the risks of surgery often outweigh the potential benefits of a brief course of antibiotics. Most enlarged lymph nodes are caused by an infectious process. If aspects of the clinical picture suggest malignancy, such as persistent fevers or weight loss, biopsy should be pursued sooner.
Management of superior vena cava syndrome requires emergency care, including chemotherapy and possibly radiation therapy.
Surgical Care
Surgical care usually involves a biopsy. If lymphadenitis is present, aspirate may be needed for culture, and removal of the affected node may be indicated.
Consultations
Consultation with a pediatric hematologist, pediatric oncologist, or both is often useful, especially if the adenopathy seems to be more than reactive. Often, the most important decision for these children is whether further evaluation is necessary at all; experience in evaluating these children is frequently very helpful. The ability to provide a careful assessment of the peripheral blood smear may be particularly important.
Surgical consultation is usually helpful for lymph node biopsy, needle aspiration for culture, and for incision and drainage of obviously infected fluctuant nodes.
Diet
Diet plays little role in the pathophysiology of lymphadenopathy.
Internationally, many of the infectious etiologies may be associated with a higher risk of malnutrition.
Activity
Limitations on activity usually involve associated acute-onset splenomegaly. Any patient with an acutely enlarged spleen may need to be restricted from contact sports.
In infectious mononucleosis, rupture of the spleen can occur with relatively little trauma and can be fatal.
Medication
No specific medical therapy for lymphadenopathy is acknowledged.
Therapy is directed at the specific diagnosis, once established, and when appropriate.
13

Lymphadenitis
Author: Ulfat Shaikh, MD, MPH, Assistant Professor of Pediatrics, Department of Pediatrics, University of California Davis Medical CenterCoauthor(s): Dean A Blumberg MD, Associate Professor of Pediatrics, Section of Pediatric Infectious Disease, University of California Davis School of Medicine; Acting Chief, Section of Pediatric Infectious Disease, UC Davis Medical CenterContributor Information and Disclosures
Updated: Apr 23, 2010
Introduction
Background
Lymphadenitis is the inflammation and/or enlargement of a lymph node. Lymph node enlargement is common in children. Most cases represent a response to benign, local, or generalized infections (usually viral).1 Lymphadenitis may affect a single node or a localized group of nodes (regional adenopathy) and may be unilateral or bilateral. The onset and course of lymphadenitis may be acute, subacute, or chronic.2
Most children with lymphadenitis exhibit small palpable cervical, axillary, and inguinal nodes. Approximately 5% of these children have palpable suboccipital or postauricular nodes. Palpable supraclavicular, epitrochlear, and popliteal nodes are uncommon, as are mediastinal or abdominal nodes that are detected with radiographic studies.
Pathophysiology
Increased node size may be caused by the following:
Multiplication of cells within the node, including lymphocytes, plasma cells, monocytes, or histiocytes Infiltration of cells from outside the node, such as malignant cells or neutrophils Draining of a source of infection by lymph nodes
If the cause of adenopathy is not evident, consider congenital or neoplastic causes.
Frequency
United States
Lymph nodes are usually small and firm. They are palpable in the cervical, axillary, inguinal, and occipital regions of healthy infants and children. Multiple nodes, especially if present with splenomegaly, may be associated with human immunodeficiency virus (HIV) infection.
International
Tuberculous lymphadenitis can be seen in developing countries.
Mortality/Morbidity
14

Nodes may be large and may cause local pain and tenderness. Overlying skin may be erythematous. Neck stiffness and torticollis may occur because of cervical lymphadenopathy. Inflammation of retropharyngeal nodes (retropharyngeal abscess) may lead to dysphagia or dyspnea.
Mediastinal lymphadenitis may cause cough, dyspnea, stridor, dysphagia, pleural effusion, and venous congestion in the upper body. Intra-abdominal (mesenteric and retroperitoneal) adenopathy may manifest as abdominal pain. Iliac lymph node involvement may cause abdominal pain and limping.
Clinical
History
The history in patients with lymphadenitis may include the following:
Upper respiratory symptoms, sore throat, earache, coryza, conjunctivitis, and impetigo Fever, irritability, and anorexia Contact with animals, especially kittens
Dental care
Submaxillary adenopathy may develop secondary to stomatitis, dental caries, or a dental abscess.
Risk factors for tuberculosis3
Generalized lymphadenopathy in a child with tuberculosis may indicate a hematogenous spread of tubercle bacilli.
Localized involvement is most common in the mediastinal, mesenteric, or anterior cervical nodes.
Acute or chronic onset
Usually, bilateral acute cervical adenitis is caused by either viral pharyngitis or infectious mononucleosis.
Chronic localized adenopathy can be attributed to a persistent regional infection.
Skin and scalp conditions
Occipital and postauricular adenopathy may accompany scalp infections, seborrheic dermatitis, or scalp pediculosis. Epitrochlear and axillary lymphadenopathy may result from infections on the arms. Inguinal and femoral adenopathy may be due to infections on the lower extremities.
Periodicity
Periodic fever, aphthous stomatitis, pharyngitis, and cervical adenitis (PFAPA) syndrome usually results in adenopathy associated with the other findings every 3-6 weeks.
History of travel
When adenopathy is caused by Yersinia pestis (bubonic plague), the patient may have visited a rural area in the western United States one week prior to the onset of illness.
Medication use
15

The following medications may have been used:
Hydantoin Mesantoin
Age
Atypical mycobacteria typically cause adenopathy in toddlers.
Physical
Physical findings may include the following:
Location
Tularemia may be accompanied by regional adenopathy, most commonly cervical.
Yersinia enterocolitica infection may cause cervical or abdominal adenopathy.
Salmonella infections may accompany generalized lymphadenopathy.
Rubella and parvovirus infection is characterized by enlarged and tender posterior auricular, posterior cervical, and occipital lymph nodes.
Atypical (environmental) mycobacteria may cause submandibular or submental adenopathy.
Mediastinal or infectious hilar adenopathy may occur in patients with tuberculosis, chronic sinusitis, histoplasmosis, tularemia, infectious mononucleosis, candidiasis, coccidioidomycosis, and bronchiectasis.
Size
Lymph nodes that are noted to increase rapidly in size may indicate potential malignancy.
Shape
Confluent lymph nodes may be indicators of malignancy.
Consistency
Descriptors may include soft, fluctuant, firm, rubbery, or hard.
In early stages, nodes in tuberculosis are well-demarcated, mobile, nontender, and firm. If the infection remains untreated, the nodes soften, become fluctuant, and adhere to the skin, which may be erythematous.
In Hodgkin disease, nodes are initially soft. They later become firm and rubbery.
Fixation of lymph nodes to the skin and soft tissue may indicate malignancy.
Tenderness
Lymph nodes of infectious etiology are usually tender.
16

Bubonic plague, caused by Y pestis, may cause extremely tender lymph node enlargement and erythema of overlying skin in the inguinal, femoral, axillary, or cervical area.
Hodgkin lymphoma may initially present as painless lymph node enlargement, especially of the cervical and supraclavicular region.
Overlying skin
The overlying skin may be erythematous in infectious etiologies.
Draining sinuses may develop in patients with tuberculous adenopathy.
Infants with atopic eczema may have generalized lymphadenopathy.
Systemic signs
Group B streptococcal cellulitis and adenitis, which may occur in infants younger than 2 months, are characterized by sudden onset of fever, anorexia, irritability, and submandibular swelling. Usually, a blood culture test demonstrates positive results.
Hepatosplenomegaly is common in patients with infectious mononucleosis.
Conjunctivitis
Preauricular adenopathy (Parinaud oculoglandular syndrome) secondary to uniocular granulomatous conjunctivitis may be caused by catscratch disease, chlamydial conjunctivitis, listeriosis, tularemia, or tuberculosis.
Adenovirus type 3 causes pharyngeal conjunctival fever. Symptoms associated with adenovirus type 3 include follicular conjunctivitis with enlarged preauricular and/or posterior cervical nodes. Adenovirus type 8 causes epidemic keratoconjunctivitis, which causes preauricular adenopathy.
PFAPA syndrome
Aphthous stomatitis and pharyngitis are associated with PFAPA syndrome.
Number
A single node or multiple nodes may be involved.
Catscratch disease
In catscratch disease, usually only a single node is involved.
Causes
Causes of lymphadenitis include the following:
Infections
Acute, one-sided, pyogenic adenitis is most common. The involved node may be firm and tender, with erythema of the overlying skin. Etiologic agents include group A beta-hemolytic streptococci, staphylococcal organisms (especially Staphylococcus aureus),4 and viruses.
17

Tularemia may be accompanied by regional adenopathy, most commonly cervical, with local tenderness, pain, and fever. Generalized lymphadenopathy may also develop.5
In a child with tuberculosis, generalized lymphadenopathy may indicate hematogenous spread of tubercle bacilli. Localized involvement is most common in the mediastinal, mesenteric, or anterior cervical nodes. Initially, the nodes are discrete, firm, mobile, and tender. If the patient remains untreated, the nodes soften, become fluctuant and matted, and adhere to overlying skin, which may become erythematous. Bilateral involvement is characteristic of this condition. Pulmonary disease is common.
Atypical mycobacteria can manifest cervical or submandibular involvement identical to that of tuberculosis, except the involvement is usually unilateral.6
Group B streptococcal cellulitis and adenitis may occur in infants younger than 2 months.
Brucellosis may accompany chronic or intermittent lymphadenopathy.
Y enterocolitica may be associated with cervical lymphadenitis.
Salmonella infection can correspond to generalized adenopathy.
Bubonic plague is caused by Y pestis.
In patients with catscratch disease, the site of the scratch determines if axillary, epitrochlear, supraclavicular, femoral, inguinal, or submaxillary lymph nodes are involved. The nodes are nontender, discrete, mobile, and moderately or greatly enlarged. Occasionally, tenderness, redness, warmth, and suppuration may occur. Bartonella henselae is the organism that causes catscratch disease.
Patients with infectious mononucleosis typically present with discrete, firm, nontender lymph nodes. Usually, anterior cervical nodes are involved. Generalized lymphadenopathy may occur, and hepatosplenomegaly is common.
Cytomegalovirus or toxoplasmosis may cause a mononucleosislike syndrome with generalized adenopathy, fever, atypical lymphocytes, and hepatosplenomegaly.
Gianotti-Crosti syndrome accompanies generalized lymphadenopathy, hepatomegaly, splenomegaly, nonicteric hepatitis, and crops of papular lesions that persist for 2-8 weeks.
Immunologic or connective tissue disorders
Juvenile rheumatoid arthritis should be considered in unexplained fever and persistent lymphadenopathy in a child.
Serum sickness can correspond with generalized tender lymphadenopathy.
Chronic graft versus host disease may occur.
Primary disease of lymphoid or reticuloendothelial tissue
These include the following:
Acute leukemia Lymphosarcoma Reticulum cell sarcoma Hodgkin disease Non-Hodgkin lymphoma Malignant histocytosis or histocytic lymphoma
18

Nonendemic Burkitt tumor Nasopharyngeal rhabdomyosarcoma Neuroblastoma 7
Thyroid carcinoma, chronic lymphocytic thyroiditis Histiocytosis X Kikuchi disease8
Benign sinus histiocytosis Angioimmunoblastic or immunoblastic lymphadenopathy Chronic pseudolymphomatous lymphadenopathy (chronic benign lymphadenopathy)
Immunodeficiency syndromes and phagocytic dysfunction
These include the following:
Chronic granulomatous disease of childhood Acquired immunodeficiency syndrome Hyperimmunoglobulin E (Job) syndrome
Metabolic and storage diseases
These include the following:
Gaucher disease Niemann-Pick disease Histiocytosis X Cystinosis
Hematopoietic diseases
These include the following:
Sickle cell anemia Thalassemia Congenital hemolytic anemia Autoimmune hemolytic anemia
Other disorders
Kawasaki disease usually presents with cervical adenopathy that is unilateral and with nodes that are firm, nontender, and greater than 1.5 cm in diameter.9 Overlying skin may be erythematous but not warm.10
PFAPA syndrome usually occurs in young children (onset almost always before age 5 y) and is remarkable because of its regular periodicity. All findings may not occur in each patient. Children are otherwise healthy between episodes and display normal growth and development. During the acute episodes, elevation of inflammatory markers (eg, WBC count, erythrocyte sedimentation rate) is often present. A recent study determined that the Gaslini diagnostic score is a useful tool in differentiating PFAPA syndrome from monogenic periodic fevers.11
Drug use can affect lymph nodes. Mesantoin use may cause enlargement of lymph nodes (most commonly in the cervical region), fever, eosinophilia, rash, and hepatosplenomegaly. Hydantoin use also may produce lymphadenopathy as an adverse effect.
Almost all patients with sarcoidosis demonstrate either generalized or hilar lymphadenopathy. When enlarged, bilateral cervical nodes are firm, rubbery, and discrete, with little tendency to coalesce. Other symptoms include
19

fatigue, cough, fever, dyspnea, and weight loss. Hyperglobulinemia and eosinophilia are common laboratory findings.
Castleman disease or benign giant lymph node hyperplasia may cause lymphadenopathy in the mediastinum, abdomen, neck, or axilla. Some patients experience fever, anemia, weight loss, and hyperglobulinemia.
Differential Diagnoses
Brucellosis NeuroblastomaCatscratch Disease Niemann-Pick DiseaseChronic Granulomatous Disease Non-Hodgkin LymphomaCystinosis PlagueCytomegalovirus Infection RhabdomyosarcomaGaucher Disease Salmonella InfectionGianotti-Crosti Syndrome SarcoidosisGraft Versus Host Disease Serum SicknessHemolytic Disease of Newborn Sickle Cell AnemiaHistiocytosis Staphylococcus Aureus InfectionHodgkin Disease Streptococcal Infection, Group
AHyperimmunoglobulinemia E (Job) Syndrome ThalassemiaJuvenile Rheumatoid Arthritis ThyroiditisKawasaki Disease TuberculosisLymphadenopathy TularemiaMononucleosis and Epstein-Barr Virus InfectionYersinia Enterocolitica Infection
Other Problems to Be Considered
LymphomaMycobacterial infectionKikuchi diseasePeriodic fever, aphthous stomatitis, pharyngitis, and cervical adenitis (PFAPA) syndrome
Workup
Laboratory Studies
The following studies may be indicated in patients with lymphadenitis:
Gram stain
Staining can be performed on aspirated tissue. Gram staining is a quick method used to evaluate bacterial etiologies.
Culture of aspirated tissue or biopsy specimen
Culturing is performed to determine the causative organism and sensitivity to antibiotics.
Monospot
Monospot (in older children) or Epstein-Barr virus (EBV) serologies are useful to confirm the diagnosis of infectious mononucleosis.
20

B henselae serologies
These can be used to confirm the diagnosis of catscratch disease.
Skin testing Purified protein derivative testing can be helpful in confirming the diagnosis of tuberculous lymphadenopathy and may be suggestive of atypical mycobacterial infection.
CBC count
A high WBC count may indicate an infectious etiology.
Erythrocyte sedimentation rate
A high erythrocyte sedimentation rate is a nonspecific indicator of inflammation.
Liver function tests
These may indicate hepatic or systemic involvement. An elevation may occur in infectious mononucleosis.
Imaging Studies
The following imaging studies may be indicated in patients with lymphadenitis:
Ultrasonography Images may be helpful in detecting the extent of the spread of lymphadenopathy.12
Chest radiography
Radiography may be helpful in determining pulmonary involvement or spread of lymphadenopathy to the chest.
Procedures
The following procedures may be indicated:
Needle aspiration13
Partial or excisional biopsy (See the image below.)
A lymph node biopsy is performed. Note that a marking pen has been used to outline the node before removal and that a silk suture has been used to provide traction to assist the removal.
[ CLOSE WINDOW ]
21
A lymph node biopsy is performed. Note that a marking pen has been used to outline the node before removal and that a silk suture has been used to provide traction to assist the removal.
Incision and drainage
Treatment
Medical Care
In patients with lymphadenitis, treatment depends on the causative agent and may include the following:
Antimicrobial therapy Expectant management: Catscratch disease is usually benign and self-limited and generally does not require
treatment with antibiotics. Chemotherapy Radiotherapy
For details on medical therapy, please refer to the eMedicine article that discusses the specific diagnosed condition, including the following:
Cytomegalovirus Toxoplasmosis Gianotti-Crosti syndrome Graft versus host disease Non-Hodgkin lymphoma Hodgkin disease Neuroblastoma Hyperimmunoglobulin E (Job) syndrome Gaucher disease Niemann-Pick disease Sickle cell anemia Thalassemia Kawasaki disease Dental abscess Pharyngitis Mononucleosis Tularemia Yersinia enterocolitica infection Salmonella infections Rubella Tuberculosis Sinusitis Histoplasmosis Candidiasis Bronchiectasis
Surgical Care
Depending on presentation, the following procedures may be appropriate:
Excisional biopsy: Lymphadenitis caused by atypical mycobacteria may have improved cosmetic outcome with surgical excision.
Aspiration
22

Incision and drainage
Consultations
Depending on the etiology, consultations with the following specialists may be appropriate:
Pediatric infectious disease specialist Surgeon Hematologist Oncologist
Medication
Therapy in patients with lymphadenitis is determined by diagnosis. Refer to the eMedicine article that discusses the diagnosed condition for information about appropriate medications. (See Causes and Treatment).
http://emedicine.medscape.com/article/960858-diagnosis
23

Lymphadenopathy and Malignancy
ANDREW W. BAZEMORE, M.D., and DOUGLAS R. SMUCKER, M.D., M.P.H
University of Cincinnati College of Medicine, Cincinnati, Ohio
Am Fam Physician. 2002 Dec 1;66(11):2103-2111.
This article exemplifies the AAFP 2002 Annual Clinical Focus on cancer: prevention, detection, management, support, and survival.
The majority of patients presenting with peripheral lymphadenopathy have easily identifiable causes that are benign or self-limited. Among primary care patients presenting with lymphadenopathy, the prevalence of malignancy has been estimated to be as low as 1.1 percent. The critical challenge for the primary care physician is to identify which cases are secondary to malignancies or other serious conditions. Key risk factors for malignancy include older age, firm, fixed nodal character, duration of greater than two weeks, and supraclavicular location. Knowledge of these risk factors is critical to determining the management of unexplained lymphadenopathy. In addition, a complete exposure history, review of associated symptoms, and a thorough regional examination help determine whether lymphadenopathy is of benign or malignant origin. Unexplained lymphadenopathy without signs or symptoms of serious disease or malignancy can be observed for one month, after which specific testing or biopsy should be performed. While modern hematopathologic technologies have improved the diagnostic yields of fine-needle aspiration, excisional biopsy remains the initial diagnostic procedure of choice. The overall evaluation of lymphadenopathy, with a focus on findings suggestive of malignancy, as well as an approach to the patient with unexplained lymphadenopathy, will be reviewed.
Lymphadenopathy, which is defined as an abnormality in the size or character of lymph nodes, is caused by the invasion or propagation of either inflammatory cells or neoplastic cells into the node. It results from a vast array of disease processes (Table 1),1 whose broad categories are easily recalled using the mnemonic acronym “MIAMI,” representing Malignancies, Infections, Autoimmune disorders, Miscellaneous and unusual conditions, and Iatrogenic causes. A common finding in the primary care outpatient setting, lymphadenopathy is typically explained by identifiable regional injury or infection. Among the serious illnesses that can present with lymphadenopathy, perhaps the most concerning to the patient and physician alike is the possibility of underlying malignancy.
TABLE 1Diagnosis of Select Causes of Lymphadenopathy
The rightsholder did not grant rights to reproduce this item in electronic media. For the missing item, see the original print version of this publication.
The prevalence of malignancy is thought to be quite low among all patients with lymphadenopathy. Few studies define the prospective risk of malignancy with adenopathy, but three case series support the suggestion that the risk is very low. In two studies,2,3 three of 238 and zero of 80 patients presenting with unexplained lymphadenopathy were determined to have malignancies, while a third study4 retrospectively found a 1.1 percent prevalence of malignancy in primary care patients presenting to the office with unexplained lymphadenopathy.
Essential to identifying the infrequent but serious causes of peripheral lymphadenopathy are the following: an awareness of lymphatic anatomy, drainage patterns, and regional differential diagnosis; a thorough history including key factors such as age, location, duration, and patient exposures; and a focused physical examination according to the location of lymphadenopathy.
Historical Clues
24

AGE AND DURATION
The rate of malignant etiologies of lymphadenopathy is very low in childhood, but increases with age. Lymph nodes are palpable as early as the neonatal period, and a majority of healthy children have palpable cervical, inguinal, and axillary adenopathy.5 The vast majority of cases of lym-phadenopathy in children is infectious or benign in etiology.6 In one series7 of 628 patients undergoing nodal biopsy, benign or self-limited causes were found in 79 percent of patients younger than 30 years of age, versus 59 percent in patients 31 to 50 years of age and 39 percent in those older than 50 years. Lymphadenopathy that lasts less than two weeks or more than one year with no progressive size increase has a very low likelihood of being neoplastic.8 The rare exceptions to the latter include low-grade Hodgkin's and non-Hodgkin's lymphomas and, occasionally, chronic lymphocytic leukemia.
EXPOSURES
A complete exposure history is essential to determining the etiology of lymphadenopathy. Exposure to animals and biting insects, chronic use of medications, infectious contacts, and a history of recurrent infections are essential in the evaluation of persistent lymphadenopathy. Travel-related exposures and immunization status should be noted, because many tropical or nonendemic diseases may be associated with persistent lymphadenopathy, including tuberculosis, trypanosomiasis, scrub typhus, leishmaniasis, tularemia, brucellosis, plague, and anthrax.
Environmental exposures such as tobacco, alcohol, and ultraviolet radiation may raise suspicion for metastatic carcinoma of the internal organs, cancers of the head and neck, and skin malignancies, respectively. Occupational exposures to silicon or beryllium may also lead to lymphadenopathy. Sexual history and orientation are important in determining potentially sexually transmitted causes of inguinal and cervical lymphadenopathy. Patients with acquired immunodeficiency syndrome (AIDS) have a broad differential of causes of lymphadenopathy, and rates of malignancies such as Kaposi's sarcoma and non-Hodg-kin's lymphoma are increased in this group.9,10 Family history may raise suspicion for certain neoplastic causes of lymphadenopathy, such as carcinomas of the breast or familial dysplastic nevus syndrome and melanoma.
ASSOCIATED SYMPTOMS
A thorough review of systems is important in the evaluation of peripheral lymphadenopathy. Constitutional symptoms such as fatigue, malaise, and fever, often associated with impressive cervical lymphadenopathy and atypical lymphocytosis, are seen most commonly with mononucleosis syndromes. Significant fever, night sweats, and unexplained weight loss of more than 10 percent of a patient's normal body weight are the “B” symptoms of Hodgkin's lymphoma, increasing in frequency from 8 percent of patients with Stage I disease to 68 percent of those with Stage IV disease.11 These symptoms are also seen in 10 percent of patients with non-Hodgkin's lymphoma.8
Symptoms such as arthralgias, muscle weakness, or unusual rash may indicate the possibility of autoimmune diseases such as rheumatoid arthritis, lupus erythematosus, or dermatomyositis. More specific review questions, such as whether pain occurs in the area of lymphadenopathy after even limited alcohol ingestion, may bring out a rare but fairly specific finding of a neoplasm such as Hodgkin's lymphoma.
Physical Examination
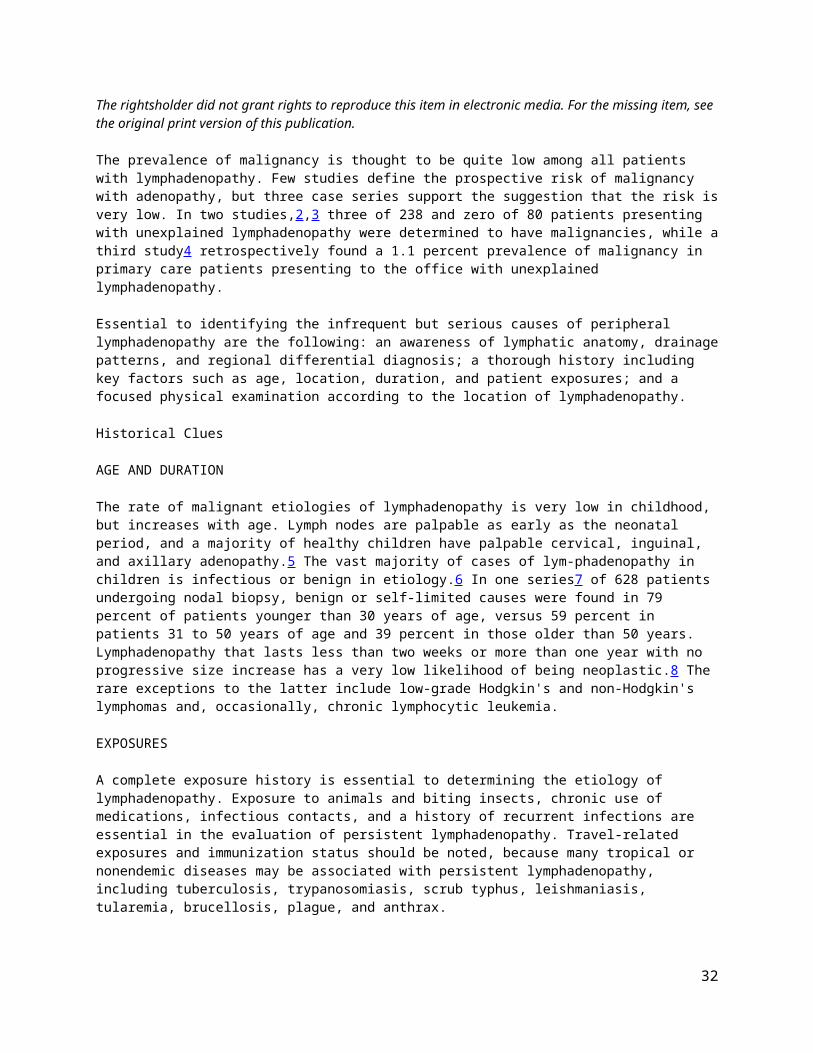
The physical examination should be regionally directed by knowledge of the lymphatic drainage patterns (Figures 1 through 3) and should include a complete lymphatic examination looking for generalized lymphadenopathy. Skin should be examined for unusual lesions that suggest malignancy and for traumatic lesions, which can be sites of infectious inoculation. Splenomegaly, while rarely associated with lymphadenopathy, focuses the differential on a limited number of disorders, most commonly infectious mononucleosis,8 but also the lymphomas, the lymphocytic leukemias, and sarcoidosis.
25

FIGURE 1.
Lymph nodes of the head and neck, and the regions that they drain.
FIGURE 2.
Axillary lymphatics and the structures that they drain.
26

FIGURE 3.
ILLUSTRATION BY CHRISTY KRAMES
Inguinal lymphatics and the structures that they drain.
HEAD AND NECK LYMPHADENOPATHY
Palpable cervical lymph nodes, which are commonly appreciable throughout childhood, were noted in 56 percent of adult physicals in one outpatient primary care study,12 although the incidence declined with age. The most common cause of cervical lymphadenopathy is infection, which in children is typically an acute and self-limited viral infection. While most cases resolve quickly, some entities such as atypical mycobacteria, cat-scratch disease, toxoplasmosis, Kikuchi's lymphadenitis, sarcoidosis, and Kawasaki's syndrome can create persistent lymphadenopathy for many months, and may be confused with neoplasms.
Among this group, supraclavicular nodes are the most likely to be malignant, and should always be investigated, even in children.5,13 Overall, the prevalence of malignancy in this presentation is unknown, but rates of 54 to 85 percent have been seen in biopsy series reports.7,14–16
AXILLARY LYMPHADENOPATHY
Because the upper extremities that axillary lymph nodes drain are commonly exposed to local infection and injury, most axillary lymphadenopathy is nonspecific or reactive in etiology. Infectious sources of prolonged lymphadenopathy such as toxoplasmosis, tuberculosis, and mononucleosis rarely manifest with lymphadenopathy alone,8 and persistent lymphadenopathy is less commonly found in the axillary nodes than in the inguinal chain.
Breast adenocarcinoma often metastasizes initially to the anterior and central axillary nodes, which may be palpable before discovery of the primary tumor. Hodgkin's and non-Hodgkin's lymphomas rarely manifest solely or initially in the axillary nodes,17 although this can be the first region discovered by the patient. Antecubital or epitrochlear lymphadenopathy can suggest lymphoma, or melanoma of the extremity, which first metastasizes to the ipsilateral regional lymph nodes.18,19
INGUINAL LYMPHADENOPATHY
Inguinal lymphadenopathy is common, with nodes enlarged up to 1 to 2 cm in diameter in many healthy adults, particularly those who spend time barefoot outdoors.19 Benign reactive lymphadenopathy and infection are the most common etiologies, and inguinal lymphadenopathy is of low suspicion for malignancy.
27

Infrequently, Hodgkin's lymphomas first present in this area,11,17 as do non-Hodgkin's lymphomas. Penile and vulvar squamous cell carcinomas, the lymphomas, and melanoma also can occur with lymphadenopathy in this area. When the overlying skin is involved, testicular carcinoma may lead to inguinal lymphadenopathy,20 which is present in 58 percent of patients diagnosed with penile or urethral carcinoma.21 In neither case is it the typical presenting finding.
GENERALIZED LYMPHADENOPATHY
Generalized lymphadenopathy, defined as lymphadenopathy found in two or more distinct anatomic regions, is more likely than localized adenopathy to result from serious infections, autoimmune diseases, and disseminated malignancy. It usually merits specific testing. Common benign causes include adenoviral illness in children, mononucleosis, and some pharmaceuticals, and these can usually be identified with a careful history and examination. Generalized adenopathy infrequently occurs in patients with neoplasms, but it is occasionally seen in patients with leukemias and lymphomas, or advanced disseminated metastatic solid tumors. Hodgkin's lymphoma and most metastatic carcinomas typically progress through nodes in anatomic sequence.
Patients who are immunocompromised and those with AIDS have a wide differential for generalized lymphadenopathy, including early human immunodeficiency virus infection, activated tuberculosis, cryptococcosis, cytomegalovirus, toxoplasmosis, and Kaposi's sarcoma, which can present with lymphadenopathy before visible skin lesions appear.22
NODAL CHARACTER AND SIZE
Lymph nodes that are hard and painless have increased significance for malignant or granulomatous disease and typically merit further investigation. For example, the nodes of nodular sclerosing Hodgkin's lymphoma are firm, fixed, circumscribed, and rubbery. This is in contrast to viral infection, which typically produces hyperplastic nodes that are bilateral, mobile, nontender, and clearly demarcated. Painful or tender lymphadenopathy is non-specific but typically represents nodal inflammation from an infection. In rare cases, painful or tender lymphadenopathy can result from hemorrhage into the necrotic center of a neoplastic node or from pressure on the nodal capsule caused by rapid tumor expansion.
Lymphadenopathy is classically described as a node larger than 1 cm, although this varies by lymphatic region. Palpable supraclavicular, iliac, or popliteal nodes of any size and epitrochlear nodes larger than 5 mm are considered abnormal.5,23 There is no uniform nodal size at which one should become suspicious of a neoplastic etiology. Two series8,13 reported maximum diameters of more than 2 cm and 1.5 cm, respectively, as an appropriate starting point for high suspicion of malignant or granulomatous disease. Increasing size and persistence over time are of greater concern for malignancy than a specific level of nodal enlargement.
DIAGNOSIS
Using the factors above as guidance, a thorough history and physical examination should allow physicians to categorize individual cases of lymphadenopathy according to the algorithm in Figure 4.1 If findings suggest benign, self-limited disease, then the patient should be reassured, concerns addressed, the natural history of the disease explained, and follow-up offered for persistent adenopathy. Specific testing is indicated if the history and examination suggest autoimmune or more serious infectious diseases (Table 1).1 If neoplasm is suspected, the work-up may involve laboratory testing or radiologic evaluation, computed tomography, magnetic resonance imaging, and ultrasonography, which has been particularly useful in distinguishing benign from malignant nodes in patients with cancer of the head and neck. However, definitive diagnosis is only obtained from biopsy.
Peripheral Lymphadenopathy
28
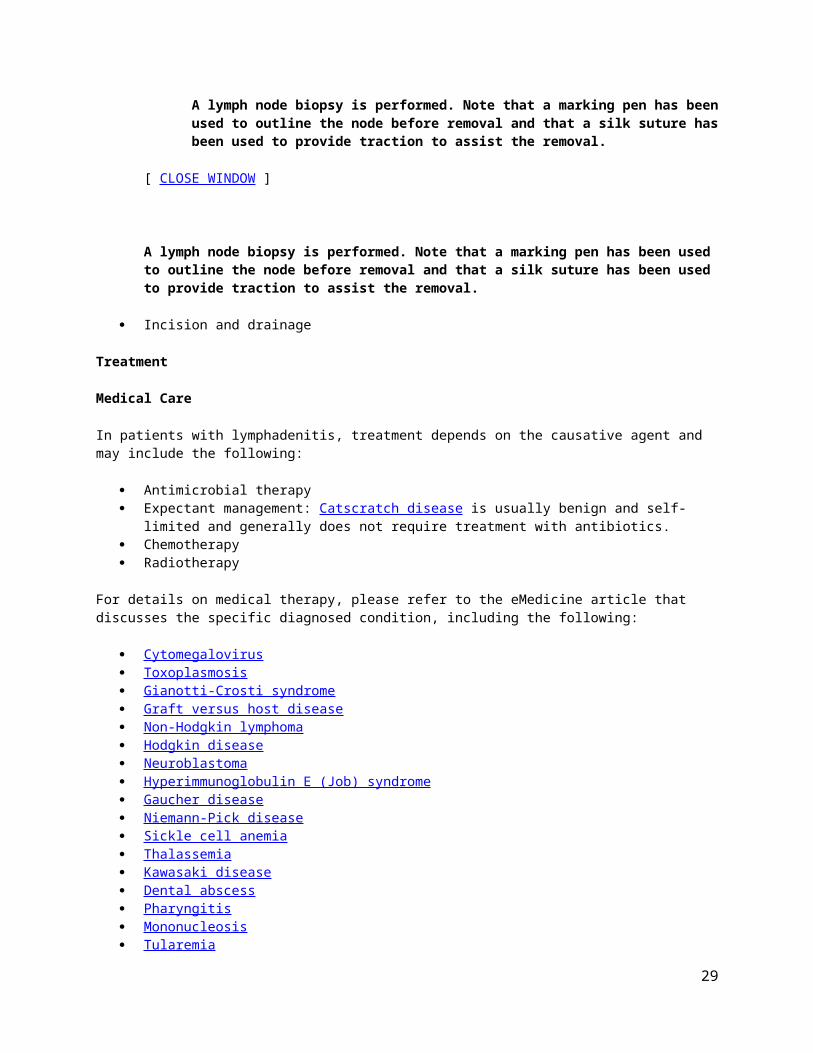
FIGURE 4.
Algorithm for the evaluation of peripheral lymphadenopathy. (CBC = complete blood count; RPR = rapid plasma reagin; PPD = purified protein derivative; HIV = human immunodeficiency virus; HbsAg = hepatitis B surface antigen; ANA = antinuclear antibody).
Adapted with permission from Ferrer R. Lymphadenopathy: differential diagnosis and evaluation. Am Fam Physician 1998;58:1315.
The most difficult task for the primary care physician occurs when the initial history and physical examination are not suggestive of a diagnosis that can be pursued with specific testing. Use of a short course of antibiotics or corticosteroids in the patient with unexplained lymphadenopathy is common. However, there is no evidence to support this practice, which should be avoided because it may hinder or delay diagnosis. The patient's level of concern should be addressed early and often, with provocative questioning, if necessary.
The first step in evaluating unexplained lymphadenopathy involves reviewing the patient's medications (Table 2 1 ,8,19), considering unusual causes of lymphadenopathy (Table 3 1 ,8,19), and reconsidering the risk factors for neoplasm discussed earlier. If a diagnosis is not suggested, and the patient is deemed low risk for neoplasm, then regional lymphadenopathy can be safely observed. Given the number of serious causes of generalized lymphadenopathy, a careful search for clues to autoimmune or infectious etiology is essential, and screening laboratory tests for several difficult diagnoses that could present with lymphadenopathy prior to other symptoms may be warranted before observation.
TABLE 2Medications That Can Cause Lymphadenopathy
29

Allopurinol (Zyloprim) Atenolol (Tenormin) Captopril (Capoten) Carbamazepine (Tegretol) Gold Hydralazine (Après line) Penicillins
Phenytoin (Dilantin) Primidone (Mysoline) Pyrimethamine (Daraprim) Quinidine Trimethoprim/sulfamethoxazole (Bactrim) Sulindac (Clinoril)
Information from references 1,8, and 19.
There is no consensus on the appropriate observation period for unexplained lymphadenopathy, although several authors1,8,19 suggest that unexplained, noninguinal lymphadenopathy lasting more than one month merits specific investigation or biopsy. Despite several attempts to create a scoring system to identify which patients who have lymphadenopathy require biopsy,13,24 it remains an inexact science. Both the physician's level of clinical suspicion for serious illness and the patient's level of concern should be considered.
TABLE 3Miscellaneous/Unusual Causes of Lymphadenopathy (SHAK)
SarcoidosisSilicosis/berylliosisStorage disease: Gaucher'sdisease, Niemann-Pickdisease, Fabry's disease, Tangier diseaseHyperthyroidismHistiocytosis XHypertriglyceridemia, severeAngiofollicular lymph node hyperplasia: Castleman's diseaseAngioimmunoblastic lymphadenopathyKawasaki syndromeKikuchi's lymphadenitisKimura's disease
Information from references 1,8, and 19.
LYMPH NODE BIOPSY
Once biopsy has been chosen, ideally the largest, most suspicious, and most accessible node is selected, taking into account differing diagnostic yields by site. Inguinal nodes offer the lowest yield, and supraclavicular nodes have the highest.14,16 Although the advent of new immunohisto-chemical analytic techniques has increased the sensitivity and specificity of fine-needle aspiration,25–29 excisional biopsy remains the diagnostic procedure of choice. The preservation of nodal architecture is critical to the proper diagnosis of lymphadenopathy, particularly when differentiating lymphoma from benign reactive hyperplasia. Higher diagnostic yields can be expected from medical centers that adhere to strict protocols on specimen handling,30,31 and from board-certified cytopathologists. Excisional biopsy has few complications, such as vessel injury and the rare spinal accessory nerve injury.32
The Authors
ANDREW W. BAZEMORE, M.D., is currently assistant professor in the Department of Family Medicine at the University of Cincinnati College of Medicine, where he also completed a faculty development fellowship and served a residency in family medicine. Dr. Bazemore received his medical degree from the University of North Carolina at Chapel Hill School of Medicine.
30

DOUGLAS R. SMUCKER, M.D., M.P.H., is associate professor and director of research in the Department of Family Medicine at the University of Cincinnati College of Medicine. Dr. Smucker completed his medical degree and served a residency in family practice at the Medical College of Ohio in Toledo. He also completed a primary care research fellowship and a residency in preventive medicine at the University of North Carolina at Chapel Hill School of Medicine.
Address correspondence to Andrew W. Bazemore, M.D., University of Cincinnati Family Practice, 2446 Kipling Ave., Cincinnati, OH 45239 (e-mail: [email protected]). Reprints are not available from the authors.
The authors indicate that they do not have any conflicts of interest. Sources of funding: none reported.
REFERENCES
1. Ferrer R. Lymphadenopathy: differential diagnosis and evaluation. Am Fam Physician. 1998;58:1313–20.
2. Allhiser J, McKnight TA, Shank JC. Lymphadenopathy in a family practice. J Fam Pract. 1981;12:27–32.
3. Williamson HA Jr. Lymphadenopathy in a family practice: a descriptive study of 249 cases. J Fam Pract. 1985;20:449–52.
4. Fijten GH, Blijham GH. Unexplained lymphadenopathy in family practice. An evaluation of the probability of malignant causes and the effectiveness of physicians' workup. J Fam Pract. 1988;27:373–6.
5. Kelly CS, Kelly RE Jr. Lymphadenopathy in children. Pediatr Clin North Am. 1998;45:875–88.
6. Knight PJ, Mulne AF, Vassy LE. When is lymph node biopsy indicated in children with enlarged peripheral nodes? Pediatrics. 1982;69:391–6.
7. Lee Y, Terry R, Lukes RJ. Lymph node biopsy for diagnosis: a statistical study. J Surg Oncol. 1980;14:53–60.
8. Pangalis GA, Vassilakopoulos TP, Boussiotis VA, Fessas P. Clinical approach to lymphadenopathy. Semin Oncol. 1993;20:570–82.
9. Rabkin CS. AIDS and cancer in the era of highly active antiretroviral therapy (HAART). Eur J Cancer. 2001;37:1316–9.
10. Vaccher E, Spina M, Tirelli U. Clinical aspects and management of Hodgkin's disease and other tumours in HIV-infected individuals. Eur J Cancer. 2001;37:1306–15.
11. Rosenburg S, Canellos G. Hodgkin's disease. In: Canellos GP, Lister TA, Sklar JL, eds. The lymphomas. Philadelphia: Saunders, 1998:305–30.
12. Linet OI, Metzler C. Practical ENT. Incidence of palpable cervical nodes in adults. Postgrad Med. 1977;62:210–3.
13. Slap GB, Brooks JS, Schwartz JS. When to perform biopsies of enlarged lymph nodes in young patients. JAMA. 1984;252:1321–6.
14. Steel BL, Schwartz MR, Ramzy I. Fine needle aspiration biopsy in the diagnosis of lymphadenopathy in 1,103 patients. Role, limitations and analysis of diagnostic pitfalls. Acta Cytol. 1995;39:76–81.
31
15. Ellison E, LaPuerta P, Martin SE. Supraclavicular masses: results of a series of 309 cases biopsied by fine needle aspiration. Head Neck. 1999;21:239–46.
16. Karadeniz C, Oguz A, Ezer U, Ozturk G, Dursun A. The etiology of peripheral lymphadenopathy in children. Pediatr Hematol Oncol. 1999;16:525–31.
17. Mauch PM, Kalish LA, Kadin M, Coleman CN, Osteen R, Hellman S. Patterns of presentation of Hodgkin disease. Implications for etiology and pathogenesis. Cancer. 1993;71:2062–71.
18. Cochran AJ. Melanoma metastases through the lymphatic system. Surg Clin North Am. 2000;80:1683–93.
19. Habermann TM, Steensma DP. Lymphadenopathy. Mayo Clin Proc. 2000;75:723–32.
20. Small EJ, Torti FM. Testes. In: Abeloff MD, ed. Clinical oncology. 2d ed. New York: Churchill Livingstone, 2000:1912.
21. Skinner DG, Leadbetter WF, Kelley SB. The surgical management of squamous cell carcinoma of the penis. J Urol. 1972;107:273–7.
22. Saif MW. Diagnosis and treatment of Kaposi's sarcoma. Resid Staff Physician. 2001;47:19–24.
23. Grossman M, Shiramizu B. Evaluation of lymphadenopathy in children. Curr Opin Pediatr. 1994;6:68–76.
24. Vassilakopoulos TP, Pangalis GA. Application of a prediction rule to select which patients presenting with lymphadenopathy should undergo a lymph node biopsy. Medicine (Baltimore). 2000;79:338–47.
25. Layfield LJ. Fine-needle aspiration of the head and neck. Pathology (Phila). 1996;4:409–38.
26. Das DK. Value and limitations of fine-needle aspiration cytology in diagnosis and classification of lymphomas: a review. Diagn Cytopathol. 1999;21:240–9.
27. Dunphy CH, Ramos R. Combining fine-needle aspiration and flow cytometric immunophenotyping in evaluation of nodal and extranodal sites for possible lymphoma: a retrospective review. Diagn Cytopathol. 1997;16:200–6.
28. Wakely PE Jr. Fine needle aspiration cytopathology of malignant lymphoma. Clin Lab Med. 1998;18:541–59.
29. Wakely PE Jr. Fine-needle aspiration cytopathology in diagnosis and classification of malignant lymphoma: accurate and reliable? Diagn Cytopathol. 2000;22:120–5.
30. Margolis IB, Matteucci D, Organ CH Jr. To improve the yield of biopsy of the lymph nodes. Surg Gynecol Obstet. 1978;147:376–8.
31. Sinclair S, Beckman E, Ellman L. Biopsy of enlarged, superficial lymph nodes. JAMA. 1974;228:602–3.
32. Battista AF. Complications of biopsy of the cervical lymph node. Surg Gynecol Obstet. 1991;173:142–6.
Copyright © 2002 by the American Academy of Family Physicians.This content is owned by the AAFP. A person viewing it online may make one printout of the material and may use that printout only for his or her personal, non-commercial reference. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later
32

invented, except as authorized in writing by the AAFP. Contact [email protected] for copyright questions and/or permission requests.
http://www.aafp.org/afp/2002/1201/p2103.html
33
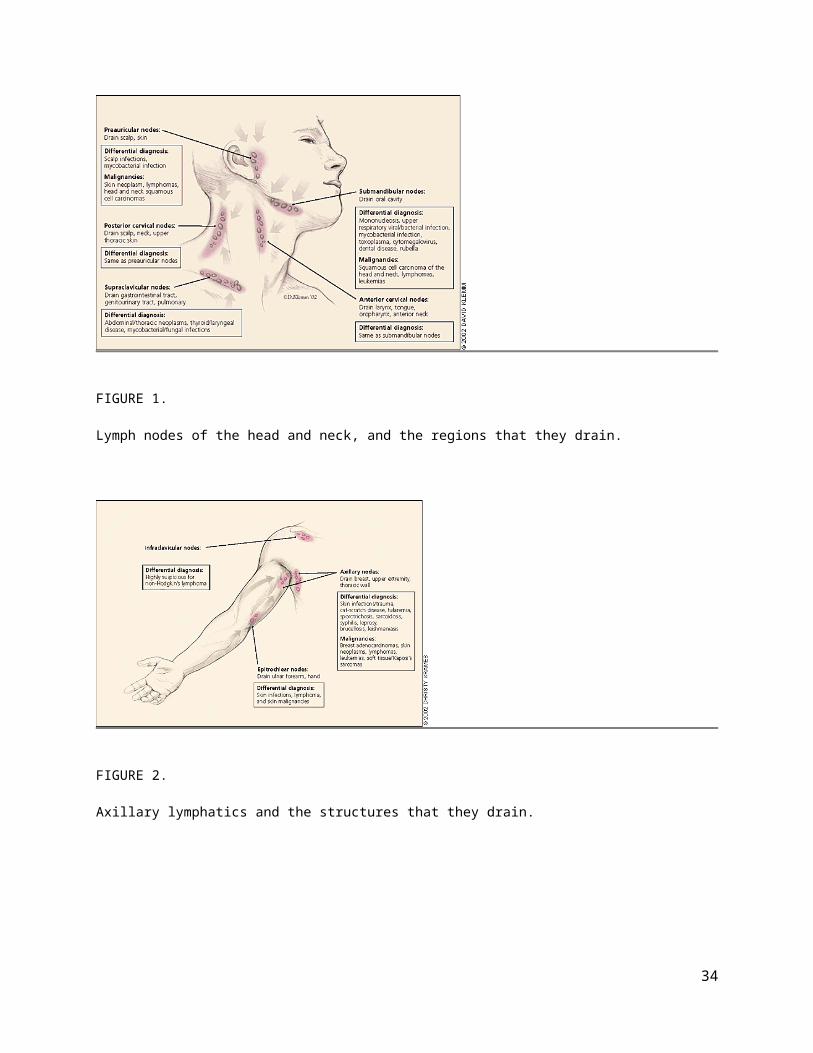
Limfadenitis DEFINISILimfadenitis adalah peradangan pada satu atau beberapa kelenjar getah bening.
PENYEBABLimfadenitis bisa disebabkan oleh infeksi dari berbagai organisme, yaitu bakteri, virus, protozoa, riketsia atau jamur. Secara khusus, infeksi menyebar ke kelenjar getah bening dari infeksi kulit, telinga, hidung atau mata.
GEJALAKelenjar getah bening yang terinfeksi akan membesar dan biasanya teraba lunak dan nyeri. Kadang-kadang kulit diatasnya tampak merah dan teraba hangat.
DIAGNOSADiagnosis ditegakkan berdasarkan gejala-gejalanya.
Untuk membantu menentukan penyebabnya, bisa dilakukan biopsi (pengangkatan jaringan untuk diperiksa di bawah mikroskop).
PENGOBATANPengobatan tergantung dari organisme penyebabnya. Untuk infeksi bakteri, biasanya diberikan antibiotik per-oral (melalui mulut) atau intravena (melalui pembuluh darah).
Untuk membantu mengurangi rasa sakit, kelenjar getah bening yang terkena bisa dikompres hangat. Biasanya jika infeksi telah diobati, kelenjar akan mengecil secara perlahan dan rasa sakit akan hilang. Kadang-kadang kelenjar yang membesar tetap keras dan tidak lagi terasa lunak pada perabaan.
PENCEGAHANMenjaga kesehatan dan kebersihan badan bisa membantu mencegah terjadinya berbagai infeksi.
http://medicastore.com/penyakit/195/Limfadenitis.html
34
Related Documents











